User login
COVID-19 and decision-making capacity; more
COVID-19 and decision-making capacity
Dr. Ryznar’s article “Evaluating patients’ decision-making capacity during COVID-19” (Evidence-Based Reviews,
For example, in a controversial 2007 case in Atlanta, Georgia, an attorney with active tuberculosis failed to heed medical advice to refrain from traveling.1 The patient’s uncooperativeness did not implicate concerns over his decisional capacity.1 However, his international and interstate travel triggered the Centers for Disease Control and Prevention’s legal authority under the Public Health Service Act to prevent the entry and spread of communicable disease.1-3 An authorized order from a duly constituted public health authority is issued and enforceable without regard to clinical determinations of capacity (and is generally subject to challenge via judicial or other due process mechanisms as a government-sanctioned deprivation of liberty to protect public welfare). State laws and local ordinances require physicians to notify the appropriate public health department when patients test positive for certain contagious diseases.
The difficulty with involuntarily detaining a cognitively intact patient due to concern over their contagion risk and erroneous beliefs runs considerably deeper than eliciting a “political backlash” or managing the qualms of hospital security officers. It is a fundamental matter of proper legal authority. Psychiatrists and other physicians assess patients’ decision-making capacity for specific treatment decisions on a case-by-case basis, seeking to preserve autonomy while practicing beneficence. Public health officers are agents of the state with designated authorities to control the spread of disease. A capacity determination in the absence of neurocognitive deficits implies the psychiatrist is evaluating the soundness of the patient’s ideas as opposed to their cognition, overlooking the reality that fully capable individuals can possess dubious—and even unsalutary—beliefs. While physicians educate patients about the risks of contracting and communicating infection, they are thankfully not tasked with arbitrating sociopolitical disputes at the bedside. Such controversies regarding pandemic response do not belong under the rubric of medical decision-making capacity. Conflating psychosomatic medicine consultations with public health orders risks unmooring capacity determinations from their medicolegal and bioethical foundations.
Charles G. Kels, JD
S Army Medical Center of Excellence
San Antonio, Texas
Disclaimer: The views expressed here are those of the author and do not necessarily reflect those of any government agency.
References
1. Tanne JH. Tuberculosis case exposes flaws in international public health systems. BMJ. 2007;334(7605):1187.
2. Public Health Service Act, 42 USC § 264-272 (1944).
3. Interstate and Foreign Quarantine, 42 CFR Parts 70-71 (2017).
The author responds
I appreciate Mr. Kels’s letter and explicit discussion of the limits of decision-making capacity. I agree that physicians should not overstep their legal authority and ethical mandate. The specific case discussed in my article was a patient who was symptomatic from COVID-19 who wanted to leave the hospital against medical advice. The contagious nature of this virus certainly falls under the risk/benefit analysis of the clinical situation because it is an important aspect of understanding the nature of the illness and treatment/recovery process (as a thought example, consider that such a patient lives with their elderly mother who has heart disease and chronic obstructive pulmonary disease, and the patient does not want their mother to die). From a medicolegal perspective, the risk of infection to others may not necessarily outweigh the benefit of autonomy, especially because decision-making capacity assessments are made with the purpose of balancing autonomy and beneficence of the patient, not others. I highlighted the relative importance of autonomy using the weight of the arrows in Figure 2 of my article. I did not task physicians with arbitrating sociopolitical disputes, but merely highlighted how the current climate can impact people’s personal views on COVID-19, which sometimes can run counter to scientific evidence. If a patient has an erroneous view about an illness, it is our duty to try to help them understand if it directly impacts their health or affects their decision-making process, especially in a high-stakes clinical scenario.
Elizabeth Ryznar, MD, MSc
Assistant Professor
Department of Psychiatry and Behavioral Sciences
Johns Hopkins School of Medicine
Baltimore, Maryland
Continue to: Olanzapine for treatment-resistant anxiety
Olanzapine for treatment-resistant anxiety
Ms. A, age 62, was a retired high school teacher. Her primary care physician referred her to me for persistent, disabling anxiety. Her condition was recently worsened by a trial of escitalopram, 5 mg/d, which led her to visit the emergency department (ED). There she was prescribed lorazepam, 0.5 mg as needed, which helped her somewhat. Her medical conditions included prominent gastrointestinal (GI) symptoms, with nausea and a restricted diet; tinnitus; and chronic bilateral hand tremors. Her initial Patient Health Questionnaire-9 (PHQ-9) score was 11, and her Generalized Anxiety Disorder-7 (GAD-7) score was 10.
Initially, I encouraged Ms. A to exercise regularly, and I changed her lorazepam from 0.5 mg as-needed to 0.5 mg twice a day. I also referred her to a psychologist for psychotherapy. She showed limited improvement. I increased her lorazepam to 1 mg 3 times a day and started sertraline, 12.5 mg/d, but she soon experienced chest tightness and was admitted to the ED for observation and a cardiac workup. After she visited the ED, Ms. A stopped taking sertraline.
When I next saw Ms. A, she agreed to a trial of olanzapine, 2.5 mg/d at bedtime. Three weeks later, she told me, “I feel so much better.” Her scores on the PHQ-9 and GAD-7 were 0 and 1, respectively. Her GI complaints decreased, she had gained a little weight, and her tinnitus bothered her less. Lorazepam was gradually decreased and stopped.
After approximately 2 years, Ms. A had experienced no long-term adverse effects. We agreed to gradually discontinue olanzapine. Over the next 4 months, Ms. A decreased and stopped taking olanzapine at her own discretion.Three weeks after she stopped taking olanzapine, Ms. A reported that her psychiatric and GI symptoms had returned. She still maintained weekly visits with her psychotherapist. Her GI specialist asked if I could prescribe her olanzapine again. I restarted Ms. A on olanzapine, 2.5 mg/d at bedtime. By the next month, she said she felt much better (PHQ-9: 0; GAD-7: 1). I last saw Ms. A approximately 1 year ago.
Over the years, I have usually prescribed low-dose olanzapine alone or with other medications for patients with treatment-resistance who had no overt psychotic symptoms, I have used this medication for patients with “soft” psychotic thinking marked by severe anxiety, obsessions, compulsivity, perfectionism, and/or rumination.1 Evidence suggests olanzapine also may be effective for anorexia nervosa.2 There is good evidence for its use in the DSM-5 diagnosis of avoidant/restrictive food intake disorder (“a food avoidance emotional disorder”).3,4 In retrospect, Ms. A also likely met the criteria for the diagnosis of unspecified eating disorder. Despite extensive GI workup and follow-up, physical signs of GI pathology were equivocal.
Among antipsychotics, olanzapine most closely resembles clozapine, the only antipsychotic that has been proved more efficacious than others for psychotic symptoms.5 There is also some research suggesting that olanzapine may be more efficacious.6 Obsessions and perfectionism are associated with dopamine D4 receptor activity, and D1, D2, and D3 receptors are involved in normalizing cognition and reward.7 There are appropriate concerns about adverse effects, especially metabolic syndrome and obesity, with olanzapine, but patients can have different profiles of receptor sensitivity. In my conversations with Ms. A’s primary care physician and GI specialist, metabolic syndrome was not an issue. Clearly, low-dose olanzapine was very helpful in her treatment.
Daniel Storch, MD
Key Point Health Services
Catonsville, Maryland
References
1. Goodnick PJ, Barrios CA. Use of olanzapine in non-psychotic psychiatric disorders. Expert Opin Pharmacother. 2001;2(4):667-680.
2. Brewerton TD. Psychopharmacologic management of eating disorders. Presented at: 25th Annual National Psychopharmacology Update; February 2020; Las Vegas, Nevada. Accessed December 8, 2020. https://legacy.audio-digest.org/pages/htmlos/pastissues.html?sub1=psychiatry&sub2=2020
3. Diagnostic and statistical manual of mental disorders, 5th ed. American Psychiatric Association; 2013.
4. Brewerton TD, D’Agostino M. Adjunctive use of olanzapine in the treatment of avoidant restrictive food intake disorder in children and adolescents in an eating disorders program. J Child Adolesc Psychopharmacol. 2017;27(10):920-922.
5. Lobos CA, Komossa K, Rummel-Kluge C, et al. Clozapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev. 2010;(11):CD006633.
6. Komossa K, Rummel-Kluge C, Hunger H, et al. Olanzapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev. 2010;(3):CD006654.
7. Bachner-Melman R, Lerer E, Zohar AH, et al. Anorexia nervosa, perfectionism, and dopamine D4 receptor (DRD4). Am J Med Genet B Neuropsychiatr Genet. 2007;144B(6):748-756.
Continue to: Neuro-politics and academic paralysis...
Neuro-politics and academic paralysis
I commend Dr. Nasrallah for his brief, precisely defined, scientific editorial “Neuro-politics: Will you vote with your cortex or limbic system?” (From the Editor,
I would like to see
Similar to a hurricane or tsunami that pushes water into a river, this retrograde shift of feedback pathways is demonstrated by emotional narratives that have flooded the public and drowned facts and evidence-based practice. Furthermore, the science of convenience has emerged, where facts are eligible only if they justify the narrative. Any discussion, debate, or questioning of the rationale of the approach is met with hostility, naming, shaming, and even loss of employment at universities. I have sadly learned from frightened colleagues and from reading reports by academicians whose publications have been either rejected or coerced for revision following acceptance by a peer-reviewed journal or even retracted post-publication due to complaints, harassment, and threats by the politically correct “thought police.” Diversity of thinking and freedom of speech—core values and principles in academic dialogue—have been violated. Academicians are as perplexed as laboratory rats that need to learn which lever to push in order to receive a reward and avoid punishment in an ever-shifting environment. People have been pondering, “Is it time for flight, fright, or fight?” As Buffalo Springfield’s legendary Vietnam 1960s–era song “For What it’s Worth” states: “There’s battle lines being drawn and nobody’s right if everybody’s wrong.”
What we have learned from history is that the majority of people exercise passivity and hope as bystanders in order to avoid becoming victims of “collateral damage.” Are there no modern Giordano Bruno (the martyr of science), Copernicus, or Michelangelo who would challenge the “Church of the People” that has created new language, terminology, and culture and is on the verge of creating nouveau scientific principles that could lead to a monopoly of one segment of society that threatens pluralism of thought. Do we need dystopic books such as 1984 or Fahrenheit 451, or the experience of the French and Russian revolution (epitomized by the guillotine and the gulag) to remind us that we are a step away from education and reprogramming camps that used to be called universities? The American Association of University Professors’ most recent announcement on academic freedom ominously avoids using terms such as freedom of speech, diversity of opinions, or even pluralism.
I hope that psychiatrists will lead the way back to sanity, starting with focus groups and forums. It would amount to a group cognitive-behavioral therapy of immense proportion following a paradigm of “Problem Solving,” according to Albert Bandura’s social learning model. There is simply no other constructive way to get to the cheese at the end of the maze.
Yifrah Kaminer, MD
Professor Emeritus of Psychiatry & Pediatrics
University of Connecticut School of Medicine
Farmington, Connecticut
Disclosures: The authors report no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
COVID-19 and decision-making capacity
Dr. Ryznar’s article “Evaluating patients’ decision-making capacity during COVID-19” (Evidence-Based Reviews,
For example, in a controversial 2007 case in Atlanta, Georgia, an attorney with active tuberculosis failed to heed medical advice to refrain from traveling.1 The patient’s uncooperativeness did not implicate concerns over his decisional capacity.1 However, his international and interstate travel triggered the Centers for Disease Control and Prevention’s legal authority under the Public Health Service Act to prevent the entry and spread of communicable disease.1-3 An authorized order from a duly constituted public health authority is issued and enforceable without regard to clinical determinations of capacity (and is generally subject to challenge via judicial or other due process mechanisms as a government-sanctioned deprivation of liberty to protect public welfare). State laws and local ordinances require physicians to notify the appropriate public health department when patients test positive for certain contagious diseases.
The difficulty with involuntarily detaining a cognitively intact patient due to concern over their contagion risk and erroneous beliefs runs considerably deeper than eliciting a “political backlash” or managing the qualms of hospital security officers. It is a fundamental matter of proper legal authority. Psychiatrists and other physicians assess patients’ decision-making capacity for specific treatment decisions on a case-by-case basis, seeking to preserve autonomy while practicing beneficence. Public health officers are agents of the state with designated authorities to control the spread of disease. A capacity determination in the absence of neurocognitive deficits implies the psychiatrist is evaluating the soundness of the patient’s ideas as opposed to their cognition, overlooking the reality that fully capable individuals can possess dubious—and even unsalutary—beliefs. While physicians educate patients about the risks of contracting and communicating infection, they are thankfully not tasked with arbitrating sociopolitical disputes at the bedside. Such controversies regarding pandemic response do not belong under the rubric of medical decision-making capacity. Conflating psychosomatic medicine consultations with public health orders risks unmooring capacity determinations from their medicolegal and bioethical foundations.
Charles G. Kels, JD
S Army Medical Center of Excellence
San Antonio, Texas
Disclaimer: The views expressed here are those of the author and do not necessarily reflect those of any government agency.
References
1. Tanne JH. Tuberculosis case exposes flaws in international public health systems. BMJ. 2007;334(7605):1187.
2. Public Health Service Act, 42 USC § 264-272 (1944).
3. Interstate and Foreign Quarantine, 42 CFR Parts 70-71 (2017).
The author responds
I appreciate Mr. Kels’s letter and explicit discussion of the limits of decision-making capacity. I agree that physicians should not overstep their legal authority and ethical mandate. The specific case discussed in my article was a patient who was symptomatic from COVID-19 who wanted to leave the hospital against medical advice. The contagious nature of this virus certainly falls under the risk/benefit analysis of the clinical situation because it is an important aspect of understanding the nature of the illness and treatment/recovery process (as a thought example, consider that such a patient lives with their elderly mother who has heart disease and chronic obstructive pulmonary disease, and the patient does not want their mother to die). From a medicolegal perspective, the risk of infection to others may not necessarily outweigh the benefit of autonomy, especially because decision-making capacity assessments are made with the purpose of balancing autonomy and beneficence of the patient, not others. I highlighted the relative importance of autonomy using the weight of the arrows in Figure 2 of my article. I did not task physicians with arbitrating sociopolitical disputes, but merely highlighted how the current climate can impact people’s personal views on COVID-19, which sometimes can run counter to scientific evidence. If a patient has an erroneous view about an illness, it is our duty to try to help them understand if it directly impacts their health or affects their decision-making process, especially in a high-stakes clinical scenario.
