User login
To MU or not to MU, that is the question
If you are still on the fence on meaningful use – our government’s motivational strategy for popularizing electronic health records – the point of no return is rapidly approaching: If you want to qualify for at least a portion of the incentive money, plus avoid a 1% penalty (eventually rising to 5%) on your Medicare Part B reimbursements, this year is your final opportunity to join the party. And, unfortunately, it is not simply a matter of adopting an electronic record system.
Each year, you must attest to demonstrating "meaningful use" (MU) of that system. To do that, you must continually monitor your progress toward meeting the necessary percentage benchmarks, making course corrections as you go. If the numbers are not there when your practice is ready to attest, it will have all been for naught, and a major waste of time and resources.
That being the case, private practitioners who have not yet taken the plunge – and those who have, but are undecided on progressing to stage 2 – must ask themselves whether the significant temporal and monetary investment is worth the trouble.
Many, apparently, have decided that it is not. While a substantial percentage of eligible practitioners signed up for stage 1, approximately 20% of them stopped participating in 2013. And according to the Centers for Medicare & Medicaid Services’ own data, only 4 hospitals and 50 individual practitioners in the entire country had attested to stage 2 through March of 2014.
The American Medical Association has little faith in the program, at least in its current form. In an open letter to the CMS in May 2014, they predicted significantly higher dropout rates unless major modifications are made. Specifically, they singled out the requirement that providers meet all requirements at each stage. Rather than "all or nothing," they proposed a 75% achievement level to receive incentive payments, and a 50% minimum to avoid financial penalties. The AMA also recommended eliminating all benchmarks beyond physicians’ control, such as the stage 2 goal of 5% patient participation on the practice’s electronic health record (EHR) portal.
Another problem that falls outside the control of physicians is maintenance of EHR software. Nearly one EHR-equipped office in five, according to the CMS, is running software that does not meet stage 2 standards. The unfortunate owners of systems that cannot be upgraded before the stage 2 deadline will – through no fault of their own – be faced with a Morton’s fork of replacing their EHR on short notice or abandoning their quest for stage 2 attestation.
While the CMS has not yet indicated whether it has any inclination to address these issues or ease any of the requirements, one official did announce that the agency will be more flexible with its hardship exemptions on a case-by-case basis. Currently, such exemptions are available to new providers, those recovering from natural disasters, and others, such as pathologists, who do not interact face-to-face with patients.
So the question remains: Is the investment of time and resources needed to capture all of the data necessary for successful MU attestation worth making? Is it justified by the promise of MU incentive dollars and the benefits to your practice and your patients? And what exactly are those purported benefits, anyway?
Proponents maintain that integrated EHR will lead to improved documentation, which in turn should lead to improvements in patient care. Errors would be more easily identified because entries from generalists, specialists, labs, and others would be available to all at any time. All involved providers, theoretically, would be on the same page with every individual patient. The downside, of course, is that the real world seldom reflects the ideal situation envisioned by bureaucrats.
Ultimately, the choice is yours: Each private practitioner must decide whether starting (or continuing) meaningful use is worth the financial and time burden in his or her particular situation. If you are still undecided, time is almost up: You must begin your 90-day stage 1 reporting period in July 2014 in order to attest by the final deadline of October 1. The last calendar quarter to begin stage 2 reporting starts on October 1 as well. Detailed instructions for meeting stage 1 and stage 2 deadlines are available from many sources, including the American Academy of Dermatology website.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
If you are still on the fence on meaningful use – our government’s motivational strategy for popularizing electronic health records – the point of no return is rapidly approaching: If you want to qualify for at least a portion of the incentive money, plus avoid a 1% penalty (eventually rising to 5%) on your Medicare Part B reimbursements, this year is your final opportunity to join the party. And, unfortunately, it is not simply a matter of adopting an electronic record system.
Each year, you must attest to demonstrating "meaningful use" (MU) of that system. To do that, you must continually monitor your progress toward meeting the necessary percentage benchmarks, making course corrections as you go. If the numbers are not there when your practice is ready to attest, it will have all been for naught, and a major waste of time and resources.
That being the case, private practitioners who have not yet taken the plunge – and those who have, but are undecided on progressing to stage 2 – must ask themselves whether the significant temporal and monetary investment is worth the trouble.
Many, apparently, have decided that it is not. While a substantial percentage of eligible practitioners signed up for stage 1, approximately 20% of them stopped participating in 2013. And according to the Centers for Medicare & Medicaid Services’ own data, only 4 hospitals and 50 individual practitioners in the entire country had attested to stage 2 through March of 2014.
The American Medical Association has little faith in the program, at least in its current form. In an open letter to the CMS in May 2014, they predicted significantly higher dropout rates unless major modifications are made. Specifically, they singled out the requirement that providers meet all requirements at each stage. Rather than "all or nothing," they proposed a 75% achievement level to receive incentive payments, and a 50% minimum to avoid financial penalties. The AMA also recommended eliminating all benchmarks beyond physicians’ control, such as the stage 2 goal of 5% patient participation on the practice’s electronic health record (EHR) portal.
Another problem that falls outside the control of physicians is maintenance of EHR software. Nearly one EHR-equipped office in five, according to the CMS, is running software that does not meet stage 2 standards. The unfortunate owners of systems that cannot be upgraded before the stage 2 deadline will – through no fault of their own – be faced with a Morton’s fork of replacing their EHR on short notice or abandoning their quest for stage 2 attestation.
While the CMS has not yet indicated whether it has any inclination to address these issues or ease any of the requirements, one official did announce that the agency will be more flexible with its hardship exemptions on a case-by-case basis. Currently, such exemptions are available to new providers, those recovering from natural disasters, and others, such as pathologists, who do not interact face-to-face with patients.
So the question remains: Is the investment of time and resources needed to capture all of the data necessary for successful MU attestation worth making? Is it justified by the promise of MU incentive dollars and the benefits to your practice and your patients? And what exactly are those purported benefits, anyway?
Proponents maintain that integrated EHR will lead to improved documentation, which in turn should lead to improvements in patient care. Errors would be more easily identified because entries from generalists, specialists, labs, and others would be available to all at any time. All involved providers, theoretically, would be on the same page with every individual patient. The downside, of course, is that the real world seldom reflects the ideal situation envisioned by bureaucrats.
Ultimately, the choice is yours: Each private practitioner must decide whether starting (or continuing) meaningful use is worth the financial and time burden in his or her particular situation. If you are still undecided, time is almost up: You must begin your 90-day stage 1 reporting period in July 2014 in order to attest by the final deadline of October 1. The last calendar quarter to begin stage 2 reporting starts on October 1 as well. Detailed instructions for meeting stage 1 and stage 2 deadlines are available from many sources, including the American Academy of Dermatology website.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.
If you are still on the fence on meaningful use – our government’s motivational strategy for popularizing electronic health records – the point of no return is rapidly approaching: If you want to qualify for at least a portion of the incentive money, plus avoid a 1% penalty (eventually rising to 5%) on your Medicare Part B reimbursements, this year is your final opportunity to join the party. And, unfortunately, it is not simply a matter of adopting an electronic record system.
Each year, you must attest to demonstrating "meaningful use" (MU) of that system. To do that, you must continually monitor your progress toward meeting the necessary percentage benchmarks, making course corrections as you go. If the numbers are not there when your practice is ready to attest, it will have all been for naught, and a major waste of time and resources.
That being the case, private practitioners who have not yet taken the plunge – and those who have, but are undecided on progressing to stage 2 – must ask themselves whether the significant temporal and monetary investment is worth the trouble.
Many, apparently, have decided that it is not. While a substantial percentage of eligible practitioners signed up for stage 1, approximately 20% of them stopped participating in 2013. And according to the Centers for Medicare & Medicaid Services’ own data, only 4 hospitals and 50 individual practitioners in the entire country had attested to stage 2 through March of 2014.
The American Medical Association has little faith in the program, at least in its current form. In an open letter to the CMS in May 2014, they predicted significantly higher dropout rates unless major modifications are made. Specifically, they singled out the requirement that providers meet all requirements at each stage. Rather than "all or nothing," they proposed a 75% achievement level to receive incentive payments, and a 50% minimum to avoid financial penalties. The AMA also recommended eliminating all benchmarks beyond physicians’ control, such as the stage 2 goal of 5% patient participation on the practice’s electronic health record (EHR) portal.
Another problem that falls outside the control of physicians is maintenance of EHR software. Nearly one EHR-equipped office in five, according to the CMS, is running software that does not meet stage 2 standards. The unfortunate owners of systems that cannot be upgraded before the stage 2 deadline will – through no fault of their own – be faced with a Morton’s fork of replacing their EHR on short notice or abandoning their quest for stage 2 attestation.
While the CMS has not yet indicated whether it has any inclination to address these issues or ease any of the requirements, one official did announce that the agency will be more flexible with its hardship exemptions on a case-by-case basis. Currently, such exemptions are available to new providers, those recovering from natural disasters, and others, such as pathologists, who do not interact face-to-face with patients.
So the question remains: Is the investment of time and resources needed to capture all of the data necessary for successful MU attestation worth making? Is it justified by the promise of MU incentive dollars and the benefits to your practice and your patients? And what exactly are those purported benefits, anyway?
Proponents maintain that integrated EHR will lead to improved documentation, which in turn should lead to improvements in patient care. Errors would be more easily identified because entries from generalists, specialists, labs, and others would be available to all at any time. All involved providers, theoretically, would be on the same page with every individual patient. The downside, of course, is that the real world seldom reflects the ideal situation envisioned by bureaucrats.
Ultimately, the choice is yours: Each private practitioner must decide whether starting (or continuing) meaningful use is worth the financial and time burden in his or her particular situation. If you are still undecided, time is almost up: You must begin your 90-day stage 1 reporting period in July 2014 in order to attest by the final deadline of October 1. The last calendar quarter to begin stage 2 reporting starts on October 1 as well. Detailed instructions for meeting stage 1 and stage 2 deadlines are available from many sources, including the American Academy of Dermatology website.
Dr. Eastern practices dermatology and dermatologic surgery in Belleville, N.J. He is the author of numerous articles and textbook chapters, and is a long-time monthly columnist for Skin & Allergy News.

Cream provides relief for leg ulcers in SCD
MILAN—Results of a phase 1 study indicate that topical sodium nitrate is safe and effective for treating leg ulcers in patients with sickle cell disease (SCD).
The cream significantly decreased the size of leg ulcers overall, healed ulcers in 6 of the 18 patients studied, and reduced pain levels, seemingly independent of wound healing.
A few patients did experience short-lived burning at the treatment site, and some experienced a temporary, asymptomatic drop in blood pressure that resolved without intervention.
But the treatment was generally well-tolerated, according to study investigator Caterina P. Minniti, MD, of the National Heart, Lung and Blood Institute in Bethesda, Maryland.
She presented these results at the 19th Congress of the European Hematology Association (EHA) as abstract S663.
“The morbidity from chronic and recurrent leg ulcers in sickle cell disease and other hematologic disorders . . . remains a clinical and economic burden,” Dr Minniti noted.
“[C]urrent therapies have limited efficacy and usually are borrowed from the treatment of venous ulcers and diabetic ulcers. There isn’t really a concerted effort to treat sickle cell leg ulcers.”
With that in mind, she and her colleagues initiated a phase 1 dose-escalation trial of topical sodium nitrate in SCD patients.
Patient characteristics and treatment
The researchers enrolled 18 patients with a median age of 39 ± 12 (range, 20-59). The median number of ulcers per patient was 1.5 (range, 1-10), and the median ulcer age was 10 months (range, 2-300).
Manual assessment suggested the median ulcer size was 7.50 ± 4.65 cm2 (range, 2.09-16.50). Digital assessment suggested the median ulcer size was 5.97± 3.40 cm2 (range, 2.51-14.66).
The mean number of prior ulcer therapies was 8. This included surgical/sharp debridement (n=18), hyperbaric chamber (n=7), skin graft (n=6), MIST therapy (n=4), and oral/parenteral antibiotics (n=11).
For this study, patients had sodium nitrate cream applied twice a week for 4 weeks on 1 leg ulcer per subject. There were 5 cohorts of escalating treatment concentrations: 0.5%, 1%, 1.5%, 1.8%, and 2%.
Adverse events
There were no serious adverse events, and none of the patients discontinued treatment. One adverse event that was likely related to treatment was short-lived burning after cream application in 4 patients. But this resolved without intervention.
Another event that may have been related to treatment was asymptomatic, short-lived, diastolic blood pressure less than 50 mmHg in 5 subjects who received treatment at the highest concentrations (2 in the 2% cohort and 3 in the 1.8% cohort). On the other hand, 3 of these 5 subjects had documented diastolic blood pressure less than 50 mmHg prior to starting the treatment.
For the most part, there were no changes in laboratory or clinical parameters before and after the trial. However, the researchers did observe a significant decrease in white blood cell counts.
Effects on ulcer size
Among all patients, there was a significant decrease in ulcer size from the first treatment application to the end of the study, both according to digital photography and assessment by wound-care nurses (P<0.001 and P<0.0001, respectively).
Although patients in all of the treatment groups experienced a decrease in wound size, there was a correlation between the decrease and the concentration of treatment.
One patient in the 1%-concentration cohort had an ulcer that progressed, but all other patients saw improvements. The 4 patients who received the 1.8% concentration had a 69.7% decrease in ulcer size at week 5, and 1 ulcer had healed by the end of treatment.
The 3 patients who received the 2% concentration had an 88.3% decrease in ulcer size at week 5, and 2 ulcers had healed by that time. An additional 3 ulcers healed within weeks or months of the study end.
Effects on pain and blood flow
One of the most interesting findings of this study, according to Dr Minniti, was the effect of the cream on patients’ pain.
There was a significant decrease in patient-reported pain for treated ulcers (P<0.006) but not for untreated ulcers (P=0.38). And there was a significant correlation with pain score and nitrate concentration (P=0.006).
Patients’ weekly total usage of opioids decreased from baseline to the end of the study, but this difference was not significant (P=0.26).
“There was a trend toward significance,” Dr Minniti noted. “It’s very hard, in 1 month, to get off your long-acting opioid.”
Finally, Dr Minniti and her colleagues found that blood flow to the wound area changed before and after treatment. According to laser speckle contrast imaging, there was a significant increase in blood flow after treatment (P<0.0002).
Based on these results, the researchers have initiated a phase 1/2, randomized trial comparing topical sodium nitrate to placebo in SCD patients. ![]()
MILAN—Results of a phase 1 study indicate that topical sodium nitrate is safe and effective for treating leg ulcers in patients with sickle cell disease (SCD).
