User login
Laser tattoo removal clinic closures: Are patients getting scammed?
A patient came into my office recently and informed me that a well-known laser tattoo removal clinic in Los Angeles that she had gone to for years had suddenly shut down. All locations closed. No one answered the phone. No information about the remainder of the money in the package she bought. After researching online, she found that the Better Business Bureau did not yet have much information but doubted she would get her money back. This particular patient had not gone to the clinic in more than a year but had a residual tattoo and had looked into returning for more treatments and using the remainder of her package. She was one of the lucky ones. Other online discussion groups had entries from numerous patients who paid for packages (some costing thousands of dollars) for multiple laser treatments. Some had paid recently and had not yet received a single treatment and were left with no information about their options or where their money had gone.

It turns out in Southern California and Texas. No notification was given to the patients in advance. Nor was any notification given to some of the staff members, who complained online that they suddenly lost their jobs. Ironically, the same clinics had posted a letter online several years ago honoring discounted first treatments and packages for patients of a different laser tattoo clinic that had suddenly shut down.
So how often is this happening? Are all these clinics owned by the same people? And what can our specialty do to protect patients from being scammed and, for that matter, receiving treatment from professionals who may not be properly trained or experienced to provide that treatment?
In a world in which insurance reimbursements keep getting cut, more and more medical professionals – physicians and nonphysicians alike – are looking to fee-for-service procedures and practice models for increasing income. Sometimes, this may involve physicians delegating procedures to nonphysicians. Franchised clinics open up with a physician to “oversee” the clinic, while extenders often perform the procedures (many times without the physician present). Physicians who are neither trained nor specialized to do certain cosmetic procedures start to perform them. Patients get used to receiving treatments from nonphysicians or from physicians who are not specialized to perform cosmetic procedures, and then may devalue the procedure, feeling it’s unnecessary for a physician or a specialized physician to perform it.


Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
A patient came into my office recently and informed me that a well-known laser tattoo removal clinic in Los Angeles that she had gone to for years had suddenly shut down. All locations closed. No one answered the phone. No information about the remainder of the money in the package she bought. After researching online, she found that the Better Business Bureau did not yet have much information but doubted she would get her money back. This particular patient had not gone to the clinic in more than a year but had a residual tattoo and had looked into returning for more treatments and using the remainder of her package. She was one of the lucky ones. Other online discussion groups had entries from numerous patients who paid for packages (some costing thousands of dollars) for multiple laser treatments. Some had paid recently and had not yet received a single treatment and were left with no information about their options or where their money had gone.
It turns out in Southern California and Texas. No notification was given to the patients in advance. Nor was any notification given to some of the staff members, who complained online that they suddenly lost their jobs. Ironically, the same clinics had posted a letter online several years ago honoring discounted first treatments and packages for patients of a different laser tattoo clinic that had suddenly shut down.
So how often is this happening? Are all these clinics owned by the same people? And what can our specialty do to protect patients from being scammed and, for that matter, receiving treatment from professionals who may not be properly trained or experienced to provide that treatment?
In a world in which insurance reimbursements keep getting cut, more and more medical professionals – physicians and nonphysicians alike – are looking to fee-for-service procedures and practice models for increasing income. Sometimes, this may involve physicians delegating procedures to nonphysicians. Franchised clinics open up with a physician to “oversee” the clinic, while extenders often perform the procedures (many times without the physician present). Physicians who are neither trained nor specialized to do certain cosmetic procedures start to perform them. Patients get used to receiving treatments from nonphysicians or from physicians who are not specialized to perform cosmetic procedures, and then may devalue the procedure, feeling it’s unnecessary for a physician or a specialized physician to perform it.
Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
A patient came into my office recently and informed me that a well-known laser tattoo removal clinic in Los Angeles that she had gone to for years had suddenly shut down. All locations closed. No one answered the phone. No information about the remainder of the money in the package she bought. After researching online, she found that the Better Business Bureau did not yet have much information but doubted she would get her money back. This particular patient had not gone to the clinic in more than a year but had a residual tattoo and had looked into returning for more treatments and using the remainder of her package. She was one of the lucky ones. Other online discussion groups had entries from numerous patients who paid for packages (some costing thousands of dollars) for multiple laser treatments. Some had paid recently and had not yet received a single treatment and were left with no information about their options or where their money had gone.
It turns out in Southern California and Texas. No notification was given to the patients in advance. Nor was any notification given to some of the staff members, who complained online that they suddenly lost their jobs. Ironically, the same clinics had posted a letter online several years ago honoring discounted first treatments and packages for patients of a different laser tattoo clinic that had suddenly shut down.
So how often is this happening? Are all these clinics owned by the same people? And what can our specialty do to protect patients from being scammed and, for that matter, receiving treatment from professionals who may not be properly trained or experienced to provide that treatment?
In a world in which insurance reimbursements keep getting cut, more and more medical professionals – physicians and nonphysicians alike – are looking to fee-for-service procedures and practice models for increasing income. Sometimes, this may involve physicians delegating procedures to nonphysicians. Franchised clinics open up with a physician to “oversee” the clinic, while extenders often perform the procedures (many times without the physician present). Physicians who are neither trained nor specialized to do certain cosmetic procedures start to perform them. Patients get used to receiving treatments from nonphysicians or from physicians who are not specialized to perform cosmetic procedures, and then may devalue the procedure, feeling it’s unnecessary for a physician or a specialized physician to perform it.
Dr. Wesley and Dr. Talakoub are co-contributors to this column. Dr. Wesley practices dermatology in Beverly Hills, Calif. Dr. Talakoub is in private practice in McLean, Va. This month’s column is by Dr. Wesley. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
SGLT2 inhibitors cut cardiovascular outcomes regardless of region
ORLANDO – Cardiovascular outcomes were significantly more favorable with sodium glucose cotransporter-2 inhibitors compared with other glucose-lowering drugs, according to data from more than 400,000 type 2 diabetes patients in the Middle East, Asia Pacific, and North America.
Data on cardiovascular outcomes from diabetes treatments in patients outside the United States and Europe are limited, said Mikhail Kosiborod, MD, of Saint Luke’s Mid-America Heart Institute and University of Missouri–Kansas City.
In fact, most patients with type 2 diabetes reside in the Asia-Pacific and the Middle East, he said in a presentation at the annual meeting of the American College of Cardiology.
Dr. Kosiborod was involved in a previous large pharmaco-epidemiologic study known as the Comparative Effectiveness of Cardiovascular Outcomes in New Users of Sodium-Glucose Cotransporter-2 Inhibitors (CVD-REAL), that showed SGLT2 inhibitor effects in a broad population of type 2 diabetes patients, but that study included only patients from Europe and North America, and focused on just two outcomes: all-cause mortality and hospitalization for heart failure.
The study population included adults aged 18 years and older diagnosed with type 2 diabetes; a total of 235,064 treated with SGLT2 inhibitors and 235,064 treated with other GLDs. The participants were selected from national databases in Australia, Canada, Israel, Japan, Singapore, and South Korea. Individuals with type 1 diabetes or gestational diabetes were excluded from the study.
Outcomes comparing SGLT2 inhibitors and other GLDs included all-cause death, all-cause death or hospitalization for heart failure, hospitalization for heart failure, myocardial infarction, and stroke. Baseline patient characteristics were similar between the two treatment groups. Exposure time for patients in the SGLT2-inhibitor group was highest by far for dapagliflozin (75%), followed by empagliflozin, ipragliflozin, canagliflozin, tofogliflozin, and luseogliflozin at 9%, 8%, 4%, 3%, and 1%, respectively. (Ipragliflozin, tofogliflozin, and luseogliflozin are approved only in Japan.)
The researchers identified 5,216 deaths from any cause. Overall, treatment with an SGLT2 inhibitor was associated with significantly lower risks of death (hazard ratio, 0.51), hospitalization for heart failure (HR, 0.64), death or hospitalization for heart failure (HR, 0.60), myocardial infarction (HR, 0.81), and stroke (HR, 0.68).
The findings remained consistent across countries and patient subgroups, and in patients with and without cardiovascular disease, Dr. Kosiborod noted.
The results were limited by several factors, including the observational nature of the study and incomplete mortality data, Dr. Kosiborod said. However, the results suggest that the SGLT2 inhibitors’ impacts on cardiovascular outcomes persist across categories of ethnicity, geography, and cardiovascular disease.
AstraZeneca supported the study. Dr. Kosiborod disclosed relationships with multiple companies including AstraZeneca, Boehringer Ingelheim, Janssen, Merck, Novartis, Novo Nordisk, Glytec, and ZS Pharma. The findings were simultaneously published online (J Am Coll Cardiol. 2018 Mar 11. doi: 10.1016/j.jacc.2018.03.009).
SOURCE: Kosiborod M. ACC 2018.
ORLANDO – Cardiovascular outcomes were significantly more favorable with sodium glucose cotransporter-2 inhibitors compared with other glucose-lowering drugs, according to data from more than 400,000 type 2 diabetes patients in the Middle East, Asia Pacific, and North America.
Data on cardiovascular outcomes from diabetes treatments in patients outside the United States and Europe are limited, said Mikhail Kosiborod, MD, of Saint Luke’s Mid-America Heart Institute and University of Missouri–Kansas City.
In fact, most patients with type 2 diabetes reside in the Asia-Pacific and the Middle East, he said in a presentation at the annual meeting of the American College of Cardiology.
Dr. Kosiborod was involved in a previous large pharmaco-epidemiologic study known as the Comparative Effectiveness of Cardiovascular Outcomes in New Users of Sodium-Glucose Cotransporter-2 Inhibitors (CVD-REAL), that showed SGLT2 inhibitor effects in a broad population of type 2 diabetes patients, but that study included only patients from Europe and North America, and focused on just two outcomes: all-cause mortality and hospitalization for heart failure.
The study population included adults aged 18 years and older diagnosed with type 2 diabetes; a total of 235,064 treated with SGLT2 inhibitors and 235,064 treated with other GLDs. The participants were selected from national databases in Australia, Canada, Israel, Japan, Singapore, and South Korea. Individuals with type 1 diabetes or gestational diabetes were excluded from the study.
Outcomes comparing SGLT2 inhibitors and other GLDs included all-cause death, all-cause death or hospitalization for heart failure, hospitalization for heart failure, myocardial infarction, and stroke. Baseline patient characteristics were similar between the two treatment groups. Exposure time for patients in the SGLT2-inhibitor group was highest by far for dapagliflozin (75%), followed by empagliflozin, ipragliflozin, canagliflozin, tofogliflozin, and luseogliflozin at 9%, 8%, 4%, 3%, and 1%, respectively. (Ipragliflozin, tofogliflozin, and luseogliflozin are approved only in Japan.)
The researchers identified 5,216 deaths from any cause. Overall, treatment with an SGLT2 inhibitor was associated with significantly lower risks of death (hazard ratio, 0.51), hospitalization for heart failure (HR, 0.64), death or hospitalization for heart failure (HR, 0.60), myocardial infarction (HR, 0.81), and stroke (HR, 0.68).
The findings remained consistent across countries and patient subgroups, and in patients with and without cardiovascular disease, Dr. Kosiborod noted.
The results were limited by several factors, including the observational nature of the study and incomplete mortality data, Dr. Kosiborod said. However, the results suggest that the SGLT2 inhibitors’ impacts on cardiovascular outcomes persist across categories of ethnicity, geography, and cardiovascular disease.
AstraZeneca supported the study. Dr. Kosiborod disclosed relationships with multiple companies including AstraZeneca, Boehringer Ingelheim, Janssen, Merck, Novartis, Novo Nordisk, Glytec, and ZS Pharma. The findings were simultaneously published online (J Am Coll Cardiol. 2018 Mar 11. doi: 10.1016/j.jacc.2018.03.009).
SOURCE: Kosiborod M. ACC 2018.
ORLANDO – Cardiovascular outcomes were significantly more favorable with sodium glucose cotransporter-2 inhibitors compared with other glucose-lowering drugs, according to data from more than 400,000 type 2 diabetes patients in the Middle East, Asia Pacific, and North America.
Data on cardiovascular outcomes from diabetes treatments in patients outside the United States and Europe are limited, said Mikhail Kosiborod, MD, of Saint Luke’s Mid-America Heart Institute and University of Missouri–Kansas City.
In fact, most patients with type 2 diabetes reside in the Asia-Pacific and the Middle East, he said in a presentation at the annual meeting of the American College of Cardiology.
Dr. Kosiborod was involved in a previous large pharmaco-epidemiologic study known as the Comparative Effectiveness of Cardiovascular Outcomes in New Users of Sodium-Glucose Cotransporter-2 Inhibitors (CVD-REAL), that showed SGLT2 inhibitor effects in a broad population of type 2 diabetes patients, but that study included only patients from Europe and North America, and focused on just two outcomes: all-cause mortality and hospitalization for heart failure.
The study population included adults aged 18 years and older diagnosed with type 2 diabetes; a total of 235,064 treated with SGLT2 inhibitors and 235,064 treated with other GLDs. The participants were selected from national databases in Australia, Canada, Israel, Japan, Singapore, and South Korea. Individuals with type 1 diabetes or gestational diabetes were excluded from the study.
Outcomes comparing SGLT2 inhibitors and other GLDs included all-cause death, all-cause death or hospitalization for heart failure, hospitalization for heart failure, myocardial infarction, and stroke. Baseline patient characteristics were similar between the two treatment groups. Exposure time for patients in the SGLT2-inhibitor group was highest by far for dapagliflozin (75%), followed by empagliflozin, ipragliflozin, canagliflozin, tofogliflozin, and luseogliflozin at 9%, 8%, 4%, 3%, and 1%, respectively. (Ipragliflozin, tofogliflozin, and luseogliflozin are approved only in Japan.)
