User login
Recurrent Cerebriform Connective Tissue Nevus on the Foot of a Patient With Proteus Syndrome
To the Editor:
A 12-year-old girl presented with discomfort and walking limitation caused by cutaneous masses on the plantar aspects of the feet with associated bone abnormalities that had started as several flesh-colored papules on the plantar surface of both feet at the age of 1 year. Over time the lesions gradually enlarged and formed irregular masses, more prominently on the right foot. At the age of 6 years, surgical correction was performed due to increased walking impairment and a skin examination that suggested connective tissue nevus. The results were good. However, the local tissue overgrowth recurred after 1 year. Slowly growing lesions were found at the surgical site, which necessitated hospitalization. Her medical history was negative for other disease. There was no family history of similar skin conditions and her parents were nonconsanguineous.
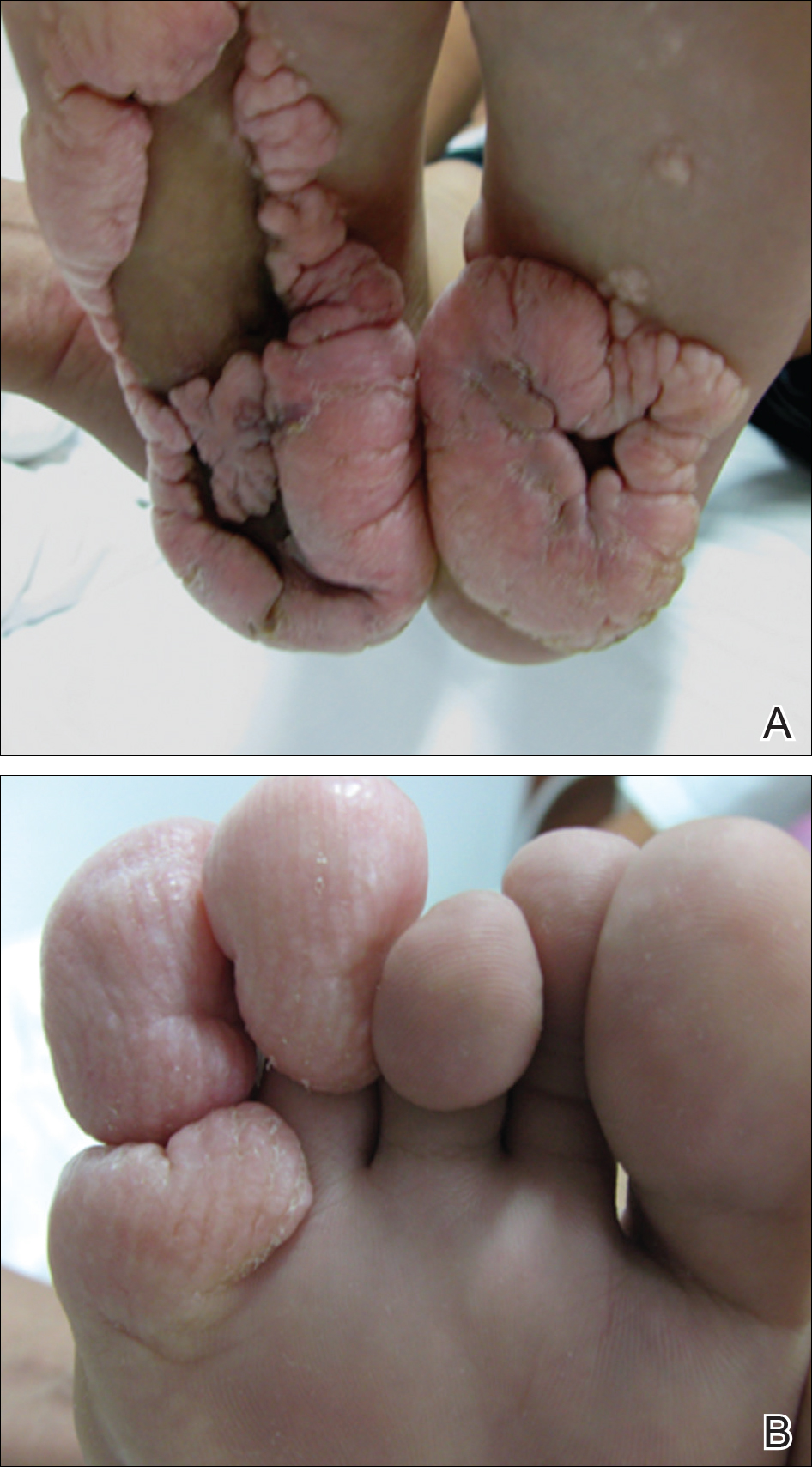
Physical examination revealed malnutrition and poor development in height as well as difficulty walking. She also had moderate scoliosis with a curve to the left. Dermatological examination showed multiple reddish cerebriform hyperplasia in both plantar areas; the right side was more severely involved (Figure 1A). There was macrodactyly of 2 toes on the right foot (Figure 1B). All results of routine blood examinations were within reference range. There were no abnormalities noted in the abdominal ultrasound and cardiac examinations. Plain radiographs of the spine and feet demonstrated scoliosis and exostosis on the calcaneus and bottom of the scaphoid. Histopathologic examination of tissue from the plantar cerebriform hyperplasia revealed hyperkeratosis, slight acanthosis and papillomatosis in the epidermis, and dense collagen bands and sparse elastic fibers in the dermis (Figure 2).

Given the clinical and radiologic manifestation, the diagnosis of Proteus syndrome (PS) was established. After taking into account the severe discomfort and the success of the first surgery, we performed a resection and full-thickness skin graft surgery once again. The feet recovered without any discomfort in daily life. The appearance of the skin graft area was normal 1 year following surgery (Figure 3). She was treated with spinal plate fixation at another institution, progressed well for 2 years, and was subsequently lost to follow-up.

Proteus syndrome is a multisystem disorder with a difficult diagnosis due to the variability of its manifestations. The worldwide incidence of this rare disorder is less than 1 per 1 million individuals, and it is thought to be caused by a somatic genetic alteration.1 Clinical characteristics include bone abnormalities, vascular malformations, dysregulation of fatty tissue, linear verrucous epidermal nevus, and cerebriform connective tissue nevus (CCTN). Although CCTN is not a common finding in patients with PS, it is considered a fairly specific sign with the greatest impact for the diagnosis of PS.2
The general feature of PS--asymmetric disproportionate overgrowth of tissues--appears at 6 to 18 months of age, which makes it challenging to diagnose disease earlier. The CCTN in our patient was present since 1 year of age.
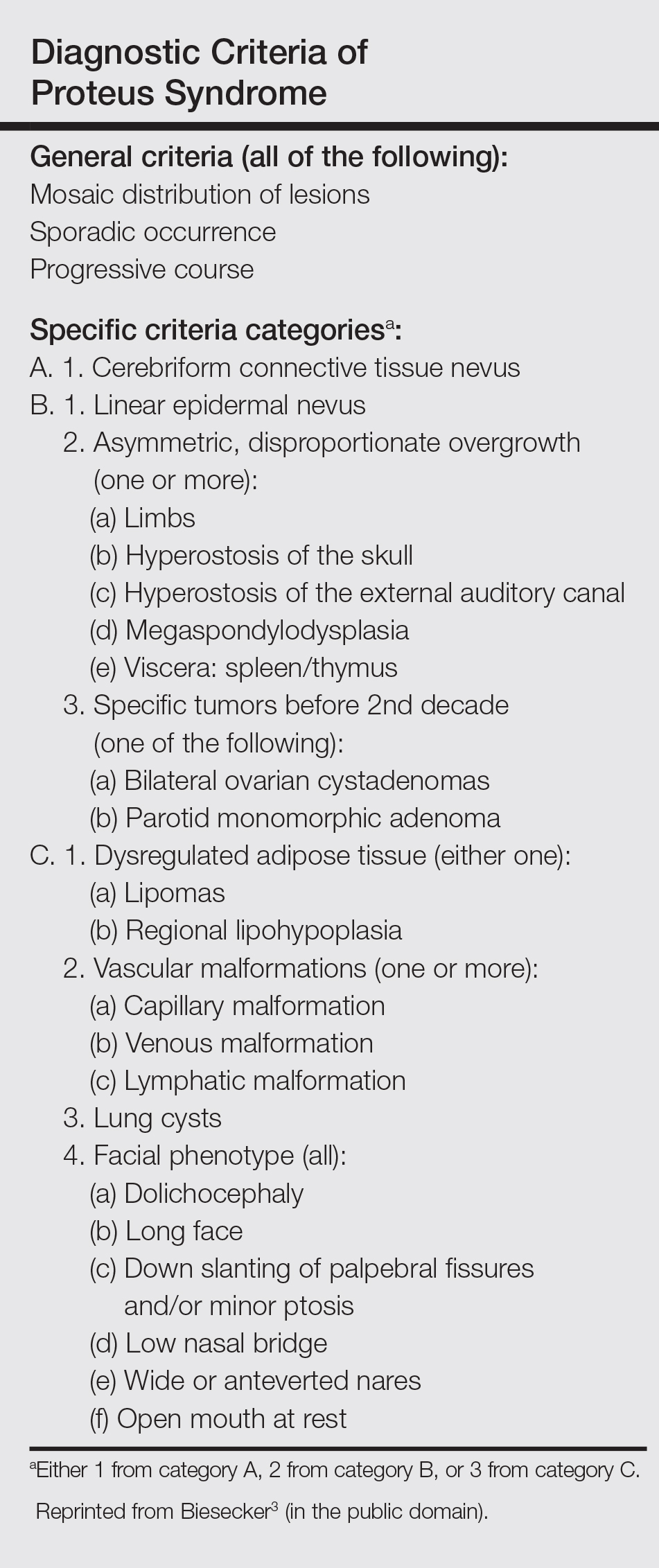
To make a diagnosis of PS, one must have all the general criteria and various specific criteria. The revised diagnostic criteria for PS are given in the Table.3 According to the diagnostic criteria, our patient fulfilled the mandatory general criteria and had plantar CCTN, epidermal nevus, and dysregulated adipose tissue. The CCTN has notable diagnostic value in mildly affected patients, as it is absent in diseases included in the differential diagnosis such as neurofibromatosis, Klippel-Trenaunay-Weber syndrome, Maffucci syndrome, and Bannayan-Riley-Ruvalcaba syndrome. Hemihyperplasia-multiple lipomatosis syndrome and CLOVES (congenital, lipomatous overgrowth, vascular malformations, epidermal nevi, and scoliosis/spinal/skeletal anomalies) syndrome also can present on the plantar surfaces, and lesions may be overgrown at birth but are softer and compressible, have wrinkles instead of deep folds, and tend to grow with the child rather than disproportionately as in PS.4
The epidermal nevi and vascular malformations generally do not spread or increase in number. In contrast, CCTN in PS grows throughout childhood but tends to remain stable in adulthood.4 Postponing surgical treatment until skin lesions stabilize appears to be the best option. However, for practical purposes, surgical intervention may be required at an earlier phase to address the severe functional and cosmetic consequences. Some patients require multiple orthopedic procedures over the ensuing years or decades to control the hyperplasia.3 New CCTN that developed from the prior surgical incision, macrodactyly of the fourth and fifth right toes, and scoliosis appeared when the patient came to our clinic for retreatment 1 year after the initial presentation. The asymmetrical and disproportionate overgrowth of tissues had moderately accelerated in that period. Considering the increasingly impaired walking, we performed a second surgery. On follow-up visits, the patient expressed improvement in daily life.
Studies had been performed to clarify the genetic bases of PS, and the somatic activating mutation in AKT1 (AKT serine/threonine kinase 1) was reported to be the cause of the disease.5,6 Germline PTEN (phosphatase and tensin homolog) mutations have been identified in some patients with overgrowth abnormalities of PS. However, given the misdiagnosis of PS with PTEN mutations and the notion that a gene alone cannot result in PS, the loss-of-function mutations of LEMD3 that have been reported in familial cutaneous collagenomas also may be related to the abnormal growth of connective and bone tissues that are typical of PS.7,8 Lindhurst et al5 concluded that PS is caused by a somatic activating mutation in AKT1, which proved the hypothesis of somatic mosaicism and implicated activation of the PI3K-AKT pathway in the characteristic clinical findings of overgrowth and tumor susceptibility in this disorder. AKT1 is activated by loss-of-function mutations in PTEN, which explains why patients with these mutations (eg, those with the segmental overgrowth, lipomatosis, arteriovenous malformation, epidermal nevus, SOLAMEN [segmental overgrowth, lipomatosis, arteriovenous malformation, and epidermal nevus] syndrome) and patients with activating mutations in AKT1 (eg, those with PS) have overlapping but distinct clinical manifestations. Molecular genetic testing may be useful to confirm the diagnosis in individuals who meet clinical criteria and to establish the diagnosis in individuals with clinical findings that are ambiguous or mild. Further studies are necessary to progress the understanding and management of PS, which will require cooperation of geneticists, surgeons, and other specialists.
- Popescu MD, Burnei G, Draghici L, et al. Proteus syndrome: a difficult diagnosis and management plan. J Med Life. 2014;7:563-566.
- Schepis C, Greco D, Siragusa M, et al. Cerebriform plantar hyperplasia: the major cutaneous feature of Proteus syndrome. Int J Dermatol. 2008;47:374-376.
- Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14:1151-1157.
- Beachkofsky TM, Sapp JC, Biesecker LG, et al. Progressive overgrowth of the cerebriform connective tissue nevus in patients with Proteus syndrome. J Am Acad Dermatol. 2010;63:799-804.
- Lindhurst MJ, Sapp JC, Teer JK, et al. A mosaic activating mutation in AKT1 associated with the Proteus syndrome. N Engl J Med. 2011;365:611-619.
- Wieland I, Tinschert S, Zenker M. High-level somatic mosaicism of AKT1 c.49G>A mutation in skin scrapings from epidermal nevi enables non-invasive molecular diagnosis in patients with Proteus syndrome. Am J Med Genet A. 2013;161A:889-891.
- Cohen MJ, Turner JT, Biesecker LG. Proteus syndrome: misdiagnosis with PTEN mutations. Am J Med Genet A. 2003;122A:323-324.
- Di Stefani A, Gabellini M, Ferlosio A, et al. Cerebriform plantar hyperplasia: the clinico-pathological hallmark of Proteus syndrome. Acta Derm Venereol. 2011;91:580-581.
To the Editor:
A 12-year-old girl presented with discomfort and walking limitation caused by cutaneous masses on the plantar aspects of the feet with associated bone abnormalities that had started as several flesh-colored papules on the plantar surface of both feet at the age of 1 year. Over time the lesions gradually enlarged and formed irregular masses, more prominently on the right foot. At the age of 6 years, surgical correction was performed due to increased walking impairment and a skin examination that suggested connective tissue nevus. The results were good. However, the local tissue overgrowth recurred after 1 year. Slowly growing lesions were found at the surgical site, which necessitated hospitalization. Her medical history was negative for other disease. There was no family history of similar skin conditions and her parents were nonconsanguineous.
Physical examination revealed malnutrition and poor development in height as well as difficulty walking. She also had moderate scoliosis with a curve to the left. Dermatological examination showed multiple reddish cerebriform hyperplasia in both plantar areas; the right side was more severely involved (Figure 1A). There was macrodactyly of 2 toes on the right foot (Figure 1B). All results of routine blood examinations were within reference range. There were no abnormalities noted in the abdominal ultrasound and cardiac examinations. Plain radiographs of the spine and feet demonstrated scoliosis and exostosis on the calcaneus and bottom of the scaphoid. Histopathologic examination of tissue from the plantar cerebriform hyperplasia revealed hyperkeratosis, slight acanthosis and papillomatosis in the epidermis, and dense collagen bands and sparse elastic fibers in the dermis (Figure 2).
Given the clinical and radiologic manifestation, the diagnosis of Proteus syndrome (PS) was established. After taking into account the severe discomfort and the success of the first surgery, we performed a resection and full-thickness skin graft surgery once again. The feet recovered without any discomfort in daily life. The appearance of the skin graft area was normal 1 year following surgery (Figure 3). She was treated with spinal plate fixation at another institution, progressed well for 2 years, and was subsequently lost to follow-up.
Proteus syndrome is a multisystem disorder with a difficult diagnosis due to the variability of its manifestations. The worldwide incidence of this rare disorder is less than 1 per 1 million individuals, and it is thought to be caused by a somatic genetic alteration.1 Clinical characteristics include bone abnormalities, vascular malformations, dysregulation of fatty tissue, linear verrucous epidermal nevus, and cerebriform connective tissue nevus (CCTN). Although CCTN is not a common finding in patients with PS, it is considered a fairly specific sign with the greatest impact for the diagnosis of PS.2
The general feature of PS--asymmetric disproportionate overgrowth of tissues--appears at 6 to 18 months of age, which makes it challenging to diagnose disease earlier. The CCTN in our patient was present since 1 year of age.