The cream significantly decreased the size of leg ulcers overall, healed ulcers in 6 of the 18 patients studied, and reduced pain levels, seemingly independent of wound healing.
A few patients did experience short-lived burning at the treatment site, and some experienced a temporary, asymptomatic drop in blood pressure that resolved without intervention.
But the treatment was generally well-tolerated, according to study investigator Caterina P. Minniti, MD, of the National Heart, Lung and Blood Institute in Bethesda, Maryland.
She presented these results at the 19th Congress of the European Hematology Association (EHA) as abstract S663.
“The morbidity from chronic and recurrent leg ulcers in sickle cell disease and other hematologic disorders . . . remains a clinical and economic burden,” Dr Minniti noted.
“[C]urrent therapies have limited efficacy and usually are borrowed from the treatment of venous ulcers and diabetic ulcers. There isn’t really a concerted effort to treat sickle cell leg ulcers.”
With that in mind, she and her colleagues initiated a phase 1 dose-escalation trial of topical sodium nitrate in SCD patients.
Patient characteristics and treatment
The researchers enrolled 18 patients with a median age of 39 ± 12 (range, 20-59). The median number of ulcers per patient was 1.5 (range, 1-10), and the median ulcer age was 10 months (range, 2-300).
Manual assessment suggested the median ulcer size was 7.50 ± 4.65 cm2 (range, 2.09-16.50). Digital assessment suggested the median ulcer size was 5.97± 3.40 cm2 (range, 2.51-14.66).
The mean number of prior ulcer therapies was 8. This included surgical/sharp debridement (n=18), hyperbaric chamber (n=7), skin graft (n=6), MIST therapy (n=4), and oral/parenteral antibiotics (n=11).
For this study, patients had sodium nitrate cream applied twice a week for 4 weeks on 1 leg ulcer per subject. There were 5 cohorts of escalating treatment concentrations: 0.5%, 1%, 1.5%, 1.8%, and 2%.
Adverse events
There were no serious adverse events, and none of the patients discontinued treatment. One adverse event that was likely related to treatment was short-lived burning after cream application in 4 patients. But this resolved without intervention.
Another event that may have been related to treatment was asymptomatic, short-lived, diastolic blood pressure less than 50 mmHg in 5 subjects who received treatment at the highest concentrations (2 in the 2% cohort and 3 in the 1.8% cohort). On the other hand, 3 of these 5 subjects had documented diastolic blood pressure less than 50 mmHg prior to starting the treatment.
For the most part, there were no changes in laboratory or clinical parameters before and after the trial. However, the researchers did observe a significant decrease in white blood cell counts.
Effects on ulcer size
Among all patients, there was a significant decrease in ulcer size from the first treatment application to the end of the study, both according to digital photography and assessment by wound-care nurses (P<0.001 and P<0.0001, respectively).
Although patients in all of the treatment groups experienced a decrease in wound size, there was a correlation between the decrease and the concentration of treatment.
One patient in the 1%-concentration cohort had an ulcer that progressed, but all other patients saw improvements. The 4 patients who received the 1.8% concentration had a 69.7% decrease in ulcer size at week 5, and 1 ulcer had healed by the end of treatment.
The 3 patients who received the 2% concentration had an 88.3% decrease in ulcer size at week 5, and 2 ulcers had healed by that time. An additional 3 ulcers healed within weeks or months of the study end.
Effects on pain and blood flow
One of the most interesting findings of this study, according to Dr Minniti, was the effect of the cream on patients’ pain.
There was a significant decrease in patient-reported pain for treated ulcers (P<0.006) but not for untreated ulcers (P=0.38). And there was a significant correlation with pain score and nitrate concentration (P=0.006).
Patients’ weekly total usage of opioids decreased from baseline to the end of the study, but this difference was not significant (P=0.26).
“There was a trend toward significance,” Dr Minniti noted. “It’s very hard, in 1 month, to get off your long-acting opioid.”
Finally, Dr Minniti and her colleagues found that blood flow to the wound area changed before and after treatment. According to laser speckle contrast imaging, there was a significant increase in blood flow after treatment (P<0.0002).
Based on these results, the researchers have initiated a phase 1/2, randomized trial comparing topical sodium nitrate to placebo in SCD patients. ![]()
MILAN—Results of a phase 1 study indicate that topical sodium nitrate is safe and effective for treating leg ulcers in patients with sickle cell disease (SCD).
The cream significantly decreased the size of leg ulcers overall, healed ulcers in 6 of the 18 patients studied, and reduced pain levels, seemingly independent of wound healing.
A few patients did experience short-lived burning at the treatment site, and some experienced a temporary, asymptomatic drop in blood pressure that resolved without intervention.
But the treatment was generally well-tolerated, according to study investigator Caterina P. Minniti, MD, of the National Heart, Lung and Blood Institute in Bethesda, Maryland.
She presented these results at the 19th Congress of the European Hematology Association (EHA) as abstract S663.
“The morbidity from chronic and recurrent leg ulcers in sickle cell disease and other hematologic disorders . . . remains a clinical and economic burden,” Dr Minniti noted.
“[C]urrent therapies have limited efficacy and usually are borrowed from the treatment of venous ulcers and diabetic ulcers. There isn’t really a concerted effort to treat sickle cell leg ulcers.”
With that in mind, she and her colleagues initiated a phase 1 dose-escalation trial of topical sodium nitrate in SCD patients.
Patient characteristics and treatment
The researchers enrolled 18 patients with a median age of 39 ± 12 (range, 20-59). The median number of ulcers per patient was 1.5 (range, 1-10), and the median ulcer age was 10 months (range, 2-300).
Manual assessment suggested the median ulcer size was 7.50 ± 4.65 cm2 (range, 2.09-16.50). Digital assessment suggested the median ulcer size was 5.97± 3.40 cm2 (range, 2.51-14.66).
The mean number of prior ulcer therapies was 8. This included surgical/sharp debridement (n=18), hyperbaric chamber (n=7), skin graft (n=6), MIST therapy (n=4), and oral/parenteral antibiotics (n=11).
For this study, patients had sodium nitrate cream applied twice a week for 4 weeks on 1 leg ulcer per subject. There were 5 cohorts of escalating treatment concentrations: 0.5%, 1%, 1.5%, 1.8%, and 2%.
Adverse events
There were no serious adverse events, and none of the patients discontinued treatment. One adverse event that was likely related to treatment was short-lived burning after cream application in 4 patients. But this resolved without intervention.
Another event that may have been related to treatment was asymptomatic, short-lived, diastolic blood pressure less than 50 mmHg in 5 subjects who received treatment at the highest concentrations (2 in the 2% cohort and 3 in the 1.8% cohort). On the other hand, 3 of these 5 subjects had documented diastolic blood pressure less than 50 mmHg prior to starting the treatment.
For the most part, there were no changes in laboratory or clinical parameters before and after the trial. However, the researchers did observe a significant decrease in white blood cell counts.
Effects on ulcer size
Among all patients, there was a significant decrease in ulcer size from the first treatment application to the end of the study, both according to digital photography and assessment by wound-care nurses (P<0.001 and P<0.0001, respectively).
Although patients in all of the treatment groups experienced a decrease in wound size, there was a correlation between the decrease and the concentration of treatment.
One patient in the 1%-concentration cohort had an ulcer that progressed, but all other patients saw improvements. The 4 patients who received the 1.8% concentration had a 69.7% decrease in ulcer size at week 5, and 1 ulcer had healed by the end of treatment.
The 3 patients who received the 2% concentration had an 88.3% decrease in ulcer size at week 5, and 2 ulcers had healed by that time. An additional 3 ulcers healed within weeks or months of the study end.
Effects on pain and blood flow
One of the most interesting findings of this study, according to Dr Minniti, was the effect of the cream on patients’ pain.
There was a significant decrease in patient-reported pain for treated ulcers (P<0.006) but not for untreated ulcers (P=0.38). And there was a significant correlation with pain score and nitrate concentration (P=0.006).
Patients’ weekly total usage of opioids decreased from baseline to the end of the study, but this difference was not significant (P=0.26).
“There was a trend toward significance,” Dr Minniti noted. “It’s very hard, in 1 month, to get off your long-acting opioid.”
Finally, Dr Minniti and her colleagues found that blood flow to the wound area changed before and after treatment. According to laser speckle contrast imaging, there was a significant increase in blood flow after treatment (P<0.0002).
Based on these results, the researchers have initiated a phase 1/2, randomized trial comparing topical sodium nitrate to placebo in SCD patients. ![]()
US ranked last in healthcare report

Credit: NIH
In a study comparing healthcare in 11 industrialized countries, the US ranked last on measures of health system quality, efficiency, access to care, equity, and healthy lives.
The other countries included in this study were Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, and the UK.
While the results revealed room for improvement in every country, the US stood out for having the highest costs and lowest performance.
For instance, the US spent $8508 per person on healthcare in 2011, compared with $3406 in the UK, which ranked first overall.
Details on expenditures and rankings derived from this study are available in the Commonwealth Fund report, Mirror, Mirror on the Wall: How the Performance of the U.S. Health Care System Compares Internationally, 2014 Update.
“It is disappointing, but not surprising, that, despite our significant investment in healthcare, the US has continued to lag behind other countries,” said lead report author Karen Davis, of the Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland.
The report was also produced in 2004, 2006, 2007, and 2010, with the US ranking last in each of those years. Four countries were added to this year’s report: Switzerland and Sweden, which followed the UK at the top of the rankings, and Norway and France, which were in the middle of the pack.
Australia, Germany, the Netherlands, New Zealand, and Norway also placed in the middle, and Canada ranked just above the US.
In addition to ranking last overall, the US ranked last on infant mortality and on deaths that were potentially preventable with timely access to effective healthcare. The country ranked second-to-last on healthy life expectancy at age 60.
The US also ranked last on every measure of cost-related access. More than one-third (37%) of US adults reported forgoing a recommended test, treatment, or follow-up care because of cost.
With regard to healthcare quality, the US fell somewhere in the middle. On 2 of 4 measures of quality—effective care and patient-centered care—the US ranked near the top (3rd and 4th of 11 countries, respectively). But it did not perform as well with regard to providing safe or coordinated care.
The US ranked last in efficiency, due to low marks on the time and dollars spent dealing with insurance administration, lack of communication among healthcare providers, and duplicative medical testing.
Forty percent of US adults who had visited an emergency room reported they could have been treated by a regular doctor if one had been available. This is more than double the rate of patients in the UK (16%).
The US also ranked last in healthcare equity. About 4 of 10 (39%) adults with below-average incomes in the US reported a medical problem but did not visit a doctor in the past year because of costs, compared with less than 1 of 10 in the UK, Sweden, Canada, and Norway.
There were also large discrepancies in the length of time US adults waited for specialist, emergency, and after-hours care. And wait times were associated with patient income.
The data for this research were drawn from the Commonwealth Fund 2011 International Health Policy Survey of Sicker Adults, the Commonwealth Fund 2012 International Health Policy Survey of Primary Care Physicians, and the Commonwealth Fund 2013 International Health Policy Survey.
The 2011 survey targeted a representative sample of “sicker adults,” defined as those who rated their health status as fair or poor, received medical care for a serious chronic illness, serious injury, or disability in the past year, or were hospitalized or underwent surgery in the previous 2 years.
The 2012 survey looked at the experiences of primary care physicians. The 2013 survey focused on the experiences of nationally representative samples of adults ages 18 and older.
Additional data on health outcomes were drawn from the Organization for Economic Cooperation and Development and the World Health Organization. ![]()
Credit: NIH
In a study comparing healthcare in 11 industrialized countries, the US ranked last on measures of health system quality, efficiency, access to care, equity, and healthy lives.
The other countries included in this study were Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, and the UK.
While the results revealed room for improvement in every country, the US stood out for having the highest costs and lowest performance.
For instance, the US spent $8508 per person on healthcare in 2011, compared with $3406 in the UK, which ranked first overall.
Details on expenditures and rankings derived from this study are available in the Commonwealth Fund report, Mirror, Mirror on the Wall: How the Performance of the U.S. Health Care System Compares Internationally, 2014 Update.
“It is disappointing, but not surprising, that, despite our significant investment in healthcare, the US has continued to lag behind other countries,” said lead report author Karen Davis, of the Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland.
The report was also produced in 2004, 2006, 2007, and 2010, with the US ranking last in each of those years. Four countries were added to this year’s report: Switzerland and Sweden, which followed the UK at the top of the rankings, and Norway and France, which were in the middle of the pack.
Australia, Germany, the Netherlands, New Zealand, and Norway also placed in the middle, and Canada ranked just above the US.
In addition to ranking last overall, the US ranked last on infant mortality and on deaths that were potentially preventable with timely access to effective healthcare. The country ranked second-to-last on healthy life expectancy at age 60.
The US also ranked last on every measure of cost-related access. More than one-third (37%) of US adults reported forgoing a recommended test, treatment, or follow-up care because of cost.
With regard to healthcare quality, the US fell somewhere in the middle. On 2 of 4 measures of quality—effective care and patient-centered care—the US ranked near the top (3rd and 4th of 11 countries, respectively). But it did not perform as well with regard to providing safe or coordinated care.
The US ranked last in efficiency, due to low marks on the time and dollars spent dealing with insurance administration, lack of communication among healthcare providers, and duplicative medical testing.
Forty percent of US adults who had visited an emergency room reported they could have been treated by a regular doctor if one had been available. This is more than double the rate of patients in the UK (16%).
The US also ranked last in healthcare equity. About 4 of 10 (39%) adults with below-average incomes in the US reported a medical problem but did not visit a doctor in the past year because of costs, compared with less than 1 of 10 in the UK, Sweden, Canada, and Norway.
There were also large discrepancies in the length of time US adults waited for specialist, emergency, and after-hours care. And wait times were associated with patient income.
The data for this research were drawn from the Commonwealth Fund 2011 International Health Policy Survey of Sicker Adults, the Commonwealth Fund 2012 International Health Policy Survey of Primary Care Physicians, and the Commonwealth Fund 2013 International Health Policy Survey.
The 2011 survey targeted a representative sample of “sicker adults,” defined as those who rated their health status as fair or poor, received medical care for a serious chronic illness, serious injury, or disability in the past year, or were hospitalized or underwent surgery in the previous 2 years.
The 2012 survey looked at the experiences of primary care physicians. The 2013 survey focused on the experiences of nationally representative samples of adults ages 18 and older.
Additional data on health outcomes were drawn from the Organization for Economic Cooperation and Development and the World Health Organization. ![]()
Credit: NIH
In a study comparing healthcare in 11 industrialized countries, the US ranked last on measures of health system quality, efficiency, access to care, equity, and healthy lives.
