User login
‘Large benefit’ in ovarian function suppression for breast cancer
“Adding ovarian suppression to tamoxifen should be considered for this population of women,” said senior author Hee Jeong Kim, MD, a breast cancer surgeon with the Asan Medical Center, Seoul, South Korea. Dr. Kim presented the data earlier this month at the annual meeting of the American Society of Clinical Oncology.
The median disease-free survival rate of 85.4% for tamoxifen plus ovarian function suppression versus 80.2% for tamoxifen alone (HR, 0.67; 95% confidence interval, 0.514-0.869; P = .0027) was consistent with recent findings from SOFT (Suppression of Ovarian Function Trial), which also showed a clear survival benefit in breast cancer events with the addition of ovarian function suppression to tamoxifen for women who remain premenopausal after chemotherapy. SOFT trial analyses of disease-free survival at 5 and 8 years demonstrated hazard ratios of 0.82 and 0.76 respectively.
Dr. Kim’s study is a post-trial follow-up of the ASTRRA trial, or the Addition of Ovarian Suppression to Tamoxifen in Young Women With Hormone-Sensitive Breast Cancer Who Remain Premenopausal or Regain Vaginal Bleeding After Chemotherapy, which randomly assigned 1,298 patients with breast cancer in a one-to-one ratio to receive tamoxifen only (n = 647) or tamoxifen plus ovarian function suppression (n = 635). The primary endpoint was disease-free survival and the secondary endpoint was overall survival.
Earlier ASTRRA analysis at 5-year follow-up had shown disease-free survival rates of 89.9% for tamoxifen plus ovarian function suppression versus 87.2% for tamoxifen alone in women with hormone-sensitive breast cancer who remained premenopausal or had premenopausal status restored after chemotherapy. Overall survival, a secondary endpoint, also favored adding ovarian function suppression (HR, 0.31; 95% CI, 0.10-0.94; P = .029). The absolute difference for disease-free survival adding ovarian function suppression at the later median follow-up of 106.4 months was 5.2%. The difference at 5 years had been 2.7%, Dr. Kim pointed out. Also, these findings were calculated from time of enrollment. When calculated from time of randomization, the disease-free survival rates were 84.1% and 78.1%, respectively, for tamoxifen plus ovarian function suppression and tamoxifen alone, with a 6.0% absolute difference (HR, 0.67; 95% CI, 0.516-0.872); P = .0025).
The benefit of adding ovarian function suppression to tamoxifen for the secondary endpoint of overall survival at 8 years (96.5% versus 95.3%) did not achieve statistical significance (HR, 0.78; 95% CI, 0.486-1.253); P = .3). “Although it’s not statistically significant, there are absolute differences between the two groups favoring tamoxifen plus ovarian function suppression,” Dr. Kim said in an interview. She pointed out also that for distant metastasis-free survival the hazard ratio was 0.71, significantly favoring tamoxifen plus ovarian function suppression. “More than 95% were still surviving at 8 years with tamoxifen plus ovarian function suppression. So, we need more events to fully evaluate the overall survival benefit.”
A study limitation, Dr. Kim acknowledged in the interview, is that safety and adverse event data were not collected. “As ovarian function suppression has been widely used in clinical practice for decades, and the side effects of its relatively short-term use were considered to be well-understood in previous studies, we focused on the oncologic efficacy of ovarian function suppression in this study,” she said.
“Adding ovarian suppression to tamoxifen should be considered for this population of women,” said senior author Hee Jeong Kim, MD, a breast cancer surgeon with the Asan Medical Center, Seoul, South Korea. Dr. Kim presented the data earlier this month at the annual meeting of the American Society of Clinical Oncology.
The median disease-free survival rate of 85.4% for tamoxifen plus ovarian function suppression versus 80.2% for tamoxifen alone (HR, 0.67; 95% confidence interval, 0.514-0.869; P = .0027) was consistent with recent findings from SOFT (Suppression of Ovarian Function Trial), which also showed a clear survival benefit in breast cancer events with the addition of ovarian function suppression to tamoxifen for women who remain premenopausal after chemotherapy. SOFT trial analyses of disease-free survival at 5 and 8 years demonstrated hazard ratios of 0.82 and 0.76 respectively.
Dr. Kim’s study is a post-trial follow-up of the ASTRRA trial, or the Addition of Ovarian Suppression to Tamoxifen in Young Women With Hormone-Sensitive Breast Cancer Who Remain Premenopausal or Regain Vaginal Bleeding After Chemotherapy, which randomly assigned 1,298 patients with breast cancer in a one-to-one ratio to receive tamoxifen only (n = 647) or tamoxifen plus ovarian function suppression (n = 635). The primary endpoint was disease-free survival and the secondary endpoint was overall survival.
Earlier ASTRRA analysis at 5-year follow-up had shown disease-free survival rates of 89.9% for tamoxifen plus ovarian function suppression versus 87.2% for tamoxifen alone in women with hormone-sensitive breast cancer who remained premenopausal or had premenopausal status restored after chemotherapy. Overall survival, a secondary endpoint, also favored adding ovarian function suppression (HR, 0.31; 95% CI, 0.10-0.94; P = .029). The absolute difference for disease-free survival adding ovarian function suppression at the later median follow-up of 106.4 months was 5.2%. The difference at 5 years had been 2.7%, Dr. Kim pointed out. Also, these findings were calculated from time of enrollment. When calculated from time of randomization, the disease-free survival rates were 84.1% and 78.1%, respectively, for tamoxifen plus ovarian function suppression and tamoxifen alone, with a 6.0% absolute difference (HR, 0.67; 95% CI, 0.516-0.872); P = .0025).
The benefit of adding ovarian function suppression to tamoxifen for the secondary endpoint of overall survival at 8 years (96.5% versus 95.3%) did not achieve statistical significance (HR, 0.78; 95% CI, 0.486-1.253); P = .3). “Although it’s not statistically significant, there are absolute differences between the two groups favoring tamoxifen plus ovarian function suppression,” Dr. Kim said in an interview. She pointed out also that for distant metastasis-free survival the hazard ratio was 0.71, significantly favoring tamoxifen plus ovarian function suppression. “More than 95% were still surviving at 8 years with tamoxifen plus ovarian function suppression. So, we need more events to fully evaluate the overall survival benefit.”
A study limitation, Dr. Kim acknowledged in the interview, is that safety and adverse event data were not collected. “As ovarian function suppression has been widely used in clinical practice for decades, and the side effects of its relatively short-term use were considered to be well-understood in previous studies, we focused on the oncologic efficacy of ovarian function suppression in this study,” she said.
“Adding ovarian suppression to tamoxifen should be considered for this population of women,” said senior author Hee Jeong Kim, MD, a breast cancer surgeon with the Asan Medical Center, Seoul, South Korea. Dr. Kim presented the data earlier this month at the annual meeting of the American Society of Clinical Oncology.
The median disease-free survival rate of 85.4% for tamoxifen plus ovarian function suppression versus 80.2% for tamoxifen alone (HR, 0.67; 95% confidence interval, 0.514-0.869; P = .0027) was consistent with recent findings from SOFT (Suppression of Ovarian Function Trial), which also showed a clear survival benefit in breast cancer events with the addition of ovarian function suppression to tamoxifen for women who remain premenopausal after chemotherapy. SOFT trial analyses of disease-free survival at 5 and 8 years demonstrated hazard ratios of 0.82 and 0.76 respectively.
Dr. Kim’s study is a post-trial follow-up of the ASTRRA trial, or the Addition of Ovarian Suppression to Tamoxifen in Young Women With Hormone-Sensitive Breast Cancer Who Remain Premenopausal or Regain Vaginal Bleeding After Chemotherapy, which randomly assigned 1,298 patients with breast cancer in a one-to-one ratio to receive tamoxifen only (n = 647) or tamoxifen plus ovarian function suppression (n = 635). The primary endpoint was disease-free survival and the secondary endpoint was overall survival.
Earlier ASTRRA analysis at 5-year follow-up had shown disease-free survival rates of 89.9% for tamoxifen plus ovarian function suppression versus 87.2% for tamoxifen alone in women with hormone-sensitive breast cancer who remained premenopausal or had premenopausal status restored after chemotherapy. Overall survival, a secondary endpoint, also favored adding ovarian function suppression (HR, 0.31; 95% CI, 0.10-0.94; P = .029). The absolute difference for disease-free survival adding ovarian function suppression at the later median follow-up of 106.4 months was 5.2%. The difference at 5 years had been 2.7%, Dr. Kim pointed out. Also, these findings were calculated from time of enrollment. When calculated from time of randomization, the disease-free survival rates were 84.1% and 78.1%, respectively, for tamoxifen plus ovarian function suppression and tamoxifen alone, with a 6.0% absolute difference (HR, 0.67; 95% CI, 0.516-0.872); P = .0025).
The benefit of adding ovarian function suppression to tamoxifen for the secondary endpoint of overall survival at 8 years (96.5% versus 95.3%) did not achieve statistical significance (HR, 0.78; 95% CI, 0.486-1.253); P = .3). “Although it’s not statistically significant, there are absolute differences between the two groups favoring tamoxifen plus ovarian function suppression,” Dr. Kim said in an interview. She pointed out also that for distant metastasis-free survival the hazard ratio was 0.71, significantly favoring tamoxifen plus ovarian function suppression. “More than 95% were still surviving at 8 years with tamoxifen plus ovarian function suppression. So, we need more events to fully evaluate the overall survival benefit.”
A study limitation, Dr. Kim acknowledged in the interview, is that safety and adverse event data were not collected. “As ovarian function suppression has been widely used in clinical practice for decades, and the side effects of its relatively short-term use were considered to be well-understood in previous studies, we focused on the oncologic efficacy of ovarian function suppression in this study,” she said.
FROM ASCO 2022
Neighborhood analysis links breast cancer outcomes to socioeconomic status
A neighborhood analysis of socioeconomic status conducted in the Pittsburgh area found worse metastatic breast cancer survival outcomes among patients of low socioeconomic status. The findings suggest that race is not a relevant factor in outcomes.
“This study demonstrates that metastatic breast cancer patients of low socioeconomic status have worse outcomes than those with higher socioeconomic status at our center. It also underscores the idea that race is not so much a biological construct but more a consequence of socioeconomic issues. The effect of race is likely mediated by lower socioeconomic status,” said Susrutha Puthanmadhom Narayanan, MD, who presented the results of her study earlier this month in Chicago at the annual meeting of the American Society of Clinical Oncology.
“The current study should make clinicians cognizant of the potential for biases in the management of metastatic breast cancer in terms of socioeconomic status and race. One should think of socioeconomic status as a predictor of bad outcomes, almost like a comorbidity, and think of [associations between race and outcomes], as a consequence of socioeconomic inequality,” said Dr. Puthanmadhom Narayanan, who is an internal medicine resident at University of Pittsburgh Medical Center.
She and her colleagues intend to dig deeper into the relationships. “We are interested in looking at utilization of different treatment options for metastatic breast cancer between the socioeconomic status groups. In the preliminary analysis, we saw that ER-positive metastatic breast cancer patients with lower socioeconomic status get treated with tamoxifen more often than aromatase inhibitors and newer agents. And, we have plans to study stress signaling and inflammation as mediators of bad outcomes in the low socioeconomic status population,” Dr. Puthanmadhom Narayanan said.
In fact, that tendency for lower socioeconomic status patients to receive older treatments should be a call to action for physicians. “This study should make clinicians cognizant of the potential for biases in management of metastatic breast cancer in terms of socioeconomic status and race,” she said.
The study is based on an analysis of data from the Neighborhood Atlas in which a Neighborhood Deprivation Index (NDI) score was calculated. An NDI score in the bottom tertile meant that patients were better off than patients with mid to high range NDI scores. In this study, socioeconomic status was described as “low deprivation” or “high depreviation.” Higher deprivation correlated with lower overall survival. And, there were more Black patients in the higher deprivation group (10.5%), compared with the low deprivation group (3.7%). In multivariate Cox proportional hazard model, socioeconomic status, but not race, had a significant effect on overall survival (HR for high deprivation was 1.19 [95% confidence interval; 1.04-1.37], P = 0.01).
It included 1,246 patients who were treated at the University of Pittsburgh Medical Center between 2000 and 2017. Of 1,246 patients, 414 patients considered in the bottom tertile of NDI as having low deprivation, while 832 patients in the middle or top tertiles were classified as having high deprivation.