Elizabeth Ryznar, MD, MSc
Assistant Professor
Department of Psychiatry and Behavioral Sciences
Johns Hopkins School of Medicine
Baltimore, Maryland
Continue to: Olanzapine for treatment-resistant anxiety
Olanzapine for treatment-resistant anxiety
Ms. A, age 62, was a retired high school teacher. Her primary care physician referred her to me for persistent, disabling anxiety. Her condition was recently worsened by a trial of escitalopram, 5 mg/d, which led her to visit the emergency department (ED). There she was prescribed lorazepam, 0.5 mg as needed, which helped her somewhat. Her medical conditions included prominent gastrointestinal (GI) symptoms, with nausea and a restricted diet; tinnitus; and chronic bilateral hand tremors. Her initial Patient Health Questionnaire-9 (PHQ-9) score was 11, and her Generalized Anxiety Disorder-7 (GAD-7) score was 10.
Initially, I encouraged Ms. A to exercise regularly, and I changed her lorazepam from 0.5 mg as-needed to 0.5 mg twice a day. I also referred her to a psychologist for psychotherapy. She showed limited improvement. I increased her lorazepam to 1 mg 3 times a day and started sertraline, 12.5 mg/d, but she soon experienced chest tightness and was admitted to the ED for observation and a cardiac workup. After she visited the ED, Ms. A stopped taking sertraline.
When I next saw Ms. A, she agreed to a trial of olanzapine, 2.5 mg/d at bedtime. Three weeks later, she told me, “I feel so much better.” Her scores on the PHQ-9 and GAD-7 were 0 and 1, respectively. Her GI complaints decreased, she had gained a little weight, and her tinnitus bothered her less. Lorazepam was gradually decreased and stopped.
After approximately 2 years, Ms. A had experienced no long-term adverse effects. We agreed to gradually discontinue olanzapine. Over the next 4 months, Ms. A decreased and stopped taking olanzapine at her own discretion.Three weeks after she stopped taking olanzapine, Ms. A reported that her psychiatric and GI symptoms had returned. She still maintained weekly visits with her psychotherapist. Her GI specialist asked if I could prescribe her olanzapine again. I restarted Ms. A on olanzapine, 2.5 mg/d at bedtime. By the next month, she said she felt much better (PHQ-9: 0; GAD-7: 1). I last saw Ms. A approximately 1 year ago.
Over the years, I have usually prescribed low-dose olanzapine alone or with other medications for patients with treatment-resistance who had no overt psychotic symptoms, I have used this medication for patients with “soft” psychotic thinking marked by severe anxiety, obsessions, compulsivity, perfectionism, and/or rumination.1 Evidence suggests olanzapine also may be effective for anorexia nervosa.2 There is good evidence for its use in the DSM-5 diagnosis of avoidant/restrictive food intake disorder (“a food avoidance emotional disorder”).3,4 In retrospect, Ms. A also likely met the criteria for the diagnosis of unspecified eating disorder. Despite extensive GI workup and follow-up, physical signs of GI pathology were equivocal.
Among antipsychotics, olanzapine most closely resembles clozapine, the only antipsychotic that has been proved more efficacious than others for psychotic symptoms.5 There is also some research suggesting that olanzapine may be more efficacious.6 Obsessions and perfectionism are associated with dopamine D4 receptor activity, and D1, D2, and D3 receptors are involved in normalizing cognition and reward.7 There are appropriate concerns about adverse effects, especially metabolic syndrome and obesity, with olanzapine, but patients can have different profiles of receptor sensitivity. In my conversations with Ms. A’s primary care physician and GI specialist, metabolic syndrome was not an issue. Clearly, low-dose olanzapine was very helpful in her treatment.
Daniel Storch, MD
Key Point Health Services
Catonsville, Maryland
References
1. Goodnick PJ, Barrios CA. Use of olanzapine in non-psychotic psychiatric disorders. Expert Opin Pharmacother. 2001;2(4):667-680.
2. Brewerton TD. Psychopharmacologic management of eating disorders. Presented at: 25th Annual National Psychopharmacology Update; February 2020; Las Vegas, Nevada. Accessed December 8, 2020. https://legacy.audio-digest.org/pages/htmlos/pastissues.html?sub1=psychiatry&sub2=2020
3. Diagnostic and statistical manual of mental disorders, 5th ed. American Psychiatric Association; 2013.
4. Brewerton TD, D’Agostino M. Adjunctive use of olanzapine in the treatment of avoidant restrictive food intake disorder in children and adolescents in an eating disorders program. J Child Adolesc Psychopharmacol. 2017;27(10):920-922.
5. Lobos CA, Komossa K, Rummel-Kluge C, et al. Clozapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev. 2010;(11):CD006633.
6. Komossa K, Rummel-Kluge C, Hunger H, et al. Olanzapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev. 2010;(3):CD006654.
7. Bachner-Melman R, Lerer E, Zohar AH, et al. Anorexia nervosa, perfectionism, and dopamine D4 receptor (DRD4). Am J Med Genet B Neuropsychiatr Genet. 2007;144B(6):748-756.
Continue to: Neuro-politics and academic paralysis...
Neuro-politics and academic paralysis
I commend Dr. Nasrallah for his brief, precisely defined, scientific editorial “Neuro-politics: Will you vote with your cortex or limbic system?” (From the Editor,
I would like to see
Similar to a hurricane or tsunami that pushes water into a river, this retrograde shift of feedback pathways is demonstrated by emotional narratives that have flooded the public and drowned facts and evidence-based practice. Furthermore, the science of convenience has emerged, where facts are eligible only if they justify the narrative. Any discussion, debate, or questioning of the rationale of the approach is met with hostility, naming, shaming, and even loss of employment at universities. I have sadly learned from frightened colleagues and from reading reports by academicians whose publications have been either rejected or coerced for revision following acceptance by a peer-reviewed journal or even retracted post-publication due to complaints, harassment, and threats by the politically correct “thought police.” Diversity of thinking and freedom of speech—core values and principles in academic dialogue—have been violated. Academicians are as perplexed as laboratory rats that need to learn which lever to push in order to receive a reward and avoid punishment in an ever-shifting environment. People have been pondering, “Is it time for flight, fright, or fight?” As Buffalo Springfield’s legendary Vietnam 1960s–era song “For What it’s Worth” states: “There’s battle lines being drawn and nobody’s right if everybody’s wrong.”
What we have learned from history is that the majority of people exercise passivity and hope as bystanders in order to avoid becoming victims of “collateral damage.” Are there no modern Giordano Bruno (the martyr of science), Copernicus, or Michelangelo who would challenge the “Church of the People” that has created new language, terminology, and culture and is on the verge of creating nouveau scientific principles that could lead to a monopoly of one segment of society that threatens pluralism of thought. Do we need dystopic books such as 1984 or Fahrenheit 451, or the experience of the French and Russian revolution (epitomized by the guillotine and the gulag) to remind us that we are a step away from education and reprogramming camps that used to be called universities? The American Association of University Professors’ most recent announcement on academic freedom ominously avoids using terms such as freedom of speech, diversity of opinions, or even pluralism.
I hope that psychiatrists will lead the way back to sanity, starting with focus groups and forums. It would amount to a group cognitive-behavioral therapy of immense proportion following a paradigm of “Problem Solving,” according to Albert Bandura’s social learning model. There is simply no other constructive way to get to the cheese at the end of the maze.
Yifrah Kaminer, MD
Professor Emeritus of Psychiatry & Pediatrics
University of Connecticut School of Medicine
Farmington, Connecticut
Disclosures: The authors report no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
COVID-19 and decision-making capacity
Dr. Ryznar’s article “Evaluating patients’ decision-making capacity during COVID-19” (Evidence-Based Reviews,
For example, in a controversial 2007 case in Atlanta, Georgia, an attorney with active tuberculosis failed to heed medical advice to refrain from traveling.1 The patient’s uncooperativeness did not implicate concerns over his decisional capacity.1 However, his international and interstate travel triggered the Centers for Disease Control and Prevention’s legal authority under the Public Health Service Act to prevent the entry and spread of communicable disease.1-3 An authorized order from a duly constituted public health authority is issued and enforceable without regard to clinical determinations of capacity (and is generally subject to challenge via judicial or other due process mechanisms as a government-sanctioned deprivation of liberty to protect public welfare). State laws and local ordinances require physicians to notify the appropriate public health department when patients test positive for certain contagious diseases.
The difficulty with involuntarily detaining a cognitively intact patient due to concern over their contagion risk and erroneous beliefs runs considerably deeper than eliciting a “political backlash” or managing the qualms of hospital security officers. It is a fundamental matter of proper legal authority. Psychiatrists and other physicians assess patients’ decision-making capacity for specific treatment decisions on a case-by-case basis, seeking to preserve autonomy while practicing beneficence. Public health officers are agents of the state with designated authorities to control the spread of disease. A capacity determination in the absence of neurocognitive deficits implies the psychiatrist is evaluating the soundness of the patient’s ideas as opposed to their cognition, overlooking the reality that fully capable individuals can possess dubious—and even unsalutary—beliefs. While physicians educate patients about the risks of contracting and communicating infection, they are thankfully not tasked with arbitrating sociopolitical disputes at the bedside. Such controversies regarding pandemic response do not belong under the rubric of medical decision-making capacity. Conflating psychosomatic medicine consultations with public health orders risks unmooring capacity determinations from their medicolegal and bioethical foundations.
Charles G. Kels, JD
S Army Medical Center of Excellence
San Antonio, Texas
Disclaimer: The views expressed here are those of the author and do not necessarily reflect those of any government agency.
References
1. Tanne JH. Tuberculosis case exposes flaws in international public health systems. BMJ. 2007;334(7605):1187.
2. Public Health Service Act, 42 USC § 264-272 (1944).
3. Interstate and Foreign Quarantine, 42 CFR Parts 70-71 (2017).
The author responds
I appreciate Mr. Kels’s letter and explicit discussion of the limits of decision-making capacity. I agree that physicians should not overstep their legal authority and ethical mandate. The specific case discussed in my article was a patient who was symptomatic from COVID-19 who wanted to leave the hospital against medical advice. The contagious nature of this virus certainly falls under the risk/benefit analysis of the clinical situation because it is an important aspect of understanding the nature of the illness and treatment/recovery process (as a thought example, consider that such a patient lives with their elderly mother who has heart disease and chronic obstructive pulmonary disease, and the patient does not want their mother to die). From a medicolegal perspective, the risk of infection to others may not necessarily outweigh the benefit of autonomy, especially because decision-making capacity assessments are made with the purpose of balancing autonomy and beneficence of the patient, not others. I highlighted the relative importance of autonomy using the weight of the arrows in Figure 2 of my article. I did not task physicians with arbitrating sociopolitical disputes, but merely highlighted how the current climate can impact people’s personal views on COVID-19, which sometimes can run counter to scientific evidence. If a patient has an erroneous view about an illness, it is our duty to try to help them understand if it directly impacts their health or affects their decision-making process, especially in a high-stakes clinical scenario.
Elizabeth Ryznar, MD, MSc
Assistant Professor
Department of Psychiatry and Behavioral Sciences
Johns Hopkins School of Medicine
Baltimore, Maryland
Continue to: Olanzapine for treatment-resistant anxiety
Olanzapine for treatment-resistant anxiety
Ms. A, age 62, was a retired high school teacher. Her primary care physician referred her to me for persistent, disabling anxiety. Her condition was recently worsened by a trial of escitalopram, 5 mg/d, which led her to visit the emergency department (ED). There she was prescribed lorazepam, 0.5 mg as needed, which helped her somewhat. Her medical conditions included prominent gastrointestinal (GI) symptoms, with nausea and a restricted diet; tinnitus; and chronic bilateral hand tremors. Her initial Patient Health Questionnaire-9 (PHQ-9) score was 11, and her Generalized Anxiety Disorder-7 (GAD-7) score was 10.
Initially, I encouraged Ms. A to exercise regularly, and I changed her lorazepam from 0.5 mg as-needed to 0.5 mg twice a day. I also referred her to a psychologist for psychotherapy. She showed limited improvement. I increased her lorazepam to 1 mg 3 times a day and started sertraline, 12.5 mg/d, but she soon experienced chest tightness and was admitted to the ED for observation and a cardiac workup. After she visited the ED, Ms. A stopped taking sertraline.
When I next saw Ms. A, she agreed to a trial of olanzapine, 2.5 mg/d at bedtime. Three weeks later, she told me, “I feel so much better.” Her scores on the PHQ-9 and GAD-7 were 0 and 1, respectively. Her GI complaints decreased, she had gained a little weight, and her tinnitus bothered her less. Lorazepam was gradually decreased and stopped.
After approximately 2 years, Ms. A had experienced no long-term adverse effects. We agreed to gradually discontinue olanzapine. Over the next 4 months, Ms. A decreased and stopped taking olanzapine at her own discretion.Three weeks after she stopped taking olanzapine, Ms. A reported that her psychiatric and GI symptoms had returned. She still maintained weekly visits with her psychotherapist. Her GI specialist asked if I could prescribe her olanzapine again. I restarted Ms. A on olanzapine, 2.5 mg/d at bedtime. By the next month, she said she felt much better (PHQ-9: 0; GAD-7: 1). I last saw Ms. A approximately 1 year ago.
Over the years, I have usually prescribed low-dose olanzapine alone or with other medications for patients with treatment-resistance who had no overt psychotic symptoms, I have used this medication for patients with “soft” psychotic thinking marked by severe anxiety, obsessions, compulsivity, perfectionism, and/or rumination.1 Evidence suggests olanzapine also may be effective for anorexia nervosa.2 There is good evidence for its use in the DSM-5 diagnosis of avoidant/restrictive food intake disorder (“a food avoidance emotional disorder”).3,4 In retrospect, Ms. A also likely met the criteria for the diagnosis of unspecified eating disorder. Despite extensive GI workup and follow-up, physical signs of GI pathology were equivocal.
Among antipsychotics, olanzapine most closely resembles clozapine, the only antipsychotic that has been proved more efficacious than others for psychotic symptoms.5 There is also some research suggesting that olanzapine may be more efficacious.6 Obsessions and perfectionism are associated with dopamine D4 receptor activity, and D1, D2, and D3 receptors are involved in normalizing cognition and reward.7 There are appropriate concerns about adverse effects, especially metabolic syndrome and obesity, with olanzapine, but patients can have different profiles of receptor sensitivity. In my conversations with Ms. A’s primary care physician and GI specialist, metabolic syndrome was not an issue. Clearly, low-dose olanzapine was very helpful in her treatment.
Daniel Storch, MD
Key Point Health Services
Catonsville, Maryland
References
1. Goodnick PJ, Barrios CA. Use of olanzapine in non-psychotic psychiatric disorders. Expert Opin Pharmacother. 2001;2(4):667-680.
