User login
Decentralized vs Centralized Pharmacist Treatment of Patients With Atrial Fibrillation Managed With Direct Oral Anticoagulants
In the U.S. about 2.7 to 6.1 million people have atrial fibrillation (AF).1 This condition affects the rhythm of the heart, causes blood in the heart to become stagnant, and puts patients at high risk for developing a systemic embolism, particularly a stroke.1 Recent studies have shown that AF accounts for at least 15% of all strokes in the U.S. and 36% of strokes in people aged > 80 years.2
For patients aged > 60 years, the gold standard of long-term anticoagulation for reducing the risk of stroke has been oral vitamin K antagonist (warfarin) therapy.2 Although overwhelming evidence exists that supports the use of warfarin in these patients, warfarin is a narrow therapeutic index medication that requires frequent laboratory monitoring of international normalized ratio (INR) for dose titration guidance. There is also strong evidence that pharmacist-run anticoagulation clinics have improved patient-centered outcomes in patients prescribed warfarin.3-5
Direct oral anticoagulants (DOACs) are recently approved oral medications used as alternatives to warfarin for anticoagulation in AF. Direct oral anticoagulants do not require INR monitoring or any laboratory test for efficacy. In 2010, the FDA approved the first DOAC, dabigatran, for use in patients with AF. In 2011, rivaroxaban received approval for the same indication. One potential drawback of these new agents relative to warfarin is the lack of availability of a reversal agent that can be used in the event of a life-threatening bleeding event. Dabigatran is the only DOAC with an FDA-approved available reversal agent. In both 2011 and 2012, dabigatran, warfarin, and other anticoagulants topped the Institute for Safe Medicine Practice list of suspect drugs related to adverse events (AEs). These data prompted the Joint Commission to incorporate anticoagulation into the 2017 National Hospital Patient Safety Goals to improve patient outcomes and reduce harm from use of anticoagulants.6
In early 2011, the VHA produced national guidance on the treatment of patients who receive DOACs; this guidance was updated most recently in September 2016.7 Patients who were receiving DOACs at the Ralph H. Johnson VAMC (RHJVAMC) were initially monitored by 12 primary care pharmacists at the main hospital or at community-based outpatient clinics (CBOCs). Ambulatory care pharmacists at RHJVAMC work under a scope of practice to prescribe and adjust certain classes of medications to provide the highest level of care to more than 65,000 veterans in South Carolina and Georgia. Historically at RHJVAMC, warfarin has been the anticoagulant most commonly used for AF, though dabigatran and rivaroxaban have gained in popularity after being added to the national VA formulary.
In November 2012, for better monitoring of patient outcomes, improved efficiency of the primary care pharmacist clinics, and increased access to care in these clinics, treatment of patients prescribed DOACs was shifted to a centralized model that involved 3 anticoagulation clinical pharmacy specialists.
Centralized pharmacy services have a small number of core team members in a specific service for a particular disease, which reduces the number of different pharmacists a patient could talk to for management of a particular condition. Centralized pharmacy services allow for streamlining anticoagulation management to a small group of individual pharmacists considered specialists in anticoagulation. This shift in management to centralized anticoagulation services was supported at RHJVAMC by findings from a study of a pharmacist-run centralized anticoagulation clinic: Patients treated by the centralized clinic were 39% less likely to experience an anticoagulation therapy complication.8
Protocol for dabigatran follow-up and monitoring at RHJVAMC was developed by clinical and supervisory pharmacy staff, to align with national VA guidance. When a provider determines a patient is a candidate for dabigatran, an outpatient consultation is entered for the clinical pharmacy specialist to review the appropriateness of the patient selection for therapy. If the patient is eligible for therapy, the pharmacist contacts the patient to set up an initial visit to confirm selection and to provide the first dabigatran prescription and counseling. For assessments, with specific emphasis on adherence and AE monitoring, the patient is contacted 2 weeks, 1 month, 3 months, and every 6 months after the initial appointment.
Although most of the literature supports pharmacist-managed anticoagulation for patients who receive warfarin, DOACs have become more integrated into practice and more evaluated. Evidence supports pharmacists' interventions on evaluation of patient education and dosing, but there is conflicting evidence regarding pharmacists' impact on adherence after 3 months of therapy.9,10 In a larger VA study of the impact of dabigatran adherence on patient-centered outcomes, patients were mostly nonadherent to prescribed dosing.11 These studies support the need for improved adherence in patients prescribed DOACs and the need for further investigation of pharmacists' roles in improving patient outcomes.
Methods
This single-center, retrospective anticoagulant-use evaluation covered 2 study periods between November 1, 2011 and October 31, 2013. Study approval was obtained from the institutional review board of the Medical University of South Carolina and the research and development committee of RHJVAMC. The study population consisted of veterans who had a diagnosis of AF and received at least 3 outpatient prescription fills of a 30-day supply of dabigatran at RHJVAMC during either or both of the study periods. Patients were excluded if they were pregnant or planning to become pregnant or were incarcerated at any time during the study period. Dabigatran was selected because it was the first DOAC added to the local VA formulary before the start of this study.
Patients who met the inclusion criteria were separated into 2 groups based on the dates of their prescription fills. The precentralization group included patients treated by primary care pharmacists from November 1, 2011 to October 31, 2012; the postcentralization group included patients treated by anticoagulation clinical pharmacy specialists from November 1, 2012 to October 31, 2013. In each group, patients were followed for 1 year during their respective study period. For analysis, patients were included in both study periods if they received at least 3 fills of dabigatran during each period.
Medication possession ratio (MPR), which was used to measure the primary endpoint of adherence, is defined as the proportion of days a patient had dabigatran. The MPR denominator is the total number of days between the first and last prescription refill dates within the 52-week study period; the numerator is calculated by summing the days' supply for all but the last filling of the medication during each respective period. Nonadherence was defined as an MPR < 0.8 (or 80%), which has been used to define poor adherence in the literature.12 The authors calculated all patients' mean MPRs and compared them to determine statistical significance by repeated-measures linear regression. Descriptive statistics on proportion of patients in each study group with MPR < 0.8 were examined. Last, the authors performed a comparative subanalysis of median MPRs to determine whether there was an adherence difference between patients initially started on dabigatran at RHJVAMC and patients who were started on dabigatran before receiving it at RHJVAMC.
The secondary focus of this study was safety outcomes, including any bleeding event or thromboembolism within either study period. A bleeding event was defined as any major or minor bleeding event recognized through ICD-9 codes or any bleeding recorded in the patient's chart and noted during chart review, as well as any serum hemoglobin (Hgb) level decrease of ≥ to 2 g/dL during the study period. Thromboembolism was defined as a thromboembolism recognized through ICD-9 codes or any thromboembolism noted during chart review. Descriptive statistics were reported for this outcome, and a chi-square test was used to compare bleeding events between groups to determine significance.
The tertiary focus of this study was clinical efficiency as determined by number of primary care pharmacist visits during each study period. Primary care pharmacist visits were included for all primary care pharmacists in primary care clinics at the main hospital and in all 6 CBOCs.
For statistical analysis α was set at 0.05, and P < .05 was considered statistically significant. SAS Enterprise Guide software (Cary, North Carolina) was used for all statistical analyses.
Results
An initial data pull was completed from the RHJVAMC prescription records database for patients who had ≥ 3 prescriptions of dabigatran filled for treatment of AF during the study period, which yielded 65 unique patients. There were 34 patients in the precentralization group and 55 patients in the postcentralization group. Twenty-four unique patients were included in both study groups.
Mean MPR was 1.01 (range, 0.59-1.41) for the precentralization study period and 0.96 (range, 0.33-1.36) for the postcentralization period (Table 1). The difference was not statistically significant (P = .91). Number of patients considered nonadherent (MPR < 0.8) was 3 (8.82%) in the precentralization group and 8 (14.6%) in the postcentralization group.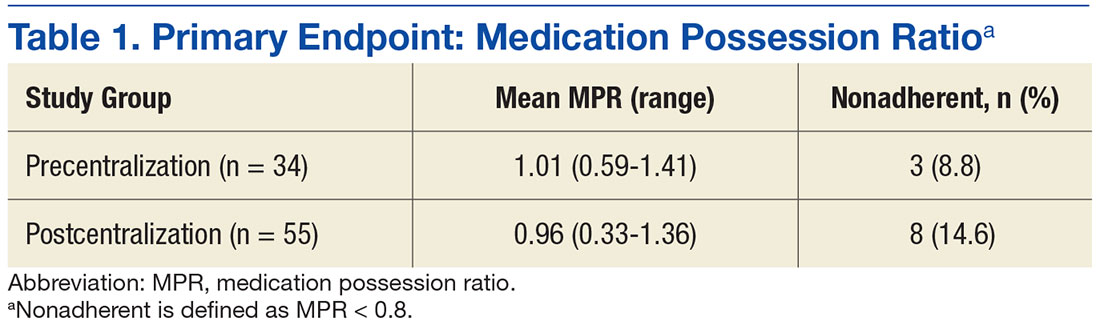
The primary endpoint subanalysis compared the median MPRs for the patients initially started on dabigatran at RHJVAMC (de novo starts) and the patients who were started on dabigatran before receiving it at RHJVAMC (prior starts). In each group, number and percentage of patients determined to be nonadherent by MPR were evaluated as well. De novo patients received initial assessment, counseling, and a dabigatran prescription from RHJVAMC pharmacists before or during the study period, and prior patients were initially prescribed dabigatran at another VA facility or at a non-VA facility (Table 2).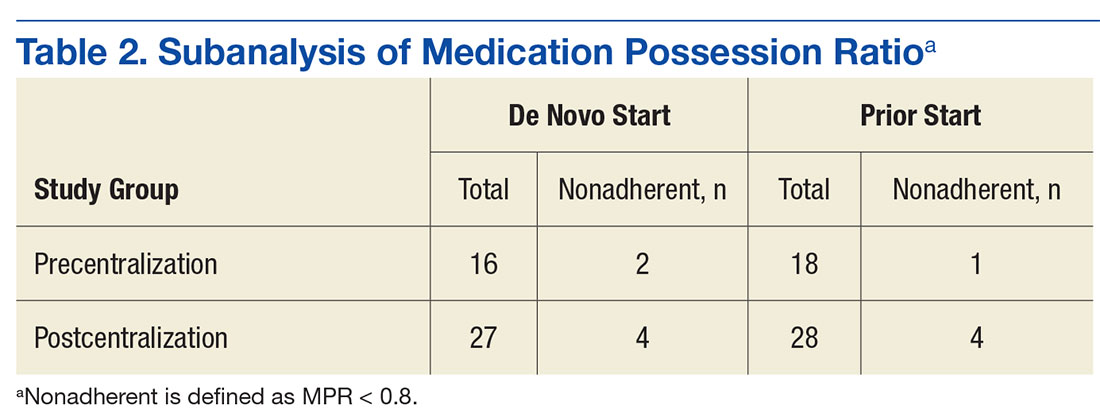
Regarding safety outcomes (secondary endpoint), a bleeding event was identified in 6 (17.7%) of the precentralization patients and 7 (12.7%) of the postcentralization patients. Of the 6 precentralization events, 1 was a case of hemoptysis, 1 was a hematoma on the forehead, 1 was a lower gastrointestinal bleed (unconfirmed), 1 was retinal hemorrhaging (noted by ophthalmologist), and 2 were serum Hgb level decreases of more than 2 g/dL (neither patient required transfusion of packed red blood cells). Of the 7 postcentralization events, 1 was persistent hematochezia caused by hemorrhoids, 1 was hematuria, 1 was a hematoma, 1 was an upper gastrointestinal bleed (required blood transfusion), and 4 were serum Hgb level decreases of more than 2 g/dL (1 of the 4 required transfusion). No precentralization patient had any evidence of thromboembolism during the study period; 1 postcentralization patient had a superficial venous thromboembolism near a hematoma on the elbow.
Discussion
In this single-center, retrospective medication-use evaluation, the authors found a high rate of adherence to dabigatran before and after centralization of outpatient DOAC management by pharmacists. There was no statistically significant difference in bleeding events between the study periods, but primary care pharmacist visits increased by 108% from precentralization to postcentralization. Although the primary outcome findings did not refute the study's null hypothesis, results support implementing centralized pharmacist DOAC management to maintain a high rate of adherence and a low incidence of adverse outcomes and providing more primary care pharmacist services to increase access to care for other chronic diseases.
Although there was no statistically significant difference in adherence rates between study periods, the 2 groups' rates were higher than the national average of 72%, as calculated by the proportion-of-days-covered (PDC) equation (median, 74%) in a 2015 large-scale study of site-level adherence in more than 5,000 VA patients.13 The authors' findings support that study's significant finding of a high rate of adherence to pharmacist-provided dabigatran treatment. This study's adherence rate also was higher than the median PDC rate reported in a 2014 study that focused on dabigatran adherence: 94% (mean, 84%; SD, 22%).11
The RHJVAMC follows national VA guidance on pharmacist follow-up for patients who receive DOACs. This follow-up focuses on frequent counseling over the first 6 months of de novo DOAC treatment and on monitoring and assessing adherence and AEs. Although there is less laboratory monitoring for DOAC treatment than for treatment with vitamin K antagonists (eg, warfarin), telephone monitoring as described in this study has been associated with a high adherence rate and minimization of AEs. The 2014 study with the 94% median PDC rate also showed an association of decreased adherence and increased harm, including combined all-cause mortality and stroke (hazard ratio, 1.13; 95% confidence interval [CI], 1.07-1.19 per 10% decrease in PDC rate).11
This study's subanalysis revealed no difference in adherence between patients initially started on dabigatran at RHJVAMC and patients who were started on dabigatran before receiving it at RHJVAMC. Each group had a high rate of adherence. Shore and colleagues found that most of the VA sites they surveyed (22/41) had anticoagulation clinics monitoring patients who were prescribed dabigatran.13 Pharmacist-led monitoring of adherence and AEs led to increased adherence to dabigatran treatment (relative risk, 1.25; 95% CI, 1.11-1.41), which was the standard of care at RHJVAMC throughout their entire study. Many of these factors may explain the very high rate of adherence found in the present study, specifically in comparison to previously reported national averages.
In addition, the authors found no statistically significant difference in bleeding outcomes between the precentralization and postcentralization groups. Their incidence of bleeding was similar to the 16.6% rate reported in the package insert for dabigatran.14 Furthermore, the safety outcomes were similar for both groups in this study, which may be attributable to the quality of patient care provided by all RHJVAMC pharmacists, particularly in the setting of dabigatran management.
Many studies have found an association between dabigatran use and an increased rate of bleeding, particularly gastrointestinal, as demonstrated in several patients in this study. Evidence of these clinically significant AEs further supports pharmacists' close monitoring to detect these AEs and working with patients' providers to determine whether an alternative anticoagulant should be used.
A significant finding of this study regarding centralization of DOAC management by pharmacists was the increased number of primary care pharmacist visits. By streamlining all anticoagulant services to anticoagulation clinical pharmacy specialists, primary care pharmacists were able to care for more veterans and increase access to care without adding staff. The centralized anticoagulation pharmacists were volunteers who held other positions within the department; they did not have to be replaced when they became anticoagulation providers. This workload reallocation helped the RHJVAMC pharmacy department increase access to care.
Limitations
This study had several potential limitations. First, MPR, a widely studied common tool for assessing adherence, has been criticized for often being imprecise when used with short study periods.12 Another commonly used adherence measure is PDC rate, which has been reported in several large-scale studies of dabigatran therapy. The authors selected MPR for the present study because MPR calculation is more practical in the patient population and because MPR and PDC rate are predicted to yield similar results in assessments of adherence to a single medication.12 It also should be noted that both MPR and PDC rate are surrogate markers for adherence and assume adherence based on the availability of medication to the patient. Assessing adherence in a retrospective study is a challenge, as more reliable adherence assessment--for example, with use of pill counts or blister packs--is not possible. This study's retrospective design was another potential limitation, as an active intervention was not used.
In addition, this study had a small sample, likely attributable to the addition of dabigatran to the VA national formulary just months before the start of the study period. Furthermore, this study was not powered to detect significant differences in safety or efficacy outcomes. Other potential study limitations included having national VA guidance regarding follow-up periods and dabigatran prescription quantity limits during both study periods. Also, there was some potential for pharmacist-initiated refills at follow-up visits, which could falsely increase MPR. Last, the study analyzed only 1 DOAC and not the entire class of medications.
Conclusion
Centralizing DOAC management by clinical pharmacy specialists at a single VA facility helped maintain high rates of dabigatran adherence, above the national average, and low rates of adverse outcomes were maintained in both study groups. In addition, centralization of anticoagulation services improved access to care through an increase in primary care pharmacist visits without the addition of staff. Centralization of DOAC management by pharmacists is a viable option for maintaining high rates of adherence and low rates of adverse outcomes in facilities where the goal is to achieve clinical efficiency.
