User login
ACR annual meeting pediatric track highlights gene sequencing, brain disease
Will gene sequencing be one of the keys to unlocking previously mysterious inflammatory disorders in children?
Yes, according to new research to be presented at the annual meeting of the American College of Rheumatology in Washington. Gene and whole-exome sequencing will change the way these disorders are categorized, diagnosed, and managed, bringing new hope to the children who suffer from these rare, and devastating illnesses.
Program cochairs Anne M. Stevens, MD, and Anthony French, MD, PhD, agree: Gene sequencing is one of the most exciting and potentially practice-changing topics that ACR’s pediatric track will explore.
A session at 11:00 a.m. on Sunday, Nov. 13, is particularly intriguing, said Dr. Stevens of Seattle Children’s Hospital. “Early-Onset Monogenic Inflammatory Diseases” features two speakers.
Hal Hoffman, MD, chief of allergy, immunology and rheumatology in the department of pediatrics at the University of California, San Diego, will speak on inflammasome-associated disorders. He’ll present a case-based lecture, “so pediatric rheumatologists will be able to recognize these diseases, identify the genes underlying them, and make a clear genetic diagnosis,” Dr. Stevens said.

“These two speakers have been successful in identifying specific genes for these illnesses that have led to very specific treatments and, in some cases, complete resolution of symptoms,” Dr. Stevens noted.
“Advances in Clinical Care through Whole Exome Sequencing,” set for 11:00 a.m. on Tuesday, Nov. 15, will explore the practical impact of gene sequencing studies. Alexei A. Grom, MD, of Cincinnati Children’s Hospital, will discuss the practicalities of whole-exome sequencing: when to order it, how to interpret the findings, and how to use the results to help patients.
Jordan S. Orange, MD, PhD, of Baylor College of Medicine, Houston, will discuss his lab’s recent project: whole-exome sequencing of hundreds of pediatric rheumatology patients. “This study hasn’t focused on a specific disease or a specific gene but looked at the entire exome in an unbiased way,” Dr. Stevens said. “So far, they have identified genes associated with inflammatory disease in about 25% of this population.”
The session is meant to be practical as well as academic, Dr. French noted. “In the last few years, these tests have become much more accessible and easier to do in the clinic, not just in a research setting, and we’re going to focus on how to use them to individualize care.”
Dr. Stevens and Dr. French are also excited about the pediatric nephrology track, which kicks off with “What a Pediatric Rheumatologist May Want to Know About the Kidneys” at 8:30 a.m. on Monday, Nov. 14.
Mark M. Mitsnefes, MD, director of clinical and translational research at Cincinnati Children’s Hospital, will focus on treating hypertension in pediatric rheumatology patients. Bradley P. Dixon, MD, director of the nephrology clinical laboratory at Cincinnati Children’s, will review the thrombotic microangiopathies and discuss new treatment options. Stephen Marks, MD, a kidney transplant expert from London, will finish the session with a detailed discussion of lupus nephritis in children, focusing on early diagnosis.
Pediatric autoimmune brain disorders are on tap for a morning session on Tuesday, Nov. 14. Dr. Stevens is particularly looking forward to this session, which begins at 8:30 a.m.
“As pediatric rheumatologists, we are more and more often being asked to consult on new-onset seizures, psychoses, hallucinations, and stroke. It’s quite a challenge to figure out whether these are related to autoimmune disorders.”
The first lecture of the series focuses on the pathogenesis of autoimmune brain disease, and how to make the diagnosis. Russell Dale, MD, of the University of Sydney will talk about therapeutic decision making in these illnesses.
Josep Obrador Dalmau, MD, of the University of Pennsylvania, Philadelphia, will discuss anti–NMDA receptor encephalitis. Hermine I. Brunner, MD, director of rheumatology at Cincinnati Children’s, will close with a diagnostic and therapeutic update of neuropsychiatric systemic lupus erythematosus.
“This is a huge challenge for us,” Dr. Stevens said. “Children with lupus can have obvious central nervous system involvement, but also not-so-obvious involvement, including depression, anxiety, and cognitive difficulties.”
Will gene sequencing be one of the keys to unlocking previously mysterious inflammatory disorders in children?
Yes, according to new research to be presented at the annual meeting of the American College of Rheumatology in Washington. Gene and whole-exome sequencing will change the way these disorders are categorized, diagnosed, and managed, bringing new hope to the children who suffer from these rare, and devastating illnesses.
Program cochairs Anne M. Stevens, MD, and Anthony French, MD, PhD, agree: Gene sequencing is one of the most exciting and potentially practice-changing topics that ACR’s pediatric track will explore.
A session at 11:00 a.m. on Sunday, Nov. 13, is particularly intriguing, said Dr. Stevens of Seattle Children’s Hospital. “Early-Onset Monogenic Inflammatory Diseases” features two speakers.
Hal Hoffman, MD, chief of allergy, immunology and rheumatology in the department of pediatrics at the University of California, San Diego, will speak on inflammasome-associated disorders. He’ll present a case-based lecture, “so pediatric rheumatologists will be able to recognize these diseases, identify the genes underlying them, and make a clear genetic diagnosis,” Dr. Stevens said.
“These two speakers have been successful in identifying specific genes for these illnesses that have led to very specific treatments and, in some cases, complete resolution of symptoms,” Dr. Stevens noted.
“Advances in Clinical Care through Whole Exome Sequencing,” set for 11:00 a.m. on Tuesday, Nov. 15, will explore the practical impact of gene sequencing studies. Alexei A. Grom, MD, of Cincinnati Children’s Hospital, will discuss the practicalities of whole-exome sequencing: when to order it, how to interpret the findings, and how to use the results to help patients.
Jordan S. Orange, MD, PhD, of Baylor College of Medicine, Houston, will discuss his lab’s recent project: whole-exome sequencing of hundreds of pediatric rheumatology patients. “This study hasn’t focused on a specific disease or a specific gene but looked at the entire exome in an unbiased way,” Dr. Stevens said. “So far, they have identified genes associated with inflammatory disease in about 25% of this population.”
The session is meant to be practical as well as academic, Dr. French noted. “In the last few years, these tests have become much more accessible and easier to do in the clinic, not just in a research setting, and we’re going to focus on how to use them to individualize care.”
Dr. Stevens and Dr. French are also excited about the pediatric nephrology track, which kicks off with “What a Pediatric Rheumatologist May Want to Know About the Kidneys” at 8:30 a.m. on Monday, Nov. 14.
Mark M. Mitsnefes, MD, director of clinical and translational research at Cincinnati Children’s Hospital, will focus on treating hypertension in pediatric rheumatology patients. Bradley P. Dixon, MD, director of the nephrology clinical laboratory at Cincinnati Children’s, will review the thrombotic microangiopathies and discuss new treatment options. Stephen Marks, MD, a kidney transplant expert from London, will finish the session with a detailed discussion of lupus nephritis in children, focusing on early diagnosis.
Pediatric autoimmune brain disorders are on tap for a morning session on Tuesday, Nov. 14. Dr. Stevens is particularly looking forward to this session, which begins at 8:30 a.m.
“As pediatric rheumatologists, we are more and more often being asked to consult on new-onset seizures, psychoses, hallucinations, and stroke. It’s quite a challenge to figure out whether these are related to autoimmune disorders.”
The first lecture of the series focuses on the pathogenesis of autoimmune brain disease, and how to make the diagnosis. Russell Dale, MD, of the University of Sydney will talk about therapeutic decision making in these illnesses.
Josep Obrador Dalmau, MD, of the University of Pennsylvania, Philadelphia, will discuss anti–NMDA receptor encephalitis. Hermine I. Brunner, MD, director of rheumatology at Cincinnati Children’s, will close with a diagnostic and therapeutic update of neuropsychiatric systemic lupus erythematosus.
“This is a huge challenge for us,” Dr. Stevens said. “Children with lupus can have obvious central nervous system involvement, but also not-so-obvious involvement, including depression, anxiety, and cognitive difficulties.”
Will gene sequencing be one of the keys to unlocking previously mysterious inflammatory disorders in children?
Yes, according to new research to be presented at the annual meeting of the American College of Rheumatology in Washington. Gene and whole-exome sequencing will change the way these disorders are categorized, diagnosed, and managed, bringing new hope to the children who suffer from these rare, and devastating illnesses.
Program cochairs Anne M. Stevens, MD, and Anthony French, MD, PhD, agree: Gene sequencing is one of the most exciting and potentially practice-changing topics that ACR’s pediatric track will explore.
A session at 11:00 a.m. on Sunday, Nov. 13, is particularly intriguing, said Dr. Stevens of Seattle Children’s Hospital. “Early-Onset Monogenic Inflammatory Diseases” features two speakers.
Hal Hoffman, MD, chief of allergy, immunology and rheumatology in the department of pediatrics at the University of California, San Diego, will speak on inflammasome-associated disorders. He’ll present a case-based lecture, “so pediatric rheumatologists will be able to recognize these diseases, identify the genes underlying them, and make a clear genetic diagnosis,” Dr. Stevens said.
“These two speakers have been successful in identifying specific genes for these illnesses that have led to very specific treatments and, in some cases, complete resolution of symptoms,” Dr. Stevens noted.
“Advances in Clinical Care through Whole Exome Sequencing,” set for 11:00 a.m. on Tuesday, Nov. 15, will explore the practical impact of gene sequencing studies. Alexei A. Grom, MD, of Cincinnati Children’s Hospital, will discuss the practicalities of whole-exome sequencing: when to order it, how to interpret the findings, and how to use the results to help patients.
Jordan S. Orange, MD, PhD, of Baylor College of Medicine, Houston, will discuss his lab’s recent project: whole-exome sequencing of hundreds of pediatric rheumatology patients. “This study hasn’t focused on a specific disease or a specific gene but looked at the entire exome in an unbiased way,” Dr. Stevens said. “So far, they have identified genes associated with inflammatory disease in about 25% of this population.”
The session is meant to be practical as well as academic, Dr. French noted. “In the last few years, these tests have become much more accessible and easier to do in the clinic, not just in a research setting, and we’re going to focus on how to use them to individualize care.”
Dr. Stevens and Dr. French are also excited about the pediatric nephrology track, which kicks off with “What a Pediatric Rheumatologist May Want to Know About the Kidneys” at 8:30 a.m. on Monday, Nov. 14.
Mark M. Mitsnefes, MD, director of clinical and translational research at Cincinnati Children’s Hospital, will focus on treating hypertension in pediatric rheumatology patients. Bradley P. Dixon, MD, director of the nephrology clinical laboratory at Cincinnati Children’s, will review the thrombotic microangiopathies and discuss new treatment options. Stephen Marks, MD, a kidney transplant expert from London, will finish the session with a detailed discussion of lupus nephritis in children, focusing on early diagnosis.
Pediatric autoimmune brain disorders are on tap for a morning session on Tuesday, Nov. 14. Dr. Stevens is particularly looking forward to this session, which begins at 8:30 a.m.
“As pediatric rheumatologists, we are more and more often being asked to consult on new-onset seizures, psychoses, hallucinations, and stroke. It’s quite a challenge to figure out whether these are related to autoimmune disorders.”
The first lecture of the series focuses on the pathogenesis of autoimmune brain disease, and how to make the diagnosis. Russell Dale, MD, of the University of Sydney will talk about therapeutic decision making in these illnesses.
Josep Obrador Dalmau, MD, of the University of Pennsylvania, Philadelphia, will discuss anti–NMDA receptor encephalitis. Hermine I. Brunner, MD, director of rheumatology at Cincinnati Children’s, will close with a diagnostic and therapeutic update of neuropsychiatric systemic lupus erythematosus.
“This is a huge challenge for us,” Dr. Stevens said. “Children with lupus can have obvious central nervous system involvement, but also not-so-obvious involvement, including depression, anxiety, and cognitive difficulties.”
FROM THE ACR ANNUAL MEETING
Topical crisaborole boosts quality of life in atopic dermatitis
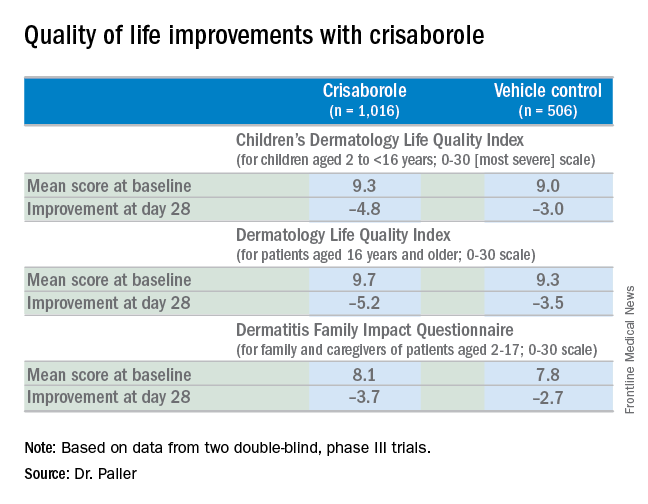
VIENNA – Topical crisaborole 2% ointment administered twice a day was consistently associated with clinically meaningful quality of life improvement scores on multiple measures in the two pivotal phase III, randomized, controlled trials of atopic dermatitis (AD) patients aged 2 years old through adulthood, Amy S. Paller, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
AD in children and adolescents is infamous for the adverse quality of life impact it imposes upon the patients’ parents, family, and caregivers. So the significant improvement seen with crisaborole, compared with its vehicle on the Dermatitis Family Impact (DFI) Questionnaire was particularly gratifying. The DFI questionnaire assesses quality of life in key domains, including family, parent, and caregiver sleep, emotional distress, relationships, family leisure, and ability to do housework or go shopping.

“If approved, crisaborole ... could improve the quality of life for patients with mild to moderate atopic dermatitis and, very importantly, for their families as well,” declared Dr. Paller, professor of dermatology and chair of the department of dermatology and professor of pediatrics at Northwestern University, Chicago.
Crisaborole’s developer, Anacor Pharmaceuticals, has filed an application for approval for treating mild to moderate AD in patients aged 2 years and older, now under review at the Food and Drug Administration.
In a separate presentation at the EADV congress, Lawrence F. Eichenfield, MD, presented the results of a long-term, open-label crisaborole safety study of 48-52 weeks duration. The long-term study involved 517 participants in the two pivotal phase III trials. There were no serious adverse events and no long-term cutaneous adverse events such as the skin atrophy or telangiectasias that can occur with topical steroids. The safety profile was favorable for long-term treatment of patients 2 years of age or older with mild to moderate AD.