2. Brewerton TD. Psychopharmacologic management of eating disorders. Presented at: 25th Annual National Psychopharmacology Update; February 2020; Las Vegas, Nevada. Accessed December 8, 2020. https://legacy.audio-digest.org/pages/htmlos/pastissues.html?sub1=psychiatry&sub2=2020
3. Diagnostic and statistical manual of mental disorders, 5th ed. American Psychiatric Association; 2013.
4. Brewerton TD, D’Agostino M. Adjunctive use of olanzapine in the treatment of avoidant restrictive food intake disorder in children and adolescents in an eating disorders program. J Child Adolesc Psychopharmacol. 2017;27(10):920-922.
5. Lobos CA, Komossa K, Rummel-Kluge C, et al. Clozapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev. 2010;(11):CD006633.
6. Komossa K, Rummel-Kluge C, Hunger H, et al. Olanzapine versus other atypical antipsychotics for schizophrenia. Cochrane Database Syst Rev. 2010;(3):CD006654.
7. Bachner-Melman R, Lerer E, Zohar AH, et al. Anorexia nervosa, perfectionism, and dopamine D4 receptor (DRD4). Am J Med Genet B Neuropsychiatr Genet. 2007;144B(6):748-756.
Continue to: Neuro-politics and academic paralysis...
Neuro-politics and academic paralysis
I commend Dr. Nasrallah for his brief, precisely defined, scientific editorial “Neuro-politics: Will you vote with your cortex or limbic system?” (From the Editor,
I would like to see
Similar to a hurricane or tsunami that pushes water into a river, this retrograde shift of feedback pathways is demonstrated by emotional narratives that have flooded the public and drowned facts and evidence-based practice. Furthermore, the science of convenience has emerged, where facts are eligible only if they justify the narrative. Any discussion, debate, or questioning of the rationale of the approach is met with hostility, naming, shaming, and even loss of employment at universities. I have sadly learned from frightened colleagues and from reading reports by academicians whose publications have been either rejected or coerced for revision following acceptance by a peer-reviewed journal or even retracted post-publication due to complaints, harassment, and threats by the politically correct “thought police.” Diversity of thinking and freedom of speech—core values and principles in academic dialogue—have been violated. Academicians are as perplexed as laboratory rats that need to learn which lever to push in order to receive a reward and avoid punishment in an ever-shifting environment. People have been pondering, “Is it time for flight, fright, or fight?” As Buffalo Springfield’s legendary Vietnam 1960s–era song “For What it’s Worth” states: “There’s battle lines being drawn and nobody’s right if everybody’s wrong.”
What we have learned from history is that the majority of people exercise passivity and hope as bystanders in order to avoid becoming victims of “collateral damage.” Are there no modern Giordano Bruno (the martyr of science), Copernicus, or Michelangelo who would challenge the “Church of the People” that has created new language, terminology, and culture and is on the verge of creating nouveau scientific principles that could lead to a monopoly of one segment of society that threatens pluralism of thought. Do we need dystopic books such as 1984 or Fahrenheit 451, or the experience of the French and Russian revolution (epitomized by the guillotine and the gulag) to remind us that we are a step away from education and reprogramming camps that used to be called universities? The American Association of University Professors’ most recent announcement on academic freedom ominously avoids using terms such as freedom of speech, diversity of opinions, or even pluralism.
I hope that psychiatrists will lead the way back to sanity, starting with focus groups and forums. It would amount to a group cognitive-behavioral therapy of immense proportion following a paradigm of “Problem Solving,” according to Albert Bandura’s social learning model. There is simply no other constructive way to get to the cheese at the end of the maze.
Yifrah Kaminer, MD
Professor Emeritus of Psychiatry & Pediatrics
University of Connecticut School of Medicine
Farmington, Connecticut
Disclosures: The authors report no financial relationships with any companies whose products are mentioned in this article, or with manufacturers of competing products.
ASH guidelines for venous thromboembolism: What family physicians need to know
Each year in the United States, approximately one to two out of every thousand people suffer from venous thromboembolism (VTE), including deep vein thrombosis and pulmonary embolism. .

These guidelines, which were recently published in Blood Advances (Ortel T L et al. Blood Adv 2020 doi: 10.1182/bloodadvances.2020001830), include 28 recommendations.
How to treat uncomplicated patients
For uncomplicated deep vein thrombosis (DVT) and/or pulmonary embolism (PE), the guidelines suggest treating patients at home rather than in the hospital. This is especially important for family physicians to note as many of these patients will now be the responsibility of the primary care doctor to treat and follow. Patients treated at home can avoid the risk of nosocomial infections, especially in the days of COVID-19. Evidence also suggests that being treated at home was shown to reduce the risk of PE versus being treated in the hospital. It is, therefore, crucial that family physicians know which patients are low versus high risk.
Further, the guidelines suggest that these patients with low risk of complications are better treated with direct oral anticoagulants (DOACs) instead of vitamin K antagonists, such as Coumadin.
Medication-related suggestions
The guidelines also suggest that no DOAC is preferred over another. Since DOACs are relatively newer agents, family doctors need to become comfortable with their use. For proximal DVTs, anticoagulation alone can be used without thrombolytics.
Family physicians are often tasked with the decision on when to stop anticoagulation. The authors recommend against using diagnostic tests such as D-Dimer or ultrasound to decide when to stop these medications in low-risk patients. In patients at risk of recurrent VTE due to chronic medical conditions, it is suggested to continue anti-coagulants indefinitely. While anticoagulant therapy effectively reduces risk of VTE, it does increase the risk of bleeding events.
The guidelines are quite extensive and specific in their recommendations and family physicians need to understand them. We are often the first ones in the medical system to diagnose VTE, and it is quite possible to keep these patients home, thereby eliminating risks they may encounter by being hospitalized. In addition, the recommendation regarding the use of DOACs may ease some of the burden of monitoring patients on long-term Coumadin. These medications do not come without risks, and we must be comfortable evaluating for any complications. In our current health care system, different insurance companies have different formularies making it necessary for us to know all these medications.
In the past, the diagnosis of PE and even a DVT would mean a hospital stay. We now know, and these guidelines reaffirm, that this is not necessary in uncomplicated cases.
In addition to diagnosing VTE, family physicians are also tasked with following up with patients who were hospitalized or started on treatment by other physicians. We need to know the plan on when to stop the medication or when to reevaluate its use. Patients often bring this question to us, and these guidelines will help us answer that question.
Many patients who have more complicated medical conditions often see multiple specialists. The ASH recommendations help standardize the care of these patients across specialties.
What the recommendations are missing
As family doctors, we often treat patients with multiple comorbidities. These guidelines do not make recommendations for patients with cancer, who are at high risk of VTE events. Some patients also have conditions that increase their risk of bleeding or have contraindications to the use of anticoagulants. It would be helpful to have more recommendations for both of these types of patients in addition to the use of inferior vena cava filter in patients with proximal DVT. The document is also missing recommendations for pregnant patients, which would be useful.
Overall, these guidelines include much of what we already do in our practices while doing a great job of incorporating the newer DOACs. These guidelines are easy for family physicians to put into practice.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
Each year in the United States, approximately one to two out of every thousand people suffer from venous thromboembolism (VTE), including deep vein thrombosis and pulmonary embolism. .
These guidelines, which were recently published in Blood Advances (Ortel T L et al. Blood Adv 2020 doi: 10.1182/bloodadvances.2020001830), include 28 recommendations.
How to treat uncomplicated patients
For uncomplicated deep vein thrombosis (DVT) and/or pulmonary embolism (PE), the guidelines suggest treating patients at home rather than in the hospital. This is especially important for family physicians to note as many of these patients will now be the responsibility of the primary care doctor to treat and follow. Patients treated at home can avoid the risk of nosocomial infections, especially in the days of COVID-19. Evidence also suggests that being treated at home was shown to reduce the risk of PE versus being treated in the hospital. It is, therefore, crucial that family physicians know which patients are low versus high risk.
Further, the guidelines suggest that these patients with low risk of complications are better treated with direct oral anticoagulants (DOACs) instead of vitamin K antagonists, such as Coumadin.
Medication-related suggestions
The guidelines also suggest that no DOAC is preferred over another. Since DOACs are relatively newer agents, family doctors need to become comfortable with their use. For proximal DVTs, anticoagulation alone can be used without thrombolytics.
Family physicians are often tasked with the decision on when to stop anticoagulation. The authors recommend against using diagnostic tests such as D-Dimer or ultrasound to decide when to stop these medications in low-risk patients. In patients at risk of recurrent VTE due to chronic medical conditions, it is suggested to continue anti-coagulants indefinitely. While anticoagulant therapy effectively reduces risk of VTE, it does increase the risk of bleeding events.
The guidelines are quite extensive and specific in their recommendations and family physicians need to understand them. We are often the first ones in the medical system to diagnose VTE, and it is quite possible to keep these patients home, thereby eliminating risks they may encounter by being hospitalized. In addition, the recommendation regarding the use of DOACs may ease some of the burden of monitoring patients on long-term Coumadin. These medications do not come without risks, and we must be comfortable evaluating for any complications. In our current health care system, different insurance companies have different formularies making it necessary for us to know all these medications.
In the past, the diagnosis of PE and even a DVT would mean a hospital stay. We now know, and these guidelines reaffirm, that this is not necessary in uncomplicated cases.
In addition to diagnosing VTE, family physicians are also tasked with following up with patients who were hospitalized or started on treatment by other physicians. We need to know the plan on when to stop the medication or when to reevaluate its use. Patients often bring this question to us, and these guidelines will help us answer that question.
Many patients who have more complicated medical conditions often see multiple specialists. The ASH recommendations help standardize the care of these patients across specialties.
What the recommendations are missing
As family doctors, we often treat patients with multiple comorbidities. These guidelines do not make recommendations for patients with cancer, who are at high risk of VTE events. Some patients also have conditions that increase their risk of bleeding or have contraindications to the use of anticoagulants. It would be helpful to have more recommendations for both of these types of patients in addition to the use of inferior vena cava filter in patients with proximal DVT. The document is also missing recommendations for pregnant patients, which would be useful.
Overall, these guidelines include much of what we already do in our practices while doing a great job of incorporating the newer DOACs. These guidelines are easy for family physicians to put into practice.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
Each year in the United States, approximately one to two out of every thousand people suffer from venous thromboembolism (VTE), including deep vein thrombosis and pulmonary embolism. .
These guidelines, which were recently published in Blood Advances (Ortel T L et al. Blood Adv 2020 doi: 10.1182/bloodadvances.2020001830), include 28 recommendations.
How to treat uncomplicated patients
For uncomplicated deep vein thrombosis (DVT) and/or pulmonary embolism (PE), the guidelines suggest treating patients at home rather than in the hospital. This is especially important for family physicians to note as many of these patients will now be the responsibility of the primary care doctor to treat and follow. Patients treated at home can avoid the risk of nosocomial infections, especially in the days of COVID-19. Evidence also suggests that being treated at home was shown to reduce the risk of PE versus being treated in the hospital. It is, therefore, crucial that family physicians know which patients are low versus high risk.
Further, the guidelines suggest that these patients with low risk of complications are better treated with direct oral anticoagulants (DOACs) instead of vitamin K antagonists, such as Coumadin.
Medication-related suggestions
The guidelines also suggest that no DOAC is preferred over another. Since DOACs are relatively newer agents, family doctors need to become comfortable with their use. For proximal DVTs, anticoagulation alone can be used without thrombolytics.
Family physicians are often tasked with the decision on when to stop anticoagulation. The authors recommend against using diagnostic tests such as D-Dimer or ultrasound to decide when to stop these medications in low-risk patients. In patients at risk of recurrent VTE due to chronic medical conditions, it is suggested to continue anti-coagulants indefinitely. While anticoagulant therapy effectively reduces risk of VTE, it does increase the risk of bleeding events.
The guidelines are quite extensive and specific in their recommendations and family physicians need to understand them. We are often the first ones in the medical system to diagnose VTE, and it is quite possible to keep these patients home, thereby eliminating risks they may encounter by being hospitalized. In addition, the recommendation regarding the use of DOACs may ease some of the burden of monitoring patients on long-term Coumadin. These medications do not come without risks, and we must be comfortable evaluating for any complications. In our current health care system, different insurance companies have different formularies making it necessary for us to know all these medications.
In the past, the diagnosis of PE and even a DVT would mean a hospital stay. We now know, and these guidelines reaffirm, that this is not necessary in uncomplicated cases.
In addition to diagnosing VTE, family physicians are also tasked with following up with patients who were hospitalized or started on treatment by other physicians. We need to know the plan on when to stop the medication or when to reevaluate its use. Patients often bring this question to us, and these guidelines will help us answer that question.
Many patients who have more complicated medical conditions often see multiple specialists. The ASH recommendations help standardize the care of these patients across specialties.
What the recommendations are missing
As family doctors, we often treat patients with multiple comorbidities. These guidelines do not make recommendations for patients with cancer, who are at high risk of VTE events. Some patients also have conditions that increase their risk of bleeding or have contraindications to the use of anticoagulants. It would be helpful to have more recommendations for both of these types of patients in addition to the use of inferior vena cava filter in patients with proximal DVT. The document is also missing recommendations for pregnant patients, which would be useful.
Overall, these guidelines include much of what we already do in our practices while doing a great job of incorporating the newer DOACs. These guidelines are easy for family physicians to put into practice.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. You can contact her at fpnews@mdedge.com.
Tackling screen time from birth
In this day and age, a new question should make its way to the top of the list for new parents and their pediatricians: How will the family approach the issue of household technology use – for their children as well as themselves?

Even the most vigilant among them will find much available guidance conflicting – and a good deal of it may feel oblivious to their day-to-day realities. This is especially true now, as many families face the daunting demands of pandemic parenting – juggling full-time jobs with childcare and distance learning.
While the American Academy of Pediatrics still specifies daily time limits by age (difficult for many families to achieve even in “normal” times), pediatricians and other child development experts now recognize that a host of factors should inform decisions about healthy screen use. There’s no one “magic number” for acceptable daily use, as not all screen time is the same (particularly during the pandemic) – and different children will experience the effects of technology usage differently.
The quality of content the child engages with; the degree of parental involvement; and the individual cognitive and behavioral considerations of a child are just some of the factors that should be considered. Given the complexities, it’s unfortunate that many parents will not have discussed screen use with their pediatrician or even their partner before their child first reaches for that glowing screen – and certainly not before they are using technology to multitask work, social connections, and day-to-day child rearing. Screen habits form early for both children and families.
An early well-visit priority
Pediatricians have an important role to play in helping families develop a more purposeful approach to household technology by providing them with trusted, evidence-based information on screens and the potential impact on children’s development. This is not information parents should receive when a child is 2 or 3 years of age. By then, toddlers are often already avid tablet users and parents may have come to rely on technology as a parenting aid.

