User login
VIDEO: Clear food labels may improve healthy habits
WASHINGTON – Application clear graphic nutrition labels on the front of packaged foods could help patients make healthier food choices, according to a study out of the George Institute of Global Health, Sydney.
Bruce Neal, PhD, senior director of the food policy division at the institute, and his colleagues asked 1,578 study participants to use a smart phone scanner to record the packaged foods they bought over the course of a week. Nutrition information from those scans was used to derive a nutrient profile score and plugged into four different food labeling systems on a randomized basis:
- Health Star Rating (HSR). A graphic label that gives the product from one to five stars.
- Multi-color Traffic Light (MTD). A graphic label that advises the participant to stop, use caution, or go.
- Daily Intake Guide (DIG). A graphic label that presents important nutrients in larger numbers.
- Nutrient Information Panel (NIP). A chart-based label listing nutrient values, similar to the U.S. Nutrition Facts label.
Nutrient information provided by HSR was found to be noninferior to the alternatives, Dr. Neal said at the annual meeting of the American College of Cardiology.
HSR earned a superiority score of 0.38, 0.1, and 0.23 when compared with MTL, DIG, and NIP labels, respectively, according to the study.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Neal attributed the “unimpressive results” in part to the use of the smart phone interface.
“The trial used a smart phone design, which is a suboptimal surrogate, compared with printed on every pack. In the real world it would work better,” he said in a video interview.
While overall mean nutrition information was found to be not inferior, HSR scored significantly higher that the alternatives in user perception. In understandability, HSR scored 0.62 (P = .005), 1.02 (P less than .001), and 0.22 (P equal .32), compared with MTL, DIG, and NIP, respectively.
HSR also scored significantly higher among participants in “value of having on all food packs,” especially against DIG, scoring 0.70 (P = .002).
“It is absolutely clear that Health Star Rating is preferred to any of the other formats by consumers,” Dr. Neal said. “It is probably [also] fair to say Health Star is now the Australian government’s strongest choice.”
Participants were on average 38 years old, overwhelmingly female (84%), and well educated with 72% reporting a tertiary education or higher. Despite this more affluent and educated population, Dr. Neal and his colleagues believe that HSR can be used with any group.
“We are embarking on a project to roll out this smart phone application with a different interface suited to other, disadvantaged groups,” Dr. Neal said. “We are also working with the [Australian] state government to use Health Star for fast food restaurants and school canteens, as well as government procurement for use in hospitals and prisons.”
The study was limited by its reliance on participants to record their own purchases, Dr. Neal added.
ezimmerman@frontlinemedcom.com
On Twitter @EAZtweets
WASHINGTON – Application clear graphic nutrition labels on the front of packaged foods could help patients make healthier food choices, according to a study out of the George Institute of Global Health, Sydney.
Bruce Neal, PhD, senior director of the food policy division at the institute, and his colleagues asked 1,578 study participants to use a smart phone scanner to record the packaged foods they bought over the course of a week. Nutrition information from those scans was used to derive a nutrient profile score and plugged into four different food labeling systems on a randomized basis:
- Health Star Rating (HSR). A graphic label that gives the product from one to five stars.
- Multi-color Traffic Light (MTD). A graphic label that advises the participant to stop, use caution, or go.
- Daily Intake Guide (DIG). A graphic label that presents important nutrients in larger numbers.
- Nutrient Information Panel (NIP). A chart-based label listing nutrient values, similar to the U.S. Nutrition Facts label.
Nutrient information provided by HSR was found to be noninferior to the alternatives, Dr. Neal said at the annual meeting of the American College of Cardiology.
HSR earned a superiority score of 0.38, 0.1, and 0.23 when compared with MTL, DIG, and NIP labels, respectively, according to the study.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Neal attributed the “unimpressive results” in part to the use of the smart phone interface.
“The trial used a smart phone design, which is a suboptimal surrogate, compared with printed on every pack. In the real world it would work better,” he said in a video interview.
While overall mean nutrition information was found to be not inferior, HSR scored significantly higher that the alternatives in user perception. In understandability, HSR scored 0.62 (P = .005), 1.02 (P less than .001), and 0.22 (P equal .32), compared with MTL, DIG, and NIP, respectively.
HSR also scored significantly higher among participants in “value of having on all food packs,” especially against DIG, scoring 0.70 (P = .002).
“It is absolutely clear that Health Star Rating is preferred to any of the other formats by consumers,” Dr. Neal said. “It is probably [also] fair to say Health Star is now the Australian government’s strongest choice.”
Participants were on average 38 years old, overwhelmingly female (84%), and well educated with 72% reporting a tertiary education or higher. Despite this more affluent and educated population, Dr. Neal and his colleagues believe that HSR can be used with any group.
“We are embarking on a project to roll out this smart phone application with a different interface suited to other, disadvantaged groups,” Dr. Neal said. “We are also working with the [Australian] state government to use Health Star for fast food restaurants and school canteens, as well as government procurement for use in hospitals and prisons.”
The study was limited by its reliance on participants to record their own purchases, Dr. Neal added.
ezimmerman@frontlinemedcom.com
On Twitter @EAZtweets
WASHINGTON – Application clear graphic nutrition labels on the front of packaged foods could help patients make healthier food choices, according to a study out of the George Institute of Global Health, Sydney.
Bruce Neal, PhD, senior director of the food policy division at the institute, and his colleagues asked 1,578 study participants to use a smart phone scanner to record the packaged foods they bought over the course of a week. Nutrition information from those scans was used to derive a nutrient profile score and plugged into four different food labeling systems on a randomized basis:
- Health Star Rating (HSR). A graphic label that gives the product from one to five stars.
- Multi-color Traffic Light (MTD). A graphic label that advises the participant to stop, use caution, or go.
- Daily Intake Guide (DIG). A graphic label that presents important nutrients in larger numbers.
- Nutrient Information Panel (NIP). A chart-based label listing nutrient values, similar to the U.S. Nutrition Facts label.
Nutrient information provided by HSR was found to be noninferior to the alternatives, Dr. Neal said at the annual meeting of the American College of Cardiology.
HSR earned a superiority score of 0.38, 0.1, and 0.23 when compared with MTL, DIG, and NIP labels, respectively, according to the study.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Dr. Neal attributed the “unimpressive results” in part to the use of the smart phone interface.
“The trial used a smart phone design, which is a suboptimal surrogate, compared with printed on every pack. In the real world it would work better,” he said in a video interview.
While overall mean nutrition information was found to be not inferior, HSR scored significantly higher that the alternatives in user perception. In understandability, HSR scored 0.62 (P = .005), 1.02 (P less than .001), and 0.22 (P equal .32), compared with MTL, DIG, and NIP, respectively.
HSR also scored significantly higher among participants in “value of having on all food packs,” especially against DIG, scoring 0.70 (P = .002).
“It is absolutely clear that Health Star Rating is preferred to any of the other formats by consumers,” Dr. Neal said. “It is probably [also] fair to say Health Star is now the Australian government’s strongest choice.”
Participants were on average 38 years old, overwhelmingly female (84%), and well educated with 72% reporting a tertiary education or higher. Despite this more affluent and educated population, Dr. Neal and his colleagues believe that HSR can be used with any group.
“We are embarking on a project to roll out this smart phone application with a different interface suited to other, disadvantaged groups,” Dr. Neal said. “We are also working with the [Australian] state government to use Health Star for fast food restaurants and school canteens, as well as government procurement for use in hospitals and prisons.”
The study was limited by its reliance on participants to record their own purchases, Dr. Neal added.
ezimmerman@frontlinemedcom.com
On Twitter @EAZtweets
AT ACC 17
Older TAVR implant devices significantly less effective than newer ones in bicuspid AS patients
Using transcatheter aortic valve replacement (TAVR) to treat bicuspid aortic valve stenosis (AS) can be significantly less effective than using TAVR to treat tricuspid AS, according to the findings of a new study presented at the annual meeting of the American College of Cardiology and published simultaneously in the Journal of the American College of Cardiology.
“There is a paucity of data comparing the clinical outcomes of TAVR in bicuspid and tricuspid AS,” wrote the authors of the study, led by Sung-Han Yoon, MD, of the Cedars-Sinai Heart Institute in Los Angeles. “Given the increasing frequency of bicuspid AS in younger patients, coupled with the worldwide shift of treating younger and lower–surgical-risk patients with TAVR, the clinical outcomes of TAVR in bicuspid AS warrants special attention.”
Dr. Yoon and his coinvestigators began by collecting data from the Bicuspid AS TAVR registry, which began in December 2013 and contains information on patients from 33 health care centers around the world. Patients who entered the database prior to the initiation of the study were screened retroactively, while those who joined afterward were followed prospectively.
Eventually, 561 bicuspid AS patients were included in the study, out of a total of 576 that were treated between April 2005 and May 2016. Twelve centers also performed tricuspid AS, with investigators able to collect data on 5,900 patients who underwent the procedure during the same period of time. Ultimately, 4,546 were included in the study.
“Given the differences in baseline clinical, echocardiographic, and procedural characteristics between patients with bicuspid and tricuspid AS, propensity-score matching was applied to identify a cohort of patients with similar baseline characteristics, and thus clinical outcomes of propensity-score matched cohorts were compared,” the authors explained.
Variables used when establishing propensity-score matches included age, sex, New York Heart Association functional class III or IV, the presence of certain conditions such as chronic lung disease and diabetes, and procedural data. Dr. Yoon and his colleagues were able to create 546 pairs of matched patients between the bicuspid AS and tricuspid AS cohorts.
The devices implanted in subjects also underwent classification by the investigators, either as early-generation or new-generation devices. The former consisted of Sapien XT and CoreValve devices, while Sapien 3, Lotus, and Evolut R devices comprised the latter classification. A total of 320 bicuspid AS and 321 tricuspid AS patients received early-generation implant devices, with 226 and 225 patients, respectively, receiving new-generation devices.
Devices were less successful in bicuspid AS patients versus tricuspid AS patients: 85.3% and 91.4%, respectively (P = .002). Furthermore, a significantly higher rate of bicuspid AS patients had to be converted to surgery, compared with tricuspid AS patients: 2.0% and 0.2%, respectively (P = .006). Early-generation implant devices had considerably higher rates of issues in bicuspid AS patients, with 4.5% of those receiving Sapien XT experiencing aortic root injury and 0% of tricuspid AS patients with the same device having the same problem (P = .015). Bicuspid AS patients who received the CoreValve implant experienced paravalvular leak 19.4% of the time, compared with 10.5% in tricuspid AS patients (P = .02); these leaks were classified as “moderate to severe.”
“In addition, patients with bicuspid AS had more frequent second valve implantation (11.6% vs. 2.9%; P = .002) [and] subsequent lower device success rates (72.1% vs. 86.0%; P = .002) than those with tricuspid AS when receiving the CoreValve,” the authors noted. “However, there were no significant differences in these adverse procedural events between groups when receiving the Sapien 3 and Lotus.”
There were also no significant differences between the bicuspid and tricuspid AS in terms of mortality rates. At 2 years postoperation, all-cause mortality rates were 17.2% for bicuspid AS patients and 19.4% for tricuspid AS patients, regardless of the type of device implant (P = .28). When comparing early and new-generation devices, results were similarly nonsignificant: early-generation bicuspid vs. tricuspid AS all-cause mortality rates were 14.5% and 13.7%, respectively (P = .80) and 4.5% vs. 7.4% (P = .64) for new-generation devices.
“The present study is the first large-scale study that compared the safety, efficacy, and clinical outcomes of TAVR in patients with bicuspid and tricuspid AS,” Dr. Yoon and his colleagues noted, adding that, in regards to the disparity in device effectiveness, “The present study showed that the initial attempt of device advancement succeeded in overcoming the procedural limitations in tricuspid AS and now go beyond the challenges in treating bicuspid AS.”
No funding source for this study was disclosed. Dr. Yoon did not report any relevant financial disclosures, but several coauthors disclosed potentially relevant financial conflicts.
Using transcatheter aortic valve replacement (TAVR) to treat bicuspid aortic valve stenosis (AS) can be significantly less effective than using TAVR to treat tricuspid AS, according to the findings of a new study presented at the annual meeting of the American College of Cardiology and published simultaneously in the Journal of the American College of Cardiology.
“There is a paucity of data comparing the clinical outcomes of TAVR in bicuspid and tricuspid AS,” wrote the authors of the study, led by Sung-Han Yoon, MD, of the Cedars-Sinai Heart Institute in Los Angeles. “Given the increasing frequency of bicuspid AS in younger patients, coupled with the worldwide shift of treating younger and lower–surgical-risk patients with TAVR, the clinical outcomes of TAVR in bicuspid AS warrants special attention.”
Dr. Yoon and his coinvestigators began by collecting data from the Bicuspid AS TAVR registry, which began in December 2013 and contains information on patients from 33 health care centers around the world. Patients who entered the database prior to the initiation of the study were screened retroactively, while those who joined afterward were followed prospectively.
