User login
Physicians Often Missing Boat on Gout Therapy
SNOWMASS, COLO. – A disturbing proportion of gout cases are mismanaged by primary care physicians, and the blame falls squarely upon rheumatologists, according to one prominent gout expert.
"As rheumatologists, gout is our disease. The cause and pathophysiology are well understood, we can make the diagnosis with absolute certainty, and we’ve got great medicines. Yet today we all see people with tophi. That’s tragic. It shouldn’t exist. One of our biggest mistakes has been not being able to educate primary care physicians that having a tophus is bad, that it’s eroding cartilage and bone, and that it’s something we can prevent if we start urate-lowering therapy soon enough," Dr. Robert L. Wortmann said at the conference.
An estimated 8.3 million Americans have gout. Yet, the pharmaceutical industry says only 3.1 million of them are prescribed urate-lowering drugs. Five different studies show that a mere 40% of those on allopurinol are prescribed a dose sufficient to drive serum uric acid below 6 mg/dL, a key tenet of gout management, noted Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
Moreover, poor treatment adherence is a huge problem in gout. A study of close to 4,200 gout patients started on urate-lowering drug therapy found that 56% of them were nonadherent (Arthritis Res. Ther. 2009;11(2):R46).
"I charge you all to go back from this meeting and try to communicate with all the primary care physicians you can about the principles of managing gout. People shouldn’t suffer from this," the rheumatologist declared.
He offered these major take home points:
Don’t prescribe urate-lowering drugs for asymptomatic hyperuricemia: This practice hasn’t been shown to prevent the future development of gout, yet it exposes patients to the risk of drug toxicities.
But don’t ignore asymptomatic hyperuricemia, either: Epidemiologic studies have linked asymptomatic hyperuricemia, defined by a serum urate in excess of 6.8 mg/dL, to increased risks of hypertension, cardiovascular disease, diabetes, chronic kidney disease, and all-cause mortality. The big unanswered question is whether using medications to lower serum urate in individuals with asymptomatic hyperuricemia reduces the risk of any of these conditions. That’s the subject of ongoing large clinical trials in high-risk patients. If those studies prove positive, clinical practice will change.
While awaiting the outcome of the prevention trials, it’s worth bearing in mind that Framingham Heart Study data indicate that individuals with a serum uric acid level above 9 mg/dL have a 22% chance of developing gout within the next 5 years. The major contributors to asymptomatic hyperuricemia include obesity, metabolic syndrome, and heavy consumption of fructose-containing beverages or alcohol. Those issues should be addressed.
Losartan is the only antihypertensive agent that’s uricosuric. Fenofibrate is the sole uricosuric drug indicated for dyslipidemia. Preferential consideration could be given to the use of these drugs in hypertensive and/or hyperlipidemic patients with asymptomatic hyperuricemia.
The important thing is not which oral agent you use for treatment of acute gout, it’s to initiate therapy as early as possible, at the first hint of an attack. Colchicine, maximum-dose NSAIDs, and oral prednisone dosed at 20 mg BID until symptoms have been gone for 1 week followed by another week at 20 mg/day – they’re all effective. And since they work by different mechanisms, they can beneficially be combined in refractory patients.
The old-school colchicine dosing regimen most physicians were taught has been cast aside of late. It had a high rate of diarrhea, an inhumane side effect in gout patients hobbled by a foot too sore to walk on. The former regimen has been replaced by 1.2 mg, given in a single dose, followed by 0.6 mg 1 hour later.
"This lower dose is just as effective as the old high-dose regimen of two 0.6-mg pills given at once and then one per hour for the next 5 hours. And the lower-dose program has the same side effect profile as placebo," Dr. Wortmann said.
Get the gout patient’s serum urate below 6 mg/dL using the lowest effective dose of the urate-lowering drug you’ve selected. Physicians have traditionally started gout patients on allopurinol at the standard dose of 300 mg/day. Recently, it has been demonstrated that the risk of developing allopurinol hypersensitivity syndrome is greatly reduced by starting off at 150 mg/day, checking the urate level 2 weeks later, then increasing to 300 mg/day if the serum urate isn’t below 6 mg/dL. After 2 weeks at 300 mg/day, check the urate again, and if it still isn’t below 6 mg/dL then bump the dose to 400 mg/day. Continue testing and titrating every 2 weeks until the serum urate is less than 6 mg/dL – and preferably less than 4 mg/dL if the patient has tophi – or until the maximum approved dose of 800 mg/day is reached.
The same start-low-and-titrate strategy applies to febuxostat, with a maximum approved dose of 80 mg/day.
"We have to educate primary care physicians to check the serum urate after starting therapy, and that, if it’s not below 6 mg/dL, they need to increase the dose. And if they don’t feel comfortable with that, they need to send the patient to us," the rheumatologist said.
Fortunately, patients who have a hypersensitivity reaction to allopurinol are very unlikely to experience one with febuxostat, and vice versa.
For patients who can’t reach the target serum urate with maximum-dose therapy, take heart: Second-line agents with impressive potency are well-along in the developmental pipeline.
Many labs now list the upper limit of normal for serum urate as 8 mg/dL or 8.5 mg/dL. Ignore that. This raised ceiling is simply the result of the changing demographics among the increasingly obese U.S. population in the last several decades. The definition of asymptomatic hyperuricemia remains unchanged: a serum urate greater than 6.8 mg/dL. And the target in patients with gout is still a serum urate less than 6 mg/dL. Merely dropping a gout patient’s urate from 10 to 8 or even 6.6 mg/dL isn’t doing any favors; the disease will continue to progress if the urate is above 6 mg/dL.
All gout is tophaceous. Even if tophi aren’t apparent on clinical examination, often they are radiographically. "This is a message that has to get out," Dr. Wortmann insisted.
Proposed American College of Rheumatology gout management guidelines call for starting urate-lowering drug therapy when a patient is experiencing three attacks per year. Dr. Wortmann takes issue with that.
"I would argue that once you’ve had a third attack of gout, period, you should be treated. Maybe even sooner. We need to prevent the erosion and bony destruction that occur with tophi," he said.
One audience member complained that his gout patients with comorbid renal insufficiency and/or cardiovascular disease often get caught in a revolving door. He titrates their allopurinol to an effective dose, but when they are later admitted to the hospital because of their comorbid condition the hospitalists, nephrologists, and/or cardiologists are shocked at the allopurinol dose and either reduce it or stop it altogether. The first that the rheumatologist learns of it is when patients reappear in his office with active gout. He then resumes their allopurinol at the previous dose, and they remain well controlled until the next hospitalization, when the same thing happens.
Dr. Wortmann responded that the solution requires convincing the nonrheumatologists in one-on-one conversation that urate-lowering therapy is not a one-size-fits-all matter. They need to understand that to get rid of gout, it’s necessary to drive the serum urate to the target of less than 6 mg/dL, and it helps to reassure them that that this will be accomplished using the lowest effective dose.
He reported serving as a consultant to Savient, Takeda, URL Pharmaceuticals, Novartis, and Ardea Biosciences.
SNOWMASS, COLO. – A disturbing proportion of gout cases are mismanaged by primary care physicians, and the blame falls squarely upon rheumatologists, according to one prominent gout expert.
"As rheumatologists, gout is our disease. The cause and pathophysiology are well understood, we can make the diagnosis with absolute certainty, and we’ve got great medicines. Yet today we all see people with tophi. That’s tragic. It shouldn’t exist. One of our biggest mistakes has been not being able to educate primary care physicians that having a tophus is bad, that it’s eroding cartilage and bone, and that it’s something we can prevent if we start urate-lowering therapy soon enough," Dr. Robert L. Wortmann said at the conference.
An estimated 8.3 million Americans have gout. Yet, the pharmaceutical industry says only 3.1 million of them are prescribed urate-lowering drugs. Five different studies show that a mere 40% of those on allopurinol are prescribed a dose sufficient to drive serum uric acid below 6 mg/dL, a key tenet of gout management, noted Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
Moreover, poor treatment adherence is a huge problem in gout. A study of close to 4,200 gout patients started on urate-lowering drug therapy found that 56% of them were nonadherent (Arthritis Res. Ther. 2009;11(2):R46).
"I charge you all to go back from this meeting and try to communicate with all the primary care physicians you can about the principles of managing gout. People shouldn’t suffer from this," the rheumatologist declared.
He offered these major take home points:
Don’t prescribe urate-lowering drugs for asymptomatic hyperuricemia: This practice hasn’t been shown to prevent the future development of gout, yet it exposes patients to the risk of drug toxicities.
But don’t ignore asymptomatic hyperuricemia, either: Epidemiologic studies have linked asymptomatic hyperuricemia, defined by a serum urate in excess of 6.8 mg/dL, to increased risks of hypertension, cardiovascular disease, diabetes, chronic kidney disease, and all-cause mortality. The big unanswered question is whether using medications to lower serum urate in individuals with asymptomatic hyperuricemia reduces the risk of any of these conditions. That’s the subject of ongoing large clinical trials in high-risk patients. If those studies prove positive, clinical practice will change.
While awaiting the outcome of the prevention trials, it’s worth bearing in mind that Framingham Heart Study data indicate that individuals with a serum uric acid level above 9 mg/dL have a 22% chance of developing gout within the next 5 years. The major contributors to asymptomatic hyperuricemia include obesity, metabolic syndrome, and heavy consumption of fructose-containing beverages or alcohol. Those issues should be addressed.
