User login
Addressing sexual health with adolescents must be a priority
You are an important source of sexual and reproductive information for adolescents, and can be instrumental in preventing unintended pregnancies and sexually transmitted infections as well as promoting healthy relationships. A new clinical report from the American Academy of Pediatrics’ Committee on Adolescence provides a variety of tools and techniques to help you with these discussions with your patients.
Confidentiality and consent are two of the most important factors to consider when discussing sexual health with adolescents, according to Arik V. Marcell, MD, and Gale R. Burstein, MD, coauthors of the report (Pediatrics. 2017. doi: 10.1542/peds.2017-2858). As confidentiality is promoted over the course of time, adolescents are more likely to return for care. Promoting a confidential environment also allows adolescent patients to feel free to communicate about sensitive topics such as sexual behaviors, partners, or gender. This is especially true for lesbian, gay, bisexual, transgender, and questioning (LGBTQ) youth, who may need more social indications that you and your office are sympathetic to sensitive issues. One way to do this is to post an office policy that details the confidential services you provide and ensure that the post is visible to all parents and adolescents. Explain this information at the beginning of the visit, starting at age 11-14 years. State laws regarding consent and confidentiality vary from state to state. The Guttmacher Institute and the Center for Adolescent Health and the Law provide resources summarizing laws for each state.
Clear and effective communication is another important feature in providing sexual health care to adolescents. Adolescence is a time of great change, and many adolescents may not feel comfortable asking questions, even though they want them answered. The AAP report recommends utilizing several interview techniques to get solid answers from adolescents.
Asking direct but open-ended questions is a great way to get useful answers from adolescents and it avoids yes/no answers. After listening to a patient’s response, use a reflection response, or one that mirrors the feeling of the patient. This allows the patient to feel that he or she is being heard. Restating and summarizing the interview also is an effective tool and allows the patient to understand what has been discussed. Asking questions that provide insight into the patient allows you to better understand the patient as a person. The use of reassuring and supportive statements is important to support patients and allow them to feel more comfortable, according to the report.
Apart from communication strategies and creating a safe and welcoming environment where confidentiality is promoted, there are several topics from the report to focus on.
• Reproductive life plans. It is important to broach this topic with adolescents. Many adolescents don’t have a pregnancy plan or understand how this would affect their lives. Asking questions concerning the desire to become pregnant, how many children the patient would like to have and when, and past and present pregnancy status will help adolescents plan and understand the issues surrounding pregnancy.
• Sexual assault and sexual abuse. These topics are particularly relevant to adolescents. Young people aged 12-34 years experience some of the highest rates of rape and sexual assault. When questioning a young person about sexual assault, questions should include whether she has been touched by anyone in an uncomfortable way, forced into unwanted sexual contact, or whether she has been “date raped” (Pediatrics. 2008. doi: 10.1542/peds.2008-1581). When dealing with sexual assault, you always should comply with state guidelines regarding abuse, rape, and incest.
• Physical exams. These exams, including breast and female and male genital exams, should be approached with care. When conducting a physical exam, you always should have a chaperone present and allow the option of letting a parent or guardian be in the room. You always should describe what areas will be examined and inform the patient that if he or she feels uncomfortable at any point to tell you to stop. Some adolescents may not feel comfortable with their bodies and with disrobing; in this event, offering a gown may help make the patient more comfortable. It is important these exams are done to identify any pathologies and indications of sexual maturity.

In addition, counseling adolescents concerning sexual health should include contraception information (Pediatrics. 2014, Oct 1. doi: 10.1542/peds.2014-2300). This should include information about condoms as well as long-acting reversible contraceptive methods, said Dr. Breuner, chairperson of the Committee on Adolescence.
None of the contributors to the report had relevant financial disclosures.
Sexual development – including puberty, dating and coitarche – is a hallmark of adolescence. By late adolescence, the majority of teens are sexually active. A recent Centers for Disease Control and Prevention report revealed that sexually transmitted infections are at an all-time high in the United States, with the majority of infections occurring in adolescents. Conversely teen birth rates are at historic lows, although it remains unclear if this trend will continue as federal funding to teen pregnancy prevention programs has been cut. Given this changing environment, pediatricians must advocate and provide education for teens and their families on sexual health and development.
National organizations have authored practice guidelines to assist clinicians in providing care for teens. Despite these efforts, recent research has demonstrated that we are frequently falling short of providing optimal care. The question remains: How can pediatricians in a busy practice integrate these guidelines?
Clinicians can learn how to create a welcoming environment for teens, including LGBTQ youth; explain confidentiality to patients and their families; obtain sensitive histories; and effectively counsel adolescents on healthy relationships, safe sex, and pregnancy prevention. This report also outlines sexually transmitted infection screening and treatment guidelines. Implementing these changes – such as asking family to step out during the confidential history – can help identify and treat underlying risk behaviors in adolescents and support the development of the teen “patient-in-training.”
Kelly Curran , MD, is assistant professor in the section of adolescent medicine in the department of pediatrics at the University of Oklahoma, Oklahoma City. She also is a member of the Pediatric News editorial advisory board. Dr. Curran was asked to comment on the AAP clinical report. Email her at pdnews@frontlinemedcom.com .
Sexual development – including puberty, dating and coitarche – is a hallmark of adolescence. By late adolescence, the majority of teens are sexually active. A recent Centers for Disease Control and Prevention report revealed that sexually transmitted infections are at an all-time high in the United States, with the majority of infections occurring in adolescents. Conversely teen birth rates are at historic lows, although it remains unclear if this trend will continue as federal funding to teen pregnancy prevention programs has been cut. Given this changing environment, pediatricians must advocate and provide education for teens and their families on sexual health and development.
National organizations have authored practice guidelines to assist clinicians in providing care for teens. Despite these efforts, recent research has demonstrated that we are frequently falling short of providing optimal care. The question remains: How can pediatricians in a busy practice integrate these guidelines?
Clinicians can learn how to create a welcoming environment for teens, including LGBTQ youth; explain confidentiality to patients and their families; obtain sensitive histories; and effectively counsel adolescents on healthy relationships, safe sex, and pregnancy prevention. This report also outlines sexually transmitted infection screening and treatment guidelines. Implementing these changes – such as asking family to step out during the confidential history – can help identify and treat underlying risk behaviors in adolescents and support the development of the teen “patient-in-training.”
Kelly Curran , MD, is assistant professor in the section of adolescent medicine in the department of pediatrics at the University of Oklahoma, Oklahoma City. She also is a member of the Pediatric News editorial advisory board. Dr. Curran was asked to comment on the AAP clinical report. Email her at pdnews@frontlinemedcom.com .
Sexual development – including puberty, dating and coitarche – is a hallmark of adolescence. By late adolescence, the majority of teens are sexually active. A recent Centers for Disease Control and Prevention report revealed that sexually transmitted infections are at an all-time high in the United States, with the majority of infections occurring in adolescents. Conversely teen birth rates are at historic lows, although it remains unclear if this trend will continue as federal funding to teen pregnancy prevention programs has been cut. Given this changing environment, pediatricians must advocate and provide education for teens and their families on sexual health and development.
National organizations have authored practice guidelines to assist clinicians in providing care for teens. Despite these efforts, recent research has demonstrated that we are frequently falling short of providing optimal care. The question remains: How can pediatricians in a busy practice integrate these guidelines?
Clinicians can learn how to create a welcoming environment for teens, including LGBTQ youth; explain confidentiality to patients and their families; obtain sensitive histories; and effectively counsel adolescents on healthy relationships, safe sex, and pregnancy prevention. This report also outlines sexually transmitted infection screening and treatment guidelines. Implementing these changes – such as asking family to step out during the confidential history – can help identify and treat underlying risk behaviors in adolescents and support the development of the teen “patient-in-training.”
Kelly Curran , MD, is assistant professor in the section of adolescent medicine in the department of pediatrics at the University of Oklahoma, Oklahoma City. She also is a member of the Pediatric News editorial advisory board. Dr. Curran was asked to comment on the AAP clinical report. Email her at pdnews@frontlinemedcom.com .
You are an important source of sexual and reproductive information for adolescents, and can be instrumental in preventing unintended pregnancies and sexually transmitted infections as well as promoting healthy relationships. A new clinical report from the American Academy of Pediatrics’ Committee on Adolescence provides a variety of tools and techniques to help you with these discussions with your patients.
Confidentiality and consent are two of the most important factors to consider when discussing sexual health with adolescents, according to Arik V. Marcell, MD, and Gale R. Burstein, MD, coauthors of the report (Pediatrics. 2017. doi: 10.1542/peds.2017-2858). As confidentiality is promoted over the course of time, adolescents are more likely to return for care. Promoting a confidential environment also allows adolescent patients to feel free to communicate about sensitive topics such as sexual behaviors, partners, or gender. This is especially true for lesbian, gay, bisexual, transgender, and questioning (LGBTQ) youth, who may need more social indications that you and your office are sympathetic to sensitive issues. One way to do this is to post an office policy that details the confidential services you provide and ensure that the post is visible to all parents and adolescents. Explain this information at the beginning of the visit, starting at age 11-14 years. State laws regarding consent and confidentiality vary from state to state. The Guttmacher Institute and the Center for Adolescent Health and the Law provide resources summarizing laws for each state.
Clear and effective communication is another important feature in providing sexual health care to adolescents. Adolescence is a time of great change, and many adolescents may not feel comfortable asking questions, even though they want them answered. The AAP report recommends utilizing several interview techniques to get solid answers from adolescents.
Asking direct but open-ended questions is a great way to get useful answers from adolescents and it avoids yes/no answers. After listening to a patient’s response, use a reflection response, or one that mirrors the feeling of the patient. This allows the patient to feel that he or she is being heard. Restating and summarizing the interview also is an effective tool and allows the patient to understand what has been discussed. Asking questions that provide insight into the patient allows you to better understand the patient as a person. The use of reassuring and supportive statements is important to support patients and allow them to feel more comfortable, according to the report.
Apart from communication strategies and creating a safe and welcoming environment where confidentiality is promoted, there are several topics from the report to focus on.
• Reproductive life plans. It is important to broach this topic with adolescents. Many adolescents don’t have a pregnancy plan or understand how this would affect their lives. Asking questions concerning the desire to become pregnant, how many children the patient would like to have and when, and past and present pregnancy status will help adolescents plan and understand the issues surrounding pregnancy.
• Sexual assault and sexual abuse. These topics are particularly relevant to adolescents. Young people aged 12-34 years experience some of the highest rates of rape and sexual assault. When questioning a young person about sexual assault, questions should include whether she has been touched by anyone in an uncomfortable way, forced into unwanted sexual contact, or whether she has been “date raped” (Pediatrics. 2008. doi: 10.1542/peds.2008-1581). When dealing with sexual assault, you always should comply with state guidelines regarding abuse, rape, and incest.
• Physical exams. These exams, including breast and female and male genital exams, should be approached with care. When conducting a physical exam, you always should have a chaperone present and allow the option of letting a parent or guardian be in the room. You always should describe what areas will be examined and inform the patient that if he or she feels uncomfortable at any point to tell you to stop. Some adolescents may not feel comfortable with their bodies and with disrobing; in this event, offering a gown may help make the patient more comfortable. It is important these exams are done to identify any pathologies and indications of sexual maturity.
In addition, counseling adolescents concerning sexual health should include contraception information (Pediatrics. 2014, Oct 1. doi: 10.1542/peds.2014-2300). This should include information about condoms as well as long-acting reversible contraceptive methods, said Dr. Breuner, chairperson of the Committee on Adolescence.
None of the contributors to the report had relevant financial disclosures.
You are an important source of sexual and reproductive information for adolescents, and can be instrumental in preventing unintended pregnancies and sexually transmitted infections as well as promoting healthy relationships. A new clinical report from the American Academy of Pediatrics’ Committee on Adolescence provides a variety of tools and techniques to help you with these discussions with your patients.
