User login
Genetic Screens Yield Potential Therapies for Neurodegenerative Diseases
SAN DIEGO—Cross-species genetic screens are helping researchers find molecules that modulate the proteins that cause adult neurodegenerative disease, according to a lecture delivered at the 142nd Annual Meeting of the American Neurological Association. Such screening thus reveals potential therapeutic targets and augments scientific understanding of the biology of these proteins.
The research raises the possibility that clinicians will be able to delay or prevent neurodegenerative disease in the future through the early administration of molecules that target these proteins. “We need to identify those at risk and begin the therapy … before the symptoms develop, just like you would treat somebody with statins if they have high cholesterol before they have a heart attack,” said Huda Y. Zoghbi, MD, an investigator with the Howard Hughes Medical Institute; Professor of Pediatrics, Molecular and Human Genetics, Neuroscience, and Neurology at Baylor College of Medicine; and Director of the Jan and Dan Duncan Neurological Research Institute in Houston.
Research Into a Rare Disorder
Studying the rare disorder spinocerebellar ataxia type 1 (SCA1) has yielded information that could be applicable to more common neurodegenerative diseases, said Dr. Zoghbi. SCA1 is characterized by a loss of Purkinje cells and brainstem neurons that impairs balance and coordination and increases the risk of premature death. In 1993, Dr. Zoghbi; Harry Orr, PhD, Professor and Tulloch Chair in Genetics at the University of Minnesota in Minneapolis; and colleagues discovered that a CAG repeat expansion in ATXN1 causes SCA1 by producing an abnormally long version of the ataxin-1 protein. They also found that neurodegeneration results if levels of normal ataxin-1 are increased by 20% or 30%. The brain thus is highly sensitive to ataxin-1 levels, said Dr. Zoghbi.

Borrowing a technique from cancer research, the investigators performed genetic screening using fruit fly and human cells to find targets that would reduce ataxin-1 levels when inhibited. They found approximately 30 relevant genes in each organism, and about 12 were common to both organisms. All of the shared genes operate in the mitogen-activated protein (MAP) kinase pathway, and inhibiting each gene lowered ataxin-1 in cells and flies.
Inhibiting Enzymes
The researchers also observed that the enzymes MSK1 and MSK2 intervene in the pathway and promote ataxin-1 accumulation. Inhibiting MSK1 produced clinical improvement in SCA1 mouse models, and inhibiting MSK1 and MSK2 together produced still more improvement. A small molecule that inhibited MSK1 therefore could help patients with SCA1, said Dr. Zoghbi.
Inhibiting enzymes such as MSK1 and MSK2 for years at a time could raise safety concerns, however. The investigators thus decided to look for other modulators of ataxin-1, on the theory that targeting modulators that function in different pathways could reduce the amount of inhibition required and decrease the risk of adverse events.
Further screening revealed that PKA1 appeared to modulate ataxin-1 by a mechanism similar to that of MSK1. An animal study indicated that inhibiting MSK1 and inhibiting PKA1 produced equivalent reductions on ataxin-1, but that inhibiting both in tandem yielded a greater reduction. The investigators then found that the PAK1 enzyme promoted ataxin-1 accumulation through a pathway different from that of MSK1 and PKA1. Inhibiting PAK1 reduced ataxin-1 levels, and inhibiting PAK1 and MSK1 simultaneously had a still greater effect.
Targeting Tauopathies
Their research into kinases and enzymes prompted Dr. Zoghbi and colleagues to consider whole genome screening as a method of targeting proteins that cause neurodegenerative diseases other than SCA1. Overexpression of tau, for example, causes neurodegeneration, regardless of whether the overexpression results from a mutation in tau-encoding genes. “Tau is a true culprit in dementias, and we thought that if we could find something to lower it, we could help patients with these disorders,” said Dr. Zoghbi.
Another genetic screen suggested that the enzyme Nuak1 stabilizes tau by phosphorylating it at Ser356. The investigators observed that inhibiting Nuak1 reduced tau levels and suppressed neurodegeneration in human cells and in fruit flies. Tau accumulation decreases fruit flies’ climbing ability, and inhibiting Nuak1 improved this ability in flies with tau accumulation.
In a subsequent mouse study, Dr. Zoghbi and colleagues found that inhibiting Nuak1 significantly reduced levels of phosphorylated tau and provided smaller reductions in total tau and endogenous tau. They also observed that mice with tauopathy took longer than wild-type mice to complete a water maze task. Inhibiting Nuak1 in mice with tauopathy improved their performance on this task. Nuak1 inhibition also restored synaptic plasticity in these mice to a level similar to that of wild-type mice. Finally, Nuak1 inhibition reduced tau tangle pathology and increased survival. Dr. Zoghbi and colleagues are now searching for small-molecule Nuak1 inhibitors that could provide protection against tauopathy.
In Search of More Targets
The investigators next looked for genes that influence tau. Successive levels of genetic screening identified 59 genes that “robustly lower tau levels,” said Dr. Zoghbi. She and her colleagues prioritized 12 of the genes for investigation.
They used adenoassociated viral vectors to deliver therapies that can knock out mouse genes for as long as a year. With this technique, the investigators confirmed that all of the initial 12 genes decreased tau levels. In principle, this strategy could enable researchers to scan the whole genome for genes that modulate tau, said Dr. Zoghbi.
—Erik Greb
Suggested Reading
Lasagna-Reeves CA, de Haro M, Hao S, et al. Reduction of Nuak1 decreases tau and reverses phenotypes in a tauopathy mouse model. Neuron. 2016; 92(2):407-418.
Park J, Al-Ramahi I, Tan Q, et al. RAS-MAPK-MSK1 pathway modulates ataxin 1 protein levels and toxicity in SCA1. Nature. 2013;498(7454):325-331.
Rousseaux MW, de Haro M, Lasagna-Reeves CA, et al. TRIM28 regulates the nuclear accumulation and toxicity of both alpha-synuclein and tau. Elife. 2016 Oct 25;5. pii: e19809
SAN DIEGO—Cross-species genetic screens are helping researchers find molecules that modulate the proteins that cause adult neurodegenerative disease, according to a lecture delivered at the 142nd Annual Meeting of the American Neurological Association. Such screening thus reveals potential therapeutic targets and augments scientific understanding of the biology of these proteins.
The research raises the possibility that clinicians will be able to delay or prevent neurodegenerative disease in the future through the early administration of molecules that target these proteins. “We need to identify those at risk and begin the therapy … before the symptoms develop, just like you would treat somebody with statins if they have high cholesterol before they have a heart attack,” said Huda Y. Zoghbi, MD, an investigator with the Howard Hughes Medical Institute; Professor of Pediatrics, Molecular and Human Genetics, Neuroscience, and Neurology at Baylor College of Medicine; and Director of the Jan and Dan Duncan Neurological Research Institute in Houston.
Research Into a Rare Disorder
Studying the rare disorder spinocerebellar ataxia type 1 (SCA1) has yielded information that could be applicable to more common neurodegenerative diseases, said Dr. Zoghbi. SCA1 is characterized by a loss of Purkinje cells and brainstem neurons that impairs balance and coordination and increases the risk of premature death. In 1993, Dr. Zoghbi; Harry Orr, PhD, Professor and Tulloch Chair in Genetics at the University of Minnesota in Minneapolis; and colleagues discovered that a CAG repeat expansion in ATXN1 causes SCA1 by producing an abnormally long version of the ataxin-1 protein. They also found that neurodegeneration results if levels of normal ataxin-1 are increased by 20% or 30%. The brain thus is highly sensitive to ataxin-1 levels, said Dr. Zoghbi.
Borrowing a technique from cancer research, the investigators performed genetic screening using fruit fly and human cells to find targets that would reduce ataxin-1 levels when inhibited. They found approximately 30 relevant genes in each organism, and about 12 were common to both organisms. All of the shared genes operate in the mitogen-activated protein (MAP) kinase pathway, and inhibiting each gene lowered ataxin-1 in cells and flies.
Inhibiting Enzymes
The researchers also observed that the enzymes MSK1 and MSK2 intervene in the pathway and promote ataxin-1 accumulation. Inhibiting MSK1 produced clinical improvement in SCA1 mouse models, and inhibiting MSK1 and MSK2 together produced still more improvement. A small molecule that inhibited MSK1 therefore could help patients with SCA1, said Dr. Zoghbi.
Inhibiting enzymes such as MSK1 and MSK2 for years at a time could raise safety concerns, however. The investigators thus decided to look for other modulators of ataxin-1, on the theory that targeting modulators that function in different pathways could reduce the amount of inhibition required and decrease the risk of adverse events.
Further screening revealed that PKA1 appeared to modulate ataxin-1 by a mechanism similar to that of MSK1. An animal study indicated that inhibiting MSK1 and inhibiting PKA1 produced equivalent reductions on ataxin-1, but that inhibiting both in tandem yielded a greater reduction. The investigators then found that the PAK1 enzyme promoted ataxin-1 accumulation through a pathway different from that of MSK1 and PKA1. Inhibiting PAK1 reduced ataxin-1 levels, and inhibiting PAK1 and MSK1 simultaneously had a still greater effect.
Targeting Tauopathies
Their research into kinases and enzymes prompted Dr. Zoghbi and colleagues to consider whole genome screening as a method of targeting proteins that cause neurodegenerative diseases other than SCA1. Overexpression of tau, for example, causes neurodegeneration, regardless of whether the overexpression results from a mutation in tau-encoding genes. “Tau is a true culprit in dementias, and we thought that if we could find something to lower it, we could help patients with these disorders,” said Dr. Zoghbi.
Another genetic screen suggested that the enzyme Nuak1 stabilizes tau by phosphorylating it at Ser356. The investigators observed that inhibiting Nuak1 reduced tau levels and suppressed neurodegeneration in human cells and in fruit flies. Tau accumulation decreases fruit flies’ climbing ability, and inhibiting Nuak1 improved this ability in flies with tau accumulation.
In a subsequent mouse study, Dr. Zoghbi and colleagues found that inhibiting Nuak1 significantly reduced levels of phosphorylated tau and provided smaller reductions in total tau and endogenous tau. They also observed that mice with tauopathy took longer than wild-type mice to complete a water maze task. Inhibiting Nuak1 in mice with tauopathy improved their performance on this task. Nuak1 inhibition also restored synaptic plasticity in these mice to a level similar to that of wild-type mice. Finally, Nuak1 inhibition reduced tau tangle pathology and increased survival. Dr. Zoghbi and colleagues are now searching for small-molecule Nuak1 inhibitors that could provide protection against tauopathy.
In Search of More Targets
The investigators next looked for genes that influence tau. Successive levels of genetic screening identified 59 genes that “robustly lower tau levels,” said Dr. Zoghbi. She and her colleagues prioritized 12 of the genes for investigation.
They used adenoassociated viral vectors to deliver therapies that can knock out mouse genes for as long as a year. With this technique, the investigators confirmed that all of the initial 12 genes decreased tau levels. In principle, this strategy could enable researchers to scan the whole genome for genes that modulate tau, said Dr. Zoghbi.
—Erik Greb
Suggested Reading
Lasagna-Reeves CA, de Haro M, Hao S, et al. Reduction of Nuak1 decreases tau and reverses phenotypes in a tauopathy mouse model. Neuron. 2016; 92(2):407-418.
Park J, Al-Ramahi I, Tan Q, et al. RAS-MAPK-MSK1 pathway modulates ataxin 1 protein levels and toxicity in SCA1. Nature. 2013;498(7454):325-331.
Rousseaux MW, de Haro M, Lasagna-Reeves CA, et al. TRIM28 regulates the nuclear accumulation and toxicity of both alpha-synuclein and tau. Elife. 2016 Oct 25;5. pii: e19809
SAN DIEGO—Cross-species genetic screens are helping researchers find molecules that modulate the proteins that cause adult neurodegenerative disease, according to a lecture delivered at the 142nd Annual Meeting of the American Neurological Association. Such screening thus reveals potential therapeutic targets and augments scientific understanding of the biology of these proteins.
The research raises the possibility that clinicians will be able to delay or prevent neurodegenerative disease in the future through the early administration of molecules that target these proteins. “We need to identify those at risk and begin the therapy … before the symptoms develop, just like you would treat somebody with statins if they have high cholesterol before they have a heart attack,” said Huda Y. Zoghbi, MD, an investigator with the Howard Hughes Medical Institute; Professor of Pediatrics, Molecular and Human Genetics, Neuroscience, and Neurology at Baylor College of Medicine; and Director of the Jan and Dan Duncan Neurological Research Institute in Houston.
Research Into a Rare Disorder
Studying the rare disorder spinocerebellar ataxia type 1 (SCA1) has yielded information that could be applicable to more common neurodegenerative diseases, said Dr. Zoghbi. SCA1 is characterized by a loss of Purkinje cells and brainstem neurons that impairs balance and coordination and increases the risk of premature death. In 1993, Dr. Zoghbi; Harry Orr, PhD, Professor and Tulloch Chair in Genetics at the University of Minnesota in Minneapolis; and colleagues discovered that a CAG repeat expansion in ATXN1 causes SCA1 by producing an abnormally long version of the ataxin-1 protein. They also found that neurodegeneration results if levels of normal ataxin-1 are increased by 20% or 30%. The brain thus is highly sensitive to ataxin-1 levels, said Dr. Zoghbi.
Borrowing a technique from cancer research, the investigators performed genetic screening using fruit fly and human cells to find targets that would reduce ataxin-1 levels when inhibited. They found approximately 30 relevant genes in each organism, and about 12 were common to both organisms. All of the shared genes operate in the mitogen-activated protein (MAP) kinase pathway, and inhibiting each gene lowered ataxin-1 in cells and flies.
Inhibiting Enzymes
The researchers also observed that the enzymes MSK1 and MSK2 intervene in the pathway and promote ataxin-1 accumulation. Inhibiting MSK1 produced clinical improvement in SCA1 mouse models, and inhibiting MSK1 and MSK2 together produced still more improvement. A small molecule that inhibited MSK1 therefore could help patients with SCA1, said Dr. Zoghbi.
Inhibiting enzymes such as MSK1 and MSK2 for years at a time could raise safety concerns, however. The investigators thus decided to look for other modulators of ataxin-1, on the theory that targeting modulators that function in different pathways could reduce the amount of inhibition required and decrease the risk of adverse events.
Further screening revealed that PKA1 appeared to modulate ataxin-1 by a mechanism similar to that of MSK1. An animal study indicated that inhibiting MSK1 and inhibiting PKA1 produced equivalent reductions on ataxin-1, but that inhibiting both in tandem yielded a greater reduction. The investigators then found that the PAK1 enzyme promoted ataxin-1 accumulation through a pathway different from that of MSK1 and PKA1. Inhibiting PAK1 reduced ataxin-1 levels, and inhibiting PAK1 and MSK1 simultaneously had a still greater effect.
Targeting Tauopathies
Their research into kinases and enzymes prompted Dr. Zoghbi and colleagues to consider whole genome screening as a method of targeting proteins that cause neurodegenerative diseases other than SCA1. Overexpression of tau, for example, causes neurodegeneration, regardless of whether the overexpression results from a mutation in tau-encoding genes. “Tau is a true culprit in dementias, and we thought that if we could find something to lower it, we could help patients with these disorders,” said Dr. Zoghbi.
Another genetic screen suggested that the enzyme Nuak1 stabilizes tau by phosphorylating it at Ser356. The investigators observed that inhibiting Nuak1 reduced tau levels and suppressed neurodegeneration in human cells and in fruit flies. Tau accumulation decreases fruit flies’ climbing ability, and inhibiting Nuak1 improved this ability in flies with tau accumulation.
In a subsequent mouse study, Dr. Zoghbi and colleagues found that inhibiting Nuak1 significantly reduced levels of phosphorylated tau and provided smaller reductions in total tau and endogenous tau. They also observed that mice with tauopathy took longer than wild-type mice to complete a water maze task. Inhibiting Nuak1 in mice with tauopathy improved their performance on this task. Nuak1 inhibition also restored synaptic plasticity in these mice to a level similar to that of wild-type mice. Finally, Nuak1 inhibition reduced tau tangle pathology and increased survival. Dr. Zoghbi and colleagues are now searching for small-molecule Nuak1 inhibitors that could provide protection against tauopathy.
In Search of More Targets
The investigators next looked for genes that influence tau. Successive levels of genetic screening identified 59 genes that “robustly lower tau levels,” said Dr. Zoghbi. She and her colleagues prioritized 12 of the genes for investigation.
They used adenoassociated viral vectors to deliver therapies that can knock out mouse genes for as long as a year. With this technique, the investigators confirmed that all of the initial 12 genes decreased tau levels. In principle, this strategy could enable researchers to scan the whole genome for genes that modulate tau, said Dr. Zoghbi.
—Erik Greb
Suggested Reading
Lasagna-Reeves CA, de Haro M, Hao S, et al. Reduction of Nuak1 decreases tau and reverses phenotypes in a tauopathy mouse model. Neuron. 2016; 92(2):407-418.
Park J, Al-Ramahi I, Tan Q, et al. RAS-MAPK-MSK1 pathway modulates ataxin 1 protein levels and toxicity in SCA1. Nature. 2013;498(7454):325-331.
Rousseaux MW, de Haro M, Lasagna-Reeves CA, et al. TRIM28 regulates the nuclear accumulation and toxicity of both alpha-synuclein and tau. Elife. 2016 Oct 25;5. pii: e19809
Psychiatric pharmacogenomics not ‘ready for prime time’
NEW YORK – Pharmacogenomics testing for guiding drug choices in psychiatric disease is “not completely ready for prime time,” based on a critical review of published guidelines and expert opinions on the use of those tests, according to Erika L. Nurmi, MD, PhD.