Losartan is the only antihypertensive agent that’s uricosuric. Fenofibrate is the sole uricosuric drug indicated for dyslipidemia. Preferential consideration could be given to the use of these drugs in hypertensive and/or hyperlipidemic patients with asymptomatic hyperuricemia.
The important thing is not which oral agent you use for treatment of acute gout, it’s to initiate therapy as early as possible, at the first hint of an attack. Colchicine, maximum-dose NSAIDs, and oral prednisone dosed at 20 mg BID until symptoms have been gone for 1 week followed by another week at 20 mg/day – they’re all effective. And since they work by different mechanisms, they can beneficially be combined in refractory patients.
The old-school colchicine dosing regimen most physicians were taught has been cast aside of late. It had a high rate of diarrhea, an inhumane side effect in gout patients hobbled by a foot too sore to walk on. The former regimen has been replaced by 1.2 mg, given in a single dose, followed by 0.6 mg 1 hour later.
"This lower dose is just as effective as the old high-dose regimen of two 0.6-mg pills given at once and then one per hour for the next 5 hours. And the lower-dose program has the same side effect profile as placebo," Dr. Wortmann said.
Get the gout patient’s serum urate below 6 mg/dL using the lowest effective dose of the urate-lowering drug you’ve selected. Physicians have traditionally started gout patients on allopurinol at the standard dose of 300 mg/day. Recently, it has been demonstrated that the risk of developing allopurinol hypersensitivity syndrome is greatly reduced by starting off at 150 mg/day, checking the urate level 2 weeks later, then increasing to 300 mg/day if the serum urate isn’t below 6 mg/dL. After 2 weeks at 300 mg/day, check the urate again, and if it still isn’t below 6 mg/dL then bump the dose to 400 mg/day. Continue testing and titrating every 2 weeks until the serum urate is less than 6 mg/dL – and preferably less than 4 mg/dL if the patient has tophi – or until the maximum approved dose of 800 mg/day is reached.
The same start-low-and-titrate strategy applies to febuxostat, with a maximum approved dose of 80 mg/day.
"We have to educate primary care physicians to check the serum urate after starting therapy, and that, if it’s not below 6 mg/dL, they need to increase the dose. And if they don’t feel comfortable with that, they need to send the patient to us," the rheumatologist said.
Fortunately, patients who have a hypersensitivity reaction to allopurinol are very unlikely to experience one with febuxostat, and vice versa.
For patients who can’t reach the target serum urate with maximum-dose therapy, take heart: Second-line agents with impressive potency are well-along in the developmental pipeline.
Many labs now list the upper limit of normal for serum urate as 8 mg/dL or 8.5 mg/dL. Ignore that. This raised ceiling is simply the result of the changing demographics among the increasingly obese U.S. population in the last several decades. The definition of asymptomatic hyperuricemia remains unchanged: a serum urate greater than 6.8 mg/dL. And the target in patients with gout is still a serum urate less than 6 mg/dL. Merely dropping a gout patient’s urate from 10 to 8 or even 6.6 mg/dL isn’t doing any favors; the disease will continue to progress if the urate is above 6 mg/dL.
All gout is tophaceous. Even if tophi aren’t apparent on clinical examination, often they are radiographically. "This is a message that has to get out," Dr. Wortmann insisted.
Proposed American College of Rheumatology gout management guidelines call for starting urate-lowering drug therapy when a patient is experiencing three attacks per year. Dr. Wortmann takes issue with that.
"I would argue that once you’ve had a third attack of gout, period, you should be treated. Maybe even sooner. We need to prevent the erosion and bony destruction that occur with tophi," he said.
One audience member complained that his gout patients with comorbid renal insufficiency and/or cardiovascular disease often get caught in a revolving door. He titrates their allopurinol to an effective dose, but when they are later admitted to the hospital because of their comorbid condition the hospitalists, nephrologists, and/or cardiologists are shocked at the allopurinol dose and either reduce it or stop it altogether. The first that the rheumatologist learns of it is when patients reappear in his office with active gout. He then resumes their allopurinol at the previous dose, and they remain well controlled until the next hospitalization, when the same thing happens.
Dr. Wortmann responded that the solution requires convincing the nonrheumatologists in one-on-one conversation that urate-lowering therapy is not a one-size-fits-all matter. They need to understand that to get rid of gout, it’s necessary to drive the serum urate to the target of less than 6 mg/dL, and it helps to reassure them that that this will be accomplished using the lowest effective dose.
He reported serving as a consultant to Savient, Takeda, URL Pharmaceuticals, Novartis, and Ardea Biosciences.
SNOWMASS, COLO. – A disturbing proportion of gout cases are mismanaged by primary care physicians, and the blame falls squarely upon rheumatologists, according to one prominent gout expert.
"As rheumatologists, gout is our disease. The cause and pathophysiology are well understood, we can make the diagnosis with absolute certainty, and we’ve got great medicines. Yet today we all see people with tophi. That’s tragic. It shouldn’t exist. One of our biggest mistakes has been not being able to educate primary care physicians that having a tophus is bad, that it’s eroding cartilage and bone, and that it’s something we can prevent if we start urate-lowering therapy soon enough," Dr. Robert L. Wortmann said at the conference.
An estimated 8.3 million Americans have gout. Yet, the pharmaceutical industry says only 3.1 million of them are prescribed urate-lowering drugs. Five different studies show that a mere 40% of those on allopurinol are prescribed a dose sufficient to drive serum uric acid below 6 mg/dL, a key tenet of gout management, noted Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
Moreover, poor treatment adherence is a huge problem in gout. A study of close to 4,200 gout patients started on urate-lowering drug therapy found that 56% of them were nonadherent (Arthritis Res. Ther. 2009;11(2):R46).
"I charge you all to go back from this meeting and try to communicate with all the primary care physicians you can about the principles of managing gout. People shouldn’t suffer from this," the rheumatologist declared.
He offered these major take home points:
Don’t prescribe urate-lowering drugs for asymptomatic hyperuricemia: This practice hasn’t been shown to prevent the future development of gout, yet it exposes patients to the risk of drug toxicities.
But don’t ignore asymptomatic hyperuricemia, either: Epidemiologic studies have linked asymptomatic hyperuricemia, defined by a serum urate in excess of 6.8 mg/dL, to increased risks of hypertension, cardiovascular disease, diabetes, chronic kidney disease, and all-cause mortality. The big unanswered question is whether using medications to lower serum urate in individuals with asymptomatic hyperuricemia reduces the risk of any of these conditions. That’s the subject of ongoing large clinical trials in high-risk patients. If those studies prove positive, clinical practice will change.
While awaiting the outcome of the prevention trials, it’s worth bearing in mind that Framingham Heart Study data indicate that individuals with a serum uric acid level above 9 mg/dL have a 22% chance of developing gout within the next 5 years. The major contributors to asymptomatic hyperuricemia include obesity, metabolic syndrome, and heavy consumption of fructose-containing beverages or alcohol. Those issues should be addressed.
Losartan is the only antihypertensive agent that’s uricosuric. Fenofibrate is the sole uricosuric drug indicated for dyslipidemia. Preferential consideration could be given to the use of these drugs in hypertensive and/or hyperlipidemic patients with asymptomatic hyperuricemia.
The important thing is not which oral agent you use for treatment of acute gout, it’s to initiate therapy as early as possible, at the first hint of an attack. Colchicine, maximum-dose NSAIDs, and oral prednisone dosed at 20 mg BID until symptoms have been gone for 1 week followed by another week at 20 mg/day – they’re all effective. And since they work by different mechanisms, they can beneficially be combined in refractory patients.
The old-school colchicine dosing regimen most physicians were taught has been cast aside of late. It had a high rate of diarrhea, an inhumane side effect in gout patients hobbled by a foot too sore to walk on. The former regimen has been replaced by 1.2 mg, given in a single dose, followed by 0.6 mg 1 hour later.
"This lower dose is just as effective as the old high-dose regimen of two 0.6-mg pills given at once and then one per hour for the next 5 hours. And the lower-dose program has the same side effect profile as placebo," Dr. Wortmann said.
Get the gout patient’s serum urate below 6 mg/dL using the lowest effective dose of the urate-lowering drug you’ve selected. Physicians have traditionally started gout patients on allopurinol at the standard dose of 300 mg/day. Recently, it has been demonstrated that the risk of developing allopurinol hypersensitivity syndrome is greatly reduced by starting off at 150 mg/day, checking the urate level 2 weeks later, then increasing to 300 mg/day if the serum urate isn’t below 6 mg/dL. After 2 weeks at 300 mg/day, check the urate again, and if it still isn’t below 6 mg/dL then bump the dose to 400 mg/day. Continue testing and titrating every 2 weeks until the serum urate is less than 6 mg/dL – and preferably less than 4 mg/dL if the patient has tophi – or until the maximum approved dose of 800 mg/day is reached.
The same start-low-and-titrate strategy applies to febuxostat, with a maximum approved dose of 80 mg/day.
"We have to educate primary care physicians to check the serum urate after starting therapy, and that, if it’s not below 6 mg/dL, they need to increase the dose. And if they don’t feel comfortable with that, they need to send the patient to us," the rheumatologist said.
Fortunately, patients who have a hypersensitivity reaction to allopurinol are very unlikely to experience one with febuxostat, and vice versa.
