User login
Treatment plan addresses circadian rhythm disorders from nighttime screen use
SAN FRANCISCO – Among the most significant concerns associated with youth’s increasing use of screen media is the impact on their sleep, according to two policy statements of the American Academy of Pediatrics on children and media use.
To help pediatricians better understand how media might affect sleep, Sujay Kansagra, MD, a pediatric neurologist at Duke University Medical Center in Durham, N.C., presented an overview of circadian rhythm disorders and how to address them during a program on electronic media at the AAP annual meeting.
Approximately 3 hours before waking, a person experiences a nadir in body temperature that designates “the point at which the light exposure flips from delaying your rhythm to advancing your rhythm,” Dr. Kansagra said. “Five minutes before this point, it delays your phase; 5 minutes after, it advances your phase.”
A significantly advanced or delayed sleep phase can become a circadian rhythm disorder, in which a person gets the normal amount and quality of sleep he or she needs – but not at the right times. “Those with circadian rhythm disorders have failed to entrain to their environmental cues,” such as light, food, and activity levels, he said.
In youth, particularly adolescents, the most common circadian rhythm disorder is delayed sleep-wake phase syndrome, defined in the International Classification of Sleep Disorders – Third Edition (ICSD-3) with four criteria:
• A significant delay in major sleep episode in relation to desired or required sleep time and waking time (often involving a sleep time around 4 a.m.).
• The symptoms are present for more than 3 months.
• When allowed to choose a schedule, the person will exhibit improved sleep quality/duration and maintain delayed phase.
• A sleep log and/or actigraphy demonstrates a delay in timing of the sleep period for at least 7 days.
Because nearly all screen media emit light, use of such media in the evenings may contribute to this disorder. “When you combine light exposure with someone who has that later chronotype, you’re setting yourself up for disaster,” Dr. Kansagra said.
Delayed sleep-wake phase disorder can greatly interfere with school, work, and normal daily activities, and Dr. Kansagra outlined the major steps in preventing and/or treating it, starting with avoiding light exposure at night, whether from the TV, tablets, laptops, or cell phones.
“If they can’t avoid light completely, the brightness is also important,” he said. “We know that the brighter the light, the more likely you are to suppress your brain’s melatonin.” Therefore, reducing the brightness on devices that must be used can mitigate the problem, as can using red- or yellow-tinted light, provided as a “night mode” on some devices, instead of the blue light emitted by the majority of devices.
Next, he recommended that individuals maintain a set bedtime and wake time each day, including on the weekends. Although he acknowledged the challenge this schedule might present, particularly in teenagers, he described how detrimental it can be to stay up late and sleep in late on the weekends. If teens stay up until 11 p.m. throughout the week, then a little later on Friday night, and then up to 2 a.m. on Saturday night, they will likely sleep in until around 11 a.m. on Sunday. But if they need to get up at 6 a.m. for school Monday morning, that’s the equivalent of flying from Hawaii to New York in terms of jet lag effects, he explained.
“They will spend the rest of the school week slowly advancing their clock until the weekend and do it all over again,” Dr. Kansagra said. “They are perpetually jet lagged. No wonder they’re so angry all the time,” he joked. “It’s social jet lag.”
Such social jet lag leads to sleepiness throughout the week, often mistaken for laziness by frustrated parents, he said.
“Sleepiness is not laziness,” he emphasized. “It’s a problem with the quality or quantity of sleep. It’s really important to get parents’ buy in on this because it’s a contentious topic in a lot of families.”
After getting the child or teen on a regular schedule, the next important step in realigning a circadian rhythm and then maintaining it is to expose the person to light early in the morning – but after that temperature nadir that occurs 3 hours before waking. Meanwhile, 2-6 hours before their sleep time, youth trying to adjust their clocks can take a low dose of melatonin, around 0.5-1 mg. But he pointed out a common misconception about how melatonin works.
“Melatonin plays no role in fixing insomnia; melatonin doesn’t make you sleepy,” Dr. Kansagra said. “Melatonin just tells your brain what to do when it’s dark. Melatonin is good for shifting your circadian rhythm.”
But all of these steps can be successful only if the pediatrician and/or parent can convince the child or teen that it’s important to adjust their circadian rhythm. This can include discussions that lead them to realize or conclude that they are unpleasant, angry, or irritable when they don’t get enough sleep. Perhaps they have been told they are rude by a classmate on days they don’t get enough sleep, or perhaps they realize they do not perform as well while playing sports when they don’t have the rest they need. Children who can make those connections can help get the buy in needed to follow all the previous steps.
Some individuals, however, can be particularly resistant to adjusting the circadian rhythm, which calls for a much more dramatic and difficult treatment called chronotherapy. This treatment begins very counterintuitively by flipping the script: The youth should now actually try to stay up later than their bedtime while playing video games, watching TV, using a computer, or engaging in similar activities. Ideally, they should stay up until 6 a.m. and then sleep in as late as they wish.
The next evening, they should stay up even later – until 8 a.m. – and again sleep in as late as they need to. Each successive day, they should go to bed 2 hours later – 10 a.m., 12 p.m., 2 p.m., and so forth – and sleep the adequate amount anyone would need, until they eventually are going to bed at the time they should be, such as 8 p.m. or 10 p.m. Although this is a dramatic treatment, it can be very effective at resetting a person’s clock when other methods have not succeeded, he said.
The key practice-altering elements of Dr. Kansagra’s talk focused on using melatonin as a “clock-shifting” medication instead of a “sleep-inducing one” and dosing children at the appropriate time, 2-6 hours before bed. If nighttime use of light cannot be eliminated, have patients reduce the brightness and duration, and change the color, of the light to lessen its effect on the brain’s melatonin release. Finally, help families understand the concept of “social jet lag” so they grasp the importance of regular sleep times and do not mistake sleepiness for laziness.
Dr. Kansagra reported no relevant financial disclosures or external funding.
SAN FRANCISCO – Among the most significant concerns associated with youth’s increasing use of screen media is the impact on their sleep, according to two policy statements of the American Academy of Pediatrics on children and media use.
To help pediatricians better understand how media might affect sleep, Sujay Kansagra, MD, a pediatric neurologist at Duke University Medical Center in Durham, N.C., presented an overview of circadian rhythm disorders and how to address them during a program on electronic media at the AAP annual meeting.
Approximately 3 hours before waking, a person experiences a nadir in body temperature that designates “the point at which the light exposure flips from delaying your rhythm to advancing your rhythm,” Dr. Kansagra said. “Five minutes before this point, it delays your phase; 5 minutes after, it advances your phase.”
A significantly advanced or delayed sleep phase can become a circadian rhythm disorder, in which a person gets the normal amount and quality of sleep he or she needs – but not at the right times. “Those with circadian rhythm disorders have failed to entrain to their environmental cues,” such as light, food, and activity levels, he said.
In youth, particularly adolescents, the most common circadian rhythm disorder is delayed sleep-wake phase syndrome, defined in the International Classification of Sleep Disorders – Third Edition (ICSD-3) with four criteria:
• A significant delay in major sleep episode in relation to desired or required sleep time and waking time (often involving a sleep time around 4 a.m.).
• The symptoms are present for more than 3 months.
• When allowed to choose a schedule, the person will exhibit improved sleep quality/duration and maintain delayed phase.
• A sleep log and/or actigraphy demonstrates a delay in timing of the sleep period for at least 7 days.
Because nearly all screen media emit light, use of such media in the evenings may contribute to this disorder. “When you combine light exposure with someone who has that later chronotype, you’re setting yourself up for disaster,” Dr. Kansagra said.
Delayed sleep-wake phase disorder can greatly interfere with school, work, and normal daily activities, and Dr. Kansagra outlined the major steps in preventing and/or treating it, starting with avoiding light exposure at night, whether from the TV, tablets, laptops, or cell phones.
“If they can’t avoid light completely, the brightness is also important,” he said. “We know that the brighter the light, the more likely you are to suppress your brain’s melatonin.” Therefore, reducing the brightness on devices that must be used can mitigate the problem, as can using red- or yellow-tinted light, provided as a “night mode” on some devices, instead of the blue light emitted by the majority of devices.
Next, he recommended that individuals maintain a set bedtime and wake time each day, including on the weekends. Although he acknowledged the challenge this schedule might present, particularly in teenagers, he described how detrimental it can be to stay up late and sleep in late on the weekends. If teens stay up until 11 p.m. throughout the week, then a little later on Friday night, and then up to 2 a.m. on Saturday night, they will likely sleep in until around 11 a.m. on Sunday. But if they need to get up at 6 a.m. for school Monday morning, that’s the equivalent of flying from Hawaii to New York in terms of jet lag effects, he explained.
“They will spend the rest of the school week slowly advancing their clock until the weekend and do it all over again,” Dr. Kansagra said. “They are perpetually jet lagged. No wonder they’re so angry all the time,” he joked. “It’s social jet lag.”
Such social jet lag leads to sleepiness throughout the week, often mistaken for laziness by frustrated parents, he said.
“Sleepiness is not laziness,” he emphasized. “It’s a problem with the quality or quantity of sleep. It’s really important to get parents’ buy in on this because it’s a contentious topic in a lot of families.”
After getting the child or teen on a regular schedule, the next important step in realigning a circadian rhythm and then maintaining it is to expose the person to light early in the morning – but after that temperature nadir that occurs 3 hours before waking. Meanwhile, 2-6 hours before their sleep time, youth trying to adjust their clocks can take a low dose of melatonin, around 0.5-1 mg. But he pointed out a common misconception about how melatonin works.
“Melatonin plays no role in fixing insomnia; melatonin doesn’t make you sleepy,” Dr. Kansagra said. “Melatonin just tells your brain what to do when it’s dark. Melatonin is good for shifting your circadian rhythm.”
But all of these steps can be successful only if the pediatrician and/or parent can convince the child or teen that it’s important to adjust their circadian rhythm. This can include discussions that lead them to realize or conclude that they are unpleasant, angry, or irritable when they don’t get enough sleep. Perhaps they have been told they are rude by a classmate on days they don’t get enough sleep, or perhaps they realize they do not perform as well while playing sports when they don’t have the rest they need. Children who can make those connections can help get the buy in needed to follow all the previous steps.
Some individuals, however, can be particularly resistant to adjusting the circadian rhythm, which calls for a much more dramatic and difficult treatment called chronotherapy. This treatment begins very counterintuitively by flipping the script: The youth should now actually try to stay up later than their bedtime while playing video games, watching TV, using a computer, or engaging in similar activities. Ideally, they should stay up until 6 a.m. and then sleep in as late as they wish.
The next evening, they should stay up even later – until 8 a.m. – and again sleep in as late as they need to. Each successive day, they should go to bed 2 hours later – 10 a.m., 12 p.m., 2 p.m., and so forth – and sleep the adequate amount anyone would need, until they eventually are going to bed at the time they should be, such as 8 p.m. or 10 p.m. Although this is a dramatic treatment, it can be very effective at resetting a person’s clock when other methods have not succeeded, he said.
The key practice-altering elements of Dr. Kansagra’s talk focused on using melatonin as a “clock-shifting” medication instead of a “sleep-inducing one” and dosing children at the appropriate time, 2-6 hours before bed. If nighttime use of light cannot be eliminated, have patients reduce the brightness and duration, and change the color, of the light to lessen its effect on the brain’s melatonin release. Finally, help families understand the concept of “social jet lag” so they grasp the importance of regular sleep times and do not mistake sleepiness for laziness.
Dr. Kansagra reported no relevant financial disclosures or external funding.
SAN FRANCISCO – Among the most significant concerns associated with youth’s increasing use of screen media is the impact on their sleep, according to two policy statements of the American Academy of Pediatrics on children and media use.
To help pediatricians better understand how media might affect sleep, Sujay Kansagra, MD, a pediatric neurologist at Duke University Medical Center in Durham, N.C., presented an overview of circadian rhythm disorders and how to address them during a program on electronic media at the AAP annual meeting.
Approximately 3 hours before waking, a person experiences a nadir in body temperature that designates “the point at which the light exposure flips from delaying your rhythm to advancing your rhythm,” Dr. Kansagra said. “Five minutes before this point, it delays your phase; 5 minutes after, it advances your phase.”
A significantly advanced or delayed sleep phase can become a circadian rhythm disorder, in which a person gets the normal amount and quality of sleep he or she needs – but not at the right times. “Those with circadian rhythm disorders have failed to entrain to their environmental cues,” such as light, food, and activity levels, he said.
In youth, particularly adolescents, the most common circadian rhythm disorder is delayed sleep-wake phase syndrome, defined in the International Classification of Sleep Disorders – Third Edition (ICSD-3) with four criteria:
• A significant delay in major sleep episode in relation to desired or required sleep time and waking time (often involving a sleep time around 4 a.m.).
• The symptoms are present for more than 3 months.
• When allowed to choose a schedule, the person will exhibit improved sleep quality/duration and maintain delayed phase.
• A sleep log and/or actigraphy demonstrates a delay in timing of the sleep period for at least 7 days.
Because nearly all screen media emit light, use of such media in the evenings may contribute to this disorder. “When you combine light exposure with someone who has that later chronotype, you’re setting yourself up for disaster,” Dr. Kansagra said.
Delayed sleep-wake phase disorder can greatly interfere with school, work, and normal daily activities, and Dr. Kansagra outlined the major steps in preventing and/or treating it, starting with avoiding light exposure at night, whether from the TV, tablets, laptops, or cell phones.
“If they can’t avoid light completely, the brightness is also important,” he said. “We know that the brighter the light, the more likely you are to suppress your brain’s melatonin.” Therefore, reducing the brightness on devices that must be used can mitigate the problem, as can using red- or yellow-tinted light, provided as a “night mode” on some devices, instead of the blue light emitted by the majority of devices.
Next, he recommended that individuals maintain a set bedtime and wake time each day, including on the weekends. Although he acknowledged the challenge this schedule might present, particularly in teenagers, he described how detrimental it can be to stay up late and sleep in late on the weekends. If teens stay up until 11 p.m. throughout the week, then a little later on Friday night, and then up to 2 a.m. on Saturday night, they will likely sleep in until around 11 a.m. on Sunday. But if they need to get up at 6 a.m. for school Monday morning, that’s the equivalent of flying from Hawaii to New York in terms of jet lag effects, he explained.
