User login
Hospitalizations for opioid poisoning tripled in preschool children
From 1997 to 2012, the annual number of hospitalizations for opioid poisoning rose 178% among children aged 1-19 years, according to data from over 13,000 discharge records.
In 2012, there were 2,918 hospitalizations for opioid poisoning among children aged 1-19, compared with 1,049 in 1997, reported Julie R. Gaither, PhD, MPH, RN, and her associates at Yale University in New Haven, Conn. (JAMA Pediatr. 2016 Oct 31. doi: 10.1001/jamapediatrics.2016.2154).
The greatest change occurred among the youngest children, as the number of those aged 1-4 years rose from 133 in 1997 to 421 in 2012 – an increase of 217%. For those aged 15-19 years, the annual number of hospitalizations went from 715 to 2,171 (204%) over that time period, which included a slight drop from 2009 to 2012, according to the investigators, who used data from 13,052 discharges in the Agency for Healthcare Research and Quality’s Kids’ Inpatient Database.
The increase in hospitalizations for prescription opioid poisoning in children aged 10-14 years was 58% from 1997 to 2012 (rising from 171 to 272), while estimates for 5- to 9-year-olds did not meet the criteria for statistical reliability and were not included in the analysis, Dr. Gaither and her associates said.
The study was supported by grants from the National Institute on Drug Abuse. The investigators did not report any conflicts of interest.
From 1997 to 2012, the annual number of hospitalizations for opioid poisoning rose 178% among children aged 1-19 years, according to data from over 13,000 discharge records.
In 2012, there were 2,918 hospitalizations for opioid poisoning among children aged 1-19, compared with 1,049 in 1997, reported Julie R. Gaither, PhD, MPH, RN, and her associates at Yale University in New Haven, Conn. (JAMA Pediatr. 2016 Oct 31. doi: 10.1001/jamapediatrics.2016.2154).
The greatest change occurred among the youngest children, as the number of those aged 1-4 years rose from 133 in 1997 to 421 in 2012 – an increase of 217%. For those aged 15-19 years, the annual number of hospitalizations went from 715 to 2,171 (204%) over that time period, which included a slight drop from 2009 to 2012, according to the investigators, who used data from 13,052 discharges in the Agency for Healthcare Research and Quality’s Kids’ Inpatient Database.
The increase in hospitalizations for prescription opioid poisoning in children aged 10-14 years was 58% from 1997 to 2012 (rising from 171 to 272), while estimates for 5- to 9-year-olds did not meet the criteria for statistical reliability and were not included in the analysis, Dr. Gaither and her associates said.
The study was supported by grants from the National Institute on Drug Abuse. The investigators did not report any conflicts of interest.
From 1997 to 2012, the annual number of hospitalizations for opioid poisoning rose 178% among children aged 1-19 years, according to data from over 13,000 discharge records.
In 2012, there were 2,918 hospitalizations for opioid poisoning among children aged 1-19, compared with 1,049 in 1997, reported Julie R. Gaither, PhD, MPH, RN, and her associates at Yale University in New Haven, Conn. (JAMA Pediatr. 2016 Oct 31. doi: 10.1001/jamapediatrics.2016.2154).
The greatest change occurred among the youngest children, as the number of those aged 1-4 years rose from 133 in 1997 to 421 in 2012 – an increase of 217%. For those aged 15-19 years, the annual number of hospitalizations went from 715 to 2,171 (204%) over that time period, which included a slight drop from 2009 to 2012, according to the investigators, who used data from 13,052 discharges in the Agency for Healthcare Research and Quality’s Kids’ Inpatient Database.
The increase in hospitalizations for prescription opioid poisoning in children aged 10-14 years was 58% from 1997 to 2012 (rising from 171 to 272), while estimates for 5- to 9-year-olds did not meet the criteria for statistical reliability and were not included in the analysis, Dr. Gaither and her associates said.
The study was supported by grants from the National Institute on Drug Abuse. The investigators did not report any conflicts of interest.
FROM JAMA PEDIATRICS
From 1997 to 2012, the annual number of hospitalizations for opioid poisoning rose 178% among children aged 1-19 years, according to data from over 13,000 discharge records.
Two cases of asymmetric papules
CASE 1 ›
A 3-year-old boy was brought to our emergency department for evaluation of skin lesions that he’d had for 7 days. The boy would sometimes scratch the lesions, which began on his right flank as erythematous micropapules and later spread to his right lateral thigh and inner arm (FIGURE 1). His lymph nodes were not palpable.
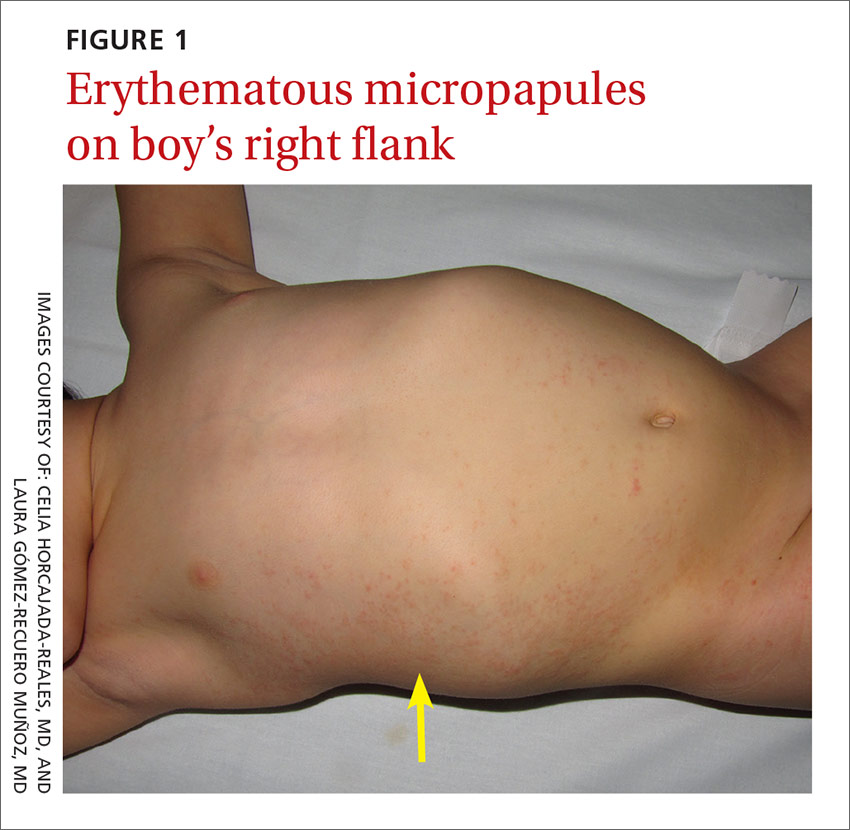
The boy’s parents had been told to use a topical corticosteroid, but the rash did not improve. His family denied fever or other previous infectious or systemic symptoms, and said that he hadn’t come into contact with any irritants or allergenic substances.
CASE 2 ›
A 13-year-old girl came to our emergency department with a pruriginous rash on her right leg and abdomen that she’d had for 4 days (FIGURE 2). The millimetric papules had also spread to the right side of her trunk, her right arm and armpit, and her inner thigh. Before the rash, she’d had a fever, otalgia, and conjunctivitis. We noted redness of her left conjunctiva, eardrum, and pharynx. The girl’s lymph nodes were not palpable. Serologic examinations for Epstein-Barr virus, cytomegalovirus, rubella, parvovirus B19, and Mycoplasma were negative.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Dx: Asymmetric periflexural exanthem of childhood
Both of these patients were given a diagnosis of asymmetric periflexural exanthem of childhood (APEC), based on the appearance and distribution of the rashes.
A rare condition that mostly affects young children
APEC is a rash of unknown cause, although epidemiologic and clinical findings support a viral etiology. Cases of this rash were first reported in 1992 by Bodemer et al, and a year later, Taïeb et al reported new cases, establishing the term “asymmetric periflexural exanthem.”1,2 Several viruses have been related to APEC (including adenovirus, parvovirus B19, parainfluenza 2 and 3, and human herpesvirus 7), but none of these has been consistently associated with the rash.3-5
APEC tends to affect children between one and 5 years of age, but adult cases have been reported.6,7 The condition occurs slightly more frequently among females and more often in winter and spring.8,9 APEC is a rare condition; since 1992, there have only been about 300 cases reported in the literature.10
What you’ll see. The erythematous rash appears as an asymmetrical or unilateral papular, scarlatiniform, or eczematous exanthema. It initially affects the axilla or groin and may then progress to the extremities and trunk. Minor lesions infrequently present on the contralateral side. Most children who are affected by APEC are otherwise healthy and asymptomatic at presentation. The exanthem is occasionally pruritic and can be preceded by short respiratory or gastrointestinal prodromes or a low-grade fever.2,9 If the rash predominantly affects the lateral thoracic wall, it may be referred to as unilateral laterothoracic exanthem.11 Regional lymphadenopathies can often be found, and there is no systemic involvement.
The distribution of the rash helps to distinguish the condition
The differential diagnosis for this type of exanthem includes drug eruptions, pityriasis rosea, miliaria, scarlet fever, papular acrodermatitis of childhood, and other viral rashes. The asymmetric distribution of APEC helps to distinguish the condition. Other possible asymmetric skin lesions, such as contact dermatitis, tinea corporis, or lichen striatus, can be differentiated by the characteristics of the cutaneous lesions. Contact dermatitis lesions are more vesicular, pruritic, and related to the contact area. Tinea corporis lesions tend to be smaller, circular, well-limited, and often have pustules. Lichen striatus starts as small pink-, red-, or flesh-colored spots that join together to form a dull red and slightly scaly linear band over the course of one or 2 weeks.12 Because APEC is self-limiting, a skin biopsy is usually not necessary.13
Lesions usually persist for one to 6 weeks and resolve with no sequelae. Only symptomatic treatment is required.9 Topical emollients, topical corticosteroids, or oral antihistamines can be used, if necessary.
Our patients. Both patients were treated with oral antihistamines and the rashes completely resolved within 2 to 3 weeks.
CORRESPONDENCE
Celia Horcajada-Reales, MD, Hospital Gregorio Marañón, Calle del Dr. Esquerdo, 46, 28007 Madrid, Spain; celiahr@hotmail.com.
1. Bodemer C, de Prost Y. Unilateral laterothoracic exanthem in children: a new disease? J Am Acad Dermatol. 1992;27:693-696.
2. Taïeb A, Mégraud F, Legrain V, et al. Asymmetric periflexural exanthem of childhood. J Am Acad Dermatol. 1993;29:391-393.
3. Al Yousef Ali A, Farhi D, De Maricourt S, et al. Asymmetric periflexural exanthema associated with HHV7 infection. Eur J Dermatol. 2010;20:230-231.
4. Coustou D, Masquelier B, Lafon ME, et al. Asymmetric periflexural exanthem of childhood: microbiologic case-control study. Pediatr Dermatol. 2000;17:169-173.
5. Harangi F, Várszegi D, Szücs G. Asymmetric periflexural exanthem of childhood and viral examinations. Pediatr Dermatol. 1995;12:112-115.
6. Zawar VP. Asymmetric periflexural exanthema: a report in an adult patient. Indian J Dermatol Venereol Leprol. 2003;69:401-404.
7. Pauluzzi P, Festini G, Gelmetti C. Asymmetric periflexural exanthem of childhood in an adult patient with parvovirus B19. J Eur Acad Dermatol Venereol. 2001;15:372-374.
8. McCuaig CC, Russo P, Powell J, et al. Unilateral laterothoracic exanthem. A clinicopathologic study of forty-eight patients. J Am Acad Dermatol. 1996;34:979-984.
9. Coustou D, Léauté-Labrèze C, Bioulac-Sage P, et al. Asymmetric periflexural exanthem of childhood: a clinical, pathologic, and epidemiologic prospective study. Arch Dermatol. 1999;135:799-803.
10. Mejía-Rodríguez SA, Ramírez-Romero VS, Valencia-Herrera A, et al. Unilateral laterothoracic exanthema of childhood. An infrequently diagnosed disease entity. Bol Med Hosp Infant Mex. 2007;64:65-68.
11. Chuh AA, Chan HH. Unilateral mediothoracic exanthem: a variant of unilateral laterothoracic exanthem. Cutis. 2006;77:29-32.
12. Chuh A, Zawar V, Law M, et al. Gianotti-Crosti syndrome, pityriasis rosea, asymmetrical periflexural exanthem, unilateral mediothoracic exanthem, eruptive pseudoangiomatosis, and papular-purpuric gloves and socks syndrome: a brief review and arguments for diagnostic criteria. Infect Dis Rep. 2012;4:e12.
13. Gelmetti C, Caputo R. Asymmetric periflexural exanthem of childhood: who are you? J Eur Acad Dermatol Venereol. 2001;15:293-294.
CASE 1 ›
A 3-year-old boy was brought to our emergency department for evaluation of skin lesions that he’d had for 7 days. The boy would sometimes scratch the lesions, which began on his right flank as erythematous micropapules and later spread to his right lateral thigh and inner arm (FIGURE 1). His lymph nodes were not palpable.
The boy’s parents had been told to use a topical corticosteroid, but the rash did not improve. His family denied fever or other previous infectious or systemic symptoms, and said that he hadn’t come into contact with any irritants or allergenic substances.
CASE 2 ›
A 13-year-old girl came to our emergency department with a pruriginous rash on her right leg and abdomen that she’d had for 4 days (FIGURE 2). The millimetric papules had also spread to the right side of her trunk, her right arm and armpit, and her inner thigh. Before the rash, she’d had a fever, otalgia, and conjunctivitis. We noted redness of her left conjunctiva, eardrum, and pharynx. The girl’s lymph nodes were not palpable. Serologic examinations for Epstein-Barr virus, cytomegalovirus, rubella, parvovirus B19, and Mycoplasma were negative.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Dx: Asymmetric periflexural exanthem of childhood
Both of these patients were given a diagnosis of asymmetric periflexural exanthem of childhood (APEC), based on the appearance and distribution of the rashes.
A rare condition that mostly affects young children
APEC is a rash of unknown cause, although epidemiologic and clinical findings support a viral etiology. Cases of this rash were first reported in 1992 by Bodemer et al, and a year later, Taïeb et al reported new cases, establishing the term “asymmetric periflexural exanthem.”1,2 Several viruses have been related to APEC (including adenovirus, parvovirus B19, parainfluenza 2 and 3, and human herpesvirus 7), but none of these has been consistently associated with the rash.3-5
APEC tends to affect children between one and 5 years of age, but adult cases have been reported.6,7 The condition occurs slightly more frequently among females and more often in winter and spring.8,9 APEC is a rare condition; since 1992, there have only been about 300 cases reported in the literature.10
What you’ll see. The erythematous rash appears as an asymmetrical or unilateral papular, scarlatiniform, or eczematous exanthema. It initially affects the axilla or groin and may then progress to the extremities and trunk. Minor lesions infrequently present on the contralateral side. Most children who are affected by APEC are otherwise healthy and asymptomatic at presentation. The exanthem is occasionally pruritic and can be preceded by short respiratory or gastrointestinal prodromes or a low-grade fever.2,9 If the rash predominantly affects the lateral thoracic wall, it may be referred to as unilateral laterothoracic exanthem.11 Regional lymphadenopathies can often be found, and there is no systemic involvement.
The distribution of the rash helps to distinguish the condition
The differential diagnosis for this type of exanthem includes drug eruptions, pityriasis rosea, miliaria, scarlet fever, papular acrodermatitis of childhood, and other viral rashes. The asymmetric distribution of APEC helps to distinguish the condition. Other possible asymmetric skin lesions, such as contact dermatitis, tinea corporis, or lichen striatus, can be differentiated by the characteristics of the cutaneous lesions. Contact dermatitis lesions are more vesicular, pruritic, and related to the contact area. Tinea corporis lesions tend to be smaller, circular, well-limited, and often have pustules. Lichen striatus starts as small pink-, red-, or flesh-colored spots that join together to form a dull red and slightly scaly linear band over the course of one or 2 weeks.12 Because APEC is self-limiting, a skin biopsy is usually not necessary.13
Lesions usually persist for one to 6 weeks and resolve with no sequelae. Only symptomatic treatment is required.9 Topical emollients, topical corticosteroids, or oral antihistamines can be used, if necessary.
Our patients. Both patients were treated with oral antihistamines and the rashes completely resolved within 2 to 3 weeks.
CORRESPONDENCE
Celia Horcajada-Reales, MD, Hospital Gregorio Marañón, Calle del Dr. Esquerdo, 46, 28007 Madrid, Spain; celiahr@hotmail.com.
CASE 1 ›
A 3-year-old boy was brought to our emergency department for evaluation of skin lesions that he’d had for 7 days. The boy would sometimes scratch the lesions, which began on his right flank as erythematous micropapules and later spread to his right lateral thigh and inner arm (FIGURE 1). His lymph nodes were not palpable.
The boy’s parents had been told to use a topical corticosteroid, but the rash did not improve. His family denied fever or other previous infectious or systemic symptoms, and said that he hadn’t come into contact with any irritants or allergenic substances.
CASE 2 ›
A 13-year-old girl came to our emergency department with a pruriginous rash on her right leg and abdomen that she’d had for 4 days (FIGURE 2). The millimetric papules had also spread to the right side of her trunk, her right arm and armpit, and her inner thigh. Before the rash, she’d had a fever, otalgia, and conjunctivitis. We noted redness of her left conjunctiva, eardrum, and pharynx. The girl’s lymph nodes were not palpable. Serologic examinations for Epstein-Barr virus, cytomegalovirus, rubella, parvovirus B19, and Mycoplasma were negative.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Dx: Asymmetric periflexural exanthem of childhood
Both of these patients were given a diagnosis of asymmetric periflexural exanthem of childhood (APEC), based on the appearance and distribution of the rashes.
A rare condition that mostly affects young children
APEC is a rash of unknown cause, although epidemiologic and clinical findings support a viral etiology. Cases of this rash were first reported in 1992 by Bodemer et al, and a year later, Taïeb et al reported new cases, establishing the term “asymmetric periflexural exanthem.”1,2 Several viruses have been related to APEC (including adenovirus, parvovirus B19, parainfluenza 2 and 3, and human herpesvirus 7), but none of these has been consistently associated with the rash.3-5
APEC tends to affect children between one and 5 years of age, but adult cases have been reported.6,7 The condition occurs slightly more frequently among females and more often in winter and spring.8,9 APEC is a rare condition; since 1992, there have only been about 300 cases reported in the literature.10
What you’ll see. The erythematous rash appears as an asymmetrical or unilateral papular, scarlatiniform, or eczematous exanthema. It initially affects the axilla or groin and may then progress to the extremities and trunk. Minor lesions infrequently present on the contralateral side. Most children who are affected by APEC are otherwise healthy and asymptomatic at presentation. The exanthem is occasionally pruritic and can be preceded by short respiratory or gastrointestinal prodromes or a low-grade fever.2,9 If the rash predominantly affects the lateral thoracic wall, it may be referred to as unilateral laterothoracic exanthem.11 Regional lymphadenopathies can often be found, and there is no systemic involvement.
The distribution of the rash helps to distinguish the condition
The differential diagnosis for this type of exanthem includes drug eruptions, pityriasis rosea, miliaria, scarlet fever, papular acrodermatitis of childhood, and other viral rashes. The asymmetric distribution of APEC helps to distinguish the condition. Other possible asymmetric skin lesions, such as contact dermatitis, tinea corporis, or lichen striatus, can be differentiated by the characteristics of the cutaneous lesions. Contact dermatitis lesions are more vesicular, pruritic, and related to the contact area. Tinea corporis lesions tend to be smaller, circular, well-limited, and often have pustules. Lichen striatus starts as small pink-, red-, or flesh-colored spots that join together to form a dull red and slightly scaly linear band over the course of one or 2 weeks.12 Because APEC is self-limiting, a skin biopsy is usually not necessary.13
Lesions usually persist for one to 6 weeks and resolve with no sequelae. Only symptomatic treatment is required.9 Topical emollients, topical corticosteroids, or oral antihistamines can be used, if necessary.
Our patients. Both patients were treated with oral antihistamines and the rashes completely resolved within 2 to 3 weeks.
CORRESPONDENCE
Celia Horcajada-Reales, MD, Hospital Gregorio Marañón, Calle del Dr. Esquerdo, 46, 28007 Madrid, Spain; celiahr@hotmail.com.
1. Bodemer C, de Prost Y. Unilateral laterothoracic exanthem in children: a new disease? J Am Acad Dermatol. 1992;27:693-696.
2. Taïeb A, Mégraud F, Legrain V, et al. Asymmetric periflexural exanthem of childhood. J Am Acad Dermatol. 1993;29:391-393.
3. Al Yousef Ali A, Farhi D, De Maricourt S, et al. Asymmetric periflexural exanthema associated with HHV7 infection. Eur J Dermatol. 2010;20:230-231.
4. Coustou D, Masquelier B, Lafon ME, et al. Asymmetric periflexural exanthem of childhood: microbiologic case-control study. Pediatr Dermatol. 2000;17:169-173.
5. Harangi F, Várszegi D, Szücs G. Asymmetric periflexural exanthem of childhood and viral examinations. Pediatr Dermatol. 1995;12:112-115.
6. Zawar VP. Asymmetric periflexural exanthema: a report in an adult patient. Indian J Dermatol Venereol Leprol. 2003;69:401-404.
7. Pauluzzi P, Festini G, Gelmetti C. Asymmetric periflexural exanthem of childhood in an adult patient with parvovirus B19. J Eur Acad Dermatol Venereol. 2001;15:372-374.
8. McCuaig CC, Russo P, Powell J, et al. Unilateral laterothoracic exanthem. A clinicopathologic study of forty-eight patients. J Am Acad Dermatol. 1996;34:979-984.
9. Coustou D, Léauté-Labrèze C, Bioulac-Sage P, et al. Asymmetric periflexural exanthem of childhood: a clinical, pathologic, and epidemiologic prospective study. Arch Dermatol. 1999;135:799-803.