The researchers identified 5,216 deaths from any cause. Overall, treatment with an SGLT2 inhibitor was associated with significantly lower risks of death (hazard ratio, 0.51), hospitalization for heart failure (HR, 0.64), death or hospitalization for heart failure (HR, 0.60), myocardial infarction (HR, 0.81), and stroke (HR, 0.68).
The findings remained consistent across countries and patient subgroups, and in patients with and without cardiovascular disease, Dr. Kosiborod noted.
The results were limited by several factors, including the observational nature of the study and incomplete mortality data, Dr. Kosiborod said. However, the results suggest that the SGLT2 inhibitors’ impacts on cardiovascular outcomes persist across categories of ethnicity, geography, and cardiovascular disease.
AstraZeneca supported the study. Dr. Kosiborod disclosed relationships with multiple companies including AstraZeneca, Boehringer Ingelheim, Janssen, Merck, Novartis, Novo Nordisk, Glytec, and ZS Pharma. The findings were simultaneously published online (J Am Coll Cardiol. 2018 Mar 11. doi: 10.1016/j.jacc.2018.03.009).
SOURCE: Kosiborod M. ACC 2018.
REPORTING FROM ACC 18
Key clinical point: SGLT2 inhibitor use was linked to a lower risk of all-cause death, hospitalization for heart failure, myocardial infarction, and stroke in a large, multinational study of adults with type 2 diabetes.
Major finding: All-cause mortality was significantly lower in patients treated with an SGLT2 inhibitor compared with other glucose lowering drugs (HR 0.51).
Study details: The data come from more than 400,000 adults with type 2 diabetes via databases in the Middle East, Asia Pacific, and North America.
Disclosures: AstraZeneca supported the study. Dr. Kosiborod disclosed relationships with AstraZeneca, Boehringer Ingelheim, Janssen, Merck, Novartis, Novo Nordisk, Glytec, and ZS Pharma.
Source: Kosiborod M. ACC 2018.
Congress tackles the opioid epidemic. But how much will it help?
The nation’s opioid epidemic has been called today’s version of the 1980s AIDS crisis.
In a New Hampshire speech on March 19, President Donald Trump pushed for a tougher federal response, emphasizing a tough-on-crime approach for drug dealers and more funding for treatment. And Congress is upping the ante, via a series of hearings – including one scheduled to last March 21-22 – to study legislation that might tackle the unyielding scourge, which has cost an estimated $1 trillion in premature deaths, health care costs, and lost wages since 2001.
Dr. Leana Wen, an emergency physician by training and the health commissioner for hard-hit Baltimore, said Capitol Hill has to help communities at risk of becoming overwhelmed.
“We haven’t seen the peak of the epidemic. We are seeing the numbers climb year after year,” she said.
Provisional data from the Centers for Disease Control and Prevention suggest that almost 45,000 Americans died from opioid overdoses in the 12-month period ending July 2017, up from about 38,000 in the previous cycle. (Those data are likely to change, since many death certificates have not yet been reported to the CDC.)
“It’s not going to get any better unless we take dramatic action,” Dr. Wen said.
And the time for most meaningful change could be dwindling. Advocates say what they need most is money, which would most likely come through the government spending bill that’s due March 23. But they aren’t holding their breath.
Show me the money
The federal budget deal, which was signed into law in early February, promised $6 billion over 2 years for initiatives to fight opioid abuse. Congress is still figuring out how to divvy up those funds. The blueprint is expected to be included in the spending bill this week.
In February, a bipartisan group of senators introduced a bill that would add another $1 billion in funding to support expanded treatment and also limit clinicians to prescribing no more than 3 days’ worth of opioids at a time.
That legislation is likely to have wide support in the Senate, but its path through the House is less certain.
This cash infusion is still not going to be enough, predicted Daniel Raymond, policy director for the Harm Reduction Coalition, a national organization that works on overdose prevention.
“It’s not clear whether there’s a real appetite to go as far as we need to see Congress go,” he said. “To have a fighting chance, we need a long-term commitment of at least $10 billion per year.” Academic experts said that assessment sounded on target.
The figure is more than 3 times what’s allocated in the budget and 10 times what even the new Senate bill would provide, and far beyond the spending levels put forth by any previous packages to fight the opioid epidemic.
The difficulty in getting funding – and a key reason why the bipartisan Senate bill might stall in the House – in part goes to the heart of Republicans’ philosophy about budgeting.
The GOP, which controls both chambers of Congress, has “always been very focused on pay-fors,” said a Republican aide to the House Energy and Commerce Committee, explaining that new funding is generally expected to be accompanied by cuts in current expenditures so that overall government spending doesn’t rise. And that could limit how much money lawmakers are ultimately willing to commit to fight opioid abuse.
Some observers worry this notion is pound-foolish.
“We have an enormous set of costs ahead of us if we don’t invest now,” said Dr. Traci Green, an associate professor of emergency medicine and community health science at Boston University, who has extensively researched the epidemic.
Ahead in Congress
Meanwhile, the House could take up its version of a separate Senate-passed proposal designed to, in certain cases, make more prominent any opioid history in a patient’s medical record. The idea is to prevent doctors from prescribing opioids to at-risk patients.
In addition, the House’s Energy and Commerce Committee in late February held a hearing focused on “enforcement” – discussing, for instance, giving the federal Drug Enforcement Administration more power in drug trafficking, and whether to treat fentanyl, a particularly potent synthetic opioid, as a controlled substance. The hearings March 21-22 will tackle a slew of public health–oriented bills, such as making sure overdose patients in the emergency room get appropriate medication and treatment upon discharge, or expanding access to buprenorphine, which is used to treat addiction.
And the House Ways and Means Committee, which has jurisdiction over Medicare – the federal insurance plan for seniors and disabled people – is working to develop strategies that limit access to opioids and make treatment more available.
These are some promising ideas, Mr. Raymond said, but it’s still “playing catch-up. … The big gap is the money, and the broader vision.”
This flurry of activity comes after Congress in 2016 passed two laws directly dealing with addiction and substance abuse disorders, the Comprehensive Addiction and Recovery Act and the 21st Century Cures Act. CARA promised $181 million – although it didn’t appropriate those dollars – while the Cures Act provided $1 billion over 2 years.
It’s playing out against the backdrop of steady policy tensions.
The Trump administration, which in October declared the opioid epidemic a public health crisis, has repeatedly pushed a more punitive approach, such as harsher sentences for drug trafficking, including the death penalty, and establishing mandatory minimum sentences. That emphasis, experts said, detracts from other parts of the plan that might highlight, say, addiction treatment.
Instead, those experts emphasized treatment and prevention as well as “harm reduction” ideas such as providing more overdose-antidote medication and funding programs like syringe exchanges.
They say focusing on punishment has been ineffective in the past and neglects the heart of the issue.
Certainly, curbing the flow of illegal drugs is important, Dr. Wen said. But it’s insufficient by itself. And the size of the problem means lawmakers need to provide quicker, more direct aid – not just proposals that tinker “around the edges.”
“We would never refuse any funding, because we need it desperately,” she said. “But ask us what we need.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The nation’s opioid epidemic has been called today’s version of the 1980s AIDS crisis.
In a New Hampshire speech on March 19, President Donald Trump pushed for a tougher federal response, emphasizing a tough-on-crime approach for drug dealers and more funding for treatment. And Congress is upping the ante, via a series of hearings – including one scheduled to last March 21-22 – to study legislation that might tackle the unyielding scourge, which has cost an estimated $1 trillion in premature deaths, health care costs, and lost wages since 2001.
Dr. Leana Wen, an emergency physician by training and the health commissioner for hard-hit Baltimore, said Capitol Hill has to help communities at risk of becoming overwhelmed.
“We haven’t seen the peak of the epidemic. We are seeing the numbers climb year after year,” she said.
Provisional data from the Centers for Disease Control and Prevention suggest that almost 45,000 Americans died from opioid overdoses in the 12-month period ending July 2017, up from about 38,000 in the previous cycle. (Those data are likely to change, since many death certificates have not yet been reported to the CDC.)
“It’s not going to get any better unless we take dramatic action,” Dr. Wen said.
And the time for most meaningful change could be dwindling. Advocates say what they need most is money, which would most likely come through the government spending bill that’s due March 23. But they aren’t holding their breath.
Show me the money
The federal budget deal, which was signed into law in early February, promised $6 billion over 2 years for initiatives to fight opioid abuse. Congress is still figuring out how to divvy up those funds. The blueprint is expected to be included in the spending bill this week.
In February, a bipartisan group of senators introduced a bill that would add another $1 billion in funding to support expanded treatment and also limit clinicians to prescribing no more than 3 days’ worth of opioids at a time.
That legislation is likely to have wide support in the Senate, but its path through the House is less certain.
This cash infusion is still not going to be enough, predicted Daniel Raymond, policy director for the Harm Reduction Coalition, a national organization that works on overdose prevention.
“It’s not clear whether there’s a real appetite to go as far as we need to see Congress go,” he said. “To have a fighting chance, we need a long-term commitment of at least $10 billion per year.” Academic experts said that assessment sounded on target.
The figure is more than 3 times what’s allocated in the budget and 10 times what even the new Senate bill would provide, and far beyond the spending levels put forth by any previous packages to fight the opioid epidemic.
The difficulty in getting funding – and a key reason why the bipartisan Senate bill might stall in the House – in part goes to the heart of Republicans’ philosophy about budgeting.
The GOP, which controls both chambers of Congress, has “always been very focused on pay-fors,” said a Republican aide to the House Energy and Commerce Committee, explaining that new funding is generally expected to be accompanied by cuts in current expenditures so that overall government spending doesn’t rise. And that could limit how much money lawmakers are ultimately willing to commit to fight opioid abuse.
Some observers worry this notion is pound-foolish.
“We have an enormous set of costs ahead of us if we don’t invest now,” said Dr. Traci Green, an associate professor of emergency medicine and community health science at Boston University, who has extensively researched the epidemic.
Ahead in Congress
Meanwhile, the House could take up its version of a separate Senate-passed proposal designed to, in certain cases, make more prominent any opioid history in a patient’s medical record. The idea is to prevent doctors from prescribing opioids to at-risk patients.
In addition, the House’s Energy and Commerce Committee in late February held a hearing focused on “enforcement” – discussing, for instance, giving the federal Drug Enforcement Administration more power in drug trafficking, and whether to treat fentanyl, a particularly potent synthetic opioid, as a controlled substance. The hearings March 21-22 will tackle a slew of public health–oriented bills, such as making sure overdose patients in the emergency room get appropriate medication and treatment upon discharge, or expanding access to buprenorphine, which is used to treat addiction.
And the House Ways and Means Committee, which has jurisdiction over Medicare – the federal insurance plan for seniors and disabled people – is working to develop strategies that limit access to opioids and make treatment more available.
These are some promising ideas, Mr. Raymond said, but it’s still “playing catch-up. … The big gap is the money, and the broader vision.”
This flurry of activity comes after Congress in 2016 passed two laws directly dealing with addiction and substance abuse disorders, the Comprehensive Addiction and Recovery Act and the 21st Century Cures Act. CARA promised $181 million – although it didn’t appropriate those dollars – while the Cures Act provided $1 billion over 2 years.
It’s playing out against the backdrop of steady policy tensions.
The Trump administration, which in October declared the opioid epidemic a public health crisis, has repeatedly pushed a more punitive approach, such as harsher sentences for drug trafficking, including the death penalty, and establishing mandatory minimum sentences. That emphasis, experts said, detracts from other parts of the plan that might highlight, say, addiction treatment.
Instead, those experts emphasized treatment and prevention as well as “harm reduction” ideas such as providing more overdose-antidote medication and funding programs like syringe exchanges.
They say focusing on punishment has been ineffective in the past and neglects the heart of the issue.
Certainly, curbing the flow of illegal drugs is important, Dr. Wen said. But it’s insufficient by itself. And the size of the problem means lawmakers need to provide quicker, more direct aid – not just proposals that tinker “around the edges.”
“We would never refuse any funding, because we need it desperately,” she said. “But ask us what we need.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
The nation’s opioid epidemic has been called today’s version of the 1980s AIDS crisis.
In a New Hampshire speech on March 19, President Donald Trump pushed for a tougher federal response, emphasizing a tough-on-crime approach for drug dealers and more funding for treatment. And Congress is upping the ante, via a series of hearings – including one scheduled to last March 21-22 – to study legislation that might tackle the unyielding scourge, which has cost an estimated $1 trillion in premature deaths, health care costs, and lost wages since 2001.
Dr. Leana Wen, an emergency physician by training and the health commissioner for hard-hit Baltimore, said Capitol Hill has to help communities at risk of becoming overwhelmed.
“We haven’t seen the peak of the epidemic. We are seeing the numbers climb year after year,” she said.
Provisional data from the Centers for Disease Control and Prevention suggest that almost 45,000 Americans died from opioid overdoses in the 12-month period ending July 2017, up from about 38,000 in the previous cycle. (Those data are likely to change, since many death certificates have not yet been reported to the CDC.)
“It’s not going to get any better unless we take dramatic action,” Dr. Wen said.
And the time for most meaningful change could be dwindling. Advocates say what they need most is money, which would most likely come through the government spending bill that’s due March 23. But they aren’t holding their breath.