“They will spend the rest of the school week slowly advancing their clock until the weekend and do it all over again,” Dr. Kansagra said. “They are perpetually jet lagged. No wonder they’re so angry all the time,” he joked. “It’s social jet lag.”
Such social jet lag leads to sleepiness throughout the week, often mistaken for laziness by frustrated parents, he said.
“Sleepiness is not laziness,” he emphasized. “It’s a problem with the quality or quantity of sleep. It’s really important to get parents’ buy in on this because it’s a contentious topic in a lot of families.”
After getting the child or teen on a regular schedule, the next important step in realigning a circadian rhythm and then maintaining it is to expose the person to light early in the morning – but after that temperature nadir that occurs 3 hours before waking. Meanwhile, 2-6 hours before their sleep time, youth trying to adjust their clocks can take a low dose of melatonin, around 0.5-1 mg. But he pointed out a common misconception about how melatonin works.
“Melatonin plays no role in fixing insomnia; melatonin doesn’t make you sleepy,” Dr. Kansagra said. “Melatonin just tells your brain what to do when it’s dark. Melatonin is good for shifting your circadian rhythm.”
But all of these steps can be successful only if the pediatrician and/or parent can convince the child or teen that it’s important to adjust their circadian rhythm. This can include discussions that lead them to realize or conclude that they are unpleasant, angry, or irritable when they don’t get enough sleep. Perhaps they have been told they are rude by a classmate on days they don’t get enough sleep, or perhaps they realize they do not perform as well while playing sports when they don’t have the rest they need. Children who can make those connections can help get the buy in needed to follow all the previous steps.
Some individuals, however, can be particularly resistant to adjusting the circadian rhythm, which calls for a much more dramatic and difficult treatment called chronotherapy. This treatment begins very counterintuitively by flipping the script: The youth should now actually try to stay up later than their bedtime while playing video games, watching TV, using a computer, or engaging in similar activities. Ideally, they should stay up until 6 a.m. and then sleep in as late as they wish.
The next evening, they should stay up even later – until 8 a.m. – and again sleep in as late as they need to. Each successive day, they should go to bed 2 hours later – 10 a.m., 12 p.m., 2 p.m., and so forth – and sleep the adequate amount anyone would need, until they eventually are going to bed at the time they should be, such as 8 p.m. or 10 p.m. Although this is a dramatic treatment, it can be very effective at resetting a person’s clock when other methods have not succeeded, he said.
The key practice-altering elements of Dr. Kansagra’s talk focused on using melatonin as a “clock-shifting” medication instead of a “sleep-inducing one” and dosing children at the appropriate time, 2-6 hours before bed. If nighttime use of light cannot be eliminated, have patients reduce the brightness and duration, and change the color, of the light to lessen its effect on the brain’s melatonin release. Finally, help families understand the concept of “social jet lag” so they grasp the importance of regular sleep times and do not mistake sleepiness for laziness.
Dr. Kansagra reported no relevant financial disclosures or external funding.
EXPERT ANALYSIS FROM AAP 16
Pediatric OSA improved with oral montelukast
The majority of children with obstructive sleep apnea (OSA) who took oral montelukast showed reductions in their apnea-hypopnea index (AHI) scores, in a randomized, double-blind placebo-controlled study.
Typically, OSA in children is treated by adenotonsillectomy, according to Leila Kheirandish-Gozal, MD, director of clinical sleep research at the University of Chicago, and her colleagues. Prior to this study, only one randomized controlled trial had showed that children with mild OSA “responded favorably” to the leukotriene modifier montelukast (Pediatrics. 2012 Aug 31. doi: 10.1542/peds.2012-0310).
Twenty (71%) of the children who received montelukast had fewer AHI events per hour of total sleep time at the end of the study. The average number of such events for these patients was 4.2 plus or minus 2.8 after taking the drug, compared with 9.2 plus or minus 4.1 at the beginning of the study (P less than .0001). Only two (6.9%) of the patients who took the placebo had lower AHI scores at the end of the study, with the average AHI score for the placebo group having been 8.7 plus or minus 4.9 events per hour of total sleep time. At baseline, the average score for patients in the placebo group was 8.2 plus or minus 5.0 AHI events per hour of total sleep time at baseline.
Another improvement seen by patients who received the drug was a decrease in the number of 3% reductions in arterial oxygen saturation per hour of sleep. At the beginning of the study, these patients had 7.2 plus or minus 3.1 of these events; by the end of the study, the number of these events was down to 2.8 plus or minus 1.8 (P less than .001). No significant decrease in the number of these events was seen among patients in the placebo group.
In this study, “montelukast emerges as favorably reducing the severity of OSA short term in children 2-10 years of age. These findings add to the existing evidence supporting a therapeutic role for anti-inflammatory approaches in the management of this highly prevalent condition in children, and clearly justify future studies targeting the long-term benefits of these approaches in children with OSA,” the researchers wrote.
All patients participated in overnight sleep studies following a referral to one of two sleep clinics by their primary care pediatrician or pediatric otolaryngologist, at the beginning of the study. Children who had been diagnosed with symptomatic snoring and had an AHI score of greater than 2 events per hour of total sleep time, and for whom adenotonsillectomy was contemplated, were included in the study.
Central, obstructive, mixed apneic events were counted and hypopneas were assessed. OSA was defined “as the absence of airflow with continued chest wall and abdominal movement for a duration of at least two breaths,” the investigators said. Hypopneas were defined “as a decrease in oronasal flow greater than 50% on either the thermistor or nasal pressure transducer signal. with a corresponding decrease in arterial oxygen saturation greater than 3% or arousal,” Dr. Kheirandish-Gozal and her coauthors said.
Patients were excluded from the study for a variety of reasons, including having severe OSA requiring early surgical intervention.
Adverse events included headache in two children, one from the experimental group and one from the placebo group, and nausea in two subjects from the placebo group and in one from the montelukast group.
Merck provided tablets used in this study. Dr. Kheirandish-Gozal reported grants from Merck and the National Institutes of Health during the conduct of the study. David Gozal, MD, is supported by the Herbert T. Abelson Chair in Pediatrics at the University of Chicago.
The majority of children with obstructive sleep apnea (OSA) who took oral montelukast showed reductions in their apnea-hypopnea index (AHI) scores, in a randomized, double-blind placebo-controlled study.
Typically, OSA in children is treated by adenotonsillectomy, according to Leila Kheirandish-Gozal, MD, director of clinical sleep research at the University of Chicago, and her colleagues. Prior to this study, only one randomized controlled trial had showed that children with mild OSA “responded favorably” to the leukotriene modifier montelukast (Pediatrics. 2012 Aug 31. doi: 10.1542/peds.2012-0310).
Twenty (71%) of the children who received montelukast had fewer AHI events per hour of total sleep time at the end of the study. The average number of such events for these patients was 4.2 plus or minus 2.8 after taking the drug, compared with 9.2 plus or minus 4.1 at the beginning of the study (P less than .0001). Only two (6.9%) of the patients who took the placebo had lower AHI scores at the end of the study, with the average AHI score for the placebo group having been 8.7 plus or minus 4.9 events per hour of total sleep time. At baseline, the average score for patients in the placebo group was 8.2 plus or minus 5.0 AHI events per hour of total sleep time at baseline.
Another improvement seen by patients who received the drug was a decrease in the number of 3% reductions in arterial oxygen saturation per hour of sleep. At the beginning of the study, these patients had 7.2 plus or minus 3.1 of these events; by the end of the study, the number of these events was down to 2.8 plus or minus 1.8 (P less than .001). No significant decrease in the number of these events was seen among patients in the placebo group.
In this study, “montelukast emerges as favorably reducing the severity of OSA short term in children 2-10 years of age. These findings add to the existing evidence supporting a therapeutic role for anti-inflammatory approaches in the management of this highly prevalent condition in children, and clearly justify future studies targeting the long-term benefits of these approaches in children with OSA,” the researchers wrote.
All patients participated in overnight sleep studies following a referral to one of two sleep clinics by their primary care pediatrician or pediatric otolaryngologist, at the beginning of the study. Children who had been diagnosed with symptomatic snoring and had an AHI score of greater than 2 events per hour of total sleep time, and for whom adenotonsillectomy was contemplated, were included in the study.
Central, obstructive, mixed apneic events were counted and hypopneas were assessed. OSA was defined “as the absence of airflow with continued chest wall and abdominal movement for a duration of at least two breaths,” the investigators said. Hypopneas were defined “as a decrease in oronasal flow greater than 50% on either the thermistor or nasal pressure transducer signal. with a corresponding decrease in arterial oxygen saturation greater than 3% or arousal,” Dr. Kheirandish-Gozal and her coauthors said.
Patients were excluded from the study for a variety of reasons, including having severe OSA requiring early surgical intervention.
Adverse events included headache in two children, one from the experimental group and one from the placebo group, and nausea in two subjects from the placebo group and in one from the montelukast group.
Merck provided tablets used in this study. Dr. Kheirandish-Gozal reported grants from Merck and the National Institutes of Health during the conduct of the study. David Gozal, MD, is supported by the Herbert T. Abelson Chair in Pediatrics at the University of Chicago.
The majority of children with obstructive sleep apnea (OSA) who took oral montelukast showed reductions in their apnea-hypopnea index (AHI) scores, in a randomized, double-blind placebo-controlled study.
Typically, OSA in children is treated by adenotonsillectomy, according to Leila Kheirandish-Gozal, MD, director of clinical sleep research at the University of Chicago, and her colleagues. Prior to this study, only one randomized controlled trial had showed that children with mild OSA “responded favorably” to the leukotriene modifier montelukast (Pediatrics. 2012 Aug 31. doi: 10.1542/peds.2012-0310).
Twenty (71%) of the children who received montelukast had fewer AHI events per hour of total sleep time at the end of the study. The average number of such events for these patients was 4.2 plus or minus 2.8 after taking the drug, compared with 9.2 plus or minus 4.1 at the beginning of the study (P less than .0001). Only two (6.9%) of the patients who took the placebo had lower AHI scores at the end of the study, with the average AHI score for the placebo group having been 8.7 plus or minus 4.9 events per hour of total sleep time. At baseline, the average score for patients in the placebo group was 8.2 plus or minus 5.0 AHI events per hour of total sleep time at baseline.
Another improvement seen by patients who received the drug was a decrease in the number of 3% reductions in arterial oxygen saturation per hour of sleep. At the beginning of the study, these patients had 7.2 plus or minus 3.1 of these events; by the end of the study, the number of these events was down to 2.8 plus or minus 1.8 (P less than .001). No significant decrease in the number of these events was seen among patients in the placebo group.
In this study, “montelukast emerges as favorably reducing the severity of OSA short term in children 2-10 years of age. These findings add to the existing evidence supporting a therapeutic role for anti-inflammatory approaches in the management of this highly prevalent condition in children, and clearly justify future studies targeting the long-term benefits of these approaches in children with OSA,” the researchers wrote.
All patients participated in overnight sleep studies following a referral to one of two sleep clinics by their primary care pediatrician or pediatric otolaryngologist, at the beginning of the study. Children who had been diagnosed with symptomatic snoring and had an AHI score of greater than 2 events per hour of total sleep time, and for whom adenotonsillectomy was contemplated, were included in the study.
Central, obstructive, mixed apneic events were counted and hypopneas were assessed. OSA was defined “as the absence of airflow with continued chest wall and abdominal movement for a duration of at least two breaths,” the investigators said. Hypopneas were defined “as a decrease in oronasal flow greater than 50% on either the thermistor or nasal pressure transducer signal. with a corresponding decrease in arterial oxygen saturation greater than 3% or arousal,” Dr. Kheirandish-Gozal and her coauthors said.
Patients were excluded from the study for a variety of reasons, including having severe OSA requiring early surgical intervention.
Adverse events included headache in two children, one from the experimental group and one from the placebo group, and nausea in two subjects from the placebo group and in one from the montelukast group.
Merck provided tablets used in this study. Dr. Kheirandish-Gozal reported grants from Merck and the National Institutes of Health during the conduct of the study. David Gozal, MD, is supported by the Herbert T. Abelson Chair in Pediatrics at the University of Chicago.
Key clinical point:
Major finding: 71% of patients who took montelukast had a significant reduction in AHI events per hour of total sleep time (P less than .0001).
Data source: A prospective, randomized, double-blind placebo-controlled study of 57 children with obstructive sleep apnea.
Disclosures: Merck provided tablets used in this study. Dr. Kheirandish-Gozal reported grants from Merck and the National Institutes of Health during the conduct of the study. David Gozal, MD, is supported by the Herbert T. Abelson Chair in Pediatrics at the University of Chicago.
USPSTF gives breastfeeding support a ‘B’ grade
The U.S. Preventive Services Task Force (USPSTF) has issued a B-level recommendation for interventions given during pregnancy and after birth to support breastfeeding.
The Task Force cites “adequate” evidence that breastfeeding provides substantial health benefits for children and moderate health benefits for women. While they found evidence to support individual-level interventions, such as education and psychosocial support, system-level interventions were not shown to be effective. The recommendation appears online in JAMA (2016 Oct 25;316[16]:1688-93).
The recommendation updates a previous one issued in 2008, in which the USPSTF also recommended breastfeeding support interventions with a grade of B. The new recommendation is based on a review of 43 studies of individual-level primary care interventions in support of breastfeeding, and nine system-level interventions. The authors evaluated the available evidence on breastfeeding initiation, duration, and exclusivity, as well as breastfeeding’s effects on child and maternal health outcomes. They determined that support from a professional lactation consultant or a peer group was effective in producing any or exclusive breastfeeding, while systemwide interventions, such as the World Health Organization’s Baby-Friendly Hospital Initiative offered inconsistent benefits. The evidence review was also published in JAMA (2016;316[16]:1694-1705).
The Initiative’s “Ten Steps to Successful Breastfeeding” program, in particular, presents a potential risk, they noted. The program recommends counseling parents to avoid use of pacifiers in the newborn period to support breastfeeding, but evidence is growing that avoiding pacifiers is not associated with any breastfeeding outcomes and pacifier use may be protective against sudden infant death syndrome.
“U.S. institutions will need to disengage from the Ten Steps if they conclude that the scientific evidence that conflicts with them is valid,” Dr. Flaherman and Dr. Von Kohorn wrote.