10. Mejía-Rodríguez SA, Ramírez-Romero VS, Valencia-Herrera A, et al. Unilateral laterothoracic exanthema of childhood. An infrequently diagnosed disease entity. Bol Med Hosp Infant Mex. 2007;64:65-68.
11. Chuh AA, Chan HH. Unilateral mediothoracic exanthem: a variant of unilateral laterothoracic exanthem. Cutis. 2006;77:29-32.
12. Chuh A, Zawar V, Law M, et al. Gianotti-Crosti syndrome, pityriasis rosea, asymmetrical periflexural exanthem, unilateral mediothoracic exanthem, eruptive pseudoangiomatosis, and papular-purpuric gloves and socks syndrome: a brief review and arguments for diagnostic criteria. Infect Dis Rep. 2012;4:e12.
13. Gelmetti C, Caputo R. Asymmetric periflexural exanthem of childhood: who are you? J Eur Acad Dermatol Venereol. 2001;15:293-294.
1. Bodemer C, de Prost Y. Unilateral laterothoracic exanthem in children: a new disease? J Am Acad Dermatol. 1992;27:693-696.
2. Taïeb A, Mégraud F, Legrain V, et al. Asymmetric periflexural exanthem of childhood. J Am Acad Dermatol. 1993;29:391-393.
3. Al Yousef Ali A, Farhi D, De Maricourt S, et al. Asymmetric periflexural exanthema associated with HHV7 infection. Eur J Dermatol. 2010;20:230-231.
4. Coustou D, Masquelier B, Lafon ME, et al. Asymmetric periflexural exanthem of childhood: microbiologic case-control study. Pediatr Dermatol. 2000;17:169-173.
5. Harangi F, Várszegi D, Szücs G. Asymmetric periflexural exanthem of childhood and viral examinations. Pediatr Dermatol. 1995;12:112-115.
6. Zawar VP. Asymmetric periflexural exanthema: a report in an adult patient. Indian J Dermatol Venereol Leprol. 2003;69:401-404.
7. Pauluzzi P, Festini G, Gelmetti C. Asymmetric periflexural exanthem of childhood in an adult patient with parvovirus B19. J Eur Acad Dermatol Venereol. 2001;15:372-374.
8. McCuaig CC, Russo P, Powell J, et al. Unilateral laterothoracic exanthem. A clinicopathologic study of forty-eight patients. J Am Acad Dermatol. 1996;34:979-984.
9. Coustou D, Léauté-Labrèze C, Bioulac-Sage P, et al. Asymmetric periflexural exanthem of childhood: a clinical, pathologic, and epidemiologic prospective study. Arch Dermatol. 1999;135:799-803.
10. Mejía-Rodríguez SA, Ramírez-Romero VS, Valencia-Herrera A, et al. Unilateral laterothoracic exanthema of childhood. An infrequently diagnosed disease entity. Bol Med Hosp Infant Mex. 2007;64:65-68.
11. Chuh AA, Chan HH. Unilateral mediothoracic exanthem: a variant of unilateral laterothoracic exanthem. Cutis. 2006;77:29-32.
12. Chuh A, Zawar V, Law M, et al. Gianotti-Crosti syndrome, pityriasis rosea, asymmetrical periflexural exanthem, unilateral mediothoracic exanthem, eruptive pseudoangiomatosis, and papular-purpuric gloves and socks syndrome: a brief review and arguments for diagnostic criteria. Infect Dis Rep. 2012;4:e12.
13. Gelmetti C, Caputo R. Asymmetric periflexural exanthem of childhood: who are you? J Eur Acad Dermatol Venereol. 2001;15:293-294.

When can infants and children benefit from probiotics?
PRACTICE RECOMMENDATIONS
› Recommend a trial of Lactobacillus reuteri for breastfed infants with colic. A
› Consider Lactobacillus and Bifidobacterium species for the prevention of upper respiratory infections (URIs) and to shorten the course of URI illness. B
› Do not recommend probiotics for the prevention of respiratory or gastrointestinal allergies. A
› Consider probiotics for the reduction of abdominal pain in pediatric irritable bowel syndrome, as well as to reduce diarrhea associated with antibiotic use and acute gastroenteritis. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Ms. B, a 26-year-old woman, presents to your office with her 3-year-old son for a well-child examination. During the course of the conversation, she asks you if she should be giving her child probiotics to improve his general health. Many of her friends, who also have their children in day care, have told her that probiotics, “are nature’s way of fighting infection.” Her son currently takes no medications, and has no history of asthma or recent gastrointestinal disturbances. He was treated for 2 ear infections last winter, approximately 3 months apart. His physical exam is normal and, after today, his immunizations will be up to date. How should you respond?
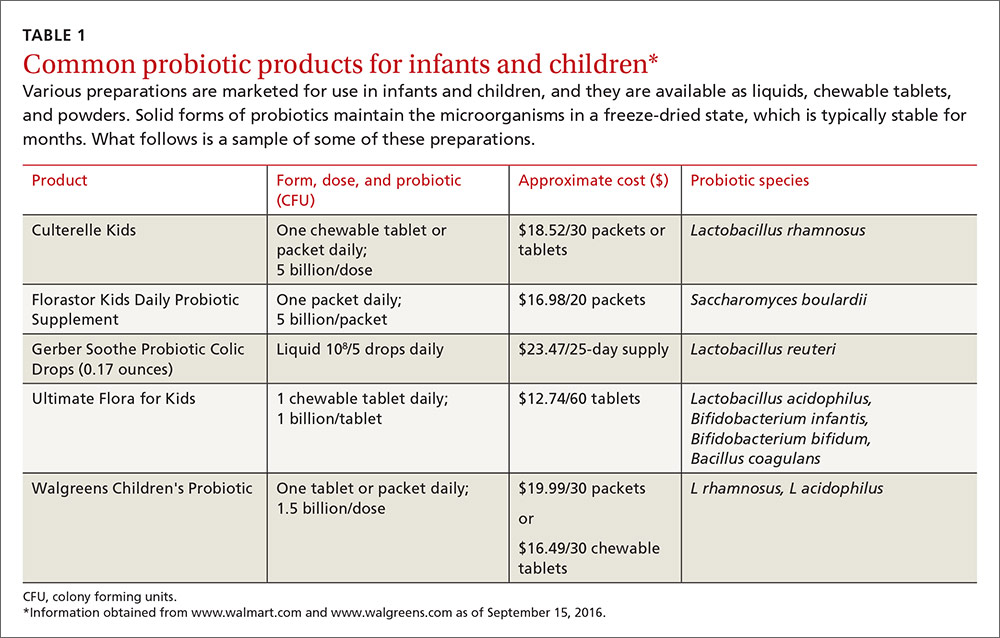
The use of probiotics as over-the-counter treatments for a variety of conditions continues to grow, with retail sales of functional probiotic foods and supplements topping $35 billion worldwide in 2014.1 In children, claims of benefit for gastrointestinal (GI) disorders, colic, and allergy prevention, as well as prevention and treatment of upper respiratory infections (URIs) have existed for over 10 years.2-4 The human gut flora develops rapidly after birth and is known to be influenced by route of delivery (vaginal vs cesarean), type of feeding (breast vs formula), and other environmental factors.5 The use of probiotics to influence the types of bacteria in a child’s intestinal tract continues to be an area of active research. (For more on probiotic formulations, see TABLE 1.)
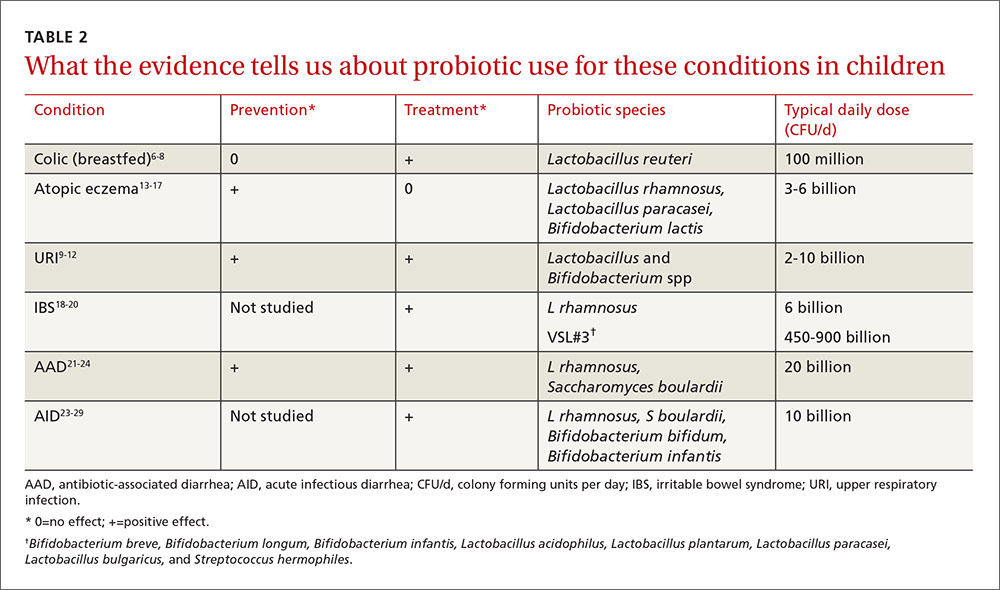
This article summarizes recent research on probiotic use in infants and children. New data support the use of probiotics for the treatment of colic and atopic eczema; however, the data on using probiotics in the management of URIs is less robust and mixed. And while probiotics improve irritable bowel syndrome (IBS) stomach pain, they do not help with related diarrhea or constipation. All of these data are summarized in TABLE 2.6-29
L reuteri improves symptoms in breastfed infants with colic
Infant colic is a relatively common condition known to negatively impact maternal mental health and the mother/child relationship.6 Numerous randomized controlled trials (RCTs) over the years have demonstrated mixed results with using probiotics to decrease crying times, with differences noted between infants who are solely breastfed and those who are not.7
In the most recent meta-analysis of 6 studies (n=427) that focused only on the probiotic Lactobacillus reuteri, breastfed infants with colic receiving a daily dose of 108 colony forming units (CFU) cried an average of 56 fewer minutes/day than those in the control group (95% confidence interval [CI], -64.4 to -47.3; P=.001) at day 21 of treatment.8 Although 2 studies in this meta-analysis included a small number of mixed-fed and formula-fed infants, the majority of trials do not show benefit for these infants. Trials assessing the use of L reuteri for prevention of colic have not shown positive results.7
Probiotics may help p
The mechanisms by which probiotics may prevent or shorten the course of URIs are not obvious. Current theories include boosting the immune function of the respiratory mucosa, acting as a competitive inhibitor for viruses, and secreting antiviral compounds.9 Multiple reviews published in the last 3 years, however, add to the evidence that the apparent benefit is real.
A 2013 meta-analysis assessed data from 4 RCTs (N=1805), which used Lactobacillus rhamnosus as the sole probiotic for prevention of URIs. In treated children, otitis media incidence was reduced by 24% (relative risk [RR] 0.76; 95% CI, 0.64-0.91) and risk of URI was reduced by 38% (RR 0.62; 95% CI, 0.50-0.78).10 The number needed to treat (NNT) was 4 for URI prevention, and the authors noted that adverse events were similar in the treatment and control groups.
A 2014 systematic review and meta-analysis of 20 RCTs examining duration of illness included 10 studies dedicated to pediatric subjects (age 12 months to 12 years).11 There were significantly fewer days of illness per person (standardized mean difference -0.31; 95% CI, -0.41 to -0.11) and each illness episode was shorter by three-quarters of a day (weighted mean difference -0.77; 95% CI, -1.5 to -0.04) in participants who received a probiotic vs those who received a placebo. Probiotics used in these studies belonged to the Lactobacillus and Bifidobacterium genera.
A 2015 systematic review of 14 RCTs assessing the benefits of probiotics, particularly Lactobacillus and Bifidobacterium strains, on URI occurrence and symptoms, showed mixed results.12 Seven of 12 studies found lowered rates of URI and otitis media incidence, 7 of 11 RCTs reported a significant reduction in severity scores for URI, and 4 of 8 RCTs reported significant reductions in school absenteeism between the probiotic and control groups. In a summary statement, the authors noted that “at least one beneficial effect of prophylactic probiotics was observed in the majority of RCTs,” and that “none of the studies reported any serious adverse events.”
Perinatal probiotics: No benefit for allergic conditions—except eczema
Allergic disease is on the rise and continues to plague children with reduced quality of life, potentially life-threatening reactions, and missed activities, including school. The gut microbiome likely influences a child’s allergic propensity through its effects on T-helper cells, transforming growth factor (TGF), and immunoglobulin A (IgA)—all known components of the allergic response. As the hygiene hypothesis suggests, the quantity and types of bacteria that inhabit the GI tract early in life play a significant role in determining a person’s later allergic responses.13
In a 2013 meta-analysis of 20 trials (N=4866), researchers looked specifically at probiotic use and the diagnosis of asthma and incident wheezing. Single and combination products of Lactobacillus and Bifidobacterium given prenatally and/or postnatally were included in the studies. The authors found no evidence to support a protective association between perinatal use of probiotics and diagnosed asthma (RR=0.99; 95% CI, 0.81-0.21) or childhood incident wheezing (RR=0.97; 95% CI, 0.87-1.09; 9 trials, 1949 infants).14
In a more recent meta-analysis (2015) conducted to inform the World Allergy Organization, 29 studies were evaluated to assess the impact of probiotics on allergic symptoms of the skin, respiratory system, and GI tract.15 No significant benefit was noted for any allergic condition except for eczema. Probiotics reduced the risk of eczema when given during the last trimester of pregnancy (RR=0.71; 95% CI, 0.60-0.84), when used by breastfeeding mothers (RR=0.57; 95% CI, 0.47-0.69), and when given to infants (RR=0.80; 95% CI, 0.68-0.94).
A 2014 systematic review and meta-analysis (N=2797) explored probiotic use specifically for the prevention of eczema.16 The pooled relative risk for all the studies was 0.74 (95% CI, 0.67-0.82). Evidence was strongest for probiotics containing the Lactobacillus species rhamnosus and paracasei, as well as for Bifidobacterium lactis. No benefit was noted with Lactobacillus acidophilus or other Bifidobacterium species. These newer reviews on eczema prevention contrast with an older Cochrane review published in 2008 (12 RCTs, N=781), which did not show significant benefit for the treatment of eczema.17
Probiotics improve IBS stomach pain, but not diarrhea or constipation
IBS is a functional disorder of the GI tract that affects up to 20% of children and teenagers and leads to a significant decrease in quality of life.18 Current theories of causation include bacterial overgrowth and neuronal hyperactivity, which may be amenable to change with supplemental probiotics.
A 2015 systematic review of non-pharmacological treatments for functional abdominal pain disorders identified 4 studies dedicated to IBS in children.19 A subgroup analysis of 3 RCTs (n=309) that looked at giving L rhamnosus to 5- to 17-year-olds with IBS showed improved abdominal pain (according to various pain scales) compared to the placebo group. Study participants received at least 3 x 109 CFU twice a day for 4 to 8 weeks. Relative risk for improvement was 1.7 (95% CI, 1.27-2.27) with an NNT of 4. None of these studies showed significant improvement in either frequency or severity of diarrhea or constipation.
A separate crossover RCT (N=59) compared placebo to VSL#3, a product containing 8 probiotics (Bifidobacterium breve, Bifidobacterium longum, Bifidobacterium infantis, L acidophilus, Lactobacillus plantarum, L paracasei, Lactobacillus bulgaricus, and Streptococcus hermophiles), given in age-dependent doses for 6 weeks to children aged 4 to 18 years.20 The frequency and intensity of abdominal pain were measured on a 5-point Likert scale. The group treated with VSL#3 dropped 1.0 ± 0.2 points vs 0.5 ± 0.2 points in the control group (P<.05) and reported an improved quality of life.
These agents reduce antibiotic-associated diarrhea
Antibiotic-associated diarrhea (AAD) occurs in 5% to 30% of children who receive antibiotic therapy.21 It occurs most frequently with the use of cephalosporins, penicillin, fluoroquinolones, and clindamycin, and is likely caused by an alteration of the normal gut flora. Colitis caused by Clostridium difficile remains the most serious antibiotic-associated GI complication.
A systematic review of the specific probiotic Saccharomyces boulardii conducted in 2015 analyzed data from 6 RCTs (n=1653) to determine the effect of co-administration of this probiotic with antibiotics.22 The pooled relative risk for AAD in children receiving the probiotic was 0.43 (95% CI, 0.3-0.6) compared to antibiotics alone. The absolute risk of AAD dropped from 20.9% to 8.8%, translating to a NNT of 8. Two of the RCTs specifically looked at rates of C difficile infection (n=579). C difficile infection rates dropped by 75% (RR=.25; 95% CI, 0.08-0.73) in the treatment group. This dramatic treatment effect was not seen in studies involving adults.
A similar systematic review focusing on L rhamnosus conducted in 2015 pooled data from 5 RCTs (n=445) to see if the probiotic would decrease AAD in children if it was co-administered with antibiotics.23 The relative risk for AAD in this treatment group was 0.48 (95% CI, 0.26-0.89) with an absolute risk reduction of 13.4% (23% compared to 9.6%), translating to an NNT of 7.
A Cochrane review published in 2015 included 23 studies (N=3938) and found similar results with an RR for AAD of 0.46 for treated children (95% CI, 0.35-0.61).24 Doses of probiotics ranged from 5 to 40 billion CFU/day. Although many probiotic species were used in these studies, S boulardii and L rhamnosus were cited as having the strongest data to support use in this context.
Probiotics reduce the duration, frequency of acute infectious diarrhea
Diarrhea remains the second leading cause of death among children one to 59 months of age worldwide.25 Current World Health Organization recommendations include oral rehydration salts, continued feeding to avoid dehydration, and zinc to decrease the duration and severity of illness.26 Multiple studies in adults confirm that a variety of probiotics decrease both the duration and severity of diarrhea in acute gastroenteritis.27
The authors of a 2013 systematic review of probiotics for the treatment of community-acquired acute diarrhea in children less than 5 years of age analyzed data from 8 RCTs (N=1755).28 Various probiotics were used including Lactobacillus species, Streptococcus thermophilus, Bifidobacterium species, and Saccharomyces boulardii for between 4 and 10 days. Six of these studies (n=1164) measured diarrhea duration and found a 14% reduction (95% CI, 3.8%-24.2%) in days of illness for those children treated vs those receiving placebo. Five studies (n=925) measured the difference in stool frequency on Day 2 of illness and reported a reduction of 13.1% (95% CI, 0.8%-5.3%) in the number of stools in the treated group vs the placebo group.
This review augments a Cochrane meta-analysis of 63 studies (N=8014) published in 2010.27 Fifty-six of these studies included infants and children. Pooled analysis of the varied probiotic treatments showed a mean reduction in duration of diarrhea of just over a day (24.76 hours; 95% CI, 15.9-33.6 hours; n=4555, trials=35) and decreased stool frequency on Day 2 of treatment (mean difference 0.80; 95% CI, 0.45-1.14; n=2751, trials=20). The authors concluded that probiotics “have clear beneficial effects in shortening the duration and reducing stool frequency in acute infectious diarrhea.”
Pediatric society weighs in. In 2014, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition issued guidelines regarding probiotic use for the treatment of acute gastroenteritis.29 In addition to rehydration therapy, these guidelines recommend the use of L rhamnosus and/or S boulardii as first-line treatments. Lower quality evidence is available for the use of L reuteri.
CASE › In response to Ms. B’s query about starting her young son on probiotics, you tell her that studies have shown that probiotics are safe for children when given in appropriate doses. They have been shown to help children recover from diarrheal illnesses and can help reduce the number of colds and ear infections when taken regularly. The reason you are giving them determines which strains you should use. You recommend giving her child a formulation of probiotic that contains Lactobacillus or Bifidobacterium with a dose range of 2 to 10 billion CFUs taken daily to reduce the risk of her child getting another ear infection.
CORRESPONDENCE
Paul Dassow, MD, MSPH, 1100 E. 3rd St, Chattanooga, TN 37403; paul.dassow@erlanger.org.
1. Euromonitor International. Global and regional trends of the probiotics and omega fatty acids market. June 23, 2015. Available at: http://uschinahpa.org/wp-content/uploads/2015/07/EMI-US-China-HPA-Probiotic-and-Omega-2015-Final.pdf. Accessed September 9, 2016.
2. Du Toit G, Lack G. Can food allergy be prevented? The current evidence. Pediatr Clin North Am. 2011;58:481-509.
3. Gerritsen J, Smidt H, Rijkers GT, et al. Intestinal microbiota in human health and disease: the impact of probiotics. Genes Nutr. 2011;6:209-240.
4. Versalovic J. The human microbiome and probiotics: implications for pediatrics. Ann Nutr Metab. 2013;63:42-52.
5. Neish AS. Microbes in gastrointestinal health and disease. Gastroenterology. 2009;136:65-80.
6. Akman I, Kușçu K, Özdemir N, et al. Mothers’ postpartum psychological adjustment and infantile colic. Arch Dis Child. 2006;91:417-419.
7. Sung V, Collett S, de Gooyer T, et al. Probiotics to prevent or treat excessive infant crying systematic review and meta-analysis. JAMA Pediatr. 2013:167:1150-1157.
8. Harb T, Matsuyama M, David M, et al. Infant colic—what works: a systematic review of interventions for breastfed infants. J Pediatr Gastroenterol Nutr. 2016;62:668-686.
9. Hill C, Guarner F, Reid G, et al. Expert consensus document: the International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. 2014;11:506-514.
10. Liu S, Hu P, Du X, et al. Lactobacillus rhamnosus GG supplementation for preventing respiratory infections in children: a meta-analysis of randomized, placebo-controlled trials. Indian Pediatr. 2013;50:377-381.