Crisaborole 2% topical ointment is a novel, boron-based, nonsteroidal inhibitor of phosphodiesterase 4 (PDE-4). AD is marked by overactivity of PDE-4, which results in decreased levels of cyclic AMP and resultant increased release of inflammatory cytokines.
Dr. Paller noted that, in the previously reported efficacy results of the two pivotal, double-blind, 28-day, phase III trials, crisaborole treatment reduced global disease severity and provided early and sustained improvement in itch severity. She presented the prespecified quality of life results for the two identically designed, parallel pivotal trials, which totaled 1,016 patients on crisaborole and 506 on its vehicle. At baseline, 39% of subjects had mild AD, and 61% had moderate AD. The mean body surface area affected was 18%. Participants’ mean age was 12.3 years, and 14% were aged 8 years old or older.
The structure of the long-term safety study suggests how crisaborole might be used in clinical practice. During the year-long, open-label study, patients were evaluated every 28 days. If their skin was deemed clear or almost clear on the basis of an Investigator’s Static Global Assessment (ISGA) score of 0 or 1, they were taken off crisaborole and could use only emollients for the next 28 days, at which time they would be reevaluated. At that point, if they had an ISGA of 2 or more, they went back on crisaborole twice a day for 28 days until their next evaluation.
Dr. Eichenfield reported that 10.2% of participants in the long-term safety study reported treatment-related adverse events, which were mild to moderate. The most frequently reported of these were mild to moderate flares of AD during a 28-day off-treatment period in 1.3% of patients, application site pain in 2.3%, and application site infection in 1.2%.
Dr. Paller and Dr. Eichenfield reported serving as consultants to Anacor Pharmaceuticals.
The FDA review of crisaborole is expected to be completed by early January 2017, according to Anacor.
VIENNA – Topical crisaborole 2% ointment administered twice a day was consistently associated with clinically meaningful quality of life improvement scores on multiple measures in the two pivotal phase III, randomized, controlled trials of atopic dermatitis (AD) patients aged 2 years old through adulthood, Amy S. Paller, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
AD in children and adolescents is infamous for the adverse quality of life impact it imposes upon the patients’ parents, family, and caregivers. So the significant improvement seen with crisaborole, compared with its vehicle on the Dermatitis Family Impact (DFI) Questionnaire was particularly gratifying. The DFI questionnaire assesses quality of life in key domains, including family, parent, and caregiver sleep, emotional distress, relationships, family leisure, and ability to do housework or go shopping.
“If approved, crisaborole ... could improve the quality of life for patients with mild to moderate atopic dermatitis and, very importantly, for their families as well,” declared Dr. Paller, professor of dermatology and chair of the department of dermatology and professor of pediatrics at Northwestern University, Chicago.
Crisaborole’s developer, Anacor Pharmaceuticals, has filed an application for approval for treating mild to moderate AD in patients aged 2 years and older, now under review at the Food and Drug Administration.
In a separate presentation at the EADV congress, Lawrence F. Eichenfield, MD, presented the results of a long-term, open-label crisaborole safety study of 48-52 weeks duration. The long-term study involved 517 participants in the two pivotal phase III trials. There were no serious adverse events and no long-term cutaneous adverse events such as the skin atrophy or telangiectasias that can occur with topical steroids. The safety profile was favorable for long-term treatment of patients 2 years of age or older with mild to moderate AD.
Crisaborole 2% topical ointment is a novel, boron-based, nonsteroidal inhibitor of phosphodiesterase 4 (PDE-4). AD is marked by overactivity of PDE-4, which results in decreased levels of cyclic AMP and resultant increased release of inflammatory cytokines.
Dr. Paller noted that, in the previously reported efficacy results of the two pivotal, double-blind, 28-day, phase III trials, crisaborole treatment reduced global disease severity and provided early and sustained improvement in itch severity. She presented the prespecified quality of life results for the two identically designed, parallel pivotal trials, which totaled 1,016 patients on crisaborole and 506 on its vehicle. At baseline, 39% of subjects had mild AD, and 61% had moderate AD. The mean body surface area affected was 18%. Participants’ mean age was 12.3 years, and 14% were aged 8 years old or older.
The structure of the long-term safety study suggests how crisaborole might be used in clinical practice. During the year-long, open-label study, patients were evaluated every 28 days. If their skin was deemed clear or almost clear on the basis of an Investigator’s Static Global Assessment (ISGA) score of 0 or 1, they were taken off crisaborole and could use only emollients for the next 28 days, at which time they would be reevaluated. At that point, if they had an ISGA of 2 or more, they went back on crisaborole twice a day for 28 days until their next evaluation.
Dr. Eichenfield reported that 10.2% of participants in the long-term safety study reported treatment-related adverse events, which were mild to moderate. The most frequently reported of these were mild to moderate flares of AD during a 28-day off-treatment period in 1.3% of patients, application site pain in 2.3%, and application site infection in 1.2%.
Dr. Paller and Dr. Eichenfield reported serving as consultants to Anacor Pharmaceuticals.
The FDA review of crisaborole is expected to be completed by early January 2017, according to Anacor.
VIENNA – Topical crisaborole 2% ointment administered twice a day was consistently associated with clinically meaningful quality of life improvement scores on multiple measures in the two pivotal phase III, randomized, controlled trials of atopic dermatitis (AD) patients aged 2 years old through adulthood, Amy S. Paller, MD, reported at the annual congress of the European Academy of Dermatology and Venereology.
AD in children and adolescents is infamous for the adverse quality of life impact it imposes upon the patients’ parents, family, and caregivers. So the significant improvement seen with crisaborole, compared with its vehicle on the Dermatitis Family Impact (DFI) Questionnaire was particularly gratifying. The DFI questionnaire assesses quality of life in key domains, including family, parent, and caregiver sleep, emotional distress, relationships, family leisure, and ability to do housework or go shopping.
“If approved, crisaborole ... could improve the quality of life for patients with mild to moderate atopic dermatitis and, very importantly, for their families as well,” declared Dr. Paller, professor of dermatology and chair of the department of dermatology and professor of pediatrics at Northwestern University, Chicago.
Crisaborole’s developer, Anacor Pharmaceuticals, has filed an application for approval for treating mild to moderate AD in patients aged 2 years and older, now under review at the Food and Drug Administration.
In a separate presentation at the EADV congress, Lawrence F. Eichenfield, MD, presented the results of a long-term, open-label crisaborole safety study of 48-52 weeks duration. The long-term study involved 517 participants in the two pivotal phase III trials. There were no serious adverse events and no long-term cutaneous adverse events such as the skin atrophy or telangiectasias that can occur with topical steroids. The safety profile was favorable for long-term treatment of patients 2 years of age or older with mild to moderate AD.
Crisaborole 2% topical ointment is a novel, boron-based, nonsteroidal inhibitor of phosphodiesterase 4 (PDE-4). AD is marked by overactivity of PDE-4, which results in decreased levels of cyclic AMP and resultant increased release of inflammatory cytokines.
Dr. Paller noted that, in the previously reported efficacy results of the two pivotal, double-blind, 28-day, phase III trials, crisaborole treatment reduced global disease severity and provided early and sustained improvement in itch severity. She presented the prespecified quality of life results for the two identically designed, parallel pivotal trials, which totaled 1,016 patients on crisaborole and 506 on its vehicle. At baseline, 39% of subjects had mild AD, and 61% had moderate AD. The mean body surface area affected was 18%. Participants’ mean age was 12.3 years, and 14% were aged 8 years old or older.
The structure of the long-term safety study suggests how crisaborole might be used in clinical practice. During the year-long, open-label study, patients were evaluated every 28 days. If their skin was deemed clear or almost clear on the basis of an Investigator’s Static Global Assessment (ISGA) score of 0 or 1, they were taken off crisaborole and could use only emollients for the next 28 days, at which time they would be reevaluated. At that point, if they had an ISGA of 2 or more, they went back on crisaborole twice a day for 28 days until their next evaluation.
Dr. Eichenfield reported that 10.2% of participants in the long-term safety study reported treatment-related adverse events, which were mild to moderate. The most frequently reported of these were mild to moderate flares of AD during a 28-day off-treatment period in 1.3% of patients, application site pain in 2.3%, and application site infection in 1.2%.
Dr. Paller and Dr. Eichenfield reported serving as consultants to Anacor Pharmaceuticals.
The FDA review of crisaborole is expected to be completed by early January 2017, according to Anacor.
EXPERT ANALYSIS FROM THE EADV CONGRESS
Body-size awareness linked with BMI decrease in obese children, teens
SAN FRANCISCO – Body-size awareness was associated with a decrease in BMI among Latino children and teens, said Grace Lim, MD, a pediatrician in King City, Calif.
Awareness of body size, as a proxy for motivation to change behavior, was based on choices of sex-specific body silhouettes in comparison to actual body mass index (BMI) z-scores. Dr. Lim and her coauthor, Dr. Nazrat Mirza, conducted a study at Children’s National Medical Center in Washington of 80 overweight or obese Latino youths aged 7-15 years who were taking part in a 12-week, community-based weight management program: 68% of study participants demonstrated awareness of overweight or obese body sizes. They were more likely to be older (P less than .001) and with higher maternal age (P = .02). Body-size awareness in the child was positively associated with a decrease in BMI during the intervention period (P less than .001).
Dr. Lim said that she had no relevant financial disclosures.
SAN FRANCISCO – Body-size awareness was associated with a decrease in BMI among Latino children and teens, said Grace Lim, MD, a pediatrician in King City, Calif.
Awareness of body size, as a proxy for motivation to change behavior, was based on choices of sex-specific body silhouettes in comparison to actual body mass index (BMI) z-scores. Dr. Lim and her coauthor, Dr. Nazrat Mirza, conducted a study at Children’s National Medical Center in Washington of 80 overweight or obese Latino youths aged 7-15 years who were taking part in a 12-week, community-based weight management program: 68% of study participants demonstrated awareness of overweight or obese body sizes. They were more likely to be older (P less than .001) and with higher maternal age (P = .02). Body-size awareness in the child was positively associated with a decrease in BMI during the intervention period (P less than .001).
Dr. Lim said that she had no relevant financial disclosures.
SAN FRANCISCO – Body-size awareness was associated with a decrease in BMI among Latino children and teens, said Grace Lim, MD, a pediatrician in King City, Calif.
Awareness of body size, as a proxy for motivation to change behavior, was based on choices of sex-specific body silhouettes in comparison to actual body mass index (BMI) z-scores. Dr. Lim and her coauthor, Dr. Nazrat Mirza, conducted a study at Children’s National Medical Center in Washington of 80 overweight or obese Latino youths aged 7-15 years who were taking part in a 12-week, community-based weight management program: 68% of study participants demonstrated awareness of overweight or obese body sizes. They were more likely to be older (P less than .001) and with higher maternal age (P = .02). Body-size awareness in the child was positively associated with a decrease in BMI during the intervention period (P less than .001).
Dr. Lim said that she had no relevant financial disclosures.
AT AAP 16
Key clinical point:
Major finding: 68% of 80 the children demonstrated awareness of overweight or obese body sizes and were more likely to drop their BMI.
Data source: A study of 80 overweight or obese Latino youths aged 7-15 years taking part in a 12-week, community-based weight management program.
Disclosures: Dr. Lim said she that had no relevant financial disclosures.
Discussing screen time with parents
The American Academy of Pediatrics released a new set of recommendations for the appropriate amount of screen time for children and adolescents in October 2016.
Among other changes, the AAP now recommends no screen time (except for video chatting) for infants and children up to 18 months old. For 18- to 24-month-olds, the AAP discourages screen time, recommending that parents introduce only selected “high-quality” programming and cowatch with their children. Likewise, for children up to 5 years old, the AAP urges parents to limit all screen time to 1 hour/day, half of its previous recommendation, and again recommends that parents cowatch with their children and use only reliable providers of quality content, such as the Public Broadcasting Service (PBS). For older children, the AAP does not set specific time limits, but recommends that parents collaborate with the children on a media plan that limits screen time so that it does not interfere with other important activities, including homework, social time, exercise, and sleep.



There also is evidence that teenagers who spend substantial time engaged passively in social media (seeing what others are doing or saying via Facebook or Instagram) report higher levels of depression and anxiety, whereas those who use social media as a platform to stay connected (via two-way communication) report lower levels of these symptoms. While many young people use social sites as a forum to find peer support, share concerns, or develop their own “voice,” some young people might be vulnerable to exploitation, cyberbullying, or even online solicitation. The key here may be for parents, who have a sense of their child’s strengths and vulnerabilities, to be aware of where their children are spending their virtual time and to check in about the kinds of connections they have there. Of course, screen time can be equally seductive for parents. And when a parent is spending time reading texts or checking for Facebook updates, they are missing opportunities to be engaged with their children, helping them with homework or simply noticing that they seem stressed, or catching an opportunity to talk with them.
The pediatrician has the opportunity to educate parents about the potential risks that unchecked screen time can pose to their children’s healthy development. But it is critical that you approach these conversations with specificity and compassion. Customize the conversation to the age and personality of the child and family. A computer in the bedroom may make sense for an academically oriented 9th grader in a demanding school who is generally well-balanced in activities and friendships. A bedroom computer may be a poor choice for an isolated 9th grader almost addicted to video games with few friends or activities.
Simply reciting recommendations may heighten a parent’s feelings of isolation and shame, and not lead to meaningful change. Instead, start by asking about the details: Where are the screens in the home? Bedrooms? Who has a computer, tablet, or smartphone? How are these screens used in the context of the child’s overall psychosocial functioning? Depending on the circumstance, a smaller change, such as “no phones while doing homework,” can make a big difference. Simple, clear rules can be easier to explain and enforce, and protect parents from the perils of daily negotiations of screen terms with their children or teenagers. Perhaps they can have a “phone zone” where phones get parked and charged once kids get home from school. Perhaps there are limits on TV or video games on school nights (for the student performing below potential, rather than the driven student who would benefit from down time). Perhaps for preteens, computer-based homework can be done only on the desktop computer that is kept in a family study, rather than a laptop in a bedroom where kids are more likely to become distracted and surf the net. Pediatricians can help families think through the right approach to screen time that may range from restriction to shared use exploring shared interests to jointly watching a favorite TV show or sporting event.
