User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
DK crush edges culotte for left main PCI
SAN FRANCISCO – The double-kissing crush approach to stenting an unprotected left main coronary artery at the distal bifurcation produced clearly better 1-year clinical outcomes than did an alternative way to stent at the bifurcation, the culotte approach, in a multicenter, randomized trial in China with 419 patients.
The survival rate of patients free of major adverse coronary events 1 year after treatment was 94% for the double kissing (DK) crush technique and 84% for the culotte technique, a statistically significant benefit for DK crush for the study’s primary endpoint, Dr. Jun-Jie Zhang reported at the American College of Cardiology/Cardiovascular Research Foundation Innovation in Intervention Summit.

This definitive clinical comparison, DKCRUSH-III (DK Crush Versus Culotte Stenting for the Treatment of Unprotected Left Main Bifurcation Lesions), is the third in a series of large randomized trials led by Dr. Zhang and his associates to compare the DK crush method of coronary bifurcation stenting with other stenting approaches. In DKCRUSH-1 they found that DK crush worked better than classical crush for treating coronary bifurcations of all types, not just in unprotected left main coronaries (Eur. J. Clin. Invest. 2008;38:361-71). In DKCRUSH-II they compared DK crush with provisional side-branch stenting in a variety of coronary artery types, and found that while DK crush was associated with significantly less restenosis it produced no significant difference in 1-year major adverse coronary events compared with provisional stenting (J. Amer. Coll. Cardiol. 2011;57:914-20).
Dr. Zhang, in collaboration with Dr. Shao-Liang Chen and their associates at Nanjing First Hospital in China, pioneered the DK crush technique, reporting results from their first 20 patients in 2005 (Chinese Med. J. 2005;118:1746-50).
Their new trial notably focused exclusively on distal bifurcations in the unprotected left main coronary artery.
"We know that left main midshaft lesions respond very well to PCI [percutaneous coronary intervention], but distal left main lesions, which represent the majority of left main lesions, have a higher 1-year event rate, mostly related to the ostium circumflex," commented Dr. Gary S. Mintz, chief medical officer of the Cardiovascular Research Foundation in Washington. "There is growing interest in stenting left main lesions among U.S. interventionalists. It is the last frontier for U.S. interventionalists but is routinely done in Asia. The goal is to get the largest cross-sectional area throughout the bifurcation, but the question is how to do that, and what produces the least amount of restenosis at the circumflex ostium? That is the Achilles heel of using two stents at the bifurcation."
While the new results seem to clearly establish the superiority of DK crush over the culotte method, the trial did not address whether stenting of the side branch is better than leaving it unstented or using a different PCI approach.
"When the bifurcation angle is more than 70 degrees, most would do neither DK crush nor culotte; if they felt they had to stent [the side branch] they would use a T stent technique," commented Dr. Gregg W. Stone, professor of medicine and director of cardiovascular research and education at Columbia University in New York.

The DKCRUSH-III trial enrolled patients between March 2009 and October 2011 at 18 Chinese centers. The patients averaged about 64 years old, and nearly four-fifths were men. Their average SYNTAX score was about 31, and their New Risk Stratification Score averaged 26. Almost two-thirds of the patients received everolimus-eluting coronary stents (J. Amer. Coll. Cardiol. Intv. 2010;3:632-41).
Quantitative coronary angiography done about 7 months after PCI in about 84% of the patients in both arms showed no significant differences in patency of the left main coronary, but the side-branch patients in the culotte group had a significantly higher rate of late lumen loss. The overall rate of side-branch restenosis at 7 months was 7% in the DK crush group and 13% in the culotte group.
The 1-year combined rate of cardiac death, myocardial infarction, or clinically driven need for target-lesion or target-vessel revascularization – the primary endpoint – was 6% in the DK crush group and 16% in the culotte group, a significant difference, reported Dr. Zhang, an interventional cardiologist at Nanjing First Hospital. The difference in the rates between the two treatment arms was primarily driven by a difference in the need for revascularization.
A set of four prespecified subgroup analyses showed that the DK crush method was significantly better than the culotte method in three of the high-risk subgroups: patients with a bifurcation angle of 70 degrees or greater, patients with a SYNTAX score of 23 or greater, and patients with a New Risk Stratification score of 20 or greater. In the fourth high-risk subgroup – patients with diabetes – DK crush was also superior, but the difference just missed statistical significance.
Concurrent with Dr. Zhang’s report at the meeting, the results were also published online (J. Am. Coll. Cardiol. 2013;61:1482-88).
Dr. Zhang said that he and his associates had no disclosures. Dr. Mintz and Dr. Stone had no relevant disclosures.
On Twitter @mitchelzoler

|
Mitchel L. Zoler/IMNG Medical Media
|
The interventionalists who participated in the DKCRUSH-III trial are to be congratulated for their excellent patient outcomes. Patients treated in this study had a 1% cardiac death rate after 1 year despite having unprotected left main disease, with 70% having triple-vessel disease. These outcomes prompt us to ask whether interventionalists should be doing more of these types of cases.
Despite this success, I am not a big fan of the crush technique. I sometimes find it difficult to assess the side branch after stenting due to x-ray artifact caused by having so much metal in place when we crush a stent placed in a side branch. My practice is to do more single-vessel stenting and leave the side branch alone.
The "one stent" technique involves stenting the main branch and just rescuing the side branch, going through the struts of the main stent to enter the circumflex and push the struts out of the way. Results from several studies have shown that this approach is just as good as using two stents and causes fewer complications, although it has not been examined specifically at the distal left main coronary bifurcation. The one-stent approach is what U.S. interventionalists most commonly use today to treat lesions at coronary bifurcations.
Dr. Cindy L. Grines, an interventional cardiologist at Detroit Medical Center, made these comments as a designated discussant for the report. She had no relevant disclosures.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The interventionalists who participated in the DKCRUSH-III trial are to be congratulated for their excellent patient outcomes. Patients treated in this study had a 1% cardiac death rate after 1 year despite having unprotected left main disease, with 70% having triple-vessel disease. These outcomes prompt us to ask whether interventionalists should be doing more of these types of cases.
Despite this success, I am not a big fan of the crush technique. I sometimes find it difficult to assess the side branch after stenting due to x-ray artifact caused by having so much metal in place when we crush a stent placed in a side branch. My practice is to do more single-vessel stenting and leave the side branch alone.
The "one stent" technique involves stenting the main branch and just rescuing the side branch, going through the struts of the main stent to enter the circumflex and push the struts out of the way. Results from several studies have shown that this approach is just as good as using two stents and causes fewer complications, although it has not been examined specifically at the distal left main coronary bifurcation. The one-stent approach is what U.S. interventionalists most commonly use today to treat lesions at coronary bifurcations.
Dr. Cindy L. Grines, an interventional cardiologist at Detroit Medical Center, made these comments as a designated discussant for the report. She had no relevant disclosures.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The interventionalists who participated in the DKCRUSH-III trial are to be congratulated for their excellent patient outcomes. Patients treated in this study had a 1% cardiac death rate after 1 year despite having unprotected left main disease, with 70% having triple-vessel disease. These outcomes prompt us to ask whether interventionalists should be doing more of these types of cases.
Despite this success, I am not a big fan of the crush technique. I sometimes find it difficult to assess the side branch after stenting due to x-ray artifact caused by having so much metal in place when we crush a stent placed in a side branch. My practice is to do more single-vessel stenting and leave the side branch alone.
The "one stent" technique involves stenting the main branch and just rescuing the side branch, going through the struts of the main stent to enter the circumflex and push the struts out of the way. Results from several studies have shown that this approach is just as good as using two stents and causes fewer complications, although it has not been examined specifically at the distal left main coronary bifurcation. The one-stent approach is what U.S. interventionalists most commonly use today to treat lesions at coronary bifurcations.
Dr. Cindy L. Grines, an interventional cardiologist at Detroit Medical Center, made these comments as a designated discussant for the report. She had no relevant disclosures.
SAN FRANCISCO – The double-kissing crush approach to stenting an unprotected left main coronary artery at the distal bifurcation produced clearly better 1-year clinical outcomes than did an alternative way to stent at the bifurcation, the culotte approach, in a multicenter, randomized trial in China with 419 patients.
The survival rate of patients free of major adverse coronary events 1 year after treatment was 94% for the double kissing (DK) crush technique and 84% for the culotte technique, a statistically significant benefit for DK crush for the study’s primary endpoint, Dr. Jun-Jie Zhang reported at the American College of Cardiology/Cardiovascular Research Foundation Innovation in Intervention Summit.
This definitive clinical comparison, DKCRUSH-III (DK Crush Versus Culotte Stenting for the Treatment of Unprotected Left Main Bifurcation Lesions), is the third in a series of large randomized trials led by Dr. Zhang and his associates to compare the DK crush method of coronary bifurcation stenting with other stenting approaches. In DKCRUSH-1 they found that DK crush worked better than classical crush for treating coronary bifurcations of all types, not just in unprotected left main coronaries (Eur. J. Clin. Invest. 2008;38:361-71). In DKCRUSH-II they compared DK crush with provisional side-branch stenting in a variety of coronary artery types, and found that while DK crush was associated with significantly less restenosis it produced no significant difference in 1-year major adverse coronary events compared with provisional stenting (J. Amer. Coll. Cardiol. 2011;57:914-20).
Dr. Zhang, in collaboration with Dr. Shao-Liang Chen and their associates at Nanjing First Hospital in China, pioneered the DK crush technique, reporting results from their first 20 patients in 2005 (Chinese Med. J. 2005;118:1746-50).
Their new trial notably focused exclusively on distal bifurcations in the unprotected left main coronary artery.
"We know that left main midshaft lesions respond very well to PCI [percutaneous coronary intervention], but distal left main lesions, which represent the majority of left main lesions, have a higher 1-year event rate, mostly related to the ostium circumflex," commented Dr. Gary S. Mintz, chief medical officer of the Cardiovascular Research Foundation in Washington. "There is growing interest in stenting left main lesions among U.S. interventionalists. It is the last frontier for U.S. interventionalists but is routinely done in Asia. The goal is to get the largest cross-sectional area throughout the bifurcation, but the question is how to do that, and what produces the least amount of restenosis at the circumflex ostium? That is the Achilles heel of using two stents at the bifurcation."
While the new results seem to clearly establish the superiority of DK crush over the culotte method, the trial did not address whether stenting of the side branch is better than leaving it unstented or using a different PCI approach.
"When the bifurcation angle is more than 70 degrees, most would do neither DK crush nor culotte; if they felt they had to stent [the side branch] they would use a T stent technique," commented Dr. Gregg W. Stone, professor of medicine and director of cardiovascular research and education at Columbia University in New York.
The DKCRUSH-III trial enrolled patients between March 2009 and October 2011 at 18 Chinese centers. The patients averaged about 64 years old, and nearly four-fifths were men. Their average SYNTAX score was about 31, and their New Risk Stratification Score averaged 26. Almost two-thirds of the patients received everolimus-eluting coronary stents (J. Amer. Coll. Cardiol. Intv. 2010;3:632-41).
Quantitative coronary angiography done about 7 months after PCI in about 84% of the patients in both arms showed no significant differences in patency of the left main coronary, but the side-branch patients in the culotte group had a significantly higher rate of late lumen loss. The overall rate of side-branch restenosis at 7 months was 7% in the DK crush group and 13% in the culotte group.
The 1-year combined rate of cardiac death, myocardial infarction, or clinically driven need for target-lesion or target-vessel revascularization – the primary endpoint – was 6% in the DK crush group and 16% in the culotte group, a significant difference, reported Dr. Zhang, an interventional cardiologist at Nanjing First Hospital. The difference in the rates between the two treatment arms was primarily driven by a difference in the need for revascularization.
A set of four prespecified subgroup analyses showed that the DK crush method was significantly better than the culotte method in three of the high-risk subgroups: patients with a bifurcation angle of 70 degrees or greater, patients with a SYNTAX score of 23 or greater, and patients with a New Risk Stratification score of 20 or greater. In the fourth high-risk subgroup – patients with diabetes – DK crush was also superior, but the difference just missed statistical significance.
Concurrent with Dr. Zhang’s report at the meeting, the results were also published online (J. Am. Coll. Cardiol. 2013;61:1482-88).
Dr. Zhang said that he and his associates had no disclosures. Dr. Mintz and Dr. Stone had no relevant disclosures.
On Twitter @mitchelzoler
SAN FRANCISCO – The double-kissing crush approach to stenting an unprotected left main coronary artery at the distal bifurcation produced clearly better 1-year clinical outcomes than did an alternative way to stent at the bifurcation, the culotte approach, in a multicenter, randomized trial in China with 419 patients.
The survival rate of patients free of major adverse coronary events 1 year after treatment was 94% for the double kissing (DK) crush technique and 84% for the culotte technique, a statistically significant benefit for DK crush for the study’s primary endpoint, Dr. Jun-Jie Zhang reported at the American College of Cardiology/Cardiovascular Research Foundation Innovation in Intervention Summit.
This definitive clinical comparison, DKCRUSH-III (DK Crush Versus Culotte Stenting for the Treatment of Unprotected Left Main Bifurcation Lesions), is the third in a series of large randomized trials led by Dr. Zhang and his associates to compare the DK crush method of coronary bifurcation stenting with other stenting approaches. In DKCRUSH-1 they found that DK crush worked better than classical crush for treating coronary bifurcations of all types, not just in unprotected left main coronaries (Eur. J. Clin. Invest. 2008;38:361-71). In DKCRUSH-II they compared DK crush with provisional side-branch stenting in a variety of coronary artery types, and found that while DK crush was associated with significantly less restenosis it produced no significant difference in 1-year major adverse coronary events compared with provisional stenting (J. Amer. Coll. Cardiol. 2011;57:914-20).
Dr. Zhang, in collaboration with Dr. Shao-Liang Chen and their associates at Nanjing First Hospital in China, pioneered the DK crush technique, reporting results from their first 20 patients in 2005 (Chinese Med. J. 2005;118:1746-50).
Their new trial notably focused exclusively on distal bifurcations in the unprotected left main coronary artery.
"We know that left main midshaft lesions respond very well to PCI [percutaneous coronary intervention], but distal left main lesions, which represent the majority of left main lesions, have a higher 1-year event rate, mostly related to the ostium circumflex," commented Dr. Gary S. Mintz, chief medical officer of the Cardiovascular Research Foundation in Washington. "There is growing interest in stenting left main lesions among U.S. interventionalists. It is the last frontier for U.S. interventionalists but is routinely done in Asia. The goal is to get the largest cross-sectional area throughout the bifurcation, but the question is how to do that, and what produces the least amount of restenosis at the circumflex ostium? That is the Achilles heel of using two stents at the bifurcation."
While the new results seem to clearly establish the superiority of DK crush over the culotte method, the trial did not address whether stenting of the side branch is better than leaving it unstented or using a different PCI approach.
"When the bifurcation angle is more than 70 degrees, most would do neither DK crush nor culotte; if they felt they had to stent [the side branch] they would use a T stent technique," commented Dr. Gregg W. Stone, professor of medicine and director of cardiovascular research and education at Columbia University in New York.
The DKCRUSH-III trial enrolled patients between March 2009 and October 2011 at 18 Chinese centers. The patients averaged about 64 years old, and nearly four-fifths were men. Their average SYNTAX score was about 31, and their New Risk Stratification Score averaged 26. Almost two-thirds of the patients received everolimus-eluting coronary stents (J. Amer. Coll. Cardiol. Intv. 2010;3:632-41).
Quantitative coronary angiography done about 7 months after PCI in about 84% of the patients in both arms showed no significant differences in patency of the left main coronary, but the side-branch patients in the culotte group had a significantly higher rate of late lumen loss. The overall rate of side-branch restenosis at 7 months was 7% in the DK crush group and 13% in the culotte group.
The 1-year combined rate of cardiac death, myocardial infarction, or clinically driven need for target-lesion or target-vessel revascularization – the primary endpoint – was 6% in the DK crush group and 16% in the culotte group, a significant difference, reported Dr. Zhang, an interventional cardiologist at Nanjing First Hospital. The difference in the rates between the two treatment arms was primarily driven by a difference in the need for revascularization.
A set of four prespecified subgroup analyses showed that the DK crush method was significantly better than the culotte method in three of the high-risk subgroups: patients with a bifurcation angle of 70 degrees or greater, patients with a SYNTAX score of 23 or greater, and patients with a New Risk Stratification score of 20 or greater. In the fourth high-risk subgroup – patients with diabetes – DK crush was also superior, but the difference just missed statistical significance.
Concurrent with Dr. Zhang’s report at the meeting, the results were also published online (J. Am. Coll. Cardiol. 2013;61:1482-88).
Dr. Zhang said that he and his associates had no disclosures. Dr. Mintz and Dr. Stone had no relevant disclosures.
On Twitter @mitchelzoler
AT THE ACC/CRF I2 SUMMIT
Major finding: After 1 year, the survival rate of patients free from major coronary events was 94% for DK crush and 84% for culotte stenting.
Data source: The DKCRUSH-III trial, which randomized 419 patients with unprotected left main coronary distal bifurcation lesions to stenting by the DK crush or culotte techniques.
Disclosures: Dr. Zhang said that he and his associates had no disclosures. Dr. Mintz and Dr. Stone had no relevant disclosures.