11. King S, Glanville J, Sanders ME, et al. Effectiveness of probiotics on the duration of illness in healthy children and adults who develop common acute respiratory infectious conditions: a systematic review and meta-analysis. Br J Nutr. 2014;112:41-54.
12. Ozen M, Kocabas Sandal G, Dinleyici EC. Probiotics for the prevention of pediatric upper respiratory tract infections: a systematic review. Expert Opin Biol Ther. 2015;15:9-20.
13. Azad MB, Konya T, Maughan H, et al. Infant gut microbiota and the hygiene hypothesis of allergic disease: impact of household pets and siblings on microbiota composition and diversity. Allergy Asthma Clin Immunol. 2013;9:15.
14. Azad MB, Coneys JG, Kozyrskyj AL, et al. Probiotic supplementation during pregnancy or infancy for the prevention of asthma and wheeze: systematic review and meta-analysis. Brit Med J. 2013;347:f6471.
15. Cuello-Garcia CA, Bro˙zek JL, Fiocchi A, et al. Probiotics for the prevention of allergy: a systematic review and meta-analysis of randomized controlled trials. J Allergy Clin Immunol. 2015;136:952-961.
16. Mansfield JA, Bergin SW, Cooper JR, et al. Comparative probiotic strain efficacy in the prevention of eczema in infants and children: a systematic review and meta-analysis. Mil Med. 2014;179:580-592.
17. Boyle RJ, Bath-Hextall FJ, Leonardi-Bee J, et al. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;(4):CD006135.
18. Chiou E, Nurko S. Management of functional abdominal pain and irritable bowel syndrome in children and adolescents. Expert Rev Gastroenterol Hepatol. 2010;4:293-304.
19. Rutten JMTM, Korterink JL, Venmans LMAJ, et al. Nonpharmacologic treatment of functional abdominal pain disorders: a systematic review. Pediatrics. 2015;135:522-535.
20. Guandalini S, Magazzù G, Chiaro A, et al. VSL#3 improves symptoms in children with irritable bowel syndrome: a multicenter, randomized, placebo-controlled, double-blind, crossover study. J Pediatr Gastroenterol Nutr. 2010;51:24-30.
21. Turck D, Bernet JP, Marx J, et al. Incidence and risk factors of oral antibiotic associated diarrhea in an outpatient pediatric population. J Pediatr Gastroenterol Nutr. 2003;37:22-26.
22. Szajewska H, Kołodziej M. Systematic review with meta-analysis: Saccharomyces boulardii in the prevention of antibiotic-associated diarrhoea. Aliment Pharmacol Ther. 2015;42:793-801.
23. Szajewska H, Kołodziej M. Systematic review with meta-analysis: Lactobacillus rhamnosus GG in the prevention of antibiotic-associated diarrhoea in children and adults. Aliment Pharmacol Ther. 2015;42:1149-1157.
24. Goldenberg JZ, Lytvyn L, Steurich J, et al. Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Cochrane Database Syst Rev. 2015;12:CD004827.
25. Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151-2161.
26. WHO/UNICEF Joint Statement: Clinical Management of Acute Diarrhea. August 2004. Available at: http://www.unicef.org/publications/files/ENAcute_Diarrhoea_reprint.pdf. Accessed September 9, 2016.
27. Allen SJ, Martinez EG, Gregorio GV, et al. Probiotics for treating acute infectious diarrhea. Cochrane Database Syst Rev. 2010;(11):CD003048.
28. Applegate JA, Fischer Walker CL, Ambikapathi R, et al. Systematic review of probiotics for the treatment of community-acquired acute diarrhea in children. BMC Public Health. 2013;13:S16.
29. Guarino A, Ashkenazi S, Gendrel D, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J Pediatr Gastroenterol Nutr. 2014;59:132-152.
PRACTICE RECOMMENDATIONS
› Recommend a trial of Lactobacillus reuteri for breastfed infants with colic. A
› Consider Lactobacillus and Bifidobacterium species for the prevention of upper respiratory infections (URIs) and to shorten the course of URI illness. B
› Do not recommend probiotics for the prevention of respiratory or gastrointestinal allergies. A
› Consider probiotics for the reduction of abdominal pain in pediatric irritable bowel syndrome, as well as to reduce diarrhea associated with antibiotic use and acute gastroenteritis. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Ms. B, a 26-year-old woman, presents to your office with her 3-year-old son for a well-child examination. During the course of the conversation, she asks you if she should be giving her child probiotics to improve his general health. Many of her friends, who also have their children in day care, have told her that probiotics, “are nature’s way of fighting infection.” Her son currently takes no medications, and has no history of asthma or recent gastrointestinal disturbances. He was treated for 2 ear infections last winter, approximately 3 months apart. His physical exam is normal and, after today, his immunizations will be up to date. How should you respond?
The use of probiotics as over-the-counter treatments for a variety of conditions continues to grow, with retail sales of functional probiotic foods and supplements topping $35 billion worldwide in 2014.1 In children, claims of benefit for gastrointestinal (GI) disorders, colic, and allergy prevention, as well as prevention and treatment of upper respiratory infections (URIs) have existed for over 10 years.2-4 The human gut flora develops rapidly after birth and is known to be influenced by route of delivery (vaginal vs cesarean), type of feeding (breast vs formula), and other environmental factors.5 The use of probiotics to influence the types of bacteria in a child’s intestinal tract continues to be an area of active research. (For more on probiotic formulations, see TABLE 1.)
This article summarizes recent research on probiotic use in infants and children. New data support the use of probiotics for the treatment of colic and atopic eczema; however, the data on using probiotics in the management of URIs is less robust and mixed. And while probiotics improve irritable bowel syndrome (IBS) stomach pain, they do not help with related diarrhea or constipation. All of these data are summarized in TABLE 2.6-29
L reuteri improves symptoms in breastfed infants with colic
Infant colic is a relatively common condition known to negatively impact maternal mental health and the mother/child relationship.6 Numerous randomized controlled trials (RCTs) over the years have demonstrated mixed results with using probiotics to decrease crying times, with differences noted between infants who are solely breastfed and those who are not.7
In the most recent meta-analysis of 6 studies (n=427) that focused only on the probiotic Lactobacillus reuteri, breastfed infants with colic receiving a daily dose of 108 colony forming units (CFU) cried an average of 56 fewer minutes/day than those in the control group (95% confidence interval [CI], -64.4 to -47.3; P=.001) at day 21 of treatment.8 Although 2 studies in this meta-analysis included a small number of mixed-fed and formula-fed infants, the majority of trials do not show benefit for these infants. Trials assessing the use of L reuteri for prevention of colic have not shown positive results.7
Probiotics may help p
The mechanisms by which probiotics may prevent or shorten the course of URIs are not obvious. Current theories include boosting the immune function of the respiratory mucosa, acting as a competitive inhibitor for viruses, and secreting antiviral compounds.9 Multiple reviews published in the last 3 years, however, add to the evidence that the apparent benefit is real.
A 2013 meta-analysis assessed data from 4 RCTs (N=1805), which used Lactobacillus rhamnosus as the sole probiotic for prevention of URIs. In treated children, otitis media incidence was reduced by 24% (relative risk [RR] 0.76; 95% CI, 0.64-0.91) and risk of URI was reduced by 38% (RR 0.62; 95% CI, 0.50-0.78).10 The number needed to treat (NNT) was 4 for URI prevention, and the authors noted that adverse events were similar in the treatment and control groups.
A 2014 systematic review and meta-analysis of 20 RCTs examining duration of illness included 10 studies dedicated to pediatric subjects (age 12 months to 12 years).11 There were significantly fewer days of illness per person (standardized mean difference -0.31; 95% CI, -0.41 to -0.11) and each illness episode was shorter by three-quarters of a day (weighted mean difference -0.77; 95% CI, -1.5 to -0.04) in participants who received a probiotic vs those who received a placebo. Probiotics used in these studies belonged to the Lactobacillus and Bifidobacterium genera.
A 2015 systematic review of 14 RCTs assessing the benefits of probiotics, particularly Lactobacillus and Bifidobacterium strains, on URI occurrence and symptoms, showed mixed results.12 Seven of 12 studies found lowered rates of URI and otitis media incidence, 7 of 11 RCTs reported a significant reduction in severity scores for URI, and 4 of 8 RCTs reported significant reductions in school absenteeism between the probiotic and control groups. In a summary statement, the authors noted that “at least one beneficial effect of prophylactic probiotics was observed in the majority of RCTs,” and that “none of the studies reported any serious adverse events.”
Perinatal probiotics: No benefit for allergic conditions—except eczema
Allergic disease is on the rise and continues to plague children with reduced quality of life, potentially life-threatening reactions, and missed activities, including school. The gut microbiome likely influences a child’s allergic propensity through its effects on T-helper cells, transforming growth factor (TGF), and immunoglobulin A (IgA)—all known components of the allergic response. As the hygiene hypothesis suggests, the quantity and types of bacteria that inhabit the GI tract early in life play a significant role in determining a person’s later allergic responses.13
In a 2013 meta-analysis of 20 trials (N=4866), researchers looked specifically at probiotic use and the diagnosis of asthma and incident wheezing. Single and combination products of Lactobacillus and Bifidobacterium given prenatally and/or postnatally were included in the studies. The authors found no evidence to support a protective association between perinatal use of probiotics and diagnosed asthma (RR=0.99; 95% CI, 0.81-0.21) or childhood incident wheezing (RR=0.97; 95% CI, 0.87-1.09; 9 trials, 1949 infants).14
In a more recent meta-analysis (2015) conducted to inform the World Allergy Organization, 29 studies were evaluated to assess the impact of probiotics on allergic symptoms of the skin, respiratory system, and GI tract.15 No significant benefit was noted for any allergic condition except for eczema. Probiotics reduced the risk of eczema when given during the last trimester of pregnancy (RR=0.71; 95% CI, 0.60-0.84), when used by breastfeeding mothers (RR=0.57; 95% CI, 0.47-0.69), and when given to infants (RR=0.80; 95% CI, 0.68-0.94).
A 2014 systematic review and meta-analysis (N=2797) explored probiotic use specifically for the prevention of eczema.16 The pooled relative risk for all the studies was 0.74 (95% CI, 0.67-0.82). Evidence was strongest for probiotics containing the Lactobacillus species rhamnosus and paracasei, as well as for Bifidobacterium lactis. No benefit was noted with Lactobacillus acidophilus or other Bifidobacterium species. These newer reviews on eczema prevention contrast with an older Cochrane review published in 2008 (12 RCTs, N=781), which did not show significant benefit for the treatment of eczema.17
Probiotics improve IBS stomach pain, but not diarrhea or constipation
IBS is a functional disorder of the GI tract that affects up to 20% of children and teenagers and leads to a significant decrease in quality of life.18 Current theories of causation include bacterial overgrowth and neuronal hyperactivity, which may be amenable to change with supplemental probiotics.
A 2015 systematic review of non-pharmacological treatments for functional abdominal pain disorders identified 4 studies dedicated to IBS in children.19 A subgroup analysis of 3 RCTs (n=309) that looked at giving L rhamnosus to 5- to 17-year-olds with IBS showed improved abdominal pain (according to various pain scales) compared to the placebo group. Study participants received at least 3 x 109 CFU twice a day for 4 to 8 weeks. Relative risk for improvement was 1.7 (95% CI, 1.27-2.27) with an NNT of 4. None of these studies showed significant improvement in either frequency or severity of diarrhea or constipation.
A separate crossover RCT (N=59) compared placebo to VSL#3, a product containing 8 probiotics (Bifidobacterium breve, Bifidobacterium longum, Bifidobacterium infantis, L acidophilus, Lactobacillus plantarum, L paracasei, Lactobacillus bulgaricus, and Streptococcus hermophiles), given in age-dependent doses for 6 weeks to children aged 4 to 18 years.20 The frequency and intensity of abdominal pain were measured on a 5-point Likert scale. The group treated with VSL#3 dropped 1.0 ± 0.2 points vs 0.5 ± 0.2 points in the control group (P<.05) and reported an improved quality of life.
These agents reduce antibiotic-associated diarrhea
Antibiotic-associated diarrhea (AAD) occurs in 5% to 30% of children who receive antibiotic therapy.21 It occurs most frequently with the use of cephalosporins, penicillin, fluoroquinolones, and clindamycin, and is likely caused by an alteration of the normal gut flora. Colitis caused by Clostridium difficile remains the most serious antibiotic-associated GI complication.
A systematic review of the specific probiotic Saccharomyces boulardii conducted in 2015 analyzed data from 6 RCTs (n=1653) to determine the effect of co-administration of this probiotic with antibiotics.22 The pooled relative risk for AAD in children receiving the probiotic was 0.43 (95% CI, 0.3-0.6) compared to antibiotics alone. The absolute risk of AAD dropped from 20.9% to 8.8%, translating to a NNT of 8. Two of the RCTs specifically looked at rates of C difficile infection (n=579). C difficile infection rates dropped by 75% (RR=.25; 95% CI, 0.08-0.73) in the treatment group. This dramatic treatment effect was not seen in studies involving adults.
A similar systematic review focusing on L rhamnosus conducted in 2015 pooled data from 5 RCTs (n=445) to see if the probiotic would decrease AAD in children if it was co-administered with antibiotics.23 The relative risk for AAD in this treatment group was 0.48 (95% CI, 0.26-0.89) with an absolute risk reduction of 13.4% (23% compared to 9.6%), translating to an NNT of 7.
A Cochrane review published in 2015 included 23 studies (N=3938) and found similar results with an RR for AAD of 0.46 for treated children (95% CI, 0.35-0.61).24 Doses of probiotics ranged from 5 to 40 billion CFU/day. Although many probiotic species were used in these studies, S boulardii and L rhamnosus were cited as having the strongest data to support use in this context.
Probiotics reduce the duration, frequency of acute infectious diarrhea
Diarrhea remains the second leading cause of death among children one to 59 months of age worldwide.25 Current World Health Organization recommendations include oral rehydration salts, continued feeding to avoid dehydration, and zinc to decrease the duration and severity of illness.26 Multiple studies in adults confirm that a variety of probiotics decrease both the duration and severity of diarrhea in acute gastroenteritis.27
The authors of a 2013 systematic review of probiotics for the treatment of community-acquired acute diarrhea in children less than 5 years of age analyzed data from 8 RCTs (N=1755).28 Various probiotics were used including Lactobacillus species, Streptococcus thermophilus, Bifidobacterium species, and Saccharomyces boulardii for between 4 and 10 days. Six of these studies (n=1164) measured diarrhea duration and found a 14% reduction (95% CI, 3.8%-24.2%) in days of illness for those children treated vs those receiving placebo. Five studies (n=925) measured the difference in stool frequency on Day 2 of illness and reported a reduction of 13.1% (95% CI, 0.8%-5.3%) in the number of stools in the treated group vs the placebo group.
This review augments a Cochrane meta-analysis of 63 studies (N=8014) published in 2010.27 Fifty-six of these studies included infants and children. Pooled analysis of the varied probiotic treatments showed a mean reduction in duration of diarrhea of just over a day (24.76 hours; 95% CI, 15.9-33.6 hours; n=4555, trials=35) and decreased stool frequency on Day 2 of treatment (mean difference 0.80; 95% CI, 0.45-1.14; n=2751, trials=20). The authors concluded that probiotics “have clear beneficial effects in shortening the duration and reducing stool frequency in acute infectious diarrhea.”
Pediatric society weighs in. In 2014, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition issued guidelines regarding probiotic use for the treatment of acute gastroenteritis.29 In addition to rehydration therapy, these guidelines recommend the use of L rhamnosus and/or S boulardii as first-line treatments. Lower quality evidence is available for the use of L reuteri.
CASE › In response to Ms. B’s query about starting her young son on probiotics, you tell her that studies have shown that probiotics are safe for children when given in appropriate doses. They have been shown to help children recover from diarrheal illnesses and can help reduce the number of colds and ear infections when taken regularly. The reason you are giving them determines which strains you should use. You recommend giving her child a formulation of probiotic that contains Lactobacillus or Bifidobacterium with a dose range of 2 to 10 billion CFUs taken daily to reduce the risk of her child getting another ear infection.
CORRESPONDENCE
Paul Dassow, MD, MSPH, 1100 E. 3rd St, Chattanooga, TN 37403; paul.dassow@erlanger.org.
PRACTICE RECOMMENDATIONS
› Recommend a trial of Lactobacillus reuteri for breastfed infants with colic. A
› Consider Lactobacillus and Bifidobacterium species for the prevention of upper respiratory infections (URIs) and to shorten the course of URI illness. B
› Do not recommend probiotics for the prevention of respiratory or gastrointestinal allergies. A
› Consider probiotics for the reduction of abdominal pain in pediatric irritable bowel syndrome, as well as to reduce diarrhea associated with antibiotic use and acute gastroenteritis. A
Strength of recommendation (SOR)
A Good-quality patient-oriented evidence
B Inconsistent or limited-quality patient-oriented evidence
C Consensus, usual practice, opinion, disease-oriented evidence, case series
CASE › Ms. B, a 26-year-old woman, presents to your office with her 3-year-old son for a well-child examination. During the course of the conversation, she asks you if she should be giving her child probiotics to improve his general health. Many of her friends, who also have their children in day care, have told her that probiotics, “are nature’s way of fighting infection.” Her son currently takes no medications, and has no history of asthma or recent gastrointestinal disturbances. He was treated for 2 ear infections last winter, approximately 3 months apart. His physical exam is normal and, after today, his immunizations will be up to date. How should you respond?
The use of probiotics as over-the-counter treatments for a variety of conditions continues to grow, with retail sales of functional probiotic foods and supplements topping $35 billion worldwide in 2014.1 In children, claims of benefit for gastrointestinal (GI) disorders, colic, and allergy prevention, as well as prevention and treatment of upper respiratory infections (URIs) have existed for over 10 years.2-4 The human gut flora develops rapidly after birth and is known to be influenced by route of delivery (vaginal vs cesarean), type of feeding (breast vs formula), and other environmental factors.5 The use of probiotics to influence the types of bacteria in a child’s intestinal tract continues to be an area of active research. (For more on probiotic formulations, see TABLE 1.)
This article summarizes recent research on probiotic use in infants and children. New data support the use of probiotics for the treatment of colic and atopic eczema; however, the data on using probiotics in the management of URIs is less robust and mixed. And while probiotics improve irritable bowel syndrome (IBS) stomach pain, they do not help with related diarrhea or constipation. All of these data are summarized in TABLE 2.6-29
L reuteri improves symptoms in breastfed infants with colic
Infant colic is a relatively common condition known to negatively impact maternal mental health and the mother/child relationship.6 Numerous randomized controlled trials (RCTs) over the years have demonstrated mixed results with using probiotics to decrease crying times, with differences noted between infants who are solely breastfed and those who are not.7
In the most recent meta-analysis of 6 studies (n=427) that focused only on the probiotic Lactobacillus reuteri, breastfed infants with colic receiving a daily dose of 108 colony forming units (CFU) cried an average of 56 fewer minutes/day than those in the control group (95% confidence interval [CI], -64.4 to -47.3; P=.001) at day 21 of treatment.8 Although 2 studies in this meta-analysis included a small number of mixed-fed and formula-fed infants, the majority of trials do not show benefit for these infants. Trials assessing the use of L reuteri for prevention of colic have not shown positive results.7
Probiotics may help p
The mechanisms by which probiotics may prevent or shorten the course of URIs are not obvious. Current theories include boosting the immune function of the respiratory mucosa, acting as a competitive inhibitor for viruses, and secreting antiviral compounds.9 Multiple reviews published in the last 3 years, however, add to the evidence that the apparent benefit is real.
A 2013 meta-analysis assessed data from 4 RCTs (N=1805), which used Lactobacillus rhamnosus as the sole probiotic for prevention of URIs. In treated children, otitis media incidence was reduced by 24% (relative risk [RR] 0.76; 95% CI, 0.64-0.91) and risk of URI was reduced by 38% (RR 0.62; 95% CI, 0.50-0.78).10 The number needed to treat (NNT) was 4 for URI prevention, and the authors noted that adverse events were similar in the treatment and control groups.
A 2014 systematic review and meta-analysis of 20 RCTs examining duration of illness included 10 studies dedicated to pediatric subjects (age 12 months to 12 years).11 There were significantly fewer days of illness per person (standardized mean difference -0.31; 95% CI, -0.41 to -0.11) and each illness episode was shorter by three-quarters of a day (weighted mean difference -0.77; 95% CI, -1.5 to -0.04) in participants who received a probiotic vs those who received a placebo. Probiotics used in these studies belonged to the Lactobacillus and Bifidobacterium genera.
A 2015 systematic review of 14 RCTs assessing the benefits of probiotics, particularly Lactobacillus and Bifidobacterium strains, on URI occurrence and symptoms, showed mixed results.12 Seven of 12 studies found lowered rates of URI and otitis media incidence, 7 of 11 RCTs reported a significant reduction in severity scores for URI, and 4 of 8 RCTs reported significant reductions in school absenteeism between the probiotic and control groups. In a summary statement, the authors noted that “at least one beneficial effect of prophylactic probiotics was observed in the majority of RCTs,” and that “none of the studies reported any serious adverse events.”
Perinatal probiotics: No benefit for allergic conditions—except eczema
Allergic disease is on the rise and continues to plague children with reduced quality of life, potentially life-threatening reactions, and missed activities, including school. The gut microbiome likely influences a child’s allergic propensity through its effects on T-helper cells, transforming growth factor (TGF), and immunoglobulin A (IgA)—all known components of the allergic response. As the hygiene hypothesis suggests, the quantity and types of bacteria that inhabit the GI tract early in life play a significant role in determining a person’s later allergic responses.13
In a 2013 meta-analysis of 20 trials (N=4866), researchers looked specifically at probiotic use and the diagnosis of asthma and incident wheezing. Single and combination products of Lactobacillus and Bifidobacterium given prenatally and/or postnatally were included in the studies. The authors found no evidence to support a protective association between perinatal use of probiotics and diagnosed asthma (RR=0.99; 95% CI, 0.81-0.21) or childhood incident wheezing (RR=0.97; 95% CI, 0.87-1.09; 9 trials, 1949 infants).14
In a more recent meta-analysis (2015) conducted to inform the World Allergy Organization, 29 studies were evaluated to assess the impact of probiotics on allergic symptoms of the skin, respiratory system, and GI tract.15 No significant benefit was noted for any allergic condition except for eczema. Probiotics reduced the risk of eczema when given during the last trimester of pregnancy (RR=0.71; 95% CI, 0.60-0.84), when used by breastfeeding mothers (RR=0.57; 95% CI, 0.47-0.69), and when given to infants (RR=0.80; 95% CI, 0.68-0.94).