To make a diagnosis of PS, one must have all the general criteria and various specific criteria. The revised diagnostic criteria for PS are given in the Table.3 According to the diagnostic criteria, our patient fulfilled the mandatory general criteria and had plantar CCTN, epidermal nevus, and dysregulated adipose tissue. The CCTN has notable diagnostic value in mildly affected patients, as it is absent in diseases included in the differential diagnosis such as neurofibromatosis, Klippel-Trenaunay-Weber syndrome, Maffucci syndrome, and Bannayan-Riley-Ruvalcaba syndrome. Hemihyperplasia-multiple lipomatosis syndrome and CLOVES (congenital, lipomatous overgrowth, vascular malformations, epidermal nevi, and scoliosis/spinal/skeletal anomalies) syndrome also can present on the plantar surfaces, and lesions may be overgrown at birth but are softer and compressible, have wrinkles instead of deep folds, and tend to grow with the child rather than disproportionately as in PS.4
The epidermal nevi and vascular malformations generally do not spread or increase in number. In contrast, CCTN in PS grows throughout childhood but tends to remain stable in adulthood.4 Postponing surgical treatment until skin lesions stabilize appears to be the best option. However, for practical purposes, surgical intervention may be required at an earlier phase to address the severe functional and cosmetic consequences. Some patients require multiple orthopedic procedures over the ensuing years or decades to control the hyperplasia.3 New CCTN that developed from the prior surgical incision, macrodactyly of the fourth and fifth right toes, and scoliosis appeared when the patient came to our clinic for retreatment 1 year after the initial presentation. The asymmetrical and disproportionate overgrowth of tissues had moderately accelerated in that period. Considering the increasingly impaired walking, we performed a second surgery. On follow-up visits, the patient expressed improvement in daily life.
Studies had been performed to clarify the genetic bases of PS, and the somatic activating mutation in AKT1 (AKT serine/threonine kinase 1) was reported to be the cause of the disease.5,6 Germline PTEN (phosphatase and tensin homolog) mutations have been identified in some patients with overgrowth abnormalities of PS. However, given the misdiagnosis of PS with PTEN mutations and the notion that a gene alone cannot result in PS, the loss-of-function mutations of LEMD3 that have been reported in familial cutaneous collagenomas also may be related to the abnormal growth of connective and bone tissues that are typical of PS.7,8 Lindhurst et al5 concluded that PS is caused by a somatic activating mutation in AKT1, which proved the hypothesis of somatic mosaicism and implicated activation of the PI3K-AKT pathway in the characteristic clinical findings of overgrowth and tumor susceptibility in this disorder. AKT1 is activated by loss-of-function mutations in PTEN, which explains why patients with these mutations (eg, those with the segmental overgrowth, lipomatosis, arteriovenous malformation, epidermal nevus, SOLAMEN [segmental overgrowth, lipomatosis, arteriovenous malformation, and epidermal nevus] syndrome) and patients with activating mutations in AKT1 (eg, those with PS) have overlapping but distinct clinical manifestations. Molecular genetic testing may be useful to confirm the diagnosis in individuals who meet clinical criteria and to establish the diagnosis in individuals with clinical findings that are ambiguous or mild. Further studies are necessary to progress the understanding and management of PS, which will require cooperation of geneticists, surgeons, and other specialists.
To the Editor:
A 12-year-old girl presented with discomfort and walking limitation caused by cutaneous masses on the plantar aspects of the feet with associated bone abnormalities that had started as several flesh-colored papules on the plantar surface of both feet at the age of 1 year. Over time the lesions gradually enlarged and formed irregular masses, more prominently on the right foot. At the age of 6 years, surgical correction was performed due to increased walking impairment and a skin examination that suggested connective tissue nevus. The results were good. However, the local tissue overgrowth recurred after 1 year. Slowly growing lesions were found at the surgical site, which necessitated hospitalization. Her medical history was negative for other disease. There was no family history of similar skin conditions and her parents were nonconsanguineous.
Physical examination revealed malnutrition and poor development in height as well as difficulty walking. She also had moderate scoliosis with a curve to the left. Dermatological examination showed multiple reddish cerebriform hyperplasia in both plantar areas; the right side was more severely involved (Figure 1A). There was macrodactyly of 2 toes on the right foot (Figure 1B). All results of routine blood examinations were within reference range. There were no abnormalities noted in the abdominal ultrasound and cardiac examinations. Plain radiographs of the spine and feet demonstrated scoliosis and exostosis on the calcaneus and bottom of the scaphoid. Histopathologic examination of tissue from the plantar cerebriform hyperplasia revealed hyperkeratosis, slight acanthosis and papillomatosis in the epidermis, and dense collagen bands and sparse elastic fibers in the dermis (Figure 2).
Given the clinical and radiologic manifestation, the diagnosis of Proteus syndrome (PS) was established. After taking into account the severe discomfort and the success of the first surgery, we performed a resection and full-thickness skin graft surgery once again. The feet recovered without any discomfort in daily life. The appearance of the skin graft area was normal 1 year following surgery (Figure 3). She was treated with spinal plate fixation at another institution, progressed well for 2 years, and was subsequently lost to follow-up.
Proteus syndrome is a multisystem disorder with a difficult diagnosis due to the variability of its manifestations. The worldwide incidence of this rare disorder is less than 1 per 1 million individuals, and it is thought to be caused by a somatic genetic alteration.1 Clinical characteristics include bone abnormalities, vascular malformations, dysregulation of fatty tissue, linear verrucous epidermal nevus, and cerebriform connective tissue nevus (CCTN). Although CCTN is not a common finding in patients with PS, it is considered a fairly specific sign with the greatest impact for the diagnosis of PS.2
The general feature of PS--asymmetric disproportionate overgrowth of tissues--appears at 6 to 18 months of age, which makes it challenging to diagnose disease earlier. The CCTN in our patient was present since 1 year of age.
To make a diagnosis of PS, one must have all the general criteria and various specific criteria. The revised diagnostic criteria for PS are given in the Table.3 According to the diagnostic criteria, our patient fulfilled the mandatory general criteria and had plantar CCTN, epidermal nevus, and dysregulated adipose tissue. The CCTN has notable diagnostic value in mildly affected patients, as it is absent in diseases included in the differential diagnosis such as neurofibromatosis, Klippel-Trenaunay-Weber syndrome, Maffucci syndrome, and Bannayan-Riley-Ruvalcaba syndrome. Hemihyperplasia-multiple lipomatosis syndrome and CLOVES (congenital, lipomatous overgrowth, vascular malformations, epidermal nevi, and scoliosis/spinal/skeletal anomalies) syndrome also can present on the plantar surfaces, and lesions may be overgrown at birth but are softer and compressible, have wrinkles instead of deep folds, and tend to grow with the child rather than disproportionately as in PS.4
The epidermal nevi and vascular malformations generally do not spread or increase in number. In contrast, CCTN in PS grows throughout childhood but tends to remain stable in adulthood.4 Postponing surgical treatment until skin lesions stabilize appears to be the best option. However, for practical purposes, surgical intervention may be required at an earlier phase to address the severe functional and cosmetic consequences. Some patients require multiple orthopedic procedures over the ensuing years or decades to control the hyperplasia.3 New CCTN that developed from the prior surgical incision, macrodactyly of the fourth and fifth right toes, and scoliosis appeared when the patient came to our clinic for retreatment 1 year after the initial presentation. The asymmetrical and disproportionate overgrowth of tissues had moderately accelerated in that period. Considering the increasingly impaired walking, we performed a second surgery. On follow-up visits, the patient expressed improvement in daily life.
Studies had been performed to clarify the genetic bases of PS, and the somatic activating mutation in AKT1 (AKT serine/threonine kinase 1) was reported to be the cause of the disease.5,6 Germline PTEN (phosphatase and tensin homolog) mutations have been identified in some patients with overgrowth abnormalities of PS. However, given the misdiagnosis of PS with PTEN mutations and the notion that a gene alone cannot result in PS, the loss-of-function mutations of LEMD3 that have been reported in familial cutaneous collagenomas also may be related to the abnormal growth of connective and bone tissues that are typical of PS.7,8 Lindhurst et al5 concluded that PS is caused by a somatic activating mutation in AKT1, which proved the hypothesis of somatic mosaicism and implicated activation of the PI3K-AKT pathway in the characteristic clinical findings of overgrowth and tumor susceptibility in this disorder. AKT1 is activated by loss-of-function mutations in PTEN, which explains why patients with these mutations (eg, those with the segmental overgrowth, lipomatosis, arteriovenous malformation, epidermal nevus, SOLAMEN [segmental overgrowth, lipomatosis, arteriovenous malformation, and epidermal nevus] syndrome) and patients with activating mutations in AKT1 (eg, those with PS) have overlapping but distinct clinical manifestations. Molecular genetic testing may be useful to confirm the diagnosis in individuals who meet clinical criteria and to establish the diagnosis in individuals with clinical findings that are ambiguous or mild. Further studies are necessary to progress the understanding and management of PS, which will require cooperation of geneticists, surgeons, and other specialists.
- Popescu MD, Burnei G, Draghici L, et al. Proteus syndrome: a difficult diagnosis and management plan. J Med Life. 2014;7:563-566.
- Schepis C, Greco D, Siragusa M, et al. Cerebriform plantar hyperplasia: the major cutaneous feature of Proteus syndrome. Int J Dermatol. 2008;47:374-376.
- Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14:1151-1157.
- Beachkofsky TM, Sapp JC, Biesecker LG, et al. Progressive overgrowth of the cerebriform connective tissue nevus in patients with Proteus syndrome. J Am Acad Dermatol. 2010;63:799-804.
- Lindhurst MJ, Sapp JC, Teer JK, et al. A mosaic activating mutation in AKT1 associated with the Proteus syndrome. N Engl J Med. 2011;365:611-619.
- Wieland I, Tinschert S, Zenker M. High-level somatic mosaicism of AKT1 c.49G>A mutation in skin scrapings from epidermal nevi enables non-invasive molecular diagnosis in patients with Proteus syndrome. Am J Med Genet A. 2013;161A:889-891.
- Cohen MJ, Turner JT, Biesecker LG. Proteus syndrome: misdiagnosis with PTEN mutations. Am J Med Genet A. 2003;122A:323-324.
- Di Stefani A, Gabellini M, Ferlosio A, et al. Cerebriform plantar hyperplasia: the clinico-pathological hallmark of Proteus syndrome. Acta Derm Venereol. 2011;91:580-581.
- Popescu MD, Burnei G, Draghici L, et al. Proteus syndrome: a difficult diagnosis and management plan. J Med Life. 2014;7:563-566.
- Schepis C, Greco D, Siragusa M, et al. Cerebriform plantar hyperplasia: the major cutaneous feature of Proteus syndrome. Int J Dermatol. 2008;47:374-376.
- Biesecker L. The challenges of Proteus syndrome: diagnosis and management. Eur J Hum Genet. 2006;14:1151-1157.
- Beachkofsky TM, Sapp JC, Biesecker LG, et al. Progressive overgrowth of the cerebriform connective tissue nevus in patients with Proteus syndrome. J Am Acad Dermatol. 2010;63:799-804.
- Lindhurst MJ, Sapp JC, Teer JK, et al. A mosaic activating mutation in AKT1 associated with the Proteus syndrome. N Engl J Med. 2011;365:611-619.
- Wieland I, Tinschert S, Zenker M. High-level somatic mosaicism of AKT1 c.49G>A mutation in skin scrapings from epidermal nevi enables non-invasive molecular diagnosis in patients with Proteus syndrome. Am J Med Genet A. 2013;161A:889-891.
- Cohen MJ, Turner JT, Biesecker LG. Proteus syndrome: misdiagnosis with PTEN mutations. Am J Med Genet A. 2003;122A:323-324.
- Di Stefani A, Gabellini M, Ferlosio A, et al. Cerebriform plantar hyperplasia: the clinico-pathological hallmark of Proteus syndrome. Acta Derm Venereol. 2011;91:580-581.
Practice Points
- Proteus syndrome (PS) is a rare mosaic condition characterized by progressive overgrowth of skin, connective tissue, brain tissue, and other tissues.
- A somatic activating mutation of the AKT1 gene has been identified as a cause for developing PS.
- Distinct cutaneous features, including cerebriform connective tissue nevi (CCTN), epidermal nevi, vascular malformations, and adipose abnormalities, can alert the dermatologist to the underlying condition before the onset of asymmetric skeletal overgrowth.
- The CCTN in PS grows throughout childhood but tends to remain stable in adulthood. Postponing surgical treatment until skin lesions stabilize appears to be the best option. However, for practical purposes, surgical intervention may be required at an earlier phase to address the severe functional and cosmetic consequences.

Atopic dermatitis prevention strategies under study
VIENNA – Diverse strategies aimed at preventing childhood atopic dermatitis (AD) now under study include installation of home water softeners, daily use of emollients starting at birth, and maternal consumption of probiotics beginning late in pregnancy, Carsten Flohr, PhD, said at a joint program of the International Eczema Council and the International Psoriasis Council held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
To date there is no effective method for preventing AD. Preventive strategies are needed sorely because the prevalence of pediatric AD worldwide is expected to increase substantially. It appears to have stabilized at roughly 20% in many affluent countries, but the global burden of the disease will climb as low-income countries – where AD is historically uncommon – become more developed and urbanized. This trend has been well documented via the International Study of Asthma and Allergies in Childhood (ISAAC), which in several phases has studied nearly 2 million children in more than 100 countries, noted Dr. Flohr of St. John’s Institute of Dermatology at King’s College London.

Dr. Flohr and coinvestigators in the Enquiring About Tolerance (EAT) study recently documented a significant association between water hardness and the risk of infant-onset AD. The investigators took advantage of the considerable variation in the amount of bedrock limestone across England, which enabled them to study the relationship between domestic water calcium carbonate concentrations and the presence of AD in 1,303 babies at 3 monthd of age drawn from the general population across the country. Filaggrin skin barrier gene mutation status was determined in all infants.
Infants whose water supply contained a calcium carbonate level above the median value were at an adjusted 46% greater risk of having visible AD at age 3 months than those whose household water calcium carbonate level was below the median. The AD risk rose by 1% for each 1 mg/L increase in calcium carbonate concentration above the median. This increased risk was confined to infants with a filaggrin skin barrier gene mutation; hard water didn’t increase early AD risk in children with the normal, wild-type version of the filaggrin gene (J Allergy Clin Immunol. 2016 Aug;138[2]:509-16).
As a result of these findings, a UK prevention trial is underway in which home water softeners are provided to families at high risk of having a baby with AD in water districts with high calcium carbonate concentrations. An earlier UK study found that installation of home water softeners didn’t reduce AD severity in children with established disease (PLoS Med. 2011 Feb 15;8[2]:e1000395), but disease prevention may be another story.
The role of the gut microbiota in development of childhood AD is an active area of investigation. Dr. Flohr said “there is a signal” that maternal intake of probiotics including lactobacilli and bifidobacteria in the third trimester and postnatally may reduce a child’s risk of developing AD by encouraging establishment of a more diverse gut microflora. He cited a meta-analysis of 14 published studies of probiotics which provided evidence of a 21% reduction in the incidence of AD in young children (Epidemiology 2012 May;23[3]:402-14). The studies have methodologic shortcomings, so multiple research groups are continuing to pursue the signal of an AD preventive effect.
Dr. Flor reported having no financial conflicts of interest regarding his presentation.
VIENNA – Diverse strategies aimed at preventing childhood atopic dermatitis (AD) now under study include installation of home water softeners, daily use of emollients starting at birth, and maternal consumption of probiotics beginning late in pregnancy, Carsten Flohr, PhD, said at a joint program of the International Eczema Council and the International Psoriasis Council held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
To date there is no effective method for preventing AD. Preventive strategies are needed sorely because the prevalence of pediatric AD worldwide is expected to increase substantially. It appears to have stabilized at roughly 20% in many affluent countries, but the global burden of the disease will climb as low-income countries – where AD is historically uncommon – become more developed and urbanized. This trend has been well documented via the International Study of Asthma and Allergies in Childhood (ISAAC), which in several phases has studied nearly 2 million children in more than 100 countries, noted Dr. Flohr of St. John’s Institute of Dermatology at King’s College London.
Dr. Flohr and coinvestigators in the Enquiring About Tolerance (EAT) study recently documented a significant association between water hardness and the risk of infant-onset AD. The investigators took advantage of the considerable variation in the amount of bedrock limestone across England, which enabled them to study the relationship between domestic water calcium carbonate concentrations and the presence of AD in 1,303 babies at 3 monthd of age drawn from the general population across the country. Filaggrin skin barrier gene mutation status was determined in all infants.