The other countries included in this study were Australia, Canada, France, Germany, the Netherlands, New Zealand, Norway, Sweden, Switzerland, and the UK.
While the results revealed room for improvement in every country, the US stood out for having the highest costs and lowest performance.
For instance, the US spent $8508 per person on healthcare in 2011, compared with $3406 in the UK, which ranked first overall.
Details on expenditures and rankings derived from this study are available in the Commonwealth Fund report, Mirror, Mirror on the Wall: How the Performance of the U.S. Health Care System Compares Internationally, 2014 Update.
“It is disappointing, but not surprising, that, despite our significant investment in healthcare, the US has continued to lag behind other countries,” said lead report author Karen Davis, of the Johns Hopkins Bloomberg School of Public Health in Baltimore, Maryland.
The report was also produced in 2004, 2006, 2007, and 2010, with the US ranking last in each of those years. Four countries were added to this year’s report: Switzerland and Sweden, which followed the UK at the top of the rankings, and Norway and France, which were in the middle of the pack.
Australia, Germany, the Netherlands, New Zealand, and Norway also placed in the middle, and Canada ranked just above the US.
In addition to ranking last overall, the US ranked last on infant mortality and on deaths that were potentially preventable with timely access to effective healthcare. The country ranked second-to-last on healthy life expectancy at age 60.
The US also ranked last on every measure of cost-related access. More than one-third (37%) of US adults reported forgoing a recommended test, treatment, or follow-up care because of cost.
With regard to healthcare quality, the US fell somewhere in the middle. On 2 of 4 measures of quality—effective care and patient-centered care—the US ranked near the top (3rd and 4th of 11 countries, respectively). But it did not perform as well with regard to providing safe or coordinated care.
The US ranked last in efficiency, due to low marks on the time and dollars spent dealing with insurance administration, lack of communication among healthcare providers, and duplicative medical testing.
Forty percent of US adults who had visited an emergency room reported they could have been treated by a regular doctor if one had been available. This is more than double the rate of patients in the UK (16%).
The US also ranked last in healthcare equity. About 4 of 10 (39%) adults with below-average incomes in the US reported a medical problem but did not visit a doctor in the past year because of costs, compared with less than 1 of 10 in the UK, Sweden, Canada, and Norway.
There were also large discrepancies in the length of time US adults waited for specialist, emergency, and after-hours care. And wait times were associated with patient income.
The data for this research were drawn from the Commonwealth Fund 2011 International Health Policy Survey of Sicker Adults, the Commonwealth Fund 2012 International Health Policy Survey of Primary Care Physicians, and the Commonwealth Fund 2013 International Health Policy Survey.
The 2011 survey targeted a representative sample of “sicker adults,” defined as those who rated their health status as fair or poor, received medical care for a serious chronic illness, serious injury, or disability in the past year, or were hospitalized or underwent surgery in the previous 2 years.
The 2012 survey looked at the experiences of primary care physicians. The 2013 survey focused on the experiences of nationally representative samples of adults ages 18 and older.
Additional data on health outcomes were drawn from the Organization for Economic Cooperation and Development and the World Health Organization. ![]()
Sequential decitabine, idarubicin combo synergistic in AML

Credit: Rhoda Baer
Researchers tested 5 anti-leukemia agents in combination with the methylation inhibitor decitabine and found that the sequential combination of decitabine and idarubicin worked synergistically to produce anti-leukemia effects.
The combination induced cell death in U937, HEL, and SKM-1 human cell lines and acute myeloid leukemia (AML) cells isolated from patients.
The researchers attributed the effects to demethylation of the Wnt/β-catenin pathway inhibitors and downregulation of the Wnt/β-catenin pathway nuclear targets.
The researchers noted that decitabine monotherapy has resulted in relatively low complete remission rates in AML and myelodysplastic syndromes (MDS). So they undertook to investigate combination therapies that would potentially improve efficacy.
Hongyan Tong, PhD, of Zhejiang University School of Medicine in Hangzhou, China, and colleagues reported their findings in the Journal of Translational Medicine.
The researchers chose 5 agents to combine, either simultaneously or sequentially, with decitabine—idarubicin, daunorubicin, aclarubicin, thalidomide, and homoharringtonine—and analyzed their effect on leukemia proliferation in the various AML cell lines mentioned above.
Using the U937 cell line first, the researchers found that when decitabine was combined simulataneously or sequentially with homharringtonine, aclarubicin, thalidomide, and daunorubicin, there was no synergistic effect. The confidence interval (CI) values of various doses were almost all over 0.8.
This was also true for the simultaneous combination of decitabine with idarubicin.
However, when they combined decitabine sequentially with idarubicin, the CI values on all 5 doses were under 0.8, indicating synergism.
In addition, when they administered decitabine twice in the sequence, the CI values were lower than a single administration.
They then confirmed the results in other AML cell lines (HEL and SKM-1) and in cells from AML patients.
Next, they confirmed the synergism of the sequential combination of decitabine and idarubicin in an AML mouse model and found that the combination inhibited tumor growth.
Tumor growth was inhibited significantly on days 4 (P<0.01), days 6 -16 (P<0.001), and started to wane by day 18 (P<0.05) after treatment.
The investigators determined that apoptosis was responsible for the combination’s decrease in leukemic cell viability. The apoptosis rates with the combination therapy were significantly increased in the U937, HEL, and SKM-1 cell lines compared with controls, (all P< 0.001).
In addition, the researchers observed that the tumor cells after treatment showed typical apoptosis characteristics, such as the absence of microvilli on cell membrane, nuclear and cell membrane blebbing, chromosome condensation, and the formation of apoptotic bodies.
The investigators used microarray expression to ascertain the differential gene expression profile of decitabine and idarubicin and found that the Wnt pathway was one of the major pathways disturbed.
Sequential treatment significantly upregulated the Wnt antagonist genes SFRP1, HDPR1, and DKK3. This in turn resulted in increased expression of these genes at the mRNA and protein levels.
In addition, treatment with idarubicin after decitabine caused significant down regulation of the expression of c-Myc, β-catenin, and cyclinD1 genes compared to treatment with decitabine or idarubicin alone.
The investigators concluded that the findings suggest clinical potential in sequential administration of decitabine and idarubicin in AML and high-risk MDS. ![]()
Credit: Rhoda Baer
Researchers tested 5 anti-leukemia agents in combination with the methylation inhibitor decitabine and found that the sequential combination of decitabine and idarubicin worked synergistically to produce anti-leukemia effects.
The combination induced cell death in U937, HEL, and SKM-1 human cell lines and acute myeloid leukemia (AML) cells isolated from patients.
The researchers attributed the effects to demethylation of the Wnt/β-catenin pathway inhibitors and downregulation of the Wnt/β-catenin pathway nuclear targets.
The researchers noted that decitabine monotherapy has resulted in relatively low complete remission rates in AML and myelodysplastic syndromes (MDS). So they undertook to investigate combination therapies that would potentially improve efficacy.
Hongyan Tong, PhD, of Zhejiang University School of Medicine in Hangzhou, China, and colleagues reported their findings in the Journal of Translational Medicine.
The researchers chose 5 agents to combine, either simultaneously or sequentially, with decitabine—idarubicin, daunorubicin, aclarubicin, thalidomide, and homoharringtonine—and analyzed their effect on leukemia proliferation in the various AML cell lines mentioned above.
Using the U937 cell line first, the researchers found that when decitabine was combined simulataneously or sequentially with homharringtonine, aclarubicin, thalidomide, and daunorubicin, there was no synergistic effect. The confidence interval (CI) values of various doses were almost all over 0.8.
This was also true for the simultaneous combination of decitabine with idarubicin.
However, when they combined decitabine sequentially with idarubicin, the CI values on all 5 doses were under 0.8, indicating synergism.
In addition, when they administered decitabine twice in the sequence, the CI values were lower than a single administration.
They then confirmed the results in other AML cell lines (HEL and SKM-1) and in cells from AML patients.
Next, they confirmed the synergism of the sequential combination of decitabine and idarubicin in an AML mouse model and found that the combination inhibited tumor growth.
Tumor growth was inhibited significantly on days 4 (P<0.01), days 6 -16 (P<0.001), and started to wane by day 18 (P<0.05) after treatment.
The investigators determined that apoptosis was responsible for the combination’s decrease in leukemic cell viability. The apoptosis rates with the combination therapy were significantly increased in the U937, HEL, and SKM-1 cell lines compared with controls, (all P< 0.001).
In addition, the researchers observed that the tumor cells after treatment showed typical apoptosis characteristics, such as the absence of microvilli on cell membrane, nuclear and cell membrane blebbing, chromosome condensation, and the formation of apoptotic bodies.
The investigators used microarray expression to ascertain the differential gene expression profile of decitabine and idarubicin and found that the Wnt pathway was one of the major pathways disturbed.
Sequential treatment significantly upregulated the Wnt antagonist genes SFRP1, HDPR1, and DKK3. This in turn resulted in increased expression of these genes at the mRNA and protein levels.
In addition, treatment with idarubicin after decitabine caused significant down regulation of the expression of c-Myc, β-catenin, and cyclinD1 genes compared to treatment with decitabine or idarubicin alone.
The investigators concluded that the findings suggest clinical potential in sequential administration of decitabine and idarubicin in AML and high-risk MDS. ![]()
Credit: Rhoda Baer
Researchers tested 5 anti-leukemia agents in combination with the methylation inhibitor decitabine and found that the sequential combination of decitabine and idarubicin worked synergistically to produce anti-leukemia effects.
The combination induced cell death in U937, HEL, and SKM-1 human cell lines and acute myeloid leukemia (AML) cells isolated from patients.
The researchers attributed the effects to demethylation of the Wnt/β-catenin pathway inhibitors and downregulation of the Wnt/β-catenin pathway nuclear targets.
The researchers noted that decitabine monotherapy has resulted in relatively low complete remission rates in AML and myelodysplastic syndromes (MDS). So they undertook to investigate combination therapies that would potentially improve efficacy.
Hongyan Tong, PhD, of Zhejiang University School of Medicine in Hangzhou, China, and colleagues reported their findings in the Journal of Translational Medicine.
The researchers chose 5 agents to combine, either simultaneously or sequentially, with decitabine—idarubicin, daunorubicin, aclarubicin, thalidomide, and homoharringtonine—and analyzed their effect on leukemia proliferation in the various AML cell lines mentioned above.
Using the U937 cell line first, the researchers found that when decitabine was combined simulataneously or sequentially with homharringtonine, aclarubicin, thalidomide, and daunorubicin, there was no synergistic effect. The confidence interval (CI) values of various doses were almost all over 0.8.
This was also true for the simultaneous combination of decitabine with idarubicin.
However, when they combined decitabine sequentially with idarubicin, the CI values on all 5 doses were under 0.8, indicating synergism.
In addition, when they administered decitabine twice in the sequence, the CI values were lower than a single administration.
They then confirmed the results in other AML cell lines (HEL and SKM-1) and in cells from AML patients.
Next, they confirmed the synergism of the sequential combination of decitabine and idarubicin in an AML mouse model and found that the combination inhibited tumor growth.
Tumor growth was inhibited significantly on days 4 (P<0.01), days 6 -16 (P<0.001), and started to wane by day 18 (P<0.05) after treatment.
The investigators determined that apoptosis was responsible for the combination’s decrease in leukemic cell viability. The apoptosis rates with the combination therapy were significantly increased in the U937, HEL, and SKM-1 cell lines compared with controls, (all P< 0.001).
In addition, the researchers observed that the tumor cells after treatment showed typical apoptosis characteristics, such as the absence of microvilli on cell membrane, nuclear and cell membrane blebbing, chromosome condensation, and the formation of apoptotic bodies.
The investigators used microarray expression to ascertain the differential gene expression profile of decitabine and idarubicin and found that the Wnt pathway was one of the major pathways disturbed.
Sequential treatment significantly upregulated the Wnt antagonist genes SFRP1, HDPR1, and DKK3. This in turn resulted in increased expression of these genes at the mRNA and protein levels.
In addition, treatment with idarubicin after decitabine caused significant down regulation of the expression of c-Myc, β-catenin, and cyclinD1 genes compared to treatment with decitabine or idarubicin alone.
The investigators concluded that the findings suggest clinical potential in sequential administration of decitabine and idarubicin in AML and high-risk MDS. ![]()
Genetic ‘barcode’ could help track malaria

Credit: James Gathany
A genetic “barcode” for malaria parasites could be used to track and contain the spread of the disease, according to research published in Nature Communications.
Investigators analyzed the DNA of more than 700 Plasmodium falciparum parasites taken from patients in East and West Africa, South East Asia, Oceania, and South America.
And this revealed several short genetic sequences that were distinct in the DNA of parasites from certain geographic regions.
The team used this information to design a genetic barcode of 23 single-nucleotide polymorphisms that can be used to identify the source of new malaria infections.
“Being able to determine the geographic origin of malaria parasites has enormous potential in containing drug-resistance and eliminating malaria,” said study author Taane Clark, DPhil, of the London School of Hygiene & Tropical Medicine in the UK.
“Our work represents a breakthrough in the genetic barcoding of P falciparum, as it reveals very specific and accurate sequences for different geographic settings. We are currently extending the barcode to include other populations, such as India, Central America, southern Africa, and the Caribbean, and plan to include genetic markers for other types malaria, such as P vivax.”
Previous candidates for malaria genetic barcodes have relied on identifying DNA markers found in the parasite’s cell nucleus, which shows too much genetic variation between individual parasites to be used accurately.
But Dr Clark and his colleagues studied the DNA found in 2 parts of the parasite’s cells outside of the nucleus—the mitochondria and the apicolasts, which are only inherited through maternal lines, so their genes remain much more stable over generations.
By identifying short sequences in the DNA of the parasite’s mitochondria and apicoplasts that were specific for different geographic locations, the investigators were able to design a genetic barcode that is 92% predictive, stable, and geographically informative over time.
“By taking finger-prick bloodspots from malaria patients and using rapid gene sequencing technologies on small amounts of parasite material, local agencies could use this new barcode to quickly and accurately identify where a form of the parasite may have come from and help in programs of malaria elimination and resistance containment,” said study author Cally Roper, PhD, also of the London School of Hygiene & Tropical Medicine.
The investigators noted, however, that this barcode is limited because their study lacks representation of the Indian sub-continent, Central America, southern Africa, and the Caribbean, owing to the scarcity of sequence data from these regions.
Additionally, there’s a need to study more samples from East Africa, a region of high genetic diversity, high migration, and poor predictive ability. ![]()
Credit: James Gathany
A genetic “barcode” for malaria parasites could be used to track and contain the spread of the disease, according to research published in Nature Communications.