A 2014 systematic review and meta-analysis (N=2797) explored probiotic use specifically for the prevention of eczema.16 The pooled relative risk for all the studies was 0.74 (95% CI, 0.67-0.82). Evidence was strongest for probiotics containing the Lactobacillus species rhamnosus and paracasei, as well as for Bifidobacterium lactis. No benefit was noted with Lactobacillus acidophilus or other Bifidobacterium species. These newer reviews on eczema prevention contrast with an older Cochrane review published in 2008 (12 RCTs, N=781), which did not show significant benefit for the treatment of eczema.17
Probiotics improve IBS stomach pain, but not diarrhea or constipation
IBS is a functional disorder of the GI tract that affects up to 20% of children and teenagers and leads to a significant decrease in quality of life.18 Current theories of causation include bacterial overgrowth and neuronal hyperactivity, which may be amenable to change with supplemental probiotics.
A 2015 systematic review of non-pharmacological treatments for functional abdominal pain disorders identified 4 studies dedicated to IBS in children.19 A subgroup analysis of 3 RCTs (n=309) that looked at giving L rhamnosus to 5- to 17-year-olds with IBS showed improved abdominal pain (according to various pain scales) compared to the placebo group. Study participants received at least 3 x 109 CFU twice a day for 4 to 8 weeks. Relative risk for improvement was 1.7 (95% CI, 1.27-2.27) with an NNT of 4. None of these studies showed significant improvement in either frequency or severity of diarrhea or constipation.
A separate crossover RCT (N=59) compared placebo to VSL#3, a product containing 8 probiotics (Bifidobacterium breve, Bifidobacterium longum, Bifidobacterium infantis, L acidophilus, Lactobacillus plantarum, L paracasei, Lactobacillus bulgaricus, and Streptococcus hermophiles), given in age-dependent doses for 6 weeks to children aged 4 to 18 years.20 The frequency and intensity of abdominal pain were measured on a 5-point Likert scale. The group treated with VSL#3 dropped 1.0 ± 0.2 points vs 0.5 ± 0.2 points in the control group (P<.05) and reported an improved quality of life.
These agents reduce antibiotic-associated diarrhea
Antibiotic-associated diarrhea (AAD) occurs in 5% to 30% of children who receive antibiotic therapy.21 It occurs most frequently with the use of cephalosporins, penicillin, fluoroquinolones, and clindamycin, and is likely caused by an alteration of the normal gut flora. Colitis caused by Clostridium difficile remains the most serious antibiotic-associated GI complication.
A systematic review of the specific probiotic Saccharomyces boulardii conducted in 2015 analyzed data from 6 RCTs (n=1653) to determine the effect of co-administration of this probiotic with antibiotics.22 The pooled relative risk for AAD in children receiving the probiotic was 0.43 (95% CI, 0.3-0.6) compared to antibiotics alone. The absolute risk of AAD dropped from 20.9% to 8.8%, translating to a NNT of 8. Two of the RCTs specifically looked at rates of C difficile infection (n=579). C difficile infection rates dropped by 75% (RR=.25; 95% CI, 0.08-0.73) in the treatment group. This dramatic treatment effect was not seen in studies involving adults.
A similar systematic review focusing on L rhamnosus conducted in 2015 pooled data from 5 RCTs (n=445) to see if the probiotic would decrease AAD in children if it was co-administered with antibiotics.23 The relative risk for AAD in this treatment group was 0.48 (95% CI, 0.26-0.89) with an absolute risk reduction of 13.4% (23% compared to 9.6%), translating to an NNT of 7.
A Cochrane review published in 2015 included 23 studies (N=3938) and found similar results with an RR for AAD of 0.46 for treated children (95% CI, 0.35-0.61).24 Doses of probiotics ranged from 5 to 40 billion CFU/day. Although many probiotic species were used in these studies, S boulardii and L rhamnosus were cited as having the strongest data to support use in this context.
Probiotics reduce the duration, frequency of acute infectious diarrhea
Diarrhea remains the second leading cause of death among children one to 59 months of age worldwide.25 Current World Health Organization recommendations include oral rehydration salts, continued feeding to avoid dehydration, and zinc to decrease the duration and severity of illness.26 Multiple studies in adults confirm that a variety of probiotics decrease both the duration and severity of diarrhea in acute gastroenteritis.27
The authors of a 2013 systematic review of probiotics for the treatment of community-acquired acute diarrhea in children less than 5 years of age analyzed data from 8 RCTs (N=1755).28 Various probiotics were used including Lactobacillus species, Streptococcus thermophilus, Bifidobacterium species, and Saccharomyces boulardii for between 4 and 10 days. Six of these studies (n=1164) measured diarrhea duration and found a 14% reduction (95% CI, 3.8%-24.2%) in days of illness for those children treated vs those receiving placebo. Five studies (n=925) measured the difference in stool frequency on Day 2 of illness and reported a reduction of 13.1% (95% CI, 0.8%-5.3%) in the number of stools in the treated group vs the placebo group.
This review augments a Cochrane meta-analysis of 63 studies (N=8014) published in 2010.27 Fifty-six of these studies included infants and children. Pooled analysis of the varied probiotic treatments showed a mean reduction in duration of diarrhea of just over a day (24.76 hours; 95% CI, 15.9-33.6 hours; n=4555, trials=35) and decreased stool frequency on Day 2 of treatment (mean difference 0.80; 95% CI, 0.45-1.14; n=2751, trials=20). The authors concluded that probiotics “have clear beneficial effects in shortening the duration and reducing stool frequency in acute infectious diarrhea.”
Pediatric society weighs in. In 2014, the European Society for Paediatric Gastroenterology, Hepatology, and Nutrition issued guidelines regarding probiotic use for the treatment of acute gastroenteritis.29 In addition to rehydration therapy, these guidelines recommend the use of L rhamnosus and/or S boulardii as first-line treatments. Lower quality evidence is available for the use of L reuteri.
CASE › In response to Ms. B’s query about starting her young son on probiotics, you tell her that studies have shown that probiotics are safe for children when given in appropriate doses. They have been shown to help children recover from diarrheal illnesses and can help reduce the number of colds and ear infections when taken regularly. The reason you are giving them determines which strains you should use. You recommend giving her child a formulation of probiotic that contains Lactobacillus or Bifidobacterium with a dose range of 2 to 10 billion CFUs taken daily to reduce the risk of her child getting another ear infection.
CORRESPONDENCE
Paul Dassow, MD, MSPH, 1100 E. 3rd St, Chattanooga, TN 37403; paul.dassow@erlanger.org.
1. Euromonitor International. Global and regional trends of the probiotics and omega fatty acids market. June 23, 2015. Available at: http://uschinahpa.org/wp-content/uploads/2015/07/EMI-US-China-HPA-Probiotic-and-Omega-2015-Final.pdf. Accessed September 9, 2016.
2. Du Toit G, Lack G. Can food allergy be prevented? The current evidence. Pediatr Clin North Am. 2011;58:481-509.
3. Gerritsen J, Smidt H, Rijkers GT, et al. Intestinal microbiota in human health and disease: the impact of probiotics. Genes Nutr. 2011;6:209-240.
4. Versalovic J. The human microbiome and probiotics: implications for pediatrics. Ann Nutr Metab. 2013;63:42-52.
5. Neish AS. Microbes in gastrointestinal health and disease. Gastroenterology. 2009;136:65-80.
6. Akman I, Kușçu K, Özdemir N, et al. Mothers’ postpartum psychological adjustment and infantile colic. Arch Dis Child. 2006;91:417-419.
7. Sung V, Collett S, de Gooyer T, et al. Probiotics to prevent or treat excessive infant crying systematic review and meta-analysis. JAMA Pediatr. 2013:167:1150-1157.
8. Harb T, Matsuyama M, David M, et al. Infant colic—what works: a systematic review of interventions for breastfed infants. J Pediatr Gastroenterol Nutr. 2016;62:668-686.
9. Hill C, Guarner F, Reid G, et al. Expert consensus document: the International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. 2014;11:506-514.
10. Liu S, Hu P, Du X, et al. Lactobacillus rhamnosus GG supplementation for preventing respiratory infections in children: a meta-analysis of randomized, placebo-controlled trials. Indian Pediatr. 2013;50:377-381.
11. King S, Glanville J, Sanders ME, et al. Effectiveness of probiotics on the duration of illness in healthy children and adults who develop common acute respiratory infectious conditions: a systematic review and meta-analysis. Br J Nutr. 2014;112:41-54.
12. Ozen M, Kocabas Sandal G, Dinleyici EC. Probiotics for the prevention of pediatric upper respiratory tract infections: a systematic review. Expert Opin Biol Ther. 2015;15:9-20.
13. Azad MB, Konya T, Maughan H, et al. Infant gut microbiota and the hygiene hypothesis of allergic disease: impact of household pets and siblings on microbiota composition and diversity. Allergy Asthma Clin Immunol. 2013;9:15.
14. Azad MB, Coneys JG, Kozyrskyj AL, et al. Probiotic supplementation during pregnancy or infancy for the prevention of asthma and wheeze: systematic review and meta-analysis. Brit Med J. 2013;347:f6471.
15. Cuello-Garcia CA, Bro˙zek JL, Fiocchi A, et al. Probiotics for the prevention of allergy: a systematic review and meta-analysis of randomized controlled trials. J Allergy Clin Immunol. 2015;136:952-961.
16. Mansfield JA, Bergin SW, Cooper JR, et al. Comparative probiotic strain efficacy in the prevention of eczema in infants and children: a systematic review and meta-analysis. Mil Med. 2014;179:580-592.
17. Boyle RJ, Bath-Hextall FJ, Leonardi-Bee J, et al. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;(4):CD006135.
18. Chiou E, Nurko S. Management of functional abdominal pain and irritable bowel syndrome in children and adolescents. Expert Rev Gastroenterol Hepatol. 2010;4:293-304.
19. Rutten JMTM, Korterink JL, Venmans LMAJ, et al. Nonpharmacologic treatment of functional abdominal pain disorders: a systematic review. Pediatrics. 2015;135:522-535.
20. Guandalini S, Magazzù G, Chiaro A, et al. VSL#3 improves symptoms in children with irritable bowel syndrome: a multicenter, randomized, placebo-controlled, double-blind, crossover study. J Pediatr Gastroenterol Nutr. 2010;51:24-30.
21. Turck D, Bernet JP, Marx J, et al. Incidence and risk factors of oral antibiotic associated diarrhea in an outpatient pediatric population. J Pediatr Gastroenterol Nutr. 2003;37:22-26.
22. Szajewska H, Kołodziej M. Systematic review with meta-analysis: Saccharomyces boulardii in the prevention of antibiotic-associated diarrhoea. Aliment Pharmacol Ther. 2015;42:793-801.
23. Szajewska H, Kołodziej M. Systematic review with meta-analysis: Lactobacillus rhamnosus GG in the prevention of antibiotic-associated diarrhoea in children and adults. Aliment Pharmacol Ther. 2015;42:1149-1157.
24. Goldenberg JZ, Lytvyn L, Steurich J, et al. Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Cochrane Database Syst Rev. 2015;12:CD004827.
25. Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151-2161.
26. WHO/UNICEF Joint Statement: Clinical Management of Acute Diarrhea. August 2004. Available at: http://www.unicef.org/publications/files/ENAcute_Diarrhoea_reprint.pdf. Accessed September 9, 2016.
27. Allen SJ, Martinez EG, Gregorio GV, et al. Probiotics for treating acute infectious diarrhea. Cochrane Database Syst Rev. 2010;(11):CD003048.
28. Applegate JA, Fischer Walker CL, Ambikapathi R, et al. Systematic review of probiotics for the treatment of community-acquired acute diarrhea in children. BMC Public Health. 2013;13:S16.
29. Guarino A, Ashkenazi S, Gendrel D, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J Pediatr Gastroenterol Nutr. 2014;59:132-152.
1. Euromonitor International. Global and regional trends of the probiotics and omega fatty acids market. June 23, 2015. Available at: http://uschinahpa.org/wp-content/uploads/2015/07/EMI-US-China-HPA-Probiotic-and-Omega-2015-Final.pdf. Accessed September 9, 2016.
2. Du Toit G, Lack G. Can food allergy be prevented? The current evidence. Pediatr Clin North Am. 2011;58:481-509.
3. Gerritsen J, Smidt H, Rijkers GT, et al. Intestinal microbiota in human health and disease: the impact of probiotics. Genes Nutr. 2011;6:209-240.
4. Versalovic J. The human microbiome and probiotics: implications for pediatrics. Ann Nutr Metab. 2013;63:42-52.
5. Neish AS. Microbes in gastrointestinal health and disease. Gastroenterology. 2009;136:65-80.
6. Akman I, Kușçu K, Özdemir N, et al. Mothers’ postpartum psychological adjustment and infantile colic. Arch Dis Child. 2006;91:417-419.
7. Sung V, Collett S, de Gooyer T, et al. Probiotics to prevent or treat excessive infant crying systematic review and meta-analysis. JAMA Pediatr. 2013:167:1150-1157.
8. Harb T, Matsuyama M, David M, et al. Infant colic—what works: a systematic review of interventions for breastfed infants. J Pediatr Gastroenterol Nutr. 2016;62:668-686.
9. Hill C, Guarner F, Reid G, et al. Expert consensus document: the International Scientific Association for Probiotics and Prebiotics consensus statement on the scope and appropriate use of the term probiotic. Nat Rev Gastroenterol Hepatol. 2014;11:506-514.
10. Liu S, Hu P, Du X, et al. Lactobacillus rhamnosus GG supplementation for preventing respiratory infections in children: a meta-analysis of randomized, placebo-controlled trials. Indian Pediatr. 2013;50:377-381.
11. King S, Glanville J, Sanders ME, et al. Effectiveness of probiotics on the duration of illness in healthy children and adults who develop common acute respiratory infectious conditions: a systematic review and meta-analysis. Br J Nutr. 2014;112:41-54.
12. Ozen M, Kocabas Sandal G, Dinleyici EC. Probiotics for the prevention of pediatric upper respiratory tract infections: a systematic review. Expert Opin Biol Ther. 2015;15:9-20.
13. Azad MB, Konya T, Maughan H, et al. Infant gut microbiota and the hygiene hypothesis of allergic disease: impact of household pets and siblings on microbiota composition and diversity. Allergy Asthma Clin Immunol. 2013;9:15.
14. Azad MB, Coneys JG, Kozyrskyj AL, et al. Probiotic supplementation during pregnancy or infancy for the prevention of asthma and wheeze: systematic review and meta-analysis. Brit Med J. 2013;347:f6471.
15. Cuello-Garcia CA, Bro˙zek JL, Fiocchi A, et al. Probiotics for the prevention of allergy: a systematic review and meta-analysis of randomized controlled trials. J Allergy Clin Immunol. 2015;136:952-961.
16. Mansfield JA, Bergin SW, Cooper JR, et al. Comparative probiotic strain efficacy in the prevention of eczema in infants and children: a systematic review and meta-analysis. Mil Med. 2014;179:580-592.
17. Boyle RJ, Bath-Hextall FJ, Leonardi-Bee J, et al. Probiotics for treating eczema. Cochrane Database Syst Rev. 2008;(4):CD006135.
18. Chiou E, Nurko S. Management of functional abdominal pain and irritable bowel syndrome in children and adolescents. Expert Rev Gastroenterol Hepatol. 2010;4:293-304.
19. Rutten JMTM, Korterink JL, Venmans LMAJ, et al. Nonpharmacologic treatment of functional abdominal pain disorders: a systematic review. Pediatrics. 2015;135:522-535.
20. Guandalini S, Magazzù G, Chiaro A, et al. VSL#3 improves symptoms in children with irritable bowel syndrome: a multicenter, randomized, placebo-controlled, double-blind, crossover study. J Pediatr Gastroenterol Nutr. 2010;51:24-30.
21. Turck D, Bernet JP, Marx J, et al. Incidence and risk factors of oral antibiotic associated diarrhea in an outpatient pediatric population. J Pediatr Gastroenterol Nutr. 2003;37:22-26.
22. Szajewska H, Kołodziej M. Systematic review with meta-analysis: Saccharomyces boulardii in the prevention of antibiotic-associated diarrhoea. Aliment Pharmacol Ther. 2015;42:793-801.
23. Szajewska H, Kołodziej M. Systematic review with meta-analysis: Lactobacillus rhamnosus GG in the prevention of antibiotic-associated diarrhoea in children and adults. Aliment Pharmacol Ther. 2015;42:1149-1157.
24. Goldenberg JZ, Lytvyn L, Steurich J, et al. Probiotics for the prevention of pediatric antibiotic-associated diarrhea. Cochrane Database Syst Rev. 2015;12:CD004827.
25. Liu L, Johnson HL, Cousens S, et al. Global, regional, and national causes of child mortality: an updated systematic analysis for 2010 with time trends since 2000. Lancet. 2012;379:2151-2161.
26. WHO/UNICEF Joint Statement: Clinical Management of Acute Diarrhea. August 2004. Available at: http://www.unicef.org/publications/files/ENAcute_Diarrhoea_reprint.pdf. Accessed September 9, 2016.
27. Allen SJ, Martinez EG, Gregorio GV, et al. Probiotics for treating acute infectious diarrhea. Cochrane Database Syst Rev. 2010;(11):CD003048.
28. Applegate JA, Fischer Walker CL, Ambikapathi R, et al. Systematic review of probiotics for the treatment of community-acquired acute diarrhea in children. BMC Public Health. 2013;13:S16.
29. Guarino A, Ashkenazi S, Gendrel D, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition/European Society for Pediatric Infectious Diseases evidence-based guidelines for the management of acute gastroenteritis in children in Europe: update 2014. J Pediatr Gastroenterol Nutr. 2014;59:132-152.

Homeless youth and risk: Untangling role of executive function
NEW YORK – Researchers studying the executive functioning ability of homeless youth have found that individuals with poor executive function report more alcohol abuse and dependence than do those with higher EF.
The results are from a study of 149 youth aged 18-22 years (53% female) living in shelters in Chicago. Subjects self-reported behaviors in a series of interviews that used three validated measures of executive function.
Scott J. Hunter, Ph.D., director of neuropsychology at the University of Chicago, presented the findings at the annual meeting of the American Academy of Child and Adolescent Psychiatry. Dr. Hunter said in an interview that the results help identify low executive functioning as both a likely contributor to risk-taking behavior and a potential target of interventions.
“We believe that the EF may be the primary concern, although the interaction [with drugs and alcohol] is something that we have to take into account,” he said. “One of the biggest issues here is how do you disentangle that executive piece with the use of substances?”
In this cohort, Dr. Hunter said, about 75% of subjects were African American and an additional 25% or so were mixed race or Latino. About half comprised a sexual minority (gay, lesbian, bisexual, or transgender). “Many had been kicked out of their homes,” he said.
Close to 80% of the youth in the study used cannabis regularly, and three-quarters used alcohol. The group with low EF used the greatest level of substances regularly. Admission of unprotected sexual intercourse was highest among the heavier substance users as well, suggesting “a reliance on substances to reduce sensitivity to the risks they were taking,” said Dr. Hunter, also a professor in the departments of psychiatry and behavioral neuroscience, and pediatrics at the university.
He said the study “is providing some support for our hypothesis that the less successful these young people are in their development of EF, particularly around inhibition, the more likely it is they are going to be engaging in risk-taking behaviors that lead to cycles of more challenge” and development of psychopathology.
The researchers are considering an intervention for this population derived from EF interventions for use with adolescents with attention-deficit/hyperactivity disorder. In their current shelter environments, he said, the youth are “already undergoing programs to learn adaptive functioning to be more successful, and we’re thinking of adding an executive component where they tie the decision-making component to what they want as outcomes.”
The prefrontal cortex of the brain, which controls executive function, is not yet fully developed in adolescence, and studies have shown that youth growing up in impoverished environments have decreases or alterations in cortical development (Front Hum Neurosci. 2012 Aug 17;6:238). “What we have to think about is that we’re still at a [developmental] point where this enhancement and myelination is taking place – into the mid-20s, in fact. We may find that [an intervention] can help them better activate that,” Dr. Hunter said.
The lead author on this study was Joshua Piche, a medical student at the University of Chicago.
Dr. Hunter also is collaborating with epidemiologist John Schneider, MD, MPH, of the University of Chicago, in a study of 600 young black men who have sex with men. The researchers are looking at drug-, alcohol-related, and sexual decision-making in that cohort, about a quarter of whom are homeless. The study includes functional magnetic resonance imaging in a subgroup of subjects.
Currently, as many as 2 million U.S. youth are estimated to be living on the streets, in shelters, or in other temporary housing environments.
NEW YORK – Researchers studying the executive functioning ability of homeless youth have found that individuals with poor executive function report more alcohol abuse and dependence than do those with higher EF.
The results are from a study of 149 youth aged 18-22 years (53% female) living in shelters in Chicago. Subjects self-reported behaviors in a series of interviews that used three validated measures of executive function.
Scott J. Hunter, Ph.D., director of neuropsychology at the University of Chicago, presented the findings at the annual meeting of the American Academy of Child and Adolescent Psychiatry. Dr. Hunter said in an interview that the results help identify low executive functioning as both a likely contributor to risk-taking behavior and a potential target of interventions.
