User login
Practical approaches to promoting brain health
More than once in his Current Psychiatry essays, Henry A. Nasrallah, MD, has stressed the seismic paradigmatic shifts in our understanding of mental illness and brain disease. He has highlighted the critical significance of processes of neurogenesis and neuroinflammation, yet little has been offered to practitioners in terms of practical approaches to promoting the brain health that he encourages.
Two of the most potent modalities for maintaining brain wellness and facilitating ongoing neurogenesis and synaptogenesis are exercise and nutrition—specifically, high-intensity interval training and a diet heavily, if not entirely, plant-based. The neuroprotective capabilities of mindfulness practice and its impact on prefrontal cortical regions also are relevant.
In society at large, it strikes me that physicians have not fared any better than the general population when it comes to maintaining a healthy diet and engaging in physical exercise. I encourage Dr. Nasrallah to continue addressing these themes, and to remind his audience of physicians to “heal thyself.”
More than once in his Current Psychiatry essays, Henry A. Nasrallah, MD, has stressed the seismic paradigmatic shifts in our understanding of mental illness and brain disease. He has highlighted the critical significance of processes of neurogenesis and neuroinflammation, yet little has been offered to practitioners in terms of practical approaches to promoting the brain health that he encourages.
Two of the most potent modalities for maintaining brain wellness and facilitating ongoing neurogenesis and synaptogenesis are exercise and nutrition—specifically, high-intensity interval training and a diet heavily, if not entirely, plant-based. The neuroprotective capabilities of mindfulness practice and its impact on prefrontal cortical regions also are relevant.
In society at large, it strikes me that physicians have not fared any better than the general population when it comes to maintaining a healthy diet and engaging in physical exercise. I encourage Dr. Nasrallah to continue addressing these themes, and to remind his audience of physicians to “heal thyself.”
More than once in his Current Psychiatry essays, Henry A. Nasrallah, MD, has stressed the seismic paradigmatic shifts in our understanding of mental illness and brain disease. He has highlighted the critical significance of processes of neurogenesis and neuroinflammation, yet little has been offered to practitioners in terms of practical approaches to promoting the brain health that he encourages.
Two of the most potent modalities for maintaining brain wellness and facilitating ongoing neurogenesis and synaptogenesis are exercise and nutrition—specifically, high-intensity interval training and a diet heavily, if not entirely, plant-based. The neuroprotective capabilities of mindfulness practice and its impact on prefrontal cortical regions also are relevant.
In society at large, it strikes me that physicians have not fared any better than the general population when it comes to maintaining a healthy diet and engaging in physical exercise. I encourage Dr. Nasrallah to continue addressing these themes, and to remind his audience of physicians to “heal thyself.”
Billing audits: The bane of a small practice
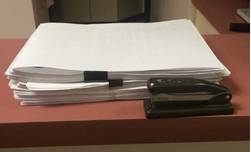
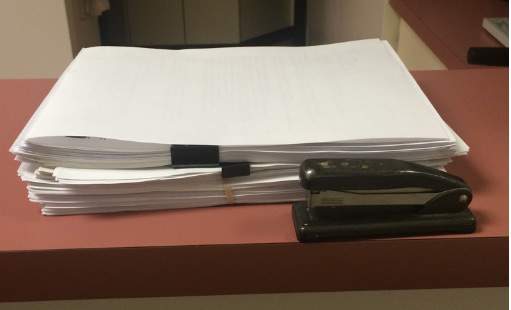
The photo you see below is a reasonably thick pile of paper, roughly 2 inches high. It’s certainly not as bad as some charts I’ve seen, especially at the VA, but still a lot of pages.
What is it?
This is, believe it or not, the stacked copies of charts we had to print in the last 30 days to fax to insurance companies for billing audits. Yeah – just the last 30 days.
Mind you, to date I don’t have any sort of actual complaints or charges against me for fraudulent billing. If anything, I tend to underbill for fear of risking the ire of insurance companies.
On one level, I understand it. The news is replete with stories of physicians who made fraudulent insurance claims, and the insurance companies want to make sure others are playing fair. Just like security cameras and magnetic tags at retailers, they’re doing what they can to avoid losses. I get that.
On the other hand, this irritates me, and it is a pain in the butt. Someone here has to print up the requested notes, organize them, fill out the accompanying forms, and fax them back. I also have to sign each note in the pile. For the number of charts they typically want, this process takes about 30-45 minutes. Then we fax them, and a 100-plus-page document ties up your office fax for a while. Incoming and outgoing faxes, such as medication refills, get put on hold. Overall, it takes maybe an hour of staff time to do this, not to mention the cost of paper and ink used.
About 25% of the time the company calls us after a few days to say they never got them (even though we have a confirmation). For this reason, we always hold onto the print-out for a month so we don’t have to start over again. Then it all has to be shredded.
In a large practice, I’m sure there are dedicated medical records staff members for this. But in my small solo world it means that someone has to let phones go to voicemail, dictations get delayed, and other work piles up, just so the insurance red tape gets done. Then we have to catch up on the more routine issues of patient care.
I can’t really refuse to send them, either. Doing so, in the insurance company’s mind, would be an admission of guilt that I never saw the patient and my claim is bogus. Then they’ll withhold payment, or ask for a refund.
This is, regrettably, a case where a few bad apples – docs filing bogus claims – have spoiled the entire barrel. Now we’re all guilty of fraud until proven innocent by sending these records. Isn’t that the reverse of the American justice system’s ideal?
I also wonder if there’s an intentional drudgery factor here. By making me do something that’s irritatingly time-wasting, is an insurance plan hoping I’ll drop them because I’m sick of this process? Does having fewer contracted neurologists work out to their benefit? It certainly isn’t to the patient’s advantage.
I don’t have an easy answer. I don’t like the wrench these requests throw into the office routine, but I also know that fraud surveillance is a necessary evil. I just wish there was a less time-consuming way of doing it.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The photo you see below is a reasonably thick pile of paper, roughly 2 inches high. It’s certainly not as bad as some charts I’ve seen, especially at the VA, but still a lot of pages.
What is it?
This is, believe it or not, the stacked copies of charts we had to print in the last 30 days to fax to insurance companies for billing audits. Yeah – just the last 30 days.
Mind you, to date I don’t have any sort of actual complaints or charges against me for fraudulent billing. If anything, I tend to underbill for fear of risking the ire of insurance companies.
On one level, I understand it. The news is replete with stories of physicians who made fraudulent insurance claims, and the insurance companies want to make sure others are playing fair. Just like security cameras and magnetic tags at retailers, they’re doing what they can to avoid losses. I get that.
On the other hand, this irritates me, and it is a pain in the butt. Someone here has to print up the requested notes, organize them, fill out the accompanying forms, and fax them back. I also have to sign each note in the pile. For the number of charts they typically want, this process takes about 30-45 minutes. Then we fax them, and a 100-plus-page document ties up your office fax for a while. Incoming and outgoing faxes, such as medication refills, get put on hold. Overall, it takes maybe an hour of staff time to do this, not to mention the cost of paper and ink used.
About 25% of the time the company calls us after a few days to say they never got them (even though we have a confirmation). For this reason, we always hold onto the print-out for a month so we don’t have to start over again. Then it all has to be shredded.
In a large practice, I’m sure there are dedicated medical records staff members for this. But in my small solo world it means that someone has to let phones go to voicemail, dictations get delayed, and other work piles up, just so the insurance red tape gets done. Then we have to catch up on the more routine issues of patient care.
I can’t really refuse to send them, either. Doing so, in the insurance company’s mind, would be an admission of guilt that I never saw the patient and my claim is bogus. Then they’ll withhold payment, or ask for a refund.
This is, regrettably, a case where a few bad apples – docs filing bogus claims – have spoiled the entire barrel. Now we’re all guilty of fraud until proven innocent by sending these records. Isn’t that the reverse of the American justice system’s ideal?
I also wonder if there’s an intentional drudgery factor here. By making me do something that’s irritatingly time-wasting, is an insurance plan hoping I’ll drop them because I’m sick of this process? Does having fewer contracted neurologists work out to their benefit? It certainly isn’t to the patient’s advantage.
I don’t have an easy answer. I don’t like the wrench these requests throw into the office routine, but I also know that fraud surveillance is a necessary evil. I just wish there was a less time-consuming way of doing it.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
The photo you see below is a reasonably thick pile of paper, roughly 2 inches high. It’s certainly not as bad as some charts I’ve seen, especially at the VA, but still a lot of pages.
What is it?
This is, believe it or not, the stacked copies of charts we had to print in the last 30 days to fax to insurance companies for billing audits. Yeah – just the last 30 days.
Mind you, to date I don’t have any sort of actual complaints or charges against me for fraudulent billing. If anything, I tend to underbill for fear of risking the ire of insurance companies.
On one level, I understand it. The news is replete with stories of physicians who made fraudulent insurance claims, and the insurance companies want to make sure others are playing fair. Just like security cameras and magnetic tags at retailers, they’re doing what they can to avoid losses. I get that.
On the other hand, this irritates me, and it is a pain in the butt. Someone here has to print up the requested notes, organize them, fill out the accompanying forms, and fax them back. I also have to sign each note in the pile. For the number of charts they typically want, this process takes about 30-45 minutes. Then we fax them, and a 100-plus-page document ties up your office fax for a while. Incoming and outgoing faxes, such as medication refills, get put on hold. Overall, it takes maybe an hour of staff time to do this, not to mention the cost of paper and ink used.
About 25% of the time the company calls us after a few days to say they never got them (even though we have a confirmation). For this reason, we always hold onto the print-out for a month so we don’t have to start over again. Then it all has to be shredded.
In a large practice, I’m sure there are dedicated medical records staff members for this. But in my small solo world it means that someone has to let phones go to voicemail, dictations get delayed, and other work piles up, just so the insurance red tape gets done. Then we have to catch up on the more routine issues of patient care.
I can’t really refuse to send them, either. Doing so, in the insurance company’s mind, would be an admission of guilt that I never saw the patient and my claim is bogus. Then they’ll withhold payment, or ask for a refund.
This is, regrettably, a case where a few bad apples – docs filing bogus claims – have spoiled the entire barrel. Now we’re all guilty of fraud until proven innocent by sending these records. Isn’t that the reverse of the American justice system’s ideal?
I also wonder if there’s an intentional drudgery factor here. By making me do something that’s irritatingly time-wasting, is an insurance plan hoping I’ll drop them because I’m sick of this process? Does having fewer contracted neurologists work out to their benefit? It certainly isn’t to the patient’s advantage.
I don’t have an easy answer. I don’t like the wrench these requests throw into the office routine, but I also know that fraud surveillance is a necessary evil. I just wish there was a less time-consuming way of doing it.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Infection prevention
Not a long ago, I received a call from a friend working in a local pediatric clinic. One of her partners had just seen a young child with an unusual rash. The diagnosis? Crusted scabies.
Sarcoptes scabiei var. hominis, the mite that causes typical scabies, also causes crusted or Norwegian scabies. These terms refer to severe infestations that occur in individuals who are immune compromised or debilitated. The rash is characterized by vesicles and thick crusts and may or may not be itchy. Because patients with crusted scabies can be infested with as many as 2 million mites, transmission from very brief skin-to-skin contact is possible, and outbreaks have occurred in health care facilities and other institutional settings.

That was the reason for my friend’s call. “What do we do for the doctors and nurses in the clinic who saw the patient?” she wanted to know.
“Everyone wore gloves, right?” I asked. There was silence on the other end of the phone.
After a quick consultation with our health department, every health care provider (HCP) who touched the patient without gloves was treated preemptively with topical permethrin. None went on to develop scabies. The experience prompted me to think about the challenges of infection prevention in ambulatory care.
Both the American Academy of Pediatrics (AAP Committee on Infectious Diseases, “Infection prevention and control in pediatric ambulatory settings,” Pediatrics 2007;20[3]:650-65) and the Centers for Disease Control and Prevention (Guide to Infection Prevention for Outpatient Settings: Minimum Expectations for Safe Care) have published recommendations for infection prevention in outpatient settings. Both organizations emphasize the importance of standard precautions. According to the CDC, standard precautions “are the minimum infection prevention practices that apply to all patient care, regardless of suspected or confirmed infection status of the patient, in any setting where health care is delivered.” They are designed to protect HCPs, as well as prevent us from spreading infections among patients. Standard precautions include:
• Hand hygiene.
• Use of personal protective equipment (gloves, gowns, masks).
• Safe injection practices.
• Safe handling of potentially contaminated equipment or surfaces in the patient environment.
• Respiratory hygiene/cough etiquette.
Some of these elements are likely second nature to office-based pediatricians. Hands must be cleaned before and after every patient encounter or an encounter with the patient’s immediate environment. “Cover your cough” signs have become ubiquitous in ambulatory care waiting rooms, even as we acknowledge the difficulties associated with expecting toddlers to wear masks or use a tissue to contain their coughs and sneezes.
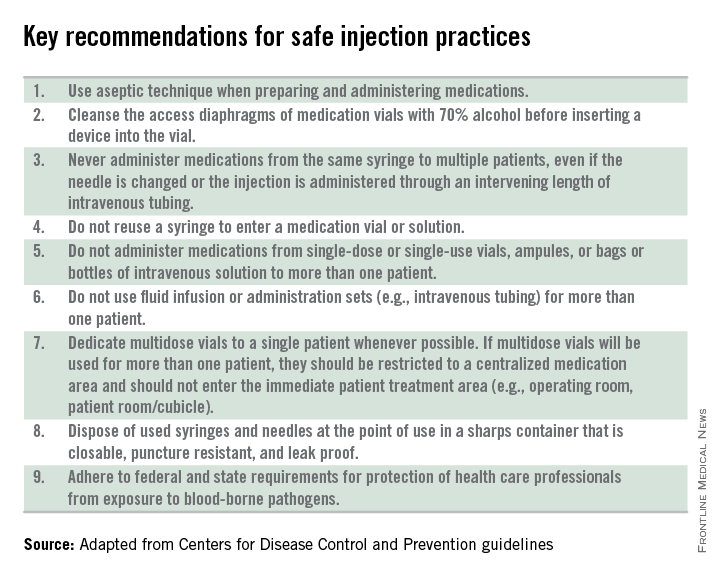
Other elements of standard precautions may receive increased attention because the consequences of noncompliance are perceived to be dangerous or severe. For example, we know that failure to reliably employ safe injection practices (see table) has resulted in transmission of blood-borne pathogens, including hepatitis B and C, in ambulatory settings.
In my experience, the use of personal protective equipment (PPE) in the ambulatory setting is the element of standard precautions that is the least understood and perhaps the most underutilized. It’s certainly easier in the inpatient setting, where we use transmission-based precautions, and colorful isolation signs instruct us to put on gown and gloves when we visit the patient with viral gastroenteritis, or gown, gloves, and mask for the child with acute viral respiratory tract infection. In the office, we expect the HCP to anticipate what kind of contact with blood or body fluids is likely and choose PPE accordingly.
Of course, anticipation can be tricky. Gowns, for example, are only required during procedures or activities when contact with blood and body fluids is likely. In routine office-based care, these sorts of procedures are uncommon. Incision and drainage of an abscess is one example of a procedure that might warrant protection of one’s clothing with a gown. Conversely, the need for a mask might arise several times a day, as these are worn to protect the mouth, nose, and eyes “during procedures that are likely to generate splashes or sprays of blood or other body fluids.” Examination of a coughing patient is a common “procedure” likely to results in sprays of saliva. Use of a mask can protect the examiner from potential exposures to Bordetella pertussis, Mycoplasma pneumoniae, and a host of respiratory viruses.
While the AAP has been careful to point out that gloves are not needed for the routine care of well children, they should be used when “there is the potential to contact blood, body fluids, mucous membranes, nonintact skin, or potentially infectious material.” In our world, potentially infectious material might include a cluster of vesicles thought to be herpes simplex, the honey-crusted lesions of impetigo, or the weeping, crusted rash of Norwegian scabies.