The two socioeconomic status groups were similar in baseline characteristics, with the exception of race: 10.5% of the high deprivation group were African American, compared with 3.7% of the low deprivation group (P =.000093).
Univariate analyses showed worse survival in both Black women and women in the lower socioeconomic status group, but a multivariate analysis found only socioeconomic status was associated with overall survival (hazard ratio for lower socioeconomic status, 1.19; P = .01).
The study had several strengths, according to Rachel Freedman, MD, MPH, who served as a discussant for the abstract. “It included both de novo and recurrent metastatic breast cancer, unlike previous studies based on the Surveillance, Epidemiology, and End Results (SEER) database that only included de novo cases. It also employed a novel tool to define socioeconomic status in the form of the Neighborhood Atlas. The study “adds more evidence that socioeconomic status likely mediates much of what we see when it comes to racial disparities,” said Dr. Freedman, who is a senior physician at Dana Farber Cancer Institute.
Nevertheless, more work needs to be done. Dr. Freedman pointed out that the current study did not include information on treatment.
“We need to standardize the way that we collect social determinants of health and act upon findings, and we need to standardize patient navigation, and we need to commit as a community to diverse clinical trial populations,” Dr. Freedman said.
Dr. Narayanan has no relevant financial disclosures. Dr. Freedman is an employee and stockholder of Firefly Health.
A neighborhood analysis of socioeconomic status conducted in the Pittsburgh area found worse metastatic breast cancer survival outcomes among patients of low socioeconomic status. The findings suggest that race is not a relevant factor in outcomes.
“This study demonstrates that metastatic breast cancer patients of low socioeconomic status have worse outcomes than those with higher socioeconomic status at our center. It also underscores the idea that race is not so much a biological construct but more a consequence of socioeconomic issues. The effect of race is likely mediated by lower socioeconomic status,” said Susrutha Puthanmadhom Narayanan, MD, who presented the results of her study earlier this month in Chicago at the annual meeting of the American Society of Clinical Oncology.
“The current study should make clinicians cognizant of the potential for biases in the management of metastatic breast cancer in terms of socioeconomic status and race. One should think of socioeconomic status as a predictor of bad outcomes, almost like a comorbidity, and think of [associations between race and outcomes], as a consequence of socioeconomic inequality,” said Dr. Puthanmadhom Narayanan, who is an internal medicine resident at University of Pittsburgh Medical Center.
She and her colleagues intend to dig deeper into the relationships. “We are interested in looking at utilization of different treatment options for metastatic breast cancer between the socioeconomic status groups. In the preliminary analysis, we saw that ER-positive metastatic breast cancer patients with lower socioeconomic status get treated with tamoxifen more often than aromatase inhibitors and newer agents. And, we have plans to study stress signaling and inflammation as mediators of bad outcomes in the low socioeconomic status population,” Dr. Puthanmadhom Narayanan said.
In fact, that tendency for lower socioeconomic status patients to receive older treatments should be a call to action for physicians. “This study should make clinicians cognizant of the potential for biases in management of metastatic breast cancer in terms of socioeconomic status and race,” she said.
The study is based on an analysis of data from the Neighborhood Atlas in which a Neighborhood Deprivation Index (NDI) score was calculated. An NDI score in the bottom tertile meant that patients were better off than patients with mid to high range NDI scores. In this study, socioeconomic status was described as “low deprivation” or “high depreviation.” Higher deprivation correlated with lower overall survival. And, there were more Black patients in the higher deprivation group (10.5%), compared with the low deprivation group (3.7%). In multivariate Cox proportional hazard model, socioeconomic status, but not race, had a significant effect on overall survival (HR for high deprivation was 1.19 [95% confidence interval; 1.04-1.37], P = 0.01).
It included 1,246 patients who were treated at the University of Pittsburgh Medical Center between 2000 and 2017. Of 1,246 patients, 414 patients considered in the bottom tertile of NDI as having low deprivation, while 832 patients in the middle or top tertiles were classified as having high deprivation.
The two socioeconomic status groups were similar in baseline characteristics, with the exception of race: 10.5% of the high deprivation group were African American, compared with 3.7% of the low deprivation group (P =.000093).
Univariate analyses showed worse survival in both Black women and women in the lower socioeconomic status group, but a multivariate analysis found only socioeconomic status was associated with overall survival (hazard ratio for lower socioeconomic status, 1.19; P = .01).
The study had several strengths, according to Rachel Freedman, MD, MPH, who served as a discussant for the abstract. “It included both de novo and recurrent metastatic breast cancer, unlike previous studies based on the Surveillance, Epidemiology, and End Results (SEER) database that only included de novo cases. It also employed a novel tool to define socioeconomic status in the form of the Neighborhood Atlas. The study “adds more evidence that socioeconomic status likely mediates much of what we see when it comes to racial disparities,” said Dr. Freedman, who is a senior physician at Dana Farber Cancer Institute.
Nevertheless, more work needs to be done. Dr. Freedman pointed out that the current study did not include information on treatment.
“We need to standardize the way that we collect social determinants of health and act upon findings, and we need to standardize patient navigation, and we need to commit as a community to diverse clinical trial populations,” Dr. Freedman said.
Dr. Narayanan has no relevant financial disclosures. Dr. Freedman is an employee and stockholder of Firefly Health.
A neighborhood analysis of socioeconomic status conducted in the Pittsburgh area found worse metastatic breast cancer survival outcomes among patients of low socioeconomic status. The findings suggest that race is not a relevant factor in outcomes.
“This study demonstrates that metastatic breast cancer patients of low socioeconomic status have worse outcomes than those with higher socioeconomic status at our center. It also underscores the idea that race is not so much a biological construct but more a consequence of socioeconomic issues. The effect of race is likely mediated by lower socioeconomic status,” said Susrutha Puthanmadhom Narayanan, MD, who presented the results of her study earlier this month in Chicago at the annual meeting of the American Society of Clinical Oncology.
“The current study should make clinicians cognizant of the potential for biases in the management of metastatic breast cancer in terms of socioeconomic status and race. One should think of socioeconomic status as a predictor of bad outcomes, almost like a comorbidity, and think of [associations between race and outcomes], as a consequence of socioeconomic inequality,” said Dr. Puthanmadhom Narayanan, who is an internal medicine resident at University of Pittsburgh Medical Center.
She and her colleagues intend to dig deeper into the relationships. “We are interested in looking at utilization of different treatment options for metastatic breast cancer between the socioeconomic status groups. In the preliminary analysis, we saw that ER-positive metastatic breast cancer patients with lower socioeconomic status get treated with tamoxifen more often than aromatase inhibitors and newer agents. And, we have plans to study stress signaling and inflammation as mediators of bad outcomes in the low socioeconomic status population,” Dr. Puthanmadhom Narayanan said.
In fact, that tendency for lower socioeconomic status patients to receive older treatments should be a call to action for physicians. “This study should make clinicians cognizant of the potential for biases in management of metastatic breast cancer in terms of socioeconomic status and race,” she said.
The study is based on an analysis of data from the Neighborhood Atlas in which a Neighborhood Deprivation Index (NDI) score was calculated. An NDI score in the bottom tertile meant that patients were better off than patients with mid to high range NDI scores. In this study, socioeconomic status was described as “low deprivation” or “high depreviation.” Higher deprivation correlated with lower overall survival. And, there were more Black patients in the higher deprivation group (10.5%), compared with the low deprivation group (3.7%). In multivariate Cox proportional hazard model, socioeconomic status, but not race, had a significant effect on overall survival (HR for high deprivation was 1.19 [95% confidence interval; 1.04-1.37], P = 0.01).
It included 1,246 patients who were treated at the University of Pittsburgh Medical Center between 2000 and 2017. Of 1,246 patients, 414 patients considered in the bottom tertile of NDI as having low deprivation, while 832 patients in the middle or top tertiles were classified as having high deprivation.
The two socioeconomic status groups were similar in baseline characteristics, with the exception of race: 10.5% of the high deprivation group were African American, compared with 3.7% of the low deprivation group (P =.000093).
Univariate analyses showed worse survival in both Black women and women in the lower socioeconomic status group, but a multivariate analysis found only socioeconomic status was associated with overall survival (hazard ratio for lower socioeconomic status, 1.19; P = .01).
The study had several strengths, according to Rachel Freedman, MD, MPH, who served as a discussant for the abstract. “It included both de novo and recurrent metastatic breast cancer, unlike previous studies based on the Surveillance, Epidemiology, and End Results (SEER) database that only included de novo cases. It also employed a novel tool to define socioeconomic status in the form of the Neighborhood Atlas. The study “adds more evidence that socioeconomic status likely mediates much of what we see when it comes to racial disparities,” said Dr. Freedman, who is a senior physician at Dana Farber Cancer Institute.
Nevertheless, more work needs to be done. Dr. Freedman pointed out that the current study did not include information on treatment.
“We need to standardize the way that we collect social determinants of health and act upon findings, and we need to standardize patient navigation, and we need to commit as a community to diverse clinical trial populations,” Dr. Freedman said.
Dr. Narayanan has no relevant financial disclosures. Dr. Freedman is an employee and stockholder of Firefly Health.
FROM ASCO 2022
Hidradenitis Suppurativa: Clinical Presentation
FDA approves setmelanotide for obesity in Bardet-Biedl syndrome
The Food and Drug Administration has approved a supplemental indication for setmelanotide (Imcivree, Rhythm Pharmaceuticals) injection for chronic weight management in adults and pediatric patients age 6 and older with obesity due to Bardet-Biedl Syndrome (BBS).

Setmelanotide, a melanocortin-4 receptor (MC4R) agonist, is the first FDA-approved therapy for BBS, a rare genetic disorder that impairs a hunger signal along the melanocortin-4 receptor (MC4R) pathway.
BBS affects an estimated 1,500-2,500 people in the United States.
Individuals with BBS typically have obesity that starts at age 1 along with insatiable hunger (hyperphagia). Available weight management options are generally unsuccessful.
Other symptoms may include retinal degeneration, reduced kidney function, or extra digits of the hands or feet.
Setmelanotide received priority review, orphan drug designation, and breakthrough designation for this new indication.
As previously reported, in November 2020, the FDA approved setmelanotide for weight management in adults and children as young as 6 years with obesity due to proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency confirmed by genetic testing – who also have impaired hunger signaling from the brain.
These individuals have a normal weight at birth but develop persistent, severe obesity within months due to hyperphagia.
The FDA approval of Imcivree for BBS “represents a significant milestone for Rhythm [Pharmaceuticals], validating our strategy of developing Imcivree for people with hyperphagia and severe obesity caused by rare MC4R-pathway diseases and allowing us to provide our precision therapy to an established community of patients living with BBS and their families who are eagerly awaiting a new treatment option,” said David Meeker, MD, chair, president and CEO of Rhythm, in a press release.
Safety, effectiveness in 66-week trial in 44 patients
The safety and effectiveness of setmelanotidewas evaluated in a 66-week phase 3 clinical trial that enrolled 44 patients age 6 and older who had a diagnosis of BBS and obesity – defined as a body mass index greater than or equal to 30 kg/m2 or greater than or equal to 97th percentile for pediatric patients.
After an initial 14-week, randomized, double-blind, placebo-controlled treatment period, patients entered a 52-week, open-label period.
The trial met its primary endpoint and all key secondary endpoints, with statistically significant reductions in weight and hunger at 52 weeks on therapy.
- After 52 weeks of treatment, patients taking setmelanotide lost, on average, 7.9% of their initial BMI.
- 61% of patients lost 5% or more of their initial BMI, and 39% lost 10% or more of their initial BMI.
- In the 14-week, placebo-controlled treatment, on average, BMI dropped by 4.6% in the 22 patients treated with the study drug and dropped 0.1% in the 22 patients treated with placebo.
- At 52 weeks, the 14 patients aged 12 and older who were able to self-report their hunger had a significant –2.1 mean change in hunger score.
Setmelanotide is associated with the following warnings and precautions:
- Spontaneous penile erections in males and sexual adverse reactions in females. Instruct males with erection lasting longer than 4 hours to seek emergency medical attention.
- Depression and suicidal ideation. Monitor patients for new onset or worsening depression or suicidal thoughts or behaviors. Consider discontinuing the drug if patients have suicidal thoughts or behaviors or clinically significant or persistent depression symptoms.
