User login
Oncologist to insurer: ‘This denial will not stand’
“Is this really the hill you want to die on?” asked Rebecca Shatsky, MD, a medical oncologist at the University of California, San Diego.
It was Nov. 18 and Dr. Shatsky was on the phone with a retired oncologist working for the health insurance company Premera Blue Cross.
Dr. Shatsky was appealing a prior authorization denial for pembrolizumab (Keytruda) to treat her patient with stage IIIc triple-negative breast cancer (TNBC). She hoped the peer-to-peer would reverse the denial. The Food and Drug Administration had approved the immunotherapy for people with high-risk TNBC both in the neoadjuvant setting alongside chemotherapy and, in her patient’s case, as a single-agent adjuvant treatment based on data from the KEYNOTE 522 trial.
In the peer-to-peer, Dr. Shatsky laid out the evidence, but she could tell the physician wasn’t going to budge.
When she pressed him further, asking why he was denying potentially lifesaving care for her patient, he said the data on whether patients really need adjuvant pembrolizumab were not clear yet.
“The man – who was not a breast oncologist – was essentially mansplaining breast oncology to me,” she said in an interview. “I don’t need a nonexpert giving me their misinterpretation of the data.”
Dr. Shatsky informed him that this decision would not stand. She would be escalating the claim.
“I’m not going to let you get in way of my patient’s survival,” Dr. Shatsky told the physician during the peer-to-peer. “We have one shot to cure this, and if we don’t do it now, patients’ average lifespan is 17 months.”
The conversation turned a few heads in her office.
“My whole office stopped and stared. But then they clapped after they realized why I was yelling,” she tweeted later that night.
She continued: “@premera picked the wrong oncologist to mess with today. I will not be letting this go. This denial. Will. Not. Stand. An insurance company should not get to tell me how to practice medicine when Phase III RCT data and @NCCN + @ASCO guideline support my decision!”
A spokesperson for Premera said in a statement that, “while we did see many of the details about the case were posted to Twitter, we cannot comment on the specifics you noted due to privacy policies.”
The spokesperson explained that Premera has “the same goal as our provider partners: ensure our members have access to quality health care,” noting that prior authorization helps health plans evaluate the medical necessity and safety of health care services given that “15%-30% of care is unnecessary.”
“We also understand that providers may not agree with our decisions, which is why we have a robust appeals process,” the spokesperson said, suggesting Dr. Shatsky could have appealed the decision a second time.
And “if the member or provider still disagrees with Premera’s coverage decision after the initial appeal, providers can request review by a medical expert outside Premera who works for an independent review organization,” and the company “will pay for” and “abide by” that decision, the spokesperson added.
The Twitter storm
After Dr. Shatsky tweeted about her experience with Premera, she received a flood of support from the Twitterverse. The thread garnered tens of thousands of likes and hundreds of comments offering support and advice.
Several people suggested asking Merck for help accessing the drug. But Dr. Shatsky said no, “I’m tired of laying down and letting [insurance companies] win. It IS worth fighting for.”
The next morning, Dr. Shatsky got a call. It was the vice president of medical management at Premera.
“We’ve talked again, and we’ll give you the drug,” Dr. Shatsky recalled the Premera vice president saying.
The next day, Monday morning, Dr. Shatsky’s patient received her first infusion of pembrolizumab.
Although relieved, Dr. Shatsky noted that it wasn’t until she posted her experience to Twitter that Premera seemed to take notice.
Plus, “an oncologist without a strong social media following may not have gotten care approved and that’s not how medicine should work,” said Dr. Anderson, assistant professor in the department of clinical pharmacy, University of Colorado at Denver, Aurora.
Tatiana Prowell, MD, expressed similar concerns in a Nov. 20 tweet: “And sadly, the patients with cancer & an even busier, more exhausted doctor who doesn’t have a big [reach] on social media will be denied appropriate care. And that’s bank for insurers.”
But, Dr. Prowell noted sarcastically: “At least a patient with cancer had her care delayed & a dedicated OncTwitter colleague’s Physician Burnout was exacerbated.”
In this case, the prior authorization process took about a week – requiring an initial prior authorization request, an appeal after the request was denied, a peer-to-peer resulting in a second denial, and finally a tweet and a phone call from a top executive at the company.
In fact, these delays have become so common that Dr. Shatsky needs to anticipate and incorporate likely delays into her workflow.
“I learn which drugs will take a long time to get prior authorization for and then plan enough time so that my patient’s care is hopefully not delayed,” Dr. Shatsky said. “It should not be so hard to get appropriate and time-sensitive care for our patients.”
A version of this article first appeared on Medscape.com.
“Is this really the hill you want to die on?” asked Rebecca Shatsky, MD, a medical oncologist at the University of California, San Diego.
It was Nov. 18 and Dr. Shatsky was on the phone with a retired oncologist working for the health insurance company Premera Blue Cross.
Dr. Shatsky was appealing a prior authorization denial for pembrolizumab (Keytruda) to treat her patient with stage IIIc triple-negative breast cancer (TNBC). She hoped the peer-to-peer would reverse the denial. The Food and Drug Administration had approved the immunotherapy for people with high-risk TNBC both in the neoadjuvant setting alongside chemotherapy and, in her patient’s case, as a single-agent adjuvant treatment based on data from the KEYNOTE 522 trial.
In the peer-to-peer, Dr. Shatsky laid out the evidence, but she could tell the physician wasn’t going to budge.
When she pressed him further, asking why he was denying potentially lifesaving care for her patient, he said the data on whether patients really need adjuvant pembrolizumab were not clear yet.
“The man – who was not a breast oncologist – was essentially mansplaining breast oncology to me,” she said in an interview. “I don’t need a nonexpert giving me their misinterpretation of the data.”
Dr. Shatsky informed him that this decision would not stand. She would be escalating the claim.
“I’m not going to let you get in way of my patient’s survival,” Dr. Shatsky told the physician during the peer-to-peer. “We have one shot to cure this, and if we don’t do it now, patients’ average lifespan is 17 months.”
The conversation turned a few heads in her office.
“My whole office stopped and stared. But then they clapped after they realized why I was yelling,” she tweeted later that night.
She continued: “@premera picked the wrong oncologist to mess with today. I will not be letting this go. This denial. Will. Not. Stand. An insurance company should not get to tell me how to practice medicine when Phase III RCT data and @NCCN + @ASCO guideline support my decision!”
A spokesperson for Premera said in a statement that, “while we did see many of the details about the case were posted to Twitter, we cannot comment on the specifics you noted due to privacy policies.”
The spokesperson explained that Premera has “the same goal as our provider partners: ensure our members have access to quality health care,” noting that prior authorization helps health plans evaluate the medical necessity and safety of health care services given that “15%-30% of care is unnecessary.”
“We also understand that providers may not agree with our decisions, which is why we have a robust appeals process,” the spokesperson said, suggesting Dr. Shatsky could have appealed the decision a second time.
And “if the member or provider still disagrees with Premera’s coverage decision after the initial appeal, providers can request review by a medical expert outside Premera who works for an independent review organization,” and the company “will pay for” and “abide by” that decision, the spokesperson added.
The Twitter storm
After Dr. Shatsky tweeted about her experience with Premera, she received a flood of support from the Twitterverse. The thread garnered tens of thousands of likes and hundreds of comments offering support and advice.
Several people suggested asking Merck for help accessing the drug. But Dr. Shatsky said no, “I’m tired of laying down and letting [insurance companies] win. It IS worth fighting for.”
The next morning, Dr. Shatsky got a call. It was the vice president of medical management at Premera.
“We’ve talked again, and we’ll give you the drug,” Dr. Shatsky recalled the Premera vice president saying.
The next day, Monday morning, Dr. Shatsky’s patient received her first infusion of pembrolizumab.
Although relieved, Dr. Shatsky noted that it wasn’t until she posted her experience to Twitter that Premera seemed to take notice.
Plus, “an oncologist without a strong social media following may not have gotten care approved and that’s not how medicine should work,” said Dr. Anderson, assistant professor in the department of clinical pharmacy, University of Colorado at Denver, Aurora.
Tatiana Prowell, MD, expressed similar concerns in a Nov. 20 tweet: “And sadly, the patients with cancer & an even busier, more exhausted doctor who doesn’t have a big [reach] on social media will be denied appropriate care. And that’s bank for insurers.”
But, Dr. Prowell noted sarcastically: “At least a patient with cancer had her care delayed & a dedicated OncTwitter colleague’s Physician Burnout was exacerbated.”
In this case, the prior authorization process took about a week – requiring an initial prior authorization request, an appeal after the request was denied, a peer-to-peer resulting in a second denial, and finally a tweet and a phone call from a top executive at the company.
In fact, these delays have become so common that Dr. Shatsky needs to anticipate and incorporate likely delays into her workflow.
“I learn which drugs will take a long time to get prior authorization for and then plan enough time so that my patient’s care is hopefully not delayed,” Dr. Shatsky said. “It should not be so hard to get appropriate and time-sensitive care for our patients.”
A version of this article first appeared on Medscape.com.
“Is this really the hill you want to die on?” asked Rebecca Shatsky, MD, a medical oncologist at the University of California, San Diego.
It was Nov. 18 and Dr. Shatsky was on the phone with a retired oncologist working for the health insurance company Premera Blue Cross.
Dr. Shatsky was appealing a prior authorization denial for pembrolizumab (Keytruda) to treat her patient with stage IIIc triple-negative breast cancer (TNBC). She hoped the peer-to-peer would reverse the denial. The Food and Drug Administration had approved the immunotherapy for people with high-risk TNBC both in the neoadjuvant setting alongside chemotherapy and, in her patient’s case, as a single-agent adjuvant treatment based on data from the KEYNOTE 522 trial.
In the peer-to-peer, Dr. Shatsky laid out the evidence, but she could tell the physician wasn’t going to budge.
When she pressed him further, asking why he was denying potentially lifesaving care for her patient, he said the data on whether patients really need adjuvant pembrolizumab were not clear yet.
“The man – who was not a breast oncologist – was essentially mansplaining breast oncology to me,” she said in an interview. “I don’t need a nonexpert giving me their misinterpretation of the data.”
Dr. Shatsky informed him that this decision would not stand. She would be escalating the claim.
“I’m not going to let you get in way of my patient’s survival,” Dr. Shatsky told the physician during the peer-to-peer. “We have one shot to cure this, and if we don’t do it now, patients’ average lifespan is 17 months.”
The conversation turned a few heads in her office.
“My whole office stopped and stared. But then they clapped after they realized why I was yelling,” she tweeted later that night.
She continued: “@premera picked the wrong oncologist to mess with today. I will not be letting this go. This denial. Will. Not. Stand. An insurance company should not get to tell me how to practice medicine when Phase III RCT data and @NCCN + @ASCO guideline support my decision!”
A spokesperson for Premera said in a statement that, “while we did see many of the details about the case were posted to Twitter, we cannot comment on the specifics you noted due to privacy policies.”
The spokesperson explained that Premera has “the same goal as our provider partners: ensure our members have access to quality health care,” noting that prior authorization helps health plans evaluate the medical necessity and safety of health care services given that “15%-30% of care is unnecessary.”
“We also understand that providers may not agree with our decisions, which is why we have a robust appeals process,” the spokesperson said, suggesting Dr. Shatsky could have appealed the decision a second time.
And “if the member or provider still disagrees with Premera’s coverage decision after the initial appeal, providers can request review by a medical expert outside Premera who works for an independent review organization,” and the company “will pay for” and “abide by” that decision, the spokesperson added.
The Twitter storm
After Dr. Shatsky tweeted about her experience with Premera, she received a flood of support from the Twitterverse. The thread garnered tens of thousands of likes and hundreds of comments offering support and advice.
Several people suggested asking Merck for help accessing the drug. But Dr. Shatsky said no, “I’m tired of laying down and letting [insurance companies] win. It IS worth fighting for.”
The next morning, Dr. Shatsky got a call. It was the vice president of medical management at Premera.
“We’ve talked again, and we’ll give you the drug,” Dr. Shatsky recalled the Premera vice president saying.
The next day, Monday morning, Dr. Shatsky’s patient received her first infusion of pembrolizumab.
Although relieved, Dr. Shatsky noted that it wasn’t until she posted her experience to Twitter that Premera seemed to take notice.
Plus, “an oncologist without a strong social media following may not have gotten care approved and that’s not how medicine should work,” said Dr. Anderson, assistant professor in the department of clinical pharmacy, University of Colorado at Denver, Aurora.
Tatiana Prowell, MD, expressed similar concerns in a Nov. 20 tweet: “And sadly, the patients with cancer & an even busier, more exhausted doctor who doesn’t have a big [reach] on social media will be denied appropriate care. And that’s bank for insurers.”
But, Dr. Prowell noted sarcastically: “At least a patient with cancer had her care delayed & a dedicated OncTwitter colleague’s Physician Burnout was exacerbated.”
In this case, the prior authorization process took about a week – requiring an initial prior authorization request, an appeal after the request was denied, a peer-to-peer resulting in a second denial, and finally a tweet and a phone call from a top executive at the company.
In fact, these delays have become so common that Dr. Shatsky needs to anticipate and incorporate likely delays into her workflow.
“I learn which drugs will take a long time to get prior authorization for and then plan enough time so that my patient’s care is hopefully not delayed,” Dr. Shatsky said. “It should not be so hard to get appropriate and time-sensitive care for our patients.”
A version of this article first appeared on Medscape.com.
Tucatinib plus trastuzumab approved for HER2+ colorectal cancer
The U.S. Food and Drug Administration has granted accelerated approval to tucatinib (Tukysa) in combination with trastuzumab for use in RAS wild-type, HER2-positive unresectable or metastatic colorectal cancer that has progressed after fluoropyrimidine, oxaliplatin, and irinotecan-based chemotherapy.
This is the first FDA-approved treatment for HER2-positive metastatic colorectal cancer, maker Seagen said in a Jan. 19 press release.
“Historically, patients with HER2-positive metastatic colorectal cancer who have progressed following frontline therapy have had poor outcomes. The FDA approval of a chemotherapy-free combination regimen that specifically targets HER2 is great news for these patients,” John Strickler, MD, associate professor of medicine at Duke University Medical Center, Durham, N.C., said in the press release.
Dr. Strickler was the lead investigator on the approval trial, dubbed MOUNTAINEER, which involved 84 patients who met the treatment criteria and who had also been treated with an anti-VEGF antibody. Participants whose tumors were deficient in mismatch repair proteins or were microsatellite instability–high must also have received a PD-1 inhibitor. Patients who received prior anti-HER2 therapy were excluded, the FDA explained in its own press release.
Participants were treated with tucatinib 300 mg orally twice daily– the recommended dose in product labeling – with trastuzumab administered at a loading dose of 8 mg/kg intravenously on day 1 of cycle 1 followed by a maintenance dose of trastuzumab 6 mg/kg on day 1 of each subsequent 21-day cycle.
Overall response rate was 38%, and median duration of response was 12.4 months.
The most common adverse events, occurring in at least 20% of study participants, were diarrhea, fatigue, rash, nausea, abdominal pain, infusion related reactions, and pyrexia. The most common laboratory abnormalities were increased creatinine, decreased lymphocytes, increased alanine aminotransferase, and decreased hemoglobin, among others.
Serious adverse reactions occurred in 22% of patients. The most common (occurring in ≥ 2% of patients) were intestinal obstruction (7%); urinary tract infection (3.5%); and pneumonia, abdominal pain, and rectal perforation (2.3% each). Adverse reactions leading to permanent discontinuation occurred in 6% of patients, including increased alanine aminotransferase in 2.3%.
Continued approval for the indication may be contingent upon verification and description of clinical benefit in confirmatory trials, the company said.
A global, randomized phase 3 clinical trial (MOUNTAINEER-03) is ongoing and is comparing tucatinib in combination with trastuzumab and mFOLFOX6 with standard of care and is intended to serve as a confirmatory trial, the company said.
Tucatinib is already approved in combination with trastuzumab and capecitabine for use in the treatment of advanced unresectable or metastatic HER2-positive breast cancer.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has granted accelerated approval to tucatinib (Tukysa) in combination with trastuzumab for use in RAS wild-type, HER2-positive unresectable or metastatic colorectal cancer that has progressed after fluoropyrimidine, oxaliplatin, and irinotecan-based chemotherapy.
This is the first FDA-approved treatment for HER2-positive metastatic colorectal cancer, maker Seagen said in a Jan. 19 press release.
“Historically, patients with HER2-positive metastatic colorectal cancer who have progressed following frontline therapy have had poor outcomes. The FDA approval of a chemotherapy-free combination regimen that specifically targets HER2 is great news for these patients,” John Strickler, MD, associate professor of medicine at Duke University Medical Center, Durham, N.C., said in the press release.
Dr. Strickler was the lead investigator on the approval trial, dubbed MOUNTAINEER, which involved 84 patients who met the treatment criteria and who had also been treated with an anti-VEGF antibody. Participants whose tumors were deficient in mismatch repair proteins or were microsatellite instability–high must also have received a PD-1 inhibitor. Patients who received prior anti-HER2 therapy were excluded, the FDA explained in its own press release.
Participants were treated with tucatinib 300 mg orally twice daily– the recommended dose in product labeling – with trastuzumab administered at a loading dose of 8 mg/kg intravenously on day 1 of cycle 1 followed by a maintenance dose of trastuzumab 6 mg/kg on day 1 of each subsequent 21-day cycle.
Overall response rate was 38%, and median duration of response was 12.4 months.
The most common adverse events, occurring in at least 20% of study participants, were diarrhea, fatigue, rash, nausea, abdominal pain, infusion related reactions, and pyrexia. The most common laboratory abnormalities were increased creatinine, decreased lymphocytes, increased alanine aminotransferase, and decreased hemoglobin, among others.
Serious adverse reactions occurred in 22% of patients. The most common (occurring in ≥ 2% of patients) were intestinal obstruction (7%); urinary tract infection (3.5%); and pneumonia, abdominal pain, and rectal perforation (2.3% each). Adverse reactions leading to permanent discontinuation occurred in 6% of patients, including increased alanine aminotransferase in 2.3%.
Continued approval for the indication may be contingent upon verification and description of clinical benefit in confirmatory trials, the company said.
A global, randomized phase 3 clinical trial (MOUNTAINEER-03) is ongoing and is comparing tucatinib in combination with trastuzumab and mFOLFOX6 with standard of care and is intended to serve as a confirmatory trial, the company said.
Tucatinib is already approved in combination with trastuzumab and capecitabine for use in the treatment of advanced unresectable or metastatic HER2-positive breast cancer.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration has granted accelerated approval to tucatinib (Tukysa) in combination with trastuzumab for use in RAS wild-type, HER2-positive unresectable or metastatic colorectal cancer that has progressed after fluoropyrimidine, oxaliplatin, and irinotecan-based chemotherapy.
This is the first FDA-approved treatment for HER2-positive metastatic colorectal cancer, maker Seagen said in a Jan. 19 press release.
“Historically, patients with HER2-positive metastatic colorectal cancer who have progressed following frontline therapy have had poor outcomes. The FDA approval of a chemotherapy-free combination regimen that specifically targets HER2 is great news for these patients,” John Strickler, MD, associate professor of medicine at Duke University Medical Center, Durham, N.C., said in the press release.
Dr. Strickler was the lead investigator on the approval trial, dubbed MOUNTAINEER, which involved 84 patients who met the treatment criteria and who had also been treated with an anti-VEGF antibody. Participants whose tumors were deficient in mismatch repair proteins or were microsatellite instability–high must also have received a PD-1 inhibitor. Patients who received prior anti-HER2 therapy were excluded, the FDA explained in its own press release.
Participants were treated with tucatinib 300 mg orally twice daily– the recommended dose in product labeling – with trastuzumab administered at a loading dose of 8 mg/kg intravenously on day 1 of cycle 1 followed by a maintenance dose of trastuzumab 6 mg/kg on day 1 of each subsequent 21-day cycle.
Overall response rate was 38%, and median duration of response was 12.4 months.
The most common adverse events, occurring in at least 20% of study participants, were diarrhea, fatigue, rash, nausea, abdominal pain, infusion related reactions, and pyrexia. The most common laboratory abnormalities were increased creatinine, decreased lymphocytes, increased alanine aminotransferase, and decreased hemoglobin, among others.
Serious adverse reactions occurred in 22% of patients. The most common (occurring in ≥ 2% of patients) were intestinal obstruction (7%); urinary tract infection (3.5%); and pneumonia, abdominal pain, and rectal perforation (2.3% each). Adverse reactions leading to permanent discontinuation occurred in 6% of patients, including increased alanine aminotransferase in 2.3%.
Continued approval for the indication may be contingent upon verification and description of clinical benefit in confirmatory trials, the company said.
A global, randomized phase 3 clinical trial (MOUNTAINEER-03) is ongoing and is comparing tucatinib in combination with trastuzumab and mFOLFOX6 with standard of care and is intended to serve as a confirmatory trial, the company said.
Tucatinib is already approved in combination with trastuzumab and capecitabine for use in the treatment of advanced unresectable or metastatic HER2-positive breast cancer.
A version of this article first appeared on Medscape.com.
Reversing abortion drug’s approval would harm public interest, FDA says
(Reuters) – President Joe Biden’s administration is urging a judge to reject a request by abortion opponents for a court order withdrawing federal approval for the drug used in medication abortions – which account for more than half of U.S. abortions – citing potential dangers to women seeking to end their pregnancies.
The U.S. Food and Drug Administration’s filing to U.S. District Judge Matthew Kacsmaryk, made available online on Tuesday, came in a lawsuit in Texas by antiabortion groups challenging the agency’s approval of the drug mifepristone in 2000 for medication abortion.
“The public interest would be dramatically harmed by effectively withdrawing from the marketplace a safe and effective drug that has lawfully been on the market for 22 years,” lawyers for the FDA said in the filing to Mr. Kacsmaryk, who is based in Amarillo.
Mifepristone is available under the brand name Mifeprex and as a generic. Used in conjunction with another drug, it is approved to terminate a pregnancy within the first 10 weeks of a pregnancy. The FDA on Jan. 3 said the government for the first time will allow mifepristone to be dispensed at retail pharmacies.
Medication abortion has drawn increasing attention since the U.S. Supreme Court last June overturned its landmark 1973 Roe v. Wade decision that had legalized abortion nationwide. Nearly all abortions, including medication abortions, are now banned in 12 states, and 16 states that permit some abortions also had laws restricting medication abortion as of November, according to the Guttmacher Institute, a research group that supports abortion rights.
“No abortion is safe, and chemical abortions are particularly dangerous,” said Julie Blake, senior counsel at the conservative legal group Alliance Defending Freedom, which represents the plaintiffs in the lawsuit. “The FDA, by approving chemical abortion drugs for home use, puts a woman or girl’s life at risk.”
The American College of Obstetricians and Gynecologists and the American Medical Association said in a joint letter to the Biden administration last June that “robust evidence exists regarding the safety of mifepristone for medication-induced abortion.”
Antiabortion groups including the Alliance for Hippocratic Medicine and the American Association of Pro-Life Obstetricians and Gynecologists sued the FDA in November, saying the agency improperly used an accelerated process to approve mifepristone and failed to study its risks for minors adequately.
In its court filing, the FDA said there was no basis for second-guessing the FDA’s judgment. The FDA said that pulling the drug would force patients seeking abortions in many cases to undergo unnecessary and more invasive surgical abortion. That would result in longer wait times and would carry risks for some patients including those intolerant to anesthesia, the FDA added.
In support of its position, the agency submitted declarations from abortion providers. For example, nonprofit Maine Family Planning said it would have to eliminate abortion services at 17 of its 18 clinics if mifepristone were no longer available.
Mifeprex maker Danco Laboratories on Friday also asked to intervene in the lawsuit to protect its ability to sell the drug.
A version of this article first appeared on Medscape.com.
(Reuters) – President Joe Biden’s administration is urging a judge to reject a request by abortion opponents for a court order withdrawing federal approval for the drug used in medication abortions – which account for more than half of U.S. abortions – citing potential dangers to women seeking to end their pregnancies.
The U.S. Food and Drug Administration’s filing to U.S. District Judge Matthew Kacsmaryk, made available online on Tuesday, came in a lawsuit in Texas by antiabortion groups challenging the agency’s approval of the drug mifepristone in 2000 for medication abortion.
“The public interest would be dramatically harmed by effectively withdrawing from the marketplace a safe and effective drug that has lawfully been on the market for 22 years,” lawyers for the FDA said in the filing to Mr. Kacsmaryk, who is based in Amarillo.
Mifepristone is available under the brand name Mifeprex and as a generic. Used in conjunction with another drug, it is approved to terminate a pregnancy within the first 10 weeks of a pregnancy. The FDA on Jan. 3 said the government for the first time will allow mifepristone to be dispensed at retail pharmacies.
Medication abortion has drawn increasing attention since the U.S. Supreme Court last June overturned its landmark 1973 Roe v. Wade decision that had legalized abortion nationwide. Nearly all abortions, including medication abortions, are now banned in 12 states, and 16 states that permit some abortions also had laws restricting medication abortion as of November, according to the Guttmacher Institute, a research group that supports abortion rights.
“No abortion is safe, and chemical abortions are particularly dangerous,” said Julie Blake, senior counsel at the conservative legal group Alliance Defending Freedom, which represents the plaintiffs in the lawsuit. “The FDA, by approving chemical abortion drugs for home use, puts a woman or girl’s life at risk.”
The American College of Obstetricians and Gynecologists and the American Medical Association said in a joint letter to the Biden administration last June that “robust evidence exists regarding the safety of mifepristone for medication-induced abortion.”
Antiabortion groups including the Alliance for Hippocratic Medicine and the American Association of Pro-Life Obstetricians and Gynecologists sued the FDA in November, saying the agency improperly used an accelerated process to approve mifepristone and failed to study its risks for minors adequately.
In its court filing, the FDA said there was no basis for second-guessing the FDA’s judgment. The FDA said that pulling the drug would force patients seeking abortions in many cases to undergo unnecessary and more invasive surgical abortion. That would result in longer wait times and would carry risks for some patients including those intolerant to anesthesia, the FDA added.
In support of its position, the agency submitted declarations from abortion providers. For example, nonprofit Maine Family Planning said it would have to eliminate abortion services at 17 of its 18 clinics if mifepristone were no longer available.
Mifeprex maker Danco Laboratories on Friday also asked to intervene in the lawsuit to protect its ability to sell the drug.
A version of this article first appeared on Medscape.com.
(Reuters) – President Joe Biden’s administration is urging a judge to reject a request by abortion opponents for a court order withdrawing federal approval for the drug used in medication abortions – which account for more than half of U.S. abortions – citing potential dangers to women seeking to end their pregnancies.
The U.S. Food and Drug Administration’s filing to U.S. District Judge Matthew Kacsmaryk, made available online on Tuesday, came in a lawsuit in Texas by antiabortion groups challenging the agency’s approval of the drug mifepristone in 2000 for medication abortion.
“The public interest would be dramatically harmed by effectively withdrawing from the marketplace a safe and effective drug that has lawfully been on the market for 22 years,” lawyers for the FDA said in the filing to Mr. Kacsmaryk, who is based in Amarillo.
Mifepristone is available under the brand name Mifeprex and as a generic. Used in conjunction with another drug, it is approved to terminate a pregnancy within the first 10 weeks of a pregnancy. The FDA on Jan. 3 said the government for the first time will allow mifepristone to be dispensed at retail pharmacies.