My own office had a powerful reminder about the importance of standard precautions last year when we were referred a young infant with recurrent fevers and a mostly dry, peeling rash. As we learned in medical school, the mucocutanous lesions of congenital syphilis can be highly contagious. In accordance with AAP recommendations, all HCPs who examined this child without the protection of gloves underwent serologic testing for syphilis. Fortunately, there were no transmissions!
Published data about infectious disease exposures and the transmission of infectious diseases in the outpatient setting, either from patients to health care workers or among patients, are largely limited to outbreak or case reports. A 1991 review identified 53 reports of infectious disease transmission in outpatient settings between 1961 and 1990 (JAMA 1991;265(18): 2377-81). Transmission occurred in medical and dental offices, clinics, emergency departments, ophthalmology offices, and alternative care settings that included chiropractic clinics and an acupuncture practice. A variety of pathogens were involved, including measles, adenovirus, hepatitis B, atypical mycobacteria, and Streptococcus pyogenes. The authors concluded that many of the outbreaks and episodes of transmission could have been prevented “if existing infection control guidelines,” including what we now consider standard precautions, had been utilized. Many reports published in the intervening 25 years have come to similar conclusions.
So why don’t HCPs yet follow standard precautions, including appropriate use of PPE? The reasons are complex and multifactorial. We’re all busy and lack of time is a common complaint. Gowns, gloves, masks, and alcohol hand gel aren’t always readily available. Some HCPs may not be knowledgeable about the elements of standard precautions while others may not understand the risks to themselves and their patients associated with nonadherence. Finally, some organizations have not established clear expectations related to infection prevention and compliance with AAP and CDC recommendations.
Several years ago, at the very beginning of the H1N1 influenza epidemic, a colleague of mine working in a pediatric practice saw a patient complaining of fever, lethargy, and myalgia. Not surprisingly, the patient’s rapid influenza test was positive. My colleague recalls that she was handed the result before she ever walked into the room – without any PPE – to see the patient.
“This was different than my usual routine at the hospital,” she told me. The expectation at the hospital was gown, gloves, and masks for any patient with influenza or influenzalike illness. At the office though, there was no such expectation, and providers did not routinely wear masks, even when seeing patients with respiratory symptoms. My colleague wasn’t reckless or rebellious. She was simply conforming to the culture in that office, and following the behavioral cues of more senior physicians in the practice. Subsequently, she developed severe influenza infection requiring a prolonged hospital stay.
It’s time to change the culture. As a first step, perform a quick audit in the office, using the AAP’s “Infection prevention and control in pediatric ambulatory settings” as a guide.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She had no relevant financial disclosures.
Not a long ago, I received a call from a friend working in a local pediatric clinic. One of her partners had just seen a young child with an unusual rash. The diagnosis? Crusted scabies.
Sarcoptes scabiei var. hominis, the mite that causes typical scabies, also causes crusted or Norwegian scabies. These terms refer to severe infestations that occur in individuals who are immune compromised or debilitated. The rash is characterized by vesicles and thick crusts and may or may not be itchy. Because patients with crusted scabies can be infested with as many as 2 million mites, transmission from very brief skin-to-skin contact is possible, and outbreaks have occurred in health care facilities and other institutional settings.
That was the reason for my friend’s call. “What do we do for the doctors and nurses in the clinic who saw the patient?” she wanted to know.
“Everyone wore gloves, right?” I asked. There was silence on the other end of the phone.
After a quick consultation with our health department, every health care provider (HCP) who touched the patient without gloves was treated preemptively with topical permethrin. None went on to develop scabies. The experience prompted me to think about the challenges of infection prevention in ambulatory care.
Both the American Academy of Pediatrics (AAP Committee on Infectious Diseases, “Infection prevention and control in pediatric ambulatory settings,” Pediatrics 2007;20[3]:650-65) and the Centers for Disease Control and Prevention (Guide to Infection Prevention for Outpatient Settings: Minimum Expectations for Safe Care) have published recommendations for infection prevention in outpatient settings. Both organizations emphasize the importance of standard precautions. According to the CDC, standard precautions “are the minimum infection prevention practices that apply to all patient care, regardless of suspected or confirmed infection status of the patient, in any setting where health care is delivered.” They are designed to protect HCPs, as well as prevent us from spreading infections among patients. Standard precautions include:
• Hand hygiene.
• Use of personal protective equipment (gloves, gowns, masks).
• Safe injection practices.
• Safe handling of potentially contaminated equipment or surfaces in the patient environment.
• Respiratory hygiene/cough etiquette.
Some of these elements are likely second nature to office-based pediatricians. Hands must be cleaned before and after every patient encounter or an encounter with the patient’s immediate environment. “Cover your cough” signs have become ubiquitous in ambulatory care waiting rooms, even as we acknowledge the difficulties associated with expecting toddlers to wear masks or use a tissue to contain their coughs and sneezes.
Other elements of standard precautions may receive increased attention because the consequences of noncompliance are perceived to be dangerous or severe. For example, we know that failure to reliably employ safe injection practices (see table) has resulted in transmission of blood-borne pathogens, including hepatitis B and C, in ambulatory settings.
In my experience, the use of personal protective equipment (PPE) in the ambulatory setting is the element of standard precautions that is the least understood and perhaps the most underutilized. It’s certainly easier in the inpatient setting, where we use transmission-based precautions, and colorful isolation signs instruct us to put on gown and gloves when we visit the patient with viral gastroenteritis, or gown, gloves, and mask for the child with acute viral respiratory tract infection. In the office, we expect the HCP to anticipate what kind of contact with blood or body fluids is likely and choose PPE accordingly.
Of course, anticipation can be tricky. Gowns, for example, are only required during procedures or activities when contact with blood and body fluids is likely. In routine office-based care, these sorts of procedures are uncommon. Incision and drainage of an abscess is one example of a procedure that might warrant protection of one’s clothing with a gown. Conversely, the need for a mask might arise several times a day, as these are worn to protect the mouth, nose, and eyes “during procedures that are likely to generate splashes or sprays of blood or other body fluids.” Examination of a coughing patient is a common “procedure” likely to results in sprays of saliva. Use of a mask can protect the examiner from potential exposures to Bordetella pertussis, Mycoplasma pneumoniae, and a host of respiratory viruses.
While the AAP has been careful to point out that gloves are not needed for the routine care of well children, they should be used when “there is the potential to contact blood, body fluids, mucous membranes, nonintact skin, or potentially infectious material.” In our world, potentially infectious material might include a cluster of vesicles thought to be herpes simplex, the honey-crusted lesions of impetigo, or the weeping, crusted rash of Norwegian scabies.
My own office had a powerful reminder about the importance of standard precautions last year when we were referred a young infant with recurrent fevers and a mostly dry, peeling rash. As we learned in medical school, the mucocutanous lesions of congenital syphilis can be highly contagious. In accordance with AAP recommendations, all HCPs who examined this child without the protection of gloves underwent serologic testing for syphilis. Fortunately, there were no transmissions!
Published data about infectious disease exposures and the transmission of infectious diseases in the outpatient setting, either from patients to health care workers or among patients, are largely limited to outbreak or case reports. A 1991 review identified 53 reports of infectious disease transmission in outpatient settings between 1961 and 1990 (JAMA 1991;265(18): 2377-81). Transmission occurred in medical and dental offices, clinics, emergency departments, ophthalmology offices, and alternative care settings that included chiropractic clinics and an acupuncture practice. A variety of pathogens were involved, including measles, adenovirus, hepatitis B, atypical mycobacteria, and Streptococcus pyogenes. The authors concluded that many of the outbreaks and episodes of transmission could have been prevented “if existing infection control guidelines,” including what we now consider standard precautions, had been utilized. Many reports published in the intervening 25 years have come to similar conclusions.
So why don’t HCPs yet follow standard precautions, including appropriate use of PPE? The reasons are complex and multifactorial. We’re all busy and lack of time is a common complaint. Gowns, gloves, masks, and alcohol hand gel aren’t always readily available. Some HCPs may not be knowledgeable about the elements of standard precautions while others may not understand the risks to themselves and their patients associated with nonadherence. Finally, some organizations have not established clear expectations related to infection prevention and compliance with AAP and CDC recommendations.
Several years ago, at the very beginning of the H1N1 influenza epidemic, a colleague of mine working in a pediatric practice saw a patient complaining of fever, lethargy, and myalgia. Not surprisingly, the patient’s rapid influenza test was positive. My colleague recalls that she was handed the result before she ever walked into the room – without any PPE – to see the patient.
“This was different than my usual routine at the hospital,” she told me. The expectation at the hospital was gown, gloves, and masks for any patient with influenza or influenzalike illness. At the office though, there was no such expectation, and providers did not routinely wear masks, even when seeing patients with respiratory symptoms. My colleague wasn’t reckless or rebellious. She was simply conforming to the culture in that office, and following the behavioral cues of more senior physicians in the practice. Subsequently, she developed severe influenza infection requiring a prolonged hospital stay.
It’s time to change the culture. As a first step, perform a quick audit in the office, using the AAP’s “Infection prevention and control in pediatric ambulatory settings” as a guide.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She had no relevant financial disclosures.
Not a long ago, I received a call from a friend working in a local pediatric clinic. One of her partners had just seen a young child with an unusual rash. The diagnosis? Crusted scabies.
Sarcoptes scabiei var. hominis, the mite that causes typical scabies, also causes crusted or Norwegian scabies. These terms refer to severe infestations that occur in individuals who are immune compromised or debilitated. The rash is characterized by vesicles and thick crusts and may or may not be itchy. Because patients with crusted scabies can be infested with as many as 2 million mites, transmission from very brief skin-to-skin contact is possible, and outbreaks have occurred in health care facilities and other institutional settings.
That was the reason for my friend’s call. “What do we do for the doctors and nurses in the clinic who saw the patient?” she wanted to know.
“Everyone wore gloves, right?” I asked. There was silence on the other end of the phone.
After a quick consultation with our health department, every health care provider (HCP) who touched the patient without gloves was treated preemptively with topical permethrin. None went on to develop scabies. The experience prompted me to think about the challenges of infection prevention in ambulatory care.
Both the American Academy of Pediatrics (AAP Committee on Infectious Diseases, “Infection prevention and control in pediatric ambulatory settings,” Pediatrics 2007;20[3]:650-65) and the Centers for Disease Control and Prevention (Guide to Infection Prevention for Outpatient Settings: Minimum Expectations for Safe Care) have published recommendations for infection prevention in outpatient settings. Both organizations emphasize the importance of standard precautions. According to the CDC, standard precautions “are the minimum infection prevention practices that apply to all patient care, regardless of suspected or confirmed infection status of the patient, in any setting where health care is delivered.” They are designed to protect HCPs, as well as prevent us from spreading infections among patients. Standard precautions include:
• Hand hygiene.
• Use of personal protective equipment (gloves, gowns, masks).
• Safe injection practices.
• Safe handling of potentially contaminated equipment or surfaces in the patient environment.
• Respiratory hygiene/cough etiquette.
Some of these elements are likely second nature to office-based pediatricians. Hands must be cleaned before and after every patient encounter or an encounter with the patient’s immediate environment. “Cover your cough” signs have become ubiquitous in ambulatory care waiting rooms, even as we acknowledge the difficulties associated with expecting toddlers to wear masks or use a tissue to contain their coughs and sneezes.
Other elements of standard precautions may receive increased attention because the consequences of noncompliance are perceived to be dangerous or severe. For example, we know that failure to reliably employ safe injection practices (see table) has resulted in transmission of blood-borne pathogens, including hepatitis B and C, in ambulatory settings.
In my experience, the use of personal protective equipment (PPE) in the ambulatory setting is the element of standard precautions that is the least understood and perhaps the most underutilized. It’s certainly easier in the inpatient setting, where we use transmission-based precautions, and colorful isolation signs instruct us to put on gown and gloves when we visit the patient with viral gastroenteritis, or gown, gloves, and mask for the child with acute viral respiratory tract infection. In the office, we expect the HCP to anticipate what kind of contact with blood or body fluids is likely and choose PPE accordingly.
Of course, anticipation can be tricky. Gowns, for example, are only required during procedures or activities when contact with blood and body fluids is likely. In routine office-based care, these sorts of procedures are uncommon. Incision and drainage of an abscess is one example of a procedure that might warrant protection of one’s clothing with a gown. Conversely, the need for a mask might arise several times a day, as these are worn to protect the mouth, nose, and eyes “during procedures that are likely to generate splashes or sprays of blood or other body fluids.” Examination of a coughing patient is a common “procedure” likely to results in sprays of saliva. Use of a mask can protect the examiner from potential exposures to Bordetella pertussis, Mycoplasma pneumoniae, and a host of respiratory viruses.
While the AAP has been careful to point out that gloves are not needed for the routine care of well children, they should be used when “there is the potential to contact blood, body fluids, mucous membranes, nonintact skin, or potentially infectious material.” In our world, potentially infectious material might include a cluster of vesicles thought to be herpes simplex, the honey-crusted lesions of impetigo, or the weeping, crusted rash of Norwegian scabies.
My own office had a powerful reminder about the importance of standard precautions last year when we were referred a young infant with recurrent fevers and a mostly dry, peeling rash. As we learned in medical school, the mucocutanous lesions of congenital syphilis can be highly contagious. In accordance with AAP recommendations, all HCPs who examined this child without the protection of gloves underwent serologic testing for syphilis. Fortunately, there were no transmissions!
Published data about infectious disease exposures and the transmission of infectious diseases in the outpatient setting, either from patients to health care workers or among patients, are largely limited to outbreak or case reports. A 1991 review identified 53 reports of infectious disease transmission in outpatient settings between 1961 and 1990 (JAMA 1991;265(18): 2377-81). Transmission occurred in medical and dental offices, clinics, emergency departments, ophthalmology offices, and alternative care settings that included chiropractic clinics and an acupuncture practice. A variety of pathogens were involved, including measles, adenovirus, hepatitis B, atypical mycobacteria, and Streptococcus pyogenes. The authors concluded that many of the outbreaks and episodes of transmission could have been prevented “if existing infection control guidelines,” including what we now consider standard precautions, had been utilized. Many reports published in the intervening 25 years have come to similar conclusions.
So why don’t HCPs yet follow standard precautions, including appropriate use of PPE? The reasons are complex and multifactorial. We’re all busy and lack of time is a common complaint. Gowns, gloves, masks, and alcohol hand gel aren’t always readily available. Some HCPs may not be knowledgeable about the elements of standard precautions while others may not understand the risks to themselves and their patients associated with nonadherence. Finally, some organizations have not established clear expectations related to infection prevention and compliance with AAP and CDC recommendations.
Several years ago, at the very beginning of the H1N1 influenza epidemic, a colleague of mine working in a pediatric practice saw a patient complaining of fever, lethargy, and myalgia. Not surprisingly, the patient’s rapid influenza test was positive. My colleague recalls that she was handed the result before she ever walked into the room – without any PPE – to see the patient.
“This was different than my usual routine at the hospital,” she told me. The expectation at the hospital was gown, gloves, and masks for any patient with influenza or influenzalike illness. At the office though, there was no such expectation, and providers did not routinely wear masks, even when seeing patients with respiratory symptoms. My colleague wasn’t reckless or rebellious. She was simply conforming to the culture in that office, and following the behavioral cues of more senior physicians in the practice. Subsequently, she developed severe influenza infection requiring a prolonged hospital stay.
It’s time to change the culture. As a first step, perform a quick audit in the office, using the AAP’s “Infection prevention and control in pediatric ambulatory settings” as a guide.
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Kosair Children’s Hospital, also in Louisville. She had no relevant financial disclosures.

Making cystoscopy accessible in gynecology
Gynecologists have used the cystoscope for decades to examine the urethra and bladder, despite urology’s traditional claim that the procedure falls under its purview.