1. January CT, Wann LS, Alpert JS, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society [published correction appears in J Am Coll Cardiol. 2014;64(21):2305-2307. J Am Coll Cardiol. 2014;64(21):e1-e76.
2. Reiffel JA. New versus traditional approaches to oral anticoagulation in patients with atrial fibrillation. Am J Med. 2014;127(4):e15.
3. Locke C, Ravnan SL, Patel R, Uchizono JA. Reduction in warfarin adverse events requiring patient hospitalization after implementation of pharmacist-managed anticoagulation service. Pharmacotherapy. 2005;25(5):685-689.
4. Poon IO, Lal L, Brown EN, Braun UK. The impact of pharmacist-managed oral anticoagulation therapy in older veterans. J Clin Pharm Ther. 2007;32(1):21-29.
5. Chiquette E, Amato MG, Bussey HI. Comparison of an anticoagulation clinic with usual medical care. Arch Intern Med. 1998;158(15):1641-1647.
6. The Joint Commission. National patient safety goals. https://www.jointcommission.org/as sets/1/6/2017_NPSG_HAP_ER.pdf. Published 2016. Accessed December 6, 2016.
7. Department of Veterans Affairs Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Direct oral anticoagulants (DOACs) (formerly called TSOACs) dabigatran (Pradaxa), rivaroxaban (Xarelto), and apixaban (Eliquis): Criteria for Use for Stroke Prevention in nonvalvular atrial fibrillation (AF) and Edoxaban (SAVAYSA). http://www.pbm.va.gov/PBM/clinicalguidance/criteriaforuse/Anticoagulants_Direct_Oral_DOACs_CFU_and_Algorithm_for_Nonvalvular_Atrial_Fibrillation_Sep_2016.pdf. Updated September 2016. Accessed December 6, 2016.
8. Witt DM, Sadler MA, Shanahan RL, Mazzoli G, Tillman DJ. Effect of a centralized clinical pharmacy anticoagulation service on the outcomes of anticoagulation therapy. Chest. 2005;127(5):1515-1522.
9. Chan LL, Crumpler WL, Jacobson AK. Implementation of pharmacist-managed anticoagulation in patients receiving newer anticoagulants. Am J Health Syst Pharm. 2013;70(15):1285-1286, 1288.
10. Lee PY, Han SY, Miyahara RK. Adherence and outcomes of patients treated with dabigatran: pharmacist-managed anticoagulation clinic versus usual care. Am J Health Syst Pharm. 2013;70(13):1154-1161.
11. Shore S, Carey EP, Turakhia MP, et al. Adherence to dabigatran therapy and longitudinal patient outcomes: insights from the Veterans Health Administration. Am Heart J. 2014;167(6):810-817.
12. Martin BC, Wiley-Exley EK, Richards S, Domino ME, Carey TS, Sleath BL. Contrasting measures of adherence with simple drug use, medication switching and therapeutic duplication. Ann Pharmacother. 2009;43(1):36-44.
13. Shore S, Ho PM, Lambert-Kerzner A, et al. Site-level variation in and practices associated with dabigatran adherence. JAMA. 2015;313(14):1443-1450.
14. Pradaxa [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2015.
In the U.S. about 2.7 to 6.1 million people have atrial fibrillation (AF).1 This condition affects the rhythm of the heart, causes blood in the heart to become stagnant, and puts patients at high risk for developing a systemic embolism, particularly a stroke.1 Recent studies have shown that AF accounts for at least 15% of all strokes in the U.S. and 36% of strokes in people aged > 80 years.2
For patients aged > 60 years, the gold standard of long-term anticoagulation for reducing the risk of stroke has been oral vitamin K antagonist (warfarin) therapy.2 Although overwhelming evidence exists that supports the use of warfarin in these patients, warfarin is a narrow therapeutic index medication that requires frequent laboratory monitoring of international normalized ratio (INR) for dose titration guidance. There is also strong evidence that pharmacist-run anticoagulation clinics have improved patient-centered outcomes in patients prescribed warfarin.3-5
Direct oral anticoagulants (DOACs) are recently approved oral medications used as alternatives to warfarin for anticoagulation in AF. Direct oral anticoagulants do not require INR monitoring or any laboratory test for efficacy. In 2010, the FDA approved the first DOAC, dabigatran, for use in patients with AF. In 2011, rivaroxaban received approval for the same indication. One potential drawback of these new agents relative to warfarin is the lack of availability of a reversal agent that can be used in the event of a life-threatening bleeding event. Dabigatran is the only DOAC with an FDA-approved available reversal agent. In both 2011 and 2012, dabigatran, warfarin, and other anticoagulants topped the Institute for Safe Medicine Practice list of suspect drugs related to adverse events (AEs). These data prompted the Joint Commission to incorporate anticoagulation into the 2017 National Hospital Patient Safety Goals to improve patient outcomes and reduce harm from use of anticoagulants.6
In early 2011, the VHA produced national guidance on the treatment of patients who receive DOACs; this guidance was updated most recently in September 2016.7 Patients who were receiving DOACs at the Ralph H. Johnson VAMC (RHJVAMC) were initially monitored by 12 primary care pharmacists at the main hospital or at community-based outpatient clinics (CBOCs). Ambulatory care pharmacists at RHJVAMC work under a scope of practice to prescribe and adjust certain classes of medications to provide the highest level of care to more than 65,000 veterans in South Carolina and Georgia. Historically at RHJVAMC, warfarin has been the anticoagulant most commonly used for AF, though dabigatran and rivaroxaban have gained in popularity after being added to the national VA formulary.
In November 2012, for better monitoring of patient outcomes, improved efficiency of the primary care pharmacist clinics, and increased access to care in these clinics, treatment of patients prescribed DOACs was shifted to a centralized model that involved 3 anticoagulation clinical pharmacy specialists.
Centralized pharmacy services have a small number of core team members in a specific service for a particular disease, which reduces the number of different pharmacists a patient could talk to for management of a particular condition. Centralized pharmacy services allow for streamlining anticoagulation management to a small group of individual pharmacists considered specialists in anticoagulation. This shift in management to centralized anticoagulation services was supported at RHJVAMC by findings from a study of a pharmacist-run centralized anticoagulation clinic: Patients treated by the centralized clinic were 39% less likely to experience an anticoagulation therapy complication.8
Protocol for dabigatran follow-up and monitoring at RHJVAMC was developed by clinical and supervisory pharmacy staff, to align with national VA guidance. When a provider determines a patient is a candidate for dabigatran, an outpatient consultation is entered for the clinical pharmacy specialist to review the appropriateness of the patient selection for therapy. If the patient is eligible for therapy, the pharmacist contacts the patient to set up an initial visit to confirm selection and to provide the first dabigatran prescription and counseling. For assessments, with specific emphasis on adherence and AE monitoring, the patient is contacted 2 weeks, 1 month, 3 months, and every 6 months after the initial appointment.
Although most of the literature supports pharmacist-managed anticoagulation for patients who receive warfarin, DOACs have become more integrated into practice and more evaluated. Evidence supports pharmacists' interventions on evaluation of patient education and dosing, but there is conflicting evidence regarding pharmacists' impact on adherence after 3 months of therapy.9,10 In a larger VA study of the impact of dabigatran adherence on patient-centered outcomes, patients were mostly nonadherent to prescribed dosing.11 These studies support the need for improved adherence in patients prescribed DOACs and the need for further investigation of pharmacists' roles in improving patient outcomes.
Methods
This single-center, retrospective anticoagulant-use evaluation covered 2 study periods between November 1, 2011 and October 31, 2013. Study approval was obtained from the institutional review board of the Medical University of South Carolina and the research and development committee of RHJVAMC. The study population consisted of veterans who had a diagnosis of AF and received at least 3 outpatient prescription fills of a 30-day supply of dabigatran at RHJVAMC during either or both of the study periods. Patients were excluded if they were pregnant or planning to become pregnant or were incarcerated at any time during the study period. Dabigatran was selected because it was the first DOAC added to the local VA formulary before the start of this study.
Patients who met the inclusion criteria were separated into 2 groups based on the dates of their prescription fills. The precentralization group included patients treated by primary care pharmacists from November 1, 2011 to October 31, 2012; the postcentralization group included patients treated by anticoagulation clinical pharmacy specialists from November 1, 2012 to October 31, 2013. In each group, patients were followed for 1 year during their respective study period. For analysis, patients were included in both study periods if they received at least 3 fills of dabigatran during each period.
Medication possession ratio (MPR), which was used to measure the primary endpoint of adherence, is defined as the proportion of days a patient had dabigatran. The MPR denominator is the total number of days between the first and last prescription refill dates within the 52-week study period; the numerator is calculated by summing the days' supply for all but the last filling of the medication during each respective period. Nonadherence was defined as an MPR < 0.8 (or 80%), which has been used to define poor adherence in the literature.12 The authors calculated all patients' mean MPRs and compared them to determine statistical significance by repeated-measures linear regression. Descriptive statistics on proportion of patients in each study group with MPR < 0.8 were examined. Last, the authors performed a comparative subanalysis of median MPRs to determine whether there was an adherence difference between patients initially started on dabigatran at RHJVAMC and patients who were started on dabigatran before receiving it at RHJVAMC.
The secondary focus of this study was safety outcomes, including any bleeding event or thromboembolism within either study period. A bleeding event was defined as any major or minor bleeding event recognized through ICD-9 codes or any bleeding recorded in the patient's chart and noted during chart review, as well as any serum hemoglobin (Hgb) level decrease of ≥ to 2 g/dL during the study period. Thromboembolism was defined as a thromboembolism recognized through ICD-9 codes or any thromboembolism noted during chart review. Descriptive statistics were reported for this outcome, and a chi-square test was used to compare bleeding events between groups to determine significance.
The tertiary focus of this study was clinical efficiency as determined by number of primary care pharmacist visits during each study period. Primary care pharmacist visits were included for all primary care pharmacists in primary care clinics at the main hospital and in all 6 CBOCs.
For statistical analysis α was set at 0.05, and P < .05 was considered statistically significant. SAS Enterprise Guide software (Cary, North Carolina) was used for all statistical analyses.
Results
An initial data pull was completed from the RHJVAMC prescription records database for patients who had ≥ 3 prescriptions of dabigatran filled for treatment of AF during the study period, which yielded 65 unique patients. There were 34 patients in the precentralization group and 55 patients in the postcentralization group. Twenty-four unique patients were included in both study groups.
Mean MPR was 1.01 (range, 0.59-1.41) for the precentralization study period and 0.96 (range, 0.33-1.36) for the postcentralization period (Table 1). The difference was not statistically significant (P = .91). Number of patients considered nonadherent (MPR < 0.8) was 3 (8.82%) in the precentralization group and 8 (14.6%) in the postcentralization group.
The primary endpoint subanalysis compared the median MPRs for the patients initially started on dabigatran at RHJVAMC (de novo starts) and the patients who were started on dabigatran before receiving it at RHJVAMC (prior starts). In each group, number and percentage of patients determined to be nonadherent by MPR were evaluated as well. De novo patients received initial assessment, counseling, and a dabigatran prescription from RHJVAMC pharmacists before or during the study period, and prior patients were initially prescribed dabigatran at another VA facility or at a non-VA facility (Table 2).
Regarding safety outcomes (secondary endpoint), a bleeding event was identified in 6 (17.7%) of the precentralization patients and 7 (12.7%) of the postcentralization patients. Of the 6 precentralization events, 1 was a case of hemoptysis, 1 was a hematoma on the forehead, 1 was a lower gastrointestinal bleed (unconfirmed), 1 was retinal hemorrhaging (noted by ophthalmologist), and 2 were serum Hgb level decreases of more than 2 g/dL (neither patient required transfusion of packed red blood cells). Of the 7 postcentralization events, 1 was persistent hematochezia caused by hemorrhoids, 1 was hematuria, 1 was a hematoma, 1 was an upper gastrointestinal bleed (required blood transfusion), and 4 were serum Hgb level decreases of more than 2 g/dL (1 of the 4 required transfusion). No precentralization patient had any evidence of thromboembolism during the study period; 1 postcentralization patient had a superficial venous thromboembolism near a hematoma on the elbow.
Discussion
In this single-center, retrospective medication-use evaluation, the authors found a high rate of adherence to dabigatran before and after centralization of outpatient DOAC management by pharmacists. There was no statistically significant difference in bleeding events between the study periods, but primary care pharmacist visits increased by 108% from precentralization to postcentralization. Although the primary outcome findings did not refute the study's null hypothesis, results support implementing centralized pharmacist DOAC management to maintain a high rate of adherence and a low incidence of adverse outcomes and providing more primary care pharmacist services to increase access to care for other chronic diseases.
Although there was no statistically significant difference in adherence rates between study periods, the 2 groups' rates were higher than the national average of 72%, as calculated by the proportion-of-days-covered (PDC) equation (median, 74%) in a 2015 large-scale study of site-level adherence in more than 5,000 VA patients.13 The authors' findings support that study's significant finding of a high rate of adherence to pharmacist-provided dabigatran treatment. This study's adherence rate also was higher than the median PDC rate reported in a 2014 study that focused on dabigatran adherence: 94% (mean, 84%; SD, 22%).11
The RHJVAMC follows national VA guidance on pharmacist follow-up for patients who receive DOACs. This follow-up focuses on frequent counseling over the first 6 months of de novo DOAC treatment and on monitoring and assessing adherence and AEs. Although there is less laboratory monitoring for DOAC treatment than for treatment with vitamin K antagonists (eg, warfarin), telephone monitoring as described in this study has been associated with a high adherence rate and minimization of AEs. The 2014 study with the 94% median PDC rate also showed an association of decreased adherence and increased harm, including combined all-cause mortality and stroke (hazard ratio, 1.13; 95% confidence interval [CI], 1.07-1.19 per 10% decrease in PDC rate).11
This study's subanalysis revealed no difference in adherence between patients initially started on dabigatran at RHJVAMC and patients who were started on dabigatran before receiving it at RHJVAMC. Each group had a high rate of adherence. Shore and colleagues found that most of the VA sites they surveyed (22/41) had anticoagulation clinics monitoring patients who were prescribed dabigatran.13 Pharmacist-led monitoring of adherence and AEs led to increased adherence to dabigatran treatment (relative risk, 1.25; 95% CI, 1.11-1.41), which was the standard of care at RHJVAMC throughout their entire study. Many of these factors may explain the very high rate of adherence found in the present study, specifically in comparison to previously reported national averages.
In addition, the authors found no statistically significant difference in bleeding outcomes between the precentralization and postcentralization groups. Their incidence of bleeding was similar to the 16.6% rate reported in the package insert for dabigatran.14 Furthermore, the safety outcomes were similar for both groups in this study, which may be attributable to the quality of patient care provided by all RHJVAMC pharmacists, particularly in the setting of dabigatran management.
Many studies have found an association between dabigatran use and an increased rate of bleeding, particularly gastrointestinal, as demonstrated in several patients in this study. Evidence of these clinically significant AEs further supports pharmacists' close monitoring to detect these AEs and working with patients' providers to determine whether an alternative anticoagulant should be used.
A significant finding of this study regarding centralization of DOAC management by pharmacists was the increased number of primary care pharmacist visits. By streamlining all anticoagulant services to anticoagulation clinical pharmacy specialists, primary care pharmacists were able to care for more veterans and increase access to care without adding staff. The centralized anticoagulation pharmacists were volunteers who held other positions within the department; they did not have to be replaced when they became anticoagulation providers. This workload reallocation helped the RHJVAMC pharmacy department increase access to care.
Limitations
This study had several potential limitations. First, MPR, a widely studied common tool for assessing adherence, has been criticized for often being imprecise when used with short study periods.12 Another commonly used adherence measure is PDC rate, which has been reported in several large-scale studies of dabigatran therapy. The authors selected MPR for the present study because MPR calculation is more practical in the patient population and because MPR and PDC rate are predicted to yield similar results in assessments of adherence to a single medication.12 It also should be noted that both MPR and PDC rate are surrogate markers for adherence and assume adherence based on the availability of medication to the patient. Assessing adherence in a retrospective study is a challenge, as more reliable adherence assessment--for example, with use of pill counts or blister packs--is not possible. This study's retrospective design was another potential limitation, as an active intervention was not used.
In addition, this study had a small sample, likely attributable to the addition of dabigatran to the VA national formulary just months before the start of the study period. Furthermore, this study was not powered to detect significant differences in safety or efficacy outcomes. Other potential study limitations included having national VA guidance regarding follow-up periods and dabigatran prescription quantity limits during both study periods. Also, there was some potential for pharmacist-initiated refills at follow-up visits, which could falsely increase MPR. Last, the study analyzed only 1 DOAC and not the entire class of medications.
