User login
Intervention helps kids stay active after cancer treatment

ORLANDO—Results of a pilot study suggest a web-based, reward-driven intervention can motivate adolescent cancer survivors to stay physically active.
Time spent performing moderate-to-vigorous physical activity (MVPA) increased by an average of 5 minutes a week for subjects who were randomized to the intervention.
For control subjects, MVPA decreased by an average of 24 minutes a week.
These findings were presented at the 2018 Cancer Survivorship Symposium (abstract 102).
“Compared to the general population, childhood cancer survivors have an increased risk for obesity and metabolic syndrome, conditions that can lead to heart disease, stroke, and diabetes, so it is really important that they are physically active,” said study investigator Carrie R. Howell, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“By intervening in this young age group, we hope to help kids develop healthy exercise habits for life.”
Dr Howell and her colleagues studied cancer survivors, ages 11 to 15, who were no longer receiving cancer treatment and were physically active less than 60 minutes a day.
The subjects were randomized to the intervention or to a control group. Controls received a wearable activity monitor and an educational handout with information about the importance of physical activity and examples of activities.
The intervention group received the handout and activity monitor but also had access to an interactive website. On at least a weekly basis, subjects would connect their monitor to a computer and log their activity through the website. Upon achieving certain thresholds of activity, they received rewards, such as T-shirts and gift cards by mail.
At the beginning and end of the study, participants visited St. Jude for an assessment of their physical fitness (strength, flexibility, and endurance) and neurocognitive measures (attention and memory), as well as health-related quality of life (assessed using the Pediatric Quality of Life Inventory questionnaire).
Results
Seventy-eight cancer survivors completed the 24-week study, 53 of them in the intervention group and 25 in the control group.
MVPA increased by an average of 4.7 minutes per week in the intervention group and decreased by an average of 24.3 minutes per week in the control group.
“In this age group, it is common to see a decrease in physical activity over time, even among healthy kids,” Dr Howell said. “Therefore, we are encouraged that our intervention was successful at maintaining physical activity levels, but a longer program may be needed to create lasting exercise habits.”
In addition to increases in MVPA, the intervention group had the following improvements in fitness:
- Increase in hand grip strength from an average of 19.9 kg to 21.0 kg
- Increase in number of push-ups from an average of 15 to 18
- Increase in number of sit-ups from an average of 11 to 14.
Furthermore, subjects in the intervention group saw their verbal fluency z-score increase by an average of 0.13 points and their general cognition z-score increase by an average of 0.23 points.
Their quality of life scores increased as well. Both overall quality of life and physical-function-related quality of life scores increased from an average of 74.2 to 78.0.
Control subjects had no significant changes in fitness, neurocognitive measures, or quality of life.
This study was supported by the National Cancer Institute, the American Lebanese Syrian Associated Charities, and HopeLab.
Based on the results of this study, the investigators have designed a larger trial (ALTE1631) to test a web-based physical activity intervention. They hope to enroll 384 survivors of childhood acute lymphoblastic leukemia at institutions across the US. The intervention will last a year, with follow-up at 18 months.
Further down the line, the investigators plan to explore the relationship between physical activity and cognition.
ORLANDO—Results of a pilot study suggest a web-based, reward-driven intervention can motivate adolescent cancer survivors to stay physically active.
Time spent performing moderate-to-vigorous physical activity (MVPA) increased by an average of 5 minutes a week for subjects who were randomized to the intervention.
For control subjects, MVPA decreased by an average of 24 minutes a week.
These findings were presented at the 2018 Cancer Survivorship Symposium (abstract 102).
“Compared to the general population, childhood cancer survivors have an increased risk for obesity and metabolic syndrome, conditions that can lead to heart disease, stroke, and diabetes, so it is really important that they are physically active,” said study investigator Carrie R. Howell, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“By intervening in this young age group, we hope to help kids develop healthy exercise habits for life.”
Dr Howell and her colleagues studied cancer survivors, ages 11 to 15, who were no longer receiving cancer treatment and were physically active less than 60 minutes a day.
The subjects were randomized to the intervention or to a control group. Controls received a wearable activity monitor and an educational handout with information about the importance of physical activity and examples of activities.
The intervention group received the handout and activity monitor but also had access to an interactive website. On at least a weekly basis, subjects would connect their monitor to a computer and log their activity through the website. Upon achieving certain thresholds of activity, they received rewards, such as T-shirts and gift cards by mail.
At the beginning and end of the study, participants visited St. Jude for an assessment of their physical fitness (strength, flexibility, and endurance) and neurocognitive measures (attention and memory), as well as health-related quality of life (assessed using the Pediatric Quality of Life Inventory questionnaire).
Results
Seventy-eight cancer survivors completed the 24-week study, 53 of them in the intervention group and 25 in the control group.
MVPA increased by an average of 4.7 minutes per week in the intervention group and decreased by an average of 24.3 minutes per week in the control group.
“In this age group, it is common to see a decrease in physical activity over time, even among healthy kids,” Dr Howell said. “Therefore, we are encouraged that our intervention was successful at maintaining physical activity levels, but a longer program may be needed to create lasting exercise habits.”
In addition to increases in MVPA, the intervention group had the following improvements in fitness:
- Increase in hand grip strength from an average of 19.9 kg to 21.0 kg
- Increase in number of push-ups from an average of 15 to 18
- Increase in number of sit-ups from an average of 11 to 14.
Furthermore, subjects in the intervention group saw their verbal fluency z-score increase by an average of 0.13 points and their general cognition z-score increase by an average of 0.23 points.
Their quality of life scores increased as well. Both overall quality of life and physical-function-related quality of life scores increased from an average of 74.2 to 78.0.
Control subjects had no significant changes in fitness, neurocognitive measures, or quality of life.
This study was supported by the National Cancer Institute, the American Lebanese Syrian Associated Charities, and HopeLab.
Based on the results of this study, the investigators have designed a larger trial (ALTE1631) to test a web-based physical activity intervention. They hope to enroll 384 survivors of childhood acute lymphoblastic leukemia at institutions across the US. The intervention will last a year, with follow-up at 18 months.
Further down the line, the investigators plan to explore the relationship between physical activity and cognition.
ORLANDO—Results of a pilot study suggest a web-based, reward-driven intervention can motivate adolescent cancer survivors to stay physically active.
Time spent performing moderate-to-vigorous physical activity (MVPA) increased by an average of 5 minutes a week for subjects who were randomized to the intervention.
For control subjects, MVPA decreased by an average of 24 minutes a week.
These findings were presented at the 2018 Cancer Survivorship Symposium (abstract 102).
“Compared to the general population, childhood cancer survivors have an increased risk for obesity and metabolic syndrome, conditions that can lead to heart disease, stroke, and diabetes, so it is really important that they are physically active,” said study investigator Carrie R. Howell, PhD, of St. Jude Children’s Research Hospital in Memphis, Tennessee.
“By intervening in this young age group, we hope to help kids develop healthy exercise habits for life.”
Dr Howell and her colleagues studied cancer survivors, ages 11 to 15, who were no longer receiving cancer treatment and were physically active less than 60 minutes a day.
The subjects were randomized to the intervention or to a control group. Controls received a wearable activity monitor and an educational handout with information about the importance of physical activity and examples of activities.
The intervention group received the handout and activity monitor but also had access to an interactive website. On at least a weekly basis, subjects would connect their monitor to a computer and log their activity through the website. Upon achieving certain thresholds of activity, they received rewards, such as T-shirts and gift cards by mail.
At the beginning and end of the study, participants visited St. Jude for an assessment of their physical fitness (strength, flexibility, and endurance) and neurocognitive measures (attention and memory), as well as health-related quality of life (assessed using the Pediatric Quality of Life Inventory questionnaire).
Results
Seventy-eight cancer survivors completed the 24-week study, 53 of them in the intervention group and 25 in the control group.
MVPA increased by an average of 4.7 minutes per week in the intervention group and decreased by an average of 24.3 minutes per week in the control group.
“In this age group, it is common to see a decrease in physical activity over time, even among healthy kids,” Dr Howell said. “Therefore, we are encouraged that our intervention was successful at maintaining physical activity levels, but a longer program may be needed to create lasting exercise habits.”
In addition to increases in MVPA, the intervention group had the following improvements in fitness:
- Increase in hand grip strength from an average of 19.9 kg to 21.0 kg
- Increase in number of push-ups from an average of 15 to 18
- Increase in number of sit-ups from an average of 11 to 14.
Furthermore, subjects in the intervention group saw their verbal fluency z-score increase by an average of 0.13 points and their general cognition z-score increase by an average of 0.23 points.
Their quality of life scores increased as well. Both overall quality of life and physical-function-related quality of life scores increased from an average of 74.2 to 78.0.
Control subjects had no significant changes in fitness, neurocognitive measures, or quality of life.
This study was supported by the National Cancer Institute, the American Lebanese Syrian Associated Charities, and HopeLab.
Based on the results of this study, the investigators have designed a larger trial (ALTE1631) to test a web-based physical activity intervention. They hope to enroll 384 survivors of childhood acute lymphoblastic leukemia at institutions across the US. The intervention will last a year, with follow-up at 18 months.
Further down the line, the investigators plan to explore the relationship between physical activity and cognition.
Topical anticholinergic improved hyperhidrosis in children
SAN DIEGO – A topical anticholinergic drug, glycopyrronium tosylate, was as safe and effective for treating hyperhidrosis in children 9-16 years old as it was in adults in two phase 3 trials that included 25 treated children, raising the prospect it could become the first drug to gain Food and Drug Administration approval for treating pediatric hyperhidrosis.
“Topical glycopyrronium tosylate treatment may provide a much needed treatment option for those with primary axillary hyperhidrosis, including pediatric patients,” Adelaide A. Hebert, MD, said at the annual meeting of the American Academy of Dermatology.

The data she reported from a post hoc analysis included 25 children. 9-16 years old, who received a daily, topical application of glycopyrronium tosylate to their underarms for 4 weeks and 19 children treated with vehicle only. The children were enrolled in either of a pair of phase 3 pivotal trials that together randomized 697 patients. In November 2017, Dermira, the company developing this drug, submitted an application to the FDA for marketing approval of the agent for adults and children at least 9 years old. A statement from the company said an FDA decision is expected by mid-2018.
Getting approval from the FDA for an effective pediatric hyperhidrosis treatment would be an important advance because nothing now exists in that space, said Dr. Hebert, professor of dermatology and pediatrics and director of pediatric dermatology at the University of Texas Health Sciences Center at Houston.
Based on past FDA actions, safety data from 25 children should be adequate to support pediatric labeling, she said in an interview, though she added that confirmatory safety data from a phase 4 study in children would be a welcome future addition. Hyperhydrosis in adolescents is “underappreciated, underdiagnosed, and is very impactful,” and currently has limited treatment options that are readily available for children, especially effective options for more severe hyperhidrosis.
The pediatric data came from the phase 3, randomized, double-blind, vehicle-controlled ATMOS-1 (DRM04 in Subjects With Axillary Hyperhidrosis) trial. The trial ran at several U.S. and German centers, although only the U.S. centers enrolled pediatric patients.
The two trials enrolled patients with “intolerable or barely tolerable” primary, axillary hyperhidrosis of at least 6 months' duration. After 4 weeks, patients treated with glycopyrronium tosylate had improvements in their daily diary account of axillary sweating and in sweat production. Dr. Hebert and her associates reported overall results from the two trials at various prior dermatology meetings, and the company reported some of the results in a press release, but the results have not yet been published in a journal.
The new, pediatric analysis that Dr. Hebert reported showed that the responder rate based on a 4 point or greater improvement in daily sweat diary assessments occurred in 60% of the actively treated children and in 13% of the controls. A 50% or greater reduction in sweat production occurred in 80% of the treated children and in 55% of controls. Quality of life, measured using the Children’s Dermatology Life Quality Index improved by an average of 8 points among the treated children, compared with an average 2-point improvement among the controls. This level of improvement among the glycopyrronium-treated patients would have been enough to move patients from the moderate-effect category at baseline to a no- or small-effect category.
The treatment was generally well tolerated, with no serious adverse effects reported and with treatment effects that were primarily as expected from an anticholinergic agent, including dry mouth, pupil dilation, and blurred vision. One of the 25 treated children withdrew because of these effects, which then resolved. Blood testing showed no systemic absorption of the drug, Dr. Hebert said.
The ATMOS-1 and ATMOS-2 trials were sponsored by Dermira, the company developing glycopyrronium tosylate. Dr. Hebert has been a consultant to and has received research funding from Dermira, and some of the coauthors of the study are Dermira employees. Dr. Hebert is an advisor to the editorial board of Dermatology News.
SOURCE: Hebert A et al. Annual meeting of the American Academy of Dermatology Abstract 6659.
SAN DIEGO – A topical anticholinergic drug, glycopyrronium tosylate, was as safe and effective for treating hyperhidrosis in children 9-16 years old as it was in adults in two phase 3 trials that included 25 treated children, raising the prospect it could become the first drug to gain Food and Drug Administration approval for treating pediatric hyperhidrosis.
“Topical glycopyrronium tosylate treatment may provide a much needed treatment option for those with primary axillary hyperhidrosis, including pediatric patients,” Adelaide A. Hebert, MD, said at the annual meeting of the American Academy of Dermatology.
The data she reported from a post hoc analysis included 25 children. 9-16 years old, who received a daily, topical application of glycopyrronium tosylate to their underarms for 4 weeks and 19 children treated with vehicle only. The children were enrolled in either of a pair of phase 3 pivotal trials that together randomized 697 patients. In November 2017, Dermira, the company developing this drug, submitted an application to the FDA for marketing approval of the agent for adults and children at least 9 years old. A statement from the company said an FDA decision is expected by mid-2018.
Getting approval from the FDA for an effective pediatric hyperhidrosis treatment would be an important advance because nothing now exists in that space, said Dr. Hebert, professor of dermatology and pediatrics and director of pediatric dermatology at the University of Texas Health Sciences Center at Houston.
Based on past FDA actions, safety data from 25 children should be adequate to support pediatric labeling, she said in an interview, though she added that confirmatory safety data from a phase 4 study in children would be a welcome future addition. Hyperhydrosis in adolescents is “underappreciated, underdiagnosed, and is very impactful,” and currently has limited treatment options that are readily available for children, especially effective options for more severe hyperhidrosis.
The pediatric data came from the phase 3, randomized, double-blind, vehicle-controlled ATMOS-1 (DRM04 in Subjects With Axillary Hyperhidrosis) trial. The trial ran at several U.S. and German centers, although only the U.S. centers enrolled pediatric patients.
The two trials enrolled patients with “intolerable or barely tolerable” primary, axillary hyperhidrosis of at least 6 months' duration. After 4 weeks, patients treated with glycopyrronium tosylate had improvements in their daily diary account of axillary sweating and in sweat production. Dr. Hebert and her associates reported overall results from the two trials at various prior dermatology meetings, and the company reported some of the results in a press release, but the results have not yet been published in a journal.
The new, pediatric analysis that Dr. Hebert reported showed that the responder rate based on a 4 point or greater improvement in daily sweat diary assessments occurred in 60% of the actively treated children and in 13% of the controls. A 50% or greater reduction in sweat production occurred in 80% of the treated children and in 55% of controls. Quality of life, measured using the Children’s Dermatology Life Quality Index improved by an average of 8 points among the treated children, compared with an average 2-point improvement among the controls. This level of improvement among the glycopyrronium-treated patients would have been enough to move patients from the moderate-effect category at baseline to a no- or small-effect category.
The treatment was generally well tolerated, with no serious adverse effects reported and with treatment effects that were primarily as expected from an anticholinergic agent, including dry mouth, pupil dilation, and blurred vision. One of the 25 treated children withdrew because of these effects, which then resolved. Blood testing showed no systemic absorption of the drug, Dr. Hebert said.
The ATMOS-1 and ATMOS-2 trials were sponsored by Dermira, the company developing glycopyrronium tosylate. Dr. Hebert has been a consultant to and has received research funding from Dermira, and some of the coauthors of the study are Dermira employees. Dr. Hebert is an advisor to the editorial board of Dermatology News.
SOURCE: Hebert A et al. Annual meeting of the American Academy of Dermatology Abstract 6659.
SAN DIEGO – A topical anticholinergic drug, glycopyrronium tosylate, was as safe and effective for treating hyperhidrosis in children 9-16 years old as it was in adults in two phase 3 trials that included 25 treated children, raising the prospect it could become the first drug to gain Food and Drug Administration approval for treating pediatric hyperhidrosis.
“Topical glycopyrronium tosylate treatment may provide a much needed treatment option for those with primary axillary hyperhidrosis, including pediatric patients,” Adelaide A. Hebert, MD, said at the annual meeting of the American Academy of Dermatology.
The data she reported from a post hoc analysis included 25 children. 9-16 years old, who received a daily, topical application of glycopyrronium tosylate to their underarms for 4 weeks and 19 children treated with vehicle only. The children were enrolled in either of a pair of phase 3 pivotal trials that together randomized 697 patients. In November 2017, Dermira, the company developing this drug, submitted an application to the FDA for marketing approval of the agent for adults and children at least 9 years old. A statement from the company said an FDA decision is expected by mid-2018.
Getting approval from the FDA for an effective pediatric hyperhidrosis treatment would be an important advance because nothing now exists in that space, said Dr. Hebert, professor of dermatology and pediatrics and director of pediatric dermatology at the University of Texas Health Sciences Center at Houston.
Based on past FDA actions, safety data from 25 children should be adequate to support pediatric labeling, she said in an interview, though she added that confirmatory safety data from a phase 4 study in children would be a welcome future addition. Hyperhydrosis in adolescents is “underappreciated, underdiagnosed, and is very impactful,” and currently has limited treatment options that are readily available for children, especially effective options for more severe hyperhidrosis.
The pediatric data came from the phase 3, randomized, double-blind, vehicle-controlled ATMOS-1 (DRM04 in Subjects With Axillary Hyperhidrosis) trial. The trial ran at several U.S. and German centers, although only the U.S. centers enrolled pediatric patients.
The two trials enrolled patients with “intolerable or barely tolerable” primary, axillary hyperhidrosis of at least 6 months' duration. After 4 weeks, patients treated with glycopyrronium tosylate had improvements in their daily diary account of axillary sweating and in sweat production. Dr. Hebert and her associates reported overall results from the two trials at various prior dermatology meetings, and the company reported some of the results in a press release, but the results have not yet been published in a journal.
The new, pediatric analysis that Dr. Hebert reported showed that the responder rate based on a 4 point or greater improvement in daily sweat diary assessments occurred in 60% of the actively treated children and in 13% of the controls. A 50% or greater reduction in sweat production occurred in 80% of the treated children and in 55% of controls. Quality of life, measured using the Children’s Dermatology Life Quality Index improved by an average of 8 points among the treated children, compared with an average 2-point improvement among the controls. This level of improvement among the glycopyrronium-treated patients would have been enough to move patients from the moderate-effect category at baseline to a no- or small-effect category.
The treatment was generally well tolerated, with no serious adverse effects reported and with treatment effects that were primarily as expected from an anticholinergic agent, including dry mouth, pupil dilation, and blurred vision. One of the 25 treated children withdrew because of these effects, which then resolved. Blood testing showed no systemic absorption of the drug, Dr. Hebert said.
The ATMOS-1 and ATMOS-2 trials were sponsored by Dermira, the company developing glycopyrronium tosylate. Dr. Hebert has been a consultant to and has received research funding from Dermira, and some of the coauthors of the study are Dermira employees. Dr. Hebert is an advisor to the editorial board of Dermatology News.
SOURCE: Hebert A et al. Annual meeting of the American Academy of Dermatology Abstract 6659.
REPORTING FROM AAD 18
Key clinical point: Max. Daily, topical glycopyrronium tosylate safely controlled pediatric hyperhidrosis.
Major finding: At least a 4-point improvement in the axillary sweating daily diary score occurred in 60% of treated patients and in 13% of controls.
Study details: Post hoc analysis of data from 44 children enrolled in either of two pivotal trials, ATMOS-1 and ATMOS-2.
Disclosures: The ATMOS-1 and ATMOS-2 trials were sponsored by Dermira, the company developing glycopyrronium tosylate. Dr. Hebert has been a consultant to and has received research funding from Dermira, and some of the coauthors of the study are Dermira employees. Dr. Hebert is an adviser to the editorial board of Dermatology News.
Source: Hebert A et al. AAD 2018, Abstract 6659.

