User login
Study spotlights body image dissatisfaction in pediatric IBD
LAS VEGAS – Among current steroid use, higher body mass index percentile, and comorbid mood disorder.
The findings come from a cross-sectional study of 664 patients enrolled in the Crohn’s & Colitis Foundation’s Partners Kids & Teens cohort, presented by Jennifer Claytor, MS, at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
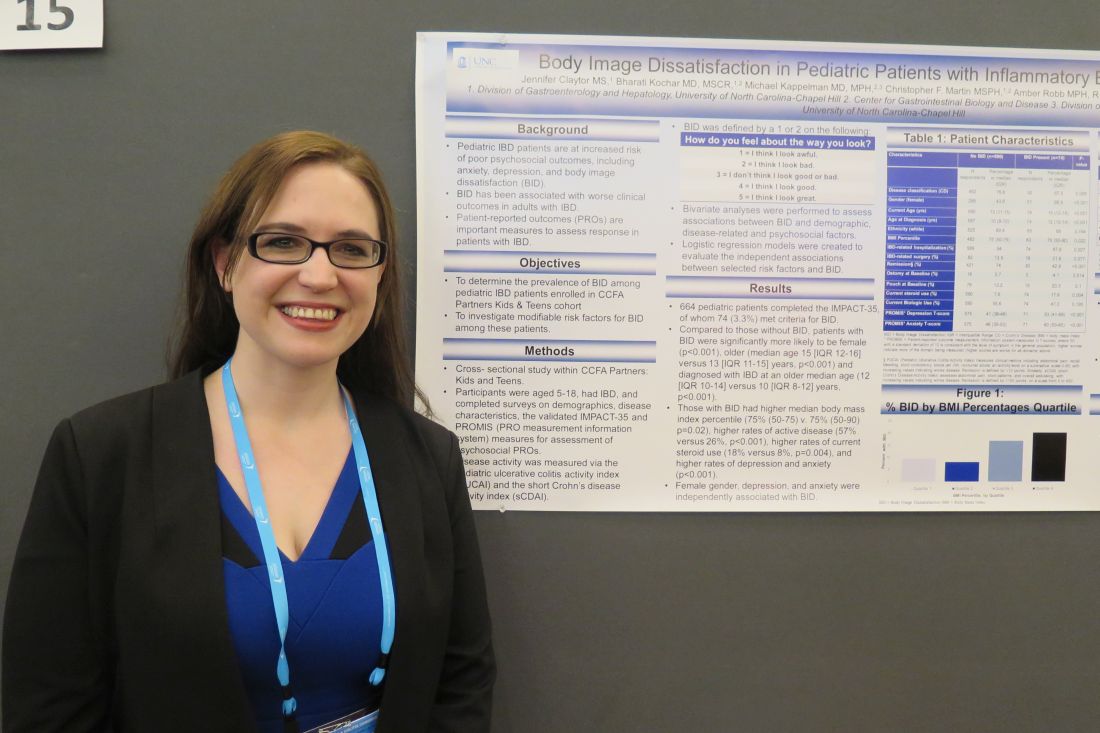
Ms. Claytor, a fourth-year medical student at the University of North Carolina at Chapel Hill, and her associates asked study participants aged 5-18 years to complete surveys on demographics, disease characteristics, and the IMPACT-35 questionnaire and Patient-Reported Outcomes Measurement Information System (PROMIS) tools for assessment of psychological patient-reported outcomes. The pediatric ulcerative colitis activity index and the short Crohn’s disease activity index were used to measure disease activity.
The researchers classified body image dissatisfaction as being present if the patients selected “I look awful” or “I look bad” from the list of possible responses to the question, “How do you feel about the way you look?” Next, they performed bivariate analyses to assess associations between body image dissatisfaction and demographic, disease-related, and psychosocial factors and created logistic regression models to evaluate independent associations between selected risk factors and body image dissatisfaction. “There has been some literature which suggests that for boys, weight and not body image dissatisfaction predicts worse psychosocial outcomes,” Ms. Claytor said. “But for girls it’s body image dissatisfaction, irrespective of weight.”
Of the 664 patients, 74 (3.3%) met criteria for body image dissatisfaction. Compared with patients who did not meet criteria for body image dissatisfaction, those who did were significantly more likely to be female (69% vs. 44%, respectively; P less than .001), older (mean age of 15 vs. 13 years; P less than .001), and diagnosed with IBD an older age (median of 12 vs. 10 years; P less than .001). Ms. Claytor and her associates also found that individuals with body image dissatisfaction had a higher median BMI percentile (P = .02), higher rates of active disease (57% vs. 26%; P less than .001), higher rates of current steroid use (18% vs. 8%; P = .004), and higher rates of depression and anxiety (P less than .001).
After adjusting for age, body mass index, remission, steroid use, and other factors, the odds for developing body image dissatisfaction was highest among those with anxiety (odds ratio, 5.42), followed by depression (OR, 4.73), female gender (OR, 2.31), and current steroid use (OR, 1.59). “I think this points to the need for enhanced counseling services and being aware of these characteristics,” Ms. Claytor said. She reported having no financial disclosures.
SOURCE: Claytor J et al. Crohn’s & Colitis Congress, Poster 15.
*This story was updated on 3/26.
LAS VEGAS – Among current steroid use, higher body mass index percentile, and comorbid mood disorder.
The findings come from a cross-sectional study of 664 patients enrolled in the Crohn’s & Colitis Foundation’s Partners Kids & Teens cohort, presented by Jennifer Claytor, MS, at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Ms. Claytor, a fourth-year medical student at the University of North Carolina at Chapel Hill, and her associates asked study participants aged 5-18 years to complete surveys on demographics, disease characteristics, and the IMPACT-35 questionnaire and Patient-Reported Outcomes Measurement Information System (PROMIS) tools for assessment of psychological patient-reported outcomes. The pediatric ulcerative colitis activity index and the short Crohn’s disease activity index were used to measure disease activity.
The researchers classified body image dissatisfaction as being present if the patients selected “I look awful” or “I look bad” from the list of possible responses to the question, “How do you feel about the way you look?” Next, they performed bivariate analyses to assess associations between body image dissatisfaction and demographic, disease-related, and psychosocial factors and created logistic regression models to evaluate independent associations between selected risk factors and body image dissatisfaction. “There has been some literature which suggests that for boys, weight and not body image dissatisfaction predicts worse psychosocial outcomes,” Ms. Claytor said. “But for girls it’s body image dissatisfaction, irrespective of weight.”
Of the 664 patients, 74 (3.3%) met criteria for body image dissatisfaction. Compared with patients who did not meet criteria for body image dissatisfaction, those who did were significantly more likely to be female (69% vs. 44%, respectively; P less than .001), older (mean age of 15 vs. 13 years; P less than .001), and diagnosed with IBD an older age (median of 12 vs. 10 years; P less than .001). Ms. Claytor and her associates also found that individuals with body image dissatisfaction had a higher median BMI percentile (P = .02), higher rates of active disease (57% vs. 26%; P less than .001), higher rates of current steroid use (18% vs. 8%; P = .004), and higher rates of depression and anxiety (P less than .001).
After adjusting for age, body mass index, remission, steroid use, and other factors, the odds for developing body image dissatisfaction was highest among those with anxiety (odds ratio, 5.42), followed by depression (OR, 4.73), female gender (OR, 2.31), and current steroid use (OR, 1.59). “I think this points to the need for enhanced counseling services and being aware of these characteristics,” Ms. Claytor said. She reported having no financial disclosures.
SOURCE: Claytor J et al. Crohn’s & Colitis Congress, Poster 15.
*This story was updated on 3/26.
LAS VEGAS – Among current steroid use, higher body mass index percentile, and comorbid mood disorder.
The findings come from a cross-sectional study of 664 patients enrolled in the Crohn’s & Colitis Foundation’s Partners Kids & Teens cohort, presented by Jennifer Claytor, MS, at the Crohn’s & Colitis Congress, a partnership of the Crohn’s & Colitis Foundation and the American Gastroenterological Association.
Ms. Claytor, a fourth-year medical student at the University of North Carolina at Chapel Hill, and her associates asked study participants aged 5-18 years to complete surveys on demographics, disease characteristics, and the IMPACT-35 questionnaire and Patient-Reported Outcomes Measurement Information System (PROMIS) tools for assessment of psychological patient-reported outcomes. The pediatric ulcerative colitis activity index and the short Crohn’s disease activity index were used to measure disease activity.
The researchers classified body image dissatisfaction as being present if the patients selected “I look awful” or “I look bad” from the list of possible responses to the question, “How do you feel about the way you look?” Next, they performed bivariate analyses to assess associations between body image dissatisfaction and demographic, disease-related, and psychosocial factors and created logistic regression models to evaluate independent associations between selected risk factors and body image dissatisfaction. “There has been some literature which suggests that for boys, weight and not body image dissatisfaction predicts worse psychosocial outcomes,” Ms. Claytor said. “But for girls it’s body image dissatisfaction, irrespective of weight.”
Of the 664 patients, 74 (3.3%) met criteria for body image dissatisfaction. Compared with patients who did not meet criteria for body image dissatisfaction, those who did were significantly more likely to be female (69% vs. 44%, respectively; P less than .001), older (mean age of 15 vs. 13 years; P less than .001), and diagnosed with IBD an older age (median of 12 vs. 10 years; P less than .001). Ms. Claytor and her associates also found that individuals with body image dissatisfaction had a higher median BMI percentile (P = .02), higher rates of active disease (57% vs. 26%; P less than .001), higher rates of current steroid use (18% vs. 8%; P = .004), and higher rates of depression and anxiety (P less than .001).
After adjusting for age, body mass index, remission, steroid use, and other factors, the odds for developing body image dissatisfaction was highest among those with anxiety (odds ratio, 5.42), followed by depression (OR, 4.73), female gender (OR, 2.31), and current steroid use (OR, 1.59). “I think this points to the need for enhanced counseling services and being aware of these characteristics,” Ms. Claytor said. She reported having no financial disclosures.
SOURCE: Claytor J et al. Crohn’s & Colitis Congress, Poster 15.
*This story was updated on 3/26.
REPORTING FROM CROHN’S & COLITIS CONGRESS
Key clinical point: Interventions to target modifiable risk factors for body image dissatisfaction may improve quality of life in pediatric IBD patients.
Major finding: The odds for developing body image dissatisfaction were highest among those with anxiety (odds ratio, 5.42), followed by depression (OR, 4.73) and female gender (OR, 2.31).
Study details: A cross-sectional study of 664 patients enrolled in the Crohn’s & Colitis Foundation’s Partners Kids & Teens cohort.
Disclosures: Ms. Claytor reported having no financial disclosures.
Source: Claytor J et al. Crohn’s & Colitis Congress, Poster 15.