Eventually, 561 bicuspid AS patients were included in the study, out of a total of 576 that were treated between April 2005 and May 2016. Twelve centers also performed tricuspid AS, with investigators able to collect data on 5,900 patients who underwent the procedure during the same period of time. Ultimately, 4,546 were included in the study.
“Given the differences in baseline clinical, echocardiographic, and procedural characteristics between patients with bicuspid and tricuspid AS, propensity-score matching was applied to identify a cohort of patients with similar baseline characteristics, and thus clinical outcomes of propensity-score matched cohorts were compared,” the authors explained.
Variables used when establishing propensity-score matches included age, sex, New York Heart Association functional class III or IV, the presence of certain conditions such as chronic lung disease and diabetes, and procedural data. Dr. Yoon and his colleagues were able to create 546 pairs of matched patients between the bicuspid AS and tricuspid AS cohorts.
The devices implanted in subjects also underwent classification by the investigators, either as early-generation or new-generation devices. The former consisted of Sapien XT and CoreValve devices, while Sapien 3, Lotus, and Evolut R devices comprised the latter classification. A total of 320 bicuspid AS and 321 tricuspid AS patients received early-generation implant devices, with 226 and 225 patients, respectively, receiving new-generation devices.
Devices were less successful in bicuspid AS patients versus tricuspid AS patients: 85.3% and 91.4%, respectively (P = .002). Furthermore, a significantly higher rate of bicuspid AS patients had to be converted to surgery, compared with tricuspid AS patients: 2.0% and 0.2%, respectively (P = .006). Early-generation implant devices had considerably higher rates of issues in bicuspid AS patients, with 4.5% of those receiving Sapien XT experiencing aortic root injury and 0% of tricuspid AS patients with the same device having the same problem (P = .015). Bicuspid AS patients who received the CoreValve implant experienced paravalvular leak 19.4% of the time, compared with 10.5% in tricuspid AS patients (P = .02); these leaks were classified as “moderate to severe.”
“In addition, patients with bicuspid AS had more frequent second valve implantation (11.6% vs. 2.9%; P = .002) [and] subsequent lower device success rates (72.1% vs. 86.0%; P = .002) than those with tricuspid AS when receiving the CoreValve,” the authors noted. “However, there were no significant differences in these adverse procedural events between groups when receiving the Sapien 3 and Lotus.”
There were also no significant differences between the bicuspid and tricuspid AS in terms of mortality rates. At 2 years postoperation, all-cause mortality rates were 17.2% for bicuspid AS patients and 19.4% for tricuspid AS patients, regardless of the type of device implant (P = .28). When comparing early and new-generation devices, results were similarly nonsignificant: early-generation bicuspid vs. tricuspid AS all-cause mortality rates were 14.5% and 13.7%, respectively (P = .80) and 4.5% vs. 7.4% (P = .64) for new-generation devices.
“The present study is the first large-scale study that compared the safety, efficacy, and clinical outcomes of TAVR in patients with bicuspid and tricuspid AS,” Dr. Yoon and his colleagues noted, adding that, in regards to the disparity in device effectiveness, “The present study showed that the initial attempt of device advancement succeeded in overcoming the procedural limitations in tricuspid AS and now go beyond the challenges in treating bicuspid AS.”
No funding source for this study was disclosed. Dr. Yoon did not report any relevant financial disclosures, but several coauthors disclosed potentially relevant financial conflicts.
Using transcatheter aortic valve replacement (TAVR) to treat bicuspid aortic valve stenosis (AS) can be significantly less effective than using TAVR to treat tricuspid AS, according to the findings of a new study presented at the annual meeting of the American College of Cardiology and published simultaneously in the Journal of the American College of Cardiology.
“There is a paucity of data comparing the clinical outcomes of TAVR in bicuspid and tricuspid AS,” wrote the authors of the study, led by Sung-Han Yoon, MD, of the Cedars-Sinai Heart Institute in Los Angeles. “Given the increasing frequency of bicuspid AS in younger patients, coupled with the worldwide shift of treating younger and lower–surgical-risk patients with TAVR, the clinical outcomes of TAVR in bicuspid AS warrants special attention.”
Dr. Yoon and his coinvestigators began by collecting data from the Bicuspid AS TAVR registry, which began in December 2013 and contains information on patients from 33 health care centers around the world. Patients who entered the database prior to the initiation of the study were screened retroactively, while those who joined afterward were followed prospectively.
Eventually, 561 bicuspid AS patients were included in the study, out of a total of 576 that were treated between April 2005 and May 2016. Twelve centers also performed tricuspid AS, with investigators able to collect data on 5,900 patients who underwent the procedure during the same period of time. Ultimately, 4,546 were included in the study.
“Given the differences in baseline clinical, echocardiographic, and procedural characteristics between patients with bicuspid and tricuspid AS, propensity-score matching was applied to identify a cohort of patients with similar baseline characteristics, and thus clinical outcomes of propensity-score matched cohorts were compared,” the authors explained.
Variables used when establishing propensity-score matches included age, sex, New York Heart Association functional class III or IV, the presence of certain conditions such as chronic lung disease and diabetes, and procedural data. Dr. Yoon and his colleagues were able to create 546 pairs of matched patients between the bicuspid AS and tricuspid AS cohorts.
The devices implanted in subjects also underwent classification by the investigators, either as early-generation or new-generation devices. The former consisted of Sapien XT and CoreValve devices, while Sapien 3, Lotus, and Evolut R devices comprised the latter classification. A total of 320 bicuspid AS and 321 tricuspid AS patients received early-generation implant devices, with 226 and 225 patients, respectively, receiving new-generation devices.
Devices were less successful in bicuspid AS patients versus tricuspid AS patients: 85.3% and 91.4%, respectively (P = .002). Furthermore, a significantly higher rate of bicuspid AS patients had to be converted to surgery, compared with tricuspid AS patients: 2.0% and 0.2%, respectively (P = .006). Early-generation implant devices had considerably higher rates of issues in bicuspid AS patients, with 4.5% of those receiving Sapien XT experiencing aortic root injury and 0% of tricuspid AS patients with the same device having the same problem (P = .015). Bicuspid AS patients who received the CoreValve implant experienced paravalvular leak 19.4% of the time, compared with 10.5% in tricuspid AS patients (P = .02); these leaks were classified as “moderate to severe.”
“In addition, patients with bicuspid AS had more frequent second valve implantation (11.6% vs. 2.9%; P = .002) [and] subsequent lower device success rates (72.1% vs. 86.0%; P = .002) than those with tricuspid AS when receiving the CoreValve,” the authors noted. “However, there were no significant differences in these adverse procedural events between groups when receiving the Sapien 3 and Lotus.”
There were also no significant differences between the bicuspid and tricuspid AS in terms of mortality rates. At 2 years postoperation, all-cause mortality rates were 17.2% for bicuspid AS patients and 19.4% for tricuspid AS patients, regardless of the type of device implant (P = .28). When comparing early and new-generation devices, results were similarly nonsignificant: early-generation bicuspid vs. tricuspid AS all-cause mortality rates were 14.5% and 13.7%, respectively (P = .80) and 4.5% vs. 7.4% (P = .64) for new-generation devices.
“The present study is the first large-scale study that compared the safety, efficacy, and clinical outcomes of TAVR in patients with bicuspid and tricuspid AS,” Dr. Yoon and his colleagues noted, adding that, in regards to the disparity in device effectiveness, “The present study showed that the initial attempt of device advancement succeeded in overcoming the procedural limitations in tricuspid AS and now go beyond the challenges in treating bicuspid AS.”
No funding source for this study was disclosed. Dr. Yoon did not report any relevant financial disclosures, but several coauthors disclosed potentially relevant financial conflicts.
From ACC 17
Key clinical point:
Major finding: Bicuspid AS patients had significantly lower device success rates than those getting tricuspid AS: 85.3% vs. 91.4% (P = .002); also were more likely to convert to surgery: 2.0% vs. 0.2% (P = .006).
Data source: Matched cohort study of 561 bicuspid AS and 4,546 tricuspid AS patients; data collected both retrospectively and prospectively.
Disclosures: No funding source disclosed. Dr. Yoon reported no relevant disclosures.
Aspirin or rivaroxaban plus P2Y12 inhibitor equals 5% bleeding risk
Clinically significant bleeding in acute coronary patients was approximately 5% when their P2Y12 inhibitor treatment was combined with either rivaroxaban or with aspirin, based on data from a randomized, multicenter study of 3,037 adults.
The findings support the use of low-dose rivaroxaban as a safe strategy and an alternative to aspirin for postacute care of coronary syndromes, wrote E. Magnus Ohman, MD, of Duke University in Durham, N.C., and his colleagues.
The study was presented at the annual meeting of the American College of Cardiology and published simultaneously in the Lancet (2017. Mar 18. doi: org/10.1016/S0140-6736[17]30751-1).
The GEMINI ACS 1 trial included patients older than 18 years, who were randomized to P2Y12 with rivaroxaban or P2Y12 with aspirin within 10 days of admission for acute coronary syndrome events, from 371 clinical centers in 21 countries. The patients received 2.5 mg of low-dose rivaroxaban twice daily plus a P2Y12 inhibitor (clopidogrel or ticagrelor, based on national availability) or 100 mg of aspirin daily plus a P2Y12 inhibitor. Patients were assessed at 30, 90, 180, and 270 days.
Overall, 154 patients (5%) met the primary endpoint of thrombolysis in myocardial infarction (TIMI) of clinically significant bleeding – 80 patients (5%) in the rivaroxaban group and 74 (5%) in the aspirin group. Baseline demographics were not significantly different between the groups, and clinically significant bleeding was not significantly different among subgroups.
TIMI bleeding that required medical attention was the most common, occurring in 4% of each group. Both groups had a low frequency of severe or major bleeding based on the TIMI bleeding definitions, the researchers noted.
The composite ischemic endpoint of cardiovascular death, myocardial infarction, stroke, or definite stent thrombosis was 5% in both groups, and both groups had a similar frequency of all-cause mortality and of each of the composite ischemic elements. Rivaroxaban was associated with a higher occurrence of the ischemic composite endpoint in the first 30 days (hazard ratio, 1.48), but this difference was not statistically significant.
“Additionally, no significant interaction was noted for the risk of clinically significant bleeding by P2Y12 inhibitor strata (ticagrelor vs. clopidogrel), but these stratified bleeding analyses were exploratory and hypothesis generating,” the researchers wrote.
The findings were limited by several factors, including a delay in randomization from the patients’ index events, a homogeneous population, and exclusion of patients treated with prasugrel, the researchers noted. However, “based upon these findings and the unmet need for improved treatments in the postacute coronary syndromes setting, further testing of the efficacy and safety of this novel dual pathway antithrombotic regimen in an adequately powered trial should be considered,” they said.
The study was funded by Janssen Research & Development and Bayer. Lead author Dr. Ohman has received research grants from Janssen and other companies. Several coauthors disclosed relationships with multiple companies, including Janssen.
“The antithrombotic effect of aspirin is largely explained by inhibition of COX [cyclo-oxygenase] 1, a central enzyme mediating platelet activation,” wrote Paul A. Gurbel, MD, and Udaya S. Tantry, PhD, in an accompanying comment. “This and pleiotropic cardioprotective properties should be considered before forsaking or replacing aspirin, particularly early in the highly prothrombotic state of a new acute coronary syndrome (panel),” they said.
The major downside of aspirin is gastrointestinal bleeding, the commenters wrote. “But, almost all bleeding metrics were nonsignificantly lower with aspirin, and a 50% increased bleed rate with rivaroxaban cannot be excluded,” they said. Also, although the frequency of major bleeding was similar between the groups, “numerically, the lowest composite ischaemic endpoint rate was noted with aspirin plus ticagrelor therapy (ticagrelor plus aspirin = 3.9%; ticagrelor plus rivaroxaban = 4.7%; clopidogrel plus rivaroxaban = 5.4%; and clopidogrel plus aspirin = 5.9%),” they said. “Thus, it might be premature to believe that a low-dose Xa inhibitor on top of a P2Y12 inhibitor can be [an] effective and safe therapy for most stabilized patients with acute coronary syndromes” (Lancet. 2017 Mar 18. doi: org/10.1016/S0140-6736[17]30760-2).
Dr. Gurbel and Dr. Tantry are affiliated with the Inova Heart and Vascular Institute, Falls Church, VA. Dr. Gurbel disclosed relationships with multiple companies including study sponsor Janssen.
“The antithrombotic effect of aspirin is largely explained by inhibition of COX [cyclo-oxygenase] 1, a central enzyme mediating platelet activation,” wrote Paul A. Gurbel, MD, and Udaya S. Tantry, PhD, in an accompanying comment. “This and pleiotropic cardioprotective properties should be considered before forsaking or replacing aspirin, particularly early in the highly prothrombotic state of a new acute coronary syndrome (panel),” they said.
