User login
Traumatic Brain Injury and CVD: What’s the Link?
The long-term impact of traumatic brain injury (TBI) on neurologic and psychiatric function is well-established, but a growing body of research is pointing to unexpected medical sequalae, including cardiovascular disease (CVD).
A recent review looked at the investigation to date into this surprising connection, not only summarizing study findings but also suggesting potential mechanisms that might account for the association.
“; consequently, they should undergo regular monitoring,” senior author Ross Zafonte, DO, president of Spaulding Rehabilitation Network, Boston, and lead author Saef Izzy, MD, MBChB, a neurologist at the Stroke and Cerebrovascular Center of Brigham and Women’s Hospital, Boston, Massachusetts, told this news organization.
“This holds significant importance for healthcare practitioners, as there exist several strategies to mitigate cardiovascular disease risk — including weight management, adopting a healthy diet, engaging in regular physical activity, and quitting smoking,” they stated.
Leslie Croll, MD, American Heart Association volunteer and assistant professor of clinical neurology at the Temple University Lewis Katz School of Medicine, Philadelphia, Pennsylvania, told this news organization that it’s “extremely important to learn more about the interplay between TBI, neurologic disease, psychiatric complications, and the cardiovascular system.”
Hopefully, she added, “future research will help us understand what kind of cardiovascular disease monitoring and prevention measures stand to give TBI patients the most benefit.”
Chronic Condition
TBI is “a major cause of long-term disability and premature death,” and is “highly prevalent among contact sports players, military personnel (eg, due to injuries sustained during conflict), and the general population (eg, due to falls and road traffic incidents),” the authors wrote.
Most studies pertaining to TBI have “primarily focused on establishing connections between single TBI, repetitive TBI, and their acute and chronic neurological and psychiatric consequences, such as Parkinson’s disease, Alzheimer’s disease, and chronic traumatic encephalopathy (CTE),” Drs. Zafonte and Izzy noted. By contrast, there has been a “notable lack of research attention given to non-neurological conditions associated with TBI.”
They pointed out that recent insights into TBI — particularly the acknowledgment of TBI as an “emerging chronic condition rather than merely an acute aftermath of brain injury” — have come to light through epidemiologic and pathologic investigations involving military veterans, professional American-style football players, and the civilian population. “This recognition opens up an opportunity to broaden our perspective and delve into the medical aspects of health that may be influenced by TBI.”
To broaden the investigation, the researchers reviewed literature published between January 1, 2001, and June 18, 2023. Of 26,335 articles, they narrowed their review down to 15 studies that investigated CVD, CVD risk factors, and cerebrovascular disease in the chronic phase of TBI, including community, military, or sport-related brain trauma, regardless of the timing of disease occurrence with respect to brain injury via TBI or repetitive head impact.
New Cardiovascular Risk
Studies that used national or local registries tended to be retrospective and predominantly conducted in people with preexisting cardiovascular conditions. In these studies, TBI was found to be an independent risk factor for myocardial dysfunction. However, although these studies do provide evidence of elevated cardiovascular risk subsequent to a single TBI, including individuals with preexisting medical comorbidities “makes it difficult to determine the timing of incident cardiovascular disease and cardiovascular risk factors subsequent to brain injury,” they wrote.
However, some studies showed that even individuals with TBI but without preexisting myocardial dysfunction at baseline had a significantly higher risk for CVD than those without a history of TBI.
In fact, several studies included populations without preexisting medical and cardiovascular comorbidities to “better refine the order and timing of CVD and other risk factors in individuals with TBI.”
For example, one study of concussion survivors without preexisting diagnoses showed that cardiovascular, endocrinological, and neuropsychiatric comorbidities occurred at a “significantly higher incidence within 5 years after concussive TBI compared with healthy individuals who were matched in terms of age, race, and sex and didn’t have a TBI exposure.” Other studies yielded similar findings.
Because cardiovascular risk factors and events become more common with age, it’s important to account for age in evaluating the effects of TBI. Although many studies of TBI and subsequent CVD didn’t stratify individuals by age, one 10-year study of people without any known cardiovascular or neuropsychiatric conditions who sustained TBI found that people as young as 18-40 years were more likely to develop hypertension, hyperlipidemia, obesity, and diabetes within 3-5 years following brain injury than matched individuals in the control group.
“Individuals who have encountered TBI, surprisingly even those who are young and in good health with no prior comorbid conditions, face an increased risk of adverse cardiovascular outcomes for an extended duration after the initial event,” Drs. Zafonte and Izzy summarized. “Therefore, it’s imperative that they receive regular and long-term screenings for CVD and associated risk factors.”
Bidirectional Relationship
Brain injury has been associated with acute cardiovascular dysfunction, including autonomic heart-brain axis dysregulation, imbalances between the sympathetic and parasympathetic nervous systems, and excessive catecholamine release, the authors noted.
Drs. Zafonte and Izzy suggested several plausible links between TBI and cardiovascular dysfunction, noting that they are “likely multifaceted, potentially encompassing risk factors that span the pre-injury, injury, and post-injury phases of the condition.”
TBI may induce alterations in neurobiological processes, which have been reported to be associated with an increased risk for CVD (eg, chronic dysfunction of the autonomic system, systemic inflammation, and modifications in the brain-gut connection).
Patients with TBI might develop additional risk factors following the injury, including conditions like posttraumatic stress disorder, depression, and other psychiatric illnesses, which are “known to augment the risk of CVD.”
TBI can lead to subsequent behavioral and lifestyle changes that place patients at an elevated risk for both cardiovascular and cognitive dysfunction when compared to the general population of TBI survivors.
There may be additional as yet undefined risks.
They believe there’s a bidirectional relationship between TBI and CVD. “On one hand, TBI has been associated with an elevated risk of CVD,” they said. “Conversely, cardiovascular risk factors such as diabetes, hypertension, hyperlipidemia, and sleep disturbances that have been demonstrated to negatively influence cognitive function and heighten the risk of dementia. Consequently, this interplay can further compound the long-term consequences of the injury.”
Their work aims to try and disentangle this “complex series of relationships.”
They recommend screening to identify diseases in their earliest and “most manageable phases” because TBI has been “unveiled as an underappreciated risk factor for CVD within contact sports, military, and community setting.”
An effective screening program “should rely on quantifiable and dependable biomarkers such as blood pressure, BMI, waist circumference, blood lipid levels, and glucose. Additionally, it should take into account other factors like smoking habits, physical activity, and dietary choices,” they recommended.
Heart-Brain Connection
Dr. Croll noted that TBI is “associated with many poorly understood physiologic changes and complications, so it’s exciting to see research aimed at clarifying this chronic disease process.”
In recent years, “we have seen a greater appreciation and understanding of the heart-brain connection,” she said. “Moving forward, more research, including TBI research, will target that connection.”
She added that there are probably “multiple mechanisms” at play underlying the connection between TBI and CVD.
Most importantly, “we are increasingly learning that TBI is not only a discrete event that requires immediate treatment but also a chronic disease process,” and when we “think about the substantial long-term morbidity associated with TBI, we should keep increased risk for CVD on top of mind,” said Dr. Croll.
The review received no funding. Izzy reported receiving grants from the US National Institutes of Health (NIH) and 2023 Stepping Strong Innovator Award. Dr. Zafonte reported receiving grants from the NIH and royalties from Springer and Demos publishing for serving as a coeditor of Brain Injury Medicine. Dr. Zafonte has also served as an adviser to Myomo, Oncare.ai, Nanodiagnostics, and Kisbee. He reported evaluating patients in the Massachusetts General Hospital Brain and Body–TRUST Program, which is funded by the NFL Players Association. The other authors’ disclosures are listed on the original paper. Dr. Croll declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
The long-term impact of traumatic brain injury (TBI) on neurologic and psychiatric function is well-established, but a growing body of research is pointing to unexpected medical sequalae, including cardiovascular disease (CVD).
A recent review looked at the investigation to date into this surprising connection, not only summarizing study findings but also suggesting potential mechanisms that might account for the association.
“; consequently, they should undergo regular monitoring,” senior author Ross Zafonte, DO, president of Spaulding Rehabilitation Network, Boston, and lead author Saef Izzy, MD, MBChB, a neurologist at the Stroke and Cerebrovascular Center of Brigham and Women’s Hospital, Boston, Massachusetts, told this news organization.
“This holds significant importance for healthcare practitioners, as there exist several strategies to mitigate cardiovascular disease risk — including weight management, adopting a healthy diet, engaging in regular physical activity, and quitting smoking,” they stated.
Leslie Croll, MD, American Heart Association volunteer and assistant professor of clinical neurology at the Temple University Lewis Katz School of Medicine, Philadelphia, Pennsylvania, told this news organization that it’s “extremely important to learn more about the interplay between TBI, neurologic disease, psychiatric complications, and the cardiovascular system.”
Hopefully, she added, “future research will help us understand what kind of cardiovascular disease monitoring and prevention measures stand to give TBI patients the most benefit.”
Chronic Condition
TBI is “a major cause of long-term disability and premature death,” and is “highly prevalent among contact sports players, military personnel (eg, due to injuries sustained during conflict), and the general population (eg, due to falls and road traffic incidents),” the authors wrote.
Most studies pertaining to TBI have “primarily focused on establishing connections between single TBI, repetitive TBI, and their acute and chronic neurological and psychiatric consequences, such as Parkinson’s disease, Alzheimer’s disease, and chronic traumatic encephalopathy (CTE),” Drs. Zafonte and Izzy noted. By contrast, there has been a “notable lack of research attention given to non-neurological conditions associated with TBI.”
They pointed out that recent insights into TBI — particularly the acknowledgment of TBI as an “emerging chronic condition rather than merely an acute aftermath of brain injury” — have come to light through epidemiologic and pathologic investigations involving military veterans, professional American-style football players, and the civilian population. “This recognition opens up an opportunity to broaden our perspective and delve into the medical aspects of health that may be influenced by TBI.”
To broaden the investigation, the researchers reviewed literature published between January 1, 2001, and June 18, 2023. Of 26,335 articles, they narrowed their review down to 15 studies that investigated CVD, CVD risk factors, and cerebrovascular disease in the chronic phase of TBI, including community, military, or sport-related brain trauma, regardless of the timing of disease occurrence with respect to brain injury via TBI or repetitive head impact.
New Cardiovascular Risk
Studies that used national or local registries tended to be retrospective and predominantly conducted in people with preexisting cardiovascular conditions. In these studies, TBI was found to be an independent risk factor for myocardial dysfunction. However, although these studies do provide evidence of elevated cardiovascular risk subsequent to a single TBI, including individuals with preexisting medical comorbidities “makes it difficult to determine the timing of incident cardiovascular disease and cardiovascular risk factors subsequent to brain injury,” they wrote.
However, some studies showed that even individuals with TBI but without preexisting myocardial dysfunction at baseline had a significantly higher risk for CVD than those without a history of TBI.
In fact, several studies included populations without preexisting medical and cardiovascular comorbidities to “better refine the order and timing of CVD and other risk factors in individuals with TBI.”
For example, one study of concussion survivors without preexisting diagnoses showed that cardiovascular, endocrinological, and neuropsychiatric comorbidities occurred at a “significantly higher incidence within 5 years after concussive TBI compared with healthy individuals who were matched in terms of age, race, and sex and didn’t have a TBI exposure.” Other studies yielded similar findings.
Because cardiovascular risk factors and events become more common with age, it’s important to account for age in evaluating the effects of TBI. Although many studies of TBI and subsequent CVD didn’t stratify individuals by age, one 10-year study of people without any known cardiovascular or neuropsychiatric conditions who sustained TBI found that people as young as 18-40 years were more likely to develop hypertension, hyperlipidemia, obesity, and diabetes within 3-5 years following brain injury than matched individuals in the control group.
“Individuals who have encountered TBI, surprisingly even those who are young and in good health with no prior comorbid conditions, face an increased risk of adverse cardiovascular outcomes for an extended duration after the initial event,” Drs. Zafonte and Izzy summarized. “Therefore, it’s imperative that they receive regular and long-term screenings for CVD and associated risk factors.”
Bidirectional Relationship
Brain injury has been associated with acute cardiovascular dysfunction, including autonomic heart-brain axis dysregulation, imbalances between the sympathetic and parasympathetic nervous systems, and excessive catecholamine release, the authors noted.
Drs. Zafonte and Izzy suggested several plausible links between TBI and cardiovascular dysfunction, noting that they are “likely multifaceted, potentially encompassing risk factors that span the pre-injury, injury, and post-injury phases of the condition.”
TBI may induce alterations in neurobiological processes, which have been reported to be associated with an increased risk for CVD (eg, chronic dysfunction of the autonomic system, systemic inflammation, and modifications in the brain-gut connection).
Patients with TBI might develop additional risk factors following the injury, including conditions like posttraumatic stress disorder, depression, and other psychiatric illnesses, which are “known to augment the risk of CVD.”
TBI can lead to subsequent behavioral and lifestyle changes that place patients at an elevated risk for both cardiovascular and cognitive dysfunction when compared to the general population of TBI survivors.
There may be additional as yet undefined risks.
They believe there’s a bidirectional relationship between TBI and CVD. “On one hand, TBI has been associated with an elevated risk of CVD,” they said. “Conversely, cardiovascular risk factors such as diabetes, hypertension, hyperlipidemia, and sleep disturbances that have been demonstrated to negatively influence cognitive function and heighten the risk of dementia. Consequently, this interplay can further compound the long-term consequences of the injury.”
Their work aims to try and disentangle this “complex series of relationships.”
They recommend screening to identify diseases in their earliest and “most manageable phases” because TBI has been “unveiled as an underappreciated risk factor for CVD within contact sports, military, and community setting.”
An effective screening program “should rely on quantifiable and dependable biomarkers such as blood pressure, BMI, waist circumference, blood lipid levels, and glucose. Additionally, it should take into account other factors like smoking habits, physical activity, and dietary choices,” they recommended.
Heart-Brain Connection
Dr. Croll noted that TBI is “associated with many poorly understood physiologic changes and complications, so it’s exciting to see research aimed at clarifying this chronic disease process.”
In recent years, “we have seen a greater appreciation and understanding of the heart-brain connection,” she said. “Moving forward, more research, including TBI research, will target that connection.”
She added that there are probably “multiple mechanisms” at play underlying the connection between TBI and CVD.
Most importantly, “we are increasingly learning that TBI is not only a discrete event that requires immediate treatment but also a chronic disease process,” and when we “think about the substantial long-term morbidity associated with TBI, we should keep increased risk for CVD on top of mind,” said Dr. Croll.
The review received no funding. Izzy reported receiving grants from the US National Institutes of Health (NIH) and 2023 Stepping Strong Innovator Award. Dr. Zafonte reported receiving grants from the NIH and royalties from Springer and Demos publishing for serving as a coeditor of Brain Injury Medicine. Dr. Zafonte has also served as an adviser to Myomo, Oncare.ai, Nanodiagnostics, and Kisbee. He reported evaluating patients in the Massachusetts General Hospital Brain and Body–TRUST Program, which is funded by the NFL Players Association. The other authors’ disclosures are listed on the original paper. Dr. Croll declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
The long-term impact of traumatic brain injury (TBI) on neurologic and psychiatric function is well-established, but a growing body of research is pointing to unexpected medical sequalae, including cardiovascular disease (CVD).
A recent review looked at the investigation to date into this surprising connection, not only summarizing study findings but also suggesting potential mechanisms that might account for the association.
“; consequently, they should undergo regular monitoring,” senior author Ross Zafonte, DO, president of Spaulding Rehabilitation Network, Boston, and lead author Saef Izzy, MD, MBChB, a neurologist at the Stroke and Cerebrovascular Center of Brigham and Women’s Hospital, Boston, Massachusetts, told this news organization.
“This holds significant importance for healthcare practitioners, as there exist several strategies to mitigate cardiovascular disease risk — including weight management, adopting a healthy diet, engaging in regular physical activity, and quitting smoking,” they stated.
Leslie Croll, MD, American Heart Association volunteer and assistant professor of clinical neurology at the Temple University Lewis Katz School of Medicine, Philadelphia, Pennsylvania, told this news organization that it’s “extremely important to learn more about the interplay between TBI, neurologic disease, psychiatric complications, and the cardiovascular system.”
Hopefully, she added, “future research will help us understand what kind of cardiovascular disease monitoring and prevention measures stand to give TBI patients the most benefit.”
Chronic Condition
TBI is “a major cause of long-term disability and premature death,” and is “highly prevalent among contact sports players, military personnel (eg, due to injuries sustained during conflict), and the general population (eg, due to falls and road traffic incidents),” the authors wrote.
Most studies pertaining to TBI have “primarily focused on establishing connections between single TBI, repetitive TBI, and their acute and chronic neurological and psychiatric consequences, such as Parkinson’s disease, Alzheimer’s disease, and chronic traumatic encephalopathy (CTE),” Drs. Zafonte and Izzy noted. By contrast, there has been a “notable lack of research attention given to non-neurological conditions associated with TBI.”
They pointed out that recent insights into TBI — particularly the acknowledgment of TBI as an “emerging chronic condition rather than merely an acute aftermath of brain injury” — have come to light through epidemiologic and pathologic investigations involving military veterans, professional American-style football players, and the civilian population. “This recognition opens up an opportunity to broaden our perspective and delve into the medical aspects of health that may be influenced by TBI.”
To broaden the investigation, the researchers reviewed literature published between January 1, 2001, and June 18, 2023. Of 26,335 articles, they narrowed their review down to 15 studies that investigated CVD, CVD risk factors, and cerebrovascular disease in the chronic phase of TBI, including community, military, or sport-related brain trauma, regardless of the timing of disease occurrence with respect to brain injury via TBI or repetitive head impact.
New Cardiovascular Risk
Studies that used national or local registries tended to be retrospective and predominantly conducted in people with preexisting cardiovascular conditions. In these studies, TBI was found to be an independent risk factor for myocardial dysfunction. However, although these studies do provide evidence of elevated cardiovascular risk subsequent to a single TBI, including individuals with preexisting medical comorbidities “makes it difficult to determine the timing of incident cardiovascular disease and cardiovascular risk factors subsequent to brain injury,” they wrote.
However, some studies showed that even individuals with TBI but without preexisting myocardial dysfunction at baseline had a significantly higher risk for CVD than those without a history of TBI.
In fact, several studies included populations without preexisting medical and cardiovascular comorbidities to “better refine the order and timing of CVD and other risk factors in individuals with TBI.”
For example, one study of concussion survivors without preexisting diagnoses showed that cardiovascular, endocrinological, and neuropsychiatric comorbidities occurred at a “significantly higher incidence within 5 years after concussive TBI compared with healthy individuals who were matched in terms of age, race, and sex and didn’t have a TBI exposure.” Other studies yielded similar findings.
Because cardiovascular risk factors and events become more common with age, it’s important to account for age in evaluating the effects of TBI. Although many studies of TBI and subsequent CVD didn’t stratify individuals by age, one 10-year study of people without any known cardiovascular or neuropsychiatric conditions who sustained TBI found that people as young as 18-40 years were more likely to develop hypertension, hyperlipidemia, obesity, and diabetes within 3-5 years following brain injury than matched individuals in the control group.
“Individuals who have encountered TBI, surprisingly even those who are young and in good health with no prior comorbid conditions, face an increased risk of adverse cardiovascular outcomes for an extended duration after the initial event,” Drs. Zafonte and Izzy summarized. “Therefore, it’s imperative that they receive regular and long-term screenings for CVD and associated risk factors.”
Bidirectional Relationship
Brain injury has been associated with acute cardiovascular dysfunction, including autonomic heart-brain axis dysregulation, imbalances between the sympathetic and parasympathetic nervous systems, and excessive catecholamine release, the authors noted.
Drs. Zafonte and Izzy suggested several plausible links between TBI and cardiovascular dysfunction, noting that they are “likely multifaceted, potentially encompassing risk factors that span the pre-injury, injury, and post-injury phases of the condition.”
TBI may induce alterations in neurobiological processes, which have been reported to be associated with an increased risk for CVD (eg, chronic dysfunction of the autonomic system, systemic inflammation, and modifications in the brain-gut connection).
Patients with TBI might develop additional risk factors following the injury, including conditions like posttraumatic stress disorder, depression, and other psychiatric illnesses, which are “known to augment the risk of CVD.”
TBI can lead to subsequent behavioral and lifestyle changes that place patients at an elevated risk for both cardiovascular and cognitive dysfunction when compared to the general population of TBI survivors.
There may be additional as yet undefined risks.
They believe there’s a bidirectional relationship between TBI and CVD. “On one hand, TBI has been associated with an elevated risk of CVD,” they said. “Conversely, cardiovascular risk factors such as diabetes, hypertension, hyperlipidemia, and sleep disturbances that have been demonstrated to negatively influence cognitive function and heighten the risk of dementia. Consequently, this interplay can further compound the long-term consequences of the injury.”
Their work aims to try and disentangle this “complex series of relationships.”
They recommend screening to identify diseases in their earliest and “most manageable phases” because TBI has been “unveiled as an underappreciated risk factor for CVD within contact sports, military, and community setting.”
An effective screening program “should rely on quantifiable and dependable biomarkers such as blood pressure, BMI, waist circumference, blood lipid levels, and glucose. Additionally, it should take into account other factors like smoking habits, physical activity, and dietary choices,” they recommended.
Heart-Brain Connection
Dr. Croll noted that TBI is “associated with many poorly understood physiologic changes and complications, so it’s exciting to see research aimed at clarifying this chronic disease process.”
In recent years, “we have seen a greater appreciation and understanding of the heart-brain connection,” she said. “Moving forward, more research, including TBI research, will target that connection.”
She added that there are probably “multiple mechanisms” at play underlying the connection between TBI and CVD.
Most importantly, “we are increasingly learning that TBI is not only a discrete event that requires immediate treatment but also a chronic disease process,” and when we “think about the substantial long-term morbidity associated with TBI, we should keep increased risk for CVD on top of mind,” said Dr. Croll.
The review received no funding. Izzy reported receiving grants from the US National Institutes of Health (NIH) and 2023 Stepping Strong Innovator Award. Dr. Zafonte reported receiving grants from the NIH and royalties from Springer and Demos publishing for serving as a coeditor of Brain Injury Medicine. Dr. Zafonte has also served as an adviser to Myomo, Oncare.ai, Nanodiagnostics, and Kisbee. He reported evaluating patients in the Massachusetts General Hospital Brain and Body–TRUST Program, which is funded by the NFL Players Association. The other authors’ disclosures are listed on the original paper. Dr. Croll declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
Chronic Fatigue Syndrome and Fibromyalgia: A Single Disease Entity?
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and fibromyalgia (FM) have overlapping neurologic symptoms — particularly profound fatigue. The similarity between these two conditions has led to the question of whether they are indeed distinct central nervous system (CNS) entities, or whether they exist along a spectrum and are actually two different manifestations of the same disease process.
A new study utilized a novel methodology — unbiased quantitative mass spectrometry-based proteomics — to investigate this question by analyzing cerebrospinal fluid (CSF) in a group of patients with ME/CFS and another group of patients diagnosed with both ME/CFS and FM.
Close to 2,100 proteins were identified, of which nearly 1,800 were common to both conditions.
“ME/CFS and fibromyalgia do not appear to be distinct entities, with respect to their cerebrospinal fluid proteins,” lead author Steven Schutzer, MD, professor of medicine, Rutgers New Jersey School of Medicine, told this news organization.
“Work is underway to solve the multiple mysteries of ME/CFS, fibromyalgia, and other neurologic-associated diseases,” he continued. “We have further affirmed that we have a precise objective discovery tool in our hands. Collectively studying multiple diseases brings clarity to each individual disease.”
The study was published in the December 2023 issue of Annals of Medicine.
Cutting-Edge Technology
“ME/CFS is characterized by disabling fatigue, and FM is an illness characterized by body-wide pain,” Dr. Schutzer said. These “medically unexplained” illnesses often coexist by current definitions, and the overlap between them has suggested that they may be part of the “same illness spectrum.”
But co-investigator Benjamin Natelson, MD, professor of neurology and director of the Pain and Fatigue Study Center, Mount Sinai, New York, and others found in previous research that there are distinct differences between the conditions, raising the possibility that there may be different pathophysiological processes.
“The physicians and scientists on our team have had longstanding interest in studying neurologic diseases with cutting-edge tools such as mass spectrometry applied to CSF,” Dr. Schutzer said. “We have had success using this message to distinguish diseases such as ME/CFS from post-treatment Lyme disease, multiple sclerosis, and healthy normal people.”
Dr. Schutzer explained that Dr. Natelson had acquired CSF samples from “well-characterized [ME/CFS] patients and controls.”
Since the cause of ME/CFS is “unknown,” it seemed “ripe to investigate it further with the discovery tool of mass spectrometry” by harnessing the “most advanced equipment in the country at the pacific Northwest National Laboratory, which is part of the US Department of Energy.”
Dr. Schutzer noted that it was the “merger of different clinical and laboratory expertise” that enabled them to address whether ME/CFS and FM are two distinct disease processes.
The choice of analyzing CSF is that it’s the fluid closest to the brain, he added. “A lot of people have studied ME/CFS peripherally because they don’t have access to spinal fluid or it’s easier to look peripherally in the blood, but that doesn’t mean that the blood is where the real ‘action’ is occurring.”
The researchers compared the CSF of 15 patients with ME/CFS only to 15 patients with ME/CFS+FM using mass spectrometry-based proteomics, which they had employed in previous research to see whether ME/CFS was distinct from persistent neurologic Lyme disease syndrome.
This technology has become the “method of choice and discovery tool to rapidly uncover protein biomarkers that can distinguish one disease from another,” the authors stated.
In particular, in unbiased quantitative mass spectrometry-based proteomics, the researchers do not have to know in advance what’s in a sample before studying it, Dr. Schutzer explained.
Shared Pathophysiology?
Both groups of patients were of similar age (41.3 ± 9.4 years and 40.1 ± 11.0 years, respectively), with no differences in gender or rates of current comorbid psychiatric diagnoses between the groups.
The researchers quantified a total of 2,083 proteins, including 1,789 that were specifically quantified in all of the CSF samples, regardless of the presence or absence of FM.
Several analyses (including an ANOVA analysis with adjusted P values, a Random Forest machine learning approach that looked at relative protein abundance changes between those with ME/CFS and ME/CFS+FM, and unsupervised hierarchical clustering analyses) did not find distinguishing differences between the groups.
the authors stated.
They noted that both conditions are “medically unexplained,” with core symptoms of pain, fatigue, sleep problems, and cognitive difficulty. The fact that these two syndromes coexist so often has led to the assumption that the “similarities between them outweigh the differences,” they wrote.
They pointed to some differences between the conditions, including an increase in substance P in the CSF of FM patients, but not in ME/CFS patients reported by others. There are also some immunological, physiological and genetic differences.
But if the conclusion that the two illnesses may share a similar pathophysiological basis is supported by other research that includes FM-only patients as comparators to those with ME/CFS, “this would support the notion that the two illnesses fall along a common illness spectrum and may be approached as a single entity — with implications for both diagnosis and the development of new treatment approaches,” they concluded.
‘Noncontributory’ Findings
Commenting on the research, Robert G. Lahita, MD, PhD, director of the Institute for Autoimmune and Rheumatic Diseases, St. Joseph Health, Wayne, New Jersey, stated that he does not regard these diseases as neurologic but rather as rheumatologic.
“Most neurologists don’t see these diseases, but as a rheumatologist, I see them every day,” said Dr. Lahita, professor of medicine at Hackensack (New Jersey) Meridian School of Medicine and a clinical professor of medicine at Rutgers New Jersey Medical School, New Brunswick. “ME/CFS isn’t as common in my practice, but we do deal with many post-COVID patients who are afflicted mostly with ME/CFS.”
He noted that an important reason for fatigue in FM is that patients generally don’t sleep, or their sleep is disrupted. This is different from the cause of fatigue in ME/CFS.
In addition, the small sample size and the lack of difference between males and females were both limitations of the current study, said Dr. Lahita, who was not involved in this research. “We know that FM disproportionately affects women — in my practice, for example, over 95% of the patients with FM are female — while ME/CFS affects both genders similarly.”
Using proteomics as a biomarker was also problematic, according to Dr. Lahita. “It would have been more valuable to investigate differences in cytokines, for example,” he suggested.
Ultimately, Dr. Lahita thinks that the study is “non-contributory to the field and, as complex as the analysis was, it does nothing to shed differentiate the two conditions or explain the syndromes themselves.”
He added that it would have been more valuable to compare ME/CFS not only to ME/CFS plus FM but also with FM without ME/CFS and to healthy controls, and perhaps to a group with an autoimmune condition, such as lupus or Hashimoto’s thyroiditis.
Dr. Schutzer acknowledged that a limitation of the current study is that his team was unable analyze the CSF of patients with only FM. He and his colleagues “combed the world’s labs” for existing CSF samples of patients with FM alone but were unable to obtain any. “We see this study as a ‘stepping stone’ and hope that future studies will include patients with FM who are willing to donate CSF samples that we can use for comparison,” he said.
The authors received support from the National Institutes of Health, National Institute of Allergy and Infectious Diseases, and National Institute of Neurological Disorders and Stroke. Dr. Schutzer, coauthors, and Dr. Lahita reported no relevant financial relationships.
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and fibromyalgia (FM) have overlapping neurologic symptoms — particularly profound fatigue. The similarity between these two conditions has led to the question of whether they are indeed distinct central nervous system (CNS) entities, or whether they exist along a spectrum and are actually two different manifestations of the same disease process.
A new study utilized a novel methodology — unbiased quantitative mass spectrometry-based proteomics — to investigate this question by analyzing cerebrospinal fluid (CSF) in a group of patients with ME/CFS and another group of patients diagnosed with both ME/CFS and FM.
Close to 2,100 proteins were identified, of which nearly 1,800 were common to both conditions.
“ME/CFS and fibromyalgia do not appear to be distinct entities, with respect to their cerebrospinal fluid proteins,” lead author Steven Schutzer, MD, professor of medicine, Rutgers New Jersey School of Medicine, told this news organization.
