User login
Primary care residents’ approach to HPV vaccine vary by specialty
SAN DIEGO – Among U.S. resident trainees in the primary care specialties, ob.gyn. and internal medicine resident physicians are the clear laggards when it comes to counseling appropriate candidates to receive the human papillomavirus (HPV) vaccine, Dr. Tiffany Zigras reported at the annual meeting of the Society of Gynecologic Oncology.
Pediatric residents led the way in self-reported “always” counseling eligible patients to receive the three-dose HPV vaccine series in her national survey, with family medicine residents in firm command of second place.

Although the HPV vaccine was approved by the Food and Drug Administration in 2006, uptake remains low. A 2014 report based upon National Health Interview Survey data concluded only 13.6% of U.S. women ages 18-26 had received all three doses of the vaccine. A national Status of Cancer report concluded that only 32% of females ages 13-17 years had been vaccinated; in the uninsured population this rate fell to a mere 14.1% (Am J Public Health. 2014 May;104(5):946-53), noted Dr. Zigras of Bridgeport (Conn.) Hospital/Yale New Haven Health.
Since physician recommendation is known to play a key role in vaccine uptake and the approach taken by primary care residents hadn’t previously been studied, Dr. Zigras and her coinvestigators created a 37-item electronic survey and sent it to residency program directors in the various primary care disciplines with a request that they share the web link with their trainees.
The survey was completed by 1,549 resident physicians. Fully 82% of the pediatric residents indicated that they “always” recommend the HPV vaccine as an important means of cancer prevention. So did 64% of family medicine residents, 39% of ob.gyn. residents, and 28% of internal medicine residents.
Overall, female primary care residents were three times more likely than their male counterparts to always recommend the HPV vaccine to their eligible patients.
Primary care residents cited parental disapproval as a major reason for vaccine refusal in 49% of cases, fear of vaccines in general as an insurmountable issue in 34%, and fear of needles as a significant factor in 14%.
Whether or not respondent residents had received education about the vaccine during medical school had no bearing on their current self-described rate of HPV vaccine recommendation. However, residents who reported receiving education about the risks, benefits, and value of the vaccine during their residency training were significantly more likely to always recommend it for eligible patients.
“Residents have a unique opportunity to capture a subset of patients who may otherwise not have an opportunity to receive the HPV vaccine,” Dr. Zigras observed. “Education about the HPV vaccine in resident curriculum is critical to improve the uptake of the HPV vaccine in the United States.”
She reported no financial conflicts with regard to her study.
SAN DIEGO – Among U.S. resident trainees in the primary care specialties, ob.gyn. and internal medicine resident physicians are the clear laggards when it comes to counseling appropriate candidates to receive the human papillomavirus (HPV) vaccine, Dr. Tiffany Zigras reported at the annual meeting of the Society of Gynecologic Oncology.
Pediatric residents led the way in self-reported “always” counseling eligible patients to receive the three-dose HPV vaccine series in her national survey, with family medicine residents in firm command of second place.
Although the HPV vaccine was approved by the Food and Drug Administration in 2006, uptake remains low. A 2014 report based upon National Health Interview Survey data concluded only 13.6% of U.S. women ages 18-26 had received all three doses of the vaccine. A national Status of Cancer report concluded that only 32% of females ages 13-17 years had been vaccinated; in the uninsured population this rate fell to a mere 14.1% (Am J Public Health. 2014 May;104(5):946-53), noted Dr. Zigras of Bridgeport (Conn.) Hospital/Yale New Haven Health.
Since physician recommendation is known to play a key role in vaccine uptake and the approach taken by primary care residents hadn’t previously been studied, Dr. Zigras and her coinvestigators created a 37-item electronic survey and sent it to residency program directors in the various primary care disciplines with a request that they share the web link with their trainees.
The survey was completed by 1,549 resident physicians. Fully 82% of the pediatric residents indicated that they “always” recommend the HPV vaccine as an important means of cancer prevention. So did 64% of family medicine residents, 39% of ob.gyn. residents, and 28% of internal medicine residents.
Overall, female primary care residents were three times more likely than their male counterparts to always recommend the HPV vaccine to their eligible patients.
Primary care residents cited parental disapproval as a major reason for vaccine refusal in 49% of cases, fear of vaccines in general as an insurmountable issue in 34%, and fear of needles as a significant factor in 14%.
Whether or not respondent residents had received education about the vaccine during medical school had no bearing on their current self-described rate of HPV vaccine recommendation. However, residents who reported receiving education about the risks, benefits, and value of the vaccine during their residency training were significantly more likely to always recommend it for eligible patients.
“Residents have a unique opportunity to capture a subset of patients who may otherwise not have an opportunity to receive the HPV vaccine,” Dr. Zigras observed. “Education about the HPV vaccine in resident curriculum is critical to improve the uptake of the HPV vaccine in the United States.”
She reported no financial conflicts with regard to her study.
SAN DIEGO – Among U.S. resident trainees in the primary care specialties, ob.gyn. and internal medicine resident physicians are the clear laggards when it comes to counseling appropriate candidates to receive the human papillomavirus (HPV) vaccine, Dr. Tiffany Zigras reported at the annual meeting of the Society of Gynecologic Oncology.
Pediatric residents led the way in self-reported “always” counseling eligible patients to receive the three-dose HPV vaccine series in her national survey, with family medicine residents in firm command of second place.
Although the HPV vaccine was approved by the Food and Drug Administration in 2006, uptake remains low. A 2014 report based upon National Health Interview Survey data concluded only 13.6% of U.S. women ages 18-26 had received all three doses of the vaccine. A national Status of Cancer report concluded that only 32% of females ages 13-17 years had been vaccinated; in the uninsured population this rate fell to a mere 14.1% (Am J Public Health. 2014 May;104(5):946-53), noted Dr. Zigras of Bridgeport (Conn.) Hospital/Yale New Haven Health.
Since physician recommendation is known to play a key role in vaccine uptake and the approach taken by primary care residents hadn’t previously been studied, Dr. Zigras and her coinvestigators created a 37-item electronic survey and sent it to residency program directors in the various primary care disciplines with a request that they share the web link with their trainees.
The survey was completed by 1,549 resident physicians. Fully 82% of the pediatric residents indicated that they “always” recommend the HPV vaccine as an important means of cancer prevention. So did 64% of family medicine residents, 39% of ob.gyn. residents, and 28% of internal medicine residents.
Overall, female primary care residents were three times more likely than their male counterparts to always recommend the HPV vaccine to their eligible patients.
Primary care residents cited parental disapproval as a major reason for vaccine refusal in 49% of cases, fear of vaccines in general as an insurmountable issue in 34%, and fear of needles as a significant factor in 14%.
Whether or not respondent residents had received education about the vaccine during medical school had no bearing on their current self-described rate of HPV vaccine recommendation. However, residents who reported receiving education about the risks, benefits, and value of the vaccine during their residency training were significantly more likely to always recommend it for eligible patients.
“Residents have a unique opportunity to capture a subset of patients who may otherwise not have an opportunity to receive the HPV vaccine,” Dr. Zigras observed. “Education about the HPV vaccine in resident curriculum is critical to improve the uptake of the HPV vaccine in the United States.”
She reported no financial conflicts with regard to her study.
AT THE ANNUAL MEETING ON WOMEN’S CANCER
Key clinical point: Nationally, pediatric and family medicine residents are tops among primary care trainees in terms of consistently recommending the HPV vaccine for eligible patients.
Major finding: Of pediatric residents, 82% report “always” recommending the HPV vaccine to appropriate candidates, compared with just 28% of internal medicine residents.
Data source: This 37-item electronic survey was completed by nearly 1,600 U.S. primary care resident physicians.
Disclosures: The study presenter reported having no financial conflicts of interest.

Rhythm control may be best for atrial fib in HFpEF
CHICAGO – Atrial fibrillation with good heart rate control in patients who have heart failure with preserved ejection fraction is independently associated with exercise intolerance, impaired contractile reserve, and a sharply higher mortality rate than in matched HFpEF patients without the arrhythmia, a retrospective analysis showed.
“Our study, the largest of its kind, provides mechanistic evidence from cardiopulmonary testing that a rhythm control strategy may potentially improve peak exercise capacity and survival in this patient population, a finding that of course requires future prospective appraisal in randomized trials comparing rate and rhythm control of atrial fibrillation in HFpEF,” Dr. Mohamed Badreldin Elshazly reported at the annual meeting of the American College of Cardiology.

In the meantime, his study also shows the useful role cardiopulmonary stress testing can play in the setting of atrial fibrillation (AF) in HFpEF, he added.
“Cardiopulmonary stress tests are cheap and easy to do. They’re a big asset for personalized medicine. Using an objective measure like cardiopulmonary stress testing to define the physiologic and hemodynamic consequences of atrial fibrillation in individual patients may help identify those in whom rhythm control may improve exercise tolerance and quality of life, and those who may be okay with rate control,” according to Dr. Elshazly of the Cleveland Clinic.
He noted that while it’s well established that atrial fibrillation is associated with exercise intolerance in patients with heart failure with reduced ejection fraction (HFrEF) and that restoration of sinus rhythm in such patients has a positive impact on exercise hemodynamics, symptom severity, and quality of life, the situation is murkier regarding AF in patients with HFpEF. Prior studies were generally small and unable to establish whether AF was independently associated with exercise intolerance or if HFpEF patients who developed AF were sicker and higher risk.
He presented a retrospective, case-control study in a cohort of 1,825 patients with HFpEF referred for maximal, symptom-limited cardiopulmonary stress testing at the Cleveland Clinic. Among these were 242 patients with AF. They were extensively propensity matched – including on the basis of heart failure etiology – to 484 HFpEF patients without AF.
“That’s what makes our study strong. We were the first to be able to do propensity matching and therefore account for other risk factors in our analysis,” Dr. Elshazly explained.
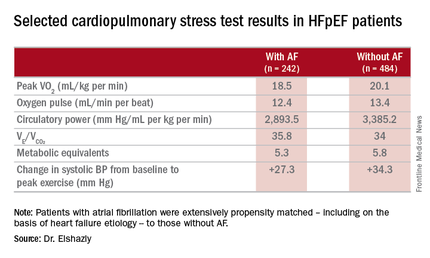
The investigators measured peak oxygen uptake (VO2), the minute ventilation–carbon dioxide production relationship (VE/VCO2) as an indicator of ventilatory efficiency, metabolic equivalents (METS), ventilatory anaerobic threshold, circulatory power as a proxy for cardiac power, peak oxygen pulse as a surrogate for stroke volume, and resting and peak heart rate and systolic blood pressure. The patients with AF were in fibrillation at the time of their cardiopulmonary stress testing.
The HFpEF patients with AF had a mean resting heart rate of 70 beats per minute and a peak rate of 130 bpm. This group showed evidence of impaired peak exercise tolerance as reflected in lower peak VO2, oxygen pulse, and circulatory power at peak exercise. Their VE/VCO2 was higher, indicating impaired ventilatory efficiency. Notably, however, their submaximal exercise capacity was similar to the non-AF controls.
“Atrial fibrillation in these patients is really more of a disease that shows itself in patients when you take them to their peak exercise capacity,” he observed.
All-cause mortality was significantly higher in the AF as compared with no-AF patients with HFpEF. The mortality curves separated early and the divergence grew larger over the course of 8 years of follow-up.
One audience member pointed out that the large mortality difference between the two groups seems disproportionate to the rather modest differences in exercise capacity.
“It brings up an interesting point,” Dr. Elshazly replied. “Maybe the increase in total mortality that we see is being driven by other things besides cardiovascular mortality. Our data doesn’t capture the specific cause of death, be it cancer, for example, but it does raise the idea that this mortality difference is not all driven by cardiovascular mortality, but by atrial fibrillation.”
Dr. Elshazly reported having no financial conflicts of interest regarding his institutionally supported study.
CHICAGO – Atrial fibrillation with good heart rate control in patients who have heart failure with preserved ejection fraction is independently associated with exercise intolerance, impaired contractile reserve, and a sharply higher mortality rate than in matched HFpEF patients without the arrhythmia, a retrospective analysis showed.
“Our study, the largest of its kind, provides mechanistic evidence from cardiopulmonary testing that a rhythm control strategy may potentially improve peak exercise capacity and survival in this patient population, a finding that of course requires future prospective appraisal in randomized trials comparing rate and rhythm control of atrial fibrillation in HFpEF,” Dr. Mohamed Badreldin Elshazly reported at the annual meeting of the American College of Cardiology.
In the meantime, his study also shows the useful role cardiopulmonary stress testing can play in the setting of atrial fibrillation (AF) in HFpEF, he added.
“Cardiopulmonary stress tests are cheap and easy to do. They’re a big asset for personalized medicine. Using an objective measure like cardiopulmonary stress testing to define the physiologic and hemodynamic consequences of atrial fibrillation in individual patients may help identify those in whom rhythm control may improve exercise tolerance and quality of life, and those who may be okay with rate control,” according to Dr. Elshazly of the Cleveland Clinic.
He noted that while it’s well established that atrial fibrillation is associated with exercise intolerance in patients with heart failure with reduced ejection fraction (HFrEF) and that restoration of sinus rhythm in such patients has a positive impact on exercise hemodynamics, symptom severity, and quality of life, the situation is murkier regarding AF in patients with HFpEF. Prior studies were generally small and unable to establish whether AF was independently associated with exercise intolerance or if HFpEF patients who developed AF were sicker and higher risk.
He presented a retrospective, case-control study in a cohort of 1,825 patients with HFpEF referred for maximal, symptom-limited cardiopulmonary stress testing at the Cleveland Clinic. Among these were 242 patients with AF. They were extensively propensity matched – including on the basis of heart failure etiology – to 484 HFpEF patients without AF.
“That’s what makes our study strong. We were the first to be able to do propensity matching and therefore account for other risk factors in our analysis,” Dr. Elshazly explained.
The investigators measured peak oxygen uptake (VO2), the minute ventilation–carbon dioxide production relationship (VE/VCO2) as an indicator of ventilatory efficiency, metabolic equivalents (METS), ventilatory anaerobic threshold, circulatory power as a proxy for cardiac power, peak oxygen pulse as a surrogate for stroke volume, and resting and peak heart rate and systolic blood pressure. The patients with AF were in fibrillation at the time of their cardiopulmonary stress testing.
The HFpEF patients with AF had a mean resting heart rate of 70 beats per minute and a peak rate of 130 bpm. This group showed evidence of impaired peak exercise tolerance as reflected in lower peak VO2, oxygen pulse, and circulatory power at peak exercise. Their VE/VCO2 was higher, indicating impaired ventilatory efficiency. Notably, however, their submaximal exercise capacity was similar to the non-AF controls.
“Atrial fibrillation in these patients is really more of a disease that shows itself in patients when you take them to their peak exercise capacity,” he observed.
All-cause mortality was significantly higher in the AF as compared with no-AF patients with HFpEF. The mortality curves separated early and the divergence grew larger over the course of 8 years of follow-up.
One audience member pointed out that the large mortality difference between the two groups seems disproportionate to the rather modest differences in exercise capacity.
“It brings up an interesting point,” Dr. Elshazly replied. “Maybe the increase in total mortality that we see is being driven by other things besides cardiovascular mortality. Our data doesn’t capture the specific cause of death, be it cancer, for example, but it does raise the idea that this mortality difference is not all driven by cardiovascular mortality, but by atrial fibrillation.”
Dr. Elshazly reported having no financial conflicts of interest regarding his institutionally supported study.
CHICAGO – Atrial fibrillation with good heart rate control in patients who have heart failure with preserved ejection fraction is independently associated with exercise intolerance, impaired contractile reserve, and a sharply higher mortality rate than in matched HFpEF patients without the arrhythmia, a retrospective analysis showed.
“Our study, the largest of its kind, provides mechanistic evidence from cardiopulmonary testing that a rhythm control strategy may potentially improve peak exercise capacity and survival in this patient population, a finding that of course requires future prospective appraisal in randomized trials comparing rate and rhythm control of atrial fibrillation in HFpEF,” Dr. Mohamed Badreldin Elshazly reported at the annual meeting of the American College of Cardiology.
In the meantime, his study also shows the useful role cardiopulmonary stress testing can play in the setting of atrial fibrillation (AF) in HFpEF, he added.
“Cardiopulmonary stress tests are cheap and easy to do. They’re a big asset for personalized medicine. Using an objective measure like cardiopulmonary stress testing to define the physiologic and hemodynamic consequences of atrial fibrillation in individual patients may help identify those in whom rhythm control may improve exercise tolerance and quality of life, and those who may be okay with rate control,” according to Dr. Elshazly of the Cleveland Clinic.
He noted that while it’s well established that atrial fibrillation is associated with exercise intolerance in patients with heart failure with reduced ejection fraction (HFrEF) and that restoration of sinus rhythm in such patients has a positive impact on exercise hemodynamics, symptom severity, and quality of life, the situation is murkier regarding AF in patients with HFpEF. Prior studies were generally small and unable to establish whether AF was independently associated with exercise intolerance or if HFpEF patients who developed AF were sicker and higher risk.
He presented a retrospective, case-control study in a cohort of 1,825 patients with HFpEF referred for maximal, symptom-limited cardiopulmonary stress testing at the Cleveland Clinic. Among these were 242 patients with AF. They were extensively propensity matched – including on the basis of heart failure etiology – to 484 HFpEF patients without AF.
“That’s what makes our study strong. We were the first to be able to do propensity matching and therefore account for other risk factors in our analysis,” Dr. Elshazly explained.
The investigators measured peak oxygen uptake (VO2), the minute ventilation–carbon dioxide production relationship (VE/VCO2) as an indicator of ventilatory efficiency, metabolic equivalents (METS), ventilatory anaerobic threshold, circulatory power as a proxy for cardiac power, peak oxygen pulse as a surrogate for stroke volume, and resting and peak heart rate and systolic blood pressure. The patients with AF were in fibrillation at the time of their cardiopulmonary stress testing.
The HFpEF patients with AF had a mean resting heart rate of 70 beats per minute and a peak rate of 130 bpm. This group showed evidence of impaired peak exercise tolerance as reflected in lower peak VO2, oxygen pulse, and circulatory power at peak exercise. Their VE/VCO2 was higher, indicating impaired ventilatory efficiency. Notably, however, their submaximal exercise capacity was similar to the non-AF controls.
“Atrial fibrillation in these patients is really more of a disease that shows itself in patients when you take them to their peak exercise capacity,” he observed.
All-cause mortality was significantly higher in the AF as compared with no-AF patients with HFpEF. The mortality curves separated early and the divergence grew larger over the course of 8 years of follow-up.
One audience member pointed out that the large mortality difference between the two groups seems disproportionate to the rather modest differences in exercise capacity.
“It brings up an interesting point,” Dr. Elshazly replied. “Maybe the increase in total mortality that we see is being driven by other things besides cardiovascular mortality. Our data doesn’t capture the specific cause of death, be it cancer, for example, but it does raise the idea that this mortality difference is not all driven by cardiovascular mortality, but by atrial fibrillation.”
Dr. Elshazly reported having no financial conflicts of interest regarding his institutionally supported study.
AT ACC 16
Key clinical point: Atrial fibrillation in patients with heart failure with preserved ejection fraction is associated with exercise intolerance and increased mortality.
Major finding: Mean peak VO2 was 18.5 mL/kg per minute in patients with HFpEF and atrial fibrillation, significantly less than the 20.1 mL/kg per minute in controls.
Data source: A retrospective, single-institution study of cardiopulmonary stress test findings and 8-year mortality in 242 patients with HFpEF and atrial fibrillation and 484 propensity-matched controls with HFpEF and no arrhythmia.
Disclosures: The presenter reported having no financial conflicts of interest regarding his institutionally supported study.