It is important to understand the limitations of such tests because many patients or family members are asking clinicians to be guided by the results of tests they have ordered on their own, said Dr. Nurmi, a researcher and clinician at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
Published guidelines and expert opinions based on objective data support these conclusions, she said. Dr. Nurmi suggested that .
“Basically, what it says is if you do not have the testing in hand, don’t order it. If you have the testing in hand when a poor metabolizer of CYP2D6 or CYP2C19 has been identified, switch to a med that is not metabolized by those enzymes. That’s it,” Dr. Nurmi reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
The guidelines from the Clinical Pharmacogenetics Implementation Consortium (CPIC) were only modestly more detailed. Only a moderate level of evidence supported most recommendations, she said, and these were labeled optional. The exception regarded treating ultrafast metabolizers of CYP2D6 who are taking paroxetine: In these, the use of a drug metabolized by a different enzyme was strongly recommended.
Similar recommendations in the CPIC guidelines were made for fluoxetine, fluvoxamine, and sertraline. In patients on citalopram or escitalopram, ultrafast metabolizers of CYP2C19 are considered candidates for a non-CYP2C19 drug. If they are poor metabolizers, the CPIC guidelines recommended a non-CYP2C19 drug or reducing the starting dose by 50%.
However, in all of these cases, pharmacogenomics testing is best reserved for patients who have had an inadequate response to therapy or, in the case of poor metabolizers, have had unacceptable adverse events.
Of the limitations Dr. Nurmi outlined for pharmacogenomics testing, one of the most important is that these tests typically focus on a single genetic variant. According to Dr. Nurmi, the problem with a single variant is that “our bodies are more complex.” She said she believes that genetic information for drug selection will not be useful until testing is able to synthesize information from multiple genetic variants and place this in context with confounders such as age and exposure to other substances, such as hormones, caffeine, or grapefruit juice.
This complexity is likely to be mastered eventually, Dr. Nurmi said, but patients now have unrealistic expectations. For their part, clinicians need to develop an understanding of the limitations of these tests in order to provide informed counsel. As pharmacogenomics testing is being marketed directly to consumers with inflated claims about its value, clinicians often must defend their decision to use or not use this information.
“Commercially available products combine variants of widely discrepant validity using proprietary, undisclosed algorithms into sweeping treatment recommendations,” said Dr. Nurmi, who noted that she has found some of her own data misappropriated to make claims. Often, the companies that develop the tests have conducted the validation studies without any replication by independent investigators. She noted that many studies have been declared positive on the basis of secondary outcomes after the primary outcome was negative.
“There are very few positive prospective, randomized, double-blind trials,” Dr. Nurmi said. Even when such trials have been conducted, they typically are not designed to show a clinically meaningful outcome.
By attempting to look at a single or a limited number of variants in which to guide choice of medication in psychiatric disease, pharmacogenomics testing is being “vastly oversimplified,” Dr. Nurmi said. Although she said she believes this field is enormously promising and that medical records for each patient eventually will contain the genome sequence, she emphasized that, at this time, pharmacogenomics testing has a very limited role to play for the management of psychiatric diseases.
Dr. Nurmi reported she had no financial relationships relevant to this topic.
NEW YORK – Pharmacogenomics testing for guiding drug choices in psychiatric disease is “not completely ready for prime time,” based on a critical review of published guidelines and expert opinions on the use of those tests, according to Erika L. Nurmi, MD, PhD.
It is important to understand the limitations of such tests because many patients or family members are asking clinicians to be guided by the results of tests they have ordered on their own, said Dr. Nurmi, a researcher and clinician at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
Published guidelines and expert opinions based on objective data support these conclusions, she said. Dr. Nurmi suggested that .
“Basically, what it says is if you do not have the testing in hand, don’t order it. If you have the testing in hand when a poor metabolizer of CYP2D6 or CYP2C19 has been identified, switch to a med that is not metabolized by those enzymes. That’s it,” Dr. Nurmi reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
The guidelines from the Clinical Pharmacogenetics Implementation Consortium (CPIC) were only modestly more detailed. Only a moderate level of evidence supported most recommendations, she said, and these were labeled optional. The exception regarded treating ultrafast metabolizers of CYP2D6 who are taking paroxetine: In these, the use of a drug metabolized by a different enzyme was strongly recommended.
Similar recommendations in the CPIC guidelines were made for fluoxetine, fluvoxamine, and sertraline. In patients on citalopram or escitalopram, ultrafast metabolizers of CYP2C19 are considered candidates for a non-CYP2C19 drug. If they are poor metabolizers, the CPIC guidelines recommended a non-CYP2C19 drug or reducing the starting dose by 50%.
However, in all of these cases, pharmacogenomics testing is best reserved for patients who have had an inadequate response to therapy or, in the case of poor metabolizers, have had unacceptable adverse events.
Of the limitations Dr. Nurmi outlined for pharmacogenomics testing, one of the most important is that these tests typically focus on a single genetic variant. According to Dr. Nurmi, the problem with a single variant is that “our bodies are more complex.” She said she believes that genetic information for drug selection will not be useful until testing is able to synthesize information from multiple genetic variants and place this in context with confounders such as age and exposure to other substances, such as hormones, caffeine, or grapefruit juice.
This complexity is likely to be mastered eventually, Dr. Nurmi said, but patients now have unrealistic expectations. For their part, clinicians need to develop an understanding of the limitations of these tests in order to provide informed counsel. As pharmacogenomics testing is being marketed directly to consumers with inflated claims about its value, clinicians often must defend their decision to use or not use this information.
“Commercially available products combine variants of widely discrepant validity using proprietary, undisclosed algorithms into sweeping treatment recommendations,” said Dr. Nurmi, who noted that she has found some of her own data misappropriated to make claims. Often, the companies that develop the tests have conducted the validation studies without any replication by independent investigators. She noted that many studies have been declared positive on the basis of secondary outcomes after the primary outcome was negative.
“There are very few positive prospective, randomized, double-blind trials,” Dr. Nurmi said. Even when such trials have been conducted, they typically are not designed to show a clinically meaningful outcome.
By attempting to look at a single or a limited number of variants in which to guide choice of medication in psychiatric disease, pharmacogenomics testing is being “vastly oversimplified,” Dr. Nurmi said. Although she said she believes this field is enormously promising and that medical records for each patient eventually will contain the genome sequence, she emphasized that, at this time, pharmacogenomics testing has a very limited role to play for the management of psychiatric diseases.
Dr. Nurmi reported she had no financial relationships relevant to this topic.
NEW YORK – Pharmacogenomics testing for guiding drug choices in psychiatric disease is “not completely ready for prime time,” based on a critical review of published guidelines and expert opinions on the use of those tests, according to Erika L. Nurmi, MD, PhD.
It is important to understand the limitations of such tests because many patients or family members are asking clinicians to be guided by the results of tests they have ordered on their own, said Dr. Nurmi, a researcher and clinician at the UCLA Semel Institute for Neuroscience and Human Behavior, Los Angeles.
Published guidelines and expert opinions based on objective data support these conclusions, she said. Dr. Nurmi suggested that .
“Basically, what it says is if you do not have the testing in hand, don’t order it. If you have the testing in hand when a poor metabolizer of CYP2D6 or CYP2C19 has been identified, switch to a med that is not metabolized by those enzymes. That’s it,” Dr. Nurmi reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
The guidelines from the Clinical Pharmacogenetics Implementation Consortium (CPIC) were only modestly more detailed. Only a moderate level of evidence supported most recommendations, she said, and these were labeled optional. The exception regarded treating ultrafast metabolizers of CYP2D6 who are taking paroxetine: In these, the use of a drug metabolized by a different enzyme was strongly recommended.
Similar recommendations in the CPIC guidelines were made for fluoxetine, fluvoxamine, and sertraline. In patients on citalopram or escitalopram, ultrafast metabolizers of CYP2C19 are considered candidates for a non-CYP2C19 drug. If they are poor metabolizers, the CPIC guidelines recommended a non-CYP2C19 drug or reducing the starting dose by 50%.
However, in all of these cases, pharmacogenomics testing is best reserved for patients who have had an inadequate response to therapy or, in the case of poor metabolizers, have had unacceptable adverse events.
Of the limitations Dr. Nurmi outlined for pharmacogenomics testing, one of the most important is that these tests typically focus on a single genetic variant. According to Dr. Nurmi, the problem with a single variant is that “our bodies are more complex.” She said she believes that genetic information for drug selection will not be useful until testing is able to synthesize information from multiple genetic variants and place this in context with confounders such as age and exposure to other substances, such as hormones, caffeine, or grapefruit juice.
This complexity is likely to be mastered eventually, Dr. Nurmi said, but patients now have unrealistic expectations. For their part, clinicians need to develop an understanding of the limitations of these tests in order to provide informed counsel. As pharmacogenomics testing is being marketed directly to consumers with inflated claims about its value, clinicians often must defend their decision to use or not use this information.
“Commercially available products combine variants of widely discrepant validity using proprietary, undisclosed algorithms into sweeping treatment recommendations,” said Dr. Nurmi, who noted that she has found some of her own data misappropriated to make claims. Often, the companies that develop the tests have conducted the validation studies without any replication by independent investigators. She noted that many studies have been declared positive on the basis of secondary outcomes after the primary outcome was negative.
“There are very few positive prospective, randomized, double-blind trials,” Dr. Nurmi said. Even when such trials have been conducted, they typically are not designed to show a clinically meaningful outcome.
By attempting to look at a single or a limited number of variants in which to guide choice of medication in psychiatric disease, pharmacogenomics testing is being “vastly oversimplified,” Dr. Nurmi said. Although she said she believes this field is enormously promising and that medical records for each patient eventually will contain the genome sequence, she emphasized that, at this time, pharmacogenomics testing has a very limited role to play for the management of psychiatric diseases.
Dr. Nurmi reported she had no financial relationships relevant to this topic.
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE
Abrupt behavior changes in autism? ID medical triggers first
NEW YORK – When treating children with autism spectrum disorder who develop an abrupt increase in symptoms, it is best to identify and treat the precipitating event or events – rather than intensify ASD drug therapy, an expert said.
“These acute behavior changes are almost always triggered by something,” Jeremy Veenstra-VanderWeele, MD, reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry. Triggers are not always identifiable, but Dr. Veenstra-VanderWeele said solutions may prove simple when they are.

In ASD patients with an acute change in behavior, caregivers typically think first of environmental triggers, including adverse interactions with peers or siblings. But Dr. Veenstra-VanderWeele emphasized that medical problems should be considered first. This makes sense because of the importance of quickly resolving health problems. However, pain and discomfort, particularly in those with difficulty verbalizing these complaints, can be overlooked.
Moreover, even highly verbal ASD patients may not volunteer physical complaints without prompting, Dr. Veenstra-VanderWeele said. Among the health issues in children, constipation and other gastrointestinal issues are “incredibly common” in ASD patients. Dr. Veenstra-VanderWeele looks for clues, such as body posturing suggesting abdominal pain or flatulence, when a history is ambiguous.
“I will order an abdominal flat plate when I hear enough symptoms to make me wonder when the family is not sure,” Dr. Veenstra-VanderWeele reported. “Almost always it comes back with evidence of constipation. We treat it, and they are less irritable like all of us would be.”
All common conditions in a pediatric population, including ear infections, dental caries, and food allergies, should be considered, according to Dr. Veenstra-VanderWeele, who recommended a practice pathway for evaluating triggers in children with ASD (Pediatrics. 2016 Feb;137 Suppl 2:S136-48). A coauthor on this pathway, Dr. Veenstra-VanderWeele emphasized the importance of pursuing a systematic approach to medical issues before considering other triggers, such as psychosocial stressors.
In adolescents, headache caused by migraine and late-onset epilepsy, often in the form of complex partial seizures, should be added to the list of potential triggers for irritation or aggression, Dr. Veenstra-VanderWeele said. Epilepsy often precedes the diagnosis of ASD in young children, and Dr. Veenstra-VanderWeele noted that a second peak incidence sometimes occurs in late adolescence.
After ruling out medical problems, helping patients recognize and verbalize stressors can serve as both diagnosis and treatment. In ASD patients with limited verbal skills who are suffering from stress, “aggression is one form of communication,” Dr. Veenstra-VanderWeele said.
However, Dr. Veenstra-VanderWeele cautioned that, even if a trigger is successfully addressed, inadvertently reinforced aggression might persist.
“Aggression can be rewarded sometimes by removing the patient from the classroom, sometimes by giving in, and then that becomes a maladaptive reinforcement pattern that needs to be broken,” Dr. Veenstra-VanderWeele said. “Even if you are treating their irritability and agitation with, say, risperidone, you still need to break the maladaptive reinforcement pattern or they will keep engaging in what has become instrumental aggression.”
Dr. Veenstra-VanderWeele reported financial relationships with Hoffmann-La Roche, Novartis, Seaside Therapeutics, and SynapDx.
NEW YORK – When treating children with autism spectrum disorder who develop an abrupt increase in symptoms, it is best to identify and treat the precipitating event or events – rather than intensify ASD drug therapy, an expert said.
“These acute behavior changes are almost always triggered by something,” Jeremy Veenstra-VanderWeele, MD, reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry. Triggers are not always identifiable, but Dr. Veenstra-VanderWeele said solutions may prove simple when they are.
In ASD patients with an acute change in behavior, caregivers typically think first of environmental triggers, including adverse interactions with peers or siblings. But Dr. Veenstra-VanderWeele emphasized that medical problems should be considered first. This makes sense because of the importance of quickly resolving health problems. However, pain and discomfort, particularly in those with difficulty verbalizing these complaints, can be overlooked.
Moreover, even highly verbal ASD patients may not volunteer physical complaints without prompting, Dr. Veenstra-VanderWeele said. Among the health issues in children, constipation and other gastrointestinal issues are “incredibly common” in ASD patients. Dr. Veenstra-VanderWeele looks for clues, such as body posturing suggesting abdominal pain or flatulence, when a history is ambiguous.
“I will order an abdominal flat plate when I hear enough symptoms to make me wonder when the family is not sure,” Dr. Veenstra-VanderWeele reported. “Almost always it comes back with evidence of constipation. We treat it, and they are less irritable like all of us would be.”
All common conditions in a pediatric population, including ear infections, dental caries, and food allergies, should be considered, according to Dr. Veenstra-VanderWeele, who recommended a practice pathway for evaluating triggers in children with ASD (Pediatrics. 2016 Feb;137 Suppl 2:S136-48). A coauthor on this pathway, Dr. Veenstra-VanderWeele emphasized the importance of pursuing a systematic approach to medical issues before considering other triggers, such as psychosocial stressors.
In adolescents, headache caused by migraine and late-onset epilepsy, often in the form of complex partial seizures, should be added to the list of potential triggers for irritation or aggression, Dr. Veenstra-VanderWeele said. Epilepsy often precedes the diagnosis of ASD in young children, and Dr. Veenstra-VanderWeele noted that a second peak incidence sometimes occurs in late adolescence.
After ruling out medical problems, helping patients recognize and verbalize stressors can serve as both diagnosis and treatment. In ASD patients with limited verbal skills who are suffering from stress, “aggression is one form of communication,” Dr. Veenstra-VanderWeele said.
However, Dr. Veenstra-VanderWeele cautioned that, even if a trigger is successfully addressed, inadvertently reinforced aggression might persist.
“Aggression can be rewarded sometimes by removing the patient from the classroom, sometimes by giving in, and then that becomes a maladaptive reinforcement pattern that needs to be broken,” Dr. Veenstra-VanderWeele said. “Even if you are treating their irritability and agitation with, say, risperidone, you still need to break the maladaptive reinforcement pattern or they will keep engaging in what has become instrumental aggression.”
Dr. Veenstra-VanderWeele reported financial relationships with Hoffmann-La Roche, Novartis, Seaside Therapeutics, and SynapDx.
NEW YORK – When treating children with autism spectrum disorder who develop an abrupt increase in symptoms, it is best to identify and treat the precipitating event or events – rather than intensify ASD drug therapy, an expert said.
“These acute behavior changes are almost always triggered by something,” Jeremy Veenstra-VanderWeele, MD, reported at a pediatric psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry. Triggers are not always identifiable, but Dr. Veenstra-VanderWeele said solutions may prove simple when they are.
In ASD patients with an acute change in behavior, caregivers typically think first of environmental triggers, including adverse interactions with peers or siblings. But Dr. Veenstra-VanderWeele emphasized that medical problems should be considered first. This makes sense because of the importance of quickly resolving health problems. However, pain and discomfort, particularly in those with difficulty verbalizing these complaints, can be overlooked.
Moreover, even highly verbal ASD patients may not volunteer physical complaints without prompting, Dr. Veenstra-VanderWeele said. Among the health issues in children, constipation and other gastrointestinal issues are “incredibly common” in ASD patients. Dr. Veenstra-VanderWeele looks for clues, such as body posturing suggesting abdominal pain or flatulence, when a history is ambiguous.
“I will order an abdominal flat plate when I hear enough symptoms to make me wonder when the family is not sure,” Dr. Veenstra-VanderWeele reported. “Almost always it comes back with evidence of constipation. We treat it, and they are less irritable like all of us would be.”