Parents also need to know that, from birth, they can influence their child’s brain and communication development through undistracted time for talking, reading, singing, and interacting with their baby. Though the way children develop speech and language skills has not changed, the level of distraction posed by technology has grown immensely. It is much more difficult for parents to notice a baby’s subtle communication attempts – a coo or a smile, for instance, and respond accordingly – with a smartphone in hand. Rather than admonish parents for overusing their devices, we can focus them on what supports healthy child development instead.
By talking to parents earlier, pediatricians can help prevent premature or excessive exposure to technology – as well as encourage parents to dedicate “unplugged” times of day with their baby, such as during feeding time or before bedtime. By accenting the positive – educating parents about how they can encourage development and growth, how they can bond with their baby, and how they can establish a loving and nurturing relationship – pediatricians can motivate them towards simple steps that limit technology’s disruption of daily developmental opportunities. They can also help them lay a solid foundation for healthy screen time habits in the long term for their family.
The critical period for speech and language development is early
The impact of screen use on a child’s communication development is a significant concern. The critical time window for the development of speech, language, and social skills is between birth and 3 years. What happens then is the precursor for later reading and writing skills that are key to academic and vocational success.

A meta-analysis published in JAMA Pediatrics in July 2020 found that greater quantity of screen use was associated with poorer language skills – while screen-use onset at later ages was also associated with stronger child language skills. A November 2019 JAMA Pediatrics study using brain imaging in pre–school age children found an association between increased screen-based media use, compared with the AAP guidelines, and lower integrity of white matter tracts supporting language and emergent literacy skills. That study also used several language and literacy tests, finding that children with higher screen exposure had poorer expressive language and worse language processing speed. A 2017 study of 900 children between 18 and 24 months found that every 30-minute increase in daily screen time was linked to a 49% increased risk of expressive speech delay. And on the parental side, numerous studies have documented decreased verbal and nonverbal interactions initiated by parents when they are using a device.
Be tech wise with baby
AAP offers many resources in its Media and Children Communication Toolkit that serve as helpful starting points for conversations, including its family media use plan templates. However, more resources tailored to parents of newborns and very young children are needed.
One new option recently developed by the American Speech-Language-Hearing Association (ASHA) and the Children’s Screen Time Action Network is Be Tech Wise With Baby! Aimed at prospective and new parents, this simple handout, available for free in English and Spanish, is an easy takeaway from early well-child visits that pediatricians and pediatric nurses can distribute.
Pediatricians have a vital role to play championing healthy, balanced screen time use for children and adults – starting from baby’s first moments of life. By guiding new parents towards simple steps, such as carving out tech-free times of day and delaying introduction of screens, they can positively influence the screen-time habits of the next generation of connected kids.
Mark Bertin, MD, is a developmental pediatrician and author of numerous parenting books, including “How Children Thrive: The Practical Science of Raising Independent, Resilient, and Happy Kids” and “Mindful Parenting for ADHD.” Diane Paul, PhD, CCC-SLP, is the director of clinical issues in speech-language pathology for the American Speech-Language-Hearing Association (ASHA) and author of numerous books, including “Talking on the Go: Everyday Activities to Enhance Speech and Language Development.” Email them at pdnews@mdedge.com.
In this day and age, a new question should make its way to the top of the list for new parents and their pediatricians: How will the family approach the issue of household technology use – for their children as well as themselves?
Even the most vigilant among them will find much available guidance conflicting – and a good deal of it may feel oblivious to their day-to-day realities. This is especially true now, as many families face the daunting demands of pandemic parenting – juggling full-time jobs with childcare and distance learning.
While the American Academy of Pediatrics still specifies daily time limits by age (difficult for many families to achieve even in “normal” times), pediatricians and other child development experts now recognize that a host of factors should inform decisions about healthy screen use. There’s no one “magic number” for acceptable daily use, as not all screen time is the same (particularly during the pandemic) – and different children will experience the effects of technology usage differently.
The quality of content the child engages with; the degree of parental involvement; and the individual cognitive and behavioral considerations of a child are just some of the factors that should be considered. Given the complexities, it’s unfortunate that many parents will not have discussed screen use with their pediatrician or even their partner before their child first reaches for that glowing screen – and certainly not before they are using technology to multitask work, social connections, and day-to-day child rearing. Screen habits form early for both children and families.
An early well-visit priority
Pediatricians have an important role to play in helping families develop a more purposeful approach to household technology by providing them with trusted, evidence-based information on screens and the potential impact on children’s development. This is not information parents should receive when a child is 2 or 3 years of age. By then, toddlers are often already avid tablet users and parents may have come to rely on technology as a parenting aid.
Parents also need to know that, from birth, they can influence their child’s brain and communication development through undistracted time for talking, reading, singing, and interacting with their baby. Though the way children develop speech and language skills has not changed, the level of distraction posed by technology has grown immensely. It is much more difficult for parents to notice a baby’s subtle communication attempts – a coo or a smile, for instance, and respond accordingly – with a smartphone in hand. Rather than admonish parents for overusing their devices, we can focus them on what supports healthy child development instead.
By talking to parents earlier, pediatricians can help prevent premature or excessive exposure to technology – as well as encourage parents to dedicate “unplugged” times of day with their baby, such as during feeding time or before bedtime. By accenting the positive – educating parents about how they can encourage development and growth, how they can bond with their baby, and how they can establish a loving and nurturing relationship – pediatricians can motivate them towards simple steps that limit technology’s disruption of daily developmental opportunities. They can also help them lay a solid foundation for healthy screen time habits in the long term for their family.
The critical period for speech and language development is early
The impact of screen use on a child’s communication development is a significant concern. The critical time window for the development of speech, language, and social skills is between birth and 3 years. What happens then is the precursor for later reading and writing skills that are key to academic and vocational success.
A meta-analysis published in JAMA Pediatrics in July 2020 found that greater quantity of screen use was associated with poorer language skills – while screen-use onset at later ages was also associated with stronger child language skills. A November 2019 JAMA Pediatrics study using brain imaging in pre–school age children found an association between increased screen-based media use, compared with the AAP guidelines, and lower integrity of white matter tracts supporting language and emergent literacy skills. That study also used several language and literacy tests, finding that children with higher screen exposure had poorer expressive language and worse language processing speed. A 2017 study of 900 children between 18 and 24 months found that every 30-minute increase in daily screen time was linked to a 49% increased risk of expressive speech delay. And on the parental side, numerous studies have documented decreased verbal and nonverbal interactions initiated by parents when they are using a device.
Be tech wise with baby
AAP offers many resources in its Media and Children Communication Toolkit that serve as helpful starting points for conversations, including its family media use plan templates. However, more resources tailored to parents of newborns and very young children are needed.
One new option recently developed by the American Speech-Language-Hearing Association (ASHA) and the Children’s Screen Time Action Network is Be Tech Wise With Baby! Aimed at prospective and new parents, this simple handout, available for free in English and Spanish, is an easy takeaway from early well-child visits that pediatricians and pediatric nurses can distribute.
Pediatricians have a vital role to play championing healthy, balanced screen time use for children and adults – starting from baby’s first moments of life. By guiding new parents towards simple steps, such as carving out tech-free times of day and delaying introduction of screens, they can positively influence the screen-time habits of the next generation of connected kids.
Mark Bertin, MD, is a developmental pediatrician and author of numerous parenting books, including “How Children Thrive: The Practical Science of Raising Independent, Resilient, and Happy Kids” and “Mindful Parenting for ADHD.” Diane Paul, PhD, CCC-SLP, is the director of clinical issues in speech-language pathology for the American Speech-Language-Hearing Association (ASHA) and author of numerous books, including “Talking on the Go: Everyday Activities to Enhance Speech and Language Development.” Email them at pdnews@mdedge.com.
In this day and age, a new question should make its way to the top of the list for new parents and their pediatricians: How will the family approach the issue of household technology use – for their children as well as themselves?
Even the most vigilant among them will find much available guidance conflicting – and a good deal of it may feel oblivious to their day-to-day realities. This is especially true now, as many families face the daunting demands of pandemic parenting – juggling full-time jobs with childcare and distance learning.
While the American Academy of Pediatrics still specifies daily time limits by age (difficult for many families to achieve even in “normal” times), pediatricians and other child development experts now recognize that a host of factors should inform decisions about healthy screen use. There’s no one “magic number” for acceptable daily use, as not all screen time is the same (particularly during the pandemic) – and different children will experience the effects of technology usage differently.
The quality of content the child engages with; the degree of parental involvement; and the individual cognitive and behavioral considerations of a child are just some of the factors that should be considered. Given the complexities, it’s unfortunate that many parents will not have discussed screen use with their pediatrician or even their partner before their child first reaches for that glowing screen – and certainly not before they are using technology to multitask work, social connections, and day-to-day child rearing. Screen habits form early for both children and families.
An early well-visit priority
Pediatricians have an important role to play in helping families develop a more purposeful approach to household technology by providing them with trusted, evidence-based information on screens and the potential impact on children’s development. This is not information parents should receive when a child is 2 or 3 years of age. By then, toddlers are often already avid tablet users and parents may have come to rely on technology as a parenting aid.
Parents also need to know that, from birth, they can influence their child’s brain and communication development through undistracted time for talking, reading, singing, and interacting with their baby. Though the way children develop speech and language skills has not changed, the level of distraction posed by technology has grown immensely. It is much more difficult for parents to notice a baby’s subtle communication attempts – a coo or a smile, for instance, and respond accordingly – with a smartphone in hand. Rather than admonish parents for overusing their devices, we can focus them on what supports healthy child development instead.
By talking to parents earlier, pediatricians can help prevent premature or excessive exposure to technology – as well as encourage parents to dedicate “unplugged” times of day with their baby, such as during feeding time or before bedtime. By accenting the positive – educating parents about how they can encourage development and growth, how they can bond with their baby, and how they can establish a loving and nurturing relationship – pediatricians can motivate them towards simple steps that limit technology’s disruption of daily developmental opportunities. They can also help them lay a solid foundation for healthy screen time habits in the long term for their family.
The critical period for speech and language development is early
The impact of screen use on a child’s communication development is a significant concern. The critical time window for the development of speech, language, and social skills is between birth and 3 years. What happens then is the precursor for later reading and writing skills that are key to academic and vocational success.
A meta-analysis published in JAMA Pediatrics in July 2020 found that greater quantity of screen use was associated with poorer language skills – while screen-use onset at later ages was also associated with stronger child language skills. A November 2019 JAMA Pediatrics study using brain imaging in pre–school age children found an association between increased screen-based media use, compared with the AAP guidelines, and lower integrity of white matter tracts supporting language and emergent literacy skills. That study also used several language and literacy tests, finding that children with higher screen exposure had poorer expressive language and worse language processing speed. A 2017 study of 900 children between 18 and 24 months found that every 30-minute increase in daily screen time was linked to a 49% increased risk of expressive speech delay. And on the parental side, numerous studies have documented decreased verbal and nonverbal interactions initiated by parents when they are using a device.
Be tech wise with baby
AAP offers many resources in its Media and Children Communication Toolkit that serve as helpful starting points for conversations, including its family media use plan templates. However, more resources tailored to parents of newborns and very young children are needed.
One new option recently developed by the American Speech-Language-Hearing Association (ASHA) and the Children’s Screen Time Action Network is Be Tech Wise With Baby! Aimed at prospective and new parents, this simple handout, available for free in English and Spanish, is an easy takeaway from early well-child visits that pediatricians and pediatric nurses can distribute.
Pediatricians have a vital role to play championing healthy, balanced screen time use for children and adults – starting from baby’s first moments of life. By guiding new parents towards simple steps, such as carving out tech-free times of day and delaying introduction of screens, they can positively influence the screen-time habits of the next generation of connected kids.
Mark Bertin, MD, is a developmental pediatrician and author of numerous parenting books, including “How Children Thrive: The Practical Science of Raising Independent, Resilient, and Happy Kids” and “Mindful Parenting for ADHD.” Diane Paul, PhD, CCC-SLP, is the director of clinical issues in speech-language pathology for the American Speech-Language-Hearing Association (ASHA) and author of numerous books, including “Talking on the Go: Everyday Activities to Enhance Speech and Language Development.” Email them at pdnews@mdedge.com.
On being an elite
Regardless of who received the most electoral votes it is pretty clear that each candidate has millions of supporters, and that they are separated by only a few percentage points. I guess one could argue that so many people being able to express their opinions is healthy. However, from my side of the divide I have difficulty understanding how so many of my fellow citizens could arrive at an opinion so diametrically opposed to my own.

Since the 2016 election I have tried to read as many articles as I could find in search of an explanation for that outcome and continuing partisan support. I have never had much interest in political science because it always sounded like an oxymoron. But I am willing to listen to anyone who claims to understand how so many other citizens can see the world so differently from the way I do. It simply may be that for whatever reason one person, in this case one man, has such charismatic power that his supporters willingly abandon the moral skeleton on which their lives had been draped. Or is this us versus them primarily a chasm between the elites and the nonelites?
I don’t know much about you but the fact that you are reading this column means that, like me, you are an elite. Even if you are a woman of color and the daughter of immigrants you have taken advantage of what opportunities you have been offered, stayed in school long enough to adopt a reverence for the scientific method, and have a job that pays well because you have acquired some expertise.
Tom Nichols, a political scientist teaching at Harvard Extension School, says that “expertise is a very exclusionary idea because it’s supposed to be: Not everybody gets a vote on how to fly the plane” (Why isn’t the right more afraid of COVID-19? by Christina Pazzanese, Harvard Gazette, Oct 30, 2020) This exclusivity may in part explain the cultural trend that has eroded faith in experts in general, but particularly around issues such as climate change. Ironically, although science continues to be held in esteem in our culture, many scientists have become targets for those citizens who wish to attack authority figures.
How is it that you and I as pediatricians have avoided those attacks and the derogatory label as “so-called experts”?
You may live and practice in a community where many of your patients’ families don’t share your political views. But you have probably been successful at maintaining a trusting relationship with them in large part because you have cast yourself in the role of an adviser and not a dictator. And, although at times it has been difficult, you have been careful to avoid sharing your advice in a manner that sounds condescending. You have succeeded in functioning as an expert while carefully disguising yourself as a nonelite.
However, you are skating on thin ice if you venture into topics that run counter to your patients’ religious beliefs. Theda Skocpol, professor of government and psychology at Harvard University, Cambridge, Mass., has observed that studies have shown that while religious conservatives are aware of the science and don’t reject the finding, “they resent the use of experts as political authorities.” This may explain why all across this diverse country, our patients are eager for and accepting of our advice on all manners of health-related issues until we step into a swampy area that threatens their political views – such as vaccination or gun control.