“Work is underway to solve the multiple mysteries of ME/CFS, fibromyalgia, and other neurologic-associated diseases,” he continued. “We have further affirmed that we have a precise objective discovery tool in our hands. Collectively studying multiple diseases brings clarity to each individual disease.”
The study was published in the December 2023 issue of Annals of Medicine.
Cutting-Edge Technology
“ME/CFS is characterized by disabling fatigue, and FM is an illness characterized by body-wide pain,” Dr. Schutzer said. These “medically unexplained” illnesses often coexist by current definitions, and the overlap between them has suggested that they may be part of the “same illness spectrum.”
But co-investigator Benjamin Natelson, MD, professor of neurology and director of the Pain and Fatigue Study Center, Mount Sinai, New York, and others found in previous research that there are distinct differences between the conditions, raising the possibility that there may be different pathophysiological processes.
“The physicians and scientists on our team have had longstanding interest in studying neurologic diseases with cutting-edge tools such as mass spectrometry applied to CSF,” Dr. Schutzer said. “We have had success using this message to distinguish diseases such as ME/CFS from post-treatment Lyme disease, multiple sclerosis, and healthy normal people.”
Dr. Schutzer explained that Dr. Natelson had acquired CSF samples from “well-characterized [ME/CFS] patients and controls.”
Since the cause of ME/CFS is “unknown,” it seemed “ripe to investigate it further with the discovery tool of mass spectrometry” by harnessing the “most advanced equipment in the country at the pacific Northwest National Laboratory, which is part of the US Department of Energy.”
Dr. Schutzer noted that it was the “merger of different clinical and laboratory expertise” that enabled them to address whether ME/CFS and FM are two distinct disease processes.
The choice of analyzing CSF is that it’s the fluid closest to the brain, he added. “A lot of people have studied ME/CFS peripherally because they don’t have access to spinal fluid or it’s easier to look peripherally in the blood, but that doesn’t mean that the blood is where the real ‘action’ is occurring.”
The researchers compared the CSF of 15 patients with ME/CFS only to 15 patients with ME/CFS+FM using mass spectrometry-based proteomics, which they had employed in previous research to see whether ME/CFS was distinct from persistent neurologic Lyme disease syndrome.
This technology has become the “method of choice and discovery tool to rapidly uncover protein biomarkers that can distinguish one disease from another,” the authors stated.
In particular, in unbiased quantitative mass spectrometry-based proteomics, the researchers do not have to know in advance what’s in a sample before studying it, Dr. Schutzer explained.
Shared Pathophysiology?
Both groups of patients were of similar age (41.3 ± 9.4 years and 40.1 ± 11.0 years, respectively), with no differences in gender or rates of current comorbid psychiatric diagnoses between the groups.
The researchers quantified a total of 2,083 proteins, including 1,789 that were specifically quantified in all of the CSF samples, regardless of the presence or absence of FM.
Several analyses (including an ANOVA analysis with adjusted P values, a Random Forest machine learning approach that looked at relative protein abundance changes between those with ME/CFS and ME/CFS+FM, and unsupervised hierarchical clustering analyses) did not find distinguishing differences between the groups.
the authors stated.
They noted that both conditions are “medically unexplained,” with core symptoms of pain, fatigue, sleep problems, and cognitive difficulty. The fact that these two syndromes coexist so often has led to the assumption that the “similarities between them outweigh the differences,” they wrote.
They pointed to some differences between the conditions, including an increase in substance P in the CSF of FM patients, but not in ME/CFS patients reported by others. There are also some immunological, physiological and genetic differences.
But if the conclusion that the two illnesses may share a similar pathophysiological basis is supported by other research that includes FM-only patients as comparators to those with ME/CFS, “this would support the notion that the two illnesses fall along a common illness spectrum and may be approached as a single entity — with implications for both diagnosis and the development of new treatment approaches,” they concluded.
‘Noncontributory’ Findings
Commenting on the research, Robert G. Lahita, MD, PhD, director of the Institute for Autoimmune and Rheumatic Diseases, St. Joseph Health, Wayne, New Jersey, stated that he does not regard these diseases as neurologic but rather as rheumatologic.
“Most neurologists don’t see these diseases, but as a rheumatologist, I see them every day,” said Dr. Lahita, professor of medicine at Hackensack (New Jersey) Meridian School of Medicine and a clinical professor of medicine at Rutgers New Jersey Medical School, New Brunswick. “ME/CFS isn’t as common in my practice, but we do deal with many post-COVID patients who are afflicted mostly with ME/CFS.”
He noted that an important reason for fatigue in FM is that patients generally don’t sleep, or their sleep is disrupted. This is different from the cause of fatigue in ME/CFS.
In addition, the small sample size and the lack of difference between males and females were both limitations of the current study, said Dr. Lahita, who was not involved in this research. “We know that FM disproportionately affects women — in my practice, for example, over 95% of the patients with FM are female — while ME/CFS affects both genders similarly.”
Using proteomics as a biomarker was also problematic, according to Dr. Lahita. “It would have been more valuable to investigate differences in cytokines, for example,” he suggested.
Ultimately, Dr. Lahita thinks that the study is “non-contributory to the field and, as complex as the analysis was, it does nothing to shed differentiate the two conditions or explain the syndromes themselves.”
He added that it would have been more valuable to compare ME/CFS not only to ME/CFS plus FM but also with FM without ME/CFS and to healthy controls, and perhaps to a group with an autoimmune condition, such as lupus or Hashimoto’s thyroiditis.
Dr. Schutzer acknowledged that a limitation of the current study is that his team was unable analyze the CSF of patients with only FM. He and his colleagues “combed the world’s labs” for existing CSF samples of patients with FM alone but were unable to obtain any. “We see this study as a ‘stepping stone’ and hope that future studies will include patients with FM who are willing to donate CSF samples that we can use for comparison,” he said.
The authors received support from the National Institutes of Health, National Institute of Allergy and Infectious Diseases, and National Institute of Neurological Disorders and Stroke. Dr. Schutzer, coauthors, and Dr. Lahita reported no relevant financial relationships.
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and fibromyalgia (FM) have overlapping neurologic symptoms — particularly profound fatigue. The similarity between these two conditions has led to the question of whether they are indeed distinct central nervous system (CNS) entities, or whether they exist along a spectrum and are actually two different manifestations of the same disease process.
A new study utilized a novel methodology — unbiased quantitative mass spectrometry-based proteomics — to investigate this question by analyzing cerebrospinal fluid (CSF) in a group of patients with ME/CFS and another group of patients diagnosed with both ME/CFS and FM.
Close to 2,100 proteins were identified, of which nearly 1,800 were common to both conditions.
“ME/CFS and fibromyalgia do not appear to be distinct entities, with respect to their cerebrospinal fluid proteins,” lead author Steven Schutzer, MD, professor of medicine, Rutgers New Jersey School of Medicine, told this news organization.
“Work is underway to solve the multiple mysteries of ME/CFS, fibromyalgia, and other neurologic-associated diseases,” he continued. “We have further affirmed that we have a precise objective discovery tool in our hands. Collectively studying multiple diseases brings clarity to each individual disease.”
The study was published in the December 2023 issue of Annals of Medicine.
Cutting-Edge Technology
“ME/CFS is characterized by disabling fatigue, and FM is an illness characterized by body-wide pain,” Dr. Schutzer said. These “medically unexplained” illnesses often coexist by current definitions, and the overlap between them has suggested that they may be part of the “same illness spectrum.”
But co-investigator Benjamin Natelson, MD, professor of neurology and director of the Pain and Fatigue Study Center, Mount Sinai, New York, and others found in previous research that there are distinct differences between the conditions, raising the possibility that there may be different pathophysiological processes.
“The physicians and scientists on our team have had longstanding interest in studying neurologic diseases with cutting-edge tools such as mass spectrometry applied to CSF,” Dr. Schutzer said. “We have had success using this message to distinguish diseases such as ME/CFS from post-treatment Lyme disease, multiple sclerosis, and healthy normal people.”
Dr. Schutzer explained that Dr. Natelson had acquired CSF samples from “well-characterized [ME/CFS] patients and controls.”
Since the cause of ME/CFS is “unknown,” it seemed “ripe to investigate it further with the discovery tool of mass spectrometry” by harnessing the “most advanced equipment in the country at the pacific Northwest National Laboratory, which is part of the US Department of Energy.”
Dr. Schutzer noted that it was the “merger of different clinical and laboratory expertise” that enabled them to address whether ME/CFS and FM are two distinct disease processes.
The choice of analyzing CSF is that it’s the fluid closest to the brain, he added. “A lot of people have studied ME/CFS peripherally because they don’t have access to spinal fluid or it’s easier to look peripherally in the blood, but that doesn’t mean that the blood is where the real ‘action’ is occurring.”
The researchers compared the CSF of 15 patients with ME/CFS only to 15 patients with ME/CFS+FM using mass spectrometry-based proteomics, which they had employed in previous research to see whether ME/CFS was distinct from persistent neurologic Lyme disease syndrome.
This technology has become the “method of choice and discovery tool to rapidly uncover protein biomarkers that can distinguish one disease from another,” the authors stated.
In particular, in unbiased quantitative mass spectrometry-based proteomics, the researchers do not have to know in advance what’s in a sample before studying it, Dr. Schutzer explained.
Shared Pathophysiology?
Both groups of patients were of similar age (41.3 ± 9.4 years and 40.1 ± 11.0 years, respectively), with no differences in gender or rates of current comorbid psychiatric diagnoses between the groups.
The researchers quantified a total of 2,083 proteins, including 1,789 that were specifically quantified in all of the CSF samples, regardless of the presence or absence of FM.
Several analyses (including an ANOVA analysis with adjusted P values, a Random Forest machine learning approach that looked at relative protein abundance changes between those with ME/CFS and ME/CFS+FM, and unsupervised hierarchical clustering analyses) did not find distinguishing differences between the groups.
the authors stated.
They noted that both conditions are “medically unexplained,” with core symptoms of pain, fatigue, sleep problems, and cognitive difficulty. The fact that these two syndromes coexist so often has led to the assumption that the “similarities between them outweigh the differences,” they wrote.
They pointed to some differences between the conditions, including an increase in substance P in the CSF of FM patients, but not in ME/CFS patients reported by others. There are also some immunological, physiological and genetic differences.
But if the conclusion that the two illnesses may share a similar pathophysiological basis is supported by other research that includes FM-only patients as comparators to those with ME/CFS, “this would support the notion that the two illnesses fall along a common illness spectrum and may be approached as a single entity — with implications for both diagnosis and the development of new treatment approaches,” they concluded.
‘Noncontributory’ Findings
Commenting on the research, Robert G. Lahita, MD, PhD, director of the Institute for Autoimmune and Rheumatic Diseases, St. Joseph Health, Wayne, New Jersey, stated that he does not regard these diseases as neurologic but rather as rheumatologic.
“Most neurologists don’t see these diseases, but as a rheumatologist, I see them every day,” said Dr. Lahita, professor of medicine at Hackensack (New Jersey) Meridian School of Medicine and a clinical professor of medicine at Rutgers New Jersey Medical School, New Brunswick. “ME/CFS isn’t as common in my practice, but we do deal with many post-COVID patients who are afflicted mostly with ME/CFS.”
He noted that an important reason for fatigue in FM is that patients generally don’t sleep, or their sleep is disrupted. This is different from the cause of fatigue in ME/CFS.
In addition, the small sample size and the lack of difference between males and females were both limitations of the current study, said Dr. Lahita, who was not involved in this research. “We know that FM disproportionately affects women — in my practice, for example, over 95% of the patients with FM are female — while ME/CFS affects both genders similarly.”
Using proteomics as a biomarker was also problematic, according to Dr. Lahita. “It would have been more valuable to investigate differences in cytokines, for example,” he suggested.
Ultimately, Dr. Lahita thinks that the study is “non-contributory to the field and, as complex as the analysis was, it does nothing to shed differentiate the two conditions or explain the syndromes themselves.”
He added that it would have been more valuable to compare ME/CFS not only to ME/CFS plus FM but also with FM without ME/CFS and to healthy controls, and perhaps to a group with an autoimmune condition, such as lupus or Hashimoto’s thyroiditis.
Dr. Schutzer acknowledged that a limitation of the current study is that his team was unable analyze the CSF of patients with only FM. He and his colleagues “combed the world’s labs” for existing CSF samples of patients with FM alone but were unable to obtain any. “We see this study as a ‘stepping stone’ and hope that future studies will include patients with FM who are willing to donate CSF samples that we can use for comparison,” he said.
The authors received support from the National Institutes of Health, National Institute of Allergy and Infectious Diseases, and National Institute of Neurological Disorders and Stroke. Dr. Schutzer, coauthors, and Dr. Lahita reported no relevant financial relationships.
Lipids and Dementia: A Complex and Evolving Story
The relationship between lipid levels and the development of dementia is an evolving but confusing landscape.
“This is an incredibly complex area, and there really isn’t a clear consensus on this subject because different lipid classes reflect different things,” according to Betsy Mills, PhD, assistant director of aging and Alzheimer’s prevention at the Alzheimer’s Drug Discovery Foundation.
Some studies suggest that excessive lipid levels may increase the risk of developing dementia and Alzheimer’s disease (AD). Others imply that elevated low-density lipoprotein (LDL) cholesterol or even triglycerides may offer some protection against subsequent dementia whereas higher levels of high-density lipoprotein (HDL) cholesterol, hitherto thought to be protective, may have a deleterious effect.
“It depends on what lipids you’re measuring, what you’re using to measure those lipids, what age the person is, and multiple other factors,” Dr. Mills told this news organization.
Teasing out the variables and potential mechanisms for the association between lipids and dementia risk necessitates understanding the role that lipids play in the healthy brain, the negative impact of brain lipid dysregulation, and the interplay between cholesterol in the central nervous system (CNS) and the cholesterol in the rest of the body.
Beyond Amyloid
The role of lipids in AD risk has historically been “overlooked,” says Scott Hansen, PhD, associate professor, Department of Molecular Medicine, Herbert Wertheim UF Scripps Institute for Biomedical Innovation and Technology, Florida.
“The common narrative is that amyloid is the culprit in AD and certainly that’s the case in familial AD,” he told this news organization. “It’s been assumed that because amyloid deposits are also found in the brains of people with late-onset AD — which is the vast majority of cases — amyloid is the cause, but that’s not clear at all.”
The “limited clinical success” of aducanumab, its “extremely small efficacy” — despite its obvious success in eradicating the amyloid plaques — suggests there’s “much more to the story than amyloid.”
He and a growing community of scientists recognize the role of inflammation and lipids. “The major finding of my lab is that cholesterol actually drives the synthesis of amyloid via inflammation. In other words, amyloid is downstream of cholesterol. Cholesterol drives the inflammation, and the inflammation drives amyloid,” he said.
‘Lipid Invasion Model’
Because the brain is an incredibly lipid-rich organ, Dr. Mills said that “any dysregulation in lipid homeostasis will impact the brain because cholesterol is needed for the myelin sheaths, cell membranes, and other functions.”
A healthy brain relies upon healthy lipid regulation, and “since the first description of AD over 100 years ago, the disease has been associated with altered lipids in the brain,” Dr. Hansen noted.
He cited the “ lipid invasion model” as a way of understanding brain lipid dysregulation. This hypothesis posits that AD is driven by external lipids that enter the brain as a result of damage to the blood-brain barrier (BBB).
“Cholesterol in the brain and cholesterol in the periphery — meaning, in the rest of the body, outside the brain — are separate,” Dr. Hansen explained. “The brain produces its own cholesterol and keeps tight control of it.”
Under normal circumstances, cholesterol from the diet doesn’t enter the brain. “Each pool of cholesterol — in the brain and in the periphery — has its own distinct regulatory mechanisms, target cells, and transport mechanisms.”
When the BBB has been compromised, it becomes permeable, allowing LDL cholesterol to enter the brain, said Dr. Hansen. Then the brain’s own lipoproteins transport the invading cholesterol, allowing it to be taken up by neurons. In turn, this causes neuronal amyloid levels to rise, ultimately leading to the creation of amyloid-b plaques. It also plays a role in tau phosphorylation. Both are key features of AD pathology.
Elevated levels of cholesterol and other lipids have been found in amyloid plaques, Dr. Hansen noted. Moreover, studies of brains of patients with AD have pointed to BBB damage.
And the risk factors for AD overlap with the risk factors for damage to the BBB (such as, aging, brain trauma, hypertension, stress, sleep deprivation, smoking, excess alcohol, obesity, diabetes, and APOE4 genotype), according to the lipid invasion model paper cited by Dr. Hansen.
‘Chicken and Egg’
“There is a strong link between the brain and the heart, and we know that cardiovascular risk factors have an overlap with dementia risk factors — especially vascular dementia,” said Dr. Mills.
She explained that an atherogenic lipid profile results in narrowing of the arteries, with less blood reaching the brain. “This can lead to stress in the brain, which drives inflammation and pathology.”
But cholesterol itself plays an important role in inflammation, Dr. Hansen said. In the periphery, it is “part of an integral response to tissue damage and infection.”
In the brain, once cholesterol is synthesized by the astrocytes, it is transported to neurons via the apolipoprotein E (APOE) protein, which plays a role in brain cholesterol homeostasis, Dr. Mills explained. Those with the ε4 allele of APOE (APOE4) tend to have faultier transport and storage of lipids in the brain, relative to the other APOE variants.
It’s known that individuals with APOE4 are particularly vulnerable to late-onset AD, Dr. Hansen observed. By contrast, APOE2 has a more protective effect. “Most people have APOE3, which is ‘in between,’ ” he said.
When there is neuronal uptake of “invading cholesterol,” not only is amyloid produced but also neuroinflammatory cytokines, further driving inflammation. A vicious cycle ensues: Cholesterol induces cytokine release; and cytokine release, in turn, induces cholesterol synthesis — which “suggests an autocatalytic function of cholesterol in the escalation of inflammation,” Dr. Hansen suggested. He noted that permeability of the BBB also allows inflammatory cytokines from elsewhere in the body to invade the brain, further driving inflammation.
Dr. Mills elaborated: “We know that generally, in dementia, there appear to be some changes in cholesterol metabolism in the brain, but it’s a chicken-and-egg question. We know that as the disease progresses, neurons are dying and getting remodeled. Do these changes have to do with the degenerative process, or are the changes in the cholesterol metabolism actually driving the degenerative disease process? It’s probably a combination, but it’s unclear at this point.”
Lipids in Plasma vs CSF
Dr. Mills explained that HDL particles in the brain differ from those in the periphery. “In the CNS, you have ‘HDL-like particles,’ which are similar in size and composition [to HDL in the periphery] but aren’t the same particles.” The brain itself generates HDL-like lipoproteins, which are produced by astrocytes and other glial cells and found in cerebrospinal fluid (CSF).
Dyslipidemia in the periphery can be a marker for cardiovascular pathology. In the brain, “it can be an indication that there is active damage going on, depending on which compartment you’re looking at.”
She noted that plasma lipid levels and brain CSF lipid levels are “very different.” Research suggests that HDL in the CSF exhibits similar heterogeneity to plasma HDL, but these CSF lipoproteins present at 100-fold lower concentrations, compared to plasma HDL and have unique combinations of protein subpopulations. Lipidomics analysis studies show that these compartments “get very different readings, in terms of the predominant lipid disease state, and they are regulated differently from the way lipids in the periphery are regulated.”
In the brain, the cholesterol “needs to get shuttled from glial cells to neurons,” so defects in the transport process can disrupt overall brain homeostasis, said Dr. Mills. But since the brain system is separate from the peripheral system, measuring plasma lipids is more likely to point to cardiovascular risks, while changes reflected in CSF lipids are “more indicative of alteration in lipid homeostasis in the brain.”
HDL and Triglycerides: A Complicated Story
Dr. Mills noted that HDL in the periphery is “very complicated,” and the idea that HDL, as a measure on its own, is “necessarily ‘good’ isn’t particularly informative.” Rather, HDL is “extremely heterogeneous, very diverse, has different lipid compositions, different classes, and different modifications.” For example, like oxidized LDL, oxidized HDL is also “bad,” preventing the HDL from having protective functions.
Similarly, the apolipoproteins associated with HDL can affect the function of the HDL. “Our understanding of the HDL-like particles in the CNS is limited, but we do understand the APOE4 link,” Dr. Mills said. “It seems that the HDL-like particles containing APOE2 or APOE3 are larger and are more effective at transferring the lipids and cholesterol linked to them relative to APOE4-containing particles.”
Because HDL is more complex than simply being “good,” measuring HDL doesn’t “give you the full story,” said Dr. Mills. She speculates that this may be why there are studies suggesting that high levels of HDL might not have protective benefits and might even be detrimental. This makes it difficult to look at population studies, where the different subclasses of HDL are not necessarily captured in depth.
Dr. Mills pointed to another confounding factor, which is that much of the risk for the development of AD appears to be related to the interaction of HDL, LDL, and triglycerides. “When you look at each of these individually, you get a lot of heterogeneity, and it’s unclear what’s driving what,” she said.
An advantage of observational studies is that they give information about which of these markers are associated with trends and disease risks in specific groups vs others.
“For example, higher levels of triglycerides are associated with cardiovascular risk more in women, relative to men,” she said. And the triglyceride-to-HDL ratio seems “particularly robust” as a measure of cardiovascular health and risk.
The interpretation of associations with triglycerides can be “tricky” and “confusing” because results differ so much between studies, she said. “There are differences between middle age and older age, which have to do with age-related changes in metabolism and lipid metabolism and not necessarily that the markers are indicating something different,” she said.
Some research has suggested that triglycerides may have a protective effect against dementia, noted Uma Naidoo, MD, director of nutritional and lifestyle psychiatry, Massachusetts General Hospital, and director of nutritional psychiatry at MGH Academy.
This may be because the brain “runs mostly on energy from burning triglycerides,” suggested Dr. Naidoo, author of the books Calm Your Mind With Food and This Is Your Brain on Food.
In addition, having higher levels of triglycerides may be linked with having overall healthier behaviors, Dr. Naidoo told this news organization.
Dr. Mills said that in middle-aged individuals, high levels of LDL-C and triglycerides are “often indicative of more atherogenic particles and risk to cardiovascular health, which is a generally negative trajectory. But in older individuals, things become more complicated because there are differences in terms of clearance of some of these particles, tissue clearance and distribution, and nutrient status. So for older individuals, it seems that fluctuations in either direction—either too high or too low—tend to be more informative that some overall dysregulation is going on the system.”
She emphasized that, in this “emerging area, looking at only one or two studies is confusing. But if you look at the spectrum of studies, you can see a pattern, which is that the regulation gets ‘off,’ as people age.”
The Potential Role of Statins
Dr. Mills speculated that there may be “neuroprotective benefits for some of the statins which appear to be related to cardiovascular benefits. But at this point, we don’t have any clear data whether statins actually directly impact brain cholesterol, since it’s a separate pool.”
They could help “by increasing blood flow and reducing narrowing of the arteries, but any direct impact on the brain is still under investigation.”
Dr. Hansen pointed to research suggesting statins taken at midlife appear to be cardioprotective and may be protective of brain health as well, whereas statins initiated in older age do not appear to have these benefits.
He speculated that one reason statins seem less helpful when initiated later in life is that the BBB has already been damaged by systemic inflammation in the periphery, and the neuroinflammatory process resulting in neuronal destruction is already underway. “I think statins aren’t going to fix that problem, so although lowering cholesterol can be helpful in some respects, it might be too late to affect cognition because the nerves have already died and won’t grow back.”
Can Dietary Approaches Help?
Dr. Naidoo said that when looking at neurologic and psychiatric disease, “it’s important to think about the ‘long game’ — how can we improve our blood and cardiovascular health earlier in life to help potentiate healthy aging?”
From a nutritional psychiatry standpoint, Dr. Naidoo focuses on nourishing the gut microbiome and decreasing inflammation. “A healthy and balanced microbiome supports cognition, while the composition of gut bacteria is actually drastically different in patients with neurological diseases, such as AD.”
She recommends a nutrient-dense, anti-inflammatory diet including probiotic-rich foods (such as kimchi, sauerkraut, plain yogurt, and miso). Moreover, “the quality and structure of our fatty acids may be relevant as well: Increasing our intake of polyunsaturated fatty acids and avoiding processed fats like trans fats and hydrogenated oils may benefit our overall brain health.”
Dr. Naidoo recommends extra-virgin olive oil as a source of healthy fat. Its consumption is linked to lower incidence of AD by way of encouraging autophagy, which she calls “our own process of “cellular cleanup.’”
Dr. Naidoo believes that clinicians’ guidance to patients should “focus on healthy nutrition and other lifestyle practices, such as exercise, outdoor time, good sleep, and stress reduction.”
Dr. Mills notes the importance of omega-3 fatty acids, such as docosahexaenoic acid (DHA) , for brain health. “DHA is a major lipid component of neuronal membranes,” she said. “Because of inefficiencies in metabolism with APOE4, people tend to metabolize more of the lipids on the membranes themselves, so they have higher lipid membrane turnover and a greater need to supplement. Supplementing particularly through diet, with foods such as fatty fish rich in omega-3, can help boost the levels to help keep neuronal membranes intact.”
What This Means for the Clinician
“At this point, we see all of these associations between lipids and dementia, but we haven’t worked out exactly what it means on the individual level for an individual patient,” said Dr. Mills. Certainly, the picture is complex, and the understanding is growing and shifting. “The clinical applications remain unclear.”
One potential clinical take-home is that clinicians might consider tracking lipid levels over time. “If you follow a patient and see an increase or decrease [in lipid levels], that can be informative.” Looking at ratios of lipids might be more useful than looking only at a change in a single measure. “If you see trends in a variety of measures that track with one another, it might be more of a sign that something is potentially wrong.”
Whether the patient should first try a lifestyle intervention or might need medication is a “personalized clinical decision, depending on the individual, their risk factors, and how their levels are going,” said Dr. Mills.
Dr. Mills, Dr. Hansen, and Dr. Naidoo declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
The relationship between lipid levels and the development of dementia is an evolving but confusing landscape.
“This is an incredibly complex area, and there really isn’t a clear consensus on this subject because different lipid classes reflect different things,” according to Betsy Mills, PhD, assistant director of aging and Alzheimer’s prevention at the Alzheimer’s Drug Discovery Foundation.
Some studies suggest that excessive lipid levels may increase the risk of developing dementia and Alzheimer’s disease (AD). Others imply that elevated low-density lipoprotein (LDL) cholesterol or even triglycerides may offer some protection against subsequent dementia whereas higher levels of high-density lipoprotein (HDL) cholesterol, hitherto thought to be protective, may have a deleterious effect.
“It depends on what lipids you’re measuring, what you’re using to measure those lipids, what age the person is, and multiple other factors,” Dr. Mills told this news organization.
Teasing out the variables and potential mechanisms for the association between lipids and dementia risk necessitates understanding the role that lipids play in the healthy brain, the negative impact of brain lipid dysregulation, and the interplay between cholesterol in the central nervous system (CNS) and the cholesterol in the rest of the body.
Beyond Amyloid
The role of lipids in AD risk has historically been “overlooked,” says Scott Hansen, PhD, associate professor, Department of Molecular Medicine, Herbert Wertheim UF Scripps Institute for Biomedical Innovation and Technology, Florida.
“The common narrative is that amyloid is the culprit in AD and certainly that’s the case in familial AD,” he told this news organization. “It’s been assumed that because amyloid deposits are also found in the brains of people with late-onset AD — which is the vast majority of cases — amyloid is the cause, but that’s not clear at all.”
The “limited clinical success” of aducanumab, its “extremely small efficacy” — despite its obvious success in eradicating the amyloid plaques — suggests there’s “much more to the story than amyloid.”
He and a growing community of scientists recognize the role of inflammation and lipids. “The major finding of my lab is that cholesterol actually drives the synthesis of amyloid via inflammation. In other words, amyloid is downstream of cholesterol. Cholesterol drives the inflammation, and the inflammation drives amyloid,” he said.
‘Lipid Invasion Model’
Because the brain is an incredibly lipid-rich organ, Dr. Mills said that “any dysregulation in lipid homeostasis will impact the brain because cholesterol is needed for the myelin sheaths, cell membranes, and other functions.”
A healthy brain relies upon healthy lipid regulation, and “since the first description of AD over 100 years ago, the disease has been associated with altered lipids in the brain,” Dr. Hansen noted.
He cited the “ lipid invasion model” as a way of understanding brain lipid dysregulation. This hypothesis posits that AD is driven by external lipids that enter the brain as a result of damage to the blood-brain barrier (BBB).
“Cholesterol in the brain and cholesterol in the periphery — meaning, in the rest of the body, outside the brain — are separate,” Dr. Hansen explained. “The brain produces its own cholesterol and keeps tight control of it.”
Under normal circumstances, cholesterol from the diet doesn’t enter the brain. “Each pool of cholesterol — in the brain and in the periphery — has its own distinct regulatory mechanisms, target cells, and transport mechanisms.”
When the BBB has been compromised, it becomes permeable, allowing LDL cholesterol to enter the brain, said Dr. Hansen. Then the brain’s own lipoproteins transport the invading cholesterol, allowing it to be taken up by neurons. In turn, this causes neuronal amyloid levels to rise, ultimately leading to the creation of amyloid-b plaques. It also plays a role in tau phosphorylation. Both are key features of AD pathology.
Elevated levels of cholesterol and other lipids have been found in amyloid plaques, Dr. Hansen noted. Moreover, studies of brains of patients with AD have pointed to BBB damage.
And the risk factors for AD overlap with the risk factors for damage to the BBB (such as, aging, brain trauma, hypertension, stress, sleep deprivation, smoking, excess alcohol, obesity, diabetes, and APOE4 genotype), according to the lipid invasion model paper cited by Dr. Hansen.
‘Chicken and Egg’
“There is a strong link between the brain and the heart, and we know that cardiovascular risk factors have an overlap with dementia risk factors — especially vascular dementia,” said Dr. Mills.