All common conditions in a pediatric population, including ear infections, dental caries, and food allergies, should be considered, according to Dr. Veenstra-VanderWeele, who recommended a practice pathway for evaluating triggers in children with ASD (Pediatrics. 2016 Feb;137 Suppl 2:S136-48). A coauthor on this pathway, Dr. Veenstra-VanderWeele emphasized the importance of pursuing a systematic approach to medical issues before considering other triggers, such as psychosocial stressors.
In adolescents, headache caused by migraine and late-onset epilepsy, often in the form of complex partial seizures, should be added to the list of potential triggers for irritation or aggression, Dr. Veenstra-VanderWeele said. Epilepsy often precedes the diagnosis of ASD in young children, and Dr. Veenstra-VanderWeele noted that a second peak incidence sometimes occurs in late adolescence.
After ruling out medical problems, helping patients recognize and verbalize stressors can serve as both diagnosis and treatment. In ASD patients with limited verbal skills who are suffering from stress, “aggression is one form of communication,” Dr. Veenstra-VanderWeele said.
However, Dr. Veenstra-VanderWeele cautioned that, even if a trigger is successfully addressed, inadvertently reinforced aggression might persist.
“Aggression can be rewarded sometimes by removing the patient from the classroom, sometimes by giving in, and then that becomes a maladaptive reinforcement pattern that needs to be broken,” Dr. Veenstra-VanderWeele said. “Even if you are treating their irritability and agitation with, say, risperidone, you still need to break the maladaptive reinforcement pattern or they will keep engaging in what has become instrumental aggression.”
Dr. Veenstra-VanderWeele reported financial relationships with Hoffmann-La Roche, Novartis, Seaside Therapeutics, and SynapDx.
EXPERT ANALYSIS FROM the PSYCHOPHARMACOLOGY UPDATE INSTITUTE
Boy, 9, With Eye Pain, Blurred Vision, and Tearing
IN THIS ARTICLE
- Diagnosis
- Management
- Outcome for the case patient
An otherwise healthy 9-year-old boy is brought to the emergency department (ED) by his father for evaluation of severe pain, blurry vision, and four hours of tearing in his right eye. The patient was in school when he experienced sudden-onset irritation and scratching pain that caused him to rub his eye. He says it “feels like there is something in my eye,” but he denies any known substance or foreign body. He has no medical or surgical history, does not wear contact lenses or eyeglasses, and denies loss of vision. There is no history of recent illness or travel.
On evaluation, the patient is in no acute distress but is holding his right eye closed due to foreign-body sensation and increased photosensitivity and tearing. There is no obvious erythema or swelling in the upper or lower eyelids bilaterally. A visual acuity test with a Snellen eye chart shows 20/20 vision in the left eye and 20/50 in the right, secondary to pain, photophobia, and excessive tearing. The patient’s right sclera is significantly injected. Intraocular pressure, measured with a tonometer, is 12 to 14 mm Hg. A fluorescein stain of the eye yields no significant findings. The globe is intact.
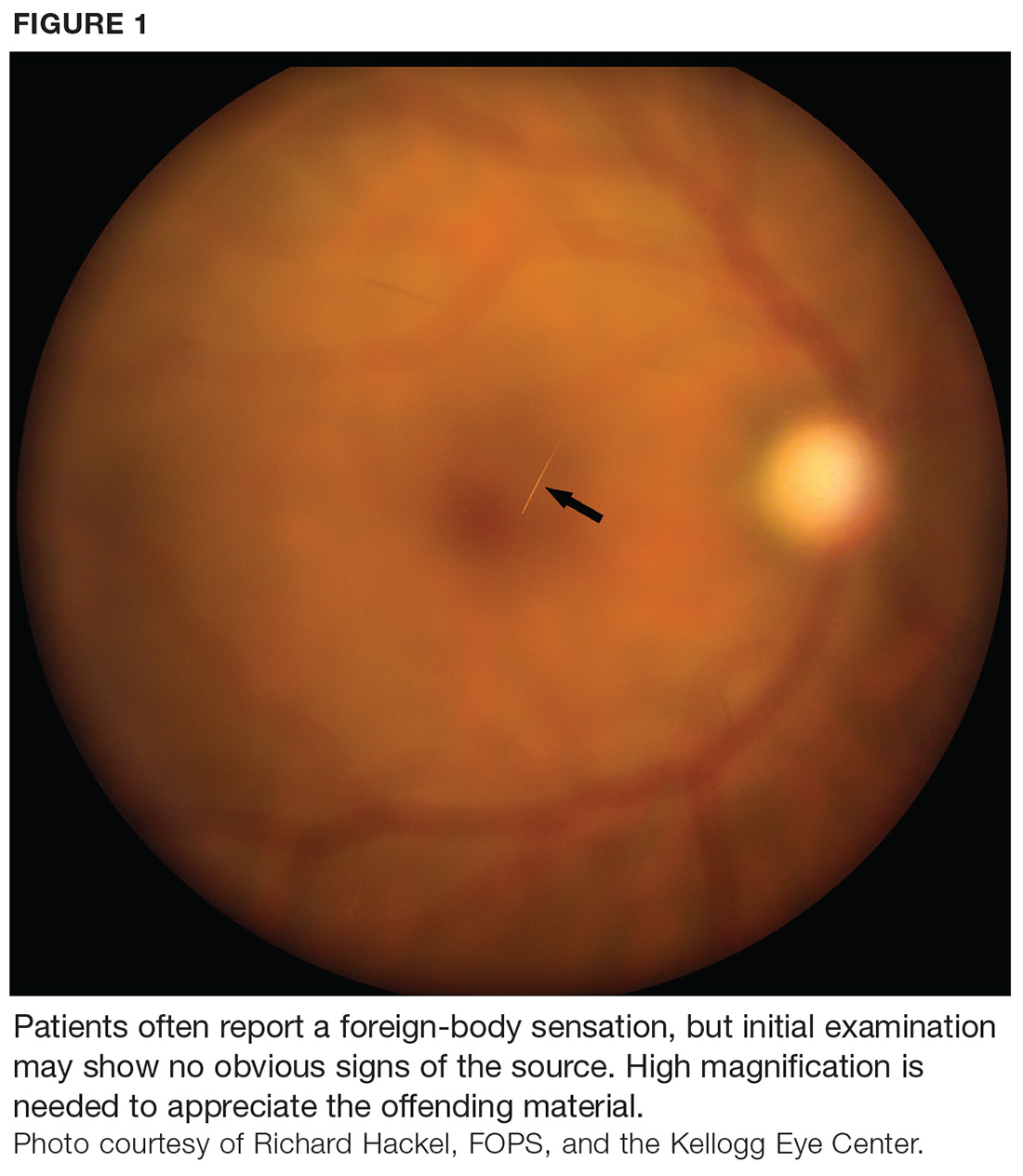
At first glance, a slit-lamp exam shows no obvious signs of a foreign body. But much higher magnification reveals substantial conjunctival injection and numerous intracorneal linear foreign bodies in the right eye (see Figure 1 for example [not the case patient]). The anterior chamber shows no inflammatory reaction, and findings in the posterior segment are unremarkable.
The initial diagnosis is simple conjunctivitis—but closer examination reveals multiple fine, barbed hairs embedded in the patient’s right cornea. Upon further questioning, the patient reports that prior to symptom onset, he had been holding the classroom pet, a Chilean Rose tarantula, in the palm of his hands.
DISCUSSION
Foreign body injury is a common cause of ocular pain and corneal damage, which can lead to challenging complications. Ophthalmic emergencies account for 2% of ED visits in the US annually and are a major cause of visual impairment.1 But when a painful eye is the chief complaint, contact with insects, plants, or spiders is rarely included in the differential. Tarantulas are popular classroom and household pets, however, and ocular injury should be suspected in anyone who has been holding a tarantula prior to onset of pain.
Ophthalmia nodosa
Tarantulas are one of the most common arachnids known to cause ophthalmia nodosa—a granulomatous reaction of the conjunctiva or cornea to an implanted plant, insect, or spider hair that typically manifests with photophobia, irritation, and chemosis.2,3 Tarantulas, when scared or defending their eggs, shoot urticating setae at the threat—a defensive mechanism largely unknown to parents, tarantula owners, and medical professionals.
Urticating setae are found in roughly 90% of tarantula species throughout tropical and subtropical regions.4 Depending on the species, setae can be located on the distal prolateral surface of the palpal femur or the dorsum of the abdomen. They can be released when the tarantula scratches its legs against the abdominal urticating setae patch or scratches the palps against the chelicerae (appendages in front of the mouth), or when direct exterior contact is made with the abdominal setae.4
There are six types of urticating hairs. Each is attached to the spider’s cuticle by either a stalk (which represents the break-off region) or a socket.4 Tarantula hairs range in size from 0.1 mm to 0.3 mm and have a sharp, pointed head and numerous barbs, which help embed them in the target.5 They are long and thin, to facilitate deep tissue penetration, and can enter the eyes, lungs, or other body parts (see Figure 2).
Ocular injury from tarantula hairs commonly involves conjunctival injection, foreign body sensation, periorbital facial rash, photophobia, and tearing.3 When a tarantula’s cloud of barbed hairs is flicked into the eye and pierces the cornea, it can cause infection, irritation, scarring on the cornea, or vision loss. Eye movement or rubbing can cause the hairs—and their toxins—to migrate over time, traveling like an arrow (the tip and barbs resist backward movement) to the anterior chamber, lens, vitreous, and retina.6,7 This can cause corneal scars, cataracts, vitritis, or macular edema, and creates the possibility for acute or chronic conjunctivitis.7
Diagnosis and management
Ophthalmic emergencies can affect the visual system and, if left untreated, can lead to permanent vision loss. Affected patients require immediate medical attention and should be referred to an ophthalmologist for follow-up care.
Diagnosis. A thorough history and physical exam are of utmost importance; tiny setae can be easily overlooked if the examiner is not diligent, and the similar symptomatology can lead to misdiagnosis as simple conjunctivitis.3 A visual acuity test and slit-lamp exam are useful for confirmation.
Treatment. Once the diagnosis is confirmed, treatment should consist of mild topical antibiotics and steroids to effectively control infection and inflammation. While topical steroids may be appropriate, local adverse events associated with their use (eg, glaucoma, cataracts) can be problematic. Gentle eye irrigation has been noted by some researchers as contraindicated, while others find it useful to flush out some of the hairs.5,8,9
Most of the visible protruding tarantula hairs can and should be removed under microscopy during slit-lamp exam. Hairs that are buried in the cornea, however, are nearly impossible to remove and pose a threat of further complications, as described. Conservative management with careful observation is therefore recommended. If the patient develops a granuloma, excision—along with a course of systemic steroids and setae removal via vitrectomy—may be needed.9
The good news is that, in many cases, deeper hairs are absorbed without complication, making their removal unnecessary.5 Factors that encourage leaving the setae untouched include a large number of hairs, deep corneal penetration, lack of patient tolerance for the procedure, and risk for perforation.3
More invasive treatments (eg, laser photocoagulation, intraocular surgery) to remove offending hairs are possible, but literature on the outcome of these interventions is limited. One report to date used argon laser photocoagulation to treat endophthalmitis from vitreous hairs.10 The laser can fragment the hairs so that they lose their barbed characteristic and cannot penetrate deeper.6
Follow-up. Close follow-up is advised, and patients should be educated on the importance of medication compliance and return visits for reevaluation. Given the potential dangers of handling these spiders, tarantula owners should be advised to use protective gloving and goggles.2,5,8,9
OUTCOME FOR THE CASE PATIENT
The case patient was sent to an ophthalmologist on day 1. Proparacaine was placed in his right eye, and all of the superficial tarantula hairs were removed using 25- and 30-gauge needles with jeweler forceps under slit-lamp microscopy. Most of the hairs were removed from the superior cornea; fewer were found in the paracentral and inferior regions of the cornea. Approximately five hairs in the paracentral area of the cornea were embedded in the midstromal depth and could not be removed. One drop of ciprofloxacin was administered.
The patient was sent home with an eye shield and instructions to use tobramycin/dexamethasone eye drops (qid in his right eye) and avoid rubbing the eye. (The eye shield, though not technically necessary, was deemed beneficial to help the patient avoid touching the eye.) He was scheduled to return to the clinic one week later.
On follow-up, a careful exam performed under microscopy showed that the five tarantula hairs were still embedded, and an additional six hairs were found in the deep stroma. Superficial punctate keratitis—an eye disorder caused by epithelial cell death on the surface of the cornea—was noted, but no anterior chamber cells were seen. The patient was instructed to continue using the eye drops as prescribed until finished, then start using loteprednol (tid) and artificial lubricating tears (every 2 h).
He returned to the clinic every two weeks for a total of 10 visits. At the end of the treatment course, the remaining tarantula hairs were unable to be removed. The patient used tapering doses of topical eye steroids and antibiotic drops secondary to flare-up.
CONCLUSION
Determining the etiology of ophthalmic emergencies is essential to timely and appropriate management. In this case, a recognized but often overlooked cause, tarantula hairs, made the diagnosis more complicated than simple conjunctivitis. When ocular injury is suspected, the provider must obtain an accurate and detailed history along with a thorough physical exam. Since patients must comply with medication regimens to prevent acute and chronic infection, a clear treatment and follow-up plan should be established. With these in place, ophthalmia nodosa caused by urticating setae can be effectively managed.
1. Fitzpatrick J, Hickman R, Alfes CM. A Guide to Mastery in Clinical Nursing: The Comprehensive Reference. New York, NY: Springer; 2018:114.
2. Lambert SR, Lyons CJ. Taylor and Hoyt’s Pediatric Ophthalmology and Strabismus. 5th ed. New York, NY: Elsevier; 2017:138.
3. Stagg BC, Ambati BK. Tarantula hairs as corneal foreign bodies. Case Rep Ophthalmol. 2011;2(3):323-326.
4. Bertani R, Guadanucci JPL. Morphology, evolution, and usage of urticating setae by tarantulas (Araneae: Theraphosidae). Zoologia (Curitiba). 2013;30(4):403-418.
5. McAnena L, Murphy C, O’Connor J. Tarantula keratitis: a case report. Ir J Med Sci. 2013;182(3):349-350.
6. Yang Y, Christakis T, Mireskandari K. Acute conjunctivitis and corneal foreign bodies secondary to tarantula hairs. CMAJ. 2016;183(3):212-214.
7. Jain N, Soong HK, Gardner TW. Ophthalmia nodosa. EyeNet Magazine. November 2013. www.aao.org/eyenet/article/blink-mystery-image-17. Accessed January 24, 2018.
8. Choi JTL, Rauf A. Ophthalmia nodosa secondary to tarantula hairs. Eye (Lond). 2003;17(3):433-434.
9. Comez AT, Tufan HA, Gencer B. Ophthalmia nodosa as an occupational disease: is it unusual or is it casual? Ocul Immunol Inflamm. 2013;21(2):144-147.
10. Marti-Huguet T, Pujol O, Cabiro I, et al. Endophthalmos caused by intravitreal caterpillar hairs. Treatment by direct photocoagulation with argon laser [article in French]. J Fr Ophthalmol. 1987;10(10):559-564.
IN THIS ARTICLE
- Diagnosis
- Management
- Outcome for the case patient
An otherwise healthy 9-year-old boy is brought to the emergency department (ED) by his father for evaluation of severe pain, blurry vision, and four hours of tearing in his right eye. The patient was in school when he experienced sudden-onset irritation and scratching pain that caused him to rub his eye. He says it “feels like there is something in my eye,” but he denies any known substance or foreign body. He has no medical or surgical history, does not wear contact lenses or eyeglasses, and denies loss of vision. There is no history of recent illness or travel.
On evaluation, the patient is in no acute distress but is holding his right eye closed due to foreign-body sensation and increased photosensitivity and tearing. There is no obvious erythema or swelling in the upper or lower eyelids bilaterally. A visual acuity test with a Snellen eye chart shows 20/20 vision in the left eye and 20/50 in the right, secondary to pain, photophobia, and excessive tearing. The patient’s right sclera is significantly injected. Intraocular pressure, measured with a tonometer, is 12 to 14 mm Hg. A fluorescein stain of the eye yields no significant findings. The globe is intact.
At first glance, a slit-lamp exam shows no obvious signs of a foreign body. But much higher magnification reveals substantial conjunctival injection and numerous intracorneal linear foreign bodies in the right eye (see Figure 1 for example [not the case patient]). The anterior chamber shows no inflammatory reaction, and findings in the posterior segment are unremarkable.
The initial diagnosis is simple conjunctivitis—but closer examination reveals multiple fine, barbed hairs embedded in the patient’s right cornea. Upon further questioning, the patient reports that prior to symptom onset, he had been holding the classroom pet, a Chilean Rose tarantula, in the palm of his hands.
DISCUSSION
Foreign body injury is a common cause of ocular pain and corneal damage, which can lead to challenging complications. Ophthalmic emergencies account for 2% of ED visits in the US annually and are a major cause of visual impairment.1 But when a painful eye is the chief complaint, contact with insects, plants, or spiders is rarely included in the differential. Tarantulas are popular classroom and household pets, however, and ocular injury should be suspected in anyone who has been holding a tarantula prior to onset of pain.
Ophthalmia nodosa
Tarantulas are one of the most common arachnids known to cause ophthalmia nodosa—a granulomatous reaction of the conjunctiva or cornea to an implanted plant, insect, or spider hair that typically manifests with photophobia, irritation, and chemosis.2,3 Tarantulas, when scared or defending their eggs, shoot urticating setae at the threat—a defensive mechanism largely unknown to parents, tarantula owners, and medical professionals.
