User login
ONLINE EXCLUSIVE: Listen to Martin Buser and Bryce Gartland discuss directors' impact on HM program success
Click here to listen to Martin Buser
Click here to listen to Dr. Gartland
Click here to listen to Martin Buser
Click here to listen to Dr. Gartland
Click here to listen to Martin Buser
Click here to listen to Dr. Gartland
ONLINE EXCLUSIVE: Listen to Lauren Doctoroff discuss BIDMC’s postdischarge clinic
Click here to listen to Dr. Doctoroff
Click here to listen to Dr. Doctoroff
Click here to listen to Dr. Doctoroff
ONLINE EXCLUSIVE: Listen to CDC expert Carolyn Gould and Emory hospitalist Ketino Kobaidze discuss C. diff prevention
Click here to listen to Dr. Gould
Click here to listen to Dr. Kobaidze
Click here to listen to Dr. Gould
Click here to listen to Dr. Kobaidze
Click here to listen to Dr. Gould
Click here to listen to Dr. Kobaidze
Gut Reaction
At 480-bed Emory University Hospital Midtown in Atlanta, the physicians and staff seemingly are doing all the right things to foil one of hospital’s archenemies: Clostridium difficile. The bacteria, better known as C. diff, is responsible for a sharp rise in hospital-acquired infections over the past decade, rivaling even MRSA.
In 2010, Emory Midtown launched a campaign to boost awareness of the importance of hand washing before and after treating patients infected with C. diff and those likely to be infected. They also began using the polymerase-chain-reaction-based assay to detect the bacteria, a test with much higher sensitivity that helps to more efficiently identify those infected so control measures can be more prompt and targeted. They use a hypochlorite mixture to clean the rooms of those infected, which is considered a must. And a committee monitors the use of antibiotics to prevent overuse—often the scapegoat for the rise of the hard-to-kill bacteria.
Still, at Emory, the rate of C. diff is about the same as the national average, says hospitalist Ketino Kobaidze, MD, assistant professor at the Emory University School of Medicine and a member of the antimicrobial stewardship and infectious disease control committees at Midtown. While Dr. Kobaidze says her institution is doing a good job of trying to keep C. diff under control, she thinks hospitalists can do more.
“My feeling is that we are not as involved as we’re supposed to be,” she says. “I think we need to be a little bit more proactive, be involved in committees and research activities across the hospital.”
—Kevin Kavanagh, MD, founder, Health Watch USA
You Are Not Alone
The experience at Emory Midtown is far from unusual—healthcare facilities, and hospitalists, across the country have seen healthcare-related C. diff cases more than double since 2001 to between 400,000 and 500,000 a year, says Carolyn Gould, MD, a medical epidemiologist in the division of healthcare quality promotion at the Centers for Disease Control and Prevention (CDC) in Atlanta.
Hospitalists, whether they realize it or not, are intimately involved in how well the C. diff outbreak is controlled. Infectious-disease (ID) specialists say hospitalists are perfectly situated to make an impact in efforts to help curb the outbreak.
“Hospitalists are critical to this effort,” Dr. Gould says. “They’re in the hospital day in and day out, and they’re constantly interacting with the patients, staff, and administration. They’re often the first on the scene to see a patient who might have suddenly developed diarrhea; they’re the first to react. I think they’re in a prime position to play a leadership role to prevent C. diff infections.”
They’re also situated well to work with infection-control experts on antimicrobial stewardship programs, she says.
“I look at hospitalists just like I would have looked at internists managing their own patients 15 years ago,” says Stuart Cohen, MD, an ID expert with the University of California at Davis and a fellow with the Infectious Diseases Society of America who was lead author of the latest published IDSA guidelines on C. diff treatment. “And so they’re the first-line people.”
continued below...
Mayo Shows How a Simple Step Can Make Big Difference in C. Diff

Sometimes even when it comes to a huge problem like widespread bacterial infections, simplicity is best.
The Mayo Clinic, in a project to cut the rate of C. diff infections, asked its workers to do one extra thing: Wipe down high-touch areas with bleach wipes. The effort worked; infections were all but eradicated in units that had been having five to seven infections per month.
The results of the project, recently published in Infectious Control and Hospital Epidemiology, show the importance of simple steps as long as they’re carried out regularly and thoroughly.1
The project began when Robert Orenstein, DO, associate professor of medicine in infectious diseases who then worked in Rochester, Minn., established a surveillance network for C. diff infections at Mayo Clinic at the time when such infections were being noted more widely throughout the U.S. and Canada. The network began tracking the cases and found that one inpatient medical unit primarily composed of patients with gastrointestinal diseases had a C. diff rate 10 times higher than the rest of the hospital. Surveillance also showed that universally gloved hematology and oncology units had substantially lower rates of C. diff infection despite high-risk patients.
Dr. Orenstein knew he had to make a change in the GI unit, but it wasn’t feasible to institute universal gloving, so he turned to bleach wipes.

Twice a day, housekeeping staff wiped down all “high-touch” areas (light switches, toilet handles, bed rails) in all of the rooms. The wipes contain 0.55% sodium hypochlorite. Within six months, the number of C. diff cases fell to almost zero.
“We were just in shock,” Dr. Orenstein says. He attributed the improvement to a reduction in the “colonization pressure”—if a high concentration of patients with C. diff can cause abundant transmissions quickly, the opposite is also true.
The greatly improved figures were shared with housekeeping, which initially complained about the smell but were encouraged to keep doors open and rooms ventilated. The bleach wipes, which Dr. Orenstein acknowledges mean an additional expense, leave a white residue when dry, so the surfaces are wiped down with water after the recommended contact time.
Dr. Orenstein notes that the results came even without a change in hand hygiene, which he had deemed not feasible because of the hospital’s lack of sinks. He isn’t diminishing the importance of hand washing, but the project does show how effective a single step can be.
The key, Dr. Orenstein adds, might be that it was just one change involving just one group of staff. “Why we think it was so effective is it was really one group that had to change their behavior and we worked with them, educated them,” he says.
He emphasizes that the wipes don’t come at the expense of other measures, like thorough cleaning of all rooms and antibiotic stewardship programs.
“You do all of those and do them well,” he says, “then you get the reduction of C. diff in the hospital.”
A Tough Bug
Believed to be aided largely by the use of broad-spectrum antibiotics that knock out the colon’s natural flora, C. diff in the hospital—as well as nursing homes and acute-care facilities—has raged for much of the past decade. Its rise is tied to the emergence of a new hypervirulent strain known as BI/NAP1/027, or NAP1 for short. The strain is highly resistant to fluoroquinolones, such as ciprofloxacin and levofloxacin, which are used often in healthcare settings.
“A fluoroquinolone will wipe out a lot of your normal flora in your gut,” Dr. Gould says. “But it won’t wipe out C. diff, in particular this hypervirulent strain. And so this strain can flourish in the presence of fluoroquinolones.” The strain produces up to 15 to 20 times more toxins than other C. diff strains, according to some data, she adds.
Vancomycin (Vanconin) and metronidazole (Flagyl) are the most common antibiotics used to treat patients infected with C. diff. Mortality rates are higher among the elderly, largely because of their weaker immune system, Dr. Gould says. Studies have generally shown mortality rates of 10% or a bit lower.1
More recent studies have shown that the number of hospital-related C. diff cases might have begun to level off in 2008 and 2009. Dr. Gould says she thinks the leveling off is for real, but there is debate over what the immediate future holds.
“There’s a lot of work and initiatives, especially state-based initiatives, that are being done in hospitals. And there’s reason to believe they’re effective,” she says, adding it’s harder to get a good picture of the problem in long-term care facilities and in the community.
Dr. Cohen with the IDSA says it’s too soon to say whether the problem is hitting a plateau. “CDC data are always a couple of years behind,” he says. “Until you see another data point, you can’t tell whether that’s just a transient flattening and whether it’s going to keep going up or not.”
Kevin Kavanagh, MD, founder of the patient advocacy group Health Watch USA and a retired otolaryngologist in Kentucky who has taken a keen interest in the C. diff problem, says he doesn’t think the end of the tunnel is within view yet.
“I think C. diff is going to get worse before it gets better,” Dr. Kavanagh says. “And that’s not necessarily because the healthcare profession isn’t doing due diligence. This is a tough organism.—it can be tough to treat and can be very tough to kill.”
The Best Defense?
Because C. diff lives within protective spores, sound hand hygiene practices and room-cleaning practices are essential for keeping infections to a minimum. Alcohol-based hand sanitizers, effective against other organisms including MRSA, do not kill C. diff. The bacteria must be mechanically removed through hand washing.
And even hand washing might not be totally effective at getting rid of the spores, which means it’s important for healthcare workers to gown and glove in high-risk rooms.
Sodium hypochlorite solutions, or bleach mixtures, have to be used to clean rooms occupied by patients with C. diff, and the prevailing thought is to clean the rooms of patients suspected of having C. diff, even if those cases might not be confirmed.
Equally important to cleaning and hand washing is systemwide emphasis on antibiotic stewardship. A 2011 study at the State University of New York Buffalo found that the risk of a C. diff infection rose with the number of antibiotics taken.2

—Carolyn Gould, MD, medical epidemiologist, division of healthcare quality promotion, Centers of Disease Control and Prevention, Atlanta
While a broad-spectrum antibiotic might be necessary at first, once the results of cultures are received, the treatment should be finely tailored to kill only the problem bacteria so that the body’s natural defenses aren’t broken down, Dr. Gould explains.
“If someone is very sick and you’re not sure what is going on, it’s very reasonable to treat them empirically with broad-spectrum antibiotics,” she says. “The important thing is that you send the appropriate cultures before so that you know what you’re treating and you can optimize those antibiotics with daily assessments.”

It’s clear why an overreliance on broad-spectrum drugs prevails in U.S. health settings, Dr. Cohen acknowledges. Recent literature suggests treating critically ill patients with wide-ranging antimicrobials as the mortality rate can be twice as high with narrower options. “I think people have gotten very quick to give broad-spectrum therapy,” he says.
continued below...
Knocking Out Clostridium Difficile

Here are the guidelines on treatment of C. diff infections (CDI) as recommended by the Infectious Diseases Society of America:
First steps:
- Discontinue therapy with the inciting antimicrobial agent(s) as soon as possible as this may influence the risk of CDI recurrence.
- When severe or complicated CDI is suspected, initiate empirical treatment as soon as the diagnosis is suspected.
- If the stool toxin assay result is negative, the decision to initiate, stop, or continue treatment must be individualized.
- If possible, avoid use of antiperistaltic agents as they may obscure symptoms and precipitate toxic megacolon.
Treatment of initial episode:
- Metronidazole is the drug of choice for the initial episode of mild to moderate CDI. The dosage is 500 mg orally three times per day for 10 to 14 days.
- Vancomycin is the drug of choice for an initial episode of severe CDI. The dosage is 125 mg orally four times per day for 10 to 14 days.
- Vancomycin administered orally (and per rectum if ileus is present) with or without intravenously administered metronidazole is the regimen of choice for the treatment of severe complicated CDI. The vancomycin dosage is 500 mg orally four times per day and 500 mg in approximately 100 mL normal saline per rectum every six hours as a retention enema, and the metronidazole dosage is 500 mg intravenously every eight hours.
Severely ill patients:
Consider colectomy for severely ill patients. Monitoring the serum lactate level and the peripheral blood white blood cell count may be helpful in prompting a decision to operate because a serum lactate level rising to 5 mmol/L and a white blood cell count rising to 50,000 cells per mL have been associated with greatly increased perioperative mortality. If surgical management is necessary, perform subtotal colectomy with preservation of the rectum.
Treatment of recurrences:
- Treatment of the first recurrence of CDI is usually with the same regimen as for the initial episode but should be stratified by disease severity (mild-to-moderate, severe, or severe complicated) as is recommended for treatment of the initial CDI episode.
- Do not use metronidazole beyond the first recurrence of CDI or for long-term chronic therapy because of potential for cumulative neurotoxicity.
- Treatment of the second or later recurrence of CDI with vancomycin therapy using a tapered and/or pulse regimen is the preferred next strategy.
Probiotics:
Administration of currently available probiotics is not recommended to prevent primary CDI as there are limited data to support this approach and there is a potential risk of bloodstream infection.
Source: Cohen SH, Gerding DH, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infection Control and Hospital Epidemiology. 2010;31(5):431–455.
National Response, Localized Attention
Dr. Kavanagh of Health Watch USA says that more information about C. diff is needed, particularly publicly available numbers of infections at hospitals. Some states require those figures to be reported, but most don’t. And there is no current federal mandate on reporting of C. diff cases, although acute-care hospitals will be required to report C. diff infection rates starting in 2013.
“We really have scant data,” he says. “There is not a lot of reporting if you look at the nation on a whole. And I think that underscores one of the reasons why you need to have data for action. You need to have reporting of these organisms to the National Healthcare Safety Network so that the CDC can monitor and can make plans and can do effective interventions.
“You want to know where the areas of highest infection are,” he adds. “You want to know what interventions work and don’t work. If you don’t have a national coordinated reporting system, it really makes it difficult to address the problem. C. diff is going to be much harder to control than MRSA or other bacteria because it changes into a hard-to-kill dormant spore stage and then re-occurs at some point.”
The Centers for Medicare & Medicaid Services (CMS) has proposed adding C. diff infections to the list of hospital-acquired conditions that will not be reimbursable. It is widely hoped that such a measure will go a long way toward stamping out the problem.
Dr. Kobaidze of Emory notes that C. diff is a dynamic problem, always adapting and posing new challenges. And hospitalists should be more involved in answering these questions through research. One recent question, she points out, is whether proton pump inhibitor use is related to the rise of C. diff.
Ultimately, though, controlling C. diff in hospitals might come down to what is done day to day inside the hospital. And hospitalists can play a big role.
Danielle Scheurer, MD, MSCR, SFHM, a hospitalist and medical director of quality at the Medical University of South Carolina in Charleston, says that a full-time pharmacist on the hospital’s antimicrobial stewardship committee is always reviewing antibiotic prescriptions and is prepared to flag cases in which a broad-spectrum is used when one with a more narrow scope might be more appropriate.
The hospital has done its best, as part of its “renovation cycle,” to standardize the layouts of rooms “so that the second you open the door you know exactly where the alcohol gel is and where the soap and the sink is going to be.” The idea is to make compliance as “mindless” as possible. Such efforts can be hampered by structural limitations though, she says.
HM group leaders, she suggests, can play an important part simply by being good role models—gowning and gloving without complaint before entering high-risk rooms and reinforcing the message that such efforts have real effects on patient safety.
But she also acknowledges that “it always sounds easy....There has to be some level of redundancy built into the hospital system. This is more of a system thing than the individual hospitalist.”
One level of redundancy at MUSC that has been particularly effective, she says, are “secret shoppers” who keep an eye out for medical teams that might not be washing their hands as they go in and out of high-risk rooms. Each unit is responsible for their hand hygiene numbers—which include both self-reported figures and those obtained by the secret onlookers—and those numbers are made available to the hospital.
Those units with the best numbers are sometimes given a reward, such as a pizza party, but it’s colleagues’ knowledge of the numbers that matters most, she says.
“That, in and of itself, is a powerful motivator,” Dr. Scheurer says. “We bring it to all of our quality operations meetings, all the administrators, the CEO, the CMO. It’s very motivating for every unit. They don’t want to be the trailing unit.”
Tom Collins is a freelance medical writer based in Miami.
References
- Orenstein R, Aronhalt KC, McManus JE Jr., Fedraw LA. A targeted strategy to wipe out Clostridium difficile. Infect Control Hosp Epidemiol. 2011;32(11):1137-1139.
- Stevens V, Dumyati G, Fine LS, Fisher SG, van Wijngaarden E. Cumulative antibiotic exposures over time and the risk of Clostridium difficile infection. Clin Infect Dis. 2011;53(1):42-48.
What Hospitalists Can Do

Here are suggestions, as provided by ID experts and hospitalist leaders, on what hospitalists can do to battle C. diff infections:
Short-term steps:
- Wash hands before entering and upon leaving rooms occupied by patients with C. diff infections and those strongly suspected of having C. diff infections.
- Continue using alcohol-based hand sanitizers in addition to hand washing to prevent other types of outbreaks.
- Ensure that infected patients, and those suspected of being infected, are isolated, possibly even for 48 hours after diarrhea resolves, as research shows the patients can still transmit the spores.
- In units with high C. diff rates, consider universal gloving, not just for patients with known infection.
- Use more highly sensitive tests, such as polymerase chain reaction, or PCR, rather than enzyme immunoassays to more efficiently identify affected patients.
- Avoid testing patients with formed stools.
- Ensure that rooms of infected patients and patients strongly suspected of being infected are cleaned with a hypochlorite solution.
- Taper the use of broad-spectrum antibiotics in non-C. diff patients after test results are obtained.
- Encourage patients to question their healthcare practitioners about hand hygiene and use of antibiotics.
Long-term steps:
- Be involved with your hospital’s antimicrobial stewardship program.
- Conduct research into C. diff to explore its causes and treatments.
- Be a good role model for the rest of your group, emphasizing good practices and a strong patient-safety message.
At 480-bed Emory University Hospital Midtown in Atlanta, the physicians and staff seemingly are doing all the right things to foil one of hospital’s archenemies: Clostridium difficile. The bacteria, better known as C. diff, is responsible for a sharp rise in hospital-acquired infections over the past decade, rivaling even MRSA.
In 2010, Emory Midtown launched a campaign to boost awareness of the importance of hand washing before and after treating patients infected with C. diff and those likely to be infected. They also began using the polymerase-chain-reaction-based assay to detect the bacteria, a test with much higher sensitivity that helps to more efficiently identify those infected so control measures can be more prompt and targeted. They use a hypochlorite mixture to clean the rooms of those infected, which is considered a must. And a committee monitors the use of antibiotics to prevent overuse—often the scapegoat for the rise of the hard-to-kill bacteria.
Still, at Emory, the rate of C. diff is about the same as the national average, says hospitalist Ketino Kobaidze, MD, assistant professor at the Emory University School of Medicine and a member of the antimicrobial stewardship and infectious disease control committees at Midtown. While Dr. Kobaidze says her institution is doing a good job of trying to keep C. diff under control, she thinks hospitalists can do more.
“My feeling is that we are not as involved as we’re supposed to be,” she says. “I think we need to be a little bit more proactive, be involved in committees and research activities across the hospital.”
—Kevin Kavanagh, MD, founder, Health Watch USA
You Are Not Alone
The experience at Emory Midtown is far from unusual—healthcare facilities, and hospitalists, across the country have seen healthcare-related C. diff cases more than double since 2001 to between 400,000 and 500,000 a year, says Carolyn Gould, MD, a medical epidemiologist in the division of healthcare quality promotion at the Centers for Disease Control and Prevention (CDC) in Atlanta.
Hospitalists, whether they realize it or not, are intimately involved in how well the C. diff outbreak is controlled. Infectious-disease (ID) specialists say hospitalists are perfectly situated to make an impact in efforts to help curb the outbreak.
“Hospitalists are critical to this effort,” Dr. Gould says. “They’re in the hospital day in and day out, and they’re constantly interacting with the patients, staff, and administration. They’re often the first on the scene to see a patient who might have suddenly developed diarrhea; they’re the first to react. I think they’re in a prime position to play a leadership role to prevent C. diff infections.”
They’re also situated well to work with infection-control experts on antimicrobial stewardship programs, she says.
“I look at hospitalists just like I would have looked at internists managing their own patients 15 years ago,” says Stuart Cohen, MD, an ID expert with the University of California at Davis and a fellow with the Infectious Diseases Society of America who was lead author of the latest published IDSA guidelines on C. diff treatment. “And so they’re the first-line people.”
continued below...
Mayo Shows How a Simple Step Can Make Big Difference in C. Diff
Sometimes even when it comes to a huge problem like widespread bacterial infections, simplicity is best.
The Mayo Clinic, in a project to cut the rate of C. diff infections, asked its workers to do one extra thing: Wipe down high-touch areas with bleach wipes. The effort worked; infections were all but eradicated in units that had been having five to seven infections per month.
The results of the project, recently published in Infectious Control and Hospital Epidemiology, show the importance of simple steps as long as they’re carried out regularly and thoroughly.1
The project began when Robert Orenstein, DO, associate professor of medicine in infectious diseases who then worked in Rochester, Minn., established a surveillance network for C. diff infections at Mayo Clinic at the time when such infections were being noted more widely throughout the U.S. and Canada. The network began tracking the cases and found that one inpatient medical unit primarily composed of patients with gastrointestinal diseases had a C. diff rate 10 times higher than the rest of the hospital. Surveillance also showed that universally gloved hematology and oncology units had substantially lower rates of C. diff infection despite high-risk patients.
Dr. Orenstein knew he had to make a change in the GI unit, but it wasn’t feasible to institute universal gloving, so he turned to bleach wipes.
Twice a day, housekeeping staff wiped down all “high-touch” areas (light switches, toilet handles, bed rails) in all of the rooms. The wipes contain 0.55% sodium hypochlorite. Within six months, the number of C. diff cases fell to almost zero.
“We were just in shock,” Dr. Orenstein says. He attributed the improvement to a reduction in the “colonization pressure”—if a high concentration of patients with C. diff can cause abundant transmissions quickly, the opposite is also true.
The greatly improved figures were shared with housekeeping, which initially complained about the smell but were encouraged to keep doors open and rooms ventilated. The bleach wipes, which Dr. Orenstein acknowledges mean an additional expense, leave a white residue when dry, so the surfaces are wiped down with water after the recommended contact time.
Dr. Orenstein notes that the results came even without a change in hand hygiene, which he had deemed not feasible because of the hospital’s lack of sinks. He isn’t diminishing the importance of hand washing, but the project does show how effective a single step can be.
The key, Dr. Orenstein adds, might be that it was just one change involving just one group of staff. “Why we think it was so effective is it was really one group that had to change their behavior and we worked with them, educated them,” he says.
He emphasizes that the wipes don’t come at the expense of other measures, like thorough cleaning of all rooms and antibiotic stewardship programs.
“You do all of those and do them well,” he says, “then you get the reduction of C. diff in the hospital.”
A Tough Bug
Believed to be aided largely by the use of broad-spectrum antibiotics that knock out the colon’s natural flora, C. diff in the hospital—as well as nursing homes and acute-care facilities—has raged for much of the past decade. Its rise is tied to the emergence of a new hypervirulent strain known as BI/NAP1/027, or NAP1 for short. The strain is highly resistant to fluoroquinolones, such as ciprofloxacin and levofloxacin, which are used often in healthcare settings.
“A fluoroquinolone will wipe out a lot of your normal flora in your gut,” Dr. Gould says. “But it won’t wipe out C. diff, in particular this hypervirulent strain. And so this strain can flourish in the presence of fluoroquinolones.” The strain produces up to 15 to 20 times more toxins than other C. diff strains, according to some data, she adds.
Vancomycin (Vanconin) and metronidazole (Flagyl) are the most common antibiotics used to treat patients infected with C. diff. Mortality rates are higher among the elderly, largely because of their weaker immune system, Dr. Gould says. Studies have generally shown mortality rates of 10% or a bit lower.1
More recent studies have shown that the number of hospital-related C. diff cases might have begun to level off in 2008 and 2009. Dr. Gould says she thinks the leveling off is for real, but there is debate over what the immediate future holds.
“There’s a lot of work and initiatives, especially state-based initiatives, that are being done in hospitals. And there’s reason to believe they’re effective,” she says, adding it’s harder to get a good picture of the problem in long-term care facilities and in the community.
Dr. Cohen with the IDSA says it’s too soon to say whether the problem is hitting a plateau. “CDC data are always a couple of years behind,” he says. “Until you see another data point, you can’t tell whether that’s just a transient flattening and whether it’s going to keep going up or not.”
Kevin Kavanagh, MD, founder of the patient advocacy group Health Watch USA and a retired otolaryngologist in Kentucky who has taken a keen interest in the C. diff problem, says he doesn’t think the end of the tunnel is within view yet.
“I think C. diff is going to get worse before it gets better,” Dr. Kavanagh says. “And that’s not necessarily because the healthcare profession isn’t doing due diligence. This is a tough organism.—it can be tough to treat and can be very tough to kill.”
The Best Defense?
Because C. diff lives within protective spores, sound hand hygiene practices and room-cleaning practices are essential for keeping infections to a minimum. Alcohol-based hand sanitizers, effective against other organisms including MRSA, do not kill C. diff. The bacteria must be mechanically removed through hand washing.
And even hand washing might not be totally effective at getting rid of the spores, which means it’s important for healthcare workers to gown and glove in high-risk rooms.
Sodium hypochlorite solutions, or bleach mixtures, have to be used to clean rooms occupied by patients with C. diff, and the prevailing thought is to clean the rooms of patients suspected of having C. diff, even if those cases might not be confirmed.
Equally important to cleaning and hand washing is systemwide emphasis on antibiotic stewardship. A 2011 study at the State University of New York Buffalo found that the risk of a C. diff infection rose with the number of antibiotics taken.2
—Carolyn Gould, MD, medical epidemiologist, division of healthcare quality promotion, Centers of Disease Control and Prevention, Atlanta
While a broad-spectrum antibiotic might be necessary at first, once the results of cultures are received, the treatment should be finely tailored to kill only the problem bacteria so that the body’s natural defenses aren’t broken down, Dr. Gould explains.
“If someone is very sick and you’re not sure what is going on, it’s very reasonable to treat them empirically with broad-spectrum antibiotics,” she says. “The important thing is that you send the appropriate cultures before so that you know what you’re treating and you can optimize those antibiotics with daily assessments.”
It’s clear why an overreliance on broad-spectrum drugs prevails in U.S. health settings, Dr. Cohen acknowledges. Recent literature suggests treating critically ill patients with wide-ranging antimicrobials as the mortality rate can be twice as high with narrower options. “I think people have gotten very quick to give broad-spectrum therapy,” he says.
continued below...
Knocking Out Clostridium Difficile
Here are the guidelines on treatment of C. diff infections (CDI) as recommended by the Infectious Diseases Society of America:
First steps:
- Discontinue therapy with the inciting antimicrobial agent(s) as soon as possible as this may influence the risk of CDI recurrence.
- When severe or complicated CDI is suspected, initiate empirical treatment as soon as the diagnosis is suspected.
- If the stool toxin assay result is negative, the decision to initiate, stop, or continue treatment must be individualized.
- If possible, avoid use of antiperistaltic agents as they may obscure symptoms and precipitate toxic megacolon.
Treatment of initial episode:
- Metronidazole is the drug of choice for the initial episode of mild to moderate CDI. The dosage is 500 mg orally three times per day for 10 to 14 days.
- Vancomycin is the drug of choice for an initial episode of severe CDI. The dosage is 125 mg orally four times per day for 10 to 14 days.
- Vancomycin administered orally (and per rectum if ileus is present) with or without intravenously administered metronidazole is the regimen of choice for the treatment of severe complicated CDI. The vancomycin dosage is 500 mg orally four times per day and 500 mg in approximately 100 mL normal saline per rectum every six hours as a retention enema, and the metronidazole dosage is 500 mg intravenously every eight hours.
Severely ill patients:
Consider colectomy for severely ill patients. Monitoring the serum lactate level and the peripheral blood white blood cell count may be helpful in prompting a decision to operate because a serum lactate level rising to 5 mmol/L and a white blood cell count rising to 50,000 cells per mL have been associated with greatly increased perioperative mortality. If surgical management is necessary, perform subtotal colectomy with preservation of the rectum.
Treatment of recurrences:
- Treatment of the first recurrence of CDI is usually with the same regimen as for the initial episode but should be stratified by disease severity (mild-to-moderate, severe, or severe complicated) as is recommended for treatment of the initial CDI episode.
- Do not use metronidazole beyond the first recurrence of CDI or for long-term chronic therapy because of potential for cumulative neurotoxicity.
- Treatment of the second or later recurrence of CDI with vancomycin therapy using a tapered and/or pulse regimen is the preferred next strategy.
Probiotics:
Administration of currently available probiotics is not recommended to prevent primary CDI as there are limited data to support this approach and there is a potential risk of bloodstream infection.
Source: Cohen SH, Gerding DH, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infection Control and Hospital Epidemiology. 2010;31(5):431–455.
National Response, Localized Attention
Dr. Kavanagh of Health Watch USA says that more information about C. diff is needed, particularly publicly available numbers of infections at hospitals. Some states require those figures to be reported, but most don’t. And there is no current federal mandate on reporting of C. diff cases, although acute-care hospitals will be required to report C. diff infection rates starting in 2013.
“We really have scant data,” he says. “There is not a lot of reporting if you look at the nation on a whole. And I think that underscores one of the reasons why you need to have data for action. You need to have reporting of these organisms to the National Healthcare Safety Network so that the CDC can monitor and can make plans and can do effective interventions.
“You want to know where the areas of highest infection are,” he adds. “You want to know what interventions work and don’t work. If you don’t have a national coordinated reporting system, it really makes it difficult to address the problem. C. diff is going to be much harder to control than MRSA or other bacteria because it changes into a hard-to-kill dormant spore stage and then re-occurs at some point.”
The Centers for Medicare & Medicaid Services (CMS) has proposed adding C. diff infections to the list of hospital-acquired conditions that will not be reimbursable. It is widely hoped that such a measure will go a long way toward stamping out the problem.
Dr. Kobaidze of Emory notes that C. diff is a dynamic problem, always adapting and posing new challenges. And hospitalists should be more involved in answering these questions through research. One recent question, she points out, is whether proton pump inhibitor use is related to the rise of C. diff.
Ultimately, though, controlling C. diff in hospitals might come down to what is done day to day inside the hospital. And hospitalists can play a big role.
Danielle Scheurer, MD, MSCR, SFHM, a hospitalist and medical director of quality at the Medical University of South Carolina in Charleston, says that a full-time pharmacist on the hospital’s antimicrobial stewardship committee is always reviewing antibiotic prescriptions and is prepared to flag cases in which a broad-spectrum is used when one with a more narrow scope might be more appropriate.
The hospital has done its best, as part of its “renovation cycle,” to standardize the layouts of rooms “so that the second you open the door you know exactly where the alcohol gel is and where the soap and the sink is going to be.” The idea is to make compliance as “mindless” as possible. Such efforts can be hampered by structural limitations though, she says.
HM group leaders, she suggests, can play an important part simply by being good role models—gowning and gloving without complaint before entering high-risk rooms and reinforcing the message that such efforts have real effects on patient safety.
But she also acknowledges that “it always sounds easy....There has to be some level of redundancy built into the hospital system. This is more of a system thing than the individual hospitalist.”
One level of redundancy at MUSC that has been particularly effective, she says, are “secret shoppers” who keep an eye out for medical teams that might not be washing their hands as they go in and out of high-risk rooms. Each unit is responsible for their hand hygiene numbers—which include both self-reported figures and those obtained by the secret onlookers—and those numbers are made available to the hospital.
Those units with the best numbers are sometimes given a reward, such as a pizza party, but it’s colleagues’ knowledge of the numbers that matters most, she says.
“That, in and of itself, is a powerful motivator,” Dr. Scheurer says. “We bring it to all of our quality operations meetings, all the administrators, the CEO, the CMO. It’s very motivating for every unit. They don’t want to be the trailing unit.”
Tom Collins is a freelance medical writer based in Miami.
References
- Orenstein R, Aronhalt KC, McManus JE Jr., Fedraw LA. A targeted strategy to wipe out Clostridium difficile. Infect Control Hosp Epidemiol. 2011;32(11):1137-1139.
- Stevens V, Dumyati G, Fine LS, Fisher SG, van Wijngaarden E. Cumulative antibiotic exposures over time and the risk of Clostridium difficile infection. Clin Infect Dis. 2011;53(1):42-48.
What Hospitalists Can Do
Here are suggestions, as provided by ID experts and hospitalist leaders, on what hospitalists can do to battle C. diff infections:
Short-term steps:
- Wash hands before entering and upon leaving rooms occupied by patients with C. diff infections and those strongly suspected of having C. diff infections.
- Continue using alcohol-based hand sanitizers in addition to hand washing to prevent other types of outbreaks.
- Ensure that infected patients, and those suspected of being infected, are isolated, possibly even for 48 hours after diarrhea resolves, as research shows the patients can still transmit the spores.
- In units with high C. diff rates, consider universal gloving, not just for patients with known infection.
- Use more highly sensitive tests, such as polymerase chain reaction, or PCR, rather than enzyme immunoassays to more efficiently identify affected patients.
- Avoid testing patients with formed stools.
- Ensure that rooms of infected patients and patients strongly suspected of being infected are cleaned with a hypochlorite solution.
- Taper the use of broad-spectrum antibiotics in non-C. diff patients after test results are obtained.
- Encourage patients to question their healthcare practitioners about hand hygiene and use of antibiotics.
Long-term steps:
- Be involved with your hospital’s antimicrobial stewardship program.
- Conduct research into C. diff to explore its causes and treatments.
- Be a good role model for the rest of your group, emphasizing good practices and a strong patient-safety message.
At 480-bed Emory University Hospital Midtown in Atlanta, the physicians and staff seemingly are doing all the right things to foil one of hospital’s archenemies: Clostridium difficile. The bacteria, better known as C. diff, is responsible for a sharp rise in hospital-acquired infections over the past decade, rivaling even MRSA.
In 2010, Emory Midtown launched a campaign to boost awareness of the importance of hand washing before and after treating patients infected with C. diff and those likely to be infected. They also began using the polymerase-chain-reaction-based assay to detect the bacteria, a test with much higher sensitivity that helps to more efficiently identify those infected so control measures can be more prompt and targeted. They use a hypochlorite mixture to clean the rooms of those infected, which is considered a must. And a committee monitors the use of antibiotics to prevent overuse—often the scapegoat for the rise of the hard-to-kill bacteria.
Still, at Emory, the rate of C. diff is about the same as the national average, says hospitalist Ketino Kobaidze, MD, assistant professor at the Emory University School of Medicine and a member of the antimicrobial stewardship and infectious disease control committees at Midtown. While Dr. Kobaidze says her institution is doing a good job of trying to keep C. diff under control, she thinks hospitalists can do more.
“My feeling is that we are not as involved as we’re supposed to be,” she says. “I think we need to be a little bit more proactive, be involved in committees and research activities across the hospital.”
—Kevin Kavanagh, MD, founder, Health Watch USA
You Are Not Alone
The experience at Emory Midtown is far from unusual—healthcare facilities, and hospitalists, across the country have seen healthcare-related C. diff cases more than double since 2001 to between 400,000 and 500,000 a year, says Carolyn Gould, MD, a medical epidemiologist in the division of healthcare quality promotion at the Centers for Disease Control and Prevention (CDC) in Atlanta.
Hospitalists, whether they realize it or not, are intimately involved in how well the C. diff outbreak is controlled. Infectious-disease (ID) specialists say hospitalists are perfectly situated to make an impact in efforts to help curb the outbreak.
“Hospitalists are critical to this effort,” Dr. Gould says. “They’re in the hospital day in and day out, and they’re constantly interacting with the patients, staff, and administration. They’re often the first on the scene to see a patient who might have suddenly developed diarrhea; they’re the first to react. I think they’re in a prime position to play a leadership role to prevent C. diff infections.”
They’re also situated well to work with infection-control experts on antimicrobial stewardship programs, she says.
“I look at hospitalists just like I would have looked at internists managing their own patients 15 years ago,” says Stuart Cohen, MD, an ID expert with the University of California at Davis and a fellow with the Infectious Diseases Society of America who was lead author of the latest published IDSA guidelines on C. diff treatment. “And so they’re the first-line people.”
continued below...
Mayo Shows How a Simple Step Can Make Big Difference in C. Diff
Sometimes even when it comes to a huge problem like widespread bacterial infections, simplicity is best.
The Mayo Clinic, in a project to cut the rate of C. diff infections, asked its workers to do one extra thing: Wipe down high-touch areas with bleach wipes. The effort worked; infections were all but eradicated in units that had been having five to seven infections per month.
The results of the project, recently published in Infectious Control and Hospital Epidemiology, show the importance of simple steps as long as they’re carried out regularly and thoroughly.1
The project began when Robert Orenstein, DO, associate professor of medicine in infectious diseases who then worked in Rochester, Minn., established a surveillance network for C. diff infections at Mayo Clinic at the time when such infections were being noted more widely throughout the U.S. and Canada. The network began tracking the cases and found that one inpatient medical unit primarily composed of patients with gastrointestinal diseases had a C. diff rate 10 times higher than the rest of the hospital. Surveillance also showed that universally gloved hematology and oncology units had substantially lower rates of C. diff infection despite high-risk patients.
Dr. Orenstein knew he had to make a change in the GI unit, but it wasn’t feasible to institute universal gloving, so he turned to bleach wipes.
Twice a day, housekeeping staff wiped down all “high-touch” areas (light switches, toilet handles, bed rails) in all of the rooms. The wipes contain 0.55% sodium hypochlorite. Within six months, the number of C. diff cases fell to almost zero.
“We were just in shock,” Dr. Orenstein says. He attributed the improvement to a reduction in the “colonization pressure”—if a high concentration of patients with C. diff can cause abundant transmissions quickly, the opposite is also true.
The greatly improved figures were shared with housekeeping, which initially complained about the smell but were encouraged to keep doors open and rooms ventilated. The bleach wipes, which Dr. Orenstein acknowledges mean an additional expense, leave a white residue when dry, so the surfaces are wiped down with water after the recommended contact time.
Dr. Orenstein notes that the results came even without a change in hand hygiene, which he had deemed not feasible because of the hospital’s lack of sinks. He isn’t diminishing the importance of hand washing, but the project does show how effective a single step can be.
The key, Dr. Orenstein adds, might be that it was just one change involving just one group of staff. “Why we think it was so effective is it was really one group that had to change their behavior and we worked with them, educated them,” he says.
He emphasizes that the wipes don’t come at the expense of other measures, like thorough cleaning of all rooms and antibiotic stewardship programs.
“You do all of those and do them well,” he says, “then you get the reduction of C. diff in the hospital.”
A Tough Bug
Believed to be aided largely by the use of broad-spectrum antibiotics that knock out the colon’s natural flora, C. diff in the hospital—as well as nursing homes and acute-care facilities—has raged for much of the past decade. Its rise is tied to the emergence of a new hypervirulent strain known as BI/NAP1/027, or NAP1 for short. The strain is highly resistant to fluoroquinolones, such as ciprofloxacin and levofloxacin, which are used often in healthcare settings.
“A fluoroquinolone will wipe out a lot of your normal flora in your gut,” Dr. Gould says. “But it won’t wipe out C. diff, in particular this hypervirulent strain. And so this strain can flourish in the presence of fluoroquinolones.” The strain produces up to 15 to 20 times more toxins than other C. diff strains, according to some data, she adds.
Vancomycin (Vanconin) and metronidazole (Flagyl) are the most common antibiotics used to treat patients infected with C. diff. Mortality rates are higher among the elderly, largely because of their weaker immune system, Dr. Gould says. Studies have generally shown mortality rates of 10% or a bit lower.1
More recent studies have shown that the number of hospital-related C. diff cases might have begun to level off in 2008 and 2009. Dr. Gould says she thinks the leveling off is for real, but there is debate over what the immediate future holds.
“There’s a lot of work and initiatives, especially state-based initiatives, that are being done in hospitals. And there’s reason to believe they’re effective,” she says, adding it’s harder to get a good picture of the problem in long-term care facilities and in the community.
Dr. Cohen with the IDSA says it’s too soon to say whether the problem is hitting a plateau. “CDC data are always a couple of years behind,” he says. “Until you see another data point, you can’t tell whether that’s just a transient flattening and whether it’s going to keep going up or not.”
Kevin Kavanagh, MD, founder of the patient advocacy group Health Watch USA and a retired otolaryngologist in Kentucky who has taken a keen interest in the C. diff problem, says he doesn’t think the end of the tunnel is within view yet.
“I think C. diff is going to get worse before it gets better,” Dr. Kavanagh says. “And that’s not necessarily because the healthcare profession isn’t doing due diligence. This is a tough organism.—it can be tough to treat and can be very tough to kill.”
The Best Defense?
Because C. diff lives within protective spores, sound hand hygiene practices and room-cleaning practices are essential for keeping infections to a minimum. Alcohol-based hand sanitizers, effective against other organisms including MRSA, do not kill C. diff. The bacteria must be mechanically removed through hand washing.
And even hand washing might not be totally effective at getting rid of the spores, which means it’s important for healthcare workers to gown and glove in high-risk rooms.
Sodium hypochlorite solutions, or bleach mixtures, have to be used to clean rooms occupied by patients with C. diff, and the prevailing thought is to clean the rooms of patients suspected of having C. diff, even if those cases might not be confirmed.
Equally important to cleaning and hand washing is systemwide emphasis on antibiotic stewardship. A 2011 study at the State University of New York Buffalo found that the risk of a C. diff infection rose with the number of antibiotics taken.2
—Carolyn Gould, MD, medical epidemiologist, division of healthcare quality promotion, Centers of Disease Control and Prevention, Atlanta
While a broad-spectrum antibiotic might be necessary at first, once the results of cultures are received, the treatment should be finely tailored to kill only the problem bacteria so that the body’s natural defenses aren’t broken down, Dr. Gould explains.
“If someone is very sick and you’re not sure what is going on, it’s very reasonable to treat them empirically with broad-spectrum antibiotics,” she says. “The important thing is that you send the appropriate cultures before so that you know what you’re treating and you can optimize those antibiotics with daily assessments.”
It’s clear why an overreliance on broad-spectrum drugs prevails in U.S. health settings, Dr. Cohen acknowledges. Recent literature suggests treating critically ill patients with wide-ranging antimicrobials as the mortality rate can be twice as high with narrower options. “I think people have gotten very quick to give broad-spectrum therapy,” he says.
continued below...
Knocking Out Clostridium Difficile
Here are the guidelines on treatment of C. diff infections (CDI) as recommended by the Infectious Diseases Society of America:
First steps:
- Discontinue therapy with the inciting antimicrobial agent(s) as soon as possible as this may influence the risk of CDI recurrence.
- When severe or complicated CDI is suspected, initiate empirical treatment as soon as the diagnosis is suspected.
- If the stool toxin assay result is negative, the decision to initiate, stop, or continue treatment must be individualized.
- If possible, avoid use of antiperistaltic agents as they may obscure symptoms and precipitate toxic megacolon.
Treatment of initial episode:
- Metronidazole is the drug of choice for the initial episode of mild to moderate CDI. The dosage is 500 mg orally three times per day for 10 to 14 days.
- Vancomycin is the drug of choice for an initial episode of severe CDI. The dosage is 125 mg orally four times per day for 10 to 14 days.
- Vancomycin administered orally (and per rectum if ileus is present) with or without intravenously administered metronidazole is the regimen of choice for the treatment of severe complicated CDI. The vancomycin dosage is 500 mg orally four times per day and 500 mg in approximately 100 mL normal saline per rectum every six hours as a retention enema, and the metronidazole dosage is 500 mg intravenously every eight hours.
Severely ill patients:
Consider colectomy for severely ill patients. Monitoring the serum lactate level and the peripheral blood white blood cell count may be helpful in prompting a decision to operate because a serum lactate level rising to 5 mmol/L and a white blood cell count rising to 50,000 cells per mL have been associated with greatly increased perioperative mortality. If surgical management is necessary, perform subtotal colectomy with preservation of the rectum.
Treatment of recurrences:
- Treatment of the first recurrence of CDI is usually with the same regimen as for the initial episode but should be stratified by disease severity (mild-to-moderate, severe, or severe complicated) as is recommended for treatment of the initial CDI episode.
- Do not use metronidazole beyond the first recurrence of CDI or for long-term chronic therapy because of potential for cumulative neurotoxicity.
- Treatment of the second or later recurrence of CDI with vancomycin therapy using a tapered and/or pulse regimen is the preferred next strategy.
Probiotics:
Administration of currently available probiotics is not recommended to prevent primary CDI as there are limited data to support this approach and there is a potential risk of bloodstream infection.
Source: Cohen SH, Gerding DH, Johnson S, et al. Clinical practice guidelines for Clostridium difficile infection in adults: 2010 update by the Society for Healthcare Epidemiology of America (SHEA) and the Infectious Diseases Society of America (IDSA). Infection Control and Hospital Epidemiology. 2010;31(5):431–455.
National Response, Localized Attention
Dr. Kavanagh of Health Watch USA says that more information about C. diff is needed, particularly publicly available numbers of infections at hospitals. Some states require those figures to be reported, but most don’t. And there is no current federal mandate on reporting of C. diff cases, although acute-care hospitals will be required to report C. diff infection rates starting in 2013.
“We really have scant data,” he says. “There is not a lot of reporting if you look at the nation on a whole. And I think that underscores one of the reasons why you need to have data for action. You need to have reporting of these organisms to the National Healthcare Safety Network so that the CDC can monitor and can make plans and can do effective interventions.