Confidentiality and consent are two of the most important factors to consider when discussing sexual health with adolescents, according to Arik V. Marcell, MD, and Gale R. Burstein, MD, coauthors of the report (Pediatrics. 2017. doi: 10.1542/peds.2017-2858). As confidentiality is promoted over the course of time, adolescents are more likely to return for care. Promoting a confidential environment also allows adolescent patients to feel free to communicate about sensitive topics such as sexual behaviors, partners, or gender. This is especially true for lesbian, gay, bisexual, transgender, and questioning (LGBTQ) youth, who may need more social indications that you and your office are sympathetic to sensitive issues. One way to do this is to post an office policy that details the confidential services you provide and ensure that the post is visible to all parents and adolescents. Explain this information at the beginning of the visit, starting at age 11-14 years. State laws regarding consent and confidentiality vary from state to state. The Guttmacher Institute and the Center for Adolescent Health and the Law provide resources summarizing laws for each state.
Clear and effective communication is another important feature in providing sexual health care to adolescents. Adolescence is a time of great change, and many adolescents may not feel comfortable asking questions, even though they want them answered. The AAP report recommends utilizing several interview techniques to get solid answers from adolescents.
Asking direct but open-ended questions is a great way to get useful answers from adolescents and it avoids yes/no answers. After listening to a patient’s response, use a reflection response, or one that mirrors the feeling of the patient. This allows the patient to feel that he or she is being heard. Restating and summarizing the interview also is an effective tool and allows the patient to understand what has been discussed. Asking questions that provide insight into the patient allows you to better understand the patient as a person. The use of reassuring and supportive statements is important to support patients and allow them to feel more comfortable, according to the report.
Apart from communication strategies and creating a safe and welcoming environment where confidentiality is promoted, there are several topics from the report to focus on.
• Reproductive life plans. It is important to broach this topic with adolescents. Many adolescents don’t have a pregnancy plan or understand how this would affect their lives. Asking questions concerning the desire to become pregnant, how many children the patient would like to have and when, and past and present pregnancy status will help adolescents plan and understand the issues surrounding pregnancy.
• Sexual assault and sexual abuse. These topics are particularly relevant to adolescents. Young people aged 12-34 years experience some of the highest rates of rape and sexual assault. When questioning a young person about sexual assault, questions should include whether she has been touched by anyone in an uncomfortable way, forced into unwanted sexual contact, or whether she has been “date raped” (Pediatrics. 2008. doi: 10.1542/peds.2008-1581). When dealing with sexual assault, you always should comply with state guidelines regarding abuse, rape, and incest.
• Physical exams. These exams, including breast and female and male genital exams, should be approached with care. When conducting a physical exam, you always should have a chaperone present and allow the option of letting a parent or guardian be in the room. You always should describe what areas will be examined and inform the patient that if he or she feels uncomfortable at any point to tell you to stop. Some adolescents may not feel comfortable with their bodies and with disrobing; in this event, offering a gown may help make the patient more comfortable. It is important these exams are done to identify any pathologies and indications of sexual maturity.
In addition, counseling adolescents concerning sexual health should include contraception information (Pediatrics. 2014, Oct 1. doi: 10.1542/peds.2014-2300). This should include information about condoms as well as long-acting reversible contraceptive methods, said Dr. Breuner, chairperson of the Committee on Adolescence.
None of the contributors to the report had relevant financial disclosures.
FROM PEDIATRICS
Lung recovery high after ECMO in near-fatal pediatric asthma
TORONTO – Extracorporeal membrane oxygenation (ECMO) is associated with lung recovery rates as high as 90% in pediatric patients with near-fatal asthma, but the risk of complications was also high and the cannulation technique employed made a significant difference to outcomes, according to a study presented at the CHEST annual meeting.
“ECMO for near-fatal asthma is a potentially life-saving intervention, however, clinicians should be aware of the potentially severe complications, particularly with veno-arterial cannulation in this population,” said Rebecca Kohlberg-Davis, MD, a pediatric resident at Connecticut Children’s Medical Center, Hartford.

ECMO is being used increasingly in the setting of near-fatal pediatric asthma but there are limited data on outcomes in this population. Dr. Kohlberg-Davis and her colleagues conducted a retrospective analysis of all children with asthma who were treated with ECMO using the Extracorporeal Life Support Organization (ELSO) registry.
Between 1988 and 2016, 371 children with status asthmaticus underwent ECMO cannulation using one of two methods. Sixty-five percent were treated with ECMO using veno-venous (VV) cannulation and 33% were treated using veno-arterial (VA) cannulation. Both VV and VA require insertion of a cannula to take deoxygenated blood from a central vein or the right atrium. VA ECMO returns the oxygenated blood, under pressure, to the arterial side of the circulation (typically to the aorta), supporting cardiac output, while VV ECMO returns oxygenated blood back to a large vein and does not support circulation.
The median age of the study participants was 7.5 years and 56% were male. The median ECMO run duration was 123 hours.
Overall, lung recovery was seen in 83% of patients, and 77% were discharged from the hospital. Of the children who received VV cannulation, 90% experienced lung recovery, while VA cannulation was associated with only a 69% rate of lung recovery and significantly more complications. Among those who experienced lung recovery, those who received VV cannulation had a 3.6-fold higher likelihood of survival (P = .006), Dr. Kohlberg-Davis reported.
At presentation, 88% of patients had hypercarbic respiratory failure, 34% had hypoxemic respiratory failure, and 27% had mixed respiratory failure. Children with hypercarbic respiratory failure were more likely to receive VV cannulation (P = .003), while children with hypoxemic or combined respiratory failure were more likely to receive VA cannulation. Those with hypoxemic respiratory failure had a significantly lower likelihood of lung recovery (odds ratio, 4.9; P less than .0001), she said.
Eighty percent of runs were associated with one or more complications and 20% had three or more complications. Of that 80%, most involved cardiovascular complications (53%), while 36% were hemorrhagic and 35% were mechanical. The most common cardiovascular complications included the need for inotropic support (in 39% of patients) and hypertension requiring vasodilators (in 18% of patients). The most common hemorrhagic complications were cannula-site bleeding (23%) and surgical-site bleeding (8%), while mechanical complications were mostly clots (19%) and cannulation problems (12%).
Children who received VA cannulation had a significantly higher rate of neurologic complications, compared with those who received VV cannulation (22% vs. 5%), and these included cerebral hemorrhage or infarct in 6% and clinical brain death in 5%.
“If early cannulation with VV ECMO could prevent the need for VA ECMO, this might lead to lower neurological complication and increased survival,” said Dr. Kohlberg-Davis. Current guidelines recommend considering cannulation at an oxygenation index – used to measure the fraction of inspired oxygen and its usage within the body – between 40 and 60. This study suggests that initiating cannulation at a lower OI is associated with better outcomes and fewer complications, she said.
The authors reported having nothing to disclose.
This is a large study looking at the use of extracorporeal membrane oxygenation (ECMO) patients dying of status asthmaticus. It is interesting that the pCO2 seemed to predict the type of ECMO used and outcomes. Of course, an ounce of prevention (i.e., appropriate asthma management) is the most important thing to say about any pediatric intensive care unit asthma study! Having said all of this, we have known that venovenous ECMO is preferred for a long time.

This is a large study looking at the use of extracorporeal membrane oxygenation (ECMO) patients dying of status asthmaticus. It is interesting that the pCO2 seemed to predict the type of ECMO used and outcomes. Of course, an ounce of prevention (i.e., appropriate asthma management) is the most important thing to say about any pediatric intensive care unit asthma study! Having said all of this, we have known that venovenous ECMO is preferred for a long time.
This is a large study looking at the use of extracorporeal membrane oxygenation (ECMO) patients dying of status asthmaticus. It is interesting that the pCO2 seemed to predict the type of ECMO used and outcomes. Of course, an ounce of prevention (i.e., appropriate asthma management) is the most important thing to say about any pediatric intensive care unit asthma study! Having said all of this, we have known that venovenous ECMO is preferred for a long time.
TORONTO – Extracorporeal membrane oxygenation (ECMO) is associated with lung recovery rates as high as 90% in pediatric patients with near-fatal asthma, but the risk of complications was also high and the cannulation technique employed made a significant difference to outcomes, according to a study presented at the CHEST annual meeting.
“ECMO for near-fatal asthma is a potentially life-saving intervention, however, clinicians should be aware of the potentially severe complications, particularly with veno-arterial cannulation in this population,” said Rebecca Kohlberg-Davis, MD, a pediatric resident at Connecticut Children’s Medical Center, Hartford.
ECMO is being used increasingly in the setting of near-fatal pediatric asthma but there are limited data on outcomes in this population. Dr. Kohlberg-Davis and her colleagues conducted a retrospective analysis of all children with asthma who were treated with ECMO using the Extracorporeal Life Support Organization (ELSO) registry.
Between 1988 and 2016, 371 children with status asthmaticus underwent ECMO cannulation using one of two methods. Sixty-five percent were treated with ECMO using veno-venous (VV) cannulation and 33% were treated using veno-arterial (VA) cannulation. Both VV and VA require insertion of a cannula to take deoxygenated blood from a central vein or the right atrium. VA ECMO returns the oxygenated blood, under pressure, to the arterial side of the circulation (typically to the aorta), supporting cardiac output, while VV ECMO returns oxygenated blood back to a large vein and does not support circulation.
The median age of the study participants was 7.5 years and 56% were male. The median ECMO run duration was 123 hours.
Overall, lung recovery was seen in 83% of patients, and 77% were discharged from the hospital. Of the children who received VV cannulation, 90% experienced lung recovery, while VA cannulation was associated with only a 69% rate of lung recovery and significantly more complications. Among those who experienced lung recovery, those who received VV cannulation had a 3.6-fold higher likelihood of survival (P = .006), Dr. Kohlberg-Davis reported.
At presentation, 88% of patients had hypercarbic respiratory failure, 34% had hypoxemic respiratory failure, and 27% had mixed respiratory failure. Children with hypercarbic respiratory failure were more likely to receive VV cannulation (P = .003), while children with hypoxemic or combined respiratory failure were more likely to receive VA cannulation. Those with hypoxemic respiratory failure had a significantly lower likelihood of lung recovery (odds ratio, 4.9; P less than .0001), she said.
Eighty percent of runs were associated with one or more complications and 20% had three or more complications. Of that 80%, most involved cardiovascular complications (53%), while 36% were hemorrhagic and 35% were mechanical. The most common cardiovascular complications included the need for inotropic support (in 39% of patients) and hypertension requiring vasodilators (in 18% of patients). The most common hemorrhagic complications were cannula-site bleeding (23%) and surgical-site bleeding (8%), while mechanical complications were mostly clots (19%) and cannulation problems (12%).
Children who received VA cannulation had a significantly higher rate of neurologic complications, compared with those who received VV cannulation (22% vs. 5%), and these included cerebral hemorrhage or infarct in 6% and clinical brain death in 5%.
“If early cannulation with VV ECMO could prevent the need for VA ECMO, this might lead to lower neurological complication and increased survival,” said Dr. Kohlberg-Davis. Current guidelines recommend considering cannulation at an oxygenation index – used to measure the fraction of inspired oxygen and its usage within the body – between 40 and 60. This study suggests that initiating cannulation at a lower OI is associated with better outcomes and fewer complications, she said.
The authors reported having nothing to disclose.
TORONTO – Extracorporeal membrane oxygenation (ECMO) is associated with lung recovery rates as high as 90% in pediatric patients with near-fatal asthma, but the risk of complications was also high and the cannulation technique employed made a significant difference to outcomes, according to a study presented at the CHEST annual meeting.
“ECMO for near-fatal asthma is a potentially life-saving intervention, however, clinicians should be aware of the potentially severe complications, particularly with veno-arterial cannulation in this population,” said Rebecca Kohlberg-Davis, MD, a pediatric resident at Connecticut Children’s Medical Center, Hartford.
ECMO is being used increasingly in the setting of near-fatal pediatric asthma but there are limited data on outcomes in this population. Dr. Kohlberg-Davis and her colleagues conducted a retrospective analysis of all children with asthma who were treated with ECMO using the Extracorporeal Life Support Organization (ELSO) registry.
Between 1988 and 2016, 371 children with status asthmaticus underwent ECMO cannulation using one of two methods. Sixty-five percent were treated with ECMO using veno-venous (VV) cannulation and 33% were treated using veno-arterial (VA) cannulation. Both VV and VA require insertion of a cannula to take deoxygenated blood from a central vein or the right atrium. VA ECMO returns the oxygenated blood, under pressure, to the arterial side of the circulation (typically to the aorta), supporting cardiac output, while VV ECMO returns oxygenated blood back to a large vein and does not support circulation.