“We believe that the EF may be the primary concern, although the interaction [with drugs and alcohol] is something that we have to take into account,” he said. “One of the biggest issues here is how do you disentangle that executive piece with the use of substances?”
In this cohort, Dr. Hunter said, about 75% of subjects were African American and an additional 25% or so were mixed race or Latino. About half comprised a sexual minority (gay, lesbian, bisexual, or transgender). “Many had been kicked out of their homes,” he said.
Close to 80% of the youth in the study used cannabis regularly, and three-quarters used alcohol. The group with low EF used the greatest level of substances regularly. Admission of unprotected sexual intercourse was highest among the heavier substance users as well, suggesting “a reliance on substances to reduce sensitivity to the risks they were taking,” said Dr. Hunter, also a professor in the departments of psychiatry and behavioral neuroscience, and pediatrics at the university.
He said the study “is providing some support for our hypothesis that the less successful these young people are in their development of EF, particularly around inhibition, the more likely it is they are going to be engaging in risk-taking behaviors that lead to cycles of more challenge” and development of psychopathology.
The researchers are considering an intervention for this population derived from EF interventions for use with adolescents with attention-deficit/hyperactivity disorder. In their current shelter environments, he said, the youth are “already undergoing programs to learn adaptive functioning to be more successful, and we’re thinking of adding an executive component where they tie the decision-making component to what they want as outcomes.”
The prefrontal cortex of the brain, which controls executive function, is not yet fully developed in adolescence, and studies have shown that youth growing up in impoverished environments have decreases or alterations in cortical development (Front Hum Neurosci. 2012 Aug 17;6:238). “What we have to think about is that we’re still at a [developmental] point where this enhancement and myelination is taking place – into the mid-20s, in fact. We may find that [an intervention] can help them better activate that,” Dr. Hunter said.
The lead author on this study was Joshua Piche, a medical student at the University of Chicago.
Dr. Hunter also is collaborating with epidemiologist John Schneider, MD, MPH, of the University of Chicago, in a study of 600 young black men who have sex with men. The researchers are looking at drug-, alcohol-related, and sexual decision-making in that cohort, about a quarter of whom are homeless. The study includes functional magnetic resonance imaging in a subgroup of subjects.
Currently, as many as 2 million U.S. youth are estimated to be living on the streets, in shelters, or in other temporary housing environments.
NEW YORK – Researchers studying the executive functioning ability of homeless youth have found that individuals with poor executive function report more alcohol abuse and dependence than do those with higher EF.
The results are from a study of 149 youth aged 18-22 years (53% female) living in shelters in Chicago. Subjects self-reported behaviors in a series of interviews that used three validated measures of executive function.
Scott J. Hunter, Ph.D., director of neuropsychology at the University of Chicago, presented the findings at the annual meeting of the American Academy of Child and Adolescent Psychiatry. Dr. Hunter said in an interview that the results help identify low executive functioning as both a likely contributor to risk-taking behavior and a potential target of interventions.
“We believe that the EF may be the primary concern, although the interaction [with drugs and alcohol] is something that we have to take into account,” he said. “One of the biggest issues here is how do you disentangle that executive piece with the use of substances?”
In this cohort, Dr. Hunter said, about 75% of subjects were African American and an additional 25% or so were mixed race or Latino. About half comprised a sexual minority (gay, lesbian, bisexual, or transgender). “Many had been kicked out of their homes,” he said.
Close to 80% of the youth in the study used cannabis regularly, and three-quarters used alcohol. The group with low EF used the greatest level of substances regularly. Admission of unprotected sexual intercourse was highest among the heavier substance users as well, suggesting “a reliance on substances to reduce sensitivity to the risks they were taking,” said Dr. Hunter, also a professor in the departments of psychiatry and behavioral neuroscience, and pediatrics at the university.
He said the study “is providing some support for our hypothesis that the less successful these young people are in their development of EF, particularly around inhibition, the more likely it is they are going to be engaging in risk-taking behaviors that lead to cycles of more challenge” and development of psychopathology.
The researchers are considering an intervention for this population derived from EF interventions for use with adolescents with attention-deficit/hyperactivity disorder. In their current shelter environments, he said, the youth are “already undergoing programs to learn adaptive functioning to be more successful, and we’re thinking of adding an executive component where they tie the decision-making component to what they want as outcomes.”
The prefrontal cortex of the brain, which controls executive function, is not yet fully developed in adolescence, and studies have shown that youth growing up in impoverished environments have decreases or alterations in cortical development (Front Hum Neurosci. 2012 Aug 17;6:238). “What we have to think about is that we’re still at a [developmental] point where this enhancement and myelination is taking place – into the mid-20s, in fact. We may find that [an intervention] can help them better activate that,” Dr. Hunter said.
The lead author on this study was Joshua Piche, a medical student at the University of Chicago.
Dr. Hunter also is collaborating with epidemiologist John Schneider, MD, MPH, of the University of Chicago, in a study of 600 young black men who have sex with men. The researchers are looking at drug-, alcohol-related, and sexual decision-making in that cohort, about a quarter of whom are homeless. The study includes functional magnetic resonance imaging in a subgroup of subjects.
Currently, as many as 2 million U.S. youth are estimated to be living on the streets, in shelters, or in other temporary housing environments.
New screen time guidelines address rapid changes in media environment
SAN FRANCISCO – A new set of policy statements on children’s media use from the American Academy of Pediatrics brings the recommendations into the 21st century.
The new guidance, released at the annual meeting of the AAP, synthesizes the most current evidence on mobile devices, interactivity, educational technology, sleep, obesity, cognitive development, and other aspects of the pervasive digital environment children now grow up in.
“I think our policy statement reflects the changes in the media landscape because not all media use is the same,” Megan A. Moreno, MD, lead author of the policy statement, “Media Use in School-Aged Children and Adolescents,” said during a press conference (Pediatrics. 2016, Oct. doi: 10.1542/peds.2016-2592).

The new statement both lowers the overall age at which parents can feel comfortable introducing their children to media and decreases the amount of screen time exposure per day. One key component of the new guidelines includes the unveiling of a new tool parents can use to create a Family Media Plan. The tool, available at https://www.healthychildren.org/English/media/Pages/default.aspx, enables parents to create a plan for each child in the household and reflects the individuality of each child’s use and age-appropriate guidelines.
After parents enter children’s names, the plan provides an editable template for each child that lays out screen-free zones, screen-free times, device curfews, recreational screen-time choices, alternative activities during non-screen time, media manners, digital citizenship, personal safety, sleep, and exercise.
Previous policy statements from the AAP relied primarily on research about television, a passive screen experience. In an age where many children and teens have interactive screens in their pockets and visit grandparents via video conferencing, however, the AAP Council on Communications and Media has likewise broadened its definition of media and noted the problems with applying research about television to other totally different types of screens.
“When we’re using media to connect, this is not what we’re traditionally calling screen time. These are tools,” Jenny S. Radesky, MD, lead author of the policy statement “Media and Young Minds,” said at the press conference (Pediatrics. 2016 Oct. doi: 10.1542/peds.2016-2592). She referred to the fact that many families who are spread across great distances, such as parents deployed overseas or grandparents in another state, use Skype, FaceTime, Google Hangouts, and similar programs to communicate and remain connected.

“We’re making sure our relationships are staying strong and not something to be discouraged with infants and toddlers, even though infants and toddlers will need their parent’s help to understand what they’re seeing on the screen,” said Dr. Radesky, a developmental-behavioral pediatrician at C.S. Mott Children’s Hospital at the University of Michigan in Ann Arbor.

The policy statement further notes that some emerging evidence has suggested children aged 2 and older can learn words from live video chatting with a responsive adult or by using an interactive touch screen that scaffolds learning.
An earlier introduction to screens
Among the most significant changes to the recommendations for children up to 5 years old is an allowance for introducing media before age 2, the previous policy’s age recommendation.
“If you want to introduce media, 18 months is the age when kids are cognitively ready to start, but we’re not saying parents need to introduce media then,” Dr. Radesky said, adding that more research is needed regarding devices such as tablets before it’s possible to know whether apps can be beneficial in toddlers that young. “There’s not enough evidence to know if interactivity helps or not right now,” she said.
The “Media and Young Minds” policy statement notes that children under age 2 years develop their cognitive, language, motor, and social-emotional skills through hands-on exploration and social interaction with trusted adults.
“Apps can’t do the things that parents’ minds can do or children’s minds can do on their own,” Dr. Radesky said. The policy notes that digital books, or eBooks, can be beneficial when used like a traditional physical book, but interactive elements to these eBooks could be distracting and decrease children’s comprehension.
When parents do choose to introduce media to their children, it’s “crucial that media be a shared experience” between the caregiving adult and the child, she said. “Think of media as a teaching tool, a way to connect and to create, not just to consume,” Dr. Radesky said.
What can preschoolers learn?
Although some laboratory research shows toddlers as young as 15 months can learn new words from touch screens, they have difficulty transferring that knowledge to the three-dimensional world. For children aged 3-5 years, however, both well-designed television programming and high-quality learning apps from Public Broadcasting Service (PBS) and the Sesame Workshop have shown benefits. In addition to early literacy, math, and personal and social development skills learned from shows such as Sesame Street, preschoolers have learned literacy skills from those programs’ apps.
But those apps are unfortunately in the minority.
“Most apps parents find under the ‘educational’ category in app stores have no such evidence of efficacy, target only rote academic skills, are not based on established curricula, and use little or no input from developmental specialists and educators,” the “Media and Young Minds” policy states. “The higher-order thinking skills and executive functions essential for school success, such as task persistence, impulse control, emotion regulation, and creative, flexible thinking, are best taught through unstructured and social (not digital) play, as well as responsive parent-child interactions.”

Risks and recommendations for preschoolers
Heavy media use among preschoolers, meanwhile, carries risks of increased weight – primarily as a result of food advertising and eating while watching TV – as well as reduced sleep and cognitive, language, and social/emotional delays.
“Content is crucial,” the “Media and Young Minds” policy notes. “Experimental evidence shows that switching from violent content to educational/prosocial content results in significant improvement in behavioral symptoms, particularly for low-income boys.”
The key points of the new statement therefore include the following recommendations:
• Limit media use to 1 hour a day in children ages 2 years and older.
• Do not use screens during mealtimes and for 1 hour before bedtime.
• Start discussing family and child media use with parents early in children’s lives.
• Educate parents about early brain development and help families develop a Family Media Use Plan.
• Discourage screen use besides video-chatting in children under 18 months old.
• Encourage caregiving adults to use screen media with children aged 18-24 months, who should not use it on their own.
• Encourage parents to rely on high-quality programming products such as PBS Kids, Sesame Workshop, and Common Sense Media.
• Help parents with challenges such as setting limits, finding alternatives to screen time, and calming children without using media.
• Avoid using screens or media to calm children except during rare extenuating circumstances, such as painful medical procedures and airplane flights.
• Encourage parents to avoid fast-paced programs, apps with distracting content, any media with violent content, and any background television, which can stunt children’s early language development.
Understanding older youth’s media use
As children move into school age and adolescence, the opportunities and utilities for media use expand – and so do the risks. Children and teens can benefit from media through gaining social support, learning about healthy behaviors, and discovering new ideas and knowledge, but youth remain at risk for obesity, sleep problems, cyberbullying, compromised privacy, and exposure to inaccurate, inappropriate or unsafe content, the “Media Use in School-Aged Children and Adolescents” policy statement reports.
Despite the wide range of media types available, TV remains the most commonly used media type among school-aged children and teens and is watched an average of 2 hours a day. Still, 91% of boys have access to a video game console, and 84% report playing games online or on a mobile phone. Further, three-quarters of teens own a smartphone and 76% use at least one social media site, with more than 70% maintaining a “social media portfolio” across several platforms.
Such social media use can provide teens with helpful support networks, particularly for those with ongoing illnesses or disabilities or those needing community support as lesbian, gay, bisexual, transgender, questioning, or intersex individuals. Social media can also promote wellness and healthy behaviors such as eating well and not smoking.
Risks for school-aged children and adolescents using media
Yet social media also can open the door to cyberbullying, leading to short-term and long-term social, academic, and health problems. It carries the risk of exploitation of youth or their images, or predation from pornographers and pedophiles. Children and teens must be made aware that the “Internet is forever” and should be taught to consider privacy and confidentiality concerns in their use of social and other media.
Another concern is teens’ “sexting,” in which they share sexually explicit messages and/or partly or fully nude photos. Exposures to unhealthy behaviors, such as substance abuse, sexual behaviors, self-injury, or disordered eating are likewise among the risks of social media, as they are with television and cinema.
In fact, TV/movie content showing alcohol use, smoking, and sexual activity is linked to earlier experimentation among children and adolescents. In addition, each extra hour of television watching is associated with increase in body mass index, as is having a TV set in the bedroom. Enjoying entertainment media while doing school work is linked to poor learning and academics.
Excessive media use may lead to problematic Internet use and Internet gaming disorder as described in the DSM-5, occurring among 4%-8.5% of children and adolescents.
“Symptoms can include a preoccupation with the activity, decreased interest in offline or ‘real life’ relationships, unsuccessful attempts to decrease use and withdrawal symptoms,” the “Media Use in School-Aged Children and Adolescents” policy statement notes.
Recommendations for older children
The policy statement advises pediatricians to help families and schools promote understanding of media’s risks and benefits, including awareness of tools to screen for sexting, cyberbullying, problematic Internet use, and Internet gaming disorder. Pediatricians should advocate for training in media literacy in the community and encourage parents to follow the media, sleep, and physical activity guidelines included in the Family Media Plan.
The research was supported by the American Academy of Pediatrics. The authors reported no disclosures.
SAN FRANCISCO – A new set of policy statements on children’s media use from the American Academy of Pediatrics brings the recommendations into the 21st century.
The new guidance, released at the annual meeting of the AAP, synthesizes the most current evidence on mobile devices, interactivity, educational technology, sleep, obesity, cognitive development, and other aspects of the pervasive digital environment children now grow up in.
“I think our policy statement reflects the changes in the media landscape because not all media use is the same,” Megan A. Moreno, MD, lead author of the policy statement, “Media Use in School-Aged Children and Adolescents,” said during a press conference (Pediatrics. 2016, Oct. doi: 10.1542/peds.2016-2592).
The new statement both lowers the overall age at which parents can feel comfortable introducing their children to media and decreases the amount of screen time exposure per day. One key component of the new guidelines includes the unveiling of a new tool parents can use to create a Family Media Plan. The tool, available at https://www.healthychildren.org/English/media/Pages/default.aspx, enables parents to create a plan for each child in the household and reflects the individuality of each child’s use and age-appropriate guidelines.
After parents enter children’s names, the plan provides an editable template for each child that lays out screen-free zones, screen-free times, device curfews, recreational screen-time choices, alternative activities during non-screen time, media manners, digital citizenship, personal safety, sleep, and exercise.
Previous policy statements from the AAP relied primarily on research about television, a passive screen experience. In an age where many children and teens have interactive screens in their pockets and visit grandparents via video conferencing, however, the AAP Council on Communications and Media has likewise broadened its definition of media and noted the problems with applying research about television to other totally different types of screens.
“When we’re using media to connect, this is not what we’re traditionally calling screen time. These are tools,” Jenny S. Radesky, MD, lead author of the policy statement “Media and Young Minds,” said at the press conference (Pediatrics. 2016 Oct. doi: 10.1542/peds.2016-2592). She referred to the fact that many families who are spread across great distances, such as parents deployed overseas or grandparents in another state, use Skype, FaceTime, Google Hangouts, and similar programs to communicate and remain connected.
“We’re making sure our relationships are staying strong and not something to be discouraged with infants and toddlers, even though infants and toddlers will need their parent’s help to understand what they’re seeing on the screen,” said Dr. Radesky, a developmental-behavioral pediatrician at C.S. Mott Children’s Hospital at the University of Michigan in Ann Arbor.
The policy statement further notes that some emerging evidence has suggested children aged 2 and older can learn words from live video chatting with a responsive adult or by using an interactive touch screen that scaffolds learning.
An earlier introduction to screens
Among the most significant changes to the recommendations for children up to 5 years old is an allowance for introducing media before age 2, the previous policy’s age recommendation.
“If you want to introduce media, 18 months is the age when kids are cognitively ready to start, but we’re not saying parents need to introduce media then,” Dr. Radesky said, adding that more research is needed regarding devices such as tablets before it’s possible to know whether apps can be beneficial in toddlers that young. “There’s not enough evidence to know if interactivity helps or not right now,” she said.
The “Media and Young Minds” policy statement notes that children under age 2 years develop their cognitive, language, motor, and social-emotional skills through hands-on exploration and social interaction with trusted adults.
“Apps can’t do the things that parents’ minds can do or children’s minds can do on their own,” Dr. Radesky said. The policy notes that digital books, or eBooks, can be beneficial when used like a traditional physical book, but interactive elements to these eBooks could be distracting and decrease children’s comprehension.
When parents do choose to introduce media to their children, it’s “crucial that media be a shared experience” between the caregiving adult and the child, she said. “Think of media as a teaching tool, a way to connect and to create, not just to consume,” Dr. Radesky said.
What can preschoolers learn?
Although some laboratory research shows toddlers as young as 15 months can learn new words from touch screens, they have difficulty transferring that knowledge to the three-dimensional world. For children aged 3-5 years, however, both well-designed television programming and high-quality learning apps from Public Broadcasting Service (PBS) and the Sesame Workshop have shown benefits. In addition to early literacy, math, and personal and social development skills learned from shows such as Sesame Street, preschoolers have learned literacy skills from those programs’ apps.
But those apps are unfortunately in the minority.
“Most apps parents find under the ‘educational’ category in app stores have no such evidence of efficacy, target only rote academic skills, are not based on established curricula, and use little or no input from developmental specialists and educators,” the “Media and Young Minds” policy states. “The higher-order thinking skills and executive functions essential for school success, such as task persistence, impulse control, emotion regulation, and creative, flexible thinking, are best taught through unstructured and social (not digital) play, as well as responsive parent-child interactions.”
Risks and recommendations for preschoolers
Heavy media use among preschoolers, meanwhile, carries risks of increased weight – primarily as a result of food advertising and eating while watching TV – as well as reduced sleep and cognitive, language, and social/emotional delays.
“Content is crucial,” the “Media and Young Minds” policy notes. “Experimental evidence shows that switching from violent content to educational/prosocial content results in significant improvement in behavioral symptoms, particularly for low-income boys.”
The key points of the new statement therefore include the following recommendations:
• Limit media use to 1 hour a day in children ages 2 years and older.
• Do not use screens during mealtimes and for 1 hour before bedtime.
• Start discussing family and child media use with parents early in children’s lives.
• Educate parents about early brain development and help families develop a Family Media Use Plan.
• Discourage screen use besides video-chatting in children under 18 months old.
• Encourage caregiving adults to use screen media with children aged 18-24 months, who should not use it on their own.
• Encourage parents to rely on high-quality programming products such as PBS Kids, Sesame Workshop, and Common Sense Media.
• Help parents with challenges such as setting limits, finding alternatives to screen time, and calming children without using media.
• Avoid using screens or media to calm children except during rare extenuating circumstances, such as painful medical procedures and airplane flights.
• Encourage parents to avoid fast-paced programs, apps with distracting content, any media with violent content, and any background television, which can stunt children’s early language development.
Understanding older youth’s media use
As children move into school age and adolescence, the opportunities and utilities for media use expand – and so do the risks. Children and teens can benefit from media through gaining social support, learning about healthy behaviors, and discovering new ideas and knowledge, but youth remain at risk for obesity, sleep problems, cyberbullying, compromised privacy, and exposure to inaccurate, inappropriate or unsafe content, the “Media Use in School-Aged Children and Adolescents” policy statement reports.
Despite the wide range of media types available, TV remains the most commonly used media type among school-aged children and teens and is watched an average of 2 hours a day. Still, 91% of boys have access to a video game console, and 84% report playing games online or on a mobile phone. Further, three-quarters of teens own a smartphone and 76% use at least one social media site, with more than 70% maintaining a “social media portfolio” across several platforms.
Such social media use can provide teens with helpful support networks, particularly for those with ongoing illnesses or disabilities or those needing community support as lesbian, gay, bisexual, transgender, questioning, or intersex individuals. Social media can also promote wellness and healthy behaviors such as eating well and not smoking.
Risks for school-aged children and adolescents using media
Yet social media also can open the door to cyberbullying, leading to short-term and long-term social, academic, and health problems. It carries the risk of exploitation of youth or their images, or predation from pornographers and pedophiles. Children and teens must be made aware that the “Internet is forever” and should be taught to consider privacy and confidentiality concerns in their use of social and other media.
Another concern is teens’ “sexting,” in which they share sexually explicit messages and/or partly or fully nude photos. Exposures to unhealthy behaviors, such as substance abuse, sexual behaviors, self-injury, or disordered eating are likewise among the risks of social media, as they are with television and cinema.
In fact, TV/movie content showing alcohol use, smoking, and sexual activity is linked to earlier experimentation among children and adolescents. In addition, each extra hour of television watching is associated with increase in body mass index, as is having a TV set in the bedroom. Enjoying entertainment media while doing school work is linked to poor learning and academics.
Excessive media use may lead to problematic Internet use and Internet gaming disorder as described in the DSM-5, occurring among 4%-8.5% of children and adolescents.
“Symptoms can include a preoccupation with the activity, decreased interest in offline or ‘real life’ relationships, unsuccessful attempts to decrease use and withdrawal symptoms,” the “Media Use in School-Aged Children and Adolescents” policy statement notes.
Recommendations for older children
The policy statement advises pediatricians to help families and schools promote understanding of media’s risks and benefits, including awareness of tools to screen for sexting, cyberbullying, problematic Internet use, and Internet gaming disorder. Pediatricians should advocate for training in media literacy in the community and encourage parents to follow the media, sleep, and physical activity guidelines included in the Family Media Plan.
The research was supported by the American Academy of Pediatrics. The authors reported no disclosures.
SAN FRANCISCO – A new set of policy statements on children’s media use from the American Academy of Pediatrics brings the recommendations into the 21st century.
