User login
Circadian rhythms, part 2: Can treating cutaneous conditions at different times of the day improve outcomes?
We continue with a focus on when possible, as well as clinical studies that may shed light on how to time skin care treatments.

It is important to remember that several studies in the last 20 years have revealed cutaneous tendencies based on the time of day. For instance, sebum production is known to be highest around noon, and pH also peaks during the day and is at its lowest at night.1-5
Skin aging
In 2019, Dong and associates showed that blue light at 410 nm reduces PER1 transcription in keratinocytes, indicating that epidermal cells have the capacity to directly sense light and regulate their own clock gene expression. With the introduction of blue light at night, circadian rhythm is disrupted as epidermal skin cells act as if it is daytime. The investigators also considered blue light–induced damage to skin cells at various doses and exposure times in comparison with cells that remained unexposed to light. The production of reactive oxygen species increased in the exposed cells, as did DNA impairment and the emergence of inflammatory mediators, all of which have the potential to hasten aging.6
Early this year, Dong and associates demonstrated that melatonin can dose-dependently stimulate PER1 clock gene expression in normal human dermal fibroblasts and normal human epidermal keratinocytes, and verified that the MT-1 melatonin receptor in such fibroblasts manifests a marked decline with age. The researchers concluded that the melatonin pathway contributes significantly in cutaneous aging and impairment, and that its relationship with skin circadian rhythm points to a possible role in slowing the rate of skin aging through the modulation of cutaneous melatonin receptors.7
Wound healing
In 2019, Walker and associates investigated the effects of dim artificial light at night on wound healing in female C57BL/6 mice, and found that those conditions prior to wounding reduced healing. They concluded that such information might warrant consideration in prescribing treatment.8
Atopic dermatitis
Vaughn and associates contended that alterations in circadian rhythm may contribute to the development of atopic dermatitis.9 A good example of the impact of circadian rhythms on cutaneous health is the nocturnal exacerbation of atopic dermatitis, particularly in children.10
Psoriasis
According to Plikus and associates, recent evidence has emerged showing that the circadian clock regulates UVB-induced DNA damage and cutaneous cancers, and it is also associated with the immune-mediated disorder psoriasis.11
Clinical studies
In 2018, Deshayes and associates conducted a clinical study to evaluate the precursors and stem cell attributes of hHF (human hair follicle keratinocytes), hEpi (human interfollicular epidermal keratinocytes), and hHFDP (hair follicle dermal papilla stem cells) in response to clock pathway changes caused by long-term deregulation of circadian rhythms. A total of 20 women participated in the study, 10 in each group (day workers were the control group and compared with shift workers). Two 3-mm fresh punch biopsies were collected from the occipital region of each participant. The investigators reported that chronic circadian rhythm deregulation influenced clock pathway protein expression and correlated with changes in hHF, hEpi, and hHFDP. They concluded that their findings represented the first data in humans suggesting that deregulation of the clock pathway modulates regenerative activity in human cutaneous and hair precursor cells.12

Later that year, Wu and associates reported on the role of the circadian clock in the transcriptional regulation of human epidermis. Investigators sampled 20 human participants through a 24-hour period and a population of 219 people once, finding a potent circadian oscillator in human epidermis at the population level, hundreds of rhythmically expressed genes, as well as a biomarker set for human epidermis that can, with one sample, highlight circadian phase within a 3-hour time frame. The team concluded that rhythms in human epidermis persist at the population level, and that they were able to present an effective single-sample circadian biomarker.13 This is important, as Morris pointed out, because the standard practice for measuring an individual’s internal clock is to use a dim-light melatonin onset assay over the course of a day.14 In 2019, Jia and associates studied the skin surface lipid profiles of young women to evaluate and characterize circadian human facial surface lipid composition. The investigators identified significant markers of circadian rhythm, with glycerolipids most affected. They ascribed changes in skin barrier function, such as variable pH and transepidermal water loss, to alterations in triacylglycerol levels as well as free fatty acid chain lengths and content that were affected by variations in circadian rhythm.15
Sleep and the timing of topicals
Based on their recent review of the literature on circadian rhythm and skin, Lyons and associates argued that an understanding of circadian rhythm helps dermatologists in recommending the optimal times for patients to apply topical medications. They added that urging patients to get sufficient sleep is important because DNA repair of the skin occurs best at that time.16
Conclusions
Doctors have known for half a century that timing drug delivery to a patient’s circadian clock can enhance outcomes. Chronobiological research into how circadian rhythms work at the cellular level, and in cutaneous cells in particular, is a fascinating and expanding area of inquiry that could help dermatologists more accurately recommend timing for skin care regimens. Much more research, especially in clinical trials, is necessary to further elucidate how to best work with the skin’s natural rhythms.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions, a company that independently tests skin care products and makes recommendations to physicians on skin care technologies. Write to her at dermnews@mdedge.com.
References
1. Mehling A et al. Skin Pharmacol Physiol. 2006;19(4):182-9.
2. Latreille J et al. Skin Pharmacol Physiol. 2004 May-Jun;17(3):133-40.
3. Le Fur I et al. J Invest Dermatol. 2001 Sep;117(3):718-24.
4. Verschoore M et al. Chronobiol Int. 1993 Oct;10(5):349-59.
5. Yosipovitch G et al. J Invest Dermatol. 1998 Jan;110(1):20-3.
6. Dong K et al. Int J Cosmet Sci. 2019 Dec;41(6):558-62.
7. Dong K et al. Int J Mol Sci. 2020 Jan 3;21(1):326.
8. Walker WH II et al. Arch Dermatol Res. 2019 Sep;311(7):573-6.
9. Vaughn AR et al. Pediatr Dermatol. 2018 Jan;35(1):152-7.
10. Fishbein AB et al. J Allergy Clin Immunol. 2015 Nov;136(5):1170-7.
11. Plikus MV et al. J Biol Rhythms. 2015 Jun;30(3):163-82.
12. Deshayes N et al. Eur J Dermatol. 2018 Aug 1;28(4):467-75.
13. Wu G et al. Proc Natl Acad Sci U S A. 2018 Nov 27;115(48):12313-8.
14. Morris A. Nat Rev Endocrinol. 2018 Dec;15(1):3.
15. Jia Y et al. Exp Dermatol. 2019 Jul;28(7):858-62.
16. Lyons AB et al. J Clin Aesthet Dermatol. 2019 Sep;12(9):42-5.
We continue with a focus on when possible, as well as clinical studies that may shed light on how to time skin care treatments.
It is important to remember that several studies in the last 20 years have revealed cutaneous tendencies based on the time of day. For instance, sebum production is known to be highest around noon, and pH also peaks during the day and is at its lowest at night.1-5
Skin aging
In 2019, Dong and associates showed that blue light at 410 nm reduces PER1 transcription in keratinocytes, indicating that epidermal cells have the capacity to directly sense light and regulate their own clock gene expression. With the introduction of blue light at night, circadian rhythm is disrupted as epidermal skin cells act as if it is daytime. The investigators also considered blue light–induced damage to skin cells at various doses and exposure times in comparison with cells that remained unexposed to light. The production of reactive oxygen species increased in the exposed cells, as did DNA impairment and the emergence of inflammatory mediators, all of which have the potential to hasten aging.6
Early this year, Dong and associates demonstrated that melatonin can dose-dependently stimulate PER1 clock gene expression in normal human dermal fibroblasts and normal human epidermal keratinocytes, and verified that the MT-1 melatonin receptor in such fibroblasts manifests a marked decline with age. The researchers concluded that the melatonin pathway contributes significantly in cutaneous aging and impairment, and that its relationship with skin circadian rhythm points to a possible role in slowing the rate of skin aging through the modulation of cutaneous melatonin receptors.7
Wound healing
In 2019, Walker and associates investigated the effects of dim artificial light at night on wound healing in female C57BL/6 mice, and found that those conditions prior to wounding reduced healing. They concluded that such information might warrant consideration in prescribing treatment.8
Atopic dermatitis
Vaughn and associates contended that alterations in circadian rhythm may contribute to the development of atopic dermatitis.9 A good example of the impact of circadian rhythms on cutaneous health is the nocturnal exacerbation of atopic dermatitis, particularly in children.10
Psoriasis
According to Plikus and associates, recent evidence has emerged showing that the circadian clock regulates UVB-induced DNA damage and cutaneous cancers, and it is also associated with the immune-mediated disorder psoriasis.11
Clinical studies
In 2018, Deshayes and associates conducted a clinical study to evaluate the precursors and stem cell attributes of hHF (human hair follicle keratinocytes), hEpi (human interfollicular epidermal keratinocytes), and hHFDP (hair follicle dermal papilla stem cells) in response to clock pathway changes caused by long-term deregulation of circadian rhythms. A total of 20 women participated in the study, 10 in each group (day workers were the control group and compared with shift workers). Two 3-mm fresh punch biopsies were collected from the occipital region of each participant. The investigators reported that chronic circadian rhythm deregulation influenced clock pathway protein expression and correlated with changes in hHF, hEpi, and hHFDP. They concluded that their findings represented the first data in humans suggesting that deregulation of the clock pathway modulates regenerative activity in human cutaneous and hair precursor cells.12
Later that year, Wu and associates reported on the role of the circadian clock in the transcriptional regulation of human epidermis. Investigators sampled 20 human participants through a 24-hour period and a population of 219 people once, finding a potent circadian oscillator in human epidermis at the population level, hundreds of rhythmically expressed genes, as well as a biomarker set for human epidermis that can, with one sample, highlight circadian phase within a 3-hour time frame. The team concluded that rhythms in human epidermis persist at the population level, and that they were able to present an effective single-sample circadian biomarker.13 This is important, as Morris pointed out, because the standard practice for measuring an individual’s internal clock is to use a dim-light melatonin onset assay over the course of a day.14 In 2019, Jia and associates studied the skin surface lipid profiles of young women to evaluate and characterize circadian human facial surface lipid composition. The investigators identified significant markers of circadian rhythm, with glycerolipids most affected. They ascribed changes in skin barrier function, such as variable pH and transepidermal water loss, to alterations in triacylglycerol levels as well as free fatty acid chain lengths and content that were affected by variations in circadian rhythm.15
Sleep and the timing of topicals
Based on their recent review of the literature on circadian rhythm and skin, Lyons and associates argued that an understanding of circadian rhythm helps dermatologists in recommending the optimal times for patients to apply topical medications. They added that urging patients to get sufficient sleep is important because DNA repair of the skin occurs best at that time.16
Conclusions
Doctors have known for half a century that timing drug delivery to a patient’s circadian clock can enhance outcomes. Chronobiological research into how circadian rhythms work at the cellular level, and in cutaneous cells in particular, is a fascinating and expanding area of inquiry that could help dermatologists more accurately recommend timing for skin care regimens. Much more research, especially in clinical trials, is necessary to further elucidate how to best work with the skin’s natural rhythms.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions, a company that independently tests skin care products and makes recommendations to physicians on skin care technologies. Write to her at dermnews@mdedge.com.
References
1. Mehling A et al. Skin Pharmacol Physiol. 2006;19(4):182-9.
2. Latreille J et al. Skin Pharmacol Physiol. 2004 May-Jun;17(3):133-40.
3. Le Fur I et al. J Invest Dermatol. 2001 Sep;117(3):718-24.
4. Verschoore M et al. Chronobiol Int. 1993 Oct;10(5):349-59.
5. Yosipovitch G et al. J Invest Dermatol. 1998 Jan;110(1):20-3.
6. Dong K et al. Int J Cosmet Sci. 2019 Dec;41(6):558-62.
7. Dong K et al. Int J Mol Sci. 2020 Jan 3;21(1):326.
8. Walker WH II et al. Arch Dermatol Res. 2019 Sep;311(7):573-6.
9. Vaughn AR et al. Pediatr Dermatol. 2018 Jan;35(1):152-7.
10. Fishbein AB et al. J Allergy Clin Immunol. 2015 Nov;136(5):1170-7.
11. Plikus MV et al. J Biol Rhythms. 2015 Jun;30(3):163-82.
12. Deshayes N et al. Eur J Dermatol. 2018 Aug 1;28(4):467-75.
13. Wu G et al. Proc Natl Acad Sci U S A. 2018 Nov 27;115(48):12313-8.
14. Morris A. Nat Rev Endocrinol. 2018 Dec;15(1):3.
15. Jia Y et al. Exp Dermatol. 2019 Jul;28(7):858-62.
16. Lyons AB et al. J Clin Aesthet Dermatol. 2019 Sep;12(9):42-5.
We continue with a focus on when possible, as well as clinical studies that may shed light on how to time skin care treatments.
It is important to remember that several studies in the last 20 years have revealed cutaneous tendencies based on the time of day. For instance, sebum production is known to be highest around noon, and pH also peaks during the day and is at its lowest at night.1-5
Skin aging
In 2019, Dong and associates showed that blue light at 410 nm reduces PER1 transcription in keratinocytes, indicating that epidermal cells have the capacity to directly sense light and regulate their own clock gene expression. With the introduction of blue light at night, circadian rhythm is disrupted as epidermal skin cells act as if it is daytime. The investigators also considered blue light–induced damage to skin cells at various doses and exposure times in comparison with cells that remained unexposed to light. The production of reactive oxygen species increased in the exposed cells, as did DNA impairment and the emergence of inflammatory mediators, all of which have the potential to hasten aging.6
Early this year, Dong and associates demonstrated that melatonin can dose-dependently stimulate PER1 clock gene expression in normal human dermal fibroblasts and normal human epidermal keratinocytes, and verified that the MT-1 melatonin receptor in such fibroblasts manifests a marked decline with age. The researchers concluded that the melatonin pathway contributes significantly in cutaneous aging and impairment, and that its relationship with skin circadian rhythm points to a possible role in slowing the rate of skin aging through the modulation of cutaneous melatonin receptors.7
Wound healing
In 2019, Walker and associates investigated the effects of dim artificial light at night on wound healing in female C57BL/6 mice, and found that those conditions prior to wounding reduced healing. They concluded that such information might warrant consideration in prescribing treatment.8
Atopic dermatitis
Vaughn and associates contended that alterations in circadian rhythm may contribute to the development of atopic dermatitis.9 A good example of the impact of circadian rhythms on cutaneous health is the nocturnal exacerbation of atopic dermatitis, particularly in children.10
Psoriasis
According to Plikus and associates, recent evidence has emerged showing that the circadian clock regulates UVB-induced DNA damage and cutaneous cancers, and it is also associated with the immune-mediated disorder psoriasis.11
Clinical studies
In 2018, Deshayes and associates conducted a clinical study to evaluate the precursors and stem cell attributes of hHF (human hair follicle keratinocytes), hEpi (human interfollicular epidermal keratinocytes), and hHFDP (hair follicle dermal papilla stem cells) in response to clock pathway changes caused by long-term deregulation of circadian rhythms. A total of 20 women participated in the study, 10 in each group (day workers were the control group and compared with shift workers). Two 3-mm fresh punch biopsies were collected from the occipital region of each participant. The investigators reported that chronic circadian rhythm deregulation influenced clock pathway protein expression and correlated with changes in hHF, hEpi, and hHFDP. They concluded that their findings represented the first data in humans suggesting that deregulation of the clock pathway modulates regenerative activity in human cutaneous and hair precursor cells.12
Later that year, Wu and associates reported on the role of the circadian clock in the transcriptional regulation of human epidermis. Investigators sampled 20 human participants through a 24-hour period and a population of 219 people once, finding a potent circadian oscillator in human epidermis at the population level, hundreds of rhythmically expressed genes, as well as a biomarker set for human epidermis that can, with one sample, highlight circadian phase within a 3-hour time frame. The team concluded that rhythms in human epidermis persist at the population level, and that they were able to present an effective single-sample circadian biomarker.13 This is important, as Morris pointed out, because the standard practice for measuring an individual’s internal clock is to use a dim-light melatonin onset assay over the course of a day.14 In 2019, Jia and associates studied the skin surface lipid profiles of young women to evaluate and characterize circadian human facial surface lipid composition. The investigators identified significant markers of circadian rhythm, with glycerolipids most affected. They ascribed changes in skin barrier function, such as variable pH and transepidermal water loss, to alterations in triacylglycerol levels as well as free fatty acid chain lengths and content that were affected by variations in circadian rhythm.15
Sleep and the timing of topicals
Based on their recent review of the literature on circadian rhythm and skin, Lyons and associates argued that an understanding of circadian rhythm helps dermatologists in recommending the optimal times for patients to apply topical medications. They added that urging patients to get sufficient sleep is important because DNA repair of the skin occurs best at that time.16
Conclusions
Doctors have known for half a century that timing drug delivery to a patient’s circadian clock can enhance outcomes. Chronobiological research into how circadian rhythms work at the cellular level, and in cutaneous cells in particular, is a fascinating and expanding area of inquiry that could help dermatologists more accurately recommend timing for skin care regimens. Much more research, especially in clinical trials, is necessary to further elucidate how to best work with the skin’s natural rhythms.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions, a company that independently tests skin care products and makes recommendations to physicians on skin care technologies. Write to her at dermnews@mdedge.com.
References
1. Mehling A et al. Skin Pharmacol Physiol. 2006;19(4):182-9.
2. Latreille J et al. Skin Pharmacol Physiol. 2004 May-Jun;17(3):133-40.
3. Le Fur I et al. J Invest Dermatol. 2001 Sep;117(3):718-24.
4. Verschoore M et al. Chronobiol Int. 1993 Oct;10(5):349-59.
5. Yosipovitch G et al. J Invest Dermatol. 1998 Jan;110(1):20-3.
6. Dong K et al. Int J Cosmet Sci. 2019 Dec;41(6):558-62.
7. Dong K et al. Int J Mol Sci. 2020 Jan 3;21(1):326.
8. Walker WH II et al. Arch Dermatol Res. 2019 Sep;311(7):573-6.
9. Vaughn AR et al. Pediatr Dermatol. 2018 Jan;35(1):152-7.
10. Fishbein AB et al. J Allergy Clin Immunol. 2015 Nov;136(5):1170-7.
11. Plikus MV et al. J Biol Rhythms. 2015 Jun;30(3):163-82.
12. Deshayes N et al. Eur J Dermatol. 2018 Aug 1;28(4):467-75.
13. Wu G et al. Proc Natl Acad Sci U S A. 2018 Nov 27;115(48):12313-8.
14. Morris A. Nat Rev Endocrinol. 2018 Dec;15(1):3.
15. Jia Y et al. Exp Dermatol. 2019 Jul;28(7):858-62.
16. Lyons AB et al. J Clin Aesthet Dermatol. 2019 Sep;12(9):42-5.
Coping with vaccine refusal
Do you accept new families into your practice who have already chosen to not have their children immunized? What about families who have been in your practice for several months or years? In 2016 the American Academy of Pediatrics published a clinical report in which it stated that, under some circumstances, dismissing families who refuse to vaccinate is permissible. Have you felt sufficiently supported by that statement and dismissed any families after multiple attempts at education on your part?

