User login
Mitchel is a reporter for MDedge based in the Philadelphia area. He started with the company in 1992, when it was International Medical News Group (IMNG), and has since covered a range of medical specialties. Mitchel trained as a virologist at Roswell Park Memorial Institute in Buffalo, and then worked briefly as a researcher at Boston Children's Hospital before pivoting to journalism as a AAAS Mass Media Fellow in 1980. His first reporting job was with Science Digest magazine, and from the mid-1980s to early-1990s he was a reporter with Medical World News. @mitchelzoler
Intratumor heterogeneity drives need for multiple biopsies
BRUSSELS – When biopsying a primary breast cancer, once is probably not enough based on accumulating evidence of primary-tumor heterogeneity, but despite this evidence, taking multiple biopsies has not yet become routine practice.
"Intra-tumor heterogeneity is one of the causes of variation during genetic profiling" of tumors, Dr. Jorge S. Reis-Fiho said. "Taking multiple biopsies from a primary tumor and putting them all together may mitigate the effect of intra-tumor heterogeneity," but taking multiple biopsies has not yet become standard of care, he said at the conference, which was sponsored by the European Society for Medical Oncology.

"I think we should start to seriously consider taking more than one biopsy. Quite a few places already do it, and our radiologists will routinely take two or three biopsies," said Dr. Fiho, a surgical pathologist at Memorial Sloan-Kettering Cancer Center in New York. "With only a single, small biopsy of the primary tumor we may not have sufficient information to predict what the metastasis will respond to," he said in an interview.
Results from two studies reported at the meeting added to the evidence favoring multiple biopsies as a way to more precisely characterize primary tumors and target the best therapy.
In one study, Dr. Michal Jarzab and his associates took three core biopsies from the primary tumors of 26 patients and assessed them genetically for estrogen receptor, progesterone receptor, and HER2-receptor mutations. Their sample included some patients with early-stage disease and others with advanced-stage cancer. The results of the three individual biopsy tests showed significant heterogeneity in seven of the 26 tumors (27%), reported Dr. Jarzab, a researcher at the Maria Sklodowska-Curie Cancer Center and Institute of Oncology in Gliwice, Poland.
The intratumor heterogeneity in these seven patients "could negatively impact genomic assessment if done with one specimen," he said.
"If other studies report similar results" on intratumor heterogeneity, "then it could become common practice to evaluate prognostic or predictive breast cancer markers from more than one primary tumour area," Dr. Angelo Di Leo, chairman of oncology at Prato (Italy) Hospital, said in a written statement.
The second study looked at the impact of assessing one, two, or three biopsies on the variance in results from four different single- or multiple-genetic tests in biopsies collected from 51 breast cancer patients. The amount of variance depended on the gene or genes tested, but, overall, using three biopsy specimens rather than one substantially reduced the variance, reported Dr. Rosanna Lau, a researcher at the University of Texas M.D. Anderson Cancer Center in Houston.
"Pooling biopsies from a single tumor reduced outlier results and reduced variance more generally for certain genes," Dr. Lau said. "Pooling biopsies is usually preferable to a single biopsy." The results showed that "we can get a comprehensive picture of the genes being expressed in the tumor by sampling multiple areas of the tumor and pooling the samples together. This increases the precision of the assay and allows us to make more reliable predictions related to the disease," she said in a written statement.
Her study also looked at the scope of analytic variance – variance caused by technical issues – in the biopsies taken from a 20-patient subgroup and found that the extent of analytic variance also varied by gene and was generally of the same magnitude as intratumor heterogeneity. The analytic variance wasn’t helped by pooling multiple biopsies, but data-processing solutions such as normalizing and scaling reduced this part of the variance, Dr. Lau said.
Dr. Reis-Fiho, Dr. Lau, Dr. Jarzab, and Dr. Di Leo had no disclosures.
BRUSSELS – When biopsying a primary breast cancer, once is probably not enough based on accumulating evidence of primary-tumor heterogeneity, but despite this evidence, taking multiple biopsies has not yet become routine practice.
"Intra-tumor heterogeneity is one of the causes of variation during genetic profiling" of tumors, Dr. Jorge S. Reis-Fiho said. "Taking multiple biopsies from a primary tumor and putting them all together may mitigate the effect of intra-tumor heterogeneity," but taking multiple biopsies has not yet become standard of care, he said at the conference, which was sponsored by the European Society for Medical Oncology.
"I think we should start to seriously consider taking more than one biopsy. Quite a few places already do it, and our radiologists will routinely take two or three biopsies," said Dr. Fiho, a surgical pathologist at Memorial Sloan-Kettering Cancer Center in New York. "With only a single, small biopsy of the primary tumor we may not have sufficient information to predict what the metastasis will respond to," he said in an interview.
Results from two studies reported at the meeting added to the evidence favoring multiple biopsies as a way to more precisely characterize primary tumors and target the best therapy.
In one study, Dr. Michal Jarzab and his associates took three core biopsies from the primary tumors of 26 patients and assessed them genetically for estrogen receptor, progesterone receptor, and HER2-receptor mutations. Their sample included some patients with early-stage disease and others with advanced-stage cancer. The results of the three individual biopsy tests showed significant heterogeneity in seven of the 26 tumors (27%), reported Dr. Jarzab, a researcher at the Maria Sklodowska-Curie Cancer Center and Institute of Oncology in Gliwice, Poland.
The intratumor heterogeneity in these seven patients "could negatively impact genomic assessment if done with one specimen," he said.
"If other studies report similar results" on intratumor heterogeneity, "then it could become common practice to evaluate prognostic or predictive breast cancer markers from more than one primary tumour area," Dr. Angelo Di Leo, chairman of oncology at Prato (Italy) Hospital, said in a written statement.
The second study looked at the impact of assessing one, two, or three biopsies on the variance in results from four different single- or multiple-genetic tests in biopsies collected from 51 breast cancer patients. The amount of variance depended on the gene or genes tested, but, overall, using three biopsy specimens rather than one substantially reduced the variance, reported Dr. Rosanna Lau, a researcher at the University of Texas M.D. Anderson Cancer Center in Houston.
"Pooling biopsies from a single tumor reduced outlier results and reduced variance more generally for certain genes," Dr. Lau said. "Pooling biopsies is usually preferable to a single biopsy." The results showed that "we can get a comprehensive picture of the genes being expressed in the tumor by sampling multiple areas of the tumor and pooling the samples together. This increases the precision of the assay and allows us to make more reliable predictions related to the disease," she said in a written statement.
Her study also looked at the scope of analytic variance – variance caused by technical issues – in the biopsies taken from a 20-patient subgroup and found that the extent of analytic variance also varied by gene and was generally of the same magnitude as intratumor heterogeneity. The analytic variance wasn’t helped by pooling multiple biopsies, but data-processing solutions such as normalizing and scaling reduced this part of the variance, Dr. Lau said.
Dr. Reis-Fiho, Dr. Lau, Dr. Jarzab, and Dr. Di Leo had no disclosures.
BRUSSELS – When biopsying a primary breast cancer, once is probably not enough based on accumulating evidence of primary-tumor heterogeneity, but despite this evidence, taking multiple biopsies has not yet become routine practice.
"Intra-tumor heterogeneity is one of the causes of variation during genetic profiling" of tumors, Dr. Jorge S. Reis-Fiho said. "Taking multiple biopsies from a primary tumor and putting them all together may mitigate the effect of intra-tumor heterogeneity," but taking multiple biopsies has not yet become standard of care, he said at the conference, which was sponsored by the European Society for Medical Oncology.
"I think we should start to seriously consider taking more than one biopsy. Quite a few places already do it, and our radiologists will routinely take two or three biopsies," said Dr. Fiho, a surgical pathologist at Memorial Sloan-Kettering Cancer Center in New York. "With only a single, small biopsy of the primary tumor we may not have sufficient information to predict what the metastasis will respond to," he said in an interview.
Results from two studies reported at the meeting added to the evidence favoring multiple biopsies as a way to more precisely characterize primary tumors and target the best therapy.
In one study, Dr. Michal Jarzab and his associates took three core biopsies from the primary tumors of 26 patients and assessed them genetically for estrogen receptor, progesterone receptor, and HER2-receptor mutations. Their sample included some patients with early-stage disease and others with advanced-stage cancer. The results of the three individual biopsy tests showed significant heterogeneity in seven of the 26 tumors (27%), reported Dr. Jarzab, a researcher at the Maria Sklodowska-Curie Cancer Center and Institute of Oncology in Gliwice, Poland.
The intratumor heterogeneity in these seven patients "could negatively impact genomic assessment if done with one specimen," he said.
"If other studies report similar results" on intratumor heterogeneity, "then it could become common practice to evaluate prognostic or predictive breast cancer markers from more than one primary tumour area," Dr. Angelo Di Leo, chairman of oncology at Prato (Italy) Hospital, said in a written statement.
The second study looked at the impact of assessing one, two, or three biopsies on the variance in results from four different single- or multiple-genetic tests in biopsies collected from 51 breast cancer patients. The amount of variance depended on the gene or genes tested, but, overall, using three biopsy specimens rather than one substantially reduced the variance, reported Dr. Rosanna Lau, a researcher at the University of Texas M.D. Anderson Cancer Center in Houston.
"Pooling biopsies from a single tumor reduced outlier results and reduced variance more generally for certain genes," Dr. Lau said. "Pooling biopsies is usually preferable to a single biopsy." The results showed that "we can get a comprehensive picture of the genes being expressed in the tumor by sampling multiple areas of the tumor and pooling the samples together. This increases the precision of the assay and allows us to make more reliable predictions related to the disease," she said in a written statement.
Her study also looked at the scope of analytic variance – variance caused by technical issues – in the biopsies taken from a 20-patient subgroup and found that the extent of analytic variance also varied by gene and was generally of the same magnitude as intratumor heterogeneity. The analytic variance wasn’t helped by pooling multiple biopsies, but data-processing solutions such as normalizing and scaling reduced this part of the variance, Dr. Lau said.
Dr. Reis-Fiho, Dr. Lau, Dr. Jarzab, and Dr. Di Leo had no disclosures.
AT IMPAKT 2013 BREAST CANCER CONFERENCE
Major finding: Significant intratumor heterogeneity occurred in the genetic-profile results from three individual biopsies for 27% of primary breast cancers tested.
Data source: Single-center study of 26 patients with either early- or advanced-stage breast cancer.
Disclosures: Dr. Reis-Fiho, Dr. Lau, Dr. Jarzab, and Dr. Di Leo had no disclosures.

Cancer-cell reprogramming poses new treatment challenge
BRUSSELS – Metastatic breast cancer cells are even more adaptable and able to evade targeted treatment than researchers suspected as recently as a few months ago, which means they present a heightened treatment challenge that in many cases may be overcome only with multiple targeted therapies delivered at the same time.
The findings were discussed at IMPAKT 2013 Breast Cancer Conference, sponsored by the European Society for Medical Oncology.

The new wrinkle in drug resistance has been dubbed reprogramming, a way that metastatic breast cancer cells (but presumably a property shared by other advanced solid tumors as well) quickly respond to a drug that shuts down an essential cell protein, a kinase, by turning on other, alternative kinases within days of drug exposure. Many of the new, targeted therapies that have successfully treated advanced-stage breast cancer and other solid tumors are kinase inhibitors, such as trastuzumab (Herceptin) and lapatinib (Tykerb).
Using a newly-developed technique for assessing many different kinases within a cell at once, Gary Johnson, Ph.D., reported that treatment of isolated, advanced breast cancer cells in vitro with a kinase inhibitor drug produced within a week a dramatic shift in the cell’s overall kinase profile, something he calls the cell’s "kinome." Part of this reprogramming response probably occurs because of new genes that the cancer cell turns on or upregulates, and part is probably driven by epigenetic changes in the cell, said Dr. Johnson, professor and chairman of pharmacology at the University of North Carolina in Chapel Hill.
Clinicians familiar with this finding quickly recognized that the phenomenon is an important, new barrier to successful treatment in patients that will require creative solutions using rational, multidrug, or multi-sequence regimens.

Dr. Lisa A. Carey, an oncologist who collaborates with Dr. Johnson, said she believes that reprogramming may explain her recent, frustrating results treating metastatic breast cancer patients with an investigational inhibitor of the epidermal growth factor receptor (EGFR), a tyrosine kinase.
"We gave the inhibitor to patients with triple-negative breast cancer, where the EGFR is clearly upregulated, a big, juicy target, and yet only 25% of the patients responded. Most of the time, the cancers had alternative mechanisms to keep the EGFR pathway active," Dr. Carey hypothesized based on Dr. Johnson’s recent findings. "The good news was that 25% of the time the treatment worked," said Dr. Carey, professor of hematology oncology at the University of North Carolina and medical director of the university’s Breast Center.
The new finding on breast-cancer cell reprogramming "helps us understand why the EGFR inhibitor didn’t work in most patients, it helps us understand what cancer cells do, and it helps us design our next approach. Most cancer drug development right now targets kinases," she said in an interview.
"One way to approach this is to use multiple agents at once, but if you add drugs you also add toxicity and expense. And in some patients the cell doesn’t reprogram. We need to understand how reprogramming works," with the potential to develop agents that block reprogramming instead of trying to deal with the changes that reprogramming causes. "This is an explanation of why patients don’t respond to even targeted treatments, and it gives us a way forward to potentially prevent it. Reprogramming is reproducible and potentially targetable. I think we can get around it."
"Limiting emergence of heterogeneity is important because heterogeneity is what defeats us," Dr. Larry Norton, director of the Breast Center at Memorial Sloan-Kettering Cancer Center. New York, said at the conference.

"I need to understand reprogramming of the kinome, what a treatment does to the cancer, and how it influences the next treatment I should use," said Dr. David Cameron, professor of oncology at Edinburgh University. "Patients with breast cancer will be treated with a sequence of agents. We treat patients longer, more effectively, and with more drugs, so we need to worry about what the first drug does to the cancer before we come in with a second.
Giving a clinician’s perspective on the significance of reprogramming in a talk at the meeting, Dr. Cameron said, "we will have to optimize therapy by understanding what one treatment does so we can give the next treatment at the optimal time. If we unravel the way the biology changes in the presence of treatment perhaps we can hone our treatments more effectively."
Dr. Johnson said that he has started a company, KinoDyn, to apply kinase-assessment to treatment, although as of now the company has no funding or employees. Dr. Carey, Dr. Norton, and Dr. Cameron had no disclosures.
Twitter: @mitchelzoler
BRUSSELS – Metastatic breast cancer cells are even more adaptable and able to evade targeted treatment than researchers suspected as recently as a few months ago, which means they present a heightened treatment challenge that in many cases may be overcome only with multiple targeted therapies delivered at the same time.
The findings were discussed at IMPAKT 2013 Breast Cancer Conference, sponsored by the European Society for Medical Oncology.
The new wrinkle in drug resistance has been dubbed reprogramming, a way that metastatic breast cancer cells (but presumably a property shared by other advanced solid tumors as well) quickly respond to a drug that shuts down an essential cell protein, a kinase, by turning on other, alternative kinases within days of drug exposure. Many of the new, targeted therapies that have successfully treated advanced-stage breast cancer and other solid tumors are kinase inhibitors, such as trastuzumab (Herceptin) and lapatinib (Tykerb).
Using a newly-developed technique for assessing many different kinases within a cell at once, Gary Johnson, Ph.D., reported that treatment of isolated, advanced breast cancer cells in vitro with a kinase inhibitor drug produced within a week a dramatic shift in the cell’s overall kinase profile, something he calls the cell’s "kinome." Part of this reprogramming response probably occurs because of new genes that the cancer cell turns on or upregulates, and part is probably driven by epigenetic changes in the cell, said Dr. Johnson, professor and chairman of pharmacology at the University of North Carolina in Chapel Hill.
Clinicians familiar with this finding quickly recognized that the phenomenon is an important, new barrier to successful treatment in patients that will require creative solutions using rational, multidrug, or multi-sequence regimens.
Dr. Lisa A. Carey, an oncologist who collaborates with Dr. Johnson, said she believes that reprogramming may explain her recent, frustrating results treating metastatic breast cancer patients with an investigational inhibitor of the epidermal growth factor receptor (EGFR), a tyrosine kinase.
"We gave the inhibitor to patients with triple-negative breast cancer, where the EGFR is clearly upregulated, a big, juicy target, and yet only 25% of the patients responded. Most of the time, the cancers had alternative mechanisms to keep the EGFR pathway active," Dr. Carey hypothesized based on Dr. Johnson’s recent findings. "The good news was that 25% of the time the treatment worked," said Dr. Carey, professor of hematology oncology at the University of North Carolina and medical director of the university’s Breast Center.
The new finding on breast-cancer cell reprogramming "helps us understand why the EGFR inhibitor didn’t work in most patients, it helps us understand what cancer cells do, and it helps us design our next approach. Most cancer drug development right now targets kinases," she said in an interview.
"One way to approach this is to use multiple agents at once, but if you add drugs you also add toxicity and expense. And in some patients the cell doesn’t reprogram. We need to understand how reprogramming works," with the potential to develop agents that block reprogramming instead of trying to deal with the changes that reprogramming causes. "This is an explanation of why patients don’t respond to even targeted treatments, and it gives us a way forward to potentially prevent it. Reprogramming is reproducible and potentially targetable. I think we can get around it."
"Limiting emergence of heterogeneity is important because heterogeneity is what defeats us," Dr. Larry Norton, director of the Breast Center at Memorial Sloan-Kettering Cancer Center. New York, said at the conference.
"I need to understand reprogramming of the kinome, what a treatment does to the cancer, and how it influences the next treatment I should use," said Dr. David Cameron, professor of oncology at Edinburgh University. "Patients with breast cancer will be treated with a sequence of agents. We treat patients longer, more effectively, and with more drugs, so we need to worry about what the first drug does to the cancer before we come in with a second.
Giving a clinician’s perspective on the significance of reprogramming in a talk at the meeting, Dr. Cameron said, "we will have to optimize therapy by understanding what one treatment does so we can give the next treatment at the optimal time. If we unravel the way the biology changes in the presence of treatment perhaps we can hone our treatments more effectively."
Dr. Johnson said that he has started a company, KinoDyn, to apply kinase-assessment to treatment, although as of now the company has no funding or employees. Dr. Carey, Dr. Norton, and Dr. Cameron had no disclosures.
Twitter: @mitchelzoler
BRUSSELS – Metastatic breast cancer cells are even more adaptable and able to evade targeted treatment than researchers suspected as recently as a few months ago, which means they present a heightened treatment challenge that in many cases may be overcome only with multiple targeted therapies delivered at the same time.
The findings were discussed at IMPAKT 2013 Breast Cancer Conference, sponsored by the European Society for Medical Oncology.
The new wrinkle in drug resistance has been dubbed reprogramming, a way that metastatic breast cancer cells (but presumably a property shared by other advanced solid tumors as well) quickly respond to a drug that shuts down an essential cell protein, a kinase, by turning on other, alternative kinases within days of drug exposure. Many of the new, targeted therapies that have successfully treated advanced-stage breast cancer and other solid tumors are kinase inhibitors, such as trastuzumab (Herceptin) and lapatinib (Tykerb).
Using a newly-developed technique for assessing many different kinases within a cell at once, Gary Johnson, Ph.D., reported that treatment of isolated, advanced breast cancer cells in vitro with a kinase inhibitor drug produced within a week a dramatic shift in the cell’s overall kinase profile, something he calls the cell’s "kinome." Part of this reprogramming response probably occurs because of new genes that the cancer cell turns on or upregulates, and part is probably driven by epigenetic changes in the cell, said Dr. Johnson, professor and chairman of pharmacology at the University of North Carolina in Chapel Hill.
Clinicians familiar with this finding quickly recognized that the phenomenon is an important, new barrier to successful treatment in patients that will require creative solutions using rational, multidrug, or multi-sequence regimens.
Dr. Lisa A. Carey, an oncologist who collaborates with Dr. Johnson, said she believes that reprogramming may explain her recent, frustrating results treating metastatic breast cancer patients with an investigational inhibitor of the epidermal growth factor receptor (EGFR), a tyrosine kinase.
"We gave the inhibitor to patients with triple-negative breast cancer, where the EGFR is clearly upregulated, a big, juicy target, and yet only 25% of the patients responded. Most of the time, the cancers had alternative mechanisms to keep the EGFR pathway active," Dr. Carey hypothesized based on Dr. Johnson’s recent findings. "The good news was that 25% of the time the treatment worked," said Dr. Carey, professor of hematology oncology at the University of North Carolina and medical director of the university’s Breast Center.
The new finding on breast-cancer cell reprogramming "helps us understand why the EGFR inhibitor didn’t work in most patients, it helps us understand what cancer cells do, and it helps us design our next approach. Most cancer drug development right now targets kinases," she said in an interview.
"One way to approach this is to use multiple agents at once, but if you add drugs you also add toxicity and expense. And in some patients the cell doesn’t reprogram. We need to understand how reprogramming works," with the potential to develop agents that block reprogramming instead of trying to deal with the changes that reprogramming causes. "This is an explanation of why patients don’t respond to even targeted treatments, and it gives us a way forward to potentially prevent it. Reprogramming is reproducible and potentially targetable. I think we can get around it."
"Limiting emergence of heterogeneity is important because heterogeneity is what defeats us," Dr. Larry Norton, director of the Breast Center at Memorial Sloan-Kettering Cancer Center. New York, said at the conference.
"I need to understand reprogramming of the kinome, what a treatment does to the cancer, and how it influences the next treatment I should use," said Dr. David Cameron, professor of oncology at Edinburgh University. "Patients with breast cancer will be treated with a sequence of agents. We treat patients longer, more effectively, and with more drugs, so we need to worry about what the first drug does to the cancer before we come in with a second.
Giving a clinician’s perspective on the significance of reprogramming in a talk at the meeting, Dr. Cameron said, "we will have to optimize therapy by understanding what one treatment does so we can give the next treatment at the optimal time. If we unravel the way the biology changes in the presence of treatment perhaps we can hone our treatments more effectively."
Dr. Johnson said that he has started a company, KinoDyn, to apply kinase-assessment to treatment, although as of now the company has no funding or employees. Dr. Carey, Dr. Norton, and Dr. Cameron had no disclosures.
Twitter: @mitchelzoler
EXPERT ANALYSIS FROM IMPAKT 2013 BREAST CANCER CONFERENCE

