User login
From the Washington Office: Advocacy in Action
Fellows frequently ask how they can get more involved in the advocacy efforts of the ACS. Whether you are new to the arena of policy and advocacy or an experienced veteran of innumerable efforts directed at ensuring access to quality surgical care, I can think of no better way to learn new skills and exercise old ones than by attending the ACS’ annual Leadership and Advocacy Summit.
The 2017 Leadership and Advocacy Summit will take place May 6–9 at the Renaissance Washington, DC Downtown Hotel. More than 300 individuals have already registered and you can join them by registering via the link found here: https://www.facs.org/advocacy/participate/summit-2017/register

The Advocacy Summit portion of the meeting will kick-off on the evening of May 7 with a reception and dinner featuring bestselling author, MSNBC political analyst, and former Communications Chief for President George W. Bush, Nicolle Wallace as the Keynote Speaker.
A robust agenda is planned for Monday, May 8. The morning will lead off with a panel entitled, Perspectives on 2017 Health Care Reform, featuring health policy experts from the Georgetown University Law Center, the George Washington University Milken Institute School of Public Health, the American Enterprise Institute, and the Heritage Foundation. The Monday agenda will also feature a panel of senior staffers from Capitol Hill discussing issues of particular interest to Fellows, a Medicare physician payment panel, and an address from a leading authority on effective communications strategies designed to make your interaction with legislators and their staff more effective.
The luncheon speaker for Monday will be Fox News contributor and Washington Examiner columnist, Lisa Boothe. The afternoon agenda will conclude with a series of issue briefings from ACS staff (in preparation for the Hill visits to legislator’s offices scheduled for Tuesday, May 9) and remarks from several United States Senators. ACSPA-SurgeonsPAC will host a reception on Monday evening, May 8 for all 2017 PAC contributors and a guest.
On Tuesday morning, May 9, attendees will be transported to Capitol Hill to visit the offices of their individual Member of Congress, Senators and staff with visits concluding in time to make flights out of Washington that afternoon.
I encourage all Fellows who are able to set aside time for the event to do so as I believe all will find the program educational and the experience rewarding.
For information about the Leadership Summit, contact Connie Bura at cbura@facs.org, or 312-919-5290. For information about the Advocacy Summit, contact Michael Carmody at mcarmody@facs.org, or 202-672-1511.
Until next month ….
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Fellows frequently ask how they can get more involved in the advocacy efforts of the ACS. Whether you are new to the arena of policy and advocacy or an experienced veteran of innumerable efforts directed at ensuring access to quality surgical care, I can think of no better way to learn new skills and exercise old ones than by attending the ACS’ annual Leadership and Advocacy Summit.
The 2017 Leadership and Advocacy Summit will take place May 6–9 at the Renaissance Washington, DC Downtown Hotel. More than 300 individuals have already registered and you can join them by registering via the link found here: https://www.facs.org/advocacy/participate/summit-2017/register
The Advocacy Summit portion of the meeting will kick-off on the evening of May 7 with a reception and dinner featuring bestselling author, MSNBC political analyst, and former Communications Chief for President George W. Bush, Nicolle Wallace as the Keynote Speaker.
A robust agenda is planned for Monday, May 8. The morning will lead off with a panel entitled, Perspectives on 2017 Health Care Reform, featuring health policy experts from the Georgetown University Law Center, the George Washington University Milken Institute School of Public Health, the American Enterprise Institute, and the Heritage Foundation. The Monday agenda will also feature a panel of senior staffers from Capitol Hill discussing issues of particular interest to Fellows, a Medicare physician payment panel, and an address from a leading authority on effective communications strategies designed to make your interaction with legislators and their staff more effective.
The luncheon speaker for Monday will be Fox News contributor and Washington Examiner columnist, Lisa Boothe. The afternoon agenda will conclude with a series of issue briefings from ACS staff (in preparation for the Hill visits to legislator’s offices scheduled for Tuesday, May 9) and remarks from several United States Senators. ACSPA-SurgeonsPAC will host a reception on Monday evening, May 8 for all 2017 PAC contributors and a guest.
On Tuesday morning, May 9, attendees will be transported to Capitol Hill to visit the offices of their individual Member of Congress, Senators and staff with visits concluding in time to make flights out of Washington that afternoon.
I encourage all Fellows who are able to set aside time for the event to do so as I believe all will find the program educational and the experience rewarding.
For information about the Leadership Summit, contact Connie Bura at cbura@facs.org, or 312-919-5290. For information about the Advocacy Summit, contact Michael Carmody at mcarmody@facs.org, or 202-672-1511.
Until next month ….
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Fellows frequently ask how they can get more involved in the advocacy efforts of the ACS. Whether you are new to the arena of policy and advocacy or an experienced veteran of innumerable efforts directed at ensuring access to quality surgical care, I can think of no better way to learn new skills and exercise old ones than by attending the ACS’ annual Leadership and Advocacy Summit.
The 2017 Leadership and Advocacy Summit will take place May 6–9 at the Renaissance Washington, DC Downtown Hotel. More than 300 individuals have already registered and you can join them by registering via the link found here: https://www.facs.org/advocacy/participate/summit-2017/register
The Advocacy Summit portion of the meeting will kick-off on the evening of May 7 with a reception and dinner featuring bestselling author, MSNBC political analyst, and former Communications Chief for President George W. Bush, Nicolle Wallace as the Keynote Speaker.
A robust agenda is planned for Monday, May 8. The morning will lead off with a panel entitled, Perspectives on 2017 Health Care Reform, featuring health policy experts from the Georgetown University Law Center, the George Washington University Milken Institute School of Public Health, the American Enterprise Institute, and the Heritage Foundation. The Monday agenda will also feature a panel of senior staffers from Capitol Hill discussing issues of particular interest to Fellows, a Medicare physician payment panel, and an address from a leading authority on effective communications strategies designed to make your interaction with legislators and their staff more effective.
The luncheon speaker for Monday will be Fox News contributor and Washington Examiner columnist, Lisa Boothe. The afternoon agenda will conclude with a series of issue briefings from ACS staff (in preparation for the Hill visits to legislator’s offices scheduled for Tuesday, May 9) and remarks from several United States Senators. ACSPA-SurgeonsPAC will host a reception on Monday evening, May 8 for all 2017 PAC contributors and a guest.
On Tuesday morning, May 9, attendees will be transported to Capitol Hill to visit the offices of their individual Member of Congress, Senators and staff with visits concluding in time to make flights out of Washington that afternoon.
I encourage all Fellows who are able to set aside time for the event to do so as I believe all will find the program educational and the experience rewarding.
For information about the Leadership Summit, contact Connie Bura at cbura@facs.org, or 312-919-5290. For information about the Advocacy Summit, contact Michael Carmody at mcarmody@facs.org, or 202-672-1511.
Until next month ….
Dr. Bailey is a pediatric surgeon, and Medical Director, Advocacy, for the Division of Advocacy and Health Policy in the ACS offices in Washington, DC.
Three days in the life of a surgeon
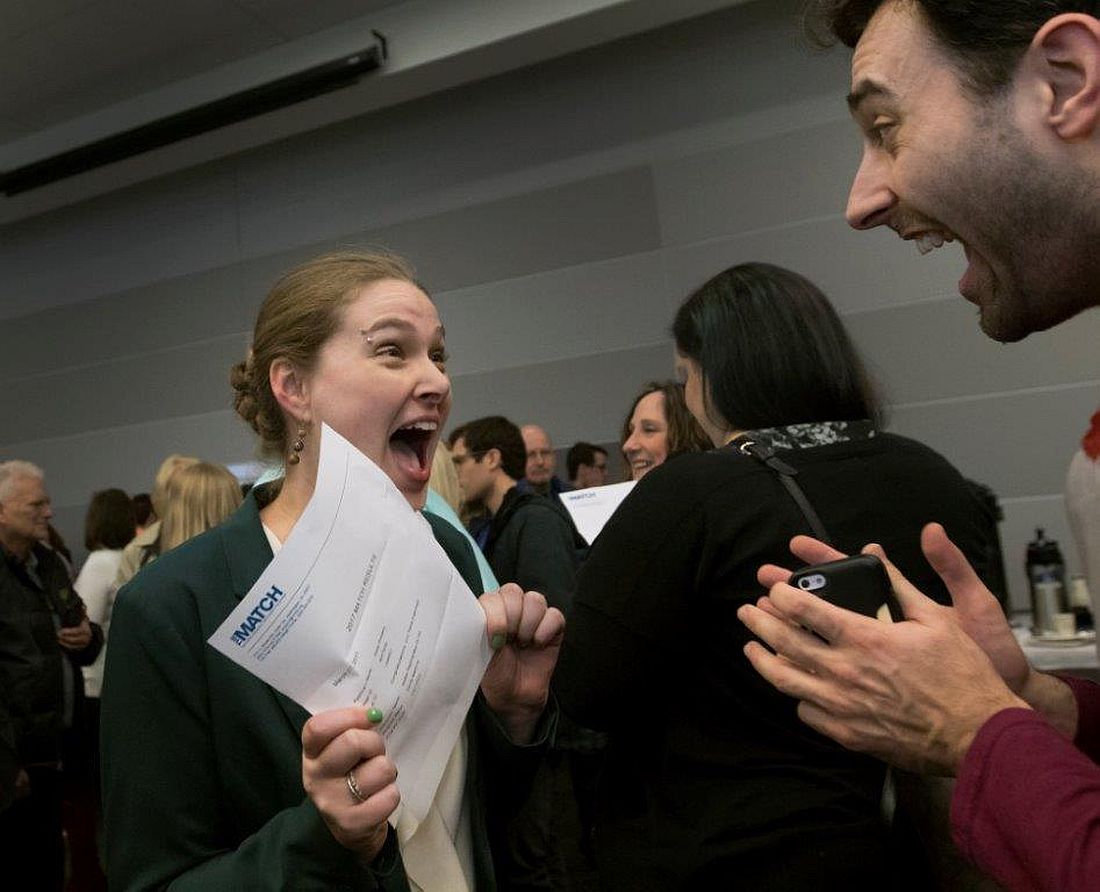
By sheer happenstance, I was visiting a surgery program on the day after “the Match.” As all of you know, four days before the official release of the placement of every new surgical trainee, both the medical students involved and the programs affected are informed as to whether they have been matched. Students don’t know where they are going, just that the last rung of training is now in place. They have a job and a relatively secure future. Those who have not been matched and those programs that did not fill all their slots now enter into a scramble (officially called SOAP) to find students for the remaining slots. This year, the scramble occurred on a Wednesday and was orchestrated by a set of rules I’d never been privy to before.