“You want to know where the areas of highest infection are,” he adds. “You want to know what interventions work and don’t work. If you don’t have a national coordinated reporting system, it really makes it difficult to address the problem. C. diff is going to be much harder to control than MRSA or other bacteria because it changes into a hard-to-kill dormant spore stage and then re-occurs at some point.”
The Centers for Medicare & Medicaid Services (CMS) has proposed adding C. diff infections to the list of hospital-acquired conditions that will not be reimbursable. It is widely hoped that such a measure will go a long way toward stamping out the problem.
Dr. Kobaidze of Emory notes that C. diff is a dynamic problem, always adapting and posing new challenges. And hospitalists should be more involved in answering these questions through research. One recent question, she points out, is whether proton pump inhibitor use is related to the rise of C. diff.
Ultimately, though, controlling C. diff in hospitals might come down to what is done day to day inside the hospital. And hospitalists can play a big role.
Danielle Scheurer, MD, MSCR, SFHM, a hospitalist and medical director of quality at the Medical University of South Carolina in Charleston, says that a full-time pharmacist on the hospital’s antimicrobial stewardship committee is always reviewing antibiotic prescriptions and is prepared to flag cases in which a broad-spectrum is used when one with a more narrow scope might be more appropriate.
The hospital has done its best, as part of its “renovation cycle,” to standardize the layouts of rooms “so that the second you open the door you know exactly where the alcohol gel is and where the soap and the sink is going to be.” The idea is to make compliance as “mindless” as possible. Such efforts can be hampered by structural limitations though, she says.
HM group leaders, she suggests, can play an important part simply by being good role models—gowning and gloving without complaint before entering high-risk rooms and reinforcing the message that such efforts have real effects on patient safety.
But she also acknowledges that “it always sounds easy....There has to be some level of redundancy built into the hospital system. This is more of a system thing than the individual hospitalist.”
One level of redundancy at MUSC that has been particularly effective, she says, are “secret shoppers” who keep an eye out for medical teams that might not be washing their hands as they go in and out of high-risk rooms. Each unit is responsible for their hand hygiene numbers—which include both self-reported figures and those obtained by the secret onlookers—and those numbers are made available to the hospital.
Those units with the best numbers are sometimes given a reward, such as a pizza party, but it’s colleagues’ knowledge of the numbers that matters most, she says.
“That, in and of itself, is a powerful motivator,” Dr. Scheurer says. “We bring it to all of our quality operations meetings, all the administrators, the CEO, the CMO. It’s very motivating for every unit. They don’t want to be the trailing unit.”
Tom Collins is a freelance medical writer based in Miami.
References
- Orenstein R, Aronhalt KC, McManus JE Jr., Fedraw LA. A targeted strategy to wipe out Clostridium difficile. Infect Control Hosp Epidemiol. 2011;32(11):1137-1139.
- Stevens V, Dumyati G, Fine LS, Fisher SG, van Wijngaarden E. Cumulative antibiotic exposures over time and the risk of Clostridium difficile infection. Clin Infect Dis. 2011;53(1):42-48.
What Hospitalists Can Do
Here are suggestions, as provided by ID experts and hospitalist leaders, on what hospitalists can do to battle C. diff infections:
Short-term steps:
- Wash hands before entering and upon leaving rooms occupied by patients with C. diff infections and those strongly suspected of having C. diff infections.
- Continue using alcohol-based hand sanitizers in addition to hand washing to prevent other types of outbreaks.
- Ensure that infected patients, and those suspected of being infected, are isolated, possibly even for 48 hours after diarrhea resolves, as research shows the patients can still transmit the spores.
- In units with high C. diff rates, consider universal gloving, not just for patients with known infection.
- Use more highly sensitive tests, such as polymerase chain reaction, or PCR, rather than enzyme immunoassays to more efficiently identify affected patients.
- Avoid testing patients with formed stools.
- Ensure that rooms of infected patients and patients strongly suspected of being infected are cleaned with a hypochlorite solution.
- Taper the use of broad-spectrum antibiotics in non-C. diff patients after test results are obtained.
- Encourage patients to question their healthcare practitioners about hand hygiene and use of antibiotics.
Long-term steps:
- Be involved with your hospital’s antimicrobial stewardship program.
- Conduct research into C. diff to explore its causes and treatments.
- Be a good role model for the rest of your group, emphasizing good practices and a strong patient-safety message.
Is a Post-Discharge Clinic in Your Hospital's Future?
The hospitalist concept was established on the foundation of timely, informative handoffs to primary-care physicians (PCPs) once a patient’s hospital stay is complete. With sicker patients and shorter hospital stays, pending test results, and complex post-discharge medication regimens to sort out, this handoff is crucial to successful discharges. But what if a discharged patient can’t get in to see the PCP, or has no established PCP?
Recent research on hospital readmissions by the Dartmouth Atlas Project found that only 42% of hospitalized Medicare patients had any contact with a primary-care clinician within 14 days of discharge.1 For patients with ongoing medical needs, such missed connections are a major contributor to hospital readmissions, and thus a target for hospitals and HM groups wanting to control their readmission rates before Medicare imposes reimbursement penalties starting in October 2012 (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
One proposed solution is the post-discharge clinic, typically located on or near a hospital’s campus and staffed by hospitalists, PCPs, or advanced-practice nurses. The patient can be seen once or a few times in the post-discharge clinic to make sure that health education started in the hospital is understood and followed, and that prescriptions ordered in the hospital are being taken on schedule.
—Lauren Doctoroff, MD, hospitalist, director, post-discharge clinic, Beth Israel Deaconess Medical Center, Boston
Mark V. Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, describes hospitalist-led post-discharge clinics as “Band-Aids for an inadequate primary-care system.” What would be better, he says, is focusing on the underlying problem and working to improve post-discharge access to primary care. Dr. Williams acknowledges, however, that sometimes a patch is needed to stanch the blood flow—e.g., to better manage care transitions—while waiting on healthcare reform and medical homes to improve care coordination throughout the system.
Working in a post-discharge clinic might seem like “a stretch for many hospitalists, especially those who chose this field because they didn’t want to do outpatient medicine,” says Lauren Doctoroff, MD, a hospitalist who directs a post-discharge clinic at Beth Israel Deaconess Medical Center (BIDMC) in Boston. “But there are times when it may be appropriate for hospital-based doctors to extend their responsibility out of the hospital.”
Dr. Doctoroff also says that working in such a clinic can be practice-changing for hospitalists. “All of a sudden, you have a different view of your hospitalized patients, and you start to ask different questions while they’re in the hospital than you ever did before,” she explains.
What is a Post-Discharge Clinic?
The post-discharge clinic, also known as a transitional-care clinic or after-care clinic, is intended to bridge medical coverage between the hospital and primary care. The clinic at BIDMC is for patients affiliated with its Health Care Associates faculty practice “discharged from either our hospital or another hospital, who need care that their PCP or specialist, because of scheduling conflicts, cannot provide within the needed time frame,” Dr. Doctoroff says.
Four hospitalists from BIDMC’s large HM group were selected to staff the clinic. The hospitalists work in one-month rotations (a total of three months on service per year), and are relieved of other responsibilities during their month in clinic. They provide five half-day clinic sessions per week, with a 40-minute-per-patient visit schedule. Thirty minutes are allotted for patients referred from the hospital’s ED who did not get admitted to the hospital but need clinical follow-up.
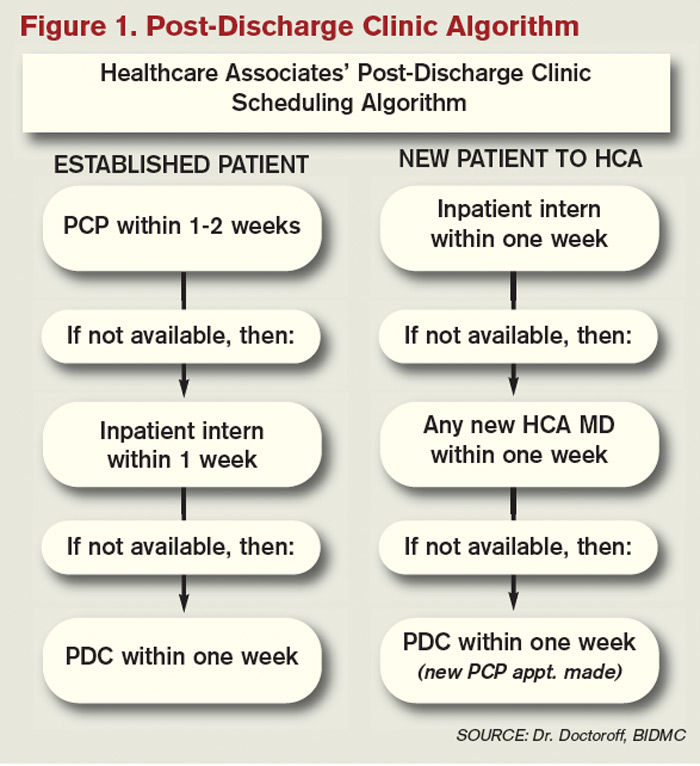
The clinic is based in a BIDMC-affiliated primary-care practice, “which allows us to use its administrative structure and logistical support,” Dr. Doctoroff explains. “A hospital-based administrative service helps set up outpatient visits prior to discharge using computerized physician order entry and a scheduling algorhythm.” (See Figure 1) Patients who can be seen by their PCP in a timely fashion are referred to the PCP office; if not, they are scheduled in the post-discharge clinic. “That helps preserve the PCP relationship, which I think is paramount,” she says.
The first two years were spent getting the clinic established, but in the near future, BIDMC will start measuring such outcomes as access to care and quality. “But not necessarily readmission rates,” Dr. Doctoroff adds. “I know many people think of post-discharge clinics in the context of preventing readmissions, although we don’t have the data yet to fully support that. In fact, some readmissions may result from seeing a doctor. If you get a closer look at some patients after discharge and they are doing badly, they are more likely to be readmitted than if they had just stayed home.” In such cases, readmission could actually be a better outcome for the patient, she notes.
Dr. Doctoroff describes a typical user of her post-discharge clinic as a non-English-speaking patient who was discharged from the hospital with severe back pain from a herniated disk. “He came back to see me 10 days later, still barely able to walk. He hadn’t been able to fill any of the prescriptions from his hospital stay. Within two hours after I saw him, we got his meds filled and outpatient services set up,” she says. “We take care of many patients like him in the hospital with acute pain issues, whom we discharge as soon as they can walk, and later we see them limping into outpatient clinics. It makes me think differently now about how I plan their discharges.”

—Shay Martinez, MD, hospitalist, medical director, Harborview Medical Center, Seattle
Who else needs these clinics? Dr. Doctoroff suggests two ways of looking at the question.
“Even for a simple patient admitted to the hospital, that can represent a significant change in the medical picture—a sort of sentinel event. In the discharge clinic, we give them an opportunity to review the hospitalization and answer their questions,” she says. “A lot of information presented to patients in the hospital is not well heard, and the initial visit may be their first time to really talk about what happened.” For other patients with conditions such as congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), or poorly controlled diabetes, treatment guidelines might dictate a pattern for post-discharge follow-up—for example, medical visits in seven or 10 days.
In Seattle, Harborview Medical Center established its After Care Clinic, staffed by hospitalists and nurse practitioners, to provide transitional care for patients discharged from inpatient wards or the ED in need of follow-up, says medical director and hospitalist Shay Martinez, MD. A second priority is to see any CHF patient within 48 hours of discharge.
“We try to limit patients to a maximum of three visits in our clinic,” she says. “At that point, we help them get established in a medical home, either here in one of our primary-care clinics, or in one of the many excellent community clinics in the area.
“This model works well with our patient population. We actually try to do primary care on the inpatient side as well. Our hospitalists are specialized in that approach, given our patient population. We see a lot of immigrants, non-English speakers, people with low health literacy, and the homeless, many of whom lack primary care,” Dr. Martinez says. “We do medication reconciliation, reassessments, and follow-ups with lab tests. We also try to assess who is more likely to be a no-show, and who needs more help with scheduling follow-up appointments.”
Clinical coverage of post-discharge clinics varies by setting, staffing, and scope. If demand is low, hospitalists or ED physicians can be called off the floor to see patients who return to the clinic, or they could staff the clinic after their hospitalist shift ends. Post-discharge clinic staff whose schedules are light can flex into providing primary-care visits in the clinic. Post-discharge can also could be provided in conjunction with—or as an alternative to—physician house calls to patients’ homes. Some post-discharge clinics work with medical call centers or telephonic case managers; some even use telemedicine.
It also could be a growth opportunity for hospitalist practices. “It is an exciting potential role for hospitalists interested in doing a little outpatient care,” Dr. Martinez says. “This is also a good way to be a safety net for your safety-net hospital.”
continued below...
What Do PCPs Think? It May Be Harder than It Looks

Although some PCPs instinctively will be suspicious of a hospitalist-run post-discharge clinic, it should be possible to clearly limit the service to short-term, immediate-post-hospital encounters focused on issues related to patients unable to get timely access to primary care, according to Dr. Doctoroff.
“I think there is a diversity of opinion by PCPs,” she says. “Some doctors really believe that it interferes with the patient-doctor relationship. But after we’ve been here for a couple of years, we’ve built up credibility with many providers.”
Charles Cutler, MD, FACP, a general internist with a practice in Norristown, Pa., and a member of the ACP’s Board of Regents, says the post-discharge clinic is “a novel idea.”
“I’d be very curious to see if this really is a way to provide better and more cost-effective care,” adds Dr. Cutler, who normally retains management of his own patients when they are hospitalized but agrees that hospitals need to find a solution for lapses in care transitions.
Even so, he says, establishing an outpatient clinic presence may be more difficult than many hospitalists appreciate. “You can’t just put a doc in a room. That physician needs equipment, scheduling, and support staff,” he says. “In our small practice, we employ one person just to ensure that each patient chart is up to date. The overhead necessary to replicate a typical medical office, even one merely providing a transition of care, could be substantial.”
Dr. Cutler emphasizes such office-based challenges as billing, which is distinctly different from hospital billing, and credentialing by insurance companies.
“There are many aspects that have to be thought through. If you see the patient, you need to make yourself available for follow-up calls, because you’ve created a relationship,” he says. “I’m a believer that hospital medicine requires a degree of specialization. But so does an office practice.”
Dr. Cutler acknowledges that some PCPs will be resentful of post-discharge clinics. “But if you don’t like a hospitalist-run discharge clinic, then you have a responsibility to rearrange your schedule to accommodate patients after their hospital discharge,” he says.
Partner with Community
Tallahassee (Fla.) Memorial Hospital (TMH) in February launched a transitional-care clinic in collaboration with faculty from Florida State University, community-based health providers, and the local Capital Health Plan. Hospitalists don’t staff the clinic, but the HM group is its major source of referrals, says Dean Watson, MD, chief medical officer at TMH. Patients can be followed for up to eight weeks, during which time they get comprehensive assessments, medication review and optimization, and referral by the clinic social worker to a PCP and to available community services.
“Three years ago, we came up with the idea for a patient population we know is at high risk for readmission. Why don’t we partner with organizations in the community, form a clinic, teach students and residents, and learn together?” Dr. Watson says. “In addition to the usual patients, TMH targets those who have been readmitted to the hospital three times or more in the past year.”
The clinic, open five days a week, is staffed by a physician, nurse practitioner, telephonic nurse, and social worker, and also has a geriatric assessment clinic.
“We set up a system to identify patients through our electronic health record, and when they come to the clinic, we focus on their social environment and other non-medical issues that might cause readmissions,” he says. The clinic has a pharmacy and funds to support medications for patients without insurance. “In our first six months, we reduced emergency room visits and readmissions for these patients by 68 percent.”
One key partner, Capital Health Plan, bought and refurbished a building, and made it available for the clinic at no cost. Capital’s motivation, says Tom Glennon, a senior vice president for the plan, is its commitment to the community and to community service.
“We’re a nonprofit HMO. We’re focused on what we can do to serve the community, and we’re looking at this as a way for the hospital to have fewer costly, unreimbursed bouncebacks,” Glennon says. “That’s a win-win for all of us.”
Most of the patients who use the clinic are not members of Capital Health Plan, Glennon adds. “If we see CHP members turning up at the transitions clinic, then we have a problem—a breakdown in our case management,” he explains. “Our goal is to have our members taken care of by primary-care providers.”
Hard Data? Not So Fast
How many post-discharge clinics are in operation today is not known. Fundamental financial data, too, are limited, but some say it is unlikely a post-discharge clinic will cover operating expenses from billing revenues alone.
Thus, such clinics will require funding from the hospital, HM group, health system, or health plans, based on the benefits the clinic provides to discharged patients and the impact on 30-day readmissions (for more about the logistical challenges post-discharge clinics present, see “What Do PCPs Think?”).
Some also suggest that many of the post-discharge clinics now in operation are too new to have demonstrated financial impact or return on investment. “We have not yet been asked to show our financial viability,” Dr. Doctoroff says. “I think the clinic leadership thinks we are fulfilling other goals for now, such as creating easier access for their patients after discharge.”
Amy Boutwell, MD, MPP, a hospitalist at Newton Wellesley Hospital in Massachusetts and founder of Collaborative Healthcare Strategies, is among the post-discharge skeptics. She agrees with Dr. Williams that the post-discharge concept is more of a temporary fix to the long-term issues in primary care. “I think the idea is getting more play than actual activity out there right now,” she says. “We need to find opportunities to manage transitions within our scope today and tomorrow while strategically looking at where we want to be in five years [as hospitals and health systems].”
Dr. Boutwell says she’s experienced the frustration of trying to make follow-up appointments with physicians who don’t have any open slots for hospitalized patients awaiting discharge. “We think of follow up as physician-led, but there are alternatives and physician extenders,” she says. “It is well-documented that our healthcare system underuses home health care and other services that might be helpful. We forget how many other opportunities there are in our communities to get another clinician to touch the patient.”
Hospitalists, as key players in the healthcare system, can speak out in support of strengthening primary-care networks and building more collaborative relationships with PCPs, according to Dr. Williams. “If you’re going to set up an outpatient clinic, ideally, have it staffed by PCPs who can funnel the patients into primary-care networks. If that’s not feasible, then hospitalists should proceed with caution, since this approach begins to take them out of their scope of practice,” he says.
With 13 years of experience in urban hospital settings, Dr. Williams is familiar with the dangers unassigned patients present at discharge. “But I don’t know that we’ve yet optimized the hospital discharge process at any hospital in the United States,” he says.
That said, Dr. Williams knows his hospital in downtown Chicago is now working to establish a post-discharge clinic. It will be staffed by PCPs and will target patients who don’t have a PCP, are on Medicaid, or lack insurance.
“Where it starts to make me uncomfortable,” Dr. Williams says, “is what happens when you follow patients out into the outpatient setting?
It’s hard to do just one visit and draw the line. Yes, you may prevent a readmission, but the patient is still left with chronic illness and the need for primary care.”
Larry Beresford is a freelance writer based in Oakland, Calif.
What Does the Research Say?

Post-discharge clinic advocates acknowledge that the research documenting outcomes from such clinics is scarce. A recent study from Northwestern University looked at 12 distinct care-transitions activities and their effect on readmission rates.2 Post-discharge clinics were not studied as a separate category, although they fit into the category of physician continuity across inpatient and outpatient settings.
“There’s definitely a hole in the literature regarding post-discharge care,” says lead author Luke Hansen, MD, MHS. The authors found that “no single intervention implemented alone was regularly associated with reduced risk for 30-day rehospitalizations.”
On the other hand, Misky et al found that discharged patients who lacked timely follow-up (within four weeks of discharge) were 10 times more likely to be readmitted than those who got the follow-up.3
Medical teams from around the world, including in Canada, the United Kingdom, Israel, and Australia, are studying readmission rates and care-transitions strategies. A study by physicians at National Taiwan University Hospital in Taipei describes its integrated transitional care to address post-discharge discontinuities and prevent rehospitalizations, including telephonic monitoring, hotline counseling, and referral to a hospital-run post-discharge clinic located within a hospitalist-managed ward.4 “Patients are treated primarily by the hospitalists who are familiar with them,” in a clinic open from 8 a.m. to 9 p.m., lead author Chin-Chung Shu, MD, wrote in an email. The clinic sees 15 to 30 patients per month; 80% of them are discharged patients without a PCP.
“We typically see patients one or two times in 30 days and then refer them to a suitable physician,” Dr. Shu says. In his study, patients who received post-discharge transitional care, including the post-discharge clinic, had lower rates of readmission and death within 30 days, 15% compared with 25% for a control group.
References
- Goodman, DC, Fisher ES, Chang C. After Hospitalization: A Dartmouth Atlas Report on Post-Acute Care for Medicare Beneficiaries. Dartmouth Atlas website. Available at: www.dartmouthatlas.org/downloads/reports/Post_discharge_events_092811.pdf. Accessed Nov. 3, 2011.
- Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 3-day rehospitalization: A systematic review. Ann Int Med. 2011;155(8): 520-528.
- Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5(7):392-397.
- Shu CC, Hsu NC, Lin YF, et al. Integrated post-discharge transitional care in Taiwan. BMC Medicine website. Available at: www.biomedcentral.com/1741-7015/9/96. Accessed Nov. 1, 2011.
The hospitalist concept was established on the foundation of timely, informative handoffs to primary-care physicians (PCPs) once a patient’s hospital stay is complete. With sicker patients and shorter hospital stays, pending test results, and complex post-discharge medication regimens to sort out, this handoff is crucial to successful discharges. But what if a discharged patient can’t get in to see the PCP, or has no established PCP?
Recent research on hospital readmissions by the Dartmouth Atlas Project found that only 42% of hospitalized Medicare patients had any contact with a primary-care clinician within 14 days of discharge.1 For patients with ongoing medical needs, such missed connections are a major contributor to hospital readmissions, and thus a target for hospitals and HM groups wanting to control their readmission rates before Medicare imposes reimbursement penalties starting in October 2012 (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
One proposed solution is the post-discharge clinic, typically located on or near a hospital’s campus and staffed by hospitalists, PCPs, or advanced-practice nurses. The patient can be seen once or a few times in the post-discharge clinic to make sure that health education started in the hospital is understood and followed, and that prescriptions ordered in the hospital are being taken on schedule.
—Lauren Doctoroff, MD, hospitalist, director, post-discharge clinic, Beth Israel Deaconess Medical Center, Boston
Mark V. Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, describes hospitalist-led post-discharge clinics as “Band-Aids for an inadequate primary-care system.” What would be better, he says, is focusing on the underlying problem and working to improve post-discharge access to primary care. Dr. Williams acknowledges, however, that sometimes a patch is needed to stanch the blood flow—e.g., to better manage care transitions—while waiting on healthcare reform and medical homes to improve care coordination throughout the system.
Working in a post-discharge clinic might seem like “a stretch for many hospitalists, especially those who chose this field because they didn’t want to do outpatient medicine,” says Lauren Doctoroff, MD, a hospitalist who directs a post-discharge clinic at Beth Israel Deaconess Medical Center (BIDMC) in Boston. “But there are times when it may be appropriate for hospital-based doctors to extend their responsibility out of the hospital.”
Dr. Doctoroff also says that working in such a clinic can be practice-changing for hospitalists. “All of a sudden, you have a different view of your hospitalized patients, and you start to ask different questions while they’re in the hospital than you ever did before,” she explains.
What is a Post-Discharge Clinic?
The post-discharge clinic, also known as a transitional-care clinic or after-care clinic, is intended to bridge medical coverage between the hospital and primary care. The clinic at BIDMC is for patients affiliated with its Health Care Associates faculty practice “discharged from either our hospital or another hospital, who need care that their PCP or specialist, because of scheduling conflicts, cannot provide within the needed time frame,” Dr. Doctoroff says.
Four hospitalists from BIDMC’s large HM group were selected to staff the clinic. The hospitalists work in one-month rotations (a total of three months on service per year), and are relieved of other responsibilities during their month in clinic. They provide five half-day clinic sessions per week, with a 40-minute-per-patient visit schedule. Thirty minutes are allotted for patients referred from the hospital’s ED who did not get admitted to the hospital but need clinical follow-up.
The clinic is based in a BIDMC-affiliated primary-care practice, “which allows us to use its administrative structure and logistical support,” Dr. Doctoroff explains. “A hospital-based administrative service helps set up outpatient visits prior to discharge using computerized physician order entry and a scheduling algorhythm.” (See Figure 1) Patients who can be seen by their PCP in a timely fashion are referred to the PCP office; if not, they are scheduled in the post-discharge clinic. “That helps preserve the PCP relationship, which I think is paramount,” she says.
The first two years were spent getting the clinic established, but in the near future, BIDMC will start measuring such outcomes as access to care and quality. “But not necessarily readmission rates,” Dr. Doctoroff adds. “I know many people think of post-discharge clinics in the context of preventing readmissions, although we don’t have the data yet to fully support that. In fact, some readmissions may result from seeing a doctor. If you get a closer look at some patients after discharge and they are doing badly, they are more likely to be readmitted than if they had just stayed home.” In such cases, readmission could actually be a better outcome for the patient, she notes.
Dr. Doctoroff describes a typical user of her post-discharge clinic as a non-English-speaking patient who was discharged from the hospital with severe back pain from a herniated disk. “He came back to see me 10 days later, still barely able to walk. He hadn’t been able to fill any of the prescriptions from his hospital stay. Within two hours after I saw him, we got his meds filled and outpatient services set up,” she says. “We take care of many patients like him in the hospital with acute pain issues, whom we discharge as soon as they can walk, and later we see them limping into outpatient clinics. It makes me think differently now about how I plan their discharges.”
—Shay Martinez, MD, hospitalist, medical director, Harborview Medical Center, Seattle
Who else needs these clinics? Dr. Doctoroff suggests two ways of looking at the question.
“Even for a simple patient admitted to the hospital, that can represent a significant change in the medical picture—a sort of sentinel event. In the discharge clinic, we give them an opportunity to review the hospitalization and answer their questions,” she says. “A lot of information presented to patients in the hospital is not well heard, and the initial visit may be their first time to really talk about what happened.” For other patients with conditions such as congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), or poorly controlled diabetes, treatment guidelines might dictate a pattern for post-discharge follow-up—for example, medical visits in seven or 10 days.
In Seattle, Harborview Medical Center established its After Care Clinic, staffed by hospitalists and nurse practitioners, to provide transitional care for patients discharged from inpatient wards or the ED in need of follow-up, says medical director and hospitalist Shay Martinez, MD. A second priority is to see any CHF patient within 48 hours of discharge.
“We try to limit patients to a maximum of three visits in our clinic,” she says. “At that point, we help them get established in a medical home, either here in one of our primary-care clinics, or in one of the many excellent community clinics in the area.
“This model works well with our patient population. We actually try to do primary care on the inpatient side as well. Our hospitalists are specialized in that approach, given our patient population. We see a lot of immigrants, non-English speakers, people with low health literacy, and the homeless, many of whom lack primary care,” Dr. Martinez says. “We do medication reconciliation, reassessments, and follow-ups with lab tests. We also try to assess who is more likely to be a no-show, and who needs more help with scheduling follow-up appointments.”
Clinical coverage of post-discharge clinics varies by setting, staffing, and scope. If demand is low, hospitalists or ED physicians can be called off the floor to see patients who return to the clinic, or they could staff the clinic after their hospitalist shift ends. Post-discharge clinic staff whose schedules are light can flex into providing primary-care visits in the clinic. Post-discharge can also could be provided in conjunction with—or as an alternative to—physician house calls to patients’ homes. Some post-discharge clinics work with medical call centers or telephonic case managers; some even use telemedicine.
It also could be a growth opportunity for hospitalist practices. “It is an exciting potential role for hospitalists interested in doing a little outpatient care,” Dr. Martinez says. “This is also a good way to be a safety net for your safety-net hospital.”
continued below...
What Do PCPs Think? It May Be Harder than It Looks
Although some PCPs instinctively will be suspicious of a hospitalist-run post-discharge clinic, it should be possible to clearly limit the service to short-term, immediate-post-hospital encounters focused on issues related to patients unable to get timely access to primary care, according to Dr. Doctoroff.
“I think there is a diversity of opinion by PCPs,” she says. “Some doctors really believe that it interferes with the patient-doctor relationship. But after we’ve been here for a couple of years, we’ve built up credibility with many providers.”
Charles Cutler, MD, FACP, a general internist with a practice in Norristown, Pa., and a member of the ACP’s Board of Regents, says the post-discharge clinic is “a novel idea.”
“I’d be very curious to see if this really is a way to provide better and more cost-effective care,” adds Dr. Cutler, who normally retains management of his own patients when they are hospitalized but agrees that hospitals need to find a solution for lapses in care transitions.
Even so, he says, establishing an outpatient clinic presence may be more difficult than many hospitalists appreciate. “You can’t just put a doc in a room. That physician needs equipment, scheduling, and support staff,” he says. “In our small practice, we employ one person just to ensure that each patient chart is up to date. The overhead necessary to replicate a typical medical office, even one merely providing a transition of care, could be substantial.”
Dr. Cutler emphasizes such office-based challenges as billing, which is distinctly different from hospital billing, and credentialing by insurance companies.
“There are many aspects that have to be thought through. If you see the patient, you need to make yourself available for follow-up calls, because you’ve created a relationship,” he says. “I’m a believer that hospital medicine requires a degree of specialization. But so does an office practice.”
Dr. Cutler acknowledges that some PCPs will be resentful of post-discharge clinics. “But if you don’t like a hospitalist-run discharge clinic, then you have a responsibility to rearrange your schedule to accommodate patients after their hospital discharge,” he says.
Partner with Community
Tallahassee (Fla.) Memorial Hospital (TMH) in February launched a transitional-care clinic in collaboration with faculty from Florida State University, community-based health providers, and the local Capital Health Plan. Hospitalists don’t staff the clinic, but the HM group is its major source of referrals, says Dean Watson, MD, chief medical officer at TMH. Patients can be followed for up to eight weeks, during which time they get comprehensive assessments, medication review and optimization, and referral by the clinic social worker to a PCP and to available community services.
“Three years ago, we came up with the idea for a patient population we know is at high risk for readmission. Why don’t we partner with organizations in the community, form a clinic, teach students and residents, and learn together?” Dr. Watson says. “In addition to the usual patients, TMH targets those who have been readmitted to the hospital three times or more in the past year.”
The clinic, open five days a week, is staffed by a physician, nurse practitioner, telephonic nurse, and social worker, and also has a geriatric assessment clinic.
“We set up a system to identify patients through our electronic health record, and when they come to the clinic, we focus on their social environment and other non-medical issues that might cause readmissions,” he says. The clinic has a pharmacy and funds to support medications for patients without insurance. “In our first six months, we reduced emergency room visits and readmissions for these patients by 68 percent.”
One key partner, Capital Health Plan, bought and refurbished a building, and made it available for the clinic at no cost. Capital’s motivation, says Tom Glennon, a senior vice president for the plan, is its commitment to the community and to community service.
“We’re a nonprofit HMO. We’re focused on what we can do to serve the community, and we’re looking at this as a way for the hospital to have fewer costly, unreimbursed bouncebacks,” Glennon says. “That’s a win-win for all of us.”
Most of the patients who use the clinic are not members of Capital Health Plan, Glennon adds. “If we see CHP members turning up at the transitions clinic, then we have a problem—a breakdown in our case management,” he explains. “Our goal is to have our members taken care of by primary-care providers.”
Hard Data? Not So Fast
How many post-discharge clinics are in operation today is not known. Fundamental financial data, too, are limited, but some say it is unlikely a post-discharge clinic will cover operating expenses from billing revenues alone.
Thus, such clinics will require funding from the hospital, HM group, health system, or health plans, based on the benefits the clinic provides to discharged patients and the impact on 30-day readmissions (for more about the logistical challenges post-discharge clinics present, see “What Do PCPs Think?”).
Some also suggest that many of the post-discharge clinics now in operation are too new to have demonstrated financial impact or return on investment. “We have not yet been asked to show our financial viability,” Dr. Doctoroff says. “I think the clinic leadership thinks we are fulfilling other goals for now, such as creating easier access for their patients after discharge.”
Amy Boutwell, MD, MPP, a hospitalist at Newton Wellesley Hospital in Massachusetts and founder of Collaborative Healthcare Strategies, is among the post-discharge skeptics. She agrees with Dr. Williams that the post-discharge concept is more of a temporary fix to the long-term issues in primary care. “I think the idea is getting more play than actual activity out there right now,” she says. “We need to find opportunities to manage transitions within our scope today and tomorrow while strategically looking at where we want to be in five years [as hospitals and health systems].”
Dr. Boutwell says she’s experienced the frustration of trying to make follow-up appointments with physicians who don’t have any open slots for hospitalized patients awaiting discharge. “We think of follow up as physician-led, but there are alternatives and physician extenders,” she says. “It is well-documented that our healthcare system underuses home health care and other services that might be helpful. We forget how many other opportunities there are in our communities to get another clinician to touch the patient.”
Hospitalists, as key players in the healthcare system, can speak out in support of strengthening primary-care networks and building more collaborative relationships with PCPs, according to Dr. Williams. “If you’re going to set up an outpatient clinic, ideally, have it staffed by PCPs who can funnel the patients into primary-care networks. If that’s not feasible, then hospitalists should proceed with caution, since this approach begins to take them out of their scope of practice,” he says.
With 13 years of experience in urban hospital settings, Dr. Williams is familiar with the dangers unassigned patients present at discharge. “But I don’t know that we’ve yet optimized the hospital discharge process at any hospital in the United States,” he says.
That said, Dr. Williams knows his hospital in downtown Chicago is now working to establish a post-discharge clinic. It will be staffed by PCPs and will target patients who don’t have a PCP, are on Medicaid, or lack insurance.
“Where it starts to make me uncomfortable,” Dr. Williams says, “is what happens when you follow patients out into the outpatient setting?
It’s hard to do just one visit and draw the line. Yes, you may prevent a readmission, but the patient is still left with chronic illness and the need for primary care.”
Larry Beresford is a freelance writer based in Oakland, Calif.
What Does the Research Say?
Post-discharge clinic advocates acknowledge that the research documenting outcomes from such clinics is scarce. A recent study from Northwestern University looked at 12 distinct care-transitions activities and their effect on readmission rates.2 Post-discharge clinics were not studied as a separate category, although they fit into the category of physician continuity across inpatient and outpatient settings.
“There’s definitely a hole in the literature regarding post-discharge care,” says lead author Luke Hansen, MD, MHS. The authors found that “no single intervention implemented alone was regularly associated with reduced risk for 30-day rehospitalizations.”
On the other hand, Misky et al found that discharged patients who lacked timely follow-up (within four weeks of discharge) were 10 times more likely to be readmitted than those who got the follow-up.3
Medical teams from around the world, including in Canada, the United Kingdom, Israel, and Australia, are studying readmission rates and care-transitions strategies. A study by physicians at National Taiwan University Hospital in Taipei describes its integrated transitional care to address post-discharge discontinuities and prevent rehospitalizations, including telephonic monitoring, hotline counseling, and referral to a hospital-run post-discharge clinic located within a hospitalist-managed ward.4 “Patients are treated primarily by the hospitalists who are familiar with them,” in a clinic open from 8 a.m. to 9 p.m., lead author Chin-Chung Shu, MD, wrote in an email. The clinic sees 15 to 30 patients per month; 80% of them are discharged patients without a PCP.
“We typically see patients one or two times in 30 days and then refer them to a suitable physician,” Dr. Shu says. In his study, patients who received post-discharge transitional care, including the post-discharge clinic, had lower rates of readmission and death within 30 days, 15% compared with 25% for a control group.
References
- Goodman, DC, Fisher ES, Chang C. After Hospitalization: A Dartmouth Atlas Report on Post-Acute Care for Medicare Beneficiaries. Dartmouth Atlas website. Available at: www.dartmouthatlas.org/downloads/reports/Post_discharge_events_092811.pdf. Accessed Nov. 3, 2011.
- Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 3-day rehospitalization: A systematic review. Ann Int Med. 2011;155(8): 520-528.
- Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5(7):392-397.
- Shu CC, Hsu NC, Lin YF, et al. Integrated post-discharge transitional care in Taiwan. BMC Medicine website. Available at: www.biomedcentral.com/1741-7015/9/96. Accessed Nov. 1, 2011.
The hospitalist concept was established on the foundation of timely, informative handoffs to primary-care physicians (PCPs) once a patient’s hospital stay is complete. With sicker patients and shorter hospital stays, pending test results, and complex post-discharge medication regimens to sort out, this handoff is crucial to successful discharges. But what if a discharged patient can’t get in to see the PCP, or has no established PCP?
Recent research on hospital readmissions by the Dartmouth Atlas Project found that only 42% of hospitalized Medicare patients had any contact with a primary-care clinician within 14 days of discharge.1 For patients with ongoing medical needs, such missed connections are a major contributor to hospital readmissions, and thus a target for hospitals and HM groups wanting to control their readmission rates before Medicare imposes reimbursement penalties starting in October 2012 (see “Value-Based Purchasing Raises the Stakes,” May 2011, p. 1).
One proposed solution is the post-discharge clinic, typically located on or near a hospital’s campus and staffed by hospitalists, PCPs, or advanced-practice nurses. The patient can be seen once or a few times in the post-discharge clinic to make sure that health education started in the hospital is understood and followed, and that prescriptions ordered in the hospital are being taken on schedule.
—Lauren Doctoroff, MD, hospitalist, director, post-discharge clinic, Beth Israel Deaconess Medical Center, Boston
Mark V. Williams, MD, FACP, FHM, professor and chief of the division of hospital medicine at Northwestern University’s Feinberg School of Medicine in Chicago, describes hospitalist-led post-discharge clinics as “Band-Aids for an inadequate primary-care system.” What would be better, he says, is focusing on the underlying problem and working to improve post-discharge access to primary care. Dr. Williams acknowledges, however, that sometimes a patch is needed to stanch the blood flow—e.g., to better manage care transitions—while waiting on healthcare reform and medical homes to improve care coordination throughout the system.
Working in a post-discharge clinic might seem like “a stretch for many hospitalists, especially those who chose this field because they didn’t want to do outpatient medicine,” says Lauren Doctoroff, MD, a hospitalist who directs a post-discharge clinic at Beth Israel Deaconess Medical Center (BIDMC) in Boston. “But there are times when it may be appropriate for hospital-based doctors to extend their responsibility out of the hospital.”
Dr. Doctoroff also says that working in such a clinic can be practice-changing for hospitalists. “All of a sudden, you have a different view of your hospitalized patients, and you start to ask different questions while they’re in the hospital than you ever did before,” she explains.
What is a Post-Discharge Clinic?
The post-discharge clinic, also known as a transitional-care clinic or after-care clinic, is intended to bridge medical coverage between the hospital and primary care. The clinic at BIDMC is for patients affiliated with its Health Care Associates faculty practice “discharged from either our hospital or another hospital, who need care that their PCP or specialist, because of scheduling conflicts, cannot provide within the needed time frame,” Dr. Doctoroff says.
Four hospitalists from BIDMC’s large HM group were selected to staff the clinic. The hospitalists work in one-month rotations (a total of three months on service per year), and are relieved of other responsibilities during their month in clinic. They provide five half-day clinic sessions per week, with a 40-minute-per-patient visit schedule. Thirty minutes are allotted for patients referred from the hospital’s ED who did not get admitted to the hospital but need clinical follow-up.
The clinic is based in a BIDMC-affiliated primary-care practice, “which allows us to use its administrative structure and logistical support,” Dr. Doctoroff explains. “A hospital-based administrative service helps set up outpatient visits prior to discharge using computerized physician order entry and a scheduling algorhythm.” (See Figure 1) Patients who can be seen by their PCP in a timely fashion are referred to the PCP office; if not, they are scheduled in the post-discharge clinic. “That helps preserve the PCP relationship, which I think is paramount,” she says.
The first two years were spent getting the clinic established, but in the near future, BIDMC will start measuring such outcomes as access to care and quality. “But not necessarily readmission rates,” Dr. Doctoroff adds. “I know many people think of post-discharge clinics in the context of preventing readmissions, although we don’t have the data yet to fully support that. In fact, some readmissions may result from seeing a doctor. If you get a closer look at some patients after discharge and they are doing badly, they are more likely to be readmitted than if they had just stayed home.” In such cases, readmission could actually be a better outcome for the patient, she notes.
Dr. Doctoroff describes a typical user of her post-discharge clinic as a non-English-speaking patient who was discharged from the hospital with severe back pain from a herniated disk. “He came back to see me 10 days later, still barely able to walk. He hadn’t been able to fill any of the prescriptions from his hospital stay. Within two hours after I saw him, we got his meds filled and outpatient services set up,” she says. “We take care of many patients like him in the hospital with acute pain issues, whom we discharge as soon as they can walk, and later we see them limping into outpatient clinics. It makes me think differently now about how I plan their discharges.”
—Shay Martinez, MD, hospitalist, medical director, Harborview Medical Center, Seattle
Who else needs these clinics? Dr. Doctoroff suggests two ways of looking at the question.
“Even for a simple patient admitted to the hospital, that can represent a significant change in the medical picture—a sort of sentinel event. In the discharge clinic, we give them an opportunity to review the hospitalization and answer their questions,” she says. “A lot of information presented to patients in the hospital is not well heard, and the initial visit may be their first time to really talk about what happened.” For other patients with conditions such as congestive heart failure (CHF), chronic obstructive pulmonary disease (COPD), or poorly controlled diabetes, treatment guidelines might dictate a pattern for post-discharge follow-up—for example, medical visits in seven or 10 days.
In Seattle, Harborview Medical Center established its After Care Clinic, staffed by hospitalists and nurse practitioners, to provide transitional care for patients discharged from inpatient wards or the ED in need of follow-up, says medical director and hospitalist Shay Martinez, MD. A second priority is to see any CHF patient within 48 hours of discharge.
“We try to limit patients to a maximum of three visits in our clinic,” she says. “At that point, we help them get established in a medical home, either here in one of our primary-care clinics, or in one of the many excellent community clinics in the area.
“This model works well with our patient population. We actually try to do primary care on the inpatient side as well. Our hospitalists are specialized in that approach, given our patient population. We see a lot of immigrants, non-English speakers, people with low health literacy, and the homeless, many of whom lack primary care,” Dr. Martinez says. “We do medication reconciliation, reassessments, and follow-ups with lab tests. We also try to assess who is more likely to be a no-show, and who needs more help with scheduling follow-up appointments.”
Clinical coverage of post-discharge clinics varies by setting, staffing, and scope. If demand is low, hospitalists or ED physicians can be called off the floor to see patients who return to the clinic, or they could staff the clinic after their hospitalist shift ends. Post-discharge clinic staff whose schedules are light can flex into providing primary-care visits in the clinic. Post-discharge can also could be provided in conjunction with—or as an alternative to—physician house calls to patients’ homes. Some post-discharge clinics work with medical call centers or telephonic case managers; some even use telemedicine.
It also could be a growth opportunity for hospitalist practices. “It is an exciting potential role for hospitalists interested in doing a little outpatient care,” Dr. Martinez says. “This is also a good way to be a safety net for your safety-net hospital.”
continued below...
What Do PCPs Think? It May Be Harder than It Looks
Although some PCPs instinctively will be suspicious of a hospitalist-run post-discharge clinic, it should be possible to clearly limit the service to short-term, immediate-post-hospital encounters focused on issues related to patients unable to get timely access to primary care, according to Dr. Doctoroff.
“I think there is a diversity of opinion by PCPs,” she says. “Some doctors really believe that it interferes with the patient-doctor relationship. But after we’ve been here for a couple of years, we’ve built up credibility with many providers.”
Charles Cutler, MD, FACP, a general internist with a practice in Norristown, Pa., and a member of the ACP’s Board of Regents, says the post-discharge clinic is “a novel idea.”
“I’d be very curious to see if this really is a way to provide better and more cost-effective care,” adds Dr. Cutler, who normally retains management of his own patients when they are hospitalized but agrees that hospitals need to find a solution for lapses in care transitions.
Even so, he says, establishing an outpatient clinic presence may be more difficult than many hospitalists appreciate. “You can’t just put a doc in a room. That physician needs equipment, scheduling, and support staff,” he says. “In our small practice, we employ one person just to ensure that each patient chart is up to date. The overhead necessary to replicate a typical medical office, even one merely providing a transition of care, could be substantial.”
Dr. Cutler emphasizes such office-based challenges as billing, which is distinctly different from hospital billing, and credentialing by insurance companies.
“There are many aspects that have to be thought through. If you see the patient, you need to make yourself available for follow-up calls, because you’ve created a relationship,” he says. “I’m a believer that hospital medicine requires a degree of specialization. But so does an office practice.”
Dr. Cutler acknowledges that some PCPs will be resentful of post-discharge clinics. “But if you don’t like a hospitalist-run discharge clinic, then you have a responsibility to rearrange your schedule to accommodate patients after their hospital discharge,” he says.
