User login
COVID-19 and youth suicide: Do the numbers match the headlines?
There’s little doubt that the COVID-19 pandemic has been hard on many children and adolescents just as it has been difficult for adults. The disruption of routines, reduced contact with friends, concern over getting ill, and financial turmoil suffered by many families is exacting a toll on our mental health, as has been documented by a number of recent surveys and studies.1,2

Quite understandably, concern about rising levels of anxiety and depression in youth prompts additional worries about suicide, the second leading cause of death in adolescents and young adults. In response, many organizations have rallied to provide additional resources to help prevent suicidal thinking and actions. Online mental health tips, support phone and text lines, and the availability of telemedicine have all been mobilized to help people cope and stay safe both physically and psychologically.
But what are the actual numbers when it comes to youth suicide during COVID-19? According to many headlines in the press, the statistics are grim and support many of distressing predictions that have been made. A December story in an Arizona newspaper, “With Teen Suicides on the Rise, Tucson Educators Struggle to Prioritize Mental Health,” described a 67% increase in teen suicides in 2020 compared with 2019 in one county.3 Another post from Psychology Today, “America is Facing a Teen Suicide Pandemic,” raised similar alarms.4 Concern over suicide has even been used politically to argue against restrictions that could reduce the spread of COVID-19 infections.
But despite this common perception shared by both health care professionals and the public, there actually is not evidence at this point that the COVID-19 pandemic has led to a broad spike in youth suicide deaths or attempts. A recent study published in the journal Pediatrics compared suicide screening results on youth presenting to emergency departments for any reason in 2020 to the same month in 2019.5 The authors found no consistent increases in reported suicidal ideation or suicide attempts with scattered elevations found in some months during 2020 compared with the previous year (including February 2020 before the pandemic really began) but not others. Internationally, newly analyzed data from 2020 with regard to suicide deaths have suggested “either no rise in suicide rates ... or a fall in the early months of the pandemic.” In my home and, admittedly small, state of Vermont, data from the Department of Health have shown 93 suicide deaths across all ages as of mid-November 2020 compared with a 5-year average of 96.
Why don’t the data match the headlines? There are a number of possibilities.
1. Suicide rates in youth were going up before the pandemic. As it takes time to verify and analyze data from large populations, many of the reports on suicide that have been published and released in 2020 summarize data from prior years. Without looking closely, a news organization can easily slap on a headline that implies that the data were obtained during the pandemic.
2. Fluctuations tend to occur from year to year. Thankfully, youth suicide remains rare (although not rare enough). With small numbers, regular variations from year to year can look huge in terms of percentages, especially if one doesn’t pull back and look at longer trends over time.
3. People are reaching out for mental health services. The public health message to access support and treatment for COVID 19–related mental health struggles appears to be having an effect, but this increased demand should not necessarily be viewed as a proxy for suicidal ideation and attempts.
While the understanding that we are not actually in the midst of a surge in COVID 19–related youth suicide is reassuring, it is important not to get complacent. Much of the data remains preliminary, and, even if these numbers hold up, there is no guarantee that things will continue this way, especially if the pandemic and it restrictions continue to drag on for many more months. And of course, whether or not the pandemic is making things significantly worse, youth suicide remains an enormous public health imperative with every one being a human tragedy.
It is also quite possible that more detailed analyses will eventually reveal a more complex association between youth suicide and COVID-19, with effects of the pandemic being realized regionally or more for some groups than others. Data from before the pandemic indicated, for example, that suicide rates are increasing more rapidly among African American youth compared with white children and adolescents.6 With the COVID-19 pandemic itself affecting disadvantaged communities more strongly, one could readily expect variable impacts in mental health related to race or socioeconomic status. A recent article voices these concerns for indigenous youth in Montana: a state with one of the highest per capita suicide rates in the country.7 The article notes, however, that the rate of suicide overall in Montana in 2020 is comparable to those of previous years.
Overall, pediatricians should not be needlessly panicked that the COVID-19 pandemic has sparked a surge in youth suicide. The data at this point simply don’t support that assertion despite many headlines to the contrary. At the same time, many children and adolescents are certainly struggling with the stresses the pandemic has created and continue to need our close monitoring and support.
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont Larner College of Medicine. Follow him on Twitter @PediPsych. His new book, “Parenting Made Complicated: What Science Really Knows About the Greatest Debates of Early Childhood,” launches Feb. 1, 2021.
References
1. Copeland WE et al. Impact of COVID-19 pandemic on college student mental health and wellness. J Am Acad Child Adolesc Psychiatry. 2020;60(1):134-41. doi: 10.1016/j.jaac.2020.08.466.
2. Qiu J et al. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen Psychiatry. 2020;33:e100213. doi: 10.1136/gpsych-2020-100213.
3. Dhmara K. With teen suicides on the rise, Tucson educators struggle to prioritize mental health. Tuscon.com. Dec. 27, 2020.
4. Chafouleas, SM. America is facing a suicide epidemic: New data confirm the urgency of confronting it now. Psychology Today blog. Sept. 4, 2020.
5. Hill RM et al. Suicide ideation and attempts in a pediatric emergency department before and after COVID-19. Pediatrics. 2020. doi: 10.1542/peds.2020-029280.
6. John A et al. Trends in suicide during the covid-19 pandemic. BMJ 2020;371:m4352. doi: 10.1136/bmj.m4352.
7. Reardon S. Health officials fear COVID-19 pandemic-related suicide spike among indigenous youth. Time Magazine. December 2020.
There’s little doubt that the COVID-19 pandemic has been hard on many children and adolescents just as it has been difficult for adults. The disruption of routines, reduced contact with friends, concern over getting ill, and financial turmoil suffered by many families is exacting a toll on our mental health, as has been documented by a number of recent surveys and studies.1,2
Quite understandably, concern about rising levels of anxiety and depression in youth prompts additional worries about suicide, the second leading cause of death in adolescents and young adults. In response, many organizations have rallied to provide additional resources to help prevent suicidal thinking and actions. Online mental health tips, support phone and text lines, and the availability of telemedicine have all been mobilized to help people cope and stay safe both physically and psychologically.
But what are the actual numbers when it comes to youth suicide during COVID-19? According to many headlines in the press, the statistics are grim and support many of distressing predictions that have been made. A December story in an Arizona newspaper, “With Teen Suicides on the Rise, Tucson Educators Struggle to Prioritize Mental Health,” described a 67% increase in teen suicides in 2020 compared with 2019 in one county.3 Another post from Psychology Today, “America is Facing a Teen Suicide Pandemic,” raised similar alarms.4 Concern over suicide has even been used politically to argue against restrictions that could reduce the spread of COVID-19 infections.
But despite this common perception shared by both health care professionals and the public, there actually is not evidence at this point that the COVID-19 pandemic has led to a broad spike in youth suicide deaths or attempts. A recent study published in the journal Pediatrics compared suicide screening results on youth presenting to emergency departments for any reason in 2020 to the same month in 2019.5 The authors found no consistent increases in reported suicidal ideation or suicide attempts with scattered elevations found in some months during 2020 compared with the previous year (including February 2020 before the pandemic really began) but not others. Internationally, newly analyzed data from 2020 with regard to suicide deaths have suggested “either no rise in suicide rates ... or a fall in the early months of the pandemic.” In my home and, admittedly small, state of Vermont, data from the Department of Health have shown 93 suicide deaths across all ages as of mid-November 2020 compared with a 5-year average of 96.
Why don’t the data match the headlines? There are a number of possibilities.
1. Suicide rates in youth were going up before the pandemic. As it takes time to verify and analyze data from large populations, many of the reports on suicide that have been published and released in 2020 summarize data from prior years. Without looking closely, a news organization can easily slap on a headline that implies that the data were obtained during the pandemic.
2. Fluctuations tend to occur from year to year. Thankfully, youth suicide remains rare (although not rare enough). With small numbers, regular variations from year to year can look huge in terms of percentages, especially if one doesn’t pull back and look at longer trends over time.
3. People are reaching out for mental health services. The public health message to access support and treatment for COVID 19–related mental health struggles appears to be having an effect, but this increased demand should not necessarily be viewed as a proxy for suicidal ideation and attempts.
While the understanding that we are not actually in the midst of a surge in COVID 19–related youth suicide is reassuring, it is important not to get complacent. Much of the data remains preliminary, and, even if these numbers hold up, there is no guarantee that things will continue this way, especially if the pandemic and it restrictions continue to drag on for many more months. And of course, whether or not the pandemic is making things significantly worse, youth suicide remains an enormous public health imperative with every one being a human tragedy.
It is also quite possible that more detailed analyses will eventually reveal a more complex association between youth suicide and COVID-19, with effects of the pandemic being realized regionally or more for some groups than others. Data from before the pandemic indicated, for example, that suicide rates are increasing more rapidly among African American youth compared with white children and adolescents.6 With the COVID-19 pandemic itself affecting disadvantaged communities more strongly, one could readily expect variable impacts in mental health related to race or socioeconomic status. A recent article voices these concerns for indigenous youth in Montana: a state with one of the highest per capita suicide rates in the country.7 The article notes, however, that the rate of suicide overall in Montana in 2020 is comparable to those of previous years.
Overall, pediatricians should not be needlessly panicked that the COVID-19 pandemic has sparked a surge in youth suicide. The data at this point simply don’t support that assertion despite many headlines to the contrary. At the same time, many children and adolescents are certainly struggling with the stresses the pandemic has created and continue to need our close monitoring and support.
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont Larner College of Medicine. Follow him on Twitter @PediPsych. His new book, “Parenting Made Complicated: What Science Really Knows About the Greatest Debates of Early Childhood,” launches Feb. 1, 2021.
References
1. Copeland WE et al. Impact of COVID-19 pandemic on college student mental health and wellness. J Am Acad Child Adolesc Psychiatry. 2020;60(1):134-41. doi: 10.1016/j.jaac.2020.08.466.
2. Qiu J et al. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen Psychiatry. 2020;33:e100213. doi: 10.1136/gpsych-2020-100213.
3. Dhmara K. With teen suicides on the rise, Tucson educators struggle to prioritize mental health. Tuscon.com. Dec. 27, 2020.
4. Chafouleas, SM. America is facing a suicide epidemic: New data confirm the urgency of confronting it now. Psychology Today blog. Sept. 4, 2020.
5. Hill RM et al. Suicide ideation and attempts in a pediatric emergency department before and after COVID-19. Pediatrics. 2020. doi: 10.1542/peds.2020-029280.
6. John A et al. Trends in suicide during the covid-19 pandemic. BMJ 2020;371:m4352. doi: 10.1136/bmj.m4352.
7. Reardon S. Health officials fear COVID-19 pandemic-related suicide spike among indigenous youth. Time Magazine. December 2020.
There’s little doubt that the COVID-19 pandemic has been hard on many children and adolescents just as it has been difficult for adults. The disruption of routines, reduced contact with friends, concern over getting ill, and financial turmoil suffered by many families is exacting a toll on our mental health, as has been documented by a number of recent surveys and studies.1,2
Quite understandably, concern about rising levels of anxiety and depression in youth prompts additional worries about suicide, the second leading cause of death in adolescents and young adults. In response, many organizations have rallied to provide additional resources to help prevent suicidal thinking and actions. Online mental health tips, support phone and text lines, and the availability of telemedicine have all been mobilized to help people cope and stay safe both physically and psychologically.
But what are the actual numbers when it comes to youth suicide during COVID-19? According to many headlines in the press, the statistics are grim and support many of distressing predictions that have been made. A December story in an Arizona newspaper, “With Teen Suicides on the Rise, Tucson Educators Struggle to Prioritize Mental Health,” described a 67% increase in teen suicides in 2020 compared with 2019 in one county.3 Another post from Psychology Today, “America is Facing a Teen Suicide Pandemic,” raised similar alarms.4 Concern over suicide has even been used politically to argue against restrictions that could reduce the spread of COVID-19 infections.
But despite this common perception shared by both health care professionals and the public, there actually is not evidence at this point that the COVID-19 pandemic has led to a broad spike in youth suicide deaths or attempts. A recent study published in the journal Pediatrics compared suicide screening results on youth presenting to emergency departments for any reason in 2020 to the same month in 2019.5 The authors found no consistent increases in reported suicidal ideation or suicide attempts with scattered elevations found in some months during 2020 compared with the previous year (including February 2020 before the pandemic really began) but not others. Internationally, newly analyzed data from 2020 with regard to suicide deaths have suggested “either no rise in suicide rates ... or a fall in the early months of the pandemic.” In my home and, admittedly small, state of Vermont, data from the Department of Health have shown 93 suicide deaths across all ages as of mid-November 2020 compared with a 5-year average of 96.
Why don’t the data match the headlines? There are a number of possibilities.
1. Suicide rates in youth were going up before the pandemic. As it takes time to verify and analyze data from large populations, many of the reports on suicide that have been published and released in 2020 summarize data from prior years. Without looking closely, a news organization can easily slap on a headline that implies that the data were obtained during the pandemic.
2. Fluctuations tend to occur from year to year. Thankfully, youth suicide remains rare (although not rare enough). With small numbers, regular variations from year to year can look huge in terms of percentages, especially if one doesn’t pull back and look at longer trends over time.
3. People are reaching out for mental health services. The public health message to access support and treatment for COVID 19–related mental health struggles appears to be having an effect, but this increased demand should not necessarily be viewed as a proxy for suicidal ideation and attempts.
While the understanding that we are not actually in the midst of a surge in COVID 19–related youth suicide is reassuring, it is important not to get complacent. Much of the data remains preliminary, and, even if these numbers hold up, there is no guarantee that things will continue this way, especially if the pandemic and it restrictions continue to drag on for many more months. And of course, whether or not the pandemic is making things significantly worse, youth suicide remains an enormous public health imperative with every one being a human tragedy.
It is also quite possible that more detailed analyses will eventually reveal a more complex association between youth suicide and COVID-19, with effects of the pandemic being realized regionally or more for some groups than others. Data from before the pandemic indicated, for example, that suicide rates are increasing more rapidly among African American youth compared with white children and adolescents.6 With the COVID-19 pandemic itself affecting disadvantaged communities more strongly, one could readily expect variable impacts in mental health related to race or socioeconomic status. A recent article voices these concerns for indigenous youth in Montana: a state with one of the highest per capita suicide rates in the country.7 The article notes, however, that the rate of suicide overall in Montana in 2020 is comparable to those of previous years.
Overall, pediatricians should not be needlessly panicked that the COVID-19 pandemic has sparked a surge in youth suicide. The data at this point simply don’t support that assertion despite many headlines to the contrary. At the same time, many children and adolescents are certainly struggling with the stresses the pandemic has created and continue to need our close monitoring and support.
Dr. Rettew is a child and adolescent psychiatrist and associate professor of psychiatry and pediatrics at the University of Vermont Larner College of Medicine. Follow him on Twitter @PediPsych. His new book, “Parenting Made Complicated: What Science Really Knows About the Greatest Debates of Early Childhood,” launches Feb. 1, 2021.
References
1. Copeland WE et al. Impact of COVID-19 pandemic on college student mental health and wellness. J Am Acad Child Adolesc Psychiatry. 2020;60(1):134-41. doi: 10.1016/j.jaac.2020.08.466.
2. Qiu J et al. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen Psychiatry. 2020;33:e100213. doi: 10.1136/gpsych-2020-100213.
3. Dhmara K. With teen suicides on the rise, Tucson educators struggle to prioritize mental health. Tuscon.com. Dec. 27, 2020.
4. Chafouleas, SM. America is facing a suicide epidemic: New data confirm the urgency of confronting it now. Psychology Today blog. Sept. 4, 2020.
5. Hill RM et al. Suicide ideation and attempts in a pediatric emergency department before and after COVID-19. Pediatrics. 2020. doi: 10.1542/peds.2020-029280.
6. John A et al. Trends in suicide during the covid-19 pandemic. BMJ 2020;371:m4352. doi: 10.1136/bmj.m4352.
7. Reardon S. Health officials fear COVID-19 pandemic-related suicide spike among indigenous youth. Time Magazine. December 2020.
Collateral damage in the war on obesity
In a recent New York Times opinion article, author Aubrey Gordon claims that since a visit to her pediatrician in fourth grade she has felt like an “enemy combatant in the nation’s war on childhood obesity.” (“Leave Fat Kids Alone,” Nov. 13, 2020).
At that unfortunate encounter, she recalls being told that “You’ll be thin and beautiful ... If you can just stay the same weight.” In retrospect she feels that the comment by her well-meaning but misguided physician “planted the seeds of depression” that have plagued her ever since.

Ms. Gordon goes on to list the many national and local initiatives that have done little to bend the curve in this country’s obesity trajectory but have succeeded in targeting bodies like hers as an epidemic and have resulted in her and thousands of other children being treated as “its virus personified.”
It is deeply troubling to read of her journey through life as collateral damage in a failed war effort, but Ms. Gordon offers little advice to us other than that we stop doing what we have been doing. It hasn’t been helping and it’s not working.
I suspect she would agree that obesity is one of our nation’s most serious public health problems. There is voluminous evidence of the association of obesity with cardiac disease, cancer, mental health challenges, and more recently COVID-19 – just to name a few. If blaming obese children who are the victims is counterproductive where do we point the finger? It is tempting to blame parents and certainly they deserve some culpability. Some parents could have created less obesity-enabling environments through healthier menu choices and done a better job discouraging sedentary behaviors. However, some families lack the access to, or the resources to, provide less calorie-dense food options. We know that many obese children have parents who have been obese themselves since childhood and we know that breaking the obesity cycle can be extremely difficult. Do we extend the sweep of our finger-pointing to include grandparents and great grandparents?
While guilt can be a powerful motivating force, obesity seems to be one of those conditions in which by the time it becomes obvious to a family, the die is cast and blaming the victim or her parents is going to do little more than engender bad feelings. We have done more than enough. In fact, Ms. Gordon’s commentary suggests we have gone too far in creating public opinion that being lean is healthy and being overweight is bad. More motivational testimonials will merely add to the shaming.
Obesity is clearly a societal problem and selectively targeting the victims is not the answer. A famine would certainly lower our national body mass index, but not even the most callous among us would include it on the list of options. Attempts at levying a hefty tax on sweetened beverages have been attempted sporadically around the country without much success. We are a nation that cherishes our personal freedoms and unfortunately this includes the freedom to do some things the aren’t in our own best interests.
You could argue that this leaves us with education as our only hope of turning the tide. However, educating without characterizing the obese among us as bad, ugly, and undisciplined people is a public relations challenge of heroic proportions. Choosing language and images that somehow convey the idea that although obesity is bad being obese doesn’t make you a bad or ugly person is walking along a fine semantic edge.
If I sound discouraged, you are reading me correctly. As pediatricians, we are left doing the few things that have been shown to make a difference. This means promoting breastfeeding and encouraging thoughtful introduction of solid foods; both strategies can be done before the child can hear our well-intentioned but misguided words of encouragement.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
In a recent New York Times opinion article, author Aubrey Gordon claims that since a visit to her pediatrician in fourth grade she has felt like an “enemy combatant in the nation’s war on childhood obesity.” (“Leave Fat Kids Alone,” Nov. 13, 2020).
At that unfortunate encounter, she recalls being told that “You’ll be thin and beautiful ... If you can just stay the same weight.” In retrospect she feels that the comment by her well-meaning but misguided physician “planted the seeds of depression” that have plagued her ever since.
Ms. Gordon goes on to list the many national and local initiatives that have done little to bend the curve in this country’s obesity trajectory but have succeeded in targeting bodies like hers as an epidemic and have resulted in her and thousands of other children being treated as “its virus personified.”
It is deeply troubling to read of her journey through life as collateral damage in a failed war effort, but Ms. Gordon offers little advice to us other than that we stop doing what we have been doing. It hasn’t been helping and it’s not working.
I suspect she would agree that obesity is one of our nation’s most serious public health problems. There is voluminous evidence of the association of obesity with cardiac disease, cancer, mental health challenges, and more recently COVID-19 – just to name a few. If blaming obese children who are the victims is counterproductive where do we point the finger? It is tempting to blame parents and certainly they deserve some culpability. Some parents could have created less obesity-enabling environments through healthier menu choices and done a better job discouraging sedentary behaviors. However, some families lack the access to, or the resources to, provide less calorie-dense food options. We know that many obese children have parents who have been obese themselves since childhood and we know that breaking the obesity cycle can be extremely difficult. Do we extend the sweep of our finger-pointing to include grandparents and great grandparents?
While guilt can be a powerful motivating force, obesity seems to be one of those conditions in which by the time it becomes obvious to a family, the die is cast and blaming the victim or her parents is going to do little more than engender bad feelings. We have done more than enough. In fact, Ms. Gordon’s commentary suggests we have gone too far in creating public opinion that being lean is healthy and being overweight is bad. More motivational testimonials will merely add to the shaming.
Obesity is clearly a societal problem and selectively targeting the victims is not the answer. A famine would certainly lower our national body mass index, but not even the most callous among us would include it on the list of options. Attempts at levying a hefty tax on sweetened beverages have been attempted sporadically around the country without much success. We are a nation that cherishes our personal freedoms and unfortunately this includes the freedom to do some things the aren’t in our own best interests.
You could argue that this leaves us with education as our only hope of turning the tide. However, educating without characterizing the obese among us as bad, ugly, and undisciplined people is a public relations challenge of heroic proportions. Choosing language and images that somehow convey the idea that although obesity is bad being obese doesn’t make you a bad or ugly person is walking along a fine semantic edge.
If I sound discouraged, you are reading me correctly. As pediatricians, we are left doing the few things that have been shown to make a difference. This means promoting breastfeeding and encouraging thoughtful introduction of solid foods; both strategies can be done before the child can hear our well-intentioned but misguided words of encouragement.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
In a recent New York Times opinion article, author Aubrey Gordon claims that since a visit to her pediatrician in fourth grade she has felt like an “enemy combatant in the nation’s war on childhood obesity.” (“Leave Fat Kids Alone,” Nov. 13, 2020).
At that unfortunate encounter, she recalls being told that “You’ll be thin and beautiful ... If you can just stay the same weight.” In retrospect she feels that the comment by her well-meaning but misguided physician “planted the seeds of depression” that have plagued her ever since.
Ms. Gordon goes on to list the many national and local initiatives that have done little to bend the curve in this country’s obesity trajectory but have succeeded in targeting bodies like hers as an epidemic and have resulted in her and thousands of other children being treated as “its virus personified.”
It is deeply troubling to read of her journey through life as collateral damage in a failed war effort, but Ms. Gordon offers little advice to us other than that we stop doing what we have been doing. It hasn’t been helping and it’s not working.
I suspect she would agree that obesity is one of our nation’s most serious public health problems. There is voluminous evidence of the association of obesity with cardiac disease, cancer, mental health challenges, and more recently COVID-19 – just to name a few. If blaming obese children who are the victims is counterproductive where do we point the finger? It is tempting to blame parents and certainly they deserve some culpability. Some parents could have created less obesity-enabling environments through healthier menu choices and done a better job discouraging sedentary behaviors. However, some families lack the access to, or the resources to, provide less calorie-dense food options. We know that many obese children have parents who have been obese themselves since childhood and we know that breaking the obesity cycle can be extremely difficult. Do we extend the sweep of our finger-pointing to include grandparents and great grandparents?
While guilt can be a powerful motivating force, obesity seems to be one of those conditions in which by the time it becomes obvious to a family, the die is cast and blaming the victim or her parents is going to do little more than engender bad feelings. We have done more than enough. In fact, Ms. Gordon’s commentary suggests we have gone too far in creating public opinion that being lean is healthy and being overweight is bad. More motivational testimonials will merely add to the shaming.
Obesity is clearly a societal problem and selectively targeting the victims is not the answer. A famine would certainly lower our national body mass index, but not even the most callous among us would include it on the list of options. Attempts at levying a hefty tax on sweetened beverages have been attempted sporadically around the country without much success. We are a nation that cherishes our personal freedoms and unfortunately this includes the freedom to do some things the aren’t in our own best interests.
You could argue that this leaves us with education as our only hope of turning the tide. However, educating without characterizing the obese among us as bad, ugly, and undisciplined people is a public relations challenge of heroic proportions. Choosing language and images that somehow convey the idea that although obesity is bad being obese doesn’t make you a bad or ugly person is walking along a fine semantic edge.
If I sound discouraged, you are reading me correctly. As pediatricians, we are left doing the few things that have been shown to make a difference. This means promoting breastfeeding and encouraging thoughtful introduction of solid foods; both strategies can be done before the child can hear our well-intentioned but misguided words of encouragement.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at pdnews@mdedge.com.
The psychiatrist and the vaccine
When the long-awaited news of a Food and Drug Administration–approved vaccine came on Dec. 11, 2020, my first thought was that I would wait. I can manage a few more months of Zooming for work, my household is down to two people, I’m not at high risk of dying from COVID, and my husband is not going to be vaccinated any time soon, so a change in my status wouldn’t “free” me. I would rather have “my” vaccine go to a 70-year-old ICU janitor or a bus driver.

The weeks have gone by. I expected there would be kinks, but it has now been a month – one in which COVID rates have soared, and hospitalizations and deaths have risen to unmanageable numbers in some places. Still, vaccines remain in freezers – people are dying while vials of prevention sit unused. I began to think that, when my “turn” came, the better thing was to be vaccinated. We need to have a large segment of the population vaccinated to squelch this virus, and it’s become much less clear to me that, if I yield my turn, it will go into the arm of a bus driver. The process has not been fair, and there are moments of media outrage when one group gets vaccinated before another, so perhaps we have reached point where the goal should not be to get the vaccine into the exact right person in the exact right order, but to get the vaccine into arms according to the protocol that has already been set. Anyone who does not end up in a hospital bed is doing the system a favor.
Mahmood Jahromi, MD, a psychiatrist in private practice in Towson, Md., described the process of vaccination as being similar to a bottleneck traffic jam. “Yes, one must be courteous to the car trying to but in, but no, don’t jam the glue because you are excessively kind. Let the traffic police do their job. When your name is called, go ahead and take it. The system needs to know people are accepting the vaccine, not by begging the authorities to be called ahead of others, but with respect for what is already designed.”
On Friday, Jan. 8, I received information on how to get vaccinated – it seems my “turn” has arrived. An email from the board of physicians informed me that I am in the “1A” category and included a link to sign up for a vaccine in Baltimore – vaccinations would be given until Jan. 29, Mondays to Thursdays from 10 a.m. to 4 p.m. and Fridays from 10 a.m. to 1 p.m. There are no weekend or evening hours, and one might think there would be enough urgency to call for this. The Maryland Psychiatric Society sent out a notice that Sheppard Pratt would be offering vaccines to all behavioral health providers in the state of Maryland during a 2-day clinic. I heard from others that health care workers can now get vaccinated at the Cow Palace (how great is that?) at the Maryland State Fairgrounds and another link was sent for those in Howard County, between Baltimore and Washington.
As I discussed this with colleagues, a couple of issues came up – the most common was one of not wanting to get the vaccine yet because there are others who need it more. Others voiced concern about a vaccine where the long-term effects remain unknown: Is this vaccine safe, might it spur autoimmune problems in the months or years to come? Is it safe for women who plan to become pregnant? Some have insisted it is safe. They say “follow the science” and have dismissed the skepticism. To my read, it makes perfect sense to be wary, but COVID spreads silently and it kills.

With a vaccine where so many are reluctant to get it, including many health care workers, Sue Kim, MD, a psychiatrist in private practice in Lutherville, Md., noted that she has concerns about the safety of the vaccine. “Getting it now is both altruistic and selfish, but letting others go first is also altruistic and selfish. In the meantime, if I get sick, I was too smart for my own good. How do you weigh this ethically?”
My personal feelings have been influenced by a few things. An article in the New York Times highlighted how New York City vaccinated 5 million people for smallpox in just 2 weeks in 1947. I am frustrated knowing that, a month after approval of the first vaccine, only 7 million people have received it in the entire United States. In that time period, millions have contracted COVID and thousands have died. Closer to home, a 45-year-old psychiatrist in Maryland died of COVID, and I have heard more stories about younger people with long-haul neurologic and vascular symptoms. The risk of COVID is feeling higher than it did, and the fact that the first vaccine was authorized after the election somehow makes me feel that it might be safer. Had it been approved right before, I would have worried – perhaps wrongly – that the authorization was a political maneuver, not one based on science.
As we think about what is best for ourselves, our families, our patients, and society as a whole, I believe that those who want the vaccine but don’t feel they should take their place in line before others who are higher risk must ask if it makes sense to wait. Each state is different. While Houston Methodist Hospital is reportedly giving its health care workers a $500 bonus to get the vaccine, Gov. Andrew Cuomo of New York announced that hospitals would be fined $100,000 if they don’t use all of their vaccines within 7 days of receipt and $1 million if they vaccinate anyone out of order. Gov. Cuomo later broadened who could be vaccinated to prevent wasting the vaccine, but there remains an element of being damned if you do and damned if you don’t.
Paul Nestadt, MD, a psychiatrist at Johns Hopkins University, Baltimore, noted that one distribution site initially had to waste unused vaccine when people did not come for their appointments. A waiting list was created for people who could come right away if called to prevent this waste. “To me, this only highlighted that the tier system, while a good idea, does not need to be written in stone. The goal needs to be getting shots in arms, building herd immunity. If there are two arms in front of you, shoot the health care worker or those who are vulnerable. But if there is a healthy arm in reach, it should get any shot made available.”