In a Pediatrics Perspective article in the December issue of Pediatrics, two philosophers and a physician make the argument that, while in some situations dismissing a family who refuses vaccines may be “an ethically acceptable option” refusing to accept a family with the same philosophy is not. It is an interesting paper and worth reading regardless of whether or not you already accept and continue to tolerate vaccine deniers in your practice.
The Pediatrics Perspective is certainly not the last word on the ethics of caring for families who deny their children care that we believe is critical to their health and the welfare of the community at large. There has been a lot of discussion about the issue but little has been written about how we as the physicians on the front line are coping emotionally with what the authors of the paper call the “burdens associated with treating” families who refuse to follow our guidance.
It is hard not to feel angry when a family you have invested valuable office time in discussing the benefits and safety of vaccines continues to disregard what you see as the facts. The time you have spent with them is not just income-generating time for your practice, it is time stolen from other families who are more willing to follow your recommendations. In how many visits will you continue to raise the issue? Unless I saw a glimmer of hope I would usually stop after two wasted encounters. But, the issue would still linger as the elephant in the examination room for as long as I continued to see the patient.
How have you expressed your anger? Have you been argumentative or rude? You may have been able maintain your composure and remain civil and appear caring, but I suspect the anger is still gnawing at you. And, there is still the frustration and feeling of impotence. You may have questioned your ability as an educator. You should get over that notion quickly. There is ample evidence that most vaccine deniers are not going to be convinced by even the most carefully presented information. I suggest you leave it to others to try their hands at education. Let them invest their time while you tend to the needs of your other patients. You can try being a fear monger and, while fear can be effective, you have better ways to spend your office day than telling horror stories.
If vaccine denial makes you feel powerless, you should get over that pretty quickly as well and accept the fact that you are simply an advisor. If you believe that most of the families in your practice are following your recommendations as though you had presented them on stone tablets, it is time for a wakeup call.
Finally, there is the most troubling emotion associated with vaccine refusal and that is fear, the fear of being sued. Establishing a relationship with a family is one that requires mutual trust and certainly vaccine refusal will put that trust in question, particularly if you have done a less than adequate job of hiding your anger and frustration with their unfortunate decision.
For now, vaccine refusal is just another one of those crosses that those of us in primary care must bear together wearing the best face we can put forward. That doesn’t mean we can’t share those emotions with our peers. Misery does love company.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Do you accept new families into your practice who have already chosen to not have their children immunized? What about families who have been in your practice for several months or years? In 2016 the American Academy of Pediatrics published a clinical report in which it stated that, under some circumstances, dismissing families who refuse to vaccinate is permissible. Have you felt sufficiently supported by that statement and dismissed any families after multiple attempts at education on your part?
In a Pediatrics Perspective article in the December issue of Pediatrics, two philosophers and a physician make the argument that, while in some situations dismissing a family who refuses vaccines may be “an ethically acceptable option” refusing to accept a family with the same philosophy is not. It is an interesting paper and worth reading regardless of whether or not you already accept and continue to tolerate vaccine deniers in your practice.
The Pediatrics Perspective is certainly not the last word on the ethics of caring for families who deny their children care that we believe is critical to their health and the welfare of the community at large. There has been a lot of discussion about the issue but little has been written about how we as the physicians on the front line are coping emotionally with what the authors of the paper call the “burdens associated with treating” families who refuse to follow our guidance.
It is hard not to feel angry when a family you have invested valuable office time in discussing the benefits and safety of vaccines continues to disregard what you see as the facts. The time you have spent with them is not just income-generating time for your practice, it is time stolen from other families who are more willing to follow your recommendations. In how many visits will you continue to raise the issue? Unless I saw a glimmer of hope I would usually stop after two wasted encounters. But, the issue would still linger as the elephant in the examination room for as long as I continued to see the patient.
How have you expressed your anger? Have you been argumentative or rude? You may have been able maintain your composure and remain civil and appear caring, but I suspect the anger is still gnawing at you. And, there is still the frustration and feeling of impotence. You may have questioned your ability as an educator. You should get over that notion quickly. There is ample evidence that most vaccine deniers are not going to be convinced by even the most carefully presented information. I suggest you leave it to others to try their hands at education. Let them invest their time while you tend to the needs of your other patients. You can try being a fear monger and, while fear can be effective, you have better ways to spend your office day than telling horror stories.
If vaccine denial makes you feel powerless, you should get over that pretty quickly as well and accept the fact that you are simply an advisor. If you believe that most of the families in your practice are following your recommendations as though you had presented them on stone tablets, it is time for a wakeup call.
Finally, there is the most troubling emotion associated with vaccine refusal and that is fear, the fear of being sued. Establishing a relationship with a family is one that requires mutual trust and certainly vaccine refusal will put that trust in question, particularly if you have done a less than adequate job of hiding your anger and frustration with their unfortunate decision.
For now, vaccine refusal is just another one of those crosses that those of us in primary care must bear together wearing the best face we can put forward. That doesn’t mean we can’t share those emotions with our peers. Misery does love company.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Do you accept new families into your practice who have already chosen to not have their children immunized? What about families who have been in your practice for several months or years? In 2016 the American Academy of Pediatrics published a clinical report in which it stated that, under some circumstances, dismissing families who refuse to vaccinate is permissible. Have you felt sufficiently supported by that statement and dismissed any families after multiple attempts at education on your part?
In a Pediatrics Perspective article in the December issue of Pediatrics, two philosophers and a physician make the argument that, while in some situations dismissing a family who refuses vaccines may be “an ethically acceptable option” refusing to accept a family with the same philosophy is not. It is an interesting paper and worth reading regardless of whether or not you already accept and continue to tolerate vaccine deniers in your practice.
The Pediatrics Perspective is certainly not the last word on the ethics of caring for families who deny their children care that we believe is critical to their health and the welfare of the community at large. There has been a lot of discussion about the issue but little has been written about how we as the physicians on the front line are coping emotionally with what the authors of the paper call the “burdens associated with treating” families who refuse to follow our guidance.
It is hard not to feel angry when a family you have invested valuable office time in discussing the benefits and safety of vaccines continues to disregard what you see as the facts. The time you have spent with them is not just income-generating time for your practice, it is time stolen from other families who are more willing to follow your recommendations. In how many visits will you continue to raise the issue? Unless I saw a glimmer of hope I would usually stop after two wasted encounters. But, the issue would still linger as the elephant in the examination room for as long as I continued to see the patient.
How have you expressed your anger? Have you been argumentative or rude? You may have been able maintain your composure and remain civil and appear caring, but I suspect the anger is still gnawing at you. And, there is still the frustration and feeling of impotence. You may have questioned your ability as an educator. You should get over that notion quickly. There is ample evidence that most vaccine deniers are not going to be convinced by even the most carefully presented information. I suggest you leave it to others to try their hands at education. Let them invest their time while you tend to the needs of your other patients. You can try being a fear monger and, while fear can be effective, you have better ways to spend your office day than telling horror stories.
If vaccine denial makes you feel powerless, you should get over that pretty quickly as well and accept the fact that you are simply an advisor. If you believe that most of the families in your practice are following your recommendations as though you had presented them on stone tablets, it is time for a wakeup call.
Finally, there is the most troubling emotion associated with vaccine refusal and that is fear, the fear of being sued. Establishing a relationship with a family is one that requires mutual trust and certainly vaccine refusal will put that trust in question, particularly if you have done a less than adequate job of hiding your anger and frustration with their unfortunate decision.
For now, vaccine refusal is just another one of those crosses that those of us in primary care must bear together wearing the best face we can put forward. That doesn’t mean we can’t share those emotions with our peers. Misery does love company.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
Waiting for the COVID 19 vaccine, or not?
A shot of relief. A shot of hope. Those are the words used to describe COVID-19 vaccines on a television commercial running in prime time in Kentucky.
“We all can’t get the vaccine at once,” the announcer says solemnly, “but we’ll all get a turn.”
For some of us, that turn came quickly. In December, the Advisory Committee on Immunization Practices recommended that health care personnel (HCP) and long-term care facility residents be the first to be immunized with COVID-19 vaccines (see table). 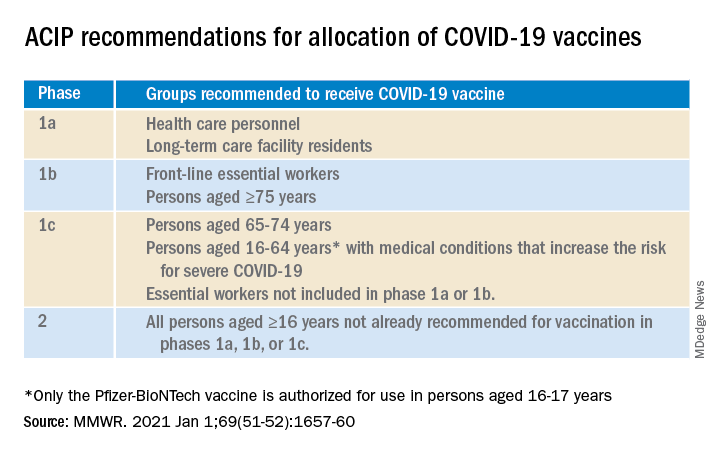
On Dec. 14, 2020, Sandra Lindsay, a nurse and director of patient care services in the intensive care unit at Long Island Jewish Medical Center, was the first person in the United States to receive a COVID-19 vaccine outside a clinical trial.
In subsequent days, social media sites were quickly flooded with photos of HCP rolling up their sleeves or flashing their immunization cards. There was jubilation ... and perhaps a little bit of jealousy. There were tears of joy and some tears of frustration.
There are more than 21 million HCP in the United States and to date, there have not been enough vaccines nor adequate infrastructure to immunize all of them. According to the Centers for Disease Control and Prevention Data Tracker, as of Jan. 7, 2021, 21,419,800 doses of vaccine had been distributed to states to immunize everyone identified in phase 1a, but only 5,919,418 people had received a first dose. Limited supply has necessitated prioritization of subgroups of HCP; those in the front of the line have varied by state, and even by hospital or health care systems within states. Both the American Academy of Pediatrics and the American Academy of Family Physicians have noted that primary care providers not employed by a hospital may have more difficulty accessing vaccine.

The mismatch between supply and demand has created an intense focus on improving supply and distribution. Soon though, we’re going to shift our attention to how we increase demand. We don’t have good data on those who being are offered COVID-19 vaccine and declining, but several studies that predate the Emergency Use Authorization for the Pfizer-BioNTech and Moderna vaccines suggest significant COVID-19 vaccine hesitancy among adults in the United States.
One large, longitudinal Internet-based study of U.S. adults found that the proportion who reported they were “somewhat or very likely” to receive COVID-19 vaccine declined from 74% in early April to 56% in early December.
In the Understanding America Study, self-reported likelihood of being vaccinated with COVID-19 vaccine was lower among Black compared to White respondents (38% vs. 59%; aRR, 0.7 [95% confidence interval, 0.6-0.8]), and lower among women compared to men (51% vs. 62%; aRR, 0.9 [95% CI, 0.8-0.9]). Those 65 years of age and older were more likely to report a willingness to be vaccinated than were those 18-49 years of age, as were those with at least a bachelor’s degree compared to those with a high school education or less.
A study conducted by the Pew Research Center in November – before any COVID-19 vaccines were available – found that only 60% of American adults said they would “definitely or probably get a vaccine for coronavirus” if one were available. That was an increase from 51% in September, but and overall decrease of 72% in May. Of the remaining 40%, just over half said they did not intend to get vaccinated and were “pretty certain” that more information would not change their minds.
Concern about acquiring a serious case of COVID-19 and trust in the vaccine development process were associated with an intent to receive vaccine, as was a personal history of receiving a flu shot annually. Willingness to be vaccinated varied by age, race, and family income, with Black respondents, women, and those with a lower family incomes less likely to accept a vaccine.
To date, few data are available about HCP and willingness to receive COVID-19 vaccine. A preprint posted at medrxiv.org reports on a cross-sectional study of more than 3,400 HCP surveyed between Oct. 7 and Nov. 9, 2020. In that study, only 36% of respondents voiced a willingness to be immunized as soon as vaccine is available. Vaccine acceptance increased with increasing age, income level, and education. As in other studies, self-reported willingness to accept vaccine was lower in women and Black individuals. While vaccine acceptance was higher in direct medical care providers than others, it was still only 49%.
So here’s the paradox: Even as limited supplies of vaccine are available and many are frustrated about lack of access, we need to promote the value of immunization to those who are hesitant. Pediatricians are trusted sources of vaccine information and we are in a good position to educate our colleagues, our staff, the parents of our patients and the community at-large.
A useful resource for those ready to take that step it is the CDC’s COVID-19 Vaccination Communication Toolkit. While this collection is designed to build vaccine confidence and promote immunization among health care providers, many of the strategies will be easily adapted for use with patients.
It’s not clear when we might have a COVID 19 vaccine for most children. The Pfizer-BioNTech vaccine emergency use authorization includes those as young as 16 years of age, and 16- and 17-year-olds with high risk medical conditions are included in phase 1c of vaccine allocation. Pfizer is currently enrolling children as young as 12 years of age in clinical trials, and Moderna and Janssen are poised to do the same. It is conceivable but far from certain that we could have a vaccine for children late this year. Are parents going to be ready to vaccinate their children?
Limited data about parental acceptance of vaccine for their children mirrors what was seen in the Understanding America Study and the Pew Research Study. In December 2020, the National Parents Union surveyed 1,008 parents of public school students enrolled in kindergarten through 12th grade. Sixty percent of parents said they would allow their children to receive a COVID-19 vaccine, while 25% would not and 15% were unsure. This suggests that now is the time to begin building vaccine confidence with parents. One conversation starter might be, “I am going to be vaccinated as soon as the vaccine is available.” Ideally, many of you will soon be able to say what I do: “I am excited to tell you that I have been immunized with the COVID-19 vaccine. I did this to protect myself, my family, and our community. I’m hopeful that vaccine will soon be available for all of us.”
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
A shot of relief. A shot of hope. Those are the words used to describe COVID-19 vaccines on a television commercial running in prime time in Kentucky.
“We all can’t get the vaccine at once,” the announcer says solemnly, “but we’ll all get a turn.”
For some of us, that turn came quickly. In December, the Advisory Committee on Immunization Practices recommended that health care personnel (HCP) and long-term care facility residents be the first to be immunized with COVID-19 vaccines (see table).
On Dec. 14, 2020, Sandra Lindsay, a nurse and director of patient care services in the intensive care unit at Long Island Jewish Medical Center, was the first person in the United States to receive a COVID-19 vaccine outside a clinical trial.
In subsequent days, social media sites were quickly flooded with photos of HCP rolling up their sleeves or flashing their immunization cards. There was jubilation ... and perhaps a little bit of jealousy. There were tears of joy and some tears of frustration.
There are more than 21 million HCP in the United States and to date, there have not been enough vaccines nor adequate infrastructure to immunize all of them. According to the Centers for Disease Control and Prevention Data Tracker, as of Jan. 7, 2021, 21,419,800 doses of vaccine had been distributed to states to immunize everyone identified in phase 1a, but only 5,919,418 people had received a first dose. Limited supply has necessitated prioritization of subgroups of HCP; those in the front of the line have varied by state, and even by hospital or health care systems within states. Both the American Academy of Pediatrics and the American Academy of Family Physicians have noted that primary care providers not employed by a hospital may have more difficulty accessing vaccine.
The mismatch between supply and demand has created an intense focus on improving supply and distribution. Soon though, we’re going to shift our attention to how we increase demand. We don’t have good data on those who being are offered COVID-19 vaccine and declining, but several studies that predate the Emergency Use Authorization for the Pfizer-BioNTech and Moderna vaccines suggest significant COVID-19 vaccine hesitancy among adults in the United States.
One large, longitudinal Internet-based study of U.S. adults found that the proportion who reported they were “somewhat or very likely” to receive COVID-19 vaccine declined from 74% in early April to 56% in early December.
In the Understanding America Study, self-reported likelihood of being vaccinated with COVID-19 vaccine was lower among Black compared to White respondents (38% vs. 59%; aRR, 0.7 [95% confidence interval, 0.6-0.8]), and lower among women compared to men (51% vs. 62%; aRR, 0.9 [95% CI, 0.8-0.9]). Those 65 years of age and older were more likely to report a willingness to be vaccinated than were those 18-49 years of age, as were those with at least a bachelor’s degree compared to those with a high school education or less.
A study conducted by the Pew Research Center in November – before any COVID-19 vaccines were available – found that only 60% of American adults said they would “definitely or probably get a vaccine for coronavirus” if one were available. That was an increase from 51% in September, but and overall decrease of 72% in May. Of the remaining 40%, just over half said they did not intend to get vaccinated and were “pretty certain” that more information would not change their minds.
Concern about acquiring a serious case of COVID-19 and trust in the vaccine development process were associated with an intent to receive vaccine, as was a personal history of receiving a flu shot annually. Willingness to be vaccinated varied by age, race, and family income, with Black respondents, women, and those with a lower family incomes less likely to accept a vaccine.
To date, few data are available about HCP and willingness to receive COVID-19 vaccine. A preprint posted at medrxiv.org reports on a cross-sectional study of more than 3,400 HCP surveyed between Oct. 7 and Nov. 9, 2020. In that study, only 36% of respondents voiced a willingness to be immunized as soon as vaccine is available. Vaccine acceptance increased with increasing age, income level, and education. As in other studies, self-reported willingness to accept vaccine was lower in women and Black individuals. While vaccine acceptance was higher in direct medical care providers than others, it was still only 49%.
So here’s the paradox: Even as limited supplies of vaccine are available and many are frustrated about lack of access, we need to promote the value of immunization to those who are hesitant. Pediatricians are trusted sources of vaccine information and we are in a good position to educate our colleagues, our staff, the parents of our patients and the community at-large.
A useful resource for those ready to take that step it is the CDC’s COVID-19 Vaccination Communication Toolkit. While this collection is designed to build vaccine confidence and promote immunization among health care providers, many of the strategies will be easily adapted for use with patients.
It’s not clear when we might have a COVID 19 vaccine for most children. The Pfizer-BioNTech vaccine emergency use authorization includes those as young as 16 years of age, and 16- and 17-year-olds with high risk medical conditions are included in phase 1c of vaccine allocation. Pfizer is currently enrolling children as young as 12 years of age in clinical trials, and Moderna and Janssen are poised to do the same. It is conceivable but far from certain that we could have a vaccine for children late this year. Are parents going to be ready to vaccinate their children?
Limited data about parental acceptance of vaccine for their children mirrors what was seen in the Understanding America Study and the Pew Research Study. In December 2020, the National Parents Union surveyed 1,008 parents of public school students enrolled in kindergarten through 12th grade. Sixty percent of parents said they would allow their children to receive a COVID-19 vaccine, while 25% would not and 15% were unsure. This suggests that now is the time to begin building vaccine confidence with parents. One conversation starter might be, “I am going to be vaccinated as soon as the vaccine is available.” Ideally, many of you will soon be able to say what I do: “I am excited to tell you that I have been immunized with the COVID-19 vaccine. I did this to protect myself, my family, and our community. I’m hopeful that vaccine will soon be available for all of us.”
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
A shot of relief. A shot of hope. Those are the words used to describe COVID-19 vaccines on a television commercial running in prime time in Kentucky.
“We all can’t get the vaccine at once,” the announcer says solemnly, “but we’ll all get a turn.”
For some of us, that turn came quickly. In December, the Advisory Committee on Immunization Practices recommended that health care personnel (HCP) and long-term care facility residents be the first to be immunized with COVID-19 vaccines (see table).
On Dec. 14, 2020, Sandra Lindsay, a nurse and director of patient care services in the intensive care unit at Long Island Jewish Medical Center, was the first person in the United States to receive a COVID-19 vaccine outside a clinical trial.
In subsequent days, social media sites were quickly flooded with photos of HCP rolling up their sleeves or flashing their immunization cards. There was jubilation ... and perhaps a little bit of jealousy. There were tears of joy and some tears of frustration.
There are more than 21 million HCP in the United States and to date, there have not been enough vaccines nor adequate infrastructure to immunize all of them. According to the Centers for Disease Control and Prevention Data Tracker, as of Jan. 7, 2021, 21,419,800 doses of vaccine had been distributed to states to immunize everyone identified in phase 1a, but only 5,919,418 people had received a first dose. Limited supply has necessitated prioritization of subgroups of HCP; those in the front of the line have varied by state, and even by hospital or health care systems within states. Both the American Academy of Pediatrics and the American Academy of Family Physicians have noted that primary care providers not employed by a hospital may have more difficulty accessing vaccine.
The mismatch between supply and demand has created an intense focus on improving supply and distribution. Soon though, we’re going to shift our attention to how we increase demand. We don’t have good data on those who being are offered COVID-19 vaccine and declining, but several studies that predate the Emergency Use Authorization for the Pfizer-BioNTech and Moderna vaccines suggest significant COVID-19 vaccine hesitancy among adults in the United States.
One large, longitudinal Internet-based study of U.S. adults found that the proportion who reported they were “somewhat or very likely” to receive COVID-19 vaccine declined from 74% in early April to 56% in early December.
In the Understanding America Study, self-reported likelihood of being vaccinated with COVID-19 vaccine was lower among Black compared to White respondents (38% vs. 59%; aRR, 0.7 [95% confidence interval, 0.6-0.8]), and lower among women compared to men (51% vs. 62%; aRR, 0.9 [95% CI, 0.8-0.9]). Those 65 years of age and older were more likely to report a willingness to be vaccinated than were those 18-49 years of age, as were those with at least a bachelor’s degree compared to those with a high school education or less.
A study conducted by the Pew Research Center in November – before any COVID-19 vaccines were available – found that only 60% of American adults said they would “definitely or probably get a vaccine for coronavirus” if one were available. That was an increase from 51% in September, but and overall decrease of 72% in May. Of the remaining 40%, just over half said they did not intend to get vaccinated and were “pretty certain” that more information would not change their minds.
Concern about acquiring a serious case of COVID-19 and trust in the vaccine development process were associated with an intent to receive vaccine, as was a personal history of receiving a flu shot annually. Willingness to be vaccinated varied by age, race, and family income, with Black respondents, women, and those with a lower family incomes less likely to accept a vaccine.
To date, few data are available about HCP and willingness to receive COVID-19 vaccine. A preprint posted at medrxiv.org reports on a cross-sectional study of more than 3,400 HCP surveyed between Oct. 7 and Nov. 9, 2020. In that study, only 36% of respondents voiced a willingness to be immunized as soon as vaccine is available. Vaccine acceptance increased with increasing age, income level, and education. As in other studies, self-reported willingness to accept vaccine was lower in women and Black individuals. While vaccine acceptance was higher in direct medical care providers than others, it was still only 49%.
So here’s the paradox: Even as limited supplies of vaccine are available and many are frustrated about lack of access, we need to promote the value of immunization to those who are hesitant. Pediatricians are trusted sources of vaccine information and we are in a good position to educate our colleagues, our staff, the parents of our patients and the community at-large.
A useful resource for those ready to take that step it is the CDC’s COVID-19 Vaccination Communication Toolkit. While this collection is designed to build vaccine confidence and promote immunization among health care providers, many of the strategies will be easily adapted for use with patients.
It’s not clear when we might have a COVID 19 vaccine for most children. The Pfizer-BioNTech vaccine emergency use authorization includes those as young as 16 years of age, and 16- and 17-year-olds with high risk medical conditions are included in phase 1c of vaccine allocation. Pfizer is currently enrolling children as young as 12 years of age in clinical trials, and Moderna and Janssen are poised to do the same. It is conceivable but far from certain that we could have a vaccine for children late this year. Are parents going to be ready to vaccinate their children?
Limited data about parental acceptance of vaccine for their children mirrors what was seen in the Understanding America Study and the Pew Research Study. In December 2020, the National Parents Union surveyed 1,008 parents of public school students enrolled in kindergarten through 12th grade. Sixty percent of parents said they would allow their children to receive a COVID-19 vaccine, while 25% would not and 15% were unsure. This suggests that now is the time to begin building vaccine confidence with parents. One conversation starter might be, “I am going to be vaccinated as soon as the vaccine is available.” Ideally, many of you will soon be able to say what I do: “I am excited to tell you that I have been immunized with the COVID-19 vaccine. I did this to protect myself, my family, and our community. I’m hopeful that vaccine will soon be available for all of us.”
Dr. Bryant is a pediatrician specializing in infectious diseases at the University of Louisville (Ky.) and Norton Children’s Hospital, also in Louisville. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
RSClin: A new tool for ‘TAILOR-ing’ treatment in early breast cancer
When results of the TAILORx trial were presented at ASCO 2018, many oncologists thought it seemed too simple that a single number from a genomic assay could separate patients who would and would not benefit from adjuvant postoperative chemotherapy.