On Tuesday night, all the programs in need of students for their open slots, whether categorical or preliminary, looked over the list of candidates remaining and made their choices. So did the students now hoping to find a place. At 10 a.m., the offers went out to students in the first round. Next, in precisely timed order, the programs found out who had accepted the offers. And, if slots were left over, the programs had a short time to put up another set of offers – and so on throughout the day until all the slots were gone. Like a game of musical chairs, the music finally stopped and the Match was over for the entering class of residents for 2017.


Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and coeditor of ACS Surgery News.
By sheer happenstance, I was visiting a surgery program on the day after “the Match.” As all of you know, four days before the official release of the placement of every new surgical trainee, both the medical students involved and the programs affected are informed as to whether they have been matched. Students don’t know where they are going, just that the last rung of training is now in place. They have a job and a relatively secure future. Those who have not been matched and those programs that did not fill all their slots now enter into a scramble (officially called SOAP) to find students for the remaining slots. This year, the scramble occurred on a Wednesday and was orchestrated by a set of rules I’d never been privy to before.
On Tuesday night, all the programs in need of students for their open slots, whether categorical or preliminary, looked over the list of candidates remaining and made their choices. So did the students now hoping to find a place. At 10 a.m., the offers went out to students in the first round. Next, in precisely timed order, the programs found out who had accepted the offers. And, if slots were left over, the programs had a short time to put up another set of offers – and so on throughout the day until all the slots were gone. Like a game of musical chairs, the music finally stopped and the Match was over for the entering class of residents for 2017.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and coeditor of ACS Surgery News.
By sheer happenstance, I was visiting a surgery program on the day after “the Match.” As all of you know, four days before the official release of the placement of every new surgical trainee, both the medical students involved and the programs affected are informed as to whether they have been matched. Students don’t know where they are going, just that the last rung of training is now in place. They have a job and a relatively secure future. Those who have not been matched and those programs that did not fill all their slots now enter into a scramble (officially called SOAP) to find students for the remaining slots. This year, the scramble occurred on a Wednesday and was orchestrated by a set of rules I’d never been privy to before.
On Tuesday night, all the programs in need of students for their open slots, whether categorical or preliminary, looked over the list of candidates remaining and made their choices. So did the students now hoping to find a place. At 10 a.m., the offers went out to students in the first round. Next, in precisely timed order, the programs found out who had accepted the offers. And, if slots were left over, the programs had a short time to put up another set of offers – and so on throughout the day until all the slots were gone. Like a game of musical chairs, the music finally stopped and the Match was over for the entering class of residents for 2017.
Dr. Hughes is clinical professor in the department of surgery and director of medical education at the Kansas University School of Medicine, Salina Campus, and coeditor of ACS Surgery News.
Combining teamwork and technology when tragedy strikes
I’m the new chief of service for the department of dermatology at Kaiser Permanente San Diego. We are hiring, so I’ve been working on my answers to astute questions about how we at Kaiser Permanente differ from other health systems and why I love our medical group. Many points of differentiation involve how we work as an integrated system and how we are compensated for effective care instead of simply volume of care.

There are more than 70 dermatologists and staff in our department, and we all play a role in meeting the access needs of our patients. When one of our docs emailed me at 4 a.m. to tell me of a terrible catastrophe that struck her family, it set off a somber day for our team. In addition to offering our sympathy to her, we got right to work to help her. She needed time off to be with her family, and like all of us, she had full schedules booked for weeks ahead.
By 6 a.m., our administrative team was aware and working to recover. We canceled her clinic, and, using scheduling software, identified dermatologists in our department who might be able to help. With a few clicks, we reassigned patients from her to me and others who immediately volunteered. This was seamless as far as the patients would be concerned. Patients coming in within hours that morning were picked up by other doctors; one by one, they added them to their schedules.
Every doctor in San Diego has a Kaiser Permanente–issued smartphone. These allowed us to quickly email, text, and message to coordinate our efforts. Each of us dermatologists connected to her in-basket in our electronic medical record and set to work sending out her biopsy results, answering her secure email messages, and calling her patients. Others volunteered to cover her call, and we reassigned her teledermatology shifts with just a click. By noon, all her responsibilities as a dermatologist had been accounted for, allowing her to focus on her family. Teamwork was enabled by our digital system of care.
This story isn’t a sales pitch. We wish it had never happened. But it might be the best answer to the question of why we love working here. When we combine team plus technology to care for our patients and to care for each other, there’s no medical group we’d rather be.
I hope this is the last tragedy to befall us as a department. And if it is not, I hope to have just this same team around me to cope.
I’m sure others have similar stories of how technology helped them work as a team. Please send them to me at dermnews@frontlinemedcom.com; I’d like to write a follow-up piece.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. He is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com.
I’m the new chief of service for the department of dermatology at Kaiser Permanente San Diego. We are hiring, so I’ve been working on my answers to astute questions about how we at Kaiser Permanente differ from other health systems and why I love our medical group. Many points of differentiation involve how we work as an integrated system and how we are compensated for effective care instead of simply volume of care.
There are more than 70 dermatologists and staff in our department, and we all play a role in meeting the access needs of our patients. When one of our docs emailed me at 4 a.m. to tell me of a terrible catastrophe that struck her family, it set off a somber day for our team. In addition to offering our sympathy to her, we got right to work to help her. She needed time off to be with her family, and like all of us, she had full schedules booked for weeks ahead.
By 6 a.m., our administrative team was aware and working to recover. We canceled her clinic, and, using scheduling software, identified dermatologists in our department who might be able to help. With a few clicks, we reassigned patients from her to me and others who immediately volunteered. This was seamless as far as the patients would be concerned. Patients coming in within hours that morning were picked up by other doctors; one by one, they added them to their schedules.
Every doctor in San Diego has a Kaiser Permanente–issued smartphone. These allowed us to quickly email, text, and message to coordinate our efforts. Each of us dermatologists connected to her in-basket in our electronic medical record and set to work sending out her biopsy results, answering her secure email messages, and calling her patients. Others volunteered to cover her call, and we reassigned her teledermatology shifts with just a click. By noon, all her responsibilities as a dermatologist had been accounted for, allowing her to focus on her family. Teamwork was enabled by our digital system of care.
This story isn’t a sales pitch. We wish it had never happened. But it might be the best answer to the question of why we love working here. When we combine team plus technology to care for our patients and to care for each other, there’s no medical group we’d rather be.
I hope this is the last tragedy to befall us as a department. And if it is not, I hope to have just this same team around me to cope.
I’m sure others have similar stories of how technology helped them work as a team. Please send them to me at dermnews@frontlinemedcom.com; I’d like to write a follow-up piece.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. He is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com.
I’m the new chief of service for the department of dermatology at Kaiser Permanente San Diego. We are hiring, so I’ve been working on my answers to astute questions about how we at Kaiser Permanente differ from other health systems and why I love our medical group. Many points of differentiation involve how we work as an integrated system and how we are compensated for effective care instead of simply volume of care.
There are more than 70 dermatologists and staff in our department, and we all play a role in meeting the access needs of our patients. When one of our docs emailed me at 4 a.m. to tell me of a terrible catastrophe that struck her family, it set off a somber day for our team. In addition to offering our sympathy to her, we got right to work to help her. She needed time off to be with her family, and like all of us, she had full schedules booked for weeks ahead.
