User login
Variation in Admission Rates From EDs Raising Eyebrows
DALLAS – Emergency departments across the United States vary widely in their admission rates for the 15 most common medical and surgical conditions resulting in hospitalization.
The variability is important from a cost perspective because ED admission is increasingly the dominant route by which patients enter the hospital, Dr. Keith E. Kocher observed at the annual meeting of the Society for Academic Emergency Medicine. "We’re talking about potentially billions of dollars that may be in play if we narrow these differences." The 15 conditions collectively account for more than $266 billion/year in hospital charges to payers.
Dr. Kocher, an emergency medicine physician at the University of Michigan, Ann Arbor, and his colleagues conducted a retrospective analysis of the Nationwide Emergency Department Sample for 2010. This database, maintained by the Agency for Healthcare Research and Quality, contains extensive records on the millions of ED visits at nearly 1,000 hospitals in 28 states.
Their analysis adjusted for the severity of case mix by incorporating demographics, comorbid conditions, primary payer, median income, and patient zip code. The researchers then determined risk-standardized admission rates – the number of predicted admissions for each ED given the institutional case mix, divided by the number of expected admissions had those patients been treated at the average ED, multiplied by the mean admission rate for the sample.
The five disorders with the least variation in admission rates among the 15 most commonly admitted conditions were heart failure, stroke, acute renal failure, acute MI, and sepsis. All are characterized by relatively high inpatient mortality.

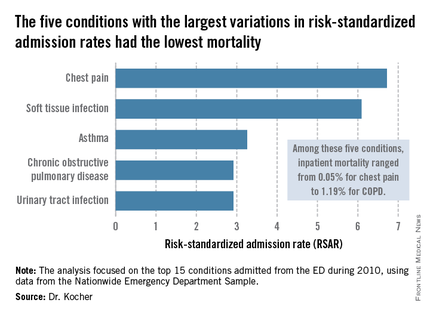
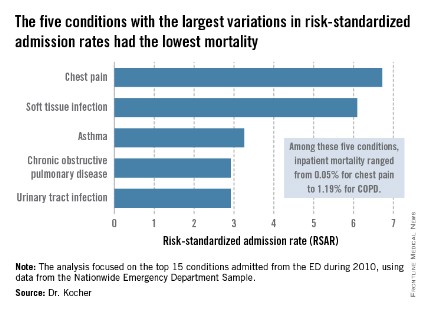
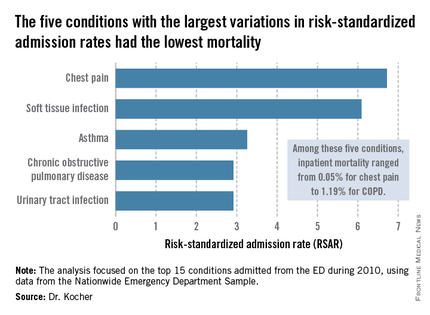
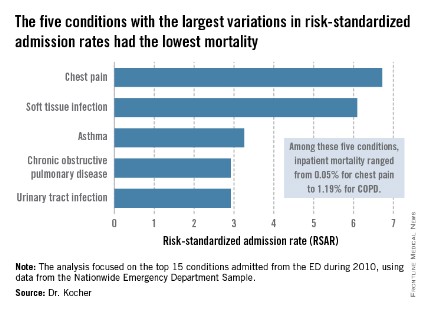
The five with the greatest variation in admission rates were chest pain, soft tissue infection, asthma, chronic obstructive pulmonary disease, and urinary tract infection. Importantly, these conditions were among those with the lowest inpatient mortality, ranging from 0.05% for patients admitted from the ED for chest pain to a high of 1.19% for those admitted for COPD.
"High-mortality/low-variation diagnoses like sepsis and MI provide little opportunity to realize meaningful spending reductions. Instead, the Big-5 high-variation/low-mortality conditions represent the greatest source of potential savings," Dr. Kocher said.
The ED could become "a workshop for developing innovative strategies for care coordination and alternatives to acute hospitalization, particularly around a select group of high-variation/low-mortality conditions" with the goal of reducing health costs, he said.
If EDs with high-risk–standardized admission rates above the median reduced admissions for the five high-variation/low-mortality conditions to the median rate, it would save an estimated $16.9 billion in charges and $5.1 billion in costs per year. Another option might be to set incentives to induce EDs with high-risk–standardized admission rates in the top quartile to reduce admissions to the 75th percentile; the resulting saving would be $7 billion less in charges and $2.1 billion less in costs per year.
Incentivizing top quartile and bottom quartile EDs to meet the median rate would yield an estimated $2.8 billion reduction in charges and a $0.8 billion decrease in costs per year.
The in-hospital mortality implications of moving admission rates toward the median are not known, Dr. Kocher acknowledged. "We’re not implying that we know the optimal rate of admission. In fact, it probably varies from condition to condition."
Further, a formal economic analysis of net expenditures would need to incorporate the increased outpatient expenditures of shifting care to ambulatory settings, he said.
The study was supported by the Agency for Healthcare Research and Quality. Dr. Kocher reported having no financial conflicts.
DALLAS – Emergency departments across the United States vary widely in their admission rates for the 15 most common medical and surgical conditions resulting in hospitalization.
The variability is important from a cost perspective because ED admission is increasingly the dominant route by which patients enter the hospital, Dr. Keith E. Kocher observed at the annual meeting of the Society for Academic Emergency Medicine. "We’re talking about potentially billions of dollars that may be in play if we narrow these differences." The 15 conditions collectively account for more than $266 billion/year in hospital charges to payers.
Dr. Kocher, an emergency medicine physician at the University of Michigan, Ann Arbor, and his colleagues conducted a retrospective analysis of the Nationwide Emergency Department Sample for 2010. This database, maintained by the Agency for Healthcare Research and Quality, contains extensive records on the millions of ED visits at nearly 1,000 hospitals in 28 states.
Their analysis adjusted for the severity of case mix by incorporating demographics, comorbid conditions, primary payer, median income, and patient zip code. The researchers then determined risk-standardized admission rates – the number of predicted admissions for each ED given the institutional case mix, divided by the number of expected admissions had those patients been treated at the average ED, multiplied by the mean admission rate for the sample.
The five disorders with the least variation in admission rates among the 15 most commonly admitted conditions were heart failure, stroke, acute renal failure, acute MI, and sepsis. All are characterized by relatively high inpatient mortality.
The five with the greatest variation in admission rates were chest pain, soft tissue infection, asthma, chronic obstructive pulmonary disease, and urinary tract infection. Importantly, these conditions were among those with the lowest inpatient mortality, ranging from 0.05% for patients admitted from the ED for chest pain to a high of 1.19% for those admitted for COPD.
"High-mortality/low-variation diagnoses like sepsis and MI provide little opportunity to realize meaningful spending reductions. Instead, the Big-5 high-variation/low-mortality conditions represent the greatest source of potential savings," Dr. Kocher said.
The ED could become "a workshop for developing innovative strategies for care coordination and alternatives to acute hospitalization, particularly around a select group of high-variation/low-mortality conditions" with the goal of reducing health costs, he said.
If EDs with high-risk–standardized admission rates above the median reduced admissions for the five high-variation/low-mortality conditions to the median rate, it would save an estimated $16.9 billion in charges and $5.1 billion in costs per year. Another option might be to set incentives to induce EDs with high-risk–standardized admission rates in the top quartile to reduce admissions to the 75th percentile; the resulting saving would be $7 billion less in charges and $2.1 billion less in costs per year.
Incentivizing top quartile and bottom quartile EDs to meet the median rate would yield an estimated $2.8 billion reduction in charges and a $0.8 billion decrease in costs per year.
The in-hospital mortality implications of moving admission rates toward the median are not known, Dr. Kocher acknowledged. "We’re not implying that we know the optimal rate of admission. In fact, it probably varies from condition to condition."
Further, a formal economic analysis of net expenditures would need to incorporate the increased outpatient expenditures of shifting care to ambulatory settings, he said.
The study was supported by the Agency for Healthcare Research and Quality. Dr. Kocher reported having no financial conflicts.
DALLAS – Emergency departments across the United States vary widely in their admission rates for the 15 most common medical and surgical conditions resulting in hospitalization.
The variability is important from a cost perspective because ED admission is increasingly the dominant route by which patients enter the hospital, Dr. Keith E. Kocher observed at the annual meeting of the Society for Academic Emergency Medicine. "We’re talking about potentially billions of dollars that may be in play if we narrow these differences." The 15 conditions collectively account for more than $266 billion/year in hospital charges to payers.
Dr. Kocher, an emergency medicine physician at the University of Michigan, Ann Arbor, and his colleagues conducted a retrospective analysis of the Nationwide Emergency Department Sample for 2010. This database, maintained by the Agency for Healthcare Research and Quality, contains extensive records on the millions of ED visits at nearly 1,000 hospitals in 28 states.
Their analysis adjusted for the severity of case mix by incorporating demographics, comorbid conditions, primary payer, median income, and patient zip code. The researchers then determined risk-standardized admission rates – the number of predicted admissions for each ED given the institutional case mix, divided by the number of expected admissions had those patients been treated at the average ED, multiplied by the mean admission rate for the sample.
The five disorders with the least variation in admission rates among the 15 most commonly admitted conditions were heart failure, stroke, acute renal failure, acute MI, and sepsis. All are characterized by relatively high inpatient mortality.
The five with the greatest variation in admission rates were chest pain, soft tissue infection, asthma, chronic obstructive pulmonary disease, and urinary tract infection. Importantly, these conditions were among those with the lowest inpatient mortality, ranging from 0.05% for patients admitted from the ED for chest pain to a high of 1.19% for those admitted for COPD.
"High-mortality/low-variation diagnoses like sepsis and MI provide little opportunity to realize meaningful spending reductions. Instead, the Big-5 high-variation/low-mortality conditions represent the greatest source of potential savings," Dr. Kocher said.
The ED could become "a workshop for developing innovative strategies for care coordination and alternatives to acute hospitalization, particularly around a select group of high-variation/low-mortality conditions" with the goal of reducing health costs, he said.
If EDs with high-risk–standardized admission rates above the median reduced admissions for the five high-variation/low-mortality conditions to the median rate, it would save an estimated $16.9 billion in charges and $5.1 billion in costs per year. Another option might be to set incentives to induce EDs with high-risk–standardized admission rates in the top quartile to reduce admissions to the 75th percentile; the resulting saving would be $7 billion less in charges and $2.1 billion less in costs per year.
Incentivizing top quartile and bottom quartile EDs to meet the median rate would yield an estimated $2.8 billion reduction in charges and a $0.8 billion decrease in costs per year.
The in-hospital mortality implications of moving admission rates toward the median are not known, Dr. Kocher acknowledged. "We’re not implying that we know the optimal rate of admission. In fact, it probably varies from condition to condition."
Further, a formal economic analysis of net expenditures would need to incorporate the increased outpatient expenditures of shifting care to ambulatory settings, he said.
The study was supported by the Agency for Healthcare Research and Quality. Dr. Kocher reported having no financial conflicts.
AT SAEM 2014
Variation in admission rates from EDs raising eyebrows
DALLAS – Emergency departments across the United States vary widely in their admission rates for the 15 most common medical and surgical conditions resulting in hospitalization.
The variability is important from a cost perspective because ED admission is increasingly the dominant route by which patients enter the hospital, Dr. Keith E. Kocher observed at the annual meeting of the Society for Academic Emergency Medicine. "We’re talking about potentially billions of dollars that may be in play if we narrow these differences." The 15 conditions collectively account for more than $266 billion/year in hospital charges to payers.
Dr. Kocher, an emergency medicine physician at the University of Michigan, Ann Arbor, and his colleagues conducted a retrospective analysis of the Nationwide Emergency Department Sample for 2010. This database, maintained by the Agency for Healthcare Research and Quality, contains extensive records on the millions of ED visits at nearly 1,000 hospitals in 28 states.
Their analysis adjusted for the severity of case mix by incorporating demographics, comorbid conditions, primary payer, median income, and patient zip code. The researchers then determined risk-standardized admission rates – the number of predicted admissions for each ED given the institutional case mix, divided by the number of expected admissions had those patients been treated at the average ED, multiplied by the mean admission rate for the sample.
The five disorders with the least variation in admission rates among the 15 most commonly admitted conditions were heart failure, stroke, acute renal failure, acute MI, and sepsis. All are characterized by relatively high inpatient mortality.