The practice of recommending that mothers do not supplement breast-milk feedings with formula is also of concern, based on mixed evidence. Since not all mothers produce adequate milk supplies during the first week postpartum, not supplementing with formula could run the risk that the infant suffers dehydration, hyperbilirubinemia, or other complications. With up to 2% of all newborns in the United States requiring hospital readmission – the risk is doubled for breastfed infants – Dr. Flaherman and Dr. Von Kohorn suggest that strict adherence to a “breast-milk only” policy has the potential to be harmful, especially given that current evidence doesn’t show that exclusive breastfeeding in the newborn period improves breastfeeding duration.
“Individual clinical judgment may be more valuable than a single rigid rule for exclusive breastfeeding for the first 6 months,” Dr. Flaherman and Dr. Von Kohorn wrote.
Based on the evidence, the USPSTF advised clinicians that they can support women before and after childbirth by promoting the benefits of breastfeeding during monthly visits, providing practical guidance on how to breastfeed, and offering psychosocial support.
“Although there is moderate certainty that breastfeeding is of moderate net benefit to women and their infants and children, not all women choose to or are able to breastfeed. Clinicians should, as with any preventive service, respect the autonomy of women and their families to make decisions that fit their specific situation, values, and preferences,” the USPSTF members wrote.
The USPSTF members reported receiving travel reimbursement and honorarium for participating in USPSTF meetings. Dr. Flaherman and Dr. Von Kohorn reported having no relevant financial disclosures.
The key to successful office-based health promotion and prevention programs is to prioritize evidence-based practices and recommendations that parents already have a predilection to follow. That is, of the myriad of topics one might discuss, why not start with the ones that caregivers are most interested in. Breastfeeding is surely one of those.
The USPSTF estimates the number needed to treat when offering breastfeeding support is 30. That is, if 30 women are offered it, 1 additional woman will breastfeed for 6 full months. This compares favorably with the NNT for antibiotics for otitis media for fever and pain reduction at 48 hours in children older than 2 years, (NNT, 20) especially when one considers the comparable benefits of each. And the breastfeeding NNT could be reduced even further if there were structural changes to workplaces and communities that helped support breastfeeding mothers.
Dimitri A. Christakis, MD, MPH , of Seattle Children’s Research Institute, is an associate editor for JAMA Pediatrics. His comments are adapted from an editorial published in JAMA Pediatrics (2016 Oct 25. doi: 10.1001/jamapediatrics.2016.3390). He reported having no relevant financial disclosures.
The key to successful office-based health promotion and prevention programs is to prioritize evidence-based practices and recommendations that parents already have a predilection to follow. That is, of the myriad of topics one might discuss, why not start with the ones that caregivers are most interested in. Breastfeeding is surely one of those.
The USPSTF estimates the number needed to treat when offering breastfeeding support is 30. That is, if 30 women are offered it, 1 additional woman will breastfeed for 6 full months. This compares favorably with the NNT for antibiotics for otitis media for fever and pain reduction at 48 hours in children older than 2 years, (NNT, 20) especially when one considers the comparable benefits of each. And the breastfeeding NNT could be reduced even further if there were structural changes to workplaces and communities that helped support breastfeeding mothers.
Dimitri A. Christakis, MD, MPH , of Seattle Children’s Research Institute, is an associate editor for JAMA Pediatrics. His comments are adapted from an editorial published in JAMA Pediatrics (2016 Oct 25. doi: 10.1001/jamapediatrics.2016.3390). He reported having no relevant financial disclosures.
The key to successful office-based health promotion and prevention programs is to prioritize evidence-based practices and recommendations that parents already have a predilection to follow. That is, of the myriad of topics one might discuss, why not start with the ones that caregivers are most interested in. Breastfeeding is surely one of those.
The USPSTF estimates the number needed to treat when offering breastfeeding support is 30. That is, if 30 women are offered it, 1 additional woman will breastfeed for 6 full months. This compares favorably with the NNT for antibiotics for otitis media for fever and pain reduction at 48 hours in children older than 2 years, (NNT, 20) especially when one considers the comparable benefits of each. And the breastfeeding NNT could be reduced even further if there were structural changes to workplaces and communities that helped support breastfeeding mothers.
Dimitri A. Christakis, MD, MPH , of Seattle Children’s Research Institute, is an associate editor for JAMA Pediatrics. His comments are adapted from an editorial published in JAMA Pediatrics (2016 Oct 25. doi: 10.1001/jamapediatrics.2016.3390). He reported having no relevant financial disclosures.
The U.S. Preventive Services Task Force (USPSTF) has issued a B-level recommendation for interventions given during pregnancy and after birth to support breastfeeding.
The Task Force cites “adequate” evidence that breastfeeding provides substantial health benefits for children and moderate health benefits for women. While they found evidence to support individual-level interventions, such as education and psychosocial support, system-level interventions were not shown to be effective. The recommendation appears online in JAMA (2016 Oct 25;316[16]:1688-93).
The recommendation updates a previous one issued in 2008, in which the USPSTF also recommended breastfeeding support interventions with a grade of B. The new recommendation is based on a review of 43 studies of individual-level primary care interventions in support of breastfeeding, and nine system-level interventions. The authors evaluated the available evidence on breastfeeding initiation, duration, and exclusivity, as well as breastfeeding’s effects on child and maternal health outcomes. They determined that support from a professional lactation consultant or a peer group was effective in producing any or exclusive breastfeeding, while systemwide interventions, such as the World Health Organization’s Baby-Friendly Hospital Initiative offered inconsistent benefits. The evidence review was also published in JAMA (2016;316[16]:1694-1705).
The Initiative’s “Ten Steps to Successful Breastfeeding” program, in particular, presents a potential risk, they noted. The program recommends counseling parents to avoid use of pacifiers in the newborn period to support breastfeeding, but evidence is growing that avoiding pacifiers is not associated with any breastfeeding outcomes and pacifier use may be protective against sudden infant death syndrome.
“U.S. institutions will need to disengage from the Ten Steps if they conclude that the scientific evidence that conflicts with them is valid,” Dr. Flaherman and Dr. Von Kohorn wrote.
The practice of recommending that mothers do not supplement breast-milk feedings with formula is also of concern, based on mixed evidence. Since not all mothers produce adequate milk supplies during the first week postpartum, not supplementing with formula could run the risk that the infant suffers dehydration, hyperbilirubinemia, or other complications. With up to 2% of all newborns in the United States requiring hospital readmission – the risk is doubled for breastfed infants – Dr. Flaherman and Dr. Von Kohorn suggest that strict adherence to a “breast-milk only” policy has the potential to be harmful, especially given that current evidence doesn’t show that exclusive breastfeeding in the newborn period improves breastfeeding duration.
“Individual clinical judgment may be more valuable than a single rigid rule for exclusive breastfeeding for the first 6 months,” Dr. Flaherman and Dr. Von Kohorn wrote.
Based on the evidence, the USPSTF advised clinicians that they can support women before and after childbirth by promoting the benefits of breastfeeding during monthly visits, providing practical guidance on how to breastfeed, and offering psychosocial support.
“Although there is moderate certainty that breastfeeding is of moderate net benefit to women and their infants and children, not all women choose to or are able to breastfeed. Clinicians should, as with any preventive service, respect the autonomy of women and their families to make decisions that fit their specific situation, values, and preferences,” the USPSTF members wrote.
The USPSTF members reported receiving travel reimbursement and honorarium for participating in USPSTF meetings. Dr. Flaherman and Dr. Von Kohorn reported having no relevant financial disclosures.
The U.S. Preventive Services Task Force (USPSTF) has issued a B-level recommendation for interventions given during pregnancy and after birth to support breastfeeding.
The Task Force cites “adequate” evidence that breastfeeding provides substantial health benefits for children and moderate health benefits for women. While they found evidence to support individual-level interventions, such as education and psychosocial support, system-level interventions were not shown to be effective. The recommendation appears online in JAMA (2016 Oct 25;316[16]:1688-93).
The recommendation updates a previous one issued in 2008, in which the USPSTF also recommended breastfeeding support interventions with a grade of B. The new recommendation is based on a review of 43 studies of individual-level primary care interventions in support of breastfeeding, and nine system-level interventions. The authors evaluated the available evidence on breastfeeding initiation, duration, and exclusivity, as well as breastfeeding’s effects on child and maternal health outcomes. They determined that support from a professional lactation consultant or a peer group was effective in producing any or exclusive breastfeeding, while systemwide interventions, such as the World Health Organization’s Baby-Friendly Hospital Initiative offered inconsistent benefits. The evidence review was also published in JAMA (2016;316[16]:1694-1705).
The Initiative’s “Ten Steps to Successful Breastfeeding” program, in particular, presents a potential risk, they noted. The program recommends counseling parents to avoid use of pacifiers in the newborn period to support breastfeeding, but evidence is growing that avoiding pacifiers is not associated with any breastfeeding outcomes and pacifier use may be protective against sudden infant death syndrome.
“U.S. institutions will need to disengage from the Ten Steps if they conclude that the scientific evidence that conflicts with them is valid,” Dr. Flaherman and Dr. Von Kohorn wrote.
The practice of recommending that mothers do not supplement breast-milk feedings with formula is also of concern, based on mixed evidence. Since not all mothers produce adequate milk supplies during the first week postpartum, not supplementing with formula could run the risk that the infant suffers dehydration, hyperbilirubinemia, or other complications. With up to 2% of all newborns in the United States requiring hospital readmission – the risk is doubled for breastfed infants – Dr. Flaherman and Dr. Von Kohorn suggest that strict adherence to a “breast-milk only” policy has the potential to be harmful, especially given that current evidence doesn’t show that exclusive breastfeeding in the newborn period improves breastfeeding duration.
“Individual clinical judgment may be more valuable than a single rigid rule for exclusive breastfeeding for the first 6 months,” Dr. Flaherman and Dr. Von Kohorn wrote.
Based on the evidence, the USPSTF advised clinicians that they can support women before and after childbirth by promoting the benefits of breastfeeding during monthly visits, providing practical guidance on how to breastfeed, and offering psychosocial support.
“Although there is moderate certainty that breastfeeding is of moderate net benefit to women and their infants and children, not all women choose to or are able to breastfeed. Clinicians should, as with any preventive service, respect the autonomy of women and their families to make decisions that fit their specific situation, values, and preferences,” the USPSTF members wrote.
The USPSTF members reported receiving travel reimbursement and honorarium for participating in USPSTF meetings. Dr. Flaherman and Dr. Von Kohorn reported having no relevant financial disclosures.
Team identifies genetic hallmarks of B-ALL subtype
Photo courtesy of St. Jude
Children’s Research Hospital
Researchers say they have uncovered a unique paradigm of transcription factor deregulation in B-precursor acute lymphoblastic leukemia (B-ALL).
The team found that deregulation of the homeobox transcription factor gene DUX4 and the ETS transcription factor gene ERG is a hallmark of a subtype of B-ALL that may comprise up to 8% of B-ALL cases.
The researchers reported these findings in Nature Genetics.
“Our work is motivated by a lack of information on the genetic basis of many B-ALL cases,” said study author Charles Mullighan, MBBS, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“We discovered a distinct gene pattern in blood samples from some patients in our study and wanted to determine the underlying molecular events behind this signal.”
The researchers studied a group of 1913 B-ALL patients (including children, adolescents, and young adults) to understand the genetic basis of the disease.
Microarray and transcriptome sequencing revealed that 7.6% of these patients had the distinctive genetic profile the researchers wanted to characterize further.
“Our work revealed that, in this type of B-ALL, there is a sequence of molecular events that involves the interplay of 2 transcription factors,” Dr Mullighan said.
The team observed rearrangement of the gene DUX4 in all cases of this subtype of B-ALL, which resulted in high-level expression of DUX4. DUX4 was shown to bind to the ERG gene, leading to deregulated expression of ERG.
The deregulation of ERG compromised the function of ERG either by deleting part of the gene or by expressing another form of ERG—ERGalt. In both cases, loss of activity was observed for the ERG transcription factor, which led to leukemia.
“These results underscore that there is still more to be learned about the genetic changes in ALL, and that this knowledge can help refine treatment for patients,” said study author Stephen Hunger, MD, of the Children’s Hospital of Philadelphia in Pennsylvania.
The researchers hope identification of the relationships between the 2 transcription factors will lead to new diagnostic tests for patients. DUX4/ERG ALL is linked to favorable outcomes even when other detrimental genetic mutations are present.
Currently, only transcriptome or genome sequencing helps identify the DUX4 rearrangements. The researchers say other detection methods, such as fluorescence hybridization or karyotyping, are not sufficient to recognize genetic changes to DUX4. ![]()
Photo courtesy of St. Jude
Children’s Research Hospital
Researchers say they have uncovered a unique paradigm of transcription factor deregulation in B-precursor acute lymphoblastic leukemia (B-ALL).
The team found that deregulation of the homeobox transcription factor gene DUX4 and the ETS transcription factor gene ERG is a hallmark of a subtype of B-ALL that may comprise up to 8% of B-ALL cases.
The researchers reported these findings in Nature Genetics.
“Our work is motivated by a lack of information on the genetic basis of many B-ALL cases,” said study author Charles Mullighan, MBBS, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“We discovered a distinct gene pattern in blood samples from some patients in our study and wanted to determine the underlying molecular events behind this signal.”
The researchers studied a group of 1913 B-ALL patients (including children, adolescents, and young adults) to understand the genetic basis of the disease.
Microarray and transcriptome sequencing revealed that 7.6% of these patients had the distinctive genetic profile the researchers wanted to characterize further.
“Our work revealed that, in this type of B-ALL, there is a sequence of molecular events that involves the interplay of 2 transcription factors,” Dr Mullighan said.
The team observed rearrangement of the gene DUX4 in all cases of this subtype of B-ALL, which resulted in high-level expression of DUX4. DUX4 was shown to bind to the ERG gene, leading to deregulated expression of ERG.
The deregulation of ERG compromised the function of ERG either by deleting part of the gene or by expressing another form of ERG—ERGalt. In both cases, loss of activity was observed for the ERG transcription factor, which led to leukemia.
“These results underscore that there is still more to be learned about the genetic changes in ALL, and that this knowledge can help refine treatment for patients,” said study author Stephen Hunger, MD, of the Children’s Hospital of Philadelphia in Pennsylvania.
The researchers hope identification of the relationships between the 2 transcription factors will lead to new diagnostic tests for patients. DUX4/ERG ALL is linked to favorable outcomes even when other detrimental genetic mutations are present.