Those oncologists were right to be skeptical. Subsequent data indicated that better predictive tools were needed.
A new tool called “RSClin” may fit the bill. RSClin integrates the prognostic and predictive value of the 21-gene Oncotype DX recurrence score (RS) with the additional prognostic information conveyed by patient age, tumor grade, and tumor size.
RSClin provides individualized estimates of distant relapse risk for women with node-negative, endocrine sensitive, HER2/neu oncogene-negative early breast cancer – and a quantification of the additive freedom from distant relapse if that patient receives adjuvant chemotherapy. The tool is now available via a tab on the professional portal at https://online.genomichealth.com/.
Details on RSClin, including how the tool was developed and validated, were presented at the 2020 San Antonio Breast Cancer Symposium by Joseph A. Sparano, MD, of Albert Einstein College of Medicine in New York.
Beyond the initial publication of TAILORx
Results from the TAILORx trial published in The New England Journal of Medicine in 2018 offered the potential for genomic risk assessment to guide the choice of postoperative therapy for many women with the most common type of primary breast cancer. The relative risk reduction with chemotherapy increased with increasing RS result.
Subsequent analyses of the TAILORx dataset, published in The New England Journal of Medicine and JAMA Oncology in 2019, examined the added effect of parameters of clinical risk (tumor size and grade) and patient age for patients with known genomic risk.
In these analyses, clinical risk was prognostic for recurrence but did not predict the absolute magnitude of chemotherapy benefit, regardless of age. There was a trend toward chemotherapy benefit in women who were younger than 50 years of age who had RS 21-15, but it was irrespective of clinical risk.
The development of RSClin
RSClin was derived from a patient-specific meta-analysis of 10,004 women with hormone receptor–positive, HER2-negative, node-negative breast cancer, of whom 9,427 participated in the TAILORx trial.
In TAILORx, which ran from 2006 to 2015, women with RS 0-11 received contemporary hormone therapy alone. Women with RS 12-25 were randomized to receive hormone therapy alone or with conventional combination chemotherapy. Women with RS above 26 received chemotherapy plus endocrine therapy.
The other patients in the meta-analysis participated in NSABP studies B-14 (tamoxifen versus placebo) and B-20 (tamoxifen versus chemotherapy plus tamoxifen).
Cox regression models were fit separately to each study with covariates of the continuous variables of RS result, tumor size, and patient age and the discrete variable of histologic tumor grade (assessed centrally in B-14 and in local laboratories in TAILORx). The prespecified endpoint was time to first distant recurrence.
RSClin estimates of distant recurrence risk were generated using baseline risk with TAILORx event rates to reflect current medical practice.
Model estimates were calculated for specified endocrine therapy with tamoxifen or aromatase inhibitors utilizing the treatment effect hazard ratio from an Early Breast Cancer Trialists’ Collaborative Group meta-analysis.
Patient-specific absolute benefit of chemotherapy was estimated by combining patient-specific meta-analysis risk estimates for distant recurrence and for relative chemotherapy benefit using the B-20 and TAILORx trials.
RSClin results and external validation
Among all patients in the meta-analysis cohort, RSClin provided a significantly more accurate prediction of distant recurrence events, in comparison with RS alone or clinical-pathologic factors alone.
External validation was performed using data from real-world outcomes from the 1,098 evaluable node-negative patients in the Clalit Health Services registry, of whom 876 received endocrine therapy alone and 222 received endocrine therapy plus chemotherapy.
RSClin estimates of distant recurrence closely approximated the observed risk in the registry (standardized hazard ratio, 1.73; 95% confidence interval, 1.40-2.15; P < .001). Within each RSClin risk quintile, the average 10-year risk estimate approached the observed Kaplan-Meier estimates in the cohort (Lin concordance correlation = 0.962).
Shared decision-making
For many years, the dilemma of whether to recommend adjuvant chemotherapy to a patient with early breast cancer has prompted the generation of tools to quantify a patient’s risk of recurrence and the magnitude of benefit for endocrine therapy and/or chemotherapy.
When the original Adjuvant! Online program was developed, genomic risk profiling was in its infancy. Genomic tools such as the 21-gene RS have subsequently demonstrated that they can help optimize the adjuvant treatment we recommend.
The RSClin tool provides more precise, individualized information than does clinical-pathological or genomic data alone. It prognosticates the risk of distant recurrence of breast cancer, which patients and providers fervently wish to minimize.
RSClin estimates the incremental benefit of contemporary adjuvant chemotherapy over modern endocrine therapy alone, in absolute values, for individual patients. This transparent, discrete, easily explained information is vital for counseling patients.
However, as highlighted in an editorial published in the Journal of Clinical Oncology, RSClin is not without its potential drawbacks. These include:
- Tumor heterogeneity leading to misleading results.
- Variable patient adherence to endocrine therapy or chemotherapy.
- The influence of comorbid conditions on the risk/benefit ratio.
- The potential of ovarian function suppression in young women to approach the magnitude of benefit associated with chemotherapy.
Accordingly, RSClin may be the latest and best available tool, but it will not be the last.
For patients with RS above 26, for older women with intermediate RS, and for younger women with a low RS and low clinical-pathologic features, RSClin may not influence treatment recommendations.
However, for the common scenario of an intermediate-risk RS and a mix of pathologic features, the accurate prognostication for distant recurrence risk and estimate of absolute benefit from chemotherapy will be terrifically helpful to oncology caregivers.
Dr. Sparano disclosed funding from the National Cancer Institute and travel support from Rhenium.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
When results of the TAILORx trial were presented at ASCO 2018, many oncologists thought it seemed too simple that a single number from a genomic assay could separate patients who would and would not benefit from adjuvant postoperative chemotherapy.
Those oncologists were right to be skeptical. Subsequent data indicated that better predictive tools were needed.
A new tool called “RSClin” may fit the bill. RSClin integrates the prognostic and predictive value of the 21-gene Oncotype DX recurrence score (RS) with the additional prognostic information conveyed by patient age, tumor grade, and tumor size.
RSClin provides individualized estimates of distant relapse risk for women with node-negative, endocrine sensitive, HER2/neu oncogene-negative early breast cancer – and a quantification of the additive freedom from distant relapse if that patient receives adjuvant chemotherapy. The tool is now available via a tab on the professional portal at https://online.genomichealth.com/.
Details on RSClin, including how the tool was developed and validated, were presented at the 2020 San Antonio Breast Cancer Symposium by Joseph A. Sparano, MD, of Albert Einstein College of Medicine in New York.
Beyond the initial publication of TAILORx
Results from the TAILORx trial published in The New England Journal of Medicine in 2018 offered the potential for genomic risk assessment to guide the choice of postoperative therapy for many women with the most common type of primary breast cancer. The relative risk reduction with chemotherapy increased with increasing RS result.
Subsequent analyses of the TAILORx dataset, published in The New England Journal of Medicine and JAMA Oncology in 2019, examined the added effect of parameters of clinical risk (tumor size and grade) and patient age for patients with known genomic risk.
In these analyses, clinical risk was prognostic for recurrence but did not predict the absolute magnitude of chemotherapy benefit, regardless of age. There was a trend toward chemotherapy benefit in women who were younger than 50 years of age who had RS 21-15, but it was irrespective of clinical risk.
The development of RSClin
RSClin was derived from a patient-specific meta-analysis of 10,004 women with hormone receptor–positive, HER2-negative, node-negative breast cancer, of whom 9,427 participated in the TAILORx trial.
In TAILORx, which ran from 2006 to 2015, women with RS 0-11 received contemporary hormone therapy alone. Women with RS 12-25 were randomized to receive hormone therapy alone or with conventional combination chemotherapy. Women with RS above 26 received chemotherapy plus endocrine therapy.
The other patients in the meta-analysis participated in NSABP studies B-14 (tamoxifen versus placebo) and B-20 (tamoxifen versus chemotherapy plus tamoxifen).
Cox regression models were fit separately to each study with covariates of the continuous variables of RS result, tumor size, and patient age and the discrete variable of histologic tumor grade (assessed centrally in B-14 and in local laboratories in TAILORx). The prespecified endpoint was time to first distant recurrence.
RSClin estimates of distant recurrence risk were generated using baseline risk with TAILORx event rates to reflect current medical practice.
Model estimates were calculated for specified endocrine therapy with tamoxifen or aromatase inhibitors utilizing the treatment effect hazard ratio from an Early Breast Cancer Trialists’ Collaborative Group meta-analysis.
Patient-specific absolute benefit of chemotherapy was estimated by combining patient-specific meta-analysis risk estimates for distant recurrence and for relative chemotherapy benefit using the B-20 and TAILORx trials.
RSClin results and external validation
Among all patients in the meta-analysis cohort, RSClin provided a significantly more accurate prediction of distant recurrence events, in comparison with RS alone or clinical-pathologic factors alone.
External validation was performed using data from real-world outcomes from the 1,098 evaluable node-negative patients in the Clalit Health Services registry, of whom 876 received endocrine therapy alone and 222 received endocrine therapy plus chemotherapy.
RSClin estimates of distant recurrence closely approximated the observed risk in the registry (standardized hazard ratio, 1.73; 95% confidence interval, 1.40-2.15; P < .001). Within each RSClin risk quintile, the average 10-year risk estimate approached the observed Kaplan-Meier estimates in the cohort (Lin concordance correlation = 0.962).
Shared decision-making
For many years, the dilemma of whether to recommend adjuvant chemotherapy to a patient with early breast cancer has prompted the generation of tools to quantify a patient’s risk of recurrence and the magnitude of benefit for endocrine therapy and/or chemotherapy.
When the original Adjuvant! Online program was developed, genomic risk profiling was in its infancy. Genomic tools such as the 21-gene RS have subsequently demonstrated that they can help optimize the adjuvant treatment we recommend.
The RSClin tool provides more precise, individualized information than does clinical-pathological or genomic data alone. It prognosticates the risk of distant recurrence of breast cancer, which patients and providers fervently wish to minimize.
RSClin estimates the incremental benefit of contemporary adjuvant chemotherapy over modern endocrine therapy alone, in absolute values, for individual patients. This transparent, discrete, easily explained information is vital for counseling patients.
However, as highlighted in an editorial published in the Journal of Clinical Oncology, RSClin is not without its potential drawbacks. These include:
- Tumor heterogeneity leading to misleading results.
- Variable patient adherence to endocrine therapy or chemotherapy.
- The influence of comorbid conditions on the risk/benefit ratio.
- The potential of ovarian function suppression in young women to approach the magnitude of benefit associated with chemotherapy.
Accordingly, RSClin may be the latest and best available tool, but it will not be the last.
For patients with RS above 26, for older women with intermediate RS, and for younger women with a low RS and low clinical-pathologic features, RSClin may not influence treatment recommendations.
However, for the common scenario of an intermediate-risk RS and a mix of pathologic features, the accurate prognostication for distant recurrence risk and estimate of absolute benefit from chemotherapy will be terrifically helpful to oncology caregivers.
Dr. Sparano disclosed funding from the National Cancer Institute and travel support from Rhenium.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
When results of the TAILORx trial were presented at ASCO 2018, many oncologists thought it seemed too simple that a single number from a genomic assay could separate patients who would and would not benefit from adjuvant postoperative chemotherapy.
Those oncologists were right to be skeptical. Subsequent data indicated that better predictive tools were needed.
A new tool called “RSClin” may fit the bill. RSClin integrates the prognostic and predictive value of the 21-gene Oncotype DX recurrence score (RS) with the additional prognostic information conveyed by patient age, tumor grade, and tumor size.
RSClin provides individualized estimates of distant relapse risk for women with node-negative, endocrine sensitive, HER2/neu oncogene-negative early breast cancer – and a quantification of the additive freedom from distant relapse if that patient receives adjuvant chemotherapy. The tool is now available via a tab on the professional portal at https://online.genomichealth.com/.
Details on RSClin, including how the tool was developed and validated, were presented at the 2020 San Antonio Breast Cancer Symposium by Joseph A. Sparano, MD, of Albert Einstein College of Medicine in New York.
Beyond the initial publication of TAILORx
Results from the TAILORx trial published in The New England Journal of Medicine in 2018 offered the potential for genomic risk assessment to guide the choice of postoperative therapy for many women with the most common type of primary breast cancer. The relative risk reduction with chemotherapy increased with increasing RS result.
Subsequent analyses of the TAILORx dataset, published in The New England Journal of Medicine and JAMA Oncology in 2019, examined the added effect of parameters of clinical risk (tumor size and grade) and patient age for patients with known genomic risk.
In these analyses, clinical risk was prognostic for recurrence but did not predict the absolute magnitude of chemotherapy benefit, regardless of age. There was a trend toward chemotherapy benefit in women who were younger than 50 years of age who had RS 21-15, but it was irrespective of clinical risk.
The development of RSClin
RSClin was derived from a patient-specific meta-analysis of 10,004 women with hormone receptor–positive, HER2-negative, node-negative breast cancer, of whom 9,427 participated in the TAILORx trial.
In TAILORx, which ran from 2006 to 2015, women with RS 0-11 received contemporary hormone therapy alone. Women with RS 12-25 were randomized to receive hormone therapy alone or with conventional combination chemotherapy. Women with RS above 26 received chemotherapy plus endocrine therapy.
The other patients in the meta-analysis participated in NSABP studies B-14 (tamoxifen versus placebo) and B-20 (tamoxifen versus chemotherapy plus tamoxifen).
Cox regression models were fit separately to each study with covariates of the continuous variables of RS result, tumor size, and patient age and the discrete variable of histologic tumor grade (assessed centrally in B-14 and in local laboratories in TAILORx). The prespecified endpoint was time to first distant recurrence.
RSClin estimates of distant recurrence risk were generated using baseline risk with TAILORx event rates to reflect current medical practice.
Model estimates were calculated for specified endocrine therapy with tamoxifen or aromatase inhibitors utilizing the treatment effect hazard ratio from an Early Breast Cancer Trialists’ Collaborative Group meta-analysis.
Patient-specific absolute benefit of chemotherapy was estimated by combining patient-specific meta-analysis risk estimates for distant recurrence and for relative chemotherapy benefit using the B-20 and TAILORx trials.
RSClin results and external validation
Among all patients in the meta-analysis cohort, RSClin provided a significantly more accurate prediction of distant recurrence events, in comparison with RS alone or clinical-pathologic factors alone.
External validation was performed using data from real-world outcomes from the 1,098 evaluable node-negative patients in the Clalit Health Services registry, of whom 876 received endocrine therapy alone and 222 received endocrine therapy plus chemotherapy.
RSClin estimates of distant recurrence closely approximated the observed risk in the registry (standardized hazard ratio, 1.73; 95% confidence interval, 1.40-2.15; P < .001). Within each RSClin risk quintile, the average 10-year risk estimate approached the observed Kaplan-Meier estimates in the cohort (Lin concordance correlation = 0.962).
Shared decision-making
For many years, the dilemma of whether to recommend adjuvant chemotherapy to a patient with early breast cancer has prompted the generation of tools to quantify a patient’s risk of recurrence and the magnitude of benefit for endocrine therapy and/or chemotherapy.
When the original Adjuvant! Online program was developed, genomic risk profiling was in its infancy. Genomic tools such as the 21-gene RS have subsequently demonstrated that they can help optimize the adjuvant treatment we recommend.
The RSClin tool provides more precise, individualized information than does clinical-pathological or genomic data alone. It prognosticates the risk of distant recurrence of breast cancer, which patients and providers fervently wish to minimize.
RSClin estimates the incremental benefit of contemporary adjuvant chemotherapy over modern endocrine therapy alone, in absolute values, for individual patients. This transparent, discrete, easily explained information is vital for counseling patients.
However, as highlighted in an editorial published in the Journal of Clinical Oncology, RSClin is not without its potential drawbacks. These include:
- Tumor heterogeneity leading to misleading results.
- Variable patient adherence to endocrine therapy or chemotherapy.
- The influence of comorbid conditions on the risk/benefit ratio.
- The potential of ovarian function suppression in young women to approach the magnitude of benefit associated with chemotherapy.
Accordingly, RSClin may be the latest and best available tool, but it will not be the last.
For patients with RS above 26, for older women with intermediate RS, and for younger women with a low RS and low clinical-pathologic features, RSClin may not influence treatment recommendations.
However, for the common scenario of an intermediate-risk RS and a mix of pathologic features, the accurate prognostication for distant recurrence risk and estimate of absolute benefit from chemotherapy will be terrifically helpful to oncology caregivers.
Dr. Sparano disclosed funding from the National Cancer Institute and travel support from Rhenium.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
FROM SABCS 2020
Helping interracial couples navigate racism
Joe and Esi were in the therapist’s office wanting help with their relationship. The therapist had just asked the BIG question: How does race impact your lives?”
Esi began with her story about her ethics class, a story that was at sufficient distance from her life. Depending on her husband’s response, she would move in closer. His somewhat patronizing response made her feel both angry and that he lacked any real understanding.