The new guidance, released at the annual meeting of the AAP, synthesizes the most current evidence on mobile devices, interactivity, educational technology, sleep, obesity, cognitive development, and other aspects of the pervasive digital environment children now grow up in.
“I think our policy statement reflects the changes in the media landscape because not all media use is the same,” Megan A. Moreno, MD, lead author of the policy statement, “Media Use in School-Aged Children and Adolescents,” said during a press conference (Pediatrics. 2016, Oct. doi: 10.1542/peds.2016-2592).
The new statement both lowers the overall age at which parents can feel comfortable introducing their children to media and decreases the amount of screen time exposure per day. One key component of the new guidelines includes the unveiling of a new tool parents can use to create a Family Media Plan. The tool, available at https://www.healthychildren.org/English/media/Pages/default.aspx, enables parents to create a plan for each child in the household and reflects the individuality of each child’s use and age-appropriate guidelines.
After parents enter children’s names, the plan provides an editable template for each child that lays out screen-free zones, screen-free times, device curfews, recreational screen-time choices, alternative activities during non-screen time, media manners, digital citizenship, personal safety, sleep, and exercise.
Previous policy statements from the AAP relied primarily on research about television, a passive screen experience. In an age where many children and teens have interactive screens in their pockets and visit grandparents via video conferencing, however, the AAP Council on Communications and Media has likewise broadened its definition of media and noted the problems with applying research about television to other totally different types of screens.
“When we’re using media to connect, this is not what we’re traditionally calling screen time. These are tools,” Jenny S. Radesky, MD, lead author of the policy statement “Media and Young Minds,” said at the press conference (Pediatrics. 2016 Oct. doi: 10.1542/peds.2016-2592). She referred to the fact that many families who are spread across great distances, such as parents deployed overseas or grandparents in another state, use Skype, FaceTime, Google Hangouts, and similar programs to communicate and remain connected.
“We’re making sure our relationships are staying strong and not something to be discouraged with infants and toddlers, even though infants and toddlers will need their parent’s help to understand what they’re seeing on the screen,” said Dr. Radesky, a developmental-behavioral pediatrician at C.S. Mott Children’s Hospital at the University of Michigan in Ann Arbor.
The policy statement further notes that some emerging evidence has suggested children aged 2 and older can learn words from live video chatting with a responsive adult or by using an interactive touch screen that scaffolds learning.
An earlier introduction to screens
Among the most significant changes to the recommendations for children up to 5 years old is an allowance for introducing media before age 2, the previous policy’s age recommendation.
“If you want to introduce media, 18 months is the age when kids are cognitively ready to start, but we’re not saying parents need to introduce media then,” Dr. Radesky said, adding that more research is needed regarding devices such as tablets before it’s possible to know whether apps can be beneficial in toddlers that young. “There’s not enough evidence to know if interactivity helps or not right now,” she said.
The “Media and Young Minds” policy statement notes that children under age 2 years develop their cognitive, language, motor, and social-emotional skills through hands-on exploration and social interaction with trusted adults.
“Apps can’t do the things that parents’ minds can do or children’s minds can do on their own,” Dr. Radesky said. The policy notes that digital books, or eBooks, can be beneficial when used like a traditional physical book, but interactive elements to these eBooks could be distracting and decrease children’s comprehension.
When parents do choose to introduce media to their children, it’s “crucial that media be a shared experience” between the caregiving adult and the child, she said. “Think of media as a teaching tool, a way to connect and to create, not just to consume,” Dr. Radesky said.
What can preschoolers learn?
Although some laboratory research shows toddlers as young as 15 months can learn new words from touch screens, they have difficulty transferring that knowledge to the three-dimensional world. For children aged 3-5 years, however, both well-designed television programming and high-quality learning apps from Public Broadcasting Service (PBS) and the Sesame Workshop have shown benefits. In addition to early literacy, math, and personal and social development skills learned from shows such as Sesame Street, preschoolers have learned literacy skills from those programs’ apps.
But those apps are unfortunately in the minority.
“Most apps parents find under the ‘educational’ category in app stores have no such evidence of efficacy, target only rote academic skills, are not based on established curricula, and use little or no input from developmental specialists and educators,” the “Media and Young Minds” policy states. “The higher-order thinking skills and executive functions essential for school success, such as task persistence, impulse control, emotion regulation, and creative, flexible thinking, are best taught through unstructured and social (not digital) play, as well as responsive parent-child interactions.”
Risks and recommendations for preschoolers
Heavy media use among preschoolers, meanwhile, carries risks of increased weight – primarily as a result of food advertising and eating while watching TV – as well as reduced sleep and cognitive, language, and social/emotional delays.
“Content is crucial,” the “Media and Young Minds” policy notes. “Experimental evidence shows that switching from violent content to educational/prosocial content results in significant improvement in behavioral symptoms, particularly for low-income boys.”
The key points of the new statement therefore include the following recommendations:
• Limit media use to 1 hour a day in children ages 2 years and older.
• Do not use screens during mealtimes and for 1 hour before bedtime.
• Start discussing family and child media use with parents early in children’s lives.
• Educate parents about early brain development and help families develop a Family Media Use Plan.
• Discourage screen use besides video-chatting in children under 18 months old.
• Encourage caregiving adults to use screen media with children aged 18-24 months, who should not use it on their own.
• Encourage parents to rely on high-quality programming products such as PBS Kids, Sesame Workshop, and Common Sense Media.
• Help parents with challenges such as setting limits, finding alternatives to screen time, and calming children without using media.
• Avoid using screens or media to calm children except during rare extenuating circumstances, such as painful medical procedures and airplane flights.
• Encourage parents to avoid fast-paced programs, apps with distracting content, any media with violent content, and any background television, which can stunt children’s early language development.
Understanding older youth’s media use
As children move into school age and adolescence, the opportunities and utilities for media use expand – and so do the risks. Children and teens can benefit from media through gaining social support, learning about healthy behaviors, and discovering new ideas and knowledge, but youth remain at risk for obesity, sleep problems, cyberbullying, compromised privacy, and exposure to inaccurate, inappropriate or unsafe content, the “Media Use in School-Aged Children and Adolescents” policy statement reports.
Despite the wide range of media types available, TV remains the most commonly used media type among school-aged children and teens and is watched an average of 2 hours a day. Still, 91% of boys have access to a video game console, and 84% report playing games online or on a mobile phone. Further, three-quarters of teens own a smartphone and 76% use at least one social media site, with more than 70% maintaining a “social media portfolio” across several platforms.
Such social media use can provide teens with helpful support networks, particularly for those with ongoing illnesses or disabilities or those needing community support as lesbian, gay, bisexual, transgender, questioning, or intersex individuals. Social media can also promote wellness and healthy behaviors such as eating well and not smoking.
Risks for school-aged children and adolescents using media
Yet social media also can open the door to cyberbullying, leading to short-term and long-term social, academic, and health problems. It carries the risk of exploitation of youth or their images, or predation from pornographers and pedophiles. Children and teens must be made aware that the “Internet is forever” and should be taught to consider privacy and confidentiality concerns in their use of social and other media.
Another concern is teens’ “sexting,” in which they share sexually explicit messages and/or partly or fully nude photos. Exposures to unhealthy behaviors, such as substance abuse, sexual behaviors, self-injury, or disordered eating are likewise among the risks of social media, as they are with television and cinema.
In fact, TV/movie content showing alcohol use, smoking, and sexual activity is linked to earlier experimentation among children and adolescents. In addition, each extra hour of television watching is associated with increase in body mass index, as is having a TV set in the bedroom. Enjoying entertainment media while doing school work is linked to poor learning and academics.
Excessive media use may lead to problematic Internet use and Internet gaming disorder as described in the DSM-5, occurring among 4%-8.5% of children and adolescents.
“Symptoms can include a preoccupation with the activity, decreased interest in offline or ‘real life’ relationships, unsuccessful attempts to decrease use and withdrawal symptoms,” the “Media Use in School-Aged Children and Adolescents” policy statement notes.
Recommendations for older children
The policy statement advises pediatricians to help families and schools promote understanding of media’s risks and benefits, including awareness of tools to screen for sexting, cyberbullying, problematic Internet use, and Internet gaming disorder. Pediatricians should advocate for training in media literacy in the community and encourage parents to follow the media, sleep, and physical activity guidelines included in the Family Media Plan.
The research was supported by the American Academy of Pediatrics. The authors reported no disclosures.

Sensory-related difficulties in children
A Google search of “sensory issues in children” reveals more than 20 million results and a wide range of terminology that can be confusing to parents, providers, and youth themselves. Phenomena such as sensory processing disorder, sensory integration disorder, sensory discrimination disorder, and sensory defensiveness are noted, and autism spectrum disorder (ASD) is a label not uncommonly attached to the former terms.
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) does not include a discrete diagnosis to apply to children who have sensory differences, (meaning that they have difficulties regulating sensory input and such difficulties affect their ability to successfully relate to the world around them), but these differences are now part of the diagnostic criteria for ASD. The literature indicates that a majority of youth with ASD demonstrate features of sensory overresponsiveness (JAMA Psychiatry. 2015 Aug;72[8]:778-86), and providers should rightfully be concerned about the possibility of autism in a youngster who is presenting with severe negative responses to auditory, visual, and/or tactile stimuli.
Notably, however, even though sensory problems are considered a feature of autism, they are not pathognomonic for the disorder, and most children with these problems are, in fact, not autistic. Children with deficits in their ability to modulate sensory stimuli can present with a wide range of emotional-behavioral problems, including externalizing behaviors and internalizing symptoms manifesting with anxiety, attention challenges, mood dysregulation, and overall poor adaptive functioning. The relationship between sensory issues (both underresponsiveness and overresponsiveness) and psychopathology is rather complicated as sensory dysfunction can exist independent of a psychiatric disorder, be a significant risk factor for the development of the disorder (J Abnorm Child Psychol. 2009 Nov;37[8]:1077-87), and have symptom overlap with the disorder.
All in all, in spite of this complexity, since the 1960’s (Am J Occup Ther. 1964 Jan-Feb;18:6-11), it’s been clear that sensory dysfunction in children is associated with impairments in development, learning, and self-regulation. Parents of these children experience elevated levels of stress (J Child Fam Stud. 2013 Oct 1;22[7]:912-21), and early identification of sensory differences, psychoeducation, and referral for treatment are critical to minimize these impacts and foster positive outcomes.
Case Summary

In gathering a history and administering the Autism Diagnostic Observation Schedule (ADOS), it became clear that Sarah did not present with the social-communicative impairments that characterize ASD, but she did demonstrate repetitive hand flapping, troubles tolerating large social get-togethers, hypersensitivities, and a vulnerability to getting stuck when attempting to transition between activities. It is not uncommon for Sarah to use “fight-and-flight” reactions when faced with internal or external discomfort. Child Behavior Checklist data revealed multi-informant endorsement of clinical range symptoms across broad-band and narrow-band domains. Additionally, the Sensory Profile–2 yielded elevated scores in categories measuring sensory seeking and sensory sensitivity. The Sensory Profile is a standardized tool that uses caregiver and teacher-completed questionnaires to examine a child’s sensory processing abilities and provide data regarding the effect of such sensory processing on functional performance. Integrating all the available data, our team certainly appreciated Sarah’s profound sensory overresponsiveness, and a diagnosis of an unspecified anxiety disorder was provided along with consideration for attention-deficit/hyperactivity disorder (ADHD) (with teacher input needed to further investigate this possibility). The family history revealed anxiety disorders occurring both maternally and paternally. Additionally, Sarah’s mother’s acknowledged having her own similar sensory issues as a child.
Discussion
Associations among anxiety, sensory overresponsiveness, and ADHD are recognized in the literature (Am J Occup Ther. 2009 Jul-Aug;63[4]:433-40) and have implications for treatment. Furthermore, there is evidence that there is a heritable aspect to sensory processing abnormalities, and tactile defensiveness is associated with fearful temperament and anxiety (J Abnorm Child Psychol. 2006 Jun;34[3]:393-407). In Sarah’s case, her intense behavioral response to ordinary sensory stimuli was striking, and she had not yet been referred for an occupational therapy evaluation, which was the primary recommendation to further assess and understand her complicated sensory profile. As one component of a comprehensive treatment plan, an occupational therapist (www.aota.org), by using evidence-based practices in a sensory-integration framework, could be helpful in addressing Sarah’s range of challenges and promoting positive outcomes related to socialization, behavioral regulation, and attention. Occupational therapists, with assistance from other team members, also could work with Sarah and her family on developing relaxation skills and use exposure and response prevention–oriented intervention strategies to address anxieties. Families, however, should be counseled about the limited data on the use of sensory-based therapies (Pediatrics. 2012 Jun;129[6]:1186-9); the use of parent-management training/family coaching should also be a treatment consideration to help promote overall regulatory functioning in the household.
Clinical pearl
When encountering youth with sensory-related challenges, a clinician’s diagnostic considerations should be more than just thinking about the possibility of an autism spectrum disorder. Symptoms of sensory overresponsiveness are associated with other emotional-behavioral conditions, but also can be seen without co-occurring psychopathology. With the latter, however, providers should be mindful that family-related impairments still may be quite noteworthy (J Am Acad Child Adolesc Psychiatry. 2011 Dec;50[12]:1210-9) and associated behavior problems could be attributed incorrectly to other diagnoses (which may lead to the recommendation of ineffective and inappropriate treatments). Much more research is needed to help develop a robust framework for diagnosing and labeling sensory issues in children and studying the efficacy of available intervention strategies.
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington, where he is director of the autism diagnostic clinic.
A Google search of “sensory issues in children” reveals more than 20 million results and a wide range of terminology that can be confusing to parents, providers, and youth themselves. Phenomena such as sensory processing disorder, sensory integration disorder, sensory discrimination disorder, and sensory defensiveness are noted, and autism spectrum disorder (ASD) is a label not uncommonly attached to the former terms.
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) does not include a discrete diagnosis to apply to children who have sensory differences, (meaning that they have difficulties regulating sensory input and such difficulties affect their ability to successfully relate to the world around them), but these differences are now part of the diagnostic criteria for ASD. The literature indicates that a majority of youth with ASD demonstrate features of sensory overresponsiveness (JAMA Psychiatry. 2015 Aug;72[8]:778-86), and providers should rightfully be concerned about the possibility of autism in a youngster who is presenting with severe negative responses to auditory, visual, and/or tactile stimuli.
Notably, however, even though sensory problems are considered a feature of autism, they are not pathognomonic for the disorder, and most children with these problems are, in fact, not autistic. Children with deficits in their ability to modulate sensory stimuli can present with a wide range of emotional-behavioral problems, including externalizing behaviors and internalizing symptoms manifesting with anxiety, attention challenges, mood dysregulation, and overall poor adaptive functioning. The relationship between sensory issues (both underresponsiveness and overresponsiveness) and psychopathology is rather complicated as sensory dysfunction can exist independent of a psychiatric disorder, be a significant risk factor for the development of the disorder (J Abnorm Child Psychol. 2009 Nov;37[8]:1077-87), and have symptom overlap with the disorder.
All in all, in spite of this complexity, since the 1960’s (Am J Occup Ther. 1964 Jan-Feb;18:6-11), it’s been clear that sensory dysfunction in children is associated with impairments in development, learning, and self-regulation. Parents of these children experience elevated levels of stress (J Child Fam Stud. 2013 Oct 1;22[7]:912-21), and early identification of sensory differences, psychoeducation, and referral for treatment are critical to minimize these impacts and foster positive outcomes.
Case Summary
In gathering a history and administering the Autism Diagnostic Observation Schedule (ADOS), it became clear that Sarah did not present with the social-communicative impairments that characterize ASD, but she did demonstrate repetitive hand flapping, troubles tolerating large social get-togethers, hypersensitivities, and a vulnerability to getting stuck when attempting to transition between activities. It is not uncommon for Sarah to use “fight-and-flight” reactions when faced with internal or external discomfort. Child Behavior Checklist data revealed multi-informant endorsement of clinical range symptoms across broad-band and narrow-band domains. Additionally, the Sensory Profile–2 yielded elevated scores in categories measuring sensory seeking and sensory sensitivity. The Sensory Profile is a standardized tool that uses caregiver and teacher-completed questionnaires to examine a child’s sensory processing abilities and provide data regarding the effect of such sensory processing on functional performance. Integrating all the available data, our team certainly appreciated Sarah’s profound sensory overresponsiveness, and a diagnosis of an unspecified anxiety disorder was provided along with consideration for attention-deficit/hyperactivity disorder (ADHD) (with teacher input needed to further investigate this possibility). The family history revealed anxiety disorders occurring both maternally and paternally. Additionally, Sarah’s mother’s acknowledged having her own similar sensory issues as a child.
Discussion
Associations among anxiety, sensory overresponsiveness, and ADHD are recognized in the literature (Am J Occup Ther. 2009 Jul-Aug;63[4]:433-40) and have implications for treatment. Furthermore, there is evidence that there is a heritable aspect to sensory processing abnormalities, and tactile defensiveness is associated with fearful temperament and anxiety (J Abnorm Child Psychol. 2006 Jun;34[3]:393-407). In Sarah’s case, her intense behavioral response to ordinary sensory stimuli was striking, and she had not yet been referred for an occupational therapy evaluation, which was the primary recommendation to further assess and understand her complicated sensory profile. As one component of a comprehensive treatment plan, an occupational therapist (www.aota.org), by using evidence-based practices in a sensory-integration framework, could be helpful in addressing Sarah’s range of challenges and promoting positive outcomes related to socialization, behavioral regulation, and attention. Occupational therapists, with assistance from other team members, also could work with Sarah and her family on developing relaxation skills and use exposure and response prevention–oriented intervention strategies to address anxieties. Families, however, should be counseled about the limited data on the use of sensory-based therapies (Pediatrics. 2012 Jun;129[6]:1186-9); the use of parent-management training/family coaching should also be a treatment consideration to help promote overall regulatory functioning in the household.
Clinical pearl
When encountering youth with sensory-related challenges, a clinician’s diagnostic considerations should be more than just thinking about the possibility of an autism spectrum disorder. Symptoms of sensory overresponsiveness are associated with other emotional-behavioral conditions, but also can be seen without co-occurring psychopathology. With the latter, however, providers should be mindful that family-related impairments still may be quite noteworthy (J Am Acad Child Adolesc Psychiatry. 2011 Dec;50[12]:1210-9) and associated behavior problems could be attributed incorrectly to other diagnoses (which may lead to the recommendation of ineffective and inappropriate treatments). Much more research is needed to help develop a robust framework for diagnosing and labeling sensory issues in children and studying the efficacy of available intervention strategies.
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington, where he is director of the autism diagnostic clinic.
A Google search of “sensory issues in children” reveals more than 20 million results and a wide range of terminology that can be confusing to parents, providers, and youth themselves. Phenomena such as sensory processing disorder, sensory integration disorder, sensory discrimination disorder, and sensory defensiveness are noted, and autism spectrum disorder (ASD) is a label not uncommonly attached to the former terms.
The fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM) does not include a discrete diagnosis to apply to children who have sensory differences, (meaning that they have difficulties regulating sensory input and such difficulties affect their ability to successfully relate to the world around them), but these differences are now part of the diagnostic criteria for ASD. The literature indicates that a majority of youth with ASD demonstrate features of sensory overresponsiveness (JAMA Psychiatry. 2015 Aug;72[8]:778-86), and providers should rightfully be concerned about the possibility of autism in a youngster who is presenting with severe negative responses to auditory, visual, and/or tactile stimuli.
Notably, however, even though sensory problems are considered a feature of autism, they are not pathognomonic for the disorder, and most children with these problems are, in fact, not autistic. Children with deficits in their ability to modulate sensory stimuli can present with a wide range of emotional-behavioral problems, including externalizing behaviors and internalizing symptoms manifesting with anxiety, attention challenges, mood dysregulation, and overall poor adaptive functioning. The relationship between sensory issues (both underresponsiveness and overresponsiveness) and psychopathology is rather complicated as sensory dysfunction can exist independent of a psychiatric disorder, be a significant risk factor for the development of the disorder (J Abnorm Child Psychol. 2009 Nov;37[8]:1077-87), and have symptom overlap with the disorder.
All in all, in spite of this complexity, since the 1960’s (Am J Occup Ther. 1964 Jan-Feb;18:6-11), it’s been clear that sensory dysfunction in children is associated with impairments in development, learning, and self-regulation. Parents of these children experience elevated levels of stress (J Child Fam Stud. 2013 Oct 1;22[7]:912-21), and early identification of sensory differences, psychoeducation, and referral for treatment are critical to minimize these impacts and foster positive outcomes.
Case Summary
In gathering a history and administering the Autism Diagnostic Observation Schedule (ADOS), it became clear that Sarah did not present with the social-communicative impairments that characterize ASD, but she did demonstrate repetitive hand flapping, troubles tolerating large social get-togethers, hypersensitivities, and a vulnerability to getting stuck when attempting to transition between activities. It is not uncommon for Sarah to use “fight-and-flight” reactions when faced with internal or external discomfort. Child Behavior Checklist data revealed multi-informant endorsement of clinical range symptoms across broad-band and narrow-band domains. Additionally, the Sensory Profile–2 yielded elevated scores in categories measuring sensory seeking and sensory sensitivity. The Sensory Profile is a standardized tool that uses caregiver and teacher-completed questionnaires to examine a child’s sensory processing abilities and provide data regarding the effect of such sensory processing on functional performance. Integrating all the available data, our team certainly appreciated Sarah’s profound sensory overresponsiveness, and a diagnosis of an unspecified anxiety disorder was provided along with consideration for attention-deficit/hyperactivity disorder (ADHD) (with teacher input needed to further investigate this possibility). The family history revealed anxiety disorders occurring both maternally and paternally. Additionally, Sarah’s mother’s acknowledged having her own similar sensory issues as a child.