The median age of the study participants was 7.5 years and 56% were male. The median ECMO run duration was 123 hours.
Overall, lung recovery was seen in 83% of patients, and 77% were discharged from the hospital. Of the children who received VV cannulation, 90% experienced lung recovery, while VA cannulation was associated with only a 69% rate of lung recovery and significantly more complications. Among those who experienced lung recovery, those who received VV cannulation had a 3.6-fold higher likelihood of survival (P = .006), Dr. Kohlberg-Davis reported.
At presentation, 88% of patients had hypercarbic respiratory failure, 34% had hypoxemic respiratory failure, and 27% had mixed respiratory failure. Children with hypercarbic respiratory failure were more likely to receive VV cannulation (P = .003), while children with hypoxemic or combined respiratory failure were more likely to receive VA cannulation. Those with hypoxemic respiratory failure had a significantly lower likelihood of lung recovery (odds ratio, 4.9; P less than .0001), she said.
Eighty percent of runs were associated with one or more complications and 20% had three or more complications. Of that 80%, most involved cardiovascular complications (53%), while 36% were hemorrhagic and 35% were mechanical. The most common cardiovascular complications included the need for inotropic support (in 39% of patients) and hypertension requiring vasodilators (in 18% of patients). The most common hemorrhagic complications were cannula-site bleeding (23%) and surgical-site bleeding (8%), while mechanical complications were mostly clots (19%) and cannulation problems (12%).
Children who received VA cannulation had a significantly higher rate of neurologic complications, compared with those who received VV cannulation (22% vs. 5%), and these included cerebral hemorrhage or infarct in 6% and clinical brain death in 5%.
“If early cannulation with VV ECMO could prevent the need for VA ECMO, this might lead to lower neurological complication and increased survival,” said Dr. Kohlberg-Davis. Current guidelines recommend considering cannulation at an oxygenation index – used to measure the fraction of inspired oxygen and its usage within the body – between 40 and 60. This study suggests that initiating cannulation at a lower OI is associated with better outcomes and fewer complications, she said.
The authors reported having nothing to disclose.
AT CHEST 2017
Key clinical point: ECMO is a life-saving option in children with asthma, but it is associated with significant complications.
Major finding: The use of ECMO resulted in lung recovery in 83% of pediatric patients with near-fatal asthma; 77% were discharged from the hospital.
Data source: Retrospective analysis of children with asthma treated with ECMO in the Extracorporeal Life Support Organization (ELSO) registry (n = 371).
Disclosures: The authors reported having nothing to disclose.
Meta-analysis confirms probiotics’ pediatric safety and efficacy
ORLANDO – Probiotics are safe and effective for treating functional abdominal pain in children, based on findings from a meta-analysis of 11 randomized studies with a total of 790 patients.
“We think there is pretty strong evidence” for the efficacy of probiotics, and “by any analysis you can throw at them probiotics are safe,” Gordon Morris, MD, said at the World Congress of Gastroenterology at ACG 2017. “The evidence is of moderate and high quality,” added Dr. Morris, a pediatric gastroenterologist at the University of Central Lancashire in Preston, England.
The most widely studied probiotic in the analysis was Lactobacillus reuteri, used in six of the studies with a total of 405 randomized patients. The next most commonly studied agent was Lactobacillus rhamnosus GG, the focus of four studies and tested in a total of 270 randomized patients. Both microbes showed statistically significant and clinically meaningful levels of pain reduction when compared with placebo in subgroup analyses, said Dr. Morris, who performed the meta-analysis as a Cochrane Review Groups systematic review.

“The pain score reductions we saw [with these two strains] could certainly have an impact. I think it matters clinically,” he explained. “Severity of pain is most important to patients.”
Both L. reuteri and L. rhamnosus GG have received “generally regarded as safe” designations from the Food and Drug Administration.
Based on these findings, “I don’t think we can justify, especially with these two main strains, any further basic efficacy studies,” Dr. Morris said. The primary focus for future clinical assessments of these probiotics should be long-term efficacy and safety and whether patients have rebound pain on withdrawal from probiotic use, he added.
The meta-analysis used studies that compared probiotics against placebo in children aged 4-18 years who received treatment for 4-16 weeks. The full analysis showed an average 0.57-unit reduction in pain scores across all 11 studies included, with an average 0.61-unit reduction using L. reuteri and an average 0.75-unit reduction using L. rhamnosus GG. All three between-group differences were statistically significant. Safety data came from eight of the included studies, and they collectively showed absolutely no safety difference between actively treated and control patients.
Dr. Morris noted that the mechanism by which probiotic bacilli relieve abdominal pain remains unclear, but suggested that both prokinetic and anti-inflammatory effects might be involved.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ORLANDO – Probiotics are safe and effective for treating functional abdominal pain in children, based on findings from a meta-analysis of 11 randomized studies with a total of 790 patients.
“We think there is pretty strong evidence” for the efficacy of probiotics, and “by any analysis you can throw at them probiotics are safe,” Gordon Morris, MD, said at the World Congress of Gastroenterology at ACG 2017. “The evidence is of moderate and high quality,” added Dr. Morris, a pediatric gastroenterologist at the University of Central Lancashire in Preston, England.
The most widely studied probiotic in the analysis was Lactobacillus reuteri, used in six of the studies with a total of 405 randomized patients. The next most commonly studied agent was Lactobacillus rhamnosus GG, the focus of four studies and tested in a total of 270 randomized patients. Both microbes showed statistically significant and clinically meaningful levels of pain reduction when compared with placebo in subgroup analyses, said Dr. Morris, who performed the meta-analysis as a Cochrane Review Groups systematic review.
“The pain score reductions we saw [with these two strains] could certainly have an impact. I think it matters clinically,” he explained. “Severity of pain is most important to patients.”
Both L. reuteri and L. rhamnosus GG have received “generally regarded as safe” designations from the Food and Drug Administration.
Based on these findings, “I don’t think we can justify, especially with these two main strains, any further basic efficacy studies,” Dr. Morris said. The primary focus for future clinical assessments of these probiotics should be long-term efficacy and safety and whether patients have rebound pain on withdrawal from probiotic use, he added.
The meta-analysis used studies that compared probiotics against placebo in children aged 4-18 years who received treatment for 4-16 weeks. The full analysis showed an average 0.57-unit reduction in pain scores across all 11 studies included, with an average 0.61-unit reduction using L. reuteri and an average 0.75-unit reduction using L. rhamnosus GG. All three between-group differences were statistically significant. Safety data came from eight of the included studies, and they collectively showed absolutely no safety difference between actively treated and control patients.
Dr. Morris noted that the mechanism by which probiotic bacilli relieve abdominal pain remains unclear, but suggested that both prokinetic and anti-inflammatory effects might be involved.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
ORLANDO – Probiotics are safe and effective for treating functional abdominal pain in children, based on findings from a meta-analysis of 11 randomized studies with a total of 790 patients.
“We think there is pretty strong evidence” for the efficacy of probiotics, and “by any analysis you can throw at them probiotics are safe,” Gordon Morris, MD, said at the World Congress of Gastroenterology at ACG 2017. “The evidence is of moderate and high quality,” added Dr. Morris, a pediatric gastroenterologist at the University of Central Lancashire in Preston, England.
The most widely studied probiotic in the analysis was Lactobacillus reuteri, used in six of the studies with a total of 405 randomized patients. The next most commonly studied agent was Lactobacillus rhamnosus GG, the focus of four studies and tested in a total of 270 randomized patients. Both microbes showed statistically significant and clinically meaningful levels of pain reduction when compared with placebo in subgroup analyses, said Dr. Morris, who performed the meta-analysis as a Cochrane Review Groups systematic review.
“The pain score reductions we saw [with these two strains] could certainly have an impact. I think it matters clinically,” he explained. “Severity of pain is most important to patients.”
Both L. reuteri and L. rhamnosus GG have received “generally regarded as safe” designations from the Food and Drug Administration.
Based on these findings, “I don’t think we can justify, especially with these two main strains, any further basic efficacy studies,” Dr. Morris said. The primary focus for future clinical assessments of these probiotics should be long-term efficacy and safety and whether patients have rebound pain on withdrawal from probiotic use, he added.
The meta-analysis used studies that compared probiotics against placebo in children aged 4-18 years who received treatment for 4-16 weeks. The full analysis showed an average 0.57-unit reduction in pain scores across all 11 studies included, with an average 0.61-unit reduction using L. reuteri and an average 0.75-unit reduction using L. rhamnosus GG. All three between-group differences were statistically significant. Safety data came from eight of the included studies, and they collectively showed absolutely no safety difference between actively treated and control patients.
Dr. Morris noted that the mechanism by which probiotic bacilli relieve abdominal pain remains unclear, but suggested that both prokinetic and anti-inflammatory effects might be involved.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
AT THE WORLD CONGRESS OF GASTROENTEROLOGY
Key clinical point:
Major finding: Probiotic treatment led to an average 0.57-unit reduction in pain intensity compared with placebo controls.
Data source: A Cochrane Group meta-analysis of 11 studies with 790 patients.
Disclosures: Dr. Morris had no disclosures.
Early referral recommended for high-risk port-wine stain cases
In high-risk port-wine stain phenotypes – forehead, hemifacial, and median – early referral to a pediatric neurologist is the best way to enable early symptom recognition of Sturge-Weber syndrome (SWS), according to results of a literature review.
If imaging is desired, electroencephalography (EEG) is cheaper and more minimally invasive than MRI (Pediatr Dermatol. 2017 Oct 16. doi: 10.1111/pde.13304).
Of the 34 studies analyzed, none examined the correlation between early detection of presymptomatic SWS and earlier seizure detection. There were also no data to verify improved outcomes with early detection, Michaela Zallmann, MD, of the department of dermatology at Eastern Health, Monash University, Box Hill, Australia, and her coauthors reported. While this indicates a need for further studies, it also shows a need for improved education and clinical monitoring as standard practice.
Additionally, negative imaging results do not obviate the possibility of SWS diagnosis, the investigators reported. In the studies that recorded false negatives, MRI was negative in 3%-6% of infants who later became symptomatic. Of the seven infants with false-negative results, four were less than 6 months old when the initial imaging was conducted. The investigators noted that it is not known at what age a negative MRI can reliably exclude SWS.
When imaging was used for early detection, EEG was shown to be safer and less expensive than MRI, according to the review. Of children who were not anesthetized for MRI, 30%-50% showed considerable distress, while EEG was shown to be minimally invasive. Findings from a retrospective chart review show that 14 MRIs were performed to detect one asymptomatic case of SWS, costing $11,768. In comparison, EEG costs $87 for a routine outpatient study.
“Demonstrating brain involvement on MRI in infants with high-risk PWS may facilitate more stringent counseling and monitoring, but … a negative MRI does not obviate the need for neurologic counseling and monitoring,” the investigators wrote. “Allaying anxiety about diagnostic uncertainty is not achieved using a scan but through detailed education, appropriate clinical monitoring, and nuanced reassurance.”
The investigators did not report any financial disclosures.
In high-risk port-wine stain phenotypes – forehead, hemifacial, and median – early referral to a pediatric neurologist is the best way to enable early symptom recognition of Sturge-Weber syndrome (SWS), according to results of a literature review.
If imaging is desired, electroencephalography (EEG) is cheaper and more minimally invasive than MRI (Pediatr Dermatol. 2017 Oct 16. doi: 10.1111/pde.13304).
Of the 34 studies analyzed, none examined the correlation between early detection of presymptomatic SWS and earlier seizure detection. There were also no data to verify improved outcomes with early detection, Michaela Zallmann, MD, of the department of dermatology at Eastern Health, Monash University, Box Hill, Australia, and her coauthors reported. While this indicates a need for further studies, it also shows a need for improved education and clinical monitoring as standard practice.
