User login
Shades of gray
If you were born in or after the 1970s, it is very likely that you have never watched a television show on a black and white set. Although the roots of its technology extend well back into the early 20th century, the first color broadcast on a national television network didn’t occur until 1954 with NBC’s coverage of the Tournament of Roses Parade.
When we compare the popularization of color television with the rapid pace at which we adopt new technology today, the popularization of color TV was glacial. In large part because of their expense, sales of color sets did not surpass black and white sets until 1972. Our family lagged behind the curve and finally caved in and junked our black and white television around 1977.
The observable change in our viewing behavior was dramatic. While programming in black and white was interesting, the color images were magnetic. We were drawn by the visual excitement and stimulation that color offered, and our family’s viewing standards took a precipitous dip. We seemed to watch anything that was colorful and moved. The quality of the content took a back seat. Viewing in color seemed to require much less cognitive effort. Ironically what attracted our attention allowed us to invest less energy in paying attention.
As a regular reader of Letters From Maine, you know that I am convinced that sleep deprivation is a major contributor to the emergence of the ADHD phenomenon. However, I can make a similar argument that the introduction of color television is an equally potent coconspirator or confounder. The magnetism inherent in a moving color image can tempt even the most health conscious among us to stay well past a brain-friendly bedtime. The invention of the electric light may have gotten the ball rolling, but the ubiquity of moving electronic color images has certainly greased what was already a very slippery slope into an abyss of unhealthy sleep habits.
There are those who argue that smartphones and tablets can open a world of creative opportunities for even very young children. And, it is obvious that parents are struggling to find a balance as they try to decide when, where, and how often to allow their infants and toddlers access to handheld electronic devices.
Recently there has been much finger-pointing at the developers and manufacturers of smartphones and tablets. How can any company with a social conscience sell a product with such dangerous attractive potential for children without providing safeguards? Isn’t it like selling a swimming pool without a gated fence?
Of course the answer to this question goes to the heart of how our society views its responsibility to protect its children. Regardless of who makes the rules and how the responsibility is assigned, it is still the child’s parents who must make sure that the gate is locked.

Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
If you were born in or after the 1970s, it is very likely that you have never watched a television show on a black and white set. Although the roots of its technology extend well back into the early 20th century, the first color broadcast on a national television network didn’t occur until 1954 with NBC’s coverage of the Tournament of Roses Parade.
When we compare the popularization of color television with the rapid pace at which we adopt new technology today, the popularization of color TV was glacial. In large part because of their expense, sales of color sets did not surpass black and white sets until 1972. Our family lagged behind the curve and finally caved in and junked our black and white television around 1977.
The observable change in our viewing behavior was dramatic. While programming in black and white was interesting, the color images were magnetic. We were drawn by the visual excitement and stimulation that color offered, and our family’s viewing standards took a precipitous dip. We seemed to watch anything that was colorful and moved. The quality of the content took a back seat. Viewing in color seemed to require much less cognitive effort. Ironically what attracted our attention allowed us to invest less energy in paying attention.
As a regular reader of Letters From Maine, you know that I am convinced that sleep deprivation is a major contributor to the emergence of the ADHD phenomenon. However, I can make a similar argument that the introduction of color television is an equally potent coconspirator or confounder. The magnetism inherent in a moving color image can tempt even the most health conscious among us to stay well past a brain-friendly bedtime. The invention of the electric light may have gotten the ball rolling, but the ubiquity of moving electronic color images has certainly greased what was already a very slippery slope into an abyss of unhealthy sleep habits.
There are those who argue that smartphones and tablets can open a world of creative opportunities for even very young children. And, it is obvious that parents are struggling to find a balance as they try to decide when, where, and how often to allow their infants and toddlers access to handheld electronic devices.
Recently there has been much finger-pointing at the developers and manufacturers of smartphones and tablets. How can any company with a social conscience sell a product with such dangerous attractive potential for children without providing safeguards? Isn’t it like selling a swimming pool without a gated fence?
Of course the answer to this question goes to the heart of how our society views its responsibility to protect its children. Regardless of who makes the rules and how the responsibility is assigned, it is still the child’s parents who must make sure that the gate is locked.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
If you were born in or after the 1970s, it is very likely that you have never watched a television show on a black and white set. Although the roots of its technology extend well back into the early 20th century, the first color broadcast on a national television network didn’t occur until 1954 with NBC’s coverage of the Tournament of Roses Parade.
When we compare the popularization of color television with the rapid pace at which we adopt new technology today, the popularization of color TV was glacial. In large part because of their expense, sales of color sets did not surpass black and white sets until 1972. Our family lagged behind the curve and finally caved in and junked our black and white television around 1977.
The observable change in our viewing behavior was dramatic. While programming in black and white was interesting, the color images were magnetic. We were drawn by the visual excitement and stimulation that color offered, and our family’s viewing standards took a precipitous dip. We seemed to watch anything that was colorful and moved. The quality of the content took a back seat. Viewing in color seemed to require much less cognitive effort. Ironically what attracted our attention allowed us to invest less energy in paying attention.
As a regular reader of Letters From Maine, you know that I am convinced that sleep deprivation is a major contributor to the emergence of the ADHD phenomenon. However, I can make a similar argument that the introduction of color television is an equally potent coconspirator or confounder. The magnetism inherent in a moving color image can tempt even the most health conscious among us to stay well past a brain-friendly bedtime. The invention of the electric light may have gotten the ball rolling, but the ubiquity of moving electronic color images has certainly greased what was already a very slippery slope into an abyss of unhealthy sleep habits.
There are those who argue that smartphones and tablets can open a world of creative opportunities for even very young children. And, it is obvious that parents are struggling to find a balance as they try to decide when, where, and how often to allow their infants and toddlers access to handheld electronic devices.
Recently there has been much finger-pointing at the developers and manufacturers of smartphones and tablets. How can any company with a social conscience sell a product with such dangerous attractive potential for children without providing safeguards? Isn’t it like selling a swimming pool without a gated fence?
Of course the answer to this question goes to the heart of how our society views its responsibility to protect its children. Regardless of who makes the rules and how the responsibility is assigned, it is still the child’s parents who must make sure that the gate is locked.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.”
Blueberry Muffin Rash Secondary to Hereditary Spherocytosis
The term blueberry muffin rash historically was used to describe the cutaneous manifestations observed in congenital rubella. The term traditionally describes the result of a postnatal dermal extramedullary hematopoiesis. Today, TORCH (toxoplasmosis, other agents, rubella, cytomegalovirus, herpes) infections and plasma cell dyscrasias are all potential causes of extramedullary hematopoiesis. Herein, we present a unique case of a neonate born with a blueberry muffin rash secondary to extramedullary hematopoiesis induced by hereditary spherocytosis.
Case Report
The dermatology department was consulted to evaluate a 2-day-old male neonate born with a “rash.” The patient was born to a 34-year-old gravida 3, para 2, woman at 39 weeks’ gestation. The mother’s prenatal laboratory values were within reference range and ultrasounds were normal, and she was compliant with her prenatal care. She underwent a normal spontaneous vaginal delivery 3 hours after rupture of membranes without complication. The amniotic fluid and umbilical cord both were clear. There was no use of forceps or any other external aiding devices during the delivery. At the time of delivery, the consulting physician noted that the patient had “skin lesions from head to toe.”
The patient’s parents reported that the rash did not seem to cause any discomfort for the patient. In the 24 hours after birth, the parents reported that the erythema seemed to slightly fade. Physical examination revealed many scattered erythematous to violaceous, nonblanching papulonodules affecting the scalp (Figure 1), face, arms, hands (Figure 2A), back (Figure 2B), buttocks, legs, and feet. Some of the papulonodules were soft while others were firm and indurated. Several lesions had a yellowish hue with some overlying crust. There was no mucosal, genital, or ocular involvement. No erosions, ulcerations, petechiae, ecchymoses, or hepatosplenomegaly were noted on examination.


The patient was otherwise healthy with an Apgar score of 8/9 at 1 and 5 minutes. His birth weight, length, and head circumference were within normal limits. There was no evidence of ABO blood group or Rhesus factor incompatibility. His temperature, vital signs, laboratory values (including calcium level and TORCH titers, which included cytomegalovirus, rubella, toxoplasmosis, and herpes simplex virus), and review of systems all were within reference range. A bone survey of the skull, spine, ribs, arms, pelvis, legs, and feet was within normal limits.
The mother’s placenta was sent for pathology and revealed a lymphoplasmacytic chronic deciduitis and acute subchorionitis consistent with a nonspecific inflammatory response, unlikely to be from an infectious etiology.
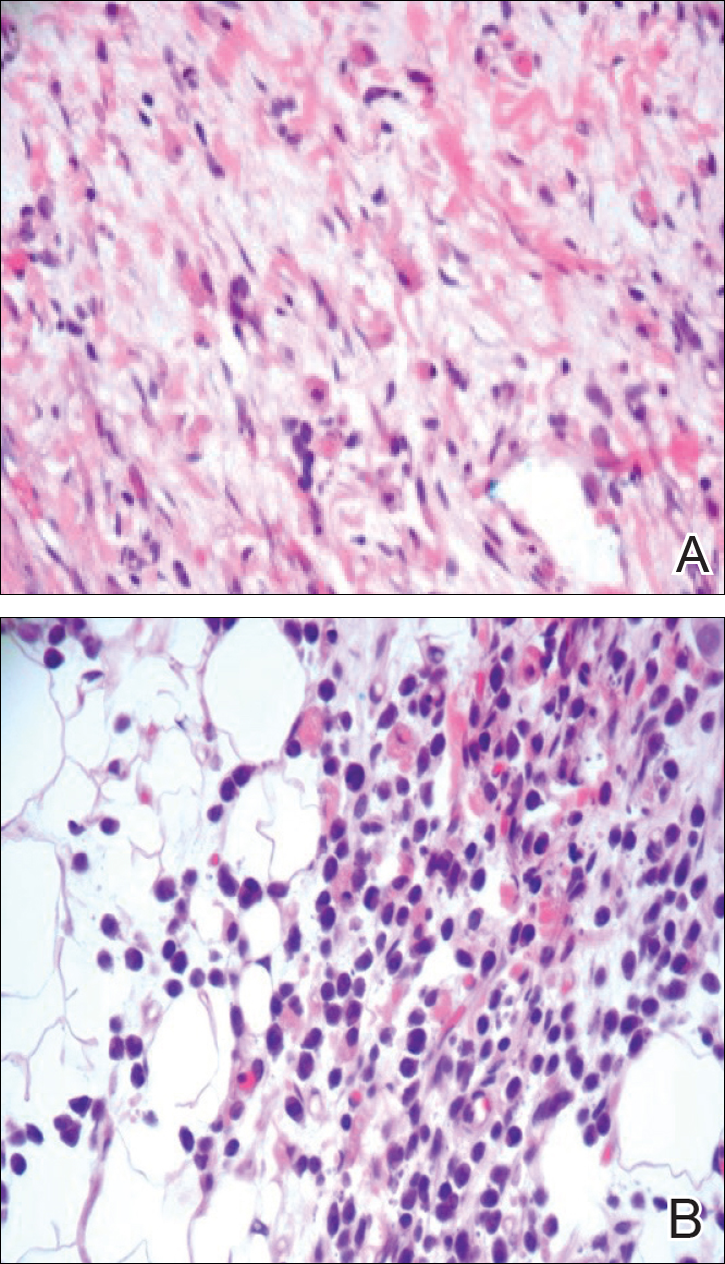
A 4-mm punch biopsy was taken from the left thigh and revealed a predominately lymphocytic infiltrate with rare eosinophils and erythrocyte precursors (Figure 3). Immunohistochemical staining was performed showing that the majority of the lymphocytes represented T lymphocytes, which stained positive for CD45 and CD3 and negative for S-100, CD1a, CD30, and CD117. There were scattered CD34+ cells, and scattered cells stained positive for myeloperoxidase. No significant CD20 immunoreactivity was noted. There were scattered eosinophils and rare normoblasts but no megakaryocytes. A complete blood cell count (CBC) with differential and reticulocyte count was within reference range.
At 1-, 3-, 8-, 12-, and 28-week follow-up visits, the patient continued to grow and feed appropriately. No new lesions developed during this time, and the preexisting lesions continued to fade into slightly hyperpigmented patches without induration (Figure 4). At 6 months of age, a CBC performed at the time of an upper respiratory infection and otitis media revealed normocytic anemia with a hemoglobin level of 9.9 g/dL (reference range, 14.0–17.5 g/dL), a reticulocyte count of 0.8% (reference range, 0.5%–1.5%), and a lactate dehydrogenase level of 424 U/L (reference range, 100–200 U/L). All red blood cell (RBC) indices were within reference range. Flow cytometry, eosin-5-maleimide, and ektacytometry were performed with results consistent with mild hereditary spherocytosis.

Comment
Dermal extramedullary hematopoiesis is a normal component of embryologic development up until the fifth month of gestation.1 The term blueberry muffin rash typically is used to describe the cutaneous manifestations of extramedullary hematopoiesis, which commonly is caused by a TORCH infection or hematologic dyscrasia.2 It has been suggested that the term be expanded to include neoplastic processes (eg, neuroblastomas) and vascular processes (eg, multiple hemangiomas, blue rubber bleb nevus syndrome, glomangiomas, multifocal lymphangionendotheliomatosis), which although not associated with an extramedullary hematopoiesis, can clinically resemble a blueberry muffin rash.
Because of the potential for serious systemic complications, a cause must be sought for all newborns presenting with a blueberry muffin rash. Our patient’s lack of cardiovascular, otic, and ocular involvement combined with a negative TORCH screen and normal CBC strongly suggested against a TORCH infection. In addition, a normal bone survey and CBC, as well as a lack of petechiae, ecchymoses, and hepatosplenomegaly, were evidence against congenital leukemia.3 With the spontaneously resolving lesions and apparent clinical resolution, a bone marrow biopsy was not performed. The skin biopsy revealed negative staining for S-100 and CD1a, making the diagnosis of congenital self-healing reticulohistiocytosis unlikely. No panniculitis was noted and calcium levels were normal, ruling out subcutaneous fat necrosis of the newborn. The predominantly T-cell lymphocytic infiltrate demonstrated on skin biopsy led us to a differential diagnosis of aleukemic leukemia cutis versus idiopathic dermal extramedullary hematopoiesis; however, normocytic anemia was later identified when the patient’s hemoglobin level dropped to 9.9 g/dL. The abnormal eosin-5-maleimide and ektacytometry results unmasked a hereditary spherocytosis.
