User login
In Case You Missed It: COVID
Clinical factors and treatment tied to COVID-19 mortality in cancer patients
according to two presentations at the European Society for Medical Oncology Virtual Congress 2020.
Two analyses of data from the COVID-19 and Cancer Consortium (CCC19) were presented at the meeting.
The data suggest that older age, male sex, more comorbidities, poor performance status, progressive cancer or multiple cancers, hematologic malignancy, and recent cancer therapy are all associated with higher mortality among patients with cancer and COVID-19. Anti-CD20 therapy is associated with an especially high mortality rate, according to an investigator.
Among hospitalized patients, increased absolute neutrophil count as well as abnormal D-dimer, high-sensitivity troponin, and C-reactive protein are associated with a higher risk of mortality.
Prior analyses of CCC19 data pointed to several factors associated with higher COVID-19 death rates, according to Petros Grivas, MD, PhD, of University of Washington, Seattle, who presented some CCC19 data at the meeting. However, the prior analyses were limited by weak statistical power and low event rates, Dr. Grivas said.
Clinical and laboratory factors: Abstract LBA72
The aim of Dr. Grivas’s analysis was to validate a priori identified demographic and clinicopathologic factors associated with 30-day all-cause mortality in patients with COVID-19 and cancer. Dr. Grivas and colleagues also explored the potential association between laboratory parameters and 30-day all-cause mortality.
The analysis included 3,899 patients with cancer and COVID-19 from 124 centers. Most centers are in the United States, but 4% are in Canada, and 2% are in Spain. About two-thirds of patients were 60 years of age or younger at baseline, half were men, 79% had solid tumors, and 21% had hematologic malignancies.
Cancer-specific factors associated with an increased risk of 30-day all-cause mortality were having progressive cancer (adjusted odds ratio, 2.9), receiving cancer therapy within 3 months (aOR, 1.2), having a hematologic versus solid tumor (aOR, 1.7), and having multiple malignancies (aOR, 1.5).
Clinical factors associated with an increased risk of 30-day all-cause mortality were Black versus White race (aOR, 1.5), older age (aOR, 1.7 per 10 years), three or more actively treated comorbidities (versus none; aOR, 2.1), and Eastern Cooperative Oncology Group performance status of 2 or more (versus 0; aOR, 4.6).
In hospitalized patients, several laboratory variables were associated with an increased risk of 30-day all-cause mortality. Having an absolute neutrophil count above the upper limit of normal doubled the risk (aOR, 2.0), while abnormal D-dimer, high-sensitivity troponin, and C-reactive protein all more than doubled the risk of mortality (aORs of 2.5, 2.5, and 2.4, respectively).
Further risk modeling with multivariable analysis will be performed after longer follow-up, Dr. Grivas noted.
Treatment-related outcomes: Abstract LBA71
An additional analysis of CCC19 data encompassed 3,654 patients. In this analysis, researchers investigated the correlation between timing of cancer treatment and COVID-19–related complications and 30-day mortality.
Mortality was highest among cancer patients treated 1-3 months prior to COVID-19 diagnosis, with all-cause mortality at 28%, said Trisha M. Wise-Draper, MD, PhD, of University of Cincinnati, when presenting the data at the meeting.
Rates for other complications (hospitalization, oxygen required, ICU admission, and mechanical ventilation) were similar regardless of treatment timing.
The unadjusted 30-day mortality rate was highest for patients treated most recently with chemoimmunotherapy (30%), followed by chemotherapy (18%), chemoradiotherapy (18%), and targeted therapy (17%).
The mortality rate was “particularly high,” at 50%, in patients receiving anti-CD20 therapy 1-3 months prior to COVID-19 diagnosis – the time period for which significant B-cell depletion develops, Dr. Wise-Draper observed.
An analysis of disease status among 1,449 patients treated within 3 months of COVID-19 diagnosis showed mortality risk increasing from 6% among patients in remission or with newly emergent disease, to 22% in patients with any active cancer, to 34% in those with progressing disease, Dr. Wise-Draper said.
Discussant Benjamin Solomon, MD, PhD, of Peter MacCallum Cancer Centre in Melbourne, made note of the high 30-day mortality rate seen in patients receiving anti-CD20 therapy as well as the elevated standardized mortality ratios with recent chemoimmunotherapy and targeted therapy.
“Although there are some limitations of this analysis, it provides the best data we have to date about the effects of treatment on early mortality in patients with COVID-19 and cancer. It points to a modest but heterogeneous effect of treatment on outcome, one which is likely to become clearer with larger cohorts and additional analysis,” Dr. Solomon said.
This research was funded by the American Cancer Society, Hope Foundation for Cancer Research, Jim and Carol O’Hare Fund, National Cancer Institute, National Human Genome Research Institute, Vanderbilt Institute for Clinical and Translational Research, and Fonds de Recherche du Quebec-Sante. Dr. Grivas disclosed relationships with many companies, but none are related to this work. Dr. Wise-Draper disclosed relationships with Merck, Bristol-Myers Squibb, Tesaro, GlaxoSmithKline, AstraZeneca, Shattuck Labs, and Rakuten. Dr. Solomon disclosed relationships with Amgen, AstraZeneca, Merck, Bristol-Myers Squibb, Novartis, Pfizer, and Roche-Genentech.
SOURCES: Grivas P et al. ESMO 2020, Abstract LBA72; Wise-Draper TM et al. ESMO 2020, Abstract LBA71.
according to two presentations at the European Society for Medical Oncology Virtual Congress 2020.
Two analyses of data from the COVID-19 and Cancer Consortium (CCC19) were presented at the meeting.
The data suggest that older age, male sex, more comorbidities, poor performance status, progressive cancer or multiple cancers, hematologic malignancy, and recent cancer therapy are all associated with higher mortality among patients with cancer and COVID-19. Anti-CD20 therapy is associated with an especially high mortality rate, according to an investigator.
Among hospitalized patients, increased absolute neutrophil count as well as abnormal D-dimer, high-sensitivity troponin, and C-reactive protein are associated with a higher risk of mortality.
Prior analyses of CCC19 data pointed to several factors associated with higher COVID-19 death rates, according to Petros Grivas, MD, PhD, of University of Washington, Seattle, who presented some CCC19 data at the meeting. However, the prior analyses were limited by weak statistical power and low event rates, Dr. Grivas said.
Clinical and laboratory factors: Abstract LBA72
The aim of Dr. Grivas’s analysis was to validate a priori identified demographic and clinicopathologic factors associated with 30-day all-cause mortality in patients with COVID-19 and cancer. Dr. Grivas and colleagues also explored the potential association between laboratory parameters and 30-day all-cause mortality.
The analysis included 3,899 patients with cancer and COVID-19 from 124 centers. Most centers are in the United States, but 4% are in Canada, and 2% are in Spain. About two-thirds of patients were 60 years of age or younger at baseline, half were men, 79% had solid tumors, and 21% had hematologic malignancies.
Cancer-specific factors associated with an increased risk of 30-day all-cause mortality were having progressive cancer (adjusted odds ratio, 2.9), receiving cancer therapy within 3 months (aOR, 1.2), having a hematologic versus solid tumor (aOR, 1.7), and having multiple malignancies (aOR, 1.5).
Clinical factors associated with an increased risk of 30-day all-cause mortality were Black versus White race (aOR, 1.5), older age (aOR, 1.7 per 10 years), three or more actively treated comorbidities (versus none; aOR, 2.1), and Eastern Cooperative Oncology Group performance status of 2 or more (versus 0; aOR, 4.6).
In hospitalized patients, several laboratory variables were associated with an increased risk of 30-day all-cause mortality. Having an absolute neutrophil count above the upper limit of normal doubled the risk (aOR, 2.0), while abnormal D-dimer, high-sensitivity troponin, and C-reactive protein all more than doubled the risk of mortality (aORs of 2.5, 2.5, and 2.4, respectively).
Further risk modeling with multivariable analysis will be performed after longer follow-up, Dr. Grivas noted.
Treatment-related outcomes: Abstract LBA71
An additional analysis of CCC19 data encompassed 3,654 patients. In this analysis, researchers investigated the correlation between timing of cancer treatment and COVID-19–related complications and 30-day mortality.
Mortality was highest among cancer patients treated 1-3 months prior to COVID-19 diagnosis, with all-cause mortality at 28%, said Trisha M. Wise-Draper, MD, PhD, of University of Cincinnati, when presenting the data at the meeting.
Rates for other complications (hospitalization, oxygen required, ICU admission, and mechanical ventilation) were similar regardless of treatment timing.
The unadjusted 30-day mortality rate was highest for patients treated most recently with chemoimmunotherapy (30%), followed by chemotherapy (18%), chemoradiotherapy (18%), and targeted therapy (17%).
The mortality rate was “particularly high,” at 50%, in patients receiving anti-CD20 therapy 1-3 months prior to COVID-19 diagnosis – the time period for which significant B-cell depletion develops, Dr. Wise-Draper observed.
An analysis of disease status among 1,449 patients treated within 3 months of COVID-19 diagnosis showed mortality risk increasing from 6% among patients in remission or with newly emergent disease, to 22% in patients with any active cancer, to 34% in those with progressing disease, Dr. Wise-Draper said.
Discussant Benjamin Solomon, MD, PhD, of Peter MacCallum Cancer Centre in Melbourne, made note of the high 30-day mortality rate seen in patients receiving anti-CD20 therapy as well as the elevated standardized mortality ratios with recent chemoimmunotherapy and targeted therapy.
“Although there are some limitations of this analysis, it provides the best data we have to date about the effects of treatment on early mortality in patients with COVID-19 and cancer. It points to a modest but heterogeneous effect of treatment on outcome, one which is likely to become clearer with larger cohorts and additional analysis,” Dr. Solomon said.
This research was funded by the American Cancer Society, Hope Foundation for Cancer Research, Jim and Carol O’Hare Fund, National Cancer Institute, National Human Genome Research Institute, Vanderbilt Institute for Clinical and Translational Research, and Fonds de Recherche du Quebec-Sante. Dr. Grivas disclosed relationships with many companies, but none are related to this work. Dr. Wise-Draper disclosed relationships with Merck, Bristol-Myers Squibb, Tesaro, GlaxoSmithKline, AstraZeneca, Shattuck Labs, and Rakuten. Dr. Solomon disclosed relationships with Amgen, AstraZeneca, Merck, Bristol-Myers Squibb, Novartis, Pfizer, and Roche-Genentech.
SOURCES: Grivas P et al. ESMO 2020, Abstract LBA72; Wise-Draper TM et al. ESMO 2020, Abstract LBA71.
according to two presentations at the European Society for Medical Oncology Virtual Congress 2020.
Two analyses of data from the COVID-19 and Cancer Consortium (CCC19) were presented at the meeting.
The data suggest that older age, male sex, more comorbidities, poor performance status, progressive cancer or multiple cancers, hematologic malignancy, and recent cancer therapy are all associated with higher mortality among patients with cancer and COVID-19. Anti-CD20 therapy is associated with an especially high mortality rate, according to an investigator.
Among hospitalized patients, increased absolute neutrophil count as well as abnormal D-dimer, high-sensitivity troponin, and C-reactive protein are associated with a higher risk of mortality.
Prior analyses of CCC19 data pointed to several factors associated with higher COVID-19 death rates, according to Petros Grivas, MD, PhD, of University of Washington, Seattle, who presented some CCC19 data at the meeting. However, the prior analyses were limited by weak statistical power and low event rates, Dr. Grivas said.
Clinical and laboratory factors: Abstract LBA72
The aim of Dr. Grivas’s analysis was to validate a priori identified demographic and clinicopathologic factors associated with 30-day all-cause mortality in patients with COVID-19 and cancer. Dr. Grivas and colleagues also explored the potential association between laboratory parameters and 30-day all-cause mortality.
The analysis included 3,899 patients with cancer and COVID-19 from 124 centers. Most centers are in the United States, but 4% are in Canada, and 2% are in Spain. About two-thirds of patients were 60 years of age or younger at baseline, half were men, 79% had solid tumors, and 21% had hematologic malignancies.
Cancer-specific factors associated with an increased risk of 30-day all-cause mortality were having progressive cancer (adjusted odds ratio, 2.9), receiving cancer therapy within 3 months (aOR, 1.2), having a hematologic versus solid tumor (aOR, 1.7), and having multiple malignancies (aOR, 1.5).
Clinical factors associated with an increased risk of 30-day all-cause mortality were Black versus White race (aOR, 1.5), older age (aOR, 1.7 per 10 years), three or more actively treated comorbidities (versus none; aOR, 2.1), and Eastern Cooperative Oncology Group performance status of 2 or more (versus 0; aOR, 4.6).
In hospitalized patients, several laboratory variables were associated with an increased risk of 30-day all-cause mortality. Having an absolute neutrophil count above the upper limit of normal doubled the risk (aOR, 2.0), while abnormal D-dimer, high-sensitivity troponin, and C-reactive protein all more than doubled the risk of mortality (aORs of 2.5, 2.5, and 2.4, respectively).
Further risk modeling with multivariable analysis will be performed after longer follow-up, Dr. Grivas noted.
Treatment-related outcomes: Abstract LBA71
An additional analysis of CCC19 data encompassed 3,654 patients. In this analysis, researchers investigated the correlation between timing of cancer treatment and COVID-19–related complications and 30-day mortality.
Mortality was highest among cancer patients treated 1-3 months prior to COVID-19 diagnosis, with all-cause mortality at 28%, said Trisha M. Wise-Draper, MD, PhD, of University of Cincinnati, when presenting the data at the meeting.
Rates for other complications (hospitalization, oxygen required, ICU admission, and mechanical ventilation) were similar regardless of treatment timing.
The unadjusted 30-day mortality rate was highest for patients treated most recently with chemoimmunotherapy (30%), followed by chemotherapy (18%), chemoradiotherapy (18%), and targeted therapy (17%).
The mortality rate was “particularly high,” at 50%, in patients receiving anti-CD20 therapy 1-3 months prior to COVID-19 diagnosis – the time period for which significant B-cell depletion develops, Dr. Wise-Draper observed.
An analysis of disease status among 1,449 patients treated within 3 months of COVID-19 diagnosis showed mortality risk increasing from 6% among patients in remission or with newly emergent disease, to 22% in patients with any active cancer, to 34% in those with progressing disease, Dr. Wise-Draper said.
Discussant Benjamin Solomon, MD, PhD, of Peter MacCallum Cancer Centre in Melbourne, made note of the high 30-day mortality rate seen in patients receiving anti-CD20 therapy as well as the elevated standardized mortality ratios with recent chemoimmunotherapy and targeted therapy.
“Although there are some limitations of this analysis, it provides the best data we have to date about the effects of treatment on early mortality in patients with COVID-19 and cancer. It points to a modest but heterogeneous effect of treatment on outcome, one which is likely to become clearer with larger cohorts and additional analysis,” Dr. Solomon said.
This research was funded by the American Cancer Society, Hope Foundation for Cancer Research, Jim and Carol O’Hare Fund, National Cancer Institute, National Human Genome Research Institute, Vanderbilt Institute for Clinical and Translational Research, and Fonds de Recherche du Quebec-Sante. Dr. Grivas disclosed relationships with many companies, but none are related to this work. Dr. Wise-Draper disclosed relationships with Merck, Bristol-Myers Squibb, Tesaro, GlaxoSmithKline, AstraZeneca, Shattuck Labs, and Rakuten. Dr. Solomon disclosed relationships with Amgen, AstraZeneca, Merck, Bristol-Myers Squibb, Novartis, Pfizer, and Roche-Genentech.
SOURCES: Grivas P et al. ESMO 2020, Abstract LBA72; Wise-Draper TM et al. ESMO 2020, Abstract LBA71.
FROM ESMO 2020
One measure of child COVID-19 may be trending downward
After increasing for several weeks, the proportion of new COVID-19 cases occurring in children has dropped for the second week in a row, according to data in a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
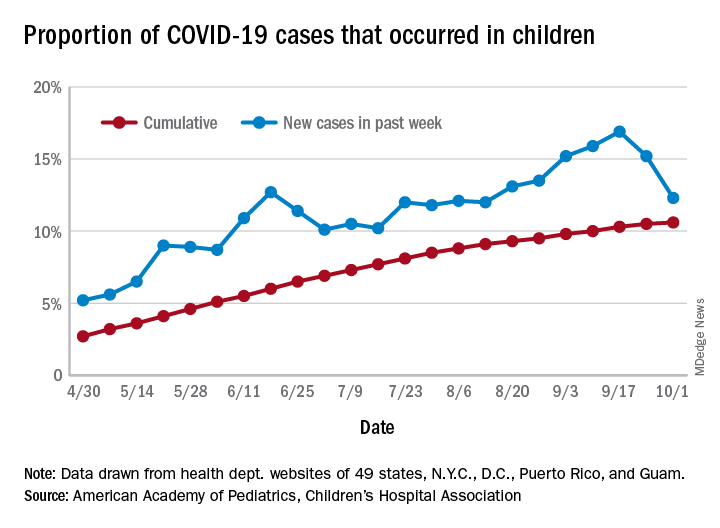
COVID-19 cases in children accounted for 12.3% of all new cases in the United States for the week ending Oct. 1, down from 15.2% the previous week. That measure had reached its highest point, 16.9%, just one week earlier (Sept. 17), the AAP and the CHA said in their weekly COVID-19 report.
based on data from the health departments of 49 states (New York does not provide ages on its website), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
The child COVID-19 rate for the United States was 874 per 100,000 children as of Oct. 1, and that figure has doubled since the end of July. At the state level, the highest rates can be found in Tennessee (2,031.4 per 100,000), North Dakota (2,029.6), and South Carolina (2,002.6), with the lowest rates in Vermont (168.9), Maine (229.1), and New Hampshire (268.3), the AAP/CHA report shows.
The children of Wyoming make up the largest share, 22.4%, of any state’s COVID-19 cases, followed by North Dakota and Tennessee, both at 18.3%. New Jersey is lower than any other state at 3.9%, although New York City is a slightly lower 3.6%, the AAP and CHA said.
“The data are limited because the states differ in how they report the data, and it is unknown how many children have been infected but not tested. It is unclear how much of the increase in child cases is due to increased testing capacity,” the AAP said in an earlier statement.
After increasing for several weeks, the proportion of new COVID-19 cases occurring in children has dropped for the second week in a row, according to data in a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
COVID-19 cases in children accounted for 12.3% of all new cases in the United States for the week ending Oct. 1, down from 15.2% the previous week. That measure had reached its highest point, 16.9%, just one week earlier (Sept. 17), the AAP and the CHA said in their weekly COVID-19 report.
based on data from the health departments of 49 states (New York does not provide ages on its website), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
The child COVID-19 rate for the United States was 874 per 100,000 children as of Oct. 1, and that figure has doubled since the end of July. At the state level, the highest rates can be found in Tennessee (2,031.4 per 100,000), North Dakota (2,029.6), and South Carolina (2,002.6), with the lowest rates in Vermont (168.9), Maine (229.1), and New Hampshire (268.3), the AAP/CHA report shows.
The children of Wyoming make up the largest share, 22.4%, of any state’s COVID-19 cases, followed by North Dakota and Tennessee, both at 18.3%. New Jersey is lower than any other state at 3.9%, although New York City is a slightly lower 3.6%, the AAP and CHA said.
“The data are limited because the states differ in how they report the data, and it is unknown how many children have been infected but not tested. It is unclear how much of the increase in child cases is due to increased testing capacity,” the AAP said in an earlier statement.
After increasing for several weeks, the proportion of new COVID-19 cases occurring in children has dropped for the second week in a row, according to data in a new report from the American Academy of Pediatrics and the Children’s Hospital Association.
COVID-19 cases in children accounted for 12.3% of all new cases in the United States for the week ending Oct. 1, down from 15.2% the previous week. That measure had reached its highest point, 16.9%, just one week earlier (Sept. 17), the AAP and the CHA said in their weekly COVID-19 report.
based on data from the health departments of 49 states (New York does not provide ages on its website), as well as the District of Columbia, New York City, Puerto Rico, and Guam.
The child COVID-19 rate for the United States was 874 per 100,000 children as of Oct. 1, and that figure has doubled since the end of July. At the state level, the highest rates can be found in Tennessee (2,031.4 per 100,000), North Dakota (2,029.6), and South Carolina (2,002.6), with the lowest rates in Vermont (168.9), Maine (229.1), and New Hampshire (268.3), the AAP/CHA report shows.
The children of Wyoming make up the largest share, 22.4%, of any state’s COVID-19 cases, followed by North Dakota and Tennessee, both at 18.3%. New Jersey is lower than any other state at 3.9%, although New York City is a slightly lower 3.6%, the AAP and CHA said.
“The data are limited because the states differ in how they report the data, and it is unknown how many children have been infected but not tested. It is unclear how much of the increase in child cases is due to increased testing capacity,” the AAP said in an earlier statement.
CMS gives hospitals 14 weeks to start daily COVID, flu reports
The federal government is giving hospitals 14 weeks to comply with daily reporting requirements for COVID-19.
The Centers for Medicare & Medicaid Services will send letters on October 7 to all 6,200 hospitals that receive reimbursement from the two federal health programs informing them of how well they are doing now, said CMS Administrator Seema Verma on a press call.
Verma would not give an estimate on how many hospitals are currently not compliant. But Deborah Birx, MD, a member of the White House Coronavirus Task Force, said on the call that 86% of hospitals are currently reporting daily.
Federal officials on the call also announced that hospitals would have the option to begin reporting certain data on influenza starting October 19, but that it would become mandatory a few weeks later.
The reporting is important “to really ensure that we’re triangulating all data to understand where this epidemic is, how it’s moving through different populations, and ensuring that we’re meeting the needs of specific hospitals and communities,” Birx said.
The federal government began a new hospital reporting system in April but did not require hospitals to participate until it quietly issued guidance in mid-July informing facilities that they should no longer report to the Centers for Disease Control and Prevention (CDC).
The move perplexed many public health experts and epidemiologists, who expressed concern that asking hospitals to use a new data system during a pandemic could result in delays and lost information. The new HHS data collection site, HHS Protect, is being managed by a private contractor, not the CDC, which also raised alarms.
The final CMS rule issued in August went into effect immediately, without any chance for comment or revision. CMS said at the time that the pandemic was reason enough to skip over the normal bureaucratic process.
Hospitals were not pleased. But Verma claimed that since then CMS had been working with hospital organizations on enforcement.
“We’re going to do everything we can to facilitate reporting, including an enforcement timeline that will provide hospitals ample opportunity to come into compliance,” she said.
Hospitals that do not comply will get a notice every 3 weeks. Three weeks after the second notice, they’ll get weekly notices for a month, and a final termination notice at 14 weeks.
The Federation of American Hospitals (FAH), however, said their members were still not happy. “It is both inappropriate and frankly overkill for CMS to tie compliance with reporting to Medicare conditions of participation,” said FAH President and CEO Chip Kahn in a statement. He called the CMS proposal “sledgehammer enforcement,” and said that the continuing data request might weaken hospitals’ response to the pandemic because it would divert time and money away from patient care.