Currently, only transcriptome or genome sequencing helps identify the DUX4 rearrangements. The researchers say other detection methods, such as fluorescence hybridization or karyotyping, are not sufficient to recognize genetic changes to DUX4. ![]()
Photo courtesy of St. Jude
Children’s Research Hospital
Researchers say they have uncovered a unique paradigm of transcription factor deregulation in B-precursor acute lymphoblastic leukemia (B-ALL).
The team found that deregulation of the homeobox transcription factor gene DUX4 and the ETS transcription factor gene ERG is a hallmark of a subtype of B-ALL that may comprise up to 8% of B-ALL cases.
The researchers reported these findings in Nature Genetics.
“Our work is motivated by a lack of information on the genetic basis of many B-ALL cases,” said study author Charles Mullighan, MBBS, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“We discovered a distinct gene pattern in blood samples from some patients in our study and wanted to determine the underlying molecular events behind this signal.”
The researchers studied a group of 1913 B-ALL patients (including children, adolescents, and young adults) to understand the genetic basis of the disease.
Microarray and transcriptome sequencing revealed that 7.6% of these patients had the distinctive genetic profile the researchers wanted to characterize further.
“Our work revealed that, in this type of B-ALL, there is a sequence of molecular events that involves the interplay of 2 transcription factors,” Dr Mullighan said.
The team observed rearrangement of the gene DUX4 in all cases of this subtype of B-ALL, which resulted in high-level expression of DUX4. DUX4 was shown to bind to the ERG gene, leading to deregulated expression of ERG.
The deregulation of ERG compromised the function of ERG either by deleting part of the gene or by expressing another form of ERG—ERGalt. In both cases, loss of activity was observed for the ERG transcription factor, which led to leukemia.
“These results underscore that there is still more to be learned about the genetic changes in ALL, and that this knowledge can help refine treatment for patients,” said study author Stephen Hunger, MD, of the Children’s Hospital of Philadelphia in Pennsylvania.
The researchers hope identification of the relationships between the 2 transcription factors will lead to new diagnostic tests for patients. DUX4/ERG ALL is linked to favorable outcomes even when other detrimental genetic mutations are present.
Currently, only transcriptome or genome sequencing helps identify the DUX4 rearrangements. The researchers say other detection methods, such as fluorescence hybridization or karyotyping, are not sufficient to recognize genetic changes to DUX4. ![]()
Children on antipsychotics show more early weight gain than adults
VIENNA – Antipsychotic-naive children and adolescents are at greater risk for clinically significant weight gain during their first 6 months on a second-generation antipsychotic agent than adults, Covadonga M. Diaz-Caneja, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
She presented what she believes to be the first prospective observational study comparing weight gain between antipsychotic-naive children and adults during their first 6 months on second-generation antipsychotics. Weight gains were significantly greater with olanzapine (Zyprexa) than risperidone (Risperdal) or quetiapine (Seroquel) in both age groups, but the magnitude and trajectory of olanzapine-related weight gain was significantly more impressive in the pediatric patients.

The study included 226 pediatric patients with a mean age of 15.2 years and 135 adults, average age 39 years. All were antipsychotic naive when placed on one of the three second-generation antipsychotics at clinician discretion. Fifty percent of the youths and 60% of adults had a psychosis diagnosis. Sixty-four percent of the pediatric group and 55% of the adults were male.
Weight gain during the first 6 months of therapy was expressed as change in body mass index z score. An increase in BMI z score of 0.5 or more is considered clinically significant.
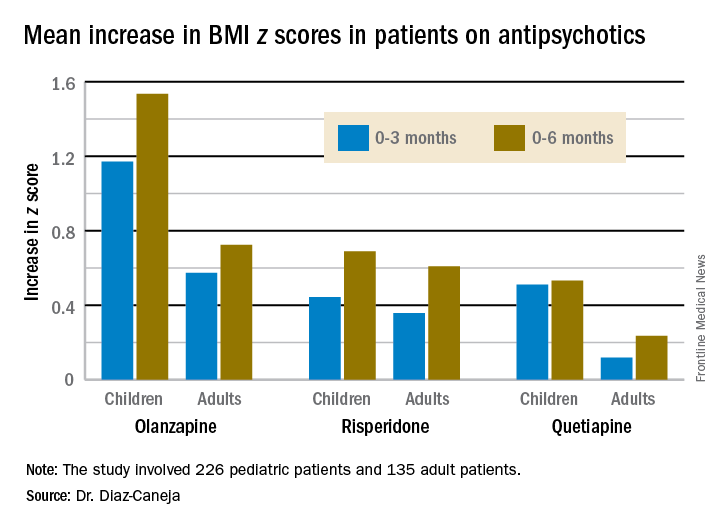
The least weight gain at 6 months occurred with quetiapine in both age groups. However, the BMI z score increased by 0.532 in the pediatric patients on the drug, more than twice the 0.236 increase in adults.
Risperidone was the only second-generation antipsychotic where the weight gain trajectories in pediatric and adult patients were not significantly different.
The study was funded by the Spanish Ministry of Economy and Competitiveness, and the European Commission. Dr. Diaz-Caneja reported having no financial conflicts of interest.
VIENNA – Antipsychotic-naive children and adolescents are at greater risk for clinically significant weight gain during their first 6 months on a second-generation antipsychotic agent than adults, Covadonga M. Diaz-Caneja, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
She presented what she believes to be the first prospective observational study comparing weight gain between antipsychotic-naive children and adults during their first 6 months on second-generation antipsychotics. Weight gains were significantly greater with olanzapine (Zyprexa) than risperidone (Risperdal) or quetiapine (Seroquel) in both age groups, but the magnitude and trajectory of olanzapine-related weight gain was significantly more impressive in the pediatric patients.
The study included 226 pediatric patients with a mean age of 15.2 years and 135 adults, average age 39 years. All were antipsychotic naive when placed on one of the three second-generation antipsychotics at clinician discretion. Fifty percent of the youths and 60% of adults had a psychosis diagnosis. Sixty-four percent of the pediatric group and 55% of the adults were male.
Weight gain during the first 6 months of therapy was expressed as change in body mass index z score. An increase in BMI z score of 0.5 or more is considered clinically significant.
The least weight gain at 6 months occurred with quetiapine in both age groups. However, the BMI z score increased by 0.532 in the pediatric patients on the drug, more than twice the 0.236 increase in adults.
Risperidone was the only second-generation antipsychotic where the weight gain trajectories in pediatric and adult patients were not significantly different.
The study was funded by the Spanish Ministry of Economy and Competitiveness, and the European Commission. Dr. Diaz-Caneja reported having no financial conflicts of interest.
VIENNA – Antipsychotic-naive children and adolescents are at greater risk for clinically significant weight gain during their first 6 months on a second-generation antipsychotic agent than adults, Covadonga M. Diaz-Caneja, MD, reported at the annual congress of the European College of Neuropsychopharmacology.
She presented what she believes to be the first prospective observational study comparing weight gain between antipsychotic-naive children and adults during their first 6 months on second-generation antipsychotics. Weight gains were significantly greater with olanzapine (Zyprexa) than risperidone (Risperdal) or quetiapine (Seroquel) in both age groups, but the magnitude and trajectory of olanzapine-related weight gain was significantly more impressive in the pediatric patients.
The study included 226 pediatric patients with a mean age of 15.2 years and 135 adults, average age 39 years. All were antipsychotic naive when placed on one of the three second-generation antipsychotics at clinician discretion. Fifty percent of the youths and 60% of adults had a psychosis diagnosis. Sixty-four percent of the pediatric group and 55% of the adults were male.
Weight gain during the first 6 months of therapy was expressed as change in body mass index z score. An increase in BMI z score of 0.5 or more is considered clinically significant.
The least weight gain at 6 months occurred with quetiapine in both age groups. However, the BMI z score increased by 0.532 in the pediatric patients on the drug, more than twice the 0.236 increase in adults.
Risperidone was the only second-generation antipsychotic where the weight gain trajectories in pediatric and adult patients were not significantly different.
The study was funded by the Spanish Ministry of Economy and Competitiveness, and the European Commission. Dr. Diaz-Caneja reported having no financial conflicts of interest.
Key clinical point:
Major finding: The BMI z score increased by 1.535 in pediatric patients during their first 6 months on olanzapine – the most weight unfriendly of the second-generation antipsychotics – compared with 0.724 in adults.
Data source: This prospective, observational study examined weight gain in 361 antipsychotic-naive children, adolescents, and adults during their first 6 months on second-generation antipsychotic agents.
Disclosures: The study was funded by the Spanish Ministry of Economy and Competitiveness and the European Commission.
Telementoring expands PCPs’ role in managing pediatric chronic disease
SAN FRANCISCO – Telementoring empowers primary care pediatric providers (PCPs) to take on a greater role in managing their patients’ chronic diseases, new data suggest. Leaders in this emerging field gave a snapshot of early experience with the model at the annual meeting of the American Academy of Pediatrics.
“About a quarter of children live with chronic health conditions, and there is an increasing need for specialty care. But many children don’t have access to the quality specialty care that they really need, particularly in rural and medically underserved areas,” explained Dr. Sucheta M. Joshi, a pediatric neurologist and epileptologist at the University of Michigan, Ann Arbor. “The goal of telementoring is to build the capacity of primary care doctors.”

“We need to empower primary care providers to work ‘at the top of their license’ because we don’t have enough specialists,” agreed Dr. David
L. Wood, a general pediatrician and chair of the department of pediatrics at East Tennessee State University in Johnson City. “We as primary care [physicians] have to shoulder more of the care of kids with chronic disease. But we need backup, we need support to do that because the science is growing rapidly, we can’t keep up.”
Telementoring first gained recognition through the University of New Mexico’s Project Extension for Community Healthcare Outcomes (ECHO), which links specialists at an academic “hub” with PCPs in local communities, or “spokes,” in a learning network.
Through regular, interactive, multisite telementoring sessions, ECHO provides training to increase PCPs’ knowledge, self-efficacy, and comfort in managing chronic diseases not typically considered within their scope of practice. Sessions combine short didactic presentations and case-based learning.
The model was initially tested in pediatrics as ECHO for Epilepsy, a partnership of the AAP and the University of New Mexico, Albuquerque. Topics covered ranged from first seizures to work-up to treatment, including when to refer to a neurologist, according to Dr. Joshi, who helped develop the curriculum. Encouraging findings among the 49 clinics participating in the first year led to expansion of the program to five more states.
Preliminary data from the full cohort show reductions from baseline to end of the program in the proportions of participants who felt not at all or not very knowledgeable about pharmacologic management of pediatric epilepsy (from 69% to 45%), related school and education issues (from 51% to 18%), pertinent state driving laws (from 69% to 45%), and when to refer to a specialist (from 34% to 0%), Dr. Joshi reported.
There were also reductions in the proportions of participants who felt not at all or not very confident about aspects of care such as medical testing in this population (from 52% to 45%), communicating with patients about the transition to adult care (from 52% to 27%), and communicating with families and caregivers about the impact of epilepsy on everyday life (from 59% to 36%).
“This has been a good demonstration to say that telementoring does improve provider knowledge and confidence,” Dr. Joshi maintained. “Everybody felt quite uniformly that the case discussions were useful, and it really fostered a sense of a community of learners and was very much an iterative process.”
The AAP has since been designated as a “superhub” for Project ECHO that can train others to start programs in specialty areas. Additional programs have been developed in pediatric endocrinology, sickle cell disease, and surgery.

The main costs of ECHO are the personnel and physician time, and financing has yet to be worked out. “Unlike traditional telemedicine, where it’s one patient and one physician, and you can actually bill for it, this is not a billable service,” Dr. Joshi noted. “What you can get is more of a downstream effect, which can take some time to become obvious.”
The key attraction for providers is obtaining CME credits, where offered. And a draw for institutions is the potential impact of ECHO in reducing provider turnover and improving value-based reimbursement.
“This is really an innovative program that can help us achieve the triple aim” of improving the patient’s experience, reducing costs, and achieving better health outcomes, Dr. Wood said. “I think this is a great enhancement to the medical home.”
Both Dr. Joshi and Dr. Wood disclosed that they had no relevant conflicts of interest.
SAN FRANCISCO – Telementoring empowers primary care pediatric providers (PCPs) to take on a greater role in managing their patients’ chronic diseases, new data suggest. Leaders in this emerging field gave a snapshot of early experience with the model at the annual meeting of the American Academy of Pediatrics.
“About a quarter of children live with chronic health conditions, and there is an increasing need for specialty care. But many children don’t have access to the quality specialty care that they really need, particularly in rural and medically underserved areas,” explained Dr. Sucheta M. Joshi, a pediatric neurologist and epileptologist at the University of Michigan, Ann Arbor. “The goal of telementoring is to build the capacity of primary care doctors.”
“We need to empower primary care providers to work ‘at the top of their license’ because we don’t have enough specialists,” agreed Dr. David
L. Wood, a general pediatrician and chair of the department of pediatrics at East Tennessee State University in Johnson City. “We as primary care [physicians] have to shoulder more of the care of kids with chronic disease. But we need backup, we need support to do that because the science is growing rapidly, we can’t keep up.”
Telementoring first gained recognition through the University of New Mexico’s Project Extension for Community Healthcare Outcomes (ECHO), which links specialists at an academic “hub” with PCPs in local communities, or “spokes,” in a learning network.
Through regular, interactive, multisite telementoring sessions, ECHO provides training to increase PCPs’ knowledge, self-efficacy, and comfort in managing chronic diseases not typically considered within their scope of practice. Sessions combine short didactic presentations and case-based learning.
The model was initially tested in pediatrics as ECHO for Epilepsy, a partnership of the AAP and the University of New Mexico, Albuquerque. Topics covered ranged from first seizures to work-up to treatment, including when to refer to a neurologist, according to Dr. Joshi, who helped develop the curriculum. Encouraging findings among the 49 clinics participating in the first year led to expansion of the program to five more states.
Preliminary data from the full cohort show reductions from baseline to end of the program in the proportions of participants who felt not at all or not very knowledgeable about pharmacologic management of pediatric epilepsy (from 69% to 45%), related school and education issues (from 51% to 18%), pertinent state driving laws (from 69% to 45%), and when to refer to a specialist (from 34% to 0%), Dr. Joshi reported.