The five with the greatest variation in admission rates were chest pain, soft tissue infection, asthma, chronic obstructive pulmonary disease, and urinary tract infection. Importantly, these conditions were among those with the lowest inpatient mortality, ranging from 0.05% for patients admitted from the ED for chest pain to a high of 1.19% for those admitted for COPD.
"High-mortality/low-variation diagnoses like sepsis and MI provide little opportunity to realize meaningful spending reductions. Instead, the Big-5 high-variation/low-mortality conditions represent the greatest source of potential savings," Dr. Kocher said.
The ED could become "a workshop for developing innovative strategies for care coordination and alternatives to acute hospitalization, particularly around a select group of high-variation/low-mortality conditions" with the goal of reducing health costs, he said.

If EDs with high-risk–standardized admission rates above the median reduced admissions for the five high-variation/low-mortality conditions to the median rate, it would save an estimated $16.9 billion in charges and $5.1 billion in costs per year. Another option might be to set incentives to induce EDs with high-risk–standardized admission rates in the top quartile to reduce admissions to the 75th percentile; the resulting saving would be $7 billion less in charges and $2.1 billion less in costs per year.
Incentivizing top quartile and bottom quartile EDs to meet the median rate would yield an estimated $2.8 billion reduction in charges and a $0.8 billion decrease in costs per year.
The in-hospital mortality implications of moving admission rates toward the median are not known, Dr. Kocher acknowledged. "We’re not implying that we know the optimal rate of admission. In fact, it probably varies from condition to condition."
Further, a formal economic analysis of net expenditures would need to incorporate the increased outpatient expenditures of shifting care to ambulatory settings, he said.
The study was supported by the Agency for Healthcare Research and Quality. Dr. Kocher reported having no financial conflicts.
DALLAS – Emergency departments across the United States vary widely in their admission rates for the 15 most common medical and surgical conditions resulting in hospitalization.
The variability is important from a cost perspective because ED admission is increasingly the dominant route by which patients enter the hospital, Dr. Keith E. Kocher observed at the annual meeting of the Society for Academic Emergency Medicine. "We’re talking about potentially billions of dollars that may be in play if we narrow these differences." The 15 conditions collectively account for more than $266 billion/year in hospital charges to payers.
Dr. Kocher, an emergency medicine physician at the University of Michigan, Ann Arbor, and his colleagues conducted a retrospective analysis of the Nationwide Emergency Department Sample for 2010. This database, maintained by the Agency for Healthcare Research and Quality, contains extensive records on the millions of ED visits at nearly 1,000 hospitals in 28 states.
Their analysis adjusted for the severity of case mix by incorporating demographics, comorbid conditions, primary payer, median income, and patient zip code. The researchers then determined risk-standardized admission rates – the number of predicted admissions for each ED given the institutional case mix, divided by the number of expected admissions had those patients been treated at the average ED, multiplied by the mean admission rate for the sample.
The five disorders with the least variation in admission rates among the 15 most commonly admitted conditions were heart failure, stroke, acute renal failure, acute MI, and sepsis. All are characterized by relatively high inpatient mortality.
The five with the greatest variation in admission rates were chest pain, soft tissue infection, asthma, chronic obstructive pulmonary disease, and urinary tract infection. Importantly, these conditions were among those with the lowest inpatient mortality, ranging from 0.05% for patients admitted from the ED for chest pain to a high of 1.19% for those admitted for COPD.
"High-mortality/low-variation diagnoses like sepsis and MI provide little opportunity to realize meaningful spending reductions. Instead, the Big-5 high-variation/low-mortality conditions represent the greatest source of potential savings," Dr. Kocher said.
The ED could become "a workshop for developing innovative strategies for care coordination and alternatives to acute hospitalization, particularly around a select group of high-variation/low-mortality conditions" with the goal of reducing health costs, he said.
If EDs with high-risk–standardized admission rates above the median reduced admissions for the five high-variation/low-mortality conditions to the median rate, it would save an estimated $16.9 billion in charges and $5.1 billion in costs per year. Another option might be to set incentives to induce EDs with high-risk–standardized admission rates in the top quartile to reduce admissions to the 75th percentile; the resulting saving would be $7 billion less in charges and $2.1 billion less in costs per year.
Incentivizing top quartile and bottom quartile EDs to meet the median rate would yield an estimated $2.8 billion reduction in charges and a $0.8 billion decrease in costs per year.
The in-hospital mortality implications of moving admission rates toward the median are not known, Dr. Kocher acknowledged. "We’re not implying that we know the optimal rate of admission. In fact, it probably varies from condition to condition."
Further, a formal economic analysis of net expenditures would need to incorporate the increased outpatient expenditures of shifting care to ambulatory settings, he said.
The study was supported by the Agency for Healthcare Research and Quality. Dr. Kocher reported having no financial conflicts.
DALLAS – Emergency departments across the United States vary widely in their admission rates for the 15 most common medical and surgical conditions resulting in hospitalization.
The variability is important from a cost perspective because ED admission is increasingly the dominant route by which patients enter the hospital, Dr. Keith E. Kocher observed at the annual meeting of the Society for Academic Emergency Medicine. "We’re talking about potentially billions of dollars that may be in play if we narrow these differences." The 15 conditions collectively account for more than $266 billion/year in hospital charges to payers.
Dr. Kocher, an emergency medicine physician at the University of Michigan, Ann Arbor, and his colleagues conducted a retrospective analysis of the Nationwide Emergency Department Sample for 2010. This database, maintained by the Agency for Healthcare Research and Quality, contains extensive records on the millions of ED visits at nearly 1,000 hospitals in 28 states.
Their analysis adjusted for the severity of case mix by incorporating demographics, comorbid conditions, primary payer, median income, and patient zip code. The researchers then determined risk-standardized admission rates – the number of predicted admissions for each ED given the institutional case mix, divided by the number of expected admissions had those patients been treated at the average ED, multiplied by the mean admission rate for the sample.
The five disorders with the least variation in admission rates among the 15 most commonly admitted conditions were heart failure, stroke, acute renal failure, acute MI, and sepsis. All are characterized by relatively high inpatient mortality.
The five with the greatest variation in admission rates were chest pain, soft tissue infection, asthma, chronic obstructive pulmonary disease, and urinary tract infection. Importantly, these conditions were among those with the lowest inpatient mortality, ranging from 0.05% for patients admitted from the ED for chest pain to a high of 1.19% for those admitted for COPD.
"High-mortality/low-variation diagnoses like sepsis and MI provide little opportunity to realize meaningful spending reductions. Instead, the Big-5 high-variation/low-mortality conditions represent the greatest source of potential savings," Dr. Kocher said.
The ED could become "a workshop for developing innovative strategies for care coordination and alternatives to acute hospitalization, particularly around a select group of high-variation/low-mortality conditions" with the goal of reducing health costs, he said.
If EDs with high-risk–standardized admission rates above the median reduced admissions for the five high-variation/low-mortality conditions to the median rate, it would save an estimated $16.9 billion in charges and $5.1 billion in costs per year. Another option might be to set incentives to induce EDs with high-risk–standardized admission rates in the top quartile to reduce admissions to the 75th percentile; the resulting saving would be $7 billion less in charges and $2.1 billion less in costs per year.
Incentivizing top quartile and bottom quartile EDs to meet the median rate would yield an estimated $2.8 billion reduction in charges and a $0.8 billion decrease in costs per year.
The in-hospital mortality implications of moving admission rates toward the median are not known, Dr. Kocher acknowledged. "We’re not implying that we know the optimal rate of admission. In fact, it probably varies from condition to condition."
Further, a formal economic analysis of net expenditures would need to incorporate the increased outpatient expenditures of shifting care to ambulatory settings, he said.
The study was supported by the Agency for Healthcare Research and Quality. Dr. Kocher reported having no financial conflicts.
AT SAEM 2014
Key clinical point: Reducing variation in admission rates from EDs for selected common conditions with low inpatient mortality rates could save billions of dollars in health care expenditures annually.
Major finding: If EDs with hospital admission rates above the national median for five target conditions were to reduce those rates to the median, payers would save an estimated $16.9 billion in charges annually.
Data source: This was a retrospective analysis of the 2010 Nationwide Emergency Department Sample, which contains detailed records on millions of ED visits at nearly 1,000 hospitals in 28 states.
Disclosures: This study was supported by the AHRQ. The presenter reported having no financial conflicts.
ECG predictors of cardiac events mandate troponin level testing in drug overdoses
DALLAS – The initial ECG is invaluable in predicting which emergency department patients with acute drug overdose will have a major cardiovascular event during hospitalization, a prospective study indicates.
"Based on our data, ECG evidence of ischemia or infarction really mandates sending for a troponin level in ED patients with overdose," Dr. Alex F. Manini said at the annual meeting of the Society for Academic Emergency Medicine.

