User login
Autonomy Now! Why PAs, Like NPs, Need Full Practice Authority
Across the nation, states are dealing with shortages of health care providers.1 The situation is expected to worsen as the physician population ages and many retire from the workforce.2 Meanwhile, the number of medical schools—and graduates from them—continue to stagnate. Even when additional residency spots are created, relatively small percentages of MDs/DOs choose to practice in primary care. Combine these circumstances with the fact that the Affordable Care Act has injected a significant number of new patients into an already overburdened health care system and you realize that new innovations are desperately needed to increase access to care for patients.
Utilizing PAs and NPs to the full extent of their training will not only help alleviate the shortages but also increase the quality and accessibility of care. NP and PA programs are proliferating across the country and producing steadily increasing numbers of graduates.3 Many of these newly minted NPs and PAs choose to enter primary care settings to practice, where they help to lower health care costs, decrease malpractice rates, and yield excellent patient outcomes and satisfaction rates.4,5
Yet physician organizations and state legislators continue to resist efforts to give these experienced and well-trained providers expanded scopes of practice and full practice authority. In many cases, physician interest groups continue to lobby for restrictive laws that are not backed with any data.6
Patients continue to suffer from a lack of access to health care because of legislative battles between groups of providers over practice territory, money, and egos. Many patients have to wait extended periods to see a provider; in some rural areas, there may be no care available at all.
In these situations, experienced PAs and NPs are held hostage and unable to practice without collaborative agreements. Often, physicians demand monthly stipends (sometimes thousands of dollars) to act as a collaborator under such an agreement. In many cases, these “collaborating” physicians provide almost no oversight. Burdensome legislation stipulating supervisory or collaborative requirements—for which there is little to no supportive evidence—keeps health care costs higher than necessary, decreases access to care, and stifles any flexibility or innovation in health care.
NPs presently have full practice authority in 21 states and the District of Columbia and are recognized for their education and clinical training.7 They must, and will, continue to lobby and fight for full practice authority in the rest of the country. PAs must join in this effort by continuing to lobby for full practice authority for experienced PAs in primary care. It’s time PAs were also recognized by state legislators for their education, clinical training, and dedication to quality patient outcomes.
PAs are graduate-level educated providers with a wealth of knowledge and experience. PAs, like our NP counterparts, have 50 years of patient outcomes data and studies that prove we are effective and safe providers. Organizations such as the VA, the FTC, and other citizen advocacy groups support PAs.8-10 These organizations have supported NP independence and will support the push for PA practice autonomy as well.
The time has come to start the movement for full practice authority for PAs on a national and state level. Experienced PAs in primary care are ready for this challenge and should lobby for legislation that would allow them the option to practice without collaborative agreements. In states that have granted independence to NPs, the wording “practice alone or in collaboration with a physician” has been used, allowing flexibility in practice environments; PAs could use the same language in their lobbying efforts.
The criteria for PA autonomy will undoubtedly be debated extensively. For our NP colleagues, many states require a specific number of hours practicing with a collaborative agreement in place before independent practice is allowed. Since very little data exist that can direct the PA profession on the number of years a PA should practice before gaining autonomy, relevant NP legislative requirements could be used as a precedent.
For example, Nevada gives NPs the ability to practice without a collaborative agreement as new graduates. Connecticut gives NPs the ability to practice independently after three years of collaboration with a physician. There is little doubt that these are arbitrary numbers that were agreed upon at the state level—but PAs will face the same negotiations when lobbying for their right to practice autonomously.
Continue for PA criteria >>
I propose several criteria as a starting point for PA autonomy discussions.11 PAs should
• Be NCCPA board-certified and eligible for state licensure
• Have three years full-time, or 6,000 hours, of practice in a primary care setting
• Have practiced at least one of the three required years within the previous two calendar years.
As I see it, PAs in a state that has passed full practice authority legislation, and met the above criteria, could start practicing without collaboration as soon as the law takes effect. Out-of-state PAs applying for licensure in a state with autonomy legislation should be permitted to use their practice experience in another state to meet the minimum requirements for autonomy.
The time has come to remove punitive legislation and supervisory burdens from hard-working, well-intentioned, quality providers. Many physicians practicing on the front lines of medicine with PAs and NPs are choosing to hire NPs who are independent, because it’s easier for them to do so. Independent NPs do not come burdened with a state-mandated list of supervisory requirements (which may create a perception of increased legal liability for the physician).
Many PAs may fear backlash from physicians over the issue of autonomy. The reality is that, yes, there will be some resistance from organized medicine. But when PA autonomy legislation is passed, organizations and physicians will continue to hire PAs—just as they continue to hire NPs. PAs who gain autonomy will be studied just as independent NPs are being studied. And, as is the case with our NP colleagues, PAs’ patient outcome data will continue to be positive.
Laws are not what make good providers. Accredited education programs, quality CME, access to technology, best practices, and team health care make good providers. America doesn’t have 20 years to wait for PAs and NPs to creep forward with baby steps in legislative sessions that last years. Our patients need us now! They need PAs and NPs to fight for their care, to be their advocates, and to be their providers.11 They need us to stand up and own our professions so we can be more effective—not for us, but for them. I hope you agree. Feel free to send your thoughts to PAEditor@frontlinemedcom.com.
REFERENCES
1. United Health Foundation. America’s Health Rankings: a Call to Action for Individuals and Their Communities (2014). http://cdnfiles.americashealthrankings.org/SiteFiles/PressReleases/Americas%20Health%20Rankings%202014%20Edition.pdf. Accessed September 9, 2015.
2. Association of American Medical Colleges Center for Workforce Studies. 2013 State Physician Workforce Data Book. https://members.aamc.org/eweb/upload/State%20Physician%20Workforce%20Data%20Book%202013%20(PDF).pdf. Accessed September 9, 2015.
3. Physician Assistant Education Association. PAEA 28th Annual Report: Physician Assistant Educational Programs in the United States, 2011-2012. www.paeaonline.org/index.php?ht=a/GetDocumentAction/i/156969. Accessed September 9, 2015.
4. Hooker RS, Nicholson JG, Le T. Does the employment of physician assistants and nurse practitioners increase liability? J Med Licensure Discipline. 2009;95(2):6-15.
5. Hooker RS, Muchow AN. Modifying state laws for NPs and PAs can reduce cost of medical services. Nurs Econ. 2015;33(2):88-94.
6. Isaacs S, Jellinek P. Accept No Substitute: A Report on Scope of Practice. The Physicians Foundation. November 2012: 14-15. www.sc.edu/study/colleges_schools/nursing/centers_institutes/center_nursing_leadership/sc_onevoice_oneplan/a_report_on_scope_of_practice.pdf. Accessed September 9, 2015.
7. American Association of Nurse Practitioners. State Practice Environment. www.aanp.org/legislation-regulation/state-legislation/state-practice-environment. Accessed September 9, 2015.
8. LeBuhn R, Swankin DA. Reforming Scopes of Practice: A White Paper. Citizen Advocacy Center. July 2010. www.cacenter.org/files/ReformingScopesofPractice-WhitePaper.pdf. Accessed September 9, 2015.
9. Department of Veteran’s Affairs, Veteran’s Health Administration. VHA DIRECTIVE 1063: Utilization of Physician Assistants, Appendix A-5. www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2958. Accessed September 9, 2015.
10. Federal Trade Commission Office of Policy Planning, Bureau of Economics, and Bureau of Competition. Letter to Representative Kirkton, April 21, 2015. www.ftc.gov/system/files/documents/advocacy_documents/ftc-staff-comment-representative-jeanne-kirkton-missouri-house-representatives-regarding-competitive/150422missourihouse.pdf. Accessed September 9, 2015.
11. Sady B. Optional Autonomy for PAs in Nevada: A White Paper. June 2015. https://app.box.com/s/6f6567b1fobkvvo1g7egfd2gq6ir1jx7. Accessed September 10, 2015.
Across the nation, states are dealing with shortages of health care providers.1 The situation is expected to worsen as the physician population ages and many retire from the workforce.2 Meanwhile, the number of medical schools—and graduates from them—continue to stagnate. Even when additional residency spots are created, relatively small percentages of MDs/DOs choose to practice in primary care. Combine these circumstances with the fact that the Affordable Care Act has injected a significant number of new patients into an already overburdened health care system and you realize that new innovations are desperately needed to increase access to care for patients.
Utilizing PAs and NPs to the full extent of their training will not only help alleviate the shortages but also increase the quality and accessibility of care. NP and PA programs are proliferating across the country and producing steadily increasing numbers of graduates.3 Many of these newly minted NPs and PAs choose to enter primary care settings to practice, where they help to lower health care costs, decrease malpractice rates, and yield excellent patient outcomes and satisfaction rates.4,5
Yet physician organizations and state legislators continue to resist efforts to give these experienced and well-trained providers expanded scopes of practice and full practice authority. In many cases, physician interest groups continue to lobby for restrictive laws that are not backed with any data.6
Patients continue to suffer from a lack of access to health care because of legislative battles between groups of providers over practice territory, money, and egos. Many patients have to wait extended periods to see a provider; in some rural areas, there may be no care available at all.
In these situations, experienced PAs and NPs are held hostage and unable to practice without collaborative agreements. Often, physicians demand monthly stipends (sometimes thousands of dollars) to act as a collaborator under such an agreement. In many cases, these “collaborating” physicians provide almost no oversight. Burdensome legislation stipulating supervisory or collaborative requirements—for which there is little to no supportive evidence—keeps health care costs higher than necessary, decreases access to care, and stifles any flexibility or innovation in health care.
NPs presently have full practice authority in 21 states and the District of Columbia and are recognized for their education and clinical training.7 They must, and will, continue to lobby and fight for full practice authority in the rest of the country. PAs must join in this effort by continuing to lobby for full practice authority for experienced PAs in primary care. It’s time PAs were also recognized by state legislators for their education, clinical training, and dedication to quality patient outcomes.
PAs are graduate-level educated providers with a wealth of knowledge and experience. PAs, like our NP counterparts, have 50 years of patient outcomes data and studies that prove we are effective and safe providers. Organizations such as the VA, the FTC, and other citizen advocacy groups support PAs.8-10 These organizations have supported NP independence and will support the push for PA practice autonomy as well.
The time has come to start the movement for full practice authority for PAs on a national and state level. Experienced PAs in primary care are ready for this challenge and should lobby for legislation that would allow them the option to practice without collaborative agreements. In states that have granted independence to NPs, the wording “practice alone or in collaboration with a physician” has been used, allowing flexibility in practice environments; PAs could use the same language in their lobbying efforts.