Show me the money
The federal budget deal, which was signed into law in early February, promised $6 billion over 2 years for initiatives to fight opioid abuse. Congress is still figuring out how to divvy up those funds. The blueprint is expected to be included in the spending bill this week.
In February, a bipartisan group of senators introduced a bill that would add another $1 billion in funding to support expanded treatment and also limit clinicians to prescribing no more than 3 days’ worth of opioids at a time.
That legislation is likely to have wide support in the Senate, but its path through the House is less certain.
This cash infusion is still not going to be enough, predicted Daniel Raymond, policy director for the Harm Reduction Coalition, a national organization that works on overdose prevention.
“It’s not clear whether there’s a real appetite to go as far as we need to see Congress go,” he said. “To have a fighting chance, we need a long-term commitment of at least $10 billion per year.” Academic experts said that assessment sounded on target.
The figure is more than 3 times what’s allocated in the budget and 10 times what even the new Senate bill would provide, and far beyond the spending levels put forth by any previous packages to fight the opioid epidemic.
The difficulty in getting funding – and a key reason why the bipartisan Senate bill might stall in the House – in part goes to the heart of Republicans’ philosophy about budgeting.
The GOP, which controls both chambers of Congress, has “always been very focused on pay-fors,” said a Republican aide to the House Energy and Commerce Committee, explaining that new funding is generally expected to be accompanied by cuts in current expenditures so that overall government spending doesn’t rise. And that could limit how much money lawmakers are ultimately willing to commit to fight opioid abuse.
Some observers worry this notion is pound-foolish.
“We have an enormous set of costs ahead of us if we don’t invest now,” said Dr. Traci Green, an associate professor of emergency medicine and community health science at Boston University, who has extensively researched the epidemic.
Ahead in Congress
Meanwhile, the House could take up its version of a separate Senate-passed proposal designed to, in certain cases, make more prominent any opioid history in a patient’s medical record. The idea is to prevent doctors from prescribing opioids to at-risk patients.
In addition, the House’s Energy and Commerce Committee in late February held a hearing focused on “enforcement” – discussing, for instance, giving the federal Drug Enforcement Administration more power in drug trafficking, and whether to treat fentanyl, a particularly potent synthetic opioid, as a controlled substance. The hearings March 21-22 will tackle a slew of public health–oriented bills, such as making sure overdose patients in the emergency room get appropriate medication and treatment upon discharge, or expanding access to buprenorphine, which is used to treat addiction.
And the House Ways and Means Committee, which has jurisdiction over Medicare – the federal insurance plan for seniors and disabled people – is working to develop strategies that limit access to opioids and make treatment more available.
These are some promising ideas, Mr. Raymond said, but it’s still “playing catch-up. … The big gap is the money, and the broader vision.”
This flurry of activity comes after Congress in 2016 passed two laws directly dealing with addiction and substance abuse disorders, the Comprehensive Addiction and Recovery Act and the 21st Century Cures Act. CARA promised $181 million – although it didn’t appropriate those dollars – while the Cures Act provided $1 billion over 2 years.
It’s playing out against the backdrop of steady policy tensions.
The Trump administration, which in October declared the opioid epidemic a public health crisis, has repeatedly pushed a more punitive approach, such as harsher sentences for drug trafficking, including the death penalty, and establishing mandatory minimum sentences. That emphasis, experts said, detracts from other parts of the plan that might highlight, say, addiction treatment.
Instead, those experts emphasized treatment and prevention as well as “harm reduction” ideas such as providing more overdose-antidote medication and funding programs like syringe exchanges.
They say focusing on punishment has been ineffective in the past and neglects the heart of the issue.
Certainly, curbing the flow of illegal drugs is important, Dr. Wen said. But it’s insufficient by itself. And the size of the problem means lawmakers need to provide quicker, more direct aid – not just proposals that tinker “around the edges.”
“We would never refuse any funding, because we need it desperately,” she said. “But ask us what we need.”
Kaiser Health News is a nonprofit news service covering health issues. It is an editorially independent program of the Kaiser Family Foundation that is not affiliated with Kaiser Permanente.
Red meat intake linked to NAFLD risk
Higher dietary intake of red meat and processed meats such as salami may increase the risk of nonalcoholic fatty liver disease and insulin resistance, new research suggests.
In a cross-sectional study, published in the March 20 edition of the Journal of Hepatology, researchers used food-frequency questionnaires to examine red and processed meat consumption in 789 adults aged 40-70 years, including information on cooking methods.
They found that those who reported a total meat intake above the median had a significant 49% higher odds of nonalcoholic fatty liver disease (NAFLD) (95% confidence interval, 1.05-2.13; P = .028) and 63% greater odds of insulin resistance (95% CI, 1.12-2.37, P = .011), even after adjustment for potential confounders such as body mass index, physical activity, smoking, alcohol, and saturated fat and cholesterol intake.
Those whose intake of red and/or processed meat was above the median had a 47% greater odds of NAFLD (P = .031), and a 55% greater odds of insulin resistance (P = .020).
Even when the analysis was limited to nondiabetic participants, the study still showed a significant relationship between higher intake of red and processed meat, and insulin resistance (J Hepatol. 2018 Mar 20. doi: 10.1016/j.jhep.2018.01.015).
“It can be claimed that the harmful association with meat may, at least partially, be related to a generally less healthy diet or lifestyle characterizing people who eat more red or processed meat, rather than a causal effect of meat,” wrote Shira Zelber-Sagi, PhD, of the department of gastroenterology at Tel Aviv Medical Center, and coauthors. “However, in the current study we meticulously adjusted the association with meat for other nutritional and lifestyle parameters to minimize confounding as much as possible.”
There was also a significant association between unhealthy cooking methods such as frying, broiling, and grilling – which are known to increase the quantity of heterocyclic amines (HCA) in the meat – and insulin resistance.
Individuals who ate one or more portions of meat cooked by these methods showed a higher incidence of insulin resistance compared with those who ate fewer than one portion per week (36.00% vs. 22.20%, P = .004). Researchers also used the food-frequency questionnaires to calculate the quantity of participants’ HCA intake, and found a significantly higher odds of insulin resistance in individuals whose HCA intake was above the median.
Even among the 305 individuals with NAFLD, higher total meat intake, and higher red and processed meat intake, the prevalence of insulin resistance was higher.
In this group, high HCA intake and high consumption of meat cooked by the unhealthy methods were associated with a fourfold higher odds of insulin resistance.
“Potential mechanisms for NAFLD may be related to the formation of reactive species during HCA metabolism, which can cause oxidation of lipids, proteins, and nucleic acids, resulting in oxidative stress, cell damage, and loss of biological function,” the authors wrote. “HCAs were also demonstrated to be bioactive in adipocytes in vitro, leading to increased expression of genes related to inflammation, diabetes and cancer risk.”
The authors noted that their findings supported the recommendations in dietary guidelines for cardiometabolic health, which suggest no more than one to two 100-g servings per week of red meat, and no more than one 50-g serving per week of processed meats.
“Although the specific effect of different types of meat and their quantities in NAFLD requires further research, these recommendations may be helpful in the treatment of patients with NAFLD at least in terms of CVD and diabetes prevention, and maybe for NAFLD prevention by reducing insulin resistance.”
The Israeli Ministry of Health supported the study. No conflicts of interest were declared.
SOURCE: Zelber-Sagi S et al. J Hepatol. 2018 Mar 20. doi: 10.1016/j.jhep.2018.01.015.
Higher dietary intake of red meat and processed meats such as salami may increase the risk of nonalcoholic fatty liver disease and insulin resistance, new research suggests.
In a cross-sectional study, published in the March 20 edition of the Journal of Hepatology, researchers used food-frequency questionnaires to examine red and processed meat consumption in 789 adults aged 40-70 years, including information on cooking methods.
They found that those who reported a total meat intake above the median had a significant 49% higher odds of nonalcoholic fatty liver disease (NAFLD) (95% confidence interval, 1.05-2.13; P = .028) and 63% greater odds of insulin resistance (95% CI, 1.12-2.37, P = .011), even after adjustment for potential confounders such as body mass index, physical activity, smoking, alcohol, and saturated fat and cholesterol intake.
Those whose intake of red and/or processed meat was above the median had a 47% greater odds of NAFLD (P = .031), and a 55% greater odds of insulin resistance (P = .020).
Even when the analysis was limited to nondiabetic participants, the study still showed a significant relationship between higher intake of red and processed meat, and insulin resistance (J Hepatol. 2018 Mar 20. doi: 10.1016/j.jhep.2018.01.015).
“It can be claimed that the harmful association with meat may, at least partially, be related to a generally less healthy diet or lifestyle characterizing people who eat more red or processed meat, rather than a causal effect of meat,” wrote Shira Zelber-Sagi, PhD, of the department of gastroenterology at Tel Aviv Medical Center, and coauthors. “However, in the current study we meticulously adjusted the association with meat for other nutritional and lifestyle parameters to minimize confounding as much as possible.”
There was also a significant association between unhealthy cooking methods such as frying, broiling, and grilling – which are known to increase the quantity of heterocyclic amines (HCA) in the meat – and insulin resistance.
Individuals who ate one or more portions of meat cooked by these methods showed a higher incidence of insulin resistance compared with those who ate fewer than one portion per week (36.00% vs. 22.20%, P = .004). Researchers also used the food-frequency questionnaires to calculate the quantity of participants’ HCA intake, and found a significantly higher odds of insulin resistance in individuals whose HCA intake was above the median.
Even among the 305 individuals with NAFLD, higher total meat intake, and higher red and processed meat intake, the prevalence of insulin resistance was higher.
In this group, high HCA intake and high consumption of meat cooked by the unhealthy methods were associated with a fourfold higher odds of insulin resistance.
“Potential mechanisms for NAFLD may be related to the formation of reactive species during HCA metabolism, which can cause oxidation of lipids, proteins, and nucleic acids, resulting in oxidative stress, cell damage, and loss of biological function,” the authors wrote. “HCAs were also demonstrated to be bioactive in adipocytes in vitro, leading to increased expression of genes related to inflammation, diabetes and cancer risk.”
The authors noted that their findings supported the recommendations in dietary guidelines for cardiometabolic health, which suggest no more than one to two 100-g servings per week of red meat, and no more than one 50-g serving per week of processed meats.
“Although the specific effect of different types of meat and their quantities in NAFLD requires further research, these recommendations may be helpful in the treatment of patients with NAFLD at least in terms of CVD and diabetes prevention, and maybe for NAFLD prevention by reducing insulin resistance.”
The Israeli Ministry of Health supported the study. No conflicts of interest were declared.
SOURCE: Zelber-Sagi S et al. J Hepatol. 2018 Mar 20. doi: 10.1016/j.jhep.2018.01.015.
Higher dietary intake of red meat and processed meats such as salami may increase the risk of nonalcoholic fatty liver disease and insulin resistance, new research suggests.
In a cross-sectional study, published in the March 20 edition of the Journal of Hepatology, researchers used food-frequency questionnaires to examine red and processed meat consumption in 789 adults aged 40-70 years, including information on cooking methods.
They found that those who reported a total meat intake above the median had a significant 49% higher odds of nonalcoholic fatty liver disease (NAFLD) (95% confidence interval, 1.05-2.13; P = .028) and 63% greater odds of insulin resistance (95% CI, 1.12-2.37, P = .011), even after adjustment for potential confounders such as body mass index, physical activity, smoking, alcohol, and saturated fat and cholesterol intake.
Those whose intake of red and/or processed meat was above the median had a 47% greater odds of NAFLD (P = .031), and a 55% greater odds of insulin resistance (P = .020).
Even when the analysis was limited to nondiabetic participants, the study still showed a significant relationship between higher intake of red and processed meat, and insulin resistance (J Hepatol. 2018 Mar 20. doi: 10.1016/j.jhep.2018.01.015).
“It can be claimed that the harmful association with meat may, at least partially, be related to a generally less healthy diet or lifestyle characterizing people who eat more red or processed meat, rather than a causal effect of meat,” wrote Shira Zelber-Sagi, PhD, of the department of gastroenterology at Tel Aviv Medical Center, and coauthors. “However, in the current study we meticulously adjusted the association with meat for other nutritional and lifestyle parameters to minimize confounding as much as possible.”
There was also a significant association between unhealthy cooking methods such as frying, broiling, and grilling – which are known to increase the quantity of heterocyclic amines (HCA) in the meat – and insulin resistance.
Individuals who ate one or more portions of meat cooked by these methods showed a higher incidence of insulin resistance compared with those who ate fewer than one portion per week (36.00% vs. 22.20%, P = .004). Researchers also used the food-frequency questionnaires to calculate the quantity of participants’ HCA intake, and found a significantly higher odds of insulin resistance in individuals whose HCA intake was above the median.
Even among the 305 individuals with NAFLD, higher total meat intake, and higher red and processed meat intake, the prevalence of insulin resistance was higher.
In this group, high HCA intake and high consumption of meat cooked by the unhealthy methods were associated with a fourfold higher odds of insulin resistance.
“Potential mechanisms for NAFLD may be related to the formation of reactive species during HCA metabolism, which can cause oxidation of lipids, proteins, and nucleic acids, resulting in oxidative stress, cell damage, and loss of biological function,” the authors wrote. “HCAs were also demonstrated to be bioactive in adipocytes in vitro, leading to increased expression of genes related to inflammation, diabetes and cancer risk.”
The authors noted that their findings supported the recommendations in dietary guidelines for cardiometabolic health, which suggest no more than one to two 100-g servings per week of red meat, and no more than one 50-g serving per week of processed meats.