By 6 a.m., our administrative team was aware and working to recover. We canceled her clinic, and, using scheduling software, identified dermatologists in our department who might be able to help. With a few clicks, we reassigned patients from her to me and others who immediately volunteered. This was seamless as far as the patients would be concerned. Patients coming in within hours that morning were picked up by other doctors; one by one, they added them to their schedules.
Every doctor in San Diego has a Kaiser Permanente–issued smartphone. These allowed us to quickly email, text, and message to coordinate our efforts. Each of us dermatologists connected to her in-basket in our electronic medical record and set to work sending out her biopsy results, answering her secure email messages, and calling her patients. Others volunteered to cover her call, and we reassigned her teledermatology shifts with just a click. By noon, all her responsibilities as a dermatologist had been accounted for, allowing her to focus on her family. Teamwork was enabled by our digital system of care.
This story isn’t a sales pitch. We wish it had never happened. But it might be the best answer to the question of why we love working here. When we combine team plus technology to care for our patients and to care for each other, there’s no medical group we’d rather be.
I hope this is the last tragedy to befall us as a department. And if it is not, I hope to have just this same team around me to cope.
I’m sure others have similar stories of how technology helped them work as a team. Please send them to me at dermnews@frontlinemedcom.com; I’d like to write a follow-up piece.
Dr. Benabio is director of Healthcare Transformation and chief of dermatology at Kaiser Permanente San Diego. He is @Dermdoc on Twitter. Write to him at dermnews@frontlinemedcom.com.
Death watch intensifies for HDL-based interventions
WASHINGTON – Is it finally time to give up on HDL cholesterol–based interventions to treat atherosclerotic disease?
The approach “is on life support,” admitted Stephen J. Nicholls, MD, a long-time leader in the field who has reported results from a series of studies during the past 10 or so years that tested various approaches to juicing HDL cholesterol activity in patients, only to see each and every candidate intervention result in an inability to budge clinical outcomes.

The latest disappointment he reported was for CER-001, an engineered HDL mimetic agent. In a placebo-controlled international study, CARAT (CER-001 Atherosclerosis Regression ACS Trial), with 301 randomized patients and 272 completers, 10 weekly infusions of CER-001 over the course of 9 weeks failed to produce discernible incremental regression of atherosclerotic plaque volume, compared with standard care measured by serial examination using intravascular ultrasound (IVUS), Dr. Nicholls reported. The absence of any detectable benefit “suggests that this is not a promising strategy,” he said during his report at the meeting.
Enthusiasm for HDL cholesterol–based interventions dates to 2003, when an IVUS study of a first-generation HDL mimetic agent, ETC-216, showed an apparent ability to produce regression of coronary atheroma after five infusions over a 2-week period, compared with placebo-treated patients (JAMA. 2003 Nov 5;290[17]:2292-300). But the successor compound to this agent, MDCO-216, flamed out in an IVUS study with 113 completing patients that Dr. Nicholls reported at the American Heart Association Scientific Sessions in November 2016.
Also lying dead on the trial trail during past years are several cholesterol ester transfer protein inhibitors – torcetrapib, dalcetrapib and evacetrapib – as well as other agents that Dr. Nicholls described in a recent review (Arch Med Sci. 2016 Oct 24;12[6]:1302-7).
“HDL wouldn’t be the first risk factor we’ve seen that is not a modifiable target. Homocysteine is a really good example” of another atherosclerotic disease risk that’s proven immune to intervention, Dr. Nicholls said in an interview at the meeting. “Ultimately we’ll come to a point when the enthusiasm [for potential HDL interventions] will wane, but we’re not quite there yet.”

“There are other players in the HDL field” that remain viable, said Dr. Nicholls, most notably CSL112, plasma-derived apoA1 – the primary functional part of HDL cholesterol – that’s infused into patients to boost HDL activity. Results from a phase II study reported in November 2016 showed it increased cholesterol efflux (Circulation 2016 Nov; doi: 10.1161/CIRCULATIONAHA.116.025687), and is now the subject of additional phase II testing. “But with every negative trial, it will get harder and harder [to fund new HDL research], and we’ll look for other targets,” he said.
One promising alternative target is triglycerides. “HDL has received more attention than triglycerides over the past decade, but I think that will start to change as HDL can’t deliver,” predicted Dr. Nicholls, professor of cardiology at the South Australian Health & Medical Research Institute in Adelaide.
Understandably “financial support is the biggest issue. Do companies and investors still believe in the [HDL] dream?” Dr. Nicholls said that, objectively, looking at the HDL research record should definitely give investors pause before they sink money into new compounds for HDL intervention.
“If I was sitting at the drawing board now, would HDL be the risk factor I’d target? Probably not,” he concluded.
Dr. Nicholls received research support from Cerenis, the company that is developing CER-001, and he has received honoraria and research support from several other companies. Dr. Bhatt has received research support from several drug companies.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
WASHINGTON – Is it finally time to give up on HDL cholesterol–based interventions to treat atherosclerotic disease?
The approach “is on life support,” admitted Stephen J. Nicholls, MD, a long-time leader in the field who has reported results from a series of studies during the past 10 or so years that tested various approaches to juicing HDL cholesterol activity in patients, only to see each and every candidate intervention result in an inability to budge clinical outcomes.
The latest disappointment he reported was for CER-001, an engineered HDL mimetic agent. In a placebo-controlled international study, CARAT (CER-001 Atherosclerosis Regression ACS Trial), with 301 randomized patients and 272 completers, 10 weekly infusions of CER-001 over the course of 9 weeks failed to produce discernible incremental regression of atherosclerotic plaque volume, compared with standard care measured by serial examination using intravascular ultrasound (IVUS), Dr. Nicholls reported. The absence of any detectable benefit “suggests that this is not a promising strategy,” he said during his report at the meeting.
Enthusiasm for HDL cholesterol–based interventions dates to 2003, when an IVUS study of a first-generation HDL mimetic agent, ETC-216, showed an apparent ability to produce regression of coronary atheroma after five infusions over a 2-week period, compared with placebo-treated patients (JAMA. 2003 Nov 5;290[17]:2292-300). But the successor compound to this agent, MDCO-216, flamed out in an IVUS study with 113 completing patients that Dr. Nicholls reported at the American Heart Association Scientific Sessions in November 2016.
Also lying dead on the trial trail during past years are several cholesterol ester transfer protein inhibitors – torcetrapib, dalcetrapib and evacetrapib – as well as other agents that Dr. Nicholls described in a recent review (Arch Med Sci. 2016 Oct 24;12[6]:1302-7).
“HDL wouldn’t be the first risk factor we’ve seen that is not a modifiable target. Homocysteine is a really good example” of another atherosclerotic disease risk that’s proven immune to intervention, Dr. Nicholls said in an interview at the meeting. “Ultimately we’ll come to a point when the enthusiasm [for potential HDL interventions] will wane, but we’re not quite there yet.”
“There are other players in the HDL field” that remain viable, said Dr. Nicholls, most notably CSL112, plasma-derived apoA1 – the primary functional part of HDL cholesterol – that’s infused into patients to boost HDL activity. Results from a phase II study reported in November 2016 showed it increased cholesterol efflux (Circulation 2016 Nov; doi: 10.1161/CIRCULATIONAHA.116.025687), and is now the subject of additional phase II testing. “But with every negative trial, it will get harder and harder [to fund new HDL research], and we’ll look for other targets,” he said.
One promising alternative target is triglycerides. “HDL has received more attention than triglycerides over the past decade, but I think that will start to change as HDL can’t deliver,” predicted Dr. Nicholls, professor of cardiology at the South Australian Health & Medical Research Institute in Adelaide.
Understandably “financial support is the biggest issue. Do companies and investors still believe in the [HDL] dream?” Dr. Nicholls said that, objectively, looking at the HDL research record should definitely give investors pause before they sink money into new compounds for HDL intervention.
“If I was sitting at the drawing board now, would HDL be the risk factor I’d target? Probably not,” he concluded.
Dr. Nicholls received research support from Cerenis, the company that is developing CER-001, and he has received honoraria and research support from several other companies. Dr. Bhatt has received research support from several drug companies.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
WASHINGTON – Is it finally time to give up on HDL cholesterol–based interventions to treat atherosclerotic disease?
The approach “is on life support,” admitted Stephen J. Nicholls, MD, a long-time leader in the field who has reported results from a series of studies during the past 10 or so years that tested various approaches to juicing HDL cholesterol activity in patients, only to see each and every candidate intervention result in an inability to budge clinical outcomes.
The latest disappointment he reported was for CER-001, an engineered HDL mimetic agent. In a placebo-controlled international study, CARAT (CER-001 Atherosclerosis Regression ACS Trial), with 301 randomized patients and 272 completers, 10 weekly infusions of CER-001 over the course of 9 weeks failed to produce discernible incremental regression of atherosclerotic plaque volume, compared with standard care measured by serial examination using intravascular ultrasound (IVUS), Dr. Nicholls reported. The absence of any detectable benefit “suggests that this is not a promising strategy,” he said during his report at the meeting.