European hypertension group endorses broad preeclampsia prophylaxis
ROME – The European Society of Hypertension is poised to endorse low-dose aspirin prophylaxis against preeclampsia for a large percent of pregnant women, according to a report at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation.
Endorsement of aspirin treatment for prophylaxis of preeclampsia in moderate- and high-risk women is part of new guidelines for managing hypertension prepared jointly by the European Society of Hypertension (ESH) and the European Society of Cardiology that will be unveiled at the hypertension society’s annual meeting in Milan in June, Dr. Renata Cifková said at the meeting.

"Aspirin, at a dosage of 75 mg/day, is recommended for the prevention of preeclampsia in women at high or moderate risk of preeclampsia from 12 weeks’ gestation until delivery," said Dr. Cifková, professor and head of the department of preventive cardiology at Thomayer University Hospital in Prague. The high- and moderate-risk categories together define a large proportion of women who become pregnant today.
The new guidelines define women at high risk who should receive aspirin prophylaxis as those who had gestational hypertension during a prior pregnancy, or women with chronic kidney disease, an autoimmune disease such as systemic lupus erythematosus or antiphospholipid syndrome, type 1 or 2 diabetes, or chronic hypertension. The guidelines also say that women should receive aspirin prophylaxis if they have two or more of these moderate-risk factors for preeclampsia: first pregnancy, age 40 years or older, a prior pregnancy interval of more than 10 years, a body mass index of 30 kg/m2 or greater, a family history of preeclampsia, or a multiple pregnancy.
These new ESH guidelines for preeclampsia prevention with aspirin follow exactly the recommendations made in August 2010 by the U.K.’s National Institute for Health and Clinical Excellence (NICE), noted Dr. Cifková. The most notable evidence supporting this approach came from a meta-analysis published in 2010 that included 27 studies involving more than 11,000 women and found that low-dose aspirin begun early in pregnancy cut the incidence of preeclampsia by about 50% (Ob.Gyn. 2010;116:402-14).
Another soon-to-appear guidance from the ESH, on appropriate patients for ambulatory blood pressure monitoring (ABPM), received a preview from Dr. Gianfranco Parati, professor of cardiovascular medicine at the University of Milan.

The new revision comes from an expert panel first convened 2 years ago by the ESH, Dr. Parati said at the meeting. The soon-to-be-published position on ABPM will not make recommendations that are as well defined as the ones for preeclampsia prophylaxis. "Is ABPM needed for every patient with hypertension? No, but it should be used in more patients," he said. Routine use of ABPM to confirm hypertension in all patients "is not suitable for every country because of its cost," he added.
Nonetheless, the new ESH consensus statement calls for using ABPM to confirm a diagnosis of hypertension or its absence, and thereby better avoid the twin nemeses of accurate hypertension assessment: white coat hypertension and masked hypertension, he said. ABPM also allows assessment of blood pressure control throughout 24 hours. The new guidelines say that ABPM is appropriate for selected elderly, children, and adolescent patients, and during pregnancy.
When high-risk patients or patients with nocturnal hypertension undergo ABPM, a follow-up, repeat examination should be done in 6 months. In most other patients, follow-up ABPM can occur after 1-2 years, Dr. Parati said.
Dr. Cifková reported no relevant financial disclosures. Dr. Parati has received honoraria from Bayer, Boegringer Ingelheim, Daiichi-Sankyo, Merck Serono, Menarini, Novartis, Recordati, Sanofi Aventis, and Takeda, and research support from Boehringer Ingelheim, Bayer, and Sanofi Aventis.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the meeting name during which these presentations were made. This version has been updated.
ROME – The European Society of Hypertension is poised to endorse low-dose aspirin prophylaxis against preeclampsia for a large percent of pregnant women, according to a report at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation.
Endorsement of aspirin treatment for prophylaxis of preeclampsia in moderate- and high-risk women is part of new guidelines for managing hypertension prepared jointly by the European Society of Hypertension (ESH) and the European Society of Cardiology that will be unveiled at the hypertension society’s annual meeting in Milan in June, Dr. Renata Cifková said at the meeting.
"Aspirin, at a dosage of 75 mg/day, is recommended for the prevention of preeclampsia in women at high or moderate risk of preeclampsia from 12 weeks’ gestation until delivery," said Dr. Cifková, professor and head of the department of preventive cardiology at Thomayer University Hospital in Prague. The high- and moderate-risk categories together define a large proportion of women who become pregnant today.
The new guidelines define women at high risk who should receive aspirin prophylaxis as those who had gestational hypertension during a prior pregnancy, or women with chronic kidney disease, an autoimmune disease such as systemic lupus erythematosus or antiphospholipid syndrome, type 1 or 2 diabetes, or chronic hypertension. The guidelines also say that women should receive aspirin prophylaxis if they have two or more of these moderate-risk factors for preeclampsia: first pregnancy, age 40 years or older, a prior pregnancy interval of more than 10 years, a body mass index of 30 kg/m2 or greater, a family history of preeclampsia, or a multiple pregnancy.
These new ESH guidelines for preeclampsia prevention with aspirin follow exactly the recommendations made in August 2010 by the U.K.’s National Institute for Health and Clinical Excellence (NICE), noted Dr. Cifková. The most notable evidence supporting this approach came from a meta-analysis published in 2010 that included 27 studies involving more than 11,000 women and found that low-dose aspirin begun early in pregnancy cut the incidence of preeclampsia by about 50% (Ob.Gyn. 2010;116:402-14).
Another soon-to-appear guidance from the ESH, on appropriate patients for ambulatory blood pressure monitoring (ABPM), received a preview from Dr. Gianfranco Parati, professor of cardiovascular medicine at the University of Milan.
The new revision comes from an expert panel first convened 2 years ago by the ESH, Dr. Parati said at the meeting. The soon-to-be-published position on ABPM will not make recommendations that are as well defined as the ones for preeclampsia prophylaxis. "Is ABPM needed for every patient with hypertension? No, but it should be used in more patients," he said. Routine use of ABPM to confirm hypertension in all patients "is not suitable for every country because of its cost," he added.
Nonetheless, the new ESH consensus statement calls for using ABPM to confirm a diagnosis of hypertension or its absence, and thereby better avoid the twin nemeses of accurate hypertension assessment: white coat hypertension and masked hypertension, he said. ABPM also allows assessment of blood pressure control throughout 24 hours. The new guidelines say that ABPM is appropriate for selected elderly, children, and adolescent patients, and during pregnancy.
When high-risk patients or patients with nocturnal hypertension undergo ABPM, a follow-up, repeat examination should be done in 6 months. In most other patients, follow-up ABPM can occur after 1-2 years, Dr. Parati said.
Dr. Cifková reported no relevant financial disclosures. Dr. Parati has received honoraria from Bayer, Boegringer Ingelheim, Daiichi-Sankyo, Merck Serono, Menarini, Novartis, Recordati, Sanofi Aventis, and Takeda, and research support from Boehringer Ingelheim, Bayer, and Sanofi Aventis.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the meeting name during which these presentations were made. This version has been updated.
ROME – The European Society of Hypertension is poised to endorse low-dose aspirin prophylaxis against preeclampsia for a large percent of pregnant women, according to a report at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation.
Endorsement of aspirin treatment for prophylaxis of preeclampsia in moderate- and high-risk women is part of new guidelines for managing hypertension prepared jointly by the European Society of Hypertension (ESH) and the European Society of Cardiology that will be unveiled at the hypertension society’s annual meeting in Milan in June, Dr. Renata Cifková said at the meeting.
"Aspirin, at a dosage of 75 mg/day, is recommended for the prevention of preeclampsia in women at high or moderate risk of preeclampsia from 12 weeks’ gestation until delivery," said Dr. Cifková, professor and head of the department of preventive cardiology at Thomayer University Hospital in Prague. The high- and moderate-risk categories together define a large proportion of women who become pregnant today.
The new guidelines define women at high risk who should receive aspirin prophylaxis as those who had gestational hypertension during a prior pregnancy, or women with chronic kidney disease, an autoimmune disease such as systemic lupus erythematosus or antiphospholipid syndrome, type 1 or 2 diabetes, or chronic hypertension. The guidelines also say that women should receive aspirin prophylaxis if they have two or more of these moderate-risk factors for preeclampsia: first pregnancy, age 40 years or older, a prior pregnancy interval of more than 10 years, a body mass index of 30 kg/m2 or greater, a family history of preeclampsia, or a multiple pregnancy.
These new ESH guidelines for preeclampsia prevention with aspirin follow exactly the recommendations made in August 2010 by the U.K.’s National Institute for Health and Clinical Excellence (NICE), noted Dr. Cifková. The most notable evidence supporting this approach came from a meta-analysis published in 2010 that included 27 studies involving more than 11,000 women and found that low-dose aspirin begun early in pregnancy cut the incidence of preeclampsia by about 50% (Ob.Gyn. 2010;116:402-14).
Another soon-to-appear guidance from the ESH, on appropriate patients for ambulatory blood pressure monitoring (ABPM), received a preview from Dr. Gianfranco Parati, professor of cardiovascular medicine at the University of Milan.
The new revision comes from an expert panel first convened 2 years ago by the ESH, Dr. Parati said at the meeting. The soon-to-be-published position on ABPM will not make recommendations that are as well defined as the ones for preeclampsia prophylaxis. "Is ABPM needed for every patient with hypertension? No, but it should be used in more patients," he said. Routine use of ABPM to confirm hypertension in all patients "is not suitable for every country because of its cost," he added.
Nonetheless, the new ESH consensus statement calls for using ABPM to confirm a diagnosis of hypertension or its absence, and thereby better avoid the twin nemeses of accurate hypertension assessment: white coat hypertension and masked hypertension, he said. ABPM also allows assessment of blood pressure control throughout 24 hours. The new guidelines say that ABPM is appropriate for selected elderly, children, and adolescent patients, and during pregnancy.
When high-risk patients or patients with nocturnal hypertension undergo ABPM, a follow-up, repeat examination should be done in 6 months. In most other patients, follow-up ABPM can occur after 1-2 years, Dr. Parati said.
Dr. Cifková reported no relevant financial disclosures. Dr. Parati has received honoraria from Bayer, Boegringer Ingelheim, Daiichi-Sankyo, Merck Serono, Menarini, Novartis, Recordati, Sanofi Aventis, and Takeda, and research support from Boehringer Ingelheim, Bayer, and Sanofi Aventis.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the meeting name during which these presentations were made. This version has been updated.
AT EUROPREVENT 2013

Primary cardiovascular prevention: Rethinking 'high risk'
Who is "high risk" when it comes to primary prevention of cardiovascular disease?
Several risk formulas now exist to calculate a person’s risk level, but maybe the best answer is rooted in clinical practice. Speaking in April at EuroPrevent 2013, cardiologist and preventive-medicine specialist Dr. Donald M. Lloyd-Jones offered this definition: "Assuming that lifestyle intervention is appropriate for everyone, ‘high risk’ may mean being at enough risk for atherosclerotic cardiovascular disease in 10 years to merit drug treatment," in a calculation that takes into account the cost-effectiveness of the treatment and its risk-to-benefit ratio.