PIANO study provides insight on safety of biologics in pregnancy
MAUI, HAWAII – The consensus among gastroenterologists with expertise in inflammatory bowel disease is that continuation of biologics or immunomodulators in affected women throughout pregnancy and breastfeeding poses no increased risks to the fetus – and therein lies a message for rheumatologists and obstetricians, Dr. Uma Mahadevan said at the 2016 Rheumatology Winter Clinical Symposium.
“The risk of uncontrolled disease must be weighed against the risk of medical therapy. And this is something that is often missed,” according to Dr. Mahadevan, professor of medicine and co–medical director of the Center for Colitis and Crohn’s Disease at the University of California, San Francisco.

Gastroenterologists – at least, those whose practices focus on inflammatory bowel disease (IBD) – have led the way within medicine in terms of establishing the safety of biologics and immunomodulators such as azathioprine in pregnant women with chronic inflammatory diseases and their babies. And having accomplished that, they have been ahead of the curve in terms of continuing such therapy throughout pregnancy and breastfeeding. That’s because active Crohn’s disease and ulcerative colitis are particularly common in women during their childbearing years. And a disease flare during pregnancy is associated with a markedly increased risk of preterm birth and other adverse outcomes.
Gastroenterologists’ longstanding interest in the safety to mother and fetus of continued use of effective, potent medications throughout pregnancy was the impetus for the ongoing prospective U.S. Pregnancy in Inflammatory Bowel Disease and Neonatal Outcomes (PIANO) study, now in its ninth year, with an enrollment of roughly 1,500 women with IBD. The study has included comparisons of outcomes of women on different medications during pregnancy versus unmedicated women.
In multiple publications, Dr. Mahadevan and other PIANO investigators have established that increased IBD activity adversely affects pregnancy outcomes, and that stabilization of disease and effective maintenance therapy throughout pregnancy is important. The PIANO group has demonstrated that IBD medication exposure well into the third trimester in patients in sustained remission was not associated with an increase in congenital anomalies, spontaneous abortions, intrauterine growth restriction, or low birth weight.
To the surprise of many gastroenterologists, the PIANO study has shown that women with Crohn’s disease generally have smoother pregnancies than do those with ulcerative colitis, who tend to get sicker and have more complications.
Since PIANO data show an increased rate of preterm birth and low birth weight in IBD patients on combination therapy with azathioprine plus a biologic throughout pregnancy, Dr. Mahadevan and others try to discontinue the azathioprine, even though the need for combination therapy is a marker for patients with more severe disease.
Anti-TNF-alpha use during third trimester
Of particular interest to rheumatologists, who rely heavily on many of the same biologic agents gastroenterologists use to treat IBD, the use of anti–tumor necrosis factor–alpha biologics in the third trimester was not associated with an increase in preterm birth or maternal disease activity in the third trimester or the first 4 months post partum. When women on certolizumab pegol (Cimzia) during the third trimester were excluded from the analysis, since this biologic uniquely does not cross the placenta at all, the most recent PIANO data show a modest yet statistically significant 35% increase in infections in infants at age 12 months whose mothers were on other biologics in the third trimester. But Dr. Mahadevan said she doesn’t yet consider this finding definitive.
“It’s still a small group of patients, and every year when we update the results the infant infection risk goes back and forth from statistically significant to nonsignificant. I think there’s a signal here; we just need to keep collecting more data,” she said.
Particularly reassuring is the finding that the offspring of PIANO participants who had in utero exposure to biologics and immunomodulators didn’t have any developmental delay, compared with unexposed babies, according to the validated Ages and Stages Questionnaire at ages 1, 2, 3, and 4 years and Denver Childhood Developmental Score at months 4, 9, and 12.
“These kids do great later in life. Actually, they have better scores than unexposed kids. Not to say that biologics make your kid smarter. It probably has to do with better IBD control,” Dr. Mahadevan said.
Effects while breastfeeding
Breastfeeding while on biologics or azathioprine didn’t adversely affect infant growth, infection rate, or developmental milestones. More specifically, levels of biologics in the mothers, babies, or cord serum were not associated with the likelihood of a neonatal intensive care unit stay, an increase in infant infections, or achievement of developmental milestones.
“Almost all the agents are detectable in breast milk, but only at the nanogram level. We tell all our patients on biologics they can breastfeed. It doesn’t matter when their last dose was, don’t worry about it,” the gastroenterologist said.
Importance of preconception counseling
Key practical lessons she has learned in taking care of large numbers of patients with severe IBD referred to her tertiary center include the importance of preconception counseling. A woman should stop methotrexate at least 3 months prior to conception. Providing information on medication safety and the risks of poorly controlled disease helps in adherence.
It’s best to communicate with the patient’s obstetrician about the importance of continuing her IBD therapy during pregnancy before she becomes pregnant.
“It’s better to have this discussion ahead of time and have a plan in place. Once a patient is pregnant it’s very difficult if her doula or someone else has told them to stop a medication to convince them to continue it,” said Dr. Mahadevan.
All women with IBD should be followed as high-risk pregnancies. Mode of delivery is at the discretion of the obstetrician unless the patient has an open rectovaginal fistula; even if it’s inactive, cesarean delivery is preferable in that situation, she said.
Steps taken in the third trimester
In the third trimester, she routinely sends a letter to the patient’s pediatrician requesting no live virus vaccines in the coming baby’s first 6 months – in the United States, that’s the rotavirus vaccine – if the infant was exposed in utero to a biologic other than certolizumab pegol, but that all other vaccines can be given on schedule. She also asks that the pediatrician monitor an exposed baby for infections.
“That being said, there have been 20-plus exposures to rotavirus vaccine in the first 6 months of life recorded in the PIANO registry in the infants of mothers on biologics and we haven’t seen any adverse events. So maybe the CDC is overstating the risk, but at this point the rule is still no live virus vaccines,” she said.
She tries to time her last dose of biologic agents during pregnancy as follows: at week 30-32 for infliximab or vedolizumab and week 36-38 for adalimumab or golimumab. As for certolizumab pegol, “they can take that on their way to labor and delivery,” she quipped.
“I give the next dose of a biologic agent soon after delivery, often while the patient is still in the hospital, 24 hours after vaginal delivery and 48 hours after a C-section, assuming no infection,” Dr. Mahadevan said.
The elements of her approach to management of the pregnant patient with IBD are in accord with a recent report, The Toronto Consensus Statements for the Management of Inflammatory Bowel Disease in Pregnancy, in which she participated (Gastroenterology. 2016 Mar;150[3]:734-57).
Rheumatologists’ habits with biologics in pregnancy