The criteria for PA autonomy will undoubtedly be debated extensively. For our NP colleagues, many states require a specific number of hours practicing with a collaborative agreement in place before independent practice is allowed. Since very little data exist that can direct the PA profession on the number of years a PA should practice before gaining autonomy, relevant NP legislative requirements could be used as a precedent.
For example, Nevada gives NPs the ability to practice without a collaborative agreement as new graduates. Connecticut gives NPs the ability to practice independently after three years of collaboration with a physician. There is little doubt that these are arbitrary numbers that were agreed upon at the state level—but PAs will face the same negotiations when lobbying for their right to practice autonomously.
Continue for PA criteria >>
I propose several criteria as a starting point for PA autonomy discussions.11 PAs should
• Be NCCPA board-certified and eligible for state licensure
• Have three years full-time, or 6,000 hours, of practice in a primary care setting
• Have practiced at least one of the three required years within the previous two calendar years.
As I see it, PAs in a state that has passed full practice authority legislation, and met the above criteria, could start practicing without collaboration as soon as the law takes effect. Out-of-state PAs applying for licensure in a state with autonomy legislation should be permitted to use their practice experience in another state to meet the minimum requirements for autonomy.
The time has come to remove punitive legislation and supervisory burdens from hard-working, well-intentioned, quality providers. Many physicians practicing on the front lines of medicine with PAs and NPs are choosing to hire NPs who are independent, because it’s easier for them to do so. Independent NPs do not come burdened with a state-mandated list of supervisory requirements (which may create a perception of increased legal liability for the physician).
Many PAs may fear backlash from physicians over the issue of autonomy. The reality is that, yes, there will be some resistance from organized medicine. But when PA autonomy legislation is passed, organizations and physicians will continue to hire PAs—just as they continue to hire NPs. PAs who gain autonomy will be studied just as independent NPs are being studied. And, as is the case with our NP colleagues, PAs’ patient outcome data will continue to be positive.
Laws are not what make good providers. Accredited education programs, quality CME, access to technology, best practices, and team health care make good providers. America doesn’t have 20 years to wait for PAs and NPs to creep forward with baby steps in legislative sessions that last years. Our patients need us now! They need PAs and NPs to fight for their care, to be their advocates, and to be their providers.11 They need us to stand up and own our professions so we can be more effective—not for us, but for them. I hope you agree. Feel free to send your thoughts to PAEditor@frontlinemedcom.com.
REFERENCES
1. United Health Foundation. America’s Health Rankings: a Call to Action for Individuals and Their Communities (2014). http://cdnfiles.americashealthrankings.org/SiteFiles/PressReleases/Americas%20Health%20Rankings%202014%20Edition.pdf. Accessed September 9, 2015.
2. Association of American Medical Colleges Center for Workforce Studies. 2013 State Physician Workforce Data Book. https://members.aamc.org/eweb/upload/State%20Physician%20Workforce%20Data%20Book%202013%20(PDF).pdf. Accessed September 9, 2015.
3. Physician Assistant Education Association. PAEA 28th Annual Report: Physician Assistant Educational Programs in the United States, 2011-2012. www.paeaonline.org/index.php?ht=a/GetDocumentAction/i/156969. Accessed September 9, 2015.
4. Hooker RS, Nicholson JG, Le T. Does the employment of physician assistants and nurse practitioners increase liability? J Med Licensure Discipline. 2009;95(2):6-15.
5. Hooker RS, Muchow AN. Modifying state laws for NPs and PAs can reduce cost of medical services. Nurs Econ. 2015;33(2):88-94.
6. Isaacs S, Jellinek P. Accept No Substitute: A Report on Scope of Practice. The Physicians Foundation. November 2012: 14-15. www.sc.edu/study/colleges_schools/nursing/centers_institutes/center_nursing_leadership/sc_onevoice_oneplan/a_report_on_scope_of_practice.pdf. Accessed September 9, 2015.
7. American Association of Nurse Practitioners. State Practice Environment. www.aanp.org/legislation-regulation/state-legislation/state-practice-environment. Accessed September 9, 2015.
8. LeBuhn R, Swankin DA. Reforming Scopes of Practice: A White Paper. Citizen Advocacy Center. July 2010. www.cacenter.org/files/ReformingScopesofPractice-WhitePaper.pdf. Accessed September 9, 2015.
9. Department of Veteran’s Affairs, Veteran’s Health Administration. VHA DIRECTIVE 1063: Utilization of Physician Assistants, Appendix A-5. www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2958. Accessed September 9, 2015.
10. Federal Trade Commission Office of Policy Planning, Bureau of Economics, and Bureau of Competition. Letter to Representative Kirkton, April 21, 2015. www.ftc.gov/system/files/documents/advocacy_documents/ftc-staff-comment-representative-jeanne-kirkton-missouri-house-representatives-regarding-competitive/150422missourihouse.pdf. Accessed September 9, 2015.
11. Sady B. Optional Autonomy for PAs in Nevada: A White Paper. June 2015. https://app.box.com/s/6f6567b1fobkvvo1g7egfd2gq6ir1jx7. Accessed September 10, 2015.
Across the nation, states are dealing with shortages of health care providers.1 The situation is expected to worsen as the physician population ages and many retire from the workforce.2 Meanwhile, the number of medical schools—and graduates from them—continue to stagnate. Even when additional residency spots are created, relatively small percentages of MDs/DOs choose to practice in primary care. Combine these circumstances with the fact that the Affordable Care Act has injected a significant number of new patients into an already overburdened health care system and you realize that new innovations are desperately needed to increase access to care for patients.
Utilizing PAs and NPs to the full extent of their training will not only help alleviate the shortages but also increase the quality and accessibility of care. NP and PA programs are proliferating across the country and producing steadily increasing numbers of graduates.3 Many of these newly minted NPs and PAs choose to enter primary care settings to practice, where they help to lower health care costs, decrease malpractice rates, and yield excellent patient outcomes and satisfaction rates.4,5
Yet physician organizations and state legislators continue to resist efforts to give these experienced and well-trained providers expanded scopes of practice and full practice authority. In many cases, physician interest groups continue to lobby for restrictive laws that are not backed with any data.6
Patients continue to suffer from a lack of access to health care because of legislative battles between groups of providers over practice territory, money, and egos. Many patients have to wait extended periods to see a provider; in some rural areas, there may be no care available at all.
In these situations, experienced PAs and NPs are held hostage and unable to practice without collaborative agreements. Often, physicians demand monthly stipends (sometimes thousands of dollars) to act as a collaborator under such an agreement. In many cases, these “collaborating” physicians provide almost no oversight. Burdensome legislation stipulating supervisory or collaborative requirements—for which there is little to no supportive evidence—keeps health care costs higher than necessary, decreases access to care, and stifles any flexibility or innovation in health care.
NPs presently have full practice authority in 21 states and the District of Columbia and are recognized for their education and clinical training.7 They must, and will, continue to lobby and fight for full practice authority in the rest of the country. PAs must join in this effort by continuing to lobby for full practice authority for experienced PAs in primary care. It’s time PAs were also recognized by state legislators for their education, clinical training, and dedication to quality patient outcomes.
PAs are graduate-level educated providers with a wealth of knowledge and experience. PAs, like our NP counterparts, have 50 years of patient outcomes data and studies that prove we are effective and safe providers. Organizations such as the VA, the FTC, and other citizen advocacy groups support PAs.8-10 These organizations have supported NP independence and will support the push for PA practice autonomy as well.
The time has come to start the movement for full practice authority for PAs on a national and state level. Experienced PAs in primary care are ready for this challenge and should lobby for legislation that would allow them the option to practice without collaborative agreements. In states that have granted independence to NPs, the wording “practice alone or in collaboration with a physician” has been used, allowing flexibility in practice environments; PAs could use the same language in their lobbying efforts.
The criteria for PA autonomy will undoubtedly be debated extensively. For our NP colleagues, many states require a specific number of hours practicing with a collaborative agreement in place before independent practice is allowed. Since very little data exist that can direct the PA profession on the number of years a PA should practice before gaining autonomy, relevant NP legislative requirements could be used as a precedent.
For example, Nevada gives NPs the ability to practice without a collaborative agreement as new graduates. Connecticut gives NPs the ability to practice independently after three years of collaboration with a physician. There is little doubt that these are arbitrary numbers that were agreed upon at the state level—but PAs will face the same negotiations when lobbying for their right to practice autonomously.
Continue for PA criteria >>
I propose several criteria as a starting point for PA autonomy discussions.11 PAs should
• Be NCCPA board-certified and eligible for state licensure
• Have three years full-time, or 6,000 hours, of practice in a primary care setting
• Have practiced at least one of the three required years within the previous two calendar years.
As I see it, PAs in a state that has passed full practice authority legislation, and met the above criteria, could start practicing without collaboration as soon as the law takes effect. Out-of-state PAs applying for licensure in a state with autonomy legislation should be permitted to use their practice experience in another state to meet the minimum requirements for autonomy.
The time has come to remove punitive legislation and supervisory burdens from hard-working, well-intentioned, quality providers. Many physicians practicing on the front lines of medicine with PAs and NPs are choosing to hire NPs who are independent, because it’s easier for them to do so. Independent NPs do not come burdened with a state-mandated list of supervisory requirements (which may create a perception of increased legal liability for the physician).
Many PAs may fear backlash from physicians over the issue of autonomy. The reality is that, yes, there will be some resistance from organized medicine. But when PA autonomy legislation is passed, organizations and physicians will continue to hire PAs—just as they continue to hire NPs. PAs who gain autonomy will be studied just as independent NPs are being studied. And, as is the case with our NP colleagues, PAs’ patient outcome data will continue to be positive.
Laws are not what make good providers. Accredited education programs, quality CME, access to technology, best practices, and team health care make good providers. America doesn’t have 20 years to wait for PAs and NPs to creep forward with baby steps in legislative sessions that last years. Our patients need us now! They need PAs and NPs to fight for their care, to be their advocates, and to be their providers.11 They need us to stand up and own our professions so we can be more effective—not for us, but for them. I hope you agree. Feel free to send your thoughts to PAEditor@frontlinemedcom.com.
REFERENCES
1. United Health Foundation. America’s Health Rankings: a Call to Action for Individuals and Their Communities (2014). http://cdnfiles.americashealthrankings.org/SiteFiles/PressReleases/Americas%20Health%20Rankings%202014%20Edition.pdf. Accessed September 9, 2015.