What I like about this definition is that it puts the meaning of high-risk in very practical terms: Is the person at enough risk to warrant a particular treatment after also taking into account its financial and adverse-effect costs?
In other words, a person may be high risk and deserve aggressive primary prevention if treated with a cheap agent, like a generic statin or aspirin, but at lower risk if treatment involves a more expensive drug, for example a brand-name statin like rosuvastatin or ezetimibe, which in the United States are only available as the brand names Crestor and Zetia. A designation of high risk that comes and goes depending in part on the cost of intervention is wonderfully adaptive to real-world circumstances.
Dr. Lloyd-Jones went a little further, elaborating on how this definition of high risk works in today’s era of generic atorvastatin, America’s first high-potency statin marketed as a generic, its status for a little over 1 year.
"In the current era when a high-potency, generic statin is $4 a month, cost is no longer an issue," he said. "All you really have to think about are the adverse events, not the cost; cost doesn’t enter into the equation."
I previously spoke to Dr. Lloyd-Jones a little less than 18 months ago, when genetic atorvastatin was on the verge of first entering the U.S. market, and at the time he excitedly called its pending availability a "game changer" for the management of patients with established cardiovascular disease. It sounds like he sees it the same way for primary prevention.
At EuroPrevent, he also talked about the need to consider a person’s long-term – either 30-year or lifetime – risk for cardiovascular disease rather than exclusively focusing on their 10-year risk calculated with one of the standard risk measurement formulas, like the Framingham Risk Score or the EuroSCORE.
Dr. Lloyd-Jones serves on the U.S. panel that’s writing America’s updated, official cholesterol-treatment guidelines, ATP IV, and he also cochairs another U.S. panel that is preparing revised guidelines on cardiovascular risk reduction. Another cardiovascular-risk expert, Dr. Peter W.F. Wilson from Emory University in Atlanta, also serves on both panels and also spoke at the same meeting session, where he said he fully agreed with Dr. Lloyd-Jones and stressed the need to take into account the net benefit that accrues when putting people on treatment.
It sounds like when the new ATP IV guidelines appear, there is a good chance they will call for more aggressive, generic-statin-based risk reduction for primary prevention than current ATP III recommendations.
On Twitter @mitchelzoler
Who is "high risk" when it comes to primary prevention of cardiovascular disease?
Several risk formulas now exist to calculate a person’s risk level, but maybe the best answer is rooted in clinical practice. Speaking in April at EuroPrevent 2013, cardiologist and preventive-medicine specialist Dr. Donald M. Lloyd-Jones offered this definition: "Assuming that lifestyle intervention is appropriate for everyone, ‘high risk’ may mean being at enough risk for atherosclerotic cardiovascular disease in 10 years to merit drug treatment," in a calculation that takes into account the cost-effectiveness of the treatment and its risk-to-benefit ratio.
What I like about this definition is that it puts the meaning of high-risk in very practical terms: Is the person at enough risk to warrant a particular treatment after also taking into account its financial and adverse-effect costs?
In other words, a person may be high risk and deserve aggressive primary prevention if treated with a cheap agent, like a generic statin or aspirin, but at lower risk if treatment involves a more expensive drug, for example a brand-name statin like rosuvastatin or ezetimibe, which in the United States are only available as the brand names Crestor and Zetia. A designation of high risk that comes and goes depending in part on the cost of intervention is wonderfully adaptive to real-world circumstances.
Dr. Lloyd-Jones went a little further, elaborating on how this definition of high risk works in today’s era of generic atorvastatin, America’s first high-potency statin marketed as a generic, its status for a little over 1 year.
"In the current era when a high-potency, generic statin is $4 a month, cost is no longer an issue," he said. "All you really have to think about are the adverse events, not the cost; cost doesn’t enter into the equation."
I previously spoke to Dr. Lloyd-Jones a little less than 18 months ago, when genetic atorvastatin was on the verge of first entering the U.S. market, and at the time he excitedly called its pending availability a "game changer" for the management of patients with established cardiovascular disease. It sounds like he sees it the same way for primary prevention.
At EuroPrevent, he also talked about the need to consider a person’s long-term – either 30-year or lifetime – risk for cardiovascular disease rather than exclusively focusing on their 10-year risk calculated with one of the standard risk measurement formulas, like the Framingham Risk Score or the EuroSCORE.
Dr. Lloyd-Jones serves on the U.S. panel that’s writing America’s updated, official cholesterol-treatment guidelines, ATP IV, and he also cochairs another U.S. panel that is preparing revised guidelines on cardiovascular risk reduction. Another cardiovascular-risk expert, Dr. Peter W.F. Wilson from Emory University in Atlanta, also serves on both panels and also spoke at the same meeting session, where he said he fully agreed with Dr. Lloyd-Jones and stressed the need to take into account the net benefit that accrues when putting people on treatment.
It sounds like when the new ATP IV guidelines appear, there is a good chance they will call for more aggressive, generic-statin-based risk reduction for primary prevention than current ATP III recommendations.
On Twitter @mitchelzoler
Who is "high risk" when it comes to primary prevention of cardiovascular disease?
Several risk formulas now exist to calculate a person’s risk level, but maybe the best answer is rooted in clinical practice. Speaking in April at EuroPrevent 2013, cardiologist and preventive-medicine specialist Dr. Donald M. Lloyd-Jones offered this definition: "Assuming that lifestyle intervention is appropriate for everyone, ‘high risk’ may mean being at enough risk for atherosclerotic cardiovascular disease in 10 years to merit drug treatment," in a calculation that takes into account the cost-effectiveness of the treatment and its risk-to-benefit ratio.
What I like about this definition is that it puts the meaning of high-risk in very practical terms: Is the person at enough risk to warrant a particular treatment after also taking into account its financial and adverse-effect costs?
In other words, a person may be high risk and deserve aggressive primary prevention if treated with a cheap agent, like a generic statin or aspirin, but at lower risk if treatment involves a more expensive drug, for example a brand-name statin like rosuvastatin or ezetimibe, which in the United States are only available as the brand names Crestor and Zetia. A designation of high risk that comes and goes depending in part on the cost of intervention is wonderfully adaptive to real-world circumstances.
Dr. Lloyd-Jones went a little further, elaborating on how this definition of high risk works in today’s era of generic atorvastatin, America’s first high-potency statin marketed as a generic, its status for a little over 1 year.
"In the current era when a high-potency, generic statin is $4 a month, cost is no longer an issue," he said. "All you really have to think about are the adverse events, not the cost; cost doesn’t enter into the equation."
I previously spoke to Dr. Lloyd-Jones a little less than 18 months ago, when genetic atorvastatin was on the verge of first entering the U.S. market, and at the time he excitedly called its pending availability a "game changer" for the management of patients with established cardiovascular disease. It sounds like he sees it the same way for primary prevention.
At EuroPrevent, he also talked about the need to consider a person’s long-term – either 30-year or lifetime – risk for cardiovascular disease rather than exclusively focusing on their 10-year risk calculated with one of the standard risk measurement formulas, like the Framingham Risk Score or the EuroSCORE.
Dr. Lloyd-Jones serves on the U.S. panel that’s writing America’s updated, official cholesterol-treatment guidelines, ATP IV, and he also cochairs another U.S. panel that is preparing revised guidelines on cardiovascular risk reduction. Another cardiovascular-risk expert, Dr. Peter W.F. Wilson from Emory University in Atlanta, also serves on both panels and also spoke at the same meeting session, where he said he fully agreed with Dr. Lloyd-Jones and stressed the need to take into account the net benefit that accrues when putting people on treatment.
It sounds like when the new ATP IV guidelines appear, there is a good chance they will call for more aggressive, generic-statin-based risk reduction for primary prevention than current ATP III recommendations.
On Twitter @mitchelzoler

