User login
‘Forever chemicals’ linked to hypertension in middle-aged women
In a large, prospective study, researchers found an association between higher blood levels of PFAS and increased risk of hypertension in middle-aged women. Women in the highest tertile of overall PFAS concentrations had a 71% increased risk of developing hypertension.
“Our findings suggest that long-term cumulative exposure, even before midlife, may increase the risk of high blood pressure, and therefore, the benefit of reducing the population exposure to PFAS and potential prevention of high blood pressure and other health conditions would be enormous,” Sung Kyun Park, ScD, MPH, University of Michigan School of Public Health, Ann Arbor, said in an interview.
The study was published online in Hypertension.
Everywhere and forever
“PFAS are forever chemicals as well as everywhere chemicals,” Dr. Park noted.
Possible sources of PFAS exposure run the gamut from nonstick cookware, food wrappers, and waterproof fabrics to cosmetics and drinking water. They have been detected in the blood of most people and have been linked to a variety of health concerns.
“A few studies showed an association between PFAS and hypertension, but those were cross-sectional and examined prevalence of hypertension. It was unclear whether PFAS are associated with the development (incidence) of hypertension,” Dr. Park explained.
For their study, the researchers examined the association between serum concentrations of PFAS and risks of incident hypertension in 1,058 initially normotensive women participating in the Study of Women’s Health Across the Nation-Multi-Pollutant Study (SWAN-MPS). They were followed annually between 1999 and 2017.
During 11,722 person-years of follow-up, 470 of the women developed hypertension, at a rate of 40.1 cases per 1,000 person-years. Hypertension was defined as blood pressure of at least 140 mm Hg systolic or at least 90 mm Hg diastolic or receiving antihypertensive treatment.
Women in the highest tertile of baseline serum concentration of perfluorooctane sulfonate (PFOS) had a 42% higher risk of developing hypertension, compared with peers in the lowest tertile (adjusted hazard ratio, 1.42; 95% confidence interval, 1.19-1.68; P trend = .01).
Similar results were found for perfluorooctanoate (PFOA) and 2-N-ethyl-perfluorooctane sulfonamido acetate (EtFOSAA), with 47% (aHR, 1.47; 95% CI, 1.24-1.75; P trend = .01) and 42% (aHR, 1.42; 95% CI, 1.19-1.70; P trend = .01) higher risks of incident hypertension, comparing the highest to the lowest tertiles.
The risks persisted after adjusting for various factors, including race, study site, education, financial strain, smoking status, alcohol use, total calorie intake, and menopausal status.
In the PFAS “mixture” analysis, women in the highest tertile of overall PFAS concentrations were 71% more likely to develop hypertension during follow-up, compared with women in the lowest tertile (aHR, 1.71; 95% CI, 1.15-2.54; P trend = .008).
“These findings suggest that PFAS might be an underappreciated contributing factor to women’s cardiovascular disease risk,” the researchers write.
They caution that the study only included middle-aged women and that it is unclear whether the findings hold for middle-aged men.
“This is an important question, but the answer is that we do not know,” Dr. Park told this news organization.
“Women become more susceptible to metabolic changes and hypertension risk during the menopausal transition. Our findings suggest that PFAS may play a role in the development of hypertension in women during this critical life stage,” Dr. Park said.
The researchers say more research is needed to confirm and expand the findings and to find ways to reduce PFAS exposure.
“If confirmed in future studies, these findings suggest that understanding human exposure to PFAS and developing effective strategies to reduce PFAS exposure may help prevent the development of hypertension and thereby reduce the global burden of CVD,” the researchers write.
‘The more we learn, the worse it gets’
This is an “interesting” study and shows that “the more we learn about PFAS, the worse it seems to get,” Ankur Shah, MD, division of kidney disease and hypertension, Warren Alpert Medical School of Brown University, Providence, R.I., said in an interview.
“This multisite, multiracial and multiethnic, community-based longitudinal study establishes an association between PFAS and hypertension,” said Dr. Shah, who wasn’t involved in the study.
“This adds to a growing literature base of associations of PFAS with illnesses, including malignancy, thyroid disorders, diabetes, ulcerative colitis, hyperlipidemia, and pregnancy-induced hypertension,” he noted.
Dr. Shah also noted that the authors adjusted for race and ethnicity, study site, education, financial strain, smoking status, environmental tobacco smoke, alcohol consumption, total calorie intake, and menopausal status “and still found a strong association.”
“Still to be determined are both whether PFAS are the causative agent or if there is an unmeasured/unadjusted for entity which has resulted in both increased PFAS exposure and hypertension, as well as if PFAS are causative, if reduction in PFAS exposure would be result in blood pressure reduction,” Dr. Shah added.
The study had no sources of funding. Dr. Park and Dr. Shah have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large, prospective study, researchers found an association between higher blood levels of PFAS and increased risk of hypertension in middle-aged women. Women in the highest tertile of overall PFAS concentrations had a 71% increased risk of developing hypertension.
“Our findings suggest that long-term cumulative exposure, even before midlife, may increase the risk of high blood pressure, and therefore, the benefit of reducing the population exposure to PFAS and potential prevention of high blood pressure and other health conditions would be enormous,” Sung Kyun Park, ScD, MPH, University of Michigan School of Public Health, Ann Arbor, said in an interview.
The study was published online in Hypertension.
Everywhere and forever
“PFAS are forever chemicals as well as everywhere chemicals,” Dr. Park noted.
Possible sources of PFAS exposure run the gamut from nonstick cookware, food wrappers, and waterproof fabrics to cosmetics and drinking water. They have been detected in the blood of most people and have been linked to a variety of health concerns.
“A few studies showed an association between PFAS and hypertension, but those were cross-sectional and examined prevalence of hypertension. It was unclear whether PFAS are associated with the development (incidence) of hypertension,” Dr. Park explained.
For their study, the researchers examined the association between serum concentrations of PFAS and risks of incident hypertension in 1,058 initially normotensive women participating in the Study of Women’s Health Across the Nation-Multi-Pollutant Study (SWAN-MPS). They were followed annually between 1999 and 2017.
During 11,722 person-years of follow-up, 470 of the women developed hypertension, at a rate of 40.1 cases per 1,000 person-years. Hypertension was defined as blood pressure of at least 140 mm Hg systolic or at least 90 mm Hg diastolic or receiving antihypertensive treatment.
Women in the highest tertile of baseline serum concentration of perfluorooctane sulfonate (PFOS) had a 42% higher risk of developing hypertension, compared with peers in the lowest tertile (adjusted hazard ratio, 1.42; 95% confidence interval, 1.19-1.68; P trend = .01).
Similar results were found for perfluorooctanoate (PFOA) and 2-N-ethyl-perfluorooctane sulfonamido acetate (EtFOSAA), with 47% (aHR, 1.47; 95% CI, 1.24-1.75; P trend = .01) and 42% (aHR, 1.42; 95% CI, 1.19-1.70; P trend = .01) higher risks of incident hypertension, comparing the highest to the lowest tertiles.
The risks persisted after adjusting for various factors, including race, study site, education, financial strain, smoking status, alcohol use, total calorie intake, and menopausal status.
In the PFAS “mixture” analysis, women in the highest tertile of overall PFAS concentrations were 71% more likely to develop hypertension during follow-up, compared with women in the lowest tertile (aHR, 1.71; 95% CI, 1.15-2.54; P trend = .008).
“These findings suggest that PFAS might be an underappreciated contributing factor to women’s cardiovascular disease risk,” the researchers write.
They caution that the study only included middle-aged women and that it is unclear whether the findings hold for middle-aged men.
“This is an important question, but the answer is that we do not know,” Dr. Park told this news organization.
“Women become more susceptible to metabolic changes and hypertension risk during the menopausal transition. Our findings suggest that PFAS may play a role in the development of hypertension in women during this critical life stage,” Dr. Park said.
The researchers say more research is needed to confirm and expand the findings and to find ways to reduce PFAS exposure.
“If confirmed in future studies, these findings suggest that understanding human exposure to PFAS and developing effective strategies to reduce PFAS exposure may help prevent the development of hypertension and thereby reduce the global burden of CVD,” the researchers write.
‘The more we learn, the worse it gets’
This is an “interesting” study and shows that “the more we learn about PFAS, the worse it seems to get,” Ankur Shah, MD, division of kidney disease and hypertension, Warren Alpert Medical School of Brown University, Providence, R.I., said in an interview.
“This multisite, multiracial and multiethnic, community-based longitudinal study establishes an association between PFAS and hypertension,” said Dr. Shah, who wasn’t involved in the study.
“This adds to a growing literature base of associations of PFAS with illnesses, including malignancy, thyroid disorders, diabetes, ulcerative colitis, hyperlipidemia, and pregnancy-induced hypertension,” he noted.
Dr. Shah also noted that the authors adjusted for race and ethnicity, study site, education, financial strain, smoking status, environmental tobacco smoke, alcohol consumption, total calorie intake, and menopausal status “and still found a strong association.”
“Still to be determined are both whether PFAS are the causative agent or if there is an unmeasured/unadjusted for entity which has resulted in both increased PFAS exposure and hypertension, as well as if PFAS are causative, if reduction in PFAS exposure would be result in blood pressure reduction,” Dr. Shah added.
The study had no sources of funding. Dr. Park and Dr. Shah have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
In a large, prospective study, researchers found an association between higher blood levels of PFAS and increased risk of hypertension in middle-aged women. Women in the highest tertile of overall PFAS concentrations had a 71% increased risk of developing hypertension.
“Our findings suggest that long-term cumulative exposure, even before midlife, may increase the risk of high blood pressure, and therefore, the benefit of reducing the population exposure to PFAS and potential prevention of high blood pressure and other health conditions would be enormous,” Sung Kyun Park, ScD, MPH, University of Michigan School of Public Health, Ann Arbor, said in an interview.
The study was published online in Hypertension.
Everywhere and forever
“PFAS are forever chemicals as well as everywhere chemicals,” Dr. Park noted.
Possible sources of PFAS exposure run the gamut from nonstick cookware, food wrappers, and waterproof fabrics to cosmetics and drinking water. They have been detected in the blood of most people and have been linked to a variety of health concerns.
“A few studies showed an association between PFAS and hypertension, but those were cross-sectional and examined prevalence of hypertension. It was unclear whether PFAS are associated with the development (incidence) of hypertension,” Dr. Park explained.
For their study, the researchers examined the association between serum concentrations of PFAS and risks of incident hypertension in 1,058 initially normotensive women participating in the Study of Women’s Health Across the Nation-Multi-Pollutant Study (SWAN-MPS). They were followed annually between 1999 and 2017.
During 11,722 person-years of follow-up, 470 of the women developed hypertension, at a rate of 40.1 cases per 1,000 person-years. Hypertension was defined as blood pressure of at least 140 mm Hg systolic or at least 90 mm Hg diastolic or receiving antihypertensive treatment.
Women in the highest tertile of baseline serum concentration of perfluorooctane sulfonate (PFOS) had a 42% higher risk of developing hypertension, compared with peers in the lowest tertile (adjusted hazard ratio, 1.42; 95% confidence interval, 1.19-1.68; P trend = .01).
Similar results were found for perfluorooctanoate (PFOA) and 2-N-ethyl-perfluorooctane sulfonamido acetate (EtFOSAA), with 47% (aHR, 1.47; 95% CI, 1.24-1.75; P trend = .01) and 42% (aHR, 1.42; 95% CI, 1.19-1.70; P trend = .01) higher risks of incident hypertension, comparing the highest to the lowest tertiles.
The risks persisted after adjusting for various factors, including race, study site, education, financial strain, smoking status, alcohol use, total calorie intake, and menopausal status.
In the PFAS “mixture” analysis, women in the highest tertile of overall PFAS concentrations were 71% more likely to develop hypertension during follow-up, compared with women in the lowest tertile (aHR, 1.71; 95% CI, 1.15-2.54; P trend = .008).
“These findings suggest that PFAS might be an underappreciated contributing factor to women’s cardiovascular disease risk,” the researchers write.
They caution that the study only included middle-aged women and that it is unclear whether the findings hold for middle-aged men.
“This is an important question, but the answer is that we do not know,” Dr. Park told this news organization.
“Women become more susceptible to metabolic changes and hypertension risk during the menopausal transition. Our findings suggest that PFAS may play a role in the development of hypertension in women during this critical life stage,” Dr. Park said.
The researchers say more research is needed to confirm and expand the findings and to find ways to reduce PFAS exposure.
“If confirmed in future studies, these findings suggest that understanding human exposure to PFAS and developing effective strategies to reduce PFAS exposure may help prevent the development of hypertension and thereby reduce the global burden of CVD,” the researchers write.
‘The more we learn, the worse it gets’
This is an “interesting” study and shows that “the more we learn about PFAS, the worse it seems to get,” Ankur Shah, MD, division of kidney disease and hypertension, Warren Alpert Medical School of Brown University, Providence, R.I., said in an interview.
“This multisite, multiracial and multiethnic, community-based longitudinal study establishes an association between PFAS and hypertension,” said Dr. Shah, who wasn’t involved in the study.
“This adds to a growing literature base of associations of PFAS with illnesses, including malignancy, thyroid disorders, diabetes, ulcerative colitis, hyperlipidemia, and pregnancy-induced hypertension,” he noted.
Dr. Shah also noted that the authors adjusted for race and ethnicity, study site, education, financial strain, smoking status, environmental tobacco smoke, alcohol consumption, total calorie intake, and menopausal status “and still found a strong association.”
“Still to be determined are both whether PFAS are the causative agent or if there is an unmeasured/unadjusted for entity which has resulted in both increased PFAS exposure and hypertension, as well as if PFAS are causative, if reduction in PFAS exposure would be result in blood pressure reduction,” Dr. Shah added.
The study had no sources of funding. Dr. Park and Dr. Shah have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM HYPERTENSION
Registered Dietitian Nutritionists’ Role in Hospital in Home
Hospital in Home (HIH) is the delivery of acute care services in a patient’s home as an alternative to hospitalization.1 Compared with traditional inpatient care, HIH programs have been associated with reduced costs, as well as patient and caregiver satisfaction, diseasespecific outcomes, and mortality rates that were similar or improved compared with inpatient admissions.1-4
The US Department of Veterans Affairs (VA) Veterans Health Administration (VHA) and other hospital systems are increasingly adopting HIH models.2-4 At the time of this writing, there were 12 HIH programs in VHA (personal communication, D. Cooper, 2/28/2022). In addition to physicians and nurses, the interdisciplinary HIH team may include a pharmacist, social worker, and registered dietitian nutritionist (RDN).2,5 HIH programs have been shown to improve nutritional status as measured by the Mini Nutritional Assessment Score, but overall, there is a paucity of published information regarding the provision of nutrition care in HIH.6 The role of the RDN has varied within VHA. Some sites, such as the Sacramento VA Medical Center in California, include a distinct RDN position on the HIH team, whereas others, such as the Spark M. Matsunaga VA Medical Center in Honolulu, Hawaii, and the James A. Haley Veterans’ Hospital in Tampa, Florida, consult clinic RDNs.
Since HIH programs typically treat conditions for which diet is an inherent part of the treatment (eg, congestive heart failure [CHF]), there is a need to precisely define the role of the RDN within the HIH model.2,3,7 Drawing from my experience as an HIH RDN, I will describe how the inclusion of an RDN position within the HIH team is optimal for health care delivery and how HIH practitioners can best utilize RDN services.
RDN Role in HIH Team
Delegating nutrition services to an RDN enhances patient care by empowering HIH team members to function at the highest level of their scope of practice. RDNs have been recognized by physicians as the most qualified health care professionals to help patients with diet-related conditions, such as obesity, and physicians also have reported a desire for additional training in nutrition.8 Although home-health nurses have frequently performed nutrition assessments and interventions, survey results have indicated that many nurses do not feel confident in teaching complex nutritional information.9 In my experience, many HIH patients are nutritionally complex, with more than one condition requiring nutrition intervention. For example, patients may be admitted to HIH for management of CHF, but they may also have diabetes mellitus (DM), obesity, and low socioeconomic status. The HIH RDN can address the nutrition aspects of these conditions, freeing time for physicians and nurses to focus on their respective areas of expertise.9,10 Moreover, the RDN can also provide dietary education to the HIH team to increase their knowledge of nutritional topics and promote consistent messaging to patients.
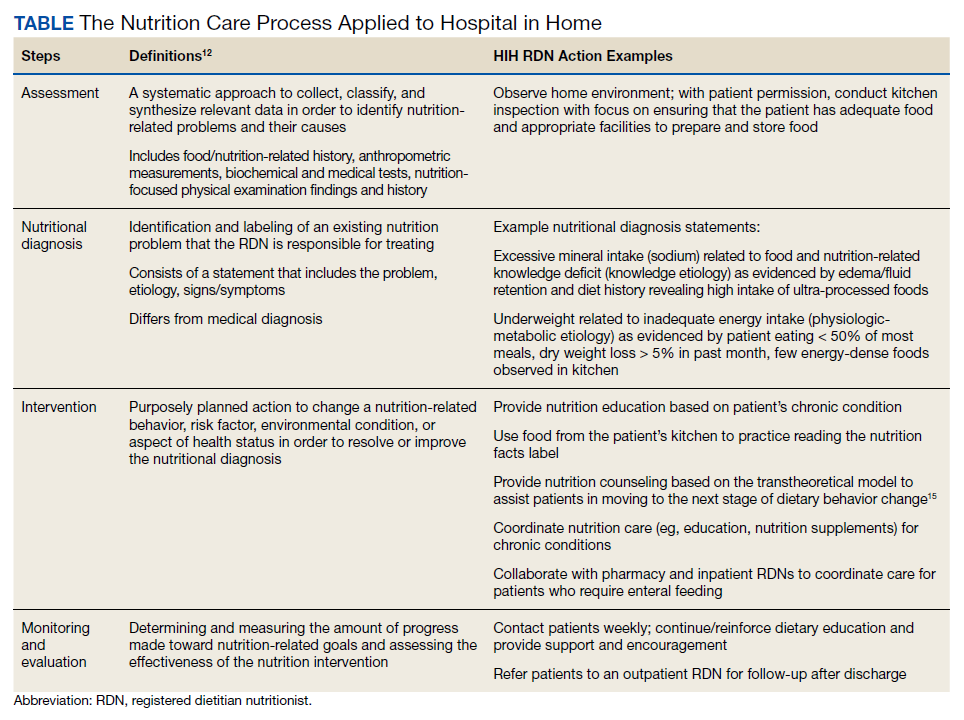
Including an RDN on the HIH team enables patients to have comprehensive, personalized nutrition care. Rather than merely offering generalized nutrition education, RDNs are trained to provide medical nutrition therapy (MNT), which has been shown to improve health outcomes and be cost-effective for conditions such as type 2 DM, chronic kidney disease, hypertension, and obesity.10,11 In MNT, RDNs use the standardized 4-stepnutrition care process (NCP).12 The Table shows examples of how the NCP can be applied in HIH settings. Furthermore, in my experience, MNT from an RDN also contributes to patient satisfaction. Subjective observations from my team have indicated that patients often express more confidence in managing their diets by the time of HIH discharge.