TAVR quickly dominates high-risk aortic stenosis
SAN FRANCISCO – It’s been barely half a year since U.S. cardiologists and cardiac surgeons first became able to routinely offer operable, high-risk patients with aortic stenosis the option of transcatheter valve replacement, yet in the first few months the transcatheter approach quickly rivaled open surgery.
But for the time being in U.S. practice, transcatheter aortic valve replacement (TAVR) remains boxed into the high-risk niche, along with the subgroup of patients who are not suitable for open surgery, king of a pair of relatively small hills.

And no matter how well TAVR performs in the current pair of trials that are comparing it with open surgical aortic valve replacement (SAVR) for intermediate-risk patients, it will remain relegated to niche status for years to come. That’s because roughly two-thirds of all operable patients with aortic stenosis who need valve replacement fall into the low-risk category, with a Society of Thoracic Surgeons (STS) risk score of less than 4%, which experts agree will remain SAVR’s exclusive territory for the foreseeable future.
The high-risk stratum of operable patients, which TAVR now dominates, constitutes about 10% of all patients who need a new aortic valve and can undergo open surgery, patients with an STS score greater than 8%. The intermediate-risk category – an STS score of 4%-8%, where TAVR now vies against open SAVR in two high-profile trials – makes up the final quarter of the operable-patient pie.
Within the high-risk and operable universe, TAVR’s rise has been meteoric, starting last October when the Food and Drug Administration gave Edwards, marketer of the SAPIEN valve system, approval for these patients. A small survey of operators from U.S. TAVR programs in March at the annual scientific session of the American College of Cardiology (ACC) revealed a uniform perception that by early 2013 a sizable majority of U.S. patients with severe aortic stenosis who are deemed operable and are at high surgical risk will wind up being treated by TAVR instead of SAVR. The cardiac surgeons who collaborate on TAVR seem to have fully conceded the advantages of TAVR for these patients.
"We generally go with TAVR. Most patients want it, and with the equivalence" in outcomes from the first PARTNER (Placement of Aortic Transcatheter Valves) cohort A (operable patients) trial (New Engl. J. Med. 2010:364:2187-98), "you usually go with the less invasive procedure," said Dr. Joseph E. Bavaria, professor of surgery and director of thoracic aortic surgery at the University of Pennsylvania in Philadelphia. The small number of high-risk patients who go to open surgery tend to be men, "because they do better with surgery, especially if their life expectancy is greater than 5-8 years," or patients with high stroke risk, Dr. Bavaria said in an interview at the annual meeting of the American College of Cardiology.
"Operable, high-risk patients get TAVR. I’m a surgeon saying that. I’ve already done the [PARTNER cohort A] trial, and I don’t want to do it again," said Dr. Michael Mack, a cardiothoracic surgeon at the Heart Hospital in Plano, Texas. "The results are the same [from TAVR and SAVR] at 30 days, 1 year, and 2 years, but boy do we beat up patients with open surgery. If it was my mom, she’d get TAVR," he said in an interview. "The tie goes to the less invasive treatment."
When high-risk, operable patients are seen by the heart team Dr. Mack works with, the only ones who go to SAVR are patients – generally men – who have a large aortic annulus and need a 29-mm-diameter valve, which is not available for the time being to U.S. TAVR patients; women with septal hypertrophy causing significant left ventricular outflow-tract obstruction; and the small percent of patients who opt for open surgery, usually because it’s the more established approach or because they fear a higher stroke risk from TAVR.
"The majority of high-risk, operable patients now go to TAVR; I think that’s pretty much true across the United States," said Dr. Jeffrey J. Popma, a cardiologist who does TAVR and is a professor of medicine at Harvard University in Boston.
Where TAVR stood in 2010 and 2011
How is TAVR performing? Performance can only be completely assessed months or years after the fact, so the impact that high-risk, operable U.S. patients received from TAVR’s use in routine practice in late 2012 and the first months of 2013 remains to be seen. The most recently treated patients now available for meaningful analysis in large numbers come from 2010 and 2011: new data reported at the ACC meeting from a U.S. program of continued TAVR access that began in late 2009 following the end of recruitment into the first PARTNER trial, and 1-year follow-up of nearly 14,000 patients who underwent TAVR in 2011 as part of routine practice in Germany and were entered into the country’s national TAVR registry.
Both databases had good news for high-risk or inoperable patients. TAVR outcomes in the first couple of years immediately following PARTNER in both the United States and Germany showed clinically meaningful improvements over the way TAVR performed during the first PARTNER trial. Less optimistic news for the low- and intermediate-risk patients who underwent TAVR in Germany, where wider device use is possible, was that in broad terms open surgery outperformed TAVR in these lower-risk patients, although TAVR’s defenders are quick to point out how tricky it is to make cross-treatment comparisons with registry data.

The nonrandomized, continued-access cohort that followed the first PARTNER trial at 22 U.S. centers, 3 sites in Canada, and 1 site in Germany included 1,017 inoperable or high-risk patients who had successful transfemoral TAVR between August 2009 and December 2011. When compared with the 415 inoperable or high-risk patients who underwent transfemoral TAVR in both cohorts of PARTNER, the more recently treated patients had a statistically significant decrease in all-cause 1-year mortality, from a 25% death rate in PARTNER to a 20% rate during the continued-access period, Dr. William F. Fearon reported at the meeting.
The continued-access patients also showed significant cuts in their rates of major vascular complications, which dropped from 15% of patients in PARTNER to 6% during continued access; and in rates of major bleeding complications, which fell from 15% in PARTNER to 7% during continued access. Strokes were also down during continued access, 5% compared with 7% during PARTNER, but this was not a statistically significant drop, reported Dr. Fearon, a cardiologist at Stanford (Calif.) University.
"Maybe these improvements are due to better patient selection, and maybe we have also gotten better at what we do," commented Dr. Popma.
The latest German experience
The 1-year German Aortic Valve Registry (GARY) results from 2011 show similar improvements compared with PARTNER. Among the 2,689 patients who underwent transvascular TAVR, the 1-year total mortality rate was 21%, and in the subset of patients with stroke data the combined rate of major and minor stroke was 5%.
But it was the way that transvascular TAVR (which includes both transfemoral and other vascular approaches but excludes the 1,181 patients who underwent transapical TAVR) stacked up against open surgical replacement that raised concern.
Of the 13,860 total patients entered into GARY during 2011, 9,985 underwent SAVR, with 6,523 of these patients undergoing an isolated procedure (the rest had valve replacement combined with coronary artery bypass). One-year mortality was 7% in patients who had isolated SAVR, dramatically below the 21% rate among the transvascular TAVR patients, Dr. Friedrich-Wilhelm Mohr reported at the meeting. The transapical TAVR patients had a 28% 1-year mortality rate.
To address the issue of between-treatment differences in patients’ underlying risk, Dr. Mohr presented two sets of analyses that stratified patients with two different risk-scoring systems, the EuroSCORE and the AKL (aortic valve surgery) score, also known as the German aortic valve score. The results showed how disparate the outcomes were when patients were subgrouped by their underlying risk. Among the patients who had lone SAVR, 80% fell into the lowest-risk level, with an AKL score of less than 3. Among the transvascular TAVR patients, only 17% had AKL scores below 3.
Among patients with AKL scores less than 3, those who underwent SAVR without bypass had a roughly 5% mortality rate after 1 year, compared with about a 15% mortality rate among the transvascular TAVR patients. Analyses in higher-risk patient subgroups showed that the survival gap between SAVR and TAVR patients progressively shrank, until in high-risk patients – as in those studied in PARTNER – the mortality rates were about the same in the SAVR and TAVR groups, said Dr. Mohr, professor and director of heart surgery at Leipzig University, Germany. He also reported similar findings when patients were stratified by their baseline EuroSCORE.
A big factor behind the worse survival among lower-risk TAVR patients is the problem of aortic regurgitation, Dr. Mohr said. Following valve replacement, 56% of the transvascular TAVR patients had grade 1 regurgitation, 7% had grade 2, and less than 1% had grade 3 leakage. These rates are way too high, he said. "Our major concern is the incidence of aortic regurgitation; more than half of the [TAVR] patients had some kind of regurgitation. Regurgitation matters whether it is mild or severe."
Despite his concern, TAVR use in Germany is accelerating. The total number of aortic valve replacements done in Germany jumped from just less than 14,000 in 2011 to more than 22,000 last year; TAVR cases more than doubled, from fewer than 4,000 in 2011 to nearly 10,000 in 2012, with a "move to intermediate-risk groups," said Dr. Mohr, who made it clear that he does not endorse this trend. "TAVR must be proven better than or equal to surgery before it’s used on a large scale," he said. The GARY results show "a clear difference [between TAVR and SAVR] in lower-risk patients. The GARY results do not support going into intermediate-risk patients."
Dr. Martin B. Leon agreed with Dr. Mohr that a definitive determination of whether TAVR is at least as good as SAVR in intermediate-risk patients must await results from the two major, ongoing multicenter trials testing this hypothesis, the PARTNER II trial, using the Edwards balloon-expandable SAPIEN XT valve system, and the SURTAVI (Safety and Efficacy Study of the Medtronic CoreValve System in the Treatment of Severe, Symptomatic Aortic Stenosis in Intermediate Risk Subjects Who Need Aortic Valve Replacement) trial. But Dr. Leon also cautioned that possible confounders might be distorting the GARY results, creating what he calls the "GARY Fallacy."
"The GARY Fallacy is the absurd notion that you can compare SAVR and TAVR in various risk strata without formal risk-adjustment methods to account for imbalances in baseline variables that are not captured in standard risk scores," he said in a talk at the meeting. "Aortic-stenosis patients were selected for TAVR based on their presumed increased risk, including many variables that are not represented in the risk algorithms, such as frailty, liver disease, porcelain aorta, a hostile chest, dementia, and severe chronic obstructive pulmonary disease. Therefore, the risk scores for TAVR patients underrepresent their true risk," Dr. Leon said.
But it’s also possible that TAVR needs more refinement before it completely catches up with SAVR, especially in patients who have the best outcomes from SAVR.