Conclusion
Centralizing DOAC management by clinical pharmacy specialists at a single VA facility helped maintain high rates of dabigatran adherence, above the national average, and low rates of adverse outcomes were maintained in both study groups. In addition, centralization of anticoagulation services improved access to care through an increase in primary care pharmacist visits without the addition of staff. Centralization of DOAC management by pharmacists is a viable option for maintaining high rates of adherence and low rates of adverse outcomes in facilities where the goal is to achieve clinical efficiency.
In the U.S. about 2.7 to 6.1 million people have atrial fibrillation (AF).1 This condition affects the rhythm of the heart, causes blood in the heart to become stagnant, and puts patients at high risk for developing a systemic embolism, particularly a stroke.1 Recent studies have shown that AF accounts for at least 15% of all strokes in the U.S. and 36% of strokes in people aged > 80 years.2
For patients aged > 60 years, the gold standard of long-term anticoagulation for reducing the risk of stroke has been oral vitamin K antagonist (warfarin) therapy.2 Although overwhelming evidence exists that supports the use of warfarin in these patients, warfarin is a narrow therapeutic index medication that requires frequent laboratory monitoring of international normalized ratio (INR) for dose titration guidance. There is also strong evidence that pharmacist-run anticoagulation clinics have improved patient-centered outcomes in patients prescribed warfarin.3-5
Direct oral anticoagulants (DOACs) are recently approved oral medications used as alternatives to warfarin for anticoagulation in AF. Direct oral anticoagulants do not require INR monitoring or any laboratory test for efficacy. In 2010, the FDA approved the first DOAC, dabigatran, for use in patients with AF. In 2011, rivaroxaban received approval for the same indication. One potential drawback of these new agents relative to warfarin is the lack of availability of a reversal agent that can be used in the event of a life-threatening bleeding event. Dabigatran is the only DOAC with an FDA-approved available reversal agent. In both 2011 and 2012, dabigatran, warfarin, and other anticoagulants topped the Institute for Safe Medicine Practice list of suspect drugs related to adverse events (AEs). These data prompted the Joint Commission to incorporate anticoagulation into the 2017 National Hospital Patient Safety Goals to improve patient outcomes and reduce harm from use of anticoagulants.6
In early 2011, the VHA produced national guidance on the treatment of patients who receive DOACs; this guidance was updated most recently in September 2016.7 Patients who were receiving DOACs at the Ralph H. Johnson VAMC (RHJVAMC) were initially monitored by 12 primary care pharmacists at the main hospital or at community-based outpatient clinics (CBOCs). Ambulatory care pharmacists at RHJVAMC work under a scope of practice to prescribe and adjust certain classes of medications to provide the highest level of care to more than 65,000 veterans in South Carolina and Georgia. Historically at RHJVAMC, warfarin has been the anticoagulant most commonly used for AF, though dabigatran and rivaroxaban have gained in popularity after being added to the national VA formulary.
In November 2012, for better monitoring of patient outcomes, improved efficiency of the primary care pharmacist clinics, and increased access to care in these clinics, treatment of patients prescribed DOACs was shifted to a centralized model that involved 3 anticoagulation clinical pharmacy specialists.
Centralized pharmacy services have a small number of core team members in a specific service for a particular disease, which reduces the number of different pharmacists a patient could talk to for management of a particular condition. Centralized pharmacy services allow for streamlining anticoagulation management to a small group of individual pharmacists considered specialists in anticoagulation. This shift in management to centralized anticoagulation services was supported at RHJVAMC by findings from a study of a pharmacist-run centralized anticoagulation clinic: Patients treated by the centralized clinic were 39% less likely to experience an anticoagulation therapy complication.8
Protocol for dabigatran follow-up and monitoring at RHJVAMC was developed by clinical and supervisory pharmacy staff, to align with national VA guidance. When a provider determines a patient is a candidate for dabigatran, an outpatient consultation is entered for the clinical pharmacy specialist to review the appropriateness of the patient selection for therapy. If the patient is eligible for therapy, the pharmacist contacts the patient to set up an initial visit to confirm selection and to provide the first dabigatran prescription and counseling. For assessments, with specific emphasis on adherence and AE monitoring, the patient is contacted 2 weeks, 1 month, 3 months, and every 6 months after the initial appointment.
Although most of the literature supports pharmacist-managed anticoagulation for patients who receive warfarin, DOACs have become more integrated into practice and more evaluated. Evidence supports pharmacists' interventions on evaluation of patient education and dosing, but there is conflicting evidence regarding pharmacists' impact on adherence after 3 months of therapy.9,10 In a larger VA study of the impact of dabigatran adherence on patient-centered outcomes, patients were mostly nonadherent to prescribed dosing.11 These studies support the need for improved adherence in patients prescribed DOACs and the need for further investigation of pharmacists' roles in improving patient outcomes.
Methods
This single-center, retrospective anticoagulant-use evaluation covered 2 study periods between November 1, 2011 and October 31, 2013. Study approval was obtained from the institutional review board of the Medical University of South Carolina and the research and development committee of RHJVAMC. The study population consisted of veterans who had a diagnosis of AF and received at least 3 outpatient prescription fills of a 30-day supply of dabigatran at RHJVAMC during either or both of the study periods. Patients were excluded if they were pregnant or planning to become pregnant or were incarcerated at any time during the study period. Dabigatran was selected because it was the first DOAC added to the local VA formulary before the start of this study.
Patients who met the inclusion criteria were separated into 2 groups based on the dates of their prescription fills. The precentralization group included patients treated by primary care pharmacists from November 1, 2011 to October 31, 2012; the postcentralization group included patients treated by anticoagulation clinical pharmacy specialists from November 1, 2012 to October 31, 2013. In each group, patients were followed for 1 year during their respective study period. For analysis, patients were included in both study periods if they received at least 3 fills of dabigatran during each period.
Medication possession ratio (MPR), which was used to measure the primary endpoint of adherence, is defined as the proportion of days a patient had dabigatran. The MPR denominator is the total number of days between the first and last prescription refill dates within the 52-week study period; the numerator is calculated by summing the days' supply for all but the last filling of the medication during each respective period. Nonadherence was defined as an MPR < 0.8 (or 80%), which has been used to define poor adherence in the literature.12 The authors calculated all patients' mean MPRs and compared them to determine statistical significance by repeated-measures linear regression. Descriptive statistics on proportion of patients in each study group with MPR < 0.8 were examined. Last, the authors performed a comparative subanalysis of median MPRs to determine whether there was an adherence difference between patients initially started on dabigatran at RHJVAMC and patients who were started on dabigatran before receiving it at RHJVAMC.
The secondary focus of this study was safety outcomes, including any bleeding event or thromboembolism within either study period. A bleeding event was defined as any major or minor bleeding event recognized through ICD-9 codes or any bleeding recorded in the patient's chart and noted during chart review, as well as any serum hemoglobin (Hgb) level decrease of ≥ to 2 g/dL during the study period. Thromboembolism was defined as a thromboembolism recognized through ICD-9 codes or any thromboembolism noted during chart review. Descriptive statistics were reported for this outcome, and a chi-square test was used to compare bleeding events between groups to determine significance.
The tertiary focus of this study was clinical efficiency as determined by number of primary care pharmacist visits during each study period. Primary care pharmacist visits were included for all primary care pharmacists in primary care clinics at the main hospital and in all 6 CBOCs.
For statistical analysis α was set at 0.05, and P < .05 was considered statistically significant. SAS Enterprise Guide software (Cary, North Carolina) was used for all statistical analyses.
Results
An initial data pull was completed from the RHJVAMC prescription records database for patients who had ≥ 3 prescriptions of dabigatran filled for treatment of AF during the study period, which yielded 65 unique patients. There were 34 patients in the precentralization group and 55 patients in the postcentralization group. Twenty-four unique patients were included in both study groups.
Mean MPR was 1.01 (range, 0.59-1.41) for the precentralization study period and 0.96 (range, 0.33-1.36) for the postcentralization period (Table 1). The difference was not statistically significant (P = .91). Number of patients considered nonadherent (MPR < 0.8) was 3 (8.82%) in the precentralization group and 8 (14.6%) in the postcentralization group.
The primary endpoint subanalysis compared the median MPRs for the patients initially started on dabigatran at RHJVAMC (de novo starts) and the patients who were started on dabigatran before receiving it at RHJVAMC (prior starts). In each group, number and percentage of patients determined to be nonadherent by MPR were evaluated as well. De novo patients received initial assessment, counseling, and a dabigatran prescription from RHJVAMC pharmacists before or during the study period, and prior patients were initially prescribed dabigatran at another VA facility or at a non-VA facility (Table 2).
Regarding safety outcomes (secondary endpoint), a bleeding event was identified in 6 (17.7%) of the precentralization patients and 7 (12.7%) of the postcentralization patients. Of the 6 precentralization events, 1 was a case of hemoptysis, 1 was a hematoma on the forehead, 1 was a lower gastrointestinal bleed (unconfirmed), 1 was retinal hemorrhaging (noted by ophthalmologist), and 2 were serum Hgb level decreases of more than 2 g/dL (neither patient required transfusion of packed red blood cells). Of the 7 postcentralization events, 1 was persistent hematochezia caused by hemorrhoids, 1 was hematuria, 1 was a hematoma, 1 was an upper gastrointestinal bleed (required blood transfusion), and 4 were serum Hgb level decreases of more than 2 g/dL (1 of the 4 required transfusion). No precentralization patient had any evidence of thromboembolism during the study period; 1 postcentralization patient had a superficial venous thromboembolism near a hematoma on the elbow.
Discussion
In this single-center, retrospective medication-use evaluation, the authors found a high rate of adherence to dabigatran before and after centralization of outpatient DOAC management by pharmacists. There was no statistically significant difference in bleeding events between the study periods, but primary care pharmacist visits increased by 108% from precentralization to postcentralization. Although the primary outcome findings did not refute the study's null hypothesis, results support implementing centralized pharmacist DOAC management to maintain a high rate of adherence and a low incidence of adverse outcomes and providing more primary care pharmacist services to increase access to care for other chronic diseases.
Although there was no statistically significant difference in adherence rates between study periods, the 2 groups' rates were higher than the national average of 72%, as calculated by the proportion-of-days-covered (PDC) equation (median, 74%) in a 2015 large-scale study of site-level adherence in more than 5,000 VA patients.13 The authors' findings support that study's significant finding of a high rate of adherence to pharmacist-provided dabigatran treatment. This study's adherence rate also was higher than the median PDC rate reported in a 2014 study that focused on dabigatran adherence: 94% (mean, 84%; SD, 22%).11
The RHJVAMC follows national VA guidance on pharmacist follow-up for patients who receive DOACs. This follow-up focuses on frequent counseling over the first 6 months of de novo DOAC treatment and on monitoring and assessing adherence and AEs. Although there is less laboratory monitoring for DOAC treatment than for treatment with vitamin K antagonists (eg, warfarin), telephone monitoring as described in this study has been associated with a high adherence rate and minimization of AEs. The 2014 study with the 94% median PDC rate also showed an association of decreased adherence and increased harm, including combined all-cause mortality and stroke (hazard ratio, 1.13; 95% confidence interval [CI], 1.07-1.19 per 10% decrease in PDC rate).11
This study's subanalysis revealed no difference in adherence between patients initially started on dabigatran at RHJVAMC and patients who were started on dabigatran before receiving it at RHJVAMC. Each group had a high rate of adherence. Shore and colleagues found that most of the VA sites they surveyed (22/41) had anticoagulation clinics monitoring patients who were prescribed dabigatran.13 Pharmacist-led monitoring of adherence and AEs led to increased adherence to dabigatran treatment (relative risk, 1.25; 95% CI, 1.11-1.41), which was the standard of care at RHJVAMC throughout their entire study. Many of these factors may explain the very high rate of adherence found in the present study, specifically in comparison to previously reported national averages.
In addition, the authors found no statistically significant difference in bleeding outcomes between the precentralization and postcentralization groups. Their incidence of bleeding was similar to the 16.6% rate reported in the package insert for dabigatran.14 Furthermore, the safety outcomes were similar for both groups in this study, which may be attributable to the quality of patient care provided by all RHJVAMC pharmacists, particularly in the setting of dabigatran management.
Many studies have found an association between dabigatran use and an increased rate of bleeding, particularly gastrointestinal, as demonstrated in several patients in this study. Evidence of these clinically significant AEs further supports pharmacists' close monitoring to detect these AEs and working with patients' providers to determine whether an alternative anticoagulant should be used.
A significant finding of this study regarding centralization of DOAC management by pharmacists was the increased number of primary care pharmacist visits. By streamlining all anticoagulant services to anticoagulation clinical pharmacy specialists, primary care pharmacists were able to care for more veterans and increase access to care without adding staff. The centralized anticoagulation pharmacists were volunteers who held other positions within the department; they did not have to be replaced when they became anticoagulation providers. This workload reallocation helped the RHJVAMC pharmacy department increase access to care.
Limitations
This study had several potential limitations. First, MPR, a widely studied common tool for assessing adherence, has been criticized for often being imprecise when used with short study periods.12 Another commonly used adherence measure is PDC rate, which has been reported in several large-scale studies of dabigatran therapy. The authors selected MPR for the present study because MPR calculation is more practical in the patient population and because MPR and PDC rate are predicted to yield similar results in assessments of adherence to a single medication.12 It also should be noted that both MPR and PDC rate are surrogate markers for adherence and assume adherence based on the availability of medication to the patient. Assessing adherence in a retrospective study is a challenge, as more reliable adherence assessment--for example, with use of pill counts or blister packs--is not possible. This study's retrospective design was another potential limitation, as an active intervention was not used.
In addition, this study had a small sample, likely attributable to the addition of dabigatran to the VA national formulary just months before the start of the study period. Furthermore, this study was not powered to detect significant differences in safety or efficacy outcomes. Other potential study limitations included having national VA guidance regarding follow-up periods and dabigatran prescription quantity limits during both study periods. Also, there was some potential for pharmacist-initiated refills at follow-up visits, which could falsely increase MPR. Last, the study analyzed only 1 DOAC and not the entire class of medications.
Conclusion
Centralizing DOAC management by clinical pharmacy specialists at a single VA facility helped maintain high rates of dabigatran adherence, above the national average, and low rates of adverse outcomes were maintained in both study groups. In addition, centralization of anticoagulation services improved access to care through an increase in primary care pharmacist visits without the addition of staff. Centralization of DOAC management by pharmacists is a viable option for maintaining high rates of adherence and low rates of adverse outcomes in facilities where the goal is to achieve clinical efficiency.
1. January CT, Wann LS, Alpert JS, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society [published correction appears in J Am Coll Cardiol. 2014;64(21):2305-2307. J Am Coll Cardiol. 2014;64(21):e1-e76.
2. Reiffel JA. New versus traditional approaches to oral anticoagulation in patients with atrial fibrillation. Am J Med. 2014;127(4):e15.
3. Locke C, Ravnan SL, Patel R, Uchizono JA. Reduction in warfarin adverse events requiring patient hospitalization after implementation of pharmacist-managed anticoagulation service. Pharmacotherapy. 2005;25(5):685-689.
4. Poon IO, Lal L, Brown EN, Braun UK. The impact of pharmacist-managed oral anticoagulation therapy in older veterans. J Clin Pharm Ther. 2007;32(1):21-29.
5. Chiquette E, Amato MG, Bussey HI. Comparison of an anticoagulation clinic with usual medical care. Arch Intern Med. 1998;158(15):1641-1647.
6. The Joint Commission. National patient safety goals. https://www.jointcommission.org/as sets/1/6/2017_NPSG_HAP_ER.pdf. Published 2016. Accessed December 6, 2016.
7. Department of Veterans Affairs Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Direct oral anticoagulants (DOACs) (formerly called TSOACs) dabigatran (Pradaxa), rivaroxaban (Xarelto), and apixaban (Eliquis): Criteria for Use for Stroke Prevention in nonvalvular atrial fibrillation (AF) and Edoxaban (SAVAYSA). http://www.pbm.va.gov/PBM/clinicalguidance/criteriaforuse/Anticoagulants_Direct_Oral_DOACs_CFU_and_Algorithm_for_Nonvalvular_Atrial_Fibrillation_Sep_2016.pdf. Updated September 2016. Accessed December 6, 2016.
8. Witt DM, Sadler MA, Shanahan RL, Mazzoli G, Tillman DJ. Effect of a centralized clinical pharmacy anticoagulation service on the outcomes of anticoagulation therapy. Chest. 2005;127(5):1515-1522.