I registered to be vaccinated. – senior citizens and essential workers are not yet eligible. In Baltimore, vaccinations are available Mondays to Thursdays from 10 a.m. to 4 p.m. and on Fridays from 10 a.m. to 1 p.m. There are no options for early morning or weekend times, but there are slots still available for the coming week. As of this writing, there are 6,100 Marylanders dead, and more than 1,800 COVID patients in hospital beds, and our governor, Larry Hogan, has commercials to “Mask On Maryland” and “Wear the Damn Mask.” I’ll offer some changes: “Wake Up, World” and “Offer the Damn Shot.”
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University, 2016). She is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, both in Baltimore. Dr. Miller has no disclosures.
When the long-awaited news of a Food and Drug Administration–approved vaccine came on Dec. 11, 2020, my first thought was that I would wait. I can manage a few more months of Zooming for work, my household is down to two people, I’m not at high risk of dying from COVID, and my husband is not going to be vaccinated any time soon, so a change in my status wouldn’t “free” me. I would rather have “my” vaccine go to a 70-year-old ICU janitor or a bus driver.
The weeks have gone by. I expected there would be kinks, but it has now been a month – one in which COVID rates have soared, and hospitalizations and deaths have risen to unmanageable numbers in some places. Still, vaccines remain in freezers – people are dying while vials of prevention sit unused. I began to think that, when my “turn” came, the better thing was to be vaccinated. We need to have a large segment of the population vaccinated to squelch this virus, and it’s become much less clear to me that, if I yield my turn, it will go into the arm of a bus driver. The process has not been fair, and there are moments of media outrage when one group gets vaccinated before another, so perhaps we have reached point where the goal should not be to get the vaccine into the exact right person in the exact right order, but to get the vaccine into arms according to the protocol that has already been set. Anyone who does not end up in a hospital bed is doing the system a favor.
Mahmood Jahromi, MD, a psychiatrist in private practice in Towson, Md., described the process of vaccination as being similar to a bottleneck traffic jam. “Yes, one must be courteous to the car trying to but in, but no, don’t jam the glue because you are excessively kind. Let the traffic police do their job. When your name is called, go ahead and take it. The system needs to know people are accepting the vaccine, not by begging the authorities to be called ahead of others, but with respect for what is already designed.”
On Friday, Jan. 8, I received information on how to get vaccinated – it seems my “turn” has arrived. An email from the board of physicians informed me that I am in the “1A” category and included a link to sign up for a vaccine in Baltimore – vaccinations would be given until Jan. 29, Mondays to Thursdays from 10 a.m. to 4 p.m. and Fridays from 10 a.m. to 1 p.m. There are no weekend or evening hours, and one might think there would be enough urgency to call for this. The Maryland Psychiatric Society sent out a notice that Sheppard Pratt would be offering vaccines to all behavioral health providers in the state of Maryland during a 2-day clinic. I heard from others that health care workers can now get vaccinated at the Cow Palace (how great is that?) at the Maryland State Fairgrounds and another link was sent for those in Howard County, between Baltimore and Washington.
As I discussed this with colleagues, a couple of issues came up – the most common was one of not wanting to get the vaccine yet because there are others who need it more. Others voiced concern about a vaccine where the long-term effects remain unknown: Is this vaccine safe, might it spur autoimmune problems in the months or years to come? Is it safe for women who plan to become pregnant? Some have insisted it is safe. They say “follow the science” and have dismissed the skepticism. To my read, it makes perfect sense to be wary, but COVID spreads silently and it kills.
With a vaccine where so many are reluctant to get it, including many health care workers, Sue Kim, MD, a psychiatrist in private practice in Lutherville, Md., noted that she has concerns about the safety of the vaccine. “Getting it now is both altruistic and selfish, but letting others go first is also altruistic and selfish. In the meantime, if I get sick, I was too smart for my own good. How do you weigh this ethically?”
My personal feelings have been influenced by a few things. An article in the New York Times highlighted how New York City vaccinated 5 million people for smallpox in just 2 weeks in 1947. I am frustrated knowing that, a month after approval of the first vaccine, only 7 million people have received it in the entire United States. In that time period, millions have contracted COVID and thousands have died. Closer to home, a 45-year-old psychiatrist in Maryland died of COVID, and I have heard more stories about younger people with long-haul neurologic and vascular symptoms. The risk of COVID is feeling higher than it did, and the fact that the first vaccine was authorized after the election somehow makes me feel that it might be safer. Had it been approved right before, I would have worried – perhaps wrongly – that the authorization was a political maneuver, not one based on science.
As we think about what is best for ourselves, our families, our patients, and society as a whole, I believe that those who want the vaccine but don’t feel they should take their place in line before others who are higher risk must ask if it makes sense to wait. Each state is different. While Houston Methodist Hospital is reportedly giving its health care workers a $500 bonus to get the vaccine, Gov. Andrew Cuomo of New York announced that hospitals would be fined $100,000 if they don’t use all of their vaccines within 7 days of receipt and $1 million if they vaccinate anyone out of order. Gov. Cuomo later broadened who could be vaccinated to prevent wasting the vaccine, but there remains an element of being damned if you do and damned if you don’t.
Paul Nestadt, MD, a psychiatrist at Johns Hopkins University, Baltimore, noted that one distribution site initially had to waste unused vaccine when people did not come for their appointments. A waiting list was created for people who could come right away if called to prevent this waste. “To me, this only highlighted that the tier system, while a good idea, does not need to be written in stone. The goal needs to be getting shots in arms, building herd immunity. If there are two arms in front of you, shoot the health care worker or those who are vulnerable. But if there is a healthy arm in reach, it should get any shot made available.”
I registered to be vaccinated. – senior citizens and essential workers are not yet eligible. In Baltimore, vaccinations are available Mondays to Thursdays from 10 a.m. to 4 p.m. and on Fridays from 10 a.m. to 1 p.m. There are no options for early morning or weekend times, but there are slots still available for the coming week. As of this writing, there are 6,100 Marylanders dead, and more than 1,800 COVID patients in hospital beds, and our governor, Larry Hogan, has commercials to “Mask On Maryland” and “Wear the Damn Mask.” I’ll offer some changes: “Wake Up, World” and “Offer the Damn Shot.”
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University, 2016). She is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, both in Baltimore. Dr. Miller has no disclosures.
When the long-awaited news of a Food and Drug Administration–approved vaccine came on Dec. 11, 2020, my first thought was that I would wait. I can manage a few more months of Zooming for work, my household is down to two people, I’m not at high risk of dying from COVID, and my husband is not going to be vaccinated any time soon, so a change in my status wouldn’t “free” me. I would rather have “my” vaccine go to a 70-year-old ICU janitor or a bus driver.
The weeks have gone by. I expected there would be kinks, but it has now been a month – one in which COVID rates have soared, and hospitalizations and deaths have risen to unmanageable numbers in some places. Still, vaccines remain in freezers – people are dying while vials of prevention sit unused. I began to think that, when my “turn” came, the better thing was to be vaccinated. We need to have a large segment of the population vaccinated to squelch this virus, and it’s become much less clear to me that, if I yield my turn, it will go into the arm of a bus driver. The process has not been fair, and there are moments of media outrage when one group gets vaccinated before another, so perhaps we have reached point where the goal should not be to get the vaccine into the exact right person in the exact right order, but to get the vaccine into arms according to the protocol that has already been set. Anyone who does not end up in a hospital bed is doing the system a favor.
Mahmood Jahromi, MD, a psychiatrist in private practice in Towson, Md., described the process of vaccination as being similar to a bottleneck traffic jam. “Yes, one must be courteous to the car trying to but in, but no, don’t jam the glue because you are excessively kind. Let the traffic police do their job. When your name is called, go ahead and take it. The system needs to know people are accepting the vaccine, not by begging the authorities to be called ahead of others, but with respect for what is already designed.”
On Friday, Jan. 8, I received information on how to get vaccinated – it seems my “turn” has arrived. An email from the board of physicians informed me that I am in the “1A” category and included a link to sign up for a vaccine in Baltimore – vaccinations would be given until Jan. 29, Mondays to Thursdays from 10 a.m. to 4 p.m. and Fridays from 10 a.m. to 1 p.m. There are no weekend or evening hours, and one might think there would be enough urgency to call for this. The Maryland Psychiatric Society sent out a notice that Sheppard Pratt would be offering vaccines to all behavioral health providers in the state of Maryland during a 2-day clinic. I heard from others that health care workers can now get vaccinated at the Cow Palace (how great is that?) at the Maryland State Fairgrounds and another link was sent for those in Howard County, between Baltimore and Washington.
As I discussed this with colleagues, a couple of issues came up – the most common was one of not wanting to get the vaccine yet because there are others who need it more. Others voiced concern about a vaccine where the long-term effects remain unknown: Is this vaccine safe, might it spur autoimmune problems in the months or years to come? Is it safe for women who plan to become pregnant? Some have insisted it is safe. They say “follow the science” and have dismissed the skepticism. To my read, it makes perfect sense to be wary, but COVID spreads silently and it kills.
With a vaccine where so many are reluctant to get it, including many health care workers, Sue Kim, MD, a psychiatrist in private practice in Lutherville, Md., noted that she has concerns about the safety of the vaccine. “Getting it now is both altruistic and selfish, but letting others go first is also altruistic and selfish. In the meantime, if I get sick, I was too smart for my own good. How do you weigh this ethically?”
My personal feelings have been influenced by a few things. An article in the New York Times highlighted how New York City vaccinated 5 million people for smallpox in just 2 weeks in 1947. I am frustrated knowing that, a month after approval of the first vaccine, only 7 million people have received it in the entire United States. In that time period, millions have contracted COVID and thousands have died. Closer to home, a 45-year-old psychiatrist in Maryland died of COVID, and I have heard more stories about younger people with long-haul neurologic and vascular symptoms. The risk of COVID is feeling higher than it did, and the fact that the first vaccine was authorized after the election somehow makes me feel that it might be safer. Had it been approved right before, I would have worried – perhaps wrongly – that the authorization was a political maneuver, not one based on science.
As we think about what is best for ourselves, our families, our patients, and society as a whole, I believe that those who want the vaccine but don’t feel they should take their place in line before others who are higher risk must ask if it makes sense to wait. Each state is different. While Houston Methodist Hospital is reportedly giving its health care workers a $500 bonus to get the vaccine, Gov. Andrew Cuomo of New York announced that hospitals would be fined $100,000 if they don’t use all of their vaccines within 7 days of receipt and $1 million if they vaccinate anyone out of order. Gov. Cuomo later broadened who could be vaccinated to prevent wasting the vaccine, but there remains an element of being damned if you do and damned if you don’t.
Paul Nestadt, MD, a psychiatrist at Johns Hopkins University, Baltimore, noted that one distribution site initially had to waste unused vaccine when people did not come for their appointments. A waiting list was created for people who could come right away if called to prevent this waste. “To me, this only highlighted that the tier system, while a good idea, does not need to be written in stone. The goal needs to be getting shots in arms, building herd immunity. If there are two arms in front of you, shoot the health care worker or those who are vulnerable. But if there is a healthy arm in reach, it should get any shot made available.”
I registered to be vaccinated. – senior citizens and essential workers are not yet eligible. In Baltimore, vaccinations are available Mondays to Thursdays from 10 a.m. to 4 p.m. and on Fridays from 10 a.m. to 1 p.m. There are no options for early morning or weekend times, but there are slots still available for the coming week. As of this writing, there are 6,100 Marylanders dead, and more than 1,800 COVID patients in hospital beds, and our governor, Larry Hogan, has commercials to “Mask On Maryland” and “Wear the Damn Mask.” I’ll offer some changes: “Wake Up, World” and “Offer the Damn Shot.”
Dr. Miller is coauthor of “Committed: The Battle Over Involuntary Psychiatric Care” (Baltimore: Johns Hopkins University, 2016). She is assistant professor of psychiatry and behavioral sciences at Johns Hopkins University, both in Baltimore. Dr. Miller has no disclosures.
Trust in a Vial
On December 11, 2020, the US Food and Drug Administration (FDA) delivered the holiday gift America was waiting for—approval of the first COVID-19 vaccine. Following the recommendation of its expert advisory panel, the FDA issued its opening emergency use authorization (EUA) for the Pfizer and BioNTech product to be distributed and administered across the country.1 A week after that historic announcement, the FDA issued an EUA to Moderna for a second COVID-19 vaccine.2
An EUA is a misunderstood concept that, like the development of the vaccine itself, appears almost like a magical federal deliverance to a nation at a time when almost every other public health effort has floundered. An EUA is a regulatory process to enable a public health emergency response with medical countermeasures including not only vaccines, but also medications. Earlier in 2020, hydroxychloroquine and remdesivir each received EUAs for treating patients with COVID-19.3 The EUA for hydroxychloroquine was later revoked when more data raised concerns for its efficacy.4 EUAs do not mean the drugs are experimental or that everyone receiving them is participating in a research trial; however, for the sake of safety and science, data continue to be collected and analyzed. Issuance of an EUA indicates that after rigorous examination and an independent advisory board review of data submitted by the manufacturer, the FDA has determined the product and situation meet key criteria: (1) There is a public health emergency that threatens health and life and requires expedited procedures; (2) there are no extant approved products able to treat or prevent the disease; and (3) the known and potential benefits of the product outweigh the known and potential risks.5
The public and even the professional press have celebrated the arrival of this technologic triumph over a virus that had vanquished staggering numbers of lives and livelihoods. Much of the media coverage aptly chose the word “hope” to capture the significance of this unprecedented accomplishment for which so many millions yearned. A Google search for “hope” on the morning of December 20, yielded 339,000,000 results. For example, a headline especially salient for Federal Practitioner readers from the New York Times read, “‘A Shot of Hope’ What the Vaccine is like for Frontline Doctors and Nurses.”6
I want to briefly argue why even though I believe hope in and for the vaccine is desperately needed if we are to survive this long, dark winter, trust in the vaccine can actually usher in the warmth of economic recovery and the light of saved lives. Trust is crucial in 3 main areas if the awe-inspiring hope of the vaccine the EUAs codify is to be fulfilled. The venerable moral and civic virtue of trust has been trivialized and commercialized mostly mentioned in advertising for insurance or real estate companies. Medical virtue-ethicists Edmund Pellegrino and David Thomasma describe trust as the binding force that keeps civilization intact. “Trust is ineradicable in human relationships. Without we could not live in society or attain even the rudiments of a fulfilling life, they explain. “Without trust we could not anticipate the future, and we would therefore be paralyzed into inaction. Yet to trust and entrust is to become vulnerable and dependent on the good will and motivations of those we trust. Trust, ineradicable as it is, is also always problematic.”7
The first area where that trust is the hardest to secure is in the federal government, the actions and messages of which have seemed so inconstant, unjust, and deceptive to many. For enough citizens to roll up their sleeves, they must believe the outgoing and the incoming administrations and legislators can make rational plans translated into sound public health policy that place the good of humanity above other interests and then mobilize the resources of the country to deliver that good with consistency, fairness, and transparency.
The second area is trust in medical science. Long before COVID-19, American attitudes toward vaccines reflected reasonable fears and ridiculous conspiracy theories—both of which are serious obstacles to the breadth of immunization required to achieve herd immunity. Ordinary people must believe that the health care professionals and scientists at the Centers for Disease Control and Prevention and the FDA will never compromise safety for political expediency. Recent polls have shown an increase in the percentage of the population willing to consider vaccination. A December Gallop poll found that 63% of Americans were willing to be vaccinated for COVID-19.8 To raise those numbers high enough to approach herd immunity will require Americans to believe that the scientists who discover the vaccines and the companies that develop them have placed people above profit and ranked the safety of society above individual scientific renown.
Groups that have been the historic objects of exploitation in research and contemporary disparities in health care understandably have more distrust of science and medicine. While public health officials insist that they have developed a system of vaccine distribution that is equitable and prioritizes the sick and old and those who care for them before the rich and powerful, we should not be surprised that our communication of this assurance is viewed with skepticism. As a recent Medscape article advised,
Third we must trust in our fellow citizens to maintain the public health measures of social distancing and mask wearing even after there is widespread vaccination. If we are to reap the benefits of a safe and effective vaccine, we must be a community of immunity, not just isolated inoculated individuals. We as health care practitioners must do all we can to educate the public that the adverse reactions to the vaccine so prominently featured in the media are expected with any new and complex biological product and do not signal risk that outweighs the deadliness of the virus.10
Fourth, and finally, we must trust in ourselves as health care professionals and administrators. We in the DoD, VA, and PHS have the knowledge and skills to endure the onslaught of pain and suffering we will all experience in one way or another in these next long months. We must believe that our courage and compassion can turn a vaccine into vaccinations sufficient to relieve the COVID-19 siege of our hospitals and intensive care units. When that day comes, hope will have been a plan we could trust.
1. US Food and Drug Administration. FDA take key action in fight against COVID-19 by issuing emergency use authorization for first COVID-19 vaccine [press release]. Published December 11, 2020. Accessed December 22, 2020. https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-covid-19-issuing-emergency-use-authorization-first-covid-19
2. US Food and Drug Administration. FDA takes additional action in fight against COVID-19 by Issuing emergency use authorization for second COVID-19 vaccine [press release]. Published December 18, 2020. Accessed December 22, 2020. https://www.fda.gov/news-events/press-announcements/fda-takes-additional-action-fight-against-covid-19-issuing-emergency-use-authorization-second-covid
3. US Food and Drug Administration. FDA approves first treatment for COVID-19 [press release]. Published October 22, 2020. Accessed December 20, 2020. https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-covid-19
4. US Food and Drug Administration. Coronavirus (COVID-19) update: FDA revokes emergency use authorization for chloroquine and hydroxychloroquine [press release]. Published June 15, 2020. Accessed December 22, 2020. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-chloroquine-and
5. US Food and Drug Administration. Emergency use authorization for vaccines explained. Updated November 20, 2020. Accessed December 22, 2020. https://www.fda.gov/vaccines-blood-biologics/vaccines/emergency-use-authorization-vaccines-explained
6. Healy J, Tompkins L, Burch ADS. ‘A shot of hope’: what the vaccine is like for frontline doctors and nurses. New York Times. Updated December 17, 2020. Accessed December 22, 2020. https://www.nytimes.com/2020/12/14/us/coronavirus-vaccine-doctors-nurses.html
7. Pellegrino E, Thomasma DC. The Virtues in Medical Practice . New York: Oxford University Press; 1993:65.
8. Brenan M. Willingness to get Covid-19 vaccine ticks up to 63% in the U.S. Published December 8, 2020. Accessed December 22, 2020. https://news.gallup.com/poll/327425/willingness-covid-vaccine-ticks.aspx
9. Eldred SM. Trusted messengers may help disenfranchised communities overcome vaccine hesitancy. Published December 17, 2020. Accessed December 22, 2020. https://www.medscape.com/viewarticle/942847
10. Chiu A. ‘Absolutely normal’: Covid vaccine side effects are not reason to avoid the shots, doctors say. Washington Post. Published December 3, 2020. Accessed December 22, 2020. https://www.washingtonpost.com/lifestyle/wellness/vaccine-side-effects-covid/2020/12/02/55bebac0-342c-11eb-8d38-6aea1adb3839_story.html
On December 11, 2020, the US Food and Drug Administration (FDA) delivered the holiday gift America was waiting for—approval of the first COVID-19 vaccine. Following the recommendation of its expert advisory panel, the FDA issued its opening emergency use authorization (EUA) for the Pfizer and BioNTech product to be distributed and administered across the country.1 A week after that historic announcement, the FDA issued an EUA to Moderna for a second COVID-19 vaccine.2
An EUA is a misunderstood concept that, like the development of the vaccine itself, appears almost like a magical federal deliverance to a nation at a time when almost every other public health effort has floundered. An EUA is a regulatory process to enable a public health emergency response with medical countermeasures including not only vaccines, but also medications. Earlier in 2020, hydroxychloroquine and remdesivir each received EUAs for treating patients with COVID-19.3 The EUA for hydroxychloroquine was later revoked when more data raised concerns for its efficacy.4 EUAs do not mean the drugs are experimental or that everyone receiving them is participating in a research trial; however, for the sake of safety and science, data continue to be collected and analyzed. Issuance of an EUA indicates that after rigorous examination and an independent advisory board review of data submitted by the manufacturer, the FDA has determined the product and situation meet key criteria: (1) There is a public health emergency that threatens health and life and requires expedited procedures; (2) there are no extant approved products able to treat or prevent the disease; and (3) the known and potential benefits of the product outweigh the known and potential risks.5
The public and even the professional press have celebrated the arrival of this technologic triumph over a virus that had vanquished staggering numbers of lives and livelihoods. Much of the media coverage aptly chose the word “hope” to capture the significance of this unprecedented accomplishment for which so many millions yearned. A Google search for “hope” on the morning of December 20, yielded 339,000,000 results. For example, a headline especially salient for Federal Practitioner readers from the New York Times read, “‘A Shot of Hope’ What the Vaccine is like for Frontline Doctors and Nurses.”6
I want to briefly argue why even though I believe hope in and for the vaccine is desperately needed if we are to survive this long, dark winter, trust in the vaccine can actually usher in the warmth of economic recovery and the light of saved lives. Trust is crucial in 3 main areas if the awe-inspiring hope of the vaccine the EUAs codify is to be fulfilled. The venerable moral and civic virtue of trust has been trivialized and commercialized mostly mentioned in advertising for insurance or real estate companies. Medical virtue-ethicists Edmund Pellegrino and David Thomasma describe trust as the binding force that keeps civilization intact. “Trust is ineradicable in human relationships. Without we could not live in society or attain even the rudiments of a fulfilling life, they explain. “Without trust we could not anticipate the future, and we would therefore be paralyzed into inaction. Yet to trust and entrust is to become vulnerable and dependent on the good will and motivations of those we trust. Trust, ineradicable as it is, is also always problematic.”7
The first area where that trust is the hardest to secure is in the federal government, the actions and messages of which have seemed so inconstant, unjust, and deceptive to many. For enough citizens to roll up their sleeves, they must believe the outgoing and the incoming administrations and legislators can make rational plans translated into sound public health policy that place the good of humanity above other interests and then mobilize the resources of the country to deliver that good with consistency, fairness, and transparency.
The second area is trust in medical science. Long before COVID-19, American attitudes toward vaccines reflected reasonable fears and ridiculous conspiracy theories—both of which are serious obstacles to the breadth of immunization required to achieve herd immunity. Ordinary people must believe that the health care professionals and scientists at the Centers for Disease Control and Prevention and the FDA will never compromise safety for political expediency. Recent polls have shown an increase in the percentage of the population willing to consider vaccination. A December Gallop poll found that 63% of Americans were willing to be vaccinated for COVID-19.8 To raise those numbers high enough to approach herd immunity will require Americans to believe that the scientists who discover the vaccines and the companies that develop them have placed people above profit and ranked the safety of society above individual scientific renown.
Groups that have been the historic objects of exploitation in research and contemporary disparities in health care understandably have more distrust of science and medicine. While public health officials insist that they have developed a system of vaccine distribution that is equitable and prioritizes the sick and old and those who care for them before the rich and powerful, we should not be surprised that our communication of this assurance is viewed with skepticism. As a recent Medscape article advised,
Third we must trust in our fellow citizens to maintain the public health measures of social distancing and mask wearing even after there is widespread vaccination. If we are to reap the benefits of a safe and effective vaccine, we must be a community of immunity, not just isolated inoculated individuals. We as health care practitioners must do all we can to educate the public that the adverse reactions to the vaccine so prominently featured in the media are expected with any new and complex biological product and do not signal risk that outweighs the deadliness of the virus.10
Fourth, and finally, we must trust in ourselves as health care professionals and administrators. We in the DoD, VA, and PHS have the knowledge and skills to endure the onslaught of pain and suffering we will all experience in one way or another in these next long months. We must believe that our courage and compassion can turn a vaccine into vaccinations sufficient to relieve the COVID-19 siege of our hospitals and intensive care units. When that day comes, hope will have been a plan we could trust.
On December 11, 2020, the US Food and Drug Administration (FDA) delivered the holiday gift America was waiting for—approval of the first COVID-19 vaccine. Following the recommendation of its expert advisory panel, the FDA issued its opening emergency use authorization (EUA) for the Pfizer and BioNTech product to be distributed and administered across the country.1 A week after that historic announcement, the FDA issued an EUA to Moderna for a second COVID-19 vaccine.2
An EUA is a misunderstood concept that, like the development of the vaccine itself, appears almost like a magical federal deliverance to a nation at a time when almost every other public health effort has floundered. An EUA is a regulatory process to enable a public health emergency response with medical countermeasures including not only vaccines, but also medications. Earlier in 2020, hydroxychloroquine and remdesivir each received EUAs for treating patients with COVID-19.3 The EUA for hydroxychloroquine was later revoked when more data raised concerns for its efficacy.4 EUAs do not mean the drugs are experimental or that everyone receiving them is participating in a research trial; however, for the sake of safety and science, data continue to be collected and analyzed. Issuance of an EUA indicates that after rigorous examination and an independent advisory board review of data submitted by the manufacturer, the FDA has determined the product and situation meet key criteria: (1) There is a public health emergency that threatens health and life and requires expedited procedures; (2) there are no extant approved products able to treat or prevent the disease; and (3) the known and potential benefits of the product outweigh the known and potential risks.5
The public and even the professional press have celebrated the arrival of this technologic triumph over a virus that had vanquished staggering numbers of lives and livelihoods. Much of the media coverage aptly chose the word “hope” to capture the significance of this unprecedented accomplishment for which so many millions yearned. A Google search for “hope” on the morning of December 20, yielded 339,000,000 results. For example, a headline especially salient for Federal Practitioner readers from the New York Times read, “‘A Shot of Hope’ What the Vaccine is like for Frontline Doctors and Nurses.”6
I want to briefly argue why even though I believe hope in and for the vaccine is desperately needed if we are to survive this long, dark winter, trust in the vaccine can actually usher in the warmth of economic recovery and the light of saved lives. Trust is crucial in 3 main areas if the awe-inspiring hope of the vaccine the EUAs codify is to be fulfilled. The venerable moral and civic virtue of trust has been trivialized and commercialized mostly mentioned in advertising for insurance or real estate companies. Medical virtue-ethicists Edmund Pellegrino and David Thomasma describe trust as the binding force that keeps civilization intact. “Trust is ineradicable in human relationships. Without we could not live in society or attain even the rudiments of a fulfilling life, they explain. “Without trust we could not anticipate the future, and we would therefore be paralyzed into inaction. Yet to trust and entrust is to become vulnerable and dependent on the good will and motivations of those we trust. Trust, ineradicable as it is, is also always problematic.”7
The first area where that trust is the hardest to secure is in the federal government, the actions and messages of which have seemed so inconstant, unjust, and deceptive to many. For enough citizens to roll up their sleeves, they must believe the outgoing and the incoming administrations and legislators can make rational plans translated into sound public health policy that place the good of humanity above other interests and then mobilize the resources of the country to deliver that good with consistency, fairness, and transparency.
The second area is trust in medical science. Long before COVID-19, American attitudes toward vaccines reflected reasonable fears and ridiculous conspiracy theories—both of which are serious obstacles to the breadth of immunization required to achieve herd immunity. Ordinary people must believe that the health care professionals and scientists at the Centers for Disease Control and Prevention and the FDA will never compromise safety for political expediency. Recent polls have shown an increase in the percentage of the population willing to consider vaccination. A December Gallop poll found that 63% of Americans were willing to be vaccinated for COVID-19.8 To raise those numbers high enough to approach herd immunity will require Americans to believe that the scientists who discover the vaccines and the companies that develop them have placed people above profit and ranked the safety of society above individual scientific renown.
Groups that have been the historic objects of exploitation in research and contemporary disparities in health care understandably have more distrust of science and medicine. While public health officials insist that they have developed a system of vaccine distribution that is equitable and prioritizes the sick and old and those who care for them before the rich and powerful, we should not be surprised that our communication of this assurance is viewed with skepticism. As a recent Medscape article advised,
Third we must trust in our fellow citizens to maintain the public health measures of social distancing and mask wearing even after there is widespread vaccination. If we are to reap the benefits of a safe and effective vaccine, we must be a community of immunity, not just isolated inoculated individuals. We as health care practitioners must do all we can to educate the public that the adverse reactions to the vaccine so prominently featured in the media are expected with any new and complex biological product and do not signal risk that outweighs the deadliness of the virus.10
Fourth, and finally, we must trust in ourselves as health care professionals and administrators. We in the DoD, VA, and PHS have the knowledge and skills to endure the onslaught of pain and suffering we will all experience in one way or another in these next long months. We must believe that our courage and compassion can turn a vaccine into vaccinations sufficient to relieve the COVID-19 siege of our hospitals and intensive care units. When that day comes, hope will have been a plan we could trust.
