User login
CHMP advocates refusal of application for SM drug

The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended refusal of the marketing authorization for masitinib (Masipro).
Masitinib is a tyrosine kinase inhibitor being developed by AB Science to treat adults with smoldering or indolent severe systemic mastocytosis (SM).
To support the application for masitinib, AB Science presented data from a study involving 135 SM patients who had severe symptoms, including at least one of the following: itching, hot flashes, depression, and tiredness.
Researchers compared masitinib to placebo in these patients, looking for improvements in any of the symptoms during the first 24 weeks of treatment.
The CHMP said it was concerned about the reliability of the study results because a routine good clinical practice inspection at the study sites revealed serious failings in the way the study had been conducted.
In addition, major changes were made to the study design while the study was underway, which made the results difficult to interpret.
Finally, data on the safety of masitinib were limited. And the CHMP was concerned about side effects, including neutropenia and harmful effects on the skin and liver, which were particularly relevant because masitinib was intended to be used long-term.
Therefore, the CHMP concluded the benefits of masitinib do not appear to outweigh the risks, and the committee recommended the drug be refused marketing authorization.
The CHMP informed AB Science of this negative opinion in May, and the company asked the committee to re-examine its opinion. However, the CHMP ultimately concluded that masitinib should be refused marketing authorization.
AB Science said this decision does not have any consequences for patients in clinical trials or compassionate use programs of masitinib.
The company also said it intends to initiate a confirmatory study in patients with smoldering or indolent severe SM that is unresponsive to optimal symptomatic treatment in order to confirm the results from the first pivotal study. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended refusal of the marketing authorization for masitinib (Masipro).
Masitinib is a tyrosine kinase inhibitor being developed by AB Science to treat adults with smoldering or indolent severe systemic mastocytosis (SM).
To support the application for masitinib, AB Science presented data from a study involving 135 SM patients who had severe symptoms, including at least one of the following: itching, hot flashes, depression, and tiredness.
Researchers compared masitinib to placebo in these patients, looking for improvements in any of the symptoms during the first 24 weeks of treatment.
The CHMP said it was concerned about the reliability of the study results because a routine good clinical practice inspection at the study sites revealed serious failings in the way the study had been conducted.
In addition, major changes were made to the study design while the study was underway, which made the results difficult to interpret.
Finally, data on the safety of masitinib were limited. And the CHMP was concerned about side effects, including neutropenia and harmful effects on the skin and liver, which were particularly relevant because masitinib was intended to be used long-term.
Therefore, the CHMP concluded the benefits of masitinib do not appear to outweigh the risks, and the committee recommended the drug be refused marketing authorization.
The CHMP informed AB Science of this negative opinion in May, and the company asked the committee to re-examine its opinion. However, the CHMP ultimately concluded that masitinib should be refused marketing authorization.
AB Science said this decision does not have any consequences for patients in clinical trials or compassionate use programs of masitinib.
The company also said it intends to initiate a confirmatory study in patients with smoldering or indolent severe SM that is unresponsive to optimal symptomatic treatment in order to confirm the results from the first pivotal study. ![]()
The European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP) has recommended refusal of the marketing authorization for masitinib (Masipro).
Masitinib is a tyrosine kinase inhibitor being developed by AB Science to treat adults with smoldering or indolent severe systemic mastocytosis (SM).
To support the application for masitinib, AB Science presented data from a study involving 135 SM patients who had severe symptoms, including at least one of the following: itching, hot flashes, depression, and tiredness.
Researchers compared masitinib to placebo in these patients, looking for improvements in any of the symptoms during the first 24 weeks of treatment.
The CHMP said it was concerned about the reliability of the study results because a routine good clinical practice inspection at the study sites revealed serious failings in the way the study had been conducted.
In addition, major changes were made to the study design while the study was underway, which made the results difficult to interpret.
Finally, data on the safety of masitinib were limited. And the CHMP was concerned about side effects, including neutropenia and harmful effects on the skin and liver, which were particularly relevant because masitinib was intended to be used long-term.
Therefore, the CHMP concluded the benefits of masitinib do not appear to outweigh the risks, and the committee recommended the drug be refused marketing authorization.
The CHMP informed AB Science of this negative opinion in May, and the company asked the committee to re-examine its opinion. However, the CHMP ultimately concluded that masitinib should be refused marketing authorization.
AB Science said this decision does not have any consequences for patients in clinical trials or compassionate use programs of masitinib.
The company also said it intends to initiate a confirmatory study in patients with smoldering or indolent severe SM that is unresponsive to optimal symptomatic treatment in order to confirm the results from the first pivotal study. ![]()
Tattooing and piercing are no longer taboo, but health concerns persist
Educate adolescents about the potential medical complications and social consequences of tattooing and body piercing as their popularity rises, an American Academy of Pediatrics clinical report recommends.
The most common complications post tattooing are bacterial and viral infections, and inflammation at the site of the tattoo. Rarely, more serious complications can arise in the form of endocarditis, gangrene, and amputations. Postprocedure care is important in preventing most complications: “Reputable tattoo parlors and piercing salons should provide a long list of do’s and don’ts on how to care for the area that was worked on, and what signs might indicate a problem,” Cora C. Breuner, MD, chairperson of the AAP Committee on Adolescence and coauthor of the report, said in a press statement. The clinical report was presented at the AAP annual meeting in Chicago and simultaneously published in the journal Pediatrics (2017 Sep 18. doi: 10.1542/peds.2017-1962).
Data concerning adolescent tattooing and piercing vary by source and age, but there is a distinct trend of adolescents getting or having an interest in body modification. In samples of adolescents attending clinics at ages 12-22 years, 10%-23% had tattoos and 27%-42% had body piercing (other than the earlobe); rates were higher among girls vs. boys and among older vs. young adolescents. “Of students with current piercings, high-ear cartilage (53%) was the most common visible piercing, followed by navel (38%), tongue (13%), and nipple and genital (9%) piercings” according to the report.
A concern that many adolescents and young adults may not consider is how tattoos affect society’s perception of tattooed and pierced people. A 2008 study found that 29% of people surveyed thought tattooed people were more likely to engage in deviant behavior; this belief had decreased to 24% by 2012 , according to a Harris Poll.
While society at large may appear more accepting of tattooed individuals, employers may be less open to hiring them. According to an executive career coach, “37% of human resource managers cite tattoos as the third physical attribute likely to limit career potential” with non-ear piercings in the top two barriers to career advancement (Am J Nurs. 2012;112[5]:15). In a 2014 survey of 2,675 people, 76% thought that tattoos and/or piercings had hurt their chances of getting a job, and 39% thought employees with tattoos and/or body piercings reflect poorly on their employers. Also, 42% of those surveyed felt visible tattoos are inappropriate at work, with 55% felt the same about body piercings.

“In most cases, teens just enjoy the look of the tattoo or piercing, but we do advise them to talk any decision over with their parents or another adult first,” David Levine, MD, coauthor of the AAP report, said in a press statement. “They may not realize how expensive it is to remove a tattoo, or how a piercing on your tongue might result in a chipped tooth.”
Laser removal of tattoos can range from $49 to $300 per square inch of treatment area, according to the report.
Some tips from the report
- You should advise adolescent patients to assess sanitary and hygienic practices of the tattoo parlors and tattoo artists, including: “use of new, disposable gloves; removal of the new needle and equipment from a sealed, sterile container; and the use of fresh, unused ink poured into a new, disposable container with each new client.”
- You should advise adolescents with tattoos to come to the office if there are signs and symptoms of infection .
- Lesions that appear to grow and/or change within a tattoo suggest a neoplasm.
- You should familiarize yourself with local laws and regulations related to tattooing so you can inform patients and parents.
- Counsel adolescents about the implications of visible tattoos on jobs.
- Use antibiotic agents with good coverage against Pseudomonas and Staphylococcus species (such as fluoroquinolones) to treat piercing-associated infections of the auricular cartilage.
- Recommend removing all jewelry during contact sports. If jewelry interferes with mouth guards or protective equipment, it should be removed before play. Have patients remove nipple jewelry prior to breastfeeding.
The authors have no relevant financial disclosures.
Educate adolescents about the potential medical complications and social consequences of tattooing and body piercing as their popularity rises, an American Academy of Pediatrics clinical report recommends.
The most common complications post tattooing are bacterial and viral infections, and inflammation at the site of the tattoo. Rarely, more serious complications can arise in the form of endocarditis, gangrene, and amputations. Postprocedure care is important in preventing most complications: “Reputable tattoo parlors and piercing salons should provide a long list of do’s and don’ts on how to care for the area that was worked on, and what signs might indicate a problem,” Cora C. Breuner, MD, chairperson of the AAP Committee on Adolescence and coauthor of the report, said in a press statement. The clinical report was presented at the AAP annual meeting in Chicago and simultaneously published in the journal Pediatrics (2017 Sep 18. doi: 10.1542/peds.2017-1962).
Data concerning adolescent tattooing and piercing vary by source and age, but there is a distinct trend of adolescents getting or having an interest in body modification. In samples of adolescents attending clinics at ages 12-22 years, 10%-23% had tattoos and 27%-42% had body piercing (other than the earlobe); rates were higher among girls vs. boys and among older vs. young adolescents. “Of students with current piercings, high-ear cartilage (53%) was the most common visible piercing, followed by navel (38%), tongue (13%), and nipple and genital (9%) piercings” according to the report.
A concern that many adolescents and young adults may not consider is how tattoos affect society’s perception of tattooed and pierced people. A 2008 study found that 29% of people surveyed thought tattooed people were more likely to engage in deviant behavior; this belief had decreased to 24% by 2012 , according to a Harris Poll.