She explained that an atherogenic lipid profile results in narrowing of the arteries, with less blood reaching the brain. “This can lead to stress in the brain, which drives inflammation and pathology.”
But cholesterol itself plays an important role in inflammation, Dr. Hansen said. In the periphery, it is “part of an integral response to tissue damage and infection.”
In the brain, once cholesterol is synthesized by the astrocytes, it is transported to neurons via the apolipoprotein E (APOE) protein, which plays a role in brain cholesterol homeostasis, Dr. Mills explained. Those with the ε4 allele of APOE (APOE4) tend to have faultier transport and storage of lipids in the brain, relative to the other APOE variants.
It’s known that individuals with APOE4 are particularly vulnerable to late-onset AD, Dr. Hansen observed. By contrast, APOE2 has a more protective effect. “Most people have APOE3, which is ‘in between,’ ” he said.
When there is neuronal uptake of “invading cholesterol,” not only is amyloid produced but also neuroinflammatory cytokines, further driving inflammation. A vicious cycle ensues: Cholesterol induces cytokine release; and cytokine release, in turn, induces cholesterol synthesis — which “suggests an autocatalytic function of cholesterol in the escalation of inflammation,” Dr. Hansen suggested. He noted that permeability of the BBB also allows inflammatory cytokines from elsewhere in the body to invade the brain, further driving inflammation.
Dr. Mills elaborated: “We know that generally, in dementia, there appear to be some changes in cholesterol metabolism in the brain, but it’s a chicken-and-egg question. We know that as the disease progresses, neurons are dying and getting remodeled. Do these changes have to do with the degenerative process, or are the changes in the cholesterol metabolism actually driving the degenerative disease process? It’s probably a combination, but it’s unclear at this point.”
Lipids in Plasma vs CSF
Dr. Mills explained that HDL particles in the brain differ from those in the periphery. “In the CNS, you have ‘HDL-like particles,’ which are similar in size and composition [to HDL in the periphery] but aren’t the same particles.” The brain itself generates HDL-like lipoproteins, which are produced by astrocytes and other glial cells and found in cerebrospinal fluid (CSF).
Dyslipidemia in the periphery can be a marker for cardiovascular pathology. In the brain, “it can be an indication that there is active damage going on, depending on which compartment you’re looking at.”
She noted that plasma lipid levels and brain CSF lipid levels are “very different.” Research suggests that HDL in the CSF exhibits similar heterogeneity to plasma HDL, but these CSF lipoproteins present at 100-fold lower concentrations, compared to plasma HDL and have unique combinations of protein subpopulations. Lipidomics analysis studies show that these compartments “get very different readings, in terms of the predominant lipid disease state, and they are regulated differently from the way lipids in the periphery are regulated.”
In the brain, the cholesterol “needs to get shuttled from glial cells to neurons,” so defects in the transport process can disrupt overall brain homeostasis, said Dr. Mills. But since the brain system is separate from the peripheral system, measuring plasma lipids is more likely to point to cardiovascular risks, while changes reflected in CSF lipids are “more indicative of alteration in lipid homeostasis in the brain.”
HDL and Triglycerides: A Complicated Story
Dr. Mills noted that HDL in the periphery is “very complicated,” and the idea that HDL, as a measure on its own, is “necessarily ‘good’ isn’t particularly informative.” Rather, HDL is “extremely heterogeneous, very diverse, has different lipid compositions, different classes, and different modifications.” For example, like oxidized LDL, oxidized HDL is also “bad,” preventing the HDL from having protective functions.
Similarly, the apolipoproteins associated with HDL can affect the function of the HDL. “Our understanding of the HDL-like particles in the CNS is limited, but we do understand the APOE4 link,” Dr. Mills said. “It seems that the HDL-like particles containing APOE2 or APOE3 are larger and are more effective at transferring the lipids and cholesterol linked to them relative to APOE4-containing particles.”
Because HDL is more complex than simply being “good,” measuring HDL doesn’t “give you the full story,” said Dr. Mills. She speculates that this may be why there are studies suggesting that high levels of HDL might not have protective benefits and might even be detrimental. This makes it difficult to look at population studies, where the different subclasses of HDL are not necessarily captured in depth.
Dr. Mills pointed to another confounding factor, which is that much of the risk for the development of AD appears to be related to the interaction of HDL, LDL, and triglycerides. “When you look at each of these individually, you get a lot of heterogeneity, and it’s unclear what’s driving what,” she said.
An advantage of observational studies is that they give information about which of these markers are associated with trends and disease risks in specific groups vs others.
“For example, higher levels of triglycerides are associated with cardiovascular risk more in women, relative to men,” she said. And the triglyceride-to-HDL ratio seems “particularly robust” as a measure of cardiovascular health and risk.
The interpretation of associations with triglycerides can be “tricky” and “confusing” because results differ so much between studies, she said. “There are differences between middle age and older age, which have to do with age-related changes in metabolism and lipid metabolism and not necessarily that the markers are indicating something different,” she said.
Some research has suggested that triglycerides may have a protective effect against dementia, noted Uma Naidoo, MD, director of nutritional and lifestyle psychiatry, Massachusetts General Hospital, and director of nutritional psychiatry at MGH Academy.
This may be because the brain “runs mostly on energy from burning triglycerides,” suggested Dr. Naidoo, author of the books Calm Your Mind With Food and This Is Your Brain on Food.
In addition, having higher levels of triglycerides may be linked with having overall healthier behaviors, Dr. Naidoo told this news organization.
Dr. Mills said that in middle-aged individuals, high levels of LDL-C and triglycerides are “often indicative of more atherogenic particles and risk to cardiovascular health, which is a generally negative trajectory. But in older individuals, things become more complicated because there are differences in terms of clearance of some of these particles, tissue clearance and distribution, and nutrient status. So for older individuals, it seems that fluctuations in either direction—either too high or too low—tend to be more informative that some overall dysregulation is going on the system.”
She emphasized that, in this “emerging area, looking at only one or two studies is confusing. But if you look at the spectrum of studies, you can see a pattern, which is that the regulation gets ‘off,’ as people age.”
The Potential Role of Statins
Dr. Mills speculated that there may be “neuroprotective benefits for some of the statins which appear to be related to cardiovascular benefits. But at this point, we don’t have any clear data whether statins actually directly impact brain cholesterol, since it’s a separate pool.”
They could help “by increasing blood flow and reducing narrowing of the arteries, but any direct impact on the brain is still under investigation.”
Dr. Hansen pointed to research suggesting statins taken at midlife appear to be cardioprotective and may be protective of brain health as well, whereas statins initiated in older age do not appear to have these benefits.
He speculated that one reason statins seem less helpful when initiated later in life is that the BBB has already been damaged by systemic inflammation in the periphery, and the neuroinflammatory process resulting in neuronal destruction is already underway. “I think statins aren’t going to fix that problem, so although lowering cholesterol can be helpful in some respects, it might be too late to affect cognition because the nerves have already died and won’t grow back.”
Can Dietary Approaches Help?
Dr. Naidoo said that when looking at neurologic and psychiatric disease, “it’s important to think about the ‘long game’ — how can we improve our blood and cardiovascular health earlier in life to help potentiate healthy aging?”
From a nutritional psychiatry standpoint, Dr. Naidoo focuses on nourishing the gut microbiome and decreasing inflammation. “A healthy and balanced microbiome supports cognition, while the composition of gut bacteria is actually drastically different in patients with neurological diseases, such as AD.”
She recommends a nutrient-dense, anti-inflammatory diet including probiotic-rich foods (such as kimchi, sauerkraut, plain yogurt, and miso). Moreover, “the quality and structure of our fatty acids may be relevant as well: Increasing our intake of polyunsaturated fatty acids and avoiding processed fats like trans fats and hydrogenated oils may benefit our overall brain health.”
Dr. Naidoo recommends extra-virgin olive oil as a source of healthy fat. Its consumption is linked to lower incidence of AD by way of encouraging autophagy, which she calls “our own process of “cellular cleanup.’”
Dr. Naidoo believes that clinicians’ guidance to patients should “focus on healthy nutrition and other lifestyle practices, such as exercise, outdoor time, good sleep, and stress reduction.”
Dr. Mills notes the importance of omega-3 fatty acids, such as docosahexaenoic acid (DHA) , for brain health. “DHA is a major lipid component of neuronal membranes,” she said. “Because of inefficiencies in metabolism with APOE4, people tend to metabolize more of the lipids on the membranes themselves, so they have higher lipid membrane turnover and a greater need to supplement. Supplementing particularly through diet, with foods such as fatty fish rich in omega-3, can help boost the levels to help keep neuronal membranes intact.”
What This Means for the Clinician
“At this point, we see all of these associations between lipids and dementia, but we haven’t worked out exactly what it means on the individual level for an individual patient,” said Dr. Mills. Certainly, the picture is complex, and the understanding is growing and shifting. “The clinical applications remain unclear.”
One potential clinical take-home is that clinicians might consider tracking lipid levels over time. “If you follow a patient and see an increase or decrease [in lipid levels], that can be informative.” Looking at ratios of lipids might be more useful than looking only at a change in a single measure. “If you see trends in a variety of measures that track with one another, it might be more of a sign that something is potentially wrong.”
Whether the patient should first try a lifestyle intervention or might need medication is a “personalized clinical decision, depending on the individual, their risk factors, and how their levels are going,” said Dr. Mills.
Dr. Mills, Dr. Hansen, and Dr. Naidoo declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
The relationship between lipid levels and the development of dementia is an evolving but confusing landscape.
“This is an incredibly complex area, and there really isn’t a clear consensus on this subject because different lipid classes reflect different things,” according to Betsy Mills, PhD, assistant director of aging and Alzheimer’s prevention at the Alzheimer’s Drug Discovery Foundation.
Some studies suggest that excessive lipid levels may increase the risk of developing dementia and Alzheimer’s disease (AD). Others imply that elevated low-density lipoprotein (LDL) cholesterol or even triglycerides may offer some protection against subsequent dementia whereas higher levels of high-density lipoprotein (HDL) cholesterol, hitherto thought to be protective, may have a deleterious effect.
“It depends on what lipids you’re measuring, what you’re using to measure those lipids, what age the person is, and multiple other factors,” Dr. Mills told this news organization.
Teasing out the variables and potential mechanisms for the association between lipids and dementia risk necessitates understanding the role that lipids play in the healthy brain, the negative impact of brain lipid dysregulation, and the interplay between cholesterol in the central nervous system (CNS) and the cholesterol in the rest of the body.
Beyond Amyloid
The role of lipids in AD risk has historically been “overlooked,” says Scott Hansen, PhD, associate professor, Department of Molecular Medicine, Herbert Wertheim UF Scripps Institute for Biomedical Innovation and Technology, Florida.
“The common narrative is that amyloid is the culprit in AD and certainly that’s the case in familial AD,” he told this news organization. “It’s been assumed that because amyloid deposits are also found in the brains of people with late-onset AD — which is the vast majority of cases — amyloid is the cause, but that’s not clear at all.”
The “limited clinical success” of aducanumab, its “extremely small efficacy” — despite its obvious success in eradicating the amyloid plaques — suggests there’s “much more to the story than amyloid.”
He and a growing community of scientists recognize the role of inflammation and lipids. “The major finding of my lab is that cholesterol actually drives the synthesis of amyloid via inflammation. In other words, amyloid is downstream of cholesterol. Cholesterol drives the inflammation, and the inflammation drives amyloid,” he said.
‘Lipid Invasion Model’
Because the brain is an incredibly lipid-rich organ, Dr. Mills said that “any dysregulation in lipid homeostasis will impact the brain because cholesterol is needed for the myelin sheaths, cell membranes, and other functions.”
A healthy brain relies upon healthy lipid regulation, and “since the first description of AD over 100 years ago, the disease has been associated with altered lipids in the brain,” Dr. Hansen noted.
He cited the “ lipid invasion model” as a way of understanding brain lipid dysregulation. This hypothesis posits that AD is driven by external lipids that enter the brain as a result of damage to the blood-brain barrier (BBB).
“Cholesterol in the brain and cholesterol in the periphery — meaning, in the rest of the body, outside the brain — are separate,” Dr. Hansen explained. “The brain produces its own cholesterol and keeps tight control of it.”
Under normal circumstances, cholesterol from the diet doesn’t enter the brain. “Each pool of cholesterol — in the brain and in the periphery — has its own distinct regulatory mechanisms, target cells, and transport mechanisms.”
When the BBB has been compromised, it becomes permeable, allowing LDL cholesterol to enter the brain, said Dr. Hansen. Then the brain’s own lipoproteins transport the invading cholesterol, allowing it to be taken up by neurons. In turn, this causes neuronal amyloid levels to rise, ultimately leading to the creation of amyloid-b plaques. It also plays a role in tau phosphorylation. Both are key features of AD pathology.
Elevated levels of cholesterol and other lipids have been found in amyloid plaques, Dr. Hansen noted. Moreover, studies of brains of patients with AD have pointed to BBB damage.
And the risk factors for AD overlap with the risk factors for damage to the BBB (such as, aging, brain trauma, hypertension, stress, sleep deprivation, smoking, excess alcohol, obesity, diabetes, and APOE4 genotype), according to the lipid invasion model paper cited by Dr. Hansen.
‘Chicken and Egg’
“There is a strong link between the brain and the heart, and we know that cardiovascular risk factors have an overlap with dementia risk factors — especially vascular dementia,” said Dr. Mills.
She explained that an atherogenic lipid profile results in narrowing of the arteries, with less blood reaching the brain. “This can lead to stress in the brain, which drives inflammation and pathology.”
But cholesterol itself plays an important role in inflammation, Dr. Hansen said. In the periphery, it is “part of an integral response to tissue damage and infection.”
In the brain, once cholesterol is synthesized by the astrocytes, it is transported to neurons via the apolipoprotein E (APOE) protein, which plays a role in brain cholesterol homeostasis, Dr. Mills explained. Those with the ε4 allele of APOE (APOE4) tend to have faultier transport and storage of lipids in the brain, relative to the other APOE variants.
It’s known that individuals with APOE4 are particularly vulnerable to late-onset AD, Dr. Hansen observed. By contrast, APOE2 has a more protective effect. “Most people have APOE3, which is ‘in between,’ ” he said.
When there is neuronal uptake of “invading cholesterol,” not only is amyloid produced but also neuroinflammatory cytokines, further driving inflammation. A vicious cycle ensues: Cholesterol induces cytokine release; and cytokine release, in turn, induces cholesterol synthesis — which “suggests an autocatalytic function of cholesterol in the escalation of inflammation,” Dr. Hansen suggested. He noted that permeability of the BBB also allows inflammatory cytokines from elsewhere in the body to invade the brain, further driving inflammation.
Dr. Mills elaborated: “We know that generally, in dementia, there appear to be some changes in cholesterol metabolism in the brain, but it’s a chicken-and-egg question. We know that as the disease progresses, neurons are dying and getting remodeled. Do these changes have to do with the degenerative process, or are the changes in the cholesterol metabolism actually driving the degenerative disease process? It’s probably a combination, but it’s unclear at this point.”
Lipids in Plasma vs CSF
Dr. Mills explained that HDL particles in the brain differ from those in the periphery. “In the CNS, you have ‘HDL-like particles,’ which are similar in size and composition [to HDL in the periphery] but aren’t the same particles.” The brain itself generates HDL-like lipoproteins, which are produced by astrocytes and other glial cells and found in cerebrospinal fluid (CSF).
Dyslipidemia in the periphery can be a marker for cardiovascular pathology. In the brain, “it can be an indication that there is active damage going on, depending on which compartment you’re looking at.”
She noted that plasma lipid levels and brain CSF lipid levels are “very different.” Research suggests that HDL in the CSF exhibits similar heterogeneity to plasma HDL, but these CSF lipoproteins present at 100-fold lower concentrations, compared to plasma HDL and have unique combinations of protein subpopulations. Lipidomics analysis studies show that these compartments “get very different readings, in terms of the predominant lipid disease state, and they are regulated differently from the way lipids in the periphery are regulated.”
In the brain, the cholesterol “needs to get shuttled from glial cells to neurons,” so defects in the transport process can disrupt overall brain homeostasis, said Dr. Mills. But since the brain system is separate from the peripheral system, measuring plasma lipids is more likely to point to cardiovascular risks, while changes reflected in CSF lipids are “more indicative of alteration in lipid homeostasis in the brain.”
HDL and Triglycerides: A Complicated Story
Dr. Mills noted that HDL in the periphery is “very complicated,” and the idea that HDL, as a measure on its own, is “necessarily ‘good’ isn’t particularly informative.” Rather, HDL is “extremely heterogeneous, very diverse, has different lipid compositions, different classes, and different modifications.” For example, like oxidized LDL, oxidized HDL is also “bad,” preventing the HDL from having protective functions.
Similarly, the apolipoproteins associated with HDL can affect the function of the HDL. “Our understanding of the HDL-like particles in the CNS is limited, but we do understand the APOE4 link,” Dr. Mills said. “It seems that the HDL-like particles containing APOE2 or APOE3 are larger and are more effective at transferring the lipids and cholesterol linked to them relative to APOE4-containing particles.”
Because HDL is more complex than simply being “good,” measuring HDL doesn’t “give you the full story,” said Dr. Mills. She speculates that this may be why there are studies suggesting that high levels of HDL might not have protective benefits and might even be detrimental. This makes it difficult to look at population studies, where the different subclasses of HDL are not necessarily captured in depth.
Dr. Mills pointed to another confounding factor, which is that much of the risk for the development of AD appears to be related to the interaction of HDL, LDL, and triglycerides. “When you look at each of these individually, you get a lot of heterogeneity, and it’s unclear what’s driving what,” she said.
An advantage of observational studies is that they give information about which of these markers are associated with trends and disease risks in specific groups vs others.
“For example, higher levels of triglycerides are associated with cardiovascular risk more in women, relative to men,” she said. And the triglyceride-to-HDL ratio seems “particularly robust” as a measure of cardiovascular health and risk.
The interpretation of associations with triglycerides can be “tricky” and “confusing” because results differ so much between studies, she said. “There are differences between middle age and older age, which have to do with age-related changes in metabolism and lipid metabolism and not necessarily that the markers are indicating something different,” she said.
Some research has suggested that triglycerides may have a protective effect against dementia, noted Uma Naidoo, MD, director of nutritional and lifestyle psychiatry, Massachusetts General Hospital, and director of nutritional psychiatry at MGH Academy.
This may be because the brain “runs mostly on energy from burning triglycerides,” suggested Dr. Naidoo, author of the books Calm Your Mind With Food and This Is Your Brain on Food.
In addition, having higher levels of triglycerides may be linked with having overall healthier behaviors, Dr. Naidoo told this news organization.
Dr. Mills said that in middle-aged individuals, high levels of LDL-C and triglycerides are “often indicative of more atherogenic particles and risk to cardiovascular health, which is a generally negative trajectory. But in older individuals, things become more complicated because there are differences in terms of clearance of some of these particles, tissue clearance and distribution, and nutrient status. So for older individuals, it seems that fluctuations in either direction—either too high or too low—tend to be more informative that some overall dysregulation is going on the system.”
She emphasized that, in this “emerging area, looking at only one or two studies is confusing. But if you look at the spectrum of studies, you can see a pattern, which is that the regulation gets ‘off,’ as people age.”
The Potential Role of Statins
Dr. Mills speculated that there may be “neuroprotective benefits for some of the statins which appear to be related to cardiovascular benefits. But at this point, we don’t have any clear data whether statins actually directly impact brain cholesterol, since it’s a separate pool.”
They could help “by increasing blood flow and reducing narrowing of the arteries, but any direct impact on the brain is still under investigation.”
Dr. Hansen pointed to research suggesting statins taken at midlife appear to be cardioprotective and may be protective of brain health as well, whereas statins initiated in older age do not appear to have these benefits.
He speculated that one reason statins seem less helpful when initiated later in life is that the BBB has already been damaged by systemic inflammation in the periphery, and the neuroinflammatory process resulting in neuronal destruction is already underway. “I think statins aren’t going to fix that problem, so although lowering cholesterol can be helpful in some respects, it might be too late to affect cognition because the nerves have already died and won’t grow back.”
Can Dietary Approaches Help?
Dr. Naidoo said that when looking at neurologic and psychiatric disease, “it’s important to think about the ‘long game’ — how can we improve our blood and cardiovascular health earlier in life to help potentiate healthy aging?”
From a nutritional psychiatry standpoint, Dr. Naidoo focuses on nourishing the gut microbiome and decreasing inflammation. “A healthy and balanced microbiome supports cognition, while the composition of gut bacteria is actually drastically different in patients with neurological diseases, such as AD.”
She recommends a nutrient-dense, anti-inflammatory diet including probiotic-rich foods (such as kimchi, sauerkraut, plain yogurt, and miso). Moreover, “the quality and structure of our fatty acids may be relevant as well: Increasing our intake of polyunsaturated fatty acids and avoiding processed fats like trans fats and hydrogenated oils may benefit our overall brain health.”
Dr. Naidoo recommends extra-virgin olive oil as a source of healthy fat. Its consumption is linked to lower incidence of AD by way of encouraging autophagy, which she calls “our own process of “cellular cleanup.’”
Dr. Naidoo believes that clinicians’ guidance to patients should “focus on healthy nutrition and other lifestyle practices, such as exercise, outdoor time, good sleep, and stress reduction.”
Dr. Mills notes the importance of omega-3 fatty acids, such as docosahexaenoic acid (DHA) , for brain health. “DHA is a major lipid component of neuronal membranes,” she said. “Because of inefficiencies in metabolism with APOE4, people tend to metabolize more of the lipids on the membranes themselves, so they have higher lipid membrane turnover and a greater need to supplement. Supplementing particularly through diet, with foods such as fatty fish rich in omega-3, can help boost the levels to help keep neuronal membranes intact.”
What This Means for the Clinician
“At this point, we see all of these associations between lipids and dementia, but we haven’t worked out exactly what it means on the individual level for an individual patient,” said Dr. Mills. Certainly, the picture is complex, and the understanding is growing and shifting. “The clinical applications remain unclear.”
One potential clinical take-home is that clinicians might consider tracking lipid levels over time. “If you follow a patient and see an increase or decrease [in lipid levels], that can be informative.” Looking at ratios of lipids might be more useful than looking only at a change in a single measure. “If you see trends in a variety of measures that track with one another, it might be more of a sign that something is potentially wrong.”
Whether the patient should first try a lifestyle intervention or might need medication is a “personalized clinical decision, depending on the individual, their risk factors, and how their levels are going,” said Dr. Mills.
Dr. Mills, Dr. Hansen, and Dr. Naidoo declared no relevant financial relationships.
A version of this article appeared on Medscape.com.
What Causes One of Stroke’s Most Common Complications?
The mechanisms underlying poststroke depression (PSD), a common and debilitating complication of stroke, are unclear. Is it neurobiological, psychosocial, or both?
Two studies offer new insight into this question. In the first, in most dimensions of depressive symptoms. But surprisingly, anhedonia was less severe in patients with PSD compared with non-stroke controls, and those with PSD also showed greater emotional dysregulation.
“Our findings support previous recommendations that clinicians should adapt the provision of psychological support to the specific needs and difficulties of stroke survivors,” said lead author Joshua Blake, DClinPsy, lecturer in clinical psychology, University of East Anglia, Norwich, United Kingdom.
The study was published online in Neuropsychology Review
A second study used a machine learning algorithm to analyze blood samples from adults who had suffered a stroke, determining whether plasma protein data could predict mood and identifying potential proteins associated with mood in these patients.
“We can now look at a stroke survivor’s blood and predict their mood,” senior author Marion Buckwalter, MD, PhD, professor of neurology and neurosurgery at Stanford Medicine, California, said in a news release. “This means there is a genuine association between what’s happening in the blood and what’s happening with a person’s mood. It also means that, down the road, we may be able to develop new treatments for PSD.”
The study was published in November 2023 in Brain, Behavior, and Immunity.
‘Surprising’ Findings
“There has long been uncertainty over whether PSD might differ in its causes, phenomenology, and treatability, due to the presence of brain injury, related biological changes, and the psychosocial context unique to this population,” Dr. Blake said. “We felt that understanding symptomatologic similarities and differences would constructively contribute to this debate.”
The researchers reviewed 12 papers that sampled both stroke and non-stroke participants. “We compared profiles of depression symptoms, correlation strengths of individual depression symptoms with general depression, and latent item severity,” Dr. Blake reported.
They extracted 38 symptoms from five standardized depression tools and then organized the symptoms into nine dimensions.
They found mostly nonsignificant differences between patients with PSD and non-stroke controls in most dimensions, including negative affect, negative cognitions, somatic features, anxiety/worry, and suicidal ideation. Those with PSD more frequently had cognitive impairment, and “work inhibition” was more common in PSD.
But the most striking finding was greater severity/prevalence of emotional dysregulation in PSD vs non-stroke depression and also less anhedonia.
Dr. Blake acknowledged being “surprised.”
One possible explanation is that stroke recovery “appears to be a highly emotional journey, with extreme findings of both positive and negative emotions reported by survivors as they psychologically adjust,” which might be protective against anhedonia, he suggested.
Moreover, neurologically driven emotional dysregulation “may similarly reduce experiences of anhedonia.”
However, there was a “considerable risk of bias in many of the included studies, meaning it’s important that these findings are experimentally confirmed before stronger conclusions about phenomenological differences can be drawn,” he cautioned.
Common, Undertreated
Dr. Buckwalter said her team was motivated to conduct the research because PSD is among the top problems reported by chronic stroke patients, and for most, it is not adequately treated.
However, “despite the high prevalence of PSD, it is very poorly studied in the chronic time period.” In particular, PSD isn’t “well understood at a molecular level.”
She added that inflammation is a “promising candidate” as a mechanism, since neuroinflammation occurs in the stroke scar for decades, and chronic peripheral inflammation can produce neuroinflammation. Aberrant immune activation has also been implicated in major depression without stroke. But large studies with broad panels of plasma biomarkers are lacking in PSD.
To address this gap, the researchers used a proteomic approach. They recruited 85 chronic stroke patients (mean age, 65 years [interquartile range, 55-71], 41.2% female, 65.9% White, 17.6% Asian, and 0% Black) from the Stanford Stroke Recovery Program. Participants were between 5 months and 9 years after an ischemic stroke.
They analyzed a comprehensive panel of 1196 proteins in plasma samples, applying a machine learning algorithm to see whether the plasma protein levels “could be used to predict mood scores, using either the proteomics data alone or adding age and time since stroke.” The proteomics data were then incorporated into multivariable regression models, along with relevant clinical features, to ascertain the model’s predictive ability.
Mood was assessed using the Stroke Impact Scale mood questionnaire, with participants’ mood dichotomized into better mood (> 63) or worse mood (≤ 63).
‘Beautiful Mechanistic Model’
Machine learning verified a relationship between plasma proteomic data and mood, with the most accurate prediction occurring when the researchers added age and time since the stroke to the analysis.
Independent univariate analyses identified 202 proteins that were most highly correlated with mood in PSD. These were then organized into functional groups, including immune proteins, integrins, growth factors, synaptic function proteins, serotonin activity-related proteins, and cell death and stress-related functional groupings.
Although no single protein could predict depression, significant changes in levels of several proteins were found in PSD patients. A high proportion (45%) were proteins previously implicated in major depression, “likely providing a link to the underlying mechanisms of chronic PSD,” the authors stated.
Moreover, 80% of correlated immune proteins were higher in the plasma of people with worse mood, and several immune proteins known to have anti-inflammatory effects were reduced in those with worse mood.
And several pro-inflammatory cytokines were implicated. For example, interleukin 6, which has been extensively studied as a potential plasma marker of major depression in non-stroke cohorts, was significantly elevated in patients with worse mood after stroke (P = .0325), «implicating a broadly overactive immune system in PSD.»
“We demonstrated for the first time that we can use plasma protein measurements to predict mood in people with chronic stroke,” Dr. Buckwalter summarized. “This means there is a biological correlate of mood but [it] doesn’t tell us causality.”
To tease out causality, the researchers used their own data, as well as information from a literature review of previous studies, to assemble a model of how the immune response following a stroke could change both serotonin and brain plasticity.
“We used the most highly correlated proteins to construct a beautiful mechanistic model of how poststroke depression may work and how it may relate to mechanisms in major depression,” Dr. Buckwalter said.
The model “posits an increased inflammatory response that leads to decreased tryptophan, serotonin, and less synaptic function, all of which contribute to symptoms of depression.”
Currently, selective serotonin reuptake inhibitors represent the “best treatment” for people with PSD, but “unfortunately they don’t work for many patients,” Dr. Buckwalter noted. The findings “provide clues as to other molecular targets that are candidates novel therapies for poststroke depression.”
Dr. Blake commented that the proteomic study “complements the work by us and others interested in understanding PSD.”
Mood disorders “must be understood in terms of the dynamic relationships between structural neurological alterations, cellular and microbiological changes, psychological processes, and the person’s interactions with their social landscape,” Dr. Blake said.
New Treatments on the Horizon?
Gustavo C. Medeiros, MD, assistant professor, Department of Psychiatry, of the University of Maryland School of Medicine, Baltimore, said that knowing which individuals are more likely to develop PSD “allows treatment teams to implement earlier and more intensive interventions in those who are at higher risk.”
The findings [of the proteomic study] may also “help clarify the neurobiological correlates of PSD…[which] may help the development of new treatments that target these neurobiological changes,” said Dr. Medeiros, who wasn’t involved with either study.
However, he warned, “we should interpret their results with caution due to methodological reasons, including the relatively small sample size.”
Also commenting, Bruce Ovbiagele, MD, MSc, MAS, MBA, MLS, professor of neurology, UCSF Weill Institute for Neurosciences, California, said the proteomic study has some “clear limitations,” including the lack of Black or African American patients in the cohort, which limits generalizability, “since we know that Black and African American people are disproportionately affected by stroke and have very high rates of PSD and very severe presentation.”
The study by Dr. Blake et al. “was interesting because the phenotype of depressive symptoms after stroke differs from what’s seen in the general population, and the authors figured out a way to better understand the nuances of such differences,” said Dr. Ovbiagele, who wasn’t involved with either study.