"I think SAVR outperforms TAVR in low-risk patients in the German registry because SAVR is a more mature procedure," said Dr. Raj R. Makkar, a TAVR operator and director of interventional cardiology at Cedars-Sinai Medical Center in Los Angeles. "Maybe this will change, as TAVR becomes safer with fewer valve leaks, strokes, and vascular complications."
Assessing patient risks
Experts also realize that the EuroSCORE, the AKL score, and the other risk-stratification tools now available have flaws when applied to TAVR patients. "Risk stratification for TAVR and SAVR is very problematic; the EuroSCORE has shown poor predictive value for mortality," Dr. Leon said. And while the AKL score was developed specifically for SAVR patients, its relevance to TAVR patients is suspect. In the first PARTNER trial, the multivariate predictors of mortality in the TAVR patients were "completely different" from the predictors in the SAVR patients, he noted.
"It’s tricky calculating scores," agreed Dr. Makkar. Both he and Dr. Mohr cited comorbidities such as pulmonary hypertension, cirrhosis, knee replacement producing impaired mobility, and porcelain aorta that each ratchet up a patient’s risk but have no effect whatsoever on a patient’s EuroSCORE or STS score.
The German cardiology and cardiac surgery societies recognize the limitations of current risk-scoring formulas and are developing a risk-stratification tool specifically designed for TAVR patients, Dr. Mohr said.
The way patients are assessed before, during, and after TAVR is receiving careful scrutiny from some investigators who reported their findings at the ACC meeting, with a particular focus on efforts to characterize and minimize aortic-valve regurgitation following TAVR.
One report, for example, reviewed 2,679 patients who underwent TAVR at any of 33 French centers and 1 in Monaco between January 2010 and October 2011, and were enrolled in the French Aortic National CoreValve and Edwards (FRANCE 2) Registry, established by the French cardiology and thoracic and cardiovascular surgery societies (N. Engl. J. Med. 2012;366:1705-15). FRANCE 2 includes nearly 1,900 patients who received the balloon-expandable Edwards SAPIEN valve, and nearly 900 treated with the self-expanding Medtronic CoreValve device.
Following TAVR, 60% of all patients in the registry had paravalvular aortic regurgitation: 45% with grade 1 regurgitation, 14% with grade 2, and 1% with grade 3 or 4. In a multivariate analysis, the self-expandable device was linked to twice the rate of higher-grade aortic regurgitation, grade 2 or higher, compared with the balloon-expandable valve; and TAVRs done via the femoral artery approach were also about twice as likely to result in higher-grade regurgitations compared with other catheterization routes, reported Dr. Eric Van Belle, a professor at the Cardiology Hospital in Lille, France.
Postprocedural paravalvular regurgitation of grade 2 or higher "was associated with a twofold increase in 1-year mortality, and was the strongest independent predictor of mortality," said Dr. Van Belle in his talk at the meeting. In addition, "annulus diameter and prosthesis diameter were major determinants of aortic regurgitation" in patients who received a balloon-expandable valve.
The FRANCE 2 results showed that postprocedural aortic regurgitation at grade 2 or higher "is a major issue and should be avoided, especially when there is no significant aortic regurgitation at baseline, or when a nonfemoral delivery approach is used." The link between nonfemoral delivery approaches and lower rates of aortic regurgitation suggests "good control of the depth of device delivery and improved catheter technology are key to reducing regurgitation rates," Dr. Van Belle said. "In addition, the prosthesis diameter relative to annulus diameter is key to preventing regurgitation with balloon-expandable devices. Prevention of aortic regurgitation is a major challenge for developing the next-generation device technology."
Minimizing aortic regurgitation
Two ways to cut aortic regurgitation rates following TAVR are to better match the valve to the annulus size, and when possible not finish a TAVR procedure until regurgitation has been minimized.
Two-dimensional transthoracic echocardiography had been the standard approach for annulus sizing as recently as 3 years ago, but it has been replaced with more accurate approaches, either three-dimensional transthoracic echo or CT. "Two-dimensional measurements are seriously limited due to variations and noncircular annular anatomy," Dr. Makkar said in a talk at the meeting. "CT provides the best overall assessment, because in addition to the cross-sectional measurement of the annulus it provides the best assessment of calcification," and three-dimensional transthoracic echo is now standard for intraprocedural assessments, he said.
The impact that a concerted effort to minimize aortic regurgitation can have on outcomes was examined in a single-center study reported by Dr. Jan-Malte Sinning, a cardiologist at University Hospital in Bonn, Germany. Last year, Dr. Sinning and his associates reported developing a quantitative measure of aortic regurgitation immediately following TAVR, the aortic regurgitation (AR) index, based on the difference between a patient’s diastolic blood pressure in the aorta and the left ventricular end-diastolic pressure (J. Am. Coll. Cardiol. 2012;59:1134-41). They then calculated the AR index immediately after TAVR in a prospective series of 167 patients, and set themselves the goal of immediately taking whatever steps were needed to bring the AR index above 25, a cutoff that seemed to correspond to no worse than mild regurgitation.
In their series, 62 patients underwent immediate post-TAVR corrective steps to reduce aortic regurgitation and bring their AR index above 25, most commonly additional balloon dilatation of the valve. The result was that while 16 patients had severe regurgitation before these steps, no patient had severe regurgitation following the corrective measures. The adjustments also cut the incidence of moderate regurgitations from 41 patients to 10, Dr. Sinning reported.
The consequence was that the 30-day stroke rate in the new cohort was 1%, compared with a 6% rate in a historical TAVR cohort at University Hospital in Bonn. The need for pacemaker implants was also cut in half by the intervention compared with the historical group, and 30-day mortality was 3% with these interventions, compared with 7% in the historical controls.
The results suggest that using the AR index as a trigger for taking corrective measures can help improve survival, and that post-TAVR dilatation can successfully decrease regurgitation without increasing patients’ stroke risk, Dr. Sinning concluded.
U.S. operators who perform TAVR say they take similar steps these days to deal with aortic regurgitation after TAVR. "We all understand that you don’t want patients to leave with a leak," said Dr. Popma. "We do everything we can to minimize leaks. When a patient leaves the lab with a moderate or severe leak, there wasn’t anything we could do about it."
Finding TAVR’s limits
Even as TAVR has become the go-to method for high-risk patients, operators have also tried to define the procedure’s outer limit, the point of disease severity when a patient is dying with aortic stenosis rather than because of aortic stenosis, and performing TAVR doesn’t make sense.
Dr. Makkar analyzed 369 inoperable patients who underwent TAVR in both the PARTNER I trial and the nonrandomized continued-access phase that followed. The patients fell into three groups: those who were inoperable because of technical reasons, such as a porcelain aorta or prior chest irradiation; patients who were inoperable because of comorbidities, such as frailty or severe lung disease; and those with both limitations. The 85 patients who were inoperable only because of a technical limitation had a 2-year mortality rate of 23% following TAVR; the other 284 patients who all had comorbidities had a 2-year mortality rate of about 43%.
Last year, Dr. Makkar reported that analysis of these 369 inoperable patients showed a 2-year mortality rate of 20% in the subgroup with an STS score of less than 5%, a mortality rate of 40% among those with a score of 5%-14.5% (but still significantly below the 60% 2-year mortality among similar inoperable patients managed by standard medical therapy only), and a 60% mortality rate among patients with a baseline STS score of 15% or more, an outcome that was no better than that of patients managed without TAVR (N. Engl. J. Med. 2012;366:1696-704).
In a multivariate analysis he recently ran on the data from these 369 patients, the likelihood of 2-year mortality rose by a statistically significant 3% for every 1% increase in the patient’s baseline STS risk score.
"It is important to remember that there are diminishing returns from TAVR in patients with more comorbidities, especially when their STS risk score is greater than 15%," said Dr. Makkar.
Dr. Sinning and Dr. Van Belle had no relevant disclosures. Dr. Mohr is a PARTNER investigator but had no other disclosures. Dr. Bavaria has been a speaker for Edwards and is a PARTNER investigator. Dr. Mack has received travel support from Edwards and is a PARTNER investigator. Dr. Popma has been a consultant to Boston Scientific, Abbott Vascular, and Covidien, and received research support from Boston Scientific, Abbott Vascular, Abiomed, Medtronic, and Cordis. Dr. Fearon has been a consultant to Heart Flow and received research support from St. Jude Medical. Dr. Leon has been a consultant to Symetis; has a major equity stake in Sadra, Claret, Valve Medical, and Apica; has received research support from Boston Scientific, Edwards, and Medtronic; and is a PARTNER investigator. Dr. Makkar has been a consultant to Cordis, Medtronic, Abbott, Entourage Medical, and Abiomed; has been a speaker for Lilly; has received research and travel support from Edwards; and is a PARTNER investigator.
On Twitter @mitchelzoler
SAN FRANCISCO – It’s been barely half a year since U.S. cardiologists and cardiac surgeons first became able to routinely offer operable, high-risk patients with aortic stenosis the option of transcatheter valve replacement, yet in the first few months the transcatheter approach quickly rivaled open surgery.
But for the time being in U.S. practice, transcatheter aortic valve replacement (TAVR) remains boxed into the high-risk niche, along with the subgroup of patients who are not suitable for open surgery, king of a pair of relatively small hills.
And no matter how well TAVR performs in the current pair of trials that are comparing it with open surgical aortic valve replacement (SAVR) for intermediate-risk patients, it will remain relegated to niche status for years to come. That’s because roughly two-thirds of all operable patients with aortic stenosis who need valve replacement fall into the low-risk category, with a Society of Thoracic Surgeons (STS) risk score of less than 4%, which experts agree will remain SAVR’s exclusive territory for the foreseeable future.
The high-risk stratum of operable patients, which TAVR now dominates, constitutes about 10% of all patients who need a new aortic valve and can undergo open surgery, patients with an STS score greater than 8%. The intermediate-risk category – an STS score of 4%-8%, where TAVR now vies against open SAVR in two high-profile trials – makes up the final quarter of the operable-patient pie.
Within the high-risk and operable universe, TAVR’s rise has been meteoric, starting last October when the Food and Drug Administration gave Edwards, marketer of the SAPIEN valve system, approval for these patients. A small survey of operators from U.S. TAVR programs in March at the annual scientific session of the American College of Cardiology (ACC) revealed a uniform perception that by early 2013 a sizable majority of U.S. patients with severe aortic stenosis who are deemed operable and are at high surgical risk will wind up being treated by TAVR instead of SAVR. The cardiac surgeons who collaborate on TAVR seem to have fully conceded the advantages of TAVR for these patients.
"We generally go with TAVR. Most patients want it, and with the equivalence" in outcomes from the first PARTNER (Placement of Aortic Transcatheter Valves) cohort A (operable patients) trial (New Engl. J. Med. 2010:364:2187-98), "you usually go with the less invasive procedure," said Dr. Joseph E. Bavaria, professor of surgery and director of thoracic aortic surgery at the University of Pennsylvania in Philadelphia. The small number of high-risk patients who go to open surgery tend to be men, "because they do better with surgery, especially if their life expectancy is greater than 5-8 years," or patients with high stroke risk, Dr. Bavaria said in an interview at the annual meeting of the American College of Cardiology.
"Operable, high-risk patients get TAVR. I’m a surgeon saying that. I’ve already done the [PARTNER cohort A] trial, and I don’t want to do it again," said Dr. Michael Mack, a cardiothoracic surgeon at the Heart Hospital in Plano, Texas. "The results are the same [from TAVR and SAVR] at 30 days, 1 year, and 2 years, but boy do we beat up patients with open surgery. If it was my mom, she’d get TAVR," he said in an interview. "The tie goes to the less invasive treatment."
When high-risk, operable patients are seen by the heart team Dr. Mack works with, the only ones who go to SAVR are patients – generally men – who have a large aortic annulus and need a 29-mm-diameter valve, which is not available for the time being to U.S. TAVR patients; women with septal hypertrophy causing significant left ventricular outflow-tract obstruction; and the small percent of patients who opt for open surgery, usually because it’s the more established approach or because they fear a higher stroke risk from TAVR.
"The majority of high-risk, operable patients now go to TAVR; I think that’s pretty much true across the United States," said Dr. Jeffrey J. Popma, a cardiologist who does TAVR and is a professor of medicine at Harvard University in Boston.
Where TAVR stood in 2010 and 2011
How is TAVR performing? Performance can only be completely assessed months or years after the fact, so the impact that high-risk, operable U.S. patients received from TAVR’s use in routine practice in late 2012 and the first months of 2013 remains to be seen. The most recently treated patients now available for meaningful analysis in large numbers come from 2010 and 2011: new data reported at the ACC meeting from a U.S. program of continued TAVR access that began in late 2009 following the end of recruitment into the first PARTNER trial, and 1-year follow-up of nearly 14,000 patients who underwent TAVR in 2011 as part of routine practice in Germany and were entered into the country’s national TAVR registry.
Both databases had good news for high-risk or inoperable patients. TAVR outcomes in the first couple of years immediately following PARTNER in both the United States and Germany showed clinically meaningful improvements over the way TAVR performed during the first PARTNER trial. Less optimistic news for the low- and intermediate-risk patients who underwent TAVR in Germany, where wider device use is possible, was that in broad terms open surgery outperformed TAVR in these lower-risk patients, although TAVR’s defenders are quick to point out how tricky it is to make cross-treatment comparisons with registry data.
The nonrandomized, continued-access cohort that followed the first PARTNER trial at 22 U.S. centers, 3 sites in Canada, and 1 site in Germany included 1,017 inoperable or high-risk patients who had successful transfemoral TAVR between August 2009 and December 2011. When compared with the 415 inoperable or high-risk patients who underwent transfemoral TAVR in both cohorts of PARTNER, the more recently treated patients had a statistically significant decrease in all-cause 1-year mortality, from a 25% death rate in PARTNER to a 20% rate during the continued-access period, Dr. William F. Fearon reported at the meeting.
The continued-access patients also showed significant cuts in their rates of major vascular complications, which dropped from 15% of patients in PARTNER to 6% during continued access; and in rates of major bleeding complications, which fell from 15% in PARTNER to 7% during continued access. Strokes were also down during continued access, 5% compared with 7% during PARTNER, but this was not a statistically significant drop, reported Dr. Fearon, a cardiologist at Stanford (Calif.) University.
"Maybe these improvements are due to better patient selection, and maybe we have also gotten better at what we do," commented Dr. Popma.
The latest German experience
The 1-year German Aortic Valve Registry (GARY) results from 2011 show similar improvements compared with PARTNER. Among the 2,689 patients who underwent transvascular TAVR, the 1-year total mortality rate was 21%, and in the subset of patients with stroke data the combined rate of major and minor stroke was 5%.
But it was the way that transvascular TAVR (which includes both transfemoral and other vascular approaches but excludes the 1,181 patients who underwent transapical TAVR) stacked up against open surgical replacement that raised concern.
Of the 13,860 total patients entered into GARY during 2011, 9,985 underwent SAVR, with 6,523 of these patients undergoing an isolated procedure (the rest had valve replacement combined with coronary artery bypass). One-year mortality was 7% in patients who had isolated SAVR, dramatically below the 21% rate among the transvascular TAVR patients, Dr. Friedrich-Wilhelm Mohr reported at the meeting. The transapical TAVR patients had a 28% 1-year mortality rate.
To address the issue of between-treatment differences in patients’ underlying risk, Dr. Mohr presented two sets of analyses that stratified patients with two different risk-scoring systems, the EuroSCORE and the AKL (aortic valve surgery) score, also known as the German aortic valve score. The results showed how disparate the outcomes were when patients were subgrouped by their underlying risk. Among the patients who had lone SAVR, 80% fell into the lowest-risk level, with an AKL score of less than 3. Among the transvascular TAVR patients, only 17% had AKL scores below 3.
Among patients with AKL scores less than 3, those who underwent SAVR without bypass had a roughly 5% mortality rate after 1 year, compared with about a 15% mortality rate among the transvascular TAVR patients. Analyses in higher-risk patient subgroups showed that the survival gap between SAVR and TAVR patients progressively shrank, until in high-risk patients – as in those studied in PARTNER – the mortality rates were about the same in the SAVR and TAVR groups, said Dr. Mohr, professor and director of heart surgery at Leipzig University, Germany. He also reported similar findings when patients were stratified by their baseline EuroSCORE.
A big factor behind the worse survival among lower-risk TAVR patients is the problem of aortic regurgitation, Dr. Mohr said. Following valve replacement, 56% of the transvascular TAVR patients had grade 1 regurgitation, 7% had grade 2, and less than 1% had grade 3 leakage. These rates are way too high, he said. "Our major concern is the incidence of aortic regurgitation; more than half of the [TAVR] patients had some kind of regurgitation. Regurgitation matters whether it is mild or severe."
Despite his concern, TAVR use in Germany is accelerating. The total number of aortic valve replacements done in Germany jumped from just less than 14,000 in 2011 to more than 22,000 last year; TAVR cases more than doubled, from fewer than 4,000 in 2011 to nearly 10,000 in 2012, with a "move to intermediate-risk groups," said Dr. Mohr, who made it clear that he does not endorse this trend. "TAVR must be proven better than or equal to surgery before it’s used on a large scale," he said. The GARY results show "a clear difference [between TAVR and SAVR] in lower-risk patients. The GARY results do not support going into intermediate-risk patients."
Dr. Martin B. Leon agreed with Dr. Mohr that a definitive determination of whether TAVR is at least as good as SAVR in intermediate-risk patients must await results from the two major, ongoing multicenter trials testing this hypothesis, the PARTNER II trial, using the Edwards balloon-expandable SAPIEN XT valve system, and the SURTAVI (Safety and Efficacy Study of the Medtronic CoreValve System in the Treatment of Severe, Symptomatic Aortic Stenosis in Intermediate Risk Subjects Who Need Aortic Valve Replacement) trial. But Dr. Leon also cautioned that possible confounders might be distorting the GARY results, creating what he calls the "GARY Fallacy."
"The GARY Fallacy is the absurd notion that you can compare SAVR and TAVR in various risk strata without formal risk-adjustment methods to account for imbalances in baseline variables that are not captured in standard risk scores," he said in a talk at the meeting. "Aortic-stenosis patients were selected for TAVR based on their presumed increased risk, including many variables that are not represented in the risk algorithms, such as frailty, liver disease, porcelain aorta, a hostile chest, dementia, and severe chronic obstructive pulmonary disease. Therefore, the risk scores for TAVR patients underrepresent their true risk," Dr. Leon said.
But it’s also possible that TAVR needs more refinement before it completely catches up with SAVR, especially in patients who have the best outcomes from SAVR.
"I think SAVR outperforms TAVR in low-risk patients in the German registry because SAVR is a more mature procedure," said Dr. Raj R. Makkar, a TAVR operator and director of interventional cardiology at Cedars-Sinai Medical Center in Los Angeles. "Maybe this will change, as TAVR becomes safer with fewer valve leaks, strokes, and vascular complications."
Assessing patient risks
Experts also realize that the EuroSCORE, the AKL score, and the other risk-stratification tools now available have flaws when applied to TAVR patients. "Risk stratification for TAVR and SAVR is very problematic; the EuroSCORE has shown poor predictive value for mortality," Dr. Leon said. And while the AKL score was developed specifically for SAVR patients, its relevance to TAVR patients is suspect. In the first PARTNER trial, the multivariate predictors of mortality in the TAVR patients were "completely different" from the predictors in the SAVR patients, he noted.
"It’s tricky calculating scores," agreed Dr. Makkar. Both he and Dr. Mohr cited comorbidities such as pulmonary hypertension, cirrhosis, knee replacement producing impaired mobility, and porcelain aorta that each ratchet up a patient’s risk but have no effect whatsoever on a patient’s EuroSCORE or STS score.
The German cardiology and cardiac surgery societies recognize the limitations of current risk-scoring formulas and are developing a risk-stratification tool specifically designed for TAVR patients, Dr. Mohr said.
The way patients are assessed before, during, and after TAVR is receiving careful scrutiny from some investigators who reported their findings at the ACC meeting, with a particular focus on efforts to characterize and minimize aortic-valve regurgitation following TAVR.
One report, for example, reviewed 2,679 patients who underwent TAVR at any of 33 French centers and 1 in Monaco between January 2010 and October 2011, and were enrolled in the French Aortic National CoreValve and Edwards (FRANCE 2) Registry, established by the French cardiology and thoracic and cardiovascular surgery societies (N. Engl. J. Med. 2012;366:1705-15). FRANCE 2 includes nearly 1,900 patients who received the balloon-expandable Edwards SAPIEN valve, and nearly 900 treated with the self-expanding Medtronic CoreValve device.
Following TAVR, 60% of all patients in the registry had paravalvular aortic regurgitation: 45% with grade 1 regurgitation, 14% with grade 2, and 1% with grade 3 or 4. In a multivariate analysis, the self-expandable device was linked to twice the rate of higher-grade aortic regurgitation, grade 2 or higher, compared with the balloon-expandable valve; and TAVRs done via the femoral artery approach were also about twice as likely to result in higher-grade regurgitations compared with other catheterization routes, reported Dr. Eric Van Belle, a professor at the Cardiology Hospital in Lille, France.
Postprocedural paravalvular regurgitation of grade 2 or higher "was associated with a twofold increase in 1-year mortality, and was the strongest independent predictor of mortality," said Dr. Van Belle in his talk at the meeting. In addition, "annulus diameter and prosthesis diameter were major determinants of aortic regurgitation" in patients who received a balloon-expandable valve.
The FRANCE 2 results showed that postprocedural aortic regurgitation at grade 2 or higher "is a major issue and should be avoided, especially when there is no significant aortic regurgitation at baseline, or when a nonfemoral delivery approach is used." The link between nonfemoral delivery approaches and lower rates of aortic regurgitation suggests "good control of the depth of device delivery and improved catheter technology are key to reducing regurgitation rates," Dr. Van Belle said. "In addition, the prosthesis diameter relative to annulus diameter is key to preventing regurgitation with balloon-expandable devices. Prevention of aortic regurgitation is a major challenge for developing the next-generation device technology."
Minimizing aortic regurgitation
Two ways to cut aortic regurgitation rates following TAVR are to better match the valve to the annulus size, and when possible not finish a TAVR procedure until regurgitation has been minimized.
Two-dimensional transthoracic echocardiography had been the standard approach for annulus sizing as recently as 3 years ago, but it has been replaced with more accurate approaches, either three-dimensional transthoracic echo or CT. "Two-dimensional measurements are seriously limited due to variations and noncircular annular anatomy," Dr. Makkar said in a talk at the meeting. "CT provides the best overall assessment, because in addition to the cross-sectional measurement of the annulus it provides the best assessment of calcification," and three-dimensional transthoracic echo is now standard for intraprocedural assessments, he said.