The major downside of aspirin is gastrointestinal bleeding, the commenters wrote. “But, almost all bleeding metrics were nonsignificantly lower with aspirin, and a 50% increased bleed rate with rivaroxaban cannot be excluded,” they said. Also, although the frequency of major bleeding was similar between the groups, “numerically, the lowest composite ischaemic endpoint rate was noted with aspirin plus ticagrelor therapy (ticagrelor plus aspirin = 3.9%; ticagrelor plus rivaroxaban = 4.7%; clopidogrel plus rivaroxaban = 5.4%; and clopidogrel plus aspirin = 5.9%),” they said. “Thus, it might be premature to believe that a low-dose Xa inhibitor on top of a P2Y12 inhibitor can be [an] effective and safe therapy for most stabilized patients with acute coronary syndromes” (Lancet. 2017 Mar 18. doi: org/10.1016/S0140-6736[17]30760-2).
Dr. Gurbel and Dr. Tantry are affiliated with the Inova Heart and Vascular Institute, Falls Church, VA. Dr. Gurbel disclosed relationships with multiple companies including study sponsor Janssen.
“The antithrombotic effect of aspirin is largely explained by inhibition of COX [cyclo-oxygenase] 1, a central enzyme mediating platelet activation,” wrote Paul A. Gurbel, MD, and Udaya S. Tantry, PhD, in an accompanying comment. “This and pleiotropic cardioprotective properties should be considered before forsaking or replacing aspirin, particularly early in the highly prothrombotic state of a new acute coronary syndrome (panel),” they said.
The major downside of aspirin is gastrointestinal bleeding, the commenters wrote. “But, almost all bleeding metrics were nonsignificantly lower with aspirin, and a 50% increased bleed rate with rivaroxaban cannot be excluded,” they said. Also, although the frequency of major bleeding was similar between the groups, “numerically, the lowest composite ischaemic endpoint rate was noted with aspirin plus ticagrelor therapy (ticagrelor plus aspirin = 3.9%; ticagrelor plus rivaroxaban = 4.7%; clopidogrel plus rivaroxaban = 5.4%; and clopidogrel plus aspirin = 5.9%),” they said. “Thus, it might be premature to believe that a low-dose Xa inhibitor on top of a P2Y12 inhibitor can be [an] effective and safe therapy for most stabilized patients with acute coronary syndromes” (Lancet. 2017 Mar 18. doi: org/10.1016/S0140-6736[17]30760-2).
Dr. Gurbel and Dr. Tantry are affiliated with the Inova Heart and Vascular Institute, Falls Church, VA. Dr. Gurbel disclosed relationships with multiple companies including study sponsor Janssen.
Clinically significant bleeding in acute coronary patients was approximately 5% when their P2Y12 inhibitor treatment was combined with either rivaroxaban or with aspirin, based on data from a randomized, multicenter study of 3,037 adults.
The findings support the use of low-dose rivaroxaban as a safe strategy and an alternative to aspirin for postacute care of coronary syndromes, wrote E. Magnus Ohman, MD, of Duke University in Durham, N.C., and his colleagues.
The study was presented at the annual meeting of the American College of Cardiology and published simultaneously in the Lancet (2017. Mar 18. doi: org/10.1016/S0140-6736[17]30751-1).
The GEMINI ACS 1 trial included patients older than 18 years, who were randomized to P2Y12 with rivaroxaban or P2Y12 with aspirin within 10 days of admission for acute coronary syndrome events, from 371 clinical centers in 21 countries. The patients received 2.5 mg of low-dose rivaroxaban twice daily plus a P2Y12 inhibitor (clopidogrel or ticagrelor, based on national availability) or 100 mg of aspirin daily plus a P2Y12 inhibitor. Patients were assessed at 30, 90, 180, and 270 days.
Overall, 154 patients (5%) met the primary endpoint of thrombolysis in myocardial infarction (TIMI) of clinically significant bleeding – 80 patients (5%) in the rivaroxaban group and 74 (5%) in the aspirin group. Baseline demographics were not significantly different between the groups, and clinically significant bleeding was not significantly different among subgroups.
TIMI bleeding that required medical attention was the most common, occurring in 4% of each group. Both groups had a low frequency of severe or major bleeding based on the TIMI bleeding definitions, the researchers noted.
The composite ischemic endpoint of cardiovascular death, myocardial infarction, stroke, or definite stent thrombosis was 5% in both groups, and both groups had a similar frequency of all-cause mortality and of each of the composite ischemic elements. Rivaroxaban was associated with a higher occurrence of the ischemic composite endpoint in the first 30 days (hazard ratio, 1.48), but this difference was not statistically significant.
“Additionally, no significant interaction was noted for the risk of clinically significant bleeding by P2Y12 inhibitor strata (ticagrelor vs. clopidogrel), but these stratified bleeding analyses were exploratory and hypothesis generating,” the researchers wrote.
The findings were limited by several factors, including a delay in randomization from the patients’ index events, a homogeneous population, and exclusion of patients treated with prasugrel, the researchers noted. However, “based upon these findings and the unmet need for improved treatments in the postacute coronary syndromes setting, further testing of the efficacy and safety of this novel dual pathway antithrombotic regimen in an adequately powered trial should be considered,” they said.
The study was funded by Janssen Research & Development and Bayer. Lead author Dr. Ohman has received research grants from Janssen and other companies. Several coauthors disclosed relationships with multiple companies, including Janssen.
Clinically significant bleeding in acute coronary patients was approximately 5% when their P2Y12 inhibitor treatment was combined with either rivaroxaban or with aspirin, based on data from a randomized, multicenter study of 3,037 adults.
The findings support the use of low-dose rivaroxaban as a safe strategy and an alternative to aspirin for postacute care of coronary syndromes, wrote E. Magnus Ohman, MD, of Duke University in Durham, N.C., and his colleagues.
The study was presented at the annual meeting of the American College of Cardiology and published simultaneously in the Lancet (2017. Mar 18. doi: org/10.1016/S0140-6736[17]30751-1).
The GEMINI ACS 1 trial included patients older than 18 years, who were randomized to P2Y12 with rivaroxaban or P2Y12 with aspirin within 10 days of admission for acute coronary syndrome events, from 371 clinical centers in 21 countries. The patients received 2.5 mg of low-dose rivaroxaban twice daily plus a P2Y12 inhibitor (clopidogrel or ticagrelor, based on national availability) or 100 mg of aspirin daily plus a P2Y12 inhibitor. Patients were assessed at 30, 90, 180, and 270 days.
Overall, 154 patients (5%) met the primary endpoint of thrombolysis in myocardial infarction (TIMI) of clinically significant bleeding – 80 patients (5%) in the rivaroxaban group and 74 (5%) in the aspirin group. Baseline demographics were not significantly different between the groups, and clinically significant bleeding was not significantly different among subgroups.
TIMI bleeding that required medical attention was the most common, occurring in 4% of each group. Both groups had a low frequency of severe or major bleeding based on the TIMI bleeding definitions, the researchers noted.
The composite ischemic endpoint of cardiovascular death, myocardial infarction, stroke, or definite stent thrombosis was 5% in both groups, and both groups had a similar frequency of all-cause mortality and of each of the composite ischemic elements. Rivaroxaban was associated with a higher occurrence of the ischemic composite endpoint in the first 30 days (hazard ratio, 1.48), but this difference was not statistically significant.
“Additionally, no significant interaction was noted for the risk of clinically significant bleeding by P2Y12 inhibitor strata (ticagrelor vs. clopidogrel), but these stratified bleeding analyses were exploratory and hypothesis generating,” the researchers wrote.
The findings were limited by several factors, including a delay in randomization from the patients’ index events, a homogeneous population, and exclusion of patients treated with prasugrel, the researchers noted. However, “based upon these findings and the unmet need for improved treatments in the postacute coronary syndromes setting, further testing of the efficacy and safety of this novel dual pathway antithrombotic regimen in an adequately powered trial should be considered,” they said.
The study was funded by Janssen Research & Development and Bayer. Lead author Dr. Ohman has received research grants from Janssen and other companies. Several coauthors disclosed relationships with multiple companies, including Janssen.
FROM ACC 17
Key clinical point: The risk of major bleeding was similar between acute coronary syndrome patients treated with a combination of low-dose rivaroxaban and P2Y12 inhibitor and those treated with aspirin and P2Y12 inhibitor.
Major finding: Clinically significant bleeding occurred in 5% of patients in each treatment group (HR, 1.09).
Data source: A double-blind, multicenter, randomized trial (GEMINI ACS 1) including 3,037 adults.
Disclosures: The study was funded by Janssen Research & Development and Bayer. Lead author Dr. Ohman has received research grants from Janssen and other companies. Several coauthors disclosed relationships with multiple companies, including Janssen.
A little rivaroxaban goes a long way
In patients with venous thromboembolism at equipoise for further anticoagulation therapy, treatment with a 10-mg dose of rivaroxaban (Xarelto) had comparable efficacy to a 20-mg dose, with both leading to fewer recurrences than treatment with aspirin. There were no statistically significant differences in clinically relevant nonmajor bleeding between the three groups.
The study’s conclusions are limited to relatively healthy patients such as the ones who were selected for the study.
The findings were presented at the annual meeting of the American College of Cardiology and published simultaneously in the New England Journal of Medicine (N Engl J Med 2017 March 18. doi: 10.1056/NEJMoa1700518).
Anticoagulants are the primary treatment for prevention of venous thromboembolism recurrences, but the medications are often stopped after 6-12 months because of concerns about bleeding. To counter that issue, physicians may prescribe lower doses of anticoagulants such as rivaroxaban, or substitute aspirin.
The work follows another recent study of apixaban (Eliquis), which showed that a 2.5-mg twice-daily dose performed the same as did a 5.0-mg twice-daily dose in the prevention of venous thromboembolism recurrence (N Engl J Med. 2013;368[8]:699-708).
“I think the story is kind of the same here,” said David Garcia, MD, professor of hematology at the University of Washington, Seattle, who was one of the principal investigators in the trial.
Patients with unprompted venous thromboembolism are increasingly being offered anticoagulant therapy to prevent recurrences. Those drugs have inherent bleeding risks, but the newer drugs and even warfarin are becoming safer. Even so, “as we embark on that, one has to remember that the risk of anticoagulants is cumulative. It may only carry a risk of 1% per year of major hemorrhage, but if the patient has to take it for 10 or 20 or 30 years, it’s a nontrivial risk of major bleeding over that time,” said Dr. Garcia.
The researchers conducted the Reduced-Dose Rivaroxaban in the Long-Term Prevention of Recurrent Symptomatic Venous Thromboembolism (EINSTEIN CHOICE) trial, in which 3,365 patients from 24 sites were randomized to receive 20 mg rivaroxaban, 10 mg rivaroxaban, or 100 mg aspirin for up to 1 year following an initial 6-12 months of treatment with anticoagulation therapy.
During a median follow-up of 1 year, 4.4% of patients on aspirin experienced a recurrence, compared with 1.5% of patients in the 20-mg rivaroxaban group (hazard ratio versus aspirin, 0.34; 95% confidence interval, 0.20-0.59; P less than .001), and 1.2% in the 10-mg rivaroxaban group (HR versus aspirin, 0.26; 95% CI, 0.14-0.47; P less than .001). There was no statistical significance between the two doses of rivaroxaban.
The rates of fatal thromboembolism were similar, at 0.2% in the 20-mg rivaroxaban group, 0% in the 10-mg group, and 0.2% in the aspirin group.
Major bleeding occurred in 0.5% of patients in the 20-mg rivaroxaban group, in 0.4% of the 10-mg rivaroxaban group, and 0.3% in the aspirin group. Nonmajor, clinically relevant bleeding was also similar between groups, at 2.7% in the 20-mg group, 2.0% in the 10-mg group, and 1.8% in the aspirin group. These differences were not statistically significant.
The study is good news for clinicians as they help patients decide whether to undergo preventive therapy. “Even before the newer agents arrived on the market, we had moved the needle a lot in terms of maximizing the safety of warfarin. I think these drugs take it to yet another level,” said Dr. Garcia.
Bayer Pharmaceuticals funded the study. Dr. Garcia has received honoraria from Bristol-Meyers Squibb, Pfizer, and Boehringer Ingelheim.
“Given the protection from recurrent venous thromboembolism afforded by reduced-dose rivaroxaban, extending treatment beyond 3 months could be considered in patients with provoked venous thromboembolism who are at average risk for bleeding and who are strongly averse to having another episode of venous thromboembolism. In light of the safety profile of low-dose rivaroxaban, the benefit of this strategy does not need to be large in order to justify the extension of therapy.
“This trial suggests that it would be helpful to evaluate the effects of reduced doses of rivaroxaban within 6 months after an episode of venous thromboembolism.
“For patients without cancer, the use of direct oral anticoagulant agents might be considered as first-line treatment for those with acute venous thromboembolism. Full-dose treatment could be continued for a minimum of 3-6 months. In patients in whom there is equipoise with respect to continuing anticoagulant therapy beyond this period, the use of a reduced-intensity direct oral anticoagulant agent might be considered. Clinicians who choose this strategy can be confident of excellent efficacy and low bleeding risk similar to that observed with aspirin or placebo” (N Engl J Med 2017 March 18. doi: 10.1056/NEJMe1701628).