1. US Food and Drug Administration. FDA take key action in fight against COVID-19 by issuing emergency use authorization for first COVID-19 vaccine [press release]. Published December 11, 2020. Accessed December 22, 2020. https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-covid-19-issuing-emergency-use-authorization-first-covid-19
2. US Food and Drug Administration. FDA takes additional action in fight against COVID-19 by Issuing emergency use authorization for second COVID-19 vaccine [press release]. Published December 18, 2020. Accessed December 22, 2020. https://www.fda.gov/news-events/press-announcements/fda-takes-additional-action-fight-against-covid-19-issuing-emergency-use-authorization-second-covid
3. US Food and Drug Administration. FDA approves first treatment for COVID-19 [press release]. Published October 22, 2020. Accessed December 20, 2020. https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-covid-19
4. US Food and Drug Administration. Coronavirus (COVID-19) update: FDA revokes emergency use authorization for chloroquine and hydroxychloroquine [press release]. Published June 15, 2020. Accessed December 22, 2020. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-chloroquine-and
5. US Food and Drug Administration. Emergency use authorization for vaccines explained. Updated November 20, 2020. Accessed December 22, 2020. https://www.fda.gov/vaccines-blood-biologics/vaccines/emergency-use-authorization-vaccines-explained
6. Healy J, Tompkins L, Burch ADS. ‘A shot of hope’: what the vaccine is like for frontline doctors and nurses. New York Times. Updated December 17, 2020. Accessed December 22, 2020. https://www.nytimes.com/2020/12/14/us/coronavirus-vaccine-doctors-nurses.html
7. Pellegrino E, Thomasma DC. The Virtues in Medical Practice . New York: Oxford University Press; 1993:65.
8. Brenan M. Willingness to get Covid-19 vaccine ticks up to 63% in the U.S. Published December 8, 2020. Accessed December 22, 2020. https://news.gallup.com/poll/327425/willingness-covid-vaccine-ticks.aspx
9. Eldred SM. Trusted messengers may help disenfranchised communities overcome vaccine hesitancy. Published December 17, 2020. Accessed December 22, 2020. https://www.medscape.com/viewarticle/942847
10. Chiu A. ‘Absolutely normal’: Covid vaccine side effects are not reason to avoid the shots, doctors say. Washington Post. Published December 3, 2020. Accessed December 22, 2020. https://www.washingtonpost.com/lifestyle/wellness/vaccine-side-effects-covid/2020/12/02/55bebac0-342c-11eb-8d38-6aea1adb3839_story.html
1. US Food and Drug Administration. FDA take key action in fight against COVID-19 by issuing emergency use authorization for first COVID-19 vaccine [press release]. Published December 11, 2020. Accessed December 22, 2020. https://www.fda.gov/news-events/press-announcements/fda-takes-key-action-fight-against-covid-19-issuing-emergency-use-authorization-first-covid-19
2. US Food and Drug Administration. FDA takes additional action in fight against COVID-19 by Issuing emergency use authorization for second COVID-19 vaccine [press release]. Published December 18, 2020. Accessed December 22, 2020. https://www.fda.gov/news-events/press-announcements/fda-takes-additional-action-fight-against-covid-19-issuing-emergency-use-authorization-second-covid
3. US Food and Drug Administration. FDA approves first treatment for COVID-19 [press release]. Published October 22, 2020. Accessed December 20, 2020. https://www.fda.gov/news-events/press-announcements/fda-approves-first-treatment-covid-19
4. US Food and Drug Administration. Coronavirus (COVID-19) update: FDA revokes emergency use authorization for chloroquine and hydroxychloroquine [press release]. Published June 15, 2020. Accessed December 22, 2020. https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-revokes-emergency-use-authorization-chloroquine-and
5. US Food and Drug Administration. Emergency use authorization for vaccines explained. Updated November 20, 2020. Accessed December 22, 2020. https://www.fda.gov/vaccines-blood-biologics/vaccines/emergency-use-authorization-vaccines-explained
6. Healy J, Tompkins L, Burch ADS. ‘A shot of hope’: what the vaccine is like for frontline doctors and nurses. New York Times. Updated December 17, 2020. Accessed December 22, 2020. https://www.nytimes.com/2020/12/14/us/coronavirus-vaccine-doctors-nurses.html
7. Pellegrino E, Thomasma DC. The Virtues in Medical Practice . New York: Oxford University Press; 1993:65.
8. Brenan M. Willingness to get Covid-19 vaccine ticks up to 63% in the U.S. Published December 8, 2020. Accessed December 22, 2020. https://news.gallup.com/poll/327425/willingness-covid-vaccine-ticks.aspx
9. Eldred SM. Trusted messengers may help disenfranchised communities overcome vaccine hesitancy. Published December 17, 2020. Accessed December 22, 2020. https://www.medscape.com/viewarticle/942847
10. Chiu A. ‘Absolutely normal’: Covid vaccine side effects are not reason to avoid the shots, doctors say. Washington Post. Published December 3, 2020. Accessed December 22, 2020. https://www.washingtonpost.com/lifestyle/wellness/vaccine-side-effects-covid/2020/12/02/55bebac0-342c-11eb-8d38-6aea1adb3839_story.html

Is it safe to be pregnant during the COVID-19 pandemic?

Pregnant women, or women considering pregnancy, want to know—is pregnancy safe in the midst of the coronavirus disease 2019 (COVID-19) pandemic? In this article, I tackle common questions facing reproductive-aged or pregnant women and their providers.
1. What are the risks of COVID-19 in pregnancy?
A large, national prospective cohort study of outpatient pregnant and recently postpartum women with the diagnosis of suspected or confirmed COVID-19 demonstrated that many affected women have mild illnesses, with typical symptoms including cough, sore throat, body aches, fever, and headache.1 Although symptoms were most common within the first 3 weeks of presentation, approximately 25% of women had a protracted course of symptoms (8 or more weeks). As this cohort disproportionately enrolled outpatients, it is important to note that many women had mild illnesses, which is the most likely course of infection in otherwise healthy, young women.
Data on the impact of COVID-19 on rates of miscarriage and birth defects are limited, yet the published reports are reassuring, with no increased risks of miscarriage, and no clear signal for birth defects.2
In a prospective cohort study across 3 New York City institutions when universal severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing was recommended upon admission for delivery, approximately 80% of women who were positive were asymptomatic.3 Maternal outcomes generally were reassuring, with no patients experiencing severe or critical illness. There were no differences in preterm delivery rates by SARS-CoV-2 status, but the rate of cesarean delivery was higher among women with COVID-19, for unclear reasons. Most notably, the rate of postpartum complications was 13% among women with COVID-19, versus 2.5% among women without COVID-19. These complications included readmission for worsening COVID-19, postpartum hypoxia, and postpartum fever.
A recent prospective cohort study from 1 institution in Texas similarly demonstrated favorable maternal outcomes with COVID-19, with 95% of women with asymptomatic or mild illness, and no differences in adverse pregnancy outcomes between COVID-19–positive and COVID-19–negative women, including cesarean delivery rate.4
Finally, certain characteristics increase the risk of COVID-19 among pregnant women and nonpregnant individuals alike. In a nationwide prospective cohort from the United Kingdom, medical comorbidities including obesity, diabetes (gestational or pregestational), hypertension, as well as Black or other minority ethnicities are associated with COVID-19.5 This is particularly notable given universal health insurance in the United Kingdom. Other data have also confirmed that women with comorbidities, women of Black or Hispanic ethnicity, and women with lower socioeconomic status, are at increased risk of COVID-19.3,6,7
2. Is COVID-19 worse in pregnancy?
Given the well-documented risks of COVID-19 outside of pregnancy, is COVID-19 worse in a pregnant woman than in a nonpregnant woman? The most recent guidance from the Centers for Disease Control and Prevention (CDC) from November 2020 suggests that pregnant women are at increased risk for severe illness.8 However, it is important to understand the design of this study in order to appreciate its implications. Laboratory confirmed SARS-CoV-2 in the United States is systematically reported to the CDC. Among women aged 15–44 years with such confirmation, data on pregnancy status were available for 35.5%, almost 90% of whom were symptomatic. Within this cohort of largely symptomatic pregnant women, risks of intensive care unit (ICU) admission, invasive ventilation, and use of extracorporeal membrane oxygenation (ECMO) were approximately 2 to 3 times higher for pregnant women than for nonpregnant women. The absolute risks, however, were low. The risk of ICU admission for symptomatic pregnant women was approximately 1%; the risk of invasive ventilation, 0.3%; and the risk of ECMO, 0.1%.
Moreover, the lack of uniform data capture on pregnancy status for all women ages 15–44 years may skew the population with known pregnancy status to be sicker and, thus, may bias the results toward increased risks. Nevertheless, there is consistency in several publications with different data sources, all of which suggest pregnancy is an independent risk factor for increased severity of COVID-19.9-11 Additionally, women with medical comorbidities (such as pregestational or gestational diabetes or obesity) are more likely to have severe COVID-19.
Continue to: 3. What are newborn outcomes if COVID-19 is diagnosed during pregnancy?...
3. What are newborn outcomes if COVID-19 is diagnosed during pregnancy?
Two large cohorts of newborns, disproportionately term infants, from the first wave of the pandemic in New York City, have reassuring news. In one cohort of 101 infants born at 2 New York City institutions to SARS-CoV-2–positive mothers, 2 neonates were diagnosed with SARS-CoV-2 during the immediate postnatal period.12 Neither infant demonstrated clinical COVID-19. In another cohort of 120 infants born at 3 other New York City institutions to SARS-CoV-2–positive mothers and tested systematically within 24 hours of life, 5–7 days of life, and 14 days of life, there were no neonates who tested positive for SARS-CoV-2 at the initial time point. Among the 79 infants who had testing at 5–7 days of life and the 72 tested at 14 days of life, there were no infants positive for SARS-CoV-2.13 It is important to note that case reports and small case series have demonstrated some convincing evidence of vertical transmission. However, the overwhelming evidence suggests this risk is very low.
4. What is a reasonable outpatient setting–approach to managing COVID-19 in a pregnant woman?
Women should be counseled to quarantine for 10 to 14 days from symptom onset or, if asymptomatic, from positive polymerase chain reaction (PCR) test. Warning signs of worsening COVID-19 disease should be reviewed. Serial telemedicine follow-up for 10 to 14 days is recommended to ensure clinical stability and continued management as an outpatient. A home pulse oximeter is also recommended. Women should be advised to check their oxygen saturation daily and to call if oxygen saturation becomes less than 93%. Supportive care is recommended.
If delay in obstetric care may result in adverse pregnancy outcomes (for instance, postponing indicated fetal surveillance), obstetric care should be delivered, with appropriate personal protective equipment for health care workers and minimization of exposure of other pregnant women to the infected patient. Appointments should be scheduled at the end of the day.
During influenza season, women should receive empiric oseltamivir treatment (75 mg twice a day) per CDC guidelines for symptoms that may also be consistent with influenza, regardless of testing.
Prophylactic anticoagulation is not indicated for pregnant antepartum women who do not require inpatient care.
If inpatient care is required, management is individualized.
The approach to prenatal care after resolution of COVID-19 is not evidence-based. At my institution, all patients have a detailed mid-trimester anatomic evaluation, but if this is not routine, a detailed anatomic ultrasound (Current Procedural Terminology code 76811) may be considered. Additionally, for women with COVID-19 we perform one third-trimester growth ultrasound to screen for fetal growth restriction, on the basis of several placental studies demonstrating clots on the fetal or maternal side of the placenta.3,14 Routine antenatal testing in the absence of growth restriction, or other comorbid conditions for which testing occurs, is not recommended.
Continue to: 5. What if asymptomatic or mild COVID-19 is diagnosed at the time of delivery?...
5. What if asymptomatic or mild COVID-19 is diagnosed at the time of delivery? What is reasonable management?
Asymptomatic or mildly symptomatic COVID-19 should not alter obstetric management, beyond appropriate use of personal protective equipment. Delayed cord clamping is also reasonable, if there are no other contraindications, as there is no documented harm associated with this practice among women with COVID-19.
Women with COVID-19 may be at higher risk for venous thromboembolic events in the postpartum period. At my institution, prophylactic postpartum anticoagulation is recommended for 2 weeks after vaginal delivery, and 6 weeks after cesarean delivery.
During the postpartum hospitalization, given reassuring data about vertical transmission and postnatal horizontal transmission risks, babies may room in with mothers in a single private room, if rooming-in is the current standard of care—as long as the mother and newborn do not require higher levels of care. Mothers should wear a mask and use hand hygiene when in contact with the baby. Skin-to-skin and breastfeeding or infant feeding of breast milk are appropriate practices to continue. There is no evidence to suggest that transmission of COVID-19 can occur via breastmilk; however, given the close contact inherent in breastfeeding, transmission through direct contact or maternal respiratory droplets is possible, and thus maternal use of masks and hand hygiene is recommended. When not feeding, the infant should be 6 feet away, and if possible, in an isolette.
6. When can individuals with COVID-19 discontinue transmission precautions or “home quarantine”?
For women with mildly symptomatic COVID-19 and without immunocompromise, home quarantine can be discontinued 10 days after onset of symptoms as long as there has been symptom improvement and no fever for at least 24 hours without the use of antipyretics. For immunocompetent women with incidentally diagnosed asymptomatic COVID-19, home quarantine can be discontinued 10 days after the positive test was obtained. Pregnancy in and of itself is not an immunocompromising condition.15,16
For women with severe or critical COVID-19, who were hospitalized due to their clinical status, home quarantine can be discontinued when at least 10 days, and up to 20 days, after onset of symptoms and with symptom improvement and with no fever for at least 24 hours, without the use of antipyretics. Local hospital infection control experts may be able to guide the recommended practice for your site better, based on local information.15,16
Repeating a PCR test to discontinue home quarantine is not recommended in most circumstances, as individuals may have prolonged shedding of noninfectious particles in their nasopharynx. Immunocompromise may be one exception to this general guidance, but consultation with local hospital infection control experts will help guide management.15,16
7. Should women get pregnant during the COVID-19 pandemic?
Every pandemic has its own set of implications for the health of the mother, fetus, or both, and COVID-19 is no exception. While there are risks, described above, to mother and fetus, these risks are not so catastrophic as to strongly and directively recommend a patient not become pregnant.17 Moreover, the last several months of the pandemic have demonstrated that consistent mask usage, social distancing, and hand hygiene, are effective methods of preventing the acquisition of COVID-19. All of these risk-reducing strategies are available to pregnant women. Finally, accessing care during a pandemic in a hospital setting does not also pose a risk for acquisition of SARS-CoV-2.18
Continue to: 8. Is the COVID-19 vaccine safe for pregnant or postpartum/lactating women?...
8. Is the COVID-19 vaccine safe for pregnant or postpartum/lactating women?
On December 11, 2020, the US Food and Drug Administration (FDA) issued emergency use authorization (EUA) for the Pfizer-BioNtech mRNA vaccine (BNT 162b2) against COVID-19, for individuals aged 16 and older as a 2-dose series given 21 days apart. Among the more than 40,000 individuals in the trial that led to this EUA, vaccine efficacy was 95%.19 Adverse effects included fatigue and headache most commonly, with 16% of vaccine recipients experiencing fever after the second dose. Follow-up regarding safety is planned for 2 years by the manufacturer, in addition to safety monitoring by pre-existing national systems.
On December 18, 2020, the FDA announced EUA for Moderna’s mRNA-based vaccine, mRNA-1273, in men and women aged 18 and older. This is a 2-dose series given 28 days apart. The vaccine efficacy has been reported at 94.5%, with the most common adverse effects being injection site pain, tiredness, headache, muscle pain, chills, joint pain, swollen lymph nodes in the same arm as the injection, nausea and vomiting, and fever.20,21 The phase 3 trial is ongoing.
Despite the speed with which these effective vaccines were developed, it is important to note that all regulatory and safety steps mandated for the development of any vaccine were met for these two, as well as for other COVID-19 vaccinations that will similarly receive EUA from the FDA.
In the EUA for BNT 162b2, the specific language regarding pregnant and lactating women recommends that patients and providers have an individualized conversation about vaccination. In the data presented to the FDA for the Pfizer-BioNtech mRNA vaccine, a limited number of pregnant women received either the vaccine (12 women) or placebo (11 women), with no long-term follow-up data available to characterize either maternal or fetal benefits and risks. The mechanism of action of an mRNA vaccine is to induce the cytoplasmic machinery within cells to create the coronavirus spike protein, which then allows the body’s immune system to create antibodies against this protein and confer protection accordingly. While the above mechanism is not theorized to result in different outcomes or different efficacy, the safety for the pregnant woman and fetus are unknown. It is not believed that vaccination during lactation would cause any adverse outcomes to a neonate, and lactating women do not need to interrupt or discontinue breast milk production in order to receive the vaccine.
The American College of Obstetricians and Gynecologists (ACOG) released a Practice Advisory on December 13, 2020, regarding their recommendations.22 ACOG recommends that vaccines against COVID-19 not be withheld from pregnant or lactating women, if they might otherwise meet criteria for and have access to vaccination. Currently, the CDC’s Advisory Committee on Immunization Practices (ACIP) stated that health care workers and long-term care facility residents represent priority groups to vaccinate in the initial phases of vaccination, given limitations in supply.23 This recommendation is likely to be updated frequently as additional vaccines become available. Shared decision-making between patient and provider may help the patient to make the best decision for herself, but provider input is not required prior to a pregnant woman being vaccinated.
Additional animal data evaluating adverse effects on the reproductive system from developmental and reproductive toxicity (DART) studies for both mRNA vaccines should be available in the coming weeks, which may aid in the counseling of reproductive-aged women.
Vaccine trials to specifically enroll pregnant women are set to begin in early 2021, and more data will certainly inform the conversation between patient and provider regarding risks and benefits.
Conclusions
While the absolute risks of COVID-19 to mothers, fetuses, and neonates is low, pregnancy is a risk factor for severe disease. Many pregnant women with COVID-19 can be safely followed as outpatients via telemedicine, and supportive care is recommended. Inpatient care should be individualized. Pregnancy during the COVID-19 pandemic should be not be absolutely discouraged; instead, a conversation about risk mitigation should be undertaken. The COVID-19 vaccine is available to pregnant and lactating women, and the decision to choose vaccination in pregnancy is in the purview of the patient, in consultation with her physician. ●
- Afshar Y, Gaw SL, Flaherman VJ, et al. Clinical presentation of coronavirus disease 2019 (COVID-19) in pregnant and recently pregnant people. Obstet Gynecol. 2020;128:1117-1125.
- Cosma S, Carosso AR, Cusato J, et al. Coronavirus disease 2019 and first-trimester spontaneous abortion: a casecontrol study of 225 pregnant patients. Am J Obstet Gynecol. 2020;S0002-9378:31177-7. doi: 10.1016/j.ajog.2020.10.005.
- Prabhu M, Cagino K, Matthews KC, et al. Pregnancy and postpartum outcomes in a universally tested population for SARS-CoV-2 in New York City: a prospective cohort study. BJOG. 2020;127:1548-1556.
- Adhikari E, Moreno W, Zofkie AC, et al. Pregnancy outcomes among women with and without severe acute respiratory syndrome coronavirus 2 infection. JAMA Netw Open. 2020;3:e2029256.
- Knight M, Bunch K, Vousden B, et al; UK Obstetric Suveillance System SARS-CoV-2 Infection in Pregnancy Collaborative Group. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: national population based cohort study. BMJ. 2020;369:m2107.
- Emeruwa UN, Ona S, Shaman JL, et al. Associations between built environment, neighborhood socioeconomic status, and SARS-CoV-2 infection among pregnant women in New York City. JAMA. 2020;324:390-392.
- Emeruwa UN, Spiegelman J, Ona S, et al. Influence of race and ethnicity on severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection rates and clinical outcomes in pregnancy. Obstet Gynecol. 2020;126:1040-1043.
- Zambrano LD, Ellington S, Strid P, et al; CDC COVID-19 response pregnancy and infant linked outcomes team. Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status–United States, January 22-October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1641-1647.
- Badr DA, Mattern J, Carlin A, et al. Are clinical outcomes worse for pregnant women at ≥20 weeks’ gestation infected with coronavirus disease 2019? A multicenter case control study with propensity score matching. Am J Obstet Gynecol. 2020;223:764-768.
- DeBolt CA, Bianco A, Limaye MA, et al. Pregnant women with severe or critical COVID-19 have increased composite morbidity compared with nonpregnant matched controls. Am J Obstet Gynecol. 2020;S0002-9378:31312-0.
- Collin J, Byström E, Carnahan A, et al. Public Health Agency of Sweden’s Brief Report: pregnant and postpartum women with severe acute respiratory syndrome coronavirus 2 infection in intensive care in Sweden. Acta Obstet Gynecol Scand. 2020;99: 819-822.
- Dumitriu D, Emeruwa UN, Hanft E, et al. Outcomes of neonates born to mothers with severe acute respiratory syndrome coronavirus 2 infection at a large medical center in New York City. JAMA Pediatr. 2020;e204298.
- Salvatore CM, Han JY, Acker KP, et al. Neonatal management and outcomes during the COVID-19 pandemic: an observational cohort study. Lancet Child Adolesc Health. 2020;4: 721-727.
- Shanes ED, Mithal LB, Otero S, et al. Placental pathology in COVID-19. Am J Clin Path. 2020;154:23-32.
- Centers for Disease Control and Prevention. Duration of isolation and precautions for adults with COVID-19. Updated October 19, 2020. https://www.cdc.gov/corona virus/2019-ncov/hcp/duration-isolation.html?CDC _AA_refVal=https%3A%2F%2Fwww.cdc.gov%2F coronavirus%2F2019-ncov%2Fcommunity%2Fstrategy -discontinue-isolation.html. Accessed December 15, 2020.
- Centers for Disease Control and Prevention. Discontinuation of transmission-based precautions and disposition of patients with COVID-19 in healthcare settings. Updated August 10, 2020. https://www.cdc.gov /coronavirus/2019-ncov/hcp/disposition-hospitalized -patients.html. Accessed December 15, 2020.
- Rasmussen SA, Lyerly AD, Jamieson DJ. Delaying pregnancy during a public health crisis–examining public health recommendations for COVID-19 and beyond. N Engl J Med. 2020;383:2097-2099.
- Reale SC, Field KG, Lumbreras-Marquez MI, et al. Association between number of in-person health care visits and SARS-CoV-2 infection in obstetrical patients. JAMA. 2020;324: 1210-1212.
- Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT 162b2 mRNA Covid-19 vaccine. N Engl J Med. December 10, 2020. doi: 10.1056/NEJMoa2034577.
- Widge AT, Rouphael NG, Jackson LA, et al. Durability of responses after SARS-CoV-2 mRNA-1273 vaccination. December 3, 2020. doi: 10.1056/NEJMc2032195.
- US Food and Drug Administration. FDA takes additional action in fight against COVID-19 by issuing emergency use authorization for second COVID-19 vaccine. December 18, 2020. https://www.fda.gov/news-events/press-announcements /fda-takes-additional-action-fight-against-covid-19-issuing -emergency-use-authorization-second-covid. Accessed December 22, 2020.
- American College of Obstetricians and Gynecologists. Practice advisory: vaccinating pregnancy and lactating patients against COVID-19. https://www.acog.org/clinical/clinical -guidance/practice-advisory/articles/2020/12/vaccinating -pregnant-and-lactating-patients-against-covid-19. Last updated December 21, 2020. Accessed December 21, 2020.
- Dooling K, McClung N, Chamberland M, et al. The Advisory Committee on Immunization Practices’ interim recommendation for allocating initial supplies of COVID-19 vaccine–United States, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1857-1859.

Dr. Prabhu is from the Division of Maternal-Fetal Medicine, Department of Obstetrics & Gynecology, Weill Cornell Medicine, New York City, New York.
The author reports no financial relationships relevant to this article.
Dr. Prabhu is from the Division of Maternal-Fetal Medicine, Department of Obstetrics & Gynecology, Weill Cornell Medicine, New York City, New York.
The author reports no financial relationships relevant to this article.
Dr. Prabhu is from the Division of Maternal-Fetal Medicine, Department of Obstetrics & Gynecology, Weill Cornell Medicine, New York City, New York.
The author reports no financial relationships relevant to this article.
Pregnant women, or women considering pregnancy, want to know—is pregnancy safe in the midst of the coronavirus disease 2019 (COVID-19) pandemic? In this article, I tackle common questions facing reproductive-aged or pregnant women and their providers.
1. What are the risks of COVID-19 in pregnancy?
A large, national prospective cohort study of outpatient pregnant and recently postpartum women with the diagnosis of suspected or confirmed COVID-19 demonstrated that many affected women have mild illnesses, with typical symptoms including cough, sore throat, body aches, fever, and headache.1 Although symptoms were most common within the first 3 weeks of presentation, approximately 25% of women had a protracted course of symptoms (8 or more weeks). As this cohort disproportionately enrolled outpatients, it is important to note that many women had mild illnesses, which is the most likely course of infection in otherwise healthy, young women.
Data on the impact of COVID-19 on rates of miscarriage and birth defects are limited, yet the published reports are reassuring, with no increased risks of miscarriage, and no clear signal for birth defects.2
In a prospective cohort study across 3 New York City institutions when universal severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing was recommended upon admission for delivery, approximately 80% of women who were positive were asymptomatic.3 Maternal outcomes generally were reassuring, with no patients experiencing severe or critical illness. There were no differences in preterm delivery rates by SARS-CoV-2 status, but the rate of cesarean delivery was higher among women with COVID-19, for unclear reasons. Most notably, the rate of postpartum complications was 13% among women with COVID-19, versus 2.5% among women without COVID-19. These complications included readmission for worsening COVID-19, postpartum hypoxia, and postpartum fever.
A recent prospective cohort study from 1 institution in Texas similarly demonstrated favorable maternal outcomes with COVID-19, with 95% of women with asymptomatic or mild illness, and no differences in adverse pregnancy outcomes between COVID-19–positive and COVID-19–negative women, including cesarean delivery rate.4
Finally, certain characteristics increase the risk of COVID-19 among pregnant women and nonpregnant individuals alike. In a nationwide prospective cohort from the United Kingdom, medical comorbidities including obesity, diabetes (gestational or pregestational), hypertension, as well as Black or other minority ethnicities are associated with COVID-19.5 This is particularly notable given universal health insurance in the United Kingdom. Other data have also confirmed that women with comorbidities, women of Black or Hispanic ethnicity, and women with lower socioeconomic status, are at increased risk of COVID-19.3,6,7
2. Is COVID-19 worse in pregnancy?
Given the well-documented risks of COVID-19 outside of pregnancy, is COVID-19 worse in a pregnant woman than in a nonpregnant woman? The most recent guidance from the Centers for Disease Control and Prevention (CDC) from November 2020 suggests that pregnant women are at increased risk for severe illness.8 However, it is important to understand the design of this study in order to appreciate its implications. Laboratory confirmed SARS-CoV-2 in the United States is systematically reported to the CDC. Among women aged 15–44 years with such confirmation, data on pregnancy status were available for 35.5%, almost 90% of whom were symptomatic. Within this cohort of largely symptomatic pregnant women, risks of intensive care unit (ICU) admission, invasive ventilation, and use of extracorporeal membrane oxygenation (ECMO) were approximately 2 to 3 times higher for pregnant women than for nonpregnant women. The absolute risks, however, were low. The risk of ICU admission for symptomatic pregnant women was approximately 1%; the risk of invasive ventilation, 0.3%; and the risk of ECMO, 0.1%.
Moreover, the lack of uniform data capture on pregnancy status for all women ages 15–44 years may skew the population with known pregnancy status to be sicker and, thus, may bias the results toward increased risks. Nevertheless, there is consistency in several publications with different data sources, all of which suggest pregnancy is an independent risk factor for increased severity of COVID-19.9-11 Additionally, women with medical comorbidities (such as pregestational or gestational diabetes or obesity) are more likely to have severe COVID-19.
Continue to: 3. What are newborn outcomes if COVID-19 is diagnosed during pregnancy?...
3. What are newborn outcomes if COVID-19 is diagnosed during pregnancy?
Two large cohorts of newborns, disproportionately term infants, from the first wave of the pandemic in New York City, have reassuring news. In one cohort of 101 infants born at 2 New York City institutions to SARS-CoV-2–positive mothers, 2 neonates were diagnosed with SARS-CoV-2 during the immediate postnatal period.12 Neither infant demonstrated clinical COVID-19. In another cohort of 120 infants born at 3 other New York City institutions to SARS-CoV-2–positive mothers and tested systematically within 24 hours of life, 5–7 days of life, and 14 days of life, there were no neonates who tested positive for SARS-CoV-2 at the initial time point. Among the 79 infants who had testing at 5–7 days of life and the 72 tested at 14 days of life, there were no infants positive for SARS-CoV-2.13 It is important to note that case reports and small case series have demonstrated some convincing evidence of vertical transmission. However, the overwhelming evidence suggests this risk is very low.
4. What is a reasonable outpatient setting–approach to managing COVID-19 in a pregnant woman?
Women should be counseled to quarantine for 10 to 14 days from symptom onset or, if asymptomatic, from positive polymerase chain reaction (PCR) test. Warning signs of worsening COVID-19 disease should be reviewed. Serial telemedicine follow-up for 10 to 14 days is recommended to ensure clinical stability and continued management as an outpatient. A home pulse oximeter is also recommended. Women should be advised to check their oxygen saturation daily and to call if oxygen saturation becomes less than 93%. Supportive care is recommended.