Biologics gaining traction in children with moderate to severe psoriasis
SAN DIEGO – Systemic therapies are increasingly being used for children with moderate to severe psoriasis; methotrexate is still the mainstay of systemic treatment, but biologics appear to achieve superior results with fewer side effects, Amy S. Paller, MD, said at the annual meeting of the American Academy of Dermatology.
Etanercept was approved in 2016 for children ages 6 and up, and ustekinumab was approved for use in patients aged 12 years or older in October 2017. Ongoing trials are examining adalimumab, apremilast, ustekinumab, and ixekizumab for use in adolescents and younger children. Trials are also being planned for other therapies that inhibit the Th17/IL-23 pathway, said Dr. Paller, the Walter J. Hamlin Professor and chair of dermatology at Northwestern University Feinberg School of Medicine, Chicago.

Further, the study found that biologic agents, primarily etanercept, were used by 27%, acitretin by nearly 15%, cyclosporine by about 8%, and fumaric acid esters by 5%. More than 1 medication was used by 19%, according to the study results.
Adverse events affected the ability to tolerate therapy, and methotrexate and biologic agents were taken for a mean duration that was 2-fold greater than the mean duration for cyclosporine or fumaric acid esters. “A prospective registry is needed to track the long-term risks of systemic agents for pediatric psoriasis,” the authors concluded.
Dr. Paller reported that, in her practice, "we're still primarily using methotrexate. It takes time to see an effect with methotrexate, and you have to let people know this up front.” She pointed to a 2015 single-site prospective study of 25 children that found just 40% achieved Psoriasis Area and Severity Index 50 at 12 weeks, with that number rising to 80% by 36 weeks. (J Derm Treat 2015; 26: 406-12)
Dr. Paller recommends baseline and annual TB testing, updated vaccinations and pregnancy counseling for all patients taking immunosuppressant therapies.
"I don't use a lot of retinoids for plaque psoriasis in kids," Dr. Paller said, "but for pustular psoriasis, I use (them) quite a bit. The beauty of retinoids is that they are not immunosuppressants, and you can start and stop them without loss of efficacy. There are many potential side effects, primarily skin and mucosal dryness."
Cyclosporine "has the greatest potential toxicity, which leaves it lower on the therapeutic ladder," Dr. Paller said. "But it has a pretty good safety record. The nice thing we can say is that (cyclosporine has) been around a long time. We have decades of experience in children, and we're using a low dose."
Benefits of biologics include convenience, infrequent dosing, and, potentially, fewer lab tests, Dr. Paller said. She added that there's no consensus about whether lab tests beyond annual TB tests are a good idea for patients on biologics.
Long-term risks are unclear, however, and drug holidays could spell trouble for efficacy when kids return to the medications.
Dr. Paller noted that biologics can cost tens of thousands of dollars for several weeks of treatment, and insurers may not cover them.
A 2014 meta-analysis of 48 randomized, controlled trials of 16,696 adult patients with psoriasis put biologics as the most effective therapies, with infliximab at the top (risk difference 76%), followed by adalimumab (RD 61%) and ustekinumab (RD 63%).
“These biologics are more effective than etanercept and all conventional treatments. Head-to-head trials indicate the superiority of adalimumab and infliximab over methotrexate (MTX), the superiority of ustekinumab over etanercept …” the meta-analysis concluded. (Br J Dermatol. 2014 Feb;170(2):274-303)
Dr. Paller disclosed that she is an investigator for Abbvie; Celgene; Eli Lilly, Janssen, Leo Foundation; Novartis. She is a consultant with honorarium for Amgen; Celgene; Eli Lilly; and Novartis.
SOURCE: Paller, A. et al, Session F025 Update on systemic therapies and emerging treatments
SAN DIEGO – Systemic therapies are increasingly being used for children with moderate to severe psoriasis; methotrexate is still the mainstay of systemic treatment, but biologics appear to achieve superior results with fewer side effects, Amy S. Paller, MD, said at the annual meeting of the American Academy of Dermatology.
Etanercept was approved in 2016 for children ages 6 and up, and ustekinumab was approved for use in patients aged 12 years or older in October 2017. Ongoing trials are examining adalimumab, apremilast, ustekinumab, and ixekizumab for use in adolescents and younger children. Trials are also being planned for other therapies that inhibit the Th17/IL-23 pathway, said Dr. Paller, the Walter J. Hamlin Professor and chair of dermatology at Northwestern University Feinberg School of Medicine, Chicago.
Further, the study found that biologic agents, primarily etanercept, were used by 27%, acitretin by nearly 15%, cyclosporine by about 8%, and fumaric acid esters by 5%. More than 1 medication was used by 19%, according to the study results.
Adverse events affected the ability to tolerate therapy, and methotrexate and biologic agents were taken for a mean duration that was 2-fold greater than the mean duration for cyclosporine or fumaric acid esters. “A prospective registry is needed to track the long-term risks of systemic agents for pediatric psoriasis,” the authors concluded.
Dr. Paller reported that, in her practice, "we're still primarily using methotrexate. It takes time to see an effect with methotrexate, and you have to let people know this up front.” She pointed to a 2015 single-site prospective study of 25 children that found just 40% achieved Psoriasis Area and Severity Index 50 at 12 weeks, with that number rising to 80% by 36 weeks. (J Derm Treat 2015; 26: 406-12)
Dr. Paller recommends baseline and annual TB testing, updated vaccinations and pregnancy counseling for all patients taking immunosuppressant therapies.
"I don't use a lot of retinoids for plaque psoriasis in kids," Dr. Paller said, "but for pustular psoriasis, I use (them) quite a bit. The beauty of retinoids is that they are not immunosuppressants, and you can start and stop them without loss of efficacy. There are many potential side effects, primarily skin and mucosal dryness."
Cyclosporine "has the greatest potential toxicity, which leaves it lower on the therapeutic ladder," Dr. Paller said. "But it has a pretty good safety record. The nice thing we can say is that (cyclosporine has) been around a long time. We have decades of experience in children, and we're using a low dose."
Benefits of biologics include convenience, infrequent dosing, and, potentially, fewer lab tests, Dr. Paller said. She added that there's no consensus about whether lab tests beyond annual TB tests are a good idea for patients on biologics.
Long-term risks are unclear, however, and drug holidays could spell trouble for efficacy when kids return to the medications.
Dr. Paller noted that biologics can cost tens of thousands of dollars for several weeks of treatment, and insurers may not cover them.
A 2014 meta-analysis of 48 randomized, controlled trials of 16,696 adult patients with psoriasis put biologics as the most effective therapies, with infliximab at the top (risk difference 76%), followed by adalimumab (RD 61%) and ustekinumab (RD 63%).
“These biologics are more effective than etanercept and all conventional treatments. Head-to-head trials indicate the superiority of adalimumab and infliximab over methotrexate (MTX), the superiority of ustekinumab over etanercept …” the meta-analysis concluded. (Br J Dermatol. 2014 Feb;170(2):274-303)
Dr. Paller disclosed that she is an investigator for Abbvie; Celgene; Eli Lilly, Janssen, Leo Foundation; Novartis. She is a consultant with honorarium for Amgen; Celgene; Eli Lilly; and Novartis.
SOURCE: Paller, A. et al, Session F025 Update on systemic therapies and emerging treatments
SAN DIEGO – Systemic therapies are increasingly being used for children with moderate to severe psoriasis; methotrexate is still the mainstay of systemic treatment, but biologics appear to achieve superior results with fewer side effects, Amy S. Paller, MD, said at the annual meeting of the American Academy of Dermatology.
Etanercept was approved in 2016 for children ages 6 and up, and ustekinumab was approved for use in patients aged 12 years or older in October 2017. Ongoing trials are examining adalimumab, apremilast, ustekinumab, and ixekizumab for use in adolescents and younger children. Trials are also being planned for other therapies that inhibit the Th17/IL-23 pathway, said Dr. Paller, the Walter J. Hamlin Professor and chair of dermatology at Northwestern University Feinberg School of Medicine, Chicago.
Further, the study found that biologic agents, primarily etanercept, were used by 27%, acitretin by nearly 15%, cyclosporine by about 8%, and fumaric acid esters by 5%. More than 1 medication was used by 19%, according to the study results.
Adverse events affected the ability to tolerate therapy, and methotrexate and biologic agents were taken for a mean duration that was 2-fold greater than the mean duration for cyclosporine or fumaric acid esters. “A prospective registry is needed to track the long-term risks of systemic agents for pediatric psoriasis,” the authors concluded.
Dr. Paller reported that, in her practice, "we're still primarily using methotrexate. It takes time to see an effect with methotrexate, and you have to let people know this up front.” She pointed to a 2015 single-site prospective study of 25 children that found just 40% achieved Psoriasis Area and Severity Index 50 at 12 weeks, with that number rising to 80% by 36 weeks. (J Derm Treat 2015; 26: 406-12)
Dr. Paller recommends baseline and annual TB testing, updated vaccinations and pregnancy counseling for all patients taking immunosuppressant therapies.
"I don't use a lot of retinoids for plaque psoriasis in kids," Dr. Paller said, "but for pustular psoriasis, I use (them) quite a bit. The beauty of retinoids is that they are not immunosuppressants, and you can start and stop them without loss of efficacy. There are many potential side effects, primarily skin and mucosal dryness."
Cyclosporine "has the greatest potential toxicity, which leaves it lower on the therapeutic ladder," Dr. Paller said. "But it has a pretty good safety record. The nice thing we can say is that (cyclosporine has) been around a long time. We have decades of experience in children, and we're using a low dose."
Benefits of biologics include convenience, infrequent dosing, and, potentially, fewer lab tests, Dr. Paller said. She added that there's no consensus about whether lab tests beyond annual TB tests are a good idea for patients on biologics.
Long-term risks are unclear, however, and drug holidays could spell trouble for efficacy when kids return to the medications.
Dr. Paller noted that biologics can cost tens of thousands of dollars for several weeks of treatment, and insurers may not cover them.
A 2014 meta-analysis of 48 randomized, controlled trials of 16,696 adult patients with psoriasis put biologics as the most effective therapies, with infliximab at the top (risk difference 76%), followed by adalimumab (RD 61%) and ustekinumab (RD 63%).
“These biologics are more effective than etanercept and all conventional treatments. Head-to-head trials indicate the superiority of adalimumab and infliximab over methotrexate (MTX), the superiority of ustekinumab over etanercept …” the meta-analysis concluded. (Br J Dermatol. 2014 Feb;170(2):274-303)
Dr. Paller disclosed that she is an investigator for Abbvie; Celgene; Eli Lilly, Janssen, Leo Foundation; Novartis. She is a consultant with honorarium for Amgen; Celgene; Eli Lilly; and Novartis.
SOURCE: Paller, A. et al, Session F025 Update on systemic therapies and emerging treatments
EXPERT ANALYSIS AT AAD 18

Screening for adolescent idiopathic scoliosis
The United States Preventive Services Task Force (USPSTF) has issued recommendations on screening for idiopathic scoliosis in asymptomatic children and adolescents aged 10-18 years.1 This recommendation concluded that the current evidence on the benefits and harms of screening is insufficient (I statement) and updated its 2004 recommendation against routine screening, in which it had concluded that the harms of screening exceeded the potential benefits (D recommendation).
Importance

Screening methods
The USPSTF concluded that currently available screening tests can accurately detect adolescent idiopathic scoliosis. Screening methods include visual inspection using the forward bend test, use of scoliometer measurement of the angle of trunk rotation during forward bend test with a rotation of 5 degrees–7 degrees recommended to be referred for radiography, and Moiré topography that enumerates asymmetric contour lines on the back (values greater than 2 are referred to radiography).
The USPSTF reviewed seven fair-quality observational studies (n = 447,243) and concluded that screening with a combination of forward bend test, scoliometer measurement and that Moiré topography had the highest sensitivity (93.8%) and specificity (99.2%), a low false-negative rate (6.2%), the lowest false-positive rate (0.8%), and the highest positive predictive value (81%). Sensitivity was lower when screening programs used only one or two screening tests, and single screening tests were associated with highest false-positive rates.
In general, the potential harms associated with false-positive results include psychological harm, chest radiation exposure, and other unnecessary treatment, but the USPSTF did not find evidence on the direct harms of screening.
Effectiveness of intervention or treatment
Bracing: The USPSTF found five studies (n = 651) that evaluated the effectiveness of treatment with three different types of braces. The average ages of participants ranged from 12 to 13 years, and their curvature severity varied from Cobb angle of 20 degrees to 30 degrees. The largest study (n = 242) was a good-quality, international, controlled clinical trial known as the Bracing in Adolescent Idiopathic Scoliosis Trial; it demonstrated significant benefit and quality-of-life outcomes associated with bracing for 18 hours/day. In this study, the rate of treatment success in the as-treated analysis was 72% in the intervention group and 48% in the control group. The rate of treatment success in the intention-to-treat analysis was 75% in the intervention group and 42% in the control group. The number needed to treat was three to prevent one case of curvature progression past 50%.
Exercise: The USPSTF found just two trials (n = 184) that evaluated the effectiveness of tailored physiotherapeutic, scoliosis-specific exercise treatments. The participants were older than 10 years and had Cobb angles ranging from 10 degrees to 25 degrees. At the 12-month follow-up, the studies showed significant improvement, including those in quality-of-life measures. In one of the trials, the intervention group had a Cobb angle reduction of 4.9 degrees while the control group had an increase of 2.8 degrees.
Harms: Only one good-quality study (n = 242) reported harms of bracing, which include skin problems, body pain, physical limitations, anxiety, and depression. The USPSTF did not find any studies that assessed the harms of treatment with exercise or surgery.
Association between spinal curvature severity and adult health outcomes
The USPSTF did not find any studies that directly addressed whether changes in the severity of spinal curvature in adolescence resulted in changes in adult health outcomes. The USPSTF did review two fair-quality retrospective, observational, long-term, follow-up analyses (n = 339) of adults diagnosed with idiopathic scoliosis in adolescence and treated with either bracing or surgery. Quality of life measurements, pulmonary consequences, and pregnancy outcomes were not significantly different between the two treatment groups or between those treated and those simply observed. However, those treated with bracing did report more negative treatment experience and body distortion.
Recommendation of others
The Scoliosis Research Society, American Academy of Orthopedic Surgeons, Pediatric Orthopedic Society of North America, and American Academy of Pediatrics issued a joint position statement in September 2015 recommending that screening examinations for scoliosis should be performed for females at ages 10 and 12 years and for males at either 13 or 14 years.2
Their rationale, articulated in the statement and in an editorial in JAMA accompanying the publication of the USPSTF statement, is primarily based on findings in the Bracing in Adolescent Idiopathic Scoliosis Trial that showed a 56% decrease in the rate of progression of moderate curves to greater than 50 degrees. The evidence that intervention works – along with concerns about costs, family burden, loss of school time, risks of surgical complications, and the 22% need for long-term revision surgery – makes avoidance of progression of curves in scoliosis a high-value issue. In addition, they reasoned, the screening trials from which the false-positive values were derived were primarily school-based screening and not done in physician offices.
The Bottom Line

Although the joint statement made by pediatric orthopedic societies and the American Academy of Pediatrics had recommended screening examinations, the USPSTF concluded that the current evidence is insufficient and that the balance of benefits and harms of screening for adolescent (aged 10-18 years) idiopathic scoliosis (Cobb angle greater than 10 degrees) cannot be determined, giving an “I” recommendation.
Dr. Aarisha Shrestha is a first-year resident in the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
References
1. US Preventive Services Task Force. JAMA. 2018;319(2):165–72.
2. HreskoMT et al. SRS/POSNA/AAOS/AAP position statement: Screening for the early detection for idiopathic scoliosis in adolescents. 2015. Accessed December 8, 2017.
The United States Preventive Services Task Force (USPSTF) has issued recommendations on screening for idiopathic scoliosis in asymptomatic children and adolescents aged 10-18 years.1 This recommendation concluded that the current evidence on the benefits and harms of screening is insufficient (I statement) and updated its 2004 recommendation against routine screening, in which it had concluded that the harms of screening exceeded the potential benefits (D recommendation).
Importance
Screening methods
The USPSTF concluded that currently available screening tests can accurately detect adolescent idiopathic scoliosis. Screening methods include visual inspection using the forward bend test, use of scoliometer measurement of the angle of trunk rotation during forward bend test with a rotation of 5 degrees–7 degrees recommended to be referred for radiography, and Moiré topography that enumerates asymmetric contour lines on the back (values greater than 2 are referred to radiography).
The USPSTF reviewed seven fair-quality observational studies (n = 447,243) and concluded that screening with a combination of forward bend test, scoliometer measurement and that Moiré topography had the highest sensitivity (93.8%) and specificity (99.2%), a low false-negative rate (6.2%), the lowest false-positive rate (0.8%), and the highest positive predictive value (81%). Sensitivity was lower when screening programs used only one or two screening tests, and single screening tests were associated with highest false-positive rates.
In general, the potential harms associated with false-positive results include psychological harm, chest radiation exposure, and other unnecessary treatment, but the USPSTF did not find evidence on the direct harms of screening.
Effectiveness of intervention or treatment
Bracing: The USPSTF found five studies (n = 651) that evaluated the effectiveness of treatment with three different types of braces. The average ages of participants ranged from 12 to 13 years, and their curvature severity varied from Cobb angle of 20 degrees to 30 degrees. The largest study (n = 242) was a good-quality, international, controlled clinical trial known as the Bracing in Adolescent Idiopathic Scoliosis Trial; it demonstrated significant benefit and quality-of-life outcomes associated with bracing for 18 hours/day. In this study, the rate of treatment success in the as-treated analysis was 72% in the intervention group and 48% in the control group. The rate of treatment success in the intention-to-treat analysis was 75% in the intervention group and 42% in the control group. The number needed to treat was three to prevent one case of curvature progression past 50%.
Exercise: The USPSTF found just two trials (n = 184) that evaluated the effectiveness of tailored physiotherapeutic, scoliosis-specific exercise treatments. The participants were older than 10 years and had Cobb angles ranging from 10 degrees to 25 degrees. At the 12-month follow-up, the studies showed significant improvement, including those in quality-of-life measures. In one of the trials, the intervention group had a Cobb angle reduction of 4.9 degrees while the control group had an increase of 2.8 degrees.
Harms: Only one good-quality study (n = 242) reported harms of bracing, which include skin problems, body pain, physical limitations, anxiety, and depression. The USPSTF did not find any studies that assessed the harms of treatment with exercise or surgery.
Association between spinal curvature severity and adult health outcomes
The USPSTF did not find any studies that directly addressed whether changes in the severity of spinal curvature in adolescence resulted in changes in adult health outcomes. The USPSTF did review two fair-quality retrospective, observational, long-term, follow-up analyses (n = 339) of adults diagnosed with idiopathic scoliosis in adolescence and treated with either bracing or surgery. Quality of life measurements, pulmonary consequences, and pregnancy outcomes were not significantly different between the two treatment groups or between those treated and those simply observed. However, those treated with bracing did report more negative treatment experience and body distortion.
Recommendation of others
The Scoliosis Research Society, American Academy of Orthopedic Surgeons, Pediatric Orthopedic Society of North America, and American Academy of Pediatrics issued a joint position statement in September 2015 recommending that screening examinations for scoliosis should be performed for females at ages 10 and 12 years and for males at either 13 or 14 years.2
Their rationale, articulated in the statement and in an editorial in JAMA accompanying the publication of the USPSTF statement, is primarily based on findings in the Bracing in Adolescent Idiopathic Scoliosis Trial that showed a 56% decrease in the rate of progression of moderate curves to greater than 50 degrees. The evidence that intervention works – along with concerns about costs, family burden, loss of school time, risks of surgical complications, and the 22% need for long-term revision surgery – makes avoidance of progression of curves in scoliosis a high-value issue. In addition, they reasoned, the screening trials from which the false-positive values were derived were primarily school-based screening and not done in physician offices.
The Bottom Line
Although the joint statement made by pediatric orthopedic societies and the American Academy of Pediatrics had recommended screening examinations, the USPSTF concluded that the current evidence is insufficient and that the balance of benefits and harms of screening for adolescent (aged 10-18 years) idiopathic scoliosis (Cobb angle greater than 10 degrees) cannot be determined, giving an “I” recommendation.
Dr. Aarisha Shrestha is a first-year resident in the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
References
1. US Preventive Services Task Force. JAMA. 2018;319(2):165–72.
2. HreskoMT et al. SRS/POSNA/AAOS/AAP position statement: Screening for the early detection for idiopathic scoliosis in adolescents. 2015. Accessed December 8, 2017.