He said he was also surprised by the finding regarding anhedonia and suggested that the findings be replicated in a study directly comparing patients with PSD and patients with depression from the general population.
The study by Bidoki et al. was funded by AHA/Paul Allen Foundation, the Leducq Stroke-IMPaCT Transatlantic Network of Excellence (MSB), the Wu Tsai Neurosciences Institute (MSB), the Alfred E. Mann Foundation (NA), and an Alzheimer’s Association Research Fellowship to one of the authors. No source of funding was listed for the study by Dr. Blake et al. The authors of both studies, Dr. Medeiros and Dr. Ovbiagele, declare no relevant financial relationships.
A version of this article appeared on Medscape.com.
The mechanisms underlying poststroke depression (PSD), a common and debilitating complication of stroke, are unclear. Is it neurobiological, psychosocial, or both?
Two studies offer new insight into this question. In the first, in most dimensions of depressive symptoms. But surprisingly, anhedonia was less severe in patients with PSD compared with non-stroke controls, and those with PSD also showed greater emotional dysregulation.
“Our findings support previous recommendations that clinicians should adapt the provision of psychological support to the specific needs and difficulties of stroke survivors,” said lead author Joshua Blake, DClinPsy, lecturer in clinical psychology, University of East Anglia, Norwich, United Kingdom.
The study was published online in Neuropsychology Review
A second study used a machine learning algorithm to analyze blood samples from adults who had suffered a stroke, determining whether plasma protein data could predict mood and identifying potential proteins associated with mood in these patients.
“We can now look at a stroke survivor’s blood and predict their mood,” senior author Marion Buckwalter, MD, PhD, professor of neurology and neurosurgery at Stanford Medicine, California, said in a news release. “This means there is a genuine association between what’s happening in the blood and what’s happening with a person’s mood. It also means that, down the road, we may be able to develop new treatments for PSD.”
The study was published in November 2023 in Brain, Behavior, and Immunity.
‘Surprising’ Findings
“There has long been uncertainty over whether PSD might differ in its causes, phenomenology, and treatability, due to the presence of brain injury, related biological changes, and the psychosocial context unique to this population,” Dr. Blake said. “We felt that understanding symptomatologic similarities and differences would constructively contribute to this debate.”
The researchers reviewed 12 papers that sampled both stroke and non-stroke participants. “We compared profiles of depression symptoms, correlation strengths of individual depression symptoms with general depression, and latent item severity,” Dr. Blake reported.
They extracted 38 symptoms from five standardized depression tools and then organized the symptoms into nine dimensions.
They found mostly nonsignificant differences between patients with PSD and non-stroke controls in most dimensions, including negative affect, negative cognitions, somatic features, anxiety/worry, and suicidal ideation. Those with PSD more frequently had cognitive impairment, and “work inhibition” was more common in PSD.
But the most striking finding was greater severity/prevalence of emotional dysregulation in PSD vs non-stroke depression and also less anhedonia.
Dr. Blake acknowledged being “surprised.”
One possible explanation is that stroke recovery “appears to be a highly emotional journey, with extreme findings of both positive and negative emotions reported by survivors as they psychologically adjust,” which might be protective against anhedonia, he suggested.
Moreover, neurologically driven emotional dysregulation “may similarly reduce experiences of anhedonia.”
However, there was a “considerable risk of bias in many of the included studies, meaning it’s important that these findings are experimentally confirmed before stronger conclusions about phenomenological differences can be drawn,” he cautioned.
Common, Undertreated
Dr. Buckwalter said her team was motivated to conduct the research because PSD is among the top problems reported by chronic stroke patients, and for most, it is not adequately treated.
However, “despite the high prevalence of PSD, it is very poorly studied in the chronic time period.” In particular, PSD isn’t “well understood at a molecular level.”
She added that inflammation is a “promising candidate” as a mechanism, since neuroinflammation occurs in the stroke scar for decades, and chronic peripheral inflammation can produce neuroinflammation. Aberrant immune activation has also been implicated in major depression without stroke. But large studies with broad panels of plasma biomarkers are lacking in PSD.
To address this gap, the researchers used a proteomic approach. They recruited 85 chronic stroke patients (mean age, 65 years [interquartile range, 55-71], 41.2% female, 65.9% White, 17.6% Asian, and 0% Black) from the Stanford Stroke Recovery Program. Participants were between 5 months and 9 years after an ischemic stroke.
They analyzed a comprehensive panel of 1196 proteins in plasma samples, applying a machine learning algorithm to see whether the plasma protein levels “could be used to predict mood scores, using either the proteomics data alone or adding age and time since stroke.” The proteomics data were then incorporated into multivariable regression models, along with relevant clinical features, to ascertain the model’s predictive ability.
Mood was assessed using the Stroke Impact Scale mood questionnaire, with participants’ mood dichotomized into better mood (> 63) or worse mood (≤ 63).
‘Beautiful Mechanistic Model’
Machine learning verified a relationship between plasma proteomic data and mood, with the most accurate prediction occurring when the researchers added age and time since the stroke to the analysis.
Independent univariate analyses identified 202 proteins that were most highly correlated with mood in PSD. These were then organized into functional groups, including immune proteins, integrins, growth factors, synaptic function proteins, serotonin activity-related proteins, and cell death and stress-related functional groupings.
Although no single protein could predict depression, significant changes in levels of several proteins were found in PSD patients. A high proportion (45%) were proteins previously implicated in major depression, “likely providing a link to the underlying mechanisms of chronic PSD,” the authors stated.
Moreover, 80% of correlated immune proteins were higher in the plasma of people with worse mood, and several immune proteins known to have anti-inflammatory effects were reduced in those with worse mood.
And several pro-inflammatory cytokines were implicated. For example, interleukin 6, which has been extensively studied as a potential plasma marker of major depression in non-stroke cohorts, was significantly elevated in patients with worse mood after stroke (P = .0325), «implicating a broadly overactive immune system in PSD.»
“We demonstrated for the first time that we can use plasma protein measurements to predict mood in people with chronic stroke,” Dr. Buckwalter summarized. “This means there is a biological correlate of mood but [it] doesn’t tell us causality.”
To tease out causality, the researchers used their own data, as well as information from a literature review of previous studies, to assemble a model of how the immune response following a stroke could change both serotonin and brain plasticity.
“We used the most highly correlated proteins to construct a beautiful mechanistic model of how poststroke depression may work and how it may relate to mechanisms in major depression,” Dr. Buckwalter said.
The model “posits an increased inflammatory response that leads to decreased tryptophan, serotonin, and less synaptic function, all of which contribute to symptoms of depression.”
Currently, selective serotonin reuptake inhibitors represent the “best treatment” for people with PSD, but “unfortunately they don’t work for many patients,” Dr. Buckwalter noted. The findings “provide clues as to other molecular targets that are candidates novel therapies for poststroke depression.”
Dr. Blake commented that the proteomic study “complements the work by us and others interested in understanding PSD.”
Mood disorders “must be understood in terms of the dynamic relationships between structural neurological alterations, cellular and microbiological changes, psychological processes, and the person’s interactions with their social landscape,” Dr. Blake said.
New Treatments on the Horizon?
Gustavo C. Medeiros, MD, assistant professor, Department of Psychiatry, of the University of Maryland School of Medicine, Baltimore, said that knowing which individuals are more likely to develop PSD “allows treatment teams to implement earlier and more intensive interventions in those who are at higher risk.”
The findings [of the proteomic study] may also “help clarify the neurobiological correlates of PSD…[which] may help the development of new treatments that target these neurobiological changes,” said Dr. Medeiros, who wasn’t involved with either study.
However, he warned, “we should interpret their results with caution due to methodological reasons, including the relatively small sample size.”
Also commenting, Bruce Ovbiagele, MD, MSc, MAS, MBA, MLS, professor of neurology, UCSF Weill Institute for Neurosciences, California, said the proteomic study has some “clear limitations,” including the lack of Black or African American patients in the cohort, which limits generalizability, “since we know that Black and African American people are disproportionately affected by stroke and have very high rates of PSD and very severe presentation.”
The study by Dr. Blake et al. “was interesting because the phenotype of depressive symptoms after stroke differs from what’s seen in the general population, and the authors figured out a way to better understand the nuances of such differences,” said Dr. Ovbiagele, who wasn’t involved with either study.
He said he was also surprised by the finding regarding anhedonia and suggested that the findings be replicated in a study directly comparing patients with PSD and patients with depression from the general population.
The study by Bidoki et al. was funded by AHA/Paul Allen Foundation, the Leducq Stroke-IMPaCT Transatlantic Network of Excellence (MSB), the Wu Tsai Neurosciences Institute (MSB), the Alfred E. Mann Foundation (NA), and an Alzheimer’s Association Research Fellowship to one of the authors. No source of funding was listed for the study by Dr. Blake et al. The authors of both studies, Dr. Medeiros and Dr. Ovbiagele, declare no relevant financial relationships.
A version of this article appeared on Medscape.com.
The mechanisms underlying poststroke depression (PSD), a common and debilitating complication of stroke, are unclear. Is it neurobiological, psychosocial, or both?
Two studies offer new insight into this question. In the first, in most dimensions of depressive symptoms. But surprisingly, anhedonia was less severe in patients with PSD compared with non-stroke controls, and those with PSD also showed greater emotional dysregulation.
“Our findings support previous recommendations that clinicians should adapt the provision of psychological support to the specific needs and difficulties of stroke survivors,” said lead author Joshua Blake, DClinPsy, lecturer in clinical psychology, University of East Anglia, Norwich, United Kingdom.
The study was published online in Neuropsychology Review
A second study used a machine learning algorithm to analyze blood samples from adults who had suffered a stroke, determining whether plasma protein data could predict mood and identifying potential proteins associated with mood in these patients.
“We can now look at a stroke survivor’s blood and predict their mood,” senior author Marion Buckwalter, MD, PhD, professor of neurology and neurosurgery at Stanford Medicine, California, said in a news release. “This means there is a genuine association between what’s happening in the blood and what’s happening with a person’s mood. It also means that, down the road, we may be able to develop new treatments for PSD.”
The study was published in November 2023 in Brain, Behavior, and Immunity.
‘Surprising’ Findings
“There has long been uncertainty over whether PSD might differ in its causes, phenomenology, and treatability, due to the presence of brain injury, related biological changes, and the psychosocial context unique to this population,” Dr. Blake said. “We felt that understanding symptomatologic similarities and differences would constructively contribute to this debate.”
The researchers reviewed 12 papers that sampled both stroke and non-stroke participants. “We compared profiles of depression symptoms, correlation strengths of individual depression symptoms with general depression, and latent item severity,” Dr. Blake reported.
They extracted 38 symptoms from five standardized depression tools and then organized the symptoms into nine dimensions.
They found mostly nonsignificant differences between patients with PSD and non-stroke controls in most dimensions, including negative affect, negative cognitions, somatic features, anxiety/worry, and suicidal ideation. Those with PSD more frequently had cognitive impairment, and “work inhibition” was more common in PSD.
But the most striking finding was greater severity/prevalence of emotional dysregulation in PSD vs non-stroke depression and also less anhedonia.
Dr. Blake acknowledged being “surprised.”
One possible explanation is that stroke recovery “appears to be a highly emotional journey, with extreme findings of both positive and negative emotions reported by survivors as they psychologically adjust,” which might be protective against anhedonia, he suggested.
Moreover, neurologically driven emotional dysregulation “may similarly reduce experiences of anhedonia.”
However, there was a “considerable risk of bias in many of the included studies, meaning it’s important that these findings are experimentally confirmed before stronger conclusions about phenomenological differences can be drawn,” he cautioned.
Common, Undertreated
Dr. Buckwalter said her team was motivated to conduct the research because PSD is among the top problems reported by chronic stroke patients, and for most, it is not adequately treated.
However, “despite the high prevalence of PSD, it is very poorly studied in the chronic time period.” In particular, PSD isn’t “well understood at a molecular level.”
She added that inflammation is a “promising candidate” as a mechanism, since neuroinflammation occurs in the stroke scar for decades, and chronic peripheral inflammation can produce neuroinflammation. Aberrant immune activation has also been implicated in major depression without stroke. But large studies with broad panels of plasma biomarkers are lacking in PSD.
To address this gap, the researchers used a proteomic approach. They recruited 85 chronic stroke patients (mean age, 65 years [interquartile range, 55-71], 41.2% female, 65.9% White, 17.6% Asian, and 0% Black) from the Stanford Stroke Recovery Program. Participants were between 5 months and 9 years after an ischemic stroke.
They analyzed a comprehensive panel of 1196 proteins in plasma samples, applying a machine learning algorithm to see whether the plasma protein levels “could be used to predict mood scores, using either the proteomics data alone or adding age and time since stroke.” The proteomics data were then incorporated into multivariable regression models, along with relevant clinical features, to ascertain the model’s predictive ability.
Mood was assessed using the Stroke Impact Scale mood questionnaire, with participants’ mood dichotomized into better mood (> 63) or worse mood (≤ 63).
‘Beautiful Mechanistic Model’
Machine learning verified a relationship between plasma proteomic data and mood, with the most accurate prediction occurring when the researchers added age and time since the stroke to the analysis.
Independent univariate analyses identified 202 proteins that were most highly correlated with mood in PSD. These were then organized into functional groups, including immune proteins, integrins, growth factors, synaptic function proteins, serotonin activity-related proteins, and cell death and stress-related functional groupings.
Although no single protein could predict depression, significant changes in levels of several proteins were found in PSD patients. A high proportion (45%) were proteins previously implicated in major depression, “likely providing a link to the underlying mechanisms of chronic PSD,” the authors stated.
Moreover, 80% of correlated immune proteins were higher in the plasma of people with worse mood, and several immune proteins known to have anti-inflammatory effects were reduced in those with worse mood.
And several pro-inflammatory cytokines were implicated. For example, interleukin 6, which has been extensively studied as a potential plasma marker of major depression in non-stroke cohorts, was significantly elevated in patients with worse mood after stroke (P = .0325), «implicating a broadly overactive immune system in PSD.»
“We demonstrated for the first time that we can use plasma protein measurements to predict mood in people with chronic stroke,” Dr. Buckwalter summarized. “This means there is a biological correlate of mood but [it] doesn’t tell us causality.”
To tease out causality, the researchers used their own data, as well as information from a literature review of previous studies, to assemble a model of how the immune response following a stroke could change both serotonin and brain plasticity.
“We used the most highly correlated proteins to construct a beautiful mechanistic model of how poststroke depression may work and how it may relate to mechanisms in major depression,” Dr. Buckwalter said.
The model “posits an increased inflammatory response that leads to decreased tryptophan, serotonin, and less synaptic function, all of which contribute to symptoms of depression.”
Currently, selective serotonin reuptake inhibitors represent the “best treatment” for people with PSD, but “unfortunately they don’t work for many patients,” Dr. Buckwalter noted. The findings “provide clues as to other molecular targets that are candidates novel therapies for poststroke depression.”
Dr. Blake commented that the proteomic study “complements the work by us and others interested in understanding PSD.”
Mood disorders “must be understood in terms of the dynamic relationships between structural neurological alterations, cellular and microbiological changes, psychological processes, and the person’s interactions with their social landscape,” Dr. Blake said.
New Treatments on the Horizon?
Gustavo C. Medeiros, MD, assistant professor, Department of Psychiatry, of the University of Maryland School of Medicine, Baltimore, said that knowing which individuals are more likely to develop PSD “allows treatment teams to implement earlier and more intensive interventions in those who are at higher risk.”
The findings [of the proteomic study] may also “help clarify the neurobiological correlates of PSD…[which] may help the development of new treatments that target these neurobiological changes,” said Dr. Medeiros, who wasn’t involved with either study.
However, he warned, “we should interpret their results with caution due to methodological reasons, including the relatively small sample size.”
Also commenting, Bruce Ovbiagele, MD, MSc, MAS, MBA, MLS, professor of neurology, UCSF Weill Institute for Neurosciences, California, said the proteomic study has some “clear limitations,” including the lack of Black or African American patients in the cohort, which limits generalizability, “since we know that Black and African American people are disproportionately affected by stroke and have very high rates of PSD and very severe presentation.”
The study by Dr. Blake et al. “was interesting because the phenotype of depressive symptoms after stroke differs from what’s seen in the general population, and the authors figured out a way to better understand the nuances of such differences,” said Dr. Ovbiagele, who wasn’t involved with either study.
He said he was also surprised by the finding regarding anhedonia and suggested that the findings be replicated in a study directly comparing patients with PSD and patients with depression from the general population.
The study by Bidoki et al. was funded by AHA/Paul Allen Foundation, the Leducq Stroke-IMPaCT Transatlantic Network of Excellence (MSB), the Wu Tsai Neurosciences Institute (MSB), the Alfred E. Mann Foundation (NA), and an Alzheimer’s Association Research Fellowship to one of the authors. No source of funding was listed for the study by Dr. Blake et al. The authors of both studies, Dr. Medeiros and Dr. Ovbiagele, declare no relevant financial relationships.
A version of this article appeared on Medscape.com.
Alcohol and CV Risk: Both Beneficial and Harmful Effects?
with evidence emerging that alcohol use may both increase and decrease the risk for CVD.
The answer may depend on the presence of circulating metabolites of alcohol, some of which may be beneficial while others may be harmful, new research suggests.
“We adopted an association analysis, looking at 60 metabolites produced during or after alcohol has been metabolized, to see whether those metabolites can link alcohol consumption with CVD,” senior author Jiantao Ma, PhD, MBBS, assistant professor, Division of Nutrition Epidemiology and Data Science, Friedman School, Tufts University, Boston, Massachusetts, said in an interview.
“We found that the relationship is quite complex, with some metabolites showing protective effects against CVD and others showing harmful effects,” said Dr. Ma. “This opens the door for future research because we think that these molecules can help [us] understand the mechanism of the relationship between alcohol and CVD.”
The study was published online in BMC Medicine.
J-Shaped Relationship?
Previous research has painted a confusing picture of the relationship between alcohol consumption and CVD. For example, some studies have suggested that moderate levels of drinking may be hazardous to cardiac health, while others have pointed to potential cardioprotective effects.
Nevertheless, “according to the latest ACC/AHA guidelines regarding alcohol consumption and its relationship to CVD, there is no level of alcohol use that is deemed safe and considered acceptable,” Saurabh Sharma, MD, program director, Internal Medicine Residency Program, and clinical assistant professor of cardiology, Geisinger Commonwealth School of Medicine, Scranton, Pennsylvania, said in an interview.
Older observational data suggested a “J-shaped” relationship between alcohol consumption and cardiovascular risk, such that a low to moderate amount might reduce risk, while higher amounts increase it, said Dr. Sharma, a member of the American College of Cardiology (ACC) Prevention of Cardiovascular Diseases Council.
“But it’s essential to note that these findings were based on observational studies. No randomized controlled trials have provided conclusive evidence supporting the idea that moderate alcohol consumption actively reduces cardiovascular risk,” he said.
The current study is also observational, but it shines a somewhat different spotlight on the subject by examining alcohol consumption–related metabolites, said Dr. Ma — that is, small molecules that are the intermediates or end-products of metabolism in many cellular processes.
Some recent research “shows that alcohol may be harmful or at least has no beneficial effect in CVD prevention,” he said. “Our motivation was to analyze the association using metabolites, genetics, and epigenetics, because we think that these molecules may help us understand some of the mechanisms that underlie the relationship between alcohol consumption and CVD, and partially answer the question of whether alcohol may be harmful or helpful.”
Caution Warranted
Although some previous studies have looked at metabolites, most analyzed alcohol consumption measured at a single time point, “which may not represent habitual or long-term alcohol consumption,” the researchers note.
The team used data derived from 2458 Framingham Heart Study Offspring participants (mean age, 56 ± 9.3 years at the fifth examination; 52% female), calculating the cumulative average alcohol consumption from total intake of beer, wine, and liquor over an average 20-year period. Most participants were overweight, close to one fifth were current smokers, and 636 developed CVD over the study period.
Participants were assessed every 4-8 years, with metabolites measured during the fifth examination.
Linear models were used to investigate the association of alcohol consumption with 211 plasma metabolites, adjusting for a variety of potential confounders, including age, sex, batch, smoking, diet, physical activity, body mass index, and familial relationship.
Sixty metabolites associated with cumulative average alcohol consumption were identified (P < .00024), after adjustment for confounders. Of these, 40 displayed positive associations with the cumulative average alcohol consumption, with the most significant metabolite being cholesteryl palmitoleate (CE16:1), a plasma cholesteryl ester involved with cholesterol metabolism.
One gram per day of higher alcohol consumption was associated with a higher-level CE16:1 in the blood (b = .023). Several other phosphatidylcholine metabolites were also positively associated with alcohol consumption.
On the other hand, 20 metabolites were negatively associated with alcohol consumption, with triacylglycerol 54:4 (TAG 54:4) displaying the most significant association (b = –.017).
The alcoholic beverages were not equal when it came to association with metabolites: 19 metabolites were significantly associated with the cumulative average consumption of beer, 30 with wine, and 32 with liquor. Seven were significantly associated with the cumulative consumption of all three types of drinks.
The researchers conducted survival analysis that identified 10 alcohol-associated metabolites associated with differential CVD risks, after adjusting for confounders. They also built two alcohol consumption–weighted metabolite scores using these 10 metabolites. After adjustment for confounders including CVD risk factors, the two scores had “comparable but opposite” associations with incident CVD, HR 1.11 (95% CI, 1.02-1.21) vs 0.88 (0.78-0.98; both P values = .02).
“We found that seven metabolites were harmful, while three were beneficial, “ Dr. Ma reported.
Dr. Ma cautioned that association “doesn’t represent causation.” On the basis of the findings, however, “we can hypothesize that if you drink a moderate amount of alcohol, you can either increase or decrease your risk of CVD.”
For people with cardiac conditions, “it would be [wise to be] cautious in recommending alcohol consumption,” he said. “For people without cardiac conditions, I would follow the recommendations of the AHA. If people don’t already drink alcohol, we don’t recommend that you start drinking it; and if you already drink, we’d recommend keeping it minimal.”
He cautioned that this is “only one study and we need more research if we are to generate a clearer message to the patient.” At present, perhaps the best message to patients is “to be cautious and warn them that there are potentially harmful effects,” he said.
Mendelian Randomization?
Dr. Sharma, who was not involved in the study, emphasized that it’s “crucial” to recognize that the study “does not alter the established understanding that any level of alcohol consumption poses harm to the heart,” and that “any amount of alcohol consumption has the potential to elevate triglyceride levels, thereby contributing to the increased risk of cardiovascular complications.”
Previously reported cardioprotective benefits “are likely influenced by confounding factors, such as lifestyle and sociodemographic elements,” he speculated.
He noted that observational studies “encounter challenges in disentangling the influence of factors like obesity, lack of exercise, and tobacco use” as well as reverse causality.
“To overcome these limitations, Mendelian randomization emerges as a robust method,” he suggested. “This approach utilizes measured genetic variations with known functions to investigate the causal effect of a modifiable exposure on disease within the framework of observational studies.”
Notably, certain studies using this approach, including one by Larsson and colleagues, and another by Biddinger and associates, “have provided valuable insights by establishing a clear and causal relationship between alcohol consumption and CVD,” he said.
The study was funded by the National Institute of Health’s National Institute on Alcohol Abuse and Alcoholism. Data collection in the Framingham Heart Study was supported by the National Heart, Lung, and Blood Institute. Dr. Ma and coauthors and Dr. Sharma disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
with evidence emerging that alcohol use may both increase and decrease the risk for CVD.
The answer may depend on the presence of circulating metabolites of alcohol, some of which may be beneficial while others may be harmful, new research suggests.
“We adopted an association analysis, looking at 60 metabolites produced during or after alcohol has been metabolized, to see whether those metabolites can link alcohol consumption with CVD,” senior author Jiantao Ma, PhD, MBBS, assistant professor, Division of Nutrition Epidemiology and Data Science, Friedman School, Tufts University, Boston, Massachusetts, said in an interview.
“We found that the relationship is quite complex, with some metabolites showing protective effects against CVD and others showing harmful effects,” said Dr. Ma. “This opens the door for future research because we think that these molecules can help [us] understand the mechanism of the relationship between alcohol and CVD.”
The study was published online in BMC Medicine.
J-Shaped Relationship?
Previous research has painted a confusing picture of the relationship between alcohol consumption and CVD. For example, some studies have suggested that moderate levels of drinking may be hazardous to cardiac health, while others have pointed to potential cardioprotective effects.
Nevertheless, “according to the latest ACC/AHA guidelines regarding alcohol consumption and its relationship to CVD, there is no level of alcohol use that is deemed safe and considered acceptable,” Saurabh Sharma, MD, program director, Internal Medicine Residency Program, and clinical assistant professor of cardiology, Geisinger Commonwealth School of Medicine, Scranton, Pennsylvania, said in an interview.
Older observational data suggested a “J-shaped” relationship between alcohol consumption and cardiovascular risk, such that a low to moderate amount might reduce risk, while higher amounts increase it, said Dr. Sharma, a member of the American College of Cardiology (ACC) Prevention of Cardiovascular Diseases Council.
“But it’s essential to note that these findings were based on observational studies. No randomized controlled trials have provided conclusive evidence supporting the idea that moderate alcohol consumption actively reduces cardiovascular risk,” he said.
The current study is also observational, but it shines a somewhat different spotlight on the subject by examining alcohol consumption–related metabolites, said Dr. Ma — that is, small molecules that are the intermediates or end-products of metabolism in many cellular processes.
Some recent research “shows that alcohol may be harmful or at least has no beneficial effect in CVD prevention,” he said. “Our motivation was to analyze the association using metabolites, genetics, and epigenetics, because we think that these molecules may help us understand some of the mechanisms that underlie the relationship between alcohol consumption and CVD, and partially answer the question of whether alcohol may be harmful or helpful.”
Caution Warranted
Although some previous studies have looked at metabolites, most analyzed alcohol consumption measured at a single time point, “which may not represent habitual or long-term alcohol consumption,” the researchers note.
The team used data derived from 2458 Framingham Heart Study Offspring participants (mean age, 56 ± 9.3 years at the fifth examination; 52% female), calculating the cumulative average alcohol consumption from total intake of beer, wine, and liquor over an average 20-year period. Most participants were overweight, close to one fifth were current smokers, and 636 developed CVD over the study period.
Participants were assessed every 4-8 years, with metabolites measured during the fifth examination.
Linear models were used to investigate the association of alcohol consumption with 211 plasma metabolites, adjusting for a variety of potential confounders, including age, sex, batch, smoking, diet, physical activity, body mass index, and familial relationship.
Sixty metabolites associated with cumulative average alcohol consumption were identified (P < .00024), after adjustment for confounders. Of these, 40 displayed positive associations with the cumulative average alcohol consumption, with the most significant metabolite being cholesteryl palmitoleate (CE16:1), a plasma cholesteryl ester involved with cholesterol metabolism.
One gram per day of higher alcohol consumption was associated with a higher-level CE16:1 in the blood (b = .023). Several other phosphatidylcholine metabolites were also positively associated with alcohol consumption.
On the other hand, 20 metabolites were negatively associated with alcohol consumption, with triacylglycerol 54:4 (TAG 54:4) displaying the most significant association (b = –.017).
The alcoholic beverages were not equal when it came to association with metabolites: 19 metabolites were significantly associated with the cumulative average consumption of beer, 30 with wine, and 32 with liquor. Seven were significantly associated with the cumulative consumption of all three types of drinks.
The researchers conducted survival analysis that identified 10 alcohol-associated metabolites associated with differential CVD risks, after adjusting for confounders. They also built two alcohol consumption–weighted metabolite scores using these 10 metabolites. After adjustment for confounders including CVD risk factors, the two scores had “comparable but opposite” associations with incident CVD, HR 1.11 (95% CI, 1.02-1.21) vs 0.88 (0.78-0.98; both P values = .02).
“We found that seven metabolites were harmful, while three were beneficial, “ Dr. Ma reported.
Dr. Ma cautioned that association “doesn’t represent causation.” On the basis of the findings, however, “we can hypothesize that if you drink a moderate amount of alcohol, you can either increase or decrease your risk of CVD.”
For people with cardiac conditions, “it would be [wise to be] cautious in recommending alcohol consumption,” he said. “For people without cardiac conditions, I would follow the recommendations of the AHA. If people don’t already drink alcohol, we don’t recommend that you start drinking it; and if you already drink, we’d recommend keeping it minimal.”
He cautioned that this is “only one study and we need more research if we are to generate a clearer message to the patient.” At present, perhaps the best message to patients is “to be cautious and warn them that there are potentially harmful effects,” he said.
Mendelian Randomization?
Dr. Sharma, who was not involved in the study, emphasized that it’s “crucial” to recognize that the study “does not alter the established understanding that any level of alcohol consumption poses harm to the heart,” and that “any amount of alcohol consumption has the potential to elevate triglyceride levels, thereby contributing to the increased risk of cardiovascular complications.”
Previously reported cardioprotective benefits “are likely influenced by confounding factors, such as lifestyle and sociodemographic elements,” he speculated.
He noted that observational studies “encounter challenges in disentangling the influence of factors like obesity, lack of exercise, and tobacco use” as well as reverse causality.
“To overcome these limitations, Mendelian randomization emerges as a robust method,” he suggested. “This approach utilizes measured genetic variations with known functions to investigate the causal effect of a modifiable exposure on disease within the framework of observational studies.”
Notably, certain studies using this approach, including one by Larsson and colleagues, and another by Biddinger and associates, “have provided valuable insights by establishing a clear and causal relationship between alcohol consumption and CVD,” he said.
The study was funded by the National Institute of Health’s National Institute on Alcohol Abuse and Alcoholism. Data collection in the Framingham Heart Study was supported by the National Heart, Lung, and Blood Institute. Dr. Ma and coauthors and Dr. Sharma disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
with evidence emerging that alcohol use may both increase and decrease the risk for CVD.
The answer may depend on the presence of circulating metabolites of alcohol, some of which may be beneficial while others may be harmful, new research suggests.