Rick Pollack, president and CEO of the American Hospital Association called the CMS rule an “overly heavy-handed approach that could jeopardize access to hospital care for all Americans.” He noted in a statement that barring hospitals from Medicare and Medicaid could harm beneficiaries and the effort to provide COVID care.
Pollack also noted that AHA has “observed errors in data processing and confusion about exactly what was being requested at the hospital, state, contractor, and federal level, and has worked diligently with the federal agencies to identify and correct those problems.”
The document that lays out U.S. Department of Health and Human Services (HHS) Protect reporting requirements were updated again on October 6 to add influenza data. The hospitals must report on total patients with laboratory-confirmed flu; previous day’s flu admissions; total ICU patients with lab-confirmed flu; total inpatients with either flu or COVID-19; and the previous day’s deaths for flu and COVID.
CDC Director Robert Redfield, MD, said on the press call that the new data will give the agency crucial hospital-level information and perhaps better estimates of the flu burden. Flu trends have been tracked using the CDC’s Influenza Hospitalization Surveillance Network (FluSurv-NET), which will not be replaced, Redfield said. But that network only tracks hospitalizations in 14 states and does not provide information in “nearly real-time,” he said.
Having the new data “will give us a true situational awareness of severe respiratory illness, provide local hospitalization trends, and help direct resources such as antiretrovirals to address potential increased impact of flu and COVID cocirculation,” Redfield said.
This article first appeared on Medscape.com.
The federal government is giving hospitals 14 weeks to comply with daily reporting requirements for COVID-19.
The Centers for Medicare & Medicaid Services will send letters on October 7 to all 6,200 hospitals that receive reimbursement from the two federal health programs informing them of how well they are doing now, said CMS Administrator Seema Verma on a press call.
Verma would not give an estimate on how many hospitals are currently not compliant. But Deborah Birx, MD, a member of the White House Coronavirus Task Force, said on the call that 86% of hospitals are currently reporting daily.
Federal officials on the call also announced that hospitals would have the option to begin reporting certain data on influenza starting October 19, but that it would become mandatory a few weeks later.
The reporting is important “to really ensure that we’re triangulating all data to understand where this epidemic is, how it’s moving through different populations, and ensuring that we’re meeting the needs of specific hospitals and communities,” Birx said.
The federal government began a new hospital reporting system in April but did not require hospitals to participate until it quietly issued guidance in mid-July informing facilities that they should no longer report to the Centers for Disease Control and Prevention (CDC).
The move perplexed many public health experts and epidemiologists, who expressed concern that asking hospitals to use a new data system during a pandemic could result in delays and lost information. The new HHS data collection site, HHS Protect, is being managed by a private contractor, not the CDC, which also raised alarms.
The final CMS rule issued in August went into effect immediately, without any chance for comment or revision. CMS said at the time that the pandemic was reason enough to skip over the normal bureaucratic process.
Hospitals were not pleased. But Verma claimed that since then CMS had been working with hospital organizations on enforcement.
“We’re going to do everything we can to facilitate reporting, including an enforcement timeline that will provide hospitals ample opportunity to come into compliance,” she said.
Hospitals that do not comply will get a notice every 3 weeks. Three weeks after the second notice, they’ll get weekly notices for a month, and a final termination notice at 14 weeks.
The Federation of American Hospitals (FAH), however, said their members were still not happy. “It is both inappropriate and frankly overkill for CMS to tie compliance with reporting to Medicare conditions of participation,” said FAH President and CEO Chip Kahn in a statement. He called the CMS proposal “sledgehammer enforcement,” and said that the continuing data request might weaken hospitals’ response to the pandemic because it would divert time and money away from patient care.
Rick Pollack, president and CEO of the American Hospital Association called the CMS rule an “overly heavy-handed approach that could jeopardize access to hospital care for all Americans.” He noted in a statement that barring hospitals from Medicare and Medicaid could harm beneficiaries and the effort to provide COVID care.
Pollack also noted that AHA has “observed errors in data processing and confusion about exactly what was being requested at the hospital, state, contractor, and federal level, and has worked diligently with the federal agencies to identify and correct those problems.”
The document that lays out U.S. Department of Health and Human Services (HHS) Protect reporting requirements were updated again on October 6 to add influenza data. The hospitals must report on total patients with laboratory-confirmed flu; previous day’s flu admissions; total ICU patients with lab-confirmed flu; total inpatients with either flu or COVID-19; and the previous day’s deaths for flu and COVID.
CDC Director Robert Redfield, MD, said on the press call that the new data will give the agency crucial hospital-level information and perhaps better estimates of the flu burden. Flu trends have been tracked using the CDC’s Influenza Hospitalization Surveillance Network (FluSurv-NET), which will not be replaced, Redfield said. But that network only tracks hospitalizations in 14 states and does not provide information in “nearly real-time,” he said.
Having the new data “will give us a true situational awareness of severe respiratory illness, provide local hospitalization trends, and help direct resources such as antiretrovirals to address potential increased impact of flu and COVID cocirculation,” Redfield said.
This article first appeared on Medscape.com.
The federal government is giving hospitals 14 weeks to comply with daily reporting requirements for COVID-19.
The Centers for Medicare & Medicaid Services will send letters on October 7 to all 6,200 hospitals that receive reimbursement from the two federal health programs informing them of how well they are doing now, said CMS Administrator Seema Verma on a press call.
Verma would not give an estimate on how many hospitals are currently not compliant. But Deborah Birx, MD, a member of the White House Coronavirus Task Force, said on the call that 86% of hospitals are currently reporting daily.
Federal officials on the call also announced that hospitals would have the option to begin reporting certain data on influenza starting October 19, but that it would become mandatory a few weeks later.
The reporting is important “to really ensure that we’re triangulating all data to understand where this epidemic is, how it’s moving through different populations, and ensuring that we’re meeting the needs of specific hospitals and communities,” Birx said.
The federal government began a new hospital reporting system in April but did not require hospitals to participate until it quietly issued guidance in mid-July informing facilities that they should no longer report to the Centers for Disease Control and Prevention (CDC).
The move perplexed many public health experts and epidemiologists, who expressed concern that asking hospitals to use a new data system during a pandemic could result in delays and lost information. The new HHS data collection site, HHS Protect, is being managed by a private contractor, not the CDC, which also raised alarms.
The final CMS rule issued in August went into effect immediately, without any chance for comment or revision. CMS said at the time that the pandemic was reason enough to skip over the normal bureaucratic process.
Hospitals were not pleased. But Verma claimed that since then CMS had been working with hospital organizations on enforcement.
“We’re going to do everything we can to facilitate reporting, including an enforcement timeline that will provide hospitals ample opportunity to come into compliance,” she said.
Hospitals that do not comply will get a notice every 3 weeks. Three weeks after the second notice, they’ll get weekly notices for a month, and a final termination notice at 14 weeks.
The Federation of American Hospitals (FAH), however, said their members were still not happy. “It is both inappropriate and frankly overkill for CMS to tie compliance with reporting to Medicare conditions of participation,” said FAH President and CEO Chip Kahn in a statement. He called the CMS proposal “sledgehammer enforcement,” and said that the continuing data request might weaken hospitals’ response to the pandemic because it would divert time and money away from patient care.
Rick Pollack, president and CEO of the American Hospital Association called the CMS rule an “overly heavy-handed approach that could jeopardize access to hospital care for all Americans.” He noted in a statement that barring hospitals from Medicare and Medicaid could harm beneficiaries and the effort to provide COVID care.
Pollack also noted that AHA has “observed errors in data processing and confusion about exactly what was being requested at the hospital, state, contractor, and federal level, and has worked diligently with the federal agencies to identify and correct those problems.”
The document that lays out U.S. Department of Health and Human Services (HHS) Protect reporting requirements were updated again on October 6 to add influenza data. The hospitals must report on total patients with laboratory-confirmed flu; previous day’s flu admissions; total ICU patients with lab-confirmed flu; total inpatients with either flu or COVID-19; and the previous day’s deaths for flu and COVID.
CDC Director Robert Redfield, MD, said on the press call that the new data will give the agency crucial hospital-level information and perhaps better estimates of the flu burden. Flu trends have been tracked using the CDC’s Influenza Hospitalization Surveillance Network (FluSurv-NET), which will not be replaced, Redfield said. But that network only tracks hospitalizations in 14 states and does not provide information in “nearly real-time,” he said.
Having the new data “will give us a true situational awareness of severe respiratory illness, provide local hospitalization trends, and help direct resources such as antiretrovirals to address potential increased impact of flu and COVID cocirculation,” Redfield said.
This article first appeared on Medscape.com.
Optimal sedation strategies for COVID-19 ICU patients: A work in progress
According to the best available evidence, analagosedation remains the focus for managing COVID-19 ICU patients, according to Steven B. Greenberg, MD, FCCP, FCCM.

“The choice of sedation and analgesia is important,” Dr. Greenberg, vice chair of education in the department of anesthesiology at Evanston Hospital, part of NorthShore University Health System, Chicago, said at a Society for Critical Care virtual meeting: COVID-19: What’s Next. “We know that the right choice of these two components may increase liberation from ventilators, earlier ICU discharge, and return to normal brain function and independent functional status.”
Analgesia first
Prior to the current pandemic, the approach to sedation of patients in the ICU was based on the PADIS Guidelines of 2018, which call for an assessment-driven, protocol-based stepwise approach to pain and sedation management in critically ill adults (Crit Care Med. 2018;46:e825-73). “” Dr. Greenberg said. “We know that pain management should be a priority of sedation, because pain may increase the risk of delirium, anxiety, and endocrine suppression, and may increase the risk of release of endogenous catecholamines, ischemia, and hypermetabolic states.”
Fentanyl appears to be the most common opioid analgesic used for patients in the ICU, “but fentanyl is a very lipophilic drug and has a long context-sensitive half-life,” he said. “There are components to fentanyl that allow it to become a very long-acting drug upon days and days of infusion. Another opioid used is remifentanil, which is typically short-acting because it is broken down in the blood by esterases, but may cause rigidity at higher doses. Dilaudid seems to be the least affected by organ dysfunction. In our very critically ill, prolonged mechanically ventilated COVID-19 patients, we’ve been using methadone for its NMDA [N-methyl-D-aspartate] antagonistic effect and its opioid-sparing effects.”
As for nonopioid analgesics, Dr. Greenberg said that clinicians have shied away from using NSAIDs because of their side effects. “Tramadol indirectly inhibits reuptake of norepinephrine and serotonin, and ketamine is being used a lot more because of its NMDA antagonist effect,” he said. “Lidocaine and gabapentin have also been used.”
In a recent systematic review and meta-analysis, researchers assessed 34 trials that examined adjuvant analgesic use with an opioid in critically ill patients versus an opioid alone (Crit Care Expl. 2020;2:e0157). They found that when using an adjuvant such as acetaminophen, clonidine, dexmedetomidine, gabapentin, ketamine, magnesium, nefopam, NSAIDs, pregabalin, and tramadol, there was a reduction in pain scores as well as a reduction in opioid consumption. “So, clinicians should consider using adjuvant agents to limit opioid exposure and improve pain scores in the critically ill,” Dr. Greenberg said.
ICU delirium: Risk factors, prevention
Delirium in COVID-19 patients treated in the ICU of particular concern. According to a systematic review of 33 studies, 11 risk factors for delirium in the ICU were supported by strong or moderate levels of evidence (Crit Care Med. 2015;43:40-7). These include age, dementia, hypertension, emergency surgery, trauma, APACHE score of II, need for mechanical ventilation, metabolic acidosis, delirium on prior day, coma, and dexmedetomidine use. Risk factors for ICU delirium among COVID-19 patients, however, “are far different,” Dr. Greenberg said. “Why? First and foremost, we are restricting visitation of family,” he said. “That family connection largely can be lost. Second, there are limitations of nonpharmacologic interventions. There is less mobility and physical therapy employed because of the risk of health care workers’ exposure to the virus. There’s also uncertainty about the global pandemic. Anxiety and depression come with that, as well as disruptions to spiritual and religious services.”
Strategies for preventing delirium remain the same as before the pandemic and in accord with recent clinical practice guidelines: Reduce the use of certain drugs such as benzodiazepines and narcotics, reorient the patients, treat dehydration, use hearing aids and eyeglasses in patients who have them, use ear plugs to cancel noise, mobilize patients, maintain sleep/awake cycles, and encourage sedation holidays (Crit Care Med. 2018;46[9]:e825-73).
A recent study from France found that among 58 patients with COVID-19, 65% had positive Confusion Assessment Method (CAM)–ICU findings and 69% had agitation (N Engl J Med 2020;382:2268-70). Most of the patients (86%) received midazolam, 47% received propofol, and all received sufentanil. “In the pre-COVID days, we would use midazolam as a second-line agent for many of these patients,” Dr. Greenberg said. “So, times really have changed.”
The fate of COVID-19 patients following discharge from the ICU remains a concern, continued Dr. Greenberg, clinical professor of anesthesiology at the University of Chicago. A recent journal article by Michelle Biehl, MD, and Denise Sese, MD, noted that post–intensive care syndrome (PICS) or new or worsening impairment in any physical, cognitive, or mental domain is of significant concern among COVID-19 patients following their ICU stay (Cleveland Clin J Med 2020 Aug doi: 10.3949/ccjm.87a.ccc055). The authors stated that COVID-19 patients may face a higher risk of PICS because of restricted family visitation, prolonged mechanical ventilation, exposure to higher amounts of sedatives, and limited physical therapy during hospital stay.
No ideal sedative agent
The 2018 PADIS Guidelines on the use of ICU sedation suggested strong evidence for modifiable risk factors producing delirium in the context of benzodiazepines and blood transfusion. They recommend a light level of sedation and the use of propofol or dexmedetomidine over benzodiazepines. They also recommend routine delirium testing such as using the CAM-ICU or Intensive Care Delirium Screening Checklist (ICDSC) and nonpharmacologic therapies such as reorientation, cognitive stimulation, sleep improvement, and mobilization.
Several sedation-related factors may be related to an increased risk of delirium. “The type, dose, duration, and mode of delivery are very important,” Dr. Greenberg said. “The ideal sedative agent has a rapid, predictable onset; is short-acting; has anxiolytic, amnestic, and analgesic properties; is soluble; has a high therapeutic index; and no toxicity. The ideal sedative is also easy to administrate, contains no active metabolites, has minimal actions with other drugs, is reversible, and is cost effective. The problem is, there really is no ideal sedative agent. There is inadequate knowledge about the drugs [used to treat COVID-19 in the ICU] available to us, the dosage, and importantly, the pharmacokinetics and dynamics of these medications.”
The classic types of sedation being used in the ICU, he said, include the benzodiazepines midazolam, lorazepam, and diazepam, as well as propofol. Alternatives include dexmedetomidine, clonidine, ketamine, and the neuroleptics – haloperidol, quetiapine, olanzapine, ziprasidone, and risperidone. “The advantages of benzos are that they are anxiolytics, amnestics, and they are good sedatives with minimal hemodynamic effects,” Dr. Greenberg said.
Advantages of propofol include its sedative, hypnotic, and anxiolytic properties, he said. It reduces the cerebral metabolic rate and can relieve bronchospasm. “However, small studies have found that its use may be associated with an increased risk of delirium,” he said. “It is a respiratory depressant, and it can cause hypotension and decreased contractility. It has no analgesic properties, and two of the big concerns of its use in COVID-19 are the potential for hypertriglyceridemia and propofol infusion syndrome, particularly at doses of greater than 5 mg/kg per hour for greater than 48 hours. It is being given in high doses because patients are requiring higher doses to maintain ventilator synchrony.”
Choosing the right drug
The keys to success for sedation of ICU patients are choosing the right drug at the right dose for the right duration and the right mode of delivery, and applying them to the right population. However, as noted in a recent study, the pandemic poses unique challenges to clinicians in how they care for critically ill COVID-19 patients who require sedation (Anesth Analg. 2020 Apr 22. doi: 10.1213/ANE.0000000000004887). The use of provisional work areas “has escalated because of the amount of patients we’ve had to care for over the past nine months,” Dr. Greenberg said. “We’ve used alternate providers who are not necessarily familiar with the sedation and analgesic protocols and how to use these specific medications. Drug shortages have been on the rise, so there’s a need to understand alternative agents that can be used.”
COVID-19 patients face the potential risk for an increase in drug-drug interactions and side effects due to the polypharmacy that is often required to provide adequate sedation during mechanical ventilation. He noted that these patients may have “unusually high” analgesia and sedation requirements, particularly when they’re mechanically ventilated. A hypothesis as to why patients with COVID-19 require so much sedation and analgesia is that they often have a high respiratory drive and ventilator dyssynchrony, which requires increased neuromuscular blockade. “They also have an intense inflammatory response, which may be linked to tolerance of specific opioids and other medications,” Dr. Greenberg said. “Many ventilated COVID-19 patients are of younger age and previously in good health, and therefore, have an excellent metabolism. Health care providers are concerned about self-extubation. This prompts bedside providers to administer more sedatives to prevent this unwanted complication. There may also be a reduction of drip modifications by health care workers because of the potential risk of contracting COVID-19 when going into the room multiple times and for long periods of time” (Anesth Analg. 2020;131[1]:e34-e35).
According to a sedation resource on the SCCM website, about 5% of COVID-19 patients require mechanical ventilation. “There has been a massive shortage of the usual drugs that we use,” Dr. Greenberg said. “The demand for sedatives has increased by approximately 91%, while the demand for analgesics has increased by 79%, and neuromuscular blocker demand has increased by 105%.”
A retrospective study of 24 COVID-19 patients who required ventilation in the ICU found that the median daily dose of benzodiazepines was significantly higher, compared with the median daily dose used in the OSCILLATE trial (a median of 270 mg vs. 199 mg, respectively; Anesth Analg. 2020;131[4]e198-e200. doi: 10.1213/ane.0000000000005131). In addition, their median daily dose of opioid was approximately three times higher, compared with patients in the OSCILLATE trial (a median of 775 mg vs. 289 mg). Other agents used included propofol (84%), dexmedetomidine (53%), and ketamine (11%).
“A potential strategy for COVID-19 ICU patient sedation should be analgesia first, as indicated in the 2018 PADIS guidelines,” Dr. Greenberg advised. “We should also apply nonpharmacologic measures to reduce delirium. In nonintubated patients, we should use light to moderate sedation, targeting a RASS of –2 to +1, using hydromorphone or fentanyl boluses for analgesia and midazolam boluses or dexmedetomidine for sedation,.”
For intubated patients, he continued, target a RASS of –3 to –4, or –4 to –5 in those who require neuromuscular blockade. “Use propofol first then intermittent boluses of benzodiazepines,” said Dr. Greenberg, editor-in-chief of the Anesthesia Patient Safety Foundation newsletter. “For heavy sedation, use midazolam and supplement with ketamine and other analgesics and sedatives such as barbiturates, methadone, and even inhalation anesthetics in some cases.”
For analgesia in intubated patients, use fentanyl boluses then infusion. “Patients can easily become tachyphylactic to fentanyl, and it has a long context-sensitive half time,” he said. “Hydromorphone may be least affected by organ dysfunction.”
Dr. Greenberg concluded his presentation by stating that more studies are required “to delineate the best analgesia/sedation strategies and monitoring modalities for COVID-19 ICU patients.”
In commenting on the presentation, Mangala Narasimhan, DO, FCCP, senior vice president and director of critical care services at Northwell Health, said that the recommendations regarding sedation highlight a struggle that ICU providers have been dealing with during the COVID-19 epidemic.

“There have been unique challenges with COVID-19 and intubated patients. We have seen severe ventilator dyssynchrony and prolonged duration of mechanical ventilation. I think we can all agree that these patients have extremely high metabolic rates, have required high levels of sedation, have an increased need for neuromuscular blockade, and have high levels of delirium for extended periods of time. The recommendations provided here are reasonable. Strategies to prevent delirium should be employed, pain management should be prioritized, analgesics can help reduce the need for opioids. Alternatives to sedation are useful in this patient population and are well tolerated. Drug shortages have provided additional challenges to these strategies and have required us to think about the use of alternative agents. The recommendations echo the experience we have had with large numbers of intubated COVID-19 patients.”
Dr. Greenberg disclosed that he receives a stipend from the Anesthesia Patient Safety Foundation for serving as editor-in-chief of the foundation’s newsletter.
According to the best available evidence, analagosedation remains the focus for managing COVID-19 ICU patients, according to Steven B. Greenberg, MD, FCCP, FCCM.
“The choice of sedation and analgesia is important,” Dr. Greenberg, vice chair of education in the department of anesthesiology at Evanston Hospital, part of NorthShore University Health System, Chicago, said at a Society for Critical Care virtual meeting: COVID-19: What’s Next. “We know that the right choice of these two components may increase liberation from ventilators, earlier ICU discharge, and return to normal brain function and independent functional status.”
Analgesia first
Prior to the current pandemic, the approach to sedation of patients in the ICU was based on the PADIS Guidelines of 2018, which call for an assessment-driven, protocol-based stepwise approach to pain and sedation management in critically ill adults (Crit Care Med. 2018;46:e825-73). “” Dr. Greenberg said. “We know that pain management should be a priority of sedation, because pain may increase the risk of delirium, anxiety, and endocrine suppression, and may increase the risk of release of endogenous catecholamines, ischemia, and hypermetabolic states.”
Fentanyl appears to be the most common opioid analgesic used for patients in the ICU, “but fentanyl is a very lipophilic drug and has a long context-sensitive half-life,” he said. “There are components to fentanyl that allow it to become a very long-acting drug upon days and days of infusion. Another opioid used is remifentanil, which is typically short-acting because it is broken down in the blood by esterases, but may cause rigidity at higher doses. Dilaudid seems to be the least affected by organ dysfunction. In our very critically ill, prolonged mechanically ventilated COVID-19 patients, we’ve been using methadone for its NMDA [N-methyl-D-aspartate] antagonistic effect and its opioid-sparing effects.”
As for nonopioid analgesics, Dr. Greenberg said that clinicians have shied away from using NSAIDs because of their side effects. “Tramadol indirectly inhibits reuptake of norepinephrine and serotonin, and ketamine is being used a lot more because of its NMDA antagonist effect,” he said. “Lidocaine and gabapentin have also been used.”
In a recent systematic review and meta-analysis, researchers assessed 34 trials that examined adjuvant analgesic use with an opioid in critically ill patients versus an opioid alone (Crit Care Expl. 2020;2:e0157). They found that when using an adjuvant such as acetaminophen, clonidine, dexmedetomidine, gabapentin, ketamine, magnesium, nefopam, NSAIDs, pregabalin, and tramadol, there was a reduction in pain scores as well as a reduction in opioid consumption. “So, clinicians should consider using adjuvant agents to limit opioid exposure and improve pain scores in the critically ill,” Dr. Greenberg said.