2. Association of American Medical Colleges Center for Workforce Studies. 2013 State Physician Workforce Data Book. https://members.aamc.org/eweb/upload/State%20Physician%20Workforce%20Data%20Book%202013%20(PDF).pdf. Accessed September 9, 2015.
3. Physician Assistant Education Association. PAEA 28th Annual Report: Physician Assistant Educational Programs in the United States, 2011-2012. www.paeaonline.org/index.php?ht=a/GetDocumentAction/i/156969. Accessed September 9, 2015.
4. Hooker RS, Nicholson JG, Le T. Does the employment of physician assistants and nurse practitioners increase liability? J Med Licensure Discipline. 2009;95(2):6-15.
5. Hooker RS, Muchow AN. Modifying state laws for NPs and PAs can reduce cost of medical services. Nurs Econ. 2015;33(2):88-94.
6. Isaacs S, Jellinek P. Accept No Substitute: A Report on Scope of Practice. The Physicians Foundation. November 2012: 14-15. www.sc.edu/study/colleges_schools/nursing/centers_institutes/center_nursing_leadership/sc_onevoice_oneplan/a_report_on_scope_of_practice.pdf. Accessed September 9, 2015.
7. American Association of Nurse Practitioners. State Practice Environment. www.aanp.org/legislation-regulation/state-legislation/state-practice-environment. Accessed September 9, 2015.
8. LeBuhn R, Swankin DA. Reforming Scopes of Practice: A White Paper. Citizen Advocacy Center. July 2010. www.cacenter.org/files/ReformingScopesofPractice-WhitePaper.pdf. Accessed September 9, 2015.
9. Department of Veteran’s Affairs, Veteran’s Health Administration. VHA DIRECTIVE 1063: Utilization of Physician Assistants, Appendix A-5. www.va.gov/vhapublications/ViewPublication.asp?pub_ID=2958. Accessed September 9, 2015.
10. Federal Trade Commission Office of Policy Planning, Bureau of Economics, and Bureau of Competition. Letter to Representative Kirkton, April 21, 2015. www.ftc.gov/system/files/documents/advocacy_documents/ftc-staff-comment-representative-jeanne-kirkton-missouri-house-representatives-regarding-competitive/150422missourihouse.pdf. Accessed September 9, 2015.
11. Sady B. Optional Autonomy for PAs in Nevada: A White Paper. June 2015. https://app.box.com/s/6f6567b1fobkvvo1g7egfd2gq6ir1jx7. Accessed September 10, 2015.
Office visits should be a “dance,” not a dictate

Last month, a group of investigators from the American Academy of Family Physicians and the University of Wisconsin led by Holman1 published a study entitled, “The myth of standardized workflow in primary care.” The researchers directly observed 20 primary care physician (PCP) visits and coded the usual tasks physicians perform during a visit. For some physicians, they observed 2 encounters to see if individual physicians followed a consistent pattern. What they found won’t surprise any of you:
“…We found no consistent workflows when analyzing visits individually or by PCP, or visits conducted at clinics with or without an [electronic medical record (EMR)]. The workflow for tasks is dictated not by the type of chart, the patient, or the physician. Instead, workflow emerges from the interaction between the patient’s and the physician’s agendas.”
This rang true for me. For example, sometimes a patient immediately pulls out her bag of pills, so I do the medication review first. Other times, social chat comes first. Often, asking, “Is there anything else you need today?” leads to another round of history-taking and test-ordering.
The physicians in this study approached patient visits as a conversation rather than adhering to a rigid protocol, as the EMR vendors imply we should do. Frankly, that has never made sense to me. Why shouldn’t the EMR companies adapt their tools to the needs of patients and physicians? It was so heartening to read that experienced family physicians are not kowtowing to EMR experts’ insistence that we change our workflow to adapt to the realities of EMRs. We still approach patient encounters in a patient-centered way, following the thread of the conversation to fully respond to our patients’ needs. (Can the same be said for medical students? See last month’s Guest Editorial, “Med students: Look up from your EMRs”.)
"Workflow" was a foreign concept to me until the advent of EMRs. I never worried much about the order in which I was performing "tasks," and I still don't.
Holman et al1 describe the interplay between physicians and patients during office visits as a “dance” in which patients and physicians take turns leading. Let’s invite EMR vendors to join our dance—and follow our lead.
Reference
1. Holman GT, Beasley JW, Karsh BT, et al. The myth of standardized workflow in primary care. J Am Med Inform Assoc. 2015. [Epub ahead of print].
Last month, a group of investigators from the American Academy of Family Physicians and the University of Wisconsin led by Holman1 published a study entitled, “The myth of standardized workflow in primary care.” The researchers directly observed 20 primary care physician (PCP) visits and coded the usual tasks physicians perform during a visit. For some physicians, they observed 2 encounters to see if individual physicians followed a consistent pattern. What they found won’t surprise any of you:
“…We found no consistent workflows when analyzing visits individually or by PCP, or visits conducted at clinics with or without an [electronic medical record (EMR)]. The workflow for tasks is dictated not by the type of chart, the patient, or the physician. Instead, workflow emerges from the interaction between the patient’s and the physician’s agendas.”
This rang true for me. For example, sometimes a patient immediately pulls out her bag of pills, so I do the medication review first. Other times, social chat comes first. Often, asking, “Is there anything else you need today?” leads to another round of history-taking and test-ordering.
The physicians in this study approached patient visits as a conversation rather than adhering to a rigid protocol, as the EMR vendors imply we should do. Frankly, that has never made sense to me. Why shouldn’t the EMR companies adapt their tools to the needs of patients and physicians? It was so heartening to read that experienced family physicians are not kowtowing to EMR experts’ insistence that we change our workflow to adapt to the realities of EMRs. We still approach patient encounters in a patient-centered way, following the thread of the conversation to fully respond to our patients’ needs. (Can the same be said for medical students? See last month’s Guest Editorial, “Med students: Look up from your EMRs”.)
"Workflow" was a foreign concept to me until the advent of EMRs. I never worried much about the order in which I was performing "tasks," and I still don't.
Holman et al1 describe the interplay between physicians and patients during office visits as a “dance” in which patients and physicians take turns leading. Let’s invite EMR vendors to join our dance—and follow our lead.
Last month, a group of investigators from the American Academy of Family Physicians and the University of Wisconsin led by Holman1 published a study entitled, “The myth of standardized workflow in primary care.” The researchers directly observed 20 primary care physician (PCP) visits and coded the usual tasks physicians perform during a visit. For some physicians, they observed 2 encounters to see if individual physicians followed a consistent pattern. What they found won’t surprise any of you:
“…We found no consistent workflows when analyzing visits individually or by PCP, or visits conducted at clinics with or without an [electronic medical record (EMR)]. The workflow for tasks is dictated not by the type of chart, the patient, or the physician. Instead, workflow emerges from the interaction between the patient’s and the physician’s agendas.”
This rang true for me. For example, sometimes a patient immediately pulls out her bag of pills, so I do the medication review first. Other times, social chat comes first. Often, asking, “Is there anything else you need today?” leads to another round of history-taking and test-ordering.
The physicians in this study approached patient visits as a conversation rather than adhering to a rigid protocol, as the EMR vendors imply we should do. Frankly, that has never made sense to me. Why shouldn’t the EMR companies adapt their tools to the needs of patients and physicians? It was so heartening to read that experienced family physicians are not kowtowing to EMR experts’ insistence that we change our workflow to adapt to the realities of EMRs. We still approach patient encounters in a patient-centered way, following the thread of the conversation to fully respond to our patients’ needs. (Can the same be said for medical students? See last month’s Guest Editorial, “Med students: Look up from your EMRs”.)
"Workflow" was a foreign concept to me until the advent of EMRs. I never worried much about the order in which I was performing "tasks," and I still don't.
Holman et al1 describe the interplay between physicians and patients during office visits as a “dance” in which patients and physicians take turns leading. Let’s invite EMR vendors to join our dance—and follow our lead.
Reference
1. Holman GT, Beasley JW, Karsh BT, et al. The myth of standardized workflow in primary care. J Am Med Inform Assoc. 2015. [Epub ahead of print].
Reference
1. Holman GT, Beasley JW, Karsh BT, et al. The myth of standardized workflow in primary care. J Am Med Inform Assoc. 2015. [Epub ahead of print].
Harold Osborn, MD, Paul Krochmal, MD, and ACEP Scientific Assembly
Several years ago, I read an op-ed piece in the New York Times about how celebrating Christmas is different for children and adults. While most children experience pure joy, adults’ joy is usually tempered with the sadness of thinking about family members and friends who were part of past celebrations but have since passed away. So too, now when I attend annual ACEP scientific assemblies, my thoughts frequently turn to some of the pioneering emergency physicians (EPs) who I no longer encounter in the convention center hallways, session rooms, and exhibition halls. |
At ACEP this year, I will be thinking a lot about Harold Osborn, MD, who died at the age of 71 after a long illness in New Rochelle, NY on April 30, 2015 (http://www.legacy.com/obituaries/nytimes/obituary.aspx?pid=175075119). “Oz” was a striking figure in the ED and in the corridors of ACEP meetings over the years, as his ponytail turned from black to white. Having embraced radical politics by the time he obtained his MD degree from Columbia University in 1970, Oz was a fierce advocate of healthcare reform, particularly emergency medicine (EM) and health issues affecting poor and minority populations. During residency training at Lincoln Hospital in the South Bronx, Oz organized and led community-oriented care initiatives, including detox and holistic medicine programs. He also was a leading advocate of more rational working conditions for house officers a decade before work-hour reform became part of the New York State health code and later nationwide ACGME standards.
At times Oz’s unrelenting zeal could make you crazy, but he would also be the first person to come to your aid, or defense, if there was a need. As an EP with a growing interest in treating overdoses and poisonings in the Bronx, Oz worked with Lewis Goldfrank, MD, with whom he coauthored many early chapters of Goldfrank’s Toxicologic Emergencies. In 1993, Oz became one of the first academic chairs of EM in the New York metropolitan area.
In a career spanning more than 30 years, Oz never hesitated to champion a health-related cause he believed in—often at great personal risk and sacrifice. His strong advocacy helped elevate the standards for New York City receiving hospital EDs, even as many worried that his moving so fast would prompt an unsympathetic healthcare establishment to take back recent EM gains. Looking back now, almost everything Oz fought for has become standard practice for EM in New York and elsewhere.