Mark Crowther, MD, is professor of medicine at McMaster University, Hamilton, Ont. Adam Cuker is assistant professor of medicine at the hospital of the University of Pennsylvania, Philadelphia.
“Given the protection from recurrent venous thromboembolism afforded by reduced-dose rivaroxaban, extending treatment beyond 3 months could be considered in patients with provoked venous thromboembolism who are at average risk for bleeding and who are strongly averse to having another episode of venous thromboembolism. In light of the safety profile of low-dose rivaroxaban, the benefit of this strategy does not need to be large in order to justify the extension of therapy.
“This trial suggests that it would be helpful to evaluate the effects of reduced doses of rivaroxaban within 6 months after an episode of venous thromboembolism.
“For patients without cancer, the use of direct oral anticoagulant agents might be considered as first-line treatment for those with acute venous thromboembolism. Full-dose treatment could be continued for a minimum of 3-6 months. In patients in whom there is equipoise with respect to continuing anticoagulant therapy beyond this period, the use of a reduced-intensity direct oral anticoagulant agent might be considered. Clinicians who choose this strategy can be confident of excellent efficacy and low bleeding risk similar to that observed with aspirin or placebo” (N Engl J Med 2017 March 18. doi: 10.1056/NEJMe1701628).
Mark Crowther, MD, is professor of medicine at McMaster University, Hamilton, Ont. Adam Cuker is assistant professor of medicine at the hospital of the University of Pennsylvania, Philadelphia.
“Given the protection from recurrent venous thromboembolism afforded by reduced-dose rivaroxaban, extending treatment beyond 3 months could be considered in patients with provoked venous thromboembolism who are at average risk for bleeding and who are strongly averse to having another episode of venous thromboembolism. In light of the safety profile of low-dose rivaroxaban, the benefit of this strategy does not need to be large in order to justify the extension of therapy.
“This trial suggests that it would be helpful to evaluate the effects of reduced doses of rivaroxaban within 6 months after an episode of venous thromboembolism.
“For patients without cancer, the use of direct oral anticoagulant agents might be considered as first-line treatment for those with acute venous thromboembolism. Full-dose treatment could be continued for a minimum of 3-6 months. In patients in whom there is equipoise with respect to continuing anticoagulant therapy beyond this period, the use of a reduced-intensity direct oral anticoagulant agent might be considered. Clinicians who choose this strategy can be confident of excellent efficacy and low bleeding risk similar to that observed with aspirin or placebo” (N Engl J Med 2017 March 18. doi: 10.1056/NEJMe1701628).
Mark Crowther, MD, is professor of medicine at McMaster University, Hamilton, Ont. Adam Cuker is assistant professor of medicine at the hospital of the University of Pennsylvania, Philadelphia.
In patients with venous thromboembolism at equipoise for further anticoagulation therapy, treatment with a 10-mg dose of rivaroxaban (Xarelto) had comparable efficacy to a 20-mg dose, with both leading to fewer recurrences than treatment with aspirin. There were no statistically significant differences in clinically relevant nonmajor bleeding between the three groups.
The study’s conclusions are limited to relatively healthy patients such as the ones who were selected for the study.
The findings were presented at the annual meeting of the American College of Cardiology and published simultaneously in the New England Journal of Medicine (N Engl J Med 2017 March 18. doi: 10.1056/NEJMoa1700518).
Anticoagulants are the primary treatment for prevention of venous thromboembolism recurrences, but the medications are often stopped after 6-12 months because of concerns about bleeding. To counter that issue, physicians may prescribe lower doses of anticoagulants such as rivaroxaban, or substitute aspirin.
The work follows another recent study of apixaban (Eliquis), which showed that a 2.5-mg twice-daily dose performed the same as did a 5.0-mg twice-daily dose in the prevention of venous thromboembolism recurrence (N Engl J Med. 2013;368[8]:699-708).
“I think the story is kind of the same here,” said David Garcia, MD, professor of hematology at the University of Washington, Seattle, who was one of the principal investigators in the trial.
Patients with unprompted venous thromboembolism are increasingly being offered anticoagulant therapy to prevent recurrences. Those drugs have inherent bleeding risks, but the newer drugs and even warfarin are becoming safer. Even so, “as we embark on that, one has to remember that the risk of anticoagulants is cumulative. It may only carry a risk of 1% per year of major hemorrhage, but if the patient has to take it for 10 or 20 or 30 years, it’s a nontrivial risk of major bleeding over that time,” said Dr. Garcia.
The researchers conducted the Reduced-Dose Rivaroxaban in the Long-Term Prevention of Recurrent Symptomatic Venous Thromboembolism (EINSTEIN CHOICE) trial, in which 3,365 patients from 24 sites were randomized to receive 20 mg rivaroxaban, 10 mg rivaroxaban, or 100 mg aspirin for up to 1 year following an initial 6-12 months of treatment with anticoagulation therapy.
During a median follow-up of 1 year, 4.4% of patients on aspirin experienced a recurrence, compared with 1.5% of patients in the 20-mg rivaroxaban group (hazard ratio versus aspirin, 0.34; 95% confidence interval, 0.20-0.59; P less than .001), and 1.2% in the 10-mg rivaroxaban group (HR versus aspirin, 0.26; 95% CI, 0.14-0.47; P less than .001). There was no statistical significance between the two doses of rivaroxaban.
The rates of fatal thromboembolism were similar, at 0.2% in the 20-mg rivaroxaban group, 0% in the 10-mg group, and 0.2% in the aspirin group.
Major bleeding occurred in 0.5% of patients in the 20-mg rivaroxaban group, in 0.4% of the 10-mg rivaroxaban group, and 0.3% in the aspirin group. Nonmajor, clinically relevant bleeding was also similar between groups, at 2.7% in the 20-mg group, 2.0% in the 10-mg group, and 1.8% in the aspirin group. These differences were not statistically significant.
The study is good news for clinicians as they help patients decide whether to undergo preventive therapy. “Even before the newer agents arrived on the market, we had moved the needle a lot in terms of maximizing the safety of warfarin. I think these drugs take it to yet another level,” said Dr. Garcia.
Bayer Pharmaceuticals funded the study. Dr. Garcia has received honoraria from Bristol-Meyers Squibb, Pfizer, and Boehringer Ingelheim.
In patients with venous thromboembolism at equipoise for further anticoagulation therapy, treatment with a 10-mg dose of rivaroxaban (Xarelto) had comparable efficacy to a 20-mg dose, with both leading to fewer recurrences than treatment with aspirin. There were no statistically significant differences in clinically relevant nonmajor bleeding between the three groups.
The study’s conclusions are limited to relatively healthy patients such as the ones who were selected for the study.
The findings were presented at the annual meeting of the American College of Cardiology and published simultaneously in the New England Journal of Medicine (N Engl J Med 2017 March 18. doi: 10.1056/NEJMoa1700518).
Anticoagulants are the primary treatment for prevention of venous thromboembolism recurrences, but the medications are often stopped after 6-12 months because of concerns about bleeding. To counter that issue, physicians may prescribe lower doses of anticoagulants such as rivaroxaban, or substitute aspirin.
The work follows another recent study of apixaban (Eliquis), which showed that a 2.5-mg twice-daily dose performed the same as did a 5.0-mg twice-daily dose in the prevention of venous thromboembolism recurrence (N Engl J Med. 2013;368[8]:699-708).
“I think the story is kind of the same here,” said David Garcia, MD, professor of hematology at the University of Washington, Seattle, who was one of the principal investigators in the trial.
Patients with unprompted venous thromboembolism are increasingly being offered anticoagulant therapy to prevent recurrences. Those drugs have inherent bleeding risks, but the newer drugs and even warfarin are becoming safer. Even so, “as we embark on that, one has to remember that the risk of anticoagulants is cumulative. It may only carry a risk of 1% per year of major hemorrhage, but if the patient has to take it for 10 or 20 or 30 years, it’s a nontrivial risk of major bleeding over that time,” said Dr. Garcia.
The researchers conducted the Reduced-Dose Rivaroxaban in the Long-Term Prevention of Recurrent Symptomatic Venous Thromboembolism (EINSTEIN CHOICE) trial, in which 3,365 patients from 24 sites were randomized to receive 20 mg rivaroxaban, 10 mg rivaroxaban, or 100 mg aspirin for up to 1 year following an initial 6-12 months of treatment with anticoagulation therapy.
During a median follow-up of 1 year, 4.4% of patients on aspirin experienced a recurrence, compared with 1.5% of patients in the 20-mg rivaroxaban group (hazard ratio versus aspirin, 0.34; 95% confidence interval, 0.20-0.59; P less than .001), and 1.2% in the 10-mg rivaroxaban group (HR versus aspirin, 0.26; 95% CI, 0.14-0.47; P less than .001). There was no statistical significance between the two doses of rivaroxaban.
The rates of fatal thromboembolism were similar, at 0.2% in the 20-mg rivaroxaban group, 0% in the 10-mg group, and 0.2% in the aspirin group.
Major bleeding occurred in 0.5% of patients in the 20-mg rivaroxaban group, in 0.4% of the 10-mg rivaroxaban group, and 0.3% in the aspirin group. Nonmajor, clinically relevant bleeding was also similar between groups, at 2.7% in the 20-mg group, 2.0% in the 10-mg group, and 1.8% in the aspirin group. These differences were not statistically significant.
The study is good news for clinicians as they help patients decide whether to undergo preventive therapy. “Even before the newer agents arrived on the market, we had moved the needle a lot in terms of maximizing the safety of warfarin. I think these drugs take it to yet another level,” said Dr. Garcia.
Bayer Pharmaceuticals funded the study. Dr. Garcia has received honoraria from Bristol-Meyers Squibb, Pfizer, and Boehringer Ingelheim.
FROM ACC 17
Key clinical point: In venous thromboembolism prevention, a 10-mg dose matched 20 mg.
Major finding: The recurrence rates were 1.2% at 10 mg versus 4.4% with aspirin.
Data source: Randomized comparison trial of 3,365 patients.
Disclosures: Bayer Pharmaceuticals funded the study. Dr. Garcia has received honoraria from Bristol-Meyers Squibb, Pfizer, and Boehringer Ingelheim.
VIDEO: SURTAVI results ‘tremendously important’ for decision making
Washington – Heart teams will have more options when making treatment decisions for patients with severe aortic stenosis who are at intermediate risk, now that the results of the SURTAVI (Surgical Replacement and Transcatheter Aortic Valve Implantation) trial have been presented.
Those results showed that transcatheter aortic valve replacement (TAVR) in patients with severe aortic stenosis at intermediate risk was not only noninferior to surgical replacement, “but in my mind superior, because you don’t get your chest cracked, you get home earlier, and you have fewer strokes [in this trial], Roxana Mehran, MD, professor and director of interventional cardiovascular research at Mount Sinai Hospital in New York, said in a video interview at the annual meeting of the American College of Cardiology.
In SURTAVI, which used Medtronic’s self-expanding CoreValve and Evolut-R bioprostheses in 863 patients randomized to TAVR, 12.6% met the study’s primary endpoint – death from any cause or disabling stroke at 24 months – versus 14% of the 796 patients randomized to surgery, a statistically nonsignificant difference. Notably, the risk of any type of stroke at 30 days was statistically superior for TAVR, 3.4%, compared with 5.6% for surgical replacement.
“It’s tremendously important to see the change in how we’re going to be evaluating patients with aortic stenosis,” Dr. Mehran said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Washington – Heart teams will have more options when making treatment decisions for patients with severe aortic stenosis who are at intermediate risk, now that the results of the SURTAVI (Surgical Replacement and Transcatheter Aortic Valve Implantation) trial have been presented.
Those results showed that transcatheter aortic valve replacement (TAVR) in patients with severe aortic stenosis at intermediate risk was not only noninferior to surgical replacement, “but in my mind superior, because you don’t get your chest cracked, you get home earlier, and you have fewer strokes [in this trial], Roxana Mehran, MD, professor and director of interventional cardiovascular research at Mount Sinai Hospital in New York, said in a video interview at the annual meeting of the American College of Cardiology.
In SURTAVI, which used Medtronic’s self-expanding CoreValve and Evolut-R bioprostheses in 863 patients randomized to TAVR, 12.6% met the study’s primary endpoint – death from any cause or disabling stroke at 24 months – versus 14% of the 796 patients randomized to surgery, a statistically nonsignificant difference. Notably, the risk of any type of stroke at 30 days was statistically superior for TAVR, 3.4%, compared with 5.6% for surgical replacement.
“It’s tremendously important to see the change in how we’re going to be evaluating patients with aortic stenosis,” Dr. Mehran said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
Washington – Heart teams will have more options when making treatment decisions for patients with severe aortic stenosis who are at intermediate risk, now that the results of the SURTAVI (Surgical Replacement and Transcatheter Aortic Valve Implantation) trial have been presented.
Those results showed that transcatheter aortic valve replacement (TAVR) in patients with severe aortic stenosis at intermediate risk was not only noninferior to surgical replacement, “but in my mind superior, because you don’t get your chest cracked, you get home earlier, and you have fewer strokes [in this trial], Roxana Mehran, MD, professor and director of interventional cardiovascular research at Mount Sinai Hospital in New York, said in a video interview at the annual meeting of the American College of Cardiology.