Medication abortion has drawn increasing attention since the U.S. Supreme Court last June overturned its landmark 1973 Roe v. Wade decision that had legalized abortion nationwide. Nearly all abortions, including medication abortions, are now banned in 12 states, and 16 states that permit some abortions also had laws restricting medication abortion as of November, according to the Guttmacher Institute, a research group that supports abortion rights.
“No abortion is safe, and chemical abortions are particularly dangerous,” said Julie Blake, senior counsel at the conservative legal group Alliance Defending Freedom, which represents the plaintiffs in the lawsuit. “The FDA, by approving chemical abortion drugs for home use, puts a woman or girl’s life at risk.”
The American College of Obstetricians and Gynecologists and the American Medical Association said in a joint letter to the Biden administration last June that “robust evidence exists regarding the safety of mifepristone for medication-induced abortion.”
Antiabortion groups including the Alliance for Hippocratic Medicine and the American Association of Pro-Life Obstetricians and Gynecologists sued the FDA in November, saying the agency improperly used an accelerated process to approve mifepristone and failed to study its risks for minors adequately.
In its court filing, the FDA said there was no basis for second-guessing the FDA’s judgment. The FDA said that pulling the drug would force patients seeking abortions in many cases to undergo unnecessary and more invasive surgical abortion. That would result in longer wait times and would carry risks for some patients including those intolerant to anesthesia, the FDA added.
In support of its position, the agency submitted declarations from abortion providers. For example, nonprofit Maine Family Planning said it would have to eliminate abortion services at 17 of its 18 clinics if mifepristone were no longer available.
Mifeprex maker Danco Laboratories on Friday also asked to intervene in the lawsuit to protect its ability to sell the drug.
A version of this article first appeared on Medscape.com.
Hope for catching infants with CP early
A new prognostic tool may help identify infants with cerebral palsy (CP) earlier, allowing them to receive therapies to improve later outcomes.
Researchers from Canada used 12 clinical variables to predict the condition. The tool accurately predicted 75% of CP cases. The study was published in JAMA Pediatrics.
The prevalence of CP in the United States is 2-3 children per 1,000, a rate that has been relatively unchanged for decades. Although recent innovations in diagnosis using motor scores and MRI scans have aided in diagnosis, these techniques have historically been reserved only for infants who were cared for in neonatal intensive care units, were born prematurely, or who had other neurologic risk factors, such as birth defects.
The tool identified 2.4 times more children with CP than would have been detected using current diagnostic methods, according to the researchers.
“We developed the prediction tool to try to make these findings accessible to any health care provider, which will hopefully help break down the long-held perception that CP is usually related to prematurity or a difficult delivery,” said Mary Dunbar, MD, an author of the study. “We know that about half of children with CP aren’t premature and didn’t have a particularly difficult birth.”
The bedside tool weighs factors such as the use by mothers of illicit drugs and tobacco; the presence of diabetes and preeclampsia during pregnancy; whether the infant is male; birth weight; and the number of miscarriages the mother had prior to the birth. The tool also factors in results from a test that measures how well the infant is adjusting to life outside the womb.
Dr. Dunbar and colleagues compared 1,265 infants with CP from the Canadian Cerebral Palsy Registry from 2003 to 2019 with a control group of 1,985 children without CP from the Alberta Pregnancy Outcomes and Nutrition longitudinal study.
The study authors hope that the prognostic tool can be integrated into existing newborn screenings and completed by nurses or physicians as part of routine care.
“Its cost is low especially in comparison to MRI and specialized neurological assessments,” said Sarah Taylor, MD, section chief of neonatal-perinatal medicine at Yale New Haven Children’s Hospital in New Haven, Conn. Health systems and doctors may be more apt to adopt the tool, since it does not require specialized equipment or training.
Surprising findings
Several clinical variables independently increased the risk of CP, including independent 5-minute Apgar test scores of <6, chorioamnionitis, and illicit drug use during the pregnancy. Dr. Dunbar and colleagues recommend that primary care clinicians provide enhanced surveillance for these infants.
“I think there are also really important public health implications to address maternal and reproductive health to support pregnant people, since this study shows that common pregnancy conditions that are potentially treatable may additively contribute to cerebral palsy risk,” said Dr. Dunbar, a pediatric neurologist and assistant professor at the University of Calgary (Alta.)
For infants identified as being at risk, the study authors also suggest that doctors conduct focused examinations for CP at 3-, 6- and 12-month well-baby visits. If results of an examination are abnormal, doctors can advise the caregiver to conduct an early expert evaluation for a general movements assessment. Interventions for children with CP usually start in the first few years of life and can include occupational therapy, use of orthotic devices, and medication.
Dr. Dunbar and colleagues acknowledge that the test is not perfect and that additional work is needed.
“As helpful as the prediction tool may be to identify cases of CP early, we know there are still a minority of CP cases that it won’t catch because they don’t have any of the known risk factors,” Dr. Dunbar said. “We’re currently working on further research about this unique group.”
The researchers cited several limitations to the dataset used in the study, including a control group that was skewed toward older patients and persons of higher socioeconomic status. In addition, the data included a greater proportion of White women than the average Canadian population.
The Canadian Cerebral Palsy Registry was supported by the NeuroDevNet, KidsBrainHealth, the Harvey Guyda Chair of McGill University, Montreal Children’s Hospital, and the Public Health Agency of Canada. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new prognostic tool may help identify infants with cerebral palsy (CP) earlier, allowing them to receive therapies to improve later outcomes.
Researchers from Canada used 12 clinical variables to predict the condition. The tool accurately predicted 75% of CP cases. The study was published in JAMA Pediatrics.
The prevalence of CP in the United States is 2-3 children per 1,000, a rate that has been relatively unchanged for decades. Although recent innovations in diagnosis using motor scores and MRI scans have aided in diagnosis, these techniques have historically been reserved only for infants who were cared for in neonatal intensive care units, were born prematurely, or who had other neurologic risk factors, such as birth defects.
The tool identified 2.4 times more children with CP than would have been detected using current diagnostic methods, according to the researchers.
“We developed the prediction tool to try to make these findings accessible to any health care provider, which will hopefully help break down the long-held perception that CP is usually related to prematurity or a difficult delivery,” said Mary Dunbar, MD, an author of the study. “We know that about half of children with CP aren’t premature and didn’t have a particularly difficult birth.”
The bedside tool weighs factors such as the use by mothers of illicit drugs and tobacco; the presence of diabetes and preeclampsia during pregnancy; whether the infant is male; birth weight; and the number of miscarriages the mother had prior to the birth. The tool also factors in results from a test that measures how well the infant is adjusting to life outside the womb.
Dr. Dunbar and colleagues compared 1,265 infants with CP from the Canadian Cerebral Palsy Registry from 2003 to 2019 with a control group of 1,985 children without CP from the Alberta Pregnancy Outcomes and Nutrition longitudinal study.
The study authors hope that the prognostic tool can be integrated into existing newborn screenings and completed by nurses or physicians as part of routine care.
“Its cost is low especially in comparison to MRI and specialized neurological assessments,” said Sarah Taylor, MD, section chief of neonatal-perinatal medicine at Yale New Haven Children’s Hospital in New Haven, Conn. Health systems and doctors may be more apt to adopt the tool, since it does not require specialized equipment or training.
Surprising findings
Several clinical variables independently increased the risk of CP, including independent 5-minute Apgar test scores of <6, chorioamnionitis, and illicit drug use during the pregnancy. Dr. Dunbar and colleagues recommend that primary care clinicians provide enhanced surveillance for these infants.
“I think there are also really important public health implications to address maternal and reproductive health to support pregnant people, since this study shows that common pregnancy conditions that are potentially treatable may additively contribute to cerebral palsy risk,” said Dr. Dunbar, a pediatric neurologist and assistant professor at the University of Calgary (Alta.)
For infants identified as being at risk, the study authors also suggest that doctors conduct focused examinations for CP at 3-, 6- and 12-month well-baby visits. If results of an examination are abnormal, doctors can advise the caregiver to conduct an early expert evaluation for a general movements assessment. Interventions for children with CP usually start in the first few years of life and can include occupational therapy, use of orthotic devices, and medication.
Dr. Dunbar and colleagues acknowledge that the test is not perfect and that additional work is needed.
“As helpful as the prediction tool may be to identify cases of CP early, we know there are still a minority of CP cases that it won’t catch because they don’t have any of the known risk factors,” Dr. Dunbar said. “We’re currently working on further research about this unique group.”
The researchers cited several limitations to the dataset used in the study, including a control group that was skewed toward older patients and persons of higher socioeconomic status. In addition, the data included a greater proportion of White women than the average Canadian population.
The Canadian Cerebral Palsy Registry was supported by the NeuroDevNet, KidsBrainHealth, the Harvey Guyda Chair of McGill University, Montreal Children’s Hospital, and the Public Health Agency of Canada. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new prognostic tool may help identify infants with cerebral palsy (CP) earlier, allowing them to receive therapies to improve later outcomes.
Researchers from Canada used 12 clinical variables to predict the condition. The tool accurately predicted 75% of CP cases. The study was published in JAMA Pediatrics.
The prevalence of CP in the United States is 2-3 children per 1,000, a rate that has been relatively unchanged for decades. Although recent innovations in diagnosis using motor scores and MRI scans have aided in diagnosis, these techniques have historically been reserved only for infants who were cared for in neonatal intensive care units, were born prematurely, or who had other neurologic risk factors, such as birth defects.
The tool identified 2.4 times more children with CP than would have been detected using current diagnostic methods, according to the researchers.
“We developed the prediction tool to try to make these findings accessible to any health care provider, which will hopefully help break down the long-held perception that CP is usually related to prematurity or a difficult delivery,” said Mary Dunbar, MD, an author of the study. “We know that about half of children with CP aren’t premature and didn’t have a particularly difficult birth.”
The bedside tool weighs factors such as the use by mothers of illicit drugs and tobacco; the presence of diabetes and preeclampsia during pregnancy; whether the infant is male; birth weight; and the number of miscarriages the mother had prior to the birth. The tool also factors in results from a test that measures how well the infant is adjusting to life outside the womb.
Dr. Dunbar and colleagues compared 1,265 infants with CP from the Canadian Cerebral Palsy Registry from 2003 to 2019 with a control group of 1,985 children without CP from the Alberta Pregnancy Outcomes and Nutrition longitudinal study.
The study authors hope that the prognostic tool can be integrated into existing newborn screenings and completed by nurses or physicians as part of routine care.
“Its cost is low especially in comparison to MRI and specialized neurological assessments,” said Sarah Taylor, MD, section chief of neonatal-perinatal medicine at Yale New Haven Children’s Hospital in New Haven, Conn. Health systems and doctors may be more apt to adopt the tool, since it does not require specialized equipment or training.
Surprising findings
Several clinical variables independently increased the risk of CP, including independent 5-minute Apgar test scores of <6, chorioamnionitis, and illicit drug use during the pregnancy. Dr. Dunbar and colleagues recommend that primary care clinicians provide enhanced surveillance for these infants.
“I think there are also really important public health implications to address maternal and reproductive health to support pregnant people, since this study shows that common pregnancy conditions that are potentially treatable may additively contribute to cerebral palsy risk,” said Dr. Dunbar, a pediatric neurologist and assistant professor at the University of Calgary (Alta.)
For infants identified as being at risk, the study authors also suggest that doctors conduct focused examinations for CP at 3-, 6- and 12-month well-baby visits. If results of an examination are abnormal, doctors can advise the caregiver to conduct an early expert evaluation for a general movements assessment. Interventions for children with CP usually start in the first few years of life and can include occupational therapy, use of orthotic devices, and medication.
Dr. Dunbar and colleagues acknowledge that the test is not perfect and that additional work is needed.
“As helpful as the prediction tool may be to identify cases of CP early, we know there are still a minority of CP cases that it won’t catch because they don’t have any of the known risk factors,” Dr. Dunbar said. “We’re currently working on further research about this unique group.”
The researchers cited several limitations to the dataset used in the study, including a control group that was skewed toward older patients and persons of higher socioeconomic status. In addition, the data included a greater proportion of White women than the average Canadian population.
The Canadian Cerebral Palsy Registry was supported by the NeuroDevNet, KidsBrainHealth, the Harvey Guyda Chair of McGill University, Montreal Children’s Hospital, and the Public Health Agency of Canada. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA PEDIATRICS
Holding out hope for ambroxol
How many of you hadn’t heard of ambroxol until the last few weeks?
How many of you have gotten at least one call asking for a prescription for it in that time?
I’ll raise my hand on both accounts.

Ambroxol seems relatively innocuous – an over-the-counter cold medication commonly used on planet Earth (though not approved in the U.S. for whatever reason). But in the last few years some interesting data have cropped up that it may help with Parkinson’s disease.
“May” being the key word here.
Now, I’m not saying it will or won’t do something. The trials that are being started will show that. It would be totally awesome if it did.
But we’ve been here before: The hope that some old, inexpensive, and widely available medication would turn out to have an amazing benefit we didn’t anticipate. We saw this with hydroxychloroquine and ivermectin during the pandemic. Before that we saw all kinds of speculative ideas that statins would be effective for diseases from multiple sclerosis to Alzheimer’s disease.
And, as with many incurable diseases, patients and their families are hoping for a breakthrough. We have plenty of treatments for Parkinson’s disease, but no cures yet. So any potentially effective drug news makes the rounds quickly on news sites, patient advocacy sites, Facebook, and others.
Like the childrens’ telephone game, each time the story is repeated it changes a bit. We’ve gone from an article saying the drug is starting clinical trials to see if it works, to it being a cure now on the marketplace.
Which is when people start calling my office. Most are disappointed to learn that its benefit (if any) is unknown and that it’s not even available. A few get confrontational, accusing me of withholding treatment, when “everyone knows” the drug works.
Believe me, if I had a cure I’d be thrilled to be able to offer it.
I understand that patients and families want a cure.
I understand hope.
I want ambroxol to work for Parkinson’s disease and make a huge difference in the lives of those affected by it. Maybe it will. Or maybe it won’t.
But these things take time to figure out. None of the amazing medications and hi-tech toys we have came about overnight. They were all years in the making.
That’s how science works, and medicine is as much a science as an art.
The art is being able to explain this to patients, and still allow them to hope.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
How many of you hadn’t heard of ambroxol until the last few weeks?
How many of you have gotten at least one call asking for a prescription for it in that time?
I’ll raise my hand on both accounts.
Ambroxol seems relatively innocuous – an over-the-counter cold medication commonly used on planet Earth (though not approved in the U.S. for whatever reason). But in the last few years some interesting data have cropped up that it may help with Parkinson’s disease.
“May” being the key word here.
Now, I’m not saying it will or won’t do something. The trials that are being started will show that. It would be totally awesome if it did.
But we’ve been here before: The hope that some old, inexpensive, and widely available medication would turn out to have an amazing benefit we didn’t anticipate. We saw this with hydroxychloroquine and ivermectin during the pandemic. Before that we saw all kinds of speculative ideas that statins would be effective for diseases from multiple sclerosis to Alzheimer’s disease.
And, as with many incurable diseases, patients and their families are hoping for a breakthrough. We have plenty of treatments for Parkinson’s disease, but no cures yet. So any potentially effective drug news makes the rounds quickly on news sites, patient advocacy sites, Facebook, and others.
Like the childrens’ telephone game, each time the story is repeated it changes a bit. We’ve gone from an article saying the drug is starting clinical trials to see if it works, to it being a cure now on the marketplace.
Which is when people start calling my office. Most are disappointed to learn that its benefit (if any) is unknown and that it’s not even available. A few get confrontational, accusing me of withholding treatment, when “everyone knows” the drug works.
Believe me, if I had a cure I’d be thrilled to be able to offer it.
I understand that patients and families want a cure.
I understand hope.
I want ambroxol to work for Parkinson’s disease and make a huge difference in the lives of those affected by it. Maybe it will. Or maybe it won’t.
But these things take time to figure out. None of the amazing medications and hi-tech toys we have came about overnight. They were all years in the making.
That’s how science works, and medicine is as much a science as an art.
The art is being able to explain this to patients, and still allow them to hope.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
How many of you hadn’t heard of ambroxol until the last few weeks?
How many of you have gotten at least one call asking for a prescription for it in that time?
I’ll raise my hand on both accounts.
Ambroxol seems relatively innocuous – an over-the-counter cold medication commonly used on planet Earth (though not approved in the U.S. for whatever reason). But in the last few years some interesting data have cropped up that it may help with Parkinson’s disease.
“May” being the key word here.
Now, I’m not saying it will or won’t do something. The trials that are being started will show that. It would be totally awesome if it did.
But we’ve been here before: The hope that some old, inexpensive, and widely available medication would turn out to have an amazing benefit we didn’t anticipate. We saw this with hydroxychloroquine and ivermectin during the pandemic. Before that we saw all kinds of speculative ideas that statins would be effective for diseases from multiple sclerosis to Alzheimer’s disease.
And, as with many incurable diseases, patients and their families are hoping for a breakthrough. We have plenty of treatments for Parkinson’s disease, but no cures yet. So any potentially effective drug news makes the rounds quickly on news sites, patient advocacy sites, Facebook, and others.
Like the childrens’ telephone game, each time the story is repeated it changes a bit. We’ve gone from an article saying the drug is starting clinical trials to see if it works, to it being a cure now on the marketplace.
Which is when people start calling my office. Most are disappointed to learn that its benefit (if any) is unknown and that it’s not even available. A few get confrontational, accusing me of withholding treatment, when “everyone knows” the drug works.
Believe me, if I had a cure I’d be thrilled to be able to offer it.
I understand that patients and families want a cure.
I understand hope.
I want ambroxol to work for Parkinson’s disease and make a huge difference in the lives of those affected by it. Maybe it will. Or maybe it won’t.
But these things take time to figure out. None of the amazing medications and hi-tech toys we have came about overnight. They were all years in the making.
That’s how science works, and medicine is as much a science as an art.
The art is being able to explain this to patients, and still allow them to hope.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Should pediatricians fret over their falling board scores?
Few pediatricians have warm, fuzzy memories about taking their initial board exam.
But many reacted strongly when they read a recent post on Twitter by Bryan Carmody, MD, who noted that the passing rate for first-time test takers had dipped to its lowest level in 5 years – hitting 81% in 2021, down from 91% 3 years earlier.
“It’s literally an awfully written exam,” replied one person who posted. Another asked: “At what point is the exam just not reflective of clinical practice?” And, inevitably, the question of the effect of COVID-19 surfaced: “Is any of this attributable to pulling early career physicians into the pandemic?”
But Dr. Carmody, an associate professor of pediatrics at the University of Eastern Virginia Medical School, Norfolk, isn’t buying that explanation. He researched board scores for internal medicine, general surgery, and family medicine for 2021. All were stable during the same period, he said, leading him to dismiss the idea that the pandemic drove the decline. “It’s not really clear to me why other specialties wouldn’t have seen similar drops,” Dr. Carmody said.
The slip has caught the attention of the American Board of Pediatrics, according to Judy Schaechter, MD, MBA, who was chair of the department of pediatrics at the University of Miami before taking her post as president and CEO of the American Board of Pediatrics in 2021.
“So, our first question was, was this within the range of what one might expect?” Dr. Schaechter said. “Were there other factors that might have come into play?”
The board performs an extensive analysis every year before releasing scores, and it didn’t uncover any changes in the difficulty or content of the test in 2021, nor did the score that was needed to pass increase. Dr. Schaechter pointed out that the passing rate that year was not unprecedented – in 2016, it also dipped to 81%.
Dr. Schaechter said COVID-19 might have affected test takers. “Remember, pediatrics was different from any other specialty during the pandemic,” she said. The census in pediatric wards around the country dropped dramatically in the first two winters of the pandemic, leaving residents with less hands-on experience with patients and mentorship from attendings – both of which can help test-takers pass the exam.
Eyal Ben-Isaac, MD, an associate professor of the department of pediatrics at the Keck School of Medicine at the University of Southern California, Los Angeles, said residents likely suffered during the pandemic, when noon lectures and grand rounds became virtual events.
“I’m sure that clearly affected a person’s ability to sit and listen and really learn the material, as opposed to either doing it hands on or learning the material from a faculty member face to face,” Dr. Ben-Isaac said.
But how much do the didactic experiences of residency programs contribute to residents’ readiness to take the boards? Thomas Welch, MD, professor and chair emeritus of the department of pediatrics at SUNY Upstate Medical University, Syracuse, credits his own success in advancing through college, medical school, pediatric residency, and nephrology fellowship to his skill as a test taker.
He confirmed his suspicions by conducting a study that evaluated correlations between residents’ performance on the United States Medical Licensing Exam (USMLE) taken during medical school and their board scores after completing residency.
Dr. Welch said he wasn’t surprised to find that “the best predictor of one’s passing the pediatric boards was not the training program in which one worked. It was their performance on Step 2 [taken during the fourth year of medical school] of the USMLE.”
Although Dr. Ben-Isaac felt that changes in residency training opportunities might have partially explained the drop in passing rates, he agreed that other factors contribute to success on boards. As director of the pediatric residency program at Children’s Hospital of Los Angeles from 1994 to 2019, one of his first goals was to increase the pass rate of graduates. He developed a board review course for residents, revising it over time on the basis of resident feedback and adding individual coaching for residents who wanted more help.
“Without a question, it raised our board pass rate to being one of the highest in the country,” he said.
Dr. Welch said that while “being up all night with a sick child teaches you a lot about medicine and certainly makes you a better doctor, it doesn’t do anything to improve your board scores.”
None of the pediatricians was too worried about a 1-year drop in scores, and the consensus was that supporting residents with review courses and coaching on how to take multiple choice tests would raise passing rates.
“There are definitely people who are amazing clinicians who did not pass the boards on their first attempt,” Dr. Ben-Isaac said.
But Dr. Schaechter defended the importance of the examination. “Our first obligation is really to the public,” she said. The ABP’s role is to ensure that pediatricians “provide the care that parents want their kids to have.”
As Dr. Welch put it, “Would I trust someone who didn’t pass the board exam to take care of my own kid? Probably not.”
A version of this article first appeared on Medscape.com.
Few pediatricians have warm, fuzzy memories about taking their initial board exam.
But many reacted strongly when they read a recent post on Twitter by Bryan Carmody, MD, who noted that the passing rate for first-time test takers had dipped to its lowest level in 5 years – hitting 81% in 2021, down from 91% 3 years earlier.
“It’s literally an awfully written exam,” replied one person who posted. Another asked: “At what point is the exam just not reflective of clinical practice?” And, inevitably, the question of the effect of COVID-19 surfaced: “Is any of this attributable to pulling early career physicians into the pandemic?”
But Dr. Carmody, an associate professor of pediatrics at the University of Eastern Virginia Medical School, Norfolk, isn’t buying that explanation. He researched board scores for internal medicine, general surgery, and family medicine for 2021. All were stable during the same period, he said, leading him to dismiss the idea that the pandemic drove the decline. “It’s not really clear to me why other specialties wouldn’t have seen similar drops,” Dr. Carmody said.
The slip has caught the attention of the American Board of Pediatrics, according to Judy Schaechter, MD, MBA, who was chair of the department of pediatrics at the University of Miami before taking her post as president and CEO of the American Board of Pediatrics in 2021.
“So, our first question was, was this within the range of what one might expect?” Dr. Schaechter said. “Were there other factors that might have come into play?”
The board performs an extensive analysis every year before releasing scores, and it didn’t uncover any changes in the difficulty or content of the test in 2021, nor did the score that was needed to pass increase. Dr. Schaechter pointed out that the passing rate that year was not unprecedented – in 2016, it also dipped to 81%.
Dr. Schaechter said COVID-19 might have affected test takers. “Remember, pediatrics was different from any other specialty during the pandemic,” she said. The census in pediatric wards around the country dropped dramatically in the first two winters of the pandemic, leaving residents with less hands-on experience with patients and mentorship from attendings – both of which can help test-takers pass the exam.
Eyal Ben-Isaac, MD, an associate professor of the department of pediatrics at the Keck School of Medicine at the University of Southern California, Los Angeles, said residents likely suffered during the pandemic, when noon lectures and grand rounds became virtual events.
“I’m sure that clearly affected a person’s ability to sit and listen and really learn the material, as opposed to either doing it hands on or learning the material from a faculty member face to face,” Dr. Ben-Isaac said.
But how much do the didactic experiences of residency programs contribute to residents’ readiness to take the boards? Thomas Welch, MD, professor and chair emeritus of the department of pediatrics at SUNY Upstate Medical University, Syracuse, credits his own success in advancing through college, medical school, pediatric residency, and nephrology fellowship to his skill as a test taker.
He confirmed his suspicions by conducting a study that evaluated correlations between residents’ performance on the United States Medical Licensing Exam (USMLE) taken during medical school and their board scores after completing residency.
Dr. Welch said he wasn’t surprised to find that “the best predictor of one’s passing the pediatric boards was not the training program in which one worked. It was their performance on Step 2 [taken during the fourth year of medical school] of the USMLE.”
Although Dr. Ben-Isaac felt that changes in residency training opportunities might have partially explained the drop in passing rates, he agreed that other factors contribute to success on boards. As director of the pediatric residency program at Children’s Hospital of Los Angeles from 1994 to 2019, one of his first goals was to increase the pass rate of graduates. He developed a board review course for residents, revising it over time on the basis of resident feedback and adding individual coaching for residents who wanted more help.
“Without a question, it raised our board pass rate to being one of the highest in the country,” he said.
Dr. Welch said that while “being up all night with a sick child teaches you a lot about medicine and certainly makes you a better doctor, it doesn’t do anything to improve your board scores.”
None of the pediatricians was too worried about a 1-year drop in scores, and the consensus was that supporting residents with review courses and coaching on how to take multiple choice tests would raise passing rates.
“There are definitely people who are amazing clinicians who did not pass the boards on their first attempt,” Dr. Ben-Isaac said.
But Dr. Schaechter defended the importance of the examination. “Our first obligation is really to the public,” she said. The ABP’s role is to ensure that pediatricians “provide the care that parents want their kids to have.”
As Dr. Welch put it, “Would I trust someone who didn’t pass the board exam to take care of my own kid? Probably not.”
A version of this article first appeared on Medscape.com.
Few pediatricians have warm, fuzzy memories about taking their initial board exam.
But many reacted strongly when they read a recent post on Twitter by Bryan Carmody, MD, who noted that the passing rate for first-time test takers had dipped to its lowest level in 5 years – hitting 81% in 2021, down from 91% 3 years earlier.
“It’s literally an awfully written exam,” replied one person who posted. Another asked: “At what point is the exam just not reflective of clinical practice?” And, inevitably, the question of the effect of COVID-19 surfaced: “Is any of this attributable to pulling early career physicians into the pandemic?”
But Dr. Carmody, an associate professor of pediatrics at the University of Eastern Virginia Medical School, Norfolk, isn’t buying that explanation. He researched board scores for internal medicine, general surgery, and family medicine for 2021. All were stable during the same period, he said, leading him to dismiss the idea that the pandemic drove the decline. “It’s not really clear to me why other specialties wouldn’t have seen similar drops,” Dr. Carmody said.
The slip has caught the attention of the American Board of Pediatrics, according to Judy Schaechter, MD, MBA, who was chair of the department of pediatrics at the University of Miami before taking her post as president and CEO of the American Board of Pediatrics in 2021.
“So, our first question was, was this within the range of what one might expect?” Dr. Schaechter said. “Were there other factors that might have come into play?”
The board performs an extensive analysis every year before releasing scores, and it didn’t uncover any changes in the difficulty or content of the test in 2021, nor did the score that was needed to pass increase. Dr. Schaechter pointed out that the passing rate that year was not unprecedented – in 2016, it also dipped to 81%.