Additionally, negative imaging results do not obviate the possibility of SWS diagnosis, the investigators reported. In the studies that recorded false negatives, MRI was negative in 3%-6% of infants who later became symptomatic. Of the seven infants with false-negative results, four were less than 6 months old when the initial imaging was conducted. The investigators noted that it is not known at what age a negative MRI can reliably exclude SWS.
When imaging was used for early detection, EEG was shown to be safer and less expensive than MRI, according to the review. Of children who were not anesthetized for MRI, 30%-50% showed considerable distress, while EEG was shown to be minimally invasive. Findings from a retrospective chart review show that 14 MRIs were performed to detect one asymptomatic case of SWS, costing $11,768. In comparison, EEG costs $87 for a routine outpatient study.
“Demonstrating brain involvement on MRI in infants with high-risk PWS may facilitate more stringent counseling and monitoring, but … a negative MRI does not obviate the need for neurologic counseling and monitoring,” the investigators wrote. “Allaying anxiety about diagnostic uncertainty is not achieved using a scan but through detailed education, appropriate clinical monitoring, and nuanced reassurance.”
The investigators did not report any financial disclosures.
In high-risk port-wine stain phenotypes – forehead, hemifacial, and median – early referral to a pediatric neurologist is the best way to enable early symptom recognition of Sturge-Weber syndrome (SWS), according to results of a literature review.
If imaging is desired, electroencephalography (EEG) is cheaper and more minimally invasive than MRI (Pediatr Dermatol. 2017 Oct 16. doi: 10.1111/pde.13304).
Of the 34 studies analyzed, none examined the correlation between early detection of presymptomatic SWS and earlier seizure detection. There were also no data to verify improved outcomes with early detection, Michaela Zallmann, MD, of the department of dermatology at Eastern Health, Monash University, Box Hill, Australia, and her coauthors reported. While this indicates a need for further studies, it also shows a need for improved education and clinical monitoring as standard practice.
Additionally, negative imaging results do not obviate the possibility of SWS diagnosis, the investigators reported. In the studies that recorded false negatives, MRI was negative in 3%-6% of infants who later became symptomatic. Of the seven infants with false-negative results, four were less than 6 months old when the initial imaging was conducted. The investigators noted that it is not known at what age a negative MRI can reliably exclude SWS.
When imaging was used for early detection, EEG was shown to be safer and less expensive than MRI, according to the review. Of children who were not anesthetized for MRI, 30%-50% showed considerable distress, while EEG was shown to be minimally invasive. Findings from a retrospective chart review show that 14 MRIs were performed to detect one asymptomatic case of SWS, costing $11,768. In comparison, EEG costs $87 for a routine outpatient study.
“Demonstrating brain involvement on MRI in infants with high-risk PWS may facilitate more stringent counseling and monitoring, but … a negative MRI does not obviate the need for neurologic counseling and monitoring,” the investigators wrote. “Allaying anxiety about diagnostic uncertainty is not achieved using a scan but through detailed education, appropriate clinical monitoring, and nuanced reassurance.”
The investigators did not report any financial disclosures.
Key clinical point:
Major finding: To identify one case of Sturge-Weber syndrome, MRI cost $11,768, compared with $87 for a routine outpatient EEG.
Data source: A literature review of 34 articles.
Disclosures: The investigators did not report any financial disclosures.
Therapy receives rare pediatric disease designation

The US Food and Drug Administration (FDA) has granted rare pediatric disease designation to ATA230 for the treatment of congenital cytomegalovirus (CMV) infection.
ATA230 is an allogeneic T-cell immunotherapy targeting antigens expressed by CMV.
Rare pediatric disease designation is granted to drugs that show promise to treat orphan diseases affecting fewer than 200,000 patients in the US, primarily patients age 18 and younger.
The designation provides incentives to advance the development of drugs for rare disease, including access to the FDA’s expedited review and approval programs.
Under the FDA’s Rare Pediatric Disease Priority Review Voucher Program, a drug developer with rare pediatric disease designation that receives an approval of a new drug application is eligible for a voucher that can be redeemed to obtain priority review for any subsequent marketing application.
The company developing ATA230 is Atara Biotherapeutics, Inc. The company also received orphan designation for ATA230.
ATA230 trials
ATA230 has been investigated in phase 1 and 2 studies of immunocompromised patients with CMV viremia or disease who are refractory or resistant to antiviral drug treatment in the post-transplant setting.
Researchers reported phase 2 results with ATA230 at the 2016 ASH Annual Meeting.
The data encompassed 15 patients with documented CMV mutations conferring resistance to antiviral therapies. The patients had received a median of 3 prior therapies.
Eleven of the 15 patients (73.3%) responded to ATA230, 6 with complete responses and 5 with partial responses.
At 6 months, the overall survival was 72.7% in responders and 25% in non-responders.
Within the 6 months of follow-up, 1 of the 11 responders died of CMV, and 3 of the 4 non-responders died of CMV.
Adverse events occurred in 6 patients. One grade 3 event and 1 grade 4 event were considered possibly related to ATA230. ![]()
The US Food and Drug Administration (FDA) has granted rare pediatric disease designation to ATA230 for the treatment of congenital cytomegalovirus (CMV) infection.
ATA230 is an allogeneic T-cell immunotherapy targeting antigens expressed by CMV.
Rare pediatric disease designation is granted to drugs that show promise to treat orphan diseases affecting fewer than 200,000 patients in the US, primarily patients age 18 and younger.
The designation provides incentives to advance the development of drugs for rare disease, including access to the FDA’s expedited review and approval programs.
Under the FDA’s Rare Pediatric Disease Priority Review Voucher Program, a drug developer with rare pediatric disease designation that receives an approval of a new drug application is eligible for a voucher that can be redeemed to obtain priority review for any subsequent marketing application.
The company developing ATA230 is Atara Biotherapeutics, Inc. The company also received orphan designation for ATA230.
ATA230 trials
ATA230 has been investigated in phase 1 and 2 studies of immunocompromised patients with CMV viremia or disease who are refractory or resistant to antiviral drug treatment in the post-transplant setting.
Researchers reported phase 2 results with ATA230 at the 2016 ASH Annual Meeting.
The data encompassed 15 patients with documented CMV mutations conferring resistance to antiviral therapies. The patients had received a median of 3 prior therapies.
Eleven of the 15 patients (73.3%) responded to ATA230, 6 with complete responses and 5 with partial responses.
At 6 months, the overall survival was 72.7% in responders and 25% in non-responders.
Within the 6 months of follow-up, 1 of the 11 responders died of CMV, and 3 of the 4 non-responders died of CMV.
Adverse events occurred in 6 patients. One grade 3 event and 1 grade 4 event were considered possibly related to ATA230. ![]()
The US Food and Drug Administration (FDA) has granted rare pediatric disease designation to ATA230 for the treatment of congenital cytomegalovirus (CMV) infection.
ATA230 is an allogeneic T-cell immunotherapy targeting antigens expressed by CMV.
Rare pediatric disease designation is granted to drugs that show promise to treat orphan diseases affecting fewer than 200,000 patients in the US, primarily patients age 18 and younger.
The designation provides incentives to advance the development of drugs for rare disease, including access to the FDA’s expedited review and approval programs.
Under the FDA’s Rare Pediatric Disease Priority Review Voucher Program, a drug developer with rare pediatric disease designation that receives an approval of a new drug application is eligible for a voucher that can be redeemed to obtain priority review for any subsequent marketing application.
The company developing ATA230 is Atara Biotherapeutics, Inc. The company also received orphan designation for ATA230.
ATA230 trials
ATA230 has been investigated in phase 1 and 2 studies of immunocompromised patients with CMV viremia or disease who are refractory or resistant to antiviral drug treatment in the post-transplant setting.
Researchers reported phase 2 results with ATA230 at the 2016 ASH Annual Meeting.
The data encompassed 15 patients with documented CMV mutations conferring resistance to antiviral therapies. The patients had received a median of 3 prior therapies.
Eleven of the 15 patients (73.3%) responded to ATA230, 6 with complete responses and 5 with partial responses.
At 6 months, the overall survival was 72.7% in responders and 25% in non-responders.
Within the 6 months of follow-up, 1 of the 11 responders died of CMV, and 3 of the 4 non-responders died of CMV.
Adverse events occurred in 6 patients. One grade 3 event and 1 grade 4 event were considered possibly related to ATA230. ![]()
ACOG advises against vaginal seeding
The practice of vaginal seeding should not be performed outside of an approved research protocol until adequate data on safety and potential benefits are available, according to a new policy statement from the American College of Obstetricians and Gynecologists.
Vaginal seeding is “the practice of inoculating a cotton gauze or a cotton swab with vaginal fluids to transfer the vaginal flora to the mouth, nose, or skin of a newborn infant,” according to ACOG.
Data from several studies have suggested babies delivered by cesarean may lack the immunologic and metabolic benefits of vaginally delivered babies because of the unique properties of vaginal fluid, and a proof-of-concept study showed changes in newborns’ microbiome profiles when they received transfers of vaginal fluid soon after a cesarean delivery. However, the impact of the fluid transfer (vaginal seeding) remains unknown, according to the ACOG committee opinion (Obstet Gynecol. 2017;130:e274-8).
Additional safety concerns include the potential transfer of pathogens from mother to neonate from undiagnosed maternal conditions such as gonorrhea, human papillomavirus, group A streptococci, and others, the committee noted.
Women who wish to perform neonatal seeding themselves should be educated about the risks and tested for infectious diseases and pathogenic bacteria, the committee emphasized. Additionally, ACOG urged ob.gyns. to document the discussion in the medical record. The infant’s physician should also be made aware of the procedure because of the potential for neonatal infection.
The research on vaginal seeding currently consists of one pilot study, with an outcome measure of neonatal microbiota. No studies of other clinical outcomes have been completed.
“The paucity of data on this subject supports the need for additional research on the safety and benefit of vaginal seeding,” the ACOG Committee on Obstetric Practice wrote.
In the meantime, ACOG recommends exclusive breastfeeding in the first 6 months, noting that there are mixed data on associations between breastfeeding and the development of asthma and atopic disease in childhood.
The practice of vaginal seeding should not be performed outside of an approved research protocol until adequate data on safety and potential benefits are available, according to a new policy statement from the American College of Obstetricians and Gynecologists.
Vaginal seeding is “the practice of inoculating a cotton gauze or a cotton swab with vaginal fluids to transfer the vaginal flora to the mouth, nose, or skin of a newborn infant,” according to ACOG.
Data from several studies have suggested babies delivered by cesarean may lack the immunologic and metabolic benefits of vaginally delivered babies because of the unique properties of vaginal fluid, and a proof-of-concept study showed changes in newborns’ microbiome profiles when they received transfers of vaginal fluid soon after a cesarean delivery. However, the impact of the fluid transfer (vaginal seeding) remains unknown, according to the ACOG committee opinion (Obstet Gynecol. 2017;130:e274-8).
Additional safety concerns include the potential transfer of pathogens from mother to neonate from undiagnosed maternal conditions such as gonorrhea, human papillomavirus, group A streptococci, and others, the committee noted.
Women who wish to perform neonatal seeding themselves should be educated about the risks and tested for infectious diseases and pathogenic bacteria, the committee emphasized. Additionally, ACOG urged ob.gyns. to document the discussion in the medical record. The infant’s physician should also be made aware of the procedure because of the potential for neonatal infection.
The research on vaginal seeding currently consists of one pilot study, with an outcome measure of neonatal microbiota. No studies of other clinical outcomes have been completed.
“The paucity of data on this subject supports the need for additional research on the safety and benefit of vaginal seeding,” the ACOG Committee on Obstetric Practice wrote.
In the meantime, ACOG recommends exclusive breastfeeding in the first 6 months, noting that there are mixed data on associations between breastfeeding and the development of asthma and atopic disease in childhood.
The practice of vaginal seeding should not be performed outside of an approved research protocol until adequate data on safety and potential benefits are available, according to a new policy statement from the American College of Obstetricians and Gynecologists.
Vaginal seeding is “the practice of inoculating a cotton gauze or a cotton swab with vaginal fluids to transfer the vaginal flora to the mouth, nose, or skin of a newborn infant,” according to ACOG.