While society at large may appear more accepting of tattooed individuals, employers may be less open to hiring them. According to an executive career coach, “37% of human resource managers cite tattoos as the third physical attribute likely to limit career potential” with non-ear piercings in the top two barriers to career advancement (Am J Nurs. 2012;112[5]:15). In a 2014 survey of 2,675 people, 76% thought that tattoos and/or piercings had hurt their chances of getting a job, and 39% thought employees with tattoos and/or body piercings reflect poorly on their employers. Also, 42% of those surveyed felt visible tattoos are inappropriate at work, with 55% felt the same about body piercings.
“In most cases, teens just enjoy the look of the tattoo or piercing, but we do advise them to talk any decision over with their parents or another adult first,” David Levine, MD, coauthor of the AAP report, said in a press statement. “They may not realize how expensive it is to remove a tattoo, or how a piercing on your tongue might result in a chipped tooth.”
Laser removal of tattoos can range from $49 to $300 per square inch of treatment area, according to the report.
Some tips from the report
- You should advise adolescent patients to assess sanitary and hygienic practices of the tattoo parlors and tattoo artists, including: “use of new, disposable gloves; removal of the new needle and equipment from a sealed, sterile container; and the use of fresh, unused ink poured into a new, disposable container with each new client.”
- You should advise adolescents with tattoos to come to the office if there are signs and symptoms of infection .
- Lesions that appear to grow and/or change within a tattoo suggest a neoplasm.
- You should familiarize yourself with local laws and regulations related to tattooing so you can inform patients and parents.
- Counsel adolescents about the implications of visible tattoos on jobs.
- Use antibiotic agents with good coverage against Pseudomonas and Staphylococcus species (such as fluoroquinolones) to treat piercing-associated infections of the auricular cartilage.
- Recommend removing all jewelry during contact sports. If jewelry interferes with mouth guards or protective equipment, it should be removed before play. Have patients remove nipple jewelry prior to breastfeeding.
The authors have no relevant financial disclosures.
Educate adolescents about the potential medical complications and social consequences of tattooing and body piercing as their popularity rises, an American Academy of Pediatrics clinical report recommends.
The most common complications post tattooing are bacterial and viral infections, and inflammation at the site of the tattoo. Rarely, more serious complications can arise in the form of endocarditis, gangrene, and amputations. Postprocedure care is important in preventing most complications: “Reputable tattoo parlors and piercing salons should provide a long list of do’s and don’ts on how to care for the area that was worked on, and what signs might indicate a problem,” Cora C. Breuner, MD, chairperson of the AAP Committee on Adolescence and coauthor of the report, said in a press statement. The clinical report was presented at the AAP annual meeting in Chicago and simultaneously published in the journal Pediatrics (2017 Sep 18. doi: 10.1542/peds.2017-1962).
Data concerning adolescent tattooing and piercing vary by source and age, but there is a distinct trend of adolescents getting or having an interest in body modification. In samples of adolescents attending clinics at ages 12-22 years, 10%-23% had tattoos and 27%-42% had body piercing (other than the earlobe); rates were higher among girls vs. boys and among older vs. young adolescents. “Of students with current piercings, high-ear cartilage (53%) was the most common visible piercing, followed by navel (38%), tongue (13%), and nipple and genital (9%) piercings” according to the report.
A concern that many adolescents and young adults may not consider is how tattoos affect society’s perception of tattooed and pierced people. A 2008 study found that 29% of people surveyed thought tattooed people were more likely to engage in deviant behavior; this belief had decreased to 24% by 2012 , according to a Harris Poll.
While society at large may appear more accepting of tattooed individuals, employers may be less open to hiring them. According to an executive career coach, “37% of human resource managers cite tattoos as the third physical attribute likely to limit career potential” with non-ear piercings in the top two barriers to career advancement (Am J Nurs. 2012;112[5]:15). In a 2014 survey of 2,675 people, 76% thought that tattoos and/or piercings had hurt their chances of getting a job, and 39% thought employees with tattoos and/or body piercings reflect poorly on their employers. Also, 42% of those surveyed felt visible tattoos are inappropriate at work, with 55% felt the same about body piercings.
“In most cases, teens just enjoy the look of the tattoo or piercing, but we do advise them to talk any decision over with their parents or another adult first,” David Levine, MD, coauthor of the AAP report, said in a press statement. “They may not realize how expensive it is to remove a tattoo, or how a piercing on your tongue might result in a chipped tooth.”
Laser removal of tattoos can range from $49 to $300 per square inch of treatment area, according to the report.
Some tips from the report
- You should advise adolescent patients to assess sanitary and hygienic practices of the tattoo parlors and tattoo artists, including: “use of new, disposable gloves; removal of the new needle and equipment from a sealed, sterile container; and the use of fresh, unused ink poured into a new, disposable container with each new client.”
- You should advise adolescents with tattoos to come to the office if there are signs and symptoms of infection .
- Lesions that appear to grow and/or change within a tattoo suggest a neoplasm.
- You should familiarize yourself with local laws and regulations related to tattooing so you can inform patients and parents.
- Counsel adolescents about the implications of visible tattoos on jobs.
- Use antibiotic agents with good coverage against Pseudomonas and Staphylococcus species (such as fluoroquinolones) to treat piercing-associated infections of the auricular cartilage.
- Recommend removing all jewelry during contact sports. If jewelry interferes with mouth guards or protective equipment, it should be removed before play. Have patients remove nipple jewelry prior to breastfeeding.
The authors have no relevant financial disclosures.
FROM AAP 2017
Oral Cues to Disease
1. A 21-year-old man complains of prolonged diarrhea with steady abdominal pain and recent weight loss. He also reports painful knee and hip joints and generalized fatigue. Physical exam reveals fissure-like ulcerations of the mandibular buccal vestibule and localized abdominal pain with fullness in the right lower quadrant.

Diagnosis: Crohn disease can affect the gastrointestinal tract anywhere from the mouth to the anus, and can manifest with oral findings that may not correlate with abdominal symptoms (eg, mucosal cobble stoning, mucosal tags, deep linear ulcerations, gingival hyperplasia, lip fissuring, aphthous ulcers, angular cheilitis). Other features may include diffuse, painless swelling of the lips and mucosal erythema.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
2. Over the past few months, this 43-year-old woman has had multiple severely painful, slow-healing oral ulcers, resulting in the erosion of the lower lip. She reports pain on swallowing and occasional bloody nose after blowing in the morning.

Diagnosis: Vesiculo-bullous lesions in the mouth may be seen with pemphigus vulgaris or bullous pemphigoid. Pemphigus vulgaris, an autoimmune intraepithelial blistering disease, often manifests as flaccid bullae or painful ulcerations in the oral cavity prior to the onset of skin lesions.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
3. A 26-year-old woman presents with fever and fatigue, as well as arthralgia in her hands. Upon examination, she has a malar rash and lichenoid inflammation of the buccal mucosa. She has a family history of autoimmune disorders.
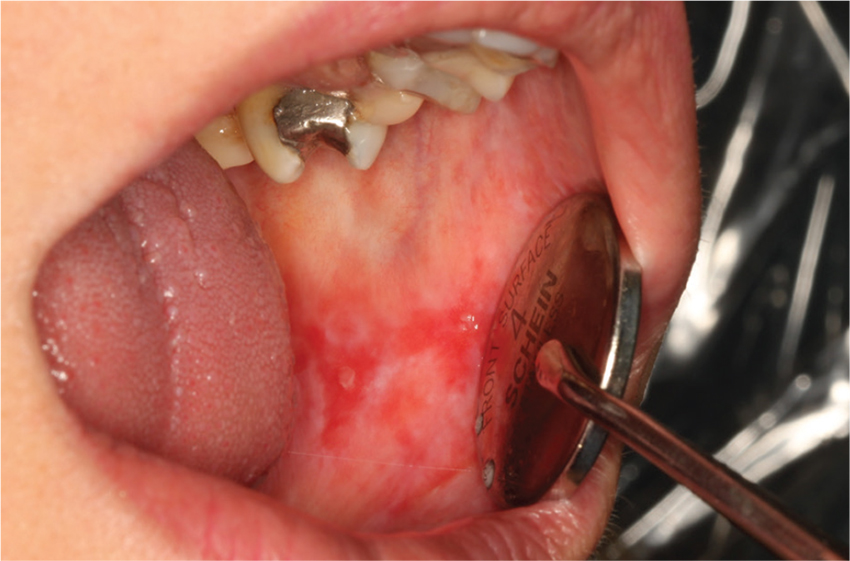
Diagnosis: Oral findings suggestive of systemic or discoid lupus erythematosus may greatly resemble those of oral lichen planus.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
4. This 14-year-old girl is concerned about the multiple ecchymoses and thrombi in her mouth. She feels fatigued and has a fever. Her history includes a tendency to bruise easily, menorrhagia, and a recent infection treated with vancomycin. Physical exam is notable for retinal hemorrhages and jaundice.

Diagnosis: Thrombocytopenia purpura may manifest with oral petechiae, purpura, oral hematomas, or hemorrhagic bullae.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
1. A 21-year-old man complains of prolonged diarrhea with steady abdominal pain and recent weight loss. He also reports painful knee and hip joints and generalized fatigue. Physical exam reveals fissure-like ulcerations of the mandibular buccal vestibule and localized abdominal pain with fullness in the right lower quadrant.
Diagnosis: Crohn disease can affect the gastrointestinal tract anywhere from the mouth to the anus, and can manifest with oral findings that may not correlate with abdominal symptoms (eg, mucosal cobble stoning, mucosal tags, deep linear ulcerations, gingival hyperplasia, lip fissuring, aphthous ulcers, angular cheilitis). Other features may include diffuse, painless swelling of the lips and mucosal erythema.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
2. Over the past few months, this 43-year-old woman has had multiple severely painful, slow-healing oral ulcers, resulting in the erosion of the lower lip. She reports pain on swallowing and occasional bloody nose after blowing in the morning.