Dr. Schaechter said COVID-19 might have affected test takers. “Remember, pediatrics was different from any other specialty during the pandemic,” she said. The census in pediatric wards around the country dropped dramatically in the first two winters of the pandemic, leaving residents with less hands-on experience with patients and mentorship from attendings – both of which can help test-takers pass the exam.
Eyal Ben-Isaac, MD, an associate professor of the department of pediatrics at the Keck School of Medicine at the University of Southern California, Los Angeles, said residents likely suffered during the pandemic, when noon lectures and grand rounds became virtual events.
“I’m sure that clearly affected a person’s ability to sit and listen and really learn the material, as opposed to either doing it hands on or learning the material from a faculty member face to face,” Dr. Ben-Isaac said.
But how much do the didactic experiences of residency programs contribute to residents’ readiness to take the boards? Thomas Welch, MD, professor and chair emeritus of the department of pediatrics at SUNY Upstate Medical University, Syracuse, credits his own success in advancing through college, medical school, pediatric residency, and nephrology fellowship to his skill as a test taker.
He confirmed his suspicions by conducting a study that evaluated correlations between residents’ performance on the United States Medical Licensing Exam (USMLE) taken during medical school and their board scores after completing residency.
Dr. Welch said he wasn’t surprised to find that “the best predictor of one’s passing the pediatric boards was not the training program in which one worked. It was their performance on Step 2 [taken during the fourth year of medical school] of the USMLE.”
Although Dr. Ben-Isaac felt that changes in residency training opportunities might have partially explained the drop in passing rates, he agreed that other factors contribute to success on boards. As director of the pediatric residency program at Children’s Hospital of Los Angeles from 1994 to 2019, one of his first goals was to increase the pass rate of graduates. He developed a board review course for residents, revising it over time on the basis of resident feedback and adding individual coaching for residents who wanted more help.
“Without a question, it raised our board pass rate to being one of the highest in the country,” he said.
Dr. Welch said that while “being up all night with a sick child teaches you a lot about medicine and certainly makes you a better doctor, it doesn’t do anything to improve your board scores.”
None of the pediatricians was too worried about a 1-year drop in scores, and the consensus was that supporting residents with review courses and coaching on how to take multiple choice tests would raise passing rates.
“There are definitely people who are amazing clinicians who did not pass the boards on their first attempt,” Dr. Ben-Isaac said.
But Dr. Schaechter defended the importance of the examination. “Our first obligation is really to the public,” she said. The ABP’s role is to ensure that pediatricians “provide the care that parents want their kids to have.”
As Dr. Welch put it, “Would I trust someone who didn’t pass the board exam to take care of my own kid? Probably not.”
A version of this article first appeared on Medscape.com.
Teamwork guides cardio-rheumatology clinics that care for unique patient population
Clinical cardiologist Heba Wassif, MD, MPH, knows the value of working with her fellow rheumatologists, surgeons, and other clinicians to establish a care plan for her patients with cardiac conditions and autoimmune diseases.
She is the cofounder of the Cleveland Clinic’s new cardio-rheumatology program, which places an emphasis on multidisciplinary care. In her role, Dr. Wassif closely follows her patients, and if she sees any inflammation or any other condition that requires the rheumatologist, she reaches out to her colleagues to adjust medications if needed.

Collaboration with a rheumatologist was important when a patient with valvular disease was prepping for surgery. The patient was on significant immunosuppressants and the surgery had to be timed appropriately, accounting for any decreases in her immunosuppression, explained Dr. Wassif, director of inpatient clinical cardiology at Cleveland Clinic in Ohio.
Cardio-rheumatology programs are “the newest child” in a series of cardiology offshoots focusing on different populations. Cardio-oncology and cardio-obstetrics took off about 6 years ago, with cardio-rheumatology clinics and interested physicians rising in number over the last several years, Dr. Wassif noted.
The relationship between cardiovascular diseases and rheumatologic conditions is certainly recognized more often, “which means more literature is being published to discuss the link,” according to Rekha Mankad, MD, a trailblazer of this model of care. She directs the Women’s Heart Clinic at Mayo Clinic in Rochester, Minn., which was one of the earliest adopters of a cardio-rheumatology clinic.

Ten years ago, “nobody was talking about the link between rheumatologic conditions and cardiovascular disease,” Dr. Mankad said. “I’ve been asked to speak on this topic, and programs have asked me to speak about establishing cardio-rheumatology practices. So, there’s been an evolution as far as a recognition that these two conditions overlap.”
Patients have come to her independent of internal referrals, which means they have done Google searches on cardiology and rheumatology. “I think that it has made a splash, at least in the world of cardiology,” Dr. Mankad observed in an interview.
Other institutions such as NYU-Langone, Yale, Stanford, Brigham and Women’s Hospital in Boston, and Women’s College Hospital in Toronto have formed similar clinics whose focus is to address the specific needs of rheumatology patients with cardiac conditions through a teamwork approach.
Challenges of treating cardiac, rheumatologic conditions
The rise in clinics addresses the longstanding connection between autoimmune disorders and cardiac conditions.
Cardiologists have known that there is an element of inflammation that contributes to atherosclerosis, said Dr. Wassif, who has researched this topic extensively. A recent study she led found a strong association between rheumatic immune-mediated inflammatory diseases (IMIDs) and high risk of acute coronary syndrome in Medicare patients.
“This particular population has a very clear increased risk for cardiovascular conditions, including valve disease and heart failure,” she emphasized.
Patients with rheumatoid arthritis and lupus have up to a twofold and eightfold higher risk of heart disease, respectively, noted Michael S. Garshick, MD, a cardiovascular disease specialist who directs the cardio-rheumatology program at NYU-Langone Health, in New York. Cardiologists “have really developed an understanding that the immune system can impact the heart, and that there’s a need for people to understand the nuance behind how the immune system can affect them and what to do about it,” Dr. Garshick said.

Caring for patients with both afflictions comes with specific challenges. Many physicians are not well trained on managing and treating patients with these dual conditions.
The “lipid paradox,” in which lipids are reduced with active inflammation in some rheumatologic conditions, can make treatment more nuanced. In addition, the traditional ASCVD (atherosclerotic cardiovascular disease) score often underestimates the cardiovascular risk of these patients, noted cardiologist Margaret Furman, MD, MPH, assistant professor and codirector of Yale’s Cardio-Rheumatology Program, New Haven, Conn.
Newer biologic medications used to treat rheumatologic diseases can alter a patient’s lipid profile, she said in an interview.
“It can be difficult to assess each individual patient’s cardiovascular risk as their disease state and treatment can vary throughout their lifetime based on their degree of inflammation. The importance of aggressive lipid management is often underestimated,” Dr. Furman added.
Cardiology and rheumatology partnerships can address gaps in care of this unique group of patients, said Vaidehi R. Chowdhary, MBBS, MD, clinical chief of the Yale Section of Rheumatology, Allergy, and Immunology at Yale University.

“The role of the rheumatologist in this dyad is to educate patients on this risk, work toward adequate control of inflammation, and minimize use of medications that contribute to increased cardiovascular risks,” said Dr. Chowdhary, who cofounded Yale’s cardio-rheumatology program with Dr. Furman.
Cardiologists in turn can assert their knowledge about medications and their impact on lipids and inflammation, Dr. Wassif said.
Many anti-inflammatory therapies are now within the cardiologist’s purview, Dr. Garshick noted. “For example, specifically with pericarditis, there’s [Food and Drug Administration]–approved anti-inflammatories or biologics. We’re the ones who feel the most comfortable giving them right now.” Cardiologists quite often are consulted about medications that are efficacious in rheumatologic conditions but could negatively impact the cardiovascular system, such as Janus kinase inhibitors, he added.
‘Reading the tea leaves’
Each program has its own unique story. For the Cleveland Clinic, the concept of a cardio-rheumatology program began during the COVID-19 pandemic in 2020. Developing such a concept and gaining institutional acceptance is always a work in process, Dr. Wassif said. “It’s not that you decide one day that you’re going to build a center, and that center is going to come into fruition overnight. You first gauge interest within your division. Who are the individuals that are interested in this area?”
Cleveland Clinic’s center is seeking to build relations between medical disciplines while spotlighting the concept of cardio-rheumatology, said Dr. Wassif, who has been providing education within the clinic and at other health institutions to ensure that patients receive appropriate attention early.
NYU-Langone launched its program amid this heightened awareness that the immune system could affect atherosclerosis, “kind of reading of the tea leaves, so to speak,” Dr. Garshick said.
Several clinical trials served as a catalyst for this movement. “A lot of clinical cardiologists were never 100% convinced that targeting the immune system reduced cardiovascular disease,” he said. Then the CANTOS clinical trial came along and showed for the first time that a therapeutic monoclonal antibody targeting interleukin-1beta, a cytokine central to inflammatory response, could in fact reduce cardiovascular disease.
Trials like this, along with epidemiologic literature connecting the rheumatologic and the autoimmune conditions with cardiovascular disease, pushed this concept to the forefront, Dr. Garshick said.
The notion that a clinic could successfully address cardiac problems in patients with rheumatic diseases yielded promising returns at Women’s College Hospital in Toronto, according to a report presented at the 2018 American College of Rheumatology annual meeting. Researchers reported that patients with rheumatologic conditions who attended a cardio-rheumatology clinic at this center saw improvements in care. The clinic identified increased cardiovascular risk and early atherosclerosis, and 53.8% of patients altered their medications after being seen in the clinic.
A total of 39.7% and 32.1% received lipid lowering and antiplatelet therapies, respectively, and 14% received antihypertensive therapy. A small percentage were treated for heart failure or placed on lifelong anticoagulation therapy for atrial fibrillation, and one patient received a percutaneous coronary stent.
Ins and outs of the referral process
Initially designed for preventive cardiac risk assessment, Yale’s program evolved into a multidisciplinary, patient-centered approach for the management of complex cardiovascular conditions in patients with autoimmune rheumatologic diseases.
The program is open to anyone who carries a diagnosis of rheumatologic disease or has elevated inflammatory markers. “Every patient, regardless of the reason for the referral, receives a cardiovascular risk assessment,” Dr. Furman said.

Most referrals come from rheumatologists, although cardiology colleagues and pulmonologists have also sent referrals. A pulmonologist, for example, may want to rule out a cardiac cause to shortness of breath. The patient’s workup, care, and follow-up are based on the reason for referral.
“We are currently referring patients with established cardiac disease, traditional risk factors, or for better risk assessment for primary prevention of coronary artery disease,” Dr. Chowdhary said. “We communicate very frequently about medication changes, and patients are aware of goals of care from both sides.”
Dr. Furman works closely with several of the rheumatology specialists taking care of patients with rheumatoid arthritis, systemic lupus erythematosus, and scleroderma.
Rheumatology follows patients every 3-6 months or more frequently based on their disease activity.
Dr. Mankad uses her sleuthing skills at Mayo Clinic to determine what the patients need. If they come in for a preventive assessment, she looks more closely at their cardiovascular risks and may order additional imaging to look for subclinical atherosclerosis. “We’re more aggressive with statin therapy in this population because of that,” she said.
If it’s valve disease, she pays extra attention to the patients’ valves in the echocardiograms and follows them a bit more regularly than someone without a rheumatologic condition and valve disease.
For patients with heart failure signs or symptoms, “it depends on how symptomatic they are,” Dr. Mankad said. In some instances, she may look for evidence of heart failure with preserved ejection fraction in patients who have rheumatoid arthritis who happen to be short of breath. “There’s so many different manifestations that patients with rheumatologic conditions can have as far as what could be affected in the heart,” she noted.
Quite frequently, Dr. Mankad identifies subclinical disease in her patients with rheumatoid arthritis. “I’ve seen many patients whose risk scores would not dictate statin therapy. But I went looking for subclinical disease by either doing coronary assessment or carotid assessment and have found atherosclerosis that would be enough to warrant statin therapy.”
A personalized assessment to reduce cardiac risk
NYU-Langone’s program offers opportunities to educate patients about the link between cardiac and rheumatologic disease.
“Their rheumatologist or their dermatologist will say, ‘Hey, have you heard about the connection between psoriasis, psoriatic or rheumatoid arthritis, and heart disease and the risk of heart attack or stroke?’ ” Dr. Garshick said.
The patients will often say they know nothing about these connections and want to learn more about how to treat it.
“We’ll say, ‘we have someone here that can help you.’ They’ll send them to myself or other colleagues like me across the country. We’ll assess blood pressure, weight, lipids, hemoglobin A1c, and other serologic and oftentimes imaging biomarkers of cardiovascular risk.” The patients will receive a personalized assessment, listing things they can do to lower their risk, whether it’s diet, exercise, or lifestyle. “Many times it can involve medications to reduce heart disease risk,” said Dr. Garshick.
In some instances, a rheumatologist or dermatologist may be concerned about starting a patient on a specific medication for the disease such as a JAK inhibitor. “We’ll help assess their risk because there’s been a lot of literature out in the rheumatology world about the risk of JAK inhibitors and heart disease and blood clots,” said Dr. Garshick.
Dr. Garshick also sees patients with rheumatologic conditions who have a specific cardiovascular concern or complaint such as shortness of breath or chest pain. “We’ll work that up with a specific knowledge of the underlying immune condition and how that may impact their heart,” he said.
Advances in research
As they continue to see patients and devise specific care plans, developers of cardio-rheumatology programs have been supplementing their work with ongoing research.
Yale’s clinic is expanding this year to include a new attending physician, Attila Feher, MD, PhD, who has conducted research in autoimmunity and microcirculation using molecular imaging and multimodality imaging techniques. Prevalence of coronary microvascular dysfunction appears to be increased in this patient population, Dr. Furman said.
Dr. Wassif recently coauthored a paper that examined patients with underlying rheumatologic conditions who undergo valvular and aortic valve replacement. “To our surprise, there was really no difference between patients with autoimmune conditions and others with nonautoimmune conditions,” she said, adding that the study had its limitations.
Other work includes data on Medicare patients with ST- and non-ST-elevation myocardial infarctions who have an underlying autoimmune disorder. Dr. Wassif and her colleagues found that their long-term outcomes are worse than those of patients without these conditions. “It’s unclear if worse outcomes are related to complications of autoimmunity versus the extent of their underlying disease. This is a work in progress and certainly an area that is ripe for research.”
Dr. Garshick and other collaborators at NYU have been focusing on the endothelium, specifically platelet biology in patients with psoriasis, psoriatic arthritis, and lupus. “We’re about to start the same research with gout as well,” he said.
“The process we’re most interested in is understanding how these diseases impact the early stages of cholesterol. And the way we’re doing that is evaluating the vasculature, specifically the endothelium,” he said.
He has finished two clinical trials that evaluate how standard heart disease medications such as aspirin and statins impact or can potentially benefit patients with psoriasis and/or psoriatic arthritis. “We have a whole list of other trials in the pipeline with other institutions across the country.”
Through a grant, Dr. Mankad is assessing whether a PET scan could detect inflammation in the hearts of rheumatoid arthritis patients. “We’re looking to see if the reason these patients have heart failure later in life is because their heart muscle actually shows evidence of inflammation, even when they have no symptoms,” she explained.
Other tests such as echocardiogram and CT scans will be used to evaluate coronary disease in about 40-50 patients. The goal of using these multiple imaging tools is to find markers indicating that the heart is affected by rheumatoid arthritis, which may indicate a higher likelihood of developing heart failure, she said.
Clinics are popping up
Through these new clinics, some collaborations have emerged. Dr. Garshick works closely with Brigham and Women’s Hospital, which has a similar cardio-rheumatology program, run by Brittany Weber, MD, to exchange ideas, discuss challenging cases, and collaborate.
“There are a lot of clinics like us popping up across the country,” he observed. Every so often, he hears from other institutions that are interested in starting their own cardio-rheumatology programs. “They ask us: How do you start, what should we look for?”
It’s an education process for both patients and providers, Dr. Garshick emphasized. “I also think it’s a bandwidth issue. Many of our rheumatology and dermatology colleagues are acutely aware of the connection, but there may not be enough time at a clinic visit to really go in depth” with these dual conditions, he said.
NYU-Langone Health for the past several years has been holding a symposium to educate people on the cardio-rheumatology connection and treating inflammation in cardiovascular disease. This year’s symposium, held in conjunction with Brigham and Women’s Hospital, is scheduled for April 28. For more information, visit the course website: nyulmc.org/cvinflammationcme.
“What we’re trying to do is help [other institutions] get that bandwidth” to adequately help and serve these patients, he said.
Dr. Garshick has received consultant fees from Abbvie and Horizon therapeutics and an unrestricted research grant from Pfizer. No other sources had relevant financial disclosures.
Clinical cardiologist Heba Wassif, MD, MPH, knows the value of working with her fellow rheumatologists, surgeons, and other clinicians to establish a care plan for her patients with cardiac conditions and autoimmune diseases.
She is the cofounder of the Cleveland Clinic’s new cardio-rheumatology program, which places an emphasis on multidisciplinary care. In her role, Dr. Wassif closely follows her patients, and if she sees any inflammation or any other condition that requires the rheumatologist, she reaches out to her colleagues to adjust medications if needed.
Collaboration with a rheumatologist was important when a patient with valvular disease was prepping for surgery. The patient was on significant immunosuppressants and the surgery had to be timed appropriately, accounting for any decreases in her immunosuppression, explained Dr. Wassif, director of inpatient clinical cardiology at Cleveland Clinic in Ohio.
Cardio-rheumatology programs are “the newest child” in a series of cardiology offshoots focusing on different populations. Cardio-oncology and cardio-obstetrics took off about 6 years ago, with cardio-rheumatology clinics and interested physicians rising in number over the last several years, Dr. Wassif noted.
The relationship between cardiovascular diseases and rheumatologic conditions is certainly recognized more often, “which means more literature is being published to discuss the link,” according to Rekha Mankad, MD, a trailblazer of this model of care. She directs the Women’s Heart Clinic at Mayo Clinic in Rochester, Minn., which was one of the earliest adopters of a cardio-rheumatology clinic.
Ten years ago, “nobody was talking about the link between rheumatologic conditions and cardiovascular disease,” Dr. Mankad said. “I’ve been asked to speak on this topic, and programs have asked me to speak about establishing cardio-rheumatology practices. So, there’s been an evolution as far as a recognition that these two conditions overlap.”
Patients have come to her independent of internal referrals, which means they have done Google searches on cardiology and rheumatology. “I think that it has made a splash, at least in the world of cardiology,” Dr. Mankad observed in an interview.
Other institutions such as NYU-Langone, Yale, Stanford, Brigham and Women’s Hospital in Boston, and Women’s College Hospital in Toronto have formed similar clinics whose focus is to address the specific needs of rheumatology patients with cardiac conditions through a teamwork approach.
Challenges of treating cardiac, rheumatologic conditions
The rise in clinics addresses the longstanding connection between autoimmune disorders and cardiac conditions.
Cardiologists have known that there is an element of inflammation that contributes to atherosclerosis, said Dr. Wassif, who has researched this topic extensively. A recent study she led found a strong association between rheumatic immune-mediated inflammatory diseases (IMIDs) and high risk of acute coronary syndrome in Medicare patients.
“This particular population has a very clear increased risk for cardiovascular conditions, including valve disease and heart failure,” she emphasized.
Patients with rheumatoid arthritis and lupus have up to a twofold and eightfold higher risk of heart disease, respectively, noted Michael S. Garshick, MD, a cardiovascular disease specialist who directs the cardio-rheumatology program at NYU-Langone Health, in New York. Cardiologists “have really developed an understanding that the immune system can impact the heart, and that there’s a need for people to understand the nuance behind how the immune system can affect them and what to do about it,” Dr. Garshick said.
Caring for patients with both afflictions comes with specific challenges. Many physicians are not well trained on managing and treating patients with these dual conditions.
The “lipid paradox,” in which lipids are reduced with active inflammation in some rheumatologic conditions, can make treatment more nuanced. In addition, the traditional ASCVD (atherosclerotic cardiovascular disease) score often underestimates the cardiovascular risk of these patients, noted cardiologist Margaret Furman, MD, MPH, assistant professor and codirector of Yale’s Cardio-Rheumatology Program, New Haven, Conn.
Newer biologic medications used to treat rheumatologic diseases can alter a patient’s lipid profile, she said in an interview.
“It can be difficult to assess each individual patient’s cardiovascular risk as their disease state and treatment can vary throughout their lifetime based on their degree of inflammation. The importance of aggressive lipid management is often underestimated,” Dr. Furman added.
Cardiology and rheumatology partnerships can address gaps in care of this unique group of patients, said Vaidehi R. Chowdhary, MBBS, MD, clinical chief of the Yale Section of Rheumatology, Allergy, and Immunology at Yale University.
“The role of the rheumatologist in this dyad is to educate patients on this risk, work toward adequate control of inflammation, and minimize use of medications that contribute to increased cardiovascular risks,” said Dr. Chowdhary, who cofounded Yale’s cardio-rheumatology program with Dr. Furman.
Cardiologists in turn can assert their knowledge about medications and their impact on lipids and inflammation, Dr. Wassif said.
Many anti-inflammatory therapies are now within the cardiologist’s purview, Dr. Garshick noted. “For example, specifically with pericarditis, there’s [Food and Drug Administration]–approved anti-inflammatories or biologics. We’re the ones who feel the most comfortable giving them right now.” Cardiologists quite often are consulted about medications that are efficacious in rheumatologic conditions but could negatively impact the cardiovascular system, such as Janus kinase inhibitors, he added.
‘Reading the tea leaves’
Each program has its own unique story. For the Cleveland Clinic, the concept of a cardio-rheumatology program began during the COVID-19 pandemic in 2020. Developing such a concept and gaining institutional acceptance is always a work in process, Dr. Wassif said. “It’s not that you decide one day that you’re going to build a center, and that center is going to come into fruition overnight. You first gauge interest within your division. Who are the individuals that are interested in this area?”
Cleveland Clinic’s center is seeking to build relations between medical disciplines while spotlighting the concept of cardio-rheumatology, said Dr. Wassif, who has been providing education within the clinic and at other health institutions to ensure that patients receive appropriate attention early.
NYU-Langone launched its program amid this heightened awareness that the immune system could affect atherosclerosis, “kind of reading of the tea leaves, so to speak,” Dr. Garshick said.
Several clinical trials served as a catalyst for this movement. “A lot of clinical cardiologists were never 100% convinced that targeting the immune system reduced cardiovascular disease,” he said. Then the CANTOS clinical trial came along and showed for the first time that a therapeutic monoclonal antibody targeting interleukin-1beta, a cytokine central to inflammatory response, could in fact reduce cardiovascular disease.
Trials like this, along with epidemiologic literature connecting the rheumatologic and the autoimmune conditions with cardiovascular disease, pushed this concept to the forefront, Dr. Garshick said.
The notion that a clinic could successfully address cardiac problems in patients with rheumatic diseases yielded promising returns at Women’s College Hospital in Toronto, according to a report presented at the 2018 American College of Rheumatology annual meeting. Researchers reported that patients with rheumatologic conditions who attended a cardio-rheumatology clinic at this center saw improvements in care. The clinic identified increased cardiovascular risk and early atherosclerosis, and 53.8% of patients altered their medications after being seen in the clinic.
A total of 39.7% and 32.1% received lipid lowering and antiplatelet therapies, respectively, and 14% received antihypertensive therapy. A small percentage were treated for heart failure or placed on lifelong anticoagulation therapy for atrial fibrillation, and one patient received a percutaneous coronary stent.
Ins and outs of the referral process
Initially designed for preventive cardiac risk assessment, Yale’s program evolved into a multidisciplinary, patient-centered approach for the management of complex cardiovascular conditions in patients with autoimmune rheumatologic diseases.
The program is open to anyone who carries a diagnosis of rheumatologic disease or has elevated inflammatory markers. “Every patient, regardless of the reason for the referral, receives a cardiovascular risk assessment,” Dr. Furman said.
Most referrals come from rheumatologists, although cardiology colleagues and pulmonologists have also sent referrals. A pulmonologist, for example, may want to rule out a cardiac cause to shortness of breath. The patient’s workup, care, and follow-up are based on the reason for referral.
“We are currently referring patients with established cardiac disease, traditional risk factors, or for better risk assessment for primary prevention of coronary artery disease,” Dr. Chowdhary said. “We communicate very frequently about medication changes, and patients are aware of goals of care from both sides.”
Dr. Furman works closely with several of the rheumatology specialists taking care of patients with rheumatoid arthritis, systemic lupus erythematosus, and scleroderma.
Rheumatology follows patients every 3-6 months or more frequently based on their disease activity.
Dr. Mankad uses her sleuthing skills at Mayo Clinic to determine what the patients need. If they come in for a preventive assessment, she looks more closely at their cardiovascular risks and may order additional imaging to look for subclinical atherosclerosis. “We’re more aggressive with statin therapy in this population because of that,” she said.
If it’s valve disease, she pays extra attention to the patients’ valves in the echocardiograms and follows them a bit more regularly than someone without a rheumatologic condition and valve disease.
For patients with heart failure signs or symptoms, “it depends on how symptomatic they are,” Dr. Mankad said. In some instances, she may look for evidence of heart failure with preserved ejection fraction in patients who have rheumatoid arthritis who happen to be short of breath. “There’s so many different manifestations that patients with rheumatologic conditions can have as far as what could be affected in the heart,” she noted.
Quite frequently, Dr. Mankad identifies subclinical disease in her patients with rheumatoid arthritis. “I’ve seen many patients whose risk scores would not dictate statin therapy. But I went looking for subclinical disease by either doing coronary assessment or carotid assessment and have found atherosclerosis that would be enough to warrant statin therapy.”
A personalized assessment to reduce cardiac risk
NYU-Langone’s program offers opportunities to educate patients about the link between cardiac and rheumatologic disease.
“Their rheumatologist or their dermatologist will say, ‘Hey, have you heard about the connection between psoriasis, psoriatic or rheumatoid arthritis, and heart disease and the risk of heart attack or stroke?’ ” Dr. Garshick said.
The patients will often say they know nothing about these connections and want to learn more about how to treat it.
“We’ll say, ‘we have someone here that can help you.’ They’ll send them to myself or other colleagues like me across the country. We’ll assess blood pressure, weight, lipids, hemoglobin A1c, and other serologic and oftentimes imaging biomarkers of cardiovascular risk.” The patients will receive a personalized assessment, listing things they can do to lower their risk, whether it’s diet, exercise, or lifestyle. “Many times it can involve medications to reduce heart disease risk,” said Dr. Garshick.
In some instances, a rheumatologist or dermatologist may be concerned about starting a patient on a specific medication for the disease such as a JAK inhibitor. “We’ll help assess their risk because there’s been a lot of literature out in the rheumatology world about the risk of JAK inhibitors and heart disease and blood clots,” said Dr. Garshick.
Dr. Garshick also sees patients with rheumatologic conditions who have a specific cardiovascular concern or complaint such as shortness of breath or chest pain. “We’ll work that up with a specific knowledge of the underlying immune condition and how that may impact their heart,” he said.
Advances in research
As they continue to see patients and devise specific care plans, developers of cardio-rheumatology programs have been supplementing their work with ongoing research.
Yale’s clinic is expanding this year to include a new attending physician, Attila Feher, MD, PhD, who has conducted research in autoimmunity and microcirculation using molecular imaging and multimodality imaging techniques. Prevalence of coronary microvascular dysfunction appears to be increased in this patient population, Dr. Furman said.