Data from several studies have suggested babies delivered by cesarean may lack the immunologic and metabolic benefits of vaginally delivered babies because of the unique properties of vaginal fluid, and a proof-of-concept study showed changes in newborns’ microbiome profiles when they received transfers of vaginal fluid soon after a cesarean delivery. However, the impact of the fluid transfer (vaginal seeding) remains unknown, according to the ACOG committee opinion (Obstet Gynecol. 2017;130:e274-8).
Additional safety concerns include the potential transfer of pathogens from mother to neonate from undiagnosed maternal conditions such as gonorrhea, human papillomavirus, group A streptococci, and others, the committee noted.
Women who wish to perform neonatal seeding themselves should be educated about the risks and tested for infectious diseases and pathogenic bacteria, the committee emphasized. Additionally, ACOG urged ob.gyns. to document the discussion in the medical record. The infant’s physician should also be made aware of the procedure because of the potential for neonatal infection.
The research on vaginal seeding currently consists of one pilot study, with an outcome measure of neonatal microbiota. No studies of other clinical outcomes have been completed.
“The paucity of data on this subject supports the need for additional research on the safety and benefit of vaginal seeding,” the ACOG Committee on Obstetric Practice wrote.
In the meantime, ACOG recommends exclusive breastfeeding in the first 6 months, noting that there are mixed data on associations between breastfeeding and the development of asthma and atopic disease in childhood.
FROM OBSTETRICS & GYNECOLOGY
Listen carefully
The widespread use of fetal ultrasound has dramatically decreased the number of delivery room surprises. In this country, most infants with a cardiac anomaly detected in utero probably are delivered at tertiary medical centers, leapfrogging over the maternity units at their local community hospitals. But infants with critical cardiac conditions continue to arrive unheralded at every hospital, both large and small. And many of these babies are asymptomatic without tachypnea or cyanosis. A study reported in the October 2017 Pediatrics by Hu et al. suggests a strategy for detecting these little masters of disguise before their lesions get them into serious trouble (doi: 10.1542/peds.2017-1154).
Pulse oximetry has been widely debated as a method for detecting congenital heart disease, because of course it misses the cases that are acyanotic. In a series of more than 150,000 asymptomatic neonates, and 92% for major congenital heart disease. Their false-positive rate for both categories was just a bit over 1%.

This may be another case in which the training of the examiner and the environment are critical to a positive result. As I think back to the conditions in which I examined newborns, I wonder how careful I was that my auscultating was being done in a quiet environment. If I was in the nursery, there may have been other babies crying, a radio playing, or nurses conversing with one another. I may have been deluding myself that, over the years in practice, I had developed the ability to cancel out those auditory distractions. It was probably dumb luck that I didn’t miss any critical murmurs.
And then there is the timing. The investigators don’t describe how soon after birth the auscultation was performed. Is there an optimum time in relation to the neonate’s transition from his/her fetal circulation? How long did the examiners listen? Were they in a rush to get back to their offices and busy waiting room or were they hospitalists?
I found this to be an interesting study, and if repeated by other investigators, it provides an example of how technology advancement doesn’t always render our old examining skills obsolete. In fact, it may demand we sharpen them.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
The widespread use of fetal ultrasound has dramatically decreased the number of delivery room surprises. In this country, most infants with a cardiac anomaly detected in utero probably are delivered at tertiary medical centers, leapfrogging over the maternity units at their local community hospitals. But infants with critical cardiac conditions continue to arrive unheralded at every hospital, both large and small. And many of these babies are asymptomatic without tachypnea or cyanosis. A study reported in the October 2017 Pediatrics by Hu et al. suggests a strategy for detecting these little masters of disguise before their lesions get them into serious trouble (doi: 10.1542/peds.2017-1154).
Pulse oximetry has been widely debated as a method for detecting congenital heart disease, because of course it misses the cases that are acyanotic. In a series of more than 150,000 asymptomatic neonates, and 92% for major congenital heart disease. Their false-positive rate for both categories was just a bit over 1%.
This may be another case in which the training of the examiner and the environment are critical to a positive result. As I think back to the conditions in which I examined newborns, I wonder how careful I was that my auscultating was being done in a quiet environment. If I was in the nursery, there may have been other babies crying, a radio playing, or nurses conversing with one another. I may have been deluding myself that, over the years in practice, I had developed the ability to cancel out those auditory distractions. It was probably dumb luck that I didn’t miss any critical murmurs.
And then there is the timing. The investigators don’t describe how soon after birth the auscultation was performed. Is there an optimum time in relation to the neonate’s transition from his/her fetal circulation? How long did the examiners listen? Were they in a rush to get back to their offices and busy waiting room or were they hospitalists?
I found this to be an interesting study, and if repeated by other investigators, it provides an example of how technology advancement doesn’t always render our old examining skills obsolete. In fact, it may demand we sharpen them.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
The widespread use of fetal ultrasound has dramatically decreased the number of delivery room surprises. In this country, most infants with a cardiac anomaly detected in utero probably are delivered at tertiary medical centers, leapfrogging over the maternity units at their local community hospitals. But infants with critical cardiac conditions continue to arrive unheralded at every hospital, both large and small. And many of these babies are asymptomatic without tachypnea or cyanosis. A study reported in the October 2017 Pediatrics by Hu et al. suggests a strategy for detecting these little masters of disguise before their lesions get them into serious trouble (doi: 10.1542/peds.2017-1154).
Pulse oximetry has been widely debated as a method for detecting congenital heart disease, because of course it misses the cases that are acyanotic. In a series of more than 150,000 asymptomatic neonates, and 92% for major congenital heart disease. Their false-positive rate for both categories was just a bit over 1%.
This may be another case in which the training of the examiner and the environment are critical to a positive result. As I think back to the conditions in which I examined newborns, I wonder how careful I was that my auscultating was being done in a quiet environment. If I was in the nursery, there may have been other babies crying, a radio playing, or nurses conversing with one another. I may have been deluding myself that, over the years in practice, I had developed the ability to cancel out those auditory distractions. It was probably dumb luck that I didn’t miss any critical murmurs.
And then there is the timing. The investigators don’t describe how soon after birth the auscultation was performed. Is there an optimum time in relation to the neonate’s transition from his/her fetal circulation? How long did the examiners listen? Were they in a rush to get back to their offices and busy waiting room or were they hospitalists?
I found this to be an interesting study, and if repeated by other investigators, it provides an example of how technology advancement doesn’t always render our old examining skills obsolete. In fact, it may demand we sharpen them.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
IDSA updates infectious diarrhea guidelines
Molecular-based diagnostic tests for enteric pathogens are highly sensitive but may require expert input to assess their clinical and public health implications, according to new guidelines from the Infectious Diseases Society of America.
Among the specific areas on which the guidelines focus are assessment of the diagnostic needs of patients who have been traveling, those in health care settings, including long-term care facilities, and dealing with immunocompromised patients, especially those with acquired immune deficiency syndrome (AIDS).
“Differentiating colonization from active infection, obtaining antimicrobial susceptibility results, providing optimal management, and preventing transmission are areas in need of additional research as nonculture diagnostics replace traditional culture-based methods,” writes Andi L. Shane, MD, of Emory University and Children’s Healthcare in Atlanta, with her associates in Clinical Infectious Diseases. Performing a complete physical exam and taking a thorough exposure history remain crucial in this era of rapid molecular tests in order to identify and treat infectious diarrhea and interrupt the chain of transmission, the experts emphasize (Clin Infect Dis. 2017 Oct 19. doi: 10.1093/cid/cix669).

The rise of culture-independent diagnostic tests also has important public health implications, the experts state. Pulsed-field gel electrophoresis and whole-genome sequencing are essential for rapidly detecting outbreaks, but they must be performed on clinical isolates. “Continuing to detect and respond to such outbreaks is a vital part of making our food and water systems safer,” the authors add. “As culture-independent diagnostic panels become used more frequently, public health departments may request that specimens be cultured in public health laboratories if unable to be cultured in the clinical diagnostic laboratory.” Clinicians should continue submitting isolates for subtyping of notifiable pathogens, such as Salmonella, Shiga toxin–producing Escherichia coli, Shigella, and Listeria, according to the guidelines.
The guidelines also recommend a broad differential diagnosis in immunocompromised people with diarrhea, and people with AIDS who have persistent diarrhea should undergo additional testing for other organisms including, Cryptosporidium, Cyclospora, Cystoisospora, Microsporidia, Mycobacterium avium complex, and Cytomegalovirus.
The IDSA last updated its guidelines on infectious diarrhea in 2001. The current iteration includes 60 specific recommendations and five tables that stratify pathogens by exposures, clinical signs and symptoms, postinfectious sequelae, laboratory diagnostics, and antimicrobial therapy. Two additional tables list other sources of guidelines and provide detailed recommendations on rehydration therapy. Most patients with diarrhea do not need to be tested for infectious pathogens, with exceptions such as children younger than 5 years, the elderly, immunocompromised patients, and patients with bloody diarrhea, severe abdominal pain or tenderness, or signs of sepsis. Even when patients do not need to be tested, they should receive oral rehydration solution to correct mild to moderate dehydration or intravenous rehydration if they cannot tolerate oral therapy.
The World Health Organization defines diarrhea as loose or liquid stools occurring three or more times in 24 hours or more often than normal. Rapid molecular tests most often identify norovirus in these patients. Infectious diarrhea remains most common in children under age 5 years, but the advent of rotavirus vaccines over the past decade has decreased its incidence in this age group.
The work was funded by IDSA. Dr. Shane disclosed research grants from the Division of Microbiology and Infectious Diseases of the National Institute of Allergy and Infectious Diseases, salary support from the Gerber Foundation, honoraria from SLACK, and travel support from International Scientific Association for Probiotics and Prebiotics.
This article was updated 11/3/17.
Molecular-based diagnostic tests for enteric pathogens are highly sensitive but may require expert input to assess their clinical and public health implications, according to new guidelines from the Infectious Diseases Society of America.
Among the specific areas on which the guidelines focus are assessment of the diagnostic needs of patients who have been traveling, those in health care settings, including long-term care facilities, and dealing with immunocompromised patients, especially those with acquired immune deficiency syndrome (AIDS).
“Differentiating colonization from active infection, obtaining antimicrobial susceptibility results, providing optimal management, and preventing transmission are areas in need of additional research as nonculture diagnostics replace traditional culture-based methods,” writes Andi L. Shane, MD, of Emory University and Children’s Healthcare in Atlanta, with her associates in Clinical Infectious Diseases. Performing a complete physical exam and taking a thorough exposure history remain crucial in this era of rapid molecular tests in order to identify and treat infectious diarrhea and interrupt the chain of transmission, the experts emphasize (Clin Infect Dis. 2017 Oct 19. doi: 10.1093/cid/cix669).
The rise of culture-independent diagnostic tests also has important public health implications, the experts state. Pulsed-field gel electrophoresis and whole-genome sequencing are essential for rapidly detecting outbreaks, but they must be performed on clinical isolates. “Continuing to detect and respond to such outbreaks is a vital part of making our food and water systems safer,” the authors add. “As culture-independent diagnostic panels become used more frequently, public health departments may request that specimens be cultured in public health laboratories if unable to be cultured in the clinical diagnostic laboratory.” Clinicians should continue submitting isolates for subtyping of notifiable pathogens, such as Salmonella, Shiga toxin–producing Escherichia coli, Shigella, and Listeria, according to the guidelines.
The guidelines also recommend a broad differential diagnosis in immunocompromised people with diarrhea, and people with AIDS who have persistent diarrhea should undergo additional testing for other organisms including, Cryptosporidium, Cyclospora, Cystoisospora, Microsporidia, Mycobacterium avium complex, and Cytomegalovirus.
The IDSA last updated its guidelines on infectious diarrhea in 2001. The current iteration includes 60 specific recommendations and five tables that stratify pathogens by exposures, clinical signs and symptoms, postinfectious sequelae, laboratory diagnostics, and antimicrobial therapy. Two additional tables list other sources of guidelines and provide detailed recommendations on rehydration therapy. Most patients with diarrhea do not need to be tested for infectious pathogens, with exceptions such as children younger than 5 years, the elderly, immunocompromised patients, and patients with bloody diarrhea, severe abdominal pain or tenderness, or signs of sepsis. Even when patients do not need to be tested, they should receive oral rehydration solution to correct mild to moderate dehydration or intravenous rehydration if they cannot tolerate oral therapy.