Infants whose water supply contained a calcium carbonate level above the median value were at an adjusted 46% greater risk of having visible AD at age 3 months than those whose household water calcium carbonate level was below the median. The AD risk rose by 1% for each 1 mg/L increase in calcium carbonate concentration above the median. This increased risk was confined to infants with a filaggrin skin barrier gene mutation; hard water didn’t increase early AD risk in children with the normal, wild-type version of the filaggrin gene (J Allergy Clin Immunol. 2016 Aug;138[2]:509-16).
As a result of these findings, a UK prevention trial is underway in which home water softeners are provided to families at high risk of having a baby with AD in water districts with high calcium carbonate concentrations. An earlier UK study found that installation of home water softeners didn’t reduce AD severity in children with established disease (PLoS Med. 2011 Feb 15;8[2]:e1000395), but disease prevention may be another story.
The role of the gut microbiota in development of childhood AD is an active area of investigation. Dr. Flohr said “there is a signal” that maternal intake of probiotics including lactobacilli and bifidobacteria in the third trimester and postnatally may reduce a child’s risk of developing AD by encouraging establishment of a more diverse gut microflora. He cited a meta-analysis of 14 published studies of probiotics which provided evidence of a 21% reduction in the incidence of AD in young children (Epidemiology 2012 May;23[3]:402-14). The studies have methodologic shortcomings, so multiple research groups are continuing to pursue the signal of an AD preventive effect.
Dr. Flor reported having no financial conflicts of interest regarding his presentation.
VIENNA – Diverse strategies aimed at preventing childhood atopic dermatitis (AD) now under study include installation of home water softeners, daily use of emollients starting at birth, and maternal consumption of probiotics beginning late in pregnancy, Carsten Flohr, PhD, said at a joint program of the International Eczema Council and the International Psoriasis Council held in conjunction with the annual congress of the European Academy of Dermatology and Venereology.
To date there is no effective method for preventing AD. Preventive strategies are needed sorely because the prevalence of pediatric AD worldwide is expected to increase substantially. It appears to have stabilized at roughly 20% in many affluent countries, but the global burden of the disease will climb as low-income countries – where AD is historically uncommon – become more developed and urbanized. This trend has been well documented via the International Study of Asthma and Allergies in Childhood (ISAAC), which in several phases has studied nearly 2 million children in more than 100 countries, noted Dr. Flohr of St. John’s Institute of Dermatology at King’s College London.
Dr. Flohr and coinvestigators in the Enquiring About Tolerance (EAT) study recently documented a significant association between water hardness and the risk of infant-onset AD. The investigators took advantage of the considerable variation in the amount of bedrock limestone across England, which enabled them to study the relationship between domestic water calcium carbonate concentrations and the presence of AD in 1,303 babies at 3 monthd of age drawn from the general population across the country. Filaggrin skin barrier gene mutation status was determined in all infants.
Infants whose water supply contained a calcium carbonate level above the median value were at an adjusted 46% greater risk of having visible AD at age 3 months than those whose household water calcium carbonate level was below the median. The AD risk rose by 1% for each 1 mg/L increase in calcium carbonate concentration above the median. This increased risk was confined to infants with a filaggrin skin barrier gene mutation; hard water didn’t increase early AD risk in children with the normal, wild-type version of the filaggrin gene (J Allergy Clin Immunol. 2016 Aug;138[2]:509-16).
As a result of these findings, a UK prevention trial is underway in which home water softeners are provided to families at high risk of having a baby with AD in water districts with high calcium carbonate concentrations. An earlier UK study found that installation of home water softeners didn’t reduce AD severity in children with established disease (PLoS Med. 2011 Feb 15;8[2]:e1000395), but disease prevention may be another story.
The role of the gut microbiota in development of childhood AD is an active area of investigation. Dr. Flohr said “there is a signal” that maternal intake of probiotics including lactobacilli and bifidobacteria in the third trimester and postnatally may reduce a child’s risk of developing AD by encouraging establishment of a more diverse gut microflora. He cited a meta-analysis of 14 published studies of probiotics which provided evidence of a 21% reduction in the incidence of AD in young children (Epidemiology 2012 May;23[3]:402-14). The studies have methodologic shortcomings, so multiple research groups are continuing to pursue the signal of an AD preventive effect.
Dr. Flor reported having no financial conflicts of interest regarding his presentation.
EXPERT ANALYSIS FROM THE EADV CONGRESS
Collaborative Approaches Improve Pediatric Discharges

Clinical Question: Can a collaborative quality improvement project improve the quality and efficiency of pediatric hospital discharges?
Background: Transitions of care, including at the time of hospital discharge, are a potential source of risk and can be associated with adverse events including medication errors and preventable readmissions. Some studies have shown that 10–20% of patients had an adverse event after discharge, and half of those were preventable; one adult study found nearly half of the discharged patients had at least one medication error.1,2 Although multiple projects to improve the discharge process have been published in adult literature, few have focused on the pediatric population. In this study, the Children’s Hospital Association (CHA) formed a pediatric quality improvement collaborative across multiple facilities to examine whether shared improvement strategies would affect failures of discharge-related care, parent-reported readiness for discharge, and readmission rates.
Study Design: Multicenter quality improvement collaborative.
Setting: 11 freestanding tertiary-care children’s hospitals in the United States.
Synopsis: Each of the 11 participating sites chose a specific target population, such as patients with sickle cell disease, asthma, or all discharged pediatric patients. Populations were selected at the discretion of the sites. A multidisciplinary expert advisory panel reviewed literature and developed a change package that included being proactive about discharge planning during hospitalization; improving throughput; arranging post-discharge treatment and support; and communicating post-discharge plan with patients, families, and providers. Each site selected elements of the change package to implement based on individual needs and preferences and incorporated via plan-do-study-act cycles during three action periods. Elements that were implemented by most or all sites included family education on diagnosis and discharge plans, use of discharge checklists, improvement of written discharge instructions, post-discharge follow-up phone calls to reinforce discharge instructions, and identifying and obtaining medications. Virtual learning conferences and monthly Web conferences were held for participants in the collaborative, and experienced improvement coaches guided teams through implementation.
The primary aim of the study was to reduce discharge-related care failures by 50% in 12 months. Failures were measured by phone calls to families two to seven days following discharge, and if any problem related to discharge occurred, the discharge was considered a failure (all-or-none measure). Components of this measure included understanding the diagnosis, receiving discharge instructions and education, complying with instructions, receiving necessary equipment, planning for follow-up pending tests, receiving help with appointments, and not requiring a related unplanned medical visit. Other measures evaluated in this study included patient/family readiness for discharge and unplanned readmission rates (72 hours and 30 days).
Overall, the rate of failures of discharge care was 34% at baseline, which decreased to 21% at the end of the collaborative, for a reduction of 40%. Some individual hospitals exceeded this mark as well. Among the hospitals reporting data on family readiness for discharge, there was a statistically significant improvement, with 85% of families at baseline rating readiness in the highest category and 91% in the last quarter of the study. There was no improvement in rates of unplanned readmission, with 72-hour readmission rates steady across the project (0.7% at onset, 1.1% at end of study; P = 0.29) and slight worsening of the 30-day rate (4.5% to 6.3%; P = 0.05).
Potential explanations for the findings related to readmission rates include seasonal variability in readmissions as well as high variability in patients included in the study. For example, one site focused on patients with sickle cell disease, another on patients with asthma, and others included all diagnoses. Overall, unplanned readmission rates were low (around 1% for 72-hour, 5% for 30-day), which is consistent with other pediatric studies.
Bottom Line: In this study, institutions using a collaborative approach improved the quality of inpatient discharges by using an intervention bundle in pediatric hospital settings. There was no improvement noted in readmission rates, although these rates were low.
Citation: Wu S, Tyler A, Logsdon T, et al. A quality improvement collaborative to improve the discharge process for hospitalized children. Pediatrics. 2016;138(2). pii:e20143604.
References:
- Moore C, Wisnivesky J, Williams S, McGinn T. Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med. 2003;18(8):646-651.
- Forster AJ, Clark HD, Menard A, et al. Adverse events among medical patients after discharge from hospital. CMAJ. 2004;170(3):345-349.
Clinical Question: Can a collaborative quality improvement project improve the quality and efficiency of pediatric hospital discharges?
Background: Transitions of care, including at the time of hospital discharge, are a potential source of risk and can be associated with adverse events including medication errors and preventable readmissions. Some studies have shown that 10–20% of patients had an adverse event after discharge, and half of those were preventable; one adult study found nearly half of the discharged patients had at least one medication error.1,2 Although multiple projects to improve the discharge process have been published in adult literature, few have focused on the pediatric population. In this study, the Children’s Hospital Association (CHA) formed a pediatric quality improvement collaborative across multiple facilities to examine whether shared improvement strategies would affect failures of discharge-related care, parent-reported readiness for discharge, and readmission rates.
Study Design: Multicenter quality improvement collaborative.
Setting: 11 freestanding tertiary-care children’s hospitals in the United States.
Synopsis: Each of the 11 participating sites chose a specific target population, such as patients with sickle cell disease, asthma, or all discharged pediatric patients. Populations were selected at the discretion of the sites. A multidisciplinary expert advisory panel reviewed literature and developed a change package that included being proactive about discharge planning during hospitalization; improving throughput; arranging post-discharge treatment and support; and communicating post-discharge plan with patients, families, and providers. Each site selected elements of the change package to implement based on individual needs and preferences and incorporated via plan-do-study-act cycles during three action periods. Elements that were implemented by most or all sites included family education on diagnosis and discharge plans, use of discharge checklists, improvement of written discharge instructions, post-discharge follow-up phone calls to reinforce discharge instructions, and identifying and obtaining medications. Virtual learning conferences and monthly Web conferences were held for participants in the collaborative, and experienced improvement coaches guided teams through implementation.
The primary aim of the study was to reduce discharge-related care failures by 50% in 12 months. Failures were measured by phone calls to families two to seven days following discharge, and if any problem related to discharge occurred, the discharge was considered a failure (all-or-none measure). Components of this measure included understanding the diagnosis, receiving discharge instructions and education, complying with instructions, receiving necessary equipment, planning for follow-up pending tests, receiving help with appointments, and not requiring a related unplanned medical visit. Other measures evaluated in this study included patient/family readiness for discharge and unplanned readmission rates (72 hours and 30 days).
Overall, the rate of failures of discharge care was 34% at baseline, which decreased to 21% at the end of the collaborative, for a reduction of 40%. Some individual hospitals exceeded this mark as well. Among the hospitals reporting data on family readiness for discharge, there was a statistically significant improvement, with 85% of families at baseline rating readiness in the highest category and 91% in the last quarter of the study. There was no improvement in rates of unplanned readmission, with 72-hour readmission rates steady across the project (0.7% at onset, 1.1% at end of study; P = 0.29) and slight worsening of the 30-day rate (4.5% to 6.3%; P = 0.05).
Potential explanations for the findings related to readmission rates include seasonal variability in readmissions as well as high variability in patients included in the study. For example, one site focused on patients with sickle cell disease, another on patients with asthma, and others included all diagnoses. Overall, unplanned readmission rates were low (around 1% for 72-hour, 5% for 30-day), which is consistent with other pediatric studies.
Bottom Line: In this study, institutions using a collaborative approach improved the quality of inpatient discharges by using an intervention bundle in pediatric hospital settings. There was no improvement noted in readmission rates, although these rates were low.
Citation: Wu S, Tyler A, Logsdon T, et al. A quality improvement collaborative to improve the discharge process for hospitalized children. Pediatrics. 2016;138(2). pii:e20143604.
References:
- Moore C, Wisnivesky J, Williams S, McGinn T. Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med. 2003;18(8):646-651.
- Forster AJ, Clark HD, Menard A, et al. Adverse events among medical patients after discharge from hospital. CMAJ. 2004;170(3):345-349.
Clinical Question: Can a collaborative quality improvement project improve the quality and efficiency of pediatric hospital discharges?
Background: Transitions of care, including at the time of hospital discharge, are a potential source of risk and can be associated with adverse events including medication errors and preventable readmissions. Some studies have shown that 10–20% of patients had an adverse event after discharge, and half of those were preventable; one adult study found nearly half of the discharged patients had at least one medication error.1,2 Although multiple projects to improve the discharge process have been published in adult literature, few have focused on the pediatric population. In this study, the Children’s Hospital Association (CHA) formed a pediatric quality improvement collaborative across multiple facilities to examine whether shared improvement strategies would affect failures of discharge-related care, parent-reported readiness for discharge, and readmission rates.
Study Design: Multicenter quality improvement collaborative.
Setting: 11 freestanding tertiary-care children’s hospitals in the United States.
Synopsis: Each of the 11 participating sites chose a specific target population, such as patients with sickle cell disease, asthma, or all discharged pediatric patients. Populations were selected at the discretion of the sites. A multidisciplinary expert advisory panel reviewed literature and developed a change package that included being proactive about discharge planning during hospitalization; improving throughput; arranging post-discharge treatment and support; and communicating post-discharge plan with patients, families, and providers. Each site selected elements of the change package to implement based on individual needs and preferences and incorporated via plan-do-study-act cycles during three action periods. Elements that were implemented by most or all sites included family education on diagnosis and discharge plans, use of discharge checklists, improvement of written discharge instructions, post-discharge follow-up phone calls to reinforce discharge instructions, and identifying and obtaining medications. Virtual learning conferences and monthly Web conferences were held for participants in the collaborative, and experienced improvement coaches guided teams through implementation.
The primary aim of the study was to reduce discharge-related care failures by 50% in 12 months. Failures were measured by phone calls to families two to seven days following discharge, and if any problem related to discharge occurred, the discharge was considered a failure (all-or-none measure). Components of this measure included understanding the diagnosis, receiving discharge instructions and education, complying with instructions, receiving necessary equipment, planning for follow-up pending tests, receiving help with appointments, and not requiring a related unplanned medical visit. Other measures evaluated in this study included patient/family readiness for discharge and unplanned readmission rates (72 hours and 30 days).
Overall, the rate of failures of discharge care was 34% at baseline, which decreased to 21% at the end of the collaborative, for a reduction of 40%. Some individual hospitals exceeded this mark as well. Among the hospitals reporting data on family readiness for discharge, there was a statistically significant improvement, with 85% of families at baseline rating readiness in the highest category and 91% in the last quarter of the study. There was no improvement in rates of unplanned readmission, with 72-hour readmission rates steady across the project (0.7% at onset, 1.1% at end of study; P = 0.29) and slight worsening of the 30-day rate (4.5% to 6.3%; P = 0.05).
Potential explanations for the findings related to readmission rates include seasonal variability in readmissions as well as high variability in patients included in the study. For example, one site focused on patients with sickle cell disease, another on patients with asthma, and others included all diagnoses. Overall, unplanned readmission rates were low (around 1% for 72-hour, 5% for 30-day), which is consistent with other pediatric studies.
Bottom Line: In this study, institutions using a collaborative approach improved the quality of inpatient discharges by using an intervention bundle in pediatric hospital settings. There was no improvement noted in readmission rates, although these rates were low.
Citation: Wu S, Tyler A, Logsdon T, et al. A quality improvement collaborative to improve the discharge process for hospitalized children. Pediatrics. 2016;138(2). pii:e20143604.
References:
- Moore C, Wisnivesky J, Williams S, McGinn T. Medical errors related to discontinuity of care from an inpatient to an outpatient setting. J Gen Intern Med. 2003;18(8):646-651.
- Forster AJ, Clark HD, Menard A, et al. Adverse events among medical patients after discharge from hospital. CMAJ. 2004;170(3):345-349.
2016 Pediatric Hospital Medicine Award Winners Announced
Congratulations to the recipients of the 2016 Pediatric Hospital Medicine Awards, who were recently recognized at the 2016 Pediatric Hospital Medicine meeting in Chicago. The awards are presented to pediatric hospitalists who make exemplary contributions to hospital medicine, quality improvement, and patient care.
The awards are presented in four categories:
Safety and Quality Improvement
Recipient: Kavita Parikh, MD, Children’s National Medical Center, Washington, D.C.
Dr. Parikh is a member of the Value in Inpatient Pediatrics Network and has worked with the group to improve the care of community-acquired pneumonia. The group has enrolled more than 50 hospitals around the country and one international site to standardize care so that all children hospitalized with pneumonia can receive the same high-quality care, including the use of narrow-spectrum antibiotics.
Educational Achievement and Innovation
Recipient: H. Barrett Fromme, MD, University of Chicago
Dr. Fromme is well known as a leader in pediatric medical education and was instrumental in establishing the Pediatric National Nighttime Curriculum, which includes approximately 75 percent of all residency programs across the U.S. She also led the Advancing Pediatric Educator Excellence Teaching Program for hospitalists, which helps develop their teaching skills. Dr. Fromme has also been named a Master Educator at the University of Chicago Academy of Distinguished Medical Educators.