Partner with Community
Tallahassee (Fla.) Memorial Hospital (TMH) in February launched a transitional-care clinic in collaboration with faculty from Florida State University, community-based health providers, and the local Capital Health Plan. Hospitalists don’t staff the clinic, but the HM group is its major source of referrals, says Dean Watson, MD, chief medical officer at TMH. Patients can be followed for up to eight weeks, during which time they get comprehensive assessments, medication review and optimization, and referral by the clinic social worker to a PCP and to available community services.
“Three years ago, we came up with the idea for a patient population we know is at high risk for readmission. Why don’t we partner with organizations in the community, form a clinic, teach students and residents, and learn together?” Dr. Watson says. “In addition to the usual patients, TMH targets those who have been readmitted to the hospital three times or more in the past year.”
The clinic, open five days a week, is staffed by a physician, nurse practitioner, telephonic nurse, and social worker, and also has a geriatric assessment clinic.
“We set up a system to identify patients through our electronic health record, and when they come to the clinic, we focus on their social environment and other non-medical issues that might cause readmissions,” he says. The clinic has a pharmacy and funds to support medications for patients without insurance. “In our first six months, we reduced emergency room visits and readmissions for these patients by 68 percent.”
One key partner, Capital Health Plan, bought and refurbished a building, and made it available for the clinic at no cost. Capital’s motivation, says Tom Glennon, a senior vice president for the plan, is its commitment to the community and to community service.
“We’re a nonprofit HMO. We’re focused on what we can do to serve the community, and we’re looking at this as a way for the hospital to have fewer costly, unreimbursed bouncebacks,” Glennon says. “That’s a win-win for all of us.”
Most of the patients who use the clinic are not members of Capital Health Plan, Glennon adds. “If we see CHP members turning up at the transitions clinic, then we have a problem—a breakdown in our case management,” he explains. “Our goal is to have our members taken care of by primary-care providers.”
Hard Data? Not So Fast
How many post-discharge clinics are in operation today is not known. Fundamental financial data, too, are limited, but some say it is unlikely a post-discharge clinic will cover operating expenses from billing revenues alone.
Thus, such clinics will require funding from the hospital, HM group, health system, or health plans, based on the benefits the clinic provides to discharged patients and the impact on 30-day readmissions (for more about the logistical challenges post-discharge clinics present, see “What Do PCPs Think?”).
Some also suggest that many of the post-discharge clinics now in operation are too new to have demonstrated financial impact or return on investment. “We have not yet been asked to show our financial viability,” Dr. Doctoroff says. “I think the clinic leadership thinks we are fulfilling other goals for now, such as creating easier access for their patients after discharge.”
Amy Boutwell, MD, MPP, a hospitalist at Newton Wellesley Hospital in Massachusetts and founder of Collaborative Healthcare Strategies, is among the post-discharge skeptics. She agrees with Dr. Williams that the post-discharge concept is more of a temporary fix to the long-term issues in primary care. “I think the idea is getting more play than actual activity out there right now,” she says. “We need to find opportunities to manage transitions within our scope today and tomorrow while strategically looking at where we want to be in five years [as hospitals and health systems].”
Dr. Boutwell says she’s experienced the frustration of trying to make follow-up appointments with physicians who don’t have any open slots for hospitalized patients awaiting discharge. “We think of follow up as physician-led, but there are alternatives and physician extenders,” she says. “It is well-documented that our healthcare system underuses home health care and other services that might be helpful. We forget how many other opportunities there are in our communities to get another clinician to touch the patient.”
Hospitalists, as key players in the healthcare system, can speak out in support of strengthening primary-care networks and building more collaborative relationships with PCPs, according to Dr. Williams. “If you’re going to set up an outpatient clinic, ideally, have it staffed by PCPs who can funnel the patients into primary-care networks. If that’s not feasible, then hospitalists should proceed with caution, since this approach begins to take them out of their scope of practice,” he says.
With 13 years of experience in urban hospital settings, Dr. Williams is familiar with the dangers unassigned patients present at discharge. “But I don’t know that we’ve yet optimized the hospital discharge process at any hospital in the United States,” he says.
That said, Dr. Williams knows his hospital in downtown Chicago is now working to establish a post-discharge clinic. It will be staffed by PCPs and will target patients who don’t have a PCP, are on Medicaid, or lack insurance.
“Where it starts to make me uncomfortable,” Dr. Williams says, “is what happens when you follow patients out into the outpatient setting?
It’s hard to do just one visit and draw the line. Yes, you may prevent a readmission, but the patient is still left with chronic illness and the need for primary care.”
Larry Beresford is a freelance writer based in Oakland, Calif.
What Does the Research Say?
Post-discharge clinic advocates acknowledge that the research documenting outcomes from such clinics is scarce. A recent study from Northwestern University looked at 12 distinct care-transitions activities and their effect on readmission rates.2 Post-discharge clinics were not studied as a separate category, although they fit into the category of physician continuity across inpatient and outpatient settings.
“There’s definitely a hole in the literature regarding post-discharge care,” says lead author Luke Hansen, MD, MHS. The authors found that “no single intervention implemented alone was regularly associated with reduced risk for 30-day rehospitalizations.”
On the other hand, Misky et al found that discharged patients who lacked timely follow-up (within four weeks of discharge) were 10 times more likely to be readmitted than those who got the follow-up.3
Medical teams from around the world, including in Canada, the United Kingdom, Israel, and Australia, are studying readmission rates and care-transitions strategies. A study by physicians at National Taiwan University Hospital in Taipei describes its integrated transitional care to address post-discharge discontinuities and prevent rehospitalizations, including telephonic monitoring, hotline counseling, and referral to a hospital-run post-discharge clinic located within a hospitalist-managed ward.4 “Patients are treated primarily by the hospitalists who are familiar with them,” in a clinic open from 8 a.m. to 9 p.m., lead author Chin-Chung Shu, MD, wrote in an email. The clinic sees 15 to 30 patients per month; 80% of them are discharged patients without a PCP.
“We typically see patients one or two times in 30 days and then refer them to a suitable physician,” Dr. Shu says. In his study, patients who received post-discharge transitional care, including the post-discharge clinic, had lower rates of readmission and death within 30 days, 15% compared with 25% for a control group.
References
- Goodman, DC, Fisher ES, Chang C. After Hospitalization: A Dartmouth Atlas Report on Post-Acute Care for Medicare Beneficiaries. Dartmouth Atlas website. Available at: www.dartmouthatlas.org/downloads/reports/Post_discharge_events_092811.pdf. Accessed Nov. 3, 2011.
- Hansen LO, Young RS, Hinami K, Leung A, Williams MV. Interventions to reduce 3-day rehospitalization: A systematic review. Ann Int Med. 2011;155(8): 520-528.
- Misky GJ, Wald HL, Coleman EA. Post-hospitalization transitions: Examining the effects of timing of primary care provider follow-up. J Hosp Med. 2010;5(7):392-397.
- Shu CC, Hsu NC, Lin YF, et al. Integrated post-discharge transitional care in Taiwan. BMC Medicine website. Available at: www.biomedcentral.com/1741-7015/9/96. Accessed Nov. 1, 2011.
What Are the Clinical Indications for Noninvasive Positive Pressure Ventilation?

Case
A 63-year-old man with severe chronic obstructive pulmonary disease (COPD) presents with one week of increasing sputum, cough, and dyspnea. His respiratory rate is 26/minute and oxygen saturation is 86% on room air (RA). He is lethargic and appears mildly uncomfortable, but he responds appropriately to questions in three- to four-word sentences. He is tachypneic with accessory muscle use and has diffuse wheezes throughout his bilateral lung fields. His initial room air arterial blood gas (ABG) is 7.32/68/86/32. Chest radiograph is notable for flattened hemidiaphragms without focal opacity. The patient is placed on oxygen and receives prednisone with nebulized albuterol and ipratropium, but his dyspnea and tachypnea persist. Due to his respiratory distress, bilevel positive airway pressure (BiPAP) is considered.
What are the clinical indications for noninvasive positive pressure ventilation (NPPV)?
Overview
NPPV assists ventilation by delivering positive expiratory and/or inspiratory pressure without the use of an endotracheal tube. Theoretically, NPPV is a preferred method of ventilation as it may eliminate the need for endotracheal intubation and its associated morbidity and mortality, including airway trauma, loss of airway defense mechanisms (ventilator-associated pneumonia), mechanical ventilation (barotrauma), and disruption of speech and swallowing.1
NPPV is generally delivered via full-face mask or nasal mask. Nasal mask is often preferred for patient comfort, though air leaks occur with mouth breathing. There is no difference between nasal and full-face masks in outcomes including intubation rates and mortality.2,3,4 NPPV can be delivered via a portable or standard ventilator using the same modes available for endotracheal intubation, though pressure-cycled ventilators utilizing continuous positive airway pressure (CPAP) and BiPAP are most common. CPAP delivers air at a continuous fixed pressure throughout the respiratory cycle. BiPAP delivers positive pressure at alternating levels—higher for inspiration and lower for expiration. Guidelines suggest choosing a mode based on the etiology and pathophysiology of the respiratory failure and leveraging local comfort and expertise.2,3
In general, good candidates for NPPV display signs of tachypnea and dyspnea due to hypoxic or hypercapnic respiratory failure but are hemodynamically stable, without excessive secretions, and can protect their airway and achieve a proper seal with the mask.3 Difficulty may arise due to patient intolerance, claustrophobia, gastric distention, and poor fit that leads to air leak or skin erosion. With initiation of NPPV, patients should be followed in a care setting with the capacity for frequent monitoring and, if needed, quick access to invasive airway management. Monitoring should include patient comfort and ability to tolerate the device, vital signs, breathing pattern, oxygen saturation, ABG, and mental status. This initial evaluation may help predict the success of NPPV (see Table 2). Appropriately chosen candidates who do well with NPPV often demonstrate respiratory turnaround in a relatively brief interval.2,3
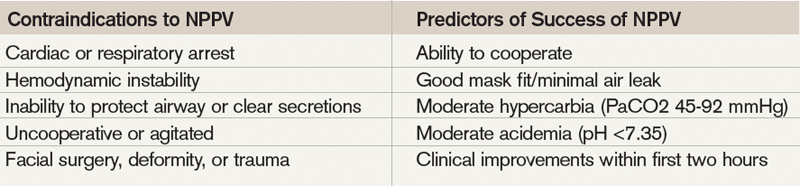
Review of the Data
NPPV is increasingly utilized in a variety of clinical situations. In 2000, the American Thoracic Society published consensus guidelines on the use of NPPV in acute respiratory failure.2 More recently, the Canadian Medical Association developed clinical guidelines for the use of NPPV in the acute-care setting.4 Clinical scenarios in which there is evidence for the efficacy of NPPV include severe exacerbations of COPD, cardiogenic pulmonary edema, immunosuppressed patients with pulmonary infiltrates, and hypoxia; it can also be used as a bridge to extubation in COPD patients.1-4
Acute exacerbation of COPD. Several randomized controlled trials (RCT) and meta-analyses have assessed the potential benefits of NPPV in patients with acute exacerbations of COPD. In COPD, NPPV improves gas exchange and facilitates respiratory muscle rest to decrease the work of breathing, which allows for respiratory recovery and time to effectiveness of standard therapies.5 Multiple trials have demonstrated that the addition of NPPV to usual care decreases intubation and mortality rates, as well as hospital lengths of stay (LOS).5-8
A Cochrane review of eight RCTs comparing NPPV with usual care noted a greater than 50% reduction in risk of intubation, and a number needed to treat (NNT) of eight patients to prevent one death.5 Quon and colleagues also compared NPPV to usual care in a meta-analysis of 14 trials.6 Eleven of these trials evaluated hospital mortality, which was decreased by 55% in patients receiving NPPV. Twelve trials assessed need for intubation, which decreased by 65%. In these trials, BiPAP was the most commonly used modality (see Table 3, for a comparison of NPPV modalities). Study patients had an average pH of 7.31 with an average PaCO2 of 68 mmHg. It was noted that the beneficial effects of NPPV increased as pH decreased. An earlier meta-analysis from Keenan and colleagues supported this notion, noting that the subgroup of patients with pH <7.3 benefited most in terms of decreased rates of intubation, hospital LOS, and hospital mortality.7 In this 2003 study, patients with relatively mild exacerbations of COPD did not benefit from the addition of NPPV to usual care. Based on the amount of positive evidence, NPPV is recommended in patients experiencing severe exacerbations of COPD as evidenced by a pH <7.35 and relative hypercarbia.1,2,4,7
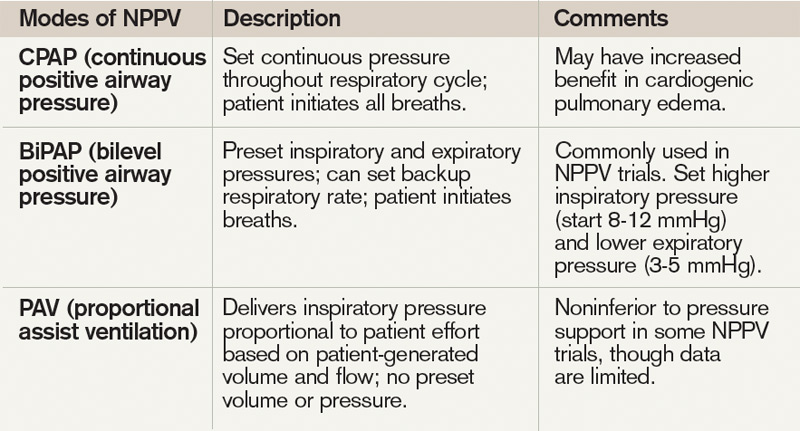
Cardiogenic pulmonary edema. In patients with acute cardiogenic pulmonary edema, NPPV has been found to be beneficial, decreasing mortality, rates of intubation, and hospital LOS. Physiologically, NPPV augments cardiac output, improves respiratory mechanics, and decreases afterload.10 Cardiogenic edema is variably defined and has a number of causes elucidated in an analysis of 11 RCTs conducted by Masip and colleagues. These causes included acute coronary syndrome (31%), hypertension (27%), congestive heart failure (14%), and a combination of respiratory infection, arrhythmia, volume overload, and treatment noncompliance (28%).9 In this analysis, CPAP and BiPAP demonstrated a combined 43% reduction in mortality and a 57% reduction in intubation. More recently, Peter and colleagues described a statistically significant reduction in hospital mortality and the need for intubation with CPAP, while BiPAP only demonstrated a statistically significant decrease in need for intubation.10 Thus, there appears to be some evidence that CPAP is the preferred NPPV mode in patients with acute cardiogenic pulmonary edema. Despite inclusion of a recent, large RCT showing no benefit of NPPV versus usual care in cardiogenic pulmonary edema, the overall positive effect of NPPV persisted, particularly when the cause of pulmonary edema was acute coronary syndrome.11
Weaning after intubation. NPPV has been evaluated as a method to facilitate early extubation, as a measure to prevent extubation failure, and as a treatment modality for respiratory failure following extubation, with mixed results.12,13 In 1998, a small trial compared the use of NPPV in COPD patients to facilitate early extubation with a standard weaning protocol. In this population, early NPPV resulted in better weaning rates with shorter times of mechanical ventilation (10 vs. 16 days), fewer days in the ICU, and improved 60-day survival rates (92% vs. 72%).3,14 In another RCT not limited to COPD patients, Grault and colleagues found that NPPV reduced the duration of intubation (4.5 vs. 7.6 days) but was not associated with benefits in ICU length of stay or survival previously described.3,15 Thus, though NPPV may be beneficial in facilitating early extubation in COPD patients, it is not recommended in other patient populations.4
NPPV has also been evaluated as a measure to prevent respiratory failure in patients at high risk for extubation failure. When applied immediately after extubation in patients with COPD and obesity, NPPV reduced reintubation rates and ICU mortality.3,4 In 2004, Esteban and colleagues examined NPPV in patients who had respiratory failure following extubation. In this setting, NPPV was ineffective at preventing reintubation and had no survival benefit.
In summary, NPPV may facilitate early extubation and prevent extubation failure in appropriate patients, such as those with COPD, but is unlikely to be beneficial and is not recommended in patients with existing respiratory failure after extubation.4,15
Immunosuppressed patients. A 2001 single-center, randomized-controlled trial by Holbert and colleagues demonstrated decreased intubation rates and mortality with the application of NPPV in immunosuppressed patients with hypoxemic respiratory failure, fever, and pulmonary infiltrates.16
In this study, immunosuppression occurred most commonly as a result of malignancy. In the group receiving NPPV alternating with oxygen (at least 45 minutes of NPPV alternated every three hours with periods of spontaneous breathing), the rate of subsequent intubation decreased to 46%, compared with 77% in those receiving oxygen alone. The mortality rate was 38% in the NPPV group, as compared with 69% in the standard treatment group.
Though the outcomes in immunocompromised patients with hypoxemia, fever, and pulmonary infiltrates were very poor (38% mortality even with NPPV), this small study and recent guidelines suggest a trial of NPPV in this population.4,16
Other indications. NPPV has been applied in multiple other clinical scenarios, including exacerbation of asthma, community-acquired pneumonia, acute lung injury, and bronchoscopy in hypoxemic patients. It has also been evaluated in the postsurgical period and in chest trauma. There are mixed and less robust data in these various applications, and larger controlled trials are lacking.
In asthma exacerbation, NPPV may improve dyspnea, but data regarding outcomes (intubation, mortality) are lacking. A 2005 Cochrane review concluded that data remain controversial due to insufficient evidence, and guidelines make no recommendations concerning NPPV in asthma exacerbation.4,17 Similarly, in community-acquired pneumonia without prior history of COPD, there is no major role for NPPV.1,3,4 Limited data suggest that NPPV lacks efficacy in preventing post-surgical respiratory failure, though it may be useful in treating existing respiratory failure or preventing intubation in patients following lung resection or abdominal surgery.1,4 In hypoxemic patients undergoing bronchoscopy, NPPV may improve oxygenation (lower respiratory rates and improved PaO2 to FiO2 ratios, compared with oxygen alone) as well as hemodynamics (minimizing the drop in mean arterial pressure). However, outcome data are lacking and the data set is small.4,18 In acute lung injury/acute respiratory distress syndrome, data are also limited, but NPPV appears to have a high failure rate and confers little benefit.1,4
Back to the Case
The patient was admitted to the hospital and placed on BiPAP for approximately 1.5 hours. The patient’s respiratory rate improved to 20/minute and he appeared increasingly comfortable and alert. A repeat ABG revealed improved hypercarbia and acidosis. He was continued on steroids and antibiotics and eventually was weaned from BiPAP and discharged home.
Bottom Line
NPPV is an effective method to decrease mortality, intubation rates, and duration of ICU stay in severe exacerbations of COPD, cardiogenic pulmonary edema, immunosuppressed patients with pulmonary infiltrates, and hypoxia, and as a bridge to extubation in COPD patients.
Dr. Kraynek is an internal medicine resident in the Department of Medicine at the University of Washington School of Medicine in Seattle. Dr. Best is assistant professor of medicine in the Division of General Internal Medicine at the University of Washington School of Medicine.
References
- Ambrosino N, Vagheggini G. Noninvasive positive pressure ventilation in the acute care setting: where are we? Euro Resp J. 2008;31:874-856.
- American Thoracic Society. International Consensus Conferences in Intensive Care Medicine: Noninvasive Positive Pressure Ventilation in Acute Respiratory Failure. Am J Respir Crit Care Med. 2001;163:283-291.
- Liesching T, Kwok H, Hill N. Acute applications of noninvasive positive pressure ventilation. Chest. 2003;124:699-713.
- Keenan S, Sinuff T, Burns K, et al. Clinical practice guidelines for the use of noninvasive positive pressure ventilation and noninvasive continuous positive airway pressure in the acute care setting. CMAJ. 2001;183:E195-E214.
- Lightowler J, Wedzicha J, Elliot M, Ram F. Noninvasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. BMJ. 2003;326:185.
- Quon B, Gan W, Sin D. Contemporary management of acute exacerbations of COPD: a systematic review of the metaanalysis. Chest. 2008;133:756-766.
- Keenan S, Sinuff T, Cook D, Hill, N. Which patients with acute exacerbation of chronic obstructive pulmonary disease benefit from noninvasive positive pressure ventilation? Ann Intern Med. 2003;138:861-870.
- Scala R, Naldi M, Archinucci I, Conigilo G, Nava S. Noninvasive positive pressure ventilation in patients with acute exacerbations of COPD and varying levels of consciousness. Chest. 2005;128:1657-1666.
- Masip J, Roque M, Sanchez B, Fernandez R, Subirana M, Exposito J. Noninvasive ventilation in acute cardiogenic pulmonary edema. JAMA. 2005;294:3124-3130.
- Peter J, Moran J, Phillips-Hughes J, Graham P, Bersten A. Effect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-anaylsis. Lancet. 2006;367:1155-1163.
- Weng C, Zhao Y, Liu Q, et al. Meta-analysis: noninvasive ventilation in acute cardiogenic pulmonary edema. Ann Intern Med. 2010;152:560-600.
- Keenan S, Sinuff T, Cook D, Hill N. Does noninvasive positive pressure ventilation improve outcome in acute hypoxemic respiratory failure? A systematic review. Crit Care Med. 2004;32:2516-2523.
- Esteban A, Frutos-Vivar F, Fergusun N, et al. Noninvasive positive pressure ventilation for respiratory failure after extubation. N Engl J Med. 2004;350:2452-2460.
- Nava S, Ambrosino N, Clinie E, et al. Noninvasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease: a randomized, controlled trial. Ann Intern Med. 1998;128:721-728.
- Grault C, Daudenthun I, Chevron V, et al. Noninvasive ventilation as a systematic extubation and weaning technique in acute on chronic respiratory failure: a prospective, randomized controlled study. Am J Respir Crit Care Med. 1999;160:86-92.
- Hilbert G, Gruson D, Vargas F, et al. Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure. N Engl J Med. 2001;344:481-487.
- Ram FSF, Wellington SR, Rowe BH, Wedzicha JA. Non-invasive positive pressure ventilation for treatment of respiratory failure due to severe acute exacerbations of asthma. Cochrane Database of Systematic Reviews. 2005, Issue 3.
- Antonelli M, Conti G, Rocco M, et al. Noninvasive positive pressure ventilation vs. conventional oxygen supplementation in hypoxemic patients undergoing diagnostic bronchoscopy. Chest. 2002;121:1149-1154.
Case
A 63-year-old man with severe chronic obstructive pulmonary disease (COPD) presents with one week of increasing sputum, cough, and dyspnea. His respiratory rate is 26/minute and oxygen saturation is 86% on room air (RA). He is lethargic and appears mildly uncomfortable, but he responds appropriately to questions in three- to four-word sentences. He is tachypneic with accessory muscle use and has diffuse wheezes throughout his bilateral lung fields. His initial room air arterial blood gas (ABG) is 7.32/68/86/32. Chest radiograph is notable for flattened hemidiaphragms without focal opacity. The patient is placed on oxygen and receives prednisone with nebulized albuterol and ipratropium, but his dyspnea and tachypnea persist. Due to his respiratory distress, bilevel positive airway pressure (BiPAP) is considered.
What are the clinical indications for noninvasive positive pressure ventilation (NPPV)?
Overview
NPPV assists ventilation by delivering positive expiratory and/or inspiratory pressure without the use of an endotracheal tube. Theoretically, NPPV is a preferred method of ventilation as it may eliminate the need for endotracheal intubation and its associated morbidity and mortality, including airway trauma, loss of airway defense mechanisms (ventilator-associated pneumonia), mechanical ventilation (barotrauma), and disruption of speech and swallowing.1
NPPV is generally delivered via full-face mask or nasal mask. Nasal mask is often preferred for patient comfort, though air leaks occur with mouth breathing. There is no difference between nasal and full-face masks in outcomes including intubation rates and mortality.2,3,4 NPPV can be delivered via a portable or standard ventilator using the same modes available for endotracheal intubation, though pressure-cycled ventilators utilizing continuous positive airway pressure (CPAP) and BiPAP are most common. CPAP delivers air at a continuous fixed pressure throughout the respiratory cycle. BiPAP delivers positive pressure at alternating levels—higher for inspiration and lower for expiration. Guidelines suggest choosing a mode based on the etiology and pathophysiology of the respiratory failure and leveraging local comfort and expertise.2,3
In general, good candidates for NPPV display signs of tachypnea and dyspnea due to hypoxic or hypercapnic respiratory failure but are hemodynamically stable, without excessive secretions, and can protect their airway and achieve a proper seal with the mask.3 Difficulty may arise due to patient intolerance, claustrophobia, gastric distention, and poor fit that leads to air leak or skin erosion. With initiation of NPPV, patients should be followed in a care setting with the capacity for frequent monitoring and, if needed, quick access to invasive airway management. Monitoring should include patient comfort and ability to tolerate the device, vital signs, breathing pattern, oxygen saturation, ABG, and mental status. This initial evaluation may help predict the success of NPPV (see Table 2). Appropriately chosen candidates who do well with NPPV often demonstrate respiratory turnaround in a relatively brief interval.2,3
Review of the Data
NPPV is increasingly utilized in a variety of clinical situations. In 2000, the American Thoracic Society published consensus guidelines on the use of NPPV in acute respiratory failure.2 More recently, the Canadian Medical Association developed clinical guidelines for the use of NPPV in the acute-care setting.4 Clinical scenarios in which there is evidence for the efficacy of NPPV include severe exacerbations of COPD, cardiogenic pulmonary edema, immunosuppressed patients with pulmonary infiltrates, and hypoxia; it can also be used as a bridge to extubation in COPD patients.1-4
Acute exacerbation of COPD. Several randomized controlled trials (RCT) and meta-analyses have assessed the potential benefits of NPPV in patients with acute exacerbations of COPD. In COPD, NPPV improves gas exchange and facilitates respiratory muscle rest to decrease the work of breathing, which allows for respiratory recovery and time to effectiveness of standard therapies.5 Multiple trials have demonstrated that the addition of NPPV to usual care decreases intubation and mortality rates, as well as hospital lengths of stay (LOS).5-8
A Cochrane review of eight RCTs comparing NPPV with usual care noted a greater than 50% reduction in risk of intubation, and a number needed to treat (NNT) of eight patients to prevent one death.5 Quon and colleagues also compared NPPV to usual care in a meta-analysis of 14 trials.6 Eleven of these trials evaluated hospital mortality, which was decreased by 55% in patients receiving NPPV. Twelve trials assessed need for intubation, which decreased by 65%. In these trials, BiPAP was the most commonly used modality (see Table 3, for a comparison of NPPV modalities). Study patients had an average pH of 7.31 with an average PaCO2 of 68 mmHg. It was noted that the beneficial effects of NPPV increased as pH decreased. An earlier meta-analysis from Keenan and colleagues supported this notion, noting that the subgroup of patients with pH <7.3 benefited most in terms of decreased rates of intubation, hospital LOS, and hospital mortality.7 In this 2003 study, patients with relatively mild exacerbations of COPD did not benefit from the addition of NPPV to usual care. Based on the amount of positive evidence, NPPV is recommended in patients experiencing severe exacerbations of COPD as evidenced by a pH <7.35 and relative hypercarbia.1,2,4,7
Cardiogenic pulmonary edema. In patients with acute cardiogenic pulmonary edema, NPPV has been found to be beneficial, decreasing mortality, rates of intubation, and hospital LOS. Physiologically, NPPV augments cardiac output, improves respiratory mechanics, and decreases afterload.10 Cardiogenic edema is variably defined and has a number of causes elucidated in an analysis of 11 RCTs conducted by Masip and colleagues. These causes included acute coronary syndrome (31%), hypertension (27%), congestive heart failure (14%), and a combination of respiratory infection, arrhythmia, volume overload, and treatment noncompliance (28%).9 In this analysis, CPAP and BiPAP demonstrated a combined 43% reduction in mortality and a 57% reduction in intubation. More recently, Peter and colleagues described a statistically significant reduction in hospital mortality and the need for intubation with CPAP, while BiPAP only demonstrated a statistically significant decrease in need for intubation.10 Thus, there appears to be some evidence that CPAP is the preferred NPPV mode in patients with acute cardiogenic pulmonary edema. Despite inclusion of a recent, large RCT showing no benefit of NPPV versus usual care in cardiogenic pulmonary edema, the overall positive effect of NPPV persisted, particularly when the cause of pulmonary edema was acute coronary syndrome.11
Weaning after intubation. NPPV has been evaluated as a method to facilitate early extubation, as a measure to prevent extubation failure, and as a treatment modality for respiratory failure following extubation, with mixed results.12,13 In 1998, a small trial compared the use of NPPV in COPD patients to facilitate early extubation with a standard weaning protocol. In this population, early NPPV resulted in better weaning rates with shorter times of mechanical ventilation (10 vs. 16 days), fewer days in the ICU, and improved 60-day survival rates (92% vs. 72%).3,14 In another RCT not limited to COPD patients, Grault and colleagues found that NPPV reduced the duration of intubation (4.5 vs. 7.6 days) but was not associated with benefits in ICU length of stay or survival previously described.3,15 Thus, though NPPV may be beneficial in facilitating early extubation in COPD patients, it is not recommended in other patient populations.4
NPPV has also been evaluated as a measure to prevent respiratory failure in patients at high risk for extubation failure. When applied immediately after extubation in patients with COPD and obesity, NPPV reduced reintubation rates and ICU mortality.3,4 In 2004, Esteban and colleagues examined NPPV in patients who had respiratory failure following extubation. In this setting, NPPV was ineffective at preventing reintubation and had no survival benefit.
In summary, NPPV may facilitate early extubation and prevent extubation failure in appropriate patients, such as those with COPD, but is unlikely to be beneficial and is not recommended in patients with existing respiratory failure after extubation.4,15
Immunosuppressed patients. A 2001 single-center, randomized-controlled trial by Holbert and colleagues demonstrated decreased intubation rates and mortality with the application of NPPV in immunosuppressed patients with hypoxemic respiratory failure, fever, and pulmonary infiltrates.16
In this study, immunosuppression occurred most commonly as a result of malignancy. In the group receiving NPPV alternating with oxygen (at least 45 minutes of NPPV alternated every three hours with periods of spontaneous breathing), the rate of subsequent intubation decreased to 46%, compared with 77% in those receiving oxygen alone. The mortality rate was 38% in the NPPV group, as compared with 69% in the standard treatment group.
Though the outcomes in immunocompromised patients with hypoxemia, fever, and pulmonary infiltrates were very poor (38% mortality even with NPPV), this small study and recent guidelines suggest a trial of NPPV in this population.4,16
Other indications. NPPV has been applied in multiple other clinical scenarios, including exacerbation of asthma, community-acquired pneumonia, acute lung injury, and bronchoscopy in hypoxemic patients. It has also been evaluated in the postsurgical period and in chest trauma. There are mixed and less robust data in these various applications, and larger controlled trials are lacking.
In asthma exacerbation, NPPV may improve dyspnea, but data regarding outcomes (intubation, mortality) are lacking. A 2005 Cochrane review concluded that data remain controversial due to insufficient evidence, and guidelines make no recommendations concerning NPPV in asthma exacerbation.4,17 Similarly, in community-acquired pneumonia without prior history of COPD, there is no major role for NPPV.1,3,4 Limited data suggest that NPPV lacks efficacy in preventing post-surgical respiratory failure, though it may be useful in treating existing respiratory failure or preventing intubation in patients following lung resection or abdominal surgery.1,4 In hypoxemic patients undergoing bronchoscopy, NPPV may improve oxygenation (lower respiratory rates and improved PaO2 to FiO2 ratios, compared with oxygen alone) as well as hemodynamics (minimizing the drop in mean arterial pressure). However, outcome data are lacking and the data set is small.4,18 In acute lung injury/acute respiratory distress syndrome, data are also limited, but NPPV appears to have a high failure rate and confers little benefit.1,4
Back to the Case
The patient was admitted to the hospital and placed on BiPAP for approximately 1.5 hours. The patient’s respiratory rate improved to 20/minute and he appeared increasingly comfortable and alert. A repeat ABG revealed improved hypercarbia and acidosis. He was continued on steroids and antibiotics and eventually was weaned from BiPAP and discharged home.
Bottom Line
NPPV is an effective method to decrease mortality, intubation rates, and duration of ICU stay in severe exacerbations of COPD, cardiogenic pulmonary edema, immunosuppressed patients with pulmonary infiltrates, and hypoxia, and as a bridge to extubation in COPD patients.
Dr. Kraynek is an internal medicine resident in the Department of Medicine at the University of Washington School of Medicine in Seattle. Dr. Best is assistant professor of medicine in the Division of General Internal Medicine at the University of Washington School of Medicine.
References
- Ambrosino N, Vagheggini G. Noninvasive positive pressure ventilation in the acute care setting: where are we? Euro Resp J. 2008;31:874-856.
- American Thoracic Society. International Consensus Conferences in Intensive Care Medicine: Noninvasive Positive Pressure Ventilation in Acute Respiratory Failure. Am J Respir Crit Care Med. 2001;163:283-291.
- Liesching T, Kwok H, Hill N. Acute applications of noninvasive positive pressure ventilation. Chest. 2003;124:699-713.
- Keenan S, Sinuff T, Burns K, et al. Clinical practice guidelines for the use of noninvasive positive pressure ventilation and noninvasive continuous positive airway pressure in the acute care setting. CMAJ. 2001;183:E195-E214.
- Lightowler J, Wedzicha J, Elliot M, Ram F. Noninvasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. BMJ. 2003;326:185.
- Quon B, Gan W, Sin D. Contemporary management of acute exacerbations of COPD: a systematic review of the metaanalysis. Chest. 2008;133:756-766.
- Keenan S, Sinuff T, Cook D, Hill, N. Which patients with acute exacerbation of chronic obstructive pulmonary disease benefit from noninvasive positive pressure ventilation? Ann Intern Med. 2003;138:861-870.
- Scala R, Naldi M, Archinucci I, Conigilo G, Nava S. Noninvasive positive pressure ventilation in patients with acute exacerbations of COPD and varying levels of consciousness. Chest. 2005;128:1657-1666.
- Masip J, Roque M, Sanchez B, Fernandez R, Subirana M, Exposito J. Noninvasive ventilation in acute cardiogenic pulmonary edema. JAMA. 2005;294:3124-3130.
- Peter J, Moran J, Phillips-Hughes J, Graham P, Bersten A. Effect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-anaylsis. Lancet. 2006;367:1155-1163.
- Weng C, Zhao Y, Liu Q, et al. Meta-analysis: noninvasive ventilation in acute cardiogenic pulmonary edema. Ann Intern Med. 2010;152:560-600.
- Keenan S, Sinuff T, Cook D, Hill N. Does noninvasive positive pressure ventilation improve outcome in acute hypoxemic respiratory failure? A systematic review. Crit Care Med. 2004;32:2516-2523.
- Esteban A, Frutos-Vivar F, Fergusun N, et al. Noninvasive positive pressure ventilation for respiratory failure after extubation. N Engl J Med. 2004;350:2452-2460.
- Nava S, Ambrosino N, Clinie E, et al. Noninvasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease: a randomized, controlled trial. Ann Intern Med. 1998;128:721-728.
- Grault C, Daudenthun I, Chevron V, et al. Noninvasive ventilation as a systematic extubation and weaning technique in acute on chronic respiratory failure: a prospective, randomized controlled study. Am J Respir Crit Care Med. 1999;160:86-92.
- Hilbert G, Gruson D, Vargas F, et al. Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure. N Engl J Med. 2001;344:481-487.
- Ram FSF, Wellington SR, Rowe BH, Wedzicha JA. Non-invasive positive pressure ventilation for treatment of respiratory failure due to severe acute exacerbations of asthma. Cochrane Database of Systematic Reviews. 2005, Issue 3.
- Antonelli M, Conti G, Rocco M, et al. Noninvasive positive pressure ventilation vs. conventional oxygen supplementation in hypoxemic patients undergoing diagnostic bronchoscopy. Chest. 2002;121:1149-1154.
Case
A 63-year-old man with severe chronic obstructive pulmonary disease (COPD) presents with one week of increasing sputum, cough, and dyspnea. His respiratory rate is 26/minute and oxygen saturation is 86% on room air (RA). He is lethargic and appears mildly uncomfortable, but he responds appropriately to questions in three- to four-word sentences. He is tachypneic with accessory muscle use and has diffuse wheezes throughout his bilateral lung fields. His initial room air arterial blood gas (ABG) is 7.32/68/86/32. Chest radiograph is notable for flattened hemidiaphragms without focal opacity. The patient is placed on oxygen and receives prednisone with nebulized albuterol and ipratropium, but his dyspnea and tachypnea persist. Due to his respiratory distress, bilevel positive airway pressure (BiPAP) is considered.
What are the clinical indications for noninvasive positive pressure ventilation (NPPV)?
Overview
NPPV assists ventilation by delivering positive expiratory and/or inspiratory pressure without the use of an endotracheal tube. Theoretically, NPPV is a preferred method of ventilation as it may eliminate the need for endotracheal intubation and its associated morbidity and mortality, including airway trauma, loss of airway defense mechanisms (ventilator-associated pneumonia), mechanical ventilation (barotrauma), and disruption of speech and swallowing.1
NPPV is generally delivered via full-face mask or nasal mask. Nasal mask is often preferred for patient comfort, though air leaks occur with mouth breathing. There is no difference between nasal and full-face masks in outcomes including intubation rates and mortality.2,3,4 NPPV can be delivered via a portable or standard ventilator using the same modes available for endotracheal intubation, though pressure-cycled ventilators utilizing continuous positive airway pressure (CPAP) and BiPAP are most common. CPAP delivers air at a continuous fixed pressure throughout the respiratory cycle. BiPAP delivers positive pressure at alternating levels—higher for inspiration and lower for expiration. Guidelines suggest choosing a mode based on the etiology and pathophysiology of the respiratory failure and leveraging local comfort and expertise.2,3
In general, good candidates for NPPV display signs of tachypnea and dyspnea due to hypoxic or hypercapnic respiratory failure but are hemodynamically stable, without excessive secretions, and can protect their airway and achieve a proper seal with the mask.3 Difficulty may arise due to patient intolerance, claustrophobia, gastric distention, and poor fit that leads to air leak or skin erosion. With initiation of NPPV, patients should be followed in a care setting with the capacity for frequent monitoring and, if needed, quick access to invasive airway management. Monitoring should include patient comfort and ability to tolerate the device, vital signs, breathing pattern, oxygen saturation, ABG, and mental status. This initial evaluation may help predict the success of NPPV (see Table 2). Appropriately chosen candidates who do well with NPPV often demonstrate respiratory turnaround in a relatively brief interval.2,3
Review of the Data
NPPV is increasingly utilized in a variety of clinical situations. In 2000, the American Thoracic Society published consensus guidelines on the use of NPPV in acute respiratory failure.2 More recently, the Canadian Medical Association developed clinical guidelines for the use of NPPV in the acute-care setting.4 Clinical scenarios in which there is evidence for the efficacy of NPPV include severe exacerbations of COPD, cardiogenic pulmonary edema, immunosuppressed patients with pulmonary infiltrates, and hypoxia; it can also be used as a bridge to extubation in COPD patients.1-4
Acute exacerbation of COPD. Several randomized controlled trials (RCT) and meta-analyses have assessed the potential benefits of NPPV in patients with acute exacerbations of COPD. In COPD, NPPV improves gas exchange and facilitates respiratory muscle rest to decrease the work of breathing, which allows for respiratory recovery and time to effectiveness of standard therapies.5 Multiple trials have demonstrated that the addition of NPPV to usual care decreases intubation and mortality rates, as well as hospital lengths of stay (LOS).5-8
A Cochrane review of eight RCTs comparing NPPV with usual care noted a greater than 50% reduction in risk of intubation, and a number needed to treat (NNT) of eight patients to prevent one death.5 Quon and colleagues also compared NPPV to usual care in a meta-analysis of 14 trials.6 Eleven of these trials evaluated hospital mortality, which was decreased by 55% in patients receiving NPPV. Twelve trials assessed need for intubation, which decreased by 65%. In these trials, BiPAP was the most commonly used modality (see Table 3, for a comparison of NPPV modalities). Study patients had an average pH of 7.31 with an average PaCO2 of 68 mmHg. It was noted that the beneficial effects of NPPV increased as pH decreased. An earlier meta-analysis from Keenan and colleagues supported this notion, noting that the subgroup of patients with pH <7.3 benefited most in terms of decreased rates of intubation, hospital LOS, and hospital mortality.7 In this 2003 study, patients with relatively mild exacerbations of COPD did not benefit from the addition of NPPV to usual care. Based on the amount of positive evidence, NPPV is recommended in patients experiencing severe exacerbations of COPD as evidenced by a pH <7.35 and relative hypercarbia.1,2,4,7
Cardiogenic pulmonary edema. In patients with acute cardiogenic pulmonary edema, NPPV has been found to be beneficial, decreasing mortality, rates of intubation, and hospital LOS. Physiologically, NPPV augments cardiac output, improves respiratory mechanics, and decreases afterload.10 Cardiogenic edema is variably defined and has a number of causes elucidated in an analysis of 11 RCTs conducted by Masip and colleagues. These causes included acute coronary syndrome (31%), hypertension (27%), congestive heart failure (14%), and a combination of respiratory infection, arrhythmia, volume overload, and treatment noncompliance (28%).9 In this analysis, CPAP and BiPAP demonstrated a combined 43% reduction in mortality and a 57% reduction in intubation. More recently, Peter and colleagues described a statistically significant reduction in hospital mortality and the need for intubation with CPAP, while BiPAP only demonstrated a statistically significant decrease in need for intubation.10 Thus, there appears to be some evidence that CPAP is the preferred NPPV mode in patients with acute cardiogenic pulmonary edema. Despite inclusion of a recent, large RCT showing no benefit of NPPV versus usual care in cardiogenic pulmonary edema, the overall positive effect of NPPV persisted, particularly when the cause of pulmonary edema was acute coronary syndrome.11
Weaning after intubation. NPPV has been evaluated as a method to facilitate early extubation, as a measure to prevent extubation failure, and as a treatment modality for respiratory failure following extubation, with mixed results.12,13 In 1998, a small trial compared the use of NPPV in COPD patients to facilitate early extubation with a standard weaning protocol. In this population, early NPPV resulted in better weaning rates with shorter times of mechanical ventilation (10 vs. 16 days), fewer days in the ICU, and improved 60-day survival rates (92% vs. 72%).3,14 In another RCT not limited to COPD patients, Grault and colleagues found that NPPV reduced the duration of intubation (4.5 vs. 7.6 days) but was not associated with benefits in ICU length of stay or survival previously described.3,15 Thus, though NPPV may be beneficial in facilitating early extubation in COPD patients, it is not recommended in other patient populations.4
NPPV has also been evaluated as a measure to prevent respiratory failure in patients at high risk for extubation failure. When applied immediately after extubation in patients with COPD and obesity, NPPV reduced reintubation rates and ICU mortality.3,4 In 2004, Esteban and colleagues examined NPPV in patients who had respiratory failure following extubation. In this setting, NPPV was ineffective at preventing reintubation and had no survival benefit.
In summary, NPPV may facilitate early extubation and prevent extubation failure in appropriate patients, such as those with COPD, but is unlikely to be beneficial and is not recommended in patients with existing respiratory failure after extubation.4,15
Immunosuppressed patients. A 2001 single-center, randomized-controlled trial by Holbert and colleagues demonstrated decreased intubation rates and mortality with the application of NPPV in immunosuppressed patients with hypoxemic respiratory failure, fever, and pulmonary infiltrates.16
In this study, immunosuppression occurred most commonly as a result of malignancy. In the group receiving NPPV alternating with oxygen (at least 45 minutes of NPPV alternated every three hours with periods of spontaneous breathing), the rate of subsequent intubation decreased to 46%, compared with 77% in those receiving oxygen alone. The mortality rate was 38% in the NPPV group, as compared with 69% in the standard treatment group.
Though the outcomes in immunocompromised patients with hypoxemia, fever, and pulmonary infiltrates were very poor (38% mortality even with NPPV), this small study and recent guidelines suggest a trial of NPPV in this population.4,16
Other indications. NPPV has been applied in multiple other clinical scenarios, including exacerbation of asthma, community-acquired pneumonia, acute lung injury, and bronchoscopy in hypoxemic patients. It has also been evaluated in the postsurgical period and in chest trauma. There are mixed and less robust data in these various applications, and larger controlled trials are lacking.