- Skin pigmentation and darkening of preexisting nevi (moles). Examine skin before and during treatment.
- Setmelanotide is not approved for use in neonates or infants. Serious and fatal adverse reactions including “gasping syndrome” can occur in neonates and low-birth-weight infants treated with benzyl alcohol-preserved drugs.
The most common adverse reactions (with an incidence greater than or equal to 20%) included skin hyperpigmentation, injection site reactions, nausea, headache, diarrhea, abdominal pain, vomiting, depression, and spontaneous penile erection.
The FDA did not approve the company’s supplemental new drug application for setmelanotide in Alström syndrome.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved a supplemental indication for setmelanotide (Imcivree, Rhythm Pharmaceuticals) injection for chronic weight management in adults and pediatric patients age 6 and older with obesity due to Bardet-Biedl Syndrome (BBS).
Setmelanotide, a melanocortin-4 receptor (MC4R) agonist, is the first FDA-approved therapy for BBS, a rare genetic disorder that impairs a hunger signal along the melanocortin-4 receptor (MC4R) pathway.
BBS affects an estimated 1,500-2,500 people in the United States.
Individuals with BBS typically have obesity that starts at age 1 along with insatiable hunger (hyperphagia). Available weight management options are generally unsuccessful.
Other symptoms may include retinal degeneration, reduced kidney function, or extra digits of the hands or feet.
Setmelanotide received priority review, orphan drug designation, and breakthrough designation for this new indication.
As previously reported, in November 2020, the FDA approved setmelanotide for weight management in adults and children as young as 6 years with obesity due to proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency confirmed by genetic testing – who also have impaired hunger signaling from the brain.
These individuals have a normal weight at birth but develop persistent, severe obesity within months due to hyperphagia.
The FDA approval of Imcivree for BBS “represents a significant milestone for Rhythm [Pharmaceuticals], validating our strategy of developing Imcivree for people with hyperphagia and severe obesity caused by rare MC4R-pathway diseases and allowing us to provide our precision therapy to an established community of patients living with BBS and their families who are eagerly awaiting a new treatment option,” said David Meeker, MD, chair, president and CEO of Rhythm, in a press release.
Safety, effectiveness in 66-week trial in 44 patients
The safety and effectiveness of setmelanotidewas evaluated in a 66-week phase 3 clinical trial that enrolled 44 patients age 6 and older who had a diagnosis of BBS and obesity – defined as a body mass index greater than or equal to 30 kg/m2 or greater than or equal to 97th percentile for pediatric patients.
After an initial 14-week, randomized, double-blind, placebo-controlled treatment period, patients entered a 52-week, open-label period.
The trial met its primary endpoint and all key secondary endpoints, with statistically significant reductions in weight and hunger at 52 weeks on therapy.
- After 52 weeks of treatment, patients taking setmelanotide lost, on average, 7.9% of their initial BMI.
- 61% of patients lost 5% or more of their initial BMI, and 39% lost 10% or more of their initial BMI.
- In the 14-week, placebo-controlled treatment, on average, BMI dropped by 4.6% in the 22 patients treated with the study drug and dropped 0.1% in the 22 patients treated with placebo.
- At 52 weeks, the 14 patients aged 12 and older who were able to self-report their hunger had a significant –2.1 mean change in hunger score.
Setmelanotide is associated with the following warnings and precautions:
- Spontaneous penile erections in males and sexual adverse reactions in females. Instruct males with erection lasting longer than 4 hours to seek emergency medical attention.
- Depression and suicidal ideation. Monitor patients for new onset or worsening depression or suicidal thoughts or behaviors. Consider discontinuing the drug if patients have suicidal thoughts or behaviors or clinically significant or persistent depression symptoms.
- Skin pigmentation and darkening of preexisting nevi (moles). Examine skin before and during treatment.
- Setmelanotide is not approved for use in neonates or infants. Serious and fatal adverse reactions including “gasping syndrome” can occur in neonates and low-birth-weight infants treated with benzyl alcohol-preserved drugs.
The most common adverse reactions (with an incidence greater than or equal to 20%) included skin hyperpigmentation, injection site reactions, nausea, headache, diarrhea, abdominal pain, vomiting, depression, and spontaneous penile erection.
The FDA did not approve the company’s supplemental new drug application for setmelanotide in Alström syndrome.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved a supplemental indication for setmelanotide (Imcivree, Rhythm Pharmaceuticals) injection for chronic weight management in adults and pediatric patients age 6 and older with obesity due to Bardet-Biedl Syndrome (BBS).
Setmelanotide, a melanocortin-4 receptor (MC4R) agonist, is the first FDA-approved therapy for BBS, a rare genetic disorder that impairs a hunger signal along the melanocortin-4 receptor (MC4R) pathway.
BBS affects an estimated 1,500-2,500 people in the United States.
Individuals with BBS typically have obesity that starts at age 1 along with insatiable hunger (hyperphagia). Available weight management options are generally unsuccessful.
Other symptoms may include retinal degeneration, reduced kidney function, or extra digits of the hands or feet.
Setmelanotide received priority review, orphan drug designation, and breakthrough designation for this new indication.
As previously reported, in November 2020, the FDA approved setmelanotide for weight management in adults and children as young as 6 years with obesity due to proopiomelanocortin (POMC), proprotein convertase subtilisin/kexin type 1 (PCSK1), or leptin receptor (LEPR) deficiency confirmed by genetic testing – who also have impaired hunger signaling from the brain.
These individuals have a normal weight at birth but develop persistent, severe obesity within months due to hyperphagia.
The FDA approval of Imcivree for BBS “represents a significant milestone for Rhythm [Pharmaceuticals], validating our strategy of developing Imcivree for people with hyperphagia and severe obesity caused by rare MC4R-pathway diseases and allowing us to provide our precision therapy to an established community of patients living with BBS and their families who are eagerly awaiting a new treatment option,” said David Meeker, MD, chair, president and CEO of Rhythm, in a press release.
Safety, effectiveness in 66-week trial in 44 patients
The safety and effectiveness of setmelanotidewas evaluated in a 66-week phase 3 clinical trial that enrolled 44 patients age 6 and older who had a diagnosis of BBS and obesity – defined as a body mass index greater than or equal to 30 kg/m2 or greater than or equal to 97th percentile for pediatric patients.
After an initial 14-week, randomized, double-blind, placebo-controlled treatment period, patients entered a 52-week, open-label period.
The trial met its primary endpoint and all key secondary endpoints, with statistically significant reductions in weight and hunger at 52 weeks on therapy.
- After 52 weeks of treatment, patients taking setmelanotide lost, on average, 7.9% of their initial BMI.
- 61% of patients lost 5% or more of their initial BMI, and 39% lost 10% or more of their initial BMI.
- In the 14-week, placebo-controlled treatment, on average, BMI dropped by 4.6% in the 22 patients treated with the study drug and dropped 0.1% in the 22 patients treated with placebo.
- At 52 weeks, the 14 patients aged 12 and older who were able to self-report their hunger had a significant –2.1 mean change in hunger score.
Setmelanotide is associated with the following warnings and precautions:
- Spontaneous penile erections in males and sexual adverse reactions in females. Instruct males with erection lasting longer than 4 hours to seek emergency medical attention.
- Depression and suicidal ideation. Monitor patients for new onset or worsening depression or suicidal thoughts or behaviors. Consider discontinuing the drug if patients have suicidal thoughts or behaviors or clinically significant or persistent depression symptoms.
- Skin pigmentation and darkening of preexisting nevi (moles). Examine skin before and during treatment.
- Setmelanotide is not approved for use in neonates or infants. Serious and fatal adverse reactions including “gasping syndrome” can occur in neonates and low-birth-weight infants treated with benzyl alcohol-preserved drugs.
The most common adverse reactions (with an incidence greater than or equal to 20%) included skin hyperpigmentation, injection site reactions, nausea, headache, diarrhea, abdominal pain, vomiting, depression, and spontaneous penile erection.
The FDA did not approve the company’s supplemental new drug application for setmelanotide in Alström syndrome.
A version of this article first appeared on Medscape.com.
Meta-analysis points to safety of acetylcholine coronary testing
Provocation testing with intracoronary acetylcholine is safe, particularly among Western patients, suggests a large systematic review that underscores the importance of functional coronary angiography to diagnose epicardial or microvascular spasm.
The results, derived from more than 12,000 patients in 16 studies, showed a 0.5% risk of major complications, defined as death, ventricular tachycardia/ventricular fibrillation, myocardial infarction, and shock requiring resuscitation.
Ventricular tachycardia/fibrillation were the most common events and mainly reported from two Japanese studies. There were no deaths.
Exploratory subgroup analyses revealed significantly fewer major complications in Western populations (0.0%; P for heterogeneity = .938), compared with Asian populations (2.3%; P for heterogeneity < .001).
The pooled positive vasospasm rate was also lower in Western versus Asian studies (37.9% vs. 50.7%; P for between-group heterogeneity = .010), as reported by the Microvascular Network in the Journal of the American College of Cardiology.
“If you look at the data between Asian studies versus others, mainly European or U.S. studies, primarily in Caucasian populations, it’s like zero percent history of major complications. So, it sounds extremely safe to do this testing in Caucasian populations,” Yuhei Kobayashi, MD, NewYork-Presbyterian Brooklyn Methodist Hospital, Weill Cornell Medicine, said.
Safety will need to be assessed in African Americans and other racial/ethnic groups, but “it makes us think we should end up testing more in the United States,” he told this news organization.
Intracoronary acetylcholine testing is daily practice in Japan but is limited in the United States and Europe to a few specialized centers due to safety concerns. Three deaths were reported in 1980 with intravenous ergonovine testing, whereas the safety of acetylcholine protocols has been studied largely in single-center retrospective studies, typically in Asian populations.
Growing recognition of myocardial infarction with nonobstructive coronary arteries (MINOCA) and ischemia with no obstructive coronary arteries (INOCA), however, is changing the landscape. In recent U.S. and European guidelines, intracoronary acetylcholine testing is indicated as a class 2a recommendation in MINOCA/INOCA.
“More and more institutions in Europe and the United States are starting to do acetylcholine testing, because now we know that chest pain isn’t necessarily coming from the blocked arteries,” Dr. Kobayashi said. “There are functional abnormalities, including coronary spasm, and if we diagnose it, we have appropriate medical regimens for this kind of disease.”
First safety meta-analysis
The present review and meta-analysis included 12,585 participants in 16 studies through November 2021. Of these, 63% were conducted in Western countries, and most were prospective studies published over the past decade in patients with MINOCA or INOCA.
Ten studies used the contemporary diagnostic criteria for epicardial spasm of at least 90% reduction in coronary diameter. Acetylcholine was administered into the left coronary artery at up to 100 mcg and 200 mcg in seven and six studies, respectively, and was used in the other three studies to assess endothelial function with a slower infusion of up to 36.4 mcg.
Major complications were significantly higher in studies following the contemporary diagnostic cutoff than in those using a lower cutoff of at least 75% diameter reduction (1.0% vs. 0.0%; P for between-group heterogeneity < .001).
The incidence of major complications was 0.2% with the slower infusion of up to 36.4 mcg, 0.8% with a maximum dose of 100 mcg, and 0.3% with a maximum dose of 200 mcg. The positive vasospasm rate was similar with the latter two protocols, at 46.3% and 41.4%, respectively.
Minor complications occurred in 3.3% of patients but were not detailed. They can include paroxysmal atrial fibrillation, ventricular ectopic beats, transient hypotension, and bradycardia requiring intervention.
As with major complications, minor complications were lower in studies using noncontemporary versus contemporary diagnostic cutoffs for epicardial spasm (1.8% vs. 4.7%) and in Western versus Asian populations (2.6% vs. 9.4%). Minor complications were similar between protocols with maximum doses of 100 mcg and 200 mcg (3.6% vs. 3.8%).
Dr. Kobayashi suggested that several factors may explain the racial differences, including previously reported smooth muscle hyperresponsiveness to provocation stimuli in Japanese patients and the inclusion of a wide range of patients in Japanese studies, such as those with obstructive coronary disease.
Japanese studies also used sequential acetylcholine injection into both the right and left coronaries, a faster injection speed of 20 seconds, and upfront placement of a temporary pacing catheter in case of acetylcholine-induced bradycardia, particularly with right coronary injection.