In SURTAVI, which used Medtronic’s self-expanding CoreValve and Evolut-R bioprostheses in 863 patients randomized to TAVR, 12.6% met the study’s primary endpoint – death from any cause or disabling stroke at 24 months – versus 14% of the 796 patients randomized to surgery, a statistically nonsignificant difference. Notably, the risk of any type of stroke at 30 days was statistically superior for TAVR, 3.4%, compared with 5.6% for surgical replacement.
“It’s tremendously important to see the change in how we’re going to be evaluating patients with aortic stenosis,” Dr. Mehran said.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ACC 17

HIV research update: Late February 2017
A great volume of HIV and AIDS research enters the medical literature every month. It can be difficult to monitor everything, so here’s a quick look at some notable news items and journal articles published over the past few weeks.
Targeted recruitment of hospitalized populations is a feasible and productive approach for finding and engaging people who live with HIV and who are newly diagnosed or out of routine care, according to a study in HIV Clinical Trials.
A recent study highlighted the need to enhance the immunogenicity of the seasonal trivalent inactivated influenza vaccine for the HIV-positive population, potentially through harnessing the innate immunity with an external adjuvant.
Greater attention is needed to build a more comprehensive understanding of the rural HIV epidemic in the United States and Canada, including research efforts, innovative approaches to care delivery, and greater community engagement in prevention and care, a recent study revealed.
Recent U.S. research supports prioritizing in-person partner services for HIV and suggests that in-person partner services for syphilis may not have major public health benefit, according to a study in Sexually Transmitted Diseases.
A multinational study of HIV/TB coinfected children highlighted the importance of early antiretroviral therapy for children with HIV/TB coinfection, and reinforced the need for implementation research to improve pediatric TB management.
Placentas of HIV-infected pregnant women under combined antiretroviral therapy containing zidovudine showed evidence of mitochondrial DNA depletion, increased oxidative stress levels, and apoptosis suggestive of secondary mitochondrial failure, all potential bases of associated adverse perinatal outcomes.
U.S. investigators observed no evidence that reporting depressive symptoms increased the likelihood of all-cause mortality in a large cohort of HIV-infected adults in care, controlling for a range of time-varying factors.
The second-generation maturation inhibitor GSK3532795 maintains potent antiviral activity toward HIV protease inhibitor-resistant clinical isolates, according to a study in JAIDS.
Pregnant adolescents must be a priority for primary HIV prevention services and expanded HIV treatment services among pregnant women to achieve an AIDS-free generation in Zimbabwe and similar high HIV burden countries, a recent study revealed.
rpizzi@frontlinemedcom.com
On Twitter @richpizzi
A great volume of HIV and AIDS research enters the medical literature every month. It can be difficult to monitor everything, so here’s a quick look at some notable news items and journal articles published over the past few weeks.
Targeted recruitment of hospitalized populations is a feasible and productive approach for finding and engaging people who live with HIV and who are newly diagnosed or out of routine care, according to a study in HIV Clinical Trials.
A recent study highlighted the need to enhance the immunogenicity of the seasonal trivalent inactivated influenza vaccine for the HIV-positive population, potentially through harnessing the innate immunity with an external adjuvant.
Greater attention is needed to build a more comprehensive understanding of the rural HIV epidemic in the United States and Canada, including research efforts, innovative approaches to care delivery, and greater community engagement in prevention and care, a recent study revealed.
Recent U.S. research supports prioritizing in-person partner services for HIV and suggests that in-person partner services for syphilis may not have major public health benefit, according to a study in Sexually Transmitted Diseases.
A multinational study of HIV/TB coinfected children highlighted the importance of early antiretroviral therapy for children with HIV/TB coinfection, and reinforced the need for implementation research to improve pediatric TB management.
Placentas of HIV-infected pregnant women under combined antiretroviral therapy containing zidovudine showed evidence of mitochondrial DNA depletion, increased oxidative stress levels, and apoptosis suggestive of secondary mitochondrial failure, all potential bases of associated adverse perinatal outcomes.
U.S. investigators observed no evidence that reporting depressive symptoms increased the likelihood of all-cause mortality in a large cohort of HIV-infected adults in care, controlling for a range of time-varying factors.
The second-generation maturation inhibitor GSK3532795 maintains potent antiviral activity toward HIV protease inhibitor-resistant clinical isolates, according to a study in JAIDS.
Pregnant adolescents must be a priority for primary HIV prevention services and expanded HIV treatment services among pregnant women to achieve an AIDS-free generation in Zimbabwe and similar high HIV burden countries, a recent study revealed.
rpizzi@frontlinemedcom.com
On Twitter @richpizzi
A great volume of HIV and AIDS research enters the medical literature every month. It can be difficult to monitor everything, so here’s a quick look at some notable news items and journal articles published over the past few weeks.
Targeted recruitment of hospitalized populations is a feasible and productive approach for finding and engaging people who live with HIV and who are newly diagnosed or out of routine care, according to a study in HIV Clinical Trials.
A recent study highlighted the need to enhance the immunogenicity of the seasonal trivalent inactivated influenza vaccine for the HIV-positive population, potentially through harnessing the innate immunity with an external adjuvant.
Greater attention is needed to build a more comprehensive understanding of the rural HIV epidemic in the United States and Canada, including research efforts, innovative approaches to care delivery, and greater community engagement in prevention and care, a recent study revealed.
Recent U.S. research supports prioritizing in-person partner services for HIV and suggests that in-person partner services for syphilis may not have major public health benefit, according to a study in Sexually Transmitted Diseases.
A multinational study of HIV/TB coinfected children highlighted the importance of early antiretroviral therapy for children with HIV/TB coinfection, and reinforced the need for implementation research to improve pediatric TB management.
Placentas of HIV-infected pregnant women under combined antiretroviral therapy containing zidovudine showed evidence of mitochondrial DNA depletion, increased oxidative stress levels, and apoptosis suggestive of secondary mitochondrial failure, all potential bases of associated adverse perinatal outcomes.
U.S. investigators observed no evidence that reporting depressive symptoms increased the likelihood of all-cause mortality in a large cohort of HIV-infected adults in care, controlling for a range of time-varying factors.
The second-generation maturation inhibitor GSK3532795 maintains potent antiviral activity toward HIV protease inhibitor-resistant clinical isolates, according to a study in JAIDS.
Pregnant adolescents must be a priority for primary HIV prevention services and expanded HIV treatment services among pregnant women to achieve an AIDS-free generation in Zimbabwe and similar high HIV burden countries, a recent study revealed.
rpizzi@frontlinemedcom.com
On Twitter @richpizzi
VIDEO: FOURIER and SPIRE show lower LDL is better for longer
WASHINGTON – With the results of two blockbuster trials in lipid-lowering PCSK9 inhibitors, the long-awaited verdict on LDL cholesterol’s effect on cardiovascular outcomes is in: Lower is better.
In a video interview at the annual meeting of the American College of Cardiology, Paul M. Ridker, MD, added that “lower is better for longer.”
Dr. Ridker presented results of the SPIRE (Studies of PCSK9 Inhibition and the Reduction of Vascular Events) program in bococizumab. Bococizumab was revealed to spur antibody responses in some patients, leading Pfizer to discontinue the SPIRE program and any further development. However, the combined endpoint for all six SPIRE trials was reduced by 25%, a trend that continued with longer treatment.
The FOURIER (Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk) trial, presented by Marc S. Sabatine, MD, of Brigham and Women’s Hospital in Boston, showed a reduction of 15% in the cardiovascular events.
Both the SPIRE and the FOURIER program have now provided evidence saying “lower is better for longer,” Dr. Ridker said in a video interview. The challenge is, “who do we want to get these drugs into first?”
For his part, Dr. Ridker, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital and professor of medicine at Harvard Medical School, Boston, will focus on his very-high-risk patients who are receiving the most aggressive therapy possible.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – With the results of two blockbuster trials in lipid-lowering PCSK9 inhibitors, the long-awaited verdict on LDL cholesterol’s effect on cardiovascular outcomes is in: Lower is better.
In a video interview at the annual meeting of the American College of Cardiology, Paul M. Ridker, MD, added that “lower is better for longer.”
Dr. Ridker presented results of the SPIRE (Studies of PCSK9 Inhibition and the Reduction of Vascular Events) program in bococizumab. Bococizumab was revealed to spur antibody responses in some patients, leading Pfizer to discontinue the SPIRE program and any further development. However, the combined endpoint for all six SPIRE trials was reduced by 25%, a trend that continued with longer treatment.
The FOURIER (Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk) trial, presented by Marc S. Sabatine, MD, of Brigham and Women’s Hospital in Boston, showed a reduction of 15% in the cardiovascular events.
Both the SPIRE and the FOURIER program have now provided evidence saying “lower is better for longer,” Dr. Ridker said in a video interview. The challenge is, “who do we want to get these drugs into first?”
For his part, Dr. Ridker, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital and professor of medicine at Harvard Medical School, Boston, will focus on his very-high-risk patients who are receiving the most aggressive therapy possible.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – With the results of two blockbuster trials in lipid-lowering PCSK9 inhibitors, the long-awaited verdict on LDL cholesterol’s effect on cardiovascular outcomes is in: Lower is better.
In a video interview at the annual meeting of the American College of Cardiology, Paul M. Ridker, MD, added that “lower is better for longer.”
Dr. Ridker presented results of the SPIRE (Studies of PCSK9 Inhibition and the Reduction of Vascular Events) program in bococizumab. Bococizumab was revealed to spur antibody responses in some patients, leading Pfizer to discontinue the SPIRE program and any further development. However, the combined endpoint for all six SPIRE trials was reduced by 25%, a trend that continued with longer treatment.
The FOURIER (Further Cardiovascular Outcomes Research with PCSK9 Inhibition in Subjects with Elevated Risk) trial, presented by Marc S. Sabatine, MD, of Brigham and Women’s Hospital in Boston, showed a reduction of 15% in the cardiovascular events.
Both the SPIRE and the FOURIER program have now provided evidence saying “lower is better for longer,” Dr. Ridker said in a video interview. The challenge is, “who do we want to get these drugs into first?”
For his part, Dr. Ridker, director of the Center for Cardiovascular Disease Prevention at Brigham and Women’s Hospital and professor of medicine at Harvard Medical School, Boston, will focus on his very-high-risk patients who are receiving the most aggressive therapy possible.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT ACC 17

Racial differences in skin cancer risk after organ transplantation
Nonwhite organ transplant recipients (OTRs) are more likely to present with inflammatory or infectious conditions after transplantation, while white organ recipients more commonly present with malignant disease, new research suggests.
While the high incidence of skin cancers has been well described in patients who undergo solid organ transplants, little is known about the risk factors, incidence, locations, and types of skin disease that occur in nonwhite OTRs, wrote Christina Lee Chung, MD, from Drexel University, Philadelphia, and her coauthors in JAMA Dermatology.
In a retrospective review, the investigators examined the medical records of 412 organ transplant recipients treated at an academic referral center during 2011-2016, of whom 154 were white, 35 were Asian, 33 were Hispanic, and 190 were black (JAMA Dermatology. 2017 Mar 8. doi: 10.1001/jamadermatol.2017.0045).
Among the white patients, malignant or premalignant disease was the most common diagnostic category (67.8%), followed by inflammatory (20.7%) and infectious processes (11.6%). However, among nonwhite organ transplant recipients, inflammatory processes were present in 48.8% of patients, infectious processes in 37.5% and the remaining 13.7% presented with malignant or premalignant lesions.
Black and Hispanic patients were more likely to present with inflammatory or infectious disease; only 8.6% presented with malignant conditions and 16% presented with premalignant disease.
Among the Asian patient population, one-third presented with malignant or premalignant, one-third presented with infectious, and one-third presented with inflammatory conditions.
“Although early detection and treatment of cancer is vital, nonwhite OTRs would also benefit from addressing nonmalignant processes that are exacerbated by immunosuppression,” the authors wrote.
Overall, 389 skin cancers were diagnosed, with squamous cell carcinoma in situ (SCC) the most common type of skin cancer diagnosed in each racial or ethnic group. The mean time between transplant and first skin cancer lesion was 12.67 years in black patients, 6.5 years in Hispanic patients, 6.13 years among white patients, and 3.75 years in Asian patients.
The vast majority of skin cancers (95.1%) were found in white patients. While the majority of lesions in white and Asian patients were found in sun-exposed areas, the few skin cancers seen in black patients were more likely to be found in sun-protected areas, particularly the genitals.
Four of the six genital SCCs tested positive for high-risk human papillomavirus strains – in one Asian patient and three black patients – while the two SCCs found on lower extremities in Hispanic patients tested negative for HPV.
Researchers also looked at skin cancer awareness among the organ transplant recipients using data from initial visit questionnaires. They found that more than 17 of the 22 (77.3%) white organ transplant recipients surveyed were aware their skin cancer risk was increased, compared with 30 of the 44 (68.2%) nonwhite patients.