You can help parents consider how they will talk about all this, acknowledging what is fun and rewarding about TV shows, social media, and the Internet alongside the problems of excessive use. Ask parents if it is hard for them to put down their own phones or tablets. They can acknowledge this explicitly with their children when establishing new media use rules. It is powerful for children, especially teenagers, to hear their parents acknowledge that “phones, tablets, and computers are powerful tools, but we all need to improve our skills at being in control of our use of them.” You might suggest that parents try this exercise: list all of the activities they wish they had time for in every day, and how much time they would spend in them. Then they should guess how much time they spend in screen-based entertainment. If they wish to protect time for screen-based entertainment, they can actively choose to do so. If you are able to help parents better understand the risks of excessive screen time and facilitate desired and appropriate use of media, you will have added to the quality of the family’s life.
The AAP has resources to help pediatricians partner with parents to create a Family Media Use Plan (www.healthychildren.org/MediaUsePlan).
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@frontlinemedcom.com.
The American Academy of Pediatrics released a new set of recommendations for the appropriate amount of screen time for children and adolescents in October 2016.
Among other changes, the AAP now recommends no screen time (except for video chatting) for infants and children up to 18 months old. For 18- to 24-month-olds, the AAP discourages screen time, recommending that parents introduce only selected “high-quality” programming and cowatch with their children. Likewise, for children up to 5 years old, the AAP urges parents to limit all screen time to 1 hour/day, half of its previous recommendation, and again recommends that parents cowatch with their children and use only reliable providers of quality content, such as the Public Broadcasting Service (PBS). For older children, the AAP does not set specific time limits, but recommends that parents collaborate with the children on a media plan that limits screen time so that it does not interfere with other important activities, including homework, social time, exercise, and sleep.
There also is evidence that teenagers who spend substantial time engaged passively in social media (seeing what others are doing or saying via Facebook or Instagram) report higher levels of depression and anxiety, whereas those who use social media as a platform to stay connected (via two-way communication) report lower levels of these symptoms. While many young people use social sites as a forum to find peer support, share concerns, or develop their own “voice,” some young people might be vulnerable to exploitation, cyberbullying, or even online solicitation. The key here may be for parents, who have a sense of their child’s strengths and vulnerabilities, to be aware of where their children are spending their virtual time and to check in about the kinds of connections they have there. Of course, screen time can be equally seductive for parents. And when a parent is spending time reading texts or checking for Facebook updates, they are missing opportunities to be engaged with their children, helping them with homework or simply noticing that they seem stressed, or catching an opportunity to talk with them.
The pediatrician has the opportunity to educate parents about the potential risks that unchecked screen time can pose to their children’s healthy development. But it is critical that you approach these conversations with specificity and compassion. Customize the conversation to the age and personality of the child and family. A computer in the bedroom may make sense for an academically oriented 9th grader in a demanding school who is generally well-balanced in activities and friendships. A bedroom computer may be a poor choice for an isolated 9th grader almost addicted to video games with few friends or activities.
Simply reciting recommendations may heighten a parent’s feelings of isolation and shame, and not lead to meaningful change. Instead, start by asking about the details: Where are the screens in the home? Bedrooms? Who has a computer, tablet, or smartphone? How are these screens used in the context of the child’s overall psychosocial functioning? Depending on the circumstance, a smaller change, such as “no phones while doing homework,” can make a big difference. Simple, clear rules can be easier to explain and enforce, and protect parents from the perils of daily negotiations of screen terms with their children or teenagers. Perhaps they can have a “phone zone” where phones get parked and charged once kids get home from school. Perhaps there are limits on TV or video games on school nights (for the student performing below potential, rather than the driven student who would benefit from down time). Perhaps for preteens, computer-based homework can be done only on the desktop computer that is kept in a family study, rather than a laptop in a bedroom where kids are more likely to become distracted and surf the net. Pediatricians can help families think through the right approach to screen time that may range from restriction to shared use exploring shared interests to jointly watching a favorite TV show or sporting event.
You can help parents consider how they will talk about all this, acknowledging what is fun and rewarding about TV shows, social media, and the Internet alongside the problems of excessive use. Ask parents if it is hard for them to put down their own phones or tablets. They can acknowledge this explicitly with their children when establishing new media use rules. It is powerful for children, especially teenagers, to hear their parents acknowledge that “phones, tablets, and computers are powerful tools, but we all need to improve our skills at being in control of our use of them.” You might suggest that parents try this exercise: list all of the activities they wish they had time for in every day, and how much time they would spend in them. Then they should guess how much time they spend in screen-based entertainment. If they wish to protect time for screen-based entertainment, they can actively choose to do so. If you are able to help parents better understand the risks of excessive screen time and facilitate desired and appropriate use of media, you will have added to the quality of the family’s life.
The AAP has resources to help pediatricians partner with parents to create a Family Media Use Plan (www.healthychildren.org/MediaUsePlan).
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@frontlinemedcom.com.
The American Academy of Pediatrics released a new set of recommendations for the appropriate amount of screen time for children and adolescents in October 2016.
Among other changes, the AAP now recommends no screen time (except for video chatting) for infants and children up to 18 months old. For 18- to 24-month-olds, the AAP discourages screen time, recommending that parents introduce only selected “high-quality” programming and cowatch with their children. Likewise, for children up to 5 years old, the AAP urges parents to limit all screen time to 1 hour/day, half of its previous recommendation, and again recommends that parents cowatch with their children and use only reliable providers of quality content, such as the Public Broadcasting Service (PBS). For older children, the AAP does not set specific time limits, but recommends that parents collaborate with the children on a media plan that limits screen time so that it does not interfere with other important activities, including homework, social time, exercise, and sleep.
There also is evidence that teenagers who spend substantial time engaged passively in social media (seeing what others are doing or saying via Facebook or Instagram) report higher levels of depression and anxiety, whereas those who use social media as a platform to stay connected (via two-way communication) report lower levels of these symptoms. While many young people use social sites as a forum to find peer support, share concerns, or develop their own “voice,” some young people might be vulnerable to exploitation, cyberbullying, or even online solicitation. The key here may be for parents, who have a sense of their child’s strengths and vulnerabilities, to be aware of where their children are spending their virtual time and to check in about the kinds of connections they have there. Of course, screen time can be equally seductive for parents. And when a parent is spending time reading texts or checking for Facebook updates, they are missing opportunities to be engaged with their children, helping them with homework or simply noticing that they seem stressed, or catching an opportunity to talk with them.
The pediatrician has the opportunity to educate parents about the potential risks that unchecked screen time can pose to their children’s healthy development. But it is critical that you approach these conversations with specificity and compassion. Customize the conversation to the age and personality of the child and family. A computer in the bedroom may make sense for an academically oriented 9th grader in a demanding school who is generally well-balanced in activities and friendships. A bedroom computer may be a poor choice for an isolated 9th grader almost addicted to video games with few friends or activities.
Simply reciting recommendations may heighten a parent’s feelings of isolation and shame, and not lead to meaningful change. Instead, start by asking about the details: Where are the screens in the home? Bedrooms? Who has a computer, tablet, or smartphone? How are these screens used in the context of the child’s overall psychosocial functioning? Depending on the circumstance, a smaller change, such as “no phones while doing homework,” can make a big difference. Simple, clear rules can be easier to explain and enforce, and protect parents from the perils of daily negotiations of screen terms with their children or teenagers. Perhaps they can have a “phone zone” where phones get parked and charged once kids get home from school. Perhaps there are limits on TV or video games on school nights (for the student performing below potential, rather than the driven student who would benefit from down time). Perhaps for preteens, computer-based homework can be done only on the desktop computer that is kept in a family study, rather than a laptop in a bedroom where kids are more likely to become distracted and surf the net. Pediatricians can help families think through the right approach to screen time that may range from restriction to shared use exploring shared interests to jointly watching a favorite TV show or sporting event.
You can help parents consider how they will talk about all this, acknowledging what is fun and rewarding about TV shows, social media, and the Internet alongside the problems of excessive use. Ask parents if it is hard for them to put down their own phones or tablets. They can acknowledge this explicitly with their children when establishing new media use rules. It is powerful for children, especially teenagers, to hear their parents acknowledge that “phones, tablets, and computers are powerful tools, but we all need to improve our skills at being in control of our use of them.” You might suggest that parents try this exercise: list all of the activities they wish they had time for in every day, and how much time they would spend in them. Then they should guess how much time they spend in screen-based entertainment. If they wish to protect time for screen-based entertainment, they can actively choose to do so. If you are able to help parents better understand the risks of excessive screen time and facilitate desired and appropriate use of media, you will have added to the quality of the family’s life.
The AAP has resources to help pediatricians partner with parents to create a Family Media Use Plan (www.healthychildren.org/MediaUsePlan).
Dr. Swick is an attending psychiatrist in the division of child psychiatry at Massachusetts General Hospital, Boston, and director of the Parenting at a Challenging Time (PACT) Program at the Vernon Cancer Center at Newton Wellesley Hospital, also in Boston. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@frontlinemedcom.com.
The culture change of assessing parents for ACEs
Several years ago, pediatricians R.J. Gillespie, MD, MHPE, and Teri Pettersen, MD, piloted the use of a questionnaire about adverse childhood experiences (ACEs) and resilience at the 4-month well-child visit.
They and six other pediatricians at The Children’s Clinic in Portland, Ore., explained in a cover letter why they were posing the questions of parents, and they ended the survey by asking them about their interest in potential resources.
[[{"fid":"172157","view_mode":"medstat_image_flush_left","fields":{"format":"medstat_image_flush_left","field_file_image_alt_text[und][0][value]":"R.J. Gillespie, MD, MHPE","field_file_image_credit[und][0][value]":"Courtesy The Children's Clinic","field_file_image_caption[und][0][value]":"Dr. R.J. Gillespie "},"type":"media","attributes":{"class":"media-element file-medstat_image_flush_left"}}]]Today, all 28 of the pediatricians at the clinic screen for ACEs and resilience, and Dr. Pettersen, now retired from the practice, travels through the state conducting training for the Oregon Pediatric Society about the impact of ACEs in parents and their children, and how to go about identifying and addressing them.
“So many of our visits are about behavioral problems or emotional disturbances, and so often at the root of these issues is some sort of trauma the child is experiencing,” Dr. Gillespie said in an interview. “What we’re seeing in many of these cases really are coping strategies for that child to deal with the toxic stress in his or her life.”
By assessing parents’ exposure to ACEs, briefly talking with them about how ACEs might impact their parenting, and tailoring their counseling and anticipatory guidance, the pediatricians hope to prevent ACEs and consequent toxic stress from developing in children.

The driving science
The term ACEs entered the medical lexicon after 1998, when a landmark study called the Adverse Childhood Experiences Study showed that traumatic experiences in childhood – abuse, neglect, and other severe dysfunctions in a household – not only are common among American adults but are associated with numerous poor health outcomes.
In the study and subsequent analyses, Dr. Vincent Felitti of Kaiser Permanente in San Diego and Dr. Robert Anda of the Centers for Disease Control and Prevention surveyed more than 17,000 patients about 10 types of ACEs and their current health status and behaviors. About two-thirds reported having at least one ACE, and one in eight reported four or more (Am J Prev Med. 1998;14[4]:245-58, www.cdc.gov/violenceprevention/acestudy/about.html).
Adults with four or more ACEs were not only significantly more likely to report health risk behaviors (smoking, substance abuse) and poor mental health outcomes (depression, suicide attempt); they were also significantly more likely to have poor physical health outcomes, with 2.2 times the risk of ischemic heart disease, 1.9 times the risk of cancer, and 3.9 times the risk of chronic bronchitis or emphysema, for instance. There was a strong dose-response relationship between ACEs and poor outcomes.
The Felitti study spawned dozens of analyses and additional research – in children as well as adults – on the associations between early-life adversity and the incidence of poor behavioral, mental, and physical outcomes, as well as on potential mechanisms.
Some research suggested a direct link between ACEs and negative outcomes, independent of whether individuals adopt risky behavior. Other studies suggested what experts in child development and mental health have long argued – that the more ACEs a parent has, the more ACEs their child will have.
And a growing body of biomedical literature linked the extreme, frequent, or prolonged activation of the body’s stress response in childhood – what has come to be known as “toxic stress” – with disruptions of the developing nervous, cardiovascular, immune, and metabolic systems.

While precise connections and mechanisms need to be clarified, “we now know that the repeated activation of the stress response leads to [negative] changes in the neuroendocrine immune pathways,” said Dr. Burke Harris, who coauthored a recent review of toxic stress in children and adolescents (Adv Pediatr. 2016;63[1]:403-28).
In January 2012, the American Academy of Pediatrics published a policy statement titled “Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician: Translating Developmental Science into Lifelong Health,” in which it urged pediatricians to consider actively screening for precipitants of toxic stress that are common in their communities (Pediatrics. 2011 Dec. doi: 10.1542/peds.2011-2662). But it stopped short of recommending particular tools or methods.
Dr. Gillespie and Dr. Pettersen did not want to wait for tools to be validated and approaches to be proven. “We’re building the plane as we fly,” Dr. Pettersen said.
The clinic’s roll-out
Dr. Pettersen learned about the ACE study and related research about 8 years ago while on a sabbatical to learn more about mental health issues. It “changed everything” about the way she viewed children and families and adversity. “I knew (we) didn’t have the infrastructure at the clinic, or the clinic’s support, to really start assessing children for what was happening to them,” she said, so she began thinking about ACE prevention and a focus on parenting.
Dr. Gillespie, in the meantime, was active in various quality improvement efforts at the state and national level, and had also become increasingly bothered by visits in which he saw children affected by maternal depression, abnormal attachment, and other problems. “I was seeing the consequences of ACEs, but I didn’t know specifically what was going on or how to talk about it,” he said.
The two pediatricians agreed to ask parents about ACEs at the 4-month well visit – a time when the families “knew us a little bit” and when “we could still influence parenting styles.”
In March 2013, they and their colleagues in the pilot group began giving parents a questionnaire that included the 10 ACE questions from Felitti’s study, questions about resilience from the Children’s Resilience Initiative, and a list of potential resources so they could understand parents’ needs.
They created a confidential field in their electronic medical record for documentation that appears during a visit, but does not print into notes and therefore will not be inadvertently released.
As they moved through the pilot phase, the pediatricians used various approaches to follow up on the assessment face-to-face. Eventually, they chose three particular questions as nonthreatening and helpful for conversation: Are there any experiences that still bother you? Of those experiences that don’t bother you, how did you get to the point where they don’t bother you? And how do these experiences affect your parenting now?
“It’s a motivational interviewing sort of style,” said Dr. Gillespie. “Parents can start identifying for themselves the solutions for the problems they’ve experienced, and they can start thinking about how their parenting might be impacted by things that have happened [or are still happening] to them.”