Although the protocol is largely settled in Japan, he said, provocation protocols need to be standardized because “depending on the country and depending on the institution, people are doing totally different things.”
A big step forward
Commenting on the study, C. Noel Bairey Merz, MD, from Cedars Sinai, Los Angeles, said it has “widespread relevance” because half of all coronary angiograms done invasively in the United States for suspected ischemia find no obstructive coronary disease. Left untreated, however, MINOCA has a 2.5% annual event rate, and a quarter of that is death.
“This is a big step forward with likely equal opportunity to improve women and men’s ischemic heart disease,” she said.

On the other hand, all studies were conducted at centers of excellence, so safety will need to be carefully watched as testing rolls out to more community care, Dr. Merz said. “And it always needs to be underscored that this is done by an interventional cardiologist because they’re familiar with wires that can dissect arteries, and they’re familiar with minor complications that could turn into major, if someone didn’t act appropriately.”
Dr. Merz also called for unifying protocols and the need to raise awareness within the general cardiology community to ask interventionalists for acetylcholine spasm testing. Randomized controlled data from within the WISE study and the CorMica study showed that diagnostic certainty leads to greater therapeutic certainty. “You do a much better job about who and how to treat,” she said.
There are also three ongoing randomized controlled trials – WARRIOR, MINOCA-BAT, and iCorMica – in the INOCA and MINOCA populations testing different treatment strategies for hard clinical outcomes like death and myocardial infarction.
“So in addition to this publication being guideline-forming for diagnosis, we anticipate in the next several years to have clinical trial evidence about therapeutics, again, for formulation of class 1 guidelines,” Dr. Merz said.
John Beltrame, BMBS, PhD, University of Adelaide, Australia, said the meta-analysis shows that intracoronary acetylcholine spasm testing is safe and should prompt greater adoption of invasive functional angiography.
Interventionalists are quite happy to do fractional flow reserve using intravenous adenosine to assess coronary microvascular dysfunction, he said, and “what we think is that functional angiography should test both – both the spasm as well as the microvasculature – and that will give us a clear direction because the treatments are slightly different when you’re treating the large arteries as compared to the microscopic arteries. It’s an important thing.”
Dr. Beltrame and colleagues further detail the benefits of comprehensive invasive functional angiography over structural angiography in a related editorial.
He also noted that the Coronary Vasomotion Disorders International Study Group published international diagnostic criteria for microvascular angina and that several protocols for acetylcholine spasm testing are in the works, including one from Australia. Australian investigators are also organizing an accreditation program for those performing the test.
“The protocol itself is relatively straightforward, but it’s not merely picking up a manual and following the instructions,” Dr. Beltrame said. “Just the same as when you train someone in angioplasty, you don’t just go out and do it. You need to develop some experience in it and so should be proctored.”
Dr. Kobayashi reported consulting agreements with Abbott Vascular. Coauthor disclosures are listed in the paper. Dr. Beltrame and colleagues have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Provocation testing with intracoronary acetylcholine is safe, particularly among Western patients, suggests a large systematic review that underscores the importance of functional coronary angiography to diagnose epicardial or microvascular spasm.
The results, derived from more than 12,000 patients in 16 studies, showed a 0.5% risk of major complications, defined as death, ventricular tachycardia/ventricular fibrillation, myocardial infarction, and shock requiring resuscitation.
Ventricular tachycardia/fibrillation were the most common events and mainly reported from two Japanese studies. There were no deaths.
Exploratory subgroup analyses revealed significantly fewer major complications in Western populations (0.0%; P for heterogeneity = .938), compared with Asian populations (2.3%; P for heterogeneity < .001).
The pooled positive vasospasm rate was also lower in Western versus Asian studies (37.9% vs. 50.7%; P for between-group heterogeneity = .010), as reported by the Microvascular Network in the Journal of the American College of Cardiology.
“If you look at the data between Asian studies versus others, mainly European or U.S. studies, primarily in Caucasian populations, it’s like zero percent history of major complications. So, it sounds extremely safe to do this testing in Caucasian populations,” Yuhei Kobayashi, MD, NewYork-Presbyterian Brooklyn Methodist Hospital, Weill Cornell Medicine, said.
Safety will need to be assessed in African Americans and other racial/ethnic groups, but “it makes us think we should end up testing more in the United States,” he told this news organization.
Intracoronary acetylcholine testing is daily practice in Japan but is limited in the United States and Europe to a few specialized centers due to safety concerns. Three deaths were reported in 1980 with intravenous ergonovine testing, whereas the safety of acetylcholine protocols has been studied largely in single-center retrospective studies, typically in Asian populations.
Growing recognition of myocardial infarction with nonobstructive coronary arteries (MINOCA) and ischemia with no obstructive coronary arteries (INOCA), however, is changing the landscape. In recent U.S. and European guidelines, intracoronary acetylcholine testing is indicated as a class 2a recommendation in MINOCA/INOCA.
“More and more institutions in Europe and the United States are starting to do acetylcholine testing, because now we know that chest pain isn’t necessarily coming from the blocked arteries,” Dr. Kobayashi said. “There are functional abnormalities, including coronary spasm, and if we diagnose it, we have appropriate medical regimens for this kind of disease.”
First safety meta-analysis
The present review and meta-analysis included 12,585 participants in 16 studies through November 2021. Of these, 63% were conducted in Western countries, and most were prospective studies published over the past decade in patients with MINOCA or INOCA.
Ten studies used the contemporary diagnostic criteria for epicardial spasm of at least 90% reduction in coronary diameter. Acetylcholine was administered into the left coronary artery at up to 100 mcg and 200 mcg in seven and six studies, respectively, and was used in the other three studies to assess endothelial function with a slower infusion of up to 36.4 mcg.
Major complications were significantly higher in studies following the contemporary diagnostic cutoff than in those using a lower cutoff of at least 75% diameter reduction (1.0% vs. 0.0%; P for between-group heterogeneity < .001).
The incidence of major complications was 0.2% with the slower infusion of up to 36.4 mcg, 0.8% with a maximum dose of 100 mcg, and 0.3% with a maximum dose of 200 mcg. The positive vasospasm rate was similar with the latter two protocols, at 46.3% and 41.4%, respectively.
Minor complications occurred in 3.3% of patients but were not detailed. They can include paroxysmal atrial fibrillation, ventricular ectopic beats, transient hypotension, and bradycardia requiring intervention.
As with major complications, minor complications were lower in studies using noncontemporary versus contemporary diagnostic cutoffs for epicardial spasm (1.8% vs. 4.7%) and in Western versus Asian populations (2.6% vs. 9.4%). Minor complications were similar between protocols with maximum doses of 100 mcg and 200 mcg (3.6% vs. 3.8%).
Dr. Kobayashi suggested that several factors may explain the racial differences, including previously reported smooth muscle hyperresponsiveness to provocation stimuli in Japanese patients and the inclusion of a wide range of patients in Japanese studies, such as those with obstructive coronary disease.
Japanese studies also used sequential acetylcholine injection into both the right and left coronaries, a faster injection speed of 20 seconds, and upfront placement of a temporary pacing catheter in case of acetylcholine-induced bradycardia, particularly with right coronary injection.
Although the protocol is largely settled in Japan, he said, provocation protocols need to be standardized because “depending on the country and depending on the institution, people are doing totally different things.”
A big step forward
Commenting on the study, C. Noel Bairey Merz, MD, from Cedars Sinai, Los Angeles, said it has “widespread relevance” because half of all coronary angiograms done invasively in the United States for suspected ischemia find no obstructive coronary disease. Left untreated, however, MINOCA has a 2.5% annual event rate, and a quarter of that is death.
“This is a big step forward with likely equal opportunity to improve women and men’s ischemic heart disease,” she said.
On the other hand, all studies were conducted at centers of excellence, so safety will need to be carefully watched as testing rolls out to more community care, Dr. Merz said. “And it always needs to be underscored that this is done by an interventional cardiologist because they’re familiar with wires that can dissect arteries, and they’re familiar with minor complications that could turn into major, if someone didn’t act appropriately.”
Dr. Merz also called for unifying protocols and the need to raise awareness within the general cardiology community to ask interventionalists for acetylcholine spasm testing. Randomized controlled data from within the WISE study and the CorMica study showed that diagnostic certainty leads to greater therapeutic certainty. “You do a much better job about who and how to treat,” she said.
There are also three ongoing randomized controlled trials – WARRIOR, MINOCA-BAT, and iCorMica – in the INOCA and MINOCA populations testing different treatment strategies for hard clinical outcomes like death and myocardial infarction.
“So in addition to this publication being guideline-forming for diagnosis, we anticipate in the next several years to have clinical trial evidence about therapeutics, again, for formulation of class 1 guidelines,” Dr. Merz said.
John Beltrame, BMBS, PhD, University of Adelaide, Australia, said the meta-analysis shows that intracoronary acetylcholine spasm testing is safe and should prompt greater adoption of invasive functional angiography.
Interventionalists are quite happy to do fractional flow reserve using intravenous adenosine to assess coronary microvascular dysfunction, he said, and “what we think is that functional angiography should test both – both the spasm as well as the microvasculature – and that will give us a clear direction because the treatments are slightly different when you’re treating the large arteries as compared to the microscopic arteries. It’s an important thing.”
Dr. Beltrame and colleagues further detail the benefits of comprehensive invasive functional angiography over structural angiography in a related editorial.
He also noted that the Coronary Vasomotion Disorders International Study Group published international diagnostic criteria for microvascular angina and that several protocols for acetylcholine spasm testing are in the works, including one from Australia. Australian investigators are also organizing an accreditation program for those performing the test.
“The protocol itself is relatively straightforward, but it’s not merely picking up a manual and following the instructions,” Dr. Beltrame said. “Just the same as when you train someone in angioplasty, you don’t just go out and do it. You need to develop some experience in it and so should be proctored.”
Dr. Kobayashi reported consulting agreements with Abbott Vascular. Coauthor disclosures are listed in the paper. Dr. Beltrame and colleagues have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Provocation testing with intracoronary acetylcholine is safe, particularly among Western patients, suggests a large systematic review that underscores the importance of functional coronary angiography to diagnose epicardial or microvascular spasm.
The results, derived from more than 12,000 patients in 16 studies, showed a 0.5% risk of major complications, defined as death, ventricular tachycardia/ventricular fibrillation, myocardial infarction, and shock requiring resuscitation.
Ventricular tachycardia/fibrillation were the most common events and mainly reported from two Japanese studies. There were no deaths.
Exploratory subgroup analyses revealed significantly fewer major complications in Western populations (0.0%; P for heterogeneity = .938), compared with Asian populations (2.3%; P for heterogeneity < .001).
The pooled positive vasospasm rate was also lower in Western versus Asian studies (37.9% vs. 50.7%; P for between-group heterogeneity = .010), as reported by the Microvascular Network in the Journal of the American College of Cardiology.
“If you look at the data between Asian studies versus others, mainly European or U.S. studies, primarily in Caucasian populations, it’s like zero percent history of major complications. So, it sounds extremely safe to do this testing in Caucasian populations,” Yuhei Kobayashi, MD, NewYork-Presbyterian Brooklyn Methodist Hospital, Weill Cornell Medicine, said.
Safety will need to be assessed in African Americans and other racial/ethnic groups, but “it makes us think we should end up testing more in the United States,” he told this news organization.
Intracoronary acetylcholine testing is daily practice in Japan but is limited in the United States and Europe to a few specialized centers due to safety concerns. Three deaths were reported in 1980 with intravenous ergonovine testing, whereas the safety of acetylcholine protocols has been studied largely in single-center retrospective studies, typically in Asian populations.
Growing recognition of myocardial infarction with nonobstructive coronary arteries (MINOCA) and ischemia with no obstructive coronary arteries (INOCA), however, is changing the landscape. In recent U.S. and European guidelines, intracoronary acetylcholine testing is indicated as a class 2a recommendation in MINOCA/INOCA.
“More and more institutions in Europe and the United States are starting to do acetylcholine testing, because now we know that chest pain isn’t necessarily coming from the blocked arteries,” Dr. Kobayashi said. “There are functional abnormalities, including coronary spasm, and if we diagnose it, we have appropriate medical regimens for this kind of disease.”
First safety meta-analysis
The present review and meta-analysis included 12,585 participants in 16 studies through November 2021. Of these, 63% were conducted in Western countries, and most were prospective studies published over the past decade in patients with MINOCA or INOCA.