Discussion
Associations among anxiety, sensory overresponsiveness, and ADHD are recognized in the literature (Am J Occup Ther. 2009 Jul-Aug;63[4]:433-40) and have implications for treatment. Furthermore, there is evidence that there is a heritable aspect to sensory processing abnormalities, and tactile defensiveness is associated with fearful temperament and anxiety (J Abnorm Child Psychol. 2006 Jun;34[3]:393-407). In Sarah’s case, her intense behavioral response to ordinary sensory stimuli was striking, and she had not yet been referred for an occupational therapy evaluation, which was the primary recommendation to further assess and understand her complicated sensory profile. As one component of a comprehensive treatment plan, an occupational therapist (www.aota.org), by using evidence-based practices in a sensory-integration framework, could be helpful in addressing Sarah’s range of challenges and promoting positive outcomes related to socialization, behavioral regulation, and attention. Occupational therapists, with assistance from other team members, also could work with Sarah and her family on developing relaxation skills and use exposure and response prevention–oriented intervention strategies to address anxieties. Families, however, should be counseled about the limited data on the use of sensory-based therapies (Pediatrics. 2012 Jun;129[6]:1186-9); the use of parent-management training/family coaching should also be a treatment consideration to help promote overall regulatory functioning in the household.
Clinical pearl
When encountering youth with sensory-related challenges, a clinician’s diagnostic considerations should be more than just thinking about the possibility of an autism spectrum disorder. Symptoms of sensory overresponsiveness are associated with other emotional-behavioral conditions, but also can be seen without co-occurring psychopathology. With the latter, however, providers should be mindful that family-related impairments still may be quite noteworthy (J Am Acad Child Adolesc Psychiatry. 2011 Dec;50[12]:1210-9) and associated behavior problems could be attributed incorrectly to other diagnoses (which may lead to the recommendation of ineffective and inappropriate treatments). Much more research is needed to help develop a robust framework for diagnosing and labeling sensory issues in children and studying the efficacy of available intervention strategies.
Dr. Dickerson, a child and adolescent psychiatrist, is assistant professor of psychiatry at the University of Vermont, Burlington, where he is director of the autism diagnostic clinic.
Obesity risk rises when kids aren’t active 1 hour a day
SAN FRANCISCO – The behavioral characteristic that correlated the most with obesity in school-age children was being active less than 1 hour per day, according to findings from a prospective study.
Meredith Johnston, DO, of Eau Claire Cooperative in Columbia, S.C., performed the study with Nirupma Sharma, MD, at Children’s Hospital of Georgia in Augusta. The prospective, questionnaire-based study was conducted with 103 children, aged 5-18 years, over a 6-month period. Dr. Johnston reported the results in a poster presentation at the annual meeting of the American Academy of Pediatrics.
“Giving a child one modifiable lifestyle factor to incorporate into their lifestyle instead of overwhelming them with multiple changes is more likely to produce significant change to prevent obesity,” Dr. Johnston said in an interview. “And finding an activity that the child enjoys will produce the best adherence and greatest long-term effects.”
Considering the findings of the study, “children should exercise 30 minutes to 1 hour a day to prevent childhood obesity,” she explained.
A recent review in the Annual Review of Public Health has shown a change in teen physical activity patterns due to an increase in screen time and a decrease in opportunities for physical activities at school and in the community. Giving patients tools for exercise such as dancing to YouTube videos or playing active video games might be a good idea, Dr. Johnston said.
Drinking more than five cans of soda in a day also was significantly associated with a higher BMI (P = .001). That lifestyle factor could be addressed at subsequent well-child visits.
Such efforts are critical, she noted, because an estimated 17% of 2- to 19-year-olds are obese, and 15% are overweight.
Dr. Johnston said she had no relevant financial disclosures.
SAN FRANCISCO – The behavioral characteristic that correlated the most with obesity in school-age children was being active less than 1 hour per day, according to findings from a prospective study.
Meredith Johnston, DO, of Eau Claire Cooperative in Columbia, S.C., performed the study with Nirupma Sharma, MD, at Children’s Hospital of Georgia in Augusta. The prospective, questionnaire-based study was conducted with 103 children, aged 5-18 years, over a 6-month period. Dr. Johnston reported the results in a poster presentation at the annual meeting of the American Academy of Pediatrics.
“Giving a child one modifiable lifestyle factor to incorporate into their lifestyle instead of overwhelming them with multiple changes is more likely to produce significant change to prevent obesity,” Dr. Johnston said in an interview. “And finding an activity that the child enjoys will produce the best adherence and greatest long-term effects.”
Considering the findings of the study, “children should exercise 30 minutes to 1 hour a day to prevent childhood obesity,” she explained.
A recent review in the Annual Review of Public Health has shown a change in teen physical activity patterns due to an increase in screen time and a decrease in opportunities for physical activities at school and in the community. Giving patients tools for exercise such as dancing to YouTube videos or playing active video games might be a good idea, Dr. Johnston said.
Drinking more than five cans of soda in a day also was significantly associated with a higher BMI (P = .001). That lifestyle factor could be addressed at subsequent well-child visits.
Such efforts are critical, she noted, because an estimated 17% of 2- to 19-year-olds are obese, and 15% are overweight.
Dr. Johnston said she had no relevant financial disclosures.
SAN FRANCISCO – The behavioral characteristic that correlated the most with obesity in school-age children was being active less than 1 hour per day, according to findings from a prospective study.
Meredith Johnston, DO, of Eau Claire Cooperative in Columbia, S.C., performed the study with Nirupma Sharma, MD, at Children’s Hospital of Georgia in Augusta. The prospective, questionnaire-based study was conducted with 103 children, aged 5-18 years, over a 6-month period. Dr. Johnston reported the results in a poster presentation at the annual meeting of the American Academy of Pediatrics.
“Giving a child one modifiable lifestyle factor to incorporate into their lifestyle instead of overwhelming them with multiple changes is more likely to produce significant change to prevent obesity,” Dr. Johnston said in an interview. “And finding an activity that the child enjoys will produce the best adherence and greatest long-term effects.”
Considering the findings of the study, “children should exercise 30 minutes to 1 hour a day to prevent childhood obesity,” she explained.
A recent review in the Annual Review of Public Health has shown a change in teen physical activity patterns due to an increase in screen time and a decrease in opportunities for physical activities at school and in the community. Giving patients tools for exercise such as dancing to YouTube videos or playing active video games might be a good idea, Dr. Johnston said.
Drinking more than five cans of soda in a day also was significantly associated with a higher BMI (P = .001). That lifestyle factor could be addressed at subsequent well-child visits.
Such efforts are critical, she noted, because an estimated 17% of 2- to 19-year-olds are obese, and 15% are overweight.
Dr. Johnston said she had no relevant financial disclosures.
AT AAP 2016
Key clinical point:
Major finding: Being active less than 1 hour per day was significantly associated with a higher body mass index in children (P = .006 for 30 minutes to 1 hour, and P = .017 for less than 30 minutes).
Data source: A prospective, questionnaire-based study involving 103 children, aged 5-18 years, over a 6-month period.
Disclosures: Dr. Johnston said she had no relevant financial disclosures.
Updated AAP safe sleep recs for infants reinforce life-saving messages
SAN FRANCISCO – At sleep time, infants should share their parents’ bedroom on a separate sleep surface without bed sharing, should be placed on their backs on a firm surface, and should have a sleep area free of blankets and soft objects, according to updated guidelines from the American Academy of Pediatrics aimed at reducing the risk of sudden infant death syndrome (SIDS) and other sleep-related infant deaths.
Drafted by a multidisciplinary task force, the set of 19 evidence-based recommendations largely reiterate messages that the academy has promoted for years such as “back to sleep for every sleep,” according to task force member Fern R. Hauck, MD, the Spencer P. Bass, MD, Twenty-First Century Professor of Family Medicine at the University of Virginia, Charlottesville. They were unveiled in a press briefing at the academy’s annual meeting and simultaneously published (Pediatrics. 2016;138[5]:e20162938).
Progress, but still a ways to go
Education campaigns that convey these and related messages to new parents and other caregivers have led to a more than halving of the rate of SIDS in recent decades. Yet, 3,500 infants are still lost each year to this syndrome and other sleep-related causes of infant death, such as unintentional suffocation, collectively called sudden unexpected infant death (SUID).

New is a recommendation for skin-to-skin care for at least the first hour of life for healthy newborns, as soon as the mother is alert enough to respond to her infant, according to Dr. Hauck. The aims here are to optimize neurodevelopment and promote temperature regulation.
There is no evidence that swaddling reduces the risk of SIDS, but parents can still use this technique if they wish as long as infants are placed on their back and it is discontinued as soon as they start to show signs of rolling over, she said. Evidence is also lacking for new technologies marketed as protective, for example, crib mattresses designed to reduce re-breathing of carbon dioxide should an infant become prone.
Sleeping in the parents’ room but on a separate surface decreases the risk of SIDS by as much as 50%, according to several studies. Bed sharing is not recommended because of the risk of suffocation, strangulation, and entrapment, the policy states.
The updated recommendations should be followed for every sleep and by every caregiver, until the child reaches 1 year of age, Dr. Hauck stressed. “This includes nap time and bedtime sleep, at home, in day care, or in any other locations where the baby is sleeping.”
“We feel that these messages need to start while the mom’s pregnant because some of the decisions that are made that are not always the best decisions, when the mother is exhausted, can occur spur of the moment,” she added. “As pediatricians, you can set up a prebirth visit to start talking about this, and obstetricians should be doing more as well to bring this up during their prenatal visits.”
Other recommendations include offering a pacifier at nap time and bedtime; avoiding smoke exposure during pregnancy and after birth; and avoiding alcohol and illicit drug use during pregnancy and after birth.
Breastfeeding issues
Although breastfeeding protects against SIDS, it can pose some problems for safe sleep practices, acknowledged Lori B. Feldman-Winter, MD, a liaison from the AAP section on breastfeeding to the task force, as well as head of the division of adolescent medicine and professor of pediatrics at Cooper University Health Care in Camden, N.J.

Bedside sleepers (also called sidecar sleepers) that attach to the parents’ bed may help facilitate the dual aims of breastfeeding and safe sleep, but they have not been formally studied to assess their impact on SIDS risk.
Raising awareness
“As a father and pediatrician, I want parents to know that their baby is safest following the AAP safe sleep recommendations, and spreading this message has become my life’s mission,” said Dr. Samuel P. Hanke, a pediatric cardiologist at the University of Cincinnati, who knows the heartbreak of SIDS firsthand.

“We know practicing safe sleep is hard. We have to be vigilant. We need to start adopting a mentality that safe sleep is not negotiable,” Dr. Hanke asserted. “We cannot emphasize enough that practicing safe sleep for every sleep is as important as buckling your child into a car seat for every drive. And just like car seats, this change won’t occur overnight.”
Federal commitment
Since the 1970s, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) in Bethesda, Md., has been supporting and performing much of the research on which the updated recommendations are based. This research continues to help identify areas where greater efforts are needed, according to acting director Catherine Y. Spong, MD.

NICHD also conducts and collaborates on related education campaigns, such as Safe to Sleep, to disseminate messages such as those in the updated AAP recommendations as widely as possible.
“I encourage all physicians, pediatricians, nurses, and other health care and child care providers to lend their authoritative voices to the Safe to Sleep effort,” Dr. Spong said. “Join us all in sharing safe infant sleep recommendations and in supporting parents and caregivers to make informed decisions that will help keep their baby safe during sleep.”
A closer look at setting
Published in conjunction with the guidelines is a study on risk factors that looked at the role of the setting in which sleep-related infant deaths occur (Pediatrics. 2016 Oct 24:e20161124).
The analysis of nearly 12,000 such deaths found that, relative to counterparts who died in their home, infants who died outside of their home were more likely to be in a stroller or car seat at the time (adjusted odds ratio, 2.6) and in other locations, such as on the floor or a futon (1.9), and to have been placed prone (1.1). They were less likely to have been sharing a bed (0.7).
The groups did not differ in terms of whether the infant was sleeping in an adult bed or on a person, on a couch or chair, or with any objects in their sleep environment.
“Caregivers should be educated on the importance of placing infants to sleep supine in cribs/bassinets to protect against sleep-related deaths, both in and out of the home,” conclude the investigators, one of whom disclosed serving as a paid expert witness in cases of sleep-related infant death.
SAN FRANCISCO – At sleep time, infants should share their parents’ bedroom on a separate sleep surface without bed sharing, should be placed on their backs on a firm surface, and should have a sleep area free of blankets and soft objects, according to updated guidelines from the American Academy of Pediatrics aimed at reducing the risk of sudden infant death syndrome (SIDS) and other sleep-related infant deaths.
Drafted by a multidisciplinary task force, the set of 19 evidence-based recommendations largely reiterate messages that the academy has promoted for years such as “back to sleep for every sleep,” according to task force member Fern R. Hauck, MD, the Spencer P. Bass, MD, Twenty-First Century Professor of Family Medicine at the University of Virginia, Charlottesville. They were unveiled in a press briefing at the academy’s annual meeting and simultaneously published (Pediatrics. 2016;138[5]:e20162938).
Progress, but still a ways to go
Education campaigns that convey these and related messages to new parents and other caregivers have led to a more than halving of the rate of SIDS in recent decades. Yet, 3,500 infants are still lost each year to this syndrome and other sleep-related causes of infant death, such as unintentional suffocation, collectively called sudden unexpected infant death (SUID).
New is a recommendation for skin-to-skin care for at least the first hour of life for healthy newborns, as soon as the mother is alert enough to respond to her infant, according to Dr. Hauck. The aims here are to optimize neurodevelopment and promote temperature regulation.
There is no evidence that swaddling reduces the risk of SIDS, but parents can still use this technique if they wish as long as infants are placed on their back and it is discontinued as soon as they start to show signs of rolling over, she said. Evidence is also lacking for new technologies marketed as protective, for example, crib mattresses designed to reduce re-breathing of carbon dioxide should an infant become prone.
Sleeping in the parents’ room but on a separate surface decreases the risk of SIDS by as much as 50%, according to several studies. Bed sharing is not recommended because of the risk of suffocation, strangulation, and entrapment, the policy states.
The updated recommendations should be followed for every sleep and by every caregiver, until the child reaches 1 year of age, Dr. Hauck stressed. “This includes nap time and bedtime sleep, at home, in day care, or in any other locations where the baby is sleeping.”
“We feel that these messages need to start while the mom’s pregnant because some of the decisions that are made that are not always the best decisions, when the mother is exhausted, can occur spur of the moment,” she added. “As pediatricians, you can set up a prebirth visit to start talking about this, and obstetricians should be doing more as well to bring this up during their prenatal visits.”
Other recommendations include offering a pacifier at nap time and bedtime; avoiding smoke exposure during pregnancy and after birth; and avoiding alcohol and illicit drug use during pregnancy and after birth.
Breastfeeding issues
Although breastfeeding protects against SIDS, it can pose some problems for safe sleep practices, acknowledged Lori B. Feldman-Winter, MD, a liaison from the AAP section on breastfeeding to the task force, as well as head of the division of adolescent medicine and professor of pediatrics at Cooper University Health Care in Camden, N.J.
Bedside sleepers (also called sidecar sleepers) that attach to the parents’ bed may help facilitate the dual aims of breastfeeding and safe sleep, but they have not been formally studied to assess their impact on SIDS risk.
Raising awareness
“As a father and pediatrician, I want parents to know that their baby is safest following the AAP safe sleep recommendations, and spreading this message has become my life’s mission,” said Dr. Samuel P. Hanke, a pediatric cardiologist at the University of Cincinnati, who knows the heartbreak of SIDS firsthand.
“We know practicing safe sleep is hard. We have to be vigilant. We need to start adopting a mentality that safe sleep is not negotiable,” Dr. Hanke asserted. “We cannot emphasize enough that practicing safe sleep for every sleep is as important as buckling your child into a car seat for every drive. And just like car seats, this change won’t occur overnight.”
Federal commitment
Since the 1970s, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) in Bethesda, Md., has been supporting and performing much of the research on which the updated recommendations are based. This research continues to help identify areas where greater efforts are needed, according to acting director Catherine Y. Spong, MD.
NICHD also conducts and collaborates on related education campaigns, such as Safe to Sleep, to disseminate messages such as those in the updated AAP recommendations as widely as possible.
“I encourage all physicians, pediatricians, nurses, and other health care and child care providers to lend their authoritative voices to the Safe to Sleep effort,” Dr. Spong said. “Join us all in sharing safe infant sleep recommendations and in supporting parents and caregivers to make informed decisions that will help keep their baby safe during sleep.”
A closer look at setting
Published in conjunction with the guidelines is a study on risk factors that looked at the role of the setting in which sleep-related infant deaths occur (Pediatrics. 2016 Oct 24:e20161124).
The analysis of nearly 12,000 such deaths found that, relative to counterparts who died in their home, infants who died outside of their home were more likely to be in a stroller or car seat at the time (adjusted odds ratio, 2.6) and in other locations, such as on the floor or a futon (1.9), and to have been placed prone (1.1). They were less likely to have been sharing a bed (0.7).
The groups did not differ in terms of whether the infant was sleeping in an adult bed or on a person, on a couch or chair, or with any objects in their sleep environment.
“Caregivers should be educated on the importance of placing infants to sleep supine in cribs/bassinets to protect against sleep-related deaths, both in and out of the home,” conclude the investigators, one of whom disclosed serving as a paid expert witness in cases of sleep-related infant death.
SAN FRANCISCO – At sleep time, infants should share their parents’ bedroom on a separate sleep surface without bed sharing, should be placed on their backs on a firm surface, and should have a sleep area free of blankets and soft objects, according to updated guidelines from the American Academy of Pediatrics aimed at reducing the risk of sudden infant death syndrome (SIDS) and other sleep-related infant deaths.
Drafted by a multidisciplinary task force, the set of 19 evidence-based recommendations largely reiterate messages that the academy has promoted for years such as “back to sleep for every sleep,” according to task force member Fern R. Hauck, MD, the Spencer P. Bass, MD, Twenty-First Century Professor of Family Medicine at the University of Virginia, Charlottesville. They were unveiled in a press briefing at the academy’s annual meeting and simultaneously published (Pediatrics. 2016;138[5]:e20162938).
Progress, but still a ways to go
Education campaigns that convey these and related messages to new parents and other caregivers have led to a more than halving of the rate of SIDS in recent decades. Yet, 3,500 infants are still lost each year to this syndrome and other sleep-related causes of infant death, such as unintentional suffocation, collectively called sudden unexpected infant death (SUID).
New is a recommendation for skin-to-skin care for at least the first hour of life for healthy newborns, as soon as the mother is alert enough to respond to her infant, according to Dr. Hauck. The aims here are to optimize neurodevelopment and promote temperature regulation.
There is no evidence that swaddling reduces the risk of SIDS, but parents can still use this technique if they wish as long as infants are placed on their back and it is discontinued as soon as they start to show signs of rolling over, she said. Evidence is also lacking for new technologies marketed as protective, for example, crib mattresses designed to reduce re-breathing of carbon dioxide should an infant become prone.
Sleeping in the parents’ room but on a separate surface decreases the risk of SIDS by as much as 50%, according to several studies. Bed sharing is not recommended because of the risk of suffocation, strangulation, and entrapment, the policy states.
The updated recommendations should be followed for every sleep and by every caregiver, until the child reaches 1 year of age, Dr. Hauck stressed. “This includes nap time and bedtime sleep, at home, in day care, or in any other locations where the baby is sleeping.”
“We feel that these messages need to start while the mom’s pregnant because some of the decisions that are made that are not always the best decisions, when the mother is exhausted, can occur spur of the moment,” she added. “As pediatricians, you can set up a prebirth visit to start talking about this, and obstetricians should be doing more as well to bring this up during their prenatal visits.”
Other recommendations include offering a pacifier at nap time and bedtime; avoiding smoke exposure during pregnancy and after birth; and avoiding alcohol and illicit drug use during pregnancy and after birth.
Breastfeeding issues
Although breastfeeding protects against SIDS, it can pose some problems for safe sleep practices, acknowledged Lori B. Feldman-Winter, MD, a liaison from the AAP section on breastfeeding to the task force, as well as head of the division of adolescent medicine and professor of pediatrics at Cooper University Health Care in Camden, N.J.
Bedside sleepers (also called sidecar sleepers) that attach to the parents’ bed may help facilitate the dual aims of breastfeeding and safe sleep, but they have not been formally studied to assess their impact on SIDS risk.
Raising awareness
“As a father and pediatrician, I want parents to know that their baby is safest following the AAP safe sleep recommendations, and spreading this message has become my life’s mission,” said Dr. Samuel P. Hanke, a pediatric cardiologist at the University of Cincinnati, who knows the heartbreak of SIDS firsthand.
“We know practicing safe sleep is hard. We have to be vigilant. We need to start adopting a mentality that safe sleep is not negotiable,” Dr. Hanke asserted. “We cannot emphasize enough that practicing safe sleep for every sleep is as important as buckling your child into a car seat for every drive. And just like car seats, this change won’t occur overnight.”
Federal commitment
Since the 1970s, the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) in Bethesda, Md., has been supporting and performing much of the research on which the updated recommendations are based. This research continues to help identify areas where greater efforts are needed, according to acting director Catherine Y. Spong, MD.
NICHD also conducts and collaborates on related education campaigns, such as Safe to Sleep, to disseminate messages such as those in the updated AAP recommendations as widely as possible.
“I encourage all physicians, pediatricians, nurses, and other health care and child care providers to lend their authoritative voices to the Safe to Sleep effort,” Dr. Spong said. “Join us all in sharing safe infant sleep recommendations and in supporting parents and caregivers to make informed decisions that will help keep their baby safe during sleep.”
A closer look at setting
Published in conjunction with the guidelines is a study on risk factors that looked at the role of the setting in which sleep-related infant deaths occur (Pediatrics. 2016 Oct 24:e20161124).