“Me and a mulatto girl were in ethics class,” said Esi, who grew in Kenya. We had a White professor. He seemed to think I had no education. If you are a woman of color, you are automatically thought to have no education and that you don’t know what you are talking about. He tried to shut me up. When I persisted, I know he thought from the tone of my voice that I was an angry Black woman, even although I am not Black and I am not angry! In this country, if you have any color to your skin, you are called Black and relegated to a certain place: The bottom. I was excited about what he was teaching us, but when everyone looked at me with a certain gaze, like something bad was going to happen, all those White people, just looking, I tightened up inside and sat back down.”

Esi looked down at her folded hands. Her husband, who was White, reached over and reassuringly patted her hands.
“Yes, Esi, they are wrong. They shouldn’t have treated you that way. White people can be insensitive.”
Then, she continued, “Joe, you do the same to me!”
“What do you mean, Esi?” responded Joe, with an innocent and anxious look scanning back and forth between her and the White male therapist.
“Well, Joe, do you really want to hear how I felt last week after we came back from that party at your sister’s house?”
“Yes, Esi.”
“But do you really? Are you sure you want to hear this?”
“Yes, Esi.”
“Remember when we went over, me and the kids sat with the other people of color and you sat with your sister and her side of the family?
“Yes, I remember. What is wrong with that?”
“Well, me and my colored friends got loud and excited, and you shot me a look, like ‘pipe down over there.’ THEN, after we got home, the next day, your sister called you and said that you had better control your wife; she is too loud. Do you remember all that?
“Yes, well you do get loud – especially when you are around your people.”
“So why is it I have to fit in with your relatives and not the other way round? Why do I have to conform to the whiteness in your sister’s world, not the other way round?”
“Well, we were in her house.”
“So if they came to our house and were too quiet, how would you feel if I called them up and said they needed to participate with more enthusiasm?”
“Esi, that’s not fair, and you know it isn’t.”
Esi stops and looks at the therapist.
“So I check myself. It is the same all over, White people imposing their values and beliefs on me, on us. I am not an angry Black woman. I am just frustrated. People, White people, always want an explanation for what they think is my loss of control. You can see when their demeanor changes, they pull back, sit up, back away, fidget, and won’t look you in the eye. All these little tics that show that they are trying to get out of the situation.”
Esi took a breath and saw that her husband and the therapist were listening.
“These signs are ingrained in your brain ... these signs ... I saw it when I first came here to this country. The first time I had a good dose of it ... was in that ethics class in college. You can’t use words that you are accustomed to, ’cause they mean something else here, something bad.”
“Oh, Esi, I am so sorry,” said Joe, looking concerned.
“You may be sorry but you are not willing to stand up for me against your sister and her White values. You want me to conform.”
“What do you want me to do?”
“I want you to call your sister out.”
“But she may not ever speak to me again!”
“OK, don’t then,” and Esi looked down at her hands. She was finished talking. Joe looked at the therapist, waiting for something.
The therapist resisted intervening on the issue. “Keep talking this through,” he instructed them.
Joe could see that Esi had done talking and that it was his move.
“Do you really want me to call my sister out, even if it means that she will not talk to me again?”
“Yes.”
“I don’t know if I can do that.”
The therapist now intervened: “What does that mean to you, Esi, that he doesn’t know if he can do that.”
“It means he doesn’t really love me or value me or even value our mulatto children. What do think our daughter is learning?”
“That’s not true, Esi.”
The therapist, Dr. Swarthmore, watched Esi, who has very a dark, blue-black skin tone, with a flawless complexion and a shapely body. She wears her hair cropped and she looks like that Black model, what’s her name. Joe was short, a little plump with ultra White skin and freckles on his nose. He had been brought up in the Midwest and had had little exposure to Africans before his internship abroad in Kenya. Dr. S. thought he had probably not really thought much about Esi’s dilemma.
Dr. Swarthmore encouraged Esi to talk about her immigration experience.
“Esi, can you talk more about what it is like to be an immigrant from Africa?”
“Well, I just have to check myself so that I can fit in with this White culture. If you want to see how I feel about it, you will have to see an angry Black woman and I have learned not to give you that satisfaction. You will just dismiss me. Please Dr. Swarthmore, can we move on?”
Dr. Swarthmore was caught between his desire to accept her wish to move on and his wish to have her express herself fully. He realized that it was not his desire that mattered; that the couple had to work this out between them if they were going to move forward. So he punted it back to them.
“Esi and Joe, you are both caught in an important dilemma. Esi, you want more respect from your husband and his family. Joe, you do not want to upset your family by confronting them. Is that right? You are both dammed if you do and dammed if you don’t.”
“I agree,” Joe and Esi both said, nodding.
“Do you want to work on this issue?”
They both agreed with equal enthusiasm.
“Ok, can you spend the next 10 minutes to work on this?”
They agreed.
“Ok, let’s start. What skills do you have that can help you resolve this important issue?”
Dr. Swarthmore framed the issue as one to be solved by the couple. The couple discussed that they are usually good at communication and solving problems. This problem is about whether or not Joe is more aligned with his White family than with Esi and their children.
Dr. Swarthmore encouraged them to think about this more deeply and over time; that this is such an important issue that it requires time and deep conversation.
“How do you think you can educate yourselves about the issues at hand?”
Esi’s reading list
1. “Why I’m No Longer Talking to White People About Race” by Reni Eddo-Lodge (London: Bloomsbury, 2018).
2. “Americanah” by Chimamanda Ngozi Adichie (New York: Alfred A. Knopf, 2013).
3. “How to be an Antiracist” by Ibram X. Kendi (New York: Random House, 2019).
Joe suggests that Esi think about what it might mean if his sister and their children were no longer part of their lives. She agrees to do this.
Dr. Swarthmore asks if they can each do their homework before they come back. They agree and thought they could manage that and the book for 2 weeks out.
Dr. Swarthmore decides that he will read one of the books Esi suggested, as he does not know much about racism and White privilege and he wants to learn more. Dr. Swarthmore demonstrates his desire to become more racially sensitive. The following steps can be taken by therapists who want to become more racially sensitive, according to TA Laszloffy and KV Hardy (Fam Process. 2000 Spring;39[1]:35-50):
1. Read and watch movies that address the experience of other cultural groups.
2. Go to and participate in cross-cultural events.
3. Engage in a racial self-exploration process. The following questions can begin the racial identity exploration process:
- How do I define myself racially?
- When did I first become aware of race/skin color in general, and mine in particular?
- What messages did I learn about race/skin color based on that first experience?
- What direct and indirect messages did I receive about race/skin color?
- How did the messages that I received about race/skin color affect how I thought and felt about myself racially?
- What benefits did I gain because of my race/skin color?
- What did I lose because of my race/skin?
- Have I ever dated cross-racially? Why or why not?
- How many friends of a different race do I have?
4. Internal commitment. This means committing to addressing racism in therapeutic encounters.
Lessons learned for psychiatrists
1. Therapeutic space is allocated to discuss the issue.
2. The time is strictly limited to 10 minutes, so the couple won’t feel that their emotions will overwhelm them.
3. The space is to focus on the strengths that they can bring to resolving the issue.
4. Give patients the impression that they can solve this and that it is an important issue.
5. Do not put yourself in the patients’ argument; take neither side.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest. Dr. Heru wrote the article in collaboration with Lynette Ramsingh Barros, artist and social commentator.
Joe and Esi were in the therapist’s office wanting help with their relationship. The therapist had just asked the BIG question: How does race impact your lives?”
Esi began with her story about her ethics class, a story that was at sufficient distance from her life. Depending on her husband’s response, she would move in closer. His somewhat patronizing response made her feel both angry and that he lacked any real understanding.
“Me and a mulatto girl were in ethics class,” said Esi, who grew in Kenya. We had a White professor. He seemed to think I had no education. If you are a woman of color, you are automatically thought to have no education and that you don’t know what you are talking about. He tried to shut me up. When I persisted, I know he thought from the tone of my voice that I was an angry Black woman, even although I am not Black and I am not angry! In this country, if you have any color to your skin, you are called Black and relegated to a certain place: The bottom. I was excited about what he was teaching us, but when everyone looked at me with a certain gaze, like something bad was going to happen, all those White people, just looking, I tightened up inside and sat back down.”
Esi looked down at her folded hands. Her husband, who was White, reached over and reassuringly patted her hands.
“Yes, Esi, they are wrong. They shouldn’t have treated you that way. White people can be insensitive.”
Then, she continued, “Joe, you do the same to me!”
“What do you mean, Esi?” responded Joe, with an innocent and anxious look scanning back and forth between her and the White male therapist.
“Well, Joe, do you really want to hear how I felt last week after we came back from that party at your sister’s house?”
“Yes, Esi.”
“But do you really? Are you sure you want to hear this?”
“Yes, Esi.”
“Remember when we went over, me and the kids sat with the other people of color and you sat with your sister and her side of the family?
“Yes, I remember. What is wrong with that?”
“Well, me and my colored friends got loud and excited, and you shot me a look, like ‘pipe down over there.’ THEN, after we got home, the next day, your sister called you and said that you had better control your wife; she is too loud. Do you remember all that?
“Yes, well you do get loud – especially when you are around your people.”
“So why is it I have to fit in with your relatives and not the other way round? Why do I have to conform to the whiteness in your sister’s world, not the other way round?”
“Well, we were in her house.”
“So if they came to our house and were too quiet, how would you feel if I called them up and said they needed to participate with more enthusiasm?”
“Esi, that’s not fair, and you know it isn’t.”
Esi stops and looks at the therapist.
“So I check myself. It is the same all over, White people imposing their values and beliefs on me, on us. I am not an angry Black woman. I am just frustrated. People, White people, always want an explanation for what they think is my loss of control. You can see when their demeanor changes, they pull back, sit up, back away, fidget, and won’t look you in the eye. All these little tics that show that they are trying to get out of the situation.”
Esi took a breath and saw that her husband and the therapist were listening.
“These signs are ingrained in your brain ... these signs ... I saw it when I first came here to this country. The first time I had a good dose of it ... was in that ethics class in college. You can’t use words that you are accustomed to, ’cause they mean something else here, something bad.”
“Oh, Esi, I am so sorry,” said Joe, looking concerned.
“You may be sorry but you are not willing to stand up for me against your sister and her White values. You want me to conform.”
“What do you want me to do?”
“I want you to call your sister out.”
“But she may not ever speak to me again!”
“OK, don’t then,” and Esi looked down at her hands. She was finished talking. Joe looked at the therapist, waiting for something.
The therapist resisted intervening on the issue. “Keep talking this through,” he instructed them.
Joe could see that Esi had done talking and that it was his move.
“Do you really want me to call my sister out, even if it means that she will not talk to me again?”
“Yes.”
“I don’t know if I can do that.”
The therapist now intervened: “What does that mean to you, Esi, that he doesn’t know if he can do that.”
“It means he doesn’t really love me or value me or even value our mulatto children. What do think our daughter is learning?”
“That’s not true, Esi.”
The therapist, Dr. Swarthmore, watched Esi, who has very a dark, blue-black skin tone, with a flawless complexion and a shapely body. She wears her hair cropped and she looks like that Black model, what’s her name. Joe was short, a little plump with ultra White skin and freckles on his nose. He had been brought up in the Midwest and had had little exposure to Africans before his internship abroad in Kenya. Dr. S. thought he had probably not really thought much about Esi’s dilemma.
Dr. Swarthmore encouraged Esi to talk about her immigration experience.
“Esi, can you talk more about what it is like to be an immigrant from Africa?”
“Well, I just have to check myself so that I can fit in with this White culture. If you want to see how I feel about it, you will have to see an angry Black woman and I have learned not to give you that satisfaction. You will just dismiss me. Please Dr. Swarthmore, can we move on?”
Dr. Swarthmore was caught between his desire to accept her wish to move on and his wish to have her express herself fully. He realized that it was not his desire that mattered; that the couple had to work this out between them if they were going to move forward. So he punted it back to them.
“Esi and Joe, you are both caught in an important dilemma. Esi, you want more respect from your husband and his family. Joe, you do not want to upset your family by confronting them. Is that right? You are both dammed if you do and dammed if you don’t.”
“I agree,” Joe and Esi both said, nodding.
“Do you want to work on this issue?”
They both agreed with equal enthusiasm.
“Ok, can you spend the next 10 minutes to work on this?”
They agreed.
“Ok, let’s start. What skills do you have that can help you resolve this important issue?”
Dr. Swarthmore framed the issue as one to be solved by the couple. The couple discussed that they are usually good at communication and solving problems. This problem is about whether or not Joe is more aligned with his White family than with Esi and their children.
Dr. Swarthmore encouraged them to think about this more deeply and over time; that this is such an important issue that it requires time and deep conversation.
“How do you think you can educate yourselves about the issues at hand?”
Esi’s reading list
1. “Why I’m No Longer Talking to White People About Race” by Reni Eddo-Lodge (London: Bloomsbury, 2018).
2. “Americanah” by Chimamanda Ngozi Adichie (New York: Alfred A. Knopf, 2013).
3. “How to be an Antiracist” by Ibram X. Kendi (New York: Random House, 2019).
Joe suggests that Esi think about what it might mean if his sister and their children were no longer part of their lives. She agrees to do this.
Dr. Swarthmore asks if they can each do their homework before they come back. They agree and thought they could manage that and the book for 2 weeks out.
Dr. Swarthmore decides that he will read one of the books Esi suggested, as he does not know much about racism and White privilege and he wants to learn more. Dr. Swarthmore demonstrates his desire to become more racially sensitive. The following steps can be taken by therapists who want to become more racially sensitive, according to TA Laszloffy and KV Hardy (Fam Process. 2000 Spring;39[1]:35-50):
1. Read and watch movies that address the experience of other cultural groups.
2. Go to and participate in cross-cultural events.
3. Engage in a racial self-exploration process. The following questions can begin the racial identity exploration process:
- How do I define myself racially?
- When did I first become aware of race/skin color in general, and mine in particular?
- What messages did I learn about race/skin color based on that first experience?
- What direct and indirect messages did I receive about race/skin color?
- How did the messages that I received about race/skin color affect how I thought and felt about myself racially?
- What benefits did I gain because of my race/skin color?
- What did I lose because of my race/skin?
- Have I ever dated cross-racially? Why or why not?
- How many friends of a different race do I have?
4. Internal commitment. This means committing to addressing racism in therapeutic encounters.
Lessons learned for psychiatrists
1. Therapeutic space is allocated to discuss the issue.
2. The time is strictly limited to 10 minutes, so the couple won’t feel that their emotions will overwhelm them.
3. The space is to focus on the strengths that they can bring to resolving the issue.
4. Give patients the impression that they can solve this and that it is an important issue.
5. Do not put yourself in the patients’ argument; take neither side.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest. Dr. Heru wrote the article in collaboration with Lynette Ramsingh Barros, artist and social commentator.
Joe and Esi were in the therapist’s office wanting help with their relationship. The therapist had just asked the BIG question: How does race impact your lives?”
Esi began with her story about her ethics class, a story that was at sufficient distance from her life. Depending on her husband’s response, she would move in closer. His somewhat patronizing response made her feel both angry and that he lacked any real understanding.
“Me and a mulatto girl were in ethics class,” said Esi, who grew in Kenya. We had a White professor. He seemed to think I had no education. If you are a woman of color, you are automatically thought to have no education and that you don’t know what you are talking about. He tried to shut me up. When I persisted, I know he thought from the tone of my voice that I was an angry Black woman, even although I am not Black and I am not angry! In this country, if you have any color to your skin, you are called Black and relegated to a certain place: The bottom. I was excited about what he was teaching us, but when everyone looked at me with a certain gaze, like something bad was going to happen, all those White people, just looking, I tightened up inside and sat back down.”
Esi looked down at her folded hands. Her husband, who was White, reached over and reassuringly patted her hands.
“Yes, Esi, they are wrong. They shouldn’t have treated you that way. White people can be insensitive.”
Then, she continued, “Joe, you do the same to me!”
“What do you mean, Esi?” responded Joe, with an innocent and anxious look scanning back and forth between her and the White male therapist.
“Well, Joe, do you really want to hear how I felt last week after we came back from that party at your sister’s house?”
“Yes, Esi.”
“But do you really? Are you sure you want to hear this?”
“Yes, Esi.”
“Remember when we went over, me and the kids sat with the other people of color and you sat with your sister and her side of the family?
“Yes, I remember. What is wrong with that?”
“Well, me and my colored friends got loud and excited, and you shot me a look, like ‘pipe down over there.’ THEN, after we got home, the next day, your sister called you and said that you had better control your wife; she is too loud. Do you remember all that?
“Yes, well you do get loud – especially when you are around your people.”
“So why is it I have to fit in with your relatives and not the other way round? Why do I have to conform to the whiteness in your sister’s world, not the other way round?”
“Well, we were in her house.”
“So if they came to our house and were too quiet, how would you feel if I called them up and said they needed to participate with more enthusiasm?”
“Esi, that’s not fair, and you know it isn’t.”
Esi stops and looks at the therapist.
“So I check myself. It is the same all over, White people imposing their values and beliefs on me, on us. I am not an angry Black woman. I am just frustrated. People, White people, always want an explanation for what they think is my loss of control. You can see when their demeanor changes, they pull back, sit up, back away, fidget, and won’t look you in the eye. All these little tics that show that they are trying to get out of the situation.”
Esi took a breath and saw that her husband and the therapist were listening.
“These signs are ingrained in your brain ... these signs ... I saw it when I first came here to this country. The first time I had a good dose of it ... was in that ethics class in college. You can’t use words that you are accustomed to, ’cause they mean something else here, something bad.”
“Oh, Esi, I am so sorry,” said Joe, looking concerned.
“You may be sorry but you are not willing to stand up for me against your sister and her White values. You want me to conform.”
“What do you want me to do?”
“I want you to call your sister out.”
“But she may not ever speak to me again!”
“OK, don’t then,” and Esi looked down at her hands. She was finished talking. Joe looked at the therapist, waiting for something.
The therapist resisted intervening on the issue. “Keep talking this through,” he instructed them.
Joe could see that Esi had done talking and that it was his move.
“Do you really want me to call my sister out, even if it means that she will not talk to me again?”
“Yes.”
“I don’t know if I can do that.”
The therapist now intervened: “What does that mean to you, Esi, that he doesn’t know if he can do that.”
“It means he doesn’t really love me or value me or even value our mulatto children. What do think our daughter is learning?”
“That’s not true, Esi.”
The therapist, Dr. Swarthmore, watched Esi, who has very a dark, blue-black skin tone, with a flawless complexion and a shapely body. She wears her hair cropped and she looks like that Black model, what’s her name. Joe was short, a little plump with ultra White skin and freckles on his nose. He had been brought up in the Midwest and had had little exposure to Africans before his internship abroad in Kenya. Dr. S. thought he had probably not really thought much about Esi’s dilemma.
Dr. Swarthmore encouraged Esi to talk about her immigration experience.
“Esi, can you talk more about what it is like to be an immigrant from Africa?”
“Well, I just have to check myself so that I can fit in with this White culture. If you want to see how I feel about it, you will have to see an angry Black woman and I have learned not to give you that satisfaction. You will just dismiss me. Please Dr. Swarthmore, can we move on?”
Dr. Swarthmore was caught between his desire to accept her wish to move on and his wish to have her express herself fully. He realized that it was not his desire that mattered; that the couple had to work this out between them if they were going to move forward. So he punted it back to them.
“Esi and Joe, you are both caught in an important dilemma. Esi, you want more respect from your husband and his family. Joe, you do not want to upset your family by confronting them. Is that right? You are both dammed if you do and dammed if you don’t.”
“I agree,” Joe and Esi both said, nodding.
“Do you want to work on this issue?”
They both agreed with equal enthusiasm.
“Ok, can you spend the next 10 minutes to work on this?”
They agreed.
“Ok, let’s start. What skills do you have that can help you resolve this important issue?”
Dr. Swarthmore framed the issue as one to be solved by the couple. The couple discussed that they are usually good at communication and solving problems. This problem is about whether or not Joe is more aligned with his White family than with Esi and their children.
Dr. Swarthmore encouraged them to think about this more deeply and over time; that this is such an important issue that it requires time and deep conversation.
“How do you think you can educate yourselves about the issues at hand?”
Esi’s reading list
1. “Why I’m No Longer Talking to White People About Race” by Reni Eddo-Lodge (London: Bloomsbury, 2018).
2. “Americanah” by Chimamanda Ngozi Adichie (New York: Alfred A. Knopf, 2013).
3. “How to be an Antiracist” by Ibram X. Kendi (New York: Random House, 2019).
Joe suggests that Esi think about what it might mean if his sister and their children were no longer part of their lives. She agrees to do this.
Dr. Swarthmore asks if they can each do their homework before they come back. They agree and thought they could manage that and the book for 2 weeks out.
Dr. Swarthmore decides that he will read one of the books Esi suggested, as he does not know much about racism and White privilege and he wants to learn more. Dr. Swarthmore demonstrates his desire to become more racially sensitive. The following steps can be taken by therapists who want to become more racially sensitive, according to TA Laszloffy and KV Hardy (Fam Process. 2000 Spring;39[1]:35-50):
1. Read and watch movies that address the experience of other cultural groups.
2. Go to and participate in cross-cultural events.
3. Engage in a racial self-exploration process. The following questions can begin the racial identity exploration process:
- How do I define myself racially?
- When did I first become aware of race/skin color in general, and mine in particular?
- What messages did I learn about race/skin color based on that first experience?
- What direct and indirect messages did I receive about race/skin color?
- How did the messages that I received about race/skin color affect how I thought and felt about myself racially?
- What benefits did I gain because of my race/skin color?
- What did I lose because of my race/skin?
- Have I ever dated cross-racially? Why or why not?
- How many friends of a different race do I have?
4. Internal commitment. This means committing to addressing racism in therapeutic encounters.
Lessons learned for psychiatrists
1. Therapeutic space is allocated to discuss the issue.
2. The time is strictly limited to 10 minutes, so the couple won’t feel that their emotions will overwhelm them.
3. The space is to focus on the strengths that they can bring to resolving the issue.
4. Give patients the impression that they can solve this and that it is an important issue.
5. Do not put yourself in the patients’ argument; take neither side.
Dr. Heru is professor of psychiatry at the University of Colorado at Denver, Aurora. She is editor of “Working With Families in Medical Settings: A Multidisciplinary Guide for Psychiatrists and Other Health Professionals” (New York: Routledge, 2013). She has no conflicts of interest. Dr. Heru wrote the article in collaboration with Lynette Ramsingh Barros, artist and social commentator.
‘The Undoing’: A dramatization of ‘You Should Have Known’
Jean Hanff Korelitz’s ironic psychological thriller, “You Should Have Known,” (New York: Grand Central Publishing, 2014) was transformed into an HBO miniseries called “The Undoing,” written and produced by David E. Kelley and directed by Susanne Bier, which premiered on Oct. 25, 2020.

