User login
Skills training improves psychosocial outcomes for young cancer patients
Compared with standard psychosocial care, a one-on-one skills-based intervention improved psychosocial outcomes in adolescents and young adults with cancer, according to results of a pilot randomized study presented at the Palliative and Supportive Care in Oncology Symposium.
The novel intervention was associated with improved patient resilience, cancer-specific quality of life, and hope, plus fewer cases of depression, said lead study author Abby R. Rosenberg, MD, director of palliative care and resilience research at Seattle Children’s Research Institute.
Brief, developmentally-targeted psychosocial interventions are promising for this population of adolescents and young adults with cancer, Dr. Rosenberg said in a press conference at the symposium, which was cosponsored by AAHPM, ASCO, ASTRO, and MASCC.
Adolescents and young adults with cancer tend to have poor psychosocial outcomes, possibly because they have not yet developed skills that would help them manage hardships they encounter as a result of having cancer, according to Dr. Rosenberg.
She and her colleagues previously designed and tested the intervention, called Promoting Resilience in Stress Management (PRISM). The intervention is brief and focuses on helping patients develop skills in stress management, goal setting, positive reframing, and benefit finding.
The clinical evaluation of PRISM presented at the symposium included 100 English-speaking patients aged 12-25 who had new or recently recurrent cancer. They were randomized to the skills-based intervention or standard psychosocial care.
In the PRISM group, the adolescents and young adults participated in four in-person one-on-one training sessions lasting 30-60 minutes, plus a facilitated family meeting. Patients were surveyed at baseline and again at 6 months to measure the impact of the intervention.
A total of 36 patients in the PRISM arm and 38 in the usual-care arm completed the study. Most attrition was due to medical complications or death, the investigators said.
Results showed that, compared with standard psychosocial care, the skills-based intervention was associated with significant improvements in resilience (+2.3; 95% confidence interval, 0.7-4.0), hope (+2.8; 95% CI, 0.5-5.1), quality of life (+6.3; 95% CI, –0.8-13.5), and a trend toward less distress (–1.6; 95% CI –3.3-0.0).
Fewer cases of depression occurred in the PRISM group compared with the standard care group (two versus eight cases), Dr. Rosenberg added.
The psychosocial toll of cancer can be significant, especially in a vulnerable population such as adolescents and young adults, according to Andrew S. Epstein, MD, of Memorial Sloan Kettering Cancer Center, New York. “The intervention by Rosenberg and her coauthors represents an important beacon of hope for improving the cancer experience for this population,” Dr. Epstein said.
Compared with standard psychosocial care, a one-on-one skills-based intervention improved psychosocial outcomes in adolescents and young adults with cancer, according to results of a pilot randomized study presented at the Palliative and Supportive Care in Oncology Symposium.
The novel intervention was associated with improved patient resilience, cancer-specific quality of life, and hope, plus fewer cases of depression, said lead study author Abby R. Rosenberg, MD, director of palliative care and resilience research at Seattle Children’s Research Institute.
Brief, developmentally-targeted psychosocial interventions are promising for this population of adolescents and young adults with cancer, Dr. Rosenberg said in a press conference at the symposium, which was cosponsored by AAHPM, ASCO, ASTRO, and MASCC.
Adolescents and young adults with cancer tend to have poor psychosocial outcomes, possibly because they have not yet developed skills that would help them manage hardships they encounter as a result of having cancer, according to Dr. Rosenberg.
She and her colleagues previously designed and tested the intervention, called Promoting Resilience in Stress Management (PRISM). The intervention is brief and focuses on helping patients develop skills in stress management, goal setting, positive reframing, and benefit finding.
The clinical evaluation of PRISM presented at the symposium included 100 English-speaking patients aged 12-25 who had new or recently recurrent cancer. They were randomized to the skills-based intervention or standard psychosocial care.
In the PRISM group, the adolescents and young adults participated in four in-person one-on-one training sessions lasting 30-60 minutes, plus a facilitated family meeting. Patients were surveyed at baseline and again at 6 months to measure the impact of the intervention.
A total of 36 patients in the PRISM arm and 38 in the usual-care arm completed the study. Most attrition was due to medical complications or death, the investigators said.
Results showed that, compared with standard psychosocial care, the skills-based intervention was associated with significant improvements in resilience (+2.3; 95% confidence interval, 0.7-4.0), hope (+2.8; 95% CI, 0.5-5.1), quality of life (+6.3; 95% CI, –0.8-13.5), and a trend toward less distress (–1.6; 95% CI –3.3-0.0).
Fewer cases of depression occurred in the PRISM group compared with the standard care group (two versus eight cases), Dr. Rosenberg added.
The psychosocial toll of cancer can be significant, especially in a vulnerable population such as adolescents and young adults, according to Andrew S. Epstein, MD, of Memorial Sloan Kettering Cancer Center, New York. “The intervention by Rosenberg and her coauthors represents an important beacon of hope for improving the cancer experience for this population,” Dr. Epstein said.
Compared with standard psychosocial care, a one-on-one skills-based intervention improved psychosocial outcomes in adolescents and young adults with cancer, according to results of a pilot randomized study presented at the Palliative and Supportive Care in Oncology Symposium.
The novel intervention was associated with improved patient resilience, cancer-specific quality of life, and hope, plus fewer cases of depression, said lead study author Abby R. Rosenberg, MD, director of palliative care and resilience research at Seattle Children’s Research Institute.
Brief, developmentally-targeted psychosocial interventions are promising for this population of adolescents and young adults with cancer, Dr. Rosenberg said in a press conference at the symposium, which was cosponsored by AAHPM, ASCO, ASTRO, and MASCC.
Adolescents and young adults with cancer tend to have poor psychosocial outcomes, possibly because they have not yet developed skills that would help them manage hardships they encounter as a result of having cancer, according to Dr. Rosenberg.
She and her colleagues previously designed and tested the intervention, called Promoting Resilience in Stress Management (PRISM). The intervention is brief and focuses on helping patients develop skills in stress management, goal setting, positive reframing, and benefit finding.
The clinical evaluation of PRISM presented at the symposium included 100 English-speaking patients aged 12-25 who had new or recently recurrent cancer. They were randomized to the skills-based intervention or standard psychosocial care.
In the PRISM group, the adolescents and young adults participated in four in-person one-on-one training sessions lasting 30-60 minutes, plus a facilitated family meeting. Patients were surveyed at baseline and again at 6 months to measure the impact of the intervention.
A total of 36 patients in the PRISM arm and 38 in the usual-care arm completed the study. Most attrition was due to medical complications or death, the investigators said.
Results showed that, compared with standard psychosocial care, the skills-based intervention was associated with significant improvements in resilience (+2.3; 95% confidence interval, 0.7-4.0), hope (+2.8; 95% CI, 0.5-5.1), quality of life (+6.3; 95% CI, –0.8-13.5), and a trend toward less distress (–1.6; 95% CI –3.3-0.0).
Fewer cases of depression occurred in the PRISM group compared with the standard care group (two versus eight cases), Dr. Rosenberg added.
The psychosocial toll of cancer can be significant, especially in a vulnerable population such as adolescents and young adults, according to Andrew S. Epstein, MD, of Memorial Sloan Kettering Cancer Center, New York. “The intervention by Rosenberg and her coauthors represents an important beacon of hope for improving the cancer experience for this population,” Dr. Epstein said.
FROM PALLONC 2017
Key clinical point: A one-on-one skills-based intervention improved psychosocial outcomes, compared with standard psychosocial care, in adolescents and young adults with cancer.
Major finding: The skills-based intervention was associated with improvements in resilience (+2.3; 95% CI, 0.7-4.0), hope (+2.8; 95% CI, 0.5-5.1), quality of life (+6.3; 95% CI, –0.8-13.5), and distress (–1.6; 95% CI –3.3-0.0).
Data source: A pilot study of 100 English-speaking cancer patients aged 12-25 who were randomly assigned to the skills-based intervention or standard psychosocial care.
Disclosures: The study was partly funded by the National Institutes of Health. The authors reported having no financial disclosures.
ACIP recommends third MMR dose, if outbreak risk
The Advisory Committee on Immunization Practices voted Oct. 25 to recommend a 3rd dose of measles, mumps, and rubella (MMR) vaccine for individuals at mumps risk from an outbreak.
The recommendation applies to individuals who already have been vaccinated with the usual two doses of MMR “who are identified by public health as at increased risk for mumps because of an outbreak,” according to draft text of the recommendation. This practice would “improve protection against mumps disease and related complications.”
Young adults are at highest risk, she said.
Key evidence supporting the ACIP’s recommendation includes one recent study suggesting a 3rd dose of MMR is effective for mumps outbreak control (N Engl J Med. 2017 Sep 7; doi: 10.1056/NEJMoa1703309).
In that study, Cristina V. Cardemil, MD, of the CDC, and her colleagues looked at college students who received a 3rd MMR dose during an outbreak of at the University of Iowa in Iowa City. Almost a quarter of students (4,783 of 20,496) enrolled in the 2015-2016 academic year received a 3rd dose. Compared with two doses of MMR, students receiving three total doses had a 78% lower risk of mumps at 28 days after vaccination, investigators reported.
“These findings suggest that the campaign to administer a 3rd dose of MMR vaccine improved mumps outbreak control and that waning immunity probably contributed to propagation of the outbreak,” Dr. Cardemil and her colleagues wrote.
The vote in favor of a 3rd dose was unanimous among 15 voting members of ACIP. The committee’s recommendations must be approved by the CDC director before they are considered official recommendations.
The Advisory Committee on Immunization Practices voted Oct. 25 to recommend a 3rd dose of measles, mumps, and rubella (MMR) vaccine for individuals at mumps risk from an outbreak.
The recommendation applies to individuals who already have been vaccinated with the usual two doses of MMR “who are identified by public health as at increased risk for mumps because of an outbreak,” according to draft text of the recommendation. This practice would “improve protection against mumps disease and related complications.”
Young adults are at highest risk, she said.
Key evidence supporting the ACIP’s recommendation includes one recent study suggesting a 3rd dose of MMR is effective for mumps outbreak control (N Engl J Med. 2017 Sep 7; doi: 10.1056/NEJMoa1703309).
In that study, Cristina V. Cardemil, MD, of the CDC, and her colleagues looked at college students who received a 3rd MMR dose during an outbreak of at the University of Iowa in Iowa City. Almost a quarter of students (4,783 of 20,496) enrolled in the 2015-2016 academic year received a 3rd dose. Compared with two doses of MMR, students receiving three total doses had a 78% lower risk of mumps at 28 days after vaccination, investigators reported.
“These findings suggest that the campaign to administer a 3rd dose of MMR vaccine improved mumps outbreak control and that waning immunity probably contributed to propagation of the outbreak,” Dr. Cardemil and her colleagues wrote.
The vote in favor of a 3rd dose was unanimous among 15 voting members of ACIP. The committee’s recommendations must be approved by the CDC director before they are considered official recommendations.
The Advisory Committee on Immunization Practices voted Oct. 25 to recommend a 3rd dose of measles, mumps, and rubella (MMR) vaccine for individuals at mumps risk from an outbreak.
The recommendation applies to individuals who already have been vaccinated with the usual two doses of MMR “who are identified by public health as at increased risk for mumps because of an outbreak,” according to draft text of the recommendation. This practice would “improve protection against mumps disease and related complications.”
Young adults are at highest risk, she said.
Key evidence supporting the ACIP’s recommendation includes one recent study suggesting a 3rd dose of MMR is effective for mumps outbreak control (N Engl J Med. 2017 Sep 7; doi: 10.1056/NEJMoa1703309).
In that study, Cristina V. Cardemil, MD, of the CDC, and her colleagues looked at college students who received a 3rd MMR dose during an outbreak of at the University of Iowa in Iowa City. Almost a quarter of students (4,783 of 20,496) enrolled in the 2015-2016 academic year received a 3rd dose. Compared with two doses of MMR, students receiving three total doses had a 78% lower risk of mumps at 28 days after vaccination, investigators reported.
“These findings suggest that the campaign to administer a 3rd dose of MMR vaccine improved mumps outbreak control and that waning immunity probably contributed to propagation of the outbreak,” Dr. Cardemil and her colleagues wrote.
The vote in favor of a 3rd dose was unanimous among 15 voting members of ACIP. The committee’s recommendations must be approved by the CDC director before they are considered official recommendations.
AT AN ACIP MEETING
Conjugate typhoid vaccine safe and effective in phase 2 trials
A new conjugate typhoid vaccine suitable for administration to infants and young children was efficacious, highly immunogenic, and well tolerated, compared with placebo, in a phase 2 study that tested the vaccine using a human typhoid infection model.
In a study that compared two formulations of typhoid vaccine to a control meningococcal vaccine, the new Vi-conjugate (Vi-TT) vaccine had an efficacy of 54.6% (95% confidence interval, 26.8-71.8) and a 100% seroconversion rate.
The study was not powered for a direct comparison of the efficacy of the Vi-TT with the efficacy of the Vi-polysaccharide (Vi-PS), the other vaccine used in the study. The Vi-PS vaccine had an efficacy of 52.0% (95% CI, 23.2-70.0), and 88.6% of the Vi-PS recipients had seroconversion.
However, “clinical manifestations of typhoid fever seemed less severe among diagnosed participants following Vi-TT vaccination,” Celina Jin, MD, and her colleagues wrote (Lancet. 2017 Sep 28: doi: 10.1016/S0140-6736[17]32149-9). Fever, defined as an oral temperature of 38° C or higher, was seen in 6 of 37 (16%) Vi-TT recipients, 17 of 31 (55%) receiving control, and 11 of 35 (31%) receiving Vi-PS.
Geometric mean titers also were significantly higher in the Vi-TT group than in the Vi-PS group, with an adjusted geometric mean titer of 562.9 EU/mL for Vi-TT and 140.5 EU/mL for Vi-PS (P less than .0001).
The study enrolled 112 healthy adult volunteers who were randomized 1:1:1 to receive Vi-PS, Vi-TT, or control meningococcal vaccine. A total of 103 of the participants eventually received one of the two study vaccines or the control vaccines, and that group was included in the per-protocol analysis.