Hereditary spherocytosis typically is inherited in an autosomal-dominant manner and may be caused by mutations in ankyrin-1, band 3, spectrin, or protein 4.2 on the erythrocyte membrane. It is the third leading cause of hemolytic anemia in newborns and the leading cause of direct Coombs-negative hemolytic anemia requiring blood transfusion in neonates. It is most common in neonates of Northern European ancestry, affecting 1 in every 1000 to 2000 births.4 Presentation may range from asymptomatic to severe anemia with hydrops fetalis. Most neonates have an elevated mean corpuscular hemoglobin and low mean corpuscular volume. Acute illness may cause hemolytic or aplastic crises, possibly explaining our patient’s normocytic anemia discovered on a CBC during an episode of an upper respiratory infection and otitis media.
Treatment options for hereditary spherocytosis include phototherapy for jaundiced neonates, folate supplementation, packed erythrocyte transfusions for symptomatic anemia, and recombinant erythropoietin in neonates.4 Splenectomy is curative for the majority of patients and requires immunization against Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitidis several weeks preoperatively. Patients with symptomatic gallstones may be treated with cholecystectomy at the time of splenectomy or by laparoscopic cholecystectomy, endoscopic sphincterotomy, cholecystostomy, or extracorporeal cholecystolithotripsy.5
Although a PubMed search of articles indexed for MEDLINE using the terms dermal hematopoiesis, extramedullary hematopoiesis, hereditary spherocytosis, and blueberry muffin rash yielded only 1 other known case of blueberry muffin rash caused by hereditary spherocytosis,6 other case reports demonstrate extramedullary hematopoiesis in hereditary spherocytosis patients in locations other than the skin. Calhoun et al7 described a case of a 9-year-old boy with hereditary spherocytosis who presented with jaundice. Pathologic examination revealed a 5-cm suprarenal mass demonstrating extramedullary hematopoiesis.7 A case reported by Xiros et al8 described a 64-year-old man with a history of hereditary spherocytosis who presented with hemothorax from paravertebral extramedullary hematopoiesis. De Backer et al9 reported a case of a 60-year-old man diagnosed with hereditary spherocytosis after an abnormal CBC who was subsequently found to have paravertebral masses containing extramedullary hematopoiesis.
There is one known case of a blueberry muffin rash caused by hereditary spherocytosis.6 A female neonate was born at 38 weeks’ gestation with multiple petechiae and faint purpuric papules. Initial complications included intracranial ventricular hemorrhage, hyperbilirubinemia, and anemia requiring blood transfusions on the first day of life. TORCH titers were negative and a skin biopsy demonstrated a diffuse infiltrate of mature RBCs, normoblasts, and pronormoblasts in the reticular dermis. She was healthy until 3 months of age when she had several days of vomiting and diarrhea. Laboratory workup revealed a hematocrit level of 20.5% (reference range, 41%–50%); a reticulocyte count of 22.6% (reference range, 0.5%–1.5%); and a peripheral blood smear demonstrating polychromatophilia, anisocytosis, and spherocytosis. She was then diagnosed with hereditary spherocytosis.6
Hereditary spherocytosis is a known, albeit rare, cause of extramedullary hematopoiesis presenting as blueberry muffin rash. Patients with mild hereditary spherocytosis may have a compensated hemolysis without anemia or spherocytes on peripheral smear, which may explain the lack of severe hemolytic anemia or RBC-predominant pathology in our patient.5 Argyle and Zone6 proposed that severe hemolysis and hypoxia were the cause of extramedullary hematopoiesis in their patient. Because our patient did not experience a notable hemolytic episode until he had an upper respiratory infection and otitis media at 6 months of age, the pathophysiology is less clear; a compensated hemolytic process may underlie the extramedullary hematopoiesis and normal RBC indices.
Regardless of the precise cause of extramedullary hematopoiesis in our patient, this case of a T lymphocyte–dominant cutaneous infiltrate in a patient with mild hereditary spherocytosis is exceptionally rare and leads us to consider that perhaps there are causes of this pathology that are unknown to us.
- Zhang IH, Zane LT, Braun BS, et al. Congenital leukemia cutis with subsequent development of leukemia. J Am Acad Dermatol. 2006;54(2 suppl):S22–S27.
- Karmegaraj B, Vijayakumar S, Ramanathan R, et al. Extramedullary haematopoiesis resembling a blueberry muffin, in a neonate. BMJ Case Rep. pii: bcr2014208473. doi: 10.1136/bcr-2014-208473.
- Handler MZ, Schwartz RA. Neonatal leukaemia cutis. J Eur Acad Dermatol Venereol. 2015;29:1884-1889.
- Christensen RD, Yaish HM, Gallagher PG. A pediatrician’s practical guide to diagnosing and treating hereditary spherocytosis in neonates. Pediatrics. 2015;135:1107-1114.
- Perrotta S, Gallagher PG, Mohandas N. Hereditary spherocytosis. Lancet. 2008;372:1411-1426.
- Argyle JC, Zone JJ. Dermal erythropoiesis in a neonate. Arch Dermatol. 1981;117:492-494.
- Calhoun SK, Murphy RC, Shariati N, et al. Extramedullary hematopoiesis in a child with hereditary spherocytosis: an uncommon cause of an adrenal mass. Pediatr Radiol. 2001;31:879-881.
- Xiros N, Economopoulos T, Papageorgiou E, et al. Massive hemothorax due to intrathoracic extramedullary hematopoiesis in a patient with hereditary spherocytosis. Ann Hematol. 2001;80:38-40.
- De Backer AI, Zachée P, Vanschoubroeck IJ, et al. Extramedullary paraspinal hematopoiesis in hereditary spherocytosis. JBR-BTR. 2002;85:206-208.
The term blueberry muffin rash historically was used to describe the cutaneous manifestations observed in congenital rubella. The term traditionally describes the result of a postnatal dermal extramedullary hematopoiesis. Today, TORCH (toxoplasmosis, other agents, rubella, cytomegalovirus, herpes) infections and plasma cell dyscrasias are all potential causes of extramedullary hematopoiesis. Herein, we present a unique case of a neonate born with a blueberry muffin rash secondary to extramedullary hematopoiesis induced by hereditary spherocytosis.
Case Report
The dermatology department was consulted to evaluate a 2-day-old male neonate born with a “rash.” The patient was born to a 34-year-old gravida 3, para 2, woman at 39 weeks’ gestation. The mother’s prenatal laboratory values were within reference range and ultrasounds were normal, and she was compliant with her prenatal care. She underwent a normal spontaneous vaginal delivery 3 hours after rupture of membranes without complication. The amniotic fluid and umbilical cord both were clear. There was no use of forceps or any other external aiding devices during the delivery. At the time of delivery, the consulting physician noted that the patient had “skin lesions from head to toe.”
The patient’s parents reported that the rash did not seem to cause any discomfort for the patient. In the 24 hours after birth, the parents reported that the erythema seemed to slightly fade. Physical examination revealed many scattered erythematous to violaceous, nonblanching papulonodules affecting the scalp (Figure 1), face, arms, hands (Figure 2A), back (Figure 2B), buttocks, legs, and feet. Some of the papulonodules were soft while others were firm and indurated. Several lesions had a yellowish hue with some overlying crust. There was no mucosal, genital, or ocular involvement. No erosions, ulcerations, petechiae, ecchymoses, or hepatosplenomegaly were noted on examination.
The patient was otherwise healthy with an Apgar score of 8/9 at 1 and 5 minutes. His birth weight, length, and head circumference were within normal limits. There was no evidence of ABO blood group or Rhesus factor incompatibility. His temperature, vital signs, laboratory values (including calcium level and TORCH titers, which included cytomegalovirus, rubella, toxoplasmosis, and herpes simplex virus), and review of systems all were within reference range. A bone survey of the skull, spine, ribs, arms, pelvis, legs, and feet was within normal limits.
The mother’s placenta was sent for pathology and revealed a lymphoplasmacytic chronic deciduitis and acute subchorionitis consistent with a nonspecific inflammatory response, unlikely to be from an infectious etiology.
A 4-mm punch biopsy was taken from the left thigh and revealed a predominately lymphocytic infiltrate with rare eosinophils and erythrocyte precursors (Figure 3). Immunohistochemical staining was performed showing that the majority of the lymphocytes represented T lymphocytes, which stained positive for CD45 and CD3 and negative for S-100, CD1a, CD30, and CD117. There were scattered CD34+ cells, and scattered cells stained positive for myeloperoxidase. No significant CD20 immunoreactivity was noted. There were scattered eosinophils and rare normoblasts but no megakaryocytes. A complete blood cell count (CBC) with differential and reticulocyte count was within reference range.
At 1-, 3-, 8-, 12-, and 28-week follow-up visits, the patient continued to grow and feed appropriately. No new lesions developed during this time, and the preexisting lesions continued to fade into slightly hyperpigmented patches without induration (Figure 4). At 6 months of age, a CBC performed at the time of an upper respiratory infection and otitis media revealed normocytic anemia with a hemoglobin level of 9.9 g/dL (reference range, 14.0–17.5 g/dL), a reticulocyte count of 0.8% (reference range, 0.5%–1.5%), and a lactate dehydrogenase level of 424 U/L (reference range, 100–200 U/L). All red blood cell (RBC) indices were within reference range. Flow cytometry, eosin-5-maleimide, and ektacytometry were performed with results consistent with mild hereditary spherocytosis.
Comment
Dermal extramedullary hematopoiesis is a normal component of embryologic development up until the fifth month of gestation.1 The term blueberry muffin rash typically is used to describe the cutaneous manifestations of extramedullary hematopoiesis, which commonly is caused by a TORCH infection or hematologic dyscrasia.2 It has been suggested that the term be expanded to include neoplastic processes (eg, neuroblastomas) and vascular processes (eg, multiple hemangiomas, blue rubber bleb nevus syndrome, glomangiomas, multifocal lymphangionendotheliomatosis), which although not associated with an extramedullary hematopoiesis, can clinically resemble a blueberry muffin rash.
Because of the potential for serious systemic complications, a cause must be sought for all newborns presenting with a blueberry muffin rash. Our patient’s lack of cardiovascular, otic, and ocular involvement combined with a negative TORCH screen and normal CBC strongly suggested against a TORCH infection. In addition, a normal bone survey and CBC, as well as a lack of petechiae, ecchymoses, and hepatosplenomegaly, were evidence against congenital leukemia.3 With the spontaneously resolving lesions and apparent clinical resolution, a bone marrow biopsy was not performed. The skin biopsy revealed negative staining for S-100 and CD1a, making the diagnosis of congenital self-healing reticulohistiocytosis unlikely. No panniculitis was noted and calcium levels were normal, ruling out subcutaneous fat necrosis of the newborn. The predominantly T-cell lymphocytic infiltrate demonstrated on skin biopsy led us to a differential diagnosis of aleukemic leukemia cutis versus idiopathic dermal extramedullary hematopoiesis; however, normocytic anemia was later identified when the patient’s hemoglobin level dropped to 9.9 g/dL. The abnormal eosin-5-maleimide and ektacytometry results unmasked a hereditary spherocytosis.
Hereditary spherocytosis typically is inherited in an autosomal-dominant manner and may be caused by mutations in ankyrin-1, band 3, spectrin, or protein 4.2 on the erythrocyte membrane. It is the third leading cause of hemolytic anemia in newborns and the leading cause of direct Coombs-negative hemolytic anemia requiring blood transfusion in neonates. It is most common in neonates of Northern European ancestry, affecting 1 in every 1000 to 2000 births.4 Presentation may range from asymptomatic to severe anemia with hydrops fetalis. Most neonates have an elevated mean corpuscular hemoglobin and low mean corpuscular volume. Acute illness may cause hemolytic or aplastic crises, possibly explaining our patient’s normocytic anemia discovered on a CBC during an episode of an upper respiratory infection and otitis media.
Treatment options for hereditary spherocytosis include phototherapy for jaundiced neonates, folate supplementation, packed erythrocyte transfusions for symptomatic anemia, and recombinant erythropoietin in neonates.4 Splenectomy is curative for the majority of patients and requires immunization against Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitidis several weeks preoperatively. Patients with symptomatic gallstones may be treated with cholecystectomy at the time of splenectomy or by laparoscopic cholecystectomy, endoscopic sphincterotomy, cholecystostomy, or extracorporeal cholecystolithotripsy.5
Although a PubMed search of articles indexed for MEDLINE using the terms dermal hematopoiesis, extramedullary hematopoiesis, hereditary spherocytosis, and blueberry muffin rash yielded only 1 other known case of blueberry muffin rash caused by hereditary spherocytosis,6 other case reports demonstrate extramedullary hematopoiesis in hereditary spherocytosis patients in locations other than the skin. Calhoun et al7 described a case of a 9-year-old boy with hereditary spherocytosis who presented with jaundice. Pathologic examination revealed a 5-cm suprarenal mass demonstrating extramedullary hematopoiesis.7 A case reported by Xiros et al8 described a 64-year-old man with a history of hereditary spherocytosis who presented with hemothorax from paravertebral extramedullary hematopoiesis. De Backer et al9 reported a case of a 60-year-old man diagnosed with hereditary spherocytosis after an abnormal CBC who was subsequently found to have paravertebral masses containing extramedullary hematopoiesis.
There is one known case of a blueberry muffin rash caused by hereditary spherocytosis.6 A female neonate was born at 38 weeks’ gestation with multiple petechiae and faint purpuric papules. Initial complications included intracranial ventricular hemorrhage, hyperbilirubinemia, and anemia requiring blood transfusions on the first day of life. TORCH titers were negative and a skin biopsy demonstrated a diffuse infiltrate of mature RBCs, normoblasts, and pronormoblasts in the reticular dermis. She was healthy until 3 months of age when she had several days of vomiting and diarrhea. Laboratory workup revealed a hematocrit level of 20.5% (reference range, 41%–50%); a reticulocyte count of 22.6% (reference range, 0.5%–1.5%); and a peripheral blood smear demonstrating polychromatophilia, anisocytosis, and spherocytosis. She was then diagnosed with hereditary spherocytosis.6
Hereditary spherocytosis is a known, albeit rare, cause of extramedullary hematopoiesis presenting as blueberry muffin rash. Patients with mild hereditary spherocytosis may have a compensated hemolysis without anemia or spherocytes on peripheral smear, which may explain the lack of severe hemolytic anemia or RBC-predominant pathology in our patient.5 Argyle and Zone6 proposed that severe hemolysis and hypoxia were the cause of extramedullary hematopoiesis in their patient. Because our patient did not experience a notable hemolytic episode until he had an upper respiratory infection and otitis media at 6 months of age, the pathophysiology is less clear; a compensated hemolytic process may underlie the extramedullary hematopoiesis and normal RBC indices.