Investigators analyzed the DNA of more than 700 Plasmodium falciparum parasites taken from patients in East and West Africa, South East Asia, Oceania, and South America.
And this revealed several short genetic sequences that were distinct in the DNA of parasites from certain geographic regions.
The team used this information to design a genetic barcode of 23 single-nucleotide polymorphisms that can be used to identify the source of new malaria infections.
“Being able to determine the geographic origin of malaria parasites has enormous potential in containing drug-resistance and eliminating malaria,” said study author Taane Clark, DPhil, of the London School of Hygiene & Tropical Medicine in the UK.
“Our work represents a breakthrough in the genetic barcoding of P falciparum, as it reveals very specific and accurate sequences for different geographic settings. We are currently extending the barcode to include other populations, such as India, Central America, southern Africa, and the Caribbean, and plan to include genetic markers for other types malaria, such as P vivax.”
Previous candidates for malaria genetic barcodes have relied on identifying DNA markers found in the parasite’s cell nucleus, which shows too much genetic variation between individual parasites to be used accurately.
But Dr Clark and his colleagues studied the DNA found in 2 parts of the parasite’s cells outside of the nucleus—the mitochondria and the apicolasts, which are only inherited through maternal lines, so their genes remain much more stable over generations.
By identifying short sequences in the DNA of the parasite’s mitochondria and apicoplasts that were specific for different geographic locations, the investigators were able to design a genetic barcode that is 92% predictive, stable, and geographically informative over time.
“By taking finger-prick bloodspots from malaria patients and using rapid gene sequencing technologies on small amounts of parasite material, local agencies could use this new barcode to quickly and accurately identify where a form of the parasite may have come from and help in programs of malaria elimination and resistance containment,” said study author Cally Roper, PhD, also of the London School of Hygiene & Tropical Medicine.
The investigators noted, however, that this barcode is limited because their study lacks representation of the Indian sub-continent, Central America, southern Africa, and the Caribbean, owing to the scarcity of sequence data from these regions.
Additionally, there’s a need to study more samples from East Africa, a region of high genetic diversity, high migration, and poor predictive ability. ![]()
Credit: James Gathany
A genetic “barcode” for malaria parasites could be used to track and contain the spread of the disease, according to research published in Nature Communications.
Investigators analyzed the DNA of more than 700 Plasmodium falciparum parasites taken from patients in East and West Africa, South East Asia, Oceania, and South America.
And this revealed several short genetic sequences that were distinct in the DNA of parasites from certain geographic regions.
The team used this information to design a genetic barcode of 23 single-nucleotide polymorphisms that can be used to identify the source of new malaria infections.
“Being able to determine the geographic origin of malaria parasites has enormous potential in containing drug-resistance and eliminating malaria,” said study author Taane Clark, DPhil, of the London School of Hygiene & Tropical Medicine in the UK.
“Our work represents a breakthrough in the genetic barcoding of P falciparum, as it reveals very specific and accurate sequences for different geographic settings. We are currently extending the barcode to include other populations, such as India, Central America, southern Africa, and the Caribbean, and plan to include genetic markers for other types malaria, such as P vivax.”
Previous candidates for malaria genetic barcodes have relied on identifying DNA markers found in the parasite’s cell nucleus, which shows too much genetic variation between individual parasites to be used accurately.
But Dr Clark and his colleagues studied the DNA found in 2 parts of the parasite’s cells outside of the nucleus—the mitochondria and the apicolasts, which are only inherited through maternal lines, so their genes remain much more stable over generations.
By identifying short sequences in the DNA of the parasite’s mitochondria and apicoplasts that were specific for different geographic locations, the investigators were able to design a genetic barcode that is 92% predictive, stable, and geographically informative over time.
“By taking finger-prick bloodspots from malaria patients and using rapid gene sequencing technologies on small amounts of parasite material, local agencies could use this new barcode to quickly and accurately identify where a form of the parasite may have come from and help in programs of malaria elimination and resistance containment,” said study author Cally Roper, PhD, also of the London School of Hygiene & Tropical Medicine.
The investigators noted, however, that this barcode is limited because their study lacks representation of the Indian sub-continent, Central America, southern Africa, and the Caribbean, owing to the scarcity of sequence data from these regions.
Additionally, there’s a need to study more samples from East Africa, a region of high genetic diversity, high migration, and poor predictive ability. ![]()
Major Depressive Disorder: June 16
This study by Sinyor et al. reviewed 56 studies of antidepressants versus placebo and found that active drugs physiologically generated more neurological, sexual and anticholinergic side effects. No differences between drug and placebo were found for generating more psychic symptoms, pain symptoms, or weight gain suggesting that if remarkable complaints exist post dosing that these may be nocebo in origin. A nocebo effect occurs when negative expectations in the patient’s mindset creates artificial or psychic-based side effects.

Interestingly in large psychotropic trials, up to a quarter of subject will discontinue the placebo treatment due to side effects. In clinical practice, this also means that many of our patients may quit their medications early or we may discontinue them early allowing for poor dosing and likely poor outcomes. More interventional research about anti-nocebo interventions (identifying those at nocebo risk, tailoring information during informed consent, positive framing of side effect percentages, etc.) are warranted and could lead to more days on drug per patient and ideally better outcomes for them as well.
Thomas L. Schwartz, MD
Senior Associate Dean of Education
Interim Chair/Professor of Psychiatry
SUNY Upstate Medical University
This study by Sinyor et al. reviewed 56 studies of antidepressants versus placebo and found that active drugs physiologically generated more neurological, sexual and anticholinergic side effects. No differences between drug and placebo were found for generating more psychic symptoms, pain symptoms, or weight gain suggesting that if remarkable complaints exist post dosing that these may be nocebo in origin. A nocebo effect occurs when negative expectations in the patient’s mindset creates artificial or psychic-based side effects.
Interestingly in large psychotropic trials, up to a quarter of subject will discontinue the placebo treatment due to side effects. In clinical practice, this also means that many of our patients may quit their medications early or we may discontinue them early allowing for poor dosing and likely poor outcomes. More interventional research about anti-nocebo interventions (identifying those at nocebo risk, tailoring information during informed consent, positive framing of side effect percentages, etc.) are warranted and could lead to more days on drug per patient and ideally better outcomes for them as well.
Thomas L. Schwartz, MD
Senior Associate Dean of Education
Interim Chair/Professor of Psychiatry
SUNY Upstate Medical University
This study by Sinyor et al. reviewed 56 studies of antidepressants versus placebo and found that active drugs physiologically generated more neurological, sexual and anticholinergic side effects. No differences between drug and placebo were found for generating more psychic symptoms, pain symptoms, or weight gain suggesting that if remarkable complaints exist post dosing that these may be nocebo in origin. A nocebo effect occurs when negative expectations in the patient’s mindset creates artificial or psychic-based side effects.
Interestingly in large psychotropic trials, up to a quarter of subject will discontinue the placebo treatment due to side effects. In clinical practice, this also means that many of our patients may quit their medications early or we may discontinue them early allowing for poor dosing and likely poor outcomes. More interventional research about anti-nocebo interventions (identifying those at nocebo risk, tailoring information during informed consent, positive framing of side effect percentages, etc.) are warranted and could lead to more days on drug per patient and ideally better outcomes for them as well.
Thomas L. Schwartz, MD
Senior Associate Dean of Education
Interim Chair/Professor of Psychiatry
SUNY Upstate Medical University
Pharmacist-Managed Collaborative Practice for Chronic Stable Angina
Coronary artery disease (CAD) continues to have a significant impact on society. The latest update by the American Heart Association estimates that 83.6 million American adults have some form of cardiovascular disease (CVD) with an anticipated 15.4 million attributed to CAD.1 A portion of patients with CAD experience predictable chest pain, which occurs as a result of physical, emotional, or mental stress, more commonly referred to as chronic stable angina (CSA). Based on the most recent estimates, the incidence of patients who experience CSA is about 565,000 and increases in the male population through the eighth decade of life.1
Although it may be common, treatment options for patients with CSA are limited, as these patients may not be ideal candidates for coronary artery bypass graft or percutaneous coronary intervention (PCI) and may often prefer less invasive treatments. It has also been demonstrated that optimal medical management results in similar cardiovascular outcomes when compared with optimal medical management combined with PCI.2,3 Therefore, optimizing medical management is a reasonable alternative for these individuals.
Pharmacists have been successful in implementing collaborative practices for the management of various conditions, including anticoagulation, diabetes, hypertension, and hyperlipidemia.4-7 Pharmacists are heavily involved with cardiovascular risk reduction and management, so it seems opportune that they also treat CSA.8 The latest estimated direct and indirect costs for CVD and stroke were well over $315 billion for 2010, and it is anticipated that the costs will continue to rise.1 Because CSA is typically a medically managed disease and due to its huge medical expense, the development of a pharmacist-managed collaborative practice for treating CSA may prove to be beneficial for both clinical and pharmacoeconomic outcomes.
Clinic Development and Practices
In June 2007, following the approval of ranolazine by the FDA, the VA adopted nonformulary criteria for ranolazine use (Appendix).9,10 In order for patients to receive ranolazine, health care providers (HCPs) within the North Florida/South Georgia Veterans Health System (NFSGVHS) network were required to submit an electronic nonformulary consult using the computerized patient record system (CPRS). Select clinical pharmacists who had knowledge of the health system’s nonformulary criteria and who were granted access to the electronic consults responded to the requests.
The consults primarily consisted of an automated template that required providers to fill out their contact information and the name of the requested nonformulary medication, dose, and clinical rationale for requesting the specified medication, including any previous treatments that the patient could not tolerate or on which the patient failed to achieve an adequate response. It was highly recommended but not required that the HCPs include other supporting information regarding the patient’s cardiovascular status, such as results from diagnostic cardiac catheterization, stress tests, electrocardiograms (ECGs), or echocardiograms if not readily available from the CPRS. If procedures or tests were conducted at outside facilities, then this information was supplied in the request or obtained with the patient’s consent. However, this information was not necessarily required in order to complete the nonformulary consult. Nonformulary requests for ranolazine were typically forwarded to the clinical pharmacists who specialized in cardiology.
A pharmacist-oriented collaborative practice was established to increase cost-effective use, improve monitoring by a HCP because of the drug’s ability to prolong the corrected QT (QTc) interval, and to more firmly establish its safety and efficacy in a veteran population. This practice operated in a clinic, which was staffed by a nurse, postdoctoral pharmacy fellow, clinical pharmacy specialist in cardiology, and a cardiologist. The nurse was responsible for obtaining the patient’s vitals and ECG and documenting them in the CPRS. The pharmacy fellow interviewed the patient and obtained pertinent medical and historical information before discussing any clinical recommendations with the clinical pharmacy specialist.
The recommendations consisted of drug initiation/discontinuation, dose adjustments, and assessing and ordering of pertinent laboratory values and ECGs, which took place under the scope of the clinical pharmacy specialist. The focus of the ECG was to assess for any evidence of excessive QTc prolongation. Due to the variable and subjective nature of CAD, a cardiologist was available at any time and was used to review any relevant information and further discuss any treatment recommendations.
Based in the NFSGVHS Malcom Randall Veterans Affairs Medical Center (VAMC) in Gainesville, Florida, clinic services were primarily offered to patients of that facility due to the limited number of cardiology providers and services offered at other NFSGVHS locations. Despite being driven by requests for ranolazine, especially after cardiac catheterization when further cardiac intervention may not have been feasible, all patients were allowed to enroll in the clinic at the discretion of their primary care provider (PCP) for optimization of their CSA regimen with the intent of adding ranolazine when appropriate.
Patients in outlying regions who met the criteria were supplied with ranolazine and continued to follow up with their HCPs as recommended by the criteria for use. Conversely, if patients from outside areas failed to meet the criteria, their PCPs were supplied with appropriate, alternative guideline-based recommendations for improving CSA with the option to resubmit the nonformulary consult.11 Recommendations regarding cardiovascular risk reduction were also sent to HCPs at that time, which included optimal endpoints for managing other conditions, such as diabetes, hypertension, and hyperlipidemia when necesary.8,11
Regardless of whether ranolazine was initiated at baseline, all patients enrolled in the clinic underwent appropriate labs and tests, including a basic metabolic panel, magnesium level, and an ECG, if not otherwise available from the CPRS or documented from outside facilities. A thorough history and description of the patient’s anginal symptoms were also taken at baseline and during follow-up visits. Once it was confirmed that the patients’ electrolytes were within normal limits and there was no evidence of prolongation in the Bazett’s QTc interval or major drug interactions, all patients who met criteria for ranolazine were initiated at 500 mg twice daily.9,12 The Seattle Angina Questionnaire (SAQ) was also completed by patients at the initiation of ranolazine and then again at follow-up visits. The SAQ is an 11-question, self-administered survey that measures functional status of patients with angina.13
All patients initiated on or ensuing dose changes with ranolazine followed up with the clinic at 1 and 3 months with labs and ECGs obtained prior to ensure that there were no electrolyte imbalances or excessive QTc prolongation. Excessive QTc prolongation was defined as an increase of ≥ 60 milliseconds (msec) from baseline or > 500 msec.14 If this boundary was exceeded, ranolazine was discontinued, or for those taking higher doses, it was reduced to the initial 500 mg twice daily as long as there was no previous excessive QTc prolongation. In cases where ranolazine was not added at baseline, doses of antianginal medications were titrated over appropriate intervals to improve angina symptoms with ranolazine subsequently added in conjunction with the nonformulary criteria.
A generalized treatment algorithm was followed by the clinic for the management of CSA (Figure). It was highly recommended that all referred patients have an active prescription in the CPRS for short-acting sublingual nitroglycerin 0.4 mg in case of any acute episodes. Although other forms of short-acting nitroglycerin were available, sublingual nitroglycerin 0.4 mg was the preferred formulary medication at the time of the study.