The World Health Organization defines diarrhea as loose or liquid stools occurring three or more times in 24 hours or more often than normal. Rapid molecular tests most often identify norovirus in these patients. Infectious diarrhea remains most common in children under age 5 years, but the advent of rotavirus vaccines over the past decade has decreased its incidence in this age group.
The work was funded by IDSA. Dr. Shane disclosed research grants from the Division of Microbiology and Infectious Diseases of the National Institute of Allergy and Infectious Diseases, salary support from the Gerber Foundation, honoraria from SLACK, and travel support from International Scientific Association for Probiotics and Prebiotics.
This article was updated 11/3/17.
Molecular-based diagnostic tests for enteric pathogens are highly sensitive but may require expert input to assess their clinical and public health implications, according to new guidelines from the Infectious Diseases Society of America.
Among the specific areas on which the guidelines focus are assessment of the diagnostic needs of patients who have been traveling, those in health care settings, including long-term care facilities, and dealing with immunocompromised patients, especially those with acquired immune deficiency syndrome (AIDS).
“Differentiating colonization from active infection, obtaining antimicrobial susceptibility results, providing optimal management, and preventing transmission are areas in need of additional research as nonculture diagnostics replace traditional culture-based methods,” writes Andi L. Shane, MD, of Emory University and Children’s Healthcare in Atlanta, with her associates in Clinical Infectious Diseases. Performing a complete physical exam and taking a thorough exposure history remain crucial in this era of rapid molecular tests in order to identify and treat infectious diarrhea and interrupt the chain of transmission, the experts emphasize (Clin Infect Dis. 2017 Oct 19. doi: 10.1093/cid/cix669).
The rise of culture-independent diagnostic tests also has important public health implications, the experts state. Pulsed-field gel electrophoresis and whole-genome sequencing are essential for rapidly detecting outbreaks, but they must be performed on clinical isolates. “Continuing to detect and respond to such outbreaks is a vital part of making our food and water systems safer,” the authors add. “As culture-independent diagnostic panels become used more frequently, public health departments may request that specimens be cultured in public health laboratories if unable to be cultured in the clinical diagnostic laboratory.” Clinicians should continue submitting isolates for subtyping of notifiable pathogens, such as Salmonella, Shiga toxin–producing Escherichia coli, Shigella, and Listeria, according to the guidelines.
The guidelines also recommend a broad differential diagnosis in immunocompromised people with diarrhea, and people with AIDS who have persistent diarrhea should undergo additional testing for other organisms including, Cryptosporidium, Cyclospora, Cystoisospora, Microsporidia, Mycobacterium avium complex, and Cytomegalovirus.
The IDSA last updated its guidelines on infectious diarrhea in 2001. The current iteration includes 60 specific recommendations and five tables that stratify pathogens by exposures, clinical signs and symptoms, postinfectious sequelae, laboratory diagnostics, and antimicrobial therapy. Two additional tables list other sources of guidelines and provide detailed recommendations on rehydration therapy. Most patients with diarrhea do not need to be tested for infectious pathogens, with exceptions such as children younger than 5 years, the elderly, immunocompromised patients, and patients with bloody diarrhea, severe abdominal pain or tenderness, or signs of sepsis. Even when patients do not need to be tested, they should receive oral rehydration solution to correct mild to moderate dehydration or intravenous rehydration if they cannot tolerate oral therapy.
The World Health Organization defines diarrhea as loose or liquid stools occurring three or more times in 24 hours or more often than normal. Rapid molecular tests most often identify norovirus in these patients. Infectious diarrhea remains most common in children under age 5 years, but the advent of rotavirus vaccines over the past decade has decreased its incidence in this age group.
The work was funded by IDSA. Dr. Shane disclosed research grants from the Division of Microbiology and Infectious Diseases of the National Institute of Allergy and Infectious Diseases, salary support from the Gerber Foundation, honoraria from SLACK, and travel support from International Scientific Association for Probiotics and Prebiotics.
This article was updated 11/3/17.
FROM CLINICAL INFECTIOUS DISEASES
Guidelines are not cookbooks
For many years I have counseled medical students and residents that half of what I was taught in medical school has since been proven obsolete or frankly wrong. I counsel them that I have no reason to believe that I am any better than my professors were. So I wish them luck sorting out what is true. Earlier in my career, that warning was mild hyperbole, but not anymore.
Upper respiratory infections (URIs) are the most common reason for an office visit during the winter. Bronchiolitis is the most frequent diagnosis for a winter admission of an infant to a community hospital. Pediatricians have nuanced assessments and many options when treating these diseases. Best practices have changed frequently over the past 3 decades, mostly by eliminating previously espoused treatments as ineffective. In infants and young children, those obsolete treatments include decongestants and cough suppressants for young children with common colds, inhaled beta-agonists and steroids for infants with bronchiolitis, and antibiotics for simple otitis media in older children. In other words, most of what I was originally taught.
There is a discontinuity between guidelines that forbid routine steroids and beta-agonists for bronchiolitis in infants, and guidelines that strongly prescribe steroids, metered dose inhalers, and asthma action plans for all discharged wheezers over age 2 years. When I worked as a hospitalist in the pulmonology department, I frequently diagnosed asthma under age 1 year. As a general pediatric hospitalist, one winter I twice ran afoul of a hospital quality metric that benchmarked 100% compliance with providing steroids, inhaled corticosteroids, and asthma action plans on discharge for all wheezers over age 2. Fortunately for both me and the quality team working on that quality dashboard, my thorough documentation of why I didn’t think a particular wheezer had asthma was detailed enough to satisfy peer review.
Historically, medical knowledge has been dependent upon these types of observation which then are taught to the next generation of physicians and, if confirmed repeatedly, become memes with some degree of reliability. An all-too-typical Cochrane library entry may challenge these memes by looking at 200 articles, finding 20 relevant studies, selecting only 2 underpowered studies as meeting their randomized controlled trial criteria, and then concluding that there is “insufficient evidence” to prove the treatment works. But absence of proof is not proof of absence. Twenty five years after coining the phrase “evidence-based medicine,” our medical knowledge base has not been purified.

In medicine, absolute certainty isn’t possible. Using 95% confidence intervals for a research paper does not even mean it is 95% likely to be right. So part of (which is tainted with confirmation bias.) It is a very imperfect art.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@frontlinemedcom.com.
For many years I have counseled medical students and residents that half of what I was taught in medical school has since been proven obsolete or frankly wrong. I counsel them that I have no reason to believe that I am any better than my professors were. So I wish them luck sorting out what is true. Earlier in my career, that warning was mild hyperbole, but not anymore.
Upper respiratory infections (URIs) are the most common reason for an office visit during the winter. Bronchiolitis is the most frequent diagnosis for a winter admission of an infant to a community hospital. Pediatricians have nuanced assessments and many options when treating these diseases. Best practices have changed frequently over the past 3 decades, mostly by eliminating previously espoused treatments as ineffective. In infants and young children, those obsolete treatments include decongestants and cough suppressants for young children with common colds, inhaled beta-agonists and steroids for infants with bronchiolitis, and antibiotics for simple otitis media in older children. In other words, most of what I was originally taught.
There is a discontinuity between guidelines that forbid routine steroids and beta-agonists for bronchiolitis in infants, and guidelines that strongly prescribe steroids, metered dose inhalers, and asthma action plans for all discharged wheezers over age 2 years. When I worked as a hospitalist in the pulmonology department, I frequently diagnosed asthma under age 1 year. As a general pediatric hospitalist, one winter I twice ran afoul of a hospital quality metric that benchmarked 100% compliance with providing steroids, inhaled corticosteroids, and asthma action plans on discharge for all wheezers over age 2. Fortunately for both me and the quality team working on that quality dashboard, my thorough documentation of why I didn’t think a particular wheezer had asthma was detailed enough to satisfy peer review.
Historically, medical knowledge has been dependent upon these types of observation which then are taught to the next generation of physicians and, if confirmed repeatedly, become memes with some degree of reliability. An all-too-typical Cochrane library entry may challenge these memes by looking at 200 articles, finding 20 relevant studies, selecting only 2 underpowered studies as meeting their randomized controlled trial criteria, and then concluding that there is “insufficient evidence” to prove the treatment works. But absence of proof is not proof of absence. Twenty five years after coining the phrase “evidence-based medicine,” our medical knowledge base has not been purified.
In medicine, absolute certainty isn’t possible. Using 95% confidence intervals for a research paper does not even mean it is 95% likely to be right. So part of (which is tainted with confirmation bias.) It is a very imperfect art.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@frontlinemedcom.com.
For many years I have counseled medical students and residents that half of what I was taught in medical school has since been proven obsolete or frankly wrong. I counsel them that I have no reason to believe that I am any better than my professors were. So I wish them luck sorting out what is true. Earlier in my career, that warning was mild hyperbole, but not anymore.
Upper respiratory infections (URIs) are the most common reason for an office visit during the winter. Bronchiolitis is the most frequent diagnosis for a winter admission of an infant to a community hospital. Pediatricians have nuanced assessments and many options when treating these diseases. Best practices have changed frequently over the past 3 decades, mostly by eliminating previously espoused treatments as ineffective. In infants and young children, those obsolete treatments include decongestants and cough suppressants for young children with common colds, inhaled beta-agonists and steroids for infants with bronchiolitis, and antibiotics for simple otitis media in older children. In other words, most of what I was originally taught.
There is a discontinuity between guidelines that forbid routine steroids and beta-agonists for bronchiolitis in infants, and guidelines that strongly prescribe steroids, metered dose inhalers, and asthma action plans for all discharged wheezers over age 2 years. When I worked as a hospitalist in the pulmonology department, I frequently diagnosed asthma under age 1 year. As a general pediatric hospitalist, one winter I twice ran afoul of a hospital quality metric that benchmarked 100% compliance with providing steroids, inhaled corticosteroids, and asthma action plans on discharge for all wheezers over age 2. Fortunately for both me and the quality team working on that quality dashboard, my thorough documentation of why I didn’t think a particular wheezer had asthma was detailed enough to satisfy peer review.
Historically, medical knowledge has been dependent upon these types of observation which then are taught to the next generation of physicians and, if confirmed repeatedly, become memes with some degree of reliability. An all-too-typical Cochrane library entry may challenge these memes by looking at 200 articles, finding 20 relevant studies, selecting only 2 underpowered studies as meeting their randomized controlled trial criteria, and then concluding that there is “insufficient evidence” to prove the treatment works. But absence of proof is not proof of absence. Twenty five years after coining the phrase “evidence-based medicine,” our medical knowledge base has not been purified.
In medicine, absolute certainty isn’t possible. Using 95% confidence intervals for a research paper does not even mean it is 95% likely to be right. So part of (which is tainted with confirmation bias.) It is a very imperfect art.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@frontlinemedcom.com.
LARCs remain best contraception for teens
CHICAGO – The steady drop in teen pregnancy rates over the past 25 years – more than a 75% decline – is directly attributed to more effective use of contraception, but it only will continue if teens use the most effective forms of contraception, explained Rachael Phelps, MD, medical director of Planned Parenthood of Central and Western New York.
Teen birth rates in the United States already remain much higher than those in other high-income countries. In fact, the 2015 U.S. rate of 22 births per 1,000 teens ages 15-19 years is barely below that of India and Rwanda – and more than triple the rates in France, Germany, Italy, and other Western European countries.

“A lot of what you’re doing for adolescents in primary care is transitioning them from being a child to being an adult,” Dr. Phelps said. “Once they’re in their 20s, they may not see a primary care doctor, so you have the opportunity to give them the skills and the knowledge they need with contraception to protect themselves not only through their teens, but through their 20s.”
Contraceptive methods’ effectiveness
The most effective forms of birth control, with a less than 1% chance of pregnancy, are long-acting reversible contraceptives (LARCs), including the implant (Nexplanon) and an intrauterine device (IUD), such as Skyla, Mirena, Liletta, and Kyleena, and the hormone-free Paragard. Sterilization also is highly effective, but is permanent and rarely an ideal option for the average teen.