Enthusiasm for HDL cholesterol–based interventions dates to 2003, when an IVUS study of a first-generation HDL mimetic agent, ETC-216, showed an apparent ability to produce regression of coronary atheroma after five infusions over a 2-week period, compared with placebo-treated patients (JAMA. 2003 Nov 5;290[17]:2292-300). But the successor compound to this agent, MDCO-216, flamed out in an IVUS study with 113 completing patients that Dr. Nicholls reported at the American Heart Association Scientific Sessions in November 2016.
Also lying dead on the trial trail during past years are several cholesterol ester transfer protein inhibitors – torcetrapib, dalcetrapib and evacetrapib – as well as other agents that Dr. Nicholls described in a recent review (Arch Med Sci. 2016 Oct 24;12[6]:1302-7).
“HDL wouldn’t be the first risk factor we’ve seen that is not a modifiable target. Homocysteine is a really good example” of another atherosclerotic disease risk that’s proven immune to intervention, Dr. Nicholls said in an interview at the meeting. “Ultimately we’ll come to a point when the enthusiasm [for potential HDL interventions] will wane, but we’re not quite there yet.”
“There are other players in the HDL field” that remain viable, said Dr. Nicholls, most notably CSL112, plasma-derived apoA1 – the primary functional part of HDL cholesterol – that’s infused into patients to boost HDL activity. Results from a phase II study reported in November 2016 showed it increased cholesterol efflux (Circulation 2016 Nov; doi: 10.1161/CIRCULATIONAHA.116.025687), and is now the subject of additional phase II testing. “But with every negative trial, it will get harder and harder [to fund new HDL research], and we’ll look for other targets,” he said.
One promising alternative target is triglycerides. “HDL has received more attention than triglycerides over the past decade, but I think that will start to change as HDL can’t deliver,” predicted Dr. Nicholls, professor of cardiology at the South Australian Health & Medical Research Institute in Adelaide.
Understandably “financial support is the biggest issue. Do companies and investors still believe in the [HDL] dream?” Dr. Nicholls said that, objectively, looking at the HDL research record should definitely give investors pause before they sink money into new compounds for HDL intervention.
“If I was sitting at the drawing board now, would HDL be the risk factor I’d target? Probably not,” he concluded.
Dr. Nicholls received research support from Cerenis, the company that is developing CER-001, and he has received honoraria and research support from several other companies. Dr. Bhatt has received research support from several drug companies.
mzoler@frontlinemedcom.com
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM ACC 17
Tapering opioids
The Centers for Disease Control and Prevention guideline for prescribing opioids for chronic pain released in March 2016 suggests that if “patients are found to be receiving high total daily dosages of opioids, clinicians should discuss their safety concerns with the patient [and] consider tapering to a safer dosage...”
All of us who prescribe opioids have had these discussions with patients. They are frequently fraught with hand-wringing and, all-too-often, a “steeling” for battle. We may have a general sense for what these discussions are like from the provider perspective, but what are they like for patients?

Interestingly, patients had an overall low self-perceived risk of opioid overdose. Patients attributed reports of overdose to intent or risky behaviors. Patients rated the importance of treatment of current pain higher than the future potential risk of opioid use and had little faith in nonopioid pain management strategies. Patients reported fear of opioid withdrawal. They also reported the importance of social support and a healthy, trusting relationship with their provider for the facilitation of tapering. None of the patients reported switching providers who had recommended tapering. Patients who had tapered off opioids reported improved quality of life and a level of pain that was largely unchanged.
This work provides critical insight into the fears and reservations of patients facing the prospect of life on lower doses of opioids or life without them altogether. Addressing these fears directly may facilitate the discussions with patients when discussing the tapering of opioids.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
The Centers for Disease Control and Prevention guideline for prescribing opioids for chronic pain released in March 2016 suggests that if “patients are found to be receiving high total daily dosages of opioids, clinicians should discuss their safety concerns with the patient [and] consider tapering to a safer dosage...”
All of us who prescribe opioids have had these discussions with patients. They are frequently fraught with hand-wringing and, all-too-often, a “steeling” for battle. We may have a general sense for what these discussions are like from the provider perspective, but what are they like for patients?
Interestingly, patients had an overall low self-perceived risk of opioid overdose. Patients attributed reports of overdose to intent or risky behaviors. Patients rated the importance of treatment of current pain higher than the future potential risk of opioid use and had little faith in nonopioid pain management strategies. Patients reported fear of opioid withdrawal. They also reported the importance of social support and a healthy, trusting relationship with their provider for the facilitation of tapering. None of the patients reported switching providers who had recommended tapering. Patients who had tapered off opioids reported improved quality of life and a level of pain that was largely unchanged.
This work provides critical insight into the fears and reservations of patients facing the prospect of life on lower doses of opioids or life without them altogether. Addressing these fears directly may facilitate the discussions with patients when discussing the tapering of opioids.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
The Centers for Disease Control and Prevention guideline for prescribing opioids for chronic pain released in March 2016 suggests that if “patients are found to be receiving high total daily dosages of opioids, clinicians should discuss their safety concerns with the patient [and] consider tapering to a safer dosage...”
All of us who prescribe opioids have had these discussions with patients. They are frequently fraught with hand-wringing and, all-too-often, a “steeling” for battle. We may have a general sense for what these discussions are like from the provider perspective, but what are they like for patients?
Interestingly, patients had an overall low self-perceived risk of opioid overdose. Patients attributed reports of overdose to intent or risky behaviors. Patients rated the importance of treatment of current pain higher than the future potential risk of opioid use and had little faith in nonopioid pain management strategies. Patients reported fear of opioid withdrawal. They also reported the importance of social support and a healthy, trusting relationship with their provider for the facilitation of tapering. None of the patients reported switching providers who had recommended tapering. Patients who had tapered off opioids reported improved quality of life and a level of pain that was largely unchanged.
This work provides critical insight into the fears and reservations of patients facing the prospect of life on lower doses of opioids or life without them altogether. Addressing these fears directly may facilitate the discussions with patients when discussing the tapering of opioids.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article.
Hard water versus your skin
Observational studies suggest that hard water is associated with the development of atopic dermatitis (AD). Studies of children in the United Kingdom, Spain, and Japan show the prevalence of AD is significantly higher in the highest water hardness categories than that in the lowest. Calcium cations in water can interfere with normal epidermal calcium gradients that are necessary for corneocyte development and proper stratum corneum barrier formation.
Water hardness, determined by the amount of dissolved calcium and magnesium in the water, varies by geography and mineral content of the water supply. The hardest water supply in the United States is mostly localized to the Upper Plains and Rocky Mountain areas. General guidelines for classification of waters are: 0-60 mg/L calcium carbonate (soft); 61-120 mg/L (moderately hard); 121-180 mg/L (hard); and more than 180 mg/L (very hard). In regions where there is hard water, the surfactants in soap, such as sodium dodecyl sulfate, react with the calcium and magnesium ions in hard water, resulting in precipitation of the surfactant – leaving a film of residue on the skin, shower tiles, pipes, glassware, etc.

Atopic dermatitis, xerosis, and pruritus are some of the common skin reactions to hard water. Other less-well-defined effects on the skin include clogged pores and acne from surfactant residue left on the skin and altered sebum production. In addition, more surfactants or cleansers are needed to clean the skin and hair in areas with hard water because the abundant cations require a much heavier lather to dissolve.
Calcium and magnesium cations left on the skin can also form free radicals. Free radicals over time can result in collagen and elastin breakdown and in the increased prevalence of fine lines and wrinkles.

Hard water and geography should be considered a possible factor when assessing patients with recalcitrant eczema, pruritus, or xerosis that cannot otherwise be reversed. Water softening treatments are a simple solution in areas where the mineral content of water is elevated or the water plays a role in clinical skin disease.
Dr. Lily Talakoub and Dr. Naissan O. Wesley and are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
References
United States Geological Survey Water Quality Information: Water Hardness and Alkalinity.
J Am Acad Dermatol. 1987 Jun;16(6):1263-4.
Contact Dermatitis. 1996 Dec;35(6):337-43.
Lancet. 1998 Aug 15;352(9127):527-31.
Contact Dermatitis. 1999;41(6):311-4.
Environ Res. 2004 Jan;94(1):33-7.
Observational studies suggest that hard water is associated with the development of atopic dermatitis (AD). Studies of children in the United Kingdom, Spain, and Japan show the prevalence of AD is significantly higher in the highest water hardness categories than that in the lowest. Calcium cations in water can interfere with normal epidermal calcium gradients that are necessary for corneocyte development and proper stratum corneum barrier formation.