The findings are important as "we’re currently undergoing the worst epidemic of drug overdoses in our nation’s history," observed Dr. Manini of the department of emergency medicine at Mount Sinai School of Medicine in New York. Poisoning is now the No. 1 cause of injury-related fatalities in the United States, and many patient series indicate 10%-15% of ED patients with an acute drug overdose experience a major cardiac event during their hospitalization.
Dr. Manini and his colleagues performed a study that validated the prognostic value of four high-risk features of the ED admission ECG in an acute drug overdose cohort: ectopy, a QTc interval of 500 msec or longer, non–sinus rhythm, and any evidence of ischemia or infarction.
Emergency physicians can readily identify those features without need for input from a cardiologist, he said.
In their study performed at two university EDs, 16% of 589 adults with acute drug overdoses experienced an acute MI, cardiogenic shock, dysrhythmia, or cardiac arrest during their hospitalization. The most common drug exposures were benzodiazepines, opioids, and acetaminophen.
Ectopy was associated with an 8.9-fold increased odds ratio for a major cardiovascular event. A QTc of 500 msec or longer was associated with an odds ratio of 11.2; a non–sinus rhythm, 8.9; and ischemia, 5.0.
The presence of one or more of these four ECG predictors was associated with 68% sensitivity and 69% specificity for a subsequent in-hospital cardiac event, with a negative predictive value of 91.9%. Dr. Manini called those sensitivity and specificity figures "modest." Thus, the ECG findings alone are not sufficient to exclude the likelihood of a cardiac event, although they certainly are useful in risk stratification. Future studies will seek to boost the predictive power by combining the ECG findings with other clinical tools, he said.
A QT dispersion of 50 msec or more also proved useful for prognosis, with an associated 2.2-fold increased risk of an in-hospital cardiac event. However, measuring QT dispersion is a fairly cumbersome process, and for this reason it needs further study before being introduced into clinical practice in busy EDs, Dr. Manini added.
In this study, any ECG evidence of ischemia or infarction – including ST depression or elevation, T wave inversion, or Q waves – had specificities of 91%-98% for an elevated troponin assay. In addition, ST depression was associated with a 6.4-fold increased odds ratio for in-hospital cardiac arrest.
The study was funded by the National Institute on Drug Abuse. Dr. Manini reported having no financial conflicts.
DALLAS – The initial ECG is invaluable in predicting which emergency department patients with acute drug overdose will have a major cardiovascular event during hospitalization, a prospective study indicates.
"Based on our data, ECG evidence of ischemia or infarction really mandates sending for a troponin level in ED patients with overdose," Dr. Alex F. Manini said at the annual meeting of the Society for Academic Emergency Medicine.
The findings are important as "we’re currently undergoing the worst epidemic of drug overdoses in our nation’s history," observed Dr. Manini of the department of emergency medicine at Mount Sinai School of Medicine in New York. Poisoning is now the No. 1 cause of injury-related fatalities in the United States, and many patient series indicate 10%-15% of ED patients with an acute drug overdose experience a major cardiac event during their hospitalization.
Dr. Manini and his colleagues performed a study that validated the prognostic value of four high-risk features of the ED admission ECG in an acute drug overdose cohort: ectopy, a QTc interval of 500 msec or longer, non–sinus rhythm, and any evidence of ischemia or infarction.
Emergency physicians can readily identify those features without need for input from a cardiologist, he said.
In their study performed at two university EDs, 16% of 589 adults with acute drug overdoses experienced an acute MI, cardiogenic shock, dysrhythmia, or cardiac arrest during their hospitalization. The most common drug exposures were benzodiazepines, opioids, and acetaminophen.
Ectopy was associated with an 8.9-fold increased odds ratio for a major cardiovascular event. A QTc of 500 msec or longer was associated with an odds ratio of 11.2; a non–sinus rhythm, 8.9; and ischemia, 5.0.
The presence of one or more of these four ECG predictors was associated with 68% sensitivity and 69% specificity for a subsequent in-hospital cardiac event, with a negative predictive value of 91.9%. Dr. Manini called those sensitivity and specificity figures "modest." Thus, the ECG findings alone are not sufficient to exclude the likelihood of a cardiac event, although they certainly are useful in risk stratification. Future studies will seek to boost the predictive power by combining the ECG findings with other clinical tools, he said.
A QT dispersion of 50 msec or more also proved useful for prognosis, with an associated 2.2-fold increased risk of an in-hospital cardiac event. However, measuring QT dispersion is a fairly cumbersome process, and for this reason it needs further study before being introduced into clinical practice in busy EDs, Dr. Manini added.
In this study, any ECG evidence of ischemia or infarction – including ST depression or elevation, T wave inversion, or Q waves – had specificities of 91%-98% for an elevated troponin assay. In addition, ST depression was associated with a 6.4-fold increased odds ratio for in-hospital cardiac arrest.
The study was funded by the National Institute on Drug Abuse. Dr. Manini reported having no financial conflicts.
DALLAS – The initial ECG is invaluable in predicting which emergency department patients with acute drug overdose will have a major cardiovascular event during hospitalization, a prospective study indicates.
"Based on our data, ECG evidence of ischemia or infarction really mandates sending for a troponin level in ED patients with overdose," Dr. Alex F. Manini said at the annual meeting of the Society for Academic Emergency Medicine.
The findings are important as "we’re currently undergoing the worst epidemic of drug overdoses in our nation’s history," observed Dr. Manini of the department of emergency medicine at Mount Sinai School of Medicine in New York. Poisoning is now the No. 1 cause of injury-related fatalities in the United States, and many patient series indicate 10%-15% of ED patients with an acute drug overdose experience a major cardiac event during their hospitalization.
Dr. Manini and his colleagues performed a study that validated the prognostic value of four high-risk features of the ED admission ECG in an acute drug overdose cohort: ectopy, a QTc interval of 500 msec or longer, non–sinus rhythm, and any evidence of ischemia or infarction.
Emergency physicians can readily identify those features without need for input from a cardiologist, he said.
In their study performed at two university EDs, 16% of 589 adults with acute drug overdoses experienced an acute MI, cardiogenic shock, dysrhythmia, or cardiac arrest during their hospitalization. The most common drug exposures were benzodiazepines, opioids, and acetaminophen.
Ectopy was associated with an 8.9-fold increased odds ratio for a major cardiovascular event. A QTc of 500 msec or longer was associated with an odds ratio of 11.2; a non–sinus rhythm, 8.9; and ischemia, 5.0.
The presence of one or more of these four ECG predictors was associated with 68% sensitivity and 69% specificity for a subsequent in-hospital cardiac event, with a negative predictive value of 91.9%. Dr. Manini called those sensitivity and specificity figures "modest." Thus, the ECG findings alone are not sufficient to exclude the likelihood of a cardiac event, although they certainly are useful in risk stratification. Future studies will seek to boost the predictive power by combining the ECG findings with other clinical tools, he said.
A QT dispersion of 50 msec or more also proved useful for prognosis, with an associated 2.2-fold increased risk of an in-hospital cardiac event. However, measuring QT dispersion is a fairly cumbersome process, and for this reason it needs further study before being introduced into clinical practice in busy EDs, Dr. Manini added.
In this study, any ECG evidence of ischemia or infarction – including ST depression or elevation, T wave inversion, or Q waves – had specificities of 91%-98% for an elevated troponin assay. In addition, ST depression was associated with a 6.4-fold increased odds ratio for in-hospital cardiac arrest.
The study was funded by the National Institute on Drug Abuse. Dr. Manini reported having no financial conflicts.
AT SAEM 2014
Key clinical point: Roughly 15% of adult ED patients with an acute drug overdose will experience a major cardiac event during their hospital stay. The ED admission ECG is helpful in risk stratification.
Major finding: Acute drug overdose patients with one or more of four key findings on their initial ECG in the ED – ectopy, a QTc interval of 500 msec or longer, non–sinus rhythm, or any evidence of ischemia or infarction – are at increased risk for a major cardiac event during their hospitalization.
Data source: This was a prospective study involving 589 adults with acute drug overdose in two university EDs.
Disclosures: The study was supported by the National Institute on Drug Abuse. The presenter reported having no financial conflicts.

Refining prognosis in small intestinal neuroendocrine tumors
CHICAGO – The extent of lymph node involvement provides independent prognostic information in patients with early-stage T1 or T2 small intestinal neuroendocrine tumors, according to a study involving nearly 3,000 lymph node–positive individuals.
This metric, best expressed as the lymph node ratio, or the number of positive nodes divided by the total number of lymph nodes examined, is not included in current European and American Joint Committee on Cancer staging classification guidelines. But it should be, Dr. Michelle K. Kim said at the annual Digestive Disease Week.

"The lymph node ratio is a readily available marker of disease progression. It’s available as part of usual clinical care; it’s not something extra you have to ask for. It may help identify patients who may require more-aggressive therapy," according to Dr. Kim of Mount Sinai School of Medicine, New York.
Current staging guidelines merely make a binary distinction: lymph node–positive or –negative. But previous studies in colon, gastric, and pancreatic cancers indicate the lymph node ratio (LNR) further differentiates outcomes in node-positive patients. The same now appears to be true for small intestinal neuroendocrine tumors (SI-NETs), which are the most common of the gastroenteropancreatic neuroendocrine tumors. Indeed, the incidence of SI-NETs has tripled during the last 3 decades, she noted.
Dr. Kim presented an analysis of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, which included 2,984 patients with surgically resected lymph node–positive, metastasis-negative SI-NETs diagnosed in 1988-2010. Dr. Kim and coinvestigators classified patients into three LNR groups: 531 were LNR 1, defined as an LNR ratio of 0.2 or less; 1,525 patients were LNR 2, with a ratio of 0.21-0.5; and 928 were LNR 3, with a ratio greater than 0.5. Patients with T1 and T2 disease were overrepresented in the LNR 1 group.
The primary outcome in the study was disease-specific survival. The more-extensive the lymph node involvement in patients with T1 or T2 disease, the poorer their disease-specific survival. For example, LNR 1 patients with T1 or T2 SI-NETs were 1.6-fold more likely to experience disease-specific mortality during 10 years of follow-up than did a reference control group of node-negative T1/T2 patients, an elevation in risk that did not achieve statistical significance. However, the risk of disease-specific mortality was increased 2.29-fold in LNR 2 patients with T1/T2 disease and 4.52-fold in LNR 3 patients with T1/T2 SI-NETs, compared with node-negative controls, and those differences were significant.
In contrast, there was no difference in disease-specific survival according to LNR status in patients with more-advanced T3 or T4 disease.
This study was funded by Mount Sinai School of Medicine and the National Center for Advancing Translational Sciences. Dr. Kim reported having no financial conflicts.
CHICAGO – The extent of lymph node involvement provides independent prognostic information in patients with early-stage T1 or T2 small intestinal neuroendocrine tumors, according to a study involving nearly 3,000 lymph node–positive individuals.
This metric, best expressed as the lymph node ratio, or the number of positive nodes divided by the total number of lymph nodes examined, is not included in current European and American Joint Committee on Cancer staging classification guidelines. But it should be, Dr. Michelle K. Kim said at the annual Digestive Disease Week.
"The lymph node ratio is a readily available marker of disease progression. It’s available as part of usual clinical care; it’s not something extra you have to ask for. It may help identify patients who may require more-aggressive therapy," according to Dr. Kim of Mount Sinai School of Medicine, New York.
Current staging guidelines merely make a binary distinction: lymph node–positive or –negative. But previous studies in colon, gastric, and pancreatic cancers indicate the lymph node ratio (LNR) further differentiates outcomes in node-positive patients. The same now appears to be true for small intestinal neuroendocrine tumors (SI-NETs), which are the most common of the gastroenteropancreatic neuroendocrine tumors. Indeed, the incidence of SI-NETs has tripled during the last 3 decades, she noted.
Dr. Kim presented an analysis of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, which included 2,984 patients with surgically resected lymph node–positive, metastasis-negative SI-NETs diagnosed in 1988-2010. Dr. Kim and coinvestigators classified patients into three LNR groups: 531 were LNR 1, defined as an LNR ratio of 0.2 or less; 1,525 patients were LNR 2, with a ratio of 0.21-0.5; and 928 were LNR 3, with a ratio greater than 0.5. Patients with T1 and T2 disease were overrepresented in the LNR 1 group.
The primary outcome in the study was disease-specific survival. The more-extensive the lymph node involvement in patients with T1 or T2 disease, the poorer their disease-specific survival. For example, LNR 1 patients with T1 or T2 SI-NETs were 1.6-fold more likely to experience disease-specific mortality during 10 years of follow-up than did a reference control group of node-negative T1/T2 patients, an elevation in risk that did not achieve statistical significance. However, the risk of disease-specific mortality was increased 2.29-fold in LNR 2 patients with T1/T2 disease and 4.52-fold in LNR 3 patients with T1/T2 SI-NETs, compared with node-negative controls, and those differences were significant.
In contrast, there was no difference in disease-specific survival according to LNR status in patients with more-advanced T3 or T4 disease.
This study was funded by Mount Sinai School of Medicine and the National Center for Advancing Translational Sciences. Dr. Kim reported having no financial conflicts.
CHICAGO – The extent of lymph node involvement provides independent prognostic information in patients with early-stage T1 or T2 small intestinal neuroendocrine tumors, according to a study involving nearly 3,000 lymph node–positive individuals.
This metric, best expressed as the lymph node ratio, or the number of positive nodes divided by the total number of lymph nodes examined, is not included in current European and American Joint Committee on Cancer staging classification guidelines. But it should be, Dr. Michelle K. Kim said at the annual Digestive Disease Week.
"The lymph node ratio is a readily available marker of disease progression. It’s available as part of usual clinical care; it’s not something extra you have to ask for. It may help identify patients who may require more-aggressive therapy," according to Dr. Kim of Mount Sinai School of Medicine, New York.
Current staging guidelines merely make a binary distinction: lymph node–positive or –negative. But previous studies in colon, gastric, and pancreatic cancers indicate the lymph node ratio (LNR) further differentiates outcomes in node-positive patients. The same now appears to be true for small intestinal neuroendocrine tumors (SI-NETs), which are the most common of the gastroenteropancreatic neuroendocrine tumors. Indeed, the incidence of SI-NETs has tripled during the last 3 decades, she noted.
Dr. Kim presented an analysis of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) database, which included 2,984 patients with surgically resected lymph node–positive, metastasis-negative SI-NETs diagnosed in 1988-2010. Dr. Kim and coinvestigators classified patients into three LNR groups: 531 were LNR 1, defined as an LNR ratio of 0.2 or less; 1,525 patients were LNR 2, with a ratio of 0.21-0.5; and 928 were LNR 3, with a ratio greater than 0.5. Patients with T1 and T2 disease were overrepresented in the LNR 1 group.
The primary outcome in the study was disease-specific survival. The more-extensive the lymph node involvement in patients with T1 or T2 disease, the poorer their disease-specific survival. For example, LNR 1 patients with T1 or T2 SI-NETs were 1.6-fold more likely to experience disease-specific mortality during 10 years of follow-up than did a reference control group of node-negative T1/T2 patients, an elevation in risk that did not achieve statistical significance. However, the risk of disease-specific mortality was increased 2.29-fold in LNR 2 patients with T1/T2 disease and 4.52-fold in LNR 3 patients with T1/T2 SI-NETs, compared with node-negative controls, and those differences were significant.
In contrast, there was no difference in disease-specific survival according to LNR status in patients with more-advanced T3 or T4 disease.
This study was funded by Mount Sinai School of Medicine and the National Center for Advancing Translational Sciences. Dr. Kim reported having no financial conflicts.
AT DDW 2014
Key clinical point: The extent of lymph node involvement provides important independent prognostic information in patients with early-stage, T1, or T2 small intestinal neuroendocrine tumors.
Major finding: The risk of disease-specific mortality jumped up to 4.5-fold depending on the extent of lymph node involvement in patients with T1 or T2 small intestinal neuroendocrine tumors.
Data source: This study involved retrospective analysis of SEER data on 2,984 patients with surgically resected lymph node-positive, metastasis-negative small intestinal neuroendocrine tumors.
Disclosures: The study was funded by Mount Sinai School of Medicine and the National Center for Advancing Translational Sciences. The presenter reported having no financial conflicts.