“Although the specific effect of different types of meat and their quantities in NAFLD requires further research, these recommendations may be helpful in the treatment of patients with NAFLD at least in terms of CVD and diabetes prevention, and maybe for NAFLD prevention by reducing insulin resistance.”
The Israeli Ministry of Health supported the study. No conflicts of interest were declared.
SOURCE: Zelber-Sagi S et al. J Hepatol. 2018 Mar 20. doi: 10.1016/j.jhep.2018.01.015.
FROM JOURNAL OF HEPATOLOGY
Key clinical point: High red meat intake increases the risk of nonalcoholic fatty liver disease.
Major finding: Higher meat intake was associated with a 49% greater odds of NAFLD.
Study details: A cross-sectional study of 789 adults.
Disclosures: The Israeli Ministry of Health supported the study. No conflicts of interest were declared.
Source: Zelber-Sagi S et al. J. Hepatol. 2018. doi: 10.1016/j.jhep.2018.01.015.
FDA approves subcutaneous immunoglobulin treatment for CIDP
The Food and Drug Administration has approved Hizentra as the first subcutaneously administered human immunoglobulin maintenance therapy for adults with chronic inflammatory demyelinating polyneuropathy (CIDP), according to a statement from its manufacturer, CSL Behring.
Immune globulin subcutaneous (human) 20% liquid (Hizentra) was approved at doses of 0.2 and 0.4 g/kg per week because of the strength of the phase 3 PATH (Polyneuropathy and Treatment with Hizentra) clinical trial and the PATH extension study, which is still ongoing. PATH is the largest and longest running randomized study of patients with CIDP. The clinical trial studied the safety, efficacy, and tolerability of the two different doses of the subcutaneous immunoglobulin in 172 patients.
There were markedly lower rates of CIDP relapse or withdrawal for any reason during Hizentra treatment among patients taking a high dose of 0.4 g/kg weekly (39%; P less than .001) and those taking a low dose of 0.2 g/kg weekly (33%; P less than .007), compared with those among patients taking placebo (63%). The adverse reactions that occurred in 5% or more of patients included local infusion-site reactions, headache, diarrhea, fatigue, and upper respiratory tract infections.
The European Commission also recently granted marketing authorization for Hizentra based on the information from the PATH trial.
Hizentra was initially approved in the United States in 2010 for primary immunodeficiency in patients aged 2 years and older.
Since Hizentra is a self-administered drug, it is important for physicians to teach their patients how to properly inject this treatment without hitting a blood vessel. Apart from issues related to self-administration, the risk of thrombosis is also present, which is not uncommon for immune globulin products.
The Food and Drug Administration has approved Hizentra as the first subcutaneously administered human immunoglobulin maintenance therapy for adults with chronic inflammatory demyelinating polyneuropathy (CIDP), according to a statement from its manufacturer, CSL Behring.
Immune globulin subcutaneous (human) 20% liquid (Hizentra) was approved at doses of 0.2 and 0.4 g/kg per week because of the strength of the phase 3 PATH (Polyneuropathy and Treatment with Hizentra) clinical trial and the PATH extension study, which is still ongoing. PATH is the largest and longest running randomized study of patients with CIDP. The clinical trial studied the safety, efficacy, and tolerability of the two different doses of the subcutaneous immunoglobulin in 172 patients.
There were markedly lower rates of CIDP relapse or withdrawal for any reason during Hizentra treatment among patients taking a high dose of 0.4 g/kg weekly (39%; P less than .001) and those taking a low dose of 0.2 g/kg weekly (33%; P less than .007), compared with those among patients taking placebo (63%). The adverse reactions that occurred in 5% or more of patients included local infusion-site reactions, headache, diarrhea, fatigue, and upper respiratory tract infections.
The European Commission also recently granted marketing authorization for Hizentra based on the information from the PATH trial.
Hizentra was initially approved in the United States in 2010 for primary immunodeficiency in patients aged 2 years and older.
Since Hizentra is a self-administered drug, it is important for physicians to teach their patients how to properly inject this treatment without hitting a blood vessel. Apart from issues related to self-administration, the risk of thrombosis is also present, which is not uncommon for immune globulin products.
The Food and Drug Administration has approved Hizentra as the first subcutaneously administered human immunoglobulin maintenance therapy for adults with chronic inflammatory demyelinating polyneuropathy (CIDP), according to a statement from its manufacturer, CSL Behring.
Immune globulin subcutaneous (human) 20% liquid (Hizentra) was approved at doses of 0.2 and 0.4 g/kg per week because of the strength of the phase 3 PATH (Polyneuropathy and Treatment with Hizentra) clinical trial and the PATH extension study, which is still ongoing. PATH is the largest and longest running randomized study of patients with CIDP. The clinical trial studied the safety, efficacy, and tolerability of the two different doses of the subcutaneous immunoglobulin in 172 patients.
There were markedly lower rates of CIDP relapse or withdrawal for any reason during Hizentra treatment among patients taking a high dose of 0.4 g/kg weekly (39%; P less than .001) and those taking a low dose of 0.2 g/kg weekly (33%; P less than .007), compared with those among patients taking placebo (63%). The adverse reactions that occurred in 5% or more of patients included local infusion-site reactions, headache, diarrhea, fatigue, and upper respiratory tract infections.
The European Commission also recently granted marketing authorization for Hizentra based on the information from the PATH trial.
Hizentra was initially approved in the United States in 2010 for primary immunodeficiency in patients aged 2 years and older.
Since Hizentra is a self-administered drug, it is important for physicians to teach their patients how to properly inject this treatment without hitting a blood vessel. Apart from issues related to self-administration, the risk of thrombosis is also present, which is not uncommon for immune globulin products.
Survey: Litigation fears drive response to FDA power morcellator warnings
ORLANDO – A 2014 Food and Drug Administration Safety Communication warning about the risk of disseminating occult cancerous tissue when using power morcellation led to a sharp decline in its use among physicians in a large health care system, a survey and records review showed.

Of 126 ob.gyns. in the Charlotte, N.C., metro area who received the 24-question e-mail survey, 58% responded, and while 75% reported that they always or sometimes used power morcellation prior to receiving the FDA communication, more than 80% reported rarely or never using it after receiving the communication, Gerald Bernard Taylor, MD, reported at the annual scientific meeting of the Society of Gynecologic Surgeons.
Fear of litigation was cited as the reason for the change in practice by 45.7% of ob.gyns., followed by lack of access to power morcellators (34.7%), and concerns about undiagnosed malignancy (11.8%) and patient safety (5.7%), said Dr. Taylor of the Carolinas HealthCare System in Charlotte.
“We also heard from physicians about the guidelines,” he added, referring to informed consent protocols developed by a group of “key opinion leaders in gynecologic oncology and minimally invasive gynecology.” Many institutions developed moratoriums against the use of power morcellation in the wake of the FDA communication, but the Carolinas HealthCare System chose to commission these opinion leaders to address the issue, he explained.
“Interestingly enough, some [survey respondents] were not aware that the guidelines were available. Most (74.6%) thought that they were helpful when they actually reviewed them, and a few said that they were not helpful,” he said, noting that most of those who found the guidelines helpful said they felt that way because the guidelines “provide a standard of care and a possible defense against litigation.”
Analyses with respect to changes in practice after the FDA communication are ongoing but suggest that changes occurred mainly in the approach to myomectomies rather than in hysterectomy routes, Dr. Taylor said.
“We’re looking to see if there was increased use of minilaparotomy, and we are looking at the use of concealed morcellation bags right now,” he said.
The FDA Safety Communication was issued April 17, 2014 and stated that power morcellation used for hysterectomy or myomectomy in women with uterine fibroids “poses a risk of spreading unsuspected cancerous tissue, notably uterine sarcomas, beyond the uterus.”
“Health care providers and patients should carefully consider available alternative treatment options for symptomatic uterine fibroids. Based on currently available information, the FDA discourages the use of laparoscopic power morcellation during hysterectomy or myomectomy for uterine fibroids,” the communication stated.
A Nov. 24, 2014 update stated that “laparoscopic power morcellators are contraindicated for removal of uterine tissue containing suspected fibroids in patients who are peri- or postmenopausal or are candidates for en bloc tissue removal, for example, through the vagina or minilaparotomy incision,” and “in gynecologic surgery in which the tissue to be morcellated is known or suspected to contain malignancy.”
The update also urged manufacturers of new and existing laparoscopic power morcellators to include the contraindications and a boxed warning in their product labeling and recommended that doctors share the information with their patients.
On Dec. 24, 2017, the FDA issued an updated assessment reinforcing their earlier communications. This latest update was based on a review of recent medical studies that, according to the FDA, suggested that “approximately 1 in 225 to 1 in 580 women who undergo surgery (hysterectomy or myomectomy) for presumed benign uterine growths (‘fibroids’) may have ‘occult’ or hidden uterine cancers known as sarcomas.” The FDA also said that “this is generally consistent with the 1 in 350 incidence estimated by the FDA in a 2014 review. The FDA also estimates the rate of occult leiomyosarcoma, a particularly aggressive type of sarcoma, to be approximately 1 in 495 to 1 in 1,100, again in general agreement with our previous assessment of 1 in 498.”
The FDA acknowledged that some health organizations have reported a lower estimate of risk but maintained its findings and recommendations, noting that it will continue to review new and relevant data.
Dr. Taylor reported having no disclosures.
SOURCE: Taylor GB et al. SGS 2018, Oral Poster 19.
ORLANDO – A 2014 Food and Drug Administration Safety Communication warning about the risk of disseminating occult cancerous tissue when using power morcellation led to a sharp decline in its use among physicians in a large health care system, a survey and records review showed.
Of 126 ob.gyns. in the Charlotte, N.C., metro area who received the 24-question e-mail survey, 58% responded, and while 75% reported that they always or sometimes used power morcellation prior to receiving the FDA communication, more than 80% reported rarely or never using it after receiving the communication, Gerald Bernard Taylor, MD, reported at the annual scientific meeting of the Society of Gynecologic Surgeons.
Fear of litigation was cited as the reason for the change in practice by 45.7% of ob.gyns., followed by lack of access to power morcellators (34.7%), and concerns about undiagnosed malignancy (11.8%) and patient safety (5.7%), said Dr. Taylor of the Carolinas HealthCare System in Charlotte.
“We also heard from physicians about the guidelines,” he added, referring to informed consent protocols developed by a group of “key opinion leaders in gynecologic oncology and minimally invasive gynecology.” Many institutions developed moratoriums against the use of power morcellation in the wake of the FDA communication, but the Carolinas HealthCare System chose to commission these opinion leaders to address the issue, he explained.
“Interestingly enough, some [survey respondents] were not aware that the guidelines were available. Most (74.6%) thought that they were helpful when they actually reviewed them, and a few said that they were not helpful,” he said, noting that most of those who found the guidelines helpful said they felt that way because the guidelines “provide a standard of care and a possible defense against litigation.”
Analyses with respect to changes in practice after the FDA communication are ongoing but suggest that changes occurred mainly in the approach to myomectomies rather than in hysterectomy routes, Dr. Taylor said.
“We’re looking to see if there was increased use of minilaparotomy, and we are looking at the use of concealed morcellation bags right now,” he said.
The FDA Safety Communication was issued April 17, 2014 and stated that power morcellation used for hysterectomy or myomectomy in women with uterine fibroids “poses a risk of spreading unsuspected cancerous tissue, notably uterine sarcomas, beyond the uterus.”
“Health care providers and patients should carefully consider available alternative treatment options for symptomatic uterine fibroids. Based on currently available information, the FDA discourages the use of laparoscopic power morcellation during hysterectomy or myomectomy for uterine fibroids,” the communication stated.
A Nov. 24, 2014 update stated that “laparoscopic power morcellators are contraindicated for removal of uterine tissue containing suspected fibroids in patients who are peri- or postmenopausal or are candidates for en bloc tissue removal, for example, through the vagina or minilaparotomy incision,” and “in gynecologic surgery in which the tissue to be morcellated is known or suspected to contain malignancy.”
The update also urged manufacturers of new and existing laparoscopic power morcellators to include the contraindications and a boxed warning in their product labeling and recommended that doctors share the information with their patients.
On Dec. 24, 2017, the FDA issued an updated assessment reinforcing their earlier communications. This latest update was based on a review of recent medical studies that, according to the FDA, suggested that “approximately 1 in 225 to 1 in 580 women who undergo surgery (hysterectomy or myomectomy) for presumed benign uterine growths (‘fibroids’) may have ‘occult’ or hidden uterine cancers known as sarcomas.” The FDA also said that “this is generally consistent with the 1 in 350 incidence estimated by the FDA in a 2014 review. The FDA also estimates the rate of occult leiomyosarcoma, a particularly aggressive type of sarcoma, to be approximately 1 in 495 to 1 in 1,100, again in general agreement with our previous assessment of 1 in 498.”
The FDA acknowledged that some health organizations have reported a lower estimate of risk but maintained its findings and recommendations, noting that it will continue to review new and relevant data.
Dr. Taylor reported having no disclosures.
SOURCE: Taylor GB et al. SGS 2018, Oral Poster 19.
ORLANDO – A 2014 Food and Drug Administration Safety Communication warning about the risk of disseminating occult cancerous tissue when using power morcellation led to a sharp decline in its use among physicians in a large health care system, a survey and records review showed.