FDA backs abuse-deterring OxyContin, thwarts generics
In an eleventh-hour action that derailed the possibility of generic formulations of controlled-release oxycodone (OxyContin) from appearing on the U.S. market anytime soon, the Food and Drug Administration announced April 16 that it withdrew its approval of the original, conventional formulation of OxyContin.
Acting on the very day that the patent on the original formulation of OxyContin, held by Purdue Pharma, was set to expire, the FDA took an additional step to support the newer formulation of OxyContin that Purdue has marketed exclusively since August 2010. The newer version includes a polymer so that, when a pill is crushed and then mixed with water it turns into a gel rather than remaining a more easily manipulated powder. The FDA approved updated labeling for OxyContin that highlights the abuse-deterring features of the newer formulation, which means that Purdue can now cite these attributes when marketing the drug.
The FDA "approved labeling for reformulated OxyContin stating that it possesses physiochemical properties that are expected to: (1) make abuse via injection difficult, and (2) reduce abuse via the intranasal route. This is the first opioid product for which FDA has approved labeling that includes statements regarding abuse-deterrence," according to a letter from FDA Commissioner Margaret A. Hamburg sent April 16 to Rep. Fred Upton (R-Mich.) and Sen. Tom Coburn (R-Okla).
"We applaud FDA Commissioner Hamburg’s announcement that the FDA will not approve any abbreviated new drug applications that rely upon the approval of original OxyContin which did not have abuse-deterrent properties," the lawmakers said in a statement. "With more than 16,000 Americans dying from opioid drug overdoses each year, Commissioner Hamburg’s announcement is a significant step forward in the federal government’s effort to reduce opioid drug abuse and protect consumers. For too long, drug abusers have been able to crush or dissolve opioid drug products in order to defeat their time-release mechanisms for snorting or injecting the drugs."
For patients, the major downside of the FDA’s action is economic. OxyContin retails for about $7.50 per tablet and had roughly $2.7 billion in U.S. sales in 2012. The patent on the abuse-deterring formulation of the drug lasts until 2025.
On Twitter @mitchelzoler
In an eleventh-hour action that derailed the possibility of generic formulations of controlled-release oxycodone (OxyContin) from appearing on the U.S. market anytime soon, the Food and Drug Administration announced April 16 that it withdrew its approval of the original, conventional formulation of OxyContin.
Acting on the very day that the patent on the original formulation of OxyContin, held by Purdue Pharma, was set to expire, the FDA took an additional step to support the newer formulation of OxyContin that Purdue has marketed exclusively since August 2010. The newer version includes a polymer so that, when a pill is crushed and then mixed with water it turns into a gel rather than remaining a more easily manipulated powder. The FDA approved updated labeling for OxyContin that highlights the abuse-deterring features of the newer formulation, which means that Purdue can now cite these attributes when marketing the drug.
The FDA "approved labeling for reformulated OxyContin stating that it possesses physiochemical properties that are expected to: (1) make abuse via injection difficult, and (2) reduce abuse via the intranasal route. This is the first opioid product for which FDA has approved labeling that includes statements regarding abuse-deterrence," according to a letter from FDA Commissioner Margaret A. Hamburg sent April 16 to Rep. Fred Upton (R-Mich.) and Sen. Tom Coburn (R-Okla).
"We applaud FDA Commissioner Hamburg’s announcement that the FDA will not approve any abbreviated new drug applications that rely upon the approval of original OxyContin which did not have abuse-deterrent properties," the lawmakers said in a statement. "With more than 16,000 Americans dying from opioid drug overdoses each year, Commissioner Hamburg’s announcement is a significant step forward in the federal government’s effort to reduce opioid drug abuse and protect consumers. For too long, drug abusers have been able to crush or dissolve opioid drug products in order to defeat their time-release mechanisms for snorting or injecting the drugs."
For patients, the major downside of the FDA’s action is economic. OxyContin retails for about $7.50 per tablet and had roughly $2.7 billion in U.S. sales in 2012. The patent on the abuse-deterring formulation of the drug lasts until 2025.
On Twitter @mitchelzoler
In an eleventh-hour action that derailed the possibility of generic formulations of controlled-release oxycodone (OxyContin) from appearing on the U.S. market anytime soon, the Food and Drug Administration announced April 16 that it withdrew its approval of the original, conventional formulation of OxyContin.
Acting on the very day that the patent on the original formulation of OxyContin, held by Purdue Pharma, was set to expire, the FDA took an additional step to support the newer formulation of OxyContin that Purdue has marketed exclusively since August 2010. The newer version includes a polymer so that, when a pill is crushed and then mixed with water it turns into a gel rather than remaining a more easily manipulated powder. The FDA approved updated labeling for OxyContin that highlights the abuse-deterring features of the newer formulation, which means that Purdue can now cite these attributes when marketing the drug.
The FDA "approved labeling for reformulated OxyContin stating that it possesses physiochemical properties that are expected to: (1) make abuse via injection difficult, and (2) reduce abuse via the intranasal route. This is the first opioid product for which FDA has approved labeling that includes statements regarding abuse-deterrence," according to a letter from FDA Commissioner Margaret A. Hamburg sent April 16 to Rep. Fred Upton (R-Mich.) and Sen. Tom Coburn (R-Okla).
"We applaud FDA Commissioner Hamburg’s announcement that the FDA will not approve any abbreviated new drug applications that rely upon the approval of original OxyContin which did not have abuse-deterrent properties," the lawmakers said in a statement. "With more than 16,000 Americans dying from opioid drug overdoses each year, Commissioner Hamburg’s announcement is a significant step forward in the federal government’s effort to reduce opioid drug abuse and protect consumers. For too long, drug abusers have been able to crush or dissolve opioid drug products in order to defeat their time-release mechanisms for snorting or injecting the drugs."
For patients, the major downside of the FDA’s action is economic. OxyContin retails for about $7.50 per tablet and had roughly $2.7 billion in U.S. sales in 2012. The patent on the abuse-deterring formulation of the drug lasts until 2025.
On Twitter @mitchelzoler
Exercise ABI aids PAD risk stratification
SAN FRANCISCO – A postexercise ankle-brachial index measure provides useful, additional risk stratification to patients with peripheral arterial disease, according to a review of more than 2,800 patients tested at one U.S. center.
"Postexercise ABI [ankle brachial index], which is not routinely tested in most vascular labs, is a very effective tool to identify patients at risk of peripheral disease," Jason Strefling, D.O., said while presenting a poster at the annual meeting of the American College of Cardiology. "Resting ABI is a pretty sensitive test, but when you add exercise you can significantly increase the sensitivity," said Dr. Strefling, a cardiologist at Texas Tech University in Lubbock.
"Patients with diabetes or renal dysfunction can have an unusually normal resting ABI," but measuring a patient’s ABI a second time, after exercise, can better stratify patients who have some level of peripheral arterial disease (PAD), he said in an interview. "Postexercise ABI should probably be measured in all patients having their ABI measured, and on all PAD patients, but most vascular labs don’t do it." Patients with depressed ABIs both at rest and after exercise have the worst outcomes, but depressed exercise ABI with a normal rest ABI may identify patients with milder but nonetheless clinically significant PAD.
The exercise can be in the form of a treadmill protocol, or as simple as a few minutes of toe lifts, he said.
Dr. Strefling and his associates reviewed 2,842 patients seen at the vascular laboratory at the Cleveland Clinic during 2005-2009 who underwent both resting and postexercise ABI measurements. "A lot of vascular surgeons and cardiologists [at the Cleveland Clinic] order an exercise ABI," he explained. The ABI, the difference in systolic pressure between the ankle and arm, is measured with a handheld continuous wave Doppler ultrasound device and a blood pressure cuff. An ABI measurement of less than 0.90 is considered diagnostic of PAD. Dr. Strefling was on the Cleveland Clinic staff when he did this analysis.
The cohort included 1,383 patients with a normal ABI, greater than 0.9, at rest and post exercise, 479 with a normal rest ABI but a depressed ABI post exercise, 0.9 or less, and 980 patients with a low ABI at both measurements.
During follow-up of up to 5 years, the mortality rate was 9% in patients with both ABIs normal, 13% in patients whose ABI was only depressed post exercise, and 21% in patients with low rest and exercise ABIs, statistically significant between-group differences. The researchers reported a similar, statistically significant risk stratification pattern for the combined outcome of death, stroke, and myocardial infarction.
A third combined outcome – death, stroke, myocardial infarction, or lower extremity revascularization or amputation – had rates of 14% in patients with normal rest and exercise ABIs, 27% in patients with a normal rest ABI but reduced postexercise ABI, and 51% in patients with a low ABI on both measures, statistically significant differences. This combined endpoint was primarily driven by episodes of revascularization or amputation, Dr. Strefling noted.
No study results have yet documented the best way to manage patients with a normal resting ABI and a depressed exercise ABI, but Dr. Strefling suggested treating these patients with at least one antiplatelet drug and possibly two of these drugs (such as aspirin and clopidogrel), aggressive statin treatment, and other treatments for risk-factor modification.
Dr. Strefling said that he had no disclosures.
Twitter: @mitchelzoler
SAN FRANCISCO – A postexercise ankle-brachial index measure provides useful, additional risk stratification to patients with peripheral arterial disease, according to a review of more than 2,800 patients tested at one U.S. center.
"Postexercise ABI [ankle brachial index], which is not routinely tested in most vascular labs, is a very effective tool to identify patients at risk of peripheral disease," Jason Strefling, D.O., said while presenting a poster at the annual meeting of the American College of Cardiology. "Resting ABI is a pretty sensitive test, but when you add exercise you can significantly increase the sensitivity," said Dr. Strefling, a cardiologist at Texas Tech University in Lubbock.
"Patients with diabetes or renal dysfunction can have an unusually normal resting ABI," but measuring a patient’s ABI a second time, after exercise, can better stratify patients who have some level of peripheral arterial disease (PAD), he said in an interview. "Postexercise ABI should probably be measured in all patients having their ABI measured, and on all PAD patients, but most vascular labs don’t do it." Patients with depressed ABIs both at rest and after exercise have the worst outcomes, but depressed exercise ABI with a normal rest ABI may identify patients with milder but nonetheless clinically significant PAD.
The exercise can be in the form of a treadmill protocol, or as simple as a few minutes of toe lifts, he said.
Dr. Strefling and his associates reviewed 2,842 patients seen at the vascular laboratory at the Cleveland Clinic during 2005-2009 who underwent both resting and postexercise ABI measurements. "A lot of vascular surgeons and cardiologists [at the Cleveland Clinic] order an exercise ABI," he explained. The ABI, the difference in systolic pressure between the ankle and arm, is measured with a handheld continuous wave Doppler ultrasound device and a blood pressure cuff. An ABI measurement of less than 0.90 is considered diagnostic of PAD. Dr. Strefling was on the Cleveland Clinic staff when he did this analysis.
The cohort included 1,383 patients with a normal ABI, greater than 0.9, at rest and post exercise, 479 with a normal rest ABI but a depressed ABI post exercise, 0.9 or less, and 980 patients with a low ABI at both measurements.
During follow-up of up to 5 years, the mortality rate was 9% in patients with both ABIs normal, 13% in patients whose ABI was only depressed post exercise, and 21% in patients with low rest and exercise ABIs, statistically significant between-group differences. The researchers reported a similar, statistically significant risk stratification pattern for the combined outcome of death, stroke, and myocardial infarction.
A third combined outcome – death, stroke, myocardial infarction, or lower extremity revascularization or amputation – had rates of 14% in patients with normal rest and exercise ABIs, 27% in patients with a normal rest ABI but reduced postexercise ABI, and 51% in patients with a low ABI on both measures, statistically significant differences. This combined endpoint was primarily driven by episodes of revascularization or amputation, Dr. Strefling noted.
No study results have yet documented the best way to manage patients with a normal resting ABI and a depressed exercise ABI, but Dr. Strefling suggested treating these patients with at least one antiplatelet drug and possibly two of these drugs (such as aspirin and clopidogrel), aggressive statin treatment, and other treatments for risk-factor modification.
Dr. Strefling said that he had no disclosures.
Twitter: @mitchelzoler
SAN FRANCISCO – A postexercise ankle-brachial index measure provides useful, additional risk stratification to patients with peripheral arterial disease, according to a review of more than 2,800 patients tested at one U.S. center.
"Postexercise ABI [ankle brachial index], which is not routinely tested in most vascular labs, is a very effective tool to identify patients at risk of peripheral disease," Jason Strefling, D.O., said while presenting a poster at the annual meeting of the American College of Cardiology. "Resting ABI is a pretty sensitive test, but when you add exercise you can significantly increase the sensitivity," said Dr. Strefling, a cardiologist at Texas Tech University in Lubbock.
"Patients with diabetes or renal dysfunction can have an unusually normal resting ABI," but measuring a patient’s ABI a second time, after exercise, can better stratify patients who have some level of peripheral arterial disease (PAD), he said in an interview. "Postexercise ABI should probably be measured in all patients having their ABI measured, and on all PAD patients, but most vascular labs don’t do it." Patients with depressed ABIs both at rest and after exercise have the worst outcomes, but depressed exercise ABI with a normal rest ABI may identify patients with milder but nonetheless clinically significant PAD.
The exercise can be in the form of a treadmill protocol, or as simple as a few minutes of toe lifts, he said.
Dr. Strefling and his associates reviewed 2,842 patients seen at the vascular laboratory at the Cleveland Clinic during 2005-2009 who underwent both resting and postexercise ABI measurements. "A lot of vascular surgeons and cardiologists [at the Cleveland Clinic] order an exercise ABI," he explained. The ABI, the difference in systolic pressure between the ankle and arm, is measured with a handheld continuous wave Doppler ultrasound device and a blood pressure cuff. An ABI measurement of less than 0.90 is considered diagnostic of PAD. Dr. Strefling was on the Cleveland Clinic staff when he did this analysis.
The cohort included 1,383 patients with a normal ABI, greater than 0.9, at rest and post exercise, 479 with a normal rest ABI but a depressed ABI post exercise, 0.9 or less, and 980 patients with a low ABI at both measurements.
During follow-up of up to 5 years, the mortality rate was 9% in patients with both ABIs normal, 13% in patients whose ABI was only depressed post exercise, and 21% in patients with low rest and exercise ABIs, statistically significant between-group differences. The researchers reported a similar, statistically significant risk stratification pattern for the combined outcome of death, stroke, and myocardial infarction.
A third combined outcome – death, stroke, myocardial infarction, or lower extremity revascularization or amputation – had rates of 14% in patients with normal rest and exercise ABIs, 27% in patients with a normal rest ABI but reduced postexercise ABI, and 51% in patients with a low ABI on both measures, statistically significant differences. This combined endpoint was primarily driven by episodes of revascularization or amputation, Dr. Strefling noted.
No study results have yet documented the best way to manage patients with a normal resting ABI and a depressed exercise ABI, but Dr. Strefling suggested treating these patients with at least one antiplatelet drug and possibly two of these drugs (such as aspirin and clopidogrel), aggressive statin treatment, and other treatments for risk-factor modification.
Dr. Strefling said that he had no disclosures.
Twitter: @mitchelzoler
AT ACC 2013
Major finding: Mortality was 9% in patients with ABIs normal at rest and post exercise and 21% in patients with low rest and low postexercise ABI.
Data source: A review of 2,842 patients at one U.S. center who underwent both rest and postexercise ankle-brachial index measurements.
Disclosures: Dr. Strefling said that he had no disclosures.
Atrial fib symptoms milder but mortality higher in men
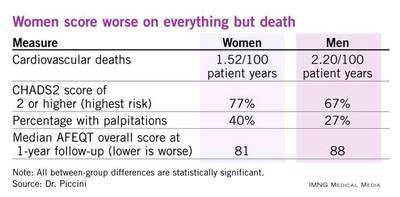
SAN FRANCISCO – Women with atrial fibrillation have significantly more debilitation than men with the disorder, but men with atrial fibrillation have double the cardiovascular death rate than their female counterparts, based on data collected from more than 10,000 U.S. patients.
During follow-up of the 5,842 men and 4,290 women with atrial fibrillation who were enrolled in the registry, women’s cumulative rate of cardiovascular death lagged 54% behind men’s, a statistically significant difference, Dr. Jonathan P. Piccini reported at the annual meeting of the American College of Cardiology.