I will also be thinking about Paul Krochmal, MD, at ACEP this year. Paul, who died unexpectedly in his sleep at the age of 67, on August 25, 2015, was one of the very first EM residents trained at Einstein/Jacobi Hospital in the Bronx, at a time when the entire residency consisted of three residents in each of 2 years. An imposing figure with a thick mustache longer then the handlebar of his BMW motorcycle, Paul was smart, skilled, gentle, and understanding. He befriended everyone he met and was an effective ambassador for EM in the days when the rest of academia had trouble figuring out who we were and how we fit in.
If you would like to read about how one EP can profoundly affect the lives of so many members of his community, and about the truly inspiring legacy Paul leaves behind, read the short obituary about him followed by more than 60 brief tributes, in the August 27, 2015 issue of the Southington Citizen (http://www.legacy.com/obituaries/thesouthingtoncitizen/obituary.aspx?pid=175654394).
As for the pure joy of youth, I still remember clearly the first ACEP Scientific Assembly I attended in San Francisco, in 1977. Registering late, I couldn’t obtain a room at any of the convention hotels and ended up staying at the Hotel California—really! I suppose it’s fair to say that, paraphrasing the song of the same name, I may have checked out after the meeting, but part of me never left.
Several years ago, I read an op-ed piece in the New York Times about how celebrating Christmas is different for children and adults. While most children experience pure joy, adults’ joy is usually tempered with the sadness of thinking about family members and friends who were part of past celebrations but have since passed away. So too, now when I attend annual ACEP scientific assemblies, my thoughts frequently turn to some of the pioneering emergency physicians (EPs) who I no longer encounter in the convention center hallways, session rooms, and exhibition halls. |
At ACEP this year, I will be thinking a lot about Harold Osborn, MD, who died at the age of 71 after a long illness in New Rochelle, NY on April 30, 2015 (http://www.legacy.com/obituaries/nytimes/obituary.aspx?pid=175075119). “Oz” was a striking figure in the ED and in the corridors of ACEP meetings over the years, as his ponytail turned from black to white. Having embraced radical politics by the time he obtained his MD degree from Columbia University in 1970, Oz was a fierce advocate of healthcare reform, particularly emergency medicine (EM) and health issues affecting poor and minority populations. During residency training at Lincoln Hospital in the South Bronx, Oz organized and led community-oriented care initiatives, including detox and holistic medicine programs. He also was a leading advocate of more rational working conditions for house officers a decade before work-hour reform became part of the New York State health code and later nationwide ACGME standards.
At times Oz’s unrelenting zeal could make you crazy, but he would also be the first person to come to your aid, or defense, if there was a need. As an EP with a growing interest in treating overdoses and poisonings in the Bronx, Oz worked with Lewis Goldfrank, MD, with whom he coauthored many early chapters of Goldfrank’s Toxicologic Emergencies. In 1993, Oz became one of the first academic chairs of EM in the New York metropolitan area.
In a career spanning more than 30 years, Oz never hesitated to champion a health-related cause he believed in—often at great personal risk and sacrifice. His strong advocacy helped elevate the standards for New York City receiving hospital EDs, even as many worried that his moving so fast would prompt an unsympathetic healthcare establishment to take back recent EM gains. Looking back now, almost everything Oz fought for has become standard practice for EM in New York and elsewhere.
I will also be thinking about Paul Krochmal, MD, at ACEP this year. Paul, who died unexpectedly in his sleep at the age of 67, on August 25, 2015, was one of the very first EM residents trained at Einstein/Jacobi Hospital in the Bronx, at a time when the entire residency consisted of three residents in each of 2 years. An imposing figure with a thick mustache longer then the handlebar of his BMW motorcycle, Paul was smart, skilled, gentle, and understanding. He befriended everyone he met and was an effective ambassador for EM in the days when the rest of academia had trouble figuring out who we were and how we fit in.
If you would like to read about how one EP can profoundly affect the lives of so many members of his community, and about the truly inspiring legacy Paul leaves behind, read the short obituary about him followed by more than 60 brief tributes, in the August 27, 2015 issue of the Southington Citizen (http://www.legacy.com/obituaries/thesouthingtoncitizen/obituary.aspx?pid=175654394).
As for the pure joy of youth, I still remember clearly the first ACEP Scientific Assembly I attended in San Francisco, in 1977. Registering late, I couldn’t obtain a room at any of the convention hotels and ended up staying at the Hotel California—really! I suppose it’s fair to say that, paraphrasing the song of the same name, I may have checked out after the meeting, but part of me never left.
Several years ago, I read an op-ed piece in the New York Times about how celebrating Christmas is different for children and adults. While most children experience pure joy, adults’ joy is usually tempered with the sadness of thinking about family members and friends who were part of past celebrations but have since passed away. So too, now when I attend annual ACEP scientific assemblies, my thoughts frequently turn to some of the pioneering emergency physicians (EPs) who I no longer encounter in the convention center hallways, session rooms, and exhibition halls. |
At ACEP this year, I will be thinking a lot about Harold Osborn, MD, who died at the age of 71 after a long illness in New Rochelle, NY on April 30, 2015 (http://www.legacy.com/obituaries/nytimes/obituary.aspx?pid=175075119). “Oz” was a striking figure in the ED and in the corridors of ACEP meetings over the years, as his ponytail turned from black to white. Having embraced radical politics by the time he obtained his MD degree from Columbia University in 1970, Oz was a fierce advocate of healthcare reform, particularly emergency medicine (EM) and health issues affecting poor and minority populations. During residency training at Lincoln Hospital in the South Bronx, Oz organized and led community-oriented care initiatives, including detox and holistic medicine programs. He also was a leading advocate of more rational working conditions for house officers a decade before work-hour reform became part of the New York State health code and later nationwide ACGME standards.
At times Oz’s unrelenting zeal could make you crazy, but he would also be the first person to come to your aid, or defense, if there was a need. As an EP with a growing interest in treating overdoses and poisonings in the Bronx, Oz worked with Lewis Goldfrank, MD, with whom he coauthored many early chapters of Goldfrank’s Toxicologic Emergencies. In 1993, Oz became one of the first academic chairs of EM in the New York metropolitan area.
In a career spanning more than 30 years, Oz never hesitated to champion a health-related cause he believed in—often at great personal risk and sacrifice. His strong advocacy helped elevate the standards for New York City receiving hospital EDs, even as many worried that his moving so fast would prompt an unsympathetic healthcare establishment to take back recent EM gains. Looking back now, almost everything Oz fought for has become standard practice for EM in New York and elsewhere.
I will also be thinking about Paul Krochmal, MD, at ACEP this year. Paul, who died unexpectedly in his sleep at the age of 67, on August 25, 2015, was one of the very first EM residents trained at Einstein/Jacobi Hospital in the Bronx, at a time when the entire residency consisted of three residents in each of 2 years. An imposing figure with a thick mustache longer then the handlebar of his BMW motorcycle, Paul was smart, skilled, gentle, and understanding. He befriended everyone he met and was an effective ambassador for EM in the days when the rest of academia had trouble figuring out who we were and how we fit in.
If you would like to read about how one EP can profoundly affect the lives of so many members of his community, and about the truly inspiring legacy Paul leaves behind, read the short obituary about him followed by more than 60 brief tributes, in the August 27, 2015 issue of the Southington Citizen (http://www.legacy.com/obituaries/thesouthingtoncitizen/obituary.aspx?pid=175654394).
As for the pure joy of youth, I still remember clearly the first ACEP Scientific Assembly I attended in San Francisco, in 1977. Registering late, I couldn’t obtain a room at any of the convention hotels and ended up staying at the Hotel California—really! I suppose it’s fair to say that, paraphrasing the song of the same name, I may have checked out after the meeting, but part of me never left.
Metabolic monitoring of antipsychotic meds
Introduction
The use of antipsychotic medications has become more common in children and adolescents over the past 2 decades (Arch Gen Psychiatry. 2012 Dec;69[12]:1247-56). Whether or not one agrees that the trend in prescribing these agents is problematic (and I do), often the prescription and monitoring of antipsychotic medication falls to the primary care clinician who may have concerns about how to manage them. Here, we present a case to illustrate just such an issue.
Case summary
James is a 17-year-old young man with a diagnosis of bipolar disorder made earlier this year after an inpatient day at a local hospital. James had a history of attention-deficit/hyperactivity disorder (ADHD) growing up, but also had a strong family history of bipolar disorder. He began having increasing difficulty during the summer after his junior year, and then had a clear manic episode with elation and grandiosity that necessitated the hospitalization. During the relatively short stay on the psychiatric unit, he was placed on lithium carbonate and risperidone to treat the mania, which did respond. Although it was recommended that he follow up with a child and adolescent psychiatrist, through a series of happenstances he missed two appointments for an intake. He is now only able to get a new intake that is 4 months off.

You have continued to prescribe for him, waiting for what always seemed to be an imminent appointment. But now he comes to the office for a follow-up visit that can no longer wait. His mood symptoms are actually doing quite well. However, you have always known James to have a relatively thin build in the 25th percentile for weight and the 75th percentile for height. Now (is it possible?) 6 months after starting the risperidone and lithium, he returns to the office in the 50th percentile for weight and remains in the 75th percentile for height. There is nothing else noted to be concerning on physical or mental status examination, but you wonder what should be done for monitoring of his weight, should you be doing it, and whether there are other metabolic parameters that you should be measuring?
Case discussion
Regardless of your stance on pediatric bipolar disorder and the treatments for it, James has been placed on medications that need to be monitored. While it appears that James will, eventually, have a prescriber who can monitor his medication for side effects, it is incumbent on all of his providers to make sure that monitoring is occurring. Recent studies have demonstrated that guidelines for monitoring of antipsychotic use are not consistently being adhered to. For example, Rettew et al. (Pediatrics. 2015 Apr;135[4]:658-65) recently reported that metabolic monitoring that included laboratory tests was reported in only 57.2% of cases where an antipsychotic was prescribed.
Children and adolescents placed on these agents should be monitored in a number of ways. First, height and weight should be taken at baseline and at follow-up visits – at least every 6 months. The American Academy of Child and Adolescent Psychiatry practice parameters state that “consideration of weight management interventions and increased regularity of blood glucose and lipid levels should be implemented if [atypical antipsychotic agent]–induced weight gain exceeds 90th percentile body mass index (BMI) for age, or a change of five BMI units in those youths who were obese at the beginning of treatment.” Fasting blood sugar, fasting triglyceride, and cholesterol panels should be done at baseline and at approximately 6-month intervals. Screening for dystonic movements with an Abnormal Involuntary Movement Scale (AIMS) should be done at 6-month intervals. In the case of risperidone, if there are any questions about gynecomastia, galactorrhea, and/or sexual dysfunction, a prolactin level should be considered. Certain other antipsychotics require specific monitoring (for example, ECG for prolonged QT interval for ziprasidone, CBC for clozapine, and an eye exam for quetiapine).