“We adopted an association analysis, looking at 60 metabolites produced during or after alcohol has been metabolized, to see whether those metabolites can link alcohol consumption with CVD,” senior author Jiantao Ma, PhD, MBBS, assistant professor, Division of Nutrition Epidemiology and Data Science, Friedman School, Tufts University, Boston, Massachusetts, said in an interview.
“We found that the relationship is quite complex, with some metabolites showing protective effects against CVD and others showing harmful effects,” said Dr. Ma. “This opens the door for future research because we think that these molecules can help [us] understand the mechanism of the relationship between alcohol and CVD.”
The study was published online in BMC Medicine.
J-Shaped Relationship?
Previous research has painted a confusing picture of the relationship between alcohol consumption and CVD. For example, some studies have suggested that moderate levels of drinking may be hazardous to cardiac health, while others have pointed to potential cardioprotective effects.
Nevertheless, “according to the latest ACC/AHA guidelines regarding alcohol consumption and its relationship to CVD, there is no level of alcohol use that is deemed safe and considered acceptable,” Saurabh Sharma, MD, program director, Internal Medicine Residency Program, and clinical assistant professor of cardiology, Geisinger Commonwealth School of Medicine, Scranton, Pennsylvania, said in an interview.
Older observational data suggested a “J-shaped” relationship between alcohol consumption and cardiovascular risk, such that a low to moderate amount might reduce risk, while higher amounts increase it, said Dr. Sharma, a member of the American College of Cardiology (ACC) Prevention of Cardiovascular Diseases Council.
“But it’s essential to note that these findings were based on observational studies. No randomized controlled trials have provided conclusive evidence supporting the idea that moderate alcohol consumption actively reduces cardiovascular risk,” he said.
The current study is also observational, but it shines a somewhat different spotlight on the subject by examining alcohol consumption–related metabolites, said Dr. Ma — that is, small molecules that are the intermediates or end-products of metabolism in many cellular processes.
Some recent research “shows that alcohol may be harmful or at least has no beneficial effect in CVD prevention,” he said. “Our motivation was to analyze the association using metabolites, genetics, and epigenetics, because we think that these molecules may help us understand some of the mechanisms that underlie the relationship between alcohol consumption and CVD, and partially answer the question of whether alcohol may be harmful or helpful.”
Caution Warranted
Although some previous studies have looked at metabolites, most analyzed alcohol consumption measured at a single time point, “which may not represent habitual or long-term alcohol consumption,” the researchers note.
The team used data derived from 2458 Framingham Heart Study Offspring participants (mean age, 56 ± 9.3 years at the fifth examination; 52% female), calculating the cumulative average alcohol consumption from total intake of beer, wine, and liquor over an average 20-year period. Most participants were overweight, close to one fifth were current smokers, and 636 developed CVD over the study period.
Participants were assessed every 4-8 years, with metabolites measured during the fifth examination.
Linear models were used to investigate the association of alcohol consumption with 211 plasma metabolites, adjusting for a variety of potential confounders, including age, sex, batch, smoking, diet, physical activity, body mass index, and familial relationship.
Sixty metabolites associated with cumulative average alcohol consumption were identified (P < .00024), after adjustment for confounders. Of these, 40 displayed positive associations with the cumulative average alcohol consumption, with the most significant metabolite being cholesteryl palmitoleate (CE16:1), a plasma cholesteryl ester involved with cholesterol metabolism.
One gram per day of higher alcohol consumption was associated with a higher-level CE16:1 in the blood (b = .023). Several other phosphatidylcholine metabolites were also positively associated with alcohol consumption.
On the other hand, 20 metabolites were negatively associated with alcohol consumption, with triacylglycerol 54:4 (TAG 54:4) displaying the most significant association (b = –.017).
The alcoholic beverages were not equal when it came to association with metabolites: 19 metabolites were significantly associated with the cumulative average consumption of beer, 30 with wine, and 32 with liquor. Seven were significantly associated with the cumulative consumption of all three types of drinks.
The researchers conducted survival analysis that identified 10 alcohol-associated metabolites associated with differential CVD risks, after adjusting for confounders. They also built two alcohol consumption–weighted metabolite scores using these 10 metabolites. After adjustment for confounders including CVD risk factors, the two scores had “comparable but opposite” associations with incident CVD, HR 1.11 (95% CI, 1.02-1.21) vs 0.88 (0.78-0.98; both P values = .02).
“We found that seven metabolites were harmful, while three were beneficial, “ Dr. Ma reported.
Dr. Ma cautioned that association “doesn’t represent causation.” On the basis of the findings, however, “we can hypothesize that if you drink a moderate amount of alcohol, you can either increase or decrease your risk of CVD.”
For people with cardiac conditions, “it would be [wise to be] cautious in recommending alcohol consumption,” he said. “For people without cardiac conditions, I would follow the recommendations of the AHA. If people don’t already drink alcohol, we don’t recommend that you start drinking it; and if you already drink, we’d recommend keeping it minimal.”
He cautioned that this is “only one study and we need more research if we are to generate a clearer message to the patient.” At present, perhaps the best message to patients is “to be cautious and warn them that there are potentially harmful effects,” he said.
Mendelian Randomization?
Dr. Sharma, who was not involved in the study, emphasized that it’s “crucial” to recognize that the study “does not alter the established understanding that any level of alcohol consumption poses harm to the heart,” and that “any amount of alcohol consumption has the potential to elevate triglyceride levels, thereby contributing to the increased risk of cardiovascular complications.”
Previously reported cardioprotective benefits “are likely influenced by confounding factors, such as lifestyle and sociodemographic elements,” he speculated.
He noted that observational studies “encounter challenges in disentangling the influence of factors like obesity, lack of exercise, and tobacco use” as well as reverse causality.
“To overcome these limitations, Mendelian randomization emerges as a robust method,” he suggested. “This approach utilizes measured genetic variations with known functions to investigate the causal effect of a modifiable exposure on disease within the framework of observational studies.”
Notably, certain studies using this approach, including one by Larsson and colleagues, and another by Biddinger and associates, “have provided valuable insights by establishing a clear and causal relationship between alcohol consumption and CVD,” he said.
The study was funded by the National Institute of Health’s National Institute on Alcohol Abuse and Alcoholism. Data collection in the Framingham Heart Study was supported by the National Heart, Lung, and Blood Institute. Dr. Ma and coauthors and Dr. Sharma disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM BMC MEDICINE
Do patients follow up on referrals after telehealth visits?
Telehealth has been a boon for modern-day patients, allowing people who might have difficulty accessing in-person appointments to continue seeing their physicians. But how many patients actually follow through on their physician’s recommendations afterward?
A new study suggests that
Investigators retrospectively examined test and referral orders for more than 4,000 patients to see how many complied with recommendations to have a colonoscopy, consult a dermatologist for a suspicious skin lesion, or undergo a cardiac stress test.
Completion of a recommended test or specialty referral was termed “diagnostic loop closure.” In particular, the researchers wanted to compare loop closure after telehealth versus in-person visits.
Rates of loop closure were low across all visit modalities but were lower for tests and referrals ordered during telehealth visits, compared with in-person visits – especially for colonoscopies.
“The take-home message for practicing clinicians is that they should be especially aware of follow-up for tests or referrals ordered during telehealth visits,” said corresponding author Maëlys Amat, MD, MBA, a primary care physician at Healthcare Associates, Beth Israel Deaconess Medical Center, Boston.
The study was published online on in JAMA Network Open.
‘Unintended side effects’
“Diagnostic errors present a huge safety concern, impacting many patient lives and costing the health care system billions of dollars, said Dr. Amat, who is also an instructor at Harvard Medical School.
“Telehealth utilization increased rapidly during the COVID pandemic, and although there are clear benefits to utilizing telehealth, our team sought to investigate unintended side effects of this technology and highlight opportunities for improvement,” she said.
To investigate the question, the researchers reviewed medical records of 4,113 patients, with a mean age of 59 years, at two Boston-based primary care sites: an urban hospital–based primary care practice and an affiliated community health center.
Orders for tests or referrals in both centers were placed electronically through the medical record. During an in-person visit, the patient was handed a form with a phone number to call to schedule the test or referral. Patients with limited English proficiency or complex needs may have received help with the scheduling the referral during check-out.
For telehealth visits, the clinician gave the patient the phone number to call to schedule the test or referral during the visit itself. In all scenarios, patients did not receive communication after the visit reminding them about the referral or test.
A loop was considered “closed” if the orders were completed within 365 days, 90 days, or 45 days for colonoscopy, dermatology visits, or cardiac stress testing, respectively.
Of the tests, 52.4% were ordered during an in-person visit, 27.8% were ordered during a telehealth visit, and 19.7% were ordered without a visit.
Tracking systems, virtual checkout
Fewer than half of the orders (42.6%) placed during a telehealth visit were completed within the designated time frame, compared with 58.4% of the orders placed during an in-person visit and 57.4% placed without a visit.
Patients who had telehealth visits were roughly half as likely as those who had in-person visits to close the loop on high-risk tests and referrals, even in an analysis that adjusted for test type, patient demographic characteristics, comorbidities, clinical site, clinician type, and patient engagement (odds ratio, 0.55; 95% confidence interval, 0.47-0.64).
Only 39.8% of colonoscopy referrals ordered during a telehealth visit were completed during the 365-day time period, compared with 56.9% ordered during an in-person visit and 56.7% ordered without a visit.
Follow-through with dermatology referrals within 90 days was roughly the same across all types of visits (63.1% for telehealth, 61.5% for in-person, and 62.9% for no visit). No significant differences were found between telehealth and in-person visits or orders placed without a visit.
Although patients seen via telehealth were less likely than those seen in person to follow through on cardiac stress tests within the 45-day window (59.1% vs. 63.2%), this difference didn’t reach statistical significance.
“Ideally, clinicians would implement automatic tracking systems to help ensure that an ordered test or referral is completed,” Dr. Amat commented. “However, if these systems aren’t yet in place, we strongly encourage clinicians to create their own work flows for tracking tests to completion.”
Additionally, “clinicians should consider implementing a virtual checkout system, similar to what is done during in-person visits, to help patients better understand recommended next steps,” she continued.
Other potentially helpful ways to improve loop closure include automatic tracking for outstanding tests, interventions such as telephone outreach to patients, automated text and email reminders, and the use of referral managers – especially in remote, rural areas or for “disadvantaged patients with limited health care access and literacy.”
Education is key
Kisha Davis, MD, MPH, member of the board of directors of the American Academy of Family Physicians, said in an interview that being able to see a provider virtually can make the difference between a person receiving or not receiving medical care. She regards telehealth as another tool in the toolkit her practice offers to provide comprehensive health care.
Dr. Davis, a family physician in Gaithersburg, Md., who wasn’t involved with the study, described a patient with hypertension who was an Uber driver. “During the pandemic, Uber rides were down, and he couldn›t afford to pass up any opportunities, so he pulled over to the side of the road after one of his rides, did his telehealth visit, reviewed his medications, and went on to his next ride.”
The key is to make sure that patients receive adequate follow-up from the office, which Dr. Davis arranged for this patient.
She noted that telehealth “is best done if there’s an established physician-patient relationship but harder to accomplish successfully if you’ve only met the patient on telehealth and never in person.”
The study didn’t specify whether the physicians had an established relationship with their patients.
During the checkout process after an in-person appointment, patients often receive a sheet of paper with the follow-up referrals. “I can see where patients are less likely to follow through if they don’t have someone handing them that paper,” she said.
In her practice, patients’ charts are color-coded “to keep track and make sure it’s not just the ‘squeaky wheels’ that get all the attention,” she said. “The onus is on the physician and the practice, in today’s world of value-based care, to make sure that patients who don’t come into the office are getting the care they need.”
This is facilitated by a “system of care coordination” in which the office team – such as a nurse or medical assistant – follows up with patients to see if they’ve “gotten everything done without barriers,” Dr. Davis said. “Did they have trouble filling that prescription? Did they have difficulty with the referral? Or do they not think it’s necessary – for example, a patient might not go to physical therapy because the injury has improved.”
Dr. Davis wasn’t surprised that patients were less likely to close the loop for colonoscopies compared with seeking out a stress test or treatment for skin lesions.
“People who have a skin lesion may be concerned about their appearance or about skin cancer, and people who need a stress test may have had cardiac symptoms or be worried about their heart.” But a routine screening such as a colonoscopy may not mobilize the patient’s concern to the same degree.
“Additionally, a colonoscopy has an ‘ick factor,’ so there aren’t a whole lot of people who are jumping to have the procedure done.” She suggested considering newer FDA-approved stool tests to screen for colon cancer.
Dr. Amat and Dr. Davis both emphasized that educating patients – both during and after the visit – and making sure they understand the importance of their referral for tests or specialists referrals are key to ensuring that they follow through on the recommendations.
The study was funded by the Agency for Healthcare Research and Quality. Dr. Amat was supported by the Arnold Tofias and Leo Condakes Quality Scholarship Program. Dr. Amat declared no relevant financial relationships. Dr. Davis is the chief health officer for Montgomery County in Maryland.
A version of this article first appeared on Medscape.com.
Telehealth has been a boon for modern-day patients, allowing people who might have difficulty accessing in-person appointments to continue seeing their physicians. But how many patients actually follow through on their physician’s recommendations afterward?
A new study suggests that
Investigators retrospectively examined test and referral orders for more than 4,000 patients to see how many complied with recommendations to have a colonoscopy, consult a dermatologist for a suspicious skin lesion, or undergo a cardiac stress test.
Completion of a recommended test or specialty referral was termed “diagnostic loop closure.” In particular, the researchers wanted to compare loop closure after telehealth versus in-person visits.
Rates of loop closure were low across all visit modalities but were lower for tests and referrals ordered during telehealth visits, compared with in-person visits – especially for colonoscopies.
“The take-home message for practicing clinicians is that they should be especially aware of follow-up for tests or referrals ordered during telehealth visits,” said corresponding author Maëlys Amat, MD, MBA, a primary care physician at Healthcare Associates, Beth Israel Deaconess Medical Center, Boston.
The study was published online on in JAMA Network Open.
‘Unintended side effects’
“Diagnostic errors present a huge safety concern, impacting many patient lives and costing the health care system billions of dollars, said Dr. Amat, who is also an instructor at Harvard Medical School.
“Telehealth utilization increased rapidly during the COVID pandemic, and although there are clear benefits to utilizing telehealth, our team sought to investigate unintended side effects of this technology and highlight opportunities for improvement,” she said.
To investigate the question, the researchers reviewed medical records of 4,113 patients, with a mean age of 59 years, at two Boston-based primary care sites: an urban hospital–based primary care practice and an affiliated community health center.
Orders for tests or referrals in both centers were placed electronically through the medical record. During an in-person visit, the patient was handed a form with a phone number to call to schedule the test or referral. Patients with limited English proficiency or complex needs may have received help with the scheduling the referral during check-out.
For telehealth visits, the clinician gave the patient the phone number to call to schedule the test or referral during the visit itself. In all scenarios, patients did not receive communication after the visit reminding them about the referral or test.
A loop was considered “closed” if the orders were completed within 365 days, 90 days, or 45 days for colonoscopy, dermatology visits, or cardiac stress testing, respectively.
Of the tests, 52.4% were ordered during an in-person visit, 27.8% were ordered during a telehealth visit, and 19.7% were ordered without a visit.
Tracking systems, virtual checkout
Fewer than half of the orders (42.6%) placed during a telehealth visit were completed within the designated time frame, compared with 58.4% of the orders placed during an in-person visit and 57.4% placed without a visit.
Patients who had telehealth visits were roughly half as likely as those who had in-person visits to close the loop on high-risk tests and referrals, even in an analysis that adjusted for test type, patient demographic characteristics, comorbidities, clinical site, clinician type, and patient engagement (odds ratio, 0.55; 95% confidence interval, 0.47-0.64).
Only 39.8% of colonoscopy referrals ordered during a telehealth visit were completed during the 365-day time period, compared with 56.9% ordered during an in-person visit and 56.7% ordered without a visit.
Follow-through with dermatology referrals within 90 days was roughly the same across all types of visits (63.1% for telehealth, 61.5% for in-person, and 62.9% for no visit). No significant differences were found between telehealth and in-person visits or orders placed without a visit.
Although patients seen via telehealth were less likely than those seen in person to follow through on cardiac stress tests within the 45-day window (59.1% vs. 63.2%), this difference didn’t reach statistical significance.
“Ideally, clinicians would implement automatic tracking systems to help ensure that an ordered test or referral is completed,” Dr. Amat commented. “However, if these systems aren’t yet in place, we strongly encourage clinicians to create their own work flows for tracking tests to completion.”
Additionally, “clinicians should consider implementing a virtual checkout system, similar to what is done during in-person visits, to help patients better understand recommended next steps,” she continued.
Other potentially helpful ways to improve loop closure include automatic tracking for outstanding tests, interventions such as telephone outreach to patients, automated text and email reminders, and the use of referral managers – especially in remote, rural areas or for “disadvantaged patients with limited health care access and literacy.”
Education is key
Kisha Davis, MD, MPH, member of the board of directors of the American Academy of Family Physicians, said in an interview that being able to see a provider virtually can make the difference between a person receiving or not receiving medical care. She regards telehealth as another tool in the toolkit her practice offers to provide comprehensive health care.
Dr. Davis, a family physician in Gaithersburg, Md., who wasn’t involved with the study, described a patient with hypertension who was an Uber driver. “During the pandemic, Uber rides were down, and he couldn›t afford to pass up any opportunities, so he pulled over to the side of the road after one of his rides, did his telehealth visit, reviewed his medications, and went on to his next ride.”
The key is to make sure that patients receive adequate follow-up from the office, which Dr. Davis arranged for this patient.
She noted that telehealth “is best done if there’s an established physician-patient relationship but harder to accomplish successfully if you’ve only met the patient on telehealth and never in person.”
The study didn’t specify whether the physicians had an established relationship with their patients.
During the checkout process after an in-person appointment, patients often receive a sheet of paper with the follow-up referrals. “I can see where patients are less likely to follow through if they don’t have someone handing them that paper,” she said.
In her practice, patients’ charts are color-coded “to keep track and make sure it’s not just the ‘squeaky wheels’ that get all the attention,” she said. “The onus is on the physician and the practice, in today’s world of value-based care, to make sure that patients who don’t come into the office are getting the care they need.”
This is facilitated by a “system of care coordination” in which the office team – such as a nurse or medical assistant – follows up with patients to see if they’ve “gotten everything done without barriers,” Dr. Davis said. “Did they have trouble filling that prescription? Did they have difficulty with the referral? Or do they not think it’s necessary – for example, a patient might not go to physical therapy because the injury has improved.”
Dr. Davis wasn’t surprised that patients were less likely to close the loop for colonoscopies compared with seeking out a stress test or treatment for skin lesions.
“People who have a skin lesion may be concerned about their appearance or about skin cancer, and people who need a stress test may have had cardiac symptoms or be worried about their heart.” But a routine screening such as a colonoscopy may not mobilize the patient’s concern to the same degree.
“Additionally, a colonoscopy has an ‘ick factor,’ so there aren’t a whole lot of people who are jumping to have the procedure done.” She suggested considering newer FDA-approved stool tests to screen for colon cancer.
Dr. Amat and Dr. Davis both emphasized that educating patients – both during and after the visit – and making sure they understand the importance of their referral for tests or specialists referrals are key to ensuring that they follow through on the recommendations.
The study was funded by the Agency for Healthcare Research and Quality. Dr. Amat was supported by the Arnold Tofias and Leo Condakes Quality Scholarship Program. Dr. Amat declared no relevant financial relationships. Dr. Davis is the chief health officer for Montgomery County in Maryland.
A version of this article first appeared on Medscape.com.
Telehealth has been a boon for modern-day patients, allowing people who might have difficulty accessing in-person appointments to continue seeing their physicians. But how many patients actually follow through on their physician’s recommendations afterward?
A new study suggests that
Investigators retrospectively examined test and referral orders for more than 4,000 patients to see how many complied with recommendations to have a colonoscopy, consult a dermatologist for a suspicious skin lesion, or undergo a cardiac stress test.
Completion of a recommended test or specialty referral was termed “diagnostic loop closure.” In particular, the researchers wanted to compare loop closure after telehealth versus in-person visits.
Rates of loop closure were low across all visit modalities but were lower for tests and referrals ordered during telehealth visits, compared with in-person visits – especially for colonoscopies.
“The take-home message for practicing clinicians is that they should be especially aware of follow-up for tests or referrals ordered during telehealth visits,” said corresponding author Maëlys Amat, MD, MBA, a primary care physician at Healthcare Associates, Beth Israel Deaconess Medical Center, Boston.
The study was published online on in JAMA Network Open.
‘Unintended side effects’
“Diagnostic errors present a huge safety concern, impacting many patient lives and costing the health care system billions of dollars, said Dr. Amat, who is also an instructor at Harvard Medical School.
“Telehealth utilization increased rapidly during the COVID pandemic, and although there are clear benefits to utilizing telehealth, our team sought to investigate unintended side effects of this technology and highlight opportunities for improvement,” she said.
To investigate the question, the researchers reviewed medical records of 4,113 patients, with a mean age of 59 years, at two Boston-based primary care sites: an urban hospital–based primary care practice and an affiliated community health center.
Orders for tests or referrals in both centers were placed electronically through the medical record. During an in-person visit, the patient was handed a form with a phone number to call to schedule the test or referral. Patients with limited English proficiency or complex needs may have received help with the scheduling the referral during check-out.
For telehealth visits, the clinician gave the patient the phone number to call to schedule the test or referral during the visit itself. In all scenarios, patients did not receive communication after the visit reminding them about the referral or test.
A loop was considered “closed” if the orders were completed within 365 days, 90 days, or 45 days for colonoscopy, dermatology visits, or cardiac stress testing, respectively.
Of the tests, 52.4% were ordered during an in-person visit, 27.8% were ordered during a telehealth visit, and 19.7% were ordered without a visit.
Tracking systems, virtual checkout
Fewer than half of the orders (42.6%) placed during a telehealth visit were completed within the designated time frame, compared with 58.4% of the orders placed during an in-person visit and 57.4% placed without a visit.
Patients who had telehealth visits were roughly half as likely as those who had in-person visits to close the loop on high-risk tests and referrals, even in an analysis that adjusted for test type, patient demographic characteristics, comorbidities, clinical site, clinician type, and patient engagement (odds ratio, 0.55; 95% confidence interval, 0.47-0.64).
Only 39.8% of colonoscopy referrals ordered during a telehealth visit were completed during the 365-day time period, compared with 56.9% ordered during an in-person visit and 56.7% ordered without a visit.
Follow-through with dermatology referrals within 90 days was roughly the same across all types of visits (63.1% for telehealth, 61.5% for in-person, and 62.9% for no visit). No significant differences were found between telehealth and in-person visits or orders placed without a visit.
Although patients seen via telehealth were less likely than those seen in person to follow through on cardiac stress tests within the 45-day window (59.1% vs. 63.2%), this difference didn’t reach statistical significance.
“Ideally, clinicians would implement automatic tracking systems to help ensure that an ordered test or referral is completed,” Dr. Amat commented. “However, if these systems aren’t yet in place, we strongly encourage clinicians to create their own work flows for tracking tests to completion.”
Additionally, “clinicians should consider implementing a virtual checkout system, similar to what is done during in-person visits, to help patients better understand recommended next steps,” she continued.
Other potentially helpful ways to improve loop closure include automatic tracking for outstanding tests, interventions such as telephone outreach to patients, automated text and email reminders, and the use of referral managers – especially in remote, rural areas or for “disadvantaged patients with limited health care access and literacy.”
Education is key
Kisha Davis, MD, MPH, member of the board of directors of the American Academy of Family Physicians, said in an interview that being able to see a provider virtually can make the difference between a person receiving or not receiving medical care. She regards telehealth as another tool in the toolkit her practice offers to provide comprehensive health care.
Dr. Davis, a family physician in Gaithersburg, Md., who wasn’t involved with the study, described a patient with hypertension who was an Uber driver. “During the pandemic, Uber rides were down, and he couldn›t afford to pass up any opportunities, so he pulled over to the side of the road after one of his rides, did his telehealth visit, reviewed his medications, and went on to his next ride.”
The key is to make sure that patients receive adequate follow-up from the office, which Dr. Davis arranged for this patient.
She noted that telehealth “is best done if there’s an established physician-patient relationship but harder to accomplish successfully if you’ve only met the patient on telehealth and never in person.”
The study didn’t specify whether the physicians had an established relationship with their patients.
During the checkout process after an in-person appointment, patients often receive a sheet of paper with the follow-up referrals. “I can see where patients are less likely to follow through if they don’t have someone handing them that paper,” she said.
In her practice, patients’ charts are color-coded “to keep track and make sure it’s not just the ‘squeaky wheels’ that get all the attention,” she said. “The onus is on the physician and the practice, in today’s world of value-based care, to make sure that patients who don’t come into the office are getting the care they need.”
This is facilitated by a “system of care coordination” in which the office team – such as a nurse or medical assistant – follows up with patients to see if they’ve “gotten everything done without barriers,” Dr. Davis said. “Did they have trouble filling that prescription? Did they have difficulty with the referral? Or do they not think it’s necessary – for example, a patient might not go to physical therapy because the injury has improved.”
Dr. Davis wasn’t surprised that patients were less likely to close the loop for colonoscopies compared with seeking out a stress test or treatment for skin lesions.
“People who have a skin lesion may be concerned about their appearance or about skin cancer, and people who need a stress test may have had cardiac symptoms or be worried about their heart.” But a routine screening such as a colonoscopy may not mobilize the patient’s concern to the same degree.
“Additionally, a colonoscopy has an ‘ick factor,’ so there aren’t a whole lot of people who are jumping to have the procedure done.” She suggested considering newer FDA-approved stool tests to screen for colon cancer.
Dr. Amat and Dr. Davis both emphasized that educating patients – both during and after the visit – and making sure they understand the importance of their referral for tests or specialists referrals are key to ensuring that they follow through on the recommendations.
The study was funded by the Agency for Healthcare Research and Quality. Dr. Amat was supported by the Arnold Tofias and Leo Condakes Quality Scholarship Program. Dr. Amat declared no relevant financial relationships. Dr. Davis is the chief health officer for Montgomery County in Maryland.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Before signing an offer letter: Read this
You’ve just received an offer letter from that job you interviewed for. Sometimes you want to let the employer know right away how interested you are. The verbiage says the letter isn’t “binding.” So you eagerly sign on the dotted line. Everything looks great ... until it isn’t.
Attorney Ericka Adler, JD, LLM, a partner at Roetzel & Andress, a Chicago-based law firm that represents physicians and health care professionals nationwide, described her client who was in this predicament. The physician, a dermatologist, left a practice where she had been employed because she had received an “amazing” offer letter that included promises about her new work location, staffing, equipment, and hours. She signed and immediately gave notice to her previous employer.
“When she received the actual employment contract, none of those details from the offer letter – which is also called a letter of intent [LOI] – were included,” Ms. Adler told this news organization. The physician wanted to have the details from the LOI formally spelled out in the contract, but the employer refused.
“Basically, they said, ‘This is our standard contract and you’ll just have to trust us that we’ll keep our word. We meant what we said in the LOI, but we cannot include those details in the actual agreement because everyone has the same form of agreement.’ “ The physician decided to sign the contract and accept the position.
She contacted Ms. Adler after she had been at her new position for a month. “She had received none of the things they had promised her in the LOI,” Ms. Adler reported. “She lacked the NP and PA support, she lacked the equipment, she didn’t have enough exam rooms. As soon as she started, someone with whom she was sharing call coverage left, and she was expected to take over. The LOI had a cap on the amount of call she would be required to take, but that verbiage didn’t make it into the contract.”
Ms. Adler tried to address this issue with the employer. “We couldn’t say they had literally breached the agreement, but we did list the things that were mentioned in the LOI but on which they hadn’t delivered. We asked them to fix the issue within 10 days.”
The employer argued “that they didn’t have to fulfill anything that wasn’t spelled out in the contract, even if it was in the LOI. In fact, the contract specified clearly that the signed employment agreement was the only agreement and replaced any previous written or oral agreements between the parties.”
The dermatologist ultimately left the new position. “She might have been able to have a legal claim against the employer for breach or perhaps ‘detrimental reliance’ – meaning, she might have argued that she had been financially harmed due to the false promises made to her. But it would have been difficult and expensive for her to litigate the issue,” said Ms. Adler.
“It also didn’t seem like the physician could remain in the job and develop a positive work relationship with the employer, given that she felt betrayed and misled, and didn’t like the terms of employment, which didn’t match her needs or expectations,” said Ms. Adler.
She added that “most employers are not as unscrupulous and dishonest as this one was. But some employers do play on the fact that younger doctors – especially residents and fellows – tend to be trusting or feel they don’t have negotiation power. They’re often excited to get an offer and sign it without a second thought.”
That’s why she advises physicians to “review the terms of the LOI carefully and make sure you’re comfortable with them before signing it; but know that the real contract to negotiate will be the actual Employment Agreement.”
She also advises physicians not to give notice at their current place of employment until they’ve signed the final contract with the new employer.
On the same page?
Anu Murthy, JD, an attorney and associate contract review specialist at Contract Diagnostics, explained that the LOI is a document that the candidate receives after an interview but before a full contract. Sometimes, the LOI is preceded by a verbal or e-mailed offer, which is less formal.
“An LOI is sometimes called a Term Sheet or Memorandum of Understanding,“ Ms. Murthy told this news organization. “Typically, it lays out key provisions, such as compensation, initial term of the contract, location, and recruitment incentives.” Sometimes it includes mention of staffing, call schedule, malpractice, noncompete covenants, and other components of the position.
Justin Nabity, founder and CEO of Physicians Thrive, a physician financial advisory group, said that LOIs are “a way for employers to gauge a prospective employee’s level of interest.”
The employer “doesn’t want to send a contract with a lot of details before determining whether the candidate is really serious about the position, so the offer letter doesn’t show the whole picture,” Mr. Nabity told this news organization.