The lines between urology and gynecology have blurred, and cystoscopy has become an even more important and natural part of gynecology’s realm.

During the past 2 decades, gynecologists have become even more involved both in evaluating problems such as overactive bladder symptoms, recurrent urinary tract infection, and bladder/pelvic pain, and in performing pelvic reconstruction procedures.
The American College of Obstetricians and Gynecologists has recommended adoption of cystoscopy by ob.gyns. for diagnostic purposes and some operative indications – most importantly for ruling out cystotomy and intravesical or intraurethral suture or mesh placement, and for verifying ureteral patency. ACOG’s 2007 committee opinion on the role of cystourethroscopy in the generalist obstetrican-gyncecologist practice was reaffirmed in 2015 (Obstet Gynecol. 2007 Jul;110[1]:221-24.).
Yet, to a large extent, cystoscopy has been a good fit in principle, rather than in practice. Training in residency programs has been limited, and traditional cystoscopy can be cumbersome and time consuming. It also is costly, requiring equipment – including a light source and camera – and service contracts that may make it too expensive for many gynecologists to set up and maintain in their offices.
Cystoscopy has therefore often required referral to urologists, resulting in additional appointments, patient inconvenience, and increased costs to the health care system. The learning curve for traditional cystoscopy has been relatively steep, and delays in diagnosis and management as a result of referrals are not uncommon.
Moreover, cystoscopes were never designed to be safe and comfortable for women. Men and women have different anatomy, yet there always has been a one-size-fits-all device. The flexible cystoscope commonly used by urologists was designed for the unique length and anatomy of the male urethra.
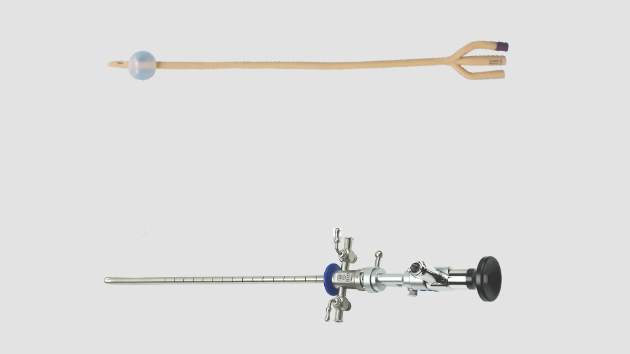
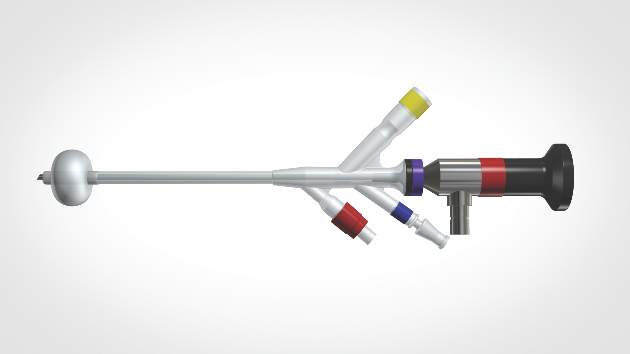
A new catheter-based system specifically for female cystoscopy and simple diagnostic visualization of the female bladder and ureters is now available. The system – called CystoSure (Emmy Medical) – comprises a single-use silicone access catheter (18 French today, 16 French in development) and a reusable 2.7 mm, 70-degree rigid-rod lens optic.
The CystoSure catheter is of shorter length than the traditional catheter is, and it adds a fourth self-sealing port; this fourth port allows it to function both as a three-way urinary catheter and as an access sheath for female cystoscopy. When the scope is not inserted, the port remains sealed. The catheter design allows for multiple passes of the Cystosure scope without additional trauma, infection risk, or discomfort.
Additionally, the distal tip of the catheter is open with a flat pancake-shaped balloon that ensures that the scope is consistently placed and fixed at the trigonal ridge. Since the scope tip cannot advance beyond the lower bladder segment, bladder perforation and trauma risk are negligible.
Comprehensive evaluation of the entire bladder lumen including the trigone and ureters is performed with a simple 360-degree rotation of the scope, with minimal manipulation, compared with the traditional in-and-out technique used to circumferentially view sections of the bladder surface.

Full evaluation of the bladder and ureters takes less than 1 minute, and the urethra can be visualized, if desired, by decompressing the distal balloon and removing the entire unit.
The new cystoscopy procedure involves no assembly and is safer, simpler and more consistent than traditional cystoscopy – factors that we hope will make it easier to perform more often in the office for evaluation of bladder conditions (with or without simple cystometrogram testing), as well as during laparoscopic surgery, hysterectomy, incontinence/prolapse surgery, and other urologic procedures to ensure that the bladder and ureters are uninjured and to verify bilateral ureteral flow.
From May 2015 through the mid-summer, we completed and reviewed 55 cases of cystoscopy with Cystosure at several Harvard hospitals, including Brigham and Women’s Faulkner Hospital, Boston, the majority of them in the operating room during sling procedures and other laparoscopic surgeries. We achieved complete bladder and ureter visualization in all cases – including a small number of procedures done in the office setting – with no complications and an extremely short learning curve. For most physicians, it was possible to learn how to perform comprehensive cystoscopy with Cystosure in just one case.
Intraoperative cystoscopy
Reported rates of ureteral and bladder injury during gynecologic procedures have varied by study, type of injury, and complexity of surgery.
In an early report on the usefulness of intra-operative cystoscopy, Dr. Sergio Ribeirio and his colleagues reported that the procedure enabled early recognition and treatment of ureteral injuries in four of a series of 118 patients (3.4%) undergoing total laparoscopic hysterectomy with vault suspension (Hum Reprod. 1999 Jul;14[7]:1727-9.)
A review of 236,392 patients who underwent various laparoscopic gynecologic operations during 1994-2000 showed a urinary tract injury rate ranging from 0.02% to 1.7% (Clin Obstet Gynecol. 2002 Jun;45[2]:469- 80.). And, in another review specifically of ureteral injury in laparoscopic pelvic surgery, incidences of injury ranged from less than 1% to 2% (Obstet Gynecol Surv. 2003 Dec;58[12]:794-9.).
Other studies on the use of cystoscopy have reported injury rates up to and above 3%. In most cases, such reports include the incidence of bladder injury, which is less uncommon. Intraoperative bladder perforation occurs in 3%-9% of cases of midurethral retropubic sling procedures, for instance, according to ACOG’s opinion paper.
In a recent chart review of almost 1,000 women who underwent uterosacral colpopexy for pelvic organ prolapse, on the other hand, the intraoperative bladder injury rate was only 1%, and the rate of ureteral kinking/obstruction requiring stitch removal was significantly higher at 4.5% (Am J Obstet Gynecol. 2015;212:603.e1-7.).
Urinary tract injuries can have serious implications in terms of morbidity and litigation. When an injury is detected intraoperatively, the surgeon can repair it immediately and reduce the risk of complications and readmissions. The ureteral kinking detected in the previously mentioned study would not have been diagnosed without routine cystoscopy; nor would most cases of inadvertent suture or mesh placement in the bladder or urethral lumen.
The advisability of performing cystoscopy routinely in all gynecologic surgical procedures has been debated and should be studied further. However, given the advantages of early detection and the new availability of relatively simple and inexpensive cystoscopy, it is now possible – and will likely be beneficial – to move toward more routine use.
Currently, cystoscopy is performed in only a minority of indicated cases. In the 2003 review cited above from Obstetrical & Gynecological Survey, the ureteral injuries that occurred were identified intraoperatively in only 8.6% of the cases. And in an additional systematic literature review of urinary tract injury from gynecologic surgery, only 17 of the 47 studies included in the review employed routine intraoperative cystoscopy (Obstet Gynecol. 2006 Jun;107[6]:1366-72.).
A survey of ob.gyn residents presented at the ACOG meeting in May 2015 similarly showed that for hysterectomy, universal cystoscopy (defined as being performed in more than 90% of cases) was performed in the residents’ training settings for only a fraction of various types of hysterectomies, from vaginal hysterectomy to total laparoscopic hysterectomy.
Yet, in looking toward their future practice, the residents indicated in the survey that they plan to perform universal cystoscopy more frequently. The majority of them – almost 80% – had been involved with a hysterectomy having a bladder or ureter injury, according to the survey.
The Cystosure system facilitates a complete check of ureteral patency and bladder integrity. The system’s three-way catheter can be placed once and used for multiple passes of the cystoscope as well as for intraoperative retrograde fill of the bladder, postoperative drainage, and IV-based hands-free backfill voiding trials prior to discharge. The catheter’s red balloon port accepts the standard 5 cc syringe, and the blue inflow port provides a universal IV/cysto tubing fitting. The yellow drainage port may be attached to a standardized urinary drainage bag.
With Cystosure, a postoperative voiding trial thus becomes simpler and more efficient than it has in the past. Our nurses can clamp the outflow port, attach the IV bag to the inflow port, and briefly turn their attention elsewhere while the bladder fills hands free. The catheter is then removed, and the patient is allowed to void.
In the office
In the office, Cystosure can similarly make the evaluation of conditions like overactive bladder, urinary incontinence, incomplete bladder emptying, and recurrent urinary tract infections much easier and less expensive, enabling more gynecologists to take the lead in diagnosis.
Currently, there are various methods for performing cystometric testing. One technique, sometimes called “poor man’s cystometry,” involves placing a Foley red rubber catheter in the bladder, attaching a large syringe with the plunger removed, filling the bladder by pour technique, and monitoring the patient’s described sensations of bladder fullness and urge to urinate. This basic test can provide useful information about bladder functioning; patients with overactive bladder feel sensation at much smaller volumes than do patients with neurogenic bladder, for instance.
Yet, while the technique is simple and cheap, it is far from precise and may be misleading. It provides for a fast fill of the bladder in that water enters the bladder as fast as gravity allows. The rapid infusion can sometimes cause an artifact in the patient’s sensation – a significant feeling of pressure or fullness that is premature.
The more-sophisticated technique, multichannel urodynamics, pumps fluid at a slower, controlled rate and provides more accurate information. Yet, it requires expensive equipment, more time, and special expertise. It has not been universally accessible and relevant to the ob.gyn.’s office.
Cystosure bridges the gap between the accurate but costly multichannel urodynamics and the simple but less accurate fast-fill testing method. The nurse can place the Cystosure catheter, attach IV tubing to the inflow port, and then control the drip rate, emulating the pump of the complex urodynamics equipment. When the patient indicates fullness and the overactive bladder/incontinence evaluation is completed, the physician may immediately proceed with simple diagnostic cystoscopy without any further urethral manipulation.
The system can also be coupled to an LED-based battery light source and/or attached to a smartphone/iPad, so that cystoscopy can be performed in any room or at bedside without large bulky equipment and cords. Images and video can be saved and shared from remote locations or used for documentation or teaching.
Dr. Kohli is medical director of Boston Urogyn in Wellesley, Mass., an ob.gyn. staff member at Brigham and Women's Hospital/Newton Wellesley Hospital, and assistant professor of ob.gyn. at Harvard Medical School in Boston. He serves as chief medical officer at Emmy Medical, Holliston, Mass., which manufactures Cystosure.
Gynecologists have used the cystoscope for decades to examine the urethra and bladder, despite urology’s traditional claim that the procedure falls under its purview.
The lines between urology and gynecology have blurred, and cystoscopy has become an even more important and natural part of gynecology’s realm.
During the past 2 decades, gynecologists have become even more involved both in evaluating problems such as overactive bladder symptoms, recurrent urinary tract infection, and bladder/pelvic pain, and in performing pelvic reconstruction procedures.
The American College of Obstetricians and Gynecologists has recommended adoption of cystoscopy by ob.gyns. for diagnostic purposes and some operative indications – most importantly for ruling out cystotomy and intravesical or intraurethral suture or mesh placement, and for verifying ureteral patency. ACOG’s 2007 committee opinion on the role of cystourethroscopy in the generalist obstetrican-gyncecologist practice was reaffirmed in 2015 (Obstet Gynecol. 2007 Jul;110[1]:221-24.).
Yet, to a large extent, cystoscopy has been a good fit in principle, rather than in practice. Training in residency programs has been limited, and traditional cystoscopy can be cumbersome and time consuming. It also is costly, requiring equipment – including a light source and camera – and service contracts that may make it too expensive for many gynecologists to set up and maintain in their offices.
Cystoscopy has therefore often required referral to urologists, resulting in additional appointments, patient inconvenience, and increased costs to the health care system. The learning curve for traditional cystoscopy has been relatively steep, and delays in diagnosis and management as a result of referrals are not uncommon.
Moreover, cystoscopes were never designed to be safe and comfortable for women. Men and women have different anatomy, yet there always has been a one-size-fits-all device. The flexible cystoscope commonly used by urologists was designed for the unique length and anatomy of the male urethra.
A new catheter-based system specifically for female cystoscopy and simple diagnostic visualization of the female bladder and ureters is now available. The system – called CystoSure (Emmy Medical) – comprises a single-use silicone access catheter (18 French today, 16 French in development) and a reusable 2.7 mm, 70-degree rigid-rod lens optic.
The CystoSure catheter is of shorter length than the traditional catheter is, and it adds a fourth self-sealing port; this fourth port allows it to function both as a three-way urinary catheter and as an access sheath for female cystoscopy. When the scope is not inserted, the port remains sealed. The catheter design allows for multiple passes of the Cystosure scope without additional trauma, infection risk, or discomfort.
Additionally, the distal tip of the catheter is open with a flat pancake-shaped balloon that ensures that the scope is consistently placed and fixed at the trigonal ridge. Since the scope tip cannot advance beyond the lower bladder segment, bladder perforation and trauma risk are negligible.
Comprehensive evaluation of the entire bladder lumen including the trigone and ureters is performed with a simple 360-degree rotation of the scope, with minimal manipulation, compared with the traditional in-and-out technique used to circumferentially view sections of the bladder surface.
Full evaluation of the bladder and ureters takes less than 1 minute, and the urethra can be visualized, if desired, by decompressing the distal balloon and removing the entire unit.
The new cystoscopy procedure involves no assembly and is safer, simpler and more consistent than traditional cystoscopy – factors that we hope will make it easier to perform more often in the office for evaluation of bladder conditions (with or without simple cystometrogram testing), as well as during laparoscopic surgery, hysterectomy, incontinence/prolapse surgery, and other urologic procedures to ensure that the bladder and ureters are uninjured and to verify bilateral ureteral flow.
From May 2015 through the mid-summer, we completed and reviewed 55 cases of cystoscopy with Cystosure at several Harvard hospitals, including Brigham and Women’s Faulkner Hospital, Boston, the majority of them in the operating room during sling procedures and other laparoscopic surgeries. We achieved complete bladder and ureter visualization in all cases – including a small number of procedures done in the office setting – with no complications and an extremely short learning curve. For most physicians, it was possible to learn how to perform comprehensive cystoscopy with Cystosure in just one case.
Intraoperative cystoscopy
Reported rates of ureteral and bladder injury during gynecologic procedures have varied by study, type of injury, and complexity of surgery.
In an early report on the usefulness of intra-operative cystoscopy, Dr. Sergio Ribeirio and his colleagues reported that the procedure enabled early recognition and treatment of ureteral injuries in four of a series of 118 patients (3.4%) undergoing total laparoscopic hysterectomy with vault suspension (Hum Reprod. 1999 Jul;14[7]:1727-9.)
A review of 236,392 patients who underwent various laparoscopic gynecologic operations during 1994-2000 showed a urinary tract injury rate ranging from 0.02% to 1.7% (Clin Obstet Gynecol. 2002 Jun;45[2]:469- 80.). And, in another review specifically of ureteral injury in laparoscopic pelvic surgery, incidences of injury ranged from less than 1% to 2% (Obstet Gynecol Surv. 2003 Dec;58[12]:794-9.).