Dr. Wassif recently coauthored a paper that examined patients with underlying rheumatologic conditions who undergo valvular and aortic valve replacement. “To our surprise, there was really no difference between patients with autoimmune conditions and others with nonautoimmune conditions,” she said, adding that the study had its limitations.
Other work includes data on Medicare patients with ST- and non-ST-elevation myocardial infarctions who have an underlying autoimmune disorder. Dr. Wassif and her colleagues found that their long-term outcomes are worse than those of patients without these conditions. “It’s unclear if worse outcomes are related to complications of autoimmunity versus the extent of their underlying disease. This is a work in progress and certainly an area that is ripe for research.”
Dr. Garshick and other collaborators at NYU have been focusing on the endothelium, specifically platelet biology in patients with psoriasis, psoriatic arthritis, and lupus. “We’re about to start the same research with gout as well,” he said.
“The process we’re most interested in is understanding how these diseases impact the early stages of cholesterol. And the way we’re doing that is evaluating the vasculature, specifically the endothelium,” he said.
He has finished two clinical trials that evaluate how standard heart disease medications such as aspirin and statins impact or can potentially benefit patients with psoriasis and/or psoriatic arthritis. “We have a whole list of other trials in the pipeline with other institutions across the country.”
Through a grant, Dr. Mankad is assessing whether a PET scan could detect inflammation in the hearts of rheumatoid arthritis patients. “We’re looking to see if the reason these patients have heart failure later in life is because their heart muscle actually shows evidence of inflammation, even when they have no symptoms,” she explained.
Other tests such as echocardiogram and CT scans will be used to evaluate coronary disease in about 40-50 patients. The goal of using these multiple imaging tools is to find markers indicating that the heart is affected by rheumatoid arthritis, which may indicate a higher likelihood of developing heart failure, she said.
Clinics are popping up
Through these new clinics, some collaborations have emerged. Dr. Garshick works closely with Brigham and Women’s Hospital, which has a similar cardio-rheumatology program, run by Brittany Weber, MD, to exchange ideas, discuss challenging cases, and collaborate.
“There are a lot of clinics like us popping up across the country,” he observed. Every so often, he hears from other institutions that are interested in starting their own cardio-rheumatology programs. “They ask us: How do you start, what should we look for?”
It’s an education process for both patients and providers, Dr. Garshick emphasized. “I also think it’s a bandwidth issue. Many of our rheumatology and dermatology colleagues are acutely aware of the connection, but there may not be enough time at a clinic visit to really go in depth” with these dual conditions, he said.
NYU-Langone Health for the past several years has been holding a symposium to educate people on the cardio-rheumatology connection and treating inflammation in cardiovascular disease. This year’s symposium, held in conjunction with Brigham and Women’s Hospital, is scheduled for April 28. For more information, visit the course website: nyulmc.org/cvinflammationcme.
“What we’re trying to do is help [other institutions] get that bandwidth” to adequately help and serve these patients, he said.
Dr. Garshick has received consultant fees from Abbvie and Horizon therapeutics and an unrestricted research grant from Pfizer. No other sources had relevant financial disclosures.
Clinical cardiologist Heba Wassif, MD, MPH, knows the value of working with her fellow rheumatologists, surgeons, and other clinicians to establish a care plan for her patients with cardiac conditions and autoimmune diseases.
She is the cofounder of the Cleveland Clinic’s new cardio-rheumatology program, which places an emphasis on multidisciplinary care. In her role, Dr. Wassif closely follows her patients, and if she sees any inflammation or any other condition that requires the rheumatologist, she reaches out to her colleagues to adjust medications if needed.
Collaboration with a rheumatologist was important when a patient with valvular disease was prepping for surgery. The patient was on significant immunosuppressants and the surgery had to be timed appropriately, accounting for any decreases in her immunosuppression, explained Dr. Wassif, director of inpatient clinical cardiology at Cleveland Clinic in Ohio.
Cardio-rheumatology programs are “the newest child” in a series of cardiology offshoots focusing on different populations. Cardio-oncology and cardio-obstetrics took off about 6 years ago, with cardio-rheumatology clinics and interested physicians rising in number over the last several years, Dr. Wassif noted.
The relationship between cardiovascular diseases and rheumatologic conditions is certainly recognized more often, “which means more literature is being published to discuss the link,” according to Rekha Mankad, MD, a trailblazer of this model of care. She directs the Women’s Heart Clinic at Mayo Clinic in Rochester, Minn., which was one of the earliest adopters of a cardio-rheumatology clinic.
Ten years ago, “nobody was talking about the link between rheumatologic conditions and cardiovascular disease,” Dr. Mankad said. “I’ve been asked to speak on this topic, and programs have asked me to speak about establishing cardio-rheumatology practices. So, there’s been an evolution as far as a recognition that these two conditions overlap.”
Patients have come to her independent of internal referrals, which means they have done Google searches on cardiology and rheumatology. “I think that it has made a splash, at least in the world of cardiology,” Dr. Mankad observed in an interview.
Other institutions such as NYU-Langone, Yale, Stanford, Brigham and Women’s Hospital in Boston, and Women’s College Hospital in Toronto have formed similar clinics whose focus is to address the specific needs of rheumatology patients with cardiac conditions through a teamwork approach.
Challenges of treating cardiac, rheumatologic conditions
The rise in clinics addresses the longstanding connection between autoimmune disorders and cardiac conditions.
Cardiologists have known that there is an element of inflammation that contributes to atherosclerosis, said Dr. Wassif, who has researched this topic extensively. A recent study she led found a strong association between rheumatic immune-mediated inflammatory diseases (IMIDs) and high risk of acute coronary syndrome in Medicare patients.
“This particular population has a very clear increased risk for cardiovascular conditions, including valve disease and heart failure,” she emphasized.
Patients with rheumatoid arthritis and lupus have up to a twofold and eightfold higher risk of heart disease, respectively, noted Michael S. Garshick, MD, a cardiovascular disease specialist who directs the cardio-rheumatology program at NYU-Langone Health, in New York. Cardiologists “have really developed an understanding that the immune system can impact the heart, and that there’s a need for people to understand the nuance behind how the immune system can affect them and what to do about it,” Dr. Garshick said.
Caring for patients with both afflictions comes with specific challenges. Many physicians are not well trained on managing and treating patients with these dual conditions.
The “lipid paradox,” in which lipids are reduced with active inflammation in some rheumatologic conditions, can make treatment more nuanced. In addition, the traditional ASCVD (atherosclerotic cardiovascular disease) score often underestimates the cardiovascular risk of these patients, noted cardiologist Margaret Furman, MD, MPH, assistant professor and codirector of Yale’s Cardio-Rheumatology Program, New Haven, Conn.
Newer biologic medications used to treat rheumatologic diseases can alter a patient’s lipid profile, she said in an interview.
“It can be difficult to assess each individual patient’s cardiovascular risk as their disease state and treatment can vary throughout their lifetime based on their degree of inflammation. The importance of aggressive lipid management is often underestimated,” Dr. Furman added.
Cardiology and rheumatology partnerships can address gaps in care of this unique group of patients, said Vaidehi R. Chowdhary, MBBS, MD, clinical chief of the Yale Section of Rheumatology, Allergy, and Immunology at Yale University.
“The role of the rheumatologist in this dyad is to educate patients on this risk, work toward adequate control of inflammation, and minimize use of medications that contribute to increased cardiovascular risks,” said Dr. Chowdhary, who cofounded Yale’s cardio-rheumatology program with Dr. Furman.
Cardiologists in turn can assert their knowledge about medications and their impact on lipids and inflammation, Dr. Wassif said.
Many anti-inflammatory therapies are now within the cardiologist’s purview, Dr. Garshick noted. “For example, specifically with pericarditis, there’s [Food and Drug Administration]–approved anti-inflammatories or biologics. We’re the ones who feel the most comfortable giving them right now.” Cardiologists quite often are consulted about medications that are efficacious in rheumatologic conditions but could negatively impact the cardiovascular system, such as Janus kinase inhibitors, he added.
‘Reading the tea leaves’
Each program has its own unique story. For the Cleveland Clinic, the concept of a cardio-rheumatology program began during the COVID-19 pandemic in 2020. Developing such a concept and gaining institutional acceptance is always a work in process, Dr. Wassif said. “It’s not that you decide one day that you’re going to build a center, and that center is going to come into fruition overnight. You first gauge interest within your division. Who are the individuals that are interested in this area?”
Cleveland Clinic’s center is seeking to build relations between medical disciplines while spotlighting the concept of cardio-rheumatology, said Dr. Wassif, who has been providing education within the clinic and at other health institutions to ensure that patients receive appropriate attention early.
NYU-Langone launched its program amid this heightened awareness that the immune system could affect atherosclerosis, “kind of reading of the tea leaves, so to speak,” Dr. Garshick said.
Several clinical trials served as a catalyst for this movement. “A lot of clinical cardiologists were never 100% convinced that targeting the immune system reduced cardiovascular disease,” he said. Then the CANTOS clinical trial came along and showed for the first time that a therapeutic monoclonal antibody targeting interleukin-1beta, a cytokine central to inflammatory response, could in fact reduce cardiovascular disease.
Trials like this, along with epidemiologic literature connecting the rheumatologic and the autoimmune conditions with cardiovascular disease, pushed this concept to the forefront, Dr. Garshick said.
The notion that a clinic could successfully address cardiac problems in patients with rheumatic diseases yielded promising returns at Women’s College Hospital in Toronto, according to a report presented at the 2018 American College of Rheumatology annual meeting. Researchers reported that patients with rheumatologic conditions who attended a cardio-rheumatology clinic at this center saw improvements in care. The clinic identified increased cardiovascular risk and early atherosclerosis, and 53.8% of patients altered their medications after being seen in the clinic.
A total of 39.7% and 32.1% received lipid lowering and antiplatelet therapies, respectively, and 14% received antihypertensive therapy. A small percentage were treated for heart failure or placed on lifelong anticoagulation therapy for atrial fibrillation, and one patient received a percutaneous coronary stent.
Ins and outs of the referral process
Initially designed for preventive cardiac risk assessment, Yale’s program evolved into a multidisciplinary, patient-centered approach for the management of complex cardiovascular conditions in patients with autoimmune rheumatologic diseases.
The program is open to anyone who carries a diagnosis of rheumatologic disease or has elevated inflammatory markers. “Every patient, regardless of the reason for the referral, receives a cardiovascular risk assessment,” Dr. Furman said.
Most referrals come from rheumatologists, although cardiology colleagues and pulmonologists have also sent referrals. A pulmonologist, for example, may want to rule out a cardiac cause to shortness of breath. The patient’s workup, care, and follow-up are based on the reason for referral.
“We are currently referring patients with established cardiac disease, traditional risk factors, or for better risk assessment for primary prevention of coronary artery disease,” Dr. Chowdhary said. “We communicate very frequently about medication changes, and patients are aware of goals of care from both sides.”
Dr. Furman works closely with several of the rheumatology specialists taking care of patients with rheumatoid arthritis, systemic lupus erythematosus, and scleroderma.
Rheumatology follows patients every 3-6 months or more frequently based on their disease activity.
Dr. Mankad uses her sleuthing skills at Mayo Clinic to determine what the patients need. If they come in for a preventive assessment, she looks more closely at their cardiovascular risks and may order additional imaging to look for subclinical atherosclerosis. “We’re more aggressive with statin therapy in this population because of that,” she said.
If it’s valve disease, she pays extra attention to the patients’ valves in the echocardiograms and follows them a bit more regularly than someone without a rheumatologic condition and valve disease.
For patients with heart failure signs or symptoms, “it depends on how symptomatic they are,” Dr. Mankad said. In some instances, she may look for evidence of heart failure with preserved ejection fraction in patients who have rheumatoid arthritis who happen to be short of breath. “There’s so many different manifestations that patients with rheumatologic conditions can have as far as what could be affected in the heart,” she noted.
Quite frequently, Dr. Mankad identifies subclinical disease in her patients with rheumatoid arthritis. “I’ve seen many patients whose risk scores would not dictate statin therapy. But I went looking for subclinical disease by either doing coronary assessment or carotid assessment and have found atherosclerosis that would be enough to warrant statin therapy.”
A personalized assessment to reduce cardiac risk
NYU-Langone’s program offers opportunities to educate patients about the link between cardiac and rheumatologic disease.
“Their rheumatologist or their dermatologist will say, ‘Hey, have you heard about the connection between psoriasis, psoriatic or rheumatoid arthritis, and heart disease and the risk of heart attack or stroke?’ ” Dr. Garshick said.
The patients will often say they know nothing about these connections and want to learn more about how to treat it.
“We’ll say, ‘we have someone here that can help you.’ They’ll send them to myself or other colleagues like me across the country. We’ll assess blood pressure, weight, lipids, hemoglobin A1c, and other serologic and oftentimes imaging biomarkers of cardiovascular risk.” The patients will receive a personalized assessment, listing things they can do to lower their risk, whether it’s diet, exercise, or lifestyle. “Many times it can involve medications to reduce heart disease risk,” said Dr. Garshick.
In some instances, a rheumatologist or dermatologist may be concerned about starting a patient on a specific medication for the disease such as a JAK inhibitor. “We’ll help assess their risk because there’s been a lot of literature out in the rheumatology world about the risk of JAK inhibitors and heart disease and blood clots,” said Dr. Garshick.
Dr. Garshick also sees patients with rheumatologic conditions who have a specific cardiovascular concern or complaint such as shortness of breath or chest pain. “We’ll work that up with a specific knowledge of the underlying immune condition and how that may impact their heart,” he said.
Advances in research
As they continue to see patients and devise specific care plans, developers of cardio-rheumatology programs have been supplementing their work with ongoing research.
Yale’s clinic is expanding this year to include a new attending physician, Attila Feher, MD, PhD, who has conducted research in autoimmunity and microcirculation using molecular imaging and multimodality imaging techniques. Prevalence of coronary microvascular dysfunction appears to be increased in this patient population, Dr. Furman said.
Dr. Wassif recently coauthored a paper that examined patients with underlying rheumatologic conditions who undergo valvular and aortic valve replacement. “To our surprise, there was really no difference between patients with autoimmune conditions and others with nonautoimmune conditions,” she said, adding that the study had its limitations.
Other work includes data on Medicare patients with ST- and non-ST-elevation myocardial infarctions who have an underlying autoimmune disorder. Dr. Wassif and her colleagues found that their long-term outcomes are worse than those of patients without these conditions. “It’s unclear if worse outcomes are related to complications of autoimmunity versus the extent of their underlying disease. This is a work in progress and certainly an area that is ripe for research.”
Dr. Garshick and other collaborators at NYU have been focusing on the endothelium, specifically platelet biology in patients with psoriasis, psoriatic arthritis, and lupus. “We’re about to start the same research with gout as well,” he said.
“The process we’re most interested in is understanding how these diseases impact the early stages of cholesterol. And the way we’re doing that is evaluating the vasculature, specifically the endothelium,” he said.
He has finished two clinical trials that evaluate how standard heart disease medications such as aspirin and statins impact or can potentially benefit patients with psoriasis and/or psoriatic arthritis. “We have a whole list of other trials in the pipeline with other institutions across the country.”
Through a grant, Dr. Mankad is assessing whether a PET scan could detect inflammation in the hearts of rheumatoid arthritis patients. “We’re looking to see if the reason these patients have heart failure later in life is because their heart muscle actually shows evidence of inflammation, even when they have no symptoms,” she explained.
Other tests such as echocardiogram and CT scans will be used to evaluate coronary disease in about 40-50 patients. The goal of using these multiple imaging tools is to find markers indicating that the heart is affected by rheumatoid arthritis, which may indicate a higher likelihood of developing heart failure, she said.
Clinics are popping up
Through these new clinics, some collaborations have emerged. Dr. Garshick works closely with Brigham and Women’s Hospital, which has a similar cardio-rheumatology program, run by Brittany Weber, MD, to exchange ideas, discuss challenging cases, and collaborate.
“There are a lot of clinics like us popping up across the country,” he observed. Every so often, he hears from other institutions that are interested in starting their own cardio-rheumatology programs. “They ask us: How do you start, what should we look for?”
It’s an education process for both patients and providers, Dr. Garshick emphasized. “I also think it’s a bandwidth issue. Many of our rheumatology and dermatology colleagues are acutely aware of the connection, but there may not be enough time at a clinic visit to really go in depth” with these dual conditions, he said.
NYU-Langone Health for the past several years has been holding a symposium to educate people on the cardio-rheumatology connection and treating inflammation in cardiovascular disease. This year’s symposium, held in conjunction with Brigham and Women’s Hospital, is scheduled for April 28. For more information, visit the course website: nyulmc.org/cvinflammationcme.
“What we’re trying to do is help [other institutions] get that bandwidth” to adequately help and serve these patients, he said.
Dr. Garshick has received consultant fees from Abbvie and Horizon therapeutics and an unrestricted research grant from Pfizer. No other sources had relevant financial disclosures.
Long-pulsed 1,064 nm Nd:YAG for nonaggressive BCC ‘effective and easy’
SAN DIEGO – After Arisa E. Ortiz, MD, and colleagues published results of a multicenter study reporting that one treatment with the long-pulsed 1,064-nm Nd:YAG laser cleared nonaggressive basal cell carcinoma (BCC) on the trunk and extremities in 90% of patients, she heard from colleagues who were skeptical of the approach.
Maybe it’s just the biopsy alone that’s clearing these tumors, some told her. Others postulated that since the energy was delivered with a 5- to 6-mm spot size at a fluence of 125-140 J/cm2 and a 7- to 10-ms pulse duration, bulk heating likely disrupted the tumors. However, treatments were generally well tolerated, required no anesthesia, and caused no significant adverse events.
“It’s almost scarless,” Dr. Ortiz, director of laser and cosmetic dermatology at the University of California, San Diego, said at the annual Masters of Aesthetics Symposium. “Sometimes the treatment does leave a mark, but I think the scars are always acceptable. We do have good histologic evidence that we can penetrate 2.15 mm, which is a lot deeper than what the pulsed-dye laser or other superficial wavelengths are able to penetrate.”
Data is well powered to reject the null hypothesis that laser treatment does not have an effect on nodular and superficial BCC lesions, she continued, noting that it is at least comparable if not superior with clearance rates reported for methyl aminolevulinate–PDT (73%), imiquimod cream (83%), and fluorouracil cream (80%). “Maybe we’re not specifically targeting the vasculature [with this approach], but we did some optical coherence tomography imaging and saw that the blood vessels in the tumor were coagulated while the vasculature in the surrounding normal skin were spared,” said Dr. Ortiz, who is also vice president of the American Society for Laser Medicine and Surgery.
In a more recent analysis, she and her colleagues retrospectively analyzed long-term outcomes in 11 patients with BCC who had 16 lesions treated with the 1,064-nm Nd:YAG laser. At a mean of 9 months, 100% of lesions remained clear as determined by clinical observation.
In a subsequent, as yet unpublished study, she and her collaborators followed 34 patients with BCC one year following laser treatment. “Of these, 33 had no recurrence at 1-year follow-up,” Dr. Ortiz said, noting that the one patient with a recurrence was on a biologic agent for Crohn’s disease.
One key advantage of using the long-pulsed 1,064-nm Nd:YAG laser for nonaggressive BCC is the potential for one treatment visit. “They don’t have to come back for suture removal,” she said. “It’s a quick procedure, takes only about 5 minutes. There’s no limitation on activity and there’s minimal wound care, light ointment, and a band-aid; that’s it.”
In addition, she said, there is a lower risk of complications, infections, and bleeding, and there is minimal scarring. It is “also an alternative for treating patients with multiple tumors or those who are poor surgical candidates, such as the elderly and those with Gorlin syndrome.”
Dr. Ortiz avoids treating aggressive subtypes “because we don’t know what margin to treat,” she added. “Avoid the face. I do make some exceptions for patients if they’re elderly or if they’ve had multiple tumors. Monitor for recurrence like you would using any other modality.”
She uses lidocaine without epinephrine to avoid vasoconstriction and treats with the 1,064-nm Nd:YAG laser as follows: a 5-mm spot size, a fluence of 140 J/cm2, and a pulse duration of 8 ms, with no cooling, which are the settings for the Excel V Laser System, she noted. “If you’re using a different Nd:YAG laser, your pulse duration may vary. I do let the device cool in between pulses to avoid bulk heating.”
The immediate endpoint to strive for is slight greying and slight contraction, and the procedure is covered by insurance, billed as malignant destruction/EDC (CPT codes 17260-17266 trunk and 17280-17283 face). “I do biopsy prior to treatment,” she said. “I like the biopsy to be healed when I’m using the laser, so I’ll treat them about a month later.”
As for future directions, Dr. Ortiz and colleagues plan to evaluate the use of gold nanoparticles to more selectively target BCC during treatment with the 1,064-nm Nd:YAG laser. For now, she sees no downside of the procedure for proper candidates. “I do think that patients really like it,” she said. “It’s effective and easy.”
Dr. Ortiz disclosed having financial relationships with several pharmaceutical and device companies. She is also cochair of the MOAS.
SAN DIEGO – After Arisa E. Ortiz, MD, and colleagues published results of a multicenter study reporting that one treatment with the long-pulsed 1,064-nm Nd:YAG laser cleared nonaggressive basal cell carcinoma (BCC) on the trunk and extremities in 90% of patients, she heard from colleagues who were skeptical of the approach.
Maybe it’s just the biopsy alone that’s clearing these tumors, some told her. Others postulated that since the energy was delivered with a 5- to 6-mm spot size at a fluence of 125-140 J/cm2 and a 7- to 10-ms pulse duration, bulk heating likely disrupted the tumors. However, treatments were generally well tolerated, required no anesthesia, and caused no significant adverse events.
“It’s almost scarless,” Dr. Ortiz, director of laser and cosmetic dermatology at the University of California, San Diego, said at the annual Masters of Aesthetics Symposium. “Sometimes the treatment does leave a mark, but I think the scars are always acceptable. We do have good histologic evidence that we can penetrate 2.15 mm, which is a lot deeper than what the pulsed-dye laser or other superficial wavelengths are able to penetrate.”
Data is well powered to reject the null hypothesis that laser treatment does not have an effect on nodular and superficial BCC lesions, she continued, noting that it is at least comparable if not superior with clearance rates reported for methyl aminolevulinate–PDT (73%), imiquimod cream (83%), and fluorouracil cream (80%). “Maybe we’re not specifically targeting the vasculature [with this approach], but we did some optical coherence tomography imaging and saw that the blood vessels in the tumor were coagulated while the vasculature in the surrounding normal skin were spared,” said Dr. Ortiz, who is also vice president of the American Society for Laser Medicine and Surgery.
In a more recent analysis, she and her colleagues retrospectively analyzed long-term outcomes in 11 patients with BCC who had 16 lesions treated with the 1,064-nm Nd:YAG laser. At a mean of 9 months, 100% of lesions remained clear as determined by clinical observation.
In a subsequent, as yet unpublished study, she and her collaborators followed 34 patients with BCC one year following laser treatment. “Of these, 33 had no recurrence at 1-year follow-up,” Dr. Ortiz said, noting that the one patient with a recurrence was on a biologic agent for Crohn’s disease.
One key advantage of using the long-pulsed 1,064-nm Nd:YAG laser for nonaggressive BCC is the potential for one treatment visit. “They don’t have to come back for suture removal,” she said. “It’s a quick procedure, takes only about 5 minutes. There’s no limitation on activity and there’s minimal wound care, light ointment, and a band-aid; that’s it.”
In addition, she said, there is a lower risk of complications, infections, and bleeding, and there is minimal scarring. It is “also an alternative for treating patients with multiple tumors or those who are poor surgical candidates, such as the elderly and those with Gorlin syndrome.”
Dr. Ortiz avoids treating aggressive subtypes “because we don’t know what margin to treat,” she added. “Avoid the face. I do make some exceptions for patients if they’re elderly or if they’ve had multiple tumors. Monitor for recurrence like you would using any other modality.”
She uses lidocaine without epinephrine to avoid vasoconstriction and treats with the 1,064-nm Nd:YAG laser as follows: a 5-mm spot size, a fluence of 140 J/cm2, and a pulse duration of 8 ms, with no cooling, which are the settings for the Excel V Laser System, she noted. “If you’re using a different Nd:YAG laser, your pulse duration may vary. I do let the device cool in between pulses to avoid bulk heating.”
The immediate endpoint to strive for is slight greying and slight contraction, and the procedure is covered by insurance, billed as malignant destruction/EDC (CPT codes 17260-17266 trunk and 17280-17283 face). “I do biopsy prior to treatment,” she said. “I like the biopsy to be healed when I’m using the laser, so I’ll treat them about a month later.”
As for future directions, Dr. Ortiz and colleagues plan to evaluate the use of gold nanoparticles to more selectively target BCC during treatment with the 1,064-nm Nd:YAG laser. For now, she sees no downside of the procedure for proper candidates. “I do think that patients really like it,” she said. “It’s effective and easy.”
Dr. Ortiz disclosed having financial relationships with several pharmaceutical and device companies. She is also cochair of the MOAS.
SAN DIEGO – After Arisa E. Ortiz, MD, and colleagues published results of a multicenter study reporting that one treatment with the long-pulsed 1,064-nm Nd:YAG laser cleared nonaggressive basal cell carcinoma (BCC) on the trunk and extremities in 90% of patients, she heard from colleagues who were skeptical of the approach.
Maybe it’s just the biopsy alone that’s clearing these tumors, some told her. Others postulated that since the energy was delivered with a 5- to 6-mm spot size at a fluence of 125-140 J/cm2 and a 7- to 10-ms pulse duration, bulk heating likely disrupted the tumors. However, treatments were generally well tolerated, required no anesthesia, and caused no significant adverse events.
“It’s almost scarless,” Dr. Ortiz, director of laser and cosmetic dermatology at the University of California, San Diego, said at the annual Masters of Aesthetics Symposium. “Sometimes the treatment does leave a mark, but I think the scars are always acceptable. We do have good histologic evidence that we can penetrate 2.15 mm, which is a lot deeper than what the pulsed-dye laser or other superficial wavelengths are able to penetrate.”
Data is well powered to reject the null hypothesis that laser treatment does not have an effect on nodular and superficial BCC lesions, she continued, noting that it is at least comparable if not superior with clearance rates reported for methyl aminolevulinate–PDT (73%), imiquimod cream (83%), and fluorouracil cream (80%). “Maybe we’re not specifically targeting the vasculature [with this approach], but we did some optical coherence tomography imaging and saw that the blood vessels in the tumor were coagulated while the vasculature in the surrounding normal skin were spared,” said Dr. Ortiz, who is also vice president of the American Society for Laser Medicine and Surgery.
In a more recent analysis, she and her colleagues retrospectively analyzed long-term outcomes in 11 patients with BCC who had 16 lesions treated with the 1,064-nm Nd:YAG laser. At a mean of 9 months, 100% of lesions remained clear as determined by clinical observation.
In a subsequent, as yet unpublished study, she and her collaborators followed 34 patients with BCC one year following laser treatment. “Of these, 33 had no recurrence at 1-year follow-up,” Dr. Ortiz said, noting that the one patient with a recurrence was on a biologic agent for Crohn’s disease.
One key advantage of using the long-pulsed 1,064-nm Nd:YAG laser for nonaggressive BCC is the potential for one treatment visit. “They don’t have to come back for suture removal,” she said. “It’s a quick procedure, takes only about 5 minutes. There’s no limitation on activity and there’s minimal wound care, light ointment, and a band-aid; that’s it.”
In addition, she said, there is a lower risk of complications, infections, and bleeding, and there is minimal scarring. It is “also an alternative for treating patients with multiple tumors or those who are poor surgical candidates, such as the elderly and those with Gorlin syndrome.”