For patients who can’t reach the target serum urate with maximum-dose therapy, take heart: Second-line agents with impressive potency are well-along in the developmental pipeline.
Many labs now list the upper limit of normal for serum urate as 8 mg/dL or 8.5 mg/dL. Ignore that. This raised ceiling is simply the result of the changing demographics among the increasingly obese U.S. population in the last several decades. The definition of asymptomatic hyperuricemia remains unchanged: a serum urate greater than 6.8 mg/dL. And the target in patients with gout is still a serum urate less than 6 mg/dL. Merely dropping a gout patient’s urate from 10 to 8 or even 6.6 mg/dL isn’t doing any favors; the disease will continue to progress if the urate is above 6 mg/dL.
All gout is tophaceous. Even if tophi aren’t apparent on clinical examination, often they are radiographically. "This is a message that has to get out," Dr. Wortmann insisted.
Proposed American College of Rheumatology gout management guidelines call for starting urate-lowering drug therapy when a patient is experiencing three attacks per year. Dr. Wortmann takes issue with that.
"I would argue that once you’ve had a third attack of gout, period, you should be treated. Maybe even sooner. We need to prevent the erosion and bony destruction that occur with tophi," he said.
One audience member complained that his gout patients with comorbid renal insufficiency and/or cardiovascular disease often get caught in a revolving door. He titrates their allopurinol to an effective dose, but when they are later admitted to the hospital because of their comorbid condition the hospitalists, nephrologists, and/or cardiologists are shocked at the allopurinol dose and either reduce it or stop it altogether. The first that the rheumatologist learns of it is when patients reappear in his office with active gout. He then resumes their allopurinol at the previous dose, and they remain well controlled until the next hospitalization, when the same thing happens.
Dr. Wortmann responded that the solution requires convincing the nonrheumatologists in one-on-one conversation that urate-lowering therapy is not a one-size-fits-all matter. They need to understand that to get rid of gout, it’s necessary to drive the serum urate to the target of less than 6 mg/dL, and it helps to reassure them that that this will be accomplished using the lowest effective dose.
He reported serving as a consultant to Savient, Takeda, URL Pharmaceuticals, Novartis, and Ardea Biosciences.
EXPERT ANALYSIS FROM A SYMPOSIUM SPONSORED BY THE AMERICAN COLLEGE OF RHEUMATOLOGY
Obesity Epidemic Is Skewing Face of Gout
SNOWMASS, COLO. – The epidemiology of gout has changed considerably in the past several decades, rendering treatment more challenging.
For example, today fully 21.4% of all U.S. adults are hyperuricemic as defined by a serum uric acid in excess of 6.8 mg/dL.

"When I was a fellow it was 5%. There’s a lot more uric acid in the world today," Dr. Robert L. Wortmann observed at the symposium.
Major contributing factors include metabolic syndrome, the obesity epidemic, increased consumption of high-fructose drinks and processed foods, and alcohol. Liquor has a twofold stronger urate-boosting effect than does wine, and beer’s impact is fourfold greater than wine, according to Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
"When I was in training uric acids above 9 mg/dL weren’t common; now, when I see a newly diagnosed gout patient with a uric acid level below 9, it’s exceptional. Gout patients today have uric acids of 10, 11, and 12 mg/dL as opposed to 7.5, 8, and 9 in decades past," he said.
Since 1964 the standard dose of allopurinol has been 300 mg/day. Back then, that was sufficient to reach the serum uric acid target of less than 6.0 mg/dL in about 90% of gout patients. Today, 300 mg/day gets only about 40% of patients to target, as has been shown in numerous studies.
Dr. Wortmann reported serving as a consultant to Ardea Biosciences, Novartis, Savient, Takeda, and URL Pharmaceuticals.
SNOWMASS, COLO. – The epidemiology of gout has changed considerably in the past several decades, rendering treatment more challenging.
For example, today fully 21.4% of all U.S. adults are hyperuricemic as defined by a serum uric acid in excess of 6.8 mg/dL.
"When I was a fellow it was 5%. There’s a lot more uric acid in the world today," Dr. Robert L. Wortmann observed at the symposium.
Major contributing factors include metabolic syndrome, the obesity epidemic, increased consumption of high-fructose drinks and processed foods, and alcohol. Liquor has a twofold stronger urate-boosting effect than does wine, and beer’s impact is fourfold greater than wine, according to Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
"When I was in training uric acids above 9 mg/dL weren’t common; now, when I see a newly diagnosed gout patient with a uric acid level below 9, it’s exceptional. Gout patients today have uric acids of 10, 11, and 12 mg/dL as opposed to 7.5, 8, and 9 in decades past," he said.
Since 1964 the standard dose of allopurinol has been 300 mg/day. Back then, that was sufficient to reach the serum uric acid target of less than 6.0 mg/dL in about 90% of gout patients. Today, 300 mg/day gets only about 40% of patients to target, as has been shown in numerous studies.
Dr. Wortmann reported serving as a consultant to Ardea Biosciences, Novartis, Savient, Takeda, and URL Pharmaceuticals.
SNOWMASS, COLO. – The epidemiology of gout has changed considerably in the past several decades, rendering treatment more challenging.
For example, today fully 21.4% of all U.S. adults are hyperuricemic as defined by a serum uric acid in excess of 6.8 mg/dL.
"When I was a fellow it was 5%. There’s a lot more uric acid in the world today," Dr. Robert L. Wortmann observed at the symposium.
Major contributing factors include metabolic syndrome, the obesity epidemic, increased consumption of high-fructose drinks and processed foods, and alcohol. Liquor has a twofold stronger urate-boosting effect than does wine, and beer’s impact is fourfold greater than wine, according to Dr. Wortmann, professor of medicine at Dartmouth Medical School in Hanover, N.H.
"When I was in training uric acids above 9 mg/dL weren’t common; now, when I see a newly diagnosed gout patient with a uric acid level below 9, it’s exceptional. Gout patients today have uric acids of 10, 11, and 12 mg/dL as opposed to 7.5, 8, and 9 in decades past," he said.
Since 1964 the standard dose of allopurinol has been 300 mg/day. Back then, that was sufficient to reach the serum uric acid target of less than 6.0 mg/dL in about 90% of gout patients. Today, 300 mg/day gets only about 40% of patients to target, as has been shown in numerous studies.
Dr. Wortmann reported serving as a consultant to Ardea Biosciences, Novartis, Savient, Takeda, and URL Pharmaceuticals.
EXPERT ANALYSIS FROM A SYMPOSIUM SPONSORED BY THE AMERICAN COLLEGE OF RHEUMATOLOGY
Survey: Steady Increase in Complementary Alternative Medicine (CAM) Offerings in U.S. Hospitals
According to a survey released last fall by the Health Forum, a subsidiary of the American Hospital Association, and the Samueli Institute of Alexandria, Va., complementary and alternative medicine (CAM) services in responding hospitals increased to 42% in 2010 from 37% in 2007.
The fourth Complementary and Alternative Medicine Survey of Hospitals is a follow-up report to the 2007 survey, which The Hospitalist featured in January 2010.
Twelve percent of 5,858 hospitals answered a 42-question instrument in 2010, according to Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author. The results, Ananth says, showed that the hospitals most likely to offer CAM were urban and tended to be either medium-size (50-299 beds) or large (500+ beds) institutions.
What’s driving the increase? She believes that hospitals are simply responding to patients’ desire to have “the best that both conventional and alternative medicine can offer.”

—Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author
Sixty-five percent of hospitals responding to the survey offer CAM therapies for pain management. That figure is echoed in a 2008 National Health Statistics report (PDF) published by the Centers for Disease Control and Prevention. Back pain, neck pain, and joint pain were the three top reasons for using CAM, according to the CDC report.
“Adjacent” Treatment
Hospitalist Sanjay Reddy, MD, assistant clinical professor of medicine in the Department of Medicine at the University of California at San Francisco (UCSF), says acupuncture can be a valuable adjunct when treating patients for pain, chemotherapy-induced nausea, and insomnia. He is a trained acupuncturist and has studied complementary therapies extensively. He also is interested in exploring ways to incorporate acupuncture into the UCSF’s Osher Center for Integrative Medicine program.
David H. Gorski, MD, PhD, FACS, associate professor of surgery and director of the Breast Cancer Multidisciplinary Team at the Barbara Ann Karmanos Cancer Institute at Wayne State University School of Medicine in Detroit, strenuously objects to the incorporation of alternative therapies (often under the moniker of “integrative medicine”) in the hospital setting.
“If you accept the premise that medicine should be based in sound science and evidence, then we have an obligation not to be offering treatments that are not based in science,” he asserts. Dr. Gorski, who also blogs on such topics, finds that many of those who endorse integrative medicine have become “true believers,” and that some are mixing pseudo-science with science.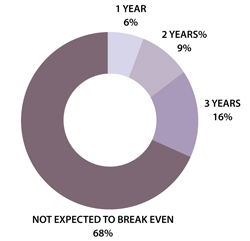
In an August 2011 post regarding the College of Physicians and Surgeons of Ontario’s draft policy on alternative treatments, Dr. Gorski wrote: “Competent adults have every right to seek out non-science-based medicine if that is what they desire. However, informed consent mandates that physicians who encounter such patients provide an honest professional assessment of such treatments based on science.”