The United States Preventive Services Task Force (USPSTF) has issued recommendations on screening for idiopathic scoliosis in asymptomatic children and adolescents aged 10-18 years.1 This recommendation concluded that the current evidence on the benefits and harms of screening is insufficient (I statement) and updated its 2004 recommendation against routine screening, in which it had concluded that the harms of screening exceeded the potential benefits (D recommendation).
Importance
Screening methods
The USPSTF concluded that currently available screening tests can accurately detect adolescent idiopathic scoliosis. Screening methods include visual inspection using the forward bend test, use of scoliometer measurement of the angle of trunk rotation during forward bend test with a rotation of 5 degrees–7 degrees recommended to be referred for radiography, and Moiré topography that enumerates asymmetric contour lines on the back (values greater than 2 are referred to radiography).
The USPSTF reviewed seven fair-quality observational studies (n = 447,243) and concluded that screening with a combination of forward bend test, scoliometer measurement and that Moiré topography had the highest sensitivity (93.8%) and specificity (99.2%), a low false-negative rate (6.2%), the lowest false-positive rate (0.8%), and the highest positive predictive value (81%). Sensitivity was lower when screening programs used only one or two screening tests, and single screening tests were associated with highest false-positive rates.
In general, the potential harms associated with false-positive results include psychological harm, chest radiation exposure, and other unnecessary treatment, but the USPSTF did not find evidence on the direct harms of screening.
Effectiveness of intervention or treatment
Bracing: The USPSTF found five studies (n = 651) that evaluated the effectiveness of treatment with three different types of braces. The average ages of participants ranged from 12 to 13 years, and their curvature severity varied from Cobb angle of 20 degrees to 30 degrees. The largest study (n = 242) was a good-quality, international, controlled clinical trial known as the Bracing in Adolescent Idiopathic Scoliosis Trial; it demonstrated significant benefit and quality-of-life outcomes associated with bracing for 18 hours/day. In this study, the rate of treatment success in the as-treated analysis was 72% in the intervention group and 48% in the control group. The rate of treatment success in the intention-to-treat analysis was 75% in the intervention group and 42% in the control group. The number needed to treat was three to prevent one case of curvature progression past 50%.
Exercise: The USPSTF found just two trials (n = 184) that evaluated the effectiveness of tailored physiotherapeutic, scoliosis-specific exercise treatments. The participants were older than 10 years and had Cobb angles ranging from 10 degrees to 25 degrees. At the 12-month follow-up, the studies showed significant improvement, including those in quality-of-life measures. In one of the trials, the intervention group had a Cobb angle reduction of 4.9 degrees while the control group had an increase of 2.8 degrees.
Harms: Only one good-quality study (n = 242) reported harms of bracing, which include skin problems, body pain, physical limitations, anxiety, and depression. The USPSTF did not find any studies that assessed the harms of treatment with exercise or surgery.
Association between spinal curvature severity and adult health outcomes
The USPSTF did not find any studies that directly addressed whether changes in the severity of spinal curvature in adolescence resulted in changes in adult health outcomes. The USPSTF did review two fair-quality retrospective, observational, long-term, follow-up analyses (n = 339) of adults diagnosed with idiopathic scoliosis in adolescence and treated with either bracing or surgery. Quality of life measurements, pulmonary consequences, and pregnancy outcomes were not significantly different between the two treatment groups or between those treated and those simply observed. However, those treated with bracing did report more negative treatment experience and body distortion.
Recommendation of others
The Scoliosis Research Society, American Academy of Orthopedic Surgeons, Pediatric Orthopedic Society of North America, and American Academy of Pediatrics issued a joint position statement in September 2015 recommending that screening examinations for scoliosis should be performed for females at ages 10 and 12 years and for males at either 13 or 14 years.2
Their rationale, articulated in the statement and in an editorial in JAMA accompanying the publication of the USPSTF statement, is primarily based on findings in the Bracing in Adolescent Idiopathic Scoliosis Trial that showed a 56% decrease in the rate of progression of moderate curves to greater than 50 degrees. The evidence that intervention works – along with concerns about costs, family burden, loss of school time, risks of surgical complications, and the 22% need for long-term revision surgery – makes avoidance of progression of curves in scoliosis a high-value issue. In addition, they reasoned, the screening trials from which the false-positive values were derived were primarily school-based screening and not done in physician offices.
The Bottom Line
Although the joint statement made by pediatric orthopedic societies and the American Academy of Pediatrics had recommended screening examinations, the USPSTF concluded that the current evidence is insufficient and that the balance of benefits and harms of screening for adolescent (aged 10-18 years) idiopathic scoliosis (Cobb angle greater than 10 degrees) cannot be determined, giving an “I” recommendation.
Dr. Aarisha Shrestha is a first-year resident in the family medicine residency program at Abington (Pa.) Jefferson Health. Dr. Skolnik is a professor of family and community medicine at Jefferson Medical College, Philadelphia, and associate director of the family medicine residency program at Abington Jefferson Health.
References
1. US Preventive Services Task Force. JAMA. 2018;319(2):165–72.
2. HreskoMT et al. SRS/POSNA/AAOS/AAP position statement: Screening for the early detection for idiopathic scoliosis in adolescents. 2015. Accessed December 8, 2017.

Mercury vapor from skin cream caused neurotoxicity in toddler
researchers at the University of Arizona, Tucson, found in the case of a toddler who presented with puzzling symptoms.
“Although mercury toxicity is rare and has variable symptoms, it is valuable for clinicians to consider this diagnosis in cases of unexplained hypertension and neurologic findings,” Michael R. Ori, MD, and his associates wrote in the Journal of Pediatrics.
U.S. federal law has prohibited mercury in cosmetics beyond trace amounts (1 mg/kg) since 1973 because of toxicity concerns, but mercury-containing skin creams remain a public health problem in the United States.
A 17-month-old previously healthy girl was seen by her pediatrician because of a 3-week history of fussiness, constipation, decreased appetite, and temperature to 37.7° C. A chest radiograph was normal, as was a urinalysis. Two days later, the child was taken to the emergency department with symptoms of rhinorrhea, congestion, fussiness, and a fever of 38.3° C. She was sent home with a presumptive diagnosis of a viral syndrome. Her symptoms had not resolved 1 week later, and she returned to the pediatrician, having developed a limp with tenderness in the right knee. A radiograph of the knee was unremarkable, repeat urinalysis showed no evidence of a urinary tract infection, and an abdominal x-ray showed a large stool burden. She had a 0.5-kg weight loss and new hypertension, and was afebrile.
The child was admitted to the hospital the next day for an endocrine work-up, but no noticeable abnormalities were found. She became increasingly fussy with a poor appetite and continued weight loss, persistent hypertension, and an inability to walk. Heavy metal screening on day 18 revealed an elevated whole blood mercury level of 26 mcg/L (normal is less than 10 mcg/L), with a random spot urine mercury level of 243 mcg/g creatinine (normal is less than 35 mcg/g creatinine). Repeated chelation with succimer was provided. On day 61, she had significant delay in receptive language and fine motor skills on a Bayley scale. On the most recent evaluation on day 222, she was shy and had stereotypical hand-flapping behavior when stressed, the investigators reported.
Multiple conversations with the patient’s mother eventually identified the source of mercury as a skin-lightening facial cream she had been using for 4 months, which she stored in the refrigerator. The cream was produced and purchased in a beauty salon in Mexico. Several containers of the cream were sent to an Arizona state laboratory; they were found to have mercury levels between 27,000 and 34,000 mg/kg. The mother and the grandmother had no symptoms or findings on physical exam, but had markedly elevated first-void urine mercury levels of 197 mcg/g creatinine for the mother and 222 mcg/g creatinine for the grandmother, the researchers reported.
Testing of the home the family rented found ambient air mercury vapor levels ranged from 1,900 to 2,800 ng/m3 for most areas. Federal agencies recommend remediation for levels greater than 1,000 ng/m3; remediation was performed in the home, with some household items disposed of in a hazardous waste landfill.
This toddler’s exposure to mercury was from contact with contaminated people, objects, and vapor, although the mercury-containing cream was not directly put on her skin. Of these sources of contact, vapor may have contributed the most. There likely was incidental dermal contact through contaminated bed linens, and she also likely had incidental oral contact from contaminated objects that she put in her mouth, Dr. Ori and his associates reported.
Over time, central nervous system penetration occurs with neurologic dysfunction; “this was the dominant feature of this patient’s presentation, with debilitating leg pain, anorexia, constipation, neurasthenia, and hypertension. Acrodynia, meaning extremity pain, is an idiosyncratic reaction to mercury exposure seen in childhood. Symptoms include irritability,weakness, paresthesias, a pink papular rash, and desquamation of the palms and soles. Our patient did not have the characteristic dermal findings but did have other symptoms consistent with acrodynia,” they noted.
The authors declared no conflicts of interest.
SOURCE: Ori MR et al. J Pediatr. 2018. doi: 10.1016/j.jpeds.2017.12.0.23.
researchers at the University of Arizona, Tucson, found in the case of a toddler who presented with puzzling symptoms.
“Although mercury toxicity is rare and has variable symptoms, it is valuable for clinicians to consider this diagnosis in cases of unexplained hypertension and neurologic findings,” Michael R. Ori, MD, and his associates wrote in the Journal of Pediatrics.
U.S. federal law has prohibited mercury in cosmetics beyond trace amounts (1 mg/kg) since 1973 because of toxicity concerns, but mercury-containing skin creams remain a public health problem in the United States.
A 17-month-old previously healthy girl was seen by her pediatrician because of a 3-week history of fussiness, constipation, decreased appetite, and temperature to 37.7° C. A chest radiograph was normal, as was a urinalysis. Two days later, the child was taken to the emergency department with symptoms of rhinorrhea, congestion, fussiness, and a fever of 38.3° C. She was sent home with a presumptive diagnosis of a viral syndrome. Her symptoms had not resolved 1 week later, and she returned to the pediatrician, having developed a limp with tenderness in the right knee. A radiograph of the knee was unremarkable, repeat urinalysis showed no evidence of a urinary tract infection, and an abdominal x-ray showed a large stool burden. She had a 0.5-kg weight loss and new hypertension, and was afebrile.
The child was admitted to the hospital the next day for an endocrine work-up, but no noticeable abnormalities were found. She became increasingly fussy with a poor appetite and continued weight loss, persistent hypertension, and an inability to walk. Heavy metal screening on day 18 revealed an elevated whole blood mercury level of 26 mcg/L (normal is less than 10 mcg/L), with a random spot urine mercury level of 243 mcg/g creatinine (normal is less than 35 mcg/g creatinine). Repeated chelation with succimer was provided. On day 61, she had significant delay in receptive language and fine motor skills on a Bayley scale. On the most recent evaluation on day 222, she was shy and had stereotypical hand-flapping behavior when stressed, the investigators reported.
Multiple conversations with the patient’s mother eventually identified the source of mercury as a skin-lightening facial cream she had been using for 4 months, which she stored in the refrigerator. The cream was produced and purchased in a beauty salon in Mexico. Several containers of the cream were sent to an Arizona state laboratory; they were found to have mercury levels between 27,000 and 34,000 mg/kg. The mother and the grandmother had no symptoms or findings on physical exam, but had markedly elevated first-void urine mercury levels of 197 mcg/g creatinine for the mother and 222 mcg/g creatinine for the grandmother, the researchers reported.
Testing of the home the family rented found ambient air mercury vapor levels ranged from 1,900 to 2,800 ng/m3 for most areas. Federal agencies recommend remediation for levels greater than 1,000 ng/m3; remediation was performed in the home, with some household items disposed of in a hazardous waste landfill.
This toddler’s exposure to mercury was from contact with contaminated people, objects, and vapor, although the mercury-containing cream was not directly put on her skin. Of these sources of contact, vapor may have contributed the most. There likely was incidental dermal contact through contaminated bed linens, and she also likely had incidental oral contact from contaminated objects that she put in her mouth, Dr. Ori and his associates reported.
Over time, central nervous system penetration occurs with neurologic dysfunction; “this was the dominant feature of this patient’s presentation, with debilitating leg pain, anorexia, constipation, neurasthenia, and hypertension. Acrodynia, meaning extremity pain, is an idiosyncratic reaction to mercury exposure seen in childhood. Symptoms include irritability,weakness, paresthesias, a pink papular rash, and desquamation of the palms and soles. Our patient did not have the characteristic dermal findings but did have other symptoms consistent with acrodynia,” they noted.
The authors declared no conflicts of interest.
SOURCE: Ori MR et al. J Pediatr. 2018. doi: 10.1016/j.jpeds.2017.12.0.23.
researchers at the University of Arizona, Tucson, found in the case of a toddler who presented with puzzling symptoms.
“Although mercury toxicity is rare and has variable symptoms, it is valuable for clinicians to consider this diagnosis in cases of unexplained hypertension and neurologic findings,” Michael R. Ori, MD, and his associates wrote in the Journal of Pediatrics.
U.S. federal law has prohibited mercury in cosmetics beyond trace amounts (1 mg/kg) since 1973 because of toxicity concerns, but mercury-containing skin creams remain a public health problem in the United States.
A 17-month-old previously healthy girl was seen by her pediatrician because of a 3-week history of fussiness, constipation, decreased appetite, and temperature to 37.7° C. A chest radiograph was normal, as was a urinalysis. Two days later, the child was taken to the emergency department with symptoms of rhinorrhea, congestion, fussiness, and a fever of 38.3° C. She was sent home with a presumptive diagnosis of a viral syndrome. Her symptoms had not resolved 1 week later, and she returned to the pediatrician, having developed a limp with tenderness in the right knee. A radiograph of the knee was unremarkable, repeat urinalysis showed no evidence of a urinary tract infection, and an abdominal x-ray showed a large stool burden. She had a 0.5-kg weight loss and new hypertension, and was afebrile.
The child was admitted to the hospital the next day for an endocrine work-up, but no noticeable abnormalities were found. She became increasingly fussy with a poor appetite and continued weight loss, persistent hypertension, and an inability to walk. Heavy metal screening on day 18 revealed an elevated whole blood mercury level of 26 mcg/L (normal is less than 10 mcg/L), with a random spot urine mercury level of 243 mcg/g creatinine (normal is less than 35 mcg/g creatinine). Repeated chelation with succimer was provided. On day 61, she had significant delay in receptive language and fine motor skills on a Bayley scale. On the most recent evaluation on day 222, she was shy and had stereotypical hand-flapping behavior when stressed, the investigators reported.
Multiple conversations with the patient’s mother eventually identified the source of mercury as a skin-lightening facial cream she had been using for 4 months, which she stored in the refrigerator. The cream was produced and purchased in a beauty salon in Mexico. Several containers of the cream were sent to an Arizona state laboratory; they were found to have mercury levels between 27,000 and 34,000 mg/kg. The mother and the grandmother had no symptoms or findings on physical exam, but had markedly elevated first-void urine mercury levels of 197 mcg/g creatinine for the mother and 222 mcg/g creatinine for the grandmother, the researchers reported.
Testing of the home the family rented found ambient air mercury vapor levels ranged from 1,900 to 2,800 ng/m3 for most areas. Federal agencies recommend remediation for levels greater than 1,000 ng/m3; remediation was performed in the home, with some household items disposed of in a hazardous waste landfill.
This toddler’s exposure to mercury was from contact with contaminated people, objects, and vapor, although the mercury-containing cream was not directly put on her skin. Of these sources of contact, vapor may have contributed the most. There likely was incidental dermal contact through contaminated bed linens, and she also likely had incidental oral contact from contaminated objects that she put in her mouth, Dr. Ori and his associates reported.
Over time, central nervous system penetration occurs with neurologic dysfunction; “this was the dominant feature of this patient’s presentation, with debilitating leg pain, anorexia, constipation, neurasthenia, and hypertension. Acrodynia, meaning extremity pain, is an idiosyncratic reaction to mercury exposure seen in childhood. Symptoms include irritability,weakness, paresthesias, a pink papular rash, and desquamation of the palms and soles. Our patient did not have the characteristic dermal findings but did have other symptoms consistent with acrodynia,” they noted.
The authors declared no conflicts of interest.
SOURCE: Ori MR et al. J Pediatr. 2018. doi: 10.1016/j.jpeds.2017.12.0.23.
FROM THE JOURNAL OF PEDIATRICS
Young kids with SCA not receiving recommended prophylaxis

Many young children with sickle cell anemia (SCA) may not be taking the recommended antibiotics to prevent invasive pneumococcal disease (IPD), according to research published in Pediatrics.
Results of a previous study indicated that daily treatment with penicillin could reduce the risk of IPD by 84% in young children with SCA.
In the current study, only 18% of young SCA patients received daily penicillin or an equivalent antibiotic as IPD prophylaxis.
“Most children with sickle cell anemia are not getting the antibiotics they should be to adequately protect against potentially deadly infections,” said study author Sarah Reeves, PhD, of the University of Michigan Medical School in Ann Arbor.
“Long-standing recommendations say children with sickle cell anemia should take antibiotics daily for their first 5 years of life. It can be life-saving.”
For this study, Dr Reeves and her colleagues analyzed data on 2821 SCA patients, ages 3 months to 5 years, living in Florida, Illinois, Louisiana, Michigan, South Carolina, and Texas.
The patients were continuously enrolled in the Medicaid program for at least 1 calendar year between 2005 and 2012. The researchers evaluated the receipt of antibiotics through the insurance claims for filled prescriptions.
The team found that, overall, 18% of patients received at least 300 days of antibiotics.
Sixteen percent of patients received at least 300 days of penicillin; 16% received at least 300 days of penicillin or erythromycin; 18% received at least 300 days of penicillin, erythromycin, or amoxicillin; and 22% received at least 300 days of any antibiotic to prevent Streptococcus pneumoniae.
On average, patients received 162 days of penicillin; 164 days of penicillin or erythromycin; 178 days of penicillin, erythromycin, or amoxicillin; and 193 days of any antibiotic to prevent S pneumoniae.
Multivariable analysis suggested that medical visits and a patient’s state of residence were associated with receiving at least 300 days of antibiotics.
The researchers said that each additional SCA-related outpatient visit and well-child visit was associated with incrementally increased odds of receiving at least 300 days of antibiotics. The odds ratio (OR) was 1.01 for SCA-related outpatient visits and 1.08 for well-child visits (P<0.05 for both).
Patients in Florida (OR=0.51, P<0.05), Louisiana (OR=0.57, P<0.05), Michigan (OR=0.60, P<0.05), and South Carolina (OR=0.62, P<0.05) had lower odds of receiving at least 300 days of antibiotics than patients in Illinois (OR=1.00) or Texas (OR=1.01).
The researchers did not investigate why children were not receiving recommended antibiotics, but Dr Reeves identified possible barriers to compliance. She noted that caregiver challenges include picking up prescriptions every 2 weeks from a pharmacy as well as remembering to administer an antibiotic to a young, healthy-appearing child twice a day.
“The types of challenges involved in making sure children get the recommended dose of antibiotics is exacerbated by the substantial burden of care already experienced by families to help control the symptoms of this disease,” Dr Reeves said.
She added that future studies should more deeply explore barriers preventing families from getting antibiotics and potential interventions to improve the rate of children receiving recommended prescriptions.
“Interventions to improve the receipt of antibiotics among children with sickle cell anemia should include enhanced collaboration between healthcare providers, pharmacists, and families,” Dr Reeves said.
“Doctors need to repeatedly discuss the importance of taking antibiotics with families of children with sickle cell anemia. Social factors that may impact receiving filled prescriptions should also be considered, such as the availability of transportation and time to travel to pharmacies to pick up the prescriptions.” ![]()
Many young children with sickle cell anemia (SCA) may not be taking the recommended antibiotics to prevent invasive pneumococcal disease (IPD), according to research published in Pediatrics.
Results of a previous study indicated that daily treatment with penicillin could reduce the risk of IPD by 84% in young children with SCA.
In the current study, only 18% of young SCA patients received daily penicillin or an equivalent antibiotic as IPD prophylaxis.
“Most children with sickle cell anemia are not getting the antibiotics they should be to adequately protect against potentially deadly infections,” said study author Sarah Reeves, PhD, of the University of Michigan Medical School in Ann Arbor.
“Long-standing recommendations say children with sickle cell anemia should take antibiotics daily for their first 5 years of life. It can be life-saving.”
For this study, Dr Reeves and her colleagues analyzed data on 2821 SCA patients, ages 3 months to 5 years, living in Florida, Illinois, Louisiana, Michigan, South Carolina, and Texas.