After vaccination (recipients and investigators were masked as to which formulation participants received), study participants kept an online diary to report any vaccination-related symptoms for 7 days, and also had clinic visits scheduled at days 1, 3, 7, and 10.
Participants received one oral dose of wild-type Salmonella enterica serovar Typhi Quailes strain bacteria about 1 month after vaccination. The dose was 1-5x104 colony forming units, and was administered immediately following a 120-mL oral bolus of sodium bicarbonate (to neutralize stomach acid).
Participants then were seen daily in an outpatient clinic for 2 weeks. At each visit, investigators monitored vital signs, performed a general assessment, and drew blood to assess for typhoid bacteremia. Participants also kept an online diary for 21 days, reporting twice-daily self-measured temperatures as well. No antipyretics were allowed before typhoid diagnosis.
Participants who met the study’s criteria for typhoid diagnosis were treated with a 2-week course of ciprofloxacin or azithromycin; patients who did not become ill were treated 14 days after the oral typhoid challenge. None of the four serious adverse events reported during the study was deemed to be related to vaccination.
That broad definition of typhoid infection was used to determine attack rates for the study’s primary outcome measure. However, Dr. Jin and her colleagues also looked at a less stringent – and perhaps more clinically pertinent – definition of 12 hours of fever of 38° C or higher followed by S. Typhi bacteremia. Using those criteria, the Vi-TT vaccine prevented up to 87% of infections.
Salmonella Typhi is the world’s leading cause of enteric fever, said Dr. Jin, of the Oxford Vaccine Group at the University of Oxford (England). Up to 20.6 million people per year are affected, with children most commonly infected and low-resource populations in Asia and Africa hardest hit.
Both prescription and over-the-counter antibiotics are used worldwide to combat typhoid fever, and S. Typhi strains are becoming increasingly antibiotic resistant in South Asia and Africa, Dr. Jin and her coauthors said.
The typhoid vaccines that are currently licensed are either not suitable for administration to infants and young children, or are insufficiently immunogenic in younger populations.
The typhoid conjugate vaccine used in the study combines the Vi-polysaccharide capsule with a protein carrier, increasing host immunologic response and making the vaccine effective in infancy.
“This human challenge study provides further evidence to support the deployment of Vi-conjugate vaccines as a control measure to reduce the burden of typhoid fever, because those individuals living in endemic regions should not be made to wait another 60 years,” wrote Dr. Jin and her coauthors.
The study was funded by the Bill & Melinda Gates Foundation and the European commission FP7 grant, Advanced Immunization Technologies.
The Oxford Vaccine Group has developed a typhoid challenge model that provides an important bridge in clinical testing and affords the possibility of significant acceleration of the vaccine development process. Despite the controversy human challenge models sometimes engender, previous human typhoid challenge studies contributed to the development of the live attenuated typhoid vaccine Ty21a.
The conjugate vaccine tested by Dr. Jin and her colleagues is a much-needed weapon in the public health armamentarium of typhoid control. Treatment options are limited in regions of South Asia and Africa where endemic typhoid shows increasing antibiotic resistance.
This human challenge study provides the first evidence that the conjugate vaccine reduces the attack rate of typhoid fever, though its use in India has shown it to be safe and immunogenic, even in children as young as 6 months of age.
The stringent definition of typhoid fever attack used in this study may result in a finding of lower efficacy than would be seen in a field trial, and a National Institutes of Health–sponsored study of another conjugate vaccine found efficacy rates of 89% among Vietnamese preschoolers followed for nearly 4 years after vaccination. When the present study’s data were reanalyzed with use of the less stringent case definition of fever followed by typhoid bacteremia, a similar efficacy of 87.1% was seen for the conjugate vaccine. A larger sample size would be needed in a challenge study that included the less stringent definition as a coprimary endpoint, but results might better correlate with real-world field trials.
Phase 3 and 4 trials for the typhoid conjugate vaccine are forthcoming, but final results will not be tallied for many years. The typhoid challenge study reported by Dr. Jin and her colleagues bolsters hopes that the candidate vaccine will help with typhoid control where it’s most needed.
Nicholas A. Feasey, MD , is at the Liverpool (England) School of Tropical Medicine. Myron M. Levine, MD , is at the University of Maryland, Baltimore. Their comments were drawn from an editorial accompanying the study (Lancet. 2017 Sep 28. doi: 10.1016/S0140-6736[17]32407-8 ).
The Oxford Vaccine Group has developed a typhoid challenge model that provides an important bridge in clinical testing and affords the possibility of significant acceleration of the vaccine development process. Despite the controversy human challenge models sometimes engender, previous human typhoid challenge studies contributed to the development of the live attenuated typhoid vaccine Ty21a.
The conjugate vaccine tested by Dr. Jin and her colleagues is a much-needed weapon in the public health armamentarium of typhoid control. Treatment options are limited in regions of South Asia and Africa where endemic typhoid shows increasing antibiotic resistance.
This human challenge study provides the first evidence that the conjugate vaccine reduces the attack rate of typhoid fever, though its use in India has shown it to be safe and immunogenic, even in children as young as 6 months of age.
The stringent definition of typhoid fever attack used in this study may result in a finding of lower efficacy than would be seen in a field trial, and a National Institutes of Health–sponsored study of another conjugate vaccine found efficacy rates of 89% among Vietnamese preschoolers followed for nearly 4 years after vaccination. When the present study’s data were reanalyzed with use of the less stringent case definition of fever followed by typhoid bacteremia, a similar efficacy of 87.1% was seen for the conjugate vaccine. A larger sample size would be needed in a challenge study that included the less stringent definition as a coprimary endpoint, but results might better correlate with real-world field trials.
Phase 3 and 4 trials for the typhoid conjugate vaccine are forthcoming, but final results will not be tallied for many years. The typhoid challenge study reported by Dr. Jin and her colleagues bolsters hopes that the candidate vaccine will help with typhoid control where it’s most needed.
Nicholas A. Feasey, MD , is at the Liverpool (England) School of Tropical Medicine. Myron M. Levine, MD , is at the University of Maryland, Baltimore. Their comments were drawn from an editorial accompanying the study (Lancet. 2017 Sep 28. doi: 10.1016/S0140-6736[17]32407-8 ).
The Oxford Vaccine Group has developed a typhoid challenge model that provides an important bridge in clinical testing and affords the possibility of significant acceleration of the vaccine development process. Despite the controversy human challenge models sometimes engender, previous human typhoid challenge studies contributed to the development of the live attenuated typhoid vaccine Ty21a.
The conjugate vaccine tested by Dr. Jin and her colleagues is a much-needed weapon in the public health armamentarium of typhoid control. Treatment options are limited in regions of South Asia and Africa where endemic typhoid shows increasing antibiotic resistance.
This human challenge study provides the first evidence that the conjugate vaccine reduces the attack rate of typhoid fever, though its use in India has shown it to be safe and immunogenic, even in children as young as 6 months of age.
The stringent definition of typhoid fever attack used in this study may result in a finding of lower efficacy than would be seen in a field trial, and a National Institutes of Health–sponsored study of another conjugate vaccine found efficacy rates of 89% among Vietnamese preschoolers followed for nearly 4 years after vaccination. When the present study’s data were reanalyzed with use of the less stringent case definition of fever followed by typhoid bacteremia, a similar efficacy of 87.1% was seen for the conjugate vaccine. A larger sample size would be needed in a challenge study that included the less stringent definition as a coprimary endpoint, but results might better correlate with real-world field trials.
Phase 3 and 4 trials for the typhoid conjugate vaccine are forthcoming, but final results will not be tallied for many years. The typhoid challenge study reported by Dr. Jin and her colleagues bolsters hopes that the candidate vaccine will help with typhoid control where it’s most needed.
Nicholas A. Feasey, MD , is at the Liverpool (England) School of Tropical Medicine. Myron M. Levine, MD , is at the University of Maryland, Baltimore. Their comments were drawn from an editorial accompanying the study (Lancet. 2017 Sep 28. doi: 10.1016/S0140-6736[17]32407-8 ).
A new conjugate typhoid vaccine suitable for administration to infants and young children was efficacious, highly immunogenic, and well tolerated, compared with placebo, in a phase 2 study that tested the vaccine using a human typhoid infection model.
In a study that compared two formulations of typhoid vaccine to a control meningococcal vaccine, the new Vi-conjugate (Vi-TT) vaccine had an efficacy of 54.6% (95% confidence interval, 26.8-71.8) and a 100% seroconversion rate.
The study was not powered for a direct comparison of the efficacy of the Vi-TT with the efficacy of the Vi-polysaccharide (Vi-PS), the other vaccine used in the study. The Vi-PS vaccine had an efficacy of 52.0% (95% CI, 23.2-70.0), and 88.6% of the Vi-PS recipients had seroconversion.
However, “clinical manifestations of typhoid fever seemed less severe among diagnosed participants following Vi-TT vaccination,” Celina Jin, MD, and her colleagues wrote (Lancet. 2017 Sep 28: doi: 10.1016/S0140-6736[17]32149-9). Fever, defined as an oral temperature of 38° C or higher, was seen in 6 of 37 (16%) Vi-TT recipients, 17 of 31 (55%) receiving control, and 11 of 35 (31%) receiving Vi-PS.
Geometric mean titers also were significantly higher in the Vi-TT group than in the Vi-PS group, with an adjusted geometric mean titer of 562.9 EU/mL for Vi-TT and 140.5 EU/mL for Vi-PS (P less than .0001).
The study enrolled 112 healthy adult volunteers who were randomized 1:1:1 to receive Vi-PS, Vi-TT, or control meningococcal vaccine. A total of 103 of the participants eventually received one of the two study vaccines or the control vaccines, and that group was included in the per-protocol analysis.
After vaccination (recipients and investigators were masked as to which formulation participants received), study participants kept an online diary to report any vaccination-related symptoms for 7 days, and also had clinic visits scheduled at days 1, 3, 7, and 10.
Participants received one oral dose of wild-type Salmonella enterica serovar Typhi Quailes strain bacteria about 1 month after vaccination. The dose was 1-5x104 colony forming units, and was administered immediately following a 120-mL oral bolus of sodium bicarbonate (to neutralize stomach acid).
Participants then were seen daily in an outpatient clinic for 2 weeks. At each visit, investigators monitored vital signs, performed a general assessment, and drew blood to assess for typhoid bacteremia. Participants also kept an online diary for 21 days, reporting twice-daily self-measured temperatures as well. No antipyretics were allowed before typhoid diagnosis.
Participants who met the study’s criteria for typhoid diagnosis were treated with a 2-week course of ciprofloxacin or azithromycin; patients who did not become ill were treated 14 days after the oral typhoid challenge. None of the four serious adverse events reported during the study was deemed to be related to vaccination.
That broad definition of typhoid infection was used to determine attack rates for the study’s primary outcome measure. However, Dr. Jin and her colleagues also looked at a less stringent – and perhaps more clinically pertinent – definition of 12 hours of fever of 38° C or higher followed by S. Typhi bacteremia. Using those criteria, the Vi-TT vaccine prevented up to 87% of infections.
Salmonella Typhi is the world’s leading cause of enteric fever, said Dr. Jin, of the Oxford Vaccine Group at the University of Oxford (England). Up to 20.6 million people per year are affected, with children most commonly infected and low-resource populations in Asia and Africa hardest hit.
Both prescription and over-the-counter antibiotics are used worldwide to combat typhoid fever, and S. Typhi strains are becoming increasingly antibiotic resistant in South Asia and Africa, Dr. Jin and her coauthors said.
The typhoid vaccines that are currently licensed are either not suitable for administration to infants and young children, or are insufficiently immunogenic in younger populations.
The typhoid conjugate vaccine used in the study combines the Vi-polysaccharide capsule with a protein carrier, increasing host immunologic response and making the vaccine effective in infancy.
“This human challenge study provides further evidence to support the deployment of Vi-conjugate vaccines as a control measure to reduce the burden of typhoid fever, because those individuals living in endemic regions should not be made to wait another 60 years,” wrote Dr. Jin and her coauthors.
The study was funded by the Bill & Melinda Gates Foundation and the European commission FP7 grant, Advanced Immunization Technologies.
A new conjugate typhoid vaccine suitable for administration to infants and young children was efficacious, highly immunogenic, and well tolerated, compared with placebo, in a phase 2 study that tested the vaccine using a human typhoid infection model.
In a study that compared two formulations of typhoid vaccine to a control meningococcal vaccine, the new Vi-conjugate (Vi-TT) vaccine had an efficacy of 54.6% (95% confidence interval, 26.8-71.8) and a 100% seroconversion rate.
The study was not powered for a direct comparison of the efficacy of the Vi-TT with the efficacy of the Vi-polysaccharide (Vi-PS), the other vaccine used in the study. The Vi-PS vaccine had an efficacy of 52.0% (95% CI, 23.2-70.0), and 88.6% of the Vi-PS recipients had seroconversion.
However, “clinical manifestations of typhoid fever seemed less severe among diagnosed participants following Vi-TT vaccination,” Celina Jin, MD, and her colleagues wrote (Lancet. 2017 Sep 28: doi: 10.1016/S0140-6736[17]32149-9). Fever, defined as an oral temperature of 38° C or higher, was seen in 6 of 37 (16%) Vi-TT recipients, 17 of 31 (55%) receiving control, and 11 of 35 (31%) receiving Vi-PS.
Geometric mean titers also were significantly higher in the Vi-TT group than in the Vi-PS group, with an adjusted geometric mean titer of 562.9 EU/mL for Vi-TT and 140.5 EU/mL for Vi-PS (P less than .0001).
The study enrolled 112 healthy adult volunteers who were randomized 1:1:1 to receive Vi-PS, Vi-TT, or control meningococcal vaccine. A total of 103 of the participants eventually received one of the two study vaccines or the control vaccines, and that group was included in the per-protocol analysis.
After vaccination (recipients and investigators were masked as to which formulation participants received), study participants kept an online diary to report any vaccination-related symptoms for 7 days, and also had clinic visits scheduled at days 1, 3, 7, and 10.