As the project rolled out, the physicians tweaked their process. They added four more ACE questions to address issues – community violence, extreme bullying, racism and prejudice, and foster care exposure – that they thought might lead to toxic stress in their population, for instance. And rather than ask on the written questionnaire for a “yes” or “no” to each of the ACE questions, they began asking the parent how many of the ACE questions applied to them. Moving away from the yes-no format to asking for a total count has led to more disclosures, Dr. Gillespie said.
To “keep the conversation going” in subsequent well-child visits, they developed a few questions to ask high-risk parents, like “How do you and your partner resolve conflict?” and “How did your parents resolve conflict in your household when you were a child?” And they provided training to all of the clinic’s staff on trauma-informed care and the need for support and compassion in their interactions with family members.
In the 3-plus years since incorporating ACEs assessments, the clinic’s pediatricians have made soft referrals to mental health professionals in only several cases – in each case, by suggesting that the parent contact their primary care physician. What most parents have wanted, says Dr. Gillespie, is recommendations for parenting classes and support groups. The clinic’s care manager assists the pediatricians in maintaining and providing links and handouts for various resources.
For Dr. Gillespie, the impact of the culture shift has been dramatic. “I’ve had 8-10 moms spontaneously reveal domestic violence to me in a subsequent visit, and say that they need a little help, because they’ve gotten the message that this is a safe place to talk about their experiences,” he said. “That had never happened to me in the previous 12 years of so of my career.”
Dr. Pettersen’s relationships with parents became “more intimate and more honest.” There was more trust. “If we can talk with parents [about ACEs] and not judge them for it,” she said, “then nothing is off the table.”
The ‘Two-Gen’ approach

“But I’d push back and say, parents know they have toxic stress but they don’t name it,” she said. “What we can do as trusted providers who want to advocate for families is to bear witness to their history by asking about it. Once they realize it’s not what’s wrong with [them], it’s what’s happened to [them], a shift occurs. That’s extremely validating for parents.”
That validation is part of a two-generation approach that she and Dr. Burke Harris see as part of a movement to break cycles of ACEs and toxic stress. At the California Pacific Medical Center’s Bayview Child Health Center in San Francisco, Dr. Burke Harris uses three ACE questionnaires – two of them ask parents (of children or teens) to report how many adverse experience types, or categories, apply to them and/or their child or teen, and one surveys adolescents themselves.
With the resources and clinical support of the Center for Youth Wellness, whose major funders include Google, Dr. Burke Harris can initiate a “warm hand-off” of patients with a high ACE score to a care coordinator or therapist. (The Center for Youth Wellness is beginning research to validate its ACE screening tools.) And in the meantime, the medical care she provides is trauma-informed.
“If a patient comes in for ADHD [attention-deficit/hyperactivity disorder] and has an ACE score of 6, my differential diagnosis and assessment will be different than if I see a patient sent by the school who has an ACE score of 0,” she said.
At the Portland Clinic, even though ACEs screening is now tied with the 4-month visit, pediatricians are much more attentive across the board to possible ACEs and toxic stress, and feel better able to converse with families, Dr. Gillespie said. One of his partners recently saw a 12-year-old boy who was failing in school and not making friends. Trauma-informed history-taking revealed at least several ACEs, and conversation turned to “all the resilience pieces… the connections he was missing and what he needed to cope,” he said.
References
• Resilience Project: This AAP project houses a “trauma toolkit” for primary care, case studies, and a variety of other tools.
• Center for Youth Wellness: The ACEs screening tools used by Dr. Burke Harris may be accessed at this website, along with a user guide containing sample scripts, and two white papers on ACEs and toxic stress.
• Resilience: The Biology of Stress and the Science of Hope: This documentary film, released in September 2016, is about ACEs and “a new movement” to treat and prevent toxic stress; it features the work of Dr. Burke Harris and others.
• Academy on Violence & Abuse: Various papers on ACEs screening and case finding in practice may be accessed here.
Several years ago, pediatricians R.J. Gillespie, MD, MHPE, and Teri Pettersen, MD, piloted the use of a questionnaire about adverse childhood experiences (ACEs) and resilience at the 4-month well-child visit.
They and six other pediatricians at The Children’s Clinic in Portland, Ore., explained in a cover letter why they were posing the questions of parents, and they ended the survey by asking them about their interest in potential resources.
[[{"fid":"172157","view_mode":"medstat_image_flush_left","fields":{"format":"medstat_image_flush_left","field_file_image_alt_text[und][0][value]":"R.J. Gillespie, MD, MHPE","field_file_image_credit[und][0][value]":"Courtesy The Children's Clinic","field_file_image_caption[und][0][value]":"Dr. R.J. Gillespie "},"type":"media","attributes":{"class":"media-element file-medstat_image_flush_left"}}]]Today, all 28 of the pediatricians at the clinic screen for ACEs and resilience, and Dr. Pettersen, now retired from the practice, travels through the state conducting training for the Oregon Pediatric Society about the impact of ACEs in parents and their children, and how to go about identifying and addressing them.
“So many of our visits are about behavioral problems or emotional disturbances, and so often at the root of these issues is some sort of trauma the child is experiencing,” Dr. Gillespie said in an interview. “What we’re seeing in many of these cases really are coping strategies for that child to deal with the toxic stress in his or her life.”
By assessing parents’ exposure to ACEs, briefly talking with them about how ACEs might impact their parenting, and tailoring their counseling and anticipatory guidance, the pediatricians hope to prevent ACEs and consequent toxic stress from developing in children.
The driving science
The term ACEs entered the medical lexicon after 1998, when a landmark study called the Adverse Childhood Experiences Study showed that traumatic experiences in childhood – abuse, neglect, and other severe dysfunctions in a household – not only are common among American adults but are associated with numerous poor health outcomes.
In the study and subsequent analyses, Dr. Vincent Felitti of Kaiser Permanente in San Diego and Dr. Robert Anda of the Centers for Disease Control and Prevention surveyed more than 17,000 patients about 10 types of ACEs and their current health status and behaviors. About two-thirds reported having at least one ACE, and one in eight reported four or more (Am J Prev Med. 1998;14[4]:245-58, www.cdc.gov/violenceprevention/acestudy/about.html).
Adults with four or more ACEs were not only significantly more likely to report health risk behaviors (smoking, substance abuse) and poor mental health outcomes (depression, suicide attempt); they were also significantly more likely to have poor physical health outcomes, with 2.2 times the risk of ischemic heart disease, 1.9 times the risk of cancer, and 3.9 times the risk of chronic bronchitis or emphysema, for instance. There was a strong dose-response relationship between ACEs and poor outcomes.
The Felitti study spawned dozens of analyses and additional research – in children as well as adults – on the associations between early-life adversity and the incidence of poor behavioral, mental, and physical outcomes, as well as on potential mechanisms.
Some research suggested a direct link between ACEs and negative outcomes, independent of whether individuals adopt risky behavior. Other studies suggested what experts in child development and mental health have long argued – that the more ACEs a parent has, the more ACEs their child will have.
And a growing body of biomedical literature linked the extreme, frequent, or prolonged activation of the body’s stress response in childhood – what has come to be known as “toxic stress” – with disruptions of the developing nervous, cardiovascular, immune, and metabolic systems.
While precise connections and mechanisms need to be clarified, “we now know that the repeated activation of the stress response leads to [negative] changes in the neuroendocrine immune pathways,” said Dr. Burke Harris, who coauthored a recent review of toxic stress in children and adolescents (Adv Pediatr. 2016;63[1]:403-28).
In January 2012, the American Academy of Pediatrics published a policy statement titled “Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician: Translating Developmental Science into Lifelong Health,” in which it urged pediatricians to consider actively screening for precipitants of toxic stress that are common in their communities (Pediatrics. 2011 Dec. doi: 10.1542/peds.2011-2662). But it stopped short of recommending particular tools or methods.
Dr. Gillespie and Dr. Pettersen did not want to wait for tools to be validated and approaches to be proven. “We’re building the plane as we fly,” Dr. Pettersen said.
The clinic’s roll-out
Dr. Pettersen learned about the ACE study and related research about 8 years ago while on a sabbatical to learn more about mental health issues. It “changed everything” about the way she viewed children and families and adversity. “I knew (we) didn’t have the infrastructure at the clinic, or the clinic’s support, to really start assessing children for what was happening to them,” she said, so she began thinking about ACE prevention and a focus on parenting.
Dr. Gillespie, in the meantime, was active in various quality improvement efforts at the state and national level, and had also become increasingly bothered by visits in which he saw children affected by maternal depression, abnormal attachment, and other problems. “I was seeing the consequences of ACEs, but I didn’t know specifically what was going on or how to talk about it,” he said.
The two pediatricians agreed to ask parents about ACEs at the 4-month well visit – a time when the families “knew us a little bit” and when “we could still influence parenting styles.”
In March 2013, they and their colleagues in the pilot group began giving parents a questionnaire that included the 10 ACE questions from Felitti’s study, questions about resilience from the Children’s Resilience Initiative, and a list of potential resources so they could understand parents’ needs.
They created a confidential field in their electronic medical record for documentation that appears during a visit, but does not print into notes and therefore will not be inadvertently released.
As they moved through the pilot phase, the pediatricians used various approaches to follow up on the assessment face-to-face. Eventually, they chose three particular questions as nonthreatening and helpful for conversation: Are there any experiences that still bother you? Of those experiences that don’t bother you, how did you get to the point where they don’t bother you? And how do these experiences affect your parenting now?
“It’s a motivational interviewing sort of style,” said Dr. Gillespie. “Parents can start identifying for themselves the solutions for the problems they’ve experienced, and they can start thinking about how their parenting might be impacted by things that have happened [or are still happening] to them.”
As the project rolled out, the physicians tweaked their process. They added four more ACE questions to address issues – community violence, extreme bullying, racism and prejudice, and foster care exposure – that they thought might lead to toxic stress in their population, for instance. And rather than ask on the written questionnaire for a “yes” or “no” to each of the ACE questions, they began asking the parent how many of the ACE questions applied to them. Moving away from the yes-no format to asking for a total count has led to more disclosures, Dr. Gillespie said.
To “keep the conversation going” in subsequent well-child visits, they developed a few questions to ask high-risk parents, like “How do you and your partner resolve conflict?” and “How did your parents resolve conflict in your household when you were a child?” And they provided training to all of the clinic’s staff on trauma-informed care and the need for support and compassion in their interactions with family members.
In the 3-plus years since incorporating ACEs assessments, the clinic’s pediatricians have made soft referrals to mental health professionals in only several cases – in each case, by suggesting that the parent contact their primary care physician. What most parents have wanted, says Dr. Gillespie, is recommendations for parenting classes and support groups. The clinic’s care manager assists the pediatricians in maintaining and providing links and handouts for various resources.
For Dr. Gillespie, the impact of the culture shift has been dramatic. “I’ve had 8-10 moms spontaneously reveal domestic violence to me in a subsequent visit, and say that they need a little help, because they’ve gotten the message that this is a safe place to talk about their experiences,” he said. “That had never happened to me in the previous 12 years of so of my career.”
Dr. Pettersen’s relationships with parents became “more intimate and more honest.” There was more trust. “If we can talk with parents [about ACEs] and not judge them for it,” she said, “then nothing is off the table.”
The ‘Two-Gen’ approach
“But I’d push back and say, parents know they have toxic stress but they don’t name it,” she said. “What we can do as trusted providers who want to advocate for families is to bear witness to their history by asking about it. Once they realize it’s not what’s wrong with [them], it’s what’s happened to [them], a shift occurs. That’s extremely validating for parents.”
That validation is part of a two-generation approach that she and Dr. Burke Harris see as part of a movement to break cycles of ACEs and toxic stress. At the California Pacific Medical Center’s Bayview Child Health Center in San Francisco, Dr. Burke Harris uses three ACE questionnaires – two of them ask parents (of children or teens) to report how many adverse experience types, or categories, apply to them and/or their child or teen, and one surveys adolescents themselves.
With the resources and clinical support of the Center for Youth Wellness, whose major funders include Google, Dr. Burke Harris can initiate a “warm hand-off” of patients with a high ACE score to a care coordinator or therapist. (The Center for Youth Wellness is beginning research to validate its ACE screening tools.) And in the meantime, the medical care she provides is trauma-informed.
“If a patient comes in for ADHD [attention-deficit/hyperactivity disorder] and has an ACE score of 6, my differential diagnosis and assessment will be different than if I see a patient sent by the school who has an ACE score of 0,” she said.
At the Portland Clinic, even though ACEs screening is now tied with the 4-month visit, pediatricians are much more attentive across the board to possible ACEs and toxic stress, and feel better able to converse with families, Dr. Gillespie said. One of his partners recently saw a 12-year-old boy who was failing in school and not making friends. Trauma-informed history-taking revealed at least several ACEs, and conversation turned to “all the resilience pieces… the connections he was missing and what he needed to cope,” he said.
References
• Resilience Project: This AAP project houses a “trauma toolkit” for primary care, case studies, and a variety of other tools.
• Center for Youth Wellness: The ACEs screening tools used by Dr. Burke Harris may be accessed at this website, along with a user guide containing sample scripts, and two white papers on ACEs and toxic stress.
• Resilience: The Biology of Stress and the Science of Hope: This documentary film, released in September 2016, is about ACEs and “a new movement” to treat and prevent toxic stress; it features the work of Dr. Burke Harris and others.
• Academy on Violence & Abuse: Various papers on ACEs screening and case finding in practice may be accessed here.
Several years ago, pediatricians R.J. Gillespie, MD, MHPE, and Teri Pettersen, MD, piloted the use of a questionnaire about adverse childhood experiences (ACEs) and resilience at the 4-month well-child visit.
They and six other pediatricians at The Children’s Clinic in Portland, Ore., explained in a cover letter why they were posing the questions of parents, and they ended the survey by asking them about their interest in potential resources.
[[{"fid":"172157","view_mode":"medstat_image_flush_left","fields":{"format":"medstat_image_flush_left","field_file_image_alt_text[und][0][value]":"R.J. Gillespie, MD, MHPE","field_file_image_credit[und][0][value]":"Courtesy The Children's Clinic","field_file_image_caption[und][0][value]":"Dr. R.J. Gillespie "},"type":"media","attributes":{"class":"media-element file-medstat_image_flush_left"}}]]Today, all 28 of the pediatricians at the clinic screen for ACEs and resilience, and Dr. Pettersen, now retired from the practice, travels through the state conducting training for the Oregon Pediatric Society about the impact of ACEs in parents and their children, and how to go about identifying and addressing them.