Regardless of the precise cause of extramedullary hematopoiesis in our patient, this case of a T lymphocyte–dominant cutaneous infiltrate in a patient with mild hereditary spherocytosis is exceptionally rare and leads us to consider that perhaps there are causes of this pathology that are unknown to us.
The term blueberry muffin rash historically was used to describe the cutaneous manifestations observed in congenital rubella. The term traditionally describes the result of a postnatal dermal extramedullary hematopoiesis. Today, TORCH (toxoplasmosis, other agents, rubella, cytomegalovirus, herpes) infections and plasma cell dyscrasias are all potential causes of extramedullary hematopoiesis. Herein, we present a unique case of a neonate born with a blueberry muffin rash secondary to extramedullary hematopoiesis induced by hereditary spherocytosis.
Case Report
The dermatology department was consulted to evaluate a 2-day-old male neonate born with a “rash.” The patient was born to a 34-year-old gravida 3, para 2, woman at 39 weeks’ gestation. The mother’s prenatal laboratory values were within reference range and ultrasounds were normal, and she was compliant with her prenatal care. She underwent a normal spontaneous vaginal delivery 3 hours after rupture of membranes without complication. The amniotic fluid and umbilical cord both were clear. There was no use of forceps or any other external aiding devices during the delivery. At the time of delivery, the consulting physician noted that the patient had “skin lesions from head to toe.”
The patient’s parents reported that the rash did not seem to cause any discomfort for the patient. In the 24 hours after birth, the parents reported that the erythema seemed to slightly fade. Physical examination revealed many scattered erythematous to violaceous, nonblanching papulonodules affecting the scalp (Figure 1), face, arms, hands (Figure 2A), back (Figure 2B), buttocks, legs, and feet. Some of the papulonodules were soft while others were firm and indurated. Several lesions had a yellowish hue with some overlying crust. There was no mucosal, genital, or ocular involvement. No erosions, ulcerations, petechiae, ecchymoses, or hepatosplenomegaly were noted on examination.
The patient was otherwise healthy with an Apgar score of 8/9 at 1 and 5 minutes. His birth weight, length, and head circumference were within normal limits. There was no evidence of ABO blood group or Rhesus factor incompatibility. His temperature, vital signs, laboratory values (including calcium level and TORCH titers, which included cytomegalovirus, rubella, toxoplasmosis, and herpes simplex virus), and review of systems all were within reference range. A bone survey of the skull, spine, ribs, arms, pelvis, legs, and feet was within normal limits.
The mother’s placenta was sent for pathology and revealed a lymphoplasmacytic chronic deciduitis and acute subchorionitis consistent with a nonspecific inflammatory response, unlikely to be from an infectious etiology.
A 4-mm punch biopsy was taken from the left thigh and revealed a predominately lymphocytic infiltrate with rare eosinophils and erythrocyte precursors (Figure 3). Immunohistochemical staining was performed showing that the majority of the lymphocytes represented T lymphocytes, which stained positive for CD45 and CD3 and negative for S-100, CD1a, CD30, and CD117. There were scattered CD34+ cells, and scattered cells stained positive for myeloperoxidase. No significant CD20 immunoreactivity was noted. There were scattered eosinophils and rare normoblasts but no megakaryocytes. A complete blood cell count (CBC) with differential and reticulocyte count was within reference range.
At 1-, 3-, 8-, 12-, and 28-week follow-up visits, the patient continued to grow and feed appropriately. No new lesions developed during this time, and the preexisting lesions continued to fade into slightly hyperpigmented patches without induration (Figure 4). At 6 months of age, a CBC performed at the time of an upper respiratory infection and otitis media revealed normocytic anemia with a hemoglobin level of 9.9 g/dL (reference range, 14.0–17.5 g/dL), a reticulocyte count of 0.8% (reference range, 0.5%–1.5%), and a lactate dehydrogenase level of 424 U/L (reference range, 100–200 U/L). All red blood cell (RBC) indices were within reference range. Flow cytometry, eosin-5-maleimide, and ektacytometry were performed with results consistent with mild hereditary spherocytosis.
Comment
Dermal extramedullary hematopoiesis is a normal component of embryologic development up until the fifth month of gestation.1 The term blueberry muffin rash typically is used to describe the cutaneous manifestations of extramedullary hematopoiesis, which commonly is caused by a TORCH infection or hematologic dyscrasia.2 It has been suggested that the term be expanded to include neoplastic processes (eg, neuroblastomas) and vascular processes (eg, multiple hemangiomas, blue rubber bleb nevus syndrome, glomangiomas, multifocal lymphangionendotheliomatosis), which although not associated with an extramedullary hematopoiesis, can clinically resemble a blueberry muffin rash.
Because of the potential for serious systemic complications, a cause must be sought for all newborns presenting with a blueberry muffin rash. Our patient’s lack of cardiovascular, otic, and ocular involvement combined with a negative TORCH screen and normal CBC strongly suggested against a TORCH infection. In addition, a normal bone survey and CBC, as well as a lack of petechiae, ecchymoses, and hepatosplenomegaly, were evidence against congenital leukemia.3 With the spontaneously resolving lesions and apparent clinical resolution, a bone marrow biopsy was not performed. The skin biopsy revealed negative staining for S-100 and CD1a, making the diagnosis of congenital self-healing reticulohistiocytosis unlikely. No panniculitis was noted and calcium levels were normal, ruling out subcutaneous fat necrosis of the newborn. The predominantly T-cell lymphocytic infiltrate demonstrated on skin biopsy led us to a differential diagnosis of aleukemic leukemia cutis versus idiopathic dermal extramedullary hematopoiesis; however, normocytic anemia was later identified when the patient’s hemoglobin level dropped to 9.9 g/dL. The abnormal eosin-5-maleimide and ektacytometry results unmasked a hereditary spherocytosis.
Hereditary spherocytosis typically is inherited in an autosomal-dominant manner and may be caused by mutations in ankyrin-1, band 3, spectrin, or protein 4.2 on the erythrocyte membrane. It is the third leading cause of hemolytic anemia in newborns and the leading cause of direct Coombs-negative hemolytic anemia requiring blood transfusion in neonates. It is most common in neonates of Northern European ancestry, affecting 1 in every 1000 to 2000 births.4 Presentation may range from asymptomatic to severe anemia with hydrops fetalis. Most neonates have an elevated mean corpuscular hemoglobin and low mean corpuscular volume. Acute illness may cause hemolytic or aplastic crises, possibly explaining our patient’s normocytic anemia discovered on a CBC during an episode of an upper respiratory infection and otitis media.
Treatment options for hereditary spherocytosis include phototherapy for jaundiced neonates, folate supplementation, packed erythrocyte transfusions for symptomatic anemia, and recombinant erythropoietin in neonates.4 Splenectomy is curative for the majority of patients and requires immunization against Streptococcus pneumoniae, Haemophilus influenzae type b, and Neisseria meningitidis several weeks preoperatively. Patients with symptomatic gallstones may be treated with cholecystectomy at the time of splenectomy or by laparoscopic cholecystectomy, endoscopic sphincterotomy, cholecystostomy, or extracorporeal cholecystolithotripsy.5
Although a PubMed search of articles indexed for MEDLINE using the terms dermal hematopoiesis, extramedullary hematopoiesis, hereditary spherocytosis, and blueberry muffin rash yielded only 1 other known case of blueberry muffin rash caused by hereditary spherocytosis,6 other case reports demonstrate extramedullary hematopoiesis in hereditary spherocytosis patients in locations other than the skin. Calhoun et al7 described a case of a 9-year-old boy with hereditary spherocytosis who presented with jaundice. Pathologic examination revealed a 5-cm suprarenal mass demonstrating extramedullary hematopoiesis.7 A case reported by Xiros et al8 described a 64-year-old man with a history of hereditary spherocytosis who presented with hemothorax from paravertebral extramedullary hematopoiesis. De Backer et al9 reported a case of a 60-year-old man diagnosed with hereditary spherocytosis after an abnormal CBC who was subsequently found to have paravertebral masses containing extramedullary hematopoiesis.
There is one known case of a blueberry muffin rash caused by hereditary spherocytosis.6 A female neonate was born at 38 weeks’ gestation with multiple petechiae and faint purpuric papules. Initial complications included intracranial ventricular hemorrhage, hyperbilirubinemia, and anemia requiring blood transfusions on the first day of life. TORCH titers were negative and a skin biopsy demonstrated a diffuse infiltrate of mature RBCs, normoblasts, and pronormoblasts in the reticular dermis. She was healthy until 3 months of age when she had several days of vomiting and diarrhea. Laboratory workup revealed a hematocrit level of 20.5% (reference range, 41%–50%); a reticulocyte count of 22.6% (reference range, 0.5%–1.5%); and a peripheral blood smear demonstrating polychromatophilia, anisocytosis, and spherocytosis. She was then diagnosed with hereditary spherocytosis.6
Hereditary spherocytosis is a known, albeit rare, cause of extramedullary hematopoiesis presenting as blueberry muffin rash. Patients with mild hereditary spherocytosis may have a compensated hemolysis without anemia or spherocytes on peripheral smear, which may explain the lack of severe hemolytic anemia or RBC-predominant pathology in our patient.5 Argyle and Zone6 proposed that severe hemolysis and hypoxia were the cause of extramedullary hematopoiesis in their patient. Because our patient did not experience a notable hemolytic episode until he had an upper respiratory infection and otitis media at 6 months of age, the pathophysiology is less clear; a compensated hemolytic process may underlie the extramedullary hematopoiesis and normal RBC indices.
Regardless of the precise cause of extramedullary hematopoiesis in our patient, this case of a T lymphocyte–dominant cutaneous infiltrate in a patient with mild hereditary spherocytosis is exceptionally rare and leads us to consider that perhaps there are causes of this pathology that are unknown to us.
- Zhang IH, Zane LT, Braun BS, et al. Congenital leukemia cutis with subsequent development of leukemia. J Am Acad Dermatol. 2006;54(2 suppl):S22–S27.
- Karmegaraj B, Vijayakumar S, Ramanathan R, et al. Extramedullary haematopoiesis resembling a blueberry muffin, in a neonate. BMJ Case Rep. pii: bcr2014208473. doi: 10.1136/bcr-2014-208473.
- Handler MZ, Schwartz RA. Neonatal leukaemia cutis. J Eur Acad Dermatol Venereol. 2015;29:1884-1889.
- Christensen RD, Yaish HM, Gallagher PG. A pediatrician’s practical guide to diagnosing and treating hereditary spherocytosis in neonates. Pediatrics. 2015;135:1107-1114.
- Perrotta S, Gallagher PG, Mohandas N. Hereditary spherocytosis. Lancet. 2008;372:1411-1426.
- Argyle JC, Zone JJ. Dermal erythropoiesis in a neonate. Arch Dermatol. 1981;117:492-494.
- Calhoun SK, Murphy RC, Shariati N, et al. Extramedullary hematopoiesis in a child with hereditary spherocytosis: an uncommon cause of an adrenal mass. Pediatr Radiol. 2001;31:879-881.
- Xiros N, Economopoulos T, Papageorgiou E, et al. Massive hemothorax due to intrathoracic extramedullary hematopoiesis in a patient with hereditary spherocytosis. Ann Hematol. 2001;80:38-40.
- De Backer AI, Zachée P, Vanschoubroeck IJ, et al. Extramedullary paraspinal hematopoiesis in hereditary spherocytosis. JBR-BTR. 2002;85:206-208.
- Zhang IH, Zane LT, Braun BS, et al. Congenital leukemia cutis with subsequent development of leukemia. J Am Acad Dermatol. 2006;54(2 suppl):S22–S27.
- Karmegaraj B, Vijayakumar S, Ramanathan R, et al. Extramedullary haematopoiesis resembling a blueberry muffin, in a neonate. BMJ Case Rep. pii: bcr2014208473. doi: 10.1136/bcr-2014-208473.
- Handler MZ, Schwartz RA. Neonatal leukaemia cutis. J Eur Acad Dermatol Venereol. 2015;29:1884-1889.
- Christensen RD, Yaish HM, Gallagher PG. A pediatrician’s practical guide to diagnosing and treating hereditary spherocytosis in neonates. Pediatrics. 2015;135:1107-1114.
- Perrotta S, Gallagher PG, Mohandas N. Hereditary spherocytosis. Lancet. 2008;372:1411-1426.
- Argyle JC, Zone JJ. Dermal erythropoiesis in a neonate. Arch Dermatol. 1981;117:492-494.
- Calhoun SK, Murphy RC, Shariati N, et al. Extramedullary hematopoiesis in a child with hereditary spherocytosis: an uncommon cause of an adrenal mass. Pediatr Radiol. 2001;31:879-881.
- Xiros N, Economopoulos T, Papageorgiou E, et al. Massive hemothorax due to intrathoracic extramedullary hematopoiesis in a patient with hereditary spherocytosis. Ann Hematol. 2001;80:38-40.
- De Backer AI, Zachée P, Vanschoubroeck IJ, et al. Extramedullary paraspinal hematopoiesis in hereditary spherocytosis. JBR-BTR. 2002;85:206-208.
Practice Points
- The term blueberry muffin rash is used to describe the clinical presentation of dermal extramedullary hematopoiesis. The common culprits of this rash include a TORCH (toxoplasmosis, other agents, rubella, cytomegalovirus, herpes) infection or hematologic dyscrasia.
- Because of the potential for serious systemic complications, a cause must be sought for all newborns presenting with a blueberry muffin rash.
- Hereditary spherocytosis typically is inherited in an autosomal-dominant manner and may be caused by mutations in ankyrin-1, band 3, spectrin, or protein 4.2 on the erythrocyte membrane. It is the third leading cause of hemolytic anemia in newborns and the leading cause of direct Coombs-negative hemolytic anemia requiring blood transfusion in neonates.
- Treatment options for hereditary spherocytosis include phototherapy for jaundiced neonates, folate supplementation, packed erythrocyte transfusions for symptomatic anemia, and recombinant erythropoietin in neonates.

Is anxiety normal or pathological? Age of onset is key
NEW YORK – Anxiety has become a common descriptor for fears, worries, or concerns, but the diagnosis of anxiety as a pathological affective disorder in children requires attention to the age of onset and the types of triggers, according to a presentation at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Normal anxiety involves predictable triggers like a test in school,” explained John T. Walkup, MD, director of the division of child and adolescent psychiatry at Children’s Hospital, Northwestern University, Chicago. In the absence of the trigger, the symptoms abate or resolve.