Dennis Hursh, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, agreed.
“Another way of putting it is that the employer wants to see whether the prospective employee is on the same page. The LOI will typically include some key components that will later appear in a more complete and formal contract, together with other topics and details. Agreeing to those key components signals that indeed you and the employer are in accord,” said Mr. Hursh.
But are you really on the same page with your prospective employer? And if you seem to be on the same page, and you sign the LOI, is that a guarantee that the employer will honor its terms?
Not necessarily, according to the experts. In fact, many LOIs contain some verbiage stating that the letter isn’t binding, which can be confusing. Others suggest that it is binding, but the candidate doesn’t realize that the letter isn’t a formal contract and that the contract may contain details not included in the LOI or may omit details mentioned in the LOI, as happened to Ms. Adler’s unfortunate client.
“One of the pitfalls I see is that doctors sign the LOI without recognizing whether it’s binding or nonbinding,” Ms. Murthy said. “If it’s binding, it creates a legal obligation on your part and could preclude you from further negotiation once you see the contract and feel you’d like to negotiate some of its terms.”
Binding letters are typically offered to candidates after some back-and-forth between the parties, and important terms have been agreed to, which can happen either verbally or via e-mail. Once these agreements have been reached, they’re summarized in a “binding” letter before being extended into a full contract.
“But even if you’ve agreed on the terms verbally, it’s still important to have someone more experienced review the offer letter before signing it,” Ms. Murthy said. “It’s important to understand the ‘legalese’ and what your rights and obligations are before agreeing to anything.”
And certainly, if you receive a binding LOI, you shouldn’t sign anything until you’re sure you’re comfortable with its contents and have more details.
Are “nonbinding” LOIs really not binding?
Even if the LOI is nonbinding, that doesn’t necessarily mean you can sign it and expect to negotiate later. “I see people tripped up when they sign the LOI, thinking they’ll negotiate later,” said Mr. Hursh. “They may not like the terms – for example, they think the compensation is too low – and they figure they’ll work it out at the contract stage, because the LOI is ‘not legally binding.’ “
But because the candidate signed the LOI, “the employer is under the impression that the compensation was acceptable, so now you’ve tied your hands – and the hands of any attorney you may consult down the road – to negotiate those terms.”
Mr. Hursh said he is often consulted by physicians who signed the contract “to get the ball rolling,” thinking that the LOI was “just a meaningless bureaucratic paper.” They need to understand “that the employer wants to make sure they’re in agreement on the basic points before getting into the details,” he said. “Large hospitals with in-house counsel may not want to use their legal department’s valuable time in redrafting terms they thought were acceptable to the candidate, and most practices don’t want to pay a lawyer to draft an LOI and then come back and say, ‘Actually, the physician wants more compensation.’ “
Mr. Nabity summarized: “The LOI is essentially a negotiation tactic to take some of the cards out of the hands of the doctor and commit him or her to something they’re not ready to commit to.” Employers may be playing on the sense of pressure and candidate’s fear that the job will slip through their fingers if they wait too long to sign. “But it’s better to wait longer at this stage before signing even a nonbinding LOI,” he said.
What to do before signing
So how should physicians relate to the LOI? Mr. Nabity advises “working through the details of the offer letter first, going through it carefully and identifying areas of concern, bearing in mind that employers never begin with their best offer.”
He pointed out that physicians “rarely know their value and usually don’t know how to work through the dynamics of compensation, call schedules, additional incentives, bonuses, and productivity,” so they need to be informed about these areas before signing anything.
Ms. Murthy recommended “going back and saying [to the prospective employer], ‘Thank you, but I need time to consider and evaluate this offer.’ Then, do some due diligence.”
At that point, you can hire an attorney to go over the offer, educate yourself about compensation benchmarks and what your worth actually is, or consult another trained professional or more experienced individual who can review the LOI before you sign it.
That’s what Dominique Cleveland, MD, a Texas-based ob.gyn., did when she received an LOI 5 years ago.
“The offer letter from the group practice contained a statement that the group wanted me to come on board, what the salary would be, and the time frame that would be covered in the contract,” she told this news organization. “It mentioned benefits and incentives and relocation, but it was only a short document – maybe one or two pages long.”
At the time that she received her LOI, Dr. Cleveland was completing her residency. She consulted experienced faculty members from her institution to find out whether the terms laid out in the LOI “were the norm and were reasonable.” She was “fairly certain” that the salary was low and this was confirmed by the faculty members she talked to. “So I felt comfortable asking for more [compensation],” she said.
The employer was receptive to her proposed changes, which were included in the more detailed contract that followed. “I can’t say there were any surprises per se in the contract because I had negotiated my salary after receiving the offer letter,” she said. She accepted the position and has been working there ever since.
Dr. Cleveland advises physicians “not to make a decision without speaking to someone who’s experienced and can help you compare what’s out there.”
She also encourages physicians to ask for what they want, whether it’s compensation or something else, such as call schedule or vacation time, without being afraid. “I’m a firm believer that you won’t know what you can get if you don’t ask for it,” she said.
Negotiation tips
Mr. Nabity recommended not agreeing to any terms until you are ready to enter into negotiation, recognizing that negotiation is an “art” that requires skill and training. “Either get trained in negotiation, perhaps taking courses to advocate for yourself – which is rare, and most doctors aren’t likely to do this – or go to a trained advocate, such as a lawyer, who can do so on your behalf.”
You might share your concerns with the person who interviewed you, with the person whose name is on the LOI, or with the recruiter who can advocate on your behalf, Ms. Murthy said. “You can reach out to the recruiter and say, ‘I really appreciate the opportunity, but there are some things in the offer letter I’d like to continue discussing.’ “
When you’re ready to negotiate, be sure to assemble all of your “asks” in a single document rather than going back to the prospective employer with “multiple individual questions multiple times,” Ms. Murthy advised. It’s more efficient and the employer or recruiter will appreciate that.
She also advised couching your request in language that expresses your appreciation for the offer and stating that you would like the agreement to serve the best interests of both parties. “Use open-ended language like that, and ask if it’s all right for you to send back some questions, ask for clarification, or share concerns.”
Most employers “will be fine with that,” Ms. Murthy said. “Most won’t say, ‘This is it, take it or leave it.’ If they do, that’s a red flag for you to reconsider whether you really want to work for this particular employer.”
Mr. Hursh suggested that if you choose to sign the LOI immediately, so as to rapidly let the prospective employer know of your interest, “you should add some type of qualification such as, ‘I’m signing this to express my interest, but accepting the position will be dependent upon a more thorough review of compensation benchmarks,’ for example.”
Mr. Nabity agreed: “You can add a handwritten note to the signed LOI expressing that you’re eager to move forward and proceed with the position, but it shouldn’t be construed as accepting the terms of the LOI until you’ve seen the full contract.
“Remember, health care can’t exist without doctors,” Mr. Nabity said. “Doctors are the star players and should go into the negotiation process recognizing their true worth.”
A version of this article appeared on Medscape.com.
You’ve just received an offer letter from that job you interviewed for. Sometimes you want to let the employer know right away how interested you are. The verbiage says the letter isn’t “binding.” So you eagerly sign on the dotted line. Everything looks great ... until it isn’t.
Attorney Ericka Adler, JD, LLM, a partner at Roetzel & Andress, a Chicago-based law firm that represents physicians and health care professionals nationwide, described her client who was in this predicament. The physician, a dermatologist, left a practice where she had been employed because she had received an “amazing” offer letter that included promises about her new work location, staffing, equipment, and hours. She signed and immediately gave notice to her previous employer.
“When she received the actual employment contract, none of those details from the offer letter – which is also called a letter of intent [LOI] – were included,” Ms. Adler told this news organization. The physician wanted to have the details from the LOI formally spelled out in the contract, but the employer refused.
“Basically, they said, ‘This is our standard contract and you’ll just have to trust us that we’ll keep our word. We meant what we said in the LOI, but we cannot include those details in the actual agreement because everyone has the same form of agreement.’ “ The physician decided to sign the contract and accept the position.
She contacted Ms. Adler after she had been at her new position for a month. “She had received none of the things they had promised her in the LOI,” Ms. Adler reported. “She lacked the NP and PA support, she lacked the equipment, she didn’t have enough exam rooms. As soon as she started, someone with whom she was sharing call coverage left, and she was expected to take over. The LOI had a cap on the amount of call she would be required to take, but that verbiage didn’t make it into the contract.”
Ms. Adler tried to address this issue with the employer. “We couldn’t say they had literally breached the agreement, but we did list the things that were mentioned in the LOI but on which they hadn’t delivered. We asked them to fix the issue within 10 days.”
The employer argued “that they didn’t have to fulfill anything that wasn’t spelled out in the contract, even if it was in the LOI. In fact, the contract specified clearly that the signed employment agreement was the only agreement and replaced any previous written or oral agreements between the parties.”
The dermatologist ultimately left the new position. “She might have been able to have a legal claim against the employer for breach or perhaps ‘detrimental reliance’ – meaning, she might have argued that she had been financially harmed due to the false promises made to her. But it would have been difficult and expensive for her to litigate the issue,” said Ms. Adler.
“It also didn’t seem like the physician could remain in the job and develop a positive work relationship with the employer, given that she felt betrayed and misled, and didn’t like the terms of employment, which didn’t match her needs or expectations,” said Ms. Adler.
She added that “most employers are not as unscrupulous and dishonest as this one was. But some employers do play on the fact that younger doctors – especially residents and fellows – tend to be trusting or feel they don’t have negotiation power. They’re often excited to get an offer and sign it without a second thought.”
That’s why she advises physicians to “review the terms of the LOI carefully and make sure you’re comfortable with them before signing it; but know that the real contract to negotiate will be the actual Employment Agreement.”
She also advises physicians not to give notice at their current place of employment until they’ve signed the final contract with the new employer.
On the same page?
Anu Murthy, JD, an attorney and associate contract review specialist at Contract Diagnostics, explained that the LOI is a document that the candidate receives after an interview but before a full contract. Sometimes, the LOI is preceded by a verbal or e-mailed offer, which is less formal.
“An LOI is sometimes called a Term Sheet or Memorandum of Understanding,“ Ms. Murthy told this news organization. “Typically, it lays out key provisions, such as compensation, initial term of the contract, location, and recruitment incentives.” Sometimes it includes mention of staffing, call schedule, malpractice, noncompete covenants, and other components of the position.
Justin Nabity, founder and CEO of Physicians Thrive, a physician financial advisory group, said that LOIs are “a way for employers to gauge a prospective employee’s level of interest.”
The employer “doesn’t want to send a contract with a lot of details before determining whether the candidate is really serious about the position, so the offer letter doesn’t show the whole picture,” Mr. Nabity told this news organization.
Dennis Hursh, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, agreed.
“Another way of putting it is that the employer wants to see whether the prospective employee is on the same page. The LOI will typically include some key components that will later appear in a more complete and formal contract, together with other topics and details. Agreeing to those key components signals that indeed you and the employer are in accord,” said Mr. Hursh.
But are you really on the same page with your prospective employer? And if you seem to be on the same page, and you sign the LOI, is that a guarantee that the employer will honor its terms?
Not necessarily, according to the experts. In fact, many LOIs contain some verbiage stating that the letter isn’t binding, which can be confusing. Others suggest that it is binding, but the candidate doesn’t realize that the letter isn’t a formal contract and that the contract may contain details not included in the LOI or may omit details mentioned in the LOI, as happened to Ms. Adler’s unfortunate client.
“One of the pitfalls I see is that doctors sign the LOI without recognizing whether it’s binding or nonbinding,” Ms. Murthy said. “If it’s binding, it creates a legal obligation on your part and could preclude you from further negotiation once you see the contract and feel you’d like to negotiate some of its terms.”
Binding letters are typically offered to candidates after some back-and-forth between the parties, and important terms have been agreed to, which can happen either verbally or via e-mail. Once these agreements have been reached, they’re summarized in a “binding” letter before being extended into a full contract.
“But even if you’ve agreed on the terms verbally, it’s still important to have someone more experienced review the offer letter before signing it,” Ms. Murthy said. “It’s important to understand the ‘legalese’ and what your rights and obligations are before agreeing to anything.”
And certainly, if you receive a binding LOI, you shouldn’t sign anything until you’re sure you’re comfortable with its contents and have more details.
Are “nonbinding” LOIs really not binding?
Even if the LOI is nonbinding, that doesn’t necessarily mean you can sign it and expect to negotiate later. “I see people tripped up when they sign the LOI, thinking they’ll negotiate later,” said Mr. Hursh. “They may not like the terms – for example, they think the compensation is too low – and they figure they’ll work it out at the contract stage, because the LOI is ‘not legally binding.’ “
But because the candidate signed the LOI, “the employer is under the impression that the compensation was acceptable, so now you’ve tied your hands – and the hands of any attorney you may consult down the road – to negotiate those terms.”
Mr. Hursh said he is often consulted by physicians who signed the contract “to get the ball rolling,” thinking that the LOI was “just a meaningless bureaucratic paper.” They need to understand “that the employer wants to make sure they’re in agreement on the basic points before getting into the details,” he said. “Large hospitals with in-house counsel may not want to use their legal department’s valuable time in redrafting terms they thought were acceptable to the candidate, and most practices don’t want to pay a lawyer to draft an LOI and then come back and say, ‘Actually, the physician wants more compensation.’ “
Mr. Nabity summarized: “The LOI is essentially a negotiation tactic to take some of the cards out of the hands of the doctor and commit him or her to something they’re not ready to commit to.” Employers may be playing on the sense of pressure and candidate’s fear that the job will slip through their fingers if they wait too long to sign. “But it’s better to wait longer at this stage before signing even a nonbinding LOI,” he said.
What to do before signing
So how should physicians relate to the LOI? Mr. Nabity advises “working through the details of the offer letter first, going through it carefully and identifying areas of concern, bearing in mind that employers never begin with their best offer.”
He pointed out that physicians “rarely know their value and usually don’t know how to work through the dynamics of compensation, call schedules, additional incentives, bonuses, and productivity,” so they need to be informed about these areas before signing anything.
Ms. Murthy recommended “going back and saying [to the prospective employer], ‘Thank you, but I need time to consider and evaluate this offer.’ Then, do some due diligence.”
At that point, you can hire an attorney to go over the offer, educate yourself about compensation benchmarks and what your worth actually is, or consult another trained professional or more experienced individual who can review the LOI before you sign it.
That’s what Dominique Cleveland, MD, a Texas-based ob.gyn., did when she received an LOI 5 years ago.
“The offer letter from the group practice contained a statement that the group wanted me to come on board, what the salary would be, and the time frame that would be covered in the contract,” she told this news organization. “It mentioned benefits and incentives and relocation, but it was only a short document – maybe one or two pages long.”
At the time that she received her LOI, Dr. Cleveland was completing her residency. She consulted experienced faculty members from her institution to find out whether the terms laid out in the LOI “were the norm and were reasonable.” She was “fairly certain” that the salary was low and this was confirmed by the faculty members she talked to. “So I felt comfortable asking for more [compensation],” she said.
The employer was receptive to her proposed changes, which were included in the more detailed contract that followed. “I can’t say there were any surprises per se in the contract because I had negotiated my salary after receiving the offer letter,” she said. She accepted the position and has been working there ever since.
Dr. Cleveland advises physicians “not to make a decision without speaking to someone who’s experienced and can help you compare what’s out there.”
She also encourages physicians to ask for what they want, whether it’s compensation or something else, such as call schedule or vacation time, without being afraid. “I’m a firm believer that you won’t know what you can get if you don’t ask for it,” she said.
Negotiation tips
Mr. Nabity recommended not agreeing to any terms until you are ready to enter into negotiation, recognizing that negotiation is an “art” that requires skill and training. “Either get trained in negotiation, perhaps taking courses to advocate for yourself – which is rare, and most doctors aren’t likely to do this – or go to a trained advocate, such as a lawyer, who can do so on your behalf.”
You might share your concerns with the person who interviewed you, with the person whose name is on the LOI, or with the recruiter who can advocate on your behalf, Ms. Murthy said. “You can reach out to the recruiter and say, ‘I really appreciate the opportunity, but there are some things in the offer letter I’d like to continue discussing.’ “
When you’re ready to negotiate, be sure to assemble all of your “asks” in a single document rather than going back to the prospective employer with “multiple individual questions multiple times,” Ms. Murthy advised. It’s more efficient and the employer or recruiter will appreciate that.
She also advised couching your request in language that expresses your appreciation for the offer and stating that you would like the agreement to serve the best interests of both parties. “Use open-ended language like that, and ask if it’s all right for you to send back some questions, ask for clarification, or share concerns.”
Most employers “will be fine with that,” Ms. Murthy said. “Most won’t say, ‘This is it, take it or leave it.’ If they do, that’s a red flag for you to reconsider whether you really want to work for this particular employer.”
Mr. Hursh suggested that if you choose to sign the LOI immediately, so as to rapidly let the prospective employer know of your interest, “you should add some type of qualification such as, ‘I’m signing this to express my interest, but accepting the position will be dependent upon a more thorough review of compensation benchmarks,’ for example.”
Mr. Nabity agreed: “You can add a handwritten note to the signed LOI expressing that you’re eager to move forward and proceed with the position, but it shouldn’t be construed as accepting the terms of the LOI until you’ve seen the full contract.
“Remember, health care can’t exist without doctors,” Mr. Nabity said. “Doctors are the star players and should go into the negotiation process recognizing their true worth.”
A version of this article appeared on Medscape.com.
You’ve just received an offer letter from that job you interviewed for. Sometimes you want to let the employer know right away how interested you are. The verbiage says the letter isn’t “binding.” So you eagerly sign on the dotted line. Everything looks great ... until it isn’t.
Attorney Ericka Adler, JD, LLM, a partner at Roetzel & Andress, a Chicago-based law firm that represents physicians and health care professionals nationwide, described her client who was in this predicament. The physician, a dermatologist, left a practice where she had been employed because she had received an “amazing” offer letter that included promises about her new work location, staffing, equipment, and hours. She signed and immediately gave notice to her previous employer.
“When she received the actual employment contract, none of those details from the offer letter – which is also called a letter of intent [LOI] – were included,” Ms. Adler told this news organization. The physician wanted to have the details from the LOI formally spelled out in the contract, but the employer refused.
“Basically, they said, ‘This is our standard contract and you’ll just have to trust us that we’ll keep our word. We meant what we said in the LOI, but we cannot include those details in the actual agreement because everyone has the same form of agreement.’ “ The physician decided to sign the contract and accept the position.
She contacted Ms. Adler after she had been at her new position for a month. “She had received none of the things they had promised her in the LOI,” Ms. Adler reported. “She lacked the NP and PA support, she lacked the equipment, she didn’t have enough exam rooms. As soon as she started, someone with whom she was sharing call coverage left, and she was expected to take over. The LOI had a cap on the amount of call she would be required to take, but that verbiage didn’t make it into the contract.”
Ms. Adler tried to address this issue with the employer. “We couldn’t say they had literally breached the agreement, but we did list the things that were mentioned in the LOI but on which they hadn’t delivered. We asked them to fix the issue within 10 days.”
The employer argued “that they didn’t have to fulfill anything that wasn’t spelled out in the contract, even if it was in the LOI. In fact, the contract specified clearly that the signed employment agreement was the only agreement and replaced any previous written or oral agreements between the parties.”
The dermatologist ultimately left the new position. “She might have been able to have a legal claim against the employer for breach or perhaps ‘detrimental reliance’ – meaning, she might have argued that she had been financially harmed due to the false promises made to her. But it would have been difficult and expensive for her to litigate the issue,” said Ms. Adler.
“It also didn’t seem like the physician could remain in the job and develop a positive work relationship with the employer, given that she felt betrayed and misled, and didn’t like the terms of employment, which didn’t match her needs or expectations,” said Ms. Adler.
She added that “most employers are not as unscrupulous and dishonest as this one was. But some employers do play on the fact that younger doctors – especially residents and fellows – tend to be trusting or feel they don’t have negotiation power. They’re often excited to get an offer and sign it without a second thought.”
That’s why she advises physicians to “review the terms of the LOI carefully and make sure you’re comfortable with them before signing it; but know that the real contract to negotiate will be the actual Employment Agreement.”
She also advises physicians not to give notice at their current place of employment until they’ve signed the final contract with the new employer.
On the same page?
Anu Murthy, JD, an attorney and associate contract review specialist at Contract Diagnostics, explained that the LOI is a document that the candidate receives after an interview but before a full contract. Sometimes, the LOI is preceded by a verbal or e-mailed offer, which is less formal.
“An LOI is sometimes called a Term Sheet or Memorandum of Understanding,“ Ms. Murthy told this news organization. “Typically, it lays out key provisions, such as compensation, initial term of the contract, location, and recruitment incentives.” Sometimes it includes mention of staffing, call schedule, malpractice, noncompete covenants, and other components of the position.
Justin Nabity, founder and CEO of Physicians Thrive, a physician financial advisory group, said that LOIs are “a way for employers to gauge a prospective employee’s level of interest.”
The employer “doesn’t want to send a contract with a lot of details before determining whether the candidate is really serious about the position, so the offer letter doesn’t show the whole picture,” Mr. Nabity told this news organization.
Dennis Hursh, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, agreed.
“Another way of putting it is that the employer wants to see whether the prospective employee is on the same page. The LOI will typically include some key components that will later appear in a more complete and formal contract, together with other topics and details. Agreeing to those key components signals that indeed you and the employer are in accord,” said Mr. Hursh.
But are you really on the same page with your prospective employer? And if you seem to be on the same page, and you sign the LOI, is that a guarantee that the employer will honor its terms?
Not necessarily, according to the experts. In fact, many LOIs contain some verbiage stating that the letter isn’t binding, which can be confusing. Others suggest that it is binding, but the candidate doesn’t realize that the letter isn’t a formal contract and that the contract may contain details not included in the LOI or may omit details mentioned in the LOI, as happened to Ms. Adler’s unfortunate client.
“One of the pitfalls I see is that doctors sign the LOI without recognizing whether it’s binding or nonbinding,” Ms. Murthy said. “If it’s binding, it creates a legal obligation on your part and could preclude you from further negotiation once you see the contract and feel you’d like to negotiate some of its terms.”
Binding letters are typically offered to candidates after some back-and-forth between the parties, and important terms have been agreed to, which can happen either verbally or via e-mail. Once these agreements have been reached, they’re summarized in a “binding” letter before being extended into a full contract.
“But even if you’ve agreed on the terms verbally, it’s still important to have someone more experienced review the offer letter before signing it,” Ms. Murthy said. “It’s important to understand the ‘legalese’ and what your rights and obligations are before agreeing to anything.”
And certainly, if you receive a binding LOI, you shouldn’t sign anything until you’re sure you’re comfortable with its contents and have more details.
Are “nonbinding” LOIs really not binding?
Even if the LOI is nonbinding, that doesn’t necessarily mean you can sign it and expect to negotiate later. “I see people tripped up when they sign the LOI, thinking they’ll negotiate later,” said Mr. Hursh. “They may not like the terms – for example, they think the compensation is too low – and they figure they’ll work it out at the contract stage, because the LOI is ‘not legally binding.’ “
But because the candidate signed the LOI, “the employer is under the impression that the compensation was acceptable, so now you’ve tied your hands – and the hands of any attorney you may consult down the road – to negotiate those terms.”
Mr. Hursh said he is often consulted by physicians who signed the contract “to get the ball rolling,” thinking that the LOI was “just a meaningless bureaucratic paper.” They need to understand “that the employer wants to make sure they’re in agreement on the basic points before getting into the details,” he said. “Large hospitals with in-house counsel may not want to use their legal department’s valuable time in redrafting terms they thought were acceptable to the candidate, and most practices don’t want to pay a lawyer to draft an LOI and then come back and say, ‘Actually, the physician wants more compensation.’ “
Mr. Nabity summarized: “The LOI is essentially a negotiation tactic to take some of the cards out of the hands of the doctor and commit him or her to something they’re not ready to commit to.” Employers may be playing on the sense of pressure and candidate’s fear that the job will slip through their fingers if they wait too long to sign. “But it’s better to wait longer at this stage before signing even a nonbinding LOI,” he said.
What to do before signing
So how should physicians relate to the LOI? Mr. Nabity advises “working through the details of the offer letter first, going through it carefully and identifying areas of concern, bearing in mind that employers never begin with their best offer.”
He pointed out that physicians “rarely know their value and usually don’t know how to work through the dynamics of compensation, call schedules, additional incentives, bonuses, and productivity,” so they need to be informed about these areas before signing anything.
Ms. Murthy recommended “going back and saying [to the prospective employer], ‘Thank you, but I need time to consider and evaluate this offer.’ Then, do some due diligence.”
At that point, you can hire an attorney to go over the offer, educate yourself about compensation benchmarks and what your worth actually is, or consult another trained professional or more experienced individual who can review the LOI before you sign it.
That’s what Dominique Cleveland, MD, a Texas-based ob.gyn., did when she received an LOI 5 years ago.
“The offer letter from the group practice contained a statement that the group wanted me to come on board, what the salary would be, and the time frame that would be covered in the contract,” she told this news organization. “It mentioned benefits and incentives and relocation, but it was only a short document – maybe one or two pages long.”
At the time that she received her LOI, Dr. Cleveland was completing her residency. She consulted experienced faculty members from her institution to find out whether the terms laid out in the LOI “were the norm and were reasonable.” She was “fairly certain” that the salary was low and this was confirmed by the faculty members she talked to. “So I felt comfortable asking for more [compensation],” she said.
The employer was receptive to her proposed changes, which were included in the more detailed contract that followed. “I can’t say there were any surprises per se in the contract because I had negotiated my salary after receiving the offer letter,” she said. She accepted the position and has been working there ever since.
Dr. Cleveland advises physicians “not to make a decision without speaking to someone who’s experienced and can help you compare what’s out there.”
She also encourages physicians to ask for what they want, whether it’s compensation or something else, such as call schedule or vacation time, without being afraid. “I’m a firm believer that you won’t know what you can get if you don’t ask for it,” she said.
Negotiation tips
Mr. Nabity recommended not agreeing to any terms until you are ready to enter into negotiation, recognizing that negotiation is an “art” that requires skill and training. “Either get trained in negotiation, perhaps taking courses to advocate for yourself – which is rare, and most doctors aren’t likely to do this – or go to a trained advocate, such as a lawyer, who can do so on your behalf.”
You might share your concerns with the person who interviewed you, with the person whose name is on the LOI, or with the recruiter who can advocate on your behalf, Ms. Murthy said. “You can reach out to the recruiter and say, ‘I really appreciate the opportunity, but there are some things in the offer letter I’d like to continue discussing.’ “
When you’re ready to negotiate, be sure to assemble all of your “asks” in a single document rather than going back to the prospective employer with “multiple individual questions multiple times,” Ms. Murthy advised. It’s more efficient and the employer or recruiter will appreciate that.
She also advised couching your request in language that expresses your appreciation for the offer and stating that you would like the agreement to serve the best interests of both parties. “Use open-ended language like that, and ask if it’s all right for you to send back some questions, ask for clarification, or share concerns.”
Most employers “will be fine with that,” Ms. Murthy said. “Most won’t say, ‘This is it, take it or leave it.’ If they do, that’s a red flag for you to reconsider whether you really want to work for this particular employer.”
Mr. Hursh suggested that if you choose to sign the LOI immediately, so as to rapidly let the prospective employer know of your interest, “you should add some type of qualification such as, ‘I’m signing this to express my interest, but accepting the position will be dependent upon a more thorough review of compensation benchmarks,’ for example.”
Mr. Nabity agreed: “You can add a handwritten note to the signed LOI expressing that you’re eager to move forward and proceed with the position, but it shouldn’t be construed as accepting the terms of the LOI until you’ve seen the full contract.
“Remember, health care can’t exist without doctors,” Mr. Nabity said. “Doctors are the star players and should go into the negotiation process recognizing their true worth.”
A version of this article appeared on Medscape.com.
Patient contact time vs. admin: Is your contract fair?
What’s in a day’s work? For doctors, it’s typically a mix of seeing patients and completing paperwork and follow-up. Often it extends well past the standard workday.
Dennis Hursh, JD, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, describes one overwhelmed ob.gyn. who recently consulted him for this problem.
“My client had accepted a position in a group practice where his contract stated he would be working during normal office hours, Monday through Friday, from 8 a.m. to 5 p.m. – in other words, a 40-hour workweek,” Mr. Hursh said.
But the distressed physician discovered that actually, he was working almost twice as many hours. “He’d get to work early to do charting, then see patients during the 40 hours, perhaps grabbing a quick sandwich for a few minutes – and then stay after 5 [p.m.] for a few more hours when he’d work on charts or other administrative tasks. Then he’d get something to eat, work on more charts, then go to bed, get up in the morning, and repeat.”
Mr. Hursh summarized the client’s life: “Eating, sleeping, practicing clinical medicine, and doing nonclinical tasks.”
It turned out that the 40-hour workweek included in the contract referred to patient-facing hours, not to all of the ancillary tasks that are part of practicing medicine in this day and age. “Unfortunately, this is far from an isolated story,” said Mr. Hursh.
Be aware of what’s in the contract
“The first draft of many standard physician employment contracts often omits mention of patient contact hour requirements and rather uses vague verbiage such as ‘full-time’ employment or ‘1.0 FTE’ – or full-time equivalent – without defining that term,” said Mr. Hursh. Typically, the 40 hours exclude call coverage, but most physicians understand that and, at least at first glance, it all sounds very reasonable.
But once charting, hours on the phone, arguing with managed care companies, sending in prescriptions, administrative meetings, and other tasks are thrown in, the work hours expand dramatically. Moreover, if your employer doesn’t utilize hospitalists, you may be expected to “round” outside of the 40 hours, which can be particularly burdensome if the employer admits patients to multiple hospitals.
Amanda Hill, JD, owner of Hill Health Law based in Austin, Texas, told this news organization that this predicament isn’t unique to physicians. Exempt employees who don’t clock in and out are often expected to work overtime – that is, to “work as long as it takes to get the job done.” It can affect NPs, PAs, and many others in the health care space. But the number of tasks that fall upon a doctor’s shoulders and the fact that patients’ health and lives are at stake up the ante and make the situation far more difficult for doctors than for employees in other industries.