Other studies on the use of cystoscopy have reported injury rates up to and above 3%. In most cases, such reports include the incidence of bladder injury, which is less uncommon. Intraoperative bladder perforation occurs in 3%-9% of cases of midurethral retropubic sling procedures, for instance, according to ACOG’s opinion paper.
In a recent chart review of almost 1,000 women who underwent uterosacral colpopexy for pelvic organ prolapse, on the other hand, the intraoperative bladder injury rate was only 1%, and the rate of ureteral kinking/obstruction requiring stitch removal was significantly higher at 4.5% (Am J Obstet Gynecol. 2015;212:603.e1-7.).
Urinary tract injuries can have serious implications in terms of morbidity and litigation. When an injury is detected intraoperatively, the surgeon can repair it immediately and reduce the risk of complications and readmissions. The ureteral kinking detected in the previously mentioned study would not have been diagnosed without routine cystoscopy; nor would most cases of inadvertent suture or mesh placement in the bladder or urethral lumen.
The advisability of performing cystoscopy routinely in all gynecologic surgical procedures has been debated and should be studied further. However, given the advantages of early detection and the new availability of relatively simple and inexpensive cystoscopy, it is now possible – and will likely be beneficial – to move toward more routine use.
Currently, cystoscopy is performed in only a minority of indicated cases. In the 2003 review cited above from Obstetrical & Gynecological Survey, the ureteral injuries that occurred were identified intraoperatively in only 8.6% of the cases. And in an additional systematic literature review of urinary tract injury from gynecologic surgery, only 17 of the 47 studies included in the review employed routine intraoperative cystoscopy (Obstet Gynecol. 2006 Jun;107[6]:1366-72.).
A survey of ob.gyn residents presented at the ACOG meeting in May 2015 similarly showed that for hysterectomy, universal cystoscopy (defined as being performed in more than 90% of cases) was performed in the residents’ training settings for only a fraction of various types of hysterectomies, from vaginal hysterectomy to total laparoscopic hysterectomy.
Yet, in looking toward their future practice, the residents indicated in the survey that they plan to perform universal cystoscopy more frequently. The majority of them – almost 80% – had been involved with a hysterectomy having a bladder or ureter injury, according to the survey.
The Cystosure system facilitates a complete check of ureteral patency and bladder integrity. The system’s three-way catheter can be placed once and used for multiple passes of the cystoscope as well as for intraoperative retrograde fill of the bladder, postoperative drainage, and IV-based hands-free backfill voiding trials prior to discharge. The catheter’s red balloon port accepts the standard 5 cc syringe, and the blue inflow port provides a universal IV/cysto tubing fitting. The yellow drainage port may be attached to a standardized urinary drainage bag.
With Cystosure, a postoperative voiding trial thus becomes simpler and more efficient than it has in the past. Our nurses can clamp the outflow port, attach the IV bag to the inflow port, and briefly turn their attention elsewhere while the bladder fills hands free. The catheter is then removed, and the patient is allowed to void.
In the office
In the office, Cystosure can similarly make the evaluation of conditions like overactive bladder, urinary incontinence, incomplete bladder emptying, and recurrent urinary tract infections much easier and less expensive, enabling more gynecologists to take the lead in diagnosis.
Currently, there are various methods for performing cystometric testing. One technique, sometimes called “poor man’s cystometry,” involves placing a Foley red rubber catheter in the bladder, attaching a large syringe with the plunger removed, filling the bladder by pour technique, and monitoring the patient’s described sensations of bladder fullness and urge to urinate. This basic test can provide useful information about bladder functioning; patients with overactive bladder feel sensation at much smaller volumes than do patients with neurogenic bladder, for instance.
Yet, while the technique is simple and cheap, it is far from precise and may be misleading. It provides for a fast fill of the bladder in that water enters the bladder as fast as gravity allows. The rapid infusion can sometimes cause an artifact in the patient’s sensation – a significant feeling of pressure or fullness that is premature.
The more-sophisticated technique, multichannel urodynamics, pumps fluid at a slower, controlled rate and provides more accurate information. Yet, it requires expensive equipment, more time, and special expertise. It has not been universally accessible and relevant to the ob.gyn.’s office.
Cystosure bridges the gap between the accurate but costly multichannel urodynamics and the simple but less accurate fast-fill testing method. The nurse can place the Cystosure catheter, attach IV tubing to the inflow port, and then control the drip rate, emulating the pump of the complex urodynamics equipment. When the patient indicates fullness and the overactive bladder/incontinence evaluation is completed, the physician may immediately proceed with simple diagnostic cystoscopy without any further urethral manipulation.
The system can also be coupled to an LED-based battery light source and/or attached to a smartphone/iPad, so that cystoscopy can be performed in any room or at bedside without large bulky equipment and cords. Images and video can be saved and shared from remote locations or used for documentation or teaching.
Dr. Kohli is medical director of Boston Urogyn in Wellesley, Mass., an ob.gyn. staff member at Brigham and Women's Hospital/Newton Wellesley Hospital, and assistant professor of ob.gyn. at Harvard Medical School in Boston. He serves as chief medical officer at Emmy Medical, Holliston, Mass., which manufactures Cystosure.
Gynecologists have used the cystoscope for decades to examine the urethra and bladder, despite urology’s traditional claim that the procedure falls under its purview.
The lines between urology and gynecology have blurred, and cystoscopy has become an even more important and natural part of gynecology’s realm.
During the past 2 decades, gynecologists have become even more involved both in evaluating problems such as overactive bladder symptoms, recurrent urinary tract infection, and bladder/pelvic pain, and in performing pelvic reconstruction procedures.
The American College of Obstetricians and Gynecologists has recommended adoption of cystoscopy by ob.gyns. for diagnostic purposes and some operative indications – most importantly for ruling out cystotomy and intravesical or intraurethral suture or mesh placement, and for verifying ureteral patency. ACOG’s 2007 committee opinion on the role of cystourethroscopy in the generalist obstetrican-gyncecologist practice was reaffirmed in 2015 (Obstet Gynecol. 2007 Jul;110[1]:221-24.).
Yet, to a large extent, cystoscopy has been a good fit in principle, rather than in practice. Training in residency programs has been limited, and traditional cystoscopy can be cumbersome and time consuming. It also is costly, requiring equipment – including a light source and camera – and service contracts that may make it too expensive for many gynecologists to set up and maintain in their offices.
Cystoscopy has therefore often required referral to urologists, resulting in additional appointments, patient inconvenience, and increased costs to the health care system. The learning curve for traditional cystoscopy has been relatively steep, and delays in diagnosis and management as a result of referrals are not uncommon.
Moreover, cystoscopes were never designed to be safe and comfortable for women. Men and women have different anatomy, yet there always has been a one-size-fits-all device. The flexible cystoscope commonly used by urologists was designed for the unique length and anatomy of the male urethra.
A new catheter-based system specifically for female cystoscopy and simple diagnostic visualization of the female bladder and ureters is now available. The system – called CystoSure (Emmy Medical) – comprises a single-use silicone access catheter (18 French today, 16 French in development) and a reusable 2.7 mm, 70-degree rigid-rod lens optic.
The CystoSure catheter is of shorter length than the traditional catheter is, and it adds a fourth self-sealing port; this fourth port allows it to function both as a three-way urinary catheter and as an access sheath for female cystoscopy. When the scope is not inserted, the port remains sealed. The catheter design allows for multiple passes of the Cystosure scope without additional trauma, infection risk, or discomfort.
Additionally, the distal tip of the catheter is open with a flat pancake-shaped balloon that ensures that the scope is consistently placed and fixed at the trigonal ridge. Since the scope tip cannot advance beyond the lower bladder segment, bladder perforation and trauma risk are negligible.
Comprehensive evaluation of the entire bladder lumen including the trigone and ureters is performed with a simple 360-degree rotation of the scope, with minimal manipulation, compared with the traditional in-and-out technique used to circumferentially view sections of the bladder surface.
Full evaluation of the bladder and ureters takes less than 1 minute, and the urethra can be visualized, if desired, by decompressing the distal balloon and removing the entire unit.
The new cystoscopy procedure involves no assembly and is safer, simpler and more consistent than traditional cystoscopy – factors that we hope will make it easier to perform more often in the office for evaluation of bladder conditions (with or without simple cystometrogram testing), as well as during laparoscopic surgery, hysterectomy, incontinence/prolapse surgery, and other urologic procedures to ensure that the bladder and ureters are uninjured and to verify bilateral ureteral flow.
From May 2015 through the mid-summer, we completed and reviewed 55 cases of cystoscopy with Cystosure at several Harvard hospitals, including Brigham and Women’s Faulkner Hospital, Boston, the majority of them in the operating room during sling procedures and other laparoscopic surgeries. We achieved complete bladder and ureter visualization in all cases – including a small number of procedures done in the office setting – with no complications and an extremely short learning curve. For most physicians, it was possible to learn how to perform comprehensive cystoscopy with Cystosure in just one case.
Intraoperative cystoscopy
Reported rates of ureteral and bladder injury during gynecologic procedures have varied by study, type of injury, and complexity of surgery.
In an early report on the usefulness of intra-operative cystoscopy, Dr. Sergio Ribeirio and his colleagues reported that the procedure enabled early recognition and treatment of ureteral injuries in four of a series of 118 patients (3.4%) undergoing total laparoscopic hysterectomy with vault suspension (Hum Reprod. 1999 Jul;14[7]:1727-9.)
A review of 236,392 patients who underwent various laparoscopic gynecologic operations during 1994-2000 showed a urinary tract injury rate ranging from 0.02% to 1.7% (Clin Obstet Gynecol. 2002 Jun;45[2]:469- 80.). And, in another review specifically of ureteral injury in laparoscopic pelvic surgery, incidences of injury ranged from less than 1% to 2% (Obstet Gynecol Surv. 2003 Dec;58[12]:794-9.).
Other studies on the use of cystoscopy have reported injury rates up to and above 3%. In most cases, such reports include the incidence of bladder injury, which is less uncommon. Intraoperative bladder perforation occurs in 3%-9% of cases of midurethral retropubic sling procedures, for instance, according to ACOG’s opinion paper.
In a recent chart review of almost 1,000 women who underwent uterosacral colpopexy for pelvic organ prolapse, on the other hand, the intraoperative bladder injury rate was only 1%, and the rate of ureteral kinking/obstruction requiring stitch removal was significantly higher at 4.5% (Am J Obstet Gynecol. 2015;212:603.e1-7.).
Urinary tract injuries can have serious implications in terms of morbidity and litigation. When an injury is detected intraoperatively, the surgeon can repair it immediately and reduce the risk of complications and readmissions. The ureteral kinking detected in the previously mentioned study would not have been diagnosed without routine cystoscopy; nor would most cases of inadvertent suture or mesh placement in the bladder or urethral lumen.
The advisability of performing cystoscopy routinely in all gynecologic surgical procedures has been debated and should be studied further. However, given the advantages of early detection and the new availability of relatively simple and inexpensive cystoscopy, it is now possible – and will likely be beneficial – to move toward more routine use.
Currently, cystoscopy is performed in only a minority of indicated cases. In the 2003 review cited above from Obstetrical & Gynecological Survey, the ureteral injuries that occurred were identified intraoperatively in only 8.6% of the cases. And in an additional systematic literature review of urinary tract injury from gynecologic surgery, only 17 of the 47 studies included in the review employed routine intraoperative cystoscopy (Obstet Gynecol. 2006 Jun;107[6]:1366-72.).
A survey of ob.gyn residents presented at the ACOG meeting in May 2015 similarly showed that for hysterectomy, universal cystoscopy (defined as being performed in more than 90% of cases) was performed in the residents’ training settings for only a fraction of various types of hysterectomies, from vaginal hysterectomy to total laparoscopic hysterectomy.
Yet, in looking toward their future practice, the residents indicated in the survey that they plan to perform universal cystoscopy more frequently. The majority of them – almost 80% – had been involved with a hysterectomy having a bladder or ureter injury, according to the survey.
The Cystosure system facilitates a complete check of ureteral patency and bladder integrity. The system’s three-way catheter can be placed once and used for multiple passes of the cystoscope as well as for intraoperative retrograde fill of the bladder, postoperative drainage, and IV-based hands-free backfill voiding trials prior to discharge. The catheter’s red balloon port accepts the standard 5 cc syringe, and the blue inflow port provides a universal IV/cysto tubing fitting. The yellow drainage port may be attached to a standardized urinary drainage bag.
With Cystosure, a postoperative voiding trial thus becomes simpler and more efficient than it has in the past. Our nurses can clamp the outflow port, attach the IV bag to the inflow port, and briefly turn their attention elsewhere while the bladder fills hands free. The catheter is then removed, and the patient is allowed to void.
In the office
In the office, Cystosure can similarly make the evaluation of conditions like overactive bladder, urinary incontinence, incomplete bladder emptying, and recurrent urinary tract infections much easier and less expensive, enabling more gynecologists to take the lead in diagnosis.
Currently, there are various methods for performing cystometric testing. One technique, sometimes called “poor man’s cystometry,” involves placing a Foley red rubber catheter in the bladder, attaching a large syringe with the plunger removed, filling the bladder by pour technique, and monitoring the patient’s described sensations of bladder fullness and urge to urinate. This basic test can provide useful information about bladder functioning; patients with overactive bladder feel sensation at much smaller volumes than do patients with neurogenic bladder, for instance.
Yet, while the technique is simple and cheap, it is far from precise and may be misleading. It provides for a fast fill of the bladder in that water enters the bladder as fast as gravity allows. The rapid infusion can sometimes cause an artifact in the patient’s sensation – a significant feeling of pressure or fullness that is premature.
The more-sophisticated technique, multichannel urodynamics, pumps fluid at a slower, controlled rate and provides more accurate information. Yet, it requires expensive equipment, more time, and special expertise. It has not been universally accessible and relevant to the ob.gyn.’s office.
Cystosure bridges the gap between the accurate but costly multichannel urodynamics and the simple but less accurate fast-fill testing method. The nurse can place the Cystosure catheter, attach IV tubing to the inflow port, and then control the drip rate, emulating the pump of the complex urodynamics equipment. When the patient indicates fullness and the overactive bladder/incontinence evaluation is completed, the physician may immediately proceed with simple diagnostic cystoscopy without any further urethral manipulation.
The system can also be coupled to an LED-based battery light source and/or attached to a smartphone/iPad, so that cystoscopy can be performed in any room or at bedside without large bulky equipment and cords. Images and video can be saved and shared from remote locations or used for documentation or teaching.
Dr. Kohli is medical director of Boston Urogyn in Wellesley, Mass., an ob.gyn. staff member at Brigham and Women's Hospital/Newton Wellesley Hospital, and assistant professor of ob.gyn. at Harvard Medical School in Boston. He serves as chief medical officer at Emmy Medical, Holliston, Mass., which manufactures Cystosure.

Cystoscopies are us
In 2012, the AAGL issued Guidelines for Intraoperative Cystoscopy in Laparoscopic Hysterectomy (J Minim Invasive Gynecol. 2012 Jul-Aug;19[4]:407-11.). In this AAGL report, a meta-analysis noted 27 published trials comprising 3,643 cases. Laparoscopic hysterectomy was associated with an increased risk of urinary tract injury when compared with abdominal hysterectomy (odds ratio, 2.61; 95% confidence interval, 1.22-5.60), according to the meta-analysis (BMJ. 2005 Jun 25;330[7506]:1478.).
As a result of this meta-analysis, as well as multiple other studies, the AAGL Guidelines Committee noted that “current evidence supports the conclusion that cystoscopic evaluation of the lower urinary tract should be readily available to gynecologic surgeons performing laparoscopic hysterectomy.” The resultant guidelines recommend that “a surgeon with appropriate education, training, and institutional privileges be available without delay to perform the task (cystoscopy).”

Besides the evaluation of the urinary tract for potential injury at hysterectomy, cystoscopy is useful in evaluation of various urogynecologic concerns, potential malignancy, and possible genitourinary fistula.