RDNs can guide physicians and pharmacists in ordering oral nutrition supplements (ONS). Within the VHA, a “food first” approach is preferred to increase caloric intake, and patients must meet specific criteria for prescription of an ONS.13 Furthermore, ONS designed for specific medical conditions (eg, chronic kidney disease) are considered nonformulary and require an RDN evaluation.13 Including an RDN on the HIH team allows this evaluation process to begin early in the patient’s admission to the program and ensures that provision of ONS is clinically appropriate and cost-effective.
Care Coordination
HIH is highly interdisciplinary. Team members perform their respective roles and communicate with the team throughout the day. RDNs can help monitor patients and alert physicians for changes in blood glucose, gastrointestinal concerns, and weight. This is especially helpful for patients who do not have a planned nursing visit on the day of an RDN evaluation. The HIH RDN can also collaborate with other team members to address patient needs. For example, for patients with limited financial resources, the HIH RDN can provide nutrition education regarding cooking on a budget, and the HIH social worker can arrange free or low-cost meal services.
Tips
When hiring an HIH RDN, seek candidates with experience in inpatient, outpatient, and home care settings. As a hybrid of these 3 areas, the HIH RDN position requires a unique combination of acute care skills and health coaching. Additionally, in my experience, the HIH RDN interacts more frequently with the HIH team than other RDN colleagues, so it is important that candidates can work independently and take initiative. This type of position would not be suitable for entry-level RDNs.
Stagger HIH team visits to prevent overwhelming the patient and caregivers. Early in our program, my team quickly learned that patients and caregivers can feel overwhelmed with too many home visits upon admission to HIH. After seeing multiple HIH team members the same day, they were often too tired to focus well on diet education during my visit. Staggering visits (eg, completing the initial nutrition assessment 1 day to 1 week after the initial medical and pharmacy visits) has been an effective strategy to address this problem. Furthermore, some patients prefer that the initial RDN appointment is conducted by telephone, with an inperson reassessment the following week. In my experience, HIH workflow is dynamic by nature, so it is crucial to remain flexible and accommodate individual patient needs as much as possible.
Dietary behavior change is a long-term process, and restrictive hospital diets can be challenging to replicate at home. In a hospital setting, clinicians can order a specialized diet (eg, low sodium with fluid restriction for CHF patients), whereas efforts to implement these restrictions in the home setting can be cumbersome and negatively impact quality of life.7,14 Nevertheless, the effectiveness of medical treatment is compromised when patients do not adhere to dietary recommendations. Meal delivery services that offer specialized diets can be a useful resource for patients and caregivers who are unable to cook, and the HIH RDN can assist patients in ordering these services.
HIH patients may vary in terms of readiness to make dietary changes, and in addition to nutrition education, nutrition counseling is usually needed to effect behavior change. My team has found that consideration of the transtheoretical/ stages of change model can be a helpful approach. 15 The HIH RDN can tailor nutrition interventions to the patient’s stage of change. For example, for patients in the precontemplation stage, the HIH RDN would focus on providing information and addressing emotional aspects of dietary change. In contrast, for patients in the action stage of change, the HIH RDN might emphasize behavioral skill training and social support.15 Particularly for patients in the early stages of change, it may be unrealistic to expect full adoption of the recommended diet within the 30 days of the HIH program. However, by acknowledging the reality of the patient’s stage of change, the HIH RDN and team can then collaborate to support the patient in moving toward the next stage. Patients who are not ready for dietary behavior change during the 30 days of HIH may benefit from longer-term support, and the HIH RDN can arrange followup care with an outpatient RDN.
Conclusions
As the HIH model continues to be adopted across the VHA and other health care systems, it is crucial to consider the value and expertise of an RDN for guiding nutrition care in the HIH setting. The HIH RDN contributes to optimal health care delivery by leading nutritional aspects of patient care, offering personalized MNT, and coordinating and collaborating with team members to meet individual patient needs. An RDN can serve as a valuable resource for nutrition information and enhance the team’s overall services, with the potential to impact clinical outcomes and patient satisfaction.
1. Levine DM, Ouchi K, Blanchfield B, et al. Hospitallevel care at home for acutely ill adults: a randomized controlled trial. Ann Intern Med. 2020;172(2):77-85. doi:10.7326/M19-0600
2. Cai S, Grubbs A, Makineni R, Kinosian B, Phibbs CS, Intrator O. Evaluation of the Cincinnati Veterans Affairs medical center hospital-in-home program. J Am Geriatr Soc. 2018;66(7):1392-1398. doi:10.1111/jgs.15382
3. Cai S, Laurel PA, Makineni R, Marks ML. Evaluation of a hospital-in-home program implemented among veterans. Am J Manag Care. 2017;23(8):482-487.
4. Conley J, O’Brien CW, Leff BA, Bolen S, Zulman D. Alternative strategies to inpatient hospitalization for acute medical conditions: a systematic review. JAMA Intern Med. 2016;176(11):1693-1702. doi:10.1001/jamainternmed.2016.5974
5. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1144: Hospital in Home program, Appendix A, Hospital in Home program standards. January 19, 2021. Accessed May 5, 2022. https://www .va.gov/VHApublications/ViewPublication.asp?pub _ID=9157
6. Tibaldi V, Isaia G, Scarafiotti C, et al. Hospital at home for elderly patients with acute decompensation of chronic heart failure: a prospective randomized controlled trial. Arch Intern Med. 2009;169(17):1569-1575. doi:10.1001/archinternmed.2009.267
7. Abshire M, Xu J, Baptiste D, et al. Nutritional interventions in heart failure: a systematic review of the literature. J Card Fail. 2015;21(12):989-999. doi:10.1016/j.cardfail.2015.10.004
8. Bleich SN, Bennett WL, Gudzune KA, Cooper LA. National survey of US primary care physicians’ perspectives about causes of obesity and solutions to improve care. BMJ Open. 2012;2(6):e001871. Published 2012 Dec 20. doi:10.1136/bmjopen-2012-001871
9. Sousa AM. Benefits of dietitian home visits. J Am Diet Assoc. 1994;94(10):1149-1151. doi:10.1016/0002-8223(94)91136-3
10. Casas-Agustench P, Megías-Rangil I, Babio N. Economic benefit of dietetic-nutritional treatment in the multidisciplinary primary care team. Beneficio económico del tratamiento dietético-nutricional en el equipo multidisciplinario de atención primaria. Nutr Hosp. 2020;37(4):863-874. doi:10.20960/nh.03025
11. Lee J, Briggs Early K, Kovesdy CP, Lancaster K, Brown N, Steiber AL. The impact of RDNs on non-communicable diseases: proceedings from The State of Food and Nutrition Series Forum. J Acad Nutr Diet. 2022;122(1):166-174. doi:10.1016/j.jand.2021.02.021
12. Academy of Nutrition and Dietetics. Evidence analysis library, nutrition care process. Accessed May 5, 2022. https://www.andeal.org/ncp
13. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1438, clinical nutrition management and therapy. Appendix A, nutrition support therapy. September 19, 2019. Accessed January 20, 2022. https://www.va.gov/VHAPUBLICATIONS/ViewPublication .asp?pub_ID=8512
14. Vogelzang JL. Fifteen ways to enhance client outcomes by using your registered dietitian. Home Healthc Nurse. 2002;20(4):227-229. doi:10.1097/00004045-200204000-00005
15. Kristal AR, Glanz K, Curry SJ, Patterson RE. How can stages of change be best used in dietary interventions?. J Am Diet Assoc. 1999;99(6):679-684. doi:10.1016/S0002-8223(99)00165-0
Hospital in Home (HIH) is the delivery of acute care services in a patient’s home as an alternative to hospitalization.1 Compared with traditional inpatient care, HIH programs have been associated with reduced costs, as well as patient and caregiver satisfaction, diseasespecific outcomes, and mortality rates that were similar or improved compared with inpatient admissions.1-4
The US Department of Veterans Affairs (VA) Veterans Health Administration (VHA) and other hospital systems are increasingly adopting HIH models.2-4 At the time of this writing, there were 12 HIH programs in VHA (personal communication, D. Cooper, 2/28/2022). In addition to physicians and nurses, the interdisciplinary HIH team may include a pharmacist, social worker, and registered dietitian nutritionist (RDN).2,5 HIH programs have been shown to improve nutritional status as measured by the Mini Nutritional Assessment Score, but overall, there is a paucity of published information regarding the provision of nutrition care in HIH.6 The role of the RDN has varied within VHA. Some sites, such as the Sacramento VA Medical Center in California, include a distinct RDN position on the HIH team, whereas others, such as the Spark M. Matsunaga VA Medical Center in Honolulu, Hawaii, and the James A. Haley Veterans’ Hospital in Tampa, Florida, consult clinic RDNs.
Since HIH programs typically treat conditions for which diet is an inherent part of the treatment (eg, congestive heart failure [CHF]), there is a need to precisely define the role of the RDN within the HIH model.2,3,7 Drawing from my experience as an HIH RDN, I will describe how the inclusion of an RDN position within the HIH team is optimal for health care delivery and how HIH practitioners can best utilize RDN services.
RDN Role in HIH Team
Delegating nutrition services to an RDN enhances patient care by empowering HIH team members to function at the highest level of their scope of practice. RDNs have been recognized by physicians as the most qualified health care professionals to help patients with diet-related conditions, such as obesity, and physicians also have reported a desire for additional training in nutrition.8 Although home-health nurses have frequently performed nutrition assessments and interventions, survey results have indicated that many nurses do not feel confident in teaching complex nutritional information.9 In my experience, many HIH patients are nutritionally complex, with more than one condition requiring nutrition intervention. For example, patients may be admitted to HIH for management of CHF, but they may also have diabetes mellitus (DM), obesity, and low socioeconomic status. The HIH RDN can address the nutrition aspects of these conditions, freeing time for physicians and nurses to focus on their respective areas of expertise.9,10 Moreover, the RDN can also provide dietary education to the HIH team to increase their knowledge of nutritional topics and promote consistent messaging to patients.
Including an RDN on the HIH team enables patients to have comprehensive, personalized nutrition care. Rather than merely offering generalized nutrition education, RDNs are trained to provide medical nutrition therapy (MNT), which has been shown to improve health outcomes and be cost-effective for conditions such as type 2 DM, chronic kidney disease, hypertension, and obesity.10,11 In MNT, RDNs use the standardized 4-stepnutrition care process (NCP).12 The Table shows examples of how the NCP can be applied in HIH settings. Furthermore, in my experience, MNT from an RDN also contributes to patient satisfaction. Subjective observations from my team have indicated that patients often express more confidence in managing their diets by the time of HIH discharge.
RDNs can guide physicians and pharmacists in ordering oral nutrition supplements (ONS). Within the VHA, a “food first” approach is preferred to increase caloric intake, and patients must meet specific criteria for prescription of an ONS.13 Furthermore, ONS designed for specific medical conditions (eg, chronic kidney disease) are considered nonformulary and require an RDN evaluation.13 Including an RDN on the HIH team allows this evaluation process to begin early in the patient’s admission to the program and ensures that provision of ONS is clinically appropriate and cost-effective.
Care Coordination
HIH is highly interdisciplinary. Team members perform their respective roles and communicate with the team throughout the day. RDNs can help monitor patients and alert physicians for changes in blood glucose, gastrointestinal concerns, and weight. This is especially helpful for patients who do not have a planned nursing visit on the day of an RDN evaluation. The HIH RDN can also collaborate with other team members to address patient needs. For example, for patients with limited financial resources, the HIH RDN can provide nutrition education regarding cooking on a budget, and the HIH social worker can arrange free or low-cost meal services.
Tips
When hiring an HIH RDN, seek candidates with experience in inpatient, outpatient, and home care settings. As a hybrid of these 3 areas, the HIH RDN position requires a unique combination of acute care skills and health coaching. Additionally, in my experience, the HIH RDN interacts more frequently with the HIH team than other RDN colleagues, so it is important that candidates can work independently and take initiative. This type of position would not be suitable for entry-level RDNs.
Stagger HIH team visits to prevent overwhelming the patient and caregivers. Early in our program, my team quickly learned that patients and caregivers can feel overwhelmed with too many home visits upon admission to HIH. After seeing multiple HIH team members the same day, they were often too tired to focus well on diet education during my visit. Staggering visits (eg, completing the initial nutrition assessment 1 day to 1 week after the initial medical and pharmacy visits) has been an effective strategy to address this problem. Furthermore, some patients prefer that the initial RDN appointment is conducted by telephone, with an inperson reassessment the following week. In my experience, HIH workflow is dynamic by nature, so it is crucial to remain flexible and accommodate individual patient needs as much as possible.
Dietary behavior change is a long-term process, and restrictive hospital diets can be challenging to replicate at home. In a hospital setting, clinicians can order a specialized diet (eg, low sodium with fluid restriction for CHF patients), whereas efforts to implement these restrictions in the home setting can be cumbersome and negatively impact quality of life.7,14 Nevertheless, the effectiveness of medical treatment is compromised when patients do not adhere to dietary recommendations. Meal delivery services that offer specialized diets can be a useful resource for patients and caregivers who are unable to cook, and the HIH RDN can assist patients in ordering these services.
HIH patients may vary in terms of readiness to make dietary changes, and in addition to nutrition education, nutrition counseling is usually needed to effect behavior change. My team has found that consideration of the transtheoretical/ stages of change model can be a helpful approach. 15 The HIH RDN can tailor nutrition interventions to the patient’s stage of change. For example, for patients in the precontemplation stage, the HIH RDN would focus on providing information and addressing emotional aspects of dietary change. In contrast, for patients in the action stage of change, the HIH RDN might emphasize behavioral skill training and social support.15 Particularly for patients in the early stages of change, it may be unrealistic to expect full adoption of the recommended diet within the 30 days of the HIH program. However, by acknowledging the reality of the patient’s stage of change, the HIH RDN and team can then collaborate to support the patient in moving toward the next stage. Patients who are not ready for dietary behavior change during the 30 days of HIH may benefit from longer-term support, and the HIH RDN can arrange followup care with an outpatient RDN.
Conclusions
As the HIH model continues to be adopted across the VHA and other health care systems, it is crucial to consider the value and expertise of an RDN for guiding nutrition care in the HIH setting. The HIH RDN contributes to optimal health care delivery by leading nutritional aspects of patient care, offering personalized MNT, and coordinating and collaborating with team members to meet individual patient needs. An RDN can serve as a valuable resource for nutrition information and enhance the team’s overall services, with the potential to impact clinical outcomes and patient satisfaction.
Hospital in Home (HIH) is the delivery of acute care services in a patient’s home as an alternative to hospitalization.1 Compared with traditional inpatient care, HIH programs have been associated with reduced costs, as well as patient and caregiver satisfaction, diseasespecific outcomes, and mortality rates that were similar or improved compared with inpatient admissions.1-4
The US Department of Veterans Affairs (VA) Veterans Health Administration (VHA) and other hospital systems are increasingly adopting HIH models.2-4 At the time of this writing, there were 12 HIH programs in VHA (personal communication, D. Cooper, 2/28/2022). In addition to physicians and nurses, the interdisciplinary HIH team may include a pharmacist, social worker, and registered dietitian nutritionist (RDN).2,5 HIH programs have been shown to improve nutritional status as measured by the Mini Nutritional Assessment Score, but overall, there is a paucity of published information regarding the provision of nutrition care in HIH.6 The role of the RDN has varied within VHA. Some sites, such as the Sacramento VA Medical Center in California, include a distinct RDN position on the HIH team, whereas others, such as the Spark M. Matsunaga VA Medical Center in Honolulu, Hawaii, and the James A. Haley Veterans’ Hospital in Tampa, Florida, consult clinic RDNs.
Since HIH programs typically treat conditions for which diet is an inherent part of the treatment (eg, congestive heart failure [CHF]), there is a need to precisely define the role of the RDN within the HIH model.2,3,7 Drawing from my experience as an HIH RDN, I will describe how the inclusion of an RDN position within the HIH team is optimal for health care delivery and how HIH practitioners can best utilize RDN services.
RDN Role in HIH Team
Delegating nutrition services to an RDN enhances patient care by empowering HIH team members to function at the highest level of their scope of practice. RDNs have been recognized by physicians as the most qualified health care professionals to help patients with diet-related conditions, such as obesity, and physicians also have reported a desire for additional training in nutrition.8 Although home-health nurses have frequently performed nutrition assessments and interventions, survey results have indicated that many nurses do not feel confident in teaching complex nutritional information.9 In my experience, many HIH patients are nutritionally complex, with more than one condition requiring nutrition intervention. For example, patients may be admitted to HIH for management of CHF, but they may also have diabetes mellitus (DM), obesity, and low socioeconomic status. The HIH RDN can address the nutrition aspects of these conditions, freeing time for physicians and nurses to focus on their respective areas of expertise.9,10 Moreover, the RDN can also provide dietary education to the HIH team to increase their knowledge of nutritional topics and promote consistent messaging to patients.
Including an RDN on the HIH team enables patients to have comprehensive, personalized nutrition care. Rather than merely offering generalized nutrition education, RDNs are trained to provide medical nutrition therapy (MNT), which has been shown to improve health outcomes and be cost-effective for conditions such as type 2 DM, chronic kidney disease, hypertension, and obesity.10,11 In MNT, RDNs use the standardized 4-stepnutrition care process (NCP).12 The Table shows examples of how the NCP can be applied in HIH settings. Furthermore, in my experience, MNT from an RDN also contributes to patient satisfaction. Subjective observations from my team have indicated that patients often express more confidence in managing their diets by the time of HIH discharge.
RDNs can guide physicians and pharmacists in ordering oral nutrition supplements (ONS). Within the VHA, a “food first” approach is preferred to increase caloric intake, and patients must meet specific criteria for prescription of an ONS.13 Furthermore, ONS designed for specific medical conditions (eg, chronic kidney disease) are considered nonformulary and require an RDN evaluation.13 Including an RDN on the HIH team allows this evaluation process to begin early in the patient’s admission to the program and ensures that provision of ONS is clinically appropriate and cost-effective.
Care Coordination
HIH is highly interdisciplinary. Team members perform their respective roles and communicate with the team throughout the day. RDNs can help monitor patients and alert physicians for changes in blood glucose, gastrointestinal concerns, and weight. This is especially helpful for patients who do not have a planned nursing visit on the day of an RDN evaluation. The HIH RDN can also collaborate with other team members to address patient needs. For example, for patients with limited financial resources, the HIH RDN can provide nutrition education regarding cooking on a budget, and the HIH social worker can arrange free or low-cost meal services.
Tips
When hiring an HIH RDN, seek candidates with experience in inpatient, outpatient, and home care settings. As a hybrid of these 3 areas, the HIH RDN position requires a unique combination of acute care skills and health coaching. Additionally, in my experience, the HIH RDN interacts more frequently with the HIH team than other RDN colleagues, so it is important that candidates can work independently and take initiative. This type of position would not be suitable for entry-level RDNs.
Stagger HIH team visits to prevent overwhelming the patient and caregivers. Early in our program, my team quickly learned that patients and caregivers can feel overwhelmed with too many home visits upon admission to HIH. After seeing multiple HIH team members the same day, they were often too tired to focus well on diet education during my visit. Staggering visits (eg, completing the initial nutrition assessment 1 day to 1 week after the initial medical and pharmacy visits) has been an effective strategy to address this problem. Furthermore, some patients prefer that the initial RDN appointment is conducted by telephone, with an inperson reassessment the following week. In my experience, HIH workflow is dynamic by nature, so it is crucial to remain flexible and accommodate individual patient needs as much as possible.