In asthma exacerbation, NPPV may improve dyspnea, but data regarding outcomes (intubation, mortality) are lacking. A 2005 Cochrane review concluded that data remain controversial due to insufficient evidence, and guidelines make no recommendations concerning NPPV in asthma exacerbation.4,17 Similarly, in community-acquired pneumonia without prior history of COPD, there is no major role for NPPV.1,3,4 Limited data suggest that NPPV lacks efficacy in preventing post-surgical respiratory failure, though it may be useful in treating existing respiratory failure or preventing intubation in patients following lung resection or abdominal surgery.1,4 In hypoxemic patients undergoing bronchoscopy, NPPV may improve oxygenation (lower respiratory rates and improved PaO2 to FiO2 ratios, compared with oxygen alone) as well as hemodynamics (minimizing the drop in mean arterial pressure). However, outcome data are lacking and the data set is small.4,18 In acute lung injury/acute respiratory distress syndrome, data are also limited, but NPPV appears to have a high failure rate and confers little benefit.1,4
Back to the Case
The patient was admitted to the hospital and placed on BiPAP for approximately 1.5 hours. The patient’s respiratory rate improved to 20/minute and he appeared increasingly comfortable and alert. A repeat ABG revealed improved hypercarbia and acidosis. He was continued on steroids and antibiotics and eventually was weaned from BiPAP and discharged home.
Bottom Line
NPPV is an effective method to decrease mortality, intubation rates, and duration of ICU stay in severe exacerbations of COPD, cardiogenic pulmonary edema, immunosuppressed patients with pulmonary infiltrates, and hypoxia, and as a bridge to extubation in COPD patients.
Dr. Kraynek is an internal medicine resident in the Department of Medicine at the University of Washington School of Medicine in Seattle. Dr. Best is assistant professor of medicine in the Division of General Internal Medicine at the University of Washington School of Medicine.
References
- Ambrosino N, Vagheggini G. Noninvasive positive pressure ventilation in the acute care setting: where are we? Euro Resp J. 2008;31:874-856.
- American Thoracic Society. International Consensus Conferences in Intensive Care Medicine: Noninvasive Positive Pressure Ventilation in Acute Respiratory Failure. Am J Respir Crit Care Med. 2001;163:283-291.
- Liesching T, Kwok H, Hill N. Acute applications of noninvasive positive pressure ventilation. Chest. 2003;124:699-713.
- Keenan S, Sinuff T, Burns K, et al. Clinical practice guidelines for the use of noninvasive positive pressure ventilation and noninvasive continuous positive airway pressure in the acute care setting. CMAJ. 2001;183:E195-E214.
- Lightowler J, Wedzicha J, Elliot M, Ram F. Noninvasive positive pressure ventilation to treat respiratory failure resulting from exacerbations of chronic obstructive pulmonary disease: Cochrane systematic review and meta-analysis. BMJ. 2003;326:185.
- Quon B, Gan W, Sin D. Contemporary management of acute exacerbations of COPD: a systematic review of the metaanalysis. Chest. 2008;133:756-766.
- Keenan S, Sinuff T, Cook D, Hill, N. Which patients with acute exacerbation of chronic obstructive pulmonary disease benefit from noninvasive positive pressure ventilation? Ann Intern Med. 2003;138:861-870.
- Scala R, Naldi M, Archinucci I, Conigilo G, Nava S. Noninvasive positive pressure ventilation in patients with acute exacerbations of COPD and varying levels of consciousness. Chest. 2005;128:1657-1666.
- Masip J, Roque M, Sanchez B, Fernandez R, Subirana M, Exposito J. Noninvasive ventilation in acute cardiogenic pulmonary edema. JAMA. 2005;294:3124-3130.
- Peter J, Moran J, Phillips-Hughes J, Graham P, Bersten A. Effect of non-invasive positive pressure ventilation (NIPPV) on mortality in patients with acute cardiogenic pulmonary oedema: a meta-anaylsis. Lancet. 2006;367:1155-1163.
- Weng C, Zhao Y, Liu Q, et al. Meta-analysis: noninvasive ventilation in acute cardiogenic pulmonary edema. Ann Intern Med. 2010;152:560-600.
- Keenan S, Sinuff T, Cook D, Hill N. Does noninvasive positive pressure ventilation improve outcome in acute hypoxemic respiratory failure? A systematic review. Crit Care Med. 2004;32:2516-2523.
- Esteban A, Frutos-Vivar F, Fergusun N, et al. Noninvasive positive pressure ventilation for respiratory failure after extubation. N Engl J Med. 2004;350:2452-2460.
- Nava S, Ambrosino N, Clinie E, et al. Noninvasive mechanical ventilation in the weaning of patients with respiratory failure due to chronic obstructive pulmonary disease: a randomized, controlled trial. Ann Intern Med. 1998;128:721-728.
- Grault C, Daudenthun I, Chevron V, et al. Noninvasive ventilation as a systematic extubation and weaning technique in acute on chronic respiratory failure: a prospective, randomized controlled study. Am J Respir Crit Care Med. 1999;160:86-92.
- Hilbert G, Gruson D, Vargas F, et al. Noninvasive ventilation in immunosuppressed patients with pulmonary infiltrates, fever, and acute respiratory failure. N Engl J Med. 2001;344:481-487.
- Ram FSF, Wellington SR, Rowe BH, Wedzicha JA. Non-invasive positive pressure ventilation for treatment of respiratory failure due to severe acute exacerbations of asthma. Cochrane Database of Systematic Reviews. 2005, Issue 3.
- Antonelli M, Conti G, Rocco M, et al. Noninvasive positive pressure ventilation vs. conventional oxygen supplementation in hypoxemic patients undergoing diagnostic bronchoscopy. Chest. 2002;121:1149-1154.
Medical Profession “Terrified” to Address Kernicterus Concerns
I read with interest this article and I must say it is inaccurate. My son was born in 2001. He had a bilirubin of 51. Having the diagnosis of kernicterus was difficult in coming. Why? Because the medical profession is terrified to admit that this is happening.
I am a proud member of PICK. My son is wheelchair-confined, he is completely deaf, visually impaired, and has cerebral palsy, epilepsy, and lung disease from the pneumonias that he suffers from almost monthly. Due to his many seizure medications, he now has a blood disease.
Please visit our website (www.pickonline.org) to do a little more research on this matter. Maybe call one of us, as parents, to find out more. My son is not from California. In fact, most of our parents are not from California. Maybe research in other states is warranted.
Christine Thau
I read with interest this article and I must say it is inaccurate. My son was born in 2001. He had a bilirubin of 51. Having the diagnosis of kernicterus was difficult in coming. Why? Because the medical profession is terrified to admit that this is happening.
I am a proud member of PICK. My son is wheelchair-confined, he is completely deaf, visually impaired, and has cerebral palsy, epilepsy, and lung disease from the pneumonias that he suffers from almost monthly. Due to his many seizure medications, he now has a blood disease.
Please visit our website (www.pickonline.org) to do a little more research on this matter. Maybe call one of us, as parents, to find out more. My son is not from California. In fact, most of our parents are not from California. Maybe research in other states is warranted.
Christine Thau
I read with interest this article and I must say it is inaccurate. My son was born in 2001. He had a bilirubin of 51. Having the diagnosis of kernicterus was difficult in coming. Why? Because the medical profession is terrified to admit that this is happening.
I am a proud member of PICK. My son is wheelchair-confined, he is completely deaf, visually impaired, and has cerebral palsy, epilepsy, and lung disease from the pneumonias that he suffers from almost monthly. Due to his many seizure medications, he now has a blood disease.
Please visit our website (www.pickonline.org) to do a little more research on this matter. Maybe call one of us, as parents, to find out more. My son is not from California. In fact, most of our parents are not from California. Maybe research in other states is warranted.
Christine Thau
Quick Diagnosis Units
In recent years, hospitals in countries with public health systems have adopted organizational changes to improve efficiency and resource allocation. Acute hospital bed utilization is a growing concern for healthcare systems in these countries, as it represents a significant share of health costs.1
Inappropriate hospitalization is a significant problem for public health systems. In Spain and other countries, due to deficiencies in outpatient services, acute beds are increasingly occupied by patients requiring diagnostic tests for nonacute but potentially severe diseases that often need no immediate treatment, thereby reducing beds for acute patients.2, 3
Reports suggest 9% to 17% of patients admitted to Spanish internal medicine units could be studied on an outpatient basis.47 However, long delays in outpatient diagnostic tests in Spain make diagnosis outside conventional hospitalization unviable, especially when rapid access to tests for suspected malignancy is required.
These shortcomings have prompted the search for alternatives to hospitalization. Alternative care models include: 1‐day hospitals (providing medical procedures requiring <24 hours of hospitalization)8; short‐stay observation units (often located adjacent to emergency departments [ED], and accommodating patients requiring brief periods of observation or therapy)912; hospital‐in‐the‐home programs (delivering a limited range of acute care services to selected patients)1013; outpatient major surgery programs (providing surgical procedures with postoperative recovery periods short enough to permit same‐day discharge);14 and, more recently, quick diagnosis units ([QDUs], outpatient diagnostic units for patients with suspected severe disease).2, 3, 15, 16
Current referral processes for diagnosis and specialized care in primary health care (PHC), especially waiting times for diagnostic procedures, are longeven in patients with suspected cancerin public health systems such as in Spain. This results in PHC physicians and patients using the ED as a voluntary shortcut.3, 6, 17
In 1996, the use and benefits of quick‐and‐early diagnosis units were first described for suspected cancer patients referred from PHC centers to the Queen Elizabeth Hospital in Birmingham, England.16 Patients were evaluated by specialists according to the suspected diagnosis (eg, patients with hematuria or testicular masses were assessed by urologists).
QDUs are a little‐reported, potentially cost‐saving alternative that allow coordinated, agile diagnostic procedures and may avoid hospital admission. QDUs increase patient comfort by allowing many to remain at home during the diagnostic process.17 QDUs have been introduced in Spain in recent years, and are mainly directed by internists (similar to hospitalists in the United States). Patients with specific symptoms, such as breast or testicular masses, are referred to, and evaluated directly by, the appropriate medical specialist.17 Apart from 2 Opinion articles on QDUs led by specialists other than internists in the United Kingdom,16 and by internists (our group) in Spain,17 there are, to our knowledge, no other English‐language reports on this healthcare model.
The aim of this study was to describe the functioning of a QDU in a Spanish public university hospital after evaluating 2000 consecutive patients. We intended to ascertain the utility and cost of the model compared to conventional hospitalization and the degree of patient satisfaction.
METHODS
We carried out a longitudinal, descriptive study in a prospective cohort of 2000 consecutive QDU patients, evaluated between December 2007 and July 2010, in a public university hospital with 840 acute beds, serving a reference population of 540,000 in Barcelona, Spain.
The QDU is composed of a specialist in internal medicine and a registered nurse who work in the QDU for 5 hours daily, 5 days a week (Monday‐Friday), assisted by specialists from other specialties. It has a consulting room and a waiting room for patients and families, and functions daily.
For comparison, we analyzed a retrospective cohort of 1454 patients diagnosed with anemia (n = 548), cachexia‐anorexia syndrome (n = 458), febrile syndrome (n = 240), and adenopathies or palpable masses (n = 208) admitted to the internal medicine department between September 2006 and June 2010. Patients were randomly selected from the 2022 consecutive patients with these diagnoses, hospitalized during this period and compared, on an unmatched basis, with all 1468 QDU patients with the same diagnoses.
Patients evaluated by the QDU have potentially severe disease that would normally require hospital admission for diagnosis, but whose health status allows outpatient study, and who have no physical or psychological disability that would make attending the hospital several times difficult. The criteria for QDU referral are agreed with central services (Table 1). In our hospital, patients with lung abnormalities (eg, pulmonary nodules) are usually evaluated quickly in the 1‐day hospital of the respiratory diseases department, however, they are not excluded from QDU evaluation.
|
| Anemia* |
| Cachexia‐anorexia syndrome |
| Febrile syndrome |
| Adenopathies and/or palpable masses |
| Unexplained severe abdominal pain |
| Chronic diarrhea |
| Rectorrhagia |
| Jaundice |
| Lung and/or pleural abnormalities |
| Unexplained dyspnea |
| Dysphagia |
| Ascites |
| Anasarca |
| Arthritis |
Our QDU protocol is based on an urgent first visit, followed by preferential programming and coordination of complementary tests, and subsequent visits until a diagnosis is made. The main diagnostic tests are normally carried out within 10 days after the first visit and, thus, visits are not consecutive but spread over a short period of time. Patients are attended on an ambulatory basis and do not stay overnight.
Inclusion Criteria
When setting up the QDU, the ED, PHC centers, outpatients and other sources of referral were informed and trained in QDU referral criteria (Table 1). All diseases selected for QDU assessment were agreed according to established guidelines. For example, only patients with severe anemia, with or without symptoms, defined as a hemoglobin concentration <8 g/L, our accepted criterion for hospitalization for diagnosis and treatment, were included.
Exclusion Criteria
Patients who fulfilled the inclusion criteria but were judged by the QDU or ED physician as requiring hospitalization or routine outpatient study (eg, active bleeding, uncompensated heart failure, impaired general status, mobility, and social problems) were excluded. Likewise, patients lost to follow‐up or hospitalized during the study due to complications, and deaths were excluded.
For each patient, in addition to clinical data, we prospectively recorded: demographic data; reason for consultation; source of referral; waiting time for the first visit; number and date of visits; waiting times between visits; time to diagnosis; type, number, and date of complementary tests; final diagnosis; and onward referral. The full diagnostic workup was done according to previously established protocols. The Charlson comorbidity index was calculated.18 Blood transfusions and the mean number of units used (SAG‐M red cell concentrates with a median volume per unit of 289 [25] ml) were recorded and administered according to hospital protocol. The time to diagnosis was defined as the time from the first visit to a definitive diagnosis, and usually coincided with the results of diagnostic tests (eg, imaging or pathology).
The same factors were recorded for hospitalized patients (retrospective cohort) except for waiting time to the first visit, number and date of visits, waiting times between visits, and time to diagnosis. In addition, we recorded the mean hospital stay for each patient. Hospital admission avoided was defined as patients who would have been admitted for a diagnostic workup if there were no QDU.
We made a cost analysis using microcosting techniques. First, we calculated the mean number of QDU visits in 150 randomly selected patients with iron‐deficiency anemia, 150 with cachexia‐anorexia syndrome, 150 with fever of unknown origin, and 150 with adenopathies and/or palpable masses. We analyzed the full direct and indirect costs, and calculated the mean cost per visit and the mean cost per process (admission to discharge). The mean length‐of‐stay, and direct and indirect costs were also calculated retrospectively for the same number of hospitalized patients in 2 internal medicine wards, as were the mean cost per daily stay and the mean cost per process (admission to discharge). In our hospital, a 25‐bed internal medicine ward is staffed by 2 consultant physicians and 4 residents, a nursing sister, and 3 teams of 3 registered nurses working 8‐hour daily shifts, 2 nursing assistants, and a full‐time secretary. In contrast, the QDU is staffed by a physician and a nurse, and receives administrative support from 2 secretaries shared with other units. All staff salaries were included in the analysis. All costs analyzed were hospital costs and not National Health Service costs.
A telephone survey was carried out in a random sample of 225 patients 3 months after the QDU intervention, based on a survey previously used and validated by our department. To respect privacy issues, all participants provided verbal consent over the telephone prior to the survey interview. Approval was obtained from the hospital Ethics Committee. The survey consisted of 20 multiple choice questions (4 options) and evaluated: perception of the care process, degree of difficulty of travel to the unit, overall satisfaction, preferential future care type, and conditions of physical space.
Statistical Analysis
The mean, standard deviation, median, and 25% and 75% percentiles were calculated for descriptive variables. Categorical variables were compared using the chi‐square test or Fisher's exact test as necessary. Continuous variables were analyzed using the Student t test for variables with a normal distribution, and the MannWhitney U nonparametric test for variables with a non‐normal distribution. The level of statistical significance was established as P = 0.05. The analysis was made using the SAS v.9.1 statistical package (SAS Institute, Cary, NC).
RESULTS
Of the 2302 patients initially evaluated, 276 were excluded due to associated conditions that made outpatient QDU management inappropriate, 7 patients were lost to follow‐up, 4 died, and 15 were hospitalized during the study due to complications. Therefore, 2000 QDU patients were finally included, of whom 1106 were female, with a mean age of 60 years (18.84).
The main reasons for consultation are shown in Table 2. The main sources of referral were the ED (1022 patients) and PHC centers (942 patients). Waiting time for the first QDU visit ranged from 2 to 8 days (mean: 3.9 days) in patients referred from PHC centers, and 0 to 4 days (mean: 2.1 days) in patients referred by the ED.
| Reasons for Consultation | n (%) |
|---|---|
| |
| Anemia* | 550 (27.5) |
| Cachexia‐anorexia syndrome | 462 (23.1) |
| Febrile syndrome | 244 (12.2) |
| Adenopathies and/or palpable masses | 212 (10.6) |
| Abdominal pain | 128 (6.4) |
| Chronic diarrhea | 108 (5.4) |
| Lung abnormalities | 50 (2.5) |
The 2000 first visits generated 4260 successive visits (ratio first/successive = 2.13). The average number of visits per patient was 3.11.
The most frequent diagnoses were cancer (both epithelial and hematological) in 526/2000 (26.3%) patients, and iron‐deficiency anemia (unrelated to malignancy) in 360 patients. The most common cancers were colon cancer and lymphomas, while the main cause of iron‐deficiency anemia was chronic gastrointestinal bleeding (148/2000 [7.4%] patients) (Table 3).
| Diagnosis | n (%) |
|---|---|
| |
| Malignant neoplasm | 526 (26.3) |
| Colon | 132 (6.6) |
| Lymphoma | 142 (7.1) |
| Gastric | 46 (2.3) |
| Lung | 37 (1.9) |
| Pancreas | 89 (4.5) |
| Other hematological* | 32 (1.6) |
| Breast | 20 (1.0) |
| Ovary | 16 (0.8) |
| UPM | 12 (0.6) |
| Iron‐deficiency anemia | 360 (18) |
| Digestive | 148 (7.4) |
| Unknown cause | 80 (4.0) |
| Heavy menstrual bleeding | 66 (3.3) |
| Multifactorial anemia | 66 (3.3) |
| Chronic liver disease | 57 (2.9) |
| Acute viral illness | 80 (4) |
| Reactive adenitis | 78 (3.9) |
| MGUS | 34 (1.7) |
The mean time to diagnosis was 9.4 days (1.78). After the diagnostic study was completed, 1232 patients were referred to PHC centers, 712 to outpatients, and 56 required hospitalization.
Taking into account previously used criteria, we estimated that 820 (41%) patients would have been candidates for conventional hospitalization (for diagnostic studies) before QDU was created. Considering that the mean length‐of‐stay of the internal medicine department (50 beds) during 2009 for patients admitted for a diagnostic workup was 10.3 days, we estimated that 12.5 beds per day during a year were freed up (ie, 4563 bed‐days saved in a year). On the other hand, 45 of 1000 (4.5%) patients required immediate or early hospitalization due to their bad health status, which impeded further QDU diagnosis.
Table 4 shows the main characteristics of QDU and hospitalized patients according to the main reasons for consultation. QDU patients with anemia were significantly younger than hospitalized patients with the same diagnosis (P < 0.0001). Other parameters, notably age, time to diagnosis versus length‐of‐stay, and Charlson comorbidity index showed no statistically significant differences in any of the 4 main reasons for consultation (Table 4).
| Anemia | QDU (n = 550) | Hospitalized (n = 548) | P Value |
|---|---|---|---|
| |||
| Age | 66.72 (15.23) 71 [59;79] | 77.18 (13.71) 79.23 [72;85] | <0.0001 |
| Female | 280 (51%) | 291 (53.1%) | |
| Male | 270 (49%) | 257 (46.9%) | |
| Time to diagnosis/HS (days) | 7.91 (1.41) 8 [6;9] | 8.66 (3.44) 8.5 [7;10] | NS |
| Hemoglobin | 75.56 (20.9) 76 [55;79] | 74.94 (19.1) 76 [61;78] | NS |
| Anemic syndrome | 509 (92.3%) | 512 (93.4%) | NS |
| Transfusion | 362 (65.8%) | 355 (64.8%) | NS |
| Charlson co. index | 1.3 (2.1) 1.5 [1;1.6] | 1.4 (2.2) 1.5 [1;1.8] | NS |
| Main diagnosis | Iron‐deficiency anemia/colon cancer | Iron‐deficiency anemia/colon cancer | |
| Cachexia‐Anorexia Syndrome | QDU (n = 462) | Hospitalized (n = 458) | P Value |
| Age | 68.32 (18.27) 69 [60;77] | 70.23 (15.23) 73.5 [68;79] | NS |
| Female | 230 (49.8%) | 236 (51.6%) | |
| Male | 232 (50.2%) | 222 (48.4%) | |
| Time to diagnosis/HS (days) | 10.21 (3.31) 11 [10;12] | 11.32 (4.12) 12 [10;13] | NS |
| Weight loss (Kg) | 9.7 (2.25) 10 [9;12] | 9.5 (1.76) 10 [8;11] | NS |
| Charlson co. index | 1.1 (2.1) 1.3 [1;1.4] | 1.2 (2.4) 1.4 [1;1.6] | NS |
| Main diagnosis | Pancreatic cancer | Pancreatic cancer | |
| Febrile Syndrome | QDU (n = 244) | Hospitalized (n = 240) | P Value |
| Age | 47.18 (15.23) 50 [45;55] | 49.34 (14.72) 53 [49;56] | NS |
| Female | 127 (52%) | 121 (50.4%) | |
| Male | 117 (48%) | 119 (49.6%) | |
| Time to diagnosis/HS (days) | 8.32 (2.23) 9 [8;10.5] | 9.11 (3.54) 10.5 [9;11.5] | NS |
| Mean duration of fever (days) | 20.15 (12.12) 24 [20;26] | 19.76 (10.54) 23 [19;25] | NS |
| Charlson co. index | 1.0 (1.5) 1.2 [1.1;1.6] | 1.2 (2.1) 1.3 [0.9;1.4] | NS |
| Main diagnosis | Lymphoma | Lymphoma | |
| Adenopathies and/or Palpable Masses | QDU (n = 212) | Hospitalized (n = 208) | P Value |
| Age | 58.23 (17.20) 59.5 [55;61] | 60.19 (13.21) 64 [58;65] | NS |
| Female | 110 (51.9%) | 106 (51%) | |
| Male | 102 (48.1%) | 102 (49%) | |
| Time to diagnosis/HS | 7.89 (2.54) 8 [7;9] | 7.77 (3.23) 9 [7.5;11] | NS |
| Charlson co. index | 1.1 (1.1) 1.3 [0.8;1.4] | 1.1 (1.7) 1.5 [1.1;1.6] | NS |
| Main diagnosis | Lymphoma | Lymphoma | |
Table 5 shows the mean costs per stay, per visit, and per process for hospitalized and QDU patients included in the 4 main reasons for consultation. In hospitalized patients, the total mean cost per day of hospital stay was 363.35 Euros, and the mean cost per process was 3153.87 (910) Euros. In contrast, the mean cost per process in the QDU was 702.33 (610) Euros.
| Cost per Process* | ||||
|---|---|---|---|---|
| Hospitalization (1‐day stay) | QDU (1 visit) | Hospitalization | QDU | |
| ||||
| Staff salary | 260.94 | 58.79 | 2264.96 | 182.84 |
| Complementary tests | 53.73 | 158.12 | 466.38 | 491.75 |
| Stock | 15.27 | 0.84 | 132.54 | 2.61 |
| Pharmacy, | 0.97 | 0.15 | 8.42 | 0.47 |
| Medical gases | 0.02 | NA | 0.17 | NA |
| Catering | 15.23 | NA | 132.20 | NA |
| Cleaning | 8.78 | 4.47 | 76.21 | 13.90 |
| Laundry | 5.11 | 0.23 | 44.35 | 0.72 |
| Maintenance | 0.47 | 0.28 | 4.08 | 0.87 |
| Communications | 0.31 | 0.29 | 2.69 | 0.90 |
| 0.00 | 0.00 | 0.00 | 0.00 | |
| Depreciation | 2.52 | 1.26 | 21.87 | 3.92 |
| Travel∥ | NA | 1.4 | NA | 4.35 |
| Total | 363.35 | 225.83 | 3153.87 (SD: 910) | 702.33 (SD: 610) |
Compliance with the patient survey was 94%. The results highlighted 3 main aspects: a) overall satisfaction with QDU care was high in 93% of cases; b) repeated travel to the hospital was not a major difficulty; and c) if further diagnostic tests were required, 84% of patients would prefer the QDU care model to hospitalization. The same results were obtained analyzing only patients with previous hospital admission. The remaining 16% indicated no preference for 1 type of care.
DISCUSSION
Our results indicate that, for diagnostic purposes, patients with potentially severe diseases can be managed similarly in a QDU or in‐hospital setting, and that the QDU model saves money compared to hospitalization. QDU patients expressed a high degree of satisfaction, with most preferring this model to hospital admission.
The only significant difference between QDU and hospitalized patients in the 4 main reasons for consultation was age in anemia patients, which may reflect the decision of the ED physician to exclude 56 patients from the initial evaluation. A separate analysis of this subgroup revealed an older age (75.3 years) and a higher number of comorbidities (Charlson index = 2.3) (data not shown).
In Spain, some patients with potentially severe diseases are hospitalized for several days for diagnostic tests without therapy. Can these patients be studied and diagnosed on an outpatient basis? Cachexia‐anorexia syndrome and severe anemia are among the main disorders for which patients are hospitalized for diagnostic tests.5, 7 In our center and others, anemia, with hemoglobin levels <8 g/L, is a criterion for hospitalization for both diagnosis and treatment.2, 3, 17 These patients are commonly evaluated initially in the ED and hospitalized in internal medicine wards, where they have a full baseline laboratory analysis (to study the type of anemia in naive conditions), a blood transfusion if necessary, and several days' hospitalization for diagnostic tests.
The motives for QDU consultation and the final diagnoses are fairly homogenous among Spanish units,2, 3, 15 allowing a profile to be drawn up of patients who could benefit from early QDU diagnosis. In 88% of our patients, the reasons for consultation were anemia, cachexia‐anorexia syndrome, febrile syndrome, adenopathies and/or palpable masses, abdominal pain, diarrhea, and lung abnormalities. The most frequent diagnosis was cancer (26.3%), although most patients showed no clear signs or symptoms of cancer at the initial consultation, suggesting that nonspecific but suspicious symptoms warrant early investigation.
QDUs seem to reduce costs, as reported by a 2004 Spanish study of patients evaluated for various conditions,3 which found that the mean cost per patient was up to 8 times cheaper than conventional hospitalization; hospitalization was avoided in 45% of patients, representing the freeing up of 7 internal medicine beds per day. In our case, and on the basis of previous criteria, avoiding hospital admission in 41% of patients evaluated resulted in the permanent freeing up of 12.5 internal medicine beds per day and a significant reduction in hospital costs. However, this does not mean the QDU system would reduce costs by permanently freeing inpatient beds, as its adoption would drive up systemic costs due to increased QDU utilization and indirect admissions from the QDU to the hospital. The cost differences between QDU and hospitalized patients (702.33 vs 3153.87 Euros) were due to differences in staffing and working hours and, to a lesser degree, fixed hospital costs (eg, catering) (Table 5). This might suggest that our internal medicine wards and QDU are overstaffed and understaffed, respectively, and that resources may be more effectively used in QDU. However, different staff dimensions between hospitals limits the extrapolation of costs and savings.
The QDU model has limitations. Using QDU resources to diagnose mild disorders could delay the diagnosis of severe disease and, therefore, clear agreement on referral criteria is essential. Likewise, although we followed approved guidelines, QDU physicians may prescribe too many diagnostic tests, searching for severe diseases the patient is unlikely to have, especially if the referral diagnosis is incorrect.17 This could be minimized by implementing standardized QDU diagnostic protocols and guidelines. In our study, the type and mean number of complementary explorations in patients with the 4 main reasons for consultation was similar between QDU and hospitalized patients (2.27 vs 2.33, respectively) (data not shown).
How and where (in‐hospital vs outpatients or PHC) patients with potentially severe disease, such as those seen in QDUs, are managed in different countries seems to vary widely. Although there are few reports on this topic,19, 20 these variations might be due, among other reasons, to guidelines for invasive diagnostic procedures and departmental and hospital traditions. Our findings may result in a shift in the paradigm of hospitalization for the diagnostic evaluation of patients with severe conditions, who are often hospitalized and, in some cases, studied in naive conditions (eg, anemia). Our results have already resulted in policy changes, since, increasingly, patients are referred directly from the ED or PHC centers to the QDU rather than being hospitalized, with the consequent savings in hospital beds and costs. Although, ideally, the QDU workup should be led by the primary care physician, waiting times for diagnostic tests are inappropriately long, as mentioned above. A successful reform would likely require better, more agile coordination between PHC and hospital settings, with quicker access to diagnostic procedures from PHC centers.
Ruling out cancer and, indirectly, easing the uncertainty and fear caused by suspected malignancy in patients awaiting diagnostic confirmation is one of the main QDU objectives.21 Cancer is the most common diagnosis (nearly 20% of patients) in Spanish QDUs.2, 3, 17 According to the Strategy on Cancer of the Spanish National Health System 2006, every patient with a well‐founded clinical suspicion of cancer must undergo a first confirmatory diagnostic test within 15 days of the suspicion.22 Our QDU patients received a final diagnosis of cancer in a mean of 11.82 days (waiting time plus evaluation period) (data not shown).
Due to unacceptable outpatient delays, most patients with suspected cancer are hospitalized directly from outpatients for the diagnostic workup,17 although this may be inappropriate in patients who are still practically asymptomatic. Inappropriate use of acute hospital beds, measured by different instruments, ranges from 6% to >20%,2326 with the most common reason being programmed hospitalization solely for diagnostic tests. Twenty‐eight percent of hospital admissions to a public hospital in England in 2000 were reported as inappropriate, mainly because diagnostic tests or treatment could have been made on an outpatient basis.25
QDU may be inappropriate outside publicly funded health systems. The QDU model could be useful, for example, in the United Kingdom, Italy, Canada, and Latin‐American countries; overcrowding and long waiting lists in PHC, and suboptimal coordination between primary and hospital care, means patients with suspected severe disease, including those in good health, are hospitalized for diagnostic tests, aggravating overcrowding and increasing costs.17 However, in countries with mainly private healthcare systems, QDUs created to reduce health costs or free hospital beds may not be as relevant. In the United States, although day hospitals and urgent care units provide similar care to QDUs (at least in urban areas), most insurers would not cover such admissions without clinical urgency, while access and efficient, streamlined care, is a major concern.
The exclusion criteria, which were based on the ED/QDU physician's judgment, are a limitation of the study. This might be circumvented by a randomized study evaluating 2 cohorts prospectively, although there would still be patients whose clinical status would require hospitalization and exclusion from QDU evaluation.
In conclusion, QDUs can manage the diagnosis of patients with potentially severe diseases equally as well as traditional hospitalization and saves costs. QDU patients expressed a high degree of satisfaction, with most preferring this model to hospitalization.
- ,,.Measuring appropriate use of acute beds. A systematic review of methods and results.Health Policy.2000;53:157–184.
- ,,,,.Rapid diagnosis unit in a third level hospital. Descriptive study of the first year and a half.Rev Clin Esp.2008;208:561–563.
- ,,, et al.Quick and early diagnostic outpatient unit: an effective and efficient model of care. Five years experience.Med Clin (Barc).2004;123:247–250.
- ,,.Study on the immediate care clinics of the internal medicine department (University Clinic Hospital of Valladolid).Rev Clin Esp.2006;206:84–89.
- ,,.Impact on hospital days of care due to unnecessary emergency admissions.Rev Esp Salud Pública.2005;79:541–549.
- ,,,.Inappropriate admissions and stays in internal medicine.Med Clin (Barc).2002;118:157.
- ,,,,.Appropriateness of hospitalization in a short stay unit of a teaching hospital. A controlled study.Med Clin (Barc).2004;122:454–456.
- ,,,.Day hospital as conventional hospitalization alternative in an internal medicine service of a first level center.An Med Interna.2007;24:613–614.
- ,,.Short‐stay units and observation medicine: a systematic review.Med J Aust.2003;178:559–563.
- ,,,.Conventional hospitalization alternatives in internal medicine.Med Clin (Barc).2005;124:620–626.
- ,,.Effectiveness of acute medical units in hospitals: a systematic review.Int J Qual Health Care.2009;21:397–407.
- ,,, et al.A hospitalist‐run short‐stay unit: features that predict length‐of‐stay and eventual admission to traditional inpatient services.J Hosp Med.2009;4:276–284.
- ,,.Hospital in the home is cost saving for appropriately selected patients: a comparison with in‐hospital care.Int J Qual Health Care.2002;14:285–293.
- ,,.Criteria for selection and contraindications of ambulatory surgery.Chirurgie.1990;116:568–572.
- ,,,,.Fast specialized ambulatory care of medical disease in an urban tertiary university hospital. Fast care consultation.Rev Clin Esp.2008;208:71–75.
- ,,.QED: quick and early diagnosis.Lancet.1996;348:528–529.
- ,,,,.Quick diagnosis units: a potentially useful alternative to conventional hospitalisation.Med J Aust.2009;191:496–498.
- ,,,.A new method of classifying prognostic comorbidity in longitudinal studies: development and validation.J Chron Dis.1987;40:373–383.
- ,,,.The role of correction of anaemia in patients with congestive heart failure: a short review.Eur J Heart Fail.2008;10:819–823.
- ,,, et al.Who makes the diagnosis? The role of clinical skills and diagnostic test results.J Eval Clin Pract.2007;13:321–325.
- .Two week wait for suspected cancer: milestone or millstone?Int J Clin Pract.2005;59:1251–1252.
- Plan de calidad para el Sistema Nacional de Salud. Estrategia en cáncer del Sistema Nacional de Salud. Ministerio de Sanidad y Consumo 2006. Available at: http://www.msc.es/organizacion/sns/planCalidadSNS/pdf/excelencia/cancer‐cardiopatia/CANCER/opsc_est1.pdf.pdf. Accessed October 17,2010.
- ,,.Alternatives to hospital care: what are they and who should decide?BMJ.1996;312:162–166.
- ,,,.The hospital of the future. Better out than in? Alternatives to acute hospital care.BMJ.1999;319:1127–1130.
- .Inappropriate admissions. Thoughts of patients and referring doctors.J R Soc Med.2001;94:628–631.
- ,,, et al.Predictors of inappropriate hospital days in a department of internal medicine.Int J Epidemiol.1998;27:513–519.
In recent years, hospitals in countries with public health systems have adopted organizational changes to improve efficiency and resource allocation. Acute hospital bed utilization is a growing concern for healthcare systems in these countries, as it represents a significant share of health costs.1
Inappropriate hospitalization is a significant problem for public health systems. In Spain and other countries, due to deficiencies in outpatient services, acute beds are increasingly occupied by patients requiring diagnostic tests for nonacute but potentially severe diseases that often need no immediate treatment, thereby reducing beds for acute patients.2, 3
Reports suggest 9% to 17% of patients admitted to Spanish internal medicine units could be studied on an outpatient basis.47 However, long delays in outpatient diagnostic tests in Spain make diagnosis outside conventional hospitalization unviable, especially when rapid access to tests for suspected malignancy is required.
These shortcomings have prompted the search for alternatives to hospitalization. Alternative care models include: 1‐day hospitals (providing medical procedures requiring <24 hours of hospitalization)8; short‐stay observation units (often located adjacent to emergency departments [ED], and accommodating patients requiring brief periods of observation or therapy)912; hospital‐in‐the‐home programs (delivering a limited range of acute care services to selected patients)1013; outpatient major surgery programs (providing surgical procedures with postoperative recovery periods short enough to permit same‐day discharge);14 and, more recently, quick diagnosis units ([QDUs], outpatient diagnostic units for patients with suspected severe disease).2, 3, 15, 16
Current referral processes for diagnosis and specialized care in primary health care (PHC), especially waiting times for diagnostic procedures, are longeven in patients with suspected cancerin public health systems such as in Spain. This results in PHC physicians and patients using the ED as a voluntary shortcut.3, 6, 17
In 1996, the use and benefits of quick‐and‐early diagnosis units were first described for suspected cancer patients referred from PHC centers to the Queen Elizabeth Hospital in Birmingham, England.16 Patients were evaluated by specialists according to the suspected diagnosis (eg, patients with hematuria or testicular masses were assessed by urologists).
QDUs are a little‐reported, potentially cost‐saving alternative that allow coordinated, agile diagnostic procedures and may avoid hospital admission. QDUs increase patient comfort by allowing many to remain at home during the diagnostic process.17 QDUs have been introduced in Spain in recent years, and are mainly directed by internists (similar to hospitalists in the United States). Patients with specific symptoms, such as breast or testicular masses, are referred to, and evaluated directly by, the appropriate medical specialist.17 Apart from 2 Opinion articles on QDUs led by specialists other than internists in the United Kingdom,16 and by internists (our group) in Spain,17 there are, to our knowledge, no other English‐language reports on this healthcare model.
The aim of this study was to describe the functioning of a QDU in a Spanish public university hospital after evaluating 2000 consecutive patients. We intended to ascertain the utility and cost of the model compared to conventional hospitalization and the degree of patient satisfaction.
METHODS
We carried out a longitudinal, descriptive study in a prospective cohort of 2000 consecutive QDU patients, evaluated between December 2007 and July 2010, in a public university hospital with 840 acute beds, serving a reference population of 540,000 in Barcelona, Spain.
The QDU is composed of a specialist in internal medicine and a registered nurse who work in the QDU for 5 hours daily, 5 days a week (Monday‐Friday), assisted by specialists from other specialties. It has a consulting room and a waiting room for patients and families, and functions daily.
For comparison, we analyzed a retrospective cohort of 1454 patients diagnosed with anemia (n = 548), cachexia‐anorexia syndrome (n = 458), febrile syndrome (n = 240), and adenopathies or palpable masses (n = 208) admitted to the internal medicine department between September 2006 and June 2010. Patients were randomly selected from the 2022 consecutive patients with these diagnoses, hospitalized during this period and compared, on an unmatched basis, with all 1468 QDU patients with the same diagnoses.
Patients evaluated by the QDU have potentially severe disease that would normally require hospital admission for diagnosis, but whose health status allows outpatient study, and who have no physical or psychological disability that would make attending the hospital several times difficult. The criteria for QDU referral are agreed with central services (Table 1). In our hospital, patients with lung abnormalities (eg, pulmonary nodules) are usually evaluated quickly in the 1‐day hospital of the respiratory diseases department, however, they are not excluded from QDU evaluation.
|
| Anemia* |
| Cachexia‐anorexia syndrome |
| Febrile syndrome |
| Adenopathies and/or palpable masses |
| Unexplained severe abdominal pain |
| Chronic diarrhea |
| Rectorrhagia |
| Jaundice |
| Lung and/or pleural abnormalities |
| Unexplained dyspnea |
| Dysphagia |
| Ascites |
| Anasarca |
| Arthritis |
Our QDU protocol is based on an urgent first visit, followed by preferential programming and coordination of complementary tests, and subsequent visits until a diagnosis is made. The main diagnostic tests are normally carried out within 10 days after the first visit and, thus, visits are not consecutive but spread over a short period of time. Patients are attended on an ambulatory basis and do not stay overnight.
Inclusion Criteria
When setting up the QDU, the ED, PHC centers, outpatients and other sources of referral were informed and trained in QDU referral criteria (Table 1). All diseases selected for QDU assessment were agreed according to established guidelines. For example, only patients with severe anemia, with or without symptoms, defined as a hemoglobin concentration <8 g/L, our accepted criterion for hospitalization for diagnosis and treatment, were included.
Exclusion Criteria
Patients who fulfilled the inclusion criteria but were judged by the QDU or ED physician as requiring hospitalization or routine outpatient study (eg, active bleeding, uncompensated heart failure, impaired general status, mobility, and social problems) were excluded. Likewise, patients lost to follow‐up or hospitalized during the study due to complications, and deaths were excluded.
For each patient, in addition to clinical data, we prospectively recorded: demographic data; reason for consultation; source of referral; waiting time for the first visit; number and date of visits; waiting times between visits; time to diagnosis; type, number, and date of complementary tests; final diagnosis; and onward referral. The full diagnostic workup was done according to previously established protocols. The Charlson comorbidity index was calculated.18 Blood transfusions and the mean number of units used (SAG‐M red cell concentrates with a median volume per unit of 289 [25] ml) were recorded and administered according to hospital protocol. The time to diagnosis was defined as the time from the first visit to a definitive diagnosis, and usually coincided with the results of diagnostic tests (eg, imaging or pathology).
The same factors were recorded for hospitalized patients (retrospective cohort) except for waiting time to the first visit, number and date of visits, waiting times between visits, and time to diagnosis. In addition, we recorded the mean hospital stay for each patient. Hospital admission avoided was defined as patients who would have been admitted for a diagnostic workup if there were no QDU.
We made a cost analysis using microcosting techniques. First, we calculated the mean number of QDU visits in 150 randomly selected patients with iron‐deficiency anemia, 150 with cachexia‐anorexia syndrome, 150 with fever of unknown origin, and 150 with adenopathies and/or palpable masses. We analyzed the full direct and indirect costs, and calculated the mean cost per visit and the mean cost per process (admission to discharge). The mean length‐of‐stay, and direct and indirect costs were also calculated retrospectively for the same number of hospitalized patients in 2 internal medicine wards, as were the mean cost per daily stay and the mean cost per process (admission to discharge). In our hospital, a 25‐bed internal medicine ward is staffed by 2 consultant physicians and 4 residents, a nursing sister, and 3 teams of 3 registered nurses working 8‐hour daily shifts, 2 nursing assistants, and a full‐time secretary. In contrast, the QDU is staffed by a physician and a nurse, and receives administrative support from 2 secretaries shared with other units. All staff salaries were included in the analysis. All costs analyzed were hospital costs and not National Health Service costs.
A telephone survey was carried out in a random sample of 225 patients 3 months after the QDU intervention, based on a survey previously used and validated by our department. To respect privacy issues, all participants provided verbal consent over the telephone prior to the survey interview. Approval was obtained from the hospital Ethics Committee. The survey consisted of 20 multiple choice questions (4 options) and evaluated: perception of the care process, degree of difficulty of travel to the unit, overall satisfaction, preferential future care type, and conditions of physical space.
Statistical Analysis
The mean, standard deviation, median, and 25% and 75% percentiles were calculated for descriptive variables. Categorical variables were compared using the chi‐square test or Fisher's exact test as necessary. Continuous variables were analyzed using the Student t test for variables with a normal distribution, and the MannWhitney U nonparametric test for variables with a non‐normal distribution. The level of statistical significance was established as P = 0.05. The analysis was made using the SAS v.9.1 statistical package (SAS Institute, Cary, NC).
RESULTS
Of the 2302 patients initially evaluated, 276 were excluded due to associated conditions that made outpatient QDU management inappropriate, 7 patients were lost to follow‐up, 4 died, and 15 were hospitalized during the study due to complications. Therefore, 2000 QDU patients were finally included, of whom 1106 were female, with a mean age of 60 years (18.84).
The main reasons for consultation are shown in Table 2. The main sources of referral were the ED (1022 patients) and PHC centers (942 patients). Waiting time for the first QDU visit ranged from 2 to 8 days (mean: 3.9 days) in patients referred from PHC centers, and 0 to 4 days (mean: 2.1 days) in patients referred by the ED.
| Reasons for Consultation | n (%) |
|---|---|
| |
| Anemia* | 550 (27.5) |
| Cachexia‐anorexia syndrome | 462 (23.1) |
| Febrile syndrome | 244 (12.2) |
| Adenopathies and/or palpable masses | 212 (10.6) |
| Abdominal pain | 128 (6.4) |
| Chronic diarrhea | 108 (5.4) |
| Lung abnormalities | 50 (2.5) |
The 2000 first visits generated 4260 successive visits (ratio first/successive = 2.13). The average number of visits per patient was 3.11.
The most frequent diagnoses were cancer (both epithelial and hematological) in 526/2000 (26.3%) patients, and iron‐deficiency anemia (unrelated to malignancy) in 360 patients. The most common cancers were colon cancer and lymphomas, while the main cause of iron‐deficiency anemia was chronic gastrointestinal bleeding (148/2000 [7.4%] patients) (Table 3).
| Diagnosis | n (%) |
|---|---|
| |
| Malignant neoplasm | 526 (26.3) |
| Colon | 132 (6.6) |
| Lymphoma | 142 (7.1) |
| Gastric | 46 (2.3) |
| Lung | 37 (1.9) |
| Pancreas | 89 (4.5) |
| Other hematological* | 32 (1.6) |
| Breast | 20 (1.0) |
| Ovary | 16 (0.8) |
| UPM | 12 (0.6) |
| Iron‐deficiency anemia | 360 (18) |
| Digestive | 148 (7.4) |
| Unknown cause | 80 (4.0) |
| Heavy menstrual bleeding | 66 (3.3) |
| Multifactorial anemia | 66 (3.3) |
| Chronic liver disease | 57 (2.9) |
| Acute viral illness | 80 (4) |
| Reactive adenitis | 78 (3.9) |
| MGUS | 34 (1.7) |
The mean time to diagnosis was 9.4 days (1.78). After the diagnostic study was completed, 1232 patients were referred to PHC centers, 712 to outpatients, and 56 required hospitalization.