The impact that a concerted effort to minimize aortic regurgitation can have on outcomes was examined in a single-center study reported by Dr. Jan-Malte Sinning, a cardiologist at University Hospital in Bonn, Germany. Last year, Dr. Sinning and his associates reported developing a quantitative measure of aortic regurgitation immediately following TAVR, the aortic regurgitation (AR) index, based on the difference between a patient’s diastolic blood pressure in the aorta and the left ventricular end-diastolic pressure (J. Am. Coll. Cardiol. 2012;59:1134-41). They then calculated the AR index immediately after TAVR in a prospective series of 167 patients, and set themselves the goal of immediately taking whatever steps were needed to bring the AR index above 25, a cutoff that seemed to correspond to no worse than mild regurgitation.
In their series, 62 patients underwent immediate post-TAVR corrective steps to reduce aortic regurgitation and bring their AR index above 25, most commonly additional balloon dilatation of the valve. The result was that while 16 patients had severe regurgitation before these steps, no patient had severe regurgitation following the corrective measures. The adjustments also cut the incidence of moderate regurgitations from 41 patients to 10, Dr. Sinning reported.
The consequence was that the 30-day stroke rate in the new cohort was 1%, compared with a 6% rate in a historical TAVR cohort at University Hospital in Bonn. The need for pacemaker implants was also cut in half by the intervention compared with the historical group, and 30-day mortality was 3% with these interventions, compared with 7% in the historical controls.
The results suggest that using the AR index as a trigger for taking corrective measures can help improve survival, and that post-TAVR dilatation can successfully decrease regurgitation without increasing patients’ stroke risk, Dr. Sinning concluded.
U.S. operators who perform TAVR say they take similar steps these days to deal with aortic regurgitation after TAVR. "We all understand that you don’t want patients to leave with a leak," said Dr. Popma. "We do everything we can to minimize leaks. When a patient leaves the lab with a moderate or severe leak, there wasn’t anything we could do about it."
Finding TAVR’s limits
Even as TAVR has become the go-to method for high-risk patients, operators have also tried to define the procedure’s outer limit, the point of disease severity when a patient is dying with aortic stenosis rather than because of aortic stenosis, and performing TAVR doesn’t make sense.
Dr. Makkar analyzed 369 inoperable patients who underwent TAVR in both the PARTNER I trial and the nonrandomized continued-access phase that followed. The patients fell into three groups: those who were inoperable because of technical reasons, such as a porcelain aorta or prior chest irradiation; patients who were inoperable because of comorbidities, such as frailty or severe lung disease; and those with both limitations. The 85 patients who were inoperable only because of a technical limitation had a 2-year mortality rate of 23% following TAVR; the other 284 patients who all had comorbidities had a 2-year mortality rate of about 43%.
Last year, Dr. Makkar reported that analysis of these 369 inoperable patients showed a 2-year mortality rate of 20% in the subgroup with an STS score of less than 5%, a mortality rate of 40% among those with a score of 5%-14.5% (but still significantly below the 60% 2-year mortality among similar inoperable patients managed by standard medical therapy only), and a 60% mortality rate among patients with a baseline STS score of 15% or more, an outcome that was no better than that of patients managed without TAVR (N. Engl. J. Med. 2012;366:1696-704).
In a multivariate analysis he recently ran on the data from these 369 patients, the likelihood of 2-year mortality rose by a statistically significant 3% for every 1% increase in the patient’s baseline STS risk score.
"It is important to remember that there are diminishing returns from TAVR in patients with more comorbidities, especially when their STS risk score is greater than 15%," said Dr. Makkar.
Dr. Sinning and Dr. Van Belle had no relevant disclosures. Dr. Mohr is a PARTNER investigator but had no other disclosures. Dr. Bavaria has been a speaker for Edwards and is a PARTNER investigator. Dr. Mack has received travel support from Edwards and is a PARTNER investigator. Dr. Popma has been a consultant to Boston Scientific, Abbott Vascular, and Covidien, and received research support from Boston Scientific, Abbott Vascular, Abiomed, Medtronic, and Cordis. Dr. Fearon has been a consultant to Heart Flow and received research support from St. Jude Medical. Dr. Leon has been a consultant to Symetis; has a major equity stake in Sadra, Claret, Valve Medical, and Apica; has received research support from Boston Scientific, Edwards, and Medtronic; and is a PARTNER investigator. Dr. Makkar has been a consultant to Cordis, Medtronic, Abbott, Entourage Medical, and Abiomed; has been a speaker for Lilly; has received research and travel support from Edwards; and is a PARTNER investigator.
On Twitter @mitchelzoler
SAN FRANCISCO – It’s been barely half a year since U.S. cardiologists and cardiac surgeons first became able to routinely offer operable, high-risk patients with aortic stenosis the option of transcatheter valve replacement, yet in the first few months the transcatheter approach quickly rivaled open surgery.
But for the time being in U.S. practice, transcatheter aortic valve replacement (TAVR) remains boxed into the high-risk niche, along with the subgroup of patients who are not suitable for open surgery, king of a pair of relatively small hills.
And no matter how well TAVR performs in the current pair of trials that are comparing it with open surgical aortic valve replacement (SAVR) for intermediate-risk patients, it will remain relegated to niche status for years to come. That’s because roughly two-thirds of all operable patients with aortic stenosis who need valve replacement fall into the low-risk category, with a Society of Thoracic Surgeons (STS) risk score of less than 4%, which experts agree will remain SAVR’s exclusive territory for the foreseeable future.
The high-risk stratum of operable patients, which TAVR now dominates, constitutes about 10% of all patients who need a new aortic valve and can undergo open surgery, patients with an STS score greater than 8%. The intermediate-risk category – an STS score of 4%-8%, where TAVR now vies against open SAVR in two high-profile trials – makes up the final quarter of the operable-patient pie.
Within the high-risk and operable universe, TAVR’s rise has been meteoric, starting last October when the Food and Drug Administration gave Edwards, marketer of the SAPIEN valve system, approval for these patients. A small survey of operators from U.S. TAVR programs in March at the annual scientific session of the American College of Cardiology (ACC) revealed a uniform perception that by early 2013 a sizable majority of U.S. patients with severe aortic stenosis who are deemed operable and are at high surgical risk will wind up being treated by TAVR instead of SAVR. The cardiac surgeons who collaborate on TAVR seem to have fully conceded the advantages of TAVR for these patients.
"We generally go with TAVR. Most patients want it, and with the equivalence" in outcomes from the first PARTNER (Placement of Aortic Transcatheter Valves) cohort A (operable patients) trial (New Engl. J. Med. 2010:364:2187-98), "you usually go with the less invasive procedure," said Dr. Joseph E. Bavaria, professor of surgery and director of thoracic aortic surgery at the University of Pennsylvania in Philadelphia. The small number of high-risk patients who go to open surgery tend to be men, "because they do better with surgery, especially if their life expectancy is greater than 5-8 years," or patients with high stroke risk, Dr. Bavaria said in an interview at the annual meeting of the American College of Cardiology.
"Operable, high-risk patients get TAVR. I’m a surgeon saying that. I’ve already done the [PARTNER cohort A] trial, and I don’t want to do it again," said Dr. Michael Mack, a cardiothoracic surgeon at the Heart Hospital in Plano, Texas. "The results are the same [from TAVR and SAVR] at 30 days, 1 year, and 2 years, but boy do we beat up patients with open surgery. If it was my mom, she’d get TAVR," he said in an interview. "The tie goes to the less invasive treatment."
When high-risk, operable patients are seen by the heart team Dr. Mack works with, the only ones who go to SAVR are patients – generally men – who have a large aortic annulus and need a 29-mm-diameter valve, which is not available for the time being to U.S. TAVR patients; women with septal hypertrophy causing significant left ventricular outflow-tract obstruction; and the small percent of patients who opt for open surgery, usually because it’s the more established approach or because they fear a higher stroke risk from TAVR.
"The majority of high-risk, operable patients now go to TAVR; I think that’s pretty much true across the United States," said Dr. Jeffrey J. Popma, a cardiologist who does TAVR and is a professor of medicine at Harvard University in Boston.
Where TAVR stood in 2010 and 2011
How is TAVR performing? Performance can only be completely assessed months or years after the fact, so the impact that high-risk, operable U.S. patients received from TAVR’s use in routine practice in late 2012 and the first months of 2013 remains to be seen. The most recently treated patients now available for meaningful analysis in large numbers come from 2010 and 2011: new data reported at the ACC meeting from a U.S. program of continued TAVR access that began in late 2009 following the end of recruitment into the first PARTNER trial, and 1-year follow-up of nearly 14,000 patients who underwent TAVR in 2011 as part of routine practice in Germany and were entered into the country’s national TAVR registry.
Both databases had good news for high-risk or inoperable patients. TAVR outcomes in the first couple of years immediately following PARTNER in both the United States and Germany showed clinically meaningful improvements over the way TAVR performed during the first PARTNER trial. Less optimistic news for the low- and intermediate-risk patients who underwent TAVR in Germany, where wider device use is possible, was that in broad terms open surgery outperformed TAVR in these lower-risk patients, although TAVR’s defenders are quick to point out how tricky it is to make cross-treatment comparisons with registry data.
The nonrandomized, continued-access cohort that followed the first PARTNER trial at 22 U.S. centers, 3 sites in Canada, and 1 site in Germany included 1,017 inoperable or high-risk patients who had successful transfemoral TAVR between August 2009 and December 2011. When compared with the 415 inoperable or high-risk patients who underwent transfemoral TAVR in both cohorts of PARTNER, the more recently treated patients had a statistically significant decrease in all-cause 1-year mortality, from a 25% death rate in PARTNER to a 20% rate during the continued-access period, Dr. William F. Fearon reported at the meeting.
The continued-access patients also showed significant cuts in their rates of major vascular complications, which dropped from 15% of patients in PARTNER to 6% during continued access; and in rates of major bleeding complications, which fell from 15% in PARTNER to 7% during continued access. Strokes were also down during continued access, 5% compared with 7% during PARTNER, but this was not a statistically significant drop, reported Dr. Fearon, a cardiologist at Stanford (Calif.) University.
"Maybe these improvements are due to better patient selection, and maybe we have also gotten better at what we do," commented Dr. Popma.
The latest German experience
The 1-year German Aortic Valve Registry (GARY) results from 2011 show similar improvements compared with PARTNER. Among the 2,689 patients who underwent transvascular TAVR, the 1-year total mortality rate was 21%, and in the subset of patients with stroke data the combined rate of major and minor stroke was 5%.
But it was the way that transvascular TAVR (which includes both transfemoral and other vascular approaches but excludes the 1,181 patients who underwent transapical TAVR) stacked up against open surgical replacement that raised concern.
Of the 13,860 total patients entered into GARY during 2011, 9,985 underwent SAVR, with 6,523 of these patients undergoing an isolated procedure (the rest had valve replacement combined with coronary artery bypass). One-year mortality was 7% in patients who had isolated SAVR, dramatically below the 21% rate among the transvascular TAVR patients, Dr. Friedrich-Wilhelm Mohr reported at the meeting. The transapical TAVR patients had a 28% 1-year mortality rate.
To address the issue of between-treatment differences in patients’ underlying risk, Dr. Mohr presented two sets of analyses that stratified patients with two different risk-scoring systems, the EuroSCORE and the AKL (aortic valve surgery) score, also known as the German aortic valve score. The results showed how disparate the outcomes were when patients were subgrouped by their underlying risk. Among the patients who had lone SAVR, 80% fell into the lowest-risk level, with an AKL score of less than 3. Among the transvascular TAVR patients, only 17% had AKL scores below 3.
Among patients with AKL scores less than 3, those who underwent SAVR without bypass had a roughly 5% mortality rate after 1 year, compared with about a 15% mortality rate among the transvascular TAVR patients. Analyses in higher-risk patient subgroups showed that the survival gap between SAVR and TAVR patients progressively shrank, until in high-risk patients – as in those studied in PARTNER – the mortality rates were about the same in the SAVR and TAVR groups, said Dr. Mohr, professor and director of heart surgery at Leipzig University, Germany. He also reported similar findings when patients were stratified by their baseline EuroSCORE.
A big factor behind the worse survival among lower-risk TAVR patients is the problem of aortic regurgitation, Dr. Mohr said. Following valve replacement, 56% of the transvascular TAVR patients had grade 1 regurgitation, 7% had grade 2, and less than 1% had grade 3 leakage. These rates are way too high, he said. "Our major concern is the incidence of aortic regurgitation; more than half of the [TAVR] patients had some kind of regurgitation. Regurgitation matters whether it is mild or severe."
Despite his concern, TAVR use in Germany is accelerating. The total number of aortic valve replacements done in Germany jumped from just less than 14,000 in 2011 to more than 22,000 last year; TAVR cases more than doubled, from fewer than 4,000 in 2011 to nearly 10,000 in 2012, with a "move to intermediate-risk groups," said Dr. Mohr, who made it clear that he does not endorse this trend. "TAVR must be proven better than or equal to surgery before it’s used on a large scale," he said. The GARY results show "a clear difference [between TAVR and SAVR] in lower-risk patients. The GARY results do not support going into intermediate-risk patients."
Dr. Martin B. Leon agreed with Dr. Mohr that a definitive determination of whether TAVR is at least as good as SAVR in intermediate-risk patients must await results from the two major, ongoing multicenter trials testing this hypothesis, the PARTNER II trial, using the Edwards balloon-expandable SAPIEN XT valve system, and the SURTAVI (Safety and Efficacy Study of the Medtronic CoreValve System in the Treatment of Severe, Symptomatic Aortic Stenosis in Intermediate Risk Subjects Who Need Aortic Valve Replacement) trial. But Dr. Leon also cautioned that possible confounders might be distorting the GARY results, creating what he calls the "GARY Fallacy."
"The GARY Fallacy is the absurd notion that you can compare SAVR and TAVR in various risk strata without formal risk-adjustment methods to account for imbalances in baseline variables that are not captured in standard risk scores," he said in a talk at the meeting. "Aortic-stenosis patients were selected for TAVR based on their presumed increased risk, including many variables that are not represented in the risk algorithms, such as frailty, liver disease, porcelain aorta, a hostile chest, dementia, and severe chronic obstructive pulmonary disease. Therefore, the risk scores for TAVR patients underrepresent their true risk," Dr. Leon said.
But it’s also possible that TAVR needs more refinement before it completely catches up with SAVR, especially in patients who have the best outcomes from SAVR.
"I think SAVR outperforms TAVR in low-risk patients in the German registry because SAVR is a more mature procedure," said Dr. Raj R. Makkar, a TAVR operator and director of interventional cardiology at Cedars-Sinai Medical Center in Los Angeles. "Maybe this will change, as TAVR becomes safer with fewer valve leaks, strokes, and vascular complications."
Assessing patient risks
Experts also realize that the EuroSCORE, the AKL score, and the other risk-stratification tools now available have flaws when applied to TAVR patients. "Risk stratification for TAVR and SAVR is very problematic; the EuroSCORE has shown poor predictive value for mortality," Dr. Leon said. And while the AKL score was developed specifically for SAVR patients, its relevance to TAVR patients is suspect. In the first PARTNER trial, the multivariate predictors of mortality in the TAVR patients were "completely different" from the predictors in the SAVR patients, he noted.
"It’s tricky calculating scores," agreed Dr. Makkar. Both he and Dr. Mohr cited comorbidities such as pulmonary hypertension, cirrhosis, knee replacement producing impaired mobility, and porcelain aorta that each ratchet up a patient’s risk but have no effect whatsoever on a patient’s EuroSCORE or STS score.
The German cardiology and cardiac surgery societies recognize the limitations of current risk-scoring formulas and are developing a risk-stratification tool specifically designed for TAVR patients, Dr. Mohr said.
The way patients are assessed before, during, and after TAVR is receiving careful scrutiny from some investigators who reported their findings at the ACC meeting, with a particular focus on efforts to characterize and minimize aortic-valve regurgitation following TAVR.
One report, for example, reviewed 2,679 patients who underwent TAVR at any of 33 French centers and 1 in Monaco between January 2010 and October 2011, and were enrolled in the French Aortic National CoreValve and Edwards (FRANCE 2) Registry, established by the French cardiology and thoracic and cardiovascular surgery societies (N. Engl. J. Med. 2012;366:1705-15). FRANCE 2 includes nearly 1,900 patients who received the balloon-expandable Edwards SAPIEN valve, and nearly 900 treated with the self-expanding Medtronic CoreValve device.
Following TAVR, 60% of all patients in the registry had paravalvular aortic regurgitation: 45% with grade 1 regurgitation, 14% with grade 2, and 1% with grade 3 or 4. In a multivariate analysis, the self-expandable device was linked to twice the rate of higher-grade aortic regurgitation, grade 2 or higher, compared with the balloon-expandable valve; and TAVRs done via the femoral artery approach were also about twice as likely to result in higher-grade regurgitations compared with other catheterization routes, reported Dr. Eric Van Belle, a professor at the Cardiology Hospital in Lille, France.
Postprocedural paravalvular regurgitation of grade 2 or higher "was associated with a twofold increase in 1-year mortality, and was the strongest independent predictor of mortality," said Dr. Van Belle in his talk at the meeting. In addition, "annulus diameter and prosthesis diameter were major determinants of aortic regurgitation" in patients who received a balloon-expandable valve.
The FRANCE 2 results showed that postprocedural aortic regurgitation at grade 2 or higher "is a major issue and should be avoided, especially when there is no significant aortic regurgitation at baseline, or when a nonfemoral delivery approach is used." The link between nonfemoral delivery approaches and lower rates of aortic regurgitation suggests "good control of the depth of device delivery and improved catheter technology are key to reducing regurgitation rates," Dr. Van Belle said. "In addition, the prosthesis diameter relative to annulus diameter is key to preventing regurgitation with balloon-expandable devices. Prevention of aortic regurgitation is a major challenge for developing the next-generation device technology."
Minimizing aortic regurgitation
Two ways to cut aortic regurgitation rates following TAVR are to better match the valve to the annulus size, and when possible not finish a TAVR procedure until regurgitation has been minimized.
Two-dimensional transthoracic echocardiography had been the standard approach for annulus sizing as recently as 3 years ago, but it has been replaced with more accurate approaches, either three-dimensional transthoracic echo or CT. "Two-dimensional measurements are seriously limited due to variations and noncircular annular anatomy," Dr. Makkar said in a talk at the meeting. "CT provides the best overall assessment, because in addition to the cross-sectional measurement of the annulus it provides the best assessment of calcification," and three-dimensional transthoracic echo is now standard for intraprocedural assessments, he said.
The impact that a concerted effort to minimize aortic regurgitation can have on outcomes was examined in a single-center study reported by Dr. Jan-Malte Sinning, a cardiologist at University Hospital in Bonn, Germany. Last year, Dr. Sinning and his associates reported developing a quantitative measure of aortic regurgitation immediately following TAVR, the aortic regurgitation (AR) index, based on the difference between a patient’s diastolic blood pressure in the aorta and the left ventricular end-diastolic pressure (J. Am. Coll. Cardiol. 2012;59:1134-41). They then calculated the AR index immediately after TAVR in a prospective series of 167 patients, and set themselves the goal of immediately taking whatever steps were needed to bring the AR index above 25, a cutoff that seemed to correspond to no worse than mild regurgitation.
In their series, 62 patients underwent immediate post-TAVR corrective steps to reduce aortic regurgitation and bring their AR index above 25, most commonly additional balloon dilatation of the valve. The result was that while 16 patients had severe regurgitation before these steps, no patient had severe regurgitation following the corrective measures. The adjustments also cut the incidence of moderate regurgitations from 41 patients to 10, Dr. Sinning reported.
The consequence was that the 30-day stroke rate in the new cohort was 1%, compared with a 6% rate in a historical TAVR cohort at University Hospital in Bonn. The need for pacemaker implants was also cut in half by the intervention compared with the historical group, and 30-day mortality was 3% with these interventions, compared with 7% in the historical controls.
The results suggest that using the AR index as a trigger for taking corrective measures can help improve survival, and that post-TAVR dilatation can successfully decrease regurgitation without increasing patients’ stroke risk, Dr. Sinning concluded.
U.S. operators who perform TAVR say they take similar steps these days to deal with aortic regurgitation after TAVR. "We all understand that you don’t want patients to leave with a leak," said Dr. Popma. "We do everything we can to minimize leaks. When a patient leaves the lab with a moderate or severe leak, there wasn’t anything we could do about it."
Finding TAVR’s limits
Even as TAVR has become the go-to method for high-risk patients, operators have also tried to define the procedure’s outer limit, the point of disease severity when a patient is dying with aortic stenosis rather than because of aortic stenosis, and performing TAVR doesn’t make sense.
Dr. Makkar analyzed 369 inoperable patients who underwent TAVR in both the PARTNER I trial and the nonrandomized continued-access phase that followed. The patients fell into three groups: those who were inoperable because of technical reasons, such as a porcelain aorta or prior chest irradiation; patients who were inoperable because of comorbidities, such as frailty or severe lung disease; and those with both limitations. The 85 patients who were inoperable only because of a technical limitation had a 2-year mortality rate of 23% following TAVR; the other 284 patients who all had comorbidities had a 2-year mortality rate of about 43%.
Last year, Dr. Makkar reported that analysis of these 369 inoperable patients showed a 2-year mortality rate of 20% in the subgroup with an STS score of less than 5%, a mortality rate of 40% among those with a score of 5%-14.5% (but still significantly below the 60% 2-year mortality among similar inoperable patients managed by standard medical therapy only), and a 60% mortality rate among patients with a baseline STS score of 15% or more, an outcome that was no better than that of patients managed without TAVR (N. Engl. J. Med. 2012;366:1696-704).
In a multivariate analysis he recently ran on the data from these 369 patients, the likelihood of 2-year mortality rose by a statistically significant 3% for every 1% increase in the patient’s baseline STS risk score.
"It is important to remember that there are diminishing returns from TAVR in patients with more comorbidities, especially when their STS risk score is greater than 15%," said Dr. Makkar.
Dr. Sinning and Dr. Van Belle had no relevant disclosures. Dr. Mohr is a PARTNER investigator but had no other disclosures. Dr. Bavaria has been a speaker for Edwards and is a PARTNER investigator. Dr. Mack has received travel support from Edwards and is a PARTNER investigator. Dr. Popma has been a consultant to Boston Scientific, Abbott Vascular, and Covidien, and received research support from Boston Scientific, Abbott Vascular, Abiomed, Medtronic, and Cordis. Dr. Fearon has been a consultant to Heart Flow and received research support from St. Jude Medical. Dr. Leon has been a consultant to Symetis; has a major equity stake in Sadra, Claret, Valve Medical, and Apica; has received research support from Boston Scientific, Edwards, and Medtronic; and is a PARTNER investigator. Dr. Makkar has been a consultant to Cordis, Medtronic, Abbott, Entourage Medical, and Abiomed; has been a speaker for Lilly; has received research and travel support from Edwards; and is a PARTNER investigator.
On Twitter @mitchelzoler
AT ACC 13