The most important kinds of monitoring are for dose and efficacy. While the antipsychotic medications may have a role, they are not a panacea and do carry longer-term risks of metabolic problems and obesity, among others. If it is possible to provide interventions to reduce the dose or duration of use, that is preferable. If not, it’s best to work with the psychiatrist (if available) to determine who will perform the monitoring and how often it will be done to stave off metabolic problems as early as possible.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at pdnews@frontlinemedcom.com.
Introduction
The use of antipsychotic medications has become more common in children and adolescents over the past 2 decades (Arch Gen Psychiatry. 2012 Dec;69[12]:1247-56). Whether or not one agrees that the trend in prescribing these agents is problematic (and I do), often the prescription and monitoring of antipsychotic medication falls to the primary care clinician who may have concerns about how to manage them. Here, we present a case to illustrate just such an issue.
Case summary
James is a 17-year-old young man with a diagnosis of bipolar disorder made earlier this year after an inpatient day at a local hospital. James had a history of attention-deficit/hyperactivity disorder (ADHD) growing up, but also had a strong family history of bipolar disorder. He began having increasing difficulty during the summer after his junior year, and then had a clear manic episode with elation and grandiosity that necessitated the hospitalization. During the relatively short stay on the psychiatric unit, he was placed on lithium carbonate and risperidone to treat the mania, which did respond. Although it was recommended that he follow up with a child and adolescent psychiatrist, through a series of happenstances he missed two appointments for an intake. He is now only able to get a new intake that is 4 months off.
You have continued to prescribe for him, waiting for what always seemed to be an imminent appointment. But now he comes to the office for a follow-up visit that can no longer wait. His mood symptoms are actually doing quite well. However, you have always known James to have a relatively thin build in the 25th percentile for weight and the 75th percentile for height. Now (is it possible?) 6 months after starting the risperidone and lithium, he returns to the office in the 50th percentile for weight and remains in the 75th percentile for height. There is nothing else noted to be concerning on physical or mental status examination, but you wonder what should be done for monitoring of his weight, should you be doing it, and whether there are other metabolic parameters that you should be measuring?
Case discussion
Regardless of your stance on pediatric bipolar disorder and the treatments for it, James has been placed on medications that need to be monitored. While it appears that James will, eventually, have a prescriber who can monitor his medication for side effects, it is incumbent on all of his providers to make sure that monitoring is occurring. Recent studies have demonstrated that guidelines for monitoring of antipsychotic use are not consistently being adhered to. For example, Rettew et al. (Pediatrics. 2015 Apr;135[4]:658-65) recently reported that metabolic monitoring that included laboratory tests was reported in only 57.2% of cases where an antipsychotic was prescribed.
Children and adolescents placed on these agents should be monitored in a number of ways. First, height and weight should be taken at baseline and at follow-up visits – at least every 6 months. The American Academy of Child and Adolescent Psychiatry practice parameters state that “consideration of weight management interventions and increased regularity of blood glucose and lipid levels should be implemented if [atypical antipsychotic agent]–induced weight gain exceeds 90th percentile body mass index (BMI) for age, or a change of five BMI units in those youths who were obese at the beginning of treatment.” Fasting blood sugar, fasting triglyceride, and cholesterol panels should be done at baseline and at approximately 6-month intervals. Screening for dystonic movements with an Abnormal Involuntary Movement Scale (AIMS) should be done at 6-month intervals. In the case of risperidone, if there are any questions about gynecomastia, galactorrhea, and/or sexual dysfunction, a prolactin level should be considered. Certain other antipsychotics require specific monitoring (for example, ECG for prolonged QT interval for ziprasidone, CBC for clozapine, and an eye exam for quetiapine).
The most important kinds of monitoring are for dose and efficacy. While the antipsychotic medications may have a role, they are not a panacea and do carry longer-term risks of metabolic problems and obesity, among others. If it is possible to provide interventions to reduce the dose or duration of use, that is preferable. If not, it’s best to work with the psychiatrist (if available) to determine who will perform the monitoring and how often it will be done to stave off metabolic problems as early as possible.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at pdnews@frontlinemedcom.com.
Introduction
The use of antipsychotic medications has become more common in children and adolescents over the past 2 decades (Arch Gen Psychiatry. 2012 Dec;69[12]:1247-56). Whether or not one agrees that the trend in prescribing these agents is problematic (and I do), often the prescription and monitoring of antipsychotic medication falls to the primary care clinician who may have concerns about how to manage them. Here, we present a case to illustrate just such an issue.
Case summary
James is a 17-year-old young man with a diagnosis of bipolar disorder made earlier this year after an inpatient day at a local hospital. James had a history of attention-deficit/hyperactivity disorder (ADHD) growing up, but also had a strong family history of bipolar disorder. He began having increasing difficulty during the summer after his junior year, and then had a clear manic episode with elation and grandiosity that necessitated the hospitalization. During the relatively short stay on the psychiatric unit, he was placed on lithium carbonate and risperidone to treat the mania, which did respond. Although it was recommended that he follow up with a child and adolescent psychiatrist, through a series of happenstances he missed two appointments for an intake. He is now only able to get a new intake that is 4 months off.
You have continued to prescribe for him, waiting for what always seemed to be an imminent appointment. But now he comes to the office for a follow-up visit that can no longer wait. His mood symptoms are actually doing quite well. However, you have always known James to have a relatively thin build in the 25th percentile for weight and the 75th percentile for height. Now (is it possible?) 6 months after starting the risperidone and lithium, he returns to the office in the 50th percentile for weight and remains in the 75th percentile for height. There is nothing else noted to be concerning on physical or mental status examination, but you wonder what should be done for monitoring of his weight, should you be doing it, and whether there are other metabolic parameters that you should be measuring?
Case discussion
Regardless of your stance on pediatric bipolar disorder and the treatments for it, James has been placed on medications that need to be monitored. While it appears that James will, eventually, have a prescriber who can monitor his medication for side effects, it is incumbent on all of his providers to make sure that monitoring is occurring. Recent studies have demonstrated that guidelines for monitoring of antipsychotic use are not consistently being adhered to. For example, Rettew et al. (Pediatrics. 2015 Apr;135[4]:658-65) recently reported that metabolic monitoring that included laboratory tests was reported in only 57.2% of cases where an antipsychotic was prescribed.
Children and adolescents placed on these agents should be monitored in a number of ways. First, height and weight should be taken at baseline and at follow-up visits – at least every 6 months. The American Academy of Child and Adolescent Psychiatry practice parameters state that “consideration of weight management interventions and increased regularity of blood glucose and lipid levels should be implemented if [atypical antipsychotic agent]–induced weight gain exceeds 90th percentile body mass index (BMI) for age, or a change of five BMI units in those youths who were obese at the beginning of treatment.” Fasting blood sugar, fasting triglyceride, and cholesterol panels should be done at baseline and at approximately 6-month intervals. Screening for dystonic movements with an Abnormal Involuntary Movement Scale (AIMS) should be done at 6-month intervals. In the case of risperidone, if there are any questions about gynecomastia, galactorrhea, and/or sexual dysfunction, a prolactin level should be considered. Certain other antipsychotics require specific monitoring (for example, ECG for prolonged QT interval for ziprasidone, CBC for clozapine, and an eye exam for quetiapine).
The most important kinds of monitoring are for dose and efficacy. While the antipsychotic medications may have a role, they are not a panacea and do carry longer-term risks of metabolic problems and obesity, among others. If it is possible to provide interventions to reduce the dose or duration of use, that is preferable. If not, it’s best to work with the psychiatrist (if available) to determine who will perform the monitoring and how often it will be done to stave off metabolic problems as early as possible.
Dr. Althoff is associate professor of psychiatry, psychology, and pediatrics at the University of Vermont, Burlington. He is director of the division of behavioral genetics and conducts research on the development of self-regulation in children. Dr. Althoff receives no funding from pharmaceutical companies or industry. He has grant funding from the National Institute of General Medical Sciences and the Klingenstein Third Generation Foundation and is employed, in part, by the nonprofit Research Center for Children, Youth, and Families that develops the Child Behavior Checklist and associated instruments. E-mail him at pdnews@frontlinemedcom.com.

Reflections on My VA Experience and Why I See the Proverbial Glass as Half Full
Veterans Health Administration (VA) hospitals have received notoriety due to episodes of misdiagnosis, poor management, and negligent care described in many recent reports and news articles.1-3 While veterans are appropriately the primary focus of these investigative reports, physicians are also challenged in this setting, as they often meet resistance when advocating for patients and attempting to improve a flawed system.2 Although my residency training includes 6 months at a VA hospital mired in controversy, the hospital has played a critical role in my training.3
Despite my many frustrations with the VA and the daily stresses incurred because of barriers impeding the timing and quality of care, I have several reasons to see the glass as “half full” when reflecting on my experiences as an orthopedic surgery resident at a VA medical center. This editorial will focus on the most important of these reasons—the special opportunity and pride associated with caring for veterans and these patients’ extremely appreciative nature.
The VA is one of the largest integrated health care systems in the United States, offering both inpatient and outpatient care to eligible veterans. Although eligibility has historically been based on military service–related medical conditions, disability, and financial need, reforms from 1996 to 2002 expanded enrollment to veteran populations previously deemed ineligible for VA care.4,5 Despite this, studies suggest that some uninsured veterans do not seek VA care, even when eligible for VA coverage. This troubling notion is further complicated by research suggesting that veterans who use the VA for all of their health care are more likely to be from poor, less-educated, and minority populations, and are more likely to report fair or poor health and seek more disability days.6
Such disheartening realities can mask the most important attributes of VA patients, which pertain to their selfless commitment to our country. Orthopedic surgery residents must appreciate these attributes as well as the tremendous need for musculoskeletal care in this setting, as musculoskeletal conditions are some of the most common reasons for patient visits at the VA.7 Although combat-related high-energy blast injuries and the reconstructive procedures used to treat them have received a lot of attention, it is the more common musculoskeletal disorders that are most responsible for the tremendous burden of musculoskeletal disease in the VA. In a study by Dominick and colleagues,8 veterans had significantly greater odds of reporting doctor-diagnosed arthritis compared with nonveterans. Furthermore, veterans are also more vulnerable to overuse injuries, a finding attributed to the intense physical activity associated with military training and service.9
The busy orthopedic surgery clinic at my VA hospital is a fulfilling experience and a reminder of the large demand for musculoskeletal care. However, it is the patient population that makes it most gratifying. Most of the veterans seeking care are appreciative, regularly expressing their gratitude. They view me and the other residents as their physicians, not simply as doctors in training, like so many other non-VA patients do. Despite the fact that VA patients sometimes have to wait several hours to be seen in clinic and several months for surgery, I have never been subjected to their inevitable disdain or frustration. This is true in even the most trying and infuriating times, such as when an operation is cancelled on the day of surgery for reasons that many surgeons in non-VA hospitals would consider trivial. And even when witness to my visible irritation with the VA system, the veterans remain respectful and understanding; if they ever share similar feelings, they most certainly never voice them to me.