Taking into account previously used criteria, we estimated that 820 (41%) patients would have been candidates for conventional hospitalization (for diagnostic studies) before QDU was created. Considering that the mean length‐of‐stay of the internal medicine department (50 beds) during 2009 for patients admitted for a diagnostic workup was 10.3 days, we estimated that 12.5 beds per day during a year were freed up (ie, 4563 bed‐days saved in a year). On the other hand, 45 of 1000 (4.5%) patients required immediate or early hospitalization due to their bad health status, which impeded further QDU diagnosis.
Table 4 shows the main characteristics of QDU and hospitalized patients according to the main reasons for consultation. QDU patients with anemia were significantly younger than hospitalized patients with the same diagnosis (P < 0.0001). Other parameters, notably age, time to diagnosis versus length‐of‐stay, and Charlson comorbidity index showed no statistically significant differences in any of the 4 main reasons for consultation (Table 4).
| Anemia | QDU (n = 550) | Hospitalized (n = 548) | P Value |
|---|---|---|---|
| |||
| Age | 66.72 (15.23) 71 [59;79] | 77.18 (13.71) 79.23 [72;85] | <0.0001 |
| Female | 280 (51%) | 291 (53.1%) | |
| Male | 270 (49%) | 257 (46.9%) | |
| Time to diagnosis/HS (days) | 7.91 (1.41) 8 [6;9] | 8.66 (3.44) 8.5 [7;10] | NS |
| Hemoglobin | 75.56 (20.9) 76 [55;79] | 74.94 (19.1) 76 [61;78] | NS |
| Anemic syndrome | 509 (92.3%) | 512 (93.4%) | NS |
| Transfusion | 362 (65.8%) | 355 (64.8%) | NS |
| Charlson co. index | 1.3 (2.1) 1.5 [1;1.6] | 1.4 (2.2) 1.5 [1;1.8] | NS |
| Main diagnosis | Iron‐deficiency anemia/colon cancer | Iron‐deficiency anemia/colon cancer | |
| Cachexia‐Anorexia Syndrome | QDU (n = 462) | Hospitalized (n = 458) | P Value |
| Age | 68.32 (18.27) 69 [60;77] | 70.23 (15.23) 73.5 [68;79] | NS |
| Female | 230 (49.8%) | 236 (51.6%) | |
| Male | 232 (50.2%) | 222 (48.4%) | |
| Time to diagnosis/HS (days) | 10.21 (3.31) 11 [10;12] | 11.32 (4.12) 12 [10;13] | NS |
| Weight loss (Kg) | 9.7 (2.25) 10 [9;12] | 9.5 (1.76) 10 [8;11] | NS |
| Charlson co. index | 1.1 (2.1) 1.3 [1;1.4] | 1.2 (2.4) 1.4 [1;1.6] | NS |
| Main diagnosis | Pancreatic cancer | Pancreatic cancer | |
| Febrile Syndrome | QDU (n = 244) | Hospitalized (n = 240) | P Value |
| Age | 47.18 (15.23) 50 [45;55] | 49.34 (14.72) 53 [49;56] | NS |
| Female | 127 (52%) | 121 (50.4%) | |
| Male | 117 (48%) | 119 (49.6%) | |
| Time to diagnosis/HS (days) | 8.32 (2.23) 9 [8;10.5] | 9.11 (3.54) 10.5 [9;11.5] | NS |
| Mean duration of fever (days) | 20.15 (12.12) 24 [20;26] | 19.76 (10.54) 23 [19;25] | NS |
| Charlson co. index | 1.0 (1.5) 1.2 [1.1;1.6] | 1.2 (2.1) 1.3 [0.9;1.4] | NS |
| Main diagnosis | Lymphoma | Lymphoma | |
| Adenopathies and/or Palpable Masses | QDU (n = 212) | Hospitalized (n = 208) | P Value |
| Age | 58.23 (17.20) 59.5 [55;61] | 60.19 (13.21) 64 [58;65] | NS |
| Female | 110 (51.9%) | 106 (51%) | |
| Male | 102 (48.1%) | 102 (49%) | |
| Time to diagnosis/HS | 7.89 (2.54) 8 [7;9] | 7.77 (3.23) 9 [7.5;11] | NS |
| Charlson co. index | 1.1 (1.1) 1.3 [0.8;1.4] | 1.1 (1.7) 1.5 [1.1;1.6] | NS |
| Main diagnosis | Lymphoma | Lymphoma | |
Table 5 shows the mean costs per stay, per visit, and per process for hospitalized and QDU patients included in the 4 main reasons for consultation. In hospitalized patients, the total mean cost per day of hospital stay was 363.35 Euros, and the mean cost per process was 3153.87 (910) Euros. In contrast, the mean cost per process in the QDU was 702.33 (610) Euros.
| Cost per Process* | ||||
|---|---|---|---|---|
| Hospitalization (1‐day stay) | QDU (1 visit) | Hospitalization | QDU | |
| ||||
| Staff salary | 260.94 | 58.79 | 2264.96 | 182.84 |
| Complementary tests | 53.73 | 158.12 | 466.38 | 491.75 |
| Stock | 15.27 | 0.84 | 132.54 | 2.61 |
| Pharmacy, | 0.97 | 0.15 | 8.42 | 0.47 |
| Medical gases | 0.02 | NA | 0.17 | NA |
| Catering | 15.23 | NA | 132.20 | NA |
| Cleaning | 8.78 | 4.47 | 76.21 | 13.90 |
| Laundry | 5.11 | 0.23 | 44.35 | 0.72 |
| Maintenance | 0.47 | 0.28 | 4.08 | 0.87 |
| Communications | 0.31 | 0.29 | 2.69 | 0.90 |
| 0.00 | 0.00 | 0.00 | 0.00 | |
| Depreciation | 2.52 | 1.26 | 21.87 | 3.92 |
| Travel∥ | NA | 1.4 | NA | 4.35 |
| Total | 363.35 | 225.83 | 3153.87 (SD: 910) | 702.33 (SD: 610) |
Compliance with the patient survey was 94%. The results highlighted 3 main aspects: a) overall satisfaction with QDU care was high in 93% of cases; b) repeated travel to the hospital was not a major difficulty; and c) if further diagnostic tests were required, 84% of patients would prefer the QDU care model to hospitalization. The same results were obtained analyzing only patients with previous hospital admission. The remaining 16% indicated no preference for 1 type of care.
DISCUSSION
Our results indicate that, for diagnostic purposes, patients with potentially severe diseases can be managed similarly in a QDU or in‐hospital setting, and that the QDU model saves money compared to hospitalization. QDU patients expressed a high degree of satisfaction, with most preferring this model to hospital admission.
The only significant difference between QDU and hospitalized patients in the 4 main reasons for consultation was age in anemia patients, which may reflect the decision of the ED physician to exclude 56 patients from the initial evaluation. A separate analysis of this subgroup revealed an older age (75.3 years) and a higher number of comorbidities (Charlson index = 2.3) (data not shown).
In Spain, some patients with potentially severe diseases are hospitalized for several days for diagnostic tests without therapy. Can these patients be studied and diagnosed on an outpatient basis? Cachexia‐anorexia syndrome and severe anemia are among the main disorders for which patients are hospitalized for diagnostic tests.5, 7 In our center and others, anemia, with hemoglobin levels <8 g/L, is a criterion for hospitalization for both diagnosis and treatment.2, 3, 17 These patients are commonly evaluated initially in the ED and hospitalized in internal medicine wards, where they have a full baseline laboratory analysis (to study the type of anemia in naive conditions), a blood transfusion if necessary, and several days' hospitalization for diagnostic tests.
The motives for QDU consultation and the final diagnoses are fairly homogenous among Spanish units,2, 3, 15 allowing a profile to be drawn up of patients who could benefit from early QDU diagnosis. In 88% of our patients, the reasons for consultation were anemia, cachexia‐anorexia syndrome, febrile syndrome, adenopathies and/or palpable masses, abdominal pain, diarrhea, and lung abnormalities. The most frequent diagnosis was cancer (26.3%), although most patients showed no clear signs or symptoms of cancer at the initial consultation, suggesting that nonspecific but suspicious symptoms warrant early investigation.
QDUs seem to reduce costs, as reported by a 2004 Spanish study of patients evaluated for various conditions,3 which found that the mean cost per patient was up to 8 times cheaper than conventional hospitalization; hospitalization was avoided in 45% of patients, representing the freeing up of 7 internal medicine beds per day. In our case, and on the basis of previous criteria, avoiding hospital admission in 41% of patients evaluated resulted in the permanent freeing up of 12.5 internal medicine beds per day and a significant reduction in hospital costs. However, this does not mean the QDU system would reduce costs by permanently freeing inpatient beds, as its adoption would drive up systemic costs due to increased QDU utilization and indirect admissions from the QDU to the hospital. The cost differences between QDU and hospitalized patients (702.33 vs 3153.87 Euros) were due to differences in staffing and working hours and, to a lesser degree, fixed hospital costs (eg, catering) (Table 5). This might suggest that our internal medicine wards and QDU are overstaffed and understaffed, respectively, and that resources may be more effectively used in QDU. However, different staff dimensions between hospitals limits the extrapolation of costs and savings.
The QDU model has limitations. Using QDU resources to diagnose mild disorders could delay the diagnosis of severe disease and, therefore, clear agreement on referral criteria is essential. Likewise, although we followed approved guidelines, QDU physicians may prescribe too many diagnostic tests, searching for severe diseases the patient is unlikely to have, especially if the referral diagnosis is incorrect.17 This could be minimized by implementing standardized QDU diagnostic protocols and guidelines. In our study, the type and mean number of complementary explorations in patients with the 4 main reasons for consultation was similar between QDU and hospitalized patients (2.27 vs 2.33, respectively) (data not shown).
How and where (in‐hospital vs outpatients or PHC) patients with potentially severe disease, such as those seen in QDUs, are managed in different countries seems to vary widely. Although there are few reports on this topic,19, 20 these variations might be due, among other reasons, to guidelines for invasive diagnostic procedures and departmental and hospital traditions. Our findings may result in a shift in the paradigm of hospitalization for the diagnostic evaluation of patients with severe conditions, who are often hospitalized and, in some cases, studied in naive conditions (eg, anemia). Our results have already resulted in policy changes, since, increasingly, patients are referred directly from the ED or PHC centers to the QDU rather than being hospitalized, with the consequent savings in hospital beds and costs. Although, ideally, the QDU workup should be led by the primary care physician, waiting times for diagnostic tests are inappropriately long, as mentioned above. A successful reform would likely require better, more agile coordination between PHC and hospital settings, with quicker access to diagnostic procedures from PHC centers.
Ruling out cancer and, indirectly, easing the uncertainty and fear caused by suspected malignancy in patients awaiting diagnostic confirmation is one of the main QDU objectives.21 Cancer is the most common diagnosis (nearly 20% of patients) in Spanish QDUs.2, 3, 17 According to the Strategy on Cancer of the Spanish National Health System 2006, every patient with a well‐founded clinical suspicion of cancer must undergo a first confirmatory diagnostic test within 15 days of the suspicion.22 Our QDU patients received a final diagnosis of cancer in a mean of 11.82 days (waiting time plus evaluation period) (data not shown).
Due to unacceptable outpatient delays, most patients with suspected cancer are hospitalized directly from outpatients for the diagnostic workup,17 although this may be inappropriate in patients who are still practically asymptomatic. Inappropriate use of acute hospital beds, measured by different instruments, ranges from 6% to >20%,2326 with the most common reason being programmed hospitalization solely for diagnostic tests. Twenty‐eight percent of hospital admissions to a public hospital in England in 2000 were reported as inappropriate, mainly because diagnostic tests or treatment could have been made on an outpatient basis.25
QDU may be inappropriate outside publicly funded health systems. The QDU model could be useful, for example, in the United Kingdom, Italy, Canada, and Latin‐American countries; overcrowding and long waiting lists in PHC, and suboptimal coordination between primary and hospital care, means patients with suspected severe disease, including those in good health, are hospitalized for diagnostic tests, aggravating overcrowding and increasing costs.17 However, in countries with mainly private healthcare systems, QDUs created to reduce health costs or free hospital beds may not be as relevant. In the United States, although day hospitals and urgent care units provide similar care to QDUs (at least in urban areas), most insurers would not cover such admissions without clinical urgency, while access and efficient, streamlined care, is a major concern.
The exclusion criteria, which were based on the ED/QDU physician's judgment, are a limitation of the study. This might be circumvented by a randomized study evaluating 2 cohorts prospectively, although there would still be patients whose clinical status would require hospitalization and exclusion from QDU evaluation.
In conclusion, QDUs can manage the diagnosis of patients with potentially severe diseases equally as well as traditional hospitalization and saves costs. QDU patients expressed a high degree of satisfaction, with most preferring this model to hospitalization.
In recent years, hospitals in countries with public health systems have adopted organizational changes to improve efficiency and resource allocation. Acute hospital bed utilization is a growing concern for healthcare systems in these countries, as it represents a significant share of health costs.1
Inappropriate hospitalization is a significant problem for public health systems. In Spain and other countries, due to deficiencies in outpatient services, acute beds are increasingly occupied by patients requiring diagnostic tests for nonacute but potentially severe diseases that often need no immediate treatment, thereby reducing beds for acute patients.2, 3
Reports suggest 9% to 17% of patients admitted to Spanish internal medicine units could be studied on an outpatient basis.47 However, long delays in outpatient diagnostic tests in Spain make diagnosis outside conventional hospitalization unviable, especially when rapid access to tests for suspected malignancy is required.
These shortcomings have prompted the search for alternatives to hospitalization. Alternative care models include: 1‐day hospitals (providing medical procedures requiring <24 hours of hospitalization)8; short‐stay observation units (often located adjacent to emergency departments [ED], and accommodating patients requiring brief periods of observation or therapy)912; hospital‐in‐the‐home programs (delivering a limited range of acute care services to selected patients)1013; outpatient major surgery programs (providing surgical procedures with postoperative recovery periods short enough to permit same‐day discharge);14 and, more recently, quick diagnosis units ([QDUs], outpatient diagnostic units for patients with suspected severe disease).2, 3, 15, 16
Current referral processes for diagnosis and specialized care in primary health care (PHC), especially waiting times for diagnostic procedures, are longeven in patients with suspected cancerin public health systems such as in Spain. This results in PHC physicians and patients using the ED as a voluntary shortcut.3, 6, 17
In 1996, the use and benefits of quick‐and‐early diagnosis units were first described for suspected cancer patients referred from PHC centers to the Queen Elizabeth Hospital in Birmingham, England.16 Patients were evaluated by specialists according to the suspected diagnosis (eg, patients with hematuria or testicular masses were assessed by urologists).
QDUs are a little‐reported, potentially cost‐saving alternative that allow coordinated, agile diagnostic procedures and may avoid hospital admission. QDUs increase patient comfort by allowing many to remain at home during the diagnostic process.17 QDUs have been introduced in Spain in recent years, and are mainly directed by internists (similar to hospitalists in the United States). Patients with specific symptoms, such as breast or testicular masses, are referred to, and evaluated directly by, the appropriate medical specialist.17 Apart from 2 Opinion articles on QDUs led by specialists other than internists in the United Kingdom,16 and by internists (our group) in Spain,17 there are, to our knowledge, no other English‐language reports on this healthcare model.
The aim of this study was to describe the functioning of a QDU in a Spanish public university hospital after evaluating 2000 consecutive patients. We intended to ascertain the utility and cost of the model compared to conventional hospitalization and the degree of patient satisfaction.
METHODS
We carried out a longitudinal, descriptive study in a prospective cohort of 2000 consecutive QDU patients, evaluated between December 2007 and July 2010, in a public university hospital with 840 acute beds, serving a reference population of 540,000 in Barcelona, Spain.
The QDU is composed of a specialist in internal medicine and a registered nurse who work in the QDU for 5 hours daily, 5 days a week (Monday‐Friday), assisted by specialists from other specialties. It has a consulting room and a waiting room for patients and families, and functions daily.
For comparison, we analyzed a retrospective cohort of 1454 patients diagnosed with anemia (n = 548), cachexia‐anorexia syndrome (n = 458), febrile syndrome (n = 240), and adenopathies or palpable masses (n = 208) admitted to the internal medicine department between September 2006 and June 2010. Patients were randomly selected from the 2022 consecutive patients with these diagnoses, hospitalized during this period and compared, on an unmatched basis, with all 1468 QDU patients with the same diagnoses.
Patients evaluated by the QDU have potentially severe disease that would normally require hospital admission for diagnosis, but whose health status allows outpatient study, and who have no physical or psychological disability that would make attending the hospital several times difficult. The criteria for QDU referral are agreed with central services (Table 1). In our hospital, patients with lung abnormalities (eg, pulmonary nodules) are usually evaluated quickly in the 1‐day hospital of the respiratory diseases department, however, they are not excluded from QDU evaluation.
|
| Anemia* |
| Cachexia‐anorexia syndrome |
| Febrile syndrome |
| Adenopathies and/or palpable masses |
| Unexplained severe abdominal pain |
| Chronic diarrhea |
| Rectorrhagia |
| Jaundice |
| Lung and/or pleural abnormalities |
| Unexplained dyspnea |
| Dysphagia |
| Ascites |
| Anasarca |
| Arthritis |
Our QDU protocol is based on an urgent first visit, followed by preferential programming and coordination of complementary tests, and subsequent visits until a diagnosis is made. The main diagnostic tests are normally carried out within 10 days after the first visit and, thus, visits are not consecutive but spread over a short period of time. Patients are attended on an ambulatory basis and do not stay overnight.
Inclusion Criteria
When setting up the QDU, the ED, PHC centers, outpatients and other sources of referral were informed and trained in QDU referral criteria (Table 1). All diseases selected for QDU assessment were agreed according to established guidelines. For example, only patients with severe anemia, with or without symptoms, defined as a hemoglobin concentration <8 g/L, our accepted criterion for hospitalization for diagnosis and treatment, were included.
Exclusion Criteria
Patients who fulfilled the inclusion criteria but were judged by the QDU or ED physician as requiring hospitalization or routine outpatient study (eg, active bleeding, uncompensated heart failure, impaired general status, mobility, and social problems) were excluded. Likewise, patients lost to follow‐up or hospitalized during the study due to complications, and deaths were excluded.
For each patient, in addition to clinical data, we prospectively recorded: demographic data; reason for consultation; source of referral; waiting time for the first visit; number and date of visits; waiting times between visits; time to diagnosis; type, number, and date of complementary tests; final diagnosis; and onward referral. The full diagnostic workup was done according to previously established protocols. The Charlson comorbidity index was calculated.18 Blood transfusions and the mean number of units used (SAG‐M red cell concentrates with a median volume per unit of 289 [25] ml) were recorded and administered according to hospital protocol. The time to diagnosis was defined as the time from the first visit to a definitive diagnosis, and usually coincided with the results of diagnostic tests (eg, imaging or pathology).
The same factors were recorded for hospitalized patients (retrospective cohort) except for waiting time to the first visit, number and date of visits, waiting times between visits, and time to diagnosis. In addition, we recorded the mean hospital stay for each patient. Hospital admission avoided was defined as patients who would have been admitted for a diagnostic workup if there were no QDU.
We made a cost analysis using microcosting techniques. First, we calculated the mean number of QDU visits in 150 randomly selected patients with iron‐deficiency anemia, 150 with cachexia‐anorexia syndrome, 150 with fever of unknown origin, and 150 with adenopathies and/or palpable masses. We analyzed the full direct and indirect costs, and calculated the mean cost per visit and the mean cost per process (admission to discharge). The mean length‐of‐stay, and direct and indirect costs were also calculated retrospectively for the same number of hospitalized patients in 2 internal medicine wards, as were the mean cost per daily stay and the mean cost per process (admission to discharge). In our hospital, a 25‐bed internal medicine ward is staffed by 2 consultant physicians and 4 residents, a nursing sister, and 3 teams of 3 registered nurses working 8‐hour daily shifts, 2 nursing assistants, and a full‐time secretary. In contrast, the QDU is staffed by a physician and a nurse, and receives administrative support from 2 secretaries shared with other units. All staff salaries were included in the analysis. All costs analyzed were hospital costs and not National Health Service costs.
A telephone survey was carried out in a random sample of 225 patients 3 months after the QDU intervention, based on a survey previously used and validated by our department. To respect privacy issues, all participants provided verbal consent over the telephone prior to the survey interview. Approval was obtained from the hospital Ethics Committee. The survey consisted of 20 multiple choice questions (4 options) and evaluated: perception of the care process, degree of difficulty of travel to the unit, overall satisfaction, preferential future care type, and conditions of physical space.
Statistical Analysis
The mean, standard deviation, median, and 25% and 75% percentiles were calculated for descriptive variables. Categorical variables were compared using the chi‐square test or Fisher's exact test as necessary. Continuous variables were analyzed using the Student t test for variables with a normal distribution, and the MannWhitney U nonparametric test for variables with a non‐normal distribution. The level of statistical significance was established as P = 0.05. The analysis was made using the SAS v.9.1 statistical package (SAS Institute, Cary, NC).
RESULTS
Of the 2302 patients initially evaluated, 276 were excluded due to associated conditions that made outpatient QDU management inappropriate, 7 patients were lost to follow‐up, 4 died, and 15 were hospitalized during the study due to complications. Therefore, 2000 QDU patients were finally included, of whom 1106 were female, with a mean age of 60 years (18.84).
The main reasons for consultation are shown in Table 2. The main sources of referral were the ED (1022 patients) and PHC centers (942 patients). Waiting time for the first QDU visit ranged from 2 to 8 days (mean: 3.9 days) in patients referred from PHC centers, and 0 to 4 days (mean: 2.1 days) in patients referred by the ED.
| Reasons for Consultation | n (%) |
|---|---|
| |
| Anemia* | 550 (27.5) |
| Cachexia‐anorexia syndrome | 462 (23.1) |
| Febrile syndrome | 244 (12.2) |
| Adenopathies and/or palpable masses | 212 (10.6) |
| Abdominal pain | 128 (6.4) |
| Chronic diarrhea | 108 (5.4) |
| Lung abnormalities | 50 (2.5) |
The 2000 first visits generated 4260 successive visits (ratio first/successive = 2.13). The average number of visits per patient was 3.11.
The most frequent diagnoses were cancer (both epithelial and hematological) in 526/2000 (26.3%) patients, and iron‐deficiency anemia (unrelated to malignancy) in 360 patients. The most common cancers were colon cancer and lymphomas, while the main cause of iron‐deficiency anemia was chronic gastrointestinal bleeding (148/2000 [7.4%] patients) (Table 3).
| Diagnosis | n (%) |
|---|---|
| |
| Malignant neoplasm | 526 (26.3) |
| Colon | 132 (6.6) |
| Lymphoma | 142 (7.1) |
| Gastric | 46 (2.3) |
| Lung | 37 (1.9) |
| Pancreas | 89 (4.5) |
| Other hematological* | 32 (1.6) |
| Breast | 20 (1.0) |
| Ovary | 16 (0.8) |
| UPM | 12 (0.6) |
| Iron‐deficiency anemia | 360 (18) |
| Digestive | 148 (7.4) |
| Unknown cause | 80 (4.0) |
| Heavy menstrual bleeding | 66 (3.3) |
| Multifactorial anemia | 66 (3.3) |
| Chronic liver disease | 57 (2.9) |
| Acute viral illness | 80 (4) |
| Reactive adenitis | 78 (3.9) |
| MGUS | 34 (1.7) |
The mean time to diagnosis was 9.4 days (1.78). After the diagnostic study was completed, 1232 patients were referred to PHC centers, 712 to outpatients, and 56 required hospitalization.
Taking into account previously used criteria, we estimated that 820 (41%) patients would have been candidates for conventional hospitalization (for diagnostic studies) before QDU was created. Considering that the mean length‐of‐stay of the internal medicine department (50 beds) during 2009 for patients admitted for a diagnostic workup was 10.3 days, we estimated that 12.5 beds per day during a year were freed up (ie, 4563 bed‐days saved in a year). On the other hand, 45 of 1000 (4.5%) patients required immediate or early hospitalization due to their bad health status, which impeded further QDU diagnosis.
Table 4 shows the main characteristics of QDU and hospitalized patients according to the main reasons for consultation. QDU patients with anemia were significantly younger than hospitalized patients with the same diagnosis (P < 0.0001). Other parameters, notably age, time to diagnosis versus length‐of‐stay, and Charlson comorbidity index showed no statistically significant differences in any of the 4 main reasons for consultation (Table 4).
| Anemia | QDU (n = 550) | Hospitalized (n = 548) | P Value |
|---|---|---|---|
| |||
| Age | 66.72 (15.23) 71 [59;79] | 77.18 (13.71) 79.23 [72;85] | <0.0001 |
| Female | 280 (51%) | 291 (53.1%) | |
| Male | 270 (49%) | 257 (46.9%) | |
| Time to diagnosis/HS (days) | 7.91 (1.41) 8 [6;9] | 8.66 (3.44) 8.5 [7;10] | NS |
| Hemoglobin | 75.56 (20.9) 76 [55;79] | 74.94 (19.1) 76 [61;78] | NS |
| Anemic syndrome | 509 (92.3%) | 512 (93.4%) | NS |
| Transfusion | 362 (65.8%) | 355 (64.8%) | NS |
| Charlson co. index | 1.3 (2.1) 1.5 [1;1.6] | 1.4 (2.2) 1.5 [1;1.8] | NS |
| Main diagnosis | Iron‐deficiency anemia/colon cancer | Iron‐deficiency anemia/colon cancer | |
| Cachexia‐Anorexia Syndrome | QDU (n = 462) | Hospitalized (n = 458) | P Value |
| Age | 68.32 (18.27) 69 [60;77] | 70.23 (15.23) 73.5 [68;79] | NS |
| Female | 230 (49.8%) | 236 (51.6%) | |
| Male | 232 (50.2%) | 222 (48.4%) | |
| Time to diagnosis/HS (days) | 10.21 (3.31) 11 [10;12] | 11.32 (4.12) 12 [10;13] | NS |
| Weight loss (Kg) | 9.7 (2.25) 10 [9;12] | 9.5 (1.76) 10 [8;11] | NS |
| Charlson co. index | 1.1 (2.1) 1.3 [1;1.4] | 1.2 (2.4) 1.4 [1;1.6] | NS |
| Main diagnosis | Pancreatic cancer | Pancreatic cancer | |
| Febrile Syndrome | QDU (n = 244) | Hospitalized (n = 240) | P Value |
| Age | 47.18 (15.23) 50 [45;55] | 49.34 (14.72) 53 [49;56] | NS |
| Female | 127 (52%) | 121 (50.4%) | |
| Male | 117 (48%) | 119 (49.6%) | |
| Time to diagnosis/HS (days) | 8.32 (2.23) 9 [8;10.5] | 9.11 (3.54) 10.5 [9;11.5] | NS |
| Mean duration of fever (days) | 20.15 (12.12) 24 [20;26] | 19.76 (10.54) 23 [19;25] | NS |
| Charlson co. index | 1.0 (1.5) 1.2 [1.1;1.6] | 1.2 (2.1) 1.3 [0.9;1.4] | NS |
| Main diagnosis | Lymphoma | Lymphoma | |
| Adenopathies and/or Palpable Masses | QDU (n = 212) | Hospitalized (n = 208) | P Value |
| Age | 58.23 (17.20) 59.5 [55;61] | 60.19 (13.21) 64 [58;65] | NS |
| Female | 110 (51.9%) | 106 (51%) | |
| Male | 102 (48.1%) | 102 (49%) | |
| Time to diagnosis/HS | 7.89 (2.54) 8 [7;9] | 7.77 (3.23) 9 [7.5;11] | NS |
| Charlson co. index | 1.1 (1.1) 1.3 [0.8;1.4] | 1.1 (1.7) 1.5 [1.1;1.6] | NS |
| Main diagnosis | Lymphoma | Lymphoma | |
Table 5 shows the mean costs per stay, per visit, and per process for hospitalized and QDU patients included in the 4 main reasons for consultation. In hospitalized patients, the total mean cost per day of hospital stay was 363.35 Euros, and the mean cost per process was 3153.87 (910) Euros. In contrast, the mean cost per process in the QDU was 702.33 (610) Euros.
| Cost per Process* | ||||
|---|---|---|---|---|
| Hospitalization (1‐day stay) | QDU (1 visit) | Hospitalization | QDU | |
| ||||
| Staff salary | 260.94 | 58.79 | 2264.96 | 182.84 |
| Complementary tests | 53.73 | 158.12 | 466.38 | 491.75 |
| Stock | 15.27 | 0.84 | 132.54 | 2.61 |
| Pharmacy, | 0.97 | 0.15 | 8.42 | 0.47 |
| Medical gases | 0.02 | NA | 0.17 | NA |
| Catering | 15.23 | NA | 132.20 | NA |
| Cleaning | 8.78 | 4.47 | 76.21 | 13.90 |
| Laundry | 5.11 | 0.23 | 44.35 | 0.72 |
| Maintenance | 0.47 | 0.28 | 4.08 | 0.87 |
| Communications | 0.31 | 0.29 | 2.69 | 0.90 |
| 0.00 | 0.00 | 0.00 | 0.00 | |
| Depreciation | 2.52 | 1.26 | 21.87 | 3.92 |
| Travel∥ | NA | 1.4 | NA | 4.35 |
| Total | 363.35 | 225.83 | 3153.87 (SD: 910) | 702.33 (SD: 610) |
Compliance with the patient survey was 94%. The results highlighted 3 main aspects: a) overall satisfaction with QDU care was high in 93% of cases; b) repeated travel to the hospital was not a major difficulty; and c) if further diagnostic tests were required, 84% of patients would prefer the QDU care model to hospitalization. The same results were obtained analyzing only patients with previous hospital admission. The remaining 16% indicated no preference for 1 type of care.
DISCUSSION
Our results indicate that, for diagnostic purposes, patients with potentially severe diseases can be managed similarly in a QDU or in‐hospital setting, and that the QDU model saves money compared to hospitalization. QDU patients expressed a high degree of satisfaction, with most preferring this model to hospital admission.
The only significant difference between QDU and hospitalized patients in the 4 main reasons for consultation was age in anemia patients, which may reflect the decision of the ED physician to exclude 56 patients from the initial evaluation. A separate analysis of this subgroup revealed an older age (75.3 years) and a higher number of comorbidities (Charlson index = 2.3) (data not shown).
In Spain, some patients with potentially severe diseases are hospitalized for several days for diagnostic tests without therapy. Can these patients be studied and diagnosed on an outpatient basis? Cachexia‐anorexia syndrome and severe anemia are among the main disorders for which patients are hospitalized for diagnostic tests.5, 7 In our center and others, anemia, with hemoglobin levels <8 g/L, is a criterion for hospitalization for both diagnosis and treatment.2, 3, 17 These patients are commonly evaluated initially in the ED and hospitalized in internal medicine wards, where they have a full baseline laboratory analysis (to study the type of anemia in naive conditions), a blood transfusion if necessary, and several days' hospitalization for diagnostic tests.
The motives for QDU consultation and the final diagnoses are fairly homogenous among Spanish units,2, 3, 15 allowing a profile to be drawn up of patients who could benefit from early QDU diagnosis. In 88% of our patients, the reasons for consultation were anemia, cachexia‐anorexia syndrome, febrile syndrome, adenopathies and/or palpable masses, abdominal pain, diarrhea, and lung abnormalities. The most frequent diagnosis was cancer (26.3%), although most patients showed no clear signs or symptoms of cancer at the initial consultation, suggesting that nonspecific but suspicious symptoms warrant early investigation.
QDUs seem to reduce costs, as reported by a 2004 Spanish study of patients evaluated for various conditions,3 which found that the mean cost per patient was up to 8 times cheaper than conventional hospitalization; hospitalization was avoided in 45% of patients, representing the freeing up of 7 internal medicine beds per day. In our case, and on the basis of previous criteria, avoiding hospital admission in 41% of patients evaluated resulted in the permanent freeing up of 12.5 internal medicine beds per day and a significant reduction in hospital costs. However, this does not mean the QDU system would reduce costs by permanently freeing inpatient beds, as its adoption would drive up systemic costs due to increased QDU utilization and indirect admissions from the QDU to the hospital. The cost differences between QDU and hospitalized patients (702.33 vs 3153.87 Euros) were due to differences in staffing and working hours and, to a lesser degree, fixed hospital costs (eg, catering) (Table 5). This might suggest that our internal medicine wards and QDU are overstaffed and understaffed, respectively, and that resources may be more effectively used in QDU. However, different staff dimensions between hospitals limits the extrapolation of costs and savings.
The QDU model has limitations. Using QDU resources to diagnose mild disorders could delay the diagnosis of severe disease and, therefore, clear agreement on referral criteria is essential. Likewise, although we followed approved guidelines, QDU physicians may prescribe too many diagnostic tests, searching for severe diseases the patient is unlikely to have, especially if the referral diagnosis is incorrect.17 This could be minimized by implementing standardized QDU diagnostic protocols and guidelines. In our study, the type and mean number of complementary explorations in patients with the 4 main reasons for consultation was similar between QDU and hospitalized patients (2.27 vs 2.33, respectively) (data not shown).
How and where (in‐hospital vs outpatients or PHC) patients with potentially severe disease, such as those seen in QDUs, are managed in different countries seems to vary widely. Although there are few reports on this topic,19, 20 these variations might be due, among other reasons, to guidelines for invasive diagnostic procedures and departmental and hospital traditions. Our findings may result in a shift in the paradigm of hospitalization for the diagnostic evaluation of patients with severe conditions, who are often hospitalized and, in some cases, studied in naive conditions (eg, anemia). Our results have already resulted in policy changes, since, increasingly, patients are referred directly from the ED or PHC centers to the QDU rather than being hospitalized, with the consequent savings in hospital beds and costs. Although, ideally, the QDU workup should be led by the primary care physician, waiting times for diagnostic tests are inappropriately long, as mentioned above. A successful reform would likely require better, more agile coordination between PHC and hospital settings, with quicker access to diagnostic procedures from PHC centers.
Ruling out cancer and, indirectly, easing the uncertainty and fear caused by suspected malignancy in patients awaiting diagnostic confirmation is one of the main QDU objectives.21 Cancer is the most common diagnosis (nearly 20% of patients) in Spanish QDUs.2, 3, 17 According to the Strategy on Cancer of the Spanish National Health System 2006, every patient with a well‐founded clinical suspicion of cancer must undergo a first confirmatory diagnostic test within 15 days of the suspicion.22 Our QDU patients received a final diagnosis of cancer in a mean of 11.82 days (waiting time plus evaluation period) (data not shown).
Due to unacceptable outpatient delays, most patients with suspected cancer are hospitalized directly from outpatients for the diagnostic workup,17 although this may be inappropriate in patients who are still practically asymptomatic. Inappropriate use of acute hospital beds, measured by different instruments, ranges from 6% to >20%,2326 with the most common reason being programmed hospitalization solely for diagnostic tests. Twenty‐eight percent of hospital admissions to a public hospital in England in 2000 were reported as inappropriate, mainly because diagnostic tests or treatment could have been made on an outpatient basis.25
QDU may be inappropriate outside publicly funded health systems. The QDU model could be useful, for example, in the United Kingdom, Italy, Canada, and Latin‐American countries; overcrowding and long waiting lists in PHC, and suboptimal coordination between primary and hospital care, means patients with suspected severe disease, including those in good health, are hospitalized for diagnostic tests, aggravating overcrowding and increasing costs.17 However, in countries with mainly private healthcare systems, QDUs created to reduce health costs or free hospital beds may not be as relevant. In the United States, although day hospitals and urgent care units provide similar care to QDUs (at least in urban areas), most insurers would not cover such admissions without clinical urgency, while access and efficient, streamlined care, is a major concern.
The exclusion criteria, which were based on the ED/QDU physician's judgment, are a limitation of the study. This might be circumvented by a randomized study evaluating 2 cohorts prospectively, although there would still be patients whose clinical status would require hospitalization and exclusion from QDU evaluation.
In conclusion, QDUs can manage the diagnosis of patients with potentially severe diseases equally as well as traditional hospitalization and saves costs. QDU patients expressed a high degree of satisfaction, with most preferring this model to hospitalization.
- ,,.Measuring appropriate use of acute beds. A systematic review of methods and results.Health Policy.2000;53:157–184.
- ,,,,.Rapid diagnosis unit in a third level hospital. Descriptive study of the first year and a half.Rev Clin Esp.2008;208:561–563.
- ,,, et al.Quick and early diagnostic outpatient unit: an effective and efficient model of care. Five years experience.Med Clin (Barc).2004;123:247–250.
- ,,.Study on the immediate care clinics of the internal medicine department (University Clinic Hospital of Valladolid).Rev Clin Esp.2006;206:84–89.
- ,,.Impact on hospital days of care due to unnecessary emergency admissions.Rev Esp Salud Pública.2005;79:541–549.
- ,,,.Inappropriate admissions and stays in internal medicine.Med Clin (Barc).2002;118:157.
- ,,,,.Appropriateness of hospitalization in a short stay unit of a teaching hospital. A controlled study.Med Clin (Barc).2004;122:454–456.
- ,,,.Day hospital as conventional hospitalization alternative in an internal medicine service of a first level center.An Med Interna.2007;24:613–614.
- ,,.Short‐stay units and observation medicine: a systematic review.Med J Aust.2003;178:559–563.
- ,,,.Conventional hospitalization alternatives in internal medicine.Med Clin (Barc).2005;124:620–626.
- ,,.Effectiveness of acute medical units in hospitals: a systematic review.Int J Qual Health Care.2009;21:397–407.
- ,,, et al.A hospitalist‐run short‐stay unit: features that predict length‐of‐stay and eventual admission to traditional inpatient services.J Hosp Med.2009;4:276–284.
- ,,.Hospital in the home is cost saving for appropriately selected patients: a comparison with in‐hospital care.Int J Qual Health Care.2002;14:285–293.
- ,,.Criteria for selection and contraindications of ambulatory surgery.Chirurgie.1990;116:568–572.
- ,,,,.Fast specialized ambulatory care of medical disease in an urban tertiary university hospital. Fast care consultation.Rev Clin Esp.2008;208:71–75.
- ,,.QED: quick and early diagnosis.Lancet.1996;348:528–529.
- ,,,,.Quick diagnosis units: a potentially useful alternative to conventional hospitalisation.Med J Aust.2009;191:496–498.
- ,,,.A new method of classifying prognostic comorbidity in longitudinal studies: development and validation.J Chron Dis.1987;40:373–383.
- ,,,.The role of correction of anaemia in patients with congestive heart failure: a short review.Eur J Heart Fail.2008;10:819–823.
- ,,, et al.Who makes the diagnosis? The role of clinical skills and diagnostic test results.J Eval Clin Pract.2007;13:321–325.
- .Two week wait for suspected cancer: milestone or millstone?Int J Clin Pract.2005;59:1251–1252.
- Plan de calidad para el Sistema Nacional de Salud. Estrategia en cáncer del Sistema Nacional de Salud. Ministerio de Sanidad y Consumo 2006. Available at: http://www.msc.es/organizacion/sns/planCalidadSNS/pdf/excelencia/cancer‐cardiopatia/CANCER/opsc_est1.pdf.pdf. Accessed October 17,2010.
- ,,.Alternatives to hospital care: what are they and who should decide?BMJ.1996;312:162–166.
- ,,,.The hospital of the future. Better out than in? Alternatives to acute hospital care.BMJ.1999;319:1127–1130.
- .Inappropriate admissions. Thoughts of patients and referring doctors.J R Soc Med.2001;94:628–631.
- ,,, et al.Predictors of inappropriate hospital days in a department of internal medicine.Int J Epidemiol.1998;27:513–519.
- ,,.Measuring appropriate use of acute beds. A systematic review of methods and results.Health Policy.2000;53:157–184.
- ,,,,.Rapid diagnosis unit in a third level hospital. Descriptive study of the first year and a half.Rev Clin Esp.2008;208:561–563.
- ,,, et al.Quick and early diagnostic outpatient unit: an effective and efficient model of care. Five years experience.Med Clin (Barc).2004;123:247–250.
- ,,.Study on the immediate care clinics of the internal medicine department (University Clinic Hospital of Valladolid).Rev Clin Esp.2006;206:84–89.
- ,,.Impact on hospital days of care due to unnecessary emergency admissions.Rev Esp Salud Pública.2005;79:541–549.
- ,,,.Inappropriate admissions and stays in internal medicine.Med Clin (Barc).2002;118:157.
- ,,,,.Appropriateness of hospitalization in a short stay unit of a teaching hospital. A controlled study.Med Clin (Barc).2004;122:454–456.
- ,,,.Day hospital as conventional hospitalization alternative in an internal medicine service of a first level center.An Med Interna.2007;24:613–614.
- ,,.Short‐stay units and observation medicine: a systematic review.Med J Aust.2003;178:559–563.
- ,,,.Conventional hospitalization alternatives in internal medicine.Med Clin (Barc).2005;124:620–626.
- ,,.Effectiveness of acute medical units in hospitals: a systematic review.Int J Qual Health Care.2009;21:397–407.
- ,,, et al.A hospitalist‐run short‐stay unit: features that predict length‐of‐stay and eventual admission to traditional inpatient services.J Hosp Med.2009;4:276–284.
- ,,.Hospital in the home is cost saving for appropriately selected patients: a comparison with in‐hospital care.Int J Qual Health Care.2002;14:285–293.
- ,,.Criteria for selection and contraindications of ambulatory surgery.Chirurgie.1990;116:568–572.
- ,,,,.Fast specialized ambulatory care of medical disease in an urban tertiary university hospital. Fast care consultation.Rev Clin Esp.2008;208:71–75.
- ,,.QED: quick and early diagnosis.Lancet.1996;348:528–529.
- ,,,,.Quick diagnosis units: a potentially useful alternative to conventional hospitalisation.Med J Aust.2009;191:496–498.
- ,,,.A new method of classifying prognostic comorbidity in longitudinal studies: development and validation.J Chron Dis.1987;40:373–383.
- ,,,.The role of correction of anaemia in patients with congestive heart failure: a short review.Eur J Heart Fail.2008;10:819–823.
- ,,, et al.Who makes the diagnosis? The role of clinical skills and diagnostic test results.J Eval Clin Pract.2007;13:321–325.
- .Two week wait for suspected cancer: milestone or millstone?Int J Clin Pract.2005;59:1251–1252.
- Plan de calidad para el Sistema Nacional de Salud. Estrategia en cáncer del Sistema Nacional de Salud. Ministerio de Sanidad y Consumo 2006. Available at: http://www.msc.es/organizacion/sns/planCalidadSNS/pdf/excelencia/cancer‐cardiopatia/CANCER/opsc_est1.pdf.pdf. Accessed October 17,2010.
- ,,.Alternatives to hospital care: what are they and who should decide?BMJ.1996;312:162–166.
- ,,,.The hospital of the future. Better out than in? Alternatives to acute hospital care.BMJ.1999;319:1127–1130.
- .Inappropriate admissions. Thoughts of patients and referring doctors.J R Soc Med.2001;94:628–631.
- ,,, et al.Predictors of inappropriate hospital days in a department of internal medicine.Int J Epidemiol.1998;27:513–519.
Copyright © 2011 Society of Hospital Medicine
Bioidentical hormone therapy: Clarifying the misconceptions
Recent product endorsements from celebrities on television have brought a new term into the vocabulary of many American women: bioidentical hormone therapy—treatment with hormone products that are identical in molecular structure to those in the human body.
Since 2002, when results of the Women’s Health Initiative1 raised questions about the safety of hormone replacement therapy, women have been inundated by commercials, talk shows, and self-help books that promote bioidentical hormone therapy as a safe and natural way to treat menopausal symptoms—and more.
Although this publicity has helped promote discussion about menopause, it has also perpetuated confusion and misinformation among the lay public and the general medical community concerning menopausal hormone therapy.
Many postmenopausal women suffering from vasomotor symptoms, vaginal dryness, and vaginal atrophy are apprehensive about seeking therapy, owing to concerns resulting from misinterpreted information derived from the Women’s Health Initiative trial.1 (See “What are the known risks of FDA-approved hormone therapy.”2–8) Many others are told to suffer through their symptoms, which may eventually pass. It is not surprising, then, that women turn to unconventional treatments that are claimed to be safer. This unfortunate situation has driven the business of many compounding pharmacies into the multibillion dollar level.
In this paper, we hope to clarify some of the misconceptions surrounding this issue. But first we need to define some terms in what has become a confusing area.

WHAT ARE BIOIDENTICAL HORMONES?
“Bioidentical” means identical in molecular structure to endogenous hormones. However, as we will see, a better distinction should be made between products that are approved and regulated by the US Food and Drug Administration (FDA) and those that are not.