Dr. Reddy notes that with appropriate disclosure, offering a modality such as acupuncture can be appropriate. For example, in the setting of pain relief, acupuncture offers a less sedative approach. He explains that Chinese diagnostics and treatment approaches are slightly different, so it’s difficult to study them in the context of randomized trials. (Click here to listen to more of Dr. Reddy’s discussion of appropriate indications for acupuncture.)
In the Health Forum/Samueli Institute survey, 57% of hospitals reported that their programs were not yet breaking even and only 16% said they'd be breaking even in three years (see Figure 1). In light of these results, Ananth says, hospitals undertaking complementary services should “start small and not have high expectations of breaking even for several years.”
Gretchen Henkel is a freelance writer in California.
Herbals another Matter
In the 2010 Health Forum/Samueli Institute survey, 82% of responding hospitals reported that they did not offer herbal supplements in their hospital pharmacies. Study author Sita Ananth surmises that most hospitals may be “playing it safe” by offering noninvasive therapies. Hospitalists are aware of the potentially dangerous interactions between herbal supplements and mainstream treatments, Dr. Reddy says.
A majority of the hospitals Ananth queried (67%) reported having existing policies regarding patients’ use of herbal and nutritional supplements during hospitalization. To avoid adverse events, “It’s really crucial that they are asking the right questions of their patients,” she says.—GH
According to a survey released last fall by the Health Forum, a subsidiary of the American Hospital Association, and the Samueli Institute of Alexandria, Va., complementary and alternative medicine (CAM) services in responding hospitals increased to 42% in 2010 from 37% in 2007.
The fourth Complementary and Alternative Medicine Survey of Hospitals is a follow-up report to the 2007 survey, which The Hospitalist featured in January 2010.
Twelve percent of 5,858 hospitals answered a 42-question instrument in 2010, according to Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author. The results, Ananth says, showed that the hospitals most likely to offer CAM were urban and tended to be either medium-size (50-299 beds) or large (500+ beds) institutions.
What’s driving the increase? She believes that hospitals are simply responding to patients’ desire to have “the best that both conventional and alternative medicine can offer.”
—Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author
Sixty-five percent of hospitals responding to the survey offer CAM therapies for pain management. That figure is echoed in a 2008 National Health Statistics report (PDF) published by the Centers for Disease Control and Prevention. Back pain, neck pain, and joint pain were the three top reasons for using CAM, according to the CDC report.
“Adjacent” Treatment
Hospitalist Sanjay Reddy, MD, assistant clinical professor of medicine in the Department of Medicine at the University of California at San Francisco (UCSF), says acupuncture can be a valuable adjunct when treating patients for pain, chemotherapy-induced nausea, and insomnia. He is a trained acupuncturist and has studied complementary therapies extensively. He also is interested in exploring ways to incorporate acupuncture into the UCSF’s Osher Center for Integrative Medicine program.
David H. Gorski, MD, PhD, FACS, associate professor of surgery and director of the Breast Cancer Multidisciplinary Team at the Barbara Ann Karmanos Cancer Institute at Wayne State University School of Medicine in Detroit, strenuously objects to the incorporation of alternative therapies (often under the moniker of “integrative medicine”) in the hospital setting.
“If you accept the premise that medicine should be based in sound science and evidence, then we have an obligation not to be offering treatments that are not based in science,” he asserts. Dr. Gorski, who also blogs on such topics, finds that many of those who endorse integrative medicine have become “true believers,” and that some are mixing pseudo-science with science.
In an August 2011 post regarding the College of Physicians and Surgeons of Ontario’s draft policy on alternative treatments, Dr. Gorski wrote: “Competent adults have every right to seek out non-science-based medicine if that is what they desire. However, informed consent mandates that physicians who encounter such patients provide an honest professional assessment of such treatments based on science.”
Dr. Reddy notes that with appropriate disclosure, offering a modality such as acupuncture can be appropriate. For example, in the setting of pain relief, acupuncture offers a less sedative approach. He explains that Chinese diagnostics and treatment approaches are slightly different, so it’s difficult to study them in the context of randomized trials. (Click here to listen to more of Dr. Reddy’s discussion of appropriate indications for acupuncture.)
In the Health Forum/Samueli Institute survey, 57% of hospitals reported that their programs were not yet breaking even and only 16% said they'd be breaking even in three years (see Figure 1). In light of these results, Ananth says, hospitals undertaking complementary services should “start small and not have high expectations of breaking even for several years.”
Gretchen Henkel is a freelance writer in California.
Herbals another Matter
In the 2010 Health Forum/Samueli Institute survey, 82% of responding hospitals reported that they did not offer herbal supplements in their hospital pharmacies. Study author Sita Ananth surmises that most hospitals may be “playing it safe” by offering noninvasive therapies. Hospitalists are aware of the potentially dangerous interactions between herbal supplements and mainstream treatments, Dr. Reddy says.
A majority of the hospitals Ananth queried (67%) reported having existing policies regarding patients’ use of herbal and nutritional supplements during hospitalization. To avoid adverse events, “It’s really crucial that they are asking the right questions of their patients,” she says.—GH
According to a survey released last fall by the Health Forum, a subsidiary of the American Hospital Association, and the Samueli Institute of Alexandria, Va., complementary and alternative medicine (CAM) services in responding hospitals increased to 42% in 2010 from 37% in 2007.
The fourth Complementary and Alternative Medicine Survey of Hospitals is a follow-up report to the 2007 survey, which The Hospitalist featured in January 2010.
Twelve percent of 5,858 hospitals answered a 42-question instrument in 2010, according to Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author. The results, Ananth says, showed that the hospitals most likely to offer CAM were urban and tended to be either medium-size (50-299 beds) or large (500+ beds) institutions.
What’s driving the increase? She believes that hospitals are simply responding to patients’ desire to have “the best that both conventional and alternative medicine can offer.”
—Sita Ananth, MHA, director of knowledge services at the Samueli Institute and study report author
Sixty-five percent of hospitals responding to the survey offer CAM therapies for pain management. That figure is echoed in a 2008 National Health Statistics report (PDF) published by the Centers for Disease Control and Prevention. Back pain, neck pain, and joint pain were the three top reasons for using CAM, according to the CDC report.
“Adjacent” Treatment
Hospitalist Sanjay Reddy, MD, assistant clinical professor of medicine in the Department of Medicine at the University of California at San Francisco (UCSF), says acupuncture can be a valuable adjunct when treating patients for pain, chemotherapy-induced nausea, and insomnia. He is a trained acupuncturist and has studied complementary therapies extensively. He also is interested in exploring ways to incorporate acupuncture into the UCSF’s Osher Center for Integrative Medicine program.
David H. Gorski, MD, PhD, FACS, associate professor of surgery and director of the Breast Cancer Multidisciplinary Team at the Barbara Ann Karmanos Cancer Institute at Wayne State University School of Medicine in Detroit, strenuously objects to the incorporation of alternative therapies (often under the moniker of “integrative medicine”) in the hospital setting.
“If you accept the premise that medicine should be based in sound science and evidence, then we have an obligation not to be offering treatments that are not based in science,” he asserts. Dr. Gorski, who also blogs on such topics, finds that many of those who endorse integrative medicine have become “true believers,” and that some are mixing pseudo-science with science.
In an August 2011 post regarding the College of Physicians and Surgeons of Ontario’s draft policy on alternative treatments, Dr. Gorski wrote: “Competent adults have every right to seek out non-science-based medicine if that is what they desire. However, informed consent mandates that physicians who encounter such patients provide an honest professional assessment of such treatments based on science.”
Dr. Reddy notes that with appropriate disclosure, offering a modality such as acupuncture can be appropriate. For example, in the setting of pain relief, acupuncture offers a less sedative approach. He explains that Chinese diagnostics and treatment approaches are slightly different, so it’s difficult to study them in the context of randomized trials. (Click here to listen to more of Dr. Reddy’s discussion of appropriate indications for acupuncture.)
In the Health Forum/Samueli Institute survey, 57% of hospitals reported that their programs were not yet breaking even and only 16% said they'd be breaking even in three years (see Figure 1). In light of these results, Ananth says, hospitals undertaking complementary services should “start small and not have high expectations of breaking even for several years.”
Gretchen Henkel is a freelance writer in California.
Herbals another Matter
In the 2010 Health Forum/Samueli Institute survey, 82% of responding hospitals reported that they did not offer herbal supplements in their hospital pharmacies. Study author Sita Ananth surmises that most hospitals may be “playing it safe” by offering noninvasive therapies. Hospitalists are aware of the potentially dangerous interactions between herbal supplements and mainstream treatments, Dr. Reddy says.
A majority of the hospitals Ananth queried (67%) reported having existing policies regarding patients’ use of herbal and nutritional supplements during hospitalization. To avoid adverse events, “It’s really crucial that they are asking the right questions of their patients,” she says.—GH
FDA Panel Nixes Decitabine for Acute Myeloid Leukemia
SILVER SPRING, MD. – The leukemia drug decitabine didn’t show robust-enough results to convince the majority of an advisory panel to support its approval by the U.S. Food and Drug Administration as a new treatment for elderly patients with acute myeloid leukemia.
Ten members of the independent Oncologic Drugs Advisory Committee (ODAC) voted no, three voted yes, and one member abstained on a question related to the proposed indication. They were asked whether decitabine (Dacogen) demonstrated a favorable risk-benefit profile for the treatment of newly diagnosed acute myeloid leukemia (AML) in patients 65 years and older who are not candidates for induction chemotherapy.