Later-life PTSD boosts vascular risk, study finds
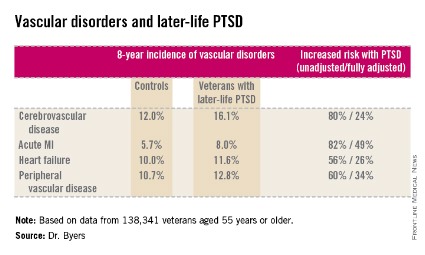
ORLANDO – Military veterans aged 55 years or older with current posttraumatic stress disorder are at significantly higher risk of developing new-onset vascular disease than are those without PTSD, according to a very large national longitudinal study.
"This study suggests the need for greater monitoring and treatment of PTSD in older veterans to assist in the prevention of vascular disorders," Amy L. Byers, Ph.D., said at the annual meeting of the American Association for Geriatric Psychiatry.
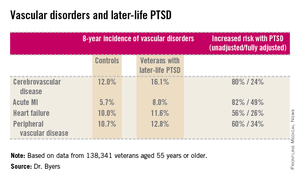
She reported on 138,341 veterans aged 55 years or older who were free of known vascular disease at baseline. During 8 years of follow-up, those with PTSD had significantly higher rates of incident cerebrovascular disease, acute MI, heart failure, and peripheral vascular disease than did those without PTSD, even after adjustment for demographics, comorbid diabetes, hypertension, cancer, chronic obstructive pulmonary disease, renal disease, traumatic brain injury, dementia, substance use disorders, and psychiatric diagnoses. The fully adjusted increased risk of each of the forms of vascular disease under study still remained significant at P less than .001, noted Dr. Byers, an epidemiologist in the psychiatry department at the University of California, San Francisco.
In a separate study led by Dr. Byers, PTSD in the general population with onset prior to and persistence beyond age 55 was a powerful independent predictor of global disability.
Dr. Byers’ study of older veterans was funded by the Department of Defense. She had no disclosures.
This paper continues to strengthen a link between PTSD and inflammatory markers. Dewleen Baker of the VA health care system in San Diego reported that there was a 10-fold increase in C-reactive protein (CRP) post deployment as compared with these same soldiers predeployment CRP levels. After adjustment for battlefield experience scores and combat exposures, those patients with PTSD symptoms had elevated CRP levels of 1.0 ng/mL versus 0.7 ng/mL without postdeployment symptoms (JAMA Psychiatry. 2014;71:423-31). So it seems that there may be a link between PTSD negative cardiovascular outcomes. And there may be a link between PTSD and elevated CRP. So, this leaves us with at least two questions: Is elevated CRP related to increased incidence of negative cardiovascular outcomes? And, which came first, the chicken (PTSD) or the egg (elevated CRP)?
Dr. Mark A. Adelman is chief of vascular and endovascular surgery at NYU Langone Medical Center, New York, and an associate medical editor for Vascular Specialist.
This paper continues to strengthen a link between PTSD and inflammatory markers. Dewleen Baker of the VA health care system in San Diego reported that there was a 10-fold increase in C-reactive protein (CRP) post deployment as compared with these same soldiers predeployment CRP levels. After adjustment for battlefield experience scores and combat exposures, those patients with PTSD symptoms had elevated CRP levels of 1.0 ng/mL versus 0.7 ng/mL without postdeployment symptoms (JAMA Psychiatry. 2014;71:423-31). So it seems that there may be a link between PTSD negative cardiovascular outcomes. And there may be a link between PTSD and elevated CRP. So, this leaves us with at least two questions: Is elevated CRP related to increased incidence of negative cardiovascular outcomes? And, which came first, the chicken (PTSD) or the egg (elevated CRP)?
Dr. Mark A. Adelman is chief of vascular and endovascular surgery at NYU Langone Medical Center, New York, and an associate medical editor for Vascular Specialist.
This paper continues to strengthen a link between PTSD and inflammatory markers. Dewleen Baker of the VA health care system in San Diego reported that there was a 10-fold increase in C-reactive protein (CRP) post deployment as compared with these same soldiers predeployment CRP levels. After adjustment for battlefield experience scores and combat exposures, those patients with PTSD symptoms had elevated CRP levels of 1.0 ng/mL versus 0.7 ng/mL without postdeployment symptoms (JAMA Psychiatry. 2014;71:423-31). So it seems that there may be a link between PTSD negative cardiovascular outcomes. And there may be a link between PTSD and elevated CRP. So, this leaves us with at least two questions: Is elevated CRP related to increased incidence of negative cardiovascular outcomes? And, which came first, the chicken (PTSD) or the egg (elevated CRP)?
Dr. Mark A. Adelman is chief of vascular and endovascular surgery at NYU Langone Medical Center, New York, and an associate medical editor for Vascular Specialist.
ORLANDO – Military veterans aged 55 years or older with current posttraumatic stress disorder are at significantly higher risk of developing new-onset vascular disease than are those without PTSD, according to a very large national longitudinal study.
"This study suggests the need for greater monitoring and treatment of PTSD in older veterans to assist in the prevention of vascular disorders," Amy L. Byers, Ph.D., said at the annual meeting of the American Association for Geriatric Psychiatry.
She reported on 138,341 veterans aged 55 years or older who were free of known vascular disease at baseline. During 8 years of follow-up, those with PTSD had significantly higher rates of incident cerebrovascular disease, acute MI, heart failure, and peripheral vascular disease than did those without PTSD, even after adjustment for demographics, comorbid diabetes, hypertension, cancer, chronic obstructive pulmonary disease, renal disease, traumatic brain injury, dementia, substance use disorders, and psychiatric diagnoses. The fully adjusted increased risk of each of the forms of vascular disease under study still remained significant at P less than .001, noted Dr. Byers, an epidemiologist in the psychiatry department at the University of California, San Francisco.
In a separate study led by Dr. Byers, PTSD in the general population with onset prior to and persistence beyond age 55 was a powerful independent predictor of global disability.
Dr. Byers’ study of older veterans was funded by the Department of Defense. She had no disclosures.
ORLANDO – Military veterans aged 55 years or older with current posttraumatic stress disorder are at significantly higher risk of developing new-onset vascular disease than are those without PTSD, according to a very large national longitudinal study.
"This study suggests the need for greater monitoring and treatment of PTSD in older veterans to assist in the prevention of vascular disorders," Amy L. Byers, Ph.D., said at the annual meeting of the American Association for Geriatric Psychiatry.
She reported on 138,341 veterans aged 55 years or older who were free of known vascular disease at baseline. During 8 years of follow-up, those with PTSD had significantly higher rates of incident cerebrovascular disease, acute MI, heart failure, and peripheral vascular disease than did those without PTSD, even after adjustment for demographics, comorbid diabetes, hypertension, cancer, chronic obstructive pulmonary disease, renal disease, traumatic brain injury, dementia, substance use disorders, and psychiatric diagnoses. The fully adjusted increased risk of each of the forms of vascular disease under study still remained significant at P less than .001, noted Dr. Byers, an epidemiologist in the psychiatry department at the University of California, San Francisco.
In a separate study led by Dr. Byers, PTSD in the general population with onset prior to and persistence beyond age 55 was a powerful independent predictor of global disability.
Dr. Byers’ study of older veterans was funded by the Department of Defense. She had no disclosures.
Major finding: Military veterans with late-life posttraumatic stress disorder were 80% more likely to develop new-onset cerebrovascular disease during 8 years of follow-up than were those without PTSD. They were also 82% more likely to have a first acute myocardial infarction, 56% more likely to develop heart failure, and 60% more likely to be diagnosed with peripheral vascular disease.
Data source: This was a longitudinal observational study in 138,341 veterans aged 55 years or older who were free of known vascular disease at baseline and were followed for 8 years.
Disclosures: Dr. Byers’ study of older veterans was funded by the Department of Defense. She reported having no financial conflicts.
Olmesartan can cause celiac disease mimicker
CHICAGO – The antihypertensive agent olmesartan is associated with increased risk of a severe sprue-like enteropathy, as highlighted in a nationwide French cohort study.
This olmesartan-related illness is characterized by villous atrophy, severe chronic diarrhea, and weight loss, with negative serology for celiac disease.