Diagnosis: Vesiculo-bullous lesions in the mouth may be seen with pemphigus vulgaris or bullous pemphigoid. Pemphigus vulgaris, an autoimmune intraepithelial blistering disease, often manifests as flaccid bullae or painful ulcerations in the oral cavity prior to the onset of skin lesions.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
3. A 26-year-old woman presents with fever and fatigue, as well as arthralgia in her hands. Upon examination, she has a malar rash and lichenoid inflammation of the buccal mucosa. She has a family history of autoimmune disorders.
Diagnosis: Oral findings suggestive of systemic or discoid lupus erythematosus may greatly resemble those of oral lichen planus.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
4. This 14-year-old girl is concerned about the multiple ecchymoses and thrombi in her mouth. She feels fatigued and has a fever. Her history includes a tendency to bruise easily, menorrhagia, and a recent infection treated with vancomycin. Physical exam is notable for retinal hemorrhages and jaundice.
Diagnosis: Thrombocytopenia purpura may manifest with oral petechiae, purpura, oral hematomas, or hemorrhagic bullae.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
1. A 21-year-old man complains of prolonged diarrhea with steady abdominal pain and recent weight loss. He also reports painful knee and hip joints and generalized fatigue. Physical exam reveals fissure-like ulcerations of the mandibular buccal vestibule and localized abdominal pain with fullness in the right lower quadrant.
Diagnosis: Crohn disease can affect the gastrointestinal tract anywhere from the mouth to the anus, and can manifest with oral findings that may not correlate with abdominal symptoms (eg, mucosal cobble stoning, mucosal tags, deep linear ulcerations, gingival hyperplasia, lip fissuring, aphthous ulcers, angular cheilitis). Other features may include diffuse, painless swelling of the lips and mucosal erythema.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
2. Over the past few months, this 43-year-old woman has had multiple severely painful, slow-healing oral ulcers, resulting in the erosion of the lower lip. She reports pain on swallowing and occasional bloody nose after blowing in the morning.
Diagnosis: Vesiculo-bullous lesions in the mouth may be seen with pemphigus vulgaris or bullous pemphigoid. Pemphigus vulgaris, an autoimmune intraepithelial blistering disease, often manifests as flaccid bullae or painful ulcerations in the oral cavity prior to the onset of skin lesions.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
3. A 26-year-old woman presents with fever and fatigue, as well as arthralgia in her hands. Upon examination, she has a malar rash and lichenoid inflammation of the buccal mucosa. She has a family history of autoimmune disorders.
Diagnosis: Oral findings suggestive of systemic or discoid lupus erythematosus may greatly resemble those of oral lichen planus.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.
4. This 14-year-old girl is concerned about the multiple ecchymoses and thrombi in her mouth. She feels fatigued and has a fever. Her history includes a tendency to bruise easily, menorrhagia, and a recent infection treated with vancomycin. Physical exam is notable for retinal hemorrhages and jaundice.
Diagnosis: Thrombocytopenia purpura may manifest with oral petechiae, purpura, oral hematomas, or hemorrhagic bullae.
For more information, see “Oral lesions you can’t afford to miss.” J Fam Pract. 2015;64(7):392-399.

COPD in Primary Care
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel

CONCEPTT: Continuous glucose monitoring during pregnancy benefits baby
LISBON – , according to the investigators of a prospective, multicenter, randomized, controlled study who found that it improved a number of neonatal outcomes.
In the open-label Continuous Glucose Monitoring in Pregnant Women with Type 1 Diabetes(CONCEPTT) study, infants born to mothers who had used continuous glucose monitoring (CGM) versus those who had not had a 49% lower chance of being large for gestational age (53% vs. 69%, odds ratio [OR] 0.51, P = .0210) and were 52% less likely to need neonatal intensive care lasting for longer than 24 hours (27% vs. 43%, OR 0.48, P = .0157).
Neonates born to mothers who used CGM during their pregnancy were also less likely to experience hypoglycemia (15% vs. 28%, OR 0.45, P = .0250) and were able to leave the hospital with their mother 1 day earlier (P = .0091) than those born to mothers who did not use CGM.However, these were secondary outcomes of the study, which first looked at how CGM affected the glycemic profile of the mother.“To the best of our knowledge, this is the first trial to demonstrate a benefit of CGM on health outcomes beyond glucose control,” Helen Murphy, MD, one of the CONCEPTT trial’s two principal investigators, said at the annual meeting of the European Association for the Study of Diabetes.

“We would suggest, on the back of these data, that CGM should be offered to all pregnant women with type 1 diabetes using intensive insulin therapy during the first trimester,” Dr. Murphy said, adding that results of the study were simultaneously published online in the Lancet (2017 Sept. 15. doi. 10.1016/S0140-6736(17)32400-5).
“The CONCEPTT study will change the future for pregnant women with diabetes,” commented Elisabeth Mathiesen, MD, who was the EASD’s invited discussant for the study, and who congratulated the investigators for “a well performed study” and being “brave,” as “performing a RCT [randomized controlled trial] in pregnancy is not easy”.
Satish Garg, MD, and Sarit Polsky, MD, of the Barbara Davis Center for Diabetes at the University of Colorado, Denver, agreed in an editorial (Lancet 2017; Sept. 12. doi: 10.1016/S0140-6736(17)32449-2) accompanying the published article that the study findings were clinically important.
“We believe that the CONCEPTT results support CGM use during pregnancy for all women with type 1 diabetes,” they wrote, adding that the mother’s “time in [glycated hemoglobin, HbA1C] range might become an important measure in pregnancies with type 1 diabetes.”
Dr. Garg and Dr. Polsky also suggested that endocrine and obstetric medical societies take note and perhaps revise accordingly their guidelines on the use of CGM during pregnancy in diabetic women.
CONCEPTT involved 325 women with type 1 diabetes; 215 were pregnant at the time of enrollment, and 110 were planning on becoming pregnant in the near future.
Co-principal investigator Denice Feig, MD, of Sinai Health System in Toronto, explained that women were eligible for inclusion in the trial if they had type 1 diabetes for at least 1 year, were aged between 18 and 40 years, and had been using daily insulin delivered by either an insulin pump or multiple daily injections (MDI). At enrollment, the participants’ insulin regimen had to been stable for at least 4 weeks before randomization to CGM with capillary glucose monitoring or capillary glucose monitoring alone and their glycemic control had to be suboptimal.
Two groups of women were studied: a “pre-pregnancy group” of women who were planning on pregnancy and wanted to optimize their glycemic control before conception, and a “pregnancy group” of women in their first trimester (less than 14 weeks’ gestation) who were due to have a live, singleton birth as confirmed by ultrasound.
The primary outcome of the trial was the change in HbA1C from baseline to 34 weeks, with pre-specified secondary outcomes of various CGM measures, neoneonatal outcomes, and patient-reported outcomes.
Pregnant women using CGM had lower HbA1C levels during the trial than women who did not have CGM monitoring, although the difference was small (–0.19%, P = .0207).
The use of CGM was associated with more time spent in target HbA1C range (68% of women using CMG vs. 61% of those not using CGM, P = .0034), with less time being hyperglycemic (27% vs. 37%, P = .0279) and comparable rates of hypoglycemia (17 vs. 21 episodes) and time spent being hypoglycemic (2% vs. 4%, P = .10).“The CGM effects were very comparable among insulin pump and MDI users and across 31 international sites,” Dr. Murphy summarized, although she noted that there was no consistent benefit of using CGM seen in women who were planning a pregnancy. Dr. Feig noted that the strengths of the study were the large sample size and that CGM was used continuously from the first trimester until delivery. Women using both pumps and MDI were included at multiple centers and countries, and HbA1C was centrally assessed, with detailed CGM measures used in an exclusively type 1 diabetes population.“Of note, one needed to treat only six women with CGM to prevent one episode of large for gestational age,” Dr. Feig reported. “One needed to treat only eight women to prevent one neonatal hypoglycemia, and six women to prevent one NICU [neonatal intensive care unit] admission over 24 hours.”
There were some limitations, of course, including: around 20% of women had missing data on their HbA1C level; women using CGM also made more unscheduled visits to their health care providers although there are no data on the frequency of self-monitoring of blood glucose or frequency of insulin bolus dosing; and the study was open label.
In her independent précis of the trial, Dr. Mathiesen, professor of endocrinology and chief physician managing pregnant women with diabetes at the Rigshospitalet University Hospital in Copenhagen, noted that there were some other downsides to using CGM in the study.

The CONCEPTT study was funded by the Juvenile Diabetes Research Foundation, the Canadian Clinical Trial Network, the National Institute for Health Research, the Center for Mother, Infant, and Child Research, and the Jaeb Center for Health Research. Medtronic also supported the study by providing the CGM sensors and systems at a reduced cost. Dr. Feig declared she had no competing interests. Dr. Murphy disclosed sitting on an advisory board for Medtronic and receiving personal fees from Novo Nordisk and Roche, unrelated to the current study. Dr. Mathiesen was the invited EASD independent commentator for the trial and did not give any disclosures. Dr. Garg has received advisory board consulting fees and research grants from Medtronic and several other pharmaceutical companies specializing in diabetes care. Dr. Polsky has received research funding from DexCom for diabetes device use in patients with diabetes paid directly to the University of Denver.
LISBON – , according to the investigators of a prospective, multicenter, randomized, controlled study who found that it improved a number of neonatal outcomes.
In the open-label Continuous Glucose Monitoring in Pregnant Women with Type 1 Diabetes(CONCEPTT) study, infants born to mothers who had used continuous glucose monitoring (CGM) versus those who had not had a 49% lower chance of being large for gestational age (53% vs. 69%, odds ratio [OR] 0.51, P = .0210) and were 52% less likely to need neonatal intensive care lasting for longer than 24 hours (27% vs. 43%, OR 0.48, P = .0157).