Dietary behavior change is a long-term process, and restrictive hospital diets can be challenging to replicate at home. In a hospital setting, clinicians can order a specialized diet (eg, low sodium with fluid restriction for CHF patients), whereas efforts to implement these restrictions in the home setting can be cumbersome and negatively impact quality of life.7,14 Nevertheless, the effectiveness of medical treatment is compromised when patients do not adhere to dietary recommendations. Meal delivery services that offer specialized diets can be a useful resource for patients and caregivers who are unable to cook, and the HIH RDN can assist patients in ordering these services.
HIH patients may vary in terms of readiness to make dietary changes, and in addition to nutrition education, nutrition counseling is usually needed to effect behavior change. My team has found that consideration of the transtheoretical/ stages of change model can be a helpful approach. 15 The HIH RDN can tailor nutrition interventions to the patient’s stage of change. For example, for patients in the precontemplation stage, the HIH RDN would focus on providing information and addressing emotional aspects of dietary change. In contrast, for patients in the action stage of change, the HIH RDN might emphasize behavioral skill training and social support.15 Particularly for patients in the early stages of change, it may be unrealistic to expect full adoption of the recommended diet within the 30 days of the HIH program. However, by acknowledging the reality of the patient’s stage of change, the HIH RDN and team can then collaborate to support the patient in moving toward the next stage. Patients who are not ready for dietary behavior change during the 30 days of HIH may benefit from longer-term support, and the HIH RDN can arrange followup care with an outpatient RDN.
Conclusions
As the HIH model continues to be adopted across the VHA and other health care systems, it is crucial to consider the value and expertise of an RDN for guiding nutrition care in the HIH setting. The HIH RDN contributes to optimal health care delivery by leading nutritional aspects of patient care, offering personalized MNT, and coordinating and collaborating with team members to meet individual patient needs. An RDN can serve as a valuable resource for nutrition information and enhance the team’s overall services, with the potential to impact clinical outcomes and patient satisfaction.
1. Levine DM, Ouchi K, Blanchfield B, et al. Hospitallevel care at home for acutely ill adults: a randomized controlled trial. Ann Intern Med. 2020;172(2):77-85. doi:10.7326/M19-0600
2. Cai S, Grubbs A, Makineni R, Kinosian B, Phibbs CS, Intrator O. Evaluation of the Cincinnati Veterans Affairs medical center hospital-in-home program. J Am Geriatr Soc. 2018;66(7):1392-1398. doi:10.1111/jgs.15382
3. Cai S, Laurel PA, Makineni R, Marks ML. Evaluation of a hospital-in-home program implemented among veterans. Am J Manag Care. 2017;23(8):482-487.
4. Conley J, O’Brien CW, Leff BA, Bolen S, Zulman D. Alternative strategies to inpatient hospitalization for acute medical conditions: a systematic review. JAMA Intern Med. 2016;176(11):1693-1702. doi:10.1001/jamainternmed.2016.5974
5. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1144: Hospital in Home program, Appendix A, Hospital in Home program standards. January 19, 2021. Accessed May 5, 2022. https://www .va.gov/VHApublications/ViewPublication.asp?pub _ID=9157
6. Tibaldi V, Isaia G, Scarafiotti C, et al. Hospital at home for elderly patients with acute decompensation of chronic heart failure: a prospective randomized controlled trial. Arch Intern Med. 2009;169(17):1569-1575. doi:10.1001/archinternmed.2009.267
7. Abshire M, Xu J, Baptiste D, et al. Nutritional interventions in heart failure: a systematic review of the literature. J Card Fail. 2015;21(12):989-999. doi:10.1016/j.cardfail.2015.10.004
8. Bleich SN, Bennett WL, Gudzune KA, Cooper LA. National survey of US primary care physicians’ perspectives about causes of obesity and solutions to improve care. BMJ Open. 2012;2(6):e001871. Published 2012 Dec 20. doi:10.1136/bmjopen-2012-001871
9. Sousa AM. Benefits of dietitian home visits. J Am Diet Assoc. 1994;94(10):1149-1151. doi:10.1016/0002-8223(94)91136-3
10. Casas-Agustench P, Megías-Rangil I, Babio N. Economic benefit of dietetic-nutritional treatment in the multidisciplinary primary care team. Beneficio económico del tratamiento dietético-nutricional en el equipo multidisciplinario de atención primaria. Nutr Hosp. 2020;37(4):863-874. doi:10.20960/nh.03025
11. Lee J, Briggs Early K, Kovesdy CP, Lancaster K, Brown N, Steiber AL. The impact of RDNs on non-communicable diseases: proceedings from The State of Food and Nutrition Series Forum. J Acad Nutr Diet. 2022;122(1):166-174. doi:10.1016/j.jand.2021.02.021
12. Academy of Nutrition and Dietetics. Evidence analysis library, nutrition care process. Accessed May 5, 2022. https://www.andeal.org/ncp
13. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1438, clinical nutrition management and therapy. Appendix A, nutrition support therapy. September 19, 2019. Accessed January 20, 2022. https://www.va.gov/VHAPUBLICATIONS/ViewPublication .asp?pub_ID=8512
14. Vogelzang JL. Fifteen ways to enhance client outcomes by using your registered dietitian. Home Healthc Nurse. 2002;20(4):227-229. doi:10.1097/00004045-200204000-00005
15. Kristal AR, Glanz K, Curry SJ, Patterson RE. How can stages of change be best used in dietary interventions?. J Am Diet Assoc. 1999;99(6):679-684. doi:10.1016/S0002-8223(99)00165-0
1. Levine DM, Ouchi K, Blanchfield B, et al. Hospitallevel care at home for acutely ill adults: a randomized controlled trial. Ann Intern Med. 2020;172(2):77-85. doi:10.7326/M19-0600
2. Cai S, Grubbs A, Makineni R, Kinosian B, Phibbs CS, Intrator O. Evaluation of the Cincinnati Veterans Affairs medical center hospital-in-home program. J Am Geriatr Soc. 2018;66(7):1392-1398. doi:10.1111/jgs.15382
3. Cai S, Laurel PA, Makineni R, Marks ML. Evaluation of a hospital-in-home program implemented among veterans. Am J Manag Care. 2017;23(8):482-487.
4. Conley J, O’Brien CW, Leff BA, Bolen S, Zulman D. Alternative strategies to inpatient hospitalization for acute medical conditions: a systematic review. JAMA Intern Med. 2016;176(11):1693-1702. doi:10.1001/jamainternmed.2016.5974
5. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1144: Hospital in Home program, Appendix A, Hospital in Home program standards. January 19, 2021. Accessed May 5, 2022. https://www .va.gov/VHApublications/ViewPublication.asp?pub _ID=9157
6. Tibaldi V, Isaia G, Scarafiotti C, et al. Hospital at home for elderly patients with acute decompensation of chronic heart failure: a prospective randomized controlled trial. Arch Intern Med. 2009;169(17):1569-1575. doi:10.1001/archinternmed.2009.267
7. Abshire M, Xu J, Baptiste D, et al. Nutritional interventions in heart failure: a systematic review of the literature. J Card Fail. 2015;21(12):989-999. doi:10.1016/j.cardfail.2015.10.004
8. Bleich SN, Bennett WL, Gudzune KA, Cooper LA. National survey of US primary care physicians’ perspectives about causes of obesity and solutions to improve care. BMJ Open. 2012;2(6):e001871. Published 2012 Dec 20. doi:10.1136/bmjopen-2012-001871
9. Sousa AM. Benefits of dietitian home visits. J Am Diet Assoc. 1994;94(10):1149-1151. doi:10.1016/0002-8223(94)91136-3
10. Casas-Agustench P, Megías-Rangil I, Babio N. Economic benefit of dietetic-nutritional treatment in the multidisciplinary primary care team. Beneficio económico del tratamiento dietético-nutricional en el equipo multidisciplinario de atención primaria. Nutr Hosp. 2020;37(4):863-874. doi:10.20960/nh.03025
11. Lee J, Briggs Early K, Kovesdy CP, Lancaster K, Brown N, Steiber AL. The impact of RDNs on non-communicable diseases: proceedings from The State of Food and Nutrition Series Forum. J Acad Nutr Diet. 2022;122(1):166-174. doi:10.1016/j.jand.2021.02.021
12. Academy of Nutrition and Dietetics. Evidence analysis library, nutrition care process. Accessed May 5, 2022. https://www.andeal.org/ncp
13. US Department of Veterans Affairs, Veterans Health Administration. VHA Directive 1438, clinical nutrition management and therapy. Appendix A, nutrition support therapy. September 19, 2019. Accessed January 20, 2022. https://www.va.gov/VHAPUBLICATIONS/ViewPublication .asp?pub_ID=8512
14. Vogelzang JL. Fifteen ways to enhance client outcomes by using your registered dietitian. Home Healthc Nurse. 2002;20(4):227-229. doi:10.1097/00004045-200204000-00005
15. Kristal AR, Glanz K, Curry SJ, Patterson RE. How can stages of change be best used in dietary interventions?. J Am Diet Assoc. 1999;99(6):679-684. doi:10.1016/S0002-8223(99)00165-0
Don’t overlook this cause of falls
I enjoyed reading “How to identify balance disorders and reduce fall risk” (J Fam Pract. 2022;71:20-30) from the January/February issue. I was, however, disappointed to see that normal pressure hydrocephalus (NPH) was not discussed in the article or tables.
Recently, I took care of a 72-year-old patient who presented after multiple falls. In conjunction with Neurology, the presumptive diagnosis of Parkinson disease was made. However, the patient continued to experience a health decline that included cognitive changes, nocturia, and the classic “magnetic gait” of NPH (mnemonic for diagnosing this triad of symptoms: weird, wet, wobbly). The presumptive diagnosis was then changed when the results of a fluorodopa F18 positron emission tomography scan (also known as a DaT scan) returned as normal, essentially excluding the diagnosis of Parkinson disease.
The patient has since seen a dramatic improvement in gait and cognitive and urinary symptoms following a high-volume lumbar puncture and placement of a ventriculoperitoneal shunt.
This case demonstrates the importance of considering NPH in the differential diagnosis for patients with balance disorders. Prompt diagnosis and management can result in a variable, but at times dramatic, reversal of symptoms.
Ernestine Lee, MD, MPH
Austin, TX
I enjoyed reading “How to identify balance disorders and reduce fall risk” (J Fam Pract. 2022;71:20-30) from the January/February issue. I was, however, disappointed to see that normal pressure hydrocephalus (NPH) was not discussed in the article or tables.
Recently, I took care of a 72-year-old patient who presented after multiple falls. In conjunction with Neurology, the presumptive diagnosis of Parkinson disease was made. However, the patient continued to experience a health decline that included cognitive changes, nocturia, and the classic “magnetic gait” of NPH (mnemonic for diagnosing this triad of symptoms: weird, wet, wobbly). The presumptive diagnosis was then changed when the results of a fluorodopa F18 positron emission tomography scan (also known as a DaT scan) returned as normal, essentially excluding the diagnosis of Parkinson disease.
The patient has since seen a dramatic improvement in gait and cognitive and urinary symptoms following a high-volume lumbar puncture and placement of a ventriculoperitoneal shunt.
This case demonstrates the importance of considering NPH in the differential diagnosis for patients with balance disorders. Prompt diagnosis and management can result in a variable, but at times dramatic, reversal of symptoms.
Ernestine Lee, MD, MPH
Austin, TX
I enjoyed reading “How to identify balance disorders and reduce fall risk” (J Fam Pract. 2022;71:20-30) from the January/February issue. I was, however, disappointed to see that normal pressure hydrocephalus (NPH) was not discussed in the article or tables.
Recently, I took care of a 72-year-old patient who presented after multiple falls. In conjunction with Neurology, the presumptive diagnosis of Parkinson disease was made. However, the patient continued to experience a health decline that included cognitive changes, nocturia, and the classic “magnetic gait” of NPH (mnemonic for diagnosing this triad of symptoms: weird, wet, wobbly). The presumptive diagnosis was then changed when the results of a fluorodopa F18 positron emission tomography scan (also known as a DaT scan) returned as normal, essentially excluding the diagnosis of Parkinson disease.
The patient has since seen a dramatic improvement in gait and cognitive and urinary symptoms following a high-volume lumbar puncture and placement of a ventriculoperitoneal shunt.
This case demonstrates the importance of considering NPH in the differential diagnosis for patients with balance disorders. Prompt diagnosis and management can result in a variable, but at times dramatic, reversal of symptoms.
Ernestine Lee, MD, MPH
Austin, TX
Findings raise questions about migraine and sleep
CHARLOTTE, N.C. – What may be the largest case-based study of patients with migraine and sleep-disordered breathing to date has found that, counter to prevailing thought, they may not be at higher risk of having obstructive sleep apnea (OSA) than nonmigraine patients, although further prospective studies are needed to validate that finding.
“This in no way for me changes the fact that, for patients that complain of headaches, sleep apnea remains to be something that should be considered as possible cause of their headaches,” neurologist and Cleveland Clinic postdoctoral fellow Eric Gruenthal, MD, said in an interview after he presented his results at the annual meeting of the Associated Professional Sleep Societies.

The study suggested that patients with migraine may have an OSA risk that “may be a little lower” than their nonmigraine counterparts, Dr. Gruenthal said. “But we have really yet to determine whether that’s true or not.”
Large case-based study
The retrospective case study included 4,783 migraine cases from the Cleveland Clinic electronic health record database who were case matched on a 1:3 basis with 14,287 controls. Patients with migraine had an average age of 47.5 years (±13.3) and body mass index of 33.7 kg/m2 (±8.6), and 76.4% were White. All patients had polysomnography (PSG) at a Cleveland Clinic facility from 1998 to 2021.
The analysis evaluated the collected data in two domains: sleep architecture, consisting of arousal index (AI), total sleep time (TST) and percentage of sleep stage time; and sleep-disordered breathing, including apnea hypopnea index (AHI) and mean oxygen saturation. The key findings of the migraine patients versus controls include:
- Lower AI, 19.6 (95% confidence interval, 12.8-30.9) versus 22.6 (95% CI, 14.7-34.9; P < .001).
- Shorter TST, 359 (95% CI, 307-421) versus 363 (95% CI, 306-432.5) minutes (P = .01).
- With regard to sleep stage, the percentage of N2 sleep was higher, 67.8% (95% CI, 59.6%-75.6%) versus 67% (95% CI, 58.4%-74.8%; P < .001); but the percentage of REM was lower at 16.7% (95% CI, 10%-22%) versus 17% (95% CI, 11.1%-22.2%; P = .012).
- Lower AHI, 7.4 (95% CI, 2.6-17) versus 9.5 (95% CI, 3.7-22.1, P < .001).
- Higher mean oxygen saturation, 93.7 (±2.4) versus 93.3% (±2.6; P < .001).
“Also,” Dr. Gruenthal added, “we found that the percentage of sleep time with oxygen saturation below 90% was lower among patients with migraine, at 1.3% versus 2.4%” (P < .001).
A unique profile?
The goal of the study was to determine whether migraine patients would have a unique PSG profile, Dr. Gruenthal said. “We were trying to overcome some of the limitations of previous studies, most notably those that use small sample sizes, and in some cases a lack of controls.”
The findings that migraine patients would have higher AI and elevated AHI ran counter to the study’s hypotheses, but fell in line with the expectation that they would have reduced TST, Dr. Gruenthal said.
Patients with migraine “may, in fact, exhibit a lower burden of sleep-disordered breathing, and that’s based on our findings such as the lower AHI and decreased burden of hypoxemia,” he said. “We theorized that this may be related to patients with migraine having a unique CGRP [calcitonin gene-related peptide] and serotonin physiology.” He noted that previously published research has shown that sleep CGRP and serotonin have a central role in causing arousal in response to rising CO2 levels during sleep, which can occur during apneas and hypopneas.
Dr. Gruenthal noted that the researchers are still analyzing the findings. “We theorized that possible indication bias may be present in our study,” he said. “It may be the case that patients with migraine are more likely to get their PSG done because of their headache and not for things like snoring and witnessed apneas, which may be more predictive of significant sleep apnea.” They’re also evaluating the “question of medicine confounding.”
Dr. Gruenthal added that “the big unanswered question out there is, if you have a patient with migraine who also has sleep apnea, by treating the sleep apnea will that improve their migraine?”
More questions than answers
Commenting on the study, Donald Bliwise, PhD, professor of neurology at Emory Sleep Center, Atlanta, said the study findings shouldn’t change how clinicians approach migraine in relation to sleep.
“It’s a case series, it’s retrospective,” said Dr. Bliwise, who was not involved in the study. “It’s the largest study that I know of that has ever looked at the diagnosis of migraine in relation to polysomnographic measures of sleep, but it’s imprecise to the extent that migraine is a clinical diagnosis, so not everyone that carries the diagnosis of migraine has the diagnosis made by a neurologist.”
The study raises more questions than it answers, he said, “but that’s not necessarily a bad thing. I think we need more prospective studies.” Those studies should be more granular in how they analyze sleep in migraine patients “Since migraine is an intermittent event, and sleep quality and length, and percentage of REM sleep and even sleep apnea can vary from night to night, it would be fascinating to look at headaches over a month in relation to sleep over a month.”
Dr. Gruenthal and Dr. Bliwise have no disclosures. The Association of Migraine Disorders provided funding for the study.
CHARLOTTE, N.C. – What may be the largest case-based study of patients with migraine and sleep-disordered breathing to date has found that, counter to prevailing thought, they may not be at higher risk of having obstructive sleep apnea (OSA) than nonmigraine patients, although further prospective studies are needed to validate that finding.
“This in no way for me changes the fact that, for patients that complain of headaches, sleep apnea remains to be something that should be considered as possible cause of their headaches,” neurologist and Cleveland Clinic postdoctoral fellow Eric Gruenthal, MD, said in an interview after he presented his results at the annual meeting of the Associated Professional Sleep Societies.
The study suggested that patients with migraine may have an OSA risk that “may be a little lower” than their nonmigraine counterparts, Dr. Gruenthal said. “But we have really yet to determine whether that’s true or not.”
Large case-based study
The retrospective case study included 4,783 migraine cases from the Cleveland Clinic electronic health record database who were case matched on a 1:3 basis with 14,287 controls. Patients with migraine had an average age of 47.5 years (±13.3) and body mass index of 33.7 kg/m2 (±8.6), and 76.4% were White. All patients had polysomnography (PSG) at a Cleveland Clinic facility from 1998 to 2021.
The analysis evaluated the collected data in two domains: sleep architecture, consisting of arousal index (AI), total sleep time (TST) and percentage of sleep stage time; and sleep-disordered breathing, including apnea hypopnea index (AHI) and mean oxygen saturation. The key findings of the migraine patients versus controls include:
- Lower AI, 19.6 (95% confidence interval, 12.8-30.9) versus 22.6 (95% CI, 14.7-34.9; P < .001).
- Shorter TST, 359 (95% CI, 307-421) versus 363 (95% CI, 306-432.5) minutes (P = .01).