Dr. John J. Cush rose from the audience to observe that the situation in rheumatology with regard to biologics in pregnancy is quite a bit different from what’s going on in gastroenterology.
“I think a lot of rheumatologists don’t let their patients get pregnant on biologics for fear of what may happen. And that’s because they don’t know the data. I think you’ve shown very clearly that you can get pregnant on biologics and do well. But for many of us who do allow our patients to get pregnant on biologic monotherapy, the practice is to stop it once they get pregnant. The idea is we want them to be in a very deep remission to increase the odds of getting pregnant and having a successful pregnancy, but then we stop the drug and we assume the disease state is going to stay the same. Often, though, it doesn’t stay the same, it gets worse. Yet this is a common practice in rheumatology. What’s your response?” asked Dr. Cush, professor of medicine and rheumatology at Baylor University Medical Center, Dallas, and director of clinical rheumatology at the Baylor Research Institute.
“I think in IBD it’s very clear that patients with active disease in pregnancy do much, much worse,” Dr. Mahadevan replied. “They have preterm birth, they get very sick, they’re hospitalized and placed on steroids. So for us, the benefit is very clear. I don’t know the data in rheumatoid arthritis – whether active disease leads to increased complication rates – but I do know from colleagues that in the postpartum period women with poorly controlled rheumatoid arthritis can’t take care of their baby because their hands are so damaged. And that’s a big deal.
“So when you see that the drugs are not associated with an increased risk of birth defects and on monotherapy there’s no increase in infections and other complications, you’d think that in the right patient continuing treatment until the late third trimester would be the way to go, especially since if you’ve put the patient on a biologic it must mean she has severe disease,” the gastroenterologist observed.
Dr. Roy Fleischmann of the University of Texas, Dallas, asked why gastroenterologists don’t put all IBD patients of childbearing age on certolizumab pegol if they need biologic therapy, since it doesn’t cross the placenta.
“Maybe IBD is different, but our biologics don’t necessarily have the longest persistence,” Dr. Mahadevan replied. “If you start a woman on certolizumab pegol at age 20 the chances of her still being on it at 28 are probably pretty low.”
Conference director Dr. Arthur Kavanaugh, professor of medicine at the University of California, San Diego, asked if the message regarding management of IBD in pregnancy being put forth by Dr. Mahadevan and the IBD in Pregnancy Consensus Group has gained wide acceptance by gastroenterologists across the country.
“I think the people who do IBD as a concentrated practice, whether in private or academic practice, are very aware of this literature,” she said.
“In general, IBD has become more and more centered among a group of people who want to take care of IBD. If you look at the big private practices, they have a hepatitis C person, an IBD person, and everyone else just wants to scope. I think the message is getting across to non-IBD gastroenterologists, but there is some confusion because the Europeans are very firm about stopping biologics at 22 weeks’ gestation if the patient is in deep remission and we in North America continue treatment,” said Dr. Mahadevan.
Her work with the PIANO study is funded by the Crohn’s and Colitis Foundation of America. In addition, Dr. Mahadevan disclosed ties to more than half a dozen pharmaceutical companies.
MAUI, HAWAII – The consensus among gastroenterologists with expertise in inflammatory bowel disease is that continuation of biologics or immunomodulators in affected women throughout pregnancy and breastfeeding poses no increased risks to the fetus – and therein lies a message for rheumatologists and obstetricians, Dr. Uma Mahadevan said at the 2016 Rheumatology Winter Clinical Symposium.
“The risk of uncontrolled disease must be weighed against the risk of medical therapy. And this is something that is often missed,” according to Dr. Mahadevan, professor of medicine and co–medical director of the Center for Colitis and Crohn’s Disease at the University of California, San Francisco.
Gastroenterologists – at least, those whose practices focus on inflammatory bowel disease (IBD) – have led the way within medicine in terms of establishing the safety of biologics and immunomodulators such as azathioprine in pregnant women with chronic inflammatory diseases and their babies. And having accomplished that, they have been ahead of the curve in terms of continuing such therapy throughout pregnancy and breastfeeding. That’s because active Crohn’s disease and ulcerative colitis are particularly common in women during their childbearing years. And a disease flare during pregnancy is associated with a markedly increased risk of preterm birth and other adverse outcomes.
Gastroenterologists’ longstanding interest in the safety to mother and fetus of continued use of effective, potent medications throughout pregnancy was the impetus for the ongoing prospective U.S. Pregnancy in Inflammatory Bowel Disease and Neonatal Outcomes (PIANO) study, now in its ninth year, with an enrollment of roughly 1,500 women with IBD. The study has included comparisons of outcomes of women on different medications during pregnancy versus unmedicated women.
In multiple publications, Dr. Mahadevan and other PIANO investigators have established that increased IBD activity adversely affects pregnancy outcomes, and that stabilization of disease and effective maintenance therapy throughout pregnancy is important. The PIANO group has demonstrated that IBD medication exposure well into the third trimester in patients in sustained remission was not associated with an increase in congenital anomalies, spontaneous abortions, intrauterine growth restriction, or low birth weight.
To the surprise of many gastroenterologists, the PIANO study has shown that women with Crohn’s disease generally have smoother pregnancies than do those with ulcerative colitis, who tend to get sicker and have more complications.
Since PIANO data show an increased rate of preterm birth and low birth weight in IBD patients on combination therapy with azathioprine plus a biologic throughout pregnancy, Dr. Mahadevan and others try to discontinue the azathioprine, even though the need for combination therapy is a marker for patients with more severe disease.
Anti-TNF-alpha use during third trimester
Of particular interest to rheumatologists, who rely heavily on many of the same biologic agents gastroenterologists use to treat IBD, the use of anti–tumor necrosis factor–alpha biologics in the third trimester was not associated with an increase in preterm birth or maternal disease activity in the third trimester or the first 4 months post partum. When women on certolizumab pegol (Cimzia) during the third trimester were excluded from the analysis, since this biologic uniquely does not cross the placenta at all, the most recent PIANO data show a modest yet statistically significant 35% increase in infections in infants at age 12 months whose mothers were on other biologics in the third trimester. But Dr. Mahadevan said she doesn’t yet consider this finding definitive.
“It’s still a small group of patients, and every year when we update the results the infant infection risk goes back and forth from statistically significant to nonsignificant. I think there’s a signal here; we just need to keep collecting more data,” she said.
Particularly reassuring is the finding that the offspring of PIANO participants who had in utero exposure to biologics and immunomodulators didn’t have any developmental delay, compared with unexposed babies, according to the validated Ages and Stages Questionnaire at ages 1, 2, 3, and 4 years and Denver Childhood Developmental Score at months 4, 9, and 12.
“These kids do great later in life. Actually, they have better scores than unexposed kids. Not to say that biologics make your kid smarter. It probably has to do with better IBD control,” Dr. Mahadevan said.
Effects while breastfeeding
Breastfeeding while on biologics or azathioprine didn’t adversely affect infant growth, infection rate, or developmental milestones. More specifically, levels of biologics in the mothers, babies, or cord serum were not associated with the likelihood of a neonatal intensive care unit stay, an increase in infant infections, or achievement of developmental milestones.
“Almost all the agents are detectable in breast milk, but only at the nanogram level. We tell all our patients on biologics they can breastfeed. It doesn’t matter when their last dose was, don’t worry about it,” the gastroenterologist said.
Importance of preconception counseling
Key practical lessons she has learned in taking care of large numbers of patients with severe IBD referred to her tertiary center include the importance of preconception counseling. A woman should stop methotrexate at least 3 months prior to conception. Providing information on medication safety and the risks of poorly controlled disease helps in adherence.
It’s best to communicate with the patient’s obstetrician about the importance of continuing her IBD therapy during pregnancy before she becomes pregnant.
“It’s better to have this discussion ahead of time and have a plan in place. Once a patient is pregnant it’s very difficult if her doula or someone else has told them to stop a medication to convince them to continue it,” said Dr. Mahadevan.
All women with IBD should be followed as high-risk pregnancies. Mode of delivery is at the discretion of the obstetrician unless the patient has an open rectovaginal fistula; even if it’s inactive, cesarean delivery is preferable in that situation, she said.
Steps taken in the third trimester
In the third trimester, she routinely sends a letter to the patient’s pediatrician requesting no live virus vaccines in the coming baby’s first 6 months – in the United States, that’s the rotavirus vaccine – if the infant was exposed in utero to a biologic other than certolizumab pegol, but that all other vaccines can be given on schedule. She also asks that the pediatrician monitor an exposed baby for infections.
“That being said, there have been 20-plus exposures to rotavirus vaccine in the first 6 months of life recorded in the PIANO registry in the infants of mothers on biologics and we haven’t seen any adverse events. So maybe the CDC is overstating the risk, but at this point the rule is still no live virus vaccines,” she said.
She tries to time her last dose of biologic agents during pregnancy as follows: at week 30-32 for infliximab or vedolizumab and week 36-38 for adalimumab or golimumab. As for certolizumab pegol, “they can take that on their way to labor and delivery,” she quipped.
“I give the next dose of a biologic agent soon after delivery, often while the patient is still in the hospital, 24 hours after vaginal delivery and 48 hours after a C-section, assuming no infection,” Dr. Mahadevan said.
The elements of her approach to management of the pregnant patient with IBD are in accord with a recent report, The Toronto Consensus Statements for the Management of Inflammatory Bowel Disease in Pregnancy, in which she participated (Gastroenterology. 2016 Mar;150[3]:734-57).
Rheumatologists’ habits with biologics in pregnancy
Dr. John J. Cush rose from the audience to observe that the situation in rheumatology with regard to biologics in pregnancy is quite a bit different from what’s going on in gastroenterology.
“I think a lot of rheumatologists don’t let their patients get pregnant on biologics for fear of what may happen. And that’s because they don’t know the data. I think you’ve shown very clearly that you can get pregnant on biologics and do well. But for many of us who do allow our patients to get pregnant on biologic monotherapy, the practice is to stop it once they get pregnant. The idea is we want them to be in a very deep remission to increase the odds of getting pregnant and having a successful pregnancy, but then we stop the drug and we assume the disease state is going to stay the same. Often, though, it doesn’t stay the same, it gets worse. Yet this is a common practice in rheumatology. What’s your response?” asked Dr. Cush, professor of medicine and rheumatology at Baylor University Medical Center, Dallas, and director of clinical rheumatology at the Baylor Research Institute.
“I think in IBD it’s very clear that patients with active disease in pregnancy do much, much worse,” Dr. Mahadevan replied. “They have preterm birth, they get very sick, they’re hospitalized and placed on steroids. So for us, the benefit is very clear. I don’t know the data in rheumatoid arthritis – whether active disease leads to increased complication rates – but I do know from colleagues that in the postpartum period women with poorly controlled rheumatoid arthritis can’t take care of their baby because their hands are so damaged. And that’s a big deal.
“So when you see that the drugs are not associated with an increased risk of birth defects and on monotherapy there’s no increase in infections and other complications, you’d think that in the right patient continuing treatment until the late third trimester would be the way to go, especially since if you’ve put the patient on a biologic it must mean she has severe disease,” the gastroenterologist observed.
Dr. Roy Fleischmann of the University of Texas, Dallas, asked why gastroenterologists don’t put all IBD patients of childbearing age on certolizumab pegol if they need biologic therapy, since it doesn’t cross the placenta.
“Maybe IBD is different, but our biologics don’t necessarily have the longest persistence,” Dr. Mahadevan replied. “If you start a woman on certolizumab pegol at age 20 the chances of her still being on it at 28 are probably pretty low.”
Conference director Dr. Arthur Kavanaugh, professor of medicine at the University of California, San Diego, asked if the message regarding management of IBD in pregnancy being put forth by Dr. Mahadevan and the IBD in Pregnancy Consensus Group has gained wide acceptance by gastroenterologists across the country.
“I think the people who do IBD as a concentrated practice, whether in private or academic practice, are very aware of this literature,” she said.
“In general, IBD has become more and more centered among a group of people who want to take care of IBD. If you look at the big private practices, they have a hepatitis C person, an IBD person, and everyone else just wants to scope. I think the message is getting across to non-IBD gastroenterologists, but there is some confusion because the Europeans are very firm about stopping biologics at 22 weeks’ gestation if the patient is in deep remission and we in North America continue treatment,” said Dr. Mahadevan.
Her work with the PIANO study is funded by the Crohn’s and Colitis Foundation of America. In addition, Dr. Mahadevan disclosed ties to more than half a dozen pharmaceutical companies.
MAUI, HAWAII – The consensus among gastroenterologists with expertise in inflammatory bowel disease is that continuation of biologics or immunomodulators in affected women throughout pregnancy and breastfeeding poses no increased risks to the fetus – and therein lies a message for rheumatologists and obstetricians, Dr. Uma Mahadevan said at the 2016 Rheumatology Winter Clinical Symposium.
“The risk of uncontrolled disease must be weighed against the risk of medical therapy. And this is something that is often missed,” according to Dr. Mahadevan, professor of medicine and co–medical director of the Center for Colitis and Crohn’s Disease at the University of California, San Francisco.
Gastroenterologists – at least, those whose practices focus on inflammatory bowel disease (IBD) – have led the way within medicine in terms of establishing the safety of biologics and immunomodulators such as azathioprine in pregnant women with chronic inflammatory diseases and their babies. And having accomplished that, they have been ahead of the curve in terms of continuing such therapy throughout pregnancy and breastfeeding. That’s because active Crohn’s disease and ulcerative colitis are particularly common in women during their childbearing years. And a disease flare during pregnancy is associated with a markedly increased risk of preterm birth and other adverse outcomes.
Gastroenterologists’ longstanding interest in the safety to mother and fetus of continued use of effective, potent medications throughout pregnancy was the impetus for the ongoing prospective U.S. Pregnancy in Inflammatory Bowel Disease and Neonatal Outcomes (PIANO) study, now in its ninth year, with an enrollment of roughly 1,500 women with IBD. The study has included comparisons of outcomes of women on different medications during pregnancy versus unmedicated women.
In multiple publications, Dr. Mahadevan and other PIANO investigators have established that increased IBD activity adversely affects pregnancy outcomes, and that stabilization of disease and effective maintenance therapy throughout pregnancy is important. The PIANO group has demonstrated that IBD medication exposure well into the third trimester in patients in sustained remission was not associated with an increase in congenital anomalies, spontaneous abortions, intrauterine growth restriction, or low birth weight.
To the surprise of many gastroenterologists, the PIANO study has shown that women with Crohn’s disease generally have smoother pregnancies than do those with ulcerative colitis, who tend to get sicker and have more complications.
Since PIANO data show an increased rate of preterm birth and low birth weight in IBD patients on combination therapy with azathioprine plus a biologic throughout pregnancy, Dr. Mahadevan and others try to discontinue the azathioprine, even though the need for combination therapy is a marker for patients with more severe disease.
Anti-TNF-alpha use during third trimester
Of particular interest to rheumatologists, who rely heavily on many of the same biologic agents gastroenterologists use to treat IBD, the use of anti–tumor necrosis factor–alpha biologics in the third trimester was not associated with an increase in preterm birth or maternal disease activity in the third trimester or the first 4 months post partum. When women on certolizumab pegol (Cimzia) during the third trimester were excluded from the analysis, since this biologic uniquely does not cross the placenta at all, the most recent PIANO data show a modest yet statistically significant 35% increase in infections in infants at age 12 months whose mothers were on other biologics in the third trimester. But Dr. Mahadevan said she doesn’t yet consider this finding definitive.
“It’s still a small group of patients, and every year when we update the results the infant infection risk goes back and forth from statistically significant to nonsignificant. I think there’s a signal here; we just need to keep collecting more data,” she said.
Particularly reassuring is the finding that the offspring of PIANO participants who had in utero exposure to biologics and immunomodulators didn’t have any developmental delay, compared with unexposed babies, according to the validated Ages and Stages Questionnaire at ages 1, 2, 3, and 4 years and Denver Childhood Developmental Score at months 4, 9, and 12.
“These kids do great later in life. Actually, they have better scores than unexposed kids. Not to say that biologics make your kid smarter. It probably has to do with better IBD control,” Dr. Mahadevan said.
Effects while breastfeeding
Breastfeeding while on biologics or azathioprine didn’t adversely affect infant growth, infection rate, or developmental milestones. More specifically, levels of biologics in the mothers, babies, or cord serum were not associated with the likelihood of a neonatal intensive care unit stay, an increase in infant infections, or achievement of developmental milestones.
“Almost all the agents are detectable in breast milk, but only at the nanogram level. We tell all our patients on biologics they can breastfeed. It doesn’t matter when their last dose was, don’t worry about it,” the gastroenterologist said.
Importance of preconception counseling
Key practical lessons she has learned in taking care of large numbers of patients with severe IBD referred to her tertiary center include the importance of preconception counseling. A woman should stop methotrexate at least 3 months prior to conception. Providing information on medication safety and the risks of poorly controlled disease helps in adherence.
It’s best to communicate with the patient’s obstetrician about the importance of continuing her IBD therapy during pregnancy before she becomes pregnant.
“It’s better to have this discussion ahead of time and have a plan in place. Once a patient is pregnant it’s very difficult if her doula or someone else has told them to stop a medication to convince them to continue it,” said Dr. Mahadevan.
All women with IBD should be followed as high-risk pregnancies. Mode of delivery is at the discretion of the obstetrician unless the patient has an open rectovaginal fistula; even if it’s inactive, cesarean delivery is preferable in that situation, she said.
Steps taken in the third trimester
In the third trimester, she routinely sends a letter to the patient’s pediatrician requesting no live virus vaccines in the coming baby’s first 6 months – in the United States, that’s the rotavirus vaccine – if the infant was exposed in utero to a biologic other than certolizumab pegol, but that all other vaccines can be given on schedule. She also asks that the pediatrician monitor an exposed baby for infections.
“That being said, there have been 20-plus exposures to rotavirus vaccine in the first 6 months of life recorded in the PIANO registry in the infants of mothers on biologics and we haven’t seen any adverse events. So maybe the CDC is overstating the risk, but at this point the rule is still no live virus vaccines,” she said.
She tries to time her last dose of biologic agents during pregnancy as follows: at week 30-32 for infliximab or vedolizumab and week 36-38 for adalimumab or golimumab. As for certolizumab pegol, “they can take that on their way to labor and delivery,” she quipped.
“I give the next dose of a biologic agent soon after delivery, often while the patient is still in the hospital, 24 hours after vaginal delivery and 48 hours after a C-section, assuming no infection,” Dr. Mahadevan said.
The elements of her approach to management of the pregnant patient with IBD are in accord with a recent report, The Toronto Consensus Statements for the Management of Inflammatory Bowel Disease in Pregnancy, in which she participated (Gastroenterology. 2016 Mar;150[3]:734-57).
Rheumatologists’ habits with biologics in pregnancy
Dr. John J. Cush rose from the audience to observe that the situation in rheumatology with regard to biologics in pregnancy is quite a bit different from what’s going on in gastroenterology.
“I think a lot of rheumatologists don’t let their patients get pregnant on biologics for fear of what may happen. And that’s because they don’t know the data. I think you’ve shown very clearly that you can get pregnant on biologics and do well. But for many of us who do allow our patients to get pregnant on biologic monotherapy, the practice is to stop it once they get pregnant. The idea is we want them to be in a very deep remission to increase the odds of getting pregnant and having a successful pregnancy, but then we stop the drug and we assume the disease state is going to stay the same. Often, though, it doesn’t stay the same, it gets worse. Yet this is a common practice in rheumatology. What’s your response?” asked Dr. Cush, professor of medicine and rheumatology at Baylor University Medical Center, Dallas, and director of clinical rheumatology at the Baylor Research Institute.
“I think in IBD it’s very clear that patients with active disease in pregnancy do much, much worse,” Dr. Mahadevan replied. “They have preterm birth, they get very sick, they’re hospitalized and placed on steroids. So for us, the benefit is very clear. I don’t know the data in rheumatoid arthritis – whether active disease leads to increased complication rates – but I do know from colleagues that in the postpartum period women with poorly controlled rheumatoid arthritis can’t take care of their baby because their hands are so damaged. And that’s a big deal.
“So when you see that the drugs are not associated with an increased risk of birth defects and on monotherapy there’s no increase in infections and other complications, you’d think that in the right patient continuing treatment until the late third trimester would be the way to go, especially since if you’ve put the patient on a biologic it must mean she has severe disease,” the gastroenterologist observed.
Dr. Roy Fleischmann of the University of Texas, Dallas, asked why gastroenterologists don’t put all IBD patients of childbearing age on certolizumab pegol if they need biologic therapy, since it doesn’t cross the placenta.
“Maybe IBD is different, but our biologics don’t necessarily have the longest persistence,” Dr. Mahadevan replied. “If you start a woman on certolizumab pegol at age 20 the chances of her still being on it at 28 are probably pretty low.”
Conference director Dr. Arthur Kavanaugh, professor of medicine at the University of California, San Diego, asked if the message regarding management of IBD in pregnancy being put forth by Dr. Mahadevan and the IBD in Pregnancy Consensus Group has gained wide acceptance by gastroenterologists across the country.
“I think the people who do IBD as a concentrated practice, whether in private or academic practice, are very aware of this literature,” she said.
“In general, IBD has become more and more centered among a group of people who want to take care of IBD. If you look at the big private practices, they have a hepatitis C person, an IBD person, and everyone else just wants to scope. I think the message is getting across to non-IBD gastroenterologists, but there is some confusion because the Europeans are very firm about stopping biologics at 22 weeks’ gestation if the patient is in deep remission and we in North America continue treatment,” said Dr. Mahadevan.
Her work with the PIANO study is funded by the Crohn’s and Colitis Foundation of America. In addition, Dr. Mahadevan disclosed ties to more than half a dozen pharmaceutical companies.
EXPERT ANALYSIS FROM RWCS 2016