If delay in obstetric care may result in adverse pregnancy outcomes (for instance, postponing indicated fetal surveillance), obstetric care should be delivered, with appropriate personal protective equipment for health care workers and minimization of exposure of other pregnant women to the infected patient. Appointments should be scheduled at the end of the day.
During influenza season, women should receive empiric oseltamivir treatment (75 mg twice a day) per CDC guidelines for symptoms that may also be consistent with influenza, regardless of testing.
Prophylactic anticoagulation is not indicated for pregnant antepartum women who do not require inpatient care.
If inpatient care is required, management is individualized.
The approach to prenatal care after resolution of COVID-19 is not evidence-based. At my institution, all patients have a detailed mid-trimester anatomic evaluation, but if this is not routine, a detailed anatomic ultrasound (Current Procedural Terminology code 76811) may be considered. Additionally, for women with COVID-19 we perform one third-trimester growth ultrasound to screen for fetal growth restriction, on the basis of several placental studies demonstrating clots on the fetal or maternal side of the placenta.3,14 Routine antenatal testing in the absence of growth restriction, or other comorbid conditions for which testing occurs, is not recommended.
Continue to: 5. What if asymptomatic or mild COVID-19 is diagnosed at the time of delivery?...
5. What if asymptomatic or mild COVID-19 is diagnosed at the time of delivery? What is reasonable management?
Asymptomatic or mildly symptomatic COVID-19 should not alter obstetric management, beyond appropriate use of personal protective equipment. Delayed cord clamping is also reasonable, if there are no other contraindications, as there is no documented harm associated with this practice among women with COVID-19.
Women with COVID-19 may be at higher risk for venous thromboembolic events in the postpartum period. At my institution, prophylactic postpartum anticoagulation is recommended for 2 weeks after vaginal delivery, and 6 weeks after cesarean delivery.
During the postpartum hospitalization, given reassuring data about vertical transmission and postnatal horizontal transmission risks, babies may room in with mothers in a single private room, if rooming-in is the current standard of care—as long as the mother and newborn do not require higher levels of care. Mothers should wear a mask and use hand hygiene when in contact with the baby. Skin-to-skin and breastfeeding or infant feeding of breast milk are appropriate practices to continue. There is no evidence to suggest that transmission of COVID-19 can occur via breastmilk; however, given the close contact inherent in breastfeeding, transmission through direct contact or maternal respiratory droplets is possible, and thus maternal use of masks and hand hygiene is recommended. When not feeding, the infant should be 6 feet away, and if possible, in an isolette.
6. When can individuals with COVID-19 discontinue transmission precautions or “home quarantine”?
For women with mildly symptomatic COVID-19 and without immunocompromise, home quarantine can be discontinued 10 days after onset of symptoms as long as there has been symptom improvement and no fever for at least 24 hours without the use of antipyretics. For immunocompetent women with incidentally diagnosed asymptomatic COVID-19, home quarantine can be discontinued 10 days after the positive test was obtained. Pregnancy in and of itself is not an immunocompromising condition.15,16
For women with severe or critical COVID-19, who were hospitalized due to their clinical status, home quarantine can be discontinued when at least 10 days, and up to 20 days, after onset of symptoms and with symptom improvement and with no fever for at least 24 hours, without the use of antipyretics. Local hospital infection control experts may be able to guide the recommended practice for your site better, based on local information.15,16
Repeating a PCR test to discontinue home quarantine is not recommended in most circumstances, as individuals may have prolonged shedding of noninfectious particles in their nasopharynx. Immunocompromise may be one exception to this general guidance, but consultation with local hospital infection control experts will help guide management.15,16
7. Should women get pregnant during the COVID-19 pandemic?
Every pandemic has its own set of implications for the health of the mother, fetus, or both, and COVID-19 is no exception. While there are risks, described above, to mother and fetus, these risks are not so catastrophic as to strongly and directively recommend a patient not become pregnant.17 Moreover, the last several months of the pandemic have demonstrated that consistent mask usage, social distancing, and hand hygiene, are effective methods of preventing the acquisition of COVID-19. All of these risk-reducing strategies are available to pregnant women. Finally, accessing care during a pandemic in a hospital setting does not also pose a risk for acquisition of SARS-CoV-2.18
Continue to: 8. Is the COVID-19 vaccine safe for pregnant or postpartum/lactating women?...
8. Is the COVID-19 vaccine safe for pregnant or postpartum/lactating women?
On December 11, 2020, the US Food and Drug Administration (FDA) issued emergency use authorization (EUA) for the Pfizer-BioNtech mRNA vaccine (BNT 162b2) against COVID-19, for individuals aged 16 and older as a 2-dose series given 21 days apart. Among the more than 40,000 individuals in the trial that led to this EUA, vaccine efficacy was 95%.19 Adverse effects included fatigue and headache most commonly, with 16% of vaccine recipients experiencing fever after the second dose. Follow-up regarding safety is planned for 2 years by the manufacturer, in addition to safety monitoring by pre-existing national systems.
On December 18, 2020, the FDA announced EUA for Moderna’s mRNA-based vaccine, mRNA-1273, in men and women aged 18 and older. This is a 2-dose series given 28 days apart. The vaccine efficacy has been reported at 94.5%, with the most common adverse effects being injection site pain, tiredness, headache, muscle pain, chills, joint pain, swollen lymph nodes in the same arm as the injection, nausea and vomiting, and fever.20,21 The phase 3 trial is ongoing.
Despite the speed with which these effective vaccines were developed, it is important to note that all regulatory and safety steps mandated for the development of any vaccine were met for these two, as well as for other COVID-19 vaccinations that will similarly receive EUA from the FDA.
In the EUA for BNT 162b2, the specific language regarding pregnant and lactating women recommends that patients and providers have an individualized conversation about vaccination. In the data presented to the FDA for the Pfizer-BioNtech mRNA vaccine, a limited number of pregnant women received either the vaccine (12 women) or placebo (11 women), with no long-term follow-up data available to characterize either maternal or fetal benefits and risks. The mechanism of action of an mRNA vaccine is to induce the cytoplasmic machinery within cells to create the coronavirus spike protein, which then allows the body’s immune system to create antibodies against this protein and confer protection accordingly. While the above mechanism is not theorized to result in different outcomes or different efficacy, the safety for the pregnant woman and fetus are unknown. It is not believed that vaccination during lactation would cause any adverse outcomes to a neonate, and lactating women do not need to interrupt or discontinue breast milk production in order to receive the vaccine.
The American College of Obstetricians and Gynecologists (ACOG) released a Practice Advisory on December 13, 2020, regarding their recommendations.22 ACOG recommends that vaccines against COVID-19 not be withheld from pregnant or lactating women, if they might otherwise meet criteria for and have access to vaccination. Currently, the CDC’s Advisory Committee on Immunization Practices (ACIP) stated that health care workers and long-term care facility residents represent priority groups to vaccinate in the initial phases of vaccination, given limitations in supply.23 This recommendation is likely to be updated frequently as additional vaccines become available. Shared decision-making between patient and provider may help the patient to make the best decision for herself, but provider input is not required prior to a pregnant woman being vaccinated.
Additional animal data evaluating adverse effects on the reproductive system from developmental and reproductive toxicity (DART) studies for both mRNA vaccines should be available in the coming weeks, which may aid in the counseling of reproductive-aged women.
Vaccine trials to specifically enroll pregnant women are set to begin in early 2021, and more data will certainly inform the conversation between patient and provider regarding risks and benefits.
Conclusions
While the absolute risks of COVID-19 to mothers, fetuses, and neonates is low, pregnancy is a risk factor for severe disease. Many pregnant women with COVID-19 can be safely followed as outpatients via telemedicine, and supportive care is recommended. Inpatient care should be individualized. Pregnancy during the COVID-19 pandemic should be not be absolutely discouraged; instead, a conversation about risk mitigation should be undertaken. The COVID-19 vaccine is available to pregnant and lactating women, and the decision to choose vaccination in pregnancy is in the purview of the patient, in consultation with her physician. ●
Pregnant women, or women considering pregnancy, want to know—is pregnancy safe in the midst of the coronavirus disease 2019 (COVID-19) pandemic? In this article, I tackle common questions facing reproductive-aged or pregnant women and their providers.
1. What are the risks of COVID-19 in pregnancy?
A large, national prospective cohort study of outpatient pregnant and recently postpartum women with the diagnosis of suspected or confirmed COVID-19 demonstrated that many affected women have mild illnesses, with typical symptoms including cough, sore throat, body aches, fever, and headache.1 Although symptoms were most common within the first 3 weeks of presentation, approximately 25% of women had a protracted course of symptoms (8 or more weeks). As this cohort disproportionately enrolled outpatients, it is important to note that many women had mild illnesses, which is the most likely course of infection in otherwise healthy, young women.
Data on the impact of COVID-19 on rates of miscarriage and birth defects are limited, yet the published reports are reassuring, with no increased risks of miscarriage, and no clear signal for birth defects.2
In a prospective cohort study across 3 New York City institutions when universal severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) testing was recommended upon admission for delivery, approximately 80% of women who were positive were asymptomatic.3 Maternal outcomes generally were reassuring, with no patients experiencing severe or critical illness. There were no differences in preterm delivery rates by SARS-CoV-2 status, but the rate of cesarean delivery was higher among women with COVID-19, for unclear reasons. Most notably, the rate of postpartum complications was 13% among women with COVID-19, versus 2.5% among women without COVID-19. These complications included readmission for worsening COVID-19, postpartum hypoxia, and postpartum fever.
A recent prospective cohort study from 1 institution in Texas similarly demonstrated favorable maternal outcomes with COVID-19, with 95% of women with asymptomatic or mild illness, and no differences in adverse pregnancy outcomes between COVID-19–positive and COVID-19–negative women, including cesarean delivery rate.4
Finally, certain characteristics increase the risk of COVID-19 among pregnant women and nonpregnant individuals alike. In a nationwide prospective cohort from the United Kingdom, medical comorbidities including obesity, diabetes (gestational or pregestational), hypertension, as well as Black or other minority ethnicities are associated with COVID-19.5 This is particularly notable given universal health insurance in the United Kingdom. Other data have also confirmed that women with comorbidities, women of Black or Hispanic ethnicity, and women with lower socioeconomic status, are at increased risk of COVID-19.3,6,7
2. Is COVID-19 worse in pregnancy?
Given the well-documented risks of COVID-19 outside of pregnancy, is COVID-19 worse in a pregnant woman than in a nonpregnant woman? The most recent guidance from the Centers for Disease Control and Prevention (CDC) from November 2020 suggests that pregnant women are at increased risk for severe illness.8 However, it is important to understand the design of this study in order to appreciate its implications. Laboratory confirmed SARS-CoV-2 in the United States is systematically reported to the CDC. Among women aged 15–44 years with such confirmation, data on pregnancy status were available for 35.5%, almost 90% of whom were symptomatic. Within this cohort of largely symptomatic pregnant women, risks of intensive care unit (ICU) admission, invasive ventilation, and use of extracorporeal membrane oxygenation (ECMO) were approximately 2 to 3 times higher for pregnant women than for nonpregnant women. The absolute risks, however, were low. The risk of ICU admission for symptomatic pregnant women was approximately 1%; the risk of invasive ventilation, 0.3%; and the risk of ECMO, 0.1%.
Moreover, the lack of uniform data capture on pregnancy status for all women ages 15–44 years may skew the population with known pregnancy status to be sicker and, thus, may bias the results toward increased risks. Nevertheless, there is consistency in several publications with different data sources, all of which suggest pregnancy is an independent risk factor for increased severity of COVID-19.9-11 Additionally, women with medical comorbidities (such as pregestational or gestational diabetes or obesity) are more likely to have severe COVID-19.
Continue to: 3. What are newborn outcomes if COVID-19 is diagnosed during pregnancy?...
3. What are newborn outcomes if COVID-19 is diagnosed during pregnancy?
Two large cohorts of newborns, disproportionately term infants, from the first wave of the pandemic in New York City, have reassuring news. In one cohort of 101 infants born at 2 New York City institutions to SARS-CoV-2–positive mothers, 2 neonates were diagnosed with SARS-CoV-2 during the immediate postnatal period.12 Neither infant demonstrated clinical COVID-19. In another cohort of 120 infants born at 3 other New York City institutions to SARS-CoV-2–positive mothers and tested systematically within 24 hours of life, 5–7 days of life, and 14 days of life, there were no neonates who tested positive for SARS-CoV-2 at the initial time point. Among the 79 infants who had testing at 5–7 days of life and the 72 tested at 14 days of life, there were no infants positive for SARS-CoV-2.13 It is important to note that case reports and small case series have demonstrated some convincing evidence of vertical transmission. However, the overwhelming evidence suggests this risk is very low.
4. What is a reasonable outpatient setting–approach to managing COVID-19 in a pregnant woman?
Women should be counseled to quarantine for 10 to 14 days from symptom onset or, if asymptomatic, from positive polymerase chain reaction (PCR) test. Warning signs of worsening COVID-19 disease should be reviewed. Serial telemedicine follow-up for 10 to 14 days is recommended to ensure clinical stability and continued management as an outpatient. A home pulse oximeter is also recommended. Women should be advised to check their oxygen saturation daily and to call if oxygen saturation becomes less than 93%. Supportive care is recommended.
If delay in obstetric care may result in adverse pregnancy outcomes (for instance, postponing indicated fetal surveillance), obstetric care should be delivered, with appropriate personal protective equipment for health care workers and minimization of exposure of other pregnant women to the infected patient. Appointments should be scheduled at the end of the day.
During influenza season, women should receive empiric oseltamivir treatment (75 mg twice a day) per CDC guidelines for symptoms that may also be consistent with influenza, regardless of testing.
Prophylactic anticoagulation is not indicated for pregnant antepartum women who do not require inpatient care.
If inpatient care is required, management is individualized.
The approach to prenatal care after resolution of COVID-19 is not evidence-based. At my institution, all patients have a detailed mid-trimester anatomic evaluation, but if this is not routine, a detailed anatomic ultrasound (Current Procedural Terminology code 76811) may be considered. Additionally, for women with COVID-19 we perform one third-trimester growth ultrasound to screen for fetal growth restriction, on the basis of several placental studies demonstrating clots on the fetal or maternal side of the placenta.3,14 Routine antenatal testing in the absence of growth restriction, or other comorbid conditions for which testing occurs, is not recommended.
Continue to: 5. What if asymptomatic or mild COVID-19 is diagnosed at the time of delivery?...
5. What if asymptomatic or mild COVID-19 is diagnosed at the time of delivery? What is reasonable management?
Asymptomatic or mildly symptomatic COVID-19 should not alter obstetric management, beyond appropriate use of personal protective equipment. Delayed cord clamping is also reasonable, if there are no other contraindications, as there is no documented harm associated with this practice among women with COVID-19.
Women with COVID-19 may be at higher risk for venous thromboembolic events in the postpartum period. At my institution, prophylactic postpartum anticoagulation is recommended for 2 weeks after vaginal delivery, and 6 weeks after cesarean delivery.
During the postpartum hospitalization, given reassuring data about vertical transmission and postnatal horizontal transmission risks, babies may room in with mothers in a single private room, if rooming-in is the current standard of care—as long as the mother and newborn do not require higher levels of care. Mothers should wear a mask and use hand hygiene when in contact with the baby. Skin-to-skin and breastfeeding or infant feeding of breast milk are appropriate practices to continue. There is no evidence to suggest that transmission of COVID-19 can occur via breastmilk; however, given the close contact inherent in breastfeeding, transmission through direct contact or maternal respiratory droplets is possible, and thus maternal use of masks and hand hygiene is recommended. When not feeding, the infant should be 6 feet away, and if possible, in an isolette.
6. When can individuals with COVID-19 discontinue transmission precautions or “home quarantine”?
For women with mildly symptomatic COVID-19 and without immunocompromise, home quarantine can be discontinued 10 days after onset of symptoms as long as there has been symptom improvement and no fever for at least 24 hours without the use of antipyretics. For immunocompetent women with incidentally diagnosed asymptomatic COVID-19, home quarantine can be discontinued 10 days after the positive test was obtained. Pregnancy in and of itself is not an immunocompromising condition.15,16
For women with severe or critical COVID-19, who were hospitalized due to their clinical status, home quarantine can be discontinued when at least 10 days, and up to 20 days, after onset of symptoms and with symptom improvement and with no fever for at least 24 hours, without the use of antipyretics. Local hospital infection control experts may be able to guide the recommended practice for your site better, based on local information.15,16
Repeating a PCR test to discontinue home quarantine is not recommended in most circumstances, as individuals may have prolonged shedding of noninfectious particles in their nasopharynx. Immunocompromise may be one exception to this general guidance, but consultation with local hospital infection control experts will help guide management.15,16
7. Should women get pregnant during the COVID-19 pandemic?
Every pandemic has its own set of implications for the health of the mother, fetus, or both, and COVID-19 is no exception. While there are risks, described above, to mother and fetus, these risks are not so catastrophic as to strongly and directively recommend a patient not become pregnant.17 Moreover, the last several months of the pandemic have demonstrated that consistent mask usage, social distancing, and hand hygiene, are effective methods of preventing the acquisition of COVID-19. All of these risk-reducing strategies are available to pregnant women. Finally, accessing care during a pandemic in a hospital setting does not also pose a risk for acquisition of SARS-CoV-2.18
Continue to: 8. Is the COVID-19 vaccine safe for pregnant or postpartum/lactating women?...
8. Is the COVID-19 vaccine safe for pregnant or postpartum/lactating women?
On December 11, 2020, the US Food and Drug Administration (FDA) issued emergency use authorization (EUA) for the Pfizer-BioNtech mRNA vaccine (BNT 162b2) against COVID-19, for individuals aged 16 and older as a 2-dose series given 21 days apart. Among the more than 40,000 individuals in the trial that led to this EUA, vaccine efficacy was 95%.19 Adverse effects included fatigue and headache most commonly, with 16% of vaccine recipients experiencing fever after the second dose. Follow-up regarding safety is planned for 2 years by the manufacturer, in addition to safety monitoring by pre-existing national systems.
On December 18, 2020, the FDA announced EUA for Moderna’s mRNA-based vaccine, mRNA-1273, in men and women aged 18 and older. This is a 2-dose series given 28 days apart. The vaccine efficacy has been reported at 94.5%, with the most common adverse effects being injection site pain, tiredness, headache, muscle pain, chills, joint pain, swollen lymph nodes in the same arm as the injection, nausea and vomiting, and fever.20,21 The phase 3 trial is ongoing.
Despite the speed with which these effective vaccines were developed, it is important to note that all regulatory and safety steps mandated for the development of any vaccine were met for these two, as well as for other COVID-19 vaccinations that will similarly receive EUA from the FDA.
In the EUA for BNT 162b2, the specific language regarding pregnant and lactating women recommends that patients and providers have an individualized conversation about vaccination. In the data presented to the FDA for the Pfizer-BioNtech mRNA vaccine, a limited number of pregnant women received either the vaccine (12 women) or placebo (11 women), with no long-term follow-up data available to characterize either maternal or fetal benefits and risks. The mechanism of action of an mRNA vaccine is to induce the cytoplasmic machinery within cells to create the coronavirus spike protein, which then allows the body’s immune system to create antibodies against this protein and confer protection accordingly. While the above mechanism is not theorized to result in different outcomes or different efficacy, the safety for the pregnant woman and fetus are unknown. It is not believed that vaccination during lactation would cause any adverse outcomes to a neonate, and lactating women do not need to interrupt or discontinue breast milk production in order to receive the vaccine.
The American College of Obstetricians and Gynecologists (ACOG) released a Practice Advisory on December 13, 2020, regarding their recommendations.22 ACOG recommends that vaccines against COVID-19 not be withheld from pregnant or lactating women, if they might otherwise meet criteria for and have access to vaccination. Currently, the CDC’s Advisory Committee on Immunization Practices (ACIP) stated that health care workers and long-term care facility residents represent priority groups to vaccinate in the initial phases of vaccination, given limitations in supply.23 This recommendation is likely to be updated frequently as additional vaccines become available. Shared decision-making between patient and provider may help the patient to make the best decision for herself, but provider input is not required prior to a pregnant woman being vaccinated.
Additional animal data evaluating adverse effects on the reproductive system from developmental and reproductive toxicity (DART) studies for both mRNA vaccines should be available in the coming weeks, which may aid in the counseling of reproductive-aged women.
Vaccine trials to specifically enroll pregnant women are set to begin in early 2021, and more data will certainly inform the conversation between patient and provider regarding risks and benefits.
Conclusions
While the absolute risks of COVID-19 to mothers, fetuses, and neonates is low, pregnancy is a risk factor for severe disease. Many pregnant women with COVID-19 can be safely followed as outpatients via telemedicine, and supportive care is recommended. Inpatient care should be individualized. Pregnancy during the COVID-19 pandemic should be not be absolutely discouraged; instead, a conversation about risk mitigation should be undertaken. The COVID-19 vaccine is available to pregnant and lactating women, and the decision to choose vaccination in pregnancy is in the purview of the patient, in consultation with her physician. ●
- Afshar Y, Gaw SL, Flaherman VJ, et al. Clinical presentation of coronavirus disease 2019 (COVID-19) in pregnant and recently pregnant people. Obstet Gynecol. 2020;128:1117-1125.
- Cosma S, Carosso AR, Cusato J, et al. Coronavirus disease 2019 and first-trimester spontaneous abortion: a casecontrol study of 225 pregnant patients. Am J Obstet Gynecol. 2020;S0002-9378:31177-7. doi: 10.1016/j.ajog.2020.10.005.
- Prabhu M, Cagino K, Matthews KC, et al. Pregnancy and postpartum outcomes in a universally tested population for SARS-CoV-2 in New York City: a prospective cohort study. BJOG. 2020;127:1548-1556.
- Adhikari E, Moreno W, Zofkie AC, et al. Pregnancy outcomes among women with and without severe acute respiratory syndrome coronavirus 2 infection. JAMA Netw Open. 2020;3:e2029256.
- Knight M, Bunch K, Vousden B, et al; UK Obstetric Suveillance System SARS-CoV-2 Infection in Pregnancy Collaborative Group. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: national population based cohort study. BMJ. 2020;369:m2107.
- Emeruwa UN, Ona S, Shaman JL, et al. Associations between built environment, neighborhood socioeconomic status, and SARS-CoV-2 infection among pregnant women in New York City. JAMA. 2020;324:390-392.
- Emeruwa UN, Spiegelman J, Ona S, et al. Influence of race and ethnicity on severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection rates and clinical outcomes in pregnancy. Obstet Gynecol. 2020;126:1040-1043.
- Zambrano LD, Ellington S, Strid P, et al; CDC COVID-19 response pregnancy and infant linked outcomes team. Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status–United States, January 22-October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1641-1647.
- Badr DA, Mattern J, Carlin A, et al. Are clinical outcomes worse for pregnant women at ≥20 weeks’ gestation infected with coronavirus disease 2019? A multicenter case control study with propensity score matching. Am J Obstet Gynecol. 2020;223:764-768.
- DeBolt CA, Bianco A, Limaye MA, et al. Pregnant women with severe or critical COVID-19 have increased composite morbidity compared with nonpregnant matched controls. Am J Obstet Gynecol. 2020;S0002-9378:31312-0.
- Collin J, Byström E, Carnahan A, et al. Public Health Agency of Sweden’s Brief Report: pregnant and postpartum women with severe acute respiratory syndrome coronavirus 2 infection in intensive care in Sweden. Acta Obstet Gynecol Scand. 2020;99: 819-822.
- Dumitriu D, Emeruwa UN, Hanft E, et al. Outcomes of neonates born to mothers with severe acute respiratory syndrome coronavirus 2 infection at a large medical center in New York City. JAMA Pediatr. 2020;e204298.
- Salvatore CM, Han JY, Acker KP, et al. Neonatal management and outcomes during the COVID-19 pandemic: an observational cohort study. Lancet Child Adolesc Health. 2020;4: 721-727.
- Shanes ED, Mithal LB, Otero S, et al. Placental pathology in COVID-19. Am J Clin Path. 2020;154:23-32.
- Centers for Disease Control and Prevention. Duration of isolation and precautions for adults with COVID-19. Updated October 19, 2020. https://www.cdc.gov/corona virus/2019-ncov/hcp/duration-isolation.html?CDC _AA_refVal=https%3A%2F%2Fwww.cdc.gov%2F coronavirus%2F2019-ncov%2Fcommunity%2Fstrategy -discontinue-isolation.html. Accessed December 15, 2020.
- Centers for Disease Control and Prevention. Discontinuation of transmission-based precautions and disposition of patients with COVID-19 in healthcare settings. Updated August 10, 2020. https://www.cdc.gov /coronavirus/2019-ncov/hcp/disposition-hospitalized -patients.html. Accessed December 15, 2020.
- Rasmussen SA, Lyerly AD, Jamieson DJ. Delaying pregnancy during a public health crisis–examining public health recommendations for COVID-19 and beyond. N Engl J Med. 2020;383:2097-2099.
- Reale SC, Field KG, Lumbreras-Marquez MI, et al. Association between number of in-person health care visits and SARS-CoV-2 infection in obstetrical patients. JAMA. 2020;324: 1210-1212.
- Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT 162b2 mRNA Covid-19 vaccine. N Engl J Med. December 10, 2020. doi: 10.1056/NEJMoa2034577.
- Widge AT, Rouphael NG, Jackson LA, et al. Durability of responses after SARS-CoV-2 mRNA-1273 vaccination. December 3, 2020. doi: 10.1056/NEJMc2032195.
- US Food and Drug Administration. FDA takes additional action in fight against COVID-19 by issuing emergency use authorization for second COVID-19 vaccine. December 18, 2020. https://www.fda.gov/news-events/press-announcements /fda-takes-additional-action-fight-against-covid-19-issuing -emergency-use-authorization-second-covid. Accessed December 22, 2020.
- American College of Obstetricians and Gynecologists. Practice advisory: vaccinating pregnancy and lactating patients against COVID-19. https://www.acog.org/clinical/clinical -guidance/practice-advisory/articles/2020/12/vaccinating -pregnant-and-lactating-patients-against-covid-19. Last updated December 21, 2020. Accessed December 21, 2020.
- Dooling K, McClung N, Chamberland M, et al. The Advisory Committee on Immunization Practices’ interim recommendation for allocating initial supplies of COVID-19 vaccine–United States, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1857-1859.
- Afshar Y, Gaw SL, Flaherman VJ, et al. Clinical presentation of coronavirus disease 2019 (COVID-19) in pregnant and recently pregnant people. Obstet Gynecol. 2020;128:1117-1125.
- Cosma S, Carosso AR, Cusato J, et al. Coronavirus disease 2019 and first-trimester spontaneous abortion: a casecontrol study of 225 pregnant patients. Am J Obstet Gynecol. 2020;S0002-9378:31177-7. doi: 10.1016/j.ajog.2020.10.005.
- Prabhu M, Cagino K, Matthews KC, et al. Pregnancy and postpartum outcomes in a universally tested population for SARS-CoV-2 in New York City: a prospective cohort study. BJOG. 2020;127:1548-1556.
- Adhikari E, Moreno W, Zofkie AC, et al. Pregnancy outcomes among women with and without severe acute respiratory syndrome coronavirus 2 infection. JAMA Netw Open. 2020;3:e2029256.
- Knight M, Bunch K, Vousden B, et al; UK Obstetric Suveillance System SARS-CoV-2 Infection in Pregnancy Collaborative Group. Characteristics and outcomes of pregnant women admitted to hospital with confirmed SARS-CoV-2 infection in UK: national population based cohort study. BMJ. 2020;369:m2107.
- Emeruwa UN, Ona S, Shaman JL, et al. Associations between built environment, neighborhood socioeconomic status, and SARS-CoV-2 infection among pregnant women in New York City. JAMA. 2020;324:390-392.
- Emeruwa UN, Spiegelman J, Ona S, et al. Influence of race and ethnicity on severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection rates and clinical outcomes in pregnancy. Obstet Gynecol. 2020;126:1040-1043.
- Zambrano LD, Ellington S, Strid P, et al; CDC COVID-19 response pregnancy and infant linked outcomes team. Update: characteristics of symptomatic women of reproductive age with laboratory-confirmed SARS-CoV-2 infection by pregnancy status–United States, January 22-October 3, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1641-1647.
- Badr DA, Mattern J, Carlin A, et al. Are clinical outcomes worse for pregnant women at ≥20 weeks’ gestation infected with coronavirus disease 2019? A multicenter case control study with propensity score matching. Am J Obstet Gynecol. 2020;223:764-768.
- DeBolt CA, Bianco A, Limaye MA, et al. Pregnant women with severe or critical COVID-19 have increased composite morbidity compared with nonpregnant matched controls. Am J Obstet Gynecol. 2020;S0002-9378:31312-0.
- Collin J, Byström E, Carnahan A, et al. Public Health Agency of Sweden’s Brief Report: pregnant and postpartum women with severe acute respiratory syndrome coronavirus 2 infection in intensive care in Sweden. Acta Obstet Gynecol Scand. 2020;99: 819-822.
- Dumitriu D, Emeruwa UN, Hanft E, et al. Outcomes of neonates born to mothers with severe acute respiratory syndrome coronavirus 2 infection at a large medical center in New York City. JAMA Pediatr. 2020;e204298.