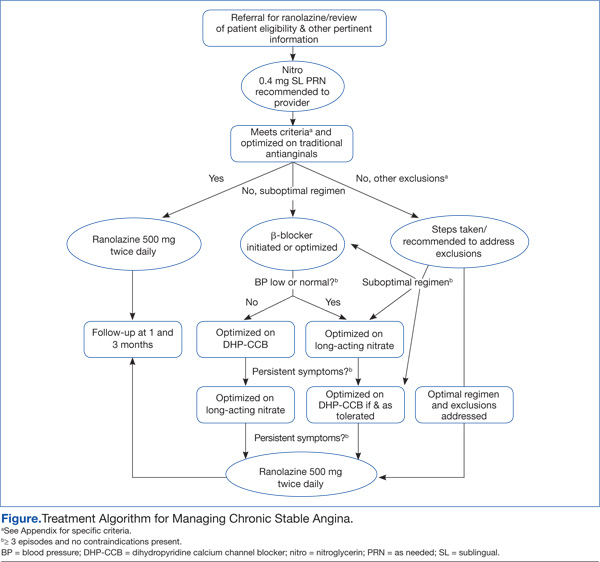
Depending on whether the patients met nonformulary inclusion or exclusion criteria, they were either initiated or optimized on ranolazine or other traditional antianginals, such as beta-blockers (BBs), dihydropyridine calcium channel blockers (DHP-CCBs), or long-acting nitrates (LANs). Beta-blockers were recommended as first-line treatment for patients with previous myocardial infarction (MI) and left ventricular dysfunction, in accordance with treatment guidelines and because of their benefits in treating patients with CSA.12,15
Once patients were optimized on BBs and/or DHP-CCBs, LANs were added if patients experienced ≥ 3 bothersome episodes of chest pain weekly. Optimization for BBs meant an ideal heart rate of at least about 60 bpm without symptoms suggestive of excessive bradycardia, whereas optimization for all 3 classes (BBs, DHP-CCBs, and LANs) consisted of dose titration until the presence of drug-related adverse effects (AEs) or symptoms suggestive of hypotension. Because LANs have lesser effects on blood pressure (BP) compared with DHP-CCBs, they were preferred in patients with persistent anginal symptoms whose BPs were considered low or normal, according to the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) guidelines.16
If patients with normal or controlled BP continued to have symptoms of angina despite optimal doses of BBs and LANs, an appropriate dose of a DHP-CCB was administered and titrated for as long as the patients tolerated the treatment. If titration of antianginal agents was limited due to the presence of other antihypertensives, then the patient’s medication regimen was modified as necessary to allow for an increased dose of the BB or DHP-CCB due to these medications’ abilities to improve angina symptoms while also lowering BP. If patients achieved an acceptable reduction in their angina symptoms, they were discharged from the clinic, whereas those with contraindications to other classes were referred to their PCP or cardiologist.
Patients successfully treated with ranolazine (defined as a noticeable reduction in angina symptoms in the absence of intolerable AEs and excessive QTc prolongation after 3 months) were discharged from the clinic and instructed to follow up with their PCP at least annually. If the patient was discharged from the clinic at the baseline dose, it was recommended to the HCP that he or she follow up within 3 months after any dose increases. Any patient whose symptoms were consistent with unstable angina (described as occurring in an unpredictable manner, as determined by the clinical pharmacy specialist, lasting longer in duration and/or increasing in frequency, and those who experience symptoms at rest) were immediately evaluated and referred to a cardiologist. Patients who continued to have unacceptable rates or episodes of angina despite an optimal medical regimen were referred to Cardiology for consideration of other treatment modalities.
Results
The initial report of this study population was described by Reeder and colleagues.17 Fifty-seven patients were evaluated for study inclusion, of which 22 were excluded due to ranolazine being managed by an outside HCP or because an SAQ was not obtained at baseline. All study participants were males with an average age of 68 years and were predominantly white (86%). All patients had a past medical history significant for hypertension and hyperlipidemia. More than half (57%) had a prior MI and multivessel disease, although only 1 patient had an ejection fraction of < 35%. The majority of patients enrolled were being treated with BBs (97%) and LANs (94%) with a little more than half prescribed CCBs (60%). A large percentage (97%) of patients were also taking aspirin and a statin.
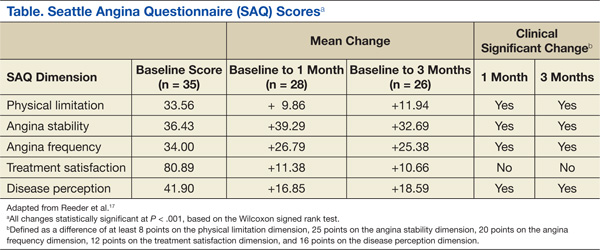
Improvements in angina symptoms as measured by the SAQ and safety measures, which included details of AEs and discontinuation rates following the initiation of ranolazine within the clinic, have previously been published.17 In summary, it was found that the addition of ranolazine to an optimal medical regimen for CSA improved all dimensions of the SAQ scores at 1 and 3 months compared with baseline (Table). Additionally, it was noted that higher doses may not have been as well tolerated in the veteran population, despite that only a small number of eligible patients were captured. This was because 5 of 7 patients whose dose was increased to 1,000 mg twice daily after 1 month required withdrawal as a result of AEs or lack of efficacy. The AEs reported included dizziness, abdominal pain, blurry vision, nausea and vomiting, dry mouth, and dyspnea.
The pharmacists were able to ensure that relevant electrolytes were replaced during the treatment period and also minimized the number of clinically significant drug interactions. Twenty-one patients received medications at baseline that had known interactions with ranolazine. Two patients required discontinuation of other medications: sotalol and diltiazem. At the time this study was conducted, diltiazem was contraindicated when given concomitantly but has since been allowed per manufacturer recommendations as long as the dose of ranolazine does not exceed 500 mg twice daily. Electrolyte replacement was also required in 3 patients, 2 of whom had hypomagnesemia.
Conclusion
Pharmacists have been influential in managing a variety of chronic diseases. When instituted into collaborative practice agreements, CSA is another unique condition that pharmacists can play a role in treating. Given that pharmacists are heavily involved with cardiovascular risk reduction, combined with the higher cost of ranolazine and the need for monitoring due to its AEs, QTc interval prolongation, and significant drug interactions, the benefits of having pharmacist-oriented clinics can ensure the safe and effective use of medications in the treatment of CSA.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
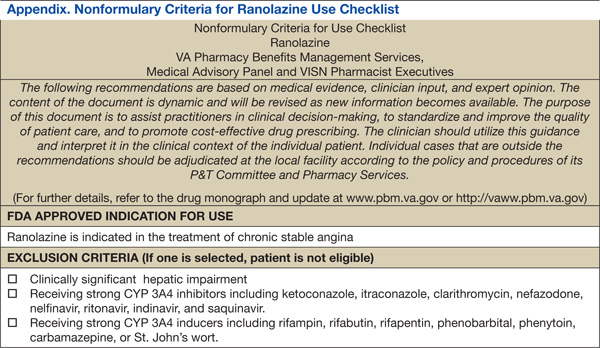
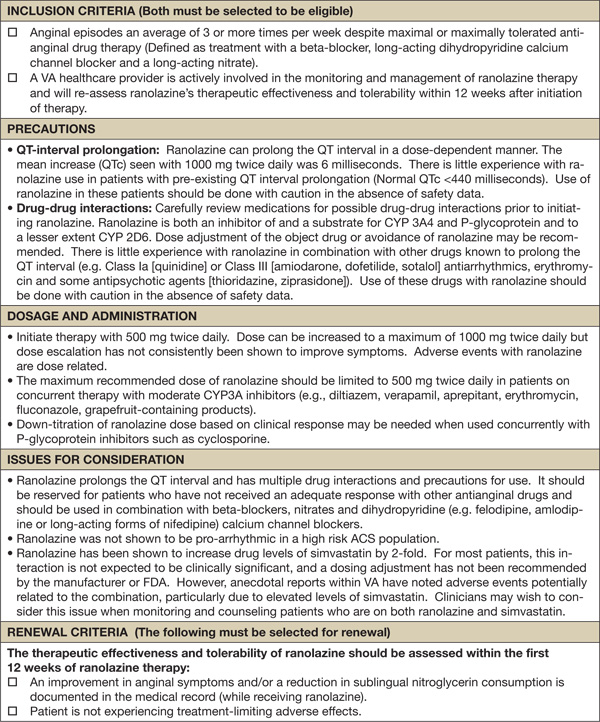
1. Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2014 update: A report from the American Heart Association. Circulation. 2014;129:e28-e292.
2. Boden WE, O’Rourke RA, Teo KK, et al; COURAGE Trial Research Group. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503-1516.
3. RITA-2 trial participants. Coronary angioplasty versus medical therapy for angina: The second Randomised Intervention Treatment of Angina (RITA-2) trial. Lancet. 1997;350(9076):461-468.
4. Norton JL, Gibson DL. Establishing an outpatient anticoagulation clinic in a community hospital. Am J Health Syst Pharm. 1996;53(10):1151-1157.
5. Morello CM, Zadvorny EB, Cording MA, Suemoto RT, Skog J, Harari A. Development and clinical outcomes of pharmacist-managed diabetes care clinics. Am J Health Syst Pharm. 2006;63(14):1325-1331.
6. Vivian EM. Improving blood pressure control in a pharmacist-managed hypertension clinic. Pharmacotherapy. 2002;22(12):1533-1540.
7. Cording MA, Engelbrecht-Zadvorny EB, Pettit BJ, Eastham JH, Sandoval R. Development of a pharmacist-managed lipid clinic. Ann Pharmacother. 2002;36(5):892-904.
8. Geber J, Parra D, Beckey NP, Korman L. Optimizing drug therapy in patients with cardiovascular disease: The impact of pharmacist-managed pharmacotherapy clinics in a primary care setting. Pharmacotherapy. 2002; 22(6):738-747.
9. Ranexa [package insert]. Foster City, CA: Gilead Sciences, Inc.; 2013.
10. VHA Pharmacy Benefits Management Strategic Healthcare Group and the Medical Advisory Panel. Ranolazine. National PBM Drug Monograph. U.S. Department of Veterans Affairs Pharmacy Benefits Management Services Website. http://www.pbm.va.gov/clinicalguidance/drugmonographs/Ranolazine.pdf. Published June 2007. Accessed May 7, 2014.
11. Fraker TD Jr, Fihn SD; writing on behalf of the 2002 Chronic Stable Angina Writing Committee. 2007 chronic angina focused update of the ACC/AHA 2002 guidelines for the management of patients with chronic stable angina: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Writing Group to develop the focused update of the 2002 guidelines for the management of patients with chronic stable angina. Circulation. 2007;116(23):2762-2772.
12. Funck-Brentano C, Jaillon P. Rate-corrected QT interval: Techniques and limitations. Am J Cardiol. 1993;72(6):17B-22B.
13. Spertus JA, Winder JA, Dewhurst TA, et al. Development and evaluation of the Seattle Angina Questionnaire: A new functional status measure for coronary artery disease. J Am Coll Cardiol. 1995;25(2):333-341.
14. Drew BJ, Ackerman MJ, Funk M, et al; American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology, the Council on Cardiovascular Nursing, and the American College of Cardiology Foundation. Prevention of torsade de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121(8):1047-1060.
15. Heidenreich PA, McDonald KM, Hastie T, et al. Meta-analysis of trials comparing beta-blockers, calcium antagonists, and nitrates for stable angina. JAMA. 1999;281(20):1927-1936.
16. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The JNC 7 report. JAMA. 2003;289(19):2560-2572.
17. Reeder DN, Gillette MA, Franck AJ, Frohnapple DJ. Clinical experience with ranolazine in a veteran population with chronic stable angina. Ann Pharmacother. 2012;46(1):42-50.
Coronary artery disease (CAD) continues to have a significant impact on society. The latest update by the American Heart Association estimates that 83.6 million American adults have some form of cardiovascular disease (CVD) with an anticipated 15.4 million attributed to CAD.1 A portion of patients with CAD experience predictable chest pain, which occurs as a result of physical, emotional, or mental stress, more commonly referred to as chronic stable angina (CSA). Based on the most recent estimates, the incidence of patients who experience CSA is about 565,000 and increases in the male population through the eighth decade of life.1
Although it may be common, treatment options for patients with CSA are limited, as these patients may not be ideal candidates for coronary artery bypass graft or percutaneous coronary intervention (PCI) and may often prefer less invasive treatments. It has also been demonstrated that optimal medical management results in similar cardiovascular outcomes when compared with optimal medical management combined with PCI.2,3 Therefore, optimizing medical management is a reasonable alternative for these individuals.
Pharmacists have been successful in implementing collaborative practices for the management of various conditions, including anticoagulation, diabetes, hypertension, and hyperlipidemia.4-7 Pharmacists are heavily involved with cardiovascular risk reduction and management, so it seems opportune that they also treat CSA.8 The latest estimated direct and indirect costs for CVD and stroke were well over $315 billion for 2010, and it is anticipated that the costs will continue to rise.1 Because CSA is typically a medically managed disease and due to its huge medical expense, the development of a pharmacist-managed collaborative practice for treating CSA may prove to be beneficial for both clinical and pharmacoeconomic outcomes.
Clinic Development and Practices
In June 2007, following the approval of ranolazine by the FDA, the VA adopted nonformulary criteria for ranolazine use (Appendix).9,10 In order for patients to receive ranolazine, health care providers (HCPs) within the North Florida/South Georgia Veterans Health System (NFSGVHS) network were required to submit an electronic nonformulary consult using the computerized patient record system (CPRS). Select clinical pharmacists who had knowledge of the health system’s nonformulary criteria and who were granted access to the electronic consults responded to the requests.
The consults primarily consisted of an automated template that required providers to fill out their contact information and the name of the requested nonformulary medication, dose, and clinical rationale for requesting the specified medication, including any previous treatments that the patient could not tolerate or on which the patient failed to achieve an adequate response. It was highly recommended but not required that the HCPs include other supporting information regarding the patient’s cardiovascular status, such as results from diagnostic cardiac catheterization, stress tests, electrocardiograms (ECGs), or echocardiograms if not readily available from the CPRS. If procedures or tests were conducted at outside facilities, then this information was supplied in the request or obtained with the patient’s consent. However, this information was not necessarily required in order to complete the nonformulary consult. Nonformulary requests for ranolazine were typically forwarded to the clinical pharmacists who specialized in cardiology.
A pharmacist-oriented collaborative practice was established to increase cost-effective use, improve monitoring by a HCP because of the drug’s ability to prolong the corrected QT (QTc) interval, and to more firmly establish its safety and efficacy in a veteran population. This practice operated in a clinic, which was staffed by a nurse, postdoctoral pharmacy fellow, clinical pharmacy specialist in cardiology, and a cardiologist. The nurse was responsible for obtaining the patient’s vitals and ECG and documenting them in the CPRS. The pharmacy fellow interviewed the patient and obtained pertinent medical and historical information before discussing any clinical recommendations with the clinical pharmacy specialist.
The recommendations consisted of drug initiation/discontinuation, dose adjustments, and assessing and ordering of pertinent laboratory values and ECGs, which took place under the scope of the clinical pharmacy specialist. The focus of the ECG was to assess for any evidence of excessive QTc prolongation. Due to the variable and subjective nature of CAD, a cardiologist was available at any time and was used to review any relevant information and further discuss any treatment recommendations.