The television drama differed from the novel in fundamental ways, but both have themes related to the therapeutic process. In the novel, a New York City–based couples therapist, Grace Reinhart Sachs, had recently written a book called “You Should Have Known,” about women who married their spouses disregarding their gut instinct that their partner was not fundamentally right for them, or might potentially cheat on them, or whose stories contained contradictions. In the miniseries, Grace (played by Nicole Kidman), is a therapist but there is no mention of her having written a book. Grace in both the novel and the miniseries is married to a pediatric oncologist, Jonathan (his ethnicity and surname were changed in the miniseries from a Jewish New Yorker in the novel to a British Dr. Jonathan Fraser in the series, played by Hugh Grant).
[Spoiler alert]: Prepandemic New York City’s Upper East Side is scandalized when a murdered mother is found by her young son the day after a lavish fund-raising auction party for a private school. Grace and Jonathan’s son, Henry, attends this school as well, and Grace had served on the auction committee with the murdered mother. When two detectives question Grace in the course of their investigation, she assumes that they are questioning her as they would any parent in the school. However, when she tries to reach her husband about the news and the investigation, she cannot. She thought he was at a medical conference in Cleveland, but she realizes that she does not know exactly what conference and exactly where. After many failed attempts at calling and texting, she hears a familiar alert sound coming from his nightstand drawer where she retrieves the cell phone that had been deliberately placed.
In the novel, Jonathan never reappears from “Cleveland,” and although it takes Grace a while to understand that her husband is not who she thought he was, she eventually does. In the miniseries, Jonathan appears in their lake house and a trial ensues with Jonathan adamantly proclaiming his innocence despite all evidence to the contrary.
The Oxford Reference defines undoing as “an emotional conflict associated with an action is dealt with by negating the action or attempting ‘magically’ to cause it not to have occurred by substituting an approximately opposite action.” It is not that the consequences of the action are attempted to be negated (as in making amends or showing remorse), but the action itself. In this way, the miniseries is aptly named since both main characters, Grace and Jonathan, use this defense mechanism. Grace has difficulty acknowledging that her husband could be capable of any wrongdoing, even as she is faced with fact after fact that contradicts this premise – and counsels others about their relationship choices. Similarly, Jonathan’s choice of profession is likely an attempt to undo his 4-year-old sister’s death that occurred on his watch when he was 14. However, even treating children’s cancer cannot undo the many indiscretions he has apparently committed in his adult life.

In the portrayal of a doctor with narcissistic, and possibly psychopathic, traits, “The Undoing” joins multiple recent podcasts that document real-life bad doctors, including Wondery’s “The Shrink Next Door,” “Dr. Death” (seasons 1 and 2), and “Do No Harm.” While most physicians go into medicine to heal and improve peoples’ lives, others, such as the character of Dr. Jonathan Fraser, appear to become physicians for ulterior and sinister motivations. Jonathan’s difficulty with empathy was present when he was a child as a character trait – rather than being attributable to any childhood traumatic event, as Grace had let herself believe.
In a Dec. 11, 2020, New York Times op-ed, Richard A. Friedman, MD, a psychiatrist affiliated with New York Presbyterian-Cornell University, discussed three “dangerous doctors” during the pandemic who are potentially harming the nation. Scott Atlas, MD, a radiologist on leave from Stanford (Calif.) University, advised President Trump on the coronavirus despite having no training in public health or infectious disease. Before resigning, he questioned the use of face masks, contradicting scientific proof of their prevention of disease. Another doctor, a cardiologist in Washington, also publicly disputed scientific evidence of the efficacy of face masks and social distancing, and a third physician promoted hydroxychloroquine as a treatment for coronavirus despite scientific evidence that it has been ineffective and possibly even harmful to patients with the virus.
Both the novel “You Should Have Known” and the series “The Undoing” will be of interest to psychiatrists, especially therapists and forensic psychiatrists, because of the themes portrayed, such as defense mechanisms, therapeutic process, and a homicide investigation – as well as the common human experience of being an expert in something in one’s professional life, yet occasionally falling short of recognizing the same phenomena in one’s personal life.
Dr. Rosenbaum is a clinical and forensic psychiatrist in private practice in New York. She is an assistant clinical professor at New York University Langone Medical Center and is on the faculty at Weill-Cornell Medical Center. She has no conflicts of interest. Dr. Friedman serves as the Phillip Resnick Professor of Forensic Psychiatry at Case Western Reserve University, Cleveland. She is also editor of Family Murder: Pathologies of Love and Hate (Washington: American Psychiatric Publishing, 2019), which was written by the Group for the Advancement of Psychiatry’s Committee on Psychiatry & Law, and which was awarded the 2020 Manfred Gutmacher Award by the American Psychiatric Association. She has no conflicts of interest.
Jean Hanff Korelitz’s ironic psychological thriller, “You Should Have Known,” (New York: Grand Central Publishing, 2014) was transformed into an HBO miniseries called “The Undoing,” written and produced by David E. Kelley and directed by Susanne Bier, which premiered on Oct. 25, 2020.
The television drama differed from the novel in fundamental ways, but both have themes related to the therapeutic process. In the novel, a New York City–based couples therapist, Grace Reinhart Sachs, had recently written a book called “You Should Have Known,” about women who married their spouses disregarding their gut instinct that their partner was not fundamentally right for them, or might potentially cheat on them, or whose stories contained contradictions. In the miniseries, Grace (played by Nicole Kidman), is a therapist but there is no mention of her having written a book. Grace in both the novel and the miniseries is married to a pediatric oncologist, Jonathan (his ethnicity and surname were changed in the miniseries from a Jewish New Yorker in the novel to a British Dr. Jonathan Fraser in the series, played by Hugh Grant).
[Spoiler alert]: Prepandemic New York City’s Upper East Side is scandalized when a murdered mother is found by her young son the day after a lavish fund-raising auction party for a private school. Grace and Jonathan’s son, Henry, attends this school as well, and Grace had served on the auction committee with the murdered mother. When two detectives question Grace in the course of their investigation, she assumes that they are questioning her as they would any parent in the school. However, when she tries to reach her husband about the news and the investigation, she cannot. She thought he was at a medical conference in Cleveland, but she realizes that she does not know exactly what conference and exactly where. After many failed attempts at calling and texting, she hears a familiar alert sound coming from his nightstand drawer where she retrieves the cell phone that had been deliberately placed.
In the novel, Jonathan never reappears from “Cleveland,” and although it takes Grace a while to understand that her husband is not who she thought he was, she eventually does. In the miniseries, Jonathan appears in their lake house and a trial ensues with Jonathan adamantly proclaiming his innocence despite all evidence to the contrary.
The Oxford Reference defines undoing as “an emotional conflict associated with an action is dealt with by negating the action or attempting ‘magically’ to cause it not to have occurred by substituting an approximately opposite action.” It is not that the consequences of the action are attempted to be negated (as in making amends or showing remorse), but the action itself. In this way, the miniseries is aptly named since both main characters, Grace and Jonathan, use this defense mechanism. Grace has difficulty acknowledging that her husband could be capable of any wrongdoing, even as she is faced with fact after fact that contradicts this premise – and counsels others about their relationship choices. Similarly, Jonathan’s choice of profession is likely an attempt to undo his 4-year-old sister’s death that occurred on his watch when he was 14. However, even treating children’s cancer cannot undo the many indiscretions he has apparently committed in his adult life.
In the portrayal of a doctor with narcissistic, and possibly psychopathic, traits, “The Undoing” joins multiple recent podcasts that document real-life bad doctors, including Wondery’s “The Shrink Next Door,” “Dr. Death” (seasons 1 and 2), and “Do No Harm.” While most physicians go into medicine to heal and improve peoples’ lives, others, such as the character of Dr. Jonathan Fraser, appear to become physicians for ulterior and sinister motivations. Jonathan’s difficulty with empathy was present when he was a child as a character trait – rather than being attributable to any childhood traumatic event, as Grace had let herself believe.
In a Dec. 11, 2020, New York Times op-ed, Richard A. Friedman, MD, a psychiatrist affiliated with New York Presbyterian-Cornell University, discussed three “dangerous doctors” during the pandemic who are potentially harming the nation. Scott Atlas, MD, a radiologist on leave from Stanford (Calif.) University, advised President Trump on the coronavirus despite having no training in public health or infectious disease. Before resigning, he questioned the use of face masks, contradicting scientific proof of their prevention of disease. Another doctor, a cardiologist in Washington, also publicly disputed scientific evidence of the efficacy of face masks and social distancing, and a third physician promoted hydroxychloroquine as a treatment for coronavirus despite scientific evidence that it has been ineffective and possibly even harmful to patients with the virus.
Both the novel “You Should Have Known” and the series “The Undoing” will be of interest to psychiatrists, especially therapists and forensic psychiatrists, because of the themes portrayed, such as defense mechanisms, therapeutic process, and a homicide investigation – as well as the common human experience of being an expert in something in one’s professional life, yet occasionally falling short of recognizing the same phenomena in one’s personal life.
Dr. Rosenbaum is a clinical and forensic psychiatrist in private practice in New York. She is an assistant clinical professor at New York University Langone Medical Center and is on the faculty at Weill-Cornell Medical Center. She has no conflicts of interest. Dr. Friedman serves as the Phillip Resnick Professor of Forensic Psychiatry at Case Western Reserve University, Cleveland. She is also editor of Family Murder: Pathologies of Love and Hate (Washington: American Psychiatric Publishing, 2019), which was written by the Group for the Advancement of Psychiatry’s Committee on Psychiatry & Law, and which was awarded the 2020 Manfred Gutmacher Award by the American Psychiatric Association. She has no conflicts of interest.
Jean Hanff Korelitz’s ironic psychological thriller, “You Should Have Known,” (New York: Grand Central Publishing, 2014) was transformed into an HBO miniseries called “The Undoing,” written and produced by David E. Kelley and directed by Susanne Bier, which premiered on Oct. 25, 2020.
The television drama differed from the novel in fundamental ways, but both have themes related to the therapeutic process. In the novel, a New York City–based couples therapist, Grace Reinhart Sachs, had recently written a book called “You Should Have Known,” about women who married their spouses disregarding their gut instinct that their partner was not fundamentally right for them, or might potentially cheat on them, or whose stories contained contradictions. In the miniseries, Grace (played by Nicole Kidman), is a therapist but there is no mention of her having written a book. Grace in both the novel and the miniseries is married to a pediatric oncologist, Jonathan (his ethnicity and surname were changed in the miniseries from a Jewish New Yorker in the novel to a British Dr. Jonathan Fraser in the series, played by Hugh Grant).
[Spoiler alert]: Prepandemic New York City’s Upper East Side is scandalized when a murdered mother is found by her young son the day after a lavish fund-raising auction party for a private school. Grace and Jonathan’s son, Henry, attends this school as well, and Grace had served on the auction committee with the murdered mother. When two detectives question Grace in the course of their investigation, she assumes that they are questioning her as they would any parent in the school. However, when she tries to reach her husband about the news and the investigation, she cannot. She thought he was at a medical conference in Cleveland, but she realizes that she does not know exactly what conference and exactly where. After many failed attempts at calling and texting, she hears a familiar alert sound coming from his nightstand drawer where she retrieves the cell phone that had been deliberately placed.
In the novel, Jonathan never reappears from “Cleveland,” and although it takes Grace a while to understand that her husband is not who she thought he was, she eventually does. In the miniseries, Jonathan appears in their lake house and a trial ensues with Jonathan adamantly proclaiming his innocence despite all evidence to the contrary.
The Oxford Reference defines undoing as “an emotional conflict associated with an action is dealt with by negating the action or attempting ‘magically’ to cause it not to have occurred by substituting an approximately opposite action.” It is not that the consequences of the action are attempted to be negated (as in making amends or showing remorse), but the action itself. In this way, the miniseries is aptly named since both main characters, Grace and Jonathan, use this defense mechanism. Grace has difficulty acknowledging that her husband could be capable of any wrongdoing, even as she is faced with fact after fact that contradicts this premise – and counsels others about their relationship choices. Similarly, Jonathan’s choice of profession is likely an attempt to undo his 4-year-old sister’s death that occurred on his watch when he was 14. However, even treating children’s cancer cannot undo the many indiscretions he has apparently committed in his adult life.
In the portrayal of a doctor with narcissistic, and possibly psychopathic, traits, “The Undoing” joins multiple recent podcasts that document real-life bad doctors, including Wondery’s “The Shrink Next Door,” “Dr. Death” (seasons 1 and 2), and “Do No Harm.” While most physicians go into medicine to heal and improve peoples’ lives, others, such as the character of Dr. Jonathan Fraser, appear to become physicians for ulterior and sinister motivations. Jonathan’s difficulty with empathy was present when he was a child as a character trait – rather than being attributable to any childhood traumatic event, as Grace had let herself believe.
In a Dec. 11, 2020, New York Times op-ed, Richard A. Friedman, MD, a psychiatrist affiliated with New York Presbyterian-Cornell University, discussed three “dangerous doctors” during the pandemic who are potentially harming the nation. Scott Atlas, MD, a radiologist on leave from Stanford (Calif.) University, advised President Trump on the coronavirus despite having no training in public health or infectious disease. Before resigning, he questioned the use of face masks, contradicting scientific proof of their prevention of disease. Another doctor, a cardiologist in Washington, also publicly disputed scientific evidence of the efficacy of face masks and social distancing, and a third physician promoted hydroxychloroquine as a treatment for coronavirus despite scientific evidence that it has been ineffective and possibly even harmful to patients with the virus.
Both the novel “You Should Have Known” and the series “The Undoing” will be of interest to psychiatrists, especially therapists and forensic psychiatrists, because of the themes portrayed, such as defense mechanisms, therapeutic process, and a homicide investigation – as well as the common human experience of being an expert in something in one’s professional life, yet occasionally falling short of recognizing the same phenomena in one’s personal life.
Dr. Rosenbaum is a clinical and forensic psychiatrist in private practice in New York. She is an assistant clinical professor at New York University Langone Medical Center and is on the faculty at Weill-Cornell Medical Center. She has no conflicts of interest. Dr. Friedman serves as the Phillip Resnick Professor of Forensic Psychiatry at Case Western Reserve University, Cleveland. She is also editor of Family Murder: Pathologies of Love and Hate (Washington: American Psychiatric Publishing, 2019), which was written by the Group for the Advancement of Psychiatry’s Committee on Psychiatry & Law, and which was awarded the 2020 Manfred Gutmacher Award by the American Psychiatric Association. She has no conflicts of interest.
Solutions to the pandemic must include public behavior
Many scientific problems are complex. Finding the solution can require the concerted efforts of a team. Producing a vaccine for COVID-19 involved a multidisciplinary team with a variety of highly specialized expertises, extensive technological resources, and a history of previous scientific discoveries upon whose shoulders today’s scientists can stand.