The hospitalization rate for this disorder is time dependent. The risk doesn’t increase significantly until after the first year on therapy but climbs steeply thereafter, Dr. Myriam Mezzarobba reported at the annual Digestive Disease Week.
Importantly, angiotensin receptor blockers other than olmesartan (Benicar) were not associated with an increased risk of severe intestinal malabsorption in the French study. Neither were ACE inhibitors, added Dr. Mezzarobba of the French National Health Insurance Fund, Paris.
A few prior reports based on relatively limited patient numbers and/or short follow-up have indicated conflicting results regarding a possible association between olmesartan and severe intestinal malabsorption. This controversy provided the impetus for Dr. Mezzarobba and coinvestigators to conduct a cohort study harnessing the database of SNIIRAM, the French national health insurance plan covering 50 million residents, with linkage to the country’s centralized hospitalization database.
The investigators zeroed in on 4.5 million patients who started on an angiotensin receptor blocker or ACE inhibitor during 2007-2012. During more than 9 million person-years of follow-up, 218 of these individuals were hospitalized with a discharge diagnosis of intestinal malabsorption.
The incidence rate for this outcome among patients on olmesartan was 2.6 cases per 100,000 person-years during their first year on the medication, rising to 6.7 per 100,000 person-years during the second year and 8.9 per 100,000 person-years after 2 years on the drug.
In contrast, the rates among patients on other angiotensin receptor blockers were 2.1, 2.0, and 1.5 per 100,000 person-years, respectively, during the same treatment duration periods. And in patients on an ACE inhibitor, the rates were 3.7, 2.0, and 0.9 cases per 100,000 person-years during the first, second, and beyond the second year on therapy.
In a regression analysis controlled for age and sex, the adjusted rate ratio for hospitalization for intestinal malabsorption in patients on olmesartan compared with those on an ACE inhibitor was 0.7 for those on medication for less than a year, 3.3 during years 1-2, and 10.3 for those on olmesartan for longer than 2 years.
The typical pattern of this disorder is clinical and histologic remission following olmesartan discontinuation, Dr. Mezzarobba noted.
Session discussant Dr. Benjamin Lebwohl stressed that the French study holds a key lesson for gastroenterologists everywhere.
"Lest we become very aggressive in our case finding for celiac disease – and many of us are now looking more closely for this disease – we need to remember that villous atrophy is not always due to celiac disease," said Dr. Lebwohl, a gastroenterologist at Columbia University, New York.
He characterized the association between olmesartan and severe intestinal malabsorption found in the French national study as "robust," adding: "Importantly, this risk was not an acute risk. It increased over time. This is not an acute drug reaction, this is something that can develop at any point, even years after starting olmesartan."
Dr. Mezzarobba and Dr. Lebwohl reported having no financial conflicts.
CHICAGO – The antihypertensive agent olmesartan is associated with increased risk of a severe sprue-like enteropathy, as highlighted in a nationwide French cohort study.
This olmesartan-related illness is characterized by villous atrophy, severe chronic diarrhea, and weight loss, with negative serology for celiac disease.
The hospitalization rate for this disorder is time dependent. The risk doesn’t increase significantly until after the first year on therapy but climbs steeply thereafter, Dr. Myriam Mezzarobba reported at the annual Digestive Disease Week.
Importantly, angiotensin receptor blockers other than olmesartan (Benicar) were not associated with an increased risk of severe intestinal malabsorption in the French study. Neither were ACE inhibitors, added Dr. Mezzarobba of the French National Health Insurance Fund, Paris.
A few prior reports based on relatively limited patient numbers and/or short follow-up have indicated conflicting results regarding a possible association between olmesartan and severe intestinal malabsorption. This controversy provided the impetus for Dr. Mezzarobba and coinvestigators to conduct a cohort study harnessing the database of SNIIRAM, the French national health insurance plan covering 50 million residents, with linkage to the country’s centralized hospitalization database.
The investigators zeroed in on 4.5 million patients who started on an angiotensin receptor blocker or ACE inhibitor during 2007-2012. During more than 9 million person-years of follow-up, 218 of these individuals were hospitalized with a discharge diagnosis of intestinal malabsorption.
The incidence rate for this outcome among patients on olmesartan was 2.6 cases per 100,000 person-years during their first year on the medication, rising to 6.7 per 100,000 person-years during the second year and 8.9 per 100,000 person-years after 2 years on the drug.
In contrast, the rates among patients on other angiotensin receptor blockers were 2.1, 2.0, and 1.5 per 100,000 person-years, respectively, during the same treatment duration periods. And in patients on an ACE inhibitor, the rates were 3.7, 2.0, and 0.9 cases per 100,000 person-years during the first, second, and beyond the second year on therapy.
In a regression analysis controlled for age and sex, the adjusted rate ratio for hospitalization for intestinal malabsorption in patients on olmesartan compared with those on an ACE inhibitor was 0.7 for those on medication for less than a year, 3.3 during years 1-2, and 10.3 for those on olmesartan for longer than 2 years.
The typical pattern of this disorder is clinical and histologic remission following olmesartan discontinuation, Dr. Mezzarobba noted.
Session discussant Dr. Benjamin Lebwohl stressed that the French study holds a key lesson for gastroenterologists everywhere.
"Lest we become very aggressive in our case finding for celiac disease – and many of us are now looking more closely for this disease – we need to remember that villous atrophy is not always due to celiac disease," said Dr. Lebwohl, a gastroenterologist at Columbia University, New York.
He characterized the association between olmesartan and severe intestinal malabsorption found in the French national study as "robust," adding: "Importantly, this risk was not an acute risk. It increased over time. This is not an acute drug reaction, this is something that can develop at any point, even years after starting olmesartan."
Dr. Mezzarobba and Dr. Lebwohl reported having no financial conflicts.
CHICAGO – The antihypertensive agent olmesartan is associated with increased risk of a severe sprue-like enteropathy, as highlighted in a nationwide French cohort study.
This olmesartan-related illness is characterized by villous atrophy, severe chronic diarrhea, and weight loss, with negative serology for celiac disease.
The hospitalization rate for this disorder is time dependent. The risk doesn’t increase significantly until after the first year on therapy but climbs steeply thereafter, Dr. Myriam Mezzarobba reported at the annual Digestive Disease Week.
Importantly, angiotensin receptor blockers other than olmesartan (Benicar) were not associated with an increased risk of severe intestinal malabsorption in the French study. Neither were ACE inhibitors, added Dr. Mezzarobba of the French National Health Insurance Fund, Paris.
A few prior reports based on relatively limited patient numbers and/or short follow-up have indicated conflicting results regarding a possible association between olmesartan and severe intestinal malabsorption. This controversy provided the impetus for Dr. Mezzarobba and coinvestigators to conduct a cohort study harnessing the database of SNIIRAM, the French national health insurance plan covering 50 million residents, with linkage to the country’s centralized hospitalization database.
The investigators zeroed in on 4.5 million patients who started on an angiotensin receptor blocker or ACE inhibitor during 2007-2012. During more than 9 million person-years of follow-up, 218 of these individuals were hospitalized with a discharge diagnosis of intestinal malabsorption.
The incidence rate for this outcome among patients on olmesartan was 2.6 cases per 100,000 person-years during their first year on the medication, rising to 6.7 per 100,000 person-years during the second year and 8.9 per 100,000 person-years after 2 years on the drug.
In contrast, the rates among patients on other angiotensin receptor blockers were 2.1, 2.0, and 1.5 per 100,000 person-years, respectively, during the same treatment duration periods. And in patients on an ACE inhibitor, the rates were 3.7, 2.0, and 0.9 cases per 100,000 person-years during the first, second, and beyond the second year on therapy.
In a regression analysis controlled for age and sex, the adjusted rate ratio for hospitalization for intestinal malabsorption in patients on olmesartan compared with those on an ACE inhibitor was 0.7 for those on medication for less than a year, 3.3 during years 1-2, and 10.3 for those on olmesartan for longer than 2 years.
The typical pattern of this disorder is clinical and histologic remission following olmesartan discontinuation, Dr. Mezzarobba noted.
Session discussant Dr. Benjamin Lebwohl stressed that the French study holds a key lesson for gastroenterologists everywhere.
"Lest we become very aggressive in our case finding for celiac disease – and many of us are now looking more closely for this disease – we need to remember that villous atrophy is not always due to celiac disease," said Dr. Lebwohl, a gastroenterologist at Columbia University, New York.
He characterized the association between olmesartan and severe intestinal malabsorption found in the French national study as "robust," adding: "Importantly, this risk was not an acute risk. It increased over time. This is not an acute drug reaction, this is something that can develop at any point, even years after starting olmesartan."
Dr. Mezzarobba and Dr. Lebwohl reported having no financial conflicts.
AT DDW 2014
Key clinical point: When patients on olmesartan develop severe intestinal malabsorption with villous atrophy in the absence of positive serology for celiac disease, think drug side effect, even with onset after years of problem-free medication use.
Major finding: The adjusted risk of hospitalization for intestinal malabsorption in patients on olmesartan was 3.3-fold greater than in individuals on an ACE inhibitor during years 1-2 of treatment and 10.3-fold greater after more than 2 years of treatment.
Data source: A French nationwide cohort study of more than 4.5 million patients on an angiotensin receptor blocker or ACE inhibitor with 9 million person-years of follow-up.
Disclosures: The study was sponsored by the University of Paris and the French National Health Insurance Fund. The presenter reported having no financial conflicts.

ZS-9 may be a safer hyperkalemia therapy
LAS VEGAS – A novel, highly selective, oral potassium ion–binding agent called ZS-9 effectively reversed hyperkalemia in patients with underlying diabetes, heart failure, or chronic kidney disease.
ZS-9’s safety and tolerability matched those of placebo in the double-blind trial, which was the largest phase III treatment trial ever conducted in patients with hyperkalemia, Dr. Bhupinder Singh said at a meeting sponsored by the National Kidney Foundation.

ZS-9 is an inorganic, microporous crystal composed of zirconium silicate. It is insoluble, highly stable, and not systemically absorbed. In vitro it is more than 125 times more selective for potassium ions than is sodium polystyrene sulfate (SPS, brand name Kayexalate), the resin-based therapy traditionally used in hyperkalemia. ZS-9 also has nine times greater potassium ion binding capacity than SPS, according to Dr. Singh, of Apex Research in Riverside, Calif.
He reported on 753 patients with serum potassium levels of 5.0-6.5 mEq/L; 60% had chronic kidney disease, 40% had heart failure, and 60% had diabetes. Two-thirds of the patients were on an ACE inhibitor or an angiotensin receptor blocker (ARB). Importantly, 28% of subjects had an estimated glomerular filtration rate below 29 mL/min per 1.73 m2.
Subjects were randomized to one of four dosing regimens of ZS-9 or to placebo. For the first 48 hours of the study, patients received oral ZS-9 at doses of 1.25, 2.5, 5, or 10 g t.i.d. or placebo. Patients whose serum potassium levels normalized after 48 hours were then switched to once-daily doses of the same strengths or to placebo for 12 days in order to evaluate ZS-9’s safety and efficacy as a maintenance therapy.
The average reduction from baseline at 48 hours in serum potassium (as measured 14 hours after the last dose) was 0.46 mEq/L in the 2.5-g t.i.d. group, 0.54 mEq/L in 5-mg t.i.d. group, and 0.73 mEq/L in the 10-mg t.i.d. group. Normokalemia was attained at a similar rate in all patient subgroups, regardless of their underlying hyperkalemia-promoting disease. ZS-9 at 1.25 g t.i.d. wasn’t significantly more effective than placebo.
The higher a patient’s baseline serum potassium, the larger the absolute drop in response to a given dose. At 10 mg t.i.d., for example, patients with a baseline serum potassium level of 5.3 mEq/L or less averaged a 0.58-mEq/L reduction. Those who started at 5.4-5.5 mEq/L averaged a 0.98-mEq/L decrease, and patients with a baseline serum potassium level in excess of 5.5 mEq/L had a 1.10-mEq/L reduction.
Of patients who were on ZS-9 at 10 mg t.i.d. for the acute phase of the study, 99% were normokalemic at 48 hours.
All told, 542 patients entered the 12-day maintenance therapy phase. The two higher dosing regimens – 5 and 10 mg once daily – provided clinically and statistically significant benefit, with serum potassium levels remaining flat throughout the study period. Those who were switched double-blind to placebo after 12 days on ZS-9 immediately experienced a rise in their serum potassium. For example, patients with a serum potassium at 4.6 mEq/L during 12 days on ZS-9 at 10 mg climbed on average to a serum potassium of 5.0 mEq/L after 1 week on placebo.
Serum sodium, magnesium, and calcium did not change, nor did blood pressure or body weight in ZS-9-treated patients. There were no cases of significant hypokalemia (values below 3.0 mEq/L) in the study. Two of 11,000 serum potassium measures were less than 3.5 mEq/L. The side-effect profile of ZS-9 was basically the same as that of placebo. The incidence of nausea, vomiting, and other gastrointestinal adverse effects was actually more than twice as high with placebo than it was with active therapy, according to Dr. Singh.
Ongoing and planned studies of ZS-9 include an open-label, 12-month study and a 1-month, randomized treatment withdrawal with long-term extension.
Dr. Singh cited two major candidates for ZS-9 in clinical practice. One is in the large subgroup of patients with heart failure, diabetic kidney disease, or proteinuric nephropathy who become hyperkalemic on optimal doses of guideline-recommended therapy with an ACE inhibitor or ARB. The other potential beneficiaries are patients who would like to follow a healthy diet emphasizing vegetables, fruits, and low-fat dairy products, many of which are quite high in potassium content.
Dr. Singh reported serving as a consultant to ZS Pharma, which is developing ZS-9, as well as to Keryx Biopharmaceuticals and Concert.