ICU delirium: Risk factors, prevention
Delirium in COVID-19 patients treated in the ICU of particular concern. According to a systematic review of 33 studies, 11 risk factors for delirium in the ICU were supported by strong or moderate levels of evidence (Crit Care Med. 2015;43:40-7). These include age, dementia, hypertension, emergency surgery, trauma, APACHE score of II, need for mechanical ventilation, metabolic acidosis, delirium on prior day, coma, and dexmedetomidine use. Risk factors for ICU delirium among COVID-19 patients, however, “are far different,” Dr. Greenberg said. “Why? First and foremost, we are restricting visitation of family,” he said. “That family connection largely can be lost. Second, there are limitations of nonpharmacologic interventions. There is less mobility and physical therapy employed because of the risk of health care workers’ exposure to the virus. There’s also uncertainty about the global pandemic. Anxiety and depression come with that, as well as disruptions to spiritual and religious services.”
Strategies for preventing delirium remain the same as before the pandemic and in accord with recent clinical practice guidelines: Reduce the use of certain drugs such as benzodiazepines and narcotics, reorient the patients, treat dehydration, use hearing aids and eyeglasses in patients who have them, use ear plugs to cancel noise, mobilize patients, maintain sleep/awake cycles, and encourage sedation holidays (Crit Care Med. 2018;46[9]:e825-73).
A recent study from France found that among 58 patients with COVID-19, 65% had positive Confusion Assessment Method (CAM)–ICU findings and 69% had agitation (N Engl J Med 2020;382:2268-70). Most of the patients (86%) received midazolam, 47% received propofol, and all received sufentanil. “In the pre-COVID days, we would use midazolam as a second-line agent for many of these patients,” Dr. Greenberg said. “So, times really have changed.”
The fate of COVID-19 patients following discharge from the ICU remains a concern, continued Dr. Greenberg, clinical professor of anesthesiology at the University of Chicago. A recent journal article by Michelle Biehl, MD, and Denise Sese, MD, noted that post–intensive care syndrome (PICS) or new or worsening impairment in any physical, cognitive, or mental domain is of significant concern among COVID-19 patients following their ICU stay (Cleveland Clin J Med 2020 Aug doi: 10.3949/ccjm.87a.ccc055). The authors stated that COVID-19 patients may face a higher risk of PICS because of restricted family visitation, prolonged mechanical ventilation, exposure to higher amounts of sedatives, and limited physical therapy during hospital stay.
No ideal sedative agent
The 2018 PADIS Guidelines on the use of ICU sedation suggested strong evidence for modifiable risk factors producing delirium in the context of benzodiazepines and blood transfusion. They recommend a light level of sedation and the use of propofol or dexmedetomidine over benzodiazepines. They also recommend routine delirium testing such as using the CAM-ICU or Intensive Care Delirium Screening Checklist (ICDSC) and nonpharmacologic therapies such as reorientation, cognitive stimulation, sleep improvement, and mobilization.
Several sedation-related factors may be related to an increased risk of delirium. “The type, dose, duration, and mode of delivery are very important,” Dr. Greenberg said. “The ideal sedative agent has a rapid, predictable onset; is short-acting; has anxiolytic, amnestic, and analgesic properties; is soluble; has a high therapeutic index; and no toxicity. The ideal sedative is also easy to administrate, contains no active metabolites, has minimal actions with other drugs, is reversible, and is cost effective. The problem is, there really is no ideal sedative agent. There is inadequate knowledge about the drugs [used to treat COVID-19 in the ICU] available to us, the dosage, and importantly, the pharmacokinetics and dynamics of these medications.”
The classic types of sedation being used in the ICU, he said, include the benzodiazepines midazolam, lorazepam, and diazepam, as well as propofol. Alternatives include dexmedetomidine, clonidine, ketamine, and the neuroleptics – haloperidol, quetiapine, olanzapine, ziprasidone, and risperidone. “The advantages of benzos are that they are anxiolytics, amnestics, and they are good sedatives with minimal hemodynamic effects,” Dr. Greenberg said.
Advantages of propofol include its sedative, hypnotic, and anxiolytic properties, he said. It reduces the cerebral metabolic rate and can relieve bronchospasm. “However, small studies have found that its use may be associated with an increased risk of delirium,” he said. “It is a respiratory depressant, and it can cause hypotension and decreased contractility. It has no analgesic properties, and two of the big concerns of its use in COVID-19 are the potential for hypertriglyceridemia and propofol infusion syndrome, particularly at doses of greater than 5 mg/kg per hour for greater than 48 hours. It is being given in high doses because patients are requiring higher doses to maintain ventilator synchrony.”
Choosing the right drug
The keys to success for sedation of ICU patients are choosing the right drug at the right dose for the right duration and the right mode of delivery, and applying them to the right population. However, as noted in a recent study, the pandemic poses unique challenges to clinicians in how they care for critically ill COVID-19 patients who require sedation (Anesth Analg. 2020 Apr 22. doi: 10.1213/ANE.0000000000004887). The use of provisional work areas “has escalated because of the amount of patients we’ve had to care for over the past nine months,” Dr. Greenberg said. “We’ve used alternate providers who are not necessarily familiar with the sedation and analgesic protocols and how to use these specific medications. Drug shortages have been on the rise, so there’s a need to understand alternative agents that can be used.”
COVID-19 patients face the potential risk for an increase in drug-drug interactions and side effects due to the polypharmacy that is often required to provide adequate sedation during mechanical ventilation. He noted that these patients may have “unusually high” analgesia and sedation requirements, particularly when they’re mechanically ventilated. A hypothesis as to why patients with COVID-19 require so much sedation and analgesia is that they often have a high respiratory drive and ventilator dyssynchrony, which requires increased neuromuscular blockade. “They also have an intense inflammatory response, which may be linked to tolerance of specific opioids and other medications,” Dr. Greenberg said. “Many ventilated COVID-19 patients are of younger age and previously in good health, and therefore, have an excellent metabolism. Health care providers are concerned about self-extubation. This prompts bedside providers to administer more sedatives to prevent this unwanted complication. There may also be a reduction of drip modifications by health care workers because of the potential risk of contracting COVID-19 when going into the room multiple times and for long periods of time” (Anesth Analg. 2020;131[1]:e34-e35).
According to a sedation resource on the SCCM website, about 5% of COVID-19 patients require mechanical ventilation. “There has been a massive shortage of the usual drugs that we use,” Dr. Greenberg said. “The demand for sedatives has increased by approximately 91%, while the demand for analgesics has increased by 79%, and neuromuscular blocker demand has increased by 105%.”
A retrospective study of 24 COVID-19 patients who required ventilation in the ICU found that the median daily dose of benzodiazepines was significantly higher, compared with the median daily dose used in the OSCILLATE trial (a median of 270 mg vs. 199 mg, respectively; Anesth Analg. 2020;131[4]e198-e200. doi: 10.1213/ane.0000000000005131). In addition, their median daily dose of opioid was approximately three times higher, compared with patients in the OSCILLATE trial (a median of 775 mg vs. 289 mg). Other agents used included propofol (84%), dexmedetomidine (53%), and ketamine (11%).
“A potential strategy for COVID-19 ICU patient sedation should be analgesia first, as indicated in the 2018 PADIS guidelines,” Dr. Greenberg advised. “We should also apply nonpharmacologic measures to reduce delirium. In nonintubated patients, we should use light to moderate sedation, targeting a RASS of –2 to +1, using hydromorphone or fentanyl boluses for analgesia and midazolam boluses or dexmedetomidine for sedation,.”
For intubated patients, he continued, target a RASS of –3 to –4, or –4 to –5 in those who require neuromuscular blockade. “Use propofol first then intermittent boluses of benzodiazepines,” said Dr. Greenberg, editor-in-chief of the Anesthesia Patient Safety Foundation newsletter. “For heavy sedation, use midazolam and supplement with ketamine and other analgesics and sedatives such as barbiturates, methadone, and even inhalation anesthetics in some cases.”
For analgesia in intubated patients, use fentanyl boluses then infusion. “Patients can easily become tachyphylactic to fentanyl, and it has a long context-sensitive half time,” he said. “Hydromorphone may be least affected by organ dysfunction.”
Dr. Greenberg concluded his presentation by stating that more studies are required “to delineate the best analgesia/sedation strategies and monitoring modalities for COVID-19 ICU patients.”
In commenting on the presentation, Mangala Narasimhan, DO, FCCP, senior vice president and director of critical care services at Northwell Health, said that the recommendations regarding sedation highlight a struggle that ICU providers have been dealing with during the COVID-19 epidemic.
“There have been unique challenges with COVID-19 and intubated patients. We have seen severe ventilator dyssynchrony and prolonged duration of mechanical ventilation. I think we can all agree that these patients have extremely high metabolic rates, have required high levels of sedation, have an increased need for neuromuscular blockade, and have high levels of delirium for extended periods of time. The recommendations provided here are reasonable. Strategies to prevent delirium should be employed, pain management should be prioritized, analgesics can help reduce the need for opioids. Alternatives to sedation are useful in this patient population and are well tolerated. Drug shortages have provided additional challenges to these strategies and have required us to think about the use of alternative agents. The recommendations echo the experience we have had with large numbers of intubated COVID-19 patients.”
Dr. Greenberg disclosed that he receives a stipend from the Anesthesia Patient Safety Foundation for serving as editor-in-chief of the foundation’s newsletter.
According to the best available evidence, analagosedation remains the focus for managing COVID-19 ICU patients, according to Steven B. Greenberg, MD, FCCP, FCCM.
“The choice of sedation and analgesia is important,” Dr. Greenberg, vice chair of education in the department of anesthesiology at Evanston Hospital, part of NorthShore University Health System, Chicago, said at a Society for Critical Care virtual meeting: COVID-19: What’s Next. “We know that the right choice of these two components may increase liberation from ventilators, earlier ICU discharge, and return to normal brain function and independent functional status.”
Analgesia first
Prior to the current pandemic, the approach to sedation of patients in the ICU was based on the PADIS Guidelines of 2018, which call for an assessment-driven, protocol-based stepwise approach to pain and sedation management in critically ill adults (Crit Care Med. 2018;46:e825-73). “” Dr. Greenberg said. “We know that pain management should be a priority of sedation, because pain may increase the risk of delirium, anxiety, and endocrine suppression, and may increase the risk of release of endogenous catecholamines, ischemia, and hypermetabolic states.”
Fentanyl appears to be the most common opioid analgesic used for patients in the ICU, “but fentanyl is a very lipophilic drug and has a long context-sensitive half-life,” he said. “There are components to fentanyl that allow it to become a very long-acting drug upon days and days of infusion. Another opioid used is remifentanil, which is typically short-acting because it is broken down in the blood by esterases, but may cause rigidity at higher doses. Dilaudid seems to be the least affected by organ dysfunction. In our very critically ill, prolonged mechanically ventilated COVID-19 patients, we’ve been using methadone for its NMDA [N-methyl-D-aspartate] antagonistic effect and its opioid-sparing effects.”
As for nonopioid analgesics, Dr. Greenberg said that clinicians have shied away from using NSAIDs because of their side effects. “Tramadol indirectly inhibits reuptake of norepinephrine and serotonin, and ketamine is being used a lot more because of its NMDA antagonist effect,” he said. “Lidocaine and gabapentin have also been used.”
In a recent systematic review and meta-analysis, researchers assessed 34 trials that examined adjuvant analgesic use with an opioid in critically ill patients versus an opioid alone (Crit Care Expl. 2020;2:e0157). They found that when using an adjuvant such as acetaminophen, clonidine, dexmedetomidine, gabapentin, ketamine, magnesium, nefopam, NSAIDs, pregabalin, and tramadol, there was a reduction in pain scores as well as a reduction in opioid consumption. “So, clinicians should consider using adjuvant agents to limit opioid exposure and improve pain scores in the critically ill,” Dr. Greenberg said.
ICU delirium: Risk factors, prevention
Delirium in COVID-19 patients treated in the ICU of particular concern. According to a systematic review of 33 studies, 11 risk factors for delirium in the ICU were supported by strong or moderate levels of evidence (Crit Care Med. 2015;43:40-7). These include age, dementia, hypertension, emergency surgery, trauma, APACHE score of II, need for mechanical ventilation, metabolic acidosis, delirium on prior day, coma, and dexmedetomidine use. Risk factors for ICU delirium among COVID-19 patients, however, “are far different,” Dr. Greenberg said. “Why? First and foremost, we are restricting visitation of family,” he said. “That family connection largely can be lost. Second, there are limitations of nonpharmacologic interventions. There is less mobility and physical therapy employed because of the risk of health care workers’ exposure to the virus. There’s also uncertainty about the global pandemic. Anxiety and depression come with that, as well as disruptions to spiritual and religious services.”
Strategies for preventing delirium remain the same as before the pandemic and in accord with recent clinical practice guidelines: Reduce the use of certain drugs such as benzodiazepines and narcotics, reorient the patients, treat dehydration, use hearing aids and eyeglasses in patients who have them, use ear plugs to cancel noise, mobilize patients, maintain sleep/awake cycles, and encourage sedation holidays (Crit Care Med. 2018;46[9]:e825-73).
A recent study from France found that among 58 patients with COVID-19, 65% had positive Confusion Assessment Method (CAM)–ICU findings and 69% had agitation (N Engl J Med 2020;382:2268-70). Most of the patients (86%) received midazolam, 47% received propofol, and all received sufentanil. “In the pre-COVID days, we would use midazolam as a second-line agent for many of these patients,” Dr. Greenberg said. “So, times really have changed.”
The fate of COVID-19 patients following discharge from the ICU remains a concern, continued Dr. Greenberg, clinical professor of anesthesiology at the University of Chicago. A recent journal article by Michelle Biehl, MD, and Denise Sese, MD, noted that post–intensive care syndrome (PICS) or new or worsening impairment in any physical, cognitive, or mental domain is of significant concern among COVID-19 patients following their ICU stay (Cleveland Clin J Med 2020 Aug doi: 10.3949/ccjm.87a.ccc055). The authors stated that COVID-19 patients may face a higher risk of PICS because of restricted family visitation, prolonged mechanical ventilation, exposure to higher amounts of sedatives, and limited physical therapy during hospital stay.
No ideal sedative agent
The 2018 PADIS Guidelines on the use of ICU sedation suggested strong evidence for modifiable risk factors producing delirium in the context of benzodiazepines and blood transfusion. They recommend a light level of sedation and the use of propofol or dexmedetomidine over benzodiazepines. They also recommend routine delirium testing such as using the CAM-ICU or Intensive Care Delirium Screening Checklist (ICDSC) and nonpharmacologic therapies such as reorientation, cognitive stimulation, sleep improvement, and mobilization.
Several sedation-related factors may be related to an increased risk of delirium. “The type, dose, duration, and mode of delivery are very important,” Dr. Greenberg said. “The ideal sedative agent has a rapid, predictable onset; is short-acting; has anxiolytic, amnestic, and analgesic properties; is soluble; has a high therapeutic index; and no toxicity. The ideal sedative is also easy to administrate, contains no active metabolites, has minimal actions with other drugs, is reversible, and is cost effective. The problem is, there really is no ideal sedative agent. There is inadequate knowledge about the drugs [used to treat COVID-19 in the ICU] available to us, the dosage, and importantly, the pharmacokinetics and dynamics of these medications.”
The classic types of sedation being used in the ICU, he said, include the benzodiazepines midazolam, lorazepam, and diazepam, as well as propofol. Alternatives include dexmedetomidine, clonidine, ketamine, and the neuroleptics – haloperidol, quetiapine, olanzapine, ziprasidone, and risperidone. “The advantages of benzos are that they are anxiolytics, amnestics, and they are good sedatives with minimal hemodynamic effects,” Dr. Greenberg said.
Advantages of propofol include its sedative, hypnotic, and anxiolytic properties, he said. It reduces the cerebral metabolic rate and can relieve bronchospasm. “However, small studies have found that its use may be associated with an increased risk of delirium,” he said. “It is a respiratory depressant, and it can cause hypotension and decreased contractility. It has no analgesic properties, and two of the big concerns of its use in COVID-19 are the potential for hypertriglyceridemia and propofol infusion syndrome, particularly at doses of greater than 5 mg/kg per hour for greater than 48 hours. It is being given in high doses because patients are requiring higher doses to maintain ventilator synchrony.”
Choosing the right drug
The keys to success for sedation of ICU patients are choosing the right drug at the right dose for the right duration and the right mode of delivery, and applying them to the right population. However, as noted in a recent study, the pandemic poses unique challenges to clinicians in how they care for critically ill COVID-19 patients who require sedation (Anesth Analg. 2020 Apr 22. doi: 10.1213/ANE.0000000000004887). The use of provisional work areas “has escalated because of the amount of patients we’ve had to care for over the past nine months,” Dr. Greenberg said. “We’ve used alternate providers who are not necessarily familiar with the sedation and analgesic protocols and how to use these specific medications. Drug shortages have been on the rise, so there’s a need to understand alternative agents that can be used.”
COVID-19 patients face the potential risk for an increase in drug-drug interactions and side effects due to the polypharmacy that is often required to provide adequate sedation during mechanical ventilation. He noted that these patients may have “unusually high” analgesia and sedation requirements, particularly when they’re mechanically ventilated. A hypothesis as to why patients with COVID-19 require so much sedation and analgesia is that they often have a high respiratory drive and ventilator dyssynchrony, which requires increased neuromuscular blockade. “They also have an intense inflammatory response, which may be linked to tolerance of specific opioids and other medications,” Dr. Greenberg said. “Many ventilated COVID-19 patients are of younger age and previously in good health, and therefore, have an excellent metabolism. Health care providers are concerned about self-extubation. This prompts bedside providers to administer more sedatives to prevent this unwanted complication. There may also be a reduction of drip modifications by health care workers because of the potential risk of contracting COVID-19 when going into the room multiple times and for long periods of time” (Anesth Analg. 2020;131[1]:e34-e35).
According to a sedation resource on the SCCM website, about 5% of COVID-19 patients require mechanical ventilation. “There has been a massive shortage of the usual drugs that we use,” Dr. Greenberg said. “The demand for sedatives has increased by approximately 91%, while the demand for analgesics has increased by 79%, and neuromuscular blocker demand has increased by 105%.”
A retrospective study of 24 COVID-19 patients who required ventilation in the ICU found that the median daily dose of benzodiazepines was significantly higher, compared with the median daily dose used in the OSCILLATE trial (a median of 270 mg vs. 199 mg, respectively; Anesth Analg. 2020;131[4]e198-e200. doi: 10.1213/ane.0000000000005131). In addition, their median daily dose of opioid was approximately three times higher, compared with patients in the OSCILLATE trial (a median of 775 mg vs. 289 mg). Other agents used included propofol (84%), dexmedetomidine (53%), and ketamine (11%).
“A potential strategy for COVID-19 ICU patient sedation should be analgesia first, as indicated in the 2018 PADIS guidelines,” Dr. Greenberg advised. “We should also apply nonpharmacologic measures to reduce delirium. In nonintubated patients, we should use light to moderate sedation, targeting a RASS of –2 to +1, using hydromorphone or fentanyl boluses for analgesia and midazolam boluses or dexmedetomidine for sedation,.”
For intubated patients, he continued, target a RASS of –3 to –4, or –4 to –5 in those who require neuromuscular blockade. “Use propofol first then intermittent boluses of benzodiazepines,” said Dr. Greenberg, editor-in-chief of the Anesthesia Patient Safety Foundation newsletter. “For heavy sedation, use midazolam and supplement with ketamine and other analgesics and sedatives such as barbiturates, methadone, and even inhalation anesthetics in some cases.”
For analgesia in intubated patients, use fentanyl boluses then infusion. “Patients can easily become tachyphylactic to fentanyl, and it has a long context-sensitive half time,” he said. “Hydromorphone may be least affected by organ dysfunction.”
Dr. Greenberg concluded his presentation by stating that more studies are required “to delineate the best analgesia/sedation strategies and monitoring modalities for COVID-19 ICU patients.”
In commenting on the presentation, Mangala Narasimhan, DO, FCCP, senior vice president and director of critical care services at Northwell Health, said that the recommendations regarding sedation highlight a struggle that ICU providers have been dealing with during the COVID-19 epidemic.
“There have been unique challenges with COVID-19 and intubated patients. We have seen severe ventilator dyssynchrony and prolonged duration of mechanical ventilation. I think we can all agree that these patients have extremely high metabolic rates, have required high levels of sedation, have an increased need for neuromuscular blockade, and have high levels of delirium for extended periods of time. The recommendations provided here are reasonable. Strategies to prevent delirium should be employed, pain management should be prioritized, analgesics can help reduce the need for opioids. Alternatives to sedation are useful in this patient population and are well tolerated. Drug shortages have provided additional challenges to these strategies and have required us to think about the use of alternative agents. The recommendations echo the experience we have had with large numbers of intubated COVID-19 patients.”
Dr. Greenberg disclosed that he receives a stipend from the Anesthesia Patient Safety Foundation for serving as editor-in-chief of the foundation’s newsletter.
FROM AN SCCM VIRTUAL MEETING
FDA posts COVID vaccine guidance amid White House pushback
while medical and trade associations called for a thorough review of any such product before approval.
The FDA took the unusual step of posting background materials much earlier than usual for its planned Oct. 22 advisory committee meeting on potential vaccines for COVID-19. The FDA also on Tuesday afternoon released a new guidance document, expanding on a previous set of recommendations the agency released in June.
In the new guidance document, FDA officials outline what will be required for even a limited clearance, known as an emergency use authorization (EUA), for a COVID-19 vaccine.
“Data from phase 3 studies should include a median follow-up duration of at least 2 months after completion of the full vaccination regimen to help provide adequate information to assess a vaccine’s benefit-risk profile,” the FDA said in the document.
FDA staff have emphasized the higher bar that drugmakers and regulators face in considering approval of a COVID-19 vaccine.
“Vaccines are complex biological products, and an EUA for a COVID-19 vaccine may allow for rapid and widespread deployment for administration of the vaccine to millions of individuals, including healthy people,” the agency staff said in the briefing documents.
The FDA’s briefing document for the Oct. 22 meeting appears to be markedly at odds with the claim Trump made in a video Monday night, in which he told the American public that “vaccines are coming momentarily.”
Trump, who is in a tightly contested presidential race against Democratic candidate Joe Biden, has repeatedly made claims of the potential arrival of COVID vaccines that are at odds with timelines offered with guarded optimism by experts in infectious diseases.
But based on these new guidelines from the FDA, it appears that the White House may now endorse the FDA’s stance, according to a Wall Street Journal report based on “people familiar with the matter.”
The publication reports that the White House, which has yet to officially comment, “endorsed the U.S. Food and Drug Administration’s plans for assessing whether a Covid-19 vaccine should be given widely, casting aside objections to requirements that would likely mean a shot won’t be cleared until after Election Day, people familiar with the matter said.”
Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, on Monday night said during a virtual appearance at the twenty-first annual New Yorker Festival that there could be evidence as early as November or December about whether one of the vaccines now in testing will work out. He declared himself to have “cautious optimism” about potential rollout of vaccines as early as late 2020 or early 2021.