“So many of our visits are about behavioral problems or emotional disturbances, and so often at the root of these issues is some sort of trauma the child is experiencing,” Dr. Gillespie said in an interview. “What we’re seeing in many of these cases really are coping strategies for that child to deal with the toxic stress in his or her life.”
By assessing parents’ exposure to ACEs, briefly talking with them about how ACEs might impact their parenting, and tailoring their counseling and anticipatory guidance, the pediatricians hope to prevent ACEs and consequent toxic stress from developing in children.
The driving science
The term ACEs entered the medical lexicon after 1998, when a landmark study called the Adverse Childhood Experiences Study showed that traumatic experiences in childhood – abuse, neglect, and other severe dysfunctions in a household – not only are common among American adults but are associated with numerous poor health outcomes.
In the study and subsequent analyses, Dr. Vincent Felitti of Kaiser Permanente in San Diego and Dr. Robert Anda of the Centers for Disease Control and Prevention surveyed more than 17,000 patients about 10 types of ACEs and their current health status and behaviors. About two-thirds reported having at least one ACE, and one in eight reported four or more (Am J Prev Med. 1998;14[4]:245-58, www.cdc.gov/violenceprevention/acestudy/about.html).
Adults with four or more ACEs were not only significantly more likely to report health risk behaviors (smoking, substance abuse) and poor mental health outcomes (depression, suicide attempt); they were also significantly more likely to have poor physical health outcomes, with 2.2 times the risk of ischemic heart disease, 1.9 times the risk of cancer, and 3.9 times the risk of chronic bronchitis or emphysema, for instance. There was a strong dose-response relationship between ACEs and poor outcomes.
The Felitti study spawned dozens of analyses and additional research – in children as well as adults – on the associations between early-life adversity and the incidence of poor behavioral, mental, and physical outcomes, as well as on potential mechanisms.
Some research suggested a direct link between ACEs and negative outcomes, independent of whether individuals adopt risky behavior. Other studies suggested what experts in child development and mental health have long argued – that the more ACEs a parent has, the more ACEs their child will have.
And a growing body of biomedical literature linked the extreme, frequent, or prolonged activation of the body’s stress response in childhood – what has come to be known as “toxic stress” – with disruptions of the developing nervous, cardiovascular, immune, and metabolic systems.
While precise connections and mechanisms need to be clarified, “we now know that the repeated activation of the stress response leads to [negative] changes in the neuroendocrine immune pathways,” said Dr. Burke Harris, who coauthored a recent review of toxic stress in children and adolescents (Adv Pediatr. 2016;63[1]:403-28).
In January 2012, the American Academy of Pediatrics published a policy statement titled “Early Childhood Adversity, Toxic Stress, and the Role of the Pediatrician: Translating Developmental Science into Lifelong Health,” in which it urged pediatricians to consider actively screening for precipitants of toxic stress that are common in their communities (Pediatrics. 2011 Dec. doi: 10.1542/peds.2011-2662). But it stopped short of recommending particular tools or methods.
Dr. Gillespie and Dr. Pettersen did not want to wait for tools to be validated and approaches to be proven. “We’re building the plane as we fly,” Dr. Pettersen said.
The clinic’s roll-out
Dr. Pettersen learned about the ACE study and related research about 8 years ago while on a sabbatical to learn more about mental health issues. It “changed everything” about the way she viewed children and families and adversity. “I knew (we) didn’t have the infrastructure at the clinic, or the clinic’s support, to really start assessing children for what was happening to them,” she said, so she began thinking about ACE prevention and a focus on parenting.
Dr. Gillespie, in the meantime, was active in various quality improvement efforts at the state and national level, and had also become increasingly bothered by visits in which he saw children affected by maternal depression, abnormal attachment, and other problems. “I was seeing the consequences of ACEs, but I didn’t know specifically what was going on or how to talk about it,” he said.
The two pediatricians agreed to ask parents about ACEs at the 4-month well visit – a time when the families “knew us a little bit” and when “we could still influence parenting styles.”
In March 2013, they and their colleagues in the pilot group began giving parents a questionnaire that included the 10 ACE questions from Felitti’s study, questions about resilience from the Children’s Resilience Initiative, and a list of potential resources so they could understand parents’ needs.
They created a confidential field in their electronic medical record for documentation that appears during a visit, but does not print into notes and therefore will not be inadvertently released.
As they moved through the pilot phase, the pediatricians used various approaches to follow up on the assessment face-to-face. Eventually, they chose three particular questions as nonthreatening and helpful for conversation: Are there any experiences that still bother you? Of those experiences that don’t bother you, how did you get to the point where they don’t bother you? And how do these experiences affect your parenting now?
“It’s a motivational interviewing sort of style,” said Dr. Gillespie. “Parents can start identifying for themselves the solutions for the problems they’ve experienced, and they can start thinking about how their parenting might be impacted by things that have happened [or are still happening] to them.”
As the project rolled out, the physicians tweaked their process. They added four more ACE questions to address issues – community violence, extreme bullying, racism and prejudice, and foster care exposure – that they thought might lead to toxic stress in their population, for instance. And rather than ask on the written questionnaire for a “yes” or “no” to each of the ACE questions, they began asking the parent how many of the ACE questions applied to them. Moving away from the yes-no format to asking for a total count has led to more disclosures, Dr. Gillespie said.
To “keep the conversation going” in subsequent well-child visits, they developed a few questions to ask high-risk parents, like “How do you and your partner resolve conflict?” and “How did your parents resolve conflict in your household when you were a child?” And they provided training to all of the clinic’s staff on trauma-informed care and the need for support and compassion in their interactions with family members.
In the 3-plus years since incorporating ACEs assessments, the clinic’s pediatricians have made soft referrals to mental health professionals in only several cases – in each case, by suggesting that the parent contact their primary care physician. What most parents have wanted, says Dr. Gillespie, is recommendations for parenting classes and support groups. The clinic’s care manager assists the pediatricians in maintaining and providing links and handouts for various resources.
For Dr. Gillespie, the impact of the culture shift has been dramatic. “I’ve had 8-10 moms spontaneously reveal domestic violence to me in a subsequent visit, and say that they need a little help, because they’ve gotten the message that this is a safe place to talk about their experiences,” he said. “That had never happened to me in the previous 12 years of so of my career.”
Dr. Pettersen’s relationships with parents became “more intimate and more honest.” There was more trust. “If we can talk with parents [about ACEs] and not judge them for it,” she said, “then nothing is off the table.”
The ‘Two-Gen’ approach
“But I’d push back and say, parents know they have toxic stress but they don’t name it,” she said. “What we can do as trusted providers who want to advocate for families is to bear witness to their history by asking about it. Once they realize it’s not what’s wrong with [them], it’s what’s happened to [them], a shift occurs. That’s extremely validating for parents.”
That validation is part of a two-generation approach that she and Dr. Burke Harris see as part of a movement to break cycles of ACEs and toxic stress. At the California Pacific Medical Center’s Bayview Child Health Center in San Francisco, Dr. Burke Harris uses three ACE questionnaires – two of them ask parents (of children or teens) to report how many adverse experience types, or categories, apply to them and/or their child or teen, and one surveys adolescents themselves.
With the resources and clinical support of the Center for Youth Wellness, whose major funders include Google, Dr. Burke Harris can initiate a “warm hand-off” of patients with a high ACE score to a care coordinator or therapist. (The Center for Youth Wellness is beginning research to validate its ACE screening tools.) And in the meantime, the medical care she provides is trauma-informed.
“If a patient comes in for ADHD [attention-deficit/hyperactivity disorder] and has an ACE score of 6, my differential diagnosis and assessment will be different than if I see a patient sent by the school who has an ACE score of 0,” she said.
At the Portland Clinic, even though ACEs screening is now tied with the 4-month visit, pediatricians are much more attentive across the board to possible ACEs and toxic stress, and feel better able to converse with families, Dr. Gillespie said. One of his partners recently saw a 12-year-old boy who was failing in school and not making friends. Trauma-informed history-taking revealed at least several ACEs, and conversation turned to “all the resilience pieces… the connections he was missing and what he needed to cope,” he said.
References
• Resilience Project: This AAP project houses a “trauma toolkit” for primary care, case studies, and a variety of other tools.
• Center for Youth Wellness: The ACEs screening tools used by Dr. Burke Harris may be accessed at this website, along with a user guide containing sample scripts, and two white papers on ACEs and toxic stress.
• Resilience: The Biology of Stress and the Science of Hope: This documentary film, released in September 2016, is about ACEs and “a new movement” to treat and prevent toxic stress; it features the work of Dr. Burke Harris and others.
• Academy on Violence & Abuse: Various papers on ACEs screening and case finding in practice may be accessed here.

New research on health-related behaviors of sexual minority youth
The Centers for Disease Control and Prevention released results from the first nationally representative study on health risk behaviors of gay, lesbian, and bisexual (GLB) high school students in August 2016.
These data were collected through the Youth Risk Behavior Survey (YRBS) questionnaire. The YRBS questionnaire was developed in 1990 as a way to monitor health-related behaviors that contribute to the leading causes of mortality and morbidity in youth and young adults. Areas covered by the survey include behaviors related to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, dietary behaviors, and physical activity. Data are collected every 2 years through national, state, territorial, tribal government, and local school-based surveys of representative samples of 9th-12th grade students.

For the study, sexual minority youth were defined as those who identified as GLB; those who reported sexual contact with members of the same sex only; and those who reported sexual contact with members of both sexes. It is important to note that the YRBS is a school-based survey and does not include youth who do not attend school, for example, homeless and runaway youth.
Exploring and identifying disparities in health behaviors that affect sexual minorities can help us as providers to better target screenings for these health behaviors at the individual level. At the population level, it is important to continue to explore why these differences exist and to continue to develop interventions that help address these differences, while educating families and communities about how to support all of their youth. It is important to note that the majority of sexual minority youth live healthy live; however, this study shows that sexual minority youth do have a higher prevalence of certain health risk behaviors, likely leading to the health disparities we see in this population. Select findings of this study are summarized in the accompanying table.
Continued study is needed to understand the health disparities that occur in sexual minority populations. In October, the National Institutes of Health designated sexual and gender minorities as a specific health disparity population for NIH research. This term encompasses lesbian, gay, bisexual, and transgender individuals as well as any individuals whose sexual identity or gender identity does not align with traditional norms. This hopefully will lead to a growing body of evidence to help all of us learn about the spectrum of sexual and gender identity and better help sexual and gender minority youth reach their full potential.
For more information about the YRBS and the report on health related behaviors in sexual minority youth visit this link:
Selected questionnaire results
Sexual identity
• 88.8% of students identified as heterosexual.
• 6.0% identified as bisexual.
• 3.2% were not sure.
• 2.0% identified as gay or lesbian.
Sexual behaviors
• 48% had had sexual contact with the opposite sex only.
• 4.6% had sexual contact with both sexes.
• 1.7% had had sexual contact with the same sex only.
• 45.7% had no sexual contact.
Mental health
Percent of students who reported making a suicide plan in the 12 months preceding the survey:
• 11.9% of heterosexual students.
• 27.9% of students not sure of sexual identity.
• 38.2% of gay, lesbian, bisexual (GLB) students.
Percent of students who attempted suicide in the 12 months preceding the survey:
• 6.4% of heterosexual students.
• 13.7% of students not sure of sexual identity.
• 29.4% of GLB students.
Sexual Behaviors
First sex before the age of 13:
• 3.4% of heterosexual students.
• 8.8% of students not sure of their sexual identity.
• 7.3% of GLB students.
Drank alcohol or used drugs before last sex:
• 20.0% of heterosexual students.
• 44.5% of students not sure of their sexual identity.
• 22.4% of GLB students.
Tested for HIV:
• 9.3% of heterosexual students.
• 12.8% of students not sure of their sexual identity.
• 18.2% of GLB students.
Substance use
Currently smoking cigarettes daily:
• 1.9% of heterosexual students.
• 7.0% of students not sure of their sexual identity.
• 4.0% of GLB students.
Current alcohol use:
• 32.1% of heterosexual students.
• 34.6% of students not sure of their sexual identity.
• 40.5% of GLB students.
Current marijuana use:
• 20.7% of heterosexual students.
• 26.0% of students not sure of their sexual identity.
• 32.0% of GLB students.
Used hallucinogenic drugs (such as LSD, acid, PCP, angel dust, mescaline, or mushrooms):
• 5.5% of heterosexual students.
• 15.7% of students not sure of their sexual identity.
• 11.5% of GLB students.
Ever used heroin:
• 1.3% of heterosexual students.
• 9.3% of students not sure of their sexual identity.
• 6.0% of GLB students.
Ever took prescription drugs without a doctor’s prescription:
15.5% of heterosexual students.
24.3% of students not sure of their sexual identity.
27.5% of GLB students.
Physical Activity
Did not participate in at least 60 minutes of physical activity on at least 1 day in past week:
• 12.6% of heterosexual students.
• 27.0% of students not sure of their sexual identity.
• 25.7% of GLB students.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
The Centers for Disease Control and Prevention released results from the first nationally representative study on health risk behaviors of gay, lesbian, and bisexual (GLB) high school students in August 2016.
These data were collected through the Youth Risk Behavior Survey (YRBS) questionnaire. The YRBS questionnaire was developed in 1990 as a way to monitor health-related behaviors that contribute to the leading causes of mortality and morbidity in youth and young adults. Areas covered by the survey include behaviors related to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, dietary behaviors, and physical activity. Data are collected every 2 years through national, state, territorial, tribal government, and local school-based surveys of representative samples of 9th-12th grade students.
For the study, sexual minority youth were defined as those who identified as GLB; those who reported sexual contact with members of the same sex only; and those who reported sexual contact with members of both sexes. It is important to note that the YRBS is a school-based survey and does not include youth who do not attend school, for example, homeless and runaway youth.
Exploring and identifying disparities in health behaviors that affect sexual minorities can help us as providers to better target screenings for these health behaviors at the individual level. At the population level, it is important to continue to explore why these differences exist and to continue to develop interventions that help address these differences, while educating families and communities about how to support all of their youth. It is important to note that the majority of sexual minority youth live healthy live; however, this study shows that sexual minority youth do have a higher prevalence of certain health risk behaviors, likely leading to the health disparities we see in this population. Select findings of this study are summarized in the accompanying table.