Genetic tests gauge breast-cancer recurrence risk
BRUSSELS – A pair of genetic tests each showed the ability to aid long-term prognosis estimates in patients with estrogen receptor–positive breast cancer, based on results from two retrospective analyses reported at IMPAKT 2013 Breast Cancer Conference.
The new results mean that a total of three different genetic tests have now shown added prognostic utility in retrospective analyses, bringing the field closer to actually using these tests in routine practice. The tests would prove particularly useful for patients with estrogen receptor–positive, node-negative breast cancer by helping to find those who are at low risk for long-term metastatic disease and who could safely stop treatment after 5 years of hormonal therapy, said Dr. Michael Gnant, professor of surgery at the University of Vienna.

But other experts stressed that it’s premature to start routinely using these tests.
"We’re getting to a point where we can offer to our patients genomic assays that are clinically validated and with demonstrated utility," Dr. W. Fraser Symmans said during the meeting. But, he added, while oncologists are "on the brink" of using the tests routinely, "we need to confirm reproducibility among labs, and that the test works in that setting," said Dr. Symmans, professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston.
None of the three genetic test panels were designed to predict late recurrences, noted Dr. Peter C. Dubsky, a surgeon at the University of Vienna and a collaborator with Dr. Gnant. "These data will need further validation before actually being incorporated into clinical decision-making concerning adjuvant endocrine therapy beyond 5 years," Dr. Dubsky said in a written statement.
The analysis reported by Dr. Gnant and Dr. Dubsky included formalin-fixed and paraffin-embedded tumor specimens from 1,478 patients who had been enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, which had the primary goal of assessing two different 5-year treatment strategies in more than 3,700 postmenopausal women with estrogen receptor–positive breast cancer (J. Clin. Oncol. 2012;30:722-8).
Dr. Gnant, Dr. Dubsky, and their associates assessed the 1,478 specimens with the Prediction Analysis of Microarray test using a 58-gene classifier panel (PAM50), a test first reported in 2009 (J. Clin. Oncol. 2009;27:1160-7) that has since been commercialized as the Prosigna assay, available in Europe but not in the United States.
Using prespecified cutoffs on the PAM50 results for classifying patients as being at low, intermediate, and high risk for long term distant recurrences, the researchers tallied the rate of actual recurrences during a median follow-up of 11 years. The 15-year disease-free survival rate was 97.6% among low-risk patients, 90.9% in intermediate-risk patients, and 82.5% in high-risk patients, Dr. Gnant reported. The between-group differences were statistically significant.
The findings suggest that high-risk patients might be good candidates for extended adjuvant therapy, while low-risk patients, with a recurrence risk of less than 2% at 5-10 years and at 10-15 years following primary therapy "can be spared the side effects of extended adjuvant therapy," he said. The PAM50 risk of recurrence score "adds prognostic information beyond established clinicopathological factors."
The second analysis reported at the meeting retrospectively used medical records and specimens collected in the Arimidex, Tamoxifen Alone or in Combination (ATAC) study, which enrolled more than 6,000 postmenopausal women with localized invasive breast cancer (Lancet Oncology 2008;9:45-53). The researchers evaluated the prognostic efficacy of five different clinical, genetic, or histochemical test panels for predicting risk of distant recurrences during a median 10 years follow-up in 891 of the enrolled patients.

All five assessment panels yielded similar prognostic information during the first 5 years of follow-up. During the next 5 years, the strongest prognostic information came via the Clinical Treatment Score, which takes into account a patient’s nodal status, tumor grade and size, patient’s age, and treatment received, said Ivana Sestak, Ph.D., a statistician and epidemiologist at the University of London. The two most important prognostic features in this panel are tumor size and nodal status, she noted. Two other assessment panels – the PAM50 genetic panel and the Breast Cancer Index, a genetic test first described in 2011 – also provided statistically significant and clinically meaningful additional prediction of distant recurrences during 5-10 years of follow-up (Br. J. Cancer 2011;104:1762-9).
The other two tests Dr. Sestak and her associates evaluated did not add further prognostic information beyond what the Clinical Treatment Score provided. The uninformative tests were a set of four immunohistochemical markers (to estrogen, progesterone, HER2, and ki67), and the Oncotype Dx recurrence score – a 21-gene panel test marketed by Genomic Health.
"The PAM50 risk of recurrence score and the Breast Cancer Index may be used to identify estrogen receptor–positive breast cancer patients who are at increased risk of late recurrence and who may benefit from extended adjuvant hormonal therapy beyond 5 years," she concluded. But "none of these scores were developed to dictate treatment," she cautioned.
These findings, together with the PAM50 analysis from the ABCSG 8 study, solidify PAM50’s position as a validated prognostic tool, Dr. Gnant said.
In addition to PAM50 and the Breast Cancer Index, a third genetic test recently shown effective for predicting long-term recurrence risk in similar patients is the EndoPredict (Ann. Oncol. 2013;24:640-7).
All three assays can now be considered validated for longer-term prognosis in patients with endocrine-responsive, lymph node–negative breast cancer, Dr. Symmans said.
The conference was sponsored by the European Society for Medical Oncology.
Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.
Twitter: @mitchelzoler
The Breast Cancer Index and the PAM50 and EndoPredict tests were all developed as prognostic assays. They were not designed to, nor have they been demonstrated to, predict patient sensitivity to an endocrine treatment or to help select a class of endocrine agent to use in therapy. Despite these limitations, the data presented on all three tests suggest that they perform well for discriminating recurrence risk among patients with hormone-receptor positive, lymph-node negative breast cancer. So far, there is not good evidence that they can predict outcomes in lymph-node positive patients.

|
Mitchel L. Zoler/IMNG Medical Media
|
The patients with the greatest potential for stopping treatment after 5 years are those who also have HER2-negative disease and grade 1 or 2 disease, similar to the women enrolled in the ABCSG 8 trial.
Another attractive feature of these tests is that they can be performed by local pathology laboratories, precluding the need to send specimens to distant testing sites. The pathology community has been waiting a long time to more fully participate in the genomic diagnostic/personalized medicine arena.
The next step is to confirm the reproducibility of these tests when used by a variety of labs, essentially guaranteeing quality control. You need a critical mass of labs working together and using these tests to be sure that everyone gets clinically valid and reproducible results. I expect this to happen during the next year.
Dr. W. Fraser Symmans is professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston. He said that he is a c-founder of, and has equity in, Nuvera Biosciences. He made these comments as an invited discussant for the reports at the meeting and in an interview.
The Breast Cancer Index and the PAM50 and EndoPredict tests were all developed as prognostic assays. They were not designed to, nor have they been demonstrated to, predict patient sensitivity to an endocrine treatment or to help select a class of endocrine agent to use in therapy. Despite these limitations, the data presented on all three tests suggest that they perform well for discriminating recurrence risk among patients with hormone-receptor positive, lymph-node negative breast cancer. So far, there is not good evidence that they can predict outcomes in lymph-node positive patients.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The patients with the greatest potential for stopping treatment after 5 years are those who also have HER2-negative disease and grade 1 or 2 disease, similar to the women enrolled in the ABCSG 8 trial.
Another attractive feature of these tests is that they can be performed by local pathology laboratories, precluding the need to send specimens to distant testing sites. The pathology community has been waiting a long time to more fully participate in the genomic diagnostic/personalized medicine arena.
The next step is to confirm the reproducibility of these tests when used by a variety of labs, essentially guaranteeing quality control. You need a critical mass of labs working together and using these tests to be sure that everyone gets clinically valid and reproducible results. I expect this to happen during the next year.
Dr. W. Fraser Symmans is professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston. He said that he is a c-founder of, and has equity in, Nuvera Biosciences. He made these comments as an invited discussant for the reports at the meeting and in an interview.
The Breast Cancer Index and the PAM50 and EndoPredict tests were all developed as prognostic assays. They were not designed to, nor have they been demonstrated to, predict patient sensitivity to an endocrine treatment or to help select a class of endocrine agent to use in therapy. Despite these limitations, the data presented on all three tests suggest that they perform well for discriminating recurrence risk among patients with hormone-receptor positive, lymph-node negative breast cancer. So far, there is not good evidence that they can predict outcomes in lymph-node positive patients.
|
|
Mitchel L. Zoler/IMNG Medical Media
|
The patients with the greatest potential for stopping treatment after 5 years are those who also have HER2-negative disease and grade 1 or 2 disease, similar to the women enrolled in the ABCSG 8 trial.
Another attractive feature of these tests is that they can be performed by local pathology laboratories, precluding the need to send specimens to distant testing sites. The pathology community has been waiting a long time to more fully participate in the genomic diagnostic/personalized medicine arena.
The next step is to confirm the reproducibility of these tests when used by a variety of labs, essentially guaranteeing quality control. You need a critical mass of labs working together and using these tests to be sure that everyone gets clinically valid and reproducible results. I expect this to happen during the next year.
Dr. W. Fraser Symmans is professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston. He said that he is a c-founder of, and has equity in, Nuvera Biosciences. He made these comments as an invited discussant for the reports at the meeting and in an interview.
BRUSSELS – A pair of genetic tests each showed the ability to aid long-term prognosis estimates in patients with estrogen receptor–positive breast cancer, based on results from two retrospective analyses reported at IMPAKT 2013 Breast Cancer Conference.
The new results mean that a total of three different genetic tests have now shown added prognostic utility in retrospective analyses, bringing the field closer to actually using these tests in routine practice. The tests would prove particularly useful for patients with estrogen receptor–positive, node-negative breast cancer by helping to find those who are at low risk for long-term metastatic disease and who could safely stop treatment after 5 years of hormonal therapy, said Dr. Michael Gnant, professor of surgery at the University of Vienna.
But other experts stressed that it’s premature to start routinely using these tests.
"We’re getting to a point where we can offer to our patients genomic assays that are clinically validated and with demonstrated utility," Dr. W. Fraser Symmans said during the meeting. But, he added, while oncologists are "on the brink" of using the tests routinely, "we need to confirm reproducibility among labs, and that the test works in that setting," said Dr. Symmans, professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston.
None of the three genetic test panels were designed to predict late recurrences, noted Dr. Peter C. Dubsky, a surgeon at the University of Vienna and a collaborator with Dr. Gnant. "These data will need further validation before actually being incorporated into clinical decision-making concerning adjuvant endocrine therapy beyond 5 years," Dr. Dubsky said in a written statement.
The analysis reported by Dr. Gnant and Dr. Dubsky included formalin-fixed and paraffin-embedded tumor specimens from 1,478 patients who had been enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, which had the primary goal of assessing two different 5-year treatment strategies in more than 3,700 postmenopausal women with estrogen receptor–positive breast cancer (J. Clin. Oncol. 2012;30:722-8).
Dr. Gnant, Dr. Dubsky, and their associates assessed the 1,478 specimens with the Prediction Analysis of Microarray test using a 58-gene classifier panel (PAM50), a test first reported in 2009 (J. Clin. Oncol. 2009;27:1160-7) that has since been commercialized as the Prosigna assay, available in Europe but not in the United States.
Using prespecified cutoffs on the PAM50 results for classifying patients as being at low, intermediate, and high risk for long term distant recurrences, the researchers tallied the rate of actual recurrences during a median follow-up of 11 years. The 15-year disease-free survival rate was 97.6% among low-risk patients, 90.9% in intermediate-risk patients, and 82.5% in high-risk patients, Dr. Gnant reported. The between-group differences were statistically significant.
The findings suggest that high-risk patients might be good candidates for extended adjuvant therapy, while low-risk patients, with a recurrence risk of less than 2% at 5-10 years and at 10-15 years following primary therapy "can be spared the side effects of extended adjuvant therapy," he said. The PAM50 risk of recurrence score "adds prognostic information beyond established clinicopathological factors."
The second analysis reported at the meeting retrospectively used medical records and specimens collected in the Arimidex, Tamoxifen Alone or in Combination (ATAC) study, which enrolled more than 6,000 postmenopausal women with localized invasive breast cancer (Lancet Oncology 2008;9:45-53). The researchers evaluated the prognostic efficacy of five different clinical, genetic, or histochemical test panels for predicting risk of distant recurrences during a median 10 years follow-up in 891 of the enrolled patients.
All five assessment panels yielded similar prognostic information during the first 5 years of follow-up. During the next 5 years, the strongest prognostic information came via the Clinical Treatment Score, which takes into account a patient’s nodal status, tumor grade and size, patient’s age, and treatment received, said Ivana Sestak, Ph.D., a statistician and epidemiologist at the University of London. The two most important prognostic features in this panel are tumor size and nodal status, she noted. Two other assessment panels – the PAM50 genetic panel and the Breast Cancer Index, a genetic test first described in 2011 – also provided statistically significant and clinically meaningful additional prediction of distant recurrences during 5-10 years of follow-up (Br. J. Cancer 2011;104:1762-9).
The other two tests Dr. Sestak and her associates evaluated did not add further prognostic information beyond what the Clinical Treatment Score provided. The uninformative tests were a set of four immunohistochemical markers (to estrogen, progesterone, HER2, and ki67), and the Oncotype Dx recurrence score – a 21-gene panel test marketed by Genomic Health.
"The PAM50 risk of recurrence score and the Breast Cancer Index may be used to identify estrogen receptor–positive breast cancer patients who are at increased risk of late recurrence and who may benefit from extended adjuvant hormonal therapy beyond 5 years," she concluded. But "none of these scores were developed to dictate treatment," she cautioned.
These findings, together with the PAM50 analysis from the ABCSG 8 study, solidify PAM50’s position as a validated prognostic tool, Dr. Gnant said.
In addition to PAM50 and the Breast Cancer Index, a third genetic test recently shown effective for predicting long-term recurrence risk in similar patients is the EndoPredict (Ann. Oncol. 2013;24:640-7).
All three assays can now be considered validated for longer-term prognosis in patients with endocrine-responsive, lymph node–negative breast cancer, Dr. Symmans said.
The conference was sponsored by the European Society for Medical Oncology.
Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.
Twitter: @mitchelzoler
BRUSSELS – A pair of genetic tests each showed the ability to aid long-term prognosis estimates in patients with estrogen receptor–positive breast cancer, based on results from two retrospective analyses reported at IMPAKT 2013 Breast Cancer Conference.
The new results mean that a total of three different genetic tests have now shown added prognostic utility in retrospective analyses, bringing the field closer to actually using these tests in routine practice. The tests would prove particularly useful for patients with estrogen receptor–positive, node-negative breast cancer by helping to find those who are at low risk for long-term metastatic disease and who could safely stop treatment after 5 years of hormonal therapy, said Dr. Michael Gnant, professor of surgery at the University of Vienna.
But other experts stressed that it’s premature to start routinely using these tests.
"We’re getting to a point where we can offer to our patients genomic assays that are clinically validated and with demonstrated utility," Dr. W. Fraser Symmans said during the meeting. But, he added, while oncologists are "on the brink" of using the tests routinely, "we need to confirm reproducibility among labs, and that the test works in that setting," said Dr. Symmans, professor of pathology at the University of Texas M.D. Anderson Cancer Center in Houston.
None of the three genetic test panels were designed to predict late recurrences, noted Dr. Peter C. Dubsky, a surgeon at the University of Vienna and a collaborator with Dr. Gnant. "These data will need further validation before actually being incorporated into clinical decision-making concerning adjuvant endocrine therapy beyond 5 years," Dr. Dubsky said in a written statement.
The analysis reported by Dr. Gnant and Dr. Dubsky included formalin-fixed and paraffin-embedded tumor specimens from 1,478 patients who had been enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial, which had the primary goal of assessing two different 5-year treatment strategies in more than 3,700 postmenopausal women with estrogen receptor–positive breast cancer (J. Clin. Oncol. 2012;30:722-8).
Dr. Gnant, Dr. Dubsky, and their associates assessed the 1,478 specimens with the Prediction Analysis of Microarray test using a 58-gene classifier panel (PAM50), a test first reported in 2009 (J. Clin. Oncol. 2009;27:1160-7) that has since been commercialized as the Prosigna assay, available in Europe but not in the United States.
Using prespecified cutoffs on the PAM50 results for classifying patients as being at low, intermediate, and high risk for long term distant recurrences, the researchers tallied the rate of actual recurrences during a median follow-up of 11 years. The 15-year disease-free survival rate was 97.6% among low-risk patients, 90.9% in intermediate-risk patients, and 82.5% in high-risk patients, Dr. Gnant reported. The between-group differences were statistically significant.
The findings suggest that high-risk patients might be good candidates for extended adjuvant therapy, while low-risk patients, with a recurrence risk of less than 2% at 5-10 years and at 10-15 years following primary therapy "can be spared the side effects of extended adjuvant therapy," he said. The PAM50 risk of recurrence score "adds prognostic information beyond established clinicopathological factors."
The second analysis reported at the meeting retrospectively used medical records and specimens collected in the Arimidex, Tamoxifen Alone or in Combination (ATAC) study, which enrolled more than 6,000 postmenopausal women with localized invasive breast cancer (Lancet Oncology 2008;9:45-53). The researchers evaluated the prognostic efficacy of five different clinical, genetic, or histochemical test panels for predicting risk of distant recurrences during a median 10 years follow-up in 891 of the enrolled patients.
All five assessment panels yielded similar prognostic information during the first 5 years of follow-up. During the next 5 years, the strongest prognostic information came via the Clinical Treatment Score, which takes into account a patient’s nodal status, tumor grade and size, patient’s age, and treatment received, said Ivana Sestak, Ph.D., a statistician and epidemiologist at the University of London. The two most important prognostic features in this panel are tumor size and nodal status, she noted. Two other assessment panels – the PAM50 genetic panel and the Breast Cancer Index, a genetic test first described in 2011 – also provided statistically significant and clinically meaningful additional prediction of distant recurrences during 5-10 years of follow-up (Br. J. Cancer 2011;104:1762-9).
The other two tests Dr. Sestak and her associates evaluated did not add further prognostic information beyond what the Clinical Treatment Score provided. The uninformative tests were a set of four immunohistochemical markers (to estrogen, progesterone, HER2, and ki67), and the Oncotype Dx recurrence score – a 21-gene panel test marketed by Genomic Health.
"The PAM50 risk of recurrence score and the Breast Cancer Index may be used to identify estrogen receptor–positive breast cancer patients who are at increased risk of late recurrence and who may benefit from extended adjuvant hormonal therapy beyond 5 years," she concluded. But "none of these scores were developed to dictate treatment," she cautioned.
These findings, together with the PAM50 analysis from the ABCSG 8 study, solidify PAM50’s position as a validated prognostic tool, Dr. Gnant said.
In addition to PAM50 and the Breast Cancer Index, a third genetic test recently shown effective for predicting long-term recurrence risk in similar patients is the EndoPredict (Ann. Oncol. 2013;24:640-7).
All three assays can now be considered validated for longer-term prognosis in patients with endocrine-responsive, lymph node–negative breast cancer, Dr. Symmans said.
The conference was sponsored by the European Society for Medical Oncology.
Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.
Twitter: @mitchelzoler
AT IMPAKT 2013 BREAST CANCER CONFERENCE
Major finding: Low-risk patients by the PAM50 test had 97.6% 15-year disease-free survival compared with 82.5% in high-risk patients.
Data source: A retrospective analysis of 1,478 women enrolled in the Austrian Breast and Colorectal Cancer Study Group (ABCSG) 8 trial.
Disclosures: Dr. Gnant disclosed ties to Amgen, Pfizer, Novartis, GlaxoSmithKline, Bayer, Sandoz, AstraZeneca, Genomic Health, NanoString Technologies, Sanofi-Aventis, and Roche. Dr. Sestak had no disclosures. Dr. Symmans is cofounder of, and has equity in, Nuvera Biosciences. Dr. Dubsky disclosed ties to AstraZeneca, Novartis, Sividon Diagnostica, and Pfizer.

Dietary antioxidants linked to reduced postoperative atrial fib
ROME – Patients undergoing cardiac surgery who ate a diet rich in antioxidants developed significantly fewer episodes of atrial fibrillation, compared with patients who consumed fewer antioxidants, in a review of 217 patients from one Italian center.
Patients in the top tertile for antioxidant consumption in their diet had roughly half the rate of new-onset atrial fibrillation following open cardiac surgery compared with the remaining patients in a multivariate adjusted analysis, Dr. Licia Iacoviello reported in a poster at the annual the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
The next step will be a prospective trial with about 700 patients to test the efficacy of an antioxidant supplement to cut the development of postoperative atrial fibrillation in patients undergoing cardiac surgery, said Dr. Iacoviello, head of the laboratory of genetic and environmental epidemiology at Catholic University, Campobasso, Italy.