Research Excellence
Recipient: Derek Williams, MD, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Nashville
Dr. Williams is a pediatric hospitalist whose research activities have focused on respiratory infections in hospitalized children. He has received multiple grants and awards from the Centers for Disease Control and Prevention, National Institutes of Health, and Patient-Centered Outcomes Research Institute and has served as the lead investigator at his institution for the CDC-sponsored study entitled Etiology of Pneumonia in the Community (EPIC), which has generated several publications, including in The New England Journal of Medicine.
Lifetime Achievement
Recipient: Ken Roberts, MD, chairman emeritus, University of North Carolina, Chapel Hill
While he is now retired, Dr. Roberts has served as a mentor to many pediatric hospitalists throughout his storied career and has more than 200 publications, including one in Pediatrics called “A Hospitalist Movement? Where to?”
Congratulations to the recipients of the 2016 Pediatric Hospital Medicine Awards, who were recently recognized at the 2016 Pediatric Hospital Medicine meeting in Chicago. The awards are presented to pediatric hospitalists who make exemplary contributions to hospital medicine, quality improvement, and patient care.
The awards are presented in four categories:
Safety and Quality Improvement
Recipient: Kavita Parikh, MD, Children’s National Medical Center, Washington, D.C.
Dr. Parikh is a member of the Value in Inpatient Pediatrics Network and has worked with the group to improve the care of community-acquired pneumonia. The group has enrolled more than 50 hospitals around the country and one international site to standardize care so that all children hospitalized with pneumonia can receive the same high-quality care, including the use of narrow-spectrum antibiotics.
Educational Achievement and Innovation
Recipient: H. Barrett Fromme, MD, University of Chicago
Dr. Fromme is well known as a leader in pediatric medical education and was instrumental in establishing the Pediatric National Nighttime Curriculum, which includes approximately 75 percent of all residency programs across the U.S. She also led the Advancing Pediatric Educator Excellence Teaching Program for hospitalists, which helps develop their teaching skills. Dr. Fromme has also been named a Master Educator at the University of Chicago Academy of Distinguished Medical Educators.
Research Excellence
Recipient: Derek Williams, MD, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Nashville
Dr. Williams is a pediatric hospitalist whose research activities have focused on respiratory infections in hospitalized children. He has received multiple grants and awards from the Centers for Disease Control and Prevention, National Institutes of Health, and Patient-Centered Outcomes Research Institute and has served as the lead investigator at his institution for the CDC-sponsored study entitled Etiology of Pneumonia in the Community (EPIC), which has generated several publications, including in The New England Journal of Medicine.
Lifetime Achievement
Recipient: Ken Roberts, MD, chairman emeritus, University of North Carolina, Chapel Hill
While he is now retired, Dr. Roberts has served as a mentor to many pediatric hospitalists throughout his storied career and has more than 200 publications, including one in Pediatrics called “A Hospitalist Movement? Where to?”
Congratulations to the recipients of the 2016 Pediatric Hospital Medicine Awards, who were recently recognized at the 2016 Pediatric Hospital Medicine meeting in Chicago. The awards are presented to pediatric hospitalists who make exemplary contributions to hospital medicine, quality improvement, and patient care.
The awards are presented in four categories:
Safety and Quality Improvement
Recipient: Kavita Parikh, MD, Children’s National Medical Center, Washington, D.C.
Dr. Parikh is a member of the Value in Inpatient Pediatrics Network and has worked with the group to improve the care of community-acquired pneumonia. The group has enrolled more than 50 hospitals around the country and one international site to standardize care so that all children hospitalized with pneumonia can receive the same high-quality care, including the use of narrow-spectrum antibiotics.
Educational Achievement and Innovation
Recipient: H. Barrett Fromme, MD, University of Chicago
Dr. Fromme is well known as a leader in pediatric medical education and was instrumental in establishing the Pediatric National Nighttime Curriculum, which includes approximately 75 percent of all residency programs across the U.S. She also led the Advancing Pediatric Educator Excellence Teaching Program for hospitalists, which helps develop their teaching skills. Dr. Fromme has also been named a Master Educator at the University of Chicago Academy of Distinguished Medical Educators.
Research Excellence
Recipient: Derek Williams, MD, Monroe Carell Jr. Children’s Hospital at Vanderbilt, Nashville
Dr. Williams is a pediatric hospitalist whose research activities have focused on respiratory infections in hospitalized children. He has received multiple grants and awards from the Centers for Disease Control and Prevention, National Institutes of Health, and Patient-Centered Outcomes Research Institute and has served as the lead investigator at his institution for the CDC-sponsored study entitled Etiology of Pneumonia in the Community (EPIC), which has generated several publications, including in The New England Journal of Medicine.
Lifetime Achievement
Recipient: Ken Roberts, MD, chairman emeritus, University of North Carolina, Chapel Hill
While he is now retired, Dr. Roberts has served as a mentor to many pediatric hospitalists throughout his storied career and has more than 200 publications, including one in Pediatrics called “A Hospitalist Movement? Where to?”
Cow’s milk allergy appears to affect more U.S. infants than thought
MONTREAL – The incidence of cow’s milk protein allergy during the first few months of life may be much more common than suggested by published studies, based on what was found is a prospective study with 700 infants seen regularly at a single, general pediatrics practice in suburban Massachusetts.
Among the 700 infants enrolled in this series, 105 (15%) were diagnosed with cow’s milk protein allergy (CMPA) when they were 5-163 days old, with a median age at diagnosis of 33 days, Victoria J. Martin, MD, said at the World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition. She and her associates confirmed that all these infants had true CMPA episodes of proctocolitis by requiring detection of blood in the stool of affected children.

The study results also suggested a protective effect against CMPA when infants received some amount of early breastfeeding, and a pilot substudy run in 47 of the enrolled infants also suggested a link between development of CMPA and abnormalities in the microbiome composition of affected infants, she reported.
While the 15% incidence rate was unexpectedly high, it “absolutely feels like what we see in routine clinical practice,” Dr. Martin said in an interview. She chalked up the much-lower figure cited in the pediatric literature as relying on strict follow-up confirmation by rechallenge of the child with cow’s milk, a step often not taken by busy clinicians. Deferring formal confirmation also often means delayed reintroduction of cow’s milk into the infant’s diet, with restriction often continuing for perhaps a year following the index episode of CMPA. Although such unnecessarily long delays in milk reintroduction have largely been considered benign, recent findings from the Learning Early About Peanut Allergy (LEAP) trial that withholding peanut exposure can increase development of peanut allergies suggests that children also might receive long-term benefit from quicker reintroduction of milk in terms of better development of the immune system and microbiome, she said.
“If we rechallenged all these infants after 1 month, I think we’d find a CMPA rate closer to 3%. Leaving infants on a mild restricted diet for 12 months is a mistake,” she added.
The Gastrointestinal Microbiome & Proctocolitis (GMAP) study enrolled 700 infants seen at a single general practice pediatric practice in suburban Massachusetts at the time of their first well-baby visit, at a median age of 8 days. During 2 years of follow-up, the researchers collected stool specimens from the enrolled children at each of up to five scheduled visits during the first 4 months. They also kept track of when children received a CMPA diagnosis confirmed by at least one bloody stool.
Analysis of CMPA correlates showed that, among infants who developed it, 17% had not received any breastfeeding soon after birth, while among infants who did not develop CMPA, 8% did not undergo early breastfeeding. The incidence of CMPA was roughly similar among infants who received an early combination of breast milk and formula and in those who received exclusively breast milk during the first days of life, showing that even partial breastfeeding is better than no breastfeeding, Dr. Martin noted.
Her analysis also includes initial results from microbial assessment of the collected serial stool specimens from a subgroup of 24 infants who developed CMPA and 23 who did not, with a total of 223 total specimens evaluated. These studies showed that the infants who developed CMPA significantly lagged in their colonization with Bifidobacteria, had significantly higher colonization levels with Enterobacteriaceae, and that in infants who did develop CMPA, their gut level of Clostridia significantly increased as their proctocolitis resolved.
Dr. Martin had no relevant financial disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
MONTREAL – The incidence of cow’s milk protein allergy during the first few months of life may be much more common than suggested by published studies, based on what was found is a prospective study with 700 infants seen regularly at a single, general pediatrics practice in suburban Massachusetts.
Among the 700 infants enrolled in this series, 105 (15%) were diagnosed with cow’s milk protein allergy (CMPA) when they were 5-163 days old, with a median age at diagnosis of 33 days, Victoria J. Martin, MD, said at the World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition. She and her associates confirmed that all these infants had true CMPA episodes of proctocolitis by requiring detection of blood in the stool of affected children.
The study results also suggested a protective effect against CMPA when infants received some amount of early breastfeeding, and a pilot substudy run in 47 of the enrolled infants also suggested a link between development of CMPA and abnormalities in the microbiome composition of affected infants, she reported.
While the 15% incidence rate was unexpectedly high, it “absolutely feels like what we see in routine clinical practice,” Dr. Martin said in an interview. She chalked up the much-lower figure cited in the pediatric literature as relying on strict follow-up confirmation by rechallenge of the child with cow’s milk, a step often not taken by busy clinicians. Deferring formal confirmation also often means delayed reintroduction of cow’s milk into the infant’s diet, with restriction often continuing for perhaps a year following the index episode of CMPA. Although such unnecessarily long delays in milk reintroduction have largely been considered benign, recent findings from the Learning Early About Peanut Allergy (LEAP) trial that withholding peanut exposure can increase development of peanut allergies suggests that children also might receive long-term benefit from quicker reintroduction of milk in terms of better development of the immune system and microbiome, she said.
“If we rechallenged all these infants after 1 month, I think we’d find a CMPA rate closer to 3%. Leaving infants on a mild restricted diet for 12 months is a mistake,” she added.
The Gastrointestinal Microbiome & Proctocolitis (GMAP) study enrolled 700 infants seen at a single general practice pediatric practice in suburban Massachusetts at the time of their first well-baby visit, at a median age of 8 days. During 2 years of follow-up, the researchers collected stool specimens from the enrolled children at each of up to five scheduled visits during the first 4 months. They also kept track of when children received a CMPA diagnosis confirmed by at least one bloody stool.
Analysis of CMPA correlates showed that, among infants who developed it, 17% had not received any breastfeeding soon after birth, while among infants who did not develop CMPA, 8% did not undergo early breastfeeding. The incidence of CMPA was roughly similar among infants who received an early combination of breast milk and formula and in those who received exclusively breast milk during the first days of life, showing that even partial breastfeeding is better than no breastfeeding, Dr. Martin noted.
Her analysis also includes initial results from microbial assessment of the collected serial stool specimens from a subgroup of 24 infants who developed CMPA and 23 who did not, with a total of 223 total specimens evaluated. These studies showed that the infants who developed CMPA significantly lagged in their colonization with Bifidobacteria, had significantly higher colonization levels with Enterobacteriaceae, and that in infants who did develop CMPA, their gut level of Clostridia significantly increased as their proctocolitis resolved.
Dr. Martin had no relevant financial disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
MONTREAL – The incidence of cow’s milk protein allergy during the first few months of life may be much more common than suggested by published studies, based on what was found is a prospective study with 700 infants seen regularly at a single, general pediatrics practice in suburban Massachusetts.
Among the 700 infants enrolled in this series, 105 (15%) were diagnosed with cow’s milk protein allergy (CMPA) when they were 5-163 days old, with a median age at diagnosis of 33 days, Victoria J. Martin, MD, said at the World Congress of Pediatric Gastroenterology, Hepatology, and Nutrition. She and her associates confirmed that all these infants had true CMPA episodes of proctocolitis by requiring detection of blood in the stool of affected children.
The study results also suggested a protective effect against CMPA when infants received some amount of early breastfeeding, and a pilot substudy run in 47 of the enrolled infants also suggested a link between development of CMPA and abnormalities in the microbiome composition of affected infants, she reported.
While the 15% incidence rate was unexpectedly high, it “absolutely feels like what we see in routine clinical practice,” Dr. Martin said in an interview. She chalked up the much-lower figure cited in the pediatric literature as relying on strict follow-up confirmation by rechallenge of the child with cow’s milk, a step often not taken by busy clinicians. Deferring formal confirmation also often means delayed reintroduction of cow’s milk into the infant’s diet, with restriction often continuing for perhaps a year following the index episode of CMPA. Although such unnecessarily long delays in milk reintroduction have largely been considered benign, recent findings from the Learning Early About Peanut Allergy (LEAP) trial that withholding peanut exposure can increase development of peanut allergies suggests that children also might receive long-term benefit from quicker reintroduction of milk in terms of better development of the immune system and microbiome, she said.
“If we rechallenged all these infants after 1 month, I think we’d find a CMPA rate closer to 3%. Leaving infants on a mild restricted diet for 12 months is a mistake,” she added.
The Gastrointestinal Microbiome & Proctocolitis (GMAP) study enrolled 700 infants seen at a single general practice pediatric practice in suburban Massachusetts at the time of their first well-baby visit, at a median age of 8 days. During 2 years of follow-up, the researchers collected stool specimens from the enrolled children at each of up to five scheduled visits during the first 4 months. They also kept track of when children received a CMPA diagnosis confirmed by at least one bloody stool.
Analysis of CMPA correlates showed that, among infants who developed it, 17% had not received any breastfeeding soon after birth, while among infants who did not develop CMPA, 8% did not undergo early breastfeeding. The incidence of CMPA was roughly similar among infants who received an early combination of breast milk and formula and in those who received exclusively breast milk during the first days of life, showing that even partial breastfeeding is better than no breastfeeding, Dr. Martin noted.
Her analysis also includes initial results from microbial assessment of the collected serial stool specimens from a subgroup of 24 infants who developed CMPA and 23 who did not, with a total of 223 total specimens evaluated. These studies showed that the infants who developed CMPA significantly lagged in their colonization with Bifidobacteria, had significantly higher colonization levels with Enterobacteriaceae, and that in infants who did develop CMPA, their gut level of Clostridia significantly increased as their proctocolitis resolved.
Dr. Martin had no relevant financial disclosures.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT WCPGHAN 2016
Key clinical point:
Major finding: Among 700 enrolled well infants, aged 5-163 days, 105 (15%) developed proctocolitis linked with cow’s milk.
Data source: Prospective observational study of 700 healthy neonates seen at a single U.S. pediatric practice.
Disclosures: Dr. Martin had no relevant financial disclosures.
Promise of effective RSV vaccines on horizon
ATLANTA – A new vaccine for respiratory syncytial virus may truly be on the horizon, given recent advances in basic science and a marked increase in interest in the pharmaceutical industry.
That’s the conclusion of Larry Anderson, MD, professor of infectious disease in the Emory University department of pediatrics, who presented the most updated research and progress on a respiratory syncytial virus (RSV) vaccine during a conference sponsored by the Centers for Disease Control and Prevention.

The high hospitalization rates of infants with RSV, also associated with later development of reactive airway disease and asthma, highlight the challenge of developing a vaccine, Dr. Anderson said.
“The infant has an immature immune system less able to respond vigorously to a vaccine,” he said. “Also, it is highly susceptible to the disease of RSV, and therefore safety becomes an issue at least in terms of the live virus vaccine.” Furthermore, RSV causes multiple repeat infections throughout life, “which underlines the difficulty in inducing a protective immune response,” he added.
But Dr. Anderson said he believes there is light at the end of the tunnel when it comes to a vaccine for the virus.
“I think in terms of [the] potential of having an RSV vaccine in the near future, now is the most promising time, recognizing that work on an RSV vaccine has been going on for over 50 years without success to date,” he said. Significant advances in basic biology, immunology, and vaccinology have led to a better understanding of the virus, and new tools such as reverse genetics make “it possible to make any live virus you want as long as you know what you want,” he added.
Dr. Anderson provided an overview of published and preliminary data on the progress of more than five dozen groups working on an RSV vaccine. About 70% of these candidates remain in preclinical research, primarily in animal models. Of the dozen in phase I, several look promising, he said. Another six vaccines are in phase II or phase III testing, and MedImmune’s Synagis is market approved. But not all target infants.
“The first and highest priority is the young infant, particularly the under 2- to 4-month-old,” he said. In infants aged 4-6 months, it’s likely easier to induce an immune response, and there’s less susceptibility to disease with replication of the virus, he said. The elderly, also at high risk for RSV, would be another target population.
Potentially “the lowest apple on the tree for immunization,” Dr. Anderson said, would be pregnant women because a vaccine could prevent infection, disease, and transmission to their infant before he might be able to be vaccinated.
“There, the primary purpose is to increase the kind of antibody that is transferred across the placenta to the fetus to protect from RSV disease” in the infant after birth, he said. Data suggest it’s possible to increase titer antibodies in infants up to 4 months from maternal immunization, possibly longer, depending on how much the vaccine can induce antibodies in the woman.