- With regard to sleep stage, the percentage of N2 sleep was higher, 67.8% (95% CI, 59.6%-75.6%) versus 67% (95% CI, 58.4%-74.8%; P < .001); but the percentage of REM was lower at 16.7% (95% CI, 10%-22%) versus 17% (95% CI, 11.1%-22.2%; P = .012).
- Lower AHI, 7.4 (95% CI, 2.6-17) versus 9.5 (95% CI, 3.7-22.1, P < .001).
- Higher mean oxygen saturation, 93.7 (±2.4) versus 93.3% (±2.6; P < .001).
“Also,” Dr. Gruenthal added, “we found that the percentage of sleep time with oxygen saturation below 90% was lower among patients with migraine, at 1.3% versus 2.4%” (P < .001).
A unique profile?
The goal of the study was to determine whether migraine patients would have a unique PSG profile, Dr. Gruenthal said. “We were trying to overcome some of the limitations of previous studies, most notably those that use small sample sizes, and in some cases a lack of controls.”
The findings that migraine patients would have higher AI and elevated AHI ran counter to the study’s hypotheses, but fell in line with the expectation that they would have reduced TST, Dr. Gruenthal said.
Patients with migraine “may, in fact, exhibit a lower burden of sleep-disordered breathing, and that’s based on our findings such as the lower AHI and decreased burden of hypoxemia,” he said. “We theorized that this may be related to patients with migraine having a unique CGRP [calcitonin gene-related peptide] and serotonin physiology.” He noted that previously published research has shown that sleep CGRP and serotonin have a central role in causing arousal in response to rising CO2 levels during sleep, which can occur during apneas and hypopneas.
Dr. Gruenthal noted that the researchers are still analyzing the findings. “We theorized that possible indication bias may be present in our study,” he said. “It may be the case that patients with migraine are more likely to get their PSG done because of their headache and not for things like snoring and witnessed apneas, which may be more predictive of significant sleep apnea.” They’re also evaluating the “question of medicine confounding.”
Dr. Gruenthal added that “the big unanswered question out there is, if you have a patient with migraine who also has sleep apnea, by treating the sleep apnea will that improve their migraine?”
More questions than answers
Commenting on the study, Donald Bliwise, PhD, professor of neurology at Emory Sleep Center, Atlanta, said the study findings shouldn’t change how clinicians approach migraine in relation to sleep.
“It’s a case series, it’s retrospective,” said Dr. Bliwise, who was not involved in the study. “It’s the largest study that I know of that has ever looked at the diagnosis of migraine in relation to polysomnographic measures of sleep, but it’s imprecise to the extent that migraine is a clinical diagnosis, so not everyone that carries the diagnosis of migraine has the diagnosis made by a neurologist.”
The study raises more questions than it answers, he said, “but that’s not necessarily a bad thing. I think we need more prospective studies.” Those studies should be more granular in how they analyze sleep in migraine patients “Since migraine is an intermittent event, and sleep quality and length, and percentage of REM sleep and even sleep apnea can vary from night to night, it would be fascinating to look at headaches over a month in relation to sleep over a month.”
Dr. Gruenthal and Dr. Bliwise have no disclosures. The Association of Migraine Disorders provided funding for the study.
CHARLOTTE, N.C. – What may be the largest case-based study of patients with migraine and sleep-disordered breathing to date has found that, counter to prevailing thought, they may not be at higher risk of having obstructive sleep apnea (OSA) than nonmigraine patients, although further prospective studies are needed to validate that finding.
“This in no way for me changes the fact that, for patients that complain of headaches, sleep apnea remains to be something that should be considered as possible cause of their headaches,” neurologist and Cleveland Clinic postdoctoral fellow Eric Gruenthal, MD, said in an interview after he presented his results at the annual meeting of the Associated Professional Sleep Societies.
The study suggested that patients with migraine may have an OSA risk that “may be a little lower” than their nonmigraine counterparts, Dr. Gruenthal said. “But we have really yet to determine whether that’s true or not.”
Large case-based study
The retrospective case study included 4,783 migraine cases from the Cleveland Clinic electronic health record database who were case matched on a 1:3 basis with 14,287 controls. Patients with migraine had an average age of 47.5 years (±13.3) and body mass index of 33.7 kg/m2 (±8.6), and 76.4% were White. All patients had polysomnography (PSG) at a Cleveland Clinic facility from 1998 to 2021.
The analysis evaluated the collected data in two domains: sleep architecture, consisting of arousal index (AI), total sleep time (TST) and percentage of sleep stage time; and sleep-disordered breathing, including apnea hypopnea index (AHI) and mean oxygen saturation. The key findings of the migraine patients versus controls include:
- Lower AI, 19.6 (95% confidence interval, 12.8-30.9) versus 22.6 (95% CI, 14.7-34.9; P < .001).
- Shorter TST, 359 (95% CI, 307-421) versus 363 (95% CI, 306-432.5) minutes (P = .01).
- With regard to sleep stage, the percentage of N2 sleep was higher, 67.8% (95% CI, 59.6%-75.6%) versus 67% (95% CI, 58.4%-74.8%; P < .001); but the percentage of REM was lower at 16.7% (95% CI, 10%-22%) versus 17% (95% CI, 11.1%-22.2%; P = .012).
- Lower AHI, 7.4 (95% CI, 2.6-17) versus 9.5 (95% CI, 3.7-22.1, P < .001).
- Higher mean oxygen saturation, 93.7 (±2.4) versus 93.3% (±2.6; P < .001).
“Also,” Dr. Gruenthal added, “we found that the percentage of sleep time with oxygen saturation below 90% was lower among patients with migraine, at 1.3% versus 2.4%” (P < .001).
A unique profile?
The goal of the study was to determine whether migraine patients would have a unique PSG profile, Dr. Gruenthal said. “We were trying to overcome some of the limitations of previous studies, most notably those that use small sample sizes, and in some cases a lack of controls.”
The findings that migraine patients would have higher AI and elevated AHI ran counter to the study’s hypotheses, but fell in line with the expectation that they would have reduced TST, Dr. Gruenthal said.
Patients with migraine “may, in fact, exhibit a lower burden of sleep-disordered breathing, and that’s based on our findings such as the lower AHI and decreased burden of hypoxemia,” he said. “We theorized that this may be related to patients with migraine having a unique CGRP [calcitonin gene-related peptide] and serotonin physiology.” He noted that previously published research has shown that sleep CGRP and serotonin have a central role in causing arousal in response to rising CO2 levels during sleep, which can occur during apneas and hypopneas.
Dr. Gruenthal noted that the researchers are still analyzing the findings. “We theorized that possible indication bias may be present in our study,” he said. “It may be the case that patients with migraine are more likely to get their PSG done because of their headache and not for things like snoring and witnessed apneas, which may be more predictive of significant sleep apnea.” They’re also evaluating the “question of medicine confounding.”
Dr. Gruenthal added that “the big unanswered question out there is, if you have a patient with migraine who also has sleep apnea, by treating the sleep apnea will that improve their migraine?”
More questions than answers
Commenting on the study, Donald Bliwise, PhD, professor of neurology at Emory Sleep Center, Atlanta, said the study findings shouldn’t change how clinicians approach migraine in relation to sleep.
“It’s a case series, it’s retrospective,” said Dr. Bliwise, who was not involved in the study. “It’s the largest study that I know of that has ever looked at the diagnosis of migraine in relation to polysomnographic measures of sleep, but it’s imprecise to the extent that migraine is a clinical diagnosis, so not everyone that carries the diagnosis of migraine has the diagnosis made by a neurologist.”
The study raises more questions than it answers, he said, “but that’s not necessarily a bad thing. I think we need more prospective studies.” Those studies should be more granular in how they analyze sleep in migraine patients “Since migraine is an intermittent event, and sleep quality and length, and percentage of REM sleep and even sleep apnea can vary from night to night, it would be fascinating to look at headaches over a month in relation to sleep over a month.”
Dr. Gruenthal and Dr. Bliwise have no disclosures. The Association of Migraine Disorders provided funding for the study.
AT SLEEP 2022
Taking the time to get it right
I cannot agree more with Dr. Hickner’s editorial, “The power of the pause to prevent diagnostic error” (J Fam Pract. 2022;71:102). In 1974, when I started at the Medical College of Virginia, I thought I was going to be a medical researcher. By mid-1978, I had completely changed my focus to family medicine. Fortunately, my drive for detail and accuracy remained, albeit at odds with a whirlwind residency and solo practice. I drove my staff (and wife) crazy because I frequently spent more than the “allotted” time with a patient. The time was not wasted; it was most important for me to gain the trust of the patient and then to get it right—or find a path to the answer.
Jeff Ginther, MD
Bristol, VA
I cannot agree more with Dr. Hickner’s editorial, “The power of the pause to prevent diagnostic error” (J Fam Pract. 2022;71:102). In 1974, when I started at the Medical College of Virginia, I thought I was going to be a medical researcher. By mid-1978, I had completely changed my focus to family medicine. Fortunately, my drive for detail and accuracy remained, albeit at odds with a whirlwind residency and solo practice. I drove my staff (and wife) crazy because I frequently spent more than the “allotted” time with a patient. The time was not wasted; it was most important for me to gain the trust of the patient and then to get it right—or find a path to the answer.
Jeff Ginther, MD
Bristol, VA
I cannot agree more with Dr. Hickner’s editorial, “The power of the pause to prevent diagnostic error” (J Fam Pract. 2022;71:102). In 1974, when I started at the Medical College of Virginia, I thought I was going to be a medical researcher. By mid-1978, I had completely changed my focus to family medicine. Fortunately, my drive for detail and accuracy remained, albeit at odds with a whirlwind residency and solo practice. I drove my staff (and wife) crazy because I frequently spent more than the “allotted” time with a patient. The time was not wasted; it was most important for me to gain the trust of the patient and then to get it right—or find a path to the answer.
Jeff Ginther, MD
Bristol, VA
Center-based childcare associated with healthier body weight
The findings of the prospective Canadian study suggest that professional childcare centers that engage in standard practices are having a positive and lasting impact on children’s health, reported lead author Michaela Kucab, RD, MHSc, of the University of Toronto and colleagues.
“Attending center-based childcare in early childhood may influence important health behaviors including nutrition, physical activity, and routines related to child growth and weight status,” the investigators wrote in their abstract, which Ms. Kucab presented at the virtual conference sponsored by the American Society for Nutrition.
Their study involved 3,503 children who attended childcare in Canada during early childhood (mean age at baseline was 2.7 years) with follow-up from ages 4-10.
Overweight/obesity risk reduced
Children who received full-time, center-based care had a 22% lower risk of overweight/obesity and a mean body mass index z score (zBMI) that was 0.11 points lower at age 4 and 7 years than those who received non–center-based care. The benefits of center-based care were even more pronounced among children from lower-income families, who, at age 10, had a 48% lower risk of overweight/obesity and a mean zBMI that was 0.32 points lower with center-based versus non–center-based care.
In a written comment, Ms. Kucab and principal author Jonathon Maguire, MD, MSc, of the University of Toronto, explained that the former difference in zBMI translates to approximately half a pound of bodyweight in an average child, whereas the larger difference in zBMI among children from lower-income families would amount to approximately three pounds. They emphasized that these are rough estimations.
Ms. Kucab and Dr. Maguire noted that body weight differences correlated with the amount of time spent in center-based care.
“There was an observed trend, whereby the estimated mean difference [in zBMI] became slightly larger (or stronger) with a higher intensity of center-based childcare compared to non–center-based childcare,” they said.
To learn more about the earliest impacts of center-based care, the investigators are conducting a clinical trial, The Nutrition Recommendation Intervention Trials in Children’s Health Care (NuRISH), which will involve 600 children aged younger than 2 years.
Center-based childcare may reduce disadvantages of low-income children
“Although more research is needed, our findings suggest that center-based childcare may help” reduce disadvantages children from low-income families experience related to their heath,” Ms. Kucab said in a press release.
Laurent Legault, MD, an associate professor specializing in endocrinology in the department of pediatrics at McGill University, Montreal, highlighted the “quite significant” sample size of more than 3,000 participants, noting that “it’s quite tough to have numerous children” involved in a study, especially with several years of follow-up.
Dr. Legault also praised the investigators for considering socioeconomic status, “which is absolutely paramount, because, unfortunately, it’s not necessarily an even playing field for these families.”
He said the findings deserve to be promoted, as they highlight the benefits of center-based care, including ones with room for physical activity, opportunities for social interaction with other children, and a structured routine.
Still, Dr. Legault said it’s “very difficult to pinpoint specifically” what led to healthier body weights. “The problem, of course, is that obesity is very multifactorial in nature,” although “early intervention is more likely to be efficient.”
Center-based care appears to be one such intervention, he said, which should “push people to make centered care more affordable and easy to access for everyone.”The investigators and Dr. Legault reported no conflicts of interest.
The findings of the prospective Canadian study suggest that professional childcare centers that engage in standard practices are having a positive and lasting impact on children’s health, reported lead author Michaela Kucab, RD, MHSc, of the University of Toronto and colleagues.
“Attending center-based childcare in early childhood may influence important health behaviors including nutrition, physical activity, and routines related to child growth and weight status,” the investigators wrote in their abstract, which Ms. Kucab presented at the virtual conference sponsored by the American Society for Nutrition.
Their study involved 3,503 children who attended childcare in Canada during early childhood (mean age at baseline was 2.7 years) with follow-up from ages 4-10.
Overweight/obesity risk reduced
Children who received full-time, center-based care had a 22% lower risk of overweight/obesity and a mean body mass index z score (zBMI) that was 0.11 points lower at age 4 and 7 years than those who received non–center-based care. The benefits of center-based care were even more pronounced among children from lower-income families, who, at age 10, had a 48% lower risk of overweight/obesity and a mean zBMI that was 0.32 points lower with center-based versus non–center-based care.
In a written comment, Ms. Kucab and principal author Jonathon Maguire, MD, MSc, of the University of Toronto, explained that the former difference in zBMI translates to approximately half a pound of bodyweight in an average child, whereas the larger difference in zBMI among children from lower-income families would amount to approximately three pounds. They emphasized that these are rough estimations.
Ms. Kucab and Dr. Maguire noted that body weight differences correlated with the amount of time spent in center-based care.
“There was an observed trend, whereby the estimated mean difference [in zBMI] became slightly larger (or stronger) with a higher intensity of center-based childcare compared to non–center-based childcare,” they said.
To learn more about the earliest impacts of center-based care, the investigators are conducting a clinical trial, The Nutrition Recommendation Intervention Trials in Children’s Health Care (NuRISH), which will involve 600 children aged younger than 2 years.
Center-based childcare may reduce disadvantages of low-income children
“Although more research is needed, our findings suggest that center-based childcare may help” reduce disadvantages children from low-income families experience related to their heath,” Ms. Kucab said in a press release.
Laurent Legault, MD, an associate professor specializing in endocrinology in the department of pediatrics at McGill University, Montreal, highlighted the “quite significant” sample size of more than 3,000 participants, noting that “it’s quite tough to have numerous children” involved in a study, especially with several years of follow-up.
Dr. Legault also praised the investigators for considering socioeconomic status, “which is absolutely paramount, because, unfortunately, it’s not necessarily an even playing field for these families.”
He said the findings deserve to be promoted, as they highlight the benefits of center-based care, including ones with room for physical activity, opportunities for social interaction with other children, and a structured routine.
Still, Dr. Legault said it’s “very difficult to pinpoint specifically” what led to healthier body weights. “The problem, of course, is that obesity is very multifactorial in nature,” although “early intervention is more likely to be efficient.”
Center-based care appears to be one such intervention, he said, which should “push people to make centered care more affordable and easy to access for everyone.”The investigators and Dr. Legault reported no conflicts of interest.
The findings of the prospective Canadian study suggest that professional childcare centers that engage in standard practices are having a positive and lasting impact on children’s health, reported lead author Michaela Kucab, RD, MHSc, of the University of Toronto and colleagues.
“Attending center-based childcare in early childhood may influence important health behaviors including nutrition, physical activity, and routines related to child growth and weight status,” the investigators wrote in their abstract, which Ms. Kucab presented at the virtual conference sponsored by the American Society for Nutrition.
Their study involved 3,503 children who attended childcare in Canada during early childhood (mean age at baseline was 2.7 years) with follow-up from ages 4-10.
Overweight/obesity risk reduced
Children who received full-time, center-based care had a 22% lower risk of overweight/obesity and a mean body mass index z score (zBMI) that was 0.11 points lower at age 4 and 7 years than those who received non–center-based care. The benefits of center-based care were even more pronounced among children from lower-income families, who, at age 10, had a 48% lower risk of overweight/obesity and a mean zBMI that was 0.32 points lower with center-based versus non–center-based care.
In a written comment, Ms. Kucab and principal author Jonathon Maguire, MD, MSc, of the University of Toronto, explained that the former difference in zBMI translates to approximately half a pound of bodyweight in an average child, whereas the larger difference in zBMI among children from lower-income families would amount to approximately three pounds. They emphasized that these are rough estimations.
Ms. Kucab and Dr. Maguire noted that body weight differences correlated with the amount of time spent in center-based care.
“There was an observed trend, whereby the estimated mean difference [in zBMI] became slightly larger (or stronger) with a higher intensity of center-based childcare compared to non–center-based childcare,” they said.
To learn more about the earliest impacts of center-based care, the investigators are conducting a clinical trial, The Nutrition Recommendation Intervention Trials in Children’s Health Care (NuRISH), which will involve 600 children aged younger than 2 years.
Center-based childcare may reduce disadvantages of low-income children
“Although more research is needed, our findings suggest that center-based childcare may help” reduce disadvantages children from low-income families experience related to their heath,” Ms. Kucab said in a press release.
Laurent Legault, MD, an associate professor specializing in endocrinology in the department of pediatrics at McGill University, Montreal, highlighted the “quite significant” sample size of more than 3,000 participants, noting that “it’s quite tough to have numerous children” involved in a study, especially with several years of follow-up.
Dr. Legault also praised the investigators for considering socioeconomic status, “which is absolutely paramount, because, unfortunately, it’s not necessarily an even playing field for these families.”
He said the findings deserve to be promoted, as they highlight the benefits of center-based care, including ones with room for physical activity, opportunities for social interaction with other children, and a structured routine.
Still, Dr. Legault said it’s “very difficult to pinpoint specifically” what led to healthier body weights. “The problem, of course, is that obesity is very multifactorial in nature,” although “early intervention is more likely to be efficient.”
Center-based care appears to be one such intervention, he said, which should “push people to make centered care more affordable and easy to access for everyone.”The investigators and Dr. Legault reported no conflicts of interest.
FROM NUTRITION 2022
FTC decision to investigate pharmacy benefit managers applauded by rheumatologists
The Federal Trade Commission’s announcement June 7 of a plan to investigate the business practices of pharmacy benefit managers (PBMs) was welcome news to rheumatologists. Widespread concern about the cost of prescription drugs and an additional 24,000 comments from the public prompted the agency’s decision to examine PBMs, which act as intermediaries between insurers, manufacturers, and pharmacies.
PBMs negotiate drug prices and rebates with manufacturers, reimburse pharmacies for drug costs, and create insurers’ drug formularies. But it’s widely held that instead of managing and leveling costs, PBMs have ratcheted up prices at multiple junctures to gain more profit.