- Salvatore CM, Han JY, Acker KP, et al. Neonatal management and outcomes during the COVID-19 pandemic: an observational cohort study. Lancet Child Adolesc Health. 2020;4: 721-727.
- Shanes ED, Mithal LB, Otero S, et al. Placental pathology in COVID-19. Am J Clin Path. 2020;154:23-32.
- Centers for Disease Control and Prevention. Duration of isolation and precautions for adults with COVID-19. Updated October 19, 2020. https://www.cdc.gov/corona virus/2019-ncov/hcp/duration-isolation.html?CDC _AA_refVal=https%3A%2F%2Fwww.cdc.gov%2F coronavirus%2F2019-ncov%2Fcommunity%2Fstrategy -discontinue-isolation.html. Accessed December 15, 2020.
- Centers for Disease Control and Prevention. Discontinuation of transmission-based precautions and disposition of patients with COVID-19 in healthcare settings. Updated August 10, 2020. https://www.cdc.gov /coronavirus/2019-ncov/hcp/disposition-hospitalized -patients.html. Accessed December 15, 2020.
- Rasmussen SA, Lyerly AD, Jamieson DJ. Delaying pregnancy during a public health crisis–examining public health recommendations for COVID-19 and beyond. N Engl J Med. 2020;383:2097-2099.
- Reale SC, Field KG, Lumbreras-Marquez MI, et al. Association between number of in-person health care visits and SARS-CoV-2 infection in obstetrical patients. JAMA. 2020;324: 1210-1212.
- Polack FP, Thomas SJ, Kitchin N, et al. Safety and efficacy of the BNT 162b2 mRNA Covid-19 vaccine. N Engl J Med. December 10, 2020. doi: 10.1056/NEJMoa2034577.
- Widge AT, Rouphael NG, Jackson LA, et al. Durability of responses after SARS-CoV-2 mRNA-1273 vaccination. December 3, 2020. doi: 10.1056/NEJMc2032195.
- US Food and Drug Administration. FDA takes additional action in fight against COVID-19 by issuing emergency use authorization for second COVID-19 vaccine. December 18, 2020. https://www.fda.gov/news-events/press-announcements /fda-takes-additional-action-fight-against-covid-19-issuing -emergency-use-authorization-second-covid. Accessed December 22, 2020.
- American College of Obstetricians and Gynecologists. Practice advisory: vaccinating pregnancy and lactating patients against COVID-19. https://www.acog.org/clinical/clinical -guidance/practice-advisory/articles/2020/12/vaccinating -pregnant-and-lactating-patients-against-covid-19. Last updated December 21, 2020. Accessed December 21, 2020.
- Dooling K, McClung N, Chamberland M, et al. The Advisory Committee on Immunization Practices’ interim recommendation for allocating initial supplies of COVID-19 vaccine–United States, 2020. MMWR Morb Mortal Wkly Rep. 2020;69:1857-1859.

Skin Cancer Management During the COVID-19 Pandemic
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome novel coronavirus 2 (SARS-CoV-2), has presented a unique challenge to providing essential care to patients. Increased demand for health care workers and medical supplies, in addition to the risk for COVID-19 infection and asymptomatic transmission of SARS-CoV-2 among health care workers and patients, prompted the delay of nonessential services during the surge of cases this summer.1 Key considerations for continuing operation included current and projected COVID-19 cases in the region, ability to implement telehealth, staffing availability, personal protective equipment availability, and office capacity.2 Providing care that is deemed essential often was determined by the urgency of the treatment or service.
The Centers for Medicare & Medicaid Services outlined a strategy to stratify patients, based on level of acuity, during the COVID-19 surge3:
- Low-acuity treatments or services: includes routine primary, specialty, or preventive care visits. They should be postponed; telehealth follow-ups should be considered.
- Intermediate-acuity treatments or services: includes pediatric and neonatal care, follow-up visits for existing conditions, and evaluation of new symptoms (including those consistent with COVID-19). These services should initially be evaluated using telehealth, then triaged to the appropriate site and level of care.
- High-acuity treatments or services: address symptoms consistent with COVID-19 or other severe disease, of which the lack of in-person evaluation would result in harm to the patient.
Employees in hospitals and health care clinics were classified as essential, but dermatologists were not given explicit direction regarding clinic operation. Many practices have restricted services, especially those in an area of higher COVID-19 prevalence. However, the challenge of determining day-to-day operation may have been left to the provider in most cases.4 As many states in the United States continue to relax restrictions, total cases and the rate of positivity of COVID-19 have been sharply rising again, after months of decline,5 which suggests increased transmission of SARS-CoV-2 and potential resurgence of the high case burden on our health care system. Furthermore, a lack of a widely distributed vaccine or herd immunity suggests we will need to take many of the same precautions as in the first surge.6
In general, patients with cancer have been found to be at greater risk for adverse outcomes and mortality after COVID-19.7 Therefore, resource rationing is particularly concerning for patients with skin cancer, including melanoma, Merkel cell carcinoma, mycosis fungoides, and keratinocyte carcinoma. Triaging patients based on level of acuity, type of skin cancer, disease burden, host immunosuppression, and risk for progression must be carefully considered in this population.2 Treatment and follow-up present additional challenges.
Guidelines provided by the National Comprehensive Cancer Network (NCCN) and the European Society for Medical Oncology (ESMO) elaborated on key considerations for the treatment of melanoma, keratinocyte carcinoma, and Merkel cell carcinoma during the COVID-19 pandemic.8-10 Guidelines from the NCCN concentrated on clear divisions between disease stages to determine provider response. Guidelines for melanoma patients proposed by the ESMO assign tiers by value-based priority in various treatment settings, which offered flexibility to providers as the COVID-19 landscape continued to change. Recommendations from the NCCN and ESMO are summarized in Tables 1 to 5.

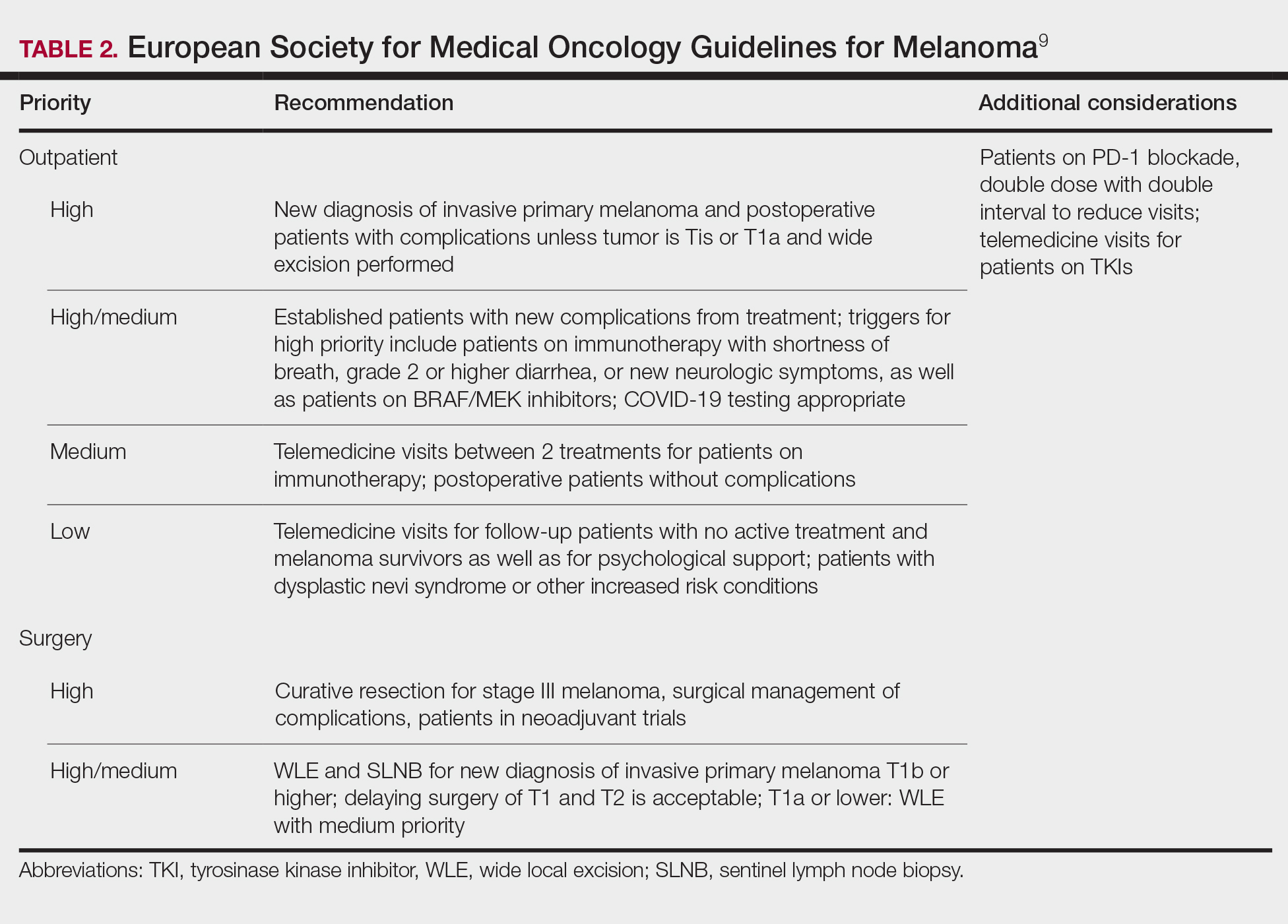

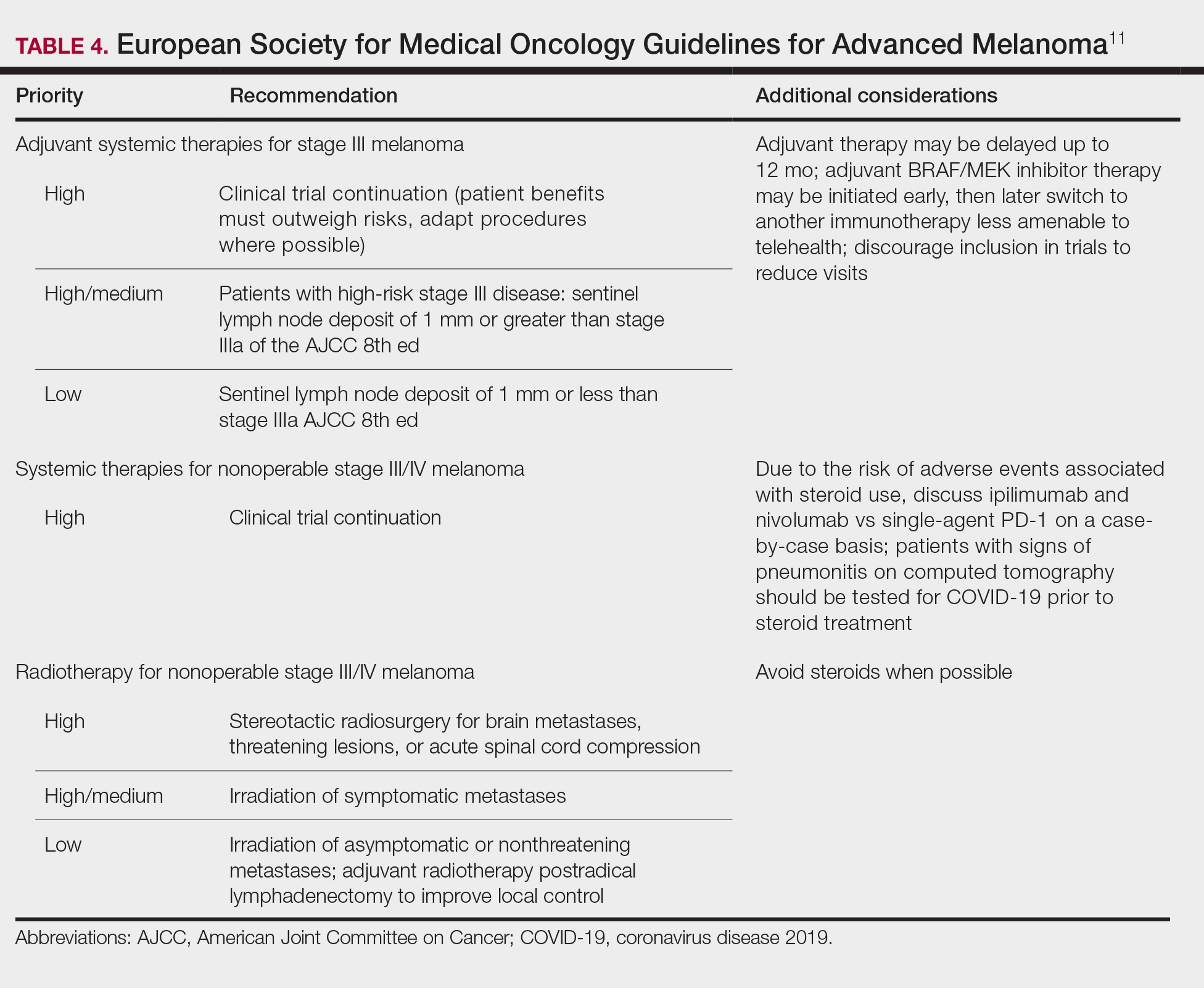
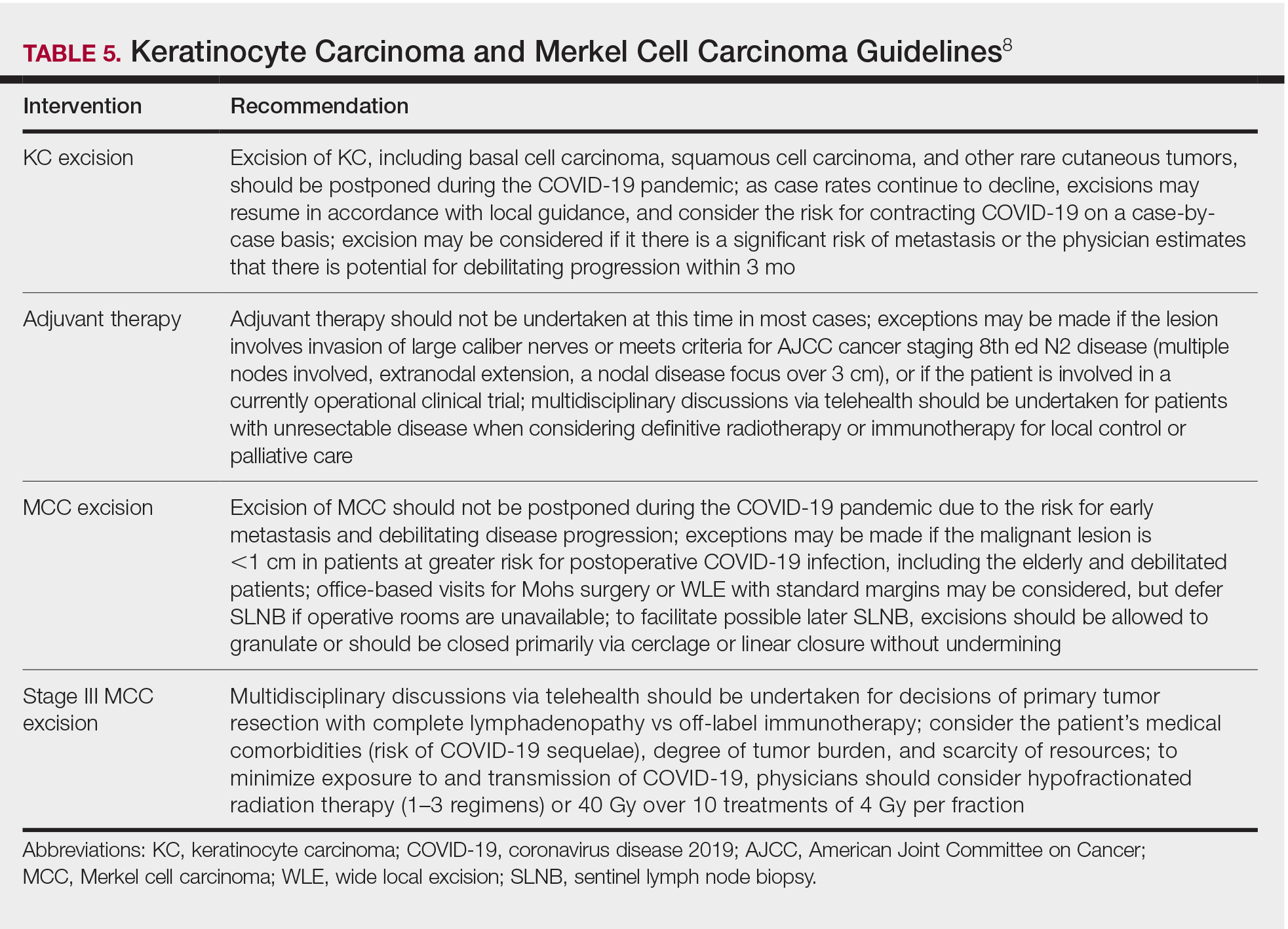
Although these guidelines initially may have been proposed to delay treatment of lower-acuity tumors, such delay might not be feasible given the unknown duration of this pandemic and future disease waves. One review of several studies, which addressed the outcomes on melanoma survival following the surgical delay recommended by the NCCN, revealed contradictory evidence.12 Further, sufficiently powered studies will be needed to better understand the impact of delaying treatment during the summer COVID-19 surge on patients with skin cancer. Therefore, physicians must triage patients accordingly to manage and treat while also preventing disease spread.
Tips for Performing Dermatologic Surgery
Careful consideration should be made to protect both the patient and staff during office-based excisional surgery during the COVID-19 pandemic. To minimize the risk of transmission of SARS-CoV-2, patients and staff should (1) be screened for symptoms of COVID-19 at least 48 hours prior to entering the office via telephone screening questions, and (2) follow proper hygiene and contact procedures once entering the office. Consider obtaining a nasal polymerase chain reaction swab or saliva test 48 hours prior to the procedure if the patient is undergoing a head and neck procedure or there is risk for transmission.
Guidelines from the ESMO recommended that all patients undergoing surgery or therapy should be swabbed for SARS-CoV-2 before each treatment.11 Patients should wear a mask, remain 6-feet apart in the waiting room, and avoid touching objects until they enter the procedure room. Objects that the patient must touch, such as pens, should be cleaned immediately after such contact with either alcohol or soap and water for 20 seconds.
Office capacity should be reduced by allowing no more than 1 person to accompany the patient and ensuring the presence of only the minimum staff needed for the procedure. Staff who are deemed necessary should wear a mask continuously and gloves during patient contact.
Once in the procedure room, providers might be at elevated risk of contracting COVID-19 or transmitting SARS-CoV-2. A properly fitted N95 respirator and a face shield are recommended, especially for facial cases. N95 respirators can be reused by following the latest Centers for Disease Control and Prevention recommendations for reuse and decontamination techniques,13 which may include protecting the N95 respirator with a surgical mask and storing it in a paper bag when not in use. Consider testing asymptomatic patients in facial cases when they cannot wear a mask.
Steps should be taken to reduce in-person visits. Dissolving sutures can help avoid return visits. Follow-up visits and postprocedural questions should be managed by telehealth. However, patients with a high-risk underlying conditions (eg, posttransplantation, immunosuppressed) should continue to obtain regular skin checks because they are at higher risk for more aggressive malignancies, such as Merkel cell carcinoma.
Conclusion
The future trajectory of the COVID-19 pandemic is uncertain. Dermatologists should continue providing care for patients with skin cancer while mitigating the risk for COVID-19 infection and transmission of SARS-CoV-2. Guidelines provided by the NCCN and ESMO should help providers triage patients. Decisions should be made case by case, keeping in mind the availability of resources and practicing in compliance with local guidance.
- Moletta L, Pierobon ES, Capovilla G, et al. International guidelines and recommendations for surgery during COVID-19 pandemic: a systematic review. Int J Surg. 2020;79:180-188.
- Ueda M, Martins R, Hendrie PC, et al. Managing cancer care during the COVID-19 pandemic: agility and collaboration toward common goal. J Natl Compr Canc Netw. 2020:1-4.
- Center for Medicare & Medicaid Services. Non-emergent, elective medical services, and treatment recommendations. Published April 7, 2020. Accessed October 15, 2020. https://www.cms.gov/files/document/cms-non-emergent-elective-medical-recommendations.pdf
- Muddasani S, Housholder A, Fleischer AB. An assessment of United States dermatology practices during the COVID-19 outbreak. J Dermatolog Treat. 2020;31:436-438.
- Coronavirus Resource Center, Johns Hopkins University & Medicine. Rate of positive tests in the US and states over time. Updated December 11, 2020. Accessed December 11, 2020. https://coronavirus.jhu.edu/testing/individual-states
- Middleton J, Lopes H, Michelson K, et al. Planning for a second wave pandemic of COVID-19 and planning for winter: a statement from the Association of Schools of Public Health in the European Region. Int J Public Health. 2020;65:1525-1527.
- Liang W, Guan W, Chen R, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21:335-337.
- National Comprehensive Cancer Network. Advisory statement for non-melanoma skin cancer care during the COVID-19 pandemic (version 4). Published May 22, 2020. Accessed December 11, 2020. https://www.nccn.org/covid-19/pdf/NCCN-NMSC.pdf
National Comprehensive Cancer Network. Short-term recommendations for cutaneous melanoma management during COVID-19 pandemic (version 3). Published May 6, 2020. Accessed December 11, 2020. www.nccn.org/covid-19/pdf/Melanoma.pdf - Conforti C, Giuffrida R, Di Meo N, et al. Management of advanced melanoma in the COVID-19 era. Dermatol Ther. 2020;33:e13444.
- ESMO [European Society for Medical Oncology]. Cancer patient management during the COVID-19 pandemic. Accessed Decemeber 11, 2020. https://www.esmo.org/guidelines/cancer-patient-management-during-the-covid-19-pandemic?hit=ehp
- Guhan S, Boland G, Tanabe K, et al. Surgical delay and mortality for primary cutaneous melanoma [published online July 22, 2020]. J Am Acad Dermatol. doi:10.1016/j.jaad.2020.07.078
- Centers for Disease Control and Prevention. Implementing filtering facepiece respirator (FFR) reuse, including reuse after decontamination, when there are known shortages of N95 respirators. Updated October 19, 2020. Accessed December 11, 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/decontamination-reuse-respirators.html
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome novel coronavirus 2 (SARS-CoV-2), has presented a unique challenge to providing essential care to patients. Increased demand for health care workers and medical supplies, in addition to the risk for COVID-19 infection and asymptomatic transmission of SARS-CoV-2 among health care workers and patients, prompted the delay of nonessential services during the surge of cases this summer.1 Key considerations for continuing operation included current and projected COVID-19 cases in the region, ability to implement telehealth, staffing availability, personal protective equipment availability, and office capacity.2 Providing care that is deemed essential often was determined by the urgency of the treatment or service.
The Centers for Medicare & Medicaid Services outlined a strategy to stratify patients, based on level of acuity, during the COVID-19 surge3:
- Low-acuity treatments or services: includes routine primary, specialty, or preventive care visits. They should be postponed; telehealth follow-ups should be considered.
- Intermediate-acuity treatments or services: includes pediatric and neonatal care, follow-up visits for existing conditions, and evaluation of new symptoms (including those consistent with COVID-19). These services should initially be evaluated using telehealth, then triaged to the appropriate site and level of care.
- High-acuity treatments or services: address symptoms consistent with COVID-19 or other severe disease, of which the lack of in-person evaluation would result in harm to the patient.
Employees in hospitals and health care clinics were classified as essential, but dermatologists were not given explicit direction regarding clinic operation. Many practices have restricted services, especially those in an area of higher COVID-19 prevalence. However, the challenge of determining day-to-day operation may have been left to the provider in most cases.4 As many states in the United States continue to relax restrictions, total cases and the rate of positivity of COVID-19 have been sharply rising again, after months of decline,5 which suggests increased transmission of SARS-CoV-2 and potential resurgence of the high case burden on our health care system. Furthermore, a lack of a widely distributed vaccine or herd immunity suggests we will need to take many of the same precautions as in the first surge.6
In general, patients with cancer have been found to be at greater risk for adverse outcomes and mortality after COVID-19.7 Therefore, resource rationing is particularly concerning for patients with skin cancer, including melanoma, Merkel cell carcinoma, mycosis fungoides, and keratinocyte carcinoma. Triaging patients based on level of acuity, type of skin cancer, disease burden, host immunosuppression, and risk for progression must be carefully considered in this population.2 Treatment and follow-up present additional challenges.
Guidelines provided by the National Comprehensive Cancer Network (NCCN) and the European Society for Medical Oncology (ESMO) elaborated on key considerations for the treatment of melanoma, keratinocyte carcinoma, and Merkel cell carcinoma during the COVID-19 pandemic.8-10 Guidelines from the NCCN concentrated on clear divisions between disease stages to determine provider response. Guidelines for melanoma patients proposed by the ESMO assign tiers by value-based priority in various treatment settings, which offered flexibility to providers as the COVID-19 landscape continued to change. Recommendations from the NCCN and ESMO are summarized in Tables 1 to 5.
Although these guidelines initially may have been proposed to delay treatment of lower-acuity tumors, such delay might not be feasible given the unknown duration of this pandemic and future disease waves. One review of several studies, which addressed the outcomes on melanoma survival following the surgical delay recommended by the NCCN, revealed contradictory evidence.12 Further, sufficiently powered studies will be needed to better understand the impact of delaying treatment during the summer COVID-19 surge on patients with skin cancer. Therefore, physicians must triage patients accordingly to manage and treat while also preventing disease spread.
Tips for Performing Dermatologic Surgery
Careful consideration should be made to protect both the patient and staff during office-based excisional surgery during the COVID-19 pandemic. To minimize the risk of transmission of SARS-CoV-2, patients and staff should (1) be screened for symptoms of COVID-19 at least 48 hours prior to entering the office via telephone screening questions, and (2) follow proper hygiene and contact procedures once entering the office. Consider obtaining a nasal polymerase chain reaction swab or saliva test 48 hours prior to the procedure if the patient is undergoing a head and neck procedure or there is risk for transmission.
Guidelines from the ESMO recommended that all patients undergoing surgery or therapy should be swabbed for SARS-CoV-2 before each treatment.11 Patients should wear a mask, remain 6-feet apart in the waiting room, and avoid touching objects until they enter the procedure room. Objects that the patient must touch, such as pens, should be cleaned immediately after such contact with either alcohol or soap and water for 20 seconds.
Office capacity should be reduced by allowing no more than 1 person to accompany the patient and ensuring the presence of only the minimum staff needed for the procedure. Staff who are deemed necessary should wear a mask continuously and gloves during patient contact.
Once in the procedure room, providers might be at elevated risk of contracting COVID-19 or transmitting SARS-CoV-2. A properly fitted N95 respirator and a face shield are recommended, especially for facial cases. N95 respirators can be reused by following the latest Centers for Disease Control and Prevention recommendations for reuse and decontamination techniques,13 which may include protecting the N95 respirator with a surgical mask and storing it in a paper bag when not in use. Consider testing asymptomatic patients in facial cases when they cannot wear a mask.
Steps should be taken to reduce in-person visits. Dissolving sutures can help avoid return visits. Follow-up visits and postprocedural questions should be managed by telehealth. However, patients with a high-risk underlying conditions (eg, posttransplantation, immunosuppressed) should continue to obtain regular skin checks because they are at higher risk for more aggressive malignancies, such as Merkel cell carcinoma.
Conclusion
The future trajectory of the COVID-19 pandemic is uncertain. Dermatologists should continue providing care for patients with skin cancer while mitigating the risk for COVID-19 infection and transmission of SARS-CoV-2. Guidelines provided by the NCCN and ESMO should help providers triage patients. Decisions should be made case by case, keeping in mind the availability of resources and practicing in compliance with local guidance.
The coronavirus disease 2019 (COVID-19) pandemic, caused by severe acute respiratory syndrome novel coronavirus 2 (SARS-CoV-2), has presented a unique challenge to providing essential care to patients. Increased demand for health care workers and medical supplies, in addition to the risk for COVID-19 infection and asymptomatic transmission of SARS-CoV-2 among health care workers and patients, prompted the delay of nonessential services during the surge of cases this summer.1 Key considerations for continuing operation included current and projected COVID-19 cases in the region, ability to implement telehealth, staffing availability, personal protective equipment availability, and office capacity.2 Providing care that is deemed essential often was determined by the urgency of the treatment or service.
The Centers for Medicare & Medicaid Services outlined a strategy to stratify patients, based on level of acuity, during the COVID-19 surge3:
- Low-acuity treatments or services: includes routine primary, specialty, or preventive care visits. They should be postponed; telehealth follow-ups should be considered.
- Intermediate-acuity treatments or services: includes pediatric and neonatal care, follow-up visits for existing conditions, and evaluation of new symptoms (including those consistent with COVID-19). These services should initially be evaluated using telehealth, then triaged to the appropriate site and level of care.
- High-acuity treatments or services: address symptoms consistent with COVID-19 or other severe disease, of which the lack of in-person evaluation would result in harm to the patient.