For young children, he noted that five live attenuated RSV vaccines are in phase I testing, and four others are in phase I that use a virus vector to deliver the F protein – three using adenovirus and one with a modified vaccinia Ankara virus. A handful of subunit vaccines have reached phase II, and Novavax is furthest along in phase III, but these target older children and adults, including pregnant women.
“There’s going to be a lot of data in the coming year on completed clinical trials, and that’s going to tell us a lot about where we are,” Dr. Anderson said. “The young infant is the most challenging for a vaccine.” But, he added, “new information on protective immunity and disease pathogenesis should help achieve or improve vaccines in the future.”
Dr. Anderson has consulted on RSV vaccines for MedImmune, Novartis, Crucell Holland, and AVC, and has served on a Moderna Therapeutics scientific advisory board. His lab also has received grant funding from Trellis RSV Holdings, and he coinvented several RSV-related vaccine and treatment patents held by the CDC.
ATLANTA – A new vaccine for respiratory syncytial virus may truly be on the horizon, given recent advances in basic science and a marked increase in interest in the pharmaceutical industry.
That’s the conclusion of Larry Anderson, MD, professor of infectious disease in the Emory University department of pediatrics, who presented the most updated research and progress on a respiratory syncytial virus (RSV) vaccine during a conference sponsored by the Centers for Disease Control and Prevention.
The high hospitalization rates of infants with RSV, also associated with later development of reactive airway disease and asthma, highlight the challenge of developing a vaccine, Dr. Anderson said.
“The infant has an immature immune system less able to respond vigorously to a vaccine,” he said. “Also, it is highly susceptible to the disease of RSV, and therefore safety becomes an issue at least in terms of the live virus vaccine.” Furthermore, RSV causes multiple repeat infections throughout life, “which underlines the difficulty in inducing a protective immune response,” he added.
But Dr. Anderson said he believes there is light at the end of the tunnel when it comes to a vaccine for the virus.
“I think in terms of [the] potential of having an RSV vaccine in the near future, now is the most promising time, recognizing that work on an RSV vaccine has been going on for over 50 years without success to date,” he said. Significant advances in basic biology, immunology, and vaccinology have led to a better understanding of the virus, and new tools such as reverse genetics make “it possible to make any live virus you want as long as you know what you want,” he added.
Dr. Anderson provided an overview of published and preliminary data on the progress of more than five dozen groups working on an RSV vaccine. About 70% of these candidates remain in preclinical research, primarily in animal models. Of the dozen in phase I, several look promising, he said. Another six vaccines are in phase II or phase III testing, and MedImmune’s Synagis is market approved. But not all target infants.
“The first and highest priority is the young infant, particularly the under 2- to 4-month-old,” he said. In infants aged 4-6 months, it’s likely easier to induce an immune response, and there’s less susceptibility to disease with replication of the virus, he said. The elderly, also at high risk for RSV, would be another target population.
Potentially “the lowest apple on the tree for immunization,” Dr. Anderson said, would be pregnant women because a vaccine could prevent infection, disease, and transmission to their infant before he might be able to be vaccinated.
“There, the primary purpose is to increase the kind of antibody that is transferred across the placenta to the fetus to protect from RSV disease” in the infant after birth, he said. Data suggest it’s possible to increase titer antibodies in infants up to 4 months from maternal immunization, possibly longer, depending on how much the vaccine can induce antibodies in the woman.
For young children, he noted that five live attenuated RSV vaccines are in phase I testing, and four others are in phase I that use a virus vector to deliver the F protein – three using adenovirus and one with a modified vaccinia Ankara virus. A handful of subunit vaccines have reached phase II, and Novavax is furthest along in phase III, but these target older children and adults, including pregnant women.
“There’s going to be a lot of data in the coming year on completed clinical trials, and that’s going to tell us a lot about where we are,” Dr. Anderson said. “The young infant is the most challenging for a vaccine.” But, he added, “new information on protective immunity and disease pathogenesis should help achieve or improve vaccines in the future.”
Dr. Anderson has consulted on RSV vaccines for MedImmune, Novartis, Crucell Holland, and AVC, and has served on a Moderna Therapeutics scientific advisory board. His lab also has received grant funding from Trellis RSV Holdings, and he coinvented several RSV-related vaccine and treatment patents held by the CDC.
ATLANTA – A new vaccine for respiratory syncytial virus may truly be on the horizon, given recent advances in basic science and a marked increase in interest in the pharmaceutical industry.
That’s the conclusion of Larry Anderson, MD, professor of infectious disease in the Emory University department of pediatrics, who presented the most updated research and progress on a respiratory syncytial virus (RSV) vaccine during a conference sponsored by the Centers for Disease Control and Prevention.
The high hospitalization rates of infants with RSV, also associated with later development of reactive airway disease and asthma, highlight the challenge of developing a vaccine, Dr. Anderson said.
“The infant has an immature immune system less able to respond vigorously to a vaccine,” he said. “Also, it is highly susceptible to the disease of RSV, and therefore safety becomes an issue at least in terms of the live virus vaccine.” Furthermore, RSV causes multiple repeat infections throughout life, “which underlines the difficulty in inducing a protective immune response,” he added.
But Dr. Anderson said he believes there is light at the end of the tunnel when it comes to a vaccine for the virus.
“I think in terms of [the] potential of having an RSV vaccine in the near future, now is the most promising time, recognizing that work on an RSV vaccine has been going on for over 50 years without success to date,” he said. Significant advances in basic biology, immunology, and vaccinology have led to a better understanding of the virus, and new tools such as reverse genetics make “it possible to make any live virus you want as long as you know what you want,” he added.
Dr. Anderson provided an overview of published and preliminary data on the progress of more than five dozen groups working on an RSV vaccine. About 70% of these candidates remain in preclinical research, primarily in animal models. Of the dozen in phase I, several look promising, he said. Another six vaccines are in phase II or phase III testing, and MedImmune’s Synagis is market approved. But not all target infants.
“The first and highest priority is the young infant, particularly the under 2- to 4-month-old,” he said. In infants aged 4-6 months, it’s likely easier to induce an immune response, and there’s less susceptibility to disease with replication of the virus, he said. The elderly, also at high risk for RSV, would be another target population.
Potentially “the lowest apple on the tree for immunization,” Dr. Anderson said, would be pregnant women because a vaccine could prevent infection, disease, and transmission to their infant before he might be able to be vaccinated.
“There, the primary purpose is to increase the kind of antibody that is transferred across the placenta to the fetus to protect from RSV disease” in the infant after birth, he said. Data suggest it’s possible to increase titer antibodies in infants up to 4 months from maternal immunization, possibly longer, depending on how much the vaccine can induce antibodies in the woman.
For young children, he noted that five live attenuated RSV vaccines are in phase I testing, and four others are in phase I that use a virus vector to deliver the F protein – three using adenovirus and one with a modified vaccinia Ankara virus. A handful of subunit vaccines have reached phase II, and Novavax is furthest along in phase III, but these target older children and adults, including pregnant women.
“There’s going to be a lot of data in the coming year on completed clinical trials, and that’s going to tell us a lot about where we are,” Dr. Anderson said. “The young infant is the most challenging for a vaccine.” But, he added, “new information on protective immunity and disease pathogenesis should help achieve or improve vaccines in the future.”
Dr. Anderson has consulted on RSV vaccines for MedImmune, Novartis, Crucell Holland, and AVC, and has served on a Moderna Therapeutics scientific advisory board. His lab also has received grant funding from Trellis RSV Holdings, and he coinvented several RSV-related vaccine and treatment patents held by the CDC.
EXPERT ANALYSIS FROM THE NATIONAL IMMUNIZATION CONFERENCE
Key clinical point: A respiratory syncytial virus vaccine is closer to reality now than at any other time.
Major finding: 62 RSV vaccines are in development, with approximately 70% in preclinical studies.
Data source: Based on a review of the current state of research into an RSV vaccine and the burden of RSV disease.
Disclosures: Dr. Anderson has consulted on RSV vaccines for MedImmune, Novartis, Crucell Holland, and AVC, and has served on a Moderna Therapeutics scientific advisory board. His lab also has received grant funding from Trellis RSV Holdings, and he coinvented several RSV-related vaccine and treatment patents held by the CDC.
Why Required Pediatric Hospital Medicine Fellowships Are Unnecessary
The Joint Council of Pediatric Hospital Medicine (JCPHM), successor to the Strategic Planning (STP) Committee, recently recommended submitting a petition for two-year pediatric hospital medicine (PHM) fellowship certification to the American Board of Pediatrics (ABP), which was completed in 2014. In December 2015, the ABP Board of Directors voted to (1) approve the proposal for a two-year PHM fellowship incorporating scholarly activity with the provision that entrustable professional activities (EPAs) be used as the framework for assessing competencies and (2) not require those who achieve and maintain PHM certification to maintain general pediatrics certification. The proposal for certification of a two-year PHM fellowship will now be submitted to the American Board of Medical Specialties (ABMS). Concerns regarding the formal certification of PHM as an ABMS-recognized subspecialty have been raised by many stakeholders, including community pediatric hospitalists, pediatric residency program directors, and med-peds physicians.
We feel that the “first, do no harm” guiding principle seems to have been forgotten by the ABP as it attempts to formalize the training of pediatric hospitalists. In December 2015, the ABP voted in favor of a two-year ACGME-accredited PHM fellowship. The intent was to “assure the best care of hospitalized children,” “assure the public,” “accelerate improvements and innovation in quality improvement,” and “raise the level of care of all hospitalized children by establishing best practices in clinical care.” To be clear, these goals are shared by all of us (although there is no indication that the public is seeking additional assurance). Prior to launching broad-scale, time-intensive, and financially costly initiatives, we should ensure that our efforts would achieve—rather than obstruct—their intended aims. In addition to a lack of evidence supporting that subspecialty certification will advance our path toward achieving these goals, there are numerous reasons a required PHM fellowship is unnecessary and potentially even harmful to the hospitalist workforce. The negative unintended consequences need to be weighed heavily.
We have found no data to support that children would receive inferior inpatient care from pediatric hospitalists due to lack of formal certification. Hospital medicine physicians are paving the way in quality improvement, high-value care, medical education, palliative care, and global health, supported in part through training in various non-accredited hospital medicine fellowships. There is nothing stopping pediatric hospitalists from establishing and disseminating best practices in clinical care. Hospitalists are already making strides in providing high-quality care at low costs, as demonstrated by the abundant PHM scholarly work described in the ABP application to the ABMS. The alleged problem of needing to build trust within the community is yet to be demonstrated, as we have leaders at local, regional, and national levels. The chief medical officer of the Centers for Medicare & Medicaid Services is a hospitalist as is our surgeon general. Hospital medicine is the fastest-growing specialty in the history of medicine,1 and we should seek to propel rather than fetter our future colleagues.
Below are our reasons for opposing this formal certification.
We already have a fellowship system.
As we all know, advanced training opportunities already exist for those interested in pursuing extra research and quality improvement training. Similar to other pediatric subspecialty fellowships, these PHM fellowships are undersubscribed (20% of PHM fellowships did not fill in 2016),2 with the majority of graduating pediatric residents transitioning to hospitalists opting not to pursue fellowship training. We should continue to let graduating pediatric residents vote with their feet without the undue influence of subspecialty certification.
Subspecialization has opportunity costs that may reduce the PHM pipeline.
Even if we assume an adequate number of fellowship programs could be developed and funded, our fear is that the decision to turn PHM into an accredited subspecialty could paradoxically reduce the pipeline of inpatient providers. Residency is already a three- to four-year endeavor (pediatrics and med-peds) that is poorly compensated and time-intensive. In the absence of evidence supporting the value of additional training, tacking on another two years seems unreasonable in the face of the student loan debt crisis, reduced compensation, and lost time for career advancement. These are significant opportunity costs. While most specialties lead to a significant pay raise to compensate for the added training time, pediatrics remains the lowest-paid physician specialty.3 Should PHM follow the trend of most pediatric subspecialties, pursuit of fellowship training would be a negative financial decision for residency graduates.4 For the health system, increasing debt-to-income ratios runs the risk of creating a medical education bubble market.5
More than 25% of med-peds graduates pursue careers in hospital medicine, a percentage that continues to grow, accounting for more than 100 new hospitalists per year.6 As a result, med-peds-trained hospitalists constitute more than 10% of the pediatric hospitalist workforce.6 Requiring PHM fellowship training may reduce this crucial pipeline of practitioners. In a 2014 unpublished survey of 225 med-peds practitioners, 78% of residents and 96% of attendings responded that they would not consider pursuing an ACGME-accredited PHM fellowship.7 This is compounded by a lack of parity with the practice of adult hospital medicine both in compensation and required training and is heightened by the fact that the training in question does not incorporate care for adult patients. There is clear consensus by 96% of med-peds hospitalists that the creation of an ACGME-certified PHM subspecialty will negatively affect the likelihood of med-peds providers pursuing PHM.7
Certification will pose a potential risk to specific patient populations.
We are also concerned that a reduced PHM workforce could disproportionately impact young adults with special healthcare needs and those children cared for in rural or community-based hospitals. Med-peds training equips providers to care for children with chronic diseases that then transition into adulthood; more than 25% provide care for young adults with special healthcare needs.6 With the increasing number of children with chronic health conditions surviving into adulthood,8 med-peds hospitalists serve essential roles in providing care and coordination for this vulnerable population. Furthermore, hospital medicine groups in medical systems that cannot support a full-time categorical pediatric hospitalist tend to employ med-peds physicians or family practitioners. Concerns with PHM certification are thus extended to those family medicine physicians who practice PHM.
Pediatric residency trains pediatricians in inpatient care.
We feel that the decision to move forward on PHM subspecialty certification calls into question the value of pediatric residency training. There is no evidence that clinical inpatient training in pediatrics residency is inadequate. If one leaves residency trained to do anything, it is practicing hospital medicine. A significant portion of residency takes place inpatient, both on wards and in the intensive care units. The 2009 ABP Foundation–funded study of PHM reported that 94% of pediatric hospitalist respondents rated their training in general clinical skills during residency as fully adequate, 85% rated their training in communication skills as fully adequate, and 73% did not believe any additional training beyond residency should be required.9 With respect to med-peds graduates, more than 90% feel equipped to care for children and adults upon residency completion.10 If the ABMS carries forward with this decision, the only clinical work one would be “certified” to do after residency is primary care. However, after completion of residency training, most of us feel at least as comfortable, if not more comfortable, caring for children in the inpatient setting.
Primary care should require subspecialty certification as well.
Furthermore, the decision to create a certified subspecialty begs the question as to why fellowship should not be mandated for those entering the field of primary care. Does the field of primary care not require research to move it forward? Does the field of primary care not require providers who can adeptly apply quality improvement methodologies to improve primary-care delivery? Does the public not require the same type of assurance? By these measures, primary care should require subspecialty certification as well. These arguments could easily be construed as an indictment of residency training.
The target should be residency training.
The PHM ABMS application describes a clinical curriculum consisting of eight core clinical rotations in various settings. That small number emphasizes the fact that extra clinical training is really not needed and that we do not require a complete overhaul of the current training system. The skills in question for the accredited PHM fellowship include communication, negotiation, leadership, quality improvement, pain management, sedation, procedures, transport, billing/coding, autonomous decision making, and scholarly practice. Are most of these not skills that we should foster in all practicing pediatricians? If graduating pediatric residents lack competence in core pediatric skills (e.g., communication, pain management, autonomous decision making), we should target improvements in residency education rather than require years of further training. Pediatrics residency training already requires training in quality improvement and is incorporating “tracks” that target areas of perceived deficiency. Those physicians who actually require specialized hospital-based skills (e.g., sedation, procedures, and transport) could receive core training during residency (e.g., through PHM tracks or electives) and further hone these skills through faculty development efforts. While non-PhD researchers may benefit from additional training in research methodologies, this training comes at the expense of time spent caring for patients on the wards and should not be required training for the majority of pediatric hospitalists pursuing purely clinical roles.
Broad-based support for a PHM subspecialty has not been demonstrated.
While approximately 40 pediatric hospitalists originated the PHM certification petition, we have not seen clear support for subspecialty certification from the community. PHM certification runs the risk of alienating the general pediatrics community, as many outpatient pediatricians continue to care for their patients in the inpatient setting. Furthermore, at tertiary-care medical centers, pediatric subspecialists often serve as hospitalists, yet this stakeholder group has not entered into this conversation. Importantly, the Association of Pediatric Program Directors (APPD) did not endorse this proposal. Many of the APPD members were quite concerned about the harm this certification could cause. While the APA Board and the AAP Board of Directors support PHM subspecialty certification, it is not clear that the rank-and-file members do. The Society of Hospital Medicine did not support or oppose certification. In an era of controversy surrounding certification requirements, prior to making a decision that will alter the direction of an entire field and impact all future residency graduates interested in entering that field, we should ensure there is broad-based support for this decision.