Urticating setae are found in roughly 90% of tarantula species throughout tropical and subtropical regions.4 Depending on the species, setae can be located on the distal prolateral surface of the palpal femur or the dorsum of the abdomen. They can be released when the tarantula scratches its legs against the abdominal urticating setae patch or scratches the palps against the chelicerae (appendages in front of the mouth), or when direct exterior contact is made with the abdominal setae.4
There are six types of urticating hairs. Each is attached to the spider’s cuticle by either a stalk (which represents the break-off region) or a socket.4 Tarantula hairs range in size from 0.1 mm to 0.3 mm and have a sharp, pointed head and numerous barbs, which help embed them in the target.5 They are long and thin, to facilitate deep tissue penetration, and can enter the eyes, lungs, or other body parts (see Figure 2).
Ocular injury from tarantula hairs commonly involves conjunctival injection, foreign body sensation, periorbital facial rash, photophobia, and tearing.3 When a tarantula’s cloud of barbed hairs is flicked into the eye and pierces the cornea, it can cause infection, irritation, scarring on the cornea, or vision loss. Eye movement or rubbing can cause the hairs—and their toxins—to migrate over time, traveling like an arrow (the tip and barbs resist backward movement) to the anterior chamber, lens, vitreous, and retina.6,7 This can cause corneal scars, cataracts, vitritis, or macular edema, and creates the possibility for acute or chronic conjunctivitis.7
Diagnosis and management
Ophthalmic emergencies can affect the visual system and, if left untreated, can lead to permanent vision loss. Affected patients require immediate medical attention and should be referred to an ophthalmologist for follow-up care.
Diagnosis. A thorough history and physical exam are of utmost importance; tiny setae can be easily overlooked if the examiner is not diligent, and the similar symptomatology can lead to misdiagnosis as simple conjunctivitis.3 A visual acuity test and slit-lamp exam are useful for confirmation.
Treatment. Once the diagnosis is confirmed, treatment should consist of mild topical antibiotics and steroids to effectively control infection and inflammation. While topical steroids may be appropriate, local adverse events associated with their use (eg, glaucoma, cataracts) can be problematic. Gentle eye irrigation has been noted by some researchers as contraindicated, while others find it useful to flush out some of the hairs.5,8,9
Most of the visible protruding tarantula hairs can and should be removed under microscopy during slit-lamp exam. Hairs that are buried in the cornea, however, are nearly impossible to remove and pose a threat of further complications, as described. Conservative management with careful observation is therefore recommended. If the patient develops a granuloma, excision—along with a course of systemic steroids and setae removal via vitrectomy—may be needed.9
The good news is that, in many cases, deeper hairs are absorbed without complication, making their removal unnecessary.5 Factors that encourage leaving the setae untouched include a large number of hairs, deep corneal penetration, lack of patient tolerance for the procedure, and risk for perforation.3
More invasive treatments (eg, laser photocoagulation, intraocular surgery) to remove offending hairs are possible, but literature on the outcome of these interventions is limited. One report to date used argon laser photocoagulation to treat endophthalmitis from vitreous hairs.10 The laser can fragment the hairs so that they lose their barbed characteristic and cannot penetrate deeper.6
Follow-up. Close follow-up is advised, and patients should be educated on the importance of medication compliance and return visits for reevaluation. Given the potential dangers of handling these spiders, tarantula owners should be advised to use protective gloving and goggles.2,5,8,9
OUTCOME FOR THE CASE PATIENT
The case patient was sent to an ophthalmologist on day 1. Proparacaine was placed in his right eye, and all of the superficial tarantula hairs were removed using 25- and 30-gauge needles with jeweler forceps under slit-lamp microscopy. Most of the hairs were removed from the superior cornea; fewer were found in the paracentral and inferior regions of the cornea. Approximately five hairs in the paracentral area of the cornea were embedded in the midstromal depth and could not be removed. One drop of ciprofloxacin was administered.
The patient was sent home with an eye shield and instructions to use tobramycin/dexamethasone eye drops (qid in his right eye) and avoid rubbing the eye. (The eye shield, though not technically necessary, was deemed beneficial to help the patient avoid touching the eye.) He was scheduled to return to the clinic one week later.
On follow-up, a careful exam performed under microscopy showed that the five tarantula hairs were still embedded, and an additional six hairs were found in the deep stroma. Superficial punctate keratitis—an eye disorder caused by epithelial cell death on the surface of the cornea—was noted, but no anterior chamber cells were seen. The patient was instructed to continue using the eye drops as prescribed until finished, then start using loteprednol (tid) and artificial lubricating tears (every 2 h).
He returned to the clinic every two weeks for a total of 10 visits. At the end of the treatment course, the remaining tarantula hairs were unable to be removed. The patient used tapering doses of topical eye steroids and antibiotic drops secondary to flare-up.
CONCLUSION
Determining the etiology of ophthalmic emergencies is essential to timely and appropriate management. In this case, a recognized but often overlooked cause, tarantula hairs, made the diagnosis more complicated than simple conjunctivitis. When ocular injury is suspected, the provider must obtain an accurate and detailed history along with a thorough physical exam. Since patients must comply with medication regimens to prevent acute and chronic infection, a clear treatment and follow-up plan should be established. With these in place, ophthalmia nodosa caused by urticating setae can be effectively managed.
IN THIS ARTICLE
- Diagnosis
- Management
- Outcome for the case patient
An otherwise healthy 9-year-old boy is brought to the emergency department (ED) by his father for evaluation of severe pain, blurry vision, and four hours of tearing in his right eye. The patient was in school when he experienced sudden-onset irritation and scratching pain that caused him to rub his eye. He says it “feels like there is something in my eye,” but he denies any known substance or foreign body. He has no medical or surgical history, does not wear contact lenses or eyeglasses, and denies loss of vision. There is no history of recent illness or travel.
On evaluation, the patient is in no acute distress but is holding his right eye closed due to foreign-body sensation and increased photosensitivity and tearing. There is no obvious erythema or swelling in the upper or lower eyelids bilaterally. A visual acuity test with a Snellen eye chart shows 20/20 vision in the left eye and 20/50 in the right, secondary to pain, photophobia, and excessive tearing. The patient’s right sclera is significantly injected. Intraocular pressure, measured with a tonometer, is 12 to 14 mm Hg. A fluorescein stain of the eye yields no significant findings. The globe is intact.
At first glance, a slit-lamp exam shows no obvious signs of a foreign body. But much higher magnification reveals substantial conjunctival injection and numerous intracorneal linear foreign bodies in the right eye (see Figure 1 for example [not the case patient]). The anterior chamber shows no inflammatory reaction, and findings in the posterior segment are unremarkable.
The initial diagnosis is simple conjunctivitis—but closer examination reveals multiple fine, barbed hairs embedded in the patient’s right cornea. Upon further questioning, the patient reports that prior to symptom onset, he had been holding the classroom pet, a Chilean Rose tarantula, in the palm of his hands.
DISCUSSION
Foreign body injury is a common cause of ocular pain and corneal damage, which can lead to challenging complications. Ophthalmic emergencies account for 2% of ED visits in the US annually and are a major cause of visual impairment.1 But when a painful eye is the chief complaint, contact with insects, plants, or spiders is rarely included in the differential. Tarantulas are popular classroom and household pets, however, and ocular injury should be suspected in anyone who has been holding a tarantula prior to onset of pain.
Ophthalmia nodosa
Tarantulas are one of the most common arachnids known to cause ophthalmia nodosa—a granulomatous reaction of the conjunctiva or cornea to an implanted plant, insect, or spider hair that typically manifests with photophobia, irritation, and chemosis.2,3 Tarantulas, when scared or defending their eggs, shoot urticating setae at the threat—a defensive mechanism largely unknown to parents, tarantula owners, and medical professionals.
Urticating setae are found in roughly 90% of tarantula species throughout tropical and subtropical regions.4 Depending on the species, setae can be located on the distal prolateral surface of the palpal femur or the dorsum of the abdomen. They can be released when the tarantula scratches its legs against the abdominal urticating setae patch or scratches the palps against the chelicerae (appendages in front of the mouth), or when direct exterior contact is made with the abdominal setae.4
There are six types of urticating hairs. Each is attached to the spider’s cuticle by either a stalk (which represents the break-off region) or a socket.4 Tarantula hairs range in size from 0.1 mm to 0.3 mm and have a sharp, pointed head and numerous barbs, which help embed them in the target.5 They are long and thin, to facilitate deep tissue penetration, and can enter the eyes, lungs, or other body parts (see Figure 2).
Ocular injury from tarantula hairs commonly involves conjunctival injection, foreign body sensation, periorbital facial rash, photophobia, and tearing.3 When a tarantula’s cloud of barbed hairs is flicked into the eye and pierces the cornea, it can cause infection, irritation, scarring on the cornea, or vision loss. Eye movement or rubbing can cause the hairs—and their toxins—to migrate over time, traveling like an arrow (the tip and barbs resist backward movement) to the anterior chamber, lens, vitreous, and retina.6,7 This can cause corneal scars, cataracts, vitritis, or macular edema, and creates the possibility for acute or chronic conjunctivitis.7
Diagnosis and management
Ophthalmic emergencies can affect the visual system and, if left untreated, can lead to permanent vision loss. Affected patients require immediate medical attention and should be referred to an ophthalmologist for follow-up care.
Diagnosis. A thorough history and physical exam are of utmost importance; tiny setae can be easily overlooked if the examiner is not diligent, and the similar symptomatology can lead to misdiagnosis as simple conjunctivitis.3 A visual acuity test and slit-lamp exam are useful for confirmation.
Treatment. Once the diagnosis is confirmed, treatment should consist of mild topical antibiotics and steroids to effectively control infection and inflammation. While topical steroids may be appropriate, local adverse events associated with their use (eg, glaucoma, cataracts) can be problematic. Gentle eye irrigation has been noted by some researchers as contraindicated, while others find it useful to flush out some of the hairs.5,8,9
Most of the visible protruding tarantula hairs can and should be removed under microscopy during slit-lamp exam. Hairs that are buried in the cornea, however, are nearly impossible to remove and pose a threat of further complications, as described. Conservative management with careful observation is therefore recommended. If the patient develops a granuloma, excision—along with a course of systemic steroids and setae removal via vitrectomy—may be needed.9
The good news is that, in many cases, deeper hairs are absorbed without complication, making their removal unnecessary.5 Factors that encourage leaving the setae untouched include a large number of hairs, deep corneal penetration, lack of patient tolerance for the procedure, and risk for perforation.3
More invasive treatments (eg, laser photocoagulation, intraocular surgery) to remove offending hairs are possible, but literature on the outcome of these interventions is limited. One report to date used argon laser photocoagulation to treat endophthalmitis from vitreous hairs.10 The laser can fragment the hairs so that they lose their barbed characteristic and cannot penetrate deeper.6
Follow-up. Close follow-up is advised, and patients should be educated on the importance of medication compliance and return visits for reevaluation. Given the potential dangers of handling these spiders, tarantula owners should be advised to use protective gloving and goggles.2,5,8,9
OUTCOME FOR THE CASE PATIENT
The case patient was sent to an ophthalmologist on day 1. Proparacaine was placed in his right eye, and all of the superficial tarantula hairs were removed using 25- and 30-gauge needles with jeweler forceps under slit-lamp microscopy. Most of the hairs were removed from the superior cornea; fewer were found in the paracentral and inferior regions of the cornea. Approximately five hairs in the paracentral area of the cornea were embedded in the midstromal depth and could not be removed. One drop of ciprofloxacin was administered.
The patient was sent home with an eye shield and instructions to use tobramycin/dexamethasone eye drops (qid in his right eye) and avoid rubbing the eye. (The eye shield, though not technically necessary, was deemed beneficial to help the patient avoid touching the eye.) He was scheduled to return to the clinic one week later.
On follow-up, a careful exam performed under microscopy showed that the five tarantula hairs were still embedded, and an additional six hairs were found in the deep stroma. Superficial punctate keratitis—an eye disorder caused by epithelial cell death on the surface of the cornea—was noted, but no anterior chamber cells were seen. The patient was instructed to continue using the eye drops as prescribed until finished, then start using loteprednol (tid) and artificial lubricating tears (every 2 h).
He returned to the clinic every two weeks for a total of 10 visits. At the end of the treatment course, the remaining tarantula hairs were unable to be removed. The patient used tapering doses of topical eye steroids and antibiotic drops secondary to flare-up.
CONCLUSION
Determining the etiology of ophthalmic emergencies is essential to timely and appropriate management. In this case, a recognized but often overlooked cause, tarantula hairs, made the diagnosis more complicated than simple conjunctivitis. When ocular injury is suspected, the provider must obtain an accurate and detailed history along with a thorough physical exam. Since patients must comply with medication regimens to prevent acute and chronic infection, a clear treatment and follow-up plan should be established. With these in place, ophthalmia nodosa caused by urticating setae can be effectively managed.
1. Fitzpatrick J, Hickman R, Alfes CM. A Guide to Mastery in Clinical Nursing: The Comprehensive Reference. New York, NY: Springer; 2018:114.
2. Lambert SR, Lyons CJ. Taylor and Hoyt’s Pediatric Ophthalmology and Strabismus. 5th ed. New York, NY: Elsevier; 2017:138.
3. Stagg BC, Ambati BK. Tarantula hairs as corneal foreign bodies. Case Rep Ophthalmol. 2011;2(3):323-326.
4. Bertani R, Guadanucci JPL. Morphology, evolution, and usage of urticating setae by tarantulas (Araneae: Theraphosidae). Zoologia (Curitiba). 2013;30(4):403-418.
5. McAnena L, Murphy C, O’Connor J. Tarantula keratitis: a case report. Ir J Med Sci. 2013;182(3):349-350.
6. Yang Y, Christakis T, Mireskandari K. Acute conjunctivitis and corneal foreign bodies secondary to tarantula hairs. CMAJ. 2016;183(3):212-214.
7. Jain N, Soong HK, Gardner TW. Ophthalmia nodosa. EyeNet Magazine. November 2013. www.aao.org/eyenet/article/blink-mystery-image-17. Accessed January 24, 2018.
8. Choi JTL, Rauf A. Ophthalmia nodosa secondary to tarantula hairs. Eye (Lond). 2003;17(3):433-434.
9. Comez AT, Tufan HA, Gencer B. Ophthalmia nodosa as an occupational disease: is it unusual or is it casual? Ocul Immunol Inflamm. 2013;21(2):144-147.
10. Marti-Huguet T, Pujol O, Cabiro I, et al. Endophthalmos caused by intravitreal caterpillar hairs. Treatment by direct photocoagulation with argon laser [article in French]. J Fr Ophthalmol. 1987;10(10):559-564.
1. Fitzpatrick J, Hickman R, Alfes CM. A Guide to Mastery in Clinical Nursing: The Comprehensive Reference. New York, NY: Springer; 2018:114.
2. Lambert SR, Lyons CJ. Taylor and Hoyt’s Pediatric Ophthalmology and Strabismus. 5th ed. New York, NY: Elsevier; 2017:138.
3. Stagg BC, Ambati BK. Tarantula hairs as corneal foreign bodies. Case Rep Ophthalmol. 2011;2(3):323-326.
4. Bertani R, Guadanucci JPL. Morphology, evolution, and usage of urticating setae by tarantulas (Araneae: Theraphosidae). Zoologia (Curitiba). 2013;30(4):403-418.
5. McAnena L, Murphy C, O’Connor J. Tarantula keratitis: a case report. Ir J Med Sci. 2013;182(3):349-350.
6. Yang Y, Christakis T, Mireskandari K. Acute conjunctivitis and corneal foreign bodies secondary to tarantula hairs. CMAJ. 2016;183(3):212-214.
7. Jain N, Soong HK, Gardner TW. Ophthalmia nodosa. EyeNet Magazine. November 2013. www.aao.org/eyenet/article/blink-mystery-image-17. Accessed January 24, 2018.
8. Choi JTL, Rauf A. Ophthalmia nodosa secondary to tarantula hairs. Eye (Lond). 2003;17(3):433-434.
9. Comez AT, Tufan HA, Gencer B. Ophthalmia nodosa as an occupational disease: is it unusual or is it casual? Ocul Immunol Inflamm. 2013;21(2):144-147.
10. Marti-Huguet T, Pujol O, Cabiro I, et al. Endophthalmos caused by intravitreal caterpillar hairs. Treatment by direct photocoagulation with argon laser [article in French]. J Fr Ophthalmol. 1987;10(10):559-564.
FDA places T-cell therapy on clinical hold

The US Food and Drug Administration (FDA) has placed BPX-501, a T-cell therapy being evaluated in patients who undergo haploidentical hematopoietic stem cell transplants (HSCTs), on clinical hold.
Three cases of encephalopathy possibly related to BPX-501 prompted the agency to impose the hold.
Bellicum Pharmaceuticals is the developer of BPX-501, and the company was conducting 4 trials in the US in children and adults with hematologic disorders.
The BPX-501 registration trial in Europe is not affected by the clinical hold.
BPX-501 is designed to fight infection, support engraftment, prevent disease relapse, and potentially stop graft-versus-host disease (GVHD) should it occur.
BPX-501 contains a safety switch, CaspaCIDe®, that can be activated with the administration of rimiducid to kill the toxic T cells in the event of GVHD.
The 3 cases of encephalopathy are complex, according to a company press release, and have confounding factors. These include prior failed transplants, prior history of immunodeficiency, concurrent infection, and administration of rimiducid in combination with other medications.