Of 126 ob.gyns. in the Charlotte, N.C., metro area who received the 24-question e-mail survey, 58% responded, and while 75% reported that they always or sometimes used power morcellation prior to receiving the FDA communication, more than 80% reported rarely or never using it after receiving the communication, Gerald Bernard Taylor, MD, reported at the annual scientific meeting of the Society of Gynecologic Surgeons.
Fear of litigation was cited as the reason for the change in practice by 45.7% of ob.gyns., followed by lack of access to power morcellators (34.7%), and concerns about undiagnosed malignancy (11.8%) and patient safety (5.7%), said Dr. Taylor of the Carolinas HealthCare System in Charlotte.
“We also heard from physicians about the guidelines,” he added, referring to informed consent protocols developed by a group of “key opinion leaders in gynecologic oncology and minimally invasive gynecology.” Many institutions developed moratoriums against the use of power morcellation in the wake of the FDA communication, but the Carolinas HealthCare System chose to commission these opinion leaders to address the issue, he explained.
“Interestingly enough, some [survey respondents] were not aware that the guidelines were available. Most (74.6%) thought that they were helpful when they actually reviewed them, and a few said that they were not helpful,” he said, noting that most of those who found the guidelines helpful said they felt that way because the guidelines “provide a standard of care and a possible defense against litigation.”
Analyses with respect to changes in practice after the FDA communication are ongoing but suggest that changes occurred mainly in the approach to myomectomies rather than in hysterectomy routes, Dr. Taylor said.
“We’re looking to see if there was increased use of minilaparotomy, and we are looking at the use of concealed morcellation bags right now,” he said.
The FDA Safety Communication was issued April 17, 2014 and stated that power morcellation used for hysterectomy or myomectomy in women with uterine fibroids “poses a risk of spreading unsuspected cancerous tissue, notably uterine sarcomas, beyond the uterus.”
“Health care providers and patients should carefully consider available alternative treatment options for symptomatic uterine fibroids. Based on currently available information, the FDA discourages the use of laparoscopic power morcellation during hysterectomy or myomectomy for uterine fibroids,” the communication stated.
A Nov. 24, 2014 update stated that “laparoscopic power morcellators are contraindicated for removal of uterine tissue containing suspected fibroids in patients who are peri- or postmenopausal or are candidates for en bloc tissue removal, for example, through the vagina or minilaparotomy incision,” and “in gynecologic surgery in which the tissue to be morcellated is known or suspected to contain malignancy.”
The update also urged manufacturers of new and existing laparoscopic power morcellators to include the contraindications and a boxed warning in their product labeling and recommended that doctors share the information with their patients.
On Dec. 24, 2017, the FDA issued an updated assessment reinforcing their earlier communications. This latest update was based on a review of recent medical studies that, according to the FDA, suggested that “approximately 1 in 225 to 1 in 580 women who undergo surgery (hysterectomy or myomectomy) for presumed benign uterine growths (‘fibroids’) may have ‘occult’ or hidden uterine cancers known as sarcomas.” The FDA also said that “this is generally consistent with the 1 in 350 incidence estimated by the FDA in a 2014 review. The FDA also estimates the rate of occult leiomyosarcoma, a particularly aggressive type of sarcoma, to be approximately 1 in 495 to 1 in 1,100, again in general agreement with our previous assessment of 1 in 498.”
The FDA acknowledged that some health organizations have reported a lower estimate of risk but maintained its findings and recommendations, noting that it will continue to review new and relevant data.
Dr. Taylor reported having no disclosures.
SOURCE: Taylor GB et al. SGS 2018, Oral Poster 19.
REPORTING FROM SGS 2018
Key clinical point: Litigation fears drove decline in power morcellation after FDA warning.
Study details: A survey of 126 physicians.
Disclosures: Dr. Taylor reported having no disclosures.
Source: Taylor GB et al. SGS 2018, Oral Poster 19.
Making structural improvements in health care
Every day, hospitalists devote time and energy to the best practices that can limit the spread of infection and the development of antibiotic resistance. Infection Prevention (IP) and Antimicrobial Stewardship (ASP) are two hospital programs that address that same goal.
But there may be a more effective approach possible, according to Jerome A. Leis, MD, MSc, FRCPC, of the Centre for Quality Improvement and Patient Safety at the University of Toronto.
“Despite the high-quality evidence supporting these IP/ASP interventions, our approach to adding these to our current practice sometimes feels like adding scaffolding to a rickety building,” he said. “It supports the underlying structure, but remove the scaffolding without fixing the building, and it may just come tumbling down.” Sometimes the work seems like an uphill battle, he added, as the same problems continue to recur.
That’s because there’s a systemic element to the problems. “Hospitalists know first hand about how the system that we work in makes it difficult to ensure that all the best IP/ASP practices are adhered to all the time,” Dr. Leis said. “Simply reminding staff to remove a urinary catheter in a timely fashion or clean their hands every single time they touch a patient or the environment can only get us so far.” That’s where improvement science comes in.
The relatively new field of improvement science provides a framework for research focused on health care improvement; its goal is to determine which improvement strategies are most effective. Dr. Leis argued that, “when our approach to IP and ASP incorporate principles of improvement science, we are more likely to be successful in achieving sustainable changes in practice.”
Rather than constantly adding extra steps and reminders for hospitalists about patient safety, he said, we need to recognize that there are systemic factors that lead to specific practices. “Our focus should be to use improvement-science methodology to understand these barriers and redesign the processes of care in a way that makes it easier for hospitalists to adhere to the best IP/ASP practices for our patients.”
These structural changes should come from collaboration among content experts in IP/ASP and those with training in improvement science, he said – many IP and ASP programs are already putting this in practice, using improvement science to create safer systems of care.
Reference
Leis J. Advancing infection prevention and antimicrobial stewardship through improvement science. BMJ Qual Saf. 2017 Jun 14. doi: 10.1136/bmjqs-2017-006793.
Every day, hospitalists devote time and energy to the best practices that can limit the spread of infection and the development of antibiotic resistance. Infection Prevention (IP) and Antimicrobial Stewardship (ASP) are two hospital programs that address that same goal.
But there may be a more effective approach possible, according to Jerome A. Leis, MD, MSc, FRCPC, of the Centre for Quality Improvement and Patient Safety at the University of Toronto.
“Despite the high-quality evidence supporting these IP/ASP interventions, our approach to adding these to our current practice sometimes feels like adding scaffolding to a rickety building,” he said. “It supports the underlying structure, but remove the scaffolding without fixing the building, and it may just come tumbling down.” Sometimes the work seems like an uphill battle, he added, as the same problems continue to recur.
That’s because there’s a systemic element to the problems. “Hospitalists know first hand about how the system that we work in makes it difficult to ensure that all the best IP/ASP practices are adhered to all the time,” Dr. Leis said. “Simply reminding staff to remove a urinary catheter in a timely fashion or clean their hands every single time they touch a patient or the environment can only get us so far.” That’s where improvement science comes in.
The relatively new field of improvement science provides a framework for research focused on health care improvement; its goal is to determine which improvement strategies are most effective. Dr. Leis argued that, “when our approach to IP and ASP incorporate principles of improvement science, we are more likely to be successful in achieving sustainable changes in practice.”
Rather than constantly adding extra steps and reminders for hospitalists about patient safety, he said, we need to recognize that there are systemic factors that lead to specific practices. “Our focus should be to use improvement-science methodology to understand these barriers and redesign the processes of care in a way that makes it easier for hospitalists to adhere to the best IP/ASP practices for our patients.”
These structural changes should come from collaboration among content experts in IP/ASP and those with training in improvement science, he said – many IP and ASP programs are already putting this in practice, using improvement science to create safer systems of care.
Reference
Leis J. Advancing infection prevention and antimicrobial stewardship through improvement science. BMJ Qual Saf. 2017 Jun 14. doi: 10.1136/bmjqs-2017-006793.
Every day, hospitalists devote time and energy to the best practices that can limit the spread of infection and the development of antibiotic resistance. Infection Prevention (IP) and Antimicrobial Stewardship (ASP) are two hospital programs that address that same goal.
But there may be a more effective approach possible, according to Jerome A. Leis, MD, MSc, FRCPC, of the Centre for Quality Improvement and Patient Safety at the University of Toronto.
“Despite the high-quality evidence supporting these IP/ASP interventions, our approach to adding these to our current practice sometimes feels like adding scaffolding to a rickety building,” he said. “It supports the underlying structure, but remove the scaffolding without fixing the building, and it may just come tumbling down.” Sometimes the work seems like an uphill battle, he added, as the same problems continue to recur.
That’s because there’s a systemic element to the problems. “Hospitalists know first hand about how the system that we work in makes it difficult to ensure that all the best IP/ASP practices are adhered to all the time,” Dr. Leis said. “Simply reminding staff to remove a urinary catheter in a timely fashion or clean their hands every single time they touch a patient or the environment can only get us so far.” That’s where improvement science comes in.
The relatively new field of improvement science provides a framework for research focused on health care improvement; its goal is to determine which improvement strategies are most effective. Dr. Leis argued that, “when our approach to IP and ASP incorporate principles of improvement science, we are more likely to be successful in achieving sustainable changes in practice.”
Rather than constantly adding extra steps and reminders for hospitalists about patient safety, he said, we need to recognize that there are systemic factors that lead to specific practices. “Our focus should be to use improvement-science methodology to understand these barriers and redesign the processes of care in a way that makes it easier for hospitalists to adhere to the best IP/ASP practices for our patients.”
These structural changes should come from collaboration among content experts in IP/ASP and those with training in improvement science, he said – many IP and ASP programs are already putting this in practice, using improvement science to create safer systems of care.
Reference
Leis J. Advancing infection prevention and antimicrobial stewardship through improvement science. BMJ Qual Saf. 2017 Jun 14. doi: 10.1136/bmjqs-2017-006793.
Brown-Black Papulonodules on the Arm
The Diagnosis: Glochid Dermatitis
Biopsy of a nodule on the upper right arm showed chronic granulomatous inflammation and polarizable foreign material consistent with plant cellulose (Figure). A diagnosis of glochid dermatitis was made. The treatment plan included follow-up skin evaluation and punch excision of persistent papules 1 month after the initial presentation. The patient reported the rash began after he fell on a cactus plant while chasing his grandson. He was seen by various clinicians and was given hydrocortisone and clobetasol, which helped with pruritis but did not resolve the rash. His grandson developed a similar rash at the site of contact with the cactus plant. The patient and his grandson did not detect the presence of any cactus spines.
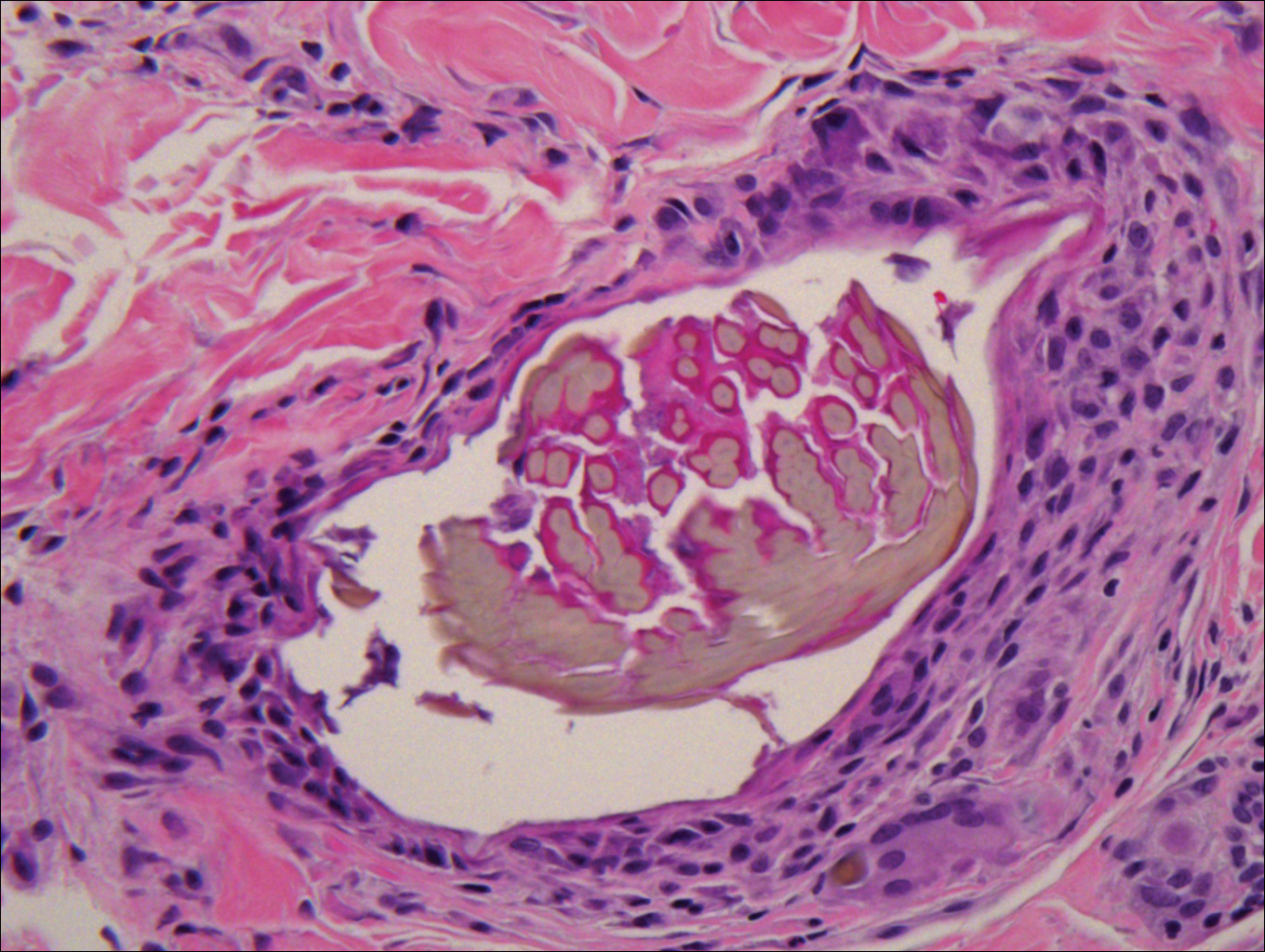
Injuries from cactus glochids most often occur due to accidental falls on cactus plants, but glochids also may be transferred from clothing to other individuals. The thin, hairlike glochids easily detach from the stem of the cactus and can become deeply embedded with virtually no pressure.1
Glochid implantation from the prickly pear cactus commonly presents as a pruritic papular eruption known as glochid dermatitis. These penetrating injuries can lead to inoculation of Clostridium tetani and Staphylococcus aureus. Additionally, unrecognized and unremoved cactus spines may be highly inflammatory and may cause chronic granulomatous inflammation.2
Initially, acute glochid dermatitis occurs due to mechanical damage caused by the detatched cactus spine and may not resolve for up to 4 months. Granuloma formation has been reported several weeks after exposure and may persist for more than 8 months.3 Although an immune mechanism has been suggested, the literature has indicated that delayed hypersensitivity reactions are a more probable cause of the granulomatous inflammation after glochid exposure.3 Madkan et al4 reported that relatively few patients developed granulomas after implantation of glochids in the skin, thus suggesting that granuloma formation is an allergic response.