Peter Lurie, MD, MPH, who earlier served as the FDA’s associate commissioner for public health strategy and analysis, described the agency’s release of the briefing document as being a positive development.
News organizations, including the New York Times, have reported that the White House had sought to block the FDA from releasing further instructions for companies developing COVID-19 vaccines. The Associated Press on Tuesday said that a senior Trump administration official confirmed that the White House had blocked earlier FDA plans to formally publish the safety guidelines based on the 2-month data requirement, arguing that there was “no clinical or medical reason” for it.
“It is an encouraging sign that, despite opposition from the White House, the Food and Drug Administration has effectively published guidelines for emergency release of a vaccine for COVID-19 by disclosing the advice it has been providing to individual sponsors,” said Dr. Lurie, who is now executive director and president of the Center for Science in the Public Interest.
In a news release, he said the White House had sought to keep the FDA guidance under wraps “so it could maintain the public fiction that a safe and effective vaccine could be available before Election Day or even so that it could force emergency authorization of a vaccine with more limited follow-up.”
“Even the pharmaceutical industry has been clamoring for the release of these guidelines. We all want a safe and effective vaccine to end the pandemic, and we want it sooner rather than later,” Dr. Lurie said. “But we can’t afford for the Trump administration to bungle vaccine review the way they’ve bungled nearly every other aspect of its pandemic response.”
Tuesday also saw a flood of statements in support of FDA officials, including tweets from the chief executive of Pfizer, which is among the leaders in the race to develop a COVID-19 vaccine. Pfizer’s Albert Bourla, DVM, PhD, said that the FDA’s “public servants are known for their high integrity and scientific expertise and we have full faith in their ability to set appropriate standards for the approval of a COVID vaccine or treatment.”
The American Medical Association on Tuesday announced a public webinar on Wednesday where its president, Susan R. Bailey, MD, will discuss the COVID-19 vaccine review process with Peter Marks, MD, PhD, director of the Center for Biologics Evaluation and Research at the FDA. The AMA described this webinar as part of work “to restore trust in science and science-based decision-making among policymakers and the public.”
“To ensure media and the physician community are continuously informed about the federal review process for COVID-19 vaccine candidates, the AMA will host a webinar series to gain fact-based insights from the nation’s highest-ranking subject matter experts working to protect the health of the public,” the organization said in announcing the webinar.
In a statement, leaders of the Association of American Medical Colleges said that the FDA’s Vaccines and Related Biological Products Advisory Committee should evaluate any COVID-19 candidate vaccines prior to the FDA issuing an EUA.
“Full approval of a new vaccine or biologic requires demonstration of safety and effectiveness through a process that includes evaluation by the VRBPAC. Their recommendations are considered by FDA staff who ultimately have the authority to approve the new product,” said AAMC chief scientific officer Ross McKinney Jr, MD, and AAMC CEO David J. Skorton, MD, in the statement.
Thomas M. File Jr., MD, president of the Infectious Diseases Society of America, said in a statement that his association again asked the White House to “follow medical and scientific expertise in efforts to combat COVID-19.”
“It is imperative that a vaccine be approved on the basis of FDA’s quality standards and that its safety and efficacy are established before it is authorized,” Dr. File said. “A vaccine that has been approved with speed, rather than safety and efficacy, at the forefront will compound the challenges posed by this pandemic. FDA guidelines for approval that set standards the American people can trust are essential to the success of a vaccine.”
Stephen J. Ubl, chief executive of the Pharmaceutical Research and Manufacturers of America, said in a statement that his association “supports any efforts by FDA to provide clarifying guidance and we have engaged with the agency to support bringing greater transparency to the review process for COVID-19 vaccines.”
“To help address this public health crisis, our companies have also taken unprecedented steps to share vaccine clinical trial protocols and data in real time,” Mr. Ubl said. “We welcome the agency’s efforts to instill confidence in the rigorous safety of these potential vaccines.”
On Oct. 1, Michelle McMurry-Heath, MD, PhD, president and chief executive of the Biotechnology Innovation Organization, released publicly her letter urging Department of Health & Human Services Secretary Alex Azar to “publicly release all new guidance” related to a COVID-19 vaccine. Such a move would bolster public confidence in the vaccine, she said.
“We cannot allow a lack of transparency to undermine confidence in the vaccine development process. The public must have full faith in the scientific process and the rigor of FDA’s regulatory oversight if we are to end the pandemic,” she wrote in the Oct. 1 letter to Azar. “Releasing any additional guidance on granting emergency use authorization for a vaccine will go a long way in accomplishing this critical goal.”
This article first appeared on Medscape.com.
while medical and trade associations called for a thorough review of any such product before approval.
The FDA took the unusual step of posting background materials much earlier than usual for its planned Oct. 22 advisory committee meeting on potential vaccines for COVID-19. The FDA also on Tuesday afternoon released a new guidance document, expanding on a previous set of recommendations the agency released in June.
In the new guidance document, FDA officials outline what will be required for even a limited clearance, known as an emergency use authorization (EUA), for a COVID-19 vaccine.
“Data from phase 3 studies should include a median follow-up duration of at least 2 months after completion of the full vaccination regimen to help provide adequate information to assess a vaccine’s benefit-risk profile,” the FDA said in the document.
FDA staff have emphasized the higher bar that drugmakers and regulators face in considering approval of a COVID-19 vaccine.
“Vaccines are complex biological products, and an EUA for a COVID-19 vaccine may allow for rapid and widespread deployment for administration of the vaccine to millions of individuals, including healthy people,” the agency staff said in the briefing documents.
The FDA’s briefing document for the Oct. 22 meeting appears to be markedly at odds with the claim Trump made in a video Monday night, in which he told the American public that “vaccines are coming momentarily.”
Trump, who is in a tightly contested presidential race against Democratic candidate Joe Biden, has repeatedly made claims of the potential arrival of COVID vaccines that are at odds with timelines offered with guarded optimism by experts in infectious diseases.
But based on these new guidelines from the FDA, it appears that the White House may now endorse the FDA’s stance, according to a Wall Street Journal report based on “people familiar with the matter.”
The publication reports that the White House, which has yet to officially comment, “endorsed the U.S. Food and Drug Administration’s plans for assessing whether a Covid-19 vaccine should be given widely, casting aside objections to requirements that would likely mean a shot won’t be cleared until after Election Day, people familiar with the matter said.”
Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, on Monday night said during a virtual appearance at the twenty-first annual New Yorker Festival that there could be evidence as early as November or December about whether one of the vaccines now in testing will work out. He declared himself to have “cautious optimism” about potential rollout of vaccines as early as late 2020 or early 2021.
Peter Lurie, MD, MPH, who earlier served as the FDA’s associate commissioner for public health strategy and analysis, described the agency’s release of the briefing document as being a positive development.
News organizations, including the New York Times, have reported that the White House had sought to block the FDA from releasing further instructions for companies developing COVID-19 vaccines. The Associated Press on Tuesday said that a senior Trump administration official confirmed that the White House had blocked earlier FDA plans to formally publish the safety guidelines based on the 2-month data requirement, arguing that there was “no clinical or medical reason” for it.
“It is an encouraging sign that, despite opposition from the White House, the Food and Drug Administration has effectively published guidelines for emergency release of a vaccine for COVID-19 by disclosing the advice it has been providing to individual sponsors,” said Dr. Lurie, who is now executive director and president of the Center for Science in the Public Interest.
In a news release, he said the White House had sought to keep the FDA guidance under wraps “so it could maintain the public fiction that a safe and effective vaccine could be available before Election Day or even so that it could force emergency authorization of a vaccine with more limited follow-up.”
“Even the pharmaceutical industry has been clamoring for the release of these guidelines. We all want a safe and effective vaccine to end the pandemic, and we want it sooner rather than later,” Dr. Lurie said. “But we can’t afford for the Trump administration to bungle vaccine review the way they’ve bungled nearly every other aspect of its pandemic response.”
Tuesday also saw a flood of statements in support of FDA officials, including tweets from the chief executive of Pfizer, which is among the leaders in the race to develop a COVID-19 vaccine. Pfizer’s Albert Bourla, DVM, PhD, said that the FDA’s “public servants are known for their high integrity and scientific expertise and we have full faith in their ability to set appropriate standards for the approval of a COVID vaccine or treatment.”
The American Medical Association on Tuesday announced a public webinar on Wednesday where its president, Susan R. Bailey, MD, will discuss the COVID-19 vaccine review process with Peter Marks, MD, PhD, director of the Center for Biologics Evaluation and Research at the FDA. The AMA described this webinar as part of work “to restore trust in science and science-based decision-making among policymakers and the public.”
“To ensure media and the physician community are continuously informed about the federal review process for COVID-19 vaccine candidates, the AMA will host a webinar series to gain fact-based insights from the nation’s highest-ranking subject matter experts working to protect the health of the public,” the organization said in announcing the webinar.
In a statement, leaders of the Association of American Medical Colleges said that the FDA’s Vaccines and Related Biological Products Advisory Committee should evaluate any COVID-19 candidate vaccines prior to the FDA issuing an EUA.
“Full approval of a new vaccine or biologic requires demonstration of safety and effectiveness through a process that includes evaluation by the VRBPAC. Their recommendations are considered by FDA staff who ultimately have the authority to approve the new product,” said AAMC chief scientific officer Ross McKinney Jr, MD, and AAMC CEO David J. Skorton, MD, in the statement.
Thomas M. File Jr., MD, president of the Infectious Diseases Society of America, said in a statement that his association again asked the White House to “follow medical and scientific expertise in efforts to combat COVID-19.”
“It is imperative that a vaccine be approved on the basis of FDA’s quality standards and that its safety and efficacy are established before it is authorized,” Dr. File said. “A vaccine that has been approved with speed, rather than safety and efficacy, at the forefront will compound the challenges posed by this pandemic. FDA guidelines for approval that set standards the American people can trust are essential to the success of a vaccine.”
Stephen J. Ubl, chief executive of the Pharmaceutical Research and Manufacturers of America, said in a statement that his association “supports any efforts by FDA to provide clarifying guidance and we have engaged with the agency to support bringing greater transparency to the review process for COVID-19 vaccines.”
“To help address this public health crisis, our companies have also taken unprecedented steps to share vaccine clinical trial protocols and data in real time,” Mr. Ubl said. “We welcome the agency’s efforts to instill confidence in the rigorous safety of these potential vaccines.”
On Oct. 1, Michelle McMurry-Heath, MD, PhD, president and chief executive of the Biotechnology Innovation Organization, released publicly her letter urging Department of Health & Human Services Secretary Alex Azar to “publicly release all new guidance” related to a COVID-19 vaccine. Such a move would bolster public confidence in the vaccine, she said.
“We cannot allow a lack of transparency to undermine confidence in the vaccine development process. The public must have full faith in the scientific process and the rigor of FDA’s regulatory oversight if we are to end the pandemic,” she wrote in the Oct. 1 letter to Azar. “Releasing any additional guidance on granting emergency use authorization for a vaccine will go a long way in accomplishing this critical goal.”
This article first appeared on Medscape.com.
while medical and trade associations called for a thorough review of any such product before approval.
The FDA took the unusual step of posting background materials much earlier than usual for its planned Oct. 22 advisory committee meeting on potential vaccines for COVID-19. The FDA also on Tuesday afternoon released a new guidance document, expanding on a previous set of recommendations the agency released in June.
In the new guidance document, FDA officials outline what will be required for even a limited clearance, known as an emergency use authorization (EUA), for a COVID-19 vaccine.
“Data from phase 3 studies should include a median follow-up duration of at least 2 months after completion of the full vaccination regimen to help provide adequate information to assess a vaccine’s benefit-risk profile,” the FDA said in the document.
FDA staff have emphasized the higher bar that drugmakers and regulators face in considering approval of a COVID-19 vaccine.
“Vaccines are complex biological products, and an EUA for a COVID-19 vaccine may allow for rapid and widespread deployment for administration of the vaccine to millions of individuals, including healthy people,” the agency staff said in the briefing documents.
The FDA’s briefing document for the Oct. 22 meeting appears to be markedly at odds with the claim Trump made in a video Monday night, in which he told the American public that “vaccines are coming momentarily.”
Trump, who is in a tightly contested presidential race against Democratic candidate Joe Biden, has repeatedly made claims of the potential arrival of COVID vaccines that are at odds with timelines offered with guarded optimism by experts in infectious diseases.
But based on these new guidelines from the FDA, it appears that the White House may now endorse the FDA’s stance, according to a Wall Street Journal report based on “people familiar with the matter.”
The publication reports that the White House, which has yet to officially comment, “endorsed the U.S. Food and Drug Administration’s plans for assessing whether a Covid-19 vaccine should be given widely, casting aside objections to requirements that would likely mean a shot won’t be cleared until after Election Day, people familiar with the matter said.”
Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, on Monday night said during a virtual appearance at the twenty-first annual New Yorker Festival that there could be evidence as early as November or December about whether one of the vaccines now in testing will work out. He declared himself to have “cautious optimism” about potential rollout of vaccines as early as late 2020 or early 2021.
Peter Lurie, MD, MPH, who earlier served as the FDA’s associate commissioner for public health strategy and analysis, described the agency’s release of the briefing document as being a positive development.
News organizations, including the New York Times, have reported that the White House had sought to block the FDA from releasing further instructions for companies developing COVID-19 vaccines. The Associated Press on Tuesday said that a senior Trump administration official confirmed that the White House had blocked earlier FDA plans to formally publish the safety guidelines based on the 2-month data requirement, arguing that there was “no clinical or medical reason” for it.
“It is an encouraging sign that, despite opposition from the White House, the Food and Drug Administration has effectively published guidelines for emergency release of a vaccine for COVID-19 by disclosing the advice it has been providing to individual sponsors,” said Dr. Lurie, who is now executive director and president of the Center for Science in the Public Interest.
In a news release, he said the White House had sought to keep the FDA guidance under wraps “so it could maintain the public fiction that a safe and effective vaccine could be available before Election Day or even so that it could force emergency authorization of a vaccine with more limited follow-up.”
“Even the pharmaceutical industry has been clamoring for the release of these guidelines. We all want a safe and effective vaccine to end the pandemic, and we want it sooner rather than later,” Dr. Lurie said. “But we can’t afford for the Trump administration to bungle vaccine review the way they’ve bungled nearly every other aspect of its pandemic response.”
Tuesday also saw a flood of statements in support of FDA officials, including tweets from the chief executive of Pfizer, which is among the leaders in the race to develop a COVID-19 vaccine. Pfizer’s Albert Bourla, DVM, PhD, said that the FDA’s “public servants are known for their high integrity and scientific expertise and we have full faith in their ability to set appropriate standards for the approval of a COVID vaccine or treatment.”
The American Medical Association on Tuesday announced a public webinar on Wednesday where its president, Susan R. Bailey, MD, will discuss the COVID-19 vaccine review process with Peter Marks, MD, PhD, director of the Center for Biologics Evaluation and Research at the FDA. The AMA described this webinar as part of work “to restore trust in science and science-based decision-making among policymakers and the public.”
“To ensure media and the physician community are continuously informed about the federal review process for COVID-19 vaccine candidates, the AMA will host a webinar series to gain fact-based insights from the nation’s highest-ranking subject matter experts working to protect the health of the public,” the organization said in announcing the webinar.
In a statement, leaders of the Association of American Medical Colleges said that the FDA’s Vaccines and Related Biological Products Advisory Committee should evaluate any COVID-19 candidate vaccines prior to the FDA issuing an EUA.
“Full approval of a new vaccine or biologic requires demonstration of safety and effectiveness through a process that includes evaluation by the VRBPAC. Their recommendations are considered by FDA staff who ultimately have the authority to approve the new product,” said AAMC chief scientific officer Ross McKinney Jr, MD, and AAMC CEO David J. Skorton, MD, in the statement.
Thomas M. File Jr., MD, president of the Infectious Diseases Society of America, said in a statement that his association again asked the White House to “follow medical and scientific expertise in efforts to combat COVID-19.”
“It is imperative that a vaccine be approved on the basis of FDA’s quality standards and that its safety and efficacy are established before it is authorized,” Dr. File said. “A vaccine that has been approved with speed, rather than safety and efficacy, at the forefront will compound the challenges posed by this pandemic. FDA guidelines for approval that set standards the American people can trust are essential to the success of a vaccine.”
Stephen J. Ubl, chief executive of the Pharmaceutical Research and Manufacturers of America, said in a statement that his association “supports any efforts by FDA to provide clarifying guidance and we have engaged with the agency to support bringing greater transparency to the review process for COVID-19 vaccines.”
“To help address this public health crisis, our companies have also taken unprecedented steps to share vaccine clinical trial protocols and data in real time,” Mr. Ubl said. “We welcome the agency’s efforts to instill confidence in the rigorous safety of these potential vaccines.”
On Oct. 1, Michelle McMurry-Heath, MD, PhD, president and chief executive of the Biotechnology Innovation Organization, released publicly her letter urging Department of Health & Human Services Secretary Alex Azar to “publicly release all new guidance” related to a COVID-19 vaccine. Such a move would bolster public confidence in the vaccine, she said.
“We cannot allow a lack of transparency to undermine confidence in the vaccine development process. The public must have full faith in the scientific process and the rigor of FDA’s regulatory oversight if we are to end the pandemic,” she wrote in the Oct. 1 letter to Azar. “Releasing any additional guidance on granting emergency use authorization for a vaccine will go a long way in accomplishing this critical goal.”
This article first appeared on Medscape.com.
Restarting breast cancer screening after disruption not so simple
according to a modeling study reported at the 12th European Breast Cancer Conference.
Fallout of the pandemic has included reductions in cancer screening and diagnosis, said study investigator Lindy M. Kregting, a PhD student in the department of public health at Erasmus Medical Center, University Medical Center Rotterdam (the Netherlands).
In the Netherlands, new breast cancer diagnoses fell dramatically from historical levels starting in February. The number in April was less than half of that expected.
Ms. Kregting and colleagues used modeling to assess the impact of four strategies for restarting breast cancer screening in the Netherlands. The strategies differed regarding the population affected, the duration of the effects, and changes in stopping age. The usual situation, without any disruption, served as the comparator.
Results showed wide variation across strategies with respect to the increase in screening capacity needed during the latter half of this year – from 0% to 100% – and the excess breast cancer mortality occurring during 2020-2030 – from as many as 181 excess breast cancer deaths to as few as 14.
“The effects of the disruption are dependent on the chosen restart strategy,” Ms. Kregting summarized. “It would be preferred to immediately catch up because this minimizes the impact, but it also requires a very high capacity, so it may not always be possible. A proper alternative would be to increase the stopping age, so no screens are omitted, because this requires a rather normal capacity, and it will result in only small effects on incidence and mortality.”
As screening programs restart in some countries, there are still a lot of unknowns that could affect outcomes, including how many women will attend given that some may stay away out of fear, Ms. Kregting cautioned.
“We plan to do further model calculations when we know exactly what has happened. ... For now, we just assumed some reasonable disruption periods, and we assumed that capacity would be back to the original, before COVID-19, but I think we can say this is probably not the case,” she added.
Study details
Ms. Kregting and colleagues used Dutch breast cancer screening program parameters (biennial digital mammography for women aged 50-75 years) and a microsimulation screening analysis model to simulate four strategies for restarting breast cancer screening after a 6-month disruption:
- “Everyone delay,” a strategy in which all screening continues in the order planned with no change in the stopping age of 75 years (so that one in four women ultimately miss a screening during their lifetime)
- “First rounds no delay,” in which there is a delay in screening except for women having their first screening
- “Continue after stopping age,” in which there is a delay in screening but temporary increasing of the stopping age (to 76.5 years) to ensure all women get their final screen
- “Catch-up after stop,” in which capacity is increased to ensure full catch-up, with all delayed screens caught up in a 6-month period (the second half of 2020).
Results showed that 5,872 women would be screened in the latter half of 2020 if screening proceeded as usual without disruption. The necessary capacity was essentially the same with all of the restarting strategies, except for the catch-up-after-stop strategy, which would require a doubling of that number.
The temporal pattern of breast cancer incidence varied according to restart strategy early on, but incidence essentially returned to that expected with undisrupted screening by 2025 for all four strategies, with some small fluctuations thereafter.
The impact on breast cancer mortality differed considerably long term. It increased slightly and transiently above the expected level with the catch-up-after-stop strategy, but there were sizable, long-lasting increases with the other strategies, with excess deaths still seen in 2060 for the everyone-delay strategy.
In absolute terms, the excess number of breast cancer deaths during 2020-2030, compared with undisrupted screening, was 181 with the everyone-delay strategy, 155 with the first-rounds-no-delay strategy, 145 with the continue-after-stopping-age strategy, and just 14 with the catch-up-after-stop strategy. Ms. Kregting declined to provide numbers for other countries, given that the model is based on the Dutch population and screening program.
Results in context
“The unprecedented burden of COVID-19 on health systems worldwide has important implications for cancer care,” said invited discussant Alessandra Gennari, MD, PhD, of the University of Eastern Piedmont and Maggiore della Carità Hospital, both in Novara, Italy.
“There is a delay in diagnosis due to the fact that screening programs and diagnostic programs have been decreased or suspended in many Western countries where this is standard of care. Patients also are more reluctant to present to health care services, delaying their diagnosis,” Dr. Gennari said.
Findings of this new study add to those of similar studies undertaken in Italy (published in In Vivo) and the United Kingdom (published in The Lancet Oncology) showing the likely marked toll of the pandemic on cancer diagnosis and mortality, Dr. Gennari noted. Taken together, the findings underscore the urgent need for policy interventions to mitigate this impact.
“These interventions should focus on increasing routine diagnostic capacity, through which up to 40% of patients with cancer are diagnosed,” Dr. Gennari recommended. “Public health messaging is needed that accurately conveys the risk of severe illness from COVID-19 versus the risks of not seeking health care advice if patients are symptomatic. Finally, there is a need for provision of evidence-based data on which clinicians can adequately base their decision on how to manage the risks of cancer patients and the risks and benefits of procedures during the pandemic.”
The current study did not have any specific funding, and Ms. Kregting disclosed no conflicts of interest. Dr. Gennari disclosed relationships with Roche, Eisai, Lilly, AstraZeneca, Daiichi Sankyo, Merck, Novartis, and Pfizer.
SOURCE: Kregting L et al. EBCC-12 Virtual Conference, Abstract 24.
according to a modeling study reported at the 12th European Breast Cancer Conference.
Fallout of the pandemic has included reductions in cancer screening and diagnosis, said study investigator Lindy M. Kregting, a PhD student in the department of public health at Erasmus Medical Center, University Medical Center Rotterdam (the Netherlands).
In the Netherlands, new breast cancer diagnoses fell dramatically from historical levels starting in February. The number in April was less than half of that expected.
Ms. Kregting and colleagues used modeling to assess the impact of four strategies for restarting breast cancer screening in the Netherlands. The strategies differed regarding the population affected, the duration of the effects, and changes in stopping age. The usual situation, without any disruption, served as the comparator.