Continued study is needed to understand the health disparities that occur in sexual minority populations. In October, the National Institutes of Health designated sexual and gender minorities as a specific health disparity population for NIH research. This term encompasses lesbian, gay, bisexual, and transgender individuals as well as any individuals whose sexual identity or gender identity does not align with traditional norms. This hopefully will lead to a growing body of evidence to help all of us learn about the spectrum of sexual and gender identity and better help sexual and gender minority youth reach their full potential.
For more information about the YRBS and the report on health related behaviors in sexual minority youth visit this link:
Selected questionnaire results
Sexual identity
• 88.8% of students identified as heterosexual.
• 6.0% identified as bisexual.
• 3.2% were not sure.
• 2.0% identified as gay or lesbian.
Sexual behaviors
• 48% had had sexual contact with the opposite sex only.
• 4.6% had sexual contact with both sexes.
• 1.7% had had sexual contact with the same sex only.
• 45.7% had no sexual contact.
Mental health
Percent of students who reported making a suicide plan in the 12 months preceding the survey:
• 11.9% of heterosexual students.
• 27.9% of students not sure of sexual identity.
• 38.2% of gay, lesbian, bisexual (GLB) students.
Percent of students who attempted suicide in the 12 months preceding the survey:
• 6.4% of heterosexual students.
• 13.7% of students not sure of sexual identity.
• 29.4% of GLB students.
Sexual Behaviors
First sex before the age of 13:
• 3.4% of heterosexual students.
• 8.8% of students not sure of their sexual identity.
• 7.3% of GLB students.
Drank alcohol or used drugs before last sex:
• 20.0% of heterosexual students.
• 44.5% of students not sure of their sexual identity.
• 22.4% of GLB students.
Tested for HIV:
• 9.3% of heterosexual students.
• 12.8% of students not sure of their sexual identity.
• 18.2% of GLB students.
Substance use
Currently smoking cigarettes daily:
• 1.9% of heterosexual students.
• 7.0% of students not sure of their sexual identity.
• 4.0% of GLB students.
Current alcohol use:
• 32.1% of heterosexual students.
• 34.6% of students not sure of their sexual identity.
• 40.5% of GLB students.
Current marijuana use:
• 20.7% of heterosexual students.
• 26.0% of students not sure of their sexual identity.
• 32.0% of GLB students.
Used hallucinogenic drugs (such as LSD, acid, PCP, angel dust, mescaline, or mushrooms):
• 5.5% of heterosexual students.
• 15.7% of students not sure of their sexual identity.
• 11.5% of GLB students.
Ever used heroin:
• 1.3% of heterosexual students.
• 9.3% of students not sure of their sexual identity.
• 6.0% of GLB students.
Ever took prescription drugs without a doctor’s prescription:
15.5% of heterosexual students.
24.3% of students not sure of their sexual identity.
27.5% of GLB students.
Physical Activity
Did not participate in at least 60 minutes of physical activity on at least 1 day in past week:
• 12.6% of heterosexual students.
• 27.0% of students not sure of their sexual identity.
• 25.7% of GLB students.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
The Centers for Disease Control and Prevention released results from the first nationally representative study on health risk behaviors of gay, lesbian, and bisexual (GLB) high school students in August 2016.
These data were collected through the Youth Risk Behavior Survey (YRBS) questionnaire. The YRBS questionnaire was developed in 1990 as a way to monitor health-related behaviors that contribute to the leading causes of mortality and morbidity in youth and young adults. Areas covered by the survey include behaviors related to unintentional injuries and violence, tobacco use, alcohol and other drug use, sexual behaviors, dietary behaviors, and physical activity. Data are collected every 2 years through national, state, territorial, tribal government, and local school-based surveys of representative samples of 9th-12th grade students.
For the study, sexual minority youth were defined as those who identified as GLB; those who reported sexual contact with members of the same sex only; and those who reported sexual contact with members of both sexes. It is important to note that the YRBS is a school-based survey and does not include youth who do not attend school, for example, homeless and runaway youth.
Exploring and identifying disparities in health behaviors that affect sexual minorities can help us as providers to better target screenings for these health behaviors at the individual level. At the population level, it is important to continue to explore why these differences exist and to continue to develop interventions that help address these differences, while educating families and communities about how to support all of their youth. It is important to note that the majority of sexual minority youth live healthy live; however, this study shows that sexual minority youth do have a higher prevalence of certain health risk behaviors, likely leading to the health disparities we see in this population. Select findings of this study are summarized in the accompanying table.
Continued study is needed to understand the health disparities that occur in sexual minority populations. In October, the National Institutes of Health designated sexual and gender minorities as a specific health disparity population for NIH research. This term encompasses lesbian, gay, bisexual, and transgender individuals as well as any individuals whose sexual identity or gender identity does not align with traditional norms. This hopefully will lead to a growing body of evidence to help all of us learn about the spectrum of sexual and gender identity and better help sexual and gender minority youth reach their full potential.
For more information about the YRBS and the report on health related behaviors in sexual minority youth visit this link:
Selected questionnaire results
Sexual identity
• 88.8% of students identified as heterosexual.
• 6.0% identified as bisexual.
• 3.2% were not sure.
• 2.0% identified as gay or lesbian.
Sexual behaviors
• 48% had had sexual contact with the opposite sex only.
• 4.6% had sexual contact with both sexes.
• 1.7% had had sexual contact with the same sex only.
• 45.7% had no sexual contact.
Mental health
Percent of students who reported making a suicide plan in the 12 months preceding the survey:
• 11.9% of heterosexual students.
• 27.9% of students not sure of sexual identity.
• 38.2% of gay, lesbian, bisexual (GLB) students.
Percent of students who attempted suicide in the 12 months preceding the survey:
• 6.4% of heterosexual students.
• 13.7% of students not sure of sexual identity.
• 29.4% of GLB students.
Sexual Behaviors
First sex before the age of 13:
• 3.4% of heterosexual students.
• 8.8% of students not sure of their sexual identity.
• 7.3% of GLB students.
Drank alcohol or used drugs before last sex:
• 20.0% of heterosexual students.
• 44.5% of students not sure of their sexual identity.
• 22.4% of GLB students.
Tested for HIV:
• 9.3% of heterosexual students.
• 12.8% of students not sure of their sexual identity.
• 18.2% of GLB students.
Substance use
Currently smoking cigarettes daily:
• 1.9% of heterosexual students.
• 7.0% of students not sure of their sexual identity.
• 4.0% of GLB students.
Current alcohol use:
• 32.1% of heterosexual students.
• 34.6% of students not sure of their sexual identity.
• 40.5% of GLB students.
Current marijuana use:
• 20.7% of heterosexual students.
• 26.0% of students not sure of their sexual identity.
• 32.0% of GLB students.
Used hallucinogenic drugs (such as LSD, acid, PCP, angel dust, mescaline, or mushrooms):
• 5.5% of heterosexual students.
• 15.7% of students not sure of their sexual identity.
• 11.5% of GLB students.
Ever used heroin:
• 1.3% of heterosexual students.
• 9.3% of students not sure of their sexual identity.
• 6.0% of GLB students.
Ever took prescription drugs without a doctor’s prescription:
15.5% of heterosexual students.
24.3% of students not sure of their sexual identity.
27.5% of GLB students.
Physical Activity
Did not participate in at least 60 minutes of physical activity on at least 1 day in past week:
• 12.6% of heterosexual students.
• 27.0% of students not sure of their sexual identity.
• 25.7% of GLB students.
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.

Fatal measles complication occurs more often than realized
NEW ORLEANS – A fatal complication of measles known as subacute sclerosing panencephalitis (SSPE) can develop years after measles infection and appears to occur much more often than published reports suggest, according to a review of cases in California from 1998 to 2015.
The findings underscore the vital importance of herd immunity by vaccination, Kristen Wendorf, MD, reported at an annual scientific meeting on infectious diseases.
The incidence of postmeasles SSPE was previously thought be about 1 in 100,000, according to an IDWeek press release.
“There is no cure for SSPE, and the only way to prevent it is to vaccinate everyone against measles,” the release stated.
The cases in the current study were among children with a clinically compatible illness, and either measles IgG antibody detected in cerebrospinal fluid, a characteristic pattern on electroencephalography, typical histologic findings on brain biopsy, or medical record documentation of SSPE-related complications. They were identified based on death certificates, reports from the Centers for Diseases Control and Prevention, or through investigations for undiagnosed neurologic disease. Twelve of the 17 affected children had a clinical history of a febrile rash illness compatible with measles, and all 12 of those experienced illness before age 15 months and before measles vaccination.
Most (67%) were living in the United States when they had measles, Dr. Wendorf said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
The median age at diagnosis of SSPE was 12 years, although the range was 3-35 years, and the mean latency period was 9.5 years. In many cases, long-standing cognitive or motor problems were experienced prior to diagnosis, she noted.
The findings suggest that SSPE is more common than previously recognized in unvaccinated children with measles during infancy, Dr. Wendorf said.
Protection of infants younger than 12-15 months of age – before the time when measles vaccine is routinely administered – and in those who can’t be vaccinated because of immune system disorders requires avoidance of travel to endemic areas. Parents also may consider early vaccination prior to such travel.
Further, clinicians should be aware of the risk of SSPE in patients with symptoms suggestive of the disease. This is true even among older patients in whom no specific history of measles infection is known, she said.
In the press release, coauthor James D. Cherry, MD, professor of pediatrics at the University of California, Los Angeles, further stressed the importance of protecting unvaccinated infants.
“Parents of infants who have not yet been vaccinated should avoid putting their children at risk. For example, they should postpone trips overseas – including to Europe – where measles is endemic and epidemic until after their baby has been vaccinated with two doses,” he said. “It’s just not worth the risk.”
The authors reported having no disclosures.
NEW ORLEANS – A fatal complication of measles known as subacute sclerosing panencephalitis (SSPE) can develop years after measles infection and appears to occur much more often than published reports suggest, according to a review of cases in California from 1998 to 2015.
The findings underscore the vital importance of herd immunity by vaccination, Kristen Wendorf, MD, reported at an annual scientific meeting on infectious diseases.
The incidence of postmeasles SSPE was previously thought be about 1 in 100,000, according to an IDWeek press release.
“There is no cure for SSPE, and the only way to prevent it is to vaccinate everyone against measles,” the release stated.
The cases in the current study were among children with a clinically compatible illness, and either measles IgG antibody detected in cerebrospinal fluid, a characteristic pattern on electroencephalography, typical histologic findings on brain biopsy, or medical record documentation of SSPE-related complications. They were identified based on death certificates, reports from the Centers for Diseases Control and Prevention, or through investigations for undiagnosed neurologic disease. Twelve of the 17 affected children had a clinical history of a febrile rash illness compatible with measles, and all 12 of those experienced illness before age 15 months and before measles vaccination.
Most (67%) were living in the United States when they had measles, Dr. Wendorf said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
The median age at diagnosis of SSPE was 12 years, although the range was 3-35 years, and the mean latency period was 9.5 years. In many cases, long-standing cognitive or motor problems were experienced prior to diagnosis, she noted.
The findings suggest that SSPE is more common than previously recognized in unvaccinated children with measles during infancy, Dr. Wendorf said.
Protection of infants younger than 12-15 months of age – before the time when measles vaccine is routinely administered – and in those who can’t be vaccinated because of immune system disorders requires avoidance of travel to endemic areas. Parents also may consider early vaccination prior to such travel.
Further, clinicians should be aware of the risk of SSPE in patients with symptoms suggestive of the disease. This is true even among older patients in whom no specific history of measles infection is known, she said.
In the press release, coauthor James D. Cherry, MD, professor of pediatrics at the University of California, Los Angeles, further stressed the importance of protecting unvaccinated infants.
“Parents of infants who have not yet been vaccinated should avoid putting their children at risk. For example, they should postpone trips overseas – including to Europe – where measles is endemic and epidemic until after their baby has been vaccinated with two doses,” he said. “It’s just not worth the risk.”
The authors reported having no disclosures.
NEW ORLEANS – A fatal complication of measles known as subacute sclerosing panencephalitis (SSPE) can develop years after measles infection and appears to occur much more often than published reports suggest, according to a review of cases in California from 1998 to 2015.
The findings underscore the vital importance of herd immunity by vaccination, Kristen Wendorf, MD, reported at an annual scientific meeting on infectious diseases.
The incidence of postmeasles SSPE was previously thought be about 1 in 100,000, according to an IDWeek press release.
“There is no cure for SSPE, and the only way to prevent it is to vaccinate everyone against measles,” the release stated.
The cases in the current study were among children with a clinically compatible illness, and either measles IgG antibody detected in cerebrospinal fluid, a characteristic pattern on electroencephalography, typical histologic findings on brain biopsy, or medical record documentation of SSPE-related complications. They were identified based on death certificates, reports from the Centers for Diseases Control and Prevention, or through investigations for undiagnosed neurologic disease. Twelve of the 17 affected children had a clinical history of a febrile rash illness compatible with measles, and all 12 of those experienced illness before age 15 months and before measles vaccination.
Most (67%) were living in the United States when they had measles, Dr. Wendorf said at the combined annual meetings of the Infectious Diseases Society of America, the Society for Healthcare Epidemiology of America, the HIV Medicine Association, and the Pediatric Infectious Diseases Society.
The median age at diagnosis of SSPE was 12 years, although the range was 3-35 years, and the mean latency period was 9.5 years. In many cases, long-standing cognitive or motor problems were experienced prior to diagnosis, she noted.
The findings suggest that SSPE is more common than previously recognized in unvaccinated children with measles during infancy, Dr. Wendorf said.
Protection of infants younger than 12-15 months of age – before the time when measles vaccine is routinely administered – and in those who can’t be vaccinated because of immune system disorders requires avoidance of travel to endemic areas. Parents also may consider early vaccination prior to such travel.
Further, clinicians should be aware of the risk of SSPE in patients with symptoms suggestive of the disease. This is true even among older patients in whom no specific history of measles infection is known, she said.
In the press release, coauthor James D. Cherry, MD, professor of pediatrics at the University of California, Los Angeles, further stressed the importance of protecting unvaccinated infants.
“Parents of infants who have not yet been vaccinated should avoid putting their children at risk. For example, they should postpone trips overseas – including to Europe – where measles is endemic and epidemic until after their baby has been vaccinated with two doses,” he said. “It’s just not worth the risk.”
The authors reported having no disclosures.
AT IDWEEK 2016
Key clinical point:
Major finding: The incidence of SSPE among measles cases was 1 in 1,367 children under age 5 years and 1 in 609 children under age 12 months at the time of measles disease.
Data source: A review of records and 17 cases of SSPE.
Disclosures: The authors reported having no disclosures.