Similarly, 72.7% of white patients surveyed were aware that sunscreen decreased the risk of cancer, compared with 59.1% of nonwhite patients; 27.3% of white patients reported using a daily sunscreen, compared with 13.6% of nonwhite patients.
“Based on our findings, we suggest that optimal posttransplant dermatologic care be determined based on the race or ethnicity of the patients; however, regardless of skin type or race or ethnicity, a baseline full-skin assessment should be performed in all patients,” the authors wrote.
They proposed that skin cancer follow-up screenings should be given to Asian and Hispanic patients immediately after transplant, but that black organ transplant recipients could delay yearly screenings.
However, they said routine skin checks should begin earlier after transplantation for all nonwhite transplant recipients with a history of, or clinically evident HPV infection.
No conflicts of interest were declared.
Nonwhite organ transplant recipients (OTRs) are more likely to present with inflammatory or infectious conditions after transplantation, while white organ recipients more commonly present with malignant disease, new research suggests.
While the high incidence of skin cancers has been well described in patients who undergo solid organ transplants, little is known about the risk factors, incidence, locations, and types of skin disease that occur in nonwhite OTRs, wrote Christina Lee Chung, MD, from Drexel University, Philadelphia, and her coauthors in JAMA Dermatology.
In a retrospective review, the investigators examined the medical records of 412 organ transplant recipients treated at an academic referral center during 2011-2016, of whom 154 were white, 35 were Asian, 33 were Hispanic, and 190 were black (JAMA Dermatology. 2017 Mar 8. doi: 10.1001/jamadermatol.2017.0045).
Among the white patients, malignant or premalignant disease was the most common diagnostic category (67.8%), followed by inflammatory (20.7%) and infectious processes (11.6%). However, among nonwhite organ transplant recipients, inflammatory processes were present in 48.8% of patients, infectious processes in 37.5% and the remaining 13.7% presented with malignant or premalignant lesions.
Black and Hispanic patients were more likely to present with inflammatory or infectious disease; only 8.6% presented with malignant conditions and 16% presented with premalignant disease.
Among the Asian patient population, one-third presented with malignant or premalignant, one-third presented with infectious, and one-third presented with inflammatory conditions.
“Although early detection and treatment of cancer is vital, nonwhite OTRs would also benefit from addressing nonmalignant processes that are exacerbated by immunosuppression,” the authors wrote.
Overall, 389 skin cancers were diagnosed, with squamous cell carcinoma in situ (SCC) the most common type of skin cancer diagnosed in each racial or ethnic group. The mean time between transplant and first skin cancer lesion was 12.67 years in black patients, 6.5 years in Hispanic patients, 6.13 years among white patients, and 3.75 years in Asian patients.
The vast majority of skin cancers (95.1%) were found in white patients. While the majority of lesions in white and Asian patients were found in sun-exposed areas, the few skin cancers seen in black patients were more likely to be found in sun-protected areas, particularly the genitals.
Four of the six genital SCCs tested positive for high-risk human papillomavirus strains – in one Asian patient and three black patients – while the two SCCs found on lower extremities in Hispanic patients tested negative for HPV.
Researchers also looked at skin cancer awareness among the organ transplant recipients using data from initial visit questionnaires. They found that more than 17 of the 22 (77.3%) white organ transplant recipients surveyed were aware their skin cancer risk was increased, compared with 30 of the 44 (68.2%) nonwhite patients.
Similarly, 72.7% of white patients surveyed were aware that sunscreen decreased the risk of cancer, compared with 59.1% of nonwhite patients; 27.3% of white patients reported using a daily sunscreen, compared with 13.6% of nonwhite patients.
“Based on our findings, we suggest that optimal posttransplant dermatologic care be determined based on the race or ethnicity of the patients; however, regardless of skin type or race or ethnicity, a baseline full-skin assessment should be performed in all patients,” the authors wrote.
They proposed that skin cancer follow-up screenings should be given to Asian and Hispanic patients immediately after transplant, but that black organ transplant recipients could delay yearly screenings.
However, they said routine skin checks should begin earlier after transplantation for all nonwhite transplant recipients with a history of, or clinically evident HPV infection.
No conflicts of interest were declared.
Nonwhite organ transplant recipients (OTRs) are more likely to present with inflammatory or infectious conditions after transplantation, while white organ recipients more commonly present with malignant disease, new research suggests.
While the high incidence of skin cancers has been well described in patients who undergo solid organ transplants, little is known about the risk factors, incidence, locations, and types of skin disease that occur in nonwhite OTRs, wrote Christina Lee Chung, MD, from Drexel University, Philadelphia, and her coauthors in JAMA Dermatology.
In a retrospective review, the investigators examined the medical records of 412 organ transplant recipients treated at an academic referral center during 2011-2016, of whom 154 were white, 35 were Asian, 33 were Hispanic, and 190 were black (JAMA Dermatology. 2017 Mar 8. doi: 10.1001/jamadermatol.2017.0045).
Among the white patients, malignant or premalignant disease was the most common diagnostic category (67.8%), followed by inflammatory (20.7%) and infectious processes (11.6%). However, among nonwhite organ transplant recipients, inflammatory processes were present in 48.8% of patients, infectious processes in 37.5% and the remaining 13.7% presented with malignant or premalignant lesions.
Black and Hispanic patients were more likely to present with inflammatory or infectious disease; only 8.6% presented with malignant conditions and 16% presented with premalignant disease.
Among the Asian patient population, one-third presented with malignant or premalignant, one-third presented with infectious, and one-third presented with inflammatory conditions.
“Although early detection and treatment of cancer is vital, nonwhite OTRs would also benefit from addressing nonmalignant processes that are exacerbated by immunosuppression,” the authors wrote.
Overall, 389 skin cancers were diagnosed, with squamous cell carcinoma in situ (SCC) the most common type of skin cancer diagnosed in each racial or ethnic group. The mean time between transplant and first skin cancer lesion was 12.67 years in black patients, 6.5 years in Hispanic patients, 6.13 years among white patients, and 3.75 years in Asian patients.
The vast majority of skin cancers (95.1%) were found in white patients. While the majority of lesions in white and Asian patients were found in sun-exposed areas, the few skin cancers seen in black patients were more likely to be found in sun-protected areas, particularly the genitals.
Four of the six genital SCCs tested positive for high-risk human papillomavirus strains – in one Asian patient and three black patients – while the two SCCs found on lower extremities in Hispanic patients tested negative for HPV.
Researchers also looked at skin cancer awareness among the organ transplant recipients using data from initial visit questionnaires. They found that more than 17 of the 22 (77.3%) white organ transplant recipients surveyed were aware their skin cancer risk was increased, compared with 30 of the 44 (68.2%) nonwhite patients.
Similarly, 72.7% of white patients surveyed were aware that sunscreen decreased the risk of cancer, compared with 59.1% of nonwhite patients; 27.3% of white patients reported using a daily sunscreen, compared with 13.6% of nonwhite patients.
“Based on our findings, we suggest that optimal posttransplant dermatologic care be determined based on the race or ethnicity of the patients; however, regardless of skin type or race or ethnicity, a baseline full-skin assessment should be performed in all patients,” the authors wrote.
They proposed that skin cancer follow-up screenings should be given to Asian and Hispanic patients immediately after transplant, but that black organ transplant recipients could delay yearly screenings.
However, they said routine skin checks should begin earlier after transplantation for all nonwhite transplant recipients with a history of, or clinically evident HPV infection.
No conflicts of interest were declared.
FROM JAMA DERMATOLOGY
Key clinical point: Nonwhite organ transplant recipients are more likely than are white recipients to present with inflammatory or infectious conditions than with skin cancer after transplantation.
Major finding: Malignant or premalignant disease was seen in 67.8% of white organ transplant recipients but just 13.7% of nonwhite recipients.
Data source: A retrospective review of medical records from 412 organ transplant recipients.
Disclosures: No conflicts of interest were declared.
Primary Cutaneous Cryptococcosis Presenting as an Extensive Eroded Plaque
To the Editor:
Primary cutaneous cryptococcal infection is rare. Cryptococcal skin infections, either primary or disseminated, can be highly pleomorphic and mimic entities such as basal cell carcinoma or even severe dermatitis, as in our case.
An 80-year-old woman who was residing in a nursing facility presented to the emergency department with an itchy nontender rash on the left arm of 2 to 3 weeks' duration that gradually spread. The patient had not started any new topical or oral medications and was otherwise healthy. A review of symptoms was negative for fever, weight loss, or new cough. Her medical history was notable for congestive heart failure, chronic obstructive pulmonary disease requiring chronic low-dose prednisone, hypothyroidism, atrial fibrillation, hypertension, and dementia. On physical examination the patient had a large, well-demarcated, pink, scaly plaque with areas of ulceration extending from the dorsal aspect of the hand and fingers to the mid upper arm. There was minimal overlying yellow-brown crust (Figure 1). A potassium hydroxide preparation from a superficial scraping was negative. A punch biopsy specimen was obtained from the lesion and microscopic examination revealed histiocytes with innumerable intracytoplasmic yeast forms demonstrating small buds (Figure 2). The organisms were highlighted by periodic acid-Schiff and Grocott-Gomori methenamine-silver stains (Figure 3), while acid-fast bacillus and Fite stains were negative. The presumptive diagnosis of cutaneous cryptococcosis was made, and subsequent culture and latex agglutination test was positive for Cryptococcus neoformans. A chest radiograph showed no evidence of active disease. Infectious disease specialists were consulted and ordered additional laboratory studies, which were negative for human immunodeficiency virus, hepatitis, and fungemia. The patient had a low CD4 count of 119 cells/μL (reference range, 496-2186 cells/μL). Workup for systemic Cryptococcus, including head computed tomography, cerebral spinal fluid analysis, and bone marrow biopsy were all negative. Epstein-Barr virus and human T lymphotropic virus tests were both negative. The source of the patient's low CD4 count was never discovered. She gradually began to improve with diligent wound care and continued fluconazole 400 mg daily. The patient's history did reveal working on a chicken farm as an adult many years ago.