9. Chan LL, Crumpler WL, Jacobson AK. Implementation of pharmacist-managed anticoagulation in patients receiving newer anticoagulants. Am J Health Syst Pharm. 2013;70(15):1285-1286, 1288.
10. Lee PY, Han SY, Miyahara RK. Adherence and outcomes of patients treated with dabigatran: pharmacist-managed anticoagulation clinic versus usual care. Am J Health Syst Pharm. 2013;70(13):1154-1161.
11. Shore S, Carey EP, Turakhia MP, et al. Adherence to dabigatran therapy and longitudinal patient outcomes: insights from the Veterans Health Administration. Am Heart J. 2014;167(6):810-817.
12. Martin BC, Wiley-Exley EK, Richards S, Domino ME, Carey TS, Sleath BL. Contrasting measures of adherence with simple drug use, medication switching and therapeutic duplication. Ann Pharmacother. 2009;43(1):36-44.
13. Shore S, Ho PM, Lambert-Kerzner A, et al. Site-level variation in and practices associated with dabigatran adherence. JAMA. 2015;313(14):1443-1450.
14. Pradaxa [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2015.
1. January CT, Wann LS, Alpert JS, et al; American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society [published correction appears in J Am Coll Cardiol. 2014;64(21):2305-2307. J Am Coll Cardiol. 2014;64(21):e1-e76.
2. Reiffel JA. New versus traditional approaches to oral anticoagulation in patients with atrial fibrillation. Am J Med. 2014;127(4):e15.
3. Locke C, Ravnan SL, Patel R, Uchizono JA. Reduction in warfarin adverse events requiring patient hospitalization after implementation of pharmacist-managed anticoagulation service. Pharmacotherapy. 2005;25(5):685-689.
4. Poon IO, Lal L, Brown EN, Braun UK. The impact of pharmacist-managed oral anticoagulation therapy in older veterans. J Clin Pharm Ther. 2007;32(1):21-29.
5. Chiquette E, Amato MG, Bussey HI. Comparison of an anticoagulation clinic with usual medical care. Arch Intern Med. 1998;158(15):1641-1647.
6. The Joint Commission. National patient safety goals. https://www.jointcommission.org/as sets/1/6/2017_NPSG_HAP_ER.pdf. Published 2016. Accessed December 6, 2016.
7. Department of Veterans Affairs Pharmacy Benefits Management Services, Medical Advisory Panel, and VISN Pharmacist Executives. Direct oral anticoagulants (DOACs) (formerly called TSOACs) dabigatran (Pradaxa), rivaroxaban (Xarelto), and apixaban (Eliquis): Criteria for Use for Stroke Prevention in nonvalvular atrial fibrillation (AF) and Edoxaban (SAVAYSA). http://www.pbm.va.gov/PBM/clinicalguidance/criteriaforuse/Anticoagulants_Direct_Oral_DOACs_CFU_and_Algorithm_for_Nonvalvular_Atrial_Fibrillation_Sep_2016.pdf. Updated September 2016. Accessed December 6, 2016.
8. Witt DM, Sadler MA, Shanahan RL, Mazzoli G, Tillman DJ. Effect of a centralized clinical pharmacy anticoagulation service on the outcomes of anticoagulation therapy. Chest. 2005;127(5):1515-1522.
9. Chan LL, Crumpler WL, Jacobson AK. Implementation of pharmacist-managed anticoagulation in patients receiving newer anticoagulants. Am J Health Syst Pharm. 2013;70(15):1285-1286, 1288.
10. Lee PY, Han SY, Miyahara RK. Adherence and outcomes of patients treated with dabigatran: pharmacist-managed anticoagulation clinic versus usual care. Am J Health Syst Pharm. 2013;70(13):1154-1161.
11. Shore S, Carey EP, Turakhia MP, et al. Adherence to dabigatran therapy and longitudinal patient outcomes: insights from the Veterans Health Administration. Am Heart J. 2014;167(6):810-817.
12. Martin BC, Wiley-Exley EK, Richards S, Domino ME, Carey TS, Sleath BL. Contrasting measures of adherence with simple drug use, medication switching and therapeutic duplication. Ann Pharmacother. 2009;43(1):36-44.
13. Shore S, Ho PM, Lambert-Kerzner A, et al. Site-level variation in and practices associated with dabigatran adherence. JAMA. 2015;313(14):1443-1450.
14. Pradaxa [package insert]. Ridgefield, CT: Boehringer Ingelheim Pharmaceuticals; 2015.
Shingles Strikes With a Vengeance
1. A 16-year-old girl presents with a rash manifesting several weeks ago that became enlarged and more symptomatic after she applied hydrogen peroxide and scrubbed with antibacterial soap. Large, annular, honey-colored crusts are focally located around the left eye, and faint pinkness is noted peripherally around the lesions. Modest but palpable adenopathy is detected in the pretragal and submental nodal areas.

Diagnosis: Impetigo has also been called impetiginized dermatitis because it almost always starts with minor breaks in the skin as a result of conditions such as eczema, acne, contact dermatitis, or insect bite. Thus provided with access to deeper portions of the epithelial surface, bacterial organisms that normally cause no problems on intact skin are able to create the minor but annoying condition we call impetigo. Rarely associated with morbidity, it tends to resolve in two to three weeks at most, even without treatment.
For more information, see “Is It Ringworm, Herpes— Or Something Else Entirely?” Clinician Reviews. 2014;24(11):8-9.
2. A 38-year-old man presents with an itchy, blistery rash that usually appears in the summer, getting worse each year. The lesions are collections of vesicles with faint underlying erythema that crisscross his legs in linear configurations. Smaller but similar lesions are scattered over his arms and trunk.

Diagnosis: The rash produced by poison ivy exposure can be severe and can last six weeks or more without treatment. Poison ivy is not contagious, cannot be spread by scratching, and (despite its name) is not poisonous in any way. The number of poison ivy plants has doubled in the past 50 years and is expected to double again within 20 years. The potency of the plant’s allergen is also expected to increase. The patient (height, 6’3”; weight, > 300 lb) was treated with a 60-mg IM injection of triamcinolone, a two-week, 40-mg taper of prednisone, and twice-daily application of betamethasone cream. This, of course, followed a discussion of the risks versus benefits of such a course of action.
For more information, see “He Tried So Hard to Avoid It … .” Clinician Reviews. 2015 July;25(7):W2.
3. For several months, a 69-year-old woman has had a rash around her eyes. It is terribly symptomatic, burning and itching regardless of any type of OTC treatment. She finally requests referral to dermatology from her primary care provider.

Diagnosis: Eyelid dermatitis, or irritant contact dermatitis, is an extremely common complaint, and this patient’s history is quite typical: The worse the problem gets, the more attempts the patient makes to relieve symptoms.
When this patient presented to dermatology, she was applying six different products (all OTC) to the affected areas. None helped, and in fact, most seemed to worsen the problem. Even if one had helped, she would never have known which. But desperation drives patients to do irrational things, especially when the problem is out in the open for the whole world to see.
For more information, see “The Eyes Have It, and It Itches Like Crazy.” Clinician Reviews. 2015;25(9):W1.
4. A 58-year-old man seeks care for burning in his right eye and a skin eruption on his forehead and scalp with progressive worsening over the past 10 days. The patient has decreased vision in his right eye, as well as fever, chills, photophobia, and headache. A physical exam reveals vesicles on an erythematous base on his right scalp, forehead, upper and lower eyelids, dorsum of his nose, and cheek distributed along the ophthalmic branch of the trigeminal nerve.

Diagnosis: Herpes zoster ophthalmicus, confirmed by an ophthalmologic exam. This serious condition has been linked to reactivation of the varicella-zoster virus (VZV) within the trigeminal ganglion. Primary infection with VZV results in varicella (chickenpox), whereas reactivation of a latent VZV infection within the sensory ganglia is known as herpes zoster.
For more information, see “Painful rash on face.” J Fam Pract. 2015;64(11):E1-E3.
RELATED ARTICLE
Jacobsen E, Hull CE. “Herpes Zoster Infection.” Clinician Reviews. 2013;23(8):42-49.
1. A 16-year-old girl presents with a rash manifesting several weeks ago that became enlarged and more symptomatic after she applied hydrogen peroxide and scrubbed with antibacterial soap. Large, annular, honey-colored crusts are focally located around the left eye, and faint pinkness is noted peripherally around the lesions. Modest but palpable adenopathy is detected in the pretragal and submental nodal areas.
Diagnosis: Impetigo has also been called impetiginized dermatitis because it almost always starts with minor breaks in the skin as a result of conditions such as eczema, acne, contact dermatitis, or insect bite. Thus provided with access to deeper portions of the epithelial surface, bacterial organisms that normally cause no problems on intact skin are able to create the minor but annoying condition we call impetigo. Rarely associated with morbidity, it tends to resolve in two to three weeks at most, even without treatment.
For more information, see “Is It Ringworm, Herpes— Or Something Else Entirely?” Clinician Reviews. 2014;24(11):8-9.
2. A 38-year-old man presents with an itchy, blistery rash that usually appears in the summer, getting worse each year. The lesions are collections of vesicles with faint underlying erythema that crisscross his legs in linear configurations. Smaller but similar lesions are scattered over his arms and trunk.
Diagnosis: The rash produced by poison ivy exposure can be severe and can last six weeks or more without treatment. Poison ivy is not contagious, cannot be spread by scratching, and (despite its name) is not poisonous in any way. The number of poison ivy plants has doubled in the past 50 years and is expected to double again within 20 years. The potency of the plant’s allergen is also expected to increase. The patient (height, 6’3”; weight, > 300 lb) was treated with a 60-mg IM injection of triamcinolone, a two-week, 40-mg taper of prednisone, and twice-daily application of betamethasone cream. This, of course, followed a discussion of the risks versus benefits of such a course of action.
For more information, see “He Tried So Hard to Avoid It … .” Clinician Reviews. 2015 July;25(7):W2.
3. For several months, a 69-year-old woman has had a rash around her eyes. It is terribly symptomatic, burning and itching regardless of any type of OTC treatment. She finally requests referral to dermatology from her primary care provider.
Diagnosis: Eyelid dermatitis, or irritant contact dermatitis, is an extremely common complaint, and this patient’s history is quite typical: The worse the problem gets, the more attempts the patient makes to relieve symptoms.
When this patient presented to dermatology, she was applying six different products (all OTC) to the affected areas. None helped, and in fact, most seemed to worsen the problem. Even if one had helped, she would never have known which. But desperation drives patients to do irrational things, especially when the problem is out in the open for the whole world to see.
For more information, see “The Eyes Have It, and It Itches Like Crazy.” Clinician Reviews. 2015;25(9):W1.
4. A 58-year-old man seeks care for burning in his right eye and a skin eruption on his forehead and scalp with progressive worsening over the past 10 days. The patient has decreased vision in his right eye, as well as fever, chills, photophobia, and headache. A physical exam reveals vesicles on an erythematous base on his right scalp, forehead, upper and lower eyelids, dorsum of his nose, and cheek distributed along the ophthalmic branch of the trigeminal nerve.
Diagnosis: Herpes zoster ophthalmicus, confirmed by an ophthalmologic exam. This serious condition has been linked to reactivation of the varicella-zoster virus (VZV) within the trigeminal ganglion. Primary infection with VZV results in varicella (chickenpox), whereas reactivation of a latent VZV infection within the sensory ganglia is known as herpes zoster.
For more information, see “Painful rash on face.” J Fam Pract. 2015;64(11):E1-E3.
RELATED ARTICLE
Jacobsen E, Hull CE. “Herpes Zoster Infection.” Clinician Reviews. 2013;23(8):42-49.
1. A 16-year-old girl presents with a rash manifesting several weeks ago that became enlarged and more symptomatic after she applied hydrogen peroxide and scrubbed with antibacterial soap. Large, annular, honey-colored crusts are focally located around the left eye, and faint pinkness is noted peripherally around the lesions. Modest but palpable adenopathy is detected in the pretragal and submental nodal areas.
Diagnosis: Impetigo has also been called impetiginized dermatitis because it almost always starts with minor breaks in the skin as a result of conditions such as eczema, acne, contact dermatitis, or insect bite. Thus provided with access to deeper portions of the epithelial surface, bacterial organisms that normally cause no problems on intact skin are able to create the minor but annoying condition we call impetigo. Rarely associated with morbidity, it tends to resolve in two to three weeks at most, even without treatment.
For more information, see “Is It Ringworm, Herpes— Or Something Else Entirely?” Clinician Reviews. 2014;24(11):8-9.
2. A 38-year-old man presents with an itchy, blistery rash that usually appears in the summer, getting worse each year. The lesions are collections of vesicles with faint underlying erythema that crisscross his legs in linear configurations. Smaller but similar lesions are scattered over his arms and trunk.
Diagnosis: The rash produced by poison ivy exposure can be severe and can last six weeks or more without treatment. Poison ivy is not contagious, cannot be spread by scratching, and (despite its name) is not poisonous in any way. The number of poison ivy plants has doubled in the past 50 years and is expected to double again within 20 years. The potency of the plant’s allergen is also expected to increase. The patient (height, 6’3”; weight, > 300 lb) was treated with a 60-mg IM injection of triamcinolone, a two-week, 40-mg taper of prednisone, and twice-daily application of betamethasone cream. This, of course, followed a discussion of the risks versus benefits of such a course of action.
For more information, see “He Tried So Hard to Avoid It … .” Clinician Reviews. 2015 July;25(7):W2.
3. For several months, a 69-year-old woman has had a rash around her eyes. It is terribly symptomatic, burning and itching regardless of any type of OTC treatment. She finally requests referral to dermatology from her primary care provider.
Diagnosis: Eyelid dermatitis, or irritant contact dermatitis, is an extremely common complaint, and this patient’s history is quite typical: The worse the problem gets, the more attempts the patient makes to relieve symptoms.
When this patient presented to dermatology, she was applying six different products (all OTC) to the affected areas. None helped, and in fact, most seemed to worsen the problem. Even if one had helped, she would never have known which. But desperation drives patients to do irrational things, especially when the problem is out in the open for the whole world to see.
For more information, see “The Eyes Have It, and It Itches Like Crazy.” Clinician Reviews. 2015;25(9):W1.
4. A 58-year-old man seeks care for burning in his right eye and a skin eruption on his forehead and scalp with progressive worsening over the past 10 days. The patient has decreased vision in his right eye, as well as fever, chills, photophobia, and headache. A physical exam reveals vesicles on an erythematous base on his right scalp, forehead, upper and lower eyelids, dorsum of his nose, and cheek distributed along the ophthalmic branch of the trigeminal nerve.
Diagnosis: Herpes zoster ophthalmicus, confirmed by an ophthalmologic exam. This serious condition has been linked to reactivation of the varicella-zoster virus (VZV) within the trigeminal ganglion. Primary infection with VZV results in varicella (chickenpox), whereas reactivation of a latent VZV infection within the sensory ganglia is known as herpes zoster.
For more information, see “Painful rash on face.” J Fam Pract. 2015;64(11):E1-E3.
RELATED ARTICLE
Jacobsen E, Hull CE. “Herpes Zoster Infection.” Clinician Reviews. 2013;23(8):42-49.
David Henry's JCSO podcast, January-February 2017
For the January-February issue of the Journal of Community and Supportive Oncology, the Editor in Chief, Dr David Henry, highlights a thought-provoking article by JCSO Editor, Dr Thomas Strouse, on end-of-life options and legal pathways to physician-assisted dying. He also features a guide by Dr Adam Bagg on the diagnosis and classification of lymphomas, and an in-depth examination of blood-based biopsies by Jane de Lartigue. Three Original Reports hone in on patient care and support and quality of care: a report on the Florida CaPCaS study documents the experiences and needs of black men at the point of prostate cancer diagnosis; another, among Spanish-speaking Latinas with breast cancer, addresses the posttreatment survivorship care needs of that population; and a third looks at strategies to improve the quality of care among head and neck cancer patients. Among the Journal’s regular offerings, the Community Translations section features the approvals of atezolizumab as a therapy for bladder cancer (the first in more than 30 years) and lenvatinib for renal cell carcinoma, and there are two Case Report, one on a patient with breast cancer who experienced severe hyponatremia with seizures associated with single-, low-dose cyclophosphamide, and another about paraneoplastic leukemoid reaction as a poor prognostic marker in a patient with urothelial bladder carcinoma.
Listen to the podcast below.