Dr. Ortiz avoids treating aggressive subtypes “because we don’t know what margin to treat,” she added. “Avoid the face. I do make some exceptions for patients if they’re elderly or if they’ve had multiple tumors. Monitor for recurrence like you would using any other modality.”
She uses lidocaine without epinephrine to avoid vasoconstriction and treats with the 1,064-nm Nd:YAG laser as follows: a 5-mm spot size, a fluence of 140 J/cm2, and a pulse duration of 8 ms, with no cooling, which are the settings for the Excel V Laser System, she noted. “If you’re using a different Nd:YAG laser, your pulse duration may vary. I do let the device cool in between pulses to avoid bulk heating.”
The immediate endpoint to strive for is slight greying and slight contraction, and the procedure is covered by insurance, billed as malignant destruction/EDC (CPT codes 17260-17266 trunk and 17280-17283 face). “I do biopsy prior to treatment,” she said. “I like the biopsy to be healed when I’m using the laser, so I’ll treat them about a month later.”
As for future directions, Dr. Ortiz and colleagues plan to evaluate the use of gold nanoparticles to more selectively target BCC during treatment with the 1,064-nm Nd:YAG laser. For now, she sees no downside of the procedure for proper candidates. “I do think that patients really like it,” she said. “It’s effective and easy.”
Dr. Ortiz disclosed having financial relationships with several pharmaceutical and device companies. She is also cochair of the MOAS.
AT MOAS 2022
Mpox: Dermatology registry data pinpoints unique signs
that frequently appeared before systemic illness and a much lower overall numbers of lesions.
“Just these two findings alone show how important it is to remain clinically vigilant as dermatologists,” Esther Freeman, MD, PhD, director of global health dermatology at Massachusetts General Hospital, Boston, said in an interview. She is the corresponding author of the study, which analyzed 101 mpox cases from 13 countries and was published online on in the Journal of the American Academy of Dermatology.
“Mpox appeared to manifest differently than in previous outbreaks with morphologic and clinical evolutions much different than previously reported in endemic and prior outbreaks,” added Dr. Freeman. “Dermatologists should continue to keep mpox on the differential as it continues to circulate at low levels in the population and is a mimicker of many other common skin diseases.”
According to the Centers for Disease Control and Prevention, as of Jan. 20, 2023, there have been 30,061 cases of mpox in the United States during the outbreak that began in 2022; 23 people died. Worldwide, the number of cases neared 85,000.

Most of the affected cases were among gay, bisexual, and other men who have sex with men. A vaccination effort began last summer, and the number of cases soon plummeted. The national daily case count in January has been in the single digits.
For the new report, dermatologists tracked cases via the American Academy of Dermatology/International League of Dermatologic Societies (AAD/ILDS) Dermatology COVID-19, Monkeypox (mpox), and Emerging Infections Registry. The new report includes data about cases entered from Aug. 4 to Nov. 13. Of these cases, 97% were male, median age was 35 years, 62% were White, 20% were Hispanic, and 11% were Black.
Just over half (54%) of patients reported skin lesions as the first sign of disease, while others had signs such as fever (16%) and malaise (9%). “This is a sharp contrast to endemic or prior outbreaks in which a ‘flu-like’ prodrome preceded lesions,” Dr. Freeman said. “Dermatologists should be aware that patients may come in with mpox skin lesions as their only initial symptoms.”
In contrast to past outbreaks where patients may have had dozens or hundreds of lesions, 20% had only 1 lesion, while 52% had 2-5 lesions, and 20% had 6-20 lesions. “There may be only a few lesions, so index of suspicion needs to be high,” Dr. Freeman said.
According to the study, “the most common skin lesion morphologies and secondary characteristics reported included papules, vesicles/blisters, pustules, erosions/ulcers and crust/scabs.” Dr. Freeman cautioned that “lesions may not go through the ‘typical’ progression from papule to pustule. The initial lesion could even be an ulceration or a crust. For dermatologists, this means you need to have a high index of suspicion, especially if you see a new onset lesion in the groin or perianal area, though they can also start elsewhere.”
She added that “the lesion you see on exam could be a classic pustule/pseudopustule, but it might not be – it could be a small perianal erosion or ulceration. If you have any concern it could be mpox, it’s a good idea to test by PCR.”
Morbilliform rash, scarring reported
The study also highlighted 10 cases of morbilliform rash. “A morbilliform exanthem is pretty nonspecific, and usually cases of mpox have more specific features,” dermatologist and study coauthor Misha Rosenbach, MD, of the University of Pennsylvania, Philadelphia, said in an interview.

“Given the current low rates of mpox, I do not think most dermatologists need to worry about mpox when evaluating morbilliform exanthems. However, in high-risk patients or patients with other morphologies, it is worth noting that there’s a chance that this may be related.”
Emory University dermatologist Howa Yeung, MD, MSc, who wasn’t involved with the study, said in an interview that morbilliform rashes in the mouth/tongue area, mostly on days 1-5, should be considered a possible sign of mpox. “While I didn’t typically think of monkeypox virus as a cause of viral exanthems, I will now add it to my differential diagnoses.”

In the report, 13% of patients had scarring, “an outcome underemphasized in the current literature” that could have long-term emotional and mental effects, the authors noted. “Some patients, particularly immunosuppressed patients, have had very large and/or ulceronecrotic lesions,” Dr. Rosenbach said. “Their scarring can be quite significant. There is, to date, very little guidance for clinicians or patients on how to mitigate this risk and, if scarring is developing, how best to manage it.”
As for lessons from the findings, Dr. Yeung said, “dermatologists need to be aware that patients with mpox can have multiple morphologies at the same time and lesions can skip stages.” And, he pointed out, it’s clear that wound care is important to prevent scarring.
The AAD has a resource page on skin care in patients with mpox that includes information about preventing scarring. Examples of mpox rashes are available on the CDC website.
The study was supported by a grant from the International League of Dermatologic Societies and in-kind support from the American Academy of Dermatology. Dr. Freeman is a coauthor for UpToDate. Dr. Freeman and Dr. Rosenbach are members of the AAD Ad Hoc Task Force to Create Monkeypox Content. Study authors reported no other disclosures, and Dr. Yeung has no disclosures.
that frequently appeared before systemic illness and a much lower overall numbers of lesions.
“Just these two findings alone show how important it is to remain clinically vigilant as dermatologists,” Esther Freeman, MD, PhD, director of global health dermatology at Massachusetts General Hospital, Boston, said in an interview. She is the corresponding author of the study, which analyzed 101 mpox cases from 13 countries and was published online on in the Journal of the American Academy of Dermatology.
“Mpox appeared to manifest differently than in previous outbreaks with morphologic and clinical evolutions much different than previously reported in endemic and prior outbreaks,” added Dr. Freeman. “Dermatologists should continue to keep mpox on the differential as it continues to circulate at low levels in the population and is a mimicker of many other common skin diseases.”
According to the Centers for Disease Control and Prevention, as of Jan. 20, 2023, there have been 30,061 cases of mpox in the United States during the outbreak that began in 2022; 23 people died. Worldwide, the number of cases neared 85,000.
Most of the affected cases were among gay, bisexual, and other men who have sex with men. A vaccination effort began last summer, and the number of cases soon plummeted. The national daily case count in January has been in the single digits.
For the new report, dermatologists tracked cases via the American Academy of Dermatology/International League of Dermatologic Societies (AAD/ILDS) Dermatology COVID-19, Monkeypox (mpox), and Emerging Infections Registry. The new report includes data about cases entered from Aug. 4 to Nov. 13. Of these cases, 97% were male, median age was 35 years, 62% were White, 20% were Hispanic, and 11% were Black.
Just over half (54%) of patients reported skin lesions as the first sign of disease, while others had signs such as fever (16%) and malaise (9%). “This is a sharp contrast to endemic or prior outbreaks in which a ‘flu-like’ prodrome preceded lesions,” Dr. Freeman said. “Dermatologists should be aware that patients may come in with mpox skin lesions as their only initial symptoms.”
In contrast to past outbreaks where patients may have had dozens or hundreds of lesions, 20% had only 1 lesion, while 52% had 2-5 lesions, and 20% had 6-20 lesions. “There may be only a few lesions, so index of suspicion needs to be high,” Dr. Freeman said.
According to the study, “the most common skin lesion morphologies and secondary characteristics reported included papules, vesicles/blisters, pustules, erosions/ulcers and crust/scabs.” Dr. Freeman cautioned that “lesions may not go through the ‘typical’ progression from papule to pustule. The initial lesion could even be an ulceration or a crust. For dermatologists, this means you need to have a high index of suspicion, especially if you see a new onset lesion in the groin or perianal area, though they can also start elsewhere.”
She added that “the lesion you see on exam could be a classic pustule/pseudopustule, but it might not be – it could be a small perianal erosion or ulceration. If you have any concern it could be mpox, it’s a good idea to test by PCR.”
Morbilliform rash, scarring reported
The study also highlighted 10 cases of morbilliform rash. “A morbilliform exanthem is pretty nonspecific, and usually cases of mpox have more specific features,” dermatologist and study coauthor Misha Rosenbach, MD, of the University of Pennsylvania, Philadelphia, said in an interview.
“Given the current low rates of mpox, I do not think most dermatologists need to worry about mpox when evaluating morbilliform exanthems. However, in high-risk patients or patients with other morphologies, it is worth noting that there’s a chance that this may be related.”
Emory University dermatologist Howa Yeung, MD, MSc, who wasn’t involved with the study, said in an interview that morbilliform rashes in the mouth/tongue area, mostly on days 1-5, should be considered a possible sign of mpox. “While I didn’t typically think of monkeypox virus as a cause of viral exanthems, I will now add it to my differential diagnoses.”
In the report, 13% of patients had scarring, “an outcome underemphasized in the current literature” that could have long-term emotional and mental effects, the authors noted. “Some patients, particularly immunosuppressed patients, have had very large and/or ulceronecrotic lesions,” Dr. Rosenbach said. “Their scarring can be quite significant. There is, to date, very little guidance for clinicians or patients on how to mitigate this risk and, if scarring is developing, how best to manage it.”
As for lessons from the findings, Dr. Yeung said, “dermatologists need to be aware that patients with mpox can have multiple morphologies at the same time and lesions can skip stages.” And, he pointed out, it’s clear that wound care is important to prevent scarring.
The AAD has a resource page on skin care in patients with mpox that includes information about preventing scarring. Examples of mpox rashes are available on the CDC website.
The study was supported by a grant from the International League of Dermatologic Societies and in-kind support from the American Academy of Dermatology. Dr. Freeman is a coauthor for UpToDate. Dr. Freeman and Dr. Rosenbach are members of the AAD Ad Hoc Task Force to Create Monkeypox Content. Study authors reported no other disclosures, and Dr. Yeung has no disclosures.
that frequently appeared before systemic illness and a much lower overall numbers of lesions.
“Just these two findings alone show how important it is to remain clinically vigilant as dermatologists,” Esther Freeman, MD, PhD, director of global health dermatology at Massachusetts General Hospital, Boston, said in an interview. She is the corresponding author of the study, which analyzed 101 mpox cases from 13 countries and was published online on in the Journal of the American Academy of Dermatology.
“Mpox appeared to manifest differently than in previous outbreaks with morphologic and clinical evolutions much different than previously reported in endemic and prior outbreaks,” added Dr. Freeman. “Dermatologists should continue to keep mpox on the differential as it continues to circulate at low levels in the population and is a mimicker of many other common skin diseases.”
According to the Centers for Disease Control and Prevention, as of Jan. 20, 2023, there have been 30,061 cases of mpox in the United States during the outbreak that began in 2022; 23 people died. Worldwide, the number of cases neared 85,000.
Most of the affected cases were among gay, bisexual, and other men who have sex with men. A vaccination effort began last summer, and the number of cases soon plummeted. The national daily case count in January has been in the single digits.
For the new report, dermatologists tracked cases via the American Academy of Dermatology/International League of Dermatologic Societies (AAD/ILDS) Dermatology COVID-19, Monkeypox (mpox), and Emerging Infections Registry. The new report includes data about cases entered from Aug. 4 to Nov. 13. Of these cases, 97% were male, median age was 35 years, 62% were White, 20% were Hispanic, and 11% were Black.
Just over half (54%) of patients reported skin lesions as the first sign of disease, while others had signs such as fever (16%) and malaise (9%). “This is a sharp contrast to endemic or prior outbreaks in which a ‘flu-like’ prodrome preceded lesions,” Dr. Freeman said. “Dermatologists should be aware that patients may come in with mpox skin lesions as their only initial symptoms.”
In contrast to past outbreaks where patients may have had dozens or hundreds of lesions, 20% had only 1 lesion, while 52% had 2-5 lesions, and 20% had 6-20 lesions. “There may be only a few lesions, so index of suspicion needs to be high,” Dr. Freeman said.
According to the study, “the most common skin lesion morphologies and secondary characteristics reported included papules, vesicles/blisters, pustules, erosions/ulcers and crust/scabs.” Dr. Freeman cautioned that “lesions may not go through the ‘typical’ progression from papule to pustule. The initial lesion could even be an ulceration or a crust. For dermatologists, this means you need to have a high index of suspicion, especially if you see a new onset lesion in the groin or perianal area, though they can also start elsewhere.”
She added that “the lesion you see on exam could be a classic pustule/pseudopustule, but it might not be – it could be a small perianal erosion or ulceration. If you have any concern it could be mpox, it’s a good idea to test by PCR.”
Morbilliform rash, scarring reported
The study also highlighted 10 cases of morbilliform rash. “A morbilliform exanthem is pretty nonspecific, and usually cases of mpox have more specific features,” dermatologist and study coauthor Misha Rosenbach, MD, of the University of Pennsylvania, Philadelphia, said in an interview.
“Given the current low rates of mpox, I do not think most dermatologists need to worry about mpox when evaluating morbilliform exanthems. However, in high-risk patients or patients with other morphologies, it is worth noting that there’s a chance that this may be related.”
Emory University dermatologist Howa Yeung, MD, MSc, who wasn’t involved with the study, said in an interview that morbilliform rashes in the mouth/tongue area, mostly on days 1-5, should be considered a possible sign of mpox. “While I didn’t typically think of monkeypox virus as a cause of viral exanthems, I will now add it to my differential diagnoses.”
In the report, 13% of patients had scarring, “an outcome underemphasized in the current literature” that could have long-term emotional and mental effects, the authors noted. “Some patients, particularly immunosuppressed patients, have had very large and/or ulceronecrotic lesions,” Dr. Rosenbach said. “Their scarring can be quite significant. There is, to date, very little guidance for clinicians or patients on how to mitigate this risk and, if scarring is developing, how best to manage it.”
As for lessons from the findings, Dr. Yeung said, “dermatologists need to be aware that patients with mpox can have multiple morphologies at the same time and lesions can skip stages.” And, he pointed out, it’s clear that wound care is important to prevent scarring.
The AAD has a resource page on skin care in patients with mpox that includes information about preventing scarring. Examples of mpox rashes are available on the CDC website.
The study was supported by a grant from the International League of Dermatologic Societies and in-kind support from the American Academy of Dermatology. Dr. Freeman is a coauthor for UpToDate. Dr. Freeman and Dr. Rosenbach are members of the AAD Ad Hoc Task Force to Create Monkeypox Content. Study authors reported no other disclosures, and Dr. Yeung has no disclosures.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
One Expert’s Approach in Transplant-Ineligible, Newly Diagnosed Multiple Myeloma

1. The treatment of multiple myeloma has evolved significantly in recent years. What are some of the most important things you consider in the treatment of your newly diagnosed, transplant-ineligible patients?
We’ve seen great progress in the treatment of multiple myeloma over the last decade, and outcomes continue to improve for many patients.1 Still, it is important to keep in mind that more than 34,000 patients will be diagnosed and more than 12,000 people will die from the disease this year.2 We may have the greatest opportunity to impact the course of disease in the treatment of newly diagnosed patients due to the nature of this cancer:
- Multiple myeloma is characterized by relapse, and we know the length of remission generally decreases with each relapse and subsequent line of therapy.3
- Patients often become refractory to treatment over time.
When I meet with a patient who has been diagnosed with multiple myeloma, the first thing I consider is their eligibility for autologous stem cell transplant (ASCT). In my opinion, the introduction of ASCT is one of the biggest advancements in the last few decades, and we’ve found that ASCT followed by maintenance therapy with targeted tools improves progression-free survival (PFS).4
Unfortunately, many newly diagnosed patients are not eligible for ASCT–either because of comorbidities or other complexities related to the presentation of their disease.
For patients who are transplant-ineligible (TIE), it is important to have treatment options that are proven effective in extending PFS and overall survival (OS), and capable of producing deep and durable responses.
2. What are the challenges associated with treating newly diagnosed patients who are not eligible for ASCT?
We still consider multiple myeloma to be an incurable disease but, in my opinion, the treatment of TIE patients is less challenging today than a decade ago due to the emergence of novel therapies. That said, TIE patients are typically older and present with more advanced disease and comorbidities, including diabetes or cardiovascular events.5
A retrospective analysis published in 2020 by Rafael Fonseca examined frontline treatment patterns and attrition rates by line of therapy among newly diagnosed multiple myeloma (NDMM) patients who are TIE. More than 22,000 patients were identified from three patient-level databases between 2000 and 2018 - the OPTUM Commercial Claims database, the OPTUM Electronic Medical Records database, and the Surveillance, Epidemiology, and End Results-Meidcare Linked database. Patients included had to have a multiple myeloma diagnosis on or after January 1, 2007. Results showed that attrition rates among newly diagnosed, TIE patients with multiple myeloma increase with each line of therapy, with the proportion of patients who receive a second line of therapy decreasing by 50 percent with each subsequent line.3
3. Can you provide more detail on the goals of therapy for newly diagnosed, transplant-ineligible patients?
When I discuss treatment goals with TIE patients, I feel it is important to emphasize managing side effects and achieving deep and durable responses. I have the benefit of being in an academic setting, where I regularly exchange information with my colleagues about what we’re learning from the clinical studies in which we participate. Choosing which treatment to administer is complex and involves other considerations. For example, if two regimens have comparable efficacy, I may recommend the regimen with a more established safety profile or more robust evidence so I can properly anticipate and manage toxicities in my patients. Overall survival is one of the most important endpoints I consider, in addition to depth of response and PFS. In recent years, we’ve seen increasing evidence pointing to the importance of using a proven effective treatment in frontline patients that are ineligible for transplant.
4. A key study in newly-diagnosed, transplant-ineligible multiple myeloma is the Phase 3 MAIA study. Can you share the key takeaways from this study and discuss how the results have shaped treatment for this patient population?
Of course. The MAIA study is a randomized Phase 3 study evaluating DARZALEX® (daratumumab) intravenous injection in combination with lenalidomide and dexamethasone (D-Rd) compared with Rd in 737 adult patients with newly diagnosed, transplant-ineligible multiple myeloma. The median age of patients participating in the MAIA study was 73 (range 45-90), an important consideration since the median age for multiple myeloma diagnosis is approximately 66-70 years of age.6 The study evaluated PFS as the primary endpoint, and overall survival as a key secondary endpoint, and supported the FDA approval of DARZALEX® in combination with lenalidomide and dexamethasone for adult patients with newly diagnosed, multiple myeloma who are ineligible for ASCT.
MAIA study design7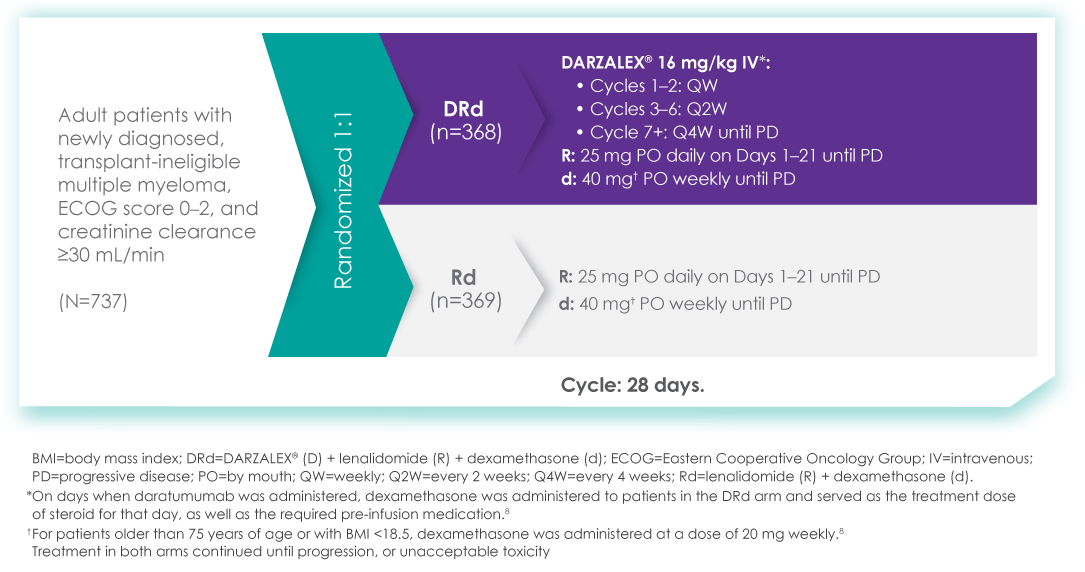
The baseline demographic and disease characteristics were similar between the 2 treatment groups. Forty-four percent of the patients were ≥75 years of age. Fifty-two percent (52%) of patients were male, 92% White, 4% Black or African American, and 1% Asian. Three percent (3%) of patients reported an ethnicity of Hispanic or Latino. Thirty-four (34%) had an Eastern Cooperative Oncology Group (ECOG) performance score of 0, 50% had an ECOG performance score of 1, and 17% had an ECOG performance score of ≥2. Twenty-seven percent had International Staging System (ISS) Stage I, 43% had ISS Stage II, and 29% had ISS Stage III disease.
Select Important Safety Information:
CONTRAINDICATIONS
DARZALEX® is contraindicated in patients with a history of severe hypersensitivity (eg, anaphylactic reactions) to daratumumab or any of the components of the formulation.
WARNINGS AND PRECAUTIONS
Infusion-Related Reactions: DARZALEX® can cause severe and/or serious infusion-related reactions including anaphylactic reactions.
These reactions can be life-threatening, and fatal outcomes have been reported. Please scroll down to read Important Safety Information for DARZALEX®.
Primary findings from the study, which were published in 2019, showed an improvement in PFS in patients receiving D-Rd compared with those receiving Rd alone.7 The median PFS was not reached in the D-Rd arm and was reached at 31.9 months in the Rd arm (HR 0.56; 95% CI 0.43-0.73; P<0.0001).7 At a median of 30 months of follow-up, the data showed the clinical benefit of D-Rd therapy, with a 44% reduction in the risk of disease progression or death in patients receiving D-Rd compared with Rd alone.7
Progression-free survival in TIE NDMM after ~30 months of treatment with D-Rd7,8
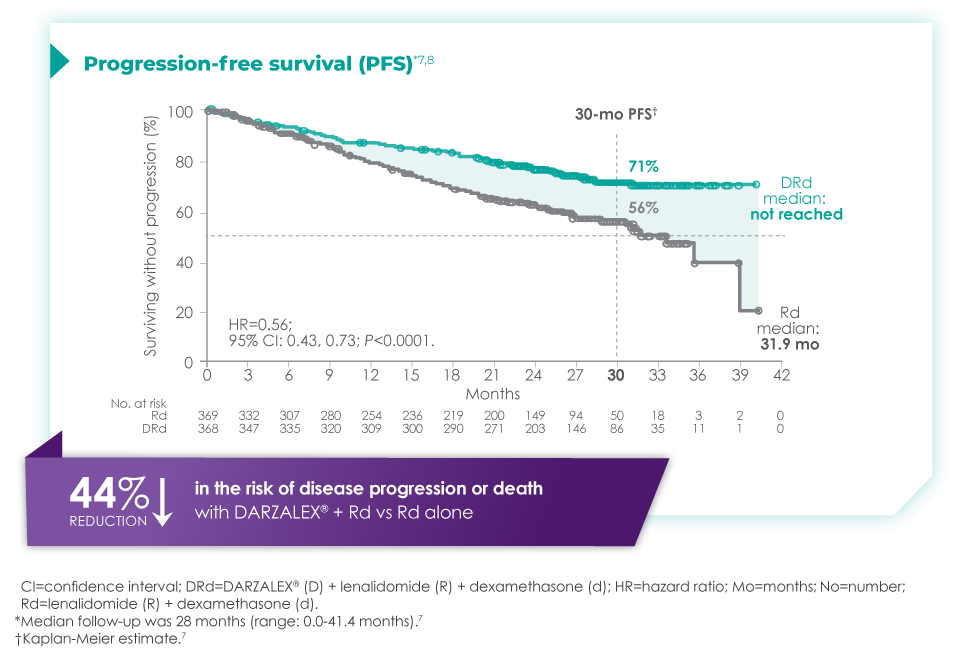
Additionally, 70.6% of patients (95% CI, 65.0-75.4) had no progressive disease with D-Rd treatment at median 30 months of follow-up, compared with 55.6% (95% CI, 49.5-61.3) of patients in the Rd group.7
In terms of depth of response, the percentage of patients with a complete response or better was 47.6% in patients receiving D-Rd compared with 24.9% in the Rd group.7
Overall response rate with D-Rd in TIE NDMM at ~30 months of follow-up8
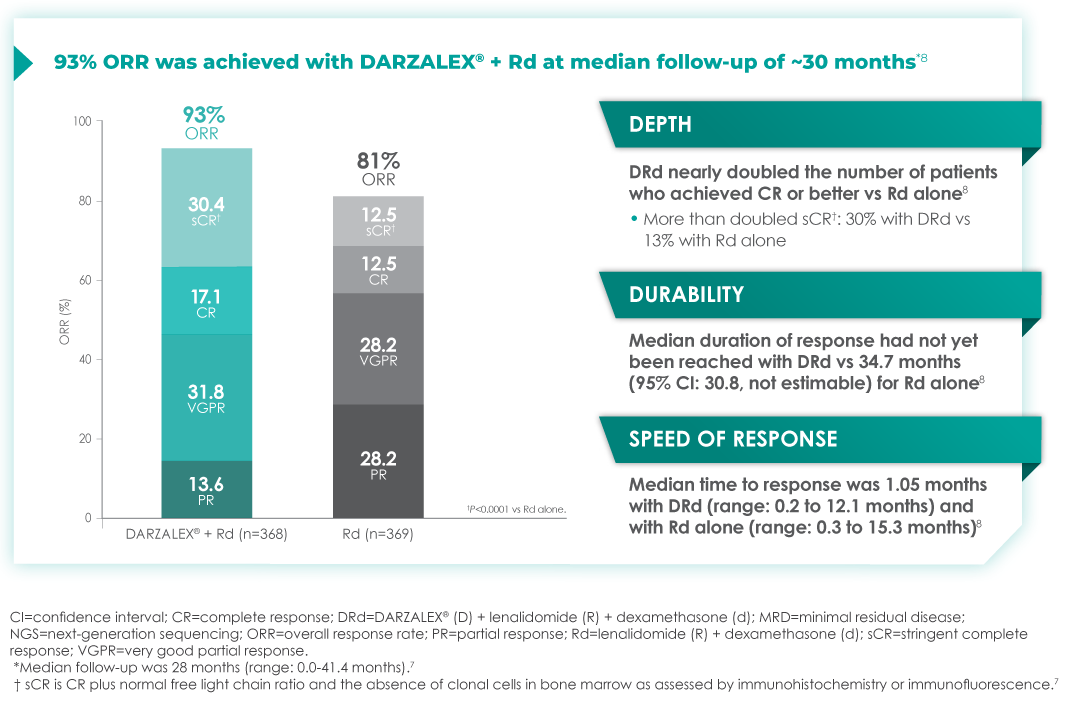
An overview of the most frequent adverse events at 30-months of follow-up are provided below. The most frequent adverse reactions were reported in ≥20% of patients, with at least a 5% greater frequency in the D-Rd arm compared with Rd alone.8
Most frequent adverse events at ~30 months of follow-up with D-Rd in TIE NDMM8
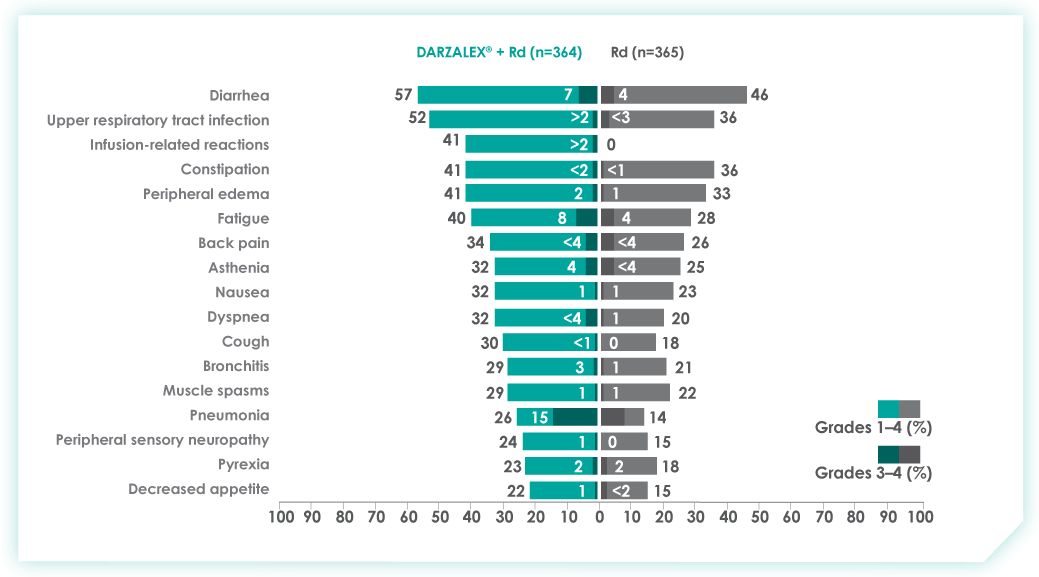
Most frequent hematologic laboratory abnormalities with D-Rd in TIE NDMM at ~30 months8
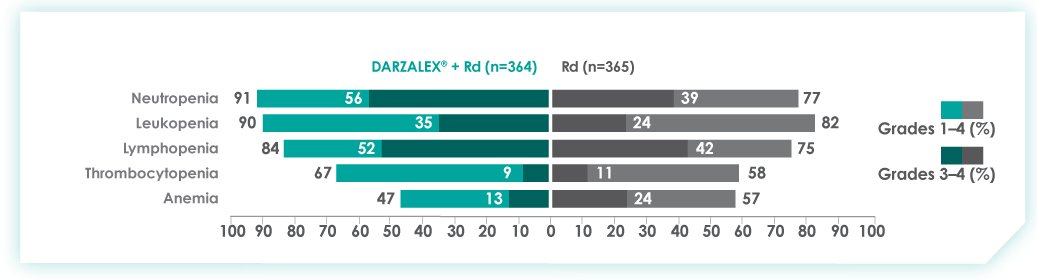
Serious adverse reactions with a 2% greater incidence in the D-Rd arm compared with the Rd arm were pneumonia (D-Rd 15% vs Rd 8%), bronchitis (D-Rd 4% vs Rd 2%), and dehydration (D-Rd 2% vs Rd <1).