Employees in hospitals and health care clinics were classified as essential, but dermatologists were not given explicit direction regarding clinic operation. Many practices have restricted services, especially those in an area of higher COVID-19 prevalence. However, the challenge of determining day-to-day operation may have been left to the provider in most cases.4 As many states in the United States continue to relax restrictions, total cases and the rate of positivity of COVID-19 have been sharply rising again, after months of decline,5 which suggests increased transmission of SARS-CoV-2 and potential resurgence of the high case burden on our health care system. Furthermore, a lack of a widely distributed vaccine or herd immunity suggests we will need to take many of the same precautions as in the first surge.6
In general, patients with cancer have been found to be at greater risk for adverse outcomes and mortality after COVID-19.7 Therefore, resource rationing is particularly concerning for patients with skin cancer, including melanoma, Merkel cell carcinoma, mycosis fungoides, and keratinocyte carcinoma. Triaging patients based on level of acuity, type of skin cancer, disease burden, host immunosuppression, and risk for progression must be carefully considered in this population.2 Treatment and follow-up present additional challenges.
Guidelines provided by the National Comprehensive Cancer Network (NCCN) and the European Society for Medical Oncology (ESMO) elaborated on key considerations for the treatment of melanoma, keratinocyte carcinoma, and Merkel cell carcinoma during the COVID-19 pandemic.8-10 Guidelines from the NCCN concentrated on clear divisions between disease stages to determine provider response. Guidelines for melanoma patients proposed by the ESMO assign tiers by value-based priority in various treatment settings, which offered flexibility to providers as the COVID-19 landscape continued to change. Recommendations from the NCCN and ESMO are summarized in Tables 1 to 5.
Although these guidelines initially may have been proposed to delay treatment of lower-acuity tumors, such delay might not be feasible given the unknown duration of this pandemic and future disease waves. One review of several studies, which addressed the outcomes on melanoma survival following the surgical delay recommended by the NCCN, revealed contradictory evidence.12 Further, sufficiently powered studies will be needed to better understand the impact of delaying treatment during the summer COVID-19 surge on patients with skin cancer. Therefore, physicians must triage patients accordingly to manage and treat while also preventing disease spread.
Tips for Performing Dermatologic Surgery
Careful consideration should be made to protect both the patient and staff during office-based excisional surgery during the COVID-19 pandemic. To minimize the risk of transmission of SARS-CoV-2, patients and staff should (1) be screened for symptoms of COVID-19 at least 48 hours prior to entering the office via telephone screening questions, and (2) follow proper hygiene and contact procedures once entering the office. Consider obtaining a nasal polymerase chain reaction swab or saliva test 48 hours prior to the procedure if the patient is undergoing a head and neck procedure or there is risk for transmission.
Guidelines from the ESMO recommended that all patients undergoing surgery or therapy should be swabbed for SARS-CoV-2 before each treatment.11 Patients should wear a mask, remain 6-feet apart in the waiting room, and avoid touching objects until they enter the procedure room. Objects that the patient must touch, such as pens, should be cleaned immediately after such contact with either alcohol or soap and water for 20 seconds.
Office capacity should be reduced by allowing no more than 1 person to accompany the patient and ensuring the presence of only the minimum staff needed for the procedure. Staff who are deemed necessary should wear a mask continuously and gloves during patient contact.
Once in the procedure room, providers might be at elevated risk of contracting COVID-19 or transmitting SARS-CoV-2. A properly fitted N95 respirator and a face shield are recommended, especially for facial cases. N95 respirators can be reused by following the latest Centers for Disease Control and Prevention recommendations for reuse and decontamination techniques,13 which may include protecting the N95 respirator with a surgical mask and storing it in a paper bag when not in use. Consider testing asymptomatic patients in facial cases when they cannot wear a mask.
Steps should be taken to reduce in-person visits. Dissolving sutures can help avoid return visits. Follow-up visits and postprocedural questions should be managed by telehealth. However, patients with a high-risk underlying conditions (eg, posttransplantation, immunosuppressed) should continue to obtain regular skin checks because they are at higher risk for more aggressive malignancies, such as Merkel cell carcinoma.
Conclusion
The future trajectory of the COVID-19 pandemic is uncertain. Dermatologists should continue providing care for patients with skin cancer while mitigating the risk for COVID-19 infection and transmission of SARS-CoV-2. Guidelines provided by the NCCN and ESMO should help providers triage patients. Decisions should be made case by case, keeping in mind the availability of resources and practicing in compliance with local guidance.
- Moletta L, Pierobon ES, Capovilla G, et al. International guidelines and recommendations for surgery during COVID-19 pandemic: a systematic review. Int J Surg. 2020;79:180-188.
- Ueda M, Martins R, Hendrie PC, et al. Managing cancer care during the COVID-19 pandemic: agility and collaboration toward common goal. J Natl Compr Canc Netw. 2020:1-4.
- Center for Medicare & Medicaid Services. Non-emergent, elective medical services, and treatment recommendations. Published April 7, 2020. Accessed October 15, 2020. https://www.cms.gov/files/document/cms-non-emergent-elective-medical-recommendations.pdf
- Muddasani S, Housholder A, Fleischer AB. An assessment of United States dermatology practices during the COVID-19 outbreak. J Dermatolog Treat. 2020;31:436-438.
- Coronavirus Resource Center, Johns Hopkins University & Medicine. Rate of positive tests in the US and states over time. Updated December 11, 2020. Accessed December 11, 2020. https://coronavirus.jhu.edu/testing/individual-states
- Middleton J, Lopes H, Michelson K, et al. Planning for a second wave pandemic of COVID-19 and planning for winter: a statement from the Association of Schools of Public Health in the European Region. Int J Public Health. 2020;65:1525-1527.
- Liang W, Guan W, Chen R, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21:335-337.
- National Comprehensive Cancer Network. Advisory statement for non-melanoma skin cancer care during the COVID-19 pandemic (version 4). Published May 22, 2020. Accessed December 11, 2020. https://www.nccn.org/covid-19/pdf/NCCN-NMSC.pdf
National Comprehensive Cancer Network. Short-term recommendations for cutaneous melanoma management during COVID-19 pandemic (version 3). Published May 6, 2020. Accessed December 11, 2020. www.nccn.org/covid-19/pdf/Melanoma.pdf - Conforti C, Giuffrida R, Di Meo N, et al. Management of advanced melanoma in the COVID-19 era. Dermatol Ther. 2020;33:e13444.
- ESMO [European Society for Medical Oncology]. Cancer patient management during the COVID-19 pandemic. Accessed Decemeber 11, 2020. https://www.esmo.org/guidelines/cancer-patient-management-during-the-covid-19-pandemic?hit=ehp
- Guhan S, Boland G, Tanabe K, et al. Surgical delay and mortality for primary cutaneous melanoma [published online July 22, 2020]. J Am Acad Dermatol. doi:10.1016/j.jaad.2020.07.078
- Centers for Disease Control and Prevention. Implementing filtering facepiece respirator (FFR) reuse, including reuse after decontamination, when there are known shortages of N95 respirators. Updated October 19, 2020. Accessed December 11, 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/decontamination-reuse-respirators.html
- Moletta L, Pierobon ES, Capovilla G, et al. International guidelines and recommendations for surgery during COVID-19 pandemic: a systematic review. Int J Surg. 2020;79:180-188.
- Ueda M, Martins R, Hendrie PC, et al. Managing cancer care during the COVID-19 pandemic: agility and collaboration toward common goal. J Natl Compr Canc Netw. 2020:1-4.
- Center for Medicare & Medicaid Services. Non-emergent, elective medical services, and treatment recommendations. Published April 7, 2020. Accessed October 15, 2020. https://www.cms.gov/files/document/cms-non-emergent-elective-medical-recommendations.pdf
- Muddasani S, Housholder A, Fleischer AB. An assessment of United States dermatology practices during the COVID-19 outbreak. J Dermatolog Treat. 2020;31:436-438.
- Coronavirus Resource Center, Johns Hopkins University & Medicine. Rate of positive tests in the US and states over time. Updated December 11, 2020. Accessed December 11, 2020. https://coronavirus.jhu.edu/testing/individual-states
- Middleton J, Lopes H, Michelson K, et al. Planning for a second wave pandemic of COVID-19 and planning for winter: a statement from the Association of Schools of Public Health in the European Region. Int J Public Health. 2020;65:1525-1527.
- Liang W, Guan W, Chen R, et al. Cancer patients in SARS-CoV-2 infection: a nationwide analysis in China. Lancet Oncol. 2020;21:335-337.
- National Comprehensive Cancer Network. Advisory statement for non-melanoma skin cancer care during the COVID-19 pandemic (version 4). Published May 22, 2020. Accessed December 11, 2020. https://www.nccn.org/covid-19/pdf/NCCN-NMSC.pdf
National Comprehensive Cancer Network. Short-term recommendations for cutaneous melanoma management during COVID-19 pandemic (version 3). Published May 6, 2020. Accessed December 11, 2020. www.nccn.org/covid-19/pdf/Melanoma.pdf - Conforti C, Giuffrida R, Di Meo N, et al. Management of advanced melanoma in the COVID-19 era. Dermatol Ther. 2020;33:e13444.
- ESMO [European Society for Medical Oncology]. Cancer patient management during the COVID-19 pandemic. Accessed Decemeber 11, 2020. https://www.esmo.org/guidelines/cancer-patient-management-during-the-covid-19-pandemic?hit=ehp
- Guhan S, Boland G, Tanabe K, et al. Surgical delay and mortality for primary cutaneous melanoma [published online July 22, 2020]. J Am Acad Dermatol. doi:10.1016/j.jaad.2020.07.078
- Centers for Disease Control and Prevention. Implementing filtering facepiece respirator (FFR) reuse, including reuse after decontamination, when there are known shortages of N95 respirators. Updated October 19, 2020. Accessed December 11, 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/decontamination-reuse-respirators.html
Practice Points
- Consider the rate of cases and transmission in your area during a pandemic surge when triaging surgical and nonsurgical cases.
- If performing head and neck surgical procedures or cosmetic procedures in which the patient cannot wear a mask, consider testing them 24 to 48 hours before the procedure.
- Follow Centers for Disease Control and Prevention (CDC) guidelines concerning screening asymptomatic patients. Also, follow CDC guidelines on testing patients who have had prior infections.
- Ensure proper personal protective equipment for yourself and staff, including the use of properly fitting N95 respirators and face shields.
TRANSforming gynecology: An introduction to hormone therapy for the obstetrician/gynecologist
Incorporating gender-nonconforming patients into practice can seem like a daunting task at first. However, obstetricians/gynecologists, midwives, and other advanced women’s health care practitioners can provide quality care for both transgender men and women. Basic preventative services such as routine health and cancer screening and testing for sexually transmitted infections does not require specialized training in transgender health. In fact, administration of hormonal therapy and some surgical interventions are well within the scope of practice of the general obstetrician/gynecologist, as long as the provider has undergone appropriate training to achieve expertise. For example, organizations such as the World Professional Association for Transgender Health (WPATH) not only provides standards of care regarding the treatment of transgender individuals, but they also have training and educational opportunities targeted at providers who wish to become certified in more advanced care of the transgender patient. If an obstetrician/gynecologist is interested in prescribing hormone therapy, seeking further training within the field is a must.

It is important to remember that the process by which transgender individuals express their gender is a spectrum. Not all patients who identify as transgender will seek hormone therapy or surgical procedures. However, even if a provider has not undergone more specific training to administer hormone therapy, it is still very important to have a basic understanding of the hormones, routes of administration, and side effects.
While cross-sex hormone therapy does differ in practice, compared with hormone replacement therapy in cisgender counterparts, the principles are relatively similar. Testosterone therapy is the mainstay treatment for transgender men who desire medical transition.1,2 The overall goal of therapy is to achieve testosterone levels within the cisgender male physiologic range (300-1000 ng/dL). While the most common route of administration is subcutaneous or intramuscular injections in weekly, biweekly, or quarterly intervals, other routes may include daily transdermal patches and gels or oral formulations.1 Within the first few months of use, patients will notice signs of masculinization such as increased facial and body hair, increased muscle mass, increased libido, and amenorrhea. Other changes include male-pattern hair loss, clitoromegaly, redistribution of fat, voice deepening, and mood changes.1
Hormone therapy for transgender women is a bit more complicated as estrogen alone will often not achieve feminizing characteristics that are satisfying for patients.3 Estrogen therapy can include oral formulations of 17-beta estradiol or conjugated estrogens, although the latter is typically avoided because of the marked increase in thromboembolic events. Estrogens can also be administered in sublingual, intramuscular, or transdermal forms. Antiandrogens are often required to help decrease endogenous testosterone levels to cisgender female levels (30-100 ng/dL).3 Spironolactone is most commonly prescribed as an adjunct to estrogen therapy. Finasteride and GnRH agonists like leuprolide acetate can also be added if spironolactone is not effective or not tolerated by the patient. Feminizing effects of estrogen can take several months and most commonly include decreased spontaneous erections, decreased libido, breast growth, redistribution of fat to the waist and hips, decreased skin oiliness, and softening of the skin.3
Overall, hormone therapy for both transgender men and women is considered effective, safe, and well tolerated.4 Monitoring is typically performed every 3 months within the first year after initiating hormone therapy, and then continued every 6-12 months thereafter. Routine screening for all organs and tissues present (e.g. prostate, breast) should be undertaken.3 While this simply highlights the therapy and surveillance for patients, it is important to remember that many transgender men and women will see an obstetrician/gynecologist at some interval during their transition. Ultimately, it is paramount that we as obstetricians/gynecologists have a basic understanding of the treatments available so we can provide our patients with competent and compassionate care.
Dr. Brandt is an obstetrician/gynecologist and a plastic surgeon at Reading Hospital/Tower Health System in West Reading, Pa., where she has developed a gender-affirming medical and surgical clinic for ob.gyn. residents and plastic surgeon fellows.
References
1. World Professional Association for Transgender Health. Standards of care for the health of transsexual, transgender, and gender nonconforming people. 7th version. Accessed 10/15/20.
2. Joint meeting of the International Society of Endocrinology and the Endocrine Society 2014; ICE/ENDO 2014, Paper 14354. Accessed 01/08/16.
3. Qian R, Safer JD. Hormone treatment for the adult transgender patient, in “Comprehensive Care of the Transgender Patient,” 1st ed. Philadelphia: Elsevier, 2020, pp. 34-6.
4. Weinand JD and Safer JD. Hormone therapy in transgender adults is safe with provider supervision: A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol. 2015;2(2):55-60.
Incorporating gender-nonconforming patients into practice can seem like a daunting task at first. However, obstetricians/gynecologists, midwives, and other advanced women’s health care practitioners can provide quality care for both transgender men and women. Basic preventative services such as routine health and cancer screening and testing for sexually transmitted infections does not require specialized training in transgender health. In fact, administration of hormonal therapy and some surgical interventions are well within the scope of practice of the general obstetrician/gynecologist, as long as the provider has undergone appropriate training to achieve expertise. For example, organizations such as the World Professional Association for Transgender Health (WPATH) not only provides standards of care regarding the treatment of transgender individuals, but they also have training and educational opportunities targeted at providers who wish to become certified in more advanced care of the transgender patient. If an obstetrician/gynecologist is interested in prescribing hormone therapy, seeking further training within the field is a must.
It is important to remember that the process by which transgender individuals express their gender is a spectrum. Not all patients who identify as transgender will seek hormone therapy or surgical procedures. However, even if a provider has not undergone more specific training to administer hormone therapy, it is still very important to have a basic understanding of the hormones, routes of administration, and side effects.
While cross-sex hormone therapy does differ in practice, compared with hormone replacement therapy in cisgender counterparts, the principles are relatively similar. Testosterone therapy is the mainstay treatment for transgender men who desire medical transition.1,2 The overall goal of therapy is to achieve testosterone levels within the cisgender male physiologic range (300-1000 ng/dL). While the most common route of administration is subcutaneous or intramuscular injections in weekly, biweekly, or quarterly intervals, other routes may include daily transdermal patches and gels or oral formulations.1 Within the first few months of use, patients will notice signs of masculinization such as increased facial and body hair, increased muscle mass, increased libido, and amenorrhea. Other changes include male-pattern hair loss, clitoromegaly, redistribution of fat, voice deepening, and mood changes.1
Hormone therapy for transgender women is a bit more complicated as estrogen alone will often not achieve feminizing characteristics that are satisfying for patients.3 Estrogen therapy can include oral formulations of 17-beta estradiol or conjugated estrogens, although the latter is typically avoided because of the marked increase in thromboembolic events. Estrogens can also be administered in sublingual, intramuscular, or transdermal forms. Antiandrogens are often required to help decrease endogenous testosterone levels to cisgender female levels (30-100 ng/dL).3 Spironolactone is most commonly prescribed as an adjunct to estrogen therapy. Finasteride and GnRH agonists like leuprolide acetate can also be added if spironolactone is not effective or not tolerated by the patient. Feminizing effects of estrogen can take several months and most commonly include decreased spontaneous erections, decreased libido, breast growth, redistribution of fat to the waist and hips, decreased skin oiliness, and softening of the skin.3
Overall, hormone therapy for both transgender men and women is considered effective, safe, and well tolerated.4 Monitoring is typically performed every 3 months within the first year after initiating hormone therapy, and then continued every 6-12 months thereafter. Routine screening for all organs and tissues present (e.g. prostate, breast) should be undertaken.3 While this simply highlights the therapy and surveillance for patients, it is important to remember that many transgender men and women will see an obstetrician/gynecologist at some interval during their transition. Ultimately, it is paramount that we as obstetricians/gynecologists have a basic understanding of the treatments available so we can provide our patients with competent and compassionate care.
Dr. Brandt is an obstetrician/gynecologist and a plastic surgeon at Reading Hospital/Tower Health System in West Reading, Pa., where she has developed a gender-affirming medical and surgical clinic for ob.gyn. residents and plastic surgeon fellows.
References
1. World Professional Association for Transgender Health. Standards of care for the health of transsexual, transgender, and gender nonconforming people. 7th version. Accessed 10/15/20.
2. Joint meeting of the International Society of Endocrinology and the Endocrine Society 2014; ICE/ENDO 2014, Paper 14354. Accessed 01/08/16.
3. Qian R, Safer JD. Hormone treatment for the adult transgender patient, in “Comprehensive Care of the Transgender Patient,” 1st ed. Philadelphia: Elsevier, 2020, pp. 34-6.
4. Weinand JD and Safer JD. Hormone therapy in transgender adults is safe with provider supervision: A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol. 2015;2(2):55-60.
Incorporating gender-nonconforming patients into practice can seem like a daunting task at first. However, obstetricians/gynecologists, midwives, and other advanced women’s health care practitioners can provide quality care for both transgender men and women. Basic preventative services such as routine health and cancer screening and testing for sexually transmitted infections does not require specialized training in transgender health. In fact, administration of hormonal therapy and some surgical interventions are well within the scope of practice of the general obstetrician/gynecologist, as long as the provider has undergone appropriate training to achieve expertise. For example, organizations such as the World Professional Association for Transgender Health (WPATH) not only provides standards of care regarding the treatment of transgender individuals, but they also have training and educational opportunities targeted at providers who wish to become certified in more advanced care of the transgender patient. If an obstetrician/gynecologist is interested in prescribing hormone therapy, seeking further training within the field is a must.
It is important to remember that the process by which transgender individuals express their gender is a spectrum. Not all patients who identify as transgender will seek hormone therapy or surgical procedures. However, even if a provider has not undergone more specific training to administer hormone therapy, it is still very important to have a basic understanding of the hormones, routes of administration, and side effects.
While cross-sex hormone therapy does differ in practice, compared with hormone replacement therapy in cisgender counterparts, the principles are relatively similar. Testosterone therapy is the mainstay treatment for transgender men who desire medical transition.1,2 The overall goal of therapy is to achieve testosterone levels within the cisgender male physiologic range (300-1000 ng/dL). While the most common route of administration is subcutaneous or intramuscular injections in weekly, biweekly, or quarterly intervals, other routes may include daily transdermal patches and gels or oral formulations.1 Within the first few months of use, patients will notice signs of masculinization such as increased facial and body hair, increased muscle mass, increased libido, and amenorrhea. Other changes include male-pattern hair loss, clitoromegaly, redistribution of fat, voice deepening, and mood changes.1
Hormone therapy for transgender women is a bit more complicated as estrogen alone will often not achieve feminizing characteristics that are satisfying for patients.3 Estrogen therapy can include oral formulations of 17-beta estradiol or conjugated estrogens, although the latter is typically avoided because of the marked increase in thromboembolic events. Estrogens can also be administered in sublingual, intramuscular, or transdermal forms. Antiandrogens are often required to help decrease endogenous testosterone levels to cisgender female levels (30-100 ng/dL).3 Spironolactone is most commonly prescribed as an adjunct to estrogen therapy. Finasteride and GnRH agonists like leuprolide acetate can also be added if spironolactone is not effective or not tolerated by the patient. Feminizing effects of estrogen can take several months and most commonly include decreased spontaneous erections, decreased libido, breast growth, redistribution of fat to the waist and hips, decreased skin oiliness, and softening of the skin.3
Overall, hormone therapy for both transgender men and women is considered effective, safe, and well tolerated.4 Monitoring is typically performed every 3 months within the first year after initiating hormone therapy, and then continued every 6-12 months thereafter. Routine screening for all organs and tissues present (e.g. prostate, breast) should be undertaken.3 While this simply highlights the therapy and surveillance for patients, it is important to remember that many transgender men and women will see an obstetrician/gynecologist at some interval during their transition. Ultimately, it is paramount that we as obstetricians/gynecologists have a basic understanding of the treatments available so we can provide our patients with competent and compassionate care.
Dr. Brandt is an obstetrician/gynecologist and a plastic surgeon at Reading Hospital/Tower Health System in West Reading, Pa., where she has developed a gender-affirming medical and surgical clinic for ob.gyn. residents and plastic surgeon fellows.
References
1. World Professional Association for Transgender Health. Standards of care for the health of transsexual, transgender, and gender nonconforming people. 7th version. Accessed 10/15/20.
2. Joint meeting of the International Society of Endocrinology and the Endocrine Society 2014; ICE/ENDO 2014, Paper 14354. Accessed 01/08/16.
3. Qian R, Safer JD. Hormone treatment for the adult transgender patient, in “Comprehensive Care of the Transgender Patient,” 1st ed. Philadelphia: Elsevier, 2020, pp. 34-6.
4. Weinand JD and Safer JD. Hormone therapy in transgender adults is safe with provider supervision: A review of hormone therapy sequelae for transgender individuals. J Clin Transl Endocrinol. 2015;2(2):55-60.
Reproductive Rounds: Understanding antimüllerian hormone in ovarian-age testing
In reproductive medicine, there are few, if any, more pressing concerns from our patients than the biological clock, i.e., ovarian aging. While addressing this issue with women can be challenging, particularly for those who are anxious regarding their advanced maternal age, gynecologists must possess a thorough understanding of available diagnostic testing. This article will review the various methods to assess ovarian age and appropriate clinical management.

Ovarian reserve tests
Ovarian reserve represents the quality and quantity of oocytes. The former is defined by the woman’s chronologic age, which is the greatest predictor of fertility. From a peak monthly fecundity rate at age 30 of approximately 20%, the slow and steady decline of fertility ensues. Quantity represents the number of oocytes remaining from the original cohort.
Ovarian reserve is most provocatively gauged by the follicle response to gonadotropin stimulation, typically during an in vitro fertilization (IVF) cycle.
Several biomarkers have been used to assess ovarian age. These include FSH, estradiol, and inhibin B. In general, these tests are more specific than sensitive, i.e., “normal” results do not necessarily exclude decreased ovarian reserve. But as a screening tool for decreased ovarian reserve, the most important factor is the positive predictive value (PPV). Statistically, in a population of women at low risk for decreased ovarian reserve, the PPV will be low despite sensitivity and specificity.
While inhibin B is a more direct and earlier reflection of ovarian function produced by granulose cells, assays lacked consistent results and a standardized cut-off value. FSH is the last biomarker to be affected by decreased ovarian reserve so elevations reflect more “end-stage” ovarian aging.
Additional tests for decreased ovarian reserve include antral follicle count (AFC) and the clomiphene citrate challenge test (CCCT). AFC is determined by using transvaginal ultrasound to count the number of follicular cysts in the 2- to 9-mm range. While AFC can be performed on any day of the cycle, the ovary is most optimally measured on menses because of less cystic activity. A combined AFC of 3-6 is considered severe decreased ovarian reserve. The CCCT involves prescribing clomiphene citrate 100 mg daily from cycle day 5-9 to measure FSH on cycle days 3 and 10. An FSH level greater than 10 IU/L or any elevation in FSH following CCCT is considered decreased ovarian reserve.
FSH had been the standard but levels may dramatically change monthly, making testing only valuable if it is elevated. Consequently, antimüllerian hormone (AMH) and AFC are considered the most useful tools to determine decreased ovarian reserve because of less variability. The other distinct advantage is the ability to obtain AMH any day in the menstrual cycle. Recently, in women undergoing IVF, AMH was superior to FSH in predicting live birth, particularly when their values were discordant (J Ovarian Res. 2018;11:60). While there is no established consensus, the ideal interval for repeating AMH appears to be approximately 3 months (Obstet Gynecol 2016;127:65S-6S).
AMH
AMH is expressed in the embryo at 8 weeks by the Sertoli cells of the testis causing the female reproductive internal system (müllerian) to regress. Without AMH expression, the müllerian system remains and the male (woffian duct system) regresses. The discovery of AMH production by the granulosa cells of the ovary launched a new era in the evaluation and management of infertile women. First reported in Fertility & Sterility in 2002 as a much earlier potential marker of ovarian aging, low levels of AMH predict a lower number of eggs in IVF.
AMH levels are produced in the embryo at 36 weeks’ gestation and increase up to the age of 24.5 years, decreasing thereafter. AMH reflects primordial (early) follicles that are FSH independent. The median AMH level decreases per year according to age groups are: 0.25 ng/mL in ages 26-30; 0.2 ng/mL in ages 31-36 years; and 0.1 ng/mL above age 36. (PLOS ONE 2015 doi: 10.1371/journal.pone.0125216).
AMH has also been studied as a potential biomarker to diagnose PCOS. While many women with PCOS have elevated AMH levels (typically greater than 3 ng/mL), there is no consensus on an AMH value that would be a criterion.
Many women, particularly those electing to defer fertility, express interest in obtaining their AMH level to consider planned oocyte cryopreservation, AKA, social egg freezing. While it is possible the results of AMH screening may compel women to electively freeze their eggs, extensive counseling on the implications and pitfalls of AMH levels is essential. Further, AMH cannot be used to accurately predict menopause.
Predicting outcomes
No biomarker is necessarily predictive of pregnancy but more a gauge of gonadotropin dosage to induce multifollicular development. AMH is a great predictor of oocyte yield with IVF (J Assist Reprod Genet. 2009;26[7]:383-9). However, in women older than 35 undergoing IVF, low AMH levels have been shown to reduce pregnancy rates (J Hum Reprod Sci. 2017;10:24–30). During IVF cycle attempts, an ultra-low AMH (≤0.4) resulted in high cancellation rates, reduced the number of oocytes retrieved and embryos developed, and lowered pregnancy rates in women of advanced reproductive age.
Alternatively, a study of 750 women who were not infertile and were actively trying to conceive demonstrated no difference in natural pregnancy rates in women aged 30-44 irrespective of AMH levels (JAMA. 2017;318[14]:1367-76).
A special consideration is for cancer patients who are status postgonadotoxic chemotherapy. Their oocyte attrition can be accelerated and AMH levels can become profoundly low. In those patients, current data suggest there is a modest recovery of postchemotherapy AMH levels up to 1 year. Further, oocyte yield following stimulation may be higher than expected despite a poor AMH level.
Conclusion
Ovarian aging is currently best measured by combining chronologic age, AFC, and AMH. There is no current evidence that AMH levels should be used to exclude patients from undergoing IVF or to recommend egg donation. Random screening of AMH levels in a low-risk population for decreased ovarian reserve may result in unnecessary alarm.
Dr. Trolice is director of Fertility CARE - The IVF Center in Winter Park, Fla., and associate professor of obstetrics and gynecology at the University of Central Florida, Orlando.
In reproductive medicine, there are few, if any, more pressing concerns from our patients than the biological clock, i.e., ovarian aging. While addressing this issue with women can be challenging, particularly for those who are anxious regarding their advanced maternal age, gynecologists must possess a thorough understanding of available diagnostic testing. This article will review the various methods to assess ovarian age and appropriate clinical management.
Ovarian reserve tests
Ovarian reserve represents the quality and quantity of oocytes. The former is defined by the woman’s chronologic age, which is the greatest predictor of fertility. From a peak monthly fecundity rate at age 30 of approximately 20%, the slow and steady decline of fertility ensues. Quantity represents the number of oocytes remaining from the original cohort.
Ovarian reserve is most provocatively gauged by the follicle response to gonadotropin stimulation, typically during an in vitro fertilization (IVF) cycle.
Several biomarkers have been used to assess ovarian age. These include FSH, estradiol, and inhibin B. In general, these tests are more specific than sensitive, i.e., “normal” results do not necessarily exclude decreased ovarian reserve. But as a screening tool for decreased ovarian reserve, the most important factor is the positive predictive value (PPV). Statistically, in a population of women at low risk for decreased ovarian reserve, the PPV will be low despite sensitivity and specificity.