I cannot refute the notion that the VA must change and that the veterans deserve an improved health care system. However, this editorial is not written as a call to action. Instead, I hope it helps to humanize the patients of the VA, serving as a reminder to residents and other providers that the VA is a unique and extraordinary opportunity to give back and say thank you to veterans.
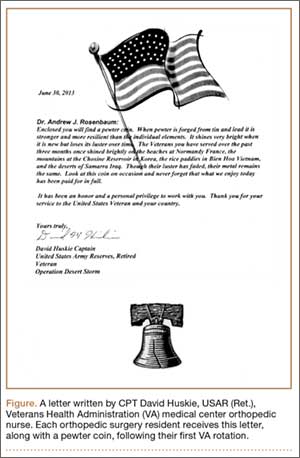
This editorial is dedicated to CPT David Huskie, USAR (Ret.), a veteran of Operation Desert Storm and orthopedic nurse at my VA hospital. It was he who first reminded me, and the other orthopedic residents, of the importance of our time at the VA. The Figure depicts the letter he gives to orthopedic residents at our program, along with a pewter coin, after their first VA rotation.
1. Pearson M. The VA’s troubled history. Cable News Network (CNN) website. http://www.cnn.com/2014/05/23/politics/va-scandals-timeline. Updated May 30, 2014. Accessed August 28, 2015.
2. Scherz H. Doctors’ war stories from VA hospitals. The Wall Street Journal website. http://www.wsj.com/articles/hal-scherz-doctors-war-stories-from-va-hospitals-1401233147. Published May 27, 2014. Accessed August 28, 2015.
3. Riviello V. Nurse exposes VA hospital: stolen drugs, tortured veterans. New York Post website. http://nypost.com/2014/07/12/nurse-exposes-va-hospital-stolen-drugs-tortured-veterans. Published July 12, 2014. Accessed August 28, 2015.
4. Enrollment—provision of hospital and outpatient care to veterans—VA. Proposed rule. Fed Regist. 1998;63(132):37299-37307.
5. US Department of Veterans Affairs, Veterans Health Administration, Office of Assistant Deputy Under Secretary for Health for Policy and Planning. 2003 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Comparisons to the 1999 and 2002 Surveys. US Department of Veterans Affairs website. www.va.gov/healthpolicyplanning/Docs/SOE2003_Report.pdf. Published December 2004. Accessed August 28, 2015.
6. Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93-100.
7. Wasserman GM, Martin BL, Hyams KC, Merrill BR, Oaks HG, McAdoo HA. A survey of outpatient visits in a United States Army forward unit during Operation Desert Shield. Mil Med. 1997;162(6):374-379.
8. Dominick KL, Golightly YM, Jackson GL. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J Rheumatol. 2006;33(2):348-354.
9. West SG. Rheumatic disorders during Operation Desert Storm. Arthritis Rheum. 1993;36(10):1487-1488.
Veterans Health Administration (VA) hospitals have received notoriety due to episodes of misdiagnosis, poor management, and negligent care described in many recent reports and news articles.1-3 While veterans are appropriately the primary focus of these investigative reports, physicians are also challenged in this setting, as they often meet resistance when advocating for patients and attempting to improve a flawed system.2 Although my residency training includes 6 months at a VA hospital mired in controversy, the hospital has played a critical role in my training.3
Despite my many frustrations with the VA and the daily stresses incurred because of barriers impeding the timing and quality of care, I have several reasons to see the glass as “half full” when reflecting on my experiences as an orthopedic surgery resident at a VA medical center. This editorial will focus on the most important of these reasons—the special opportunity and pride associated with caring for veterans and these patients’ extremely appreciative nature.
The VA is one of the largest integrated health care systems in the United States, offering both inpatient and outpatient care to eligible veterans. Although eligibility has historically been based on military service–related medical conditions, disability, and financial need, reforms from 1996 to 2002 expanded enrollment to veteran populations previously deemed ineligible for VA care.4,5 Despite this, studies suggest that some uninsured veterans do not seek VA care, even when eligible for VA coverage. This troubling notion is further complicated by research suggesting that veterans who use the VA for all of their health care are more likely to be from poor, less-educated, and minority populations, and are more likely to report fair or poor health and seek more disability days.6
Such disheartening realities can mask the most important attributes of VA patients, which pertain to their selfless commitment to our country. Orthopedic surgery residents must appreciate these attributes as well as the tremendous need for musculoskeletal care in this setting, as musculoskeletal conditions are some of the most common reasons for patient visits at the VA.7 Although combat-related high-energy blast injuries and the reconstructive procedures used to treat them have received a lot of attention, it is the more common musculoskeletal disorders that are most responsible for the tremendous burden of musculoskeletal disease in the VA. In a study by Dominick and colleagues,8 veterans had significantly greater odds of reporting doctor-diagnosed arthritis compared with nonveterans. Furthermore, veterans are also more vulnerable to overuse injuries, a finding attributed to the intense physical activity associated with military training and service.9
The busy orthopedic surgery clinic at my VA hospital is a fulfilling experience and a reminder of the large demand for musculoskeletal care. However, it is the patient population that makes it most gratifying. Most of the veterans seeking care are appreciative, regularly expressing their gratitude. They view me and the other residents as their physicians, not simply as doctors in training, like so many other non-VA patients do. Despite the fact that VA patients sometimes have to wait several hours to be seen in clinic and several months for surgery, I have never been subjected to their inevitable disdain or frustration. This is true in even the most trying and infuriating times, such as when an operation is cancelled on the day of surgery for reasons that many surgeons in non-VA hospitals would consider trivial. And even when witness to my visible irritation with the VA system, the veterans remain respectful and understanding; if they ever share similar feelings, they most certainly never voice them to me.
I cannot refute the notion that the VA must change and that the veterans deserve an improved health care system. However, this editorial is not written as a call to action. Instead, I hope it helps to humanize the patients of the VA, serving as a reminder to residents and other providers that the VA is a unique and extraordinary opportunity to give back and say thank you to veterans.
This editorial is dedicated to CPT David Huskie, USAR (Ret.), a veteran of Operation Desert Storm and orthopedic nurse at my VA hospital. It was he who first reminded me, and the other orthopedic residents, of the importance of our time at the VA. The Figure depicts the letter he gives to orthopedic residents at our program, along with a pewter coin, after their first VA rotation.
Veterans Health Administration (VA) hospitals have received notoriety due to episodes of misdiagnosis, poor management, and negligent care described in many recent reports and news articles.1-3 While veterans are appropriately the primary focus of these investigative reports, physicians are also challenged in this setting, as they often meet resistance when advocating for patients and attempting to improve a flawed system.2 Although my residency training includes 6 months at a VA hospital mired in controversy, the hospital has played a critical role in my training.3
Despite my many frustrations with the VA and the daily stresses incurred because of barriers impeding the timing and quality of care, I have several reasons to see the glass as “half full” when reflecting on my experiences as an orthopedic surgery resident at a VA medical center. This editorial will focus on the most important of these reasons—the special opportunity and pride associated with caring for veterans and these patients’ extremely appreciative nature.
The VA is one of the largest integrated health care systems in the United States, offering both inpatient and outpatient care to eligible veterans. Although eligibility has historically been based on military service–related medical conditions, disability, and financial need, reforms from 1996 to 2002 expanded enrollment to veteran populations previously deemed ineligible for VA care.4,5 Despite this, studies suggest that some uninsured veterans do not seek VA care, even when eligible for VA coverage. This troubling notion is further complicated by research suggesting that veterans who use the VA for all of their health care are more likely to be from poor, less-educated, and minority populations, and are more likely to report fair or poor health and seek more disability days.6
Such disheartening realities can mask the most important attributes of VA patients, which pertain to their selfless commitment to our country. Orthopedic surgery residents must appreciate these attributes as well as the tremendous need for musculoskeletal care in this setting, as musculoskeletal conditions are some of the most common reasons for patient visits at the VA.7 Although combat-related high-energy blast injuries and the reconstructive procedures used to treat them have received a lot of attention, it is the more common musculoskeletal disorders that are most responsible for the tremendous burden of musculoskeletal disease in the VA. In a study by Dominick and colleagues,8 veterans had significantly greater odds of reporting doctor-diagnosed arthritis compared with nonveterans. Furthermore, veterans are also more vulnerable to overuse injuries, a finding attributed to the intense physical activity associated with military training and service.9
The busy orthopedic surgery clinic at my VA hospital is a fulfilling experience and a reminder of the large demand for musculoskeletal care. However, it is the patient population that makes it most gratifying. Most of the veterans seeking care are appreciative, regularly expressing their gratitude. They view me and the other residents as their physicians, not simply as doctors in training, like so many other non-VA patients do. Despite the fact that VA patients sometimes have to wait several hours to be seen in clinic and several months for surgery, I have never been subjected to their inevitable disdain or frustration. This is true in even the most trying and infuriating times, such as when an operation is cancelled on the day of surgery for reasons that many surgeons in non-VA hospitals would consider trivial. And even when witness to my visible irritation with the VA system, the veterans remain respectful and understanding; if they ever share similar feelings, they most certainly never voice them to me.
I cannot refute the notion that the VA must change and that the veterans deserve an improved health care system. However, this editorial is not written as a call to action. Instead, I hope it helps to humanize the patients of the VA, serving as a reminder to residents and other providers that the VA is a unique and extraordinary opportunity to give back and say thank you to veterans.
This editorial is dedicated to CPT David Huskie, USAR (Ret.), a veteran of Operation Desert Storm and orthopedic nurse at my VA hospital. It was he who first reminded me, and the other orthopedic residents, of the importance of our time at the VA. The Figure depicts the letter he gives to orthopedic residents at our program, along with a pewter coin, after their first VA rotation.
1. Pearson M. The VA’s troubled history. Cable News Network (CNN) website. http://www.cnn.com/2014/05/23/politics/va-scandals-timeline. Updated May 30, 2014. Accessed August 28, 2015.