• Discontinuation rates due to any adverse event: 7% with D-Rd vs 16% with Rd
• Infusion-related reactions (IRRs) with D-Rd occurred in 41% of patients; 2% were Grade 3 and <1% were Grade 4
• IRRs of any grade or severity may require management by interruption, modification, and/or discontinuation of the infusion
• Most IRRs occurred during first infusion
5. Thanks for that overview. In addition to these results, The Lancet Oncology has published updated overall survival data from a 5-year follow-up on the MAIA study. Can you provide an overview of these data and insights on their potential for patients?
The MAIA trial was an important study, and for me, the results were practice changing. We see that after a median of nearly 5 years of follow-up, D-Rd significantly improved OS in TIE NDMM patients who were treated to progression compared with Rd alone (66.3% vs. 53.1% [HR=0.68; 95% CI, 0.53-0.86; P=0.0013]).9 This equates to approximately a 32% reduction in death when DARZALEX® was added to a two-drug regimen, which is a meaningful consideration when selecting the most appropriate regimens for my newly diagnosed, transplant-ineligible patients.9
Overall survival data at ~5 years with D-Rd compared to Rd alone in TIE NDMM9
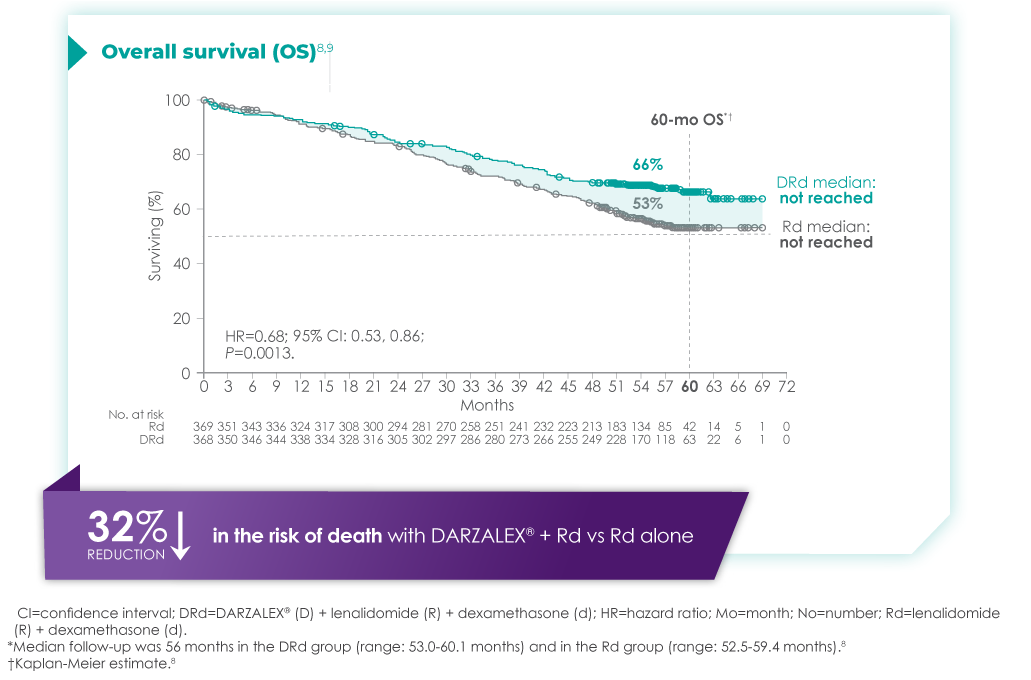
Importantly, efficacy that resulted from longer treatment with D-Rd is also supported by approximately 5 years of safety evaluation. Below is information from a follow-up analysis of the MAIA study. This information is not included in the current Prescribing Information and has not been evaluated by the FDA. Treatment-emergent adverse events are reported as observed. These analyses have not been adjusted for multiple comparisons and no conclusions should be drawn. In what I’ve observed through published data and in my practice, longer treatment has not revealed new safety signals.
Most frequent treatment-emergent adverse events (any grade reported in ≥30% of patients and/or Grade 3/4 reported in ≥10% of patients) at ~5 years9
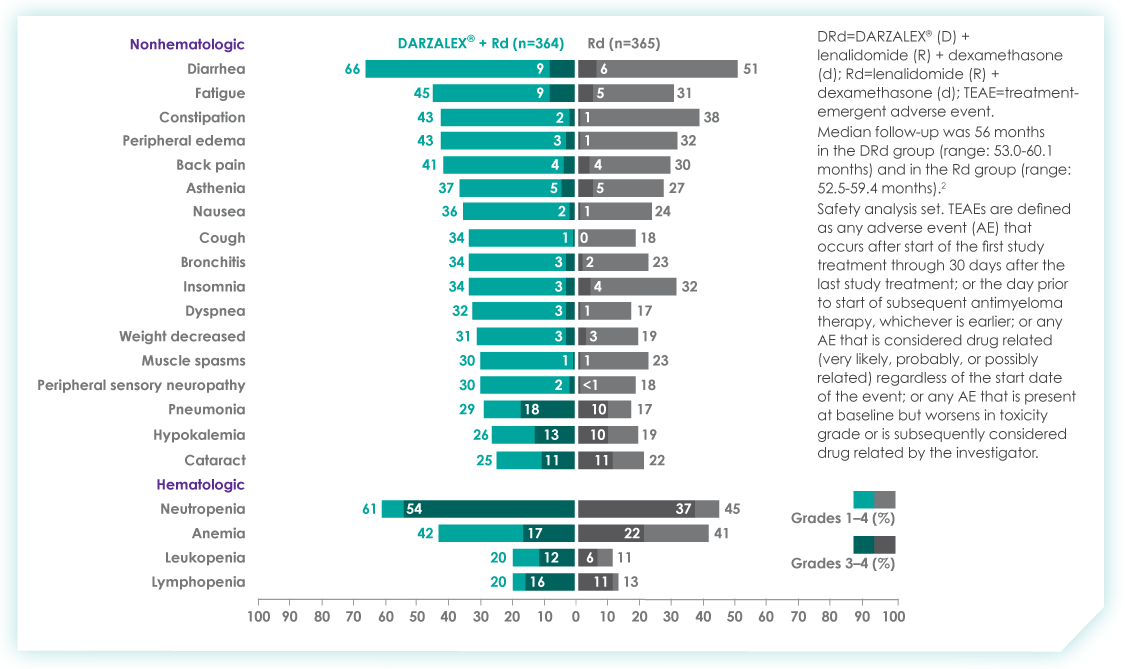
Select Important Safety Information:
DARZALEX® can cause severe and/or serious infusion-related reactions including anaphylactic reactions. These reactions can be life threatening, and fatal outcomes have been reported. In clinical trials (monotherapy and combination: N=2066), infusion-related reactions occurred in 37% of patients with the Week 1 (16 mg/kg) infusion, 2% with the Week 2 infusion, and cumulatively 6% with subsequent infusions. Less than 1% of patients had a Grade 3/4 infusion-related reaction at Week 2 or subsequent infusions. The median time to onset was 1.5 hours (range: 0 to 73 hours). Nearly all reactions occurred during infusion or within 4 hours of completing DARZALEX®. Severe reactions have occurred, including bronchospasm, hypoxia, dyspnea, hypertension, tachycardia, headache, laryngeal edema, pulmonary edema, and ocular adverse reactions, including choroidal effusion, acute myopia, and acute angle closure glaucoma. Signs and symptoms may include respiratory symptoms, such as nasal congestion, cough, throat irritation, as well as chills, vomiting, and nausea. Less common signs and symptoms were wheezing, allergic rhinitis, pyrexia, chest discomfort, pruritus, hypotension and blurred vision. Please scroll down to see Important Safety Information for DARZALEX®.
6. Does the availability of OS data influence your decisions on treatment selection in TIE NDMM?
Overall survival absolutely remains the gold standard and informs my practice. Prior to OS data being available, I will often look at other efficacy endpoints that are available sooner. In MAIA, I was encouraged by efficacy endpoints in earlier data, which were later confirmed by the latest data on OS.
7. The MAIA study shows that treating to disease progression or unacceptable toxicity is important. How does that impact your approach to treatment?
It's important to keep in mind that the MAIA trial was designed to evaluate treatment until progression or unacceptable toxicity. The results revealed a significant difference between the DR-d and Rd treatment arms, but results observed in this study are contingent on this treatment approach. From a clinical perspective, unless there is considerable toxicity, I advocate for treating with D-Rd to progression.
In the clinic, we also see that TIE patients who have higher frailty scores are more likely to discontinue treatment prior to progression.10 There can be other reasons too – such as a patient simply wanting to have a break from treatment. These conversations are not always easy, but it is important to have an honest dialogue with patients.
8. What can we learn from studies like the MAIA trial that included a wide range of patient populations including patients who are elderly, frail, or had high cytogenetic risk?
Several patient subgroups were analyzed as part of the MAIA study. It is important to note that these subgroup analyses are not included in the Prescribing Information for DARZALEX®. These analyses were not adjusted for multiple comparisons, and there are insufficient numbers of patients per subgroup to make definitive conclusions of efficacy among the subgroups.
As mentioned above, the MAIA study evaluated a wide range of patients (n=737). The baseline demographic and disease characteristics were similar between the D-Rd and Rd treatment groups and the median age was 73 (range: 45-90) years, with 44% of the patients ≥75 years of age.
In the various patient subgroups that were analyzed as part of the MAIA study, it was found that at ~3-years of follow-up the PFS numerically favored DRd compared with Rd alone in most subgroups (see table below).
Median progression-free survival by sub-population at ~3 year follow-up8
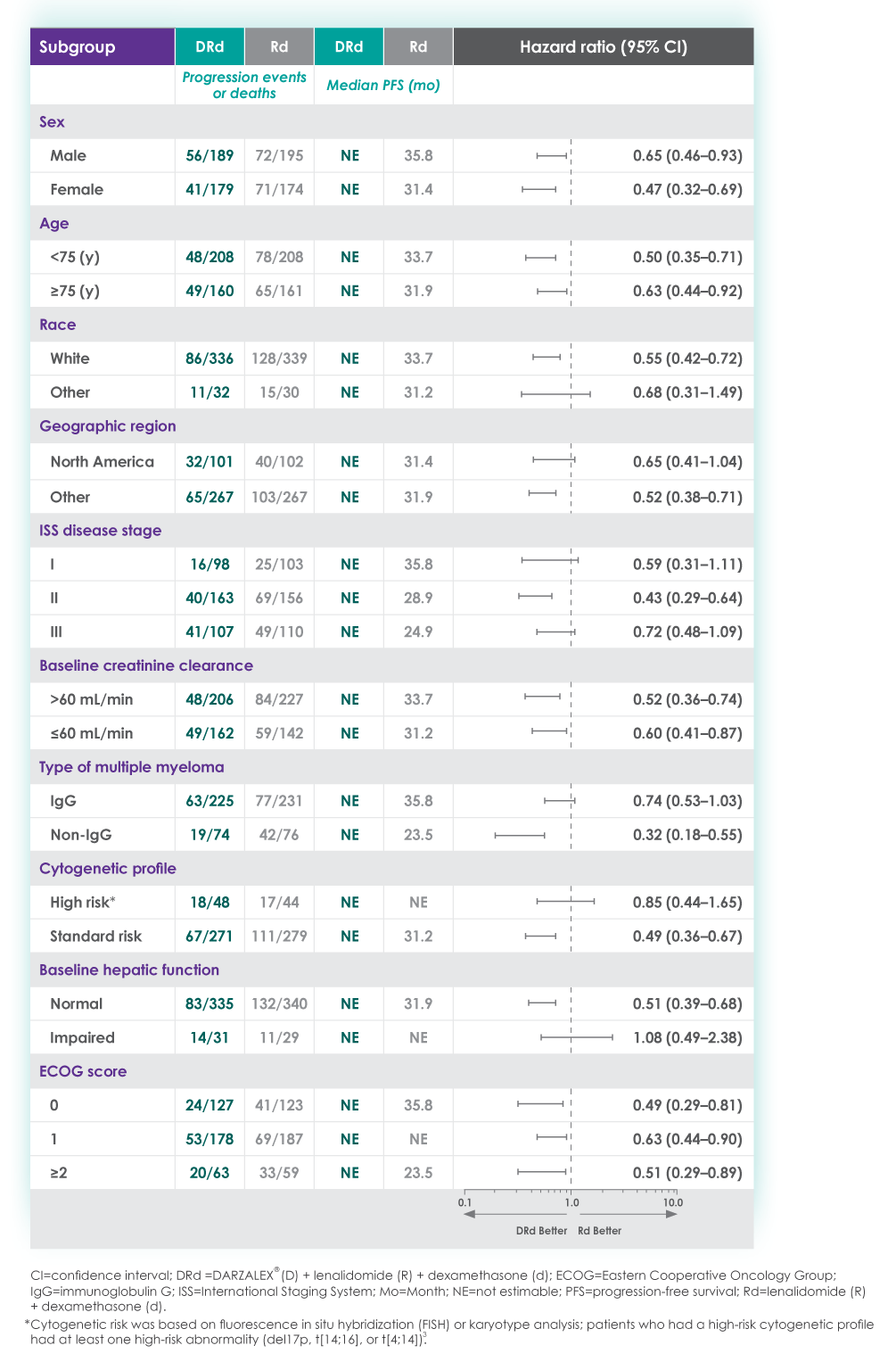
The MAIA trial also included patients who were frail and a post hoc analysis was conducted in this subgroup of patients. These analyses are not included in the Prescribing Information for DARZALEX®. These analyses were conducted post hoc and there are insufficient numbers of patients per subgroup to make definitive conclusions of efficacy among the subgroups.
A frailty assessment was performed retrospectively using age, the Charlson Comorbidity Index (CCI) – which is calculated based on a retrospective review of the patient’s medical history to predict the 10-year mortality – and the baseline Eastern Cooperative Oncology Group (ECOG) performance status score, used to measure a patient’s level of functioning in terms of their ability to care for themselves, daily activity, and physical activity. The frailty scores were then added up to classify patients into fit (0), intermediate (1), or frail (≥2). Frailty status was further simplified into 2 categories: non-frail (0-1) and frail (≥2). The median age in the frail subgroup was 77 years (range: 57-80 years), with 88% of patients having ECOG performance score ≥1. CCI was calculated based on retrospective review of each patient’s medical history.12
The charts below illustrate the frailty scoring system with an overview of the patient population included in the 3-year post hoc analysis, PFS rate, and adverse events.
MAIA post hoc subgroup analysis by frailty status score12
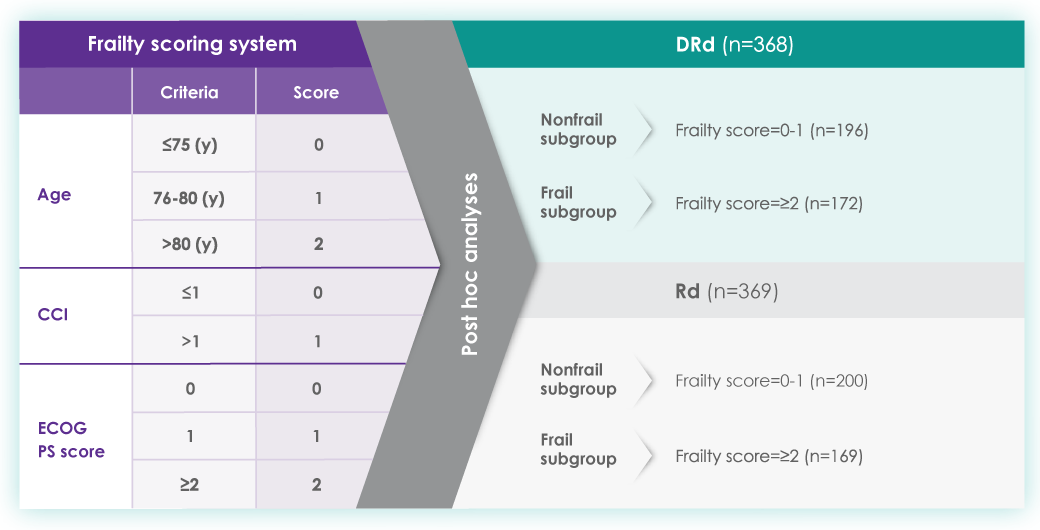
The retrospective assessment of frailty score was a limitation of this study. Retrospective CCI calculations were based on reported medical history, which may contain missing data and result in underestimating or overestimating the number of patients in each frailty subgroup. The ECOG PS score parameter used for frailty score calculations in the study is more subjective, with susceptibility to intra- and inter-observer bias, compared with the ADL (activities of daily living) and IADL (instrumental activities of daily living) scales used in the IMWG scoring system. While the frailty scale used in the study is based on parameters that are routinely assessed in clinical practice for clinical use, the use of comprehensive frailty assessments that more accurately reflect biological or functional frailty will remain important for the further optimization of treatment strategies for frail patients. Patients with an ECOG PS score ≥3 and patients with comorbidities that may interfere with the study procedures were excluded from MAIA; the inclusion and exclusion criteria for the study limits the generalizability of these results to more frail patients seen in clinical practice.
Progression-free survival in a ~3-year subgroup analysis of frail patients following treatment with D-Rd in TIE NDMM12
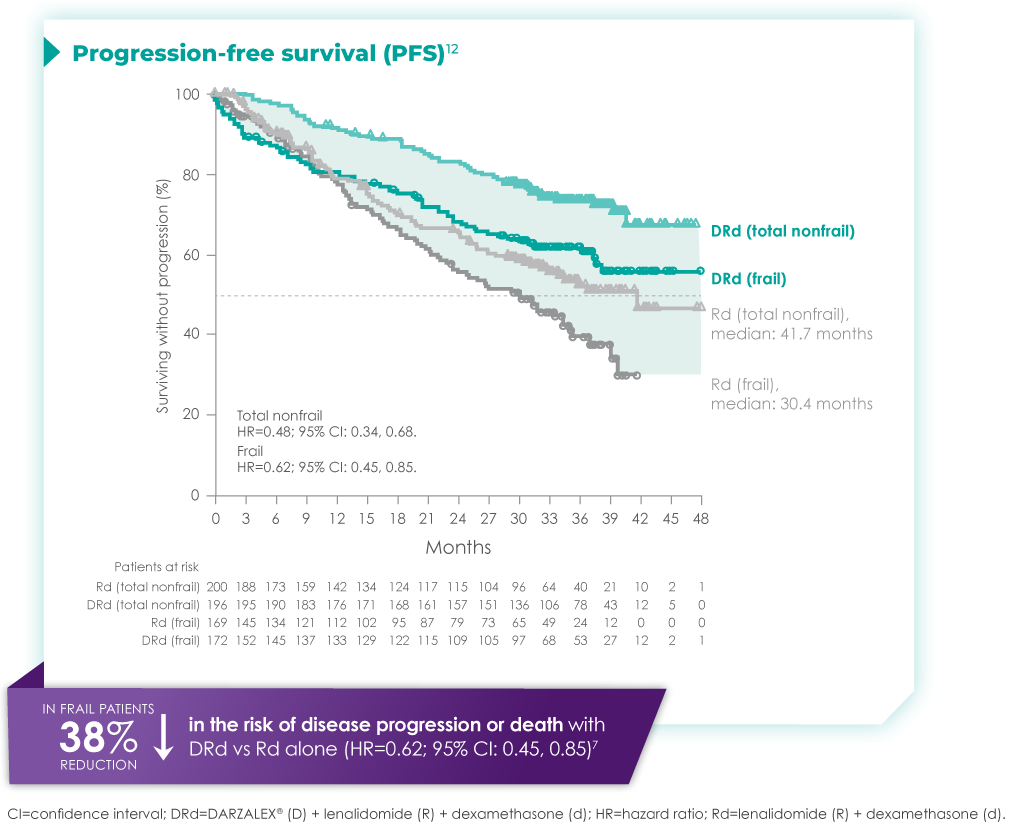
Most frequent Grade 3/4 treatment-emergent adverse events (≥10%) in frail patients at ~3 year follow-up of MAIA trial12
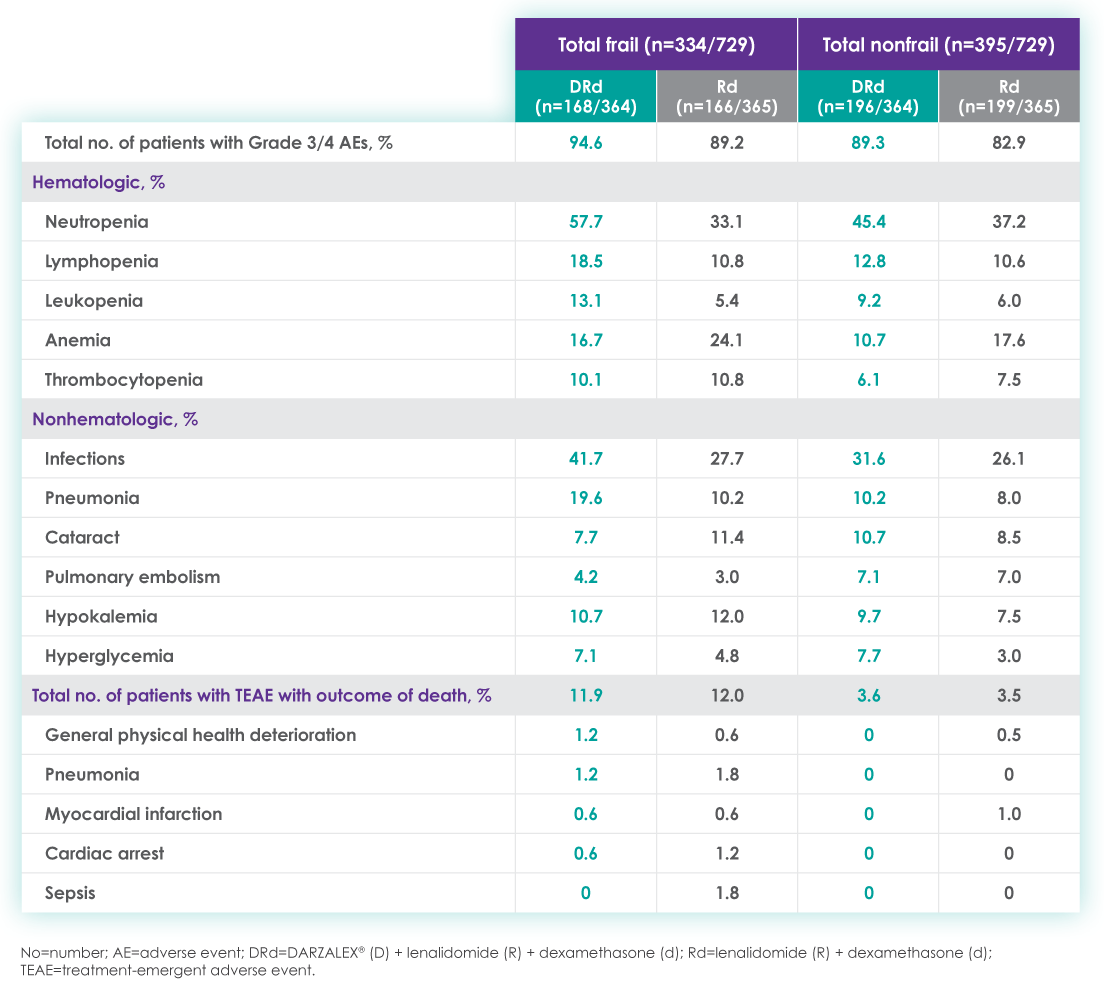
Please see additional Important Safety Information for DARZALEX® below.