Other hormonal options are second best, with 94%-99% effectiveness, but require more frequent replacement. Whereas the implant lasts 3 years and the IUDs last anywhere from 3 to 12 years depending on the type, the pill must be taken daily. The patch is replaced each week, the ring is replaced each month, and Depo-Provera shots are required every 3 months.
The least effective methods of birth control include withdrawal, natural family planning (fertility planning), and barrier methods such as condoms and diaphragms. Depending on the method, 12-24 women out of 100 will get pregnant each year using these methods, although that’s better than the 90% or more of women who get pregnant each year when using no contraception.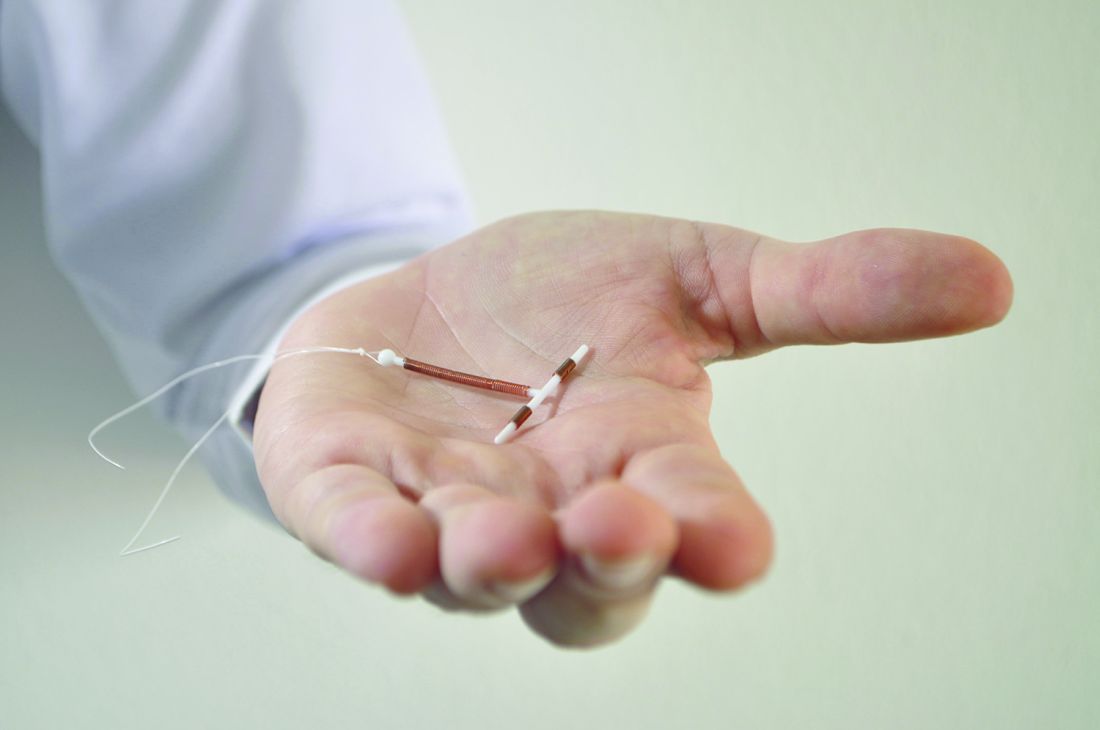
“The problem is, if you try pills first and see how that goes, the way you’re going to find out it didn’t go so well is she’s going to be pregnant,” Dr. Phelps said. “When you think about an IUD or an implant being invasive, you need to think about the alternative, which is pregnancy.”
Just over half of teens using contraception use oral contraceptives (54%), according to the Centers for Disease Control and Prevention, yet research shows only a third of women remember to take their pill every day in their first month. By their third month, just one in five women have remembered the pill every day, and more than half (51%) have forgotten three or more pills (Fam Plann Perspect. 1996 Jul-Aug;28[4]:154-8).
“When we talk about risk, we often think about the risk of the method versus not using the method,” Dr. Phelps said. “But what we should be thinking about is the risk of the method versus the risk of pregnancy. That’s the true comparison because they’re not going to stop having sex.”
After oral contraception, condoms are most popular (23%), followed by 9% using Depo-Provera, and the remaining 10% split across withdrawal, the ring, and the patch, she said.
LARCs preferred by teens and organizations
The AAP, the American College of Obstetricians and Gynecologists (ACOG), and the American Academy of Family Physicians (AAFP) all recommend LARCs as first-line contraceptive choices.
Teens also prefer LARCs to the short-term, less effective methods as well, found the Contraceptive Choice Project study. Given a choice of any birth control method without cost or other access barriers, 72% of teens would choose a LARC, compared with 28% of teens who would choose a short-acting method, Dr. Phelps said.
Satisfaction rates with LARCs, ranging from 78% with the implant to 86% with a hormonal IUD, also far exceeded satisfaction with other hormonal contraception, ranging from 42% for the patch to 54% for Depo-Provera and oral contraceptives, the study found. And LARCs are among the safest contraceptive choices because they contain no estrogen and have few contraindications.
Understanding LARC and hormonal options
The two types of IUDs are an levonorgestrel IUD and a copper-T IUD. The levonorgestrel IUD contains progestin only, released at 20 mcg per day, and is effective up to 3-7 years. Most patients have light spotting initially, lasting 6 months in about 25% of patients and up to a year in 10%. By 6 months, 44% don’t have periods, which increases to 50% by 1 year (“Contraceptive Technology,” 19ed. [London: Ardent Media, 2007]).
The copper-T IUD contains copper ions but no hormones and is effective up to 12 years, starting immediately. Women have regular periods, but they may be heavier, longer, or with more cramps for the first 6 months.
Both IUDs and implants are safe in nulliparous, postpartum, and breastfeeding teens as well as those with obesity, cervical intraepithelial neoplasia, diabetes, HIV, depression, stroke/myocardial infarction/deep vein thrombosis/pulmonary embolism, pelvic inflammatory disease, and sexually transmitted infections.
Dr. Phelps reviewed insertion for both IUDs and the implant, but also said providers can refer teens for LARCs using http://larc.arhp.org to find someone. She also recommended the Managing Contraception pocket-sized book, available at www.managingcontraception.com and free for medical students and residents. Further, the U.S. Medical Eligibility Criteria provides all necessary information on contraindications and is available as a mobile app.
All the hormonal options, including the levonorgestrel IUD, become effective 1 week after starting. The implant, costing $300-$600, contains only progesterone, is effective up to 4 years and works by inhibiting ovulation. Just over one in five girls (22%) have no period, 34% have infrequent light bleeding, and 11% discontinue it because of frequent bleeding.
Depo-Provera contains progestin only and involves an injection every 12-14 weeks; irregular bleeding is initially common, after which most patients experience amenorrhea.
Patients using the patch, containing both estrogen and progestin, should change it once a week for 3 weeks and then take 1 week off for their period. Providers should advise teens to stick the patch directly on clean, dry skin of the arm, torso, buttocks, or stomach, but not to their breasts.
The ring similarly contains estrogen and progestin and has 1 off week after 3 weeks of use, but it is changed out monthly. Patients pinch the ring and place it into the vagina in any location, going deeper if it is uncomfortable.
Emergency contraception
Of the two emergency contraception options, ulipristal acetate – prescription only as 30 mg used up to 120 hours after unprotected sex – is always more effective than levonorgestrel – over-the-counter as 1.5 mg used up to 72 hours after unprotected sex. Both, however, are less effective in those with obesity (ulipristal acetate if BMI great than 30 and levonorgestrel if BMI greater than 25), Dr. Phelps said. If the patient had unprotected sex 3-5 days earlier and/or has a higher BMI, ulipristal acetate is preferred. Ideally, teens should be provided emergency contraception ahead of time, thereby increasing earlier use and use overall when it’s needed without increasing risk-taking behavior.
Common misconceptions
Dr. Phelps also reviewed some of the key myths that providers and teens often believe about LARCs and other contraceptive methods.
“When providers or patients hold misperceptions about the risks associated with contraception, teens’ choices are unnecessarily limited,” she said.
Key facts to know about IUDs are that even nulliparous teens can use them, teens can tolerate IUD placement, and IUDs do not increase the risk of pelvic inflammatory disease or infertility. Even teens with multiple partners and/or a history of sexually transmitted infections, pelvic inflammatory disease, or ectopic pregnancy can use IUDs, Dr. Phelps emphasized.
Although Depo-Provera can lead to 3%-5% bone loss, similar to pregnancy and breastfeeding, in the first 1-2 years, the loss is temporary and reversible. No research has shown Depo-Provera to increase risk of fracture or other negative clinical outcomes, no limits to its duration of use exist, and measuring bone mass density is not recommended.
Although Depo-Provera does cause excessive weight gain in 25% of users – an average 15 pounds over 3 years – the risk of increase is evident at 6 months. All other hormonal options – IUDs, the implant, pill, patch, or ring – do not cause weight gain. Finally, obesity does not decrease the effectiveness of IUDs, the implant, patch, pill, or ring.
No funding was used for this presentation. Dr. Phelps reported having done clinical training and speaking for Merck.
CHICAGO – The steady drop in teen pregnancy rates over the past 25 years – more than a 75% decline – is directly attributed to more effective use of contraception, but it only will continue if teens use the most effective forms of contraception, explained Rachael Phelps, MD, medical director of Planned Parenthood of Central and Western New York.
Teen birth rates in the United States already remain much higher than those in other high-income countries. In fact, the 2015 U.S. rate of 22 births per 1,000 teens ages 15-19 years is barely below that of India and Rwanda – and more than triple the rates in France, Germany, Italy, and other Western European countries.
“A lot of what you’re doing for adolescents in primary care is transitioning them from being a child to being an adult,” Dr. Phelps said. “Once they’re in their 20s, they may not see a primary care doctor, so you have the opportunity to give them the skills and the knowledge they need with contraception to protect themselves not only through their teens, but through their 20s.”
Contraceptive methods’ effectiveness
The most effective forms of birth control, with a less than 1% chance of pregnancy, are long-acting reversible contraceptives (LARCs), including the implant (Nexplanon) and an intrauterine device (IUD), such as Skyla, Mirena, Liletta, and Kyleena, and the hormone-free Paragard. Sterilization also is highly effective, but is permanent and rarely an ideal option for the average teen.
Other hormonal options are second best, with 94%-99% effectiveness, but require more frequent replacement. Whereas the implant lasts 3 years and the IUDs last anywhere from 3 to 12 years depending on the type, the pill must be taken daily. The patch is replaced each week, the ring is replaced each month, and Depo-Provera shots are required every 3 months.
The least effective methods of birth control include withdrawal, natural family planning (fertility planning), and barrier methods such as condoms and diaphragms. Depending on the method, 12-24 women out of 100 will get pregnant each year using these methods, although that’s better than the 90% or more of women who get pregnant each year when using no contraception.
“The problem is, if you try pills first and see how that goes, the way you’re going to find out it didn’t go so well is she’s going to be pregnant,” Dr. Phelps said. “When you think about an IUD or an implant being invasive, you need to think about the alternative, which is pregnancy.”
Just over half of teens using contraception use oral contraceptives (54%), according to the Centers for Disease Control and Prevention, yet research shows only a third of women remember to take their pill every day in their first month. By their third month, just one in five women have remembered the pill every day, and more than half (51%) have forgotten three or more pills (Fam Plann Perspect. 1996 Jul-Aug;28[4]:154-8).
“When we talk about risk, we often think about the risk of the method versus not using the method,” Dr. Phelps said. “But what we should be thinking about is the risk of the method versus the risk of pregnancy. That’s the true comparison because they’re not going to stop having sex.”
After oral contraception, condoms are most popular (23%), followed by 9% using Depo-Provera, and the remaining 10% split across withdrawal, the ring, and the patch, she said.
LARCs preferred by teens and organizations
The AAP, the American College of Obstetricians and Gynecologists (ACOG), and the American Academy of Family Physicians (AAFP) all recommend LARCs as first-line contraceptive choices.
Teens also prefer LARCs to the short-term, less effective methods as well, found the Contraceptive Choice Project study. Given a choice of any birth control method without cost or other access barriers, 72% of teens would choose a LARC, compared with 28% of teens who would choose a short-acting method, Dr. Phelps said.