Encephalopathy had not emerged as an adverse event in 240 patients treated with the cell therapy, until now.
BPX-501 had produced encouraging results, according to trial data presented at EHA 2017 and ASH 2017 (abstract 211*).
In this trial, 112 pediatric patients were transfused with BPX-501 cells about 2 weeks after transplant. Patients had acute leukemia (n=53), primary immune deficiencies (n=26), erythroid disorders (n=17), Fanconi anemia (n=7), and other diseases (n=9).
Investigators reported that infused cells expanded and persisted, with peak expansion reached at 9 months after infusion. Investigators continued to detect BPX-501 cells after 2 years.
The European Commission granted BPX-501 orphan drug designation for the agent for treatment in HSCT, and for the activator agent rimiducid for the treatment of GVHD.
And the FDA had granted the agents orphan drug status as a combination replacement T-cell therapy for the treatment of immunodeficiency and GVHD after HSCT.
Bellicum says it is working with the FDA to evaluate the risk of encephalopathy in patients receiving BPX-501. ![]()
* Data in the abstract were updated in the oral presentation and reported on the company’s website.
The US Food and Drug Administration (FDA) has placed BPX-501, a T-cell therapy being evaluated in patients who undergo haploidentical hematopoietic stem cell transplants (HSCTs), on clinical hold.
Three cases of encephalopathy possibly related to BPX-501 prompted the agency to impose the hold.
Bellicum Pharmaceuticals is the developer of BPX-501, and the company was conducting 4 trials in the US in children and adults with hematologic disorders.
The BPX-501 registration trial in Europe is not affected by the clinical hold.
BPX-501 is designed to fight infection, support engraftment, prevent disease relapse, and potentially stop graft-versus-host disease (GVHD) should it occur.
BPX-501 contains a safety switch, CaspaCIDe®, that can be activated with the administration of rimiducid to kill the toxic T cells in the event of GVHD.
The 3 cases of encephalopathy are complex, according to a company press release, and have confounding factors. These include prior failed transplants, prior history of immunodeficiency, concurrent infection, and administration of rimiducid in combination with other medications.
Encephalopathy had not emerged as an adverse event in 240 patients treated with the cell therapy, until now.
BPX-501 had produced encouraging results, according to trial data presented at EHA 2017 and ASH 2017 (abstract 211*).
In this trial, 112 pediatric patients were transfused with BPX-501 cells about 2 weeks after transplant. Patients had acute leukemia (n=53), primary immune deficiencies (n=26), erythroid disorders (n=17), Fanconi anemia (n=7), and other diseases (n=9).
Investigators reported that infused cells expanded and persisted, with peak expansion reached at 9 months after infusion. Investigators continued to detect BPX-501 cells after 2 years.
The European Commission granted BPX-501 orphan drug designation for the agent for treatment in HSCT, and for the activator agent rimiducid for the treatment of GVHD.
And the FDA had granted the agents orphan drug status as a combination replacement T-cell therapy for the treatment of immunodeficiency and GVHD after HSCT.
Bellicum says it is working with the FDA to evaluate the risk of encephalopathy in patients receiving BPX-501. ![]()
* Data in the abstract were updated in the oral presentation and reported on the company’s website.
The US Food and Drug Administration (FDA) has placed BPX-501, a T-cell therapy being evaluated in patients who undergo haploidentical hematopoietic stem cell transplants (HSCTs), on clinical hold.
Three cases of encephalopathy possibly related to BPX-501 prompted the agency to impose the hold.
Bellicum Pharmaceuticals is the developer of BPX-501, and the company was conducting 4 trials in the US in children and adults with hematologic disorders.
The BPX-501 registration trial in Europe is not affected by the clinical hold.
BPX-501 is designed to fight infection, support engraftment, prevent disease relapse, and potentially stop graft-versus-host disease (GVHD) should it occur.
BPX-501 contains a safety switch, CaspaCIDe®, that can be activated with the administration of rimiducid to kill the toxic T cells in the event of GVHD.
The 3 cases of encephalopathy are complex, according to a company press release, and have confounding factors. These include prior failed transplants, prior history of immunodeficiency, concurrent infection, and administration of rimiducid in combination with other medications.
Encephalopathy had not emerged as an adverse event in 240 patients treated with the cell therapy, until now.
BPX-501 had produced encouraging results, according to trial data presented at EHA 2017 and ASH 2017 (abstract 211*).
In this trial, 112 pediatric patients were transfused with BPX-501 cells about 2 weeks after transplant. Patients had acute leukemia (n=53), primary immune deficiencies (n=26), erythroid disorders (n=17), Fanconi anemia (n=7), and other diseases (n=9).
Investigators reported that infused cells expanded and persisted, with peak expansion reached at 9 months after infusion. Investigators continued to detect BPX-501 cells after 2 years.
The European Commission granted BPX-501 orphan drug designation for the agent for treatment in HSCT, and for the activator agent rimiducid for the treatment of GVHD.
And the FDA had granted the agents orphan drug status as a combination replacement T-cell therapy for the treatment of immunodeficiency and GVHD after HSCT.
Bellicum says it is working with the FDA to evaluate the risk of encephalopathy in patients receiving BPX-501. ![]()
* Data in the abstract were updated in the oral presentation and reported on the company’s website.
Does fish oil during pregnancy help prevent asthma in kids?
ILLUSTRATIVE CASE
A 24-year-old G2P1 at 24 weeks’ gestation presents to your clinic for a routine prenatal visit. Her older daughter has asthma and she is inquiring as to whether there is anything she can do to lower the risk of her second child developing asthma in the future. What do you recommend?
Asthma is the most common chronic disease in children in resource-rich countries such as the United States.2 The Centers for Disease Control and Prevention (CDC) reported that 8.4% of children were diagnosed with asthma in 2015.3
Omega-3 fatty acids, found naturally in fish oil, are thought to confer anti-inflammatory properties that offer protection against asthma. Clinical trials have shown that fish oil supplementation in pregnancy results in higher levels of omega-3 fatty acids, along with anti-inflammatory changes, in offspring.4 Previous epidemiologic studies have also found that consumption of omega-3 fatty acids decreased the risk of atopy and asthma in offspring.5,6
A Cochrane review published in 2015, however, concluded that omega-3 supplementation during pregnancy had no benefit on wheeze or asthma in offspring.7 Five RCTs were included in the analysis. The largest trial by Palmer et al, which included 706 women, showed no benefit for omega-3 supplementation.8 The second largest by Olsen et al, which included 533 women, did show a benefit (hazard ratio [HR]=0.37; 95% confidence interval [CI], 0.15-0.92; number needed to treat [NNT]=19.6).9
These results, however, were limited by heterogeneity in the amount of fish oil supplemented and duration of follow-up. For example, the children in the Palmer study were followed only until 3 years of age, which is around the time that asthma can be formally diagnosed, potentially leading to under-reporting.8 In addition, the diagnosis of asthma was based on parent report of 3 episodes of wheezing, use of daily asthma medication, or use of a national registry—all of which can underestimate the incidence of asthma. The reported rate of childhood asthma with IgE-sensitization (they did not report the rate without sensitization) was 1.8% in both arms, which is much lower than the CDC’s rate of 8.4%, suggesting underdiagnosis.3,8 Due to these biases and other potential confounders, no firm conclusions can be drawn from the Cochrane review.
STUDY SUMMARY
Maternal fish oil supplementation reduces incidence of asthma in children
This single-center, double-blinded RCT of 736 pregnant women evaluated the effect of 2.4 g/d of n-3 long-chain polyunsaturated fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) or placebo (olive oil), starting at an estimated gestational age of 24 to 26 weeks, on wheeze or asthma incidence in their offspring.1
Eligible women were between 22 and 26 weeks’ pregnant at the time of recruitment. Exclusion criteria included supplementation of 600 IU/d or more of vitamin D, or having any endocrine, cardiac, or renal disorders. The investigators randomized the women in a 1:1 ratio to either fish oil or placebo. Maternal EPA and DHA blood levels were tested at the time of randomization and one week after birth.
The primary outcome was persistent wheeze or asthma (after 3 years of age, the diagnosis of persistent wheeze was termed asthma) based on daily diary recordings of 5 episodes of troublesome lung symptoms within the last 6 months (each lasting for at least 3 consecutive days), rescue use of inhaled beta2-agonists, and/or relapse after a 3-month course of inhaled glucocorticoids. Secondary outcomes included lower respiratory tract infections, asthma exacerbations, eczema, and allergic sensitization.
In total, 695 offspring were included in the study with 95.5% follow-up at 3 years and 93.1% follow-up at 5 years. The children had scheduled pediatric visits at 1 week; 1, 3, 6, 12, 18, 24, 30, and 36 months; and at 4 and 5 years, and acute visits for any pulmonary, allergic, or dermatologic symptoms that arose.
Results. The investigators found that the children of the mothers who received the fish oil had a lower risk of persistent wheeze or asthma at ages 3 to 5 years compared to those who received placebo (16.9% vs 23.7%; HR=0.69; 95% CI, 0.49-0.97; P=.035; NNT=14.7). But the effect of the fish oil supplementation was significant only in the children of the mothers with baseline EPA and DHA levels in the lowest third (17.5% vs 34.1%; HR=0.46; 95% CI, 0.25-0.83; P=.011; NNT=5.6). Similarly, in mothers who consumed the least EPA and DHA before the start of the study, fish oil supplementation had a greater benefit in terms of decreased wheeze and asthma (18.5% vs 32.4%; HR=0.55; 95% CI, 0.30-0.98; P=.043; NNT=7.2).
As for the secondary outcomes, only a reduction in lower respiratory tract infections was associated with the fish oil supplementation vs the control (38.8% vs 45.5%; HR=0.77; 95% CI, 0.61-0.99; P=.041; NNT=14.9). There was no reduction in asthma exacerbations, eczema, or risk of sensitization in the fish oil group.
WHAT'S NEW?
Study adds fuel to the fire
This study strengthens the case for fish oil supplementation during pregnancy to reduce the risk of asthma in offspring, despite the recent Cochrane review that showed no benefit.1,7 The Palmer study used a much lower amount of omega-3s (900 mg/d fish oil vs 2400 mg/d in the current trial).1,8 Olsen et al supplemented with a greater amount of omega-3s (2700 mg/d) and did find a benefit.9 The NNT from the Olsen study (19.6) is consistent with that of the current investigation, suggesting that a higher dosage may be necessary to prevent the onset of asthma.
Additionally, this study followed children for a longer period than did the Palmer study, which may have led to more accurate diagnoses of asthma.1,8 Lastly, the diagnosis of asthma in the Palmer study was based on parent survey data and use of daily asthma medicine rather than on daily diary cards, which are often more accurate.
Consider fish consumption. Both this study and the Olsen trial were performed in Denmark.1,9 While Denmark and the United States have had a relatively similar level of fish consumption since the 1990s, women in Denmark may eat a higher proportion of oily fish than women in the United States, given the more common inclusion of mackerel and herring in their diet.10 Thus, the effect of supplementation may be more pronounced in women in the United States.
CAVEATS
Questions remain: Ideal dose and which women to treat?
The US Food and Drug Administration currently recommends 8 to 12 ounces of fish per week for pregnant women, but there are no guidelines on the ideal amount of fish oil to be consumed.11 The Palmer study,8 using 900 mg/d fish oil, did not show a benefit, whereas there did appear to be benefit in this study (2400 mg/d)1 and the Olsen study (2700 mg/d).9 Further research is needed to determine the optimal dosage.
The decreased risk of persistent wheeze or asthma was seen only in the children of the women whose EPA and DHA blood levels were in the lowest third of the study population. Thus, only women whose blood levels are low to begin with will likely benefit from this intervention. Currently, EPA and DHA levels are not routinely checked, but there may be some benefit to doing so.
One proxy for blood levels is maternal intake of fish at baseline. The investigators found that there was an association between dietary intake of fish and blood levels of EPA and DHA (r=0.32; P<.001).1 Therefore, additional screening questions to determine fish consumption would be useful for identifying women most likely to benefit from supplementation.
CHALLENGES TO IMPLEMENTATION
Multiple pills and additional cost
Since omega-3 fatty acids are relatively safe and the NNT in the general population is low, it may be worth supplementing all pregnant women, even without a commercially-available blood test for EPA or DHA. Nevertheless, some women may find it challenging to take up to an additional 4 pills/d for 13 or more weeks. Also, there is an associated cost with these supplements, although it is low.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Bisgaard H, Stokholm J, Chawes BL, et al. Fish oil-derived fatty acids in pregnancy and wheeze and asthma in offspring. N Engl J Med. 2016;375:2530-2539.
2. Masoli M, Fabian D, Holt S, et al. The global burden of asthma: executive summary of the GINA Dessemination Committee Report. Allergy. 2004;59:469-478.
3. Centers for Disease Control and Prevention. Asthma. Available at: https://www.cdc.gov/asthma/most_recent_data.htm. Accessed October 9, 2017.
4. Miyata J, Arita M. Role of omega-3 fatty acids and their metabolites in asthma and allergic diseases. Allergol Int. 2015;64:27-34.
5. Salam MT, Li YF, Langholz B, et al. Maternal fish consumption during pregnancy and risk of early childhood asthma. J Asthma. 2005;42:513-518.
6. Calvani M, Alessandri C, Sopo SM, et al. Consumption of fish, butter and margarine during pregnancy and development of allergic sensitizations in the offspring: role of maternal atopy. Pediatr Allergy Immunol. 2006;17:94-102.
7. Gunaratne AW, Makrides M, Collins CT. Maternal prenatal and/or postnatal n-3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood. Cochrane Database Syst Rev. 2015;22:CD010085.
8. Palmer D, Sullivan T, Gold M, et al. Randomized controlled trial of fish oil supplementation in pregnancy on childhood allergies. Allergy. 2013;68:1370-1376.
9. Olsen SF, Østerdal ML, Salvig JD, et al. Fish oil intake compared with olive oil intake in late pregnancy and asthma in the offspring: 16 y of registry-based follow-up from a randomized controlled trial. Am J Clin Nutr. 2008;88:167-175.
10. Helgi Library. Fish consumption per capita by country. Available at: http://www.helgilibrary.com/indicators/fish-consumption-per-capita/. Accessed September 27, 2017.
11. FDA Advice About Eating Fish, From the Environmental Protection Agency and Food and Drug Administration; Revised Fish Advice; Availability. Federal Register.2017;82:6571-6574.
ILLUSTRATIVE CASE
A 24-year-old G2P1 at 24 weeks’ gestation presents to your clinic for a routine prenatal visit. Her older daughter has asthma and she is inquiring as to whether there is anything she can do to lower the risk of her second child developing asthma in the future. What do you recommend?
Asthma is the most common chronic disease in children in resource-rich countries such as the United States.2 The Centers for Disease Control and Prevention (CDC) reported that 8.4% of children were diagnosed with asthma in 2015.3
Omega-3 fatty acids, found naturally in fish oil, are thought to confer anti-inflammatory properties that offer protection against asthma. Clinical trials have shown that fish oil supplementation in pregnancy results in higher levels of omega-3 fatty acids, along with anti-inflammatory changes, in offspring.4 Previous epidemiologic studies have also found that consumption of omega-3 fatty acids decreased the risk of atopy and asthma in offspring.5,6
A Cochrane review published in 2015, however, concluded that omega-3 supplementation during pregnancy had no benefit on wheeze or asthma in offspring.7 Five RCTs were included in the analysis. The largest trial by Palmer et al, which included 706 women, showed no benefit for omega-3 supplementation.8 The second largest by Olsen et al, which included 533 women, did show a benefit (hazard ratio [HR]=0.37; 95% confidence interval [CI], 0.15-0.92; number needed to treat [NNT]=19.6).9
These results, however, were limited by heterogeneity in the amount of fish oil supplemented and duration of follow-up. For example, the children in the Palmer study were followed only until 3 years of age, which is around the time that asthma can be formally diagnosed, potentially leading to under-reporting.8 In addition, the diagnosis of asthma was based on parent report of 3 episodes of wheezing, use of daily asthma medication, or use of a national registry—all of which can underestimate the incidence of asthma. The reported rate of childhood asthma with IgE-sensitization (they did not report the rate without sensitization) was 1.8% in both arms, which is much lower than the CDC’s rate of 8.4%, suggesting underdiagnosis.3,8 Due to these biases and other potential confounders, no firm conclusions can be drawn from the Cochrane review.
STUDY SUMMARY
Maternal fish oil supplementation reduces incidence of asthma in children
This single-center, double-blinded RCT of 736 pregnant women evaluated the effect of 2.4 g/d of n-3 long-chain polyunsaturated fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) or placebo (olive oil), starting at an estimated gestational age of 24 to 26 weeks, on wheeze or asthma incidence in their offspring.1
Eligible women were between 22 and 26 weeks’ pregnant at the time of recruitment. Exclusion criteria included supplementation of 600 IU/d or more of vitamin D, or having any endocrine, cardiac, or renal disorders. The investigators randomized the women in a 1:1 ratio to either fish oil or placebo. Maternal EPA and DHA blood levels were tested at the time of randomization and one week after birth.
The primary outcome was persistent wheeze or asthma (after 3 years of age, the diagnosis of persistent wheeze was termed asthma) based on daily diary recordings of 5 episodes of troublesome lung symptoms within the last 6 months (each lasting for at least 3 consecutive days), rescue use of inhaled beta2-agonists, and/or relapse after a 3-month course of inhaled glucocorticoids. Secondary outcomes included lower respiratory tract infections, asthma exacerbations, eczema, and allergic sensitization.