Water hardness, determined by the amount of dissolved calcium and magnesium in the water, varies by geography and mineral content of the water supply. The hardest water supply in the United States is mostly localized to the Upper Plains and Rocky Mountain areas. General guidelines for classification of waters are: 0-60 mg/L calcium carbonate (soft); 61-120 mg/L (moderately hard); 121-180 mg/L (hard); and more than 180 mg/L (very hard). In regions where there is hard water, the surfactants in soap, such as sodium dodecyl sulfate, react with the calcium and magnesium ions in hard water, resulting in precipitation of the surfactant – leaving a film of residue on the skin, shower tiles, pipes, glassware, etc.
Atopic dermatitis, xerosis, and pruritus are some of the common skin reactions to hard water. Other less-well-defined effects on the skin include clogged pores and acne from surfactant residue left on the skin and altered sebum production. In addition, more surfactants or cleansers are needed to clean the skin and hair in areas with hard water because the abundant cations require a much heavier lather to dissolve.
Calcium and magnesium cations left on the skin can also form free radicals. Free radicals over time can result in collagen and elastin breakdown and in the increased prevalence of fine lines and wrinkles.
Hard water and geography should be considered a possible factor when assessing patients with recalcitrant eczema, pruritus, or xerosis that cannot otherwise be reversed. Water softening treatments are a simple solution in areas where the mineral content of water is elevated or the water plays a role in clinical skin disease.
Dr. Lily Talakoub and Dr. Naissan O. Wesley and are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
References
United States Geological Survey Water Quality Information: Water Hardness and Alkalinity.
J Am Acad Dermatol. 1987 Jun;16(6):1263-4.
Contact Dermatitis. 1996 Dec;35(6):337-43.
Lancet. 1998 Aug 15;352(9127):527-31.
Contact Dermatitis. 1999;41(6):311-4.
Environ Res. 2004 Jan;94(1):33-7.
Observational studies suggest that hard water is associated with the development of atopic dermatitis (AD). Studies of children in the United Kingdom, Spain, and Japan show the prevalence of AD is significantly higher in the highest water hardness categories than that in the lowest. Calcium cations in water can interfere with normal epidermal calcium gradients that are necessary for corneocyte development and proper stratum corneum barrier formation.
Water hardness, determined by the amount of dissolved calcium and magnesium in the water, varies by geography and mineral content of the water supply. The hardest water supply in the United States is mostly localized to the Upper Plains and Rocky Mountain areas. General guidelines for classification of waters are: 0-60 mg/L calcium carbonate (soft); 61-120 mg/L (moderately hard); 121-180 mg/L (hard); and more than 180 mg/L (very hard). In regions where there is hard water, the surfactants in soap, such as sodium dodecyl sulfate, react with the calcium and magnesium ions in hard water, resulting in precipitation of the surfactant – leaving a film of residue on the skin, shower tiles, pipes, glassware, etc.
Atopic dermatitis, xerosis, and pruritus are some of the common skin reactions to hard water. Other less-well-defined effects on the skin include clogged pores and acne from surfactant residue left on the skin and altered sebum production. In addition, more surfactants or cleansers are needed to clean the skin and hair in areas with hard water because the abundant cations require a much heavier lather to dissolve.
Calcium and magnesium cations left on the skin can also form free radicals. Free radicals over time can result in collagen and elastin breakdown and in the increased prevalence of fine lines and wrinkles.
Hard water and geography should be considered a possible factor when assessing patients with recalcitrant eczema, pruritus, or xerosis that cannot otherwise be reversed. Water softening treatments are a simple solution in areas where the mineral content of water is elevated or the water plays a role in clinical skin disease.
Dr. Lily Talakoub and Dr. Naissan O. Wesley and are cocontributors to this column. Dr. Talakoub is in private practice in McLean, Va. Dr. Wesley practices dermatology in Beverly Hills, Calif. This month’s column is by Dr. Talakoub. Write to them at dermnews@frontlinemedcom.com. They had no relevant disclosures.
References
United States Geological Survey Water Quality Information: Water Hardness and Alkalinity.
J Am Acad Dermatol. 1987 Jun;16(6):1263-4.
Contact Dermatitis. 1996 Dec;35(6):337-43.
Lancet. 1998 Aug 15;352(9127):527-31.
Contact Dermatitis. 1999;41(6):311-4.
Environ Res. 2004 Jan;94(1):33-7.
Don’t ask
You walk into an examining room and discover a 3-year-old in his underpants wearing a fireman’s hat and what must be his older sister’s rubber boots. You have to ask: “Are you going to be a firefighter when you grow up?” If he is a sensitive kid he will resist answering, “What do you think, Dr. Obvious?” and instead he politely replies, “Yes, and an EMT [emergency medical technician] too.”
Adults, even ones who have devoted their professional lives to the care of children, can’t seem to stifle the urge ask every young person they meet about his or her career plans. It is a strange sort of obsession, and may simply reflect the fact that most adults are at a loss for conversation starters when it comes to talking with young people. Children don’t seem to have much concern about the weather. And most of them don’t have opinions about the current political situation. They don’t have stories about their grandchildren they would love to bore you with. You could ask if the child has a pet, but that may be picking the scab of an unresolved family issue.

Most adults realize that their career plans prior to adolescence have no relationship to their present situation. Thinking back on this disconnect in their own lives may provide them with a good chuckle. But they also may hope to store away the child’s naive answer as ammunition for a future embarrassing challenge. “Do you remember that you once told me you were going to be a forest ranger?”
It may be that the child’s answer will give the adults an opportunity to share their “wisdom” based on their own career decisions. How lucky for the child who has stumbled on an unsolicited life coach.
For the most part, these interrogations about career planning are just idle banter. But as children get older, reality begins shining its harsh light on choices and decisions. What was once a seemingly harmless question about the distant future may no longer be so innocuous. I try to sound apologetic when I say to high school juniors and seniors, “I’m sure everyone is asking you, but what about college?” However, after reading a story in The Wall Street Journal, I now wonder whether I should be skipping the apology and just simply not raising the subject of college (“What’s Worse Than Waiting to Hear From Colleges? Getting Interrogated About It,” by Sue Shellenbarger, March 8, 2017).
In communities where most high school graduates have been on a college track since middle school, tension and anxiety hangs over the older adolescents like a cloud that darkens as application deadlines herald the long and painful wait for acceptance/rejection letters and emails. High school seniors are tired of thinking about the process and certainly don’t want to talk about. They consider questions about their future an invasion of their privacy. Redbubble, an online marketplace based in Australia, is seeing rising sales of T-shirts that read “Don’t ask me about college. Thanks.”
The unwelcome interrogations don’t stop with college acceptance. Adults want to know, “Have you chosen a major?” And as college graduation nears they can’t resist asking, “Do you have any job offers?”
Most adolescents and many 20-somethings don’t seem to have a career goal. It may be that they are afraid that the process of setting a goal will make them more vulnerable to failure. It also may be that revealing, “I’ve always wanted to be a ...” will label them as being a bit childish and weird.
Where does all this adolescent discomfort with the near future leave us pediatricians? The complete evaluation of a high school–age patient should include a question or questions about how our patient is weathering the college and career planning process. The challenge is how to present those questions in a manner that makes it clear that we aren’t just another one of those career-obsessed nosy adults.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
You walk into an examining room and discover a 3-year-old in his underpants wearing a fireman’s hat and what must be his older sister’s rubber boots. You have to ask: “Are you going to be a firefighter when you grow up?” If he is a sensitive kid he will resist answering, “What do you think, Dr. Obvious?” and instead he politely replies, “Yes, and an EMT [emergency medical technician] too.”
Adults, even ones who have devoted their professional lives to the care of children, can’t seem to stifle the urge ask every young person they meet about his or her career plans. It is a strange sort of obsession, and may simply reflect the fact that most adults are at a loss for conversation starters when it comes to talking with young people. Children don’t seem to have much concern about the weather. And most of them don’t have opinions about the current political situation. They don’t have stories about their grandchildren they would love to bore you with. You could ask if the child has a pet, but that may be picking the scab of an unresolved family issue.
Most adults realize that their career plans prior to adolescence have no relationship to their present situation. Thinking back on this disconnect in their own lives may provide them with a good chuckle. But they also may hope to store away the child’s naive answer as ammunition for a future embarrassing challenge. “Do you remember that you once told me you were going to be a forest ranger?”
It may be that the child’s answer will give the adults an opportunity to share their “wisdom” based on their own career decisions. How lucky for the child who has stumbled on an unsolicited life coach.
For the most part, these interrogations about career planning are just idle banter. But as children get older, reality begins shining its harsh light on choices and decisions. What was once a seemingly harmless question about the distant future may no longer be so innocuous. I try to sound apologetic when I say to high school juniors and seniors, “I’m sure everyone is asking you, but what about college?” However, after reading a story in The Wall Street Journal, I now wonder whether I should be skipping the apology and just simply not raising the subject of college (“What’s Worse Than Waiting to Hear From Colleges? Getting Interrogated About It,” by Sue Shellenbarger, March 8, 2017).