Many ethical problems are also complex. Finding the ideal, multifaceted answer that addresses all the nuances of a social problem requires brilliant minds, a refined ability for logical analysis and rhetoric, the empowerment of the voices of all stakeholders, and attention to social values such as diversity and justice.
In both endeavors, the typical scientists and ethicists involved tend to presume that if they can determine an ideal solution, it will be rapidly and enthusiastically adopted and implemented for the betterment of society. That is, after all, exactly how those researchers would choose to act. Scientists see moral actions as having two steps. The hard part is deciding what is right. Doing the right thing is the easier task. This delusion is ubiquitous. Many scientists and ethicists recognize the delusion of the existence of a rational society, but proceed anyhow as if one exists.
There is a chorus of voices capable of debunking this delusion. Any priest who hears confessions will testify that the vast majority of harm comes from the failure to do what people already know is right, not from uncertainty, confusion, or ignorance. Psychologists and substance abuse counselors are inundated with people who are stuck doing harmful and self-destructive acts. Internists discuss diet and exercise with their patients, but find the advice is infrequently adopted. Master in business administration programs are devoted to training graduates in methods of motivating people to do what is right.
The response of the scientific establishment to the COVID-19 pandemic was imperfect. There were gaps in knowledge and some early information from China was misleading. The initial CDC test kit production was flawed. The early appeal for the public not to buy masks was strongly driven by a desire to preserve supplies for health care workers. Despite these missteps, the overall advice of scientists was wildly successful and beneficial. The goal was to flatten the curve, and a comparison of the April-June time frame with the November-January period shows markedly fewer COVID-19 cases, hospitalizations, and deaths. Confronted with the pandemic of the century, my assessment is that scientific establishment has performed well.
I am far more negative in my assessment of the institutions that support morality, form the social order, establish justice, and promote the general welfare. For instance, misinformation on social media is rampant, including conspiracy theories and outright denials of the pandemic. Scientific advice has been undercut and impugned. Policy recommendations of esteemed scientific institutions have been ignored. The public’s cooperation has fatigued. Laws on public gatherings, quarantines, and social distancing have been broken. Communitarian ethics and devotion to the common good have been left in a trash heap. The consequences have been hundreds of thousands of lives lost in 2020 and some states are on the brink of much worse.
Medical ethicists have debated in fine detail how to triage ventilators, ration antibody treatments, and prioritize vaccinations. Those policy recommendations have had limited influence. Medical ethics has inadequately addressed the age old problem of morality, which is getting people to behave as they know they ought. Modern medical ethics may have exacerbated the deviancy. Medical ethics for 50 years has emphasized replacing paternalism with autonomy, but it has not adequately promoted communitarian virtues, self-regulation, and personal integrity.
There were many accomplishments and many people to admire in 2020 when compared to historical actions by the health care professionals during crises. Doctors, confronted with the COVID-19 plague, have not abandoned the cities as happened in prior centuries. Patients have not been shunned like lepers, though the total-body protective equipment and the no-visitor policies come very close. Nurses have heroically provided bedside care, though I am haunted by one dissident nurse during a protest carrying a sign saying “Don’t call me a hero. I am being martyred against my will.”
As a scientist, I am prone to the delusion that, if I can build a better mouse trap, people will use it. I’ve lived with that delusion for decades. It carries over into my medical ethics work. Yet I see hospitals in California being overwhelmed by the surge on top of a surge due to unwise and unsafe holiday travel. I can see that optimized solutions aren’t the answer – it is better behavior by the public. I recall when I was a child, my mother would simply command, “Behave yourself.” And never, in any of those recollections, was I in doubt about which correct behavior she meant.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
Many scientific problems are complex. Finding the solution can require the concerted efforts of a team. Producing a vaccine for COVID-19 involved a multidisciplinary team with a variety of highly specialized expertises, extensive technological resources, and a history of previous scientific discoveries upon whose shoulders today’s scientists can stand.
Many ethical problems are also complex. Finding the ideal, multifaceted answer that addresses all the nuances of a social problem requires brilliant minds, a refined ability for logical analysis and rhetoric, the empowerment of the voices of all stakeholders, and attention to social values such as diversity and justice.
In both endeavors, the typical scientists and ethicists involved tend to presume that if they can determine an ideal solution, it will be rapidly and enthusiastically adopted and implemented for the betterment of society. That is, after all, exactly how those researchers would choose to act. Scientists see moral actions as having two steps. The hard part is deciding what is right. Doing the right thing is the easier task. This delusion is ubiquitous. Many scientists and ethicists recognize the delusion of the existence of a rational society, but proceed anyhow as if one exists.
There is a chorus of voices capable of debunking this delusion. Any priest who hears confessions will testify that the vast majority of harm comes from the failure to do what people already know is right, not from uncertainty, confusion, or ignorance. Psychologists and substance abuse counselors are inundated with people who are stuck doing harmful and self-destructive acts. Internists discuss diet and exercise with their patients, but find the advice is infrequently adopted. Master in business administration programs are devoted to training graduates in methods of motivating people to do what is right.
The response of the scientific establishment to the COVID-19 pandemic was imperfect. There were gaps in knowledge and some early information from China was misleading. The initial CDC test kit production was flawed. The early appeal for the public not to buy masks was strongly driven by a desire to preserve supplies for health care workers. Despite these missteps, the overall advice of scientists was wildly successful and beneficial. The goal was to flatten the curve, and a comparison of the April-June time frame with the November-January period shows markedly fewer COVID-19 cases, hospitalizations, and deaths. Confronted with the pandemic of the century, my assessment is that scientific establishment has performed well.
I am far more negative in my assessment of the institutions that support morality, form the social order, establish justice, and promote the general welfare. For instance, misinformation on social media is rampant, including conspiracy theories and outright denials of the pandemic. Scientific advice has been undercut and impugned. Policy recommendations of esteemed scientific institutions have been ignored. The public’s cooperation has fatigued. Laws on public gatherings, quarantines, and social distancing have been broken. Communitarian ethics and devotion to the common good have been left in a trash heap. The consequences have been hundreds of thousands of lives lost in 2020 and some states are on the brink of much worse.
Medical ethicists have debated in fine detail how to triage ventilators, ration antibody treatments, and prioritize vaccinations. Those policy recommendations have had limited influence. Medical ethics has inadequately addressed the age old problem of morality, which is getting people to behave as they know they ought. Modern medical ethics may have exacerbated the deviancy. Medical ethics for 50 years has emphasized replacing paternalism with autonomy, but it has not adequately promoted communitarian virtues, self-regulation, and personal integrity.
There were many accomplishments and many people to admire in 2020 when compared to historical actions by the health care professionals during crises. Doctors, confronted with the COVID-19 plague, have not abandoned the cities as happened in prior centuries. Patients have not been shunned like lepers, though the total-body protective equipment and the no-visitor policies come very close. Nurses have heroically provided bedside care, though I am haunted by one dissident nurse during a protest carrying a sign saying “Don’t call me a hero. I am being martyred against my will.”
As a scientist, I am prone to the delusion that, if I can build a better mouse trap, people will use it. I’ve lived with that delusion for decades. It carries over into my medical ethics work. Yet I see hospitals in California being overwhelmed by the surge on top of a surge due to unwise and unsafe holiday travel. I can see that optimized solutions aren’t the answer – it is better behavior by the public. I recall when I was a child, my mother would simply command, “Behave yourself.” And never, in any of those recollections, was I in doubt about which correct behavior she meant.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
Many scientific problems are complex. Finding the solution can require the concerted efforts of a team. Producing a vaccine for COVID-19 involved a multidisciplinary team with a variety of highly specialized expertises, extensive technological resources, and a history of previous scientific discoveries upon whose shoulders today’s scientists can stand.
Many ethical problems are also complex. Finding the ideal, multifaceted answer that addresses all the nuances of a social problem requires brilliant minds, a refined ability for logical analysis and rhetoric, the empowerment of the voices of all stakeholders, and attention to social values such as diversity and justice.
In both endeavors, the typical scientists and ethicists involved tend to presume that if they can determine an ideal solution, it will be rapidly and enthusiastically adopted and implemented for the betterment of society. That is, after all, exactly how those researchers would choose to act. Scientists see moral actions as having two steps. The hard part is deciding what is right. Doing the right thing is the easier task. This delusion is ubiquitous. Many scientists and ethicists recognize the delusion of the existence of a rational society, but proceed anyhow as if one exists.
There is a chorus of voices capable of debunking this delusion. Any priest who hears confessions will testify that the vast majority of harm comes from the failure to do what people already know is right, not from uncertainty, confusion, or ignorance. Psychologists and substance abuse counselors are inundated with people who are stuck doing harmful and self-destructive acts. Internists discuss diet and exercise with their patients, but find the advice is infrequently adopted. Master in business administration programs are devoted to training graduates in methods of motivating people to do what is right.
The response of the scientific establishment to the COVID-19 pandemic was imperfect. There were gaps in knowledge and some early information from China was misleading. The initial CDC test kit production was flawed. The early appeal for the public not to buy masks was strongly driven by a desire to preserve supplies for health care workers. Despite these missteps, the overall advice of scientists was wildly successful and beneficial. The goal was to flatten the curve, and a comparison of the April-June time frame with the November-January period shows markedly fewer COVID-19 cases, hospitalizations, and deaths. Confronted with the pandemic of the century, my assessment is that scientific establishment has performed well.
I am far more negative in my assessment of the institutions that support morality, form the social order, establish justice, and promote the general welfare. For instance, misinformation on social media is rampant, including conspiracy theories and outright denials of the pandemic. Scientific advice has been undercut and impugned. Policy recommendations of esteemed scientific institutions have been ignored. The public’s cooperation has fatigued. Laws on public gatherings, quarantines, and social distancing have been broken. Communitarian ethics and devotion to the common good have been left in a trash heap. The consequences have been hundreds of thousands of lives lost in 2020 and some states are on the brink of much worse.
Medical ethicists have debated in fine detail how to triage ventilators, ration antibody treatments, and prioritize vaccinations. Those policy recommendations have had limited influence. Medical ethics has inadequately addressed the age old problem of morality, which is getting people to behave as they know they ought. Modern medical ethics may have exacerbated the deviancy. Medical ethics for 50 years has emphasized replacing paternalism with autonomy, but it has not adequately promoted communitarian virtues, self-regulation, and personal integrity.
There were many accomplishments and many people to admire in 2020 when compared to historical actions by the health care professionals during crises. Doctors, confronted with the COVID-19 plague, have not abandoned the cities as happened in prior centuries. Patients have not been shunned like lepers, though the total-body protective equipment and the no-visitor policies come very close. Nurses have heroically provided bedside care, though I am haunted by one dissident nurse during a protest carrying a sign saying “Don’t call me a hero. I am being martyred against my will.”
As a scientist, I am prone to the delusion that, if I can build a better mouse trap, people will use it. I’ve lived with that delusion for decades. It carries over into my medical ethics work. Yet I see hospitals in California being overwhelmed by the surge on top of a surge due to unwise and unsafe holiday travel. I can see that optimized solutions aren’t the answer – it is better behavior by the public. I recall when I was a child, my mother would simply command, “Behave yourself.” And never, in any of those recollections, was I in doubt about which correct behavior she meant.
Dr. Powell is a pediatric hospitalist and clinical ethics consultant living in St. Louis. Email him at pdnews@mdedge.com.
Polydoctoring: The case against fragmented psychiatric care
How many providers does it take to depersonalize a patient? Nine? 1. A psychiatrist for transcranial magnetic stimulation (TMS). 2. A psychiatrist for ketamine. 3. A psychiatrist who specializes in substance use disorder medication. 4. A psychiatrist for the rest of the psychotropic medication. 5. An alternative medicine provider who prescribes supplements. 6. A therapist for depression who uses cognitive-behavioral therapy. 7. A therapist for posttraumatic stress disorder who uses eye movement desensitization and reprocessing. 8. An addiction counselor. 9. An equine therapist.