The patients were continuously enrolled in the Medicaid program for at least 1 calendar year between 2005 and 2012. The researchers evaluated the receipt of antibiotics through the insurance claims for filled prescriptions.
The team found that, overall, 18% of patients received at least 300 days of antibiotics.
Sixteen percent of patients received at least 300 days of penicillin; 16% received at least 300 days of penicillin or erythromycin; 18% received at least 300 days of penicillin, erythromycin, or amoxicillin; and 22% received at least 300 days of any antibiotic to prevent Streptococcus pneumoniae.
On average, patients received 162 days of penicillin; 164 days of penicillin or erythromycin; 178 days of penicillin, erythromycin, or amoxicillin; and 193 days of any antibiotic to prevent S pneumoniae.
Multivariable analysis suggested that medical visits and a patient’s state of residence were associated with receiving at least 300 days of antibiotics.
The researchers said that each additional SCA-related outpatient visit and well-child visit was associated with incrementally increased odds of receiving at least 300 days of antibiotics. The odds ratio (OR) was 1.01 for SCA-related outpatient visits and 1.08 for well-child visits (P<0.05 for both).
Patients in Florida (OR=0.51, P<0.05), Louisiana (OR=0.57, P<0.05), Michigan (OR=0.60, P<0.05), and South Carolina (OR=0.62, P<0.05) had lower odds of receiving at least 300 days of antibiotics than patients in Illinois (OR=1.00) or Texas (OR=1.01).
The researchers did not investigate why children were not receiving recommended antibiotics, but Dr Reeves identified possible barriers to compliance. She noted that caregiver challenges include picking up prescriptions every 2 weeks from a pharmacy as well as remembering to administer an antibiotic to a young, healthy-appearing child twice a day.
“The types of challenges involved in making sure children get the recommended dose of antibiotics is exacerbated by the substantial burden of care already experienced by families to help control the symptoms of this disease,” Dr Reeves said.
She added that future studies should more deeply explore barriers preventing families from getting antibiotics and potential interventions to improve the rate of children receiving recommended prescriptions.
“Interventions to improve the receipt of antibiotics among children with sickle cell anemia should include enhanced collaboration between healthcare providers, pharmacists, and families,” Dr Reeves said.
“Doctors need to repeatedly discuss the importance of taking antibiotics with families of children with sickle cell anemia. Social factors that may impact receiving filled prescriptions should also be considered, such as the availability of transportation and time to travel to pharmacies to pick up the prescriptions.” ![]()
Many young children with sickle cell anemia (SCA) may not be taking the recommended antibiotics to prevent invasive pneumococcal disease (IPD), according to research published in Pediatrics.
Results of a previous study indicated that daily treatment with penicillin could reduce the risk of IPD by 84% in young children with SCA.
In the current study, only 18% of young SCA patients received daily penicillin or an equivalent antibiotic as IPD prophylaxis.
“Most children with sickle cell anemia are not getting the antibiotics they should be to adequately protect against potentially deadly infections,” said study author Sarah Reeves, PhD, of the University of Michigan Medical School in Ann Arbor.
“Long-standing recommendations say children with sickle cell anemia should take antibiotics daily for their first 5 years of life. It can be life-saving.”
For this study, Dr Reeves and her colleagues analyzed data on 2821 SCA patients, ages 3 months to 5 years, living in Florida, Illinois, Louisiana, Michigan, South Carolina, and Texas.
The patients were continuously enrolled in the Medicaid program for at least 1 calendar year between 2005 and 2012. The researchers evaluated the receipt of antibiotics through the insurance claims for filled prescriptions.
The team found that, overall, 18% of patients received at least 300 days of antibiotics.
Sixteen percent of patients received at least 300 days of penicillin; 16% received at least 300 days of penicillin or erythromycin; 18% received at least 300 days of penicillin, erythromycin, or amoxicillin; and 22% received at least 300 days of any antibiotic to prevent Streptococcus pneumoniae.
On average, patients received 162 days of penicillin; 164 days of penicillin or erythromycin; 178 days of penicillin, erythromycin, or amoxicillin; and 193 days of any antibiotic to prevent S pneumoniae.
Multivariable analysis suggested that medical visits and a patient’s state of residence were associated with receiving at least 300 days of antibiotics.
The researchers said that each additional SCA-related outpatient visit and well-child visit was associated with incrementally increased odds of receiving at least 300 days of antibiotics. The odds ratio (OR) was 1.01 for SCA-related outpatient visits and 1.08 for well-child visits (P<0.05 for both).
Patients in Florida (OR=0.51, P<0.05), Louisiana (OR=0.57, P<0.05), Michigan (OR=0.60, P<0.05), and South Carolina (OR=0.62, P<0.05) had lower odds of receiving at least 300 days of antibiotics than patients in Illinois (OR=1.00) or Texas (OR=1.01).
The researchers did not investigate why children were not receiving recommended antibiotics, but Dr Reeves identified possible barriers to compliance. She noted that caregiver challenges include picking up prescriptions every 2 weeks from a pharmacy as well as remembering to administer an antibiotic to a young, healthy-appearing child twice a day.
“The types of challenges involved in making sure children get the recommended dose of antibiotics is exacerbated by the substantial burden of care already experienced by families to help control the symptoms of this disease,” Dr Reeves said.
She added that future studies should more deeply explore barriers preventing families from getting antibiotics and potential interventions to improve the rate of children receiving recommended prescriptions.
“Interventions to improve the receipt of antibiotics among children with sickle cell anemia should include enhanced collaboration between healthcare providers, pharmacists, and families,” Dr Reeves said.
“Doctors need to repeatedly discuss the importance of taking antibiotics with families of children with sickle cell anemia. Social factors that may impact receiving filled prescriptions should also be considered, such as the availability of transportation and time to travel to pharmacies to pick up the prescriptions.” ![]()
Child’s cancer diagnosis can affect mother’s income long-term

A study conducted in Sweden revealed that social benefits can ease financial burdens for parents of children recently diagnosed with cancer.
However, the study also showed that mothers experienced persistently lower income after benefits diminished.
Ayako Hiyoshi, PhD, of Örebro University in Örebro, Sweden, and her colleagues detailed these findings in Cancer.
The researchers gathered information from Swedish national registers and examined the trajectories of parents’ income from different sources.
Parents of children with cancer diagnosed between 2004 and 2009 were identified and matched with parents of children without cancer (reference parents).
In total, 20,091 families were followed from the year before cancer diagnosis to a maximum of 8 years.
The researchers noted that, around the time of a child’s cancer diagnosis, total income (from all sources) was, on average, higher in mothers of children with cancer than in reference mothers.
The ratio of mean total income for mothers of children with cancer, compared to reference mothers, was 1.032 at 1 year prior to the child’s diagnosis and 1.064 the year of diagnosis.
For fathers of children with cancer, total income was slightly lower than reference fathers’ income. The ratios were 0.987 at 1 year prior to diagnosis and 0.995 the year of diagnosis.
The researchers also noted that parents’ income from work was at its lowest around the time of a child’s cancer diagnosis but increased with time.
At cancer diagnosis, the ratio of mean income from work was 0.642 for mothers and 0.858 for fathers. One year later, the ratios were 0.786 and 0.956, respectively. At 3 years, the ratios were 0.876 and 0.986, respectively. At 6 years, the ratios were 0.856 and 1.058, respectively.
The researchers pointed out that sickness and childcare-related benefits, which compensated for income loss, were greater for parents of children with cancer than for reference parents. However, social benefits diminished over time.
One year prior to cancer diagnosis, the ratio of sickness benefits was 3.495 for mothers and 5.213 for fathers. The year of diagnosis, the ratios were 4.785 and 5.795, respectively. At 3 years, the ratios were 1.404 and 1.339, respectively. And at 6 years, the ratios were 0.931 and 1.421, respectively.
One year prior to cancer diagnosis, the ratio of childcare-related benefits was 2.830 for mothers and 3.514 for fathers. The year of diagnosis, the ratios were 4.553 and 4.930, respectively. At 3 years, the ratios were 2.225 and 1.948, respectively. And at 6 years, the ratios were 1.272 and 1.095, respectively.
The decline of social benefits over time meant that cancer mothers’ total income became lower than that of reference mothers, and this difference persisted over the period studied. This was not the case for cancer fathers, however.
The ratio of income from all sources for cancer mothers compared to reference mothers was 1.064 the year of diagnosis, 0.985 at 2 years, 0.966 at 4 years, and 0.934 at 6 years.
The ratio of income from all sources for cancer fathers compared to reference fathers was 0.995 the year of diagnosis, 0.993 at 2 years, 0.998 at 4 years, and 1.029 at 6 years.
“A significant and unexpected finding was that, although income from employment stayed lower for several years for mothers, total income was higher for mothers of children with cancer around the time of the child’s cancer diagnosis when the compensation from social benefits were included,” Dr Hiyoshi said.
“The persistently lower income from employment for mothers of children with cancer compared with mothers of cancer-free children implies potential long-term consequences for the mothers of children with cancer, including their career and future pension in old age.” ![]()
A study conducted in Sweden revealed that social benefits can ease financial burdens for parents of children recently diagnosed with cancer.
However, the study also showed that mothers experienced persistently lower income after benefits diminished.
Ayako Hiyoshi, PhD, of Örebro University in Örebro, Sweden, and her colleagues detailed these findings in Cancer.
The researchers gathered information from Swedish national registers and examined the trajectories of parents’ income from different sources.
Parents of children with cancer diagnosed between 2004 and 2009 were identified and matched with parents of children without cancer (reference parents).
In total, 20,091 families were followed from the year before cancer diagnosis to a maximum of 8 years.
The researchers noted that, around the time of a child’s cancer diagnosis, total income (from all sources) was, on average, higher in mothers of children with cancer than in reference mothers.
The ratio of mean total income for mothers of children with cancer, compared to reference mothers, was 1.032 at 1 year prior to the child’s diagnosis and 1.064 the year of diagnosis.
For fathers of children with cancer, total income was slightly lower than reference fathers’ income. The ratios were 0.987 at 1 year prior to diagnosis and 0.995 the year of diagnosis.
The researchers also noted that parents’ income from work was at its lowest around the time of a child’s cancer diagnosis but increased with time.
At cancer diagnosis, the ratio of mean income from work was 0.642 for mothers and 0.858 for fathers. One year later, the ratios were 0.786 and 0.956, respectively. At 3 years, the ratios were 0.876 and 0.986, respectively. At 6 years, the ratios were 0.856 and 1.058, respectively.
The researchers pointed out that sickness and childcare-related benefits, which compensated for income loss, were greater for parents of children with cancer than for reference parents. However, social benefits diminished over time.
One year prior to cancer diagnosis, the ratio of sickness benefits was 3.495 for mothers and 5.213 for fathers. The year of diagnosis, the ratios were 4.785 and 5.795, respectively. At 3 years, the ratios were 1.404 and 1.339, respectively. And at 6 years, the ratios were 0.931 and 1.421, respectively.
One year prior to cancer diagnosis, the ratio of childcare-related benefits was 2.830 for mothers and 3.514 for fathers. The year of diagnosis, the ratios were 4.553 and 4.930, respectively. At 3 years, the ratios were 2.225 and 1.948, respectively. And at 6 years, the ratios were 1.272 and 1.095, respectively.
The decline of social benefits over time meant that cancer mothers’ total income became lower than that of reference mothers, and this difference persisted over the period studied. This was not the case for cancer fathers, however.
The ratio of income from all sources for cancer mothers compared to reference mothers was 1.064 the year of diagnosis, 0.985 at 2 years, 0.966 at 4 years, and 0.934 at 6 years.
The ratio of income from all sources for cancer fathers compared to reference fathers was 0.995 the year of diagnosis, 0.993 at 2 years, 0.998 at 4 years, and 1.029 at 6 years.
“A significant and unexpected finding was that, although income from employment stayed lower for several years for mothers, total income was higher for mothers of children with cancer around the time of the child’s cancer diagnosis when the compensation from social benefits were included,” Dr Hiyoshi said.
“The persistently lower income from employment for mothers of children with cancer compared with mothers of cancer-free children implies potential long-term consequences for the mothers of children with cancer, including their career and future pension in old age.” ![]()
A study conducted in Sweden revealed that social benefits can ease financial burdens for parents of children recently diagnosed with cancer.
However, the study also showed that mothers experienced persistently lower income after benefits diminished.
Ayako Hiyoshi, PhD, of Örebro University in Örebro, Sweden, and her colleagues detailed these findings in Cancer.
The researchers gathered information from Swedish national registers and examined the trajectories of parents’ income from different sources.
Parents of children with cancer diagnosed between 2004 and 2009 were identified and matched with parents of children without cancer (reference parents).
In total, 20,091 families were followed from the year before cancer diagnosis to a maximum of 8 years.
The researchers noted that, around the time of a child’s cancer diagnosis, total income (from all sources) was, on average, higher in mothers of children with cancer than in reference mothers.
The ratio of mean total income for mothers of children with cancer, compared to reference mothers, was 1.032 at 1 year prior to the child’s diagnosis and 1.064 the year of diagnosis.
For fathers of children with cancer, total income was slightly lower than reference fathers’ income. The ratios were 0.987 at 1 year prior to diagnosis and 0.995 the year of diagnosis.
The researchers also noted that parents’ income from work was at its lowest around the time of a child’s cancer diagnosis but increased with time.
At cancer diagnosis, the ratio of mean income from work was 0.642 for mothers and 0.858 for fathers. One year later, the ratios were 0.786 and 0.956, respectively. At 3 years, the ratios were 0.876 and 0.986, respectively. At 6 years, the ratios were 0.856 and 1.058, respectively.
The researchers pointed out that sickness and childcare-related benefits, which compensated for income loss, were greater for parents of children with cancer than for reference parents. However, social benefits diminished over time.
One year prior to cancer diagnosis, the ratio of sickness benefits was 3.495 for mothers and 5.213 for fathers. The year of diagnosis, the ratios were 4.785 and 5.795, respectively. At 3 years, the ratios were 1.404 and 1.339, respectively. And at 6 years, the ratios were 0.931 and 1.421, respectively.
One year prior to cancer diagnosis, the ratio of childcare-related benefits was 2.830 for mothers and 3.514 for fathers. The year of diagnosis, the ratios were 4.553 and 4.930, respectively. At 3 years, the ratios were 2.225 and 1.948, respectively. And at 6 years, the ratios were 1.272 and 1.095, respectively.
The decline of social benefits over time meant that cancer mothers’ total income became lower than that of reference mothers, and this difference persisted over the period studied. This was not the case for cancer fathers, however.
The ratio of income from all sources for cancer mothers compared to reference mothers was 1.064 the year of diagnosis, 0.985 at 2 years, 0.966 at 4 years, and 0.934 at 6 years.
The ratio of income from all sources for cancer fathers compared to reference fathers was 0.995 the year of diagnosis, 0.993 at 2 years, 0.998 at 4 years, and 1.029 at 6 years.
“A significant and unexpected finding was that, although income from employment stayed lower for several years for mothers, total income was higher for mothers of children with cancer around the time of the child’s cancer diagnosis when the compensation from social benefits were included,” Dr Hiyoshi said.
“The persistently lower income from employment for mothers of children with cancer compared with mothers of cancer-free children implies potential long-term consequences for the mothers of children with cancer, including their career and future pension in old age.” ![]()
Antibiotic Overprescribing: Still a Major Concern

Despite universal agreement that antibiotic overprescribing is a problem, the practice continues to vex us. Antibiotic use—whether appropriate or not—has been linked to rising rates of antimicrobial resistance, disruption of the gut microbiome leading to Clostridium difficile infections (CDI), allergic reactions, and increased health care costs (see Table 1).1-6 And yet, clinicians continue to overprescribe this class of medication.
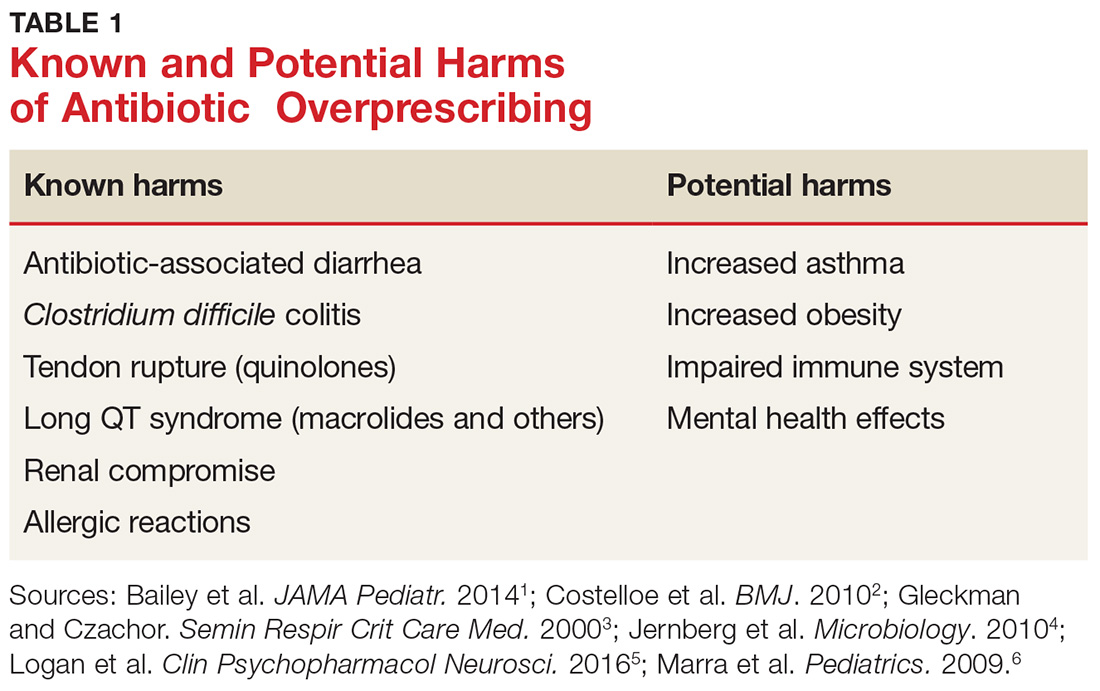
A 2016 report from the CDC estimates that at least 30% of antibiotics prescribed in US outpatient settings are unnecessary.7 Another report cites a slightly higher figure across a variety of health care settings.8 Pair these findings with the fact that there are currently few new drugs in development to target resistant bacteria, and you have the potential for a postantibiotic era in which common infections could become lethal.7
In 2003, the CDC launched its “Get Smart: Know When Antibiotics Work” program (now known as “Be Antibiotics Aware”), focused on decreasing inappropriate antibiotic use in the outpatient setting.9 In 2015, the White House released the National Action Plan for Combating Antibiotic-Resistant Bacteria, with a goal of decreasing inappropriate outpatient antibiotic use by 50% and inappropriate inpatient use by 20% by 2020.10 And, on an international level, the World Health Organization (WHO) in 2015 developed a five-year strategic framework for implementing its Global Action Plan on Antimicrobial Resistance.11
Family practitioners are on the front lines of this battle. Here’s what we can do now.
WHEN AND WHERE ARE ANTIBIOTICS MOST OFTEN INAPPROPRIATELY PRESCRIBED?
The diagnosis leading to the most frequent inappropriate prescribing of antibiotics is acute respiratory tract infection (ARTI), which includes bronchitis, otitis media, pharyngitis, sinusitis, tonsillitis, the common cold, and pneumonia. Up to 40% of antibiotic prescriptions for these conditions are unnecessary.8,12 Bronchitis is the most common ARTI diagnosis associated with inappropriate antibiotic prescriptions, while sinusitis, suppurative otitis media, and pharyngitis are the diagnoses associated with the lion’s share of all (appropriate and inappropriate) antibiotic prescriptions within the ARTI category.8,9,12,13 Refer to national clinical guidelines, which delineate when antibiotic treatment is appropriate for these conditions.14-16
With respect to setting, there are conflicting findings as to whether antibiotic prescribing differs in office-based versus emergency department (ED) settings.
- One study found a higher rate of antibiotic prescribing during ED visits than office visits (21% vs 9%), even though, between 2007 and 2009, more antibiotic prescriptions were written for adults in primary care offices than in either outpatient hospital clinics or EDs.17
- In a cross-sectional study using data from 2005 to 2010 National Ambulatory Medical Care Surveys (NAMCS) and National Hospital Ambulatory Medical Care Surveys (NHAMCS), more than half of patients with uncomplicated acute rhinosinusitis received a prescription for antibiotics, but there was no overall difference in antibiotic prescriptions between primary care and ED presentation.18
- A retrospective analysis found that between 2006 and 2010, outpatient hospital practices (56%) and community-practice offices (60%) prescribed more antibiotics for ARTIs than EDs did (51%).12
STICK TO NARROW-SPECTRUM AGENTS WHEN POSSIBLE
Using broad-spectrum antibiotics, such as quinolones or imipenem, firstline, contributes more to the problem of antibiotic resistance than does prescribing narrow-spectrum antibiotics such as amoxicillin, cephalexin, or trimethoprim-sulfamethoxazole.7 Yet between 2007 and 2009, broad-spectrum agents were prescribed for 61% of outpatient adult visits in which patients received an antibiotic prescription.17 Quinolones (25%), macrolides (20%), and aminopenicillins (12%) were most commonly prescribed, and antibiotic prescriptions were most often written for respiratory conditions, such as bronchitis, for which we now know antibiotics are rarely indicated.17
Between 2006 and 2008, pediatric patients who received antibiotic prescriptions were given broad-spectrum agents 50% of the time, of which macrolides were the class most commonly prescribed.13
More recently, researchers examined the frequency with which clinicians prescribe narrow-spectrum, firstline antibiotics for otitis media, sinusitis, and pharyngitis using 2010 to 2011 NAMCS/NHAMCS data. They found that providers used firstline agents recommended by professional guidelines 52% of the time, although it was estimated that they would have been appropriate in 80% of cases; pediatric patients were more likely to receive appropriate firstline antibiotics than adult patients.19 Macrolides, especially azithromycin, were the most common non-firstline antibiotics prescribed.19,20 The bottom line is that when antibiotics are indicated for upper respiratory infections (otitis media, sinusitis, and pharyngitis), clinicians should prescribe a narrow-spectrum antibiotic first.
ANTIBIOTIC OVERPRESCIBING AFFECTS THE GUT AND BEYOND
The human intestinal microbiome is composed of a diverse array of bacteria, viruses, and parasites.21 The main functions of the gut microbiome include interacting with the immune system and participating in biochemical reactions in the gut, such as absorption of fat-soluble vitamins and the production of vitamin K.
As we know, antibiotics decrease the diversity of gut bacteria, which, in turn, can cause less efficient nutrient extraction, as well as vulnerability to enteric infections.21 It is well known, for example, that the bacterial gut microbiome can either inhibit or promote diarrheal illnesses such as those caused by CDI. CDI is now the most common health care-related infection, accounting for about a half-million health care facility infections per year.22 It extends hospital stays an average of almost 10 days and is estimated to cost the health care system $6.3 billion annually.23
Antibiotics can also eliminate antibiotic-susceptible organisms, allowing resistant organisms to proliferate.4 They also promote the transmission of genes for antibiotic resistance between gut bacteria.4
Beyond the gut
Less well known is that gut bacteria can promote or inhibit extraintestinal infections.
Gut bacteria and HIV. In early HIV infections, for example, gut populations of Lactobacillus and Bifidobacteria are reduced, and the gut barrier becomes compromised.24 Increasing translocation of bacterial products is associated with HIV disease progression. Preservation of Lactobacillus populations in the gut is associated with markers predictive of better HIV outcomes, including a higher CD4 count, a lower viral load, and less evidence of gut microbial translocation.24 This underscores the importance of maintaining healthy gut flora in patients with HIV, using such steps as avoiding unnecessary antibiotics.
Gut bacteria and stress, depression. Antibiotics directly induce the expression of key genes that affect the stress response.25 While causative studies are lacking, there is a growing body of evidence suggesting that the gut microbiome is involved in two-way communication with the brain and can affect, and be affected by, stress and depression.21,26-30 Diseases and conditions that seem to have a putative connection to a disordered microbiome (dysbiosis) include depression, anxiety, Crohn disease, type 2 diabetes, and obesity. (For a discussion of the relationship between the gut microbiome and diabetes, see Endocrine Consult: The Gut Microbiome in Type 2 Diabetes.)
Gut bacteria and childhood obesity. Repeated use of broader-spectrum antibiotics in children younger than 24 months of age increases the risk for childhood obesity.1,6 One theory for the association is that the effects of broad-spectrum antibiotics on the intestinal flora of young children may alter long-term energy homeostasis, resulting in a higher risk for obesity.1
Gut bacteria and asthma. Studies demonstrate differences in the gut microbiomes of asthmatic and nonasthmatic patients. These differences affect the activities of helper T-cell subsets (Th1 and Th2), which in turn affect the development of immune tolerance.31
Although additional studies are needed to confirm these findings, the evidence collected thus far should make us all pause before prescribing drugs that can alter our microbiome in complex and only partially understood ways.
WHAT CAN WE DO RIGHT NOW?
The issues created by the inappropriate prescribing of antibiotics have been known for decades, and multiple attempts have been made to find solutions and implement change. Although some small successes have occurred, little overall progress has been made in reducing antibiotic prescribing in the general population. A historical review of why clinicians prescribe antibiotics inappropriately and the interventions that have successfully reduced this prescribing may prove valuable as we continue to look for new, effective answers.
Why do we overprescribe antibiotics? A 2015 systematic literature review found that patient demand, pharmaceutical company marketing activities, limited up-to-date information sources, and fear of losing patients are major reasons providers cite for prescribing antibiotics.32
In a separate study that explored antibiotic prescribing habits for acute bronchitis, clinicians cited “patient demand” as the major reason for prescribing antibiotics. Respondents also reported that “other physicians were responsible for inappropriate antibiotic prescribing.”33
Strategies that work
Some early intervention programs directed at reducing antibiotic prescribing demonstrated success (see Table 2).34-36 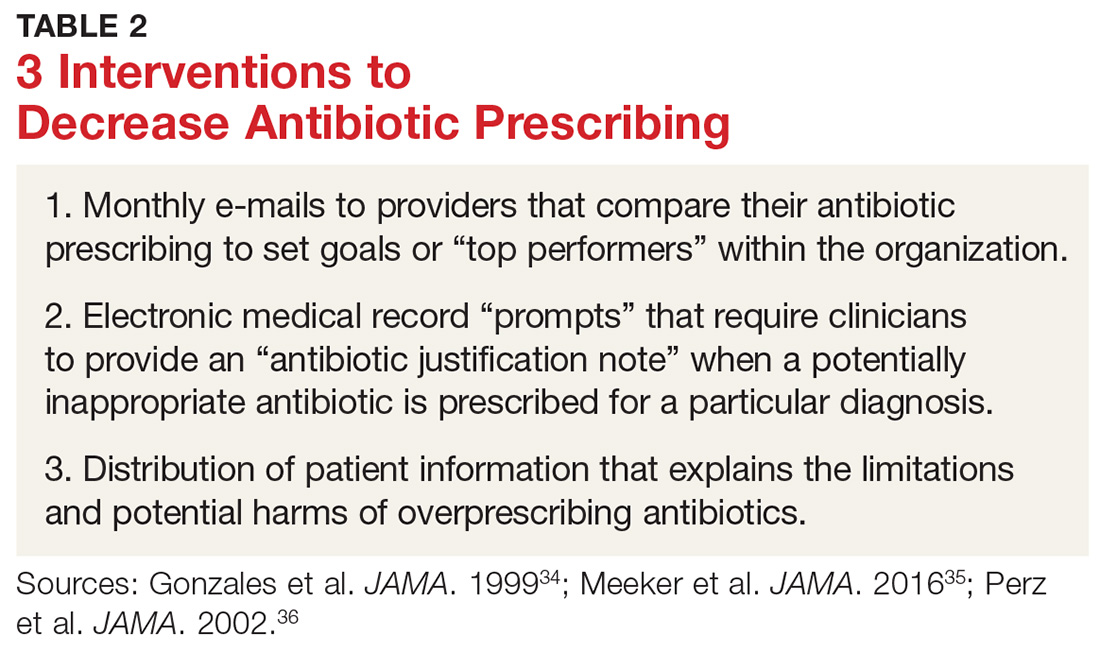
One example comes from a 1996-1998 study of four primary care practices.34 Researchers evaluated the impact of a multidimensional intervention effort targeted at clinicians and patients and aimed at lowering the use of antimicrobial agents for acute uncomplicated bronchitis in adults. It incorporated multiple elements, including office-based and household patient educational materials and a clinician intervention involving education, practice profiling, and academic detailing. Clinicians in this program reduced their rates of antibiotic prescribing for uncomplicated bronchitis from 74% to 48%.34
Employing EMRs. A more recent study focused on use of electronic medical records (EMRs) and communications to modify clinician antibiotic prescribing.35 By sending clinicians monthly emails comparing their prescribing patterns to those of peers and “typical top performers,” inappropriate antibiotic prescriptions for ARTIs went from 19.9% to 3.7%.35
In another effort, the same researchers modified providers’ EMRs to detect when potentially inappropriate antibiotics were prescribed. The system then prompted the clinician to provide an “antibiotic justification note,” which remained visible in the patient’s chart. This approach, which encouraged providers to follow prescribing guidelines by capitalizing on their concerns about their reputations, produced a 77% reduction in antibiotic prescribing.35
Focusing on the public. Studies have also examined the effectiveness of educating the public about when antibiotics are not likely to be helpful and of the harms of unnecessary antibiotics.
Studies conducted in Tennessee and Wisconsin that combined prescriber and community education about unnecessary antibiotics for children found that the intervention reduced antibiotic prescribing in both locations by about 19%, compared with about a 9% reduction in the control groups.36,37
DOES PRESCRIBING ANTIBIOTICS AFFECT PATIENT SATISFACTION?
The results are mixed as to whether prescribing antibiotics affects patient satisfaction. Two studies in the early 2000s found that both patients and parents reported higher satisfaction with clinicians who explained why antibiotics were not indicated versus those who simply prescribed them—and that such explanations do not need to take a lot of time (see Table 3 for patient care tips).37,38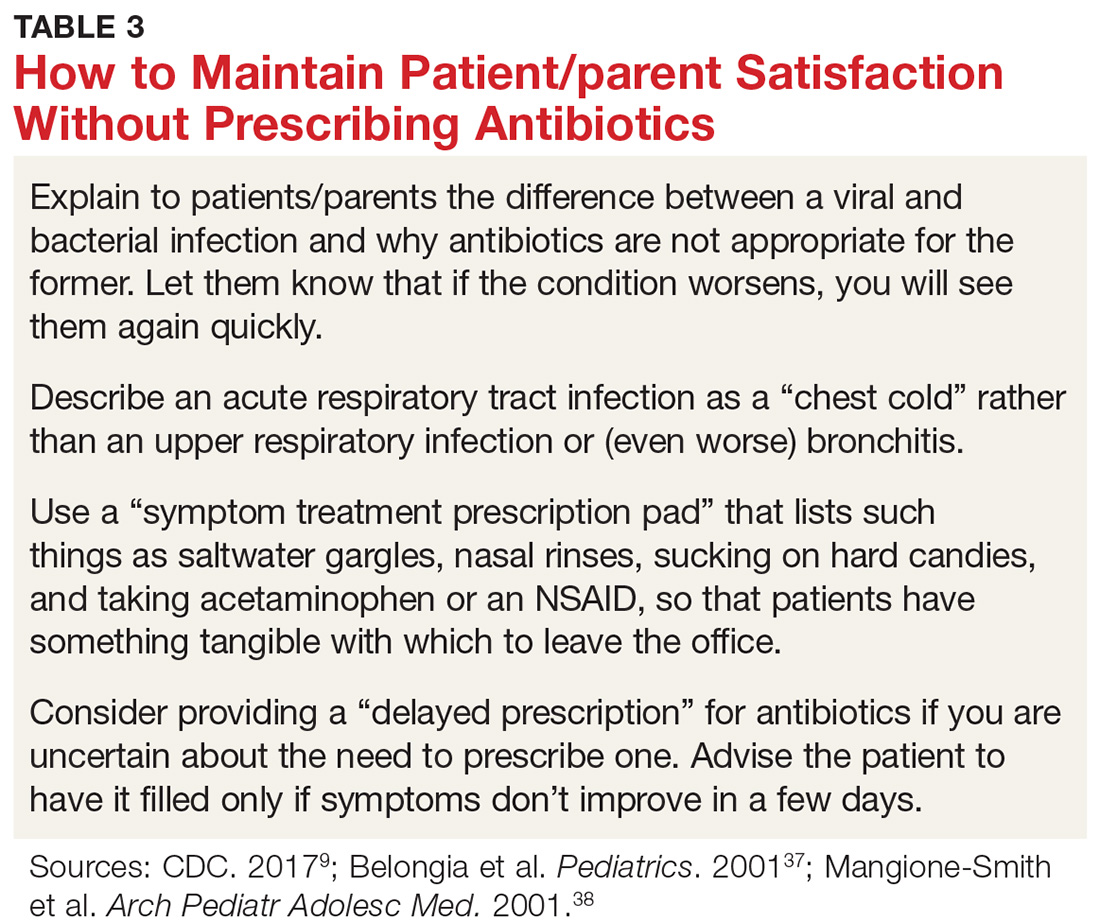
A more recent study found that higher antibiotic prescribing practices in Britain were associated with modestly higher patient satisfaction ratings.39 The authors of this study noted, however, that reduced antibiotic prescribing may be a proxy for other practice patterns that affected satisfaction ratings.
REDUCING ANTIBIOTIC PRESCRIBING REDUCES RESISTANCE
There is also strong evidence that when clinicians decrease antibiotic prescribing, antimicrobial resistance follows suit. One of the earlier landmark studies to demonstrate this was a Finnish study published in 1997.40 The authors found that a reduction of macrolide antibiotic consumption in Finland led to a reduction in streptococci macrolide resistance from 16.5% to 8.6%.40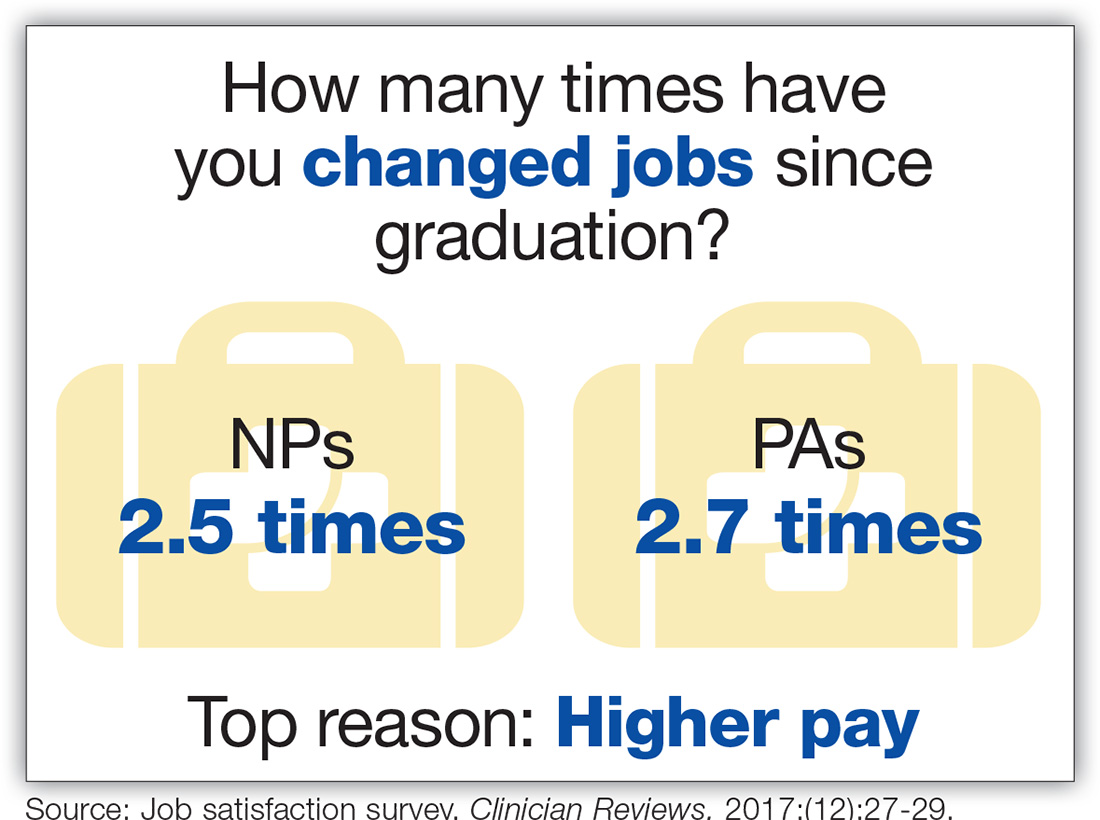
Multiple studies have since demonstrated similar results for both respiratory and urinary tract infections.41,42 A 2017 meta-analysis of 32 studies found that antibiotic stewardship programs reduced the incidence of infections and colonization with multidrug-resistant Gram-negative bacteria (by 51%), extended-spectrum beta-lactamase–producing Gram-negative bacteria (48%), and methicillin-resistant Staphylococcus aureus (37%). There was also a reduction in the incidence of CDI (32%).43
1. Bailey LC, Forrest CB, Zhang P, et al. Association of antibiotics in infancy with early childhood obesity. JAMA Pediatr. 2014;168:1063-1069.
2. Costelloe C, Metcalfe C, Lovering A, et al. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340:c2096.
3. Gleckman RA, Czachor JS. Antibiotic side effects. Semin Respir Crit Care Med. 2000;21:53-60.
4. Jernberg C, Löfmark S, Edlund C, et al. Long-term impacts of antibiotic exposure on the human intestinal microbiota. Microbiology. 2010;156:3216-3223.
5. Logan AC, Jacka FN, Craig JM, et al. The microbiome and mental health: looking back, moving forward with lessons from allergic diseases. Clin Psychopharmacol Neurosci. 2016;14:131-147.
6. Marra F, Marra CA, Richardson K, et al. Antibiotic use in children is associated with increased risk of asthma. Pediatrics. 2009;123:1003-1010.
7. Harris AM, Hicks LA, Qaseem A; the High Value Care Task Force of the American College of Physicians and the CDC. Appropriate antibiotic use for acute respiratory tract infection in adults: advice for high-value care from the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med. 2016; 164:425-434.
8. Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010-2011. JAMA. 2016;315: 1864-1873.
9. CDC. Antibiotic prescribing and use. www.cdc.gov/antibiotic-use/index.html. Accessed January 16, 2018.
10. The White House. National action plan for combating antibiotic-resistant bacteria. March 2015:1-63. https://obamawhitehouse.archives.gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf. Accessed January 16, 2018.
11. World Health Organization. Global action plan on antimicrobial resistance (2015). www.who.int/antimicrobial-resistance/global-action-plan/en/. Accessed January 16, 2018.
12. Barlam TF, Soria-Saucedo R, Cabral HJ, et al. Unnecessary antibiotics for acute respiratory tract infections: association with care setting and patient demographics. Open Forum Infect Dis. 2016;3:1-7.
13. Hersh AL, Shapiro DJ, Pavia AT, et al. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics. 2011;128:1053-1061.
14. Chow AW, Benninger MS, Brook I, et al. Executive summary: IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:1041-1045.
15. Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 suppl):S1-S39.
16. Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55:1279-1282.
17. Shapiro DJ, Hicks LA, Pavia AT, et al. Antibiotic prescribing for adults in ambulatory care in the USA, 2007-09. J Antimicrob Chemother. 2014;69:234-240.
18. Bergmark RW, Sedaghat AR. Antibiotic prescription for acute rhinosinusitis: emergency departments versus primary care providers. Laryngoscope. 2016;126:2439-2444.
19. Hersh AL, Fleming-Dutra KE, Shapiro DJ, et al. Frequency of first-line antibiotic selection among US ambulatory care visits for otitis media, sinusitis, and pharyngitis. JAMA Intern Med. 2016;176:1870-1872.
20. Hicks LA, Bartoces MG, Roberts RM, et al. US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clin Infect Dis. 2015;60:1308-1316.
21. Langdon A, Crook N, Dantas G. The effects of antibiotics on the microbiome throughout development and alternative approaches for therapeutic modulation. Genome Med. 2016;8:39.
22. Lessa FC, Gould CV, McDonald CL. Current status of Clostridium difficile infection epidemiology. Clin Infect Dis. 2012;55(suppl 2):S65-S70.
23. Zhang S, Palazuelos-Munoz S, Balsells EM, et al. Cost of hospital management of Clostridium difficile infection in United States—a meta-analysis and modelling study. BMC Infect Dis. 2016;16:447.
24. Pérez-Santiago J, Gianella S, Massanella M, et al. Gut lactobacillales are associated with higher CD4 and less microbial translocation during HIV infection. AIDS. 2013;27:1921-1931.
25. Maurice CF, Haiser HJ, Turnbaugh PJ. Xenobiotics shape the physiology and gene expression of the active human gut microbiome. Cell. 2013;152:39-50.
26. Bravo JA, Julio-Pieper M, Forsythe P, et al. Communication between gastrointestinal bacteria and the nervous system. Curr Opin Pharmacol. 2012;12:667-672.
27. Clemente JC, Ursell LK, Parfrey LW, et al. The impact of the gut microbiota on human health: an integrative view. Cell. 2012;148:1258-1270.
28. Dinan TG, Cryan JF. Regulation of the stress response by the gut microbiota: implications for psychoneuroendocrinology. Psychoneuroendocrinology. 2012;37:1369-1378.
29. Foster JA, McVey Neufeld KA. Gut-brain axis: how the microbiome influences anxiety and depression. Trends Neurosci. 2013;36:305-312.
30. Wang Y, Kasper LH. The role of microbiome in central nervous system disorders. Brain Behav Immun. 2014; 38:1-12.31. Riiser A. The human microbiome, asthma, and allergy. Allergy Asthma Clin Immunol. 2015;11:35.
32. Md Rezal RS, Hassali MA, Alrasheedy AA, et al. Physicians’ knowledge, perceptions and behaviour towards antibiotic prescribing: a systematic review of the literature. Expert Rev Anti Infect Ther. 2015;13:665-680.
33. Dempsey PP, Businger AC, Whaley LE, et al. Primary care clinicians’ perceptions about antibiotic prescribing for acute bronchitis: a qualitative study. BMC Fam Pract . 2014;15:194.
34. Gonzales R, Steiner JF, Lum A, et al. Decreasing antibiotic use in ambulatory practice. JAMA . 1999;281:1512-1519.
35. Meeker D, Linder JA, Fox CR, et al. Effect of behavioral interventions on inappropriate antibiotic prescribing among primary care practices: a randomized clinical trial. JAMA . 2016;315:562-570.
36. Perz JF, Craig AS, Coffey CS, et al. Changes in antibiotic prescribing for children after a community-wide campaign. JAMA . 2002;287:3103-3109.
37. Belongia EA, Sullivan BJ, Chyou PH, et al. A community intervention trial to promote judicious antibiotic use and reduce penicillin-resistant Streptococcus pneumoniae carriage in children. Pediatrics . 2001;108:575-583.
38. Mangione-Smith R, McGlynn EA, Elliott MN, et al. Parent expectations for antibiotics, physician-parent communication, and satisfaction. Arch Pediatr Adolesc Med. 2001;155:800-806.
39. Ashworth M, White P, Jongsma H, et al. Antibiotic prescribing and patient satisfaction in primary care in England: cross-sectional analysis of national patient survey data and prescribing data. Br J Gen Pract . 2016;66:e40-e46.
40. Seppälä H, Klaukka T, Vuopio-Varkila J, et al. The effect of changes in the consumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. N Engl J Med. 1997;337:441-446.
41. Guillemot D, Varon E, Bernède C, et al. Reduction of antibiotic use in the community reduces the rate of colonization with penicillin g–nonsusceptible Streptococcus pneumoniae . Clin Infect Dis. 2005;41:930-938.
42. Butler CC, Dunstan F, Heginbothom M, et al. Containing antibiotic resistance: decreased antibiotic-resistant coliform urinary tract infections with reduction in antibiotic prescribing by general practices. Br J Gen Pract. 2007; 57:785-792.
43. Baur D, Gladstone BP, Burkert F, et al. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17:990-1001.
Despite universal agreement that antibiotic overprescribing is a problem, the practice continues to vex us. Antibiotic use—whether appropriate or not—has been linked to rising rates of antimicrobial resistance, disruption of the gut microbiome leading to Clostridium difficile infections (CDI), allergic reactions, and increased health care costs (see Table 1).1-6 And yet, clinicians continue to overprescribe this class of medication.
A 2016 report from the CDC estimates that at least 30% of antibiotics prescribed in US outpatient settings are unnecessary.7 Another report cites a slightly higher figure across a variety of health care settings.8 Pair these findings with the fact that there are currently few new drugs in development to target resistant bacteria, and you have the potential for a postantibiotic era in which common infections could become lethal.7
In 2003, the CDC launched its “Get Smart: Know When Antibiotics Work” program (now known as “Be Antibiotics Aware”), focused on decreasing inappropriate antibiotic use in the outpatient setting.9 In 2015, the White House released the National Action Plan for Combating Antibiotic-Resistant Bacteria, with a goal of decreasing inappropriate outpatient antibiotic use by 50% and inappropriate inpatient use by 20% by 2020.10 And, on an international level, the World Health Organization (WHO) in 2015 developed a five-year strategic framework for implementing its Global Action Plan on Antimicrobial Resistance.11
Family practitioners are on the front lines of this battle. Here’s what we can do now.
WHEN AND WHERE ARE ANTIBIOTICS MOST OFTEN INAPPROPRIATELY PRESCRIBED?
The diagnosis leading to the most frequent inappropriate prescribing of antibiotics is acute respiratory tract infection (ARTI), which includes bronchitis, otitis media, pharyngitis, sinusitis, tonsillitis, the common cold, and pneumonia. Up to 40% of antibiotic prescriptions for these conditions are unnecessary.8,12 Bronchitis is the most common ARTI diagnosis associated with inappropriate antibiotic prescriptions, while sinusitis, suppurative otitis media, and pharyngitis are the diagnoses associated with the lion’s share of all (appropriate and inappropriate) antibiotic prescriptions within the ARTI category.8,9,12,13 Refer to national clinical guidelines, which delineate when antibiotic treatment is appropriate for these conditions.14-16
With respect to setting, there are conflicting findings as to whether antibiotic prescribing differs in office-based versus emergency department (ED) settings.
- One study found a higher rate of antibiotic prescribing during ED visits than office visits (21% vs 9%), even though, between 2007 and 2009, more antibiotic prescriptions were written for adults in primary care offices than in either outpatient hospital clinics or EDs.17
- In a cross-sectional study using data from 2005 to 2010 National Ambulatory Medical Care Surveys (NAMCS) and National Hospital Ambulatory Medical Care Surveys (NHAMCS), more than half of patients with uncomplicated acute rhinosinusitis received a prescription for antibiotics, but there was no overall difference in antibiotic prescriptions between primary care and ED presentation.18
- A retrospective analysis found that between 2006 and 2010, outpatient hospital practices (56%) and community-practice offices (60%) prescribed more antibiotics for ARTIs than EDs did (51%).12
STICK TO NARROW-SPECTRUM AGENTS WHEN POSSIBLE
Using broad-spectrum antibiotics, such as quinolones or imipenem, firstline, contributes more to the problem of antibiotic resistance than does prescribing narrow-spectrum antibiotics such as amoxicillin, cephalexin, or trimethoprim-sulfamethoxazole.7 Yet between 2007 and 2009, broad-spectrum agents were prescribed for 61% of outpatient adult visits in which patients received an antibiotic prescription.17 Quinolones (25%), macrolides (20%), and aminopenicillins (12%) were most commonly prescribed, and antibiotic prescriptions were most often written for respiratory conditions, such as bronchitis, for which we now know antibiotics are rarely indicated.17
Between 2006 and 2008, pediatric patients who received antibiotic prescriptions were given broad-spectrum agents 50% of the time, of which macrolides were the class most commonly prescribed.13
More recently, researchers examined the frequency with which clinicians prescribe narrow-spectrum, firstline antibiotics for otitis media, sinusitis, and pharyngitis using 2010 to 2011 NAMCS/NHAMCS data. They found that providers used firstline agents recommended by professional guidelines 52% of the time, although it was estimated that they would have been appropriate in 80% of cases; pediatric patients were more likely to receive appropriate firstline antibiotics than adult patients.19 Macrolides, especially azithromycin, were the most common non-firstline antibiotics prescribed.19,20 The bottom line is that when antibiotics are indicated for upper respiratory infections (otitis media, sinusitis, and pharyngitis), clinicians should prescribe a narrow-spectrum antibiotic first.
ANTIBIOTIC OVERPRESCIBING AFFECTS THE GUT AND BEYOND
The human intestinal microbiome is composed of a diverse array of bacteria, viruses, and parasites.21 The main functions of the gut microbiome include interacting with the immune system and participating in biochemical reactions in the gut, such as absorption of fat-soluble vitamins and the production of vitamin K.
As we know, antibiotics decrease the diversity of gut bacteria, which, in turn, can cause less efficient nutrient extraction, as well as vulnerability to enteric infections.21 It is well known, for example, that the bacterial gut microbiome can either inhibit or promote diarrheal illnesses such as those caused by CDI. CDI is now the most common health care-related infection, accounting for about a half-million health care facility infections per year.22 It extends hospital stays an average of almost 10 days and is estimated to cost the health care system $6.3 billion annually.23
Antibiotics can also eliminate antibiotic-susceptible organisms, allowing resistant organisms to proliferate.4 They also promote the transmission of genes for antibiotic resistance between gut bacteria.4
Beyond the gut
Less well known is that gut bacteria can promote or inhibit extraintestinal infections.
Gut bacteria and HIV. In early HIV infections, for example, gut populations of Lactobacillus and Bifidobacteria are reduced, and the gut barrier becomes compromised.24 Increasing translocation of bacterial products is associated with HIV disease progression. Preservation of Lactobacillus populations in the gut is associated with markers predictive of better HIV outcomes, including a higher CD4 count, a lower viral load, and less evidence of gut microbial translocation.24 This underscores the importance of maintaining healthy gut flora in patients with HIV, using such steps as avoiding unnecessary antibiotics.
Gut bacteria and stress, depression. Antibiotics directly induce the expression of key genes that affect the stress response.25 While causative studies are lacking, there is a growing body of evidence suggesting that the gut microbiome is involved in two-way communication with the brain and can affect, and be affected by, stress and depression.21,26-30 Diseases and conditions that seem to have a putative connection to a disordered microbiome (dysbiosis) include depression, anxiety, Crohn disease, type 2 diabetes, and obesity. (For a discussion of the relationship between the gut microbiome and diabetes, see Endocrine Consult: The Gut Microbiome in Type 2 Diabetes.)
Gut bacteria and childhood obesity. Repeated use of broader-spectrum antibiotics in children younger than 24 months of age increases the risk for childhood obesity.1,6 One theory for the association is that the effects of broad-spectrum antibiotics on the intestinal flora of young children may alter long-term energy homeostasis, resulting in a higher risk for obesity.1
Gut bacteria and asthma. Studies demonstrate differences in the gut microbiomes of asthmatic and nonasthmatic patients. These differences affect the activities of helper T-cell subsets (Th1 and Th2), which in turn affect the development of immune tolerance.31
Although additional studies are needed to confirm these findings, the evidence collected thus far should make us all pause before prescribing drugs that can alter our microbiome in complex and only partially understood ways.
WHAT CAN WE DO RIGHT NOW?
The issues created by the inappropriate prescribing of antibiotics have been known for decades, and multiple attempts have been made to find solutions and implement change. Although some small successes have occurred, little overall progress has been made in reducing antibiotic prescribing in the general population. A historical review of why clinicians prescribe antibiotics inappropriately and the interventions that have successfully reduced this prescribing may prove valuable as we continue to look for new, effective answers.
Why do we overprescribe antibiotics? A 2015 systematic literature review found that patient demand, pharmaceutical company marketing activities, limited up-to-date information sources, and fear of losing patients are major reasons providers cite for prescribing antibiotics.32
In a separate study that explored antibiotic prescribing habits for acute bronchitis, clinicians cited “patient demand” as the major reason for prescribing antibiotics. Respondents also reported that “other physicians were responsible for inappropriate antibiotic prescribing.”33
Strategies that work
Some early intervention programs directed at reducing antibiotic prescribing demonstrated success (see Table 2).34-36
One example comes from a 1996-1998 study of four primary care practices.34 Researchers evaluated the impact of a multidimensional intervention effort targeted at clinicians and patients and aimed at lowering the use of antimicrobial agents for acute uncomplicated bronchitis in adults. It incorporated multiple elements, including office-based and household patient educational materials and a clinician intervention involving education, practice profiling, and academic detailing. Clinicians in this program reduced their rates of antibiotic prescribing for uncomplicated bronchitis from 74% to 48%.34
Employing EMRs. A more recent study focused on use of electronic medical records (EMRs) and communications to modify clinician antibiotic prescribing.35 By sending clinicians monthly emails comparing their prescribing patterns to those of peers and “typical top performers,” inappropriate antibiotic prescriptions for ARTIs went from 19.9% to 3.7%.35
In another effort, the same researchers modified providers’ EMRs to detect when potentially inappropriate antibiotics were prescribed. The system then prompted the clinician to provide an “antibiotic justification note,” which remained visible in the patient’s chart. This approach, which encouraged providers to follow prescribing guidelines by capitalizing on their concerns about their reputations, produced a 77% reduction in antibiotic prescribing.35
Focusing on the public. Studies have also examined the effectiveness of educating the public about when antibiotics are not likely to be helpful and of the harms of unnecessary antibiotics.
Studies conducted in Tennessee and Wisconsin that combined prescriber and community education about unnecessary antibiotics for children found that the intervention reduced antibiotic prescribing in both locations by about 19%, compared with about a 9% reduction in the control groups.36,37
DOES PRESCRIBING ANTIBIOTICS AFFECT PATIENT SATISFACTION?
The results are mixed as to whether prescribing antibiotics affects patient satisfaction. Two studies in the early 2000s found that both patients and parents reported higher satisfaction with clinicians who explained why antibiotics were not indicated versus those who simply prescribed them—and that such explanations do not need to take a lot of time (see Table 3 for patient care tips).37,38
A more recent study found that higher antibiotic prescribing practices in Britain were associated with modestly higher patient satisfaction ratings.39 The authors of this study noted, however, that reduced antibiotic prescribing may be a proxy for other practice patterns that affected satisfaction ratings.
REDUCING ANTIBIOTIC PRESCRIBING REDUCES RESISTANCE
There is also strong evidence that when clinicians decrease antibiotic prescribing, antimicrobial resistance follows suit. One of the earlier landmark studies to demonstrate this was a Finnish study published in 1997.40 The authors found that a reduction of macrolide antibiotic consumption in Finland led to a reduction in streptococci macrolide resistance from 16.5% to 8.6%.40
Multiple studies have since demonstrated similar results for both respiratory and urinary tract infections.41,42 A 2017 meta-analysis of 32 studies found that antibiotic stewardship programs reduced the incidence of infections and colonization with multidrug-resistant Gram-negative bacteria (by 51%), extended-spectrum beta-lactamase–producing Gram-negative bacteria (48%), and methicillin-resistant Staphylococcus aureus (37%). There was also a reduction in the incidence of CDI (32%).43
Despite universal agreement that antibiotic overprescribing is a problem, the practice continues to vex us. Antibiotic use—whether appropriate or not—has been linked to rising rates of antimicrobial resistance, disruption of the gut microbiome leading to Clostridium difficile infections (CDI), allergic reactions, and increased health care costs (see Table 1).1-6 And yet, clinicians continue to overprescribe this class of medication.
A 2016 report from the CDC estimates that at least 30% of antibiotics prescribed in US outpatient settings are unnecessary.7 Another report cites a slightly higher figure across a variety of health care settings.8 Pair these findings with the fact that there are currently few new drugs in development to target resistant bacteria, and you have the potential for a postantibiotic era in which common infections could become lethal.7
In 2003, the CDC launched its “Get Smart: Know When Antibiotics Work” program (now known as “Be Antibiotics Aware”), focused on decreasing inappropriate antibiotic use in the outpatient setting.9 In 2015, the White House released the National Action Plan for Combating Antibiotic-Resistant Bacteria, with a goal of decreasing inappropriate outpatient antibiotic use by 50% and inappropriate inpatient use by 20% by 2020.10 And, on an international level, the World Health Organization (WHO) in 2015 developed a five-year strategic framework for implementing its Global Action Plan on Antimicrobial Resistance.11
Family practitioners are on the front lines of this battle. Here’s what we can do now.
WHEN AND WHERE ARE ANTIBIOTICS MOST OFTEN INAPPROPRIATELY PRESCRIBED?
The diagnosis leading to the most frequent inappropriate prescribing of antibiotics is acute respiratory tract infection (ARTI), which includes bronchitis, otitis media, pharyngitis, sinusitis, tonsillitis, the common cold, and pneumonia. Up to 40% of antibiotic prescriptions for these conditions are unnecessary.8,12 Bronchitis is the most common ARTI diagnosis associated with inappropriate antibiotic prescriptions, while sinusitis, suppurative otitis media, and pharyngitis are the diagnoses associated with the lion’s share of all (appropriate and inappropriate) antibiotic prescriptions within the ARTI category.8,9,12,13 Refer to national clinical guidelines, which delineate when antibiotic treatment is appropriate for these conditions.14-16
With respect to setting, there are conflicting findings as to whether antibiotic prescribing differs in office-based versus emergency department (ED) settings.
- One study found a higher rate of antibiotic prescribing during ED visits than office visits (21% vs 9%), even though, between 2007 and 2009, more antibiotic prescriptions were written for adults in primary care offices than in either outpatient hospital clinics or EDs.17
- In a cross-sectional study using data from 2005 to 2010 National Ambulatory Medical Care Surveys (NAMCS) and National Hospital Ambulatory Medical Care Surveys (NHAMCS), more than half of patients with uncomplicated acute rhinosinusitis received a prescription for antibiotics, but there was no overall difference in antibiotic prescriptions between primary care and ED presentation.18
- A retrospective analysis found that between 2006 and 2010, outpatient hospital practices (56%) and community-practice offices (60%) prescribed more antibiotics for ARTIs than EDs did (51%).12
STICK TO NARROW-SPECTRUM AGENTS WHEN POSSIBLE
Using broad-spectrum antibiotics, such as quinolones or imipenem, firstline, contributes more to the problem of antibiotic resistance than does prescribing narrow-spectrum antibiotics such as amoxicillin, cephalexin, or trimethoprim-sulfamethoxazole.7 Yet between 2007 and 2009, broad-spectrum agents were prescribed for 61% of outpatient adult visits in which patients received an antibiotic prescription.17 Quinolones (25%), macrolides (20%), and aminopenicillins (12%) were most commonly prescribed, and antibiotic prescriptions were most often written for respiratory conditions, such as bronchitis, for which we now know antibiotics are rarely indicated.17
Between 2006 and 2008, pediatric patients who received antibiotic prescriptions were given broad-spectrum agents 50% of the time, of which macrolides were the class most commonly prescribed.13
More recently, researchers examined the frequency with which clinicians prescribe narrow-spectrum, firstline antibiotics for otitis media, sinusitis, and pharyngitis using 2010 to 2011 NAMCS/NHAMCS data. They found that providers used firstline agents recommended by professional guidelines 52% of the time, although it was estimated that they would have been appropriate in 80% of cases; pediatric patients were more likely to receive appropriate firstline antibiotics than adult patients.19 Macrolides, especially azithromycin, were the most common non-firstline antibiotics prescribed.19,20 The bottom line is that when antibiotics are indicated for upper respiratory infections (otitis media, sinusitis, and pharyngitis), clinicians should prescribe a narrow-spectrum antibiotic first.
ANTIBIOTIC OVERPRESCIBING AFFECTS THE GUT AND BEYOND
The human intestinal microbiome is composed of a diverse array of bacteria, viruses, and parasites.21 The main functions of the gut microbiome include interacting with the immune system and participating in biochemical reactions in the gut, such as absorption of fat-soluble vitamins and the production of vitamin K.
As we know, antibiotics decrease the diversity of gut bacteria, which, in turn, can cause less efficient nutrient extraction, as well as vulnerability to enteric infections.21 It is well known, for example, that the bacterial gut microbiome can either inhibit or promote diarrheal illnesses such as those caused by CDI. CDI is now the most common health care-related infection, accounting for about a half-million health care facility infections per year.22 It extends hospital stays an average of almost 10 days and is estimated to cost the health care system $6.3 billion annually.23
Antibiotics can also eliminate antibiotic-susceptible organisms, allowing resistant organisms to proliferate.4 They also promote the transmission of genes for antibiotic resistance between gut bacteria.4
Beyond the gut
Less well known is that gut bacteria can promote or inhibit extraintestinal infections.
Gut bacteria and HIV. In early HIV infections, for example, gut populations of Lactobacillus and Bifidobacteria are reduced, and the gut barrier becomes compromised.24 Increasing translocation of bacterial products is associated with HIV disease progression. Preservation of Lactobacillus populations in the gut is associated with markers predictive of better HIV outcomes, including a higher CD4 count, a lower viral load, and less evidence of gut microbial translocation.24 This underscores the importance of maintaining healthy gut flora in patients with HIV, using such steps as avoiding unnecessary antibiotics.
Gut bacteria and stress, depression. Antibiotics directly induce the expression of key genes that affect the stress response.25 While causative studies are lacking, there is a growing body of evidence suggesting that the gut microbiome is involved in two-way communication with the brain and can affect, and be affected by, stress and depression.21,26-30 Diseases and conditions that seem to have a putative connection to a disordered microbiome (dysbiosis) include depression, anxiety, Crohn disease, type 2 diabetes, and obesity. (For a discussion of the relationship between the gut microbiome and diabetes, see Endocrine Consult: The Gut Microbiome in Type 2 Diabetes.)
Gut bacteria and childhood obesity. Repeated use of broader-spectrum antibiotics in children younger than 24 months of age increases the risk for childhood obesity.1,6 One theory for the association is that the effects of broad-spectrum antibiotics on the intestinal flora of young children may alter long-term energy homeostasis, resulting in a higher risk for obesity.1
Gut bacteria and asthma. Studies demonstrate differences in the gut microbiomes of asthmatic and nonasthmatic patients. These differences affect the activities of helper T-cell subsets (Th1 and Th2), which in turn affect the development of immune tolerance.31
Although additional studies are needed to confirm these findings, the evidence collected thus far should make us all pause before prescribing drugs that can alter our microbiome in complex and only partially understood ways.
WHAT CAN WE DO RIGHT NOW?
The issues created by the inappropriate prescribing of antibiotics have been known for decades, and multiple attempts have been made to find solutions and implement change. Although some small successes have occurred, little overall progress has been made in reducing antibiotic prescribing in the general population. A historical review of why clinicians prescribe antibiotics inappropriately and the interventions that have successfully reduced this prescribing may prove valuable as we continue to look for new, effective answers.
Why do we overprescribe antibiotics? A 2015 systematic literature review found that patient demand, pharmaceutical company marketing activities, limited up-to-date information sources, and fear of losing patients are major reasons providers cite for prescribing antibiotics.32
In a separate study that explored antibiotic prescribing habits for acute bronchitis, clinicians cited “patient demand” as the major reason for prescribing antibiotics. Respondents also reported that “other physicians were responsible for inappropriate antibiotic prescribing.”33
Strategies that work
Some early intervention programs directed at reducing antibiotic prescribing demonstrated success (see Table 2).34-36
One example comes from a 1996-1998 study of four primary care practices.34 Researchers evaluated the impact of a multidimensional intervention effort targeted at clinicians and patients and aimed at lowering the use of antimicrobial agents for acute uncomplicated bronchitis in adults. It incorporated multiple elements, including office-based and household patient educational materials and a clinician intervention involving education, practice profiling, and academic detailing. Clinicians in this program reduced their rates of antibiotic prescribing for uncomplicated bronchitis from 74% to 48%.34
Employing EMRs. A more recent study focused on use of electronic medical records (EMRs) and communications to modify clinician antibiotic prescribing.35 By sending clinicians monthly emails comparing their prescribing patterns to those of peers and “typical top performers,” inappropriate antibiotic prescriptions for ARTIs went from 19.9% to 3.7%.35
In another effort, the same researchers modified providers’ EMRs to detect when potentially inappropriate antibiotics were prescribed. The system then prompted the clinician to provide an “antibiotic justification note,” which remained visible in the patient’s chart. This approach, which encouraged providers to follow prescribing guidelines by capitalizing on their concerns about their reputations, produced a 77% reduction in antibiotic prescribing.35
Focusing on the public. Studies have also examined the effectiveness of educating the public about when antibiotics are not likely to be helpful and of the harms of unnecessary antibiotics.
Studies conducted in Tennessee and Wisconsin that combined prescriber and community education about unnecessary antibiotics for children found that the intervention reduced antibiotic prescribing in both locations by about 19%, compared with about a 9% reduction in the control groups.36,37
DOES PRESCRIBING ANTIBIOTICS AFFECT PATIENT SATISFACTION?
The results are mixed as to whether prescribing antibiotics affects patient satisfaction. Two studies in the early 2000s found that both patients and parents reported higher satisfaction with clinicians who explained why antibiotics were not indicated versus those who simply prescribed them—and that such explanations do not need to take a lot of time (see Table 3 for patient care tips).37,38
A more recent study found that higher antibiotic prescribing practices in Britain were associated with modestly higher patient satisfaction ratings.39 The authors of this study noted, however, that reduced antibiotic prescribing may be a proxy for other practice patterns that affected satisfaction ratings.
REDUCING ANTIBIOTIC PRESCRIBING REDUCES RESISTANCE
There is also strong evidence that when clinicians decrease antibiotic prescribing, antimicrobial resistance follows suit. One of the earlier landmark studies to demonstrate this was a Finnish study published in 1997.40 The authors found that a reduction of macrolide antibiotic consumption in Finland led to a reduction in streptococci macrolide resistance from 16.5% to 8.6%.40
Multiple studies have since demonstrated similar results for both respiratory and urinary tract infections.41,42 A 2017 meta-analysis of 32 studies found that antibiotic stewardship programs reduced the incidence of infections and colonization with multidrug-resistant Gram-negative bacteria (by 51%), extended-spectrum beta-lactamase–producing Gram-negative bacteria (48%), and methicillin-resistant Staphylococcus aureus (37%). There was also a reduction in the incidence of CDI (32%).43
1. Bailey LC, Forrest CB, Zhang P, et al. Association of antibiotics in infancy with early childhood obesity. JAMA Pediatr. 2014;168:1063-1069.
2. Costelloe C, Metcalfe C, Lovering A, et al. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340:c2096.
3. Gleckman RA, Czachor JS. Antibiotic side effects. Semin Respir Crit Care Med. 2000;21:53-60.
4. Jernberg C, Löfmark S, Edlund C, et al. Long-term impacts of antibiotic exposure on the human intestinal microbiota. Microbiology. 2010;156:3216-3223.
5. Logan AC, Jacka FN, Craig JM, et al. The microbiome and mental health: looking back, moving forward with lessons from allergic diseases. Clin Psychopharmacol Neurosci. 2016;14:131-147.
6. Marra F, Marra CA, Richardson K, et al. Antibiotic use in children is associated with increased risk of asthma. Pediatrics. 2009;123:1003-1010.
7. Harris AM, Hicks LA, Qaseem A; the High Value Care Task Force of the American College of Physicians and the CDC. Appropriate antibiotic use for acute respiratory tract infection in adults: advice for high-value care from the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med. 2016; 164:425-434.
8. Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010-2011. JAMA. 2016;315: 1864-1873.
9. CDC. Antibiotic prescribing and use. www.cdc.gov/antibiotic-use/index.html. Accessed January 16, 2018.
10. The White House. National action plan for combating antibiotic-resistant bacteria. March 2015:1-63. https://obamawhitehouse.archives.gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf. Accessed January 16, 2018.
11. World Health Organization. Global action plan on antimicrobial resistance (2015). www.who.int/antimicrobial-resistance/global-action-plan/en/. Accessed January 16, 2018.
12. Barlam TF, Soria-Saucedo R, Cabral HJ, et al. Unnecessary antibiotics for acute respiratory tract infections: association with care setting and patient demographics. Open Forum Infect Dis. 2016;3:1-7.
13. Hersh AL, Shapiro DJ, Pavia AT, et al. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics. 2011;128:1053-1061.
14. Chow AW, Benninger MS, Brook I, et al. Executive summary: IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:1041-1045.
15. Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 suppl):S1-S39.
16. Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55:1279-1282.
17. Shapiro DJ, Hicks LA, Pavia AT, et al. Antibiotic prescribing for adults in ambulatory care in the USA, 2007-09. J Antimicrob Chemother. 2014;69:234-240.
18. Bergmark RW, Sedaghat AR. Antibiotic prescription for acute rhinosinusitis: emergency departments versus primary care providers. Laryngoscope. 2016;126:2439-2444.
19. Hersh AL, Fleming-Dutra KE, Shapiro DJ, et al. Frequency of first-line antibiotic selection among US ambulatory care visits for otitis media, sinusitis, and pharyngitis. JAMA Intern Med. 2016;176:1870-1872.
20. Hicks LA, Bartoces MG, Roberts RM, et al. US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clin Infect Dis. 2015;60:1308-1316.
21. Langdon A, Crook N, Dantas G. The effects of antibiotics on the microbiome throughout development and alternative approaches for therapeutic modulation. Genome Med. 2016;8:39.
22. Lessa FC, Gould CV, McDonald CL. Current status of Clostridium difficile infection epidemiology. Clin Infect Dis. 2012;55(suppl 2):S65-S70.
23. Zhang S, Palazuelos-Munoz S, Balsells EM, et al. Cost of hospital management of Clostridium difficile infection in United States—a meta-analysis and modelling study. BMC Infect Dis. 2016;16:447.
24. Pérez-Santiago J, Gianella S, Massanella M, et al. Gut lactobacillales are associated with higher CD4 and less microbial translocation during HIV infection. AIDS. 2013;27:1921-1931.
25. Maurice CF, Haiser HJ, Turnbaugh PJ. Xenobiotics shape the physiology and gene expression of the active human gut microbiome. Cell. 2013;152:39-50.
26. Bravo JA, Julio-Pieper M, Forsythe P, et al. Communication between gastrointestinal bacteria and the nervous system. Curr Opin Pharmacol. 2012;12:667-672.
27. Clemente JC, Ursell LK, Parfrey LW, et al. The impact of the gut microbiota on human health: an integrative view. Cell. 2012;148:1258-1270.
28. Dinan TG, Cryan JF. Regulation of the stress response by the gut microbiota: implications for psychoneuroendocrinology. Psychoneuroendocrinology. 2012;37:1369-1378.
29. Foster JA, McVey Neufeld KA. Gut-brain axis: how the microbiome influences anxiety and depression. Trends Neurosci. 2013;36:305-312.
30. Wang Y, Kasper LH. The role of microbiome in central nervous system disorders. Brain Behav Immun. 2014; 38:1-12.31. Riiser A. The human microbiome, asthma, and allergy. Allergy Asthma Clin Immunol. 2015;11:35.
32. Md Rezal RS, Hassali MA, Alrasheedy AA, et al. Physicians’ knowledge, perceptions and behaviour towards antibiotic prescribing: a systematic review of the literature. Expert Rev Anti Infect Ther. 2015;13:665-680.
33. Dempsey PP, Businger AC, Whaley LE, et al. Primary care clinicians’ perceptions about antibiotic prescribing for acute bronchitis: a qualitative study. BMC Fam Pract . 2014;15:194.
34. Gonzales R, Steiner JF, Lum A, et al. Decreasing antibiotic use in ambulatory practice. JAMA . 1999;281:1512-1519.
35. Meeker D, Linder JA, Fox CR, et al. Effect of behavioral interventions on inappropriate antibiotic prescribing among primary care practices: a randomized clinical trial. JAMA . 2016;315:562-570.
36. Perz JF, Craig AS, Coffey CS, et al. Changes in antibiotic prescribing for children after a community-wide campaign. JAMA . 2002;287:3103-3109.
37. Belongia EA, Sullivan BJ, Chyou PH, et al. A community intervention trial to promote judicious antibiotic use and reduce penicillin-resistant Streptococcus pneumoniae carriage in children. Pediatrics . 2001;108:575-583.
38. Mangione-Smith R, McGlynn EA, Elliott MN, et al. Parent expectations for antibiotics, physician-parent communication, and satisfaction. Arch Pediatr Adolesc Med. 2001;155:800-806.
39. Ashworth M, White P, Jongsma H, et al. Antibiotic prescribing and patient satisfaction in primary care in England: cross-sectional analysis of national patient survey data and prescribing data. Br J Gen Pract . 2016;66:e40-e46.
40. Seppälä H, Klaukka T, Vuopio-Varkila J, et al. The effect of changes in the consumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. N Engl J Med. 1997;337:441-446.
41. Guillemot D, Varon E, Bernède C, et al. Reduction of antibiotic use in the community reduces the rate of colonization with penicillin g–nonsusceptible Streptococcus pneumoniae . Clin Infect Dis. 2005;41:930-938.
42. Butler CC, Dunstan F, Heginbothom M, et al. Containing antibiotic resistance: decreased antibiotic-resistant coliform urinary tract infections with reduction in antibiotic prescribing by general practices. Br J Gen Pract. 2007; 57:785-792.
43. Baur D, Gladstone BP, Burkert F, et al. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17:990-1001.
1. Bailey LC, Forrest CB, Zhang P, et al. Association of antibiotics in infancy with early childhood obesity. JAMA Pediatr. 2014;168:1063-1069.
2. Costelloe C, Metcalfe C, Lovering A, et al. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ. 2010;340:c2096.
3. Gleckman RA, Czachor JS. Antibiotic side effects. Semin Respir Crit Care Med. 2000;21:53-60.
4. Jernberg C, Löfmark S, Edlund C, et al. Long-term impacts of antibiotic exposure on the human intestinal microbiota. Microbiology. 2010;156:3216-3223.
5. Logan AC, Jacka FN, Craig JM, et al. The microbiome and mental health: looking back, moving forward with lessons from allergic diseases. Clin Psychopharmacol Neurosci. 2016;14:131-147.
6. Marra F, Marra CA, Richardson K, et al. Antibiotic use in children is associated with increased risk of asthma. Pediatrics. 2009;123:1003-1010.
7. Harris AM, Hicks LA, Qaseem A; the High Value Care Task Force of the American College of Physicians and the CDC. Appropriate antibiotic use for acute respiratory tract infection in adults: advice for high-value care from the American College of Physicians and the Centers for Disease Control and Prevention. Ann Intern Med. 2016; 164:425-434.
8. Fleming-Dutra KE, Hersh AL, Shapiro DJ, et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010-2011. JAMA. 2016;315: 1864-1873.
9. CDC. Antibiotic prescribing and use. www.cdc.gov/antibiotic-use/index.html. Accessed January 16, 2018.
10. The White House. National action plan for combating antibiotic-resistant bacteria. March 2015:1-63. https://obamawhitehouse.archives.gov/sites/default/files/docs/national_action_plan_for_combating_antibotic-resistant_bacteria.pdf. Accessed January 16, 2018.
11. World Health Organization. Global action plan on antimicrobial resistance (2015). www.who.int/antimicrobial-resistance/global-action-plan/en/. Accessed January 16, 2018.
12. Barlam TF, Soria-Saucedo R, Cabral HJ, et al. Unnecessary antibiotics for acute respiratory tract infections: association with care setting and patient demographics. Open Forum Infect Dis. 2016;3:1-7.
13. Hersh AL, Shapiro DJ, Pavia AT, et al. Antibiotic prescribing in ambulatory pediatrics in the United States. Pediatrics. 2011;128:1053-1061.
14. Chow AW, Benninger MS, Brook I, et al. Executive summary: IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clin Infect Dis. 2012;54:1041-1045.
15. Rosenfeld RM, Piccirillo JF, Chandrasekhar SS, et al. Clinical practice guideline (update): adult sinusitis. Otolaryngol Head Neck Surg. 2015;152(2 suppl):S1-S39.
16. Shulman ST, Bisno AL, Clegg HW, et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clin Infect Dis. 2012;55:1279-1282.
17. Shapiro DJ, Hicks LA, Pavia AT, et al. Antibiotic prescribing for adults in ambulatory care in the USA, 2007-09. J Antimicrob Chemother. 2014;69:234-240.
18. Bergmark RW, Sedaghat AR. Antibiotic prescription for acute rhinosinusitis: emergency departments versus primary care providers. Laryngoscope. 2016;126:2439-2444.
19. Hersh AL, Fleming-Dutra KE, Shapiro DJ, et al. Frequency of first-line antibiotic selection among US ambulatory care visits for otitis media, sinusitis, and pharyngitis. JAMA Intern Med. 2016;176:1870-1872.
20. Hicks LA, Bartoces MG, Roberts RM, et al. US outpatient antibiotic prescribing variation according to geography, patient population, and provider specialty in 2011. Clin Infect Dis. 2015;60:1308-1316.
21. Langdon A, Crook N, Dantas G. The effects of antibiotics on the microbiome throughout development and alternative approaches for therapeutic modulation. Genome Med. 2016;8:39.
22. Lessa FC, Gould CV, McDonald CL. Current status of Clostridium difficile infection epidemiology. Clin Infect Dis. 2012;55(suppl 2):S65-S70.
23. Zhang S, Palazuelos-Munoz S, Balsells EM, et al. Cost of hospital management of Clostridium difficile infection in United States—a meta-analysis and modelling study. BMC Infect Dis. 2016;16:447.
24. Pérez-Santiago J, Gianella S, Massanella M, et al. Gut lactobacillales are associated with higher CD4 and less microbial translocation during HIV infection. AIDS. 2013;27:1921-1931.
25. Maurice CF, Haiser HJ, Turnbaugh PJ. Xenobiotics shape the physiology and gene expression of the active human gut microbiome. Cell. 2013;152:39-50.
26. Bravo JA, Julio-Pieper M, Forsythe P, et al. Communication between gastrointestinal bacteria and the nervous system. Curr Opin Pharmacol. 2012;12:667-672.
27. Clemente JC, Ursell LK, Parfrey LW, et al. The impact of the gut microbiota on human health: an integrative view. Cell. 2012;148:1258-1270.
28. Dinan TG, Cryan JF. Regulation of the stress response by the gut microbiota: implications for psychoneuroendocrinology. Psychoneuroendocrinology. 2012;37:1369-1378.
29. Foster JA, McVey Neufeld KA. Gut-brain axis: how the microbiome influences anxiety and depression. Trends Neurosci. 2013;36:305-312.
30. Wang Y, Kasper LH. The role of microbiome in central nervous system disorders. Brain Behav Immun. 2014; 38:1-12.31. Riiser A. The human microbiome, asthma, and allergy. Allergy Asthma Clin Immunol. 2015;11:35.
32. Md Rezal RS, Hassali MA, Alrasheedy AA, et al. Physicians’ knowledge, perceptions and behaviour towards antibiotic prescribing: a systematic review of the literature. Expert Rev Anti Infect Ther. 2015;13:665-680.
33. Dempsey PP, Businger AC, Whaley LE, et al. Primary care clinicians’ perceptions about antibiotic prescribing for acute bronchitis: a qualitative study. BMC Fam Pract . 2014;15:194.
34. Gonzales R, Steiner JF, Lum A, et al. Decreasing antibiotic use in ambulatory practice. JAMA . 1999;281:1512-1519.
35. Meeker D, Linder JA, Fox CR, et al. Effect of behavioral interventions on inappropriate antibiotic prescribing among primary care practices: a randomized clinical trial. JAMA . 2016;315:562-570.
36. Perz JF, Craig AS, Coffey CS, et al. Changes in antibiotic prescribing for children after a community-wide campaign. JAMA . 2002;287:3103-3109.
37. Belongia EA, Sullivan BJ, Chyou PH, et al. A community intervention trial to promote judicious antibiotic use and reduce penicillin-resistant Streptococcus pneumoniae carriage in children. Pediatrics . 2001;108:575-583.
38. Mangione-Smith R, McGlynn EA, Elliott MN, et al. Parent expectations for antibiotics, physician-parent communication, and satisfaction. Arch Pediatr Adolesc Med. 2001;155:800-806.
39. Ashworth M, White P, Jongsma H, et al. Antibiotic prescribing and patient satisfaction in primary care in England: cross-sectional analysis of national patient survey data and prescribing data. Br J Gen Pract . 2016;66:e40-e46.
40. Seppälä H, Klaukka T, Vuopio-Varkila J, et al. The effect of changes in the consumption of macrolide antibiotics on erythromycin resistance in group A streptococci in Finland. N Engl J Med. 1997;337:441-446.
41. Guillemot D, Varon E, Bernède C, et al. Reduction of antibiotic use in the community reduces the rate of colonization with penicillin g–nonsusceptible Streptococcus pneumoniae . Clin Infect Dis. 2005;41:930-938.