In communities where most high school graduates have been on a college track since middle school, tension and anxiety hangs over the older adolescents like a cloud that darkens as application deadlines herald the long and painful wait for acceptance/rejection letters and emails. High school seniors are tired of thinking about the process and certainly don’t want to talk about. They consider questions about their future an invasion of their privacy. Redbubble, an online marketplace based in Australia, is seeing rising sales of T-shirts that read “Don’t ask me about college. Thanks.”
The unwelcome interrogations don’t stop with college acceptance. Adults want to know, “Have you chosen a major?” And as college graduation nears they can’t resist asking, “Do you have any job offers?”
Most adolescents and many 20-somethings don’t seem to have a career goal. It may be that they are afraid that the process of setting a goal will make them more vulnerable to failure. It also may be that revealing, “I’ve always wanted to be a ...” will label them as being a bit childish and weird.
Where does all this adolescent discomfort with the near future leave us pediatricians? The complete evaluation of a high school–age patient should include a question or questions about how our patient is weathering the college and career planning process. The challenge is how to present those questions in a manner that makes it clear that we aren’t just another one of those career-obsessed nosy adults.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
You walk into an examining room and discover a 3-year-old in his underpants wearing a fireman’s hat and what must be his older sister’s rubber boots. You have to ask: “Are you going to be a firefighter when you grow up?” If he is a sensitive kid he will resist answering, “What do you think, Dr. Obvious?” and instead he politely replies, “Yes, and an EMT [emergency medical technician] too.”
Adults, even ones who have devoted their professional lives to the care of children, can’t seem to stifle the urge ask every young person they meet about his or her career plans. It is a strange sort of obsession, and may simply reflect the fact that most adults are at a loss for conversation starters when it comes to talking with young people. Children don’t seem to have much concern about the weather. And most of them don’t have opinions about the current political situation. They don’t have stories about their grandchildren they would love to bore you with. You could ask if the child has a pet, but that may be picking the scab of an unresolved family issue.
Most adults realize that their career plans prior to adolescence have no relationship to their present situation. Thinking back on this disconnect in their own lives may provide them with a good chuckle. But they also may hope to store away the child’s naive answer as ammunition for a future embarrassing challenge. “Do you remember that you once told me you were going to be a forest ranger?”
It may be that the child’s answer will give the adults an opportunity to share their “wisdom” based on their own career decisions. How lucky for the child who has stumbled on an unsolicited life coach.
For the most part, these interrogations about career planning are just idle banter. But as children get older, reality begins shining its harsh light on choices and decisions. What was once a seemingly harmless question about the distant future may no longer be so innocuous. I try to sound apologetic when I say to high school juniors and seniors, “I’m sure everyone is asking you, but what about college?” However, after reading a story in The Wall Street Journal, I now wonder whether I should be skipping the apology and just simply not raising the subject of college (“What’s Worse Than Waiting to Hear From Colleges? Getting Interrogated About It,” by Sue Shellenbarger, March 8, 2017).
In communities where most high school graduates have been on a college track since middle school, tension and anxiety hangs over the older adolescents like a cloud that darkens as application deadlines herald the long and painful wait for acceptance/rejection letters and emails. High school seniors are tired of thinking about the process and certainly don’t want to talk about. They consider questions about their future an invasion of their privacy. Redbubble, an online marketplace based in Australia, is seeing rising sales of T-shirts that read “Don’t ask me about college. Thanks.”
The unwelcome interrogations don’t stop with college acceptance. Adults want to know, “Have you chosen a major?” And as college graduation nears they can’t resist asking, “Do you have any job offers?”
Most adolescents and many 20-somethings don’t seem to have a career goal. It may be that they are afraid that the process of setting a goal will make them more vulnerable to failure. It also may be that revealing, “I’ve always wanted to be a ...” will label them as being a bit childish and weird.
Where does all this adolescent discomfort with the near future leave us pediatricians? The complete evaluation of a high school–age patient should include a question or questions about how our patient is weathering the college and career planning process. The challenge is how to present those questions in a manner that makes it clear that we aren’t just another one of those career-obsessed nosy adults.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com.
Rumors about the death of tPA are exaggerated
Where do we go from here?
More than 20 years after IV tissue plasminogen activator was officially approved for use in acute ischemic stroke, now data suggest mechanical thrombectomy is superior, regardless of whether tPA is given.
Granted, these are preliminary trials, and a lot more research needs to be done: randomized studies, determinations of which patients are the best candidates, which devices are most useful, etc.

Of course, it’s not that simple. The data thus far suggest thrombectomy is best when used in anterior circulation strokes, with a National Institutes of Health Stroke Scale score of greater than 6, so obviously we shouldn’t be calling them in on every case.
You have to balance that against legal issues. It certainly isn’t too far-fetched to imagine being sued because you didn’t call an interventionalist, or another neurologist testifying that you fell below the standard of care by not doing so. The right person will say that about anything, regardless of clinical data.
This is still up in the air right now, as I doubt the interventionalists want to take acute ischemic stroke off our hands, nor do we want to give it up, either. It’s a disorder of the brain, and that is what we deal with, isn’t it?
The bottom line is that rumors about the death of tPA in acute ischemic stroke are greatly exaggerated. Only time will tell.
Medicine, for better or worse, is an inexact science. No one can predict outcomes, adverse reactions, or complications with 100% certainty. Which treatment will work best for which patient is never known. That’s why we need controlled trials to know which odds are best overall, and take it from there. Preliminary trials can be very helpful at pointing us in the right directions, but are for from definitive. As with so many other things, your mileage may vary.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Where do we go from here?
More than 20 years after IV tissue plasminogen activator was officially approved for use in acute ischemic stroke, now data suggest mechanical thrombectomy is superior, regardless of whether tPA is given.
Granted, these are preliminary trials, and a lot more research needs to be done: randomized studies, determinations of which patients are the best candidates, which devices are most useful, etc.
Of course, it’s not that simple. The data thus far suggest thrombectomy is best when used in anterior circulation strokes, with a National Institutes of Health Stroke Scale score of greater than 6, so obviously we shouldn’t be calling them in on every case.
You have to balance that against legal issues. It certainly isn’t too far-fetched to imagine being sued because you didn’t call an interventionalist, or another neurologist testifying that you fell below the standard of care by not doing so. The right person will say that about anything, regardless of clinical data.
This is still up in the air right now, as I doubt the interventionalists want to take acute ischemic stroke off our hands, nor do we want to give it up, either. It’s a disorder of the brain, and that is what we deal with, isn’t it?
The bottom line is that rumors about the death of tPA in acute ischemic stroke are greatly exaggerated. Only time will tell.
Medicine, for better or worse, is an inexact science. No one can predict outcomes, adverse reactions, or complications with 100% certainty. Which treatment will work best for which patient is never known. That’s why we need controlled trials to know which odds are best overall, and take it from there. Preliminary trials can be very helpful at pointing us in the right directions, but are for from definitive. As with so many other things, your mileage may vary.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Where do we go from here?
More than 20 years after IV tissue plasminogen activator was officially approved for use in acute ischemic stroke, now data suggest mechanical thrombectomy is superior, regardless of whether tPA is given.
Granted, these are preliminary trials, and a lot more research needs to be done: randomized studies, determinations of which patients are the best candidates, which devices are most useful, etc.
Of course, it’s not that simple. The data thus far suggest thrombectomy is best when used in anterior circulation strokes, with a National Institutes of Health Stroke Scale score of greater than 6, so obviously we shouldn’t be calling them in on every case.
You have to balance that against legal issues. It certainly isn’t too far-fetched to imagine being sued because you didn’t call an interventionalist, or another neurologist testifying that you fell below the standard of care by not doing so. The right person will say that about anything, regardless of clinical data.
This is still up in the air right now, as I doubt the interventionalists want to take acute ischemic stroke off our hands, nor do we want to give it up, either. It’s a disorder of the brain, and that is what we deal with, isn’t it?
The bottom line is that rumors about the death of tPA in acute ischemic stroke are greatly exaggerated. Only time will tell.
Medicine, for better or worse, is an inexact science. No one can predict outcomes, adverse reactions, or complications with 100% certainty. Which treatment will work best for which patient is never known. That’s why we need controlled trials to know which odds are best overall, and take it from there. Preliminary trials can be very helpful at pointing us in the right directions, but are for from definitive. As with so many other things, your mileage may vary.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Pardon the interruption?
Your first patient of the afternoon is a 9-year-old boy who moved to town several months ago. Mercifully, the second patient of the afternoon has canceled, giving you a few more minutes to get acquainted with this young man whose chief complaint is listed as “behavior problem.” You learn quickly that this family has relocated from a town just 20 miles away because they are seeking a school that is a “better fit” for your new patient.
Due to some miscommunications, the child’s old records have not arrived at your office. The mother says that her son is not taking any medication, and she isn’t sure if he has ever been given a diagnosis. You learn that he likes to argue and is prone to violent temper tantrums. Your initial brief exam does not suggest any cognitive deficits, but he exudes an aura of anger and discontent. You tell his mother that you will be glad to try to help, but you will need his old records and another longer visit before you can make any recommendations.