She said that she is planning such a trial with her colleagues, but she acknowledged that an antioxidant supplement may not deliver the same materials as a diet rich in antioxidant-containing nutrients. However, intervention based on a controlled diet is difficult to standardize and run, she said in an interview.
Her report involved 217 consecutive patients who underwent coronary artery bypass grafting (CABG), cardiac valve repair or replacement surgery, or a combination of both procedures during January 2010–June 2012. The patients agreed to participate in the study and supplied full information on their diet during the year before surgery. Dr. Iacoviello and her associates analyzed the dietary questionnaire results with several tools that assess antioxidant content, including the trolox equivalent antioxidant capacity (TEAC) (J. Nutr. 2007;137:93-8). The most commonly consumed antioxidant-containing item in their diet was wine, which supplied 46% of antioxidant content, followed by coffee, which kicked in another 30%, and then fruit and fruit juices, which supplied 8% of everyone’s antioxidant consumption. The average age of the patients was 68 years; 110 (51%) underwent isolated CABG, 54 (25%) underwent isolated valve surgery, and the remaining patients had a combined procedure.
During follow-up, 84 patients (39%) developed atrial fibrillation that produced either clinically identifiable symptoms or persisted for more than 5 minutes on an ECG recording. Incident atrial fibrillation occurred in 20 (27%) of 73 patients in the highest tertile for antioxidant consumption based on their TEAC, and in 64 (44%) of the other 144 patients.
In a multivariable analysis that controlled for age, sex, diabetes treatment, a prior diagnosis of atrial fibrillation, and total energy intake, patients in the highest TEAC tertile had a statistically significant, 51% lower risk for developing atrial fibrillation, compared with patients with lower TEAC levels, Dr. Iacoviello reported.
A second analysis that focused only on the 110 patients who underwent isolated CABG showed a similar relationship. In this subgroup, the 39 patients with higher TEAC scores had a 73% reduced risk for new-onset atrial fibrillation following CABG, compared with the remaining 71 with TEAC levels in the two lowest tertiles for the overall group, a statistically significant difference.
These findings provide the first clinical evidence that high dietary levels of antioxidants may play a role in suppressing development of atrial fibrillation following cardiac surgery, said Dr. Giovanni de Gaetano, a coinvestigator on the study and director of research laboratories at Catholic University in Campobasso.
Dr. Iacoviello and Dr. de Gaetano said that they had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
ROME – Patients undergoing cardiac surgery who ate a diet rich in antioxidants developed significantly fewer episodes of atrial fibrillation, compared with patients who consumed fewer antioxidants, in a review of 217 patients from one Italian center.
Patients in the top tertile for antioxidant consumption in their diet had roughly half the rate of new-onset atrial fibrillation following open cardiac surgery compared with the remaining patients in a multivariate adjusted analysis, Dr. Licia Iacoviello reported in a poster at the annual the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
The next step will be a prospective trial with about 700 patients to test the efficacy of an antioxidant supplement to cut the development of postoperative atrial fibrillation in patients undergoing cardiac surgery, said Dr. Iacoviello, head of the laboratory of genetic and environmental epidemiology at Catholic University, Campobasso, Italy.
She said that she is planning such a trial with her colleagues, but she acknowledged that an antioxidant supplement may not deliver the same materials as a diet rich in antioxidant-containing nutrients. However, intervention based on a controlled diet is difficult to standardize and run, she said in an interview.
Her report involved 217 consecutive patients who underwent coronary artery bypass grafting (CABG), cardiac valve repair or replacement surgery, or a combination of both procedures during January 2010–June 2012. The patients agreed to participate in the study and supplied full information on their diet during the year before surgery. Dr. Iacoviello and her associates analyzed the dietary questionnaire results with several tools that assess antioxidant content, including the trolox equivalent antioxidant capacity (TEAC) (J. Nutr. 2007;137:93-8). The most commonly consumed antioxidant-containing item in their diet was wine, which supplied 46% of antioxidant content, followed by coffee, which kicked in another 30%, and then fruit and fruit juices, which supplied 8% of everyone’s antioxidant consumption. The average age of the patients was 68 years; 110 (51%) underwent isolated CABG, 54 (25%) underwent isolated valve surgery, and the remaining patients had a combined procedure.
During follow-up, 84 patients (39%) developed atrial fibrillation that produced either clinically identifiable symptoms or persisted for more than 5 minutes on an ECG recording. Incident atrial fibrillation occurred in 20 (27%) of 73 patients in the highest tertile for antioxidant consumption based on their TEAC, and in 64 (44%) of the other 144 patients.
In a multivariable analysis that controlled for age, sex, diabetes treatment, a prior diagnosis of atrial fibrillation, and total energy intake, patients in the highest TEAC tertile had a statistically significant, 51% lower risk for developing atrial fibrillation, compared with patients with lower TEAC levels, Dr. Iacoviello reported.
A second analysis that focused only on the 110 patients who underwent isolated CABG showed a similar relationship. In this subgroup, the 39 patients with higher TEAC scores had a 73% reduced risk for new-onset atrial fibrillation following CABG, compared with the remaining 71 with TEAC levels in the two lowest tertiles for the overall group, a statistically significant difference.
These findings provide the first clinical evidence that high dietary levels of antioxidants may play a role in suppressing development of atrial fibrillation following cardiac surgery, said Dr. Giovanni de Gaetano, a coinvestigator on the study and director of research laboratories at Catholic University in Campobasso.
Dr. Iacoviello and Dr. de Gaetano said that they had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
ROME – Patients undergoing cardiac surgery who ate a diet rich in antioxidants developed significantly fewer episodes of atrial fibrillation, compared with patients who consumed fewer antioxidants, in a review of 217 patients from one Italian center.
Patients in the top tertile for antioxidant consumption in their diet had roughly half the rate of new-onset atrial fibrillation following open cardiac surgery compared with the remaining patients in a multivariate adjusted analysis, Dr. Licia Iacoviello reported in a poster at the annual the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*.
The next step will be a prospective trial with about 700 patients to test the efficacy of an antioxidant supplement to cut the development of postoperative atrial fibrillation in patients undergoing cardiac surgery, said Dr. Iacoviello, head of the laboratory of genetic and environmental epidemiology at Catholic University, Campobasso, Italy.
She said that she is planning such a trial with her colleagues, but she acknowledged that an antioxidant supplement may not deliver the same materials as a diet rich in antioxidant-containing nutrients. However, intervention based on a controlled diet is difficult to standardize and run, she said in an interview.
Her report involved 217 consecutive patients who underwent coronary artery bypass grafting (CABG), cardiac valve repair or replacement surgery, or a combination of both procedures during January 2010–June 2012. The patients agreed to participate in the study and supplied full information on their diet during the year before surgery. Dr. Iacoviello and her associates analyzed the dietary questionnaire results with several tools that assess antioxidant content, including the trolox equivalent antioxidant capacity (TEAC) (J. Nutr. 2007;137:93-8). The most commonly consumed antioxidant-containing item in their diet was wine, which supplied 46% of antioxidant content, followed by coffee, which kicked in another 30%, and then fruit and fruit juices, which supplied 8% of everyone’s antioxidant consumption. The average age of the patients was 68 years; 110 (51%) underwent isolated CABG, 54 (25%) underwent isolated valve surgery, and the remaining patients had a combined procedure.
During follow-up, 84 patients (39%) developed atrial fibrillation that produced either clinically identifiable symptoms or persisted for more than 5 minutes on an ECG recording. Incident atrial fibrillation occurred in 20 (27%) of 73 patients in the highest tertile for antioxidant consumption based on their TEAC, and in 64 (44%) of the other 144 patients.
In a multivariable analysis that controlled for age, sex, diabetes treatment, a prior diagnosis of atrial fibrillation, and total energy intake, patients in the highest TEAC tertile had a statistically significant, 51% lower risk for developing atrial fibrillation, compared with patients with lower TEAC levels, Dr. Iacoviello reported.
A second analysis that focused only on the 110 patients who underwent isolated CABG showed a similar relationship. In this subgroup, the 39 patients with higher TEAC scores had a 73% reduced risk for new-onset atrial fibrillation following CABG, compared with the remaining 71 with TEAC levels in the two lowest tertiles for the overall group, a statistically significant difference.
These findings provide the first clinical evidence that high dietary levels of antioxidants may play a role in suppressing development of atrial fibrillation following cardiac surgery, said Dr. Giovanni de Gaetano, a coinvestigator on the study and director of research laboratories at Catholic University in Campobasso.
Dr. Iacoviello and Dr. de Gaetano said that they had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the meeting name.
AT EUROPREVENT 2013
Major finding: Patients in the top tertile for dietary antioxidant consumption developed 51% fewer postoperative atrial fibrillation cases, compared with other patients.
Data source: A review of 217 consecutive patients who underwent cardiac surgery at one Italian center.
Disclosures: Dr. Iacoviello and Dr. de Gaetano said that they had no disclosures.

Telemonitored cardiac rehabilitation boosts compliance
ROME – A home-based cardiac rehabilitation program that relies on telemonitoring safely allowed effective training of about 800 elderly cardiac patients at one center in Poland since 2006.
"The advantages of telerehabilitation are the convenience and easy access for elderly patients," Dr. Ewa Piotrowicz said at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*. Telerehabilitation "fosters greater patient independence than hospital-based exercise training, and may reduce patient commute time and costs. Telemedicine may overcome some of the barriers related to aging.
"In our opinion, home-based cardiac rehabilitation is the best option" for older patients, said Dr. Piotrowicz, a cardiologist and head of the telecardiology center of the Institute of Cardiology in Warsaw.

A key to safe and successful home-based rehabilitation training for elderly cardiac patients is a thorough baseline examination to assess cardiac stability. "We don’t do telerehabilitation on unstable patients," she said in an interview. The other major feature is thorough monitoring by a telephone conversation and telephone transmission of vital recordings immediately before and after each at-home rehabilitation session. "Before and after every session the patient sends an ECG recording and answers a series of questions," she explained.
During the 7 years that the institute has run the program, it has enrolled about 500 lower-risk and 300 higher-risk patients, with about 50 in the program at any given time. At entry, each patient undergoes assessment by ECG, an echocardiography examination, 24-hour Holter blood pressure monitoring, and a cardiopulmonary exercise test.
The rehabilitation program involves an individualized exercise training program, and launches with a few sessions at the hospital along with educational sessions. The patient then continues the basic phase of the program with five daily sessions per week for 8 weeks. The program includes walking, running, interval training, and breathing training. Before and immediately after each daily session the patient speaks with a physician at the center, answering questions and sending information on ECG, heart rate, blood pressure, weight, oxygen saturation, respiration rate, and medications taken. Patients must receive approval from a physician before each exercise session starts.
The program achieved a high compliance level. Dr. Piotrowicz said that 95% of the 800 participants completed their 8-week programs. Following that, patients are encouraged to continue exercising on their own.
In 2010, she and her associates reported results from a formal, controlled assessment of compliance among 152 patients with heart failure who were randomized to either a home-based, telemonitored rehabilitation program or a more conventional outpatient program. The home-based telemonitored program produced similar clinical and quality of life improvements compared with the program for the control patients, and the 77 patients randomized to telemonitoring had 100% compliance with the 8-week rehabilitation program, compared with a 20% attrition rate among the patients enrolled in a standard outpatient rehabilitation program (Eur. J. Heart Fail. 2010;12:164-71). Dr. Piotrowicz attributed the high compliance to the daily contact that patients maintain with their health care providers.
"Telerehabilitation is a chance for implementing cardiac rehabilitation, especially in chronic heart failure patients," she said. The next step is a multicenter study of this approach, she added.
Dr. Piotrowicz said that she had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation.
ROME – A home-based cardiac rehabilitation program that relies on telemonitoring safely allowed effective training of about 800 elderly cardiac patients at one center in Poland since 2006.
"The advantages of telerehabilitation are the convenience and easy access for elderly patients," Dr. Ewa Piotrowicz said at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*. Telerehabilitation "fosters greater patient independence than hospital-based exercise training, and may reduce patient commute time and costs. Telemedicine may overcome some of the barriers related to aging.
"In our opinion, home-based cardiac rehabilitation is the best option" for older patients, said Dr. Piotrowicz, a cardiologist and head of the telecardiology center of the Institute of Cardiology in Warsaw.
A key to safe and successful home-based rehabilitation training for elderly cardiac patients is a thorough baseline examination to assess cardiac stability. "We don’t do telerehabilitation on unstable patients," she said in an interview. The other major feature is thorough monitoring by a telephone conversation and telephone transmission of vital recordings immediately before and after each at-home rehabilitation session. "Before and after every session the patient sends an ECG recording and answers a series of questions," she explained.
During the 7 years that the institute has run the program, it has enrolled about 500 lower-risk and 300 higher-risk patients, with about 50 in the program at any given time. At entry, each patient undergoes assessment by ECG, an echocardiography examination, 24-hour Holter blood pressure monitoring, and a cardiopulmonary exercise test.
The rehabilitation program involves an individualized exercise training program, and launches with a few sessions at the hospital along with educational sessions. The patient then continues the basic phase of the program with five daily sessions per week for 8 weeks. The program includes walking, running, interval training, and breathing training. Before and immediately after each daily session the patient speaks with a physician at the center, answering questions and sending information on ECG, heart rate, blood pressure, weight, oxygen saturation, respiration rate, and medications taken. Patients must receive approval from a physician before each exercise session starts.
The program achieved a high compliance level. Dr. Piotrowicz said that 95% of the 800 participants completed their 8-week programs. Following that, patients are encouraged to continue exercising on their own.
In 2010, she and her associates reported results from a formal, controlled assessment of compliance among 152 patients with heart failure who were randomized to either a home-based, telemonitored rehabilitation program or a more conventional outpatient program. The home-based telemonitored program produced similar clinical and quality of life improvements compared with the program for the control patients, and the 77 patients randomized to telemonitoring had 100% compliance with the 8-week rehabilitation program, compared with a 20% attrition rate among the patients enrolled in a standard outpatient rehabilitation program (Eur. J. Heart Fail. 2010;12:164-71). Dr. Piotrowicz attributed the high compliance to the daily contact that patients maintain with their health care providers.
"Telerehabilitation is a chance for implementing cardiac rehabilitation, especially in chronic heart failure patients," she said. The next step is a multicenter study of this approach, she added.
Dr. Piotrowicz said that she had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation.
ROME – A home-based cardiac rehabilitation program that relies on telemonitoring safely allowed effective training of about 800 elderly cardiac patients at one center in Poland since 2006.
"The advantages of telerehabilitation are the convenience and easy access for elderly patients," Dr. Ewa Piotrowicz said at the annual meeting of the European Association for Cardiovascular Prevention and Rehabilitation*. Telerehabilitation "fosters greater patient independence than hospital-based exercise training, and may reduce patient commute time and costs. Telemedicine may overcome some of the barriers related to aging.
"In our opinion, home-based cardiac rehabilitation is the best option" for older patients, said Dr. Piotrowicz, a cardiologist and head of the telecardiology center of the Institute of Cardiology in Warsaw.
A key to safe and successful home-based rehabilitation training for elderly cardiac patients is a thorough baseline examination to assess cardiac stability. "We don’t do telerehabilitation on unstable patients," she said in an interview. The other major feature is thorough monitoring by a telephone conversation and telephone transmission of vital recordings immediately before and after each at-home rehabilitation session. "Before and after every session the patient sends an ECG recording and answers a series of questions," she explained.
During the 7 years that the institute has run the program, it has enrolled about 500 lower-risk and 300 higher-risk patients, with about 50 in the program at any given time. At entry, each patient undergoes assessment by ECG, an echocardiography examination, 24-hour Holter blood pressure monitoring, and a cardiopulmonary exercise test.
The rehabilitation program involves an individualized exercise training program, and launches with a few sessions at the hospital along with educational sessions. The patient then continues the basic phase of the program with five daily sessions per week for 8 weeks. The program includes walking, running, interval training, and breathing training. Before and immediately after each daily session the patient speaks with a physician at the center, answering questions and sending information on ECG, heart rate, blood pressure, weight, oxygen saturation, respiration rate, and medications taken. Patients must receive approval from a physician before each exercise session starts.
The program achieved a high compliance level. Dr. Piotrowicz said that 95% of the 800 participants completed their 8-week programs. Following that, patients are encouraged to continue exercising on their own.
In 2010, she and her associates reported results from a formal, controlled assessment of compliance among 152 patients with heart failure who were randomized to either a home-based, telemonitored rehabilitation program or a more conventional outpatient program. The home-based telemonitored program produced similar clinical and quality of life improvements compared with the program for the control patients, and the 77 patients randomized to telemonitoring had 100% compliance with the 8-week rehabilitation program, compared with a 20% attrition rate among the patients enrolled in a standard outpatient rehabilitation program (Eur. J. Heart Fail. 2010;12:164-71). Dr. Piotrowicz attributed the high compliance to the daily contact that patients maintain with their health care providers.
"Telerehabilitation is a chance for implementing cardiac rehabilitation, especially in chronic heart failure patients," she said. The next step is a multicenter study of this approach, she added.
Dr. Piotrowicz said that she had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation.
AT EUROPREVENT 2013
Major finding: Telemedicine achieved 95% compliance with at-home cardiac rehabilitation among elderly cardiac patients.
Data source: A review of about 800 patients treated by home-based telerehabilitation at one center in Poland during 7 years.
Disclosures: Dr. Piotrowicz said that she had no disclosures.

Acute MI patients benefit from early rehabilitation
ROME – Starting cardiac rehabilitation sessions within 2 weeks of an acute myocardial infarction is safe and can improve cardiac perfusion and function, according to results of a randomized, controlled study of 46 patients who had residual myocardial ischemia following an MI and percutaneous coronary revascularization.
"Exercise-induced changes in myocardial perfusion and function were associated with an absence of unfavorable left-ventricular remodeling and an improved cardiovascular functional capacity," Dr. Francesco Giallauria said at the European Association for Cardiovascular Prevention and Rehabilitation* annual meeting. He hypothesized that exercise training begun soon after an MI improves myocardial perfusion by inducing coronary vascular adaptation or enhancing development of collateral cardiac vessels.