IMPORTANT SAFETY INFORMATION
CONTRAINDICATIONS
DARZALEX® is contraindicated in patients with a history of severe hypersensitivity (eg, anaphylactic reactions) to daratumumab or any of the components of the formulation.
WARNINGS AND PRECAUTIONS
Infusion-Related Reactions
DARZALEX® can cause severe and/or serious infusion-related reactions including anaphylactic reactions. These reactions can be life‑threatening, and fatal outcomes have been reported. In clinical trials (monotherapy and combination: N=2066), infusion-related reactions occurred in 37% of patients with the Week 1 (16 mg/kg) infusion, 2% with the Week 2 infusion, and cumulatively 6% with subsequent infusions. Less than 1% of patients had a Grade 3/4 infusion-related reaction at Week 2 or subsequent infusions. The median time to onset was 1.5 hours (range: 0 to 73 hours). Nearly all reactions occurred during infusion or within 4 hours of completing DARZALEX®. Severe reactions have occurred, including bronchospasm, hypoxia, dyspnea, hypertension, tachycardia, headache, laryngeal edema, pulmonary edema, and ocular adverse reactions, including choroidal effusion, acute myopia, and acute angle closure glaucoma. Signs and symptoms may include respiratory symptoms, such as nasal congestion, cough, throat irritation, as well as chills, vomiting, and nausea. Less common signs and symptoms were wheezing, allergic rhinitis, pyrexia, chest discomfort, pruritus, hypotension and blurred vision.
When DARZALEX® dosing was interrupted in the setting of ASCT (CASSIOPEIA) for a median of 3.75 months (range: 2.4 to 6.9 months), upon re-initiation of DARZALEX®, the incidence of infusion-related reactions was 11% for the first infusion following ASCT. Infusion-related reactions occurring at re-initiation of DARZALEX® following ASCT were consistent in terms of symptoms and severity (Grade 3 or 4: <1%) with those reported in previous studies at Week 2 or subsequent infusions. In EQUULEUS, patients receiving combination treatment (n=97) were administered the first 16 mg/kg dose at Week 1 split over two days, ie, 8 mg/kg on Day 1 and Day 2, respectively. The incidence of any grade infusion-related reactions was 42%, with 36% of patients experiencing infusion-related reactions on Day 1 of Week 1, 4% on Day 2 of Week 1, and 8% with subsequent infusions.
Pre-medicate patients with antihistamines, antipyretics, and corticosteroids. Frequently monitor patients during the entire infusion. Interrupt DARZALEX® infusion for reactions of any severity and institute medical management as needed. Permanently discontinue DARZALEX® therapy if an anaphylactic reaction or life-threatening (Grade 4) reaction occurs and institute appropriate emergency care. For patients with Grade 1, 2, or 3 reactions, reduce the infusion rate when re-starting the infusion.
To reduce the risk of delayed infusion-related reactions, administer oral corticosteroids to all patients following DARZALEX® infusions. Patients with a history of chronic obstructive pulmonary disease may require additional post-infusion medications to manage respiratory complications. Consider prescribing short- and long-acting bronchodilators and inhaled corticosteroids for patients with chronic obstructive pulmonary disease.
Ocular adverse reactions, including acute myopia and narrowing of the anterior chamber angle due to ciliochoroidal effusions with potential for increased intraocular pressure or glaucoma, have occurred with DARZALEX infusion. If ocular symptoms occur, interrupt DARZALEX infusion and seek immediate ophthalmologic evaluation prior to restarting DARZALEX.
Interference With Serological Testing
Daratumumab binds to CD38 on red blood cells (RBCs) and results in a positive indirect antiglobulin test (indirect Coombs test). Daratumumab-mediated positive indirect antiglobulin test may persist for up to 6 months after the last daratumumab infusion. Daratumumab bound to RBCs masks detection of antibodies to minor antigens in the patient’s serum. The determination of a patient’s ABO and Rh blood type is not impacted. Notify blood transfusion centers of this interference with serological testing and inform blood banks that a patient has received DARZALEX®. Type and screen patients prior to starting DARZALEX®.
Neutropenia and Thrombocytopenia
DARZALEX® may increase neutropenia and thrombocytopenia induced by background therapy. Monitor complete blood cell counts periodically during treatment according to manufacturer’s prescribing information for background therapies. Monitor patients with neutropenia for signs of infection. Consider withholding DARZALEX® until recovery of neutrophils or for recovery of platelets.
Interference With Determination of Complete Response
Daratumumab is a human immunoglobulin G (IgG) kappa monoclonal antibody that can be detected on both the serum protein electrophoresis (SPE) and immunofixation (IFE) assays used for the clinical monitoring of endogenous M-protein. This interference can impact the determination of complete response and of disease progression in some patients with IgG kappa myeloma protein.
Embryo-Fetal Toxicity
Based on the mechanism of action, DARZALEX® can cause fetal harm when administered to a pregnant woman. DARZALEX® may cause depletion of fetal immune cells and decreased bone density. Advise pregnant women of the potential risk to a fetus. Advise females with reproductive potential to use effective contraception during treatment with DARZALEX® and for 3 months after the last dose.
The combination of DARZALEX® with lenalidomide, pomalidomide, or thalidomide is contraindicated in pregnant women because lenalidomide, pomalidomide, and thalidomide may cause birth defects and death of the unborn child. Refer to the lenalidomide, pomalidomide, or thalidomide prescribing information on use during pregnancy.
ADVERSE REACTIONS
The most frequently reported adverse reactions (incidence ≥20%) were: upper respiratory infection, neutropenia, infusion‑related reactions, thrombocytopenia, diarrhea, constipation, anemia, peripheral sensory neuropathy, fatigue, peripheral edema, nausea, cough, pyrexia, dyspnea, and asthenia. The most common hematologic laboratory abnormalities (≥40%) with DARZALEX® are: neutropenia, lymphopenia, thrombocytopenia, leukopenia, and anemia.
INDICATIONS
DARZALEX® (daratumumab) is indicated for the treatment of adult patients with multiple myeloma:
- In combination with lenalidomide and dexamethasone in newly diagnosed patients who are ineligible for autologous stem cell transplant and in patients with relapsed or refractory multiple myeloma who have received at least one prior therapy
- In combination with bortezomib, melphalan, and prednisone in newly diagnosed patients who are ineligible for autologous stem cell transplant
- In combination with bortezomib, thalidomide, and dexamethasone in newly diagnosed patients who are eligible for autologous stem cell transplant
- In combination with bortezomib and dexamethasone in patients who have received at least one prior therapy
- In combination with carfilzomib and dexamethasone in patients with relapsed or refractory multiple myeloma who have received one to three prior lines of therapy
- In combination with pomalidomide and dexamethasone in patients who have received at least two prior therapies including lenalidomide and a proteasome inhibitor
- As monotherapy in patients who have received at least three prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory agent or who are double-refractory to a PI and an immunomodulatory agent
Please click here to see the full Prescribing Information.
1. Richardson PG, San Miguel JF, Moreau P, et al. Interpreting clinical trial data in multiple myeloma: translating findings to the real-world setting. Blood Cancer J. 2018;8(11). doi:10.1038/s41408-018-0141-0
2. Key Statistics About Multiple Myeloma. Cancer.org. Published 2019. https://www.cancer.org/cancer/multiple-myeloma/about/key-statistics.html
3. Fonseca R, Usmani SZ, Mehra M, et al. Frontline treatment patterns and attrition rates by subsequent lines of therapy in patients with newly diagnosed multiple myeloma. BMC Cancer. 2020;20(1). doi:10.1186/s12885-020-07503-y
4. Devarakonda S, Efebera Y, Sharma N. Role of Stem Cell Transplantation in Multiple Myeloma. Cancers. 2021;13(4):863. doi:10.3390/cancers13040863
5. Derudas D, Capraro F, Martinelli G, Cerchione C. How I manage frontline transplant-ineligible multiple myeloma. Hematol Rep. 2020;12(s1). doi:10.4081/hr.2020.8956
6. Kazandjian D. Multiple myeloma epidemiology and survival: A unique malignancy. Semin Oncl. 2016;43(6):676-681. doi:10.1053/j.seminoncol.2016.11.004
7. Facon T, Kumar S, Plesner T, et al. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. N. Engl. J. Med. 2019;380(22):2104-2115. doi:10.1056/nejmoa1817249
8. DARZALEX® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
9. Facon T, Kumar SK, Plesner T, et al. Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(11):1582-1596. doi:10.1016/s1470-2045(21)00466-6
10. Facon T, Dimopoulos MA, Meuleman N, et al. A simplified frailty scale predicts outcomes in transplant-ineligible patients with newly diagnosed multiple myeloma treated in the FIRST (MM-020) trial. Leukemia. 2019;34(1):224-233. doi:10.1038/s41375-019-0539-0
11. Facon T, Kumar SK, Plesner T, et al. Supplement to: Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(11):1582-1596.
12. Facon T, Cook G, Usmani SZ, et al. Daratumumab plus lenalidomide and dexamethasone in transplant-ineligible newly diagnosed multiple myeloma: frailty subgroup analysis of MAIA. Leukemia. 2022;36(4):1066-1077. doi:10.1038/s41375-021-01488-8
© Janssen Biotech, Inc. 2022 All rights reserved. 12/22 cp-333446v1
1. The treatment of multiple myeloma has evolved significantly in recent years. What are some of the most important things you consider in the treatment of your newly diagnosed, transplant-ineligible patients?
We’ve seen great progress in the treatment of multiple myeloma over the last decade, and outcomes continue to improve for many patients.1 Still, it is important to keep in mind that more than 34,000 patients will be diagnosed and more than 12,000 people will die from the disease this year.2 We may have the greatest opportunity to impact the course of disease in the treatment of newly diagnosed patients due to the nature of this cancer:
- Multiple myeloma is characterized by relapse, and we know the length of remission generally decreases with each relapse and subsequent line of therapy.3
- Patients often become refractory to treatment over time.
When I meet with a patient who has been diagnosed with multiple myeloma, the first thing I consider is their eligibility for autologous stem cell transplant (ASCT). In my opinion, the introduction of ASCT is one of the biggest advancements in the last few decades, and we’ve found that ASCT followed by maintenance therapy with targeted tools improves progression-free survival (PFS).4
Unfortunately, many newly diagnosed patients are not eligible for ASCT–either because of comorbidities or other complexities related to the presentation of their disease.
For patients who are transplant-ineligible (TIE), it is important to have treatment options that are proven effective in extending PFS and overall survival (OS), and capable of producing deep and durable responses.
2. What are the challenges associated with treating newly diagnosed patients who are not eligible for ASCT?
We still consider multiple myeloma to be an incurable disease but, in my opinion, the treatment of TIE patients is less challenging today than a decade ago due to the emergence of novel therapies. That said, TIE patients are typically older and present with more advanced disease and comorbidities, including diabetes or cardiovascular events.5
A retrospective analysis published in 2020 by Rafael Fonseca examined frontline treatment patterns and attrition rates by line of therapy among newly diagnosed multiple myeloma (NDMM) patients who are TIE. More than 22,000 patients were identified from three patient-level databases between 2000 and 2018 - the OPTUM Commercial Claims database, the OPTUM Electronic Medical Records database, and the Surveillance, Epidemiology, and End Results-Meidcare Linked database. Patients included had to have a multiple myeloma diagnosis on or after January 1, 2007. Results showed that attrition rates among newly diagnosed, TIE patients with multiple myeloma increase with each line of therapy, with the proportion of patients who receive a second line of therapy decreasing by 50 percent with each subsequent line.3
3. Can you provide more detail on the goals of therapy for newly diagnosed, transplant-ineligible patients?
When I discuss treatment goals with TIE patients, I feel it is important to emphasize managing side effects and achieving deep and durable responses. I have the benefit of being in an academic setting, where I regularly exchange information with my colleagues about what we’re learning from the clinical studies in which we participate. Choosing which treatment to administer is complex and involves other considerations. For example, if two regimens have comparable efficacy, I may recommend the regimen with a more established safety profile or more robust evidence so I can properly anticipate and manage toxicities in my patients. Overall survival is one of the most important endpoints I consider, in addition to depth of response and PFS. In recent years, we’ve seen increasing evidence pointing to the importance of using a proven effective treatment in frontline patients that are ineligible for transplant.
4. A key study in newly-diagnosed, transplant-ineligible multiple myeloma is the Phase 3 MAIA study. Can you share the key takeaways from this study and discuss how the results have shaped treatment for this patient population?
Of course. The MAIA study is a randomized Phase 3 study evaluating DARZALEX® (daratumumab) intravenous injection in combination with lenalidomide and dexamethasone (D-Rd) compared with Rd in 737 adult patients with newly diagnosed, transplant-ineligible multiple myeloma. The median age of patients participating in the MAIA study was 73 (range 45-90), an important consideration since the median age for multiple myeloma diagnosis is approximately 66-70 years of age.6 The study evaluated PFS as the primary endpoint, and overall survival as a key secondary endpoint, and supported the FDA approval of DARZALEX® in combination with lenalidomide and dexamethasone for adult patients with newly diagnosed, multiple myeloma who are ineligible for ASCT.
MAIA study design7
The baseline demographic and disease characteristics were similar between the 2 treatment groups. Forty-four percent of the patients were ≥75 years of age. Fifty-two percent (52%) of patients were male, 92% White, 4% Black or African American, and 1% Asian. Three percent (3%) of patients reported an ethnicity of Hispanic or Latino. Thirty-four (34%) had an Eastern Cooperative Oncology Group (ECOG) performance score of 0, 50% had an ECOG performance score of 1, and 17% had an ECOG performance score of ≥2. Twenty-seven percent had International Staging System (ISS) Stage I, 43% had ISS Stage II, and 29% had ISS Stage III disease.
Select Important Safety Information:
CONTRAINDICATIONS
DARZALEX® is contraindicated in patients with a history of severe hypersensitivity (eg, anaphylactic reactions) to daratumumab or any of the components of the formulation.
WARNINGS AND PRECAUTIONS
Infusion-Related Reactions: DARZALEX® can cause severe and/or serious infusion-related reactions including anaphylactic reactions.
These reactions can be life-threatening, and fatal outcomes have been reported. Please scroll down to read Important Safety Information for DARZALEX®.
Primary findings from the study, which were published in 2019, showed an improvement in PFS in patients receiving D-Rd compared with those receiving Rd alone.7 The median PFS was not reached in the D-Rd arm and was reached at 31.9 months in the Rd arm (HR 0.56; 95% CI 0.43-0.73; P<0.0001).7 At a median of 30 months of follow-up, the data showed the clinical benefit of D-Rd therapy, with a 44% reduction in the risk of disease progression or death in patients receiving D-Rd compared with Rd alone.7
Progression-free survival in TIE NDMM after ~30 months of treatment with D-Rd7,8
Additionally, 70.6% of patients (95% CI, 65.0-75.4) had no progressive disease with D-Rd treatment at median 30 months of follow-up, compared with 55.6% (95% CI, 49.5-61.3) of patients in the Rd group.7
In terms of depth of response, the percentage of patients with a complete response or better was 47.6% in patients receiving D-Rd compared with 24.9% in the Rd group.7
Overall response rate with D-Rd in TIE NDMM at ~30 months of follow-up8
An overview of the most frequent adverse events at 30-months of follow-up are provided below. The most frequent adverse reactions were reported in ≥20% of patients, with at least a 5% greater frequency in the D-Rd arm compared with Rd alone.8
Most frequent adverse events at ~30 months of follow-up with D-Rd in TIE NDMM8
Most frequent hematologic laboratory abnormalities with D-Rd in TIE NDMM at ~30 months8
Serious adverse reactions with a 2% greater incidence in the D-Rd arm compared with the Rd arm were pneumonia (D-Rd 15% vs Rd 8%), bronchitis (D-Rd 4% vs Rd 2%), and dehydration (D-Rd 2% vs Rd <1).
• Discontinuation rates due to any adverse event: 7% with D-Rd vs 16% with Rd
• Infusion-related reactions (IRRs) with D-Rd occurred in 41% of patients; 2% were Grade 3 and <1% were Grade 4
• IRRs of any grade or severity may require management by interruption, modification, and/or discontinuation of the infusion
• Most IRRs occurred during first infusion
5. Thanks for that overview. In addition to these results, The Lancet Oncology has published updated overall survival data from a 5-year follow-up on the MAIA study. Can you provide an overview of these data and insights on their potential for patients?
The MAIA trial was an important study, and for me, the results were practice changing. We see that after a median of nearly 5 years of follow-up, D-Rd significantly improved OS in TIE NDMM patients who were treated to progression compared with Rd alone (66.3% vs. 53.1% [HR=0.68; 95% CI, 0.53-0.86; P=0.0013]).9 This equates to approximately a 32% reduction in death when DARZALEX® was added to a two-drug regimen, which is a meaningful consideration when selecting the most appropriate regimens for my newly diagnosed, transplant-ineligible patients.9
Overall survival data at ~5 years with D-Rd compared to Rd alone in TIE NDMM9
Importantly, efficacy that resulted from longer treatment with D-Rd is also supported by approximately 5 years of safety evaluation. Below is information from a follow-up analysis of the MAIA study. This information is not included in the current Prescribing Information and has not been evaluated by the FDA. Treatment-emergent adverse events are reported as observed. These analyses have not been adjusted for multiple comparisons and no conclusions should be drawn. In what I’ve observed through published data and in my practice, longer treatment has not revealed new safety signals.
Most frequent treatment-emergent adverse events (any grade reported in ≥30% of patients and/or Grade 3/4 reported in ≥10% of patients) at ~5 years9
Select Important Safety Information:
DARZALEX® can cause severe and/or serious infusion-related reactions including anaphylactic reactions. These reactions can be life threatening, and fatal outcomes have been reported. In clinical trials (monotherapy and combination: N=2066), infusion-related reactions occurred in 37% of patients with the Week 1 (16 mg/kg) infusion, 2% with the Week 2 infusion, and cumulatively 6% with subsequent infusions. Less than 1% of patients had a Grade 3/4 infusion-related reaction at Week 2 or subsequent infusions. The median time to onset was 1.5 hours (range: 0 to 73 hours). Nearly all reactions occurred during infusion or within 4 hours of completing DARZALEX®. Severe reactions have occurred, including bronchospasm, hypoxia, dyspnea, hypertension, tachycardia, headache, laryngeal edema, pulmonary edema, and ocular adverse reactions, including choroidal effusion, acute myopia, and acute angle closure glaucoma. Signs and symptoms may include respiratory symptoms, such as nasal congestion, cough, throat irritation, as well as chills, vomiting, and nausea. Less common signs and symptoms were wheezing, allergic rhinitis, pyrexia, chest discomfort, pruritus, hypotension and blurred vision. Please scroll down to see Important Safety Information for DARZALEX®.
6. Does the availability of OS data influence your decisions on treatment selection in TIE NDMM?
Overall survival absolutely remains the gold standard and informs my practice. Prior to OS data being available, I will often look at other efficacy endpoints that are available sooner. In MAIA, I was encouraged by efficacy endpoints in earlier data, which were later confirmed by the latest data on OS.
7. The MAIA study shows that treating to disease progression or unacceptable toxicity is important. How does that impact your approach to treatment?
It's important to keep in mind that the MAIA trial was designed to evaluate treatment until progression or unacceptable toxicity. The results revealed a significant difference between the DR-d and Rd treatment arms, but results observed in this study are contingent on this treatment approach. From a clinical perspective, unless there is considerable toxicity, I advocate for treating with D-Rd to progression.
In the clinic, we also see that TIE patients who have higher frailty scores are more likely to discontinue treatment prior to progression.10 There can be other reasons too – such as a patient simply wanting to have a break from treatment. These conversations are not always easy, but it is important to have an honest dialogue with patients.
8. What can we learn from studies like the MAIA trial that included a wide range of patient populations including patients who are elderly, frail, or had high cytogenetic risk?
Several patient subgroups were analyzed as part of the MAIA study. It is important to note that these subgroup analyses are not included in the Prescribing Information for DARZALEX®. These analyses were not adjusted for multiple comparisons, and there are insufficient numbers of patients per subgroup to make definitive conclusions of efficacy among the subgroups.
As mentioned above, the MAIA study evaluated a wide range of patients (n=737). The baseline demographic and disease characteristics were similar between the D-Rd and Rd treatment groups and the median age was 73 (range: 45-90) years, with 44% of the patients ≥75 years of age.
In the various patient subgroups that were analyzed as part of the MAIA study, it was found that at ~3-years of follow-up the PFS numerically favored DRd compared with Rd alone in most subgroups (see table below).
Median progression-free survival by sub-population at ~3 year follow-up8
The MAIA trial also included patients who were frail and a post hoc analysis was conducted in this subgroup of patients. These analyses are not included in the Prescribing Information for DARZALEX®. These analyses were conducted post hoc and there are insufficient numbers of patients per subgroup to make definitive conclusions of efficacy among the subgroups.
A frailty assessment was performed retrospectively using age, the Charlson Comorbidity Index (CCI) – which is calculated based on a retrospective review of the patient’s medical history to predict the 10-year mortality – and the baseline Eastern Cooperative Oncology Group (ECOG) performance status score, used to measure a patient’s level of functioning in terms of their ability to care for themselves, daily activity, and physical activity. The frailty scores were then added up to classify patients into fit (0), intermediate (1), or frail (≥2). Frailty status was further simplified into 2 categories: non-frail (0-1) and frail (≥2). The median age in the frail subgroup was 77 years (range: 57-80 years), with 88% of patients having ECOG performance score ≥1. CCI was calculated based on retrospective review of each patient’s medical history.12
The charts below illustrate the frailty scoring system with an overview of the patient population included in the 3-year post hoc analysis, PFS rate, and adverse events.
MAIA post hoc subgroup analysis by frailty status score12
The retrospective assessment of frailty score was a limitation of this study. Retrospective CCI calculations were based on reported medical history, which may contain missing data and result in underestimating or overestimating the number of patients in each frailty subgroup. The ECOG PS score parameter used for frailty score calculations in the study is more subjective, with susceptibility to intra- and inter-observer bias, compared with the ADL (activities of daily living) and IADL (instrumental activities of daily living) scales used in the IMWG scoring system. While the frailty scale used in the study is based on parameters that are routinely assessed in clinical practice for clinical use, the use of comprehensive frailty assessments that more accurately reflect biological or functional frailty will remain important for the further optimization of treatment strategies for frail patients. Patients with an ECOG PS score ≥3 and patients with comorbidities that may interfere with the study procedures were excluded from MAIA; the inclusion and exclusion criteria for the study limits the generalizability of these results to more frail patients seen in clinical practice.
Progression-free survival in a ~3-year subgroup analysis of frail patients following treatment with D-Rd in TIE NDMM12
Most frequent Grade 3/4 treatment-emergent adverse events (≥10%) in frail patients at ~3 year follow-up of MAIA trial12
Please see additional Important Safety Information for DARZALEX® below.
IMPORTANT SAFETY INFORMATION
CONTRAINDICATIONS
DARZALEX® is contraindicated in patients with a history of severe hypersensitivity (eg, anaphylactic reactions) to daratumumab or any of the components of the formulation.
WARNINGS AND PRECAUTIONS
Infusion-Related Reactions
DARZALEX® can cause severe and/or serious infusion-related reactions including anaphylactic reactions. These reactions can be life‑threatening, and fatal outcomes have been reported. In clinical trials (monotherapy and combination: N=2066), infusion-related reactions occurred in 37% of patients with the Week 1 (16 mg/kg) infusion, 2% with the Week 2 infusion, and cumulatively 6% with subsequent infusions. Less than 1% of patients had a Grade 3/4 infusion-related reaction at Week 2 or subsequent infusions. The median time to onset was 1.5 hours (range: 0 to 73 hours). Nearly all reactions occurred during infusion or within 4 hours of completing DARZALEX®. Severe reactions have occurred, including bronchospasm, hypoxia, dyspnea, hypertension, tachycardia, headache, laryngeal edema, pulmonary edema, and ocular adverse reactions, including choroidal effusion, acute myopia, and acute angle closure glaucoma. Signs and symptoms may include respiratory symptoms, such as nasal congestion, cough, throat irritation, as well as chills, vomiting, and nausea. Less common signs and symptoms were wheezing, allergic rhinitis, pyrexia, chest discomfort, pruritus, hypotension and blurred vision.
When DARZALEX® dosing was interrupted in the setting of ASCT (CASSIOPEIA) for a median of 3.75 months (range: 2.4 to 6.9 months), upon re-initiation of DARZALEX®, the incidence of infusion-related reactions was 11% for the first infusion following ASCT. Infusion-related reactions occurring at re-initiation of DARZALEX® following ASCT were consistent in terms of symptoms and severity (Grade 3 or 4: <1%) with those reported in previous studies at Week 2 or subsequent infusions. In EQUULEUS, patients receiving combination treatment (n=97) were administered the first 16 mg/kg dose at Week 1 split over two days, ie, 8 mg/kg on Day 1 and Day 2, respectively. The incidence of any grade infusion-related reactions was 42%, with 36% of patients experiencing infusion-related reactions on Day 1 of Week 1, 4% on Day 2 of Week 1, and 8% with subsequent infusions.
Pre-medicate patients with antihistamines, antipyretics, and corticosteroids. Frequently monitor patients during the entire infusion. Interrupt DARZALEX® infusion for reactions of any severity and institute medical management as needed. Permanently discontinue DARZALEX® therapy if an anaphylactic reaction or life-threatening (Grade 4) reaction occurs and institute appropriate emergency care. For patients with Grade 1, 2, or 3 reactions, reduce the infusion rate when re-starting the infusion.
To reduce the risk of delayed infusion-related reactions, administer oral corticosteroids to all patients following DARZALEX® infusions. Patients with a history of chronic obstructive pulmonary disease may require additional post-infusion medications to manage respiratory complications. Consider prescribing short- and long-acting bronchodilators and inhaled corticosteroids for patients with chronic obstructive pulmonary disease.
Ocular adverse reactions, including acute myopia and narrowing of the anterior chamber angle due to ciliochoroidal effusions with potential for increased intraocular pressure or glaucoma, have occurred with DARZALEX infusion. If ocular symptoms occur, interrupt DARZALEX infusion and seek immediate ophthalmologic evaluation prior to restarting DARZALEX.
Interference With Serological Testing
Daratumumab binds to CD38 on red blood cells (RBCs) and results in a positive indirect antiglobulin test (indirect Coombs test). Daratumumab-mediated positive indirect antiglobulin test may persist for up to 6 months after the last daratumumab infusion. Daratumumab bound to RBCs masks detection of antibodies to minor antigens in the patient’s serum. The determination of a patient’s ABO and Rh blood type is not impacted. Notify blood transfusion centers of this interference with serological testing and inform blood banks that a patient has received DARZALEX®. Type and screen patients prior to starting DARZALEX®.
Neutropenia and Thrombocytopenia
DARZALEX® may increase neutropenia and thrombocytopenia induced by background therapy. Monitor complete blood cell counts periodically during treatment according to manufacturer’s prescribing information for background therapies. Monitor patients with neutropenia for signs of infection. Consider withholding DARZALEX® until recovery of neutrophils or for recovery of platelets.
Interference With Determination of Complete Response
Daratumumab is a human immunoglobulin G (IgG) kappa monoclonal antibody that can be detected on both the serum protein electrophoresis (SPE) and immunofixation (IFE) assays used for the clinical monitoring of endogenous M-protein. This interference can impact the determination of complete response and of disease progression in some patients with IgG kappa myeloma protein.