Satisfaction rates with LARCs, ranging from 78% with the implant to 86% with a hormonal IUD, also far exceeded satisfaction with other hormonal contraception, ranging from 42% for the patch to 54% for Depo-Provera and oral contraceptives, the study found. And LARCs are among the safest contraceptive choices because they contain no estrogen and have few contraindications.
Understanding LARC and hormonal options
The two types of IUDs are an levonorgestrel IUD and a copper-T IUD. The levonorgestrel IUD contains progestin only, released at 20 mcg per day, and is effective up to 3-7 years. Most patients have light spotting initially, lasting 6 months in about 25% of patients and up to a year in 10%. By 6 months, 44% don’t have periods, which increases to 50% by 1 year (“Contraceptive Technology,” 19ed. [London: Ardent Media, 2007]).
The copper-T IUD contains copper ions but no hormones and is effective up to 12 years, starting immediately. Women have regular periods, but they may be heavier, longer, or with more cramps for the first 6 months.
Both IUDs and implants are safe in nulliparous, postpartum, and breastfeeding teens as well as those with obesity, cervical intraepithelial neoplasia, diabetes, HIV, depression, stroke/myocardial infarction/deep vein thrombosis/pulmonary embolism, pelvic inflammatory disease, and sexually transmitted infections.
Dr. Phelps reviewed insertion for both IUDs and the implant, but also said providers can refer teens for LARCs using http://larc.arhp.org to find someone. She also recommended the Managing Contraception pocket-sized book, available at www.managingcontraception.com and free for medical students and residents. Further, the U.S. Medical Eligibility Criteria provides all necessary information on contraindications and is available as a mobile app.
All the hormonal options, including the levonorgestrel IUD, become effective 1 week after starting. The implant, costing $300-$600, contains only progesterone, is effective up to 4 years and works by inhibiting ovulation. Just over one in five girls (22%) have no period, 34% have infrequent light bleeding, and 11% discontinue it because of frequent bleeding.
Depo-Provera contains progestin only and involves an injection every 12-14 weeks; irregular bleeding is initially common, after which most patients experience amenorrhea.
Patients using the patch, containing both estrogen and progestin, should change it once a week for 3 weeks and then take 1 week off for their period. Providers should advise teens to stick the patch directly on clean, dry skin of the arm, torso, buttocks, or stomach, but not to their breasts.
The ring similarly contains estrogen and progestin and has 1 off week after 3 weeks of use, but it is changed out monthly. Patients pinch the ring and place it into the vagina in any location, going deeper if it is uncomfortable.
Emergency contraception
Of the two emergency contraception options, ulipristal acetate – prescription only as 30 mg used up to 120 hours after unprotected sex – is always more effective than levonorgestrel – over-the-counter as 1.5 mg used up to 72 hours after unprotected sex. Both, however, are less effective in those with obesity (ulipristal acetate if BMI great than 30 and levonorgestrel if BMI greater than 25), Dr. Phelps said. If the patient had unprotected sex 3-5 days earlier and/or has a higher BMI, ulipristal acetate is preferred. Ideally, teens should be provided emergency contraception ahead of time, thereby increasing earlier use and use overall when it’s needed without increasing risk-taking behavior.
Common misconceptions
Dr. Phelps also reviewed some of the key myths that providers and teens often believe about LARCs and other contraceptive methods.
“When providers or patients hold misperceptions about the risks associated with contraception, teens’ choices are unnecessarily limited,” she said.
Key facts to know about IUDs are that even nulliparous teens can use them, teens can tolerate IUD placement, and IUDs do not increase the risk of pelvic inflammatory disease or infertility. Even teens with multiple partners and/or a history of sexually transmitted infections, pelvic inflammatory disease, or ectopic pregnancy can use IUDs, Dr. Phelps emphasized.
Although Depo-Provera can lead to 3%-5% bone loss, similar to pregnancy and breastfeeding, in the first 1-2 years, the loss is temporary and reversible. No research has shown Depo-Provera to increase risk of fracture or other negative clinical outcomes, no limits to its duration of use exist, and measuring bone mass density is not recommended.
Although Depo-Provera does cause excessive weight gain in 25% of users – an average 15 pounds over 3 years – the risk of increase is evident at 6 months. All other hormonal options – IUDs, the implant, pill, patch, or ring – do not cause weight gain. Finally, obesity does not decrease the effectiveness of IUDs, the implant, patch, pill, or ring.
No funding was used for this presentation. Dr. Phelps reported having done clinical training and speaking for Merck.
CHICAGO – The steady drop in teen pregnancy rates over the past 25 years – more than a 75% decline – is directly attributed to more effective use of contraception, but it only will continue if teens use the most effective forms of contraception, explained Rachael Phelps, MD, medical director of Planned Parenthood of Central and Western New York.
Teen birth rates in the United States already remain much higher than those in other high-income countries. In fact, the 2015 U.S. rate of 22 births per 1,000 teens ages 15-19 years is barely below that of India and Rwanda – and more than triple the rates in France, Germany, Italy, and other Western European countries.
“A lot of what you’re doing for adolescents in primary care is transitioning them from being a child to being an adult,” Dr. Phelps said. “Once they’re in their 20s, they may not see a primary care doctor, so you have the opportunity to give them the skills and the knowledge they need with contraception to protect themselves not only through their teens, but through their 20s.”
Contraceptive methods’ effectiveness
The most effective forms of birth control, with a less than 1% chance of pregnancy, are long-acting reversible contraceptives (LARCs), including the implant (Nexplanon) and an intrauterine device (IUD), such as Skyla, Mirena, Liletta, and Kyleena, and the hormone-free Paragard. Sterilization also is highly effective, but is permanent and rarely an ideal option for the average teen.
Other hormonal options are second best, with 94%-99% effectiveness, but require more frequent replacement. Whereas the implant lasts 3 years and the IUDs last anywhere from 3 to 12 years depending on the type, the pill must be taken daily. The patch is replaced each week, the ring is replaced each month, and Depo-Provera shots are required every 3 months.
The least effective methods of birth control include withdrawal, natural family planning (fertility planning), and barrier methods such as condoms and diaphragms. Depending on the method, 12-24 women out of 100 will get pregnant each year using these methods, although that’s better than the 90% or more of women who get pregnant each year when using no contraception.
“The problem is, if you try pills first and see how that goes, the way you’re going to find out it didn’t go so well is she’s going to be pregnant,” Dr. Phelps said. “When you think about an IUD or an implant being invasive, you need to think about the alternative, which is pregnancy.”
Just over half of teens using contraception use oral contraceptives (54%), according to the Centers for Disease Control and Prevention, yet research shows only a third of women remember to take their pill every day in their first month. By their third month, just one in five women have remembered the pill every day, and more than half (51%) have forgotten three or more pills (Fam Plann Perspect. 1996 Jul-Aug;28[4]:154-8).
“When we talk about risk, we often think about the risk of the method versus not using the method,” Dr. Phelps said. “But what we should be thinking about is the risk of the method versus the risk of pregnancy. That’s the true comparison because they’re not going to stop having sex.”
After oral contraception, condoms are most popular (23%), followed by 9% using Depo-Provera, and the remaining 10% split across withdrawal, the ring, and the patch, she said.
LARCs preferred by teens and organizations
The AAP, the American College of Obstetricians and Gynecologists (ACOG), and the American Academy of Family Physicians (AAFP) all recommend LARCs as first-line contraceptive choices.
Teens also prefer LARCs to the short-term, less effective methods as well, found the Contraceptive Choice Project study. Given a choice of any birth control method without cost or other access barriers, 72% of teens would choose a LARC, compared with 28% of teens who would choose a short-acting method, Dr. Phelps said.
Satisfaction rates with LARCs, ranging from 78% with the implant to 86% with a hormonal IUD, also far exceeded satisfaction with other hormonal contraception, ranging from 42% for the patch to 54% for Depo-Provera and oral contraceptives, the study found. And LARCs are among the safest contraceptive choices because they contain no estrogen and have few contraindications.
Understanding LARC and hormonal options
The two types of IUDs are an levonorgestrel IUD and a copper-T IUD. The levonorgestrel IUD contains progestin only, released at 20 mcg per day, and is effective up to 3-7 years. Most patients have light spotting initially, lasting 6 months in about 25% of patients and up to a year in 10%. By 6 months, 44% don’t have periods, which increases to 50% by 1 year (“Contraceptive Technology,” 19ed. [London: Ardent Media, 2007]).
The copper-T IUD contains copper ions but no hormones and is effective up to 12 years, starting immediately. Women have regular periods, but they may be heavier, longer, or with more cramps for the first 6 months.
Both IUDs and implants are safe in nulliparous, postpartum, and breastfeeding teens as well as those with obesity, cervical intraepithelial neoplasia, diabetes, HIV, depression, stroke/myocardial infarction/deep vein thrombosis/pulmonary embolism, pelvic inflammatory disease, and sexually transmitted infections.
Dr. Phelps reviewed insertion for both IUDs and the implant, but also said providers can refer teens for LARCs using http://larc.arhp.org to find someone. She also recommended the Managing Contraception pocket-sized book, available at www.managingcontraception.com and free for medical students and residents. Further, the U.S. Medical Eligibility Criteria provides all necessary information on contraindications and is available as a mobile app.
All the hormonal options, including the levonorgestrel IUD, become effective 1 week after starting. The implant, costing $300-$600, contains only progesterone, is effective up to 4 years and works by inhibiting ovulation. Just over one in five girls (22%) have no period, 34% have infrequent light bleeding, and 11% discontinue it because of frequent bleeding.
Depo-Provera contains progestin only and involves an injection every 12-14 weeks; irregular bleeding is initially common, after which most patients experience amenorrhea.
Patients using the patch, containing both estrogen and progestin, should change it once a week for 3 weeks and then take 1 week off for their period. Providers should advise teens to stick the patch directly on clean, dry skin of the arm, torso, buttocks, or stomach, but not to their breasts.
The ring similarly contains estrogen and progestin and has 1 off week after 3 weeks of use, but it is changed out monthly. Patients pinch the ring and place it into the vagina in any location, going deeper if it is uncomfortable.
Emergency contraception
Of the two emergency contraception options, ulipristal acetate – prescription only as 30 mg used up to 120 hours after unprotected sex – is always more effective than levonorgestrel – over-the-counter as 1.5 mg used up to 72 hours after unprotected sex. Both, however, are less effective in those with obesity (ulipristal acetate if BMI great than 30 and levonorgestrel if BMI greater than 25), Dr. Phelps said. If the patient had unprotected sex 3-5 days earlier and/or has a higher BMI, ulipristal acetate is preferred. Ideally, teens should be provided emergency contraception ahead of time, thereby increasing earlier use and use overall when it’s needed without increasing risk-taking behavior.
Common misconceptions
Dr. Phelps also reviewed some of the key myths that providers and teens often believe about LARCs and other contraceptive methods.
“When providers or patients hold misperceptions about the risks associated with contraception, teens’ choices are unnecessarily limited,” she said.
Key facts to know about IUDs are that even nulliparous teens can use them, teens can tolerate IUD placement, and IUDs do not increase the risk of pelvic inflammatory disease or infertility. Even teens with multiple partners and/or a history of sexually transmitted infections, pelvic inflammatory disease, or ectopic pregnancy can use IUDs, Dr. Phelps emphasized.
Although Depo-Provera can lead to 3%-5% bone loss, similar to pregnancy and breastfeeding, in the first 1-2 years, the loss is temporary and reversible. No research has shown Depo-Provera to increase risk of fracture or other negative clinical outcomes, no limits to its duration of use exist, and measuring bone mass density is not recommended.
Although Depo-Provera does cause excessive weight gain in 25% of users – an average 15 pounds over 3 years – the risk of increase is evident at 6 months. All other hormonal options – IUDs, the implant, pill, patch, or ring – do not cause weight gain. Finally, obesity does not decrease the effectiveness of IUDs, the implant, patch, pill, or ring.
No funding was used for this presentation. Dr. Phelps reported having done clinical training and speaking for Merck.
EXPERT ANALYSIS FROM AAP 2017