Ten studies used the contemporary diagnostic criteria for epicardial spasm of at least 90% reduction in coronary diameter. Acetylcholine was administered into the left coronary artery at up to 100 mcg and 200 mcg in seven and six studies, respectively, and was used in the other three studies to assess endothelial function with a slower infusion of up to 36.4 mcg.
Major complications were significantly higher in studies following the contemporary diagnostic cutoff than in those using a lower cutoff of at least 75% diameter reduction (1.0% vs. 0.0%; P for between-group heterogeneity < .001).
The incidence of major complications was 0.2% with the slower infusion of up to 36.4 mcg, 0.8% with a maximum dose of 100 mcg, and 0.3% with a maximum dose of 200 mcg. The positive vasospasm rate was similar with the latter two protocols, at 46.3% and 41.4%, respectively.
Minor complications occurred in 3.3% of patients but were not detailed. They can include paroxysmal atrial fibrillation, ventricular ectopic beats, transient hypotension, and bradycardia requiring intervention.
As with major complications, minor complications were lower in studies using noncontemporary versus contemporary diagnostic cutoffs for epicardial spasm (1.8% vs. 4.7%) and in Western versus Asian populations (2.6% vs. 9.4%). Minor complications were similar between protocols with maximum doses of 100 mcg and 200 mcg (3.6% vs. 3.8%).
Dr. Kobayashi suggested that several factors may explain the racial differences, including previously reported smooth muscle hyperresponsiveness to provocation stimuli in Japanese patients and the inclusion of a wide range of patients in Japanese studies, such as those with obstructive coronary disease.
Japanese studies also used sequential acetylcholine injection into both the right and left coronaries, a faster injection speed of 20 seconds, and upfront placement of a temporary pacing catheter in case of acetylcholine-induced bradycardia, particularly with right coronary injection.
Although the protocol is largely settled in Japan, he said, provocation protocols need to be standardized because “depending on the country and depending on the institution, people are doing totally different things.”
A big step forward
Commenting on the study, C. Noel Bairey Merz, MD, from Cedars Sinai, Los Angeles, said it has “widespread relevance” because half of all coronary angiograms done invasively in the United States for suspected ischemia find no obstructive coronary disease. Left untreated, however, MINOCA has a 2.5% annual event rate, and a quarter of that is death.
“This is a big step forward with likely equal opportunity to improve women and men’s ischemic heart disease,” she said.
On the other hand, all studies were conducted at centers of excellence, so safety will need to be carefully watched as testing rolls out to more community care, Dr. Merz said. “And it always needs to be underscored that this is done by an interventional cardiologist because they’re familiar with wires that can dissect arteries, and they’re familiar with minor complications that could turn into major, if someone didn’t act appropriately.”
Dr. Merz also called for unifying protocols and the need to raise awareness within the general cardiology community to ask interventionalists for acetylcholine spasm testing. Randomized controlled data from within the WISE study and the CorMica study showed that diagnostic certainty leads to greater therapeutic certainty. “You do a much better job about who and how to treat,” she said.
There are also three ongoing randomized controlled trials – WARRIOR, MINOCA-BAT, and iCorMica – in the INOCA and MINOCA populations testing different treatment strategies for hard clinical outcomes like death and myocardial infarction.
“So in addition to this publication being guideline-forming for diagnosis, we anticipate in the next several years to have clinical trial evidence about therapeutics, again, for formulation of class 1 guidelines,” Dr. Merz said.
John Beltrame, BMBS, PhD, University of Adelaide, Australia, said the meta-analysis shows that intracoronary acetylcholine spasm testing is safe and should prompt greater adoption of invasive functional angiography.
Interventionalists are quite happy to do fractional flow reserve using intravenous adenosine to assess coronary microvascular dysfunction, he said, and “what we think is that functional angiography should test both – both the spasm as well as the microvasculature – and that will give us a clear direction because the treatments are slightly different when you’re treating the large arteries as compared to the microscopic arteries. It’s an important thing.”
Dr. Beltrame and colleagues further detail the benefits of comprehensive invasive functional angiography over structural angiography in a related editorial.
He also noted that the Coronary Vasomotion Disorders International Study Group published international diagnostic criteria for microvascular angina and that several protocols for acetylcholine spasm testing are in the works, including one from Australia. Australian investigators are also organizing an accreditation program for those performing the test.
“The protocol itself is relatively straightforward, but it’s not merely picking up a manual and following the instructions,” Dr. Beltrame said. “Just the same as when you train someone in angioplasty, you don’t just go out and do it. You need to develop some experience in it and so should be proctored.”
Dr. Kobayashi reported consulting agreements with Abbott Vascular. Coauthor disclosures are listed in the paper. Dr. Beltrame and colleagues have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
“How long, how long to sing this song?”
“My soul is in deep anguish. How long, Lord, how long?” – Psalm 6
. A once-common word in the 1800s, it fell steeply in popularity in the 20th century. Lately, I see it everywhere. It’s a beautiful word, capturing not only sorrow, but also weariness. It is also audacious, facing injustice and acknowledging that it ought not be this way, and communal, bearing witness to the shared hardship of being human. The Hebrew scriptures captured the experience of lament in the form of psalms, from the Greek, psalmoi or “words to accompany the music.” A few thousand years later, the words still resonate, especially in times of grief. “I am weary with my groaning; all the night make I my bed to swim; I water my couch with my tears.”
“Hair loss” is not the chief complaint you want to see when running behind in clinic – it’s never a 15-minute visit. A woman in her late 30s with wavy, light-brown hair that grew to her waistline was seated on the exam chair. When I sat across from her, I couldn’t see her scalp. No erythema or scale. No frontal band of hair loss. Just a bit thin everywhere. Perhaps another post-COVID telogen? This might be easy. I blew right by her mother, who was sitting in the corner of the room. Her black and white horizontal striped shirt seemed to match her gray and white hair. She looked worried.

Having perused my patient’s labs and done an exam, I announced that the diagnosis was telogen effluvium. “There are many possible causes, stress is a common one. Have you been under a lot of stress lately?” (The answer is always yes, thus providing a good foothold to climb out of a hair-loss visit). “Yes. My 1-year-old daughter died last year. She had choked on a cashew from a granola bar given by her sister.” I gasped and turned from her green eyes to her mom’s. Without saying a word, mom pleaded with me to help. “I don’t know what to say,” I said, “I’m so sorry.” Neither replied.
On the commute home that day I listened to a live recording of the U2 song, “40.” I had recently read about it in a touching essay about lament by Enuma Okoro of the Financial Times. I thought about my patient’s suffering and the brutal injustice of fate. It feels like it’s everywhere lately. Reporting from the events in Ukraine, Buffalo, Uvalde, Tulsa has put agonized faces like hers in the public square for us all to gape at and quietly mourn.
Even from a secular lens, it can be seen that a beauty of psalms is how they move from despair to hope. Prayers will be answered. Things will get better. Turn up the volume and feel the urgency and pathos Bono injects into your soul as he sings the refrain; “How long, how long? How long to sing this song?” In the live version we the audience take over for him. The words accompanying the music swell over the crowd. How much longer? How much more suffering? My patient’s hair will grow back. It will take years. All we can do is lament with her.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
“My soul is in deep anguish. How long, Lord, how long?” – Psalm 6
. A once-common word in the 1800s, it fell steeply in popularity in the 20th century. Lately, I see it everywhere. It’s a beautiful word, capturing not only sorrow, but also weariness. It is also audacious, facing injustice and acknowledging that it ought not be this way, and communal, bearing witness to the shared hardship of being human. The Hebrew scriptures captured the experience of lament in the form of psalms, from the Greek, psalmoi or “words to accompany the music.” A few thousand years later, the words still resonate, especially in times of grief. “I am weary with my groaning; all the night make I my bed to swim; I water my couch with my tears.”
“Hair loss” is not the chief complaint you want to see when running behind in clinic – it’s never a 15-minute visit. A woman in her late 30s with wavy, light-brown hair that grew to her waistline was seated on the exam chair. When I sat across from her, I couldn’t see her scalp. No erythema or scale. No frontal band of hair loss. Just a bit thin everywhere. Perhaps another post-COVID telogen? This might be easy. I blew right by her mother, who was sitting in the corner of the room. Her black and white horizontal striped shirt seemed to match her gray and white hair. She looked worried.
Having perused my patient’s labs and done an exam, I announced that the diagnosis was telogen effluvium. “There are many possible causes, stress is a common one. Have you been under a lot of stress lately?” (The answer is always yes, thus providing a good foothold to climb out of a hair-loss visit). “Yes. My 1-year-old daughter died last year. She had choked on a cashew from a granola bar given by her sister.” I gasped and turned from her green eyes to her mom’s. Without saying a word, mom pleaded with me to help. “I don’t know what to say,” I said, “I’m so sorry.” Neither replied.
On the commute home that day I listened to a live recording of the U2 song, “40.” I had recently read about it in a touching essay about lament by Enuma Okoro of the Financial Times. I thought about my patient’s suffering and the brutal injustice of fate. It feels like it’s everywhere lately. Reporting from the events in Ukraine, Buffalo, Uvalde, Tulsa has put agonized faces like hers in the public square for us all to gape at and quietly mourn.
Even from a secular lens, it can be seen that a beauty of psalms is how they move from despair to hope. Prayers will be answered. Things will get better. Turn up the volume and feel the urgency and pathos Bono injects into your soul as he sings the refrain; “How long, how long? How long to sing this song?” In the live version we the audience take over for him. The words accompanying the music swell over the crowd. How much longer? How much more suffering? My patient’s hair will grow back. It will take years. All we can do is lament with her.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
“My soul is in deep anguish. How long, Lord, how long?” – Psalm 6
. A once-common word in the 1800s, it fell steeply in popularity in the 20th century. Lately, I see it everywhere. It’s a beautiful word, capturing not only sorrow, but also weariness. It is also audacious, facing injustice and acknowledging that it ought not be this way, and communal, bearing witness to the shared hardship of being human. The Hebrew scriptures captured the experience of lament in the form of psalms, from the Greek, psalmoi or “words to accompany the music.” A few thousand years later, the words still resonate, especially in times of grief. “I am weary with my groaning; all the night make I my bed to swim; I water my couch with my tears.”
“Hair loss” is not the chief complaint you want to see when running behind in clinic – it’s never a 15-minute visit. A woman in her late 30s with wavy, light-brown hair that grew to her waistline was seated on the exam chair. When I sat across from her, I couldn’t see her scalp. No erythema or scale. No frontal band of hair loss. Just a bit thin everywhere. Perhaps another post-COVID telogen? This might be easy. I blew right by her mother, who was sitting in the corner of the room. Her black and white horizontal striped shirt seemed to match her gray and white hair. She looked worried.
Having perused my patient’s labs and done an exam, I announced that the diagnosis was telogen effluvium. “There are many possible causes, stress is a common one. Have you been under a lot of stress lately?” (The answer is always yes, thus providing a good foothold to climb out of a hair-loss visit). “Yes. My 1-year-old daughter died last year. She had choked on a cashew from a granola bar given by her sister.” I gasped and turned from her green eyes to her mom’s. Without saying a word, mom pleaded with me to help. “I don’t know what to say,” I said, “I’m so sorry.” Neither replied.
On the commute home that day I listened to a live recording of the U2 song, “40.” I had recently read about it in a touching essay about lament by Enuma Okoro of the Financial Times. I thought about my patient’s suffering and the brutal injustice of fate. It feels like it’s everywhere lately. Reporting from the events in Ukraine, Buffalo, Uvalde, Tulsa has put agonized faces like hers in the public square for us all to gape at and quietly mourn.
Even from a secular lens, it can be seen that a beauty of psalms is how they move from despair to hope. Prayers will be answered. Things will get better. Turn up the volume and feel the urgency and pathos Bono injects into your soul as he sings the refrain; “How long, how long? How long to sing this song?” In the live version we the audience take over for him. The words accompanying the music swell over the crowd. How much longer? How much more suffering? My patient’s hair will grow back. It will take years. All we can do is lament with her.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. The opinions expressed in this column are his own and do not represent those of Kaiser Permanente. Dr. Benabio is @Dermdoc on Twitter. Write to him at dermnews@mdedge.com.