2. Scherz H. Doctors’ war stories from VA hospitals. The Wall Street Journal website. http://www.wsj.com/articles/hal-scherz-doctors-war-stories-from-va-hospitals-1401233147. Published May 27, 2014. Accessed August 28, 2015.
3. Riviello V. Nurse exposes VA hospital: stolen drugs, tortured veterans. New York Post website. http://nypost.com/2014/07/12/nurse-exposes-va-hospital-stolen-drugs-tortured-veterans. Published July 12, 2014. Accessed August 28, 2015.
4. Enrollment—provision of hospital and outpatient care to veterans—VA. Proposed rule. Fed Regist. 1998;63(132):37299-37307.
5. US Department of Veterans Affairs, Veterans Health Administration, Office of Assistant Deputy Under Secretary for Health for Policy and Planning. 2003 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Comparisons to the 1999 and 2002 Surveys. US Department of Veterans Affairs website. www.va.gov/healthpolicyplanning/Docs/SOE2003_Report.pdf. Published December 2004. Accessed August 28, 2015.
6. Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93-100.
7. Wasserman GM, Martin BL, Hyams KC, Merrill BR, Oaks HG, McAdoo HA. A survey of outpatient visits in a United States Army forward unit during Operation Desert Shield. Mil Med. 1997;162(6):374-379.
8. Dominick KL, Golightly YM, Jackson GL. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J Rheumatol. 2006;33(2):348-354.
9. West SG. Rheumatic disorders during Operation Desert Storm. Arthritis Rheum. 1993;36(10):1487-1488.
1. Pearson M. The VA’s troubled history. Cable News Network (CNN) website. http://www.cnn.com/2014/05/23/politics/va-scandals-timeline. Updated May 30, 2014. Accessed August 28, 2015.
2. Scherz H. Doctors’ war stories from VA hospitals. The Wall Street Journal website. http://www.wsj.com/articles/hal-scherz-doctors-war-stories-from-va-hospitals-1401233147. Published May 27, 2014. Accessed August 28, 2015.
3. Riviello V. Nurse exposes VA hospital: stolen drugs, tortured veterans. New York Post website. http://nypost.com/2014/07/12/nurse-exposes-va-hospital-stolen-drugs-tortured-veterans. Published July 12, 2014. Accessed August 28, 2015.
4. Enrollment—provision of hospital and outpatient care to veterans—VA. Proposed rule. Fed Regist. 1998;63(132):37299-37307.
5. US Department of Veterans Affairs, Veterans Health Administration, Office of Assistant Deputy Under Secretary for Health for Policy and Planning. 2003 Survey of Veteran Enrollees’ Health and Reliance Upon VA With Selected Comparisons to the 1999 and 2002 Surveys. US Department of Veterans Affairs website. www.va.gov/healthpolicyplanning/Docs/SOE2003_Report.pdf. Published December 2004. Accessed August 28, 2015.
6. Nelson KM, Starkebaum GA, Reiber GE. Veterans using and uninsured veterans not using Veterans Affairs (VA) health care. Public Health Rep. 2007;122(1):93-100.
7. Wasserman GM, Martin BL, Hyams KC, Merrill BR, Oaks HG, McAdoo HA. A survey of outpatient visits in a United States Army forward unit during Operation Desert Shield. Mil Med. 1997;162(6):374-379.
8. Dominick KL, Golightly YM, Jackson GL. Arthritis prevalence and symptoms among US non-veterans, veterans, and veterans receiving Department of Veterans Affairs Healthcare. J Rheumatol. 2006;33(2):348-354.
9. West SG. Rheumatic disorders during Operation Desert Storm. Arthritis Rheum. 1993;36(10):1487-1488.

ACS Surgery News September issue digital version is available
The September issue of ACS Surgery News is available online -- use the mobile app to download or view as a pdf.
This month's issue features news about intragastric balloons now approved by the FDA, commentary by Dr. Mark Weissler on the rich variety of learning and networking opportunities at the upcoming Clinical Congress, and an update on the implications of a recent court ruling on the number of lawsuits brought against doctors.
The September issue of ACS Surgery News is available online -- use the mobile app to download or view as a pdf.
This month's issue features news about intragastric balloons now approved by the FDA, commentary by Dr. Mark Weissler on the rich variety of learning and networking opportunities at the upcoming Clinical Congress, and an update on the implications of a recent court ruling on the number of lawsuits brought against doctors.
The September issue of ACS Surgery News is available online -- use the mobile app to download or view as a pdf.
This month's issue features news about intragastric balloons now approved by the FDA, commentary by Dr. Mark Weissler on the rich variety of learning and networking opportunities at the upcoming Clinical Congress, and an update on the implications of a recent court ruling on the number of lawsuits brought against doctors.
Bullying
Back to school brings, as it does every year, an increased focus on school issues. Parents and children may feel uncomfortable discussing many of these concerns or may not realize that their pediatrician can be a source of help and support. One topic in particular, bullying, is an important and difficult issue that affects a large number of children and adolescents, yet unfortunately, often goes undetected.
More than half of teens have been either the victims or perpetrators of some type of bullying; for one in five, this takes the form of actual physical bullying or violence. Bullying can happen to anyone, from any socioeconomic status, in any school or neighborhood. Even children who are seemingly well adjusted and “popular” at school can be victimized. The dramatic increase in technology use, smartphones and social media only increases the vulnerability of youth to bullying – cyberbullying can be incredibly damaging and difficult to detect and address.

Pediatric providers can help in many ways. First, don’t hesitate to bring up the issue of bullying during well visits or sports physicals when discussing school performance or school readiness. While I admit – given the large range of topics that need to be covered – I don’t discuss this at every visit, I often do ask about friendships at school and have a low threshold for bringing up the issue of bullying with families.
Second, be alert to possible signs that your patients may be bullied. Nonspecific symptoms – such as headaches, stomach pains, fatigue, or behavior or mood changes – can be manifestations of the distress associated with being bullied. When evaluating children for these concerns, it is important to take a detailed history that includes potential psychosocial stressors or changes, such as bullying. Equally as important is to approach this history-taking in a culturally sensitive and trauma-informed way and to recognize that your patients may not immediately disclose concerns. However, by demonstrating that you are a trusted source of support, you can open the door for future conversations.
Lastly, be prepared to respond in a nonthreatening and nonjudgmental way when concerns arise. These are very challenging situations, and it is important to engage families – and the child or teen – in the best way to address them. Youth may feel a great loss of control in the bullying relationship, and thus, to avoid further trauma, it is critically important for their family and professionals to give them as much control as possible in dealing with it. Of course, there are times when the child’s safety could be compromised, and more directive intervention is needed, but even in those situations the provider and family can help by being open and communicative.
Typically, other support systems will also need to be involved – for example, the school (if that is where the bullying is taking place) or trained mental health providers. Families may need help thinking about the best way to approach or initiate these discussions, especially as they themselves may be angry or in denial. Providers can even serve as a resource to schools and communities in thinking about the best way to prevent and address bullying, either in individual situations or more generally. The U.S. Department of Health & Human Services offers comprehensive resources to providers and families faced with the issue of bullying (www.stopbullying.gov).
As partners with the family, patient, and community, pediatric providers can play an important role in preventing and addressing bullying, which can have a lifelong impact on the health of a child.
Dr. Beers is assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, both in Washington.
Back to school brings, as it does every year, an increased focus on school issues. Parents and children may feel uncomfortable discussing many of these concerns or may not realize that their pediatrician can be a source of help and support. One topic in particular, bullying, is an important and difficult issue that affects a large number of children and adolescents, yet unfortunately, often goes undetected.
More than half of teens have been either the victims or perpetrators of some type of bullying; for one in five, this takes the form of actual physical bullying or violence. Bullying can happen to anyone, from any socioeconomic status, in any school or neighborhood. Even children who are seemingly well adjusted and “popular” at school can be victimized. The dramatic increase in technology use, smartphones and social media only increases the vulnerability of youth to bullying – cyberbullying can be incredibly damaging and difficult to detect and address.
Pediatric providers can help in many ways. First, don’t hesitate to bring up the issue of bullying during well visits or sports physicals when discussing school performance or school readiness. While I admit – given the large range of topics that need to be covered – I don’t discuss this at every visit, I often do ask about friendships at school and have a low threshold for bringing up the issue of bullying with families.
Second, be alert to possible signs that your patients may be bullied. Nonspecific symptoms – such as headaches, stomach pains, fatigue, or behavior or mood changes – can be manifestations of the distress associated with being bullied. When evaluating children for these concerns, it is important to take a detailed history that includes potential psychosocial stressors or changes, such as bullying. Equally as important is to approach this history-taking in a culturally sensitive and trauma-informed way and to recognize that your patients may not immediately disclose concerns. However, by demonstrating that you are a trusted source of support, you can open the door for future conversations.
Lastly, be prepared to respond in a nonthreatening and nonjudgmental way when concerns arise. These are very challenging situations, and it is important to engage families – and the child or teen – in the best way to address them. Youth may feel a great loss of control in the bullying relationship, and thus, to avoid further trauma, it is critically important for their family and professionals to give them as much control as possible in dealing with it. Of course, there are times when the child’s safety could be compromised, and more directive intervention is needed, but even in those situations the provider and family can help by being open and communicative.
Typically, other support systems will also need to be involved – for example, the school (if that is where the bullying is taking place) or trained mental health providers. Families may need help thinking about the best way to approach or initiate these discussions, especially as they themselves may be angry or in denial. Providers can even serve as a resource to schools and communities in thinking about the best way to prevent and address bullying, either in individual situations or more generally. The U.S. Department of Health & Human Services offers comprehensive resources to providers and families faced with the issue of bullying (www.stopbullying.gov).
As partners with the family, patient, and community, pediatric providers can play an important role in preventing and addressing bullying, which can have a lifelong impact on the health of a child.
Dr. Beers is assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, both in Washington.
Back to school brings, as it does every year, an increased focus on school issues. Parents and children may feel uncomfortable discussing many of these concerns or may not realize that their pediatrician can be a source of help and support. One topic in particular, bullying, is an important and difficult issue that affects a large number of children and adolescents, yet unfortunately, often goes undetected.
More than half of teens have been either the victims or perpetrators of some type of bullying; for one in five, this takes the form of actual physical bullying or violence. Bullying can happen to anyone, from any socioeconomic status, in any school or neighborhood. Even children who are seemingly well adjusted and “popular” at school can be victimized. The dramatic increase in technology use, smartphones and social media only increases the vulnerability of youth to bullying – cyberbullying can be incredibly damaging and difficult to detect and address.