There were also reductions in the proportions of participants who felt not at all or not very confident about aspects of care such as medical testing in this population (from 52% to 45%), communicating with patients about the transition to adult care (from 52% to 27%), and communicating with families and caregivers about the impact of epilepsy on everyday life (from 59% to 36%).
“This has been a good demonstration to say that telementoring does improve provider knowledge and confidence,” Dr. Joshi maintained. “Everybody felt quite uniformly that the case discussions were useful, and it really fostered a sense of a community of learners and was very much an iterative process.”
The AAP has since been designated as a “superhub” for Project ECHO that can train others to start programs in specialty areas. Additional programs have been developed in pediatric endocrinology, sickle cell disease, and surgery.
The main costs of ECHO are the personnel and physician time, and financing has yet to be worked out. “Unlike traditional telemedicine, where it’s one patient and one physician, and you can actually bill for it, this is not a billable service,” Dr. Joshi noted. “What you can get is more of a downstream effect, which can take some time to become obvious.”
The key attraction for providers is obtaining CME credits, where offered. And a draw for institutions is the potential impact of ECHO in reducing provider turnover and improving value-based reimbursement.
“This is really an innovative program that can help us achieve the triple aim” of improving the patient’s experience, reducing costs, and achieving better health outcomes, Dr. Wood said. “I think this is a great enhancement to the medical home.”
Both Dr. Joshi and Dr. Wood disclosed that they had no relevant conflicts of interest.
SAN FRANCISCO – Telementoring empowers primary care pediatric providers (PCPs) to take on a greater role in managing their patients’ chronic diseases, new data suggest. Leaders in this emerging field gave a snapshot of early experience with the model at the annual meeting of the American Academy of Pediatrics.
“About a quarter of children live with chronic health conditions, and there is an increasing need for specialty care. But many children don’t have access to the quality specialty care that they really need, particularly in rural and medically underserved areas,” explained Dr. Sucheta M. Joshi, a pediatric neurologist and epileptologist at the University of Michigan, Ann Arbor. “The goal of telementoring is to build the capacity of primary care doctors.”
“We need to empower primary care providers to work ‘at the top of their license’ because we don’t have enough specialists,” agreed Dr. David
L. Wood, a general pediatrician and chair of the department of pediatrics at East Tennessee State University in Johnson City. “We as primary care [physicians] have to shoulder more of the care of kids with chronic disease. But we need backup, we need support to do that because the science is growing rapidly, we can’t keep up.”
Telementoring first gained recognition through the University of New Mexico’s Project Extension for Community Healthcare Outcomes (ECHO), which links specialists at an academic “hub” with PCPs in local communities, or “spokes,” in a learning network.
Through regular, interactive, multisite telementoring sessions, ECHO provides training to increase PCPs’ knowledge, self-efficacy, and comfort in managing chronic diseases not typically considered within their scope of practice. Sessions combine short didactic presentations and case-based learning.
The model was initially tested in pediatrics as ECHO for Epilepsy, a partnership of the AAP and the University of New Mexico, Albuquerque. Topics covered ranged from first seizures to work-up to treatment, including when to refer to a neurologist, according to Dr. Joshi, who helped develop the curriculum. Encouraging findings among the 49 clinics participating in the first year led to expansion of the program to five more states.
Preliminary data from the full cohort show reductions from baseline to end of the program in the proportions of participants who felt not at all or not very knowledgeable about pharmacologic management of pediatric epilepsy (from 69% to 45%), related school and education issues (from 51% to 18%), pertinent state driving laws (from 69% to 45%), and when to refer to a specialist (from 34% to 0%), Dr. Joshi reported.
There were also reductions in the proportions of participants who felt not at all or not very confident about aspects of care such as medical testing in this population (from 52% to 45%), communicating with patients about the transition to adult care (from 52% to 27%), and communicating with families and caregivers about the impact of epilepsy on everyday life (from 59% to 36%).
“This has been a good demonstration to say that telementoring does improve provider knowledge and confidence,” Dr. Joshi maintained. “Everybody felt quite uniformly that the case discussions were useful, and it really fostered a sense of a community of learners and was very much an iterative process.”
The AAP has since been designated as a “superhub” for Project ECHO that can train others to start programs in specialty areas. Additional programs have been developed in pediatric endocrinology, sickle cell disease, and surgery.
The main costs of ECHO are the personnel and physician time, and financing has yet to be worked out. “Unlike traditional telemedicine, where it’s one patient and one physician, and you can actually bill for it, this is not a billable service,” Dr. Joshi noted. “What you can get is more of a downstream effect, which can take some time to become obvious.”
The key attraction for providers is obtaining CME credits, where offered. And a draw for institutions is the potential impact of ECHO in reducing provider turnover and improving value-based reimbursement.
“This is really an innovative program that can help us achieve the triple aim” of improving the patient’s experience, reducing costs, and achieving better health outcomes, Dr. Wood said. “I think this is a great enhancement to the medical home.”
Both Dr. Joshi and Dr. Wood disclosed that they had no relevant conflicts of interest.
EXPERT ANALYSIS FROM AAP 16
Tap the power of words when counseling about divorce
SAN FRANCISCO – By choosing your words carefully, counseling families about divorce can tactfully address sensitive issues and help parents and children better cope with this life transition, Nerissa S. Bauer, MD, said at the annual meeting of the American Academy of Pediatrics.
About one in five children born within a marriage and one in two of those born within a cohabiting union will experience breakup of that relationship by the age of 9 years, she said.

You must, therefore, be prepared to monitor for and identify outcomes that commonly result from divorce, and to counsel families about how to help children cope and manage. Yet, you may feel uneasy or ill-prepared to do so.
“Turn this thought of ‘I wasn’t trained for this’ into ‘I can help,’ ” recommended Dr. Bauer, who is a specialist in behavioral pediatrics at the Indiana University in Indianapolis.
Risk and protective factors
Divorce can have an impact on all facets of a child’s life: behavior, physical and mental health, academic performance, social relationships, delinquency, substance use, and more. A variety of factors determine how well kids adjust to this stressor, for better or worse.
Marital conflict, both during and after divorce, is a more important predictor than the divorce itself. “The biggest risk factor to consider is the ongoing parental fighting and how that plays out,” Dr. Bauer elaborated. Although parents may report that they try to limit altercations in front of their children, kids usually sense what is going on anyway.
“One of the ways that I like to phrase this when I’m trying to figure out how bad the conflict is in the household is, ‘Has Johnny ever witnessed your arguments, and if so, have those arguments ever been more than just yelling?’ Or another way to say it is, ‘How do adults in your home resolve conflicts?’ ” she shared.
Divorce may negatively affect children through its impact on the household’s socioeconomic status too. For example, the standard of living often declines and the mother’s economic resources can take a hit, possibly forcing a move to a less expensive neighborhood with weaker schools and more crime.
To sound parents out on this sensitive issue, “You can say something like, ‘I’m really sorry that you’re going through this right now. Sometimes, it can cause a lot of stress and strain, especially when it comes to making ends meet, making sure you can get food on the table, and making sure you’re paying the bills. Do you have worries like this now?’ ” Dr. Bauer suggested.
Factors that are known to protect children from adverse divorce outcomes include a good relationship with at least one parent or caregiver, parental warmth, sibling support, and for teens, good self-esteem and peer support. Joint custody with shared decision making and greater paternal involvement also are protective.
“I like to say, ‘So I can understand how this affects your daily life, can you describe what your current arrangements are between you and your ex?’ just to sort of probe into that custody situation,” she said. “Or, ‘How are you (parents) handling this?’ ”
Surveillance and monitoring
“Perform surveillance on family structure and conflict at all well-child visits, as well as with any new family that comes to your practice,” Dr. Bauer recommended. You can do this by simply chatting with the family or by using screening tools such as the Family Psychosocial Screen or the Finding Your ACE Score.
Once you know that a family is dealing with divorce, perform ongoing monitoring for warning signs in the child: sleep problems; school problems, such as poor concentration, acting out, or not doing schoolwork; angry outbursts; withdrawal; and no longer participating in activities once enjoyed.
You may worry about getting dragged into the conflict. “You may feel that you’re in this position of being the mediator, but that’s not really your role. And you shouldn’t offer legal advice,” she cautioned. “You should make it clear that although you are there to support the child and the parents, your role is really to monitor how the child responds and adjusts.”
Parents will sometimes ask whether and how best to tell their children about the divorce. “I oftentimes coach parents to use kid-friendly terms, saying things such as, ‘Mommy and Daddy are having a hard time getting along, and you’ve probably noticed we argue or fight a lot.’ Just throwing it out there and pausing and waiting to see what the child says, and then always following that by answering their questions as they bring them up,” Dr. Bauer said.
Parents should be counseled not to rush children as they will vary in the time needed to process information. Additionally, they should be forewarned that children’s reactions can vary widely and that their feelings can change and resurface at any moment, particularly as they mature and at events that stir up emotions.
Messages of reassurance are essential. “The messages should always contain, ‘We are always going to be your parents no matter what’ and ‘We love you no matter what,’ and probably the most important, ‘This is not your fault.’ This is a message that kids need to hear again and again,” Dr. Bauer said.
Ongoing counseling
Over time, parents may consult you about specific situations that arise because of the divorce. For example, they may become frustrated by differences in how things are handled in the two households.
“The most important message to convey is that we can control only what we can control,” Dr. Bauer said. “Regardless of divorce or separation, kids thrive on structure and routine. Divorce is often messy, and it sometimes means that families have to find a new rhythm between households, but routines in each house should be as consistent as possible.”
Acrimony between the mother and father may persist or escalate. As children don’t want to have to choose between parents, parents should be encouraged not to undermine or talk negatively about each other in front of the child. If necessary, you can arrange to have time separately with parents to allow them to air their grievances.
If parents give permission to broach the topic of divorce, you can role model conversational strategies during visits. “You can say something like, ‘I understand there are a lot of changes going on. Through it all, your mom and dad will always be your parents. I know this isn’t easy for anybody, especially for you. Kids in this situation feel a lot of things from sadness to anger but know that you can always talk to me or your parents about your feelings,’” Dr. Bauer elaborated.
“Listening is key,” she stressed; therefore, parents should be encouraged to just sit in silence and let their children process their feelings. “In these types of situations, there’s no right or wrong: When the child has feelings, they have feelings. We can’t force them to feel a certain way, we have to acknowledge that. So tell parents to try this: ‘Thanks for telling me how you feel. I want you to know that you can always come to me when you feel this way.’ See what happens.”
Parents should be advised not to be too quick to dismiss their child’s concerns, Dr. Bauer recommended. “So, instead of saying, ‘Oh honey, you don’t have to worry about that, I’ll take care of it,’ try this: ‘It sounds like you are sad and upset right now. What can I do to help?’ Sometimes a kid will say, ‘I don’t know,’ but that’s okay. Then the parent can respond in kind and say, ‘I don’t know either, but how about a hug? Let’s start there.’ ”
Some kids simply aren’t talkers and shouldn’t be forced to share, she pointed out. This group can be given other ways to express their feelings, such as journaling, drawing, art, music, yoga, or writing a letter that they then throw away or put in a drawer.
Finally, “reminding parents that even giving children a little control with daily things – what they wear, how they do their chores, and homework, and what to make for dinner – can also help,” she noted. “Those little things can represent a lot for children who don’t feel like they have any control.”
Building resources
Explore various media and online tools to develop a set of resources on divorce for families, Dr. Bauer recommended.
Books on the topic can be great conversation starters, and many are available for various age-groups, she noted. Examples include “Was It the Chocolate Pudding? A Story for Little Kids About Divorce” (Washington: Magination Press, 2005) for ages 4-7 years, “Divorced but Still My Parents” (Longmont, Colo. : Springboard Publications, 1997) for ages 6-12 years, and “My Mom and Dad Don’t Live Together Anymore: A Drawing Book for Children of Separated or Divorced Parents” (Washington: Magination Press, 2002) for ages 8-12 years.
Sesame Street has a toolkit on divorce that offers printable materials, songs, and an app that features conversation starters and vignettes, according to Dr. Bauer; go to sesamestreet.org and type in “divorce.” Additionally, the documentary SPLIT at splitfilm.org follows real families going through divorce and helps show the child’s perspective.
When parents ask about legal references, they can be referred to the UpToParents website, a free resource and curriculum developed by attorneys on topics such as divorce, in both English and Spanish.
Finally, familiarize yourself with resources available in your local community, such as divorce education programs, and services offered for divorce and custody mediation, so that you can link parents to them as needed.
Dr. Bauer said she has no relevant financial disclosures.
SAN FRANCISCO – By choosing your words carefully, counseling families about divorce can tactfully address sensitive issues and help parents and children better cope with this life transition, Nerissa S. Bauer, MD, said at the annual meeting of the American Academy of Pediatrics.
About one in five children born within a marriage and one in two of those born within a cohabiting union will experience breakup of that relationship by the age of 9 years, she said.
You must, therefore, be prepared to monitor for and identify outcomes that commonly result from divorce, and to counsel families about how to help children cope and manage. Yet, you may feel uneasy or ill-prepared to do so.
“Turn this thought of ‘I wasn’t trained for this’ into ‘I can help,’ ” recommended Dr. Bauer, who is a specialist in behavioral pediatrics at the Indiana University in Indianapolis.
Risk and protective factors
Divorce can have an impact on all facets of a child’s life: behavior, physical and mental health, academic performance, social relationships, delinquency, substance use, and more. A variety of factors determine how well kids adjust to this stressor, for better or worse.
Marital conflict, both during and after divorce, is a more important predictor than the divorce itself. “The biggest risk factor to consider is the ongoing parental fighting and how that plays out,” Dr. Bauer elaborated. Although parents may report that they try to limit altercations in front of their children, kids usually sense what is going on anyway.
“One of the ways that I like to phrase this when I’m trying to figure out how bad the conflict is in the household is, ‘Has Johnny ever witnessed your arguments, and if so, have those arguments ever been more than just yelling?’ Or another way to say it is, ‘How do adults in your home resolve conflicts?’ ” she shared.
Divorce may negatively affect children through its impact on the household’s socioeconomic status too. For example, the standard of living often declines and the mother’s economic resources can take a hit, possibly forcing a move to a less expensive neighborhood with weaker schools and more crime.
To sound parents out on this sensitive issue, “You can say something like, ‘I’m really sorry that you’re going through this right now. Sometimes, it can cause a lot of stress and strain, especially when it comes to making ends meet, making sure you can get food on the table, and making sure you’re paying the bills. Do you have worries like this now?’ ” Dr. Bauer suggested.