The FTC’s investigation will focus on the six largest PBMs: CVS Caremark, Express Scripts, OptumRx, Humana, Prime Therapeutics, and MedImpact Healthcare Systems. CVS Caremark is owned by CVS, Express Scripts is owned by Cigna, and OptumRx is owned by UnitedHealth. The companies will have 90 days to respond to the commission’s official request for information.
Some of the information the FTC plans to ask about includes how the companies may be pushing patients toward using PBM-owned pharmacies and how rebates affect insurers’ formularies and the cost of drugs for patients.
The purchase or establishment of PBMs by the largest insurance companies – known as vertical integration – makes it nearly impossible for outsiders to determine what’s really causing price increases for prescription drugs. “The black box of secretive contracts and monies changing hands between manufacturers and PBMs has grown quite large since the Department of Justice and the FTC allowed the big three PBMs to be part of the three largest health insurance companies,” Madelaine A. Feldman, MD, a rheumatologist at the Rheumatology Group, New Orleans, and president of the Coalition of State Rheumatology Organizations, told this news organization.

Dr. Feldman and fellow rheumatologists at the American College of Rheumatology are happy that the FTC has decided to pursue this investigation. They note that rheumatologists have been calling for action for years and are eager to see change.
This probe aims to determine not only how the PBM industry affects pharmacists but also how their practices create ripple effects across the prescription drug industry, said Dr. Feldman. “I was very happy to see that they will be investigating how rebates and other manufacturer price concessions affect formulary construction and utilization management tools, ultimately increasing drug prices and patient cost share.”
A version of this article first appeared on Medscape.com.
The Federal Trade Commission’s announcement June 7 of a plan to investigate the business practices of pharmacy benefit managers (PBMs) was welcome news to rheumatologists. Widespread concern about the cost of prescription drugs and an additional 24,000 comments from the public prompted the agency’s decision to examine PBMs, which act as intermediaries between insurers, manufacturers, and pharmacies.
PBMs negotiate drug prices and rebates with manufacturers, reimburse pharmacies for drug costs, and create insurers’ drug formularies. But it’s widely held that instead of managing and leveling costs, PBMs have ratcheted up prices at multiple junctures to gain more profit.
The FTC’s investigation will focus on the six largest PBMs: CVS Caremark, Express Scripts, OptumRx, Humana, Prime Therapeutics, and MedImpact Healthcare Systems. CVS Caremark is owned by CVS, Express Scripts is owned by Cigna, and OptumRx is owned by UnitedHealth. The companies will have 90 days to respond to the commission’s official request for information.
Some of the information the FTC plans to ask about includes how the companies may be pushing patients toward using PBM-owned pharmacies and how rebates affect insurers’ formularies and the cost of drugs for patients.
The purchase or establishment of PBMs by the largest insurance companies – known as vertical integration – makes it nearly impossible for outsiders to determine what’s really causing price increases for prescription drugs. “The black box of secretive contracts and monies changing hands between manufacturers and PBMs has grown quite large since the Department of Justice and the FTC allowed the big three PBMs to be part of the three largest health insurance companies,” Madelaine A. Feldman, MD, a rheumatologist at the Rheumatology Group, New Orleans, and president of the Coalition of State Rheumatology Organizations, told this news organization.
Dr. Feldman and fellow rheumatologists at the American College of Rheumatology are happy that the FTC has decided to pursue this investigation. They note that rheumatologists have been calling for action for years and are eager to see change.
This probe aims to determine not only how the PBM industry affects pharmacists but also how their practices create ripple effects across the prescription drug industry, said Dr. Feldman. “I was very happy to see that they will be investigating how rebates and other manufacturer price concessions affect formulary construction and utilization management tools, ultimately increasing drug prices and patient cost share.”
A version of this article first appeared on Medscape.com.
The Federal Trade Commission’s announcement June 7 of a plan to investigate the business practices of pharmacy benefit managers (PBMs) was welcome news to rheumatologists. Widespread concern about the cost of prescription drugs and an additional 24,000 comments from the public prompted the agency’s decision to examine PBMs, which act as intermediaries between insurers, manufacturers, and pharmacies.
PBMs negotiate drug prices and rebates with manufacturers, reimburse pharmacies for drug costs, and create insurers’ drug formularies. But it’s widely held that instead of managing and leveling costs, PBMs have ratcheted up prices at multiple junctures to gain more profit.
The FTC’s investigation will focus on the six largest PBMs: CVS Caremark, Express Scripts, OptumRx, Humana, Prime Therapeutics, and MedImpact Healthcare Systems. CVS Caremark is owned by CVS, Express Scripts is owned by Cigna, and OptumRx is owned by UnitedHealth. The companies will have 90 days to respond to the commission’s official request for information.
Some of the information the FTC plans to ask about includes how the companies may be pushing patients toward using PBM-owned pharmacies and how rebates affect insurers’ formularies and the cost of drugs for patients.
The purchase or establishment of PBMs by the largest insurance companies – known as vertical integration – makes it nearly impossible for outsiders to determine what’s really causing price increases for prescription drugs. “The black box of secretive contracts and monies changing hands between manufacturers and PBMs has grown quite large since the Department of Justice and the FTC allowed the big three PBMs to be part of the three largest health insurance companies,” Madelaine A. Feldman, MD, a rheumatologist at the Rheumatology Group, New Orleans, and president of the Coalition of State Rheumatology Organizations, told this news organization.
Dr. Feldman and fellow rheumatologists at the American College of Rheumatology are happy that the FTC has decided to pursue this investigation. They note that rheumatologists have been calling for action for years and are eager to see change.
This probe aims to determine not only how the PBM industry affects pharmacists but also how their practices create ripple effects across the prescription drug industry, said Dr. Feldman. “I was very happy to see that they will be investigating how rebates and other manufacturer price concessions affect formulary construction and utilization management tools, ultimately increasing drug prices and patient cost share.”
A version of this article first appeared on Medscape.com.
Is nonoperative treatment effective for acute Achilles tendon rupture?
Evidence summary
Surgical repair: Re-injury risk goes down, complications risk goes up
A 2021 network meta-analysis including 38 RCTs (N = 2480) reported outcomes in patients ages 18 and older with acute Achilles tendon rupture (AATR) and 3 or more months of follow-up.1 A significant increase in re-rupture rate was shown in patients who underwent nonoperative vs open repair (risk ratio [RR] = 2.41; 95% CI, 1.12-5.18). There was a significant decrease in wound-related complications in nonoperative vs open-repair patients (RR = 0.23; 95% CI, 0.06-0.88). There was also a significant difference in incidence of sural nerve injury in nonoperative vs open repair (RR = 0.27; 95% CI, 0.08-0.94). There were no significant differences in return to sport between open repair and nonoperative repair (RR = 0.62; 95% CI, 0.22-1.77). Insufficient data were reported to calculate the number needed to treat (NNT) and number needed to harm (NNH) for these outcomes.
Additionally, the authors looked at traditional standard rehabilitation and accelerated functional rehabilitation in both the operative and the nonoperative setting. The type of rehabilitation program did not have a significant impact on complications of re-rupture, wound, or sural nerve injury.
The included studies had an overall low risk of publication bias based on Begg’s funnel plot test (Pr > |z| = 0.86). The highest risk was performance bias, as neither the participants nor personnel were blinded to treatment in 71% of the studies.
Functional outcomes are similar for surgical vs nonoperative repair
In a 2019 meta-analysis of 9 RCTs (N = 822), adults ages 18 and older with AATR and a minimum of 12 months’ follow-up were randomized to either operative or nonoperative repair. There was a decreased rate of rupture with surgical repair and an associated increased rate of complications (ie, superficial wound infections and nerve injury). However, there was no significant difference in Physical Activity Scale (PAS) score between the 2 groups (mean difference, –0.05; 95% CI, –0.37 to 0.27).2 With surgical intervention, the NNT for Achilles tendon re-rupture was 15, and the NNH for superficial wound infection and nerve injury, respectively, were 22 and 28. Limitations of the study included different operative techniques and rehab protocols, which may have affected the results of the included studies.
A third meta-analysis consisted of 10 RCTs and 19 observational studies (N = 15,862) with patients ages 16 years and older treated operatively vs nonoperatively. Function and return-to-activity rates in both the short term (≤ 1 year) and long term (> 1 year) were evaluated using the Achilles tendon Total Rupture Score (ATRS).3 Surgical management was associated with decreased re-rupture rates but increased complication rates. However, when the analysis was limited to studies using accelerated functional rehabilitation programs, there was no significant difference in re-rupture rate (RR = 0.26 to 1.37; P = .23). Only 1 observational study found a statistically significant difference in short-term functional outcomes favoring operative management, and no studies found a significant difference in long-term functional outcomes. These functional outcomes were not pooled for statistical analysis due to high interrater variability of the ATRS.
An RCT showed equal “customer satisfaction”
One RCT randomized 61 patients to either surgical or nonsurgical management and followed them for a mean of 15.7 years.4 Patient-reported outcomes of function, symptoms, and impact on daily life were measured using various surveys. There was no statistically significant difference in the function and impact on daily life after treatment according to the Short Musculoskeletal Function Assessment or the ATRS (P = .289 and .313, respectively). When assessed using the Net Promoter Score (a single-question metric used in consumer industry to assess whether an individual would recommend the product to others), there was no statistical significance for the patients to recommend one treatment over another: 79% of operatively managed patients vs 87% of nonoperatively managed patients would recommend their treatment to others (P = .225).
Recommendations from others
The American College of Foot and Ankle Surgeons consensus statement finds no difference between operative and nonoperative management with regard to complications, functional outcome, and return to activity long term, when looking at available Level 1 evidence.5 They do acknowledge that although some Level III studies suggest operative intervention will return high-functioning patients to full activity sooner, there should be discussion regarding the risks and complications of both operative and nonoperative management. Patients with increased risk factors for postoperative complications (diabetes, obesity, cigarette smoking) should have special considerations regarding the decision to operate.
Editor’s takeaway
Large data sets with consistent results show that nonoperative treatment of Achilles tendon rupture is an excellent option. However, we cannot say if it is better or worse than operative treatment, because both options have advantages and disadvantages. One must weigh the alternatives with individual patient preferences and circumstances.
1. Shi F, Wu S, Cai W, et al. Multiple comparisons of the efficacy and safety for six treatments in acute Achilles tendon rupture patients: a systematic review and network meta-analysis. Foot Ankle Surg. 2021;27:468-479. doi: 10.1016/j.fas.2020.07.004
2. Reda Y, Farouk A, Abdelmonem I, et al. Surgical versus non-surgical treatment for acute Achilles tendon rupture. A systematic review of literature and meta-analysis. Foot Ankle Surg. 2020;26:280-288. doi: 10.1016/j.fas.2019.03.010
3. Ochen Y, Beks RB, van Heijl M, et al. Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis. BMJ. 2019;364:k5120. doi: 10.1136/bmj.k5120
4. Maempel JF, Clement ND, Wickramasinghe NR, et al. Operative repair of acute Achilles tendon rupture does not give superior patient-reported outcomes to nonoperative management. Bone Joint J. 2020;102-B:933-940. doi: 10.1302/0301-620x.102b7.bjj-2019-0783.r3
5. Naldo J, Agnew P, Brucato M, et al. ACFAS clinical consensus statement: acute Achilles tendon pathology. J Foot Ankle Surg. 2021;60:93-101. doi: 10.1053/j.jfas.2020.02.006
Evidence summary
Surgical repair: Re-injury risk goes down, complications risk goes up
A 2021 network meta-analysis including 38 RCTs (N = 2480) reported outcomes in patients ages 18 and older with acute Achilles tendon rupture (AATR) and 3 or more months of follow-up.1 A significant increase in re-rupture rate was shown in patients who underwent nonoperative vs open repair (risk ratio [RR] = 2.41; 95% CI, 1.12-5.18). There was a significant decrease in wound-related complications in nonoperative vs open-repair patients (RR = 0.23; 95% CI, 0.06-0.88). There was also a significant difference in incidence of sural nerve injury in nonoperative vs open repair (RR = 0.27; 95% CI, 0.08-0.94). There were no significant differences in return to sport between open repair and nonoperative repair (RR = 0.62; 95% CI, 0.22-1.77). Insufficient data were reported to calculate the number needed to treat (NNT) and number needed to harm (NNH) for these outcomes.
Additionally, the authors looked at traditional standard rehabilitation and accelerated functional rehabilitation in both the operative and the nonoperative setting. The type of rehabilitation program did not have a significant impact on complications of re-rupture, wound, or sural nerve injury.
The included studies had an overall low risk of publication bias based on Begg’s funnel plot test (Pr > |z| = 0.86). The highest risk was performance bias, as neither the participants nor personnel were blinded to treatment in 71% of the studies.
Functional outcomes are similar for surgical vs nonoperative repair
In a 2019 meta-analysis of 9 RCTs (N = 822), adults ages 18 and older with AATR and a minimum of 12 months’ follow-up were randomized to either operative or nonoperative repair. There was a decreased rate of rupture with surgical repair and an associated increased rate of complications (ie, superficial wound infections and nerve injury). However, there was no significant difference in Physical Activity Scale (PAS) score between the 2 groups (mean difference, –0.05; 95% CI, –0.37 to 0.27).2 With surgical intervention, the NNT for Achilles tendon re-rupture was 15, and the NNH for superficial wound infection and nerve injury, respectively, were 22 and 28. Limitations of the study included different operative techniques and rehab protocols, which may have affected the results of the included studies.
A third meta-analysis consisted of 10 RCTs and 19 observational studies (N = 15,862) with patients ages 16 years and older treated operatively vs nonoperatively. Function and return-to-activity rates in both the short term (≤ 1 year) and long term (> 1 year) were evaluated using the Achilles tendon Total Rupture Score (ATRS).3 Surgical management was associated with decreased re-rupture rates but increased complication rates. However, when the analysis was limited to studies using accelerated functional rehabilitation programs, there was no significant difference in re-rupture rate (RR = 0.26 to 1.37; P = .23). Only 1 observational study found a statistically significant difference in short-term functional outcomes favoring operative management, and no studies found a significant difference in long-term functional outcomes. These functional outcomes were not pooled for statistical analysis due to high interrater variability of the ATRS.
An RCT showed equal “customer satisfaction”
One RCT randomized 61 patients to either surgical or nonsurgical management and followed them for a mean of 15.7 years.4 Patient-reported outcomes of function, symptoms, and impact on daily life were measured using various surveys. There was no statistically significant difference in the function and impact on daily life after treatment according to the Short Musculoskeletal Function Assessment or the ATRS (P = .289 and .313, respectively). When assessed using the Net Promoter Score (a single-question metric used in consumer industry to assess whether an individual would recommend the product to others), there was no statistical significance for the patients to recommend one treatment over another: 79% of operatively managed patients vs 87% of nonoperatively managed patients would recommend their treatment to others (P = .225).
Recommendations from others
The American College of Foot and Ankle Surgeons consensus statement finds no difference between operative and nonoperative management with regard to complications, functional outcome, and return to activity long term, when looking at available Level 1 evidence.5 They do acknowledge that although some Level III studies suggest operative intervention will return high-functioning patients to full activity sooner, there should be discussion regarding the risks and complications of both operative and nonoperative management. Patients with increased risk factors for postoperative complications (diabetes, obesity, cigarette smoking) should have special considerations regarding the decision to operate.
Editor’s takeaway
Large data sets with consistent results show that nonoperative treatment of Achilles tendon rupture is an excellent option. However, we cannot say if it is better or worse than operative treatment, because both options have advantages and disadvantages. One must weigh the alternatives with individual patient preferences and circumstances.
Evidence summary
Surgical repair: Re-injury risk goes down, complications risk goes up
A 2021 network meta-analysis including 38 RCTs (N = 2480) reported outcomes in patients ages 18 and older with acute Achilles tendon rupture (AATR) and 3 or more months of follow-up.1 A significant increase in re-rupture rate was shown in patients who underwent nonoperative vs open repair (risk ratio [RR] = 2.41; 95% CI, 1.12-5.18). There was a significant decrease in wound-related complications in nonoperative vs open-repair patients (RR = 0.23; 95% CI, 0.06-0.88). There was also a significant difference in incidence of sural nerve injury in nonoperative vs open repair (RR = 0.27; 95% CI, 0.08-0.94). There were no significant differences in return to sport between open repair and nonoperative repair (RR = 0.62; 95% CI, 0.22-1.77). Insufficient data were reported to calculate the number needed to treat (NNT) and number needed to harm (NNH) for these outcomes.
Additionally, the authors looked at traditional standard rehabilitation and accelerated functional rehabilitation in both the operative and the nonoperative setting. The type of rehabilitation program did not have a significant impact on complications of re-rupture, wound, or sural nerve injury.
The included studies had an overall low risk of publication bias based on Begg’s funnel plot test (Pr > |z| = 0.86). The highest risk was performance bias, as neither the participants nor personnel were blinded to treatment in 71% of the studies.
Functional outcomes are similar for surgical vs nonoperative repair
In a 2019 meta-analysis of 9 RCTs (N = 822), adults ages 18 and older with AATR and a minimum of 12 months’ follow-up were randomized to either operative or nonoperative repair. There was a decreased rate of rupture with surgical repair and an associated increased rate of complications (ie, superficial wound infections and nerve injury). However, there was no significant difference in Physical Activity Scale (PAS) score between the 2 groups (mean difference, –0.05; 95% CI, –0.37 to 0.27).2 With surgical intervention, the NNT for Achilles tendon re-rupture was 15, and the NNH for superficial wound infection and nerve injury, respectively, were 22 and 28. Limitations of the study included different operative techniques and rehab protocols, which may have affected the results of the included studies.
A third meta-analysis consisted of 10 RCTs and 19 observational studies (N = 15,862) with patients ages 16 years and older treated operatively vs nonoperatively. Function and return-to-activity rates in both the short term (≤ 1 year) and long term (> 1 year) were evaluated using the Achilles tendon Total Rupture Score (ATRS).3 Surgical management was associated with decreased re-rupture rates but increased complication rates. However, when the analysis was limited to studies using accelerated functional rehabilitation programs, there was no significant difference in re-rupture rate (RR = 0.26 to 1.37; P = .23). Only 1 observational study found a statistically significant difference in short-term functional outcomes favoring operative management, and no studies found a significant difference in long-term functional outcomes. These functional outcomes were not pooled for statistical analysis due to high interrater variability of the ATRS.
An RCT showed equal “customer satisfaction”
One RCT randomized 61 patients to either surgical or nonsurgical management and followed them for a mean of 15.7 years.4 Patient-reported outcomes of function, symptoms, and impact on daily life were measured using various surveys. There was no statistically significant difference in the function and impact on daily life after treatment according to the Short Musculoskeletal Function Assessment or the ATRS (P = .289 and .313, respectively). When assessed using the Net Promoter Score (a single-question metric used in consumer industry to assess whether an individual would recommend the product to others), there was no statistical significance for the patients to recommend one treatment over another: 79% of operatively managed patients vs 87% of nonoperatively managed patients would recommend their treatment to others (P = .225).