Heart failure: Medicare cost sharing may put quadruple therapy out of reach
Out-of-pocket (OOP) costs for Medicare enrollees receiving quadruple drug therapy for heart failure with reduced ejection fraction were “substantially higher than regimens limited to generically available medications,” according to a new analysis of prescription drug plans.
“Despite the clinical benefit of quadruple therapy” consisting of beta-blockers, angiotensin receptor-neprilysin inhibitors (ARNIs), mineralocorticoid receptor antagonists (MRAs), and sodium-glucose cotransporter-2 (SGLT2) inhibitors, “coverage was restricted primarily through cost sharing, and estimated annual OOP costs for beneficiaries were [over $2,000] per year under most plans,” wrote Kamil F. Faridi, MD, and associates. The findings were published in the Journal of the American College of Cardiology.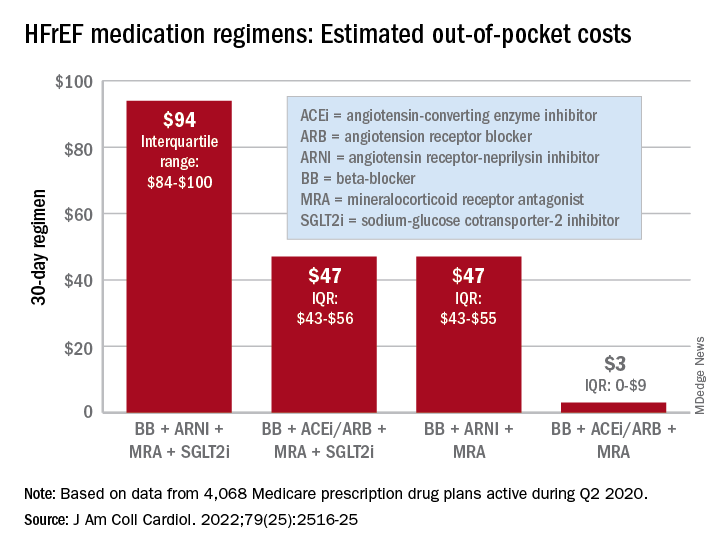
For just 1 month of quadruple drug therapy for heart failure with reduced ejection fraction (HFrEF), the estimated median OOP cost was $94 for individuals covered by a Medicare prescription drug plan during the second quarter of 2020, with the majority coming from the ARNI (median, $47) and the SGLT2 inhibitor (median, $45). Alternative HFrEF regimens were significantly less costly, ranging from $3 to $47 OOP, the investigators reported.
Almost all of the 4,068 plans participating in Medicare at that time covered quadruple therapy for HFrEF, but more than 99% restricted coverage by instituting cost sharing for medications at tier level 3 and above on the drug formularies. Such restrictions for ARNIs and SGLT2 inhibitors “might not be readily apparent to prescribing physicians,” wrote Dr. Faridi of Yale University, New Haven, Conn., and associates.
Other methods of regulating coverage were less common. Prior authorization of ARNIs was invoked by about a quarter of the plans, but none required authorization for any of the other drugs involved, and few plans used step therapy-requirements involving lower-cost alternatives, they noted.
“The use of cost sharing restricts access through high OOP costs for patients. Furthermore, these policies likely disadvantage relatively poorer patients (although the poorest Medicare patients will tend to be dual-enrolled in Medicaid and protected from cost sharing),” Jason H. Wasfy, MD, and Anna C. O’Kelly, MD, said in an accompanying editorial comment .
Since acceptable cost-effectiveness has been demonstrated for dapagliflozin, an SGLT1 inhibitor, and for the ARNIs, and because these medications have no generic equivalents, health plans should “use the discretion they have under Medicare Part D to reduce cost sharing for patients with HFrEF,” Dr. Wasfy and Dr. O’Kelly wrote, adding that the current study “demonstrates that without consensus on cost effectiveness from the societal perspective, costs can be imposed directly on patients in ways that slow uptake of cost-effective drugs.”
Data for all Medicare Advantage plans (n = 3,167) and standalone Part D plans (n = 901) came from the Medicare Prescription Drug Plan Formulary and Pricing Information Files. Annual OOP costs were estimated “using each phase of a 2020 Medicare part D standard benefit,” including deductible, standard coverage, coverage gap, and catastrophic coverage, the investigators explained.
Dr. Faridi and associates did not report any direct funding sources for their study. Dr Faridi received a grant from the National Institutes of Health outside the scope of the present work, and other investigators disclosed ties to the Food and Drug Administration, the Centers for Medicare and Medicaid Services, Johnson & Johnson, AstraZeneca, Boehringer Ingelheim, Amgen, Cytokinetics, and the Institute for Clinical and Economic Review.
Dr. Wasfy is supported by the American Heart Association and has received consulting fees from Pfizer and honoraria from the Institute for Clinical and Economic Review. Dr. O’Kelly has no relevant disclosures.
Out-of-pocket (OOP) costs for Medicare enrollees receiving quadruple drug therapy for heart failure with reduced ejection fraction were “substantially higher than regimens limited to generically available medications,” according to a new analysis of prescription drug plans.
“Despite the clinical benefit of quadruple therapy” consisting of beta-blockers, angiotensin receptor-neprilysin inhibitors (ARNIs), mineralocorticoid receptor antagonists (MRAs), and sodium-glucose cotransporter-2 (SGLT2) inhibitors, “coverage was restricted primarily through cost sharing, and estimated annual OOP costs for beneficiaries were [over $2,000] per year under most plans,” wrote Kamil F. Faridi, MD, and associates. The findings were published in the Journal of the American College of Cardiology.
For just 1 month of quadruple drug therapy for heart failure with reduced ejection fraction (HFrEF), the estimated median OOP cost was $94 for individuals covered by a Medicare prescription drug plan during the second quarter of 2020, with the majority coming from the ARNI (median, $47) and the SGLT2 inhibitor (median, $45). Alternative HFrEF regimens were significantly less costly, ranging from $3 to $47 OOP, the investigators reported.
Almost all of the 4,068 plans participating in Medicare at that time covered quadruple therapy for HFrEF, but more than 99% restricted coverage by instituting cost sharing for medications at tier level 3 and above on the drug formularies. Such restrictions for ARNIs and SGLT2 inhibitors “might not be readily apparent to prescribing physicians,” wrote Dr. Faridi of Yale University, New Haven, Conn., and associates.
Other methods of regulating coverage were less common. Prior authorization of ARNIs was invoked by about a quarter of the plans, but none required authorization for any of the other drugs involved, and few plans used step therapy-requirements involving lower-cost alternatives, they noted.
“The use of cost sharing restricts access through high OOP costs for patients. Furthermore, these policies likely disadvantage relatively poorer patients (although the poorest Medicare patients will tend to be dual-enrolled in Medicaid and protected from cost sharing),” Jason H. Wasfy, MD, and Anna C. O’Kelly, MD, said in an accompanying editorial comment .
Since acceptable cost-effectiveness has been demonstrated for dapagliflozin, an SGLT1 inhibitor, and for the ARNIs, and because these medications have no generic equivalents, health plans should “use the discretion they have under Medicare Part D to reduce cost sharing for patients with HFrEF,” Dr. Wasfy and Dr. O’Kelly wrote, adding that the current study “demonstrates that without consensus on cost effectiveness from the societal perspective, costs can be imposed directly on patients in ways that slow uptake of cost-effective drugs.”
Data for all Medicare Advantage plans (n = 3,167) and standalone Part D plans (n = 901) came from the Medicare Prescription Drug Plan Formulary and Pricing Information Files. Annual OOP costs were estimated “using each phase of a 2020 Medicare part D standard benefit,” including deductible, standard coverage, coverage gap, and catastrophic coverage, the investigators explained.
Dr. Faridi and associates did not report any direct funding sources for their study. Dr Faridi received a grant from the National Institutes of Health outside the scope of the present work, and other investigators disclosed ties to the Food and Drug Administration, the Centers for Medicare and Medicaid Services, Johnson & Johnson, AstraZeneca, Boehringer Ingelheim, Amgen, Cytokinetics, and the Institute for Clinical and Economic Review.
Dr. Wasfy is supported by the American Heart Association and has received consulting fees from Pfizer and honoraria from the Institute for Clinical and Economic Review. Dr. O’Kelly has no relevant disclosures.
Out-of-pocket (OOP) costs for Medicare enrollees receiving quadruple drug therapy for heart failure with reduced ejection fraction were “substantially higher than regimens limited to generically available medications,” according to a new analysis of prescription drug plans.
“Despite the clinical benefit of quadruple therapy” consisting of beta-blockers, angiotensin receptor-neprilysin inhibitors (ARNIs), mineralocorticoid receptor antagonists (MRAs), and sodium-glucose cotransporter-2 (SGLT2) inhibitors, “coverage was restricted primarily through cost sharing, and estimated annual OOP costs for beneficiaries were [over $2,000] per year under most plans,” wrote Kamil F. Faridi, MD, and associates. The findings were published in the Journal of the American College of Cardiology.
For just 1 month of quadruple drug therapy for heart failure with reduced ejection fraction (HFrEF), the estimated median OOP cost was $94 for individuals covered by a Medicare prescription drug plan during the second quarter of 2020, with the majority coming from the ARNI (median, $47) and the SGLT2 inhibitor (median, $45). Alternative HFrEF regimens were significantly less costly, ranging from $3 to $47 OOP, the investigators reported.
Almost all of the 4,068 plans participating in Medicare at that time covered quadruple therapy for HFrEF, but more than 99% restricted coverage by instituting cost sharing for medications at tier level 3 and above on the drug formularies. Such restrictions for ARNIs and SGLT2 inhibitors “might not be readily apparent to prescribing physicians,” wrote Dr. Faridi of Yale University, New Haven, Conn., and associates.
Other methods of regulating coverage were less common. Prior authorization of ARNIs was invoked by about a quarter of the plans, but none required authorization for any of the other drugs involved, and few plans used step therapy-requirements involving lower-cost alternatives, they noted.
“The use of cost sharing restricts access through high OOP costs for patients. Furthermore, these policies likely disadvantage relatively poorer patients (although the poorest Medicare patients will tend to be dual-enrolled in Medicaid and protected from cost sharing),” Jason H. Wasfy, MD, and Anna C. O’Kelly, MD, said in an accompanying editorial comment .
Since acceptable cost-effectiveness has been demonstrated for dapagliflozin, an SGLT1 inhibitor, and for the ARNIs, and because these medications have no generic equivalents, health plans should “use the discretion they have under Medicare Part D to reduce cost sharing for patients with HFrEF,” Dr. Wasfy and Dr. O’Kelly wrote, adding that the current study “demonstrates that without consensus on cost effectiveness from the societal perspective, costs can be imposed directly on patients in ways that slow uptake of cost-effective drugs.”
Data for all Medicare Advantage plans (n = 3,167) and standalone Part D plans (n = 901) came from the Medicare Prescription Drug Plan Formulary and Pricing Information Files. Annual OOP costs were estimated “using each phase of a 2020 Medicare part D standard benefit,” including deductible, standard coverage, coverage gap, and catastrophic coverage, the investigators explained.
Dr. Faridi and associates did not report any direct funding sources for their study. Dr Faridi received a grant from the National Institutes of Health outside the scope of the present work, and other investigators disclosed ties to the Food and Drug Administration, the Centers for Medicare and Medicaid Services, Johnson & Johnson, AstraZeneca, Boehringer Ingelheim, Amgen, Cytokinetics, and the Institute for Clinical and Economic Review.
Dr. Wasfy is supported by the American Heart Association and has received consulting fees from Pfizer and honoraria from the Institute for Clinical and Economic Review. Dr. O’Kelly has no relevant disclosures.
FROM THE JOURNAL Of the AMERICAN COLLEGE OF CARDIOLOGY
How we treat acute pain could be wrong
In a surprising discovery that flies in the face of conventional medicine,
The paper, published in Science Translational Medicine, suggests that inflammation, a normal part of injury recovery, helps resolve acute pain and prevents it from becoming chronic. Blocking that inflammation may interfere with this process, leading to harder-to-treat pain.
“What we’ve been doing for decades not only appears to be wrong, but appears to be 180 degrees wrong,” says senior study author Jeffrey Mogil, PhD, a professor in the department of psychology at McGill University in Montreal. “You should not be blocking inflammation. You should be letting inflammation happen. That’s what stops chronic pain.”
Inflammation: Nature’s pain reliever
Wanting to know why pain goes away for some but drags on (and on) for others, the researchers looked at pain mechanisms in both humans and mice. They found that a type of white blood cell known as a neutrophil seems to play a key role.