Factors that are known to protect children from adverse divorce outcomes include a good relationship with at least one parent or caregiver, parental warmth, sibling support, and for teens, good self-esteem and peer support. Joint custody with shared decision making and greater paternal involvement also are protective.
“I like to say, ‘So I can understand how this affects your daily life, can you describe what your current arrangements are between you and your ex?’ just to sort of probe into that custody situation,” she said. “Or, ‘How are you (parents) handling this?’ ”
Surveillance and monitoring
“Perform surveillance on family structure and conflict at all well-child visits, as well as with any new family that comes to your practice,” Dr. Bauer recommended. You can do this by simply chatting with the family or by using screening tools such as the Family Psychosocial Screen or the Finding Your ACE Score.
Once you know that a family is dealing with divorce, perform ongoing monitoring for warning signs in the child: sleep problems; school problems, such as poor concentration, acting out, or not doing schoolwork; angry outbursts; withdrawal; and no longer participating in activities once enjoyed.
You may worry about getting dragged into the conflict. “You may feel that you’re in this position of being the mediator, but that’s not really your role. And you shouldn’t offer legal advice,” she cautioned. “You should make it clear that although you are there to support the child and the parents, your role is really to monitor how the child responds and adjusts.”
Parents will sometimes ask whether and how best to tell their children about the divorce. “I oftentimes coach parents to use kid-friendly terms, saying things such as, ‘Mommy and Daddy are having a hard time getting along, and you’ve probably noticed we argue or fight a lot.’ Just throwing it out there and pausing and waiting to see what the child says, and then always following that by answering their questions as they bring them up,” Dr. Bauer said.
Parents should be counseled not to rush children as they will vary in the time needed to process information. Additionally, they should be forewarned that children’s reactions can vary widely and that their feelings can change and resurface at any moment, particularly as they mature and at events that stir up emotions.
Messages of reassurance are essential. “The messages should always contain, ‘We are always going to be your parents no matter what’ and ‘We love you no matter what,’ and probably the most important, ‘This is not your fault.’ This is a message that kids need to hear again and again,” Dr. Bauer said.
Ongoing counseling
Over time, parents may consult you about specific situations that arise because of the divorce. For example, they may become frustrated by differences in how things are handled in the two households.
“The most important message to convey is that we can control only what we can control,” Dr. Bauer said. “Regardless of divorce or separation, kids thrive on structure and routine. Divorce is often messy, and it sometimes means that families have to find a new rhythm between households, but routines in each house should be as consistent as possible.”
Acrimony between the mother and father may persist or escalate. As children don’t want to have to choose between parents, parents should be encouraged not to undermine or talk negatively about each other in front of the child. If necessary, you can arrange to have time separately with parents to allow them to air their grievances.
If parents give permission to broach the topic of divorce, you can role model conversational strategies during visits. “You can say something like, ‘I understand there are a lot of changes going on. Through it all, your mom and dad will always be your parents. I know this isn’t easy for anybody, especially for you. Kids in this situation feel a lot of things from sadness to anger but know that you can always talk to me or your parents about your feelings,’” Dr. Bauer elaborated.
“Listening is key,” she stressed; therefore, parents should be encouraged to just sit in silence and let their children process their feelings. “In these types of situations, there’s no right or wrong: When the child has feelings, they have feelings. We can’t force them to feel a certain way, we have to acknowledge that. So tell parents to try this: ‘Thanks for telling me how you feel. I want you to know that you can always come to me when you feel this way.’ See what happens.”
Parents should be advised not to be too quick to dismiss their child’s concerns, Dr. Bauer recommended. “So, instead of saying, ‘Oh honey, you don’t have to worry about that, I’ll take care of it,’ try this: ‘It sounds like you are sad and upset right now. What can I do to help?’ Sometimes a kid will say, ‘I don’t know,’ but that’s okay. Then the parent can respond in kind and say, ‘I don’t know either, but how about a hug? Let’s start there.’ ”
Some kids simply aren’t talkers and shouldn’t be forced to share, she pointed out. This group can be given other ways to express their feelings, such as journaling, drawing, art, music, yoga, or writing a letter that they then throw away or put in a drawer.
Finally, “reminding parents that even giving children a little control with daily things – what they wear, how they do their chores, and homework, and what to make for dinner – can also help,” she noted. “Those little things can represent a lot for children who don’t feel like they have any control.”
Building resources
Explore various media and online tools to develop a set of resources on divorce for families, Dr. Bauer recommended.
Books on the topic can be great conversation starters, and many are available for various age-groups, she noted. Examples include “Was It the Chocolate Pudding? A Story for Little Kids About Divorce” (Washington: Magination Press, 2005) for ages 4-7 years, “Divorced but Still My Parents” (Longmont, Colo. : Springboard Publications, 1997) for ages 6-12 years, and “My Mom and Dad Don’t Live Together Anymore: A Drawing Book for Children of Separated or Divorced Parents” (Washington: Magination Press, 2002) for ages 8-12 years.
Sesame Street has a toolkit on divorce that offers printable materials, songs, and an app that features conversation starters and vignettes, according to Dr. Bauer; go to sesamestreet.org and type in “divorce.” Additionally, the documentary SPLIT at splitfilm.org follows real families going through divorce and helps show the child’s perspective.
When parents ask about legal references, they can be referred to the UpToParents website, a free resource and curriculum developed by attorneys on topics such as divorce, in both English and Spanish.
Finally, familiarize yourself with resources available in your local community, such as divorce education programs, and services offered for divorce and custody mediation, so that you can link parents to them as needed.
Dr. Bauer said she has no relevant financial disclosures.
SAN FRANCISCO – By choosing your words carefully, counseling families about divorce can tactfully address sensitive issues and help parents and children better cope with this life transition, Nerissa S. Bauer, MD, said at the annual meeting of the American Academy of Pediatrics.
About one in five children born within a marriage and one in two of those born within a cohabiting union will experience breakup of that relationship by the age of 9 years, she said.
You must, therefore, be prepared to monitor for and identify outcomes that commonly result from divorce, and to counsel families about how to help children cope and manage. Yet, you may feel uneasy or ill-prepared to do so.
“Turn this thought of ‘I wasn’t trained for this’ into ‘I can help,’ ” recommended Dr. Bauer, who is a specialist in behavioral pediatrics at the Indiana University in Indianapolis.
Risk and protective factors
Divorce can have an impact on all facets of a child’s life: behavior, physical and mental health, academic performance, social relationships, delinquency, substance use, and more. A variety of factors determine how well kids adjust to this stressor, for better or worse.
Marital conflict, both during and after divorce, is a more important predictor than the divorce itself. “The biggest risk factor to consider is the ongoing parental fighting and how that plays out,” Dr. Bauer elaborated. Although parents may report that they try to limit altercations in front of their children, kids usually sense what is going on anyway.
“One of the ways that I like to phrase this when I’m trying to figure out how bad the conflict is in the household is, ‘Has Johnny ever witnessed your arguments, and if so, have those arguments ever been more than just yelling?’ Or another way to say it is, ‘How do adults in your home resolve conflicts?’ ” she shared.
Divorce may negatively affect children through its impact on the household’s socioeconomic status too. For example, the standard of living often declines and the mother’s economic resources can take a hit, possibly forcing a move to a less expensive neighborhood with weaker schools and more crime.
To sound parents out on this sensitive issue, “You can say something like, ‘I’m really sorry that you’re going through this right now. Sometimes, it can cause a lot of stress and strain, especially when it comes to making ends meet, making sure you can get food on the table, and making sure you’re paying the bills. Do you have worries like this now?’ ” Dr. Bauer suggested.
Factors that are known to protect children from adverse divorce outcomes include a good relationship with at least one parent or caregiver, parental warmth, sibling support, and for teens, good self-esteem and peer support. Joint custody with shared decision making and greater paternal involvement also are protective.
“I like to say, ‘So I can understand how this affects your daily life, can you describe what your current arrangements are between you and your ex?’ just to sort of probe into that custody situation,” she said. “Or, ‘How are you (parents) handling this?’ ”
Surveillance and monitoring
“Perform surveillance on family structure and conflict at all well-child visits, as well as with any new family that comes to your practice,” Dr. Bauer recommended. You can do this by simply chatting with the family or by using screening tools such as the Family Psychosocial Screen or the Finding Your ACE Score.
Once you know that a family is dealing with divorce, perform ongoing monitoring for warning signs in the child: sleep problems; school problems, such as poor concentration, acting out, or not doing schoolwork; angry outbursts; withdrawal; and no longer participating in activities once enjoyed.
You may worry about getting dragged into the conflict. “You may feel that you’re in this position of being the mediator, but that’s not really your role. And you shouldn’t offer legal advice,” she cautioned. “You should make it clear that although you are there to support the child and the parents, your role is really to monitor how the child responds and adjusts.”
Parents will sometimes ask whether and how best to tell their children about the divorce. “I oftentimes coach parents to use kid-friendly terms, saying things such as, ‘Mommy and Daddy are having a hard time getting along, and you’ve probably noticed we argue or fight a lot.’ Just throwing it out there and pausing and waiting to see what the child says, and then always following that by answering their questions as they bring them up,” Dr. Bauer said.
Parents should be counseled not to rush children as they will vary in the time needed to process information. Additionally, they should be forewarned that children’s reactions can vary widely and that their feelings can change and resurface at any moment, particularly as they mature and at events that stir up emotions.
Messages of reassurance are essential. “The messages should always contain, ‘We are always going to be your parents no matter what’ and ‘We love you no matter what,’ and probably the most important, ‘This is not your fault.’ This is a message that kids need to hear again and again,” Dr. Bauer said.
Ongoing counseling
Over time, parents may consult you about specific situations that arise because of the divorce. For example, they may become frustrated by differences in how things are handled in the two households.
“The most important message to convey is that we can control only what we can control,” Dr. Bauer said. “Regardless of divorce or separation, kids thrive on structure and routine. Divorce is often messy, and it sometimes means that families have to find a new rhythm between households, but routines in each house should be as consistent as possible.”
Acrimony between the mother and father may persist or escalate. As children don’t want to have to choose between parents, parents should be encouraged not to undermine or talk negatively about each other in front of the child. If necessary, you can arrange to have time separately with parents to allow them to air their grievances.
If parents give permission to broach the topic of divorce, you can role model conversational strategies during visits. “You can say something like, ‘I understand there are a lot of changes going on. Through it all, your mom and dad will always be your parents. I know this isn’t easy for anybody, especially for you. Kids in this situation feel a lot of things from sadness to anger but know that you can always talk to me or your parents about your feelings,’” Dr. Bauer elaborated.
“Listening is key,” she stressed; therefore, parents should be encouraged to just sit in silence and let their children process their feelings. “In these types of situations, there’s no right or wrong: When the child has feelings, they have feelings. We can’t force them to feel a certain way, we have to acknowledge that. So tell parents to try this: ‘Thanks for telling me how you feel. I want you to know that you can always come to me when you feel this way.’ See what happens.”
Parents should be advised not to be too quick to dismiss their child’s concerns, Dr. Bauer recommended. “So, instead of saying, ‘Oh honey, you don’t have to worry about that, I’ll take care of it,’ try this: ‘It sounds like you are sad and upset right now. What can I do to help?’ Sometimes a kid will say, ‘I don’t know,’ but that’s okay. Then the parent can respond in kind and say, ‘I don’t know either, but how about a hug? Let’s start there.’ ”
Some kids simply aren’t talkers and shouldn’t be forced to share, she pointed out. This group can be given other ways to express their feelings, such as journaling, drawing, art, music, yoga, or writing a letter that they then throw away or put in a drawer.
Finally, “reminding parents that even giving children a little control with daily things – what they wear, how they do their chores, and homework, and what to make for dinner – can also help,” she noted. “Those little things can represent a lot for children who don’t feel like they have any control.”
Building resources
Explore various media and online tools to develop a set of resources on divorce for families, Dr. Bauer recommended.
Books on the topic can be great conversation starters, and many are available for various age-groups, she noted. Examples include “Was It the Chocolate Pudding? A Story for Little Kids About Divorce” (Washington: Magination Press, 2005) for ages 4-7 years, “Divorced but Still My Parents” (Longmont, Colo. : Springboard Publications, 1997) for ages 6-12 years, and “My Mom and Dad Don’t Live Together Anymore: A Drawing Book for Children of Separated or Divorced Parents” (Washington: Magination Press, 2002) for ages 8-12 years.
Sesame Street has a toolkit on divorce that offers printable materials, songs, and an app that features conversation starters and vignettes, according to Dr. Bauer; go to sesamestreet.org and type in “divorce.” Additionally, the documentary SPLIT at splitfilm.org follows real families going through divorce and helps show the child’s perspective.
When parents ask about legal references, they can be referred to the UpToParents website, a free resource and curriculum developed by attorneys on topics such as divorce, in both English and Spanish.
Finally, familiarize yourself with resources available in your local community, such as divorce education programs, and services offered for divorce and custody mediation, so that you can link parents to them as needed.
Dr. Bauer said she has no relevant financial disclosures.
EXPERT ANALYSIS FROM AAP 16
Lyme disease spirochete helps babesiosis gain a foothold
BOSTON – The spirochete that causes Lyme disease in humans may be lending a helping hand to the weaker protozoan that causes babesiosis, escalating the rate of human babesiosis cases in regions where both are endemic.
Peter Krause, MD, a research scientist in epidemiology, medicine, and pediatrics at Yale University School of Public Health, New Haven, Conn., reviewed what’s known about babesiosis–Lyme disease coinfections at the annual meeting of the American Society for Microbiology.

Understanding the entire cycle is necessary, he said, because the effects of coinfection will be different depending on the stage of the cycle, and upon the coinfection pathogens.
Over the course of many years, Dr. Krause and his collaborators have used an interdisciplinary, multi-modal approach to try to understand the interplay between these pathogens, their hosts, and environmental, demographic, and ecologic factors.
One arm of their research has taken them to the lab, where they have modeled coinfection and transmission of Borrelia burgdorferi and Babesia microti from their reservoir host, the white-footed mouse (Peromyscus leucopus), to the vector, the deer tick (Ixodes scapularis), which can transmit both diseases to humans.