Neonates born to mothers who used CGM during their pregnancy were also less likely to experience hypoglycemia (15% vs. 28%, OR 0.45, P = .0250) and were able to leave the hospital with their mother 1 day earlier (P = .0091) than those born to mothers who did not use CGM.However, these were secondary outcomes of the study, which first looked at how CGM affected the glycemic profile of the mother.“To the best of our knowledge, this is the first trial to demonstrate a benefit of CGM on health outcomes beyond glucose control,” Helen Murphy, MD, one of the CONCEPTT trial’s two principal investigators, said at the annual meeting of the European Association for the Study of Diabetes.
“We would suggest, on the back of these data, that CGM should be offered to all pregnant women with type 1 diabetes using intensive insulin therapy during the first trimester,” Dr. Murphy said, adding that results of the study were simultaneously published online in the Lancet (2017 Sept. 15. doi. 10.1016/S0140-6736(17)32400-5).
“The CONCEPTT study will change the future for pregnant women with diabetes,” commented Elisabeth Mathiesen, MD, who was the EASD’s invited discussant for the study, and who congratulated the investigators for “a well performed study” and being “brave,” as “performing a RCT [randomized controlled trial] in pregnancy is not easy”.
Satish Garg, MD, and Sarit Polsky, MD, of the Barbara Davis Center for Diabetes at the University of Colorado, Denver, agreed in an editorial (Lancet 2017; Sept. 12. doi: 10.1016/S0140-6736(17)32449-2) accompanying the published article that the study findings were clinically important.
“We believe that the CONCEPTT results support CGM use during pregnancy for all women with type 1 diabetes,” they wrote, adding that the mother’s “time in [glycated hemoglobin, HbA1C] range might become an important measure in pregnancies with type 1 diabetes.”
Dr. Garg and Dr. Polsky also suggested that endocrine and obstetric medical societies take note and perhaps revise accordingly their guidelines on the use of CGM during pregnancy in diabetic women.
CONCEPTT involved 325 women with type 1 diabetes; 215 were pregnant at the time of enrollment, and 110 were planning on becoming pregnant in the near future.
Co-principal investigator Denice Feig, MD, of Sinai Health System in Toronto, explained that women were eligible for inclusion in the trial if they had type 1 diabetes for at least 1 year, were aged between 18 and 40 years, and had been using daily insulin delivered by either an insulin pump or multiple daily injections (MDI). At enrollment, the participants’ insulin regimen had to been stable for at least 4 weeks before randomization to CGM with capillary glucose monitoring or capillary glucose monitoring alone and their glycemic control had to be suboptimal.
Two groups of women were studied: a “pre-pregnancy group” of women who were planning on pregnancy and wanted to optimize their glycemic control before conception, and a “pregnancy group” of women in their first trimester (less than 14 weeks’ gestation) who were due to have a live, singleton birth as confirmed by ultrasound.
The primary outcome of the trial was the change in HbA1C from baseline to 34 weeks, with pre-specified secondary outcomes of various CGM measures, neoneonatal outcomes, and patient-reported outcomes.
Pregnant women using CGM had lower HbA1C levels during the trial than women who did not have CGM monitoring, although the difference was small (–0.19%, P = .0207).
The use of CGM was associated with more time spent in target HbA1C range (68% of women using CMG vs. 61% of those not using CGM, P = .0034), with less time being hyperglycemic (27% vs. 37%, P = .0279) and comparable rates of hypoglycemia (17 vs. 21 episodes) and time spent being hypoglycemic (2% vs. 4%, P = .10).“The CGM effects were very comparable among insulin pump and MDI users and across 31 international sites,” Dr. Murphy summarized, although she noted that there was no consistent benefit of using CGM seen in women who were planning a pregnancy. Dr. Feig noted that the strengths of the study were the large sample size and that CGM was used continuously from the first trimester until delivery. Women using both pumps and MDI were included at multiple centers and countries, and HbA1C was centrally assessed, with detailed CGM measures used in an exclusively type 1 diabetes population.“Of note, one needed to treat only six women with CGM to prevent one episode of large for gestational age,” Dr. Feig reported. “One needed to treat only eight women to prevent one neonatal hypoglycemia, and six women to prevent one NICU [neonatal intensive care unit] admission over 24 hours.”
There were some limitations, of course, including: around 20% of women had missing data on their HbA1C level; women using CGM also made more unscheduled visits to their health care providers although there are no data on the frequency of self-monitoring of blood glucose or frequency of insulin bolus dosing; and the study was open label.
In her independent précis of the trial, Dr. Mathiesen, professor of endocrinology and chief physician managing pregnant women with diabetes at the Rigshospitalet University Hospital in Copenhagen, noted that there were some other downsides to using CGM in the study.
The CONCEPTT study was funded by the Juvenile Diabetes Research Foundation, the Canadian Clinical Trial Network, the National Institute for Health Research, the Center for Mother, Infant, and Child Research, and the Jaeb Center for Health Research. Medtronic also supported the study by providing the CGM sensors and systems at a reduced cost. Dr. Feig declared she had no competing interests. Dr. Murphy disclosed sitting on an advisory board for Medtronic and receiving personal fees from Novo Nordisk and Roche, unrelated to the current study. Dr. Mathiesen was the invited EASD independent commentator for the trial and did not give any disclosures. Dr. Garg has received advisory board consulting fees and research grants from Medtronic and several other pharmaceutical companies specializing in diabetes care. Dr. Polsky has received research funding from DexCom for diabetes device use in patients with diabetes paid directly to the University of Denver.
LISBON – , according to the investigators of a prospective, multicenter, randomized, controlled study who found that it improved a number of neonatal outcomes.
In the open-label Continuous Glucose Monitoring in Pregnant Women with Type 1 Diabetes(CONCEPTT) study, infants born to mothers who had used continuous glucose monitoring (CGM) versus those who had not had a 49% lower chance of being large for gestational age (53% vs. 69%, odds ratio [OR] 0.51, P = .0210) and were 52% less likely to need neonatal intensive care lasting for longer than 24 hours (27% vs. 43%, OR 0.48, P = .0157).
Neonates born to mothers who used CGM during their pregnancy were also less likely to experience hypoglycemia (15% vs. 28%, OR 0.45, P = .0250) and were able to leave the hospital with their mother 1 day earlier (P = .0091) than those born to mothers who did not use CGM.However, these were secondary outcomes of the study, which first looked at how CGM affected the glycemic profile of the mother.“To the best of our knowledge, this is the first trial to demonstrate a benefit of CGM on health outcomes beyond glucose control,” Helen Murphy, MD, one of the CONCEPTT trial’s two principal investigators, said at the annual meeting of the European Association for the Study of Diabetes.
“We would suggest, on the back of these data, that CGM should be offered to all pregnant women with type 1 diabetes using intensive insulin therapy during the first trimester,” Dr. Murphy said, adding that results of the study were simultaneously published online in the Lancet (2017 Sept. 15. doi. 10.1016/S0140-6736(17)32400-5).
“The CONCEPTT study will change the future for pregnant women with diabetes,” commented Elisabeth Mathiesen, MD, who was the EASD’s invited discussant for the study, and who congratulated the investigators for “a well performed study” and being “brave,” as “performing a RCT [randomized controlled trial] in pregnancy is not easy”.
Satish Garg, MD, and Sarit Polsky, MD, of the Barbara Davis Center for Diabetes at the University of Colorado, Denver, agreed in an editorial (Lancet 2017; Sept. 12. doi: 10.1016/S0140-6736(17)32449-2) accompanying the published article that the study findings were clinically important.
“We believe that the CONCEPTT results support CGM use during pregnancy for all women with type 1 diabetes,” they wrote, adding that the mother’s “time in [glycated hemoglobin, HbA1C] range might become an important measure in pregnancies with type 1 diabetes.”
Dr. Garg and Dr. Polsky also suggested that endocrine and obstetric medical societies take note and perhaps revise accordingly their guidelines on the use of CGM during pregnancy in diabetic women.
CONCEPTT involved 325 women with type 1 diabetes; 215 were pregnant at the time of enrollment, and 110 were planning on becoming pregnant in the near future.
Co-principal investigator Denice Feig, MD, of Sinai Health System in Toronto, explained that women were eligible for inclusion in the trial if they had type 1 diabetes for at least 1 year, were aged between 18 and 40 years, and had been using daily insulin delivered by either an insulin pump or multiple daily injections (MDI). At enrollment, the participants’ insulin regimen had to been stable for at least 4 weeks before randomization to CGM with capillary glucose monitoring or capillary glucose monitoring alone and their glycemic control had to be suboptimal.
Two groups of women were studied: a “pre-pregnancy group” of women who were planning on pregnancy and wanted to optimize their glycemic control before conception, and a “pregnancy group” of women in their first trimester (less than 14 weeks’ gestation) who were due to have a live, singleton birth as confirmed by ultrasound.
The primary outcome of the trial was the change in HbA1C from baseline to 34 weeks, with pre-specified secondary outcomes of various CGM measures, neoneonatal outcomes, and patient-reported outcomes.
Pregnant women using CGM had lower HbA1C levels during the trial than women who did not have CGM monitoring, although the difference was small (–0.19%, P = .0207).