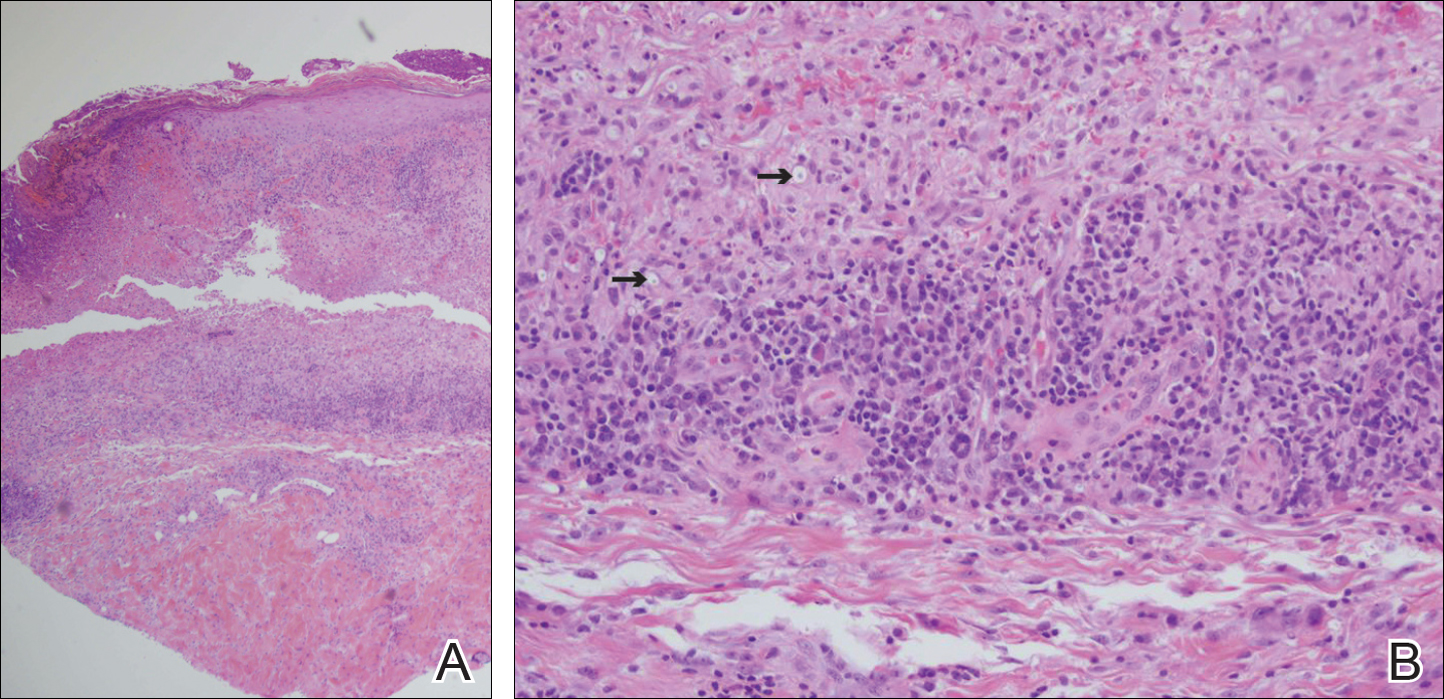
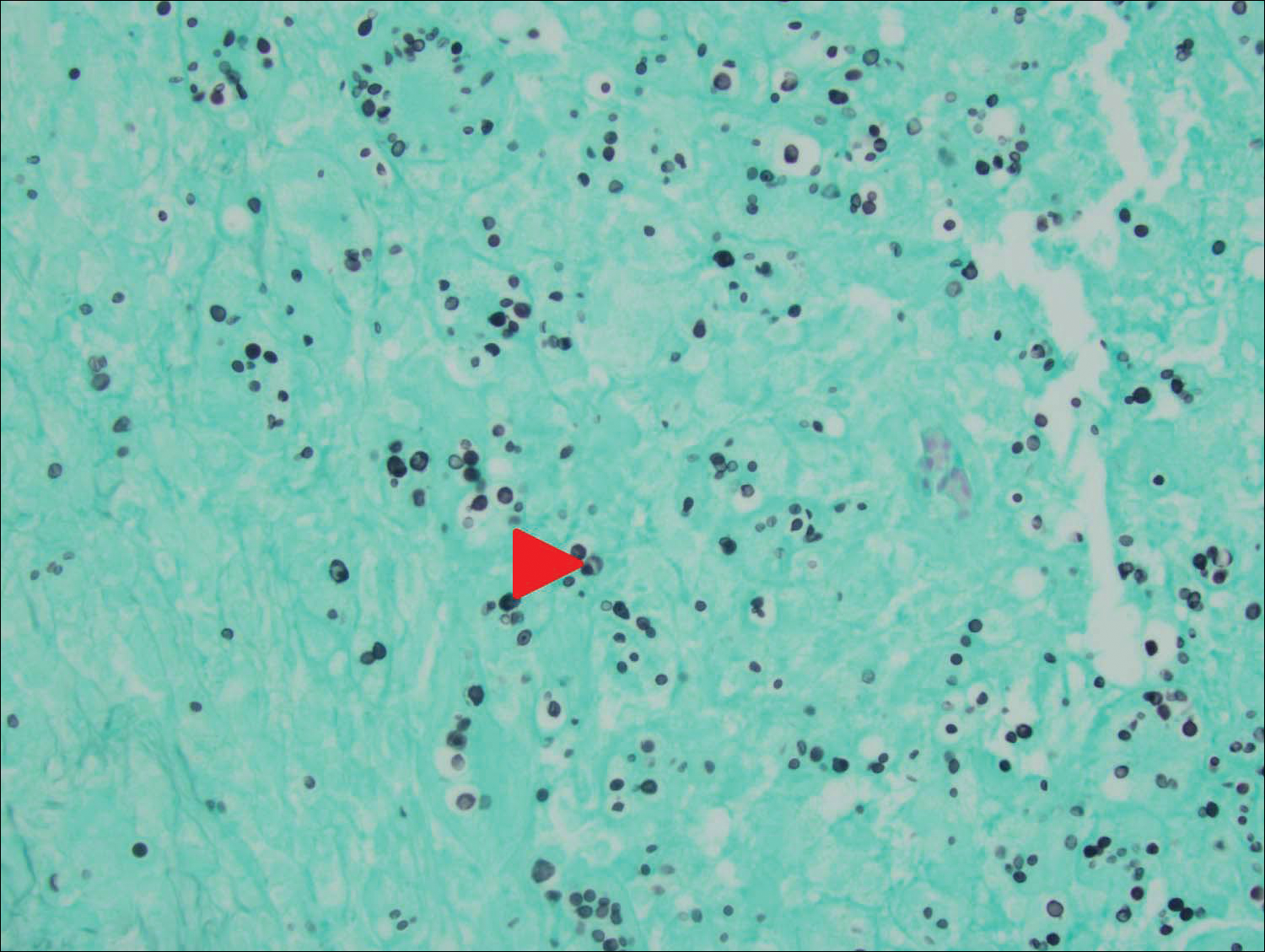
Cryptococcus is a yeast that causes infection primarily through airborne spores that lead to pulmonary infection. Cryptococcus neoformans is the most common pathogenic strain, though infection with other strains such as Cryptococcus albidus1 and Cryptococcus laurentii2 have been reported. Primary cutaneous cryptococcosis is an exceedingly rare entity, with the majority of cases of cutaneous cryptococcosis originating from primary pulmonary infection with hematogenous dissemination to the skin. Primary cutaneous cryptococcosis rarely can be caused by inoculation in nonimmunosuppressed hosts and infection of nonimmunosuppressed hosts is more common in men than in women.3 Manifestations of cutaneous cryptococcosis can be incredibly varied and diagnosis requires a high index of suspicion along with appropriate histological and serological confirmation. Cutaneous cryptococcosis can present in various clinical ways, including molluscumlike lesions, which are more common in patients with AIDS; acneform lesions; vesicles; dermal plaques or nodules; and rarely cellulitis with ulcerations, as in our patient. Cryptococcosis also can imitate basal cell carcinoma, nummular and follicular eczema, and Kaposi sarcoma.4
Histologic examination reveals either a gelatinous or granulomatous pattern based on the number of organisms present. The gelatinous pattern is characterized by little inflammation and a large number of phagocytosed organisms floating in mucin. The granulomatous pattern shows prominent inflammation with lymphocytes, histiocytes, and giant cells, as well as associated necrosis.
Treatment depends on the type of infection and host immunological status. Immunocompetent hosts with cutaneous infection may spontaneously heal. Treatment consists of surgical excision, if possible, followed by fluconazole or itraconazole. For disseminated cryptococcal infections in immunosuppressed hosts, the standard of care is amphotericin B with or without flucytosine.3
- Hoang JK, Burruss J. Localized cutaneous Cryptococcus albidus infection in a 14-year-old boy on etanercept therapy [published online June 5, 2007]. Pediatr Dermatol. 2007;24:285-288. doi:10.1111/j.1525-1470.2007.00404.x.
- Vlchkova-Lashkoska M, Kamberova S, Starova A, et al. Cutaneous Cryptococcus laurentii infection in a human immunodeficiency virus-negative subject. J Eur Acad Dermatol Venereol. 2004;18:99-100.
- Antony SA, Antony SJ. Primary cutaneous Cryptococcus in nonimmunocompromised patients. Cutis. 1995;56:96-98.
- Murakawa GJ, Kerschmann R, Berger T. Cutaneous Cryptococcus infection and AIDS. report of 12 cases and review of the literature. Arch Dermatol. 1996;132:545-548.
To the Editor:
Primary cutaneous cryptococcal infection is rare. Cryptococcal skin infections, either primary or disseminated, can be highly pleomorphic and mimic entities such as basal cell carcinoma or even severe dermatitis, as in our case.
An 80-year-old woman who was residing in a nursing facility presented to the emergency department with an itchy nontender rash on the left arm of 2 to 3 weeks' duration that gradually spread. The patient had not started any new topical or oral medications and was otherwise healthy. A review of symptoms was negative for fever, weight loss, or new cough. Her medical history was notable for congestive heart failure, chronic obstructive pulmonary disease requiring chronic low-dose prednisone, hypothyroidism, atrial fibrillation, hypertension, and dementia. On physical examination the patient had a large, well-demarcated, pink, scaly plaque with areas of ulceration extending from the dorsal aspect of the hand and fingers to the mid upper arm. There was minimal overlying yellow-brown crust (Figure 1). A potassium hydroxide preparation from a superficial scraping was negative. A punch biopsy specimen was obtained from the lesion and microscopic examination revealed histiocytes with innumerable intracytoplasmic yeast forms demonstrating small buds (Figure 2). The organisms were highlighted by periodic acid-Schiff and Grocott-Gomori methenamine-silver stains (Figure 3), while acid-fast bacillus and Fite stains were negative. The presumptive diagnosis of cutaneous cryptococcosis was made, and subsequent culture and latex agglutination test was positive for Cryptococcus neoformans. A chest radiograph showed no evidence of active disease. Infectious disease specialists were consulted and ordered additional laboratory studies, which were negative for human immunodeficiency virus, hepatitis, and fungemia. The patient had a low CD4 count of 119 cells/μL (reference range, 496-2186 cells/μL). Workup for systemic Cryptococcus, including head computed tomography, cerebral spinal fluid analysis, and bone marrow biopsy were all negative. Epstein-Barr virus and human T lymphotropic virus tests were both negative. The source of the patient's low CD4 count was never discovered. She gradually began to improve with diligent wound care and continued fluconazole 400 mg daily. The patient's history did reveal working on a chicken farm as an adult many years ago.
Cryptococcus is a yeast that causes infection primarily through airborne spores that lead to pulmonary infection. Cryptococcus neoformans is the most common pathogenic strain, though infection with other strains such as Cryptococcus albidus1 and Cryptococcus laurentii2 have been reported. Primary cutaneous cryptococcosis is an exceedingly rare entity, with the majority of cases of cutaneous cryptococcosis originating from primary pulmonary infection with hematogenous dissemination to the skin. Primary cutaneous cryptococcosis rarely can be caused by inoculation in nonimmunosuppressed hosts and infection of nonimmunosuppressed hosts is more common in men than in women.3 Manifestations of cutaneous cryptococcosis can be incredibly varied and diagnosis requires a high index of suspicion along with appropriate histological and serological confirmation. Cutaneous cryptococcosis can present in various clinical ways, including molluscumlike lesions, which are more common in patients with AIDS; acneform lesions; vesicles; dermal plaques or nodules; and rarely cellulitis with ulcerations, as in our patient. Cryptococcosis also can imitate basal cell carcinoma, nummular and follicular eczema, and Kaposi sarcoma.4
Histologic examination reveals either a gelatinous or granulomatous pattern based on the number of organisms present. The gelatinous pattern is characterized by little inflammation and a large number of phagocytosed organisms floating in mucin. The granulomatous pattern shows prominent inflammation with lymphocytes, histiocytes, and giant cells, as well as associated necrosis.
Treatment depends on the type of infection and host immunological status. Immunocompetent hosts with cutaneous infection may spontaneously heal. Treatment consists of surgical excision, if possible, followed by fluconazole or itraconazole. For disseminated cryptococcal infections in immunosuppressed hosts, the standard of care is amphotericin B with or without flucytosine.3
To the Editor:
Primary cutaneous cryptococcal infection is rare. Cryptococcal skin infections, either primary or disseminated, can be highly pleomorphic and mimic entities such as basal cell carcinoma or even severe dermatitis, as in our case.
An 80-year-old woman who was residing in a nursing facility presented to the emergency department with an itchy nontender rash on the left arm of 2 to 3 weeks' duration that gradually spread. The patient had not started any new topical or oral medications and was otherwise healthy. A review of symptoms was negative for fever, weight loss, or new cough. Her medical history was notable for congestive heart failure, chronic obstructive pulmonary disease requiring chronic low-dose prednisone, hypothyroidism, atrial fibrillation, hypertension, and dementia. On physical examination the patient had a large, well-demarcated, pink, scaly plaque with areas of ulceration extending from the dorsal aspect of the hand and fingers to the mid upper arm. There was minimal overlying yellow-brown crust (Figure 1). A potassium hydroxide preparation from a superficial scraping was negative. A punch biopsy specimen was obtained from the lesion and microscopic examination revealed histiocytes with innumerable intracytoplasmic yeast forms demonstrating small buds (Figure 2). The organisms were highlighted by periodic acid-Schiff and Grocott-Gomori methenamine-silver stains (Figure 3), while acid-fast bacillus and Fite stains were negative. The presumptive diagnosis of cutaneous cryptococcosis was made, and subsequent culture and latex agglutination test was positive for Cryptococcus neoformans. A chest radiograph showed no evidence of active disease. Infectious disease specialists were consulted and ordered additional laboratory studies, which were negative for human immunodeficiency virus, hepatitis, and fungemia. The patient had a low CD4 count of 119 cells/μL (reference range, 496-2186 cells/μL). Workup for systemic Cryptococcus, including head computed tomography, cerebral spinal fluid analysis, and bone marrow biopsy were all negative. Epstein-Barr virus and human T lymphotropic virus tests were both negative. The source of the patient's low CD4 count was never discovered. She gradually began to improve with diligent wound care and continued fluconazole 400 mg daily. The patient's history did reveal working on a chicken farm as an adult many years ago.