“Age of onset is an important clue,” said Dr. Walkup, reporting that signs of pathological anxiety typically develop between the ages of 6 and 12 years. In comparison, symptoms of ADHD and autism spectrum disorder typically begin at younger ages, while the onset of affective disorders, such as depression or bipolar disease, typically occur at older ages.
Persistent symptoms may not be limited to children with pathological anxiety. Dr. Walkup said many children contend with “bad schools, troubled homes, and interpersonal violence,” creating “a huge population that meets the criteria for anxiety disorder,” even when the solution is eliminating the triggers rather than seeking an underlying psychiatric disorder.
Conversely, families of children with clear manifestations of anxiety might resist this diagnostic label.
“Parents tell me that their kids are not anxious; they are stressed out,” Dr. Walkup recounted. “These families see the external world as the problem for a kid who actually has internal problems regulating their anxious state.”
Rather than quibbling about terminology, patients should be educated about the very real threat posed by persistent and untreated symptoms, Dr. Walkup suggested. Pathological anxiety, regardless of the term used, is not a phase.
“Some of these kids do recover from childhood onset anxiety, but more often, the condition tracks to adolescence or adulthood,” Dr. Walkup said. . He contended that many adults with personality disorders are experiencing the consequences of distorted thinking and problematic emotional responses that began with childhood anxiety.

“Children with anxiety need to learn to cope. If you medicate them to control the anxiety, it does not necessarily mean that they will learn how to live anxiety free,” Dr. Walkup said, reiterating that pathological anxiety often persists indefinitely even after effective therapy diminishes the symptom burden. To improve a supportive family environment for an anxious child, he encouraged educating parents about the condition.
“One of the many books published on childhood anxiety may be all they need,” said Dr. Walkup, listing several examples, such as “You and Your Anxious Child” (New York: Avery, 2013) coauthored by Anne Marie Albano, PhD, a professor of child psychiatry at Columbia University in New York.
As anxiety is such a ubiquitous human experience, many parents trivialize the pathological variety, Dr. Walkup said. Educating patients about the immediate and long-term risks of pathological anxiety is important. The associated symptoms are not a phase, as some parents are likely to contend. He believes that early diagnosis and effective management can change the trajectory of a lifelong threat.
Dr. Walkup reported no potential conflicts of interest.
NEW YORK – Anxiety has become a common descriptor for fears, worries, or concerns, but the diagnosis of anxiety as a pathological affective disorder in children requires attention to the age of onset and the types of triggers, according to a presentation at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Normal anxiety involves predictable triggers like a test in school,” explained John T. Walkup, MD, director of the division of child and adolescent psychiatry at Children’s Hospital, Northwestern University, Chicago. In the absence of the trigger, the symptoms abate or resolve.
“Age of onset is an important clue,” said Dr. Walkup, reporting that signs of pathological anxiety typically develop between the ages of 6 and 12 years. In comparison, symptoms of ADHD and autism spectrum disorder typically begin at younger ages, while the onset of affective disorders, such as depression or bipolar disease, typically occur at older ages.
Persistent symptoms may not be limited to children with pathological anxiety. Dr. Walkup said many children contend with “bad schools, troubled homes, and interpersonal violence,” creating “a huge population that meets the criteria for anxiety disorder,” even when the solution is eliminating the triggers rather than seeking an underlying psychiatric disorder.
Conversely, families of children with clear manifestations of anxiety might resist this diagnostic label.
“Parents tell me that their kids are not anxious; they are stressed out,” Dr. Walkup recounted. “These families see the external world as the problem for a kid who actually has internal problems regulating their anxious state.”
Rather than quibbling about terminology, patients should be educated about the very real threat posed by persistent and untreated symptoms, Dr. Walkup suggested. Pathological anxiety, regardless of the term used, is not a phase.
“Some of these kids do recover from childhood onset anxiety, but more often, the condition tracks to adolescence or adulthood,” Dr. Walkup said. . He contended that many adults with personality disorders are experiencing the consequences of distorted thinking and problematic emotional responses that began with childhood anxiety.
“Children with anxiety need to learn to cope. If you medicate them to control the anxiety, it does not necessarily mean that they will learn how to live anxiety free,” Dr. Walkup said, reiterating that pathological anxiety often persists indefinitely even after effective therapy diminishes the symptom burden. To improve a supportive family environment for an anxious child, he encouraged educating parents about the condition.
“One of the many books published on childhood anxiety may be all they need,” said Dr. Walkup, listing several examples, such as “You and Your Anxious Child” (New York: Avery, 2013) coauthored by Anne Marie Albano, PhD, a professor of child psychiatry at Columbia University in New York.
As anxiety is such a ubiquitous human experience, many parents trivialize the pathological variety, Dr. Walkup said. Educating patients about the immediate and long-term risks of pathological anxiety is important. The associated symptoms are not a phase, as some parents are likely to contend. He believes that early diagnosis and effective management can change the trajectory of a lifelong threat.
Dr. Walkup reported no potential conflicts of interest.
NEW YORK – Anxiety has become a common descriptor for fears, worries, or concerns, but the diagnosis of anxiety as a pathological affective disorder in children requires attention to the age of onset and the types of triggers, according to a presentation at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
“Normal anxiety involves predictable triggers like a test in school,” explained John T. Walkup, MD, director of the division of child and adolescent psychiatry at Children’s Hospital, Northwestern University, Chicago. In the absence of the trigger, the symptoms abate or resolve.
“Age of onset is an important clue,” said Dr. Walkup, reporting that signs of pathological anxiety typically develop between the ages of 6 and 12 years. In comparison, symptoms of ADHD and autism spectrum disorder typically begin at younger ages, while the onset of affective disorders, such as depression or bipolar disease, typically occur at older ages.
Persistent symptoms may not be limited to children with pathological anxiety. Dr. Walkup said many children contend with “bad schools, troubled homes, and interpersonal violence,” creating “a huge population that meets the criteria for anxiety disorder,” even when the solution is eliminating the triggers rather than seeking an underlying psychiatric disorder.
Conversely, families of children with clear manifestations of anxiety might resist this diagnostic label.
“Parents tell me that their kids are not anxious; they are stressed out,” Dr. Walkup recounted. “These families see the external world as the problem for a kid who actually has internal problems regulating their anxious state.”
Rather than quibbling about terminology, patients should be educated about the very real threat posed by persistent and untreated symptoms, Dr. Walkup suggested. Pathological anxiety, regardless of the term used, is not a phase.
“Some of these kids do recover from childhood onset anxiety, but more often, the condition tracks to adolescence or adulthood,” Dr. Walkup said. . He contended that many adults with personality disorders are experiencing the consequences of distorted thinking and problematic emotional responses that began with childhood anxiety.
“Children with anxiety need to learn to cope. If you medicate them to control the anxiety, it does not necessarily mean that they will learn how to live anxiety free,” Dr. Walkup said, reiterating that pathological anxiety often persists indefinitely even after effective therapy diminishes the symptom burden. To improve a supportive family environment for an anxious child, he encouraged educating parents about the condition.
“One of the many books published on childhood anxiety may be all they need,” said Dr. Walkup, listing several examples, such as “You and Your Anxious Child” (New York: Avery, 2013) coauthored by Anne Marie Albano, PhD, a professor of child psychiatry at Columbia University in New York.
As anxiety is such a ubiquitous human experience, many parents trivialize the pathological variety, Dr. Walkup said. Educating patients about the immediate and long-term risks of pathological anxiety is important. The associated symptoms are not a phase, as some parents are likely to contend. He believes that early diagnosis and effective management can change the trajectory of a lifelong threat.
Dr. Walkup reported no potential conflicts of interest.
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE
Can a Model Predict Pediatric SUDEP Risk?
WASHINGTON, DC—In a pediatric epilepsy population, number of antiepileptic drugs (AEDs) used and prior epilepsy surgery may predict sudden unexpected death in epilepsy (SUDEP), according to a study presented at the 71st Annual Meeting of the American Epilepsy Society.
Kishore Vedala, a medical student at the Medical College of Georgia at Augusta University, and colleagues sought to develop a predictive model for at-risk pediatric patients by conducting a matched case–control study.
Using records from the Medical College of Georgia, the researchers identified 11 SUDEP cases that occurred between 2007 and 2017. They compared the cases with 53 controls matched for age, epilepsy duration, and gender. The researchers used a conditional logistic regression model to evaluate the following nine potential predictor variables: mental retardation, seizure frequency, seizure type, prior status epilepticus, number of AEDs, prior epilepsy surgery, vagus nerve stimulator therapy, seizure progression, and awake interictal heart rate variability. They identified the optimum predictor models using Akaike’s information criterion and evaluated model performance using receiver operating characteristic area under the curve (AUC).
Prior status epilepticus (ie, having had a seizure that lasted longer than five minutes), prior epilepsy surgery, and having received three or more AEDs at the same time were significant predictors of SUDEP (odds ratios, 7.83, 4.23, and 4.7, respectively), whereas the other variables were not. The best model used number of AEDs and prior epilepsy surgery (AUC, 0.855). The second-best model used number of AEDs and prior status epilepticus (AUC, 0.839). The third-best model used number of AEDs alone (AUC, 0.807).

The risk factors likely reflect epilepsy that is difficult to control.
—Jake Remaly
WASHINGTON, DC—In a pediatric epilepsy population, number of antiepileptic drugs (AEDs) used and prior epilepsy surgery may predict sudden unexpected death in epilepsy (SUDEP), according to a study presented at the 71st Annual Meeting of the American Epilepsy Society.
Kishore Vedala, a medical student at the Medical College of Georgia at Augusta University, and colleagues sought to develop a predictive model for at-risk pediatric patients by conducting a matched case–control study.
Using records from the Medical College of Georgia, the researchers identified 11 SUDEP cases that occurred between 2007 and 2017. They compared the cases with 53 controls matched for age, epilepsy duration, and gender. The researchers used a conditional logistic regression model to evaluate the following nine potential predictor variables: mental retardation, seizure frequency, seizure type, prior status epilepticus, number of AEDs, prior epilepsy surgery, vagus nerve stimulator therapy, seizure progression, and awake interictal heart rate variability. They identified the optimum predictor models using Akaike’s information criterion and evaluated model performance using receiver operating characteristic area under the curve (AUC).
Prior status epilepticus (ie, having had a seizure that lasted longer than five minutes), prior epilepsy surgery, and having received three or more AEDs at the same time were significant predictors of SUDEP (odds ratios, 7.83, 4.23, and 4.7, respectively), whereas the other variables were not. The best model used number of AEDs and prior epilepsy surgery (AUC, 0.855). The second-best model used number of AEDs and prior status epilepticus (AUC, 0.839). The third-best model used number of AEDs alone (AUC, 0.807).
The risk factors likely reflect epilepsy that is difficult to control.
—Jake Remaly
WASHINGTON, DC—In a pediatric epilepsy population, number of antiepileptic drugs (AEDs) used and prior epilepsy surgery may predict sudden unexpected death in epilepsy (SUDEP), according to a study presented at the 71st Annual Meeting of the American Epilepsy Society.
Kishore Vedala, a medical student at the Medical College of Georgia at Augusta University, and colleagues sought to develop a predictive model for at-risk pediatric patients by conducting a matched case–control study.
Using records from the Medical College of Georgia, the researchers identified 11 SUDEP cases that occurred between 2007 and 2017. They compared the cases with 53 controls matched for age, epilepsy duration, and gender. The researchers used a conditional logistic regression model to evaluate the following nine potential predictor variables: mental retardation, seizure frequency, seizure type, prior status epilepticus, number of AEDs, prior epilepsy surgery, vagus nerve stimulator therapy, seizure progression, and awake interictal heart rate variability. They identified the optimum predictor models using Akaike’s information criterion and evaluated model performance using receiver operating characteristic area under the curve (AUC).
Prior status epilepticus (ie, having had a seizure that lasted longer than five minutes), prior epilepsy surgery, and having received three or more AEDs at the same time were significant predictors of SUDEP (odds ratios, 7.83, 4.23, and 4.7, respectively), whereas the other variables were not. The best model used number of AEDs and prior epilepsy surgery (AUC, 0.855). The second-best model used number of AEDs and prior status epilepticus (AUC, 0.839). The third-best model used number of AEDs alone (AUC, 0.807).
The risk factors likely reflect epilepsy that is difficult to control.
—Jake Remaly
Mass Psychogenic Illness: Risk Factors and Treatment
KANSAS CITY, MO—Mass psychogenic illness is a condition where signs and symptoms spread rapidly between members of a cohesive group. The illness may entail loss or alteration of function, and patients unconsciously manifest physical symptoms. “Our brains are wired to be empathetic and to pick up on the symptoms of others,” said Jonathan W. Mink, MD, PhD, at the 46th Annual Meeting of the Child Neurology Society. “In mass psychogenic illness, those symptoms persist, and there is that contagion from individual to individual.”
A recent occurrence of mass psychogenic illness in Le Roy, New York, suggests that news media attention and patients’ use of social media may play a role in the spread and perpetuation of symptoms. Few descriptions of mass psychogenic illness have been published in pediatric neurology journals, but prior cases may provide useful information about the condition, its risk factors, and treatment, Dr. Mink said.

“It has been argued whether this is a subcategory of conversion disorder. There has been some discussion of whether some of this is … factitious or malingering. I would argue that it does not really matter,” said Dr. Mink, Professor of Pediatric Neurology at the University of Rochester in New York. “What matters is that we understand that this is an entity. Exactly why [it occurs] may not be relevant to treatment.”
Teens With Tic-Like Movements
Between August 2011 and January 2012, 19 teenage students at Le Roy Junior–Senior High School developed a sudden onset of tic-like movements. Two had a prior diagnosis of a tic disorder: one had Tourette syndrome, and one had chronic motor tic disorder. Eighteen of the 19 were girls. Six of the 19 had additional symptoms (eg, syncope and paroxysmal nonepileptic attacks), and 10 had clearly identified significant life stressors. All of the patients had otherwise normal neurologic exams. The movements “were not tics,” Dr. Mink said. “They had no premonitory urge. They were not suppressible. They were not stereotyped. But they were often referred to as tic-like.”
The cases drew national and local media attention. News reports portrayed the cases as mysterious and suggested that the symptoms could have autoimmune or environmental causes. Furthermore, social media may have contributed to the spread of symptoms. “It has often been said that mass psychogenic illness, or what was formerly called mass hysteria, was conveyed by line-of-sight transmission. It was seeing the symptoms of other people,” Dr. Mink said. “Many of these girls had posted videos or detailed descriptions of their symptoms.”
Most of the patients were seen at the Dent Neurologic Institute in Buffalo. To help confirm the diagnosis, a majority of the patients also were seen at Dr. Mink’s center in Rochester.