With one misstep in the wrong direction, you can go from being a compassionate adviser to an elitist “so-called expert.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Regardless of who received the most electoral votes it is pretty clear that each candidate has millions of supporters, and that they are separated by only a few percentage points. I guess one could argue that so many people being able to express their opinions is healthy. However, from my side of the divide I have difficulty understanding how so many of my fellow citizens could arrive at an opinion so diametrically opposed to my own.
Since the 2016 election I have tried to read as many articles as I could find in search of an explanation for that outcome and continuing partisan support. I have never had much interest in political science because it always sounded like an oxymoron. But I am willing to listen to anyone who claims to understand how so many other citizens can see the world so differently from the way I do. It simply may be that for whatever reason one person, in this case one man, has such charismatic power that his supporters willingly abandon the moral skeleton on which their lives had been draped. Or is this us versus them primarily a chasm between the elites and the nonelites?
I don’t know much about you but the fact that you are reading this column means that, like me, you are an elite. Even if you are a woman of color and the daughter of immigrants you have taken advantage of what opportunities you have been offered, stayed in school long enough to adopt a reverence for the scientific method, and have a job that pays well because you have acquired some expertise.
Tom Nichols, a political scientist teaching at Harvard Extension School, says that “expertise is a very exclusionary idea because it’s supposed to be: Not everybody gets a vote on how to fly the plane” (Why isn’t the right more afraid of COVID-19? by Christina Pazzanese, Harvard Gazette, Oct 30, 2020) This exclusivity may in part explain the cultural trend that has eroded faith in experts in general, but particularly around issues such as climate change. Ironically, although science continues to be held in esteem in our culture, many scientists have become targets for those citizens who wish to attack authority figures.
How is it that you and I as pediatricians have avoided those attacks and the derogatory label as “so-called experts”?
You may live and practice in a community where many of your patients’ families don’t share your political views. But you have probably been successful at maintaining a trusting relationship with them in large part because you have cast yourself in the role of an adviser and not a dictator. And, although at times it has been difficult, you have been careful to avoid sharing your advice in a manner that sounds condescending. You have succeeded in functioning as an expert while carefully disguising yourself as a nonelite.
However, you are skating on thin ice if you venture into topics that run counter to your patients’ religious beliefs. Theda Skocpol, professor of government and psychology at Harvard University, Cambridge, Mass., has observed that studies have shown that while religious conservatives are aware of the science and don’t reject the finding, “they resent the use of experts as political authorities.” This may explain why all across this diverse country, our patients are eager for and accepting of our advice on all manners of health-related issues until we step into a swampy area that threatens their political views – such as vaccination or gun control.
With one misstep in the wrong direction, you can go from being a compassionate adviser to an elitist “so-called expert.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Regardless of who received the most electoral votes it is pretty clear that each candidate has millions of supporters, and that they are separated by only a few percentage points. I guess one could argue that so many people being able to express their opinions is healthy. However, from my side of the divide I have difficulty understanding how so many of my fellow citizens could arrive at an opinion so diametrically opposed to my own.
Since the 2016 election I have tried to read as many articles as I could find in search of an explanation for that outcome and continuing partisan support. I have never had much interest in political science because it always sounded like an oxymoron. But I am willing to listen to anyone who claims to understand how so many other citizens can see the world so differently from the way I do. It simply may be that for whatever reason one person, in this case one man, has such charismatic power that his supporters willingly abandon the moral skeleton on which their lives had been draped. Or is this us versus them primarily a chasm between the elites and the nonelites?
I don’t know much about you but the fact that you are reading this column means that, like me, you are an elite. Even if you are a woman of color and the daughter of immigrants you have taken advantage of what opportunities you have been offered, stayed in school long enough to adopt a reverence for the scientific method, and have a job that pays well because you have acquired some expertise.
Tom Nichols, a political scientist teaching at Harvard Extension School, says that “expertise is a very exclusionary idea because it’s supposed to be: Not everybody gets a vote on how to fly the plane” (Why isn’t the right more afraid of COVID-19? by Christina Pazzanese, Harvard Gazette, Oct 30, 2020) This exclusivity may in part explain the cultural trend that has eroded faith in experts in general, but particularly around issues such as climate change. Ironically, although science continues to be held in esteem in our culture, many scientists have become targets for those citizens who wish to attack authority figures.
How is it that you and I as pediatricians have avoided those attacks and the derogatory label as “so-called experts”?
You may live and practice in a community where many of your patients’ families don’t share your political views. But you have probably been successful at maintaining a trusting relationship with them in large part because you have cast yourself in the role of an adviser and not a dictator. And, although at times it has been difficult, you have been careful to avoid sharing your advice in a manner that sounds condescending. You have succeeded in functioning as an expert while carefully disguising yourself as a nonelite.
However, you are skating on thin ice if you venture into topics that run counter to your patients’ religious beliefs. Theda Skocpol, professor of government and psychology at Harvard University, Cambridge, Mass., has observed that studies have shown that while religious conservatives are aware of the science and don’t reject the finding, “they resent the use of experts as political authorities.” This may explain why all across this diverse country, our patients are eager for and accepting of our advice on all manners of health-related issues until we step into a swampy area that threatens their political views – such as vaccination or gun control.
With one misstep in the wrong direction, you can go from being a compassionate adviser to an elitist “so-called expert.”
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
COVID-19 vaccines and cancer patients: 4 things to know
Earlier this week, Medscape spoke with Nora Disis, MD, about vaccinating cancer patients. Disis is a medical oncologist and director of both the Institute of Translational Health Sciences and the Cancer Vaccine Institute, the University of Washington, Seattle, Washington. As editor-in-chief of JAMA Oncology, she has watched COVID-19 developments in the oncology community over the past year.
Here are a few themes that Disis said oncologists should be aware of as vaccines eventually begin reaching cancer patients.
We should expect cancer patients to respond to vaccines. Historically, some believed that cancer patients would be unable to mount an immune response to vaccines. Data on other viral vaccines have shown otherwise. For example, there has been a long history of studies of flu vaccination in cancer patients, and in general, those vaccines confer protection. Likewise for pneumococcal vaccine, which, generally speaking, cancer patients should receive.
Special cases may include hematologic malignancies in which the immune system has been destroyed and profound immunosuppression occurs. Data on immunization during this immunosuppressed period are scarce, but what data are available suggest that once cancer patients are through this immunosuppressed period, they can be vaccinated successfully.
The type of vaccine will probably be important for cancer patients. Currently, there are 61 coronavirus vaccines in human clinical trials, and 17 have reached the final stages of testing. At least 85 preclinical vaccines are under active investigation in animals.
Both the Pfizer-BioNTech and Moderna COVID vaccines are mRNA type. There are many other types, including protein-based vaccines, viral vector vaccines based on adenoviruses, and inactivated or attenuated coronavirus vaccines.
The latter vaccines, particularly attenuated live virus vaccines, may not be a good choice for cancer patients. Especially in those with rapidly progressing disease or on chemotherapy, attenuated live viruses may cause a low-grade infection.
Incidentally, the technology used in the genetic, or mRNA, vaccines developed by both Pfizer-BioNTech and Moderna was initially developed for fighting cancer, and studies have shown that patients can generate immune responses to cancer-associated proteins with this type of vaccine.
These genetic vaccines could turn out to be the most effective for cancer patients, especially those with solid tumors.
Our understanding is very limited right now. Neither the Pfizer-BioNTech nor the Moderna early data discuss cancer patients. Two of the most important questions for cancer patients are dosing and booster scheduling. Potential defects in lymphocyte function among cancer patients may require unique initial dosing and booster schedules. In terms of timing, it is unclear how active therapy might affect a patient’s immune response to vaccination and whether vaccines should be timed with therapy cycles.
Vaccine access may depend on whether cancer patients are viewed as a vulnerable population. Those at higher risk for severe COVID-19 clearly have a greater need for vaccination. While there are data suggesting that cancer patients are at higher risk, they are a bit murky, in part because cancer patients are a heterogeneous group. For example, there are data suggesting that lung and blood cancer patients fare worse. There is also a suggestion that, like in the general population, COVID risk in cancer patients remains driven by comorbidities.
It is likely, then, that personalized risk factors such as type of cancer therapy, site of disease, and comorbidities will shape individual choices about vaccination among cancer patients.
A version of this article first appeared on Medscape.com.
Earlier this week, Medscape spoke with Nora Disis, MD, about vaccinating cancer patients. Disis is a medical oncologist and director of both the Institute of Translational Health Sciences and the Cancer Vaccine Institute, the University of Washington, Seattle, Washington. As editor-in-chief of JAMA Oncology, she has watched COVID-19 developments in the oncology community over the past year.
Here are a few themes that Disis said oncologists should be aware of as vaccines eventually begin reaching cancer patients.
We should expect cancer patients to respond to vaccines. Historically, some believed that cancer patients would be unable to mount an immune response to vaccines. Data on other viral vaccines have shown otherwise. For example, there has been a long history of studies of flu vaccination in cancer patients, and in general, those vaccines confer protection. Likewise for pneumococcal vaccine, which, generally speaking, cancer patients should receive.
Special cases may include hematologic malignancies in which the immune system has been destroyed and profound immunosuppression occurs. Data on immunization during this immunosuppressed period are scarce, but what data are available suggest that once cancer patients are through this immunosuppressed period, they can be vaccinated successfully.
The type of vaccine will probably be important for cancer patients. Currently, there are 61 coronavirus vaccines in human clinical trials, and 17 have reached the final stages of testing. At least 85 preclinical vaccines are under active investigation in animals.
Both the Pfizer-BioNTech and Moderna COVID vaccines are mRNA type. There are many other types, including protein-based vaccines, viral vector vaccines based on adenoviruses, and inactivated or attenuated coronavirus vaccines.
The latter vaccines, particularly attenuated live virus vaccines, may not be a good choice for cancer patients. Especially in those with rapidly progressing disease or on chemotherapy, attenuated live viruses may cause a low-grade infection.
Incidentally, the technology used in the genetic, or mRNA, vaccines developed by both Pfizer-BioNTech and Moderna was initially developed for fighting cancer, and studies have shown that patients can generate immune responses to cancer-associated proteins with this type of vaccine.
These genetic vaccines could turn out to be the most effective for cancer patients, especially those with solid tumors.
Our understanding is very limited right now. Neither the Pfizer-BioNTech nor the Moderna early data discuss cancer patients. Two of the most important questions for cancer patients are dosing and booster scheduling. Potential defects in lymphocyte function among cancer patients may require unique initial dosing and booster schedules. In terms of timing, it is unclear how active therapy might affect a patient’s immune response to vaccination and whether vaccines should be timed with therapy cycles.
Vaccine access may depend on whether cancer patients are viewed as a vulnerable population. Those at higher risk for severe COVID-19 clearly have a greater need for vaccination. While there are data suggesting that cancer patients are at higher risk, they are a bit murky, in part because cancer patients are a heterogeneous group. For example, there are data suggesting that lung and blood cancer patients fare worse. There is also a suggestion that, like in the general population, COVID risk in cancer patients remains driven by comorbidities.
It is likely, then, that personalized risk factors such as type of cancer therapy, site of disease, and comorbidities will shape individual choices about vaccination among cancer patients.
A version of this article first appeared on Medscape.com.
Earlier this week, Medscape spoke with Nora Disis, MD, about vaccinating cancer patients. Disis is a medical oncologist and director of both the Institute of Translational Health Sciences and the Cancer Vaccine Institute, the University of Washington, Seattle, Washington. As editor-in-chief of JAMA Oncology, she has watched COVID-19 developments in the oncology community over the past year.
Here are a few themes that Disis said oncologists should be aware of as vaccines eventually begin reaching cancer patients.
We should expect cancer patients to respond to vaccines. Historically, some believed that cancer patients would be unable to mount an immune response to vaccines. Data on other viral vaccines have shown otherwise. For example, there has been a long history of studies of flu vaccination in cancer patients, and in general, those vaccines confer protection. Likewise for pneumococcal vaccine, which, generally speaking, cancer patients should receive.
Special cases may include hematologic malignancies in which the immune system has been destroyed and profound immunosuppression occurs. Data on immunization during this immunosuppressed period are scarce, but what data are available suggest that once cancer patients are through this immunosuppressed period, they can be vaccinated successfully.
The type of vaccine will probably be important for cancer patients. Currently, there are 61 coronavirus vaccines in human clinical trials, and 17 have reached the final stages of testing. At least 85 preclinical vaccines are under active investigation in animals.
Both the Pfizer-BioNTech and Moderna COVID vaccines are mRNA type. There are many other types, including protein-based vaccines, viral vector vaccines based on adenoviruses, and inactivated or attenuated coronavirus vaccines.
The latter vaccines, particularly attenuated live virus vaccines, may not be a good choice for cancer patients. Especially in those with rapidly progressing disease or on chemotherapy, attenuated live viruses may cause a low-grade infection.
Incidentally, the technology used in the genetic, or mRNA, vaccines developed by both Pfizer-BioNTech and Moderna was initially developed for fighting cancer, and studies have shown that patients can generate immune responses to cancer-associated proteins with this type of vaccine.
These genetic vaccines could turn out to be the most effective for cancer patients, especially those with solid tumors.
Our understanding is very limited right now. Neither the Pfizer-BioNTech nor the Moderna early data discuss cancer patients. Two of the most important questions for cancer patients are dosing and booster scheduling. Potential defects in lymphocyte function among cancer patients may require unique initial dosing and booster schedules. In terms of timing, it is unclear how active therapy might affect a patient’s immune response to vaccination and whether vaccines should be timed with therapy cycles.
Vaccine access may depend on whether cancer patients are viewed as a vulnerable population. Those at higher risk for severe COVID-19 clearly have a greater need for vaccination. While there are data suggesting that cancer patients are at higher risk, they are a bit murky, in part because cancer patients are a heterogeneous group. For example, there are data suggesting that lung and blood cancer patients fare worse. There is also a suggestion that, like in the general population, COVID risk in cancer patients remains driven by comorbidities.
It is likely, then, that personalized risk factors such as type of cancer therapy, site of disease, and comorbidities will shape individual choices about vaccination among cancer patients.
A version of this article first appeared on Medscape.com.
Distinguishing between joy and pleasure during the pandemic
You can now buy vegan eggnog, made from almond milk. The fact that someone created this wasn’t a surprise – plant milks are taking over. That it gave me such pleasure was. It’s rich, and if you love eggnog, like all normal people, it’s amazingly satisfying when mixed in a Nespresso latte swirled creamy white and brown. It seems some things, like Netflix’s The Crown, my Peloton spin classes, long Sunday walks on the beach, and the best mushroom risotto I ever made were still pleasurable this year, despite all. I’d daresay, there was joy even in the time of COVID.
.