In total, 695 offspring were included in the study with 95.5% follow-up at 3 years and 93.1% follow-up at 5 years. The children had scheduled pediatric visits at 1 week; 1, 3, 6, 12, 18, 24, 30, and 36 months; and at 4 and 5 years, and acute visits for any pulmonary, allergic, or dermatologic symptoms that arose.
Results. The investigators found that the children of the mothers who received the fish oil had a lower risk of persistent wheeze or asthma at ages 3 to 5 years compared to those who received placebo (16.9% vs 23.7%; HR=0.69; 95% CI, 0.49-0.97; P=.035; NNT=14.7). But the effect of the fish oil supplementation was significant only in the children of the mothers with baseline EPA and DHA levels in the lowest third (17.5% vs 34.1%; HR=0.46; 95% CI, 0.25-0.83; P=.011; NNT=5.6). Similarly, in mothers who consumed the least EPA and DHA before the start of the study, fish oil supplementation had a greater benefit in terms of decreased wheeze and asthma (18.5% vs 32.4%; HR=0.55; 95% CI, 0.30-0.98; P=.043; NNT=7.2).
As for the secondary outcomes, only a reduction in lower respiratory tract infections was associated with the fish oil supplementation vs the control (38.8% vs 45.5%; HR=0.77; 95% CI, 0.61-0.99; P=.041; NNT=14.9). There was no reduction in asthma exacerbations, eczema, or risk of sensitization in the fish oil group.
WHAT'S NEW?
Study adds fuel to the fire
This study strengthens the case for fish oil supplementation during pregnancy to reduce the risk of asthma in offspring, despite the recent Cochrane review that showed no benefit.1,7 The Palmer study used a much lower amount of omega-3s (900 mg/d fish oil vs 2400 mg/d in the current trial).1,8 Olsen et al supplemented with a greater amount of omega-3s (2700 mg/d) and did find a benefit.9 The NNT from the Olsen study (19.6) is consistent with that of the current investigation, suggesting that a higher dosage may be necessary to prevent the onset of asthma.
Additionally, this study followed children for a longer period than did the Palmer study, which may have led to more accurate diagnoses of asthma.1,8 Lastly, the diagnosis of asthma in the Palmer study was based on parent survey data and use of daily asthma medicine rather than on daily diary cards, which are often more accurate.
Consider fish consumption. Both this study and the Olsen trial were performed in Denmark.1,9 While Denmark and the United States have had a relatively similar level of fish consumption since the 1990s, women in Denmark may eat a higher proportion of oily fish than women in the United States, given the more common inclusion of mackerel and herring in their diet.10 Thus, the effect of supplementation may be more pronounced in women in the United States.
CAVEATS
Questions remain: Ideal dose and which women to treat?
The US Food and Drug Administration currently recommends 8 to 12 ounces of fish per week for pregnant women, but there are no guidelines on the ideal amount of fish oil to be consumed.11 The Palmer study,8 using 900 mg/d fish oil, did not show a benefit, whereas there did appear to be benefit in this study (2400 mg/d)1 and the Olsen study (2700 mg/d).9 Further research is needed to determine the optimal dosage.
The decreased risk of persistent wheeze or asthma was seen only in the children of the women whose EPA and DHA blood levels were in the lowest third of the study population. Thus, only women whose blood levels are low to begin with will likely benefit from this intervention. Currently, EPA and DHA levels are not routinely checked, but there may be some benefit to doing so.
One proxy for blood levels is maternal intake of fish at baseline. The investigators found that there was an association between dietary intake of fish and blood levels of EPA and DHA (r=0.32; P<.001).1 Therefore, additional screening questions to determine fish consumption would be useful for identifying women most likely to benefit from supplementation.
CHALLENGES TO IMPLEMENTATION
Multiple pills and additional cost
Since omega-3 fatty acids are relatively safe and the NNT in the general population is low, it may be worth supplementing all pregnant women, even without a commercially-available blood test for EPA or DHA. Nevertheless, some women may find it challenging to take up to an additional 4 pills/d for 13 or more weeks. Also, there is an associated cost with these supplements, although it is low.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
ILLUSTRATIVE CASE
A 24-year-old G2P1 at 24 weeks’ gestation presents to your clinic for a routine prenatal visit. Her older daughter has asthma and she is inquiring as to whether there is anything she can do to lower the risk of her second child developing asthma in the future. What do you recommend?
Asthma is the most common chronic disease in children in resource-rich countries such as the United States.2 The Centers for Disease Control and Prevention (CDC) reported that 8.4% of children were diagnosed with asthma in 2015.3
Omega-3 fatty acids, found naturally in fish oil, are thought to confer anti-inflammatory properties that offer protection against asthma. Clinical trials have shown that fish oil supplementation in pregnancy results in higher levels of omega-3 fatty acids, along with anti-inflammatory changes, in offspring.4 Previous epidemiologic studies have also found that consumption of omega-3 fatty acids decreased the risk of atopy and asthma in offspring.5,6
A Cochrane review published in 2015, however, concluded that omega-3 supplementation during pregnancy had no benefit on wheeze or asthma in offspring.7 Five RCTs were included in the analysis. The largest trial by Palmer et al, which included 706 women, showed no benefit for omega-3 supplementation.8 The second largest by Olsen et al, which included 533 women, did show a benefit (hazard ratio [HR]=0.37; 95% confidence interval [CI], 0.15-0.92; number needed to treat [NNT]=19.6).9
These results, however, were limited by heterogeneity in the amount of fish oil supplemented and duration of follow-up. For example, the children in the Palmer study were followed only until 3 years of age, which is around the time that asthma can be formally diagnosed, potentially leading to under-reporting.8 In addition, the diagnosis of asthma was based on parent report of 3 episodes of wheezing, use of daily asthma medication, or use of a national registry—all of which can underestimate the incidence of asthma. The reported rate of childhood asthma with IgE-sensitization (they did not report the rate without sensitization) was 1.8% in both arms, which is much lower than the CDC’s rate of 8.4%, suggesting underdiagnosis.3,8 Due to these biases and other potential confounders, no firm conclusions can be drawn from the Cochrane review.
STUDY SUMMARY
Maternal fish oil supplementation reduces incidence of asthma in children
This single-center, double-blinded RCT of 736 pregnant women evaluated the effect of 2.4 g/d of n-3 long-chain polyunsaturated fatty acids (eicosapentaenoic acid [EPA] and docosahexaenoic acid [DHA]) or placebo (olive oil), starting at an estimated gestational age of 24 to 26 weeks, on wheeze or asthma incidence in their offspring.1
Eligible women were between 22 and 26 weeks’ pregnant at the time of recruitment. Exclusion criteria included supplementation of 600 IU/d or more of vitamin D, or having any endocrine, cardiac, or renal disorders. The investigators randomized the women in a 1:1 ratio to either fish oil or placebo. Maternal EPA and DHA blood levels were tested at the time of randomization and one week after birth.
The primary outcome was persistent wheeze or asthma (after 3 years of age, the diagnosis of persistent wheeze was termed asthma) based on daily diary recordings of 5 episodes of troublesome lung symptoms within the last 6 months (each lasting for at least 3 consecutive days), rescue use of inhaled beta2-agonists, and/or relapse after a 3-month course of inhaled glucocorticoids. Secondary outcomes included lower respiratory tract infections, asthma exacerbations, eczema, and allergic sensitization.
In total, 695 offspring were included in the study with 95.5% follow-up at 3 years and 93.1% follow-up at 5 years. The children had scheduled pediatric visits at 1 week; 1, 3, 6, 12, 18, 24, 30, and 36 months; and at 4 and 5 years, and acute visits for any pulmonary, allergic, or dermatologic symptoms that arose.
Results. The investigators found that the children of the mothers who received the fish oil had a lower risk of persistent wheeze or asthma at ages 3 to 5 years compared to those who received placebo (16.9% vs 23.7%; HR=0.69; 95% CI, 0.49-0.97; P=.035; NNT=14.7). But the effect of the fish oil supplementation was significant only in the children of the mothers with baseline EPA and DHA levels in the lowest third (17.5% vs 34.1%; HR=0.46; 95% CI, 0.25-0.83; P=.011; NNT=5.6). Similarly, in mothers who consumed the least EPA and DHA before the start of the study, fish oil supplementation had a greater benefit in terms of decreased wheeze and asthma (18.5% vs 32.4%; HR=0.55; 95% CI, 0.30-0.98; P=.043; NNT=7.2).
As for the secondary outcomes, only a reduction in lower respiratory tract infections was associated with the fish oil supplementation vs the control (38.8% vs 45.5%; HR=0.77; 95% CI, 0.61-0.99; P=.041; NNT=14.9). There was no reduction in asthma exacerbations, eczema, or risk of sensitization in the fish oil group.
WHAT'S NEW?
Study adds fuel to the fire
This study strengthens the case for fish oil supplementation during pregnancy to reduce the risk of asthma in offspring, despite the recent Cochrane review that showed no benefit.1,7 The Palmer study used a much lower amount of omega-3s (900 mg/d fish oil vs 2400 mg/d in the current trial).1,8 Olsen et al supplemented with a greater amount of omega-3s (2700 mg/d) and did find a benefit.9 The NNT from the Olsen study (19.6) is consistent with that of the current investigation, suggesting that a higher dosage may be necessary to prevent the onset of asthma.
Additionally, this study followed children for a longer period than did the Palmer study, which may have led to more accurate diagnoses of asthma.1,8 Lastly, the diagnosis of asthma in the Palmer study was based on parent survey data and use of daily asthma medicine rather than on daily diary cards, which are often more accurate.
Consider fish consumption. Both this study and the Olsen trial were performed in Denmark.1,9 While Denmark and the United States have had a relatively similar level of fish consumption since the 1990s, women in Denmark may eat a higher proportion of oily fish than women in the United States, given the more common inclusion of mackerel and herring in their diet.10 Thus, the effect of supplementation may be more pronounced in women in the United States.
CAVEATS
Questions remain: Ideal dose and which women to treat?
The US Food and Drug Administration currently recommends 8 to 12 ounces of fish per week for pregnant women, but there are no guidelines on the ideal amount of fish oil to be consumed.11 The Palmer study,8 using 900 mg/d fish oil, did not show a benefit, whereas there did appear to be benefit in this study (2400 mg/d)1 and the Olsen study (2700 mg/d).9 Further research is needed to determine the optimal dosage.
The decreased risk of persistent wheeze or asthma was seen only in the children of the women whose EPA and DHA blood levels were in the lowest third of the study population. Thus, only women whose blood levels are low to begin with will likely benefit from this intervention. Currently, EPA and DHA levels are not routinely checked, but there may be some benefit to doing so.
One proxy for blood levels is maternal intake of fish at baseline. The investigators found that there was an association between dietary intake of fish and blood levels of EPA and DHA (r=0.32; P<.001).1 Therefore, additional screening questions to determine fish consumption would be useful for identifying women most likely to benefit from supplementation.
CHALLENGES TO IMPLEMENTATION
Multiple pills and additional cost
Since omega-3 fatty acids are relatively safe and the NNT in the general population is low, it may be worth supplementing all pregnant women, even without a commercially-available blood test for EPA or DHA. Nevertheless, some women may find it challenging to take up to an additional 4 pills/d for 13 or more weeks. Also, there is an associated cost with these supplements, although it is low.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Bisgaard H, Stokholm J, Chawes BL, et al. Fish oil-derived fatty acids in pregnancy and wheeze and asthma in offspring. N Engl J Med. 2016;375:2530-2539.
2. Masoli M, Fabian D, Holt S, et al. The global burden of asthma: executive summary of the GINA Dessemination Committee Report. Allergy. 2004;59:469-478.
3. Centers for Disease Control and Prevention. Asthma. Available at: https://www.cdc.gov/asthma/most_recent_data.htm. Accessed October 9, 2017.
4. Miyata J, Arita M. Role of omega-3 fatty acids and their metabolites in asthma and allergic diseases. Allergol Int. 2015;64:27-34.
5. Salam MT, Li YF, Langholz B, et al. Maternal fish consumption during pregnancy and risk of early childhood asthma. J Asthma. 2005;42:513-518.
6. Calvani M, Alessandri C, Sopo SM, et al. Consumption of fish, butter and margarine during pregnancy and development of allergic sensitizations in the offspring: role of maternal atopy. Pediatr Allergy Immunol. 2006;17:94-102.
7. Gunaratne AW, Makrides M, Collins CT. Maternal prenatal and/or postnatal n-3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood. Cochrane Database Syst Rev. 2015;22:CD010085.
8. Palmer D, Sullivan T, Gold M, et al. Randomized controlled trial of fish oil supplementation in pregnancy on childhood allergies. Allergy. 2013;68:1370-1376.
9. Olsen SF, Østerdal ML, Salvig JD, et al. Fish oil intake compared with olive oil intake in late pregnancy and asthma in the offspring: 16 y of registry-based follow-up from a randomized controlled trial. Am J Clin Nutr. 2008;88:167-175.
10. Helgi Library. Fish consumption per capita by country. Available at: http://www.helgilibrary.com/indicators/fish-consumption-per-capita/. Accessed September 27, 2017.
11. FDA Advice About Eating Fish, From the Environmental Protection Agency and Food and Drug Administration; Revised Fish Advice; Availability. Federal Register.2017;82:6571-6574.
1. Bisgaard H, Stokholm J, Chawes BL, et al. Fish oil-derived fatty acids in pregnancy and wheeze and asthma in offspring. N Engl J Med. 2016;375:2530-2539.
2. Masoli M, Fabian D, Holt S, et al. The global burden of asthma: executive summary of the GINA Dessemination Committee Report. Allergy. 2004;59:469-478.
3. Centers for Disease Control and Prevention. Asthma. Available at: https://www.cdc.gov/asthma/most_recent_data.htm. Accessed October 9, 2017.
4. Miyata J, Arita M. Role of omega-3 fatty acids and their metabolites in asthma and allergic diseases. Allergol Int. 2015;64:27-34.
5. Salam MT, Li YF, Langholz B, et al. Maternal fish consumption during pregnancy and risk of early childhood asthma. J Asthma. 2005;42:513-518.
6. Calvani M, Alessandri C, Sopo SM, et al. Consumption of fish, butter and margarine during pregnancy and development of allergic sensitizations in the offspring: role of maternal atopy. Pediatr Allergy Immunol. 2006;17:94-102.
7. Gunaratne AW, Makrides M, Collins CT. Maternal prenatal and/or postnatal n-3 long chain polyunsaturated fatty acids (LCPUFA) supplementation for preventing allergies in early childhood. Cochrane Database Syst Rev. 2015;22:CD010085.
8. Palmer D, Sullivan T, Gold M, et al. Randomized controlled trial of fish oil supplementation in pregnancy on childhood allergies. Allergy. 2013;68:1370-1376.
9. Olsen SF, Østerdal ML, Salvig JD, et al. Fish oil intake compared with olive oil intake in late pregnancy and asthma in the offspring: 16 y of registry-based follow-up from a randomized controlled trial. Am J Clin Nutr. 2008;88:167-175.
10. Helgi Library. Fish consumption per capita by country. Available at: http://www.helgilibrary.com/indicators/fish-consumption-per-capita/. Accessed September 27, 2017.
11. FDA Advice About Eating Fish, From the Environmental Protection Agency and Food and Drug Administration; Revised Fish Advice; Availability. Federal Register.2017;82:6571-6574.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
PRACTICE CHANGER
Fish oil supplementation taken by women in the third trimester of pregnancy can reduce the risk of persistent wheeze, asthma, and infections of the lower respiratory tract in their children.1
STRENGTH OF RECOMMENDATION
B: Based on 2 double-blinded randomized controlled trials (RCTs).
Bisgaard H, Stokholm J, Chawes BL, et al. Fish oil-derived fatty acids in pregnancy and wheeze and asthma in offspring. N Engl J Med. 2016;375:2530-2539.1

Tisagenlecleucel looks effective in phase 2 study of young ALL patients
Tisagenlecleucel was associated with durable remission and long-term persistence for younger patients with relapsed or refractory B-cell acute lymphoblastic leukemia (ALL), according to the results of a multicenter, multicontinent, phase 2 trial published in the New England Journal of Medicine.
Shannon L. Maude, MD, PhD, of the Children’s Hospital of Philadelphia and her coauthors reported that the anti-CD19 chimeric antigen receptor (CAR) therapy was highly toxic, but the effects were usually mitigated. Additionally, the investigators showed feasibility of a global supply chain for distribution of the therapy.
The investigators evaluated data from 75 patients with at least 5% lymphoblasts in their bone marrow at the time of screening. Patients were aged 3 years or older at the time of screening but were no older than 21 years of age at the time of diagnosis.
For 50 patients evaluated at the interim analysis, the primary endpoint of overall remission at 3 months was met, and the overall remission rate was 82% (P less than .001).
An updated analysis showed that 81% of 75 patients who had at least 3 months of follow-up experienced overall remission (95% confidence interval, 71-89). A total of 45 of those patients experienced complete remission, and 16 had complete remission with incomplete hematologic recovery.
Event-free survival was experienced by 73% of patients at 6 months and 50% of patients at 12 months. Overall survival was 90% at 6 months and 76% at 12 months, the investigators reported.
Before tisagenlecleucel infusion, 96% of patients received lymphodepleting chemotherapy. The administration of chemotherapy was not done at the discretion of the investigator if a patient had leukopenia.
The median duration of remission was not reached, and the persistence of tisagenlecleucel in the blood was observed for as long as 20 months.