Results showed wide variation across strategies with respect to the increase in screening capacity needed during the latter half of this year – from 0% to 100% – and the excess breast cancer mortality occurring during 2020-2030 – from as many as 181 excess breast cancer deaths to as few as 14.
“The effects of the disruption are dependent on the chosen restart strategy,” Ms. Kregting summarized. “It would be preferred to immediately catch up because this minimizes the impact, but it also requires a very high capacity, so it may not always be possible. A proper alternative would be to increase the stopping age, so no screens are omitted, because this requires a rather normal capacity, and it will result in only small effects on incidence and mortality.”
As screening programs restart in some countries, there are still a lot of unknowns that could affect outcomes, including how many women will attend given that some may stay away out of fear, Ms. Kregting cautioned.
“We plan to do further model calculations when we know exactly what has happened. ... For now, we just assumed some reasonable disruption periods, and we assumed that capacity would be back to the original, before COVID-19, but I think we can say this is probably not the case,” she added.
Study details
Ms. Kregting and colleagues used Dutch breast cancer screening program parameters (biennial digital mammography for women aged 50-75 years) and a microsimulation screening analysis model to simulate four strategies for restarting breast cancer screening after a 6-month disruption:
- “Everyone delay,” a strategy in which all screening continues in the order planned with no change in the stopping age of 75 years (so that one in four women ultimately miss a screening during their lifetime)
- “First rounds no delay,” in which there is a delay in screening except for women having their first screening
- “Continue after stopping age,” in which there is a delay in screening but temporary increasing of the stopping age (to 76.5 years) to ensure all women get their final screen
- “Catch-up after stop,” in which capacity is increased to ensure full catch-up, with all delayed screens caught up in a 6-month period (the second half of 2020).
Results showed that 5,872 women would be screened in the latter half of 2020 if screening proceeded as usual without disruption. The necessary capacity was essentially the same with all of the restarting strategies, except for the catch-up-after-stop strategy, which would require a doubling of that number.
The temporal pattern of breast cancer incidence varied according to restart strategy early on, but incidence essentially returned to that expected with undisrupted screening by 2025 for all four strategies, with some small fluctuations thereafter.
The impact on breast cancer mortality differed considerably long term. It increased slightly and transiently above the expected level with the catch-up-after-stop strategy, but there were sizable, long-lasting increases with the other strategies, with excess deaths still seen in 2060 for the everyone-delay strategy.
In absolute terms, the excess number of breast cancer deaths during 2020-2030, compared with undisrupted screening, was 181 with the everyone-delay strategy, 155 with the first-rounds-no-delay strategy, 145 with the continue-after-stopping-age strategy, and just 14 with the catch-up-after-stop strategy. Ms. Kregting declined to provide numbers for other countries, given that the model is based on the Dutch population and screening program.
Results in context
“The unprecedented burden of COVID-19 on health systems worldwide has important implications for cancer care,” said invited discussant Alessandra Gennari, MD, PhD, of the University of Eastern Piedmont and Maggiore della Carità Hospital, both in Novara, Italy.
“There is a delay in diagnosis due to the fact that screening programs and diagnostic programs have been decreased or suspended in many Western countries where this is standard of care. Patients also are more reluctant to present to health care services, delaying their diagnosis,” Dr. Gennari said.
Findings of this new study add to those of similar studies undertaken in Italy (published in In Vivo) and the United Kingdom (published in The Lancet Oncology) showing the likely marked toll of the pandemic on cancer diagnosis and mortality, Dr. Gennari noted. Taken together, the findings underscore the urgent need for policy interventions to mitigate this impact.
“These interventions should focus on increasing routine diagnostic capacity, through which up to 40% of patients with cancer are diagnosed,” Dr. Gennari recommended. “Public health messaging is needed that accurately conveys the risk of severe illness from COVID-19 versus the risks of not seeking health care advice if patients are symptomatic. Finally, there is a need for provision of evidence-based data on which clinicians can adequately base their decision on how to manage the risks of cancer patients and the risks and benefits of procedures during the pandemic.”
The current study did not have any specific funding, and Ms. Kregting disclosed no conflicts of interest. Dr. Gennari disclosed relationships with Roche, Eisai, Lilly, AstraZeneca, Daiichi Sankyo, Merck, Novartis, and Pfizer.
SOURCE: Kregting L et al. EBCC-12 Virtual Conference, Abstract 24.
according to a modeling study reported at the 12th European Breast Cancer Conference.
Fallout of the pandemic has included reductions in cancer screening and diagnosis, said study investigator Lindy M. Kregting, a PhD student in the department of public health at Erasmus Medical Center, University Medical Center Rotterdam (the Netherlands).
In the Netherlands, new breast cancer diagnoses fell dramatically from historical levels starting in February. The number in April was less than half of that expected.
Ms. Kregting and colleagues used modeling to assess the impact of four strategies for restarting breast cancer screening in the Netherlands. The strategies differed regarding the population affected, the duration of the effects, and changes in stopping age. The usual situation, without any disruption, served as the comparator.
Results showed wide variation across strategies with respect to the increase in screening capacity needed during the latter half of this year – from 0% to 100% – and the excess breast cancer mortality occurring during 2020-2030 – from as many as 181 excess breast cancer deaths to as few as 14.
“The effects of the disruption are dependent on the chosen restart strategy,” Ms. Kregting summarized. “It would be preferred to immediately catch up because this minimizes the impact, but it also requires a very high capacity, so it may not always be possible. A proper alternative would be to increase the stopping age, so no screens are omitted, because this requires a rather normal capacity, and it will result in only small effects on incidence and mortality.”
As screening programs restart in some countries, there are still a lot of unknowns that could affect outcomes, including how many women will attend given that some may stay away out of fear, Ms. Kregting cautioned.
“We plan to do further model calculations when we know exactly what has happened. ... For now, we just assumed some reasonable disruption periods, and we assumed that capacity would be back to the original, before COVID-19, but I think we can say this is probably not the case,” she added.
Study details
Ms. Kregting and colleagues used Dutch breast cancer screening program parameters (biennial digital mammography for women aged 50-75 years) and a microsimulation screening analysis model to simulate four strategies for restarting breast cancer screening after a 6-month disruption:
- “Everyone delay,” a strategy in which all screening continues in the order planned with no change in the stopping age of 75 years (so that one in four women ultimately miss a screening during their lifetime)
- “First rounds no delay,” in which there is a delay in screening except for women having their first screening
- “Continue after stopping age,” in which there is a delay in screening but temporary increasing of the stopping age (to 76.5 years) to ensure all women get their final screen
- “Catch-up after stop,” in which capacity is increased to ensure full catch-up, with all delayed screens caught up in a 6-month period (the second half of 2020).
Results showed that 5,872 women would be screened in the latter half of 2020 if screening proceeded as usual without disruption. The necessary capacity was essentially the same with all of the restarting strategies, except for the catch-up-after-stop strategy, which would require a doubling of that number.
The temporal pattern of breast cancer incidence varied according to restart strategy early on, but incidence essentially returned to that expected with undisrupted screening by 2025 for all four strategies, with some small fluctuations thereafter.
The impact on breast cancer mortality differed considerably long term. It increased slightly and transiently above the expected level with the catch-up-after-stop strategy, but there were sizable, long-lasting increases with the other strategies, with excess deaths still seen in 2060 for the everyone-delay strategy.
In absolute terms, the excess number of breast cancer deaths during 2020-2030, compared with undisrupted screening, was 181 with the everyone-delay strategy, 155 with the first-rounds-no-delay strategy, 145 with the continue-after-stopping-age strategy, and just 14 with the catch-up-after-stop strategy. Ms. Kregting declined to provide numbers for other countries, given that the model is based on the Dutch population and screening program.
Results in context
“The unprecedented burden of COVID-19 on health systems worldwide has important implications for cancer care,” said invited discussant Alessandra Gennari, MD, PhD, of the University of Eastern Piedmont and Maggiore della Carità Hospital, both in Novara, Italy.
“There is a delay in diagnosis due to the fact that screening programs and diagnostic programs have been decreased or suspended in many Western countries where this is standard of care. Patients also are more reluctant to present to health care services, delaying their diagnosis,” Dr. Gennari said.
Findings of this new study add to those of similar studies undertaken in Italy (published in In Vivo) and the United Kingdom (published in The Lancet Oncology) showing the likely marked toll of the pandemic on cancer diagnosis and mortality, Dr. Gennari noted. Taken together, the findings underscore the urgent need for policy interventions to mitigate this impact.
“These interventions should focus on increasing routine diagnostic capacity, through which up to 40% of patients with cancer are diagnosed,” Dr. Gennari recommended. “Public health messaging is needed that accurately conveys the risk of severe illness from COVID-19 versus the risks of not seeking health care advice if patients are symptomatic. Finally, there is a need for provision of evidence-based data on which clinicians can adequately base their decision on how to manage the risks of cancer patients and the risks and benefits of procedures during the pandemic.”
The current study did not have any specific funding, and Ms. Kregting disclosed no conflicts of interest. Dr. Gennari disclosed relationships with Roche, Eisai, Lilly, AstraZeneca, Daiichi Sankyo, Merck, Novartis, and Pfizer.
SOURCE: Kregting L et al. EBCC-12 Virtual Conference, Abstract 24.
FROM EBCC-12 VIRTUAL CONFERENCE
The Other Pandemic: Addiction
May 20 of this plague year, Reuters reported the death of a 32-year-old Florida nurse who had worked tirelessly to treat patients with COVID-19.1 The presumption is that, like so many selfless health care providers (HCPs), this nurse was exposed to and then sadly succumbed to the virus. That presumption would be wrong: COVID-19 did not take his young life. The other pandemic—addiction— did. Bereaved friends and family reported that the nurse had been in recovery from opioid use disorder (OUD) before the onslaught of the public health crisis. The chronicle of his relapse is instructive for the devastating effect COVID-19 has had on persons struggling with addiction, even those like the nurse who was in sustained remission from OUD with a bright future.
Many of the themes are familiar to HCPs and have been the subject of prior columns in this COVID-19 series. The nurse experienced acute stress symptoms, such as nightmares from the repeated crises of sick and dying patients in the intensive care unit where he worked.2 Like so many other HCPs, while he was desperately trying to save others, he also worried about having sufficient access to appropriate personal protective equipment (PPE).
Most relevant to this column, the caregiver was unable to access his primary source of support for his sobriety—attendance at 12-step meetings. Social distancing, which is one of the only proven means we have of reducing transmission of the virus, has had unintended consequences. Although many have found virtual connections rewarding, this nurse needed the curtailed face-to-face contact. The courage that had led him to volunteer for hazardous duty unwontedly resulted in his estrangement: Friends feared that he would expose them to the virus, and he worried that he would expose his family to danger. As in the 1918 flu pandemic, the humans we depend on for reality testing and companionship have been cruelly transformed into potential vectors of the virus.3
Isolation is the worst of all possible counselors as the great Spanish philosopher of alienation Miguel de Unamuno has argued. The deceptive promise of a rapid deliverance from anxiety and pain that substances of abuse proffer apparently led the nurse back to opioids. The virtue of being clean permitted the dirty drug to take advantage of the nurses’ reduced physiologic tolerance to opioids. It is suspected but not confirmed that he fatally overdosed alone in his car.
This Florida nurse is an especially tragic example of a terrible phenomenon being repeated all over the country. And the epidemic of substance use disorders (SUDs) related to COVID-19 is not confined to the US; there are similar reports from other afflicted nations, making addiction truly the other pandemic.4 The Centers for Disease Control and Prevention reported that 13.3% of American adults have started or increased their substance use as a means of managing the negative emotions associated with the pandemic.5 Also from March to May 2020, researchers in Baltimore found a 17.6% increase in suspected overdoses in counties advising social distancing and/or mandating stay at home orders.5
These data reinforce a well-known maxim in the addiction community that “addiction is a disease of isolation.”6-8 The burden of the lockdown falls harder on many of the patients we treat in the federal health care system whose other mental and physical health conditions, including chronic pain, depression, and posttraumatic stress disorder already placed them at elevated risk of SUDs.9 Director of the National Institute of Drug Abuse Nora Volkow, MD, recently traced the well-known arc from isolation to increased use of drugs and alcohol.10 Isolation is stressful and amplifies negative thoughts, dysphoria, and fearful emotions, which are recognized triggers for the use of substances of abuse. The usually available means of coping with craving, and in many cases withdrawal, such as prescribed medications, visits to therapists, participation in support groups are either not available or much more difficult to access.10 Nor are those without a current or even historical SUD immune to the psychosocial pressures of the pandemic: Isolation also constitutes a risk for the development of de novo addiction particularly among already marginalized groups, such as the elderly and disabled.
The federal government has initiated several important measures to reduce the adverse impact of isolation on persons with SUDs. The Drug Enforcement Administration is exempting qualified practitioners of medication-assisted treatment from the in-person evaluation that is usually required for the prescription of controlled substances, including buprenorphine. This exemption applies to both established patient prescriptions for buprenorphine and new buprenorphine patient prescriptions.11 These and other administrative contingencies at the federal government level can assist persons with OUD to continue to receive medicationassisted treatment.
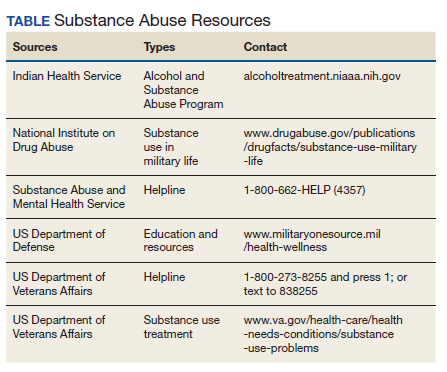
As individual clinicians in federal practice, we alone cannot engineer such major policy accommodations in response to COVID-19, yet we can still make a difference in the lives of our patients. We can focus a few minutes of our telehealth interactions on checking in with patients who have a history or a current SUD. We can remember to use evidence-based screens for these patients and those with other risk factors to detect drug or alcohol use before it becomes a disorder. And we can identify and refer not only patients but also our beleaguered colleagues who feel alone at sea—to the many lifelines our agencies have cast into what other commentators have referred to as a Perfect Storm of COVID-19 and the opioid crisis (Table).12
1. Borter G. A nurse struggled with COVID-19 trauma. He was found dead in his car. Reuters. May 20, 2020. https:// www.reuters.com/article/us-health-coronavirus-nurse -death-insigh/a-nurse-struggled-with-covid-19-trauma-he -was-found-dead-in-his-car-idUSKBN22W1JD Accessed September 15, 2020.
2. Geppert CMA. The duty to care and its exceptions in a pandemic. Fed Pract. 2020;37(5):210-211.
3. Kim NY. How the 1918 pandemic frayed social bonds. The Atlantic. March 31, 2020. https://www.theatlantic.com /family/archive/2020/03/coronavirus-loneliness-and-mistrust -1918-flu-pandemic-quarantine/609163. Accessed September 18, 2020.
4. Jemberie WB, Stewart Williams J, Eriksson M, et al. Substance use disorders and COVID-19: multi-faceted problems which require multi-pronged solutions. Front Psychiatry. 2020;11:714. Published 2020 Jul 21. doi:10.3389/fpsyt.2020.00714
5. Alter A, Yeager C. COVID-19 impact on US national overdose crises. http://www.odmap.org/Content/docs/news/2020 /ODMAP-Report-June-2020.pdf. Published May 2020. Accessed September 18, 2020.
6. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1049-1057. Published 2020 Aug 14. doi:10.15585/mmwr.mm6932a1
7. Grinspoon P. A tale of two epidemics: when COVID-19 and opioid addiction collide. https://www.health.harvard.edu /blog/a-tale-of-two-epidemics-when-covid-19-and-opioid -addiction-collide-2020042019569. Published April 20, 2020. Accessed September 16, 2020
8. Bebinger M. Addiction is “a disease of isolation”—so pandemic puts recovery at risk. https://khn.org/news/addiction -is-a-disease-of-isolation-so-pandemic-puts-recovery-at-risk. Published March 30, 2020. Accessed September 23, 2020.
9. National Institute of Drug Abuse. Substance abuse and military life. DrugFacts. https://www.drugabuse.gov/publications /drugfacts/substance-use-military-life. Published October 2019. Accessed September 16, 2020.
10. Volkow ND. Collision of the COVID-19 and addiction epidemics. Ann Intern Med. 2020;173(1):61-62. doi:10.7326/M20-1212
11. Substance Abuse and Mental Health Administration. FAQS: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID-19 emergency. https:// www.samhsa.gov/sites/default/files/faqs-for-oud-prescribing -and-dispensing.pdf. Updated April 21, 2020. Accessed September 22, 2020.
12. Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance usedisorders-the perfect storm. Am J Psychiatry. 2020;177(9):805-807. doi:10.1176/appi. ajp.2020.20040417
May 20 of this plague year, Reuters reported the death of a 32-year-old Florida nurse who had worked tirelessly to treat patients with COVID-19.1 The presumption is that, like so many selfless health care providers (HCPs), this nurse was exposed to and then sadly succumbed to the virus. That presumption would be wrong: COVID-19 did not take his young life. The other pandemic—addiction— did. Bereaved friends and family reported that the nurse had been in recovery from opioid use disorder (OUD) before the onslaught of the public health crisis. The chronicle of his relapse is instructive for the devastating effect COVID-19 has had on persons struggling with addiction, even those like the nurse who was in sustained remission from OUD with a bright future.
Many of the themes are familiar to HCPs and have been the subject of prior columns in this COVID-19 series. The nurse experienced acute stress symptoms, such as nightmares from the repeated crises of sick and dying patients in the intensive care unit where he worked.2 Like so many other HCPs, while he was desperately trying to save others, he also worried about having sufficient access to appropriate personal protective equipment (PPE).
Most relevant to this column, the caregiver was unable to access his primary source of support for his sobriety—attendance at 12-step meetings. Social distancing, which is one of the only proven means we have of reducing transmission of the virus, has had unintended consequences. Although many have found virtual connections rewarding, this nurse needed the curtailed face-to-face contact. The courage that had led him to volunteer for hazardous duty unwontedly resulted in his estrangement: Friends feared that he would expose them to the virus, and he worried that he would expose his family to danger. As in the 1918 flu pandemic, the humans we depend on for reality testing and companionship have been cruelly transformed into potential vectors of the virus.3
Isolation is the worst of all possible counselors as the great Spanish philosopher of alienation Miguel de Unamuno has argued. The deceptive promise of a rapid deliverance from anxiety and pain that substances of abuse proffer apparently led the nurse back to opioids. The virtue of being clean permitted the dirty drug to take advantage of the nurses’ reduced physiologic tolerance to opioids. It is suspected but not confirmed that he fatally overdosed alone in his car.
This Florida nurse is an especially tragic example of a terrible phenomenon being repeated all over the country. And the epidemic of substance use disorders (SUDs) related to COVID-19 is not confined to the US; there are similar reports from other afflicted nations, making addiction truly the other pandemic.4 The Centers for Disease Control and Prevention reported that 13.3% of American adults have started or increased their substance use as a means of managing the negative emotions associated with the pandemic.5 Also from March to May 2020, researchers in Baltimore found a 17.6% increase in suspected overdoses in counties advising social distancing and/or mandating stay at home orders.5
These data reinforce a well-known maxim in the addiction community that “addiction is a disease of isolation.”6-8 The burden of the lockdown falls harder on many of the patients we treat in the federal health care system whose other mental and physical health conditions, including chronic pain, depression, and posttraumatic stress disorder already placed them at elevated risk of SUDs.9 Director of the National Institute of Drug Abuse Nora Volkow, MD, recently traced the well-known arc from isolation to increased use of drugs and alcohol.10 Isolation is stressful and amplifies negative thoughts, dysphoria, and fearful emotions, which are recognized triggers for the use of substances of abuse. The usually available means of coping with craving, and in many cases withdrawal, such as prescribed medications, visits to therapists, participation in support groups are either not available or much more difficult to access.10 Nor are those without a current or even historical SUD immune to the psychosocial pressures of the pandemic: Isolation also constitutes a risk for the development of de novo addiction particularly among already marginalized groups, such as the elderly and disabled.
The federal government has initiated several important measures to reduce the adverse impact of isolation on persons with SUDs. The Drug Enforcement Administration is exempting qualified practitioners of medication-assisted treatment from the in-person evaluation that is usually required for the prescription of controlled substances, including buprenorphine. This exemption applies to both established patient prescriptions for buprenorphine and new buprenorphine patient prescriptions.11 These and other administrative contingencies at the federal government level can assist persons with OUD to continue to receive medicationassisted treatment.
As individual clinicians in federal practice, we alone cannot engineer such major policy accommodations in response to COVID-19, yet we can still make a difference in the lives of our patients. We can focus a few minutes of our telehealth interactions on checking in with patients who have a history or a current SUD. We can remember to use evidence-based screens for these patients and those with other risk factors to detect drug or alcohol use before it becomes a disorder. And we can identify and refer not only patients but also our beleaguered colleagues who feel alone at sea—to the many lifelines our agencies have cast into what other commentators have referred to as a Perfect Storm of COVID-19 and the opioid crisis (Table).12
May 20 of this plague year, Reuters reported the death of a 32-year-old Florida nurse who had worked tirelessly to treat patients with COVID-19.1 The presumption is that, like so many selfless health care providers (HCPs), this nurse was exposed to and then sadly succumbed to the virus. That presumption would be wrong: COVID-19 did not take his young life. The other pandemic—addiction— did. Bereaved friends and family reported that the nurse had been in recovery from opioid use disorder (OUD) before the onslaught of the public health crisis. The chronicle of his relapse is instructive for the devastating effect COVID-19 has had on persons struggling with addiction, even those like the nurse who was in sustained remission from OUD with a bright future.
Many of the themes are familiar to HCPs and have been the subject of prior columns in this COVID-19 series. The nurse experienced acute stress symptoms, such as nightmares from the repeated crises of sick and dying patients in the intensive care unit where he worked.2 Like so many other HCPs, while he was desperately trying to save others, he also worried about having sufficient access to appropriate personal protective equipment (PPE).
Most relevant to this column, the caregiver was unable to access his primary source of support for his sobriety—attendance at 12-step meetings. Social distancing, which is one of the only proven means we have of reducing transmission of the virus, has had unintended consequences. Although many have found virtual connections rewarding, this nurse needed the curtailed face-to-face contact. The courage that had led him to volunteer for hazardous duty unwontedly resulted in his estrangement: Friends feared that he would expose them to the virus, and he worried that he would expose his family to danger. As in the 1918 flu pandemic, the humans we depend on for reality testing and companionship have been cruelly transformed into potential vectors of the virus.3
Isolation is the worst of all possible counselors as the great Spanish philosopher of alienation Miguel de Unamuno has argued. The deceptive promise of a rapid deliverance from anxiety and pain that substances of abuse proffer apparently led the nurse back to opioids. The virtue of being clean permitted the dirty drug to take advantage of the nurses’ reduced physiologic tolerance to opioids. It is suspected but not confirmed that he fatally overdosed alone in his car.