The rate of all-cause death ran a relative 31% lower in women compared with men, but this difference seemed mostly due to the cardiovascular-death disparity because rates of noncardiovascular deaths in women and men with atrial fibrillation were virtually identical, said Dr. Piccini, an electrophysiology cardiologist at Duke University in Durham, N.C.
Despite this survival advantage, women with atrial fibrillation fare worse than men by several other measures. Women report worse symptoms, more functional impairment, and worse quality of life; they also spend significantly less time in their target anticoagulant range and they have a higher stroke risk than men, he reported.
"When we see women with atrial fibrillation, we should be aware that they are more likely to have worse symptoms and quality of life. Symptoms need to be treated; when a patient persists in having symptoms, treatment to control the symptoms is very important," he said in an interview. "We need to investigate the registry data to see why women have more symptoms and worse quality of life. This is the largest quality of life study ever done in atrial fibrillation."
Among the 10,132 patients enrolled in the registry, 1,339 participated in a substudy that serially measured quality of life using the Atrial Fibrillation Effect on Quality of Life (AFEQT) questionnaire (Circ. Arrhythm. Electrophysiol. 2011;4:15-25). "We have the power to look at the effects of different treatments so we can assess how changing treatment affects quality of life," Dr. Piccini said.
The Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT AF) enrolled both prevalent and new-onset atrial fibrillation patients at 184 diverse practice settings, including primary care, cardiology, and electrophysiology offices, between June 2010 and August 2011. The enrolled men were an average of 73 years old, while the women averaged 77 years of age.
Coronary disease was present in 39% of men and 23% of the women, but 17% of the women had a history of stroke or transient ischemic attack, compared with 14% of the men. Both sexes had a similar distribution of atrial fibrillation type, but women had clearly higher CHADS2 scores, a measure of stroke risk. The percentage of patients with a score of 0 or 1, the lowest-risk patients, was 33% among men and 23% among women.
Every symptom assessed was more common among women, led by the most frequent symptom, palpitations, which affected 40% of women and 27% of men. The next most common symptoms – exertional dyspnea, fatigue, and lightheadedness – were each several percentage points more common in women than men, all statistically significant differences.
Reassuringly, use of rate and rhythm-control treatments and oral anticoagulation were very similar among men and women, but women more frequently had a prolonged gap between their anticoagulation checkups, and their time spent within the target international normalized ratio of 2.0-3.0 was 65%, significantly below the 68% rate in men.
The rate of new heart failure during follow-up was the same in the men and women. Women had higher stroke risk based on their CHADS2 scores, but their stroke rate, while numerically greater than in men, was not significantly higher.
AFEQT results from the registry subset showed that women had significantly worse (lower) scores than men overall and for each of four AFEQT component scores tallied at both baseline and 1-year follow-up: symptoms, daily activity, treatment concern, and treatment satisfaction.
The ORBIT AF registry is sponsored by Janssen. Dr. Piccini said that he has financial relationships with Boston Scientific, GE Healthcare, Janssen, Johnson & Johnson, Medtronic, and Pfizer Bristol-Myers Squibb.
On Twitter @mitchelzoler
SAN FRANCISCO – Women with atrial fibrillation have significantly more debilitation than men with the disorder, but men with atrial fibrillation have double the cardiovascular death rate than their female counterparts, based on data collected from more than 10,000 U.S. patients.
During follow-up of the 5,842 men and 4,290 women with atrial fibrillation who were enrolled in the registry, women’s cumulative rate of cardiovascular death lagged 54% behind men’s, a statistically significant difference, Dr. Jonathan P. Piccini reported at the annual meeting of the American College of Cardiology.
The rate of all-cause death ran a relative 31% lower in women compared with men, but this difference seemed mostly due to the cardiovascular-death disparity because rates of noncardiovascular deaths in women and men with atrial fibrillation were virtually identical, said Dr. Piccini, an electrophysiology cardiologist at Duke University in Durham, N.C.
Despite this survival advantage, women with atrial fibrillation fare worse than men by several other measures. Women report worse symptoms, more functional impairment, and worse quality of life; they also spend significantly less time in their target anticoagulant range and they have a higher stroke risk than men, he reported.
"When we see women with atrial fibrillation, we should be aware that they are more likely to have worse symptoms and quality of life. Symptoms need to be treated; when a patient persists in having symptoms, treatment to control the symptoms is very important," he said in an interview. "We need to investigate the registry data to see why women have more symptoms and worse quality of life. This is the largest quality of life study ever done in atrial fibrillation."
Among the 10,132 patients enrolled in the registry, 1,339 participated in a substudy that serially measured quality of life using the Atrial Fibrillation Effect on Quality of Life (AFEQT) questionnaire (Circ. Arrhythm. Electrophysiol. 2011;4:15-25). "We have the power to look at the effects of different treatments so we can assess how changing treatment affects quality of life," Dr. Piccini said.
The Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT AF) enrolled both prevalent and new-onset atrial fibrillation patients at 184 diverse practice settings, including primary care, cardiology, and electrophysiology offices, between June 2010 and August 2011. The enrolled men were an average of 73 years old, while the women averaged 77 years of age.
Coronary disease was present in 39% of men and 23% of the women, but 17% of the women had a history of stroke or transient ischemic attack, compared with 14% of the men. Both sexes had a similar distribution of atrial fibrillation type, but women had clearly higher CHADS2 scores, a measure of stroke risk. The percentage of patients with a score of 0 or 1, the lowest-risk patients, was 33% among men and 23% among women.
Every symptom assessed was more common among women, led by the most frequent symptom, palpitations, which affected 40% of women and 27% of men. The next most common symptoms – exertional dyspnea, fatigue, and lightheadedness – were each several percentage points more common in women than men, all statistically significant differences.
Reassuringly, use of rate and rhythm-control treatments and oral anticoagulation were very similar among men and women, but women more frequently had a prolonged gap between their anticoagulation checkups, and their time spent within the target international normalized ratio of 2.0-3.0 was 65%, significantly below the 68% rate in men.
The rate of new heart failure during follow-up was the same in the men and women. Women had higher stroke risk based on their CHADS2 scores, but their stroke rate, while numerically greater than in men, was not significantly higher.
AFEQT results from the registry subset showed that women had significantly worse (lower) scores than men overall and for each of four AFEQT component scores tallied at both baseline and 1-year follow-up: symptoms, daily activity, treatment concern, and treatment satisfaction.
The ORBIT AF registry is sponsored by Janssen. Dr. Piccini said that he has financial relationships with Boston Scientific, GE Healthcare, Janssen, Johnson & Johnson, Medtronic, and Pfizer Bristol-Myers Squibb.
On Twitter @mitchelzoler
SAN FRANCISCO – Women with atrial fibrillation have significantly more debilitation than men with the disorder, but men with atrial fibrillation have double the cardiovascular death rate than their female counterparts, based on data collected from more than 10,000 U.S. patients.
During follow-up of the 5,842 men and 4,290 women with atrial fibrillation who were enrolled in the registry, women’s cumulative rate of cardiovascular death lagged 54% behind men’s, a statistically significant difference, Dr. Jonathan P. Piccini reported at the annual meeting of the American College of Cardiology.
The rate of all-cause death ran a relative 31% lower in women compared with men, but this difference seemed mostly due to the cardiovascular-death disparity because rates of noncardiovascular deaths in women and men with atrial fibrillation were virtually identical, said Dr. Piccini, an electrophysiology cardiologist at Duke University in Durham, N.C.
Despite this survival advantage, women with atrial fibrillation fare worse than men by several other measures. Women report worse symptoms, more functional impairment, and worse quality of life; they also spend significantly less time in their target anticoagulant range and they have a higher stroke risk than men, he reported.
"When we see women with atrial fibrillation, we should be aware that they are more likely to have worse symptoms and quality of life. Symptoms need to be treated; when a patient persists in having symptoms, treatment to control the symptoms is very important," he said in an interview. "We need to investigate the registry data to see why women have more symptoms and worse quality of life. This is the largest quality of life study ever done in atrial fibrillation."
Among the 10,132 patients enrolled in the registry, 1,339 participated in a substudy that serially measured quality of life using the Atrial Fibrillation Effect on Quality of Life (AFEQT) questionnaire (Circ. Arrhythm. Electrophysiol. 2011;4:15-25). "We have the power to look at the effects of different treatments so we can assess how changing treatment affects quality of life," Dr. Piccini said.
The Outcomes Registry for Better Informed Treatment of Atrial Fibrillation (ORBIT AF) enrolled both prevalent and new-onset atrial fibrillation patients at 184 diverse practice settings, including primary care, cardiology, and electrophysiology offices, between June 2010 and August 2011. The enrolled men were an average of 73 years old, while the women averaged 77 years of age.
Coronary disease was present in 39% of men and 23% of the women, but 17% of the women had a history of stroke or transient ischemic attack, compared with 14% of the men. Both sexes had a similar distribution of atrial fibrillation type, but women had clearly higher CHADS2 scores, a measure of stroke risk. The percentage of patients with a score of 0 or 1, the lowest-risk patients, was 33% among men and 23% among women.
Every symptom assessed was more common among women, led by the most frequent symptom, palpitations, which affected 40% of women and 27% of men. The next most common symptoms – exertional dyspnea, fatigue, and lightheadedness – were each several percentage points more common in women than men, all statistically significant differences.
Reassuringly, use of rate and rhythm-control treatments and oral anticoagulation were very similar among men and women, but women more frequently had a prolonged gap between their anticoagulation checkups, and their time spent within the target international normalized ratio of 2.0-3.0 was 65%, significantly below the 68% rate in men.
The rate of new heart failure during follow-up was the same in the men and women. Women had higher stroke risk based on their CHADS2 scores, but their stroke rate, while numerically greater than in men, was not significantly higher.
AFEQT results from the registry subset showed that women had significantly worse (lower) scores than men overall and for each of four AFEQT component scores tallied at both baseline and 1-year follow-up: symptoms, daily activity, treatment concern, and treatment satisfaction.
The ORBIT AF registry is sponsored by Janssen. Dr. Piccini said that he has financial relationships with Boston Scientific, GE Healthcare, Janssen, Johnson & Johnson, Medtronic, and Pfizer Bristol-Myers Squibb.
On Twitter @mitchelzoler
AT ACC 13
Major finding: Cardiovascular death in women with atrial fibrillation was 54% lower than affected men after adjustment for clinical differences.
Data source: ORBIT AF registry, which included 10,132 adults enrolled at 184 U.S. sites.
Disclosures: The ORBIT AF registry is sponsored by Janssen. Dr. Piccini said that he has financial relationships with Boston Scientific, GE Healthcare, Janssen, Johnson & Johnson, Medtronic, and Pfizer Bristol-Myers Squibb.

Can digoxin get another chance for heart failure?
One of the late-breaker reports at the American College of Cardiology’s annual meeting in March had results from a post hoc analysis of 16-year-old data from the DIG trial, by far the largest study to ever assess digoxin for heart failure, a treatment that precipitously dropped out of favor during the decade following the initial DIG report in 1997. Not your typical back story for a late breaker.
The researchers who ran the new analysis of the old DIG data also took what seem like two sizable leaps by framing their new look as a way to get a sense whether digoxin treatment could cut the large number of Medicare patients with heart failure who need rehospitalization within a month after a hospital discharge.