The use of CGM was associated with more time spent in target HbA1C range (68% of women using CMG vs. 61% of those not using CGM, P = .0034), with less time being hyperglycemic (27% vs. 37%, P = .0279) and comparable rates of hypoglycemia (17 vs. 21 episodes) and time spent being hypoglycemic (2% vs. 4%, P = .10).“The CGM effects were very comparable among insulin pump and MDI users and across 31 international sites,” Dr. Murphy summarized, although she noted that there was no consistent benefit of using CGM seen in women who were planning a pregnancy. Dr. Feig noted that the strengths of the study were the large sample size and that CGM was used continuously from the first trimester until delivery. Women using both pumps and MDI were included at multiple centers and countries, and HbA1C was centrally assessed, with detailed CGM measures used in an exclusively type 1 diabetes population.“Of note, one needed to treat only six women with CGM to prevent one episode of large for gestational age,” Dr. Feig reported. “One needed to treat only eight women to prevent one neonatal hypoglycemia, and six women to prevent one NICU [neonatal intensive care unit] admission over 24 hours.”
There were some limitations, of course, including: around 20% of women had missing data on their HbA1C level; women using CGM also made more unscheduled visits to their health care providers although there are no data on the frequency of self-monitoring of blood glucose or frequency of insulin bolus dosing; and the study was open label.
In her independent précis of the trial, Dr. Mathiesen, professor of endocrinology and chief physician managing pregnant women with diabetes at the Rigshospitalet University Hospital in Copenhagen, noted that there were some other downsides to using CGM in the study.
The CONCEPTT study was funded by the Juvenile Diabetes Research Foundation, the Canadian Clinical Trial Network, the National Institute for Health Research, the Center for Mother, Infant, and Child Research, and the Jaeb Center for Health Research. Medtronic also supported the study by providing the CGM sensors and systems at a reduced cost. Dr. Feig declared she had no competing interests. Dr. Murphy disclosed sitting on an advisory board for Medtronic and receiving personal fees from Novo Nordisk and Roche, unrelated to the current study. Dr. Mathiesen was the invited EASD independent commentator for the trial and did not give any disclosures. Dr. Garg has received advisory board consulting fees and research grants from Medtronic and several other pharmaceutical companies specializing in diabetes care. Dr. Polsky has received research funding from DexCom for diabetes device use in patients with diabetes paid directly to the University of Denver.
AT EASD 2017
Key clinical point: Continuous glucose monitoring should be offered to women with type 1 diabetes on intensive insulin therapy during their pregnancy.
Major finding: Neonatal outcomes were significantly better if women used CGM while they were pregnant than if they did not. Some maternal outcomes were also improved.
Data source: CONCEPTT: a prospective, multicenter, open-label, randomized controlled trial of 325 women with type 1 diabetes: 215 were pregnant; 110 were planning a pregnancy.
Disclosures: The study was funded by the Juvenile Diabetes Research Foundation, the Canadian Clinical Trial Network, the National Institute for Health Research, the Center for Mother, Infant, and Child Research, and the Jaeb Center for Health Research. Medtronic also supported the study by providing the CGM sensors and systems at a reduced cost. One of the study presenters disclosed sitting on an advisory board for Medtronic.
How can pediatricians help prevent preschool expulsions?
CHICAGO –
Young African American boys are particularly at risk, said Claire Lerner, a senior parenting specialist with the nonprofit organization Zero to Three in Washington.
Speaking at the annual meeting of the American Academy of Pediatrics, Ms. Lerner cited data from 2005 showing that 10.4% of prekindergarten (preK) teachers had expelled at least one child for behavior problems during the previous year, yielding a preK expulsion rate of 6.7 per 1,000 students. This contrasts with a K-12 expulsion rate of 2.1 per 1,000 students.

“What I would say to you is that if a parent, or school, or caregiver comes to you and says, ‘The teacher’s concerned about X,’ don’t dismiss it. I cannot tell you how many times parents have come to me and said, ‘Well, the pediatrician says he’s totally fine. He’s just two.’”
This is not to blame pediatricians, said Ms. Lerner. Rather, “it’s to help you remember that teachers are smart, and they’re with these kids in a natural environment all day long. ...You are seeing such a random, finite, artificial experience in that room that you don’t see what’s going on in the classroom.” The child’s interactions with other children -- usually the impetus for disciplinary action -- will not necessarily be apparent in the pediatrician’s office.
Often, said Ms. Lerner, the child in question isn’t picking up on verbal and physical clues from other children, leading to behavior that’s seen as inappropriate or aggressive by other children -- and by staff. “A lot of these kids have motor planning problems, meaning they don’t know how to take their idea and execute it, so they’re the ones who are knocking down towers, and in kids’ faces. ...Those are the things that I’m talking about that are very unlikely to be picked up in a pediatric well-child visit,” she said.
“The evidence tells us that gender and race matter” in preschool suspensions and expulsions, said Ms. Lerner, noting that black preschool children are 3.6 times as likely as white children to be given an out-of-school suspension.
Black boys, she said, are 19% of male preschool attendees but make up 45% of the preschool children who receive out-of-school suspensions. Black girls make up 20% of female preschool attendees, but 54% of preschool girls who receive out-of-school suspensions are black.
In public preschools, 78% of those suspended are boys, though they make up just 54% of the attendees.
Aside from the home and work disruption caused by these suspensions, Ms. Lerner said that later outcomes are much worse for young students who are expelled or suspended, stacking the deck further against success. Rates of dropping out of high school, grade retention, and incarceration may be up to 10 times higher for these children.
Many school-related factors, including a higher child-teacher ratio and a longer school day, are associated with higher rates of preschool expulsion. Also, teachers who report more job stress are more likely to mete out suspensions or expulsions. By contrast, the availability of behavioral consultations reduces the risk of expulsion.
Within the realistic constraints of a busy pediatric practice, what can a physician do?
At the very least, said Ms. Lerner, pay attention when a parent comes to you and says, “My child’s getting in trouble in the classroom, and I’m afraid he’s going to get kicked out.” At that point, she said, the pediatrician should get in touch with the school. An approach that can be used in communicating with the school is to say, “We’re not seeing that, but we want to learn more,” said Ms. Lerner.
Just the fact that a pediatrician or his or her team members would reach out to the teacher for collaboration helps the teacher and school or daycare center realize that the family is taking the concerns seriously, said Ms. Lerner. “I will tell you that even just that phone call changes what happens for that kid,” she said.
Facilitating appropriate behavioral and mental health evaluations allows those professionals to become part of the problem-solving team for the child, school, and family.
Physicians can also help children and families by being familiar with the Americans with Disabilities Act safeguards for children with an Individualized Education Program (IEP) or a 504 Plan and making sure that families know about these protections.
Within the larger context of the school district and the community, a pediatrician’s voice can be a powerful advocacy tool to lobby against zero tolerance policies, and for stronger prevention and outreach strategies to help avoid out-of-school suspensions and expulsions for the very young. “There are things you can do -- starting tomorrow -- that will change the course for these children,” said Ms. Lerner.
Ms. Lerner is employed by Zero to Three. She reported no conflicts of interest.
CHICAGO –
Young African American boys are particularly at risk, said Claire Lerner, a senior parenting specialist with the nonprofit organization Zero to Three in Washington.
Speaking at the annual meeting of the American Academy of Pediatrics, Ms. Lerner cited data from 2005 showing that 10.4% of prekindergarten (preK) teachers had expelled at least one child for behavior problems during the previous year, yielding a preK expulsion rate of 6.7 per 1,000 students. This contrasts with a K-12 expulsion rate of 2.1 per 1,000 students.
“What I would say to you is that if a parent, or school, or caregiver comes to you and says, ‘The teacher’s concerned about X,’ don’t dismiss it. I cannot tell you how many times parents have come to me and said, ‘Well, the pediatrician says he’s totally fine. He’s just two.’”
This is not to blame pediatricians, said Ms. Lerner. Rather, “it’s to help you remember that teachers are smart, and they’re with these kids in a natural environment all day long. ...You are seeing such a random, finite, artificial experience in that room that you don’t see what’s going on in the classroom.” The child’s interactions with other children -- usually the impetus for disciplinary action -- will not necessarily be apparent in the pediatrician’s office.
Often, said Ms. Lerner, the child in question isn’t picking up on verbal and physical clues from other children, leading to behavior that’s seen as inappropriate or aggressive by other children -- and by staff. “A lot of these kids have motor planning problems, meaning they don’t know how to take their idea and execute it, so they’re the ones who are knocking down towers, and in kids’ faces. ...Those are the things that I’m talking about that are very unlikely to be picked up in a pediatric well-child visit,” she said.
“The evidence tells us that gender and race matter” in preschool suspensions and expulsions, said Ms. Lerner, noting that black preschool children are 3.6 times as likely as white children to be given an out-of-school suspension.
Black boys, she said, are 19% of male preschool attendees but make up 45% of the preschool children who receive out-of-school suspensions. Black girls make up 20% of female preschool attendees, but 54% of preschool girls who receive out-of-school suspensions are black.
In public preschools, 78% of those suspended are boys, though they make up just 54% of the attendees.
Aside from the home and work disruption caused by these suspensions, Ms. Lerner said that later outcomes are much worse for young students who are expelled or suspended, stacking the deck further against success. Rates of dropping out of high school, grade retention, and incarceration may be up to 10 times higher for these children.
Many school-related factors, including a higher child-teacher ratio and a longer school day, are associated with higher rates of preschool expulsion. Also, teachers who report more job stress are more likely to mete out suspensions or expulsions. By contrast, the availability of behavioral consultations reduces the risk of expulsion.
Within the realistic constraints of a busy pediatric practice, what can a physician do?
At the very least, said Ms. Lerner, pay attention when a parent comes to you and says, “My child’s getting in trouble in the classroom, and I’m afraid he’s going to get kicked out.” At that point, she said, the pediatrician should get in touch with the school. An approach that can be used in communicating with the school is to say, “We’re not seeing that, but we want to learn more,” said Ms. Lerner.
Just the fact that a pediatrician or his or her team members would reach out to the teacher for collaboration helps the teacher and school or daycare center realize that the family is taking the concerns seriously, said Ms. Lerner. “I will tell you that even just that phone call changes what happens for that kid,” she said.