An alternative path has already been established and validated.
A more prudent, cost-effective, and universally acceptable approach would be to follow in the footsteps of the American Board of Internal Medicine (ABIM) and American Board of Family Medicine (ABFM) in establishing a Focused Practice in Pediatric Hospital Medicine program. This approach respects the unique body of knowledge required of those who care for hospitalized children while maintaining the required flexibility to nurture and help to mature existing training pipelines. Core hospital medicine skills should be further honed through residency curricular changes and faculty development efforts, while hospital-based physicians interested in developing niche skills could still do so via already existing fellowships.
When it comes to pediatric hospital medicine, first, do no harm.
Pediatric hospitalists are inpatient generalists by training and clinical approach. Our practices vary from large academic medical centers with every imaginable subspecialty consult service available to remote rural settings that require hospitalists to possess unique and specific skills. Some pediatric hospitalists participate in newborn care, some perform sedations, and some perform a variety of diagnostic and therapeutic procedures. The current system is meeting the needs of the vast majority of our PHM community. Changes to the residency curriculum that are already under way can address any clinical and quality improvement gaps. More than enough PHM fellowships are available to those who choose to pursue them. The public is not requesting reassurance, and the field is already advancing at a rapid rate both clinically and scholarly. Subspecialty recognition is not necessary and will likely lead to negative unintended consequences. Given the financial constraints on our current system and the need for pediatric hospitalists to be stewards of high-value care, we should make collective decisions that will clearly benefit our patients and health system. As medical professionals, our priority should always be first, do no harm.
Weijen W. Chang, MD, is chief of the Division of Pediatric Hospital Medicine at Baystate Children’s Hospital and associate professor of pediatrics at the University of Massachusetts Medical School.
Leonard Samuel Feldman, MD, is director of the Medicine-Pediatrics Urban Health Residency Program and associate professor of medicine and pediatrics at Johns Hopkins School of Medicine.
Bradley Monash, MD, is associate chief of medicine at University of California, San Francisco and assistant clinical professor of medicine and pediatrics at UCSF School of Medicine.
Archna Eniasivam, MD, is assistant clinical professor of medicine at UCSF School of Medicine.
References
- Chen C, Eagle S. “Should Pediatric HM Pursue Subspecialty Certification, Required Fellowship Training?” The Hospitalist. July 31, 2012
- Results and Data: Specialties Matching Service 2016 Appointment Year. National Resident Matching Program website. Accessed May 15, 2016.
- Medscape Pediatrician Compensation Report 2015. Medscape website. Accessed April 29, 2016.
- Rochlin JM, Simon HK. Does fellowship pay: what is the long-term financial impact of subspecialty training in pediatrics? Pediatrics. 2001;127(2):254-260.
- Asch DA, Nicholson S, Vujicic M. Are we in a medical education bubble market? N Engl J Med. 2013;369(21):1973-1975.
- O’Toole JK, Friedland AR, Gonzaga AM, et al. The practice patterns of recently graduated internal medicine-pediatric hospitalists. Hosp Pediatr. 2015;5(6):309-314.
- Society of Hospital Medicine: Survey of Med-Peds Physicians about PHM Certification. May 2014 (unpublished).
- Goodman DM, Hall M, Levin A, et al. Adults with chronic health conditions originating in childhood: inpatient experience in children’s hospitals. Pediatrics. 2011;128(1):5-13.
- Freed GL, Dunham KM, Research Advisory Committee of the American Board of P. Pediatric hospitalists: training, current practice, and career goals. J Hosp Med. 2009;4(3):179-186.
- Donnelly MJ, Lubrano L, Radabaugh CL, Lukela MP, Friedland AR, Ruch-Ross HS. The med-peds hospitalist workforce: results from the American Academy of Pediatrics Workforce Survey. Hosp Pediatr. 2015;5(11):574-579.
The Joint Council of Pediatric Hospital Medicine (JCPHM), successor to the Strategic Planning (STP) Committee, recently recommended submitting a petition for two-year pediatric hospital medicine (PHM) fellowship certification to the American Board of Pediatrics (ABP), which was completed in 2014. In December 2015, the ABP Board of Directors voted to (1) approve the proposal for a two-year PHM fellowship incorporating scholarly activity with the provision that entrustable professional activities (EPAs) be used as the framework for assessing competencies and (2) not require those who achieve and maintain PHM certification to maintain general pediatrics certification. The proposal for certification of a two-year PHM fellowship will now be submitted to the American Board of Medical Specialties (ABMS). Concerns regarding the formal certification of PHM as an ABMS-recognized subspecialty have been raised by many stakeholders, including community pediatric hospitalists, pediatric residency program directors, and med-peds physicians.
We feel that the “first, do no harm” guiding principle seems to have been forgotten by the ABP as it attempts to formalize the training of pediatric hospitalists. In December 2015, the ABP voted in favor of a two-year ACGME-accredited PHM fellowship. The intent was to “assure the best care of hospitalized children,” “assure the public,” “accelerate improvements and innovation in quality improvement,” and “raise the level of care of all hospitalized children by establishing best practices in clinical care.” To be clear, these goals are shared by all of us (although there is no indication that the public is seeking additional assurance). Prior to launching broad-scale, time-intensive, and financially costly initiatives, we should ensure that our efforts would achieve—rather than obstruct—their intended aims. In addition to a lack of evidence supporting that subspecialty certification will advance our path toward achieving these goals, there are numerous reasons a required PHM fellowship is unnecessary and potentially even harmful to the hospitalist workforce. The negative unintended consequences need to be weighed heavily.
We have found no data to support that children would receive inferior inpatient care from pediatric hospitalists due to lack of formal certification. Hospital medicine physicians are paving the way in quality improvement, high-value care, medical education, palliative care, and global health, supported in part through training in various non-accredited hospital medicine fellowships. There is nothing stopping pediatric hospitalists from establishing and disseminating best practices in clinical care. Hospitalists are already making strides in providing high-quality care at low costs, as demonstrated by the abundant PHM scholarly work described in the ABP application to the ABMS. The alleged problem of needing to build trust within the community is yet to be demonstrated, as we have leaders at local, regional, and national levels. The chief medical officer of the Centers for Medicare & Medicaid Services is a hospitalist as is our surgeon general. Hospital medicine is the fastest-growing specialty in the history of medicine,1 and we should seek to propel rather than fetter our future colleagues.
Below are our reasons for opposing this formal certification.
We already have a fellowship system.
As we all know, advanced training opportunities already exist for those interested in pursuing extra research and quality improvement training. Similar to other pediatric subspecialty fellowships, these PHM fellowships are undersubscribed (20% of PHM fellowships did not fill in 2016),2 with the majority of graduating pediatric residents transitioning to hospitalists opting not to pursue fellowship training. We should continue to let graduating pediatric residents vote with their feet without the undue influence of subspecialty certification.
Subspecialization has opportunity costs that may reduce the PHM pipeline.
Even if we assume an adequate number of fellowship programs could be developed and funded, our fear is that the decision to turn PHM into an accredited subspecialty could paradoxically reduce the pipeline of inpatient providers. Residency is already a three- to four-year endeavor (pediatrics and med-peds) that is poorly compensated and time-intensive. In the absence of evidence supporting the value of additional training, tacking on another two years seems unreasonable in the face of the student loan debt crisis, reduced compensation, and lost time for career advancement. These are significant opportunity costs. While most specialties lead to a significant pay raise to compensate for the added training time, pediatrics remains the lowest-paid physician specialty.3 Should PHM follow the trend of most pediatric subspecialties, pursuit of fellowship training would be a negative financial decision for residency graduates.4 For the health system, increasing debt-to-income ratios runs the risk of creating a medical education bubble market.5
More than 25% of med-peds graduates pursue careers in hospital medicine, a percentage that continues to grow, accounting for more than 100 new hospitalists per year.6 As a result, med-peds-trained hospitalists constitute more than 10% of the pediatric hospitalist workforce.6 Requiring PHM fellowship training may reduce this crucial pipeline of practitioners. In a 2014 unpublished survey of 225 med-peds practitioners, 78% of residents and 96% of attendings responded that they would not consider pursuing an ACGME-accredited PHM fellowship.7 This is compounded by a lack of parity with the practice of adult hospital medicine both in compensation and required training and is heightened by the fact that the training in question does not incorporate care for adult patients. There is clear consensus by 96% of med-peds hospitalists that the creation of an ACGME-certified PHM subspecialty will negatively affect the likelihood of med-peds providers pursuing PHM.7
Certification will pose a potential risk to specific patient populations.
We are also concerned that a reduced PHM workforce could disproportionately impact young adults with special healthcare needs and those children cared for in rural or community-based hospitals. Med-peds training equips providers to care for children with chronic diseases that then transition into adulthood; more than 25% provide care for young adults with special healthcare needs.6 With the increasing number of children with chronic health conditions surviving into adulthood,8 med-peds hospitalists serve essential roles in providing care and coordination for this vulnerable population. Furthermore, hospital medicine groups in medical systems that cannot support a full-time categorical pediatric hospitalist tend to employ med-peds physicians or family practitioners. Concerns with PHM certification are thus extended to those family medicine physicians who practice PHM.
Pediatric residency trains pediatricians in inpatient care.
We feel that the decision to move forward on PHM subspecialty certification calls into question the value of pediatric residency training. There is no evidence that clinical inpatient training in pediatrics residency is inadequate. If one leaves residency trained to do anything, it is practicing hospital medicine. A significant portion of residency takes place inpatient, both on wards and in the intensive care units. The 2009 ABP Foundation–funded study of PHM reported that 94% of pediatric hospitalist respondents rated their training in general clinical skills during residency as fully adequate, 85% rated their training in communication skills as fully adequate, and 73% did not believe any additional training beyond residency should be required.9 With respect to med-peds graduates, more than 90% feel equipped to care for children and adults upon residency completion.10 If the ABMS carries forward with this decision, the only clinical work one would be “certified” to do after residency is primary care. However, after completion of residency training, most of us feel at least as comfortable, if not more comfortable, caring for children in the inpatient setting.
Primary care should require subspecialty certification as well.
Furthermore, the decision to create a certified subspecialty begs the question as to why fellowship should not be mandated for those entering the field of primary care. Does the field of primary care not require research to move it forward? Does the field of primary care not require providers who can adeptly apply quality improvement methodologies to improve primary-care delivery? Does the public not require the same type of assurance? By these measures, primary care should require subspecialty certification as well. These arguments could easily be construed as an indictment of residency training.
The target should be residency training.
The PHM ABMS application describes a clinical curriculum consisting of eight core clinical rotations in various settings. That small number emphasizes the fact that extra clinical training is really not needed and that we do not require a complete overhaul of the current training system. The skills in question for the accredited PHM fellowship include communication, negotiation, leadership, quality improvement, pain management, sedation, procedures, transport, billing/coding, autonomous decision making, and scholarly practice. Are most of these not skills that we should foster in all practicing pediatricians? If graduating pediatric residents lack competence in core pediatric skills (e.g., communication, pain management, autonomous decision making), we should target improvements in residency education rather than require years of further training. Pediatrics residency training already requires training in quality improvement and is incorporating “tracks” that target areas of perceived deficiency. Those physicians who actually require specialized hospital-based skills (e.g., sedation, procedures, and transport) could receive core training during residency (e.g., through PHM tracks or electives) and further hone these skills through faculty development efforts. While non-PhD researchers may benefit from additional training in research methodologies, this training comes at the expense of time spent caring for patients on the wards and should not be required training for the majority of pediatric hospitalists pursuing purely clinical roles.
Broad-based support for a PHM subspecialty has not been demonstrated.
While approximately 40 pediatric hospitalists originated the PHM certification petition, we have not seen clear support for subspecialty certification from the community. PHM certification runs the risk of alienating the general pediatrics community, as many outpatient pediatricians continue to care for their patients in the inpatient setting. Furthermore, at tertiary-care medical centers, pediatric subspecialists often serve as hospitalists, yet this stakeholder group has not entered into this conversation. Importantly, the Association of Pediatric Program Directors (APPD) did not endorse this proposal. Many of the APPD members were quite concerned about the harm this certification could cause. While the APA Board and the AAP Board of Directors support PHM subspecialty certification, it is not clear that the rank-and-file members do. The Society of Hospital Medicine did not support or oppose certification. In an era of controversy surrounding certification requirements, prior to making a decision that will alter the direction of an entire field and impact all future residency graduates interested in entering that field, we should ensure there is broad-based support for this decision.
An alternative path has already been established and validated.
A more prudent, cost-effective, and universally acceptable approach would be to follow in the footsteps of the American Board of Internal Medicine (ABIM) and American Board of Family Medicine (ABFM) in establishing a Focused Practice in Pediatric Hospital Medicine program. This approach respects the unique body of knowledge required of those who care for hospitalized children while maintaining the required flexibility to nurture and help to mature existing training pipelines. Core hospital medicine skills should be further honed through residency curricular changes and faculty development efforts, while hospital-based physicians interested in developing niche skills could still do so via already existing fellowships.
When it comes to pediatric hospital medicine, first, do no harm.
Pediatric hospitalists are inpatient generalists by training and clinical approach. Our practices vary from large academic medical centers with every imaginable subspecialty consult service available to remote rural settings that require hospitalists to possess unique and specific skills. Some pediatric hospitalists participate in newborn care, some perform sedations, and some perform a variety of diagnostic and therapeutic procedures. The current system is meeting the needs of the vast majority of our PHM community. Changes to the residency curriculum that are already under way can address any clinical and quality improvement gaps. More than enough PHM fellowships are available to those who choose to pursue them. The public is not requesting reassurance, and the field is already advancing at a rapid rate both clinically and scholarly. Subspecialty recognition is not necessary and will likely lead to negative unintended consequences. Given the financial constraints on our current system and the need for pediatric hospitalists to be stewards of high-value care, we should make collective decisions that will clearly benefit our patients and health system. As medical professionals, our priority should always be first, do no harm.
Weijen W. Chang, MD, is chief of the Division of Pediatric Hospital Medicine at Baystate Children’s Hospital and associate professor of pediatrics at the University of Massachusetts Medical School.
Leonard Samuel Feldman, MD, is director of the Medicine-Pediatrics Urban Health Residency Program and associate professor of medicine and pediatrics at Johns Hopkins School of Medicine.
Bradley Monash, MD, is associate chief of medicine at University of California, San Francisco and assistant clinical professor of medicine and pediatrics at UCSF School of Medicine.
Archna Eniasivam, MD, is assistant clinical professor of medicine at UCSF School of Medicine.
References
- Chen C, Eagle S. “Should Pediatric HM Pursue Subspecialty Certification, Required Fellowship Training?” The Hospitalist. July 31, 2012
- Results and Data: Specialties Matching Service 2016 Appointment Year. National Resident Matching Program website. Accessed May 15, 2016.
- Medscape Pediatrician Compensation Report 2015. Medscape website. Accessed April 29, 2016.
- Rochlin JM, Simon HK. Does fellowship pay: what is the long-term financial impact of subspecialty training in pediatrics? Pediatrics. 2001;127(2):254-260.
- Asch DA, Nicholson S, Vujicic M. Are we in a medical education bubble market? N Engl J Med. 2013;369(21):1973-1975.
- O’Toole JK, Friedland AR, Gonzaga AM, et al. The practice patterns of recently graduated internal medicine-pediatric hospitalists. Hosp Pediatr. 2015;5(6):309-314.
- Society of Hospital Medicine: Survey of Med-Peds Physicians about PHM Certification. May 2014 (unpublished).
- Goodman DM, Hall M, Levin A, et al. Adults with chronic health conditions originating in childhood: inpatient experience in children’s hospitals. Pediatrics. 2011;128(1):5-13.
- Freed GL, Dunham KM, Research Advisory Committee of the American Board of P. Pediatric hospitalists: training, current practice, and career goals. J Hosp Med. 2009;4(3):179-186.
- Donnelly MJ, Lubrano L, Radabaugh CL, Lukela MP, Friedland AR, Ruch-Ross HS. The med-peds hospitalist workforce: results from the American Academy of Pediatrics Workforce Survey. Hosp Pediatr. 2015;5(11):574-579.
The Joint Council of Pediatric Hospital Medicine (JCPHM), successor to the Strategic Planning (STP) Committee, recently recommended submitting a petition for two-year pediatric hospital medicine (PHM) fellowship certification to the American Board of Pediatrics (ABP), which was completed in 2014. In December 2015, the ABP Board of Directors voted to (1) approve the proposal for a two-year PHM fellowship incorporating scholarly activity with the provision that entrustable professional activities (EPAs) be used as the framework for assessing competencies and (2) not require those who achieve and maintain PHM certification to maintain general pediatrics certification. The proposal for certification of a two-year PHM fellowship will now be submitted to the American Board of Medical Specialties (ABMS). Concerns regarding the formal certification of PHM as an ABMS-recognized subspecialty have been raised by many stakeholders, including community pediatric hospitalists, pediatric residency program directors, and med-peds physicians.