Pediatric providers can help in many ways. First, don’t hesitate to bring up the issue of bullying during well visits or sports physicals when discussing school performance or school readiness. While I admit – given the large range of topics that need to be covered – I don’t discuss this at every visit, I often do ask about friendships at school and have a low threshold for bringing up the issue of bullying with families.
Second, be alert to possible signs that your patients may be bullied. Nonspecific symptoms – such as headaches, stomach pains, fatigue, or behavior or mood changes – can be manifestations of the distress associated with being bullied. When evaluating children for these concerns, it is important to take a detailed history that includes potential psychosocial stressors or changes, such as bullying. Equally as important is to approach this history-taking in a culturally sensitive and trauma-informed way and to recognize that your patients may not immediately disclose concerns. However, by demonstrating that you are a trusted source of support, you can open the door for future conversations.
Lastly, be prepared to respond in a nonthreatening and nonjudgmental way when concerns arise. These are very challenging situations, and it is important to engage families – and the child or teen – in the best way to address them. Youth may feel a great loss of control in the bullying relationship, and thus, to avoid further trauma, it is critically important for their family and professionals to give them as much control as possible in dealing with it. Of course, there are times when the child’s safety could be compromised, and more directive intervention is needed, but even in those situations the provider and family can help by being open and communicative.
Typically, other support systems will also need to be involved – for example, the school (if that is where the bullying is taking place) or trained mental health providers. Families may need help thinking about the best way to approach or initiate these discussions, especially as they themselves may be angry or in denial. Providers can even serve as a resource to schools and communities in thinking about the best way to prevent and address bullying, either in individual situations or more generally. The U.S. Department of Health & Human Services offers comprehensive resources to providers and families faced with the issue of bullying (www.stopbullying.gov).
As partners with the family, patient, and community, pediatric providers can play an important role in preventing and addressing bullying, which can have a lifelong impact on the health of a child.
Dr. Beers is assistant professor of pediatrics at Children’s National Medical Center and the George Washington University Medical Center, both in Washington.

Big changes in practice, but none for the better
Dr. Nasrallah’s approach to psychiatry, especially to the real problems confronting us, is both professionally astute and realistic.
I have been in practice for more than 60 years and have seen tremendous changes—none for the better— in the intrusion of insurance tyranny and government overregulation. Dr. Nasrallah’s comments about obstacles created from the system, regardless of so-called “parity,” hit the mark. The insurance companies control everything by setting fees so low and documentation requirements so high that there is little time to focus on the dynamics of the patient population. Unqualified people are deciding whether or not the medications we prescribe will be paid for.
To illustrate what I think of some of the changes, here is what I have observed:
• Electroconvulsive therapy for severe depression has been “rediscovered,” but for decades those of us who used it selectively, with good results, were considered to be practicing quackery.
• Dr. Nasrallah’s recent article on development of immediate treatment plans for a patient given a diagnosis of schizophrenia (Current Psychiatry. 2015;14(5):32-34,36-40,42 [http://bit.ly/1GLGtrZ]) reminds me of a time when it was thought that you couldn’t diagnose schizophrenia until symptoms had been present for 6 months. (Had they ever heard of the work of Eugen Bleuler?)
• At a national meeting 20 years ago, I raised the question of why every other specialty of medicine stressed early diagnosis and treatment but psychiatry did not—and, instead, was doing the opposite. The speaker did not have the courtesy to answer my question.
Keep up the good work! We need people such as Dr. Nasrallah to educate the public about how government and insurance companies are destroying our specialty.
Dr. Nasrallah’s approach to psychiatry, especially to the real problems confronting us, is both professionally astute and realistic.
I have been in practice for more than 60 years and have seen tremendous changes—none for the better— in the intrusion of insurance tyranny and government overregulation. Dr. Nasrallah’s comments about obstacles created from the system, regardless of so-called “parity,” hit the mark. The insurance companies control everything by setting fees so low and documentation requirements so high that there is little time to focus on the dynamics of the patient population. Unqualified people are deciding whether or not the medications we prescribe will be paid for.
To illustrate what I think of some of the changes, here is what I have observed:
• Electroconvulsive therapy for severe depression has been “rediscovered,” but for decades those of us who used it selectively, with good results, were considered to be practicing quackery.
• Dr. Nasrallah’s recent article on development of immediate treatment plans for a patient given a diagnosis of schizophrenia (Current Psychiatry. 2015;14(5):32-34,36-40,42 [http://bit.ly/1GLGtrZ]) reminds me of a time when it was thought that you couldn’t diagnose schizophrenia until symptoms had been present for 6 months. (Had they ever heard of the work of Eugen Bleuler?)
• At a national meeting 20 years ago, I raised the question of why every other specialty of medicine stressed early diagnosis and treatment but psychiatry did not—and, instead, was doing the opposite. The speaker did not have the courtesy to answer my question.
Keep up the good work! We need people such as Dr. Nasrallah to educate the public about how government and insurance companies are destroying our specialty.
Dr. Nasrallah’s approach to psychiatry, especially to the real problems confronting us, is both professionally astute and realistic.
I have been in practice for more than 60 years and have seen tremendous changes—none for the better— in the intrusion of insurance tyranny and government overregulation. Dr. Nasrallah’s comments about obstacles created from the system, regardless of so-called “parity,” hit the mark. The insurance companies control everything by setting fees so low and documentation requirements so high that there is little time to focus on the dynamics of the patient population. Unqualified people are deciding whether or not the medications we prescribe will be paid for.
To illustrate what I think of some of the changes, here is what I have observed:
• Electroconvulsive therapy for severe depression has been “rediscovered,” but for decades those of us who used it selectively, with good results, were considered to be practicing quackery.
• Dr. Nasrallah’s recent article on development of immediate treatment plans for a patient given a diagnosis of schizophrenia (Current Psychiatry. 2015;14(5):32-34,36-40,42 [http://bit.ly/1GLGtrZ]) reminds me of a time when it was thought that you couldn’t diagnose schizophrenia until symptoms had been present for 6 months. (Had they ever heard of the work of Eugen Bleuler?)
• At a national meeting 20 years ago, I raised the question of why every other specialty of medicine stressed early diagnosis and treatment but psychiatry did not—and, instead, was doing the opposite. The speaker did not have the courtesy to answer my question.
Keep up the good work! We need people such as Dr. Nasrallah to educate the public about how government and insurance companies are destroying our specialty.
A nod to a ‘psychiatry great’
In his recent editorial, “Is there only 1 neurobiologic psychiatric disorder, with different clinical expressions?” (Current Psychiatry. 2015;14(7):10-12 [http://bit.ly/1INCvxw]), Dr. Nasrallah presents convincing evidence for such a conclusion. However, he did not mention that a somewhat similar concept was established by one of psychiatry’s greats, Karl Menninger, MD, more than 50 years ago. I’m referring to Menninger’s unitary concept of mental illness, espoused in his book, The Vital Balance.1 Dr. Menninger was, of course, founder of the Menninger Clinic in Topeka, Kansas, which now thrives in Houston, Texas, at Baylor College of Medicine. Like Freud, who predicted that advances in viewing the brain will someday help us understand it better than he could at the time, Dr. Menninger perhaps was ahead of his time in his perspective on mental illness.
We should appreciate Dr. Nasrallah for putting together the research that provides an updated, somewhat revised view of Dr. Menninger’s theory.
Reference
1. Menninger K. The vital balance. New York, NY: Viking; 1963.
In his recent editorial, “Is there only 1 neurobiologic psychiatric disorder, with different clinical expressions?” (Current Psychiatry. 2015;14(7):10-12 [http://bit.ly/1INCvxw]), Dr. Nasrallah presents convincing evidence for such a conclusion. However, he did not mention that a somewhat similar concept was established by one of psychiatry’s greats, Karl Menninger, MD, more than 50 years ago. I’m referring to Menninger’s unitary concept of mental illness, espoused in his book, The Vital Balance.1 Dr. Menninger was, of course, founder of the Menninger Clinic in Topeka, Kansas, which now thrives in Houston, Texas, at Baylor College of Medicine. Like Freud, who predicted that advances in viewing the brain will someday help us understand it better than he could at the time, Dr. Menninger perhaps was ahead of his time in his perspective on mental illness.
We should appreciate Dr. Nasrallah for putting together the research that provides an updated, somewhat revised view of Dr. Menninger’s theory.
In his recent editorial, “Is there only 1 neurobiologic psychiatric disorder, with different clinical expressions?” (Current Psychiatry. 2015;14(7):10-12 [http://bit.ly/1INCvxw]), Dr. Nasrallah presents convincing evidence for such a conclusion. However, he did not mention that a somewhat similar concept was established by one of psychiatry’s greats, Karl Menninger, MD, more than 50 years ago. I’m referring to Menninger’s unitary concept of mental illness, espoused in his book, The Vital Balance.1 Dr. Menninger was, of course, founder of the Menninger Clinic in Topeka, Kansas, which now thrives in Houston, Texas, at Baylor College of Medicine. Like Freud, who predicted that advances in viewing the brain will someday help us understand it better than he could at the time, Dr. Menninger perhaps was ahead of his time in his perspective on mental illness.
We should appreciate Dr. Nasrallah for putting together the research that provides an updated, somewhat revised view of Dr. Menninger’s theory.
Reference
1. Menninger K. The vital balance. New York, NY: Viking; 1963.
Reference
1. Menninger K. The vital balance. New York, NY: Viking; 1963.
‘Appreciate the editorials’
I appreciate Dr. Nasrallah’s editorial on the so-called abdominal brain (Current Psychiatry. 2015;14(5):10- 11 [http://bit.ly/1PcxFNP]). Current Psychiatry is a journal with useful reports of advances, reviews, and opinion of research and treatment in our specialty. The selections and editing are always pertinent and thoughtful.
I appreciate Dr. Nasrallah’s editorial on the so-called abdominal brain (Current Psychiatry. 2015;14(5):10- 11 [http://bit.ly/1PcxFNP]). Current Psychiatry is a journal with useful reports of advances, reviews, and opinion of research and treatment in our specialty. The selections and editing are always pertinent and thoughtful.
I appreciate Dr. Nasrallah’s editorial on the so-called abdominal brain (Current Psychiatry. 2015;14(5):10- 11 [http://bit.ly/1PcxFNP]). Current Psychiatry is a journal with useful reports of advances, reviews, and opinion of research and treatment in our specialty. The selections and editing are always pertinent and thoughtful.