Cryptococcus is a yeast that causes infection primarily through airborne spores that lead to pulmonary infection. Cryptococcus neoformans is the most common pathogenic strain, though infection with other strains such as Cryptococcus albidus1 and Cryptococcus laurentii2 have been reported. Primary cutaneous cryptococcosis is an exceedingly rare entity, with the majority of cases of cutaneous cryptococcosis originating from primary pulmonary infection with hematogenous dissemination to the skin. Primary cutaneous cryptococcosis rarely can be caused by inoculation in nonimmunosuppressed hosts and infection of nonimmunosuppressed hosts is more common in men than in women.3 Manifestations of cutaneous cryptococcosis can be incredibly varied and diagnosis requires a high index of suspicion along with appropriate histological and serological confirmation. Cutaneous cryptococcosis can present in various clinical ways, including molluscumlike lesions, which are more common in patients with AIDS; acneform lesions; vesicles; dermal plaques or nodules; and rarely cellulitis with ulcerations, as in our patient. Cryptococcosis also can imitate basal cell carcinoma, nummular and follicular eczema, and Kaposi sarcoma.4
Histologic examination reveals either a gelatinous or granulomatous pattern based on the number of organisms present. The gelatinous pattern is characterized by little inflammation and a large number of phagocytosed organisms floating in mucin. The granulomatous pattern shows prominent inflammation with lymphocytes, histiocytes, and giant cells, as well as associated necrosis.
Treatment depends on the type of infection and host immunological status. Immunocompetent hosts with cutaneous infection may spontaneously heal. Treatment consists of surgical excision, if possible, followed by fluconazole or itraconazole. For disseminated cryptococcal infections in immunosuppressed hosts, the standard of care is amphotericin B with or without flucytosine.3
- Hoang JK, Burruss J. Localized cutaneous Cryptococcus albidus infection in a 14-year-old boy on etanercept therapy [published online June 5, 2007]. Pediatr Dermatol. 2007;24:285-288. doi:10.1111/j.1525-1470.2007.00404.x.
- Vlchkova-Lashkoska M, Kamberova S, Starova A, et al. Cutaneous Cryptococcus laurentii infection in a human immunodeficiency virus-negative subject. J Eur Acad Dermatol Venereol. 2004;18:99-100.
- Antony SA, Antony SJ. Primary cutaneous Cryptococcus in nonimmunocompromised patients. Cutis. 1995;56:96-98.
- Murakawa GJ, Kerschmann R, Berger T. Cutaneous Cryptococcus infection and AIDS. report of 12 cases and review of the literature. Arch Dermatol. 1996;132:545-548.
- Hoang JK, Burruss J. Localized cutaneous Cryptococcus albidus infection in a 14-year-old boy on etanercept therapy [published online June 5, 2007]. Pediatr Dermatol. 2007;24:285-288. doi:10.1111/j.1525-1470.2007.00404.x.
- Vlchkova-Lashkoska M, Kamberova S, Starova A, et al. Cutaneous Cryptococcus laurentii infection in a human immunodeficiency virus-negative subject. J Eur Acad Dermatol Venereol. 2004;18:99-100.
- Antony SA, Antony SJ. Primary cutaneous Cryptococcus in nonimmunocompromised patients. Cutis. 1995;56:96-98.
- Murakawa GJ, Kerschmann R, Berger T. Cutaneous Cryptococcus infection and AIDS. report of 12 cases and review of the literature. Arch Dermatol. 1996;132:545-548.
Practice Points
- Primary cutaneous cryptococcosis is rare in nonimmunosuppressed patients.
- Primary cutaneous cryptococcosis secondary to inoculation can have a clinical presentation similar to more common conditions, such as molluscum, acne, and dermatitis.

How will crisaborole for atopic dermatitis fit into clinical practice?
WAILEA, HAWAII – With the recent approval of crisaborole ointment 2% for the treatment of atopic dermatitis, the question of how to best utilize this novel drug in daily clinical practice was put to two atopic dermatitis experts at the Hawaii Dermatology Seminar sponsored by the Global Academy for Medical Education/Skin Disease Research Foundation.
Two of these experts, Lawrence F. Eichenfield, MD, and Wynnis L. Tom, MD, have garnered extensive clinical trials experience with crisaborole (Eucrisa), which, in December 2016, became the first prescription drug approved by the Food and Drug Administration for atopic dermatitis (AD) in more than 10 years. The topical phosphodiesterase-4 inhibitor is indicated for twice-daily treatment of patients aged 2 years and older with mild to moderate AD.

“Topical steroids are the most cost-effective medicine for the management of acute flares of atopic dermatitis. And if I can then take patients down to only intermittent use of topical corticosteroids of mid-strength or lower, depending on patient age, I’ll probably hang in and do just that,” said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital-San Diego.
“But, when I have patients with more persistent disease, frequent flaring where I can’t get by with just twice-a-week topical steroids, or ... sensitive areas where I need to avoid steroid atrophy, that’s when I’m likely to incorporate a nonsteroidal agent into regimens of care. Traditionally, over the past 15-18 years, that’s been either with topical tacrolimus [Protopic] or pimecrolimus [Elidel]. And now crisaborole will fit right in there,” he continued.
As for how long to keep patients on crisaborole, Dr. Eichenfield noted that the package labeling “is pretty open.” It doesn’t address the question of treatment duration, and the patient handout that accompanies the tube of ointment simply states, “Use [crisaborole] Eucrisa exactly as your health care provider tells you to use it.”
“In a no-data situation such as this, I’ll probably try to see if use a few times a week or in a mix/match between corticosteroids, a topical calcineurin inhibitor, and crisaborole will provide decent long-term disease control,” Dr. Eichenfield said.
The important, remaining questions regarding crisaborole include, Is it comparatively efficient? – a question that will require head-to-head clinical trials. Is it cost effective? Will it be effective and safe in children younger than 2 years of age? Is it safe beyond 1 year of use? – a particularly important question, given that the phase III clinical trials were only a month long, the dermatologist added.
Dr. Eichenfield emphasized that he was offering only his personal opinion on the use of crisaborole in response to audience questions. Eventually, guidelines committees will formally address how to incorporate the new drug into a sound treatment strategy.
Dr. Tom, like Dr. Eichenfield, was a coauthor of the two pivotal phase III randomized trials of crisaborole, which found infrequent and minimal side effects along with significant improvement of formal quality of life measures (J Am Acad Dermatol. 2016 Sep;75[3]:494-503.e4).
She said that one way she’ll immediately put the new topical agent to work is in treating disease on the face and other sensitive skin areas. The drug’s steroid-sparing ability is also a major asset, given how many parents of children with AD are steroid phobic.
“I’m certainly not going to give up on topical steroids, but anything that enables me to lessen their use is a comfort for parents. That’s really important,” observed Dr. Tom of the University of California, San Diego, and Rady Children’s Hospital.
Both pediatric dermatologists reported having received research grants from or serving as consultants to roughly half-a-dozen pharmaceutical companies, including Anacor/Pfizer, which markets crisaborole.
SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – With the recent approval of crisaborole ointment 2% for the treatment of atopic dermatitis, the question of how to best utilize this novel drug in daily clinical practice was put to two atopic dermatitis experts at the Hawaii Dermatology Seminar sponsored by the Global Academy for Medical Education/Skin Disease Research Foundation.
Two of these experts, Lawrence F. Eichenfield, MD, and Wynnis L. Tom, MD, have garnered extensive clinical trials experience with crisaborole (Eucrisa), which, in December 2016, became the first prescription drug approved by the Food and Drug Administration for atopic dermatitis (AD) in more than 10 years. The topical phosphodiesterase-4 inhibitor is indicated for twice-daily treatment of patients aged 2 years and older with mild to moderate AD.
“Topical steroids are the most cost-effective medicine for the management of acute flares of atopic dermatitis. And if I can then take patients down to only intermittent use of topical corticosteroids of mid-strength or lower, depending on patient age, I’ll probably hang in and do just that,” said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital-San Diego.
“But, when I have patients with more persistent disease, frequent flaring where I can’t get by with just twice-a-week topical steroids, or ... sensitive areas where I need to avoid steroid atrophy, that’s when I’m likely to incorporate a nonsteroidal agent into regimens of care. Traditionally, over the past 15-18 years, that’s been either with topical tacrolimus [Protopic] or pimecrolimus [Elidel]. And now crisaborole will fit right in there,” he continued.
As for how long to keep patients on crisaborole, Dr. Eichenfield noted that the package labeling “is pretty open.” It doesn’t address the question of treatment duration, and the patient handout that accompanies the tube of ointment simply states, “Use [crisaborole] Eucrisa exactly as your health care provider tells you to use it.”
“In a no-data situation such as this, I’ll probably try to see if use a few times a week or in a mix/match between corticosteroids, a topical calcineurin inhibitor, and crisaborole will provide decent long-term disease control,” Dr. Eichenfield said.
The important, remaining questions regarding crisaborole include, Is it comparatively efficient? – a question that will require head-to-head clinical trials. Is it cost effective? Will it be effective and safe in children younger than 2 years of age? Is it safe beyond 1 year of use? – a particularly important question, given that the phase III clinical trials were only a month long, the dermatologist added.
Dr. Eichenfield emphasized that he was offering only his personal opinion on the use of crisaborole in response to audience questions. Eventually, guidelines committees will formally address how to incorporate the new drug into a sound treatment strategy.
Dr. Tom, like Dr. Eichenfield, was a coauthor of the two pivotal phase III randomized trials of crisaborole, which found infrequent and minimal side effects along with significant improvement of formal quality of life measures (J Am Acad Dermatol. 2016 Sep;75[3]:494-503.e4).
She said that one way she’ll immediately put the new topical agent to work is in treating disease on the face and other sensitive skin areas. The drug’s steroid-sparing ability is also a major asset, given how many parents of children with AD are steroid phobic.
“I’m certainly not going to give up on topical steroids, but anything that enables me to lessen their use is a comfort for parents. That’s really important,” observed Dr. Tom of the University of California, San Diego, and Rady Children’s Hospital.
Both pediatric dermatologists reported having received research grants from or serving as consultants to roughly half-a-dozen pharmaceutical companies, including Anacor/Pfizer, which markets crisaborole.
SDEF and this news organization are owned by the same parent company.
WAILEA, HAWAII – With the recent approval of crisaborole ointment 2% for the treatment of atopic dermatitis, the question of how to best utilize this novel drug in daily clinical practice was put to two atopic dermatitis experts at the Hawaii Dermatology Seminar sponsored by the Global Academy for Medical Education/Skin Disease Research Foundation.
Two of these experts, Lawrence F. Eichenfield, MD, and Wynnis L. Tom, MD, have garnered extensive clinical trials experience with crisaborole (Eucrisa), which, in December 2016, became the first prescription drug approved by the Food and Drug Administration for atopic dermatitis (AD) in more than 10 years. The topical phosphodiesterase-4 inhibitor is indicated for twice-daily treatment of patients aged 2 years and older with mild to moderate AD.
“Topical steroids are the most cost-effective medicine for the management of acute flares of atopic dermatitis. And if I can then take patients down to only intermittent use of topical corticosteroids of mid-strength or lower, depending on patient age, I’ll probably hang in and do just that,” said Dr. Eichenfield, professor of dermatology and pediatrics at the University of California, San Diego, and chief of pediatric and adolescent dermatology at Rady Children’s Hospital-San Diego.
“But, when I have patients with more persistent disease, frequent flaring where I can’t get by with just twice-a-week topical steroids, or ... sensitive areas where I need to avoid steroid atrophy, that’s when I’m likely to incorporate a nonsteroidal agent into regimens of care. Traditionally, over the past 15-18 years, that’s been either with topical tacrolimus [Protopic] or pimecrolimus [Elidel]. And now crisaborole will fit right in there,” he continued.
As for how long to keep patients on crisaborole, Dr. Eichenfield noted that the package labeling “is pretty open.” It doesn’t address the question of treatment duration, and the patient handout that accompanies the tube of ointment simply states, “Use [crisaborole] Eucrisa exactly as your health care provider tells you to use it.”
“In a no-data situation such as this, I’ll probably try to see if use a few times a week or in a mix/match between corticosteroids, a topical calcineurin inhibitor, and crisaborole will provide decent long-term disease control,” Dr. Eichenfield said.
The important, remaining questions regarding crisaborole include, Is it comparatively efficient? – a question that will require head-to-head clinical trials. Is it cost effective? Will it be effective and safe in children younger than 2 years of age? Is it safe beyond 1 year of use? – a particularly important question, given that the phase III clinical trials were only a month long, the dermatologist added.
Dr. Eichenfield emphasized that he was offering only his personal opinion on the use of crisaborole in response to audience questions. Eventually, guidelines committees will formally address how to incorporate the new drug into a sound treatment strategy.
Dr. Tom, like Dr. Eichenfield, was a coauthor of the two pivotal phase III randomized trials of crisaborole, which found infrequent and minimal side effects along with significant improvement of formal quality of life measures (J Am Acad Dermatol. 2016 Sep;75[3]:494-503.e4).
She said that one way she’ll immediately put the new topical agent to work is in treating disease on the face and other sensitive skin areas. The drug’s steroid-sparing ability is also a major asset, given how many parents of children with AD are steroid phobic.
“I’m certainly not going to give up on topical steroids, but anything that enables me to lessen their use is a comfort for parents. That’s really important,” observed Dr. Tom of the University of California, San Diego, and Rady Children’s Hospital.
Both pediatric dermatologists reported having received research grants from or serving as consultants to roughly half-a-dozen pharmaceutical companies, including Anacor/Pfizer, which markets crisaborole.
SDEF and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM THE SDEF HAWAII DERMATOLOGY SEMINAR