So it’s important to nail down precise terms in the contract and, if possible, negotiate for a more humane schedule by specifying how the working hours will be used.
“It’s true that a 1.0 FTE definition is too vague,” Ms. Hill said. “I’ve negotiated a lot of contracts where we nail down in writing that the in-office schedule equals 34 hours per week, so the physician is guaranteed an additional 6 hours for administrative time.”
Mr. Hursh usually asks for 32 hours of patient contact per week, which leaves 1 full day per week to catch up on basic administrative tasks. “It’s important for employers to recognize that seeing patients isn’t the only thing a doctor does and there’s a lot of work in addition to face-to-face time,” he said.
But he hasn’t always been successful. One physician client was seeking a workweek consisting of 36 patient contact hours, “which is 90% of the usual FTE of a 40-hour week,” said Mr. Hursh. “But the employer called it ‘part-time,’ as if the doctor were planning to be lying in the sun for the other 4 hours.”
The client decided to accept a 10% pay cut and 10% less vacation to guarantee that she had those extra hours for administrative tasks. “She’s probably working way more than 36 hours a week, but maybe closer to 50 or 60 instead of 70 or more,” he said.
Clarify call coverage
Call coverage is typically not included in the hours a physician is contracted to work on a weekly basis. “Most contracts have call, and it’s usually evenly distributed among parties in a practice, but call can expand if another doctor is out sick, for example,” said Ms. Hill.
Sometimes the language in the contract is vague regarding call coverage. “I ask, how many shifts per year is the doctor is expected to work? Then, I try to negotiate extra pay if more shifts arise,” she said. “The hospital or practice may not demand extra call because they don’t want to pay extra money to the physician.”
On the other hand, some physicians may be eager to take extra call if it means extra income.
Ms. Hill stated that one of her clients was being paid as a “part-time, 2-day-a-week provider” but was asked to be on call and take night and weekend work. When you added it all up, she was putting in almost 30 hours a week.
“This is abusive to a provider that works so hard for patients,” Ms. Hill said. “We have to protect them through the contract language, so they have something hard and fast to point to when their administrator pushes them too hard. Doctors should get value for their time.”
Ms. Hill and her client pushed for more money, and the employer gave in. “All we had to do was to point out how many hours she was actually working. She didn’t mind all the extra call, but she wanted to be compensated.” The doctor’s salary was hiked by $25,000.
Differences in specialties and settings
There are some specialties where it might be easier to have more defined hours, while other specialties are more challenging. Anu Murthy, Esq., an attorney and associate contract review specialist at Contract Diagnostics (a national firm that reviews physician contracts) told this news organization that the work of hospitalists, intensivists, and emergency department physicians, for example, is done in shifts, which tend to be fixed hours.
“They need to get their charting completed so that whoever takes over on the next shift has access to the most recent notes about the patient,” she said. By contrast, surgeons can’t always account for how long a given surgery will take. “It could be as long as 9 hours,” she said. Notes need to be written immediately for the sake of the patient’s postsurgical care.
Dermatologists tend to deal with fewer emergencies, compared with other specialists, and it’s easier for their patients to be slotted into an organized schedule. On the other hand, primary care doctors – internists, family practice physicians, and pediatricians – may be seeing 40-50 patients a day, one every 15 minutes.
Practice setting also makes a difference, said Ms. Murthy. Veterans Administration (VA) hospitals or government-run clinics tend to have more rigidly defined hours, compared with other settings, so if you’re in a VA hospital or government-run clinic, work-life balance tends to be better.
Physicians who work remotely via telehealth also tend to have a better work-life balance, compared with those who see patients in person, Ms. Murthy said. But the difference may be in not having to spend extra time commuting to work or interacting with others in the work environment, since some research has suggested that telehealth physicians may actually spend more time engaged in charting after hours, compared with their in-person counterparts.
Using scribes to maximize your time
Elliott Trotter, MD, is an emergency medicine physician, associate clinical professor of emergency medicine at Texas Christian University Medical Schools, and founder of the ScribeNest, a Texas-based company that trains health care scribes. He told this news organization that there are ways to maximize one’s time during shifts so that much of the charting can be accomplished during working hours.
“About 28 years ago, I realized that the documentation load for physicians was enormous and at that time I developed the Modern Scribe, using premed students for ‘elbow support’ to help with the workload by documenting the ED encounters in real time during the encounter so I wouldn’t have to do so later.”
Over the years, as EHRs have become more ubiquitous and onerous, the role of the scribe has “evolved from a luxury to a necessity,” said Dr. Trotter. The scribes can actually record the encounter directly into the EHR so that the physician doesn’t have to do so later and doesn’t have to look at a computer screen but can look at the patient during the encounter.
“This enhances communication and has been shown to improve patient care,” he said.
Dr. Trotter said he rarely, if ever, needs to do documentation after hours. “But one of my physician colleagues had over 500 charts in his in-basket on a regular basis, which was overwhelming and untenable.”
The use of AI in health care is rapidly growing. Tools to help hasten the process of taking notes through use of AI-generated summaries is something appealing to many doctors. Ms. Hill warned physicians to “be careful not to rely so heavily on AI that you trust it over your own words.” She noted that it can make mistakes, and the liability always remains with the clinician.
Creating time-efficient strategies
Wilfrid Noel Raby, PhD, MD, a psychiatrist in private practice in Teaneck, N.J., was formerly a psychiatrist in the substance abuse unit at Montefiore Hospital, New York. He told this news organization that he developed a system whereby he rarely had to take work home with him. “I was working only 20 hours a week, but I was usually able to do my charting during those hours, as well as seeing patients,” he said. “I scheduled my appointments and structured a little ‘buffer time’ between them so that I had time to document the first appointment before moving on to the next one.”
There were days when this wasn’t possible because there were too many patients who needed to be seen back-to-back. “So I developed my own template where I could take rapid, very standardized notes that fit into the format of the EHR and met those expectations.” Then, when he had finished seeing patients, he could quickly enter the content of his notes into the EHR. If necessary, he completed his charting on a different day.
Viwek Bisen, DO, assistant professor of psychiatry, Hackensack (N.J.) University Medical Center, is a psychiatrist in the emergency department. “My contract is based on a traditional 40-hour workweek, with 80% of my time allotted to seeing patients and 20% of my time allotted to administration.”
But the way his time actually plays out is that he’s seeing patients during about half of the 32 hours. “The rest of the time, I’m charting, speaking to family members of patients, writing notes, engaging in team meetings, and dealing with insurance companies.” Dr. Bisen has developed his own system of completing his notes while still in the hospital. “I’ve learned to be efficient and manage my time better, so I no longer have to take work home with me.”
“At the end of the day, doctors are people,” Ms. Hill said. “They are not machines. Maybe in residency and fellowship they may grind out impossible shifts with little sleep, but this pace isn’t tenable for an entire career.”
A version of this article first appeared on Medscape.com.
What’s in a day’s work? For doctors, it’s typically a mix of seeing patients and completing paperwork and follow-up. Often it extends well past the standard workday.
Dennis Hursh, JD, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, describes one overwhelmed ob.gyn. who recently consulted him for this problem.
“My client had accepted a position in a group practice where his contract stated he would be working during normal office hours, Monday through Friday, from 8 a.m. to 5 p.m. – in other words, a 40-hour workweek,” Mr. Hursh said.
But the distressed physician discovered that actually, he was working almost twice as many hours. “He’d get to work early to do charting, then see patients during the 40 hours, perhaps grabbing a quick sandwich for a few minutes – and then stay after 5 [p.m.] for a few more hours when he’d work on charts or other administrative tasks. Then he’d get something to eat, work on more charts, then go to bed, get up in the morning, and repeat.”
Mr. Hursh summarized the client’s life: “Eating, sleeping, practicing clinical medicine, and doing nonclinical tasks.”
It turned out that the 40-hour workweek included in the contract referred to patient-facing hours, not to all of the ancillary tasks that are part of practicing medicine in this day and age. “Unfortunately, this is far from an isolated story,” said Mr. Hursh.
Be aware of what’s in the contract
“The first draft of many standard physician employment contracts often omits mention of patient contact hour requirements and rather uses vague verbiage such as ‘full-time’ employment or ‘1.0 FTE’ – or full-time equivalent – without defining that term,” said Mr. Hursh. Typically, the 40 hours exclude call coverage, but most physicians understand that and, at least at first glance, it all sounds very reasonable.
But once charting, hours on the phone, arguing with managed care companies, sending in prescriptions, administrative meetings, and other tasks are thrown in, the work hours expand dramatically. Moreover, if your employer doesn’t utilize hospitalists, you may be expected to “round” outside of the 40 hours, which can be particularly burdensome if the employer admits patients to multiple hospitals.
Amanda Hill, JD, owner of Hill Health Law based in Austin, Texas, told this news organization that this predicament isn’t unique to physicians. Exempt employees who don’t clock in and out are often expected to work overtime – that is, to “work as long as it takes to get the job done.” It can affect NPs, PAs, and many others in the health care space. But the number of tasks that fall upon a doctor’s shoulders and the fact that patients’ health and lives are at stake up the ante and make the situation far more difficult for doctors than for employees in other industries.
So it’s important to nail down precise terms in the contract and, if possible, negotiate for a more humane schedule by specifying how the working hours will be used.
“It’s true that a 1.0 FTE definition is too vague,” Ms. Hill said. “I’ve negotiated a lot of contracts where we nail down in writing that the in-office schedule equals 34 hours per week, so the physician is guaranteed an additional 6 hours for administrative time.”
Mr. Hursh usually asks for 32 hours of patient contact per week, which leaves 1 full day per week to catch up on basic administrative tasks. “It’s important for employers to recognize that seeing patients isn’t the only thing a doctor does and there’s a lot of work in addition to face-to-face time,” he said.
But he hasn’t always been successful. One physician client was seeking a workweek consisting of 36 patient contact hours, “which is 90% of the usual FTE of a 40-hour week,” said Mr. Hursh. “But the employer called it ‘part-time,’ as if the doctor were planning to be lying in the sun for the other 4 hours.”
The client decided to accept a 10% pay cut and 10% less vacation to guarantee that she had those extra hours for administrative tasks. “She’s probably working way more than 36 hours a week, but maybe closer to 50 or 60 instead of 70 or more,” he said.
Clarify call coverage
Call coverage is typically not included in the hours a physician is contracted to work on a weekly basis. “Most contracts have call, and it’s usually evenly distributed among parties in a practice, but call can expand if another doctor is out sick, for example,” said Ms. Hill.
Sometimes the language in the contract is vague regarding call coverage. “I ask, how many shifts per year is the doctor is expected to work? Then, I try to negotiate extra pay if more shifts arise,” she said. “The hospital or practice may not demand extra call because they don’t want to pay extra money to the physician.”
On the other hand, some physicians may be eager to take extra call if it means extra income.
Ms. Hill stated that one of her clients was being paid as a “part-time, 2-day-a-week provider” but was asked to be on call and take night and weekend work. When you added it all up, she was putting in almost 30 hours a week.
“This is abusive to a provider that works so hard for patients,” Ms. Hill said. “We have to protect them through the contract language, so they have something hard and fast to point to when their administrator pushes them too hard. Doctors should get value for their time.”
Ms. Hill and her client pushed for more money, and the employer gave in. “All we had to do was to point out how many hours she was actually working. She didn’t mind all the extra call, but she wanted to be compensated.” The doctor’s salary was hiked by $25,000.
Differences in specialties and settings
There are some specialties where it might be easier to have more defined hours, while other specialties are more challenging. Anu Murthy, Esq., an attorney and associate contract review specialist at Contract Diagnostics (a national firm that reviews physician contracts) told this news organization that the work of hospitalists, intensivists, and emergency department physicians, for example, is done in shifts, which tend to be fixed hours.
“They need to get their charting completed so that whoever takes over on the next shift has access to the most recent notes about the patient,” she said. By contrast, surgeons can’t always account for how long a given surgery will take. “It could be as long as 9 hours,” she said. Notes need to be written immediately for the sake of the patient’s postsurgical care.
Dermatologists tend to deal with fewer emergencies, compared with other specialists, and it’s easier for their patients to be slotted into an organized schedule. On the other hand, primary care doctors – internists, family practice physicians, and pediatricians – may be seeing 40-50 patients a day, one every 15 minutes.
Practice setting also makes a difference, said Ms. Murthy. Veterans Administration (VA) hospitals or government-run clinics tend to have more rigidly defined hours, compared with other settings, so if you’re in a VA hospital or government-run clinic, work-life balance tends to be better.
Physicians who work remotely via telehealth also tend to have a better work-life balance, compared with those who see patients in person, Ms. Murthy said. But the difference may be in not having to spend extra time commuting to work or interacting with others in the work environment, since some research has suggested that telehealth physicians may actually spend more time engaged in charting after hours, compared with their in-person counterparts.
Using scribes to maximize your time
Elliott Trotter, MD, is an emergency medicine physician, associate clinical professor of emergency medicine at Texas Christian University Medical Schools, and founder of the ScribeNest, a Texas-based company that trains health care scribes. He told this news organization that there are ways to maximize one’s time during shifts so that much of the charting can be accomplished during working hours.
“About 28 years ago, I realized that the documentation load for physicians was enormous and at that time I developed the Modern Scribe, using premed students for ‘elbow support’ to help with the workload by documenting the ED encounters in real time during the encounter so I wouldn’t have to do so later.”
Over the years, as EHRs have become more ubiquitous and onerous, the role of the scribe has “evolved from a luxury to a necessity,” said Dr. Trotter. The scribes can actually record the encounter directly into the EHR so that the physician doesn’t have to do so later and doesn’t have to look at a computer screen but can look at the patient during the encounter.
“This enhances communication and has been shown to improve patient care,” he said.
Dr. Trotter said he rarely, if ever, needs to do documentation after hours. “But one of my physician colleagues had over 500 charts in his in-basket on a regular basis, which was overwhelming and untenable.”
The use of AI in health care is rapidly growing. Tools to help hasten the process of taking notes through use of AI-generated summaries is something appealing to many doctors. Ms. Hill warned physicians to “be careful not to rely so heavily on AI that you trust it over your own words.” She noted that it can make mistakes, and the liability always remains with the clinician.
Creating time-efficient strategies
Wilfrid Noel Raby, PhD, MD, a psychiatrist in private practice in Teaneck, N.J., was formerly a psychiatrist in the substance abuse unit at Montefiore Hospital, New York. He told this news organization that he developed a system whereby he rarely had to take work home with him. “I was working only 20 hours a week, but I was usually able to do my charting during those hours, as well as seeing patients,” he said. “I scheduled my appointments and structured a little ‘buffer time’ between them so that I had time to document the first appointment before moving on to the next one.”
There were days when this wasn’t possible because there were too many patients who needed to be seen back-to-back. “So I developed my own template where I could take rapid, very standardized notes that fit into the format of the EHR and met those expectations.” Then, when he had finished seeing patients, he could quickly enter the content of his notes into the EHR. If necessary, he completed his charting on a different day.
Viwek Bisen, DO, assistant professor of psychiatry, Hackensack (N.J.) University Medical Center, is a psychiatrist in the emergency department. “My contract is based on a traditional 40-hour workweek, with 80% of my time allotted to seeing patients and 20% of my time allotted to administration.”
But the way his time actually plays out is that he’s seeing patients during about half of the 32 hours. “The rest of the time, I’m charting, speaking to family members of patients, writing notes, engaging in team meetings, and dealing with insurance companies.” Dr. Bisen has developed his own system of completing his notes while still in the hospital. “I’ve learned to be efficient and manage my time better, so I no longer have to take work home with me.”
“At the end of the day, doctors are people,” Ms. Hill said. “They are not machines. Maybe in residency and fellowship they may grind out impossible shifts with little sleep, but this pace isn’t tenable for an entire career.”
A version of this article first appeared on Medscape.com.
What’s in a day’s work? For doctors, it’s typically a mix of seeing patients and completing paperwork and follow-up. Often it extends well past the standard workday.
Dennis Hursh, JD, managing partner of Physician Agreements Health Law, a Pennsylvania-based law firm that represents physicians, describes one overwhelmed ob.gyn. who recently consulted him for this problem.
“My client had accepted a position in a group practice where his contract stated he would be working during normal office hours, Monday through Friday, from 8 a.m. to 5 p.m. – in other words, a 40-hour workweek,” Mr. Hursh said.
But the distressed physician discovered that actually, he was working almost twice as many hours. “He’d get to work early to do charting, then see patients during the 40 hours, perhaps grabbing a quick sandwich for a few minutes – and then stay after 5 [p.m.] for a few more hours when he’d work on charts or other administrative tasks. Then he’d get something to eat, work on more charts, then go to bed, get up in the morning, and repeat.”
Mr. Hursh summarized the client’s life: “Eating, sleeping, practicing clinical medicine, and doing nonclinical tasks.”
It turned out that the 40-hour workweek included in the contract referred to patient-facing hours, not to all of the ancillary tasks that are part of practicing medicine in this day and age. “Unfortunately, this is far from an isolated story,” said Mr. Hursh.
Be aware of what’s in the contract
“The first draft of many standard physician employment contracts often omits mention of patient contact hour requirements and rather uses vague verbiage such as ‘full-time’ employment or ‘1.0 FTE’ – or full-time equivalent – without defining that term,” said Mr. Hursh. Typically, the 40 hours exclude call coverage, but most physicians understand that and, at least at first glance, it all sounds very reasonable.
But once charting, hours on the phone, arguing with managed care companies, sending in prescriptions, administrative meetings, and other tasks are thrown in, the work hours expand dramatically. Moreover, if your employer doesn’t utilize hospitalists, you may be expected to “round” outside of the 40 hours, which can be particularly burdensome if the employer admits patients to multiple hospitals.
Amanda Hill, JD, owner of Hill Health Law based in Austin, Texas, told this news organization that this predicament isn’t unique to physicians. Exempt employees who don’t clock in and out are often expected to work overtime – that is, to “work as long as it takes to get the job done.” It can affect NPs, PAs, and many others in the health care space. But the number of tasks that fall upon a doctor’s shoulders and the fact that patients’ health and lives are at stake up the ante and make the situation far more difficult for doctors than for employees in other industries.
So it’s important to nail down precise terms in the contract and, if possible, negotiate for a more humane schedule by specifying how the working hours will be used.
“It’s true that a 1.0 FTE definition is too vague,” Ms. Hill said. “I’ve negotiated a lot of contracts where we nail down in writing that the in-office schedule equals 34 hours per week, so the physician is guaranteed an additional 6 hours for administrative time.”
Mr. Hursh usually asks for 32 hours of patient contact per week, which leaves 1 full day per week to catch up on basic administrative tasks. “It’s important for employers to recognize that seeing patients isn’t the only thing a doctor does and there’s a lot of work in addition to face-to-face time,” he said.
But he hasn’t always been successful. One physician client was seeking a workweek consisting of 36 patient contact hours, “which is 90% of the usual FTE of a 40-hour week,” said Mr. Hursh. “But the employer called it ‘part-time,’ as if the doctor were planning to be lying in the sun for the other 4 hours.”
The client decided to accept a 10% pay cut and 10% less vacation to guarantee that she had those extra hours for administrative tasks. “She’s probably working way more than 36 hours a week, but maybe closer to 50 or 60 instead of 70 or more,” he said.
Clarify call coverage
Call coverage is typically not included in the hours a physician is contracted to work on a weekly basis. “Most contracts have call, and it’s usually evenly distributed among parties in a practice, but call can expand if another doctor is out sick, for example,” said Ms. Hill.
Sometimes the language in the contract is vague regarding call coverage. “I ask, how many shifts per year is the doctor is expected to work? Then, I try to negotiate extra pay if more shifts arise,” she said. “The hospital or practice may not demand extra call because they don’t want to pay extra money to the physician.”
On the other hand, some physicians may be eager to take extra call if it means extra income.
Ms. Hill stated that one of her clients was being paid as a “part-time, 2-day-a-week provider” but was asked to be on call and take night and weekend work. When you added it all up, she was putting in almost 30 hours a week.
“This is abusive to a provider that works so hard for patients,” Ms. Hill said. “We have to protect them through the contract language, so they have something hard and fast to point to when their administrator pushes them too hard. Doctors should get value for their time.”
Ms. Hill and her client pushed for more money, and the employer gave in. “All we had to do was to point out how many hours she was actually working. She didn’t mind all the extra call, but she wanted to be compensated.” The doctor’s salary was hiked by $25,000.
Differences in specialties and settings
There are some specialties where it might be easier to have more defined hours, while other specialties are more challenging. Anu Murthy, Esq., an attorney and associate contract review specialist at Contract Diagnostics (a national firm that reviews physician contracts) told this news organization that the work of hospitalists, intensivists, and emergency department physicians, for example, is done in shifts, which tend to be fixed hours.
“They need to get their charting completed so that whoever takes over on the next shift has access to the most recent notes about the patient,” she said. By contrast, surgeons can’t always account for how long a given surgery will take. “It could be as long as 9 hours,” she said. Notes need to be written immediately for the sake of the patient’s postsurgical care.
Dermatologists tend to deal with fewer emergencies, compared with other specialists, and it’s easier for their patients to be slotted into an organized schedule. On the other hand, primary care doctors – internists, family practice physicians, and pediatricians – may be seeing 40-50 patients a day, one every 15 minutes.
Practice setting also makes a difference, said Ms. Murthy. Veterans Administration (VA) hospitals or government-run clinics tend to have more rigidly defined hours, compared with other settings, so if you’re in a VA hospital or government-run clinic, work-life balance tends to be better.
Physicians who work remotely via telehealth also tend to have a better work-life balance, compared with those who see patients in person, Ms. Murthy said. But the difference may be in not having to spend extra time commuting to work or interacting with others in the work environment, since some research has suggested that telehealth physicians may actually spend more time engaged in charting after hours, compared with their in-person counterparts.
Using scribes to maximize your time
Elliott Trotter, MD, is an emergency medicine physician, associate clinical professor of emergency medicine at Texas Christian University Medical Schools, and founder of the ScribeNest, a Texas-based company that trains health care scribes. He told this news organization that there are ways to maximize one’s time during shifts so that much of the charting can be accomplished during working hours.
“About 28 years ago, I realized that the documentation load for physicians was enormous and at that time I developed the Modern Scribe, using premed students for ‘elbow support’ to help with the workload by documenting the ED encounters in real time during the encounter so I wouldn’t have to do so later.”
Over the years, as EHRs have become more ubiquitous and onerous, the role of the scribe has “evolved from a luxury to a necessity,” said Dr. Trotter. The scribes can actually record the encounter directly into the EHR so that the physician doesn’t have to do so later and doesn’t have to look at a computer screen but can look at the patient during the encounter.
“This enhances communication and has been shown to improve patient care,” he said.
Dr. Trotter said he rarely, if ever, needs to do documentation after hours. “But one of my physician colleagues had over 500 charts in his in-basket on a regular basis, which was overwhelming and untenable.”
The use of AI in health care is rapidly growing. Tools to help hasten the process of taking notes through use of AI-generated summaries is something appealing to many doctors. Ms. Hill warned physicians to “be careful not to rely so heavily on AI that you trust it over your own words.” She noted that it can make mistakes, and the liability always remains with the clinician.
Creating time-efficient strategies
Wilfrid Noel Raby, PhD, MD, a psychiatrist in private practice in Teaneck, N.J., was formerly a psychiatrist in the substance abuse unit at Montefiore Hospital, New York. He told this news organization that he developed a system whereby he rarely had to take work home with him. “I was working only 20 hours a week, but I was usually able to do my charting during those hours, as well as seeing patients,” he said. “I scheduled my appointments and structured a little ‘buffer time’ between them so that I had time to document the first appointment before moving on to the next one.”
There were days when this wasn’t possible because there were too many patients who needed to be seen back-to-back. “So I developed my own template where I could take rapid, very standardized notes that fit into the format of the EHR and met those expectations.” Then, when he had finished seeing patients, he could quickly enter the content of his notes into the EHR. If necessary, he completed his charting on a different day.
Viwek Bisen, DO, assistant professor of psychiatry, Hackensack (N.J.) University Medical Center, is a psychiatrist in the emergency department. “My contract is based on a traditional 40-hour workweek, with 80% of my time allotted to seeing patients and 20% of my time allotted to administration.”
But the way his time actually plays out is that he’s seeing patients during about half of the 32 hours. “The rest of the time, I’m charting, speaking to family members of patients, writing notes, engaging in team meetings, and dealing with insurance companies.” Dr. Bisen has developed his own system of completing his notes while still in the hospital. “I’ve learned to be efficient and manage my time better, so I no longer have to take work home with me.”
“At the end of the day, doctors are people,” Ms. Hill said. “They are not machines. Maybe in residency and fellowship they may grind out impossible shifts with little sleep, but this pace isn’t tenable for an entire career.”
A version of this article first appeared on Medscape.com.
How does lecanemab work in Alzheimer’s?
Lecanemab (Lequembi, Esai), an amyloid-beta–directed antibody therapy, is approved by the Food and Drug Administration for the treatment of Alzheimer’s disease (AD). But exactly how the drug clears amyloid-beta wasn’t clear.
The investigators tested the effectiveness of various forms of amyloid-beta in activating the plasma contact system and found that amyloid-beta protofibrils, known to be the most toxic form of amyloid-beta, promoted the activation of this molecular cascade and that lecanemab inhibited pathway activation.
“In our study, we looked at lecanemab and found it can block the activation of the contact system, which could be one of the reasons that it works so well for AD,” study coinvestigator Erin Norris, PhD, research associate professor, Rockefeller University, New York, said in an interview.
The study was published online in the Proceedings of the National Academy of Science.
Unknown mechanism
“Many years ago, we started looking at the involvement of vascular dysfunction in AD,” Dr. Norris said. “We wanted to see whether or not irregular blood clotting or problems with blood flow was problematic in Alzheimer’s patients.”
The researchers found that fibrin, a major component involved in blood clotting, can extravasate into the brain.
“The blood-brain barrier can break down in Alzheimer’s, so things from the blood can move into the brain and deposit there,” she added. Fibrin then interacts with amyloid-beta, the major pathogenic protein in AD.
Dr. Norris explained that fibrin clots can form in two different ways. One is through the normal process that occurs when there’s an injury and bleeding. The second is through intrinsic clotting, which takes place through the contact system.
“We started looking into this system and found that the plasma of Alzheimer’s patients showed irregular levels of these enzymes and proteins that are part of the intrinsic clotting system compared to those of normal controls,” said Dr. Norris.
“This paper was an extension of years studying this pathway and these mechanisms. It was also inspired by the approval of lecanemab and its release for use in Alzheimer’s patients,” she added.
In previous research, the same researchers found that amyloid-beta has different forms. “It’s normally soluble, and it’s a very tiny molecule,” Dr. Norris said. “But over time, and in different situations, it can start to aggregate, becoming bigger and bigger.”
Implications beyond Alzheimer’s
Postmortem tissue analysis has found fibrillar plaques that are “clumped together.” These are insoluble and hard to get rid of, she said. “Protofibrils are the step before amyloid-beta forms fibrils and are considered to be the most toxic form, although the mechanism behind why it’s so toxic is not understood.”
Previous research has already shown that amyloid-beta can activate the contact system. The contact system has two “arms,” the first of which is involved with clotting, and the second with inflammation, Dr. Norris said. In fact, it’s the plasma contact system that links vascular and inflammatory pathways.
The plasma contact system leads to the clotting of fibrin, Dr. Norris continued. It activates factor XII, which leads to blood clotting by binding to coagulation factor XI.
The contact system also causes inflammation – the second “arm.” Bradykinin, a potent inflammatory molecule, is released by binding to high-molecular-weight kininogen (HK). In addition to inflammation, bradykinin can cause edema and blood-brain barrier permeability.
Although it’s been known that amyloid-beta can activate the contact system, the particular form of amyloid-beta implicated in this cascade has not been identified. And so, the researchers incubated amyloid-beta42 with human plasma, testing various types of amyloid-beta – monomers, oligomers, protofibrils, and fibrils – to see which would activate the contact system.
Amyloid-beta protofibrils promoted the activation of the contact system, as evidenced by several reactions, including activation of factor XII, while other forms of amyloid-beta did not. HK also “bound tightly” to amyloid-beta protofibrils, with “weaker” binding to other amyloid-beta species, the authors reported, confirming that amyloid-beta protofibrils bind to HK and factor XII.
Bradykinin levels were increased by amyloid-beta protofibrils, which also induced faster clotting, compared with other forms of amyloid-beta.
The researchers introduced lecanemab into the picture and found it “dramatically inhibited” contact system activation induced by amyloid-beta protofibrils. For example, it blocked the binding of factor XII to amyloid-beta. By contrast, human IgG (which the researchers used as a control) had no effect.
Additionally, lecanemab also prevented accelerated intrinsic coagulation in normal human plasma mediated by amyloid-beta protofibril.
Senior author Sidney Strickland, PhD, the Zachary and Elizabeth M. Fisher professor in Alzheimer’s and neurodegenerative disease, Rockefeller University, said in an interview: “One of the strong motivators for conducting this study was the fact that this drug, which is effective in AD, targets this specific form of amyloid-beta; but no one knows why it›s more toxic. We thought we could see if we could tie it to what we›re working on, and we found it ties in beautifully.”
The findings have implications that go beyond AD, Dr. Strickland said. “The contact system is implicated in lots of different pathologies, including sickle cell anemia, sepsis, inflammatory bowel disease, and so on.” Blocking the contact system might be a helpful approach in these conditions too.
Innovative, plausible, but still preliminary
In a comment, Heather M. Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, called the investigation “innovative,” with ideas that are “certainly plausible.” However, “at this time, the work is preliminary and not conclusive.”
The hypothesized mechanisms for why amyloid (lecanemab’s target) is toxic to the brain “does incorporate important AD-related brain changes that have been observed in other studies, including inflammatory/immune changes and vascular-related changes,” said Dr. Snyder, who was not involved with the current study.