In this edition of the Master Class in Gynecologic Surgery, I have asked urogynecologist Dr. Neeraj Kohli to discuss the use of cystoscopy in gynecology, as well as to present new instrumentation to aide in the performance of the procedure.
Dr. Kohli is in private practice as medical director of Boston Urogyn in Wellesley, Mass., an ob.gyn. staff member at Brigham Women’s Hospital/Newton Wellesley Hospital, and assistant professor of ob.gyn. at Harvard Medical School in Boston.
Dr. Kohli is a nationally recognized leader in the field of urogynecology and reconstructive pelvic surgery, specializing in the treatment of pelvic prolapse, urinary incontinence, and advanced pelvic surgery. He has authored more than 100 scientific articles, book chapters, research abstracts, clinical presentations and multimedia educational tools.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill; and the medical editor of this column, Master Class. Dr. Miller reported having no financial disclosures relevant to this Master Class.
In 2012, the AAGL issued Guidelines for Intraoperative Cystoscopy in Laparoscopic Hysterectomy (J Minim Invasive Gynecol. 2012 Jul-Aug;19[4]:407-11.). In this AAGL report, a meta-analysis noted 27 published trials comprising 3,643 cases. Laparoscopic hysterectomy was associated with an increased risk of urinary tract injury when compared with abdominal hysterectomy (odds ratio, 2.61; 95% confidence interval, 1.22-5.60), according to the meta-analysis (BMJ. 2005 Jun 25;330[7506]:1478.).
As a result of this meta-analysis, as well as multiple other studies, the AAGL Guidelines Committee noted that “current evidence supports the conclusion that cystoscopic evaluation of the lower urinary tract should be readily available to gynecologic surgeons performing laparoscopic hysterectomy.” The resultant guidelines recommend that “a surgeon with appropriate education, training, and institutional privileges be available without delay to perform the task (cystoscopy).”
Besides the evaluation of the urinary tract for potential injury at hysterectomy, cystoscopy is useful in evaluation of various urogynecologic concerns, potential malignancy, and possible genitourinary fistula.
In this edition of the Master Class in Gynecologic Surgery, I have asked urogynecologist Dr. Neeraj Kohli to discuss the use of cystoscopy in gynecology, as well as to present new instrumentation to aide in the performance of the procedure.
Dr. Kohli is in private practice as medical director of Boston Urogyn in Wellesley, Mass., an ob.gyn. staff member at Brigham Women’s Hospital/Newton Wellesley Hospital, and assistant professor of ob.gyn. at Harvard Medical School in Boston.
Dr. Kohli is a nationally recognized leader in the field of urogynecology and reconstructive pelvic surgery, specializing in the treatment of pelvic prolapse, urinary incontinence, and advanced pelvic surgery. He has authored more than 100 scientific articles, book chapters, research abstracts, clinical presentations and multimedia educational tools.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill; and the medical editor of this column, Master Class. Dr. Miller reported having no financial disclosures relevant to this Master Class.
In 2012, the AAGL issued Guidelines for Intraoperative Cystoscopy in Laparoscopic Hysterectomy (J Minim Invasive Gynecol. 2012 Jul-Aug;19[4]:407-11.). In this AAGL report, a meta-analysis noted 27 published trials comprising 3,643 cases. Laparoscopic hysterectomy was associated with an increased risk of urinary tract injury when compared with abdominal hysterectomy (odds ratio, 2.61; 95% confidence interval, 1.22-5.60), according to the meta-analysis (BMJ. 2005 Jun 25;330[7506]:1478.).
As a result of this meta-analysis, as well as multiple other studies, the AAGL Guidelines Committee noted that “current evidence supports the conclusion that cystoscopic evaluation of the lower urinary tract should be readily available to gynecologic surgeons performing laparoscopic hysterectomy.” The resultant guidelines recommend that “a surgeon with appropriate education, training, and institutional privileges be available without delay to perform the task (cystoscopy).”
Besides the evaluation of the urinary tract for potential injury at hysterectomy, cystoscopy is useful in evaluation of various urogynecologic concerns, potential malignancy, and possible genitourinary fistula.
In this edition of the Master Class in Gynecologic Surgery, I have asked urogynecologist Dr. Neeraj Kohli to discuss the use of cystoscopy in gynecology, as well as to present new instrumentation to aide in the performance of the procedure.
Dr. Kohli is in private practice as medical director of Boston Urogyn in Wellesley, Mass., an ob.gyn. staff member at Brigham Women’s Hospital/Newton Wellesley Hospital, and assistant professor of ob.gyn. at Harvard Medical School in Boston.
Dr. Kohli is a nationally recognized leader in the field of urogynecology and reconstructive pelvic surgery, specializing in the treatment of pelvic prolapse, urinary incontinence, and advanced pelvic surgery. He has authored more than 100 scientific articles, book chapters, research abstracts, clinical presentations and multimedia educational tools.
Dr. Miller is a clinical associate professor at the University of Illinois at Chicago, immediate past president of the International Society for Gynecologic Endoscopy (ISGE), and a past president of the AAGL. He is a reproductive endocrinologist and minimally invasive gynecologic surgeon in private practice in Naperville, Ill., and Schaumburg, Ill.; director of minimally invasive gynecologic surgery and the director of the AAGL/SRS fellowship in minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, Ill; and the medical editor of this column, Master Class. Dr. Miller reported having no financial disclosures relevant to this Master Class.

Commentary to "Measurement of Resource Utilization for Total and Reverse Shoulder Arthroplasty"
In this month’s issue of The American Journal of Orthopedics, Tannenbaum and colleagues present a “5 Points” article on “Measurement of Resource Utilization for Total and Reverse Shoulder Arthroplasty.” This is an excellent article that summarizes the authors’ methodology of determining not only the overall cost of hospital care for shoulder replacement but a detailed analysis of many components contributing to that cost.
The steps are fairly straightforward: identify the various components of the cost, gather the data contributing to those costs, and then analyze what are the major expenditures that contribute to the overall cost. Sounds simple, but, in practice, it is anything but!
As health care expenditures in the United States continue to increase and approach 20% of the gross domestic product, every sector of the health care industry is searching for ways to curtail and eventually decrease the cost of health care. However, one cannot control costs without accurate data that defines those costs. In this article, Tannenbaum and colleagues have provided a methodology to help both hospital administrators and surgeons determine the overall cost of shoulder arthroplasty, but their principles of analysis can be applied to all aspects of hospital care.
Such efforts are gaining the attention of many leaders of the health care industry. For example, in the September 8, 2015, edition of The New York Times, I was very interested to read the article “What are a Hospital’s Costs? Utah System Is Trying to Learn.”1 The article reviewed the efforts of Dr. Vivian Lee, chief executive at University of Utah Health Care, to determine the actual cost of all care provided by the university hospital, the same goal as the present 5 Points article on shoulder arthroplasty but on a vastly greater scale. Analyzing those costs guided Dr. Lee and her colleagues to alter clinical programs, which led to a decrease of 30% in hospital expenditures and fewer complications.1
We are all indebted to Mr. Tannenbaum and his coauthors for providing the journal’s readers with a clear map that we can use to both understand and navigate the current maze of hospital costs. Using such a guide, we will be able to gather information that not only saves money, but will improve care by directing resources to services that actually benefit our patients.
Reference
1. Kolata G. What are a hospital’s costs? Utah system is trying to learn. New York Times. September 8, 2015:A1. http://www.nytimes.com/2015/09/08/health/what-are-a-hospitals-costs-utah-system-is-trying-to-learn.html. Accessed September 17, 2015.
In this month’s issue of The American Journal of Orthopedics, Tannenbaum and colleagues present a “5 Points” article on “Measurement of Resource Utilization for Total and Reverse Shoulder Arthroplasty.” This is an excellent article that summarizes the authors’ methodology of determining not only the overall cost of hospital care for shoulder replacement but a detailed analysis of many components contributing to that cost.
The steps are fairly straightforward: identify the various components of the cost, gather the data contributing to those costs, and then analyze what are the major expenditures that contribute to the overall cost. Sounds simple, but, in practice, it is anything but!
As health care expenditures in the United States continue to increase and approach 20% of the gross domestic product, every sector of the health care industry is searching for ways to curtail and eventually decrease the cost of health care. However, one cannot control costs without accurate data that defines those costs. In this article, Tannenbaum and colleagues have provided a methodology to help both hospital administrators and surgeons determine the overall cost of shoulder arthroplasty, but their principles of analysis can be applied to all aspects of hospital care.
Such efforts are gaining the attention of many leaders of the health care industry. For example, in the September 8, 2015, edition of The New York Times, I was very interested to read the article “What are a Hospital’s Costs? Utah System Is Trying to Learn.”1 The article reviewed the efforts of Dr. Vivian Lee, chief executive at University of Utah Health Care, to determine the actual cost of all care provided by the university hospital, the same goal as the present 5 Points article on shoulder arthroplasty but on a vastly greater scale. Analyzing those costs guided Dr. Lee and her colleagues to alter clinical programs, which led to a decrease of 30% in hospital expenditures and fewer complications.1
We are all indebted to Mr. Tannenbaum and his coauthors for providing the journal’s readers with a clear map that we can use to both understand and navigate the current maze of hospital costs. Using such a guide, we will be able to gather information that not only saves money, but will improve care by directing resources to services that actually benefit our patients.
In this month’s issue of The American Journal of Orthopedics, Tannenbaum and colleagues present a “5 Points” article on “Measurement of Resource Utilization for Total and Reverse Shoulder Arthroplasty.” This is an excellent article that summarizes the authors’ methodology of determining not only the overall cost of hospital care for shoulder replacement but a detailed analysis of many components contributing to that cost.
The steps are fairly straightforward: identify the various components of the cost, gather the data contributing to those costs, and then analyze what are the major expenditures that contribute to the overall cost. Sounds simple, but, in practice, it is anything but!
As health care expenditures in the United States continue to increase and approach 20% of the gross domestic product, every sector of the health care industry is searching for ways to curtail and eventually decrease the cost of health care. However, one cannot control costs without accurate data that defines those costs. In this article, Tannenbaum and colleagues have provided a methodology to help both hospital administrators and surgeons determine the overall cost of shoulder arthroplasty, but their principles of analysis can be applied to all aspects of hospital care.
Such efforts are gaining the attention of many leaders of the health care industry. For example, in the September 8, 2015, edition of The New York Times, I was very interested to read the article “What are a Hospital’s Costs? Utah System Is Trying to Learn.”1 The article reviewed the efforts of Dr. Vivian Lee, chief executive at University of Utah Health Care, to determine the actual cost of all care provided by the university hospital, the same goal as the present 5 Points article on shoulder arthroplasty but on a vastly greater scale. Analyzing those costs guided Dr. Lee and her colleagues to alter clinical programs, which led to a decrease of 30% in hospital expenditures and fewer complications.1
We are all indebted to Mr. Tannenbaum and his coauthors for providing the journal’s readers with a clear map that we can use to both understand and navigate the current maze of hospital costs. Using such a guide, we will be able to gather information that not only saves money, but will improve care by directing resources to services that actually benefit our patients.
Reference
1. Kolata G. What are a hospital’s costs? Utah system is trying to learn. New York Times. September 8, 2015:A1. http://www.nytimes.com/2015/09/08/health/what-are-a-hospitals-costs-utah-system-is-trying-to-learn.html. Accessed September 17, 2015.
Reference
1. Kolata G. What are a hospital’s costs? Utah system is trying to learn. New York Times. September 8, 2015:A1. http://www.nytimes.com/2015/09/08/health/what-are-a-hospitals-costs-utah-system-is-trying-to-learn.html. Accessed September 17, 2015.

Breast reductions
Adolescent medicine presents a unique challenge. Many pediatricians find themselves extrapolating treatment of childhood issues or modifying adult treatment to address adolescent issues. But the reality is adolescents are not big kids or little adults. They are a unique group that require special considerations and analysis for appropriate treatment.
Macromastia, enlarged breast, is a condition that affects many teenagers. It impacts their self-esteem, limits physical ability, and causes musculoskeletal and dermatologic issues, and yet most pediatricians cannot recall a specific lesson that covered the evaluation and treatment of this condition. Juvenile, or virginal, gigantomastia is a rare condition that consists of a period of rapid breast tissue growth followed by sustained growth in the peripubertal years. Growth can be symmetrical or asymmetrical. Either condition can lead to disfigurement, social anxiety, unwanted attention, and withdrawal. Therefore, acknowledging the condition and intervening are essential.
With obesity on the rise, the issue of macromastia continues to grow. Although macromastia and obesity can occur independently, obesity certainly augments the condition, and more and more physicians are confronted with complaints of neck, back, and shoulder pain. Left untreated, macromastia can cause physical limitation leading to further morbidity. The exact etiology is unknown, but it is presumed to be associated with a hypersensitivity of the mammary estrogen receptors and exposure to exogenous estrogen through food, drugs, or the environment.
Although a patient who has significant discomfort may benefit from physical therapy and strengthening exercises to improve posture, the definitive treatment for macromastia and juvenile gigantomastia is surgical breast reduction, even in adolescence. Medical management with injections of tamoxifen will halt the continued growth, but it will not reduce the size, and therefore will not correct the associated side effects. Weight loss may reduce the general appearance, but it will do little to reduce the actual size of the breast tissue itself.
Because breast development arrests before adulthood, delaying surgical intervention to adulthood is not necessary. In a retrospective study, recurrence took place with juvenile gigantomastia only if intervention was done in early adolescence and did not take place at all with macromastia (Mayo Clin Proc. 2001;76:503-10).
Indications for surgical intervention are chronic shoulder, neck, and back pain; shoulder grooving; skin irritation and skin breakdown underneath the breast; and social stress. It is important that the growth of the breast has ceased for at least a year, and a psychological assessment of the impact of the condition is performed.
Misconceptions associated with breast reduction include that it is for cosmetic purposes only; that macromastia can be reduced by weight loss, and therefore a surgical intervention is not necessary; that lactation is not possible after the procedure; and that insurance will not cover this procedure. As explained previously, there is an identifiable negative impact of macromastia on the musculoskeletal system as well as huge self-esteem and social issues.
Decades ago, breast reduction was seen as a cosmetic surgery. Surprisingly, many insurance companies will now cover the procedure if the morbidity is well documented.
Inability to breastfeed was the initial concern with early surgical intervention. Several studies have evaluated this, and all have come to the same conclusion: Although milk production may be reduced, postsurgical patients can breastfeed without difficulty. Given that lactation is not inhibited and continued stress on the musculoskeletal system causes further harm, early intervention is imperative.
Breast reduction surgery is safe. There is a risk of bleeding, infection, fat necrosis, and loss of sensation, but there is no higher incidence of these adverse effects in adolescents than there is in adults (J Pediatr Adolesc Gynecol. 2013;26[4]:228-33).
Macromastia clearly impacts the emotional, social, and physical well-being of an adolescent, and it likely will not be addressed by the young patient because of embarrassment. Therefore, it is up to the pediatrician to inquire about body image with all routine health exams, and to keep up to date with the latest recommendations to ensure the best outcomes.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com.
Adolescent medicine presents a unique challenge. Many pediatricians find themselves extrapolating treatment of childhood issues or modifying adult treatment to address adolescent issues. But the reality is adolescents are not big kids or little adults. They are a unique group that require special considerations and analysis for appropriate treatment.
Macromastia, enlarged breast, is a condition that affects many teenagers. It impacts their self-esteem, limits physical ability, and causes musculoskeletal and dermatologic issues, and yet most pediatricians cannot recall a specific lesson that covered the evaluation and treatment of this condition. Juvenile, or virginal, gigantomastia is a rare condition that consists of a period of rapid breast tissue growth followed by sustained growth in the peripubertal years. Growth can be symmetrical or asymmetrical. Either condition can lead to disfigurement, social anxiety, unwanted attention, and withdrawal. Therefore, acknowledging the condition and intervening are essential.