We feel that the “first, do no harm” guiding principle seems to have been forgotten by the ABP as it attempts to formalize the training of pediatric hospitalists. In December 2015, the ABP voted in favor of a two-year ACGME-accredited PHM fellowship. The intent was to “assure the best care of hospitalized children,” “assure the public,” “accelerate improvements and innovation in quality improvement,” and “raise the level of care of all hospitalized children by establishing best practices in clinical care.” To be clear, these goals are shared by all of us (although there is no indication that the public is seeking additional assurance). Prior to launching broad-scale, time-intensive, and financially costly initiatives, we should ensure that our efforts would achieve—rather than obstruct—their intended aims. In addition to a lack of evidence supporting that subspecialty certification will advance our path toward achieving these goals, there are numerous reasons a required PHM fellowship is unnecessary and potentially even harmful to the hospitalist workforce. The negative unintended consequences need to be weighed heavily.
We have found no data to support that children would receive inferior inpatient care from pediatric hospitalists due to lack of formal certification. Hospital medicine physicians are paving the way in quality improvement, high-value care, medical education, palliative care, and global health, supported in part through training in various non-accredited hospital medicine fellowships. There is nothing stopping pediatric hospitalists from establishing and disseminating best practices in clinical care. Hospitalists are already making strides in providing high-quality care at low costs, as demonstrated by the abundant PHM scholarly work described in the ABP application to the ABMS. The alleged problem of needing to build trust within the community is yet to be demonstrated, as we have leaders at local, regional, and national levels. The chief medical officer of the Centers for Medicare & Medicaid Services is a hospitalist as is our surgeon general. Hospital medicine is the fastest-growing specialty in the history of medicine,1 and we should seek to propel rather than fetter our future colleagues.
Below are our reasons for opposing this formal certification.
We already have a fellowship system.
As we all know, advanced training opportunities already exist for those interested in pursuing extra research and quality improvement training. Similar to other pediatric subspecialty fellowships, these PHM fellowships are undersubscribed (20% of PHM fellowships did not fill in 2016),2 with the majority of graduating pediatric residents transitioning to hospitalists opting not to pursue fellowship training. We should continue to let graduating pediatric residents vote with their feet without the undue influence of subspecialty certification.
Subspecialization has opportunity costs that may reduce the PHM pipeline.
Even if we assume an adequate number of fellowship programs could be developed and funded, our fear is that the decision to turn PHM into an accredited subspecialty could paradoxically reduce the pipeline of inpatient providers. Residency is already a three- to four-year endeavor (pediatrics and med-peds) that is poorly compensated and time-intensive. In the absence of evidence supporting the value of additional training, tacking on another two years seems unreasonable in the face of the student loan debt crisis, reduced compensation, and lost time for career advancement. These are significant opportunity costs. While most specialties lead to a significant pay raise to compensate for the added training time, pediatrics remains the lowest-paid physician specialty.3 Should PHM follow the trend of most pediatric subspecialties, pursuit of fellowship training would be a negative financial decision for residency graduates.4 For the health system, increasing debt-to-income ratios runs the risk of creating a medical education bubble market.5
More than 25% of med-peds graduates pursue careers in hospital medicine, a percentage that continues to grow, accounting for more than 100 new hospitalists per year.6 As a result, med-peds-trained hospitalists constitute more than 10% of the pediatric hospitalist workforce.6 Requiring PHM fellowship training may reduce this crucial pipeline of practitioners. In a 2014 unpublished survey of 225 med-peds practitioners, 78% of residents and 96% of attendings responded that they would not consider pursuing an ACGME-accredited PHM fellowship.7 This is compounded by a lack of parity with the practice of adult hospital medicine both in compensation and required training and is heightened by the fact that the training in question does not incorporate care for adult patients. There is clear consensus by 96% of med-peds hospitalists that the creation of an ACGME-certified PHM subspecialty will negatively affect the likelihood of med-peds providers pursuing PHM.7
Certification will pose a potential risk to specific patient populations.
We are also concerned that a reduced PHM workforce could disproportionately impact young adults with special healthcare needs and those children cared for in rural or community-based hospitals. Med-peds training equips providers to care for children with chronic diseases that then transition into adulthood; more than 25% provide care for young adults with special healthcare needs.6 With the increasing number of children with chronic health conditions surviving into adulthood,8 med-peds hospitalists serve essential roles in providing care and coordination for this vulnerable population. Furthermore, hospital medicine groups in medical systems that cannot support a full-time categorical pediatric hospitalist tend to employ med-peds physicians or family practitioners. Concerns with PHM certification are thus extended to those family medicine physicians who practice PHM.
Pediatric residency trains pediatricians in inpatient care.
We feel that the decision to move forward on PHM subspecialty certification calls into question the value of pediatric residency training. There is no evidence that clinical inpatient training in pediatrics residency is inadequate. If one leaves residency trained to do anything, it is practicing hospital medicine. A significant portion of residency takes place inpatient, both on wards and in the intensive care units. The 2009 ABP Foundation–funded study of PHM reported that 94% of pediatric hospitalist respondents rated their training in general clinical skills during residency as fully adequate, 85% rated their training in communication skills as fully adequate, and 73% did not believe any additional training beyond residency should be required.9 With respect to med-peds graduates, more than 90% feel equipped to care for children and adults upon residency completion.10 If the ABMS carries forward with this decision, the only clinical work one would be “certified” to do after residency is primary care. However, after completion of residency training, most of us feel at least as comfortable, if not more comfortable, caring for children in the inpatient setting.
Primary care should require subspecialty certification as well.
Furthermore, the decision to create a certified subspecialty begs the question as to why fellowship should not be mandated for those entering the field of primary care. Does the field of primary care not require research to move it forward? Does the field of primary care not require providers who can adeptly apply quality improvement methodologies to improve primary-care delivery? Does the public not require the same type of assurance? By these measures, primary care should require subspecialty certification as well. These arguments could easily be construed as an indictment of residency training.
The target should be residency training.
The PHM ABMS application describes a clinical curriculum consisting of eight core clinical rotations in various settings. That small number emphasizes the fact that extra clinical training is really not needed and that we do not require a complete overhaul of the current training system. The skills in question for the accredited PHM fellowship include communication, negotiation, leadership, quality improvement, pain management, sedation, procedures, transport, billing/coding, autonomous decision making, and scholarly practice. Are most of these not skills that we should foster in all practicing pediatricians? If graduating pediatric residents lack competence in core pediatric skills (e.g., communication, pain management, autonomous decision making), we should target improvements in residency education rather than require years of further training. Pediatrics residency training already requires training in quality improvement and is incorporating “tracks” that target areas of perceived deficiency. Those physicians who actually require specialized hospital-based skills (e.g., sedation, procedures, and transport) could receive core training during residency (e.g., through PHM tracks or electives) and further hone these skills through faculty development efforts. While non-PhD researchers may benefit from additional training in research methodologies, this training comes at the expense of time spent caring for patients on the wards and should not be required training for the majority of pediatric hospitalists pursuing purely clinical roles.
Broad-based support for a PHM subspecialty has not been demonstrated.
While approximately 40 pediatric hospitalists originated the PHM certification petition, we have not seen clear support for subspecialty certification from the community. PHM certification runs the risk of alienating the general pediatrics community, as many outpatient pediatricians continue to care for their patients in the inpatient setting. Furthermore, at tertiary-care medical centers, pediatric subspecialists often serve as hospitalists, yet this stakeholder group has not entered into this conversation. Importantly, the Association of Pediatric Program Directors (APPD) did not endorse this proposal. Many of the APPD members were quite concerned about the harm this certification could cause. While the APA Board and the AAP Board of Directors support PHM subspecialty certification, it is not clear that the rank-and-file members do. The Society of Hospital Medicine did not support or oppose certification. In an era of controversy surrounding certification requirements, prior to making a decision that will alter the direction of an entire field and impact all future residency graduates interested in entering that field, we should ensure there is broad-based support for this decision.
An alternative path has already been established and validated.
A more prudent, cost-effective, and universally acceptable approach would be to follow in the footsteps of the American Board of Internal Medicine (ABIM) and American Board of Family Medicine (ABFM) in establishing a Focused Practice in Pediatric Hospital Medicine program. This approach respects the unique body of knowledge required of those who care for hospitalized children while maintaining the required flexibility to nurture and help to mature existing training pipelines. Core hospital medicine skills should be further honed through residency curricular changes and faculty development efforts, while hospital-based physicians interested in developing niche skills could still do so via already existing fellowships.
When it comes to pediatric hospital medicine, first, do no harm.
Pediatric hospitalists are inpatient generalists by training and clinical approach. Our practices vary from large academic medical centers with every imaginable subspecialty consult service available to remote rural settings that require hospitalists to possess unique and specific skills. Some pediatric hospitalists participate in newborn care, some perform sedations, and some perform a variety of diagnostic and therapeutic procedures. The current system is meeting the needs of the vast majority of our PHM community. Changes to the residency curriculum that are already under way can address any clinical and quality improvement gaps. More than enough PHM fellowships are available to those who choose to pursue them. The public is not requesting reassurance, and the field is already advancing at a rapid rate both clinically and scholarly. Subspecialty recognition is not necessary and will likely lead to negative unintended consequences. Given the financial constraints on our current system and the need for pediatric hospitalists to be stewards of high-value care, we should make collective decisions that will clearly benefit our patients and health system. As medical professionals, our priority should always be first, do no harm.
Weijen W. Chang, MD, is chief of the Division of Pediatric Hospital Medicine at Baystate Children’s Hospital and associate professor of pediatrics at the University of Massachusetts Medical School.
Leonard Samuel Feldman, MD, is director of the Medicine-Pediatrics Urban Health Residency Program and associate professor of medicine and pediatrics at Johns Hopkins School of Medicine.
Bradley Monash, MD, is associate chief of medicine at University of California, San Francisco and assistant clinical professor of medicine and pediatrics at UCSF School of Medicine.
Archna Eniasivam, MD, is assistant clinical professor of medicine at UCSF School of Medicine.
References
- Chen C, Eagle S. “Should Pediatric HM Pursue Subspecialty Certification, Required Fellowship Training?” The Hospitalist. July 31, 2012
- Results and Data: Specialties Matching Service 2016 Appointment Year. National Resident Matching Program website. Accessed May 15, 2016.
- Medscape Pediatrician Compensation Report 2015. Medscape website. Accessed April 29, 2016.
- Rochlin JM, Simon HK. Does fellowship pay: what is the long-term financial impact of subspecialty training in pediatrics? Pediatrics. 2001;127(2):254-260.
- Asch DA, Nicholson S, Vujicic M. Are we in a medical education bubble market? N Engl J Med. 2013;369(21):1973-1975.
- O’Toole JK, Friedland AR, Gonzaga AM, et al. The practice patterns of recently graduated internal medicine-pediatric hospitalists. Hosp Pediatr. 2015;5(6):309-314.
- Society of Hospital Medicine: Survey of Med-Peds Physicians about PHM Certification. May 2014 (unpublished).
- Goodman DM, Hall M, Levin A, et al. Adults with chronic health conditions originating in childhood: inpatient experience in children’s hospitals. Pediatrics. 2011;128(1):5-13.
- Freed GL, Dunham KM, Research Advisory Committee of the American Board of P. Pediatric hospitalists: training, current practice, and career goals. J Hosp Med. 2009;4(3):179-186.
- Donnelly MJ, Lubrano L, Radabaugh CL, Lukela MP, Friedland AR, Ruch-Ross HS. The med-peds hospitalist workforce: results from the American Academy of Pediatrics Workforce Survey. Hosp Pediatr. 2015;5(11):574-579.
Reassuring findings on neurodevelopmental outcomes in HIV-exposed children
DURBAN, SOUTH AFRICA – Children exposed to HIV in utero but uninfected at birth have neurodevelopmental test scores at age 24 months that are comparable with those of unexposed children, based on a study conducted in Botswana and presented by Jean Leidner at the 21st International AIDS Conference.
“These results provide reassurance regarding the potential effects of in-utero HIV and antiretroviral exposure,” declared Ms. Leidner, CEO of Goodtables Data Consulting in Norman, Okla., and the Botswana Harvard AIDS Institute Partnership.

The two groups of children had virtually identical scores on the cognitive, gross motor, fine motor, expressive language, and receptive language domains measured in the Bayley-III. The same was true for scores on the fine motor, locomotor, language, and personal-social elements of the Developmental Milestone Checklist.
The two groups of children differed in other ways; 17% of the uninfected children exposed to HIV in utero and 8% of the controls were low birth weight. The HIV-exposed children are being raised in a more challenging environment: just 49% have electricity in the home, compared with 64% of control families. Moreover, 53% of the HIV-exposed children and 33% of the controls live under conditions of moderate-to-severe food uncertainty.
Only 8% of the HIV-infected mothers breastfed, whereas breastfeeding was universal among the control group.
More than 99% of the HIV-infected mothers took antiretroviral medication antenatally. Roughly two-thirds were on zidovudine (Retrovir) monotherapy, the rest on a three-drug regimen of nevirapine (Viramune) plus lamivudine/zidovudine (Combivir). These are older antiretrovirals. Additional neurodevelopmental studies are warranted in children with in-utero exposure to newer agents, as well as in older children, Ms. Leidner said.
She reported having no financial conflicts regarding this study, which was funded by the National Institute of Mental Health.
DURBAN, SOUTH AFRICA – Children exposed to HIV in utero but uninfected at birth have neurodevelopmental test scores at age 24 months that are comparable with those of unexposed children, based on a study conducted in Botswana and presented by Jean Leidner at the 21st International AIDS Conference.
“These results provide reassurance regarding the potential effects of in-utero HIV and antiretroviral exposure,” declared Ms. Leidner, CEO of Goodtables Data Consulting in Norman, Okla., and the Botswana Harvard AIDS Institute Partnership.
The two groups of children had virtually identical scores on the cognitive, gross motor, fine motor, expressive language, and receptive language domains measured in the Bayley-III. The same was true for scores on the fine motor, locomotor, language, and personal-social elements of the Developmental Milestone Checklist.
The two groups of children differed in other ways; 17% of the uninfected children exposed to HIV in utero and 8% of the controls were low birth weight. The HIV-exposed children are being raised in a more challenging environment: just 49% have electricity in the home, compared with 64% of control families. Moreover, 53% of the HIV-exposed children and 33% of the controls live under conditions of moderate-to-severe food uncertainty.
Only 8% of the HIV-infected mothers breastfed, whereas breastfeeding was universal among the control group.
More than 99% of the HIV-infected mothers took antiretroviral medication antenatally. Roughly two-thirds were on zidovudine (Retrovir) monotherapy, the rest on a three-drug regimen of nevirapine (Viramune) plus lamivudine/zidovudine (Combivir). These are older antiretrovirals. Additional neurodevelopmental studies are warranted in children with in-utero exposure to newer agents, as well as in older children, Ms. Leidner said.
She reported having no financial conflicts regarding this study, which was funded by the National Institute of Mental Health.
DURBAN, SOUTH AFRICA – Children exposed to HIV in utero but uninfected at birth have neurodevelopmental test scores at age 24 months that are comparable with those of unexposed children, based on a study conducted in Botswana and presented by Jean Leidner at the 21st International AIDS Conference.
“These results provide reassurance regarding the potential effects of in-utero HIV and antiretroviral exposure,” declared Ms. Leidner, CEO of Goodtables Data Consulting in Norman, Okla., and the Botswana Harvard AIDS Institute Partnership.
The two groups of children had virtually identical scores on the cognitive, gross motor, fine motor, expressive language, and receptive language domains measured in the Bayley-III. The same was true for scores on the fine motor, locomotor, language, and personal-social elements of the Developmental Milestone Checklist.
The two groups of children differed in other ways; 17% of the uninfected children exposed to HIV in utero and 8% of the controls were low birth weight. The HIV-exposed children are being raised in a more challenging environment: just 49% have electricity in the home, compared with 64% of control families. Moreover, 53% of the HIV-exposed children and 33% of the controls live under conditions of moderate-to-severe food uncertainty.
Only 8% of the HIV-infected mothers breastfed, whereas breastfeeding was universal among the control group.
More than 99% of the HIV-infected mothers took antiretroviral medication antenatally. Roughly two-thirds were on zidovudine (Retrovir) monotherapy, the rest on a three-drug regimen of nevirapine (Viramune) plus lamivudine/zidovudine (Combivir). These are older antiretrovirals. Additional neurodevelopmental studies are warranted in children with in-utero exposure to newer agents, as well as in older children, Ms. Leidner said.