Recommendations from others
The American College of Foot and Ankle Surgeons consensus statement finds no difference between operative and nonoperative management with regard to complications, functional outcome, and return to activity long term, when looking at available Level 1 evidence.5 They do acknowledge that although some Level III studies suggest operative intervention will return high-functioning patients to full activity sooner, there should be discussion regarding the risks and complications of both operative and nonoperative management. Patients with increased risk factors for postoperative complications (diabetes, obesity, cigarette smoking) should have special considerations regarding the decision to operate.
Editor’s takeaway
Large data sets with consistent results show that nonoperative treatment of Achilles tendon rupture is an excellent option. However, we cannot say if it is better or worse than operative treatment, because both options have advantages and disadvantages. One must weigh the alternatives with individual patient preferences and circumstances.
1. Shi F, Wu S, Cai W, et al. Multiple comparisons of the efficacy and safety for six treatments in acute Achilles tendon rupture patients: a systematic review and network meta-analysis. Foot Ankle Surg. 2021;27:468-479. doi: 10.1016/j.fas.2020.07.004
2. Reda Y, Farouk A, Abdelmonem I, et al. Surgical versus non-surgical treatment for acute Achilles tendon rupture. A systematic review of literature and meta-analysis. Foot Ankle Surg. 2020;26:280-288. doi: 10.1016/j.fas.2019.03.010
3. Ochen Y, Beks RB, van Heijl M, et al. Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis. BMJ. 2019;364:k5120. doi: 10.1136/bmj.k5120
4. Maempel JF, Clement ND, Wickramasinghe NR, et al. Operative repair of acute Achilles tendon rupture does not give superior patient-reported outcomes to nonoperative management. Bone Joint J. 2020;102-B:933-940. doi: 10.1302/0301-620x.102b7.bjj-2019-0783.r3
5. Naldo J, Agnew P, Brucato M, et al. ACFAS clinical consensus statement: acute Achilles tendon pathology. J Foot Ankle Surg. 2021;60:93-101. doi: 10.1053/j.jfas.2020.02.006
1. Shi F, Wu S, Cai W, et al. Multiple comparisons of the efficacy and safety for six treatments in acute Achilles tendon rupture patients: a systematic review and network meta-analysis. Foot Ankle Surg. 2021;27:468-479. doi: 10.1016/j.fas.2020.07.004
2. Reda Y, Farouk A, Abdelmonem I, et al. Surgical versus non-surgical treatment for acute Achilles tendon rupture. A systematic review of literature and meta-analysis. Foot Ankle Surg. 2020;26:280-288. doi: 10.1016/j.fas.2019.03.010
3. Ochen Y, Beks RB, van Heijl M, et al. Operative treatment versus nonoperative treatment of Achilles tendon ruptures: systematic review and meta-analysis. BMJ. 2019;364:k5120. doi: 10.1136/bmj.k5120
4. Maempel JF, Clement ND, Wickramasinghe NR, et al. Operative repair of acute Achilles tendon rupture does not give superior patient-reported outcomes to nonoperative management. Bone Joint J. 2020;102-B:933-940. doi: 10.1302/0301-620x.102b7.bjj-2019-0783.r3
5. Naldo J, Agnew P, Brucato M, et al. ACFAS clinical consensus statement: acute Achilles tendon pathology. J Foot Ankle Surg. 2021;60:93-101. doi: 10.1053/j.jfas.2020.02.006
EVIDENCE-BASED ANSWER:
YES. Nonoperative and open sur- gical interventions provide equal long-term functional outcomes of the affected Achilles tendon and ankle (strength of recommendation [SOR], A; based on 2 meta-analyses and a separate randomized controlled trial [RCT]). Although nonoperative management is associated with increased risk of re-rupture, it confers lower risk for complications including wound infection and nerve injury (SOR, A; based on meta-analysis and separate RCT).
Select individuals—high-performing athletes or those who otherwise require near-baseline strength and function of their Achilles tendon—would likely benefit from surgical intervention (SOR, A; based on meta-analysis and consensus recommendations).
Patients with comorbid conditions that would put them at greater risk for postoperative complications should be advised to consider nonoperative treatment of acute Achilles tendon rupture (SOR, C; based on consensus opinion).

Helping patients move forward following traumatic brain injury
THE CASE
Declan M*, a 42-year-old man, presents as a new patient for general medical care. One year ago, he sustained a severe frontal traumatic brain injury (TBI) when he was hit by a car while crossing a street. He developed a subdural hematoma and was in a coma for 6 days. He also had fractured ribs and a fractured left foot. When he regained consciousness, he had posttraumatic amnesia. He also had executive function deficits and memory difficulties, so a guardian was appointed.
Mr. M no longer works as an auto mechanic, a career he once greatly enjoyed. Mr. M’s guardian reports that recently, Mr. M has lost interest in activities he’d previously enjoyed, is frequently irritable, has poor sleep, is socially isolated, and is spending increasing amounts of time at home. When his new primary care physician (PCP) enters the examining room, Mr. M is seated in a chair with his arms folded across his chest. He states that he is “fine” and just needs to “get a doctor.”
●
*This patient is an amalgam of patients for whom the author has provided care.
TBI ranges from mild to severe and can produce a number of profound effects that are a direct—or indirect—result of the physical injury.1 The location and the severity of the injury affect symptoms.2 Even mild TBI can cause impairment, and severe TBI can lead to broad cognitive, behavioral, and physical difficulties. As numbers of TBI cases increase globally, primary care providers need to recognize the symptoms and assess accordingly.1 The Acute Concussion Evaluation (ACE; Physician/Clinician Office Version) facilitates a structured evaluation for patients presenting with possible TBI symptoms. It can easily be accessed on the Centers for Disease Control and Prevention website.3
Direct effects of TBI include impulsivity, depression, reduced frustration tolerance, reduced motivation, low awareness, and insomnia and other sleep difficulties.4,5 Depression may also result indirectly from, or be exacerbated by, new posttraumatic limitations and lifestyle changes as well as loss of career and community.4 Both direct and indirect depression often manifest as feelings of hopelessness and worthlessness and a lack of interest in once enjoyable activities. Depression can worsen other TBI sequelae such as difficulty concentrating, lack of initiation, flat affect, irritability, reduced independence, reduced functional performance, loss of inhibition, and physical pain.6
Nationwide, most mental health concerns continue to be addressed in the primary care setting.7 Individuals with TBI experience major depression at a rate 5 to 6 times higher than those in the general population, with a prevalence rate of 45%.8
Suicide. The subject of suicide must be explored with survivors of TBI; evidence suggests a correlation between TBI, depression, and increased risk for suicide.9 Among those who have TBI, as many as 22% experience suicidal ideation; the risk of suicide in survivors of severe TBI is 3 to 4 times the risk in the general population.10 Additionally, suicidality in this context appears to be a chronic concern; therefore, carefully assess for its presence no matter how long ago the TBI occurred.10
Additional TBI-associated health concerns
Grief and loss. We so often focus on death as the only cause for grief, but grief can occur for other types of loss, as well. Individuals with TBI often experience a radical negative change in self-concept after their injury, which is associated with feelings of grief.11 Helping patients recognize that they are grieving the loss of the person they once were can help set a framework for their experience.
Continue to: Relationship loss
Relationship loss. Many people with TBI lose close relationships.12 This can be due to life changes such as job loss, loss of function or ability to do previously enjoyed activities, or personality changes. These relationship losses can affect a person profoundly.12 Going forward, they may have difficulty trusting others, for example.
Existential issues. Many people with TBI also find that cognitive deficits prevent them from engaging in formerly meaningful work. For example, Mr. M lost his longstanding career as an auto mechanic and therefore part of his identity. Not being able to find purpose and meaning can be a strong contributor to coping difficulties in those with TBI.13
Chronic pain. More than half of people with TBI experience chronic pain. Headaches are the most common pain condition among all TBI survivors.14
Substance use disorders. The directionality of substance use disorders and TBI is not always clear; however, most evidence suggests that substance abuse is highly prevalent, premorbid, and often a contributing factor in TBI (eg, car accidents).15 Alcohol abuse is the most common risk factor, followed by drug abuse.16 Substance abuse may be exacerbated after TBI when it becomes a coping mechanism under worsening stressors; additionally, executive function deficits or other neurologic problems may result in poor decision-making with regard to substance use.15 While substance abuse may decline in the immediate post-TBI period, it can return to pre-injury levels within a year.17
Selective serotonin reuptake inhibitors may help
Few studies have explored the efficacy of antidepressant medication in TBI survivors. In a controlled study of patients with TBI, Fann and colleagues18 found no significant improvement in depression symptoms between sertraline and a placebo. However, they did note some possibilities for this lack of significance: socially isolated TBI survivors in the placebo group may have demonstrated improvement in depression symptoms because of increased social interaction;
Continue to: Other research has found...
Other research has found that sertraline improved both depression and quality of life for men with post-TBI depression.19 In a meta-analysis of 4 studies, Paraschakis and Katsanos20 found that sertraline demonstrated a “trend toward significance” in the treatment of depression among patients with TBI. Silverberg and Panenka21 argue that selective serotonin reuptake inhibitors should be used as first-line treatment for depression in survivors of TBI. They note that in non-randomized studies, treatment effects with antidepressants are significant. Additionally, patients who do not respond to the first antidepressant prescribed will often respond to adjunctive or different medications. Finally, they argue that depression measures can capture symptoms related to the physical brain injury, in addition to symptoms of depression, thus confounding results.
THE CASE
Mr. M’s chart showed that he was not taking any medication and that he had no history of substance abuse or tobacco use. He refused to fill out the Patient Health Questionnaire (PHQ)-2. His guardian said that Mr. M was spending much of his time at home, and that he used to be an avid painter and guitar player but had not engaged in either activity for months. Furthermore, Mr. M used to enjoy working out but did so rarely now.
During the interview, the PCP was careful to make eye contact with Mr. M as well as his guardian, thereby making sure Mr. M was part of the conversation about his care. Pacing of questions was deliberate and unhurried; a return visit would be scheduled to further explore any concerns not covered in this visit. This collaborative, inclusive, patient-centered approach to the clinical interview seemed to place Mr. M at ease. When his guardian said he thought Mr. M was depressed, Mr. M agreed. Although Mr. M still refused to fill out the PHQ-2, he was now willing to answer questions about depression. He acknowledged that he was feeling hopeless and took little pleasure in activities he used to enjoy, thereby indicating a positive screen for depression.
The PCP opted to read the PHQ-9 questions aloud, and Mr. M agreed with most of the items but strongly denied suicidal ideation, citing his religious faith.
The PCP determined that Mr. M’s depression was likely a combination of the direct and indirect effects of his TBI. A quantitative estimate based on Mr. M’s report yielded a PHQ-9 score of 17, indicating moderately severe depression.
Continue to: In addition to building rapport...
In addition to building rapport, careful listening garnered important information about Mr. M. For example, until his accident and subsequent depression, Mr. M had long prioritized his physical health through diet and exercise. He followed a vegetarian diet but recently had little appetite and was eating one microwaveable meal a day. He had an irregular sleep schedule and struggled with insomnia. He lost his closest long-term relationship after his accident due to difficulties with affect regulation. He also lost his job as he could no longer cognitively handle the tasks required.
Hearing Mr. M’s story provided the opportunity to customize education about self-management skills including regular diet, exercise, and sleep hygiene. Due to limited visit time, the PCP elected to use this first visit to focus on sleep and depression. As cognitive behavioral therapy (CBT) for insomnia is first-line treatment for both primary insomnia and insomnia due to a medical condition such as TBI,5 a sleep aid was not prescribed. Fortunately, the clinic psychologist who offered CBT was able to join the interview to meet Mr. M and explain the treatment.
Mr. M expressed some initial reluctance to try an antidepressant. However, acknowledging he “just hasn’t been the same” since his TBI, he agreed to a prescription for sertraline and said he hoped it could make him “more like [he] was.”
RETURN VISIT
Four weeks after Mr. M began taking sertraline and participating in weekly CBT sessions, he returned for a follow-up visit with his PCP. He had a noticeably brighter affect, and his guardian reported that he had been playing the guitar again. Mr. M said that he had more energy as a result of improved sleep and mood, and that he felt like his “thinking was clearer.” Mr. M noted that he never thought he would meet with a psychologist but was finding CBT for insomnia helpful.
The psychologist’s notes proposed a treatment plan that would also include targeted grief and existential therapies to address Mr. M’s sudden life changes. At this visit, Mr. M admitted that his reading comprehension and speed were negatively affected by the accident and said this is why he did not wish to fill out the PHQ-2. But he was again willing to have the PHQ-9 questions read to him with his guardian’s support. Results showed a score of 6, indicating mild depression.
A follow-up appointment with Mr. M was scheduled for 6 weeks later, and the team was confident he was getting the behavioral and mental health support he needed through medication and therapy.
CORRESPONDENCE
Elizabeth Imbesi, PhD, VA Ann Arbor Healthcare System, 2215 Fuller Road, Ann Arbor, MI 48105; elizabeth.imbesi@va.gov
1. CDC. Traumatic brain injury & concussion. 2020. Accessed May 19, 2022. www.cdc.gov/traumaticbraininjury/index.html
2. Finset A, Anderson S. Coping strategies in patients with acquired brain injury: relationships between coping, apathy, depression and lesion location. Brain Inj. 2009;14:887-905. doi: 10.1080/026990500445718
3. CDC. Gioia G, Collins M. Acute concussion evaluation. 2006. Accessed May 19, 2022. www.cdc.gov/headsup/pdfs/providers/ace_v2-a.pdf
4. Prigatano GP. Psychotherapy and the process of coping with a brain disorder. Oral presentation at: American Psychological Association annual convention. August 2015; Toronto, Canada.
5. Ouellet M, Beaulieu-Bonneau S, Savard J, Morin C. Insomnia and Fatigue After Traumatic Brain Injury: A CBT Approach to Assessment and Treatment. Elsevier Academic Press: 2019.
6. Lewis FD, Horn GH. Depression following traumatic brain injury: impact on post-hospital residential rehabilitation outcomes. NeuroRehabilitation. 2017;40:401-410. doi: 10.3233/NRE-161427
7. Barkil-Oteo A. Collaborative care for depression in primary care: how psychiatry could “troubleshoot” current treatments and practices. Yale J Bio Med. 2013;86:139-146.
8. Whelan-Goodinson R, Ponsford J, Johnston L, et al. Psychiatric disorders following traumatic brain injury: their nature and frequency. J Head Trauma Rehabil. 2009;24:324-332. doi: 10.1097/HTR.0b013e3181a712aa
9. Reeves RR, Laizer JT. Traumatic brain injury and suicide. J Psychosoc Nurs Ment Health Serv. 2012;50:32-38. doi: 10.3928/02793695-20120207-02
10. Simpson G, Tate R. Suicidality in people surviving a traumatic brain injury: Prevalence, risk factors and implications for clinical management. Brain Inj. 2007;21:1335-1351. doi: 10.1080/02699050701785542
11. Carroll E, Coetzer R. Identity, grief and self-awareness after traumatic brain injury. Neuropsychol Rehabil. 2011;21:289-305. doi: 10.1080/09602011.2011.555972
12. Salas CE, Casassus M, Rowlands L, et al. “Relating through sameness”: a qualitative study of friendship and social isolation in chronic traumatic brain injury. Neuropsychol Rehabil. 2018;28:1161-1178. doi: 10.1080/09602011.2016.1247730
13. Hinkebein JA, Stucky R. Coping with traumatic brain injury: existential challenges and managing hope. In: Martz E, Livneh H, eds. Coping with Chronic Illness and Disability: Theoretical, Empirical, and Clinical Aspects. Springer Science & Business Media; 2007:389-409.
14. Khoury S, Benavides R. Pain with traumatic brain injury and psychological disorders. Prog Neuropsychopharmacol and Biol Psychiatry. 2018;87:224-233. doi: 10.1016/j.pnpbp.2017.06.007
15. Bjork JM, Grant SJ. Does traumatic brain injury increase risk for substance abuse? J Neurotrauma. 2009;26:1077-1082. doi: 10.1089/neu.2008.0849
16. Unsworth DJ, Mathias JL. Traumatic brain injury and alcohol/substance abuse: a Bayesian meta-analysis comparing the outcomes of people with and without a history of abuse. J Clin Exp Neuropsychol. 2017,39:547-562. doi: 10.1080/13803395.2016.1248812
17. Beaulieu-Bonneau S, St-Onge F, Blackburn M, et al. Alcohol and drug use before and during the first year after traumatic brain injury. J Head Trauma Rehabil. 2018;33:E51-E60. doi: 10.1097/HTR.0000000000000341
18. Fann JR, Bombardier CH, Temkin N, et al. Sertraline for major depression during the year following traumatic brain injury: a randomized control trial. J Head Trauma Rehabil. 2017;32:332-342. doi: 10.1097/HTR.0000000000000322
19. Ansari A, Jain A, Sharma A, et al. Role of sertraline in posttraumatic brain injury depression and quality of life in TBI. Asian J Neurosurg. 2014;9:182-188. doi: 10.4103/1793-5482.146597
20. Paraschakis A, Katsanos AH. Antidepressants for depression associated with traumatic brain injury: a meta-analytical study of randomized control trials. East Asian Arch Psychiatry. 2017;27:142-149.
21. Silverberg ND, Panenka WJ. Antidepressants for depression after concussion and traumatic brain injury are still best practice. BMC Psychiatry. 2019;19:100. doi: 10.1186/s12888-019-2076-9
THE CASE
Declan M*, a 42-year-old man, presents as a new patient for general medical care. One year ago, he sustained a severe frontal traumatic brain injury (TBI) when he was hit by a car while crossing a street. He developed a subdural hematoma and was in a coma for 6 days. He also had fractured ribs and a fractured left foot. When he regained consciousness, he had posttraumatic amnesia. He also had executive function deficits and memory difficulties, so a guardian was appointed.
Mr. M no longer works as an auto mechanic, a career he once greatly enjoyed. Mr. M’s guardian reports that recently, Mr. M has lost interest in activities he’d previously enjoyed, is frequently irritable, has poor sleep, is socially isolated, and is spending increasing amounts of time at home. When his new primary care physician (PCP) enters the examining room, Mr. M is seated in a chair with his arms folded across his chest. He states that he is “fine” and just needs to “get a doctor.”
●
*This patient is an amalgam of patients for whom the author has provided care.