With regard to the pathogenesis of glochid dermatitis, the initial response to foreign plant matter in the dermis involves a neutrophilic infiltrate, which later is replaced by histiocytes; however, the foreign material remains undegraded in the macrophage cytoplasm.5 Activated macrophages secrete cytokines that intensify the inflammatory response, resulting in formation of a granuloma around the foreign body. The granuloma acts as a wall to isolate the foreign matter from the rest of the body.5
Regarding treatment of chronic granulomas, Madkan et al4 reported a case that showed some improvement with clobetasol ointment; however, clinical lesions resolved only after punch biopsies were performed to confirm the diagnosis of cactus spine granuloma. In a controlled study in rabbits, glochids were successfully removed by first detaching the larger clumps with tweezers then applying glue and gauze to the affected area.6 After the glue dried, the gauze was peeled off, resulting in the removal of 95% of the implanted glochids. Overall, removal of embedded spines is difficult because the glochids typically radiate in several directions.7 Treatment of foreign body granulomas caused by cactus spines can be achieved by expulsion of plant matter remnants and symptomatic treatment using midpotency topical steroids twice daily.4 Uncovering and performing punch biopsies of papules also can result in rapid healing of the lesions. Without manual removal of the glochid, lesions can persist for 2 to 8 months until gradual resolution with possible postinflammatory hyperpigmentation.4
- Suzuki H, Baba S. Cactus granuloma of the skin. J Dermatol. 1993;20:424-427.
- Suárez A, Freeman S, Puls L, et al. Unusual presentation of cactus spines in the flank of an elderly man: a case report. J Med Case Rep. 2010;4:152.
- Spoerke DG, Spoerke SE. Granuloma formation induced by spines of the cactus, Opuntia acanthocarpa. Vet Hum Toxicol. 1991;33:342-344.
- Madkan VK, Abraham T, Lesher JL Jr. Cactus spine granuloma. Cutis. 2007;79:208-210.
- Molina-Ruiz AM, Requena L. Foreign body granulomas. Dermatol Clin. 2015;33:497-523.
- McGovern TW, Barkley TM. Botanical dermatology. Int J Dermatol. 1998;37:321-334.
- Lindsey D, Lindsey WE. Cactus spine injuries. Am J Emerg Med. 1988;6:362-369.
The Diagnosis: Glochid Dermatitis
Biopsy of a nodule on the upper right arm showed chronic granulomatous inflammation and polarizable foreign material consistent with plant cellulose (Figure). A diagnosis of glochid dermatitis was made. The treatment plan included follow-up skin evaluation and punch excision of persistent papules 1 month after the initial presentation. The patient reported the rash began after he fell on a cactus plant while chasing his grandson. He was seen by various clinicians and was given hydrocortisone and clobetasol, which helped with pruritis but did not resolve the rash. His grandson developed a similar rash at the site of contact with the cactus plant. The patient and his grandson did not detect the presence of any cactus spines.
Injuries from cactus glochids most often occur due to accidental falls on cactus plants, but glochids also may be transferred from clothing to other individuals. The thin, hairlike glochids easily detach from the stem of the cactus and can become deeply embedded with virtually no pressure.1
Glochid implantation from the prickly pear cactus commonly presents as a pruritic papular eruption known as glochid dermatitis. These penetrating injuries can lead to inoculation of Clostridium tetani and Staphylococcus aureus. Additionally, unrecognized and unremoved cactus spines may be highly inflammatory and may cause chronic granulomatous inflammation.2
Initially, acute glochid dermatitis occurs due to mechanical damage caused by the detatched cactus spine and may not resolve for up to 4 months. Granuloma formation has been reported several weeks after exposure and may persist for more than 8 months.3 Although an immune mechanism has been suggested, the literature has indicated that delayed hypersensitivity reactions are a more probable cause of the granulomatous inflammation after glochid exposure.3 Madkan et al4 reported that relatively few patients developed granulomas after implantation of glochids in the skin, thus suggesting that granuloma formation is an allergic response.
With regard to the pathogenesis of glochid dermatitis, the initial response to foreign plant matter in the dermis involves a neutrophilic infiltrate, which later is replaced by histiocytes; however, the foreign material remains undegraded in the macrophage cytoplasm.5 Activated macrophages secrete cytokines that intensify the inflammatory response, resulting in formation of a granuloma around the foreign body. The granuloma acts as a wall to isolate the foreign matter from the rest of the body.5
Regarding treatment of chronic granulomas, Madkan et al4 reported a case that showed some improvement with clobetasol ointment; however, clinical lesions resolved only after punch biopsies were performed to confirm the diagnosis of cactus spine granuloma. In a controlled study in rabbits, glochids were successfully removed by first detaching the larger clumps with tweezers then applying glue and gauze to the affected area.6 After the glue dried, the gauze was peeled off, resulting in the removal of 95% of the implanted glochids. Overall, removal of embedded spines is difficult because the glochids typically radiate in several directions.7 Treatment of foreign body granulomas caused by cactus spines can be achieved by expulsion of plant matter remnants and symptomatic treatment using midpotency topical steroids twice daily.4 Uncovering and performing punch biopsies of papules also can result in rapid healing of the lesions. Without manual removal of the glochid, lesions can persist for 2 to 8 months until gradual resolution with possible postinflammatory hyperpigmentation.4
The Diagnosis: Glochid Dermatitis
Biopsy of a nodule on the upper right arm showed chronic granulomatous inflammation and polarizable foreign material consistent with plant cellulose (Figure). A diagnosis of glochid dermatitis was made. The treatment plan included follow-up skin evaluation and punch excision of persistent papules 1 month after the initial presentation. The patient reported the rash began after he fell on a cactus plant while chasing his grandson. He was seen by various clinicians and was given hydrocortisone and clobetasol, which helped with pruritis but did not resolve the rash. His grandson developed a similar rash at the site of contact with the cactus plant. The patient and his grandson did not detect the presence of any cactus spines.
Injuries from cactus glochids most often occur due to accidental falls on cactus plants, but glochids also may be transferred from clothing to other individuals. The thin, hairlike glochids easily detach from the stem of the cactus and can become deeply embedded with virtually no pressure.1
Glochid implantation from the prickly pear cactus commonly presents as a pruritic papular eruption known as glochid dermatitis. These penetrating injuries can lead to inoculation of Clostridium tetani and Staphylococcus aureus. Additionally, unrecognized and unremoved cactus spines may be highly inflammatory and may cause chronic granulomatous inflammation.2
Initially, acute glochid dermatitis occurs due to mechanical damage caused by the detatched cactus spine and may not resolve for up to 4 months. Granuloma formation has been reported several weeks after exposure and may persist for more than 8 months.3 Although an immune mechanism has been suggested, the literature has indicated that delayed hypersensitivity reactions are a more probable cause of the granulomatous inflammation after glochid exposure.3 Madkan et al4 reported that relatively few patients developed granulomas after implantation of glochids in the skin, thus suggesting that granuloma formation is an allergic response.
With regard to the pathogenesis of glochid dermatitis, the initial response to foreign plant matter in the dermis involves a neutrophilic infiltrate, which later is replaced by histiocytes; however, the foreign material remains undegraded in the macrophage cytoplasm.5 Activated macrophages secrete cytokines that intensify the inflammatory response, resulting in formation of a granuloma around the foreign body. The granuloma acts as a wall to isolate the foreign matter from the rest of the body.5
Regarding treatment of chronic granulomas, Madkan et al4 reported a case that showed some improvement with clobetasol ointment; however, clinical lesions resolved only after punch biopsies were performed to confirm the diagnosis of cactus spine granuloma. In a controlled study in rabbits, glochids were successfully removed by first detaching the larger clumps with tweezers then applying glue and gauze to the affected area.6 After the glue dried, the gauze was peeled off, resulting in the removal of 95% of the implanted glochids. Overall, removal of embedded spines is difficult because the glochids typically radiate in several directions.7 Treatment of foreign body granulomas caused by cactus spines can be achieved by expulsion of plant matter remnants and symptomatic treatment using midpotency topical steroids twice daily.4 Uncovering and performing punch biopsies of papules also can result in rapid healing of the lesions. Without manual removal of the glochid, lesions can persist for 2 to 8 months until gradual resolution with possible postinflammatory hyperpigmentation.4
- Suzuki H, Baba S. Cactus granuloma of the skin. J Dermatol. 1993;20:424-427.
- Suárez A, Freeman S, Puls L, et al. Unusual presentation of cactus spines in the flank of an elderly man: a case report. J Med Case Rep. 2010;4:152.
- Spoerke DG, Spoerke SE. Granuloma formation induced by spines of the cactus, Opuntia acanthocarpa. Vet Hum Toxicol. 1991;33:342-344.
- Madkan VK, Abraham T, Lesher JL Jr. Cactus spine granuloma. Cutis. 2007;79:208-210.
- Molina-Ruiz AM, Requena L. Foreign body granulomas. Dermatol Clin. 2015;33:497-523.
- McGovern TW, Barkley TM. Botanical dermatology. Int J Dermatol. 1998;37:321-334.
- Lindsey D, Lindsey WE. Cactus spine injuries. Am J Emerg Med. 1988;6:362-369.
- Suzuki H, Baba S. Cactus granuloma of the skin. J Dermatol. 1993;20:424-427.
- Suárez A, Freeman S, Puls L, et al. Unusual presentation of cactus spines in the flank of an elderly man: a case report. J Med Case Rep. 2010;4:152.
- Spoerke DG, Spoerke SE. Granuloma formation induced by spines of the cactus, Opuntia acanthocarpa. Vet Hum Toxicol. 1991;33:342-344.
- Madkan VK, Abraham T, Lesher JL Jr. Cactus spine granuloma. Cutis. 2007;79:208-210.
- Molina-Ruiz AM, Requena L. Foreign body granulomas. Dermatol Clin. 2015;33:497-523.
- McGovern TW, Barkley TM. Botanical dermatology. Int J Dermatol. 1998;37:321-334.
- Lindsey D, Lindsey WE. Cactus spine injuries. Am J Emerg Med. 1988;6:362-369.