The study began with patients who underwent percutaneous coronary intervention (PCI) following an acute ST-elevation MI who were then assessed by dipyridamole stress and gated single-photon emission CT (SPECT) using labeled sestamibi. All 46 included patients had a significant amount of residual myocardial ischemia despite PCI, presumably caused by inadequate perfusion in myocardial regions not vascularized by the PCI-treated coronaries, said Dr. Giallauria, a cardiologist at the University of Naples (Italy). All patients also underwent a cardiopulmonary exercise test at baseline to determine their peak exercise capacity.
The researchers then randomized the patients. Twenty-five entered a hospital outpatient program of supervised, 30-minutes sessions of bicycle exercise three times a week, with an exercise target during each session of 60%-70% of their peak exercise capacity. The program began within 2 weeks of their acute MI. The remaining 21 patients served as controls and received just instructions about maintaining physical exercise and lifestyle modification.
The exercise rehabilitation program continued for 6 months, when all 46 patients underwent a follow-up examination of their myocardial perfusion with gated SPECT and follow-up cardiopulmonary stress testing. The average age of the patients was 54 years, and 87% were men.
The results showed that after 6 months, patients who underwent exercise training had an average 29% increase in peak exercise capacity and a 10% average rise in their peak heart rate compared with baseline, both statistically significant differences. Results from the serial SPECT studies showed that left ventricular ejection fraction rose from an average of 48% at baseline to 52% in the patients who underwent exercise training, a statistically significant rise, and their wall motion and wall thickness scores showed improvements in cardiac shape and function compared with baseline, all differences that were statistically significant. In contrast, the control patients had no significant changes for any of these exercise or cardiac measures during the 6 months of follow-up.
In addition, the SPECT imaging showed that at follow-up the extent of myocardial perfusion defect and ischemia fell by about 50% in the exercise group while remaining virtually unchanged in the control patients.
Dr. Giallauria said that he had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation annual conference.
ROME – Starting cardiac rehabilitation sessions within 2 weeks of an acute myocardial infarction is safe and can improve cardiac perfusion and function, according to results of a randomized, controlled study of 46 patients who had residual myocardial ischemia following an MI and percutaneous coronary revascularization.
"Exercise-induced changes in myocardial perfusion and function were associated with an absence of unfavorable left-ventricular remodeling and an improved cardiovascular functional capacity," Dr. Francesco Giallauria said at the European Association for Cardiovascular Prevention and Rehabilitation* annual meeting. He hypothesized that exercise training begun soon after an MI improves myocardial perfusion by inducing coronary vascular adaptation or enhancing development of collateral cardiac vessels.
The study began with patients who underwent percutaneous coronary intervention (PCI) following an acute ST-elevation MI who were then assessed by dipyridamole stress and gated single-photon emission CT (SPECT) using labeled sestamibi. All 46 included patients had a significant amount of residual myocardial ischemia despite PCI, presumably caused by inadequate perfusion in myocardial regions not vascularized by the PCI-treated coronaries, said Dr. Giallauria, a cardiologist at the University of Naples (Italy). All patients also underwent a cardiopulmonary exercise test at baseline to determine their peak exercise capacity.
The researchers then randomized the patients. Twenty-five entered a hospital outpatient program of supervised, 30-minutes sessions of bicycle exercise three times a week, with an exercise target during each session of 60%-70% of their peak exercise capacity. The program began within 2 weeks of their acute MI. The remaining 21 patients served as controls and received just instructions about maintaining physical exercise and lifestyle modification.
The exercise rehabilitation program continued for 6 months, when all 46 patients underwent a follow-up examination of their myocardial perfusion with gated SPECT and follow-up cardiopulmonary stress testing. The average age of the patients was 54 years, and 87% were men.
The results showed that after 6 months, patients who underwent exercise training had an average 29% increase in peak exercise capacity and a 10% average rise in their peak heart rate compared with baseline, both statistically significant differences. Results from the serial SPECT studies showed that left ventricular ejection fraction rose from an average of 48% at baseline to 52% in the patients who underwent exercise training, a statistically significant rise, and their wall motion and wall thickness scores showed improvements in cardiac shape and function compared with baseline, all differences that were statistically significant. In contrast, the control patients had no significant changes for any of these exercise or cardiac measures during the 6 months of follow-up.
In addition, the SPECT imaging showed that at follow-up the extent of myocardial perfusion defect and ischemia fell by about 50% in the exercise group while remaining virtually unchanged in the control patients.
Dr. Giallauria said that he had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation annual conference.
ROME – Starting cardiac rehabilitation sessions within 2 weeks of an acute myocardial infarction is safe and can improve cardiac perfusion and function, according to results of a randomized, controlled study of 46 patients who had residual myocardial ischemia following an MI and percutaneous coronary revascularization.
"Exercise-induced changes in myocardial perfusion and function were associated with an absence of unfavorable left-ventricular remodeling and an improved cardiovascular functional capacity," Dr. Francesco Giallauria said at the European Association for Cardiovascular Prevention and Rehabilitation* annual meeting. He hypothesized that exercise training begun soon after an MI improves myocardial perfusion by inducing coronary vascular adaptation or enhancing development of collateral cardiac vessels.
The study began with patients who underwent percutaneous coronary intervention (PCI) following an acute ST-elevation MI who were then assessed by dipyridamole stress and gated single-photon emission CT (SPECT) using labeled sestamibi. All 46 included patients had a significant amount of residual myocardial ischemia despite PCI, presumably caused by inadequate perfusion in myocardial regions not vascularized by the PCI-treated coronaries, said Dr. Giallauria, a cardiologist at the University of Naples (Italy). All patients also underwent a cardiopulmonary exercise test at baseline to determine their peak exercise capacity.
The researchers then randomized the patients. Twenty-five entered a hospital outpatient program of supervised, 30-minutes sessions of bicycle exercise three times a week, with an exercise target during each session of 60%-70% of their peak exercise capacity. The program began within 2 weeks of their acute MI. The remaining 21 patients served as controls and received just instructions about maintaining physical exercise and lifestyle modification.
The exercise rehabilitation program continued for 6 months, when all 46 patients underwent a follow-up examination of their myocardial perfusion with gated SPECT and follow-up cardiopulmonary stress testing. The average age of the patients was 54 years, and 87% were men.
The results showed that after 6 months, patients who underwent exercise training had an average 29% increase in peak exercise capacity and a 10% average rise in their peak heart rate compared with baseline, both statistically significant differences. Results from the serial SPECT studies showed that left ventricular ejection fraction rose from an average of 48% at baseline to 52% in the patients who underwent exercise training, a statistically significant rise, and their wall motion and wall thickness scores showed improvements in cardiac shape and function compared with baseline, all differences that were statistically significant. In contrast, the control patients had no significant changes for any of these exercise or cardiac measures during the 6 months of follow-up.
In addition, the SPECT imaging showed that at follow-up the extent of myocardial perfusion defect and ischemia fell by about 50% in the exercise group while remaining virtually unchanged in the control patients.
Dr. Giallauria said that he had no disclosures.
On Twitter @mitchelzoler
*Correction, 5/29/2013: An earlier version of this story misstated the name of the European Association for Cardiovascular Prevention and Rehabilitation annual conference.
AT EUROPREVENT 2013
Major finding: Six months of exercise cardiac rehabilitation, started soon after an acute MI, safely boosted exercise capacity by 29%.
Data source: A randomized, controlled, single-center study of 46 patients.
Disclosures: Dr. Giallauria said that he had no disclosures.

Panel cuts coronary-intervention case load for competency
The panel of cardiologists who revised U.S. competency standards for coronary interventionalists acknowledged prevailing case-volume realities and cut the minimum number of cases recommended for active operators to 50 per year, down from a long-standing recommendation of 75 coronary interventions annually.
The Clinical Competence and Training Task Force, assembled by the American College of Cardiology, the American Heart Association, and the Society for Cardiovascular Angiography and Interventions (SCAI), also made the linked change of halving prior recommended coronary-case volumes for catheterization-laboratory centers, with a new recommended minimum target of 200 cases per year per site, down from the 400 annual cases called for in the 2007 version of the clinical competence statement for cardiac interventions.
The 2013 revision, with a focus specifically on coronary-artery interventions, appeared online on May 8 on the websites of all three organizations (J. Am. Coll. Cardiol. 2013 [doi:10.1016/j.jacc.2013.05.002]).
Although the revised case numbers will likely be what first captures the attention of interventionalists and cath lab administrators, these changes were not the most central to the new revision, said Dr. Theodore A. Bass, professor and chief of cardiology at the University of Florida, Jacksonville, and vice chair of the task force. He focused on the diverse, 35-item list of core competency components that is the backbone of the new revision.
"It’s a much broader view of what competency involves," he said in an interview. "In the past, competency was taking an exam, or having a certain knowledge base. But now we realize that other skills are also extremely important," such as appropriate patient selection, using technologies in a safe and appropriate manner, and delivering patient-centered care, said Dr. Bass, who is also president-elect of SCAI.
The new statement "is the first cardiovascular competency statement to fully utilize the six-domains structure promulgated by the Accreditation Council of Graduate Medical Education and adopted and endorsed by the American Board of Internal Medicine," Dr. John Gordon Harold, chair of the writing committee, said in a written statement.
"It goes beyond medical knowledge and procedure performance to include the important issues of leading an interdisciplinary team, working in a complex system, communicating effectively, engaging in continuous quality improvement at individual and system levels, adhering to evidence-based medicine, and demonstrating the highest levels of professionalism," said Dr. Harold, who is also ACC president and a cardiologist at Cedars-Sinai Heart Institute in Los Angeles.
Although the new statement is wide ranging, the case-number issue stands out as something the task force worked on at length, with a quarter of the statement devoted to various aspects of the issue for both individual operators and for cath labs.
"Volume has been used as a surrogate for quality because it measurable, but there has never been clear data that there is a strong correlation," said Dr. Bass. Plus, the original individual volume number, the venerable figure of 75 cases per year that has been around since at least 1990, when it appeared in the first clinical competency statement, "was not data based, it was judgment based," he noted. "Volume is not the be all and end all. We thought that 100 cases over 2 years seemed in the sweet spot for all considerations."
"Low-volume operators can self restrict what they do and get very good outcomes with less volume," said Dr. Christopher J. White, professor and chair for cardiovascular diseases at the Ochsner Clinic, New Orleans, and a member of the task force. "Rather than use an arbitrary volume as a surrogate for quality, it is more useful to actually measure quality, with a tool like the NCDR [National Cardiovascular Data Registry] for CathPCI."
Another issue is the feasibility of calling for annual rates of 75 cases individually and 400 per center, given recent trends with substantially fewer U.S. percutaneous coronary interventions (PCI), compared with the mid-2000s, and the growing number of interventionalists. The statement notes that "a majority of interventional cardiologists in the United States are not achieving the previously recommended threshold of 75 PCIs annually."
Also, these days most interventional cardiologists perform other types of procedures that may not count as PCIs but still keep their skills sharp – things like peripheral vascular procedures, carotid stenting, and transcatheter aortic valve replacements, Dr. Bass said. And there is the issue of society’s need to have important acute-care services like primary PCI for myocardial infarctions available in even remote areas, where higher case volumes are hard to maintain.
"Cath labs with fewer than 200 cases per year should examine what they do and have stringent quality assurance measures in place," he said.
Two other notable changes in the 2013 competency revision are the inclusion for the first time of radial-artery access as an identified competency. Radial access "is still just under 20% of all U.S. PCI, but that’s up exponentially from a few years ago," Dr. Bass said. "There is a huge amount of patient preference for it, and the next generation is now trained in it. Radial access is the future."
The new revision focused exclusively on coronary artery interventions, with other common cardiac percutaneous procedures like valvuloplasty on hold for a different competency task force that will deal with structural and noncoronary interventions, Dr. Bass said.
Dr. Bass, Dr. Harold, and Dr. White had no relevant disclosures.
On Twitter @mitchelzoler
The panel of cardiologists who revised U.S. competency standards for coronary interventionalists acknowledged prevailing case-volume realities and cut the minimum number of cases recommended for active operators to 50 per year, down from a long-standing recommendation of 75 coronary interventions annually.
The Clinical Competence and Training Task Force, assembled by the American College of Cardiology, the American Heart Association, and the Society for Cardiovascular Angiography and Interventions (SCAI), also made the linked change of halving prior recommended coronary-case volumes for catheterization-laboratory centers, with a new recommended minimum target of 200 cases per year per site, down from the 400 annual cases called for in the 2007 version of the clinical competence statement for cardiac interventions.
The 2013 revision, with a focus specifically on coronary-artery interventions, appeared online on May 8 on the websites of all three organizations (J. Am. Coll. Cardiol. 2013 [doi:10.1016/j.jacc.2013.05.002]).
Although the revised case numbers will likely be what first captures the attention of interventionalists and cath lab administrators, these changes were not the most central to the new revision, said Dr. Theodore A. Bass, professor and chief of cardiology at the University of Florida, Jacksonville, and vice chair of the task force. He focused on the diverse, 35-item list of core competency components that is the backbone of the new revision.
"It’s a much broader view of what competency involves," he said in an interview. "In the past, competency was taking an exam, or having a certain knowledge base. But now we realize that other skills are also extremely important," such as appropriate patient selection, using technologies in a safe and appropriate manner, and delivering patient-centered care, said Dr. Bass, who is also president-elect of SCAI.
The new statement "is the first cardiovascular competency statement to fully utilize the six-domains structure promulgated by the Accreditation Council of Graduate Medical Education and adopted and endorsed by the American Board of Internal Medicine," Dr. John Gordon Harold, chair of the writing committee, said in a written statement.
"It goes beyond medical knowledge and procedure performance to include the important issues of leading an interdisciplinary team, working in a complex system, communicating effectively, engaging in continuous quality improvement at individual and system levels, adhering to evidence-based medicine, and demonstrating the highest levels of professionalism," said Dr. Harold, who is also ACC president and a cardiologist at Cedars-Sinai Heart Institute in Los Angeles.
Although the new statement is wide ranging, the case-number issue stands out as something the task force worked on at length, with a quarter of the statement devoted to various aspects of the issue for both individual operators and for cath labs.
"Volume has been used as a surrogate for quality because it measurable, but there has never been clear data that there is a strong correlation," said Dr. Bass. Plus, the original individual volume number, the venerable figure of 75 cases per year that has been around since at least 1990, when it appeared in the first clinical competency statement, "was not data based, it was judgment based," he noted. "Volume is not the be all and end all. We thought that 100 cases over 2 years seemed in the sweet spot for all considerations."
"Low-volume operators can self restrict what they do and get very good outcomes with less volume," said Dr. Christopher J. White, professor and chair for cardiovascular diseases at the Ochsner Clinic, New Orleans, and a member of the task force. "Rather than use an arbitrary volume as a surrogate for quality, it is more useful to actually measure quality, with a tool like the NCDR [National Cardiovascular Data Registry] for CathPCI."
Another issue is the feasibility of calling for annual rates of 75 cases individually and 400 per center, given recent trends with substantially fewer U.S. percutaneous coronary interventions (PCI), compared with the mid-2000s, and the growing number of interventionalists. The statement notes that "a majority of interventional cardiologists in the United States are not achieving the previously recommended threshold of 75 PCIs annually."
Also, these days most interventional cardiologists perform other types of procedures that may not count as PCIs but still keep their skills sharp – things like peripheral vascular procedures, carotid stenting, and transcatheter aortic valve replacements, Dr. Bass said. And there is the issue of society’s need to have important acute-care services like primary PCI for myocardial infarctions available in even remote areas, where higher case volumes are hard to maintain.
"Cath labs with fewer than 200 cases per year should examine what they do and have stringent quality assurance measures in place," he said.
Two other notable changes in the 2013 competency revision are the inclusion for the first time of radial-artery access as an identified competency. Radial access "is still just under 20% of all U.S. PCI, but that’s up exponentially from a few years ago," Dr. Bass said. "There is a huge amount of patient preference for it, and the next generation is now trained in it. Radial access is the future."
The new revision focused exclusively on coronary artery interventions, with other common cardiac percutaneous procedures like valvuloplasty on hold for a different competency task force that will deal with structural and noncoronary interventions, Dr. Bass said.
Dr. Bass, Dr. Harold, and Dr. White had no relevant disclosures.
On Twitter @mitchelzoler
The panel of cardiologists who revised U.S. competency standards for coronary interventionalists acknowledged prevailing case-volume realities and cut the minimum number of cases recommended for active operators to 50 per year, down from a long-standing recommendation of 75 coronary interventions annually.
The Clinical Competence and Training Task Force, assembled by the American College of Cardiology, the American Heart Association, and the Society for Cardiovascular Angiography and Interventions (SCAI), also made the linked change of halving prior recommended coronary-case volumes for catheterization-laboratory centers, with a new recommended minimum target of 200 cases per year per site, down from the 400 annual cases called for in the 2007 version of the clinical competence statement for cardiac interventions.
The 2013 revision, with a focus specifically on coronary-artery interventions, appeared online on May 8 on the websites of all three organizations (J. Am. Coll. Cardiol. 2013 [doi:10.1016/j.jacc.2013.05.002]).
Although the revised case numbers will likely be what first captures the attention of interventionalists and cath lab administrators, these changes were not the most central to the new revision, said Dr. Theodore A. Bass, professor and chief of cardiology at the University of Florida, Jacksonville, and vice chair of the task force. He focused on the diverse, 35-item list of core competency components that is the backbone of the new revision.
"It’s a much broader view of what competency involves," he said in an interview. "In the past, competency was taking an exam, or having a certain knowledge base. But now we realize that other skills are also extremely important," such as appropriate patient selection, using technologies in a safe and appropriate manner, and delivering patient-centered care, said Dr. Bass, who is also president-elect of SCAI.
The new statement "is the first cardiovascular competency statement to fully utilize the six-domains structure promulgated by the Accreditation Council of Graduate Medical Education and adopted and endorsed by the American Board of Internal Medicine," Dr. John Gordon Harold, chair of the writing committee, said in a written statement.
"It goes beyond medical knowledge and procedure performance to include the important issues of leading an interdisciplinary team, working in a complex system, communicating effectively, engaging in continuous quality improvement at individual and system levels, adhering to evidence-based medicine, and demonstrating the highest levels of professionalism," said Dr. Harold, who is also ACC president and a cardiologist at Cedars-Sinai Heart Institute in Los Angeles.
Although the new statement is wide ranging, the case-number issue stands out as something the task force worked on at length, with a quarter of the statement devoted to various aspects of the issue for both individual operators and for cath labs.
"Volume has been used as a surrogate for quality because it measurable, but there has never been clear data that there is a strong correlation," said Dr. Bass. Plus, the original individual volume number, the venerable figure of 75 cases per year that has been around since at least 1990, when it appeared in the first clinical competency statement, "was not data based, it was judgment based," he noted. "Volume is not the be all and end all. We thought that 100 cases over 2 years seemed in the sweet spot for all considerations."
"Low-volume operators can self restrict what they do and get very good outcomes with less volume," said Dr. Christopher J. White, professor and chair for cardiovascular diseases at the Ochsner Clinic, New Orleans, and a member of the task force. "Rather than use an arbitrary volume as a surrogate for quality, it is more useful to actually measure quality, with a tool like the NCDR [National Cardiovascular Data Registry] for CathPCI."
Another issue is the feasibility of calling for annual rates of 75 cases individually and 400 per center, given recent trends with substantially fewer U.S. percutaneous coronary interventions (PCI), compared with the mid-2000s, and the growing number of interventionalists. The statement notes that "a majority of interventional cardiologists in the United States are not achieving the previously recommended threshold of 75 PCIs annually."
Also, these days most interventional cardiologists perform other types of procedures that may not count as PCIs but still keep their skills sharp – things like peripheral vascular procedures, carotid stenting, and transcatheter aortic valve replacements, Dr. Bass said. And there is the issue of society’s need to have important acute-care services like primary PCI for myocardial infarctions available in even remote areas, where higher case volumes are hard to maintain.
"Cath labs with fewer than 200 cases per year should examine what they do and have stringent quality assurance measures in place," he said.
Two other notable changes in the 2013 competency revision are the inclusion for the first time of radial-artery access as an identified competency. Radial access "is still just under 20% of all U.S. PCI, but that’s up exponentially from a few years ago," Dr. Bass said. "There is a huge amount of patient preference for it, and the next generation is now trained in it. Radial access is the future."
The new revision focused exclusively on coronary artery interventions, with other common cardiac percutaneous procedures like valvuloplasty on hold for a different competency task force that will deal with structural and noncoronary interventions, Dr. Bass said.
Dr. Bass, Dr. Harold, and Dr. White had no relevant disclosures.
On Twitter @mitchelzoler
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
ECG keys pre-sport participation screening
ROME – Efficient screening for potentially dangerous arrhythmias in adolescent and young-adult athletes requires the participant’s history, a physical examination, and results from a 12-lead ECG examination, based on experience with more than 15,000 screenings at one U.K. center.
"You need to use symptoms and the ECG results together," Jakir Ullah said at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation. "Either technique by itself is not best." Symptoms in sport participants who underwent screening were not associated with underlying cardiac pathology unless they occurred along with a group 2 ECG abnormality, said Mr. Ullah, a researcher at St. George’s University in London.
Most potentially dangerous cardiac abnormalities in adolescent or young-adult sport participants are asymptomatic, said Dr. Saqib Ghani, a cardiologist at St. George’s and a coinvestigator on the study. "ECG is more helpful than symptoms because you can miss the condition if it’s asymptomatic, and symptoms are very subjective," Dr. Ghani said in an interview.
An expert panel organized by the European Association for Cardiovascular Prevention and Rehabilitation and the European Society of Cardiology compiled a list of 13 uncommon, potentially pathological ECG abnormalities, known as group 2 abnormalities, in 2010 (Eur. J. Cardiol. 2010;31:243-59). The list includes T-wave inversion, left atrial enlargement, a long QT interval, and right ventricular hypertrophy.
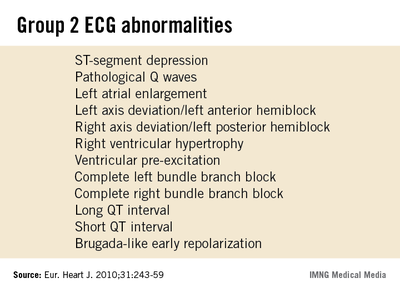
Together, these abnormalities occur in fewer than 5% of people screened by ECG prior to starting sport participation, according to data collected on more than 32,000 Italians aged 8-78 years who underwent pre–sport participation screening during 2003 (Eur. Heart J. 2007:28:2006-10).
Although many sports organizations call for preparticipation screening regardless of age or intensity level, cardiologists at St. George’s focused on people 14-35 years old because children under age 14 often show transient ECG abnormalities, while among adults over age 35 the main cardiac threat during sport participation comes from coronary artery disease rather than an abnormality, Dr. Ghani said.