She reported having no financial conflicts regarding this study, which was funded by the National Institute of Mental Health.
Key clinical point:
Major finding: In-utero exposure to maternal HIV and antiretroviral drugs had no measurable adverse neurodevelopmental effects at age 24 months in uninfected children.
Data source: 337 uninfected children exposed to HIV in-utero and 387 children unexposed to HIV in utero.
Disclosures: The National Institute of Mental Health funded the study. The presenter reported having no financial conflicts of interest.
Hypertension in children linked to lower neurocognitive performance
Children with primary hypertension demonstrated significantly lower performance on neurocognitive testing, compared with children without primary hypertension, according to Marc B. Lande, MD, of the University of Rochester (N.Y.), and his associates.

In the study, 75 children with newly diagnosed untreated primary hypertension and 75 normotensive control subjects were examined. Hypertension was linked with worse performances on neurocognitive measures of attention, learning, memory, and fine motor dexterity, compared with the controls. There also was an association between increased disordered sleep and worse executive function. This was more pronounced in children with hypertension than in normotensive children. Hypertension and control groups did not differ significantly in age, sex, maternal education, income, race, ethnicity, obesity, anxiety, depression, cholesterol, glucose, insulin, and C-reactive protein.
“These results suggest that hypertension in youth may have an impact on brain function, and perhaps brain development, in childhood,” the researchers concluded. “Future results from this study will assess the degree to which these effects can be minimized or reversed with antihypertensive therapies.”
Find the full study in the Journal of Pediatrics (2016 Sept 29. doi: 10.1016/j.jpeds.2016.08.076).
Children with primary hypertension demonstrated significantly lower performance on neurocognitive testing, compared with children without primary hypertension, according to Marc B. Lande, MD, of the University of Rochester (N.Y.), and his associates.
In the study, 75 children with newly diagnosed untreated primary hypertension and 75 normotensive control subjects were examined. Hypertension was linked with worse performances on neurocognitive measures of attention, learning, memory, and fine motor dexterity, compared with the controls. There also was an association between increased disordered sleep and worse executive function. This was more pronounced in children with hypertension than in normotensive children. Hypertension and control groups did not differ significantly in age, sex, maternal education, income, race, ethnicity, obesity, anxiety, depression, cholesterol, glucose, insulin, and C-reactive protein.
“These results suggest that hypertension in youth may have an impact on brain function, and perhaps brain development, in childhood,” the researchers concluded. “Future results from this study will assess the degree to which these effects can be minimized or reversed with antihypertensive therapies.”
Find the full study in the Journal of Pediatrics (2016 Sept 29. doi: 10.1016/j.jpeds.2016.08.076).
Children with primary hypertension demonstrated significantly lower performance on neurocognitive testing, compared with children without primary hypertension, according to Marc B. Lande, MD, of the University of Rochester (N.Y.), and his associates.
In the study, 75 children with newly diagnosed untreated primary hypertension and 75 normotensive control subjects were examined. Hypertension was linked with worse performances on neurocognitive measures of attention, learning, memory, and fine motor dexterity, compared with the controls. There also was an association between increased disordered sleep and worse executive function. This was more pronounced in children with hypertension than in normotensive children. Hypertension and control groups did not differ significantly in age, sex, maternal education, income, race, ethnicity, obesity, anxiety, depression, cholesterol, glucose, insulin, and C-reactive protein.
“These results suggest that hypertension in youth may have an impact on brain function, and perhaps brain development, in childhood,” the researchers concluded. “Future results from this study will assess the degree to which these effects can be minimized or reversed with antihypertensive therapies.”
Find the full study in the Journal of Pediatrics (2016 Sept 29. doi: 10.1016/j.jpeds.2016.08.076).

Immunotherapy produces CRs in kids with rel/ref ALL
The bispecific T-cell engager (BiTE®) antibody blinatumomab can produce complete responses (CRs) in pediatric patients with relapsed/refractory B-cell precursor acute lymphoblastic leukemia (ALL), according to a phase 1/2 study published in the Journal of Clinical Oncology.
Of the patients who received the recommended dosage of blinatumomab, 39% achieved a CR within the first 2 treatment cycles.
And 52% of these patients achieved a complete minimal residual disease (MRD) response.
“This study showed that [blinatumomab] can induce deep molecular remissions in children with highly refractory, multiply relapsed ALL,” said study author Lia Gore, MD, of University of Colorado Anschutz Medical Campus in Aurora, Colorado.
However, most of these remissions did not last. Although a few of the complete responders were still alive and in CR at the study’s 2-year follow-up, more than half had relapsed, and two-thirds had died.
This trial, known as Study ‘205, was supported by Amgen.
Study ‘205 included 93 pediatric patients with relapsed or refractory B-cell precursor ALL. Patients received blinatumomab as a continuous intravenous infusion—49 patients in the phase 1 portion of the trial and 44 in phase 2. The patients were followed for 2 years.
Toxicities and recommended dose
There were 4 dose-limiting toxicities during the phase 1 portion of the trial, and 2 of these events were fatal. One patient treated at 15 μg/m2/day developed grade 4 cytokine release syndrome (CRS), which was deemed related to grade 4 gastrointestinal hemorrhage.
Two patients treated at 30 μg/m2/day had grade 4 CRS. One case was attributed to grade 5 cardiac failure, and the other was treated successfully with tocilizumab.
One patient treated at 15 μg/m2/day had grade 5 respiratory failure with cardiac arrest after hypotonia and muscle weakness after 7 days of infusion with blinatumomab. This patient experienced febrile neutropenia and pneumonia shortly before the start of the infusion.
Based on these toxicities, the maximum-tolerated dose of blinatumomab was 15 μg/m2/day, but a step-wise dosage was recommended to reduce the risk of CRS.
So the recommended dose was 5 μg/m2/day on days 1-7 and 15 μg/m2/day on days 8-28 for cycle 1, and 15 μg/m2/day on days 1-28 for subsequent cycles.
Dose adjustment was possible in case of adverse events. Patients who responded to blinatumomab but later relapsed had the option to be retreated with blinatumomab.
Treatment at recommended dose
Seventy patients received at least 1 infusion of blinatumomab at the recommended dose. The median number of treatment cycles was 1 (range, 1 to 5).
The patients’ median age was 8 years (range, 7 months to 17 years). Forty patients (57%) had undergone allogeneic transplant prior to receiving blinatumomab, and 39 (56%) had refractory disease. Four patients had less than the 25% bone marrow blasts required for protocol entry but had more than 5% blasts.
Adverse events
The most common adverse events among the patients who received the recommended dose of blinatumomab were pyrexia (80%), anemia (41%), nausea (33%), and headache (30%).
The most frequent grade 3 or higher events were anemia (36%), thrombocytopenia (21%), febrile neutropenia (17%), hypokalemia (17%), and neutropenia (17%).
Eight patients developed CRS. Three had grade 3 and 1 had grade 4 CRS. Two of these patients had treatment interruptions, and 2 discontinued treatment permanently. All 4 patients achieved a CR.
Ten patients (14%) had treatment interruptions due to adverse events, and 4 (6%) discontinued treatment permanently because of adverse events.
Six patients had fatal adverse events. Three died after they went on to allogeneic transplant—1 of multiorgan failure, 1 of sepsis, and 1 of respiratory failure. The 3 other deaths were due to fungal infection, multiorgan failure, and thrombocytopenia.
Response and follow-up
Among the 70 patients who received the recommended dose of blinatumomab, 27 (39%) achieved a CR within the first 2 cycles. Fourteen of these patients (52%) achieved complete MRD response.
CRs were achieved across subgroups, and complete MRD response rates were similar across subgroups.
Thirteen of the 27 patients (48%) who achieved a CR went on to receive an allogeneic transplant.
At the end of the 2-year follow-up, 4 of the 27 complete responders were still in remission.
Two of the patients had relapsed but were still alive, 3 had withdrawn consent (1 in CR and 2 after relapse), 3 had died in CR after transplant, and 15 had relapsed and died.
Of the 43 patients who did not achieve a CR within the first 2 treatment cycles, 8 were still alive at the end of the 2-year follow-up. ![]()
The bispecific T-cell engager (BiTE®) antibody blinatumomab can produce complete responses (CRs) in pediatric patients with relapsed/refractory B-cell precursor acute lymphoblastic leukemia (ALL), according to a phase 1/2 study published in the Journal of Clinical Oncology.
Of the patients who received the recommended dosage of blinatumomab, 39% achieved a CR within the first 2 treatment cycles.
And 52% of these patients achieved a complete minimal residual disease (MRD) response.
“This study showed that [blinatumomab] can induce deep molecular remissions in children with highly refractory, multiply relapsed ALL,” said study author Lia Gore, MD, of University of Colorado Anschutz Medical Campus in Aurora, Colorado.
However, most of these remissions did not last. Although a few of the complete responders were still alive and in CR at the study’s 2-year follow-up, more than half had relapsed, and two-thirds had died.
This trial, known as Study ‘205, was supported by Amgen.
Study ‘205 included 93 pediatric patients with relapsed or refractory B-cell precursor ALL. Patients received blinatumomab as a continuous intravenous infusion—49 patients in the phase 1 portion of the trial and 44 in phase 2. The patients were followed for 2 years.
Toxicities and recommended dose
There were 4 dose-limiting toxicities during the phase 1 portion of the trial, and 2 of these events were fatal. One patient treated at 15 μg/m2/day developed grade 4 cytokine release syndrome (CRS), which was deemed related to grade 4 gastrointestinal hemorrhage.
Two patients treated at 30 μg/m2/day had grade 4 CRS. One case was attributed to grade 5 cardiac failure, and the other was treated successfully with tocilizumab.
One patient treated at 15 μg/m2/day had grade 5 respiratory failure with cardiac arrest after hypotonia and muscle weakness after 7 days of infusion with blinatumomab. This patient experienced febrile neutropenia and pneumonia shortly before the start of the infusion.
Based on these toxicities, the maximum-tolerated dose of blinatumomab was 15 μg/m2/day, but a step-wise dosage was recommended to reduce the risk of CRS.
So the recommended dose was 5 μg/m2/day on days 1-7 and 15 μg/m2/day on days 8-28 for cycle 1, and 15 μg/m2/day on days 1-28 for subsequent cycles.
Dose adjustment was possible in case of adverse events. Patients who responded to blinatumomab but later relapsed had the option to be retreated with blinatumomab.
Treatment at recommended dose
Seventy patients received at least 1 infusion of blinatumomab at the recommended dose. The median number of treatment cycles was 1 (range, 1 to 5).
The patients’ median age was 8 years (range, 7 months to 17 years). Forty patients (57%) had undergone allogeneic transplant prior to receiving blinatumomab, and 39 (56%) had refractory disease. Four patients had less than the 25% bone marrow blasts required for protocol entry but had more than 5% blasts.
Adverse events
The most common adverse events among the patients who received the recommended dose of blinatumomab were pyrexia (80%), anemia (41%), nausea (33%), and headache (30%).
The most frequent grade 3 or higher events were anemia (36%), thrombocytopenia (21%), febrile neutropenia (17%), hypokalemia (17%), and neutropenia (17%).
Eight patients developed CRS. Three had grade 3 and 1 had grade 4 CRS. Two of these patients had treatment interruptions, and 2 discontinued treatment permanently. All 4 patients achieved a CR.
Ten patients (14%) had treatment interruptions due to adverse events, and 4 (6%) discontinued treatment permanently because of adverse events.
Six patients had fatal adverse events. Three died after they went on to allogeneic transplant—1 of multiorgan failure, 1 of sepsis, and 1 of respiratory failure. The 3 other deaths were due to fungal infection, multiorgan failure, and thrombocytopenia.
Response and follow-up
Among the 70 patients who received the recommended dose of blinatumomab, 27 (39%) achieved a CR within the first 2 cycles. Fourteen of these patients (52%) achieved complete MRD response.
CRs were achieved across subgroups, and complete MRD response rates were similar across subgroups.
Thirteen of the 27 patients (48%) who achieved a CR went on to receive an allogeneic transplant.
At the end of the 2-year follow-up, 4 of the 27 complete responders were still in remission.
Two of the patients had relapsed but were still alive, 3 had withdrawn consent (1 in CR and 2 after relapse), 3 had died in CR after transplant, and 15 had relapsed and died.
Of the 43 patients who did not achieve a CR within the first 2 treatment cycles, 8 were still alive at the end of the 2-year follow-up. ![]()
The bispecific T-cell engager (BiTE®) antibody blinatumomab can produce complete responses (CRs) in pediatric patients with relapsed/refractory B-cell precursor acute lymphoblastic leukemia (ALL), according to a phase 1/2 study published in the Journal of Clinical Oncology.
Of the patients who received the recommended dosage of blinatumomab, 39% achieved a CR within the first 2 treatment cycles.
And 52% of these patients achieved a complete minimal residual disease (MRD) response.
“This study showed that [blinatumomab] can induce deep molecular remissions in children with highly refractory, multiply relapsed ALL,” said study author Lia Gore, MD, of University of Colorado Anschutz Medical Campus in Aurora, Colorado.
However, most of these remissions did not last. Although a few of the complete responders were still alive and in CR at the study’s 2-year follow-up, more than half had relapsed, and two-thirds had died.
This trial, known as Study ‘205, was supported by Amgen.
Study ‘205 included 93 pediatric patients with relapsed or refractory B-cell precursor ALL. Patients received blinatumomab as a continuous intravenous infusion—49 patients in the phase 1 portion of the trial and 44 in phase 2. The patients were followed for 2 years.
Toxicities and recommended dose
There were 4 dose-limiting toxicities during the phase 1 portion of the trial, and 2 of these events were fatal. One patient treated at 15 μg/m2/day developed grade 4 cytokine release syndrome (CRS), which was deemed related to grade 4 gastrointestinal hemorrhage.
Two patients treated at 30 μg/m2/day had grade 4 CRS. One case was attributed to grade 5 cardiac failure, and the other was treated successfully with tocilizumab.
One patient treated at 15 μg/m2/day had grade 5 respiratory failure with cardiac arrest after hypotonia and muscle weakness after 7 days of infusion with blinatumomab. This patient experienced febrile neutropenia and pneumonia shortly before the start of the infusion.
Based on these toxicities, the maximum-tolerated dose of blinatumomab was 15 μg/m2/day, but a step-wise dosage was recommended to reduce the risk of CRS.
So the recommended dose was 5 μg/m2/day on days 1-7 and 15 μg/m2/day on days 8-28 for cycle 1, and 15 μg/m2/day on days 1-28 for subsequent cycles.
Dose adjustment was possible in case of adverse events. Patients who responded to blinatumomab but later relapsed had the option to be retreated with blinatumomab.
Treatment at recommended dose
Seventy patients received at least 1 infusion of blinatumomab at the recommended dose. The median number of treatment cycles was 1 (range, 1 to 5).
The patients’ median age was 8 years (range, 7 months to 17 years). Forty patients (57%) had undergone allogeneic transplant prior to receiving blinatumomab, and 39 (56%) had refractory disease. Four patients had less than the 25% bone marrow blasts required for protocol entry but had more than 5% blasts.
Adverse events
The most common adverse events among the patients who received the recommended dose of blinatumomab were pyrexia (80%), anemia (41%), nausea (33%), and headache (30%).
The most frequent grade 3 or higher events were anemia (36%), thrombocytopenia (21%), febrile neutropenia (17%), hypokalemia (17%), and neutropenia (17%).
Eight patients developed CRS. Three had grade 3 and 1 had grade 4 CRS. Two of these patients had treatment interruptions, and 2 discontinued treatment permanently. All 4 patients achieved a CR.
Ten patients (14%) had treatment interruptions due to adverse events, and 4 (6%) discontinued treatment permanently because of adverse events.
Six patients had fatal adverse events. Three died after they went on to allogeneic transplant—1 of multiorgan failure, 1 of sepsis, and 1 of respiratory failure. The 3 other deaths were due to fungal infection, multiorgan failure, and thrombocytopenia.
Response and follow-up
Among the 70 patients who received the recommended dose of blinatumomab, 27 (39%) achieved a CR within the first 2 cycles. Fourteen of these patients (52%) achieved complete MRD response.
CRs were achieved across subgroups, and complete MRD response rates were similar across subgroups.
Thirteen of the 27 patients (48%) who achieved a CR went on to receive an allogeneic transplant.
At the end of the 2-year follow-up, 4 of the 27 complete responders were still in remission.
Two of the patients had relapsed but were still alive, 3 had withdrawn consent (1 in CR and 2 after relapse), 3 had died in CR after transplant, and 15 had relapsed and died.
Of the 43 patients who did not achieve a CR within the first 2 treatment cycles, 8 were still alive at the end of the 2-year follow-up. ![]()