Embryo-Fetal Toxicity
Based on the mechanism of action, DARZALEX® can cause fetal harm when administered to a pregnant woman. DARZALEX® may cause depletion of fetal immune cells and decreased bone density. Advise pregnant women of the potential risk to a fetus. Advise females with reproductive potential to use effective contraception during treatment with DARZALEX® and for 3 months after the last dose.
The combination of DARZALEX® with lenalidomide, pomalidomide, or thalidomide is contraindicated in pregnant women because lenalidomide, pomalidomide, and thalidomide may cause birth defects and death of the unborn child. Refer to the lenalidomide, pomalidomide, or thalidomide prescribing information on use during pregnancy.
ADVERSE REACTIONS
The most frequently reported adverse reactions (incidence ≥20%) were: upper respiratory infection, neutropenia, infusion‑related reactions, thrombocytopenia, diarrhea, constipation, anemia, peripheral sensory neuropathy, fatigue, peripheral edema, nausea, cough, pyrexia, dyspnea, and asthenia. The most common hematologic laboratory abnormalities (≥40%) with DARZALEX® are: neutropenia, lymphopenia, thrombocytopenia, leukopenia, and anemia.
INDICATIONS
DARZALEX® (daratumumab) is indicated for the treatment of adult patients with multiple myeloma:
- In combination with lenalidomide and dexamethasone in newly diagnosed patients who are ineligible for autologous stem cell transplant and in patients with relapsed or refractory multiple myeloma who have received at least one prior therapy
- In combination with bortezomib, melphalan, and prednisone in newly diagnosed patients who are ineligible for autologous stem cell transplant
- In combination with bortezomib, thalidomide, and dexamethasone in newly diagnosed patients who are eligible for autologous stem cell transplant
- In combination with bortezomib and dexamethasone in patients who have received at least one prior therapy
- In combination with carfilzomib and dexamethasone in patients with relapsed or refractory multiple myeloma who have received one to three prior lines of therapy
- In combination with pomalidomide and dexamethasone in patients who have received at least two prior therapies including lenalidomide and a proteasome inhibitor
- As monotherapy in patients who have received at least three prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory agent or who are double-refractory to a PI and an immunomodulatory agent
Please click here to see the full Prescribing Information.
1. Richardson PG, San Miguel JF, Moreau P, et al. Interpreting clinical trial data in multiple myeloma: translating findings to the real-world setting. Blood Cancer J. 2018;8(11). doi:10.1038/s41408-018-0141-0
2. Key Statistics About Multiple Myeloma. Cancer.org. Published 2019. https://www.cancer.org/cancer/multiple-myeloma/about/key-statistics.html
3. Fonseca R, Usmani SZ, Mehra M, et al. Frontline treatment patterns and attrition rates by subsequent lines of therapy in patients with newly diagnosed multiple myeloma. BMC Cancer. 2020;20(1). doi:10.1186/s12885-020-07503-y
4. Devarakonda S, Efebera Y, Sharma N. Role of Stem Cell Transplantation in Multiple Myeloma. Cancers. 2021;13(4):863. doi:10.3390/cancers13040863
5. Derudas D, Capraro F, Martinelli G, Cerchione C. How I manage frontline transplant-ineligible multiple myeloma. Hematol Rep. 2020;12(s1). doi:10.4081/hr.2020.8956
6. Kazandjian D. Multiple myeloma epidemiology and survival: A unique malignancy. Semin Oncl. 2016;43(6):676-681. doi:10.1053/j.seminoncol.2016.11.004
7. Facon T, Kumar S, Plesner T, et al. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. N. Engl. J. Med. 2019;380(22):2104-2115. doi:10.1056/nejmoa1817249
8. DARZALEX® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
9. Facon T, Kumar SK, Plesner T, et al. Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(11):1582-1596. doi:10.1016/s1470-2045(21)00466-6
10. Facon T, Dimopoulos MA, Meuleman N, et al. A simplified frailty scale predicts outcomes in transplant-ineligible patients with newly diagnosed multiple myeloma treated in the FIRST (MM-020) trial. Leukemia. 2019;34(1):224-233. doi:10.1038/s41375-019-0539-0
11. Facon T, Kumar SK, Plesner T, et al. Supplement to: Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(11):1582-1596.
12. Facon T, Cook G, Usmani SZ, et al. Daratumumab plus lenalidomide and dexamethasone in transplant-ineligible newly diagnosed multiple myeloma: frailty subgroup analysis of MAIA. Leukemia. 2022;36(4):1066-1077. doi:10.1038/s41375-021-01488-8
© Janssen Biotech, Inc. 2022 All rights reserved. 12/22 cp-333446v1
1. The treatment of multiple myeloma has evolved significantly in recent years. What are some of the most important things you consider in the treatment of your newly diagnosed, transplant-ineligible patients?
We’ve seen great progress in the treatment of multiple myeloma over the last decade, and outcomes continue to improve for many patients.1 Still, it is important to keep in mind that more than 34,000 patients will be diagnosed and more than 12,000 people will die from the disease this year.2 We may have the greatest opportunity to impact the course of disease in the treatment of newly diagnosed patients due to the nature of this cancer:
- Multiple myeloma is characterized by relapse, and we know the length of remission generally decreases with each relapse and subsequent line of therapy.3
- Patients often become refractory to treatment over time.
When I meet with a patient who has been diagnosed with multiple myeloma, the first thing I consider is their eligibility for autologous stem cell transplant (ASCT). In my opinion, the introduction of ASCT is one of the biggest advancements in the last few decades, and we’ve found that ASCT followed by maintenance therapy with targeted tools improves progression-free survival (PFS).4
Unfortunately, many newly diagnosed patients are not eligible for ASCT–either because of comorbidities or other complexities related to the presentation of their disease.
For patients who are transplant-ineligible (TIE), it is important to have treatment options that are proven effective in extending PFS and overall survival (OS), and capable of producing deep and durable responses.
2. What are the challenges associated with treating newly diagnosed patients who are not eligible for ASCT?
We still consider multiple myeloma to be an incurable disease but, in my opinion, the treatment of TIE patients is less challenging today than a decade ago due to the emergence of novel therapies. That said, TIE patients are typically older and present with more advanced disease and comorbidities, including diabetes or cardiovascular events.5
A retrospective analysis published in 2020 by Rafael Fonseca examined frontline treatment patterns and attrition rates by line of therapy among newly diagnosed multiple myeloma (NDMM) patients who are TIE. More than 22,000 patients were identified from three patient-level databases between 2000 and 2018 - the OPTUM Commercial Claims database, the OPTUM Electronic Medical Records database, and the Surveillance, Epidemiology, and End Results-Meidcare Linked database. Patients included had to have a multiple myeloma diagnosis on or after January 1, 2007. Results showed that attrition rates among newly diagnosed, TIE patients with multiple myeloma increase with each line of therapy, with the proportion of patients who receive a second line of therapy decreasing by 50 percent with each subsequent line.3
3. Can you provide more detail on the goals of therapy for newly diagnosed, transplant-ineligible patients?
When I discuss treatment goals with TIE patients, I feel it is important to emphasize managing side effects and achieving deep and durable responses. I have the benefit of being in an academic setting, where I regularly exchange information with my colleagues about what we’re learning from the clinical studies in which we participate. Choosing which treatment to administer is complex and involves other considerations. For example, if two regimens have comparable efficacy, I may recommend the regimen with a more established safety profile or more robust evidence so I can properly anticipate and manage toxicities in my patients. Overall survival is one of the most important endpoints I consider, in addition to depth of response and PFS. In recent years, we’ve seen increasing evidence pointing to the importance of using a proven effective treatment in frontline patients that are ineligible for transplant.
4. A key study in newly-diagnosed, transplant-ineligible multiple myeloma is the Phase 3 MAIA study. Can you share the key takeaways from this study and discuss how the results have shaped treatment for this patient population?
Of course. The MAIA study is a randomized Phase 3 study evaluating DARZALEX® (daratumumab) intravenous injection in combination with lenalidomide and dexamethasone (D-Rd) compared with Rd in 737 adult patients with newly diagnosed, transplant-ineligible multiple myeloma. The median age of patients participating in the MAIA study was 73 (range 45-90), an important consideration since the median age for multiple myeloma diagnosis is approximately 66-70 years of age.6 The study evaluated PFS as the primary endpoint, and overall survival as a key secondary endpoint, and supported the FDA approval of DARZALEX® in combination with lenalidomide and dexamethasone for adult patients with newly diagnosed, multiple myeloma who are ineligible for ASCT.
MAIA study design7
The baseline demographic and disease characteristics were similar between the 2 treatment groups. Forty-four percent of the patients were ≥75 years of age. Fifty-two percent (52%) of patients were male, 92% White, 4% Black or African American, and 1% Asian. Three percent (3%) of patients reported an ethnicity of Hispanic or Latino. Thirty-four (34%) had an Eastern Cooperative Oncology Group (ECOG) performance score of 0, 50% had an ECOG performance score of 1, and 17% had an ECOG performance score of ≥2. Twenty-seven percent had International Staging System (ISS) Stage I, 43% had ISS Stage II, and 29% had ISS Stage III disease.
Select Important Safety Information:
CONTRAINDICATIONS
DARZALEX® is contraindicated in patients with a history of severe hypersensitivity (eg, anaphylactic reactions) to daratumumab or any of the components of the formulation.
WARNINGS AND PRECAUTIONS
Infusion-Related Reactions: DARZALEX® can cause severe and/or serious infusion-related reactions including anaphylactic reactions.
These reactions can be life-threatening, and fatal outcomes have been reported. Please scroll down to read Important Safety Information for DARZALEX®.
Primary findings from the study, which were published in 2019, showed an improvement in PFS in patients receiving D-Rd compared with those receiving Rd alone.7 The median PFS was not reached in the D-Rd arm and was reached at 31.9 months in the Rd arm (HR 0.56; 95% CI 0.43-0.73; P<0.0001).7 At a median of 30 months of follow-up, the data showed the clinical benefit of D-Rd therapy, with a 44% reduction in the risk of disease progression or death in patients receiving D-Rd compared with Rd alone.7
Progression-free survival in TIE NDMM after ~30 months of treatment with D-Rd7,8
Additionally, 70.6% of patients (95% CI, 65.0-75.4) had no progressive disease with D-Rd treatment at median 30 months of follow-up, compared with 55.6% (95% CI, 49.5-61.3) of patients in the Rd group.7
In terms of depth of response, the percentage of patients with a complete response or better was 47.6% in patients receiving D-Rd compared with 24.9% in the Rd group.7
Overall response rate with D-Rd in TIE NDMM at ~30 months of follow-up8
An overview of the most frequent adverse events at 30-months of follow-up are provided below. The most frequent adverse reactions were reported in ≥20% of patients, with at least a 5% greater frequency in the D-Rd arm compared with Rd alone.8
Most frequent adverse events at ~30 months of follow-up with D-Rd in TIE NDMM8
Most frequent hematologic laboratory abnormalities with D-Rd in TIE NDMM at ~30 months8
Serious adverse reactions with a 2% greater incidence in the D-Rd arm compared with the Rd arm were pneumonia (D-Rd 15% vs Rd 8%), bronchitis (D-Rd 4% vs Rd 2%), and dehydration (D-Rd 2% vs Rd <1).
• Discontinuation rates due to any adverse event: 7% with D-Rd vs 16% with Rd
• Infusion-related reactions (IRRs) with D-Rd occurred in 41% of patients; 2% were Grade 3 and <1% were Grade 4
• IRRs of any grade or severity may require management by interruption, modification, and/or discontinuation of the infusion
• Most IRRs occurred during first infusion
5. Thanks for that overview. In addition to these results, The Lancet Oncology has published updated overall survival data from a 5-year follow-up on the MAIA study. Can you provide an overview of these data and insights on their potential for patients?
The MAIA trial was an important study, and for me, the results were practice changing. We see that after a median of nearly 5 years of follow-up, D-Rd significantly improved OS in TIE NDMM patients who were treated to progression compared with Rd alone (66.3% vs. 53.1% [HR=0.68; 95% CI, 0.53-0.86; P=0.0013]).9 This equates to approximately a 32% reduction in death when DARZALEX® was added to a two-drug regimen, which is a meaningful consideration when selecting the most appropriate regimens for my newly diagnosed, transplant-ineligible patients.9
Overall survival data at ~5 years with D-Rd compared to Rd alone in TIE NDMM9
Importantly, efficacy that resulted from longer treatment with D-Rd is also supported by approximately 5 years of safety evaluation. Below is information from a follow-up analysis of the MAIA study. This information is not included in the current Prescribing Information and has not been evaluated by the FDA. Treatment-emergent adverse events are reported as observed. These analyses have not been adjusted for multiple comparisons and no conclusions should be drawn. In what I’ve observed through published data and in my practice, longer treatment has not revealed new safety signals.
Most frequent treatment-emergent adverse events (any grade reported in ≥30% of patients and/or Grade 3/4 reported in ≥10% of patients) at ~5 years9
Select Important Safety Information:
DARZALEX® can cause severe and/or serious infusion-related reactions including anaphylactic reactions. These reactions can be life threatening, and fatal outcomes have been reported. In clinical trials (monotherapy and combination: N=2066), infusion-related reactions occurred in 37% of patients with the Week 1 (16 mg/kg) infusion, 2% with the Week 2 infusion, and cumulatively 6% with subsequent infusions. Less than 1% of patients had a Grade 3/4 infusion-related reaction at Week 2 or subsequent infusions. The median time to onset was 1.5 hours (range: 0 to 73 hours). Nearly all reactions occurred during infusion or within 4 hours of completing DARZALEX®. Severe reactions have occurred, including bronchospasm, hypoxia, dyspnea, hypertension, tachycardia, headache, laryngeal edema, pulmonary edema, and ocular adverse reactions, including choroidal effusion, acute myopia, and acute angle closure glaucoma. Signs and symptoms may include respiratory symptoms, such as nasal congestion, cough, throat irritation, as well as chills, vomiting, and nausea. Less common signs and symptoms were wheezing, allergic rhinitis, pyrexia, chest discomfort, pruritus, hypotension and blurred vision. Please scroll down to see Important Safety Information for DARZALEX®.
6. Does the availability of OS data influence your decisions on treatment selection in TIE NDMM?
Overall survival absolutely remains the gold standard and informs my practice. Prior to OS data being available, I will often look at other efficacy endpoints that are available sooner. In MAIA, I was encouraged by efficacy endpoints in earlier data, which were later confirmed by the latest data on OS.
7. The MAIA study shows that treating to disease progression or unacceptable toxicity is important. How does that impact your approach to treatment?
It's important to keep in mind that the MAIA trial was designed to evaluate treatment until progression or unacceptable toxicity. The results revealed a significant difference between the DR-d and Rd treatment arms, but results observed in this study are contingent on this treatment approach. From a clinical perspective, unless there is considerable toxicity, I advocate for treating with D-Rd to progression.
In the clinic, we also see that TIE patients who have higher frailty scores are more likely to discontinue treatment prior to progression.10 There can be other reasons too – such as a patient simply wanting to have a break from treatment. These conversations are not always easy, but it is important to have an honest dialogue with patients.
8. What can we learn from studies like the MAIA trial that included a wide range of patient populations including patients who are elderly, frail, or had high cytogenetic risk?
Several patient subgroups were analyzed as part of the MAIA study. It is important to note that these subgroup analyses are not included in the Prescribing Information for DARZALEX®. These analyses were not adjusted for multiple comparisons, and there are insufficient numbers of patients per subgroup to make definitive conclusions of efficacy among the subgroups.
As mentioned above, the MAIA study evaluated a wide range of patients (n=737). The baseline demographic and disease characteristics were similar between the D-Rd and Rd treatment groups and the median age was 73 (range: 45-90) years, with 44% of the patients ≥75 years of age.
In the various patient subgroups that were analyzed as part of the MAIA study, it was found that at ~3-years of follow-up the PFS numerically favored DRd compared with Rd alone in most subgroups (see table below).
Median progression-free survival by sub-population at ~3 year follow-up8
The MAIA trial also included patients who were frail and a post hoc analysis was conducted in this subgroup of patients. These analyses are not included in the Prescribing Information for DARZALEX®. These analyses were conducted post hoc and there are insufficient numbers of patients per subgroup to make definitive conclusions of efficacy among the subgroups.
A frailty assessment was performed retrospectively using age, the Charlson Comorbidity Index (CCI) – which is calculated based on a retrospective review of the patient’s medical history to predict the 10-year mortality – and the baseline Eastern Cooperative Oncology Group (ECOG) performance status score, used to measure a patient’s level of functioning in terms of their ability to care for themselves, daily activity, and physical activity. The frailty scores were then added up to classify patients into fit (0), intermediate (1), or frail (≥2). Frailty status was further simplified into 2 categories: non-frail (0-1) and frail (≥2). The median age in the frail subgroup was 77 years (range: 57-80 years), with 88% of patients having ECOG performance score ≥1. CCI was calculated based on retrospective review of each patient’s medical history.12
The charts below illustrate the frailty scoring system with an overview of the patient population included in the 3-year post hoc analysis, PFS rate, and adverse events.
MAIA post hoc subgroup analysis by frailty status score12
The retrospective assessment of frailty score was a limitation of this study. Retrospective CCI calculations were based on reported medical history, which may contain missing data and result in underestimating or overestimating the number of patients in each frailty subgroup. The ECOG PS score parameter used for frailty score calculations in the study is more subjective, with susceptibility to intra- and inter-observer bias, compared with the ADL (activities of daily living) and IADL (instrumental activities of daily living) scales used in the IMWG scoring system. While the frailty scale used in the study is based on parameters that are routinely assessed in clinical practice for clinical use, the use of comprehensive frailty assessments that more accurately reflect biological or functional frailty will remain important for the further optimization of treatment strategies for frail patients. Patients with an ECOG PS score ≥3 and patients with comorbidities that may interfere with the study procedures were excluded from MAIA; the inclusion and exclusion criteria for the study limits the generalizability of these results to more frail patients seen in clinical practice.
Progression-free survival in a ~3-year subgroup analysis of frail patients following treatment with D-Rd in TIE NDMM12
Most frequent Grade 3/4 treatment-emergent adverse events (≥10%) in frail patients at ~3 year follow-up of MAIA trial12
Please see additional Important Safety Information for DARZALEX® below.
IMPORTANT SAFETY INFORMATION
CONTRAINDICATIONS
DARZALEX® is contraindicated in patients with a history of severe hypersensitivity (eg, anaphylactic reactions) to daratumumab or any of the components of the formulation.
WARNINGS AND PRECAUTIONS
Infusion-Related Reactions
DARZALEX® can cause severe and/or serious infusion-related reactions including anaphylactic reactions. These reactions can be life‑threatening, and fatal outcomes have been reported. In clinical trials (monotherapy and combination: N=2066), infusion-related reactions occurred in 37% of patients with the Week 1 (16 mg/kg) infusion, 2% with the Week 2 infusion, and cumulatively 6% with subsequent infusions. Less than 1% of patients had a Grade 3/4 infusion-related reaction at Week 2 or subsequent infusions. The median time to onset was 1.5 hours (range: 0 to 73 hours). Nearly all reactions occurred during infusion or within 4 hours of completing DARZALEX®. Severe reactions have occurred, including bronchospasm, hypoxia, dyspnea, hypertension, tachycardia, headache, laryngeal edema, pulmonary edema, and ocular adverse reactions, including choroidal effusion, acute myopia, and acute angle closure glaucoma. Signs and symptoms may include respiratory symptoms, such as nasal congestion, cough, throat irritation, as well as chills, vomiting, and nausea. Less common signs and symptoms were wheezing, allergic rhinitis, pyrexia, chest discomfort, pruritus, hypotension and blurred vision.
When DARZALEX® dosing was interrupted in the setting of ASCT (CASSIOPEIA) for a median of 3.75 months (range: 2.4 to 6.9 months), upon re-initiation of DARZALEX®, the incidence of infusion-related reactions was 11% for the first infusion following ASCT. Infusion-related reactions occurring at re-initiation of DARZALEX® following ASCT were consistent in terms of symptoms and severity (Grade 3 or 4: <1%) with those reported in previous studies at Week 2 or subsequent infusions. In EQUULEUS, patients receiving combination treatment (n=97) were administered the first 16 mg/kg dose at Week 1 split over two days, ie, 8 mg/kg on Day 1 and Day 2, respectively. The incidence of any grade infusion-related reactions was 42%, with 36% of patients experiencing infusion-related reactions on Day 1 of Week 1, 4% on Day 2 of Week 1, and 8% with subsequent infusions.
Pre-medicate patients with antihistamines, antipyretics, and corticosteroids. Frequently monitor patients during the entire infusion. Interrupt DARZALEX® infusion for reactions of any severity and institute medical management as needed. Permanently discontinue DARZALEX® therapy if an anaphylactic reaction or life-threatening (Grade 4) reaction occurs and institute appropriate emergency care. For patients with Grade 1, 2, or 3 reactions, reduce the infusion rate when re-starting the infusion.
To reduce the risk of delayed infusion-related reactions, administer oral corticosteroids to all patients following DARZALEX® infusions. Patients with a history of chronic obstructive pulmonary disease may require additional post-infusion medications to manage respiratory complications. Consider prescribing short- and long-acting bronchodilators and inhaled corticosteroids for patients with chronic obstructive pulmonary disease.
Ocular adverse reactions, including acute myopia and narrowing of the anterior chamber angle due to ciliochoroidal effusions with potential for increased intraocular pressure or glaucoma, have occurred with DARZALEX infusion. If ocular symptoms occur, interrupt DARZALEX infusion and seek immediate ophthalmologic evaluation prior to restarting DARZALEX.
Interference With Serological Testing
Daratumumab binds to CD38 on red blood cells (RBCs) and results in a positive indirect antiglobulin test (indirect Coombs test). Daratumumab-mediated positive indirect antiglobulin test may persist for up to 6 months after the last daratumumab infusion. Daratumumab bound to RBCs masks detection of antibodies to minor antigens in the patient’s serum. The determination of a patient’s ABO and Rh blood type is not impacted. Notify blood transfusion centers of this interference with serological testing and inform blood banks that a patient has received DARZALEX®. Type and screen patients prior to starting DARZALEX®.
Neutropenia and Thrombocytopenia
DARZALEX® may increase neutropenia and thrombocytopenia induced by background therapy. Monitor complete blood cell counts periodically during treatment according to manufacturer’s prescribing information for background therapies. Monitor patients with neutropenia for signs of infection. Consider withholding DARZALEX® until recovery of neutrophils or for recovery of platelets.
Interference With Determination of Complete Response
Daratumumab is a human immunoglobulin G (IgG) kappa monoclonal antibody that can be detected on both the serum protein electrophoresis (SPE) and immunofixation (IFE) assays used for the clinical monitoring of endogenous M-protein. This interference can impact the determination of complete response and of disease progression in some patients with IgG kappa myeloma protein.
Embryo-Fetal Toxicity
Based on the mechanism of action, DARZALEX® can cause fetal harm when administered to a pregnant woman. DARZALEX® may cause depletion of fetal immune cells and decreased bone density. Advise pregnant women of the potential risk to a fetus. Advise females with reproductive potential to use effective contraception during treatment with DARZALEX® and for 3 months after the last dose.
The combination of DARZALEX® with lenalidomide, pomalidomide, or thalidomide is contraindicated in pregnant women because lenalidomide, pomalidomide, and thalidomide may cause birth defects and death of the unborn child. Refer to the lenalidomide, pomalidomide, or thalidomide prescribing information on use during pregnancy.
ADVERSE REACTIONS
The most frequently reported adverse reactions (incidence ≥20%) were: upper respiratory infection, neutropenia, infusion‑related reactions, thrombocytopenia, diarrhea, constipation, anemia, peripheral sensory neuropathy, fatigue, peripheral edema, nausea, cough, pyrexia, dyspnea, and asthenia. The most common hematologic laboratory abnormalities (≥40%) with DARZALEX® are: neutropenia, lymphopenia, thrombocytopenia, leukopenia, and anemia.
INDICATIONS
DARZALEX® (daratumumab) is indicated for the treatment of adult patients with multiple myeloma:
- In combination with lenalidomide and dexamethasone in newly diagnosed patients who are ineligible for autologous stem cell transplant and in patients with relapsed or refractory multiple myeloma who have received at least one prior therapy
- In combination with bortezomib, melphalan, and prednisone in newly diagnosed patients who are ineligible for autologous stem cell transplant
- In combination with bortezomib, thalidomide, and dexamethasone in newly diagnosed patients who are eligible for autologous stem cell transplant
- In combination with bortezomib and dexamethasone in patients who have received at least one prior therapy
- In combination with carfilzomib and dexamethasone in patients with relapsed or refractory multiple myeloma who have received one to three prior lines of therapy
- In combination with pomalidomide and dexamethasone in patients who have received at least two prior therapies including lenalidomide and a proteasome inhibitor
- As monotherapy in patients who have received at least three prior lines of therapy including a proteasome inhibitor (PI) and an immunomodulatory agent or who are double-refractory to a PI and an immunomodulatory agent
Please click here to see the full Prescribing Information.
1. Richardson PG, San Miguel JF, Moreau P, et al. Interpreting clinical trial data in multiple myeloma: translating findings to the real-world setting. Blood Cancer J. 2018;8(11). doi:10.1038/s41408-018-0141-0
2. Key Statistics About Multiple Myeloma. Cancer.org. Published 2019. https://www.cancer.org/cancer/multiple-myeloma/about/key-statistics.html
3. Fonseca R, Usmani SZ, Mehra M, et al. Frontline treatment patterns and attrition rates by subsequent lines of therapy in patients with newly diagnosed multiple myeloma. BMC Cancer. 2020;20(1). doi:10.1186/s12885-020-07503-y
4. Devarakonda S, Efebera Y, Sharma N. Role of Stem Cell Transplantation in Multiple Myeloma. Cancers. 2021;13(4):863. doi:10.3390/cancers13040863
5. Derudas D, Capraro F, Martinelli G, Cerchione C. How I manage frontline transplant-ineligible multiple myeloma. Hematol Rep. 2020;12(s1). doi:10.4081/hr.2020.8956
6. Kazandjian D. Multiple myeloma epidemiology and survival: A unique malignancy. Semin Oncl. 2016;43(6):676-681. doi:10.1053/j.seminoncol.2016.11.004
7. Facon T, Kumar S, Plesner T, et al. Daratumumab plus lenalidomide and dexamethasone for untreated myeloma. N. Engl. J. Med. 2019;380(22):2104-2115. doi:10.1056/nejmoa1817249
8. DARZALEX® [Prescribing Information]. Horsham, PA: Janssen Biotech, Inc.
9. Facon T, Kumar SK, Plesner T, et al. Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(11):1582-1596. doi:10.1016/s1470-2045(21)00466-6
10. Facon T, Dimopoulos MA, Meuleman N, et al. A simplified frailty scale predicts outcomes in transplant-ineligible patients with newly diagnosed multiple myeloma treated in the FIRST (MM-020) trial. Leukemia. 2019;34(1):224-233. doi:10.1038/s41375-019-0539-0
11. Facon T, Kumar SK, Plesner T, et al. Supplement to: Daratumumab, lenalidomide, and dexamethasone versus lenalidomide and dexamethasone alone in newly diagnosed multiple myeloma (MAIA): overall survival results from a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(11):1582-1596.
12. Facon T, Cook G, Usmani SZ, et al. Daratumumab plus lenalidomide and dexamethasone in transplant-ineligible newly diagnosed multiple myeloma: frailty subgroup analysis of MAIA. Leukemia. 2022;36(4):1066-1077. doi:10.1038/s41375-021-01488-8
© Janssen Biotech, Inc. 2022 All rights reserved. 12/22 cp-333446v1