TBI ranges from mild to severe and can produce a number of profound effects that are a direct—or indirect—result of the physical injury.1 The location and the severity of the injury affect symptoms.2 Even mild TBI can cause impairment, and severe TBI can lead to broad cognitive, behavioral, and physical difficulties. As numbers of TBI cases increase globally, primary care providers need to recognize the symptoms and assess accordingly.1 The Acute Concussion Evaluation (ACE; Physician/Clinician Office Version) facilitates a structured evaluation for patients presenting with possible TBI symptoms. It can easily be accessed on the Centers for Disease Control and Prevention website.3
Direct effects of TBI include impulsivity, depression, reduced frustration tolerance, reduced motivation, low awareness, and insomnia and other sleep difficulties.4,5 Depression may also result indirectly from, or be exacerbated by, new posttraumatic limitations and lifestyle changes as well as loss of career and community.4 Both direct and indirect depression often manifest as feelings of hopelessness and worthlessness and a lack of interest in once enjoyable activities. Depression can worsen other TBI sequelae such as difficulty concentrating, lack of initiation, flat affect, irritability, reduced independence, reduced functional performance, loss of inhibition, and physical pain.6
Nationwide, most mental health concerns continue to be addressed in the primary care setting.7 Individuals with TBI experience major depression at a rate 5 to 6 times higher than those in the general population, with a prevalence rate of 45%.8
Suicide. The subject of suicide must be explored with survivors of TBI; evidence suggests a correlation between TBI, depression, and increased risk for suicide.9 Among those who have TBI, as many as 22% experience suicidal ideation; the risk of suicide in survivors of severe TBI is 3 to 4 times the risk in the general population.10 Additionally, suicidality in this context appears to be a chronic concern; therefore, carefully assess for its presence no matter how long ago the TBI occurred.10
Additional TBI-associated health concerns
Grief and loss. We so often focus on death as the only cause for grief, but grief can occur for other types of loss, as well. Individuals with TBI often experience a radical negative change in self-concept after their injury, which is associated with feelings of grief.11 Helping patients recognize that they are grieving the loss of the person they once were can help set a framework for their experience.
Continue to: Relationship loss
Relationship loss. Many people with TBI lose close relationships.12 This can be due to life changes such as job loss, loss of function or ability to do previously enjoyed activities, or personality changes. These relationship losses can affect a person profoundly.12 Going forward, they may have difficulty trusting others, for example.
Existential issues. Many people with TBI also find that cognitive deficits prevent them from engaging in formerly meaningful work. For example, Mr. M lost his longstanding career as an auto mechanic and therefore part of his identity. Not being able to find purpose and meaning can be a strong contributor to coping difficulties in those with TBI.13
Chronic pain. More than half of people with TBI experience chronic pain. Headaches are the most common pain condition among all TBI survivors.14
Substance use disorders. The directionality of substance use disorders and TBI is not always clear; however, most evidence suggests that substance abuse is highly prevalent, premorbid, and often a contributing factor in TBI (eg, car accidents).15 Alcohol abuse is the most common risk factor, followed by drug abuse.16 Substance abuse may be exacerbated after TBI when it becomes a coping mechanism under worsening stressors; additionally, executive function deficits or other neurologic problems may result in poor decision-making with regard to substance use.15 While substance abuse may decline in the immediate post-TBI period, it can return to pre-injury levels within a year.17
Selective serotonin reuptake inhibitors may help
Few studies have explored the efficacy of antidepressant medication in TBI survivors. In a controlled study of patients with TBI, Fann and colleagues18 found no significant improvement in depression symptoms between sertraline and a placebo. However, they did note some possibilities for this lack of significance: socially isolated TBI survivors in the placebo group may have demonstrated improvement in depression symptoms because of increased social interaction;
Continue to: Other research has found...
Other research has found that sertraline improved both depression and quality of life for men with post-TBI depression.19 In a meta-analysis of 4 studies, Paraschakis and Katsanos20 found that sertraline demonstrated a “trend toward significance” in the treatment of depression among patients with TBI. Silverberg and Panenka21 argue that selective serotonin reuptake inhibitors should be used as first-line treatment for depression in survivors of TBI. They note that in non-randomized studies, treatment effects with antidepressants are significant. Additionally, patients who do not respond to the first antidepressant prescribed will often respond to adjunctive or different medications. Finally, they argue that depression measures can capture symptoms related to the physical brain injury, in addition to symptoms of depression, thus confounding results.
THE CASE
Mr. M’s chart showed that he was not taking any medication and that he had no history of substance abuse or tobacco use. He refused to fill out the Patient Health Questionnaire (PHQ)-2. His guardian said that Mr. M was spending much of his time at home, and that he used to be an avid painter and guitar player but had not engaged in either activity for months. Furthermore, Mr. M used to enjoy working out but did so rarely now.
During the interview, the PCP was careful to make eye contact with Mr. M as well as his guardian, thereby making sure Mr. M was part of the conversation about his care. Pacing of questions was deliberate and unhurried; a return visit would be scheduled to further explore any concerns not covered in this visit. This collaborative, inclusive, patient-centered approach to the clinical interview seemed to place Mr. M at ease. When his guardian said he thought Mr. M was depressed, Mr. M agreed. Although Mr. M still refused to fill out the PHQ-2, he was now willing to answer questions about depression. He acknowledged that he was feeling hopeless and took little pleasure in activities he used to enjoy, thereby indicating a positive screen for depression.
The PCP opted to read the PHQ-9 questions aloud, and Mr. M agreed with most of the items but strongly denied suicidal ideation, citing his religious faith.
The PCP determined that Mr. M’s depression was likely a combination of the direct and indirect effects of his TBI. A quantitative estimate based on Mr. M’s report yielded a PHQ-9 score of 17, indicating moderately severe depression.
Continue to: In addition to building rapport...
In addition to building rapport, careful listening garnered important information about Mr. M. For example, until his accident and subsequent depression, Mr. M had long prioritized his physical health through diet and exercise. He followed a vegetarian diet but recently had little appetite and was eating one microwaveable meal a day. He had an irregular sleep schedule and struggled with insomnia. He lost his closest long-term relationship after his accident due to difficulties with affect regulation. He also lost his job as he could no longer cognitively handle the tasks required.
Hearing Mr. M’s story provided the opportunity to customize education about self-management skills including regular diet, exercise, and sleep hygiene. Due to limited visit time, the PCP elected to use this first visit to focus on sleep and depression. As cognitive behavioral therapy (CBT) for insomnia is first-line treatment for both primary insomnia and insomnia due to a medical condition such as TBI,5 a sleep aid was not prescribed. Fortunately, the clinic psychologist who offered CBT was able to join the interview to meet Mr. M and explain the treatment.
Mr. M expressed some initial reluctance to try an antidepressant. However, acknowledging he “just hasn’t been the same” since his TBI, he agreed to a prescription for sertraline and said he hoped it could make him “more like [he] was.”
RETURN VISIT
Four weeks after Mr. M began taking sertraline and participating in weekly CBT sessions, he returned for a follow-up visit with his PCP. He had a noticeably brighter affect, and his guardian reported that he had been playing the guitar again. Mr. M said that he had more energy as a result of improved sleep and mood, and that he felt like his “thinking was clearer.” Mr. M noted that he never thought he would meet with a psychologist but was finding CBT for insomnia helpful.
The psychologist’s notes proposed a treatment plan that would also include targeted grief and existential therapies to address Mr. M’s sudden life changes. At this visit, Mr. M admitted that his reading comprehension and speed were negatively affected by the accident and said this is why he did not wish to fill out the PHQ-2. But he was again willing to have the PHQ-9 questions read to him with his guardian’s support. Results showed a score of 6, indicating mild depression.
A follow-up appointment with Mr. M was scheduled for 6 weeks later, and the team was confident he was getting the behavioral and mental health support he needed through medication and therapy.
CORRESPONDENCE
Elizabeth Imbesi, PhD, VA Ann Arbor Healthcare System, 2215 Fuller Road, Ann Arbor, MI 48105; elizabeth.imbesi@va.gov
THE CASE
Declan M*, a 42-year-old man, presents as a new patient for general medical care. One year ago, he sustained a severe frontal traumatic brain injury (TBI) when he was hit by a car while crossing a street. He developed a subdural hematoma and was in a coma for 6 days. He also had fractured ribs and a fractured left foot. When he regained consciousness, he had posttraumatic amnesia. He also had executive function deficits and memory difficulties, so a guardian was appointed.
Mr. M no longer works as an auto mechanic, a career he once greatly enjoyed. Mr. M’s guardian reports that recently, Mr. M has lost interest in activities he’d previously enjoyed, is frequently irritable, has poor sleep, is socially isolated, and is spending increasing amounts of time at home. When his new primary care physician (PCP) enters the examining room, Mr. M is seated in a chair with his arms folded across his chest. He states that he is “fine” and just needs to “get a doctor.”
●
*This patient is an amalgam of patients for whom the author has provided care.
TBI ranges from mild to severe and can produce a number of profound effects that are a direct—or indirect—result of the physical injury.1 The location and the severity of the injury affect symptoms.2 Even mild TBI can cause impairment, and severe TBI can lead to broad cognitive, behavioral, and physical difficulties. As numbers of TBI cases increase globally, primary care providers need to recognize the symptoms and assess accordingly.1 The Acute Concussion Evaluation (ACE; Physician/Clinician Office Version) facilitates a structured evaluation for patients presenting with possible TBI symptoms. It can easily be accessed on the Centers for Disease Control and Prevention website.3
Direct effects of TBI include impulsivity, depression, reduced frustration tolerance, reduced motivation, low awareness, and insomnia and other sleep difficulties.4,5 Depression may also result indirectly from, or be exacerbated by, new posttraumatic limitations and lifestyle changes as well as loss of career and community.4 Both direct and indirect depression often manifest as feelings of hopelessness and worthlessness and a lack of interest in once enjoyable activities. Depression can worsen other TBI sequelae such as difficulty concentrating, lack of initiation, flat affect, irritability, reduced independence, reduced functional performance, loss of inhibition, and physical pain.6
Nationwide, most mental health concerns continue to be addressed in the primary care setting.7 Individuals with TBI experience major depression at a rate 5 to 6 times higher than those in the general population, with a prevalence rate of 45%.8
Suicide. The subject of suicide must be explored with survivors of TBI; evidence suggests a correlation between TBI, depression, and increased risk for suicide.9 Among those who have TBI, as many as 22% experience suicidal ideation; the risk of suicide in survivors of severe TBI is 3 to 4 times the risk in the general population.10 Additionally, suicidality in this context appears to be a chronic concern; therefore, carefully assess for its presence no matter how long ago the TBI occurred.10
Additional TBI-associated health concerns
Grief and loss. We so often focus on death as the only cause for grief, but grief can occur for other types of loss, as well. Individuals with TBI often experience a radical negative change in self-concept after their injury, which is associated with feelings of grief.11 Helping patients recognize that they are grieving the loss of the person they once were can help set a framework for their experience.
Continue to: Relationship loss
Relationship loss. Many people with TBI lose close relationships.12 This can be due to life changes such as job loss, loss of function or ability to do previously enjoyed activities, or personality changes. These relationship losses can affect a person profoundly.12 Going forward, they may have difficulty trusting others, for example.
Existential issues. Many people with TBI also find that cognitive deficits prevent them from engaging in formerly meaningful work. For example, Mr. M lost his longstanding career as an auto mechanic and therefore part of his identity. Not being able to find purpose and meaning can be a strong contributor to coping difficulties in those with TBI.13
Chronic pain. More than half of people with TBI experience chronic pain. Headaches are the most common pain condition among all TBI survivors.14
Substance use disorders. The directionality of substance use disorders and TBI is not always clear; however, most evidence suggests that substance abuse is highly prevalent, premorbid, and often a contributing factor in TBI (eg, car accidents).15 Alcohol abuse is the most common risk factor, followed by drug abuse.16 Substance abuse may be exacerbated after TBI when it becomes a coping mechanism under worsening stressors; additionally, executive function deficits or other neurologic problems may result in poor decision-making with regard to substance use.15 While substance abuse may decline in the immediate post-TBI period, it can return to pre-injury levels within a year.17
Selective serotonin reuptake inhibitors may help
Few studies have explored the efficacy of antidepressant medication in TBI survivors. In a controlled study of patients with TBI, Fann and colleagues18 found no significant improvement in depression symptoms between sertraline and a placebo. However, they did note some possibilities for this lack of significance: socially isolated TBI survivors in the placebo group may have demonstrated improvement in depression symptoms because of increased social interaction;
Continue to: Other research has found...
Other research has found that sertraline improved both depression and quality of life for men with post-TBI depression.19 In a meta-analysis of 4 studies, Paraschakis and Katsanos20 found that sertraline demonstrated a “trend toward significance” in the treatment of depression among patients with TBI. Silverberg and Panenka21 argue that selective serotonin reuptake inhibitors should be used as first-line treatment for depression in survivors of TBI. They note that in non-randomized studies, treatment effects with antidepressants are significant. Additionally, patients who do not respond to the first antidepressant prescribed will often respond to adjunctive or different medications. Finally, they argue that depression measures can capture symptoms related to the physical brain injury, in addition to symptoms of depression, thus confounding results.
THE CASE
Mr. M’s chart showed that he was not taking any medication and that he had no history of substance abuse or tobacco use. He refused to fill out the Patient Health Questionnaire (PHQ)-2. His guardian said that Mr. M was spending much of his time at home, and that he used to be an avid painter and guitar player but had not engaged in either activity for months. Furthermore, Mr. M used to enjoy working out but did so rarely now.
During the interview, the PCP was careful to make eye contact with Mr. M as well as his guardian, thereby making sure Mr. M was part of the conversation about his care. Pacing of questions was deliberate and unhurried; a return visit would be scheduled to further explore any concerns not covered in this visit. This collaborative, inclusive, patient-centered approach to the clinical interview seemed to place Mr. M at ease. When his guardian said he thought Mr. M was depressed, Mr. M agreed. Although Mr. M still refused to fill out the PHQ-2, he was now willing to answer questions about depression. He acknowledged that he was feeling hopeless and took little pleasure in activities he used to enjoy, thereby indicating a positive screen for depression.
The PCP opted to read the PHQ-9 questions aloud, and Mr. M agreed with most of the items but strongly denied suicidal ideation, citing his religious faith.
The PCP determined that Mr. M’s depression was likely a combination of the direct and indirect effects of his TBI. A quantitative estimate based on Mr. M’s report yielded a PHQ-9 score of 17, indicating moderately severe depression.
Continue to: In addition to building rapport...
In addition to building rapport, careful listening garnered important information about Mr. M. For example, until his accident and subsequent depression, Mr. M had long prioritized his physical health through diet and exercise. He followed a vegetarian diet but recently had little appetite and was eating one microwaveable meal a day. He had an irregular sleep schedule and struggled with insomnia. He lost his closest long-term relationship after his accident due to difficulties with affect regulation. He also lost his job as he could no longer cognitively handle the tasks required.
Hearing Mr. M’s story provided the opportunity to customize education about self-management skills including regular diet, exercise, and sleep hygiene. Due to limited visit time, the PCP elected to use this first visit to focus on sleep and depression. As cognitive behavioral therapy (CBT) for insomnia is first-line treatment for both primary insomnia and insomnia due to a medical condition such as TBI,5 a sleep aid was not prescribed. Fortunately, the clinic psychologist who offered CBT was able to join the interview to meet Mr. M and explain the treatment.
Mr. M expressed some initial reluctance to try an antidepressant. However, acknowledging he “just hasn’t been the same” since his TBI, he agreed to a prescription for sertraline and said he hoped it could make him “more like [he] was.”
RETURN VISIT
Four weeks after Mr. M began taking sertraline and participating in weekly CBT sessions, he returned for a follow-up visit with his PCP. He had a noticeably brighter affect, and his guardian reported that he had been playing the guitar again. Mr. M said that he had more energy as a result of improved sleep and mood, and that he felt like his “thinking was clearer.” Mr. M noted that he never thought he would meet with a psychologist but was finding CBT for insomnia helpful.
The psychologist’s notes proposed a treatment plan that would also include targeted grief and existential therapies to address Mr. M’s sudden life changes. At this visit, Mr. M admitted that his reading comprehension and speed were negatively affected by the accident and said this is why he did not wish to fill out the PHQ-2. But he was again willing to have the PHQ-9 questions read to him with his guardian’s support. Results showed a score of 6, indicating mild depression.
A follow-up appointment with Mr. M was scheduled for 6 weeks later, and the team was confident he was getting the behavioral and mental health support he needed through medication and therapy.
CORRESPONDENCE
Elizabeth Imbesi, PhD, VA Ann Arbor Healthcare System, 2215 Fuller Road, Ann Arbor, MI 48105; elizabeth.imbesi@va.gov
1. CDC. Traumatic brain injury & concussion. 2020. Accessed May 19, 2022. www.cdc.gov/traumaticbraininjury/index.html
2. Finset A, Anderson S. Coping strategies in patients with acquired brain injury: relationships between coping, apathy, depression and lesion location. Brain Inj. 2009;14:887-905. doi: 10.1080/026990500445718
3. CDC. Gioia G, Collins M. Acute concussion evaluation. 2006. Accessed May 19, 2022. www.cdc.gov/headsup/pdfs/providers/ace_v2-a.pdf
4. Prigatano GP. Psychotherapy and the process of coping with a brain disorder. Oral presentation at: American Psychological Association annual convention. August 2015; Toronto, Canada.
5. Ouellet M, Beaulieu-Bonneau S, Savard J, Morin C. Insomnia and Fatigue After Traumatic Brain Injury: A CBT Approach to Assessment and Treatment. Elsevier Academic Press: 2019.
6. Lewis FD, Horn GH. Depression following traumatic brain injury: impact on post-hospital residential rehabilitation outcomes. NeuroRehabilitation. 2017;40:401-410. doi: 10.3233/NRE-161427
7. Barkil-Oteo A. Collaborative care for depression in primary care: how psychiatry could “troubleshoot” current treatments and practices. Yale J Bio Med. 2013;86:139-146.
8. Whelan-Goodinson R, Ponsford J, Johnston L, et al. Psychiatric disorders following traumatic brain injury: their nature and frequency. J Head Trauma Rehabil. 2009;24:324-332. doi: 10.1097/HTR.0b013e3181a712aa
9. Reeves RR, Laizer JT. Traumatic brain injury and suicide. J Psychosoc Nurs Ment Health Serv. 2012;50:32-38. doi: 10.3928/02793695-20120207-02
10. Simpson G, Tate R. Suicidality in people surviving a traumatic brain injury: Prevalence, risk factors and implications for clinical management. Brain Inj. 2007;21:1335-1351. doi: 10.1080/02699050701785542
11. Carroll E, Coetzer R. Identity, grief and self-awareness after traumatic brain injury. Neuropsychol Rehabil. 2011;21:289-305. doi: 10.1080/09602011.2011.555972
12. Salas CE, Casassus M, Rowlands L, et al. “Relating through sameness”: a qualitative study of friendship and social isolation in chronic traumatic brain injury. Neuropsychol Rehabil. 2018;28:1161-1178. doi: 10.1080/09602011.2016.1247730
13. Hinkebein JA, Stucky R. Coping with traumatic brain injury: existential challenges and managing hope. In: Martz E, Livneh H, eds. Coping with Chronic Illness and Disability: Theoretical, Empirical, and Clinical Aspects. Springer Science & Business Media; 2007:389-409.