“The remissions were durable, with a 6-month relapse-free survival rate of 80%,” the investigators wrote. “The durability of the clinical response was associated with persistence of tisagenlecleucel in peripheral blood and with persistent B-cell aplasia.”
The phase 1 study of tisagenlecleucel infusion therapy for younger patients with B-cell ALL showed the toxic nature of the therapy, so investigators were not surprised by the safety data they found. Nearly three-quarters of patients who were evaluated in the study experienced a grade 3 or 4 tisagenlecleucel-related adverse event. Cytokine release syndrome occurred in 77% of patients.
Previously reported data regarding anti-CD19 CAR T-cell therapy for ALL came from single-center studies where manufacturing occurred on site, but the current study employed a global, multicenter supply chain, according to the investigators.
“The toxicity and efficacy of tisagenlecleucel [in this study] were consistent with those in the single-center study, and the feasibility of a global supply chain was demonstrated,” they wrote. “Because this study used cryopreserved leukapheresis product, it did not require fresh product and an open manufacture slot for enrollment.”
This research was sponsored and designed by Novartis Pharmaceuticals. Dr. Maude reported having received personal fees from Novartis as well as grant funding from St. Baldrick’s Foundation.
hematologynews@frontlinemedcom.com
SOURCE: Maude SL, et al. N Engl J Med. 2018;378:439-48.
Tisagenlecleucel was associated with durable remission and long-term persistence for younger patients with relapsed or refractory B-cell acute lymphoblastic leukemia (ALL), according to the results of a multicenter, multicontinent, phase 2 trial published in the New England Journal of Medicine.
Shannon L. Maude, MD, PhD, of the Children’s Hospital of Philadelphia and her coauthors reported that the anti-CD19 chimeric antigen receptor (CAR) therapy was highly toxic, but the effects were usually mitigated. Additionally, the investigators showed feasibility of a global supply chain for distribution of the therapy.
The investigators evaluated data from 75 patients with at least 5% lymphoblasts in their bone marrow at the time of screening. Patients were aged 3 years or older at the time of screening but were no older than 21 years of age at the time of diagnosis.
For 50 patients evaluated at the interim analysis, the primary endpoint of overall remission at 3 months was met, and the overall remission rate was 82% (P less than .001).
An updated analysis showed that 81% of 75 patients who had at least 3 months of follow-up experienced overall remission (95% confidence interval, 71-89). A total of 45 of those patients experienced complete remission, and 16 had complete remission with incomplete hematologic recovery.
Event-free survival was experienced by 73% of patients at 6 months and 50% of patients at 12 months. Overall survival was 90% at 6 months and 76% at 12 months, the investigators reported.
Before tisagenlecleucel infusion, 96% of patients received lymphodepleting chemotherapy. The administration of chemotherapy was not done at the discretion of the investigator if a patient had leukopenia.
The median duration of remission was not reached, and the persistence of tisagenlecleucel in the blood was observed for as long as 20 months.
“The remissions were durable, with a 6-month relapse-free survival rate of 80%,” the investigators wrote. “The durability of the clinical response was associated with persistence of tisagenlecleucel in peripheral blood and with persistent B-cell aplasia.”
The phase 1 study of tisagenlecleucel infusion therapy for younger patients with B-cell ALL showed the toxic nature of the therapy, so investigators were not surprised by the safety data they found. Nearly three-quarters of patients who were evaluated in the study experienced a grade 3 or 4 tisagenlecleucel-related adverse event. Cytokine release syndrome occurred in 77% of patients.
Previously reported data regarding anti-CD19 CAR T-cell therapy for ALL came from single-center studies where manufacturing occurred on site, but the current study employed a global, multicenter supply chain, according to the investigators.
“The toxicity and efficacy of tisagenlecleucel [in this study] were consistent with those in the single-center study, and the feasibility of a global supply chain was demonstrated,” they wrote. “Because this study used cryopreserved leukapheresis product, it did not require fresh product and an open manufacture slot for enrollment.”
This research was sponsored and designed by Novartis Pharmaceuticals. Dr. Maude reported having received personal fees from Novartis as well as grant funding from St. Baldrick’s Foundation.
hematologynews@frontlinemedcom.com
SOURCE: Maude SL, et al. N Engl J Med. 2018;378:439-48.
Tisagenlecleucel was associated with durable remission and long-term persistence for younger patients with relapsed or refractory B-cell acute lymphoblastic leukemia (ALL), according to the results of a multicenter, multicontinent, phase 2 trial published in the New England Journal of Medicine.
Shannon L. Maude, MD, PhD, of the Children’s Hospital of Philadelphia and her coauthors reported that the anti-CD19 chimeric antigen receptor (CAR) therapy was highly toxic, but the effects were usually mitigated. Additionally, the investigators showed feasibility of a global supply chain for distribution of the therapy.
The investigators evaluated data from 75 patients with at least 5% lymphoblasts in their bone marrow at the time of screening. Patients were aged 3 years or older at the time of screening but were no older than 21 years of age at the time of diagnosis.
For 50 patients evaluated at the interim analysis, the primary endpoint of overall remission at 3 months was met, and the overall remission rate was 82% (P less than .001).
An updated analysis showed that 81% of 75 patients who had at least 3 months of follow-up experienced overall remission (95% confidence interval, 71-89). A total of 45 of those patients experienced complete remission, and 16 had complete remission with incomplete hematologic recovery.
Event-free survival was experienced by 73% of patients at 6 months and 50% of patients at 12 months. Overall survival was 90% at 6 months and 76% at 12 months, the investigators reported.
Before tisagenlecleucel infusion, 96% of patients received lymphodepleting chemotherapy. The administration of chemotherapy was not done at the discretion of the investigator if a patient had leukopenia.
The median duration of remission was not reached, and the persistence of tisagenlecleucel in the blood was observed for as long as 20 months.
“The remissions were durable, with a 6-month relapse-free survival rate of 80%,” the investigators wrote. “The durability of the clinical response was associated with persistence of tisagenlecleucel in peripheral blood and with persistent B-cell aplasia.”
The phase 1 study of tisagenlecleucel infusion therapy for younger patients with B-cell ALL showed the toxic nature of the therapy, so investigators were not surprised by the safety data they found. Nearly three-quarters of patients who were evaluated in the study experienced a grade 3 or 4 tisagenlecleucel-related adverse event. Cytokine release syndrome occurred in 77% of patients.
Previously reported data regarding anti-CD19 CAR T-cell therapy for ALL came from single-center studies where manufacturing occurred on site, but the current study employed a global, multicenter supply chain, according to the investigators.
“The toxicity and efficacy of tisagenlecleucel [in this study] were consistent with those in the single-center study, and the feasibility of a global supply chain was demonstrated,” they wrote. “Because this study used cryopreserved leukapheresis product, it did not require fresh product and an open manufacture slot for enrollment.”
This research was sponsored and designed by Novartis Pharmaceuticals. Dr. Maude reported having received personal fees from Novartis as well as grant funding from St. Baldrick’s Foundation.
hematologynews@frontlinemedcom.com
SOURCE: Maude SL, et al. N Engl J Med. 2018;378:439-48.
Key clinical point:
Major finding: The overall remission rate was 81% at 3 months, and 73% of patients experienced grade 3 or 4 adverse events.
Study details: A multicenter, phase 2 study of 75 patients.
Disclosures: Novartis designed and sponsored this research. Dr. Maude reported receiving fees from Novartis and grant funding from St. Baldrick’s Foundation.
Source: Maude SL et al. N Engl J Med. 2018;378:439-48.
Children’s behavioral problems tied to mothers’ postpartum depression
Persistent and severe postpartum depression in mothers may be associated with behavioral problems, poor mathematics grades, and a higher risk of depression in their offspring, research published Jan. 31 in JAMA Psychiatry showed.
In the study, Elena Netsi, DPhil, and her associates presented an analysis of data from 9,848 mothers and 8,287 children enrolled in the observational Avon Longitudinal Study of Parents and Children.
This analysis revealed that postpartum depression of any severity or level of persistence was associated with a two- to fourfold increase in the risk of children showing behavioral problems at age 3.5 years. In women with marked but not persistent postpartum depression, the odds ratio for child behavioral disturbance was 1.91, in mothers with severe but not persistent depression it was 2.39, and in mothers with severe persistent depression, the odds ratio was 4.84 – all of which were highly significant (P less than .001).
However, the authors reported.
It was associated with a 2.65-fold increase in the likelihood of a child having mathematics grades of D or below (P = .01), and a more than sevenfold increase in the prevalence of depression in offspring at 18 years (P less than .001). There also was a 2.3-fold increase in depression at 18 years in the children of mothers who experienced marked but not persistent postpartum depression (P = .04).
Dr. Netsi of the department of psychiatry at the University of Oxford (England) and her coauthors noted that, in women with persistent postpartum depression, mean Edinburgh Postpartum Depression Scale scores remained relatively stable, from 21 months to 11 years, suggesting an increased risk for prolonged depression.
“Identification of women with [postpartum depression] may be associated with increased treatment costs, but the overall cost to the public sector of perinatal mental health problems is five times more than the cost of improving services, further highlighting that early intervention and effective treatment of perinatal depression are a public health priority,” they wrote.
However, they acknowledged that there were mixed findings in the literature with respect to the impact on child outcomes of treating maternal depression.
“Treatments for [postpartum depression] have been relatively brief in duration and moderate in intensity; therefore, it is perhaps unsurprising that such interventions have not shown long-term benefits for either the mother or the child,” the investigators wrote.
The Avon Longitudinal Study of Parents and Children is supported by the U.K. Medical Research Council, the Wellcome Trust, and the University of Bristol. This study was supported by the Wellcome Trust, the National Institute for Health Research Biomedical Research Centre, the University of Bristol, and the NIHR Oxford Health Biomedical Research Centre. No conflicts of interest were declared.
SOURCE: Netsi E et al. JAMA Psychiatry. 2018 Jan 31. doi: 10.1001/jamapsychiatry.2017.4363.
This study raises new and interesting questions about the clinical effects of maternal depression on offspring, and identifies a particularly vulnerable group of mothers and their offspring. If anything, the findings are likely an underestimation of the true effect, because of high rates of study attrition, especially within the most vulnerable group.
However, this does not answer the question of what interventions to use, whom to treat, when to do so, and how to treat. Some would argue that clinicians should treat maternal depression first, as a woman with acute depression needs care before she can be helped with parenting. Others suggest that a better approach is to engage the unique mother-infant experience, as this can be a positive therapeutic interaction in itself.
Whatever the approach, the treatment of maternal depression should be evidence based and available early, particularly in new mothers with persistent depression.
Myrna M. Weissman, PhD, is affiliated with the division of epidemiology at Columbia University, New York. These comments are taken from an accompanying editorial (JAMA Psychiatry. 2018 Jan 31. doi: 10.1001/jamapsychiatry.2017.4265). Dr. Weissman declared funding from a variety of funding bodies and publishing companies outside the submitted work.
This study raises new and interesting questions about the clinical effects of maternal depression on offspring, and identifies a particularly vulnerable group of mothers and their offspring. If anything, the findings are likely an underestimation of the true effect, because of high rates of study attrition, especially within the most vulnerable group.
However, this does not answer the question of what interventions to use, whom to treat, when to do so, and how to treat. Some would argue that clinicians should treat maternal depression first, as a woman with acute depression needs care before she can be helped with parenting. Others suggest that a better approach is to engage the unique mother-infant experience, as this can be a positive therapeutic interaction in itself.
Whatever the approach, the treatment of maternal depression should be evidence based and available early, particularly in new mothers with persistent depression.
Myrna M. Weissman, PhD, is affiliated with the division of epidemiology at Columbia University, New York. These comments are taken from an accompanying editorial (JAMA Psychiatry. 2018 Jan 31. doi: 10.1001/jamapsychiatry.2017.4265). Dr. Weissman declared funding from a variety of funding bodies and publishing companies outside the submitted work.
This study raises new and interesting questions about the clinical effects of maternal depression on offspring, and identifies a particularly vulnerable group of mothers and their offspring. If anything, the findings are likely an underestimation of the true effect, because of high rates of study attrition, especially within the most vulnerable group.
However, this does not answer the question of what interventions to use, whom to treat, when to do so, and how to treat. Some would argue that clinicians should treat maternal depression first, as a woman with acute depression needs care before she can be helped with parenting. Others suggest that a better approach is to engage the unique mother-infant experience, as this can be a positive therapeutic interaction in itself.
Whatever the approach, the treatment of maternal depression should be evidence based and available early, particularly in new mothers with persistent depression.
Myrna M. Weissman, PhD, is affiliated with the division of epidemiology at Columbia University, New York. These comments are taken from an accompanying editorial (JAMA Psychiatry. 2018 Jan 31. doi: 10.1001/jamapsychiatry.2017.4265). Dr. Weissman declared funding from a variety of funding bodies and publishing companies outside the submitted work.
Persistent and severe postpartum depression in mothers may be associated with behavioral problems, poor mathematics grades, and a higher risk of depression in their offspring, research published Jan. 31 in JAMA Psychiatry showed.
In the study, Elena Netsi, DPhil, and her associates presented an analysis of data from 9,848 mothers and 8,287 children enrolled in the observational Avon Longitudinal Study of Parents and Children.
This analysis revealed that postpartum depression of any severity or level of persistence was associated with a two- to fourfold increase in the risk of children showing behavioral problems at age 3.5 years. In women with marked but not persistent postpartum depression, the odds ratio for child behavioral disturbance was 1.91, in mothers with severe but not persistent depression it was 2.39, and in mothers with severe persistent depression, the odds ratio was 4.84 – all of which were highly significant (P less than .001).
However, the authors reported.
It was associated with a 2.65-fold increase in the likelihood of a child having mathematics grades of D or below (P = .01), and a more than sevenfold increase in the prevalence of depression in offspring at 18 years (P less than .001). There also was a 2.3-fold increase in depression at 18 years in the children of mothers who experienced marked but not persistent postpartum depression (P = .04).
Dr. Netsi of the department of psychiatry at the University of Oxford (England) and her coauthors noted that, in women with persistent postpartum depression, mean Edinburgh Postpartum Depression Scale scores remained relatively stable, from 21 months to 11 years, suggesting an increased risk for prolonged depression.
“Identification of women with [postpartum depression] may be associated with increased treatment costs, but the overall cost to the public sector of perinatal mental health problems is five times more than the cost of improving services, further highlighting that early intervention and effective treatment of perinatal depression are a public health priority,” they wrote.
However, they acknowledged that there were mixed findings in the literature with respect to the impact on child outcomes of treating maternal depression.
“Treatments for [postpartum depression] have been relatively brief in duration and moderate in intensity; therefore, it is perhaps unsurprising that such interventions have not shown long-term benefits for either the mother or the child,” the investigators wrote.
The Avon Longitudinal Study of Parents and Children is supported by the U.K. Medical Research Council, the Wellcome Trust, and the University of Bristol. This study was supported by the Wellcome Trust, the National Institute for Health Research Biomedical Research Centre, the University of Bristol, and the NIHR Oxford Health Biomedical Research Centre. No conflicts of interest were declared.
SOURCE: Netsi E et al. JAMA Psychiatry. 2018 Jan 31. doi: 10.1001/jamapsychiatry.2017.4363.
Persistent and severe postpartum depression in mothers may be associated with behavioral problems, poor mathematics grades, and a higher risk of depression in their offspring, research published Jan. 31 in JAMA Psychiatry showed.
In the study, Elena Netsi, DPhil, and her associates presented an analysis of data from 9,848 mothers and 8,287 children enrolled in the observational Avon Longitudinal Study of Parents and Children.
This analysis revealed that postpartum depression of any severity or level of persistence was associated with a two- to fourfold increase in the risk of children showing behavioral problems at age 3.5 years. In women with marked but not persistent postpartum depression, the odds ratio for child behavioral disturbance was 1.91, in mothers with severe but not persistent depression it was 2.39, and in mothers with severe persistent depression, the odds ratio was 4.84 – all of which were highly significant (P less than .001).
However, the authors reported.
It was associated with a 2.65-fold increase in the likelihood of a child having mathematics grades of D or below (P = .01), and a more than sevenfold increase in the prevalence of depression in offspring at 18 years (P less than .001). There also was a 2.3-fold increase in depression at 18 years in the children of mothers who experienced marked but not persistent postpartum depression (P = .04).
Dr. Netsi of the department of psychiatry at the University of Oxford (England) and her coauthors noted that, in women with persistent postpartum depression, mean Edinburgh Postpartum Depression Scale scores remained relatively stable, from 21 months to 11 years, suggesting an increased risk for prolonged depression.
“Identification of women with [postpartum depression] may be associated with increased treatment costs, but the overall cost to the public sector of perinatal mental health problems is five times more than the cost of improving services, further highlighting that early intervention and effective treatment of perinatal depression are a public health priority,” they wrote.
However, they acknowledged that there were mixed findings in the literature with respect to the impact on child outcomes of treating maternal depression.
“Treatments for [postpartum depression] have been relatively brief in duration and moderate in intensity; therefore, it is perhaps unsurprising that such interventions have not shown long-term benefits for either the mother or the child,” the investigators wrote.
The Avon Longitudinal Study of Parents and Children is supported by the U.K. Medical Research Council, the Wellcome Trust, and the University of Bristol. This study was supported by the Wellcome Trust, the National Institute for Health Research Biomedical Research Centre, the University of Bristol, and the NIHR Oxford Health Biomedical Research Centre. No conflicts of interest were declared.