While inhibin B is a more direct and earlier reflection of ovarian function produced by granulose cells, assays lacked consistent results and a standardized cut-off value. FSH is the last biomarker to be affected by decreased ovarian reserve so elevations reflect more “end-stage” ovarian aging.
Additional tests for decreased ovarian reserve include antral follicle count (AFC) and the clomiphene citrate challenge test (CCCT). AFC is determined by using transvaginal ultrasound to count the number of follicular cysts in the 2- to 9-mm range. While AFC can be performed on any day of the cycle, the ovary is most optimally measured on menses because of less cystic activity. A combined AFC of 3-6 is considered severe decreased ovarian reserve. The CCCT involves prescribing clomiphene citrate 100 mg daily from cycle day 5-9 to measure FSH on cycle days 3 and 10. An FSH level greater than 10 IU/L or any elevation in FSH following CCCT is considered decreased ovarian reserve.
FSH had been the standard but levels may dramatically change monthly, making testing only valuable if it is elevated. Consequently, antimüllerian hormone (AMH) and AFC are considered the most useful tools to determine decreased ovarian reserve because of less variability. The other distinct advantage is the ability to obtain AMH any day in the menstrual cycle. Recently, in women undergoing IVF, AMH was superior to FSH in predicting live birth, particularly when their values were discordant (J Ovarian Res. 2018;11:60). While there is no established consensus, the ideal interval for repeating AMH appears to be approximately 3 months (Obstet Gynecol 2016;127:65S-6S).
AMH
AMH is expressed in the embryo at 8 weeks by the Sertoli cells of the testis causing the female reproductive internal system (müllerian) to regress. Without AMH expression, the müllerian system remains and the male (woffian duct system) regresses. The discovery of AMH production by the granulosa cells of the ovary launched a new era in the evaluation and management of infertile women. First reported in Fertility & Sterility in 2002 as a much earlier potential marker of ovarian aging, low levels of AMH predict a lower number of eggs in IVF.
AMH levels are produced in the embryo at 36 weeks’ gestation and increase up to the age of 24.5 years, decreasing thereafter. AMH reflects primordial (early) follicles that are FSH independent. The median AMH level decreases per year according to age groups are: 0.25 ng/mL in ages 26-30; 0.2 ng/mL in ages 31-36 years; and 0.1 ng/mL above age 36. (PLOS ONE 2015 doi: 10.1371/journal.pone.0125216).
AMH has also been studied as a potential biomarker to diagnose PCOS. While many women with PCOS have elevated AMH levels (typically greater than 3 ng/mL), there is no consensus on an AMH value that would be a criterion.
Many women, particularly those electing to defer fertility, express interest in obtaining their AMH level to consider planned oocyte cryopreservation, AKA, social egg freezing. While it is possible the results of AMH screening may compel women to electively freeze their eggs, extensive counseling on the implications and pitfalls of AMH levels is essential. Further, AMH cannot be used to accurately predict menopause.
Predicting outcomes
No biomarker is necessarily predictive of pregnancy but more a gauge of gonadotropin dosage to induce multifollicular development. AMH is a great predictor of oocyte yield with IVF (J Assist Reprod Genet. 2009;26[7]:383-9). However, in women older than 35 undergoing IVF, low AMH levels have been shown to reduce pregnancy rates (J Hum Reprod Sci. 2017;10:24–30). During IVF cycle attempts, an ultra-low AMH (≤0.4) resulted in high cancellation rates, reduced the number of oocytes retrieved and embryos developed, and lowered pregnancy rates in women of advanced reproductive age.
Alternatively, a study of 750 women who were not infertile and were actively trying to conceive demonstrated no difference in natural pregnancy rates in women aged 30-44 irrespective of AMH levels (JAMA. 2017;318[14]:1367-76).
A special consideration is for cancer patients who are status postgonadotoxic chemotherapy. Their oocyte attrition can be accelerated and AMH levels can become profoundly low. In those patients, current data suggest there is a modest recovery of postchemotherapy AMH levels up to 1 year. Further, oocyte yield following stimulation may be higher than expected despite a poor AMH level.
Conclusion
Ovarian aging is currently best measured by combining chronologic age, AFC, and AMH. There is no current evidence that AMH levels should be used to exclude patients from undergoing IVF or to recommend egg donation. Random screening of AMH levels in a low-risk population for decreased ovarian reserve may result in unnecessary alarm.
Dr. Trolice is director of Fertility CARE - The IVF Center in Winter Park, Fla., and associate professor of obstetrics and gynecology at the University of Central Florida, Orlando.
In reproductive medicine, there are few, if any, more pressing concerns from our patients than the biological clock, i.e., ovarian aging. While addressing this issue with women can be challenging, particularly for those who are anxious regarding their advanced maternal age, gynecologists must possess a thorough understanding of available diagnostic testing. This article will review the various methods to assess ovarian age and appropriate clinical management.
Ovarian reserve tests
Ovarian reserve represents the quality and quantity of oocytes. The former is defined by the woman’s chronologic age, which is the greatest predictor of fertility. From a peak monthly fecundity rate at age 30 of approximately 20%, the slow and steady decline of fertility ensues. Quantity represents the number of oocytes remaining from the original cohort.
Ovarian reserve is most provocatively gauged by the follicle response to gonadotropin stimulation, typically during an in vitro fertilization (IVF) cycle.
Several biomarkers have been used to assess ovarian age. These include FSH, estradiol, and inhibin B. In general, these tests are more specific than sensitive, i.e., “normal” results do not necessarily exclude decreased ovarian reserve. But as a screening tool for decreased ovarian reserve, the most important factor is the positive predictive value (PPV). Statistically, in a population of women at low risk for decreased ovarian reserve, the PPV will be low despite sensitivity and specificity.
While inhibin B is a more direct and earlier reflection of ovarian function produced by granulose cells, assays lacked consistent results and a standardized cut-off value. FSH is the last biomarker to be affected by decreased ovarian reserve so elevations reflect more “end-stage” ovarian aging.
Additional tests for decreased ovarian reserve include antral follicle count (AFC) and the clomiphene citrate challenge test (CCCT). AFC is determined by using transvaginal ultrasound to count the number of follicular cysts in the 2- to 9-mm range. While AFC can be performed on any day of the cycle, the ovary is most optimally measured on menses because of less cystic activity. A combined AFC of 3-6 is considered severe decreased ovarian reserve. The CCCT involves prescribing clomiphene citrate 100 mg daily from cycle day 5-9 to measure FSH on cycle days 3 and 10. An FSH level greater than 10 IU/L or any elevation in FSH following CCCT is considered decreased ovarian reserve.
FSH had been the standard but levels may dramatically change monthly, making testing only valuable if it is elevated. Consequently, antimüllerian hormone (AMH) and AFC are considered the most useful tools to determine decreased ovarian reserve because of less variability. The other distinct advantage is the ability to obtain AMH any day in the menstrual cycle. Recently, in women undergoing IVF, AMH was superior to FSH in predicting live birth, particularly when their values were discordant (J Ovarian Res. 2018;11:60). While there is no established consensus, the ideal interval for repeating AMH appears to be approximately 3 months (Obstet Gynecol 2016;127:65S-6S).
AMH
AMH is expressed in the embryo at 8 weeks by the Sertoli cells of the testis causing the female reproductive internal system (müllerian) to regress. Without AMH expression, the müllerian system remains and the male (woffian duct system) regresses. The discovery of AMH production by the granulosa cells of the ovary launched a new era in the evaluation and management of infertile women. First reported in Fertility & Sterility in 2002 as a much earlier potential marker of ovarian aging, low levels of AMH predict a lower number of eggs in IVF.
AMH levels are produced in the embryo at 36 weeks’ gestation and increase up to the age of 24.5 years, decreasing thereafter. AMH reflects primordial (early) follicles that are FSH independent. The median AMH level decreases per year according to age groups are: 0.25 ng/mL in ages 26-30; 0.2 ng/mL in ages 31-36 years; and 0.1 ng/mL above age 36. (PLOS ONE 2015 doi: 10.1371/journal.pone.0125216).
AMH has also been studied as a potential biomarker to diagnose PCOS. While many women with PCOS have elevated AMH levels (typically greater than 3 ng/mL), there is no consensus on an AMH value that would be a criterion.
Many women, particularly those electing to defer fertility, express interest in obtaining their AMH level to consider planned oocyte cryopreservation, AKA, social egg freezing. While it is possible the results of AMH screening may compel women to electively freeze their eggs, extensive counseling on the implications and pitfalls of AMH levels is essential. Further, AMH cannot be used to accurately predict menopause.
Predicting outcomes
No biomarker is necessarily predictive of pregnancy but more a gauge of gonadotropin dosage to induce multifollicular development. AMH is a great predictor of oocyte yield with IVF (J Assist Reprod Genet. 2009;26[7]:383-9). However, in women older than 35 undergoing IVF, low AMH levels have been shown to reduce pregnancy rates (J Hum Reprod Sci. 2017;10:24–30). During IVF cycle attempts, an ultra-low AMH (≤0.4) resulted in high cancellation rates, reduced the number of oocytes retrieved and embryos developed, and lowered pregnancy rates in women of advanced reproductive age.
Alternatively, a study of 750 women who were not infertile and were actively trying to conceive demonstrated no difference in natural pregnancy rates in women aged 30-44 irrespective of AMH levels (JAMA. 2017;318[14]:1367-76).
A special consideration is for cancer patients who are status postgonadotoxic chemotherapy. Their oocyte attrition can be accelerated and AMH levels can become profoundly low. In those patients, current data suggest there is a modest recovery of postchemotherapy AMH levels up to 1 year. Further, oocyte yield following stimulation may be higher than expected despite a poor AMH level.
Conclusion
Ovarian aging is currently best measured by combining chronologic age, AFC, and AMH. There is no current evidence that AMH levels should be used to exclude patients from undergoing IVF or to recommend egg donation. Random screening of AMH levels in a low-risk population for decreased ovarian reserve may result in unnecessary alarm.
Dr. Trolice is director of Fertility CARE - The IVF Center in Winter Park, Fla., and associate professor of obstetrics and gynecology at the University of Central Florida, Orlando.
Recent Developments in Psychodermatology and Psychopharmacology for Delusional Patients
The management of delusional infestation (DI), also known as Morgellons disease or delusional parasitosis, can lead to some of the most difficult and stressful patient encounters in dermatology. As a specialty, dermatology providers are trained to respect scientific objectivity and pride themselves on their visual diagnostic acumen. Therefore, having to accommodate a patient’s erroneous ideations and potentially treat a psychiatric pathology poses a challenge for many dermatology providers because it requires shifting their mindset to where the subjective reality becomes the primary issue during the visit. This disconnect may lead to strife between the patient and the provider. All of these issues may make it difficult for dermatologists to connect with DI patients with the usual courtesy and consideration given to other patients. Moreover, some dermatologists find it difficult to respect the chief concern, which often is seen as purely psychological because there may be some lingering bias where psychological concerns perhaps are not seen as bona fide or legitimate disorders.
Is There a Biologic Basis for DI? A New Theory on the Etiology of Delusional Parasitosis
It is important to distinguish DI phenomenology into primary and secondary causes. Primary DI refers to cases where the delusion and formication occur spontaneously. In contrast, in secondary DI the delusion and other manifestations (eg, formication) happen secondarily to underlying broader diagnoses such as illicit substance abuse, primary psychiatric conditions including schizophrenia, organic brain syndrome, and vitamin B12 deficiency.
It is well known that primary DI overwhelmingly occurs in older women, whereas secondary DI does not show this same predilection. It has been a big unanswered question as to why primary DI so often occurs not only in women but specifically in older women. The latest theory that has been advancing in Europe and is supported by some data, including magnetic resonance imaging of the brain, involves the dopamine transporter (DAT) system, which is important in making sure the dopamine level in the intersynaptic space is not excessive.1 The DAT system is much more prominent in woman vs men and deteriorates with age due to declining estrogen levels. This age-related loss of striatal DAT is thought to be one possible etiology of DI. It has been hypothesized that decreased DAT functioning may cause an increase in extracellular striatal dopamine levels in the synapse that can lead to tactile hallucinations and delusions, which are hallmark symptoms seen in DI. Given that women experience a greater age-related DAT decline in striatal subregions than men, it is thought that primary DI mainly affects older women due to the decline of neuroprotective effects of estrogen on DAT activity with age.2 Further studies should evaluate the possibility of estrogen replacement therapy for treatment of DI.
Improving Care of Psychodermatology Patients in Clinic
There are several medications that are known to be effective for the treatment of DI, including pimozide, risperidone, aripiprazole, and olanzapine, among others. Pimozide is uniquely accepted by DI patients because it has no official psychiatric indication from the US Food and Drug Administration (FDA); it is only indicated in the United States for Tourette syndrome, which is a neurologic disorder. Therefore, pimozide arguably can be disregarded as a true antipsychotic agent. The fact that its chemical structure is similar to those of bona fide antipsychotic medications does not necessarily put it in this same category, as there also are antiemetic and antitussive medications (eg, prochlorperazine, promethazine) with chemical structures similar to antipsychotics, but clinicians generally do not think of these drugs as antipsychotics despite the similarities. This nuanced and admittedly somewhat arbitrary categorization is critical to patient care; in our clinic, we have found that patients who categorically refuse to consider all psychiatric medications are much more willing to try pimozide for this very reason, that this medication can uniquely be presented to the DI patient as an agent not used in psychiatry. We have found great success in treatment with pimozide, even with relatively low doses.3,4
One of the main reasons dermatologists are reluctant to prescribe antipsychotic medications or even pimozide is the concern for side effects, especially tardive dyskinesia (TD), which is thought to be irreversible and untreatable. However, after a half century of worldwide use of pimozide in dermatology, a PubMed search of English-language articles indexed for MEDLINE using the terms pimozide and tardive dyskinesia, tardive dyskinesia and delusions of parasitosis, tardive dyskinesia and dermatology, and tardive dyskinesia and delusional infestation/Morgellons disease yielded only 1 known case of TD reported in dermatologic use for DI.5 In this particular case, TD-like symptoms did not appear until after pimozide had been discontinued for 1 month. Therefore, it is not clear if this case was true TD or a condition known as withdrawal dyskinesia, which mimics TD and usually is self-limiting.5
The senior author (J.K.) has been using pimozide for treatment of DI for more than 30 years and has not encountered TD or any other notable side effects. The reason for this extremely low incidence of side effects may be due to its high efficacy in treating DI; hence, only a low dose of pimozide usually is needed. At the University of California, San Francisco, Psychodermatology Clinic, pimozide typically is used to treat DI at a low dose of 3 mg or less daily, starting with 0.5 or 1 mg and slowly titrating upward until a clinically effective dose is reached. Pimozide rarely is used long-term; after the resolution of symptoms, the dose usually is continued at the clinically effective dose for a few months and then is slowly tapered off. In contrast, for a condition such as schizophrenia, an antipsychotic medication often is needed at high doses for life, resulting in higher TD occurrences being reported. Therefore, even though the newer antipsychotic agents are preferable to pimozide because of their somewhat lower risk for TD, in actual clinical practice many, if not most, DI patients detest any suggestion of taking a medication for “crazy people.” Thus, we find that pimozide’s inherent superior acceptability among DI patients often is critical to enabling any effective treatment to occur at all due to the fact that the provider can honestly say that pimozide has no FDA psychiatric indication.
Still, one of the biggest apprehensions with initiating and continuing these medications in dermatology is fear of TD. Now, dermatologists can be made aware that if this very rare side effect occurs, there are medications approved to treat TD, even if the anti-TD therapy is administered by a neurologist. For the first time, 2 medications were approved by the FDA for treatment of TD in 2017, namely valbenazine and deutetrabenazine. These medications represent a class known as vesicular monoamine transporter type 2 inhibitors and function by ultimately reducing the amount of dopamine released from the presynaptic dopaminergic neurons. In phase 3 trials for valbenazine and deutetrabenazine, 40% (N=234) and 34% (N=222) of patients, respectively, achieved a response, which was defined as at least a 50% decrease from baseline on the abnormal involuntary movement scale dyskinesia score in 6 to 12 weeks compared to 9% and 12%, respectively, with placebo.Discontinuation because of an adverse event was seldom encountered with both medications.6
Conclusion
The recent developments in psychodermatology with regard to DI are encouraging. The advent of new evidence and theories suggestive of an organic basis for DI could help this condition become more respected in the eyes of the dermatologist as a bona fide disorder. Moreover, the new developments and availability of medications that can treat TD can further make it easier for dermatologists to consider offering DI patients truly meaningful treatment that they desperately need. Therefore, both of these developments are welcomed for our specialty.
- Huber M, Kirchler E, Karner M, et al. Delusional parasitosis and the dopamine transporter. a new insight of etiology? Med Hypotheses. 2007;68:1351-1358.
- Chan SY, Koo J. Sex differences in primary delusional infestation: an insight into etiology and potential novel therapy. Int J Women Dermatol. 2020;6:226.
- Lorenzo CR, Koo J. Pimozide in dermatologic practice: a comprehensive review. Am J Clin Dermatol. 2004;5:339-349.
- Brownstone ND, Beck K, Sekhon S, et al. Morgellons Disease. 2nd ed. Kindle Direct Publishing; 2020.
- Thomson AM, Wallace J, Kobylecki C. Tardive dyskinesia after drug withdrawal in two older adults: clinical features, complications and management. Geriatr Gerontol Int. 2019;19:563-564.
- Citrome L. Tardive dyskinesia: placing vesicular monoamine transporter type 2 (VMAT2) inhibitors into clinical perspective. Expert Rev Neurother. 2018;18:323-332.
The management of delusional infestation (DI), also known as Morgellons disease or delusional parasitosis, can lead to some of the most difficult and stressful patient encounters in dermatology. As a specialty, dermatology providers are trained to respect scientific objectivity and pride themselves on their visual diagnostic acumen. Therefore, having to accommodate a patient’s erroneous ideations and potentially treat a psychiatric pathology poses a challenge for many dermatology providers because it requires shifting their mindset to where the subjective reality becomes the primary issue during the visit. This disconnect may lead to strife between the patient and the provider. All of these issues may make it difficult for dermatologists to connect with DI patients with the usual courtesy and consideration given to other patients. Moreover, some dermatologists find it difficult to respect the chief concern, which often is seen as purely psychological because there may be some lingering bias where psychological concerns perhaps are not seen as bona fide or legitimate disorders.
Is There a Biologic Basis for DI? A New Theory on the Etiology of Delusional Parasitosis
It is important to distinguish DI phenomenology into primary and secondary causes. Primary DI refers to cases where the delusion and formication occur spontaneously. In contrast, in secondary DI the delusion and other manifestations (eg, formication) happen secondarily to underlying broader diagnoses such as illicit substance abuse, primary psychiatric conditions including schizophrenia, organic brain syndrome, and vitamin B12 deficiency.
It is well known that primary DI overwhelmingly occurs in older women, whereas secondary DI does not show this same predilection. It has been a big unanswered question as to why primary DI so often occurs not only in women but specifically in older women. The latest theory that has been advancing in Europe and is supported by some data, including magnetic resonance imaging of the brain, involves the dopamine transporter (DAT) system, which is important in making sure the dopamine level in the intersynaptic space is not excessive.1 The DAT system is much more prominent in woman vs men and deteriorates with age due to declining estrogen levels. This age-related loss of striatal DAT is thought to be one possible etiology of DI. It has been hypothesized that decreased DAT functioning may cause an increase in extracellular striatal dopamine levels in the synapse that can lead to tactile hallucinations and delusions, which are hallmark symptoms seen in DI. Given that women experience a greater age-related DAT decline in striatal subregions than men, it is thought that primary DI mainly affects older women due to the decline of neuroprotective effects of estrogen on DAT activity with age.2 Further studies should evaluate the possibility of estrogen replacement therapy for treatment of DI.
Improving Care of Psychodermatology Patients in Clinic
There are several medications that are known to be effective for the treatment of DI, including pimozide, risperidone, aripiprazole, and olanzapine, among others. Pimozide is uniquely accepted by DI patients because it has no official psychiatric indication from the US Food and Drug Administration (FDA); it is only indicated in the United States for Tourette syndrome, which is a neurologic disorder. Therefore, pimozide arguably can be disregarded as a true antipsychotic agent. The fact that its chemical structure is similar to those of bona fide antipsychotic medications does not necessarily put it in this same category, as there also are antiemetic and antitussive medications (eg, prochlorperazine, promethazine) with chemical structures similar to antipsychotics, but clinicians generally do not think of these drugs as antipsychotics despite the similarities. This nuanced and admittedly somewhat arbitrary categorization is critical to patient care; in our clinic, we have found that patients who categorically refuse to consider all psychiatric medications are much more willing to try pimozide for this very reason, that this medication can uniquely be presented to the DI patient as an agent not used in psychiatry. We have found great success in treatment with pimozide, even with relatively low doses.3,4
One of the main reasons dermatologists are reluctant to prescribe antipsychotic medications or even pimozide is the concern for side effects, especially tardive dyskinesia (TD), which is thought to be irreversible and untreatable. However, after a half century of worldwide use of pimozide in dermatology, a PubMed search of English-language articles indexed for MEDLINE using the terms pimozide and tardive dyskinesia, tardive dyskinesia and delusions of parasitosis, tardive dyskinesia and dermatology, and tardive dyskinesia and delusional infestation/Morgellons disease yielded only 1 known case of TD reported in dermatologic use for DI.5 In this particular case, TD-like symptoms did not appear until after pimozide had been discontinued for 1 month. Therefore, it is not clear if this case was true TD or a condition known as withdrawal dyskinesia, which mimics TD and usually is self-limiting.5
The senior author (J.K.) has been using pimozide for treatment of DI for more than 30 years and has not encountered TD or any other notable side effects. The reason for this extremely low incidence of side effects may be due to its high efficacy in treating DI; hence, only a low dose of pimozide usually is needed. At the University of California, San Francisco, Psychodermatology Clinic, pimozide typically is used to treat DI at a low dose of 3 mg or less daily, starting with 0.5 or 1 mg and slowly titrating upward until a clinically effective dose is reached. Pimozide rarely is used long-term; after the resolution of symptoms, the dose usually is continued at the clinically effective dose for a few months and then is slowly tapered off. In contrast, for a condition such as schizophrenia, an antipsychotic medication often is needed at high doses for life, resulting in higher TD occurrences being reported. Therefore, even though the newer antipsychotic agents are preferable to pimozide because of their somewhat lower risk for TD, in actual clinical practice many, if not most, DI patients detest any suggestion of taking a medication for “crazy people.” Thus, we find that pimozide’s inherent superior acceptability among DI patients often is critical to enabling any effective treatment to occur at all due to the fact that the provider can honestly say that pimozide has no FDA psychiatric indication.
Still, one of the biggest apprehensions with initiating and continuing these medications in dermatology is fear of TD. Now, dermatologists can be made aware that if this very rare side effect occurs, there are medications approved to treat TD, even if the anti-TD therapy is administered by a neurologist. For the first time, 2 medications were approved by the FDA for treatment of TD in 2017, namely valbenazine and deutetrabenazine. These medications represent a class known as vesicular monoamine transporter type 2 inhibitors and function by ultimately reducing the amount of dopamine released from the presynaptic dopaminergic neurons. In phase 3 trials for valbenazine and deutetrabenazine, 40% (N=234) and 34% (N=222) of patients, respectively, achieved a response, which was defined as at least a 50% decrease from baseline on the abnormal involuntary movement scale dyskinesia score in 6 to 12 weeks compared to 9% and 12%, respectively, with placebo.Discontinuation because of an adverse event was seldom encountered with both medications.6
Conclusion
The recent developments in psychodermatology with regard to DI are encouraging. The advent of new evidence and theories suggestive of an organic basis for DI could help this condition become more respected in the eyes of the dermatologist as a bona fide disorder. Moreover, the new developments and availability of medications that can treat TD can further make it easier for dermatologists to consider offering DI patients truly meaningful treatment that they desperately need. Therefore, both of these developments are welcomed for our specialty.
The management of delusional infestation (DI), also known as Morgellons disease or delusional parasitosis, can lead to some of the most difficult and stressful patient encounters in dermatology. As a specialty, dermatology providers are trained to respect scientific objectivity and pride themselves on their visual diagnostic acumen. Therefore, having to accommodate a patient’s erroneous ideations and potentially treat a psychiatric pathology poses a challenge for many dermatology providers because it requires shifting their mindset to where the subjective reality becomes the primary issue during the visit. This disconnect may lead to strife between the patient and the provider. All of these issues may make it difficult for dermatologists to connect with DI patients with the usual courtesy and consideration given to other patients. Moreover, some dermatologists find it difficult to respect the chief concern, which often is seen as purely psychological because there may be some lingering bias where psychological concerns perhaps are not seen as bona fide or legitimate disorders.
Is There a Biologic Basis for DI? A New Theory on the Etiology of Delusional Parasitosis
It is important to distinguish DI phenomenology into primary and secondary causes. Primary DI refers to cases where the delusion and formication occur spontaneously. In contrast, in secondary DI the delusion and other manifestations (eg, formication) happen secondarily to underlying broader diagnoses such as illicit substance abuse, primary psychiatric conditions including schizophrenia, organic brain syndrome, and vitamin B12 deficiency.
It is well known that primary DI overwhelmingly occurs in older women, whereas secondary DI does not show this same predilection. It has been a big unanswered question as to why primary DI so often occurs not only in women but specifically in older women. The latest theory that has been advancing in Europe and is supported by some data, including magnetic resonance imaging of the brain, involves the dopamine transporter (DAT) system, which is important in making sure the dopamine level in the intersynaptic space is not excessive.1 The DAT system is much more prominent in woman vs men and deteriorates with age due to declining estrogen levels. This age-related loss of striatal DAT is thought to be one possible etiology of DI. It has been hypothesized that decreased DAT functioning may cause an increase in extracellular striatal dopamine levels in the synapse that can lead to tactile hallucinations and delusions, which are hallmark symptoms seen in DI. Given that women experience a greater age-related DAT decline in striatal subregions than men, it is thought that primary DI mainly affects older women due to the decline of neuroprotective effects of estrogen on DAT activity with age.2 Further studies should evaluate the possibility of estrogen replacement therapy for treatment of DI.
Improving Care of Psychodermatology Patients in Clinic
There are several medications that are known to be effective for the treatment of DI, including pimozide, risperidone, aripiprazole, and olanzapine, among others. Pimozide is uniquely accepted by DI patients because it has no official psychiatric indication from the US Food and Drug Administration (FDA); it is only indicated in the United States for Tourette syndrome, which is a neurologic disorder. Therefore, pimozide arguably can be disregarded as a true antipsychotic agent. The fact that its chemical structure is similar to those of bona fide antipsychotic medications does not necessarily put it in this same category, as there also are antiemetic and antitussive medications (eg, prochlorperazine, promethazine) with chemical structures similar to antipsychotics, but clinicians generally do not think of these drugs as antipsychotics despite the similarities. This nuanced and admittedly somewhat arbitrary categorization is critical to patient care; in our clinic, we have found that patients who categorically refuse to consider all psychiatric medications are much more willing to try pimozide for this very reason, that this medication can uniquely be presented to the DI patient as an agent not used in psychiatry. We have found great success in treatment with pimozide, even with relatively low doses.3,4
One of the main reasons dermatologists are reluctant to prescribe antipsychotic medications or even pimozide is the concern for side effects, especially tardive dyskinesia (TD), which is thought to be irreversible and untreatable. However, after a half century of worldwide use of pimozide in dermatology, a PubMed search of English-language articles indexed for MEDLINE using the terms pimozide and tardive dyskinesia, tardive dyskinesia and delusions of parasitosis, tardive dyskinesia and dermatology, and tardive dyskinesia and delusional infestation/Morgellons disease yielded only 1 known case of TD reported in dermatologic use for DI.5 In this particular case, TD-like symptoms did not appear until after pimozide had been discontinued for 1 month. Therefore, it is not clear if this case was true TD or a condition known as withdrawal dyskinesia, which mimics TD and usually is self-limiting.5
The senior author (J.K.) has been using pimozide for treatment of DI for more than 30 years and has not encountered TD or any other notable side effects. The reason for this extremely low incidence of side effects may be due to its high efficacy in treating DI; hence, only a low dose of pimozide usually is needed. At the University of California, San Francisco, Psychodermatology Clinic, pimozide typically is used to treat DI at a low dose of 3 mg or less daily, starting with 0.5 or 1 mg and slowly titrating upward until a clinically effective dose is reached. Pimozide rarely is used long-term; after the resolution of symptoms, the dose usually is continued at the clinically effective dose for a few months and then is slowly tapered off. In contrast, for a condition such as schizophrenia, an antipsychotic medication often is needed at high doses for life, resulting in higher TD occurrences being reported. Therefore, even though the newer antipsychotic agents are preferable to pimozide because of their somewhat lower risk for TD, in actual clinical practice many, if not most, DI patients detest any suggestion of taking a medication for “crazy people.” Thus, we find that pimozide’s inherent superior acceptability among DI patients often is critical to enabling any effective treatment to occur at all due to the fact that the provider can honestly say that pimozide has no FDA psychiatric indication.