42. Butler CC, Dunstan F, Heginbothom M, et al. Containing antibiotic resistance: decreased antibiotic-resistant coliform urinary tract infections with reduction in antibiotic prescribing by general practices. Br J Gen Pract. 2007; 57:785-792.
43. Baur D, Gladstone BP, Burkert F, et al. Effect of antibiotic stewardship on the incidence of infection and colonisation with antibiotic-resistant bacteria and Clostridium difficile infection: a systematic review and meta-analysis. Lancet Infect Dis. 2017;17:990-1001.

More time with digital media impacts childhood well-being
In school-aged children, according to Stephanie Ruest, MD, of Hasbro Children’s Hospital, Providence, R.I., and her associates.
In a study surveying parents from the 2011-2012 National Survey of Children’s Health, behavior of 64,464 children aged 6-17 years was examined. Results found that 31% of children were reported to have a combined daily digital media exposure (DME) of less than 2 hours/day, 36% had 2-4 hours, 17% had 4-6 hours, and 16% had at least 6 hours/day of DME. Among the children with less than 2 hours of DME, 38% had access to media devices in their bedroom, compared with 73% in the greater than 6-hour exposure group.
Additionally, children who had 2-4 hours of DME per weekday not related to schoolwork had 22% lower odds of always/usually finishing their homework, compared with children who had less than 2 hours. Children with 4-6 hours/day had 46% lower odds and those with greater than 6 hours/day had 57% lower odds of demonstrating this marker, compared with children with less than 2 hours (P less than .001). “There was a similar decrease in odds seen with each of the remaining four flourishing markers (test for trend P less than .001 for each marker),” Dr. Ruest and her associates said.
“DME, when measured in combined daily hours, is inversely associated with behaviors and attitudes that have been identified as markers of childhood flourishing in a dose-dependent manner,” the researchers concluded. “Future studies should continue to work towards elucidating the complex relationship between total DME time in conjunction with the content of the media and how the interplay affects childhood flourishing.”
SOURCE: Ruest S et al. J Pediatr. 2018 Feb 1. doi: 10.1016/j.jpeds.2017.12.016.
In school-aged children, according to Stephanie Ruest, MD, of Hasbro Children’s Hospital, Providence, R.I., and her associates.
In a study surveying parents from the 2011-2012 National Survey of Children’s Health, behavior of 64,464 children aged 6-17 years was examined. Results found that 31% of children were reported to have a combined daily digital media exposure (DME) of less than 2 hours/day, 36% had 2-4 hours, 17% had 4-6 hours, and 16% had at least 6 hours/day of DME. Among the children with less than 2 hours of DME, 38% had access to media devices in their bedroom, compared with 73% in the greater than 6-hour exposure group.
Additionally, children who had 2-4 hours of DME per weekday not related to schoolwork had 22% lower odds of always/usually finishing their homework, compared with children who had less than 2 hours. Children with 4-6 hours/day had 46% lower odds and those with greater than 6 hours/day had 57% lower odds of demonstrating this marker, compared with children with less than 2 hours (P less than .001). “There was a similar decrease in odds seen with each of the remaining four flourishing markers (test for trend P less than .001 for each marker),” Dr. Ruest and her associates said.
“DME, when measured in combined daily hours, is inversely associated with behaviors and attitudes that have been identified as markers of childhood flourishing in a dose-dependent manner,” the researchers concluded. “Future studies should continue to work towards elucidating the complex relationship between total DME time in conjunction with the content of the media and how the interplay affects childhood flourishing.”
SOURCE: Ruest S et al. J Pediatr. 2018 Feb 1. doi: 10.1016/j.jpeds.2017.12.016.
In school-aged children, according to Stephanie Ruest, MD, of Hasbro Children’s Hospital, Providence, R.I., and her associates.
In a study surveying parents from the 2011-2012 National Survey of Children’s Health, behavior of 64,464 children aged 6-17 years was examined. Results found that 31% of children were reported to have a combined daily digital media exposure (DME) of less than 2 hours/day, 36% had 2-4 hours, 17% had 4-6 hours, and 16% had at least 6 hours/day of DME. Among the children with less than 2 hours of DME, 38% had access to media devices in their bedroom, compared with 73% in the greater than 6-hour exposure group.
Additionally, children who had 2-4 hours of DME per weekday not related to schoolwork had 22% lower odds of always/usually finishing their homework, compared with children who had less than 2 hours. Children with 4-6 hours/day had 46% lower odds and those with greater than 6 hours/day had 57% lower odds of demonstrating this marker, compared with children with less than 2 hours (P less than .001). “There was a similar decrease in odds seen with each of the remaining four flourishing markers (test for trend P less than .001 for each marker),” Dr. Ruest and her associates said.
“DME, when measured in combined daily hours, is inversely associated with behaviors and attitudes that have been identified as markers of childhood flourishing in a dose-dependent manner,” the researchers concluded. “Future studies should continue to work towards elucidating the complex relationship between total DME time in conjunction with the content of the media and how the interplay affects childhood flourishing.”
SOURCE: Ruest S et al. J Pediatr. 2018 Feb 1. doi: 10.1016/j.jpeds.2017.12.016.
FROM THE JOURNAL OF PEDIATRICS
Dermoscopy will help diagnose pediatric melanomas
Adding dermoscopy to the classic and modified melanoma ABCD criteria will help speed detection of melanoma in children, said Cristina Carrera, MD, of the University of Barcelona, and her associates.
Pediatric melanomas make up less than 3% of pediatric cancers and 1%-4% of all melanomas, occurring more commonly in adolescents than in children aged 5-9 years. These cancers often are thicker when first seen because of delay in diagnosis and/or differences in growth dynamics. Delay in diagnosis may occur because of the low incidence of pediatric melanoma and because classic melanoma criteria – ABCD: asymmetry, border irregularity, multiple colors, diameter (6 mm) – don’t always apply, they said.
A modified clinical ABCD rule of ‘‘amelanotic, bleeding bump, color uniformity, and de novo lesion of any diameter’’ was proposed to improve early detection of pediatric melanoma. And because dermoscopy improves melanoma diagnosis in adults, researchers decided to examine clinical and dermascopic findings in a group of pediatric melanoma cases.
Fifty-two pediatric melanoma cases from 51 patients were collected from pigmented lesion clinics across nine countries (Australia, Belgium, Brazil, France, Israel, Italy, Serbia, Spain, and the United States), and clinical and dermoscopic specimens were examined by two experienced reviewers.
The mean age of the patients was 15 years, and 26 of the patients were female. Histopathologically, 28% of the pediatric melanomas were classified as spitzoid and 72% as nonspitzoid. Patients with a spitzoid melanoma were significantly younger than those with nonspitzoid melanoma (12.5 vs. 16 years, P = .004). All of the spitzoid tumors were invasive, and they were significantly thicker than the nonspitzoid melanomas (2.6 vs. 1.2 mm, P = .004). Also, these lesions more frequently were ulcerated than nonspitzoid melanomas (29% vs. 8%, P = .06). Melanomas associated with a nevus more often were among nonspitzoid than spitzoid melanomas (62% vs. 27% P = .02), and the congenital type of nevus was linked most often with nonspitzoid melanomas (25 of 27 [92.6%]), Dr. Carrera and her associates reported.
The pediatric melanomas in this study appeared most frequently on the lower extremities (31%), followed by the back (27%). Spitzoid melanomas most often appeared on the limbs (73%); nonspitzoid melanomas were likely to occur on the torso (52%).
In the majority of cases (52%), the overall clinical morphology was considered to fulfill the classic melanoma ABCD criteria. The remaining lesions that did not fulfill the conventional ABCD criteria were called benign-appearing tumors or nodular/polypoid tumors. Spitzoid melanomas most often were nodular/ polypoid (47%), while most nonspitzoid melanomas (59%) were melanoma-like. Only 21% of the pediatric melanomas fulfilled the modified melanoma ABCD criteria, they noted.
On dermoscopy, which was available in 49 cases, a multicomponent pattern seen in 24 cases mostly was associated with nonspitzoid melanoma (88%, P less than.03); a nevus-like pattern in 9 cases was seen only among nonspitzoid melanomas. A vascular pink Spitz-like pattern in seven cases mostly was associated with spitzoid melanomas (86%, P less than .002). A pigmented Reed-like pattern seen in seven cases occurred more often among spitzoid melanomas, but this did not reach statistical significance, the investigators wrote.
In terms of appearance, “red and white colors, milky red areas, polymorphous vessels, and shiny white structures were associated with spitzoid melanoma. Dark brown color, atypical network, and structureless areas were associated with nonspitzoid melanomas,” Dr. Carrera and her associates said.
Dermoscopic patterns that were pink spitzoid or Reed-like were more likely to be histopathologically classified as spitzoid. These pediatric melanomas were linked with younger age, occurrence on the limbs, and de novo development. On the other hand, dermoscopic patterns that were multicomponent or nevus-like were likely to be histopathologically classified as nonspitzoid. These lesions were linked with older age, fair skin phenotype, family history of melanoma, and a preexisting nevus, the researchers said.
“In contrast to previous reports, the present study highlights the fact that the majority of melanomas diagnosed in patients younger than 20 years look similar to melanomas found in adults. Nonspitzoid melanomas were associated with adolescence and with the presence of melanoma risk factors. All nonspitzoid melanomas displayed dermoscopic features associated with melanoma. Spitzoid melanomas were associated with younger age, location on the extremities, and nodular/polypoid clinical morphology. Dermoscopy of spitzoid melanomas revealed atypical vessels and shiny white lines (if amelanotic) or an asymmetric starburst pattern (if pigmented),” Dr. Carrera and her associates concluded.
The investigators had no relevant financial disclosures. The study was supported in part through a grant from the National Institutes of Health/ National Cancer Institute. The research at the melanoma unit in Barcelona was partially funded by grants from the Spanish Fondo de Investigaciones Sanitarias and CIBER de Enfermedades Raras of the Instituto de Salud Carlos III, Spain; it was confinanced by numerous other grants.
SOURCE: Carrera C et al. J Am Acad Dermatol. 2018;78(2):278-88. doi: 10.1016/j.jaad.2017.09.065.
Adding dermoscopy to the classic and modified melanoma ABCD criteria will help speed detection of melanoma in children, said Cristina Carrera, MD, of the University of Barcelona, and her associates.
Pediatric melanomas make up less than 3% of pediatric cancers and 1%-4% of all melanomas, occurring more commonly in adolescents than in children aged 5-9 years. These cancers often are thicker when first seen because of delay in diagnosis and/or differences in growth dynamics. Delay in diagnosis may occur because of the low incidence of pediatric melanoma and because classic melanoma criteria – ABCD: asymmetry, border irregularity, multiple colors, diameter (6 mm) – don’t always apply, they said.
A modified clinical ABCD rule of ‘‘amelanotic, bleeding bump, color uniformity, and de novo lesion of any diameter’’ was proposed to improve early detection of pediatric melanoma. And because dermoscopy improves melanoma diagnosis in adults, researchers decided to examine clinical and dermascopic findings in a group of pediatric melanoma cases.
Fifty-two pediatric melanoma cases from 51 patients were collected from pigmented lesion clinics across nine countries (Australia, Belgium, Brazil, France, Israel, Italy, Serbia, Spain, and the United States), and clinical and dermoscopic specimens were examined by two experienced reviewers.
The mean age of the patients was 15 years, and 26 of the patients were female. Histopathologically, 28% of the pediatric melanomas were classified as spitzoid and 72% as nonspitzoid. Patients with a spitzoid melanoma were significantly younger than those with nonspitzoid melanoma (12.5 vs. 16 years, P = .004). All of the spitzoid tumors were invasive, and they were significantly thicker than the nonspitzoid melanomas (2.6 vs. 1.2 mm, P = .004). Also, these lesions more frequently were ulcerated than nonspitzoid melanomas (29% vs. 8%, P = .06). Melanomas associated with a nevus more often were among nonspitzoid than spitzoid melanomas (62% vs. 27% P = .02), and the congenital type of nevus was linked most often with nonspitzoid melanomas (25 of 27 [92.6%]), Dr. Carrera and her associates reported.
The pediatric melanomas in this study appeared most frequently on the lower extremities (31%), followed by the back (27%). Spitzoid melanomas most often appeared on the limbs (73%); nonspitzoid melanomas were likely to occur on the torso (52%).
In the majority of cases (52%), the overall clinical morphology was considered to fulfill the classic melanoma ABCD criteria. The remaining lesions that did not fulfill the conventional ABCD criteria were called benign-appearing tumors or nodular/polypoid tumors. Spitzoid melanomas most often were nodular/ polypoid (47%), while most nonspitzoid melanomas (59%) were melanoma-like. Only 21% of the pediatric melanomas fulfilled the modified melanoma ABCD criteria, they noted.
On dermoscopy, which was available in 49 cases, a multicomponent pattern seen in 24 cases mostly was associated with nonspitzoid melanoma (88%, P less than.03); a nevus-like pattern in 9 cases was seen only among nonspitzoid melanomas. A vascular pink Spitz-like pattern in seven cases mostly was associated with spitzoid melanomas (86%, P less than .002). A pigmented Reed-like pattern seen in seven cases occurred more often among spitzoid melanomas, but this did not reach statistical significance, the investigators wrote.
In terms of appearance, “red and white colors, milky red areas, polymorphous vessels, and shiny white structures were associated with spitzoid melanoma. Dark brown color, atypical network, and structureless areas were associated with nonspitzoid melanomas,” Dr. Carrera and her associates said.
Dermoscopic patterns that were pink spitzoid or Reed-like were more likely to be histopathologically classified as spitzoid. These pediatric melanomas were linked with younger age, occurrence on the limbs, and de novo development. On the other hand, dermoscopic patterns that were multicomponent or nevus-like were likely to be histopathologically classified as nonspitzoid. These lesions were linked with older age, fair skin phenotype, family history of melanoma, and a preexisting nevus, the researchers said.
“In contrast to previous reports, the present study highlights the fact that the majority of melanomas diagnosed in patients younger than 20 years look similar to melanomas found in adults. Nonspitzoid melanomas were associated with adolescence and with the presence of melanoma risk factors. All nonspitzoid melanomas displayed dermoscopic features associated with melanoma. Spitzoid melanomas were associated with younger age, location on the extremities, and nodular/polypoid clinical morphology. Dermoscopy of spitzoid melanomas revealed atypical vessels and shiny white lines (if amelanotic) or an asymmetric starburst pattern (if pigmented),” Dr. Carrera and her associates concluded.
The investigators had no relevant financial disclosures. The study was supported in part through a grant from the National Institutes of Health/ National Cancer Institute. The research at the melanoma unit in Barcelona was partially funded by grants from the Spanish Fondo de Investigaciones Sanitarias and CIBER de Enfermedades Raras of the Instituto de Salud Carlos III, Spain; it was confinanced by numerous other grants.
SOURCE: Carrera C et al. J Am Acad Dermatol. 2018;78(2):278-88. doi: 10.1016/j.jaad.2017.09.065.
Adding dermoscopy to the classic and modified melanoma ABCD criteria will help speed detection of melanoma in children, said Cristina Carrera, MD, of the University of Barcelona, and her associates.
Pediatric melanomas make up less than 3% of pediatric cancers and 1%-4% of all melanomas, occurring more commonly in adolescents than in children aged 5-9 years. These cancers often are thicker when first seen because of delay in diagnosis and/or differences in growth dynamics. Delay in diagnosis may occur because of the low incidence of pediatric melanoma and because classic melanoma criteria – ABCD: asymmetry, border irregularity, multiple colors, diameter (6 mm) – don’t always apply, they said.
A modified clinical ABCD rule of ‘‘amelanotic, bleeding bump, color uniformity, and de novo lesion of any diameter’’ was proposed to improve early detection of pediatric melanoma. And because dermoscopy improves melanoma diagnosis in adults, researchers decided to examine clinical and dermascopic findings in a group of pediatric melanoma cases.
Fifty-two pediatric melanoma cases from 51 patients were collected from pigmented lesion clinics across nine countries (Australia, Belgium, Brazil, France, Israel, Italy, Serbia, Spain, and the United States), and clinical and dermoscopic specimens were examined by two experienced reviewers.
The mean age of the patients was 15 years, and 26 of the patients were female. Histopathologically, 28% of the pediatric melanomas were classified as spitzoid and 72% as nonspitzoid. Patients with a spitzoid melanoma were significantly younger than those with nonspitzoid melanoma (12.5 vs. 16 years, P = .004). All of the spitzoid tumors were invasive, and they were significantly thicker than the nonspitzoid melanomas (2.6 vs. 1.2 mm, P = .004). Also, these lesions more frequently were ulcerated than nonspitzoid melanomas (29% vs. 8%, P = .06). Melanomas associated with a nevus more often were among nonspitzoid than spitzoid melanomas (62% vs. 27% P = .02), and the congenital type of nevus was linked most often with nonspitzoid melanomas (25 of 27 [92.6%]), Dr. Carrera and her associates reported.
The pediatric melanomas in this study appeared most frequently on the lower extremities (31%), followed by the back (27%). Spitzoid melanomas most often appeared on the limbs (73%); nonspitzoid melanomas were likely to occur on the torso (52%).
In the majority of cases (52%), the overall clinical morphology was considered to fulfill the classic melanoma ABCD criteria. The remaining lesions that did not fulfill the conventional ABCD criteria were called benign-appearing tumors or nodular/polypoid tumors. Spitzoid melanomas most often were nodular/ polypoid (47%), while most nonspitzoid melanomas (59%) were melanoma-like. Only 21% of the pediatric melanomas fulfilled the modified melanoma ABCD criteria, they noted.
On dermoscopy, which was available in 49 cases, a multicomponent pattern seen in 24 cases mostly was associated with nonspitzoid melanoma (88%, P less than.03); a nevus-like pattern in 9 cases was seen only among nonspitzoid melanomas. A vascular pink Spitz-like pattern in seven cases mostly was associated with spitzoid melanomas (86%, P less than .002). A pigmented Reed-like pattern seen in seven cases occurred more often among spitzoid melanomas, but this did not reach statistical significance, the investigators wrote.
In terms of appearance, “red and white colors, milky red areas, polymorphous vessels, and shiny white structures were associated with spitzoid melanoma. Dark brown color, atypical network, and structureless areas were associated with nonspitzoid melanomas,” Dr. Carrera and her associates said.
Dermoscopic patterns that were pink spitzoid or Reed-like were more likely to be histopathologically classified as spitzoid. These pediatric melanomas were linked with younger age, occurrence on the limbs, and de novo development. On the other hand, dermoscopic patterns that were multicomponent or nevus-like were likely to be histopathologically classified as nonspitzoid. These lesions were linked with older age, fair skin phenotype, family history of melanoma, and a preexisting nevus, the researchers said.
“In contrast to previous reports, the present study highlights the fact that the majority of melanomas diagnosed in patients younger than 20 years look similar to melanomas found in adults. Nonspitzoid melanomas were associated with adolescence and with the presence of melanoma risk factors. All nonspitzoid melanomas displayed dermoscopic features associated with melanoma. Spitzoid melanomas were associated with younger age, location on the extremities, and nodular/polypoid clinical morphology. Dermoscopy of spitzoid melanomas revealed atypical vessels and shiny white lines (if amelanotic) or an asymmetric starburst pattern (if pigmented),” Dr. Carrera and her associates concluded.
The investigators had no relevant financial disclosures. The study was supported in part through a grant from the National Institutes of Health/ National Cancer Institute. The research at the melanoma unit in Barcelona was partially funded by grants from the Spanish Fondo de Investigaciones Sanitarias and CIBER de Enfermedades Raras of the Instituto de Salud Carlos III, Spain; it was confinanced by numerous other grants.
SOURCE: Carrera C et al. J Am Acad Dermatol. 2018;78(2):278-88. doi: 10.1016/j.jaad.2017.09.065.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Key clinical point:
Major finding: On dermoscopy, a multicomponent pattern seen in 24 cases mostly was associated with nonspitzoid melanoma (88%, P less than.03).
Data source: Fifty-two pediatric melanoma cases from 51 patients were collected from pigmented lesion clinics across 9 countries.
Disclosures: The investigators had no relevant financial disclosures. The study was supported in part through a grant from the National Institutes of Health/ National Cancer Institute. The research at the melanoma unit in Barcelona was partially funded by grants from the Spanish Fondo de Investigaciones Sanitarias and CIBER de Enfermedades Raras of the Instituto de Salud Carlos III, Spain; it was cofinanced by numerous other grants.
Source: Carrera C et al. J Am Acad Dermatol. 2018;78(2):278-88.