Two days later you see a fourth-grader you have known since birth. He rarely comes to the office with problems, but you understand that he is a good student, a competent athlete, and socially engaged. His chief complaint for this visit is “hair loss,” but you soon discover that he has trichotillomania and has recently begun having nightmares and experiencing enuresis. All of these symptoms began a month ago with arrival of a new student in his class whose violent outbursts have become increasingly more physical. I have borrowed this child’s scenario from a similar case study in a recent supplement to the Journal of Developmental & Behavioral Pediatrics titled, “Behavioral Changes Associated with a Disruptive New Student in the Classroom,” (J Dev Behav Pediatr. Feb/Mar 2017. doi: 10.1097/DBP.0000000000000175).
The afternoon following your visit with the hair-pulling fourth-grader, you receive the new patient’s records for which you have been waiting. The circle is completed as you read that this is his third school in 18 months, and the reports of his behavior make it clear that your two patients are classmates. This scenario of coincidence could easily have occurred in a small town like Brunswick, Maine, where I practiced, but I have manufactured it to raise several questions about social priorities and professional ethics.
Forty years ago, institutions housing individuals with Down syndrome started closing and the process of integrating children with a variety of cognitive and physical disabilities into traditional classrooms began. To the surprise of some people, this mainstreaming has generally gone well. Unfortunately, funding hasn’t always caught up with the demand for services. For the most part, children readily accept their challenged classmates who look, move, and sound different. The flailing and grunting of the child with spastic choreoathetosis using a wheelchair isn’t considered an interruption because “that’s just the way she is.”
However, there seems to be an invisible line that separates those children who seem to be incapable of stopping their potentially disruptive behavior from those children we assume “ought to know better” or whose parents we believe have failed at instilling even the most basic discipline. You can certainly question the validity of those assumptions. But it is clear that your new patient’s disruptive behavior is interfering with his classmates’ education, and in some cases threatening their health. Your patient with trichotillomania is probably the canary in a very unsettled mine.
Your dilemma as the pediatrician for these two boys is the same we face as a society. How do you effectively advocate for a positive educational atmosphere for children with a variety of special needs, some of which seem to be in direct conflict? You can ask the school system to be patient as you help the disruptive child get connected with the services he needs. But you know that could take several months at a minimum. Meanwhile your hair-pulling patient and his classmates are losing valuable educational opportunities by the day.
I don’t have the answer, but I suspect that somehow it is going to come down to affordability. Counseling, psychiatrists, and one on one classroom aids don’t come cheap, nor does the tuition for a special school in another school district. But we can’t discount the value of an education free of disruption.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com
Your first patient of the afternoon is a 9-year-old boy who moved to town several months ago. Mercifully, the second patient of the afternoon has canceled, giving you a few more minutes to get acquainted with this young man whose chief complaint is listed as “behavior problem.” You learn quickly that this family has relocated from a town just 20 miles away because they are seeking a school that is a “better fit” for your new patient.
Due to some miscommunications, the child’s old records have not arrived at your office. The mother says that her son is not taking any medication, and she isn’t sure if he has ever been given a diagnosis. You learn that he likes to argue and is prone to violent temper tantrums. Your initial brief exam does not suggest any cognitive deficits, but he exudes an aura of anger and discontent. You tell his mother that you will be glad to try to help, but you will need his old records and another longer visit before you can make any recommendations.
Two days later you see a fourth-grader you have known since birth. He rarely comes to the office with problems, but you understand that he is a good student, a competent athlete, and socially engaged. His chief complaint for this visit is “hair loss,” but you soon discover that he has trichotillomania and has recently begun having nightmares and experiencing enuresis. All of these symptoms began a month ago with arrival of a new student in his class whose violent outbursts have become increasingly more physical. I have borrowed this child’s scenario from a similar case study in a recent supplement to the Journal of Developmental & Behavioral Pediatrics titled, “Behavioral Changes Associated with a Disruptive New Student in the Classroom,” (J Dev Behav Pediatr. Feb/Mar 2017. doi: 10.1097/DBP.0000000000000175).
The afternoon following your visit with the hair-pulling fourth-grader, you receive the new patient’s records for which you have been waiting. The circle is completed as you read that this is his third school in 18 months, and the reports of his behavior make it clear that your two patients are classmates. This scenario of coincidence could easily have occurred in a small town like Brunswick, Maine, where I practiced, but I have manufactured it to raise several questions about social priorities and professional ethics.
Forty years ago, institutions housing individuals with Down syndrome started closing and the process of integrating children with a variety of cognitive and physical disabilities into traditional classrooms began. To the surprise of some people, this mainstreaming has generally gone well. Unfortunately, funding hasn’t always caught up with the demand for services. For the most part, children readily accept their challenged classmates who look, move, and sound different. The flailing and grunting of the child with spastic choreoathetosis using a wheelchair isn’t considered an interruption because “that’s just the way she is.”
However, there seems to be an invisible line that separates those children who seem to be incapable of stopping their potentially disruptive behavior from those children we assume “ought to know better” or whose parents we believe have failed at instilling even the most basic discipline. You can certainly question the validity of those assumptions. But it is clear that your new patient’s disruptive behavior is interfering with his classmates’ education, and in some cases threatening their health. Your patient with trichotillomania is probably the canary in a very unsettled mine.
Your dilemma as the pediatrician for these two boys is the same we face as a society. How do you effectively advocate for a positive educational atmosphere for children with a variety of special needs, some of which seem to be in direct conflict? You can ask the school system to be patient as you help the disruptive child get connected with the services he needs. But you know that could take several months at a minimum. Meanwhile your hair-pulling patient and his classmates are losing valuable educational opportunities by the day.
I don’t have the answer, but I suspect that somehow it is going to come down to affordability. Counseling, psychiatrists, and one on one classroom aids don’t come cheap, nor does the tuition for a special school in another school district. But we can’t discount the value of an education free of disruption.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com
Your first patient of the afternoon is a 9-year-old boy who moved to town several months ago. Mercifully, the second patient of the afternoon has canceled, giving you a few more minutes to get acquainted with this young man whose chief complaint is listed as “behavior problem.” You learn quickly that this family has relocated from a town just 20 miles away because they are seeking a school that is a “better fit” for your new patient.
Due to some miscommunications, the child’s old records have not arrived at your office. The mother says that her son is not taking any medication, and she isn’t sure if he has ever been given a diagnosis. You learn that he likes to argue and is prone to violent temper tantrums. Your initial brief exam does not suggest any cognitive deficits, but he exudes an aura of anger and discontent. You tell his mother that you will be glad to try to help, but you will need his old records and another longer visit before you can make any recommendations.
Two days later you see a fourth-grader you have known since birth. He rarely comes to the office with problems, but you understand that he is a good student, a competent athlete, and socially engaged. His chief complaint for this visit is “hair loss,” but you soon discover that he has trichotillomania and has recently begun having nightmares and experiencing enuresis. All of these symptoms began a month ago with arrival of a new student in his class whose violent outbursts have become increasingly more physical. I have borrowed this child’s scenario from a similar case study in a recent supplement to the Journal of Developmental & Behavioral Pediatrics titled, “Behavioral Changes Associated with a Disruptive New Student in the Classroom,” (J Dev Behav Pediatr. Feb/Mar 2017. doi: 10.1097/DBP.0000000000000175).
The afternoon following your visit with the hair-pulling fourth-grader, you receive the new patient’s records for which you have been waiting. The circle is completed as you read that this is his third school in 18 months, and the reports of his behavior make it clear that your two patients are classmates. This scenario of coincidence could easily have occurred in a small town like Brunswick, Maine, where I practiced, but I have manufactured it to raise several questions about social priorities and professional ethics.
Forty years ago, institutions housing individuals with Down syndrome started closing and the process of integrating children with a variety of cognitive and physical disabilities into traditional classrooms began. To the surprise of some people, this mainstreaming has generally gone well. Unfortunately, funding hasn’t always caught up with the demand for services. For the most part, children readily accept their challenged classmates who look, move, and sound different. The flailing and grunting of the child with spastic choreoathetosis using a wheelchair isn’t considered an interruption because “that’s just the way she is.”
However, there seems to be an invisible line that separates those children who seem to be incapable of stopping their potentially disruptive behavior from those children we assume “ought to know better” or whose parents we believe have failed at instilling even the most basic discipline. You can certainly question the validity of those assumptions. But it is clear that your new patient’s disruptive behavior is interfering with his classmates’ education, and in some cases threatening their health. Your patient with trichotillomania is probably the canary in a very unsettled mine.
Your dilemma as the pediatrician for these two boys is the same we face as a society. How do you effectively advocate for a positive educational atmosphere for children with a variety of special needs, some of which seem to be in direct conflict? You can ask the school system to be patient as you help the disruptive child get connected with the services he needs. But you know that could take several months at a minimum. Meanwhile your hair-pulling patient and his classmates are losing valuable educational opportunities by the day.