Prompt antidepressant treatment swiftly chops cardiovascular risk
CHICAGO – Prompt, effective treatment for depression in the primary care setting appears to swiftly reduce the elevated cardiovascular risk known to be tied to the mood disorder, Heidi Thomas May, Ph.D., reported at the annual meeting of the American College of Cardiology.
“We know that depression is a risk factor for long-term adverse cardiovascular outcomes. Our study shows that it can also have immediate effects on someone’s cardiovascular health. I think our study highlights the importance of screening for depression in the primary care setting – and if someone’s depressed, they need to be treated,” said Dr. May, a cardiovascular and genetic epidemiologist at Intermountain Medical Center in Murray, Utah.

She presented an observational study of the electronic medical records of 7,559 Intermountain Healthcare patients over age 40 years who completed the Patient Health Questionnaire-9 (PHQ-9) depression screening tool during a visit to an Intermountain primary care clinic for any reason. They completed another PHQ-9 a median of 2.7 years later. Under the Intermountain system, a PHQ-9 score of 10 or more triggers implementation of a depression treatment pathway, the specifics of which vary depending upon the severity of symptoms.
On the basis of their two PHQ-9 scores, all patients were classified into one of four groups: The “nondepressed” group of 3,286 patients had a score of 9 or less on both occasions; the “remained depressed” cohort of 1,987 patients scored 10 or more on both PHQ-9s; the “no longer depressed” group of 1,542 patients scored at least 10 but subsequently improved by at least 5 points to a score of 9 or less; and the 735 patients in the “became depressed” group first scored 9 or less on the PHQ-9 but subsequently had at least a 5-point increase to a score of 10 or more.
The subjects were then followed for major adverse cardiovascular events, or MACE – defined as a composite of death, diagnosis of coronary artery disease, acute MI, stroke, and heart failure hospitalization – for a median of 208 days after completing their second PHQ-9.
The MACE rate was 4.8% in the nondepressed group and similar at 4.6% in the “no longer depressed” group, Dr. May reported. Both groups fared significantly better than the “remained depressed” and “became depressed” groups, which had MACE rates of 6% and 6.4%, respectively.
In a multivariate regression analysis adjusted for demographics, cardiovascular risk factors, prior disease diagnoses, medications, and other potential confounders, the “remained depressed” group was 33% more likely to experience a cardiovascular event than was the nondepressed group, she said. The “became depressed” group had a 44% increase in risk, compared with the nondepressed individuals. In contrast, the MACE risk in patients in the “no longer depressed” group was not significantly different from that of patients who weren’t depressed at either time point. And the MACE risk of patients who became depressed during the course of the study was no different from that of patients who remained depressed at both time points.
This is the first study of its kind, Dr. May said. Hence, the results require confirmation, ideally in a randomized clinical trial.
She reported having no financial conflicts regarding the study, which was supported by Intermountain Healthcare.
CHICAGO – Prompt, effective treatment for depression in the primary care setting appears to swiftly reduce the elevated cardiovascular risk known to be tied to the mood disorder, Heidi Thomas May, Ph.D., reported at the annual meeting of the American College of Cardiology.
“We know that depression is a risk factor for long-term adverse cardiovascular outcomes. Our study shows that it can also have immediate effects on someone’s cardiovascular health. I think our study highlights the importance of screening for depression in the primary care setting – and if someone’s depressed, they need to be treated,” said Dr. May, a cardiovascular and genetic epidemiologist at Intermountain Medical Center in Murray, Utah.
She presented an observational study of the electronic medical records of 7,559 Intermountain Healthcare patients over age 40 years who completed the Patient Health Questionnaire-9 (PHQ-9) depression screening tool during a visit to an Intermountain primary care clinic for any reason. They completed another PHQ-9 a median of 2.7 years later. Under the Intermountain system, a PHQ-9 score of 10 or more triggers implementation of a depression treatment pathway, the specifics of which vary depending upon the severity of symptoms.
On the basis of their two PHQ-9 scores, all patients were classified into one of four groups: The “nondepressed” group of 3,286 patients had a score of 9 or less on both occasions; the “remained depressed” cohort of 1,987 patients scored 10 or more on both PHQ-9s; the “no longer depressed” group of 1,542 patients scored at least 10 but subsequently improved by at least 5 points to a score of 9 or less; and the 735 patients in the “became depressed” group first scored 9 or less on the PHQ-9 but subsequently had at least a 5-point increase to a score of 10 or more.
The subjects were then followed for major adverse cardiovascular events, or MACE – defined as a composite of death, diagnosis of coronary artery disease, acute MI, stroke, and heart failure hospitalization – for a median of 208 days after completing their second PHQ-9.
The MACE rate was 4.8% in the nondepressed group and similar at 4.6% in the “no longer depressed” group, Dr. May reported. Both groups fared significantly better than the “remained depressed” and “became depressed” groups, which had MACE rates of 6% and 6.4%, respectively.
In a multivariate regression analysis adjusted for demographics, cardiovascular risk factors, prior disease diagnoses, medications, and other potential confounders, the “remained depressed” group was 33% more likely to experience a cardiovascular event than was the nondepressed group, she said. The “became depressed” group had a 44% increase in risk, compared with the nondepressed individuals. In contrast, the MACE risk in patients in the “no longer depressed” group was not significantly different from that of patients who weren’t depressed at either time point. And the MACE risk of patients who became depressed during the course of the study was no different from that of patients who remained depressed at both time points.
This is the first study of its kind, Dr. May said. Hence, the results require confirmation, ideally in a randomized clinical trial.
She reported having no financial conflicts regarding the study, which was supported by Intermountain Healthcare.
CHICAGO – Prompt, effective treatment for depression in the primary care setting appears to swiftly reduce the elevated cardiovascular risk known to be tied to the mood disorder, Heidi Thomas May, Ph.D., reported at the annual meeting of the American College of Cardiology.
“We know that depression is a risk factor for long-term adverse cardiovascular outcomes. Our study shows that it can also have immediate effects on someone’s cardiovascular health. I think our study highlights the importance of screening for depression in the primary care setting – and if someone’s depressed, they need to be treated,” said Dr. May, a cardiovascular and genetic epidemiologist at Intermountain Medical Center in Murray, Utah.
She presented an observational study of the electronic medical records of 7,559 Intermountain Healthcare patients over age 40 years who completed the Patient Health Questionnaire-9 (PHQ-9) depression screening tool during a visit to an Intermountain primary care clinic for any reason. They completed another PHQ-9 a median of 2.7 years later. Under the Intermountain system, a PHQ-9 score of 10 or more triggers implementation of a depression treatment pathway, the specifics of which vary depending upon the severity of symptoms.
On the basis of their two PHQ-9 scores, all patients were classified into one of four groups: The “nondepressed” group of 3,286 patients had a score of 9 or less on both occasions; the “remained depressed” cohort of 1,987 patients scored 10 or more on both PHQ-9s; the “no longer depressed” group of 1,542 patients scored at least 10 but subsequently improved by at least 5 points to a score of 9 or less; and the 735 patients in the “became depressed” group first scored 9 or less on the PHQ-9 but subsequently had at least a 5-point increase to a score of 10 or more.
The subjects were then followed for major adverse cardiovascular events, or MACE – defined as a composite of death, diagnosis of coronary artery disease, acute MI, stroke, and heart failure hospitalization – for a median of 208 days after completing their second PHQ-9.
The MACE rate was 4.8% in the nondepressed group and similar at 4.6% in the “no longer depressed” group, Dr. May reported. Both groups fared significantly better than the “remained depressed” and “became depressed” groups, which had MACE rates of 6% and 6.4%, respectively.
In a multivariate regression analysis adjusted for demographics, cardiovascular risk factors, prior disease diagnoses, medications, and other potential confounders, the “remained depressed” group was 33% more likely to experience a cardiovascular event than was the nondepressed group, she said. The “became depressed” group had a 44% increase in risk, compared with the nondepressed individuals. In contrast, the MACE risk in patients in the “no longer depressed” group was not significantly different from that of patients who weren’t depressed at either time point. And the MACE risk of patients who became depressed during the course of the study was no different from that of patients who remained depressed at both time points.
This is the first study of its kind, Dr. May said. Hence, the results require confirmation, ideally in a randomized clinical trial.
She reported having no financial conflicts regarding the study, which was supported by Intermountain Healthcare.
AT ACC 16
Key clinical point: Event rate was no different in “no longer depressed” group than in “never depressed.”
Major finding: Major adverse cardiovascular events were 44% more likely in primary care patients who became depressed during a median 2.7-year period, compared with those who weren’t depressed at either time point.
Data source: An observational study of 7,550 patients screened for depression in primary care clinics.
Disclosures: The study was supported by Intermountain Healthcare. Dr. May reported having no financial conflicts of interest.

Exercise Is Protective but Underutilized in Atrial Fib Patients
CHICAGO – Efforts to encourage even modest amounts of physical activity in sedentary patients with atrial fibrillation are likely to pay off in reduced risks of cardiovascular and all-cause mortality, according to a report from the EurObservational Research Program Pilot Survey on Atrial Fibrillation General Registry.
“Clearly we would recommend regular physical activity for patients with atrial fibrillation on the basis of the mortality benefit we see in the registry. If we give patients with atrial fibrillation oral anticoagulation, they are protected against stroke risk, but clearly they are still dying a lot,” Dr. Marco Proietti said at the annual meeting of the American College of Cardiology.