The St. George’s series consisted of 15,027 people who were examined during 2007-2012. More than half of them were free of any ECG abnormality or symptoms and received immediate clearance for participation. But 6,598 people required further assessment, with 5,415 reporting symptoms, and 1,183 found with a group 2 ECG abnormality. The 8% prevalence rate for a group 2 abnormality, higher than in Italy, matches the somewhat higher U.K. prevalence rates reported by others, he added.
Among the 5,415 people investigated because of symptoms, none were found to have any underlying pathology that precluded sports participation, Mr. Ullah said. Symptoms included chest pain, syncope, palpitations, and dyspnea.
In contrast, among the 1,183 people identified for further assessment because of a group 2 ECG abnormality, the examination identified a clinically important underlying pathology in 67, 0.4% of everyone screened; another 44 people continue to undergo evaluations, and 1,072 people were found free of any sports-limiting condition. Among the 67 with an ECG abnormality and confirmed cardiac pathology, 25 (37%) also had symptoms. The most common cardiac pathology was Wolff-Parkinson-White syndrome, in 29 people, followed by a long QT interval in 8.
Dr. Ghani also stressed that ideally, pre–sport participation screening should occur for all sport participants regardless of the intensity of training or competition. "You only hear about sudden death in high-level athletes, but that is just the tip of the iceberg," he said. "We never know about the sudden death that happens to someone who is just running on the road."
Dr. Ghani and Mr. Ullah had no disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting during which these presentations were given. This story has been updated.
ROME – Efficient screening for potentially dangerous arrhythmias in adolescent and young-adult athletes requires the participant’s history, a physical examination, and results from a 12-lead ECG examination, based on experience with more than 15,000 screenings at one U.K. center.
"You need to use symptoms and the ECG results together," Jakir Ullah said at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation. "Either technique by itself is not best." Symptoms in sport participants who underwent screening were not associated with underlying cardiac pathology unless they occurred along with a group 2 ECG abnormality, said Mr. Ullah, a researcher at St. George’s University in London.
Most potentially dangerous cardiac abnormalities in adolescent or young-adult sport participants are asymptomatic, said Dr. Saqib Ghani, a cardiologist at St. George’s and a coinvestigator on the study. "ECG is more helpful than symptoms because you can miss the condition if it’s asymptomatic, and symptoms are very subjective," Dr. Ghani said in an interview.
An expert panel organized by the European Association for Cardiovascular Prevention and Rehabilitation and the European Society of Cardiology compiled a list of 13 uncommon, potentially pathological ECG abnormalities, known as group 2 abnormalities, in 2010 (Eur. J. Cardiol. 2010;31:243-59). The list includes T-wave inversion, left atrial enlargement, a long QT interval, and right ventricular hypertrophy.
Together, these abnormalities occur in fewer than 5% of people screened by ECG prior to starting sport participation, according to data collected on more than 32,000 Italians aged 8-78 years who underwent pre–sport participation screening during 2003 (Eur. Heart J. 2007:28:2006-10).
Although many sports organizations call for preparticipation screening regardless of age or intensity level, cardiologists at St. George’s focused on people 14-35 years old because children under age 14 often show transient ECG abnormalities, while among adults over age 35 the main cardiac threat during sport participation comes from coronary artery disease rather than an abnormality, Dr. Ghani said.
The St. George’s series consisted of 15,027 people who were examined during 2007-2012. More than half of them were free of any ECG abnormality or symptoms and received immediate clearance for participation. But 6,598 people required further assessment, with 5,415 reporting symptoms, and 1,183 found with a group 2 ECG abnormality. The 8% prevalence rate for a group 2 abnormality, higher than in Italy, matches the somewhat higher U.K. prevalence rates reported by others, he added.
Among the 5,415 people investigated because of symptoms, none were found to have any underlying pathology that precluded sports participation, Mr. Ullah said. Symptoms included chest pain, syncope, palpitations, and dyspnea.
In contrast, among the 1,183 people identified for further assessment because of a group 2 ECG abnormality, the examination identified a clinically important underlying pathology in 67, 0.4% of everyone screened; another 44 people continue to undergo evaluations, and 1,072 people were found free of any sports-limiting condition. Among the 67 with an ECG abnormality and confirmed cardiac pathology, 25 (37%) also had symptoms. The most common cardiac pathology was Wolff-Parkinson-White syndrome, in 29 people, followed by a long QT interval in 8.
Dr. Ghani also stressed that ideally, pre–sport participation screening should occur for all sport participants regardless of the intensity of training or competition. "You only hear about sudden death in high-level athletes, but that is just the tip of the iceberg," he said. "We never know about the sudden death that happens to someone who is just running on the road."
Dr. Ghani and Mr. Ullah had no disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting during which these presentations were given. This story has been updated.
ROME – Efficient screening for potentially dangerous arrhythmias in adolescent and young-adult athletes requires the participant’s history, a physical examination, and results from a 12-lead ECG examination, based on experience with more than 15,000 screenings at one U.K. center.
"You need to use symptoms and the ECG results together," Jakir Ullah said at the annual meeting of the *European Association for Cardiovascular Prevention and Rehabilitation. "Either technique by itself is not best." Symptoms in sport participants who underwent screening were not associated with underlying cardiac pathology unless they occurred along with a group 2 ECG abnormality, said Mr. Ullah, a researcher at St. George’s University in London.
Most potentially dangerous cardiac abnormalities in adolescent or young-adult sport participants are asymptomatic, said Dr. Saqib Ghani, a cardiologist at St. George’s and a coinvestigator on the study. "ECG is more helpful than symptoms because you can miss the condition if it’s asymptomatic, and symptoms are very subjective," Dr. Ghani said in an interview.
An expert panel organized by the European Association for Cardiovascular Prevention and Rehabilitation and the European Society of Cardiology compiled a list of 13 uncommon, potentially pathological ECG abnormalities, known as group 2 abnormalities, in 2010 (Eur. J. Cardiol. 2010;31:243-59). The list includes T-wave inversion, left atrial enlargement, a long QT interval, and right ventricular hypertrophy.
Together, these abnormalities occur in fewer than 5% of people screened by ECG prior to starting sport participation, according to data collected on more than 32,000 Italians aged 8-78 years who underwent pre–sport participation screening during 2003 (Eur. Heart J. 2007:28:2006-10).
Although many sports organizations call for preparticipation screening regardless of age or intensity level, cardiologists at St. George’s focused on people 14-35 years old because children under age 14 often show transient ECG abnormalities, while among adults over age 35 the main cardiac threat during sport participation comes from coronary artery disease rather than an abnormality, Dr. Ghani said.
The St. George’s series consisted of 15,027 people who were examined during 2007-2012. More than half of them were free of any ECG abnormality or symptoms and received immediate clearance for participation. But 6,598 people required further assessment, with 5,415 reporting symptoms, and 1,183 found with a group 2 ECG abnormality. The 8% prevalence rate for a group 2 abnormality, higher than in Italy, matches the somewhat higher U.K. prevalence rates reported by others, he added.
Among the 5,415 people investigated because of symptoms, none were found to have any underlying pathology that precluded sports participation, Mr. Ullah said. Symptoms included chest pain, syncope, palpitations, and dyspnea.
In contrast, among the 1,183 people identified for further assessment because of a group 2 ECG abnormality, the examination identified a clinically important underlying pathology in 67, 0.4% of everyone screened; another 44 people continue to undergo evaluations, and 1,072 people were found free of any sports-limiting condition. Among the 67 with an ECG abnormality and confirmed cardiac pathology, 25 (37%) also had symptoms. The most common cardiac pathology was Wolff-Parkinson-White syndrome, in 29 people, followed by a long QT interval in 8.
Dr. Ghani also stressed that ideally, pre–sport participation screening should occur for all sport participants regardless of the intensity of training or competition. "You only hear about sudden death in high-level athletes, but that is just the tip of the iceberg," he said. "We never know about the sudden death that happens to someone who is just running on the road."
Dr. Ghani and Mr. Ullah had no disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting during which these presentations were given. This story has been updated.
AT EUROPREVENT 2013
Major finding: Cardiac symptoms with no group 2 ECG abnormality were associated with no cases of dangerous cardiac pathology.
Data source: Data came from screening 15,027 people 14-35 years old at one U.K. hospital during 2007-2012.
Disclosures: Dr. Ghani and Mr. Ullah had no disclosures.
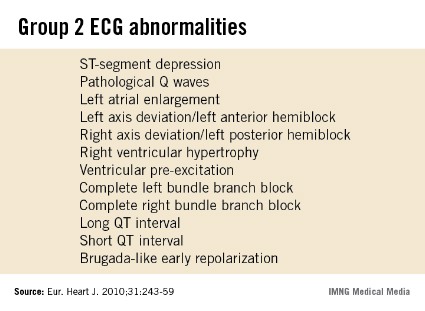
Heart rate linked to men's heart failure
ROME – Otherwise healthy, older men with a heart rate of 79 beats per minute or higher had a roughly 50% increased risk of developing heart failure, compared with men with slower heart rates, in a population-based cohort of more than 1,800 Dutch men.
The finding suggests that heart rate, independent of any other cardiovascular risk factor, could boost the risk for developing heart failure, and raises the possibility of trying to dampen this effect by using interventions to reduce heart rate, Dr. David Nanchen said at the annual meeting of the * European Association for Cardiovascular Prevention and Rehabilitation.

But the apparent link between resting heart rate and a boosted incidence of heart failure during follow-up occurred only in men. The analysis also included 2,939 women, who showed no suggestion of an association between baseline heart rate and subsequent development of heart failure.
The work reported by Dr. Nanchen also included an analysis that censored men who had an incident myocardial infarction during a median follow-up of 15 years, thereby eliminating cases of heart failure that occurred following an MI. In this analysis, men with a baseline heart rate of 79 beats per minute or greater had a statistically significant, 56% increased incidence of heart failure compared with men with an entry heart rate of less than 69 beats per minute, said Dr. Nanchen, head of the cardiovascular preventative clinic of the University of Lausanne (Switzerland).
Ruling out MI as a mediator between high heart rate and the development of heart failure means some other pathologic sequence is involved. One possibility is that patients with high heart rates develop tachycardia-induced cardiomyopathy that progresses to heart failure, Dr. Nanchen said in an interview."
His study included 4,768 people aged 55 or older enrolled in the Rotterdam Study from among apparently healthy people living in the Rotterdam area. During a median follow-up of 15 years, 656 enrollees developed heart failure. The analysis excluded people who at baseline had heart failure, coronary heart disease, atrial fibrillation, atrioventricular block, or a pacemaker, or were taking a beta-blocker or calcium channel blocker.
Among the 1,829 men in the study, every increment of 10 beats per minute in resting heart rate at entry into the study was linked with a statistically significant, 16% relative increase in the incidence of heart failure, an association not seen in women. When the researchers divided the men into tertiles based on their baseline heart rate, those in the top tertile with a rate of 79 beats per minute or greater had a 51% increased incidence of heart failure during follow-up, compared with men in the lowest tertile, with a rate of less than 69 beats per minute.
The analysis adjusted for age, smoking status, systolic blood pressure, diabetes, body mass index, total cholesterol level, HDL cholesterol level, and antihypertensive treatment.
The absence of this heart rate and heart failure link in women was a "surprise," Dr. Nanchen said. It’s possible that women’s hearts are more resilient to high heart rates, he suggested.
For the time being, the only intervention to offer otherwise healthy men older than 55 with a high heart rate is intensified control of lifestyle risk factors. Trial results showed that treatment with the heart rate–lowering drug ivabradine (Prooralan) in heart failure patients led to a reduction in heart failure–related hospitalizations (Lancet 2010;376:875-85).That experience makes it attractive to speculate that ivabradine treatment might also improve outcomes in men with high heart rates and no heart failure, but Dr. Nanchen said he had no immediate plans to test that hypothesis.
U.S. physicians won’t get the chance to study ivabradine in clinical practice for some time. Its manufacturer, Servier, has not disclosed any plans to submit a new drug application to the Food and Drug Administration.
Dr. Nanchen said he had no relevant financial disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting from which this presentation was made. This version has been updated.
ROME – Otherwise healthy, older men with a heart rate of 79 beats per minute or higher had a roughly 50% increased risk of developing heart failure, compared with men with slower heart rates, in a population-based cohort of more than 1,800 Dutch men.
The finding suggests that heart rate, independent of any other cardiovascular risk factor, could boost the risk for developing heart failure, and raises the possibility of trying to dampen this effect by using interventions to reduce heart rate, Dr. David Nanchen said at the annual meeting of the * European Association for Cardiovascular Prevention and Rehabilitation.
But the apparent link between resting heart rate and a boosted incidence of heart failure during follow-up occurred only in men. The analysis also included 2,939 women, who showed no suggestion of an association between baseline heart rate and subsequent development of heart failure.
The work reported by Dr. Nanchen also included an analysis that censored men who had an incident myocardial infarction during a median follow-up of 15 years, thereby eliminating cases of heart failure that occurred following an MI. In this analysis, men with a baseline heart rate of 79 beats per minute or greater had a statistically significant, 56% increased incidence of heart failure compared with men with an entry heart rate of less than 69 beats per minute, said Dr. Nanchen, head of the cardiovascular preventative clinic of the University of Lausanne (Switzerland).
Ruling out MI as a mediator between high heart rate and the development of heart failure means some other pathologic sequence is involved. One possibility is that patients with high heart rates develop tachycardia-induced cardiomyopathy that progresses to heart failure, Dr. Nanchen said in an interview."
His study included 4,768 people aged 55 or older enrolled in the Rotterdam Study from among apparently healthy people living in the Rotterdam area. During a median follow-up of 15 years, 656 enrollees developed heart failure. The analysis excluded people who at baseline had heart failure, coronary heart disease, atrial fibrillation, atrioventricular block, or a pacemaker, or were taking a beta-blocker or calcium channel blocker.
Among the 1,829 men in the study, every increment of 10 beats per minute in resting heart rate at entry into the study was linked with a statistically significant, 16% relative increase in the incidence of heart failure, an association not seen in women. When the researchers divided the men into tertiles based on their baseline heart rate, those in the top tertile with a rate of 79 beats per minute or greater had a 51% increased incidence of heart failure during follow-up, compared with men in the lowest tertile, with a rate of less than 69 beats per minute.
The analysis adjusted for age, smoking status, systolic blood pressure, diabetes, body mass index, total cholesterol level, HDL cholesterol level, and antihypertensive treatment.
The absence of this heart rate and heart failure link in women was a "surprise," Dr. Nanchen said. It’s possible that women’s hearts are more resilient to high heart rates, he suggested.
For the time being, the only intervention to offer otherwise healthy men older than 55 with a high heart rate is intensified control of lifestyle risk factors. Trial results showed that treatment with the heart rate–lowering drug ivabradine (Prooralan) in heart failure patients led to a reduction in heart failure–related hospitalizations (Lancet 2010;376:875-85).That experience makes it attractive to speculate that ivabradine treatment might also improve outcomes in men with high heart rates and no heart failure, but Dr. Nanchen said he had no immediate plans to test that hypothesis.
U.S. physicians won’t get the chance to study ivabradine in clinical practice for some time. Its manufacturer, Servier, has not disclosed any plans to submit a new drug application to the Food and Drug Administration.
Dr. Nanchen said he had no relevant financial disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting from which this presentation was made. This version has been updated.
ROME – Otherwise healthy, older men with a heart rate of 79 beats per minute or higher had a roughly 50% increased risk of developing heart failure, compared with men with slower heart rates, in a population-based cohort of more than 1,800 Dutch men.
The finding suggests that heart rate, independent of any other cardiovascular risk factor, could boost the risk for developing heart failure, and raises the possibility of trying to dampen this effect by using interventions to reduce heart rate, Dr. David Nanchen said at the annual meeting of the * European Association for Cardiovascular Prevention and Rehabilitation.
But the apparent link between resting heart rate and a boosted incidence of heart failure during follow-up occurred only in men. The analysis also included 2,939 women, who showed no suggestion of an association between baseline heart rate and subsequent development of heart failure.
The work reported by Dr. Nanchen also included an analysis that censored men who had an incident myocardial infarction during a median follow-up of 15 years, thereby eliminating cases of heart failure that occurred following an MI. In this analysis, men with a baseline heart rate of 79 beats per minute or greater had a statistically significant, 56% increased incidence of heart failure compared with men with an entry heart rate of less than 69 beats per minute, said Dr. Nanchen, head of the cardiovascular preventative clinic of the University of Lausanne (Switzerland).
Ruling out MI as a mediator between high heart rate and the development of heart failure means some other pathologic sequence is involved. One possibility is that patients with high heart rates develop tachycardia-induced cardiomyopathy that progresses to heart failure, Dr. Nanchen said in an interview."
His study included 4,768 people aged 55 or older enrolled in the Rotterdam Study from among apparently healthy people living in the Rotterdam area. During a median follow-up of 15 years, 656 enrollees developed heart failure. The analysis excluded people who at baseline had heart failure, coronary heart disease, atrial fibrillation, atrioventricular block, or a pacemaker, or were taking a beta-blocker or calcium channel blocker.
Among the 1,829 men in the study, every increment of 10 beats per minute in resting heart rate at entry into the study was linked with a statistically significant, 16% relative increase in the incidence of heart failure, an association not seen in women. When the researchers divided the men into tertiles based on their baseline heart rate, those in the top tertile with a rate of 79 beats per minute or greater had a 51% increased incidence of heart failure during follow-up, compared with men in the lowest tertile, with a rate of less than 69 beats per minute.
The analysis adjusted for age, smoking status, systolic blood pressure, diabetes, body mass index, total cholesterol level, HDL cholesterol level, and antihypertensive treatment.
The absence of this heart rate and heart failure link in women was a "surprise," Dr. Nanchen said. It’s possible that women’s hearts are more resilient to high heart rates, he suggested.
For the time being, the only intervention to offer otherwise healthy men older than 55 with a high heart rate is intensified control of lifestyle risk factors. Trial results showed that treatment with the heart rate–lowering drug ivabradine (Prooralan) in heart failure patients led to a reduction in heart failure–related hospitalizations (Lancet 2010;376:875-85).That experience makes it attractive to speculate that ivabradine treatment might also improve outcomes in men with high heart rates and no heart failure, but Dr. Nanchen said he had no immediate plans to test that hypothesis.
U.S. physicians won’t get the chance to study ivabradine in clinical practice for some time. Its manufacturer, Servier, has not disclosed any plans to submit a new drug application to the Food and Drug Administration.
Dr. Nanchen said he had no relevant financial disclosures.
On Twitter @mitchelzoler
*Correction (5/29/13): A previous version of this story misstated the name of the meeting from which this presentation was made. This version has been updated.
AT EUROPREVENT 2013
Major finding: Among healthy men, heart rates of at least 79 beats per minute were linked with a 51% increased incidence of heart failure.
Data source: A prospective follow-up of a population-based cohort of 4,768 people enrolled in the Rotterdam Study.
Disclosures: Dr. Nanchen said he had no relevant financial disclosures.