Endogenous reproductive hormones
Women produce various reproductive hormones, including three estrogens—estradiol, estrone, and estriol—as well as progesterone and testosterone.9
17-beta estradiol (E2) is the most bioactive endogenous estrogen. It is primarily produced by the dominant ovarian follicle and the corpus luteum and is synthesized intracellularly through aromatase activity.10,11 The rest of the circulating estradiol is derived from peripheral conversion of estrone to estradiol, and this is the primary source in postmenopausal women not on hormone therapy.11
In postmenopausal women, serum estradiol levels are often below 15 pg/mL. Many physiologic effects of the cellular compartmentalized estradiol contribute to an over-riding force in certain tissues even after menopause.10 With the loss of estradiol, many tissues in postmenopausal women can be affected, particularly resulting in genitourinary atrophy and bone loss.
Estrone (E1), the second dominant human estrogen, is primarily derived from the metabolism of estradiol and from the aromatization of androstenedione in adipose tissue, with a small quantity being secreted directly by the ovary and the adrenal glands.9 In postmenopausal women, mean estrone levels are about 30 pg/mL.11
Estriol (E3), the least active of the endogenous estrogens, is very short-acting.
Progesterone is a 21-carbon steroid secreted by the human ovary.9 It is formed during the transformation of cholesterol to estrogens and androgens and is no longer produced after menopause.9
Testosterone. In premenopausal women, the androgen testosterone is synthesized by the ovary, the adrenal cortex, and the peripheral conversion of circulating androstenedione and dehydroepiandrosterone (DHEA).9 Over a woman’s life span, her androgen levels decline progressively.10 The rate of decline has not been shown to be appreciably affected by the onset of menopause.10
All these hormone therapy products are synthesized
Many nonmedical women’s health books erroneously classify the forms of estrogen used in hormone therapy as either bioidentical or synthetic. In fact, they are all man-made.
Bioidentical hormones are synthesized by chemically extracting diosgenin from plants such as yams and soy.12 Diosgenin is chemically modified to yield the precursor progesterone, which is then used to synthesize bioidentical estrogens and androgens.10
Nonbioidentical estrogen products include conjugated equine estrogens (CEE), which is extracted from the urine of pregnant mares. The two predominant estrogens found in CEE are equilin sulfate (native to horses) and estrone sulfate.10
Other nonbioidentical products include ethinyl estradiol, which is used in most combined oral contraceptives. It is formed after a minor chemical modification of estradiol that makes it one of the most potent estrogens. The ethinyl group at carbon 17 of ring D of the steroid nucleus greatly slows the hepatic and enzymatic degradation of the molecule and, thereby, makes oral ethinyl estradiol 15 to 20 times more active than oral estradiol.
Mestranol is an inactive prodrug that is converted in the body to ethinyl estradiol.
While many women may find the idea of natural bioidentical hormones derived from sweet potatoes or soybeans more acceptable than taking one made from horse’s urine, all the products undergo extensive chemical processing and modification.
Misconception: FDA-regulated products are not bioidentical
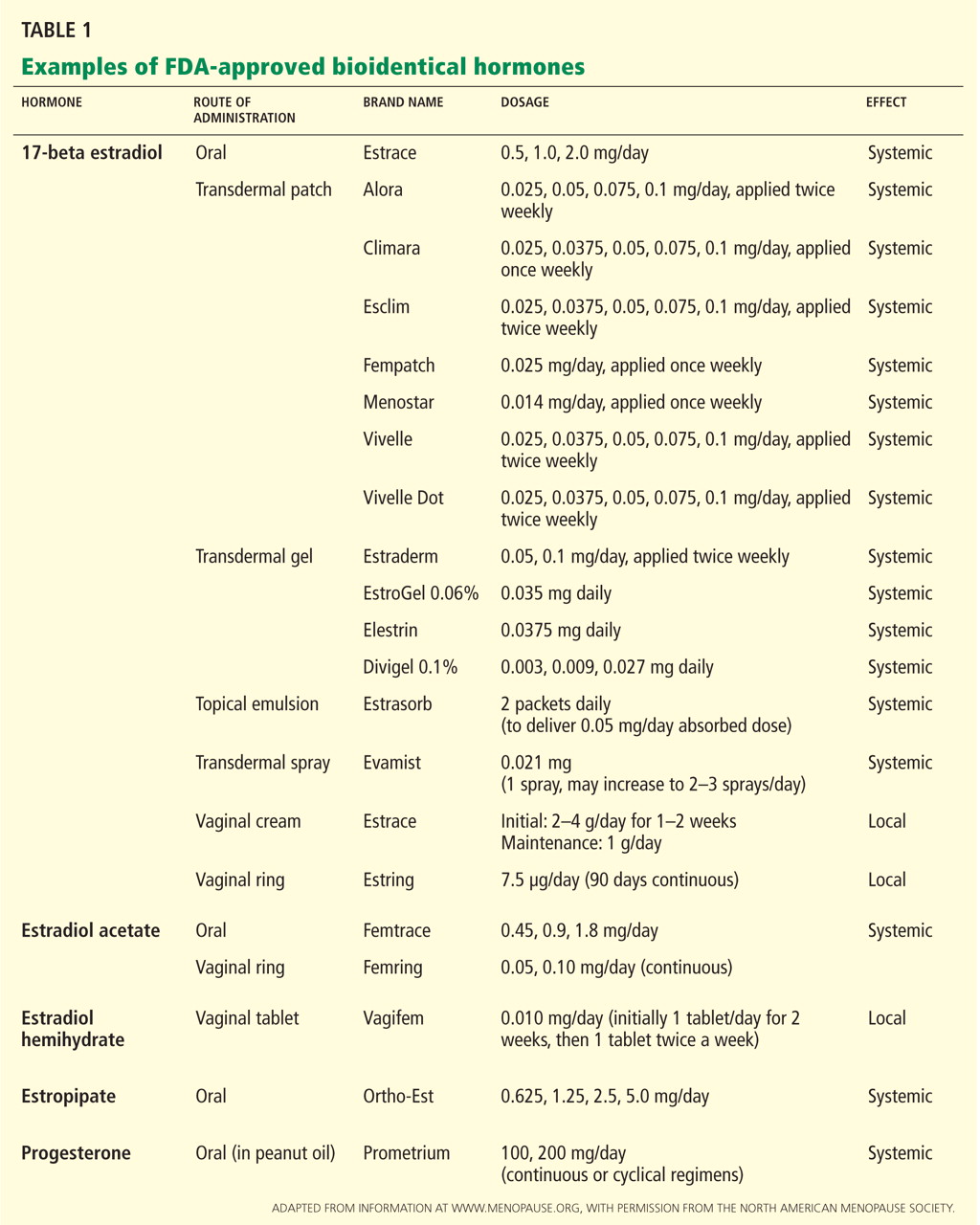
WHAT IS CUSTOMIZED COMPOUNDED HORMONAL THERAPY?
There is often confusion between the terms “bioidentical hormones” and “customized compounded therapy,” which are often used interchangeably. Compounded therapy combines ratios of bioidentical hormones into a particular recipe or mixture. Customized compounding can be done by local compounding pharmacies.2
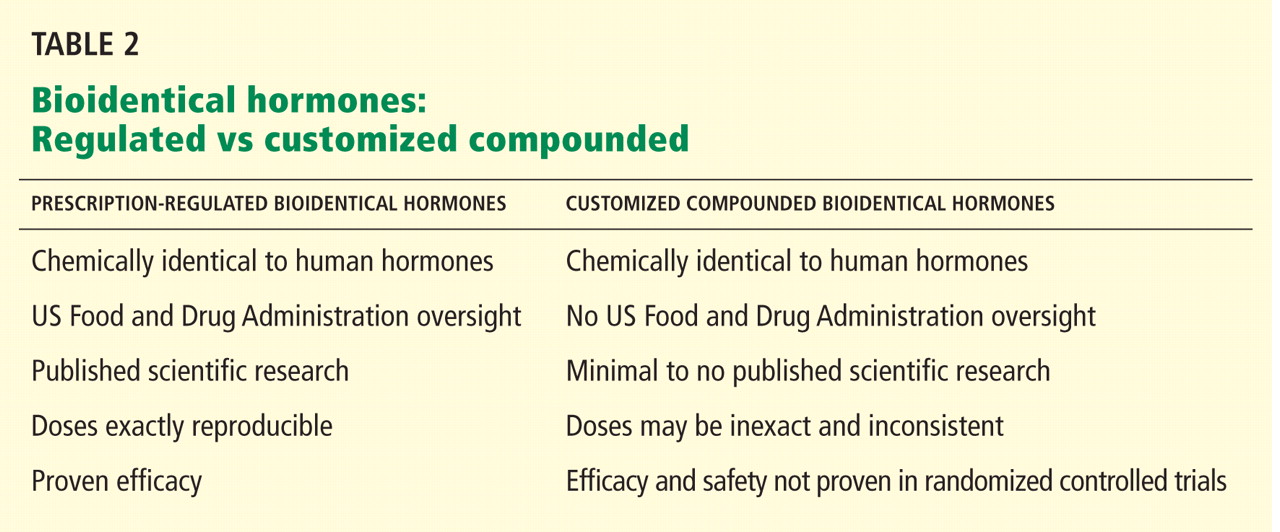
Compounded bioidentical estrogen products
There are several commonly marketed compounded products.
Tri-estrogen (tri-est) is a compounded hormone preparation made up of a mixture of 80% estriol, 10% estrone, and 10% estradiol.12
Bi-estrogen (bi-est) contains estriol and estradiol in a ratio of 8:1 or 9:1.
Although both tri-est and bi-est are largely composed of estriol, given the low potency of estriol, the effects of these products may be solely mediated by their major bioactive component, estradiol.10,12 No large prospective, well-controlled clinical trial has investigated the compounded ratios of these mixtures of estrogens.10
Tri-est and bi-est are frequently promoted as posing less risk of breast or endometrial cancer than FDA-approved agents, although there is no research to back up this claim.12 In fact, estriol may have a stimulatory effect on the breast and endometrium.9
In addition to these “standard” compounded preparations, women can receive more customized compounds.
Valid uses for customized compounded formulations
Some clinical providers use customized compounded formulations when prescribing hormone therapy to women who have allergies to certain ingredients, such as peanut oil (found in the FDA-regulated oral product Prometrium). Customized compounded formulations have also been used when prescribing hormones currently not FDA-approved for women, such as testosterone and DHEA.12 Before oral micronized progesterone was marketed in the United States as Prometrium, it was frequently prescribed as a compounded hormone.
HORMONE THERAPY COMES IN VARIOUS FORMS
Both FDA-regulated hormone therapy and unregulated compounded hormone therapy come in various doses and dosage forms administered by different routes, allowing for individualization for each woman’s specific characteristics.
Estrogens: Oral, transdermal, others
Estrogen therapy can be given orally, transvaginally (as creams, tablets, and rings), transdermally (as patches, gels, and creams), subcutaneously in pellets, intranasally (in Europe), and by injection.11
Most oral contraceptives contain the synthetic estrogen ethinyl estradiol. Ethinyl estradiol is more potent than human estrogens,11 specifically in increasing the production of hepatic proteins (sex-hormone-binding globulin, renin substrate, corticosteroid-binding globulin, and thyroid-binding globulin).11
Bioidentical estradiol, taken orally in tablet form, is first processed through the liver and converted into estrone.12 This stimulates proteins such as C-reactive protein, activated protein C, and clotting factors, which may increase the risk of clotting.12 Estradiol given transdermally by patch or gel or vaginally bypasses the liver and enters the bloodstream as 17-beta estradiol, therefore avoiding stimulation of these proteins.12 Case-control data have shown an associated lower risk of deep venous thromboembolism with transdermal therapy.3
Subcutaneous pellet therapy is a less common, non-FDA-approved method of hormone therapy to relieve postmenopausal symptoms.10 In an outpatient procedure, the pellet is inserted into the subcutaneous fat of the abdomen.10 The crystalline pellet is biodegradable and contains a mixture of testosterone and 17-beta estradiol.10 It is important to remember that endometrial stimulation may be prolonged with this form of therapy and levels may be supraphysiologic.
Progestogens can also be given by different routes
Oral progesterone has poor gastrointestinal absorption and a short half-life.10 Therefore, it is micronized with oil for better absorption. Reported side effects include sedative and anesthetic effects; therefore, it is recommended that oral progesterone be taken at bedtime.9 Medroxyprogesterone acetate may interfere more with estrogen’s positive effects on cholesterol than micronized progesterone does.13
Topical progesterone preparations vary widely in dosage and formulation. Over-the-counter progesterone creams vary in concentration from no active ingredient to 450 mg or more of progesterone per ounce. Application sites for progesterone cream include the inner arm, chest, and inner thigh. No transdermal hormone should be applied to areas of the body that may allow possible contact and transference to others.
Progestogen products
Progestogen products include “natural” progesterone and synthetic progestins. They should be given concurrently with estrogen therapy in women who have an intact uterus to prevent endometrial hyperplasia.9
Bioidentical progesterone is micronized in the laboratory for better absorption in the gut.2
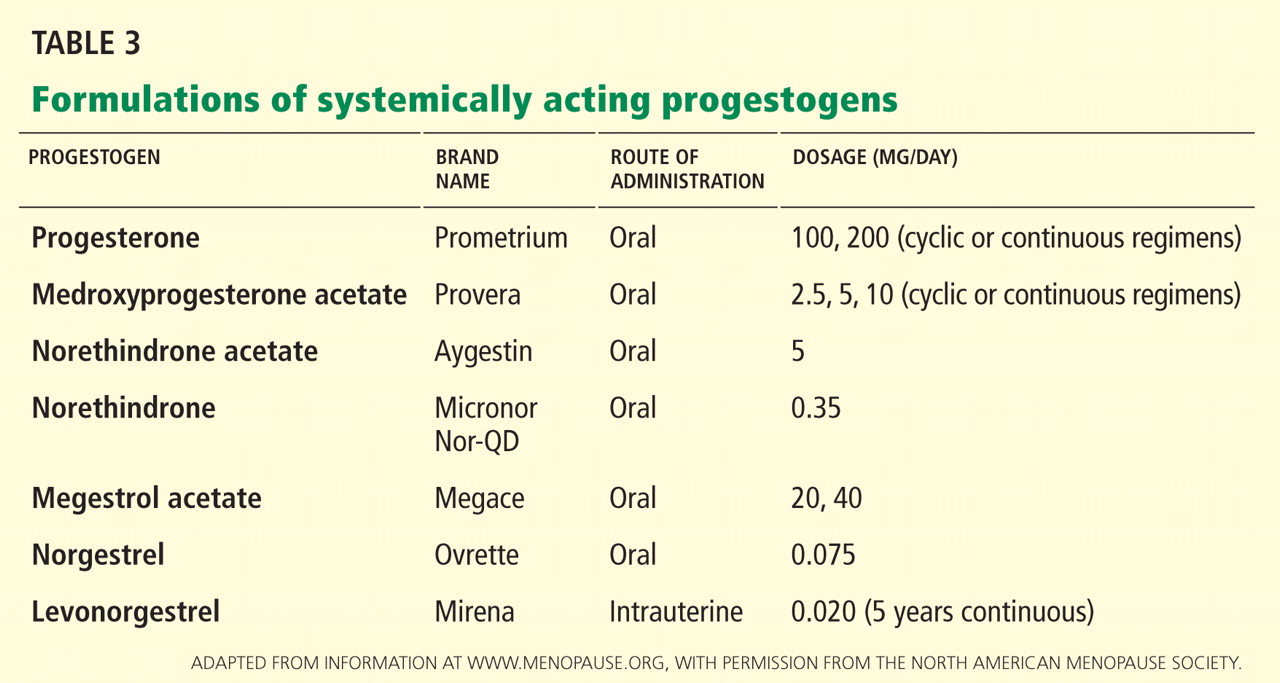
Misconception: Transdermal progesterone protects the endometrium
In general, transdermal progesterone should be avoided, as it does not protect against endometrial cancer.
Many forms of progesterone are available by prescription at compounding pharmacies as lotions, gels, creams, capsules, trochees, and suppositories.9 Transdermal progesterone creams are also available over the counter at health stores. Some of these creams contain only diosgenin, a progesterone precursor derived from wild yams.10 Diosgenin cannot be converted into progesterone within the body and thus does not provide an adequate amount of absorbable progesterone.9 Therefore, progesterone cream that contains only diosgenin is not effective in preventing endometrial hyperplasia and cancer.
To achieve a physiologic response, progesterone levels must be at least in the nanogram range.10 Transdermal progesterone cream has not been shown to reach this level and may not significantly improve vasomotor symptoms.12 Some practitioners prescribe cream that contains more than 400 mg progesterone per ounce. This may achieve physiologic levels of progesterone, but no improvement has been proven for bone mineral density or endometrial protection. In general, no transdermal progesterone cream can be assumed to protect the endometrium against the stimulatory effects of estrogen.
CUSTOM COMPOUNDING AND SALIVA TESTING TO INDIVIDUALIZE THERAPY
Some clinicians who prescribe compounded hormones order saliva tests. They argue the tests help them to establish which hormones are deficient and therefore to customize therapy.12 The basis for this is that saliva is similar to an ultrafiltrate of blood and, theoretically, hormone levels in saliva should represent the bioavailable hormone in serum.10
Unfortunately, this testing is often unreliable due to poor stability of samples in storage and large interassay variability.10 Many factors may alter hormone levels in saliva and make test results unreproducible, including the time of day the sample is collected and dietary habits.10 The FDA states that there is no scientific basis for using salivary testing to adjust hormone levels.2
Levels of drugs with clearance that varies depending on hepatic enzyme activity and plasma binding (capacity-limited metabolism) such as estradiol and testosterone can be monitored with total blood serum concentrations.10 However, many physiologic effects of estrogens are determined intracellularly at the level of tissues.10 Therefore, although levels during therapy with bioidentical estrogens can be monitored more precisely, the FDA states that hormone therapy should be guided by symptom response and findings on physical examination and not by hormone levels alone.2,12 It may be reasonable to order serum levels of estradiol in women being treated with therapeutic doses of bioidentical estrogen but still not achieving symptom relief. If women are being treated with conjugated equine estrogens, serum levels cannot be monitored. Total estrogen can be monitored as a send-out laboratory test.
MISCONCEPTION: HORMONE THERAPY IS A FOUNTAIN OF YOUTH
Customized compounded hormonal therapy is marketed as being able to help with rejuvenation, improve memory, sexual function, and reverse the aging process, essentially promising to be an elixir or fountain of youth.
These claims are not substantiated. However, the actual benefits of hormone therapy in women who have menopausal symptoms include alleviation of moderate to severe vasomotor symptoms and vaginal atrophy that can result in dyspareunia. By alleviating their symptoms, hormone therapy improves women’s quality of life. It also reduces the incidence of postmenopausal osteoporotic fractures.
A research finding that is often overlooked is that postmenopausal women younger than 60 years who started estrogen or estrogenprogestin therapy soon after menopause had a 30% lower rate of death from all causes.2,14 This difference was statistically significant when the estrogen and estrogen-progestin therapy groups were combined. No reduction in the mortality rate was seen if therapy was started after age 60.
MISCONCEPTION: COMPOUNDED THERAPY IS SAFER
Compounded hormone therapy is often marketed as a safer or more effective alternative to government-regulated and approved therapy. Unfortunately, these claims are often false and misleading, and safety information is not consistently provided to patients as is required with FDA-regulated hormone therapy.2
Since these compounds have not been approved by the FDA, there is no guarantee that the ingredients have been tested for purity, potency, and efficacy. There is no batch standardization. These unregulated therapies may use unapproved ingredients, routes of administration, and mixtures with contaminants such as dyes and preservatives.2
Also, custom-compounded prescriptions are considered experimental. Therefore, they are often not covered by insurance, and many women must pay for them out of pocket.11
The North American Menopause Society does not recommend custom-mixed products over well-tested, government-approved commercial products for most women.2 All bioidentical hormone prescriptions should include a patient package insert,11 identical to that required of FDA-approved products.2
- Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002; 288:321–333.
- North American Menopause Society. Estrogen and progestogen use in postmenopausal women: 2010 position statement of the North American Menopause Society. Menopause 2010; 17:242–255.
- Canonico M, Oger E, Plu-Bureau G; Estrogen and Thromboembolism Risk (ESTHER) Study Group. Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of estrogen administration and progestogens: the ESTHER study. Circulation 2007; 115:840–845.
- Risks of postmenopausal hormone replacement (letters). JAMA 2002; 288:2819–2825.
- Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA 2007; 297:1465–1477.
- Grodstein F, Manson JE, Colditz GA, Willett WC, Speizer FE, Stampfer MJ. A prospective, observational study of postmenopausal hormone therapy and primary prevention of cardiovascular disease. Ann Intern Med 2000; 133:933–941.
- Shumaker SA, Legault C, Rapp SR, et al; WHIMS Investigators. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women’s Health Initiative Memory Study: a randomized controlled trial. JAMA 2003; 289:2651–2662.
- Chlebowski RT, Anderson GL, Gass M, et al; WHI Investigators. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA 2010; 304:1684–1692.
- Lobo RA. Treatment of the Postmenopausal Woman: Basic and Clinical Aspects. 3rd ed. Burlington, MA: Academic Press; 2007.
- Cirigliano M. Bioidentical hormone therapy: a review of the evidence. J Womens Health (Larchmt) 2007; 16:600–631.
- Menopause Practice: A Clinician’s Guide. 4th ed. Cleveland, OH: The North American Menopause Society; 2010.
- What are bioidentical hormones? Natural. Bioidentical. Compounded. Confusion about these terms is only adding to the confusion over hormone therapy. Harv Womens Health Watch 2006; 13:1–3.
- The Writing Group for the PEPI Trial. Effects of estrogen or estrogen/progestin regimens on heart disease risk factors in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA 1995; 273:199–208.
- Hodis HN, Mack WJ. Postmenopausal hormone therapy in clinical perspective. Menopause 2007; 14:944–957.
Recent product endorsements from celebrities on television have brought a new term into the vocabulary of many American women: bioidentical hormone therapy—treatment with hormone products that are identical in molecular structure to those in the human body.
Since 2002, when results of the Women’s Health Initiative1 raised questions about the safety of hormone replacement therapy, women have been inundated by commercials, talk shows, and self-help books that promote bioidentical hormone therapy as a safe and natural way to treat menopausal symptoms—and more.
Although this publicity has helped promote discussion about menopause, it has also perpetuated confusion and misinformation among the lay public and the general medical community concerning menopausal hormone therapy.
Many postmenopausal women suffering from vasomotor symptoms, vaginal dryness, and vaginal atrophy are apprehensive about seeking therapy, owing to concerns resulting from misinterpreted information derived from the Women’s Health Initiative trial.1 (See “What are the known risks of FDA-approved hormone therapy.”2–8) Many others are told to suffer through their symptoms, which may eventually pass. It is not surprising, then, that women turn to unconventional treatments that are claimed to be safer. This unfortunate situation has driven the business of many compounding pharmacies into the multibillion dollar level.
In this paper, we hope to clarify some of the misconceptions surrounding this issue. But first we need to define some terms in what has become a confusing area.
WHAT ARE BIOIDENTICAL HORMONES?
“Bioidentical” means identical in molecular structure to endogenous hormones. However, as we will see, a better distinction should be made between products that are approved and regulated by the US Food and Drug Administration (FDA) and those that are not.
Endogenous reproductive hormones
Women produce various reproductive hormones, including three estrogens—estradiol, estrone, and estriol—as well as progesterone and testosterone.9
17-beta estradiol (E2) is the most bioactive endogenous estrogen. It is primarily produced by the dominant ovarian follicle and the corpus luteum and is synthesized intracellularly through aromatase activity.10,11 The rest of the circulating estradiol is derived from peripheral conversion of estrone to estradiol, and this is the primary source in postmenopausal women not on hormone therapy.11
In postmenopausal women, serum estradiol levels are often below 15 pg/mL. Many physiologic effects of the cellular compartmentalized estradiol contribute to an over-riding force in certain tissues even after menopause.10 With the loss of estradiol, many tissues in postmenopausal women can be affected, particularly resulting in genitourinary atrophy and bone loss.
Estrone (E1), the second dominant human estrogen, is primarily derived from the metabolism of estradiol and from the aromatization of androstenedione in adipose tissue, with a small quantity being secreted directly by the ovary and the adrenal glands.9 In postmenopausal women, mean estrone levels are about 30 pg/mL.11
Estriol (E3), the least active of the endogenous estrogens, is very short-acting.
Progesterone is a 21-carbon steroid secreted by the human ovary.9 It is formed during the transformation of cholesterol to estrogens and androgens and is no longer produced after menopause.9
Testosterone. In premenopausal women, the androgen testosterone is synthesized by the ovary, the adrenal cortex, and the peripheral conversion of circulating androstenedione and dehydroepiandrosterone (DHEA).9 Over a woman’s life span, her androgen levels decline progressively.10 The rate of decline has not been shown to be appreciably affected by the onset of menopause.10
All these hormone therapy products are synthesized
Many nonmedical women’s health books erroneously classify the forms of estrogen used in hormone therapy as either bioidentical or synthetic. In fact, they are all man-made.
Bioidentical hormones are synthesized by chemically extracting diosgenin from plants such as yams and soy.12 Diosgenin is chemically modified to yield the precursor progesterone, which is then used to synthesize bioidentical estrogens and androgens.10
Nonbioidentical estrogen products include conjugated equine estrogens (CEE), which is extracted from the urine of pregnant mares. The two predominant estrogens found in CEE are equilin sulfate (native to horses) and estrone sulfate.10
Other nonbioidentical products include ethinyl estradiol, which is used in most combined oral contraceptives. It is formed after a minor chemical modification of estradiol that makes it one of the most potent estrogens. The ethinyl group at carbon 17 of ring D of the steroid nucleus greatly slows the hepatic and enzymatic degradation of the molecule and, thereby, makes oral ethinyl estradiol 15 to 20 times more active than oral estradiol.
Mestranol is an inactive prodrug that is converted in the body to ethinyl estradiol.
While many women may find the idea of natural bioidentical hormones derived from sweet potatoes or soybeans more acceptable than taking one made from horse’s urine, all the products undergo extensive chemical processing and modification.
Misconception: FDA-regulated products are not bioidentical
WHAT IS CUSTOMIZED COMPOUNDED HORMONAL THERAPY?
There is often confusion between the terms “bioidentical hormones” and “customized compounded therapy,” which are often used interchangeably. Compounded therapy combines ratios of bioidentical hormones into a particular recipe or mixture. Customized compounding can be done by local compounding pharmacies.2
Compounded bioidentical estrogen products
There are several commonly marketed compounded products.
Tri-estrogen (tri-est) is a compounded hormone preparation made up of a mixture of 80% estriol, 10% estrone, and 10% estradiol.12
Bi-estrogen (bi-est) contains estriol and estradiol in a ratio of 8:1 or 9:1.
Although both tri-est and bi-est are largely composed of estriol, given the low potency of estriol, the effects of these products may be solely mediated by their major bioactive component, estradiol.10,12 No large prospective, well-controlled clinical trial has investigated the compounded ratios of these mixtures of estrogens.10
Tri-est and bi-est are frequently promoted as posing less risk of breast or endometrial cancer than FDA-approved agents, although there is no research to back up this claim.12 In fact, estriol may have a stimulatory effect on the breast and endometrium.9
In addition to these “standard” compounded preparations, women can receive more customized compounds.
Valid uses for customized compounded formulations
Some clinical providers use customized compounded formulations when prescribing hormone therapy to women who have allergies to certain ingredients, such as peanut oil (found in the FDA-regulated oral product Prometrium). Customized compounded formulations have also been used when prescribing hormones currently not FDA-approved for women, such as testosterone and DHEA.12 Before oral micronized progesterone was marketed in the United States as Prometrium, it was frequently prescribed as a compounded hormone.
HORMONE THERAPY COMES IN VARIOUS FORMS
Both FDA-regulated hormone therapy and unregulated compounded hormone therapy come in various doses and dosage forms administered by different routes, allowing for individualization for each woman’s specific characteristics.
Estrogens: Oral, transdermal, others
Estrogen therapy can be given orally, transvaginally (as creams, tablets, and rings), transdermally (as patches, gels, and creams), subcutaneously in pellets, intranasally (in Europe), and by injection.11
Most oral contraceptives contain the synthetic estrogen ethinyl estradiol. Ethinyl estradiol is more potent than human estrogens,11 specifically in increasing the production of hepatic proteins (sex-hormone-binding globulin, renin substrate, corticosteroid-binding globulin, and thyroid-binding globulin).11
Bioidentical estradiol, taken orally in tablet form, is first processed through the liver and converted into estrone.12 This stimulates proteins such as C-reactive protein, activated protein C, and clotting factors, which may increase the risk of clotting.12 Estradiol given transdermally by patch or gel or vaginally bypasses the liver and enters the bloodstream as 17-beta estradiol, therefore avoiding stimulation of these proteins.12 Case-control data have shown an associated lower risk of deep venous thromboembolism with transdermal therapy.3
Subcutaneous pellet therapy is a less common, non-FDA-approved method of hormone therapy to relieve postmenopausal symptoms.10 In an outpatient procedure, the pellet is inserted into the subcutaneous fat of the abdomen.10 The crystalline pellet is biodegradable and contains a mixture of testosterone and 17-beta estradiol.10 It is important to remember that endometrial stimulation may be prolonged with this form of therapy and levels may be supraphysiologic.
Progestogens can also be given by different routes
Oral progesterone has poor gastrointestinal absorption and a short half-life.10 Therefore, it is micronized with oil for better absorption. Reported side effects include sedative and anesthetic effects; therefore, it is recommended that oral progesterone be taken at bedtime.9 Medroxyprogesterone acetate may interfere more with estrogen’s positive effects on cholesterol than micronized progesterone does.13
Topical progesterone preparations vary widely in dosage and formulation. Over-the-counter progesterone creams vary in concentration from no active ingredient to 450 mg or more of progesterone per ounce. Application sites for progesterone cream include the inner arm, chest, and inner thigh. No transdermal hormone should be applied to areas of the body that may allow possible contact and transference to others.
Progestogen products
Progestogen products include “natural” progesterone and synthetic progestins. They should be given concurrently with estrogen therapy in women who have an intact uterus to prevent endometrial hyperplasia.9
Bioidentical progesterone is micronized in the laboratory for better absorption in the gut.2
Misconception: Transdermal progesterone protects the endometrium
In general, transdermal progesterone should be avoided, as it does not protect against endometrial cancer.
Many forms of progesterone are available by prescription at compounding pharmacies as lotions, gels, creams, capsules, trochees, and suppositories.9 Transdermal progesterone creams are also available over the counter at health stores. Some of these creams contain only diosgenin, a progesterone precursor derived from wild yams.10 Diosgenin cannot be converted into progesterone within the body and thus does not provide an adequate amount of absorbable progesterone.9 Therefore, progesterone cream that contains only diosgenin is not effective in preventing endometrial hyperplasia and cancer.
To achieve a physiologic response, progesterone levels must be at least in the nanogram range.10 Transdermal progesterone cream has not been shown to reach this level and may not significantly improve vasomotor symptoms.12 Some practitioners prescribe cream that contains more than 400 mg progesterone per ounce. This may achieve physiologic levels of progesterone, but no improvement has been proven for bone mineral density or endometrial protection. In general, no transdermal progesterone cream can be assumed to protect the endometrium against the stimulatory effects of estrogen.
CUSTOM COMPOUNDING AND SALIVA TESTING TO INDIVIDUALIZE THERAPY
Some clinicians who prescribe compounded hormones order saliva tests. They argue the tests help them to establish which hormones are deficient and therefore to customize therapy.12 The basis for this is that saliva is similar to an ultrafiltrate of blood and, theoretically, hormone levels in saliva should represent the bioavailable hormone in serum.10
Unfortunately, this testing is often unreliable due to poor stability of samples in storage and large interassay variability.10 Many factors may alter hormone levels in saliva and make test results unreproducible, including the time of day the sample is collected and dietary habits.10 The FDA states that there is no scientific basis for using salivary testing to adjust hormone levels.2
Levels of drugs with clearance that varies depending on hepatic enzyme activity and plasma binding (capacity-limited metabolism) such as estradiol and testosterone can be monitored with total blood serum concentrations.10 However, many physiologic effects of estrogens are determined intracellularly at the level of tissues.10 Therefore, although levels during therapy with bioidentical estrogens can be monitored more precisely, the FDA states that hormone therapy should be guided by symptom response and findings on physical examination and not by hormone levels alone.2,12 It may be reasonable to order serum levels of estradiol in women being treated with therapeutic doses of bioidentical estrogen but still not achieving symptom relief. If women are being treated with conjugated equine estrogens, serum levels cannot be monitored. Total estrogen can be monitored as a send-out laboratory test.
MISCONCEPTION: HORMONE THERAPY IS A FOUNTAIN OF YOUTH
Customized compounded hormonal therapy is marketed as being able to help with rejuvenation, improve memory, sexual function, and reverse the aging process, essentially promising to be an elixir or fountain of youth.
These claims are not substantiated. However, the actual benefits of hormone therapy in women who have menopausal symptoms include alleviation of moderate to severe vasomotor symptoms and vaginal atrophy that can result in dyspareunia. By alleviating their symptoms, hormone therapy improves women’s quality of life. It also reduces the incidence of postmenopausal osteoporotic fractures.
A research finding that is often overlooked is that postmenopausal women younger than 60 years who started estrogen or estrogenprogestin therapy soon after menopause had a 30% lower rate of death from all causes.2,14 This difference was statistically significant when the estrogen and estrogen-progestin therapy groups were combined. No reduction in the mortality rate was seen if therapy was started after age 60.
MISCONCEPTION: COMPOUNDED THERAPY IS SAFER
Compounded hormone therapy is often marketed as a safer or more effective alternative to government-regulated and approved therapy. Unfortunately, these claims are often false and misleading, and safety information is not consistently provided to patients as is required with FDA-regulated hormone therapy.2
Since these compounds have not been approved by the FDA, there is no guarantee that the ingredients have been tested for purity, potency, and efficacy. There is no batch standardization. These unregulated therapies may use unapproved ingredients, routes of administration, and mixtures with contaminants such as dyes and preservatives.2
Also, custom-compounded prescriptions are considered experimental. Therefore, they are often not covered by insurance, and many women must pay for them out of pocket.11
The North American Menopause Society does not recommend custom-mixed products over well-tested, government-approved commercial products for most women.2 All bioidentical hormone prescriptions should include a patient package insert,11 identical to that required of FDA-approved products.2
Recent product endorsements from celebrities on television have brought a new term into the vocabulary of many American women: bioidentical hormone therapy—treatment with hormone products that are identical in molecular structure to those in the human body.
Since 2002, when results of the Women’s Health Initiative1 raised questions about the safety of hormone replacement therapy, women have been inundated by commercials, talk shows, and self-help books that promote bioidentical hormone therapy as a safe and natural way to treat menopausal symptoms—and more.
Although this publicity has helped promote discussion about menopause, it has also perpetuated confusion and misinformation among the lay public and the general medical community concerning menopausal hormone therapy.
Many postmenopausal women suffering from vasomotor symptoms, vaginal dryness, and vaginal atrophy are apprehensive about seeking therapy, owing to concerns resulting from misinterpreted information derived from the Women’s Health Initiative trial.1 (See “What are the known risks of FDA-approved hormone therapy.”2–8) Many others are told to suffer through their symptoms, which may eventually pass. It is not surprising, then, that women turn to unconventional treatments that are claimed to be safer. This unfortunate situation has driven the business of many compounding pharmacies into the multibillion dollar level.
In this paper, we hope to clarify some of the misconceptions surrounding this issue. But first we need to define some terms in what has become a confusing area.
WHAT ARE BIOIDENTICAL HORMONES?
“Bioidentical” means identical in molecular structure to endogenous hormones. However, as we will see, a better distinction should be made between products that are approved and regulated by the US Food and Drug Administration (FDA) and those that are not.
Endogenous reproductive hormones
Women produce various reproductive hormones, including three estrogens—estradiol, estrone, and estriol—as well as progesterone and testosterone.9
17-beta estradiol (E2) is the most bioactive endogenous estrogen. It is primarily produced by the dominant ovarian follicle and the corpus luteum and is synthesized intracellularly through aromatase activity.10,11 The rest of the circulating estradiol is derived from peripheral conversion of estrone to estradiol, and this is the primary source in postmenopausal women not on hormone therapy.11
In postmenopausal women, serum estradiol levels are often below 15 pg/mL. Many physiologic effects of the cellular compartmentalized estradiol contribute to an over-riding force in certain tissues even after menopause.10 With the loss of estradiol, many tissues in postmenopausal women can be affected, particularly resulting in genitourinary atrophy and bone loss.
Estrone (E1), the second dominant human estrogen, is primarily derived from the metabolism of estradiol and from the aromatization of androstenedione in adipose tissue, with a small quantity being secreted directly by the ovary and the adrenal glands.9 In postmenopausal women, mean estrone levels are about 30 pg/mL.11
Estriol (E3), the least active of the endogenous estrogens, is very short-acting.
Progesterone is a 21-carbon steroid secreted by the human ovary.9 It is formed during the transformation of cholesterol to estrogens and androgens and is no longer produced after menopause.9
Testosterone. In premenopausal women, the androgen testosterone is synthesized by the ovary, the adrenal cortex, and the peripheral conversion of circulating androstenedione and dehydroepiandrosterone (DHEA).9 Over a woman’s life span, her androgen levels decline progressively.10 The rate of decline has not been shown to be appreciably affected by the onset of menopause.10
All these hormone therapy products are synthesized
Many nonmedical women’s health books erroneously classify the forms of estrogen used in hormone therapy as either bioidentical or synthetic. In fact, they are all man-made.
Bioidentical hormones are synthesized by chemically extracting diosgenin from plants such as yams and soy.12 Diosgenin is chemically modified to yield the precursor progesterone, which is then used to synthesize bioidentical estrogens and androgens.10
Nonbioidentical estrogen products include conjugated equine estrogens (CEE), which is extracted from the urine of pregnant mares. The two predominant estrogens found in CEE are equilin sulfate (native to horses) and estrone sulfate.10
Other nonbioidentical products include ethinyl estradiol, which is used in most combined oral contraceptives. It is formed after a minor chemical modification of estradiol that makes it one of the most potent estrogens. The ethinyl group at carbon 17 of ring D of the steroid nucleus greatly slows the hepatic and enzymatic degradation of the molecule and, thereby, makes oral ethinyl estradiol 15 to 20 times more active than oral estradiol.
Mestranol is an inactive prodrug that is converted in the body to ethinyl estradiol.
While many women may find the idea of natural bioidentical hormones derived from sweet potatoes or soybeans more acceptable than taking one made from horse’s urine, all the products undergo extensive chemical processing and modification.
Misconception: FDA-regulated products are not bioidentical
WHAT IS CUSTOMIZED COMPOUNDED HORMONAL THERAPY?
There is often confusion between the terms “bioidentical hormones” and “customized compounded therapy,” which are often used interchangeably. Compounded therapy combines ratios of bioidentical hormones into a particular recipe or mixture. Customized compounding can be done by local compounding pharmacies.2
Compounded bioidentical estrogen products
There are several commonly marketed compounded products.
Tri-estrogen (tri-est) is a compounded hormone preparation made up of a mixture of 80% estriol, 10% estrone, and 10% estradiol.12
Bi-estrogen (bi-est) contains estriol and estradiol in a ratio of 8:1 or 9:1.
Although both tri-est and bi-est are largely composed of estriol, given the low potency of estriol, the effects of these products may be solely mediated by their major bioactive component, estradiol.10,12 No large prospective, well-controlled clinical trial has investigated the compounded ratios of these mixtures of estrogens.10
Tri-est and bi-est are frequently promoted as posing less risk of breast or endometrial cancer than FDA-approved agents, although there is no research to back up this claim.12 In fact, estriol may have a stimulatory effect on the breast and endometrium.9
In addition to these “standard” compounded preparations, women can receive more customized compounds.
Valid uses for customized compounded formulations
Some clinical providers use customized compounded formulations when prescribing hormone therapy to women who have allergies to certain ingredients, such as peanut oil (found in the FDA-regulated oral product Prometrium). Customized compounded formulations have also been used when prescribing hormones currently not FDA-approved for women, such as testosterone and DHEA.12 Before oral micronized progesterone was marketed in the United States as Prometrium, it was frequently prescribed as a compounded hormone.
HORMONE THERAPY COMES IN VARIOUS FORMS
Both FDA-regulated hormone therapy and unregulated compounded hormone therapy come in various doses and dosage forms administered by different routes, allowing for individualization for each woman’s specific characteristics.
Estrogens: Oral, transdermal, others
Estrogen therapy can be given orally, transvaginally (as creams, tablets, and rings), transdermally (as patches, gels, and creams), subcutaneously in pellets, intranasally (in Europe), and by injection.11
Most oral contraceptives contain the synthetic estrogen ethinyl estradiol. Ethinyl estradiol is more potent than human estrogens,11 specifically in increasing the production of hepatic proteins (sex-hormone-binding globulin, renin substrate, corticosteroid-binding globulin, and thyroid-binding globulin).11
Bioidentical estradiol, taken orally in tablet form, is first processed through the liver and converted into estrone.12 This stimulates proteins such as C-reactive protein, activated protein C, and clotting factors, which may increase the risk of clotting.12 Estradiol given transdermally by patch or gel or vaginally bypasses the liver and enters the bloodstream as 17-beta estradiol, therefore avoiding stimulation of these proteins.12 Case-control data have shown an associated lower risk of deep venous thromboembolism with transdermal therapy.3
Subcutaneous pellet therapy is a less common, non-FDA-approved method of hormone therapy to relieve postmenopausal symptoms.10 In an outpatient procedure, the pellet is inserted into the subcutaneous fat of the abdomen.10 The crystalline pellet is biodegradable and contains a mixture of testosterone and 17-beta estradiol.10 It is important to remember that endometrial stimulation may be prolonged with this form of therapy and levels may be supraphysiologic.
Progestogens can also be given by different routes
Oral progesterone has poor gastrointestinal absorption and a short half-life.10 Therefore, it is micronized with oil for better absorption. Reported side effects include sedative and anesthetic effects; therefore, it is recommended that oral progesterone be taken at bedtime.9 Medroxyprogesterone acetate may interfere more with estrogen’s positive effects on cholesterol than micronized progesterone does.13
Topical progesterone preparations vary widely in dosage and formulation. Over-the-counter progesterone creams vary in concentration from no active ingredient to 450 mg or more of progesterone per ounce. Application sites for progesterone cream include the inner arm, chest, and inner thigh. No transdermal hormone should be applied to areas of the body that may allow possible contact and transference to others.
Progestogen products
Progestogen products include “natural” progesterone and synthetic progestins. They should be given concurrently with estrogen therapy in women who have an intact uterus to prevent endometrial hyperplasia.9
Bioidentical progesterone is micronized in the laboratory for better absorption in the gut.2
Misconception: Transdermal progesterone protects the endometrium
In general, transdermal progesterone should be avoided, as it does not protect against endometrial cancer.
Many forms of progesterone are available by prescription at compounding pharmacies as lotions, gels, creams, capsules, trochees, and suppositories.9 Transdermal progesterone creams are also available over the counter at health stores. Some of these creams contain only diosgenin, a progesterone precursor derived from wild yams.10 Diosgenin cannot be converted into progesterone within the body and thus does not provide an adequate amount of absorbable progesterone.9 Therefore, progesterone cream that contains only diosgenin is not effective in preventing endometrial hyperplasia and cancer.
To achieve a physiologic response, progesterone levels must be at least in the nanogram range.10 Transdermal progesterone cream has not been shown to reach this level and may not significantly improve vasomotor symptoms.12 Some practitioners prescribe cream that contains more than 400 mg progesterone per ounce. This may achieve physiologic levels of progesterone, but no improvement has been proven for bone mineral density or endometrial protection. In general, no transdermal progesterone cream can be assumed to protect the endometrium against the stimulatory effects of estrogen.
CUSTOM COMPOUNDING AND SALIVA TESTING TO INDIVIDUALIZE THERAPY
Some clinicians who prescribe compounded hormones order saliva tests. They argue the tests help them to establish which hormones are deficient and therefore to customize therapy.12 The basis for this is that saliva is similar to an ultrafiltrate of blood and, theoretically, hormone levels in saliva should represent the bioavailable hormone in serum.10
Unfortunately, this testing is often unreliable due to poor stability of samples in storage and large interassay variability.10 Many factors may alter hormone levels in saliva and make test results unreproducible, including the time of day the sample is collected and dietary habits.10 The FDA states that there is no scientific basis for using salivary testing to adjust hormone levels.2
Levels of drugs with clearance that varies depending on hepatic enzyme activity and plasma binding (capacity-limited metabolism) such as estradiol and testosterone can be monitored with total blood serum concentrations.10 However, many physiologic effects of estrogens are determined intracellularly at the level of tissues.10 Therefore, although levels during therapy with bioidentical estrogens can be monitored more precisely, the FDA states that hormone therapy should be guided by symptom response and findings on physical examination and not by hormone levels alone.2,12 It may be reasonable to order serum levels of estradiol in women being treated with therapeutic doses of bioidentical estrogen but still not achieving symptom relief. If women are being treated with conjugated equine estrogens, serum levels cannot be monitored. Total estrogen can be monitored as a send-out laboratory test.