Those who voted no said they didn't find the results of a key study convincing and were not comfortable drawing any solid conclusions. The yea-sayers said they looked beyond the fact that the study didn’t meet its end point and instead erred on the side of adding another treatment choice for doctors and their patients.
The FDA considers the panel’s recommendations, but doesn’t necessarily follow them.
Drugmaker Eisai sought the drug’s approval by filing an application to the FDA in May 2011, with the goal of meeting the "unmet medical need" of older adults with AML who are not candidates for induction therapy.
Although the company’s trials didn’t reach a statistically significant result, its officials made the argument that aggregate clinical data from a randomized trial and a single-arm study showed that the drug was well tolerated, had good efficacy and safety profiles, and would provide a clinically meaningful benefit to older patients with AML who are not candidates for induction chemotherapy.
But FDA officials made the case that the "primary end point of overall survival was not met and any further analyses are expiatory and inflate the false-positive rate." They also pointed out that they defined efficacy as a statistically significant survival rate or a rigorous analysis that shows noninferiority.
AML is mainly a disease of the elderly, with an onset at the median age of 69 years. Because of poorer outcomes among this age group, one-third of patients don’t receive chemotherapy.
Decitabine, a hypomethylating agent, was FDA approved in 2006 for the treatment of myelodysplastic syndromes.
A 2009 randomized, open-label, multinational phase III trial, conducted by Eisai, enrolled 485 patients, with a median age of 73. Patients were randomized to decitabine (242) or treatment of choice (low-dose cytarabine or supportive care) (243), with the primary end point of overall survival, prespecified as a 25% reduction in mortality risk.
Patients in the decitabine arm had a median overall survival of 7.7 months, compared with 5 months in the treatment of choice group, (hazard ratio, 0.85; P = .11). A 2010 post hoc analysis showed the median overall survival was unchanged, but the difference became statistically significant (HR, 0.82; P = .037).
FDA officials argued that, "given the final analysis results, post hoc analysis results could be due to chance," adding that the false-positive rate is greater than 5%.
Eisai also conducted a phase II supportive study, which was a single-arm trial that enrolled 55 patients with a median age of 60 years or older. The efficacy and safety results were similar to those of the randomized trial. The safety profile of decitabine was comparable to that in the label for myelodysplastic syndrome, Eisai officials reported.
"Elderly patients [with AML] are desperate for new treatments," said Dr. Mikkael Sekeres, an ODAC member from the department of hematologic oncology and blood disorders at the Cleveland Clinic Taussig Cancer Institute who voted no. "Unfortunately this drug didn’t do the job."
Dr. Wyndham Wilson, ODAC chair and chief of the lymphoma therapeutics section at the National Institutes of Health, voted yes and said he looked at the totality of the data and thought that they favored its approval.
"I see it as a rare setting, where we really have no good drugs. I couldn’t get stuck on that the primary end point wasn’t met. I feel that I wanted to err on the side of choice," he said. "For me the data was sufficiently robust to approve the drug and have the choice available for physicians and patients."
Dr. Ralph Freedman of the University of Texas M.D. Anderson Cancer Center in Houston – the only ODAC member who abstained from voting – said it was his first time doing so, and he expressed his ambivalence on the risks and benefits of the drug based on the study’s results.
Meanwhile, the issue at hand highlights the fact that the standard of care for treating older adults with AML is not clearly defined, said Dr. Sekeres. Their treatment options currently range from induction chemotherapy to aggressive supportive care, with low-dose cytarabine therapy as a middle-of-the-road therapy.
There are currently four FDA-approved first-line drugs for AML. The last drug was idarubicin, approved in 1990.
Another issue highlighted during the discussions was the available treatments for the growing aging population. The medical community is entering somewhat of an uncharted territory and such trials are important, said Dr. William Kevin Kelly, a voting member of ODAC and professor of medical oncology and urology at Thomas Jefferson University, Philadelphia who voted no.
Panelists were cleared of potential conflicts before voting on decitabine.
SILVER SPRING, MD. – The leukemia drug decitabine didn’t show robust-enough results to convince the majority of an advisory panel to support its approval by the U.S. Food and Drug Administration as a new treatment for elderly patients with acute myeloid leukemia.
Ten members of the independent Oncologic Drugs Advisory Committee (ODAC) voted no, three voted yes, and one member abstained on a question related to the proposed indication. They were asked whether decitabine (Dacogen) demonstrated a favorable risk-benefit profile for the treatment of newly diagnosed acute myeloid leukemia (AML) in patients 65 years and older who are not candidates for induction chemotherapy.
Those who voted no said they didn't find the results of a key study convincing and were not comfortable drawing any solid conclusions. The yea-sayers said they looked beyond the fact that the study didn’t meet its end point and instead erred on the side of adding another treatment choice for doctors and their patients.
The FDA considers the panel’s recommendations, but doesn’t necessarily follow them.
Drugmaker Eisai sought the drug’s approval by filing an application to the FDA in May 2011, with the goal of meeting the "unmet medical need" of older adults with AML who are not candidates for induction therapy.
Although the company’s trials didn’t reach a statistically significant result, its officials made the argument that aggregate clinical data from a randomized trial and a single-arm study showed that the drug was well tolerated, had good efficacy and safety profiles, and would provide a clinically meaningful benefit to older patients with AML who are not candidates for induction chemotherapy.
But FDA officials made the case that the "primary end point of overall survival was not met and any further analyses are expiatory and inflate the false-positive rate." They also pointed out that they defined efficacy as a statistically significant survival rate or a rigorous analysis that shows noninferiority.
AML is mainly a disease of the elderly, with an onset at the median age of 69 years. Because of poorer outcomes among this age group, one-third of patients don’t receive chemotherapy.
Decitabine, a hypomethylating agent, was FDA approved in 2006 for the treatment of myelodysplastic syndromes.
A 2009 randomized, open-label, multinational phase III trial, conducted by Eisai, enrolled 485 patients, with a median age of 73. Patients were randomized to decitabine (242) or treatment of choice (low-dose cytarabine or supportive care) (243), with the primary end point of overall survival, prespecified as a 25% reduction in mortality risk.
Patients in the decitabine arm had a median overall survival of 7.7 months, compared with 5 months in the treatment of choice group, (hazard ratio, 0.85; P = .11). A 2010 post hoc analysis showed the median overall survival was unchanged, but the difference became statistically significant (HR, 0.82; P = .037).
FDA officials argued that, "given the final analysis results, post hoc analysis results could be due to chance," adding that the false-positive rate is greater than 5%.
Eisai also conducted a phase II supportive study, which was a single-arm trial that enrolled 55 patients with a median age of 60 years or older. The efficacy and safety results were similar to those of the randomized trial. The safety profile of decitabine was comparable to that in the label for myelodysplastic syndrome, Eisai officials reported.
"Elderly patients [with AML] are desperate for new treatments," said Dr. Mikkael Sekeres, an ODAC member from the department of hematologic oncology and blood disorders at the Cleveland Clinic Taussig Cancer Institute who voted no. "Unfortunately this drug didn’t do the job."
Dr. Wyndham Wilson, ODAC chair and chief of the lymphoma therapeutics section at the National Institutes of Health, voted yes and said he looked at the totality of the data and thought that they favored its approval.
"I see it as a rare setting, where we really have no good drugs. I couldn’t get stuck on that the primary end point wasn’t met. I feel that I wanted to err on the side of choice," he said. "For me the data was sufficiently robust to approve the drug and have the choice available for physicians and patients."
Dr. Ralph Freedman of the University of Texas M.D. Anderson Cancer Center in Houston – the only ODAC member who abstained from voting – said it was his first time doing so, and he expressed his ambivalence on the risks and benefits of the drug based on the study’s results.
Meanwhile, the issue at hand highlights the fact that the standard of care for treating older adults with AML is not clearly defined, said Dr. Sekeres. Their treatment options currently range from induction chemotherapy to aggressive supportive care, with low-dose cytarabine therapy as a middle-of-the-road therapy.
There are currently four FDA-approved first-line drugs for AML. The last drug was idarubicin, approved in 1990.
Another issue highlighted during the discussions was the available treatments for the growing aging population. The medical community is entering somewhat of an uncharted territory and such trials are important, said Dr. William Kevin Kelly, a voting member of ODAC and professor of medical oncology and urology at Thomas Jefferson University, Philadelphia who voted no.
Panelists were cleared of potential conflicts before voting on decitabine.
SILVER SPRING, MD. – The leukemia drug decitabine didn’t show robust-enough results to convince the majority of an advisory panel to support its approval by the U.S. Food and Drug Administration as a new treatment for elderly patients with acute myeloid leukemia.
Ten members of the independent Oncologic Drugs Advisory Committee (ODAC) voted no, three voted yes, and one member abstained on a question related to the proposed indication. They were asked whether decitabine (Dacogen) demonstrated a favorable risk-benefit profile for the treatment of newly diagnosed acute myeloid leukemia (AML) in patients 65 years and older who are not candidates for induction chemotherapy.
Those who voted no said they didn't find the results of a key study convincing and were not comfortable drawing any solid conclusions. The yea-sayers said they looked beyond the fact that the study didn’t meet its end point and instead erred on the side of adding another treatment choice for doctors and their patients.