This Florida nurse is an especially tragic example of a terrible phenomenon being repeated all over the country. And the epidemic of substance use disorders (SUDs) related to COVID-19 is not confined to the US; there are similar reports from other afflicted nations, making addiction truly the other pandemic.4 The Centers for Disease Control and Prevention reported that 13.3% of American adults have started or increased their substance use as a means of managing the negative emotions associated with the pandemic.5 Also from March to May 2020, researchers in Baltimore found a 17.6% increase in suspected overdoses in counties advising social distancing and/or mandating stay at home orders.5
These data reinforce a well-known maxim in the addiction community that “addiction is a disease of isolation.”6-8 The burden of the lockdown falls harder on many of the patients we treat in the federal health care system whose other mental and physical health conditions, including chronic pain, depression, and posttraumatic stress disorder already placed them at elevated risk of SUDs.9 Director of the National Institute of Drug Abuse Nora Volkow, MD, recently traced the well-known arc from isolation to increased use of drugs and alcohol.10 Isolation is stressful and amplifies negative thoughts, dysphoria, and fearful emotions, which are recognized triggers for the use of substances of abuse. The usually available means of coping with craving, and in many cases withdrawal, such as prescribed medications, visits to therapists, participation in support groups are either not available or much more difficult to access.10 Nor are those without a current or even historical SUD immune to the psychosocial pressures of the pandemic: Isolation also constitutes a risk for the development of de novo addiction particularly among already marginalized groups, such as the elderly and disabled.
The federal government has initiated several important measures to reduce the adverse impact of isolation on persons with SUDs. The Drug Enforcement Administration is exempting qualified practitioners of medication-assisted treatment from the in-person evaluation that is usually required for the prescription of controlled substances, including buprenorphine. This exemption applies to both established patient prescriptions for buprenorphine and new buprenorphine patient prescriptions.11 These and other administrative contingencies at the federal government level can assist persons with OUD to continue to receive medicationassisted treatment.
As individual clinicians in federal practice, we alone cannot engineer such major policy accommodations in response to COVID-19, yet we can still make a difference in the lives of our patients. We can focus a few minutes of our telehealth interactions on checking in with patients who have a history or a current SUD. We can remember to use evidence-based screens for these patients and those with other risk factors to detect drug or alcohol use before it becomes a disorder. And we can identify and refer not only patients but also our beleaguered colleagues who feel alone at sea—to the many lifelines our agencies have cast into what other commentators have referred to as a Perfect Storm of COVID-19 and the opioid crisis (Table).12
1. Borter G. A nurse struggled with COVID-19 trauma. He was found dead in his car. Reuters. May 20, 2020. https:// www.reuters.com/article/us-health-coronavirus-nurse -death-insigh/a-nurse-struggled-with-covid-19-trauma-he -was-found-dead-in-his-car-idUSKBN22W1JD Accessed September 15, 2020.
2. Geppert CMA. The duty to care and its exceptions in a pandemic. Fed Pract. 2020;37(5):210-211.
3. Kim NY. How the 1918 pandemic frayed social bonds. The Atlantic. March 31, 2020. https://www.theatlantic.com /family/archive/2020/03/coronavirus-loneliness-and-mistrust -1918-flu-pandemic-quarantine/609163. Accessed September 18, 2020.
4. Jemberie WB, Stewart Williams J, Eriksson M, et al. Substance use disorders and COVID-19: multi-faceted problems which require multi-pronged solutions. Front Psychiatry. 2020;11:714. Published 2020 Jul 21. doi:10.3389/fpsyt.2020.00714
5. Alter A, Yeager C. COVID-19 impact on US national overdose crises. http://www.odmap.org/Content/docs/news/2020 /ODMAP-Report-June-2020.pdf. Published May 2020. Accessed September 18, 2020.
6. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1049-1057. Published 2020 Aug 14. doi:10.15585/mmwr.mm6932a1
7. Grinspoon P. A tale of two epidemics: when COVID-19 and opioid addiction collide. https://www.health.harvard.edu /blog/a-tale-of-two-epidemics-when-covid-19-and-opioid -addiction-collide-2020042019569. Published April 20, 2020. Accessed September 16, 2020
8. Bebinger M. Addiction is “a disease of isolation”—so pandemic puts recovery at risk. https://khn.org/news/addiction -is-a-disease-of-isolation-so-pandemic-puts-recovery-at-risk. Published March 30, 2020. Accessed September 23, 2020.
9. National Institute of Drug Abuse. Substance abuse and military life. DrugFacts. https://www.drugabuse.gov/publications /drugfacts/substance-use-military-life. Published October 2019. Accessed September 16, 2020.
10. Volkow ND. Collision of the COVID-19 and addiction epidemics. Ann Intern Med. 2020;173(1):61-62. doi:10.7326/M20-1212
11. Substance Abuse and Mental Health Administration. FAQS: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID-19 emergency. https:// www.samhsa.gov/sites/default/files/faqs-for-oud-prescribing -and-dispensing.pdf. Updated April 21, 2020. Accessed September 22, 2020.
12. Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance usedisorders-the perfect storm. Am J Psychiatry. 2020;177(9):805-807. doi:10.1176/appi. ajp.2020.20040417
1. Borter G. A nurse struggled with COVID-19 trauma. He was found dead in his car. Reuters. May 20, 2020. https:// www.reuters.com/article/us-health-coronavirus-nurse -death-insigh/a-nurse-struggled-with-covid-19-trauma-he -was-found-dead-in-his-car-idUSKBN22W1JD Accessed September 15, 2020.
2. Geppert CMA. The duty to care and its exceptions in a pandemic. Fed Pract. 2020;37(5):210-211.
3. Kim NY. How the 1918 pandemic frayed social bonds. The Atlantic. March 31, 2020. https://www.theatlantic.com /family/archive/2020/03/coronavirus-loneliness-and-mistrust -1918-flu-pandemic-quarantine/609163. Accessed September 18, 2020.
4. Jemberie WB, Stewart Williams J, Eriksson M, et al. Substance use disorders and COVID-19: multi-faceted problems which require multi-pronged solutions. Front Psychiatry. 2020;11:714. Published 2020 Jul 21. doi:10.3389/fpsyt.2020.00714
5. Alter A, Yeager C. COVID-19 impact on US national overdose crises. http://www.odmap.org/Content/docs/news/2020 /ODMAP-Report-June-2020.pdf. Published May 2020. Accessed September 18, 2020.
6. Czeisler MÉ, Lane RI, Petrosky E, et al. Mental health, substance use, and suicidal ideation during the COVID-19 pandemic - United States, June 24-30, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(32):1049-1057. Published 2020 Aug 14. doi:10.15585/mmwr.mm6932a1
7. Grinspoon P. A tale of two epidemics: when COVID-19 and opioid addiction collide. https://www.health.harvard.edu /blog/a-tale-of-two-epidemics-when-covid-19-and-opioid -addiction-collide-2020042019569. Published April 20, 2020. Accessed September 16, 2020
8. Bebinger M. Addiction is “a disease of isolation”—so pandemic puts recovery at risk. https://khn.org/news/addiction -is-a-disease-of-isolation-so-pandemic-puts-recovery-at-risk. Published March 30, 2020. Accessed September 23, 2020.
9. National Institute of Drug Abuse. Substance abuse and military life. DrugFacts. https://www.drugabuse.gov/publications /drugfacts/substance-use-military-life. Published October 2019. Accessed September 16, 2020.
10. Volkow ND. Collision of the COVID-19 and addiction epidemics. Ann Intern Med. 2020;173(1):61-62. doi:10.7326/M20-1212
11. Substance Abuse and Mental Health Administration. FAQS: Provision of methadone and buprenorphine for the treatment of opioid use disorder in the COVID-19 emergency. https:// www.samhsa.gov/sites/default/files/faqs-for-oud-prescribing -and-dispensing.pdf. Updated April 21, 2020. Accessed September 22, 2020.
12. Spagnolo PA, Montemitro C, Leggio L. New challenges in addiction medicine: COVID-19 infection in patients with alcohol and substance usedisorders-the perfect storm. Am J Psychiatry. 2020;177(9):805-807. doi:10.1176/appi. ajp.2020.20040417

{kind=link}
HM20 Virtual: Key takeaways for the pediatric hospitalist
The HM20 Virtual conference in August was filled with excellent content that can be applied by all hospitalists. This article summarizes key concepts and takeaways for the pediatric hospitalist.
Racism and bias in medicine
HM20 Virtual session: Structural Racism and Bias in Hospital Medicine During Two Pandemics
Presenters: Nathan Chomilo, MD, FAAP, and Benji K. Mathews, MD, SFHM

Dr. Nathan Chomilo, of HealthPartners in Minneapolis, opened the session sharing how racial disparities were a symptom of racism. The presenters explained how structural racism has been propagated in medicine with the Hospital Survey and Construction Act of 1964 that allowed segregated hospitals, as well as the racism that exists within the “hidden curriculum.”
Dr. Chomilo discussed how personal experiences of racism can lead to worse health outcomes, including depression, obesity, and overall poor health. Dr. Mathews, also of HealthPartners, discussed how implicit biases can be addressed at the individual level, the organizational level, and simultaneously at both levels to create an antiracist culture. He presented strategies to mitigate individual biases; recognizing when biases may be triggered, checking biases at the door, connecting with others from different backgrounds as equals, and practicing antiracism by being an active bystander. Dr. Chomilo concluded the session by sharing that we can all grow by addressing racism at “our houses” (health care systems, medical schools, payer systems) with the goal to create an antiracist system.
Key takeaways
- Racial disparities are a symptom of structural racism that has been propagated in medicine for centuries.
- Addressing implicit biases at the individual level, organization level, and simultaneously at both levels can help leaders model and promote an antiracism culture.
HM20 Virtual session: When Grief and Crises Intersect: Perspectives of a Black Physician in the Time of Two Pandemics
Presenter: Kimberly Manning, MD, FACP, FAAP
Dr. Kimberly Manning, of Emory University in Atlanta, discussed the dual pandemics of COVID-19 and the racism that we are currently experiencing and tried to describe the unique perspective of Black Americans. Though it is easy to see that COVID-19 is a pandemic, racism is not always seen in this way. Dr. Manning demonstrated that, when a pandemic is defined as “that which occurs over a wide geographic area and affects a high proportion of the population,” racism is absolutely a pandemic. Black Americans have been disproportionately affected by COVID-19. Dr. Manning said we often hear that we are in unprecedented times but as far as racism is concerned, there is nothing new about this. She shared stories of personal milestones and how each of these instances, though marked by something beautiful, was also marked by something truly awful. Each time she had a reason to smile, there was something awful going on in the country that showed how racism was still present. Dr. Manning described that, though these were her stories, all Black Americans can recount the same stories, emotions, and feelings of grief.
Dr. Manning concluded by sharing how we can “Do The Work” to combat the pandemic of racism: broaden our funds of knowledge, remember that people are grieving, explore our implicit biases, be brave bystanders, and avoid performative allyship
Key takeaways
- Though the COVID19 pandemic is unprecedented, the pandemic of racism is not.
- We must “Do The Work” to combat everyday racism and to be cognizant of what our Black colleagues are going through every day.
Immigrant hospitalist challenges
HM20 Virtual session: The Immigrant Hospitalist: Navigating the Uncertain Terrain During COVID-19
Presenters: Manpreet S. Malik, MD, FHM, and Benji K. Mathews, MD, SFHM
Dr. Malik of Emory University in Atlanta, and Dr. Mathews of HealthPartners, opened this session by sharing their personal stories as immigrant physicians in the United States. Dr. Malik noted that physicians born outside the United States make up 29% of U.S. physicians, and 32% of hospitalists are international medical graduates.
The presenters revealed the structural hurdles immigrant physicians face, including lack of empowerment until achieving permanent residency status; limited leadership, administrative, and academic roles; concerns for job security and financial stability; and experiencing micro- and macroaggressions at work. The presenters shared a framework for a developmental orientation inclined toward cultural competency beginning with denial, followed by polarization, progressing to minimization, advancing to acceptance, and culminating in adaptation.
They concluded the session by stressing the importance of advocacy for immigrant physicians and encouraged colleagues to become engaged in efforts within their professional organizations.
Key takeaway
- Immigrant physicians experience structural challenges to their professional advancement because of their residency status.
Learner supervision
HM20 Virtual session: Call Me Maybe: Balancing Resident Autonomy With Sensible Supervision
Presenter: Daniel Steinberg, MD, SFHM, FACP

Dr. Steinberg, based at Mount Sinai in New York, explained that resident supervision is driven by three factors: what residents need, what residents want, and what the supervisor can provide. Although data is mixed as to whether supervision improves patient outcomes, supervision is essential for patient care and resident education. Dr. Steinberg showcased several relevant medical education studies related to supervision and focused on a key question: Do you trust the resident? The review of medical education literature discussed the meaning and development of trust, oral case presentations to determine trust, and the influence of supervisor experience.
Key takeaways
- Resident supervision is driven by what residents need, what residents want, and what the supervisor can provide.
- Trust can be determined from direct supervision, oral presentations, and remote access of electronic medical records, but is also influenced by attending experience and style.
Balancing personal and professional life
HM20 Virtual session: Being a Hospitalist and a Parent: Balancing Roles With Grace
Presenters: Heather E. Nye, MD, PhD, SFHM, and David Alfandre, MD, MSPH
Dr. Nye of the University of California, San Francisco, and Dr. Alfandre of New York University shared their challenges as hospitalists, parents, and partners before and during the COVID-19 pandemic. They described their feelings of guilt during the pandemic related to increasing their families’ infection risks, as well as the gratitude they felt for having stable jobs during the crisis. They shared solutions that worked for their families, including cooperating with their partners, expressing their scheduling needs, and negotiating to meet those needs with their employers.
Dr. Nye and Dr. Alfandre recommended staying connected with others for help, including partners, institutions, neighbors, and colleagues. They also recommended supporting, sharing, collaborating, and connecting with their partners and colleagues to maintain a balanced professional and personal life.
Key takeaway:
- Stay connected and support, collaborate, and share with your colleagues and partner at home.
Dr. Kumar is the pediatric editor of The Hospitalist. She is clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University and a pediatric hospitalist at Cleveland Clinic Children’s. Dr. Doraiswamy is an assistant professor of medicine and pediatrics and a med-peds hospitalist at The Ohio State University and Nationwide Children’s Hospital, both in Columbus. Dr. Tantoco is an academic med-peds hospitalist practicing in Northwestern Memorial Hospital, Chicago, and Ann & Robert H. Lurie Children’s Hospital of Chicago.
The HM20 Virtual conference in August was filled with excellent content that can be applied by all hospitalists. This article summarizes key concepts and takeaways for the pediatric hospitalist.
Racism and bias in medicine
HM20 Virtual session: Structural Racism and Bias in Hospital Medicine During Two Pandemics
Presenters: Nathan Chomilo, MD, FAAP, and Benji K. Mathews, MD, SFHM
Dr. Nathan Chomilo, of HealthPartners in Minneapolis, opened the session sharing how racial disparities were a symptom of racism. The presenters explained how structural racism has been propagated in medicine with the Hospital Survey and Construction Act of 1964 that allowed segregated hospitals, as well as the racism that exists within the “hidden curriculum.”
Dr. Chomilo discussed how personal experiences of racism can lead to worse health outcomes, including depression, obesity, and overall poor health. Dr. Mathews, also of HealthPartners, discussed how implicit biases can be addressed at the individual level, the organizational level, and simultaneously at both levels to create an antiracist culture. He presented strategies to mitigate individual biases; recognizing when biases may be triggered, checking biases at the door, connecting with others from different backgrounds as equals, and practicing antiracism by being an active bystander. Dr. Chomilo concluded the session by sharing that we can all grow by addressing racism at “our houses” (health care systems, medical schools, payer systems) with the goal to create an antiracist system.
Key takeaways
- Racial disparities are a symptom of structural racism that has been propagated in medicine for centuries.
- Addressing implicit biases at the individual level, organization level, and simultaneously at both levels can help leaders model and promote an antiracism culture.
HM20 Virtual session: When Grief and Crises Intersect: Perspectives of a Black Physician in the Time of Two Pandemics
Presenter: Kimberly Manning, MD, FACP, FAAP
Dr. Kimberly Manning, of Emory University in Atlanta, discussed the dual pandemics of COVID-19 and the racism that we are currently experiencing and tried to describe the unique perspective of Black Americans. Though it is easy to see that COVID-19 is a pandemic, racism is not always seen in this way. Dr. Manning demonstrated that, when a pandemic is defined as “that which occurs over a wide geographic area and affects a high proportion of the population,” racism is absolutely a pandemic. Black Americans have been disproportionately affected by COVID-19. Dr. Manning said we often hear that we are in unprecedented times but as far as racism is concerned, there is nothing new about this. She shared stories of personal milestones and how each of these instances, though marked by something beautiful, was also marked by something truly awful. Each time she had a reason to smile, there was something awful going on in the country that showed how racism was still present. Dr. Manning described that, though these were her stories, all Black Americans can recount the same stories, emotions, and feelings of grief.
Dr. Manning concluded by sharing how we can “Do The Work” to combat the pandemic of racism: broaden our funds of knowledge, remember that people are grieving, explore our implicit biases, be brave bystanders, and avoid performative allyship
Key takeaways
- Though the COVID19 pandemic is unprecedented, the pandemic of racism is not.
- We must “Do The Work” to combat everyday racism and to be cognizant of what our Black colleagues are going through every day.
Immigrant hospitalist challenges
HM20 Virtual session: The Immigrant Hospitalist: Navigating the Uncertain Terrain During COVID-19
Presenters: Manpreet S. Malik, MD, FHM, and Benji K. Mathews, MD, SFHM
Dr. Malik of Emory University in Atlanta, and Dr. Mathews of HealthPartners, opened this session by sharing their personal stories as immigrant physicians in the United States. Dr. Malik noted that physicians born outside the United States make up 29% of U.S. physicians, and 32% of hospitalists are international medical graduates.
The presenters revealed the structural hurdles immigrant physicians face, including lack of empowerment until achieving permanent residency status; limited leadership, administrative, and academic roles; concerns for job security and financial stability; and experiencing micro- and macroaggressions at work. The presenters shared a framework for a developmental orientation inclined toward cultural competency beginning with denial, followed by polarization, progressing to minimization, advancing to acceptance, and culminating in adaptation.
They concluded the session by stressing the importance of advocacy for immigrant physicians and encouraged colleagues to become engaged in efforts within their professional organizations.
Key takeaway
- Immigrant physicians experience structural challenges to their professional advancement because of their residency status.
Learner supervision
HM20 Virtual session: Call Me Maybe: Balancing Resident Autonomy With Sensible Supervision
Presenter: Daniel Steinberg, MD, SFHM, FACP
Dr. Steinberg, based at Mount Sinai in New York, explained that resident supervision is driven by three factors: what residents need, what residents want, and what the supervisor can provide. Although data is mixed as to whether supervision improves patient outcomes, supervision is essential for patient care and resident education. Dr. Steinberg showcased several relevant medical education studies related to supervision and focused on a key question: Do you trust the resident? The review of medical education literature discussed the meaning and development of trust, oral case presentations to determine trust, and the influence of supervisor experience.
Key takeaways
- Resident supervision is driven by what residents need, what residents want, and what the supervisor can provide.
- Trust can be determined from direct supervision, oral presentations, and remote access of electronic medical records, but is also influenced by attending experience and style.
Balancing personal and professional life
HM20 Virtual session: Being a Hospitalist and a Parent: Balancing Roles With Grace
Presenters: Heather E. Nye, MD, PhD, SFHM, and David Alfandre, MD, MSPH
Dr. Nye of the University of California, San Francisco, and Dr. Alfandre of New York University shared their challenges as hospitalists, parents, and partners before and during the COVID-19 pandemic. They described their feelings of guilt during the pandemic related to increasing their families’ infection risks, as well as the gratitude they felt for having stable jobs during the crisis. They shared solutions that worked for their families, including cooperating with their partners, expressing their scheduling needs, and negotiating to meet those needs with their employers.
Dr. Nye and Dr. Alfandre recommended staying connected with others for help, including partners, institutions, neighbors, and colleagues. They also recommended supporting, sharing, collaborating, and connecting with their partners and colleagues to maintain a balanced professional and personal life.
Key takeaway:
- Stay connected and support, collaborate, and share with your colleagues and partner at home.
Dr. Kumar is the pediatric editor of The Hospitalist. She is clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University and a pediatric hospitalist at Cleveland Clinic Children’s. Dr. Doraiswamy is an assistant professor of medicine and pediatrics and a med-peds hospitalist at The Ohio State University and Nationwide Children’s Hospital, both in Columbus. Dr. Tantoco is an academic med-peds hospitalist practicing in Northwestern Memorial Hospital, Chicago, and Ann & Robert H. Lurie Children’s Hospital of Chicago.
The HM20 Virtual conference in August was filled with excellent content that can be applied by all hospitalists. This article summarizes key concepts and takeaways for the pediatric hospitalist.
Racism and bias in medicine
HM20 Virtual session: Structural Racism and Bias in Hospital Medicine During Two Pandemics
Presenters: Nathan Chomilo, MD, FAAP, and Benji K. Mathews, MD, SFHM
Dr. Nathan Chomilo, of HealthPartners in Minneapolis, opened the session sharing how racial disparities were a symptom of racism. The presenters explained how structural racism has been propagated in medicine with the Hospital Survey and Construction Act of 1964 that allowed segregated hospitals, as well as the racism that exists within the “hidden curriculum.”
Dr. Chomilo discussed how personal experiences of racism can lead to worse health outcomes, including depression, obesity, and overall poor health. Dr. Mathews, also of HealthPartners, discussed how implicit biases can be addressed at the individual level, the organizational level, and simultaneously at both levels to create an antiracist culture. He presented strategies to mitigate individual biases; recognizing when biases may be triggered, checking biases at the door, connecting with others from different backgrounds as equals, and practicing antiracism by being an active bystander. Dr. Chomilo concluded the session by sharing that we can all grow by addressing racism at “our houses” (health care systems, medical schools, payer systems) with the goal to create an antiracist system.
Key takeaways
- Racial disparities are a symptom of structural racism that has been propagated in medicine for centuries.
- Addressing implicit biases at the individual level, organization level, and simultaneously at both levels can help leaders model and promote an antiracism culture.
HM20 Virtual session: When Grief and Crises Intersect: Perspectives of a Black Physician in the Time of Two Pandemics
Presenter: Kimberly Manning, MD, FACP, FAAP
Dr. Kimberly Manning, of Emory University in Atlanta, discussed the dual pandemics of COVID-19 and the racism that we are currently experiencing and tried to describe the unique perspective of Black Americans. Though it is easy to see that COVID-19 is a pandemic, racism is not always seen in this way. Dr. Manning demonstrated that, when a pandemic is defined as “that which occurs over a wide geographic area and affects a high proportion of the population,” racism is absolutely a pandemic. Black Americans have been disproportionately affected by COVID-19. Dr. Manning said we often hear that we are in unprecedented times but as far as racism is concerned, there is nothing new about this. She shared stories of personal milestones and how each of these instances, though marked by something beautiful, was also marked by something truly awful. Each time she had a reason to smile, there was something awful going on in the country that showed how racism was still present. Dr. Manning described that, though these were her stories, all Black Americans can recount the same stories, emotions, and feelings of grief.