MISCONCEPTION: HORMONE THERAPY IS A FOUNTAIN OF YOUTH
Customized compounded hormonal therapy is marketed as being able to help with rejuvenation, improve memory, sexual function, and reverse the aging process, essentially promising to be an elixir or fountain of youth.
These claims are not substantiated. However, the actual benefits of hormone therapy in women who have menopausal symptoms include alleviation of moderate to severe vasomotor symptoms and vaginal atrophy that can result in dyspareunia. By alleviating their symptoms, hormone therapy improves women’s quality of life. It also reduces the incidence of postmenopausal osteoporotic fractures.
A research finding that is often overlooked is that postmenopausal women younger than 60 years who started estrogen or estrogenprogestin therapy soon after menopause had a 30% lower rate of death from all causes.2,14 This difference was statistically significant when the estrogen and estrogen-progestin therapy groups were combined. No reduction in the mortality rate was seen if therapy was started after age 60.
MISCONCEPTION: COMPOUNDED THERAPY IS SAFER
Compounded hormone therapy is often marketed as a safer or more effective alternative to government-regulated and approved therapy. Unfortunately, these claims are often false and misleading, and safety information is not consistently provided to patients as is required with FDA-regulated hormone therapy.2
Since these compounds have not been approved by the FDA, there is no guarantee that the ingredients have been tested for purity, potency, and efficacy. There is no batch standardization. These unregulated therapies may use unapproved ingredients, routes of administration, and mixtures with contaminants such as dyes and preservatives.2
Also, custom-compounded prescriptions are considered experimental. Therefore, they are often not covered by insurance, and many women must pay for them out of pocket.11
The North American Menopause Society does not recommend custom-mixed products over well-tested, government-approved commercial products for most women.2 All bioidentical hormone prescriptions should include a patient package insert,11 identical to that required of FDA-approved products.2
- Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002; 288:321–333.
- North American Menopause Society. Estrogen and progestogen use in postmenopausal women: 2010 position statement of the North American Menopause Society. Menopause 2010; 17:242–255.
- Canonico M, Oger E, Plu-Bureau G; Estrogen and Thromboembolism Risk (ESTHER) Study Group. Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of estrogen administration and progestogens: the ESTHER study. Circulation 2007; 115:840–845.
- Risks of postmenopausal hormone replacement (letters). JAMA 2002; 288:2819–2825.
- Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA 2007; 297:1465–1477.
- Grodstein F, Manson JE, Colditz GA, Willett WC, Speizer FE, Stampfer MJ. A prospective, observational study of postmenopausal hormone therapy and primary prevention of cardiovascular disease. Ann Intern Med 2000; 133:933–941.
- Shumaker SA, Legault C, Rapp SR, et al; WHIMS Investigators. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women’s Health Initiative Memory Study: a randomized controlled trial. JAMA 2003; 289:2651–2662.
- Chlebowski RT, Anderson GL, Gass M, et al; WHI Investigators. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA 2010; 304:1684–1692.
- Lobo RA. Treatment of the Postmenopausal Woman: Basic and Clinical Aspects. 3rd ed. Burlington, MA: Academic Press; 2007.
- Cirigliano M. Bioidentical hormone therapy: a review of the evidence. J Womens Health (Larchmt) 2007; 16:600–631.
- Menopause Practice: A Clinician’s Guide. 4th ed. Cleveland, OH: The North American Menopause Society; 2010.
- What are bioidentical hormones? Natural. Bioidentical. Compounded. Confusion about these terms is only adding to the confusion over hormone therapy. Harv Womens Health Watch 2006; 13:1–3.
- The Writing Group for the PEPI Trial. Effects of estrogen or estrogen/progestin regimens on heart disease risk factors in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA 1995; 273:199–208.
- Hodis HN, Mack WJ. Postmenopausal hormone therapy in clinical perspective. Menopause 2007; 14:944–957.
- Rossouw JE, Anderson GL, Prentice RL, et al. Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women’s Health Initiative randomized controlled trial. JAMA 2002; 288:321–333.
- North American Menopause Society. Estrogen and progestogen use in postmenopausal women: 2010 position statement of the North American Menopause Society. Menopause 2010; 17:242–255.
- Canonico M, Oger E, Plu-Bureau G; Estrogen and Thromboembolism Risk (ESTHER) Study Group. Hormone therapy and venous thromboembolism among postmenopausal women: impact of the route of estrogen administration and progestogens: the ESTHER study. Circulation 2007; 115:840–845.
- Risks of postmenopausal hormone replacement (letters). JAMA 2002; 288:2819–2825.
- Rossouw JE, Prentice RL, Manson JE, et al. Postmenopausal hormone therapy and risk of cardiovascular disease by age and years since menopause. JAMA 2007; 297:1465–1477.
- Grodstein F, Manson JE, Colditz GA, Willett WC, Speizer FE, Stampfer MJ. A prospective, observational study of postmenopausal hormone therapy and primary prevention of cardiovascular disease. Ann Intern Med 2000; 133:933–941.
- Shumaker SA, Legault C, Rapp SR, et al; WHIMS Investigators. Estrogen plus progestin and the incidence of dementia and mild cognitive impairment in postmenopausal women: the Women’s Health Initiative Memory Study: a randomized controlled trial. JAMA 2003; 289:2651–2662.
- Chlebowski RT, Anderson GL, Gass M, et al; WHI Investigators. Estrogen plus progestin and breast cancer incidence and mortality in postmenopausal women. JAMA 2010; 304:1684–1692.
- Lobo RA. Treatment of the Postmenopausal Woman: Basic and Clinical Aspects. 3rd ed. Burlington, MA: Academic Press; 2007.
- Cirigliano M. Bioidentical hormone therapy: a review of the evidence. J Womens Health (Larchmt) 2007; 16:600–631.
- Menopause Practice: A Clinician’s Guide. 4th ed. Cleveland, OH: The North American Menopause Society; 2010.
- What are bioidentical hormones? Natural. Bioidentical. Compounded. Confusion about these terms is only adding to the confusion over hormone therapy. Harv Womens Health Watch 2006; 13:1–3.
- The Writing Group for the PEPI Trial. Effects of estrogen or estrogen/progestin regimens on heart disease risk factors in postmenopausal women. The Postmenopausal Estrogen/Progestin Interventions (PEPI) Trial. JAMA 1995; 273:199–208.
- Hodis HN, Mack WJ. Postmenopausal hormone therapy in clinical perspective. Menopause 2007; 14:944–957.
KEY POINTS
- Hormone therapy is indicated for relief of menopausal symptoms; claims of reversal of the aging process are unsubstantiated.
- Products that are custom-compounded are not regulated by the US Food and Drug Administration and therefore carry no assurance of purity, safety, or efficacy.
- Transdermal progesterone creams do not achieve high enough serum levels to protect the endometrium.
- Hormone therapy is titrated on the basis of symptom response. Measuring hormone levels in saliva is not called for and is probably not reliable.
Essential tremor: Choosing the right management plan for your patient
Essential tremor, one of the most common movement disorders, affects about 4% of adults 40 years of age and older.1 It is often referred to as familial tremor in patients with a family history of tremor. It has also been called benign tremor to differentiate it from tremor associated with neurodegenerative diseases, particularly Parkinson disease, but this condition is certainly not benign, as it can cause substantial functional impairment and difficulties with routine activities of daily living. The terms “essential” and “idiopathic” refer to the primary nature of the disorder and differentiate it from tremor that is a feature of a distinct neurologic entity or is secondary to a metabolic disease or drug therapy.
Successful management entails exclusion of secondary causes and careful selection of drug therapy. To date, there is no cure for essential tremor; all currently available treatments are purely symptomatic.
In this review, we outline the major diagnostic and therapeutic principles of managing essential tremor, indications for referral to specialists, and alternative and advanced therapeutic options.
CLINICAL PICTURE
Tremor is defined as rhythmic to-and-fro movement in any body part. It can be slow or fast, and its amplitude can be large and coarse, or small or even “fine.” It can appear at rest, with action, or during a sustained posture. In contrast to parkinsonian tremor (which presents mainly at rest), essential tremor is typically but not exclusively postural, kinetic, or both.
Postural tremor refers to tremor seen when the patient holds the affected limb (commonly the arm) unsupported against gravity. Kinetic tremor refers to tremor that appears with active movements. This is often demonstrated clinically by the finger-nose-finger test. Patients with essential tremor commonly have both postural and kinetic tremor.
The tremor commonly involves the arms, hands, and fingers.2 Less commonly, it involves the head, the lips, the tongue, the legs, and the voice. In contrast to parkinsonian tremor, which typically affects one side of the body first, bilateral involvement is the general rule in essential tremor. However, one side of the body may be affected first, or may be more affected than the other. The frequency of the tremor ranges from 4 to 12 Hz (ie, beats per second).
The tremor usually starts in middle age and progresses slowly over time,3 but onset in old age or childhood is also possible.4 Both sexes are equally affected.
The tremor usually gets worse with anxiety, stress, and caffeine intake. It usually gets temporarily better with the consumption of small amounts of alcohol.
The functional impact of essential tremor is judged by its effect on different daily activities, especially writing, eating, drinking, dressing, manual work, and household chores.
In addition to motor dysfunction, the tremor can also have a significant psychological impact on the patient, because it usually gets worse in social situations.
Although it has long been thought that tremor is the sole neurologic sign of essential tremor, recent studies have shown that many patients have additional subtle findings, such as mild gait difficulty,5 slight incoordination,6 mild cognitive impairment,7 and decreased hearing,8 and are more likely to have anxiety and social phobia.9
Although different studies have varied in their findings, it is generally thought that about 50% of patients with essential tremor have a positive family history, often in a first-degree relative, suggesting autosomal dominant inheritance with variable penetrance.10,11 Polygenetic and sporadic variants are also common.
DIFFERENTIAL DIAGNOSIS
Resting tremor
Resting tremor is typically an extrapyramidal sign and, when accompanied by rigidity and bradykinesia, is often part of a parkinsonian syndrome. It is most pronounced at rest when the affected body part is fully supported and stationary. The tremor tends to improve with action or posture. It usually has a “pill-rolling” character and, as mentioned, is associated with other extrapyramidal signs, such as rigidity, slowness, and, later on, postural instability.
About 20% of patients with essential tremor have resting tremor. These patients usually suffer from severe or long-standing disease.12 However, the resting element in these cases is often milder than the postural and kinetic components, and it is typically not associated with other extrapyramidal signs. Also, some patients may have both essential tremor and Parkinson disease.13
Intentional tremor
Pure intentional tremor is usually seen with cerebellar pathology, which includes tumors, stroke, multiple sclerosis, trauma, and spinocerebellar degeneration. The amplitude of this type of tremor increases as the affected limb approaches the final target. It can best be demonstrated clinically by the finger-nose-finger test. The frequency of intentional tremor is slow (2 to 4 Hz) and is usually associated with other cerebellar signs, such as dysmetria, decomposition, rebound, and dysdiadochokinesia (ie, the inability to perform rapid alternating movements in a smooth and coordinated manner).
About 50% of patients with essential tremor have an intentional component to their tremor,6 or it can be mildly present in the form of a slight gait difficulty. However, in essential tremor, other features of cerebellar dysfunction are either absent or only very slight.
Secondary causes of postural-kinetic tremor
Enhanced physiologic tremor. A very mild postural tremor is present in almost all people and is considered “physiologic” since it has almost no clinical significance. This type of tremor is often invisible, but when “enhanced,” it can be visually demonstrated by placing a piece of paper over the stretched hands and watching the ripple from the paper.
Certain conditions can aggravate this physiologic tremor and can make it symptomatic. Common causes include anxiety, sleep deprivation, hypoglycemia, hyperthyroidism, pheochromocytoma, serotonin syndrome, and carcinoid syndrome.
Metabolic tremor. Hyperammonemia can cause tremor in patients with hepatic encephalopathy, and uremia can cause tremor in patients with renal failure. These metabolic conditions classically result in “flappy” tremor (asterixis), a special form of postural tremor characterized by jerking movements with high amplitude. It is best seen when the patient stretches out the arms and extends the wrists as if trying to stop traffic. But even though it may look like tremor, asterixis is thought to be a form of “negative” myoclonus.
Drug-related tremor. Postural-kinetic tremor can be induced by drugs, including lithium (Lithobid), valproate (Depakote), amiodarone (Cordarone), central nervous system stimulants, beta agonists (including inhalers), and some antidepressants. Tremor can also occur with alcohol or sedative withdrawal.
Psychogenic tremor. Tremor can be seen as part of a somatoform disorder commonly referred to as conversion disorder or conversion reaction. Psychogenic tremor is characterized by acute onset, commonly following a psychosocial stressor; it is often atypical, variable in frequency, amplitude, and body-part involvement, and it can readily be interrupted on examination by distracting the patient.
Neurologic disorders. The postural and kinetic elements of essential tremor may also be seen in the following neurologic conditions:
- Holmes (rubral) tremor, a combination of resting, postural, kinetic, and intentional tremor of low frequency and high amplitude. It usually has a proximal component and is often unilateral. It commonly is due to a lesion that involves the brainstem, eg, red nucleus, inferior olive, cerebellum, or thalamus. Common causes include stroke, prolonged hypoxia, and head trauma (including closed-head trauma with negative imaging). This type of tremor is usually associated with ataxia.14
- Dystonic tremor is predominantly postural and is associated with abnormal dystonic posturing of the affected body part, commonly the head, hands, or feet. Unlike the rhythmic oscillations of essential tremor, dystonic tremor is often irregular in rhythm.
- Multiple sclerosis can present with a combination of postural, kinetic, and intentional tremor. Patients usually have a clear history of recurrent neurologic deficits and show a combination of pyramidal, cerebellar, and sensory signs on examination consistent with multiple sclerosis.15
- Neuropathic tremor is seen in a small proportion of patients with peripheral neuropathy, especially demyelinating neuropathy.16 The tremor is usually posturalkinetic and is associated with signs of neuropathy, such as a glove-and-stocking pattern of hypoesthesia, reduced reflexes, and sensory ataxia (including intentional tremor when the eyes are closed).
- Posttraumatic tremor can occur after severe or even mild head trauma, especially in children. It is commonly rubral, but other types have been reported, including a presentation resembling essential tremor.17
- Monosymptomatic or isolated tremor. A number of conditions related to essential tremor with location-specific or task-specific tremor have been described. These rare conditions historically have been classified as “possible essential tremor” or “essential tremor variants” but are now considered separate entities. These include task-specific tremor (eg, writing tremor), isolated head tremor, isolated voice tremor, and orthostatic tremor (tremor in the legs and trunk upon standing in place, but not when sitting or walking).18,19
DIAGNOSIS IS CLINICAL
Essential tremor is a clinical diagnosis. After a thorough review of the medical history and medication exposures, laboratory and imaging tests may be ordered to rule out a secondary cause. A complete metabolic panel, including blood glucose and thyroid-stimulating hormone levels, is usually sufficient. Brain imaging or other imaging is ordered for patients with an atypical presentation.
TREATMENT IS SYMPTOMATIC
Treatment of essential tremor is symptomatic. Several drugs of different pharmacologic classes can reduce the severity of the tremor and improve function.
Choosing the appropriate treatment depends on the type of tremor and the presence of associated conditions. The response to treatment and the development of side effects guide further adjustments. The following is a brief description of the available antitremor agents.
FIRST-LINE AGENTS
Propranolol
Propranolol (Inderal), a nonselective beta blocker, is the most widely used antitremor drug and the only agent approved by the US Food and Drug Administration for essential tremor. It should be started at a low dose and titrated upward gradually. The usual starting dose is 10 mg three times daily. The average effective dose is 120 mg daily. The dose can be increased up to 320 mg if needed and tolerated.
Sustained-release preparations are equally effective and are given as a single daily dose to improve compliance.20
Propranolol improves tremor in 50% to 70% of patients with essential tremor and achieves an average tremor reduction of 50% to 60%.1,21–25 Side effects include bronchoconstriction, bradycardia, hypotension, depression, impotence, fatigue, and gastrointestinal disturbances.
Other beta-blockers, such as nadolol (Corgard) and timolol, are also effective against tremor but are less potent than propranolol.26,27 The selective beta-1-blocker metoprolol (Lopressor) may be effective and has fewer noncardiac side effects than propranolol.28 It can be used in patients who discontinue propranolol because of adverse effects. Atenolol (Tenormin) and pindolol (Visken) have little or no effect on tremor.29
A good candidate for propranolol therapy in essential tremor is:
- A patient with no known contraindication to propranolol
- A patient with hypertension, coronary heart disease, or tachyarrhythmia
- A patient with anxiety or social phobia.
Absolute contraindications to propranolol are:
- Moderate to severe bronchial asthma
- Significant bradycardia or heart block
- Symptomatic hypotension
- End-stage heart failure
- Concurrent use of a calcium channel blocker.
Relative contraindications are:
- Wheezing (eg, chronic obstructive pulmonary disease)
- Depression
- Diabetes mellitus in a patient more prone to hypoglycemia (propranolol masks the warning signs of hypoglycemia)
- Reduced sexual potency in a male patient.
Primidone
Primidone (Mysoline) is an antiepileptic drug structurally similar to barbiturates. Its antitremor effect is equal to that of propranolol, though some studies suggest it is slightly more efficacious.30,31
It should be started at a low dose, ie, 25 mg once daily at bedtime. The dose should then be increased gradually until satisfactory and tolerable tremor control is achieved. Most patients respond to doses of around 250 mg per day.1,22,24–25 The dose can be increased if needed and tolerated.
Primidone reduces tremor by about 50% to 60%.1,22,24–25 Side effects include sedation, dizziness, fatigue, nausea, and depression, as well as ataxia and confusion in severe cases.
A good candidate for primidone in essential tremor is:
- A patient with no known contraindication to primidone
- A patient with contraindications to propranolol
- A younger patient
- A patient with epilepsy.
Absolute contraindications to primidone include:
- Confusion or dementia
- Oral anticoagulant therapy with difficulty controlling the International Normalized Ratio (primidone is a potent enzyme inducer).
Relative contraindications to primidone in essential tremor are:
- Depression
- Alcohol abuse
- Ongoing therapy with sedating drugs
- Ataxia or vertigo.
SECOND-LINE AGENTS
Other antiepileptics
Topiramate (Topamax) is a broad-spectrum antiepileptic shown to be significantly effective against essential tremor.32 It is usually started at a single daily dose of 25 mg and increased gradually to the most effective dose, usually around 300 mg.
Side effects include reduced appetite, weight loss, cognitive dysfunction, and paresthesia.
Favorable candidates include patients who are epileptic or overweight. Contraindications include cognitive impairment and low body weight. It is also not recommended in children so as to avoid any possible negative effect on cognitive development. In rare cases, topiramate has been reported to cause significant visual disturbances.
Gabapentin (Neurontin) is an antiepileptic that is now more often used as a symptomatic treatment for neuropathic pain. Studies have suggested a beneficial effect on essential tremor,33,34 but some investigators have questioned its efficacy.35
Like other antitremor agents, it should be started at a low dose, ie, around 300 mg, and escalated gradually until the tremor is controlled. The usual effective dose is 1,200 mg.
Gabapentin is generally well tolerated, and side effects such as dizziness, drowsiness, sedation, and unsteadiness are rare and usually mild.
The favorable candidate is a patient with associated neuropathy or multiple comorbidities. Gabapentin has also been reported to alleviate neuropathic tremor.
Contraindications are minimal and include intolerability or hypersensitivity to the drug. It also should be avoided in patients at a high risk of falling.
Levetiracetam (Keppra) is a novel antiepileptic effective against partial seizures. Studies have shown contradictory results regarding its antitremor effect. One double-blind, placebo-controlled study demonstrated significant reduction in essential tremor with 1,000 mg of levetiracetam.36 However, its effect on tremor is believed to be short-lived, and some studies argue against its efficacy.37 It has a favorable side-effect profile and is generally very well tolerated. It can be used as an adjunct to other antitremor agents and is preferred for patients with coexisting partial seizures or myoclonus.
Benzodiazepines. Minor tranquilizers are often used to control tremor, especially in coexisting anxiety or insomnia. Alprazolam (Xanax) is the one most widely used for this indication.38 It can be started in a dose of 0.25 mg once at bedtime and increased gradually up to 0.75 to 2 mg. Clonazepam (Klonopin) is particularly useful for orthostatic tremor, a variant of essential tremor characterized by tremor of the legs and trunk upon standing.39
Common side effects of benzodiazepines include sedation, cognitive dysfunction, hypotension, respiratory inhibition, and addiction after prolonged use. In the elderly, they can lead to confusion and disinhibition and can increase the risk of falling. They should be avoided in the elderly and in alcoholic patients and those with a high risk of substance abuse.
Stopping benzodiazepines should be done gradually to avoid withdrawal symptoms, including aggravation of tremor.
THIRD-LINE AGENTS
Clozapine
Clozapine (Clozaril) is a novel antipsychotic drug with no extrapyramidal side effects. It has been reported effective in essential tremor and drug-induced tremor,40,41 but the results of these early studies have not been confirmed.
Clozapine is started as a single daily dose of 12.5 mg and is increased up to 75 mg or 100 mg. It is an attractive option for patients with coexisting psychosis, bipolar disorder, or chorea. Its main side effects are sedation, salivation, weight gain, hypertension, diabetes, and seizures.
One especially serious side effect is agranulocytosis. This potentially fatal effect is rare, occurring in about 1.3% of patients receiving this drug. Weekly monitoring of the white blood cell count is mandated during treatment with clozapine, and this has made clozapine a less attractive option for the routine treatment of essential tremor.
Mirtazapine
Mirtazapine (Remeron) is a novel antidepressant widely used in Parkinson disease as both an antidepressant and a sleeping aid. Case studies have reported efficacy in both essential tremor and parkinsonian tremor,42 but controlled studies have not confirmed this.43 Mirtazapine is a reasonable option in patients with coexisting depression or insomnia. It is usually given as a single bedtime dose of 15 to 30 mg.
Other drugs
Studies of other agents for the treatment of essential tremor—eg, carbonic anhydrase enzyme inhibitors, calcium channel blockers, isoniazid (Tubizid), clonidine (Catapres), phenobarbital, and theophylline—have yielded highly contradictory results. Thus, they are not recommended as first- or second-line agents for essential tremor.
SPECIALTY-LEVEL CARE
When essential tremor does not respond to drug therapy or the patient cannot tolerate drug therapy, the patient should be referred to a center specializing in movement disorders for more advanced treatment options, ie, botulinum toxin injection and deep brain stimulation surgery.
Botulinum toxin
Botulinum toxin type A has been studied for the treatment of essential tremor with variable degrees of success. It has been effective in reducing hand tremor in essential tremor, but without a concomitant improvement in functional disability.44 This limited functional improvement has been attributed to the development of muscle weakness after injection of the neurotoxin. This has also raised questions about unintentional unblinding when interpreting study results. Therefore, most clinicians restrict its use to focal forms of tremor such as voice tremor,45 head tremor, and task-specific tremor.
Side effects are limited and temporary and include muscle weakness, pain at the injection site, dysphagia (when injected for head or voice tremor), and a breathy vocal quality (when injected for voice tremor). Botulinum toxin injection is the treatment of choice for focal dystonia, and therefore would be a good option for dystonic tremor.
Thalamic deep brain stimulation
This technique involves stereotactic implantation of a stimulation lead in the ventral intermediate nucleus of the thalamus. The lead connects via a subcutaneous wire to an intermittent pulse generator, implanted subcutaneously in the infraclavicular region. The stimulation lead produces continuous stimulation of the ventralis intermedius nucleus that is functionally equal to lesional surgery, thus antagonizing the relay of tremor signals at the thalamus.
The battery of the pulse generator must be replaced every 4 to 7 years depending on usage and stimulation parameters. Battery replacement can be performed with minor surgery at the infraclavicular region.
Thalamic deep brain stimulation is indicated for patients with severe, disabling essential tremor who have tremor resistant to drug therapy or who cannot tolerate drug therapy.
The procedure has been shown to provide benefit in 90% of patients, with more than an 80% improvement in tremor severity and functional impact.46–49 Deep brain stimulation is effective against tremor affecting parts of the body other than the limbs, including the head; an exception to this is voice tremor, which usually does not improve dramatically. The procedure can be done unilaterally or bilaterally, depending on symptoms. Patients with asymmetrical tremor and those at risk of side effects can undergo unilateral surgery. Bilateral treatment is recommended for patients with symmetric tremor or significant head tremor, or who are young and healthy.
Surgical risks include brain hemorrhage and infection. Side effects of the stimulation include paresthesias, paresis, imbalance, dysarthria, and, in rare cases, dysphagia.
CHOOSING THE BEST MANAGEMENT PLAN FOR YOUR PATIENT
The choice of treatment may be challenging, given the multiple treatment options and the variability of tremor severity from one patient to another. The following guidelines can be used to help make this decision.
All patients should be advised to reduce caffeine intake, to have sufficient hours of sleep, and to avoid stressful situations.
Patients with minor, nondisabling tremor can be left untreated if the tremors are not bothersome or if the patient prefers not to pursue active treatment.
In patients who have bothersome tremor only when anxious or in certain social situations, give propranolol or alprazolam (or both) to be taken as needed. Relaxation techniques and meditation are also useful for these patients.
Patients with constant bothersome tremor should be started on either propranolol or primidone based on the patient’s profile and propensity to develop side effects from each of these drugs. The dosing should be optimized gradually according to the patient’s response and the drug’s tolerability.
If essential tremor is not sufficiently controlled with one first-line agent (propranolol or primidone), try combining the two first-line agents if the patient finds it tolerable.
A second-line agent can be added to either of the first-line agents or to the combination of both if tremor control is not yet sufficient. A second-line or third-line agent can also be used as the primary treatment if both first-line agents are contraindicated or intolerable. Combining two or more second- and third-line agents is another option. The choice of second- or third-line agent should be guided by the patient’s characteristics and comorbidities in relation to the agent’s side effects and contraindications as detailed in the above section.
Patients should be referred to a movement disorders specialist in cases of resistant tremor, intolerance to oral medications, severe disability, and atypical presentation. Types of tremor known to be poorly responsive to oral medications (eg, head tremor, voice tremor) deserve a specialist evaluation if they contribute significantly to the patient’s morbidity.
The usual specialist treatment of severe voice tremor and head tremor is botulinum toxin injection. Patients with resistant and disabling hand tremor are evaluated for thalamic deep brain stimulation.
Patients with residual disability despite medical and surgical treatment should be referred for occupational therapy. Occupational therapy can improve quality of life through the use of special utensils, pens, computer gadgets, and arm weights, among other devices.
- Zesiewicz TA, Chari A, Jahan I, et al. Overview of essential tremor. Neuropsychiatr Dis Treat 2010; 6:401–408.
- Elble RJ. Essential tremor frequency decreases with time. Neurology 2000; 55:1547–1551.
- Louis ED, Ottman R, Hauser WA. How common is the most common adult movement disorder? Estimates of the prevalence of essential tremor throughout the world. Mov Disord 1998; 13:5–10.
- Louis ED, Dure LS, Pullman S. Essential tremor in childhood: a series of nineteen cases. Mov Disord 2001; 16:921–923.
- Singer C, Sanchez-Ramos J, Weiner WJ. Gait abnormality in essential tremor. Mov Disord 1994; 9:193–196.
- Deuschl G, Wenzelburger R, Löffler K, et al. Essential tremor and cerebellar dysfunction. Clinical and kinematic analysis of intention tremor. Brain 2000; 123:1568–1580.
- Louis ED. Functional correlates of lower cognitive test scores in essential tremor. Mov Disord 2010; 25:481–485.
- Ondo WG, Sutton L, Dat Vuong K, et al. Hearing impairment in essential tremor. Neurology 2003; 61:1093–1097.
- Schneier FR, Barnes LF, Albert SM, et al. Characteristics of social phobia among persons with essential tremor. J Clin Psychiatry 2001; 62:367–372.
- Whaley NR, Putzke JD, Baba Y, et al. Essential tremor: phenotypic expression in a clinical cohort. Parkinsonism Relat Disord 2007; 13:333–339.
- Deng H, Le W, Jankovic J. Genetics of essential tremor. Brain 2007; 130:1456–1464.
- Cohen O, Pullman S, Jurewicz E, et al. Rest tremor in patients with essential tremor: prevalence, clinical correlates, and electrophysiologic characteristics. Arch Neurol 2003; 60:405–410.
- Shahed J, Jankovic J. Exploring the relationship between essential tremor and Parkinson’s disease. Parkinsonism Relat Disord 2007; 13:67–76.
- Yang YW, Chang FC, Tsai CH, et al. Clinical and magnetic resonance imaging manifestations of Holmes tremor. Acta Neurol Taiwan 2005; 14:9–15.
- Alusi SH, Worthington J, Glickman S, et al. A study of tremor in multiple sclerosis. Brain 2001; 124:720–730.
- Breit S, Wächter T, Schöls L, et al. Effective thalamic deep brain stimulation for neuropathic tremor in a patient with severe demyelinating neuropathy. J Neurol Neurosurg Psychiatry 2009; 80:235–236.
- Koller WC, Wong GF, Lang A. Posttraumatic movement disorders: a review. Mov Disord 1989; 4:20–36.
- Jankovic J. Essential tremor: a heterogenous disorder. Mov Disord 2002; 17:638–644.
- Deuschl G, Bain P, Brin M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov Disord 1998; 13(suppl 3):2–23.
- Calzetti S, Findley LJ, Gresty MA, et al. Effect of a single oral dose of propranolol on essential tremor: a double-blind controlled study. Ann Neurol 1983; 13:165–171.
- Larsen TA, Teräväinen H, Calne DB. Atenolol vs propranolol in essential tremor. A controlled, quantitative study. Acta Neurol Scand 1982; 66:547–554.
- Zesiewicz TA, Elble R, Louis ED, et al. Practice parameter: therapies for essential tremor: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2005; 64:2008–2020.
- Lyons KE, Pahwa R, Comella CL, et al.Benefits and risks of pharmacological treatments for essential tremor. Drug Saf 2003; 26:461–481.
- Pahwa R, Lyons KE. Essential tremor: differential diagnosis and current therapy. Am J Med 2003; 115:134–142.
- Louis ED. Clinical practice. Essential tremor. N Engl J Med 2001; 345:887–891.
- Koller WC. Nadolol in essential tremor. Neurology 1983; 33:1076–1077.
- Dietrichson P, Espen E. Effects of timolol and atenolol on benign essential tremor: placebo-controlled studies based on quantitative tremor recording. J Neurol Neurosurg Psychiatry 1981; 44:677–683.
- Calzetti S, Findley LJ, Gresty MA, et al. Metoprolol and propranolol in essential tremor: a double-blind, controlled study. J Neurol Neurosurg Psychiatry 1981; 44:814–819.
- Teravainen H, Larsen A, Fogelholm R. Comparison between the effects of pindolol and propranolol on essential tremor. Neurology 1977; 27:439–442.
- Gorman WP, Cooper R, Pocock P, et al. A comparison of primidone, propranolol, and placebo in essential tremor, using quantitative analysis. J Neurol Neurosurg Psychiatry 1986; 49:64–68.
- Koller WC, Royse VL. Efficacy of primidone in essential tremor. Neurology 1986; 36:121–124.
- Connor GS. A double-blind placebo-controlled trial of topiramate treatment for essential tremor. Neurology 2002; 59:132–134.
- Gironell A, Kulisevsky J, Barbanoj M, et al. A randomized placebo-controlled comparative trial of gabapentin and propranolol in essential tremor. Arch Neurol 1999; 56:475–480.
- Ondo W, Hunter C, Vuong KD, et al. Gabapentin for essential tremor: a multiple-dose, double-blind, placebo-controlled trial. Mov Disord 2000; 15:678–682.
- Pahwa R, Lyons K, Hubble JP, et al. Double-blind controlled trial of gabapentin in essential tremor. Mov Disord 1998; 13:465–467.
- Bushara KO, Malik T, Exconde RE. The effect of levetiracetam on essential tremor. Neurology 2005; 64:1078–1080.
- Sullivan KL, Hauser RA, Zesiewicz TA. Levetiracetam for the treatment of essential tremor. Mov Disord 2005; 20:640.
- Huber SJ, Paulson GW. Efficacy of alprazolam for essential tremor. Neurology 1988; 38:241–243.
- McManis PG, Sharbrough FW. Orthostatic tremor: clinical and electrophysiologic characteristics. Muscle Nerve 1993; 16:1254–1260.
- Ceravolo R, Salvetti S, Piccini P, et al. Acute and chronic effects of clozapine in essential tremor. Mov Disord 1999; 14:468–472.
- Pakkenberg H, Pakkenberg B. Clozapine in the treatment of tremor. Acta Neurol Scand 1986; 73:295–297.
- Pact V, Giduz T. Mirtazapine treats resting tremor, essential tremor, and levodopa-induced dyskinesias. Neurology 1999; 53:1154.
- Lyons KE, Pahwa R. A double-blind, placebo-controlled, pilot study of mirtazapine in essential tremor. Presented at the 54th Annual Meeting of the American Academy of Neurology, Denver, Colorado. Neurology 2002; 58(suppl 3):A254.
- Brin MF, Lyons KE, Doucette J, et al. A randomized, double masked, controlled trial of botulinum toxin type A in essential hand tremor. Neurology 2001; 56:1523–1528.
- Blitzer A, Brin MF, Stewart C, et al. Abductor laryngeal dystonia: a series treated with botulinum toxin. Laryngoscope 1992; 102:163–167.
- Schuurman PR, Bosch DA, Bossuyt PM, et al. A comparison of continuous thalamic stimulation and thalamotomy for suppression of severe tremor. N Engl J Med 2000; 342:461–468.
- Flora ED, Perera CL, Cameron AL, et al. Deep brain stimulation for essential tremor: a systematic review. Mov Disord 2010; 25:1550–1559.
- Nagaseki Y, Shibazaki T, Hirai T, et al. Long-term follow-up results of selective VIM-thalamotomy. J Neurosurg 1986; 65:296–302.
- Zirh A, Reich SG, Dougherty PM, et al. Stereotactic thalamotomy in the treatment of essential tremor of the upper extremity: reassessment including a blinded measure of outcome. J Neurol Neurosurg Psychiatry 1999; 66:772–775.
Essential tremor, one of the most common movement disorders, affects about 4% of adults 40 years of age and older.1 It is often referred to as familial tremor in patients with a family history of tremor. It has also been called benign tremor to differentiate it from tremor associated with neurodegenerative diseases, particularly Parkinson disease, but this condition is certainly not benign, as it can cause substantial functional impairment and difficulties with routine activities of daily living. The terms “essential” and “idiopathic” refer to the primary nature of the disorder and differentiate it from tremor that is a feature of a distinct neurologic entity or is secondary to a metabolic disease or drug therapy.
Successful management entails exclusion of secondary causes and careful selection of drug therapy. To date, there is no cure for essential tremor; all currently available treatments are purely symptomatic.
In this review, we outline the major diagnostic and therapeutic principles of managing essential tremor, indications for referral to specialists, and alternative and advanced therapeutic options.
CLINICAL PICTURE
Tremor is defined as rhythmic to-and-fro movement in any body part. It can be slow or fast, and its amplitude can be large and coarse, or small or even “fine.” It can appear at rest, with action, or during a sustained posture. In contrast to parkinsonian tremor (which presents mainly at rest), essential tremor is typically but not exclusively postural, kinetic, or both.
Postural tremor refers to tremor seen when the patient holds the affected limb (commonly the arm) unsupported against gravity. Kinetic tremor refers to tremor that appears with active movements. This is often demonstrated clinically by the finger-nose-finger test. Patients with essential tremor commonly have both postural and kinetic tremor.
The tremor commonly involves the arms, hands, and fingers.2 Less commonly, it involves the head, the lips, the tongue, the legs, and the voice. In contrast to parkinsonian tremor, which typically affects one side of the body first, bilateral involvement is the general rule in essential tremor. However, one side of the body may be affected first, or may be more affected than the other. The frequency of the tremor ranges from 4 to 12 Hz (ie, beats per second).
The tremor usually starts in middle age and progresses slowly over time,3 but onset in old age or childhood is also possible.4 Both sexes are equally affected.
The tremor usually gets worse with anxiety, stress, and caffeine intake. It usually gets temporarily better with the consumption of small amounts of alcohol.
The functional impact of essential tremor is judged by its effect on different daily activities, especially writing, eating, drinking, dressing, manual work, and household chores.
In addition to motor dysfunction, the tremor can also have a significant psychological impact on the patient, because it usually gets worse in social situations.
Although it has long been thought that tremor is the sole neurologic sign of essential tremor, recent studies have shown that many patients have additional subtle findings, such as mild gait difficulty,5 slight incoordination,6 mild cognitive impairment,7 and decreased hearing,8 and are more likely to have anxiety and social phobia.9
Although different studies have varied in their findings, it is generally thought that about 50% of patients with essential tremor have a positive family history, often in a first-degree relative, suggesting autosomal dominant inheritance with variable penetrance.10,11 Polygenetic and sporadic variants are also common.
DIFFERENTIAL DIAGNOSIS
Resting tremor
Resting tremor is typically an extrapyramidal sign and, when accompanied by rigidity and bradykinesia, is often part of a parkinsonian syndrome. It is most pronounced at rest when the affected body part is fully supported and stationary. The tremor tends to improve with action or posture. It usually has a “pill-rolling” character and, as mentioned, is associated with other extrapyramidal signs, such as rigidity, slowness, and, later on, postural instability.
About 20% of patients with essential tremor have resting tremor. These patients usually suffer from severe or long-standing disease.12 However, the resting element in these cases is often milder than the postural and kinetic components, and it is typically not associated with other extrapyramidal signs. Also, some patients may have both essential tremor and Parkinson disease.13
Intentional tremor
Pure intentional tremor is usually seen with cerebellar pathology, which includes tumors, stroke, multiple sclerosis, trauma, and spinocerebellar degeneration. The amplitude of this type of tremor increases as the affected limb approaches the final target. It can best be demonstrated clinically by the finger-nose-finger test. The frequency of intentional tremor is slow (2 to 4 Hz) and is usually associated with other cerebellar signs, such as dysmetria, decomposition, rebound, and dysdiadochokinesia (ie, the inability to perform rapid alternating movements in a smooth and coordinated manner).
About 50% of patients with essential tremor have an intentional component to their tremor,6 or it can be mildly present in the form of a slight gait difficulty. However, in essential tremor, other features of cerebellar dysfunction are either absent or only very slight.
Secondary causes of postural-kinetic tremor
Enhanced physiologic tremor. A very mild postural tremor is present in almost all people and is considered “physiologic” since it has almost no clinical significance. This type of tremor is often invisible, but when “enhanced,” it can be visually demonstrated by placing a piece of paper over the stretched hands and watching the ripple from the paper.
Certain conditions can aggravate this physiologic tremor and can make it symptomatic. Common causes include anxiety, sleep deprivation, hypoglycemia, hyperthyroidism, pheochromocytoma, serotonin syndrome, and carcinoid syndrome.
Metabolic tremor. Hyperammonemia can cause tremor in patients with hepatic encephalopathy, and uremia can cause tremor in patients with renal failure. These metabolic conditions classically result in “flappy” tremor (asterixis), a special form of postural tremor characterized by jerking movements with high amplitude. It is best seen when the patient stretches out the arms and extends the wrists as if trying to stop traffic. But even though it may look like tremor, asterixis is thought to be a form of “negative” myoclonus.
Drug-related tremor. Postural-kinetic tremor can be induced by drugs, including lithium (Lithobid), valproate (Depakote), amiodarone (Cordarone), central nervous system stimulants, beta agonists (including inhalers), and some antidepressants. Tremor can also occur with alcohol or sedative withdrawal.
Psychogenic tremor. Tremor can be seen as part of a somatoform disorder commonly referred to as conversion disorder or conversion reaction. Psychogenic tremor is characterized by acute onset, commonly following a psychosocial stressor; it is often atypical, variable in frequency, amplitude, and body-part involvement, and it can readily be interrupted on examination by distracting the patient.
Neurologic disorders. The postural and kinetic elements of essential tremor may also be seen in the following neurologic conditions:
- Holmes (rubral) tremor, a combination of resting, postural, kinetic, and intentional tremor of low frequency and high amplitude. It usually has a proximal component and is often unilateral. It commonly is due to a lesion that involves the brainstem, eg, red nucleus, inferior olive, cerebellum, or thalamus. Common causes include stroke, prolonged hypoxia, and head trauma (including closed-head trauma with negative imaging). This type of tremor is usually associated with ataxia.14
- Dystonic tremor is predominantly postural and is associated with abnormal dystonic posturing of the affected body part, commonly the head, hands, or feet. Unlike the rhythmic oscillations of essential tremor, dystonic tremor is often irregular in rhythm.
- Multiple sclerosis can present with a combination of postural, kinetic, and intentional tremor. Patients usually have a clear history of recurrent neurologic deficits and show a combination of pyramidal, cerebellar, and sensory signs on examination consistent with multiple sclerosis.15
- Neuropathic tremor is seen in a small proportion of patients with peripheral neuropathy, especially demyelinating neuropathy.16 The tremor is usually posturalkinetic and is associated with signs of neuropathy, such as a glove-and-stocking pattern of hypoesthesia, reduced reflexes, and sensory ataxia (including intentional tremor when the eyes are closed).
- Posttraumatic tremor can occur after severe or even mild head trauma, especially in children. It is commonly rubral, but other types have been reported, including a presentation resembling essential tremor.17
- Monosymptomatic or isolated tremor. A number of conditions related to essential tremor with location-specific or task-specific tremor have been described. These rare conditions historically have been classified as “possible essential tremor” or “essential tremor variants” but are now considered separate entities. These include task-specific tremor (eg, writing tremor), isolated head tremor, isolated voice tremor, and orthostatic tremor (tremor in the legs and trunk upon standing in place, but not when sitting or walking).18,19
DIAGNOSIS IS CLINICAL
Essential tremor is a clinical diagnosis. After a thorough review of the medical history and medication exposures, laboratory and imaging tests may be ordered to rule out a secondary cause. A complete metabolic panel, including blood glucose and thyroid-stimulating hormone levels, is usually sufficient. Brain imaging or other imaging is ordered for patients with an atypical presentation.
TREATMENT IS SYMPTOMATIC
Treatment of essential tremor is symptomatic. Several drugs of different pharmacologic classes can reduce the severity of the tremor and improve function.
Choosing the appropriate treatment depends on the type of tremor and the presence of associated conditions. The response to treatment and the development of side effects guide further adjustments. The following is a brief description of the available antitremor agents.
FIRST-LINE AGENTS
Propranolol
Propranolol (Inderal), a nonselective beta blocker, is the most widely used antitremor drug and the only agent approved by the US Food and Drug Administration for essential tremor. It should be started at a low dose and titrated upward gradually. The usual starting dose is 10 mg three times daily. The average effective dose is 120 mg daily. The dose can be increased up to 320 mg if needed and tolerated.
Sustained-release preparations are equally effective and are given as a single daily dose to improve compliance.20
Propranolol improves tremor in 50% to 70% of patients with essential tremor and achieves an average tremor reduction of 50% to 60%.1,21–25 Side effects include bronchoconstriction, bradycardia, hypotension, depression, impotence, fatigue, and gastrointestinal disturbances.
Other beta-blockers, such as nadolol (Corgard) and timolol, are also effective against tremor but are less potent than propranolol.26,27 The selective beta-1-blocker metoprolol (Lopressor) may be effective and has fewer noncardiac side effects than propranolol.28 It can be used in patients who discontinue propranolol because of adverse effects. Atenolol (Tenormin) and pindolol (Visken) have little or no effect on tremor.29
A good candidate for propranolol therapy in essential tremor is:
- A patient with no known contraindication to propranolol
- A patient with hypertension, coronary heart disease, or tachyarrhythmia
- A patient with anxiety or social phobia.
Absolute contraindications to propranolol are:
- Moderate to severe bronchial asthma
- Significant bradycardia or heart block
- Symptomatic hypotension
- End-stage heart failure
- Concurrent use of a calcium channel blocker.
Relative contraindications are:
- Wheezing (eg, chronic obstructive pulmonary disease)
- Depression
- Diabetes mellitus in a patient more prone to hypoglycemia (propranolol masks the warning signs of hypoglycemia)
- Reduced sexual potency in a male patient.
Primidone
Primidone (Mysoline) is an antiepileptic drug structurally similar to barbiturates. Its antitremor effect is equal to that of propranolol, though some studies suggest it is slightly more efficacious.30,31
It should be started at a low dose, ie, 25 mg once daily at bedtime. The dose should then be increased gradually until satisfactory and tolerable tremor control is achieved. Most patients respond to doses of around 250 mg per day.1,22,24–25 The dose can be increased if needed and tolerated.