“In analyzing the genes of people suffering from lower back pain, we observed active changes in genes over time in people whose pain went away,” says Luda Diatchenko, PhD, a professor in the faculty of medicine and Canada excellence research chair in human pain genetics at McGill. “Changes in the blood cells and their activity seemed to be the most important factor, especially in cells called neutrophils.”
To test this link, the researchers blocked neutrophils in mice and found the pain lasted 2-10 times longer than normal. Anti-inflammatory drugs, despite providing short-term relief, had the same pain-prolonging effect – though injecting neutrophils into the mice seemed to keep that from happening.
The findings are supported by a separate analysis of 500,000 people in the United Kingdom that showed those taking anti-inflammatory drugs to treat their pain were more likely to have pain 2-10 years later.
“Inflammation occurs for a reason,” says Dr. Mogil, “and it looks like it’s dangerous to interfere with it.”
Rethinking how we treat pain
Neutrophils arrive early during inflammation, at the onset of injury – just when many of us reach for pain medication. This research suggests it might be better not to block inflammation, instead letting the neutrophils “do their thing.” Taking an analgesic that alleviates pain without blocking neutrophils, like acetaminophen, may be better than taking an anti-inflammatory drug or steroid, says Dr. Mogil.
Still, while the findings are compelling, clinical trials are needed to directly compare anti-inflammatory drugs to other painkillers, the researchers said. This research may also lay the groundwork for new drug development for chronic pain patients, Dr. Mogil says.
“Our data strongly suggests that neutrophils act like analgesics themselves, which is potentially useful in terms of analgesic development,” Dr. Mogil says. “And of course, we need new analgesics.”
A version of this article first appeared on WebMD.com.
In a surprising discovery that flies in the face of conventional medicine,
The paper, published in Science Translational Medicine, suggests that inflammation, a normal part of injury recovery, helps resolve acute pain and prevents it from becoming chronic. Blocking that inflammation may interfere with this process, leading to harder-to-treat pain.
“What we’ve been doing for decades not only appears to be wrong, but appears to be 180 degrees wrong,” says senior study author Jeffrey Mogil, PhD, a professor in the department of psychology at McGill University in Montreal. “You should not be blocking inflammation. You should be letting inflammation happen. That’s what stops chronic pain.”
Inflammation: Nature’s pain reliever
Wanting to know why pain goes away for some but drags on (and on) for others, the researchers looked at pain mechanisms in both humans and mice. They found that a type of white blood cell known as a neutrophil seems to play a key role.
“In analyzing the genes of people suffering from lower back pain, we observed active changes in genes over time in people whose pain went away,” says Luda Diatchenko, PhD, a professor in the faculty of medicine and Canada excellence research chair in human pain genetics at McGill. “Changes in the blood cells and their activity seemed to be the most important factor, especially in cells called neutrophils.”
To test this link, the researchers blocked neutrophils in mice and found the pain lasted 2-10 times longer than normal. Anti-inflammatory drugs, despite providing short-term relief, had the same pain-prolonging effect – though injecting neutrophils into the mice seemed to keep that from happening.
The findings are supported by a separate analysis of 500,000 people in the United Kingdom that showed those taking anti-inflammatory drugs to treat their pain were more likely to have pain 2-10 years later.
“Inflammation occurs for a reason,” says Dr. Mogil, “and it looks like it’s dangerous to interfere with it.”
Rethinking how we treat pain
Neutrophils arrive early during inflammation, at the onset of injury – just when many of us reach for pain medication. This research suggests it might be better not to block inflammation, instead letting the neutrophils “do their thing.” Taking an analgesic that alleviates pain without blocking neutrophils, like acetaminophen, may be better than taking an anti-inflammatory drug or steroid, says Dr. Mogil.
Still, while the findings are compelling, clinical trials are needed to directly compare anti-inflammatory drugs to other painkillers, the researchers said. This research may also lay the groundwork for new drug development for chronic pain patients, Dr. Mogil says.
“Our data strongly suggests that neutrophils act like analgesics themselves, which is potentially useful in terms of analgesic development,” Dr. Mogil says. “And of course, we need new analgesics.”
A version of this article first appeared on WebMD.com.
In a surprising discovery that flies in the face of conventional medicine,
The paper, published in Science Translational Medicine, suggests that inflammation, a normal part of injury recovery, helps resolve acute pain and prevents it from becoming chronic. Blocking that inflammation may interfere with this process, leading to harder-to-treat pain.
“What we’ve been doing for decades not only appears to be wrong, but appears to be 180 degrees wrong,” says senior study author Jeffrey Mogil, PhD, a professor in the department of psychology at McGill University in Montreal. “You should not be blocking inflammation. You should be letting inflammation happen. That’s what stops chronic pain.”
Inflammation: Nature’s pain reliever
Wanting to know why pain goes away for some but drags on (and on) for others, the researchers looked at pain mechanisms in both humans and mice. They found that a type of white blood cell known as a neutrophil seems to play a key role.
“In analyzing the genes of people suffering from lower back pain, we observed active changes in genes over time in people whose pain went away,” says Luda Diatchenko, PhD, a professor in the faculty of medicine and Canada excellence research chair in human pain genetics at McGill. “Changes in the blood cells and their activity seemed to be the most important factor, especially in cells called neutrophils.”
To test this link, the researchers blocked neutrophils in mice and found the pain lasted 2-10 times longer than normal. Anti-inflammatory drugs, despite providing short-term relief, had the same pain-prolonging effect – though injecting neutrophils into the mice seemed to keep that from happening.
The findings are supported by a separate analysis of 500,000 people in the United Kingdom that showed those taking anti-inflammatory drugs to treat their pain were more likely to have pain 2-10 years later.
“Inflammation occurs for a reason,” says Dr. Mogil, “and it looks like it’s dangerous to interfere with it.”
Rethinking how we treat pain
Neutrophils arrive early during inflammation, at the onset of injury – just when many of us reach for pain medication. This research suggests it might be better not to block inflammation, instead letting the neutrophils “do their thing.” Taking an analgesic that alleviates pain without blocking neutrophils, like acetaminophen, may be better than taking an anti-inflammatory drug or steroid, says Dr. Mogil.
Still, while the findings are compelling, clinical trials are needed to directly compare anti-inflammatory drugs to other painkillers, the researchers said. This research may also lay the groundwork for new drug development for chronic pain patients, Dr. Mogil says.
“Our data strongly suggests that neutrophils act like analgesics themselves, which is potentially useful in terms of analgesic development,” Dr. Mogil says. “And of course, we need new analgesics.”
A version of this article first appeared on WebMD.com.
FROM SCIENCE TRANSLATIONAL MEDICINE
Longer circadian rhythms linked to severe depression in teens
, according to results from a European study.
A range of psychiatric symptoms and conditions has been linked to sleep pathologies, wrote Liisa Kuula, PhD, of the University of Helsinki, Finland, and colleagues. Some research suggests that late circadian rhythms and irregular sleep patterns increase the risk for psychiatric conditions, but the association has not been well studied, especially in adolescents, although the onset of psychiatric problems often occurs at this age, they said.

In a study published in the Journal of Psychiatric Research (2022 Apr 4. doi: 10.1016/j.jpsychires.2022.03.056.), the investigators reviewed data from 342 adolescents who were part of SleepHelsinki! a large cohort study of delayed sleep phase disorder (DSPD) in adolescents. The mean age of the participants was 17.4 years, and 70% were female.
The participants completed the Mini International Neuropsychiatric Interview (MINI) and wore temperature loggers for 3 days to assess circadian rhythms. The primary outcome was the impact of circadian dynamics on different psychiatric problems. Delayed Sleep Phase (DSP) behavior was defined as going to sleep later than 1 a.m. at least three times a week.
Circadian length was determined through the temperature loggers worn for 3 days. Most participants also completed 1-week GeneActiv Original actigraphy measurements (wearing the actigraph for 1 week) and responded to the Morningness-Eveningness Questionnaire, which divided participants into three circadian preference groups: morning, intermediate, and evening. Sleep duration was calculated as total sleep time, sleep quality was estimated by sleep efficiency, and sleep timing was assessed by the midpoint of the sleep period.
Overall, the MINI interview results suggested that approximately one-third (36%) of the teens had at least one psychiatric problem, and 21% had comorbid conditions.
Severe depression was significantly associated with a longer circadian period (P = .002), while suicidality was significantly associated with a later midpoint and more irregular sleep (P = .007 for both).
Participants with agoraphobia slept longer than did those without, the researchers noted (P = .013). However, sleep duration was not significantly associated with other psychiatric conditions.
Manic episodes and psychotic disorders were associated with irregular sleep timing (P < .018 and P < .017, respectively).
When the researchers examined DSP and circadian preferences, they found that 21.5% of individuals with suicidality had characteristics of DSP, as did 21.5% of those with panic disorder.
Individuals with a preference for eveningness were significantly more likely to meet criteria for severe depression, panic disorder, generalized anxiety disorder, and obsessive-compulsive disorder than were those without a preference for eveningness, the researchers noted.
“Our findings are the first to encompass diverse circadian measures alongside an array of psychiatric symptoms in such a focused age range,” the researchers wrote in their discussion. The data reflect results from other studies and extend the likely role of circadian patterns in mental wellbeing, they said.
The study findings were limited by several factors including the lack of actual diagnoses from medical records and use of self-reported symptoms, the researchers noted. Other limitations included the lack of polysomnography data and small size of subgroups of the study sample.
However, the results were strengthened by the heterogenous study population and use of multiple measures to examine sleep and circadian rhythms, as well as consideration of personal circadian preferences, the researchers said.
“The importance of overall synchronization with environment is perhaps best highlighted by response to treatment: most psychopathologic symptoms benefit from sleep-targeted therapeutic approaches,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
, according to results from a European study.
A range of psychiatric symptoms and conditions has been linked to sleep pathologies, wrote Liisa Kuula, PhD, of the University of Helsinki, Finland, and colleagues. Some research suggests that late circadian rhythms and irregular sleep patterns increase the risk for psychiatric conditions, but the association has not been well studied, especially in adolescents, although the onset of psychiatric problems often occurs at this age, they said.
In a study published in the Journal of Psychiatric Research (2022 Apr 4. doi: 10.1016/j.jpsychires.2022.03.056.), the investigators reviewed data from 342 adolescents who were part of SleepHelsinki! a large cohort study of delayed sleep phase disorder (DSPD) in adolescents. The mean age of the participants was 17.4 years, and 70% were female.
The participants completed the Mini International Neuropsychiatric Interview (MINI) and wore temperature loggers for 3 days to assess circadian rhythms. The primary outcome was the impact of circadian dynamics on different psychiatric problems. Delayed Sleep Phase (DSP) behavior was defined as going to sleep later than 1 a.m. at least three times a week.
Circadian length was determined through the temperature loggers worn for 3 days. Most participants also completed 1-week GeneActiv Original actigraphy measurements (wearing the actigraph for 1 week) and responded to the Morningness-Eveningness Questionnaire, which divided participants into three circadian preference groups: morning, intermediate, and evening. Sleep duration was calculated as total sleep time, sleep quality was estimated by sleep efficiency, and sleep timing was assessed by the midpoint of the sleep period.
Overall, the MINI interview results suggested that approximately one-third (36%) of the teens had at least one psychiatric problem, and 21% had comorbid conditions.
Severe depression was significantly associated with a longer circadian period (P = .002), while suicidality was significantly associated with a later midpoint and more irregular sleep (P = .007 for both).
Participants with agoraphobia slept longer than did those without, the researchers noted (P = .013). However, sleep duration was not significantly associated with other psychiatric conditions.
Manic episodes and psychotic disorders were associated with irregular sleep timing (P < .018 and P < .017, respectively).
When the researchers examined DSP and circadian preferences, they found that 21.5% of individuals with suicidality had characteristics of DSP, as did 21.5% of those with panic disorder.
Individuals with a preference for eveningness were significantly more likely to meet criteria for severe depression, panic disorder, generalized anxiety disorder, and obsessive-compulsive disorder than were those without a preference for eveningness, the researchers noted.
“Our findings are the first to encompass diverse circadian measures alongside an array of psychiatric symptoms in such a focused age range,” the researchers wrote in their discussion. The data reflect results from other studies and extend the likely role of circadian patterns in mental wellbeing, they said.