Based in the NFSGVHS Malcom Randall Veterans Affairs Medical Center (VAMC) in Gainesville, Florida, clinic services were primarily offered to patients of that facility due to the limited number of cardiology providers and services offered at other NFSGVHS locations. Despite being driven by requests for ranolazine, especially after cardiac catheterization when further cardiac intervention may not have been feasible, all patients were allowed to enroll in the clinic at the discretion of their primary care provider (PCP) for optimization of their CSA regimen with the intent of adding ranolazine when appropriate.
Patients in outlying regions who met the criteria were supplied with ranolazine and continued to follow up with their HCPs as recommended by the criteria for use. Conversely, if patients from outside areas failed to meet the criteria, their PCPs were supplied with appropriate, alternative guideline-based recommendations for improving CSA with the option to resubmit the nonformulary consult.11 Recommendations regarding cardiovascular risk reduction were also sent to HCPs at that time, which included optimal endpoints for managing other conditions, such as diabetes, hypertension, and hyperlipidemia when necesary.8,11
Regardless of whether ranolazine was initiated at baseline, all patients enrolled in the clinic underwent appropriate labs and tests, including a basic metabolic panel, magnesium level, and an ECG, if not otherwise available from the CPRS or documented from outside facilities. A thorough history and description of the patient’s anginal symptoms were also taken at baseline and during follow-up visits. Once it was confirmed that the patients’ electrolytes were within normal limits and there was no evidence of prolongation in the Bazett’s QTc interval or major drug interactions, all patients who met criteria for ranolazine were initiated at 500 mg twice daily.9,12 The Seattle Angina Questionnaire (SAQ) was also completed by patients at the initiation of ranolazine and then again at follow-up visits. The SAQ is an 11-question, self-administered survey that measures functional status of patients with angina.13
All patients initiated on or ensuing dose changes with ranolazine followed up with the clinic at 1 and 3 months with labs and ECGs obtained prior to ensure that there were no electrolyte imbalances or excessive QTc prolongation. Excessive QTc prolongation was defined as an increase of ≥ 60 milliseconds (msec) from baseline or > 500 msec.14 If this boundary was exceeded, ranolazine was discontinued, or for those taking higher doses, it was reduced to the initial 500 mg twice daily as long as there was no previous excessive QTc prolongation. In cases where ranolazine was not added at baseline, doses of antianginal medications were titrated over appropriate intervals to improve angina symptoms with ranolazine subsequently added in conjunction with the nonformulary criteria.
A generalized treatment algorithm was followed by the clinic for the management of CSA (Figure). It was highly recommended that all referred patients have an active prescription in the CPRS for short-acting sublingual nitroglycerin 0.4 mg in case of any acute episodes. Although other forms of short-acting nitroglycerin were available, sublingual nitroglycerin 0.4 mg was the preferred formulary medication at the time of the study.
Depending on whether the patients met nonformulary inclusion or exclusion criteria, they were either initiated or optimized on ranolazine or other traditional antianginals, such as beta-blockers (BBs), dihydropyridine calcium channel blockers (DHP-CCBs), or long-acting nitrates (LANs). Beta-blockers were recommended as first-line treatment for patients with previous myocardial infarction (MI) and left ventricular dysfunction, in accordance with treatment guidelines and because of their benefits in treating patients with CSA.12,15
Once patients were optimized on BBs and/or DHP-CCBs, LANs were added if patients experienced ≥ 3 bothersome episodes of chest pain weekly. Optimization for BBs meant an ideal heart rate of at least about 60 bpm without symptoms suggestive of excessive bradycardia, whereas optimization for all 3 classes (BBs, DHP-CCBs, and LANs) consisted of dose titration until the presence of drug-related adverse effects (AEs) or symptoms suggestive of hypotension. Because LANs have lesser effects on blood pressure (BP) compared with DHP-CCBs, they were preferred in patients with persistent anginal symptoms whose BPs were considered low or normal, according to the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) guidelines.16
If patients with normal or controlled BP continued to have symptoms of angina despite optimal doses of BBs and LANs, an appropriate dose of a DHP-CCB was administered and titrated for as long as the patients tolerated the treatment. If titration of antianginal agents was limited due to the presence of other antihypertensives, then the patient’s medication regimen was modified as necessary to allow for an increased dose of the BB or DHP-CCB due to these medications’ abilities to improve angina symptoms while also lowering BP. If patients achieved an acceptable reduction in their angina symptoms, they were discharged from the clinic, whereas those with contraindications to other classes were referred to their PCP or cardiologist.
Patients successfully treated with ranolazine (defined as a noticeable reduction in angina symptoms in the absence of intolerable AEs and excessive QTc prolongation after 3 months) were discharged from the clinic and instructed to follow up with their PCP at least annually. If the patient was discharged from the clinic at the baseline dose, it was recommended to the HCP that he or she follow up within 3 months after any dose increases. Any patient whose symptoms were consistent with unstable angina (described as occurring in an unpredictable manner, as determined by the clinical pharmacy specialist, lasting longer in duration and/or increasing in frequency, and those who experience symptoms at rest) were immediately evaluated and referred to a cardiologist. Patients who continued to have unacceptable rates or episodes of angina despite an optimal medical regimen were referred to Cardiology for consideration of other treatment modalities.
Results
The initial report of this study population was described by Reeder and colleagues.17 Fifty-seven patients were evaluated for study inclusion, of which 22 were excluded due to ranolazine being managed by an outside HCP or because an SAQ was not obtained at baseline. All study participants were males with an average age of 68 years and were predominantly white (86%). All patients had a past medical history significant for hypertension and hyperlipidemia. More than half (57%) had a prior MI and multivessel disease, although only 1 patient had an ejection fraction of < 35%. The majority of patients enrolled were being treated with BBs (97%) and LANs (94%) with a little more than half prescribed CCBs (60%). A large percentage (97%) of patients were also taking aspirin and a statin.
Improvements in angina symptoms as measured by the SAQ and safety measures, which included details of AEs and discontinuation rates following the initiation of ranolazine within the clinic, have previously been published.17 In summary, it was found that the addition of ranolazine to an optimal medical regimen for CSA improved all dimensions of the SAQ scores at 1 and 3 months compared with baseline (Table). Additionally, it was noted that higher doses may not have been as well tolerated in the veteran population, despite that only a small number of eligible patients were captured. This was because 5 of 7 patients whose dose was increased to 1,000 mg twice daily after 1 month required withdrawal as a result of AEs or lack of efficacy. The AEs reported included dizziness, abdominal pain, blurry vision, nausea and vomiting, dry mouth, and dyspnea.
The pharmacists were able to ensure that relevant electrolytes were replaced during the treatment period and also minimized the number of clinically significant drug interactions. Twenty-one patients received medications at baseline that had known interactions with ranolazine. Two patients required discontinuation of other medications: sotalol and diltiazem. At the time this study was conducted, diltiazem was contraindicated when given concomitantly but has since been allowed per manufacturer recommendations as long as the dose of ranolazine does not exceed 500 mg twice daily. Electrolyte replacement was also required in 3 patients, 2 of whom had hypomagnesemia.
Conclusion
Pharmacists have been influential in managing a variety of chronic diseases. When instituted into collaborative practice agreements, CSA is another unique condition that pharmacists can play a role in treating. Given that pharmacists are heavily involved with cardiovascular risk reduction, combined with the higher cost of ranolazine and the need for monitoring due to its AEs, QTc interval prolongation, and significant drug interactions, the benefits of having pharmacist-oriented clinics can ensure the safe and effective use of medications in the treatment of CSA.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
Coronary artery disease (CAD) continues to have a significant impact on society. The latest update by the American Heart Association estimates that 83.6 million American adults have some form of cardiovascular disease (CVD) with an anticipated 15.4 million attributed to CAD.1 A portion of patients with CAD experience predictable chest pain, which occurs as a result of physical, emotional, or mental stress, more commonly referred to as chronic stable angina (CSA). Based on the most recent estimates, the incidence of patients who experience CSA is about 565,000 and increases in the male population through the eighth decade of life.1
Although it may be common, treatment options for patients with CSA are limited, as these patients may not be ideal candidates for coronary artery bypass graft or percutaneous coronary intervention (PCI) and may often prefer less invasive treatments. It has also been demonstrated that optimal medical management results in similar cardiovascular outcomes when compared with optimal medical management combined with PCI.2,3 Therefore, optimizing medical management is a reasonable alternative for these individuals.
Pharmacists have been successful in implementing collaborative practices for the management of various conditions, including anticoagulation, diabetes, hypertension, and hyperlipidemia.4-7 Pharmacists are heavily involved with cardiovascular risk reduction and management, so it seems opportune that they also treat CSA.8 The latest estimated direct and indirect costs for CVD and stroke were well over $315 billion for 2010, and it is anticipated that the costs will continue to rise.1 Because CSA is typically a medically managed disease and due to its huge medical expense, the development of a pharmacist-managed collaborative practice for treating CSA may prove to be beneficial for both clinical and pharmacoeconomic outcomes.
Clinic Development and Practices
In June 2007, following the approval of ranolazine by the FDA, the VA adopted nonformulary criteria for ranolazine use (Appendix).9,10 In order for patients to receive ranolazine, health care providers (HCPs) within the North Florida/South Georgia Veterans Health System (NFSGVHS) network were required to submit an electronic nonformulary consult using the computerized patient record system (CPRS). Select clinical pharmacists who had knowledge of the health system’s nonformulary criteria and who were granted access to the electronic consults responded to the requests.
The consults primarily consisted of an automated template that required providers to fill out their contact information and the name of the requested nonformulary medication, dose, and clinical rationale for requesting the specified medication, including any previous treatments that the patient could not tolerate or on which the patient failed to achieve an adequate response. It was highly recommended but not required that the HCPs include other supporting information regarding the patient’s cardiovascular status, such as results from diagnostic cardiac catheterization, stress tests, electrocardiograms (ECGs), or echocardiograms if not readily available from the CPRS. If procedures or tests were conducted at outside facilities, then this information was supplied in the request or obtained with the patient’s consent. However, this information was not necessarily required in order to complete the nonformulary consult. Nonformulary requests for ranolazine were typically forwarded to the clinical pharmacists who specialized in cardiology.
A pharmacist-oriented collaborative practice was established to increase cost-effective use, improve monitoring by a HCP because of the drug’s ability to prolong the corrected QT (QTc) interval, and to more firmly establish its safety and efficacy in a veteran population. This practice operated in a clinic, which was staffed by a nurse, postdoctoral pharmacy fellow, clinical pharmacy specialist in cardiology, and a cardiologist. The nurse was responsible for obtaining the patient’s vitals and ECG and documenting them in the CPRS. The pharmacy fellow interviewed the patient and obtained pertinent medical and historical information before discussing any clinical recommendations with the clinical pharmacy specialist.
The recommendations consisted of drug initiation/discontinuation, dose adjustments, and assessing and ordering of pertinent laboratory values and ECGs, which took place under the scope of the clinical pharmacy specialist. The focus of the ECG was to assess for any evidence of excessive QTc prolongation. Due to the variable and subjective nature of CAD, a cardiologist was available at any time and was used to review any relevant information and further discuss any treatment recommendations.
Based in the NFSGVHS Malcom Randall Veterans Affairs Medical Center (VAMC) in Gainesville, Florida, clinic services were primarily offered to patients of that facility due to the limited number of cardiology providers and services offered at other NFSGVHS locations. Despite being driven by requests for ranolazine, especially after cardiac catheterization when further cardiac intervention may not have been feasible, all patients were allowed to enroll in the clinic at the discretion of their primary care provider (PCP) for optimization of their CSA regimen with the intent of adding ranolazine when appropriate.
Patients in outlying regions who met the criteria were supplied with ranolazine and continued to follow up with their HCPs as recommended by the criteria for use. Conversely, if patients from outside areas failed to meet the criteria, their PCPs were supplied with appropriate, alternative guideline-based recommendations for improving CSA with the option to resubmit the nonformulary consult.11 Recommendations regarding cardiovascular risk reduction were also sent to HCPs at that time, which included optimal endpoints for managing other conditions, such as diabetes, hypertension, and hyperlipidemia when necesary.8,11
Regardless of whether ranolazine was initiated at baseline, all patients enrolled in the clinic underwent appropriate labs and tests, including a basic metabolic panel, magnesium level, and an ECG, if not otherwise available from the CPRS or documented from outside facilities. A thorough history and description of the patient’s anginal symptoms were also taken at baseline and during follow-up visits. Once it was confirmed that the patients’ electrolytes were within normal limits and there was no evidence of prolongation in the Bazett’s QTc interval or major drug interactions, all patients who met criteria for ranolazine were initiated at 500 mg twice daily.9,12 The Seattle Angina Questionnaire (SAQ) was also completed by patients at the initiation of ranolazine and then again at follow-up visits. The SAQ is an 11-question, self-administered survey that measures functional status of patients with angina.13
All patients initiated on or ensuing dose changes with ranolazine followed up with the clinic at 1 and 3 months with labs and ECGs obtained prior to ensure that there were no electrolyte imbalances or excessive QTc prolongation. Excessive QTc prolongation was defined as an increase of ≥ 60 milliseconds (msec) from baseline or > 500 msec.14 If this boundary was exceeded, ranolazine was discontinued, or for those taking higher doses, it was reduced to the initial 500 mg twice daily as long as there was no previous excessive QTc prolongation. In cases where ranolazine was not added at baseline, doses of antianginal medications were titrated over appropriate intervals to improve angina symptoms with ranolazine subsequently added in conjunction with the nonformulary criteria.
A generalized treatment algorithm was followed by the clinic for the management of CSA (Figure). It was highly recommended that all referred patients have an active prescription in the CPRS for short-acting sublingual nitroglycerin 0.4 mg in case of any acute episodes. Although other forms of short-acting nitroglycerin were available, sublingual nitroglycerin 0.4 mg was the preferred formulary medication at the time of the study.
Depending on whether the patients met nonformulary inclusion or exclusion criteria, they were either initiated or optimized on ranolazine or other traditional antianginals, such as beta-blockers (BBs), dihydropyridine calcium channel blockers (DHP-CCBs), or long-acting nitrates (LANs). Beta-blockers were recommended as first-line treatment for patients with previous myocardial infarction (MI) and left ventricular dysfunction, in accordance with treatment guidelines and because of their benefits in treating patients with CSA.12,15
Once patients were optimized on BBs and/or DHP-CCBs, LANs were added if patients experienced ≥ 3 bothersome episodes of chest pain weekly. Optimization for BBs meant an ideal heart rate of at least about 60 bpm without symptoms suggestive of excessive bradycardia, whereas optimization for all 3 classes (BBs, DHP-CCBs, and LANs) consisted of dose titration until the presence of drug-related adverse effects (AEs) or symptoms suggestive of hypotension. Because LANs have lesser effects on blood pressure (BP) compared with DHP-CCBs, they were preferred in patients with persistent anginal symptoms whose BPs were considered low or normal, according to the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (JNC 7) guidelines.16
If patients with normal or controlled BP continued to have symptoms of angina despite optimal doses of BBs and LANs, an appropriate dose of a DHP-CCB was administered and titrated for as long as the patients tolerated the treatment. If titration of antianginal agents was limited due to the presence of other antihypertensives, then the patient’s medication regimen was modified as necessary to allow for an increased dose of the BB or DHP-CCB due to these medications’ abilities to improve angina symptoms while also lowering BP. If patients achieved an acceptable reduction in their angina symptoms, they were discharged from the clinic, whereas those with contraindications to other classes were referred to their PCP or cardiologist.