This doesn’t include other providers and professionals who likely contribute to one’s mental well-being, including yoga instructors and personal trainers. In addition, any one of those psychiatrists may have one or more nurse practitioners who routinely step in to attend to appointments.
In our uncertain and lonely times, the value of human contact and interaction has become exponentially more precious. I long to see my patients in my private practice office. I am now much more aware of their grounding effect on my life, and I suspect I had a similar grounding effect on theirs. Few things provide me more comfort than sitting on my lounge chair with a curious gaze waiting for the patient to start the visit. I often wonder what makes a patient choose to go see a private practice physician. Yet a common reason offered is, “Wait! You do everything? Therapy and meds if I need them? You’ll see me every week?”
While I am realistic about the need and use of split-care, I have never been enamored with the concept. I think that few medical students choose psychiatry with the goal of referring all psychotherapeutic needs and intervention to “allied mental health providers” as my prior managed care organization liked to refer to psychologists, social workers, marriage and family therapists, and other counselors. I remember particularly as a chief resident being bombarded by complaints of therapists complaining about psychiatry residents. All of their patients’ symptoms allegedly required medication adjustment and residents were supposedly dismissing them. In return, residents would complain that the therapists did not address the psychological manifestations of the patient’s ailments. Herein lies my problem with split-care, it encourages psychotherapy to be about medication management, and medication management to be about psychotherapy.
However, this is not an article against split-treatment. Psychiatrists, for a variety of reasons, are not suited to perform psychotherapy in most management care models. The main reason being that psychiatrists’ time is too expensive to justify the expense, and psychiatrists are (for the most part), the only ones able to prescribe medications for which the wait-list is already long enough. This article is about the absurd levels at which we have fragmented care of certain patients. Split-treatment is relevant in that its negative side effects, we are almost all familiar with, exemplify the problem of the fragmentation of modern psychiatry. In many ways this fragmentation of care is similar to polypharmacy – the premise for each psychotropic intervention may be sound, but the end result is often incoherent.
My main concern with the fragmentation of modern psychiatry stems from my belief that the most important facet of our work is our relationship with our patients. It is the duty we owe them, the attention we give them, the unique nature of interactions. Who among the nine providers is responsible for writing a discharge summary? Who is responsible for calling an emergency contact in a critical situation? Who communicates with the new provider when someone is taken off an insurance panel? Who makes the patient feel cared for? I am often confronted by this situation when TMS or ketamine providers say, “I just give the procedure/medication that was ordered by the referring psychiatrist.” This response disturbs me in that I could not imagine myself being so hands off in the care of a patient. There is an implication of projected immunity and lack of responsibility that bothers me.
But my concerns are also practical. From my forensic experience, I am well aware that the larger the number of providers treating a patient, the larger the number of inconsistent diagnoses, the more likely medication reconciliations are not kept up to date or incorrect, and the more likely intervention recommendations are contrary to one another. A disengaged ketamine provider may not realize that the patient was more recently enrolled in a substance use disorder program, a potential contraindication for ketamine, if not well-abreast of the patient’s continued evolution. A substance use disorder psychiatric specialist may be at odds with a substance use disorder counselor who worries about the message of treating psychiatric symptoms with chemical substances if they don’t communicate.
As with polypharmacy, “polydoctoring” has negative effects. While the field of psychiatry’s advancing knowledge may encourage providers to specialize, patients still desire and benefit from an intimate and close relationship with one provider who is warm, concerned, and hopeful. Those traits can theoretically be provided by anyone and there is not something inherently wrong with having more than one provider. However, psychiatry would be wise to recognize this concerning trend, especially at a time when we all feel lonely, disconnected, and depersonalized.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com.
How many providers does it take to depersonalize a patient? Nine? 1. A psychiatrist for transcranial magnetic stimulation (TMS). 2. A psychiatrist for ketamine. 3. A psychiatrist who specializes in substance use disorder medication. 4. A psychiatrist for the rest of the psychotropic medication. 5. An alternative medicine provider who prescribes supplements. 6. A therapist for depression who uses cognitive-behavioral therapy. 7. A therapist for posttraumatic stress disorder who uses eye movement desensitization and reprocessing. 8. An addiction counselor. 9. An equine therapist.
This doesn’t include other providers and professionals who likely contribute to one’s mental well-being, including yoga instructors and personal trainers. In addition, any one of those psychiatrists may have one or more nurse practitioners who routinely step in to attend to appointments.
In our uncertain and lonely times, the value of human contact and interaction has become exponentially more precious. I long to see my patients in my private practice office. I am now much more aware of their grounding effect on my life, and I suspect I had a similar grounding effect on theirs. Few things provide me more comfort than sitting on my lounge chair with a curious gaze waiting for the patient to start the visit. I often wonder what makes a patient choose to go see a private practice physician. Yet a common reason offered is, “Wait! You do everything? Therapy and meds if I need them? You’ll see me every week?”
While I am realistic about the need and use of split-care, I have never been enamored with the concept. I think that few medical students choose psychiatry with the goal of referring all psychotherapeutic needs and intervention to “allied mental health providers” as my prior managed care organization liked to refer to psychologists, social workers, marriage and family therapists, and other counselors. I remember particularly as a chief resident being bombarded by complaints of therapists complaining about psychiatry residents. All of their patients’ symptoms allegedly required medication adjustment and residents were supposedly dismissing them. In return, residents would complain that the therapists did not address the psychological manifestations of the patient’s ailments. Herein lies my problem with split-care, it encourages psychotherapy to be about medication management, and medication management to be about psychotherapy.
However, this is not an article against split-treatment. Psychiatrists, for a variety of reasons, are not suited to perform psychotherapy in most management care models. The main reason being that psychiatrists’ time is too expensive to justify the expense, and psychiatrists are (for the most part), the only ones able to prescribe medications for which the wait-list is already long enough. This article is about the absurd levels at which we have fragmented care of certain patients. Split-treatment is relevant in that its negative side effects, we are almost all familiar with, exemplify the problem of the fragmentation of modern psychiatry. In many ways this fragmentation of care is similar to polypharmacy – the premise for each psychotropic intervention may be sound, but the end result is often incoherent.
My main concern with the fragmentation of modern psychiatry stems from my belief that the most important facet of our work is our relationship with our patients. It is the duty we owe them, the attention we give them, the unique nature of interactions. Who among the nine providers is responsible for writing a discharge summary? Who is responsible for calling an emergency contact in a critical situation? Who communicates with the new provider when someone is taken off an insurance panel? Who makes the patient feel cared for? I am often confronted by this situation when TMS or ketamine providers say, “I just give the procedure/medication that was ordered by the referring psychiatrist.” This response disturbs me in that I could not imagine myself being so hands off in the care of a patient. There is an implication of projected immunity and lack of responsibility that bothers me.
But my concerns are also practical. From my forensic experience, I am well aware that the larger the number of providers treating a patient, the larger the number of inconsistent diagnoses, the more likely medication reconciliations are not kept up to date or incorrect, and the more likely intervention recommendations are contrary to one another. A disengaged ketamine provider may not realize that the patient was more recently enrolled in a substance use disorder program, a potential contraindication for ketamine, if not well-abreast of the patient’s continued evolution. A substance use disorder psychiatric specialist may be at odds with a substance use disorder counselor who worries about the message of treating psychiatric symptoms with chemical substances if they don’t communicate.
As with polypharmacy, “polydoctoring” has negative effects. While the field of psychiatry’s advancing knowledge may encourage providers to specialize, patients still desire and benefit from an intimate and close relationship with one provider who is warm, concerned, and hopeful. Those traits can theoretically be provided by anyone and there is not something inherently wrong with having more than one provider. However, psychiatry would be wise to recognize this concerning trend, especially at a time when we all feel lonely, disconnected, and depersonalized.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com.
How many providers does it take to depersonalize a patient? Nine? 1. A psychiatrist for transcranial magnetic stimulation (TMS). 2. A psychiatrist for ketamine. 3. A psychiatrist who specializes in substance use disorder medication. 4. A psychiatrist for the rest of the psychotropic medication. 5. An alternative medicine provider who prescribes supplements. 6. A therapist for depression who uses cognitive-behavioral therapy. 7. A therapist for posttraumatic stress disorder who uses eye movement desensitization and reprocessing. 8. An addiction counselor. 9. An equine therapist.
This doesn’t include other providers and professionals who likely contribute to one’s mental well-being, including yoga instructors and personal trainers. In addition, any one of those psychiatrists may have one or more nurse practitioners who routinely step in to attend to appointments.
In our uncertain and lonely times, the value of human contact and interaction has become exponentially more precious. I long to see my patients in my private practice office. I am now much more aware of their grounding effect on my life, and I suspect I had a similar grounding effect on theirs. Few things provide me more comfort than sitting on my lounge chair with a curious gaze waiting for the patient to start the visit. I often wonder what makes a patient choose to go see a private practice physician. Yet a common reason offered is, “Wait! You do everything? Therapy and meds if I need them? You’ll see me every week?”
While I am realistic about the need and use of split-care, I have never been enamored with the concept. I think that few medical students choose psychiatry with the goal of referring all psychotherapeutic needs and intervention to “allied mental health providers” as my prior managed care organization liked to refer to psychologists, social workers, marriage and family therapists, and other counselors. I remember particularly as a chief resident being bombarded by complaints of therapists complaining about psychiatry residents. All of their patients’ symptoms allegedly required medication adjustment and residents were supposedly dismissing them. In return, residents would complain that the therapists did not address the psychological manifestations of the patient’s ailments. Herein lies my problem with split-care, it encourages psychotherapy to be about medication management, and medication management to be about psychotherapy.
However, this is not an article against split-treatment. Psychiatrists, for a variety of reasons, are not suited to perform psychotherapy in most management care models. The main reason being that psychiatrists’ time is too expensive to justify the expense, and psychiatrists are (for the most part), the only ones able to prescribe medications for which the wait-list is already long enough. This article is about the absurd levels at which we have fragmented care of certain patients. Split-treatment is relevant in that its negative side effects, we are almost all familiar with, exemplify the problem of the fragmentation of modern psychiatry. In many ways this fragmentation of care is similar to polypharmacy – the premise for each psychotropic intervention may be sound, but the end result is often incoherent.
My main concern with the fragmentation of modern psychiatry stems from my belief that the most important facet of our work is our relationship with our patients. It is the duty we owe them, the attention we give them, the unique nature of interactions. Who among the nine providers is responsible for writing a discharge summary? Who is responsible for calling an emergency contact in a critical situation? Who communicates with the new provider when someone is taken off an insurance panel? Who makes the patient feel cared for? I am often confronted by this situation when TMS or ketamine providers say, “I just give the procedure/medication that was ordered by the referring psychiatrist.” This response disturbs me in that I could not imagine myself being so hands off in the care of a patient. There is an implication of projected immunity and lack of responsibility that bothers me.
But my concerns are also practical. From my forensic experience, I am well aware that the larger the number of providers treating a patient, the larger the number of inconsistent diagnoses, the more likely medication reconciliations are not kept up to date or incorrect, and the more likely intervention recommendations are contrary to one another. A disengaged ketamine provider may not realize that the patient was more recently enrolled in a substance use disorder program, a potential contraindication for ketamine, if not well-abreast of the patient’s continued evolution. A substance use disorder psychiatric specialist may be at odds with a substance use disorder counselor who worries about the message of treating psychiatric symptoms with chemical substances if they don’t communicate.
As with polypharmacy, “polydoctoring” has negative effects. While the field of psychiatry’s advancing knowledge may encourage providers to specialize, patients still desire and benefit from an intimate and close relationship with one provider who is warm, concerned, and hopeful. Those traits can theoretically be provided by anyone and there is not something inherently wrong with having more than one provider. However, psychiatry would be wise to recognize this concerning trend, especially at a time when we all feel lonely, disconnected, and depersonalized.
Dr. Badre is a clinical and forensic psychiatrist in San Diego. He holds teaching positions at the University of California, San Diego, and the University of San Diego. He teaches medical education, psychopharmacology, ethics in psychiatry, and correctional care. Dr. Badre can be reached at his website, BadreMD.com.
Arguing with doctors
They think people should accept what experts advise. After all, experts work hard to learn accurate facts to promote the public’s best interests.

Those who disagree and justify their reluctance – to be vaccinated against COVID-19, for instance – are unrepentant. First of all, they are not so sure experts are public spirited. Perhaps doctors have something to gain from illness and approve vaccines for political reasons, or assign certain diagnoses to get higher reimbursement.
In this contentious climate, peculiar treatments and unproved “cures” are claimed to deserve more respect than so-called experts are willing to grant them: hydroxychloroquine, bleach, and so on.
From my perspective, what is notable about such public disputes with medical experts is not that they exist but that they are public. In private, people have always argued with doctors. Most of those arguments don’t reach public notice. They are not interesting enough.
For instance, as I think back over the years, I can recall:
- A man who preferred to treat his eczema using topical yogurt. And not just any yogurt: only low-fat, plain Market Basket. He had tried them all.
- The woman with perioral scarring. She had let an unlicensed practitioner apply a painful acid on her face – he never told her what the acid was, and she hadn’t asked – as she lay on a neighbor’s living room floor to have her “skin cancer” treated.
- The man with an obvious melanoma on his chest. He did not want to treat it, because his faith healer in Milwaukee, whom he had never met in person, assured him that “it’s all taken care of.”
I could go on.
I cite these examples only because they are striking. They are far from unique.
People argue with doctors for the same reason they argue with anybody – because they think they know better. They may have heard otherwise from a friend, a magazine article, a blog, a different kind of practitioner.
Many such disagreements are never spoken out loud, because people who expect to argue usually don’t show up at their doctors’ offices. They either stay home or see a different kind of healer. If they do visit a doctor whose point of view differs from their own, most keep disagreements to themselves, because few people relish in-person confrontation. Instead they go home and ignore medical advice there.
Even when overt disagreements do erupt at a medical visit, the doctor can often find a way to convince the patient to reconsider, or somehow deflect the clash. The physician has to at least try to convince a patient who thinks his melanoma has “been taken care of” to have it removed. Whereas if someone really prefers low-fat yogurt to topical steroids, there is no need to win the argument. If the patient decides at some point that his eczema is out of control, he can call and request a prescription. He usually won’t.
For dermatologists, medical arguments rarely involve stakes high enough to force the doctor to try changing patients’ minds or discharging them from the practice. Had I stayed in my original field of pediatrics, I would have confronted patients who refused to vaccinate their children. I would have had to negotiate a compromise – vaccinate “more slowly” – or else part ways with the family.
I always advised medical students, when they found themselves argued with, to separate patients’ needs from their own egos. Being challenged in a small room can be challenging. Still, what matters is how the patient fares, not how the doctor feels.
Public disputes with scientists during the COVID-19 pandemic strike me as being motivated by the same factors behind private disputes in physicians’ offices: skepticism, resentment, suspicion, and – often underlying all these – fear.
Public disputes carried out over social media allow for posturing and aggression. A tweet is a better medium behind which to cloak opinions in the mantle of a noble cause, such as personal freedom. It is also easier to express derision and hostility toward opponents, expert or otherwise, from behind the screen of a Twitter handle.
Fortunately, in everyday medical practice, in-your-face disputes don’t happen very often.
You do remember them, though.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at online. Write to him at dermnews@mdedge.com.
They think people should accept what experts advise. After all, experts work hard to learn accurate facts to promote the public’s best interests.
Those who disagree and justify their reluctance – to be vaccinated against COVID-19, for instance – are unrepentant. First of all, they are not so sure experts are public spirited. Perhaps doctors have something to gain from illness and approve vaccines for political reasons, or assign certain diagnoses to get higher reimbursement.
In this contentious climate, peculiar treatments and unproved “cures” are claimed to deserve more respect than so-called experts are willing to grant them: hydroxychloroquine, bleach, and so on.
From my perspective, what is notable about such public disputes with medical experts is not that they exist but that they are public. In private, people have always argued with doctors. Most of those arguments don’t reach public notice. They are not interesting enough.
For instance, as I think back over the years, I can recall:
- A man who preferred to treat his eczema using topical yogurt. And not just any yogurt: only low-fat, plain Market Basket. He had tried them all.
- The woman with perioral scarring. She had let an unlicensed practitioner apply a painful acid on her face – he never told her what the acid was, and she hadn’t asked – as she lay on a neighbor’s living room floor to have her “skin cancer” treated.
- The man with an obvious melanoma on his chest. He did not want to treat it, because his faith healer in Milwaukee, whom he had never met in person, assured him that “it’s all taken care of.”
I could go on.
I cite these examples only because they are striking. They are far from unique.
People argue with doctors for the same reason they argue with anybody – because they think they know better. They may have heard otherwise from a friend, a magazine article, a blog, a different kind of practitioner.
Many such disagreements are never spoken out loud, because people who expect to argue usually don’t show up at their doctors’ offices. They either stay home or see a different kind of healer. If they do visit a doctor whose point of view differs from their own, most keep disagreements to themselves, because few people relish in-person confrontation. Instead they go home and ignore medical advice there.
Even when overt disagreements do erupt at a medical visit, the doctor can often find a way to convince the patient to reconsider, or somehow deflect the clash. The physician has to at least try to convince a patient who thinks his melanoma has “been taken care of” to have it removed. Whereas if someone really prefers low-fat yogurt to topical steroids, there is no need to win the argument. If the patient decides at some point that his eczema is out of control, he can call and request a prescription. He usually won’t.
For dermatologists, medical arguments rarely involve stakes high enough to force the doctor to try changing patients’ minds or discharging them from the practice. Had I stayed in my original field of pediatrics, I would have confronted patients who refused to vaccinate their children. I would have had to negotiate a compromise – vaccinate “more slowly” – or else part ways with the family.
I always advised medical students, when they found themselves argued with, to separate patients’ needs from their own egos. Being challenged in a small room can be challenging. Still, what matters is how the patient fares, not how the doctor feels.
Public disputes with scientists during the COVID-19 pandemic strike me as being motivated by the same factors behind private disputes in physicians’ offices: skepticism, resentment, suspicion, and – often underlying all these – fear.
Public disputes carried out over social media allow for posturing and aggression. A tweet is a better medium behind which to cloak opinions in the mantle of a noble cause, such as personal freedom. It is also easier to express derision and hostility toward opponents, expert or otherwise, from behind the screen of a Twitter handle.
Fortunately, in everyday medical practice, in-your-face disputes don’t happen very often.
You do remember them, though.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at online. Write to him at dermnews@mdedge.com.
They think people should accept what experts advise. After all, experts work hard to learn accurate facts to promote the public’s best interests.
Those who disagree and justify their reluctance – to be vaccinated against COVID-19, for instance – are unrepentant. First of all, they are not so sure experts are public spirited. Perhaps doctors have something to gain from illness and approve vaccines for political reasons, or assign certain diagnoses to get higher reimbursement.
In this contentious climate, peculiar treatments and unproved “cures” are claimed to deserve more respect than so-called experts are willing to grant them: hydroxychloroquine, bleach, and so on.
From my perspective, what is notable about such public disputes with medical experts is not that they exist but that they are public. In private, people have always argued with doctors. Most of those arguments don’t reach public notice. They are not interesting enough.
For instance, as I think back over the years, I can recall:
- A man who preferred to treat his eczema using topical yogurt. And not just any yogurt: only low-fat, plain Market Basket. He had tried them all.
- The woman with perioral scarring. She had let an unlicensed practitioner apply a painful acid on her face – he never told her what the acid was, and she hadn’t asked – as she lay on a neighbor’s living room floor to have her “skin cancer” treated.
- The man with an obvious melanoma on his chest. He did not want to treat it, because his faith healer in Milwaukee, whom he had never met in person, assured him that “it’s all taken care of.”
I could go on.
I cite these examples only because they are striking. They are far from unique.
People argue with doctors for the same reason they argue with anybody – because they think they know better. They may have heard otherwise from a friend, a magazine article, a blog, a different kind of practitioner.
Many such disagreements are never spoken out loud, because people who expect to argue usually don’t show up at their doctors’ offices. They either stay home or see a different kind of healer. If they do visit a doctor whose point of view differs from their own, most keep disagreements to themselves, because few people relish in-person confrontation. Instead they go home and ignore medical advice there.
Even when overt disagreements do erupt at a medical visit, the doctor can often find a way to convince the patient to reconsider, or somehow deflect the clash. The physician has to at least try to convince a patient who thinks his melanoma has “been taken care of” to have it removed. Whereas if someone really prefers low-fat yogurt to topical steroids, there is no need to win the argument. If the patient decides at some point that his eczema is out of control, he can call and request a prescription. He usually won’t.
For dermatologists, medical arguments rarely involve stakes high enough to force the doctor to try changing patients’ minds or discharging them from the practice. Had I stayed in my original field of pediatrics, I would have confronted patients who refused to vaccinate their children. I would have had to negotiate a compromise – vaccinate “more slowly” – or else part ways with the family.
I always advised medical students, when they found themselves argued with, to separate patients’ needs from their own egos. Being challenged in a small room can be challenging. Still, what matters is how the patient fares, not how the doctor feels.
Public disputes with scientists during the COVID-19 pandemic strike me as being motivated by the same factors behind private disputes in physicians’ offices: skepticism, resentment, suspicion, and – often underlying all these – fear.
Public disputes carried out over social media allow for posturing and aggression. A tweet is a better medium behind which to cloak opinions in the mantle of a noble cause, such as personal freedom. It is also easier to express derision and hostility toward opponents, expert or otherwise, from behind the screen of a Twitter handle.
Fortunately, in everyday medical practice, in-your-face disputes don’t happen very often.
You do remember them, though.
Dr. Rockoff, who wrote the Dermatology News column “Under My Skin,” is now semiretired, after 40 years of practice in Brookline, Mass. He served on the clinical faculty at Tufts University, Boston, and taught senior medical students and other trainees for 30 years. His second book, “Act Like a Doctor, Think Like a Patient,” is available at online. Write to him at dermnews@mdedge.com.
Overcoming the challenges of COVID-19 for Alzheimer’s patients in long-term care, research
An alarming number of additional Alzheimer’s disease (AD) deaths have been reported across various states within the past several months, according to the Alzheimer’s Association. Centers for Disease Control and Prevention data indicate that no less than 31,000 additional people with the neurodegenerative condition had died from the beginning of the pandemic through the end of September 2020. We know that long-term care facilities have been hit hardest, and access to adequate and/or prompt testing has been cited as the most pressing issue during the onset of the pandemic.1

When ADLs become a matter of survival
For individuals affected with Alzheimer’s disease and other types of dementia, performing routine tasks may seem cumbersome and overwhelming. Many of these patients are dependent upon caregivers and family support to facilitate their activities of daily living (ADLs).
Transitioning into the “new normal” set by the pandemic milieu is not an easy task for the average AD individual, because they are now expected to comply with numerous safety instructions (for example, maintaining hygiene, social distancing, etc.). They are also expected to monitor and communicate information about the onset of any suspected symptom to their caregiver or health care clinician.
The additional tasks added to their list of ADLs are particularly distressing given their already compromised short-term memory and overall cognitive decline. Individuals with AD may also be dealing with a host of psychobehavioral challenges, such as the presence of depression, anxiety, and/or agitation amid self-isolation. Enforced social isolation tied to COVID-19 may compound those issues.
Resource diversion and mitigation strategies
Unfortunately, any disruption in services within a long-term care setting may lead to a suboptimal therapeutic environment for patients. The Washington State LTC, for example, reported experiencing a case fatality rate (CFR) exceeding more than a third of its residents; essential staff and health care clinicians were duly affected from exposure to the virus (the risk of transmission increases considerably during transport between facilities). Access to personal protective equipment (PPE) might have been hindered by availability.