He presented 1-year follow-up data on 2,442 “real world” patients enrolled in the nine-country, observational, prospective registry, known as EORP-AF, shortly after being diagnosed with AF. One of the goals of EORP-AF is to learn whether physical exercise protects against cardiovascular events and all-cause mortality in AF patients, as has been well established in the general population and in patients at high cardiovascular risk.
One striking finding was that nearly 40% of patients in EORP-AF reported engaging in no physical activity, defined for study purposes as zero to less than 3 hours of physical activity per week for less than 2 years.
The other three categories employed by investigators were “occasional,” meaning less than 3 hours per week but for 2 years or more; “regular,” defined as at least 3 hours weekly for at least 2 years; and “intense,” which required more than 7 hours of physical activity per week for at least 2 years. Levels of cardiovascular and stroke risk factors decreased progressively with increasing levels of physical activity. Only 5% of the AF patients met the ‘intense’ standard, noted Dr. Proietti of the University of Birmingham (England).
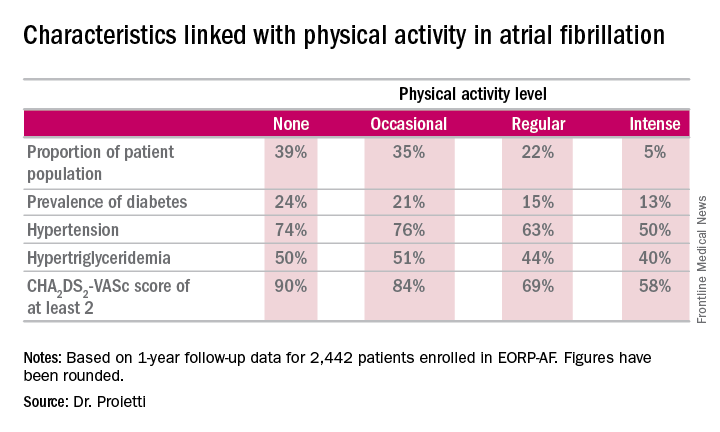
The 1-year cardiovascular mortality rate approached 6% in the no physical activity group and hovered around 1% in the other three groups. The 1-year all-cause mortality rate exceeded 12% in the no-exercise group, was 4%% in the occasional exercisers, and 1%-2% in the groups reporting regular or intense physical activity.
The 1-year composite endpoint of cardiovascular death, any thromboembolism, or a bleeding event occurred in 12% of the sedentary patients, a rate two-to-three times higher than in the others.
Updated outcomes are to be reported from the EORP-AF pilot registry after 2 and 3 years of follow-up. Meanwhile, on the basis of the success of the pilot registry, more than 10,000 patients with AF have been enrolled in the EORP-AF main registry, according to Dr. Proietti.
A study limitation, he conceded, is that the registry includes no objective measure of physical capacity, such as METS.
Session co-chair Dr. Brian Olshansky, emeritus professor of internal medicine at the University of Iowa, Iowa City, observed that the registry data raise a classic chicken-versus-egg issue: Do the sedentary patients do worse because they’re inactive, or are they inactive because they are sicker and hence have worse outcomes?
Dr. Proietti said the registry data provide some support for the latter idea, since the no-physical-activity group had higher prevalences of coronary artery disease and heart failure.
Dr. Olshansky raised another point: “It’s interesting to me that there’s a whole bunch of literature showing that elite endurance athletes – bike racers, cross country skiers – have a very high incidence of atrial fibrillation. It seems to be either an inflammatory or an autonomic issue.”
Dr. Proietti replied that he’s familiar with that extensive literature, but the EORP-AF data through 1 year don’t provide validation. While the intense physical activity group tended to have more symptomatic AF than the other groups, they were no more likely to show progression from paroxysmal to permanent AF. The much larger main registry now underway may be able to better clarify the relationship between physical activity and incidence and progression of AF, including the possibility of a U-shaped dose-response curve.
The EORP-AF registry is supported by the European Society of Cardiology. Dr. Proietti reported having no financial conflicts of interest.
CHICAGO – Efforts to encourage even modest amounts of physical activity in sedentary patients with atrial fibrillation are likely to pay off in reduced risks of cardiovascular and all-cause mortality, according to a report from the EurObservational Research Program Pilot Survey on Atrial Fibrillation General Registry.
“Clearly we would recommend regular physical activity for patients with atrial fibrillation on the basis of the mortality benefit we see in the registry. If we give patients with atrial fibrillation oral anticoagulation, they are protected against stroke risk, but clearly they are still dying a lot,” Dr. Marco Proietti said at the annual meeting of the American College of Cardiology.
He presented 1-year follow-up data on 2,442 “real world” patients enrolled in the nine-country, observational, prospective registry, known as EORP-AF, shortly after being diagnosed with AF. One of the goals of EORP-AF is to learn whether physical exercise protects against cardiovascular events and all-cause mortality in AF patients, as has been well established in the general population and in patients at high cardiovascular risk.
One striking finding was that nearly 40% of patients in EORP-AF reported engaging in no physical activity, defined for study purposes as zero to less than 3 hours of physical activity per week for less than 2 years.
The other three categories employed by investigators were “occasional,” meaning less than 3 hours per week but for 2 years or more; “regular,” defined as at least 3 hours weekly for at least 2 years; and “intense,” which required more than 7 hours of physical activity per week for at least 2 years. Levels of cardiovascular and stroke risk factors decreased progressively with increasing levels of physical activity. Only 5% of the AF patients met the ‘intense’ standard, noted Dr. Proietti of the University of Birmingham (England).
The 1-year cardiovascular mortality rate approached 6% in the no physical activity group and hovered around 1% in the other three groups. The 1-year all-cause mortality rate exceeded 12% in the no-exercise group, was 4%% in the occasional exercisers, and 1%-2% in the groups reporting regular or intense physical activity.
The 1-year composite endpoint of cardiovascular death, any thromboembolism, or a bleeding event occurred in 12% of the sedentary patients, a rate two-to-three times higher than in the others.
Updated outcomes are to be reported from the EORP-AF pilot registry after 2 and 3 years of follow-up. Meanwhile, on the basis of the success of the pilot registry, more than 10,000 patients with AF have been enrolled in the EORP-AF main registry, according to Dr. Proietti.
A study limitation, he conceded, is that the registry includes no objective measure of physical capacity, such as METS.
Session co-chair Dr. Brian Olshansky, emeritus professor of internal medicine at the University of Iowa, Iowa City, observed that the registry data raise a classic chicken-versus-egg issue: Do the sedentary patients do worse because they’re inactive, or are they inactive because they are sicker and hence have worse outcomes?
Dr. Proietti said the registry data provide some support for the latter idea, since the no-physical-activity group had higher prevalences of coronary artery disease and heart failure.
Dr. Olshansky raised another point: “It’s interesting to me that there’s a whole bunch of literature showing that elite endurance athletes – bike racers, cross country skiers – have a very high incidence of atrial fibrillation. It seems to be either an inflammatory or an autonomic issue.”
Dr. Proietti replied that he’s familiar with that extensive literature, but the EORP-AF data through 1 year don’t provide validation. While the intense physical activity group tended to have more symptomatic AF than the other groups, they were no more likely to show progression from paroxysmal to permanent AF. The much larger main registry now underway may be able to better clarify the relationship between physical activity and incidence and progression of AF, including the possibility of a U-shaped dose-response curve.
The EORP-AF registry is supported by the European Society of Cardiology. Dr. Proietti reported having no financial conflicts of interest.
CHICAGO – Efforts to encourage even modest amounts of physical activity in sedentary patients with atrial fibrillation are likely to pay off in reduced risks of cardiovascular and all-cause mortality, according to a report from the EurObservational Research Program Pilot Survey on Atrial Fibrillation General Registry.
“Clearly we would recommend regular physical activity for patients with atrial fibrillation on the basis of the mortality benefit we see in the registry. If we give patients with atrial fibrillation oral anticoagulation, they are protected against stroke risk, but clearly they are still dying a lot,” Dr. Marco Proietti said at the annual meeting of the American College of Cardiology.
He presented 1-year follow-up data on 2,442 “real world” patients enrolled in the nine-country, observational, prospective registry, known as EORP-AF, shortly after being diagnosed with AF. One of the goals of EORP-AF is to learn whether physical exercise protects against cardiovascular events and all-cause mortality in AF patients, as has been well established in the general population and in patients at high cardiovascular risk.
One striking finding was that nearly 40% of patients in EORP-AF reported engaging in no physical activity, defined for study purposes as zero to less than 3 hours of physical activity per week for less than 2 years.
The other three categories employed by investigators were “occasional,” meaning less than 3 hours per week but for 2 years or more; “regular,” defined as at least 3 hours weekly for at least 2 years; and “intense,” which required more than 7 hours of physical activity per week for at least 2 years. Levels of cardiovascular and stroke risk factors decreased progressively with increasing levels of physical activity. Only 5% of the AF patients met the ‘intense’ standard, noted Dr. Proietti of the University of Birmingham (England).
The 1-year cardiovascular mortality rate approached 6% in the no physical activity group and hovered around 1% in the other three groups. The 1-year all-cause mortality rate exceeded 12% in the no-exercise group, was 4%% in the occasional exercisers, and 1%-2% in the groups reporting regular or intense physical activity.
The 1-year composite endpoint of cardiovascular death, any thromboembolism, or a bleeding event occurred in 12% of the sedentary patients, a rate two-to-three times higher than in the others.
Updated outcomes are to be reported from the EORP-AF pilot registry after 2 and 3 years of follow-up. Meanwhile, on the basis of the success of the pilot registry, more than 10,000 patients with AF have been enrolled in the EORP-AF main registry, according to Dr. Proietti.
A study limitation, he conceded, is that the registry includes no objective measure of physical capacity, such as METS.
Session co-chair Dr. Brian Olshansky, emeritus professor of internal medicine at the University of Iowa, Iowa City, observed that the registry data raise a classic chicken-versus-egg issue: Do the sedentary patients do worse because they’re inactive, or are they inactive because they are sicker and hence have worse outcomes?
Dr. Proietti said the registry data provide some support for the latter idea, since the no-physical-activity group had higher prevalences of coronary artery disease and heart failure.
Dr. Olshansky raised another point: “It’s interesting to me that there’s a whole bunch of literature showing that elite endurance athletes – bike racers, cross country skiers – have a very high incidence of atrial fibrillation. It seems to be either an inflammatory or an autonomic issue.”
Dr. Proietti replied that he’s familiar with that extensive literature, but the EORP-AF data through 1 year don’t provide validation. While the intense physical activity group tended to have more symptomatic AF than the other groups, they were no more likely to show progression from paroxysmal to permanent AF. The much larger main registry now underway may be able to better clarify the relationship between physical activity and incidence and progression of AF, including the possibility of a U-shaped dose-response curve.
The EORP-AF registry is supported by the European Society of Cardiology. Dr. Proietti reported having no financial conflicts of interest.
AT ACC 16

Exercise is protective but underutilized in atrial fib patients
CHICAGO – Efforts to encourage even modest amounts of physical activity in sedentary patients with atrial fibrillation are likely to pay off in reduced risks of cardiovascular and all-cause mortality, according to a report from the EurObservational Research Program Pilot Survey on Atrial Fibrillation General Registry.
“Clearly we would recommend regular physical activity for patients with atrial fibrillation on the basis of the mortality benefit we see in the registry. If we give patients with atrial fibrillation oral anticoagulation, they are protected against stroke risk, but clearly they are still dying a lot,” Dr. Marco Proietti said at the annual meeting of the American College of Cardiology.