The analysis of nearly 12,000 such deaths found that, relative to counterparts who died in their home, infants who died outside of their home were more likely to be in a stroller or car seat at the time (adjusted odds ratio, 2.6) and in other locations, such as on the floor or a futon (1.9), and to have been placed prone (1.1). They were less likely to have been sharing a bed (0.7).
The groups did not differ in terms of whether the infant was sleeping in an adult bed or on a person, on a couch or chair, or with any objects in their sleep environment.
“Caregivers should be educated on the importance of placing infants to sleep supine in cribs/bassinets to protect against sleep-related deaths, both in and out of the home,” conclude the investigators, one of whom disclosed serving as a paid expert witness in cases of sleep-related infant death.
EXPERT ANALYSIS FROM AAP 16
Choosing Wisely Initiative Helps Physicians Provide Appropriate Care
HILTON HEAD, SC—Physicians sometimes order unnecessary medical tests and procedures for their patients, which results in wasteful spending and inappropriate care. Following medical associations’ practice recommendations, which have been collected by the Choosing Wisely initiative, can help physicians reduce waste in the health care system and provide appropriate treatment for patients, according to an overview presented at the 39th Annual Contemporary Clinical Neurology Symposium.
Avoiding Unnecessary Treatments and Tests
The American Board of Internal Medicine Foundation created the Choosing Wisely website to encourage dialogue between physicians and patients about the overuse of treatments and tests. An additional goal was to empower patients to make informed treatment decisions. More than 70 societies, including the American Academy of Neurology (AAN) and the American Headache Society, submitted recommendations to advise patients and clinicians about proper healthcare. “You can find a list of all the organizations that contributed on the Choosing Wisely website, and each one was asked to contribute five different topics for Choosing Wisely,” said Peter Donofrio, MD, Professor of Neurology at Vanderbilt University in Nashville.

The AAN recommends that clinicians not perform an EEG for headaches. In addition, the organization recommends that physicians not perform imaging of the carotid arteries for simple syncope without other neurologic symptoms. For patients with migraine, opioids or butalbital treatment should be a last resort. The AAN also recommends that doctors not prescribe interferon-beta or glatiramer acetate for patients with disability resulting from progressive, nonrelapsing forms of multiple sclerosis, because the drugs are ineffective. Finally, it advises doctors not to recommend carotid endarterectomy for asymptomatic carotid stenosis unless the complication rate from surgery is less than 3%.
The American Association of Neuromuscular and Electrodiagnostic Medicine recommends that physicians not perform MRI scans of the brain or spine for patients with peripheral neuropathy without signs of cerebral or spinal cord disease. In addition, the association discourages physicians from performing nerve conduction studies (NCSs) without a needle EMG for radiculopathy assessment. It also recommends that physicians not order or perform four-limb EMG/NCS testing for neck or back pain after trauma.
Treating Acute Low Back Pain and Headache
Other medical associations have made recommendations regarding the assessment and treatment of acute low back pain and headache. The North American Spine Society does not recommend advanced imaging of the spine within the first six weeks in patients with nonspecific acute low back pain in the absence of red flags.
The American Headache Society (AHS) recommends that physicians avoid advising prolonged or frequent use of over-the-counter pain medications for headache. The organization also discourages physicians from prescribing opioid or butalbital-containing medications as first-line treatment for recurrent headache disorders. Furthermore, it does not recommend surgical deactivation of migraine trigger points outside of a clinical trial. In addition, the society advises physicians not to perform CT imaging for headache when an MRI is available, except in emergency settings. The society also recommends that physicians should not perform neuroimaging studies for patients with stable headaches that meet migraine criteria.
When CT Scans Are Unnecessary in Children
The American Academy of Pediatrics (AAP) advises that CT scans and MRI scans are not necessary in a child with simple febrile seizure. The AAP also does not recommend CT scans for the immediate evaluation of minor head injuries; clinical observation and Pediatric Emergency Care Applied Research Network (PECARN) criteria should be used to determine whether imaging is indicated.
Treating Insomnia and Sleep Disorders
The American Academy of Sleep Medicine advises doctors not to prescribe medication for childhood insomnia, which usually arises from parent–child interactions and responds to behavioral intervention. In addition, the academy does no
—Erica Tricarico
Suggested Reading
Callaghan BC, De Lott LB, Kerber KA, et al. Neurology Choosing Wisely recommendations: 74 and growing. Neurol Clin Pract. 2015;5(5):439-447.
Langer-Gould AM, Anderson WE, Armstrong MJ, et al. The American Academy of Neurology’s top five choosing wisely recommendations. Neurology. 2013;81(11):1004-1011.
Loder E, Weisenbaum E, Fishberg B, et al. Choosing wisely in headache medicine: the American Headache Society’s list of five things physicians and patients should question. Headache. 2013;53(10):1651-1659.
HILTON HEAD, SC—Physicians sometimes order unnecessary medical tests and procedures for their patients, which results in wasteful spending and inappropriate care. Following medical associations’ practice recommendations, which have been collected by the Choosing Wisely initiative, can help physicians reduce waste in the health care system and provide appropriate treatment for patients, according to an overview presented at the 39th Annual Contemporary Clinical Neurology Symposium.
Avoiding Unnecessary Treatments and Tests
The American Board of Internal Medicine Foundation created the Choosing Wisely website to encourage dialogue between physicians and patients about the overuse of treatments and tests. An additional goal was to empower patients to make informed treatment decisions. More than 70 societies, including the American Academy of Neurology (AAN) and the American Headache Society, submitted recommendations to advise patients and clinicians about proper healthcare. “You can find a list of all the organizations that contributed on the Choosing Wisely website, and each one was asked to contribute five different topics for Choosing Wisely,” said Peter Donofrio, MD, Professor of Neurology at Vanderbilt University in Nashville.
The AAN recommends that clinicians not perform an EEG for headaches. In addition, the organization recommends that physicians not perform imaging of the carotid arteries for simple syncope without other neurologic symptoms. For patients with migraine, opioids or butalbital treatment should be a last resort. The AAN also recommends that doctors not prescribe interferon-beta or glatiramer acetate for patients with disability resulting from progressive, nonrelapsing forms of multiple sclerosis, because the drugs are ineffective. Finally, it advises doctors not to recommend carotid endarterectomy for asymptomatic carotid stenosis unless the complication rate from surgery is less than 3%.
The American Association of Neuromuscular and Electrodiagnostic Medicine recommends that physicians not perform MRI scans of the brain or spine for patients with peripheral neuropathy without signs of cerebral or spinal cord disease. In addition, the association discourages physicians from performing nerve conduction studies (NCSs) without a needle EMG for radiculopathy assessment. It also recommends that physicians not order or perform four-limb EMG/NCS testing for neck or back pain after trauma.
Treating Acute Low Back Pain and Headache
Other medical associations have made recommendations regarding the assessment and treatment of acute low back pain and headache. The North American Spine Society does not recommend advanced imaging of the spine within the first six weeks in patients with nonspecific acute low back pain in the absence of red flags.
The American Headache Society (AHS) recommends that physicians avoid advising prolonged or frequent use of over-the-counter pain medications for headache. The organization also discourages physicians from prescribing opioid or butalbital-containing medications as first-line treatment for recurrent headache disorders. Furthermore, it does not recommend surgical deactivation of migraine trigger points outside of a clinical trial. In addition, the society advises physicians not to perform CT imaging for headache when an MRI is available, except in emergency settings. The society also recommends that physicians should not perform neuroimaging studies for patients with stable headaches that meet migraine criteria.
When CT Scans Are Unnecessary in Children
The American Academy of Pediatrics (AAP) advises that CT scans and MRI scans are not necessary in a child with simple febrile seizure. The AAP also does not recommend CT scans for the immediate evaluation of minor head injuries; clinical observation and Pediatric Emergency Care Applied Research Network (PECARN) criteria should be used to determine whether imaging is indicated.
Treating Insomnia and Sleep Disorders
The American Academy of Sleep Medicine advises doctors not to prescribe medication for childhood insomnia, which usually arises from parent–child interactions and responds to behavioral intervention. In addition, the academy does no
—Erica Tricarico
Suggested Reading
Callaghan BC, De Lott LB, Kerber KA, et al. Neurology Choosing Wisely recommendations: 74 and growing. Neurol Clin Pract. 2015;5(5):439-447.
Langer-Gould AM, Anderson WE, Armstrong MJ, et al. The American Academy of Neurology’s top five choosing wisely recommendations. Neurology. 2013;81(11):1004-1011.
Loder E, Weisenbaum E, Fishberg B, et al. Choosing wisely in headache medicine: the American Headache Society’s list of five things physicians and patients should question. Headache. 2013;53(10):1651-1659.
HILTON HEAD, SC—Physicians sometimes order unnecessary medical tests and procedures for their patients, which results in wasteful spending and inappropriate care. Following medical associations’ practice recommendations, which have been collected by the Choosing Wisely initiative, can help physicians reduce waste in the health care system and provide appropriate treatment for patients, according to an overview presented at the 39th Annual Contemporary Clinical Neurology Symposium.
Avoiding Unnecessary Treatments and Tests
The American Board of Internal Medicine Foundation created the Choosing Wisely website to encourage dialogue between physicians and patients about the overuse of treatments and tests. An additional goal was to empower patients to make informed treatment decisions. More than 70 societies, including the American Academy of Neurology (AAN) and the American Headache Society, submitted recommendations to advise patients and clinicians about proper healthcare. “You can find a list of all the organizations that contributed on the Choosing Wisely website, and each one was asked to contribute five different topics for Choosing Wisely,” said Peter Donofrio, MD, Professor of Neurology at Vanderbilt University in Nashville.
The AAN recommends that clinicians not perform an EEG for headaches. In addition, the organization recommends that physicians not perform imaging of the carotid arteries for simple syncope without other neurologic symptoms. For patients with migraine, opioids or butalbital treatment should be a last resort. The AAN also recommends that doctors not prescribe interferon-beta or glatiramer acetate for patients with disability resulting from progressive, nonrelapsing forms of multiple sclerosis, because the drugs are ineffective. Finally, it advises doctors not to recommend carotid endarterectomy for asymptomatic carotid stenosis unless the complication rate from surgery is less than 3%.
The American Association of Neuromuscular and Electrodiagnostic Medicine recommends that physicians not perform MRI scans of the brain or spine for patients with peripheral neuropathy without signs of cerebral or spinal cord disease. In addition, the association discourages physicians from performing nerve conduction studies (NCSs) without a needle EMG for radiculopathy assessment. It also recommends that physicians not order or perform four-limb EMG/NCS testing for neck or back pain after trauma.
Treating Acute Low Back Pain and Headache
Other medical associations have made recommendations regarding the assessment and treatment of acute low back pain and headache. The North American Spine Society does not recommend advanced imaging of the spine within the first six weeks in patients with nonspecific acute low back pain in the absence of red flags.
The American Headache Society (AHS) recommends that physicians avoid advising prolonged or frequent use of over-the-counter pain medications for headache. The organization also discourages physicians from prescribing opioid or butalbital-containing medications as first-line treatment for recurrent headache disorders. Furthermore, it does not recommend surgical deactivation of migraine trigger points outside of a clinical trial. In addition, the society advises physicians not to perform CT imaging for headache when an MRI is available, except in emergency settings. The society also recommends that physicians should not perform neuroimaging studies for patients with stable headaches that meet migraine criteria.
When CT Scans Are Unnecessary in Children
The American Academy of Pediatrics (AAP) advises that CT scans and MRI scans are not necessary in a child with simple febrile seizure. The AAP also does not recommend CT scans for the immediate evaluation of minor head injuries; clinical observation and Pediatric Emergency Care Applied Research Network (PECARN) criteria should be used to determine whether imaging is indicated.
Treating Insomnia and Sleep Disorders
The American Academy of Sleep Medicine advises doctors not to prescribe medication for childhood insomnia, which usually arises from parent–child interactions and responds to behavioral intervention. In addition, the academy does no
—Erica Tricarico
Suggested Reading
Callaghan BC, De Lott LB, Kerber KA, et al. Neurology Choosing Wisely recommendations: 74 and growing. Neurol Clin Pract. 2015;5(5):439-447.
Langer-Gould AM, Anderson WE, Armstrong MJ, et al. The American Academy of Neurology’s top five choosing wisely recommendations. Neurology. 2013;81(11):1004-1011.
Loder E, Weisenbaum E, Fishberg B, et al. Choosing wisely in headache medicine: the American Headache Society’s list of five things physicians and patients should question. Headache. 2013;53(10):1651-1659.

Two migraine prevention drugs prove no better than placebo in children
Two commonly used drugs to prevent migraine in adults, amitriptyline and topiramate, proved no better than placebo at preventing migraine in children and adolescents and also were associated with more adverse events in the double-blind, randomized Childhood and Adolescent Migraine Prevention (CHAMP) trial.
The findings of the trial, which was stopped early for futility following a recommendation from a data and safety monitoring board, suggest the adult model of migraine treatment in which both drugs have been effective may not apply to pediatric patients, according to the investigators (N Engl J Med 2016 Oct 27. doi: 10.1056/NEJMoa1610384). The study was published simultaneously with its presentation at the annual meeting of the Child Neurology Society in Vancouver.
The 24-week, multicenter trial involved 328 children and adolescents aged 8-17 years who were diagnosed with migraine with or without aura or chronic migraine without continuous headache. They were randomized on a 2:2:1 ratio to receive oral amitriptyline (n = 132), topiramate (n = 130), or placebo (n = 66) according to age (8-12 years vs. 13-17 years). The target dose in the study was 1 mg/kg of body weight per day for amitriptyline and 2 mg/kg for topiramate. Doses were escalated every 2 weeks over an 8-week period and dose modifications were made according to side effects.
Overall, 52% on amitriptyline, 55% on topiramate, and 61% on placebo reached the study’s primary endpoint of a relative reduction of 50% or more in the number of headache days from baseline to the last 28 days of the trial; the outcomes were not significantly different from one another. The participants recorded the number of headache days they experienced in a diary kept during and after the 28-day baseline period of the study.
No significant differences were seen between the groups in the secondary outcomes of headache-related disability, headache days, or the number of patients who completed the trial.
However, the authors observed higher rates of adverse events overall in the active treatment groups, compared with placebo. Amitriptyline users significantly more often reported fatigue (30% vs. 14%, P = .01) and dry mouth (25% vs. 12%, P = .03), whereas topiramate users significantly more often reported paresthesia (31% vs. 8%, P less than .001) and weight loss (8% vs. 0%, P = .02).
Other adverse events among topiramate users were fatigue (25%), dry mouth (18%), memory impairment (17%), aphasia (16%), cognitive disorder (16%), and upper respiratory tract infection (12%).
Serious adverse events included altered mood in three patients in the amitriptyline group and one suicide attempt in the topiramate group.
“Given the null outcome in this trial and the adverse events and serious adverse events reported in the amitriptyline and topiramate groups, the data do not show a favorable risk-benefit profile for the use of these therapies in pediatric migraine prevention, at least over the 24-week duration of the trial,” the study authors concluded.
They noted that during their trial, the Food and Drug Administration approved topiramate for the treatment of episodic migraine in adolescents aged 12-17 years.
“Although our trial included patients outside this age range and included those with either episodic or chronic migraine, the trial results suggest that prevention medication for pediatric migraine might be reexamined,” they wrote.
The high placebo response seen in the study suggested the placebo effect might be advantageous for children and adolescents with migraine, they added.
The trial was supported by grants from the National Institute of Neurological Disorders and Stroke and the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The authors had no relevant financial disclosures.
Two commonly used drugs to prevent migraine in adults, amitriptyline and topiramate, proved no better than placebo at preventing migraine in children and adolescents and also were associated with more adverse events in the double-blind, randomized Childhood and Adolescent Migraine Prevention (CHAMP) trial.
The findings of the trial, which was stopped early for futility following a recommendation from a data and safety monitoring board, suggest the adult model of migraine treatment in which both drugs have been effective may not apply to pediatric patients, according to the investigators (N Engl J Med 2016 Oct 27. doi: 10.1056/NEJMoa1610384). The study was published simultaneously with its presentation at the annual meeting of the Child Neurology Society in Vancouver.
The 24-week, multicenter trial involved 328 children and adolescents aged 8-17 years who were diagnosed with migraine with or without aura or chronic migraine without continuous headache. They were randomized on a 2:2:1 ratio to receive oral amitriptyline (n = 132), topiramate (n = 130), or placebo (n = 66) according to age (8-12 years vs. 13-17 years). The target dose in the study was 1 mg/kg of body weight per day for amitriptyline and 2 mg/kg for topiramate. Doses were escalated every 2 weeks over an 8-week period and dose modifications were made according to side effects.
Overall, 52% on amitriptyline, 55% on topiramate, and 61% on placebo reached the study’s primary endpoint of a relative reduction of 50% or more in the number of headache days from baseline to the last 28 days of the trial; the outcomes were not significantly different from one another. The participants recorded the number of headache days they experienced in a diary kept during and after the 28-day baseline period of the study.
No significant differences were seen between the groups in the secondary outcomes of headache-related disability, headache days, or the number of patients who completed the trial.
However, the authors observed higher rates of adverse events overall in the active treatment groups, compared with placebo. Amitriptyline users significantly more often reported fatigue (30% vs. 14%, P = .01) and dry mouth (25% vs. 12%, P = .03), whereas topiramate users significantly more often reported paresthesia (31% vs. 8%, P less than .001) and weight loss (8% vs. 0%, P = .02).
Other adverse events among topiramate users were fatigue (25%), dry mouth (18%), memory impairment (17%), aphasia (16%), cognitive disorder (16%), and upper respiratory tract infection (12%).
Serious adverse events included altered mood in three patients in the amitriptyline group and one suicide attempt in the topiramate group.
“Given the null outcome in this trial and the adverse events and serious adverse events reported in the amitriptyline and topiramate groups, the data do not show a favorable risk-benefit profile for the use of these therapies in pediatric migraine prevention, at least over the 24-week duration of the trial,” the study authors concluded.
They noted that during their trial, the Food and Drug Administration approved topiramate for the treatment of episodic migraine in adolescents aged 12-17 years.
“Although our trial included patients outside this age range and included those with either episodic or chronic migraine, the trial results suggest that prevention medication for pediatric migraine might be reexamined,” they wrote.
The high placebo response seen in the study suggested the placebo effect might be advantageous for children and adolescents with migraine, they added.
The trial was supported by grants from the National Institute of Neurological Disorders and Stroke and the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The authors had no relevant financial disclosures.
Two commonly used drugs to prevent migraine in adults, amitriptyline and topiramate, proved no better than placebo at preventing migraine in children and adolescents and also were associated with more adverse events in the double-blind, randomized Childhood and Adolescent Migraine Prevention (CHAMP) trial.
The findings of the trial, which was stopped early for futility following a recommendation from a data and safety monitoring board, suggest the adult model of migraine treatment in which both drugs have been effective may not apply to pediatric patients, according to the investigators (N Engl J Med 2016 Oct 27. doi: 10.1056/NEJMoa1610384). The study was published simultaneously with its presentation at the annual meeting of the Child Neurology Society in Vancouver.
The 24-week, multicenter trial involved 328 children and adolescents aged 8-17 years who were diagnosed with migraine with or without aura or chronic migraine without continuous headache. They were randomized on a 2:2:1 ratio to receive oral amitriptyline (n = 132), topiramate (n = 130), or placebo (n = 66) according to age (8-12 years vs. 13-17 years). The target dose in the study was 1 mg/kg of body weight per day for amitriptyline and 2 mg/kg for topiramate. Doses were escalated every 2 weeks over an 8-week period and dose modifications were made according to side effects.
Overall, 52% on amitriptyline, 55% on topiramate, and 61% on placebo reached the study’s primary endpoint of a relative reduction of 50% or more in the number of headache days from baseline to the last 28 days of the trial; the outcomes were not significantly different from one another. The participants recorded the number of headache days they experienced in a diary kept during and after the 28-day baseline period of the study.
No significant differences were seen between the groups in the secondary outcomes of headache-related disability, headache days, or the number of patients who completed the trial.
However, the authors observed higher rates of adverse events overall in the active treatment groups, compared with placebo. Amitriptyline users significantly more often reported fatigue (30% vs. 14%, P = .01) and dry mouth (25% vs. 12%, P = .03), whereas topiramate users significantly more often reported paresthesia (31% vs. 8%, P less than .001) and weight loss (8% vs. 0%, P = .02).
Other adverse events among topiramate users were fatigue (25%), dry mouth (18%), memory impairment (17%), aphasia (16%), cognitive disorder (16%), and upper respiratory tract infection (12%).
Serious adverse events included altered mood in three patients in the amitriptyline group and one suicide attempt in the topiramate group.
“Given the null outcome in this trial and the adverse events and serious adverse events reported in the amitriptyline and topiramate groups, the data do not show a favorable risk-benefit profile for the use of these therapies in pediatric migraine prevention, at least over the 24-week duration of the trial,” the study authors concluded.
They noted that during their trial, the Food and Drug Administration approved topiramate for the treatment of episodic migraine in adolescents aged 12-17 years.
“Although our trial included patients outside this age range and included those with either episodic or chronic migraine, the trial results suggest that prevention medication for pediatric migraine might be reexamined,” they wrote.
The high placebo response seen in the study suggested the placebo effect might be advantageous for children and adolescents with migraine, they added.
The trial was supported by grants from the National Institute of Neurological Disorders and Stroke and the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The authors had no relevant financial disclosures.
FROM CNS 2016
Key clinical point:
Main finding: Fifty-two percent, 55%, and 61% of patients randomized to amitriptyline, topiramate, and placebo groups, respectively, reached the study primary endpoint of a relative reduction of 50% or more in the number of headache days from baseline to the last 28 days of the 24-week trial.
Data source: A phase III, randomized, placebo-controlled trial of 328 children and adolescents aged 8-17 years who were diagnosed with migraine with or without aura or chronic migraine without continuous headache.
Disclosures: The trial was supported by grants from the National Institute of Neurological Disorders and Stroke and the Eunice Kennedy Shriver National Institute of Child Health and Human Development. The authors had no relevant financial disclosures.