Dr. Manning concluded by sharing how we can “Do The Work” to combat the pandemic of racism: broaden our funds of knowledge, remember that people are grieving, explore our implicit biases, be brave bystanders, and avoid performative allyship
Key takeaways
- Though the COVID19 pandemic is unprecedented, the pandemic of racism is not.
- We must “Do The Work” to combat everyday racism and to be cognizant of what our Black colleagues are going through every day.
Immigrant hospitalist challenges
HM20 Virtual session: The Immigrant Hospitalist: Navigating the Uncertain Terrain During COVID-19
Presenters: Manpreet S. Malik, MD, FHM, and Benji K. Mathews, MD, SFHM
Dr. Malik of Emory University in Atlanta, and Dr. Mathews of HealthPartners, opened this session by sharing their personal stories as immigrant physicians in the United States. Dr. Malik noted that physicians born outside the United States make up 29% of U.S. physicians, and 32% of hospitalists are international medical graduates.
The presenters revealed the structural hurdles immigrant physicians face, including lack of empowerment until achieving permanent residency status; limited leadership, administrative, and academic roles; concerns for job security and financial stability; and experiencing micro- and macroaggressions at work. The presenters shared a framework for a developmental orientation inclined toward cultural competency beginning with denial, followed by polarization, progressing to minimization, advancing to acceptance, and culminating in adaptation.
They concluded the session by stressing the importance of advocacy for immigrant physicians and encouraged colleagues to become engaged in efforts within their professional organizations.
Key takeaway
- Immigrant physicians experience structural challenges to their professional advancement because of their residency status.
Learner supervision
HM20 Virtual session: Call Me Maybe: Balancing Resident Autonomy With Sensible Supervision
Presenter: Daniel Steinberg, MD, SFHM, FACP
Dr. Steinberg, based at Mount Sinai in New York, explained that resident supervision is driven by three factors: what residents need, what residents want, and what the supervisor can provide. Although data is mixed as to whether supervision improves patient outcomes, supervision is essential for patient care and resident education. Dr. Steinberg showcased several relevant medical education studies related to supervision and focused on a key question: Do you trust the resident? The review of medical education literature discussed the meaning and development of trust, oral case presentations to determine trust, and the influence of supervisor experience.
Key takeaways
- Resident supervision is driven by what residents need, what residents want, and what the supervisor can provide.
- Trust can be determined from direct supervision, oral presentations, and remote access of electronic medical records, but is also influenced by attending experience and style.
Balancing personal and professional life
HM20 Virtual session: Being a Hospitalist and a Parent: Balancing Roles With Grace
Presenters: Heather E. Nye, MD, PhD, SFHM, and David Alfandre, MD, MSPH
Dr. Nye of the University of California, San Francisco, and Dr. Alfandre of New York University shared their challenges as hospitalists, parents, and partners before and during the COVID-19 pandemic. They described their feelings of guilt during the pandemic related to increasing their families’ infection risks, as well as the gratitude they felt for having stable jobs during the crisis. They shared solutions that worked for their families, including cooperating with their partners, expressing their scheduling needs, and negotiating to meet those needs with their employers.
Dr. Nye and Dr. Alfandre recommended staying connected with others for help, including partners, institutions, neighbors, and colleagues. They also recommended supporting, sharing, collaborating, and connecting with their partners and colleagues to maintain a balanced professional and personal life.
Key takeaway:
- Stay connected and support, collaborate, and share with your colleagues and partner at home.
Dr. Kumar is the pediatric editor of The Hospitalist. She is clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine at Case Western Reserve University and a pediatric hospitalist at Cleveland Clinic Children’s. Dr. Doraiswamy is an assistant professor of medicine and pediatrics and a med-peds hospitalist at The Ohio State University and Nationwide Children’s Hospital, both in Columbus. Dr. Tantoco is an academic med-peds hospitalist practicing in Northwestern Memorial Hospital, Chicago, and Ann & Robert H. Lurie Children’s Hospital of Chicago.
COVID-19 risks are no higher in patients with multiple sclerosis
new U.S. data suggest. A separate study from the United Kingdom also found similar trends of rates of COVID-19 infection in patients with MS and the general population.
Both studies were presented Sept. 26 at a special session on multiple sclerosis and COVID-19 at a final “Encore” event as part of the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
The U.S. data appear consistent with studies from several other countries, in that worse COVID-19 outcomes increase with age and higher disability levels, both of which would be expected from findings in the general population.
The U.S. data also show a clear effect of race in MS, with higher rates of adverse COVID-19 outcomes in Black patients, again in line with what is seen in the general population.
“I would say the results from our study and in general do not suggest that MS itself is associated with higher risks of severe COVID-19 outcomes, compared with the general population,” said Amber Salter, PhD.
Dr. Salter, who is assistant professor of biostatistics at Washington University, St. Louis, presented data from the COViMS North American registry, set up for health care providers to report persons with MS who are infected with COVID-19.
The COViMS registry so far has information on 858 patients with MS who have COVID-19 (80% verified by a positive test), as reported from 150 different health care providers in the United States and Canada. The average age was 48 years, with average disease duration of 13.6 years. MS clinical course was reported as relapsing remitting in 78%, secondary progressive in 15%, and primary progressive in 5%. Most patients (72%) were fully ambulatory, 16% could walk with assistance, and 12% were nonambulatory.
Severe COVID-19 outcomes were classified as mortality (which occurred in 5.7% of the cohort), mortality/ICU admission (13.6%) and mortality/ICU admission/hospitalization (30.2%).
Results were adjusted for many different covariates, including sex, age, smoking, MS clinical course (relapsing, progressive), disease duration, ambulation, individual comorbidities (cardiovascular disease, cerebrovascular disease, chronic kidney disease, chronic lung disease, diabetes, hypertension, morbid obesity), and disease-modifying therapy use.
In multivariable logistic regression analyses, older age, having chronic renal disease, and being nonambulatory were consistently associated with increased odds of poorer outcomes. Chronic kidney disease had the strongest association with mortality (odds ratio, 28.6; P < .001). Other factors associated with mortality included cardiovascular disease (OR, 4.35; P = .009); age (OR per 10 years, 1.91; P = .012), and male sex (OR, 2.60; P = .041).
Patients who were nonambulatory had a higher risk of mortality/ICU admission/hospitalization (OR, 3.32; P = .003). This endpoint was also increased in patients on anti-CD20 drugs, compared with other disease-modifying treatment (OR, 2.31; P = .002), consistent with results from at least two other studies.
Disease-modifying therapy in general was not associated with an increased risk of worse outcomes. “There was some concern at the outset about the effect of disease-modifying therapies on COVID-19 outcomes, but most studies have not found an increased risk of worse outcomes in patients on such drug treatments, with the possible exception of anti-CD20 drugs,” Dr. Salter said.
“Some disease-modifying therapies may actually be protective (particularly interferon) and studies are investigating whether they may have a role in the treatment of COVID-19,” she added.
“The factors in MS patients that we and others have found to be associated with worse COVID-19 outcomes may not be specific to MS. Older age is known to be a primary risk factor for worse COVID-19 outcomes in the general population, and increasing disability presumably tracks with worse general heath,” Dr. Salter commented.
“I would say the overall data are fairly reassuring for MS patents,” she concluded.
Black patients have higher risk
One worrying finding in the North American data, however, was the effect of race. “We found an independent effect of race for worse COVID-19 outcomes in MS patients,” Dr. Slater said.
Of the 858 patients in the COViMS registry, 65.7% were White and 26.1% were Black. Black individuals were more likely to be younger, never smokers, have shorter MS duration, a relapsing MS course, and have comorbidities, compared with White patients. A higher proportion of Black patients had hypertension (40.2% vs 19.5%) and morbid obesity (17% vs. 9.5%).
Results showed that mortality rates were not statistically different between White and Black patients, but Black race was associated with increased risk of mortality and/or ICU admission, compared with White patients (16.9% vs. 12.8%), and multivariate logistic regression analysis showed Black race was independently associated with mortality/ICU admission after adjustments for covariates (OR, 3.7; P = .002).
Black race was also associated with increased risk of mortality/ICU admission/hospital admission (35.8% vs. 30.2%), and after adjustment for covariates this was found to be an independent predictor (OR, 1.7; P = .04).
“This higher COVID-19 risk in Black individuals is also seen in the general population, so these results are not that surprising and it doesn’t appear to be an effect specific to MS patients,” Dr. Salter commented.
U.K. data on risk of contracting COVID-19
A U.K. study also suggested race to be an independent predictor in the risk of contracting COVID-19 in patients with MS.
The study of more than 5,000 patients with MS showed that those from a Black, Asian, and Minority Ethnic group were twice as likely to report having COVID-19 than those who were White.
The study, which was conducted during the U.K. lockdown, also found that the trend of COVID-19 infection in patients with MS is comparable with that of the U.K. general population.
Presenting the data, Afagh Garjani, MD, concluded: “During a period with strict physical distancing measures, patients with MS are not at an increased risk of contracting COVID-19.”
Dr. Garjani, a neurology clinical research fellow at the University of Nottingham, (England), explained that the COVID-19 pandemic has introduced uncertainties into the MS community, and the focus so far has been the severity of infection among people with MS who have COVID-19.
“This approach has left questions about the risk of contracting disease in people with MS unanswered, which has implications as society gradually returns to normal,” she said.
Dr. Garjani presented data from the United Kingdom MS Register (UKMSR), which has been collecting demographic and MS-related data since 2011 from patients with MS throughout the United Kingdom.
On March 17 – just before the lockdown in United Kingdom – existing participants of the UKMSR were asked to join the COVID-19 study. The study was also advertised through social media. In this ongoing study, people with MS answered a COVID-19–related survey at participation and a different follow-up survey every 2 weeks depending on whether they contracted COVID-19.
The COVID-19 study included 5,309 patients with MS. The mean age of the study population was 52.4 years, 76.1% were female, and 95.7% were White. Of the 5,309 patients, 535 (10%) reported a self-diagnosis of COVID-19. Because of limited availability of tests in the United Kingdom at the time, only 75 patents had a positive polymerase chain reaction result.
“To our knowledge, this is the largest community-based study of COVID-19 in patients with MS worldwide,” Dr. Garjani said. She presented results from the period March 23 to June 24, when the United Kingdom was in a period of lockdown with vulnerable groups encouraged to self-isolate completely.
In this MS cohort, 47% reported self-isolating at some point. Those at older age and higher Expanded Disability Status Scale (EDSS) score were more likely to have self-isolated.
The researchers did not find that patients with progressive MS or those on disease-modifying therapies in general isolated more, but patients on monoclonal antibody drugs and fingolimod were more likely to self-isolate versus those on other therapies. “This may be because there are concerns about infection with these drugs and patients on these therapies may be more concerned about contracting COVID-19,” Dr. Garjani suggested.
In terms of contracting COVID, the researchers found a reduced risk of COVID-19 (self-diagnosed) in patients with older age and higher EDSS. “This is not really surprising that these patients were more likely to self-isolate,” Dr. Garjani commented.
No association was seen between type of MS, disease duration, disease-modifying therapy in general, and risk of COVID-19. No individual drug treatment increased risk versus no therapy or versus self-injectables. But there was an increased risk of contracting the virus in patients whose race was Black, Asian, or Minority Ethnic (OR, 2.2), which is in line with findings from the general population.
“This study is unique – the denominator is all people with MS. We are looking primarily at the risk of contracting COVID-19. Other studies are focusing more on people with MS who have COVID and assessing risk of a severe COVID outcome. Our results are not contradicting the findings from those studies,” Dr. Garjani said.
The results were similar only when patients with a confirmed COVID-19 test were considered.
In terms of outcomes in those who reported COVID-19 infection, preliminary results have not shown any MS factors – such as EDSS, age, type of MS, drug therapy in general – to be associated with outcome.
“Since the COVID-19 outbreak started there has been concern among MS patients, especially among those on disease-modifying therapies, about whether they are at increased risk of infection and severe disease,” Dr. Garjani said.
“We found similar trends of rates of infection in MS patients and the general population, and no signal of increased risks in those with higher EDSS or progressive MS. The caveat is that this study was conducted in a period of lockdown, but we adjusted for self-isolating behavior in the multivariable regression analysis,” she noted.
Dr. Salter is a statistical editor for the American Heart Association journal Circulation: Cardiovascular Imaging. Dr. Garjani has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new U.S. data suggest. A separate study from the United Kingdom also found similar trends of rates of COVID-19 infection in patients with MS and the general population.
Both studies were presented Sept. 26 at a special session on multiple sclerosis and COVID-19 at a final “Encore” event as part of the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
The U.S. data appear consistent with studies from several other countries, in that worse COVID-19 outcomes increase with age and higher disability levels, both of which would be expected from findings in the general population.
The U.S. data also show a clear effect of race in MS, with higher rates of adverse COVID-19 outcomes in Black patients, again in line with what is seen in the general population.
“I would say the results from our study and in general do not suggest that MS itself is associated with higher risks of severe COVID-19 outcomes, compared with the general population,” said Amber Salter, PhD.
Dr. Salter, who is assistant professor of biostatistics at Washington University, St. Louis, presented data from the COViMS North American registry, set up for health care providers to report persons with MS who are infected with COVID-19.
The COViMS registry so far has information on 858 patients with MS who have COVID-19 (80% verified by a positive test), as reported from 150 different health care providers in the United States and Canada. The average age was 48 years, with average disease duration of 13.6 years. MS clinical course was reported as relapsing remitting in 78%, secondary progressive in 15%, and primary progressive in 5%. Most patients (72%) were fully ambulatory, 16% could walk with assistance, and 12% were nonambulatory.
Severe COVID-19 outcomes were classified as mortality (which occurred in 5.7% of the cohort), mortality/ICU admission (13.6%) and mortality/ICU admission/hospitalization (30.2%).
Results were adjusted for many different covariates, including sex, age, smoking, MS clinical course (relapsing, progressive), disease duration, ambulation, individual comorbidities (cardiovascular disease, cerebrovascular disease, chronic kidney disease, chronic lung disease, diabetes, hypertension, morbid obesity), and disease-modifying therapy use.
In multivariable logistic regression analyses, older age, having chronic renal disease, and being nonambulatory were consistently associated with increased odds of poorer outcomes. Chronic kidney disease had the strongest association with mortality (odds ratio, 28.6; P < .001). Other factors associated with mortality included cardiovascular disease (OR, 4.35; P = .009); age (OR per 10 years, 1.91; P = .012), and male sex (OR, 2.60; P = .041).
Patients who were nonambulatory had a higher risk of mortality/ICU admission/hospitalization (OR, 3.32; P = .003). This endpoint was also increased in patients on anti-CD20 drugs, compared with other disease-modifying treatment (OR, 2.31; P = .002), consistent with results from at least two other studies.
Disease-modifying therapy in general was not associated with an increased risk of worse outcomes. “There was some concern at the outset about the effect of disease-modifying therapies on COVID-19 outcomes, but most studies have not found an increased risk of worse outcomes in patients on such drug treatments, with the possible exception of anti-CD20 drugs,” Dr. Salter said.
“Some disease-modifying therapies may actually be protective (particularly interferon) and studies are investigating whether they may have a role in the treatment of COVID-19,” she added.
“The factors in MS patients that we and others have found to be associated with worse COVID-19 outcomes may not be specific to MS. Older age is known to be a primary risk factor for worse COVID-19 outcomes in the general population, and increasing disability presumably tracks with worse general heath,” Dr. Salter commented.
“I would say the overall data are fairly reassuring for MS patents,” she concluded.
Black patients have higher risk
One worrying finding in the North American data, however, was the effect of race. “We found an independent effect of race for worse COVID-19 outcomes in MS patients,” Dr. Slater said.
Of the 858 patients in the COViMS registry, 65.7% were White and 26.1% were Black. Black individuals were more likely to be younger, never smokers, have shorter MS duration, a relapsing MS course, and have comorbidities, compared with White patients. A higher proportion of Black patients had hypertension (40.2% vs 19.5%) and morbid obesity (17% vs. 9.5%).
Results showed that mortality rates were not statistically different between White and Black patients, but Black race was associated with increased risk of mortality and/or ICU admission, compared with White patients (16.9% vs. 12.8%), and multivariate logistic regression analysis showed Black race was independently associated with mortality/ICU admission after adjustments for covariates (OR, 3.7; P = .002).
Black race was also associated with increased risk of mortality/ICU admission/hospital admission (35.8% vs. 30.2%), and after adjustment for covariates this was found to be an independent predictor (OR, 1.7; P = .04).
“This higher COVID-19 risk in Black individuals is also seen in the general population, so these results are not that surprising and it doesn’t appear to be an effect specific to MS patients,” Dr. Salter commented.
U.K. data on risk of contracting COVID-19
A U.K. study also suggested race to be an independent predictor in the risk of contracting COVID-19 in patients with MS.
The study of more than 5,000 patients with MS showed that those from a Black, Asian, and Minority Ethnic group were twice as likely to report having COVID-19 than those who were White.
The study, which was conducted during the U.K. lockdown, also found that the trend of COVID-19 infection in patients with MS is comparable with that of the U.K. general population.
Presenting the data, Afagh Garjani, MD, concluded: “During a period with strict physical distancing measures, patients with MS are not at an increased risk of contracting COVID-19.”
Dr. Garjani, a neurology clinical research fellow at the University of Nottingham, (England), explained that the COVID-19 pandemic has introduced uncertainties into the MS community, and the focus so far has been the severity of infection among people with MS who have COVID-19.
“This approach has left questions about the risk of contracting disease in people with MS unanswered, which has implications as society gradually returns to normal,” she said.
Dr. Garjani presented data from the United Kingdom MS Register (UKMSR), which has been collecting demographic and MS-related data since 2011 from patients with MS throughout the United Kingdom.
On March 17 – just before the lockdown in United Kingdom – existing participants of the UKMSR were asked to join the COVID-19 study. The study was also advertised through social media. In this ongoing study, people with MS answered a COVID-19–related survey at participation and a different follow-up survey every 2 weeks depending on whether they contracted COVID-19.
The COVID-19 study included 5,309 patients with MS. The mean age of the study population was 52.4 years, 76.1% were female, and 95.7% were White. Of the 5,309 patients, 535 (10%) reported a self-diagnosis of COVID-19. Because of limited availability of tests in the United Kingdom at the time, only 75 patents had a positive polymerase chain reaction result.
“To our knowledge, this is the largest community-based study of COVID-19 in patients with MS worldwide,” Dr. Garjani said. She presented results from the period March 23 to June 24, when the United Kingdom was in a period of lockdown with vulnerable groups encouraged to self-isolate completely.
In this MS cohort, 47% reported self-isolating at some point. Those at older age and higher Expanded Disability Status Scale (EDSS) score were more likely to have self-isolated.
The researchers did not find that patients with progressive MS or those on disease-modifying therapies in general isolated more, but patients on monoclonal antibody drugs and fingolimod were more likely to self-isolate versus those on other therapies. “This may be because there are concerns about infection with these drugs and patients on these therapies may be more concerned about contracting COVID-19,” Dr. Garjani suggested.
In terms of contracting COVID, the researchers found a reduced risk of COVID-19 (self-diagnosed) in patients with older age and higher EDSS. “This is not really surprising that these patients were more likely to self-isolate,” Dr. Garjani commented.
No association was seen between type of MS, disease duration, disease-modifying therapy in general, and risk of COVID-19. No individual drug treatment increased risk versus no therapy or versus self-injectables. But there was an increased risk of contracting the virus in patients whose race was Black, Asian, or Minority Ethnic (OR, 2.2), which is in line with findings from the general population.
“This study is unique – the denominator is all people with MS. We are looking primarily at the risk of contracting COVID-19. Other studies are focusing more on people with MS who have COVID and assessing risk of a severe COVID outcome. Our results are not contradicting the findings from those studies,” Dr. Garjani said.
The results were similar only when patients with a confirmed COVID-19 test were considered.
In terms of outcomes in those who reported COVID-19 infection, preliminary results have not shown any MS factors – such as EDSS, age, type of MS, drug therapy in general – to be associated with outcome.
“Since the COVID-19 outbreak started there has been concern among MS patients, especially among those on disease-modifying therapies, about whether they are at increased risk of infection and severe disease,” Dr. Garjani said.
“We found similar trends of rates of infection in MS patients and the general population, and no signal of increased risks in those with higher EDSS or progressive MS. The caveat is that this study was conducted in a period of lockdown, but we adjusted for self-isolating behavior in the multivariable regression analysis,” she noted.
Dr. Salter is a statistical editor for the American Heart Association journal Circulation: Cardiovascular Imaging. Dr. Garjani has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
new U.S. data suggest. A separate study from the United Kingdom also found similar trends of rates of COVID-19 infection in patients with MS and the general population.
Both studies were presented Sept. 26 at a special session on multiple sclerosis and COVID-19 at a final “Encore” event as part of the Joint European Committee for Treatment and Research in Multiple Sclerosis–Americas Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS-ACTRIMS) 2020, this year known as MSVirtual2020.
The U.S. data appear consistent with studies from several other countries, in that worse COVID-19 outcomes increase with age and higher disability levels, both of which would be expected from findings in the general population.
The U.S. data also show a clear effect of race in MS, with higher rates of adverse COVID-19 outcomes in Black patients, again in line with what is seen in the general population.
“I would say the results from our study and in general do not suggest that MS itself is associated with higher risks of severe COVID-19 outcomes, compared with the general population,” said Amber Salter, PhD.
Dr. Salter, who is assistant professor of biostatistics at Washington University, St. Louis, presented data from the COViMS North American registry, set up for health care providers to report persons with MS who are infected with COVID-19.
The COViMS registry so far has information on 858 patients with MS who have COVID-19 (80% verified by a positive test), as reported from 150 different health care providers in the United States and Canada. The average age was 48 years, with average disease duration of 13.6 years. MS clinical course was reported as relapsing remitting in 78%, secondary progressive in 15%, and primary progressive in 5%. Most patients (72%) were fully ambulatory, 16% could walk with assistance, and 12% were nonambulatory.
Severe COVID-19 outcomes were classified as mortality (which occurred in 5.7% of the cohort), mortality/ICU admission (13.6%) and mortality/ICU admission/hospitalization (30.2%).
Results were adjusted for many different covariates, including sex, age, smoking, MS clinical course (relapsing, progressive), disease duration, ambulation, individual comorbidities (cardiovascular disease, cerebrovascular disease, chronic kidney disease, chronic lung disease, diabetes, hypertension, morbid obesity), and disease-modifying therapy use.