Pleasure is pretty constant. It pops up even in the worst times. It seems, there’s plenty to be found even now. Unless, perhaps it’s just me. The label my mother pinned on me as a boy has remained into adulthood: “Easy to please.” There’s hardly a movie I’ve seen that I didn’t like. I’m quite comfortable in the middle seat. I thought the EPIC updates this year were nice. I’ve liked the vast majority of pizzas I’ve ever eaten – even those contaminated with Truffle salt. Easy to please is a gift, not something I’ve acquired through hours of meditation or aesthetic fasts. But surely pleasure isn’t the same as joy. No one has tears of pleasure. (Not to mention, pleasure as a verb has obvious NSFW connotations; not true of joy).
No, joy is waaay bigger. Joy is shared. Joy is to the whole world. Joy is what happens when you have a baby. Pleasure is what happens when you remembered to put a burp cloth in the car. Pleasure is when three patients in a row take merely 5 minutes each. Joy is when an itchy patient is cured.
2020 was one of the most miserable years in the last century. We didn’t expect it, but we ought to have. I mean really, how many plagues have we endured? How many times has inequality led to social unrest? Many times. We, by luck and dint of hard work, have always managed to get through. Although suffering would surely have been greater during those times of sickness and loss, I don’t believe joy would have been less. Indeed, maybe it is those difficulties and that suffering that allows us to feel joy in the first place. It is only once you summit that you experience joy. The run-up is just pain.
It is no coincidence that it is now during this cold, dark, difficult part of the year that we wish joy. We’ve made it. We light the darkness with candles to joyously celebrate Mawlid, Diwali, then Hanukkah and Christmas. Had malls been open now, you’d hear amongst the din of ringing bells Rejoice! Rejoice! O Emmanuel! You’d sing along, “Joy to the world, now we sing, let the Angel voices ring.” Joy: A pleasure so great and so deserved, it is shared by all. It is good news, hope, gratitude.

A joy shared amongst us all is also coming. Through the wrenching pain of watching patients suffocate, fogged shields, and bleached masks, through canceled Thanksgivings, through weekends spent in the OR on the backlog of patients, after months spent sitting in empty clinics, though the long, orange-cone-winding lines of testing, at last, at last a vaccine is here to light the darkness.
Let the sea resound, and everything in it,
Let the rivers clap their hands,
let the mountains sing together for joy.
Joy to the world.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
You can now buy vegan eggnog, made from almond milk. The fact that someone created this wasn’t a surprise – plant milks are taking over. That it gave me such pleasure was. It’s rich, and if you love eggnog, like all normal people, it’s amazingly satisfying when mixed in a Nespresso latte swirled creamy white and brown. It seems some things, like Netflix’s The Crown, my Peloton spin classes, long Sunday walks on the beach, and the best mushroom risotto I ever made were still pleasurable this year, despite all. I’d daresay, there was joy even in the time of COVID.
.
Pleasure is pretty constant. It pops up even in the worst times. It seems, there’s plenty to be found even now. Unless, perhaps it’s just me. The label my mother pinned on me as a boy has remained into adulthood: “Easy to please.” There’s hardly a movie I’ve seen that I didn’t like. I’m quite comfortable in the middle seat. I thought the EPIC updates this year were nice. I’ve liked the vast majority of pizzas I’ve ever eaten – even those contaminated with Truffle salt. Easy to please is a gift, not something I’ve acquired through hours of meditation or aesthetic fasts. But surely pleasure isn’t the same as joy. No one has tears of pleasure. (Not to mention, pleasure as a verb has obvious NSFW connotations; not true of joy).
No, joy is waaay bigger. Joy is shared. Joy is to the whole world. Joy is what happens when you have a baby. Pleasure is what happens when you remembered to put a burp cloth in the car. Pleasure is when three patients in a row take merely 5 minutes each. Joy is when an itchy patient is cured.
2020 was one of the most miserable years in the last century. We didn’t expect it, but we ought to have. I mean really, how many plagues have we endured? How many times has inequality led to social unrest? Many times. We, by luck and dint of hard work, have always managed to get through. Although suffering would surely have been greater during those times of sickness and loss, I don’t believe joy would have been less. Indeed, maybe it is those difficulties and that suffering that allows us to feel joy in the first place. It is only once you summit that you experience joy. The run-up is just pain.
It is no coincidence that it is now during this cold, dark, difficult part of the year that we wish joy. We’ve made it. We light the darkness with candles to joyously celebrate Mawlid, Diwali, then Hanukkah and Christmas. Had malls been open now, you’d hear amongst the din of ringing bells Rejoice! Rejoice! O Emmanuel! You’d sing along, “Joy to the world, now we sing, let the Angel voices ring.” Joy: A pleasure so great and so deserved, it is shared by all. It is good news, hope, gratitude.
A joy shared amongst us all is also coming. Through the wrenching pain of watching patients suffocate, fogged shields, and bleached masks, through canceled Thanksgivings, through weekends spent in the OR on the backlog of patients, after months spent sitting in empty clinics, though the long, orange-cone-winding lines of testing, at last, at last a vaccine is here to light the darkness.
Let the sea resound, and everything in it,
Let the rivers clap their hands,
let the mountains sing together for joy.
Joy to the world.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
You can now buy vegan eggnog, made from almond milk. The fact that someone created this wasn’t a surprise – plant milks are taking over. That it gave me such pleasure was. It’s rich, and if you love eggnog, like all normal people, it’s amazingly satisfying when mixed in a Nespresso latte swirled creamy white and brown. It seems some things, like Netflix’s The Crown, my Peloton spin classes, long Sunday walks on the beach, and the best mushroom risotto I ever made were still pleasurable this year, despite all. I’d daresay, there was joy even in the time of COVID.
.
Pleasure is pretty constant. It pops up even in the worst times. It seems, there’s plenty to be found even now. Unless, perhaps it’s just me. The label my mother pinned on me as a boy has remained into adulthood: “Easy to please.” There’s hardly a movie I’ve seen that I didn’t like. I’m quite comfortable in the middle seat. I thought the EPIC updates this year were nice. I’ve liked the vast majority of pizzas I’ve ever eaten – even those contaminated with Truffle salt. Easy to please is a gift, not something I’ve acquired through hours of meditation or aesthetic fasts. But surely pleasure isn’t the same as joy. No one has tears of pleasure. (Not to mention, pleasure as a verb has obvious NSFW connotations; not true of joy).
No, joy is waaay bigger. Joy is shared. Joy is to the whole world. Joy is what happens when you have a baby. Pleasure is what happens when you remembered to put a burp cloth in the car. Pleasure is when three patients in a row take merely 5 minutes each. Joy is when an itchy patient is cured.
2020 was one of the most miserable years in the last century. We didn’t expect it, but we ought to have. I mean really, how many plagues have we endured? How many times has inequality led to social unrest? Many times. We, by luck and dint of hard work, have always managed to get through. Although suffering would surely have been greater during those times of sickness and loss, I don’t believe joy would have been less. Indeed, maybe it is those difficulties and that suffering that allows us to feel joy in the first place. It is only once you summit that you experience joy. The run-up is just pain.
It is no coincidence that it is now during this cold, dark, difficult part of the year that we wish joy. We’ve made it. We light the darkness with candles to joyously celebrate Mawlid, Diwali, then Hanukkah and Christmas. Had malls been open now, you’d hear amongst the din of ringing bells Rejoice! Rejoice! O Emmanuel! You’d sing along, “Joy to the world, now we sing, let the Angel voices ring.” Joy: A pleasure so great and so deserved, it is shared by all. It is good news, hope, gratitude.
A joy shared amongst us all is also coming. Through the wrenching pain of watching patients suffocate, fogged shields, and bleached masks, through canceled Thanksgivings, through weekends spent in the OR on the backlog of patients, after months spent sitting in empty clinics, though the long, orange-cone-winding lines of testing, at last, at last a vaccine is here to light the darkness.
Let the sea resound, and everything in it,
Let the rivers clap their hands,
let the mountains sing together for joy.
Joy to the world.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Can patients record office visits?
Recently I posted a simple question on several social media pages and internet blogs populated exclusively by board-certified dermatologists and dermatologic surgeons: How would you respond to a patient asking (or demanding) to record all or part of their office visit? (Or, if you have encountered such a situation, how did you respond?)

The question was simple, but the answers were somewhat complicated.
First, I noticed a fundamental misunderstanding of applicable laws: Many practitioners apparently believe that taping or recording a private conversation is per se illegal. Perhaps they are conflating with wiretapping laws, which don’t apply in this situation. HIPAA laws don’t apply either, because the patient, by definition, is waiving the right to privacy by initiating the recording in the first place.
In fact, and only 11 states (California, Florida, Illinois, Maryland, Massachusetts, Michigan, Montana, New Hampshire, Oregon, Pennsylvania, and Washington) require the consent of both parties. All other states and territories actually allow it even if one party has not given consent. And some patients don’t ask permission at all; they just do it.
Another misconception was the perceived frequency of such situations. Recordings of conversations in the doctor’s office are by no means rare. A 2014 survey in the United Kingdom revealed that 15% of the public had secretly recorded a clinic visit, and a further 11% were aware of someone else doing the same, a topic discussed by a Dartmouth group in the Aug. 8, 2017, issue of JAMA.
In general, younger respondents to my (admittedly unscientific) informal survey tended to be less receptive to being recorded. “I do not allow recordings by patients because I can’t control how they may be used later and it’s just creepy,” wrote one. “It just seems a strange way to begin a trusting, transparent patient/doctor relationship … this is not Instagram.”
“I will sometimes let them take a photo of a specimen or a defect but I don’t allow recording,” wrote another. “Same reasons; creepy and out of my control. I worry about it happening surreptitiously, but what can you do?”
You can proactively prohibit all office recordings by posting a “no recording” sign in your waiting room in the name of confidentiality and privacy. Should a patient initiate a covert recording anyway, you have the option of terminating the visit with a warning that a repeat attempt will result in discharge. If you practice in one of the 39 one-party states, the recording would still be admissible, but your notice gives your attorney an argument – specifically, that the patient made the recording after being expressly directed not to do so – if anyone ever tries to use the recording against you, or without your permission.
Older, more experienced practitioners in the survey tended to be more sanguine about recordings. “I have allowed patients to record all or parts of the visit,” wrote one. “I even allowed a patient to film a [liposuction] procedure. My decision … was that the patient might think I had something to hide, which I [did not].”
Another reported, “I have no problem with patients or family recording office visits or procedures. When someone is recording a procedure, I have no problem ignoring them.”
“We don’t have anything to hide, after all,” affirmed another. “In the era of telemedicine, many things can be recorded, even without permission.”
Several other veteran practitioners summarized my own philosophy on the subject: Patients have a right to record visits in my state (New Jersey), whether I like it or not, so I simply assume I’m being recorded during every visit, and conduct myself accordingly.
Risk managers and malpractice carriers are divided on recordings. At one neurology clinic in Arizona, patients are routinely offered videos of their visits, and clinicians who participate in these recordings receive a 10% reduction in the cost of their medical defense and extra liability coverage. There are clear advantages to having a permanent record of a doctor’s professional opinion. Other carriers are not as supportive, discouraging their insureds from allowing recordings to be made.
In the end, like it or not, recordings are here to stay, and the omnipresence of modern communications devices such as smartphones, tablets, etc., will only increase their prevalence. My advice: Familiarize yourself with the laws in your state, and never say anything during an office visit that you would not stand behind, if it ever turns out to have been recorded.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
Recently I posted a simple question on several social media pages and internet blogs populated exclusively by board-certified dermatologists and dermatologic surgeons: How would you respond to a patient asking (or demanding) to record all or part of their office visit? (Or, if you have encountered such a situation, how did you respond?)
The question was simple, but the answers were somewhat complicated.
First, I noticed a fundamental misunderstanding of applicable laws: Many practitioners apparently believe that taping or recording a private conversation is per se illegal. Perhaps they are conflating with wiretapping laws, which don’t apply in this situation. HIPAA laws don’t apply either, because the patient, by definition, is waiving the right to privacy by initiating the recording in the first place.
In fact, and only 11 states (California, Florida, Illinois, Maryland, Massachusetts, Michigan, Montana, New Hampshire, Oregon, Pennsylvania, and Washington) require the consent of both parties. All other states and territories actually allow it even if one party has not given consent. And some patients don’t ask permission at all; they just do it.
Another misconception was the perceived frequency of such situations. Recordings of conversations in the doctor’s office are by no means rare. A 2014 survey in the United Kingdom revealed that 15% of the public had secretly recorded a clinic visit, and a further 11% were aware of someone else doing the same, a topic discussed by a Dartmouth group in the Aug. 8, 2017, issue of JAMA.
In general, younger respondents to my (admittedly unscientific) informal survey tended to be less receptive to being recorded. “I do not allow recordings by patients because I can’t control how they may be used later and it’s just creepy,” wrote one. “It just seems a strange way to begin a trusting, transparent patient/doctor relationship … this is not Instagram.”
“I will sometimes let them take a photo of a specimen or a defect but I don’t allow recording,” wrote another. “Same reasons; creepy and out of my control. I worry about it happening surreptitiously, but what can you do?”
You can proactively prohibit all office recordings by posting a “no recording” sign in your waiting room in the name of confidentiality and privacy. Should a patient initiate a covert recording anyway, you have the option of terminating the visit with a warning that a repeat attempt will result in discharge. If you practice in one of the 39 one-party states, the recording would still be admissible, but your notice gives your attorney an argument – specifically, that the patient made the recording after being expressly directed not to do so – if anyone ever tries to use the recording against you, or without your permission.
Older, more experienced practitioners in the survey tended to be more sanguine about recordings. “I have allowed patients to record all or parts of the visit,” wrote one. “I even allowed a patient to film a [liposuction] procedure. My decision … was that the patient might think I had something to hide, which I [did not].”
Another reported, “I have no problem with patients or family recording office visits or procedures. When someone is recording a procedure, I have no problem ignoring them.”
“We don’t have anything to hide, after all,” affirmed another. “In the era of telemedicine, many things can be recorded, even without permission.”
Several other veteran practitioners summarized my own philosophy on the subject: Patients have a right to record visits in my state (New Jersey), whether I like it or not, so I simply assume I’m being recorded during every visit, and conduct myself accordingly.
Risk managers and malpractice carriers are divided on recordings. At one neurology clinic in Arizona, patients are routinely offered videos of their visits, and clinicians who participate in these recordings receive a 10% reduction in the cost of their medical defense and extra liability coverage. There are clear advantages to having a permanent record of a doctor’s professional opinion. Other carriers are not as supportive, discouraging their insureds from allowing recordings to be made.