In an experimental design that mimicked the natural reservoir-vector ecology, Dr. Krause and his collaborators first infected mice with 5 to 10 nymphal ticks, to approximate the average number of ticks that feed on an individual mouse in the wild. The researchers then tracked the effect of coinfection on transmission of each pathogen to ticks during the larval feeds, finding that B. burgdorferi increased B. microti parasitemia in mice who were coinfected. Coinfection also increases B. microti transmission from mice to ticks. This effect happens at least partly because of the increased parasitemia, Dr. Krause said.
The downstream effect on humans is to increase the risk of babesiosis for those who live in regions where both B. microti and B. burgdorferi are endemic, Dr. Krause said.
B. microti is less “ecologically fit” than B. burgdorferi, Dr. Krause said, noting that there are more ticks and humans infected with the latter, as well as more reservoir mice carrying B. burgdorferi. Also, the rate of geographic expansion is more rapid for B. burgdorferi. “B. microti is only endemic in areas where B. burgdorferi is already endemic; it may not be ‘fit’ enough to establish endemic sites on its own,” Dr. Krause said.
The increased rate of B. microti transmission via ticks from mice, if the mice are coinfected with B. burgdorferi, may help explain the greater-than-expected rate of babesiosis in humans in areas of New England where coinfection is common. “This paradox might be explained by the enhancement of B. microti survival and spread by the coinfecting presence of Borrelia burgdorferi,” Dr. Krause said.
This naturalistic experiment has ecological implications in terms of the human impact as well: “Coinfection may help enhance geographic spread of B. microti to new areas,” Dr. Krause said.
Clinicians in geographic areas where both pathogens are endemic should maintain a high level of suspicion for coinfection, especially for the most ill patients. “Anaplasmosis and/or babesiosis coinfection increases the severity of Lyme disease,” Dr. Krause said. “Health care workers should consider anaplasmosis and/or babesiosis coinfection in Lyme disease patients who have more severe illness or who do not respond to antibiotic therapy.”
Understanding the complex interspecies interplay will be increasingly important as more cases of tick-borne illness are seen, Dr. Krause concluded. “Research on coinfections acquired from Ixodes scapularis has just begun.”
Dr. Krause reported no relevant conflicts of interest.
koakes@frontlinemedcom.com
On Twitter @karioakes
BOSTON – The spirochete that causes Lyme disease in humans may be lending a helping hand to the weaker protozoan that causes babesiosis, escalating the rate of human babesiosis cases in regions where both are endemic.
Peter Krause, MD, a research scientist in epidemiology, medicine, and pediatrics at Yale University School of Public Health, New Haven, Conn., reviewed what’s known about babesiosis–Lyme disease coinfections at the annual meeting of the American Society for Microbiology.
Understanding the entire cycle is necessary, he said, because the effects of coinfection will be different depending on the stage of the cycle, and upon the coinfection pathogens.
Over the course of many years, Dr. Krause and his collaborators have used an interdisciplinary, multi-modal approach to try to understand the interplay between these pathogens, their hosts, and environmental, demographic, and ecologic factors.
One arm of their research has taken them to the lab, where they have modeled coinfection and transmission of Borrelia burgdorferi and Babesia microti from their reservoir host, the white-footed mouse (Peromyscus leucopus), to the vector, the deer tick (Ixodes scapularis), which can transmit both diseases to humans.
In an experimental design that mimicked the natural reservoir-vector ecology, Dr. Krause and his collaborators first infected mice with 5 to 10 nymphal ticks, to approximate the average number of ticks that feed on an individual mouse in the wild. The researchers then tracked the effect of coinfection on transmission of each pathogen to ticks during the larval feeds, finding that B. burgdorferi increased B. microti parasitemia in mice who were coinfected. Coinfection also increases B. microti transmission from mice to ticks. This effect happens at least partly because of the increased parasitemia, Dr. Krause said.
The downstream effect on humans is to increase the risk of babesiosis for those who live in regions where both B. microti and B. burgdorferi are endemic, Dr. Krause said.
B. microti is less “ecologically fit” than B. burgdorferi, Dr. Krause said, noting that there are more ticks and humans infected with the latter, as well as more reservoir mice carrying B. burgdorferi. Also, the rate of geographic expansion is more rapid for B. burgdorferi. “B. microti is only endemic in areas where B. burgdorferi is already endemic; it may not be ‘fit’ enough to establish endemic sites on its own,” Dr. Krause said.
The increased rate of B. microti transmission via ticks from mice, if the mice are coinfected with B. burgdorferi, may help explain the greater-than-expected rate of babesiosis in humans in areas of New England where coinfection is common. “This paradox might be explained by the enhancement of B. microti survival and spread by the coinfecting presence of Borrelia burgdorferi,” Dr. Krause said.
This naturalistic experiment has ecological implications in terms of the human impact as well: “Coinfection may help enhance geographic spread of B. microti to new areas,” Dr. Krause said.
Clinicians in geographic areas where both pathogens are endemic should maintain a high level of suspicion for coinfection, especially for the most ill patients. “Anaplasmosis and/or babesiosis coinfection increases the severity of Lyme disease,” Dr. Krause said. “Health care workers should consider anaplasmosis and/or babesiosis coinfection in Lyme disease patients who have more severe illness or who do not respond to antibiotic therapy.”
Understanding the complex interspecies interplay will be increasingly important as more cases of tick-borne illness are seen, Dr. Krause concluded. “Research on coinfections acquired from Ixodes scapularis has just begun.”
Dr. Krause reported no relevant conflicts of interest.
koakes@frontlinemedcom.com
On Twitter @karioakes
BOSTON – The spirochete that causes Lyme disease in humans may be lending a helping hand to the weaker protozoan that causes babesiosis, escalating the rate of human babesiosis cases in regions where both are endemic.
Peter Krause, MD, a research scientist in epidemiology, medicine, and pediatrics at Yale University School of Public Health, New Haven, Conn., reviewed what’s known about babesiosis–Lyme disease coinfections at the annual meeting of the American Society for Microbiology.
Understanding the entire cycle is necessary, he said, because the effects of coinfection will be different depending on the stage of the cycle, and upon the coinfection pathogens.
Over the course of many years, Dr. Krause and his collaborators have used an interdisciplinary, multi-modal approach to try to understand the interplay between these pathogens, their hosts, and environmental, demographic, and ecologic factors.
One arm of their research has taken them to the lab, where they have modeled coinfection and transmission of Borrelia burgdorferi and Babesia microti from their reservoir host, the white-footed mouse (Peromyscus leucopus), to the vector, the deer tick (Ixodes scapularis), which can transmit both diseases to humans.
In an experimental design that mimicked the natural reservoir-vector ecology, Dr. Krause and his collaborators first infected mice with 5 to 10 nymphal ticks, to approximate the average number of ticks that feed on an individual mouse in the wild. The researchers then tracked the effect of coinfection on transmission of each pathogen to ticks during the larval feeds, finding that B. burgdorferi increased B. microti parasitemia in mice who were coinfected. Coinfection also increases B. microti transmission from mice to ticks. This effect happens at least partly because of the increased parasitemia, Dr. Krause said.
The downstream effect on humans is to increase the risk of babesiosis for those who live in regions where both B. microti and B. burgdorferi are endemic, Dr. Krause said.
B. microti is less “ecologically fit” than B. burgdorferi, Dr. Krause said, noting that there are more ticks and humans infected with the latter, as well as more reservoir mice carrying B. burgdorferi. Also, the rate of geographic expansion is more rapid for B. burgdorferi. “B. microti is only endemic in areas where B. burgdorferi is already endemic; it may not be ‘fit’ enough to establish endemic sites on its own,” Dr. Krause said.
The increased rate of B. microti transmission via ticks from mice, if the mice are coinfected with B. burgdorferi, may help explain the greater-than-expected rate of babesiosis in humans in areas of New England where coinfection is common. “This paradox might be explained by the enhancement of B. microti survival and spread by the coinfecting presence of Borrelia burgdorferi,” Dr. Krause said.
This naturalistic experiment has ecological implications in terms of the human impact as well: “Coinfection may help enhance geographic spread of B. microti to new areas,” Dr. Krause said.
Clinicians in geographic areas where both pathogens are endemic should maintain a high level of suspicion for coinfection, especially for the most ill patients. “Anaplasmosis and/or babesiosis coinfection increases the severity of Lyme disease,” Dr. Krause said. “Health care workers should consider anaplasmosis and/or babesiosis coinfection in Lyme disease patients who have more severe illness or who do not respond to antibiotic therapy.”
Understanding the complex interspecies interplay will be increasingly important as more cases of tick-borne illness are seen, Dr. Krause concluded. “Research on coinfections acquired from Ixodes scapularis has just begun.”
Dr. Krause reported no relevant conflicts of interest.
koakes@frontlinemedcom.com
On Twitter @karioakes
EXPERT ANALYSIS FROM ASM 2016
ACIP approves changes to HPV, Tdap, DTaP, MenB vaccination guidance
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices approved a series of minor changes to the current guidance for meningococcal, Tdap, DTaP, and human papillomavirus vaccination schedules.
Regarding meningococcal vaccinations, the committee voted to change the recommendations to state that individuals who are at an increased risk of contracting the disease should receive a three-dose regimen of Trumenba at 0 months, 1-2 months, and 6 months. The same regimen also should apply during any outbreaks of serogroup B meningococcal virus. In addition, a two-dose regimen at 0 and 6 months should be given to adolescents who are not considered high risk, and if the second dose is given fewer than 6 months following the first, then a third dose must be given within 6 months of the initial dose. 
“This new recommendation enables flexible vaccination dosing intervals depending on one’s risk of exposure to meningococcal group B disease, also known as MenB, which makes it easier for health care providers to help protect adolescents and young adults from this uncommon but life-threatening disease,” the CDC announced in a statement.
For Tdap and DTaP vaccines, changes to the language of the recommendations were approved unanimously by the committee. These changes will contain the routine recommendations for DTaP, Tdap, and TB, which previously were published as separate statements, along with Tdap recommendations made after the 2005 recommendations and published in Morbidity and Mortality Weekly Report policy notes.
“This statement also contains updates, such as DTaP vaccines that became available after the 1997 DTaP statement, and updates to the label indications on various DTaP and Tdap products,” Jennifer Liang, DVM, of the CDC’s National Center for Immunization and Respiratory Diseases, explained at the ACIP meeting. “Also included in the statement are the following updates: mention of the discontinuation of monovalent tetanus toxoid vaccine, the contraindications and precautions for DTaP are now consistent with the [American Academy of Pediatrics’] Red Book, and for persons aged 7-10 years who received a dose of Tdap as part of the catchup series, an adolescent Tdap dose may be given at age 11-12 years.”
Dr. Liang added that these updated changes would bring the guidance in line with the recommendations for children who are administered Tdap inadvertently.
With one recusal, changes to the HPV vaccination guidance also were unanimously approved. No changes were proposed to the routine and catch-up age groups for HPV vaccination, and for contraindications and precautions. Major additions were made, however, to the sections on dosing schedules, and people with prior vaccination. Clarifying language was added for the sections on interrupted schedules, special populations, and medical conditions.
For individuals initiating vaccination before the 15th birthday, the recommended immunization schedule is two doses of HPV vaccine. The second dose should be administered 6-12 months after the first dose (0 months, 6-12 months schedule). For people initiating vaccination on or after the 15th birthday, the recommendations remain the same as before: three doses of HPV vaccine, with the second dose administered 1-2 months after the first dose, and the third dose administered within 6 months of the first dose.
Those with prior vaccinations who initiated with 9-valent HPV, 4-valent HPV, or 2-valent HPV before their 15th birthday and received either two or three doses at the recommended dosing schedule should be considered adequately vaccinated. Those who initiated any of those three HPV vaccinations on or after their 15th birthday and received three doses at the currently recommended dosing schedule should be considered adequately vaccinated, too.
With regard to the minimum intervals, the proposed change was to add a footnote defining minimum intervals: in a two-dose series of HPV vaccines, the minimum interval is 5 months between the first and second dose, and in a three-dose series, 5 months between the first and third dose. All other language remains as is. Special population language also was changed to “gay, bisexual, and other” men rather than simply men who have sex with men, to broaden the scope of the language. Language also will be amended to include transgender patients.
Finally, for those with other medical conditions, ACIP still recommends that all immunocompromised males and females aged 9-26 years get a three-dose HPV vaccination at 0, 1-2, and 6 months, but now the language change will read that “Persons who should receive three doses are those with primary or secondary immunocompromising conditions that might reduce cell-mediated or humoral immunity, such as B lymphocyte antibody deficiencies, T lymphocyte complete or partial defects, HIV infection, malignant neoplasm, transplantation, autoimmune disease, or immunosuppressive therapy, since response to vaccination may be attenuated.”
In addition, there will be a footnote stating that these recommendations for a three-dose schedule do not apply to children under the age of 15 years with asplenia, asthma, chronic granulomatous disease, chronic heart/liver/lung/renal disease, central nervous system anatomic barrier defects, complement deficiency, diabetes, or sickle cell disease.”
The recommendations agreed upon will be submitted for approval to CDC Director Tom Frieden, MD. If approved, the recommendations will be published by Jan. 1, 2017, at which point, they will go into effect.
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices approved a series of minor changes to the current guidance for meningococcal, Tdap, DTaP, and human papillomavirus vaccination schedules.
Regarding meningococcal vaccinations, the committee voted to change the recommendations to state that individuals who are at an increased risk of contracting the disease should receive a three-dose regimen of Trumenba at 0 months, 1-2 months, and 6 months. The same regimen also should apply during any outbreaks of serogroup B meningococcal virus. In addition, a two-dose regimen at 0 and 6 months should be given to adolescents who are not considered high risk, and if the second dose is given fewer than 6 months following the first, then a third dose must be given within 6 months of the initial dose.
“This new recommendation enables flexible vaccination dosing intervals depending on one’s risk of exposure to meningococcal group B disease, also known as MenB, which makes it easier for health care providers to help protect adolescents and young adults from this uncommon but life-threatening disease,” the CDC announced in a statement.
For Tdap and DTaP vaccines, changes to the language of the recommendations were approved unanimously by the committee. These changes will contain the routine recommendations for DTaP, Tdap, and TB, which previously were published as separate statements, along with Tdap recommendations made after the 2005 recommendations and published in Morbidity and Mortality Weekly Report policy notes.