Still, one of the biggest apprehensions with initiating and continuing these medications in dermatology is fear of TD. Now, dermatologists can be made aware that if this very rare side effect occurs, there are medications approved to treat TD, even if the anti-TD therapy is administered by a neurologist. For the first time, 2 medications were approved by the FDA for treatment of TD in 2017, namely valbenazine and deutetrabenazine. These medications represent a class known as vesicular monoamine transporter type 2 inhibitors and function by ultimately reducing the amount of dopamine released from the presynaptic dopaminergic neurons. In phase 3 trials for valbenazine and deutetrabenazine, 40% (N=234) and 34% (N=222) of patients, respectively, achieved a response, which was defined as at least a 50% decrease from baseline on the abnormal involuntary movement scale dyskinesia score in 6 to 12 weeks compared to 9% and 12%, respectively, with placebo.Discontinuation because of an adverse event was seldom encountered with both medications.6
Conclusion
The recent developments in psychodermatology with regard to DI are encouraging. The advent of new evidence and theories suggestive of an organic basis for DI could help this condition become more respected in the eyes of the dermatologist as a bona fide disorder. Moreover, the new developments and availability of medications that can treat TD can further make it easier for dermatologists to consider offering DI patients truly meaningful treatment that they desperately need. Therefore, both of these developments are welcomed for our specialty.
- Huber M, Kirchler E, Karner M, et al. Delusional parasitosis and the dopamine transporter. a new insight of etiology? Med Hypotheses. 2007;68:1351-1358.
- Chan SY, Koo J. Sex differences in primary delusional infestation: an insight into etiology and potential novel therapy. Int J Women Dermatol. 2020;6:226.
- Lorenzo CR, Koo J. Pimozide in dermatologic practice: a comprehensive review. Am J Clin Dermatol. 2004;5:339-349.
- Brownstone ND, Beck K, Sekhon S, et al. Morgellons Disease. 2nd ed. Kindle Direct Publishing; 2020.
- Thomson AM, Wallace J, Kobylecki C. Tardive dyskinesia after drug withdrawal in two older adults: clinical features, complications and management. Geriatr Gerontol Int. 2019;19:563-564.
- Citrome L. Tardive dyskinesia: placing vesicular monoamine transporter type 2 (VMAT2) inhibitors into clinical perspective. Expert Rev Neurother. 2018;18:323-332.
- Huber M, Kirchler E, Karner M, et al. Delusional parasitosis and the dopamine transporter. a new insight of etiology? Med Hypotheses. 2007;68:1351-1358.
- Chan SY, Koo J. Sex differences in primary delusional infestation: an insight into etiology and potential novel therapy. Int J Women Dermatol. 2020;6:226.
- Lorenzo CR, Koo J. Pimozide in dermatologic practice: a comprehensive review. Am J Clin Dermatol. 2004;5:339-349.
- Brownstone ND, Beck K, Sekhon S, et al. Morgellons Disease. 2nd ed. Kindle Direct Publishing; 2020.
- Thomson AM, Wallace J, Kobylecki C. Tardive dyskinesia after drug withdrawal in two older adults: clinical features, complications and management. Geriatr Gerontol Int. 2019;19:563-564.
- Citrome L. Tardive dyskinesia: placing vesicular monoamine transporter type 2 (VMAT2) inhibitors into clinical perspective. Expert Rev Neurother. 2018;18:323-332.

Skin Cancer Screening and Prevention During the COVID-19 Pandemic
On March 11, 2020, the World Health Organization declared the outbreak of coronavirus disease 2019 (COVID-19) a pandemic, leading to an abrupt widespread shift to teledermatology, with postponement of nonessential in-office medical and surgical services, according to American Academy of Dermatology (AAD) recommendations.1 Perspectives have been offered regarding skin cancer management during the pandemic2; however, the current literature is lacking guidance on skin cancer screening and prevention during the COVID-19 era.
Preliminary data show a 34.3% reduction in skin cancer referrals from February to April 2020 compared to the same period in 2019. The authors also presented a subsequent reduction in the number of skin cancer diagnoses in March 2020 compared to March 2019.3 Although the COVID-19 public health emergency should be prioritized by all health care workers, the duty to maintain disease prevention remains.
We aim to provide recommendations for this urgent topic. Our goal is finding balance in preventing an increase in the incidence of and mortality from skin cancer that results from delayed detection, while conserving personalprotective equipment and minimizing exposure, by patients and clinical personnel, to the severe acute respiratory syndrome coronavirus 2. A primary benefit of skin cancer screening lies in the ability to detect melanoma, which is associated with higher mortality than the more common nonmelanoma skin cancers, basal and cutaneous squamous cell carcinomas. We place preeminence on screening directed toward detecting melanoma. The main screening method that dermatologists employ is the total-body skin examination (TBSE). Another widely encouraged and utilized component in skin cancer prevention is patient education, emphasizing avoidance of risk factors, undertaking protective factors, and providing clear instructions for performing the patient-led skin self-examination (SSE).
Teledermatology Essentials for Skin Cancer Screening
Arguably, dermatology possesses the most potential for successfully utilizing telemedicine. Teledermatology has become widely implemented across the United States, secondary to the implications of the current pandemic. A report by Perkins and colleagues4 provided a positive outlook in the preliminary transition to teledermatology beginning in March 2020, though reported time of use was relatively short (3 weeks). A May 2020 article in Dermatology News provided tips for implementing telemedicine for practices.5
We agree with the comprehensive screening algorithm for teledermatology presented by Perkins and colleagues4 (Figure 1A in their report) and recommend the following for the screening and prevention of skin cancer:
• Patients with any characteristics of increased risk, including a personal or family history of melanoma, large congenital nevi, many melanotic nevi, dysplastic nevi, and Fitzpatrick skin types I and II,6 should be prioritized for an in-person visit for TBSE.
• Immunosuppressed patients, particularly organ transplant recipients and those with a history of skin cancer, should be prioritized for an in-person visit for TBSE.
• Established patients evaluated and determined to be at average risk for skin cancer should be offered a teledermatology visit. Suspicious findings during these visits should be prioritized for an in-person visit, with subsequent biopsy and follow-up.
• New patients should be offered a teledermatology visit.
These recommendations must be reviewed alongside each patient’s risk for travel and being present in person as well as other factors that might place the patient at increased risk for COVID-19.
Total-body skin examination, a widely used tool in the dermatologist’s tool kit, presents minimal risk to patients while providing important data for each dermatology patient’s profile, ultimately directing patient care. The role of TBSE in skin cancer screening and prevention has been in discussion even prior to the current pandemic. The US Preventive Services Task Force (USPSTF) has not declared a role for TBSE in recent years; however, USPSTF recommendations are formulated using data from all forms of screening, not only dermatologist-led interventions. Accordingly, USPSTF recommendations target primary care. The AAD has released statements addressing the role of TBSE and skin cancer prevention in the past, when necessary, to provide clarity.7
There is no clear definition of SSE or guidelines on how to educate a patient to perform regular SSE; however, the AAD provides patients with resources on how to perform an SSE.8 Just as dermatologists would provide education, advice, and guidance by directing patients to the AAD website for the SSE during an in-person visit, we encourage dermatologists to continue this practice during all teledermatology visits.
The role of teledermatology in skin cancer screening and prevention is limited; dermatologists will not be able to adequately perform TBSE as it would be done at in-person visits. Furthermore, the true implications of teledermatology compared to in-person visits during the COVID-19 pandemic have yet to be realized and analyzed. It is nonetheless important to appreciate that teledermatology holds great promise of benefit in skin cancer prevention, especially in the form of patient education by dermatologists. Practices in the realm of screening and prevention by health care professionals should be continually addressed during the pandemic; it is important to consider the implications associated with delays in diagnosis and treatment.
Teledermatology Limitations and Recommendations for High-Quality Visits
A benefit of video consultation (VC) vs telephone visits is visual interaction—the crux of dermatology. A 2019 study investigated VC experiences among providers and patients in the primary care setting. Benefits of VC were reported to include convenience for working patients and patients with mobility or mental health problems, visual cues, building rapport, and improving communication.9
Despite these benefits, VC is not without limitations. Many technical factors create variability in the quality of teledermatology VCs for a melanocytic lesion, including patient environment and lighting, color distortion, video resolution, and Internet connection. We make the following recommendations:
• Environment: Locate or create a dedicated space for teledermatology visits that is well lit, private, and has minimal background noise. Place the device on a level surface, center yourself in the frame, and keep the camera at eye level.
• Lighting: Use neutral lighting, placing the light source in front of you but behind the camera of the device. Avoid placing light sources, such as a window, behind you.
• Video resolution: Regardless of the type of camera (eg, integrated webcam, external camera), close out all other running software programs to optimize bandwidth during the visit.
• Internet connection: Use a wired connection (via an Ethernet cable) instead of a Wi-Fi connection to greatly decrease the chance of losing the connection during the visit. It also is faster than Wi-Fi.
• Addressing specific lesions: Patients should keep the device in place, repositioning themselves to show the lesions rather than moving the device by hand.
• Video capacity: Test your device’s video capacity beforehand, which can be as simple as video-calling a family member or friend from your designated space. Feedback regarding video and audio quality will help fine-tune your setup.
• Instructions to the patient: Provide clear instructions to the patient when photographs of specific lesions are needed for further review. Specify what view(s) you need and whether size or bilateral comparison is needed. A web post by VisualDx10 provides advice to patients on taking high-quality photographs.
Final Thoughts
Teledermatology indubitably presents a learning curve for dermatologists and patients. As with other technological advances in society, we are optimistic that, first, the confidence level in teledermatology use will increase, and, second, evidence-based data will pave the way to enhance this experience. We realize the inherent limitation of accessibility to certain technologies, which is regrettably far from equitable. Patients need a personal device equipped with audio and video; access to a high-quality Internet connection; some degree of technological literacy; and a quiet private location.
We hope to learn from all experiences during the current pandemic. Future innovation in teledermatology and in telemedicine generally should aim to address technological inequities to allow for the delivery of quality care to as many patients as possible.
- American Academy of Dermatology. Everyday health and preparedness steps in clinic Updated April 4, 2020. Accessed December 17, 2020. https://assets.ctfassets.net/1ny4yoiyrqia/4LNCNjucOonbQx7aC970x/b56b540957ddad94dcc61949b8e3acc9/COVID-19_Preparedness_30Apr2020.pdf
- Geskin LJ, Trager MH, Aasi SZ, et al. Perspectives on the recommendations for skin cancer management during the COVID-19 pandemic. J Am Acad Dermatol. 2020;83:295-296.
- Earnshaw CH, Hunter HJA, McMullen E, et al. Reduction in skin cancer diagnosis, and overall cancer referrals, during the COVID-19 pandemic. Br J Dermatol. 2020;183:792-794.
- Perkins S, Cohen JM, Nelson CA, et al. Teledermatology in the era of COVID-19: experience of an academic department of dermatology. J Am Acad Dermatol. 2020;83:E43-E44.
- Marina F. COVID-19: telehealth at the forefront of the pandemic. Dermatology News. May 12, 2020. Accessed December 17, 2020. www.mdedge.com/dermatology/article/222089/coronavirus-updates/covid-19-telehealth-forefront-pandemic?channel=52
- Watts CG, Dieng M, Morton RL, et al. Clinical practice guidelines for identification, screening and follow-up of individuals at high risk of primary cutaneous melanoma: a systematic review. Br J Dermatol. 2015;172:33-47.
- Rosamilia LL. “Doctor, do I need a skin check?” Cutis. 2019;103:290-291.
- Detect skin cancer: how to perform a skin self-exam. American Academy of Dermatology. Accessed December 17, 2020. www.aad.org/public/diseases/skin-cancer/find/check-skin
- Donaghy E, Atherton H, Hammersley V, et al. Acceptability, benefits, and challenges of video consulting: a qualitative study in primary care. Br J Gen Pract. 2019;69:E586-E594.
- How to take the best photos for teledermatology. VisualDx. Accessed December 17, 2020. https://info.visualdx.com/l/11412/2020-03-31/6h4hdz
On March 11, 2020, the World Health Organization declared the outbreak of coronavirus disease 2019 (COVID-19) a pandemic, leading to an abrupt widespread shift to teledermatology, with postponement of nonessential in-office medical and surgical services, according to American Academy of Dermatology (AAD) recommendations.1 Perspectives have been offered regarding skin cancer management during the pandemic2; however, the current literature is lacking guidance on skin cancer screening and prevention during the COVID-19 era.
Preliminary data show a 34.3% reduction in skin cancer referrals from February to April 2020 compared to the same period in 2019. The authors also presented a subsequent reduction in the number of skin cancer diagnoses in March 2020 compared to March 2019.3 Although the COVID-19 public health emergency should be prioritized by all health care workers, the duty to maintain disease prevention remains.
We aim to provide recommendations for this urgent topic. Our goal is finding balance in preventing an increase in the incidence of and mortality from skin cancer that results from delayed detection, while conserving personalprotective equipment and minimizing exposure, by patients and clinical personnel, to the severe acute respiratory syndrome coronavirus 2. A primary benefit of skin cancer screening lies in the ability to detect melanoma, which is associated with higher mortality than the more common nonmelanoma skin cancers, basal and cutaneous squamous cell carcinomas. We place preeminence on screening directed toward detecting melanoma. The main screening method that dermatologists employ is the total-body skin examination (TBSE). Another widely encouraged and utilized component in skin cancer prevention is patient education, emphasizing avoidance of risk factors, undertaking protective factors, and providing clear instructions for performing the patient-led skin self-examination (SSE).
Teledermatology Essentials for Skin Cancer Screening
Arguably, dermatology possesses the most potential for successfully utilizing telemedicine. Teledermatology has become widely implemented across the United States, secondary to the implications of the current pandemic. A report by Perkins and colleagues4 provided a positive outlook in the preliminary transition to teledermatology beginning in March 2020, though reported time of use was relatively short (3 weeks). A May 2020 article in Dermatology News provided tips for implementing telemedicine for practices.5
We agree with the comprehensive screening algorithm for teledermatology presented by Perkins and colleagues4 (Figure 1A in their report) and recommend the following for the screening and prevention of skin cancer:
• Patients with any characteristics of increased risk, including a personal or family history of melanoma, large congenital nevi, many melanotic nevi, dysplastic nevi, and Fitzpatrick skin types I and II,6 should be prioritized for an in-person visit for TBSE.
• Immunosuppressed patients, particularly organ transplant recipients and those with a history of skin cancer, should be prioritized for an in-person visit for TBSE.
• Established patients evaluated and determined to be at average risk for skin cancer should be offered a teledermatology visit. Suspicious findings during these visits should be prioritized for an in-person visit, with subsequent biopsy and follow-up.
• New patients should be offered a teledermatology visit.
These recommendations must be reviewed alongside each patient’s risk for travel and being present in person as well as other factors that might place the patient at increased risk for COVID-19.
Total-body skin examination, a widely used tool in the dermatologist’s tool kit, presents minimal risk to patients while providing important data for each dermatology patient’s profile, ultimately directing patient care. The role of TBSE in skin cancer screening and prevention has been in discussion even prior to the current pandemic. The US Preventive Services Task Force (USPSTF) has not declared a role for TBSE in recent years; however, USPSTF recommendations are formulated using data from all forms of screening, not only dermatologist-led interventions. Accordingly, USPSTF recommendations target primary care. The AAD has released statements addressing the role of TBSE and skin cancer prevention in the past, when necessary, to provide clarity.7
There is no clear definition of SSE or guidelines on how to educate a patient to perform regular SSE; however, the AAD provides patients with resources on how to perform an SSE.8 Just as dermatologists would provide education, advice, and guidance by directing patients to the AAD website for the SSE during an in-person visit, we encourage dermatologists to continue this practice during all teledermatology visits.
The role of teledermatology in skin cancer screening and prevention is limited; dermatologists will not be able to adequately perform TBSE as it would be done at in-person visits. Furthermore, the true implications of teledermatology compared to in-person visits during the COVID-19 pandemic have yet to be realized and analyzed. It is nonetheless important to appreciate that teledermatology holds great promise of benefit in skin cancer prevention, especially in the form of patient education by dermatologists. Practices in the realm of screening and prevention by health care professionals should be continually addressed during the pandemic; it is important to consider the implications associated with delays in diagnosis and treatment.
Teledermatology Limitations and Recommendations for High-Quality Visits
A benefit of video consultation (VC) vs telephone visits is visual interaction—the crux of dermatology. A 2019 study investigated VC experiences among providers and patients in the primary care setting. Benefits of VC were reported to include convenience for working patients and patients with mobility or mental health problems, visual cues, building rapport, and improving communication.9
Despite these benefits, VC is not without limitations. Many technical factors create variability in the quality of teledermatology VCs for a melanocytic lesion, including patient environment and lighting, color distortion, video resolution, and Internet connection. We make the following recommendations:
• Environment: Locate or create a dedicated space for teledermatology visits that is well lit, private, and has minimal background noise. Place the device on a level surface, center yourself in the frame, and keep the camera at eye level.
• Lighting: Use neutral lighting, placing the light source in front of you but behind the camera of the device. Avoid placing light sources, such as a window, behind you.
• Video resolution: Regardless of the type of camera (eg, integrated webcam, external camera), close out all other running software programs to optimize bandwidth during the visit.
• Internet connection: Use a wired connection (via an Ethernet cable) instead of a Wi-Fi connection to greatly decrease the chance of losing the connection during the visit. It also is faster than Wi-Fi.
• Addressing specific lesions: Patients should keep the device in place, repositioning themselves to show the lesions rather than moving the device by hand.
• Video capacity: Test your device’s video capacity beforehand, which can be as simple as video-calling a family member or friend from your designated space. Feedback regarding video and audio quality will help fine-tune your setup.
• Instructions to the patient: Provide clear instructions to the patient when photographs of specific lesions are needed for further review. Specify what view(s) you need and whether size or bilateral comparison is needed. A web post by VisualDx10 provides advice to patients on taking high-quality photographs.
Final Thoughts
Teledermatology indubitably presents a learning curve for dermatologists and patients. As with other technological advances in society, we are optimistic that, first, the confidence level in teledermatology use will increase, and, second, evidence-based data will pave the way to enhance this experience. We realize the inherent limitation of accessibility to certain technologies, which is regrettably far from equitable. Patients need a personal device equipped with audio and video; access to a high-quality Internet connection; some degree of technological literacy; and a quiet private location.
We hope to learn from all experiences during the current pandemic. Future innovation in teledermatology and in telemedicine generally should aim to address technological inequities to allow for the delivery of quality care to as many patients as possible.
On March 11, 2020, the World Health Organization declared the outbreak of coronavirus disease 2019 (COVID-19) a pandemic, leading to an abrupt widespread shift to teledermatology, with postponement of nonessential in-office medical and surgical services, according to American Academy of Dermatology (AAD) recommendations.1 Perspectives have been offered regarding skin cancer management during the pandemic2; however, the current literature is lacking guidance on skin cancer screening and prevention during the COVID-19 era.
Preliminary data show a 34.3% reduction in skin cancer referrals from February to April 2020 compared to the same period in 2019. The authors also presented a subsequent reduction in the number of skin cancer diagnoses in March 2020 compared to March 2019.3 Although the COVID-19 public health emergency should be prioritized by all health care workers, the duty to maintain disease prevention remains.
We aim to provide recommendations for this urgent topic. Our goal is finding balance in preventing an increase in the incidence of and mortality from skin cancer that results from delayed detection, while conserving personalprotective equipment and minimizing exposure, by patients and clinical personnel, to the severe acute respiratory syndrome coronavirus 2. A primary benefit of skin cancer screening lies in the ability to detect melanoma, which is associated with higher mortality than the more common nonmelanoma skin cancers, basal and cutaneous squamous cell carcinomas. We place preeminence on screening directed toward detecting melanoma. The main screening method that dermatologists employ is the total-body skin examination (TBSE). Another widely encouraged and utilized component in skin cancer prevention is patient education, emphasizing avoidance of risk factors, undertaking protective factors, and providing clear instructions for performing the patient-led skin self-examination (SSE).
Teledermatology Essentials for Skin Cancer Screening
Arguably, dermatology possesses the most potential for successfully utilizing telemedicine. Teledermatology has become widely implemented across the United States, secondary to the implications of the current pandemic. A report by Perkins and colleagues4 provided a positive outlook in the preliminary transition to teledermatology beginning in March 2020, though reported time of use was relatively short (3 weeks). A May 2020 article in Dermatology News provided tips for implementing telemedicine for practices.5
We agree with the comprehensive screening algorithm for teledermatology presented by Perkins and colleagues4 (Figure 1A in their report) and recommend the following for the screening and prevention of skin cancer:
• Patients with any characteristics of increased risk, including a personal or family history of melanoma, large congenital nevi, many melanotic nevi, dysplastic nevi, and Fitzpatrick skin types I and II,6 should be prioritized for an in-person visit for TBSE.
• Immunosuppressed patients, particularly organ transplant recipients and those with a history of skin cancer, should be prioritized for an in-person visit for TBSE.
• Established patients evaluated and determined to be at average risk for skin cancer should be offered a teledermatology visit. Suspicious findings during these visits should be prioritized for an in-person visit, with subsequent biopsy and follow-up.
• New patients should be offered a teledermatology visit.
These recommendations must be reviewed alongside each patient’s risk for travel and being present in person as well as other factors that might place the patient at increased risk for COVID-19.
Total-body skin examination, a widely used tool in the dermatologist’s tool kit, presents minimal risk to patients while providing important data for each dermatology patient’s profile, ultimately directing patient care. The role of TBSE in skin cancer screening and prevention has been in discussion even prior to the current pandemic. The US Preventive Services Task Force (USPSTF) has not declared a role for TBSE in recent years; however, USPSTF recommendations are formulated using data from all forms of screening, not only dermatologist-led interventions. Accordingly, USPSTF recommendations target primary care. The AAD has released statements addressing the role of TBSE and skin cancer prevention in the past, when necessary, to provide clarity.7
There is no clear definition of SSE or guidelines on how to educate a patient to perform regular SSE; however, the AAD provides patients with resources on how to perform an SSE.8 Just as dermatologists would provide education, advice, and guidance by directing patients to the AAD website for the SSE during an in-person visit, we encourage dermatologists to continue this practice during all teledermatology visits.
The role of teledermatology in skin cancer screening and prevention is limited; dermatologists will not be able to adequately perform TBSE as it would be done at in-person visits. Furthermore, the true implications of teledermatology compared to in-person visits during the COVID-19 pandemic have yet to be realized and analyzed. It is nonetheless important to appreciate that teledermatology holds great promise of benefit in skin cancer prevention, especially in the form of patient education by dermatologists. Practices in the realm of screening and prevention by health care professionals should be continually addressed during the pandemic; it is important to consider the implications associated with delays in diagnosis and treatment.
Teledermatology Limitations and Recommendations for High-Quality Visits
A benefit of video consultation (VC) vs telephone visits is visual interaction—the crux of dermatology. A 2019 study investigated VC experiences among providers and patients in the primary care setting. Benefits of VC were reported to include convenience for working patients and patients with mobility or mental health problems, visual cues, building rapport, and improving communication.9
Despite these benefits, VC is not without limitations. Many technical factors create variability in the quality of teledermatology VCs for a melanocytic lesion, including patient environment and lighting, color distortion, video resolution, and Internet connection. We make the following recommendations:
• Environment: Locate or create a dedicated space for teledermatology visits that is well lit, private, and has minimal background noise. Place the device on a level surface, center yourself in the frame, and keep the camera at eye level.
• Lighting: Use neutral lighting, placing the light source in front of you but behind the camera of the device. Avoid placing light sources, such as a window, behind you.
• Video resolution: Regardless of the type of camera (eg, integrated webcam, external camera), close out all other running software programs to optimize bandwidth during the visit.
• Internet connection: Use a wired connection (via an Ethernet cable) instead of a Wi-Fi connection to greatly decrease the chance of losing the connection during the visit. It also is faster than Wi-Fi.
• Addressing specific lesions: Patients should keep the device in place, repositioning themselves to show the lesions rather than moving the device by hand.
• Video capacity: Test your device’s video capacity beforehand, which can be as simple as video-calling a family member or friend from your designated space. Feedback regarding video and audio quality will help fine-tune your setup.
• Instructions to the patient: Provide clear instructions to the patient when photographs of specific lesions are needed for further review. Specify what view(s) you need and whether size or bilateral comparison is needed. A web post by VisualDx10 provides advice to patients on taking high-quality photographs.
Final Thoughts
Teledermatology indubitably presents a learning curve for dermatologists and patients. As with other technological advances in society, we are optimistic that, first, the confidence level in teledermatology use will increase, and, second, evidence-based data will pave the way to enhance this experience. We realize the inherent limitation of accessibility to certain technologies, which is regrettably far from equitable. Patients need a personal device equipped with audio and video; access to a high-quality Internet connection; some degree of technological literacy; and a quiet private location.
We hope to learn from all experiences during the current pandemic. Future innovation in teledermatology and in telemedicine generally should aim to address technological inequities to allow for the delivery of quality care to as many patients as possible.
- American Academy of Dermatology. Everyday health and preparedness steps in clinic Updated April 4, 2020. Accessed December 17, 2020. https://assets.ctfassets.net/1ny4yoiyrqia/4LNCNjucOonbQx7aC970x/b56b540957ddad94dcc61949b8e3acc9/COVID-19_Preparedness_30Apr2020.pdf
- Geskin LJ, Trager MH, Aasi SZ, et al. Perspectives on the recommendations for skin cancer management during the COVID-19 pandemic. J Am Acad Dermatol. 2020;83:295-296.
- Earnshaw CH, Hunter HJA, McMullen E, et al. Reduction in skin cancer diagnosis, and overall cancer referrals, during the COVID-19 pandemic. Br J Dermatol. 2020;183:792-794.
- Perkins S, Cohen JM, Nelson CA, et al. Teledermatology in the era of COVID-19: experience of an academic department of dermatology. J Am Acad Dermatol. 2020;83:E43-E44.
- Marina F. COVID-19: telehealth at the forefront of the pandemic. Dermatology News. May 12, 2020. Accessed December 17, 2020. www.mdedge.com/dermatology/article/222089/coronavirus-updates/covid-19-telehealth-forefront-pandemic?channel=52
- Watts CG, Dieng M, Morton RL, et al. Clinical practice guidelines for identification, screening and follow-up of individuals at high risk of primary cutaneous melanoma: a systematic review. Br J Dermatol. 2015;172:33-47.
- Rosamilia LL. “Doctor, do I need a skin check?” Cutis. 2019;103:290-291.
- Detect skin cancer: how to perform a skin self-exam. American Academy of Dermatology. Accessed December 17, 2020. www.aad.org/public/diseases/skin-cancer/find/check-skin
- Donaghy E, Atherton H, Hammersley V, et al. Acceptability, benefits, and challenges of video consulting: a qualitative study in primary care. Br J Gen Pract. 2019;69:E586-E594.
- How to take the best photos for teledermatology. VisualDx. Accessed December 17, 2020. https://info.visualdx.com/l/11412/2020-03-31/6h4hdz
- American Academy of Dermatology. Everyday health and preparedness steps in clinic Updated April 4, 2020. Accessed December 17, 2020. https://assets.ctfassets.net/1ny4yoiyrqia/4LNCNjucOonbQx7aC970x/b56b540957ddad94dcc61949b8e3acc9/COVID-19_Preparedness_30Apr2020.pdf
- Geskin LJ, Trager MH, Aasi SZ, et al. Perspectives on the recommendations for skin cancer management during the COVID-19 pandemic. J Am Acad Dermatol. 2020;83:295-296.
- Earnshaw CH, Hunter HJA, McMullen E, et al. Reduction in skin cancer diagnosis, and overall cancer referrals, during the COVID-19 pandemic. Br J Dermatol. 2020;183:792-794.
- Perkins S, Cohen JM, Nelson CA, et al. Teledermatology in the era of COVID-19: experience of an academic department of dermatology. J Am Acad Dermatol. 2020;83:E43-E44.
- Marina F. COVID-19: telehealth at the forefront of the pandemic. Dermatology News. May 12, 2020. Accessed December 17, 2020. www.mdedge.com/dermatology/article/222089/coronavirus-updates/covid-19-telehealth-forefront-pandemic?channel=52
- Watts CG, Dieng M, Morton RL, et al. Clinical practice guidelines for identification, screening and follow-up of individuals at high risk of primary cutaneous melanoma: a systematic review. Br J Dermatol. 2015;172:33-47.
- Rosamilia LL. “Doctor, do I need a skin check?” Cutis. 2019;103:290-291.
- Detect skin cancer: how to perform a skin self-exam. American Academy of Dermatology. Accessed December 17, 2020. www.aad.org/public/diseases/skin-cancer/find/check-skin
- Donaghy E, Atherton H, Hammersley V, et al. Acceptability, benefits, and challenges of video consulting: a qualitative study in primary care. Br J Gen Pract. 2019;69:E586-E594.
- How to take the best photos for teledermatology. VisualDx. Accessed December 17, 2020. https://info.visualdx.com/l/11412/2020-03-31/6h4hdz
Practice Points
- It is important for dermatologists to maintain skin cancer screening and prevention efforts during the coronavirus disease 2019 pandemic.
- Patient populations at increased risk for skin cancer should be prioritized for in-person evaluations, but teledermatology should be considered for initial examination in new patients and patients at average risk for skin cancer.
- Teledermatology presents a learning curve for dermatologists and patients, but the confidence level will increase, and evidence-based data will pave the way to enhance this experience.