For the January-February issue of the Journal of Community and Supportive Oncology, the Editor in Chief, Dr David Henry, highlights a thought-provoking article by JCSO Editor, Dr Thomas Strouse, on end-of-life options and legal pathways to physician-assisted dying. He also features a guide by Dr Adam Bagg on the diagnosis and classification of lymphomas, and an in-depth examination of blood-based biopsies by Jane de Lartigue. Three Original Reports hone in on patient care and support and quality of care: a report on the Florida CaPCaS study documents the experiences and needs of black men at the point of prostate cancer diagnosis; another, among Spanish-speaking Latinas with breast cancer, addresses the posttreatment survivorship care needs of that population; and a third looks at strategies to improve the quality of care among head and neck cancer patients. Among the Journal’s regular offerings, the Community Translations section features the approvals of atezolizumab as a therapy for bladder cancer (the first in more than 30 years) and lenvatinib for renal cell carcinoma, and there are two Case Report, one on a patient with breast cancer who experienced severe hyponatremia with seizures associated with single-, low-dose cyclophosphamide, and another about paraneoplastic leukemoid reaction as a poor prognostic marker in a patient with urothelial bladder carcinoma.
Listen to the podcast below.
For the January-February issue of the Journal of Community and Supportive Oncology, the Editor in Chief, Dr David Henry, highlights a thought-provoking article by JCSO Editor, Dr Thomas Strouse, on end-of-life options and legal pathways to physician-assisted dying. He also features a guide by Dr Adam Bagg on the diagnosis and classification of lymphomas, and an in-depth examination of blood-based biopsies by Jane de Lartigue. Three Original Reports hone in on patient care and support and quality of care: a report on the Florida CaPCaS study documents the experiences and needs of black men at the point of prostate cancer diagnosis; another, among Spanish-speaking Latinas with breast cancer, addresses the posttreatment survivorship care needs of that population; and a third looks at strategies to improve the quality of care among head and neck cancer patients. Among the Journal’s regular offerings, the Community Translations section features the approvals of atezolizumab as a therapy for bladder cancer (the first in more than 30 years) and lenvatinib for renal cell carcinoma, and there are two Case Report, one on a patient with breast cancer who experienced severe hyponatremia with seizures associated with single-, low-dose cyclophosphamide, and another about paraneoplastic leukemoid reaction as a poor prognostic marker in a patient with urothelial bladder carcinoma.
Listen to the podcast below.
Drug could treat IDA in patients with NDD CKD

Photo courtesy of CDC
Results of a phase 3 trial suggest oral ferric citrate could be an alternative to intravenous iron for treating iron deficiency anemia (IDA) in patients with non-dialysis-dependent (NDD) chronic kidney disease (CKD).
Slightly more than half of patients receiving ferric citrate in this study experienced a significant boost in hemoglobin levels.
A treatment effect was seen as early as 1 to 2 weeks after patients started ferric citrate, and responses were durable.
Patients enrolled in the trial had not adequately responded to or could not tolerate prior treatment with oral iron.
Ferric citrate was generally well tolerated in this trial. Adverse events (AEs) were consistent with the drug’s known safety profile, with diarrhea being reported as the most common AE.
These results were published in the Journal of the American Society of Nephrology. The study was sponsored by Keryx Biopharmaceuticals, Inc., the company marketing ferric citrate as Auryxia.
The drug is currently approved in the US as a phosphate binder for the control of serum phosphorus levels in patients with CKD who are on dialysis.
Researchers conducted this phase 3 trial to determine if ferric citrate might be a safe and effective alternative to intravenous iron in patients with NDD CKD.
The study enrolled NDD-CKD patients with hemoglobin levels between 9.0 g/dL and 11.5 g/dL who were intolerant to or had inadequate response to oral iron supplements.
The patients were randomized 1:1 to receive ferric citrate (n=117) or placebo (n=116). Baseline characteristics were similar between the treatment arms.
The study had a 16-week, double-blind efficacy period, followed by an 8-week, open-label, safety extension period in which all patients remaining in the study, including the placebo group, received ferric citrate.
During the 16-week efficacy period, ferric citrate was administered at a starting dose of 3 tablets per day with food and could be titrated every 4 weeks by an additional 3 tablets for up to 12 tablets per day. The mean dose received in ferric citrate-treated patients was 5 tablets per day.
Efficacy
The study’s primary endpoint was the proportion of patients achieving a ≥1 g/dL increase in hemoglobin at any point during the 16-week efficacy period.
A significantly higher proportion of patients in the ferric citrate arm achieved the primary endpoint—52.1%, compared to 19.1% of patients receiving placebo (P<0.001).
The mean relative change in hemoglobin (for ferric citrate vs placebo) at week 16 was 0.84 g/dL (P<0.001).
Patients who received ferric citrate were significantly more likely to experience a sustained increase in hemoglobin—48.7%, compared to 14.8% for those receiving placebo (P<0.001).
“Not only did ferric citrate deliver a clinically meaningful 1 g/dL increase in hemoglobin levels for the majority of patients . . ., increases were seen as early as 1 to 2 weeks after start of treatment and were sustained for the majority of patients who achieved the primary endpoint,” said study author Steven Fishbane, MD, of Hofstra Northwell School of Medicine in Mineola, New York.
Safety
Treatment-emergent AEs occurred in 79.5% of patients in the ferric citrate arm and 64.7% of those in the placebo arm.
Common AEs (in the ferric citrate and placebo arms, respectively) included diarrhea (20.5% and 16.4%), constipation (18.8% and 12.9%), discolored feces (14.5% and 0%), nausea (11.1% and 2.6%), abdominal pain (6% and 1.7%), fatigue (0% and 5.2%), hyperkalemia (6.8% and 3.4%), and hypertension (4.3% and 5.2%).
Rates of serious AE were similar in the ferric citrate and placebo arms—12.0% and 11.2%, respectively. None of the serious AEs were considered treatment-related.
There were 2 deaths in the ferric citrate arm (and none in the placebo arm), but neither were considered treatment-related.
“The results shown in this pivotal study demonstrated that ferric citrate, if approved for this indication, could provide an important new treatment option for people living with chronic kidney disease and iron deficiency anemia who are not on dialysis,” Dr Fishbane said.
Keryx Biopharmaceuticals recently submitted a supplemental new drug application with these data to the US Food and Drug Administration. ![]()
Photo courtesy of CDC
Results of a phase 3 trial suggest oral ferric citrate could be an alternative to intravenous iron for treating iron deficiency anemia (IDA) in patients with non-dialysis-dependent (NDD) chronic kidney disease (CKD).
Slightly more than half of patients receiving ferric citrate in this study experienced a significant boost in hemoglobin levels.
A treatment effect was seen as early as 1 to 2 weeks after patients started ferric citrate, and responses were durable.
Patients enrolled in the trial had not adequately responded to or could not tolerate prior treatment with oral iron.
Ferric citrate was generally well tolerated in this trial. Adverse events (AEs) were consistent with the drug’s known safety profile, with diarrhea being reported as the most common AE.
These results were published in the Journal of the American Society of Nephrology. The study was sponsored by Keryx Biopharmaceuticals, Inc., the company marketing ferric citrate as Auryxia.
The drug is currently approved in the US as a phosphate binder for the control of serum phosphorus levels in patients with CKD who are on dialysis.
Researchers conducted this phase 3 trial to determine if ferric citrate might be a safe and effective alternative to intravenous iron in patients with NDD CKD.
The study enrolled NDD-CKD patients with hemoglobin levels between 9.0 g/dL and 11.5 g/dL who were intolerant to or had inadequate response to oral iron supplements.
The patients were randomized 1:1 to receive ferric citrate (n=117) or placebo (n=116). Baseline characteristics were similar between the treatment arms.
The study had a 16-week, double-blind efficacy period, followed by an 8-week, open-label, safety extension period in which all patients remaining in the study, including the placebo group, received ferric citrate.
During the 16-week efficacy period, ferric citrate was administered at a starting dose of 3 tablets per day with food and could be titrated every 4 weeks by an additional 3 tablets for up to 12 tablets per day. The mean dose received in ferric citrate-treated patients was 5 tablets per day.
Efficacy
The study’s primary endpoint was the proportion of patients achieving a ≥1 g/dL increase in hemoglobin at any point during the 16-week efficacy period.
A significantly higher proportion of patients in the ferric citrate arm achieved the primary endpoint—52.1%, compared to 19.1% of patients receiving placebo (P<0.001).
The mean relative change in hemoglobin (for ferric citrate vs placebo) at week 16 was 0.84 g/dL (P<0.001).
Patients who received ferric citrate were significantly more likely to experience a sustained increase in hemoglobin—48.7%, compared to 14.8% for those receiving placebo (P<0.001).
“Not only did ferric citrate deliver a clinically meaningful 1 g/dL increase in hemoglobin levels for the majority of patients . . ., increases were seen as early as 1 to 2 weeks after start of treatment and were sustained for the majority of patients who achieved the primary endpoint,” said study author Steven Fishbane, MD, of Hofstra Northwell School of Medicine in Mineola, New York.
Safety
Treatment-emergent AEs occurred in 79.5% of patients in the ferric citrate arm and 64.7% of those in the placebo arm.
Common AEs (in the ferric citrate and placebo arms, respectively) included diarrhea (20.5% and 16.4%), constipation (18.8% and 12.9%), discolored feces (14.5% and 0%), nausea (11.1% and 2.6%), abdominal pain (6% and 1.7%), fatigue (0% and 5.2%), hyperkalemia (6.8% and 3.4%), and hypertension (4.3% and 5.2%).
Rates of serious AE were similar in the ferric citrate and placebo arms—12.0% and 11.2%, respectively. None of the serious AEs were considered treatment-related.
There were 2 deaths in the ferric citrate arm (and none in the placebo arm), but neither were considered treatment-related.
“The results shown in this pivotal study demonstrated that ferric citrate, if approved for this indication, could provide an important new treatment option for people living with chronic kidney disease and iron deficiency anemia who are not on dialysis,” Dr Fishbane said.
Keryx Biopharmaceuticals recently submitted a supplemental new drug application with these data to the US Food and Drug Administration. ![]()
Photo courtesy of CDC
Results of a phase 3 trial suggest oral ferric citrate could be an alternative to intravenous iron for treating iron deficiency anemia (IDA) in patients with non-dialysis-dependent (NDD) chronic kidney disease (CKD).
Slightly more than half of patients receiving ferric citrate in this study experienced a significant boost in hemoglobin levels.
A treatment effect was seen as early as 1 to 2 weeks after patients started ferric citrate, and responses were durable.
Patients enrolled in the trial had not adequately responded to or could not tolerate prior treatment with oral iron.
Ferric citrate was generally well tolerated in this trial. Adverse events (AEs) were consistent with the drug’s known safety profile, with diarrhea being reported as the most common AE.
These results were published in the Journal of the American Society of Nephrology. The study was sponsored by Keryx Biopharmaceuticals, Inc., the company marketing ferric citrate as Auryxia.
The drug is currently approved in the US as a phosphate binder for the control of serum phosphorus levels in patients with CKD who are on dialysis.
Researchers conducted this phase 3 trial to determine if ferric citrate might be a safe and effective alternative to intravenous iron in patients with NDD CKD.
The study enrolled NDD-CKD patients with hemoglobin levels between 9.0 g/dL and 11.5 g/dL who were intolerant to or had inadequate response to oral iron supplements.
The patients were randomized 1:1 to receive ferric citrate (n=117) or placebo (n=116). Baseline characteristics were similar between the treatment arms.
The study had a 16-week, double-blind efficacy period, followed by an 8-week, open-label, safety extension period in which all patients remaining in the study, including the placebo group, received ferric citrate.
During the 16-week efficacy period, ferric citrate was administered at a starting dose of 3 tablets per day with food and could be titrated every 4 weeks by an additional 3 tablets for up to 12 tablets per day. The mean dose received in ferric citrate-treated patients was 5 tablets per day.
Efficacy
The study’s primary endpoint was the proportion of patients achieving a ≥1 g/dL increase in hemoglobin at any point during the 16-week efficacy period.
A significantly higher proportion of patients in the ferric citrate arm achieved the primary endpoint—52.1%, compared to 19.1% of patients receiving placebo (P<0.001).
The mean relative change in hemoglobin (for ferric citrate vs placebo) at week 16 was 0.84 g/dL (P<0.001).
Patients who received ferric citrate were significantly more likely to experience a sustained increase in hemoglobin—48.7%, compared to 14.8% for those receiving placebo (P<0.001).
“Not only did ferric citrate deliver a clinically meaningful 1 g/dL increase in hemoglobin levels for the majority of patients . . ., increases were seen as early as 1 to 2 weeks after start of treatment and were sustained for the majority of patients who achieved the primary endpoint,” said study author Steven Fishbane, MD, of Hofstra Northwell School of Medicine in Mineola, New York.
Safety
Treatment-emergent AEs occurred in 79.5% of patients in the ferric citrate arm and 64.7% of those in the placebo arm.
Common AEs (in the ferric citrate and placebo arms, respectively) included diarrhea (20.5% and 16.4%), constipation (18.8% and 12.9%), discolored feces (14.5% and 0%), nausea (11.1% and 2.6%), abdominal pain (6% and 1.7%), fatigue (0% and 5.2%), hyperkalemia (6.8% and 3.4%), and hypertension (4.3% and 5.2%).
Rates of serious AE were similar in the ferric citrate and placebo arms—12.0% and 11.2%, respectively. None of the serious AEs were considered treatment-related.
There were 2 deaths in the ferric citrate arm (and none in the placebo arm), but neither were considered treatment-related.
“The results shown in this pivotal study demonstrated that ferric citrate, if approved for this indication, could provide an important new treatment option for people living with chronic kidney disease and iron deficiency anemia who are not on dialysis,” Dr Fishbane said.
Keryx Biopharmaceuticals recently submitted a supplemental new drug application with these data to the US Food and Drug Administration. ![]()
FDA issues CRL for IV formulation of antiemetic agent

chemotherapy
Photo by Rhoda Baer
The US Food and Drug Administration (FDA) has issued a complete response letter (CRL) regarding the new drug application (NDA) for an intravenous (IV) formulation of rolapitant.
An oral formulation of rolapitant, marketed as VARUBI®, is FDA-approved for use in combination with other antiemetic agents to prevent delayed nausea and vomiting associated with initial and repeat courses of emetogenic cancer chemotherapy in adults.
The NDA for rolapitant IV is for the same indication.
The FDA requested additional information regarding the in vitro method utilized to demonstrate comparability of drug product produced at the 2 proposed commercial manufacturers for rolapitant IV that were included in the NDA.
TESARO Inc., the company developing rolapitant IV, said it is working to provide the requested information.
The CRL did not identify concerns related to the safety or efficacy of rolapitant IV or request additional clinical studies. No concerns were raised regarding the active pharmaceutical ingredient, which is also used for VARUBI®.
TESARO identified potential deficiencies at the original contract manufacturer for rolapitant IV, secured a second drug product supplier, and included data from this manufacturer in the NDA.
During the NDA review, the FDA requested and TESARO provided in vitro data to demonstrate comparability of drug product made at the 2 manufacturing sites.
“TESARO is committed to bringing this new intravenous formulation of rolapitant to physicians and patients to enable additional flexibility and choice of antiemetic regimens, and we plan to address FDA’s questions expeditiously and complete this application, which we expect to enable approval in the first half of 2017,” said Mary Lynne Hedley, PhD, president and chief operating officer of TESARO. ![]()
chemotherapy
Photo by Rhoda Baer
The US Food and Drug Administration (FDA) has issued a complete response letter (CRL) regarding the new drug application (NDA) for an intravenous (IV) formulation of rolapitant.
An oral formulation of rolapitant, marketed as VARUBI®, is FDA-approved for use in combination with other antiemetic agents to prevent delayed nausea and vomiting associated with initial and repeat courses of emetogenic cancer chemotherapy in adults.
The NDA for rolapitant IV is for the same indication.
The FDA requested additional information regarding the in vitro method utilized to demonstrate comparability of drug product produced at the 2 proposed commercial manufacturers for rolapitant IV that were included in the NDA.
TESARO Inc., the company developing rolapitant IV, said it is working to provide the requested information.
The CRL did not identify concerns related to the safety or efficacy of rolapitant IV or request additional clinical studies. No concerns were raised regarding the active pharmaceutical ingredient, which is also used for VARUBI®.
TESARO identified potential deficiencies at the original contract manufacturer for rolapitant IV, secured a second drug product supplier, and included data from this manufacturer in the NDA.
During the NDA review, the FDA requested and TESARO provided in vitro data to demonstrate comparability of drug product made at the 2 manufacturing sites.
“TESARO is committed to bringing this new intravenous formulation of rolapitant to physicians and patients to enable additional flexibility and choice of antiemetic regimens, and we plan to address FDA’s questions expeditiously and complete this application, which we expect to enable approval in the first half of 2017,” said Mary Lynne Hedley, PhD, president and chief operating officer of TESARO. ![]()
chemotherapy
Photo by Rhoda Baer
The US Food and Drug Administration (FDA) has issued a complete response letter (CRL) regarding the new drug application (NDA) for an intravenous (IV) formulation of rolapitant.