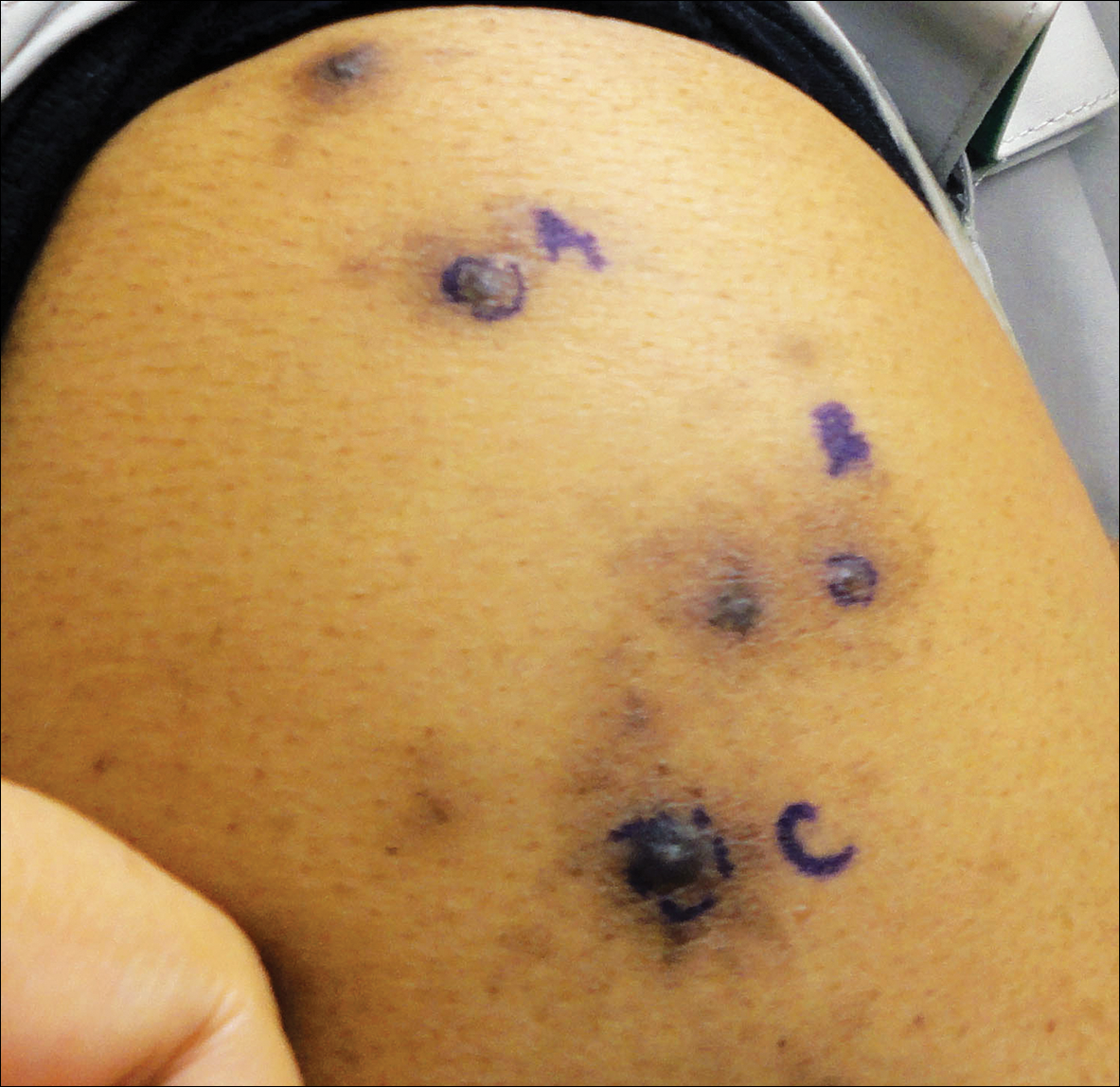
A 63-year-old man presented with a pruritic rash on the right arm of approximately 3 months' duration. On physical examination, several discrete, 4- to 5-mm, brown-black papulonodules with a central punctum were identified along the extensor aspects of the upper and lower right arm. No foreign bodies were appreciated. Biopsies of nodules on the right upper arm were performed (sites marked with letters).
Use of Urinalysis to Assess Adherence to Prescribed Cardiovascular Medications: Focus on Hypertension
Click here to read the supplement

Topics include:
- Common problem of nonadherence to CV medications
- Nonadherence as a contributor to poor CV outcomes
- Improvement of adherence in meeting quality payment program criteria
- Urinalysis as a tool to support adherence
- Benefits of using the KardiAssure™ urinalysis test
Click here to read the supplement
Click here to read the supplement
Topics include:
- Common problem of nonadherence to CV medications
- Nonadherence as a contributor to poor CV outcomes
- Improvement of adherence in meeting quality payment program criteria
- Urinalysis as a tool to support adherence
- Benefits of using the KardiAssure™ urinalysis test
Click here to read the supplement
Click here to read the supplement
Topics include:
- Common problem of nonadherence to CV medications
- Nonadherence as a contributor to poor CV outcomes
- Improvement of adherence in meeting quality payment program criteria
- Urinalysis as a tool to support adherence
- Benefits of using the KardiAssure™ urinalysis test
Click here to read the supplement

The Long and Winding Road: PTCL 10 Years from Now

Release Date: March 20, 2018
Expiration Date: March 19, 2019
Note: This activity is no longer available for credit
Agenda
New targeted agents for PTCL
(Duration: 20 minutes)
Pier Luigi Zinzani, MD, PhD
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Recently approved therapies for PTCL in Asia:
What have we learned from the US experience?
(Duration: 18 minutes)
Won Seog Kim, MD, PhD
Samsung Medical Center
Seoul, Republic of Korea
Novel combination therapies:
Where are we now and where are we going?
(Duration: 23 minutes)
Owen A. O’Connor, MD, PhD
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Provided by:
![]()
Original activity supported by an educational grant from:
Spectrum Pharmaceuticals
Learning Objectives
At the conclusion of this educational activity, the healthcare team will be better able to:
- Discuss the treatment and management of peripheral T-cell lymphoma
- Appraise how U.S. T-cell lymphoma treatment experience can impact practice in Asia
- Summarize the importance of combination therapy in peripheral T-cell lymphoma
Target Audience
Hematologists, oncologists, and other clinicians and scientists with an interest in T-cell lymphoma
Statement of Need
Peripheral T-cell lymphomas (PTCL) are rare, heterogeneous and aggressive neoplasms that are associated with a poor prognosis. In addition, with current therapies, up to 70% of patients undergo relapse or develop refractory disease. Recent evidence has indicated an increase in the incidence of PTCLs and hence current challenges including pathobiology, clinical management, new drug testing as well as clinical trial accrual, need to be addressed. This activity will provide the healthcare team with the ideal foundation to facilitate progress in PTCL treatment and management.
Won Seog Kim, MD, PhD (Presenter)
Samsung Medical Center
Seoul, Republic of Korea
Disclosure: Consulting fees: Celltrion; Contracted research: Takeda; Kyowa-Kirin; J & J; Merck; Donga; Novartis; Celltrion
Owen A. O’Connor, MD, PhD (Presenter)
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Disclosure: Contracted research: Celgene; Merck; Spectrum; Agensys
Pier Luigi Zinzani, MD, PhD (Presenter)
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Disclosure: Speakers Bureau: Janssen; Merck; Servier; Gilead; Verastem; BMS; Sandoz; Mundipharma
Permissions
Won Seog Kim presentation
Slide 4: Frequency of T and NK-cell lymphomas in Asia
Park S, Ko YH. Peripheral T cell lymphoma in Asia. Int J Hematol 2014;99:227-239. Reprinted with permission of the Japanese Society of Hematology.
Slide 29: Off-label use: 100mg of pembrolizumab, HK, Singapore, Korea
Republished with permission of the American Society of Hematology, from Kwong YL, et al. PD1 blockade with pembrolizumab is highly effective in relapsed or refractory NK/T-cell lymphoma failing L-asparaginase. Blood. 2017;129(17):2437-2442; permission conveyed through Copyright Clearance Center, Inc.
Owen A. O’Connor presentation
Slide 12: Schematic of study design, patient disposition, and thrombocytopenia as a function of schedule & dose
Republished with permission of American Society of Hematology, from Amengual JE…O’Connor OA. A phase 1 study of romidepsin and pralatrexate reveals marked activity in relapsed and refractory T-cell lymphoma. Blood 2018;131:397-407; permission conveyed through Copyright Clearance Center, Inc.
Slide 13: Summary of response rates across study population for patients treated with romidepsin and pralatrexate
Same as slide above.
Slide 14: Pharmacokinetic parameters for pralatrexate and romidepsin in the study population
Same as slide above.
Slide 15: PFS and OS as a function of treatment in study population
Same as slide above.
Slide 19: The combination of HoME and HDAC inhibitor synergistically produces apoptosis across panel of T-cell lymphomas: tCTCL H9
Marchi E . . . O’Connor OA.The combination of hypomethylating agents and histone deacetylase inhibitors produce marked synergy in preclinical models of T-cell lymphoma. Br J Haematol 2015; 171:215-226.
Slide 20: Supervised hierarchial clustering based on GEP
Same as slide above.
Slide 27: Panobinostat plus bortezomib in PTCL
Reprinted from Lancet Haematol, Tan D, et al. Panobinostat in combination with bortezomib in patients with relapsed or refractory peripheral T-cell lymphoma: an open-label, multicentre phase 2 trial. 2015; 2(8):e326-e333, with permission from Elsevier.
Pier Luigi Zinzani presentation
Slides 4, 11: New agents in T-cell lymphomas (2), Belinostat (2)
O’Connor OA, et al. Belinostat in patients with relapsed or refractory peripheral T-cell lymphoma: Results of the pivotal phase II BELIEF (CLN-19) study. J Clin Oncol 2015; 33: 2492-2499. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.
Slides 5, 8, 10, 12, 18, 20: Pralatrexate (1), Romidepsin (1), Belinostat (1), Brentuximab vedotin – Anaplastic large cell lymphoma (1), Brentuximab vedotin – CD30+ peripheral T-cell lymphoma (1), Off-label compounds in peripheral T-cell lymphomas
Reprinted from Cancer Treat Rev, volume 60, Broccoli A, Argnani L, Zinzani PL. Peripheral T-cell lymphomas: Focusing on novel agents in relapsed and refractory disease, pp 120-129, © 2017, with permission from Elsevier.
Slides 6, 7: Pralatrexate (2) and Pralatrexate (3)
O’Connor OA, et al. Pralatrexate in patients with relapsed or refractory peripheral T-cell lymphoma: results from the pivotal PROPEL study. J Clin Oncol, 2011; 29: 1182-1189. Reprinted with permission. © 2011 American Society of Clinical Oncology. All rights reserved.
Slide 9: Romidepsin (2)
Coiffier B, et al. J Clin Oncol 2012; 30: 631-636. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 13, 14: Brentuximab vedotin – Anaplastic large cell lymphoma (2), Brentulximab vedotin — Anaplastic large cell lymphoma (3)
Pro B, et al. J Clin Oncol 2012; 30: 2190-2196. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 16, 17: Brentuximab vedotin – Anaplastic large cell lymphoma (5), Brentuximab vedotin – Anaplastic large cell lymphoma (6)
Broccoli A, et al. Italian real-life experience with brentuximab vedotin: results of a large observational study of 40 cases of relapsed/refractory systemic anaplastic large cell lymphoma. Haematologica 2017; 102: 1931-1935. Obtained from the Haematologica Journal website http://www.haematologica.org
Slide 19: Brentuximab vedotin –CD30+ peripheral T-cell lymphomas (2)
Horwitz SM, et al. Blood 2014; 123: 3095-3100. Permission conveyed through Copyright Clearance Center, Inc.
Slide 21: Gemcitabine in peripheral T-cell lymphomas
Zinzani PL, et al. Ann Oncol 2010; 21: 860-863. European Society of Medical Oncology licensee.
Slide 23: Lenalidomide in T-cell lymphomas (2)
Reprinted from Morschhauser F, et al. A phase 2, multicentre, single-arm, open-label study to evaluate the safety and efficacy of single-agent lenalidomide (Revlimid) in subjects with relapsed or refractory peripheral T-cell non-Hodgkin lymphoma: the EXPECT trial. Eur J Cancer 2013, with permission from Elsevier.
Slides 24, 25: Bendamustine in T-cell lymphomas (1), Bendamustine in T-cell lymphomas (2)
Damaj G, et al. J Clin Oncol 2012; 31: 104-110. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Disclaimer
The content and views presented in this educational activity are those of the authors and do not necessarily reflect those of Hemedicus, the supporter, or Frontline Medical Communications. This material is prepared based upon a review of multiple sources of information, but it is not exhaustive of the subject matter. Therefore, healthcare professionals and other individuals should review and consider other publications and materials on the subject matter before relying solely upon the information contained within this educational activity.
Release Date: March 20, 2018
Expiration Date: March 19, 2019
Note: This activity is no longer available for credit
Agenda
New targeted agents for PTCL
(Duration: 20 minutes)
Pier Luigi Zinzani, MD, PhD
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Recently approved therapies for PTCL in Asia:
What have we learned from the US experience?
(Duration: 18 minutes)
Won Seog Kim, MD, PhD
Samsung Medical Center
Seoul, Republic of Korea
Novel combination therapies:
Where are we now and where are we going?
(Duration: 23 minutes)
Owen A. O’Connor, MD, PhD
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Provided by:
![]()
Original activity supported by an educational grant from:
Spectrum Pharmaceuticals
Learning Objectives
At the conclusion of this educational activity, the healthcare team will be better able to:
- Discuss the treatment and management of peripheral T-cell lymphoma
- Appraise how U.S. T-cell lymphoma treatment experience can impact practice in Asia
- Summarize the importance of combination therapy in peripheral T-cell lymphoma
Target Audience
Hematologists, oncologists, and other clinicians and scientists with an interest in T-cell lymphoma
Statement of Need
Peripheral T-cell lymphomas (PTCL) are rare, heterogeneous and aggressive neoplasms that are associated with a poor prognosis. In addition, with current therapies, up to 70% of patients undergo relapse or develop refractory disease. Recent evidence has indicated an increase in the incidence of PTCLs and hence current challenges including pathobiology, clinical management, new drug testing as well as clinical trial accrual, need to be addressed. This activity will provide the healthcare team with the ideal foundation to facilitate progress in PTCL treatment and management.
Won Seog Kim, MD, PhD (Presenter)
Samsung Medical Center
Seoul, Republic of Korea
Disclosure: Consulting fees: Celltrion; Contracted research: Takeda; Kyowa-Kirin; J & J; Merck; Donga; Novartis; Celltrion
Owen A. O’Connor, MD, PhD (Presenter)
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Disclosure: Contracted research: Celgene; Merck; Spectrum; Agensys
Pier Luigi Zinzani, MD, PhD (Presenter)
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Disclosure: Speakers Bureau: Janssen; Merck; Servier; Gilead; Verastem; BMS; Sandoz; Mundipharma
Permissions
Won Seog Kim presentation
Slide 4: Frequency of T and NK-cell lymphomas in Asia
Park S, Ko YH. Peripheral T cell lymphoma in Asia. Int J Hematol 2014;99:227-239. Reprinted with permission of the Japanese Society of Hematology.