He presented 1-year follow-up data on 2,442 “real world” patients enrolled in the nine-country, observational, prospective registry, known as EORP-AF, shortly after being diagnosed with AF. One of the goals of EORP-AF is to learn whether physical exercise protects against cardiovascular events and all-cause mortality in AF patients, as has been well established in the general population and in patients at high cardiovascular risk.
One striking finding was that nearly 40% of patients in EORP-AF reported engaging in no physical activity, defined for study purposes as zero to less than 3 hours of physical activity per week for less than 2 years.
The other three categories employed by investigators were “occasional,” meaning less than 3 hours per week but for 2 years or more; “regular,” defined as at least 3 hours weekly for at least 2 years; and “intense,” which required more than 7 hours of physical activity per week for at least 2 years. Levels of cardiovascular and stroke risk factors decreased progressively with increasing levels of physical activity. Only 5% of the AF patients met the ‘intense’ standard, noted Dr. Proietti of the University of Birmingham (England).
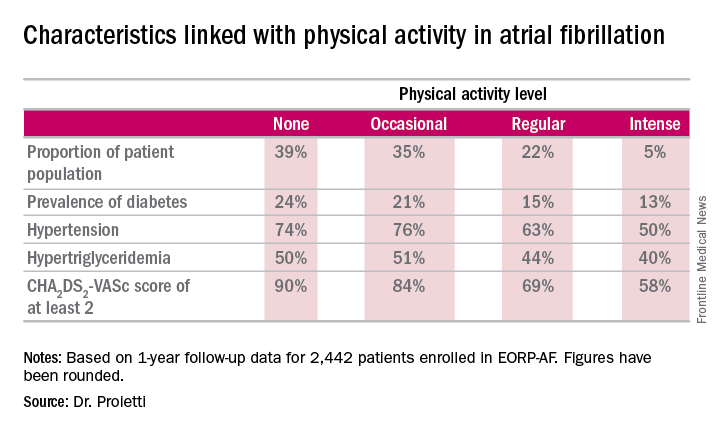
The 1-year cardiovascular mortality rate approached 6% in the no physical activity group and hovered around 1% in the other three groups. The 1-year all-cause mortality rate exceeded 12% in the no-exercise group, was 4%% in the occasional exercisers, and 1%-2% in the groups reporting regular or intense physical activity.
The 1-year composite endpoint of cardiovascular death, any thromboembolism, or a bleeding event occurred in 12% of the sedentary patients, a rate two-to-three times higher than in the others.
Updated outcomes are to be reported from the EORP-AF pilot registry after 2 and 3 years of follow-up. Meanwhile, on the basis of the success of the pilot registry, more than 10,000 patients with AF have been enrolled in the EORP-AF main registry, according to Dr. Proietti.
A study limitation, he conceded, is that the registry includes no objective measure of physical capacity, such as METS.
Session co-chair Dr. Brian Olshansky, emeritus professor of internal medicine at the University of Iowa, Iowa City, observed that the registry data raise a classic chicken-versus-egg issue: Do the sedentary patients do worse because they’re inactive, or are they inactive because they are sicker and hence have worse outcomes?
Dr. Proietti said the registry data provide some support for the latter idea, since the no-physical-activity group had higher prevalences of coronary artery disease and heart failure.
Dr. Olshansky raised another point: “It’s interesting to me that there’s a whole bunch of literature showing that elite endurance athletes – bike racers, cross country skiers – have a very high incidence of atrial fibrillation. It seems to be either an inflammatory or an autonomic issue.”
Dr. Proietti replied that he’s familiar with that extensive literature, but the EORP-AF data through 1 year don’t provide validation. While the intense physical activity group tended to have more symptomatic AF than the other groups, they were no more likely to show progression from paroxysmal to permanent AF. The much larger main registry now underway may be able to better clarify the relationship between physical activity and incidence and progression of AF, including the possibility of a U-shaped dose-response curve.
The EORP-AF registry is supported by the European Society of Cardiology. Dr. Proietti reported having no financial conflicts of interest.
CHICAGO – Efforts to encourage even modest amounts of physical activity in sedentary patients with atrial fibrillation are likely to pay off in reduced risks of cardiovascular and all-cause mortality, according to a report from the EurObservational Research Program Pilot Survey on Atrial Fibrillation General Registry.
“Clearly we would recommend regular physical activity for patients with atrial fibrillation on the basis of the mortality benefit we see in the registry. If we give patients with atrial fibrillation oral anticoagulation, they are protected against stroke risk, but clearly they are still dying a lot,” Dr. Marco Proietti said at the annual meeting of the American College of Cardiology.
He presented 1-year follow-up data on 2,442 “real world” patients enrolled in the nine-country, observational, prospective registry, known as EORP-AF, shortly after being diagnosed with AF. One of the goals of EORP-AF is to learn whether physical exercise protects against cardiovascular events and all-cause mortality in AF patients, as has been well established in the general population and in patients at high cardiovascular risk.
One striking finding was that nearly 40% of patients in EORP-AF reported engaging in no physical activity, defined for study purposes as zero to less than 3 hours of physical activity per week for less than 2 years.
The other three categories employed by investigators were “occasional,” meaning less than 3 hours per week but for 2 years or more; “regular,” defined as at least 3 hours weekly for at least 2 years; and “intense,” which required more than 7 hours of physical activity per week for at least 2 years. Levels of cardiovascular and stroke risk factors decreased progressively with increasing levels of physical activity. Only 5% of the AF patients met the ‘intense’ standard, noted Dr. Proietti of the University of Birmingham (England).
The 1-year cardiovascular mortality rate approached 6% in the no physical activity group and hovered around 1% in the other three groups. The 1-year all-cause mortality rate exceeded 12% in the no-exercise group, was 4%% in the occasional exercisers, and 1%-2% in the groups reporting regular or intense physical activity.
The 1-year composite endpoint of cardiovascular death, any thromboembolism, or a bleeding event occurred in 12% of the sedentary patients, a rate two-to-three times higher than in the others.
Updated outcomes are to be reported from the EORP-AF pilot registry after 2 and 3 years of follow-up. Meanwhile, on the basis of the success of the pilot registry, more than 10,000 patients with AF have been enrolled in the EORP-AF main registry, according to Dr. Proietti.
A study limitation, he conceded, is that the registry includes no objective measure of physical capacity, such as METS.
Session co-chair Dr. Brian Olshansky, emeritus professor of internal medicine at the University of Iowa, Iowa City, observed that the registry data raise a classic chicken-versus-egg issue: Do the sedentary patients do worse because they’re inactive, or are they inactive because they are sicker and hence have worse outcomes?
Dr. Proietti said the registry data provide some support for the latter idea, since the no-physical-activity group had higher prevalences of coronary artery disease and heart failure.
Dr. Olshansky raised another point: “It’s interesting to me that there’s a whole bunch of literature showing that elite endurance athletes – bike racers, cross country skiers – have a very high incidence of atrial fibrillation. It seems to be either an inflammatory or an autonomic issue.”
Dr. Proietti replied that he’s familiar with that extensive literature, but the EORP-AF data through 1 year don’t provide validation. While the intense physical activity group tended to have more symptomatic AF than the other groups, they were no more likely to show progression from paroxysmal to permanent AF. The much larger main registry now underway may be able to better clarify the relationship between physical activity and incidence and progression of AF, including the possibility of a U-shaped dose-response curve.
The EORP-AF registry is supported by the European Society of Cardiology. Dr. Proietti reported having no financial conflicts of interest.
CHICAGO – Efforts to encourage even modest amounts of physical activity in sedentary patients with atrial fibrillation are likely to pay off in reduced risks of cardiovascular and all-cause mortality, according to a report from the EurObservational Research Program Pilot Survey on Atrial Fibrillation General Registry.
“Clearly we would recommend regular physical activity for patients with atrial fibrillation on the basis of the mortality benefit we see in the registry. If we give patients with atrial fibrillation oral anticoagulation, they are protected against stroke risk, but clearly they are still dying a lot,” Dr. Marco Proietti said at the annual meeting of the American College of Cardiology.
He presented 1-year follow-up data on 2,442 “real world” patients enrolled in the nine-country, observational, prospective registry, known as EORP-AF, shortly after being diagnosed with AF. One of the goals of EORP-AF is to learn whether physical exercise protects against cardiovascular events and all-cause mortality in AF patients, as has been well established in the general population and in patients at high cardiovascular risk.
One striking finding was that nearly 40% of patients in EORP-AF reported engaging in no physical activity, defined for study purposes as zero to less than 3 hours of physical activity per week for less than 2 years.
The other three categories employed by investigators were “occasional,” meaning less than 3 hours per week but for 2 years or more; “regular,” defined as at least 3 hours weekly for at least 2 years; and “intense,” which required more than 7 hours of physical activity per week for at least 2 years. Levels of cardiovascular and stroke risk factors decreased progressively with increasing levels of physical activity. Only 5% of the AF patients met the ‘intense’ standard, noted Dr. Proietti of the University of Birmingham (England).
The 1-year cardiovascular mortality rate approached 6% in the no physical activity group and hovered around 1% in the other three groups. The 1-year all-cause mortality rate exceeded 12% in the no-exercise group, was 4%% in the occasional exercisers, and 1%-2% in the groups reporting regular or intense physical activity.
The 1-year composite endpoint of cardiovascular death, any thromboembolism, or a bleeding event occurred in 12% of the sedentary patients, a rate two-to-three times higher than in the others.
Updated outcomes are to be reported from the EORP-AF pilot registry after 2 and 3 years of follow-up. Meanwhile, on the basis of the success of the pilot registry, more than 10,000 patients with AF have been enrolled in the EORP-AF main registry, according to Dr. Proietti.
A study limitation, he conceded, is that the registry includes no objective measure of physical capacity, such as METS.
Session co-chair Dr. Brian Olshansky, emeritus professor of internal medicine at the University of Iowa, Iowa City, observed that the registry data raise a classic chicken-versus-egg issue: Do the sedentary patients do worse because they’re inactive, or are they inactive because they are sicker and hence have worse outcomes?
Dr. Proietti said the registry data provide some support for the latter idea, since the no-physical-activity group had higher prevalences of coronary artery disease and heart failure.
Dr. Olshansky raised another point: “It’s interesting to me that there’s a whole bunch of literature showing that elite endurance athletes – bike racers, cross country skiers – have a very high incidence of atrial fibrillation. It seems to be either an inflammatory or an autonomic issue.”
Dr. Proietti replied that he’s familiar with that extensive literature, but the EORP-AF data through 1 year don’t provide validation. While the intense physical activity group tended to have more symptomatic AF than the other groups, they were no more likely to show progression from paroxysmal to permanent AF. The much larger main registry now underway may be able to better clarify the relationship between physical activity and incidence and progression of AF, including the possibility of a U-shaped dose-response curve.
The EORP-AF registry is supported by the European Society of Cardiology. Dr. Proietti reported having no financial conflicts of interest.
AT ACC 16
Key clinical point: Atrial fibrillation patients who report engaging in even occasional physical activity have a markedly lower risk of all-cause mortality than those who are sedentary.
Major finding: The 1-year composite outcome of cardiovascular death, any thromboembolism, or a bleeding event occurred in 12% in patients with atrial fibrillation who were sedentary, a rate two to three times greater than in those who engaged in various amounts of physical activity.
Data source: An analysis of 1-year outcomes in 2,442 patients with AF enrolled in the prospective, observational EORP-AF pilot registry.
Disclosures: The EORP-AF registry is supported by the European Society of Cardiology. The presenter reported having no financial conflicts of interest.

Which ECG criteria are best for screening adolescent athletes?
CHICAGO – Results of the first-ever large study of ECG-based criteria for use in sports preparticipation screening in adolescent athletes demonstrate that the so-called Refined criteria decisively outperform the European Society of Cardiology and Seattle criteria, Dr. Aneil Malhotra reported at the annual meeting of the American College of Cardiology.
All three sets of 12-lead ECG criteria maintained an overall 92% sensitivity for the detection of serious cardiac pathology. However, the Refined criteria provided a major boost in specificity – and a markedly lower false positive rate, according to Dr. Malhotra of St. George’s, University of London.