The study findings were limited by several factors including the lack of actual diagnoses from medical records and use of self-reported symptoms, the researchers noted. Other limitations included the lack of polysomnography data and small size of subgroups of the study sample.
However, the results were strengthened by the heterogenous study population and use of multiple measures to examine sleep and circadian rhythms, as well as consideration of personal circadian preferences, the researchers said.
“The importance of overall synchronization with environment is perhaps best highlighted by response to treatment: most psychopathologic symptoms benefit from sleep-targeted therapeutic approaches,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
, according to results from a European study.
A range of psychiatric symptoms and conditions has been linked to sleep pathologies, wrote Liisa Kuula, PhD, of the University of Helsinki, Finland, and colleagues. Some research suggests that late circadian rhythms and irregular sleep patterns increase the risk for psychiatric conditions, but the association has not been well studied, especially in adolescents, although the onset of psychiatric problems often occurs at this age, they said.
In a study published in the Journal of Psychiatric Research (2022 Apr 4. doi: 10.1016/j.jpsychires.2022.03.056.), the investigators reviewed data from 342 adolescents who were part of SleepHelsinki! a large cohort study of delayed sleep phase disorder (DSPD) in adolescents. The mean age of the participants was 17.4 years, and 70% were female.
The participants completed the Mini International Neuropsychiatric Interview (MINI) and wore temperature loggers for 3 days to assess circadian rhythms. The primary outcome was the impact of circadian dynamics on different psychiatric problems. Delayed Sleep Phase (DSP) behavior was defined as going to sleep later than 1 a.m. at least three times a week.
Circadian length was determined through the temperature loggers worn for 3 days. Most participants also completed 1-week GeneActiv Original actigraphy measurements (wearing the actigraph for 1 week) and responded to the Morningness-Eveningness Questionnaire, which divided participants into three circadian preference groups: morning, intermediate, and evening. Sleep duration was calculated as total sleep time, sleep quality was estimated by sleep efficiency, and sleep timing was assessed by the midpoint of the sleep period.
Overall, the MINI interview results suggested that approximately one-third (36%) of the teens had at least one psychiatric problem, and 21% had comorbid conditions.
Severe depression was significantly associated with a longer circadian period (P = .002), while suicidality was significantly associated with a later midpoint and more irregular sleep (P = .007 for both).
Participants with agoraphobia slept longer than did those without, the researchers noted (P = .013). However, sleep duration was not significantly associated with other psychiatric conditions.
Manic episodes and psychotic disorders were associated with irregular sleep timing (P < .018 and P < .017, respectively).
When the researchers examined DSP and circadian preferences, they found that 21.5% of individuals with suicidality had characteristics of DSP, as did 21.5% of those with panic disorder.
Individuals with a preference for eveningness were significantly more likely to meet criteria for severe depression, panic disorder, generalized anxiety disorder, and obsessive-compulsive disorder than were those without a preference for eveningness, the researchers noted.
“Our findings are the first to encompass diverse circadian measures alongside an array of psychiatric symptoms in such a focused age range,” the researchers wrote in their discussion. The data reflect results from other studies and extend the likely role of circadian patterns in mental wellbeing, they said.
The study findings were limited by several factors including the lack of actual diagnoses from medical records and use of self-reported symptoms, the researchers noted. Other limitations included the lack of polysomnography data and small size of subgroups of the study sample.
However, the results were strengthened by the heterogenous study population and use of multiple measures to examine sleep and circadian rhythms, as well as consideration of personal circadian preferences, the researchers said.
“The importance of overall synchronization with environment is perhaps best highlighted by response to treatment: most psychopathologic symptoms benefit from sleep-targeted therapeutic approaches,” they concluded.
The study received no outside funding. The researchers had no financial conflicts to disclose.
FROM THE JOURNAL OF PSYCHIATRIC RESEARCH
Bariatric surgery can be a tool to relieve migraine
DENVER – , a neurologist told colleagues at the annual meeting of the American Headache Society. “There’s evidence-based medicine to support bariatric surgery, a lot of it, and the outcomes are actually pretty good,” said Jennifer McVige, MD, MA, of Dent Neurologic Institute in Buffalo, N.Y.
As Dr. McVige noted, research has linked obesity to migraine even after adjustment for comorbidities. A 2007 analysis of a survey of 30,215 participants, for example, found that “the proportion of subjects with severe headache pain increased with BMI, doubling in the morbidly obese relative to the normally weighted (odds ratio [OR] = 1.9).” And a 2011 study of 3,733 pregnant women found that risk of migraine increased in line with level of obesity: “obese women had a 1.48-fold increased odds of migraine (OR = 1.48; 95% confidence interval [CI], 1.12-1.96). Severely obese (OR = 2.07; 95% CI, 1.27-3.39) and morbidly obese (OR = 2.75; 95% CI, 1.60-4.70) had the highest odds of migraines.”
The link between obesity and headaches is unclear, she said, but there are hints at possible factors. For one, calcitonin gene-related peptide (CGRP) is increased in people with obesity and is an important factor in migraines. Additionally, nausea is quite common in people with migraine, suggesting a possible gut-brain interaction – or not.
“Nausea is associated with a lot of the medicines that we give patients with migraine. Is it the nausea that’s associated with the migraine medicine, or is nausea occurring at the end of the migraine?” she asked. “That’s always been kind of a conundrum for us.”
Whatever the case, she said, bariatric surgery appears to be helpful for patients with headache. Some studies have been small, but a 2021 analysis of 1,680 patients with migraine found that 55% experienced remission with no need for medication at 180 days post surgery. Women, older patients, and those taking more migraine medications were less likely to reach remission.
Research also suggests that bariatric surgery can relieve headache symptoms in patients with idiopathic intracranial hypertension.
Dr. McVige cautioned, however, that medical professionals must take special care when they talk to patients about their weight. “I’ve learned from conversations with my patients that they don’t like hearing ‘obese,’ or ‘fat,’ or ‘diet,’ or ‘losing weight.’ What they do like is ‘maybe we could try to find ways to be more healthy, to help your body to look the way that you would like it to look in the future. Let me help you. Maybe we can talk about nutrition. Maybe we can talk about exercise. Let’s talk about energy. Let’s talk about those types of things.’”
Unfortunately, there’s little research into how to have these conversations, Dr. McVige said. Still, “we need to be the first people to come forward and say, ‘This is a tough topic for me to talk about too. It makes me uncomfortable as well. I know you’re uncomfortable, but I have to talk to you because I care about you as a patient.’”
She also advised colleagues to not bring up weight right out of the gate. “It’s easier to say some of those things after you develop a relationship,” she said, “when they know you care about them.”
Dr. McVige reported multiple disclosures related to research funding and speaker fees.
DENVER – , a neurologist told colleagues at the annual meeting of the American Headache Society. “There’s evidence-based medicine to support bariatric surgery, a lot of it, and the outcomes are actually pretty good,” said Jennifer McVige, MD, MA, of Dent Neurologic Institute in Buffalo, N.Y.
As Dr. McVige noted, research has linked obesity to migraine even after adjustment for comorbidities. A 2007 analysis of a survey of 30,215 participants, for example, found that “the proportion of subjects with severe headache pain increased with BMI, doubling in the morbidly obese relative to the normally weighted (odds ratio [OR] = 1.9).” And a 2011 study of 3,733 pregnant women found that risk of migraine increased in line with level of obesity: “obese women had a 1.48-fold increased odds of migraine (OR = 1.48; 95% confidence interval [CI], 1.12-1.96). Severely obese (OR = 2.07; 95% CI, 1.27-3.39) and morbidly obese (OR = 2.75; 95% CI, 1.60-4.70) had the highest odds of migraines.”
The link between obesity and headaches is unclear, she said, but there are hints at possible factors. For one, calcitonin gene-related peptide (CGRP) is increased in people with obesity and is an important factor in migraines. Additionally, nausea is quite common in people with migraine, suggesting a possible gut-brain interaction – or not.
“Nausea is associated with a lot of the medicines that we give patients with migraine. Is it the nausea that’s associated with the migraine medicine, or is nausea occurring at the end of the migraine?” she asked. “That’s always been kind of a conundrum for us.”
Whatever the case, she said, bariatric surgery appears to be helpful for patients with headache. Some studies have been small, but a 2021 analysis of 1,680 patients with migraine found that 55% experienced remission with no need for medication at 180 days post surgery. Women, older patients, and those taking more migraine medications were less likely to reach remission.
Research also suggests that bariatric surgery can relieve headache symptoms in patients with idiopathic intracranial hypertension.
Dr. McVige cautioned, however, that medical professionals must take special care when they talk to patients about their weight. “I’ve learned from conversations with my patients that they don’t like hearing ‘obese,’ or ‘fat,’ or ‘diet,’ or ‘losing weight.’ What they do like is ‘maybe we could try to find ways to be more healthy, to help your body to look the way that you would like it to look in the future. Let me help you. Maybe we can talk about nutrition. Maybe we can talk about exercise. Let’s talk about energy. Let’s talk about those types of things.’”
Unfortunately, there’s little research into how to have these conversations, Dr. McVige said. Still, “we need to be the first people to come forward and say, ‘This is a tough topic for me to talk about too. It makes me uncomfortable as well. I know you’re uncomfortable, but I have to talk to you because I care about you as a patient.’”
She also advised colleagues to not bring up weight right out of the gate. “It’s easier to say some of those things after you develop a relationship,” she said, “when they know you care about them.”
Dr. McVige reported multiple disclosures related to research funding and speaker fees.
DENVER – , a neurologist told colleagues at the annual meeting of the American Headache Society. “There’s evidence-based medicine to support bariatric surgery, a lot of it, and the outcomes are actually pretty good,” said Jennifer McVige, MD, MA, of Dent Neurologic Institute in Buffalo, N.Y.
As Dr. McVige noted, research has linked obesity to migraine even after adjustment for comorbidities. A 2007 analysis of a survey of 30,215 participants, for example, found that “the proportion of subjects with severe headache pain increased with BMI, doubling in the morbidly obese relative to the normally weighted (odds ratio [OR] = 1.9).” And a 2011 study of 3,733 pregnant women found that risk of migraine increased in line with level of obesity: “obese women had a 1.48-fold increased odds of migraine (OR = 1.48; 95% confidence interval [CI], 1.12-1.96). Severely obese (OR = 2.07; 95% CI, 1.27-3.39) and morbidly obese (OR = 2.75; 95% CI, 1.60-4.70) had the highest odds of migraines.”
The link between obesity and headaches is unclear, she said, but there are hints at possible factors. For one, calcitonin gene-related peptide (CGRP) is increased in people with obesity and is an important factor in migraines. Additionally, nausea is quite common in people with migraine, suggesting a possible gut-brain interaction – or not.
“Nausea is associated with a lot of the medicines that we give patients with migraine. Is it the nausea that’s associated with the migraine medicine, or is nausea occurring at the end of the migraine?” she asked. “That’s always been kind of a conundrum for us.”
Whatever the case, she said, bariatric surgery appears to be helpful for patients with headache. Some studies have been small, but a 2021 analysis of 1,680 patients with migraine found that 55% experienced remission with no need for medication at 180 days post surgery. Women, older patients, and those taking more migraine medications were less likely to reach remission.
Research also suggests that bariatric surgery can relieve headache symptoms in patients with idiopathic intracranial hypertension.
Dr. McVige cautioned, however, that medical professionals must take special care when they talk to patients about their weight. “I’ve learned from conversations with my patients that they don’t like hearing ‘obese,’ or ‘fat,’ or ‘diet,’ or ‘losing weight.’ What they do like is ‘maybe we could try to find ways to be more healthy, to help your body to look the way that you would like it to look in the future. Let me help you. Maybe we can talk about nutrition. Maybe we can talk about exercise. Let’s talk about energy. Let’s talk about those types of things.’”
Unfortunately, there’s little research into how to have these conversations, Dr. McVige said. Still, “we need to be the first people to come forward and say, ‘This is a tough topic for me to talk about too. It makes me uncomfortable as well. I know you’re uncomfortable, but I have to talk to you because I care about you as a patient.’”
She also advised colleagues to not bring up weight right out of the gate. “It’s easier to say some of those things after you develop a relationship,” she said, “when they know you care about them.”
Dr. McVige reported multiple disclosures related to research funding and speaker fees.
AT AHS 2022