The FDA considers the panel’s recommendations, but doesn’t necessarily follow them.
Drugmaker Eisai sought the drug’s approval by filing an application to the FDA in May 2011, with the goal of meeting the "unmet medical need" of older adults with AML who are not candidates for induction therapy.
Although the company’s trials didn’t reach a statistically significant result, its officials made the argument that aggregate clinical data from a randomized trial and a single-arm study showed that the drug was well tolerated, had good efficacy and safety profiles, and would provide a clinically meaningful benefit to older patients with AML who are not candidates for induction chemotherapy.
But FDA officials made the case that the "primary end point of overall survival was not met and any further analyses are expiatory and inflate the false-positive rate." They also pointed out that they defined efficacy as a statistically significant survival rate or a rigorous analysis that shows noninferiority.
AML is mainly a disease of the elderly, with an onset at the median age of 69 years. Because of poorer outcomes among this age group, one-third of patients don’t receive chemotherapy.
Decitabine, a hypomethylating agent, was FDA approved in 2006 for the treatment of myelodysplastic syndromes.
A 2009 randomized, open-label, multinational phase III trial, conducted by Eisai, enrolled 485 patients, with a median age of 73. Patients were randomized to decitabine (242) or treatment of choice (low-dose cytarabine or supportive care) (243), with the primary end point of overall survival, prespecified as a 25% reduction in mortality risk.
Patients in the decitabine arm had a median overall survival of 7.7 months, compared with 5 months in the treatment of choice group, (hazard ratio, 0.85; P = .11). A 2010 post hoc analysis showed the median overall survival was unchanged, but the difference became statistically significant (HR, 0.82; P = .037).
FDA officials argued that, "given the final analysis results, post hoc analysis results could be due to chance," adding that the false-positive rate is greater than 5%.
Eisai also conducted a phase II supportive study, which was a single-arm trial that enrolled 55 patients with a median age of 60 years or older. The efficacy and safety results were similar to those of the randomized trial. The safety profile of decitabine was comparable to that in the label for myelodysplastic syndrome, Eisai officials reported.
"Elderly patients [with AML] are desperate for new treatments," said Dr. Mikkael Sekeres, an ODAC member from the department of hematologic oncology and blood disorders at the Cleveland Clinic Taussig Cancer Institute who voted no. "Unfortunately this drug didn’t do the job."
Dr. Wyndham Wilson, ODAC chair and chief of the lymphoma therapeutics section at the National Institutes of Health, voted yes and said he looked at the totality of the data and thought that they favored its approval.
"I see it as a rare setting, where we really have no good drugs. I couldn’t get stuck on that the primary end point wasn’t met. I feel that I wanted to err on the side of choice," he said. "For me the data was sufficiently robust to approve the drug and have the choice available for physicians and patients."
Dr. Ralph Freedman of the University of Texas M.D. Anderson Cancer Center in Houston – the only ODAC member who abstained from voting – said it was his first time doing so, and he expressed his ambivalence on the risks and benefits of the drug based on the study’s results.
Meanwhile, the issue at hand highlights the fact that the standard of care for treating older adults with AML is not clearly defined, said Dr. Sekeres. Their treatment options currently range from induction chemotherapy to aggressive supportive care, with low-dose cytarabine therapy as a middle-of-the-road therapy.
There are currently four FDA-approved first-line drugs for AML. The last drug was idarubicin, approved in 1990.
Another issue highlighted during the discussions was the available treatments for the growing aging population. The medical community is entering somewhat of an uncharted territory and such trials are important, said Dr. William Kevin Kelly, a voting member of ODAC and professor of medical oncology and urology at Thomas Jefferson University, Philadelphia who voted no.
Panelists were cleared of potential conflicts before voting on decitabine.
FROM A MEETING OF THE FOOD AND DRUG ADMINISTRATION'S ONCOLOGIC DRUGS ADVISORY COMMITTEE
New Studies Show Increased MI, ACS Risks in Dabigatran Patients
A pair of new studies suggest that dabigatran etexilate (Pradaxa), the first new oral anticoagulant approved in 56 years, increases the risk of myocardial infarction (MI) and acute coronary syndrome (ACS) in patients. But the author of one of the reports says the drug's benefits may be worth the risks.
"Yes, there's an increase, but that tends to be the headline," says Ken Uchino, MD, FAHA, program director of the Vascular Neurology Fellowship at the Cleveland Clinic's Cerebrovascular Center. "We have to think about the benefits and the risk balance. So far, it is favorable."
Dr. Uchino and a colleague's meta-analysis, "Dabigatran Association with Higher Risk of Acute Coronary Events," was published last month on the Archives of Internal Medicine's website. The report found dabigatran, which was approved last year, was significantly associated with a higher risk of MI or ACS when measured against multiple control groups.
A separate study, "Myocardial Ischemic Events in Patients with Atrial Fibrillation Treated with Dabigatran or Warfarin in the RE-LY Trial," published on Circulation's website, reported a nonsignificant increase in MI with dabigatran compared with warfarin, but other myocardial ischemic events were not increased.
Both reports come as the FDA evaluates post-marketing reports of serious bleeds in patients taking the drug.
Dr. Uchino believes that, taken together, the two studies are important, but more research would need to be completed to sway public opinion on whether dabigatran and other new anticoagulation therapies can unseat warfarin as the go-to treatment.
"Warfarin is such a cumbersome medication, we have all been waiting for a new medication," he adds. "So there are clear advantages to dabigatran and other newer anticoagulants. ... Our study puts us at a caution, but we should continue to gather data and continue to assess risk and benefits."
A pair of new studies suggest that dabigatran etexilate (Pradaxa), the first new oral anticoagulant approved in 56 years, increases the risk of myocardial infarction (MI) and acute coronary syndrome (ACS) in patients. But the author of one of the reports says the drug's benefits may be worth the risks.
"Yes, there's an increase, but that tends to be the headline," says Ken Uchino, MD, FAHA, program director of the Vascular Neurology Fellowship at the Cleveland Clinic's Cerebrovascular Center. "We have to think about the benefits and the risk balance. So far, it is favorable."
Dr. Uchino and a colleague's meta-analysis, "Dabigatran Association with Higher Risk of Acute Coronary Events," was published last month on the Archives of Internal Medicine's website. The report found dabigatran, which was approved last year, was significantly associated with a higher risk of MI or ACS when measured against multiple control groups.
A separate study, "Myocardial Ischemic Events in Patients with Atrial Fibrillation Treated with Dabigatran or Warfarin in the RE-LY Trial," published on Circulation's website, reported a nonsignificant increase in MI with dabigatran compared with warfarin, but other myocardial ischemic events were not increased.
Both reports come as the FDA evaluates post-marketing reports of serious bleeds in patients taking the drug.
Dr. Uchino believes that, taken together, the two studies are important, but more research would need to be completed to sway public opinion on whether dabigatran and other new anticoagulation therapies can unseat warfarin as the go-to treatment.
"Warfarin is such a cumbersome medication, we have all been waiting for a new medication," he adds. "So there are clear advantages to dabigatran and other newer anticoagulants. ... Our study puts us at a caution, but we should continue to gather data and continue to assess risk and benefits."
A pair of new studies suggest that dabigatran etexilate (Pradaxa), the first new oral anticoagulant approved in 56 years, increases the risk of myocardial infarction (MI) and acute coronary syndrome (ACS) in patients. But the author of one of the reports says the drug's benefits may be worth the risks.
"Yes, there's an increase, but that tends to be the headline," says Ken Uchino, MD, FAHA, program director of the Vascular Neurology Fellowship at the Cleveland Clinic's Cerebrovascular Center. "We have to think about the benefits and the risk balance. So far, it is favorable."
Dr. Uchino and a colleague's meta-analysis, "Dabigatran Association with Higher Risk of Acute Coronary Events," was published last month on the Archives of Internal Medicine's website. The report found dabigatran, which was approved last year, was significantly associated with a higher risk of MI or ACS when measured against multiple control groups.
A separate study, "Myocardial Ischemic Events in Patients with Atrial Fibrillation Treated with Dabigatran or Warfarin in the RE-LY Trial," published on Circulation's website, reported a nonsignificant increase in MI with dabigatran compared with warfarin, but other myocardial ischemic events were not increased.
Both reports come as the FDA evaluates post-marketing reports of serious bleeds in patients taking the drug.
Dr. Uchino believes that, taken together, the two studies are important, but more research would need to be completed to sway public opinion on whether dabigatran and other new anticoagulation therapies can unseat warfarin as the go-to treatment.
"Warfarin is such a cumbersome medication, we have all been waiting for a new medication," he adds. "So there are clear advantages to dabigatran and other newer anticoagulants. ... Our study puts us at a caution, but we should continue to gather data and continue to assess risk and benefits."
In the Literature: Research You Need to Know
Clinical question: What is the relationship between well-being and demographic factors, educational debt, and medical knowledge in internal-medicine residents?
Background: Physician distress during training is common and can negatively impact patient care. There has never been a study of internal-medicine residents nationally that examined the patterns of distress across demographic factors or the association of these factors with medical knowledge.
Study design: Cross-sectional study.
Setting: U.S. internal-medicine residency programs.