Facilitating appropriate behavioral and mental health evaluations allows those professionals to become part of the problem-solving team for the child, school, and family.
Physicians can also help children and families by being familiar with the Americans with Disabilities Act safeguards for children with an Individualized Education Program (IEP) or a 504 Plan and making sure that families know about these protections.
Within the larger context of the school district and the community, a pediatrician’s voice can be a powerful advocacy tool to lobby against zero tolerance policies, and for stronger prevention and outreach strategies to help avoid out-of-school suspensions and expulsions for the very young. “There are things you can do -- starting tomorrow -- that will change the course for these children,” said Ms. Lerner.
Ms. Lerner is employed by Zero to Three. She reported no conflicts of interest.
CHICAGO –
Young African American boys are particularly at risk, said Claire Lerner, a senior parenting specialist with the nonprofit organization Zero to Three in Washington.
Speaking at the annual meeting of the American Academy of Pediatrics, Ms. Lerner cited data from 2005 showing that 10.4% of prekindergarten (preK) teachers had expelled at least one child for behavior problems during the previous year, yielding a preK expulsion rate of 6.7 per 1,000 students. This contrasts with a K-12 expulsion rate of 2.1 per 1,000 students.
“What I would say to you is that if a parent, or school, or caregiver comes to you and says, ‘The teacher’s concerned about X,’ don’t dismiss it. I cannot tell you how many times parents have come to me and said, ‘Well, the pediatrician says he’s totally fine. He’s just two.’”
This is not to blame pediatricians, said Ms. Lerner. Rather, “it’s to help you remember that teachers are smart, and they’re with these kids in a natural environment all day long. ...You are seeing such a random, finite, artificial experience in that room that you don’t see what’s going on in the classroom.” The child’s interactions with other children -- usually the impetus for disciplinary action -- will not necessarily be apparent in the pediatrician’s office.
Often, said Ms. Lerner, the child in question isn’t picking up on verbal and physical clues from other children, leading to behavior that’s seen as inappropriate or aggressive by other children -- and by staff. “A lot of these kids have motor planning problems, meaning they don’t know how to take their idea and execute it, so they’re the ones who are knocking down towers, and in kids’ faces. ...Those are the things that I’m talking about that are very unlikely to be picked up in a pediatric well-child visit,” she said.
“The evidence tells us that gender and race matter” in preschool suspensions and expulsions, said Ms. Lerner, noting that black preschool children are 3.6 times as likely as white children to be given an out-of-school suspension.
Black boys, she said, are 19% of male preschool attendees but make up 45% of the preschool children who receive out-of-school suspensions. Black girls make up 20% of female preschool attendees, but 54% of preschool girls who receive out-of-school suspensions are black.
In public preschools, 78% of those suspended are boys, though they make up just 54% of the attendees.
Aside from the home and work disruption caused by these suspensions, Ms. Lerner said that later outcomes are much worse for young students who are expelled or suspended, stacking the deck further against success. Rates of dropping out of high school, grade retention, and incarceration may be up to 10 times higher for these children.
Many school-related factors, including a higher child-teacher ratio and a longer school day, are associated with higher rates of preschool expulsion. Also, teachers who report more job stress are more likely to mete out suspensions or expulsions. By contrast, the availability of behavioral consultations reduces the risk of expulsion.
Within the realistic constraints of a busy pediatric practice, what can a physician do?
At the very least, said Ms. Lerner, pay attention when a parent comes to you and says, “My child’s getting in trouble in the classroom, and I’m afraid he’s going to get kicked out.” At that point, she said, the pediatrician should get in touch with the school. An approach that can be used in communicating with the school is to say, “We’re not seeing that, but we want to learn more,” said Ms. Lerner.
Just the fact that a pediatrician or his or her team members would reach out to the teacher for collaboration helps the teacher and school or daycare center realize that the family is taking the concerns seriously, said Ms. Lerner. “I will tell you that even just that phone call changes what happens for that kid,” she said.
Facilitating appropriate behavioral and mental health evaluations allows those professionals to become part of the problem-solving team for the child, school, and family.
Physicians can also help children and families by being familiar with the Americans with Disabilities Act safeguards for children with an Individualized Education Program (IEP) or a 504 Plan and making sure that families know about these protections.
Within the larger context of the school district and the community, a pediatrician’s voice can be a powerful advocacy tool to lobby against zero tolerance policies, and for stronger prevention and outreach strategies to help avoid out-of-school suspensions and expulsions for the very young. “There are things you can do -- starting tomorrow -- that will change the course for these children,” said Ms. Lerner.
Ms. Lerner is employed by Zero to Three. She reported no conflicts of interest.
EXPERT ANALYSIS FROM AAP 2017
EMR pop-up aims to boost HPV vaccination rates
An electronic pop-up placed on clinicians’ electronic medical record may have had a positive impact on the human papillomavirus vaccination rates in a Texas pediatric clinic, according to a study presented at the annual meeting of the American Academy of Pediatrics.

HPV vaccination rates grew from 34% before the installation of the reminder to 53% afterwards. “We’ve had a lot of success in increasing the rates,” said lead researcher Kimberly Ferris, a fourth-year medical student at Texas Tech’s Paul L. Foster School of Medicine.
Ms. Ferris said that the medical center is located near Mexico, and the patient population includes children and adolescents from Juarez. “We still have a lot of young women who are dying from cervical cancer. Really honing in on this population will have a long term effect. ...Pediatrics is really where it starts. This is where you want to capture them.”
The plan is to keep the pop-up reminder in place and continue its use to educate staff and families, said co-author Maria Theresa Villanos, MD, director of ambulatory pediatrics at Texas Tech. Part of the success of their project is “there is no missed opportunity. This pop-up reminder appears during well child visits as well as any time a child comes in sick or for acute care,” she said.
“The major barrier that needs to be addressed is probably pop-up fatigue,” Ms. Ferris said. Because the prompt is new, people are still reading it each time it comes up, but that behavior could wane over time, she said. “It would be interesting to look at long-term vaccination rates and whether the numbers stay the same or if there is a decline.”
Ms. Ferris and Dr. Villanos had no relevant financial disclosures.
An electronic pop-up placed on clinicians’ electronic medical record may have had a positive impact on the human papillomavirus vaccination rates in a Texas pediatric clinic, according to a study presented at the annual meeting of the American Academy of Pediatrics.
HPV vaccination rates grew from 34% before the installation of the reminder to 53% afterwards. “We’ve had a lot of success in increasing the rates,” said lead researcher Kimberly Ferris, a fourth-year medical student at Texas Tech’s Paul L. Foster School of Medicine.
Ms. Ferris said that the medical center is located near Mexico, and the patient population includes children and adolescents from Juarez. “We still have a lot of young women who are dying from cervical cancer. Really honing in on this population will have a long term effect. ...Pediatrics is really where it starts. This is where you want to capture them.”
The plan is to keep the pop-up reminder in place and continue its use to educate staff and families, said co-author Maria Theresa Villanos, MD, director of ambulatory pediatrics at Texas Tech. Part of the success of their project is “there is no missed opportunity. This pop-up reminder appears during well child visits as well as any time a child comes in sick or for acute care,” she said.
“The major barrier that needs to be addressed is probably pop-up fatigue,” Ms. Ferris said. Because the prompt is new, people are still reading it each time it comes up, but that behavior could wane over time, she said. “It would be interesting to look at long-term vaccination rates and whether the numbers stay the same or if there is a decline.”
Ms. Ferris and Dr. Villanos had no relevant financial disclosures.
An electronic pop-up placed on clinicians’ electronic medical record may have had a positive impact on the human papillomavirus vaccination rates in a Texas pediatric clinic, according to a study presented at the annual meeting of the American Academy of Pediatrics.
HPV vaccination rates grew from 34% before the installation of the reminder to 53% afterwards. “We’ve had a lot of success in increasing the rates,” said lead researcher Kimberly Ferris, a fourth-year medical student at Texas Tech’s Paul L. Foster School of Medicine.
Ms. Ferris said that the medical center is located near Mexico, and the patient population includes children and adolescents from Juarez. “We still have a lot of young women who are dying from cervical cancer. Really honing in on this population will have a long term effect. ...Pediatrics is really where it starts. This is where you want to capture them.”
The plan is to keep the pop-up reminder in place and continue its use to educate staff and families, said co-author Maria Theresa Villanos, MD, director of ambulatory pediatrics at Texas Tech. Part of the success of their project is “there is no missed opportunity. This pop-up reminder appears during well child visits as well as any time a child comes in sick or for acute care,” she said.
“The major barrier that needs to be addressed is probably pop-up fatigue,” Ms. Ferris said. Because the prompt is new, people are still reading it each time it comes up, but that behavior could wane over time, she said. “It would be interesting to look at long-term vaccination rates and whether the numbers stay the same or if there is a decline.”
Ms. Ferris and Dr. Villanos had no relevant financial disclosures.
AT AAP 2017
Key clinical point: Vaccination of patients for HPV jumped nearly 20% following the installation of a reminder to an electronic medical record system.
Major finding: HPV vaccination rates jumped from 33.5% to 52.9% after addition of a pop-up reminder.
Data source: Random chart audit comparing periods before and after intervention.
Disclosures: Ms. Ferris and Dr. Villanos had no relevant financial disclosures.
Soccer-playing girls 5 times more likely to return to same-day play after concussion
CHICAGO – , according to a study presented at the annual meeting of the American Academy of Pediatrics.
Records from 87 soccer players aged 7-18 years (median, 14 years) were examined in a retrospective review of patients seen over a 2-year period by a single physician at a pediatric sports medicine center. Of these, two thirds (n = 58) were girls.