Insights From Prior Research
In 2004, Roach and Langley described an occurrence of mass psychogenic illness among a cohort of 10 teenage girls at a school in rural North Carolina. The patients developed paroxysmal episodes that resembled epilepsy or syncope. The episodes were relatively infrequent and typically occurred between classes. Four patients underwent video-EEG monitoring, which showed that the seizures were not epileptic. Symptoms mostly resolved after a two-week holiday break from school. “More than half of them had been treated with one or more antiepileptic medications,” Dr. Mink said.
A study of environmental chemical incidents in the United Kingdom found that a substantial minority of cases could involve mass psychogenic illness. Page et al examined incidents over a 15-month period between 2007 and 2008. Of 965 total incidents, 747 were eligible for inclusion in the study, and 280 were selected randomly for detailed evaluation.
The British researchers’ criteria for diagnosing mass psychogenic illness included the presence of somatic symptoms, a preexisting social connection between two or more of the affected people, the spread of symptoms from person to person, and the attribution of symptoms by affected individuals or by their parents or caregivers to a threatening external agent of a physical or spiritual nature. Finally, the symptoms and signs were not compatible with environmental exposures that reasonably could have been expected to be present at the time.
Nineteen of the 280 incidents were classified as probable or highly probable mass psychogenic illness (six highly probable and 13 probable), which represented 7% of the incidents and 16% of incidents in which people reported symptoms that were attributed to the chemical incident. Factors that were more common among cases of mass psychogenic illness included the presence of a nonsmoke odor and occurrence in a school or health care facility.
Experimental Induction of Mass Psychogenic Illness
Broderick et al in 2011 described a randomized controlled experimental induction of mass psychogenic illness. Their study included 39 healthy adults with a mean age of 42. A little more than half were women, half were college graduates, and almost 80% were Caucasian.
A control group sat in a room and engaged in quiet activity, while two psychogenic illness induction groups received a pill. One of the induction groups was shown a video (ie, the pill-plus-media group).
Researchers told participants in the pill groups that the study was designed to further evaluate the side effects of a new carrier compound for an antiviral medication. The participants were told that the compound contained only cellulose and did not produce serious side effects.
In the pill groups, confederates (one man and one woman) feigned illness (eg, nausea, dizziness, and headache) about 20 minutes after participants took the pills. Nurses attended to the confederates and to any participant who simulated or experienced symptoms, by taking their blood pressure and pulse, providing cool cloths for their foreheads, supplying bowls for potential vomiting, and sometimes putting participants with symptoms on gurneys outside the room within view of the other participants. An hour after taking the pills, the pill-plus-media group watched a public television documentary about the 1918 flu pandemic.
All three groups were assessed at baseline, at one hour, and at two hours. Participants rated their current symptoms by questionnaire, and nurses measured participants’ heart rate and blood pressure. Researchers debriefed all participants after the third assessment, and participants completed a psychosocial risk factor battery within a week of the initial experiment.
The primary outcome was symptom score. Participants in all three groups had some symptoms at baseline (eg, elevated heart rate and slight discomfort). At one hour, the control group had reduced symptoms, whereas the pill groups had increased symptom scores. At two hours, the control group still had few symptoms, but the psychogenic illness induction groups’ symptoms increased further. Symptoms did not differ between the pill-only and pill-plus-media groups, however.
An analysis of the psychosocial risk factor questionnaires found that participants’ total number of traumatic life events was positively associated with increased symptoms, but this relationship was not particularly strong. “It seems that the most important thing is … being exposed to people who are feigning symptoms or displaying symptoms in the setting of being told that there is a potential agent that might cause those symptoms,” Dr. Mink said.
Outcomes in Le Roy
Amid media coverage of the cases in Le Roy, Dr. Mink declined daily invitations to appear on television. “The last time I talked to the producer, I said, ‘You know, you would do these girls a big favor if you would just leave them alone,’” he said. “While the media attention persisted for another week, the improvement of their symptoms did coincide with reduced media attention, so one can speculate that that might have played a role.”
The patients in Le Roy received varying therapies, including cognitive behavioral therapy and supportive psychotherapy. They all received education about functional neurologic disorders. Some received pharmacothe
At last follow-up about two years ago, five of the 19 no longer had symptoms. Six of the 19 had experienced a greater than 85% improvement. A couple of patients continued to have symptoms, including the patients with a prior diagnosis of a chronic tic disorder. Two patients who had not improved sued the school district and alleged environmental toxins as the cause of their symptoms. The other patients were lost to follow up.
Treatment Principles
When treating patients with mass psychogenic illness, “First of all, you have to be an ally of your patient and not challenge the veracity,” Dr. Mink said. “For some of these girls, I think that there was some factitious component,” but this factor was not especially relevant to treatment recommendations.
“For mass psychogenic illness, reducing attention from social media groups and perhaps finding a way to disrupt the social cohesiveness of that group, at least until the symptoms can improve,” may be beneficial, he said. “Regular follow-up is helpful for all conversion disorders…. You do not want the patient to have to get worse to be able to see their doctor.”
Once neurologists have confirmed the diagnosis of mass psychogenic illness, they should “reinforce the certainty of the diagnosis” to occupational therapists, physical therapists, psychotherapists, and others on the health care team who treat these patients, Dr. Mink said. In addition,“It is important to prepare the therapist, particularly in an unusual situation like this where there has been a lot of media attention.”
—Jake Remaly
Suggested Reading
Bartholomew RE, Wessely S, Rubin GJ. Mass psychogenic illness and the social network: is it changing the pattern of outbreaks? J R Soc Med. 2012;105(12):509-512.
Broderick JE, Kaplan-Liss E, Bass E. Experimental induction of psychogenic illness in the context of a medical event and media exposure. Am J Disaster Med. 2011;6(3):163-172.
Page LA, Keshishian C, Leonardi G, et al. Frequency and predictors of mass psychogenic illness. Epidemiology. 2010;21(5):744-747.
Roach ES, Langley RL. Episodic neurological dysfunction due to mass hysteria. Arch Neurol. 2004;61(8):1269-1272.
KANSAS CITY, MO—Mass psychogenic illness is a condition where signs and symptoms spread rapidly between members of a cohesive group. The illness may entail loss or alteration of function, and patients unconsciously manifest physical symptoms. “Our brains are wired to be empathetic and to pick up on the symptoms of others,” said Jonathan W. Mink, MD, PhD, at the 46th Annual Meeting of the Child Neurology Society. “In mass psychogenic illness, those symptoms persist, and there is that contagion from individual to individual.”
A recent occurrence of mass psychogenic illness in Le Roy, New York, suggests that news media attention and patients’ use of social media may play a role in the spread and perpetuation of symptoms. Few descriptions of mass psychogenic illness have been published in pediatric neurology journals, but prior cases may provide useful information about the condition, its risk factors, and treatment, Dr. Mink said.
“It has been argued whether this is a subcategory of conversion disorder. There has been some discussion of whether some of this is … factitious or malingering. I would argue that it does not really matter,” said Dr. Mink, Professor of Pediatric Neurology at the University of Rochester in New York. “What matters is that we understand that this is an entity. Exactly why [it occurs] may not be relevant to treatment.”
Teens With Tic-Like Movements
Between August 2011 and January 2012, 19 teenage students at Le Roy Junior–Senior High School developed a sudden onset of tic-like movements. Two had a prior diagnosis of a tic disorder: one had Tourette syndrome, and one had chronic motor tic disorder. Eighteen of the 19 were girls. Six of the 19 had additional symptoms (eg, syncope and paroxysmal nonepileptic attacks), and 10 had clearly identified significant life stressors. All of the patients had otherwise normal neurologic exams. The movements “were not tics,” Dr. Mink said. “They had no premonitory urge. They were not suppressible. They were not stereotyped. But they were often referred to as tic-like.”
The cases drew national and local media attention. News reports portrayed the cases as mysterious and suggested that the symptoms could have autoimmune or environmental causes. Furthermore, social media may have contributed to the spread of symptoms. “It has often been said that mass psychogenic illness, or what was formerly called mass hysteria, was conveyed by line-of-sight transmission. It was seeing the symptoms of other people,” Dr. Mink said. “Many of these girls had posted videos or detailed descriptions of their symptoms.”
Most of the patients were seen at the Dent Neurologic Institute in Buffalo. To help confirm the diagnosis, a majority of the patients also were seen at Dr. Mink’s center in Rochester.
Insights From Prior Research
In 2004, Roach and Langley described an occurrence of mass psychogenic illness among a cohort of 10 teenage girls at a school in rural North Carolina. The patients developed paroxysmal episodes that resembled epilepsy or syncope. The episodes were relatively infrequent and typically occurred between classes. Four patients underwent video-EEG monitoring, which showed that the seizures were not epileptic. Symptoms mostly resolved after a two-week holiday break from school. “More than half of them had been treated with one or more antiepileptic medications,” Dr. Mink said.
A study of environmental chemical incidents in the United Kingdom found that a substantial minority of cases could involve mass psychogenic illness. Page et al examined incidents over a 15-month period between 2007 and 2008. Of 965 total incidents, 747 were eligible for inclusion in the study, and 280 were selected randomly for detailed evaluation.
The British researchers’ criteria for diagnosing mass psychogenic illness included the presence of somatic symptoms, a preexisting social connection between two or more of the affected people, the spread of symptoms from person to person, and the attribution of symptoms by affected individuals or by their parents or caregivers to a threatening external agent of a physical or spiritual nature. Finally, the symptoms and signs were not compatible with environmental exposures that reasonably could have been expected to be present at the time.
Nineteen of the 280 incidents were classified as probable or highly probable mass psychogenic illness (six highly probable and 13 probable), which represented 7% of the incidents and 16% of incidents in which people reported symptoms that were attributed to the chemical incident. Factors that were more common among cases of mass psychogenic illness included the presence of a nonsmoke odor and occurrence in a school or health care facility.
Experimental Induction of Mass Psychogenic Illness
Broderick et al in 2011 described a randomized controlled experimental induction of mass psychogenic illness. Their study included 39 healthy adults with a mean age of 42. A little more than half were women, half were college graduates, and almost 80% were Caucasian.
A control group sat in a room and engaged in quiet activity, while two psychogenic illness induction groups received a pill. One of the induction groups was shown a video (ie, the pill-plus-media group).
Researchers told participants in the pill groups that the study was designed to further evaluate the side effects of a new carrier compound for an antiviral medication. The participants were told that the compound contained only cellulose and did not produce serious side effects.
In the pill groups, confederates (one man and one woman) feigned illness (eg, nausea, dizziness, and headache) about 20 minutes after participants took the pills. Nurses attended to the confederates and to any participant who simulated or experienced symptoms, by taking their blood pressure and pulse, providing cool cloths for their foreheads, supplying bowls for potential vomiting, and sometimes putting participants with symptoms on gurneys outside the room within view of the other participants. An hour after taking the pills, the pill-plus-media group watched a public television documentary about the 1918 flu pandemic.
All three groups were assessed at baseline, at one hour, and at two hours. Participants rated their current symptoms by questionnaire, and nurses measured participants’ heart rate and blood pressure. Researchers debriefed all participants after the third assessment, and participants completed a psychosocial risk factor battery within a week of the initial experiment.
The primary outcome was symptom score. Participants in all three groups had some symptoms at baseline (eg, elevated heart rate and slight discomfort). At one hour, the control group had reduced symptoms, whereas the pill groups had increased symptom scores. At two hours, the control group still had few symptoms, but the psychogenic illness induction groups’ symptoms increased further. Symptoms did not differ between the pill-only and pill-plus-media groups, however.
An analysis of the psychosocial risk factor questionnaires found that participants’ total number of traumatic life events was positively associated with increased symptoms, but this relationship was not particularly strong. “It seems that the most important thing is … being exposed to people who are feigning symptoms or displaying symptoms in the setting of being told that there is a potential agent that might cause those symptoms,” Dr. Mink said.
Outcomes in Le Roy
Amid media coverage of the cases in Le Roy, Dr. Mink declined daily invitations to appear on television. “The last time I talked to the producer, I said, ‘You know, you would do these girls a big favor if you would just leave them alone,’” he said. “While the media attention persisted for another week, the improvement of their symptoms did coincide with reduced media attention, so one can speculate that that might have played a role.”
The patients in Le Roy received varying therapies, including cognitive behavioral therapy and supportive psychotherapy. They all received education about functional neurologic disorders. Some received pharmacothe
At last follow-up about two years ago, five of the 19 no longer had symptoms. Six of the 19 had experienced a greater than 85% improvement. A couple of patients continued to have symptoms, including the patients with a prior diagnosis of a chronic tic disorder. Two patients who had not improved sued the school district and alleged environmental toxins as the cause of their symptoms. The other patients were lost to follow up.
Treatment Principles
When treating patients with mass psychogenic illness, “First of all, you have to be an ally of your patient and not challenge the veracity,” Dr. Mink said. “For some of these girls, I think that there was some factitious component,” but this factor was not especially relevant to treatment recommendations.
“For mass psychogenic illness, reducing attention from social media groups and perhaps finding a way to disrupt the social cohesiveness of that group, at least until the symptoms can improve,” may be beneficial, he said. “Regular follow-up is helpful for all conversion disorders…. You do not want the patient to have to get worse to be able to see their doctor.”
Once neurologists have confirmed the diagnosis of mass psychogenic illness, they should “reinforce the certainty of the diagnosis” to occupational therapists, physical therapists, psychotherapists, and others on the health care team who treat these patients, Dr. Mink said. In addition,“It is important to prepare the therapist, particularly in an unusual situation like this where there has been a lot of media attention.”
—Jake Remaly
Suggested Reading
Bartholomew RE, Wessely S, Rubin GJ. Mass psychogenic illness and the social network: is it changing the pattern of outbreaks? J R Soc Med. 2012;105(12):509-512.
Broderick JE, Kaplan-Liss E, Bass E. Experimental induction of psychogenic illness in the context of a medical event and media exposure. Am J Disaster Med. 2011;6(3):163-172.
Page LA, Keshishian C, Leonardi G, et al. Frequency and predictors of mass psychogenic illness. Epidemiology. 2010;21(5):744-747.
Roach ES, Langley RL. Episodic neurological dysfunction due to mass hysteria. Arch Neurol. 2004;61(8):1269-1272.
KANSAS CITY, MO—Mass psychogenic illness is a condition where signs and symptoms spread rapidly between members of a cohesive group. The illness may entail loss or alteration of function, and patients unconsciously manifest physical symptoms. “Our brains are wired to be empathetic and to pick up on the symptoms of others,” said Jonathan W. Mink, MD, PhD, at the 46th Annual Meeting of the Child Neurology Society. “In mass psychogenic illness, those symptoms persist, and there is that contagion from individual to individual.”