The Refined criteria performed particularly well in the black adolescent athletes. That’s important because of black athletes’ historically high false positive rates with other ECG criteria, which lead to the time and expense of further testing, needless anxiety for the athletes and their families, and susceptibility to erroneous disqualification, he added.
The ESC recommendations for ECG interpretation in athletes were published in 2010 (Eur Heart J. 2010 Jan;31[2]:243-59). Because of their high false positive rates and the fact that the ESC criteria were derived exclusively from white athletes, an international consensus panel subsequently issued the Seattle criteria, which were developed based upon data from both black and white athletes (Br J Sports Med. 2013 Feb;47[3]:122-4).
While the Seattle criteria performed better than the ESC criteria, many sports cardiologists felt there was further room for improvement in setting criteria that differentiate between physiologic ECG patterns and those indicative of serious cardiac disease. Thus, another international expert consensus panel came up with the Refined criteria. And while the Refined criteria clearly outperformed the ESC and Seattle criteria when applied to a large group of young adult athletes (Circulation. 2014 Apr 22;129[16]:1637-49), the fact is that all three sets of criteria were developed with data from adult athletes. None had been tested in adolescent athletes, even though they are vastly more numerous than were adult athletes in every country. It was the need to validate the applicability of the adult-based criteria in adolescent athletes that was the impetus for Dr. Malhotra’s retrospective study.
He and his coinvestigators applied all three sets of criteria to a unique data set: 10,156 elite adolescent soccer players in the English Football Association’s program for the development of soccer professionals. The cohort consisted of 9,262 white and 894 black players, making this the largest-ever study conducted in adolescent black athletes. The subjects averaged just over 16 years in age and trained on average for more than 12 hours per week.
The English Football Association’s preparticipation screening program included a full history and physical examination, a 12-lead ECG, and – most importantly – an echocardiogram for every athlete, which enabled investigators to validate the ECG findings. The cost of echocardiography in young English footballers is covered by Cardiac Risk in the Young, a charitable organization.
Application of the ESC criteria resulted in an abnormal ECG requiring further investigation in 12.9% of the white athletes. With the Seattle criteria, this rate dropped to 4.2%. With the Refined criteria, it fell further to 2.8%.
In black adolescent athletes, the abnormal ECG rate was 16.2% with the ESC criteria, 5.8% with the Seattle criteria, and 3.8% using the Refined criteria.
A total of 36 cases of cardiac conditions predisposing to sudden cardiac death were identified in the overall cohort. Thirty-three of the 36 affected athletes were correctly identified by all three sets of ECG criteria, including all 28 cases of Wolf-Parkinson-White syndrome and the three cases of hypertrophic cardiomyopathy.
Armed with the true positive rates, the investigators were able to determine that the false positive ECG rates were 12.6% in whites and 15.5% in blacks with the ESC criteria, 3.9% in whites and 5.3% in blacks with the Seattle criteria, and 2.5% in whites and 3.1% in blacks by the Refined criteria.
The positive predictive value of the 12-lead ECG was more than fourfold higher with the Refined as compared with the ESC criteria: 11% versus 2.5% with the ESC and 7.5% with the Seattle criteria, Dr. Malhotra continued.
He explained that the Refined criteria differ from the other two sets of criteria as follows: There are a series of normal ECG findings in the adolescent athletes that are unrelated to training, and that experts agree don’t warrant further evaluation, such as incomplete right bundle branch block or sinus bradycardia. And there are well established ECG abnormalities that necessitate further testing. The Refined criteria establish an evidence-based set of borderline ECG findings that are deemed normal in isolation: atrial enlargement, axis deviation, and complete bundle branch block. Only if two or more of these findings are present is the ECG deemed abnormal.
The Refined criteria have been adopted by the sports cardiologists who perform preparticipation screening for the English Football Association and other UK athletic organizations. But Dr. Malhotra and his coinvestigators also tested a further refinement of the Refined criteria in the adolescent soccer players and found it further improved the results. The refinement involved incorporation of one element of the Seattle criteria, which deems T wave inversion in the V1 and V2 leads as normal in all athletes.
When Dr. Malhotra and colleagues applied this additional refinement to the study cohort of more than 10,000 elite adolescent soccer players, they found the updated Refined criteria reduced the overall abnormal ECG rate from 2.9% to 2.1% while maintaining a specificity in excess of 96% for the detection of serious cardiac pathology. These updated Refined criteria will soon be routinely used in preparticipation screening for the Football Association’s youth development program, he added.
Session co-chair Dr. John A. Spertus was favorably impressed.
“This is really terrific work. Congratulations. I love studies that declare and define waste in effort and resources, and worry for patients, and can eliminate that,” said Dr. Spertus, professor of medicine and director of cardiovascular education and outcomes research at the Mid America Heart Institute and University of Missouri, Kansas City.
The American Academy of Pediatrics and other U.S. medical societies do not routinely recommend a preparticipation ECG at this time, but rather a preparticipation physical evaluation involving a targeted history and physical exam available at www.aap.org by searching “ppe-4 forms.”
This study was funded by Cardiac Risk in the Young and the English Football Association. Dr. Malhotra reported having no financial conflicts of interest.
CHICAGO – Results of the first-ever large study of ECG-based criteria for use in sports preparticipation screening in adolescent athletes demonstrate that the so-called Refined criteria decisively outperform the European Society of Cardiology and Seattle criteria, Dr. Aneil Malhotra reported at the annual meeting of the American College of Cardiology.
All three sets of 12-lead ECG criteria maintained an overall 92% sensitivity for the detection of serious cardiac pathology. However, the Refined criteria provided a major boost in specificity – and a markedly lower false positive rate, according to Dr. Malhotra of St. George’s, University of London.
The Refined criteria performed particularly well in the black adolescent athletes. That’s important because of black athletes’ historically high false positive rates with other ECG criteria, which lead to the time and expense of further testing, needless anxiety for the athletes and their families, and susceptibility to erroneous disqualification, he added.
The ESC recommendations for ECG interpretation in athletes were published in 2010 (Eur Heart J. 2010 Jan;31[2]:243-59). Because of their high false positive rates and the fact that the ESC criteria were derived exclusively from white athletes, an international consensus panel subsequently issued the Seattle criteria, which were developed based upon data from both black and white athletes (Br J Sports Med. 2013 Feb;47[3]:122-4).
While the Seattle criteria performed better than the ESC criteria, many sports cardiologists felt there was further room for improvement in setting criteria that differentiate between physiologic ECG patterns and those indicative of serious cardiac disease. Thus, another international expert consensus panel came up with the Refined criteria. And while the Refined criteria clearly outperformed the ESC and Seattle criteria when applied to a large group of young adult athletes (Circulation. 2014 Apr 22;129[16]:1637-49), the fact is that all three sets of criteria were developed with data from adult athletes. None had been tested in adolescent athletes, even though they are vastly more numerous than were adult athletes in every country. It was the need to validate the applicability of the adult-based criteria in adolescent athletes that was the impetus for Dr. Malhotra’s retrospective study.
He and his coinvestigators applied all three sets of criteria to a unique data set: 10,156 elite adolescent soccer players in the English Football Association’s program for the development of soccer professionals. The cohort consisted of 9,262 white and 894 black players, making this the largest-ever study conducted in adolescent black athletes. The subjects averaged just over 16 years in age and trained on average for more than 12 hours per week.
The English Football Association’s preparticipation screening program included a full history and physical examination, a 12-lead ECG, and – most importantly – an echocardiogram for every athlete, which enabled investigators to validate the ECG findings. The cost of echocardiography in young English footballers is covered by Cardiac Risk in the Young, a charitable organization.
Application of the ESC criteria resulted in an abnormal ECG requiring further investigation in 12.9% of the white athletes. With the Seattle criteria, this rate dropped to 4.2%. With the Refined criteria, it fell further to 2.8%.
In black adolescent athletes, the abnormal ECG rate was 16.2% with the ESC criteria, 5.8% with the Seattle criteria, and 3.8% using the Refined criteria.
A total of 36 cases of cardiac conditions predisposing to sudden cardiac death were identified in the overall cohort. Thirty-three of the 36 affected athletes were correctly identified by all three sets of ECG criteria, including all 28 cases of Wolf-Parkinson-White syndrome and the three cases of hypertrophic cardiomyopathy.
Armed with the true positive rates, the investigators were able to determine that the false positive ECG rates were 12.6% in whites and 15.5% in blacks with the ESC criteria, 3.9% in whites and 5.3% in blacks with the Seattle criteria, and 2.5% in whites and 3.1% in blacks by the Refined criteria.
The positive predictive value of the 12-lead ECG was more than fourfold higher with the Refined as compared with the ESC criteria: 11% versus 2.5% with the ESC and 7.5% with the Seattle criteria, Dr. Malhotra continued.
He explained that the Refined criteria differ from the other two sets of criteria as follows: There are a series of normal ECG findings in the adolescent athletes that are unrelated to training, and that experts agree don’t warrant further evaluation, such as incomplete right bundle branch block or sinus bradycardia. And there are well established ECG abnormalities that necessitate further testing. The Refined criteria establish an evidence-based set of borderline ECG findings that are deemed normal in isolation: atrial enlargement, axis deviation, and complete bundle branch block. Only if two or more of these findings are present is the ECG deemed abnormal.
The Refined criteria have been adopted by the sports cardiologists who perform preparticipation screening for the English Football Association and other UK athletic organizations. But Dr. Malhotra and his coinvestigators also tested a further refinement of the Refined criteria in the adolescent soccer players and found it further improved the results. The refinement involved incorporation of one element of the Seattle criteria, which deems T wave inversion in the V1 and V2 leads as normal in all athletes.
When Dr. Malhotra and colleagues applied this additional refinement to the study cohort of more than 10,000 elite adolescent soccer players, they found the updated Refined criteria reduced the overall abnormal ECG rate from 2.9% to 2.1% while maintaining a specificity in excess of 96% for the detection of serious cardiac pathology. These updated Refined criteria will soon be routinely used in preparticipation screening for the Football Association’s youth development program, he added.
Session co-chair Dr. John A. Spertus was favorably impressed.
“This is really terrific work. Congratulations. I love studies that declare and define waste in effort and resources, and worry for patients, and can eliminate that,” said Dr. Spertus, professor of medicine and director of cardiovascular education and outcomes research at the Mid America Heart Institute and University of Missouri, Kansas City.
The American Academy of Pediatrics and other U.S. medical societies do not routinely recommend a preparticipation ECG at this time, but rather a preparticipation physical evaluation involving a targeted history and physical exam available at www.aap.org by searching “ppe-4 forms.”
This study was funded by Cardiac Risk in the Young and the English Football Association. Dr. Malhotra reported having no financial conflicts of interest.
CHICAGO – Results of the first-ever large study of ECG-based criteria for use in sports preparticipation screening in adolescent athletes demonstrate that the so-called Refined criteria decisively outperform the European Society of Cardiology and Seattle criteria, Dr. Aneil Malhotra reported at the annual meeting of the American College of Cardiology.
All three sets of 12-lead ECG criteria maintained an overall 92% sensitivity for the detection of serious cardiac pathology. However, the Refined criteria provided a major boost in specificity – and a markedly lower false positive rate, according to Dr. Malhotra of St. George’s, University of London.
The Refined criteria performed particularly well in the black adolescent athletes. That’s important because of black athletes’ historically high false positive rates with other ECG criteria, which lead to the time and expense of further testing, needless anxiety for the athletes and their families, and susceptibility to erroneous disqualification, he added.
The ESC recommendations for ECG interpretation in athletes were published in 2010 (Eur Heart J. 2010 Jan;31[2]:243-59). Because of their high false positive rates and the fact that the ESC criteria were derived exclusively from white athletes, an international consensus panel subsequently issued the Seattle criteria, which were developed based upon data from both black and white athletes (Br J Sports Med. 2013 Feb;47[3]:122-4).
While the Seattle criteria performed better than the ESC criteria, many sports cardiologists felt there was further room for improvement in setting criteria that differentiate between physiologic ECG patterns and those indicative of serious cardiac disease. Thus, another international expert consensus panel came up with the Refined criteria. And while the Refined criteria clearly outperformed the ESC and Seattle criteria when applied to a large group of young adult athletes (Circulation. 2014 Apr 22;129[16]:1637-49), the fact is that all three sets of criteria were developed with data from adult athletes. None had been tested in adolescent athletes, even though they are vastly more numerous than were adult athletes in every country. It was the need to validate the applicability of the adult-based criteria in adolescent athletes that was the impetus for Dr. Malhotra’s retrospective study.
He and his coinvestigators applied all three sets of criteria to a unique data set: 10,156 elite adolescent soccer players in the English Football Association’s program for the development of soccer professionals. The cohort consisted of 9,262 white and 894 black players, making this the largest-ever study conducted in adolescent black athletes. The subjects averaged just over 16 years in age and trained on average for more than 12 hours per week.
The English Football Association’s preparticipation screening program included a full history and physical examination, a 12-lead ECG, and – most importantly – an echocardiogram for every athlete, which enabled investigators to validate the ECG findings. The cost of echocardiography in young English footballers is covered by Cardiac Risk in the Young, a charitable organization.
Application of the ESC criteria resulted in an abnormal ECG requiring further investigation in 12.9% of the white athletes. With the Seattle criteria, this rate dropped to 4.2%. With the Refined criteria, it fell further to 2.8%.
In black adolescent athletes, the abnormal ECG rate was 16.2% with the ESC criteria, 5.8% with the Seattle criteria, and 3.8% using the Refined criteria.
A total of 36 cases of cardiac conditions predisposing to sudden cardiac death were identified in the overall cohort. Thirty-three of the 36 affected athletes were correctly identified by all three sets of ECG criteria, including all 28 cases of Wolf-Parkinson-White syndrome and the three cases of hypertrophic cardiomyopathy.
Armed with the true positive rates, the investigators were able to determine that the false positive ECG rates were 12.6% in whites and 15.5% in blacks with the ESC criteria, 3.9% in whites and 5.3% in blacks with the Seattle criteria, and 2.5% in whites and 3.1% in blacks by the Refined criteria.
The positive predictive value of the 12-lead ECG was more than fourfold higher with the Refined as compared with the ESC criteria: 11% versus 2.5% with the ESC and 7.5% with the Seattle criteria, Dr. Malhotra continued.
He explained that the Refined criteria differ from the other two sets of criteria as follows: There are a series of normal ECG findings in the adolescent athletes that are unrelated to training, and that experts agree don’t warrant further evaluation, such as incomplete right bundle branch block or sinus bradycardia. And there are well established ECG abnormalities that necessitate further testing. The Refined criteria establish an evidence-based set of borderline ECG findings that are deemed normal in isolation: atrial enlargement, axis deviation, and complete bundle branch block. Only if two or more of these findings are present is the ECG deemed abnormal.
The Refined criteria have been adopted by the sports cardiologists who perform preparticipation screening for the English Football Association and other UK athletic organizations. But Dr. Malhotra and his coinvestigators also tested a further refinement of the Refined criteria in the adolescent soccer players and found it further improved the results. The refinement involved incorporation of one element of the Seattle criteria, which deems T wave inversion in the V1 and V2 leads as normal in all athletes.
When Dr. Malhotra and colleagues applied this additional refinement to the study cohort of more than 10,000 elite adolescent soccer players, they found the updated Refined criteria reduced the overall abnormal ECG rate from 2.9% to 2.1% while maintaining a specificity in excess of 96% for the detection of serious cardiac pathology. These updated Refined criteria will soon be routinely used in preparticipation screening for the Football Association’s youth development program, he added.
Session co-chair Dr. John A. Spertus was favorably impressed.
“This is really terrific work. Congratulations. I love studies that declare and define waste in effort and resources, and worry for patients, and can eliminate that,” said Dr. Spertus, professor of medicine and director of cardiovascular education and outcomes research at the Mid America Heart Institute and University of Missouri, Kansas City.
The American Academy of Pediatrics and other U.S. medical societies do not routinely recommend a preparticipation ECG at this time, but rather a preparticipation physical evaluation involving a targeted history and physical exam available at www.aap.org by searching “ppe-4 forms.”
This study was funded by Cardiac Risk in the Young and the English Football Association. Dr. Malhotra reported having no financial conflicts of interest.
AT ACC 16
Key clinical point: So-called Refined criteria outperform Seattle and ESC criteria for detection of cardiac abnormalities in teen elite athletes.
Major finding: The overall abnormal screening ECG rate was 13.2% with the ESC criteria, 4.3% with the Seattle criteria, and 2.9% with the Refined criteria.
Data source: A retrospective study that applied three different sets of 12-lead ECG interpretation criteria to preparticipation screening of more than 10,000 elite adolescent United Kingdom soccer players.
Disclosures: This study was funded by Cardiac Risk in the Young and the English Football Association. The presenter reported having no financial conflicts of interest.