The soccer players included children participating in recreational, club, and school-sponsored soccer, said senior author Shane M. Miller, MD, in an interview. All patients were assessed according to a standardized concussion protocol that involved a neurologic exam and validated concussion evaluation testing, including the ImPACT and the Sports Concussion Assessment Tool (SCAT) tests.
As soccer has grown in popularity as a youth sport, so has the number of reported concussions. “The incidence of reported concussions has increased 1,600% from 1990 to 2014,” wrote Dr. Miller and his coauthors in the abstract accompanying the presentation. Dr. Miller said that girls are 1.5 times more likely than boys to sustain a concussion while playing soccer.
While seeing the patients who were the subject of the study, Dr. Miller realized that most of the soccer players had not come out of play for evaluation after the head impact. Rather, they had continued to play, only later reporting concussion symptoms to coaches, trainers, or parents.
“The athletes may have chosen not to say anything because they didn’t want to come out of the game,” said Dr. Miller, a sports medicine physician at Texas Scottish Rite Hospital for Children, Dallas.
“I was surprised by the significant degree of difference” between male and female soccer players, said Dr. Miller. The study was not designed to get at the reason for the discrepancy, so Dr. Miller could not say with certainty whether awareness of concussion symptoms is significantly lower for female athletes, or whether the athletic culture more strongly encourages minimization of symptoms for girls than boys. In any case, he said, there is room for education of players, coaches, and families to raise awareness of the importance to recognize and report concussion, and then remove the affected athlete from play,
Dr. Miller said that future research directions include collaboration with other facilities to conduct prospective research using a concussion registry. This will allow more robust statistical analysis, and help ascertain the degree of regional variation in pediatric sports concussion management.
“Current education efforts may not be enough to help athletes, parents, and coaches identify concussion symptoms, know the guidelines for immediate removal from play, and understand the risks of returning to play after an injury. More research is needed on how to better spread this message intended to protect the health of young athletes…” Aaron Zynda, the study’s first author and clinical research coordinator at Texas Scottish Rite, said in a press release accompanying the abstract. “Concussion recognition and identification is a team effort,” he said.
Neither Mr. Zynda nor Dr. Miller had any relevant conflicts of interest.
koakes@frontlinemedcom.com
CHICAGO – , according to a study presented at the annual meeting of the American Academy of Pediatrics.
Records from 87 soccer players aged 7-18 years (median, 14 years) were examined in a retrospective review of patients seen over a 2-year period by a single physician at a pediatric sports medicine center. Of these, two thirds (n = 58) were girls.
The soccer players included children participating in recreational, club, and school-sponsored soccer, said senior author Shane M. Miller, MD, in an interview. All patients were assessed according to a standardized concussion protocol that involved a neurologic exam and validated concussion evaluation testing, including the ImPACT and the Sports Concussion Assessment Tool (SCAT) tests.
As soccer has grown in popularity as a youth sport, so has the number of reported concussions. “The incidence of reported concussions has increased 1,600% from 1990 to 2014,” wrote Dr. Miller and his coauthors in the abstract accompanying the presentation. Dr. Miller said that girls are 1.5 times more likely than boys to sustain a concussion while playing soccer.
While seeing the patients who were the subject of the study, Dr. Miller realized that most of the soccer players had not come out of play for evaluation after the head impact. Rather, they had continued to play, only later reporting concussion symptoms to coaches, trainers, or parents.
“The athletes may have chosen not to say anything because they didn’t want to come out of the game,” said Dr. Miller, a sports medicine physician at Texas Scottish Rite Hospital for Children, Dallas.
“I was surprised by the significant degree of difference” between male and female soccer players, said Dr. Miller. The study was not designed to get at the reason for the discrepancy, so Dr. Miller could not say with certainty whether awareness of concussion symptoms is significantly lower for female athletes, or whether the athletic culture more strongly encourages minimization of symptoms for girls than boys. In any case, he said, there is room for education of players, coaches, and families to raise awareness of the importance to recognize and report concussion, and then remove the affected athlete from play,
Dr. Miller said that future research directions include collaboration with other facilities to conduct prospective research using a concussion registry. This will allow more robust statistical analysis, and help ascertain the degree of regional variation in pediatric sports concussion management.
“Current education efforts may not be enough to help athletes, parents, and coaches identify concussion symptoms, know the guidelines for immediate removal from play, and understand the risks of returning to play after an injury. More research is needed on how to better spread this message intended to protect the health of young athletes…” Aaron Zynda, the study’s first author and clinical research coordinator at Texas Scottish Rite, said in a press release accompanying the abstract. “Concussion recognition and identification is a team effort,” he said.
Neither Mr. Zynda nor Dr. Miller had any relevant conflicts of interest.
koakes@frontlinemedcom.com
CHICAGO – , according to a study presented at the annual meeting of the American Academy of Pediatrics.
Records from 87 soccer players aged 7-18 years (median, 14 years) were examined in a retrospective review of patients seen over a 2-year period by a single physician at a pediatric sports medicine center. Of these, two thirds (n = 58) were girls.
The soccer players included children participating in recreational, club, and school-sponsored soccer, said senior author Shane M. Miller, MD, in an interview. All patients were assessed according to a standardized concussion protocol that involved a neurologic exam and validated concussion evaluation testing, including the ImPACT and the Sports Concussion Assessment Tool (SCAT) tests.
As soccer has grown in popularity as a youth sport, so has the number of reported concussions. “The incidence of reported concussions has increased 1,600% from 1990 to 2014,” wrote Dr. Miller and his coauthors in the abstract accompanying the presentation. Dr. Miller said that girls are 1.5 times more likely than boys to sustain a concussion while playing soccer.
While seeing the patients who were the subject of the study, Dr. Miller realized that most of the soccer players had not come out of play for evaluation after the head impact. Rather, they had continued to play, only later reporting concussion symptoms to coaches, trainers, or parents.
“The athletes may have chosen not to say anything because they didn’t want to come out of the game,” said Dr. Miller, a sports medicine physician at Texas Scottish Rite Hospital for Children, Dallas.
“I was surprised by the significant degree of difference” between male and female soccer players, said Dr. Miller. The study was not designed to get at the reason for the discrepancy, so Dr. Miller could not say with certainty whether awareness of concussion symptoms is significantly lower for female athletes, or whether the athletic culture more strongly encourages minimization of symptoms for girls than boys. In any case, he said, there is room for education of players, coaches, and families to raise awareness of the importance to recognize and report concussion, and then remove the affected athlete from play,
Dr. Miller said that future research directions include collaboration with other facilities to conduct prospective research using a concussion registry. This will allow more robust statistical analysis, and help ascertain the degree of regional variation in pediatric sports concussion management.
“Current education efforts may not be enough to help athletes, parents, and coaches identify concussion symptoms, know the guidelines for immediate removal from play, and understand the risks of returning to play after an injury. More research is needed on how to better spread this message intended to protect the health of young athletes…” Aaron Zynda, the study’s first author and clinical research coordinator at Texas Scottish Rite, said in a press release accompanying the abstract. “Concussion recognition and identification is a team effort,” he said.
Neither Mr. Zynda nor Dr. Miller had any relevant conflicts of interest.
koakes@frontlinemedcom.com
At AAP 2017
Key clinical point: Girls who played soccer were five times as likely as boys to return to play on the same day of concussion.
Major finding: Thirty of 58 girls with concussion returned to same-day play, compared with 5 of 29 boys.
Study details: Retrospective single-site study of 87 soccer players with concussion, median age 14 years.
Disclosures: None of the study authors had relevant conflicts of interest.
Application for pegfilgrastim biosimilar withdrawn

Mylan S.A.S. has withdrawn the European marketing authorization application for its pegfilgrastim biosimilar Fulphila, according to the European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP).
Fulphila was intended to be used to reduce the duration of neutropenia and the incidence of febrile neutropenia in adults receiving cytotoxic therapy for malignancy (except chronic myeloid leukemia and myelodysplastic syndromes).
Fulphila was intended to be highly similar to Neulasta, a solution for injection that contains the active substance pegfilgrastim.
To support the application for Fulphila, Mylan S.A.S. presented results of studies designed to show that Fulphila is highly similar to Neulasta in terms of chemical structure, purity, mechanism, safety, effectiveness, and immunogenicity.
Mylan S.A.S withdrew the application for Fulphila after the CHMP had evaluated the initial documentation the company provided on the drug and formulated a list of questions. The CHMP was assessing the company’s responses to the questions when the application was withdrawn.
At the time of the withdrawal, the CHMP had some concerns and was of the provisional opinion that Fulphila could not have been approved.
One of the CHMP’s main concerns was the lack of a certificate of Good Manufacturing Practice for the manufacturing site of the product. Other concerns related to the description of the manufacturing process, the control of impurities in the active substance, and the sterilization of the final product.
In a letter to the European Medicines Agency, Mylan S.A.S said it withdrew the application for Fulphila because a Good Manufacturing Practice certificate for the manufacturing site could not be obtained in the time available.
The application withdrawal does not impact ongoing clinical trials of Fulphila, and there are no compassionate use programs for the drug.
Mylan S.A.S said it plans to resubmit the application for Fulphila as soon as possible. The company is working to ensure “inspection readiness” at the Fulphila manufacturing site by October 2017. ![]()
Mylan S.A.S. has withdrawn the European marketing authorization application for its pegfilgrastim biosimilar Fulphila, according to the European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP).
Fulphila was intended to be used to reduce the duration of neutropenia and the incidence of febrile neutropenia in adults receiving cytotoxic therapy for malignancy (except chronic myeloid leukemia and myelodysplastic syndromes).
Fulphila was intended to be highly similar to Neulasta, a solution for injection that contains the active substance pegfilgrastim.