SOURCE: Netsi E et al. JAMA Psychiatry. 2018 Jan 31. doi: 10.1001/jamapsychiatry.2017.4363.
FROM JAMA PSYCHIATRY
Key clinical point: Persistent and severe postpartum depression in mothers is associated with behavioral problems, poor mathematics grades, and a higher risk of depression in their offspring.
Major finding: Maternal postpartum depression of any severity or level of persistence was associated with a two- to fourfold increase in the risk of children showing behavioral problems at age 3.5 years.
Data source: An analysis of data from 9,848 mothers and 8,287 children enrolled in the observational Avon Longitudinal Study of Parents and Children.
Disclosures: The Avon Longitudinal Study of Parents and Children is supported by the U.K. Medical Research Council, the Wellcome Trust, and the University of Bristol. This study was supported by the Wellcome Trust, the National Institute for Health Research Biomedical Research Centre, the University of Bristol, and the NIHR Oxford Health Biomedical Research Centre. No conflicts of interest were declared.
Source: Netsi E et al. JAMA Psychiatry. 2018 Jan 31. doi: 10.1001/jamapsychiatry.2017.4363.
JAK inhibitors look good for severe alopecia areata treatment
said Lucy Yichu Liu, MD, and Brett Andrew King, MD, of Yale University, New Haven, Conn.
Standard medical therapies for alopecia areata – usually topical or injected corticosteroids and allergic contact sensitization – are not very effective for severe disease, particularly alopecia totalis and alopecia universalis. The Janus kinase (JAK) pathway recently has been suggested as a target for treatment.
Dr. Liu and Dr. King reviewed several studies, including a retrospective cohort study of 13 patients aged 12-17 years, in which 7 patients had 100% hair loss and 6 had 20%-70% scalp hair loss. The adolescents were treated with the JAK1/3 inhibitor tofacitinib citrate 5 mg twice daily for 2-16 months (median, 5 months). That led to 93% median improvement in Severity of Alopecia Tool (SALT) score (range, 1%-100%) from baseline. Nine patients experienced hair regrowth. There were mild adverse effects, such as upper respiratory infections and headaches.

In a retrospective cohort study of 90 adults taking tofacitinib at a dosage of 5-10 mg twice daily for 4 months or longer with or without prednisone (300 mg once monthly for three doses), patients were divided into those who were more or less likely to respond based on duration of disease. Of 65 patients with alopecia totalis, or alopecia universalis that had lasted 10 years or less, or alopecia areata, 77% had some hair regrowth; 58% had more than 50% improvement from baseline, and 20% achieved full regrowth of hair, Dr. Liu and Dr. King reported in the Journal of Investigative Dermatology Symposium Proceedings.
“Given the finding in adults that complete scalp hair loss for more than 10 years is less likely to respond to treatment, there may be merit to pursuing treatment, even if only intermittently, in adolescents or even younger patients with stable, severe alopecia areata, to prevent irreversible hair loss in the future,” they wrote.
A patient with alopecia universalis achieved partial scalp hair regrowth and complete eyebrow regrowth with compounded ruxolitinib, a topical JAK inhibitor, according to a 2016 case report. Dr. Liu and Dr. King reported that clinical trials with topical JAK inhibitors, including topical tofacitinib and topical ruxolitinib, currently are ongoing.
SOURCE: Liu LY et al. J Investig Dermatol Symp Proc. 2018 Jan. doi: 10.1016/j.jisp.2017.10.003.
said Lucy Yichu Liu, MD, and Brett Andrew King, MD, of Yale University, New Haven, Conn.
Standard medical therapies for alopecia areata – usually topical or injected corticosteroids and allergic contact sensitization – are not very effective for severe disease, particularly alopecia totalis and alopecia universalis. The Janus kinase (JAK) pathway recently has been suggested as a target for treatment.
Dr. Liu and Dr. King reviewed several studies, including a retrospective cohort study of 13 patients aged 12-17 years, in which 7 patients had 100% hair loss and 6 had 20%-70% scalp hair loss. The adolescents were treated with the JAK1/3 inhibitor tofacitinib citrate 5 mg twice daily for 2-16 months (median, 5 months). That led to 93% median improvement in Severity of Alopecia Tool (SALT) score (range, 1%-100%) from baseline. Nine patients experienced hair regrowth. There were mild adverse effects, such as upper respiratory infections and headaches.
In a retrospective cohort study of 90 adults taking tofacitinib at a dosage of 5-10 mg twice daily for 4 months or longer with or without prednisone (300 mg once monthly for three doses), patients were divided into those who were more or less likely to respond based on duration of disease. Of 65 patients with alopecia totalis, or alopecia universalis that had lasted 10 years or less, or alopecia areata, 77% had some hair regrowth; 58% had more than 50% improvement from baseline, and 20% achieved full regrowth of hair, Dr. Liu and Dr. King reported in the Journal of Investigative Dermatology Symposium Proceedings.
“Given the finding in adults that complete scalp hair loss for more than 10 years is less likely to respond to treatment, there may be merit to pursuing treatment, even if only intermittently, in adolescents or even younger patients with stable, severe alopecia areata, to prevent irreversible hair loss in the future,” they wrote.
A patient with alopecia universalis achieved partial scalp hair regrowth and complete eyebrow regrowth with compounded ruxolitinib, a topical JAK inhibitor, according to a 2016 case report. Dr. Liu and Dr. King reported that clinical trials with topical JAK inhibitors, including topical tofacitinib and topical ruxolitinib, currently are ongoing.
SOURCE: Liu LY et al. J Investig Dermatol Symp Proc. 2018 Jan. doi: 10.1016/j.jisp.2017.10.003.
said Lucy Yichu Liu, MD, and Brett Andrew King, MD, of Yale University, New Haven, Conn.
Standard medical therapies for alopecia areata – usually topical or injected corticosteroids and allergic contact sensitization – are not very effective for severe disease, particularly alopecia totalis and alopecia universalis. The Janus kinase (JAK) pathway recently has been suggested as a target for treatment.
Dr. Liu and Dr. King reviewed several studies, including a retrospective cohort study of 13 patients aged 12-17 years, in which 7 patients had 100% hair loss and 6 had 20%-70% scalp hair loss. The adolescents were treated with the JAK1/3 inhibitor tofacitinib citrate 5 mg twice daily for 2-16 months (median, 5 months). That led to 93% median improvement in Severity of Alopecia Tool (SALT) score (range, 1%-100%) from baseline. Nine patients experienced hair regrowth. There were mild adverse effects, such as upper respiratory infections and headaches.
In a retrospective cohort study of 90 adults taking tofacitinib at a dosage of 5-10 mg twice daily for 4 months or longer with or without prednisone (300 mg once monthly for three doses), patients were divided into those who were more or less likely to respond based on duration of disease. Of 65 patients with alopecia totalis, or alopecia universalis that had lasted 10 years or less, or alopecia areata, 77% had some hair regrowth; 58% had more than 50% improvement from baseline, and 20% achieved full regrowth of hair, Dr. Liu and Dr. King reported in the Journal of Investigative Dermatology Symposium Proceedings.
“Given the finding in adults that complete scalp hair loss for more than 10 years is less likely to respond to treatment, there may be merit to pursuing treatment, even if only intermittently, in adolescents or even younger patients with stable, severe alopecia areata, to prevent irreversible hair loss in the future,” they wrote.
A patient with alopecia universalis achieved partial scalp hair regrowth and complete eyebrow regrowth with compounded ruxolitinib, a topical JAK inhibitor, according to a 2016 case report. Dr. Liu and Dr. King reported that clinical trials with topical JAK inhibitors, including topical tofacitinib and topical ruxolitinib, currently are ongoing.
SOURCE: Liu LY et al. J Investig Dermatol Symp Proc. 2018 Jan. doi: 10.1016/j.jisp.2017.10.003.
FROM JOURNAL OF INVESTIGATIVE DERMATOLOGY SYMPOSIUM PROCEEDINGS

Study finds rising use of newer DMTs in pediatric-onset MS
Newer disease-modifying therapies are often used in patients with pediatric-onset MS, and they appear to have short-term side effect profiles similar to those observed in adults, a study of data from multiple clinics demonstrated.
“There are limited studies of MS treatments in pediatric-onset MS (onset before 18 years) as the main trials used to approve disease-modifying therapies [DMTs] are performed in adults,” lead study author Kristen Krysko, MD, said in an interview prior to a meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis in San Diego. “This makes it difficult to treat children with MS as there is limited high-quality evidence for safety and effectiveness of treatments.”

DMTs considered to be “newer” include dimethyl fumarate (Tecfidera), fingolimod (Gilenya), teriflunomide (Aubagio), natalizumab (Tysabri), rituximab (Rituxan), ocrelizumab (Ocrevus), alemtuzumab (Lemtrada), and daclizumab (Zinbryta). DMTs were classified as injectable (glatiramer acetate, beta-interferons), oral (dimethyl fumarate, fingolimod, teriflunomide) or intravenous (natalizumab, rituximab, alemtuzumab, ocrelizumab).
Dr. Krysko, a multiple sclerosis clinical research fellow at the University of California, San Francisco, and her associates reported findings from 749 pediatric patients with MS and 274 with clinically-isolated syndrome whose data had been entered into the network as of August 2017 and who were followed for a mean of 3.3 years. The majority of patients were female (65%) with a mean age at disease onset of 12.9 years. Over time, the researchers observed increasing overall and first-line use of newer oral and intravenous DMTs in those younger than and older than 12 years of age at the start of a DMT (P less than .001).
Of the 618 patients who received a DMT before 18 years of age, 259 (42%) received a newer DMT and 104 (17%) received a newer DMT as first-line therapy. Dimethyl fumarate was the newer DMT used most often (ever in 100, as a first-line therapy in 36), followed by natalizumab (ever in 101, as a first-line therapy in 30), rituximab (ever in 57, as a first-line therapy in 22), fingolimod (ever in 37, as a first-line therapy in 14), daclizumab (ever in 5, as a first-line therapy in none), and teriflunomide (ever in 3, as a first-line therapy in 2).
The overall side effect profiles of newer DMTs were not different from those reported with the same agents in adults. Specifically, the number of side effects was greatest for dimethyl fumarate (37.7 per 100 person-years), followed by rituximab (20.1 per 100 person-years), natalizumab (15.7 per 100 person-years), and daclizumab (9.6 per 100 person-years).
“We found that newer medications are being prescribed more often in children with MS over time,” Dr. Krysko said. “Even children who were quite young (younger than 12 years old) received newer MS treatments in some cases, although older children (12 years and older) were more likely to receive newer treatments than were the very young children. We did not find new safety concerns with these medications compared to adults.”
She acknowledged certain limitations of the study, including the “likely underestimate” of side effects and the lack of access to laboratory results of children while on these medications. “Thus, further investigation of the safety of these newer medications in children is needed,” she said.
The National MS Society funded the study. Dr. Krysko disclosed that she is funded by the society as a Sylvia Lawry Physician Fellow.
Newer disease-modifying therapies are often used in patients with pediatric-onset MS, and they appear to have short-term side effect profiles similar to those observed in adults, a study of data from multiple clinics demonstrated.
“There are limited studies of MS treatments in pediatric-onset MS (onset before 18 years) as the main trials used to approve disease-modifying therapies [DMTs] are performed in adults,” lead study author Kristen Krysko, MD, said in an interview prior to a meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis in San Diego. “This makes it difficult to treat children with MS as there is limited high-quality evidence for safety and effectiveness of treatments.”
DMTs considered to be “newer” include dimethyl fumarate (Tecfidera), fingolimod (Gilenya), teriflunomide (Aubagio), natalizumab (Tysabri), rituximab (Rituxan), ocrelizumab (Ocrevus), alemtuzumab (Lemtrada), and daclizumab (Zinbryta). DMTs were classified as injectable (glatiramer acetate, beta-interferons), oral (dimethyl fumarate, fingolimod, teriflunomide) or intravenous (natalizumab, rituximab, alemtuzumab, ocrelizumab).
Dr. Krysko, a multiple sclerosis clinical research fellow at the University of California, San Francisco, and her associates reported findings from 749 pediatric patients with MS and 274 with clinically-isolated syndrome whose data had been entered into the network as of August 2017 and who were followed for a mean of 3.3 years. The majority of patients were female (65%) with a mean age at disease onset of 12.9 years. Over time, the researchers observed increasing overall and first-line use of newer oral and intravenous DMTs in those younger than and older than 12 years of age at the start of a DMT (P less than .001).
Of the 618 patients who received a DMT before 18 years of age, 259 (42%) received a newer DMT and 104 (17%) received a newer DMT as first-line therapy. Dimethyl fumarate was the newer DMT used most often (ever in 100, as a first-line therapy in 36), followed by natalizumab (ever in 101, as a first-line therapy in 30), rituximab (ever in 57, as a first-line therapy in 22), fingolimod (ever in 37, as a first-line therapy in 14), daclizumab (ever in 5, as a first-line therapy in none), and teriflunomide (ever in 3, as a first-line therapy in 2).
The overall side effect profiles of newer DMTs were not different from those reported with the same agents in adults. Specifically, the number of side effects was greatest for dimethyl fumarate (37.7 per 100 person-years), followed by rituximab (20.1 per 100 person-years), natalizumab (15.7 per 100 person-years), and daclizumab (9.6 per 100 person-years).
“We found that newer medications are being prescribed more often in children with MS over time,” Dr. Krysko said. “Even children who were quite young (younger than 12 years old) received newer MS treatments in some cases, although older children (12 years and older) were more likely to receive newer treatments than were the very young children. We did not find new safety concerns with these medications compared to adults.”
She acknowledged certain limitations of the study, including the “likely underestimate” of side effects and the lack of access to laboratory results of children while on these medications. “Thus, further investigation of the safety of these newer medications in children is needed,” she said.
The National MS Society funded the study. Dr. Krysko disclosed that she is funded by the society as a Sylvia Lawry Physician Fellow.
Newer disease-modifying therapies are often used in patients with pediatric-onset MS, and they appear to have short-term side effect profiles similar to those observed in adults, a study of data from multiple clinics demonstrated.
“There are limited studies of MS treatments in pediatric-onset MS (onset before 18 years) as the main trials used to approve disease-modifying therapies [DMTs] are performed in adults,” lead study author Kristen Krysko, MD, said in an interview prior to a meeting held by the Americas Committee for Treatment and Research in Multiple Sclerosis in San Diego. “This makes it difficult to treat children with MS as there is limited high-quality evidence for safety and effectiveness of treatments.”
DMTs considered to be “newer” include dimethyl fumarate (Tecfidera), fingolimod (Gilenya), teriflunomide (Aubagio), natalizumab (Tysabri), rituximab (Rituxan), ocrelizumab (Ocrevus), alemtuzumab (Lemtrada), and daclizumab (Zinbryta). DMTs were classified as injectable (glatiramer acetate, beta-interferons), oral (dimethyl fumarate, fingolimod, teriflunomide) or intravenous (natalizumab, rituximab, alemtuzumab, ocrelizumab).
Dr. Krysko, a multiple sclerosis clinical research fellow at the University of California, San Francisco, and her associates reported findings from 749 pediatric patients with MS and 274 with clinically-isolated syndrome whose data had been entered into the network as of August 2017 and who were followed for a mean of 3.3 years. The majority of patients were female (65%) with a mean age at disease onset of 12.9 years. Over time, the researchers observed increasing overall and first-line use of newer oral and intravenous DMTs in those younger than and older than 12 years of age at the start of a DMT (P less than .001).
Of the 618 patients who received a DMT before 18 years of age, 259 (42%) received a newer DMT and 104 (17%) received a newer DMT as first-line therapy. Dimethyl fumarate was the newer DMT used most often (ever in 100, as a first-line therapy in 36), followed by natalizumab (ever in 101, as a first-line therapy in 30), rituximab (ever in 57, as a first-line therapy in 22), fingolimod (ever in 37, as a first-line therapy in 14), daclizumab (ever in 5, as a first-line therapy in none), and teriflunomide (ever in 3, as a first-line therapy in 2).
The overall side effect profiles of newer DMTs were not different from those reported with the same agents in adults. Specifically, the number of side effects was greatest for dimethyl fumarate (37.7 per 100 person-years), followed by rituximab (20.1 per 100 person-years), natalizumab (15.7 per 100 person-years), and daclizumab (9.6 per 100 person-years).
“We found that newer medications are being prescribed more often in children with MS over time,” Dr. Krysko said. “Even children who were quite young (younger than 12 years old) received newer MS treatments in some cases, although older children (12 years and older) were more likely to receive newer treatments than were the very young children. We did not find new safety concerns with these medications compared to adults.”
She acknowledged certain limitations of the study, including the “likely underestimate” of side effects and the lack of access to laboratory results of children while on these medications. “Thus, further investigation of the safety of these newer medications in children is needed,” she said.
The National MS Society funded the study. Dr. Krysko disclosed that she is funded by the society as a Sylvia Lawry Physician Fellow.
FROM ACTRIMS FORUM 2018
Key clinical point: Newer DMTs are often used in individuals with pediatric MS.
Major finding: Among pediatric MS patients, the first agent used was a newer DMT in 17% of cases.
Study details: A retrospective review of prospectively collected data on 1,023 pediatric patients with MS.
Disclosures: The National MS Society funded the study. Dr. Krysko disclosed that she is funded by the society as a Sylvia Lawry Physician Fellow.
Source: Krysko K et al. ACTRIMS Forum 2018 Poster 68.