Synopsis: Of the 21,208 U.S. internal-medicine residents who completed the 2008 in-training examination, 77.3% had both survey and demographic data available for analysis. Nearly 15% of these 16,394 residents rated quality of life “as bad as it can be” or “somewhat bad,” and 32.9% felt somewhat or very dissatisfied with work-life balance.
Overall burnout, high levels of weekly emotional exhaustion, and weekly depersonalization were reported by 51.5%, 45.8%, and 28.9% of residents, respectively. Symptoms of emotional exhaustion decreased as training increased, while depersonalization increased after the first postgraduate year. Residents reporting quality of life “as bad as it can be,” emotional exhaustion, or debt greater than $200,000 had mean exam scores 2.7, 4.2, and 5 points, respectively, lower than others surveyed.
Although unlikely given the study design, nonresponse bias could affect these results. Not all demographic variables or domains of well-being were studied, and self-reported educational debt could have been misclassified. Nonetheless, findings suggest that distress remains among residents despite the changes made to duty-hour regulations in 2003.
Bottom line: Suboptimal quality of life and burnout were common among internal-medicine residents nationally; symptoms of burnout were associated with higher debt and lower exam scores.
Citation: West CP, Shanafelt TD, Kolars JC. Quality of life, burnout, educational debt, and medical knowledge among internal medicine residents. JAMA. 2011;306:952-960.
Visit our website for more physician reviews of HM-related research.
Clinical question: What is the relationship between well-being and demographic factors, educational debt, and medical knowledge in internal-medicine residents?
Background: Physician distress during training is common and can negatively impact patient care. There has never been a study of internal-medicine residents nationally that examined the patterns of distress across demographic factors or the association of these factors with medical knowledge.
Study design: Cross-sectional study.
Setting: U.S. internal-medicine residency programs.
Synopsis: Of the 21,208 U.S. internal-medicine residents who completed the 2008 in-training examination, 77.3% had both survey and demographic data available for analysis. Nearly 15% of these 16,394 residents rated quality of life “as bad as it can be” or “somewhat bad,” and 32.9% felt somewhat or very dissatisfied with work-life balance.
Overall burnout, high levels of weekly emotional exhaustion, and weekly depersonalization were reported by 51.5%, 45.8%, and 28.9% of residents, respectively. Symptoms of emotional exhaustion decreased as training increased, while depersonalization increased after the first postgraduate year. Residents reporting quality of life “as bad as it can be,” emotional exhaustion, or debt greater than $200,000 had mean exam scores 2.7, 4.2, and 5 points, respectively, lower than others surveyed.
Although unlikely given the study design, nonresponse bias could affect these results. Not all demographic variables or domains of well-being were studied, and self-reported educational debt could have been misclassified. Nonetheless, findings suggest that distress remains among residents despite the changes made to duty-hour regulations in 2003.
Bottom line: Suboptimal quality of life and burnout were common among internal-medicine residents nationally; symptoms of burnout were associated with higher debt and lower exam scores.
Citation: West CP, Shanafelt TD, Kolars JC. Quality of life, burnout, educational debt, and medical knowledge among internal medicine residents. JAMA. 2011;306:952-960.
Visit our website for more physician reviews of HM-related research.
Clinical question: What is the relationship between well-being and demographic factors, educational debt, and medical knowledge in internal-medicine residents?
Background: Physician distress during training is common and can negatively impact patient care. There has never been a study of internal-medicine residents nationally that examined the patterns of distress across demographic factors or the association of these factors with medical knowledge.
Study design: Cross-sectional study.
Setting: U.S. internal-medicine residency programs.
Synopsis: Of the 21,208 U.S. internal-medicine residents who completed the 2008 in-training examination, 77.3% had both survey and demographic data available for analysis. Nearly 15% of these 16,394 residents rated quality of life “as bad as it can be” or “somewhat bad,” and 32.9% felt somewhat or very dissatisfied with work-life balance.
Overall burnout, high levels of weekly emotional exhaustion, and weekly depersonalization were reported by 51.5%, 45.8%, and 28.9% of residents, respectively. Symptoms of emotional exhaustion decreased as training increased, while depersonalization increased after the first postgraduate year. Residents reporting quality of life “as bad as it can be,” emotional exhaustion, or debt greater than $200,000 had mean exam scores 2.7, 4.2, and 5 points, respectively, lower than others surveyed.
Although unlikely given the study design, nonresponse bias could affect these results. Not all demographic variables or domains of well-being were studied, and self-reported educational debt could have been misclassified. Nonetheless, findings suggest that distress remains among residents despite the changes made to duty-hour regulations in 2003.
Bottom line: Suboptimal quality of life and burnout were common among internal-medicine residents nationally; symptoms of burnout were associated with higher debt and lower exam scores.
Citation: West CP, Shanafelt TD, Kolars JC. Quality of life, burnout, educational debt, and medical knowledge among internal medicine residents. JAMA. 2011;306:952-960.
Visit our website for more physician reviews of HM-related research.
The EHR Report Podcast: Integrated Smartphones and EHRs
Welcome to the EHR Report Podcast!

In this edition of the EHR Report Podcast, Dr. Neil Skolnik and Dr. Chris Notte take a look at how handheld devices such as smartphones, tablets, and PDAs can fit into an EHR system.
To download this podcast, click here.
To listen via this Web page, click on the player below:
Welcome to the EHR Report Podcast!
In this edition of the EHR Report Podcast, Dr. Neil Skolnik and Dr. Chris Notte take a look at how handheld devices such as smartphones, tablets, and PDAs can fit into an EHR system.
To download this podcast, click here.
To listen via this Web page, click on the player below:
Welcome to the EHR Report Podcast!
In this edition of the EHR Report Podcast, Dr. Neil Skolnik and Dr. Chris Notte take a look at how handheld devices such as smartphones, tablets, and PDAs can fit into an EHR system.
To download this podcast, click here.
To listen via this Web page, click on the player below:
Join Team Hospitalist
Team Hospitalist is the only reader-involvement program of its kind in hospital medicine. The 12-member advisory panel provides invaluable information about the current state of hospital medicine, including the daily issues facing hospitalists, group leaders, and their patients. Team members offer ideas for articles, assist writers with contacts and expert sources, and participate in monthly conference calls to discuss new ideas.
The team will seat new members for tw0-year terms at HM12 in San Diego, April 1-4. Team members must be an SHM member in good standing and be able to attend SHM's annual meetings. To apply, email the editors your CV and a letter of interest no later than Feb. 15, 2012.
Team Hospitalist is the only reader-involvement program of its kind in hospital medicine. The 12-member advisory panel provides invaluable information about the current state of hospital medicine, including the daily issues facing hospitalists, group leaders, and their patients. Team members offer ideas for articles, assist writers with contacts and expert sources, and participate in monthly conference calls to discuss new ideas.
The team will seat new members for tw0-year terms at HM12 in San Diego, April 1-4. Team members must be an SHM member in good standing and be able to attend SHM's annual meetings. To apply, email the editors your CV and a letter of interest no later than Feb. 15, 2012.
Team Hospitalist is the only reader-involvement program of its kind in hospital medicine. The 12-member advisory panel provides invaluable information about the current state of hospital medicine, including the daily issues facing hospitalists, group leaders, and their patients. Team members offer ideas for articles, assist writers with contacts and expert sources, and participate in monthly conference calls to discuss new ideas.
The team will seat new members for tw0-year terms at HM12 in San Diego, April 1-4. Team members must be an SHM member in good standing and be able to attend SHM's annual meetings. To apply, email the editors your CV and a letter of interest no later than Feb. 15, 2012.
ONLINE EXCLUSIVE: Med-Peds Physicians Make their Mark
Every day in the life of an internist and pediatrician, clinical questions arise. For HM practitioners, treating patients with chronic illnesses who are also on the cusp of adulthood presents a new set of challenges.
That’s when physicians trained in both internal medicine and pediatrics (med-peds) can lend their expertise. Once a physician successfully completes a four-year combined med-peds residency program, he or she may take the board certification exams in both internal medicine and pediatrics. Med-peds programs are now accredited by the Accreditation Council for Graduate Medical Education (ACGME) as a combined program instead of separate accreditation in internal medicine and pediatrics.
“The best solution would be to have more med-peds specialists as hospitalists,” says Moises Auron, MD, an assistant professor of medicine and pediatrics at Cleveland Clinic. They “can facilitate the transition by identifying these patients and providing an increased sensibility to the pediatric provider to ‘let the patient go’ and to open new insights to the adult providers to welcome those patients,” he says.
Broad-Based Training
—Moises Auron, MD, assistant professor of medicine and pediatrics, Cleveland Clinic
A med-peds physician can care for people of all ages—from newborns to geriatric patients. He or she is prepared for the demands of private practice, academic medicine, hospitalist programs, and fellowships, according to the National Med-Peds Residents’ Association.
While med-peds residency offers exceptional training for primary care, it also leaves open the option of pursuing a subspecialty in either internal medicine or pediatrics, or both. Subspecialties include cardiology, infectious disease, pulmonary/critical care, women’s health, and sports medicine.
Med-peds celebrated its 40th anniversary as a formal training option in 2007. There are currently about 1,400 med-peds residents in training and about 6,300 med-peds physicians in practice, according to the American Academy of Pediatrics’ section on med-peds.
This broad-based training helps ensure smoother transitions of care. “It’s incumbent upon adult physicians to make the pediatric physicians aware of what services they offer, and also for the pediatricians to reach out with specific patients and refer them to adult physicians,” says W. Benjamin Rothwell, MD, associate program director of the med-peds residency at Tulane University School of Medicine in New Orleans.