Patients successfully treated with ranolazine (defined as a noticeable reduction in angina symptoms in the absence of intolerable AEs and excessive QTc prolongation after 3 months) were discharged from the clinic and instructed to follow up with their PCP at least annually. If the patient was discharged from the clinic at the baseline dose, it was recommended to the HCP that he or she follow up within 3 months after any dose increases. Any patient whose symptoms were consistent with unstable angina (described as occurring in an unpredictable manner, as determined by the clinical pharmacy specialist, lasting longer in duration and/or increasing in frequency, and those who experience symptoms at rest) were immediately evaluated and referred to a cardiologist. Patients who continued to have unacceptable rates or episodes of angina despite an optimal medical regimen were referred to Cardiology for consideration of other treatment modalities.
Results
The initial report of this study population was described by Reeder and colleagues.17 Fifty-seven patients were evaluated for study inclusion, of which 22 were excluded due to ranolazine being managed by an outside HCP or because an SAQ was not obtained at baseline. All study participants were males with an average age of 68 years and were predominantly white (86%). All patients had a past medical history significant for hypertension and hyperlipidemia. More than half (57%) had a prior MI and multivessel disease, although only 1 patient had an ejection fraction of < 35%. The majority of patients enrolled were being treated with BBs (97%) and LANs (94%) with a little more than half prescribed CCBs (60%). A large percentage (97%) of patients were also taking aspirin and a statin.
Improvements in angina symptoms as measured by the SAQ and safety measures, which included details of AEs and discontinuation rates following the initiation of ranolazine within the clinic, have previously been published.17 In summary, it was found that the addition of ranolazine to an optimal medical regimen for CSA improved all dimensions of the SAQ scores at 1 and 3 months compared with baseline (Table). Additionally, it was noted that higher doses may not have been as well tolerated in the veteran population, despite that only a small number of eligible patients were captured. This was because 5 of 7 patients whose dose was increased to 1,000 mg twice daily after 1 month required withdrawal as a result of AEs or lack of efficacy. The AEs reported included dizziness, abdominal pain, blurry vision, nausea and vomiting, dry mouth, and dyspnea.
The pharmacists were able to ensure that relevant electrolytes were replaced during the treatment period and also minimized the number of clinically significant drug interactions. Twenty-one patients received medications at baseline that had known interactions with ranolazine. Two patients required discontinuation of other medications: sotalol and diltiazem. At the time this study was conducted, diltiazem was contraindicated when given concomitantly but has since been allowed per manufacturer recommendations as long as the dose of ranolazine does not exceed 500 mg twice daily. Electrolyte replacement was also required in 3 patients, 2 of whom had hypomagnesemia.
Conclusion
Pharmacists have been influential in managing a variety of chronic diseases. When instituted into collaborative practice agreements, CSA is another unique condition that pharmacists can play a role in treating. Given that pharmacists are heavily involved with cardiovascular risk reduction, combined with the higher cost of ranolazine and the need for monitoring due to its AEs, QTc interval prolongation, and significant drug interactions, the benefits of having pharmacist-oriented clinics can ensure the safe and effective use of medications in the treatment of CSA.
Author disclosures
The authors report no actual or potential conflicts of interest with regard to this article.
Disclaimer
The opinions expressed herein are those of the authors and do not necessarily reflect those of Federal Practitioner, Frontline Medical Communications Inc., the U.S. Government, or any of its agencies. This article may discuss unlabeled or investigational use of certain drugs. Please review complete prescribing information for specific drugs or drug combinations—including indications, contraindications, warnings, and adverse effects—before administering pharmacologic therapy to patients.
1. Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2014 update: A report from the American Heart Association. Circulation. 2014;129:e28-e292.
2. Boden WE, O’Rourke RA, Teo KK, et al; COURAGE Trial Research Group. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503-1516.
3. RITA-2 trial participants. Coronary angioplasty versus medical therapy for angina: The second Randomised Intervention Treatment of Angina (RITA-2) trial. Lancet. 1997;350(9076):461-468.
4. Norton JL, Gibson DL. Establishing an outpatient anticoagulation clinic in a community hospital. Am J Health Syst Pharm. 1996;53(10):1151-1157.
5. Morello CM, Zadvorny EB, Cording MA, Suemoto RT, Skog J, Harari A. Development and clinical outcomes of pharmacist-managed diabetes care clinics. Am J Health Syst Pharm. 2006;63(14):1325-1331.
6. Vivian EM. Improving blood pressure control in a pharmacist-managed hypertension clinic. Pharmacotherapy. 2002;22(12):1533-1540.
7. Cording MA, Engelbrecht-Zadvorny EB, Pettit BJ, Eastham JH, Sandoval R. Development of a pharmacist-managed lipid clinic. Ann Pharmacother. 2002;36(5):892-904.
8. Geber J, Parra D, Beckey NP, Korman L. Optimizing drug therapy in patients with cardiovascular disease: The impact of pharmacist-managed pharmacotherapy clinics in a primary care setting. Pharmacotherapy. 2002; 22(6):738-747.
9. Ranexa [package insert]. Foster City, CA: Gilead Sciences, Inc.; 2013.
10. VHA Pharmacy Benefits Management Strategic Healthcare Group and the Medical Advisory Panel. Ranolazine. National PBM Drug Monograph. U.S. Department of Veterans Affairs Pharmacy Benefits Management Services Website. http://www.pbm.va.gov/clinicalguidance/drugmonographs/Ranolazine.pdf. Published June 2007. Accessed May 7, 2014.
11. Fraker TD Jr, Fihn SD; writing on behalf of the 2002 Chronic Stable Angina Writing Committee. 2007 chronic angina focused update of the ACC/AHA 2002 guidelines for the management of patients with chronic stable angina: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Writing Group to develop the focused update of the 2002 guidelines for the management of patients with chronic stable angina. Circulation. 2007;116(23):2762-2772.
12. Funck-Brentano C, Jaillon P. Rate-corrected QT interval: Techniques and limitations. Am J Cardiol. 1993;72(6):17B-22B.
13. Spertus JA, Winder JA, Dewhurst TA, et al. Development and evaluation of the Seattle Angina Questionnaire: A new functional status measure for coronary artery disease. J Am Coll Cardiol. 1995;25(2):333-341.
14. Drew BJ, Ackerman MJ, Funk M, et al; American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology, the Council on Cardiovascular Nursing, and the American College of Cardiology Foundation. Prevention of torsade de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121(8):1047-1060.
15. Heidenreich PA, McDonald KM, Hastie T, et al. Meta-analysis of trials comparing beta-blockers, calcium antagonists, and nitrates for stable angina. JAMA. 1999;281(20):1927-1936.
16. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The JNC 7 report. JAMA. 2003;289(19):2560-2572.
17. Reeder DN, Gillette MA, Franck AJ, Frohnapple DJ. Clinical experience with ranolazine in a veteran population with chronic stable angina. Ann Pharmacother. 2012;46(1):42-50.
1. Go AS, Mozaffarian D, Roger VL, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics–2014 update: A report from the American Heart Association. Circulation. 2014;129:e28-e292.
2. Boden WE, O’Rourke RA, Teo KK, et al; COURAGE Trial Research Group. Optimal medical therapy with or without PCI for stable coronary disease. N Engl J Med. 2007;356(15):1503-1516.
3. RITA-2 trial participants. Coronary angioplasty versus medical therapy for angina: The second Randomised Intervention Treatment of Angina (RITA-2) trial. Lancet. 1997;350(9076):461-468.
4. Norton JL, Gibson DL. Establishing an outpatient anticoagulation clinic in a community hospital. Am J Health Syst Pharm. 1996;53(10):1151-1157.
5. Morello CM, Zadvorny EB, Cording MA, Suemoto RT, Skog J, Harari A. Development and clinical outcomes of pharmacist-managed diabetes care clinics. Am J Health Syst Pharm. 2006;63(14):1325-1331.
6. Vivian EM. Improving blood pressure control in a pharmacist-managed hypertension clinic. Pharmacotherapy. 2002;22(12):1533-1540.
7. Cording MA, Engelbrecht-Zadvorny EB, Pettit BJ, Eastham JH, Sandoval R. Development of a pharmacist-managed lipid clinic. Ann Pharmacother. 2002;36(5):892-904.
8. Geber J, Parra D, Beckey NP, Korman L. Optimizing drug therapy in patients with cardiovascular disease: The impact of pharmacist-managed pharmacotherapy clinics in a primary care setting. Pharmacotherapy. 2002; 22(6):738-747.
9. Ranexa [package insert]. Foster City, CA: Gilead Sciences, Inc.; 2013.
10. VHA Pharmacy Benefits Management Strategic Healthcare Group and the Medical Advisory Panel. Ranolazine. National PBM Drug Monograph. U.S. Department of Veterans Affairs Pharmacy Benefits Management Services Website. http://www.pbm.va.gov/clinicalguidance/drugmonographs/Ranolazine.pdf. Published June 2007. Accessed May 7, 2014.
11. Fraker TD Jr, Fihn SD; writing on behalf of the 2002 Chronic Stable Angina Writing Committee. 2007 chronic angina focused update of the ACC/AHA 2002 guidelines for the management of patients with chronic stable angina: A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines Writing Group to develop the focused update of the 2002 guidelines for the management of patients with chronic stable angina. Circulation. 2007;116(23):2762-2772.
12. Funck-Brentano C, Jaillon P. Rate-corrected QT interval: Techniques and limitations. Am J Cardiol. 1993;72(6):17B-22B.
13. Spertus JA, Winder JA, Dewhurst TA, et al. Development and evaluation of the Seattle Angina Questionnaire: A new functional status measure for coronary artery disease. J Am Coll Cardiol. 1995;25(2):333-341.
14. Drew BJ, Ackerman MJ, Funk M, et al; American Heart Association Acute Cardiac Care Committee of the Council on Clinical Cardiology, the Council on Cardiovascular Nursing, and the American College of Cardiology Foundation. Prevention of torsade de pointes in hospital settings: A scientific statement from the American Heart Association and the American College of Cardiology Foundation. Circulation. 2010;121(8):1047-1060.
15. Heidenreich PA, McDonald KM, Hastie T, et al. Meta-analysis of trials comparing beta-blockers, calcium antagonists, and nitrates for stable angina. JAMA. 1999;281(20):1927-1936.
16. Chobanian AV, Bakris GL, Black HR, et al; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. The JNC 7 report. JAMA. 2003;289(19):2560-2572.
17. Reeder DN, Gillette MA, Franck AJ, Frohnapple DJ. Clinical experience with ranolazine in a veteran population with chronic stable angina. Ann Pharmacother. 2012;46(1):42-50.
Regulator of hepcidin discovered

which secrete erythroferrone
Credit: Leon Kautz/UCLA
Researchers have discovered a new hormone, called erythroferrone, which regulates hepcidin, the main iron hormone that controls iron absorption and distribution in the body.
Using a mouse model, reseachers determined that erythroferrone is made by red blood-cell progenitors in the bone marrow, and its levels vary according to the demand for red blood cells.
“Modulating the activity of erythroferrone,” said study author Tomas Ganz, MD, PhD, of the David Geffen School of Medicine at UCLA, “could be a viable strategy for the treatment of iron disorders of both overabundance and scarcity.”
Higher levels of erythroferrone suppress hepcidin, thereby allowing more iron to be made available for red blood-cell production. Erythroferrone, or drugs acting like it, could suppress hepcidin and make more iron available for red blood-cell production.
The team began their inquiry by studying the impact of hemorrhage on the bone marrow. That led them to focus on a specific protein that was secreted in the blood. The protein belonged to a family of proteins involved in cell-to-cell communication.
They used recombinant DNA technology and found that the hormone suppressed the production of hepcidin, which affected iron metabolism.
Erythroferrone-deficient mice do not suppress hepcidin quickly after hemorrhage and consequently have delayed recovery from blood loss.
The investigators also found that erythroferrone expression is greatly increased in Hbbth3/+ mice with thalassemia intermedia, indicating that the hormone contributes to the suppression of hepcidin and iron overload characteristic of the disease.
“Overproduction of erythroferrone may be a major cause of iron overload in untransfused patients and may contribute to iron overload in transfused patients,” said study author Elizabeta Nemeth, PhD, also of the David Geffen School of Medicine at UCLA.
“The identification of erythroferrone can potentially allow researchers and drug developers to target the hormone for specific treatment to prevent iron overload in Cooley’s anemia,” she said.
The investigators reported their findings recently in Nature Genetics.
They noted that further research is needed to understand the role of the new hormone in various blood diseases and to study the mechanisms through which erythroferrone regulates hepcidin. ![]()
which secrete erythroferrone
Credit: Leon Kautz/UCLA
Researchers have discovered a new hormone, called erythroferrone, which regulates hepcidin, the main iron hormone that controls iron absorption and distribution in the body.
Using a mouse model, reseachers determined that erythroferrone is made by red blood-cell progenitors in the bone marrow, and its levels vary according to the demand for red blood cells.
“Modulating the activity of erythroferrone,” said study author Tomas Ganz, MD, PhD, of the David Geffen School of Medicine at UCLA, “could be a viable strategy for the treatment of iron disorders of both overabundance and scarcity.”
Higher levels of erythroferrone suppress hepcidin, thereby allowing more iron to be made available for red blood-cell production. Erythroferrone, or drugs acting like it, could suppress hepcidin and make more iron available for red blood-cell production.
The team began their inquiry by studying the impact of hemorrhage on the bone marrow. That led them to focus on a specific protein that was secreted in the blood. The protein belonged to a family of proteins involved in cell-to-cell communication.
They used recombinant DNA technology and found that the hormone suppressed the production of hepcidin, which affected iron metabolism.
Erythroferrone-deficient mice do not suppress hepcidin quickly after hemorrhage and consequently have delayed recovery from blood loss.
The investigators also found that erythroferrone expression is greatly increased in Hbbth3/+ mice with thalassemia intermedia, indicating that the hormone contributes to the suppression of hepcidin and iron overload characteristic of the disease.