With obesity on the rise, the issue of macromastia continues to grow. Although macromastia and obesity can occur independently, obesity certainly augments the condition, and more and more physicians are confronted with complaints of neck, back, and shoulder pain. Left untreated, macromastia can cause physical limitation leading to further morbidity. The exact etiology is unknown, but it is presumed to be associated with a hypersensitivity of the mammary estrogen receptors and exposure to exogenous estrogen through food, drugs, or the environment.
Although a patient who has significant discomfort may benefit from physical therapy and strengthening exercises to improve posture, the definitive treatment for macromastia and juvenile gigantomastia is surgical breast reduction, even in adolescence. Medical management with injections of tamoxifen will halt the continued growth, but it will not reduce the size, and therefore will not correct the associated side effects. Weight loss may reduce the general appearance, but it will do little to reduce the actual size of the breast tissue itself.
Because breast development arrests before adulthood, delaying surgical intervention to adulthood is not necessary. In a retrospective study, recurrence took place with juvenile gigantomastia only if intervention was done in early adolescence and did not take place at all with macromastia (Mayo Clin Proc. 2001;76:503-10).
Indications for surgical intervention are chronic shoulder, neck, and back pain; shoulder grooving; skin irritation and skin breakdown underneath the breast; and social stress. It is important that the growth of the breast has ceased for at least a year, and a psychological assessment of the impact of the condition is performed.
Misconceptions associated with breast reduction include that it is for cosmetic purposes only; that macromastia can be reduced by weight loss, and therefore a surgical intervention is not necessary; that lactation is not possible after the procedure; and that insurance will not cover this procedure. As explained previously, there is an identifiable negative impact of macromastia on the musculoskeletal system as well as huge self-esteem and social issues.
Decades ago, breast reduction was seen as a cosmetic surgery. Surprisingly, many insurance companies will now cover the procedure if the morbidity is well documented.
Inability to breastfeed was the initial concern with early surgical intervention. Several studies have evaluated this, and all have come to the same conclusion: Although milk production may be reduced, postsurgical patients can breastfeed without difficulty. Given that lactation is not inhibited and continued stress on the musculoskeletal system causes further harm, early intervention is imperative.
Breast reduction surgery is safe. There is a risk of bleeding, infection, fat necrosis, and loss of sensation, but there is no higher incidence of these adverse effects in adolescents than there is in adults (J Pediatr Adolesc Gynecol. 2013;26[4]:228-33).
Macromastia clearly impacts the emotional, social, and physical well-being of an adolescent, and it likely will not be addressed by the young patient because of embarrassment. Therefore, it is up to the pediatrician to inquire about body image with all routine health exams, and to keep up to date with the latest recommendations to ensure the best outcomes.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com.
Adolescent medicine presents a unique challenge. Many pediatricians find themselves extrapolating treatment of childhood issues or modifying adult treatment to address adolescent issues. But the reality is adolescents are not big kids or little adults. They are a unique group that require special considerations and analysis for appropriate treatment.
Macromastia, enlarged breast, is a condition that affects many teenagers. It impacts their self-esteem, limits physical ability, and causes musculoskeletal and dermatologic issues, and yet most pediatricians cannot recall a specific lesson that covered the evaluation and treatment of this condition. Juvenile, or virginal, gigantomastia is a rare condition that consists of a period of rapid breast tissue growth followed by sustained growth in the peripubertal years. Growth can be symmetrical or asymmetrical. Either condition can lead to disfigurement, social anxiety, unwanted attention, and withdrawal. Therefore, acknowledging the condition and intervening are essential.
With obesity on the rise, the issue of macromastia continues to grow. Although macromastia and obesity can occur independently, obesity certainly augments the condition, and more and more physicians are confronted with complaints of neck, back, and shoulder pain. Left untreated, macromastia can cause physical limitation leading to further morbidity. The exact etiology is unknown, but it is presumed to be associated with a hypersensitivity of the mammary estrogen receptors and exposure to exogenous estrogen through food, drugs, or the environment.
Although a patient who has significant discomfort may benefit from physical therapy and strengthening exercises to improve posture, the definitive treatment for macromastia and juvenile gigantomastia is surgical breast reduction, even in adolescence. Medical management with injections of tamoxifen will halt the continued growth, but it will not reduce the size, and therefore will not correct the associated side effects. Weight loss may reduce the general appearance, but it will do little to reduce the actual size of the breast tissue itself.
Because breast development arrests before adulthood, delaying surgical intervention to adulthood is not necessary. In a retrospective study, recurrence took place with juvenile gigantomastia only if intervention was done in early adolescence and did not take place at all with macromastia (Mayo Clin Proc. 2001;76:503-10).
Indications for surgical intervention are chronic shoulder, neck, and back pain; shoulder grooving; skin irritation and skin breakdown underneath the breast; and social stress. It is important that the growth of the breast has ceased for at least a year, and a psychological assessment of the impact of the condition is performed.
Misconceptions associated with breast reduction include that it is for cosmetic purposes only; that macromastia can be reduced by weight loss, and therefore a surgical intervention is not necessary; that lactation is not possible after the procedure; and that insurance will not cover this procedure. As explained previously, there is an identifiable negative impact of macromastia on the musculoskeletal system as well as huge self-esteem and social issues.
Decades ago, breast reduction was seen as a cosmetic surgery. Surprisingly, many insurance companies will now cover the procedure if the morbidity is well documented.
Inability to breastfeed was the initial concern with early surgical intervention. Several studies have evaluated this, and all have come to the same conclusion: Although milk production may be reduced, postsurgical patients can breastfeed without difficulty. Given that lactation is not inhibited and continued stress on the musculoskeletal system causes further harm, early intervention is imperative.
Breast reduction surgery is safe. There is a risk of bleeding, infection, fat necrosis, and loss of sensation, but there is no higher incidence of these adverse effects in adolescents than there is in adults (J Pediatr Adolesc Gynecol. 2013;26[4]:228-33).
Macromastia clearly impacts the emotional, social, and physical well-being of an adolescent, and it likely will not be addressed by the young patient because of embarrassment. Therefore, it is up to the pediatrician to inquire about body image with all routine health exams, and to keep up to date with the latest recommendations to ensure the best outcomes.
Dr. Pearce is a pediatrician in Frankfort, Ill. E-mail her at pdnews@frontlinemedcom.com.

From the Washington Office
This month I am writing to encourage Fellows to contact their representatives and senators to ask that they support the Critical Access Hospital Relief Act, H.R. 169 and S. 258.
Approximately 2 years ago, surgeons working at Critical Access Hospitals (CAHs) began to encounter a new barrier to caring for their patients and in some cases have been forced to send patients to other hospitals far from their homes to receive care. The barrier responsible is contained in legislation originally passed in the Balanced Budget Act of 1997, the same legislation responsible for the sustainable growth rate (SGR) and the current caps on Medicare-sponsored graduate medical education positions.

Under current law, for facilities to qualify for Medicare certification and thus participate in the Medicare program itself, CAHs must meet minimum health and safety standards known as conditions of participation. In addition, the Centers for Medicare & Medicaid Services (CMS) imposes certain Medicare conditions of payment that must be met for a CAH to receive Medicare Part A reimbursement.
The CAH 96-hour rule imposes both a condition of participation and a condition of payment on CAHs. As mentioned above, though this provision has been in the law since 1997, it was not until fall of 2013 that the condition of payment began to be enforced. Prior to that time, only the condition of participation, requiring that acute inpatient care not exceed 96 hours per patient on an average basis, had been enforced by the CMS. Despite being written in the same legislation passed in 1997, the condition of payment was virtually unknown until September of 2013 when the CMS released a statement in a document pertaining to a related policy. At that time, it was indicated that the condition of payment in the 96-hour rule would be more strictly enforced. That condition of payment states that CAHs will receive Medicare Part A reimbursement only if the admitting physician certifies, at the time of admission, that the patient can reasonably be expected to be discharged or transferred within 96 hours. This was the first time many CAHs and the surgeons and other physicians working in such facilities had ever heard of the 96-hour rule’s condition of payment certification requirement.
Since the advisory was released, administrators at some CAHs have begun requiring surgeons to sign certifications upon admission stating that the patient being admitted can reasonably be expected to be discharged or transferred within 96 hours of admission. Obviously, this has caused great concern for surgeons and other providers serving populations who receive care in CAHs. Many surgeons practicing in such rural settings routinely perform procedures and provide care for surgical patients in those CAHs with expected stays likely to exceed 4 days. On the other hand, while any individual patient may require inpatient admission exceeding 96 hours, CAHs have generally not had difficulty maintaining the 96-hour average required by the condition of participation.
In response to the CMS notice on enforcement of the 96-hour rule, Representative Adrian Smith (R-Neb.) and Senator Pat Roberts (R-Kan.) introduced the Critical Access Hospital Relief Act (H.R. 169/S. 258). The legislation proposes to simply remove the 96-hour rule condition of payment, leaving in place the currently enforced 96-hour average patient stay required by the condition of participation. As of Aug. 26, 2015, there were 75 cosponsors (58 R and 17 D) in the House of Representatives for H.R. 169 and 30 cosponsors (19 R and 11 D) in the Senate for S. 258.
While it is unlikely this legislation will progress to the floor of either the House or Senate as a “standalone” bill, it is entirely possible that the Critical Access Hospital Relief Act could be included in a larger package of legislation moving in the coming months before Congress recesses for the holidays.
The American College of Surgeons strongly supports this straightforward legislation and we would urge Fellows, especially those who either serve populations receiving care in CAHs or those practicing in states with large numbers of CAHs, to contact their representatives and senators to request that they sign on as cosponsors of H.R. 169 or S. 258 and support the inclusion of the bill in any legislation coming to the floor of either chamber for a vote this year.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy, in the ACS offices in Washington.
This month I am writing to encourage Fellows to contact their representatives and senators to ask that they support the Critical Access Hospital Relief Act, H.R. 169 and S. 258.
Approximately 2 years ago, surgeons working at Critical Access Hospitals (CAHs) began to encounter a new barrier to caring for their patients and in some cases have been forced to send patients to other hospitals far from their homes to receive care. The barrier responsible is contained in legislation originally passed in the Balanced Budget Act of 1997, the same legislation responsible for the sustainable growth rate (SGR) and the current caps on Medicare-sponsored graduate medical education positions.
Under current law, for facilities to qualify for Medicare certification and thus participate in the Medicare program itself, CAHs must meet minimum health and safety standards known as conditions of participation. In addition, the Centers for Medicare & Medicaid Services (CMS) imposes certain Medicare conditions of payment that must be met for a CAH to receive Medicare Part A reimbursement.
The CAH 96-hour rule imposes both a condition of participation and a condition of payment on CAHs. As mentioned above, though this provision has been in the law since 1997, it was not until fall of 2013 that the condition of payment began to be enforced. Prior to that time, only the condition of participation, requiring that acute inpatient care not exceed 96 hours per patient on an average basis, had been enforced by the CMS. Despite being written in the same legislation passed in 1997, the condition of payment was virtually unknown until September of 2013 when the CMS released a statement in a document pertaining to a related policy. At that time, it was indicated that the condition of payment in the 96-hour rule would be more strictly enforced. That condition of payment states that CAHs will receive Medicare Part A reimbursement only if the admitting physician certifies, at the time of admission, that the patient can reasonably be expected to be discharged or transferred within 96 hours. This was the first time many CAHs and the surgeons and other physicians working in such facilities had ever heard of the 96-hour rule’s condition of payment certification requirement.
Since the advisory was released, administrators at some CAHs have begun requiring surgeons to sign certifications upon admission stating that the patient being admitted can reasonably be expected to be discharged or transferred within 96 hours of admission. Obviously, this has caused great concern for surgeons and other providers serving populations who receive care in CAHs. Many surgeons practicing in such rural settings routinely perform procedures and provide care for surgical patients in those CAHs with expected stays likely to exceed 4 days. On the other hand, while any individual patient may require inpatient admission exceeding 96 hours, CAHs have generally not had difficulty maintaining the 96-hour average required by the condition of participation.
In response to the CMS notice on enforcement of the 96-hour rule, Representative Adrian Smith (R-Neb.) and Senator Pat Roberts (R-Kan.) introduced the Critical Access Hospital Relief Act (H.R. 169/S. 258). The legislation proposes to simply remove the 96-hour rule condition of payment, leaving in place the currently enforced 96-hour average patient stay required by the condition of participation. As of Aug. 26, 2015, there were 75 cosponsors (58 R and 17 D) in the House of Representatives for H.R. 169 and 30 cosponsors (19 R and 11 D) in the Senate for S. 258.
While it is unlikely this legislation will progress to the floor of either the House or Senate as a “standalone” bill, it is entirely possible that the Critical Access Hospital Relief Act could be included in a larger package of legislation moving in the coming months before Congress recesses for the holidays.
The American College of Surgeons strongly supports this straightforward legislation and we would urge Fellows, especially those who either serve populations receiving care in CAHs or those practicing in states with large numbers of CAHs, to contact their representatives and senators to request that they sign on as cosponsors of H.R. 169 or S. 258 and support the inclusion of the bill in any legislation coming to the floor of either chamber for a vote this year.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy, in the ACS offices in Washington.
This month I am writing to encourage Fellows to contact their representatives and senators to ask that they support the Critical Access Hospital Relief Act, H.R. 169 and S. 258.
Approximately 2 years ago, surgeons working at Critical Access Hospitals (CAHs) began to encounter a new barrier to caring for their patients and in some cases have been forced to send patients to other hospitals far from their homes to receive care. The barrier responsible is contained in legislation originally passed in the Balanced Budget Act of 1997, the same legislation responsible for the sustainable growth rate (SGR) and the current caps on Medicare-sponsored graduate medical education positions.
Under current law, for facilities to qualify for Medicare certification and thus participate in the Medicare program itself, CAHs must meet minimum health and safety standards known as conditions of participation. In addition, the Centers for Medicare & Medicaid Services (CMS) imposes certain Medicare conditions of payment that must be met for a CAH to receive Medicare Part A reimbursement.
The CAH 96-hour rule imposes both a condition of participation and a condition of payment on CAHs. As mentioned above, though this provision has been in the law since 1997, it was not until fall of 2013 that the condition of payment began to be enforced. Prior to that time, only the condition of participation, requiring that acute inpatient care not exceed 96 hours per patient on an average basis, had been enforced by the CMS. Despite being written in the same legislation passed in 1997, the condition of payment was virtually unknown until September of 2013 when the CMS released a statement in a document pertaining to a related policy. At that time, it was indicated that the condition of payment in the 96-hour rule would be more strictly enforced. That condition of payment states that CAHs will receive Medicare Part A reimbursement only if the admitting physician certifies, at the time of admission, that the patient can reasonably be expected to be discharged or transferred within 96 hours. This was the first time many CAHs and the surgeons and other physicians working in such facilities had ever heard of the 96-hour rule’s condition of payment certification requirement.
Since the advisory was released, administrators at some CAHs have begun requiring surgeons to sign certifications upon admission stating that the patient being admitted can reasonably be expected to be discharged or transferred within 96 hours of admission. Obviously, this has caused great concern for surgeons and other providers serving populations who receive care in CAHs. Many surgeons practicing in such rural settings routinely perform procedures and provide care for surgical patients in those CAHs with expected stays likely to exceed 4 days. On the other hand, while any individual patient may require inpatient admission exceeding 96 hours, CAHs have generally not had difficulty maintaining the 96-hour average required by the condition of participation.
In response to the CMS notice on enforcement of the 96-hour rule, Representative Adrian Smith (R-Neb.) and Senator Pat Roberts (R-Kan.) introduced the Critical Access Hospital Relief Act (H.R. 169/S. 258). The legislation proposes to simply remove the 96-hour rule condition of payment, leaving in place the currently enforced 96-hour average patient stay required by the condition of participation. As of Aug. 26, 2015, there were 75 cosponsors (58 R and 17 D) in the House of Representatives for H.R. 169 and 30 cosponsors (19 R and 11 D) in the Senate for S. 258.