A recent occurrence of mass psychogenic illness in Le Roy, New York, suggests that news media attention and patients’ use of social media may play a role in the spread and perpetuation of symptoms. Few descriptions of mass psychogenic illness have been published in pediatric neurology journals, but prior cases may provide useful information about the condition, its risk factors, and treatment, Dr. Mink said.
“It has been argued whether this is a subcategory of conversion disorder. There has been some discussion of whether some of this is … factitious or malingering. I would argue that it does not really matter,” said Dr. Mink, Professor of Pediatric Neurology at the University of Rochester in New York. “What matters is that we understand that this is an entity. Exactly why [it occurs] may not be relevant to treatment.”
Teens With Tic-Like Movements
Between August 2011 and January 2012, 19 teenage students at Le Roy Junior–Senior High School developed a sudden onset of tic-like movements. Two had a prior diagnosis of a tic disorder: one had Tourette syndrome, and one had chronic motor tic disorder. Eighteen of the 19 were girls. Six of the 19 had additional symptoms (eg, syncope and paroxysmal nonepileptic attacks), and 10 had clearly identified significant life stressors. All of the patients had otherwise normal neurologic exams. The movements “were not tics,” Dr. Mink said. “They had no premonitory urge. They were not suppressible. They were not stereotyped. But they were often referred to as tic-like.”
The cases drew national and local media attention. News reports portrayed the cases as mysterious and suggested that the symptoms could have autoimmune or environmental causes. Furthermore, social media may have contributed to the spread of symptoms. “It has often been said that mass psychogenic illness, or what was formerly called mass hysteria, was conveyed by line-of-sight transmission. It was seeing the symptoms of other people,” Dr. Mink said. “Many of these girls had posted videos or detailed descriptions of their symptoms.”
Most of the patients were seen at the Dent Neurologic Institute in Buffalo. To help confirm the diagnosis, a majority of the patients also were seen at Dr. Mink’s center in Rochester.
Insights From Prior Research
In 2004, Roach and Langley described an occurrence of mass psychogenic illness among a cohort of 10 teenage girls at a school in rural North Carolina. The patients developed paroxysmal episodes that resembled epilepsy or syncope. The episodes were relatively infrequent and typically occurred between classes. Four patients underwent video-EEG monitoring, which showed that the seizures were not epileptic. Symptoms mostly resolved after a two-week holiday break from school. “More than half of them had been treated with one or more antiepileptic medications,” Dr. Mink said.
A study of environmental chemical incidents in the United Kingdom found that a substantial minority of cases could involve mass psychogenic illness. Page et al examined incidents over a 15-month period between 2007 and 2008. Of 965 total incidents, 747 were eligible for inclusion in the study, and 280 were selected randomly for detailed evaluation.
The British researchers’ criteria for diagnosing mass psychogenic illness included the presence of somatic symptoms, a preexisting social connection between two or more of the affected people, the spread of symptoms from person to person, and the attribution of symptoms by affected individuals or by their parents or caregivers to a threatening external agent of a physical or spiritual nature. Finally, the symptoms and signs were not compatible with environmental exposures that reasonably could have been expected to be present at the time.
Nineteen of the 280 incidents were classified as probable or highly probable mass psychogenic illness (six highly probable and 13 probable), which represented 7% of the incidents and 16% of incidents in which people reported symptoms that were attributed to the chemical incident. Factors that were more common among cases of mass psychogenic illness included the presence of a nonsmoke odor and occurrence in a school or health care facility.
Experimental Induction of Mass Psychogenic Illness
Broderick et al in 2011 described a randomized controlled experimental induction of mass psychogenic illness. Their study included 39 healthy adults with a mean age of 42. A little more than half were women, half were college graduates, and almost 80% were Caucasian.
A control group sat in a room and engaged in quiet activity, while two psychogenic illness induction groups received a pill. One of the induction groups was shown a video (ie, the pill-plus-media group).
Researchers told participants in the pill groups that the study was designed to further evaluate the side effects of a new carrier compound for an antiviral medication. The participants were told that the compound contained only cellulose and did not produce serious side effects.
In the pill groups, confederates (one man and one woman) feigned illness (eg, nausea, dizziness, and headache) about 20 minutes after participants took the pills. Nurses attended to the confederates and to any participant who simulated or experienced symptoms, by taking their blood pressure and pulse, providing cool cloths for their foreheads, supplying bowls for potential vomiting, and sometimes putting participants with symptoms on gurneys outside the room within view of the other participants. An hour after taking the pills, the pill-plus-media group watched a public television documentary about the 1918 flu pandemic.
All three groups were assessed at baseline, at one hour, and at two hours. Participants rated their current symptoms by questionnaire, and nurses measured participants’ heart rate and blood pressure. Researchers debriefed all participants after the third assessment, and participants completed a psychosocial risk factor battery within a week of the initial experiment.
The primary outcome was symptom score. Participants in all three groups had some symptoms at baseline (eg, elevated heart rate and slight discomfort). At one hour, the control group had reduced symptoms, whereas the pill groups had increased symptom scores. At two hours, the control group still had few symptoms, but the psychogenic illness induction groups’ symptoms increased further. Symptoms did not differ between the pill-only and pill-plus-media groups, however.
An analysis of the psychosocial risk factor questionnaires found that participants’ total number of traumatic life events was positively associated with increased symptoms, but this relationship was not particularly strong. “It seems that the most important thing is … being exposed to people who are feigning symptoms or displaying symptoms in the setting of being told that there is a potential agent that might cause those symptoms,” Dr. Mink said.
Outcomes in Le Roy
Amid media coverage of the cases in Le Roy, Dr. Mink declined daily invitations to appear on television. “The last time I talked to the producer, I said, ‘You know, you would do these girls a big favor if you would just leave them alone,’” he said. “While the media attention persisted for another week, the improvement of their symptoms did coincide with reduced media attention, so one can speculate that that might have played a role.”
The patients in Le Roy received varying therapies, including cognitive behavioral therapy and supportive psychotherapy. They all received education about functional neurologic disorders. Some received pharmacothe
At last follow-up about two years ago, five of the 19 no longer had symptoms. Six of the 19 had experienced a greater than 85% improvement. A couple of patients continued to have symptoms, including the patients with a prior diagnosis of a chronic tic disorder. Two patients who had not improved sued the school district and alleged environmental toxins as the cause of their symptoms. The other patients were lost to follow up.
Treatment Principles
When treating patients with mass psychogenic illness, “First of all, you have to be an ally of your patient and not challenge the veracity,” Dr. Mink said. “For some of these girls, I think that there was some factitious component,” but this factor was not especially relevant to treatment recommendations.
“For mass psychogenic illness, reducing attention from social media groups and perhaps finding a way to disrupt the social cohesiveness of that group, at least until the symptoms can improve,” may be beneficial, he said. “Regular follow-up is helpful for all conversion disorders…. You do not want the patient to have to get worse to be able to see their doctor.”
Once neurologists have confirmed the diagnosis of mass psychogenic illness, they should “reinforce the certainty of the diagnosis” to occupational therapists, physical therapists, psychotherapists, and others on the health care team who treat these patients, Dr. Mink said. In addition,“It is important to prepare the therapist, particularly in an unusual situation like this where there has been a lot of media attention.”
—Jake Remaly
Suggested Reading
Bartholomew RE, Wessely S, Rubin GJ. Mass psychogenic illness and the social network: is it changing the pattern of outbreaks? J R Soc Med. 2012;105(12):509-512.
Broderick JE, Kaplan-Liss E, Bass E. Experimental induction of psychogenic illness in the context of a medical event and media exposure. Am J Disaster Med. 2011;6(3):163-172.
Page LA, Keshishian C, Leonardi G, et al. Frequency and predictors of mass psychogenic illness. Epidemiology. 2010;21(5):744-747.
Roach ES, Langley RL. Episodic neurological dysfunction due to mass hysteria. Arch Neurol. 2004;61(8):1269-1272.
Satisfaction is high for cantharidin in molluscum contagiosum
said Marla N. Jahnke, MD, of the Henry Ford Health System, Detroit, and her associates.
It is important to be careful when applying or handling cantharidin near the eyes, they noted. Also, parents must be counseled about possible side effects such as painful blistering, dyspigmentation, scarring, and itching, and that multiple treatment sessions may be needed.
The researchers did a retrospective chart review on patients under age 18 years treated with a cantharidin 0.7% solution between March 2013 and March 2014 at their institution, and performed a telephone survey to collect treatment outcomes from caregivers. Of the 62 caregivers contacted, the pediatric patients’ median age was 5 years (range 1.7-13), and 45% of the patients were white, 26% were black, 20% were Middle Eastern, 6% were Latino, and 3% were Asian, Pacific Islander, or Indian.
After cantharidin treatment, the caregivers most often described temporary discoloration (18%), severe blistering (10%), and pain that was excessive or greater than the caregiver expected (10%). Other outcomes described included itching (8%), scarring (6%), irritation (5%), bleeding (3%), and spreading of lesions (2%).
“Two patients returned to the office within 1 week of treatment because of excessive localized blistering that healed without long-term complications when topical emollients were used. ... Caregivers often could not confirm that they had washed off the cantharidin as recommended (1.5-2 hours after in-office application),” Dr. Jahnke and her associates noted in a research letter, which was published in the Journal of the American Academy of Dermatology.
Treatment satisfaction was high, with 94% of caregivers saying they would request cantharidin again if molluscum contagiosum were to recur on the child’s face, and 92% saying they would recommend it to others whose children had facial molluscum contagiosum. On a scale of 1 to 10, the average treatment satisfaction score was 8.7. The caregivers said that cantharidin was well tolerated by their children because it was painless when applied. The need for multiple office visits was the biggest complaint, the researchers revealed.
SOURCE: J Am Acad Dermatol. 2018 Jan. doi: 10.1016/j.jaad.2017.09.006.
said Marla N. Jahnke, MD, of the Henry Ford Health System, Detroit, and her associates.
It is important to be careful when applying or handling cantharidin near the eyes, they noted. Also, parents must be counseled about possible side effects such as painful blistering, dyspigmentation, scarring, and itching, and that multiple treatment sessions may be needed.
The researchers did a retrospective chart review on patients under age 18 years treated with a cantharidin 0.7% solution between March 2013 and March 2014 at their institution, and performed a telephone survey to collect treatment outcomes from caregivers. Of the 62 caregivers contacted, the pediatric patients’ median age was 5 years (range 1.7-13), and 45% of the patients were white, 26% were black, 20% were Middle Eastern, 6% were Latino, and 3% were Asian, Pacific Islander, or Indian.
After cantharidin treatment, the caregivers most often described temporary discoloration (18%), severe blistering (10%), and pain that was excessive or greater than the caregiver expected (10%). Other outcomes described included itching (8%), scarring (6%), irritation (5%), bleeding (3%), and spreading of lesions (2%).
“Two patients returned to the office within 1 week of treatment because of excessive localized blistering that healed without long-term complications when topical emollients were used. ... Caregivers often could not confirm that they had washed off the cantharidin as recommended (1.5-2 hours after in-office application),” Dr. Jahnke and her associates noted in a research letter, which was published in the Journal of the American Academy of Dermatology.
Treatment satisfaction was high, with 94% of caregivers saying they would request cantharidin again if molluscum contagiosum were to recur on the child’s face, and 92% saying they would recommend it to others whose children had facial molluscum contagiosum. On a scale of 1 to 10, the average treatment satisfaction score was 8.7. The caregivers said that cantharidin was well tolerated by their children because it was painless when applied. The need for multiple office visits was the biggest complaint, the researchers revealed.
SOURCE: J Am Acad Dermatol. 2018 Jan. doi: 10.1016/j.jaad.2017.09.006.
said Marla N. Jahnke, MD, of the Henry Ford Health System, Detroit, and her associates.
It is important to be careful when applying or handling cantharidin near the eyes, they noted. Also, parents must be counseled about possible side effects such as painful blistering, dyspigmentation, scarring, and itching, and that multiple treatment sessions may be needed.
The researchers did a retrospective chart review on patients under age 18 years treated with a cantharidin 0.7% solution between March 2013 and March 2014 at their institution, and performed a telephone survey to collect treatment outcomes from caregivers. Of the 62 caregivers contacted, the pediatric patients’ median age was 5 years (range 1.7-13), and 45% of the patients were white, 26% were black, 20% were Middle Eastern, 6% were Latino, and 3% were Asian, Pacific Islander, or Indian.
After cantharidin treatment, the caregivers most often described temporary discoloration (18%), severe blistering (10%), and pain that was excessive or greater than the caregiver expected (10%). Other outcomes described included itching (8%), scarring (6%), irritation (5%), bleeding (3%), and spreading of lesions (2%).
“Two patients returned to the office within 1 week of treatment because of excessive localized blistering that healed without long-term complications when topical emollients were used. ... Caregivers often could not confirm that they had washed off the cantharidin as recommended (1.5-2 hours after in-office application),” Dr. Jahnke and her associates noted in a research letter, which was published in the Journal of the American Academy of Dermatology.
Treatment satisfaction was high, with 94% of caregivers saying they would request cantharidin again if molluscum contagiosum were to recur on the child’s face, and 92% saying they would recommend it to others whose children had facial molluscum contagiosum. On a scale of 1 to 10, the average treatment satisfaction score was 8.7. The caregivers said that cantharidin was well tolerated by their children because it was painless when applied. The need for multiple office visits was the biggest complaint, the researchers revealed.
SOURCE: J Am Acad Dermatol. 2018 Jan. doi: 10.1016/j.jaad.2017.09.006.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Teen tanning bed bans keep patients from phototherapy
said Daniel J. Lewis and Madeleine Duvic, MD, of the University of Texas MD Anderson Cancer Center, Houston.
To prevent skin cancer, many states and the District of Columbia have set in place age restrictions on the use of commercial tanning beds and banned minors from indoor tanning; another 12 states put in place bans at younger ages. The Food and Drug Administration proposed a policy in 2015 that would keep all minors from indoor tanning, according to Mr. Lewis and Dr. Duvic.
Phototherapy is known to be an effective treatment for psoriasis, mycosis fungoides, and vitiligo. Phototherapy usually is given in physician offices and administered in ultraviolet B for treatment of psoriasis, but studies have found that tanning beds, which emit primarily ultraviolet A, can produce a clinical response in 80% of psoriasis patients, and 53% of patients report using tanning beds for psoriasis treatment, Mr. Lewis and Dr. Duvic said in a letter to the editor in Clinics in Dermatology.
The demanding schedule of visiting a physician’s office three times a week for phototherapy can be hard for some patients, especially children attending school during regular office hours and patients in rural areas. High copayments also can limit access, the authors said.