Another issue with far-reaching consequences is diversion of resources for urgent care. Health care professionals may simply not be readily available for those with chronic care needs because of the enormous scale of the impact of COVID-19 upon health care systems.
Continuity of therapy might include evaluations or follow-up services via teleconferencing modalities, but an exhaustive initial onsite physical examination is often necessary for accurate diagnostics and care. Medication management for the newly diagnosed AD or dementia patient necessitates a thorough screening process involving appropriate in-person blood or laboratory work. It is for this reason that clinicians will need to plan ahead by preparing a contingency plan with the corresponding mitigation strategies (for example, telemedicine, proposed solutions to anticipated disruption of services, extended support, and feedback from family members, etc.).2
Resilience and recovery in a retrospective study
A research team from Wuhan Red Cross Hospital in China performed a retrospective cohort study on a sample of patients (n = 42) to determine the severity and prognostic features of COVID-19 pneumonia; 19 AD patients (as per National Institute on Aging/Alzheimer’s Association diagnostic guidelines) were directly compared with 23 age-matched non-AD COVID-19 patients in a similar treatment context.

The study yielded some rather unexpected findings, namely, AD patients experienced remarkably shorter hospital stays and better appetites, especially with respect to their non-AD counterparts. This is even more puzzling when considering that previous studies indicated that dementia patients with concomitant COVID-19 pneumonia are twice as likely to die as those without neurodegenerative compromise.
Aside from a seemingly inexplicable interest in food, the observable positive changes may be attributable to such factors that are particular to the nursing home – residents have immediate access to health care services, which generally allows for timely diagnosis and care. However, the authors of the study speculate that the pathophysiological response of angiotensin-converting enzyme 2 (ACE2) confers to AD patients a therapeutic advantage as they have reduced expression.3 Despite the notoriously high mortality rates of COVID-19 pneumonia among the elderly population, , which underscores the importance of early diagnosis and intervention.
Genetic and environmental susceptibility
One of the more devastating observations about the ongoing pandemic environment is that a whopping 80% of dying patients committed to a long-term facility also include those with AD; it has been reported that almost half of all patients in nursing homes and related services have the neurodegenerative condition. The grim scenario is brought about by several factors, chief of which is the proximity of shared living arrangements within the context of a residential care setting. It should be noted that patients with AD exhibit comorbid conditions (for example, diabetes, cardiovascular disease, and/or respiratory issues) that immediately put them at high risk for COVID exposure. Interestingly enough, the ApoE4 genotype, which is associated with an increased susceptibility for AD, is also correlated with COVID-19 prognosis and severity. Although exact numbers are difficult to come by, it is of utmost importance for clinicians to evaluate the overall scope of the situation, identify at-risk patients such as individuals with AD and related dementias, and work with caregivers to afford care to patients who need it the most.4
Transcending research design
The elderly population, unsurprisingly, experiences the highest COVID-19 mortality rate because of the presence of multiple risk factors, namely, compromised immunity and difficulties maintaining ADLs, and thereby adhering to safety protocols. As far as Alzheimer’s patients are concerned, numerous hurdles affect the domain of neurodegenerative research.
To safeguard the health and well-being of the participants and caregivers, site sponsors and investigators must explore various communication avenues with the goal of facilitating health education (for example, mitigation strategies, adverse effects monitoring, etc.), as well as implementing contingency plans in the event that a site becomes inaccessible (for example, site closure, traveling regulations, lockdowns, etc.).
Alternatives such as telemedicine present viable solutions for ensuring completion of studies. Given the nature of the pandemic, there is a possibility that a research participant may contract the virus, necessitating a break from the established protocol. It is for this reason that site sponsors and corresponding regulatory bodies are advised to proactively engage in dialogue and transparent communications with respect to ensuing protocol deviations. Institutional Review Boards can expedite the review process by making the necessary changes in a timely manner.5
References
1. Ritchie K. KJZZ. 2020 Nov 16.
2. Brown EE et al. Am J Geriatr Psychiatry. 2020 Jul;28(7):712-21.
3. Li J et al. J Alzheimers Dis. 2020;77(1):67-73.
4. Perry G. J Alzheimers Dis. 2020 Jan 1;76(1):1.
5. Alzheimers Dement. 2020 Apr;16(4):587-8.
Dr. Islam is a medical adviser for the International Maternal and Child Health Foundation, Montreal, and is based in New York. He also is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships.
Dr. Dhillon is a staff neurologist at Brigham and Women’s Hospital in Boston. Dr. Dhillon is currently on the speaker bureau/advisory board for Biogen, Bristol Myers Squibb, Genzyme, and Teva Neuroscience.
Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the International Maternal and Child Health Foundation. He has no disclosures.
An alarming number of additional Alzheimer’s disease (AD) deaths have been reported across various states within the past several months, according to the Alzheimer’s Association. Centers for Disease Control and Prevention data indicate that no less than 31,000 additional people with the neurodegenerative condition had died from the beginning of the pandemic through the end of September 2020. We know that long-term care facilities have been hit hardest, and access to adequate and/or prompt testing has been cited as the most pressing issue during the onset of the pandemic.1
When ADLs become a matter of survival
For individuals affected with Alzheimer’s disease and other types of dementia, performing routine tasks may seem cumbersome and overwhelming. Many of these patients are dependent upon caregivers and family support to facilitate their activities of daily living (ADLs).
Transitioning into the “new normal” set by the pandemic milieu is not an easy task for the average AD individual, because they are now expected to comply with numerous safety instructions (for example, maintaining hygiene, social distancing, etc.). They are also expected to monitor and communicate information about the onset of any suspected symptom to their caregiver or health care clinician.
The additional tasks added to their list of ADLs are particularly distressing given their already compromised short-term memory and overall cognitive decline. Individuals with AD may also be dealing with a host of psychobehavioral challenges, such as the presence of depression, anxiety, and/or agitation amid self-isolation. Enforced social isolation tied to COVID-19 may compound those issues.
Resource diversion and mitigation strategies
Unfortunately, any disruption in services within a long-term care setting may lead to a suboptimal therapeutic environment for patients. The Washington State LTC, for example, reported experiencing a case fatality rate (CFR) exceeding more than a third of its residents; essential staff and health care clinicians were duly affected from exposure to the virus (the risk of transmission increases considerably during transport between facilities). Access to personal protective equipment (PPE) might have been hindered by availability.
Another issue with far-reaching consequences is diversion of resources for urgent care. Health care professionals may simply not be readily available for those with chronic care needs because of the enormous scale of the impact of COVID-19 upon health care systems.
Continuity of therapy might include evaluations or follow-up services via teleconferencing modalities, but an exhaustive initial onsite physical examination is often necessary for accurate diagnostics and care. Medication management for the newly diagnosed AD or dementia patient necessitates a thorough screening process involving appropriate in-person blood or laboratory work. It is for this reason that clinicians will need to plan ahead by preparing a contingency plan with the corresponding mitigation strategies (for example, telemedicine, proposed solutions to anticipated disruption of services, extended support, and feedback from family members, etc.).2
Resilience and recovery in a retrospective study
A research team from Wuhan Red Cross Hospital in China performed a retrospective cohort study on a sample of patients (n = 42) to determine the severity and prognostic features of COVID-19 pneumonia; 19 AD patients (as per National Institute on Aging/Alzheimer’s Association diagnostic guidelines) were directly compared with 23 age-matched non-AD COVID-19 patients in a similar treatment context.
The study yielded some rather unexpected findings, namely, AD patients experienced remarkably shorter hospital stays and better appetites, especially with respect to their non-AD counterparts. This is even more puzzling when considering that previous studies indicated that dementia patients with concomitant COVID-19 pneumonia are twice as likely to die as those without neurodegenerative compromise.
Aside from a seemingly inexplicable interest in food, the observable positive changes may be attributable to such factors that are particular to the nursing home – residents have immediate access to health care services, which generally allows for timely diagnosis and care. However, the authors of the study speculate that the pathophysiological response of angiotensin-converting enzyme 2 (ACE2) confers to AD patients a therapeutic advantage as they have reduced expression.3 Despite the notoriously high mortality rates of COVID-19 pneumonia among the elderly population, , which underscores the importance of early diagnosis and intervention.
Genetic and environmental susceptibility
One of the more devastating observations about the ongoing pandemic environment is that a whopping 80% of dying patients committed to a long-term facility also include those with AD; it has been reported that almost half of all patients in nursing homes and related services have the neurodegenerative condition. The grim scenario is brought about by several factors, chief of which is the proximity of shared living arrangements within the context of a residential care setting. It should be noted that patients with AD exhibit comorbid conditions (for example, diabetes, cardiovascular disease, and/or respiratory issues) that immediately put them at high risk for COVID exposure. Interestingly enough, the ApoE4 genotype, which is associated with an increased susceptibility for AD, is also correlated with COVID-19 prognosis and severity. Although exact numbers are difficult to come by, it is of utmost importance for clinicians to evaluate the overall scope of the situation, identify at-risk patients such as individuals with AD and related dementias, and work with caregivers to afford care to patients who need it the most.4
Transcending research design
The elderly population, unsurprisingly, experiences the highest COVID-19 mortality rate because of the presence of multiple risk factors, namely, compromised immunity and difficulties maintaining ADLs, and thereby adhering to safety protocols. As far as Alzheimer’s patients are concerned, numerous hurdles affect the domain of neurodegenerative research.
To safeguard the health and well-being of the participants and caregivers, site sponsors and investigators must explore various communication avenues with the goal of facilitating health education (for example, mitigation strategies, adverse effects monitoring, etc.), as well as implementing contingency plans in the event that a site becomes inaccessible (for example, site closure, traveling regulations, lockdowns, etc.).
Alternatives such as telemedicine present viable solutions for ensuring completion of studies. Given the nature of the pandemic, there is a possibility that a research participant may contract the virus, necessitating a break from the established protocol. It is for this reason that site sponsors and corresponding regulatory bodies are advised to proactively engage in dialogue and transparent communications with respect to ensuing protocol deviations. Institutional Review Boards can expedite the review process by making the necessary changes in a timely manner.5
References
1. Ritchie K. KJZZ. 2020 Nov 16.
2. Brown EE et al. Am J Geriatr Psychiatry. 2020 Jul;28(7):712-21.
3. Li J et al. J Alzheimers Dis. 2020;77(1):67-73.
4. Perry G. J Alzheimers Dis. 2020 Jan 1;76(1):1.
5. Alzheimers Dement. 2020 Apr;16(4):587-8.
Dr. Islam is a medical adviser for the International Maternal and Child Health Foundation, Montreal, and is based in New York. He also is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships.
Dr. Dhillon is a staff neurologist at Brigham and Women’s Hospital in Boston. Dr. Dhillon is currently on the speaker bureau/advisory board for Biogen, Bristol Myers Squibb, Genzyme, and Teva Neuroscience.
Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the International Maternal and Child Health Foundation. He has no disclosures.
An alarming number of additional Alzheimer’s disease (AD) deaths have been reported across various states within the past several months, according to the Alzheimer’s Association. Centers for Disease Control and Prevention data indicate that no less than 31,000 additional people with the neurodegenerative condition had died from the beginning of the pandemic through the end of September 2020. We know that long-term care facilities have been hit hardest, and access to adequate and/or prompt testing has been cited as the most pressing issue during the onset of the pandemic.1
When ADLs become a matter of survival
For individuals affected with Alzheimer’s disease and other types of dementia, performing routine tasks may seem cumbersome and overwhelming. Many of these patients are dependent upon caregivers and family support to facilitate their activities of daily living (ADLs).
Transitioning into the “new normal” set by the pandemic milieu is not an easy task for the average AD individual, because they are now expected to comply with numerous safety instructions (for example, maintaining hygiene, social distancing, etc.). They are also expected to monitor and communicate information about the onset of any suspected symptom to their caregiver or health care clinician.
The additional tasks added to their list of ADLs are particularly distressing given their already compromised short-term memory and overall cognitive decline. Individuals with AD may also be dealing with a host of psychobehavioral challenges, such as the presence of depression, anxiety, and/or agitation amid self-isolation. Enforced social isolation tied to COVID-19 may compound those issues.
Resource diversion and mitigation strategies
Unfortunately, any disruption in services within a long-term care setting may lead to a suboptimal therapeutic environment for patients. The Washington State LTC, for example, reported experiencing a case fatality rate (CFR) exceeding more than a third of its residents; essential staff and health care clinicians were duly affected from exposure to the virus (the risk of transmission increases considerably during transport between facilities). Access to personal protective equipment (PPE) might have been hindered by availability.
Another issue with far-reaching consequences is diversion of resources for urgent care. Health care professionals may simply not be readily available for those with chronic care needs because of the enormous scale of the impact of COVID-19 upon health care systems.
Continuity of therapy might include evaluations or follow-up services via teleconferencing modalities, but an exhaustive initial onsite physical examination is often necessary for accurate diagnostics and care. Medication management for the newly diagnosed AD or dementia patient necessitates a thorough screening process involving appropriate in-person blood or laboratory work. It is for this reason that clinicians will need to plan ahead by preparing a contingency plan with the corresponding mitigation strategies (for example, telemedicine, proposed solutions to anticipated disruption of services, extended support, and feedback from family members, etc.).2
Resilience and recovery in a retrospective study
A research team from Wuhan Red Cross Hospital in China performed a retrospective cohort study on a sample of patients (n = 42) to determine the severity and prognostic features of COVID-19 pneumonia; 19 AD patients (as per National Institute on Aging/Alzheimer’s Association diagnostic guidelines) were directly compared with 23 age-matched non-AD COVID-19 patients in a similar treatment context.
The study yielded some rather unexpected findings, namely, AD patients experienced remarkably shorter hospital stays and better appetites, especially with respect to their non-AD counterparts. This is even more puzzling when considering that previous studies indicated that dementia patients with concomitant COVID-19 pneumonia are twice as likely to die as those without neurodegenerative compromise.
Aside from a seemingly inexplicable interest in food, the observable positive changes may be attributable to such factors that are particular to the nursing home – residents have immediate access to health care services, which generally allows for timely diagnosis and care. However, the authors of the study speculate that the pathophysiological response of angiotensin-converting enzyme 2 (ACE2) confers to AD patients a therapeutic advantage as they have reduced expression.3 Despite the notoriously high mortality rates of COVID-19 pneumonia among the elderly population, , which underscores the importance of early diagnosis and intervention.
Genetic and environmental susceptibility
One of the more devastating observations about the ongoing pandemic environment is that a whopping 80% of dying patients committed to a long-term facility also include those with AD; it has been reported that almost half of all patients in nursing homes and related services have the neurodegenerative condition. The grim scenario is brought about by several factors, chief of which is the proximity of shared living arrangements within the context of a residential care setting. It should be noted that patients with AD exhibit comorbid conditions (for example, diabetes, cardiovascular disease, and/or respiratory issues) that immediately put them at high risk for COVID exposure. Interestingly enough, the ApoE4 genotype, which is associated with an increased susceptibility for AD, is also correlated with COVID-19 prognosis and severity. Although exact numbers are difficult to come by, it is of utmost importance for clinicians to evaluate the overall scope of the situation, identify at-risk patients such as individuals with AD and related dementias, and work with caregivers to afford care to patients who need it the most.4
Transcending research design
The elderly population, unsurprisingly, experiences the highest COVID-19 mortality rate because of the presence of multiple risk factors, namely, compromised immunity and difficulties maintaining ADLs, and thereby adhering to safety protocols. As far as Alzheimer’s patients are concerned, numerous hurdles affect the domain of neurodegenerative research.
To safeguard the health and well-being of the participants and caregivers, site sponsors and investigators must explore various communication avenues with the goal of facilitating health education (for example, mitigation strategies, adverse effects monitoring, etc.), as well as implementing contingency plans in the event that a site becomes inaccessible (for example, site closure, traveling regulations, lockdowns, etc.).
Alternatives such as telemedicine present viable solutions for ensuring completion of studies. Given the nature of the pandemic, there is a possibility that a research participant may contract the virus, necessitating a break from the established protocol. It is for this reason that site sponsors and corresponding regulatory bodies are advised to proactively engage in dialogue and transparent communications with respect to ensuing protocol deviations. Institutional Review Boards can expedite the review process by making the necessary changes in a timely manner.5
References
1. Ritchie K. KJZZ. 2020 Nov 16.
2. Brown EE et al. Am J Geriatr Psychiatry. 2020 Jul;28(7):712-21.
3. Li J et al. J Alzheimers Dis. 2020;77(1):67-73.
4. Perry G. J Alzheimers Dis. 2020 Jan 1;76(1):1.
5. Alzheimers Dement. 2020 Apr;16(4):587-8.
Dr. Islam is a medical adviser for the International Maternal and Child Health Foundation, Montreal, and is based in New York. He also is a postdoctoral fellow, psychopharmacologist, and a board-certified medical affairs specialist. Dr. Islam disclosed no relevant financial relationships.
Dr. Dhillon is a staff neurologist at Brigham and Women’s Hospital in Boston. Dr. Dhillon is currently on the speaker bureau/advisory board for Biogen, Bristol Myers Squibb, Genzyme, and Teva Neuroscience.
Dr. Choudhry is the chief scientific officer and head of the department of mental health and clinical research at the International Maternal and Child Health Foundation. He has no disclosures.