14. Khoury S, Benavides R. Pain with traumatic brain injury and psychological disorders. Prog Neuropsychopharmacol and Biol Psychiatry. 2018;87:224-233. doi: 10.1016/j.pnpbp.2017.06.007
15. Bjork JM, Grant SJ. Does traumatic brain injury increase risk for substance abuse? J Neurotrauma. 2009;26:1077-1082. doi: 10.1089/neu.2008.0849
16. Unsworth DJ, Mathias JL. Traumatic brain injury and alcohol/substance abuse: a Bayesian meta-analysis comparing the outcomes of people with and without a history of abuse. J Clin Exp Neuropsychol. 2017,39:547-562. doi: 10.1080/13803395.2016.1248812
17. Beaulieu-Bonneau S, St-Onge F, Blackburn M, et al. Alcohol and drug use before and during the first year after traumatic brain injury. J Head Trauma Rehabil. 2018;33:E51-E60. doi: 10.1097/HTR.0000000000000341
18. Fann JR, Bombardier CH, Temkin N, et al. Sertraline for major depression during the year following traumatic brain injury: a randomized control trial. J Head Trauma Rehabil. 2017;32:332-342. doi: 10.1097/HTR.0000000000000322
19. Ansari A, Jain A, Sharma A, et al. Role of sertraline in posttraumatic brain injury depression and quality of life in TBI. Asian J Neurosurg. 2014;9:182-188. doi: 10.4103/1793-5482.146597
20. Paraschakis A, Katsanos AH. Antidepressants for depression associated with traumatic brain injury: a meta-analytical study of randomized control trials. East Asian Arch Psychiatry. 2017;27:142-149.
21. Silverberg ND, Panenka WJ. Antidepressants for depression after concussion and traumatic brain injury are still best practice. BMC Psychiatry. 2019;19:100. doi: 10.1186/s12888-019-2076-9
1. CDC. Traumatic brain injury & concussion. 2020. Accessed May 19, 2022. www.cdc.gov/traumaticbraininjury/index.html
2. Finset A, Anderson S. Coping strategies in patients with acquired brain injury: relationships between coping, apathy, depression and lesion location. Brain Inj. 2009;14:887-905. doi: 10.1080/026990500445718
3. CDC. Gioia G, Collins M. Acute concussion evaluation. 2006. Accessed May 19, 2022. www.cdc.gov/headsup/pdfs/providers/ace_v2-a.pdf
4. Prigatano GP. Psychotherapy and the process of coping with a brain disorder. Oral presentation at: American Psychological Association annual convention. August 2015; Toronto, Canada.
5. Ouellet M, Beaulieu-Bonneau S, Savard J, Morin C. Insomnia and Fatigue After Traumatic Brain Injury: A CBT Approach to Assessment and Treatment. Elsevier Academic Press: 2019.
6. Lewis FD, Horn GH. Depression following traumatic brain injury: impact on post-hospital residential rehabilitation outcomes. NeuroRehabilitation. 2017;40:401-410. doi: 10.3233/NRE-161427
7. Barkil-Oteo A. Collaborative care for depression in primary care: how psychiatry could “troubleshoot” current treatments and practices. Yale J Bio Med. 2013;86:139-146.
8. Whelan-Goodinson R, Ponsford J, Johnston L, et al. Psychiatric disorders following traumatic brain injury: their nature and frequency. J Head Trauma Rehabil. 2009;24:324-332. doi: 10.1097/HTR.0b013e3181a712aa
9. Reeves RR, Laizer JT. Traumatic brain injury and suicide. J Psychosoc Nurs Ment Health Serv. 2012;50:32-38. doi: 10.3928/02793695-20120207-02
10. Simpson G, Tate R. Suicidality in people surviving a traumatic brain injury: Prevalence, risk factors and implications for clinical management. Brain Inj. 2007;21:1335-1351. doi: 10.1080/02699050701785542
11. Carroll E, Coetzer R. Identity, grief and self-awareness after traumatic brain injury. Neuropsychol Rehabil. 2011;21:289-305. doi: 10.1080/09602011.2011.555972
12. Salas CE, Casassus M, Rowlands L, et al. “Relating through sameness”: a qualitative study of friendship and social isolation in chronic traumatic brain injury. Neuropsychol Rehabil. 2018;28:1161-1178. doi: 10.1080/09602011.2016.1247730
13. Hinkebein JA, Stucky R. Coping with traumatic brain injury: existential challenges and managing hope. In: Martz E, Livneh H, eds. Coping with Chronic Illness and Disability: Theoretical, Empirical, and Clinical Aspects. Springer Science & Business Media; 2007:389-409.
14. Khoury S, Benavides R. Pain with traumatic brain injury and psychological disorders. Prog Neuropsychopharmacol and Biol Psychiatry. 2018;87:224-233. doi: 10.1016/j.pnpbp.2017.06.007
15. Bjork JM, Grant SJ. Does traumatic brain injury increase risk for substance abuse? J Neurotrauma. 2009;26:1077-1082. doi: 10.1089/neu.2008.0849
16. Unsworth DJ, Mathias JL. Traumatic brain injury and alcohol/substance abuse: a Bayesian meta-analysis comparing the outcomes of people with and without a history of abuse. J Clin Exp Neuropsychol. 2017,39:547-562. doi: 10.1080/13803395.2016.1248812
17. Beaulieu-Bonneau S, St-Onge F, Blackburn M, et al. Alcohol and drug use before and during the first year after traumatic brain injury. J Head Trauma Rehabil. 2018;33:E51-E60. doi: 10.1097/HTR.0000000000000341
18. Fann JR, Bombardier CH, Temkin N, et al. Sertraline for major depression during the year following traumatic brain injury: a randomized control trial. J Head Trauma Rehabil. 2017;32:332-342. doi: 10.1097/HTR.0000000000000322
19. Ansari A, Jain A, Sharma A, et al. Role of sertraline in posttraumatic brain injury depression and quality of life in TBI. Asian J Neurosurg. 2014;9:182-188. doi: 10.4103/1793-5482.146597
20. Paraschakis A, Katsanos AH. Antidepressants for depression associated with traumatic brain injury: a meta-analytical study of randomized control trials. East Asian Arch Psychiatry. 2017;27:142-149.
21. Silverberg ND, Panenka WJ. Antidepressants for depression after concussion and traumatic brain injury are still best practice. BMC Psychiatry. 2019;19:100. doi: 10.1186/s12888-019-2076-9

Long-term erratic sleep may foretell cognitive problems
CHARLOTTE, N.C. – Erratic sleep patterns over years or even decades, along with a patient’s age and history of depression, may be harbingers of cognitive impairment later in life, an analysis of decades of data from a large sleep study has found.
“What we were a little surprised to find in this model was that sleep duration, whether short, long or average, was not significant, but the sleep variability – the change in sleep across those time measurements—was significantly impacting the incidence of cognitive impairment,” Samantha Keil, PhD, a postdoctoral fellow at the University of Washington, Seattle, reported at the at the annual meeting of the Associated Professional Sleep Societies.

The researchers analyzed sleep and cognition data collected over decades on 1,104 adults who participated in the Seattle Longitudinal Study. Study participants ranged from age 55 to over 100, with almost 80% of the study cohort aged 65 and older.
The Seattle Longitudinal Study first started gathering data in the 1950s. Participants in the study cohort underwent an extensive cognitive battery, which was added to the study in 1984 and gathered every 5-7 years, and completed a health behavioral questionnaire (HBQ), which was added in 1993 and administered every 3-5 years, Dr. Keil said. The HBQ included a question on average nightly sleep duration.
The study used a multivariable Cox proportional hazard regression model to evaluate the overall effect of average sleep duration and changes in sleep duration over time on cognitive impairment. Covariates used in the model included apolipoprotein E4 (APOE4) genotype, gender, years of education, ethnicity, and depression.
Dr. Keil said the model found, as expected, that the demographic variables of education, APOE status, and depression were significantly associated with cognitive impairment (hazard ratios of 1.11; 95% confidence interval [CI], 1.02-1.21; P = .01; and 2.08; 95% CI, 1.31-3.31; P < .005; and 1.08; 95% CI, 1.04-1.13; P < .005, respectively). Importantly, when evaluating the duration, change and variability of sleep, the researchers found that increased sleep variability was significantly associated with cognitive impairment (HR, 3.15; 95% CI, 1.69-5.87; P < .005).
Under this analysis, “sleep variability over time and not median sleep duration was associated with cognitive impairment,” she said. When sleep variability was added into the model, it improved the concordance score – a value that reflects the ability of a model to predict an outcome better than random chance – from .63 to .73 (a value of .5 indicates the model is no better at predicting an outcome than a random chance model; a value of .7 or greater indicates a good model).
Identification of sleep variability as a sleep pattern of interest in longitudinal studies is important, Dr. Keil said, because simply evaluating mean or median sleep duration across time might not account for a subject’s variable sleep phenotype. Most importantly, further evaluation of sleep variability with a linear regression prediction analysis (F statistic 8.796, P < .0001, adjusted R-squared .235) found that increased age, depression, and sleep variability significantly predicted cognitive impairment 10 years downstream. “Longitudinal sleep variability is perhaps for the first time being reported as significantly associated with the development of downstream cognitive impairment,” Dr. Keil said.
What makes this study unique, Dr. Keil said in an interview, is that it used self-reported longitudinal data gathered at 3- to 5-year intervals for up to 25 years, allowing for the assessment of variation of sleep duration across this entire time frame. “If you could use that shift in sleep duration as a point of therapeutic intervention, that would be really exciting,” she said.
Future research will evaluate how sleep variability and cognitive function are impacted by other variables gathered in the Seattle Longitudinal Study over the years, including factors such as diabetes and hypertension status, diet, alcohol and tobacco use, and marital and family status. Follow-up studies will be investigating the impact of sleep variability on neuropathologic disease progression and lymphatic system impairment, Dr. Keil said.
A newer approach
By linking sleep variability and daytime functioning, the study employs a “newer approach,” said Joseph M. Dzierzewski, PhD, director of behavioral medicine concentration in the department of psychology at Virginia Commonwealth University in Richmond. “While some previous work has examined night-to-night fluctuation in various sleep characteristics and cognitive functioning, what differentiates the present study from these previous works is the duration of the investigation,” he said. The “richness of data” in the Seattle Longitudinal Study and how it tracks sleep and cognition over years make it “quite unique and novel.”

Future studies, he said, should be deliberate in how they evaluate sleep and neurocognitive function across years. “Disentangling short-term moment-to-moment and day-to-day fluctuation, which may be more reversible in nature, from long-term, enduring month-to-month or year-to-year fluctuation, which may be more permanent, will be important for continuing to advance our understanding of these complex phenomena,” Dr. Dzierzewski said. “An additional important area of future investigation would be to continue the hunt for a common biological factor underpinning both sleep variability and Alzheimer’s disease.” That, he said, may help identify potential intervention targets.
Dr. Keil and Dr. Dzierzewski have no relevant disclosures.
CHARLOTTE, N.C. – Erratic sleep patterns over years or even decades, along with a patient’s age and history of depression, may be harbingers of cognitive impairment later in life, an analysis of decades of data from a large sleep study has found.
“What we were a little surprised to find in this model was that sleep duration, whether short, long or average, was not significant, but the sleep variability – the change in sleep across those time measurements—was significantly impacting the incidence of cognitive impairment,” Samantha Keil, PhD, a postdoctoral fellow at the University of Washington, Seattle, reported at the at the annual meeting of the Associated Professional Sleep Societies.
The researchers analyzed sleep and cognition data collected over decades on 1,104 adults who participated in the Seattle Longitudinal Study. Study participants ranged from age 55 to over 100, with almost 80% of the study cohort aged 65 and older.
The Seattle Longitudinal Study first started gathering data in the 1950s. Participants in the study cohort underwent an extensive cognitive battery, which was added to the study in 1984 and gathered every 5-7 years, and completed a health behavioral questionnaire (HBQ), which was added in 1993 and administered every 3-5 years, Dr. Keil said. The HBQ included a question on average nightly sleep duration.
The study used a multivariable Cox proportional hazard regression model to evaluate the overall effect of average sleep duration and changes in sleep duration over time on cognitive impairment. Covariates used in the model included apolipoprotein E4 (APOE4) genotype, gender, years of education, ethnicity, and depression.
Dr. Keil said the model found, as expected, that the demographic variables of education, APOE status, and depression were significantly associated with cognitive impairment (hazard ratios of 1.11; 95% confidence interval [CI], 1.02-1.21; P = .01; and 2.08; 95% CI, 1.31-3.31; P < .005; and 1.08; 95% CI, 1.04-1.13; P < .005, respectively). Importantly, when evaluating the duration, change and variability of sleep, the researchers found that increased sleep variability was significantly associated with cognitive impairment (HR, 3.15; 95% CI, 1.69-5.87; P < .005).
Under this analysis, “sleep variability over time and not median sleep duration was associated with cognitive impairment,” she said. When sleep variability was added into the model, it improved the concordance score – a value that reflects the ability of a model to predict an outcome better than random chance – from .63 to .73 (a value of .5 indicates the model is no better at predicting an outcome than a random chance model; a value of .7 or greater indicates a good model).
Identification of sleep variability as a sleep pattern of interest in longitudinal studies is important, Dr. Keil said, because simply evaluating mean or median sleep duration across time might not account for a subject’s variable sleep phenotype. Most importantly, further evaluation of sleep variability with a linear regression prediction analysis (F statistic 8.796, P < .0001, adjusted R-squared .235) found that increased age, depression, and sleep variability significantly predicted cognitive impairment 10 years downstream. “Longitudinal sleep variability is perhaps for the first time being reported as significantly associated with the development of downstream cognitive impairment,” Dr. Keil said.
What makes this study unique, Dr. Keil said in an interview, is that it used self-reported longitudinal data gathered at 3- to 5-year intervals for up to 25 years, allowing for the assessment of variation of sleep duration across this entire time frame. “If you could use that shift in sleep duration as a point of therapeutic intervention, that would be really exciting,” she said.
Future research will evaluate how sleep variability and cognitive function are impacted by other variables gathered in the Seattle Longitudinal Study over the years, including factors such as diabetes and hypertension status, diet, alcohol and tobacco use, and marital and family status. Follow-up studies will be investigating the impact of sleep variability on neuropathologic disease progression and lymphatic system impairment, Dr. Keil said.
A newer approach
By linking sleep variability and daytime functioning, the study employs a “newer approach,” said Joseph M. Dzierzewski, PhD, director of behavioral medicine concentration in the department of psychology at Virginia Commonwealth University in Richmond. “While some previous work has examined night-to-night fluctuation in various sleep characteristics and cognitive functioning, what differentiates the present study from these previous works is the duration of the investigation,” he said. The “richness of data” in the Seattle Longitudinal Study and how it tracks sleep and cognition over years make it “quite unique and novel.”
Future studies, he said, should be deliberate in how they evaluate sleep and neurocognitive function across years. “Disentangling short-term moment-to-moment and day-to-day fluctuation, which may be more reversible in nature, from long-term, enduring month-to-month or year-to-year fluctuation, which may be more permanent, will be important for continuing to advance our understanding of these complex phenomena,” Dr. Dzierzewski said. “An additional important area of future investigation would be to continue the hunt for a common biological factor underpinning both sleep variability and Alzheimer’s disease.” That, he said, may help identify potential intervention targets.
Dr. Keil and Dr. Dzierzewski have no relevant disclosures.
CHARLOTTE, N.C. – Erratic sleep patterns over years or even decades, along with a patient’s age and history of depression, may be harbingers of cognitive impairment later in life, an analysis of decades of data from a large sleep study has found.
“What we were a little surprised to find in this model was that sleep duration, whether short, long or average, was not significant, but the sleep variability – the change in sleep across those time measurements—was significantly impacting the incidence of cognitive impairment,” Samantha Keil, PhD, a postdoctoral fellow at the University of Washington, Seattle, reported at the at the annual meeting of the Associated Professional Sleep Societies.
The researchers analyzed sleep and cognition data collected over decades on 1,104 adults who participated in the Seattle Longitudinal Study. Study participants ranged from age 55 to over 100, with almost 80% of the study cohort aged 65 and older.
The Seattle Longitudinal Study first started gathering data in the 1950s. Participants in the study cohort underwent an extensive cognitive battery, which was added to the study in 1984 and gathered every 5-7 years, and completed a health behavioral questionnaire (HBQ), which was added in 1993 and administered every 3-5 years, Dr. Keil said. The HBQ included a question on average nightly sleep duration.
The study used a multivariable Cox proportional hazard regression model to evaluate the overall effect of average sleep duration and changes in sleep duration over time on cognitive impairment. Covariates used in the model included apolipoprotein E4 (APOE4) genotype, gender, years of education, ethnicity, and depression.
Dr. Keil said the model found, as expected, that the demographic variables of education, APOE status, and depression were significantly associated with cognitive impairment (hazard ratios of 1.11; 95% confidence interval [CI], 1.02-1.21; P = .01; and 2.08; 95% CI, 1.31-3.31; P < .005; and 1.08; 95% CI, 1.04-1.13; P < .005, respectively). Importantly, when evaluating the duration, change and variability of sleep, the researchers found that increased sleep variability was significantly associated with cognitive impairment (HR, 3.15; 95% CI, 1.69-5.87; P < .005).
Under this analysis, “sleep variability over time and not median sleep duration was associated with cognitive impairment,” she said. When sleep variability was added into the model, it improved the concordance score – a value that reflects the ability of a model to predict an outcome better than random chance – from .63 to .73 (a value of .5 indicates the model is no better at predicting an outcome than a random chance model; a value of .7 or greater indicates a good model).
Identification of sleep variability as a sleep pattern of interest in longitudinal studies is important, Dr. Keil said, because simply evaluating mean or median sleep duration across time might not account for a subject’s variable sleep phenotype. Most importantly, further evaluation of sleep variability with a linear regression prediction analysis (F statistic 8.796, P < .0001, adjusted R-squared .235) found that increased age, depression, and sleep variability significantly predicted cognitive impairment 10 years downstream. “Longitudinal sleep variability is perhaps for the first time being reported as significantly associated with the development of downstream cognitive impairment,” Dr. Keil said.
What makes this study unique, Dr. Keil said in an interview, is that it used self-reported longitudinal data gathered at 3- to 5-year intervals for up to 25 years, allowing for the assessment of variation of sleep duration across this entire time frame. “If you could use that shift in sleep duration as a point of therapeutic intervention, that would be really exciting,” she said.
Future research will evaluate how sleep variability and cognitive function are impacted by other variables gathered in the Seattle Longitudinal Study over the years, including factors such as diabetes and hypertension status, diet, alcohol and tobacco use, and marital and family status. Follow-up studies will be investigating the impact of sleep variability on neuropathologic disease progression and lymphatic system impairment, Dr. Keil said.
A newer approach
By linking sleep variability and daytime functioning, the study employs a “newer approach,” said Joseph M. Dzierzewski, PhD, director of behavioral medicine concentration in the department of psychology at Virginia Commonwealth University in Richmond. “While some previous work has examined night-to-night fluctuation in various sleep characteristics and cognitive functioning, what differentiates the present study from these previous works is the duration of the investigation,” he said. The “richness of data” in the Seattle Longitudinal Study and how it tracks sleep and cognition over years make it “quite unique and novel.”
Future studies, he said, should be deliberate in how they evaluate sleep and neurocognitive function across years. “Disentangling short-term moment-to-moment and day-to-day fluctuation, which may be more reversible in nature, from long-term, enduring month-to-month or year-to-year fluctuation, which may be more permanent, will be important for continuing to advance our understanding of these complex phenomena,” Dr. Dzierzewski said. “An additional important area of future investigation would be to continue the hunt for a common biological factor underpinning both sleep variability and Alzheimer’s disease.” That, he said, may help identify potential intervention targets.
Dr. Keil and Dr. Dzierzewski have no relevant disclosures.
AT SLEEP 2022