“This statement also contains updates, such as DTaP vaccines that became available after the 1997 DTaP statement, and updates to the label indications on various DTaP and Tdap products,” Jennifer Liang, DVM, of the CDC’s National Center for Immunization and Respiratory Diseases, explained at the ACIP meeting. “Also included in the statement are the following updates: mention of the discontinuation of monovalent tetanus toxoid vaccine, the contraindications and precautions for DTaP are now consistent with the [American Academy of Pediatrics’] Red Book, and for persons aged 7-10 years who received a dose of Tdap as part of the catchup series, an adolescent Tdap dose may be given at age 11-12 years.”
Dr. Liang added that these updated changes would bring the guidance in line with the recommendations for children who are administered Tdap inadvertently.
With one recusal, changes to the HPV vaccination guidance also were unanimously approved. No changes were proposed to the routine and catch-up age groups for HPV vaccination, and for contraindications and precautions. Major additions were made, however, to the sections on dosing schedules, and people with prior vaccination. Clarifying language was added for the sections on interrupted schedules, special populations, and medical conditions.
For individuals initiating vaccination before the 15th birthday, the recommended immunization schedule is two doses of HPV vaccine. The second dose should be administered 6-12 months after the first dose (0 months, 6-12 months schedule). For people initiating vaccination on or after the 15th birthday, the recommendations remain the same as before: three doses of HPV vaccine, with the second dose administered 1-2 months after the first dose, and the third dose administered within 6 months of the first dose.
Those with prior vaccinations who initiated with 9-valent HPV, 4-valent HPV, or 2-valent HPV before their 15th birthday and received either two or three doses at the recommended dosing schedule should be considered adequately vaccinated. Those who initiated any of those three HPV vaccinations on or after their 15th birthday and received three doses at the currently recommended dosing schedule should be considered adequately vaccinated, too.
With regard to the minimum intervals, the proposed change was to add a footnote defining minimum intervals: in a two-dose series of HPV vaccines, the minimum interval is 5 months between the first and second dose, and in a three-dose series, 5 months between the first and third dose. All other language remains as is. Special population language also was changed to “gay, bisexual, and other” men rather than simply men who have sex with men, to broaden the scope of the language. Language also will be amended to include transgender patients.
Finally, for those with other medical conditions, ACIP still recommends that all immunocompromised males and females aged 9-26 years get a three-dose HPV vaccination at 0, 1-2, and 6 months, but now the language change will read that “Persons who should receive three doses are those with primary or secondary immunocompromising conditions that might reduce cell-mediated or humoral immunity, such as B lymphocyte antibody deficiencies, T lymphocyte complete or partial defects, HIV infection, malignant neoplasm, transplantation, autoimmune disease, or immunosuppressive therapy, since response to vaccination may be attenuated.”
In addition, there will be a footnote stating that these recommendations for a three-dose schedule do not apply to children under the age of 15 years with asplenia, asthma, chronic granulomatous disease, chronic heart/liver/lung/renal disease, central nervous system anatomic barrier defects, complement deficiency, diabetes, or sickle cell disease.”
The recommendations agreed upon will be submitted for approval to CDC Director Tom Frieden, MD. If approved, the recommendations will be published by Jan. 1, 2017, at which point, they will go into effect.
The Centers for Disease Control and Prevention’s Advisory Committee on Immunization Practices approved a series of minor changes to the current guidance for meningococcal, Tdap, DTaP, and human papillomavirus vaccination schedules.
Regarding meningococcal vaccinations, the committee voted to change the recommendations to state that individuals who are at an increased risk of contracting the disease should receive a three-dose regimen of Trumenba at 0 months, 1-2 months, and 6 months. The same regimen also should apply during any outbreaks of serogroup B meningococcal virus. In addition, a two-dose regimen at 0 and 6 months should be given to adolescents who are not considered high risk, and if the second dose is given fewer than 6 months following the first, then a third dose must be given within 6 months of the initial dose.
“This new recommendation enables flexible vaccination dosing intervals depending on one’s risk of exposure to meningococcal group B disease, also known as MenB, which makes it easier for health care providers to help protect adolescents and young adults from this uncommon but life-threatening disease,” the CDC announced in a statement.
For Tdap and DTaP vaccines, changes to the language of the recommendations were approved unanimously by the committee. These changes will contain the routine recommendations for DTaP, Tdap, and TB, which previously were published as separate statements, along with Tdap recommendations made after the 2005 recommendations and published in Morbidity and Mortality Weekly Report policy notes.
“This statement also contains updates, such as DTaP vaccines that became available after the 1997 DTaP statement, and updates to the label indications on various DTaP and Tdap products,” Jennifer Liang, DVM, of the CDC’s National Center for Immunization and Respiratory Diseases, explained at the ACIP meeting. “Also included in the statement are the following updates: mention of the discontinuation of monovalent tetanus toxoid vaccine, the contraindications and precautions for DTaP are now consistent with the [American Academy of Pediatrics’] Red Book, and for persons aged 7-10 years who received a dose of Tdap as part of the catchup series, an adolescent Tdap dose may be given at age 11-12 years.”
Dr. Liang added that these updated changes would bring the guidance in line with the recommendations for children who are administered Tdap inadvertently.
With one recusal, changes to the HPV vaccination guidance also were unanimously approved. No changes were proposed to the routine and catch-up age groups for HPV vaccination, and for contraindications and precautions. Major additions were made, however, to the sections on dosing schedules, and people with prior vaccination. Clarifying language was added for the sections on interrupted schedules, special populations, and medical conditions.
For individuals initiating vaccination before the 15th birthday, the recommended immunization schedule is two doses of HPV vaccine. The second dose should be administered 6-12 months after the first dose (0 months, 6-12 months schedule). For people initiating vaccination on or after the 15th birthday, the recommendations remain the same as before: three doses of HPV vaccine, with the second dose administered 1-2 months after the first dose, and the third dose administered within 6 months of the first dose.
Those with prior vaccinations who initiated with 9-valent HPV, 4-valent HPV, or 2-valent HPV before their 15th birthday and received either two or three doses at the recommended dosing schedule should be considered adequately vaccinated. Those who initiated any of those three HPV vaccinations on or after their 15th birthday and received three doses at the currently recommended dosing schedule should be considered adequately vaccinated, too.
With regard to the minimum intervals, the proposed change was to add a footnote defining minimum intervals: in a two-dose series of HPV vaccines, the minimum interval is 5 months between the first and second dose, and in a three-dose series, 5 months between the first and third dose. All other language remains as is. Special population language also was changed to “gay, bisexual, and other” men rather than simply men who have sex with men, to broaden the scope of the language. Language also will be amended to include transgender patients.
Finally, for those with other medical conditions, ACIP still recommends that all immunocompromised males and females aged 9-26 years get a three-dose HPV vaccination at 0, 1-2, and 6 months, but now the language change will read that “Persons who should receive three doses are those with primary or secondary immunocompromising conditions that might reduce cell-mediated or humoral immunity, such as B lymphocyte antibody deficiencies, T lymphocyte complete or partial defects, HIV infection, malignant neoplasm, transplantation, autoimmune disease, or immunosuppressive therapy, since response to vaccination may be attenuated.”
In addition, there will be a footnote stating that these recommendations for a three-dose schedule do not apply to children under the age of 15 years with asplenia, asthma, chronic granulomatous disease, chronic heart/liver/lung/renal disease, central nervous system anatomic barrier defects, complement deficiency, diabetes, or sickle cell disease.”
The recommendations agreed upon will be submitted for approval to CDC Director Tom Frieden, MD. If approved, the recommendations will be published by Jan. 1, 2017, at which point, they will go into effect.
FROM AN ACIP MEETING
Psych issues adding to pediatric hospitalization costs
Although pediatric hospitalizations are driven mostly by medical costs, comorbid psychiatric problems are increasingly adding to the expense, according to a review of 3,114,099 hospitalizations at 33 children’s hospitals in the United States from 2005 to 2014.
For pediatric hospitalizations without a psychiatric diagnosis, costs rose from $3,696 to $4,150 per day over the past decade. For medical stays with a psychiatric diagnosis, the price rose from $2,694 to $3,393 per day, a higher percent change. Overall, the cost of hospitalizing sick children with comorbid psychiatric diagnoses increased from $671 million to $1.6 billion.
The “strategic planning to meet the rising demand for psychiatric care in tertiary care children’s hospitals should place high priority on the needs of children with a primary medical condition and co-occurring psychiatric disorders,” said investigators led by Bonnie Zima, MD, from the University of California, Los Angeles, Semel Institute for Neuroscience and Human Behavior (Pediatrics. 2016 Oct 21. doi: 10.1542/peds.2016-0909).
“From 2005 through 2014 ... there was significant cumulative percent increase in total number of hospitalizations, hospital days, and hospital costs for all patients. Of the total hospitalizations, 18.3% (568,449) were associated with a psychiatric disorder, either primary or secondary,” they noted.
Meanwhile, hospitalizations for psychiatric-only diagnoses were minimal, just 3.6% of the total with the most common problems again being depression, anxiety, and suicide and self-injury. “Hospital resource use for only psychiatric disorders declined, consistent with the national shift to managed care for behavioral health services,” the investigators said.
“Collectively, these data will further guide strategic planning by children’s hospitals as they strive to integrate mental health care into their health care systems. Together, these findings … underscore the need for quality improvement interventions that target improving linkage with community mental health care after pediatric hospitalization,” they said.
The National Institutes of Health funded the study. Dr. Zima was supported by the National Institute of Mental Health and Behavioral Health Centers of Excellence for California. Dr. Naomi S. Bardach and Dr. Tumaini R. Coker were supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Jay G. Berry was supported by the Agency for Healthcare Research and Quality. The authors had no conflicts of interest.
Although pediatric hospitalizations are driven mostly by medical costs, comorbid psychiatric problems are increasingly adding to the expense, according to a review of 3,114,099 hospitalizations at 33 children’s hospitals in the United States from 2005 to 2014.
For pediatric hospitalizations without a psychiatric diagnosis, costs rose from $3,696 to $4,150 per day over the past decade. For medical stays with a psychiatric diagnosis, the price rose from $2,694 to $3,393 per day, a higher percent change. Overall, the cost of hospitalizing sick children with comorbid psychiatric diagnoses increased from $671 million to $1.6 billion.
The “strategic planning to meet the rising demand for psychiatric care in tertiary care children’s hospitals should place high priority on the needs of children with a primary medical condition and co-occurring psychiatric disorders,” said investigators led by Bonnie Zima, MD, from the University of California, Los Angeles, Semel Institute for Neuroscience and Human Behavior (Pediatrics. 2016 Oct 21. doi: 10.1542/peds.2016-0909).
“From 2005 through 2014 ... there was significant cumulative percent increase in total number of hospitalizations, hospital days, and hospital costs for all patients. Of the total hospitalizations, 18.3% (568,449) were associated with a psychiatric disorder, either primary or secondary,” they noted.
Meanwhile, hospitalizations for psychiatric-only diagnoses were minimal, just 3.6% of the total with the most common problems again being depression, anxiety, and suicide and self-injury. “Hospital resource use for only psychiatric disorders declined, consistent with the national shift to managed care for behavioral health services,” the investigators said.
“Collectively, these data will further guide strategic planning by children’s hospitals as they strive to integrate mental health care into their health care systems. Together, these findings … underscore the need for quality improvement interventions that target improving linkage with community mental health care after pediatric hospitalization,” they said.
The National Institutes of Health funded the study. Dr. Zima was supported by the National Institute of Mental Health and Behavioral Health Centers of Excellence for California. Dr. Naomi S. Bardach and Dr. Tumaini R. Coker were supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Jay G. Berry was supported by the Agency for Healthcare Research and Quality. The authors had no conflicts of interest.
Although pediatric hospitalizations are driven mostly by medical costs, comorbid psychiatric problems are increasingly adding to the expense, according to a review of 3,114,099 hospitalizations at 33 children’s hospitals in the United States from 2005 to 2014.
For pediatric hospitalizations without a psychiatric diagnosis, costs rose from $3,696 to $4,150 per day over the past decade. For medical stays with a psychiatric diagnosis, the price rose from $2,694 to $3,393 per day, a higher percent change. Overall, the cost of hospitalizing sick children with comorbid psychiatric diagnoses increased from $671 million to $1.6 billion.
The “strategic planning to meet the rising demand for psychiatric care in tertiary care children’s hospitals should place high priority on the needs of children with a primary medical condition and co-occurring psychiatric disorders,” said investigators led by Bonnie Zima, MD, from the University of California, Los Angeles, Semel Institute for Neuroscience and Human Behavior (Pediatrics. 2016 Oct 21. doi: 10.1542/peds.2016-0909).
“From 2005 through 2014 ... there was significant cumulative percent increase in total number of hospitalizations, hospital days, and hospital costs for all patients. Of the total hospitalizations, 18.3% (568,449) were associated with a psychiatric disorder, either primary or secondary,” they noted.
Meanwhile, hospitalizations for psychiatric-only diagnoses were minimal, just 3.6% of the total with the most common problems again being depression, anxiety, and suicide and self-injury. “Hospital resource use for only psychiatric disorders declined, consistent with the national shift to managed care for behavioral health services,” the investigators said.
“Collectively, these data will further guide strategic planning by children’s hospitals as they strive to integrate mental health care into their health care systems. Together, these findings … underscore the need for quality improvement interventions that target improving linkage with community mental health care after pediatric hospitalization,” they said.
The National Institutes of Health funded the study. Dr. Zima was supported by the National Institute of Mental Health and Behavioral Health Centers of Excellence for California. Dr. Naomi S. Bardach and Dr. Tumaini R. Coker were supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Jay G. Berry was supported by the Agency for Healthcare Research and Quality. The authors had no conflicts of interest.
FROM PEDIATRICS
Key clinical point:
Major finding: For pediatric hospitalizations without a psychiatric diagnosis, costs rose during the past decade from $3,696 to $4,150 per day. For medical stays with a psychiatric diagnosis, the price rose from $2,694 to $3,393 per day.
Data source: Review of 3,114,099 hospitalizations at 33 children’s hospitals in the United States during 2005-2014
Disclosures: The National Institutes of Health funded the study. Dr. Zima was supported by the National Institute of Mental Health and Behavioral Health Centers of Excellence for California. Dr. Naomi S. Bardach and Dr. Tumaini R. Coker were supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development. Dr. Jay G. Berry was supported by the Agency for Healthcare Research and Quality. The authors had no conflicts of interest.