An oral formulation of rolapitant, marketed as VARUBI®, is FDA-approved for use in combination with other antiemetic agents to prevent delayed nausea and vomiting associated with initial and repeat courses of emetogenic cancer chemotherapy in adults.
The NDA for rolapitant IV is for the same indication.
The FDA requested additional information regarding the in vitro method utilized to demonstrate comparability of drug product produced at the 2 proposed commercial manufacturers for rolapitant IV that were included in the NDA.
TESARO Inc., the company developing rolapitant IV, said it is working to provide the requested information.
The CRL did not identify concerns related to the safety or efficacy of rolapitant IV or request additional clinical studies. No concerns were raised regarding the active pharmaceutical ingredient, which is also used for VARUBI®.
TESARO identified potential deficiencies at the original contract manufacturer for rolapitant IV, secured a second drug product supplier, and included data from this manufacturer in the NDA.
During the NDA review, the FDA requested and TESARO provided in vitro data to demonstrate comparability of drug product made at the 2 manufacturing sites.
“TESARO is committed to bringing this new intravenous formulation of rolapitant to physicians and patients to enable additional flexibility and choice of antiemetic regimens, and we plan to address FDA’s questions expeditiously and complete this application, which we expect to enable approval in the first half of 2017,” said Mary Lynne Hedley, PhD, president and chief operating officer of TESARO. ![]()
Pulmonary rehabilitation helps wide range of COPD patients
Participation in at least 20 days of pulmonary rehabilitation by patients with chronic obstructive pulmonary disease (COPD) resulted in statistically significant improvements in quality of life, perception of health status, functional capacity, dyspnea, and depression, in a retrospective analysis.
Furthermore, improvements were seen regardless of the degree of exercise function, dyspnea, or lung function at baseline, reported lead investigator Praful Schroff.
The analysis focused on 229 COPD patients enrolled in the pulmonary rehabilitation program at UAB during 1996-2013, all of whom completed questionnaires both at enrollment and after completion of their respective exercise programs. The mean forced expiratory volume in 1 second (FEV1) percent predicted for the cohort was 46.3%.The researchers used pulmonary function data from tests performed within 2 years of enrollment. Change in quality of life and perception of health status were measured using the 36-item Short Form Health Survey (SF-36), dyspnea was assessed using the San Diego Shortness of Breath Questionnaire (SOBQ), depression was assessed using the Beck Depression Inventory (BDI)-II, and functional capacity was assessed using the 6-minute-walk-distance (6MWD) test. On average, the patients reported clinically significant improvements in most components of the SF-36, including an 11.5-unit, a 16.4-U, and a 12.4-U increase in physical function, social function, and vitality, respectively (P less than .001 for all three). The patients also experienced clinically important improvements in the 6MWD test (increase of 52.4 m; P less than .001) and dyspnea (decrease of 9.1 U in the SOBQ; P less than .001). On average, patients’ depression decreased by 3 U, using the BDI II (P less than .001).
When patients in this study were divided into groups based on various aspects of their health at baseline, the levels of improvements seen by each group in most components of the SF-36, the 6MWD, the SOBQ, and the BDI-II were almost always similar.
“We add to the literature by comparing outcomes across quartiles of baseline exercise capacity and showing that patients benefit independent of underlying functional capacity,” said Mr. Schroff and his colleagues.
A few differences in the outcomes following pulmonary rehabilitation were observed between these baseline characteristics–based groups. When patients were grouped by exercise capacity, for example, those with the lowest baseline exercise capacity (as measured by the 6MWD) experienced the largest incremental improvement in the 6MWD. Additionally, when patients were grouped by dyspnea score, those with the worst baseline dyspnea experienced the greatest reduction in dyspnea. However, those with the lowest lung function made the smallest improvement in the 6MWD. Another of these differences was observed between the patients with the lowest baseline lung function and the patients in the other lung function-based quartiles. Those with the worst lung function made the smallest improvement in the 6MWD, which was 39.0 m, on average. All of these subgroups achieved clinically significant improvements in the 6MWD and SOBQ (Ann Am Thorac Soc. 2017 Jan 1;14[1]:26-32).
Each exercise session included aerobic exercises, resistance training, and breathing techniques. Cardiovascular exercise was prescribed starting at 20-30 minutes of continuous or interval bouts and was gradually increasing until 30-45 minutes of exercise was achieved. Patients also received education sessions lasting 40-60 minutes on understanding their disease, smoking cessation counseling, appropriate use of inhalers, diet and nutrition, and stress management. Subjects with other concurrent chronic respiratory diseases were excluded from the analysis.
The researchers noted that their findings may not be generalizable to patients with disease burdens causing them to drop out of the study. “Although we have previously shown that baseline levels of dyspnea, FEV1, and exercise capacity did not influence dropout rates, this could be a source of bias,” they noted.
“Patients with COPD experienced meaningful improvements in quality of life, dyspnea, exercise capacity, and depression, regardless of baseline lung function, dyspnea, and exercise capacity. Current guidelines should be amended to recommend pulmonary rehabilitation to all patients with COPD, regardless of their baseline level of disease burden,” the analysis’ authors said.
Three of the study’s authors reported receiving grants and other fees or a single grant from various sources. The other authors, including Mr. Schroff, said they had nothing to disclose.

Participation in at least 20 days of pulmonary rehabilitation by patients with chronic obstructive pulmonary disease (COPD) resulted in statistically significant improvements in quality of life, perception of health status, functional capacity, dyspnea, and depression, in a retrospective analysis.
Furthermore, improvements were seen regardless of the degree of exercise function, dyspnea, or lung function at baseline, reported lead investigator Praful Schroff.
The analysis focused on 229 COPD patients enrolled in the pulmonary rehabilitation program at UAB during 1996-2013, all of whom completed questionnaires both at enrollment and after completion of their respective exercise programs. The mean forced expiratory volume in 1 second (FEV1) percent predicted for the cohort was 46.3%.The researchers used pulmonary function data from tests performed within 2 years of enrollment. Change in quality of life and perception of health status were measured using the 36-item Short Form Health Survey (SF-36), dyspnea was assessed using the San Diego Shortness of Breath Questionnaire (SOBQ), depression was assessed using the Beck Depression Inventory (BDI)-II, and functional capacity was assessed using the 6-minute-walk-distance (6MWD) test. On average, the patients reported clinically significant improvements in most components of the SF-36, including an 11.5-unit, a 16.4-U, and a 12.4-U increase in physical function, social function, and vitality, respectively (P less than .001 for all three). The patients also experienced clinically important improvements in the 6MWD test (increase of 52.4 m; P less than .001) and dyspnea (decrease of 9.1 U in the SOBQ; P less than .001). On average, patients’ depression decreased by 3 U, using the BDI II (P less than .001).
When patients in this study were divided into groups based on various aspects of their health at baseline, the levels of improvements seen by each group in most components of the SF-36, the 6MWD, the SOBQ, and the BDI-II were almost always similar.
“We add to the literature by comparing outcomes across quartiles of baseline exercise capacity and showing that patients benefit independent of underlying functional capacity,” said Mr. Schroff and his colleagues.
A few differences in the outcomes following pulmonary rehabilitation were observed between these baseline characteristics–based groups. When patients were grouped by exercise capacity, for example, those with the lowest baseline exercise capacity (as measured by the 6MWD) experienced the largest incremental improvement in the 6MWD. Additionally, when patients were grouped by dyspnea score, those with the worst baseline dyspnea experienced the greatest reduction in dyspnea. However, those with the lowest lung function made the smallest improvement in the 6MWD. Another of these differences was observed between the patients with the lowest baseline lung function and the patients in the other lung function-based quartiles. Those with the worst lung function made the smallest improvement in the 6MWD, which was 39.0 m, on average. All of these subgroups achieved clinically significant improvements in the 6MWD and SOBQ (Ann Am Thorac Soc. 2017 Jan 1;14[1]:26-32).
Each exercise session included aerobic exercises, resistance training, and breathing techniques. Cardiovascular exercise was prescribed starting at 20-30 minutes of continuous or interval bouts and was gradually increasing until 30-45 minutes of exercise was achieved. Patients also received education sessions lasting 40-60 minutes on understanding their disease, smoking cessation counseling, appropriate use of inhalers, diet and nutrition, and stress management. Subjects with other concurrent chronic respiratory diseases were excluded from the analysis.
The researchers noted that their findings may not be generalizable to patients with disease burdens causing them to drop out of the study. “Although we have previously shown that baseline levels of dyspnea, FEV1, and exercise capacity did not influence dropout rates, this could be a source of bias,” they noted.
“Patients with COPD experienced meaningful improvements in quality of life, dyspnea, exercise capacity, and depression, regardless of baseline lung function, dyspnea, and exercise capacity. Current guidelines should be amended to recommend pulmonary rehabilitation to all patients with COPD, regardless of their baseline level of disease burden,” the analysis’ authors said.
Three of the study’s authors reported receiving grants and other fees or a single grant from various sources. The other authors, including Mr. Schroff, said they had nothing to disclose.
Participation in at least 20 days of pulmonary rehabilitation by patients with chronic obstructive pulmonary disease (COPD) resulted in statistically significant improvements in quality of life, perception of health status, functional capacity, dyspnea, and depression, in a retrospective analysis.
Furthermore, improvements were seen regardless of the degree of exercise function, dyspnea, or lung function at baseline, reported lead investigator Praful Schroff.
The analysis focused on 229 COPD patients enrolled in the pulmonary rehabilitation program at UAB during 1996-2013, all of whom completed questionnaires both at enrollment and after completion of their respective exercise programs. The mean forced expiratory volume in 1 second (FEV1) percent predicted for the cohort was 46.3%.The researchers used pulmonary function data from tests performed within 2 years of enrollment. Change in quality of life and perception of health status were measured using the 36-item Short Form Health Survey (SF-36), dyspnea was assessed using the San Diego Shortness of Breath Questionnaire (SOBQ), depression was assessed using the Beck Depression Inventory (BDI)-II, and functional capacity was assessed using the 6-minute-walk-distance (6MWD) test. On average, the patients reported clinically significant improvements in most components of the SF-36, including an 11.5-unit, a 16.4-U, and a 12.4-U increase in physical function, social function, and vitality, respectively (P less than .001 for all three). The patients also experienced clinically important improvements in the 6MWD test (increase of 52.4 m; P less than .001) and dyspnea (decrease of 9.1 U in the SOBQ; P less than .001). On average, patients’ depression decreased by 3 U, using the BDI II (P less than .001).
When patients in this study were divided into groups based on various aspects of their health at baseline, the levels of improvements seen by each group in most components of the SF-36, the 6MWD, the SOBQ, and the BDI-II were almost always similar.
“We add to the literature by comparing outcomes across quartiles of baseline exercise capacity and showing that patients benefit independent of underlying functional capacity,” said Mr. Schroff and his colleagues.
A few differences in the outcomes following pulmonary rehabilitation were observed between these baseline characteristics–based groups. When patients were grouped by exercise capacity, for example, those with the lowest baseline exercise capacity (as measured by the 6MWD) experienced the largest incremental improvement in the 6MWD. Additionally, when patients were grouped by dyspnea score, those with the worst baseline dyspnea experienced the greatest reduction in dyspnea. However, those with the lowest lung function made the smallest improvement in the 6MWD. Another of these differences was observed between the patients with the lowest baseline lung function and the patients in the other lung function-based quartiles. Those with the worst lung function made the smallest improvement in the 6MWD, which was 39.0 m, on average. All of these subgroups achieved clinically significant improvements in the 6MWD and SOBQ (Ann Am Thorac Soc. 2017 Jan 1;14[1]:26-32).
Each exercise session included aerobic exercises, resistance training, and breathing techniques. Cardiovascular exercise was prescribed starting at 20-30 minutes of continuous or interval bouts and was gradually increasing until 30-45 minutes of exercise was achieved. Patients also received education sessions lasting 40-60 minutes on understanding their disease, smoking cessation counseling, appropriate use of inhalers, diet and nutrition, and stress management. Subjects with other concurrent chronic respiratory diseases were excluded from the analysis.
The researchers noted that their findings may not be generalizable to patients with disease burdens causing them to drop out of the study. “Although we have previously shown that baseline levels of dyspnea, FEV1, and exercise capacity did not influence dropout rates, this could be a source of bias,” they noted.
“Patients with COPD experienced meaningful improvements in quality of life, dyspnea, exercise capacity, and depression, regardless of baseline lung function, dyspnea, and exercise capacity. Current guidelines should be amended to recommend pulmonary rehabilitation to all patients with COPD, regardless of their baseline level of disease burden,” the analysis’ authors said.
Three of the study’s authors reported receiving grants and other fees or a single grant from various sources. The other authors, including Mr. Schroff, said they had nothing to disclose.
Key clinical point: COPD patients with a variety of baseline health characteristics experienced clinically significant improvements in quality of life, functional capacity, and dyspnea following at least 20 days of pulmonary rehabilitation.
Major finding: The patients experienced clinically important improvements in the 6-minute-walk-distance test (an average increase of 52.4 m; P less than .001) and dyspnea (an average decrease of 9.1 U in the San Diego Shortness of Breath Questionnaire, P less than .001).
Data source: A retrospective analysis of 229 COPD patients from a prospectively maintained database.
Disclosures: Three of the study’s authors reported receiving grants and other fees or a single grant from various sources. The other authors, including Mr. Schroff, said they had nothing to disclose.
Screen opioid users for depression, study recommends
Depression combined with chronic opioid analgesic use involves more symptoms and comorbidities than depression without chronic opioid use, according to a study of Department of Veterans Affairs patients seen between 2000 and 2012.
“Screening and treatment of depression in non–cancer pain patients may limit risk of persistent mood disorder and subsequent suicidal ideation,” wrote Jeffrey F. Scherrer, PhD, and his coauthors. “Opioid prescribing for pain management should be coupled with careful screening and treatment of emerging depression.”
“Eligible patients were cancer free, HIV free. ... Because we were interested in characterizing severity of new-onset [new depression episodes] and not predictors of NDE, we measured incident substance use and psychiatric comorbidities that occurred at the same time or after NDE. Therefore, eligible patients were free of psychiatric and substance use disorders before NDE. Patients whose opioid use began after NDE and patients without NDE in follow-up were excluded,” wrote Dr. Scherrer of Saint Louis University and his coauthors (J Affect Disord. 2017 Mar 1;210:125-9).
This process left the researchers with a sample size of 4,758 patients. Of those, 4,314 developed NDE without receiving an opioid, while the remaining 444 developed NDE after opioid use of more than 90 days.
Looking at raw figures prior to the application of inverse probability of treatment weighting (IPTW), the opioid use group was more likely than was the nonopioid use group to have comorbid posttraumatic stress disorder (17.3% vs. 11.9%), opioid (4.3% vs. 0.5%) and other drug abuse/dependence (11.3% vs. 4.8%), all pain-related conditions, obesity (48.2% vs. 37.4%), and nicotine abuse/dependence (52.5% vs. 30.5%). The further calculations were made “to assess whether differences between the groups were irrespective of pain-related variables.”
With IPTW adjustments made, the differences in pain-related comorbidities went away. Opioid-using patients had higher depression severity as measured by Patient Health Questionnaire–9 scores (P = .012). They also were more likely to have had antidepressant treatment for at least 12 weeks (P less than .0001). Nonopioid use patients were more likely to have anxiety disorders other than PTSD (P = .014).
Dr. Scherrer had no conflicts of interest. The study received funding support from the National Institute of Mental Health. The views reflected in the article are those of the authors and not necessarily those of the VA, the researchers reported.
Depression combined with chronic opioid analgesic use involves more symptoms and comorbidities than depression without chronic opioid use, according to a study of Department of Veterans Affairs patients seen between 2000 and 2012.
“Screening and treatment of depression in non–cancer pain patients may limit risk of persistent mood disorder and subsequent suicidal ideation,” wrote Jeffrey F. Scherrer, PhD, and his coauthors. “Opioid prescribing for pain management should be coupled with careful screening and treatment of emerging depression.”
“Eligible patients were cancer free, HIV free. ... Because we were interested in characterizing severity of new-onset [new depression episodes] and not predictors of NDE, we measured incident substance use and psychiatric comorbidities that occurred at the same time or after NDE. Therefore, eligible patients were free of psychiatric and substance use disorders before NDE. Patients whose opioid use began after NDE and patients without NDE in follow-up were excluded,” wrote Dr. Scherrer of Saint Louis University and his coauthors (J Affect Disord. 2017 Mar 1;210:125-9).