“Overproduction of erythroferrone may be a major cause of iron overload in untransfused patients and may contribute to iron overload in transfused patients,” said study author Elizabeta Nemeth, PhD, also of the David Geffen School of Medicine at UCLA.
“The identification of erythroferrone can potentially allow researchers and drug developers to target the hormone for specific treatment to prevent iron overload in Cooley’s anemia,” she said.
The investigators reported their findings recently in Nature Genetics.
They noted that further research is needed to understand the role of the new hormone in various blood diseases and to study the mechanisms through which erythroferrone regulates hepcidin. ![]()
which secrete erythroferrone
Credit: Leon Kautz/UCLA
Researchers have discovered a new hormone, called erythroferrone, which regulates hepcidin, the main iron hormone that controls iron absorption and distribution in the body.
Using a mouse model, reseachers determined that erythroferrone is made by red blood-cell progenitors in the bone marrow, and its levels vary according to the demand for red blood cells.
“Modulating the activity of erythroferrone,” said study author Tomas Ganz, MD, PhD, of the David Geffen School of Medicine at UCLA, “could be a viable strategy for the treatment of iron disorders of both overabundance and scarcity.”
Higher levels of erythroferrone suppress hepcidin, thereby allowing more iron to be made available for red blood-cell production. Erythroferrone, or drugs acting like it, could suppress hepcidin and make more iron available for red blood-cell production.
The team began their inquiry by studying the impact of hemorrhage on the bone marrow. That led them to focus on a specific protein that was secreted in the blood. The protein belonged to a family of proteins involved in cell-to-cell communication.
They used recombinant DNA technology and found that the hormone suppressed the production of hepcidin, which affected iron metabolism.
Erythroferrone-deficient mice do not suppress hepcidin quickly after hemorrhage and consequently have delayed recovery from blood loss.
The investigators also found that erythroferrone expression is greatly increased in Hbbth3/+ mice with thalassemia intermedia, indicating that the hormone contributes to the suppression of hepcidin and iron overload characteristic of the disease.
“Overproduction of erythroferrone may be a major cause of iron overload in untransfused patients and may contribute to iron overload in transfused patients,” said study author Elizabeta Nemeth, PhD, also of the David Geffen School of Medicine at UCLA.
“The identification of erythroferrone can potentially allow researchers and drug developers to target the hormone for specific treatment to prevent iron overload in Cooley’s anemia,” she said.
The investigators reported their findings recently in Nature Genetics.
They noted that further research is needed to understand the role of the new hormone in various blood diseases and to study the mechanisms through which erythroferrone regulates hepcidin. ![]()
Preoperative angiotensin axis blockade therapy, intraoperative hypotension, and the risks of postoperative acute kidney injury
We read with interest the analysis by Nielson et al., which concluded that patients undergoing major elective orthopedic surgery, who receive preoperative angiotensin axis blockade (AAB) therapy, have an associated increased risk of postinduction hypotension and postoperative acute kidney injury (AKI), with greater hospital length of stay.[1] We could not agree more with this conclusion.
Recently, we reported in the British Medical Journal our experiences with 2 patients who developed moderately severe AKI following surgical procedures while on concurrent AAB therapy, which led to prolonged hospital stays.[2, 3] The second patient was a 46‐year‐old obese Caucasian hypertensive male on triple‐whammy medications who developed intraoperative hypotension following an elective right‐hip arthroplasty.[3] Baseline serum creatinine more than doubled to 2.58 mg/dL within 36 hours. Hospital stay was prolonged. He improved with treatment before discharge.[3] We dubbed a new syndrome of quadruple whammy to represent perioperative AKI following intraoperative hypotension in patients on concurrent triple whammy medications.[2, 3]
We therefore support calls for the preemptive withholding of AAB before major elective surgical procedures, especially cardiovascular and orthopedic ones.[4] This is the cornerstone of a preventative nephrology paradigm called renoprevention, which we have repeatedly espoused since 2009.[5]
- , , , . Angiotensin axis blockade, hypotension, and acute kidney injury in elective major orthopedic surgery. J Hosp Med. 2014;9(5):283–288.
- , . “Quadruple whammy,” a new syndrome of potentially preventable yet iatrogenic acute kidney injury in the ICU. BMJ 2013: Rapid Response, Published online February 25, 2013. http://www.bmj.com/content/346/bmj.f678/rr/632570.
- , . A second case of “quadruple whammy” in a week in a northwestern Wisconsin hospital. BMJ. 2013: Rapid Response, Published online March 1, 2013. http://www.bmj.com/content/346/bmj.f678/rr/633687.
- , , , , , . Acute kidney injury and death associated with renin angiotensin system blockade in cardiothoracic surgery: a meta‐analysis of observational studies. Am J Kidney Dis. 2013;62(6):1077–1086.
- . Reno‐prevention vs. reno‐protection: a critical re‐appraisal of the evidence‐base from the large RAAS blockade trials after ONTARGET—a call for more circumspection. QJM. 2009;102:155–167.
We read with interest the analysis by Nielson et al., which concluded that patients undergoing major elective orthopedic surgery, who receive preoperative angiotensin axis blockade (AAB) therapy, have an associated increased risk of postinduction hypotension and postoperative acute kidney injury (AKI), with greater hospital length of stay.[1] We could not agree more with this conclusion.
Recently, we reported in the British Medical Journal our experiences with 2 patients who developed moderately severe AKI following surgical procedures while on concurrent AAB therapy, which led to prolonged hospital stays.[2, 3] The second patient was a 46‐year‐old obese Caucasian hypertensive male on triple‐whammy medications who developed intraoperative hypotension following an elective right‐hip arthroplasty.[3] Baseline serum creatinine more than doubled to 2.58 mg/dL within 36 hours. Hospital stay was prolonged. He improved with treatment before discharge.[3] We dubbed a new syndrome of quadruple whammy to represent perioperative AKI following intraoperative hypotension in patients on concurrent triple whammy medications.[2, 3]
We therefore support calls for the preemptive withholding of AAB before major elective surgical procedures, especially cardiovascular and orthopedic ones.[4] This is the cornerstone of a preventative nephrology paradigm called renoprevention, which we have repeatedly espoused since 2009.[5]
We read with interest the analysis by Nielson et al., which concluded that patients undergoing major elective orthopedic surgery, who receive preoperative angiotensin axis blockade (AAB) therapy, have an associated increased risk of postinduction hypotension and postoperative acute kidney injury (AKI), with greater hospital length of stay.[1] We could not agree more with this conclusion.
Recently, we reported in the British Medical Journal our experiences with 2 patients who developed moderately severe AKI following surgical procedures while on concurrent AAB therapy, which led to prolonged hospital stays.[2, 3] The second patient was a 46‐year‐old obese Caucasian hypertensive male on triple‐whammy medications who developed intraoperative hypotension following an elective right‐hip arthroplasty.[3] Baseline serum creatinine more than doubled to 2.58 mg/dL within 36 hours. Hospital stay was prolonged. He improved with treatment before discharge.[3] We dubbed a new syndrome of quadruple whammy to represent perioperative AKI following intraoperative hypotension in patients on concurrent triple whammy medications.[2, 3]
We therefore support calls for the preemptive withholding of AAB before major elective surgical procedures, especially cardiovascular and orthopedic ones.[4] This is the cornerstone of a preventative nephrology paradigm called renoprevention, which we have repeatedly espoused since 2009.[5]
- , , , . Angiotensin axis blockade, hypotension, and acute kidney injury in elective major orthopedic surgery. J Hosp Med. 2014;9(5):283–288.
- , . “Quadruple whammy,” a new syndrome of potentially preventable yet iatrogenic acute kidney injury in the ICU. BMJ 2013: Rapid Response, Published online February 25, 2013. http://www.bmj.com/content/346/bmj.f678/rr/632570.
- , . A second case of “quadruple whammy” in a week in a northwestern Wisconsin hospital. BMJ. 2013: Rapid Response, Published online March 1, 2013. http://www.bmj.com/content/346/bmj.f678/rr/633687.
- , , , , , . Acute kidney injury and death associated with renin angiotensin system blockade in cardiothoracic surgery: a meta‐analysis of observational studies. Am J Kidney Dis. 2013;62(6):1077–1086.
- . Reno‐prevention vs. reno‐protection: a critical re‐appraisal of the evidence‐base from the large RAAS blockade trials after ONTARGET—a call for more circumspection. QJM. 2009;102:155–167.
- , , , . Angiotensin axis blockade, hypotension, and acute kidney injury in elective major orthopedic surgery. J Hosp Med. 2014;9(5):283–288.
- , . “Quadruple whammy,” a new syndrome of potentially preventable yet iatrogenic acute kidney injury in the ICU. BMJ 2013: Rapid Response, Published online February 25, 2013. http://www.bmj.com/content/346/bmj.f678/rr/632570.
- , . A second case of “quadruple whammy” in a week in a northwestern Wisconsin hospital. BMJ. 2013: Rapid Response, Published online March 1, 2013. http://www.bmj.com/content/346/bmj.f678/rr/633687.
- , , , , , . Acute kidney injury and death associated with renin angiotensin system blockade in cardiothoracic surgery: a meta‐analysis of observational studies. Am J Kidney Dis. 2013;62(6):1077–1086.
- . Reno‐prevention vs. reno‐protection: a critical re‐appraisal of the evidence‐base from the large RAAS blockade trials after ONTARGET—a call for more circumspection. QJM. 2009;102:155–167.
In response to “Preoperative angiotensin axis blockade therapy, intraoperative hypotension, and the risks of postoperative acute kidney injury”
We are pleased to note the response of Onuigbo et al. to our article demonstrating an increase in acute kidney injury (AKI) associated with angiotensin axis blockade (AAB) in major orthopedic surgery.[1] Like Onuigbo et al., we also noted that intraoperative hypotension and AAB are associated with AKI.[2] In addition, we found that AAB‐associated AKI occurred independently of intraoperative hypotension. Because of our findings, we withhold angiotensin‐converting enzyme inhibitors and angiotensin receptor blockers on the day of surgery in all patients presenting for major orthopedic surgery whose blood pressure is well controlled preoperatively. We were concerned that this practice might increase the incidence of pre‐ and postoperative hypertension in such patients, but we have been reassured by a recent article demonstrating that this does not occur in outpatient surgical patients.[3]
We caution, however, that the common sense approach of stopping AAB preoperatively to avoid possible AKI still requires evaluation by a properly conducted randomized controlled trial. Because of the prolonged systemic half‐life and duration of tissue activity (>24 hours) of many AAB agents,[4] the required preoperative cessation period of AAB may vary considerably.
- , , , . Angiotensin axis blockade, hypotension, and acute kidney injury in elective major orthopedic surgery. J Hosp Med. 2014;9:283–288.
- , . A second case of “quadruple whammy” in a week in a northwestern Wisconsin hospital. BMJ. 2013;346:f678.
- , , , . The risk of hypertension after preoperative discontinuation of angiotensin‐converting enzyme inhibitors or angiotensin receptor antagonists in ambulatory and same‐day admission patients. Anesth Analg. 2014;118:938–944.
- . Management of hypotension associated with angiotensin‐axis blockade and general anesthesia administration. J Cardiothorac Vasc Anesth. 2013;27:156–167.
We are pleased to note the response of Onuigbo et al. to our article demonstrating an increase in acute kidney injury (AKI) associated with angiotensin axis blockade (AAB) in major orthopedic surgery.[1] Like Onuigbo et al., we also noted that intraoperative hypotension and AAB are associated with AKI.[2] In addition, we found that AAB‐associated AKI occurred independently of intraoperative hypotension. Because of our findings, we withhold angiotensin‐converting enzyme inhibitors and angiotensin receptor blockers on the day of surgery in all patients presenting for major orthopedic surgery whose blood pressure is well controlled preoperatively. We were concerned that this practice might increase the incidence of pre‐ and postoperative hypertension in such patients, but we have been reassured by a recent article demonstrating that this does not occur in outpatient surgical patients.[3]
We caution, however, that the common sense approach of stopping AAB preoperatively to avoid possible AKI still requires evaluation by a properly conducted randomized controlled trial. Because of the prolonged systemic half‐life and duration of tissue activity (>24 hours) of many AAB agents,[4] the required preoperative cessation period of AAB may vary considerably.
We are pleased to note the response of Onuigbo et al. to our article demonstrating an increase in acute kidney injury (AKI) associated with angiotensin axis blockade (AAB) in major orthopedic surgery.[1] Like Onuigbo et al., we also noted that intraoperative hypotension and AAB are associated with AKI.[2] In addition, we found that AAB‐associated AKI occurred independently of intraoperative hypotension. Because of our findings, we withhold angiotensin‐converting enzyme inhibitors and angiotensin receptor blockers on the day of surgery in all patients presenting for major orthopedic surgery whose blood pressure is well controlled preoperatively. We were concerned that this practice might increase the incidence of pre‐ and postoperative hypertension in such patients, but we have been reassured by a recent article demonstrating that this does not occur in outpatient surgical patients.[3]
We caution, however, that the common sense approach of stopping AAB preoperatively to avoid possible AKI still requires evaluation by a properly conducted randomized controlled trial. Because of the prolonged systemic half‐life and duration of tissue activity (>24 hours) of many AAB agents,[4] the required preoperative cessation period of AAB may vary considerably.
- , , , . Angiotensin axis blockade, hypotension, and acute kidney injury in elective major orthopedic surgery. J Hosp Med. 2014;9:283–288.
- , . A second case of “quadruple whammy” in a week in a northwestern Wisconsin hospital. BMJ. 2013;346:f678.
- , , , . The risk of hypertension after preoperative discontinuation of angiotensin‐converting enzyme inhibitors or angiotensin receptor antagonists in ambulatory and same‐day admission patients. Anesth Analg. 2014;118:938–944.
- . Management of hypotension associated with angiotensin‐axis blockade and general anesthesia administration. J Cardiothorac Vasc Anesth. 2013;27:156–167.
- , , , . Angiotensin axis blockade, hypotension, and acute kidney injury in elective major orthopedic surgery. J Hosp Med. 2014;9:283–288.
- , . A second case of “quadruple whammy” in a week in a northwestern Wisconsin hospital. BMJ. 2013;346:f678.
- , , , . The risk of hypertension after preoperative discontinuation of angiotensin‐converting enzyme inhibitors or angiotensin receptor antagonists in ambulatory and same‐day admission patients. Anesth Analg. 2014;118:938–944.
- . Management of hypotension associated with angiotensin‐axis blockade and general anesthesia administration. J Cardiothorac Vasc Anesth. 2013;27:156–167.