|
|
The phase III ZS-9 results are extremely encouraging. There is a major unmet need for a safe and effective agent for acute and chronic management of hyperkalemia. Concern is mounting regarding chronic use of sodium polystyrene sulfate. A systematic review of published reports highlighted the risk of potentially fatal colonic necrosis and other gastrointestinal injuries with this traditional therapy (Am. J. Med. 2013;126:264.e9-e.24).
This information calls into question the use of SPS as a chronic therapy. So we need other options, and we perhaps have some on the horizon with ZS-9. Patiromer is another novel therapy well along in the developmental pipeline. This high-capacity, nonabsorbed, oral ion-exchange polymer also performed well in a phase III randomized trial presented by Dr. Matthew Weir of the University of Maryland, Baltimore, last fall at the annual meeting of the American Society of Nephrology.
Dr. John P. Middleton, a nephrologist at Duke University in Durham, N.C., made these remarks in a separate presentation at the meeting. Dr. Middleton reported having no financial conflicts.
|
|
|
The phase III ZS-9 results are extremely encouraging. There is a major unmet need for a safe and effective agent for acute and chronic management of hyperkalemia. Concern is mounting regarding chronic use of sodium polystyrene sulfate. A systematic review of published reports highlighted the risk of potentially fatal colonic necrosis and other gastrointestinal injuries with this traditional therapy (Am. J. Med. 2013;126:264.e9-e.24).
This information calls into question the use of SPS as a chronic therapy. So we need other options, and we perhaps have some on the horizon with ZS-9. Patiromer is another novel therapy well along in the developmental pipeline. This high-capacity, nonabsorbed, oral ion-exchange polymer also performed well in a phase III randomized trial presented by Dr. Matthew Weir of the University of Maryland, Baltimore, last fall at the annual meeting of the American Society of Nephrology.
Dr. John P. Middleton, a nephrologist at Duke University in Durham, N.C., made these remarks in a separate presentation at the meeting. Dr. Middleton reported having no financial conflicts.
|
|
|
The phase III ZS-9 results are extremely encouraging. There is a major unmet need for a safe and effective agent for acute and chronic management of hyperkalemia. Concern is mounting regarding chronic use of sodium polystyrene sulfate. A systematic review of published reports highlighted the risk of potentially fatal colonic necrosis and other gastrointestinal injuries with this traditional therapy (Am. J. Med. 2013;126:264.e9-e.24).
This information calls into question the use of SPS as a chronic therapy. So we need other options, and we perhaps have some on the horizon with ZS-9. Patiromer is another novel therapy well along in the developmental pipeline. This high-capacity, nonabsorbed, oral ion-exchange polymer also performed well in a phase III randomized trial presented by Dr. Matthew Weir of the University of Maryland, Baltimore, last fall at the annual meeting of the American Society of Nephrology.
Dr. John P. Middleton, a nephrologist at Duke University in Durham, N.C., made these remarks in a separate presentation at the meeting. Dr. Middleton reported having no financial conflicts.
LAS VEGAS – A novel, highly selective, oral potassium ion–binding agent called ZS-9 effectively reversed hyperkalemia in patients with underlying diabetes, heart failure, or chronic kidney disease.
ZS-9’s safety and tolerability matched those of placebo in the double-blind trial, which was the largest phase III treatment trial ever conducted in patients with hyperkalemia, Dr. Bhupinder Singh said at a meeting sponsored by the National Kidney Foundation.
ZS-9 is an inorganic, microporous crystal composed of zirconium silicate. It is insoluble, highly stable, and not systemically absorbed. In vitro it is more than 125 times more selective for potassium ions than is sodium polystyrene sulfate (SPS, brand name Kayexalate), the resin-based therapy traditionally used in hyperkalemia. ZS-9 also has nine times greater potassium ion binding capacity than SPS, according to Dr. Singh, of Apex Research in Riverside, Calif.
He reported on 753 patients with serum potassium levels of 5.0-6.5 mEq/L; 60% had chronic kidney disease, 40% had heart failure, and 60% had diabetes. Two-thirds of the patients were on an ACE inhibitor or an angiotensin receptor blocker (ARB). Importantly, 28% of subjects had an estimated glomerular filtration rate below 29 mL/min per 1.73 m2.
Subjects were randomized to one of four dosing regimens of ZS-9 or to placebo. For the first 48 hours of the study, patients received oral ZS-9 at doses of 1.25, 2.5, 5, or 10 g t.i.d. or placebo. Patients whose serum potassium levels normalized after 48 hours were then switched to once-daily doses of the same strengths or to placebo for 12 days in order to evaluate ZS-9’s safety and efficacy as a maintenance therapy.
The average reduction from baseline at 48 hours in serum potassium (as measured 14 hours after the last dose) was 0.46 mEq/L in the 2.5-g t.i.d. group, 0.54 mEq/L in 5-mg t.i.d. group, and 0.73 mEq/L in the 10-mg t.i.d. group. Normokalemia was attained at a similar rate in all patient subgroups, regardless of their underlying hyperkalemia-promoting disease. ZS-9 at 1.25 g t.i.d. wasn’t significantly more effective than placebo.
The higher a patient’s baseline serum potassium, the larger the absolute drop in response to a given dose. At 10 mg t.i.d., for example, patients with a baseline serum potassium level of 5.3 mEq/L or less averaged a 0.58-mEq/L reduction. Those who started at 5.4-5.5 mEq/L averaged a 0.98-mEq/L decrease, and patients with a baseline serum potassium level in excess of 5.5 mEq/L had a 1.10-mEq/L reduction.
Of patients who were on ZS-9 at 10 mg t.i.d. for the acute phase of the study, 99% were normokalemic at 48 hours.
All told, 542 patients entered the 12-day maintenance therapy phase. The two higher dosing regimens – 5 and 10 mg once daily – provided clinically and statistically significant benefit, with serum potassium levels remaining flat throughout the study period. Those who were switched double-blind to placebo after 12 days on ZS-9 immediately experienced a rise in their serum potassium. For example, patients with a serum potassium at 4.6 mEq/L during 12 days on ZS-9 at 10 mg climbed on average to a serum potassium of 5.0 mEq/L after 1 week on placebo.
Serum sodium, magnesium, and calcium did not change, nor did blood pressure or body weight in ZS-9-treated patients. There were no cases of significant hypokalemia (values below 3.0 mEq/L) in the study. Two of 11,000 serum potassium measures were less than 3.5 mEq/L. The side-effect profile of ZS-9 was basically the same as that of placebo. The incidence of nausea, vomiting, and other gastrointestinal adverse effects was actually more than twice as high with placebo than it was with active therapy, according to Dr. Singh.
Ongoing and planned studies of ZS-9 include an open-label, 12-month study and a 1-month, randomized treatment withdrawal with long-term extension.
Dr. Singh cited two major candidates for ZS-9 in clinical practice. One is in the large subgroup of patients with heart failure, diabetic kidney disease, or proteinuric nephropathy who become hyperkalemic on optimal doses of guideline-recommended therapy with an ACE inhibitor or ARB. The other potential beneficiaries are patients who would like to follow a healthy diet emphasizing vegetables, fruits, and low-fat dairy products, many of which are quite high in potassium content.
Dr. Singh reported serving as a consultant to ZS Pharma, which is developing ZS-9, as well as to Keryx Biopharmaceuticals and Concert.
LAS VEGAS – A novel, highly selective, oral potassium ion–binding agent called ZS-9 effectively reversed hyperkalemia in patients with underlying diabetes, heart failure, or chronic kidney disease.
ZS-9’s safety and tolerability matched those of placebo in the double-blind trial, which was the largest phase III treatment trial ever conducted in patients with hyperkalemia, Dr. Bhupinder Singh said at a meeting sponsored by the National Kidney Foundation.
ZS-9 is an inorganic, microporous crystal composed of zirconium silicate. It is insoluble, highly stable, and not systemically absorbed. In vitro it is more than 125 times more selective for potassium ions than is sodium polystyrene sulfate (SPS, brand name Kayexalate), the resin-based therapy traditionally used in hyperkalemia. ZS-9 also has nine times greater potassium ion binding capacity than SPS, according to Dr. Singh, of Apex Research in Riverside, Calif.
He reported on 753 patients with serum potassium levels of 5.0-6.5 mEq/L; 60% had chronic kidney disease, 40% had heart failure, and 60% had diabetes. Two-thirds of the patients were on an ACE inhibitor or an angiotensin receptor blocker (ARB). Importantly, 28% of subjects had an estimated glomerular filtration rate below 29 mL/min per 1.73 m2.
Subjects were randomized to one of four dosing regimens of ZS-9 or to placebo. For the first 48 hours of the study, patients received oral ZS-9 at doses of 1.25, 2.5, 5, or 10 g t.i.d. or placebo. Patients whose serum potassium levels normalized after 48 hours were then switched to once-daily doses of the same strengths or to placebo for 12 days in order to evaluate ZS-9’s safety and efficacy as a maintenance therapy.
The average reduction from baseline at 48 hours in serum potassium (as measured 14 hours after the last dose) was 0.46 mEq/L in the 2.5-g t.i.d. group, 0.54 mEq/L in 5-mg t.i.d. group, and 0.73 mEq/L in the 10-mg t.i.d. group. Normokalemia was attained at a similar rate in all patient subgroups, regardless of their underlying hyperkalemia-promoting disease. ZS-9 at 1.25 g t.i.d. wasn’t significantly more effective than placebo.
The higher a patient’s baseline serum potassium, the larger the absolute drop in response to a given dose. At 10 mg t.i.d., for example, patients with a baseline serum potassium level of 5.3 mEq/L or less averaged a 0.58-mEq/L reduction. Those who started at 5.4-5.5 mEq/L averaged a 0.98-mEq/L decrease, and patients with a baseline serum potassium level in excess of 5.5 mEq/L had a 1.10-mEq/L reduction.
Of patients who were on ZS-9 at 10 mg t.i.d. for the acute phase of the study, 99% were normokalemic at 48 hours.
All told, 542 patients entered the 12-day maintenance therapy phase. The two higher dosing regimens – 5 and 10 mg once daily – provided clinically and statistically significant benefit, with serum potassium levels remaining flat throughout the study period. Those who were switched double-blind to placebo after 12 days on ZS-9 immediately experienced a rise in their serum potassium. For example, patients with a serum potassium at 4.6 mEq/L during 12 days on ZS-9 at 10 mg climbed on average to a serum potassium of 5.0 mEq/L after 1 week on placebo.
Serum sodium, magnesium, and calcium did not change, nor did blood pressure or body weight in ZS-9-treated patients. There were no cases of significant hypokalemia (values below 3.0 mEq/L) in the study. Two of 11,000 serum potassium measures were less than 3.5 mEq/L. The side-effect profile of ZS-9 was basically the same as that of placebo. The incidence of nausea, vomiting, and other gastrointestinal adverse effects was actually more than twice as high with placebo than it was with active therapy, according to Dr. Singh.
Ongoing and planned studies of ZS-9 include an open-label, 12-month study and a 1-month, randomized treatment withdrawal with long-term extension.
Dr. Singh cited two major candidates for ZS-9 in clinical practice. One is in the large subgroup of patients with heart failure, diabetic kidney disease, or proteinuric nephropathy who become hyperkalemic on optimal doses of guideline-recommended therapy with an ACE inhibitor or ARB. The other potential beneficiaries are patients who would like to follow a healthy diet emphasizing vegetables, fruits, and low-fat dairy products, many of which are quite high in potassium content.
Dr. Singh reported serving as a consultant to ZS Pharma, which is developing ZS-9, as well as to Keryx Biopharmaceuticals and Concert.
AT SCM 14
Key clinical point: ZS-9 may become a safer treatment alternative to sodium polystyrene sulfate.
Major finding: After 48 hours on the investigational selective potassium ion trapper known as ZS-9 at 10 mg t.i.d., 99% of initially hyperkalemic patients with chronic kidney disease, diabetes, and/or heart failure were normokalemic.
Data source: This phase III, double-blind trial included 753 hyperkalemic patients randomized to one of four doses of ZS-9 or to placebo.
Disclosures: The study was sponsored by ZS Pharma. Dr. Singh reported serving as a consultant to ZS Pharma, which is developing ZS-9.

Depression linked to increased mortality in dialysis patients
LAS VEGAS – Depression in patients with chronic kidney disease is common, underrecognized, and undertreated, Dr. Daniel E. Weiner asserted at a meeting sponsored by the National Kidney Foundation.
Moreover, a recent meta-analysis by University of Toronto researchers demonstrated that the presence of depressive symptoms in patients on long-term dialysis was independently associated with a 51% increase in mortality, noted Dr. Weiner, a nephrologist at Tufts University, Boston.