This process left the researchers with a sample size of 4,758 patients. Of those, 4,314 developed NDE without receiving an opioid, while the remaining 444 developed NDE after opioid use of more than 90 days.
Looking at raw figures prior to the application of inverse probability of treatment weighting (IPTW), the opioid use group was more likely than was the nonopioid use group to have comorbid posttraumatic stress disorder (17.3% vs. 11.9%), opioid (4.3% vs. 0.5%) and other drug abuse/dependence (11.3% vs. 4.8%), all pain-related conditions, obesity (48.2% vs. 37.4%), and nicotine abuse/dependence (52.5% vs. 30.5%). The further calculations were made “to assess whether differences between the groups were irrespective of pain-related variables.”
With IPTW adjustments made, the differences in pain-related comorbidities went away. Opioid-using patients had higher depression severity as measured by Patient Health Questionnaire–9 scores (P = .012). They also were more likely to have had antidepressant treatment for at least 12 weeks (P less than .0001). Nonopioid use patients were more likely to have anxiety disorders other than PTSD (P = .014).
Dr. Scherrer had no conflicts of interest. The study received funding support from the National Institute of Mental Health. The views reflected in the article are those of the authors and not necessarily those of the VA, the researchers reported.
Depression combined with chronic opioid analgesic use involves more symptoms and comorbidities than depression without chronic opioid use, according to a study of Department of Veterans Affairs patients seen between 2000 and 2012.
“Screening and treatment of depression in non–cancer pain patients may limit risk of persistent mood disorder and subsequent suicidal ideation,” wrote Jeffrey F. Scherrer, PhD, and his coauthors. “Opioid prescribing for pain management should be coupled with careful screening and treatment of emerging depression.”
“Eligible patients were cancer free, HIV free. ... Because we were interested in characterizing severity of new-onset [new depression episodes] and not predictors of NDE, we measured incident substance use and psychiatric comorbidities that occurred at the same time or after NDE. Therefore, eligible patients were free of psychiatric and substance use disorders before NDE. Patients whose opioid use began after NDE and patients without NDE in follow-up were excluded,” wrote Dr. Scherrer of Saint Louis University and his coauthors (J Affect Disord. 2017 Mar 1;210:125-9).
This process left the researchers with a sample size of 4,758 patients. Of those, 4,314 developed NDE without receiving an opioid, while the remaining 444 developed NDE after opioid use of more than 90 days.
Looking at raw figures prior to the application of inverse probability of treatment weighting (IPTW), the opioid use group was more likely than was the nonopioid use group to have comorbid posttraumatic stress disorder (17.3% vs. 11.9%), opioid (4.3% vs. 0.5%) and other drug abuse/dependence (11.3% vs. 4.8%), all pain-related conditions, obesity (48.2% vs. 37.4%), and nicotine abuse/dependence (52.5% vs. 30.5%). The further calculations were made “to assess whether differences between the groups were irrespective of pain-related variables.”
With IPTW adjustments made, the differences in pain-related comorbidities went away. Opioid-using patients had higher depression severity as measured by Patient Health Questionnaire–9 scores (P = .012). They also were more likely to have had antidepressant treatment for at least 12 weeks (P less than .0001). Nonopioid use patients were more likely to have anxiety disorders other than PTSD (P = .014).
Dr. Scherrer had no conflicts of interest. The study received funding support from the National Institute of Mental Health. The views reflected in the article are those of the authors and not necessarily those of the VA, the researchers reported.
Lower BDNF levels found in older adults with bipolar I
Older patients with bipolar I disorder appear to have lower serum levels of brain-deprived neurotrophic factor than similarly aged adults without bipolar I, a study showed.
At the beginning of the study, Aline T. Soares, MD, and her colleagues recruited 118 patients from clinics in the United States and Canada with bipolar disorder who were aged 50 and over and a similar control group of 76 healthy patients. Twenty-seven of the 118 patients had type II bipolar disorder, and 91 had type I bipolar disorder; all had been clinically euthymic for at least 4 weeks when they were evaluated, reported Dr. Soares of the department of internal medicine at the University of São Paulo (Brazil).
The results showed that patients positively identified with bipolar I disorder had lowered brain-deprived neurotrophic factor (BDNF) levels, compared with their control group counterparts. Lower levels of BDNF were not detected in those with bipolar II disorder, the investigators reported (Am J Geriatr Psychiatry. 2016 Aug;24[8]:596-601).
“Our study represents a continuation of the [bipolar disorder] and BDNF story: Prolonged bipolar illness appears to lead to decreased BDNF, even in the euthymic state,” Dr. Soares and her colleagues wrote. “This reduces the brain’s capacity for neurogenesis and neuroplasticity and theoretically increases the risk of hippocampal shrinkage, cognitive deficits, and dementia.”
Future studies are needed to look into how BDNF levels affect mood, cognitive abilities, and other areas of life related to bipolar disorder, they said.
Dr. Soares and her colleagues reported that they had no conflicts to disclose.
To read more about the study, click here.
Older patients with bipolar I disorder appear to have lower serum levels of brain-deprived neurotrophic factor than similarly aged adults without bipolar I, a study showed.
At the beginning of the study, Aline T. Soares, MD, and her colleagues recruited 118 patients from clinics in the United States and Canada with bipolar disorder who were aged 50 and over and a similar control group of 76 healthy patients. Twenty-seven of the 118 patients had type II bipolar disorder, and 91 had type I bipolar disorder; all had been clinically euthymic for at least 4 weeks when they were evaluated, reported Dr. Soares of the department of internal medicine at the University of São Paulo (Brazil).
The results showed that patients positively identified with bipolar I disorder had lowered brain-deprived neurotrophic factor (BDNF) levels, compared with their control group counterparts. Lower levels of BDNF were not detected in those with bipolar II disorder, the investigators reported (Am J Geriatr Psychiatry. 2016 Aug;24[8]:596-601).
“Our study represents a continuation of the [bipolar disorder] and BDNF story: Prolonged bipolar illness appears to lead to decreased BDNF, even in the euthymic state,” Dr. Soares and her colleagues wrote. “This reduces the brain’s capacity for neurogenesis and neuroplasticity and theoretically increases the risk of hippocampal shrinkage, cognitive deficits, and dementia.”
Future studies are needed to look into how BDNF levels affect mood, cognitive abilities, and other areas of life related to bipolar disorder, they said.
Dr. Soares and her colleagues reported that they had no conflicts to disclose.
To read more about the study, click here.
Older patients with bipolar I disorder appear to have lower serum levels of brain-deprived neurotrophic factor than similarly aged adults without bipolar I, a study showed.
At the beginning of the study, Aline T. Soares, MD, and her colleagues recruited 118 patients from clinics in the United States and Canada with bipolar disorder who were aged 50 and over and a similar control group of 76 healthy patients. Twenty-seven of the 118 patients had type II bipolar disorder, and 91 had type I bipolar disorder; all had been clinically euthymic for at least 4 weeks when they were evaluated, reported Dr. Soares of the department of internal medicine at the University of São Paulo (Brazil).
The results showed that patients positively identified with bipolar I disorder had lowered brain-deprived neurotrophic factor (BDNF) levels, compared with their control group counterparts. Lower levels of BDNF were not detected in those with bipolar II disorder, the investigators reported (Am J Geriatr Psychiatry. 2016 Aug;24[8]:596-601).
“Our study represents a continuation of the [bipolar disorder] and BDNF story: Prolonged bipolar illness appears to lead to decreased BDNF, even in the euthymic state,” Dr. Soares and her colleagues wrote. “This reduces the brain’s capacity for neurogenesis and neuroplasticity and theoretically increases the risk of hippocampal shrinkage, cognitive deficits, and dementia.”
Future studies are needed to look into how BDNF levels affect mood, cognitive abilities, and other areas of life related to bipolar disorder, they said.
Dr. Soares and her colleagues reported that they had no conflicts to disclose.
To read more about the study, click here.
FROM THE AMERICAN JOURNAL OF GERIATRIC PSYCHIATRY
When primary anti-TNF fails in axial spondyloarthritis, consider comorbidities or second anti-TNF
Most of the minority of axial spondyloarthritis patients who do not respond to their first tumor necrosis factor inhibitor still meet classification criteria for the condition 5-10 years later, but more than half respond to a second TNFi and most also have comorbidities that could affect the spondyloarthritis evaluation, according to findings from a single-center cohort study.
The study’s finding of TNFi primary inefficacy in 27 (12%) of 222 patients with axial spondyloarthritis (axSpA) who were given their first TNFi during 2004-2009 is in line with previous results of about 5%-15% primary inefficacy for a first TNFi in axSpA. However, the French investigators, led by Sandra Kossi of Cochin Hospital in Paris, noted that the difficulty of making an axSpA diagnosis and the presence of certain comorbidities “could interfere either with the activity of SpA (falsely heightened disease activity) or with the response to TNFi (falsely heightened inefficacy).” They sought to report the characteristics of axSpA patients with primary inefficacy after their first TNFi in the 5- to 10-year period after their prescription (Rheumatology [Oxford]. 2017 Jan 9. doi: 10.1093/rheumatology/kew456).
A total of 25 of the patients with primary inefficacy underwent re-evaluation 5-10 years (mean of 6 years) later. The investigators defined primary inefficacy as “treatment interruption 3-4 months after treatment onset, with a rheumatologist assessment in the medical file citing lack of efficacy as primary reason for drug interruption.”
The patients with primary TNFi inefficacy had a mean age of 53 years at the time of follow-up, and about half were female. All the patients still had symptoms and back pain, but symptoms were moderate based on a mean Bath Ankylosing Spondylitis Disease Activity Index score of 42. Overall, nine were taking a TNFi and nine were taking nonsteroidal anti-inflammatory drugs, while others used analgesics or nonpharmacologic measures.
Primary TNFi inefficacy occurred significantly more often occurred among females (48% vs. 27%; P = .04), older aged patients at first TNFi use (45 vs. 39 years; P = .04), patients with higher mean Bath Ankylosing Spondylitis Functional Index scores (68 vs. 42; P = .03), and in those who did not have an abnormally elevated C-reactive protein level (33% vs. 63%; P = .02). Patients with primary TNFi inefficacy had lower rates of HLAB27 positivity (56% vs. 72%) or radiographic sacroiliitis (67% vs. 81%), but the differences were not statistically significant.
At follow-up, 21 (84%) patients met Assessment of Spondyloarthritis International Society classification criteria for axSpA, and 20 (80%) met the axSpA diagnosis according to the rheumatologists’ opinion, with 17 (68%) fulfilling both.
A total of 18 (72%) had at least one of the following comorbidities: widespread pain syndrome, osteoarthritis, or depression. Five patients – all females – had widespread pain syndrome according to the Fibromyalgia Rapid Screening Tool questionnaire. Another 10 patients had osteoarthritis of lower-limb peripheral joints or of the spine, while an additional 8 had self-declared depression, for which 3 were taking antidepressants.
By the time of follow-up, 16 (64%) had switched to another TNFi, including 9 who had received two TNFi drugs and 7 who had received three or more. The second TNFi was considered efficacious in nine patients. The retention rate of the second TNFi at 1 year among those with primary inefficacy was 50%, and overall, nine patients were still prescribed a TNFi at the time of follow-up.
The fact that most of the patients with primary inefficacy to their first TNFi had confirmed axSpA but also had comorbidities that could affect axSpA evaluation “is important because practitioners might consider that primary inefficacy to TNFi leads to reconsidering the diagnosis of SpA (i.e. the notion of a TNFi prescription being used as the diagnostic test). We suggest here that primary inefficacy should not be considered as equivalent to a diagnostic error, and that a second prescription of TNFi may be of use in such patients, although painful comorbidities should certainly be screened for and taken into account.”
The study was funded by the Assistance Publique des Hôpitaux de Paris. The investigators had no conflicts of interest to declare.
Most of the minority of axial spondyloarthritis patients who do not respond to their first tumor necrosis factor inhibitor still meet classification criteria for the condition 5-10 years later, but more than half respond to a second TNFi and most also have comorbidities that could affect the spondyloarthritis evaluation, according to findings from a single-center cohort study.
The study’s finding of TNFi primary inefficacy in 27 (12%) of 222 patients with axial spondyloarthritis (axSpA) who were given their first TNFi during 2004-2009 is in line with previous results of about 5%-15% primary inefficacy for a first TNFi in axSpA. However, the French investigators, led by Sandra Kossi of Cochin Hospital in Paris, noted that the difficulty of making an axSpA diagnosis and the presence of certain comorbidities “could interfere either with the activity of SpA (falsely heightened disease activity) or with the response to TNFi (falsely heightened inefficacy).” They sought to report the characteristics of axSpA patients with primary inefficacy after their first TNFi in the 5- to 10-year period after their prescription (Rheumatology [Oxford]. 2017 Jan 9. doi: 10.1093/rheumatology/kew456).
A total of 25 of the patients with primary inefficacy underwent re-evaluation 5-10 years (mean of 6 years) later. The investigators defined primary inefficacy as “treatment interruption 3-4 months after treatment onset, with a rheumatologist assessment in the medical file citing lack of efficacy as primary reason for drug interruption.”
The patients with primary TNFi inefficacy had a mean age of 53 years at the time of follow-up, and about half were female. All the patients still had symptoms and back pain, but symptoms were moderate based on a mean Bath Ankylosing Spondylitis Disease Activity Index score of 42. Overall, nine were taking a TNFi and nine were taking nonsteroidal anti-inflammatory drugs, while others used analgesics or nonpharmacologic measures.
Primary TNFi inefficacy occurred significantly more often occurred among females (48% vs. 27%; P = .04), older aged patients at first TNFi use (45 vs. 39 years; P = .04), patients with higher mean Bath Ankylosing Spondylitis Functional Index scores (68 vs. 42; P = .03), and in those who did not have an abnormally elevated C-reactive protein level (33% vs. 63%; P = .02). Patients with primary TNFi inefficacy had lower rates of HLAB27 positivity (56% vs. 72%) or radiographic sacroiliitis (67% vs. 81%), but the differences were not statistically significant.
At follow-up, 21 (84%) patients met Assessment of Spondyloarthritis International Society classification criteria for axSpA, and 20 (80%) met the axSpA diagnosis according to the rheumatologists’ opinion, with 17 (68%) fulfilling both.
A total of 18 (72%) had at least one of the following comorbidities: widespread pain syndrome, osteoarthritis, or depression. Five patients – all females – had widespread pain syndrome according to the Fibromyalgia Rapid Screening Tool questionnaire. Another 10 patients had osteoarthritis of lower-limb peripheral joints or of the spine, while an additional 8 had self-declared depression, for which 3 were taking antidepressants.
By the time of follow-up, 16 (64%) had switched to another TNFi, including 9 who had received two TNFi drugs and 7 who had received three or more. The second TNFi was considered efficacious in nine patients. The retention rate of the second TNFi at 1 year among those with primary inefficacy was 50%, and overall, nine patients were still prescribed a TNFi at the time of follow-up.
The fact that most of the patients with primary inefficacy to their first TNFi had confirmed axSpA but also had comorbidities that could affect axSpA evaluation “is important because practitioners might consider that primary inefficacy to TNFi leads to reconsidering the diagnosis of SpA (i.e. the notion of a TNFi prescription being used as the diagnostic test). We suggest here that primary inefficacy should not be considered as equivalent to a diagnostic error, and that a second prescription of TNFi may be of use in such patients, although painful comorbidities should certainly be screened for and taken into account.”
The study was funded by the Assistance Publique des Hôpitaux de Paris. The investigators had no conflicts of interest to declare.
Most of the minority of axial spondyloarthritis patients who do not respond to their first tumor necrosis factor inhibitor still meet classification criteria for the condition 5-10 years later, but more than half respond to a second TNFi and most also have comorbidities that could affect the spondyloarthritis evaluation, according to findings from a single-center cohort study.
The study’s finding of TNFi primary inefficacy in 27 (12%) of 222 patients with axial spondyloarthritis (axSpA) who were given their first TNFi during 2004-2009 is in line with previous results of about 5%-15% primary inefficacy for a first TNFi in axSpA. However, the French investigators, led by Sandra Kossi of Cochin Hospital in Paris, noted that the difficulty of making an axSpA diagnosis and the presence of certain comorbidities “could interfere either with the activity of SpA (falsely heightened disease activity) or with the response to TNFi (falsely heightened inefficacy).” They sought to report the characteristics of axSpA patients with primary inefficacy after their first TNFi in the 5- to 10-year period after their prescription (Rheumatology [Oxford]. 2017 Jan 9. doi: 10.1093/rheumatology/kew456).