Dr. Ali Ahmed, a cardiologist from the University of Alabama, Birmingham, who presented this ACC late breaker, noted how clinicians and hospital officials are eager to find safe and effective treatments for cutting heart failure readmissions, especially since last Oct. 1 when the Centers for Medicare and Medicaid Services began penalizing hospitals that accumulate high heart failure readmission numbers.
One leap was that the patients in the 1990s enrolled in the Digitalis Investigation Group (DIG) trial all had chronic, stable heart failure, without recent hospitalization. Although the post hoc analysis that Dr. Ahmed presented showed that the half of the DIG patients who were aged 65 or older had their heart failure hospitalization rate cut by a third while on digoxin, compared with patients on placebo, a statistically significant difference for the analysis’ primary endpoint, Dr. Ahmed admitted in his talk that the relevance of his findings to the new Medicare penalties was doubly limited. First, because the DIG population comprised ambulatory patients rather than ones just out of the hospital, and second because the endpoint examined in DIG was index hospital admission rather than readmission. Two pretty important differences.
On top of that, many heart failure experts who heard the results were quick to question the meaning in 2013 of data collected from heart failure patients back in the mid-1990s whose background regimens completely lacked beta-blockers, aldosterone receptor antagonists (spironolactone and eplerenone), and implanted cardiac devices, treatments that have since become cornerstones of heart failure management.
Digoxin "is not a therapy we should embrace wholeheartedly until there is a new trial with contemporary management," commented Dr. Mariell L. Jessup, a heart failure specialist at the University of Pennsylvania, Philadelphia, who cochaired the late-breaker session in which Dr. Ahmed spoke.
But if it was so questionable to use 16-year old, clearly outdated data to address in a post hoc way an issue – 30-day hospital readmissions for heart failure – with at best tangential relevance to what was examined in the DIG trial, what else might be behind this curious report from a large group of prominent heart-failure specialists? (You can see all their names in the article published online simultaneous to Dr. Ahmed’s ACC report [Am. J. Med. 2013;126 (doi:10.1016/j.amjmed.2013.02.001)]).
The answer seems to be their desire to promote digoxin, keep it current in cardiology chatter, and build pressure for a new, prospective study that reexamines the incremental benefit of digoxin on top everything else that heart failure patients receive today. They see current heart failure management, especially efforts to cut hospitalizations for acute decompensation and also cut the rate at which decompensated patients wind up back in the hospital a second time, as woefully inadequate and stand discouraged after many new agents have failed to make a dent in this problem.
"Dismissing digoxin, which was approved by the FDA only 10 years ago and has been used for 2,000 years, in the face of a high event rate [among heart failure patients] when we cannot find any new drugs, is not a wise clinical decision," said Dr. Mihai Gheorghiade, a cardiologist with Northwestern University, Evanston, Ill., who coauthored the new analysis and is a leader of the movement to resurrect digoxin. Using digoxin "isn’t controversial if you see benefit from it and if we are desperate to find something for these patients," he said during a press conference at the meeting.
Efforts to rehabilitate and reevaluate digoxin in heart failure have been going on since the mid-2000s. Dr. Ahmed, Dr. Gheorghiade, and their associates published their first reanalysis of the DIG data in 2005 (Eur. Heart J. 2006;27:178-86), which was recognized by an editorialist at the time as a call to "rehabilitate" digoxin (Eur. Heart J. 2006;27:127-9). In 2006, Dr. Gheorghiade lamented digoxin’s neglect and fall from standard heart failure management, having been muscled out by treatments with big-pocket backers – beta-blockers, ACE inhibitors, and cardiac resynchronization devices; concerns over digoxin’s safety (which he says is obviated by using low dosages), and most of all the absence of any company with enough of a financial interest in digoxin to promote it and fund more studies (Circulation 2006;113:2556-64).
Houston heart failure expert Dr. Biykem Bozkurt saw the new DIG analysis as part of this decade-long rehabilitation effort. The new analysis "is a call for the reexamination of digoxin in acute heart failure," she said as an ACC panelist who discussed the study.
Digoxin’s proponents seem to recognize their big challenge: A large, new study of dioxin on top of today’s standard treatments is the key to convincing skeptical colleagues, but who will pay for it? "The problem with digoxin is that no company sponsors it," Dr. Gheorghiade said.
Twitter @mitchelzoler
One of the late-breaker reports at the American College of Cardiology’s annual meeting in March had results from a post hoc analysis of 16-year-old data from the DIG trial, by far the largest study to ever assess digoxin for heart failure, a treatment that precipitously dropped out of favor during the decade following the initial DIG report in 1997. Not your typical back story for a late breaker.
The researchers who ran the new analysis of the old DIG data also took what seem like two sizable leaps by framing their new look as a way to get a sense whether digoxin treatment could cut the large number of Medicare patients with heart failure who need rehospitalization within a month after a hospital discharge.
Dr. Ali Ahmed, a cardiologist from the University of Alabama, Birmingham, who presented this ACC late breaker, noted how clinicians and hospital officials are eager to find safe and effective treatments for cutting heart failure readmissions, especially since last Oct. 1 when the Centers for Medicare and Medicaid Services began penalizing hospitals that accumulate high heart failure readmission numbers.
One leap was that the patients in the 1990s enrolled in the Digitalis Investigation Group (DIG) trial all had chronic, stable heart failure, without recent hospitalization. Although the post hoc analysis that Dr. Ahmed presented showed that the half of the DIG patients who were aged 65 or older had their heart failure hospitalization rate cut by a third while on digoxin, compared with patients on placebo, a statistically significant difference for the analysis’ primary endpoint, Dr. Ahmed admitted in his talk that the relevance of his findings to the new Medicare penalties was doubly limited. First, because the DIG population comprised ambulatory patients rather than ones just out of the hospital, and second because the endpoint examined in DIG was index hospital admission rather than readmission. Two pretty important differences.
On top of that, many heart failure experts who heard the results were quick to question the meaning in 2013 of data collected from heart failure patients back in the mid-1990s whose background regimens completely lacked beta-blockers, aldosterone receptor antagonists (spironolactone and eplerenone), and implanted cardiac devices, treatments that have since become cornerstones of heart failure management.
Digoxin "is not a therapy we should embrace wholeheartedly until there is a new trial with contemporary management," commented Dr. Mariell L. Jessup, a heart failure specialist at the University of Pennsylvania, Philadelphia, who cochaired the late-breaker session in which Dr. Ahmed spoke.
But if it was so questionable to use 16-year old, clearly outdated data to address in a post hoc way an issue – 30-day hospital readmissions for heart failure – with at best tangential relevance to what was examined in the DIG trial, what else might be behind this curious report from a large group of prominent heart-failure specialists? (You can see all their names in the article published online simultaneous to Dr. Ahmed’s ACC report [Am. J. Med. 2013;126 (doi:10.1016/j.amjmed.2013.02.001)]).
The answer seems to be their desire to promote digoxin, keep it current in cardiology chatter, and build pressure for a new, prospective study that reexamines the incremental benefit of digoxin on top everything else that heart failure patients receive today. They see current heart failure management, especially efforts to cut hospitalizations for acute decompensation and also cut the rate at which decompensated patients wind up back in the hospital a second time, as woefully inadequate and stand discouraged after many new agents have failed to make a dent in this problem.
"Dismissing digoxin, which was approved by the FDA only 10 years ago and has been used for 2,000 years, in the face of a high event rate [among heart failure patients] when we cannot find any new drugs, is not a wise clinical decision," said Dr. Mihai Gheorghiade, a cardiologist with Northwestern University, Evanston, Ill., who coauthored the new analysis and is a leader of the movement to resurrect digoxin. Using digoxin "isn’t controversial if you see benefit from it and if we are desperate to find something for these patients," he said during a press conference at the meeting.
Efforts to rehabilitate and reevaluate digoxin in heart failure have been going on since the mid-2000s. Dr. Ahmed, Dr. Gheorghiade, and their associates published their first reanalysis of the DIG data in 2005 (Eur. Heart J. 2006;27:178-86), which was recognized by an editorialist at the time as a call to "rehabilitate" digoxin (Eur. Heart J. 2006;27:127-9). In 2006, Dr. Gheorghiade lamented digoxin’s neglect and fall from standard heart failure management, having been muscled out by treatments with big-pocket backers – beta-blockers, ACE inhibitors, and cardiac resynchronization devices; concerns over digoxin’s safety (which he says is obviated by using low dosages), and most of all the absence of any company with enough of a financial interest in digoxin to promote it and fund more studies (Circulation 2006;113:2556-64).
Houston heart failure expert Dr. Biykem Bozkurt saw the new DIG analysis as part of this decade-long rehabilitation effort. The new analysis "is a call for the reexamination of digoxin in acute heart failure," she said as an ACC panelist who discussed the study.
Digoxin’s proponents seem to recognize their big challenge: A large, new study of dioxin on top of today’s standard treatments is the key to convincing skeptical colleagues, but who will pay for it? "The problem with digoxin is that no company sponsors it," Dr. Gheorghiade said.
Twitter @mitchelzoler
One of the late-breaker reports at the American College of Cardiology’s annual meeting in March had results from a post hoc analysis of 16-year-old data from the DIG trial, by far the largest study to ever assess digoxin for heart failure, a treatment that precipitously dropped out of favor during the decade following the initial DIG report in 1997. Not your typical back story for a late breaker.
The researchers who ran the new analysis of the old DIG data also took what seem like two sizable leaps by framing their new look as a way to get a sense whether digoxin treatment could cut the large number of Medicare patients with heart failure who need rehospitalization within a month after a hospital discharge.
Dr. Ali Ahmed, a cardiologist from the University of Alabama, Birmingham, who presented this ACC late breaker, noted how clinicians and hospital officials are eager to find safe and effective treatments for cutting heart failure readmissions, especially since last Oct. 1 when the Centers for Medicare and Medicaid Services began penalizing hospitals that accumulate high heart failure readmission numbers.
One leap was that the patients in the 1990s enrolled in the Digitalis Investigation Group (DIG) trial all had chronic, stable heart failure, without recent hospitalization. Although the post hoc analysis that Dr. Ahmed presented showed that the half of the DIG patients who were aged 65 or older had their heart failure hospitalization rate cut by a third while on digoxin, compared with patients on placebo, a statistically significant difference for the analysis’ primary endpoint, Dr. Ahmed admitted in his talk that the relevance of his findings to the new Medicare penalties was doubly limited. First, because the DIG population comprised ambulatory patients rather than ones just out of the hospital, and second because the endpoint examined in DIG was index hospital admission rather than readmission. Two pretty important differences.
On top of that, many heart failure experts who heard the results were quick to question the meaning in 2013 of data collected from heart failure patients back in the mid-1990s whose background regimens completely lacked beta-blockers, aldosterone receptor antagonists (spironolactone and eplerenone), and implanted cardiac devices, treatments that have since become cornerstones of heart failure management.
Digoxin "is not a therapy we should embrace wholeheartedly until there is a new trial with contemporary management," commented Dr. Mariell L. Jessup, a heart failure specialist at the University of Pennsylvania, Philadelphia, who cochaired the late-breaker session in which Dr. Ahmed spoke.
But if it was so questionable to use 16-year old, clearly outdated data to address in a post hoc way an issue – 30-day hospital readmissions for heart failure – with at best tangential relevance to what was examined in the DIG trial, what else might be behind this curious report from a large group of prominent heart-failure specialists? (You can see all their names in the article published online simultaneous to Dr. Ahmed’s ACC report [Am. J. Med. 2013;126 (doi:10.1016/j.amjmed.2013.02.001)]).
The answer seems to be their desire to promote digoxin, keep it current in cardiology chatter, and build pressure for a new, prospective study that reexamines the incremental benefit of digoxin on top everything else that heart failure patients receive today. They see current heart failure management, especially efforts to cut hospitalizations for acute decompensation and also cut the rate at which decompensated patients wind up back in the hospital a second time, as woefully inadequate and stand discouraged after many new agents have failed to make a dent in this problem.
"Dismissing digoxin, which was approved by the FDA only 10 years ago and has been used for 2,000 years, in the face of a high event rate [among heart failure patients] when we cannot find any new drugs, is not a wise clinical decision," said Dr. Mihai Gheorghiade, a cardiologist with Northwestern University, Evanston, Ill., who coauthored the new analysis and is a leader of the movement to resurrect digoxin. Using digoxin "isn’t controversial if you see benefit from it and if we are desperate to find something for these patients," he said during a press conference at the meeting.
Efforts to rehabilitate and reevaluate digoxin in heart failure have been going on since the mid-2000s. Dr. Ahmed, Dr. Gheorghiade, and their associates published their first reanalysis of the DIG data in 2005 (Eur. Heart J. 2006;27:178-86), which was recognized by an editorialist at the time as a call to "rehabilitate" digoxin (Eur. Heart J. 2006;27:127-9). In 2006, Dr. Gheorghiade lamented digoxin’s neglect and fall from standard heart failure management, having been muscled out by treatments with big-pocket backers – beta-blockers, ACE inhibitors, and cardiac resynchronization devices; concerns over digoxin’s safety (which he says is obviated by using low dosages), and most of all the absence of any company with enough of a financial interest in digoxin to promote it and fund more studies (Circulation 2006;113:2556-64).
Houston heart failure expert Dr. Biykem Bozkurt saw the new DIG analysis as part of this decade-long rehabilitation effort. The new analysis "is a call for the reexamination of digoxin in acute heart failure," she said as an ACC panelist who discussed the study.
Digoxin’s proponents seem to recognize their big challenge: A large, new study of dioxin on top of today’s standard treatments is the key to convincing skeptical colleagues, but who will pay for it? "The problem with digoxin is that no company sponsors it," Dr. Gheorghiade said.
Twitter @mitchelzoler