Follow-Up of Infants With Zika Virus Identifies Several Neurologic Impairments
A report on 11 infants in Brazil suggests the term “congenital Zika syndrome” be used to describe the abnormalities associated with Zika virus infection because microcephaly is only one clinical sign of this congenital malformation disorder. The report was published online ahead of print October 3 in JAMA Neurology.
“To our knowledge,” the researchers wrote, “most reports to date have focused on select aspects of the maternal or fetal infection and fetal effects.” To provide a fuller description, the researchers sought to characterize the prenatal evolution and perinatal outcomes of 11 neonates who had developmental abnormalities and neurologic damage associated with Zika infection.
Follow-Up of 11 Neonates
Amilcar Tanuri, MD, PhD, Professor of Genetics and Chief of the Laboratory of Molecular Virology at the Institute of Biology, Federal University of Rio de Janeiro, and coauthors observed 11 infants with congenital Zika infection from gestation to six months in the state of Paraíba, Brazil. Cases were referred between October 2015 and February 2016. Ten of 11 women included in the study presented with symptoms of Zika infection during the first half of pregnancy, and all 11 had laboratory evidence of infection in several tissues by serology or polymerase chain reaction. Brain damage was confirmed through intrauterine ultrasonography and was complemented by MRI. Histopathologic analysis was performed on the placenta and brain tissue from infants who died. The ZIKV genome was investigated in several tissues and sequenced for further phylogenetic analysis.
Of the 11 infants, seven (63.6%) were female, and the median maternal age at delivery was 25. Three of the neonates died, giving a perinatal mortality rate of 27.3%. Zika virus was identified in amniotic fluid, placenta, cord blood, and neonatal tissues collected post mortem in the three babies who died within 48 hours of delivery.
Brain damage and neurologic impairments were identified in all patients, including microcephaly, a reduction in cerebral volume, ventriculomegaly, cerebellar hypoplasia, lissencephaly with hydrocephalus, and fetal akinesia deformation sequence. Testing for other causes of microcephaly, such as genetic disorders and infections, was negative. The ZIKV virus genome was found in tissues of the mothers and their babies.
“Combined findings from clinical, laboratory, imaging, and pathologic examinations provided a more complete picture of the severe damage and developmental abnormalities caused by ZIKV infection than has been previously reported,” Dr. Tanuri and colleagues said.
Formulating a Plan of Action
“Although we have limited ways to stop emerging pathogens, we now have powerful techniques to quickly identify the culprit, such as polymerase chain reaction and whole genome sequencing,” said Raymond P. Roos, MD, Marjorie and Robert E. Straus Professor in Neurologic Science in the Department of Neurology at the University of Chicago, in an accompanying editorial. “We also have novel methods to control vectors and produce vaccines in an accelerated time frame.”
But many unanswered questions remain, said Dr. Roos. Among those questions is what neurologists can do about the Zika virus. “It would be valuable to have adult and pediatric neurologists network with the US Centers for Disease Control and Prevention to establish a surveillance system that could track Zika virus-induced Guillain-Barré syndrome (GBS) and CNS disease. This [cooperation] would facilitate the identification and characterization of disorders, the formation of a registry, and the mounting of comprehensive epidemiologic studies. This approach would also help to identify long-term sequelae of intrauterine infection and clarify effective treatments of the GBS syndrome.”
—Glenn S. Williams
Suggested Reading
Melo AS, Aguiar RS, Amorim MM, et al. Congenital Zika virus infection: beyond neonatal microcephaly. JAMA Neurol. 2016 Oct 3 [Epub ahead of print].
Roos RP. Zika virus-a public health emergency of international concern. JAMA Neurol. 2016 Oct 3 [Epub ahead of print].
A report on 11 infants in Brazil suggests the term “congenital Zika syndrome” be used to describe the abnormalities associated with Zika virus infection because microcephaly is only one clinical sign of this congenital malformation disorder. The report was published online ahead of print October 3 in JAMA Neurology.
“To our knowledge,” the researchers wrote, “most reports to date have focused on select aspects of the maternal or fetal infection and fetal effects.” To provide a fuller description, the researchers sought to characterize the prenatal evolution and perinatal outcomes of 11 neonates who had developmental abnormalities and neurologic damage associated with Zika infection.
Follow-Up of 11 Neonates
Amilcar Tanuri, MD, PhD, Professor of Genetics and Chief of the Laboratory of Molecular Virology at the Institute of Biology, Federal University of Rio de Janeiro, and coauthors observed 11 infants with congenital Zika infection from gestation to six months in the state of Paraíba, Brazil. Cases were referred between October 2015 and February 2016. Ten of 11 women included in the study presented with symptoms of Zika infection during the first half of pregnancy, and all 11 had laboratory evidence of infection in several tissues by serology or polymerase chain reaction. Brain damage was confirmed through intrauterine ultrasonography and was complemented by MRI. Histopathologic analysis was performed on the placenta and brain tissue from infants who died. The ZIKV genome was investigated in several tissues and sequenced for further phylogenetic analysis.
Of the 11 infants, seven (63.6%) were female, and the median maternal age at delivery was 25. Three of the neonates died, giving a perinatal mortality rate of 27.3%. Zika virus was identified in amniotic fluid, placenta, cord blood, and neonatal tissues collected post mortem in the three babies who died within 48 hours of delivery.
Brain damage and neurologic impairments were identified in all patients, including microcephaly, a reduction in cerebral volume, ventriculomegaly, cerebellar hypoplasia, lissencephaly with hydrocephalus, and fetal akinesia deformation sequence. Testing for other causes of microcephaly, such as genetic disorders and infections, was negative. The ZIKV virus genome was found in tissues of the mothers and their babies.
“Combined findings from clinical, laboratory, imaging, and pathologic examinations provided a more complete picture of the severe damage and developmental abnormalities caused by ZIKV infection than has been previously reported,” Dr. Tanuri and colleagues said.
Formulating a Plan of Action
“Although we have limited ways to stop emerging pathogens, we now have powerful techniques to quickly identify the culprit, such as polymerase chain reaction and whole genome sequencing,” said Raymond P. Roos, MD, Marjorie and Robert E. Straus Professor in Neurologic Science in the Department of Neurology at the University of Chicago, in an accompanying editorial. “We also have novel methods to control vectors and produce vaccines in an accelerated time frame.”
But many unanswered questions remain, said Dr. Roos. Among those questions is what neurologists can do about the Zika virus. “It would be valuable to have adult and pediatric neurologists network with the US Centers for Disease Control and Prevention to establish a surveillance system that could track Zika virus-induced Guillain-Barré syndrome (GBS) and CNS disease. This [cooperation] would facilitate the identification and characterization of disorders, the formation of a registry, and the mounting of comprehensive epidemiologic studies. This approach would also help to identify long-term sequelae of intrauterine infection and clarify effective treatments of the GBS syndrome.”
—Glenn S. Williams
Suggested Reading
Melo AS, Aguiar RS, Amorim MM, et al. Congenital Zika virus infection: beyond neonatal microcephaly. JAMA Neurol. 2016 Oct 3 [Epub ahead of print].
Roos RP. Zika virus-a public health emergency of international concern. JAMA Neurol. 2016 Oct 3 [Epub ahead of print].
A report on 11 infants in Brazil suggests the term “congenital Zika syndrome” be used to describe the abnormalities associated with Zika virus infection because microcephaly is only one clinical sign of this congenital malformation disorder. The report was published online ahead of print October 3 in JAMA Neurology.
“To our knowledge,” the researchers wrote, “most reports to date have focused on select aspects of the maternal or fetal infection and fetal effects.” To provide a fuller description, the researchers sought to characterize the prenatal evolution and perinatal outcomes of 11 neonates who had developmental abnormalities and neurologic damage associated with Zika infection.
Follow-Up of 11 Neonates
Amilcar Tanuri, MD, PhD, Professor of Genetics and Chief of the Laboratory of Molecular Virology at the Institute of Biology, Federal University of Rio de Janeiro, and coauthors observed 11 infants with congenital Zika infection from gestation to six months in the state of Paraíba, Brazil. Cases were referred between October 2015 and February 2016. Ten of 11 women included in the study presented with symptoms of Zika infection during the first half of pregnancy, and all 11 had laboratory evidence of infection in several tissues by serology or polymerase chain reaction. Brain damage was confirmed through intrauterine ultrasonography and was complemented by MRI. Histopathologic analysis was performed on the placenta and brain tissue from infants who died. The ZIKV genome was investigated in several tissues and sequenced for further phylogenetic analysis.
Of the 11 infants, seven (63.6%) were female, and the median maternal age at delivery was 25. Three of the neonates died, giving a perinatal mortality rate of 27.3%. Zika virus was identified in amniotic fluid, placenta, cord blood, and neonatal tissues collected post mortem in the three babies who died within 48 hours of delivery.
Brain damage and neurologic impairments were identified in all patients, including microcephaly, a reduction in cerebral volume, ventriculomegaly, cerebellar hypoplasia, lissencephaly with hydrocephalus, and fetal akinesia deformation sequence. Testing for other causes of microcephaly, such as genetic disorders and infections, was negative. The ZIKV virus genome was found in tissues of the mothers and their babies.
“Combined findings from clinical, laboratory, imaging, and pathologic examinations provided a more complete picture of the severe damage and developmental abnormalities caused by ZIKV infection than has been previously reported,” Dr. Tanuri and colleagues said.
Formulating a Plan of Action
“Although we have limited ways to stop emerging pathogens, we now have powerful techniques to quickly identify the culprit, such as polymerase chain reaction and whole genome sequencing,” said Raymond P. Roos, MD, Marjorie and Robert E. Straus Professor in Neurologic Science in the Department of Neurology at the University of Chicago, in an accompanying editorial. “We also have novel methods to control vectors and produce vaccines in an accelerated time frame.”
But many unanswered questions remain, said Dr. Roos. Among those questions is what neurologists can do about the Zika virus. “It would be valuable to have adult and pediatric neurologists network with the US Centers for Disease Control and Prevention to establish a surveillance system that could track Zika virus-induced Guillain-Barré syndrome (GBS) and CNS disease. This [cooperation] would facilitate the identification and characterization of disorders, the formation of a registry, and the mounting of comprehensive epidemiologic studies. This approach would also help to identify long-term sequelae of intrauterine infection and clarify effective treatments of the GBS syndrome.”
—Glenn S. Williams
Suggested Reading
Melo AS, Aguiar RS, Amorim MM, et al. Congenital Zika virus infection: beyond neonatal microcephaly. JAMA Neurol. 2016 Oct 3 [Epub ahead of print].
Roos RP. Zika virus-a public health emergency of international concern. JAMA Neurol. 2016 Oct 3 [Epub ahead of print].
Newborns with CHD have reduced cerebral oxygen delivery
Using a newer form of MRI to investigate oxygen levels in newborns with congenital heart disease, researchers in Canada reported that these patients may have impaired brain growth and development in the first weeks of life because of significantly lower cerebral oxygen delivery levels.
These findings suggest that oxygen delivery may impact brain growth, particularly in newborns with single-ventricle physiology, reported Jessie Mei Lim, BSc, of the University of Toronto, and her colleagues from McGill University, Montreal, and the Hospital for Sick Children, Toronto. The findings were published in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:1095-103). Ms. Lim and her colleagues used cine phase-contrast (PC) MRI to measure cerebral blood flow in newborns with congenital heard disease (CHD). Previous studies used optical measures of tissue oxygenation and MRI arterial spin labeling to suggests that newborns with severe CHD have impaired CBF and cerebral oxygen delivery (CDO2) and CBF.
This single-center study involved 63 newborns from June 2013 to April 2015 at the Hospital for Sick Children. These subjects received an MRI of the head before surgery at an average of age 7.5 days. The scans were done without sedation or contrast while the infants were asleep. The study compared 31 age-matched controls with 32 subjects with various forms of CHD – 12 were managed surgically along a single-ventricle pathway (SVP), 4 had coarctation of the aorta, 13 had transposition of the great arteries (TGA), and 3 had other forms of CHD.
The researchers validated their method by reporting similarities between flows in the basilar and vertebral arteries in 14 controls, “suggesting good consistency and accuracy of our method for measuring CBF,” Ms. Lim and her coauthors noted. A comparison of CBF measured with an unpaired Student t test revealed no significant differences between the CHD group and controls. The average net CBF in CHD patients was 103.5 mL/min vs. 119.7 mL/min in controls.
However, when evaluating CDO2 using a Student t test, the researchers found significantly lower levels in the CHD group – an average of 1,1881 mLO2/min. vs. 2,712 mL O2/min in controls (P less than .0001). And when the researchers indexed CDO2 to brain volume yielding indexed oxygen delivery, the difference between the two groups was still significant: an average of 523.1 mL O2/min-1 .100 g-1 in the CHD group and 685.6 mL O2/min-1.100 g-1 in controls (P = .0006).
Among the CHD group, those with SVP and TGA had significantly lower CDO2 than that of controls. Brain volumes were also lower in those with CHD (mean of 338.5 mL vs. 377.7 mL in controls, P = .002).
The MRI findings were telling in the study population, Ms. Lim and her coauthors said. Five subjects in the CHD group had a combination of diffuse excessive high-signal intensity (DEHSI) and white-matter injury (WMI), 10 had an isolated finding of DEHSI, two had WMI alone and five others had other minor brain abnormalities. But the control group had no abnormal findings on conventional brain MRI.
The researchers acknowledged that, while the impact of reduced cerebral oxygen delivery is unknown, “theoretical reasons for thinking it might adversely impact ongoing brain growth and development during this period of rapid brain growth are considered.”
Cardiovascular surgeons should consider these findings when deciding on when to operate on newborns with CHD, the researchers said. “Further support for the concept that such a mechanism could lead to irreversible deficits in brain growth and development might result in attempts to expedite surgical repair of congenital cardiac lesions, which have conventionally not been addressed in the neonatal period,” they wrote.
Ms. Lim and her coauthors had no financial relationships to disclose.
Congenital heart disease (CHD) is heterogeneous and different types of lesions may cause different hemodynamics, Caitlin K. Rollins, MD, of Boston Children’s Hospital and Harvard Medical School said in her invited commentary (J Thorac Cardiovasc Surg. 2016;152-960-1).