Despite the risks, making tanning beds “uniformly illegal for minors would be a disservice to patients with limited access to phototherapy. A more effective approach might be to collaborate with the tanning industry to achieve reasonable limits on age and exposure as opposed to an outright ban. At the very least, patients who receive a prescription from a dermatologist should be exempted from a universal ban,” they concluded.
SOURCE: Lewis, DJ and Duvic, M. Clin Dermatol. 2018 Jan-Feb;36(1):104-5
said Daniel J. Lewis and Madeleine Duvic, MD, of the University of Texas MD Anderson Cancer Center, Houston.
To prevent skin cancer, many states and the District of Columbia have set in place age restrictions on the use of commercial tanning beds and banned minors from indoor tanning; another 12 states put in place bans at younger ages. The Food and Drug Administration proposed a policy in 2015 that would keep all minors from indoor tanning, according to Mr. Lewis and Dr. Duvic.
Phototherapy is known to be an effective treatment for psoriasis, mycosis fungoides, and vitiligo. Phototherapy usually is given in physician offices and administered in ultraviolet B for treatment of psoriasis, but studies have found that tanning beds, which emit primarily ultraviolet A, can produce a clinical response in 80% of psoriasis patients, and 53% of patients report using tanning beds for psoriasis treatment, Mr. Lewis and Dr. Duvic said in a letter to the editor in Clinics in Dermatology.
The demanding schedule of visiting a physician’s office three times a week for phototherapy can be hard for some patients, especially children attending school during regular office hours and patients in rural areas. High copayments also can limit access, the authors said.
Despite the risks, making tanning beds “uniformly illegal for minors would be a disservice to patients with limited access to phototherapy. A more effective approach might be to collaborate with the tanning industry to achieve reasonable limits on age and exposure as opposed to an outright ban. At the very least, patients who receive a prescription from a dermatologist should be exempted from a universal ban,” they concluded.
SOURCE: Lewis, DJ and Duvic, M. Clin Dermatol. 2018 Jan-Feb;36(1):104-5
said Daniel J. Lewis and Madeleine Duvic, MD, of the University of Texas MD Anderson Cancer Center, Houston.
To prevent skin cancer, many states and the District of Columbia have set in place age restrictions on the use of commercial tanning beds and banned minors from indoor tanning; another 12 states put in place bans at younger ages. The Food and Drug Administration proposed a policy in 2015 that would keep all minors from indoor tanning, according to Mr. Lewis and Dr. Duvic.
Phototherapy is known to be an effective treatment for psoriasis, mycosis fungoides, and vitiligo. Phototherapy usually is given in physician offices and administered in ultraviolet B for treatment of psoriasis, but studies have found that tanning beds, which emit primarily ultraviolet A, can produce a clinical response in 80% of psoriasis patients, and 53% of patients report using tanning beds for psoriasis treatment, Mr. Lewis and Dr. Duvic said in a letter to the editor in Clinics in Dermatology.
The demanding schedule of visiting a physician’s office three times a week for phototherapy can be hard for some patients, especially children attending school during regular office hours and patients in rural areas. High copayments also can limit access, the authors said.
Despite the risks, making tanning beds “uniformly illegal for minors would be a disservice to patients with limited access to phototherapy. A more effective approach might be to collaborate with the tanning industry to achieve reasonable limits on age and exposure as opposed to an outright ban. At the very least, patients who receive a prescription from a dermatologist should be exempted from a universal ban,” they concluded.
SOURCE: Lewis, DJ and Duvic, M. Clin Dermatol. 2018 Jan-Feb;36(1):104-5
FROM CLINICS IN DERMATOLOGY
Topical steroid reduces atopic dermatitis relapse in children
according to Elena Rubio-Gomis of the Consorcio Hospital General Universitario de Valencia, Spain, and her associates.
Most atopic disease management is based on managing active disease, but atopic dermatitis is a chronic relapsing disease for which long-term maintenance therapies are being sought.
“Fluticasone 0.05% cream is a potent topical corticosteroid with a low systemic absorption and rapid metabolism and clearance,” which argues for low likelihood of causing systemic side effects and possible use in preventing atopic dermatitis relapse, the investigators wrote. And it is not very expensive.
In a randomized, double-blind, placebo-controlled study of 54 children with mild to moderate atopic dermatitis treated with twice-daily fluticasone propionate 0.05% cream up to 2 weeks, 49 children aged 2-10 years entered the second phase of the study. These children were randomly assigned to receive fluticasone propionate or vehicle twice weekly on consecutive days for 16 weeks; treatment was stopped then or at relapse.
Children treated with fluticasone propionate had a 2.7-fold lower risk of relapse than that of children treated with vehicle; 7 of 26 (27%) in the fluticasone propionate group and 13 of 23 patients (57%) in the vehicle group experienced relapse, the investigators wrote. The report was published in Allergologia et Immunopathologia. The median time to relapse with fluticasone propionate exceeded 16 weeks (the duration of the study), while in the vehicle group it was 65 days (a little over 9 weeks).
The treatment with fluticasone propionate and vehicle both were well tolerated. During the second phase of the study, 9 patients (35%) reported at least one adverse event in the fluticasone propionate group and 11 (48%) in the vehicle group. None of these were believed to be related to the drug studied, the investigators said.
SOURCE: Rubio-Gomis E et al. Allergol Immunopathol (Madr). 2018. doi: 10.1016/j.aller.2017.12.001.
according to Elena Rubio-Gomis of the Consorcio Hospital General Universitario de Valencia, Spain, and her associates.
Most atopic disease management is based on managing active disease, but atopic dermatitis is a chronic relapsing disease for which long-term maintenance therapies are being sought.
“Fluticasone 0.05% cream is a potent topical corticosteroid with a low systemic absorption and rapid metabolism and clearance,” which argues for low likelihood of causing systemic side effects and possible use in preventing atopic dermatitis relapse, the investigators wrote. And it is not very expensive.
In a randomized, double-blind, placebo-controlled study of 54 children with mild to moderate atopic dermatitis treated with twice-daily fluticasone propionate 0.05% cream up to 2 weeks, 49 children aged 2-10 years entered the second phase of the study. These children were randomly assigned to receive fluticasone propionate or vehicle twice weekly on consecutive days for 16 weeks; treatment was stopped then or at relapse.
Children treated with fluticasone propionate had a 2.7-fold lower risk of relapse than that of children treated with vehicle; 7 of 26 (27%) in the fluticasone propionate group and 13 of 23 patients (57%) in the vehicle group experienced relapse, the investigators wrote. The report was published in Allergologia et Immunopathologia. The median time to relapse with fluticasone propionate exceeded 16 weeks (the duration of the study), while in the vehicle group it was 65 days (a little over 9 weeks).
The treatment with fluticasone propionate and vehicle both were well tolerated. During the second phase of the study, 9 patients (35%) reported at least one adverse event in the fluticasone propionate group and 11 (48%) in the vehicle group. None of these were believed to be related to the drug studied, the investigators said.
SOURCE: Rubio-Gomis E et al. Allergol Immunopathol (Madr). 2018. doi: 10.1016/j.aller.2017.12.001.
according to Elena Rubio-Gomis of the Consorcio Hospital General Universitario de Valencia, Spain, and her associates.
Most atopic disease management is based on managing active disease, but atopic dermatitis is a chronic relapsing disease for which long-term maintenance therapies are being sought.
“Fluticasone 0.05% cream is a potent topical corticosteroid with a low systemic absorption and rapid metabolism and clearance,” which argues for low likelihood of causing systemic side effects and possible use in preventing atopic dermatitis relapse, the investigators wrote. And it is not very expensive.
In a randomized, double-blind, placebo-controlled study of 54 children with mild to moderate atopic dermatitis treated with twice-daily fluticasone propionate 0.05% cream up to 2 weeks, 49 children aged 2-10 years entered the second phase of the study. These children were randomly assigned to receive fluticasone propionate or vehicle twice weekly on consecutive days for 16 weeks; treatment was stopped then or at relapse.
Children treated with fluticasone propionate had a 2.7-fold lower risk of relapse than that of children treated with vehicle; 7 of 26 (27%) in the fluticasone propionate group and 13 of 23 patients (57%) in the vehicle group experienced relapse, the investigators wrote. The report was published in Allergologia et Immunopathologia. The median time to relapse with fluticasone propionate exceeded 16 weeks (the duration of the study), while in the vehicle group it was 65 days (a little over 9 weeks).
The treatment with fluticasone propionate and vehicle both were well tolerated. During the second phase of the study, 9 patients (35%) reported at least one adverse event in the fluticasone propionate group and 11 (48%) in the vehicle group. None of these were believed to be related to the drug studied, the investigators said.
SOURCE: Rubio-Gomis E et al. Allergol Immunopathol (Madr). 2018. doi: 10.1016/j.aller.2017.12.001.
FROM ALLERGOLOGIA ET IMMUNOPATHOLOGIA
Latest PANS trials suggest cause may be treatable
NEW YORK – New controlled trials in the treatment of pediatric acute neuropsychiatric syndrome (PANS) support the hypothesis that the cause may, in fact, be treatable, an expert said at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
PANS and pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS) are controversial diagnoses. But ongoing research has expanded the body of literature describing symptoms and evaluating treatments, according to an overview from Barbara J. Coffey, MD, division chief in child and adolescent psychiatry at the University of Miami.
PANS and PANDAS, which are clinical diagnoses of exclusion, are characterized by an abrupt onset of one or more neuropsychiatric symptoms in children that can include signs of obsessive-compulsive disorder (OCD), tics, anxiety, irritability, and behavioral changes. Despite more than 15 years of clinical and experimental studies, almost all aspects of PANS and PANDAS remain controversial, Dr. Coffey said.
“Many pediatricians I work with do not want to see these kids, because they really do not know what to do,” she reported.
This prevailing conception has led to treatment trials with antibiotics for the underlying infection and, most recently, with intravenous immunoglobulins (IVIG) to prevent cross-reactive antibodies induced by infection. Dr. Coffey, reviewing several recently published studies, noted that there have been signals of activity suggesting “there may be something there.” However, she cautioned that the data are inconclusive.
Of recent studies, a trial with azithromycin in children with PANS generated somewhat positive findings (J Child Adolesc Psychopharmacol. 2017;27[7]:640-51). In this study, 31 children aged 4-14 years were randomized to receive azithromycin or placebo for 4 weeks. They were evaluated via the Children’s Yale–Brown Obsessive Compulsive Scale (CY-BOCS) and the OCD Clinical Global Impression Severity (CGI-S OCD) scale.
The study associated azithromycin with a significant reduction in symptoms as measured with CGI-S OCD (41.2% vs. 7.1%; P = .045), but no difference was found in response as measured with the CY-BOCS, which Dr. Coffey described as the more conservative measure. Even when measured with the CGI-S OCD scale, symptom improvements were modest. But the authors concluded that azithromycin “may be helpful” for the control of neuropsychiatric symptoms.
In a trial with IVIG, 35 children with PANDAS were randomized to IVIG or placebo (J Am Acad Child Adolesc Psychiatry. 2016;55[10]:860-7). The primary outcome was at least a 30% reduction in CY-BOCS at 12 weeks. Nonresponders at 12 weeks were permitted 12 more weeks of treatment with open-label IVIG.
Twice as many patients receiving IVIG, compared with those on placebo, reached the primary outcome (24% vs. 12%), but the study was small and the difference did not reach significance. However, the authors reported that the mean CY-BOCS improvement from baseline on IVIG, which was well tolerated, was 55% at week 12 and 62% at week 24. The authors suggested that larger trials are warranted.
“One critique of this study is that all of the patients were placed on prophylactic antibiotics, which may have attenuated the response,” Dr. Coffey said. In outlining these results, she emphasized: “This is not something I am recommending. I just want to acquaint you with what is going on out there.”
None of the most recent trials provide conclusive support for therapy targeted at infection or an autoimmune process in PANS or PANDAS, but Dr. Coffey indicated that . One of the most recent sets of data come from a recently published Scandinavian cohort study with 17 years of follow-up (JAMA Psychiatry. 2017;74[7]:740-6). That study associated pediatric infections of any kind, not just streptococcal infections, with an elevated risk of mental disorders – particularly OCD and tics.
Overall, the evidence base is growing to suggest “antibiotics and immune therapy may be beneficial, but the jury is not in yet for which patients, how much, and how long,” Dr. Coffey said. She is aware of clinicians who are now using antibiotics empirically to control neuropsychiatric symptoms in PANDAS but cautioned that more investigation is needed.
Dr. Coffey reports financial relationships with Genco Sciences, Neurocrine Biosciences, Shire, and Teva/Nuvelution.
NEW YORK – New controlled trials in the treatment of pediatric acute neuropsychiatric syndrome (PANS) support the hypothesis that the cause may, in fact, be treatable, an expert said at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
PANS and pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS) are controversial diagnoses. But ongoing research has expanded the body of literature describing symptoms and evaluating treatments, according to an overview from Barbara J. Coffey, MD, division chief in child and adolescent psychiatry at the University of Miami.
PANS and PANDAS, which are clinical diagnoses of exclusion, are characterized by an abrupt onset of one or more neuropsychiatric symptoms in children that can include signs of obsessive-compulsive disorder (OCD), tics, anxiety, irritability, and behavioral changes. Despite more than 15 years of clinical and experimental studies, almost all aspects of PANS and PANDAS remain controversial, Dr. Coffey said.
“Many pediatricians I work with do not want to see these kids, because they really do not know what to do,” she reported.
This prevailing conception has led to treatment trials with antibiotics for the underlying infection and, most recently, with intravenous immunoglobulins (IVIG) to prevent cross-reactive antibodies induced by infection. Dr. Coffey, reviewing several recently published studies, noted that there have been signals of activity suggesting “there may be something there.” However, she cautioned that the data are inconclusive.
Of recent studies, a trial with azithromycin in children with PANS generated somewhat positive findings (J Child Adolesc Psychopharmacol. 2017;27[7]:640-51). In this study, 31 children aged 4-14 years were randomized to receive azithromycin or placebo for 4 weeks. They were evaluated via the Children’s Yale–Brown Obsessive Compulsive Scale (CY-BOCS) and the OCD Clinical Global Impression Severity (CGI-S OCD) scale.
The study associated azithromycin with a significant reduction in symptoms as measured with CGI-S OCD (41.2% vs. 7.1%; P = .045), but no difference was found in response as measured with the CY-BOCS, which Dr. Coffey described as the more conservative measure. Even when measured with the CGI-S OCD scale, symptom improvements were modest. But the authors concluded that azithromycin “may be helpful” for the control of neuropsychiatric symptoms.