Strong gender difference for stroke in diabetes patients with restless legs syndrome
CHICAGO – Stroke risk in diabetic women with restless legs syndrome (RLS) is triple that of diabetic men with the sensorimotor disease, Zoe Heis reported at the annual meeting of the American College of Cardiology.
The mechanism underlying this marked gender discrepancy in risk requires further investigation, as does the highly practical question of whether improved diabetic control can reduce the stroke risk, said Ms. Heis of the Center for Integrative Research on Cardiovascular Aging at Aurora Health Care in Milwaukee.
She presented a retrospective cohort study of 385 patients diagnosed with RLS during 2011-2013 at a community sleep center using the International RLS Study Group criteria. Along with 770 propensity-matched controls, they were followed until mid-2015. At baseline, 40% of the RLS patients had diabetes and 70% had hypertension, as did 32% and 63% of controls, respectively.
Stroke occurred in 7.5% of the RLS group and 4.2% of matched controls. The presence of diabetes more than doubled the stroke risk in both groups.
The risk of stroke was 18.2% in diabetic women with RLS and 7% in diabetic men with RLS. In a multivariate analysis that controlled for potential confounding factors, this translated to a threefold increased stroke risk.
Diabetes was associated with a doubling of stroke risk in subjects without RLS, but the risk was similar in men and women, according to Ms. Heis.
In addition to diabetes and female gender, the other major predictor of increased stroke risk in patients with RLS was, not surprisingly, hypertension. It was associated with a 13-fold increased likelihood of stroke, she noted.
RLS was initially linked to increased risk of coronary heart disease in a report from the Nurses’ Health Study (Circulation. 2012 Oct 2;126[14]:1689-94). In 2015, another research group linked more severe RLS to an increased risk of stroke. Ms. Heis and her coinvestigators carried out the current study to test their hypothesis that, since diabetes is a condition that accelerates cardiovascular disease, the endocrine disorder would boost stroke risk more in subjects with RLS than in those without it.
Ms. Heis reported having no financial conflicts regarding her study, which was conducted free of commercial support.
CHICAGO – Stroke risk in diabetic women with restless legs syndrome (RLS) is triple that of diabetic men with the sensorimotor disease, Zoe Heis reported at the annual meeting of the American College of Cardiology.
The mechanism underlying this marked gender discrepancy in risk requires further investigation, as does the highly practical question of whether improved diabetic control can reduce the stroke risk, said Ms. Heis of the Center for Integrative Research on Cardiovascular Aging at Aurora Health Care in Milwaukee.
She presented a retrospective cohort study of 385 patients diagnosed with RLS during 2011-2013 at a community sleep center using the International RLS Study Group criteria. Along with 770 propensity-matched controls, they were followed until mid-2015. At baseline, 40% of the RLS patients had diabetes and 70% had hypertension, as did 32% and 63% of controls, respectively.
Stroke occurred in 7.5% of the RLS group and 4.2% of matched controls. The presence of diabetes more than doubled the stroke risk in both groups.
The risk of stroke was 18.2% in diabetic women with RLS and 7% in diabetic men with RLS. In a multivariate analysis that controlled for potential confounding factors, this translated to a threefold increased stroke risk.
Diabetes was associated with a doubling of stroke risk in subjects without RLS, but the risk was similar in men and women, according to Ms. Heis.
In addition to diabetes and female gender, the other major predictor of increased stroke risk in patients with RLS was, not surprisingly, hypertension. It was associated with a 13-fold increased likelihood of stroke, she noted.
RLS was initially linked to increased risk of coronary heart disease in a report from the Nurses’ Health Study (Circulation. 2012 Oct 2;126[14]:1689-94). In 2015, another research group linked more severe RLS to an increased risk of stroke. Ms. Heis and her coinvestigators carried out the current study to test their hypothesis that, since diabetes is a condition that accelerates cardiovascular disease, the endocrine disorder would boost stroke risk more in subjects with RLS than in those without it.
Ms. Heis reported having no financial conflicts regarding her study, which was conducted free of commercial support.
CHICAGO – Stroke risk in diabetic women with restless legs syndrome (RLS) is triple that of diabetic men with the sensorimotor disease, Zoe Heis reported at the annual meeting of the American College of Cardiology.
The mechanism underlying this marked gender discrepancy in risk requires further investigation, as does the highly practical question of whether improved diabetic control can reduce the stroke risk, said Ms. Heis of the Center for Integrative Research on Cardiovascular Aging at Aurora Health Care in Milwaukee.
She presented a retrospective cohort study of 385 patients diagnosed with RLS during 2011-2013 at a community sleep center using the International RLS Study Group criteria. Along with 770 propensity-matched controls, they were followed until mid-2015. At baseline, 40% of the RLS patients had diabetes and 70% had hypertension, as did 32% and 63% of controls, respectively.
Stroke occurred in 7.5% of the RLS group and 4.2% of matched controls. The presence of diabetes more than doubled the stroke risk in both groups.
The risk of stroke was 18.2% in diabetic women with RLS and 7% in diabetic men with RLS. In a multivariate analysis that controlled for potential confounding factors, this translated to a threefold increased stroke risk.
Diabetes was associated with a doubling of stroke risk in subjects without RLS, but the risk was similar in men and women, according to Ms. Heis.
In addition to diabetes and female gender, the other major predictor of increased stroke risk in patients with RLS was, not surprisingly, hypertension. It was associated with a 13-fold increased likelihood of stroke, she noted.
RLS was initially linked to increased risk of coronary heart disease in a report from the Nurses’ Health Study (Circulation. 2012 Oct 2;126[14]:1689-94). In 2015, another research group linked more severe RLS to an increased risk of stroke. Ms. Heis and her coinvestigators carried out the current study to test their hypothesis that, since diabetes is a condition that accelerates cardiovascular disease, the endocrine disorder would boost stroke risk more in subjects with RLS than in those without it.
Ms. Heis reported having no financial conflicts regarding her study, which was conducted free of commercial support.
AT ACC 16
Key clinical point: Diabetic women who have restless legs syndrome face a sharply elevated risk of stroke.
Major finding: Stroke occurred in 18.2% of diabetic women with restless legs syndrome, compared with 7% of men.
Data source: This retrospective cohort study included 385 patients with restless legs syndrome and 770 propensity-matched controls.
Disclosures: This study was conducted free of commercial support. The presenter reported having no financial conflicts.
Strong gender difference for stroke in diabetes patients with restless legs syndrome
CHICAGO – Stroke risk in diabetic women with restless legs syndrome (RLS) is triple that of diabetic men with the sensorimotor disease, Zoe Heis reported at the annual meeting of the American College of Cardiology.
The mechanism underlying this marked gender discrepancy in risk requires further investigation, as does the highly practical question of whether improved diabetic control can reduce the stroke risk, said Ms. Heis of the Center for Integrative Research on Cardiovascular Aging at Aurora Health Care in Milwaukee.
She presented a retrospective cohort study of 385 patients diagnosed with RLS during 2011-2013 at a community sleep center using the International RLS Study Group criteria. Along with 770 propensity-matched controls, they were followed until mid-2015. At baseline, 40% of the RLS patients had diabetes and 70% had hypertension, as did 32% and 63% of controls, respectively.
Stroke occurred in 7.5% of the RLS group and 4.2% of matched controls. The presence of diabetes more than doubled the stroke risk in both groups.
The risk of stroke was 18.2% in diabetic women with RLS and 7% in diabetic men with RLS. In a multivariate analysis that controlled for potential confounding factors, this translated to a threefold increased stroke risk.
Diabetes was associated with a doubling of stroke risk in subjects without RLS, but the risk was similar in men and women, according to Ms. Heis.
In addition to diabetes and female gender, the other major predictor of increased stroke risk in patients with RLS was, not surprisingly, hypertension. It was associated with a 13-fold increased likelihood of stroke, she noted.
RLS was initially linked to increased risk of coronary heart disease in a report from the Nurses’ Health Study (Circulation. 2012 Oct 2;126[14]:1689-94). In 2015, another research group linked more severe RLS to an increased risk of stroke. Ms. Heis and her coinvestigators carried out the current study to test their hypothesis that, since diabetes is a condition that accelerates cardiovascular disease, the endocrine disorder would boost stroke risk more in subjects with RLS than in those without it.
Ms. Heis reported having no financial conflicts regarding her study, which was conducted free of commercial support.
CHICAGO – Stroke risk in diabetic women with restless legs syndrome (RLS) is triple that of diabetic men with the sensorimotor disease, Zoe Heis reported at the annual meeting of the American College of Cardiology.
The mechanism underlying this marked gender discrepancy in risk requires further investigation, as does the highly practical question of whether improved diabetic control can reduce the stroke risk, said Ms. Heis of the Center for Integrative Research on Cardiovascular Aging at Aurora Health Care in Milwaukee.
She presented a retrospective cohort study of 385 patients diagnosed with RLS during 2011-2013 at a community sleep center using the International RLS Study Group criteria. Along with 770 propensity-matched controls, they were followed until mid-2015. At baseline, 40% of the RLS patients had diabetes and 70% had hypertension, as did 32% and 63% of controls, respectively.
Stroke occurred in 7.5% of the RLS group and 4.2% of matched controls. The presence of diabetes more than doubled the stroke risk in both groups.
The risk of stroke was 18.2% in diabetic women with RLS and 7% in diabetic men with RLS. In a multivariate analysis that controlled for potential confounding factors, this translated to a threefold increased stroke risk.
Diabetes was associated with a doubling of stroke risk in subjects without RLS, but the risk was similar in men and women, according to Ms. Heis.
In addition to diabetes and female gender, the other major predictor of increased stroke risk in patients with RLS was, not surprisingly, hypertension. It was associated with a 13-fold increased likelihood of stroke, she noted.
RLS was initially linked to increased risk of coronary heart disease in a report from the Nurses’ Health Study (Circulation. 2012 Oct 2;126[14]:1689-94). In 2015, another research group linked more severe RLS to an increased risk of stroke. Ms. Heis and her coinvestigators carried out the current study to test their hypothesis that, since diabetes is a condition that accelerates cardiovascular disease, the endocrine disorder would boost stroke risk more in subjects with RLS than in those without it.
Ms. Heis reported having no financial conflicts regarding her study, which was conducted free of commercial support.
CHICAGO – Stroke risk in diabetic women with restless legs syndrome (RLS) is triple that of diabetic men with the sensorimotor disease, Zoe Heis reported at the annual meeting of the American College of Cardiology.
The mechanism underlying this marked gender discrepancy in risk requires further investigation, as does the highly practical question of whether improved diabetic control can reduce the stroke risk, said Ms. Heis of the Center for Integrative Research on Cardiovascular Aging at Aurora Health Care in Milwaukee.
She presented a retrospective cohort study of 385 patients diagnosed with RLS during 2011-2013 at a community sleep center using the International RLS Study Group criteria. Along with 770 propensity-matched controls, they were followed until mid-2015. At baseline, 40% of the RLS patients had diabetes and 70% had hypertension, as did 32% and 63% of controls, respectively.
Stroke occurred in 7.5% of the RLS group and 4.2% of matched controls. The presence of diabetes more than doubled the stroke risk in both groups.
The risk of stroke was 18.2% in diabetic women with RLS and 7% in diabetic men with RLS. In a multivariate analysis that controlled for potential confounding factors, this translated to a threefold increased stroke risk.
Diabetes was associated with a doubling of stroke risk in subjects without RLS, but the risk was similar in men and women, according to Ms. Heis.
In addition to diabetes and female gender, the other major predictor of increased stroke risk in patients with RLS was, not surprisingly, hypertension. It was associated with a 13-fold increased likelihood of stroke, she noted.
RLS was initially linked to increased risk of coronary heart disease in a report from the Nurses’ Health Study (Circulation. 2012 Oct 2;126[14]:1689-94). In 2015, another research group linked more severe RLS to an increased risk of stroke. Ms. Heis and her coinvestigators carried out the current study to test their hypothesis that, since diabetes is a condition that accelerates cardiovascular disease, the endocrine disorder would boost stroke risk more in subjects with RLS than in those without it.
Ms. Heis reported having no financial conflicts regarding her study, which was conducted free of commercial support.
AT ACC 16
Key clinical point: Diabetic women who have restless legs syndrome face a sharply elevated risk of stroke.
Major finding: Stroke occurred in 18.2% of diabetic women with restless legs syndrome, compared with 7% of men.
Data source: This retrospective cohort study included 385 patients with restless legs syndrome and 770 propensity-matched controls.
Disclosures: This study was conducted free of commercial support. The presenter reported having no financial conflicts.
Drilling down on end-of-life health care costs in heart failure
CHICAGO – Health care costs for heart failure patients spike dramatically in the last 6 months of life, with lack of adherence to guideline-directed outpatient medical therapy being the major modifiable factor driving the costs, Jason P. Swindle, Ph.D., reported at the annual meeting of the American College of Cardiology.
He presented a retrospective study of heart failure–related and total health care costs during the final 24 months of life for 48,026 Medicare Advantage managed care plan members with heart failure.
The researchers were interested in exploring possible racial/ethnic differences in costs, particularly in light of evidence that African Americans have a higher risk of heart failure and higher all-cause mortality. And while a first look at the data indicated racial differences in the size of end-of-life cost spikes, those differences lost their significance in multivariate analysis.
“Lack of guideline-directed outpatient heart failure therapy was a key. Also older age and the presence of coronary heart disease – those were really the big three items that were driving the spike in costs,” said Dr. Swindle of the Chicago office of Optum, a health care consulting group.
He was quick to add that, since the study was based upon administrative data, the lack of adherence to guideline-directed therapy may be unrelated to physician prescribing.
“We see the prescriptions that patients are actually filling. Patients may very well be seeing their cardiologist and being prescribed a medication, but they simply don’t fill the prescription,” he explained in an interview.
Over patients’ final 2 years of life, semiannual all-cause health care costs climbed from a baseline of roughly $10,000 during months 24-19 before death by about 4-fold during months 6-1 before death. Heart failure–related medical costs jumped 10-fold in Asians, 7.8-fold in Hispanics, 6.6-fold in African Americans, and 6.7-fold in whites. Most of the increases occurred in the final 6 months.
Zeroing in on the final 6 months of life, the mean cumulative total medical costs were $44,599, with heart failure–related medical costs accounting for $24,818 of that figure. Total medical costs averaged just under $5,000 during month 6 prior to death and rose roughly 3.5-fold over the remaining months.
This study was supported by Novartis Pharmaceuticals.
CHICAGO – Health care costs for heart failure patients spike dramatically in the last 6 months of life, with lack of adherence to guideline-directed outpatient medical therapy being the major modifiable factor driving the costs, Jason P. Swindle, Ph.D., reported at the annual meeting of the American College of Cardiology.
He presented a retrospective study of heart failure–related and total health care costs during the final 24 months of life for 48,026 Medicare Advantage managed care plan members with heart failure.
The researchers were interested in exploring possible racial/ethnic differences in costs, particularly in light of evidence that African Americans have a higher risk of heart failure and higher all-cause mortality. And while a first look at the data indicated racial differences in the size of end-of-life cost spikes, those differences lost their significance in multivariate analysis.
“Lack of guideline-directed outpatient heart failure therapy was a key. Also older age and the presence of coronary heart disease – those were really the big three items that were driving the spike in costs,” said Dr. Swindle of the Chicago office of Optum, a health care consulting group.
He was quick to add that, since the study was based upon administrative data, the lack of adherence to guideline-directed therapy may be unrelated to physician prescribing.
“We see the prescriptions that patients are actually filling. Patients may very well be seeing their cardiologist and being prescribed a medication, but they simply don’t fill the prescription,” he explained in an interview.
Over patients’ final 2 years of life, semiannual all-cause health care costs climbed from a baseline of roughly $10,000 during months 24-19 before death by about 4-fold during months 6-1 before death. Heart failure–related medical costs jumped 10-fold in Asians, 7.8-fold in Hispanics, 6.6-fold in African Americans, and 6.7-fold in whites. Most of the increases occurred in the final 6 months.
Zeroing in on the final 6 months of life, the mean cumulative total medical costs were $44,599, with heart failure–related medical costs accounting for $24,818 of that figure. Total medical costs averaged just under $5,000 during month 6 prior to death and rose roughly 3.5-fold over the remaining months.
This study was supported by Novartis Pharmaceuticals.
CHICAGO – Health care costs for heart failure patients spike dramatically in the last 6 months of life, with lack of adherence to guideline-directed outpatient medical therapy being the major modifiable factor driving the costs, Jason P. Swindle, Ph.D., reported at the annual meeting of the American College of Cardiology.
He presented a retrospective study of heart failure–related and total health care costs during the final 24 months of life for 48,026 Medicare Advantage managed care plan members with heart failure.
The researchers were interested in exploring possible racial/ethnic differences in costs, particularly in light of evidence that African Americans have a higher risk of heart failure and higher all-cause mortality. And while a first look at the data indicated racial differences in the size of end-of-life cost spikes, those differences lost their significance in multivariate analysis.
“Lack of guideline-directed outpatient heart failure therapy was a key. Also older age and the presence of coronary heart disease – those were really the big three items that were driving the spike in costs,” said Dr. Swindle of the Chicago office of Optum, a health care consulting group.
He was quick to add that, since the study was based upon administrative data, the lack of adherence to guideline-directed therapy may be unrelated to physician prescribing.
“We see the prescriptions that patients are actually filling. Patients may very well be seeing their cardiologist and being prescribed a medication, but they simply don’t fill the prescription,” he explained in an interview.
Over patients’ final 2 years of life, semiannual all-cause health care costs climbed from a baseline of roughly $10,000 during months 24-19 before death by about 4-fold during months 6-1 before death. Heart failure–related medical costs jumped 10-fold in Asians, 7.8-fold in Hispanics, 6.6-fold in African Americans, and 6.7-fold in whites. Most of the increases occurred in the final 6 months.
Zeroing in on the final 6 months of life, the mean cumulative total medical costs were $44,599, with heart failure–related medical costs accounting for $24,818 of that figure. Total medical costs averaged just under $5,000 during month 6 prior to death and rose roughly 3.5-fold over the remaining months.
This study was supported by Novartis Pharmaceuticals.
AT ACC 16
Key clinical point: Addressing lack of adherence to guideline-directed medical therapy could curb end-of-life health care costs in heart failure.
Major finding: Total monthly medical costs in heart failure patients during their final 6 months of life climbed roughly 3.5-fold.
Data source: This was a retrospective study of total and heart failure–related health care costs during the final 24 months of life for more than 48,000 patients with heart failure.
Disclosures: This study was supported by Novartis Pharmaceuticals. Dr. Swindle is an employee of Optum, which conducted the research.