Slide 29: Off-label use: 100mg of pembrolizumab, HK, Singapore, Korea
Republished with permission of the American Society of Hematology, from Kwong YL, et al. PD1 blockade with pembrolizumab is highly effective in relapsed or refractory NK/T-cell lymphoma failing L-asparaginase. Blood. 2017;129(17):2437-2442; permission conveyed through Copyright Clearance Center, Inc.
Owen A. O’Connor presentation
Slide 12: Schematic of study design, patient disposition, and thrombocytopenia as a function of schedule & dose
Republished with permission of American Society of Hematology, from Amengual JE…O’Connor OA. A phase 1 study of romidepsin and pralatrexate reveals marked activity in relapsed and refractory T-cell lymphoma. Blood 2018;131:397-407; permission conveyed through Copyright Clearance Center, Inc.
Slide 13: Summary of response rates across study population for patients treated with romidepsin and pralatrexate
Same as slide above.
Slide 14: Pharmacokinetic parameters for pralatrexate and romidepsin in the study population
Same as slide above.
Slide 15: PFS and OS as a function of treatment in study population
Same as slide above.
Slide 19: The combination of HoME and HDAC inhibitor synergistically produces apoptosis across panel of T-cell lymphomas: tCTCL H9
Marchi E . . . O’Connor OA.The combination of hypomethylating agents and histone deacetylase inhibitors produce marked synergy in preclinical models of T-cell lymphoma. Br J Haematol 2015; 171:215-226.
Slide 20: Supervised hierarchial clustering based on GEP
Same as slide above.
Slide 27: Panobinostat plus bortezomib in PTCL
Reprinted from Lancet Haematol, Tan D, et al. Panobinostat in combination with bortezomib in patients with relapsed or refractory peripheral T-cell lymphoma: an open-label, multicentre phase 2 trial. 2015; 2(8):e326-e333, with permission from Elsevier.
Pier Luigi Zinzani presentation
Slides 4, 11: New agents in T-cell lymphomas (2), Belinostat (2)
O’Connor OA, et al. Belinostat in patients with relapsed or refractory peripheral T-cell lymphoma: Results of the pivotal phase II BELIEF (CLN-19) study. J Clin Oncol 2015; 33: 2492-2499. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.
Slides 5, 8, 10, 12, 18, 20: Pralatrexate (1), Romidepsin (1), Belinostat (1), Brentuximab vedotin – Anaplastic large cell lymphoma (1), Brentuximab vedotin – CD30+ peripheral T-cell lymphoma (1), Off-label compounds in peripheral T-cell lymphomas
Reprinted from Cancer Treat Rev, volume 60, Broccoli A, Argnani L, Zinzani PL. Peripheral T-cell lymphomas: Focusing on novel agents in relapsed and refractory disease, pp 120-129, © 2017, with permission from Elsevier.
Slides 6, 7: Pralatrexate (2) and Pralatrexate (3)
O’Connor OA, et al. Pralatrexate in patients with relapsed or refractory peripheral T-cell lymphoma: results from the pivotal PROPEL study. J Clin Oncol, 2011; 29: 1182-1189. Reprinted with permission. © 2011 American Society of Clinical Oncology. All rights reserved.
Slide 9: Romidepsin (2)
Coiffier B, et al. J Clin Oncol 2012; 30: 631-636. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 13, 14: Brentuximab vedotin – Anaplastic large cell lymphoma (2), Brentulximab vedotin — Anaplastic large cell lymphoma (3)
Pro B, et al. J Clin Oncol 2012; 30: 2190-2196. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 16, 17: Brentuximab vedotin – Anaplastic large cell lymphoma (5), Brentuximab vedotin – Anaplastic large cell lymphoma (6)
Broccoli A, et al. Italian real-life experience with brentuximab vedotin: results of a large observational study of 40 cases of relapsed/refractory systemic anaplastic large cell lymphoma. Haematologica 2017; 102: 1931-1935. Obtained from the Haematologica Journal website http://www.haematologica.org
Slide 19: Brentuximab vedotin –CD30+ peripheral T-cell lymphomas (2)
Horwitz SM, et al. Blood 2014; 123: 3095-3100. Permission conveyed through Copyright Clearance Center, Inc.
Slide 21: Gemcitabine in peripheral T-cell lymphomas
Zinzani PL, et al. Ann Oncol 2010; 21: 860-863. European Society of Medical Oncology licensee.
Slide 23: Lenalidomide in T-cell lymphomas (2)
Reprinted from Morschhauser F, et al. A phase 2, multicentre, single-arm, open-label study to evaluate the safety and efficacy of single-agent lenalidomide (Revlimid) in subjects with relapsed or refractory peripheral T-cell non-Hodgkin lymphoma: the EXPECT trial. Eur J Cancer 2013, with permission from Elsevier.
Slides 24, 25: Bendamustine in T-cell lymphomas (1), Bendamustine in T-cell lymphomas (2)
Damaj G, et al. J Clin Oncol 2012; 31: 104-110. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Disclaimer
The content and views presented in this educational activity are those of the authors and do not necessarily reflect those of Hemedicus, the supporter, or Frontline Medical Communications. This material is prepared based upon a review of multiple sources of information, but it is not exhaustive of the subject matter. Therefore, healthcare professionals and other individuals should review and consider other publications and materials on the subject matter before relying solely upon the information contained within this educational activity.
Release Date: March 20, 2018
Expiration Date: March 19, 2019
Note: This activity is no longer available for credit
Agenda
New targeted agents for PTCL
(Duration: 20 minutes)
Pier Luigi Zinzani, MD, PhD
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Recently approved therapies for PTCL in Asia:
What have we learned from the US experience?
(Duration: 18 minutes)
Won Seog Kim, MD, PhD
Samsung Medical Center
Seoul, Republic of Korea
Novel combination therapies:
Where are we now and where are we going?
(Duration: 23 minutes)
Owen A. O’Connor, MD, PhD
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Provided by:
![]()
Original activity supported by an educational grant from:
Spectrum Pharmaceuticals
Learning Objectives
At the conclusion of this educational activity, the healthcare team will be better able to:
- Discuss the treatment and management of peripheral T-cell lymphoma
- Appraise how U.S. T-cell lymphoma treatment experience can impact practice in Asia
- Summarize the importance of combination therapy in peripheral T-cell lymphoma
Target Audience
Hematologists, oncologists, and other clinicians and scientists with an interest in T-cell lymphoma
Statement of Need
Peripheral T-cell lymphomas (PTCL) are rare, heterogeneous and aggressive neoplasms that are associated with a poor prognosis. In addition, with current therapies, up to 70% of patients undergo relapse or develop refractory disease. Recent evidence has indicated an increase in the incidence of PTCLs and hence current challenges including pathobiology, clinical management, new drug testing as well as clinical trial accrual, need to be addressed. This activity will provide the healthcare team with the ideal foundation to facilitate progress in PTCL treatment and management.
Won Seog Kim, MD, PhD (Presenter)
Samsung Medical Center
Seoul, Republic of Korea
Disclosure: Consulting fees: Celltrion; Contracted research: Takeda; Kyowa-Kirin; J & J; Merck; Donga; Novartis; Celltrion
Owen A. O’Connor, MD, PhD (Presenter)
Columbia University Medical Center
The New York Presbyterian Hospital
New York, NY USA
Disclosure: Contracted research: Celgene; Merck; Spectrum; Agensys
Pier Luigi Zinzani, MD, PhD (Presenter)
Bologna University
Institute of Hematology “Seragnoli”
Bologna, Italy
Disclosure: Speakers Bureau: Janssen; Merck; Servier; Gilead; Verastem; BMS; Sandoz; Mundipharma
Permissions
Won Seog Kim presentation
Slide 4: Frequency of T and NK-cell lymphomas in Asia
Park S, Ko YH. Peripheral T cell lymphoma in Asia. Int J Hematol 2014;99:227-239. Reprinted with permission of the Japanese Society of Hematology.
Slide 29: Off-label use: 100mg of pembrolizumab, HK, Singapore, Korea
Republished with permission of the American Society of Hematology, from Kwong YL, et al. PD1 blockade with pembrolizumab is highly effective in relapsed or refractory NK/T-cell lymphoma failing L-asparaginase. Blood. 2017;129(17):2437-2442; permission conveyed through Copyright Clearance Center, Inc.
Owen A. O’Connor presentation
Slide 12: Schematic of study design, patient disposition, and thrombocytopenia as a function of schedule & dose
Republished with permission of American Society of Hematology, from Amengual JE…O’Connor OA. A phase 1 study of romidepsin and pralatrexate reveals marked activity in relapsed and refractory T-cell lymphoma. Blood 2018;131:397-407; permission conveyed through Copyright Clearance Center, Inc.
Slide 13: Summary of response rates across study population for patients treated with romidepsin and pralatrexate
Same as slide above.
Slide 14: Pharmacokinetic parameters for pralatrexate and romidepsin in the study population
Same as slide above.
Slide 15: PFS and OS as a function of treatment in study population
Same as slide above.
Slide 19: The combination of HoME and HDAC inhibitor synergistically produces apoptosis across panel of T-cell lymphomas: tCTCL H9
Marchi E . . . O’Connor OA.The combination of hypomethylating agents and histone deacetylase inhibitors produce marked synergy in preclinical models of T-cell lymphoma. Br J Haematol 2015; 171:215-226.
Slide 20: Supervised hierarchial clustering based on GEP
Same as slide above.
Slide 27: Panobinostat plus bortezomib in PTCL
Reprinted from Lancet Haematol, Tan D, et al. Panobinostat in combination with bortezomib in patients with relapsed or refractory peripheral T-cell lymphoma: an open-label, multicentre phase 2 trial. 2015; 2(8):e326-e333, with permission from Elsevier.
Pier Luigi Zinzani presentation
Slides 4, 11: New agents in T-cell lymphomas (2), Belinostat (2)
O’Connor OA, et al. Belinostat in patients with relapsed or refractory peripheral T-cell lymphoma: Results of the pivotal phase II BELIEF (CLN-19) study. J Clin Oncol 2015; 33: 2492-2499. Reprinted with permission. © 2015 American Society of Clinical Oncology. All rights reserved.
Slides 5, 8, 10, 12, 18, 20: Pralatrexate (1), Romidepsin (1), Belinostat (1), Brentuximab vedotin – Anaplastic large cell lymphoma (1), Brentuximab vedotin – CD30+ peripheral T-cell lymphoma (1), Off-label compounds in peripheral T-cell lymphomas
Reprinted from Cancer Treat Rev, volume 60, Broccoli A, Argnani L, Zinzani PL. Peripheral T-cell lymphomas: Focusing on novel agents in relapsed and refractory disease, pp 120-129, © 2017, with permission from Elsevier.
Slides 6, 7: Pralatrexate (2) and Pralatrexate (3)
O’Connor OA, et al. Pralatrexate in patients with relapsed or refractory peripheral T-cell lymphoma: results from the pivotal PROPEL study. J Clin Oncol, 2011; 29: 1182-1189. Reprinted with permission. © 2011 American Society of Clinical Oncology. All rights reserved.
Slide 9: Romidepsin (2)
Coiffier B, et al. J Clin Oncol 2012; 30: 631-636. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 13, 14: Brentuximab vedotin – Anaplastic large cell lymphoma (2), Brentulximab vedotin — Anaplastic large cell lymphoma (3)
Pro B, et al. J Clin Oncol 2012; 30: 2190-2196. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Slides 16, 17: Brentuximab vedotin – Anaplastic large cell lymphoma (5), Brentuximab vedotin – Anaplastic large cell lymphoma (6)
Broccoli A, et al. Italian real-life experience with brentuximab vedotin: results of a large observational study of 40 cases of relapsed/refractory systemic anaplastic large cell lymphoma. Haematologica 2017; 102: 1931-1935. Obtained from the Haematologica Journal website http://www.haematologica.org
Slide 19: Brentuximab vedotin –CD30+ peripheral T-cell lymphomas (2)
Horwitz SM, et al. Blood 2014; 123: 3095-3100. Permission conveyed through Copyright Clearance Center, Inc.
Slide 21: Gemcitabine in peripheral T-cell lymphomas
Zinzani PL, et al. Ann Oncol 2010; 21: 860-863. European Society of Medical Oncology licensee.
Slide 23: Lenalidomide in T-cell lymphomas (2)
Reprinted from Morschhauser F, et al. A phase 2, multicentre, single-arm, open-label study to evaluate the safety and efficacy of single-agent lenalidomide (Revlimid) in subjects with relapsed or refractory peripheral T-cell non-Hodgkin lymphoma: the EXPECT trial. Eur J Cancer 2013, with permission from Elsevier.
Slides 24, 25: Bendamustine in T-cell lymphomas (1), Bendamustine in T-cell lymphomas (2)
Damaj G, et al. J Clin Oncol 2012; 31: 104-110. Reprinted with permission. © 2012 American Society of Clinical Oncology. All rights reserved.
Disclaimer
The content and views presented in this educational activity are those of the authors and do not necessarily reflect those of Hemedicus, the supporter, or Frontline Medical Communications. This material is prepared based upon a review of multiple sources of information, but it is not exhaustive of the subject matter. Therefore, healthcare professionals and other individuals should review and consider other publications and materials on the subject matter before relying solely upon the information contained within this educational activity.