I don’t have the answer, but I suspect that somehow it is going to come down to affordability. Counseling, psychiatrists, and one on one classroom aids don’t come cheap, nor does the tuition for a special school in another school district. But we can’t discount the value of an education free of disruption.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@frontlinemedcom.com
How’s your postacute network doing?
By now, nearly all hospitals are developing networks of postacute facilities for some or all of their patients, such as those in ACOs, bundled payments, or other value-based programs. Commonly referred to as preferred providers, performance networks, narrow networks, or similar, these networks of skilled nursing facilities (SNFs) and other entities that provide postacute care (like home health agencies) are usually chosen because they have demonstrated that they provide high quality, cost-effective care for patients after they leave the hospital.
While case managers are often the ones who counsel patients and caregivers on the details of the network, hospitalists should have at least a high-level grasp of which facilities are on the list and what the network selection criteria are. I would argue that hospitalists should lead the discussion with patients on postacute facility selection as it relates to which facilities are in the network and why going to a network facility is advantageous. Why? Because as hospitalist practices begin to share clinical and financial risk for patients, or at least become eligible to share in savings as MACRA encourages, they will have a vested interest in network facilities’ performance.
Postacute care network selection criteria
There is a range of criteria – usually incorporating measures of quality and efficiency – for including providers like SNFs in networks. In terms of quality, criteria can include physician/provider availability, star ratings on Nursing Home Compare, care transitions measures, Department of Public Health inspection survey scores, Joint Commission accreditation, etc.

A few caveats regarding specific selection criteria:
Star ratings on Nursing Home Compare
These are derived from nursing staffing ratios, health inspections, and 16 quality measures. More than half of the quality measures pertain to long-stay residents who typically are not in the ACO or bundled payment program for which the network was created (these are usually short-stay patients).
SNF length of stay
High readmission rates from a SNF can actually lower its length of stay, so including “balancing” measures such as readmissions should be considered.
What about patient choice?
Narrow postacute networks are not only becoming the norm, but there is also broad recognition from CMS, MedPAC, and industry leaders that value-based payment programs require such networks to succeed. That said, case managers and other discharge planners may still resist networks on the grounds that they might be perceived as restricting patient choice. One approach to balancing differing views on patient choice is to give patients the traditional longer list of available postacute providers, and also furnish the shorter network list accompanied by an explanation of why certain SNFs are in the network. Thankfully, as ACOs and bundles become widespread, resistance to narrow networks is dying down.
What role should hospitalists play in network referrals?
High functioning hospitalist practices should lead the discussion with patients and the health care team on referrals to network SNFs. Why? Patients are looking for their doctors to guide them on such decisions. Only if the physician opts not to have the discussion will patients look to the case manager for direction on which postacute facility to choose. A better option still would be for the hospitalists to partner with case managers to have the conversation with patients. In such a scenario, the hospitalist can begin the discussion and cover the major points, and the case manager can follow with more detailed information. For less mature hospitalist practices, the case manager can play a larger role in the discussion. In any case, as value-based models become ubiquitous, and shared savings become a driver of hospitalist revenue, hospitalists’ knowledge of and active participation in conversations around narrow networks and referrals will be necessary.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn. He is a cofounder and past president of SHM.
By now, nearly all hospitals are developing networks of postacute facilities for some or all of their patients, such as those in ACOs, bundled payments, or other value-based programs. Commonly referred to as preferred providers, performance networks, narrow networks, or similar, these networks of skilled nursing facilities (SNFs) and other entities that provide postacute care (like home health agencies) are usually chosen because they have demonstrated that they provide high quality, cost-effective care for patients after they leave the hospital.
While case managers are often the ones who counsel patients and caregivers on the details of the network, hospitalists should have at least a high-level grasp of which facilities are on the list and what the network selection criteria are. I would argue that hospitalists should lead the discussion with patients on postacute facility selection as it relates to which facilities are in the network and why going to a network facility is advantageous. Why? Because as hospitalist practices begin to share clinical and financial risk for patients, or at least become eligible to share in savings as MACRA encourages, they will have a vested interest in network facilities’ performance.
Postacute care network selection criteria
There is a range of criteria – usually incorporating measures of quality and efficiency – for including providers like SNFs in networks. In terms of quality, criteria can include physician/provider availability, star ratings on Nursing Home Compare, care transitions measures, Department of Public Health inspection survey scores, Joint Commission accreditation, etc.
A few caveats regarding specific selection criteria:
Star ratings on Nursing Home Compare
These are derived from nursing staffing ratios, health inspections, and 16 quality measures. More than half of the quality measures pertain to long-stay residents who typically are not in the ACO or bundled payment program for which the network was created (these are usually short-stay patients).
SNF length of stay
High readmission rates from a SNF can actually lower its length of stay, so including “balancing” measures such as readmissions should be considered.
What about patient choice?
Narrow postacute networks are not only becoming the norm, but there is also broad recognition from CMS, MedPAC, and industry leaders that value-based payment programs require such networks to succeed. That said, case managers and other discharge planners may still resist networks on the grounds that they might be perceived as restricting patient choice. One approach to balancing differing views on patient choice is to give patients the traditional longer list of available postacute providers, and also furnish the shorter network list accompanied by an explanation of why certain SNFs are in the network. Thankfully, as ACOs and bundles become widespread, resistance to narrow networks is dying down.
What role should hospitalists play in network referrals?
High functioning hospitalist practices should lead the discussion with patients and the health care team on referrals to network SNFs. Why? Patients are looking for their doctors to guide them on such decisions. Only if the physician opts not to have the discussion will patients look to the case manager for direction on which postacute facility to choose. A better option still would be for the hospitalists to partner with case managers to have the conversation with patients. In such a scenario, the hospitalist can begin the discussion and cover the major points, and the case manager can follow with more detailed information. For less mature hospitalist practices, the case manager can play a larger role in the discussion. In any case, as value-based models become ubiquitous, and shared savings become a driver of hospitalist revenue, hospitalists’ knowledge of and active participation in conversations around narrow networks and referrals will be necessary.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn. He is a cofounder and past president of SHM.
By now, nearly all hospitals are developing networks of postacute facilities for some or all of their patients, such as those in ACOs, bundled payments, or other value-based programs. Commonly referred to as preferred providers, performance networks, narrow networks, or similar, these networks of skilled nursing facilities (SNFs) and other entities that provide postacute care (like home health agencies) are usually chosen because they have demonstrated that they provide high quality, cost-effective care for patients after they leave the hospital.
While case managers are often the ones who counsel patients and caregivers on the details of the network, hospitalists should have at least a high-level grasp of which facilities are on the list and what the network selection criteria are. I would argue that hospitalists should lead the discussion with patients on postacute facility selection as it relates to which facilities are in the network and why going to a network facility is advantageous. Why? Because as hospitalist practices begin to share clinical and financial risk for patients, or at least become eligible to share in savings as MACRA encourages, they will have a vested interest in network facilities’ performance.
Postacute care network selection criteria
There is a range of criteria – usually incorporating measures of quality and efficiency – for including providers like SNFs in networks. In terms of quality, criteria can include physician/provider availability, star ratings on Nursing Home Compare, care transitions measures, Department of Public Health inspection survey scores, Joint Commission accreditation, etc.
A few caveats regarding specific selection criteria:
Star ratings on Nursing Home Compare
These are derived from nursing staffing ratios, health inspections, and 16 quality measures. More than half of the quality measures pertain to long-stay residents who typically are not in the ACO or bundled payment program for which the network was created (these are usually short-stay patients).
SNF length of stay
High readmission rates from a SNF can actually lower its length of stay, so including “balancing” measures such as readmissions should be considered.
What about patient choice?
Narrow postacute networks are not only becoming the norm, but there is also broad recognition from CMS, MedPAC, and industry leaders that value-based payment programs require such networks to succeed. That said, case managers and other discharge planners may still resist networks on the grounds that they might be perceived as restricting patient choice. One approach to balancing differing views on patient choice is to give patients the traditional longer list of available postacute providers, and also furnish the shorter network list accompanied by an explanation of why certain SNFs are in the network. Thankfully, as ACOs and bundles become widespread, resistance to narrow networks is dying down.
What role should hospitalists play in network referrals?
High functioning hospitalist practices should lead the discussion with patients and the health care team on referrals to network SNFs. Why? Patients are looking for their doctors to guide them on such decisions. Only if the physician opts not to have the discussion will patients look to the case manager for direction on which postacute facility to choose. A better option still would be for the hospitalists to partner with case managers to have the conversation with patients. In such a scenario, the hospitalist can begin the discussion and cover the major points, and the case manager can follow with more detailed information. For less mature hospitalist practices, the case manager can play a larger role in the discussion. In any case, as value-based models become ubiquitous, and shared savings become a driver of hospitalist revenue, hospitalists’ knowledge of and active participation in conversations around narrow networks and referrals will be necessary.
Dr. Whitcomb is chief medical officer at Remedy Partners in Darien, Conn. He is a cofounder and past president of SHM.