In multivariable logistic regression analyses, older age, having chronic renal disease, and being nonambulatory were consistently associated with increased odds of poorer outcomes. Chronic kidney disease had the strongest association with mortality (odds ratio, 28.6; P < .001). Other factors associated with mortality included cardiovascular disease (OR, 4.35; P = .009); age (OR per 10 years, 1.91; P = .012), and male sex (OR, 2.60; P = .041).
Patients who were nonambulatory had a higher risk of mortality/ICU admission/hospitalization (OR, 3.32; P = .003). This endpoint was also increased in patients on anti-CD20 drugs, compared with other disease-modifying treatment (OR, 2.31; P = .002), consistent with results from at least two other studies.
Disease-modifying therapy in general was not associated with an increased risk of worse outcomes. “There was some concern at the outset about the effect of disease-modifying therapies on COVID-19 outcomes, but most studies have not found an increased risk of worse outcomes in patients on such drug treatments, with the possible exception of anti-CD20 drugs,” Dr. Salter said.
“Some disease-modifying therapies may actually be protective (particularly interferon) and studies are investigating whether they may have a role in the treatment of COVID-19,” she added.
“The factors in MS patients that we and others have found to be associated with worse COVID-19 outcomes may not be specific to MS. Older age is known to be a primary risk factor for worse COVID-19 outcomes in the general population, and increasing disability presumably tracks with worse general heath,” Dr. Salter commented.
“I would say the overall data are fairly reassuring for MS patents,” she concluded.
Black patients have higher risk
One worrying finding in the North American data, however, was the effect of race. “We found an independent effect of race for worse COVID-19 outcomes in MS patients,” Dr. Slater said.
Of the 858 patients in the COViMS registry, 65.7% were White and 26.1% were Black. Black individuals were more likely to be younger, never smokers, have shorter MS duration, a relapsing MS course, and have comorbidities, compared with White patients. A higher proportion of Black patients had hypertension (40.2% vs 19.5%) and morbid obesity (17% vs. 9.5%).
Results showed that mortality rates were not statistically different between White and Black patients, but Black race was associated with increased risk of mortality and/or ICU admission, compared with White patients (16.9% vs. 12.8%), and multivariate logistic regression analysis showed Black race was independently associated with mortality/ICU admission after adjustments for covariates (OR, 3.7; P = .002).
Black race was also associated with increased risk of mortality/ICU admission/hospital admission (35.8% vs. 30.2%), and after adjustment for covariates this was found to be an independent predictor (OR, 1.7; P = .04).
“This higher COVID-19 risk in Black individuals is also seen in the general population, so these results are not that surprising and it doesn’t appear to be an effect specific to MS patients,” Dr. Salter commented.
U.K. data on risk of contracting COVID-19
A U.K. study also suggested race to be an independent predictor in the risk of contracting COVID-19 in patients with MS.
The study of more than 5,000 patients with MS showed that those from a Black, Asian, and Minority Ethnic group were twice as likely to report having COVID-19 than those who were White.
The study, which was conducted during the U.K. lockdown, also found that the trend of COVID-19 infection in patients with MS is comparable with that of the U.K. general population.
Presenting the data, Afagh Garjani, MD, concluded: “During a period with strict physical distancing measures, patients with MS are not at an increased risk of contracting COVID-19.”
Dr. Garjani, a neurology clinical research fellow at the University of Nottingham, (England), explained that the COVID-19 pandemic has introduced uncertainties into the MS community, and the focus so far has been the severity of infection among people with MS who have COVID-19.
“This approach has left questions about the risk of contracting disease in people with MS unanswered, which has implications as society gradually returns to normal,” she said.
Dr. Garjani presented data from the United Kingdom MS Register (UKMSR), which has been collecting demographic and MS-related data since 2011 from patients with MS throughout the United Kingdom.
On March 17 – just before the lockdown in United Kingdom – existing participants of the UKMSR were asked to join the COVID-19 study. The study was also advertised through social media. In this ongoing study, people with MS answered a COVID-19–related survey at participation and a different follow-up survey every 2 weeks depending on whether they contracted COVID-19.
The COVID-19 study included 5,309 patients with MS. The mean age of the study population was 52.4 years, 76.1% were female, and 95.7% were White. Of the 5,309 patients, 535 (10%) reported a self-diagnosis of COVID-19. Because of limited availability of tests in the United Kingdom at the time, only 75 patents had a positive polymerase chain reaction result.
“To our knowledge, this is the largest community-based study of COVID-19 in patients with MS worldwide,” Dr. Garjani said. She presented results from the period March 23 to June 24, when the United Kingdom was in a period of lockdown with vulnerable groups encouraged to self-isolate completely.
In this MS cohort, 47% reported self-isolating at some point. Those at older age and higher Expanded Disability Status Scale (EDSS) score were more likely to have self-isolated.
The researchers did not find that patients with progressive MS or those on disease-modifying therapies in general isolated more, but patients on monoclonal antibody drugs and fingolimod were more likely to self-isolate versus those on other therapies. “This may be because there are concerns about infection with these drugs and patients on these therapies may be more concerned about contracting COVID-19,” Dr. Garjani suggested.
In terms of contracting COVID, the researchers found a reduced risk of COVID-19 (self-diagnosed) in patients with older age and higher EDSS. “This is not really surprising that these patients were more likely to self-isolate,” Dr. Garjani commented.
No association was seen between type of MS, disease duration, disease-modifying therapy in general, and risk of COVID-19. No individual drug treatment increased risk versus no therapy or versus self-injectables. But there was an increased risk of contracting the virus in patients whose race was Black, Asian, or Minority Ethnic (OR, 2.2), which is in line with findings from the general population.
“This study is unique – the denominator is all people with MS. We are looking primarily at the risk of contracting COVID-19. Other studies are focusing more on people with MS who have COVID and assessing risk of a severe COVID outcome. Our results are not contradicting the findings from those studies,” Dr. Garjani said.
The results were similar only when patients with a confirmed COVID-19 test were considered.
In terms of outcomes in those who reported COVID-19 infection, preliminary results have not shown any MS factors – such as EDSS, age, type of MS, drug therapy in general – to be associated with outcome.
“Since the COVID-19 outbreak started there has been concern among MS patients, especially among those on disease-modifying therapies, about whether they are at increased risk of infection and severe disease,” Dr. Garjani said.
“We found similar trends of rates of infection in MS patients and the general population, and no signal of increased risks in those with higher EDSS or progressive MS. The caveat is that this study was conducted in a period of lockdown, but we adjusted for self-isolating behavior in the multivariable regression analysis,” she noted.
Dr. Salter is a statistical editor for the American Heart Association journal Circulation: Cardiovascular Imaging. Dr. Garjani has disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM MSVIRTUAL2020
Primary care isn’t bouncing back
published by the Primary Care Collaborative (PCC) and Larry A. Green Center.
Since mid-March these organizations have issued short weekly and biweekly surveys to U.S. primary care physicians in an attempt to find the pulse of the county’s first line of care. “There is not a federal office for primary care, and it’s been anemically funded for decades,” Rebecca Etz, PhD, said in an interview. Yet these clinics represent the front lines of U.S. health care, and it’s where most Americans go for care and COVID-19 care, said Dr. Etz, director of the Virginia-based Larry A. Green Center, which is devoted to primary care research, development, and advocacy.
The latest survey responses, collected between Sept. 4 and 6, confirm what researchers had suspected: Primary care isn’t on solid footing. Eighty-one percent of respondents disagreed emphatically that primary care has bounced back, and another 13% said things were better than earlier this year but not normal.
Meanwhile, 35% of respondents said that revenue and pay are significantly lower than they were before the pandemic and net losses threaten their practices’ viability. Almost half (49%) said their mental exhaustion from work was at an all-time high.
“Because of how our system is set up – it’s a fee-for-service model – the more patients you see, the more money you get,” said Yalda Jabbarpour, MD, medical director at the Graham Center, a leading think tank on family medicine and health care policy. But the stay-at-home order, aversion to telehealth, and fear of in-person visits have been keeping patients away – and driving primary care revenue down. Even when practices transition to and expand their telehealth, payer reimbursement is not yet on parity with in-person visits.
Right now, primary care physicians are doing fewer procedures and spending more time on video visits. “So you may have the same overhead and time investment but you’re getting paid a fraction,” Dr. Etz said. In August, 50% of primary care physicians reported they were working the same or more hours per week as they did before the pandemic but for less money, according to an earlier survey from the Green Center and the PCC. That loss of revenue is compounded by the need for expensive personal protective equipment and preparation for the upcoming flu season, Dr. Etz said.
Ongoing surveys reveal stress
Over the last 20 weeks or so, the Green Center and PCC together have disseminated weekly (through June) or biweekly surveys to 100 professional organizations. Because there isn’t an entity that represents all of primary care and claims data take years to process, these surveys are intended to get real-time feedback from clinicians who are providing a lot of patient care during the pandemic.
The sample sizes are admittedly small, with the most recent survey including 489 clinicians. Dr. Jabbarpour noted, “489 – it’s a good number, but you would want more.” Generally, for a great survey response you’d want 20%-30% of the physician population because then you could assume you’re getting a good mix of geographies, practice sizes, and settings, she said.
Respondents to the most recent survey were from 49 different states; 70% identified their practice as family medicine. One-third had between one and three physicians in their practice and 40% had 10 or more clinicians. “It’s not perfect, but it sounds pretty representative of the primary care workforce,” Dr. Jabbarpour continued.
The latest Green Center-PCC survey, published last week, also found that one in five physicians surveyed said at least one clinician in their practice had opted for early retirement or left practice as a direct result of the pandemic. These declines in clinician staffing come as school reopenings threaten to cause a resurgence of COVID-19 cases and the 2021 flu season could complicate COVID-19 care and testing.
Shortfall could cascade to other specialties
News that primary care is both struggling and shrinking doesn’t come as a surprise to those who research this area, according to Dr. Jabbarpour. Yet it matters “because primary care is where the majority of Americans get their health care.” According to the Centers for Disease Control and Prevention, primary care accounts for 50% of all office visits. But the sector only encompasses 30% of the clinician workforce, according to a 2019 study of physician supply, and accounts for just 7% of national health expenditures, according to a separate 2019 study that measured primary care investment.
If primary care doesn’t bounce back, the shortfall could overwhelm the rest of the health care system, Dr. Jabbarpour said. “If primary care shortages increase, then urgent cares, ERs, and hospitals will become overwhelmed.”
Or public health could suffer as people don’t seek care at all. A study published earlier this summer found that up to 35% of excess deaths during the pandemic were not caused by COVID-19. Instead, they can be attributed to treatable causes, like heart disease, diabetes, and Alzheimers, the researchers concluded. In Dr. Etz’s estimation, this high cost is a glimpse of what happens when there isn’t adequate access to primary care.
When asked about the frequency of the PCC/Green Center surveys, Bianca Frogner, PhD, a health economist and deputy director at the University of Washington Primary Care Innovation Lab in Seattle, said it’s unusual to have this regularity. Also, it’s unique in that it offers a constant mix of physicians. “It’s a small sample, but it still gives a voice where there isn’t one.”
Smaller weekly surveys and secondary analysis projects from the Graham Center, an American Academy of Family Physicians affiliated research center, reinforce findings of the Green Center. The Graham Center surveys also found primary care is taking a financial hit, staff is being furloughed, and patient volume is down, according to Dr. Jabbarpour, who has been involved in most of the Graham Center’s work on COVID.
Dr. Frogner, Dr. Etz, and Dr. Jabbarpour agree that, as a nation, the United States has chronically underinvested in primary care, and now the system is in crisis. The hope is that the survey data gives policymakers, state leaders, and the federal government a better idea of what’s happening on the ground.
It’s also important for researchers “keeping an eye out for the available supply of primary care for certain populations,” Dr. Frogner said. The current conditions are especially a threat to rural and underserved areas, she added.
If primary health care isn’t near recovery that’s a problem for the entire population, Dr. Etz said. And what happens if there’s another surge of COVID-19 or even a second pandemic in our lifetime? Her recommendation: Treat it like disaster recovery. Step one is “Stop the hemorrhaging – they need immediate cash flow.”
A version of this article originally appeared on Medscape.com.
published by the Primary Care Collaborative (PCC) and Larry A. Green Center.
Since mid-March these organizations have issued short weekly and biweekly surveys to U.S. primary care physicians in an attempt to find the pulse of the county’s first line of care. “There is not a federal office for primary care, and it’s been anemically funded for decades,” Rebecca Etz, PhD, said in an interview. Yet these clinics represent the front lines of U.S. health care, and it’s where most Americans go for care and COVID-19 care, said Dr. Etz, director of the Virginia-based Larry A. Green Center, which is devoted to primary care research, development, and advocacy.
The latest survey responses, collected between Sept. 4 and 6, confirm what researchers had suspected: Primary care isn’t on solid footing. Eighty-one percent of respondents disagreed emphatically that primary care has bounced back, and another 13% said things were better than earlier this year but not normal.
Meanwhile, 35% of respondents said that revenue and pay are significantly lower than they were before the pandemic and net losses threaten their practices’ viability. Almost half (49%) said their mental exhaustion from work was at an all-time high.
“Because of how our system is set up – it’s a fee-for-service model – the more patients you see, the more money you get,” said Yalda Jabbarpour, MD, medical director at the Graham Center, a leading think tank on family medicine and health care policy. But the stay-at-home order, aversion to telehealth, and fear of in-person visits have been keeping patients away – and driving primary care revenue down. Even when practices transition to and expand their telehealth, payer reimbursement is not yet on parity with in-person visits.
Right now, primary care physicians are doing fewer procedures and spending more time on video visits. “So you may have the same overhead and time investment but you’re getting paid a fraction,” Dr. Etz said. In August, 50% of primary care physicians reported they were working the same or more hours per week as they did before the pandemic but for less money, according to an earlier survey from the Green Center and the PCC. That loss of revenue is compounded by the need for expensive personal protective equipment and preparation for the upcoming flu season, Dr. Etz said.
Ongoing surveys reveal stress
Over the last 20 weeks or so, the Green Center and PCC together have disseminated weekly (through June) or biweekly surveys to 100 professional organizations. Because there isn’t an entity that represents all of primary care and claims data take years to process, these surveys are intended to get real-time feedback from clinicians who are providing a lot of patient care during the pandemic.
The sample sizes are admittedly small, with the most recent survey including 489 clinicians. Dr. Jabbarpour noted, “489 – it’s a good number, but you would want more.” Generally, for a great survey response you’d want 20%-30% of the physician population because then you could assume you’re getting a good mix of geographies, practice sizes, and settings, she said.
Respondents to the most recent survey were from 49 different states; 70% identified their practice as family medicine. One-third had between one and three physicians in their practice and 40% had 10 or more clinicians. “It’s not perfect, but it sounds pretty representative of the primary care workforce,” Dr. Jabbarpour continued.
The latest Green Center-PCC survey, published last week, also found that one in five physicians surveyed said at least one clinician in their practice had opted for early retirement or left practice as a direct result of the pandemic. These declines in clinician staffing come as school reopenings threaten to cause a resurgence of COVID-19 cases and the 2021 flu season could complicate COVID-19 care and testing.
Shortfall could cascade to other specialties
News that primary care is both struggling and shrinking doesn’t come as a surprise to those who research this area, according to Dr. Jabbarpour. Yet it matters “because primary care is where the majority of Americans get their health care.” According to the Centers for Disease Control and Prevention, primary care accounts for 50% of all office visits. But the sector only encompasses 30% of the clinician workforce, according to a 2019 study of physician supply, and accounts for just 7% of national health expenditures, according to a separate 2019 study that measured primary care investment.
If primary care doesn’t bounce back, the shortfall could overwhelm the rest of the health care system, Dr. Jabbarpour said. “If primary care shortages increase, then urgent cares, ERs, and hospitals will become overwhelmed.”
Or public health could suffer as people don’t seek care at all. A study published earlier this summer found that up to 35% of excess deaths during the pandemic were not caused by COVID-19. Instead, they can be attributed to treatable causes, like heart disease, diabetes, and Alzheimers, the researchers concluded. In Dr. Etz’s estimation, this high cost is a glimpse of what happens when there isn’t adequate access to primary care.
When asked about the frequency of the PCC/Green Center surveys, Bianca Frogner, PhD, a health economist and deputy director at the University of Washington Primary Care Innovation Lab in Seattle, said it’s unusual to have this regularity. Also, it’s unique in that it offers a constant mix of physicians. “It’s a small sample, but it still gives a voice where there isn’t one.”
Smaller weekly surveys and secondary analysis projects from the Graham Center, an American Academy of Family Physicians affiliated research center, reinforce findings of the Green Center. The Graham Center surveys also found primary care is taking a financial hit, staff is being furloughed, and patient volume is down, according to Dr. Jabbarpour, who has been involved in most of the Graham Center’s work on COVID.
Dr. Frogner, Dr. Etz, and Dr. Jabbarpour agree that, as a nation, the United States has chronically underinvested in primary care, and now the system is in crisis. The hope is that the survey data gives policymakers, state leaders, and the federal government a better idea of what’s happening on the ground.
It’s also important for researchers “keeping an eye out for the available supply of primary care for certain populations,” Dr. Frogner said. The current conditions are especially a threat to rural and underserved areas, she added.
If primary health care isn’t near recovery that’s a problem for the entire population, Dr. Etz said. And what happens if there’s another surge of COVID-19 or even a second pandemic in our lifetime? Her recommendation: Treat it like disaster recovery. Step one is “Stop the hemorrhaging – they need immediate cash flow.”
A version of this article originally appeared on Medscape.com.
published by the Primary Care Collaborative (PCC) and Larry A. Green Center.
Since mid-March these organizations have issued short weekly and biweekly surveys to U.S. primary care physicians in an attempt to find the pulse of the county’s first line of care. “There is not a federal office for primary care, and it’s been anemically funded for decades,” Rebecca Etz, PhD, said in an interview. Yet these clinics represent the front lines of U.S. health care, and it’s where most Americans go for care and COVID-19 care, said Dr. Etz, director of the Virginia-based Larry A. Green Center, which is devoted to primary care research, development, and advocacy.
The latest survey responses, collected between Sept. 4 and 6, confirm what researchers had suspected: Primary care isn’t on solid footing. Eighty-one percent of respondents disagreed emphatically that primary care has bounced back, and another 13% said things were better than earlier this year but not normal.
Meanwhile, 35% of respondents said that revenue and pay are significantly lower than they were before the pandemic and net losses threaten their practices’ viability. Almost half (49%) said their mental exhaustion from work was at an all-time high.
“Because of how our system is set up – it’s a fee-for-service model – the more patients you see, the more money you get,” said Yalda Jabbarpour, MD, medical director at the Graham Center, a leading think tank on family medicine and health care policy. But the stay-at-home order, aversion to telehealth, and fear of in-person visits have been keeping patients away – and driving primary care revenue down. Even when practices transition to and expand their telehealth, payer reimbursement is not yet on parity with in-person visits.
Right now, primary care physicians are doing fewer procedures and spending more time on video visits. “So you may have the same overhead and time investment but you’re getting paid a fraction,” Dr. Etz said. In August, 50% of primary care physicians reported they were working the same or more hours per week as they did before the pandemic but for less money, according to an earlier survey from the Green Center and the PCC. That loss of revenue is compounded by the need for expensive personal protective equipment and preparation for the upcoming flu season, Dr. Etz said.
Ongoing surveys reveal stress
Over the last 20 weeks or so, the Green Center and PCC together have disseminated weekly (through June) or biweekly surveys to 100 professional organizations. Because there isn’t an entity that represents all of primary care and claims data take years to process, these surveys are intended to get real-time feedback from clinicians who are providing a lot of patient care during the pandemic.
The sample sizes are admittedly small, with the most recent survey including 489 clinicians. Dr. Jabbarpour noted, “489 – it’s a good number, but you would want more.” Generally, for a great survey response you’d want 20%-30% of the physician population because then you could assume you’re getting a good mix of geographies, practice sizes, and settings, she said.
Respondents to the most recent survey were from 49 different states; 70% identified their practice as family medicine. One-third had between one and three physicians in their practice and 40% had 10 or more clinicians. “It’s not perfect, but it sounds pretty representative of the primary care workforce,” Dr. Jabbarpour continued.
The latest Green Center-PCC survey, published last week, also found that one in five physicians surveyed said at least one clinician in their practice had opted for early retirement or left practice as a direct result of the pandemic. These declines in clinician staffing come as school reopenings threaten to cause a resurgence of COVID-19 cases and the 2021 flu season could complicate COVID-19 care and testing.
Shortfall could cascade to other specialties
News that primary care is both struggling and shrinking doesn’t come as a surprise to those who research this area, according to Dr. Jabbarpour. Yet it matters “because primary care is where the majority of Americans get their health care.” According to the Centers for Disease Control and Prevention, primary care accounts for 50% of all office visits. But the sector only encompasses 30% of the clinician workforce, according to a 2019 study of physician supply, and accounts for just 7% of national health expenditures, according to a separate 2019 study that measured primary care investment.
If primary care doesn’t bounce back, the shortfall could overwhelm the rest of the health care system, Dr. Jabbarpour said. “If primary care shortages increase, then urgent cares, ERs, and hospitals will become overwhelmed.”
Or public health could suffer as people don’t seek care at all. A study published earlier this summer found that up to 35% of excess deaths during the pandemic were not caused by COVID-19. Instead, they can be attributed to treatable causes, like heart disease, diabetes, and Alzheimers, the researchers concluded. In Dr. Etz’s estimation, this high cost is a glimpse of what happens when there isn’t adequate access to primary care.
When asked about the frequency of the PCC/Green Center surveys, Bianca Frogner, PhD, a health economist and deputy director at the University of Washington Primary Care Innovation Lab in Seattle, said it’s unusual to have this regularity. Also, it’s unique in that it offers a constant mix of physicians. “It’s a small sample, but it still gives a voice where there isn’t one.”
Smaller weekly surveys and secondary analysis projects from the Graham Center, an American Academy of Family Physicians affiliated research center, reinforce findings of the Green Center. The Graham Center surveys also found primary care is taking a financial hit, staff is being furloughed, and patient volume is down, according to Dr. Jabbarpour, who has been involved in most of the Graham Center’s work on COVID.
Dr. Frogner, Dr. Etz, and Dr. Jabbarpour agree that, as a nation, the United States has chronically underinvested in primary care, and now the system is in crisis. The hope is that the survey data gives policymakers, state leaders, and the federal government a better idea of what’s happening on the ground.
It’s also important for researchers “keeping an eye out for the available supply of primary care for certain populations,” Dr. Frogner said. The current conditions are especially a threat to rural and underserved areas, she added.
If primary health care isn’t near recovery that’s a problem for the entire population, Dr. Etz said. And what happens if there’s another surge of COVID-19 or even a second pandemic in our lifetime? Her recommendation: Treat it like disaster recovery. Step one is “Stop the hemorrhaging – they need immediate cash flow.”
A version of this article originally appeared on Medscape.com.