While it is unlikely this legislation will progress to the floor of either the House or Senate as a “standalone” bill, it is entirely possible that the Critical Access Hospital Relief Act could be included in a larger package of legislation moving in the coming months before Congress recesses for the holidays.
The American College of Surgeons strongly supports this straightforward legislation and we would urge Fellows, especially those who either serve populations receiving care in CAHs or those practicing in states with large numbers of CAHs, to contact their representatives and senators to request that they sign on as cosponsors of H.R. 169 or S. 258 and support the inclusion of the bill in any legislation coming to the floor of either chamber for a vote this year.
Until next month …
Dr. Bailey is a pediatric surgeon and Medical Director, Advocacy, for the Division of Advocacy and Health Policy, in the ACS offices in Washington.

ACS Clinical Congress: Something for everyone
Every year I am amazed by the breadth of knowledge and information presented at the annual Clinical Congress. I find it deeply satisfying to realize how much I can still enjoy and learn from the wide variety of topics presented from all the surgical specialties.
First, there is so much new to absorb in each of our specialties and the Clinical Congress is a must in terms of hearing firsthand about innovation and change. The technical aspects of surgical techniques seemingly unrelated to my own area of specialization often have parallels to my own practice and raise questions or possible answers to problems I face in my own field.

Second, the vast amount of information about topics germane to all surgeons, such as surgical ethics, professionalism, critical care, surgical fundamentals, information technology, new surgical technology, advocacy and more, really can’t be found in any other venue.
The College has worked hard to offer learning environments that meet a variety of needs. The Town Hall meetings give groups of surgeons with a common interest the opportunity to freely discuss a wide variety of topics in a relatively unstructured environment. There will be 20 Town Hall meetings this year ranging from “Development of a Rural Track in Residency” to “The Surgeon Specific Registry (SSR): Maintenance of Certification (MOC), Physician Quality Reporting System (PQRS) and other Mandates,” to 18 additional sessions on such topics as incorporating surgical ethics into your practice, MOC, surgical education, and others.
Named Lectures are generally given by carefully chosen experts in a field and include the Martin Memorial Lecture during the opening ceremony, which this year will be given by Dr. John Meara: “Addressing Unmet Surgical Need: The Role of Academic Surgery.” Among the 10 other Named Lectures will be the Charles G. Drake History of Surgery Lecture, the Scudder Oration on Trauma, and the John J. Conley Ethics and Philosophy Lecture, to name but a few. These lectures often turn out to be highly memorable, groundbreaking explorations of critical issues in our profession and all attendees should try to hear one or more.
For those looking for an in-depth experience in a focused surgical topic, the Post Graduate Courses offer both didactic/experiential courses and surgical skills courses. Offerings this year include a General Surgery Review Course in the didactic format along with 14 others, and 15 surgical skills courses including courses on palliative surgical care, thyroid and parathyroid ultrasonography, advanced hepatopancreaticobiliary ultrasonography, laparoscopic inguinal and ventral hernia repair, total mesorectal excision, and many others.
There will be 48 Meet the Expert Luncheons, which offer a small group of participants the opportunity to sit down in a nonformal environment and engage in a case-based discussion of a wide variety of surgical issues. These luncheons can be a wonderful networking opportunity and a setting in which like-minded colleagues can interact face to face. A Meet the Expert conversation can be the beginning of a friendship or a professional relationship built around mutual interests.
Of course, there will also be the more traditional panel discussion sessions, the scientific forum for the presentation of scientific papers, and the video-based education sessions.
The point of all this is that the Clinical Congress offers a huge variety of ways in which to learn and interact with your fellow surgeons. Different learners prefer different formats, and the College offers something for everyone. In addition, the Clinical Congress offers unparalleled CME and other credit to address regulatory mandates with content specific to ethics, patient safety, pain management, palliative care, and trauma and critical care. Self-assessment credit can be earned to meet requirements of MOC part II.
Finally, part of the purpose of the Clinical Congress is to encourage social and networking interaction among our surgical sisters and brothers and to encourage the advancement of our profession as a group of individuals bound together by a bond of special knowledge and skill and a dedication to our fellow surgeons and our patients. Together in congress we advance the interests of our profession and our patients. See you in Chicago.
Dr. Weissler is the Joseph P. Riddle Distinguished Professor, department of otolaryngology–head and neck surgery, and chief, division of head and neck surgery, University of North Carolina (UNC) School of Medicine, Chapel Hill, and the chair of the ACS Board of Regents.
Every year I am amazed by the breadth of knowledge and information presented at the annual Clinical Congress. I find it deeply satisfying to realize how much I can still enjoy and learn from the wide variety of topics presented from all the surgical specialties.
First, there is so much new to absorb in each of our specialties and the Clinical Congress is a must in terms of hearing firsthand about innovation and change. The technical aspects of surgical techniques seemingly unrelated to my own area of specialization often have parallels to my own practice and raise questions or possible answers to problems I face in my own field.
Second, the vast amount of information about topics germane to all surgeons, such as surgical ethics, professionalism, critical care, surgical fundamentals, information technology, new surgical technology, advocacy and more, really can’t be found in any other venue.
The College has worked hard to offer learning environments that meet a variety of needs. The Town Hall meetings give groups of surgeons with a common interest the opportunity to freely discuss a wide variety of topics in a relatively unstructured environment. There will be 20 Town Hall meetings this year ranging from “Development of a Rural Track in Residency” to “The Surgeon Specific Registry (SSR): Maintenance of Certification (MOC), Physician Quality Reporting System (PQRS) and other Mandates,” to 18 additional sessions on such topics as incorporating surgical ethics into your practice, MOC, surgical education, and others.
Named Lectures are generally given by carefully chosen experts in a field and include the Martin Memorial Lecture during the opening ceremony, which this year will be given by Dr. John Meara: “Addressing Unmet Surgical Need: The Role of Academic Surgery.” Among the 10 other Named Lectures will be the Charles G. Drake History of Surgery Lecture, the Scudder Oration on Trauma, and the John J. Conley Ethics and Philosophy Lecture, to name but a few. These lectures often turn out to be highly memorable, groundbreaking explorations of critical issues in our profession and all attendees should try to hear one or more.
For those looking for an in-depth experience in a focused surgical topic, the Post Graduate Courses offer both didactic/experiential courses and surgical skills courses. Offerings this year include a General Surgery Review Course in the didactic format along with 14 others, and 15 surgical skills courses including courses on palliative surgical care, thyroid and parathyroid ultrasonography, advanced hepatopancreaticobiliary ultrasonography, laparoscopic inguinal and ventral hernia repair, total mesorectal excision, and many others.
There will be 48 Meet the Expert Luncheons, which offer a small group of participants the opportunity to sit down in a nonformal environment and engage in a case-based discussion of a wide variety of surgical issues. These luncheons can be a wonderful networking opportunity and a setting in which like-minded colleagues can interact face to face. A Meet the Expert conversation can be the beginning of a friendship or a professional relationship built around mutual interests.
Of course, there will also be the more traditional panel discussion sessions, the scientific forum for the presentation of scientific papers, and the video-based education sessions.
The point of all this is that the Clinical Congress offers a huge variety of ways in which to learn and interact with your fellow surgeons. Different learners prefer different formats, and the College offers something for everyone. In addition, the Clinical Congress offers unparalleled CME and other credit to address regulatory mandates with content specific to ethics, patient safety, pain management, palliative care, and trauma and critical care. Self-assessment credit can be earned to meet requirements of MOC part II.
Finally, part of the purpose of the Clinical Congress is to encourage social and networking interaction among our surgical sisters and brothers and to encourage the advancement of our profession as a group of individuals bound together by a bond of special knowledge and skill and a dedication to our fellow surgeons and our patients. Together in congress we advance the interests of our profession and our patients. See you in Chicago.
Dr. Weissler is the Joseph P. Riddle Distinguished Professor, department of otolaryngology–head and neck surgery, and chief, division of head and neck surgery, University of North Carolina (UNC) School of Medicine, Chapel Hill, and the chair of the ACS Board of Regents.
Every year I am amazed by the breadth of knowledge and information presented at the annual Clinical Congress. I find it deeply satisfying to realize how much I can still enjoy and learn from the wide variety of topics presented from all the surgical specialties.
First, there is so much new to absorb in each of our specialties and the Clinical Congress is a must in terms of hearing firsthand about innovation and change. The technical aspects of surgical techniques seemingly unrelated to my own area of specialization often have parallels to my own practice and raise questions or possible answers to problems I face in my own field.
Second, the vast amount of information about topics germane to all surgeons, such as surgical ethics, professionalism, critical care, surgical fundamentals, information technology, new surgical technology, advocacy and more, really can’t be found in any other venue.
The College has worked hard to offer learning environments that meet a variety of needs. The Town Hall meetings give groups of surgeons with a common interest the opportunity to freely discuss a wide variety of topics in a relatively unstructured environment. There will be 20 Town Hall meetings this year ranging from “Development of a Rural Track in Residency” to “The Surgeon Specific Registry (SSR): Maintenance of Certification (MOC), Physician Quality Reporting System (PQRS) and other Mandates,” to 18 additional sessions on such topics as incorporating surgical ethics into your practice, MOC, surgical education, and others.
Named Lectures are generally given by carefully chosen experts in a field and include the Martin Memorial Lecture during the opening ceremony, which this year will be given by Dr. John Meara: “Addressing Unmet Surgical Need: The Role of Academic Surgery.” Among the 10 other Named Lectures will be the Charles G. Drake History of Surgery Lecture, the Scudder Oration on Trauma, and the John J. Conley Ethics and Philosophy Lecture, to name but a few. These lectures often turn out to be highly memorable, groundbreaking explorations of critical issues in our profession and all attendees should try to hear one or more.
For those looking for an in-depth experience in a focused surgical topic, the Post Graduate Courses offer both didactic/experiential courses and surgical skills courses. Offerings this year include a General Surgery Review Course in the didactic format along with 14 others, and 15 surgical skills courses including courses on palliative surgical care, thyroid and parathyroid ultrasonography, advanced hepatopancreaticobiliary ultrasonography, laparoscopic inguinal and ventral hernia repair, total mesorectal excision, and many others.
There will be 48 Meet the Expert Luncheons, which offer a small group of participants the opportunity to sit down in a nonformal environment and engage in a case-based discussion of a wide variety of surgical issues. These luncheons can be a wonderful networking opportunity and a setting in which like-minded colleagues can interact face to face. A Meet the Expert conversation can be the beginning of a friendship or a professional relationship built around mutual interests.
Of course, there will also be the more traditional panel discussion sessions, the scientific forum for the presentation of scientific papers, and the video-based education sessions.
The point of all this is that the Clinical Congress offers a huge variety of ways in which to learn and interact with your fellow surgeons. Different learners prefer different formats, and the College offers something for everyone. In addition, the Clinical Congress offers unparalleled CME and other credit to address regulatory mandates with content specific to ethics, patient safety, pain management, palliative care, and trauma and critical care. Self-assessment credit can be earned to meet requirements of MOC part II.
Finally, part of the purpose of the Clinical Congress is to encourage social and networking interaction among our surgical sisters and brothers and to encourage the advancement of our profession as a group of individuals bound together by a bond of special knowledge and skill and a dedication to our fellow surgeons and our patients. Together in congress we advance the interests of our profession and our patients. See you in Chicago.
Dr. Weissler is the Joseph P. Riddle Distinguished Professor, department of otolaryngology–head and neck surgery, and chief, division of head and neck surgery, University of North Carolina (UNC) School of Medicine, Chapel Hill, and the chair of the ACS Board of Regents.

ADHD and comorbidities
No pediatrician thinks caring for children with attention-deficit/hyperactivity disorder (ADHD) is easy, but some of these patients are far easier than others! The difference between your patients with ADHD who give you nightmares and those you are eager to see at return visits is usually the presence of comorbidities (not counting parent issues!).
Comorbidities are very common with ADHD, occurring in nearly half of all patients. One of the tricky things about comorbidities in ADHD is that several of them, or medicines used to treat them, also are potential explanations for the ADHD symptoms themselves.
The most common comorbid conditions are learning disabilities, which are present in 12% when narrowly defined, but school underachievement occurs in up to 60% of children with ADHD. Children with learning difficulties that are not adequately accommodated can present with “ADHD symptoms.” These children can be inattentive, fidgety, or out of their seats; may do classwork slowly or poorly; and may ultimately be disruptive in class. What child wouldn’t act this way if he or she couldn’t understand the work? Remember that a child will do anything to “save face.” Acting up and getting sent out of class is a last resort, but not a bad option over being humiliated by looking dumb, being teased, or being embarrassed in front of peers.
Some clues that learning disabilities are responsible for symptoms include behaviors that occur selectively during specific subjects, reports of disliking the subject, or refusal to do homework for certain subjects. One would think that poor grades would point to learning disabilities, but this is not always true either because the teacher is not that discerning or because a bright child compensates while still struggling. Be sure to have some grade-level assessment you can administer yourself such as the Einstein Evaluation of School-Related Skills or the WRAT (Wide Range Achievement Test). A large proportion of children with ADHD have a reading disability so having standard paragraphs available is important in deciding who needs complete psychological testing.
With this high prevalence of reading disabilities, it should not surprise you that language disorders also are comorbid with ADHD, occurring in 4% of these children. Because language disorder is among the developmental issues most amenable to intervention, detection and referral are especially important. If a child does not answer your questions with the grammar, vocabulary, or flow of ideas you expect at a particular age, consider using the Sentence Repetition Test to check for understanding. There are no easy screens for the complex language expected of school-aged children, so consider referral to a speech-language pathologist if you are suspicious.
Anxiety is comorbid with ADHD in 21% of children, but most importantly, it the most-often-missed diagnosis causing ADHD symptoms. Consider anxiety when a child is too nervous to pay attention, is distracted by worry, is concerned about what peers think to the point of having to listen in on their conversations, is unable to come up with an answer for a teacher that is perceived as critical, or is perfectionistic about work so it never gets done on time. Although children with ADHD are rather poor observers of their own symptoms, I always ask, “Is it hard to pay attention in class?” and follow up on a “yes” by asking, “What is going through your mind when you are not paying attention?” Reports of daydreams about skateboarding are one thing, but if children say they are thinking about their mother or worrying about an upcoming test, then further evaluation for anxiety is in order. Using a screening self-report tool such as the SCARED (Screen for Childhood Anxiety and Related Disorders) or the Pediatric Anxiety Rating Scale have rather low sensitivity, but can help the conversation to define anxiety symptoms, something children do not find easy to do if asked directly.
Remember that anxiety disorders do not “fly alone” either: Children with one anxiety disorder have a greater than 60% chance of having two, and children with two have a 30% chance of having three or more anxiety disorders. That means that children with generalized anxiety disorder may well have obsessive-compulsive disorder or a specific phobia as well. Just watching for general worrying is not enough. Add to this that the parent coming in worried about their child may be the genetic source with an anxiety disorder themselves, potentially contributing to the child’s distress and making it harder for you to assess the severity of either the anxiety or the ADHD symptoms!
I am sometimes grateful that a child with ADHD has excessive anxiety because it may protect him from jumping out of windows! But the combination has downsides in making the child even less preferred by peers and more likely to have hostile bias attribution – the tendency to see others as a threat. This combination can result in impulsive proactive aggression. Recognizing the role of anxiety in the aggressive episodes, and helping the child and parent to identify it, also is crucial to successful management. Anxiety is rarely perceived by parents, teachers, or children themselves as a cause of oppositional or aggressive behavior, so you need to probe for this connection. There is no substitute for debriefing a specific example of aggression and asking the child, “What were you thinking right before this happened?” You may suspect anxiety simply by watching the child’s reaction to what the parent says in the interview. Having the child draw a picture of a child, tell a story about “What happens next?” and then “How does the story end?” can be another adjunct to detecting anxiety.