In the end, like it or not, recordings are here to stay, and the omnipresence of modern communications devices such as smartphones, tablets, etc., will only increase their prevalence. My advice: Familiarize yourself with the laws in your state, and never say anything during an office visit that you would not stand behind, if it ever turns out to have been recorded.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.
Recently I posted a simple question on several social media pages and internet blogs populated exclusively by board-certified dermatologists and dermatologic surgeons: How would you respond to a patient asking (or demanding) to record all or part of their office visit? (Or, if you have encountered such a situation, how did you respond?)
The question was simple, but the answers were somewhat complicated.
First, I noticed a fundamental misunderstanding of applicable laws: Many practitioners apparently believe that taping or recording a private conversation is per se illegal. Perhaps they are conflating with wiretapping laws, which don’t apply in this situation. HIPAA laws don’t apply either, because the patient, by definition, is waiving the right to privacy by initiating the recording in the first place.
In fact, and only 11 states (California, Florida, Illinois, Maryland, Massachusetts, Michigan, Montana, New Hampshire, Oregon, Pennsylvania, and Washington) require the consent of both parties. All other states and territories actually allow it even if one party has not given consent. And some patients don’t ask permission at all; they just do it.
Another misconception was the perceived frequency of such situations. Recordings of conversations in the doctor’s office are by no means rare. A 2014 survey in the United Kingdom revealed that 15% of the public had secretly recorded a clinic visit, and a further 11% were aware of someone else doing the same, a topic discussed by a Dartmouth group in the Aug. 8, 2017, issue of JAMA.
In general, younger respondents to my (admittedly unscientific) informal survey tended to be less receptive to being recorded. “I do not allow recordings by patients because I can’t control how they may be used later and it’s just creepy,” wrote one. “It just seems a strange way to begin a trusting, transparent patient/doctor relationship … this is not Instagram.”
“I will sometimes let them take a photo of a specimen or a defect but I don’t allow recording,” wrote another. “Same reasons; creepy and out of my control. I worry about it happening surreptitiously, but what can you do?”
You can proactively prohibit all office recordings by posting a “no recording” sign in your waiting room in the name of confidentiality and privacy. Should a patient initiate a covert recording anyway, you have the option of terminating the visit with a warning that a repeat attempt will result in discharge. If you practice in one of the 39 one-party states, the recording would still be admissible, but your notice gives your attorney an argument – specifically, that the patient made the recording after being expressly directed not to do so – if anyone ever tries to use the recording against you, or without your permission.
Older, more experienced practitioners in the survey tended to be more sanguine about recordings. “I have allowed patients to record all or parts of the visit,” wrote one. “I even allowed a patient to film a [liposuction] procedure. My decision … was that the patient might think I had something to hide, which I [did not].”
Another reported, “I have no problem with patients or family recording office visits or procedures. When someone is recording a procedure, I have no problem ignoring them.”
“We don’t have anything to hide, after all,” affirmed another. “In the era of telemedicine, many things can be recorded, even without permission.”
Several other veteran practitioners summarized my own philosophy on the subject: Patients have a right to record visits in my state (New Jersey), whether I like it or not, so I simply assume I’m being recorded during every visit, and conduct myself accordingly.
Risk managers and malpractice carriers are divided on recordings. At one neurology clinic in Arizona, patients are routinely offered videos of their visits, and clinicians who participate in these recordings receive a 10% reduction in the cost of their medical defense and extra liability coverage. There are clear advantages to having a permanent record of a doctor’s professional opinion. Other carriers are not as supportive, discouraging their insureds from allowing recordings to be made.
In the end, like it or not, recordings are here to stay, and the omnipresence of modern communications devices such as smartphones, tablets, etc., will only increase their prevalence. My advice: Familiarize yourself with the laws in your state, and never say anything during an office visit that you would not stand behind, if it ever turns out to have been recorded.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a longtime monthly columnist for Dermatology News. Write to him at dermnews@mdedge.com.

Six big changes coming for office-visit coding
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to gtwachtman@mdedge.com.
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
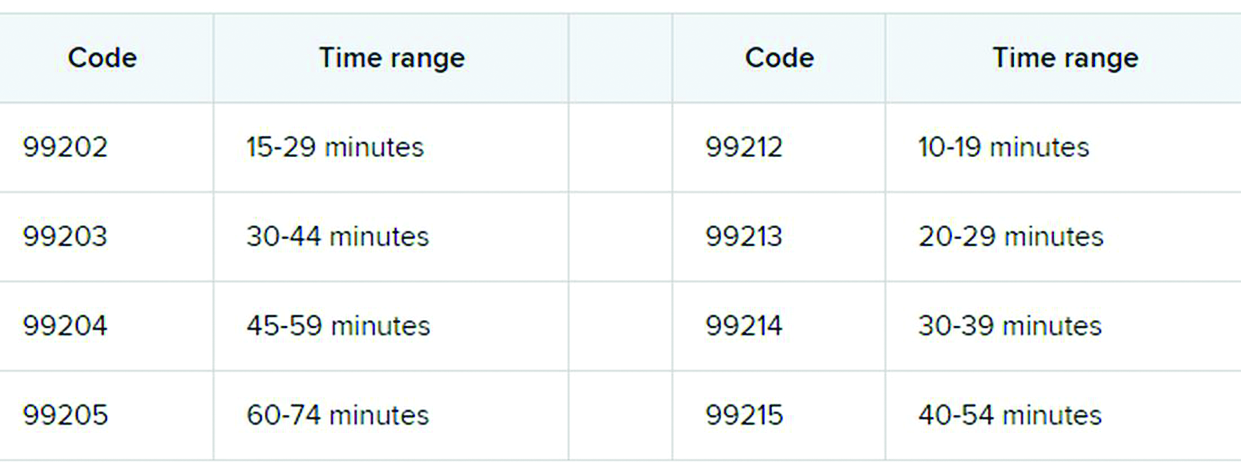
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to gtwachtman@mdedge.com.
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to gtwachtman@mdedge.com.
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Etonogestrel implants may be bent, fractured by trauma or during sports
In 2017, Global Pediatric Health published a case report series associated with the use of long-acting reversible contraceptives, specifically the etonogestrel implant.
In November 2020, the makers of the etonogestrel implant (Merck) recommended a change in practice with the release of a notice to health care providers certified in the training of this product. This mass marketing blast included an updated warning and cautions for prescribers as well as patient information on the potential risks of migration, fracture, and bent devices attributable to trauma or sports. “Broken or Bent Implant (Section 5.16). The addition of the following underlined language: “There have been reports of broken or bent implants, which may be related to external forces (e.g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm.”
Clearly the etonogestrel subdermal hormonal implant is an effective form of contraception and particularly beneficial in nonadherent sexually active teens who struggle to remember oral contraceptives. But it is important to be aware of this alert. Little is known about the type of trauma or rate of external force required to cause migration, fracture, or bend implants. This update requires adequate counseling of potential risks and complications of the etonogestrel implant, including the risk of migration, fracture, or bent devices specifically in the event of contact sports and trauma.
Ms. Thew is medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She had no relevant financial disclosures. Email Ms. Thew at pdnews@mdedge.com.
In 2017, Global Pediatric Health published a case report series associated with the use of long-acting reversible contraceptives, specifically the etonogestrel implant.
In November 2020, the makers of the etonogestrel implant (Merck) recommended a change in practice with the release of a notice to health care providers certified in the training of this product. This mass marketing blast included an updated warning and cautions for prescribers as well as patient information on the potential risks of migration, fracture, and bent devices attributable to trauma or sports. “Broken or Bent Implant (Section 5.16). The addition of the following underlined language: “There have been reports of broken or bent implants, which may be related to external forces (e.g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm.”
Clearly the etonogestrel subdermal hormonal implant is an effective form of contraception and particularly beneficial in nonadherent sexually active teens who struggle to remember oral contraceptives. But it is important to be aware of this alert. Little is known about the type of trauma or rate of external force required to cause migration, fracture, or bend implants. This update requires adequate counseling of potential risks and complications of the etonogestrel implant, including the risk of migration, fracture, or bent devices specifically in the event of contact sports and trauma.
Ms. Thew is medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She had no relevant financial disclosures. Email Ms. Thew at pdnews@mdedge.com.
In 2017, Global Pediatric Health published a case report series associated with the use of long-acting reversible contraceptives, specifically the etonogestrel implant.
In November 2020, the makers of the etonogestrel implant (Merck) recommended a change in practice with the release of a notice to health care providers certified in the training of this product. This mass marketing blast included an updated warning and cautions for prescribers as well as patient information on the potential risks of migration, fracture, and bent devices attributable to trauma or sports. “Broken or Bent Implant (Section 5.16). The addition of the following underlined language: “There have been reports of broken or bent implants, which may be related to external forces (e.g., manipulation of the implant or contact sports) while in the patient’s arm. There have also been reports of migration of a broken implant fragment within the arm.”
Clearly the etonogestrel subdermal hormonal implant is an effective form of contraception and particularly beneficial in nonadherent sexually active teens who struggle to remember oral contraceptives. But it is important to be aware of this alert. Little is known about the type of trauma or rate of external force required to cause migration, fracture, or bend implants. This update requires adequate counseling of potential risks and complications of the etonogestrel implant, including the risk of migration, fracture, or bent devices specifically in the event of contact sports and trauma.
Ms. Thew is medical director of the department of adolescent medicine at Children’s Wisconsin in Milwaukee. She is a member of the Pediatric News editorial advisory board. She had no relevant financial disclosures. Email Ms. Thew at pdnews@mdedge.com.
To vape or not to vape: Is that really a question?
All pediatricians are relieved that the rates of children smoking cigarettes has dropped steadily since 2011. This decline seems to be associated with education on the dangers of cigarettes and fewer parents smoking. Perhaps less modeling of cigarette use in movies (although it increased again from 2010 to 2019) and lawsuits against advertisements targeting children also has helped.

“Whew,” we may have said, “we can relax our efforts to convince children to avoid smoking.” But, as is commonly true in medicine, the next threat was right around the corner – in this case vaping or e-cigarettes, also called vapes, e-hookahs, vape pens, tank systems, mods, and electronic nicotine delivery systems. And the size of the problem is huge – over 20% of high school students report using e-cigarettes – and immediate, as vaping can kill in the short term as well as causing long-term harm.
“E-cigarette, or vaping, product use–associated Lung Injury” – EVALI for short – has killed 68 vapers and hospitalized thousands. EVALI is thought to be caused by a vitamin E acetate additive used when vaping marijuana, particularly from informal sources like friends, family, or in-person or online dealers.
Vaping increases the risk of severe COVID-19 disease
While EVALI deaths dropped in months after being explained, the COVID-19 epidemic is now a much greater threat to vapers. Vaping increases risk of severe COVID-19 disease because of its immediate paralysis of lung cilia. Sharing vape devices and touching one’s lips while using also increase the risk of virus transmission. Vaping and smoking increase the number of ACE2 receptors to which the SARS-CoV-2 virus attaches causing the characteristic cell damage, and suppresses macrophages and neutrophils, resulting in more smokers testing positive, being twice as likely to develop a severe illness and get hospitalized because of pneumonia from COVID-19, and being less likely to recover. Unfortunately, addressing this new threat to the immediate and long-term health of our patients appears to be more complicated than for addressing smoking tobacco. First of all, vaping is much more difficult to detect than smelly cigarettes sending smoke signals from behind the garage or in the school bathrooms. Many, if not most, adults do not recognize the vaping devices when they see them, as many are tiny and some look like computer thumb drives. The aerosol emitted when in use, while containing dangerous toxins, has less odor than tobacco smoke. Vaping equipment and ads have been designed to attract youth, including linking them to sports and music events. Vaping has been advertised as a way to wean off nicotine addiction, a claim that has some scientific evidence in adults, but at a lower dose of nicotine. Warning children about the dangers of marijuana vaping has been made less credible by the rapid expansion of legalization of marijuana around the United States, eliciting “I told you it was fine” reactions from youth. And the person vaping does not know what or how much of the psychoactive components are being delivered into their bodies. One Juul pod, for example, has the equivalent in nicotine of an entire pack of 20 cigarettes. They are highly addictive, especially to the developing brain, such that youth who vape are more likely to become addicted and to smoke cigarettes in the future.
Help from federal regulation has been weak
While all 50 states ban sales to youth, adults can still buy. Food and Drug Administration limitations on kid-friendly ads, and use of sweet, fruity, and mint flavorings that are most preferred by children, apply only to new producers. The FDA does not yet regulate content of vaping solutions.

So we pediatricians are on the front line for this new threat to prevent vaping or convince youth to cut down or quit. The first step in addressing vaping is being knowledgeable about its many known and emerging health risks. It may seem obvious that the dangers of vaping microscopic particles depends on the contents. Water vapor alone is not dangerous; in fact, we prescribe it in nebulizers. Unfortunately, the contents of different vaping products vary and are not well defined in different vape products. The process of using an electric current to vaporize a substance can make it more toxic than the precursor, and teens have little idea about the substances they are inhaling. The psychoactive components vary from nicotine to tetrahydrocannabinol in varying amounts. These have the well known effects of stimulation or a high, but also the potential adverse effects of poor concentration, agitation, and even psychosis. Most e-cigarettes contain nicotine, which is highly addictive and can harm adolescent brain development, which continues into the early- to mid-20s. About two-thirds of Juul users aged 15-24 years did not know that it always contains nicotine, as do 99% of all vape solutions (Centers for Disease Control and Prevention, 2020). Earlier use of nicotine is more highly associated with later addiction to tobacco products that cause lung damage, acid reflux, insulin resistance, harm to the testes, harm to fetuses, cancer, and heart disease.
E-cigarette aerosols also contain dozens of other harmful substances besides nicotine ranging from acetone, propylene glycol, and metals to formaldehyde and ethyl benzene. These same chemicals are part of familiar toxic substances such as antifreeze, paint thinner, and pesticides. These cause ear, eye and throat irritation, and impairments in the cardiovascular system reducing athletic ability – at the least. Some flavorings in vape fluids also are toxic. Even the residual left on furniture and floors is harmful to those coming in contact, including pets.
How to encourage teens not to vaping
Trying to scare youth about health hazards is not generally effective in stopping risk behaviors since adolescence is a time of perceived singularity (it does not apply to me) and even a sense of immortality. Teens also see peers who vape as being unaffected and decide on using based on this small personal sample instead of valid statistics.
But teens do pay some attention to peer models or influencers saying why they do not use. One source of such testimony you can refer to is videos of inspiring athletes, musicians, and other “cool” young adults found on the naturalhigh.org website. You may know other examples of community teens desisting you can reference.