The meta-analysis included 12 observational studies in which formal depression scales were utilized in more than 21,000 dialysis patients. Even after adjusting for potential publication bias, the presence of depressive symptoms was associated with a 45% increased risk of mortality (Am. J. Kidney Dis. 2014;63:623-35).
The prevalence of depression is elevated among patients across the spectrum of chronic kidney disease (CKD) severity. This was highlighted in a study in which 272 consecutive non–dialysis dependent patients with stage 2-5 CKD underwent screening for depression using the structured Mini International Neuropsychiatric Interview. One in five met criteria for an ongoing major depressive episode. The prevalence of depression didn’t vary significantly by CKD stage (Am. J. Kidney Dis. 2009;54:424-32).
Depression is even more common among patients on dialysis for end-stage renal disease, with prevalence rates of up to 42% reported, Dr. Weiner continued.
He urged physicians to routinely screen for depression in patients with CKD. Studies indicate that’s not widely being done at present, probably in part because the evidence for therapeutic benefit is spotty because the large randomized controlled trials of antidepressant medications have generally excluded patients with advanced CKD.
Dr. Weiner, however, argued that routine screening in patients with CKD is warranted given that the yield is markedly higher than in the general population, depression is associated with increased mortality in dialysis-dependent patients, and it is a treatable disorder. There is evidence from small studies that the selective serotonin reuptake inhibitors (SSRIs) are safe in patients with CKD. Cognitive-behavioral therapy and exercise-based treatment regimens also are backed by supporting evidence.
Dr. Weiner reported having no financial conflicts regarding his presentation.
LAS VEGAS – Depression in patients with chronic kidney disease is common, underrecognized, and undertreated, Dr. Daniel E. Weiner asserted at a meeting sponsored by the National Kidney Foundation.
Moreover, a recent meta-analysis by University of Toronto researchers demonstrated that the presence of depressive symptoms in patients on long-term dialysis was independently associated with a 51% increase in mortality, noted Dr. Weiner, a nephrologist at Tufts University, Boston.
The meta-analysis included 12 observational studies in which formal depression scales were utilized in more than 21,000 dialysis patients. Even after adjusting for potential publication bias, the presence of depressive symptoms was associated with a 45% increased risk of mortality (Am. J. Kidney Dis. 2014;63:623-35).
The prevalence of depression is elevated among patients across the spectrum of chronic kidney disease (CKD) severity. This was highlighted in a study in which 272 consecutive non–dialysis dependent patients with stage 2-5 CKD underwent screening for depression using the structured Mini International Neuropsychiatric Interview. One in five met criteria for an ongoing major depressive episode. The prevalence of depression didn’t vary significantly by CKD stage (Am. J. Kidney Dis. 2009;54:424-32).
Depression is even more common among patients on dialysis for end-stage renal disease, with prevalence rates of up to 42% reported, Dr. Weiner continued.
He urged physicians to routinely screen for depression in patients with CKD. Studies indicate that’s not widely being done at present, probably in part because the evidence for therapeutic benefit is spotty because the large randomized controlled trials of antidepressant medications have generally excluded patients with advanced CKD.
Dr. Weiner, however, argued that routine screening in patients with CKD is warranted given that the yield is markedly higher than in the general population, depression is associated with increased mortality in dialysis-dependent patients, and it is a treatable disorder. There is evidence from small studies that the selective serotonin reuptake inhibitors (SSRIs) are safe in patients with CKD. Cognitive-behavioral therapy and exercise-based treatment regimens also are backed by supporting evidence.
Dr. Weiner reported having no financial conflicts regarding his presentation.
LAS VEGAS – Depression in patients with chronic kidney disease is common, underrecognized, and undertreated, Dr. Daniel E. Weiner asserted at a meeting sponsored by the National Kidney Foundation.
Moreover, a recent meta-analysis by University of Toronto researchers demonstrated that the presence of depressive symptoms in patients on long-term dialysis was independently associated with a 51% increase in mortality, noted Dr. Weiner, a nephrologist at Tufts University, Boston.
The meta-analysis included 12 observational studies in which formal depression scales were utilized in more than 21,000 dialysis patients. Even after adjusting for potential publication bias, the presence of depressive symptoms was associated with a 45% increased risk of mortality (Am. J. Kidney Dis. 2014;63:623-35).
The prevalence of depression is elevated among patients across the spectrum of chronic kidney disease (CKD) severity. This was highlighted in a study in which 272 consecutive non–dialysis dependent patients with stage 2-5 CKD underwent screening for depression using the structured Mini International Neuropsychiatric Interview. One in five met criteria for an ongoing major depressive episode. The prevalence of depression didn’t vary significantly by CKD stage (Am. J. Kidney Dis. 2009;54:424-32).
Depression is even more common among patients on dialysis for end-stage renal disease, with prevalence rates of up to 42% reported, Dr. Weiner continued.
He urged physicians to routinely screen for depression in patients with CKD. Studies indicate that’s not widely being done at present, probably in part because the evidence for therapeutic benefit is spotty because the large randomized controlled trials of antidepressant medications have generally excluded patients with advanced CKD.
Dr. Weiner, however, argued that routine screening in patients with CKD is warranted given that the yield is markedly higher than in the general population, depression is associated with increased mortality in dialysis-dependent patients, and it is a treatable disorder. There is evidence from small studies that the selective serotonin reuptake inhibitors (SSRIs) are safe in patients with CKD. Cognitive-behavioral therapy and exercise-based treatment regimens also are backed by supporting evidence.
Dr. Weiner reported having no financial conflicts regarding his presentation.
EXPERT ANALYSIS FROM SCM 14

Resuming aspirin for cardioprotection after GI bleed tied to 38% cut in CV risk
CHICAGO – New data shine a light on the trade-offs involved in resuming low-dose aspirin therapy for secondary cardiovascular prevention following a lower gastrointestinal bleeding event.
Going back onto daily low-dose aspirin was associated with a 2.7-fold greater risk of recurrent lower GI bleeding than no use of aspirin during 5 years of follow-up. However, the risk of a major cardiovascular event – nonfatal myocardial infarction or stroke or death due to a vascular cause – was reduced by 38%. Moreover, the rate of death due to nonvascular causes was 3.2-fold lower among the aspirin-using group, Dr. Francis K.L. Chan reported at the annual Digestive Disease Week.

He presented a single-center retrospective cohort study involving 295 patients who developed endoscopically confirmed lower GI bleeding while on low-dose aspirin for secondary cardiovascular prevention. A total of 174 subjects in this observational study resumed aspirin and 121 did not.
The two groups were similar in terms of their cardiovascular risk profiles based upon conventional risk factors. However, the aspirin nonusers, with a mean age of 76 years, were on average 3 years older than those who resumed aspirin. The nonusers were also more likely to have had a severe index lower GI bleed requiring transfusion of more than 2 units of blood products, by a margin of 55%-40%. An upper GI bleeding source was excluded by endoscopy in all participants, noted Dr. Chan of the Chinese University of Hong Kong.
The 5-year cumulative incidence of recurrent lower GI bleeding was 18.9% among the aspirin users, compared with 6.9% in the nonusers. The incidence of a major cardiovascular event was 22.8% in the aspirin group versus 36.5% among aspirin nonusers. And the 5-year incidence of death due to nonvascular causes was 8.2% in the aspirin users, compared with 26.7% in nonusers.
The nature of the Hong Kong health care system is such that all outcomes of interest were reliably captured. Eighty-four percent of patients in the aspirin user group received prescriptions for aspirin during at least 75% of the follow-up period, while 87% of the nonuser group received aspirin during 10% or less of the study period.
Audience members praised Dr. Chan for providing "clear-cut" and "very significant" findings addressing the previously unanswered but clinically important question of the risks and benefits of aspirin resumption versus nonuse following a lower GI bleed occurring while on therapy.
The study was carried out with institutional funds. Dr. Chan is on speakers bureaus for AstraZeneca, Pfizer, Takeda, and Eisai.
CHICAGO – New data shine a light on the trade-offs involved in resuming low-dose aspirin therapy for secondary cardiovascular prevention following a lower gastrointestinal bleeding event.
Going back onto daily low-dose aspirin was associated with a 2.7-fold greater risk of recurrent lower GI bleeding than no use of aspirin during 5 years of follow-up. However, the risk of a major cardiovascular event – nonfatal myocardial infarction or stroke or death due to a vascular cause – was reduced by 38%. Moreover, the rate of death due to nonvascular causes was 3.2-fold lower among the aspirin-using group, Dr. Francis K.L. Chan reported at the annual Digestive Disease Week.
He presented a single-center retrospective cohort study involving 295 patients who developed endoscopically confirmed lower GI bleeding while on low-dose aspirin for secondary cardiovascular prevention. A total of 174 subjects in this observational study resumed aspirin and 121 did not.
The two groups were similar in terms of their cardiovascular risk profiles based upon conventional risk factors. However, the aspirin nonusers, with a mean age of 76 years, were on average 3 years older than those who resumed aspirin. The nonusers were also more likely to have had a severe index lower GI bleed requiring transfusion of more than 2 units of blood products, by a margin of 55%-40%. An upper GI bleeding source was excluded by endoscopy in all participants, noted Dr. Chan of the Chinese University of Hong Kong.
The 5-year cumulative incidence of recurrent lower GI bleeding was 18.9% among the aspirin users, compared with 6.9% in the nonusers. The incidence of a major cardiovascular event was 22.8% in the aspirin group versus 36.5% among aspirin nonusers. And the 5-year incidence of death due to nonvascular causes was 8.2% in the aspirin users, compared with 26.7% in nonusers.
The nature of the Hong Kong health care system is such that all outcomes of interest were reliably captured. Eighty-four percent of patients in the aspirin user group received prescriptions for aspirin during at least 75% of the follow-up period, while 87% of the nonuser group received aspirin during 10% or less of the study period.
Audience members praised Dr. Chan for providing "clear-cut" and "very significant" findings addressing the previously unanswered but clinically important question of the risks and benefits of aspirin resumption versus nonuse following a lower GI bleed occurring while on therapy.
The study was carried out with institutional funds. Dr. Chan is on speakers bureaus for AstraZeneca, Pfizer, Takeda, and Eisai.
CHICAGO – New data shine a light on the trade-offs involved in resuming low-dose aspirin therapy for secondary cardiovascular prevention following a lower gastrointestinal bleeding event.
Going back onto daily low-dose aspirin was associated with a 2.7-fold greater risk of recurrent lower GI bleeding than no use of aspirin during 5 years of follow-up. However, the risk of a major cardiovascular event – nonfatal myocardial infarction or stroke or death due to a vascular cause – was reduced by 38%. Moreover, the rate of death due to nonvascular causes was 3.2-fold lower among the aspirin-using group, Dr. Francis K.L. Chan reported at the annual Digestive Disease Week.
He presented a single-center retrospective cohort study involving 295 patients who developed endoscopically confirmed lower GI bleeding while on low-dose aspirin for secondary cardiovascular prevention. A total of 174 subjects in this observational study resumed aspirin and 121 did not.
The two groups were similar in terms of their cardiovascular risk profiles based upon conventional risk factors. However, the aspirin nonusers, with a mean age of 76 years, were on average 3 years older than those who resumed aspirin. The nonusers were also more likely to have had a severe index lower GI bleed requiring transfusion of more than 2 units of blood products, by a margin of 55%-40%. An upper GI bleeding source was excluded by endoscopy in all participants, noted Dr. Chan of the Chinese University of Hong Kong.
The 5-year cumulative incidence of recurrent lower GI bleeding was 18.9% among the aspirin users, compared with 6.9% in the nonusers. The incidence of a major cardiovascular event was 22.8% in the aspirin group versus 36.5% among aspirin nonusers. And the 5-year incidence of death due to nonvascular causes was 8.2% in the aspirin users, compared with 26.7% in nonusers.
The nature of the Hong Kong health care system is such that all outcomes of interest were reliably captured. Eighty-four percent of patients in the aspirin user group received prescriptions for aspirin during at least 75% of the follow-up period, while 87% of the nonuser group received aspirin during 10% or less of the study period.
Audience members praised Dr. Chan for providing "clear-cut" and "very significant" findings addressing the previously unanswered but clinically important question of the risks and benefits of aspirin resumption versus nonuse following a lower GI bleed occurring while on therapy.
The study was carried out with institutional funds. Dr. Chan is on speakers bureaus for AstraZeneca, Pfizer, Takeda, and Eisai.
AT DDW 2014
Key clinical point: What’s the risk/benefit balance in restarting low-dose aspirin for secondary cardioprevention following a lower GI bleed? New data provide the answer to this common clinical dilemma.
Major finding: Resuming low-dose aspirin in patients after a lower GI bleed was associated with a 2.7-fold increased risk of a recurrent bleed within 5 years, but a 38% reduction in the risk of a major cardiovascular event, compared with aspirin discontinuation.
Data source: This was a single-center retrospective cohort study involving 295 patients with a history of a lower GI bleed while on low-dose aspirin for secondary cardiovascular prophylaxis.
Disclosures: The study was carried out with institutional funds. Dr. Chan is on speakers bureaus for AstraZeneca, Pfizer, Takeda, and Eisai.