To support the application for Fulphila, Mylan S.A.S. presented results of studies designed to show that Fulphila is highly similar to Neulasta in terms of chemical structure, purity, mechanism, safety, effectiveness, and immunogenicity.
Mylan S.A.S withdrew the application for Fulphila after the CHMP had evaluated the initial documentation the company provided on the drug and formulated a list of questions. The CHMP was assessing the company’s responses to the questions when the application was withdrawn.
At the time of the withdrawal, the CHMP had some concerns and was of the provisional opinion that Fulphila could not have been approved.
One of the CHMP’s main concerns was the lack of a certificate of Good Manufacturing Practice for the manufacturing site of the product. Other concerns related to the description of the manufacturing process, the control of impurities in the active substance, and the sterilization of the final product.
In a letter to the European Medicines Agency, Mylan S.A.S said it withdrew the application for Fulphila because a Good Manufacturing Practice certificate for the manufacturing site could not be obtained in the time available.
The application withdrawal does not impact ongoing clinical trials of Fulphila, and there are no compassionate use programs for the drug.
Mylan S.A.S said it plans to resubmit the application for Fulphila as soon as possible. The company is working to ensure “inspection readiness” at the Fulphila manufacturing site by October 2017. ![]()
Mylan S.A.S. has withdrawn the European marketing authorization application for its pegfilgrastim biosimilar Fulphila, according to the European Medicines Agency’s Committee for Medicinal Products for Human Use (CHMP).
Fulphila was intended to be used to reduce the duration of neutropenia and the incidence of febrile neutropenia in adults receiving cytotoxic therapy for malignancy (except chronic myeloid leukemia and myelodysplastic syndromes).
Fulphila was intended to be highly similar to Neulasta, a solution for injection that contains the active substance pegfilgrastim.
To support the application for Fulphila, Mylan S.A.S. presented results of studies designed to show that Fulphila is highly similar to Neulasta in terms of chemical structure, purity, mechanism, safety, effectiveness, and immunogenicity.
Mylan S.A.S withdrew the application for Fulphila after the CHMP had evaluated the initial documentation the company provided on the drug and formulated a list of questions. The CHMP was assessing the company’s responses to the questions when the application was withdrawn.
At the time of the withdrawal, the CHMP had some concerns and was of the provisional opinion that Fulphila could not have been approved.
One of the CHMP’s main concerns was the lack of a certificate of Good Manufacturing Practice for the manufacturing site of the product. Other concerns related to the description of the manufacturing process, the control of impurities in the active substance, and the sterilization of the final product.
In a letter to the European Medicines Agency, Mylan S.A.S said it withdrew the application for Fulphila because a Good Manufacturing Practice certificate for the manufacturing site could not be obtained in the time available.
The application withdrawal does not impact ongoing clinical trials of Fulphila, and there are no compassionate use programs for the drug.
Mylan S.A.S said it plans to resubmit the application for Fulphila as soon as possible. The company is working to ensure “inspection readiness” at the Fulphila manufacturing site by October 2017. ![]()
Duke’s Criteria help guide echocardiography decision in suspected infective endocarditis
CHICAGO – In screening children with suspected endocarditis, clinicians should first apply Duke’s Criteria to assess risk and guide the decision of whether to order an echocardiogram.
Nancy Hua, DO, a first-year pediatric cardiology fellow at Doernbecher Children’s Hospital/ Oregon Health & Science University in Portland, and fellow researchers evaluated the appropriateness and effectiveness of 300 echocardiograms ordered at their institution over 10 years for suspected infective endocarditis in pediatric patients. Patients were younger than 21 years and all had structurally normal hearts. “We did notice there have been a lot of people ordering echocardiograms because of a concern about infective endocarditis,” Dr. Hua said. “But echocardiograms are expensive and require the patients to lay still for half an hour to an hour with a probe on their chest to obtain the images.”

A total of 10, or 3%, of echocardiograms were positive for a mass, abscess, thrombus, or new valve regurgitation consistent with infective endocarditis. Eight of the 300 patients screened with echocardiography were diagnosed with infective endocarditis. Of the two remaining patients, one had negative blood cultures, so clinicians did not administer antibiotics or diagnose infective endocarditis. The other patient presented with a new, mild mitral valve regurgitation; however, the echocardiography results appeared within normal limits, according to a cardiology consultation. This patient was ultimately treated for bacteremia.
“If the patient doesn’t really have the appropriate risk factors [for infective endocarditis], do they really need to go for this echo?” Dr. Hua asked here at the annual meeting of the American Academy of Pediatrics. The researchers suggest considering an echocardiogram when a patient has two or more persistent positive blood cultures, persistent fever on antibiotic therapy, and/or a new pathologic murmur.
Dr. Hua and her colleagues plan to launch a quality improvement project to target more appropriate echocardiogram use. Specifically, they are developing an elecronic health record order set to remind clinicians about appropriate criteria for ordering the imaging when they suspect infective endocarditis. “Does the patient fulfill the criteria? If the answer is no, they can reconsider if they want to order the echo at that point. Or if they are still worried for any reason at all, they can consult pediatric cardiology.” She added, “If we think it’s still warranted, we’ll order the echo ourselves.”
Dr. Hua reported having no financial disclosures.
CHICAGO – In screening children with suspected endocarditis, clinicians should first apply Duke’s Criteria to assess risk and guide the decision of whether to order an echocardiogram.
Nancy Hua, DO, a first-year pediatric cardiology fellow at Doernbecher Children’s Hospital/ Oregon Health & Science University in Portland, and fellow researchers evaluated the appropriateness and effectiveness of 300 echocardiograms ordered at their institution over 10 years for suspected infective endocarditis in pediatric patients. Patients were younger than 21 years and all had structurally normal hearts. “We did notice there have been a lot of people ordering echocardiograms because of a concern about infective endocarditis,” Dr. Hua said. “But echocardiograms are expensive and require the patients to lay still for half an hour to an hour with a probe on their chest to obtain the images.”
A total of 10, or 3%, of echocardiograms were positive for a mass, abscess, thrombus, or new valve regurgitation consistent with infective endocarditis. Eight of the 300 patients screened with echocardiography were diagnosed with infective endocarditis. Of the two remaining patients, one had negative blood cultures, so clinicians did not administer antibiotics or diagnose infective endocarditis. The other patient presented with a new, mild mitral valve regurgitation; however, the echocardiography results appeared within normal limits, according to a cardiology consultation. This patient was ultimately treated for bacteremia.
“If the patient doesn’t really have the appropriate risk factors [for infective endocarditis], do they really need to go for this echo?” Dr. Hua asked here at the annual meeting of the American Academy of Pediatrics. The researchers suggest considering an echocardiogram when a patient has two or more persistent positive blood cultures, persistent fever on antibiotic therapy, and/or a new pathologic murmur.
Dr. Hua and her colleagues plan to launch a quality improvement project to target more appropriate echocardiogram use. Specifically, they are developing an elecronic health record order set to remind clinicians about appropriate criteria for ordering the imaging when they suspect infective endocarditis. “Does the patient fulfill the criteria? If the answer is no, they can reconsider if they want to order the echo at that point. Or if they are still worried for any reason at all, they can consult pediatric cardiology.” She added, “If we think it’s still warranted, we’ll order the echo ourselves.”
Dr. Hua reported having no financial disclosures.
CHICAGO – In screening children with suspected endocarditis, clinicians should first apply Duke’s Criteria to assess risk and guide the decision of whether to order an echocardiogram.
Nancy Hua, DO, a first-year pediatric cardiology fellow at Doernbecher Children’s Hospital/ Oregon Health & Science University in Portland, and fellow researchers evaluated the appropriateness and effectiveness of 300 echocardiograms ordered at their institution over 10 years for suspected infective endocarditis in pediatric patients. Patients were younger than 21 years and all had structurally normal hearts. “We did notice there have been a lot of people ordering echocardiograms because of a concern about infective endocarditis,” Dr. Hua said. “But echocardiograms are expensive and require the patients to lay still for half an hour to an hour with a probe on their chest to obtain the images.”
A total of 10, or 3%, of echocardiograms were positive for a mass, abscess, thrombus, or new valve regurgitation consistent with infective endocarditis. Eight of the 300 patients screened with echocardiography were diagnosed with infective endocarditis. Of the two remaining patients, one had negative blood cultures, so clinicians did not administer antibiotics or diagnose infective endocarditis. The other patient presented with a new, mild mitral valve regurgitation; however, the echocardiography results appeared within normal limits, according to a cardiology consultation. This patient was ultimately treated for bacteremia.
“If the patient doesn’t really have the appropriate risk factors [for infective endocarditis], do they really need to go for this echo?” Dr. Hua asked here at the annual meeting of the American Academy of Pediatrics. The researchers suggest considering an echocardiogram when a patient has two or more persistent positive blood cultures, persistent fever on antibiotic therapy, and/or a new pathologic murmur.
Dr. Hua and her colleagues plan to launch a quality improvement project to target more appropriate echocardiogram use. Specifically, they are developing an elecronic health record order set to remind clinicians about appropriate criteria for ordering the imaging when they suspect infective endocarditis. “Does the patient fulfill the criteria? If the answer is no, they can reconsider if they want to order the echo at that point. Or if they are still worried for any reason at all, they can consult pediatric cardiology.” She added, “If we think it’s still warranted, we’ll order the echo ourselves.”
Dr. Hua reported having no financial disclosures.
AT AAP 2017
Key clinical point: Duke’s Criteria should be used to establish whether echocardiograms is needed to screen for infective endocarditis.
Major finding: A total 3% of echocardiograms were positive for mass, abscess, thrombus, or new valve regurgitation consistent with infective endocarditis.
Data source: Review of 300 patients who had an echocardiogram for suspected infective endocarditis between 2005 and 2015.
Disclosures: Dr. Hua reported having no financial disclosures.