U.S. post-PCI cardiac rehabilitation referrals lag
SAN FRANCISCO – U.S. patients are not getting referred to cardiac rehabilitation programs following percutaneous coronary interventions, despite clear guidelines calling for it.
A review of more than 1.4 million Americans who underwent percutaneous coronary intervention at more than 1,300 U.S. hospitals during 2009-2011 showed that 59% received cardiac rehabilitation referral, a rate that lagged far behind several other post-PCI interventions, Dr. Krishna G. Aragam and his associates reported in a poster at the annual meeting of the American College of Cardiology.
"Rates of cardiac rehabilitation referral are well below those of other acute myocardial infarction quality-of-care measures with little change over the past 3 years," said Dr. Aragam, a cardiologist at the University of Pennsylvania, Philadelphia, and his associates.
Analysis of data collected in the CathPCI Registry of the National Cardiovascular Data Registry of the ACC also showed "considerable" interhospital variation in the rates of rehabilitation referral, with a majority of hospitals having rates that either ran greater than 80% or less than 20%.
A relatively low rate of rehabilitation referral reflects inferior patient care based on the endorsements that rehabilitation programs have received for post-PCI patients. The most recent PCI guidelines of the ACC and other professional societies rate cardiac rehabilitation following PCI a class 1A recommendation, saying that cardiac rehabilitation "should be recommended to patients after PCI." (Circulation 2011:124:2574-609). And last year the Centers for Medicare and Medicaid Services announced that starting in 2014 it would make referral to cardiac rehabilitation for patients following PCI or a myocardial infarction a hospital-performance measure.
If the numbers collected following PCIs as recently as 2011 are a guide, many hospitals will need to act quickly to make rehabilitation referral routine.
Data from 1,432,399 PCIs done at 1,310 U.S. hospitals during the 3 years starting in 2009 showed that discharge referrals to a cardiac rehabilitation program occurred for about 57% of PCI patients in 2009, which upticked to 61% in 2011. The analysis excluded patients who died while hospitalized, and those discharged to a nursing home, acute-care hospital, or hospice.
In contrast, data reported by Dr. Aragam and his associates showed that the next-lowest level of compliance with post-PCI recommendations was discharge prescription of an ACE inhibitor or angiotensin-receptor blocker in patients with a left-ventricular ejection fraction of less than 40%, which happened for about 80% of patients. At discharge, 95% of patients received an aspirin prescription, 90% received a statin prescription, and 85% were prescribed a beta-blocker.
The analysis also identified several factors that significantly linked with either an increased or decreased likelihood of referral to cardiac rehabilitation. Factors linked with rehab being less likely included older age, diabetes, peripheral artery disease, or prior revascularization. Factors that boosted the likelihood that patients received a rehabilitation referral included having an ST elevation MI, which boosted the referral rate by 66% compared with other PCI patients, and having a non-ST elevation MI, which raised the referral rate by 38%.
Dr. Aragam said that he had no disclosures.
SAN FRANCISCO – U.S. patients are not getting referred to cardiac rehabilitation programs following percutaneous coronary interventions, despite clear guidelines calling for it.
A review of more than 1.4 million Americans who underwent percutaneous coronary intervention at more than 1,300 U.S. hospitals during 2009-2011 showed that 59% received cardiac rehabilitation referral, a rate that lagged far behind several other post-PCI interventions, Dr. Krishna G. Aragam and his associates reported in a poster at the annual meeting of the American College of Cardiology.
"Rates of cardiac rehabilitation referral are well below those of other acute myocardial infarction quality-of-care measures with little change over the past 3 years," said Dr. Aragam, a cardiologist at the University of Pennsylvania, Philadelphia, and his associates.
Analysis of data collected in the CathPCI Registry of the National Cardiovascular Data Registry of the ACC also showed "considerable" interhospital variation in the rates of rehabilitation referral, with a majority of hospitals having rates that either ran greater than 80% or less than 20%.
A relatively low rate of rehabilitation referral reflects inferior patient care based on the endorsements that rehabilitation programs have received for post-PCI patients. The most recent PCI guidelines of the ACC and other professional societies rate cardiac rehabilitation following PCI a class 1A recommendation, saying that cardiac rehabilitation "should be recommended to patients after PCI." (Circulation 2011:124:2574-609). And last year the Centers for Medicare and Medicaid Services announced that starting in 2014 it would make referral to cardiac rehabilitation for patients following PCI or a myocardial infarction a hospital-performance measure.
If the numbers collected following PCIs as recently as 2011 are a guide, many hospitals will need to act quickly to make rehabilitation referral routine.
Data from 1,432,399 PCIs done at 1,310 U.S. hospitals during the 3 years starting in 2009 showed that discharge referrals to a cardiac rehabilitation program occurred for about 57% of PCI patients in 2009, which upticked to 61% in 2011. The analysis excluded patients who died while hospitalized, and those discharged to a nursing home, acute-care hospital, or hospice.
In contrast, data reported by Dr. Aragam and his associates showed that the next-lowest level of compliance with post-PCI recommendations was discharge prescription of an ACE inhibitor or angiotensin-receptor blocker in patients with a left-ventricular ejection fraction of less than 40%, which happened for about 80% of patients. At discharge, 95% of patients received an aspirin prescription, 90% received a statin prescription, and 85% were prescribed a beta-blocker.
The analysis also identified several factors that significantly linked with either an increased or decreased likelihood of referral to cardiac rehabilitation. Factors linked with rehab being less likely included older age, diabetes, peripheral artery disease, or prior revascularization. Factors that boosted the likelihood that patients received a rehabilitation referral included having an ST elevation MI, which boosted the referral rate by 66% compared with other PCI patients, and having a non-ST elevation MI, which raised the referral rate by 38%.
Dr. Aragam said that he had no disclosures.
SAN FRANCISCO – U.S. patients are not getting referred to cardiac rehabilitation programs following percutaneous coronary interventions, despite clear guidelines calling for it.
A review of more than 1.4 million Americans who underwent percutaneous coronary intervention at more than 1,300 U.S. hospitals during 2009-2011 showed that 59% received cardiac rehabilitation referral, a rate that lagged far behind several other post-PCI interventions, Dr. Krishna G. Aragam and his associates reported in a poster at the annual meeting of the American College of Cardiology.
"Rates of cardiac rehabilitation referral are well below those of other acute myocardial infarction quality-of-care measures with little change over the past 3 years," said Dr. Aragam, a cardiologist at the University of Pennsylvania, Philadelphia, and his associates.
Analysis of data collected in the CathPCI Registry of the National Cardiovascular Data Registry of the ACC also showed "considerable" interhospital variation in the rates of rehabilitation referral, with a majority of hospitals having rates that either ran greater than 80% or less than 20%.
A relatively low rate of rehabilitation referral reflects inferior patient care based on the endorsements that rehabilitation programs have received for post-PCI patients. The most recent PCI guidelines of the ACC and other professional societies rate cardiac rehabilitation following PCI a class 1A recommendation, saying that cardiac rehabilitation "should be recommended to patients after PCI." (Circulation 2011:124:2574-609). And last year the Centers for Medicare and Medicaid Services announced that starting in 2014 it would make referral to cardiac rehabilitation for patients following PCI or a myocardial infarction a hospital-performance measure.
If the numbers collected following PCIs as recently as 2011 are a guide, many hospitals will need to act quickly to make rehabilitation referral routine.
Data from 1,432,399 PCIs done at 1,310 U.S. hospitals during the 3 years starting in 2009 showed that discharge referrals to a cardiac rehabilitation program occurred for about 57% of PCI patients in 2009, which upticked to 61% in 2011. The analysis excluded patients who died while hospitalized, and those discharged to a nursing home, acute-care hospital, or hospice.
In contrast, data reported by Dr. Aragam and his associates showed that the next-lowest level of compliance with post-PCI recommendations was discharge prescription of an ACE inhibitor or angiotensin-receptor blocker in patients with a left-ventricular ejection fraction of less than 40%, which happened for about 80% of patients. At discharge, 95% of patients received an aspirin prescription, 90% received a statin prescription, and 85% were prescribed a beta-blocker.
The analysis also identified several factors that significantly linked with either an increased or decreased likelihood of referral to cardiac rehabilitation. Factors linked with rehab being less likely included older age, diabetes, peripheral artery disease, or prior revascularization. Factors that boosted the likelihood that patients received a rehabilitation referral included having an ST elevation MI, which boosted the referral rate by 66% compared with other PCI patients, and having a non-ST elevation MI, which raised the referral rate by 38%.
Dr. Aragam said that he had no disclosures.
AT ACC 13
Major finding: During 2009-2011, 59% of all U.S. PCI patients received a discharge referral to cardiac rehabilitation.
Data source: More than 1.4 million U.S. PCI patients during 2009-2011 enrolled in the CathPCI Registry of the National Cardiovascular data Registry of the American College of Cardiology.
Disclosures: Dr. Aragam said that he had no disclosures.
BNP screening effectively targets heart failure prevention
SAN FRANCISCO – Targeting a comprehensive cardiac-risk reduction program to adults with elevated natriuretic peptide significantly cut the rate of new left ventricular dysfunction, heart failure, and other cardiovascular events in a randomized trial with more than 1,300 patients.
"I think it was the structure of the intervention, the cohesion of care, rather than a specific intervention" that improved clinical outcomes, Dr. Kenneth M. McDonald said at the annual meeting of the American College of Cardiology. "Undoubtedly, a patient’s knowledge [of a high B-type natriuretic peptide level] improved their adherence to therapy." He and his associates ran the study at 39 primary care practices around Dublin that worked in collaboration with the cardiology department at St. Vincent’s University Hospital in Dublin.

The primary care physicians looked for patients at least 40 years old with at least one identified cardiovascular risk factor whose B-type natriuretic peptide (BNP) level rose above 50 pg/mL on an annual screening test. They referred these patients to St. Vincent’s for an intensified testing and management program similar to "the disease management structure we’ve used for several years for patients with heart failure," said Dr. McDonald, a professor of cardiology at St. Vincent’s and director of the heart failure unit. The program included a cardiology review and regular follow-up, echocardiography with Doppler and other cardiovascular investigations as needed, and nurse coaching.
"Routine BNP screening is not recommended in current guidelines. Perhaps this finding is the first step to get guidelines committees to address the use of BNP for screening," commented Dr. Sanjay Kaul, director of the vascular physiology and thrombosis research laboratory at the Burns and Allen Research Institute at Cedars Sinai Medical Center in Los Angeles.
Among the 1,374 patients enrolled in the STOP-HF (Screening to Prevent Heart Failure) trial, annual BNP measurement found 498 (36%) with a BNP level that rose above 50 pg/mL in at least one annual test. This included 235 patients randomized to the control arm and 263 randomized to the intervention group. The overall age of patients in the study averaged 65 years, but the age of those with elevated BNP averaged closer to 70 years.
During average follow-up of just over 4 years, patients referred to the cardiology program had 25 cases (10%) of heart failure or asymptomatic left ventricular dysfunction, compared with 44 cases (19%) in the control arm, a 54% odds ratio reduction that was statistically significant for the study’s primary endpoint. For the entire study group of 1,374 randomized patients, participation in the group eligible for referred care cut the primary endpoint by a relative 41%, compared with the controls, a statistically significant difference.

A secondary efficacy analysis that tallied the combined rate of incident heart failure, arrhythmia, myocardial infarction, unstable angina, cerebrovascular events, peripheral thrombosis, or pulmonary embolism found 51 events (7%) in the entire intervention group compared with 71 events (10%) in the control group, a 46% odds rate reduction that was statistically significant.
A study limitation was the large percentage of patients in both arms either lost to follow-up, 10%; or who withdrew their consent to participate, another 16%. "It challenges interpretation of the results," commented Dr. Kaul.
But Dr. McDonald and his associates were convinced by their findings.
"We believe the results are conclusive enough to roll this out as a clinical program," he said in an interview. "We are now extending this to another region of Ireland, and we will try to get this disseminated nationally."
He also foresees additional refinements to the program, possibly identifying other risk markers that can compliment BNP and further focus intervention.
"We have shown benefit, but a question is the cost of getting that benefit. BNP is clearly a step up from where we were, but that doesn’t mean we are as good as we could make it."
Dr. McDonald said that he had no disclosures.
On Twitter @mitchelzoler
SAN FRANCISCO – Targeting a comprehensive cardiac-risk reduction program to adults with elevated natriuretic peptide significantly cut the rate of new left ventricular dysfunction, heart failure, and other cardiovascular events in a randomized trial with more than 1,300 patients.
"I think it was the structure of the intervention, the cohesion of care, rather than a specific intervention" that improved clinical outcomes, Dr. Kenneth M. McDonald said at the annual meeting of the American College of Cardiology. "Undoubtedly, a patient’s knowledge [of a high B-type natriuretic peptide level] improved their adherence to therapy." He and his associates ran the study at 39 primary care practices around Dublin that worked in collaboration with the cardiology department at St. Vincent’s University Hospital in Dublin.
The primary care physicians looked for patients at least 40 years old with at least one identified cardiovascular risk factor whose B-type natriuretic peptide (BNP) level rose above 50 pg/mL on an annual screening test. They referred these patients to St. Vincent’s for an intensified testing and management program similar to "the disease management structure we’ve used for several years for patients with heart failure," said Dr. McDonald, a professor of cardiology at St. Vincent’s and director of the heart failure unit. The program included a cardiology review and regular follow-up, echocardiography with Doppler and other cardiovascular investigations as needed, and nurse coaching.
"Routine BNP screening is not recommended in current guidelines. Perhaps this finding is the first step to get guidelines committees to address the use of BNP for screening," commented Dr. Sanjay Kaul, director of the vascular physiology and thrombosis research laboratory at the Burns and Allen Research Institute at Cedars Sinai Medical Center in Los Angeles.
Among the 1,374 patients enrolled in the STOP-HF (Screening to Prevent Heart Failure) trial, annual BNP measurement found 498 (36%) with a BNP level that rose above 50 pg/mL in at least one annual test. This included 235 patients randomized to the control arm and 263 randomized to the intervention group. The overall age of patients in the study averaged 65 years, but the age of those with elevated BNP averaged closer to 70 years.
During average follow-up of just over 4 years, patients referred to the cardiology program had 25 cases (10%) of heart failure or asymptomatic left ventricular dysfunction, compared with 44 cases (19%) in the control arm, a 54% odds ratio reduction that was statistically significant for the study’s primary endpoint. For the entire study group of 1,374 randomized patients, participation in the group eligible for referred care cut the primary endpoint by a relative 41%, compared with the controls, a statistically significant difference.
A secondary efficacy analysis that tallied the combined rate of incident heart failure, arrhythmia, myocardial infarction, unstable angina, cerebrovascular events, peripheral thrombosis, or pulmonary embolism found 51 events (7%) in the entire intervention group compared with 71 events (10%) in the control group, a 46% odds rate reduction that was statistically significant.
A study limitation was the large percentage of patients in both arms either lost to follow-up, 10%; or who withdrew their consent to participate, another 16%. "It challenges interpretation of the results," commented Dr. Kaul.
But Dr. McDonald and his associates were convinced by their findings.
"We believe the results are conclusive enough to roll this out as a clinical program," he said in an interview. "We are now extending this to another region of Ireland, and we will try to get this disseminated nationally."
He also foresees additional refinements to the program, possibly identifying other risk markers that can compliment BNP and further focus intervention.
"We have shown benefit, but a question is the cost of getting that benefit. BNP is clearly a step up from where we were, but that doesn’t mean we are as good as we could make it."
Dr. McDonald said that he had no disclosures.
On Twitter @mitchelzoler
SAN FRANCISCO – Targeting a comprehensive cardiac-risk reduction program to adults with elevated natriuretic peptide significantly cut the rate of new left ventricular dysfunction, heart failure, and other cardiovascular events in a randomized trial with more than 1,300 patients.
"I think it was the structure of the intervention, the cohesion of care, rather than a specific intervention" that improved clinical outcomes, Dr. Kenneth M. McDonald said at the annual meeting of the American College of Cardiology. "Undoubtedly, a patient’s knowledge [of a high B-type natriuretic peptide level] improved their adherence to therapy." He and his associates ran the study at 39 primary care practices around Dublin that worked in collaboration with the cardiology department at St. Vincent’s University Hospital in Dublin.
The primary care physicians looked for patients at least 40 years old with at least one identified cardiovascular risk factor whose B-type natriuretic peptide (BNP) level rose above 50 pg/mL on an annual screening test. They referred these patients to St. Vincent’s for an intensified testing and management program similar to "the disease management structure we’ve used for several years for patients with heart failure," said Dr. McDonald, a professor of cardiology at St. Vincent’s and director of the heart failure unit. The program included a cardiology review and regular follow-up, echocardiography with Doppler and other cardiovascular investigations as needed, and nurse coaching.
"Routine BNP screening is not recommended in current guidelines. Perhaps this finding is the first step to get guidelines committees to address the use of BNP for screening," commented Dr. Sanjay Kaul, director of the vascular physiology and thrombosis research laboratory at the Burns and Allen Research Institute at Cedars Sinai Medical Center in Los Angeles.
Among the 1,374 patients enrolled in the STOP-HF (Screening to Prevent Heart Failure) trial, annual BNP measurement found 498 (36%) with a BNP level that rose above 50 pg/mL in at least one annual test. This included 235 patients randomized to the control arm and 263 randomized to the intervention group. The overall age of patients in the study averaged 65 years, but the age of those with elevated BNP averaged closer to 70 years.
During average follow-up of just over 4 years, patients referred to the cardiology program had 25 cases (10%) of heart failure or asymptomatic left ventricular dysfunction, compared with 44 cases (19%) in the control arm, a 54% odds ratio reduction that was statistically significant for the study’s primary endpoint. For the entire study group of 1,374 randomized patients, participation in the group eligible for referred care cut the primary endpoint by a relative 41%, compared with the controls, a statistically significant difference.
A secondary efficacy analysis that tallied the combined rate of incident heart failure, arrhythmia, myocardial infarction, unstable angina, cerebrovascular events, peripheral thrombosis, or pulmonary embolism found 51 events (7%) in the entire intervention group compared with 71 events (10%) in the control group, a 46% odds rate reduction that was statistically significant.
A study limitation was the large percentage of patients in both arms either lost to follow-up, 10%; or who withdrew their consent to participate, another 16%. "It challenges interpretation of the results," commented Dr. Kaul.
But Dr. McDonald and his associates were convinced by their findings.
"We believe the results are conclusive enough to roll this out as a clinical program," he said in an interview. "We are now extending this to another region of Ireland, and we will try to get this disseminated nationally."
He also foresees additional refinements to the program, possibly identifying other risk markers that can compliment BNP and further focus intervention.
"We have shown benefit, but a question is the cost of getting that benefit. BNP is clearly a step up from where we were, but that doesn’t mean we are as good as we could make it."
Dr. McDonald said that he had no disclosures.
On Twitter @mitchelzoler
AT ACC 13
Major finding: BNP-driven referral to intensive preventive care cut heart failures and left ventricular dysfunctions 54%, compared with standard care.
Data source: The STOP-HF trial, which randomized 1,374 adults in 39 primary-care practices around Dublin, Ireland.
Disclosures: Dr. McDonald said that he had no disclosures.
One-year outcomes support emergency department CCTA
SAN FRANCISCO – Coronary CT angiography works better than traditional rule-out approaches for identifying emergency department patients with chest pain who are free of significant coronary disease, according to 1-year results from a randomized comparison of more than 1,300 patients.
The results also show that relying on coronary CT angiography (CCTA) for emergency department assessment of coronary disease is safe, with a 1-year rate of death or myocardial infarction substantially below 1% in patients judged negative for coronary disease by CCTA, Dr. Judd E. Hollander said at the annual meeting of the American College of Cardiology.