In a trial with IVIG, 35 children with PANDAS were randomized to IVIG or placebo (J Am Acad Child Adolesc Psychiatry. 2016;55[10]:860-7). The primary outcome was at least a 30% reduction in CY-BOCS at 12 weeks. Nonresponders at 12 weeks were permitted 12 more weeks of treatment with open-label IVIG.
Twice as many patients receiving IVIG, compared with those on placebo, reached the primary outcome (24% vs. 12%), but the study was small and the difference did not reach significance. However, the authors reported that the mean CY-BOCS improvement from baseline on IVIG, which was well tolerated, was 55% at week 12 and 62% at week 24. The authors suggested that larger trials are warranted.
“One critique of this study is that all of the patients were placed on prophylactic antibiotics, which may have attenuated the response,” Dr. Coffey said. In outlining these results, she emphasized: “This is not something I am recommending. I just want to acquaint you with what is going on out there.”
None of the most recent trials provide conclusive support for therapy targeted at infection or an autoimmune process in PANS or PANDAS, but Dr. Coffey indicated that . One of the most recent sets of data come from a recently published Scandinavian cohort study with 17 years of follow-up (JAMA Psychiatry. 2017;74[7]:740-6). That study associated pediatric infections of any kind, not just streptococcal infections, with an elevated risk of mental disorders – particularly OCD and tics.
Overall, the evidence base is growing to suggest “antibiotics and immune therapy may be beneficial, but the jury is not in yet for which patients, how much, and how long,” Dr. Coffey said. She is aware of clinicians who are now using antibiotics empirically to control neuropsychiatric symptoms in PANDAS but cautioned that more investigation is needed.
Dr. Coffey reports financial relationships with Genco Sciences, Neurocrine Biosciences, Shire, and Teva/Nuvelution.
NEW YORK – New controlled trials in the treatment of pediatric acute neuropsychiatric syndrome (PANS) support the hypothesis that the cause may, in fact, be treatable, an expert said at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
PANS and pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections (PANDAS) are controversial diagnoses. But ongoing research has expanded the body of literature describing symptoms and evaluating treatments, according to an overview from Barbara J. Coffey, MD, division chief in child and adolescent psychiatry at the University of Miami.
PANS and PANDAS, which are clinical diagnoses of exclusion, are characterized by an abrupt onset of one or more neuropsychiatric symptoms in children that can include signs of obsessive-compulsive disorder (OCD), tics, anxiety, irritability, and behavioral changes. Despite more than 15 years of clinical and experimental studies, almost all aspects of PANS and PANDAS remain controversial, Dr. Coffey said.
“Many pediatricians I work with do not want to see these kids, because they really do not know what to do,” she reported.
This prevailing conception has led to treatment trials with antibiotics for the underlying infection and, most recently, with intravenous immunoglobulins (IVIG) to prevent cross-reactive antibodies induced by infection. Dr. Coffey, reviewing several recently published studies, noted that there have been signals of activity suggesting “there may be something there.” However, she cautioned that the data are inconclusive.
Of recent studies, a trial with azithromycin in children with PANS generated somewhat positive findings (J Child Adolesc Psychopharmacol. 2017;27[7]:640-51). In this study, 31 children aged 4-14 years were randomized to receive azithromycin or placebo for 4 weeks. They were evaluated via the Children’s Yale–Brown Obsessive Compulsive Scale (CY-BOCS) and the OCD Clinical Global Impression Severity (CGI-S OCD) scale.
The study associated azithromycin with a significant reduction in symptoms as measured with CGI-S OCD (41.2% vs. 7.1%; P = .045), but no difference was found in response as measured with the CY-BOCS, which Dr. Coffey described as the more conservative measure. Even when measured with the CGI-S OCD scale, symptom improvements were modest. But the authors concluded that azithromycin “may be helpful” for the control of neuropsychiatric symptoms.
In a trial with IVIG, 35 children with PANDAS were randomized to IVIG or placebo (J Am Acad Child Adolesc Psychiatry. 2016;55[10]:860-7). The primary outcome was at least a 30% reduction in CY-BOCS at 12 weeks. Nonresponders at 12 weeks were permitted 12 more weeks of treatment with open-label IVIG.
Twice as many patients receiving IVIG, compared with those on placebo, reached the primary outcome (24% vs. 12%), but the study was small and the difference did not reach significance. However, the authors reported that the mean CY-BOCS improvement from baseline on IVIG, which was well tolerated, was 55% at week 12 and 62% at week 24. The authors suggested that larger trials are warranted.
“One critique of this study is that all of the patients were placed on prophylactic antibiotics, which may have attenuated the response,” Dr. Coffey said. In outlining these results, she emphasized: “This is not something I am recommending. I just want to acquaint you with what is going on out there.”
None of the most recent trials provide conclusive support for therapy targeted at infection or an autoimmune process in PANS or PANDAS, but Dr. Coffey indicated that . One of the most recent sets of data come from a recently published Scandinavian cohort study with 17 years of follow-up (JAMA Psychiatry. 2017;74[7]:740-6). That study associated pediatric infections of any kind, not just streptococcal infections, with an elevated risk of mental disorders – particularly OCD and tics.
Overall, the evidence base is growing to suggest “antibiotics and immune therapy may be beneficial, but the jury is not in yet for which patients, how much, and how long,” Dr. Coffey said. She is aware of clinicians who are now using antibiotics empirically to control neuropsychiatric symptoms in PANDAS but cautioned that more investigation is needed.
Dr. Coffey reports financial relationships with Genco Sciences, Neurocrine Biosciences, Shire, and Teva/Nuvelution.
REPORTING FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE

Antihistamines still are prescribed inappropriately for atopic dermatitis
said Alice He, MD, at the Center for Dermatology Research, Wake Forest University, Winston-Salem, N.C., and her associates.
Results of double-blind, randomized trials have found that oral antihistamines do not effectively treat itch associated with atopic dermatitis (AD), and American Academy of Dermatology guidelines state that intermittent short-term use of sedating antihistamines may help insomnia secondary to itch, but should not be substituted for topical treatments in atopic dermatitis management (J Am Acad Dermatol. 2014;71[2]:327-49), the investigators said. Nonetheless, physicians continue to prescribe antihistamines to AD patients.
Sedating antihistamines accounted for the majority of antihistamines prescribed by pediatricians (58%) and dermatologists (70%) for AD. Nonsedating antihistamines accounted for the majority of the antihistamines prescribed by family physicians (84%), internists (100%), and other specialists (55%), the investigators said.
(The sedating antihistamines prescribed included hydroxyzine, diphenhydramine, chlorpheniramine, brompheniramine, and cyproheptadine; nonsedating antihistamines include cetirizine, desloratadine, levocetirizine, loratadine, and fexofenadine.)
Although the AAD guidelines allow intermittent, short-term use of sedating antihistamines to treat AD-associated itch, these medications may be harmful to sleep in terms of reduced sleep quality and decreased REM sleep. Also, studies have shown that their effects can persist into the daytime and have the potential to impair cognitive function, including learning and memory.
“Physicians should consider the potential risks when prescribing sedating antihistamines as adjunctive treatment for atopic dermatitis,” Dr. He and her associates warned in the article in the Journal of the American Academy of Dermatology.
The researchers took a look at the top ten comorbidities reported among visits for AD, because nonsedating antihistamines might have been prescribed for a different diagnosis. There were three conditions for which antihistamines may be indicated: allergic rhinitis (13%), dermatitis attributable to food (8.5%), and conjunctivitis (3%). This “validates antihistamine prescriptions for a maximum of only 24.5% of patients who received antihistamines, indicating that a large proportion of antihistamine prescriptions were prescribed specifically for AD,” they said.
The authors said that, “while histamine does not play a role in AD via H1R [histamine-1 receptor], it may still be relevant in AD pathogenesis through actions on its most recently described receptor, histamine-4 receptor (H4R).”
“The advent of new targeted systemic therapies, such as T-helper 2 cytokine antagonists and H4R antagonists,” may one day help fill “the unmet need for effective treatments for atopic dermatitis,” Dr. He and her associates concluded.
The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories. Dr. He listed no other relevant financial disclosures. Her coauthors disclosed research, speaking, and/or consulting support from a variety of pharmaceutical companies; one author is an employee of Abbvie.
SOURCE: He A et al. J Amer Acad of Dermatol. 2008. doi: 10.1016/j.jaad.2017.12.077.
said Alice He, MD, at the Center for Dermatology Research, Wake Forest University, Winston-Salem, N.C., and her associates.
Results of double-blind, randomized trials have found that oral antihistamines do not effectively treat itch associated with atopic dermatitis (AD), and American Academy of Dermatology guidelines state that intermittent short-term use of sedating antihistamines may help insomnia secondary to itch, but should not be substituted for topical treatments in atopic dermatitis management (J Am Acad Dermatol. 2014;71[2]:327-49), the investigators said. Nonetheless, physicians continue to prescribe antihistamines to AD patients.
Sedating antihistamines accounted for the majority of antihistamines prescribed by pediatricians (58%) and dermatologists (70%) for AD. Nonsedating antihistamines accounted for the majority of the antihistamines prescribed by family physicians (84%), internists (100%), and other specialists (55%), the investigators said.
(The sedating antihistamines prescribed included hydroxyzine, diphenhydramine, chlorpheniramine, brompheniramine, and cyproheptadine; nonsedating antihistamines include cetirizine, desloratadine, levocetirizine, loratadine, and fexofenadine.)
Although the AAD guidelines allow intermittent, short-term use of sedating antihistamines to treat AD-associated itch, these medications may be harmful to sleep in terms of reduced sleep quality and decreased REM sleep. Also, studies have shown that their effects can persist into the daytime and have the potential to impair cognitive function, including learning and memory.
“Physicians should consider the potential risks when prescribing sedating antihistamines as adjunctive treatment for atopic dermatitis,” Dr. He and her associates warned in the article in the Journal of the American Academy of Dermatology.
The researchers took a look at the top ten comorbidities reported among visits for AD, because nonsedating antihistamines might have been prescribed for a different diagnosis. There were three conditions for which antihistamines may be indicated: allergic rhinitis (13%), dermatitis attributable to food (8.5%), and conjunctivitis (3%). This “validates antihistamine prescriptions for a maximum of only 24.5% of patients who received antihistamines, indicating that a large proportion of antihistamine prescriptions were prescribed specifically for AD,” they said.
The authors said that, “while histamine does not play a role in AD via H1R [histamine-1 receptor], it may still be relevant in AD pathogenesis through actions on its most recently described receptor, histamine-4 receptor (H4R).”
“The advent of new targeted systemic therapies, such as T-helper 2 cytokine antagonists and H4R antagonists,” may one day help fill “the unmet need for effective treatments for atopic dermatitis,” Dr. He and her associates concluded.
The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories. Dr. He listed no other relevant financial disclosures. Her coauthors disclosed research, speaking, and/or consulting support from a variety of pharmaceutical companies; one author is an employee of Abbvie.
SOURCE: He A et al. J Amer Acad of Dermatol. 2008. doi: 10.1016/j.jaad.2017.12.077.
said Alice He, MD, at the Center for Dermatology Research, Wake Forest University, Winston-Salem, N.C., and her associates.
Results of double-blind, randomized trials have found that oral antihistamines do not effectively treat itch associated with atopic dermatitis (AD), and American Academy of Dermatology guidelines state that intermittent short-term use of sedating antihistamines may help insomnia secondary to itch, but should not be substituted for topical treatments in atopic dermatitis management (J Am Acad Dermatol. 2014;71[2]:327-49), the investigators said. Nonetheless, physicians continue to prescribe antihistamines to AD patients.
Sedating antihistamines accounted for the majority of antihistamines prescribed by pediatricians (58%) and dermatologists (70%) for AD. Nonsedating antihistamines accounted for the majority of the antihistamines prescribed by family physicians (84%), internists (100%), and other specialists (55%), the investigators said.
(The sedating antihistamines prescribed included hydroxyzine, diphenhydramine, chlorpheniramine, brompheniramine, and cyproheptadine; nonsedating antihistamines include cetirizine, desloratadine, levocetirizine, loratadine, and fexofenadine.)
Although the AAD guidelines allow intermittent, short-term use of sedating antihistamines to treat AD-associated itch, these medications may be harmful to sleep in terms of reduced sleep quality and decreased REM sleep. Also, studies have shown that their effects can persist into the daytime and have the potential to impair cognitive function, including learning and memory.
“Physicians should consider the potential risks when prescribing sedating antihistamines as adjunctive treatment for atopic dermatitis,” Dr. He and her associates warned in the article in the Journal of the American Academy of Dermatology.
The researchers took a look at the top ten comorbidities reported among visits for AD, because nonsedating antihistamines might have been prescribed for a different diagnosis. There were three conditions for which antihistamines may be indicated: allergic rhinitis (13%), dermatitis attributable to food (8.5%), and conjunctivitis (3%). This “validates antihistamine prescriptions for a maximum of only 24.5% of patients who received antihistamines, indicating that a large proportion of antihistamine prescriptions were prescribed specifically for AD,” they said.
The authors said that, “while histamine does not play a role in AD via H1R [histamine-1 receptor], it may still be relevant in AD pathogenesis through actions on its most recently described receptor, histamine-4 receptor (H4R).”
“The advent of new targeted systemic therapies, such as T-helper 2 cytokine antagonists and H4R antagonists,” may one day help fill “the unmet need for effective treatments for atopic dermatitis,” Dr. He and her associates concluded.
The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories. Dr. He listed no other relevant financial disclosures. Her coauthors disclosed research, speaking, and/or consulting support from a variety of pharmaceutical companies; one author is an employee of Abbvie.
SOURCE: He A et al. J Amer Acad of Dermatol. 2008. doi: 10.1016/j.jaad.2017.12.077.
FROM JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
Key clinical point: Physicians should consider the potential risks when prescribing sedating antihistamines as adjunctive treatment for atopic dermatitis.
Major finding: Physicians from specialties other than dermatology prescribed antihistamines at a greater proportion of AD visits than dermatologists (26%-44% of visits vs. 22%), with the exception of pediatricians (16%).
Study details: Data from the National Ambulatory Medical Care Survey on 9.9 million physician visits for AD from 2003 to 2012.
Disclosures: The Center for Dermatology Research is supported by an unrestricted educational grant from Galderma Laboratories. Dr. He listed no other relevant financial disclosures. Her associates disclosed research, speaking and/or consulting support from a variety of pharmaceutical companies. One author was an employee of Abbvie.
Source: He A et al. J Amer Acad of Dermatol. 2008. doi: 10.1016/j.jaad.2017.12.077.