However, “additional studies that look both in model systems and in humans are needed to further illuminate these relationships,” Dr. Snyder said.
The study was supported by grants from the National Institutes of Health as well as the Robertson Therapeutic Development Fund, Samuel Newhouse Foundation, John A. Herrmann, and the May and Samuel Rudin Family Foundation. Dr. Norris, Dr. Strickland, and Dr. Snyder declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Lecanemab (Lequembi, Esai), an amyloid-beta–directed antibody therapy, is approved by the Food and Drug Administration for the treatment of Alzheimer’s disease (AD). But exactly how the drug clears amyloid-beta wasn’t clear.
The investigators tested the effectiveness of various forms of amyloid-beta in activating the plasma contact system and found that amyloid-beta protofibrils, known to be the most toxic form of amyloid-beta, promoted the activation of this molecular cascade and that lecanemab inhibited pathway activation.
“In our study, we looked at lecanemab and found it can block the activation of the contact system, which could be one of the reasons that it works so well for AD,” study coinvestigator Erin Norris, PhD, research associate professor, Rockefeller University, New York, said in an interview.
The study was published online in the Proceedings of the National Academy of Science.
Unknown mechanism
“Many years ago, we started looking at the involvement of vascular dysfunction in AD,” Dr. Norris said. “We wanted to see whether or not irregular blood clotting or problems with blood flow was problematic in Alzheimer’s patients.”
The researchers found that fibrin, a major component involved in blood clotting, can extravasate into the brain.
“The blood-brain barrier can break down in Alzheimer’s, so things from the blood can move into the brain and deposit there,” she added. Fibrin then interacts with amyloid-beta, the major pathogenic protein in AD.
Dr. Norris explained that fibrin clots can form in two different ways. One is through the normal process that occurs when there’s an injury and bleeding. The second is through intrinsic clotting, which takes place through the contact system.
“We started looking into this system and found that the plasma of Alzheimer’s patients showed irregular levels of these enzymes and proteins that are part of the intrinsic clotting system compared to those of normal controls,” said Dr. Norris.
“This paper was an extension of years studying this pathway and these mechanisms. It was also inspired by the approval of lecanemab and its release for use in Alzheimer’s patients,” she added.
In previous research, the same researchers found that amyloid-beta has different forms. “It’s normally soluble, and it’s a very tiny molecule,” Dr. Norris said. “But over time, and in different situations, it can start to aggregate, becoming bigger and bigger.”
Implications beyond Alzheimer’s
Postmortem tissue analysis has found fibrillar plaques that are “clumped together.” These are insoluble and hard to get rid of, she said. “Protofibrils are the step before amyloid-beta forms fibrils and are considered to be the most toxic form, although the mechanism behind why it’s so toxic is not understood.”
Previous research has already shown that amyloid-beta can activate the contact system. The contact system has two “arms,” the first of which is involved with clotting, and the second with inflammation, Dr. Norris said. In fact, it’s the plasma contact system that links vascular and inflammatory pathways.
The plasma contact system leads to the clotting of fibrin, Dr. Norris continued. It activates factor XII, which leads to blood clotting by binding to coagulation factor XI.
The contact system also causes inflammation – the second “arm.” Bradykinin, a potent inflammatory molecule, is released by binding to high-molecular-weight kininogen (HK). In addition to inflammation, bradykinin can cause edema and blood-brain barrier permeability.
Although it’s been known that amyloid-beta can activate the contact system, the particular form of amyloid-beta implicated in this cascade has not been identified. And so, the researchers incubated amyloid-beta42 with human plasma, testing various types of amyloid-beta – monomers, oligomers, protofibrils, and fibrils – to see which would activate the contact system.
Amyloid-beta protofibrils promoted the activation of the contact system, as evidenced by several reactions, including activation of factor XII, while other forms of amyloid-beta did not. HK also “bound tightly” to amyloid-beta protofibrils, with “weaker” binding to other amyloid-beta species, the authors reported, confirming that amyloid-beta protofibrils bind to HK and factor XII.
Bradykinin levels were increased by amyloid-beta protofibrils, which also induced faster clotting, compared with other forms of amyloid-beta.
The researchers introduced lecanemab into the picture and found it “dramatically inhibited” contact system activation induced by amyloid-beta protofibrils. For example, it blocked the binding of factor XII to amyloid-beta. By contrast, human IgG (which the researchers used as a control) had no effect.
Additionally, lecanemab also prevented accelerated intrinsic coagulation in normal human plasma mediated by amyloid-beta protofibril.
Senior author Sidney Strickland, PhD, the Zachary and Elizabeth M. Fisher professor in Alzheimer’s and neurodegenerative disease, Rockefeller University, said in an interview: “One of the strong motivators for conducting this study was the fact that this drug, which is effective in AD, targets this specific form of amyloid-beta; but no one knows why it›s more toxic. We thought we could see if we could tie it to what we›re working on, and we found it ties in beautifully.”
The findings have implications that go beyond AD, Dr. Strickland said. “The contact system is implicated in lots of different pathologies, including sickle cell anemia, sepsis, inflammatory bowel disease, and so on.” Blocking the contact system might be a helpful approach in these conditions too.
Innovative, plausible, but still preliminary
In a comment, Heather M. Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, called the investigation “innovative,” with ideas that are “certainly plausible.” However, “at this time, the work is preliminary and not conclusive.”
The hypothesized mechanisms for why amyloid (lecanemab’s target) is toxic to the brain “does incorporate important AD-related brain changes that have been observed in other studies, including inflammatory/immune changes and vascular-related changes,” said Dr. Snyder, who was not involved with the current study.
However, “additional studies that look both in model systems and in humans are needed to further illuminate these relationships,” Dr. Snyder said.
The study was supported by grants from the National Institutes of Health as well as the Robertson Therapeutic Development Fund, Samuel Newhouse Foundation, John A. Herrmann, and the May and Samuel Rudin Family Foundation. Dr. Norris, Dr. Strickland, and Dr. Snyder declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Lecanemab (Lequembi, Esai), an amyloid-beta–directed antibody therapy, is approved by the Food and Drug Administration for the treatment of Alzheimer’s disease (AD). But exactly how the drug clears amyloid-beta wasn’t clear.
The investigators tested the effectiveness of various forms of amyloid-beta in activating the plasma contact system and found that amyloid-beta protofibrils, known to be the most toxic form of amyloid-beta, promoted the activation of this molecular cascade and that lecanemab inhibited pathway activation.
“In our study, we looked at lecanemab and found it can block the activation of the contact system, which could be one of the reasons that it works so well for AD,” study coinvestigator Erin Norris, PhD, research associate professor, Rockefeller University, New York, said in an interview.
The study was published online in the Proceedings of the National Academy of Science.
Unknown mechanism
“Many years ago, we started looking at the involvement of vascular dysfunction in AD,” Dr. Norris said. “We wanted to see whether or not irregular blood clotting or problems with blood flow was problematic in Alzheimer’s patients.”
The researchers found that fibrin, a major component involved in blood clotting, can extravasate into the brain.
“The blood-brain barrier can break down in Alzheimer’s, so things from the blood can move into the brain and deposit there,” she added. Fibrin then interacts with amyloid-beta, the major pathogenic protein in AD.
Dr. Norris explained that fibrin clots can form in two different ways. One is through the normal process that occurs when there’s an injury and bleeding. The second is through intrinsic clotting, which takes place through the contact system.
“We started looking into this system and found that the plasma of Alzheimer’s patients showed irregular levels of these enzymes and proteins that are part of the intrinsic clotting system compared to those of normal controls,” said Dr. Norris.
“This paper was an extension of years studying this pathway and these mechanisms. It was also inspired by the approval of lecanemab and its release for use in Alzheimer’s patients,” she added.
In previous research, the same researchers found that amyloid-beta has different forms. “It’s normally soluble, and it’s a very tiny molecule,” Dr. Norris said. “But over time, and in different situations, it can start to aggregate, becoming bigger and bigger.”
Implications beyond Alzheimer’s
Postmortem tissue analysis has found fibrillar plaques that are “clumped together.” These are insoluble and hard to get rid of, she said. “Protofibrils are the step before amyloid-beta forms fibrils and are considered to be the most toxic form, although the mechanism behind why it’s so toxic is not understood.”
Previous research has already shown that amyloid-beta can activate the contact system. The contact system has two “arms,” the first of which is involved with clotting, and the second with inflammation, Dr. Norris said. In fact, it’s the plasma contact system that links vascular and inflammatory pathways.
The plasma contact system leads to the clotting of fibrin, Dr. Norris continued. It activates factor XII, which leads to blood clotting by binding to coagulation factor XI.
The contact system also causes inflammation – the second “arm.” Bradykinin, a potent inflammatory molecule, is released by binding to high-molecular-weight kininogen (HK). In addition to inflammation, bradykinin can cause edema and blood-brain barrier permeability.
Although it’s been known that amyloid-beta can activate the contact system, the particular form of amyloid-beta implicated in this cascade has not been identified. And so, the researchers incubated amyloid-beta42 with human plasma, testing various types of amyloid-beta – monomers, oligomers, protofibrils, and fibrils – to see which would activate the contact system.
Amyloid-beta protofibrils promoted the activation of the contact system, as evidenced by several reactions, including activation of factor XII, while other forms of amyloid-beta did not. HK also “bound tightly” to amyloid-beta protofibrils, with “weaker” binding to other amyloid-beta species, the authors reported, confirming that amyloid-beta protofibrils bind to HK and factor XII.
Bradykinin levels were increased by amyloid-beta protofibrils, which also induced faster clotting, compared with other forms of amyloid-beta.
The researchers introduced lecanemab into the picture and found it “dramatically inhibited” contact system activation induced by amyloid-beta protofibrils. For example, it blocked the binding of factor XII to amyloid-beta. By contrast, human IgG (which the researchers used as a control) had no effect.
Additionally, lecanemab also prevented accelerated intrinsic coagulation in normal human plasma mediated by amyloid-beta protofibril.
Senior author Sidney Strickland, PhD, the Zachary and Elizabeth M. Fisher professor in Alzheimer’s and neurodegenerative disease, Rockefeller University, said in an interview: “One of the strong motivators for conducting this study was the fact that this drug, which is effective in AD, targets this specific form of amyloid-beta; but no one knows why it›s more toxic. We thought we could see if we could tie it to what we›re working on, and we found it ties in beautifully.”
The findings have implications that go beyond AD, Dr. Strickland said. “The contact system is implicated in lots of different pathologies, including sickle cell anemia, sepsis, inflammatory bowel disease, and so on.” Blocking the contact system might be a helpful approach in these conditions too.
Innovative, plausible, but still preliminary
In a comment, Heather M. Snyder, PhD, vice president of medical and scientific relations at the Alzheimer’s Association, called the investigation “innovative,” with ideas that are “certainly plausible.” However, “at this time, the work is preliminary and not conclusive.”
The hypothesized mechanisms for why amyloid (lecanemab’s target) is toxic to the brain “does incorporate important AD-related brain changes that have been observed in other studies, including inflammatory/immune changes and vascular-related changes,” said Dr. Snyder, who was not involved with the current study.
However, “additional studies that look both in model systems and in humans are needed to further illuminate these relationships,” Dr. Snyder said.
The study was supported by grants from the National Institutes of Health as well as the Robertson Therapeutic Development Fund, Samuel Newhouse Foundation, John A. Herrmann, and the May and Samuel Rudin Family Foundation. Dr. Norris, Dr. Strickland, and Dr. Snyder declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PROCEEDINGS OF THE NATIONAL ACADEMY OF SCIENCE
Suicidal behavior tied to increased all-cause mortality in MDD
Investigators studied close to 143,000 patients, encompassing more than 150,000 MDD episodes. Episodes of depression with suicidal behavior (MDD-SB) were compared to MDD episodes without suicidal behavior (MDD-non-SB).
Suicidal behavior was associated with a 2.6-fold higher rate of all-cause mortality, as well as considerably higher health care resource utilization (HCRU) and work loss, compared with matched controls.
Patients with depression who had attempted suicide were younger and more commonly suffering from other psychiatric comorbidities, such as anxiety and addiction. Important risk factors for suicidal acts within a year after the onset of a depressive episode were previous suicide attempts, substance use disorder, anxiety, and sleeping disorders.
“The findings tell us that the care provided for this particular group needs to be developed,” lead author Johan Lundberg, MD, PhD, adjunct professor in psychiatry and senior physician in psychiatry, Karolinska Institute, Stockholm, told this news organization.
“The take-home message is that, when treating patients with increased risk of suicidal behavior, one should offer treatments with this in mind,” said Dr. Lundberg, also the head of the section of mood disorders, Northern Stockholm Psychiatry Clinic. “One possible option is lithium augmentation.”
The study was published online in JAMA Psychiatry.
Identifying subgroups
Depression is associated with increased all-cause mortality, the authors write. Suicidal behavior and previous suicide attempts are known to increase the risk of suicide-associated mortality, with up to 13% of patients with nonfatal suicide attempts dying of suicide at a later time.
Previous studies investigating the association between suicidal behavior and mortality have been limited by nonrandom sampling due to “nonuniversal access to health care and/or exclusion of primary care data,” they state.
For this reason, it’s not established to what extent these estimates actually represent patients with MDD as a whole, or to what extent suicidal behavior is a risk factor for all-cause mortality.
“We think there is a need to identify subgroups within the very large group of individuals with MDD in order to improve treatment outcomes,” Dr. Lundberg said.
To do so, the researchers turned to data from the Stockholm MDD Cohort (SMC), which comprises all patients diagnosed with MDD in any health care setting in the regions of Stockholm from 2010 to 2018. They identified 5 years of recorded MDD episodes (n = 158,169) in patients aged 18 years and older (n = 145,577). A single patient could contribute more than one episode.
At index, MDD-SB patients (n = 2,219; mean age, 41 years) were matched with MDD-non-SB patients (9,574; mean age, 41 years) based on age, sex, year of MDD diagnosis, and socioeconomic status. In total, 2,219 episodes (63.2% in women, 36.8% in men) were compared to 11,109 episodes (63.4% in women, 36.6% in men), respectively.
Enhanced monitoring, optimized treatment
The median time from the start of the episode until the first suicidal behavior was 165 days.
The all-cause mortality rate in the MDD-SB and MDD-non-SB groups was 2.5 per 100 person-years vs. 1 per 100 person-years, respectively (based on 466 deaths), corresponding to a hazard ratio of 2.62 (95% confidence interval, 2.15-3.20).
Patients in the MDD-SB group were younger, were more frequently diagnosed while in specialized care, and had sustained more work loss than their counterparts in the MDD-non-SB group. They also showed a gradual increase in the prevalence of comorbid conditions from about 12 months before index, with this increase being “most pronounced” for anxiety, stress, substance use, and personality disorders.
MDD-SB episodes were associated with higher HCRU and more work loss, compared with MDD-non-SB episodes.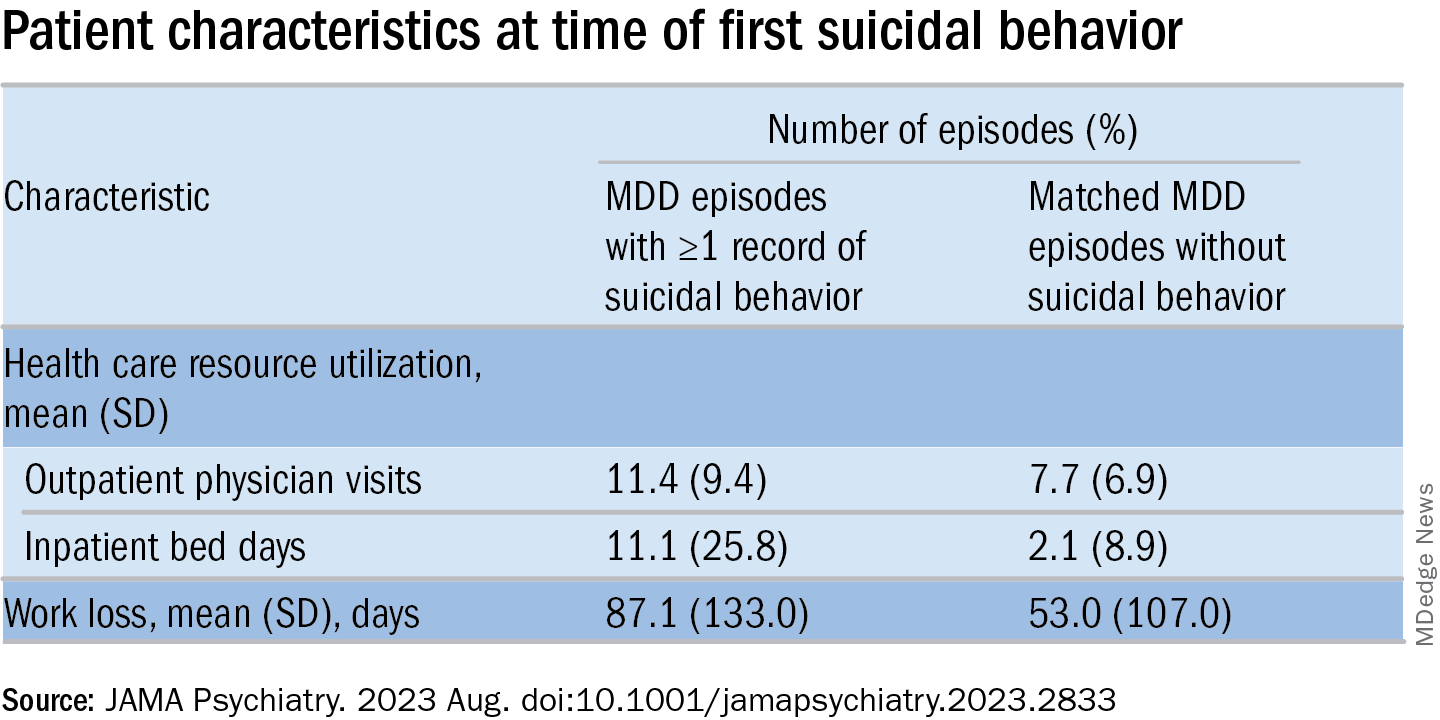
The researchers calculated a risk score for factors associated with suicidal behavior within 1 year after the start of an MDD episode (outcome). The two most important risk factors for suicidal behavior were a history of suicidal behavior together with age, which had a “U-shaped association” with the outcome, they write, with individuals younger than age 20 and older than age 70 having the highest risks.
The final risk score included additional factors that increased the risk of the outcome (in descending order): history of substance use, history of sleep disorders, health care level in which MDD was diagnosed, history of antidepressant use, and history of anxiety disorders.
These results “indicate that patients at risk for suicidal behavior can be identified at an early stage to allow for enhanced monitoring and optimized treatment with the goal of preventing suicidal behavior and reducing mortality,” the authors state.
The specific causes of death weren’t analyzed in this particular paper, Dr. Lundberg noted. A previous study conducted by the same group found the risk of death was doubled in MDD patients, compared with controls.
“We don’t speculate about which causes other than suicide might explain the difference” and account for the increased mortality risk, he said. “This should be studied in future projects.”
Complicated family of destructive behaviors
In a comment, Russell Copelan, MD, a former emergency department psychiatrist at the University of Colorado Affiliated Hospital and currently an expert consultant to the American Association of Suicidology, said a take-home message of the study is that suicide is “a complex and complicated family of destructive behaviors.”
The findings “should not suggest a wait-and-see clinical approach,” warned Dr. Copelan, who wasn’t involved with the study.
Underrecognized or misdiagnosed anxiety, agitation, and insomnia may be “barriers to remission and treatment response,” he noted.
Dr. Copelan, who is also the founder and CEO of eMed Logic, which offers assessment tools for suicide and violence, encouraged clinicians “not to minimize the proportion of patients who experience anxiety, agitation, and insomnia in response to what some may consider a personal misfortune, such as interpersonal, employment, or financial crisis.”
A version of this article first appeared on Medscape.com.
Investigators studied close to 143,000 patients, encompassing more than 150,000 MDD episodes. Episodes of depression with suicidal behavior (MDD-SB) were compared to MDD episodes without suicidal behavior (MDD-non-SB).
Suicidal behavior was associated with a 2.6-fold higher rate of all-cause mortality, as well as considerably higher health care resource utilization (HCRU) and work loss, compared with matched controls.
Patients with depression who had attempted suicide were younger and more commonly suffering from other psychiatric comorbidities, such as anxiety and addiction. Important risk factors for suicidal acts within a year after the onset of a depressive episode were previous suicide attempts, substance use disorder, anxiety, and sleeping disorders.
“The findings tell us that the care provided for this particular group needs to be developed,” lead author Johan Lundberg, MD, PhD, adjunct professor in psychiatry and senior physician in psychiatry, Karolinska Institute, Stockholm, told this news organization.
“The take-home message is that, when treating patients with increased risk of suicidal behavior, one should offer treatments with this in mind,” said Dr. Lundberg, also the head of the section of mood disorders, Northern Stockholm Psychiatry Clinic. “One possible option is lithium augmentation.”
The study was published online in JAMA Psychiatry.
Identifying subgroups
Depression is associated with increased all-cause mortality, the authors write. Suicidal behavior and previous suicide attempts are known to increase the risk of suicide-associated mortality, with up to 13% of patients with nonfatal suicide attempts dying of suicide at a later time.
Previous studies investigating the association between suicidal behavior and mortality have been limited by nonrandom sampling due to “nonuniversal access to health care and/or exclusion of primary care data,” they state.
For this reason, it’s not established to what extent these estimates actually represent patients with MDD as a whole, or to what extent suicidal behavior is a risk factor for all-cause mortality.
“We think there is a need to identify subgroups within the very large group of individuals with MDD in order to improve treatment outcomes,” Dr. Lundberg said.
To do so, the researchers turned to data from the Stockholm MDD Cohort (SMC), which comprises all patients diagnosed with MDD in any health care setting in the regions of Stockholm from 2010 to 2018. They identified 5 years of recorded MDD episodes (n = 158,169) in patients aged 18 years and older (n = 145,577). A single patient could contribute more than one episode.
At index, MDD-SB patients (n = 2,219; mean age, 41 years) were matched with MDD-non-SB patients (9,574; mean age, 41 years) based on age, sex, year of MDD diagnosis, and socioeconomic status. In total, 2,219 episodes (63.2% in women, 36.8% in men) were compared to 11,109 episodes (63.4% in women, 36.6% in men), respectively.
Enhanced monitoring, optimized treatment
The median time from the start of the episode until the first suicidal behavior was 165 days.
The all-cause mortality rate in the MDD-SB and MDD-non-SB groups was 2.5 per 100 person-years vs. 1 per 100 person-years, respectively (based on 466 deaths), corresponding to a hazard ratio of 2.62 (95% confidence interval, 2.15-3.20).
Patients in the MDD-SB group were younger, were more frequently diagnosed while in specialized care, and had sustained more work loss than their counterparts in the MDD-non-SB group. They also showed a gradual increase in the prevalence of comorbid conditions from about 12 months before index, with this increase being “most pronounced” for anxiety, stress, substance use, and personality disorders.
MDD-SB episodes were associated with higher HCRU and more work loss, compared with MDD-non-SB episodes.
The researchers calculated a risk score for factors associated with suicidal behavior within 1 year after the start of an MDD episode (outcome). The two most important risk factors for suicidal behavior were a history of suicidal behavior together with age, which had a “U-shaped association” with the outcome, they write, with individuals younger than age 20 and older than age 70 having the highest risks.
The final risk score included additional factors that increased the risk of the outcome (in descending order): history of substance use, history of sleep disorders, health care level in which MDD was diagnosed, history of antidepressant use, and history of anxiety disorders.
These results “indicate that patients at risk for suicidal behavior can be identified at an early stage to allow for enhanced monitoring and optimized treatment with the goal of preventing suicidal behavior and reducing mortality,” the authors state.
The specific causes of death weren’t analyzed in this particular paper, Dr. Lundberg noted. A previous study conducted by the same group found the risk of death was doubled in MDD patients, compared with controls.
“We don’t speculate about which causes other than suicide might explain the difference” and account for the increased mortality risk, he said. “This should be studied in future projects.”
Complicated family of destructive behaviors
In a comment, Russell Copelan, MD, a former emergency department psychiatrist at the University of Colorado Affiliated Hospital and currently an expert consultant to the American Association of Suicidology, said a take-home message of the study is that suicide is “a complex and complicated family of destructive behaviors.”
The findings “should not suggest a wait-and-see clinical approach,” warned Dr. Copelan, who wasn’t involved with the study.
Underrecognized or misdiagnosed anxiety, agitation, and insomnia may be “barriers to remission and treatment response,” he noted.
Dr. Copelan, who is also the founder and CEO of eMed Logic, which offers assessment tools for suicide and violence, encouraged clinicians “not to minimize the proportion of patients who experience anxiety, agitation, and insomnia in response to what some may consider a personal misfortune, such as interpersonal, employment, or financial crisis.”
A version of this article first appeared on Medscape.com.
Investigators studied close to 143,000 patients, encompassing more than 150,000 MDD episodes. Episodes of depression with suicidal behavior (MDD-SB) were compared to MDD episodes without suicidal behavior (MDD-non-SB).
Suicidal behavior was associated with a 2.6-fold higher rate of all-cause mortality, as well as considerably higher health care resource utilization (HCRU) and work loss, compared with matched controls.
Patients with depression who had attempted suicide were younger and more commonly suffering from other psychiatric comorbidities, such as anxiety and addiction. Important risk factors for suicidal acts within a year after the onset of a depressive episode were previous suicide attempts, substance use disorder, anxiety, and sleeping disorders.
“The findings tell us that the care provided for this particular group needs to be developed,” lead author Johan Lundberg, MD, PhD, adjunct professor in psychiatry and senior physician in psychiatry, Karolinska Institute, Stockholm, told this news organization.
“The take-home message is that, when treating patients with increased risk of suicidal behavior, one should offer treatments with this in mind,” said Dr. Lundberg, also the head of the section of mood disorders, Northern Stockholm Psychiatry Clinic. “One possible option is lithium augmentation.”
The study was published online in JAMA Psychiatry.
Identifying subgroups
Depression is associated with increased all-cause mortality, the authors write. Suicidal behavior and previous suicide attempts are known to increase the risk of suicide-associated mortality, with up to 13% of patients with nonfatal suicide attempts dying of suicide at a later time.
Previous studies investigating the association between suicidal behavior and mortality have been limited by nonrandom sampling due to “nonuniversal access to health care and/or exclusion of primary care data,” they state.
For this reason, it’s not established to what extent these estimates actually represent patients with MDD as a whole, or to what extent suicidal behavior is a risk factor for all-cause mortality.
“We think there is a need to identify subgroups within the very large group of individuals with MDD in order to improve treatment outcomes,” Dr. Lundberg said.
To do so, the researchers turned to data from the Stockholm MDD Cohort (SMC), which comprises all patients diagnosed with MDD in any health care setting in the regions of Stockholm from 2010 to 2018. They identified 5 years of recorded MDD episodes (n = 158,169) in patients aged 18 years and older (n = 145,577). A single patient could contribute more than one episode.
At index, MDD-SB patients (n = 2,219; mean age, 41 years) were matched with MDD-non-SB patients (9,574; mean age, 41 years) based on age, sex, year of MDD diagnosis, and socioeconomic status. In total, 2,219 episodes (63.2% in women, 36.8% in men) were compared to 11,109 episodes (63.4% in women, 36.6% in men), respectively.
Enhanced monitoring, optimized treatment
The median time from the start of the episode until the first suicidal behavior was 165 days.
The all-cause mortality rate in the MDD-SB and MDD-non-SB groups was 2.5 per 100 person-years vs. 1 per 100 person-years, respectively (based on 466 deaths), corresponding to a hazard ratio of 2.62 (95% confidence interval, 2.15-3.20).
Patients in the MDD-SB group were younger, were more frequently diagnosed while in specialized care, and had sustained more work loss than their counterparts in the MDD-non-SB group. They also showed a gradual increase in the prevalence of comorbid conditions from about 12 months before index, with this increase being “most pronounced” for anxiety, stress, substance use, and personality disorders.
MDD-SB episodes were associated with higher HCRU and more work loss, compared with MDD-non-SB episodes.
The researchers calculated a risk score for factors associated with suicidal behavior within 1 year after the start of an MDD episode (outcome). The two most important risk factors for suicidal behavior were a history of suicidal behavior together with age, which had a “U-shaped association” with the outcome, they write, with individuals younger than age 20 and older than age 70 having the highest risks.
The final risk score included additional factors that increased the risk of the outcome (in descending order): history of substance use, history of sleep disorders, health care level in which MDD was diagnosed, history of antidepressant use, and history of anxiety disorders.
These results “indicate that patients at risk for suicidal behavior can be identified at an early stage to allow for enhanced monitoring and optimized treatment with the goal of preventing suicidal behavior and reducing mortality,” the authors state.
The specific causes of death weren’t analyzed in this particular paper, Dr. Lundberg noted. A previous study conducted by the same group found the risk of death was doubled in MDD patients, compared with controls.
“We don’t speculate about which causes other than suicide might explain the difference” and account for the increased mortality risk, he said. “This should be studied in future projects.”
Complicated family of destructive behaviors
In a comment, Russell Copelan, MD, a former emergency department psychiatrist at the University of Colorado Affiliated Hospital and currently an expert consultant to the American Association of Suicidology, said a take-home message of the study is that suicide is “a complex and complicated family of destructive behaviors.”
The findings “should not suggest a wait-and-see clinical approach,” warned Dr. Copelan, who wasn’t involved with the study.
Underrecognized or misdiagnosed anxiety, agitation, and insomnia may be “barriers to remission and treatment response,” he noted.
Dr. Copelan, who is also the founder and CEO of eMed Logic, which offers assessment tools for suicide and violence, encouraged clinicians “not to minimize the proportion of patients who experience anxiety, agitation, and insomnia in response to what some may consider a personal misfortune, such as interpersonal, employment, or financial crisis.”
A version of this article first appeared on Medscape.com.
FROM JAMA PSYCHIATRY