Parent rules, and less so advice, against smoking have been shown to be effective in deterring youth cigarette smoking. Because parents are less aware of vaping and its dangers, another step we can take is educating parents in our practices about vaping, its variable forms, its effects, and dangers, supplying authoritative materials, and advising them to talk with their children. Other steps the American Academy of Pediatrics recommends regarding smoking is for parents to be a role model of not using or try to quit, designate the house and car as smoking free, avoid children viewing smoking in media, tell their children about the side effects, and encourage their children who use to quit. Parents also can encourage schools to teach and have rules about smoking and vaping (e.g., med.stanford.edu/tobaccopreventiontoolkit.html).
Another approach we have been using is to not only screen for all substance use, but also to gather information about the teen’s strengths, activities, and life goals both to enhance rapport and to reference during motivational interviewing as reasons to avoid, reduce, or quit vaping. Motivational interviewing has been shown to help patients make healthier lifestyle choices by nonjudgmentally exploring their pros and cons in a conversation that takes into account readiness to change. This fits well with the stage of developing autonomy when teens want above all to make their own decisions. The cons of using can be discussed as including the effects and side effects of vaping interfering with their favored activities and moving towards their identified goals. Praising abstinence and asking them to show you how they could decline offers to vape are valuable reinforcement you can provide.
Finally, we all know that teens hate being manipulated. Vaping education we provide can make it clear that youth are being tricked by companies – most being large cigarette producers who know the dangers of vaping – into getting addicted so these companies can get rich on their money.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication is as a paid expert to MDedge News. Email her at pdnews@mdedge.com.
All pediatricians are relieved that the rates of children smoking cigarettes has dropped steadily since 2011. This decline seems to be associated with education on the dangers of cigarettes and fewer parents smoking. Perhaps less modeling of cigarette use in movies (although it increased again from 2010 to 2019) and lawsuits against advertisements targeting children also has helped.
“Whew,” we may have said, “we can relax our efforts to convince children to avoid smoking.” But, as is commonly true in medicine, the next threat was right around the corner – in this case vaping or e-cigarettes, also called vapes, e-hookahs, vape pens, tank systems, mods, and electronic nicotine delivery systems. And the size of the problem is huge – over 20% of high school students report using e-cigarettes – and immediate, as vaping can kill in the short term as well as causing long-term harm.
“E-cigarette, or vaping, product use–associated Lung Injury” – EVALI for short – has killed 68 vapers and hospitalized thousands. EVALI is thought to be caused by a vitamin E acetate additive used when vaping marijuana, particularly from informal sources like friends, family, or in-person or online dealers.
Vaping increases the risk of severe COVID-19 disease
While EVALI deaths dropped in months after being explained, the COVID-19 epidemic is now a much greater threat to vapers. Vaping increases risk of severe COVID-19 disease because of its immediate paralysis of lung cilia. Sharing vape devices and touching one’s lips while using also increase the risk of virus transmission. Vaping and smoking increase the number of ACE2 receptors to which the SARS-CoV-2 virus attaches causing the characteristic cell damage, and suppresses macrophages and neutrophils, resulting in more smokers testing positive, being twice as likely to develop a severe illness and get hospitalized because of pneumonia from COVID-19, and being less likely to recover. Unfortunately, addressing this new threat to the immediate and long-term health of our patients appears to be more complicated than for addressing smoking tobacco. First of all, vaping is much more difficult to detect than smelly cigarettes sending smoke signals from behind the garage or in the school bathrooms. Many, if not most, adults do not recognize the vaping devices when they see them, as many are tiny and some look like computer thumb drives. The aerosol emitted when in use, while containing dangerous toxins, has less odor than tobacco smoke. Vaping equipment and ads have been designed to attract youth, including linking them to sports and music events. Vaping has been advertised as a way to wean off nicotine addiction, a claim that has some scientific evidence in adults, but at a lower dose of nicotine. Warning children about the dangers of marijuana vaping has been made less credible by the rapid expansion of legalization of marijuana around the United States, eliciting “I told you it was fine” reactions from youth. And the person vaping does not know what or how much of the psychoactive components are being delivered into their bodies. One Juul pod, for example, has the equivalent in nicotine of an entire pack of 20 cigarettes. They are highly addictive, especially to the developing brain, such that youth who vape are more likely to become addicted and to smoke cigarettes in the future.
Help from federal regulation has been weak
While all 50 states ban sales to youth, adults can still buy. Food and Drug Administration limitations on kid-friendly ads, and use of sweet, fruity, and mint flavorings that are most preferred by children, apply only to new producers. The FDA does not yet regulate content of vaping solutions.
So we pediatricians are on the front line for this new threat to prevent vaping or convince youth to cut down or quit. The first step in addressing vaping is being knowledgeable about its many known and emerging health risks. It may seem obvious that the dangers of vaping microscopic particles depends on the contents. Water vapor alone is not dangerous; in fact, we prescribe it in nebulizers. Unfortunately, the contents of different vaping products vary and are not well defined in different vape products. The process of using an electric current to vaporize a substance can make it more toxic than the precursor, and teens have little idea about the substances they are inhaling. The psychoactive components vary from nicotine to tetrahydrocannabinol in varying amounts. These have the well known effects of stimulation or a high, but also the potential adverse effects of poor concentration, agitation, and even psychosis. Most e-cigarettes contain nicotine, which is highly addictive and can harm adolescent brain development, which continues into the early- to mid-20s. About two-thirds of Juul users aged 15-24 years did not know that it always contains nicotine, as do 99% of all vape solutions (Centers for Disease Control and Prevention, 2020). Earlier use of nicotine is more highly associated with later addiction to tobacco products that cause lung damage, acid reflux, insulin resistance, harm to the testes, harm to fetuses, cancer, and heart disease.
E-cigarette aerosols also contain dozens of other harmful substances besides nicotine ranging from acetone, propylene glycol, and metals to formaldehyde and ethyl benzene. These same chemicals are part of familiar toxic substances such as antifreeze, paint thinner, and pesticides. These cause ear, eye and throat irritation, and impairments in the cardiovascular system reducing athletic ability – at the least. Some flavorings in vape fluids also are toxic. Even the residual left on furniture and floors is harmful to those coming in contact, including pets.
How to encourage teens not to vaping
Trying to scare youth about health hazards is not generally effective in stopping risk behaviors since adolescence is a time of perceived singularity (it does not apply to me) and even a sense of immortality. Teens also see peers who vape as being unaffected and decide on using based on this small personal sample instead of valid statistics.
But teens do pay some attention to peer models or influencers saying why they do not use. One source of such testimony you can refer to is videos of inspiring athletes, musicians, and other “cool” young adults found on the naturalhigh.org website. You may know other examples of community teens desisting you can reference.
Parent rules, and less so advice, against smoking have been shown to be effective in deterring youth cigarette smoking. Because parents are less aware of vaping and its dangers, another step we can take is educating parents in our practices about vaping, its variable forms, its effects, and dangers, supplying authoritative materials, and advising them to talk with their children. Other steps the American Academy of Pediatrics recommends regarding smoking is for parents to be a role model of not using or try to quit, designate the house and car as smoking free, avoid children viewing smoking in media, tell their children about the side effects, and encourage their children who use to quit. Parents also can encourage schools to teach and have rules about smoking and vaping (e.g., med.stanford.edu/tobaccopreventiontoolkit.html).
Another approach we have been using is to not only screen for all substance use, but also to gather information about the teen’s strengths, activities, and life goals both to enhance rapport and to reference during motivational interviewing as reasons to avoid, reduce, or quit vaping. Motivational interviewing has been shown to help patients make healthier lifestyle choices by nonjudgmentally exploring their pros and cons in a conversation that takes into account readiness to change. This fits well with the stage of developing autonomy when teens want above all to make their own decisions. The cons of using can be discussed as including the effects and side effects of vaping interfering with their favored activities and moving towards their identified goals. Praising abstinence and asking them to show you how they could decline offers to vape are valuable reinforcement you can provide.
Finally, we all know that teens hate being manipulated. Vaping education we provide can make it clear that youth are being tricked by companies – most being large cigarette producers who know the dangers of vaping – into getting addicted so these companies can get rich on their money.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication is as a paid expert to MDedge News. Email her at pdnews@mdedge.com.
All pediatricians are relieved that the rates of children smoking cigarettes has dropped steadily since 2011. This decline seems to be associated with education on the dangers of cigarettes and fewer parents smoking. Perhaps less modeling of cigarette use in movies (although it increased again from 2010 to 2019) and lawsuits against advertisements targeting children also has helped.
“Whew,” we may have said, “we can relax our efforts to convince children to avoid smoking.” But, as is commonly true in medicine, the next threat was right around the corner – in this case vaping or e-cigarettes, also called vapes, e-hookahs, vape pens, tank systems, mods, and electronic nicotine delivery systems. And the size of the problem is huge – over 20% of high school students report using e-cigarettes – and immediate, as vaping can kill in the short term as well as causing long-term harm.
“E-cigarette, or vaping, product use–associated Lung Injury” – EVALI for short – has killed 68 vapers and hospitalized thousands. EVALI is thought to be caused by a vitamin E acetate additive used when vaping marijuana, particularly from informal sources like friends, family, or in-person or online dealers.
Vaping increases the risk of severe COVID-19 disease
While EVALI deaths dropped in months after being explained, the COVID-19 epidemic is now a much greater threat to vapers. Vaping increases risk of severe COVID-19 disease because of its immediate paralysis of lung cilia. Sharing vape devices and touching one’s lips while using also increase the risk of virus transmission. Vaping and smoking increase the number of ACE2 receptors to which the SARS-CoV-2 virus attaches causing the characteristic cell damage, and suppresses macrophages and neutrophils, resulting in more smokers testing positive, being twice as likely to develop a severe illness and get hospitalized because of pneumonia from COVID-19, and being less likely to recover. Unfortunately, addressing this new threat to the immediate and long-term health of our patients appears to be more complicated than for addressing smoking tobacco. First of all, vaping is much more difficult to detect than smelly cigarettes sending smoke signals from behind the garage or in the school bathrooms. Many, if not most, adults do not recognize the vaping devices when they see them, as many are tiny and some look like computer thumb drives. The aerosol emitted when in use, while containing dangerous toxins, has less odor than tobacco smoke. Vaping equipment and ads have been designed to attract youth, including linking them to sports and music events. Vaping has been advertised as a way to wean off nicotine addiction, a claim that has some scientific evidence in adults, but at a lower dose of nicotine. Warning children about the dangers of marijuana vaping has been made less credible by the rapid expansion of legalization of marijuana around the United States, eliciting “I told you it was fine” reactions from youth. And the person vaping does not know what or how much of the psychoactive components are being delivered into their bodies. One Juul pod, for example, has the equivalent in nicotine of an entire pack of 20 cigarettes. They are highly addictive, especially to the developing brain, such that youth who vape are more likely to become addicted and to smoke cigarettes in the future.
Help from federal regulation has been weak
While all 50 states ban sales to youth, adults can still buy. Food and Drug Administration limitations on kid-friendly ads, and use of sweet, fruity, and mint flavorings that are most preferred by children, apply only to new producers. The FDA does not yet regulate content of vaping solutions.
So we pediatricians are on the front line for this new threat to prevent vaping or convince youth to cut down or quit. The first step in addressing vaping is being knowledgeable about its many known and emerging health risks. It may seem obvious that the dangers of vaping microscopic particles depends on the contents. Water vapor alone is not dangerous; in fact, we prescribe it in nebulizers. Unfortunately, the contents of different vaping products vary and are not well defined in different vape products. The process of using an electric current to vaporize a substance can make it more toxic than the precursor, and teens have little idea about the substances they are inhaling. The psychoactive components vary from nicotine to tetrahydrocannabinol in varying amounts. These have the well known effects of stimulation or a high, but also the potential adverse effects of poor concentration, agitation, and even psychosis. Most e-cigarettes contain nicotine, which is highly addictive and can harm adolescent brain development, which continues into the early- to mid-20s. About two-thirds of Juul users aged 15-24 years did not know that it always contains nicotine, as do 99% of all vape solutions (Centers for Disease Control and Prevention, 2020). Earlier use of nicotine is more highly associated with later addiction to tobacco products that cause lung damage, acid reflux, insulin resistance, harm to the testes, harm to fetuses, cancer, and heart disease.
E-cigarette aerosols also contain dozens of other harmful substances besides nicotine ranging from acetone, propylene glycol, and metals to formaldehyde and ethyl benzene. These same chemicals are part of familiar toxic substances such as antifreeze, paint thinner, and pesticides. These cause ear, eye and throat irritation, and impairments in the cardiovascular system reducing athletic ability – at the least. Some flavorings in vape fluids also are toxic. Even the residual left on furniture and floors is harmful to those coming in contact, including pets.
How to encourage teens not to vaping
Trying to scare youth about health hazards is not generally effective in stopping risk behaviors since adolescence is a time of perceived singularity (it does not apply to me) and even a sense of immortality. Teens also see peers who vape as being unaffected and decide on using based on this small personal sample instead of valid statistics.
But teens do pay some attention to peer models or influencers saying why they do not use. One source of such testimony you can refer to is videos of inspiring athletes, musicians, and other “cool” young adults found on the naturalhigh.org website. You may know other examples of community teens desisting you can reference.
Parent rules, and less so advice, against smoking have been shown to be effective in deterring youth cigarette smoking. Because parents are less aware of vaping and its dangers, another step we can take is educating parents in our practices about vaping, its variable forms, its effects, and dangers, supplying authoritative materials, and advising them to talk with their children. Other steps the American Academy of Pediatrics recommends regarding smoking is for parents to be a role model of not using or try to quit, designate the house and car as smoking free, avoid children viewing smoking in media, tell their children about the side effects, and encourage their children who use to quit. Parents also can encourage schools to teach and have rules about smoking and vaping (e.g., med.stanford.edu/tobaccopreventiontoolkit.html).
Another approach we have been using is to not only screen for all substance use, but also to gather information about the teen’s strengths, activities, and life goals both to enhance rapport and to reference during motivational interviewing as reasons to avoid, reduce, or quit vaping. Motivational interviewing has been shown to help patients make healthier lifestyle choices by nonjudgmentally exploring their pros and cons in a conversation that takes into account readiness to change. This fits well with the stage of developing autonomy when teens want above all to make their own decisions. The cons of using can be discussed as including the effects and side effects of vaping interfering with their favored activities and moving towards their identified goals. Praising abstinence and asking them to show you how they could decline offers to vape are valuable reinforcement you can provide.
Finally, we all know that teens hate being manipulated. Vaping education we provide can make it clear that youth are being tricked by companies – most being large cigarette producers who know the dangers of vaping – into getting addicted so these companies can get rich on their money.
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University, Baltimore, and creator of CHADIS (www.CHADIS.com). She has no other relevant disclosures. Dr. Howard’s contribution to this publication is as a paid expert to MDedge News. Email her at pdnews@mdedge.com.