Sometimes the treatment of ADHD makes the comorbid condition worse or vice versa. A prime example where treatment of one exacerbates the other is the use of stimulants, especially amphetamines, which can produce or worsen anxiety. Even though the reported side effects of stimulants do not state that there is more anxiety with amphetamines, I often prefer to prescribe dexmethylphenidate when both ADHD and anxiety coexist. The longer-acting preparations such as methylphenidate in a long-acting liquid or patch also seem to allow for finer tuning of dose with less anxiety exacerbation than shorter-acting preparations. Nonstimulants such as long-acting guanfacine or atomoxetine as treatment for the ADHD may be needed alone or in combination to allow a lower dose when the side effects of the stimulants on the anxiety outweigh their benefits. On the other hand, if the child is on selective serotonin reuptake inhibitors for anxiety (not the first-line treatment, which is cognitive-behavior therapy), he or she may experience behavioral activation that looks a lot like worsening ADHD!
Depression is “the other side” of anxiety – often developing at a later age after an earlier diagnosis of anxiety disorder – and another common comorbidity to ADHD occurring in 18% of children. Depression is less likely to masquerade as ADHD, but still may present as inattention or poor performance. Remember that children with depression may act irritable or aggressive rather than lethargic. Depression screens such as the Patient Health Questionnaire–9 can help sort this out.
Oppositional-defiant disorder (32%) and conduct disorder (25%) are more commonly comorbid with ADHD than are the conditions just discussed, but because they are “acting-out” conditions they are of great concern to parents and thus not likely to be missed in your office visits. Other medical conditions such as tics, enuresis, encopresis and even asthma also are comorbid and should be asked about.
The Vanderbilt Initial questionnaires have a few items for anxiety, depression, and conduct as well as performance items about academic functioning. A general screening tool such as the Pediatric Symptom Checklist, perhaps followed by a diagnostic tool such as the CHADIS DSM questionnaire, can be completed by parents online or on paper to detect and help diagnose any of these comorbidities before visits.
Pediatricians are the main clinicians diagnosing (for 53% of children with ADHD) and managing this condition (Natl. Health Stat Report. 2015 Sep;81:1-8). You should be proud of how well we have recently risen to the occasion and are now identifying and treating ADHD using evidence-based tools (90%) and attempting to collect data from schools (82%) as well as parents. The biggest gap in effective primary care management of ADHD now is detecting and managing its comorbidities.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical Communications. E-mail her at pdnews@frontlinemedcom.com.
No pediatrician thinks caring for children with attention-deficit/hyperactivity disorder (ADHD) is easy, but some of these patients are far easier than others! The difference between your patients with ADHD who give you nightmares and those you are eager to see at return visits is usually the presence of comorbidities (not counting parent issues!).
Comorbidities are very common with ADHD, occurring in nearly half of all patients. One of the tricky things about comorbidities in ADHD is that several of them, or medicines used to treat them, also are potential explanations for the ADHD symptoms themselves.
The most common comorbid conditions are learning disabilities, which are present in 12% when narrowly defined, but school underachievement occurs in up to 60% of children with ADHD. Children with learning difficulties that are not adequately accommodated can present with “ADHD symptoms.” These children can be inattentive, fidgety, or out of their seats; may do classwork slowly or poorly; and may ultimately be disruptive in class. What child wouldn’t act this way if he or she couldn’t understand the work? Remember that a child will do anything to “save face.” Acting up and getting sent out of class is a last resort, but not a bad option over being humiliated by looking dumb, being teased, or being embarrassed in front of peers.
Some clues that learning disabilities are responsible for symptoms include behaviors that occur selectively during specific subjects, reports of disliking the subject, or refusal to do homework for certain subjects. One would think that poor grades would point to learning disabilities, but this is not always true either because the teacher is not that discerning or because a bright child compensates while still struggling. Be sure to have some grade-level assessment you can administer yourself such as the Einstein Evaluation of School-Related Skills or the WRAT (Wide Range Achievement Test). A large proportion of children with ADHD have a reading disability so having standard paragraphs available is important in deciding who needs complete psychological testing.
With this high prevalence of reading disabilities, it should not surprise you that language disorders also are comorbid with ADHD, occurring in 4% of these children. Because language disorder is among the developmental issues most amenable to intervention, detection and referral are especially important. If a child does not answer your questions with the grammar, vocabulary, or flow of ideas you expect at a particular age, consider using the Sentence Repetition Test to check for understanding. There are no easy screens for the complex language expected of school-aged children, so consider referral to a speech-language pathologist if you are suspicious.
Anxiety is comorbid with ADHD in 21% of children, but most importantly, it the most-often-missed diagnosis causing ADHD symptoms. Consider anxiety when a child is too nervous to pay attention, is distracted by worry, is concerned about what peers think to the point of having to listen in on their conversations, is unable to come up with an answer for a teacher that is perceived as critical, or is perfectionistic about work so it never gets done on time. Although children with ADHD are rather poor observers of their own symptoms, I always ask, “Is it hard to pay attention in class?” and follow up on a “yes” by asking, “What is going through your mind when you are not paying attention?” Reports of daydreams about skateboarding are one thing, but if children say they are thinking about their mother or worrying about an upcoming test, then further evaluation for anxiety is in order. Using a screening self-report tool such as the SCARED (Screen for Childhood Anxiety and Related Disorders) or the Pediatric Anxiety Rating Scale have rather low sensitivity, but can help the conversation to define anxiety symptoms, something children do not find easy to do if asked directly.
Remember that anxiety disorders do not “fly alone” either: Children with one anxiety disorder have a greater than 60% chance of having two, and children with two have a 30% chance of having three or more anxiety disorders. That means that children with generalized anxiety disorder may well have obsessive-compulsive disorder or a specific phobia as well. Just watching for general worrying is not enough. Add to this that the parent coming in worried about their child may be the genetic source with an anxiety disorder themselves, potentially contributing to the child’s distress and making it harder for you to assess the severity of either the anxiety or the ADHD symptoms!
I am sometimes grateful that a child with ADHD has excessive anxiety because it may protect him from jumping out of windows! But the combination has downsides in making the child even less preferred by peers and more likely to have hostile bias attribution – the tendency to see others as a threat. This combination can result in impulsive proactive aggression. Recognizing the role of anxiety in the aggressive episodes, and helping the child and parent to identify it, also is crucial to successful management. Anxiety is rarely perceived by parents, teachers, or children themselves as a cause of oppositional or aggressive behavior, so you need to probe for this connection. There is no substitute for debriefing a specific example of aggression and asking the child, “What were you thinking right before this happened?” You may suspect anxiety simply by watching the child’s reaction to what the parent says in the interview. Having the child draw a picture of a child, tell a story about “What happens next?” and then “How does the story end?” can be another adjunct to detecting anxiety.
Sometimes the treatment of ADHD makes the comorbid condition worse or vice versa. A prime example where treatment of one exacerbates the other is the use of stimulants, especially amphetamines, which can produce or worsen anxiety. Even though the reported side effects of stimulants do not state that there is more anxiety with amphetamines, I often prefer to prescribe dexmethylphenidate when both ADHD and anxiety coexist. The longer-acting preparations such as methylphenidate in a long-acting liquid or patch also seem to allow for finer tuning of dose with less anxiety exacerbation than shorter-acting preparations. Nonstimulants such as long-acting guanfacine or atomoxetine as treatment for the ADHD may be needed alone or in combination to allow a lower dose when the side effects of the stimulants on the anxiety outweigh their benefits. On the other hand, if the child is on selective serotonin reuptake inhibitors for anxiety (not the first-line treatment, which is cognitive-behavior therapy), he or she may experience behavioral activation that looks a lot like worsening ADHD!
Depression is “the other side” of anxiety – often developing at a later age after an earlier diagnosis of anxiety disorder – and another common comorbidity to ADHD occurring in 18% of children. Depression is less likely to masquerade as ADHD, but still may present as inattention or poor performance. Remember that children with depression may act irritable or aggressive rather than lethargic. Depression screens such as the Patient Health Questionnaire–9 can help sort this out.
Oppositional-defiant disorder (32%) and conduct disorder (25%) are more commonly comorbid with ADHD than are the conditions just discussed, but because they are “acting-out” conditions they are of great concern to parents and thus not likely to be missed in your office visits. Other medical conditions such as tics, enuresis, encopresis and even asthma also are comorbid and should be asked about.
The Vanderbilt Initial questionnaires have a few items for anxiety, depression, and conduct as well as performance items about academic functioning. A general screening tool such as the Pediatric Symptom Checklist, perhaps followed by a diagnostic tool such as the CHADIS DSM questionnaire, can be completed by parents online or on paper to detect and help diagnose any of these comorbidities before visits.
Pediatricians are the main clinicians diagnosing (for 53% of children with ADHD) and managing this condition (Natl. Health Stat Report. 2015 Sep;81:1-8). You should be proud of how well we have recently risen to the occasion and are now identifying and treating ADHD using evidence-based tools (90%) and attempting to collect data from schools (82%) as well as parents. The biggest gap in effective primary care management of ADHD now is detecting and managing its comorbidities.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical Communications. E-mail her at pdnews@frontlinemedcom.com.
No pediatrician thinks caring for children with attention-deficit/hyperactivity disorder (ADHD) is easy, but some of these patients are far easier than others! The difference between your patients with ADHD who give you nightmares and those you are eager to see at return visits is usually the presence of comorbidities (not counting parent issues!).
Comorbidities are very common with ADHD, occurring in nearly half of all patients. One of the tricky things about comorbidities in ADHD is that several of them, or medicines used to treat them, also are potential explanations for the ADHD symptoms themselves.
The most common comorbid conditions are learning disabilities, which are present in 12% when narrowly defined, but school underachievement occurs in up to 60% of children with ADHD. Children with learning difficulties that are not adequately accommodated can present with “ADHD symptoms.” These children can be inattentive, fidgety, or out of their seats; may do classwork slowly or poorly; and may ultimately be disruptive in class. What child wouldn’t act this way if he or she couldn’t understand the work? Remember that a child will do anything to “save face.” Acting up and getting sent out of class is a last resort, but not a bad option over being humiliated by looking dumb, being teased, or being embarrassed in front of peers.
Some clues that learning disabilities are responsible for symptoms include behaviors that occur selectively during specific subjects, reports of disliking the subject, or refusal to do homework for certain subjects. One would think that poor grades would point to learning disabilities, but this is not always true either because the teacher is not that discerning or because a bright child compensates while still struggling. Be sure to have some grade-level assessment you can administer yourself such as the Einstein Evaluation of School-Related Skills or the WRAT (Wide Range Achievement Test). A large proportion of children with ADHD have a reading disability so having standard paragraphs available is important in deciding who needs complete psychological testing.
With this high prevalence of reading disabilities, it should not surprise you that language disorders also are comorbid with ADHD, occurring in 4% of these children. Because language disorder is among the developmental issues most amenable to intervention, detection and referral are especially important. If a child does not answer your questions with the grammar, vocabulary, or flow of ideas you expect at a particular age, consider using the Sentence Repetition Test to check for understanding. There are no easy screens for the complex language expected of school-aged children, so consider referral to a speech-language pathologist if you are suspicious.
Anxiety is comorbid with ADHD in 21% of children, but most importantly, it the most-often-missed diagnosis causing ADHD symptoms. Consider anxiety when a child is too nervous to pay attention, is distracted by worry, is concerned about what peers think to the point of having to listen in on their conversations, is unable to come up with an answer for a teacher that is perceived as critical, or is perfectionistic about work so it never gets done on time. Although children with ADHD are rather poor observers of their own symptoms, I always ask, “Is it hard to pay attention in class?” and follow up on a “yes” by asking, “What is going through your mind when you are not paying attention?” Reports of daydreams about skateboarding are one thing, but if children say they are thinking about their mother or worrying about an upcoming test, then further evaluation for anxiety is in order. Using a screening self-report tool such as the SCARED (Screen for Childhood Anxiety and Related Disorders) or the Pediatric Anxiety Rating Scale have rather low sensitivity, but can help the conversation to define anxiety symptoms, something children do not find easy to do if asked directly.
Remember that anxiety disorders do not “fly alone” either: Children with one anxiety disorder have a greater than 60% chance of having two, and children with two have a 30% chance of having three or more anxiety disorders. That means that children with generalized anxiety disorder may well have obsessive-compulsive disorder or a specific phobia as well. Just watching for general worrying is not enough. Add to this that the parent coming in worried about their child may be the genetic source with an anxiety disorder themselves, potentially contributing to the child’s distress and making it harder for you to assess the severity of either the anxiety or the ADHD symptoms!
I am sometimes grateful that a child with ADHD has excessive anxiety because it may protect him from jumping out of windows! But the combination has downsides in making the child even less preferred by peers and more likely to have hostile bias attribution – the tendency to see others as a threat. This combination can result in impulsive proactive aggression. Recognizing the role of anxiety in the aggressive episodes, and helping the child and parent to identify it, also is crucial to successful management. Anxiety is rarely perceived by parents, teachers, or children themselves as a cause of oppositional or aggressive behavior, so you need to probe for this connection. There is no substitute for debriefing a specific example of aggression and asking the child, “What were you thinking right before this happened?” You may suspect anxiety simply by watching the child’s reaction to what the parent says in the interview. Having the child draw a picture of a child, tell a story about “What happens next?” and then “How does the story end?” can be another adjunct to detecting anxiety.
Sometimes the treatment of ADHD makes the comorbid condition worse or vice versa. A prime example where treatment of one exacerbates the other is the use of stimulants, especially amphetamines, which can produce or worsen anxiety. Even though the reported side effects of stimulants do not state that there is more anxiety with amphetamines, I often prefer to prescribe dexmethylphenidate when both ADHD and anxiety coexist. The longer-acting preparations such as methylphenidate in a long-acting liquid or patch also seem to allow for finer tuning of dose with less anxiety exacerbation than shorter-acting preparations. Nonstimulants such as long-acting guanfacine or atomoxetine as treatment for the ADHD may be needed alone or in combination to allow a lower dose when the side effects of the stimulants on the anxiety outweigh their benefits. On the other hand, if the child is on selective serotonin reuptake inhibitors for anxiety (not the first-line treatment, which is cognitive-behavior therapy), he or she may experience behavioral activation that looks a lot like worsening ADHD!
Depression is “the other side” of anxiety – often developing at a later age after an earlier diagnosis of anxiety disorder – and another common comorbidity to ADHD occurring in 18% of children. Depression is less likely to masquerade as ADHD, but still may present as inattention or poor performance. Remember that children with depression may act irritable or aggressive rather than lethargic. Depression screens such as the Patient Health Questionnaire–9 can help sort this out.
Oppositional-defiant disorder (32%) and conduct disorder (25%) are more commonly comorbid with ADHD than are the conditions just discussed, but because they are “acting-out” conditions they are of great concern to parents and thus not likely to be missed in your office visits. Other medical conditions such as tics, enuresis, encopresis and even asthma also are comorbid and should be asked about.
The Vanderbilt Initial questionnaires have a few items for anxiety, depression, and conduct as well as performance items about academic functioning. A general screening tool such as the Pediatric Symptom Checklist, perhaps followed by a diagnostic tool such as the CHADIS DSM questionnaire, can be completed by parents online or on paper to detect and help diagnose any of these comorbidities before visits.
Pediatricians are the main clinicians diagnosing (for 53% of children with ADHD) and managing this condition (Natl. Health Stat Report. 2015 Sep;81:1-8). You should be proud of how well we have recently risen to the occasion and are now identifying and treating ADHD using evidence-based tools (90%) and attempting to collect data from schools (82%) as well as parents. The biggest gap in effective primary care management of ADHD now is detecting and managing its comorbidities.
Dr. Howard is assistant professor of pediatrics at the Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS (www.CHADIS.com). She had no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical Communications. E-mail her at pdnews@frontlinemedcom.com.