Primidone reduces tremor by about 50% to 60%.1,22,24–25 Side effects include sedation, dizziness, fatigue, nausea, and depression, as well as ataxia and confusion in severe cases.
A good candidate for primidone in essential tremor is:
- A patient with no known contraindication to primidone
- A patient with contraindications to propranolol
- A younger patient
- A patient with epilepsy.
Absolute contraindications to primidone include:
- Confusion or dementia
- Oral anticoagulant therapy with difficulty controlling the International Normalized Ratio (primidone is a potent enzyme inducer).
Relative contraindications to primidone in essential tremor are:
- Depression
- Alcohol abuse
- Ongoing therapy with sedating drugs
- Ataxia or vertigo.
SECOND-LINE AGENTS
Other antiepileptics
Topiramate (Topamax) is a broad-spectrum antiepileptic shown to be significantly effective against essential tremor.32 It is usually started at a single daily dose of 25 mg and increased gradually to the most effective dose, usually around 300 mg.
Side effects include reduced appetite, weight loss, cognitive dysfunction, and paresthesia.
Favorable candidates include patients who are epileptic or overweight. Contraindications include cognitive impairment and low body weight. It is also not recommended in children so as to avoid any possible negative effect on cognitive development. In rare cases, topiramate has been reported to cause significant visual disturbances.
Gabapentin (Neurontin) is an antiepileptic that is now more often used as a symptomatic treatment for neuropathic pain. Studies have suggested a beneficial effect on essential tremor,33,34 but some investigators have questioned its efficacy.35
Like other antitremor agents, it should be started at a low dose, ie, around 300 mg, and escalated gradually until the tremor is controlled. The usual effective dose is 1,200 mg.
Gabapentin is generally well tolerated, and side effects such as dizziness, drowsiness, sedation, and unsteadiness are rare and usually mild.
The favorable candidate is a patient with associated neuropathy or multiple comorbidities. Gabapentin has also been reported to alleviate neuropathic tremor.
Contraindications are minimal and include intolerability or hypersensitivity to the drug. It also should be avoided in patients at a high risk of falling.
Levetiracetam (Keppra) is a novel antiepileptic effective against partial seizures. Studies have shown contradictory results regarding its antitremor effect. One double-blind, placebo-controlled study demonstrated significant reduction in essential tremor with 1,000 mg of levetiracetam.36 However, its effect on tremor is believed to be short-lived, and some studies argue against its efficacy.37 It has a favorable side-effect profile and is generally very well tolerated. It can be used as an adjunct to other antitremor agents and is preferred for patients with coexisting partial seizures or myoclonus.
Benzodiazepines. Minor tranquilizers are often used to control tremor, especially in coexisting anxiety or insomnia. Alprazolam (Xanax) is the one most widely used for this indication.38 It can be started in a dose of 0.25 mg once at bedtime and increased gradually up to 0.75 to 2 mg. Clonazepam (Klonopin) is particularly useful for orthostatic tremor, a variant of essential tremor characterized by tremor of the legs and trunk upon standing.39
Common side effects of benzodiazepines include sedation, cognitive dysfunction, hypotension, respiratory inhibition, and addiction after prolonged use. In the elderly, they can lead to confusion and disinhibition and can increase the risk of falling. They should be avoided in the elderly and in alcoholic patients and those with a high risk of substance abuse.
Stopping benzodiazepines should be done gradually to avoid withdrawal symptoms, including aggravation of tremor.
THIRD-LINE AGENTS
Clozapine
Clozapine (Clozaril) is a novel antipsychotic drug with no extrapyramidal side effects. It has been reported effective in essential tremor and drug-induced tremor,40,41 but the results of these early studies have not been confirmed.
Clozapine is started as a single daily dose of 12.5 mg and is increased up to 75 mg or 100 mg. It is an attractive option for patients with coexisting psychosis, bipolar disorder, or chorea. Its main side effects are sedation, salivation, weight gain, hypertension, diabetes, and seizures.
One especially serious side effect is agranulocytosis. This potentially fatal effect is rare, occurring in about 1.3% of patients receiving this drug. Weekly monitoring of the white blood cell count is mandated during treatment with clozapine, and this has made clozapine a less attractive option for the routine treatment of essential tremor.
Mirtazapine
Mirtazapine (Remeron) is a novel antidepressant widely used in Parkinson disease as both an antidepressant and a sleeping aid. Case studies have reported efficacy in both essential tremor and parkinsonian tremor,42 but controlled studies have not confirmed this.43 Mirtazapine is a reasonable option in patients with coexisting depression or insomnia. It is usually given as a single bedtime dose of 15 to 30 mg.
Other drugs
Studies of other agents for the treatment of essential tremor—eg, carbonic anhydrase enzyme inhibitors, calcium channel blockers, isoniazid (Tubizid), clonidine (Catapres), phenobarbital, and theophylline—have yielded highly contradictory results. Thus, they are not recommended as first- or second-line agents for essential tremor.
SPECIALTY-LEVEL CARE
When essential tremor does not respond to drug therapy or the patient cannot tolerate drug therapy, the patient should be referred to a center specializing in movement disorders for more advanced treatment options, ie, botulinum toxin injection and deep brain stimulation surgery.
Botulinum toxin
Botulinum toxin type A has been studied for the treatment of essential tremor with variable degrees of success. It has been effective in reducing hand tremor in essential tremor, but without a concomitant improvement in functional disability.44 This limited functional improvement has been attributed to the development of muscle weakness after injection of the neurotoxin. This has also raised questions about unintentional unblinding when interpreting study results. Therefore, most clinicians restrict its use to focal forms of tremor such as voice tremor,45 head tremor, and task-specific tremor.
Side effects are limited and temporary and include muscle weakness, pain at the injection site, dysphagia (when injected for head or voice tremor), and a breathy vocal quality (when injected for voice tremor). Botulinum toxin injection is the treatment of choice for focal dystonia, and therefore would be a good option for dystonic tremor.
Thalamic deep brain stimulation
This technique involves stereotactic implantation of a stimulation lead in the ventral intermediate nucleus of the thalamus. The lead connects via a subcutaneous wire to an intermittent pulse generator, implanted subcutaneously in the infraclavicular region. The stimulation lead produces continuous stimulation of the ventralis intermedius nucleus that is functionally equal to lesional surgery, thus antagonizing the relay of tremor signals at the thalamus.
The battery of the pulse generator must be replaced every 4 to 7 years depending on usage and stimulation parameters. Battery replacement can be performed with minor surgery at the infraclavicular region.
Thalamic deep brain stimulation is indicated for patients with severe, disabling essential tremor who have tremor resistant to drug therapy or who cannot tolerate drug therapy.
The procedure has been shown to provide benefit in 90% of patients, with more than an 80% improvement in tremor severity and functional impact.46–49 Deep brain stimulation is effective against tremor affecting parts of the body other than the limbs, including the head; an exception to this is voice tremor, which usually does not improve dramatically. The procedure can be done unilaterally or bilaterally, depending on symptoms. Patients with asymmetrical tremor and those at risk of side effects can undergo unilateral surgery. Bilateral treatment is recommended for patients with symmetric tremor or significant head tremor, or who are young and healthy.
Surgical risks include brain hemorrhage and infection. Side effects of the stimulation include paresthesias, paresis, imbalance, dysarthria, and, in rare cases, dysphagia.
CHOOSING THE BEST MANAGEMENT PLAN FOR YOUR PATIENT
The choice of treatment may be challenging, given the multiple treatment options and the variability of tremor severity from one patient to another. The following guidelines can be used to help make this decision.
All patients should be advised to reduce caffeine intake, to have sufficient hours of sleep, and to avoid stressful situations.
Patients with minor, nondisabling tremor can be left untreated if the tremors are not bothersome or if the patient prefers not to pursue active treatment.
In patients who have bothersome tremor only when anxious or in certain social situations, give propranolol or alprazolam (or both) to be taken as needed. Relaxation techniques and meditation are also useful for these patients.
Patients with constant bothersome tremor should be started on either propranolol or primidone based on the patient’s profile and propensity to develop side effects from each of these drugs. The dosing should be optimized gradually according to the patient’s response and the drug’s tolerability.
If essential tremor is not sufficiently controlled with one first-line agent (propranolol or primidone), try combining the two first-line agents if the patient finds it tolerable.
A second-line agent can be added to either of the first-line agents or to the combination of both if tremor control is not yet sufficient. A second-line or third-line agent can also be used as the primary treatment if both first-line agents are contraindicated or intolerable. Combining two or more second- and third-line agents is another option. The choice of second- or third-line agent should be guided by the patient’s characteristics and comorbidities in relation to the agent’s side effects and contraindications as detailed in the above section.
Patients should be referred to a movement disorders specialist in cases of resistant tremor, intolerance to oral medications, severe disability, and atypical presentation. Types of tremor known to be poorly responsive to oral medications (eg, head tremor, voice tremor) deserve a specialist evaluation if they contribute significantly to the patient’s morbidity.
The usual specialist treatment of severe voice tremor and head tremor is botulinum toxin injection. Patients with resistant and disabling hand tremor are evaluated for thalamic deep brain stimulation.
Patients with residual disability despite medical and surgical treatment should be referred for occupational therapy. Occupational therapy can improve quality of life through the use of special utensils, pens, computer gadgets, and arm weights, among other devices.
Essential tremor, one of the most common movement disorders, affects about 4% of adults 40 years of age and older.1 It is often referred to as familial tremor in patients with a family history of tremor. It has also been called benign tremor to differentiate it from tremor associated with neurodegenerative diseases, particularly Parkinson disease, but this condition is certainly not benign, as it can cause substantial functional impairment and difficulties with routine activities of daily living. The terms “essential” and “idiopathic” refer to the primary nature of the disorder and differentiate it from tremor that is a feature of a distinct neurologic entity or is secondary to a metabolic disease or drug therapy.
Successful management entails exclusion of secondary causes and careful selection of drug therapy. To date, there is no cure for essential tremor; all currently available treatments are purely symptomatic.
In this review, we outline the major diagnostic and therapeutic principles of managing essential tremor, indications for referral to specialists, and alternative and advanced therapeutic options.
CLINICAL PICTURE
Tremor is defined as rhythmic to-and-fro movement in any body part. It can be slow or fast, and its amplitude can be large and coarse, or small or even “fine.” It can appear at rest, with action, or during a sustained posture. In contrast to parkinsonian tremor (which presents mainly at rest), essential tremor is typically but not exclusively postural, kinetic, or both.
Postural tremor refers to tremor seen when the patient holds the affected limb (commonly the arm) unsupported against gravity. Kinetic tremor refers to tremor that appears with active movements. This is often demonstrated clinically by the finger-nose-finger test. Patients with essential tremor commonly have both postural and kinetic tremor.
The tremor commonly involves the arms, hands, and fingers.2 Less commonly, it involves the head, the lips, the tongue, the legs, and the voice. In contrast to parkinsonian tremor, which typically affects one side of the body first, bilateral involvement is the general rule in essential tremor. However, one side of the body may be affected first, or may be more affected than the other. The frequency of the tremor ranges from 4 to 12 Hz (ie, beats per second).
The tremor usually starts in middle age and progresses slowly over time,3 but onset in old age or childhood is also possible.4 Both sexes are equally affected.
The tremor usually gets worse with anxiety, stress, and caffeine intake. It usually gets temporarily better with the consumption of small amounts of alcohol.
The functional impact of essential tremor is judged by its effect on different daily activities, especially writing, eating, drinking, dressing, manual work, and household chores.
In addition to motor dysfunction, the tremor can also have a significant psychological impact on the patient, because it usually gets worse in social situations.
Although it has long been thought that tremor is the sole neurologic sign of essential tremor, recent studies have shown that many patients have additional subtle findings, such as mild gait difficulty,5 slight incoordination,6 mild cognitive impairment,7 and decreased hearing,8 and are more likely to have anxiety and social phobia.9
Although different studies have varied in their findings, it is generally thought that about 50% of patients with essential tremor have a positive family history, often in a first-degree relative, suggesting autosomal dominant inheritance with variable penetrance.10,11 Polygenetic and sporadic variants are also common.
DIFFERENTIAL DIAGNOSIS
Resting tremor
Resting tremor is typically an extrapyramidal sign and, when accompanied by rigidity and bradykinesia, is often part of a parkinsonian syndrome. It is most pronounced at rest when the affected body part is fully supported and stationary. The tremor tends to improve with action or posture. It usually has a “pill-rolling” character and, as mentioned, is associated with other extrapyramidal signs, such as rigidity, slowness, and, later on, postural instability.
About 20% of patients with essential tremor have resting tremor. These patients usually suffer from severe or long-standing disease.12 However, the resting element in these cases is often milder than the postural and kinetic components, and it is typically not associated with other extrapyramidal signs. Also, some patients may have both essential tremor and Parkinson disease.13
Intentional tremor
Pure intentional tremor is usually seen with cerebellar pathology, which includes tumors, stroke, multiple sclerosis, trauma, and spinocerebellar degeneration. The amplitude of this type of tremor increases as the affected limb approaches the final target. It can best be demonstrated clinically by the finger-nose-finger test. The frequency of intentional tremor is slow (2 to 4 Hz) and is usually associated with other cerebellar signs, such as dysmetria, decomposition, rebound, and dysdiadochokinesia (ie, the inability to perform rapid alternating movements in a smooth and coordinated manner).
About 50% of patients with essential tremor have an intentional component to their tremor,6 or it can be mildly present in the form of a slight gait difficulty. However, in essential tremor, other features of cerebellar dysfunction are either absent or only very slight.
Secondary causes of postural-kinetic tremor
Enhanced physiologic tremor. A very mild postural tremor is present in almost all people and is considered “physiologic” since it has almost no clinical significance. This type of tremor is often invisible, but when “enhanced,” it can be visually demonstrated by placing a piece of paper over the stretched hands and watching the ripple from the paper.
Certain conditions can aggravate this physiologic tremor and can make it symptomatic. Common causes include anxiety, sleep deprivation, hypoglycemia, hyperthyroidism, pheochromocytoma, serotonin syndrome, and carcinoid syndrome.
Metabolic tremor. Hyperammonemia can cause tremor in patients with hepatic encephalopathy, and uremia can cause tremor in patients with renal failure. These metabolic conditions classically result in “flappy” tremor (asterixis), a special form of postural tremor characterized by jerking movements with high amplitude. It is best seen when the patient stretches out the arms and extends the wrists as if trying to stop traffic. But even though it may look like tremor, asterixis is thought to be a form of “negative” myoclonus.
Drug-related tremor. Postural-kinetic tremor can be induced by drugs, including lithium (Lithobid), valproate (Depakote), amiodarone (Cordarone), central nervous system stimulants, beta agonists (including inhalers), and some antidepressants. Tremor can also occur with alcohol or sedative withdrawal.
Psychogenic tremor. Tremor can be seen as part of a somatoform disorder commonly referred to as conversion disorder or conversion reaction. Psychogenic tremor is characterized by acute onset, commonly following a psychosocial stressor; it is often atypical, variable in frequency, amplitude, and body-part involvement, and it can readily be interrupted on examination by distracting the patient.
Neurologic disorders. The postural and kinetic elements of essential tremor may also be seen in the following neurologic conditions:
- Holmes (rubral) tremor, a combination of resting, postural, kinetic, and intentional tremor of low frequency and high amplitude. It usually has a proximal component and is often unilateral. It commonly is due to a lesion that involves the brainstem, eg, red nucleus, inferior olive, cerebellum, or thalamus. Common causes include stroke, prolonged hypoxia, and head trauma (including closed-head trauma with negative imaging). This type of tremor is usually associated with ataxia.14
- Dystonic tremor is predominantly postural and is associated with abnormal dystonic posturing of the affected body part, commonly the head, hands, or feet. Unlike the rhythmic oscillations of essential tremor, dystonic tremor is often irregular in rhythm.
- Multiple sclerosis can present with a combination of postural, kinetic, and intentional tremor. Patients usually have a clear history of recurrent neurologic deficits and show a combination of pyramidal, cerebellar, and sensory signs on examination consistent with multiple sclerosis.15
- Neuropathic tremor is seen in a small proportion of patients with peripheral neuropathy, especially demyelinating neuropathy.16 The tremor is usually posturalkinetic and is associated with signs of neuropathy, such as a glove-and-stocking pattern of hypoesthesia, reduced reflexes, and sensory ataxia (including intentional tremor when the eyes are closed).
- Posttraumatic tremor can occur after severe or even mild head trauma, especially in children. It is commonly rubral, but other types have been reported, including a presentation resembling essential tremor.17
- Monosymptomatic or isolated tremor. A number of conditions related to essential tremor with location-specific or task-specific tremor have been described. These rare conditions historically have been classified as “possible essential tremor” or “essential tremor variants” but are now considered separate entities. These include task-specific tremor (eg, writing tremor), isolated head tremor, isolated voice tremor, and orthostatic tremor (tremor in the legs and trunk upon standing in place, but not when sitting or walking).18,19
DIAGNOSIS IS CLINICAL
Essential tremor is a clinical diagnosis. After a thorough review of the medical history and medication exposures, laboratory and imaging tests may be ordered to rule out a secondary cause. A complete metabolic panel, including blood glucose and thyroid-stimulating hormone levels, is usually sufficient. Brain imaging or other imaging is ordered for patients with an atypical presentation.
TREATMENT IS SYMPTOMATIC
Treatment of essential tremor is symptomatic. Several drugs of different pharmacologic classes can reduce the severity of the tremor and improve function.
Choosing the appropriate treatment depends on the type of tremor and the presence of associated conditions. The response to treatment and the development of side effects guide further adjustments. The following is a brief description of the available antitremor agents.
FIRST-LINE AGENTS
Propranolol
Propranolol (Inderal), a nonselective beta blocker, is the most widely used antitremor drug and the only agent approved by the US Food and Drug Administration for essential tremor. It should be started at a low dose and titrated upward gradually. The usual starting dose is 10 mg three times daily. The average effective dose is 120 mg daily. The dose can be increased up to 320 mg if needed and tolerated.
Sustained-release preparations are equally effective and are given as a single daily dose to improve compliance.20
Propranolol improves tremor in 50% to 70% of patients with essential tremor and achieves an average tremor reduction of 50% to 60%.1,21–25 Side effects include bronchoconstriction, bradycardia, hypotension, depression, impotence, fatigue, and gastrointestinal disturbances.
Other beta-blockers, such as nadolol (Corgard) and timolol, are also effective against tremor but are less potent than propranolol.26,27 The selective beta-1-blocker metoprolol (Lopressor) may be effective and has fewer noncardiac side effects than propranolol.28 It can be used in patients who discontinue propranolol because of adverse effects. Atenolol (Tenormin) and pindolol (Visken) have little or no effect on tremor.29
A good candidate for propranolol therapy in essential tremor is:
- A patient with no known contraindication to propranolol
- A patient with hypertension, coronary heart disease, or tachyarrhythmia
- A patient with anxiety or social phobia.
Absolute contraindications to propranolol are:
- Moderate to severe bronchial asthma
- Significant bradycardia or heart block
- Symptomatic hypotension
- End-stage heart failure
- Concurrent use of a calcium channel blocker.
Relative contraindications are:
- Wheezing (eg, chronic obstructive pulmonary disease)
- Depression
- Diabetes mellitus in a patient more prone to hypoglycemia (propranolol masks the warning signs of hypoglycemia)
- Reduced sexual potency in a male patient.
Primidone
Primidone (Mysoline) is an antiepileptic drug structurally similar to barbiturates. Its antitremor effect is equal to that of propranolol, though some studies suggest it is slightly more efficacious.30,31
It should be started at a low dose, ie, 25 mg once daily at bedtime. The dose should then be increased gradually until satisfactory and tolerable tremor control is achieved. Most patients respond to doses of around 250 mg per day.1,22,24–25 The dose can be increased if needed and tolerated.
Primidone reduces tremor by about 50% to 60%.1,22,24–25 Side effects include sedation, dizziness, fatigue, nausea, and depression, as well as ataxia and confusion in severe cases.
A good candidate for primidone in essential tremor is:
- A patient with no known contraindication to primidone
- A patient with contraindications to propranolol
- A younger patient
- A patient with epilepsy.
Absolute contraindications to primidone include:
- Confusion or dementia
- Oral anticoagulant therapy with difficulty controlling the International Normalized Ratio (primidone is a potent enzyme inducer).
Relative contraindications to primidone in essential tremor are:
- Depression
- Alcohol abuse
- Ongoing therapy with sedating drugs
- Ataxia or vertigo.
SECOND-LINE AGENTS
Other antiepileptics
Topiramate (Topamax) is a broad-spectrum antiepileptic shown to be significantly effective against essential tremor.32 It is usually started at a single daily dose of 25 mg and increased gradually to the most effective dose, usually around 300 mg.
Side effects include reduced appetite, weight loss, cognitive dysfunction, and paresthesia.
Favorable candidates include patients who are epileptic or overweight. Contraindications include cognitive impairment and low body weight. It is also not recommended in children so as to avoid any possible negative effect on cognitive development. In rare cases, topiramate has been reported to cause significant visual disturbances.
Gabapentin (Neurontin) is an antiepileptic that is now more often used as a symptomatic treatment for neuropathic pain. Studies have suggested a beneficial effect on essential tremor,33,34 but some investigators have questioned its efficacy.35
Like other antitremor agents, it should be started at a low dose, ie, around 300 mg, and escalated gradually until the tremor is controlled. The usual effective dose is 1,200 mg.
Gabapentin is generally well tolerated, and side effects such as dizziness, drowsiness, sedation, and unsteadiness are rare and usually mild.
The favorable candidate is a patient with associated neuropathy or multiple comorbidities. Gabapentin has also been reported to alleviate neuropathic tremor.
Contraindications are minimal and include intolerability or hypersensitivity to the drug. It also should be avoided in patients at a high risk of falling.
Levetiracetam (Keppra) is a novel antiepileptic effective against partial seizures. Studies have shown contradictory results regarding its antitremor effect. One double-blind, placebo-controlled study demonstrated significant reduction in essential tremor with 1,000 mg of levetiracetam.36 However, its effect on tremor is believed to be short-lived, and some studies argue against its efficacy.37 It has a favorable side-effect profile and is generally very well tolerated. It can be used as an adjunct to other antitremor agents and is preferred for patients with coexisting partial seizures or myoclonus.
Benzodiazepines. Minor tranquilizers are often used to control tremor, especially in coexisting anxiety or insomnia. Alprazolam (Xanax) is the one most widely used for this indication.38 It can be started in a dose of 0.25 mg once at bedtime and increased gradually up to 0.75 to 2 mg. Clonazepam (Klonopin) is particularly useful for orthostatic tremor, a variant of essential tremor characterized by tremor of the legs and trunk upon standing.39
Common side effects of benzodiazepines include sedation, cognitive dysfunction, hypotension, respiratory inhibition, and addiction after prolonged use. In the elderly, they can lead to confusion and disinhibition and can increase the risk of falling. They should be avoided in the elderly and in alcoholic patients and those with a high risk of substance abuse.
Stopping benzodiazepines should be done gradually to avoid withdrawal symptoms, including aggravation of tremor.
THIRD-LINE AGENTS
Clozapine
Clozapine (Clozaril) is a novel antipsychotic drug with no extrapyramidal side effects. It has been reported effective in essential tremor and drug-induced tremor,40,41 but the results of these early studies have not been confirmed.
Clozapine is started as a single daily dose of 12.5 mg and is increased up to 75 mg or 100 mg. It is an attractive option for patients with coexisting psychosis, bipolar disorder, or chorea. Its main side effects are sedation, salivation, weight gain, hypertension, diabetes, and seizures.
One especially serious side effect is agranulocytosis. This potentially fatal effect is rare, occurring in about 1.3% of patients receiving this drug. Weekly monitoring of the white blood cell count is mandated during treatment with clozapine, and this has made clozapine a less attractive option for the routine treatment of essential tremor.
Mirtazapine
Mirtazapine (Remeron) is a novel antidepressant widely used in Parkinson disease as both an antidepressant and a sleeping aid. Case studies have reported efficacy in both essential tremor and parkinsonian tremor,42 but controlled studies have not confirmed this.43 Mirtazapine is a reasonable option in patients with coexisting depression or insomnia. It is usually given as a single bedtime dose of 15 to 30 mg.
Other drugs
Studies of other agents for the treatment of essential tremor—eg, carbonic anhydrase enzyme inhibitors, calcium channel blockers, isoniazid (Tubizid), clonidine (Catapres), phenobarbital, and theophylline—have yielded highly contradictory results. Thus, they are not recommended as first- or second-line agents for essential tremor.
SPECIALTY-LEVEL CARE
When essential tremor does not respond to drug therapy or the patient cannot tolerate drug therapy, the patient should be referred to a center specializing in movement disorders for more advanced treatment options, ie, botulinum toxin injection and deep brain stimulation surgery.
Botulinum toxin
Botulinum toxin type A has been studied for the treatment of essential tremor with variable degrees of success. It has been effective in reducing hand tremor in essential tremor, but without a concomitant improvement in functional disability.44 This limited functional improvement has been attributed to the development of muscle weakness after injection of the neurotoxin. This has also raised questions about unintentional unblinding when interpreting study results. Therefore, most clinicians restrict its use to focal forms of tremor such as voice tremor,45 head tremor, and task-specific tremor.
Side effects are limited and temporary and include muscle weakness, pain at the injection site, dysphagia (when injected for head or voice tremor), and a breathy vocal quality (when injected for voice tremor). Botulinum toxin injection is the treatment of choice for focal dystonia, and therefore would be a good option for dystonic tremor.
Thalamic deep brain stimulation
This technique involves stereotactic implantation of a stimulation lead in the ventral intermediate nucleus of the thalamus. The lead connects via a subcutaneous wire to an intermittent pulse generator, implanted subcutaneously in the infraclavicular region. The stimulation lead produces continuous stimulation of the ventralis intermedius nucleus that is functionally equal to lesional surgery, thus antagonizing the relay of tremor signals at the thalamus.
The battery of the pulse generator must be replaced every 4 to 7 years depending on usage and stimulation parameters. Battery replacement can be performed with minor surgery at the infraclavicular region.
Thalamic deep brain stimulation is indicated for patients with severe, disabling essential tremor who have tremor resistant to drug therapy or who cannot tolerate drug therapy.
The procedure has been shown to provide benefit in 90% of patients, with more than an 80% improvement in tremor severity and functional impact.46–49 Deep brain stimulation is effective against tremor affecting parts of the body other than the limbs, including the head; an exception to this is voice tremor, which usually does not improve dramatically. The procedure can be done unilaterally or bilaterally, depending on symptoms. Patients with asymmetrical tremor and those at risk of side effects can undergo unilateral surgery. Bilateral treatment is recommended for patients with symmetric tremor or significant head tremor, or who are young and healthy.
Surgical risks include brain hemorrhage and infection. Side effects of the stimulation include paresthesias, paresis, imbalance, dysarthria, and, in rare cases, dysphagia.
CHOOSING THE BEST MANAGEMENT PLAN FOR YOUR PATIENT
The choice of treatment may be challenging, given the multiple treatment options and the variability of tremor severity from one patient to another. The following guidelines can be used to help make this decision.
All patients should be advised to reduce caffeine intake, to have sufficient hours of sleep, and to avoid stressful situations.
Patients with minor, nondisabling tremor can be left untreated if the tremors are not bothersome or if the patient prefers not to pursue active treatment.
In patients who have bothersome tremor only when anxious or in certain social situations, give propranolol or alprazolam (or both) to be taken as needed. Relaxation techniques and meditation are also useful for these patients.
Patients with constant bothersome tremor should be started on either propranolol or primidone based on the patient’s profile and propensity to develop side effects from each of these drugs. The dosing should be optimized gradually according to the patient’s response and the drug’s tolerability.
If essential tremor is not sufficiently controlled with one first-line agent (propranolol or primidone), try combining the two first-line agents if the patient finds it tolerable.
A second-line agent can be added to either of the first-line agents or to the combination of both if tremor control is not yet sufficient. A second-line or third-line agent can also be used as the primary treatment if both first-line agents are contraindicated or intolerable. Combining two or more second- and third-line agents is another option. The choice of second- or third-line agent should be guided by the patient’s characteristics and comorbidities in relation to the agent’s side effects and contraindications as detailed in the above section.
Patients should be referred to a movement disorders specialist in cases of resistant tremor, intolerance to oral medications, severe disability, and atypical presentation. Types of tremor known to be poorly responsive to oral medications (eg, head tremor, voice tremor) deserve a specialist evaluation if they contribute significantly to the patient’s morbidity.
The usual specialist treatment of severe voice tremor and head tremor is botulinum toxin injection. Patients with resistant and disabling hand tremor are evaluated for thalamic deep brain stimulation.
Patients with residual disability despite medical and surgical treatment should be referred for occupational therapy. Occupational therapy can improve quality of life through the use of special utensils, pens, computer gadgets, and arm weights, among other devices.
- Zesiewicz TA, Chari A, Jahan I, et al. Overview of essential tremor. Neuropsychiatr Dis Treat 2010; 6:401–408.
- Elble RJ. Essential tremor frequency decreases with time. Neurology 2000; 55:1547–1551.
- Louis ED, Ottman R, Hauser WA. How common is the most common adult movement disorder? Estimates of the prevalence of essential tremor throughout the world. Mov Disord 1998; 13:5–10.
- Louis ED, Dure LS, Pullman S. Essential tremor in childhood: a series of nineteen cases. Mov Disord 2001; 16:921–923.
- Singer C, Sanchez-Ramos J, Weiner WJ. Gait abnormality in essential tremor. Mov Disord 1994; 9:193–196.
- Deuschl G, Wenzelburger R, Löffler K, et al. Essential tremor and cerebellar dysfunction. Clinical and kinematic analysis of intention tremor. Brain 2000; 123:1568–1580.
- Louis ED. Functional correlates of lower cognitive test scores in essential tremor. Mov Disord 2010; 25:481–485.
- Ondo WG, Sutton L, Dat Vuong K, et al. Hearing impairment in essential tremor. Neurology 2003; 61:1093–1097.
- Schneier FR, Barnes LF, Albert SM, et al. Characteristics of social phobia among persons with essential tremor. J Clin Psychiatry 2001; 62:367–372.
- Whaley NR, Putzke JD, Baba Y, et al. Essential tremor: phenotypic expression in a clinical cohort. Parkinsonism Relat Disord 2007; 13:333–339.
- Deng H, Le W, Jankovic J. Genetics of essential tremor. Brain 2007; 130:1456–1464.
- Cohen O, Pullman S, Jurewicz E, et al. Rest tremor in patients with essential tremor: prevalence, clinical correlates, and electrophysiologic characteristics. Arch Neurol 2003; 60:405–410.
- Shahed J, Jankovic J. Exploring the relationship between essential tremor and Parkinson’s disease. Parkinsonism Relat Disord 2007; 13:67–76.
- Yang YW, Chang FC, Tsai CH, et al. Clinical and magnetic resonance imaging manifestations of Holmes tremor. Acta Neurol Taiwan 2005; 14:9–15.
- Alusi SH, Worthington J, Glickman S, et al. A study of tremor in multiple sclerosis. Brain 2001; 124:720–730.
- Breit S, Wächter T, Schöls L, et al. Effective thalamic deep brain stimulation for neuropathic tremor in a patient with severe demyelinating neuropathy. J Neurol Neurosurg Psychiatry 2009; 80:235–236.
- Koller WC, Wong GF, Lang A. Posttraumatic movement disorders: a review. Mov Disord 1989; 4:20–36.
- Jankovic J. Essential tremor: a heterogenous disorder. Mov Disord 2002; 17:638–644.
- Deuschl G, Bain P, Brin M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov Disord 1998; 13(suppl 3):2–23.
- Calzetti S, Findley LJ, Gresty MA, et al. Effect of a single oral dose of propranolol on essential tremor: a double-blind controlled study. Ann Neurol 1983; 13:165–171.
- Larsen TA, Teräväinen H, Calne DB. Atenolol vs propranolol in essential tremor. A controlled, quantitative study. Acta Neurol Scand 1982; 66:547–554.
- Zesiewicz TA, Elble R, Louis ED, et al. Practice parameter: therapies for essential tremor: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2005; 64:2008–2020.
- Lyons KE, Pahwa R, Comella CL, et al.Benefits and risks of pharmacological treatments for essential tremor. Drug Saf 2003; 26:461–481.
- Pahwa R, Lyons KE. Essential tremor: differential diagnosis and current therapy. Am J Med 2003; 115:134–142.
- Louis ED. Clinical practice. Essential tremor. N Engl J Med 2001; 345:887–891.
- Koller WC. Nadolol in essential tremor. Neurology 1983; 33:1076–1077.
- Dietrichson P, Espen E. Effects of timolol and atenolol on benign essential tremor: placebo-controlled studies based on quantitative tremor recording. J Neurol Neurosurg Psychiatry 1981; 44:677–683.
- Calzetti S, Findley LJ, Gresty MA, et al. Metoprolol and propranolol in essential tremor: a double-blind, controlled study. J Neurol Neurosurg Psychiatry 1981; 44:814–819.
- Teravainen H, Larsen A, Fogelholm R. Comparison between the effects of pindolol and propranolol on essential tremor. Neurology 1977; 27:439–442.
- Gorman WP, Cooper R, Pocock P, et al. A comparison of primidone, propranolol, and placebo in essential tremor, using quantitative analysis. J Neurol Neurosurg Psychiatry 1986; 49:64–68.
- Koller WC, Royse VL. Efficacy of primidone in essential tremor. Neurology 1986; 36:121–124.
- Connor GS. A double-blind placebo-controlled trial of topiramate treatment for essential tremor. Neurology 2002; 59:132–134.
- Gironell A, Kulisevsky J, Barbanoj M, et al. A randomized placebo-controlled comparative trial of gabapentin and propranolol in essential tremor. Arch Neurol 1999; 56:475–480.
- Ondo W, Hunter C, Vuong KD, et al. Gabapentin for essential tremor: a multiple-dose, double-blind, placebo-controlled trial. Mov Disord 2000; 15:678–682.
- Pahwa R, Lyons K, Hubble JP, et al. Double-blind controlled trial of gabapentin in essential tremor. Mov Disord 1998; 13:465–467.
- Bushara KO, Malik T, Exconde RE. The effect of levetiracetam on essential tremor. Neurology 2005; 64:1078–1080.
- Sullivan KL, Hauser RA, Zesiewicz TA. Levetiracetam for the treatment of essential tremor. Mov Disord 2005; 20:640.
- Huber SJ, Paulson GW. Efficacy of alprazolam for essential tremor. Neurology 1988; 38:241–243.
- McManis PG, Sharbrough FW. Orthostatic tremor: clinical and electrophysiologic characteristics. Muscle Nerve 1993; 16:1254–1260.
- Ceravolo R, Salvetti S, Piccini P, et al. Acute and chronic effects of clozapine in essential tremor. Mov Disord 1999; 14:468–472.
- Pakkenberg H, Pakkenberg B. Clozapine in the treatment of tremor. Acta Neurol Scand 1986; 73:295–297.
- Pact V, Giduz T. Mirtazapine treats resting tremor, essential tremor, and levodopa-induced dyskinesias. Neurology 1999; 53:1154.
- Lyons KE, Pahwa R. A double-blind, placebo-controlled, pilot study of mirtazapine in essential tremor. Presented at the 54th Annual Meeting of the American Academy of Neurology, Denver, Colorado. Neurology 2002; 58(suppl 3):A254.
- Brin MF, Lyons KE, Doucette J, et al. A randomized, double masked, controlled trial of botulinum toxin type A in essential hand tremor. Neurology 2001; 56:1523–1528.
- Blitzer A, Brin MF, Stewart C, et al. Abductor laryngeal dystonia: a series treated with botulinum toxin. Laryngoscope 1992; 102:163–167.
- Schuurman PR, Bosch DA, Bossuyt PM, et al. A comparison of continuous thalamic stimulation and thalamotomy for suppression of severe tremor. N Engl J Med 2000; 342:461–468.
- Flora ED, Perera CL, Cameron AL, et al. Deep brain stimulation for essential tremor: a systematic review. Mov Disord 2010; 25:1550–1559.
- Nagaseki Y, Shibazaki T, Hirai T, et al. Long-term follow-up results of selective VIM-thalamotomy. J Neurosurg 1986; 65:296–302.
- Zirh A, Reich SG, Dougherty PM, et al. Stereotactic thalamotomy in the treatment of essential tremor of the upper extremity: reassessment including a blinded measure of outcome. J Neurol Neurosurg Psychiatry 1999; 66:772–775.
- Zesiewicz TA, Chari A, Jahan I, et al. Overview of essential tremor. Neuropsychiatr Dis Treat 2010; 6:401–408.
- Elble RJ. Essential tremor frequency decreases with time. Neurology 2000; 55:1547–1551.
- Louis ED, Ottman R, Hauser WA. How common is the most common adult movement disorder? Estimates of the prevalence of essential tremor throughout the world. Mov Disord 1998; 13:5–10.
- Louis ED, Dure LS, Pullman S. Essential tremor in childhood: a series of nineteen cases. Mov Disord 2001; 16:921–923.
- Singer C, Sanchez-Ramos J, Weiner WJ. Gait abnormality in essential tremor. Mov Disord 1994; 9:193–196.
- Deuschl G, Wenzelburger R, Löffler K, et al. Essential tremor and cerebellar dysfunction. Clinical and kinematic analysis of intention tremor. Brain 2000; 123:1568–1580.
- Louis ED. Functional correlates of lower cognitive test scores in essential tremor. Mov Disord 2010; 25:481–485.
- Ondo WG, Sutton L, Dat Vuong K, et al. Hearing impairment in essential tremor. Neurology 2003; 61:1093–1097.
- Schneier FR, Barnes LF, Albert SM, et al. Characteristics of social phobia among persons with essential tremor. J Clin Psychiatry 2001; 62:367–372.
- Whaley NR, Putzke JD, Baba Y, et al. Essential tremor: phenotypic expression in a clinical cohort. Parkinsonism Relat Disord 2007; 13:333–339.
- Deng H, Le W, Jankovic J. Genetics of essential tremor. Brain 2007; 130:1456–1464.
- Cohen O, Pullman S, Jurewicz E, et al. Rest tremor in patients with essential tremor: prevalence, clinical correlates, and electrophysiologic characteristics. Arch Neurol 2003; 60:405–410.
- Shahed J, Jankovic J. Exploring the relationship between essential tremor and Parkinson’s disease. Parkinsonism Relat Disord 2007; 13:67–76.
- Yang YW, Chang FC, Tsai CH, et al. Clinical and magnetic resonance imaging manifestations of Holmes tremor. Acta Neurol Taiwan 2005; 14:9–15.
- Alusi SH, Worthington J, Glickman S, et al. A study of tremor in multiple sclerosis. Brain 2001; 124:720–730.
- Breit S, Wächter T, Schöls L, et al. Effective thalamic deep brain stimulation for neuropathic tremor in a patient with severe demyelinating neuropathy. J Neurol Neurosurg Psychiatry 2009; 80:235–236.
- Koller WC, Wong GF, Lang A. Posttraumatic movement disorders: a review. Mov Disord 1989; 4:20–36.
- Jankovic J. Essential tremor: a heterogenous disorder. Mov Disord 2002; 17:638–644.
- Deuschl G, Bain P, Brin M. Consensus statement of the Movement Disorder Society on Tremor. Ad Hoc Scientific Committee. Mov Disord 1998; 13(suppl 3):2–23.
- Calzetti S, Findley LJ, Gresty MA, et al. Effect of a single oral dose of propranolol on essential tremor: a double-blind controlled study. Ann Neurol 1983; 13:165–171.
- Larsen TA, Teräväinen H, Calne DB. Atenolol vs propranolol in essential tremor. A controlled, quantitative study. Acta Neurol Scand 1982; 66:547–554.
- Zesiewicz TA, Elble R, Louis ED, et al. Practice parameter: therapies for essential tremor: report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2005; 64:2008–2020.
- Lyons KE, Pahwa R, Comella CL, et al.Benefits and risks of pharmacological treatments for essential tremor. Drug Saf 2003; 26:461–481.
- Pahwa R, Lyons KE. Essential tremor: differential diagnosis and current therapy. Am J Med 2003; 115:134–142.
- Louis ED. Clinical practice. Essential tremor. N Engl J Med 2001; 345:887–891.
- Koller WC. Nadolol in essential tremor. Neurology 1983; 33:1076–1077.
- Dietrichson P, Espen E. Effects of timolol and atenolol on benign essential tremor: placebo-controlled studies based on quantitative tremor recording. J Neurol Neurosurg Psychiatry 1981; 44:677–683.
- Calzetti S, Findley LJ, Gresty MA, et al. Metoprolol and propranolol in essential tremor: a double-blind, controlled study. J Neurol Neurosurg Psychiatry 1981; 44:814–819.
- Teravainen H, Larsen A, Fogelholm R. Comparison between the effects of pindolol and propranolol on essential tremor. Neurology 1977; 27:439–442.
- Gorman WP, Cooper R, Pocock P, et al. A comparison of primidone, propranolol, and placebo in essential tremor, using quantitative analysis. J Neurol Neurosurg Psychiatry 1986; 49:64–68.
- Koller WC, Royse VL. Efficacy of primidone in essential tremor. Neurology 1986; 36:121–124.
- Connor GS. A double-blind placebo-controlled trial of topiramate treatment for essential tremor. Neurology 2002; 59:132–134.
- Gironell A, Kulisevsky J, Barbanoj M, et al. A randomized placebo-controlled comparative trial of gabapentin and propranolol in essential tremor. Arch Neurol 1999; 56:475–480.
- Ondo W, Hunter C, Vuong KD, et al. Gabapentin for essential tremor: a multiple-dose, double-blind, placebo-controlled trial. Mov Disord 2000; 15:678–682.
- Pahwa R, Lyons K, Hubble JP, et al. Double-blind controlled trial of gabapentin in essential tremor. Mov Disord 1998; 13:465–467.
- Bushara KO, Malik T, Exconde RE. The effect of levetiracetam on essential tremor. Neurology 2005; 64:1078–1080.
- Sullivan KL, Hauser RA, Zesiewicz TA. Levetiracetam for the treatment of essential tremor. Mov Disord 2005; 20:640.
- Huber SJ, Paulson GW. Efficacy of alprazolam for essential tremor. Neurology 1988; 38:241–243.
- McManis PG, Sharbrough FW. Orthostatic tremor: clinical and electrophysiologic characteristics. Muscle Nerve 1993; 16:1254–1260.
- Ceravolo R, Salvetti S, Piccini P, et al. Acute and chronic effects of clozapine in essential tremor. Mov Disord 1999; 14:468–472.
- Pakkenberg H, Pakkenberg B. Clozapine in the treatment of tremor. Acta Neurol Scand 1986; 73:295–297.
- Pact V, Giduz T. Mirtazapine treats resting tremor, essential tremor, and levodopa-induced dyskinesias. Neurology 1999; 53:1154.
- Lyons KE, Pahwa R. A double-blind, placebo-controlled, pilot study of mirtazapine in essential tremor. Presented at the 54th Annual Meeting of the American Academy of Neurology, Denver, Colorado. Neurology 2002; 58(suppl 3):A254.
- Brin MF, Lyons KE, Doucette J, et al. A randomized, double masked, controlled trial of botulinum toxin type A in essential hand tremor. Neurology 2001; 56:1523–1528.
- Blitzer A, Brin MF, Stewart C, et al. Abductor laryngeal dystonia: a series treated with botulinum toxin. Laryngoscope 1992; 102:163–167.
- Schuurman PR, Bosch DA, Bossuyt PM, et al. A comparison of continuous thalamic stimulation and thalamotomy for suppression of severe tremor. N Engl J Med 2000; 342:461–468.
- Flora ED, Perera CL, Cameron AL, et al. Deep brain stimulation for essential tremor: a systematic review. Mov Disord 2010; 25:1550–1559.
- Nagaseki Y, Shibazaki T, Hirai T, et al. Long-term follow-up results of selective VIM-thalamotomy. J Neurosurg 1986; 65:296–302.
- Zirh A, Reich SG, Dougherty PM, et al. Stereotactic thalamotomy in the treatment of essential tremor of the upper extremity: reassessment including a blinded measure of outcome. J Neurol Neurosurg Psychiatry 1999; 66:772–775.
KEY POINTS
- In addition to motor dysfunction, the tremor can also have a significant psychological impact on the patient, especially since it usually gets worse in social situations.
- Essential tremor is a clinical diagnosis. After a thorough review of the medical history and medication exposures, laboratory and imaging tests may be ordered to rule out a secondary cause.
- The two first-line agents in drug therapy for essential tremor are the nonselective beta-blocker propranolol (Inderal) and the antiepileptic primidone (Mysoline). They can be used alone or in combination.
- Botulinum toxin injection and deep brain stimulation are reserved for resistant tremor or for patients who do not tolerate drug therapy.