The findings confirmed and extended the 30-day results reported a year ago from the same study, the American College of Radiology Imaging Network (ACRIN) PA 4005 study, which randomized 1,370 low- to intermediate-risk patients who presented with chest pain and possible acute coronary syndrome at any of five U.S. emergency departments.
Two-thirds of the patients were randomized to assessment that included CCTA when deemed necessary, while the remaining third underwent more traditional assessment that could include an exercise treadmill test, a stress test with imaging, and stress echocardiography.
While the results supported a role for routine use of CCTA for assessing the types of patients enrolled in the study, Dr. Hollander stressed that a CCTA is not needed for every ED patient with questionable chest pain.
"We try to use this as an exclusionary test for patients who need an exclusionary test," said Dr. Hollander, professor and clinical research director in the department of emergency medicine at the University of Pennsylvania in Philadelphia.
"We want to avoid making this like a d-dimer test [for thrombus] or CT perfusion [for stroke patients], where everyone who comes into the ED with appropriate signs and symptoms gets one. We don’t use CCTA on patients we normally discharge. There is the risk from radiation. You need to ask how much do you need to find out what is going on with the patient sooner rather than later," he said.
During year-long follow-up on 1,368 of the starting ACRIN patients (one patient was lost to follow-up from each randomization group), one cardiac death and one myocardial infarction occurred among the 825 patients randomized to the CCTA arm and declared free of coronary disease, a 0.2% rate that fell within the study’s prespecified safety criterion of less than 1%.
CCTA’s 1-year safety came without any boost in resource use compared with ED chest-pain patients assessed by conventional means. Overall use of cardiac testing, hospital readmissions, revascularization, and ED visits was similar during 1-year follow-up in the two treatment arms, Dr. Hollander said. Further breakdown of the resource-use data showed that the majority of medical activity following the index hospitalization occurred in the 9% of the initial patients identified with coronary disease by CCTA. Fewer resources were used in patients who had questionable coronary disease following CCTA, and the least amount of resource use occurred in patients without coronary disease by CCTA.
Because CCTA categorized 9% of patients in that study arm as having coronary disease compared with 3% of the control group, and since 77% of patients in the CCTA arm were judged free of coronary disease compared with 61% in the control arm, CCTA "shifts resources to where they are most useful, with more coronary artery disease identified and treated and more patients without disease not receiving treatment," Dr. Hollander said.
The initial, 30-day ACRIN report said that 50% of patients managed in the CCTA arm were discharged early from the ED, compared with 23% of the control group (N. Engl. J. Med. 2012;366:1393-403). Patients in the CCTA group also had a substantially shorter average length of stay during their initial hospital visit.
The ACRIN PA 4005 study was sponsored by the Pennsylvania Department of Health and the ACRIN Foundation. Dr. Hollander said that he has also been a consultant to Behring, Janssen, Luitpold, and Radiometer, and that he has received research funding from Abbott, Alere, Brahms, and Siemens.
On Twitter @mitchelzoler
SAN FRANCISCO – Coronary CT angiography works better than traditional rule-out approaches for identifying emergency department patients with chest pain who are free of significant coronary disease, according to 1-year results from a randomized comparison of more than 1,300 patients.
The results also show that relying on coronary CT angiography (CCTA) for emergency department assessment of coronary disease is safe, with a 1-year rate of death or myocardial infarction substantially below 1% in patients judged negative for coronary disease by CCTA, Dr. Judd E. Hollander said at the annual meeting of the American College of Cardiology.
The findings confirmed and extended the 30-day results reported a year ago from the same study, the American College of Radiology Imaging Network (ACRIN) PA 4005 study, which randomized 1,370 low- to intermediate-risk patients who presented with chest pain and possible acute coronary syndrome at any of five U.S. emergency departments.
Two-thirds of the patients were randomized to assessment that included CCTA when deemed necessary, while the remaining third underwent more traditional assessment that could include an exercise treadmill test, a stress test with imaging, and stress echocardiography.
While the results supported a role for routine use of CCTA for assessing the types of patients enrolled in the study, Dr. Hollander stressed that a CCTA is not needed for every ED patient with questionable chest pain.
"We try to use this as an exclusionary test for patients who need an exclusionary test," said Dr. Hollander, professor and clinical research director in the department of emergency medicine at the University of Pennsylvania in Philadelphia.
"We want to avoid making this like a d-dimer test [for thrombus] or CT perfusion [for stroke patients], where everyone who comes into the ED with appropriate signs and symptoms gets one. We don’t use CCTA on patients we normally discharge. There is the risk from radiation. You need to ask how much do you need to find out what is going on with the patient sooner rather than later," he said.
During year-long follow-up on 1,368 of the starting ACRIN patients (one patient was lost to follow-up from each randomization group), one cardiac death and one myocardial infarction occurred among the 825 patients randomized to the CCTA arm and declared free of coronary disease, a 0.2% rate that fell within the study’s prespecified safety criterion of less than 1%.
CCTA’s 1-year safety came without any boost in resource use compared with ED chest-pain patients assessed by conventional means. Overall use of cardiac testing, hospital readmissions, revascularization, and ED visits was similar during 1-year follow-up in the two treatment arms, Dr. Hollander said. Further breakdown of the resource-use data showed that the majority of medical activity following the index hospitalization occurred in the 9% of the initial patients identified with coronary disease by CCTA. Fewer resources were used in patients who had questionable coronary disease following CCTA, and the least amount of resource use occurred in patients without coronary disease by CCTA.
Because CCTA categorized 9% of patients in that study arm as having coronary disease compared with 3% of the control group, and since 77% of patients in the CCTA arm were judged free of coronary disease compared with 61% in the control arm, CCTA "shifts resources to where they are most useful, with more coronary artery disease identified and treated and more patients without disease not receiving treatment," Dr. Hollander said.
The initial, 30-day ACRIN report said that 50% of patients managed in the CCTA arm were discharged early from the ED, compared with 23% of the control group (N. Engl. J. Med. 2012;366:1393-403). Patients in the CCTA group also had a substantially shorter average length of stay during their initial hospital visit.
The ACRIN PA 4005 study was sponsored by the Pennsylvania Department of Health and the ACRIN Foundation. Dr. Hollander said that he has also been a consultant to Behring, Janssen, Luitpold, and Radiometer, and that he has received research funding from Abbott, Alere, Brahms, and Siemens.
On Twitter @mitchelzoler
SAN FRANCISCO – Coronary CT angiography works better than traditional rule-out approaches for identifying emergency department patients with chest pain who are free of significant coronary disease, according to 1-year results from a randomized comparison of more than 1,300 patients.
The results also show that relying on coronary CT angiography (CCTA) for emergency department assessment of coronary disease is safe, with a 1-year rate of death or myocardial infarction substantially below 1% in patients judged negative for coronary disease by CCTA, Dr. Judd E. Hollander said at the annual meeting of the American College of Cardiology.
The findings confirmed and extended the 30-day results reported a year ago from the same study, the American College of Radiology Imaging Network (ACRIN) PA 4005 study, which randomized 1,370 low- to intermediate-risk patients who presented with chest pain and possible acute coronary syndrome at any of five U.S. emergency departments.
Two-thirds of the patients were randomized to assessment that included CCTA when deemed necessary, while the remaining third underwent more traditional assessment that could include an exercise treadmill test, a stress test with imaging, and stress echocardiography.
While the results supported a role for routine use of CCTA for assessing the types of patients enrolled in the study, Dr. Hollander stressed that a CCTA is not needed for every ED patient with questionable chest pain.
"We try to use this as an exclusionary test for patients who need an exclusionary test," said Dr. Hollander, professor and clinical research director in the department of emergency medicine at the University of Pennsylvania in Philadelphia.
"We want to avoid making this like a d-dimer test [for thrombus] or CT perfusion [for stroke patients], where everyone who comes into the ED with appropriate signs and symptoms gets one. We don’t use CCTA on patients we normally discharge. There is the risk from radiation. You need to ask how much do you need to find out what is going on with the patient sooner rather than later," he said.
During year-long follow-up on 1,368 of the starting ACRIN patients (one patient was lost to follow-up from each randomization group), one cardiac death and one myocardial infarction occurred among the 825 patients randomized to the CCTA arm and declared free of coronary disease, a 0.2% rate that fell within the study’s prespecified safety criterion of less than 1%.
CCTA’s 1-year safety came without any boost in resource use compared with ED chest-pain patients assessed by conventional means. Overall use of cardiac testing, hospital readmissions, revascularization, and ED visits was similar during 1-year follow-up in the two treatment arms, Dr. Hollander said. Further breakdown of the resource-use data showed that the majority of medical activity following the index hospitalization occurred in the 9% of the initial patients identified with coronary disease by CCTA. Fewer resources were used in patients who had questionable coronary disease following CCTA, and the least amount of resource use occurred in patients without coronary disease by CCTA.
Because CCTA categorized 9% of patients in that study arm as having coronary disease compared with 3% of the control group, and since 77% of patients in the CCTA arm were judged free of coronary disease compared with 61% in the control arm, CCTA "shifts resources to where they are most useful, with more coronary artery disease identified and treated and more patients without disease not receiving treatment," Dr. Hollander said.
The initial, 30-day ACRIN report said that 50% of patients managed in the CCTA arm were discharged early from the ED, compared with 23% of the control group (N. Engl. J. Med. 2012;366:1393-403). Patients in the CCTA group also had a substantially shorter average length of stay during their initial hospital visit.
The ACRIN PA 4005 study was sponsored by the Pennsylvania Department of Health and the ACRIN Foundation. Dr. Hollander said that he has also been a consultant to Behring, Janssen, Luitpold, and Radiometer, and that he has received research funding from Abbott, Alere, Brahms, and Siemens.
On Twitter @mitchelzoler
AT ACC 13
Major finding: Patients negative for coronary disease by CT angiography had a 0.2% rate of cardiac death or myocardial infarction at 1-year follow-up.
Data source: The ACRIN PA 4005 study, which followed 1,368 chest-pain patients for 1 year after randomization to coronary CT angiography or conventional emergency department assessment.
Disclosures: The ACRIN PA 4005 study was sponsored by the Pennsylvania Department of Health and the ACRIN Foundation. Dr. Hollander said that he has also been a consultant to Behring, Janssen, Luitpold, and Radiometer, and that he has received research funding from Abbott, Alere, Brahms, and Siemens.