ED doc survey: 22% of advanced imaging is ‘medically unnecessary’
DALLAS – On average, 22% of the CTs and MRIs ordered by emergency physicians are "medically unnecessary," based on responses by 435 emergency physicians participating in a national survey.
"The overwhelming majority of physicians in our sample recognized the issue of overimaging in the ED, and it’s not just something they felt was going on among others in their group. It’s something they personally acknowledged participating in," Dr. Hemal K. Kanzaria said at the annual meeting of the Society for Academic Emergency Medicine.

The two most common reasons for ordering "medically unnecessary" advanced diagnostic imaging studies were fear of missing a diagnosis despite low pretest probability, cited by 69% of respondents, and fear of litigation, cited by 64%, noted Dr. Kanzaria, a Robert Woods Johnson Foundation Clinical Scholar and emergency medicine fellow at the University of California, Los Angeles.
Patient and family expectations were identified as a driving force in ordering medically unnecessary imaging, 40% of respondents said. A mere 1% of respondents cited administrative pressure to increase group reimbursement as a main contributor, he added.
Advanced diagnostic imaging in EDs has increased appreciably in recent years, with little evidence of a resultant improvement in patient outcomes. The trend has drawn scrutiny from health policy experts in light of estimates that the U.S. annually spends $210 billion on unnecessary medical tests, procedures, and services. Yet there are little data on emergency physicians’ perceptions regarding overordering of CTs and MRIs, the causes, and the potential solutions.
"Basically, we need to know what physicians are thinking (about the issue), and that’s why we did this study," Dr. Kanzaria explained.
Two focus groups of multispecialty physicians and expert opinion from physicians who have researched overordering of diagnostic imaging were used to create the questions, which were then revised in response to a pilot study conducted among 16 emergency physicians.
The resulting 19-item survey took about 10 minutes to complete. The survey defined a "medically unnecessary" imaging study as "one you wouldn’t order if you had no external pressure and were only concerned about providing optimal medical care."
The nonrandom sample for the survey included 478 academic and community practice emergency physicians in 29 states; the completion rate was a whopping 91% (435 respondents). Respondents’ average age was 42 years with a mean 14 years in clinical practice; 68% were board-certified in emergency medicine. The pattern of survey responses did not differ based upon physician age, years in practice, or board certification status.
More than 85% of the emergency physicians said they believe too many diagnostic tests are ordered in their own ED. More specifically, a similarly lofty percentage believe medically unnecessary CTs and MRIs are ordered in their ED under common clinical scenarios described in the survey, such as head CTs for nontraumatic headaches and pan scans for trauma patients. Fully 97% of EPs acknowledged ordering medically unnecessary CTs and MRIs.
More than 50% of respondents identified as "extremely or very helpful" proposed solutions to "medically unnecessary" advanced imaging in the ED.
Topping the options was tort reform, which 79% of emergency physicians thought would make a major difference. However, Dr. Kanzaria called malpractice reform necessary but not sufficient to change practice. "Recent studies on tort reform efforts have not actually shown subsequent significant effects on cost reduction or a change in test-ordering behavior."
A more promising option may be shared decision making with patients regarding diagnostic testing for low-probability outcomes, he said. "The literature on shared decision making is still in its infancy, but what’s out there [indicates this option] is really promising as an avenue to improve communication and potentially to reduce overuse. So, I think we should consider ways to incorporate shared decision making into emergency care," Dr. Kanzaria said.
Another popular suggestion was to provide feedback to emergency physicians regarding their own test ordering behavior compared to that of their peers, something Dr. Kanzaria called "incredibly simple to do."
Education aimed at steering patients, families, and referring physicians away from the prevailing "no miss" attitude in favor of greater understanding of the probabilistic limits of diagnostic testing was also widely endorsed by the survey respondents.
Dr. Kanzaria’s research is funded by the Robert Wood Johnson Foundation Clinical Scholars Program. He reported having no financial conflicts.
DALLAS – On average, 22% of the CTs and MRIs ordered by emergency physicians are "medically unnecessary," based on responses by 435 emergency physicians participating in a national survey.
"The overwhelming majority of physicians in our sample recognized the issue of overimaging in the ED, and it’s not just something they felt was going on among others in their group. It’s something they personally acknowledged participating in," Dr. Hemal K. Kanzaria said at the annual meeting of the Society for Academic Emergency Medicine.
The two most common reasons for ordering "medically unnecessary" advanced diagnostic imaging studies were fear of missing a diagnosis despite low pretest probability, cited by 69% of respondents, and fear of litigation, cited by 64%, noted Dr. Kanzaria, a Robert Woods Johnson Foundation Clinical Scholar and emergency medicine fellow at the University of California, Los Angeles.
Patient and family expectations were identified as a driving force in ordering medically unnecessary imaging, 40% of respondents said. A mere 1% of respondents cited administrative pressure to increase group reimbursement as a main contributor, he added.
Advanced diagnostic imaging in EDs has increased appreciably in recent years, with little evidence of a resultant improvement in patient outcomes. The trend has drawn scrutiny from health policy experts in light of estimates that the U.S. annually spends $210 billion on unnecessary medical tests, procedures, and services. Yet there are little data on emergency physicians’ perceptions regarding overordering of CTs and MRIs, the causes, and the potential solutions.
"Basically, we need to know what physicians are thinking (about the issue), and that’s why we did this study," Dr. Kanzaria explained.
Two focus groups of multispecialty physicians and expert opinion from physicians who have researched overordering of diagnostic imaging were used to create the questions, which were then revised in response to a pilot study conducted among 16 emergency physicians.
The resulting 19-item survey took about 10 minutes to complete. The survey defined a "medically unnecessary" imaging study as "one you wouldn’t order if you had no external pressure and were only concerned about providing optimal medical care."
The nonrandom sample for the survey included 478 academic and community practice emergency physicians in 29 states; the completion rate was a whopping 91% (435 respondents). Respondents’ average age was 42 years with a mean 14 years in clinical practice; 68% were board-certified in emergency medicine. The pattern of survey responses did not differ based upon physician age, years in practice, or board certification status.
More than 85% of the emergency physicians said they believe too many diagnostic tests are ordered in their own ED. More specifically, a similarly lofty percentage believe medically unnecessary CTs and MRIs are ordered in their ED under common clinical scenarios described in the survey, such as head CTs for nontraumatic headaches and pan scans for trauma patients. Fully 97% of EPs acknowledged ordering medically unnecessary CTs and MRIs.
More than 50% of respondents identified as "extremely or very helpful" proposed solutions to "medically unnecessary" advanced imaging in the ED.
Topping the options was tort reform, which 79% of emergency physicians thought would make a major difference. However, Dr. Kanzaria called malpractice reform necessary but not sufficient to change practice. "Recent studies on tort reform efforts have not actually shown subsequent significant effects on cost reduction or a change in test-ordering behavior."
A more promising option may be shared decision making with patients regarding diagnostic testing for low-probability outcomes, he said. "The literature on shared decision making is still in its infancy, but what’s out there [indicates this option] is really promising as an avenue to improve communication and potentially to reduce overuse. So, I think we should consider ways to incorporate shared decision making into emergency care," Dr. Kanzaria said.
Another popular suggestion was to provide feedback to emergency physicians regarding their own test ordering behavior compared to that of their peers, something Dr. Kanzaria called "incredibly simple to do."
Education aimed at steering patients, families, and referring physicians away from the prevailing "no miss" attitude in favor of greater understanding of the probabilistic limits of diagnostic testing was also widely endorsed by the survey respondents.
Dr. Kanzaria’s research is funded by the Robert Wood Johnson Foundation Clinical Scholars Program. He reported having no financial conflicts.
DALLAS – On average, 22% of the CTs and MRIs ordered by emergency physicians are "medically unnecessary," based on responses by 435 emergency physicians participating in a national survey.
"The overwhelming majority of physicians in our sample recognized the issue of overimaging in the ED, and it’s not just something they felt was going on among others in their group. It’s something they personally acknowledged participating in," Dr. Hemal K. Kanzaria said at the annual meeting of the Society for Academic Emergency Medicine.
The two most common reasons for ordering "medically unnecessary" advanced diagnostic imaging studies were fear of missing a diagnosis despite low pretest probability, cited by 69% of respondents, and fear of litigation, cited by 64%, noted Dr. Kanzaria, a Robert Woods Johnson Foundation Clinical Scholar and emergency medicine fellow at the University of California, Los Angeles.
Patient and family expectations were identified as a driving force in ordering medically unnecessary imaging, 40% of respondents said. A mere 1% of respondents cited administrative pressure to increase group reimbursement as a main contributor, he added.
Advanced diagnostic imaging in EDs has increased appreciably in recent years, with little evidence of a resultant improvement in patient outcomes. The trend has drawn scrutiny from health policy experts in light of estimates that the U.S. annually spends $210 billion on unnecessary medical tests, procedures, and services. Yet there are little data on emergency physicians’ perceptions regarding overordering of CTs and MRIs, the causes, and the potential solutions.
"Basically, we need to know what physicians are thinking (about the issue), and that’s why we did this study," Dr. Kanzaria explained.
Two focus groups of multispecialty physicians and expert opinion from physicians who have researched overordering of diagnostic imaging were used to create the questions, which were then revised in response to a pilot study conducted among 16 emergency physicians.
The resulting 19-item survey took about 10 minutes to complete. The survey defined a "medically unnecessary" imaging study as "one you wouldn’t order if you had no external pressure and were only concerned about providing optimal medical care."
The nonrandom sample for the survey included 478 academic and community practice emergency physicians in 29 states; the completion rate was a whopping 91% (435 respondents). Respondents’ average age was 42 years with a mean 14 years in clinical practice; 68% were board-certified in emergency medicine. The pattern of survey responses did not differ based upon physician age, years in practice, or board certification status.
More than 85% of the emergency physicians said they believe too many diagnostic tests are ordered in their own ED. More specifically, a similarly lofty percentage believe medically unnecessary CTs and MRIs are ordered in their ED under common clinical scenarios described in the survey, such as head CTs for nontraumatic headaches and pan scans for trauma patients. Fully 97% of EPs acknowledged ordering medically unnecessary CTs and MRIs.
More than 50% of respondents identified as "extremely or very helpful" proposed solutions to "medically unnecessary" advanced imaging in the ED.
Topping the options was tort reform, which 79% of emergency physicians thought would make a major difference. However, Dr. Kanzaria called malpractice reform necessary but not sufficient to change practice. "Recent studies on tort reform efforts have not actually shown subsequent significant effects on cost reduction or a change in test-ordering behavior."
A more promising option may be shared decision making with patients regarding diagnostic testing for low-probability outcomes, he said. "The literature on shared decision making is still in its infancy, but what’s out there [indicates this option] is really promising as an avenue to improve communication and potentially to reduce overuse. So, I think we should consider ways to incorporate shared decision making into emergency care," Dr. Kanzaria said.
Another popular suggestion was to provide feedback to emergency physicians regarding their own test ordering behavior compared to that of their peers, something Dr. Kanzaria called "incredibly simple to do."
Education aimed at steering patients, families, and referring physicians away from the prevailing "no miss" attitude in favor of greater understanding of the probabilistic limits of diagnostic testing was also widely endorsed by the survey respondents.
Dr. Kanzaria’s research is funded by the Robert Wood Johnson Foundation Clinical Scholars Program. He reported having no financial conflicts.
AT SAEM 2014