Susan Kreimer is a freelance medical writer based in New York.
Every day in the life of an internist and pediatrician, clinical questions arise. For HM practitioners, treating patients with chronic illnesses who are also on the cusp of adulthood presents a new set of challenges.
That’s when physicians trained in both internal medicine and pediatrics (med-peds) can lend their expertise. Once a physician successfully completes a four-year combined med-peds residency program, he or she may take the board certification exams in both internal medicine and pediatrics. Med-peds programs are now accredited by the Accreditation Council for Graduate Medical Education (ACGME) as a combined program instead of separate accreditation in internal medicine and pediatrics.
“The best solution would be to have more med-peds specialists as hospitalists,” says Moises Auron, MD, an assistant professor of medicine and pediatrics at Cleveland Clinic. They “can facilitate the transition by identifying these patients and providing an increased sensibility to the pediatric provider to ‘let the patient go’ and to open new insights to the adult providers to welcome those patients,” he says.
Broad-Based Training
—Moises Auron, MD, assistant professor of medicine and pediatrics, Cleveland Clinic
A med-peds physician can care for people of all ages—from newborns to geriatric patients. He or she is prepared for the demands of private practice, academic medicine, hospitalist programs, and fellowships, according to the National Med-Peds Residents’ Association.
While med-peds residency offers exceptional training for primary care, it also leaves open the option of pursuing a subspecialty in either internal medicine or pediatrics, or both. Subspecialties include cardiology, infectious disease, pulmonary/critical care, women’s health, and sports medicine.
Med-peds celebrated its 40th anniversary as a formal training option in 2007. There are currently about 1,400 med-peds residents in training and about 6,300 med-peds physicians in practice, according to the American Academy of Pediatrics’ section on med-peds.
This broad-based training helps ensure smoother transitions of care. “It’s incumbent upon adult physicians to make the pediatric physicians aware of what services they offer, and also for the pediatricians to reach out with specific patients and refer them to adult physicians,” says W. Benjamin Rothwell, MD, associate program director of the med-peds residency at Tulane University School of Medicine in New Orleans.
Susan Kreimer is a freelance medical writer based in New York.
Every day in the life of an internist and pediatrician, clinical questions arise. For HM practitioners, treating patients with chronic illnesses who are also on the cusp of adulthood presents a new set of challenges.
That’s when physicians trained in both internal medicine and pediatrics (med-peds) can lend their expertise. Once a physician successfully completes a four-year combined med-peds residency program, he or she may take the board certification exams in both internal medicine and pediatrics. Med-peds programs are now accredited by the Accreditation Council for Graduate Medical Education (ACGME) as a combined program instead of separate accreditation in internal medicine and pediatrics.
“The best solution would be to have more med-peds specialists as hospitalists,” says Moises Auron, MD, an assistant professor of medicine and pediatrics at Cleveland Clinic. They “can facilitate the transition by identifying these patients and providing an increased sensibility to the pediatric provider to ‘let the patient go’ and to open new insights to the adult providers to welcome those patients,” he says.
Broad-Based Training
—Moises Auron, MD, assistant professor of medicine and pediatrics, Cleveland Clinic
A med-peds physician can care for people of all ages—from newborns to geriatric patients. He or she is prepared for the demands of private practice, academic medicine, hospitalist programs, and fellowships, according to the National Med-Peds Residents’ Association.
While med-peds residency offers exceptional training for primary care, it also leaves open the option of pursuing a subspecialty in either internal medicine or pediatrics, or both. Subspecialties include cardiology, infectious disease, pulmonary/critical care, women’s health, and sports medicine.
Med-peds celebrated its 40th anniversary as a formal training option in 2007. There are currently about 1,400 med-peds residents in training and about 6,300 med-peds physicians in practice, according to the American Academy of Pediatrics’ section on med-peds.
This broad-based training helps ensure smoother transitions of care. “It’s incumbent upon adult physicians to make the pediatric physicians aware of what services they offer, and also for the pediatricians to reach out with specific patients and refer them to adult physicians,” says W. Benjamin Rothwell, MD, associate program director of the med-peds residency at Tulane University School of Medicine in New Orleans.
Susan Kreimer is a freelance medical writer based in New York.
ONLINE EXCLUSIVE: Shifting Strategies Can Make Physician Workloads Manageable
As hospitalists have learned, sometimes a workload problem is related to how that work is apportioned. The trick is to devise a solution that’s good for patients, doctors, and the hospital.
Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company, has long advocated changing from a shift-based model to a more full-time model that expands the number of days worked per month. Although the concept has faced resistance from many rank-and-file hospitalists, Dr. Singer argues that the latter model means that more staff will be available to care for patients on any given day, leading to a lower and more manageable average census. Dr. Singer concedes that switching to a full-time model can be a “painful process,” but it’s one that has led to improved patient outcomes, higher revenues, and more sustainable workloads.
John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., agrees that titrating the same annual workload over more shifts is desirable. “If you work a small number of days in a year, then every day you work, you’re going to get smacked,” says Dr. Nelson, co-founder of SHM and longtime practice management columnist for The Hospitalist. “It’s going to be hard. And that’s just not smart. It’s not a good idea.”
—John Nelson, MD, MHM, FACP, medical director of the hospitalist practice, Overlake Hospital Medical Center, Bellevue, Wash., SHM co-founder
Dr. Nelson worries that a straightforward, Monday-to-Friday model with periodic weekend responsibilities, though, can be disruptive to doctor-patient continuity. Another strategy, he says, is to take each doctor’s workload preferences into account when devising a practice’s schedule, with compensation distributed accordingly. At one practice in the Pacific Northwest, for example, the hospitalists all decided they wanted to work about half as much as they were. Their pay dropped accordingly, Dr. Nelson says, providing the necessary funds for hiring new doctors to pick up the slack.
Bryn Nelson is a freelance medical journalist in Seattle.
As hospitalists have learned, sometimes a workload problem is related to how that work is apportioned. The trick is to devise a solution that’s good for patients, doctors, and the hospital.
Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company, has long advocated changing from a shift-based model to a more full-time model that expands the number of days worked per month. Although the concept has faced resistance from many rank-and-file hospitalists, Dr. Singer argues that the latter model means that more staff will be available to care for patients on any given day, leading to a lower and more manageable average census. Dr. Singer concedes that switching to a full-time model can be a “painful process,” but it’s one that has led to improved patient outcomes, higher revenues, and more sustainable workloads.
John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., agrees that titrating the same annual workload over more shifts is desirable. “If you work a small number of days in a year, then every day you work, you’re going to get smacked,” says Dr. Nelson, co-founder of SHM and longtime practice management columnist for The Hospitalist. “It’s going to be hard. And that’s just not smart. It’s not a good idea.”
—John Nelson, MD, MHM, FACP, medical director of the hospitalist practice, Overlake Hospital Medical Center, Bellevue, Wash., SHM co-founder
Dr. Nelson worries that a straightforward, Monday-to-Friday model with periodic weekend responsibilities, though, can be disruptive to doctor-patient continuity. Another strategy, he says, is to take each doctor’s workload preferences into account when devising a practice’s schedule, with compensation distributed accordingly. At one practice in the Pacific Northwest, for example, the hospitalists all decided they wanted to work about half as much as they were. Their pay dropped accordingly, Dr. Nelson says, providing the necessary funds for hiring new doctors to pick up the slack.
Bryn Nelson is a freelance medical journalist in Seattle.
As hospitalists have learned, sometimes a workload problem is related to how that work is apportioned. The trick is to devise a solution that’s good for patients, doctors, and the hospital.
Adam Singer, MD, CEO of North Hollywood, Calif.-based IPC: The Hospitalist Company, has long advocated changing from a shift-based model to a more full-time model that expands the number of days worked per month. Although the concept has faced resistance from many rank-and-file hospitalists, Dr. Singer argues that the latter model means that more staff will be available to care for patients on any given day, leading to a lower and more manageable average census. Dr. Singer concedes that switching to a full-time model can be a “painful process,” but it’s one that has led to improved patient outcomes, higher revenues, and more sustainable workloads.
John Nelson, MD, MHM, FACP, medical director of the hospitalist practice at Overlake Hospital Medical Center in Bellevue, Wash., agrees that titrating the same annual workload over more shifts is desirable. “If you work a small number of days in a year, then every day you work, you’re going to get smacked,” says Dr. Nelson, co-founder of SHM and longtime practice management columnist for The Hospitalist. “It’s going to be hard. And that’s just not smart. It’s not a good idea.”
—John Nelson, MD, MHM, FACP, medical director of the hospitalist practice, Overlake Hospital Medical Center, Bellevue, Wash., SHM co-founder
Dr. Nelson worries that a straightforward, Monday-to-Friday model with periodic weekend responsibilities, though, can be disruptive to doctor-patient continuity. Another strategy, he says, is to take each doctor’s workload preferences into account when devising a practice’s schedule, with compensation distributed accordingly. At one practice in the Pacific Northwest, for example, the hospitalists all decided they wanted to work about half as much as they were. Their pay dropped accordingly, Dr. Nelson says, providing the necessary funds for hiring new doctors to pick up the slack.
Bryn Nelson is a freelance medical journalist in Seattle.