VIDEO: With tinea capitis, don’t be fooled by a Wood’s lamp
KAUAI, HAWAII – When it comes to diagnosing tinea capitis, you really can’t rely on a Wood’s lamp, according to pediatric dermatologist Robert Silverman, MD.
The Wood’s lamp generally misses the most common cause of tinea capitis in urban and suburban environments today, Trichophyton tonsurans, said Dr. Silverman, a pediatric dermatologist and clinical associate professor in the department of pediatrics at Georgetown University, Washington.
The dermatoscope, which “will allow you to see what is called the black dots of tinea capitis very, very closely,” is far better, he said in an interview at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation
He explained the limitations of the Wood’s lamp in this setting, and what to look for with a dermatoscope. He had other tips to share, too, from years of experience treating the condition, including how to differentiate tinea capitis on exam from its most common mimics, why it’s best to include a counter stain when using potassium hydroxide, and how to motivate parents to wash their child’s hair more frequently to reduce spores on the hair and scalp.
Dr. Silverman disclosed relationships with Pierre Fabre, Pfizer, and Regeneron.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – When it comes to diagnosing tinea capitis, you really can’t rely on a Wood’s lamp, according to pediatric dermatologist Robert Silverman, MD.
The Wood’s lamp generally misses the most common cause of tinea capitis in urban and suburban environments today, Trichophyton tonsurans, said Dr. Silverman, a pediatric dermatologist and clinical associate professor in the department of pediatrics at Georgetown University, Washington.
The dermatoscope, which “will allow you to see what is called the black dots of tinea capitis very, very closely,” is far better, he said in an interview at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation
He explained the limitations of the Wood’s lamp in this setting, and what to look for with a dermatoscope. He had other tips to share, too, from years of experience treating the condition, including how to differentiate tinea capitis on exam from its most common mimics, why it’s best to include a counter stain when using potassium hydroxide, and how to motivate parents to wash their child’s hair more frequently to reduce spores on the hair and scalp.
Dr. Silverman disclosed relationships with Pierre Fabre, Pfizer, and Regeneron.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – When it comes to diagnosing tinea capitis, you really can’t rely on a Wood’s lamp, according to pediatric dermatologist Robert Silverman, MD.
The Wood’s lamp generally misses the most common cause of tinea capitis in urban and suburban environments today, Trichophyton tonsurans, said Dr. Silverman, a pediatric dermatologist and clinical associate professor in the department of pediatrics at Georgetown University, Washington.
The dermatoscope, which “will allow you to see what is called the black dots of tinea capitis very, very closely,” is far better, he said in an interview at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation
He explained the limitations of the Wood’s lamp in this setting, and what to look for with a dermatoscope. He had other tips to share, too, from years of experience treating the condition, including how to differentiate tinea capitis on exam from its most common mimics, why it’s best to include a counter stain when using potassium hydroxide, and how to motivate parents to wash their child’s hair more frequently to reduce spores on the hair and scalp.
Dr. Silverman disclosed relationships with Pierre Fabre, Pfizer, and Regeneron.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
REPORTING FROM SDEF HAWAII DERMATOLOGY SEMINAR

Exploding e-cigs can cause grievous injuries
With the increasing use of e-cigarettes among adolescents, explosions involving these devices are a growing concern because they can cause serious injuries.
One such incident, described by Elizabeth Ackley, MD, of the University of Colorado at Denver, Aurora, and her coauthors, involved a 17-year-old youth whose electronic nicotine-delivery systems (ENDS) exploded as he was about to take a puff. He presented with a burned left thumb with sensory loss, reduced motor control, and heavy bleeding. He underwent debridement, multiple antibiotic courses, and six operative procedures that ultimately led to removal of the lateral aspect of his thumb.
Dr. Ackley and her associates emphasized. This can occur with overheating, water exposure, excessive charging, improper charging with incompatible devices, contact with metallic objects such as keys or coins, or damage of the battery.
Mineral oil should be used for initial wound irrigation, the authors advise, and “surgical debridement is the definitive treatment for injuries and should remove any remaining alkaline material from tissues.” Delay use of water-based irrigation until after surgical debridement, and one report suggests probing the wound with litmus paper to ensure the pH is no longer alkaline prior to using water irrigation.
Although there are other talking points pediatricians may use when counseling teens about use of e-cigs and other tobacco products, the authors suggested that “the potential for major and disfiguring injury from ENDS explosions may be a more compelling talking point with teens instead of long-term or other nebulous adverse effects of ENDS and tobacco products.”
Read more about the subject at J Pediatr. 2018. doi: 10.1016/j.jpeds.2017.12.032.
With the increasing use of e-cigarettes among adolescents, explosions involving these devices are a growing concern because they can cause serious injuries.
One such incident, described by Elizabeth Ackley, MD, of the University of Colorado at Denver, Aurora, and her coauthors, involved a 17-year-old youth whose electronic nicotine-delivery systems (ENDS) exploded as he was about to take a puff. He presented with a burned left thumb with sensory loss, reduced motor control, and heavy bleeding. He underwent debridement, multiple antibiotic courses, and six operative procedures that ultimately led to removal of the lateral aspect of his thumb.
Dr. Ackley and her associates emphasized. This can occur with overheating, water exposure, excessive charging, improper charging with incompatible devices, contact with metallic objects such as keys or coins, or damage of the battery.
Mineral oil should be used for initial wound irrigation, the authors advise, and “surgical debridement is the definitive treatment for injuries and should remove any remaining alkaline material from tissues.” Delay use of water-based irrigation until after surgical debridement, and one report suggests probing the wound with litmus paper to ensure the pH is no longer alkaline prior to using water irrigation.
Although there are other talking points pediatricians may use when counseling teens about use of e-cigs and other tobacco products, the authors suggested that “the potential for major and disfiguring injury from ENDS explosions may be a more compelling talking point with teens instead of long-term or other nebulous adverse effects of ENDS and tobacco products.”
Read more about the subject at J Pediatr. 2018. doi: 10.1016/j.jpeds.2017.12.032.
With the increasing use of e-cigarettes among adolescents, explosions involving these devices are a growing concern because they can cause serious injuries.
One such incident, described by Elizabeth Ackley, MD, of the University of Colorado at Denver, Aurora, and her coauthors, involved a 17-year-old youth whose electronic nicotine-delivery systems (ENDS) exploded as he was about to take a puff. He presented with a burned left thumb with sensory loss, reduced motor control, and heavy bleeding. He underwent debridement, multiple antibiotic courses, and six operative procedures that ultimately led to removal of the lateral aspect of his thumb.
Dr. Ackley and her associates emphasized. This can occur with overheating, water exposure, excessive charging, improper charging with incompatible devices, contact with metallic objects such as keys or coins, or damage of the battery.
Mineral oil should be used for initial wound irrigation, the authors advise, and “surgical debridement is the definitive treatment for injuries and should remove any remaining alkaline material from tissues.” Delay use of water-based irrigation until after surgical debridement, and one report suggests probing the wound with litmus paper to ensure the pH is no longer alkaline prior to using water irrigation.
Although there are other talking points pediatricians may use when counseling teens about use of e-cigs and other tobacco products, the authors suggested that “the potential for major and disfiguring injury from ENDS explosions may be a more compelling talking point with teens instead of long-term or other nebulous adverse effects of ENDS and tobacco products.”
Read more about the subject at J Pediatr. 2018. doi: 10.1016/j.jpeds.2017.12.032.
This is what a flu pandemic looks like
For the week ending Feb. 3, 2018, the proportion of outpatient visits for influenza-like illness (ILI) was 7.7%, which would appear to equal the mark of 7.7% set in October of 2009. The earlier 7.7%, however, is rounded down from 7.715%, while the current mark is rounded up from 7.653%, data from the CDC’s Fluview website show.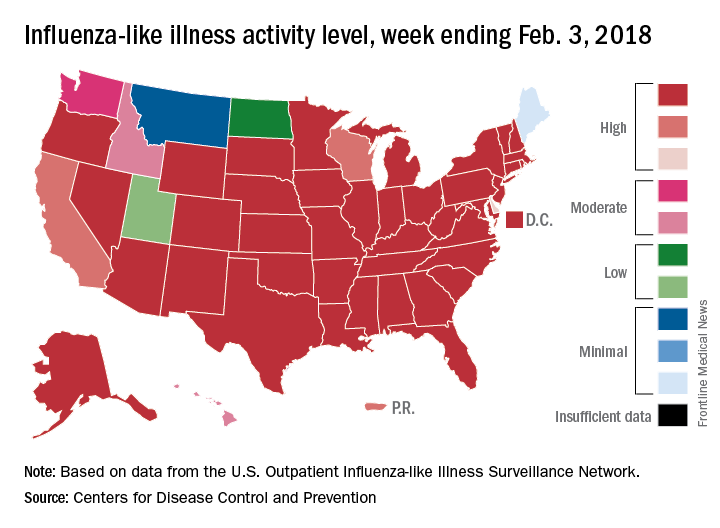
Deaths attributed to pneumonia and influenza were above the epidemic threshold set by the National Center for Health Statistics Mortality Surveillance system, acting CDC director Anne Schuchat, MD, said in a teleconference sponsored by the agency.
ILI activity was at level 10 on the CDC’s 1-10 scale in 41 states, compared with 34 the week before, and was categorized in the “high” range (levels 8-10) in another 3 states and Puerto Rico, according to data from the CDC’s Outpatient Influenza-like Illness Surveillance Network. In California, which was noted as a possible bright spot last week by Dr. Schuchat because activity there had been decreasing, the ILI level went back up to level 9 after being at 7 the week before.
Flu-related hospitalizations are continuing to rise at a record clip, with the cumulative rate for the week of Feb. 3 at 59.9 per 100,000 population, the CDC reported. A total of 1 in 10 hospital-based deaths last week were related to influenza. At this point in the 2014-2015 flu season – which has the highest number of hospitalizations at 710,000 – the hospitalization rate was only 50.9 per 100,000 population.
There were 10 pediatric deaths reported for the week ending Feb. 3, although 9 occurred in previous weeks. There have been 63 flu-related deaths among children so far during the 2017-2018 season.
Dr. Schuchat continued to recommend members of the public to get a flu shot and to stay home if they are feeling sick.
“What could be mild symptoms for you could be deadly for someone else,” Dr. Schuchat said, adding that antiviral medications remain important. “Physicians do not have to wait for confirmatory flu testing. They should begin treatment with antiviral drugs immediately in they suspect they have a severely ill or a high risk patient.”
“Flu vaccines often have lower effectiveness against H3N1 viruses. However, some protection is better than none. The vaccine’s effectiveness against other flu viruses, like B and H1N1, is better. Because of the ongoing intensity of the flu season and the increasing circulation of influenza B and h1n1, we do continue to recommend vaccination even this late in the season.”
Dr. Schuchat stressed the importance of the pneumococcal pneumonia vaccine. “Flu can make people more vulnerable to secondary infections like bacterial pneumonia. We recommend people aged 65 and over get a pneumococcal pneumonia vaccine,” she said.
For the week ending Feb. 3, 2018, the proportion of outpatient visits for influenza-like illness (ILI) was 7.7%, which would appear to equal the mark of 7.7% set in October of 2009. The earlier 7.7%, however, is rounded down from 7.715%, while the current mark is rounded up from 7.653%, data from the CDC’s Fluview website show.
Deaths attributed to pneumonia and influenza were above the epidemic threshold set by the National Center for Health Statistics Mortality Surveillance system, acting CDC director Anne Schuchat, MD, said in a teleconference sponsored by the agency.
ILI activity was at level 10 on the CDC’s 1-10 scale in 41 states, compared with 34 the week before, and was categorized in the “high” range (levels 8-10) in another 3 states and Puerto Rico, according to data from the CDC’s Outpatient Influenza-like Illness Surveillance Network. In California, which was noted as a possible bright spot last week by Dr. Schuchat because activity there had been decreasing, the ILI level went back up to level 9 after being at 7 the week before.
Flu-related hospitalizations are continuing to rise at a record clip, with the cumulative rate for the week of Feb. 3 at 59.9 per 100,000 population, the CDC reported. A total of 1 in 10 hospital-based deaths last week were related to influenza. At this point in the 2014-2015 flu season – which has the highest number of hospitalizations at 710,000 – the hospitalization rate was only 50.9 per 100,000 population.
There were 10 pediatric deaths reported for the week ending Feb. 3, although 9 occurred in previous weeks. There have been 63 flu-related deaths among children so far during the 2017-2018 season.
Dr. Schuchat continued to recommend members of the public to get a flu shot and to stay home if they are feeling sick.
“What could be mild symptoms for you could be deadly for someone else,” Dr. Schuchat said, adding that antiviral medications remain important. “Physicians do not have to wait for confirmatory flu testing. They should begin treatment with antiviral drugs immediately in they suspect they have a severely ill or a high risk patient.”
“Flu vaccines often have lower effectiveness against H3N1 viruses. However, some protection is better than none. The vaccine’s effectiveness against other flu viruses, like B and H1N1, is better. Because of the ongoing intensity of the flu season and the increasing circulation of influenza B and h1n1, we do continue to recommend vaccination even this late in the season.”
Dr. Schuchat stressed the importance of the pneumococcal pneumonia vaccine. “Flu can make people more vulnerable to secondary infections like bacterial pneumonia. We recommend people aged 65 and over get a pneumococcal pneumonia vaccine,” she said.
For the week ending Feb. 3, 2018, the proportion of outpatient visits for influenza-like illness (ILI) was 7.7%, which would appear to equal the mark of 7.7% set in October of 2009. The earlier 7.7%, however, is rounded down from 7.715%, while the current mark is rounded up from 7.653%, data from the CDC’s Fluview website show.
Deaths attributed to pneumonia and influenza were above the epidemic threshold set by the National Center for Health Statistics Mortality Surveillance system, acting CDC director Anne Schuchat, MD, said in a teleconference sponsored by the agency.
ILI activity was at level 10 on the CDC’s 1-10 scale in 41 states, compared with 34 the week before, and was categorized in the “high” range (levels 8-10) in another 3 states and Puerto Rico, according to data from the CDC’s Outpatient Influenza-like Illness Surveillance Network. In California, which was noted as a possible bright spot last week by Dr. Schuchat because activity there had been decreasing, the ILI level went back up to level 9 after being at 7 the week before.
Flu-related hospitalizations are continuing to rise at a record clip, with the cumulative rate for the week of Feb. 3 at 59.9 per 100,000 population, the CDC reported. A total of 1 in 10 hospital-based deaths last week were related to influenza. At this point in the 2014-2015 flu season – which has the highest number of hospitalizations at 710,000 – the hospitalization rate was only 50.9 per 100,000 population.
There were 10 pediatric deaths reported for the week ending Feb. 3, although 9 occurred in previous weeks. There have been 63 flu-related deaths among children so far during the 2017-2018 season.
Dr. Schuchat continued to recommend members of the public to get a flu shot and to stay home if they are feeling sick.
“What could be mild symptoms for you could be deadly for someone else,” Dr. Schuchat said, adding that antiviral medications remain important. “Physicians do not have to wait for confirmatory flu testing. They should begin treatment with antiviral drugs immediately in they suspect they have a severely ill or a high risk patient.”
“Flu vaccines often have lower effectiveness against H3N1 viruses. However, some protection is better than none. The vaccine’s effectiveness against other flu viruses, like B and H1N1, is better. Because of the ongoing intensity of the flu season and the increasing circulation of influenza B and h1n1, we do continue to recommend vaccination even this late in the season.”
Dr. Schuchat stressed the importance of the pneumococcal pneumonia vaccine. “Flu can make people more vulnerable to secondary infections like bacterial pneumonia. We recommend people aged 65 and over get a pneumococcal pneumonia vaccine,” she said.
FROM A CDC TELECONFERENCE
ACR sounds more welcoming tone in new biosimilars position paper
The American College of Rheumatology has shifted from a more cautious stance toward the use of biosimilars in clinical practice to now recommend in a new position statement that health care providers incorporate biosimilars, where appropriate, into treatment regimens for their patients living with rheumatic diseases.
“Now that biosimilars have been used successfully in Europe, with rigorously acquired data supporting their broader use, and , S. Louis Bridges Jr., MD, PhD, chair of the ACR Committee on Research, wrote with seven other authors of the position statement in Arthritis & Rheumatology.
The ACR position statement addresses the issues of immunogenicity, extrapolation of indications, interchangeability, substitution, switching, and cost surrounding biosimilars.
The position statement’s authors said they expect switching and nonmedical substitution to become as common in the United States as it is in the rest of the world. They do not anticipate efficacy and safety issues for biosimilars based on available data regarding switching between reference products and biosimilars and their understanding of product drift.
“However, we encourage vigorous postmarketing surveillance of both biosimilars and their reference products as we enter the era where patients may undergo multiple switches as a result of insurance company and [pharmacy benefits manager] formulary preferences,” they said.
Immunogenicity
Concerns about immunogenicity for biosimilars approved in the United States have mostly been well addressed through studies showing similar frequencies of binding and neutralizing antidrug antibodies (ADA) in biosimilars and their reference products. Furthermore, no safety signals between biosimilars and their reference products have been observed that suggest a differential effect of ADA on efficacy, safety, or patient outcomes, the authors said. But they noted that “if immunogenicity findings are to be extrapolated from one disease to additional indications, the subjects being studied should be those most likely to develop ADA, such as subjects not receiving concomitant immunosuppressive medications.” The results of comparative immunogenicity studies carried out to date also indicate that “a patient who develops ADA to a reference drug with resultant loss of clinical response should not be switched to its biosimilar.”
Again, the authors said postmarketing pharmacovigilance using observational registry data would be critical to assessing the effect of switching on immunogenicity.
Extrapolation of indications
The extrapolation of biosimilars to reference product indications for which the biosimilar was not assessed in clinical trials continues to “be an area of uneasiness” among clinicians “who are surprised to find” that a biosimilar can be approved for inflammatory bowel disease in the absence of clinical trials in the relevant patient populations, the authors said. In geographic areas where it is not mandatory to use biosimilars, this lack of confidence in extrapolation of indications may limit their acceptance, the authors wrote, but data from studies such as NOR-SWITCH and DANBIO have provided reassuring evidence to support regulated extrapolation of indication for biosimilars.
However, since extrapolation of indications also applies to pediatric patients who often metabolize drugs faster than adults, the position paper says that “it may be important” to conduct pharmacodynamic and pharmacokinetic studies in children as well as postmarketing surveillance “since potential immunogenicity may be of particular importance in these younger patients with chronic diseases who might encounter several biological agents during their lifetime.”
Substitution, interchangeability, and switching
The “interchangeability” regulatory pathway in the United States that would allow substitution at the point of dispensing has not been finalized, but most states have enacted, or are in the process of enacting, legislation to regulate the practice, the statement says.
While substitution describes a change made by someone other than the prescriber, the authors note that switching defines the “intentional change initiated by a health care provider in partnership with the patient” for economic or medical reasons. Switching has been studied most often in open-label extension studies of biosimilar clinic trials and has shown no loss of efficacy or increase in adverse events.
Dr. Fleischmann contended that substitution, extrapolation, and interchangeability of biosimilars in clinical practice remain gray areas. For example, in a clinical trial, patients switching from a reference product to a biosimilar may show equivalency of clinical response and adverse events. “But as rheumatologists, we don’t treat groups of patients; we treat individual patients and here the results may be different,” he wrote in Arthritis & Rheumatology.
While the white paper appropriately points out that interchangeability among multiple biosimilars is a question that should be answered in postmarketing registries, Dr. Fleischmann noted that no interchangeability study has been reported, even though the FDA has issued guidance on how a study should be done.
“Although interchangeability may be safe and effective in many patients, until the results of such a study are available and properly analyzed, it is only conjecture that interchangeability is appropriate and safe,” he said.
Costs
The white paper acknowledged that the “only anticipated advantage” of a biosimilar over its reference product was lower cost, since both drugs should be therapeutically equivalent. “The degree to which the availability of biosimilars in the U.S. will drive down the cost of biologic therapy, and who will benefit from any cost reductions remains to be seen,” the authors wrote.
“To incentivize the use of biosimilars,” the authors suggested that “commercial and government insurance programs could harmonize drug prices with patients’ out-of-pocket costs and provider reimbursement. Currently, however, patients with commercial insurance are likely to have similar copayments for both biosimilars and originator biologics because of [pharmacy benefits manager]– or plan-mandated patient cost sharing. Also, patients’ out-of-pocket costs for biosimilars in the Medicare Part D (self-administered drug) program likely will be higher than for originator biologics because of a flaw that maintains, rather than reduces, biosimilar patient cost sharing in the coverage gap (also known as the “donut hole”) until 2020.”
It is not at all clear that a biosimilar would be cheaper for the individual patient, Dr. Fleischmann said. “It may be cheaper to the pharmacy benefit management firm, but this may not really help patient access to these medications. It is also not clear that nonmedical substitution will be effective in every patient nor has it been demonstrated that extrapolation is effective,” he wrote.
No disclosures were listed for the authors of the position statement. Dr. Fleischmann is a consultant for AbbVie, Amgen, Bristol-Myers Squibb, Celltrion, Eli Lilly, GlaxoSmithKline, Novartis, Pfizer, Sanofi Aventis, and UCB.
SOURCES: Bridges S et al. Arthritis Rheumatol. 2018 Feb 7. doi: 10.1002/art.40388; and Fleischmann R. Arthritis Rheumatol. 2018 Feb 7. doi: 10.1002/art.40402
The American College of Rheumatology has shifted from a more cautious stance toward the use of biosimilars in clinical practice to now recommend in a new position statement that health care providers incorporate biosimilars, where appropriate, into treatment regimens for their patients living with rheumatic diseases.
“Now that biosimilars have been used successfully in Europe, with rigorously acquired data supporting their broader use, and , S. Louis Bridges Jr., MD, PhD, chair of the ACR Committee on Research, wrote with seven other authors of the position statement in Arthritis & Rheumatology.
The ACR position statement addresses the issues of immunogenicity, extrapolation of indications, interchangeability, substitution, switching, and cost surrounding biosimilars.
The position statement’s authors said they expect switching and nonmedical substitution to become as common in the United States as it is in the rest of the world. They do not anticipate efficacy and safety issues for biosimilars based on available data regarding switching between reference products and biosimilars and their understanding of product drift.
“However, we encourage vigorous postmarketing surveillance of both biosimilars and their reference products as we enter the era where patients may undergo multiple switches as a result of insurance company and [pharmacy benefits manager] formulary preferences,” they said.
Immunogenicity
Concerns about immunogenicity for biosimilars approved in the United States have mostly been well addressed through studies showing similar frequencies of binding and neutralizing antidrug antibodies (ADA) in biosimilars and their reference products. Furthermore, no safety signals between biosimilars and their reference products have been observed that suggest a differential effect of ADA on efficacy, safety, or patient outcomes, the authors said. But they noted that “if immunogenicity findings are to be extrapolated from one disease to additional indications, the subjects being studied should be those most likely to develop ADA, such as subjects not receiving concomitant immunosuppressive medications.” The results of comparative immunogenicity studies carried out to date also indicate that “a patient who develops ADA to a reference drug with resultant loss of clinical response should not be switched to its biosimilar.”
Again, the authors said postmarketing pharmacovigilance using observational registry data would be critical to assessing the effect of switching on immunogenicity.
Extrapolation of indications
The extrapolation of biosimilars to reference product indications for which the biosimilar was not assessed in clinical trials continues to “be an area of uneasiness” among clinicians “who are surprised to find” that a biosimilar can be approved for inflammatory bowel disease in the absence of clinical trials in the relevant patient populations, the authors said. In geographic areas where it is not mandatory to use biosimilars, this lack of confidence in extrapolation of indications may limit their acceptance, the authors wrote, but data from studies such as NOR-SWITCH and DANBIO have provided reassuring evidence to support regulated extrapolation of indication for biosimilars.
However, since extrapolation of indications also applies to pediatric patients who often metabolize drugs faster than adults, the position paper says that “it may be important” to conduct pharmacodynamic and pharmacokinetic studies in children as well as postmarketing surveillance “since potential immunogenicity may be of particular importance in these younger patients with chronic diseases who might encounter several biological agents during their lifetime.”
Substitution, interchangeability, and switching
The “interchangeability” regulatory pathway in the United States that would allow substitution at the point of dispensing has not been finalized, but most states have enacted, or are in the process of enacting, legislation to regulate the practice, the statement says.
While substitution describes a change made by someone other than the prescriber, the authors note that switching defines the “intentional change initiated by a health care provider in partnership with the patient” for economic or medical reasons. Switching has been studied most often in open-label extension studies of biosimilar clinic trials and has shown no loss of efficacy or increase in adverse events.
Dr. Fleischmann contended that substitution, extrapolation, and interchangeability of biosimilars in clinical practice remain gray areas. For example, in a clinical trial, patients switching from a reference product to a biosimilar may show equivalency of clinical response and adverse events. “But as rheumatologists, we don’t treat groups of patients; we treat individual patients and here the results may be different,” he wrote in Arthritis & Rheumatology.
While the white paper appropriately points out that interchangeability among multiple biosimilars is a question that should be answered in postmarketing registries, Dr. Fleischmann noted that no interchangeability study has been reported, even though the FDA has issued guidance on how a study should be done.
“Although interchangeability may be safe and effective in many patients, until the results of such a study are available and properly analyzed, it is only conjecture that interchangeability is appropriate and safe,” he said.
Costs
The white paper acknowledged that the “only anticipated advantage” of a biosimilar over its reference product was lower cost, since both drugs should be therapeutically equivalent. “The degree to which the availability of biosimilars in the U.S. will drive down the cost of biologic therapy, and who will benefit from any cost reductions remains to be seen,” the authors wrote.
“To incentivize the use of biosimilars,” the authors suggested that “commercial and government insurance programs could harmonize drug prices with patients’ out-of-pocket costs and provider reimbursement. Currently, however, patients with commercial insurance are likely to have similar copayments for both biosimilars and originator biologics because of [pharmacy benefits manager]– or plan-mandated patient cost sharing. Also, patients’ out-of-pocket costs for biosimilars in the Medicare Part D (self-administered drug) program likely will be higher than for originator biologics because of a flaw that maintains, rather than reduces, biosimilar patient cost sharing in the coverage gap (also known as the “donut hole”) until 2020.”
It is not at all clear that a biosimilar would be cheaper for the individual patient, Dr. Fleischmann said. “It may be cheaper to the pharmacy benefit management firm, but this may not really help patient access to these medications. It is also not clear that nonmedical substitution will be effective in every patient nor has it been demonstrated that extrapolation is effective,” he wrote.
No disclosures were listed for the authors of the position statement. Dr. Fleischmann is a consultant for AbbVie, Amgen, Bristol-Myers Squibb, Celltrion, Eli Lilly, GlaxoSmithKline, Novartis, Pfizer, Sanofi Aventis, and UCB.
SOURCES: Bridges S et al. Arthritis Rheumatol. 2018 Feb 7. doi: 10.1002/art.40388; and Fleischmann R. Arthritis Rheumatol. 2018 Feb 7. doi: 10.1002/art.40402
The American College of Rheumatology has shifted from a more cautious stance toward the use of biosimilars in clinical practice to now recommend in a new position statement that health care providers incorporate biosimilars, where appropriate, into treatment regimens for their patients living with rheumatic diseases.
“Now that biosimilars have been used successfully in Europe, with rigorously acquired data supporting their broader use, and , S. Louis Bridges Jr., MD, PhD, chair of the ACR Committee on Research, wrote with seven other authors of the position statement in Arthritis & Rheumatology.
The ACR position statement addresses the issues of immunogenicity, extrapolation of indications, interchangeability, substitution, switching, and cost surrounding biosimilars.
The position statement’s authors said they expect switching and nonmedical substitution to become as common in the United States as it is in the rest of the world. They do not anticipate efficacy and safety issues for biosimilars based on available data regarding switching between reference products and biosimilars and their understanding of product drift.
“However, we encourage vigorous postmarketing surveillance of both biosimilars and their reference products as we enter the era where patients may undergo multiple switches as a result of insurance company and [pharmacy benefits manager] formulary preferences,” they said.
Immunogenicity
Concerns about immunogenicity for biosimilars approved in the United States have mostly been well addressed through studies showing similar frequencies of binding and neutralizing antidrug antibodies (ADA) in biosimilars and their reference products. Furthermore, no safety signals between biosimilars and their reference products have been observed that suggest a differential effect of ADA on efficacy, safety, or patient outcomes, the authors said. But they noted that “if immunogenicity findings are to be extrapolated from one disease to additional indications, the subjects being studied should be those most likely to develop ADA, such as subjects not receiving concomitant immunosuppressive medications.” The results of comparative immunogenicity studies carried out to date also indicate that “a patient who develops ADA to a reference drug with resultant loss of clinical response should not be switched to its biosimilar.”
Again, the authors said postmarketing pharmacovigilance using observational registry data would be critical to assessing the effect of switching on immunogenicity.
Extrapolation of indications
The extrapolation of biosimilars to reference product indications for which the biosimilar was not assessed in clinical trials continues to “be an area of uneasiness” among clinicians “who are surprised to find” that a biosimilar can be approved for inflammatory bowel disease in the absence of clinical trials in the relevant patient populations, the authors said. In geographic areas where it is not mandatory to use biosimilars, this lack of confidence in extrapolation of indications may limit their acceptance, the authors wrote, but data from studies such as NOR-SWITCH and DANBIO have provided reassuring evidence to support regulated extrapolation of indication for biosimilars.
However, since extrapolation of indications also applies to pediatric patients who often metabolize drugs faster than adults, the position paper says that “it may be important” to conduct pharmacodynamic and pharmacokinetic studies in children as well as postmarketing surveillance “since potential immunogenicity may be of particular importance in these younger patients with chronic diseases who might encounter several biological agents during their lifetime.”
Substitution, interchangeability, and switching
The “interchangeability” regulatory pathway in the United States that would allow substitution at the point of dispensing has not been finalized, but most states have enacted, or are in the process of enacting, legislation to regulate the practice, the statement says.
While substitution describes a change made by someone other than the prescriber, the authors note that switching defines the “intentional change initiated by a health care provider in partnership with the patient” for economic or medical reasons. Switching has been studied most often in open-label extension studies of biosimilar clinic trials and has shown no loss of efficacy or increase in adverse events.
Dr. Fleischmann contended that substitution, extrapolation, and interchangeability of biosimilars in clinical practice remain gray areas. For example, in a clinical trial, patients switching from a reference product to a biosimilar may show equivalency of clinical response and adverse events. “But as rheumatologists, we don’t treat groups of patients; we treat individual patients and here the results may be different,” he wrote in Arthritis & Rheumatology.
While the white paper appropriately points out that interchangeability among multiple biosimilars is a question that should be answered in postmarketing registries, Dr. Fleischmann noted that no interchangeability study has been reported, even though the FDA has issued guidance on how a study should be done.
“Although interchangeability may be safe and effective in many patients, until the results of such a study are available and properly analyzed, it is only conjecture that interchangeability is appropriate and safe,” he said.
Costs
The white paper acknowledged that the “only anticipated advantage” of a biosimilar over its reference product was lower cost, since both drugs should be therapeutically equivalent. “The degree to which the availability of biosimilars in the U.S. will drive down the cost of biologic therapy, and who will benefit from any cost reductions remains to be seen,” the authors wrote.
“To incentivize the use of biosimilars,” the authors suggested that “commercial and government insurance programs could harmonize drug prices with patients’ out-of-pocket costs and provider reimbursement. Currently, however, patients with commercial insurance are likely to have similar copayments for both biosimilars and originator biologics because of [pharmacy benefits manager]– or plan-mandated patient cost sharing. Also, patients’ out-of-pocket costs for biosimilars in the Medicare Part D (self-administered drug) program likely will be higher than for originator biologics because of a flaw that maintains, rather than reduces, biosimilar patient cost sharing in the coverage gap (also known as the “donut hole”) until 2020.”
It is not at all clear that a biosimilar would be cheaper for the individual patient, Dr. Fleischmann said. “It may be cheaper to the pharmacy benefit management firm, but this may not really help patient access to these medications. It is also not clear that nonmedical substitution will be effective in every patient nor has it been demonstrated that extrapolation is effective,” he wrote.
No disclosures were listed for the authors of the position statement. Dr. Fleischmann is a consultant for AbbVie, Amgen, Bristol-Myers Squibb, Celltrion, Eli Lilly, GlaxoSmithKline, Novartis, Pfizer, Sanofi Aventis, and UCB.
SOURCES: Bridges S et al. Arthritis Rheumatol. 2018 Feb 7. doi: 10.1002/art.40388; and Fleischmann R. Arthritis Rheumatol. 2018 Feb 7. doi: 10.1002/art.40402
FROM ARTHRITIS & RHEUMATOLOGY
VIDEO: Off-label dupilumab finding a home in pediatric AD
KAUAI, HAWAII – Pediatric dermatologists aren’t waiting for Food and Drug Administration approval to try dupilumab (Dupixent) for their patients with severe atopic dermatitis.
It’s not approved in children, but the possibility of good control without the side effects of cyclosporine and other alternatives is too much to resist. A phase 2, company-sponsored study reported Eczema Area and Severity Index score improvements of up to 76% in pediatric patients treated with dupilumab, an interleukin-4 and IL-13 signaling blocker approved in 2017 for moderate to severe AD in adults.
Large pediatric trials are pending, but with results like that, “many of us just feel if it was our own kid, and we could get dupilumab, we would like to do that first,” said Lawrence Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego.
It’s not just dupilumab that’s causing excitement. With almost 20 biologics in the pipeline, eczema seems poised to undergo a revolution in treatment much like psoriasis has in recent years.
Dr. Eichenfield explained (Eucrisa), a topical nonsteroidal phosphodiesterase-4 inhibitor approved for mild to moderate AD for children and adults ages two and older in December 2016, which doesn’t seem to have the duration limits of steroids, he said in an interview at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Treatment of pediatric AD is “going to be a very different picture over the next few years,” he said.
Dr. Eichenfield is a consultant or investigator for many companies, including Regeneron/Sanofi, Genentech, Novartis, Pfizer, Lilly, and Allergan.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – Pediatric dermatologists aren’t waiting for Food and Drug Administration approval to try dupilumab (Dupixent) for their patients with severe atopic dermatitis.
It’s not approved in children, but the possibility of good control without the side effects of cyclosporine and other alternatives is too much to resist. A phase 2, company-sponsored study reported Eczema Area and Severity Index score improvements of up to 76% in pediatric patients treated with dupilumab, an interleukin-4 and IL-13 signaling blocker approved in 2017 for moderate to severe AD in adults.
Large pediatric trials are pending, but with results like that, “many of us just feel if it was our own kid, and we could get dupilumab, we would like to do that first,” said Lawrence Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego.
It’s not just dupilumab that’s causing excitement. With almost 20 biologics in the pipeline, eczema seems poised to undergo a revolution in treatment much like psoriasis has in recent years.
Dr. Eichenfield explained (Eucrisa), a topical nonsteroidal phosphodiesterase-4 inhibitor approved for mild to moderate AD for children and adults ages two and older in December 2016, which doesn’t seem to have the duration limits of steroids, he said in an interview at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Treatment of pediatric AD is “going to be a very different picture over the next few years,” he said.
Dr. Eichenfield is a consultant or investigator for many companies, including Regeneron/Sanofi, Genentech, Novartis, Pfizer, Lilly, and Allergan.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – Pediatric dermatologists aren’t waiting for Food and Drug Administration approval to try dupilumab (Dupixent) for their patients with severe atopic dermatitis.
It’s not approved in children, but the possibility of good control without the side effects of cyclosporine and other alternatives is too much to resist. A phase 2, company-sponsored study reported Eczema Area and Severity Index score improvements of up to 76% in pediatric patients treated with dupilumab, an interleukin-4 and IL-13 signaling blocker approved in 2017 for moderate to severe AD in adults.
Large pediatric trials are pending, but with results like that, “many of us just feel if it was our own kid, and we could get dupilumab, we would like to do that first,” said Lawrence Eichenfield, MD, professor of dermatology and pediatrics at the University of California, San Diego.
It’s not just dupilumab that’s causing excitement. With almost 20 biologics in the pipeline, eczema seems poised to undergo a revolution in treatment much like psoriasis has in recent years.
Dr. Eichenfield explained (Eucrisa), a topical nonsteroidal phosphodiesterase-4 inhibitor approved for mild to moderate AD for children and adults ages two and older in December 2016, which doesn’t seem to have the duration limits of steroids, he said in an interview at the Hawaii Dermatology Seminar provided by the Global Academy for Medical Education/Skin Disease Education Foundation.
Treatment of pediatric AD is “going to be a very different picture over the next few years,” he said.
Dr. Eichenfield is a consultant or investigator for many companies, including Regeneron/Sanofi, Genentech, Novartis, Pfizer, Lilly, and Allergan.
SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
REPORTING FROM SDEF HAWAII DERMATOLOGY SEMINAR

Fetal alcohol spectrum disorders incidence exceeds previous estimates
, according to a cross-sectional study.
Philip A. May, PhD, of the University of North Carolina, Gillings School of Global Public Health, and his coauthors assessed 6,639 first-grade children from four communities in the Rocky Mountain, Midwestern, Southeastern, and Pacific Southwestern regions of the United States.
In their report, published Feb. 6 in JAMA, they identified 222 cases of fetal alcohol spectrum disorders, representing conservative prevalence estimates ranging from 11.3 to 50 cases per 1,000 children (JAMA 2018;319[5]:474-82. doi: 10.1001/jama.2017.21896).
Of these children, 27 met the criteria for fetal alcohol syndrome, 104 met the criteria for partial fetal alcohol syndrome, and 91 met the criteria for alcohol-related neurodevelopmental disorder.
“These prevalence estimates are consistent with mounting evidence that harmful fetal alcohol exposure is common in the United States today and highlight the public health burden due to fetal alcohol spectrum disorders,” the authors wrote.
The finding was much higher than previous estimates of the prevalence of fetal alcohol spectrum disorders in the United States. The authors pointed out that routine surveillance methods may have previously underestimated the prevalence because so many children are either misdiagnosed or not diagnosed at all. But even two previous single-site, active-case ascertainment studies conducted in the United States found prevalence rates of 10 and 24 per 1,000 children.
“This consortium study, to our knowledge, was the first to apply active case ascertainment, common methodology, a single classification system, and expert in-person evaluation for a continuum of fetal alcohol spectrum disorders including alcohol-related neurodevelopmental disorder to a large number of children from communities across the United States,” the authors wrote. “These data have highlighted the need for a larger study with broader representation of U.S. communities with general population samples.”
Only 2 of the 222 children had actually been previously diagnosed with a fetal alcohol spectrum disorder, “although many parents and guardians were aware of the learning and behavioral challenges facing their children,” the researchers noted.
“These data confirm that missed diagnoses and misdiagnoses of children are common,” the authors wrote, pointing to a previous study in U.S. schoolchildren that found only one in seven children identified as having fetal alcohol syndrome had been previously diagnosed.
The assessment of fetal alcohol spectrum disorder was based on four domains: growth, dysmorphology, neurodevelopment, and prenatal alcohol exposure – the latter being assessed by interviewing the mother in person or by telephone.
The lowest prevalence – 11.3 per 1,000 children – was seen in the Midwestern community, while the highest – 50 per 1,000 – was in the Rocky Mountain community.
The main weakness of the study was that no individual sample included the entire eligible population because of differing policies on access to children for recruitment and variability in willingness to consent.
“Consent rates for screening ranged from 36.9% to 92.5% in individual samples and overall consent rates for screening averaged only 59.9% of eligible children,” the authors wrote. “If nonconsented children differed from consented, this could have biased prevalence estimates in either direction.”
The researchers acknowledged that the absence of a definitive biomarker for fetal alcohol spectrum disorder meant it was impossible to know for certain that the observed deficits were actually the result of fetal alcohol exposure, and that the prevalence estimates may therefore be overestimated.
The study was funded by grants from the National Institute on Alcohol Abuse and Alcoholism. One author declared grant support from the National Institute on Alcohol Abuse and Alcoholism and personal fees and honorarium from the Alcohol Center. No conflicts of interest were declared.
SOURCE: May, P et al. JAMA 2018;319[5]:474-82. doi: 10.1001/jama.2017.21896.
The finding of higher-than-expected prevalence estimates for fetal alcohol spectrum disorder has significant implications for clinicians and for public health. Many cases are misdiagnosed or not diagnosed, which may be the result of unknown or unconfirmed prenatal alcohol exposure, overlapping diagnostic criteria with other neurodevelopmental disorders, high rates of comorbidity, and the presence of a number of different clinical diagnostic guidelines. There is, therefore, a need for a universal diagnostic approach and the identification of novel and reliable biomarkers for detecting fetal alcohol effects.
In addition, the high prevalence of these disorders points to a need for better education of girls and women of childbearing age about the detrimental effects of alcohol consumption during pregnancy. Primary care clinicians should routinely include appropriate screening for alcohol use in all women of childbearing age in preconceptual health promotion and in contraceptive counseling and refer anyone identified as having an alcohol use disorder to substance abuse programs.
Shannon Lange, MPH, Jurgen Rehm, PhD, and Svetlana Popova, PhD, are with the Institute for Mental Health Policy Research at the Centre for Addiction and Mental Health in Toronto and the University of Toronto. These comments are taken from an accompanying editorial (JAMA 2018, 319[5]:448-9. doi: 10.1001/jama.2017.21895). No conflicts of interest were declared.
The finding of higher-than-expected prevalence estimates for fetal alcohol spectrum disorder has significant implications for clinicians and for public health. Many cases are misdiagnosed or not diagnosed, which may be the result of unknown or unconfirmed prenatal alcohol exposure, overlapping diagnostic criteria with other neurodevelopmental disorders, high rates of comorbidity, and the presence of a number of different clinical diagnostic guidelines. There is, therefore, a need for a universal diagnostic approach and the identification of novel and reliable biomarkers for detecting fetal alcohol effects.
In addition, the high prevalence of these disorders points to a need for better education of girls and women of childbearing age about the detrimental effects of alcohol consumption during pregnancy. Primary care clinicians should routinely include appropriate screening for alcohol use in all women of childbearing age in preconceptual health promotion and in contraceptive counseling and refer anyone identified as having an alcohol use disorder to substance abuse programs.
Shannon Lange, MPH, Jurgen Rehm, PhD, and Svetlana Popova, PhD, are with the Institute for Mental Health Policy Research at the Centre for Addiction and Mental Health in Toronto and the University of Toronto. These comments are taken from an accompanying editorial (JAMA 2018, 319[5]:448-9. doi: 10.1001/jama.2017.21895). No conflicts of interest were declared.
The finding of higher-than-expected prevalence estimates for fetal alcohol spectrum disorder has significant implications for clinicians and for public health. Many cases are misdiagnosed or not diagnosed, which may be the result of unknown or unconfirmed prenatal alcohol exposure, overlapping diagnostic criteria with other neurodevelopmental disorders, high rates of comorbidity, and the presence of a number of different clinical diagnostic guidelines. There is, therefore, a need for a universal diagnostic approach and the identification of novel and reliable biomarkers for detecting fetal alcohol effects.
In addition, the high prevalence of these disorders points to a need for better education of girls and women of childbearing age about the detrimental effects of alcohol consumption during pregnancy. Primary care clinicians should routinely include appropriate screening for alcohol use in all women of childbearing age in preconceptual health promotion and in contraceptive counseling and refer anyone identified as having an alcohol use disorder to substance abuse programs.
Shannon Lange, MPH, Jurgen Rehm, PhD, and Svetlana Popova, PhD, are with the Institute for Mental Health Policy Research at the Centre for Addiction and Mental Health in Toronto and the University of Toronto. These comments are taken from an accompanying editorial (JAMA 2018, 319[5]:448-9. doi: 10.1001/jama.2017.21895). No conflicts of interest were declared.
, according to a cross-sectional study.
Philip A. May, PhD, of the University of North Carolina, Gillings School of Global Public Health, and his coauthors assessed 6,639 first-grade children from four communities in the Rocky Mountain, Midwestern, Southeastern, and Pacific Southwestern regions of the United States.
In their report, published Feb. 6 in JAMA, they identified 222 cases of fetal alcohol spectrum disorders, representing conservative prevalence estimates ranging from 11.3 to 50 cases per 1,000 children (JAMA 2018;319[5]:474-82. doi: 10.1001/jama.2017.21896).
Of these children, 27 met the criteria for fetal alcohol syndrome, 104 met the criteria for partial fetal alcohol syndrome, and 91 met the criteria for alcohol-related neurodevelopmental disorder.
“These prevalence estimates are consistent with mounting evidence that harmful fetal alcohol exposure is common in the United States today and highlight the public health burden due to fetal alcohol spectrum disorders,” the authors wrote.
The finding was much higher than previous estimates of the prevalence of fetal alcohol spectrum disorders in the United States. The authors pointed out that routine surveillance methods may have previously underestimated the prevalence because so many children are either misdiagnosed or not diagnosed at all. But even two previous single-site, active-case ascertainment studies conducted in the United States found prevalence rates of 10 and 24 per 1,000 children.
“This consortium study, to our knowledge, was the first to apply active case ascertainment, common methodology, a single classification system, and expert in-person evaluation for a continuum of fetal alcohol spectrum disorders including alcohol-related neurodevelopmental disorder to a large number of children from communities across the United States,” the authors wrote. “These data have highlighted the need for a larger study with broader representation of U.S. communities with general population samples.”
Only 2 of the 222 children had actually been previously diagnosed with a fetal alcohol spectrum disorder, “although many parents and guardians were aware of the learning and behavioral challenges facing their children,” the researchers noted.
“These data confirm that missed diagnoses and misdiagnoses of children are common,” the authors wrote, pointing to a previous study in U.S. schoolchildren that found only one in seven children identified as having fetal alcohol syndrome had been previously diagnosed.
The assessment of fetal alcohol spectrum disorder was based on four domains: growth, dysmorphology, neurodevelopment, and prenatal alcohol exposure – the latter being assessed by interviewing the mother in person or by telephone.
The lowest prevalence – 11.3 per 1,000 children – was seen in the Midwestern community, while the highest – 50 per 1,000 – was in the Rocky Mountain community.
The main weakness of the study was that no individual sample included the entire eligible population because of differing policies on access to children for recruitment and variability in willingness to consent.
“Consent rates for screening ranged from 36.9% to 92.5% in individual samples and overall consent rates for screening averaged only 59.9% of eligible children,” the authors wrote. “If nonconsented children differed from consented, this could have biased prevalence estimates in either direction.”
The researchers acknowledged that the absence of a definitive biomarker for fetal alcohol spectrum disorder meant it was impossible to know for certain that the observed deficits were actually the result of fetal alcohol exposure, and that the prevalence estimates may therefore be overestimated.
The study was funded by grants from the National Institute on Alcohol Abuse and Alcoholism. One author declared grant support from the National Institute on Alcohol Abuse and Alcoholism and personal fees and honorarium from the Alcohol Center. No conflicts of interest were declared.
SOURCE: May, P et al. JAMA 2018;319[5]:474-82. doi: 10.1001/jama.2017.21896.
, according to a cross-sectional study.
Philip A. May, PhD, of the University of North Carolina, Gillings School of Global Public Health, and his coauthors assessed 6,639 first-grade children from four communities in the Rocky Mountain, Midwestern, Southeastern, and Pacific Southwestern regions of the United States.
In their report, published Feb. 6 in JAMA, they identified 222 cases of fetal alcohol spectrum disorders, representing conservative prevalence estimates ranging from 11.3 to 50 cases per 1,000 children (JAMA 2018;319[5]:474-82. doi: 10.1001/jama.2017.21896).
Of these children, 27 met the criteria for fetal alcohol syndrome, 104 met the criteria for partial fetal alcohol syndrome, and 91 met the criteria for alcohol-related neurodevelopmental disorder.
“These prevalence estimates are consistent with mounting evidence that harmful fetal alcohol exposure is common in the United States today and highlight the public health burden due to fetal alcohol spectrum disorders,” the authors wrote.
The finding was much higher than previous estimates of the prevalence of fetal alcohol spectrum disorders in the United States. The authors pointed out that routine surveillance methods may have previously underestimated the prevalence because so many children are either misdiagnosed or not diagnosed at all. But even two previous single-site, active-case ascertainment studies conducted in the United States found prevalence rates of 10 and 24 per 1,000 children.
“This consortium study, to our knowledge, was the first to apply active case ascertainment, common methodology, a single classification system, and expert in-person evaluation for a continuum of fetal alcohol spectrum disorders including alcohol-related neurodevelopmental disorder to a large number of children from communities across the United States,” the authors wrote. “These data have highlighted the need for a larger study with broader representation of U.S. communities with general population samples.”
Only 2 of the 222 children had actually been previously diagnosed with a fetal alcohol spectrum disorder, “although many parents and guardians were aware of the learning and behavioral challenges facing their children,” the researchers noted.
“These data confirm that missed diagnoses and misdiagnoses of children are common,” the authors wrote, pointing to a previous study in U.S. schoolchildren that found only one in seven children identified as having fetal alcohol syndrome had been previously diagnosed.
The assessment of fetal alcohol spectrum disorder was based on four domains: growth, dysmorphology, neurodevelopment, and prenatal alcohol exposure – the latter being assessed by interviewing the mother in person or by telephone.
The lowest prevalence – 11.3 per 1,000 children – was seen in the Midwestern community, while the highest – 50 per 1,000 – was in the Rocky Mountain community.
The main weakness of the study was that no individual sample included the entire eligible population because of differing policies on access to children for recruitment and variability in willingness to consent.
“Consent rates for screening ranged from 36.9% to 92.5% in individual samples and overall consent rates for screening averaged only 59.9% of eligible children,” the authors wrote. “If nonconsented children differed from consented, this could have biased prevalence estimates in either direction.”
The researchers acknowledged that the absence of a definitive biomarker for fetal alcohol spectrum disorder meant it was impossible to know for certain that the observed deficits were actually the result of fetal alcohol exposure, and that the prevalence estimates may therefore be overestimated.
The study was funded by grants from the National Institute on Alcohol Abuse and Alcoholism. One author declared grant support from the National Institute on Alcohol Abuse and Alcoholism and personal fees and honorarium from the Alcohol Center. No conflicts of interest were declared.
SOURCE: May, P et al. JAMA 2018;319[5]:474-82. doi: 10.1001/jama.2017.21896.
FROM JAMA
Key clinical point: The prevalence of fetal alcohol spectrum disorder in first-grade children in the United States may be as high as 1 in 20.
Major finding: The prevalence of fetal alcohol spectrum disorder ranged from 11.3 to 50 children per 1,000.
Data source: Cross-sectional study of 6,639 first-grade children.
Disclosures: The study was funded by grants from the National Institute on Alcohol Abuse and Alcoholism. One author declared grant support from the National Institute on Alcohol Abuse and Alcoholism and personal fees and honorarium from the Alcohol Center. No conflicts of interest were declared.
Source: May, P et al. JAMA 2018;319[5]:474-82. doi: 10.1001/jama.2017.21896.
Macrophage activation syndrome’s impact in childhood SLE felt mostly early
Nearly 10% of children with systemic lupus erythematosus (SLE) developed macrophage activation syndrome (MAS) at some point during a mean follow-up time of more than 3 years at one center, and most were concomitantly diagnosed with the syndrome.
Although the investigators from the University of Toronto reported significantly higher mortality among patients with MAS, most cases were successfully treated with corticosteroids, and no relapses were observed during follow-up.
MAS was first identified in patients with juvenile idiopathic arthritis and is most well known as a complication of that broadly named disease, but data on outcomes and disease course in SLE patients are limited, first author Roberto Ezequiel Borgia, MD, and his colleagues wrote in their report in Arthritis & Rheumatology.
The researchers identified 403 children with SLE seen at the Hospital for Sick Children in Toronto during 2002-2012. Overall, 38 patients (9%) had MAS; of those patients, 68% received a MAS diagnosis within 7 days of the SLE diagnosis – termed “concomitant” diagnosis – while another 29% received a MAS diagnosis within 180 days of their SLE diagnosis.
The researchers explained that “since there are no validated nor universally accepted diagnostic criteria for MAS in SLE, the definition of MAS was based on the treating pediatric rheumatologist’s expert opinion at the time of the initial presentation.” The most common presenting feature of MAS was fever (100%), followed by generalized lymphadenopathy (24%), hepatomegaly (18%), CNS dysfunction secondary to MAS (18%), hemorrhage (13%), and splenomegaly (10%).
The average age of the children at diagnosis was nearly 14 years, and 79% were female. The average follow-up was 3.5 years. There were no significant differences in the demographic features of children with and without MAS nor were there any in variables used to assess lupus outcomes, which included immunosuppressive drug use, average daily corticosteroid dose (18.3 mg/day with MAS vs. 18.6 mg/day without MAS), and the number of pediatric ICU visits (incidence rate ratio for MAS vs. non-MAS, 1.60 [95% CI, 0.74-3.18]).
Mortality was significantly higher in children with MAS, compared with those without MAS (5.3% vs. 0.3%; P = .02), although the overall number of deaths in the cohort was small (n = 3). Apart from the “acute illness which was associated with 2 deaths secondary to MAS,” the investigators said that they “did not find any significant differences in the number of deaths or damage accrual between the cohorts, including overall SLICC [Systemic Lupus International Collaborating Clinics] damage score or any specific damage feature within the score.”
The study findings were limited by several factors including the lack of validated MAS criteria for children with SLE and a lack of follow-up data on the patients beyond 18 years of age, the researchers said.
The results suggest that MAS remains a life-threatening complication in children with SLE and should be considered an important cause of mortality for them, but “if the initial presentation does not result in death, the long-term outcome seem[s] to be comparable to those without MAS,” the investigators wrote.
The researchers had no financial conflicts to disclose.
SOURCE: Borgia R et al. Arthritis Rheumatol. 2018 Jan 17. doi: 10.1002/art.40417
As we learn more about the role of macrophage activation syndrome (MAS), a secondary form of hemophagocytic lymphohistiocytosis in rheumatic diseases, it has become clear that patients may develop this syndrome in a variety of settings. The most common presentation of MAS is in association with systemic onset juvenile idiopathic arthritis, but is has been described in other forms of childhood rheumatic diseases, including other types of juvenile idiopathic arthritis, lupus, mixed connective tissue disease, Kawasaki disease, and sarcoidosis. Study of secondary MAS has led to suggested diagnostic criteria; however, those criteria are very similar to the presentation of adult and childhood systemic lupus with cytopenias, hepatitis, and coagulopathy.

The work by Borgia et al. encourages us to look for evidence of MAS in our lupus patients as it allows us to identify patients at risk for poor outcomes and to provide interventions to reduce those risks.
Marisa S. Klein-Gitelman, MD , is a professor of pediatrics at Northwestern University, Chicago, and is a pediatric rheumatologist at the Ann & Robert H. Lurie Children’s Hospital of Chicago. She has no relevant disclosures.
As we learn more about the role of macrophage activation syndrome (MAS), a secondary form of hemophagocytic lymphohistiocytosis in rheumatic diseases, it has become clear that patients may develop this syndrome in a variety of settings. The most common presentation of MAS is in association with systemic onset juvenile idiopathic arthritis, but is has been described in other forms of childhood rheumatic diseases, including other types of juvenile idiopathic arthritis, lupus, mixed connective tissue disease, Kawasaki disease, and sarcoidosis. Study of secondary MAS has led to suggested diagnostic criteria; however, those criteria are very similar to the presentation of adult and childhood systemic lupus with cytopenias, hepatitis, and coagulopathy.
The work by Borgia et al. encourages us to look for evidence of MAS in our lupus patients as it allows us to identify patients at risk for poor outcomes and to provide interventions to reduce those risks.
Marisa S. Klein-Gitelman, MD , is a professor of pediatrics at Northwestern University, Chicago, and is a pediatric rheumatologist at the Ann & Robert H. Lurie Children’s Hospital of Chicago. She has no relevant disclosures.
As we learn more about the role of macrophage activation syndrome (MAS), a secondary form of hemophagocytic lymphohistiocytosis in rheumatic diseases, it has become clear that patients may develop this syndrome in a variety of settings. The most common presentation of MAS is in association with systemic onset juvenile idiopathic arthritis, but is has been described in other forms of childhood rheumatic diseases, including other types of juvenile idiopathic arthritis, lupus, mixed connective tissue disease, Kawasaki disease, and sarcoidosis. Study of secondary MAS has led to suggested diagnostic criteria; however, those criteria are very similar to the presentation of adult and childhood systemic lupus with cytopenias, hepatitis, and coagulopathy.
The work by Borgia et al. encourages us to look for evidence of MAS in our lupus patients as it allows us to identify patients at risk for poor outcomes and to provide interventions to reduce those risks.
Marisa S. Klein-Gitelman, MD , is a professor of pediatrics at Northwestern University, Chicago, and is a pediatric rheumatologist at the Ann & Robert H. Lurie Children’s Hospital of Chicago. She has no relevant disclosures.
Nearly 10% of children with systemic lupus erythematosus (SLE) developed macrophage activation syndrome (MAS) at some point during a mean follow-up time of more than 3 years at one center, and most were concomitantly diagnosed with the syndrome.
Although the investigators from the University of Toronto reported significantly higher mortality among patients with MAS, most cases were successfully treated with corticosteroids, and no relapses were observed during follow-up.
MAS was first identified in patients with juvenile idiopathic arthritis and is most well known as a complication of that broadly named disease, but data on outcomes and disease course in SLE patients are limited, first author Roberto Ezequiel Borgia, MD, and his colleagues wrote in their report in Arthritis & Rheumatology.
The researchers identified 403 children with SLE seen at the Hospital for Sick Children in Toronto during 2002-2012. Overall, 38 patients (9%) had MAS; of those patients, 68% received a MAS diagnosis within 7 days of the SLE diagnosis – termed “concomitant” diagnosis – while another 29% received a MAS diagnosis within 180 days of their SLE diagnosis.
The researchers explained that “since there are no validated nor universally accepted diagnostic criteria for MAS in SLE, the definition of MAS was based on the treating pediatric rheumatologist’s expert opinion at the time of the initial presentation.” The most common presenting feature of MAS was fever (100%), followed by generalized lymphadenopathy (24%), hepatomegaly (18%), CNS dysfunction secondary to MAS (18%), hemorrhage (13%), and splenomegaly (10%).
The average age of the children at diagnosis was nearly 14 years, and 79% were female. The average follow-up was 3.5 years. There were no significant differences in the demographic features of children with and without MAS nor were there any in variables used to assess lupus outcomes, which included immunosuppressive drug use, average daily corticosteroid dose (18.3 mg/day with MAS vs. 18.6 mg/day without MAS), and the number of pediatric ICU visits (incidence rate ratio for MAS vs. non-MAS, 1.60 [95% CI, 0.74-3.18]).
Mortality was significantly higher in children with MAS, compared with those without MAS (5.3% vs. 0.3%; P = .02), although the overall number of deaths in the cohort was small (n = 3). Apart from the “acute illness which was associated with 2 deaths secondary to MAS,” the investigators said that they “did not find any significant differences in the number of deaths or damage accrual between the cohorts, including overall SLICC [Systemic Lupus International Collaborating Clinics] damage score or any specific damage feature within the score.”
The study findings were limited by several factors including the lack of validated MAS criteria for children with SLE and a lack of follow-up data on the patients beyond 18 years of age, the researchers said.
The results suggest that MAS remains a life-threatening complication in children with SLE and should be considered an important cause of mortality for them, but “if the initial presentation does not result in death, the long-term outcome seem[s] to be comparable to those without MAS,” the investigators wrote.
The researchers had no financial conflicts to disclose.
SOURCE: Borgia R et al. Arthritis Rheumatol. 2018 Jan 17. doi: 10.1002/art.40417
Nearly 10% of children with systemic lupus erythematosus (SLE) developed macrophage activation syndrome (MAS) at some point during a mean follow-up time of more than 3 years at one center, and most were concomitantly diagnosed with the syndrome.
Although the investigators from the University of Toronto reported significantly higher mortality among patients with MAS, most cases were successfully treated with corticosteroids, and no relapses were observed during follow-up.
MAS was first identified in patients with juvenile idiopathic arthritis and is most well known as a complication of that broadly named disease, but data on outcomes and disease course in SLE patients are limited, first author Roberto Ezequiel Borgia, MD, and his colleagues wrote in their report in Arthritis & Rheumatology.
The researchers identified 403 children with SLE seen at the Hospital for Sick Children in Toronto during 2002-2012. Overall, 38 patients (9%) had MAS; of those patients, 68% received a MAS diagnosis within 7 days of the SLE diagnosis – termed “concomitant” diagnosis – while another 29% received a MAS diagnosis within 180 days of their SLE diagnosis.
The researchers explained that “since there are no validated nor universally accepted diagnostic criteria for MAS in SLE, the definition of MAS was based on the treating pediatric rheumatologist’s expert opinion at the time of the initial presentation.” The most common presenting feature of MAS was fever (100%), followed by generalized lymphadenopathy (24%), hepatomegaly (18%), CNS dysfunction secondary to MAS (18%), hemorrhage (13%), and splenomegaly (10%).
The average age of the children at diagnosis was nearly 14 years, and 79% were female. The average follow-up was 3.5 years. There were no significant differences in the demographic features of children with and without MAS nor were there any in variables used to assess lupus outcomes, which included immunosuppressive drug use, average daily corticosteroid dose (18.3 mg/day with MAS vs. 18.6 mg/day without MAS), and the number of pediatric ICU visits (incidence rate ratio for MAS vs. non-MAS, 1.60 [95% CI, 0.74-3.18]).
Mortality was significantly higher in children with MAS, compared with those without MAS (5.3% vs. 0.3%; P = .02), although the overall number of deaths in the cohort was small (n = 3). Apart from the “acute illness which was associated with 2 deaths secondary to MAS,” the investigators said that they “did not find any significant differences in the number of deaths or damage accrual between the cohorts, including overall SLICC [Systemic Lupus International Collaborating Clinics] damage score or any specific damage feature within the score.”
The study findings were limited by several factors including the lack of validated MAS criteria for children with SLE and a lack of follow-up data on the patients beyond 18 years of age, the researchers said.
The results suggest that MAS remains a life-threatening complication in children with SLE and should be considered an important cause of mortality for them, but “if the initial presentation does not result in death, the long-term outcome seem[s] to be comparable to those without MAS,” the investigators wrote.
The researchers had no financial conflicts to disclose.
SOURCE: Borgia R et al. Arthritis Rheumatol. 2018 Jan 17. doi: 10.1002/art.40417
FROM ARTHRITIS & RHEUMATOLOGY
Key clinical point: Nearly 10% of children with SLE developed MAS at some point during a mean follow-up time of more than 3 years, but many outcomes were the same in patients with and without MAS.
Major finding: Mortality was 5.3% in children with MAS, compared with 0.3% in those without MAS (P = .02), over a 3.5-year follow-up period.
Study details: The data come from 403 children with SLE seen at a single center during 2002-2012.
Disclosures: The researchers had no financial conflicts to disclose.
Source: Borgia R et al. Arthritis Rheumatol. 2018 Jan 17. doi: 10.1002/art.40417.

Advocating for reality
Our first daughter was born during my last year in medical school, and our second was born as I was finishing my second year in residency. Seeing those two little darlings grow and develop was a critical supplement to my pediatric training. And, watching my wife initially struggle and then succeed with breastfeeding provided a very personal experience and education about lactation that my interactions in the hospital and outpatient clinics didn’t offer.
We considered ourselves lucky because my wife wasn’t facing the additional challenge of returning to an out-of-the-home job. However, our good fortune did not confer immunity against the anxiety, insecurity, discomfort, and sleep deprivation–induced frustrations of breastfeeding. Watching my wife navigate the choppy waters of lactation certainly influenced my approach to counseling new mothers over my subsequent 4 decades of practice. I think I was a more sympathetic and realistic adviser based on my first-hand observations.
In a different survey of American Academy of Pediatrics fellows, more of the 832 pediatricians responding reported having had a personal experience with breastfeeding in 2014 than of the 620 responding in 1995 (68% vs. 42%). However, it is interesting that fewer of the respondents in 2014 felt that any mother can succeed at breastfeeding (predicted value = 70% in 1995, PV = 56% in 2014; P less than .05), and fewer in 2014 believed that the advantages of breastfeeding outweighed the difficulties than among those surveyed in 1995 (PV = 70% in 1995, PV = 50% in 2014; P less than .05) (Pediatrics. 2017 Oct;140[4]. pii: e20171229). These results suggest that, as more pediatricians gained personal experience with breastfeeding, more may have realized that the American Academy of Pediatrics recommendations for breastfeeding are unrealistic and may contribute to the negative experiences of some women, including pediatric trainees.
An implied assumption in the AAP News article is that a pediatrician who has had a negative breastfeeding experience is less likely to be a strong advocate for breastfeeding. I would argue that a pediatrician who has witnessed or personally experienced difficulties is more likely to be a sympathetic and realistic advocate of breastfeeding.

We must walk that fine line between actively advocating for lactation-friendly hospitals and work environments and supporting mothers who, due to circumstances beyond their control, can’t meet the expectations we have created for them.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Our first daughter was born during my last year in medical school, and our second was born as I was finishing my second year in residency. Seeing those two little darlings grow and develop was a critical supplement to my pediatric training. And, watching my wife initially struggle and then succeed with breastfeeding provided a very personal experience and education about lactation that my interactions in the hospital and outpatient clinics didn’t offer.
We considered ourselves lucky because my wife wasn’t facing the additional challenge of returning to an out-of-the-home job. However, our good fortune did not confer immunity against the anxiety, insecurity, discomfort, and sleep deprivation–induced frustrations of breastfeeding. Watching my wife navigate the choppy waters of lactation certainly influenced my approach to counseling new mothers over my subsequent 4 decades of practice. I think I was a more sympathetic and realistic adviser based on my first-hand observations.
In a different survey of American Academy of Pediatrics fellows, more of the 832 pediatricians responding reported having had a personal experience with breastfeeding in 2014 than of the 620 responding in 1995 (68% vs. 42%). However, it is interesting that fewer of the respondents in 2014 felt that any mother can succeed at breastfeeding (predicted value = 70% in 1995, PV = 56% in 2014; P less than .05), and fewer in 2014 believed that the advantages of breastfeeding outweighed the difficulties than among those surveyed in 1995 (PV = 70% in 1995, PV = 50% in 2014; P less than .05) (Pediatrics. 2017 Oct;140[4]. pii: e20171229). These results suggest that, as more pediatricians gained personal experience with breastfeeding, more may have realized that the American Academy of Pediatrics recommendations for breastfeeding are unrealistic and may contribute to the negative experiences of some women, including pediatric trainees.
An implied assumption in the AAP News article is that a pediatrician who has had a negative breastfeeding experience is less likely to be a strong advocate for breastfeeding. I would argue that a pediatrician who has witnessed or personally experienced difficulties is more likely to be a sympathetic and realistic advocate of breastfeeding.
We must walk that fine line between actively advocating for lactation-friendly hospitals and work environments and supporting mothers who, due to circumstances beyond their control, can’t meet the expectations we have created for them.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Our first daughter was born during my last year in medical school, and our second was born as I was finishing my second year in residency. Seeing those two little darlings grow and develop was a critical supplement to my pediatric training. And, watching my wife initially struggle and then succeed with breastfeeding provided a very personal experience and education about lactation that my interactions in the hospital and outpatient clinics didn’t offer.
We considered ourselves lucky because my wife wasn’t facing the additional challenge of returning to an out-of-the-home job. However, our good fortune did not confer immunity against the anxiety, insecurity, discomfort, and sleep deprivation–induced frustrations of breastfeeding. Watching my wife navigate the choppy waters of lactation certainly influenced my approach to counseling new mothers over my subsequent 4 decades of practice. I think I was a more sympathetic and realistic adviser based on my first-hand observations.
In a different survey of American Academy of Pediatrics fellows, more of the 832 pediatricians responding reported having had a personal experience with breastfeeding in 2014 than of the 620 responding in 1995 (68% vs. 42%). However, it is interesting that fewer of the respondents in 2014 felt that any mother can succeed at breastfeeding (predicted value = 70% in 1995, PV = 56% in 2014; P less than .05), and fewer in 2014 believed that the advantages of breastfeeding outweighed the difficulties than among those surveyed in 1995 (PV = 70% in 1995, PV = 50% in 2014; P less than .05) (Pediatrics. 2017 Oct;140[4]. pii: e20171229). These results suggest that, as more pediatricians gained personal experience with breastfeeding, more may have realized that the American Academy of Pediatrics recommendations for breastfeeding are unrealistic and may contribute to the negative experiences of some women, including pediatric trainees.
An implied assumption in the AAP News article is that a pediatrician who has had a negative breastfeeding experience is less likely to be a strong advocate for breastfeeding. I would argue that a pediatrician who has witnessed or personally experienced difficulties is more likely to be a sympathetic and realistic advocate of breastfeeding.
We must walk that fine line between actively advocating for lactation-friendly hospitals and work environments and supporting mothers who, due to circumstances beyond their control, can’t meet the expectations we have created for them.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
… What comes naturally
When we were invited to a family gathering to celebrate a 60th birthday, we expected to hear an abundance of news about grandchildren. They are natural, and seldom controversial, topics of discussion. If there is a child still waiting in utero and destined to be the first grandchild on one or both sides of the family, the impending adventure in parenthood will dominate the conversation.
To our great surprise, despite the presence of one very pregnant young woman, who in 6 weeks would be giving birth to the first grandchild in my nephew’s family, my wife and I can recall only one brief dialogue in which I was asked about how one might go about selecting a pediatrician.
I’m not sure why the blessed event to come was being ignored, but I found the oversight unusual and refreshing. It is possible that there had been so much hype about the pregnancy on her side of the family that the couple relished its absence from the birthday party’s topics for discussion.
In the spirit of full disclosure, I must add that, as a result of my frequent claims of ignorance when asked about medically related topics, I am often referred to by the extended family as “Dr. I-Don’t-Know.” It may be that my presence influenced the conversation, but regardless of the reason, I was impressed with the ease at which this couple was approaching the birth of their first child.
I am sure they harbor some anxieties, and I am sure they have listened to some horror stories from their peers about sleep and breastfeeding problems. They are bright people who acknowledge that they are going to encounter some bumps along the road of parenthood. However, they seem to be immune to the epidemic of anxiety that for decades has been sweeping over cohorts of North Americans entering their family-building years.
The young couple my wife and I encountered are just as clueless about what parenthood has in store as their anxiety-driven peers are. The difference is that they are enjoying their pregnancy in blissful ignorance buffered by their refreshing confidence that, however they do it, they will be doing it naturally.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
When we were invited to a family gathering to celebrate a 60th birthday, we expected to hear an abundance of news about grandchildren. They are natural, and seldom controversial, topics of discussion. If there is a child still waiting in utero and destined to be the first grandchild on one or both sides of the family, the impending adventure in parenthood will dominate the conversation.
To our great surprise, despite the presence of one very pregnant young woman, who in 6 weeks would be giving birth to the first grandchild in my nephew’s family, my wife and I can recall only one brief dialogue in which I was asked about how one might go about selecting a pediatrician.
I’m not sure why the blessed event to come was being ignored, but I found the oversight unusual and refreshing. It is possible that there had been so much hype about the pregnancy on her side of the family that the couple relished its absence from the birthday party’s topics for discussion.
In the spirit of full disclosure, I must add that, as a result of my frequent claims of ignorance when asked about medically related topics, I am often referred to by the extended family as “Dr. I-Don’t-Know.” It may be that my presence influenced the conversation, but regardless of the reason, I was impressed with the ease at which this couple was approaching the birth of their first child.
I am sure they harbor some anxieties, and I am sure they have listened to some horror stories from their peers about sleep and breastfeeding problems. They are bright people who acknowledge that they are going to encounter some bumps along the road of parenthood. However, they seem to be immune to the epidemic of anxiety that for decades has been sweeping over cohorts of North Americans entering their family-building years.
The young couple my wife and I encountered are just as clueless about what parenthood has in store as their anxiety-driven peers are. The difference is that they are enjoying their pregnancy in blissful ignorance buffered by their refreshing confidence that, however they do it, they will be doing it naturally.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
When we were invited to a family gathering to celebrate a 60th birthday, we expected to hear an abundance of news about grandchildren. They are natural, and seldom controversial, topics of discussion. If there is a child still waiting in utero and destined to be the first grandchild on one or both sides of the family, the impending adventure in parenthood will dominate the conversation.
To our great surprise, despite the presence of one very pregnant young woman, who in 6 weeks would be giving birth to the first grandchild in my nephew’s family, my wife and I can recall only one brief dialogue in which I was asked about how one might go about selecting a pediatrician.
I’m not sure why the blessed event to come was being ignored, but I found the oversight unusual and refreshing. It is possible that there had been so much hype about the pregnancy on her side of the family that the couple relished its absence from the birthday party’s topics for discussion.
In the spirit of full disclosure, I must add that, as a result of my frequent claims of ignorance when asked about medically related topics, I am often referred to by the extended family as “Dr. I-Don’t-Know.” It may be that my presence influenced the conversation, but regardless of the reason, I was impressed with the ease at which this couple was approaching the birth of their first child.
I am sure they harbor some anxieties, and I am sure they have listened to some horror stories from their peers about sleep and breastfeeding problems. They are bright people who acknowledge that they are going to encounter some bumps along the road of parenthood. However, they seem to be immune to the epidemic of anxiety that for decades has been sweeping over cohorts of North Americans entering their family-building years.
The young couple my wife and I encountered are just as clueless about what parenthood has in store as their anxiety-driven peers are. The difference is that they are enjoying their pregnancy in blissful ignorance buffered by their refreshing confidence that, however they do it, they will be doing it naturally.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”