Participants received one oral dose of wild-type Salmonella enterica serovar Typhi Quailes strain bacteria about 1 month after vaccination. The dose was 1-5x104 colony forming units, and was administered immediately following a 120-mL oral bolus of sodium bicarbonate (to neutralize stomach acid).
Participants then were seen daily in an outpatient clinic for 2 weeks. At each visit, investigators monitored vital signs, performed a general assessment, and drew blood to assess for typhoid bacteremia. Participants also kept an online diary for 21 days, reporting twice-daily self-measured temperatures as well. No antipyretics were allowed before typhoid diagnosis.
Participants who met the study’s criteria for typhoid diagnosis were treated with a 2-week course of ciprofloxacin or azithromycin; patients who did not become ill were treated 14 days after the oral typhoid challenge. None of the four serious adverse events reported during the study was deemed to be related to vaccination.
That broad definition of typhoid infection was used to determine attack rates for the study’s primary outcome measure. However, Dr. Jin and her colleagues also looked at a less stringent – and perhaps more clinically pertinent – definition of 12 hours of fever of 38° C or higher followed by S. Typhi bacteremia. Using those criteria, the Vi-TT vaccine prevented up to 87% of infections.
Salmonella Typhi is the world’s leading cause of enteric fever, said Dr. Jin, of the Oxford Vaccine Group at the University of Oxford (England). Up to 20.6 million people per year are affected, with children most commonly infected and low-resource populations in Asia and Africa hardest hit.
Both prescription and over-the-counter antibiotics are used worldwide to combat typhoid fever, and S. Typhi strains are becoming increasingly antibiotic resistant in South Asia and Africa, Dr. Jin and her coauthors said.
The typhoid vaccines that are currently licensed are either not suitable for administration to infants and young children, or are insufficiently immunogenic in younger populations.
The typhoid conjugate vaccine used in the study combines the Vi-polysaccharide capsule with a protein carrier, increasing host immunologic response and making the vaccine effective in infancy.
“This human challenge study provides further evidence to support the deployment of Vi-conjugate vaccines as a control measure to reduce the burden of typhoid fever, because those individuals living in endemic regions should not be made to wait another 60 years,” wrote Dr. Jin and her coauthors.
The study was funded by the Bill & Melinda Gates Foundation and the European commission FP7 grant, Advanced Immunization Technologies.
FROM THE LANCET
Key clinical point: A conjugate typhoid vaccine significantly reduced typhoid fever rates under a stringent case definition.
Major finding: Efficacy was 54.6% for the Vi-conjugate vaccine, with 100% seroconversion.
Study details: Randomized, controlled phase 2b trial of 112 participants receiving one of two typhoid vaccines, or control meningococcal vaccine.
Disclosures: The study was funded by the Bill & Melinda Gates Foundation and the European Commission FP7 grant, Advanced Immunization Technologies.
CHEST Physician’s planned coverage of CHEST 2017
CHEST Physician is providing on-site coverage of the CHEST annual meeting in Toronto from Oct. 29 through Nov. 1.
We are planning to share findings from the latest research on treating COPD, sleep apnea, pulmonary hypertension, severe asthma, and other diseases that are part of pulmonary, critical care, and sleep medicine. Any improved methods for managing an ICU and updated recommendations on screening for lung cancer will also be on our radar.
The meeting’s agenda includes presentations of hundreds of study abstracts, and we thought you would be interested in hearing which ones grabbed the attention of some of CHEST Physician’s editorial advisory board members.
Board member Susan L. Millard, MD, FCCP, suggested attendees check out presentations of the following two studies:
- Impact of Race on Quality of Life of Families of Children with Asthma when Asthma Guidelines are Followed: Long-Term Follow-Up
- Results Of A Phase 3, Multicenter, Randomized, Placebo-controlled Trial of Remimazolam: A New Ultra Short Acting Benzodiazepine for Bronchoscopy
The first study is part of a session entitled Pediatrics, scheduled to run from 3:15 to 4:15 p.m. on Sunday, Oct. 29, in Convention Center - 606. Shahid Sheikh, MD, of Nationwide Children’s Hospital in New Albany, Ohio, is scheduled to present the abstract at 4:00 p.m.
Dr. Millard, who is Therapeutic Development Network director for the Pediatric CF Care Center and director of research for pediatric pulmonary and sleep medicine at the Helen DeVos Children’s Hospital in Grand Rapids, Mich., noted that she is interested in Dr. Sheikh’s research, “because cultural diversity is such a hot topic in general.”
Her other recommendation is part of the Late Breaking Abstracts 2 session, scheduled to occur on Wednesday, Nov. 1, from 2:45 to 4:15 p.m. in Convention Center - 603. CHEST President, Gerard A. Silvestri, MD, MS, FCCP, will present the abstract at 4:00 p.m.
Dr. Millard said she is interested in this study, because new drug options are so helpful for the frequently performed bronchoscopy.
Two sleep medicine experts on CHEST Physician’s editorial advisory board also selected a few presentations they expect to be newsworthy.
David Schulman, MD, MPH, FCCP, and professor of medicine at Emory University School of Medicine in Atlanta suggested CHEST Physician cover the following studies:
- Results of a Randomized, Placebo-Controlled, Double-Blind, 12-Week, Multicenter Study of JZP-110 for the Treatment Of Excessive Sleepiness in Patients with OSA, scheduled to be presented on Sunday, Oct. 29, at 1:30 p.m. in Convention Center - 601A. Dr. Kingman Strohl, MD, FCCP, of University Hospitals Case Medical Center-Sleep Center in Shaker Heights, Ohio, will present this research during a session entitled, Obstructive Sleep Apnea: Insights & Management, running from 1:30 to 3:00 p.m.
- History of Sleep Apnea and Cardiovascular Disease may Portend Improved Mortality in Patients With Acute Ischemic Stroke, scheduled to be presented on Tuesday, Oct. 31, at 11:15 a.m., in Convention Center - 601A. Nura Festic will present this research during the session, “Sleep, Heart, Brain and More,” running from 11:00 a.m. to 12:15 p.m.
- Ischemic Preconditioning in OSA Patients Manifested after Surviving a Cardiac Arrest? John Moss, MD, of Jacksonville, Fla., will present this study on Tuesday, Oct. 31, at 11:30 a.m., in Convention Center - 601A as part of the session “Sleep, Heart, Brain and More.”
Krishna M. Sundar, MD, FCCP, also recommended that CHEST Physician cover “A Prospective Cohort Study of Endothelial Function and its Relationship to Aspirin Responsiveness in OSA Patients.” Lirim Krveshi is scheduled to present this study on Sunday, Oct. 29, at 1:45 p.m. in Convention Center - 601A. This presentation is part of the Obstructive Sleep Apnea: Insights & Management session.
Dr. Sundar is an associate clinical professor of pulmonary, critical care and sleep medicine and medical director of the Sleep-Wake Center at the University of Utah, Salt Lake City.
To view the full agenda of the CHEST annual meeting, visit: chestmeeting.chestnet.org.
Look for CHEST Physician’s coverage of CHEST 2017 on our conference coverage page.
CHEST Physician is providing on-site coverage of the CHEST annual meeting in Toronto from Oct. 29 through Nov. 1.
We are planning to share findings from the latest research on treating COPD, sleep apnea, pulmonary hypertension, severe asthma, and other diseases that are part of pulmonary, critical care, and sleep medicine. Any improved methods for managing an ICU and updated recommendations on screening for lung cancer will also be on our radar.
The meeting’s agenda includes presentations of hundreds of study abstracts, and we thought you would be interested in hearing which ones grabbed the attention of some of CHEST Physician’s editorial advisory board members.
Board member Susan L. Millard, MD, FCCP, suggested attendees check out presentations of the following two studies:
- Impact of Race on Quality of Life of Families of Children with Asthma when Asthma Guidelines are Followed: Long-Term Follow-Up
- Results Of A Phase 3, Multicenter, Randomized, Placebo-controlled Trial of Remimazolam: A New Ultra Short Acting Benzodiazepine for Bronchoscopy
The first study is part of a session entitled Pediatrics, scheduled to run from 3:15 to 4:15 p.m. on Sunday, Oct. 29, in Convention Center - 606. Shahid Sheikh, MD, of Nationwide Children’s Hospital in New Albany, Ohio, is scheduled to present the abstract at 4:00 p.m.
Dr. Millard, who is Therapeutic Development Network director for the Pediatric CF Care Center and director of research for pediatric pulmonary and sleep medicine at the Helen DeVos Children’s Hospital in Grand Rapids, Mich., noted that she is interested in Dr. Sheikh’s research, “because cultural diversity is such a hot topic in general.”
Her other recommendation is part of the Late Breaking Abstracts 2 session, scheduled to occur on Wednesday, Nov. 1, from 2:45 to 4:15 p.m. in Convention Center - 603. CHEST President, Gerard A. Silvestri, MD, MS, FCCP, will present the abstract at 4:00 p.m.
Dr. Millard said she is interested in this study, because new drug options are so helpful for the frequently performed bronchoscopy.
Two sleep medicine experts on CHEST Physician’s editorial advisory board also selected a few presentations they expect to be newsworthy.
David Schulman, MD, MPH, FCCP, and professor of medicine at Emory University School of Medicine in Atlanta suggested CHEST Physician cover the following studies:
- Results of a Randomized, Placebo-Controlled, Double-Blind, 12-Week, Multicenter Study of JZP-110 for the Treatment Of Excessive Sleepiness in Patients with OSA, scheduled to be presented on Sunday, Oct. 29, at 1:30 p.m. in Convention Center - 601A. Dr. Kingman Strohl, MD, FCCP, of University Hospitals Case Medical Center-Sleep Center in Shaker Heights, Ohio, will present this research during a session entitled, Obstructive Sleep Apnea: Insights & Management, running from 1:30 to 3:00 p.m.
- History of Sleep Apnea and Cardiovascular Disease may Portend Improved Mortality in Patients With Acute Ischemic Stroke, scheduled to be presented on Tuesday, Oct. 31, at 11:15 a.m., in Convention Center - 601A. Nura Festic will present this research during the session, “Sleep, Heart, Brain and More,” running from 11:00 a.m. to 12:15 p.m.
- Ischemic Preconditioning in OSA Patients Manifested after Surviving a Cardiac Arrest? John Moss, MD, of Jacksonville, Fla., will present this study on Tuesday, Oct. 31, at 11:30 a.m., in Convention Center - 601A as part of the session “Sleep, Heart, Brain and More.”
Krishna M. Sundar, MD, FCCP, also recommended that CHEST Physician cover “A Prospective Cohort Study of Endothelial Function and its Relationship to Aspirin Responsiveness in OSA Patients.” Lirim Krveshi is scheduled to present this study on Sunday, Oct. 29, at 1:45 p.m. in Convention Center - 601A. This presentation is part of the Obstructive Sleep Apnea: Insights & Management session.
Dr. Sundar is an associate clinical professor of pulmonary, critical care and sleep medicine and medical director of the Sleep-Wake Center at the University of Utah, Salt Lake City.
To view the full agenda of the CHEST annual meeting, visit: chestmeeting.chestnet.org.
Look for CHEST Physician’s coverage of CHEST 2017 on our conference coverage page.
CHEST Physician is providing on-site coverage of the CHEST annual meeting in Toronto from Oct. 29 through Nov. 1.
We are planning to share findings from the latest research on treating COPD, sleep apnea, pulmonary hypertension, severe asthma, and other diseases that are part of pulmonary, critical care, and sleep medicine. Any improved methods for managing an ICU and updated recommendations on screening for lung cancer will also be on our radar.
The meeting’s agenda includes presentations of hundreds of study abstracts, and we thought you would be interested in hearing which ones grabbed the attention of some of CHEST Physician’s editorial advisory board members.
Board member Susan L. Millard, MD, FCCP, suggested attendees check out presentations of the following two studies:
- Impact of Race on Quality of Life of Families of Children with Asthma when Asthma Guidelines are Followed: Long-Term Follow-Up
- Results Of A Phase 3, Multicenter, Randomized, Placebo-controlled Trial of Remimazolam: A New Ultra Short Acting Benzodiazepine for Bronchoscopy
The first study is part of a session entitled Pediatrics, scheduled to run from 3:15 to 4:15 p.m. on Sunday, Oct. 29, in Convention Center - 606. Shahid Sheikh, MD, of Nationwide Children’s Hospital in New Albany, Ohio, is scheduled to present the abstract at 4:00 p.m.
Dr. Millard, who is Therapeutic Development Network director for the Pediatric CF Care Center and director of research for pediatric pulmonary and sleep medicine at the Helen DeVos Children’s Hospital in Grand Rapids, Mich., noted that she is interested in Dr. Sheikh’s research, “because cultural diversity is such a hot topic in general.”
Her other recommendation is part of the Late Breaking Abstracts 2 session, scheduled to occur on Wednesday, Nov. 1, from 2:45 to 4:15 p.m. in Convention Center - 603. CHEST President, Gerard A. Silvestri, MD, MS, FCCP, will present the abstract at 4:00 p.m.
Dr. Millard said she is interested in this study, because new drug options are so helpful for the frequently performed bronchoscopy.
Two sleep medicine experts on CHEST Physician’s editorial advisory board also selected a few presentations they expect to be newsworthy.
David Schulman, MD, MPH, FCCP, and professor of medicine at Emory University School of Medicine in Atlanta suggested CHEST Physician cover the following studies:
- Results of a Randomized, Placebo-Controlled, Double-Blind, 12-Week, Multicenter Study of JZP-110 for the Treatment Of Excessive Sleepiness in Patients with OSA, scheduled to be presented on Sunday, Oct. 29, at 1:30 p.m. in Convention Center - 601A. Dr. Kingman Strohl, MD, FCCP, of University Hospitals Case Medical Center-Sleep Center in Shaker Heights, Ohio, will present this research during a session entitled, Obstructive Sleep Apnea: Insights & Management, running from 1:30 to 3:00 p.m.
- History of Sleep Apnea and Cardiovascular Disease may Portend Improved Mortality in Patients With Acute Ischemic Stroke, scheduled to be presented on Tuesday, Oct. 31, at 11:15 a.m., in Convention Center - 601A. Nura Festic will present this research during the session, “Sleep, Heart, Brain and More,” running from 11:00 a.m. to 12:15 p.m.
- Ischemic Preconditioning in OSA Patients Manifested after Surviving a Cardiac Arrest? John Moss, MD, of Jacksonville, Fla., will present this study on Tuesday, Oct. 31, at 11:30 a.m., in Convention Center - 601A as part of the session “Sleep, Heart, Brain and More.”
Krishna M. Sundar, MD, FCCP, also recommended that CHEST Physician cover “A Prospective Cohort Study of Endothelial Function and its Relationship to Aspirin Responsiveness in OSA Patients.” Lirim Krveshi is scheduled to present this study on Sunday, Oct. 29, at 1:45 p.m. in Convention Center - 601A. This presentation is part of the Obstructive Sleep Apnea: Insights & Management session.
Dr. Sundar is an associate clinical professor of pulmonary, critical care and sleep medicine and medical director of the Sleep-Wake Center at the University of Utah, Salt Lake City.
To view the full agenda of the CHEST annual meeting, visit: chestmeeting.chestnet.org.
Look for CHEST Physician’s coverage of CHEST 2017 on our conference coverage page.
FROM CHEST 2017
Vaccine renaissance
In 1967, pediatric patients were vaccinated routinely against eight diseases with 10 vaccines: smallpox; diphtheria; tetanus and pertussis; polio serotypes 1, 2, and 3; measles; rubella; and mumps. Then in 1989, vaccine discovery took a dramatic upward trend. For the physicians and scientists involved in vaccine discovery, the driving force may have been a passion for scientific discovery and a humanitarian motivation, but what drove this major change in pediatric infectious diseases was economics.

I believe The hiatus of more than 20 years between the introduction of the mumps vaccine in 1967 and that of the Hib vaccine in 1989 in my view was because the economic incentives to develop vaccines were absent. In fact, in the 1970s and early 1980s, vaccine manufacturers were drawing back from making vaccines because they were losing money selling them at a few dollars per dose.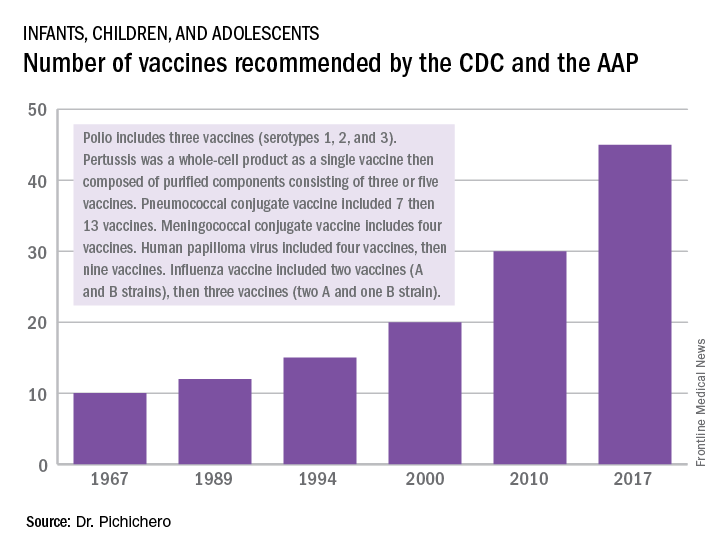
A trailblazing path had been created, and more and more vaccines have been discovered and come to market since then. Combination vaccines and vaccines for adolescents and adults have followed. The biggest blockbuster is Prevnar13 (actually 13 vaccines contained in a single combination), now with annual sales in excess of $7 billion worldwide and growing. Other vaccines with sales of a billion dollars or more are also on the market; anything in excess of $1 billion is considered a blockbuster in the pharmaceutical industry and gets the attention of CEOs (and investors) in a big way.

Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute at Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. He has received funding awarded to his institution for vaccine research from GlaxoSmithKline, Merck, Pfizer, and Sanofi Pasteur. Email him at pdnews@frontlinemedcom.com.
In 1967, pediatric patients were vaccinated routinely against eight diseases with 10 vaccines: smallpox; diphtheria; tetanus and pertussis; polio serotypes 1, 2, and 3; measles; rubella; and mumps. Then in 1989, vaccine discovery took a dramatic upward trend. For the physicians and scientists involved in vaccine discovery, the driving force may have been a passion for scientific discovery and a humanitarian motivation, but what drove this major change in pediatric infectious diseases was economics.
I believe The hiatus of more than 20 years between the introduction of the mumps vaccine in 1967 and that of the Hib vaccine in 1989 in my view was because the economic incentives to develop vaccines were absent. In fact, in the 1970s and early 1980s, vaccine manufacturers were drawing back from making vaccines because they were losing money selling them at a few dollars per dose.
A trailblazing path had been created, and more and more vaccines have been discovered and come to market since then. Combination vaccines and vaccines for adolescents and adults have followed. The biggest blockbuster is Prevnar13 (actually 13 vaccines contained in a single combination), now with annual sales in excess of $7 billion worldwide and growing. Other vaccines with sales of a billion dollars or more are also on the market; anything in excess of $1 billion is considered a blockbuster in the pharmaceutical industry and gets the attention of CEOs (and investors) in a big way.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute at Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. He has received funding awarded to his institution for vaccine research from GlaxoSmithKline, Merck, Pfizer, and Sanofi Pasteur. Email him at pdnews@frontlinemedcom.com.
In 1967, pediatric patients were vaccinated routinely against eight diseases with 10 vaccines: smallpox; diphtheria; tetanus and pertussis; polio serotypes 1, 2, and 3; measles; rubella; and mumps. Then in 1989, vaccine discovery took a dramatic upward trend. For the physicians and scientists involved in vaccine discovery, the driving force may have been a passion for scientific discovery and a humanitarian motivation, but what drove this major change in pediatric infectious diseases was economics.
I believe The hiatus of more than 20 years between the introduction of the mumps vaccine in 1967 and that of the Hib vaccine in 1989 in my view was because the economic incentives to develop vaccines were absent. In fact, in the 1970s and early 1980s, vaccine manufacturers were drawing back from making vaccines because they were losing money selling them at a few dollars per dose.
A trailblazing path had been created, and more and more vaccines have been discovered and come to market since then. Combination vaccines and vaccines for adolescents and adults have followed. The biggest blockbuster is Prevnar13 (actually 13 vaccines contained in a single combination), now with annual sales in excess of $7 billion worldwide and growing. Other vaccines with sales of a billion dollars or more are also on the market; anything in excess of $1 billion is considered a blockbuster in the pharmaceutical industry and gets the attention of CEOs (and investors) in a big way.
Dr. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute at Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. He has received funding awarded to his institution for vaccine research from GlaxoSmithKline, Merck, Pfizer, and Sanofi Pasteur. Email him at pdnews@frontlinemedcom.com.
Artemisinin: Its global impact on the treatment of malaria
Malaria remains a major international public health concern. In 2015, the World Health Organization estimated that 212 million individuals were infected and that there were 429,000 deaths. This represents a 21% decline in incidence globally and a 29% decline in global mortality between 2010 and 2015. In 2016, malaria was endemic in 91 countries and territories, down from 108 in 2000. Although malaria has been eliminated from the United States since the early 1950s, approximately 1,700 cases are reported annually, most of which occur in returned travelers, according to the Centers for Disease Control and Prevention.

Five species of Plasmodium (P. falciparum, P. vivax, P. malariae, P. ovale, and, more recently, P. knowelsi) account for most of the infections in humans and are transmitted by the bite of an infected female Anopheles mosquito. The disease is rarely acquired by blood transfusion, by needle sharing, by organ transplantation, or congenitally. Once diagnosed, malaria can be treated; however, delay in initiating therapy can lead to both serious and fatal outcomes.
Treatment
Historically, drug development was driven by the need to protect the military. While quinine was isolated from the bark of the cinchona tree in 1820, chloroquine, proguanil, mefloquine, and atovaquone each were developed during or after a military conflict during 1945-1985. Tetracycline/doxycycline and clindamycin also have antimalarial activity. Use of any of these agents as monotherapy has led to drug resistance and treatment failure.
Artemisinin
Artemisinin (also known as qinghao su) and its derivatives are a new class of antimalarials derived from the sweet wormwood plant Artemisia annua. Initially developed in China in the 1970s, this class gained global attention in the 1990s. and have the fastest parasite clearance time, rapid resolution of symptoms, and an excellent safety profile. They have activity against all Plasmodium species.
Because of artemisinins’ rapid elimination, they are used in combination with an agent that also kills blood parasites but has a slower elimination rate and a different mechanism of action. The goal is to prevent and delay the development of resistance and reduce recrudescence. The superiority of artemisinin-based combination therapy (ACT) over monotherapies has been documented.

Resistance, always a concern, has remained limited to specific areas in Southeast Asia since reported in 2008. Monitoring drug efficacy, safety, quality of antimalarials is ongoing, as is discouraging monotherapy use of these agents. Globally, artemisinins are the mainstay of treatment. Spread of resistance would be a major setback for both malaria control and elimination.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Malaria remains a major international public health concern. In 2015, the World Health Organization estimated that 212 million individuals were infected and that there were 429,000 deaths. This represents a 21% decline in incidence globally and a 29% decline in global mortality between 2010 and 2015. In 2016, malaria was endemic in 91 countries and territories, down from 108 in 2000. Although malaria has been eliminated from the United States since the early 1950s, approximately 1,700 cases are reported annually, most of which occur in returned travelers, according to the Centers for Disease Control and Prevention.
Five species of Plasmodium (P. falciparum, P. vivax, P. malariae, P. ovale, and, more recently, P. knowelsi) account for most of the infections in humans and are transmitted by the bite of an infected female Anopheles mosquito. The disease is rarely acquired by blood transfusion, by needle sharing, by organ transplantation, or congenitally. Once diagnosed, malaria can be treated; however, delay in initiating therapy can lead to both serious and fatal outcomes.
Treatment
Historically, drug development was driven by the need to protect the military. While quinine was isolated from the bark of the cinchona tree in 1820, chloroquine, proguanil, mefloquine, and atovaquone each were developed during or after a military conflict during 1945-1985. Tetracycline/doxycycline and clindamycin also have antimalarial activity. Use of any of these agents as monotherapy has led to drug resistance and treatment failure.
Artemisinin
Artemisinin (also known as qinghao su) and its derivatives are a new class of antimalarials derived from the sweet wormwood plant Artemisia annua. Initially developed in China in the 1970s, this class gained global attention in the 1990s. and have the fastest parasite clearance time, rapid resolution of symptoms, and an excellent safety profile. They have activity against all Plasmodium species.
Because of artemisinins’ rapid elimination, they are used in combination with an agent that also kills blood parasites but has a slower elimination rate and a different mechanism of action. The goal is to prevent and delay the development of resistance and reduce recrudescence. The superiority of artemisinin-based combination therapy (ACT) over monotherapies has been documented.
Resistance, always a concern, has remained limited to specific areas in Southeast Asia since reported in 2008. Monitoring drug efficacy, safety, quality of antimalarials is ongoing, as is discouraging monotherapy use of these agents. Globally, artemisinins are the mainstay of treatment. Spread of resistance would be a major setback for both malaria control and elimination.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
Malaria remains a major international public health concern. In 2015, the World Health Organization estimated that 212 million individuals were infected and that there were 429,000 deaths. This represents a 21% decline in incidence globally and a 29% decline in global mortality between 2010 and 2015. In 2016, malaria was endemic in 91 countries and territories, down from 108 in 2000. Although malaria has been eliminated from the United States since the early 1950s, approximately 1,700 cases are reported annually, most of which occur in returned travelers, according to the Centers for Disease Control and Prevention.
Five species of Plasmodium (P. falciparum, P. vivax, P. malariae, P. ovale, and, more recently, P. knowelsi) account for most of the infections in humans and are transmitted by the bite of an infected female Anopheles mosquito. The disease is rarely acquired by blood transfusion, by needle sharing, by organ transplantation, or congenitally. Once diagnosed, malaria can be treated; however, delay in initiating therapy can lead to both serious and fatal outcomes.
Treatment
Historically, drug development was driven by the need to protect the military. While quinine was isolated from the bark of the cinchona tree in 1820, chloroquine, proguanil, mefloquine, and atovaquone each were developed during or after a military conflict during 1945-1985. Tetracycline/doxycycline and clindamycin also have antimalarial activity. Use of any of these agents as monotherapy has led to drug resistance and treatment failure.
Artemisinin
Artemisinin (also known as qinghao su) and its derivatives are a new class of antimalarials derived from the sweet wormwood plant Artemisia annua. Initially developed in China in the 1970s, this class gained global attention in the 1990s. and have the fastest parasite clearance time, rapid resolution of symptoms, and an excellent safety profile. They have activity against all Plasmodium species.
Because of artemisinins’ rapid elimination, they are used in combination with an agent that also kills blood parasites but has a slower elimination rate and a different mechanism of action. The goal is to prevent and delay the development of resistance and reduce recrudescence. The superiority of artemisinin-based combination therapy (ACT) over monotherapies has been documented.
Resistance, always a concern, has remained limited to specific areas in Southeast Asia since reported in 2008. Monitoring drug efficacy, safety, quality of antimalarials is ongoing, as is discouraging monotherapy use of these agents. Globally, artemisinins are the mainstay of treatment. Spread of resistance would be a major setback for both malaria control and elimination.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@frontlinemedcom.com.
You can help with behavior of children with autism spectrum disorder
There are lots of reasons you may be eager to refer children with autism spectrum disorder (ASD) to specialty agencies. You want the fastest possible entry for the child into intervention and the families into a support system. , as well as the general health care, of their children.
“Wait!” you say, “I do not have the special knowledge to help with behavior of children with autism! There is much you can and should do, however, as the specialist(s) may not provide such guidance, entry into behavioral services may take months, and behavior issues may feel urgent to families.

So pick an example of a behavior that is concerning to the family. One problem might be lack of cooperation with activities of daily living such as eating. In this case, the A is being asked to stop playing and sit at the table; the B may be refusing to eat what is served or even to sit very long, ending in a tantrum that disrupts the family meal; and the C could be the child being sent from the table to play on their iPad. But what is the G?
Lack of social communication skills, restrictive interests, hypersensitivity, lack of coordination, and ADHD all may be playing a role. Lack of communication skills makes the social aspect of meals uninteresting. Giving verbal reasons for joining the family may not be effective. Hypersensitivity often is associated with extremes of food selectivity. Lack of fine motor coordination makes eating soup a challenge. And ADHD makes sitting for a long time difficult!

But what about that tantrum? Tantrums that are reinforced by allowing the child to leave and play on the iPad easily can turn into a chronic escape mechanism. Instead, parents need to watch for increasing restlessness, and allow the child to signal “all done” and be “excused” before any tantrum begins. Use of the iPad (a reward) should not be allowed until the family meal is over for everyone. Such accommodations are best decided on by all caregivers in advance, ideally also involving the higher-functioning child. A caregiver who persists in thinking that the child “should” be able to behave may be in denial or grief, and deserves counseling on ASD.
But he is so rigid, the parents say! The tendency of children with ASD to like sameness can be an asset to easing behavior. The key is to design and stick to routines as much as possible, 7 days per week. If the meal is at the same time each day, in the same seat, with the same plate, with no iPad, and the child is allowed to leave only after requesting to, the entire sequence is likely to be smoother. While flexibility does not come easily, it is acquired from the natural variability in family life, but only gradually and over time.
Creating and rehearsing “social stories” is an evidence-based way to help children with ASD have acceptable behaviors. Books, storyboards, and visual schedulers can be purchased to help. But even taking photos or a video of the components of a task and posting this online (private YouTube channel) or on the refrigerator, to review before, during, and/or after the activity, builds an internal image for the child. Children with ASD often watch the same YouTube videos over and over again, and even memorize and use chunks of the speech or songs at other times. Families can capitalize on this kind of repetition by using routines and songs to improve skills.
What to do when she only cares about her iPad? It is sometimes difficult to identify reinforcers to use to strengthen desired behaviors in a child with ASD. A smile or a hug or even candy may not be valued. Help parents think about an object, song, or touch the child tends to like. Media are a strong reinforcer, but need to be used sparingly, in specific situations, and kept under parental control, or else removing them can become a major source of upsets.
When a child with ASD gets upset or even violent, the behavior may be interpreted as defiance; it may scare or upset the whole family, and is not conducive to problem solving. Siblings may start screaming or begging for the parents to stop the behavior. While this creates a crisis, you can advise parents to first ensure that everyone is safe, take deep breaths, and then think about which gap is being stressed. A subtle change from what the child expected – new furniture, a guest at the table, a day off from school, or being interrupted mid video – can cause panic, especially for anxious children. Children with ASD also may act up when uncomfortable from a headache, tooth pain, constipation, hunger, or lack of sleep, but often are unable to vocalize the reason, even if they are verbal. Having parents make a few notes about the As, Bs, Cs, and Gs of each event (the essence of a functional behavioral assessment) to review with the child, each other, the teacher, or you is key to understanding the child with ASD and successfully shifting his behavior.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
There are lots of reasons you may be eager to refer children with autism spectrum disorder (ASD) to specialty agencies. You want the fastest possible entry for the child into intervention and the families into a support system. , as well as the general health care, of their children.
“Wait!” you say, “I do not have the special knowledge to help with behavior of children with autism! There is much you can and should do, however, as the specialist(s) may not provide such guidance, entry into behavioral services may take months, and behavior issues may feel urgent to families.
So pick an example of a behavior that is concerning to the family. One problem might be lack of cooperation with activities of daily living such as eating. In this case, the A is being asked to stop playing and sit at the table; the B may be refusing to eat what is served or even to sit very long, ending in a tantrum that disrupts the family meal; and the C could be the child being sent from the table to play on their iPad. But what is the G?
Lack of social communication skills, restrictive interests, hypersensitivity, lack of coordination, and ADHD all may be playing a role. Lack of communication skills makes the social aspect of meals uninteresting. Giving verbal reasons for joining the family may not be effective. Hypersensitivity often is associated with extremes of food selectivity. Lack of fine motor coordination makes eating soup a challenge. And ADHD makes sitting for a long time difficult!
But what about that tantrum? Tantrums that are reinforced by allowing the child to leave and play on the iPad easily can turn into a chronic escape mechanism. Instead, parents need to watch for increasing restlessness, and allow the child to signal “all done” and be “excused” before any tantrum begins. Use of the iPad (a reward) should not be allowed until the family meal is over for everyone. Such accommodations are best decided on by all caregivers in advance, ideally also involving the higher-functioning child. A caregiver who persists in thinking that the child “should” be able to behave may be in denial or grief, and deserves counseling on ASD.
But he is so rigid, the parents say! The tendency of children with ASD to like sameness can be an asset to easing behavior. The key is to design and stick to routines as much as possible, 7 days per week. If the meal is at the same time each day, in the same seat, with the same plate, with no iPad, and the child is allowed to leave only after requesting to, the entire sequence is likely to be smoother. While flexibility does not come easily, it is acquired from the natural variability in family life, but only gradually and over time.
Creating and rehearsing “social stories” is an evidence-based way to help children with ASD have acceptable behaviors. Books, storyboards, and visual schedulers can be purchased to help. But even taking photos or a video of the components of a task and posting this online (private YouTube channel) or on the refrigerator, to review before, during, and/or after the activity, builds an internal image for the child. Children with ASD often watch the same YouTube videos over and over again, and even memorize and use chunks of the speech or songs at other times. Families can capitalize on this kind of repetition by using routines and songs to improve skills.
What to do when she only cares about her iPad? It is sometimes difficult to identify reinforcers to use to strengthen desired behaviors in a child with ASD. A smile or a hug or even candy may not be valued. Help parents think about an object, song, or touch the child tends to like. Media are a strong reinforcer, but need to be used sparingly, in specific situations, and kept under parental control, or else removing them can become a major source of upsets.
When a child with ASD gets upset or even violent, the behavior may be interpreted as defiance; it may scare or upset the whole family, and is not conducive to problem solving. Siblings may start screaming or begging for the parents to stop the behavior. While this creates a crisis, you can advise parents to first ensure that everyone is safe, take deep breaths, and then think about which gap is being stressed. A subtle change from what the child expected – new furniture, a guest at the table, a day off from school, or being interrupted mid video – can cause panic, especially for anxious children. Children with ASD also may act up when uncomfortable from a headache, tooth pain, constipation, hunger, or lack of sleep, but often are unable to vocalize the reason, even if they are verbal. Having parents make a few notes about the As, Bs, Cs, and Gs of each event (the essence of a functional behavioral assessment) to review with the child, each other, the teacher, or you is key to understanding the child with ASD and successfully shifting his behavior.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
There are lots of reasons you may be eager to refer children with autism spectrum disorder (ASD) to specialty agencies. You want the fastest possible entry for the child into intervention and the families into a support system. , as well as the general health care, of their children.
“Wait!” you say, “I do not have the special knowledge to help with behavior of children with autism! There is much you can and should do, however, as the specialist(s) may not provide such guidance, entry into behavioral services may take months, and behavior issues may feel urgent to families.
So pick an example of a behavior that is concerning to the family. One problem might be lack of cooperation with activities of daily living such as eating. In this case, the A is being asked to stop playing and sit at the table; the B may be refusing to eat what is served or even to sit very long, ending in a tantrum that disrupts the family meal; and the C could be the child being sent from the table to play on their iPad. But what is the G?
Lack of social communication skills, restrictive interests, hypersensitivity, lack of coordination, and ADHD all may be playing a role. Lack of communication skills makes the social aspect of meals uninteresting. Giving verbal reasons for joining the family may not be effective. Hypersensitivity often is associated with extremes of food selectivity. Lack of fine motor coordination makes eating soup a challenge. And ADHD makes sitting for a long time difficult!
But what about that tantrum? Tantrums that are reinforced by allowing the child to leave and play on the iPad easily can turn into a chronic escape mechanism. Instead, parents need to watch for increasing restlessness, and allow the child to signal “all done” and be “excused” before any tantrum begins. Use of the iPad (a reward) should not be allowed until the family meal is over for everyone. Such accommodations are best decided on by all caregivers in advance, ideally also involving the higher-functioning child. A caregiver who persists in thinking that the child “should” be able to behave may be in denial or grief, and deserves counseling on ASD.
But he is so rigid, the parents say! The tendency of children with ASD to like sameness can be an asset to easing behavior. The key is to design and stick to routines as much as possible, 7 days per week. If the meal is at the same time each day, in the same seat, with the same plate, with no iPad, and the child is allowed to leave only after requesting to, the entire sequence is likely to be smoother. While flexibility does not come easily, it is acquired from the natural variability in family life, but only gradually and over time.
Creating and rehearsing “social stories” is an evidence-based way to help children with ASD have acceptable behaviors. Books, storyboards, and visual schedulers can be purchased to help. But even taking photos or a video of the components of a task and posting this online (private YouTube channel) or on the refrigerator, to review before, during, and/or after the activity, builds an internal image for the child. Children with ASD often watch the same YouTube videos over and over again, and even memorize and use chunks of the speech or songs at other times. Families can capitalize on this kind of repetition by using routines and songs to improve skills.
What to do when she only cares about her iPad? It is sometimes difficult to identify reinforcers to use to strengthen desired behaviors in a child with ASD. A smile or a hug or even candy may not be valued. Help parents think about an object, song, or touch the child tends to like. Media are a strong reinforcer, but need to be used sparingly, in specific situations, and kept under parental control, or else removing them can become a major source of upsets.
When a child with ASD gets upset or even violent, the behavior may be interpreted as defiance; it may scare or upset the whole family, and is not conducive to problem solving. Siblings may start screaming or begging for the parents to stop the behavior. While this creates a crisis, you can advise parents to first ensure that everyone is safe, take deep breaths, and then think about which gap is being stressed. A subtle change from what the child expected – new furniture, a guest at the table, a day off from school, or being interrupted mid video – can cause panic, especially for anxious children. Children with ASD also may act up when uncomfortable from a headache, tooth pain, constipation, hunger, or lack of sleep, but often are unable to vocalize the reason, even if they are verbal. Having parents make a few notes about the As, Bs, Cs, and Gs of each event (the essence of a functional behavioral assessment) to review with the child, each other, the teacher, or you is key to understanding the child with ASD and successfully shifting his behavior.
Dr. Howard is an assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News.
CCSs more likely to stay at jobs to keep health insurance

Survey results suggest childhood cancer survivors (CCSs) in the US are more likely than individuals without a history of cancer to experience “job lock,” or staying at a job to keep work-related health insurance.
CCSs are also more likely than individuals without a history of cancer to report problems paying medical bills and being denied health insurance.
Anne Kirchhoff, PhD, of Huntsman Cancer Institute at the University of Utah in Salt Lake City, and her colleagues reported these findings in JAMA Oncology.
The researchers analyzed 394 CCSs from pediatric oncology institutions across the US, along with 128 of their siblings who had no history of cancer. All study participants worked 35 hours or more per week.
The most common cancer diagnosis among CCSs was leukemia (35.4%), followed by Hodgkin lymphoma (14.9%). Most patients had undergone chemotherapy (77.2%), radiotherapy (63.9%), and surgery (81.1%).
Overall, sociodemographic and clinical characteristics were similar between CCSs and siblings. However, CCSs were more likely than siblings to have severe, disabling, or life-threatening chronic conditions—33.9% and 17.7%, respectively (P<0.001).
Most CCSs (88.0%) and siblings (88.5%) had employer-sponsored health insurance. Three percent of siblings and 5.3% of CCSs had individual insurance; 1.9% and 2.3%, respectively, had public insurance; and 6.7% and 4.4%, respectively, were uninsured.
Results
CCSs were more likely than siblings to report:
- Job lock—23.2% and 16.9%, respectively (P=0.16)
- Problems paying medical bills—20.1% and 12.9%, respectively (P=0.09)
- Denial of health insurance—13.4% and 1.8%, respectively (P<0.001).
In a multivariable analysis, insurance denial remained significantly more common among CCSs than siblings (relative risk [RR]=7.38).
In another multivariable analysis, 38% of CCSs with a previous insurance denial reported job lock, compared with 20% of those who never experienced insurance denial (RR=1.60). And 44% of CCSs who reported problems paying their medical bills also reported job lock, compared to 16% of those who had no problems paying medical bills (RR=2.43).
The researchers also found that female CCSs (RR=1.70) and CCSs with severe, disabling, or life-threatening chronic conditions (RR=1.72) were more likely to report job lock.
“This information gives us a feel for high-risk groups of survivors who may need more information about insurance,” Dr Kirchhoff said. “Many people experience a gap in education and literacy around insurance, and it’s important for people to understand their options—even those who are employed and consistently had access to insurance through work. We want to know what their concerns are so we can help patients and survivors. Getting healthcare should not be a worry for cancer survivors.”
“Survivors have been through a lot when they were younger and understand the importance of making sure they can get healthcare when they need it. I think a lot of them also saw what their parents and families went through in terms of the financial stress and burden of dealing with a health crisis. So they’re just primed to understand the importance of health insurance.”
Dr Kirchhoff noted that this study was conducted as the Affordable Care Act was rolling out. Therefore, she would like to do a follow-up study to see if the insurance exchanges and Medicaid expansion lessened job-related insurance worries. ![]()
Survey results suggest childhood cancer survivors (CCSs) in the US are more likely than individuals without a history of cancer to experience “job lock,” or staying at a job to keep work-related health insurance.
CCSs are also more likely than individuals without a history of cancer to report problems paying medical bills and being denied health insurance.
Anne Kirchhoff, PhD, of Huntsman Cancer Institute at the University of Utah in Salt Lake City, and her colleagues reported these findings in JAMA Oncology.
The researchers analyzed 394 CCSs from pediatric oncology institutions across the US, along with 128 of their siblings who had no history of cancer. All study participants worked 35 hours or more per week.
The most common cancer diagnosis among CCSs was leukemia (35.4%), followed by Hodgkin lymphoma (14.9%). Most patients had undergone chemotherapy (77.2%), radiotherapy (63.9%), and surgery (81.1%).
Overall, sociodemographic and clinical characteristics were similar between CCSs and siblings. However, CCSs were more likely than siblings to have severe, disabling, or life-threatening chronic conditions—33.9% and 17.7%, respectively (P<0.001).
Most CCSs (88.0%) and siblings (88.5%) had employer-sponsored health insurance. Three percent of siblings and 5.3% of CCSs had individual insurance; 1.9% and 2.3%, respectively, had public insurance; and 6.7% and 4.4%, respectively, were uninsured.
Results
CCSs were more likely than siblings to report:
- Job lock—23.2% and 16.9%, respectively (P=0.16)
- Problems paying medical bills—20.1% and 12.9%, respectively (P=0.09)
- Denial of health insurance—13.4% and 1.8%, respectively (P<0.001).
In a multivariable analysis, insurance denial remained significantly more common among CCSs than siblings (relative risk [RR]=7.38).
In another multivariable analysis, 38% of CCSs with a previous insurance denial reported job lock, compared with 20% of those who never experienced insurance denial (RR=1.60). And 44% of CCSs who reported problems paying their medical bills also reported job lock, compared to 16% of those who had no problems paying medical bills (RR=2.43).
The researchers also found that female CCSs (RR=1.70) and CCSs with severe, disabling, or life-threatening chronic conditions (RR=1.72) were more likely to report job lock.
“This information gives us a feel for high-risk groups of survivors who may need more information about insurance,” Dr Kirchhoff said. “Many people experience a gap in education and literacy around insurance, and it’s important for people to understand their options—even those who are employed and consistently had access to insurance through work. We want to know what their concerns are so we can help patients and survivors. Getting healthcare should not be a worry for cancer survivors.”
“Survivors have been through a lot when they were younger and understand the importance of making sure they can get healthcare when they need it. I think a lot of them also saw what their parents and families went through in terms of the financial stress and burden of dealing with a health crisis. So they’re just primed to understand the importance of health insurance.”
Dr Kirchhoff noted that this study was conducted as the Affordable Care Act was rolling out. Therefore, she would like to do a follow-up study to see if the insurance exchanges and Medicaid expansion lessened job-related insurance worries. ![]()
Survey results suggest childhood cancer survivors (CCSs) in the US are more likely than individuals without a history of cancer to experience “job lock,” or staying at a job to keep work-related health insurance.
CCSs are also more likely than individuals without a history of cancer to report problems paying medical bills and being denied health insurance.
Anne Kirchhoff, PhD, of Huntsman Cancer Institute at the University of Utah in Salt Lake City, and her colleagues reported these findings in JAMA Oncology.
The researchers analyzed 394 CCSs from pediatric oncology institutions across the US, along with 128 of their siblings who had no history of cancer. All study participants worked 35 hours or more per week.
The most common cancer diagnosis among CCSs was leukemia (35.4%), followed by Hodgkin lymphoma (14.9%). Most patients had undergone chemotherapy (77.2%), radiotherapy (63.9%), and surgery (81.1%).
Overall, sociodemographic and clinical characteristics were similar between CCSs and siblings. However, CCSs were more likely than siblings to have severe, disabling, or life-threatening chronic conditions—33.9% and 17.7%, respectively (P<0.001).
Most CCSs (88.0%) and siblings (88.5%) had employer-sponsored health insurance. Three percent of siblings and 5.3% of CCSs had individual insurance; 1.9% and 2.3%, respectively, had public insurance; and 6.7% and 4.4%, respectively, were uninsured.
Results
CCSs were more likely than siblings to report:
- Job lock—23.2% and 16.9%, respectively (P=0.16)
- Problems paying medical bills—20.1% and 12.9%, respectively (P=0.09)
- Denial of health insurance—13.4% and 1.8%, respectively (P<0.001).
In a multivariable analysis, insurance denial remained significantly more common among CCSs than siblings (relative risk [RR]=7.38).
In another multivariable analysis, 38% of CCSs with a previous insurance denial reported job lock, compared with 20% of those who never experienced insurance denial (RR=1.60). And 44% of CCSs who reported problems paying their medical bills also reported job lock, compared to 16% of those who had no problems paying medical bills (RR=2.43).
The researchers also found that female CCSs (RR=1.70) and CCSs with severe, disabling, or life-threatening chronic conditions (RR=1.72) were more likely to report job lock.
“This information gives us a feel for high-risk groups of survivors who may need more information about insurance,” Dr Kirchhoff said. “Many people experience a gap in education and literacy around insurance, and it’s important for people to understand their options—even those who are employed and consistently had access to insurance through work. We want to know what their concerns are so we can help patients and survivors. Getting healthcare should not be a worry for cancer survivors.”
“Survivors have been through a lot when they were younger and understand the importance of making sure they can get healthcare when they need it. I think a lot of them also saw what their parents and families went through in terms of the financial stress and burden of dealing with a health crisis. So they’re just primed to understand the importance of health insurance.”
Dr Kirchhoff noted that this study was conducted as the Affordable Care Act was rolling out. Therefore, she would like to do a follow-up study to see if the insurance exchanges and Medicaid expansion lessened job-related insurance worries. ![]()
Pediatric Dermatology Consult - November 2017
The patient was diagnosed with Henoch-Schönlein purpura (HSP) based on clinical presentation of the lesions and associated symptoms of arthralgia and abdominal pain. Urinalysis was obtained and found to be unremarkable, at presentation and follow-up, and treatment with naproxen 5 mg/kg divided into two doses per day was started for pain relief. A prednisone taper starting at 1 mg/kg per day for 3 weeks also was started due to the presence of severe abdominal pain and bullae on exam. The patient was followed with regular urine studies and blood pressure checks for 2 months, and these also were within normal limits.
HSP, also known as anaphylactoid purpura and immunoglobulin A (IgA) vasculitis, is a small vessel leukocytoclastic vasculitis characterized by the perivascular deposition of IgA1-based immune complexes in the walls of arterioles and postcapillary venules.1 In the vast majority of cases, the condition resolves spontaneously in 4-6 weeks and does not require any specific treatment,2 although NSAIDs and systemic corticosteroids can be used for mild-to-moderate and severe pain, respectively.3
HSP is the most common vasculitis in children, with a peak incidence in boys under the age of 5 years. It occurs worldwide, more commonly among whites and Asians, less commonly among blacks, and recent studies from the Czech Republic,4 Taiwan,5 Spain,6 France,7 South Korea,8 and the United Kingdom9 have shown similar incidence rates of 10-20 per 100,000 children. HSP does occur in adults, but is less common, and is known to carry a worse prognosis – in particular, a higher risk of progression to chronic kidney disease. The disease is more commonly seen in winter months,1 unsurprisingly as upper respiratory tract infections also are more common in these months.10
Pathogenesis
The exact pathogenesis of HSP is the subject of ongoing investigation and continued controversy. Mutations and polymorphisms in mannose-binding lectin, interleukins 1 and 8, vascular endothelial growth factor, and alpha-1-antitrypsin have been associated with HSP.3 Immunoglobulin A (IgA) normally exists in two heavily glycosylated forms – IgA1 and IgA2. Abnormal glycosylation, particularly undergalactosylation, of IgA1, the predominant form of IgA in serum and mucosal secretions, has been linked to HSP.11 HSP has been associated with group A streptococcal infections, Bartonella henselae (cat scratch fever) and numerous drugs,12 although no definitive causal or mechanistic explanation has been identified.
Diagnosis
Two major diagnostic criteria for HSP are widely in use, one developed by the American College of Rheumatology (ACR) in 199013 and the other by the European League Against Rheumatism (EULAR) in 2005.14 Both the ACR and EULAR criteria include acute abdominal pain, purpura, and microscopic evidence of vasculitis. Almost all patients with HSP have cutaneous purpura, and many of these patients have palpable purpura, which is pathognomonic of a leukocytoclastic vasculitis, but palpable purpura is not needed for diagnosis. The ACR criteria additionally include age of 20 years or younger, while the EULAR criteria include arthralgias and the presence of hematuria or proteinuria. Ancillary testing usually is not required to make the diagnosis, but when the diagnosis is not clear histopathologic analysis of a skin sample can identify leukocytoclastic vasculitis. Other laboratory studies that may be needed to rule out other conditions, as well as other organ involvement, include a complete blood count, which can be done to rule out thrombocytopenia as a cause of purpura, a metabolic panel, coagulation studies, occult blood test of stool, abdominal imaging, and urinalysis (UA), which can identify proteinuria or hematuria.
Abdominal pain in HSP is believed to be a result of vasculitis of the gastric, mesenteric, and/or colic vasculature. Bleeding from the inflamed vasculature rarely can lead to gross hematochezia, frank melena, or hematemesis. One serious, potential complication of HSP-related mesenteric vasculitis is intussusception, which is otherwise rare in children older than 2 years. Intussusception should be suspected if features of the classic triad of episodic abdominal pain, sausage-shaped abdominal mass, and currant jelly stool are present. Abdominal ultrasound can help to determine whether intussusception is present.
The purpura in HSP presents in waves or crops, and crops last 5-10 days each. Complete resolution takes 4-6 weeks. If biopsy is desired to confirm the diagnosis, it should be done on a lesion less than 24 hours old. This allows for identification of perivascular IgA on histopathology: beyond 24 hours, IgG and IgM also leak out, contributing to a less specific histopathologic picture.
Accurate diagnosis of HSP is important to guide therapy and anticipate potential complications. Wegener’s granulomatosis (A), also known as granulomatosis with polyangiitis, classically involves the upper and lower respiratory tract and the kidneys, leading to a presentation of epistaxis, cough, and hypertension. It occurs more commonly in adults than children. Finkelstein disease (B), also known as acute hemorrhagic edema of infancy (AHEI), is characterized by the development of petechial, urticarial, or targetoid plaques over 24-48 hours with tender edema and fever in children aged less than 2 years. Unlike HSP, AHEI typically does not involve the gastrointestinal tract, kidneys, or joints. Biopsy of skin lesions of AHEI reveals IgA deposition and leukocytoclastic vasculitis, leading some authors to consider it a closely related entity to HSP. Microscopic polyangiitis (D) is an uncommon pauci-immune vasculitis similar to Wegener’s granulomatosis, but lacking granulomas. It presents typically in the 5th decade of life with fever, fatigue, weight loss, and renal involvement. IgA nephropathy (E), also known as synpharyngitic nephritis and Berger disease, is less likely than HSP to cause a rash, joint pain, or abdominal pain. The nomenclature of HSP (whose alternate name is IgA vasculitis) reflects the multi-organ nature of HSP in comparison to IgA nephropathy, which is more likely to be limited to the kidneys.
Treatment
Aside from intussusception and renal disease, which may result from HSP, treatment is not typically required for HSP as it resolves spontaneously. Patients with significant arthralgias are likely to benefit from NSAIDs such as naproxen 5-20 mg/kg per day, although NSAIDs should be avoided if there is significant renal dysfunction or GI bleeding. Patients with severe abdominal pain or joint pain may be more likely to benefit from oral corticosteroids, particularly prednisone 1-2 mg/kg per day. A meta-analysis showed that corticosteroids significantly reduce the duration of symptoms if given early in the course of disease.15
The prognosis is usually excellent, except for a very small sample of the population (5%) that can develop end-stage renal disease. It is recommended that all children with HSP continue monitoring blood pressure and UA either weekly or biweekly for the first 2 months and then once a month for 6-12 months.16
First described in 1801 by a British physician, HSP is a common and usually self-limited disease for which our understanding has advanced greatly over the past 2 centuries, yet for which many important questions regarding pathophysiology remain unanswered. No diagnostic tests or treatments are needed for the majority of patients. Providers should include HSP in the differential diagnosis for the child with unexplained abdominal pain, renal dysfunction, or nonthrombocytopenic purpura.
Mr. Kusari is a medical student at the University of California, San Diego. Dr. Matiz is a practicing dermatologist at Southern California Permanente Medical Group in La Mesa, California. Dr. Matiz and Mr. Kusari said they had no relevant financial disclosures. Email them at pdnews@frontlinemedcom.com.
References
1. “Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence”, 5th ed. (New York: Elsevier, 2016).
2. Lancet. 2007;369(9566):976-8.
3. “Dermatology”, 3rd ed. (Philadelphia: Elsevier Saunders, 2012).
4. J Rheumatol. 2004 Nov;31(11):2295-9.
5. Rheumatology (Oxford). 2005 May;44(5):618-22.
6. Medicine (Baltimore). 2014 Mar;93(2):106-13.
7. Rheumatology (Oxford). 2017;56(8):1358-66.
8. J Korean Med Sci. 2014 Feb;29(2):198-203.
9. Lancet. 2002 Oct 19;360(9341):1197-202.
10. Rhinology. 2015 Jun;53(2):99-106.
11. PLoS One. 2016 Nov 21;11(11):e0166700.
12. Pediatr Infect Dis J. 2002 Jan;21(1):28-31.
13. Arthritis Rheum. 1990 Aug;33(8):1114-21.
14. Ann Rheum Dis. 2006 Jul;65(7):936-41.
15. Pediatrics. 2007 Nov;120(5):1079-87.
16. Arch Dis Child. 2010 Nov;95(11):877-82.
The patient was diagnosed with Henoch-Schönlein purpura (HSP) based on clinical presentation of the lesions and associated symptoms of arthralgia and abdominal pain. Urinalysis was obtained and found to be unremarkable, at presentation and follow-up, and treatment with naproxen 5 mg/kg divided into two doses per day was started for pain relief. A prednisone taper starting at 1 mg/kg per day for 3 weeks also was started due to the presence of severe abdominal pain and bullae on exam. The patient was followed with regular urine studies and blood pressure checks for 2 months, and these also were within normal limits.
HSP, also known as anaphylactoid purpura and immunoglobulin A (IgA) vasculitis, is a small vessel leukocytoclastic vasculitis characterized by the perivascular deposition of IgA1-based immune complexes in the walls of arterioles and postcapillary venules.1 In the vast majority of cases, the condition resolves spontaneously in 4-6 weeks and does not require any specific treatment,2 although NSAIDs and systemic corticosteroids can be used for mild-to-moderate and severe pain, respectively.3
HSP is the most common vasculitis in children, with a peak incidence in boys under the age of 5 years. It occurs worldwide, more commonly among whites and Asians, less commonly among blacks, and recent studies from the Czech Republic,4 Taiwan,5 Spain,6 France,7 South Korea,8 and the United Kingdom9 have shown similar incidence rates of 10-20 per 100,000 children. HSP does occur in adults, but is less common, and is known to carry a worse prognosis – in particular, a higher risk of progression to chronic kidney disease. The disease is more commonly seen in winter months,1 unsurprisingly as upper respiratory tract infections also are more common in these months.10
Pathogenesis
The exact pathogenesis of HSP is the subject of ongoing investigation and continued controversy. Mutations and polymorphisms in mannose-binding lectin, interleukins 1 and 8, vascular endothelial growth factor, and alpha-1-antitrypsin have been associated with HSP.3 Immunoglobulin A (IgA) normally exists in two heavily glycosylated forms – IgA1 and IgA2. Abnormal glycosylation, particularly undergalactosylation, of IgA1, the predominant form of IgA in serum and mucosal secretions, has been linked to HSP.11 HSP has been associated with group A streptococcal infections, Bartonella henselae (cat scratch fever) and numerous drugs,12 although no definitive causal or mechanistic explanation has been identified.
Diagnosis
Two major diagnostic criteria for HSP are widely in use, one developed by the American College of Rheumatology (ACR) in 199013 and the other by the European League Against Rheumatism (EULAR) in 2005.14 Both the ACR and EULAR criteria include acute abdominal pain, purpura, and microscopic evidence of vasculitis. Almost all patients with HSP have cutaneous purpura, and many of these patients have palpable purpura, which is pathognomonic of a leukocytoclastic vasculitis, but palpable purpura is not needed for diagnosis. The ACR criteria additionally include age of 20 years or younger, while the EULAR criteria include arthralgias and the presence of hematuria or proteinuria. Ancillary testing usually is not required to make the diagnosis, but when the diagnosis is not clear histopathologic analysis of a skin sample can identify leukocytoclastic vasculitis. Other laboratory studies that may be needed to rule out other conditions, as well as other organ involvement, include a complete blood count, which can be done to rule out thrombocytopenia as a cause of purpura, a metabolic panel, coagulation studies, occult blood test of stool, abdominal imaging, and urinalysis (UA), which can identify proteinuria or hematuria.
Abdominal pain in HSP is believed to be a result of vasculitis of the gastric, mesenteric, and/or colic vasculature. Bleeding from the inflamed vasculature rarely can lead to gross hematochezia, frank melena, or hematemesis. One serious, potential complication of HSP-related mesenteric vasculitis is intussusception, which is otherwise rare in children older than 2 years. Intussusception should be suspected if features of the classic triad of episodic abdominal pain, sausage-shaped abdominal mass, and currant jelly stool are present. Abdominal ultrasound can help to determine whether intussusception is present.
The purpura in HSP presents in waves or crops, and crops last 5-10 days each. Complete resolution takes 4-6 weeks. If biopsy is desired to confirm the diagnosis, it should be done on a lesion less than 24 hours old. This allows for identification of perivascular IgA on histopathology: beyond 24 hours, IgG and IgM also leak out, contributing to a less specific histopathologic picture.
Accurate diagnosis of HSP is important to guide therapy and anticipate potential complications. Wegener’s granulomatosis (A), also known as granulomatosis with polyangiitis, classically involves the upper and lower respiratory tract and the kidneys, leading to a presentation of epistaxis, cough, and hypertension. It occurs more commonly in adults than children. Finkelstein disease (B), also known as acute hemorrhagic edema of infancy (AHEI), is characterized by the development of petechial, urticarial, or targetoid plaques over 24-48 hours with tender edema and fever in children aged less than 2 years. Unlike HSP, AHEI typically does not involve the gastrointestinal tract, kidneys, or joints. Biopsy of skin lesions of AHEI reveals IgA deposition and leukocytoclastic vasculitis, leading some authors to consider it a closely related entity to HSP. Microscopic polyangiitis (D) is an uncommon pauci-immune vasculitis similar to Wegener’s granulomatosis, but lacking granulomas. It presents typically in the 5th decade of life with fever, fatigue, weight loss, and renal involvement. IgA nephropathy (E), also known as synpharyngitic nephritis and Berger disease, is less likely than HSP to cause a rash, joint pain, or abdominal pain. The nomenclature of HSP (whose alternate name is IgA vasculitis) reflects the multi-organ nature of HSP in comparison to IgA nephropathy, which is more likely to be limited to the kidneys.
Treatment
Aside from intussusception and renal disease, which may result from HSP, treatment is not typically required for HSP as it resolves spontaneously. Patients with significant arthralgias are likely to benefit from NSAIDs such as naproxen 5-20 mg/kg per day, although NSAIDs should be avoided if there is significant renal dysfunction or GI bleeding. Patients with severe abdominal pain or joint pain may be more likely to benefit from oral corticosteroids, particularly prednisone 1-2 mg/kg per day. A meta-analysis showed that corticosteroids significantly reduce the duration of symptoms if given early in the course of disease.15
The prognosis is usually excellent, except for a very small sample of the population (5%) that can develop end-stage renal disease. It is recommended that all children with HSP continue monitoring blood pressure and UA either weekly or biweekly for the first 2 months and then once a month for 6-12 months.16
First described in 1801 by a British physician, HSP is a common and usually self-limited disease for which our understanding has advanced greatly over the past 2 centuries, yet for which many important questions regarding pathophysiology remain unanswered. No diagnostic tests or treatments are needed for the majority of patients. Providers should include HSP in the differential diagnosis for the child with unexplained abdominal pain, renal dysfunction, or nonthrombocytopenic purpura.
Mr. Kusari is a medical student at the University of California, San Diego. Dr. Matiz is a practicing dermatologist at Southern California Permanente Medical Group in La Mesa, California. Dr. Matiz and Mr. Kusari said they had no relevant financial disclosures. Email them at pdnews@frontlinemedcom.com.
References
1. “Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence”, 5th ed. (New York: Elsevier, 2016).
2. Lancet. 2007;369(9566):976-8.
3. “Dermatology”, 3rd ed. (Philadelphia: Elsevier Saunders, 2012).
4. J Rheumatol. 2004 Nov;31(11):2295-9.
5. Rheumatology (Oxford). 2005 May;44(5):618-22.
6. Medicine (Baltimore). 2014 Mar;93(2):106-13.
7. Rheumatology (Oxford). 2017;56(8):1358-66.
8. J Korean Med Sci. 2014 Feb;29(2):198-203.
9. Lancet. 2002 Oct 19;360(9341):1197-202.
10. Rhinology. 2015 Jun;53(2):99-106.
11. PLoS One. 2016 Nov 21;11(11):e0166700.
12. Pediatr Infect Dis J. 2002 Jan;21(1):28-31.
13. Arthritis Rheum. 1990 Aug;33(8):1114-21.
14. Ann Rheum Dis. 2006 Jul;65(7):936-41.
15. Pediatrics. 2007 Nov;120(5):1079-87.
16. Arch Dis Child. 2010 Nov;95(11):877-82.
The patient was diagnosed with Henoch-Schönlein purpura (HSP) based on clinical presentation of the lesions and associated symptoms of arthralgia and abdominal pain. Urinalysis was obtained and found to be unremarkable, at presentation and follow-up, and treatment with naproxen 5 mg/kg divided into two doses per day was started for pain relief. A prednisone taper starting at 1 mg/kg per day for 3 weeks also was started due to the presence of severe abdominal pain and bullae on exam. The patient was followed with regular urine studies and blood pressure checks for 2 months, and these also were within normal limits.
HSP, also known as anaphylactoid purpura and immunoglobulin A (IgA) vasculitis, is a small vessel leukocytoclastic vasculitis characterized by the perivascular deposition of IgA1-based immune complexes in the walls of arterioles and postcapillary venules.1 In the vast majority of cases, the condition resolves spontaneously in 4-6 weeks and does not require any specific treatment,2 although NSAIDs and systemic corticosteroids can be used for mild-to-moderate and severe pain, respectively.3
HSP is the most common vasculitis in children, with a peak incidence in boys under the age of 5 years. It occurs worldwide, more commonly among whites and Asians, less commonly among blacks, and recent studies from the Czech Republic,4 Taiwan,5 Spain,6 France,7 South Korea,8 and the United Kingdom9 have shown similar incidence rates of 10-20 per 100,000 children. HSP does occur in adults, but is less common, and is known to carry a worse prognosis – in particular, a higher risk of progression to chronic kidney disease. The disease is more commonly seen in winter months,1 unsurprisingly as upper respiratory tract infections also are more common in these months.10
Pathogenesis
The exact pathogenesis of HSP is the subject of ongoing investigation and continued controversy. Mutations and polymorphisms in mannose-binding lectin, interleukins 1 and 8, vascular endothelial growth factor, and alpha-1-antitrypsin have been associated with HSP.3 Immunoglobulin A (IgA) normally exists in two heavily glycosylated forms – IgA1 and IgA2. Abnormal glycosylation, particularly undergalactosylation, of IgA1, the predominant form of IgA in serum and mucosal secretions, has been linked to HSP.11 HSP has been associated with group A streptococcal infections, Bartonella henselae (cat scratch fever) and numerous drugs,12 although no definitive causal or mechanistic explanation has been identified.
Diagnosis
Two major diagnostic criteria for HSP are widely in use, one developed by the American College of Rheumatology (ACR) in 199013 and the other by the European League Against Rheumatism (EULAR) in 2005.14 Both the ACR and EULAR criteria include acute abdominal pain, purpura, and microscopic evidence of vasculitis. Almost all patients with HSP have cutaneous purpura, and many of these patients have palpable purpura, which is pathognomonic of a leukocytoclastic vasculitis, but palpable purpura is not needed for diagnosis. The ACR criteria additionally include age of 20 years or younger, while the EULAR criteria include arthralgias and the presence of hematuria or proteinuria. Ancillary testing usually is not required to make the diagnosis, but when the diagnosis is not clear histopathologic analysis of a skin sample can identify leukocytoclastic vasculitis. Other laboratory studies that may be needed to rule out other conditions, as well as other organ involvement, include a complete blood count, which can be done to rule out thrombocytopenia as a cause of purpura, a metabolic panel, coagulation studies, occult blood test of stool, abdominal imaging, and urinalysis (UA), which can identify proteinuria or hematuria.
Abdominal pain in HSP is believed to be a result of vasculitis of the gastric, mesenteric, and/or colic vasculature. Bleeding from the inflamed vasculature rarely can lead to gross hematochezia, frank melena, or hematemesis. One serious, potential complication of HSP-related mesenteric vasculitis is intussusception, which is otherwise rare in children older than 2 years. Intussusception should be suspected if features of the classic triad of episodic abdominal pain, sausage-shaped abdominal mass, and currant jelly stool are present. Abdominal ultrasound can help to determine whether intussusception is present.
The purpura in HSP presents in waves or crops, and crops last 5-10 days each. Complete resolution takes 4-6 weeks. If biopsy is desired to confirm the diagnosis, it should be done on a lesion less than 24 hours old. This allows for identification of perivascular IgA on histopathology: beyond 24 hours, IgG and IgM also leak out, contributing to a less specific histopathologic picture.
Accurate diagnosis of HSP is important to guide therapy and anticipate potential complications. Wegener’s granulomatosis (A), also known as granulomatosis with polyangiitis, classically involves the upper and lower respiratory tract and the kidneys, leading to a presentation of epistaxis, cough, and hypertension. It occurs more commonly in adults than children. Finkelstein disease (B), also known as acute hemorrhagic edema of infancy (AHEI), is characterized by the development of petechial, urticarial, or targetoid plaques over 24-48 hours with tender edema and fever in children aged less than 2 years. Unlike HSP, AHEI typically does not involve the gastrointestinal tract, kidneys, or joints. Biopsy of skin lesions of AHEI reveals IgA deposition and leukocytoclastic vasculitis, leading some authors to consider it a closely related entity to HSP. Microscopic polyangiitis (D) is an uncommon pauci-immune vasculitis similar to Wegener’s granulomatosis, but lacking granulomas. It presents typically in the 5th decade of life with fever, fatigue, weight loss, and renal involvement. IgA nephropathy (E), also known as synpharyngitic nephritis and Berger disease, is less likely than HSP to cause a rash, joint pain, or abdominal pain. The nomenclature of HSP (whose alternate name is IgA vasculitis) reflects the multi-organ nature of HSP in comparison to IgA nephropathy, which is more likely to be limited to the kidneys.
Treatment
Aside from intussusception and renal disease, which may result from HSP, treatment is not typically required for HSP as it resolves spontaneously. Patients with significant arthralgias are likely to benefit from NSAIDs such as naproxen 5-20 mg/kg per day, although NSAIDs should be avoided if there is significant renal dysfunction or GI bleeding. Patients with severe abdominal pain or joint pain may be more likely to benefit from oral corticosteroids, particularly prednisone 1-2 mg/kg per day. A meta-analysis showed that corticosteroids significantly reduce the duration of symptoms if given early in the course of disease.15
The prognosis is usually excellent, except for a very small sample of the population (5%) that can develop end-stage renal disease. It is recommended that all children with HSP continue monitoring blood pressure and UA either weekly or biweekly for the first 2 months and then once a month for 6-12 months.16
First described in 1801 by a British physician, HSP is a common and usually self-limited disease for which our understanding has advanced greatly over the past 2 centuries, yet for which many important questions regarding pathophysiology remain unanswered. No diagnostic tests or treatments are needed for the majority of patients. Providers should include HSP in the differential diagnosis for the child with unexplained abdominal pain, renal dysfunction, or nonthrombocytopenic purpura.
Mr. Kusari is a medical student at the University of California, San Diego. Dr. Matiz is a practicing dermatologist at Southern California Permanente Medical Group in La Mesa, California. Dr. Matiz and Mr. Kusari said they had no relevant financial disclosures. Email them at pdnews@frontlinemedcom.com.
References
1. “Hurwitz Clinical Pediatric Dermatology: A Textbook of Skin Disorders of Childhood and Adolescence”, 5th ed. (New York: Elsevier, 2016).
2. Lancet. 2007;369(9566):976-8.
3. “Dermatology”, 3rd ed. (Philadelphia: Elsevier Saunders, 2012).
4. J Rheumatol. 2004 Nov;31(11):2295-9.
5. Rheumatology (Oxford). 2005 May;44(5):618-22.
6. Medicine (Baltimore). 2014 Mar;93(2):106-13.
7. Rheumatology (Oxford). 2017;56(8):1358-66.
8. J Korean Med Sci. 2014 Feb;29(2):198-203.
9. Lancet. 2002 Oct 19;360(9341):1197-202.
10. Rhinology. 2015 Jun;53(2):99-106.
11. PLoS One. 2016 Nov 21;11(11):e0166700.
12. Pediatr Infect Dis J. 2002 Jan;21(1):28-31.
13. Arthritis Rheum. 1990 Aug;33(8):1114-21.
14. Ann Rheum Dis. 2006 Jul;65(7):936-41.
15. Pediatrics. 2007 Nov;120(5):1079-87.
16. Arch Dis Child. 2010 Nov;95(11):877-82.
Clinical presentation
A healthy 9-year-old boy presents with 1 week history of a rash that began as “bruises” on both ankles that subsequently ascended over a few days to the proximal lower extremities and upper extremities. The rash has been painful and pruritic at times. The patient’s mother reports regular application of hydrocortisone cream for itch and pain relief, and this has been somewhat successful.
The patient has a history of longstanding constipation and abdominal pain, but over the past week has reported abdominal pain that is different and more severe than his usual abdominal pain. This abdominal pain has limited oral intake over the past 2 days. The patient and family also report bilateral pain of the wrists and elbows, which has limited his daily activities. The patient and mother deny fevers, chills, cough, coryza, and any sick contacts.

His vital signs are stable. On physical examination there is mild conjunctival injection, no intraoral lesions, and no lymphadenopathy or hepatosplenomegaly. The abdomen is not distended but it is tender to deep palpation. Bowel sounds are present. On skin examination, there are multiple purpuric annular plaques with central clearing, some with bullae and petechiae, on the bilateral buttocks and legs. There is bilateral pedal edema. On the arms, there are a few polymorphic pink and red annular to targetoid plaques.

Evidence-backed questions can guide a GERD vs. NERD differential diagnosis
CHICAGO – when doing a differential diagnosis. Fortunately, five questions backed by increasing evidence can help you make the call.
“Everyone in the room knows babies puke, and babies can puke a lot,” Barry K. Wershil, MD, said at the annual meeting of the American Academy of Pediatrics. The approach to diagnosing GERD is age specific. “Kids who puke tend to outgrow it over time. With development, 95% or more are no longer refluxing at 18 months of age.”
“So generally there is no reason to initially refer older children and teenagers to a gastroenterologist,” Dr. Wershil said. “One of the essential things [you] do is consider all the causes of vomiting that are not GERD. If your first go-to is GERD, you’re going to miss other issues.”
Dr. Wershil reviewed the definitions: Gastroesophageal reflux is passage of gastric contents into the esophagus. GERD, on the other hand, is defined by the troublesome symptoms or complications associated with reflux of gastric material into the esophagus. In contrast, NERD is the presence of reflux symptoms with no evidence of mucosal erosion or mucosal breaks.
Considerations backed by evidence
Unfortunately, symptoms alone do not always differentiate erosive versus nonerosive esophagitis, Dr. Wershil said, although recurrent vomiting, poor weight gain, anemia, feeding problems, and respiratory problems can be signs of complicated GERD.
He recommended the following five considerations to distinguish GERD from NERD:
- Is the patient exhibiting normal weight gain? If not, ask questions about how the child is being fed. Have the parents started diluting the formula because they think that will take care of the vomiting? Have they begun limiting the amount of formula after observing that the child throws up at 4 ounces but not at 2 ounces?
- Is the patient bleeding or anemic? Hematemesis is rarely the presentation of infants with GERD, but anemia may be.
- Does the patient have respiratory problems (for example, a history of aspiration, recurring wheezing, or cough)?
- Is the patient neurologically normal? If so, that can present a special class of patients in which vomiting may not be just normal infant vomiting.
- Is the patient older than 2 years? We expect 95% of children to outgrow reflux by 18 months, and most children who have physiological reflux will outgrow it by 2 years.
“Those five questions in 1983 had little evidence, but in 2017 there is more evidence that these are the questions to focus on,” Dr. Wershil said.
The role of diagnostic testing
Diagnostic testing, such as pH monitoring, impedance testing, and endoscopy, can be useful in specific situations but carry limitations for widespread use, Dr. Wershil said. “Each test has reasons and limitations.”
An upper GI tract series looks only for anatomic anomalies, for example. pH monitoring is still used in many centers, but in general, impedance monitoring has become more common because it can detect both acid and nonacid reflux: “You can get a very detailed analysis of events happening in the esophagus over time.” One caveat Dr. Wershil added is that, “in some instances, we’re unsure how to define this in the pediatric age ranges we treat.”
Endoscopy has a limited role for the rare patients with mucosal changes or erosive esophagitis, he added. Endoscopy is ordered to detect mucosal changes that confirm esophageal erosion. “In all the kids we scope with positive pH, we rarely find erosive esophagitis,” Dr. Wershil said. “What we find more often is NERD. That really represents more of what we see in our patient population.”
“I hope this information is a good starting point to understand the algorithms that get generated,” Dr. Wershil said.
He recommended an algorithm for gastroesophageal reflux prepared by the American Academy of Pediatrics’ Section on Gastroenterology, Hepatology, and Nutrition (Pediatrics. 2013 May. doi: 10.1542/peds.2013-0421). “I think this information is really solidly grounded in evidence.”
Dr. Wershil is a consultant for Alexion Pharmaceuticals; is a member of the speakers bureau for Abbott Nutrition, Mead Johnson Nutrition, and Nutricia; and receives funding from the National Institutes of Health Consortium of Eosinophilic Gastrointestinal Disease Researchers.
CHICAGO – when doing a differential diagnosis. Fortunately, five questions backed by increasing evidence can help you make the call.
“Everyone in the room knows babies puke, and babies can puke a lot,” Barry K. Wershil, MD, said at the annual meeting of the American Academy of Pediatrics. The approach to diagnosing GERD is age specific. “Kids who puke tend to outgrow it over time. With development, 95% or more are no longer refluxing at 18 months of age.”
“So generally there is no reason to initially refer older children and teenagers to a gastroenterologist,” Dr. Wershil said. “One of the essential things [you] do is consider all the causes of vomiting that are not GERD. If your first go-to is GERD, you’re going to miss other issues.”
Dr. Wershil reviewed the definitions: Gastroesophageal reflux is passage of gastric contents into the esophagus. GERD, on the other hand, is defined by the troublesome symptoms or complications associated with reflux of gastric material into the esophagus. In contrast, NERD is the presence of reflux symptoms with no evidence of mucosal erosion or mucosal breaks.
Considerations backed by evidence
Unfortunately, symptoms alone do not always differentiate erosive versus nonerosive esophagitis, Dr. Wershil said, although recurrent vomiting, poor weight gain, anemia, feeding problems, and respiratory problems can be signs of complicated GERD.
He recommended the following five considerations to distinguish GERD from NERD:
- Is the patient exhibiting normal weight gain? If not, ask questions about how the child is being fed. Have the parents started diluting the formula because they think that will take care of the vomiting? Have they begun limiting the amount of formula after observing that the child throws up at 4 ounces but not at 2 ounces?
- Is the patient bleeding or anemic? Hematemesis is rarely the presentation of infants with GERD, but anemia may be.
- Does the patient have respiratory problems (for example, a history of aspiration, recurring wheezing, or cough)?
- Is the patient neurologically normal? If so, that can present a special class of patients in which vomiting may not be just normal infant vomiting.
- Is the patient older than 2 years? We expect 95% of children to outgrow reflux by 18 months, and most children who have physiological reflux will outgrow it by 2 years.
“Those five questions in 1983 had little evidence, but in 2017 there is more evidence that these are the questions to focus on,” Dr. Wershil said.
The role of diagnostic testing
Diagnostic testing, such as pH monitoring, impedance testing, and endoscopy, can be useful in specific situations but carry limitations for widespread use, Dr. Wershil said. “Each test has reasons and limitations.”
An upper GI tract series looks only for anatomic anomalies, for example. pH monitoring is still used in many centers, but in general, impedance monitoring has become more common because it can detect both acid and nonacid reflux: “You can get a very detailed analysis of events happening in the esophagus over time.” One caveat Dr. Wershil added is that, “in some instances, we’re unsure how to define this in the pediatric age ranges we treat.”
Endoscopy has a limited role for the rare patients with mucosal changes or erosive esophagitis, he added. Endoscopy is ordered to detect mucosal changes that confirm esophageal erosion. “In all the kids we scope with positive pH, we rarely find erosive esophagitis,” Dr. Wershil said. “What we find more often is NERD. That really represents more of what we see in our patient population.”
“I hope this information is a good starting point to understand the algorithms that get generated,” Dr. Wershil said.
He recommended an algorithm for gastroesophageal reflux prepared by the American Academy of Pediatrics’ Section on Gastroenterology, Hepatology, and Nutrition (Pediatrics. 2013 May. doi: 10.1542/peds.2013-0421). “I think this information is really solidly grounded in evidence.”
Dr. Wershil is a consultant for Alexion Pharmaceuticals; is a member of the speakers bureau for Abbott Nutrition, Mead Johnson Nutrition, and Nutricia; and receives funding from the National Institutes of Health Consortium of Eosinophilic Gastrointestinal Disease Researchers.
CHICAGO – when doing a differential diagnosis. Fortunately, five questions backed by increasing evidence can help you make the call.
“Everyone in the room knows babies puke, and babies can puke a lot,” Barry K. Wershil, MD, said at the annual meeting of the American Academy of Pediatrics. The approach to diagnosing GERD is age specific. “Kids who puke tend to outgrow it over time. With development, 95% or more are no longer refluxing at 18 months of age.”
“So generally there is no reason to initially refer older children and teenagers to a gastroenterologist,” Dr. Wershil said. “One of the essential things [you] do is consider all the causes of vomiting that are not GERD. If your first go-to is GERD, you’re going to miss other issues.”
Dr. Wershil reviewed the definitions: Gastroesophageal reflux is passage of gastric contents into the esophagus. GERD, on the other hand, is defined by the troublesome symptoms or complications associated with reflux of gastric material into the esophagus. In contrast, NERD is the presence of reflux symptoms with no evidence of mucosal erosion or mucosal breaks.
Considerations backed by evidence
Unfortunately, symptoms alone do not always differentiate erosive versus nonerosive esophagitis, Dr. Wershil said, although recurrent vomiting, poor weight gain, anemia, feeding problems, and respiratory problems can be signs of complicated GERD.
He recommended the following five considerations to distinguish GERD from NERD:
- Is the patient exhibiting normal weight gain? If not, ask questions about how the child is being fed. Have the parents started diluting the formula because they think that will take care of the vomiting? Have they begun limiting the amount of formula after observing that the child throws up at 4 ounces but not at 2 ounces?
- Is the patient bleeding or anemic? Hematemesis is rarely the presentation of infants with GERD, but anemia may be.
- Does the patient have respiratory problems (for example, a history of aspiration, recurring wheezing, or cough)?
- Is the patient neurologically normal? If so, that can present a special class of patients in which vomiting may not be just normal infant vomiting.
- Is the patient older than 2 years? We expect 95% of children to outgrow reflux by 18 months, and most children who have physiological reflux will outgrow it by 2 years.
“Those five questions in 1983 had little evidence, but in 2017 there is more evidence that these are the questions to focus on,” Dr. Wershil said.
The role of diagnostic testing
Diagnostic testing, such as pH monitoring, impedance testing, and endoscopy, can be useful in specific situations but carry limitations for widespread use, Dr. Wershil said. “Each test has reasons and limitations.”
An upper GI tract series looks only for anatomic anomalies, for example. pH monitoring is still used in many centers, but in general, impedance monitoring has become more common because it can detect both acid and nonacid reflux: “You can get a very detailed analysis of events happening in the esophagus over time.” One caveat Dr. Wershil added is that, “in some instances, we’re unsure how to define this in the pediatric age ranges we treat.”
Endoscopy has a limited role for the rare patients with mucosal changes or erosive esophagitis, he added. Endoscopy is ordered to detect mucosal changes that confirm esophageal erosion. “In all the kids we scope with positive pH, we rarely find erosive esophagitis,” Dr. Wershil said. “What we find more often is NERD. That really represents more of what we see in our patient population.”
“I hope this information is a good starting point to understand the algorithms that get generated,” Dr. Wershil said.
He recommended an algorithm for gastroesophageal reflux prepared by the American Academy of Pediatrics’ Section on Gastroenterology, Hepatology, and Nutrition (Pediatrics. 2013 May. doi: 10.1542/peds.2013-0421). “I think this information is really solidly grounded in evidence.”
Dr. Wershil is a consultant for Alexion Pharmaceuticals; is a member of the speakers bureau for Abbott Nutrition, Mead Johnson Nutrition, and Nutricia; and receives funding from the National Institutes of Health Consortium of Eosinophilic Gastrointestinal Disease Researchers.
EXPERT ANALYSIS FROM AAP 2017