A total of 25 of the patients with primary inefficacy underwent re-evaluation 5-10 years (mean of 6 years) later. The investigators defined primary inefficacy as “treatment interruption 3-4 months after treatment onset, with a rheumatologist assessment in the medical file citing lack of efficacy as primary reason for drug interruption.”
The patients with primary TNFi inefficacy had a mean age of 53 years at the time of follow-up, and about half were female. All the patients still had symptoms and back pain, but symptoms were moderate based on a mean Bath Ankylosing Spondylitis Disease Activity Index score of 42. Overall, nine were taking a TNFi and nine were taking nonsteroidal anti-inflammatory drugs, while others used analgesics or nonpharmacologic measures.
Primary TNFi inefficacy occurred significantly more often occurred among females (48% vs. 27%; P = .04), older aged patients at first TNFi use (45 vs. 39 years; P = .04), patients with higher mean Bath Ankylosing Spondylitis Functional Index scores (68 vs. 42; P = .03), and in those who did not have an abnormally elevated C-reactive protein level (33% vs. 63%; P = .02). Patients with primary TNFi inefficacy had lower rates of HLAB27 positivity (56% vs. 72%) or radiographic sacroiliitis (67% vs. 81%), but the differences were not statistically significant.
At follow-up, 21 (84%) patients met Assessment of Spondyloarthritis International Society classification criteria for axSpA, and 20 (80%) met the axSpA diagnosis according to the rheumatologists’ opinion, with 17 (68%) fulfilling both.
A total of 18 (72%) had at least one of the following comorbidities: widespread pain syndrome, osteoarthritis, or depression. Five patients – all females – had widespread pain syndrome according to the Fibromyalgia Rapid Screening Tool questionnaire. Another 10 patients had osteoarthritis of lower-limb peripheral joints or of the spine, while an additional 8 had self-declared depression, for which 3 were taking antidepressants.
By the time of follow-up, 16 (64%) had switched to another TNFi, including 9 who had received two TNFi drugs and 7 who had received three or more. The second TNFi was considered efficacious in nine patients. The retention rate of the second TNFi at 1 year among those with primary inefficacy was 50%, and overall, nine patients were still prescribed a TNFi at the time of follow-up.
The fact that most of the patients with primary inefficacy to their first TNFi had confirmed axSpA but also had comorbidities that could affect axSpA evaluation “is important because practitioners might consider that primary inefficacy to TNFi leads to reconsidering the diagnosis of SpA (i.e. the notion of a TNFi prescription being used as the diagnostic test). We suggest here that primary inefficacy should not be considered as equivalent to a diagnostic error, and that a second prescription of TNFi may be of use in such patients, although painful comorbidities should certainly be screened for and taken into account.”
The study was funded by the Assistance Publique des Hôpitaux de Paris. The investigators had no conflicts of interest to declare.
Key clinical point:
Major finding: A total of 18 (72%) of 25 patients with primary TNFi inefficacy had at least one of the following comorbidities: widespread pain syndrome, osteoarthritis, or depression.
Data source: A retrospective and prospective cohort study of 222 patients who received a first TNFi after being diagnosed with axial spondyloarthritis during 2004-2009.
Disclosures: The study was funded by the Assistance Publique des Hôpitaux de Paris. The investigators had no conflicts of interest to declare.
New data signal paradigm shift in FMD and arterial disease
CHICAGO – New data have shown that fibromuscular dysplasia is associated with high rates of dissection and/or aneurysm, and emerging recommendations call for routine imaging early on in the diagnosis of FMD to monitor for these vascular events, a researcher who developed those recommendations reported at a symposium on vascular surgery sponsored by Northwestern University.
“Given the very high rate of aneurysms in this population, it is now recommended that all patients with FMD should undergo at least one-time head-to pelvis imaging with CT angiography or MR angiography to screen for the presence of an aneurysm or to identify other areas of FMD involvement,” said Daniella Kadian-Dodov, MD, of Icahn School of Medicine at Mount Sinai in New York (J Am Coll Cardiol. 2016;68:176-85).

First described in 1938, FMD is a non-atherosclerotic, noninflammatory disease that had been thought to be a rare cause of renovascular hypertension with a classic “string-of-beads” appearance upon imaging, Dr. Kadian-Dodov noted. However, recent data from the Fibromuscular Dysplasia Society of America–sponsored U.S. registry has changed that thinking. “We now know it occurs more frequently in the carotid and renal arteries, although it has been observed in almost every artery,” she said. “The pathogenesis is still unknown but up to 10% of cases are familial.”
And manifestations of disease now extend beyond the “string-of-beads” appearance to include aneurysm, dissection, and arterial tortuosity, she said (Circulation. 2012;125:3182-90; Circulation. 2014;129:1048-78; J Am Coll Cardiol. 2016;68:176-85). The classification system for FMD has also undergone a recent change, according to Dr. Kadian-Dodov. “Traditionally, a histopathologic scheme was used to classify FMD,” she said. “Nowadays, fewer and fewer patients are undergoing surgical procedures, so the classification has changed to an angiographic system,” the most common of which is the American Heart Association system adopted in 2014 that distinguishes between multifocal, characterized by the classic “string-of-beads” appearance, and focal FMD with a single area of stenosis.
But the diagnosis of either variant of FMD is not exclusive. “Patients may have multiple areas of disease involvement and the same patient may have both focal and multifocal FMD findings,” Dr. Kadian-Dodov said.
The U.S. registry has helped clarify the thinking on FMD, Dr. Kadian-Dodov said. More than 1,400 patients are in the registry, 90% of whom are women with multifocal disease. The average age of onset of symptoms is 47 years, but 52 is the average age for diagnosis. “So these patients are experiencing several years delay to FMD diagnosis,” she said.
Manifestations depend on the vascular bed involved. “In the case of cervical artery FMD, headaches and pulsatile tinnitus are commonly reported, whereas with renal artery involvement hypertension is the most common symptom,” she said. A recent analysis showed 41.7% of the FMD population have either aneurysm and dissection or both (J Am Coll Cardiol. 2016;68:176-185).
But no specific guidelines for treatment of FMD yet exist, Dr. Kadian-Dodov said. “General guidelines should be applied for the management of dissection and aneurysm in patients with FMD,” she said. For patients with arterial dissection, that means conservative therapy comprising either anticoagulation or antiplatelet agents for 3-6 months followed by daily low-dose aspirin therapy. “Revascularization is rarely required for these patients,” she said. “Endovascular or surgical modalities should be reserved for those with continued ischemia despite conservative management or more complicated pseudoaneurysm formations.”
Daily aspirin therapy is likewise the recommendation for patients with cervical artery multifocal or focal FMD involvement without dissection or aneurysms. “We follow up with imaging every 6 months for 2 years,” Dr. Kadian-Dodov said. “If they’re stable, we switch over to annual surveillance; and if the patient has an aneurysm or dissection, that might alter the imaging and surveillance program.”
During angioplasty, determining the severity of stenosis upon visual inspection is difficult, especially in multifocal FMD. She advised measuring the gradient across the area of FMD involvement with a pressure wire to determine if angioplasty has adequately treated the lesion. “You should see obliteration of the gradient with successful treatment; you don’t have to target your therapy to a perfect angiographic result,” she said.
In patients with FMD and hypertension, she recommended renal artery angioplasty for hypertension of less than 5 years duration or in resistant or labile hypertension. “In this setting, stents are only reserved for complicated or refractory cases; angioplasty alone is sufficient,” Dr. Kadian-Dodov said. Cure rates decline with age, and hypertension in focal disease has a higher cure rate than does multifocal disease, she said (Hypertension. 2010;56:525-32).
Dr. Kadian-Dodov had no relevant financial relationships to disclose.
CHICAGO – New data have shown that fibromuscular dysplasia is associated with high rates of dissection and/or aneurysm, and emerging recommendations call for routine imaging early on in the diagnosis of FMD to monitor for these vascular events, a researcher who developed those recommendations reported at a symposium on vascular surgery sponsored by Northwestern University.
“Given the very high rate of aneurysms in this population, it is now recommended that all patients with FMD should undergo at least one-time head-to pelvis imaging with CT angiography or MR angiography to screen for the presence of an aneurysm or to identify other areas of FMD involvement,” said Daniella Kadian-Dodov, MD, of Icahn School of Medicine at Mount Sinai in New York (J Am Coll Cardiol. 2016;68:176-85).
First described in 1938, FMD is a non-atherosclerotic, noninflammatory disease that had been thought to be a rare cause of renovascular hypertension with a classic “string-of-beads” appearance upon imaging, Dr. Kadian-Dodov noted. However, recent data from the Fibromuscular Dysplasia Society of America–sponsored U.S. registry has changed that thinking. “We now know it occurs more frequently in the carotid and renal arteries, although it has been observed in almost every artery,” she said. “The pathogenesis is still unknown but up to 10% of cases are familial.”
And manifestations of disease now extend beyond the “string-of-beads” appearance to include aneurysm, dissection, and arterial tortuosity, she said (Circulation. 2012;125:3182-90; Circulation. 2014;129:1048-78; J Am Coll Cardiol. 2016;68:176-85). The classification system for FMD has also undergone a recent change, according to Dr. Kadian-Dodov. “Traditionally, a histopathologic scheme was used to classify FMD,” she said. “Nowadays, fewer and fewer patients are undergoing surgical procedures, so the classification has changed to an angiographic system,” the most common of which is the American Heart Association system adopted in 2014 that distinguishes between multifocal, characterized by the classic “string-of-beads” appearance, and focal FMD with a single area of stenosis.
But the diagnosis of either variant of FMD is not exclusive. “Patients may have multiple areas of disease involvement and the same patient may have both focal and multifocal FMD findings,” Dr. Kadian-Dodov said.
The U.S. registry has helped clarify the thinking on FMD, Dr. Kadian-Dodov said. More than 1,400 patients are in the registry, 90% of whom are women with multifocal disease. The average age of onset of symptoms is 47 years, but 52 is the average age for diagnosis. “So these patients are experiencing several years delay to FMD diagnosis,” she said.
Manifestations depend on the vascular bed involved. “In the case of cervical artery FMD, headaches and pulsatile tinnitus are commonly reported, whereas with renal artery involvement hypertension is the most common symptom,” she said. A recent analysis showed 41.7% of the FMD population have either aneurysm and dissection or both (J Am Coll Cardiol. 2016;68:176-185).
But no specific guidelines for treatment of FMD yet exist, Dr. Kadian-Dodov said. “General guidelines should be applied for the management of dissection and aneurysm in patients with FMD,” she said. For patients with arterial dissection, that means conservative therapy comprising either anticoagulation or antiplatelet agents for 3-6 months followed by daily low-dose aspirin therapy. “Revascularization is rarely required for these patients,” she said. “Endovascular or surgical modalities should be reserved for those with continued ischemia despite conservative management or more complicated pseudoaneurysm formations.”
Daily aspirin therapy is likewise the recommendation for patients with cervical artery multifocal or focal FMD involvement without dissection or aneurysms. “We follow up with imaging every 6 months for 2 years,” Dr. Kadian-Dodov said. “If they’re stable, we switch over to annual surveillance; and if the patient has an aneurysm or dissection, that might alter the imaging and surveillance program.”
During angioplasty, determining the severity of stenosis upon visual inspection is difficult, especially in multifocal FMD. She advised measuring the gradient across the area of FMD involvement with a pressure wire to determine if angioplasty has adequately treated the lesion. “You should see obliteration of the gradient with successful treatment; you don’t have to target your therapy to a perfect angiographic result,” she said.
In patients with FMD and hypertension, she recommended renal artery angioplasty for hypertension of less than 5 years duration or in resistant or labile hypertension. “In this setting, stents are only reserved for complicated or refractory cases; angioplasty alone is sufficient,” Dr. Kadian-Dodov said. Cure rates decline with age, and hypertension in focal disease has a higher cure rate than does multifocal disease, she said (Hypertension. 2010;56:525-32).
Dr. Kadian-Dodov had no relevant financial relationships to disclose.
CHICAGO – New data have shown that fibromuscular dysplasia is associated with high rates of dissection and/or aneurysm, and emerging recommendations call for routine imaging early on in the diagnosis of FMD to monitor for these vascular events, a researcher who developed those recommendations reported at a symposium on vascular surgery sponsored by Northwestern University.
“Given the very high rate of aneurysms in this population, it is now recommended that all patients with FMD should undergo at least one-time head-to pelvis imaging with CT angiography or MR angiography to screen for the presence of an aneurysm or to identify other areas of FMD involvement,” said Daniella Kadian-Dodov, MD, of Icahn School of Medicine at Mount Sinai in New York (J Am Coll Cardiol. 2016;68:176-85).
First described in 1938, FMD is a non-atherosclerotic, noninflammatory disease that had been thought to be a rare cause of renovascular hypertension with a classic “string-of-beads” appearance upon imaging, Dr. Kadian-Dodov noted. However, recent data from the Fibromuscular Dysplasia Society of America–sponsored U.S. registry has changed that thinking. “We now know it occurs more frequently in the carotid and renal arteries, although it has been observed in almost every artery,” she said. “The pathogenesis is still unknown but up to 10% of cases are familial.”
And manifestations of disease now extend beyond the “string-of-beads” appearance to include aneurysm, dissection, and arterial tortuosity, she said (Circulation. 2012;125:3182-90; Circulation. 2014;129:1048-78; J Am Coll Cardiol. 2016;68:176-85). The classification system for FMD has also undergone a recent change, according to Dr. Kadian-Dodov. “Traditionally, a histopathologic scheme was used to classify FMD,” she said. “Nowadays, fewer and fewer patients are undergoing surgical procedures, so the classification has changed to an angiographic system,” the most common of which is the American Heart Association system adopted in 2014 that distinguishes between multifocal, characterized by the classic “string-of-beads” appearance, and focal FMD with a single area of stenosis.
But the diagnosis of either variant of FMD is not exclusive. “Patients may have multiple areas of disease involvement and the same patient may have both focal and multifocal FMD findings,” Dr. Kadian-Dodov said.
The U.S. registry has helped clarify the thinking on FMD, Dr. Kadian-Dodov said. More than 1,400 patients are in the registry, 90% of whom are women with multifocal disease. The average age of onset of symptoms is 47 years, but 52 is the average age for diagnosis. “So these patients are experiencing several years delay to FMD diagnosis,” she said.
Manifestations depend on the vascular bed involved. “In the case of cervical artery FMD, headaches and pulsatile tinnitus are commonly reported, whereas with renal artery involvement hypertension is the most common symptom,” she said. A recent analysis showed 41.7% of the FMD population have either aneurysm and dissection or both (J Am Coll Cardiol. 2016;68:176-185).
But no specific guidelines for treatment of FMD yet exist, Dr. Kadian-Dodov said. “General guidelines should be applied for the management of dissection and aneurysm in patients with FMD,” she said. For patients with arterial dissection, that means conservative therapy comprising either anticoagulation or antiplatelet agents for 3-6 months followed by daily low-dose aspirin therapy. “Revascularization is rarely required for these patients,” she said. “Endovascular or surgical modalities should be reserved for those with continued ischemia despite conservative management or more complicated pseudoaneurysm formations.”
Daily aspirin therapy is likewise the recommendation for patients with cervical artery multifocal or focal FMD involvement without dissection or aneurysms. “We follow up with imaging every 6 months for 2 years,” Dr. Kadian-Dodov said. “If they’re stable, we switch over to annual surveillance; and if the patient has an aneurysm or dissection, that might alter the imaging and surveillance program.”
During angioplasty, determining the severity of stenosis upon visual inspection is difficult, especially in multifocal FMD. She advised measuring the gradient across the area of FMD involvement with a pressure wire to determine if angioplasty has adequately treated the lesion. “You should see obliteration of the gradient with successful treatment; you don’t have to target your therapy to a perfect angiographic result,” she said.
In patients with FMD and hypertension, she recommended renal artery angioplasty for hypertension of less than 5 years duration or in resistant or labile hypertension. “In this setting, stents are only reserved for complicated or refractory cases; angioplasty alone is sufficient,” Dr. Kadian-Dodov said. Cure rates decline with age, and hypertension in focal disease has a higher cure rate than does multifocal disease, she said (Hypertension. 2010;56:525-32).
Dr. Kadian-Dodov had no relevant financial relationships to disclose.
Key clinical point: Fibromuscular dysplasia was thought to be a rare cause of renovascular hypertension, but new data has challenged this thinking.
Major finding: FMD accounts for 15%-20% of patients with spontaneous carotid or vertebral artery dissection and 45%-86% of patients with spontaneous coronary artery dissection.
Data source: U.S. Registry for FMD maintained by the Fibromuscular Dystrophy Society of America.
Disclosures: Dr. Kadian-Dodov reported having no financial disclosures.