Ms. Lim and her colleagues in this study confirmed that premise with their finding that newborns with CHD and controls had similar cerebral blood flow, but that those with CHD had reduced oxygen delivery. “These differences were most apparent in the neonates with single-ventricle physiology and transposition of the great arteries,” Dr. Rollins said. The study authors’ finding of an association between reduced oxygen delivery and impaired brain development, along with this group’s previous reports (Circulation 2015;131:1313-23) suggesting preserved cerebral blood flow in the late prenatal period, differ from other studies using traditional methods to show reduced cerebral blood flow in obstructive left-sided lesions, Dr. Rollins said. “Although technical differences may in part account for the discrepancy, the contrasting results also reflect that the relative contributions of abnormal cerebral blood flow and oxygenation differ among forms of CHD,” Dr. Rollins said.
Congenital heart disease (CHD) is heterogeneous and different types of lesions may cause different hemodynamics, Caitlin K. Rollins, MD, of Boston Children’s Hospital and Harvard Medical School said in her invited commentary (J Thorac Cardiovasc Surg. 2016;152-960-1).
Ms. Lim and her colleagues in this study confirmed that premise with their finding that newborns with CHD and controls had similar cerebral blood flow, but that those with CHD had reduced oxygen delivery. “These differences were most apparent in the neonates with single-ventricle physiology and transposition of the great arteries,” Dr. Rollins said. The study authors’ finding of an association between reduced oxygen delivery and impaired brain development, along with this group’s previous reports (Circulation 2015;131:1313-23) suggesting preserved cerebral blood flow in the late prenatal period, differ from other studies using traditional methods to show reduced cerebral blood flow in obstructive left-sided lesions, Dr. Rollins said. “Although technical differences may in part account for the discrepancy, the contrasting results also reflect that the relative contributions of abnormal cerebral blood flow and oxygenation differ among forms of CHD,” Dr. Rollins said.
Congenital heart disease (CHD) is heterogeneous and different types of lesions may cause different hemodynamics, Caitlin K. Rollins, MD, of Boston Children’s Hospital and Harvard Medical School said in her invited commentary (J Thorac Cardiovasc Surg. 2016;152-960-1).
Ms. Lim and her colleagues in this study confirmed that premise with their finding that newborns with CHD and controls had similar cerebral blood flow, but that those with CHD had reduced oxygen delivery. “These differences were most apparent in the neonates with single-ventricle physiology and transposition of the great arteries,” Dr. Rollins said. The study authors’ finding of an association between reduced oxygen delivery and impaired brain development, along with this group’s previous reports (Circulation 2015;131:1313-23) suggesting preserved cerebral blood flow in the late prenatal period, differ from other studies using traditional methods to show reduced cerebral blood flow in obstructive left-sided lesions, Dr. Rollins said. “Although technical differences may in part account for the discrepancy, the contrasting results also reflect that the relative contributions of abnormal cerebral blood flow and oxygenation differ among forms of CHD,” Dr. Rollins said.
Using a newer form of MRI to investigate oxygen levels in newborns with congenital heart disease, researchers in Canada reported that these patients may have impaired brain growth and development in the first weeks of life because of significantly lower cerebral oxygen delivery levels.
These findings suggest that oxygen delivery may impact brain growth, particularly in newborns with single-ventricle physiology, reported Jessie Mei Lim, BSc, of the University of Toronto, and her colleagues from McGill University, Montreal, and the Hospital for Sick Children, Toronto. The findings were published in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:1095-103). Ms. Lim and her colleagues used cine phase-contrast (PC) MRI to measure cerebral blood flow in newborns with congenital heard disease (CHD). Previous studies used optical measures of tissue oxygenation and MRI arterial spin labeling to suggests that newborns with severe CHD have impaired CBF and cerebral oxygen delivery (CDO2) and CBF.
This single-center study involved 63 newborns from June 2013 to April 2015 at the Hospital for Sick Children. These subjects received an MRI of the head before surgery at an average of age 7.5 days. The scans were done without sedation or contrast while the infants were asleep. The study compared 31 age-matched controls with 32 subjects with various forms of CHD – 12 were managed surgically along a single-ventricle pathway (SVP), 4 had coarctation of the aorta, 13 had transposition of the great arteries (TGA), and 3 had other forms of CHD.
The researchers validated their method by reporting similarities between flows in the basilar and vertebral arteries in 14 controls, “suggesting good consistency and accuracy of our method for measuring CBF,” Ms. Lim and her coauthors noted. A comparison of CBF measured with an unpaired Student t test revealed no significant differences between the CHD group and controls. The average net CBF in CHD patients was 103.5 mL/min vs. 119.7 mL/min in controls.
However, when evaluating CDO2 using a Student t test, the researchers found significantly lower levels in the CHD group – an average of 1,1881 mLO2/min. vs. 2,712 mL O2/min in controls (P less than .0001). And when the researchers indexed CDO2 to brain volume yielding indexed oxygen delivery, the difference between the two groups was still significant: an average of 523.1 mL O2/min-1 .100 g-1 in the CHD group and 685.6 mL O2/min-1.100 g-1 in controls (P = .0006).
Among the CHD group, those with SVP and TGA had significantly lower CDO2 than that of controls. Brain volumes were also lower in those with CHD (mean of 338.5 mL vs. 377.7 mL in controls, P = .002).
The MRI findings were telling in the study population, Ms. Lim and her coauthors said. Five subjects in the CHD group had a combination of diffuse excessive high-signal intensity (DEHSI) and white-matter injury (WMI), 10 had an isolated finding of DEHSI, two had WMI alone and five others had other minor brain abnormalities. But the control group had no abnormal findings on conventional brain MRI.
The researchers acknowledged that, while the impact of reduced cerebral oxygen delivery is unknown, “theoretical reasons for thinking it might adversely impact ongoing brain growth and development during this period of rapid brain growth are considered.”
Cardiovascular surgeons should consider these findings when deciding on when to operate on newborns with CHD, the researchers said. “Further support for the concept that such a mechanism could lead to irreversible deficits in brain growth and development might result in attempts to expedite surgical repair of congenital cardiac lesions, which have conventionally not been addressed in the neonatal period,” they wrote.
Ms. Lim and her coauthors had no financial relationships to disclose.
Using a newer form of MRI to investigate oxygen levels in newborns with congenital heart disease, researchers in Canada reported that these patients may have impaired brain growth and development in the first weeks of life because of significantly lower cerebral oxygen delivery levels.
These findings suggest that oxygen delivery may impact brain growth, particularly in newborns with single-ventricle physiology, reported Jessie Mei Lim, BSc, of the University of Toronto, and her colleagues from McGill University, Montreal, and the Hospital for Sick Children, Toronto. The findings were published in the October issue of the Journal of Thoracic and Cardiovascular Surgery (2016;152:1095-103). Ms. Lim and her colleagues used cine phase-contrast (PC) MRI to measure cerebral blood flow in newborns with congenital heard disease (CHD). Previous studies used optical measures of tissue oxygenation and MRI arterial spin labeling to suggests that newborns with severe CHD have impaired CBF and cerebral oxygen delivery (CDO2) and CBF.
This single-center study involved 63 newborns from June 2013 to April 2015 at the Hospital for Sick Children. These subjects received an MRI of the head before surgery at an average of age 7.5 days. The scans were done without sedation or contrast while the infants were asleep. The study compared 31 age-matched controls with 32 subjects with various forms of CHD – 12 were managed surgically along a single-ventricle pathway (SVP), 4 had coarctation of the aorta, 13 had transposition of the great arteries (TGA), and 3 had other forms of CHD.
The researchers validated their method by reporting similarities between flows in the basilar and vertebral arteries in 14 controls, “suggesting good consistency and accuracy of our method for measuring CBF,” Ms. Lim and her coauthors noted. A comparison of CBF measured with an unpaired Student t test revealed no significant differences between the CHD group and controls. The average net CBF in CHD patients was 103.5 mL/min vs. 119.7 mL/min in controls.
However, when evaluating CDO2 using a Student t test, the researchers found significantly lower levels in the CHD group – an average of 1,1881 mLO2/min. vs. 2,712 mL O2/min in controls (P less than .0001). And when the researchers indexed CDO2 to brain volume yielding indexed oxygen delivery, the difference between the two groups was still significant: an average of 523.1 mL O2/min-1 .100 g-1 in the CHD group and 685.6 mL O2/min-1.100 g-1 in controls (P = .0006).
Among the CHD group, those with SVP and TGA had significantly lower CDO2 than that of controls. Brain volumes were also lower in those with CHD (mean of 338.5 mL vs. 377.7 mL in controls, P = .002).
The MRI findings were telling in the study population, Ms. Lim and her coauthors said. Five subjects in the CHD group had a combination of diffuse excessive high-signal intensity (DEHSI) and white-matter injury (WMI), 10 had an isolated finding of DEHSI, two had WMI alone and five others had other minor brain abnormalities. But the control group had no abnormal findings on conventional brain MRI.
The researchers acknowledged that, while the impact of reduced cerebral oxygen delivery is unknown, “theoretical reasons for thinking it might adversely impact ongoing brain growth and development during this period of rapid brain growth are considered.”
Cardiovascular surgeons should consider these findings when deciding on when to operate on newborns with CHD, the researchers said. “Further support for the concept that such a mechanism could lead to irreversible deficits in brain growth and development might result in attempts to expedite surgical repair of congenital cardiac lesions, which have conventionally not been addressed in the neonatal period,” they wrote.
Ms. Lim and her coauthors had no financial relationships to disclose.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: Cerebral blood flow is maintained but cerebral oxygen delivery is decreased in preoperative newborns with cyanotic congenital heart disease (CHD).
Major finding: Average cerebral oxygen delivery measured 1,1881 mLO2/min in the CHD group when measured with Student t testing vs. 2,712 mLO2/min in controls (P less than .0001).
Data source: Single-center study of 32 neonates with various forms of CHD 31 age-matched controls.
Disclosures: Ms. Lim and coauthors have no financial relationships to disclose.
The march of technology
Each year the American Academy of Pediatrics National Conference and Exhibition fills a huge convention hall with the latest products that can improve health and generate practice revenue.
Some products are solutions to the minor annoyances of everyday practice. For instance, there are ear curettes equipped with their own LED light and a magnifying lens. There are countless creams to treat rashes. There are new automated devices for testing hearing, vision, and attention. And at the far extreme, there are products with the potential to revolutionize clinical care or to bankrupt it. The latest technology in that category is whole exome sequencing.

A couple weeks earlier I had listened to a national meeting of pediatric ethicists discuss this technology. Some proponents discussed the possibility of doing whole exome sequencing (WES) for every newborn. Alas, many ethicists can’t do math. Even if the cost goes below $1,000 per test, at 4 million babies per year in the United States, that is $4 billion per year. That sounds like a small sum, compared with the current federal deficit, but the original budget for the entire, 10-year-long Human Genome Project (HGP) was $4.5 billion. There were complaints in that era that diverting such an enormous amount of money into the HGP would cut the funding of a lot of other very good research at the National Institutes of Health. Conversely, Medicare spends $4.5 billion on hepatitis C treatment.
Viewed differently, the yearly per capita payment to general pediatricians, excluding vaccine costs, is around $1,000. Perhaps I’m biased, but I think I provide much more value than a genetic sequence.
Precision medicine has a lot of potential. So far, it is mostly potential. One colleague related that, in the past year, he has done WES on three patients, at about $4,000 charge for each, and gotten positive results in two cases. He figures soon he will be ordering it on every child with symptoms of autism, developmental delay, or failure to thrive. Is that a wise idea? That, it seems, is the area in which there is the least illuminating research.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis.
Each year the American Academy of Pediatrics National Conference and Exhibition fills a huge convention hall with the latest products that can improve health and generate practice revenue.
Some products are solutions to the minor annoyances of everyday practice. For instance, there are ear curettes equipped with their own LED light and a magnifying lens. There are countless creams to treat rashes. There are new automated devices for testing hearing, vision, and attention. And at the far extreme, there are products with the potential to revolutionize clinical care or to bankrupt it. The latest technology in that category is whole exome sequencing.
A couple weeks earlier I had listened to a national meeting of pediatric ethicists discuss this technology. Some proponents discussed the possibility of doing whole exome sequencing (WES) for every newborn. Alas, many ethicists can’t do math. Even if the cost goes below $1,000 per test, at 4 million babies per year in the United States, that is $4 billion per year. That sounds like a small sum, compared with the current federal deficit, but the original budget for the entire, 10-year-long Human Genome Project (HGP) was $4.5 billion. There were complaints in that era that diverting such an enormous amount of money into the HGP would cut the funding of a lot of other very good research at the National Institutes of Health. Conversely, Medicare spends $4.5 billion on hepatitis C treatment.
Viewed differently, the yearly per capita payment to general pediatricians, excluding vaccine costs, is around $1,000. Perhaps I’m biased, but I think I provide much more value than a genetic sequence.
Precision medicine has a lot of potential. So far, it is mostly potential. One colleague related that, in the past year, he has done WES on three patients, at about $4,000 charge for each, and gotten positive results in two cases. He figures soon he will be ordering it on every child with symptoms of autism, developmental delay, or failure to thrive. Is that a wise idea? That, it seems, is the area in which there is the least illuminating research.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis.
Each year the American Academy of Pediatrics National Conference and Exhibition fills a huge convention hall with the latest products that can improve health and generate practice revenue.
Some products are solutions to the minor annoyances of everyday practice. For instance, there are ear curettes equipped with their own LED light and a magnifying lens. There are countless creams to treat rashes. There are new automated devices for testing hearing, vision, and attention. And at the far extreme, there are products with the potential to revolutionize clinical care or to bankrupt it. The latest technology in that category is whole exome sequencing.
A couple weeks earlier I had listened to a national meeting of pediatric ethicists discuss this technology. Some proponents discussed the possibility of doing whole exome sequencing (WES) for every newborn. Alas, many ethicists can’t do math. Even if the cost goes below $1,000 per test, at 4 million babies per year in the United States, that is $4 billion per year. That sounds like a small sum, compared with the current federal deficit, but the original budget for the entire, 10-year-long Human Genome Project (HGP) was $4.5 billion. There were complaints in that era that diverting such an enormous amount of money into the HGP would cut the funding of a lot of other very good research at the National Institutes of Health. Conversely, Medicare spends $4.5 billion on hepatitis C treatment.
Viewed differently, the yearly per capita payment to general pediatricians, excluding vaccine costs, is around $1,000. Perhaps I’m biased, but I think I provide much more value than a genetic sequence.
Precision medicine has a lot of potential. So far, it is mostly potential. One colleague related that, in the past year, he has done WES on three patients, at about $4,000 charge for each, and gotten positive results in two cases. He figures soon he will be ordering it on every child with symptoms of autism, developmental delay, or failure to thrive. Is that a wise idea? That, it seems, is the area in which there is the least illuminating research.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis.