User login
Conflicting psychiatric agendas in our polarized world
A series of case discussions recently engendered discord among colleagues of ours. The conflicts raised questions about systemic biases within our field and their possible ramifications.

The cases discussed, like many in psychiatry, involved patients with severely maladaptive coping skills who lived with punishing friends, had little rewarding purpose, and had dismissive or abusive families. The conflicts involved whether the treating psychiatrists should promote seemingly obvious life choices or whether those perspectives were based in socionormative stereotypes seeped in mistaken traditional values that do not account for the rich array of experiences our patients come from.
One such case involved a seemingly masochistic patient who repeatedly found herself in abusive relationships and whether the psychiatrist should consider criticizing her partner choices. Another case involved a severely suffering veteran who felt paralyzed at home and whether the psychiatrist should encourage employment to diminish isolation. Yet another case involved a suicidal transgender patient who was in despair when feeling little relief after receiving gender-conforming surgery and – whether the psychiatrist should or could discuss perspectives on gender.
Those cases have led to accusations of misunderstanding science on both sides – and questions about the political justifications and consequences of psychiatric recommendations.
The field of psychiatry is appropriately embarrassed by its former association to misogynistic, homophobic, and even racist schools of thought. However, we wonder whether our current attempts at penance are at times discouraging important discussions. In some cases, our lowest-functioning patients living on the fringe of society benefit the most from the stabilizing influences of family, employment, social institutions, or religious worship. This is especially true considering how much social isolation has become an increasing reality of modern life. As such, we worry when colleagues argue that the promotion of common values is inherently suspect.
This problem may be exemplified by the public attacks on Allan Josephson, MD. Dr. Josephson, a child psychiatrist at the University of Louisville (Ky.), contends that he was ostracized and later fired from his position for communicating at a Heritage Foundation forum on his concerns about current recommended treatments and approaches for gender dysphoria. It appears that, despite being a renowned and previously deeply respected expert in the field, his opinions on the subject now go beyond the acceptable discourse of psychiatry. It is not just that the establishment disagrees with him, he allegedly has gone beyond the acceptable bounds of professionalism.
This reaction is surprising from numerous perspectives. First, his opinions would have seemed mainstream to many only a few years ago. Second, there is no large body of scientific evidence that has been generated to confirm that he is promoting an unscientific perspective that should rightly get ostracized by the medical community – such as anti-vaccination. Actually, some evidence suggests that some medical approaches to gender dysphoria have not always ameliorated the distress found in some patients.

After reviewing the evidence on gender reassignment surgery a few years ago, the Centers for Medicare & Medicaid Services concluded: “Based on an extensive assessment of the clinical evidence as described above, there is not enough high-quality evidence to determine whether gender reassignment surgery improves health outcomes for Medicare beneficiaries with gender dysphoria and whether patients most likely to benefit from these types of surgical intervention can be identified prospectively.”
Whether such a diagnosis should exist at all in the DSM is a worthy topic of discussion with inclusive arguments on both sides. Pathologizing gender dysphoria is stigmatizing. At the same time, a diagnosis may permit one to receive assistance for a recognized condition. One may rightfully want to discuss the scientific merit of a diagnosis without the interference of arguments based on political or social ramifications of said diagnosis, despite their obvious existence and import.
One should be able to voice scientific opinions in a fair-minded, nonpolitically biased manner that is not designed to intimidate and harass dissenters. One should note that a debate about the appropriateness of having said diagnosis will bring up many philosophical and deeply uncomfortable questions. Those questions point out the apparent nosologic problems inherent in DSM methodology that are extraordinarily difficult to solve. If psychiatry chooses to produce or dismiss psychiatric diagnoses based on the inherent political inconvenience of said diagnoses, rather than their scientific and medical basis, the entire field will rightly be called into question.
One may deplore the static and at times oppressive nature of cultural biases. However, it should be noted that the ability to safely step outside the supportive structure of family, employment, and social and religious institution is itself a privilege, one in which some our patients do not have the luxury of engaging in.
It is not clear to us how we got to this juncture. Part of psychiatric and medical training does involve learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition may be exaggerated into a desire to solve the human condition without challenging patients’ fundamental need for a well-rounded biologic, psychological, and social recovery. It is also possible that our desire to promote utopian hopes for society has blinded us from accepting the idea that, for many of our lowest-functioning patients, fitting in and participating in society can be their best path to recovery.
Psychiatry attempts to define and alleviate the suffering that accompanies some behaviors. As such, psychiatry has always and will always address and confront behaviors that society may condemn. At times, psychiatrists will be in sync or clash with societal trends. Sometimes science will contradict societal wishes. And ultimately, psychiatrists will hopefully make decisions informed in biopsychosocial constructs that best suit the patient in front of them no matter what society may want. In a polarized environment, psychiatry should remind itself that we cannot always or ever fix society, and that maintaining reasonable cultural norms and societal stability – while avoiding the traps of superficial culture wars and utopian visions – is often the wisest path.
Dr. Lehman is an associate professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
A series of case discussions recently engendered discord among colleagues of ours. The conflicts raised questions about systemic biases within our field and their possible ramifications.
The cases discussed, like many in psychiatry, involved patients with severely maladaptive coping skills who lived with punishing friends, had little rewarding purpose, and had dismissive or abusive families. The conflicts involved whether the treating psychiatrists should promote seemingly obvious life choices or whether those perspectives were based in socionormative stereotypes seeped in mistaken traditional values that do not account for the rich array of experiences our patients come from.
One such case involved a seemingly masochistic patient who repeatedly found herself in abusive relationships and whether the psychiatrist should consider criticizing her partner choices. Another case involved a severely suffering veteran who felt paralyzed at home and whether the psychiatrist should encourage employment to diminish isolation. Yet another case involved a suicidal transgender patient who was in despair when feeling little relief after receiving gender-conforming surgery and – whether the psychiatrist should or could discuss perspectives on gender.
Those cases have led to accusations of misunderstanding science on both sides – and questions about the political justifications and consequences of psychiatric recommendations.
The field of psychiatry is appropriately embarrassed by its former association to misogynistic, homophobic, and even racist schools of thought. However, we wonder whether our current attempts at penance are at times discouraging important discussions. In some cases, our lowest-functioning patients living on the fringe of society benefit the most from the stabilizing influences of family, employment, social institutions, or religious worship. This is especially true considering how much social isolation has become an increasing reality of modern life. As such, we worry when colleagues argue that the promotion of common values is inherently suspect.
This problem may be exemplified by the public attacks on Allan Josephson, MD. Dr. Josephson, a child psychiatrist at the University of Louisville (Ky.), contends that he was ostracized and later fired from his position for communicating at a Heritage Foundation forum on his concerns about current recommended treatments and approaches for gender dysphoria. It appears that, despite being a renowned and previously deeply respected expert in the field, his opinions on the subject now go beyond the acceptable discourse of psychiatry. It is not just that the establishment disagrees with him, he allegedly has gone beyond the acceptable bounds of professionalism.
This reaction is surprising from numerous perspectives. First, his opinions would have seemed mainstream to many only a few years ago. Second, there is no large body of scientific evidence that has been generated to confirm that he is promoting an unscientific perspective that should rightly get ostracized by the medical community – such as anti-vaccination. Actually, some evidence suggests that some medical approaches to gender dysphoria have not always ameliorated the distress found in some patients.
After reviewing the evidence on gender reassignment surgery a few years ago, the Centers for Medicare & Medicaid Services concluded: “Based on an extensive assessment of the clinical evidence as described above, there is not enough high-quality evidence to determine whether gender reassignment surgery improves health outcomes for Medicare beneficiaries with gender dysphoria and whether patients most likely to benefit from these types of surgical intervention can be identified prospectively.”
Whether such a diagnosis should exist at all in the DSM is a worthy topic of discussion with inclusive arguments on both sides. Pathologizing gender dysphoria is stigmatizing. At the same time, a diagnosis may permit one to receive assistance for a recognized condition. One may rightfully want to discuss the scientific merit of a diagnosis without the interference of arguments based on political or social ramifications of said diagnosis, despite their obvious existence and import.
One should be able to voice scientific opinions in a fair-minded, nonpolitically biased manner that is not designed to intimidate and harass dissenters. One should note that a debate about the appropriateness of having said diagnosis will bring up many philosophical and deeply uncomfortable questions. Those questions point out the apparent nosologic problems inherent in DSM methodology that are extraordinarily difficult to solve. If psychiatry chooses to produce or dismiss psychiatric diagnoses based on the inherent political inconvenience of said diagnoses, rather than their scientific and medical basis, the entire field will rightly be called into question.
One may deplore the static and at times oppressive nature of cultural biases. However, it should be noted that the ability to safely step outside the supportive structure of family, employment, and social and religious institution is itself a privilege, one in which some our patients do not have the luxury of engaging in.
It is not clear to us how we got to this juncture. Part of psychiatric and medical training does involve learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition may be exaggerated into a desire to solve the human condition without challenging patients’ fundamental need for a well-rounded biologic, psychological, and social recovery. It is also possible that our desire to promote utopian hopes for society has blinded us from accepting the idea that, for many of our lowest-functioning patients, fitting in and participating in society can be their best path to recovery.
Psychiatry attempts to define and alleviate the suffering that accompanies some behaviors. As such, psychiatry has always and will always address and confront behaviors that society may condemn. At times, psychiatrists will be in sync or clash with societal trends. Sometimes science will contradict societal wishes. And ultimately, psychiatrists will hopefully make decisions informed in biopsychosocial constructs that best suit the patient in front of them no matter what society may want. In a polarized environment, psychiatry should remind itself that we cannot always or ever fix society, and that maintaining reasonable cultural norms and societal stability – while avoiding the traps of superficial culture wars and utopian visions – is often the wisest path.
Dr. Lehman is an associate professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
A series of case discussions recently engendered discord among colleagues of ours. The conflicts raised questions about systemic biases within our field and their possible ramifications.
The cases discussed, like many in psychiatry, involved patients with severely maladaptive coping skills who lived with punishing friends, had little rewarding purpose, and had dismissive or abusive families. The conflicts involved whether the treating psychiatrists should promote seemingly obvious life choices or whether those perspectives were based in socionormative stereotypes seeped in mistaken traditional values that do not account for the rich array of experiences our patients come from.
One such case involved a seemingly masochistic patient who repeatedly found herself in abusive relationships and whether the psychiatrist should consider criticizing her partner choices. Another case involved a severely suffering veteran who felt paralyzed at home and whether the psychiatrist should encourage employment to diminish isolation. Yet another case involved a suicidal transgender patient who was in despair when feeling little relief after receiving gender-conforming surgery and – whether the psychiatrist should or could discuss perspectives on gender.
Those cases have led to accusations of misunderstanding science on both sides – and questions about the political justifications and consequences of psychiatric recommendations.
The field of psychiatry is appropriately embarrassed by its former association to misogynistic, homophobic, and even racist schools of thought. However, we wonder whether our current attempts at penance are at times discouraging important discussions. In some cases, our lowest-functioning patients living on the fringe of society benefit the most from the stabilizing influences of family, employment, social institutions, or religious worship. This is especially true considering how much social isolation has become an increasing reality of modern life. As such, we worry when colleagues argue that the promotion of common values is inherently suspect.
This problem may be exemplified by the public attacks on Allan Josephson, MD. Dr. Josephson, a child psychiatrist at the University of Louisville (Ky.), contends that he was ostracized and later fired from his position for communicating at a Heritage Foundation forum on his concerns about current recommended treatments and approaches for gender dysphoria. It appears that, despite being a renowned and previously deeply respected expert in the field, his opinions on the subject now go beyond the acceptable discourse of psychiatry. It is not just that the establishment disagrees with him, he allegedly has gone beyond the acceptable bounds of professionalism.
This reaction is surprising from numerous perspectives. First, his opinions would have seemed mainstream to many only a few years ago. Second, there is no large body of scientific evidence that has been generated to confirm that he is promoting an unscientific perspective that should rightly get ostracized by the medical community – such as anti-vaccination. Actually, some evidence suggests that some medical approaches to gender dysphoria have not always ameliorated the distress found in some patients.
After reviewing the evidence on gender reassignment surgery a few years ago, the Centers for Medicare & Medicaid Services concluded: “Based on an extensive assessment of the clinical evidence as described above, there is not enough high-quality evidence to determine whether gender reassignment surgery improves health outcomes for Medicare beneficiaries with gender dysphoria and whether patients most likely to benefit from these types of surgical intervention can be identified prospectively.”
Whether such a diagnosis should exist at all in the DSM is a worthy topic of discussion with inclusive arguments on both sides. Pathologizing gender dysphoria is stigmatizing. At the same time, a diagnosis may permit one to receive assistance for a recognized condition. One may rightfully want to discuss the scientific merit of a diagnosis without the interference of arguments based on political or social ramifications of said diagnosis, despite their obvious existence and import.
One should be able to voice scientific opinions in a fair-minded, nonpolitically biased manner that is not designed to intimidate and harass dissenters. One should note that a debate about the appropriateness of having said diagnosis will bring up many philosophical and deeply uncomfortable questions. Those questions point out the apparent nosologic problems inherent in DSM methodology that are extraordinarily difficult to solve. If psychiatry chooses to produce or dismiss psychiatric diagnoses based on the inherent political inconvenience of said diagnoses, rather than their scientific and medical basis, the entire field will rightly be called into question.
One may deplore the static and at times oppressive nature of cultural biases. However, it should be noted that the ability to safely step outside the supportive structure of family, employment, and social and religious institution is itself a privilege, one in which some our patients do not have the luxury of engaging in.
It is not clear to us how we got to this juncture. Part of psychiatric and medical training does involve learning nonjudgmental approaches to human suffering and an identification with individual needs over societal demands. Our suspicion is that a nonjudgmental approach to the understanding of the human condition may be exaggerated into a desire to solve the human condition without challenging patients’ fundamental need for a well-rounded biologic, psychological, and social recovery. It is also possible that our desire to promote utopian hopes for society has blinded us from accepting the idea that, for many of our lowest-functioning patients, fitting in and participating in society can be their best path to recovery.
Psychiatry attempts to define and alleviate the suffering that accompanies some behaviors. As such, psychiatry has always and will always address and confront behaviors that society may condemn. At times, psychiatrists will be in sync or clash with societal trends. Sometimes science will contradict societal wishes. And ultimately, psychiatrists will hopefully make decisions informed in biopsychosocial constructs that best suit the patient in front of them no matter what society may want. In a polarized environment, psychiatry should remind itself that we cannot always or ever fix society, and that maintaining reasonable cultural norms and societal stability – while avoiding the traps of superficial culture wars and utopian visions – is often the wisest path.
Dr. Lehman is an associate professor of psychiatry at the University of California, San Diego. He is codirector of all acute and intensive psychiatric treatment at the Veterans Affairs Medical Center in San Diego, where he practices clinical psychiatry. He also is the course director for the UCSD third-year medical student psychiatry clerkship. Dr. Badre is a forensic psychiatrist in San Diego and an expert in correctional mental health. He holds teaching positions at UCSD and the University of San Diego. Dr. Badre can be reached at his website, BadreMD.com.
Disparity in endometrial cancer outcomes: What can we do?
While the incidence of most cancers is falling, endometrial cancer rates continue to rise, in large part because of increasing life expectancy and obesity rates. However, what is even more alarming is the observation that there is a clear disparity in outcomes between black and white women with this disease. But there are things that all health care providers, including nononcologists, can do to help to overcome this disparity.

Black women are nearly twice as likely as non-Hispanic white women to die from the endometrial cancer. The 5-year survival for stage III and IV cancer is 43% for non-Hispanic white women, yet only 25% for black women.1 For a long time, this survival disparity was assumed to be a function of the more aggressive cancer histologies, such as serous, which are more commonly seen in black women. These high-grade cancers are more likely to present in advanced stages and with poorer responses to treatments; however, the predisposition to aggressive cancers tells only part of the story of racial disparities in endometrial cancer and their presentation at later stages. Indeed, fueling the problem are the findings that black women report symptoms less, experience more delays in diagnosis or more frequent deviations from guideline-directed diagnostics, undergo more morbid surgical approaches, receive less surgical staging, are enrolled less in clinical trials, have lower socioeconomic status and lower rates of health insurance, and receive less differential administration of adjuvant therapies, as well as have a background of higher all-cause mortality and comorbidities. While this array of contributing factors may seem overwhelming, it also can be considered a guide for health care providers because most of these factors, unlike histologic cell type, are modifiable, and it is important that we all consider what role we can play in dismantling them.
Black women are less likely to receive guideline-recommended care upon presentation. Research by Kemi M. Doll, MD, from the University of Washington, Seattle, demonstrated that, among women with endometrial cancers, black women were less likely to have documented histories of postmenopausal bleeding within 2 years of the diagnosis, presumably because of factors related to underreporting and inadequate ascertainment by medical professionals of whether or not they had experienced postmenopausal bleeding.2 Additionally, when postmenopausal bleeding was reported by these women, they were less likely to receive the appropriate diagnostic work-up as described by American College of Obstetricians and Gynecologists guidelines, and their bleeding was more likely to be ascribed to nonmalignant pathologies. Her work raises the important question about how black women view the health care profession and their willingness to engage early in good faith that their concerns will be met. These concerns are understandable given the documented different responsiveness of providers to black patients’ symptoms such as pain.3
both of which are considered the standard of care.1,4 Lower rates of minimally invasive surgery expose black women to increased morbidity and are deleterious to quality of life, return to work, and functionality. If surgical staging is omitted, which is more common for these women, clinicians are less able to appropriately prescribe adjuvant therapies which might prevent lethal recurrences from unrecognized advanced cancer or they may overtreat early-stage cancers with adjuvant therapy to make up for gaps in staging information.1,5 However, adjuvant therapy is not a benign intervention, and itself is associated with morbidity.

As mentioned earlier, black women are at a higher risk for developing more aggressive cancer subtypes, and this phenomenon may appear unmodifiable. However, important research is looking at the concept of epigenetics and how modifiable environmental factors may contribute to the development of more aggressive types of cancer through gene expression. Additionally, differences in the gene mutations and gene expression of cancers more frequently acquired by black women may negatively influence how these cancers respond to conventional therapies. In the GOG210 study, which evaluated the outcomes of women with comprehensively staged endometrial cancer, black women demonstrated worse survival from cancer, even though they were more likely to receive chemotherapy.5 One explanation for this finding is that these women’s cancers were less responsive to conventional chemotherapy agents.
This raises a critical issue of disparity in clinical trial inclusion. Black women are underrepresented in clinical trials in the United States. There is a dark history in medical research and minority populations, particularly African American populations, which continues to be remembered and felt. However, not all of this underrepresentation may be from unwillingness to participate: For black women, issues of lack of access to or being considered for clinical trials is also a factor. But without adequate representation in trials of novel agents, we will not know whether they are effective for all populations, and indeed it would appear that we should not assume they are equally effective based on the results to date.
So how can we all individually help to overcome these disparities in endometrial cancer outcomes? To begin with, it is important to acknowledge that black women commonly report negative experiences with reproductive health care. From early in their lives, we must sensitively engage all of our patients and ensure they all feel heard and valued. They should know that their symptoms, including pain or bleeding, are taken and treated seriously. If we can do better with this throughout a woman’s earlier reproductive health care experiences, perhaps later in her life, when she experiences postmenopausal bleeding, she will feel comfortable raising this issue with her health care provider who in turn must take this symptom seriously and expeditiously engage all of the appropriate diagnostic resources. Health care delivery is about more than simply offering the best treatment. We also are responsible for education and shared decision making to ensure that we can deliver the best treatment.
We also can support organizations such as ECANA (Endometrial Cancer Action Network for African Americans) which serves to inform black women in their communities about the threat that endometrial cancer plays and empowers them through education about its symptoms and the need to seek care.
Systematically we must ensure black women have access to the same standards in surgical and nonsurgical management of these cancers. This includes referral of all women with cancer, including minorities, to high-volume centers with oncology specialists and explaining to those who may be reluctant to travel that this is associated with improved outcomes in the short and long term. We also must actively consider our black patients for clinical trials, sensitively educate them about their benefits, and overcome barriers to access. One simple way to do this is to explain that the treatments that we have developed for endometrial cancer have mostly been tested on white women, which may explain in part why they do not work so well for nonwhite women.
The racial disparity in endometrial cancer outcomes cannot entirely be attributed to the passive phenomenon of patient and tumor genetics, particularly with consideration that race is a social construct rather than a biological phenomenon. We can all make a difference through advocacy, access, education, and heightened awareness to combat this inequity and overcome these disparate outcomes.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She said she had no relevant financial disclosures. Email her at obnews@mdedge.com.
References
1. Gynecol Oncol. 2016 Oct;143(1):98-104.
2. Am J Obstet Gynecol. 2018 Dec;219(6):593.e1-14.
3. J Clin Oncol. 2012 Jun 1;30(16):1980-8.
4. Obstet Gynecol. 2016 Sep;128(3):526-34.
5. Am J Obstet Gynecol. 2018 Nov;219(5):459.e1-11.
While the incidence of most cancers is falling, endometrial cancer rates continue to rise, in large part because of increasing life expectancy and obesity rates. However, what is even more alarming is the observation that there is a clear disparity in outcomes between black and white women with this disease. But there are things that all health care providers, including nononcologists, can do to help to overcome this disparity.
Black women are nearly twice as likely as non-Hispanic white women to die from the endometrial cancer. The 5-year survival for stage III and IV cancer is 43% for non-Hispanic white women, yet only 25% for black women.1 For a long time, this survival disparity was assumed to be a function of the more aggressive cancer histologies, such as serous, which are more commonly seen in black women. These high-grade cancers are more likely to present in advanced stages and with poorer responses to treatments; however, the predisposition to aggressive cancers tells only part of the story of racial disparities in endometrial cancer and their presentation at later stages. Indeed, fueling the problem are the findings that black women report symptoms less, experience more delays in diagnosis or more frequent deviations from guideline-directed diagnostics, undergo more morbid surgical approaches, receive less surgical staging, are enrolled less in clinical trials, have lower socioeconomic status and lower rates of health insurance, and receive less differential administration of adjuvant therapies, as well as have a background of higher all-cause mortality and comorbidities. While this array of contributing factors may seem overwhelming, it also can be considered a guide for health care providers because most of these factors, unlike histologic cell type, are modifiable, and it is important that we all consider what role we can play in dismantling them.
Black women are less likely to receive guideline-recommended care upon presentation. Research by Kemi M. Doll, MD, from the University of Washington, Seattle, demonstrated that, among women with endometrial cancers, black women were less likely to have documented histories of postmenopausal bleeding within 2 years of the diagnosis, presumably because of factors related to underreporting and inadequate ascertainment by medical professionals of whether or not they had experienced postmenopausal bleeding.2 Additionally, when postmenopausal bleeding was reported by these women, they were less likely to receive the appropriate diagnostic work-up as described by American College of Obstetricians and Gynecologists guidelines, and their bleeding was more likely to be ascribed to nonmalignant pathologies. Her work raises the important question about how black women view the health care profession and their willingness to engage early in good faith that their concerns will be met. These concerns are understandable given the documented different responsiveness of providers to black patients’ symptoms such as pain.3
both of which are considered the standard of care.1,4 Lower rates of minimally invasive surgery expose black women to increased morbidity and are deleterious to quality of life, return to work, and functionality. If surgical staging is omitted, which is more common for these women, clinicians are less able to appropriately prescribe adjuvant therapies which might prevent lethal recurrences from unrecognized advanced cancer or they may overtreat early-stage cancers with adjuvant therapy to make up for gaps in staging information.1,5 However, adjuvant therapy is not a benign intervention, and itself is associated with morbidity.
As mentioned earlier, black women are at a higher risk for developing more aggressive cancer subtypes, and this phenomenon may appear unmodifiable. However, important research is looking at the concept of epigenetics and how modifiable environmental factors may contribute to the development of more aggressive types of cancer through gene expression. Additionally, differences in the gene mutations and gene expression of cancers more frequently acquired by black women may negatively influence how these cancers respond to conventional therapies. In the GOG210 study, which evaluated the outcomes of women with comprehensively staged endometrial cancer, black women demonstrated worse survival from cancer, even though they were more likely to receive chemotherapy.5 One explanation for this finding is that these women’s cancers were less responsive to conventional chemotherapy agents.
This raises a critical issue of disparity in clinical trial inclusion. Black women are underrepresented in clinical trials in the United States. There is a dark history in medical research and minority populations, particularly African American populations, which continues to be remembered and felt. However, not all of this underrepresentation may be from unwillingness to participate: For black women, issues of lack of access to or being considered for clinical trials is also a factor. But without adequate representation in trials of novel agents, we will not know whether they are effective for all populations, and indeed it would appear that we should not assume they are equally effective based on the results to date.
So how can we all individually help to overcome these disparities in endometrial cancer outcomes? To begin with, it is important to acknowledge that black women commonly report negative experiences with reproductive health care. From early in their lives, we must sensitively engage all of our patients and ensure they all feel heard and valued. They should know that their symptoms, including pain or bleeding, are taken and treated seriously. If we can do better with this throughout a woman’s earlier reproductive health care experiences, perhaps later in her life, when she experiences postmenopausal bleeding, she will feel comfortable raising this issue with her health care provider who in turn must take this symptom seriously and expeditiously engage all of the appropriate diagnostic resources. Health care delivery is about more than simply offering the best treatment. We also are responsible for education and shared decision making to ensure that we can deliver the best treatment.
We also can support organizations such as ECANA (Endometrial Cancer Action Network for African Americans) which serves to inform black women in their communities about the threat that endometrial cancer plays and empowers them through education about its symptoms and the need to seek care.
Systematically we must ensure black women have access to the same standards in surgical and nonsurgical management of these cancers. This includes referral of all women with cancer, including minorities, to high-volume centers with oncology specialists and explaining to those who may be reluctant to travel that this is associated with improved outcomes in the short and long term. We also must actively consider our black patients for clinical trials, sensitively educate them about their benefits, and overcome barriers to access. One simple way to do this is to explain that the treatments that we have developed for endometrial cancer have mostly been tested on white women, which may explain in part why they do not work so well for nonwhite women.
The racial disparity in endometrial cancer outcomes cannot entirely be attributed to the passive phenomenon of patient and tumor genetics, particularly with consideration that race is a social construct rather than a biological phenomenon. We can all make a difference through advocacy, access, education, and heightened awareness to combat this inequity and overcome these disparate outcomes.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She said she had no relevant financial disclosures. Email her at obnews@mdedge.com.
References
1. Gynecol Oncol. 2016 Oct;143(1):98-104.
2. Am J Obstet Gynecol. 2018 Dec;219(6):593.e1-14.
3. J Clin Oncol. 2012 Jun 1;30(16):1980-8.
4. Obstet Gynecol. 2016 Sep;128(3):526-34.
5. Am J Obstet Gynecol. 2018 Nov;219(5):459.e1-11.
While the incidence of most cancers is falling, endometrial cancer rates continue to rise, in large part because of increasing life expectancy and obesity rates. However, what is even more alarming is the observation that there is a clear disparity in outcomes between black and white women with this disease. But there are things that all health care providers, including nononcologists, can do to help to overcome this disparity.
Black women are nearly twice as likely as non-Hispanic white women to die from the endometrial cancer. The 5-year survival for stage III and IV cancer is 43% for non-Hispanic white women, yet only 25% for black women.1 For a long time, this survival disparity was assumed to be a function of the more aggressive cancer histologies, such as serous, which are more commonly seen in black women. These high-grade cancers are more likely to present in advanced stages and with poorer responses to treatments; however, the predisposition to aggressive cancers tells only part of the story of racial disparities in endometrial cancer and their presentation at later stages. Indeed, fueling the problem are the findings that black women report symptoms less, experience more delays in diagnosis or more frequent deviations from guideline-directed diagnostics, undergo more morbid surgical approaches, receive less surgical staging, are enrolled less in clinical trials, have lower socioeconomic status and lower rates of health insurance, and receive less differential administration of adjuvant therapies, as well as have a background of higher all-cause mortality and comorbidities. While this array of contributing factors may seem overwhelming, it also can be considered a guide for health care providers because most of these factors, unlike histologic cell type, are modifiable, and it is important that we all consider what role we can play in dismantling them.
Black women are less likely to receive guideline-recommended care upon presentation. Research by Kemi M. Doll, MD, from the University of Washington, Seattle, demonstrated that, among women with endometrial cancers, black women were less likely to have documented histories of postmenopausal bleeding within 2 years of the diagnosis, presumably because of factors related to underreporting and inadequate ascertainment by medical professionals of whether or not they had experienced postmenopausal bleeding.2 Additionally, when postmenopausal bleeding was reported by these women, they were less likely to receive the appropriate diagnostic work-up as described by American College of Obstetricians and Gynecologists guidelines, and their bleeding was more likely to be ascribed to nonmalignant pathologies. Her work raises the important question about how black women view the health care profession and their willingness to engage early in good faith that their concerns will be met. These concerns are understandable given the documented different responsiveness of providers to black patients’ symptoms such as pain.3
both of which are considered the standard of care.1,4 Lower rates of minimally invasive surgery expose black women to increased morbidity and are deleterious to quality of life, return to work, and functionality. If surgical staging is omitted, which is more common for these women, clinicians are less able to appropriately prescribe adjuvant therapies which might prevent lethal recurrences from unrecognized advanced cancer or they may overtreat early-stage cancers with adjuvant therapy to make up for gaps in staging information.1,5 However, adjuvant therapy is not a benign intervention, and itself is associated with morbidity.
As mentioned earlier, black women are at a higher risk for developing more aggressive cancer subtypes, and this phenomenon may appear unmodifiable. However, important research is looking at the concept of epigenetics and how modifiable environmental factors may contribute to the development of more aggressive types of cancer through gene expression. Additionally, differences in the gene mutations and gene expression of cancers more frequently acquired by black women may negatively influence how these cancers respond to conventional therapies. In the GOG210 study, which evaluated the outcomes of women with comprehensively staged endometrial cancer, black women demonstrated worse survival from cancer, even though they were more likely to receive chemotherapy.5 One explanation for this finding is that these women’s cancers were less responsive to conventional chemotherapy agents.
This raises a critical issue of disparity in clinical trial inclusion. Black women are underrepresented in clinical trials in the United States. There is a dark history in medical research and minority populations, particularly African American populations, which continues to be remembered and felt. However, not all of this underrepresentation may be from unwillingness to participate: For black women, issues of lack of access to or being considered for clinical trials is also a factor. But without adequate representation in trials of novel agents, we will not know whether they are effective for all populations, and indeed it would appear that we should not assume they are equally effective based on the results to date.
So how can we all individually help to overcome these disparities in endometrial cancer outcomes? To begin with, it is important to acknowledge that black women commonly report negative experiences with reproductive health care. From early in their lives, we must sensitively engage all of our patients and ensure they all feel heard and valued. They should know that their symptoms, including pain or bleeding, are taken and treated seriously. If we can do better with this throughout a woman’s earlier reproductive health care experiences, perhaps later in her life, when she experiences postmenopausal bleeding, she will feel comfortable raising this issue with her health care provider who in turn must take this symptom seriously and expeditiously engage all of the appropriate diagnostic resources. Health care delivery is about more than simply offering the best treatment. We also are responsible for education and shared decision making to ensure that we can deliver the best treatment.
We also can support organizations such as ECANA (Endometrial Cancer Action Network for African Americans) which serves to inform black women in their communities about the threat that endometrial cancer plays and empowers them through education about its symptoms and the need to seek care.
Systematically we must ensure black women have access to the same standards in surgical and nonsurgical management of these cancers. This includes referral of all women with cancer, including minorities, to high-volume centers with oncology specialists and explaining to those who may be reluctant to travel that this is associated with improved outcomes in the short and long term. We also must actively consider our black patients for clinical trials, sensitively educate them about their benefits, and overcome barriers to access. One simple way to do this is to explain that the treatments that we have developed for endometrial cancer have mostly been tested on white women, which may explain in part why they do not work so well for nonwhite women.
The racial disparity in endometrial cancer outcomes cannot entirely be attributed to the passive phenomenon of patient and tumor genetics, particularly with consideration that race is a social construct rather than a biological phenomenon. We can all make a difference through advocacy, access, education, and heightened awareness to combat this inequity and overcome these disparate outcomes.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She said she had no relevant financial disclosures. Email her at obnews@mdedge.com.
References
1. Gynecol Oncol. 2016 Oct;143(1):98-104.
2. Am J Obstet Gynecol. 2018 Dec;219(6):593.e1-14.
3. J Clin Oncol. 2012 Jun 1;30(16):1980-8.
4. Obstet Gynecol. 2016 Sep;128(3):526-34.
5. Am J Obstet Gynecol. 2018 Nov;219(5):459.e1-11.
‘How did I get cancer?’
We are 20 minutes into the visit. My patient is 77 years old, a retired school administrator. She was sent to the oncology clinic for a new diagnosis of lung cancer with metastases to the liver and bones.

I was asking my usual questions – how did this all begin? – and I was hearing the usual answers. The cough that didn’t get better with antibiotics. The unintentional weight loss. The chest x-ray that looked “fuzzy.”
I continue: How many packs of cigarettes a day, and for how many years? Any family history of cancer?
These were my standard questions. They were met by hers: “How did I get this?”
I recently hosted a podcast on common, difficult questions we hear in hematology and oncology. How long do I have to live? What would you do if this were your family member?
This was another. There are variations to be sure. How, why, why me, what did I do, what didn’t I do, did my doctor miss it, if I had this or that test would they have caught it sooner?
When I was an internist, I talked about prevention. Meeting a new patient meant sizing them up for risk factors. In their habits I saw opportunities for healthier choices. In their family histories I gathered warning signs.
Now, I ask the same probing questions, but the purpose is not the same. Smoking, alcohol, family history, I ask these of everyone, I reassure them. It’s no longer about assessing risk. It’s not to place blame. But they read into the fact that I am asking, because they have asked themselves the same.
They ask why.
I try not to overdo the pity. I say that I’m sorry this is happening, but I don’t dwell. What I want to convey is the opposite – it’s normalcy. What I want to convey is: I’ve seen this a million times. This is where we are, and here is where we go. We don’t dwell or regret or wonder what if. My patients don’t want sympathy – at least, not from their doctor. They want a plan.

They ask: How did I get this?
It’s bad luck, I say. It’s a genetic mutation causing a cell to replicate.
My answers do not always satisfy their questions. Because it’s not a question seeking an informational answer. The truth is, medically and existentially, I don’t know. None of us do. The question is an existential itch no medical jargon can scratch.
I have a modern Hippocratic oath tacked to a wall in my room. “I will prevent disease whenever I can, because prevention is preferable to cure,” it says. True, but that offers little solace to those who already have the illness. Yes, we need prevention. And we need a path forward when tragedy has already struck.
I am humbled when I meet a new cancer patient because the visit is a metaphor for a nonjudgmental life. There’s something beautiful about meeting someone exactly where they are, where decisions made in the past are as irrelevant to me now as they were to the cancer.
When they inevitably ask “how did I get this?” and I answer, what I’m really saying is this: I don’t care what you did, or didn’t do, or how we got here. But we are here, and so I am here with you, and from now on the only place we care about is here and now, the only direction forward.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz and listen to her each week on the Blood & Cancer podcast.
We are 20 minutes into the visit. My patient is 77 years old, a retired school administrator. She was sent to the oncology clinic for a new diagnosis of lung cancer with metastases to the liver and bones.
I was asking my usual questions – how did this all begin? – and I was hearing the usual answers. The cough that didn’t get better with antibiotics. The unintentional weight loss. The chest x-ray that looked “fuzzy.”
I continue: How many packs of cigarettes a day, and for how many years? Any family history of cancer?
These were my standard questions. They were met by hers: “How did I get this?”
I recently hosted a podcast on common, difficult questions we hear in hematology and oncology. How long do I have to live? What would you do if this were your family member?
This was another. There are variations to be sure. How, why, why me, what did I do, what didn’t I do, did my doctor miss it, if I had this or that test would they have caught it sooner?
When I was an internist, I talked about prevention. Meeting a new patient meant sizing them up for risk factors. In their habits I saw opportunities for healthier choices. In their family histories I gathered warning signs.
Now, I ask the same probing questions, but the purpose is not the same. Smoking, alcohol, family history, I ask these of everyone, I reassure them. It’s no longer about assessing risk. It’s not to place blame. But they read into the fact that I am asking, because they have asked themselves the same.
They ask why.
I try not to overdo the pity. I say that I’m sorry this is happening, but I don’t dwell. What I want to convey is the opposite – it’s normalcy. What I want to convey is: I’ve seen this a million times. This is where we are, and here is where we go. We don’t dwell or regret or wonder what if. My patients don’t want sympathy – at least, not from their doctor. They want a plan.
They ask: How did I get this?
It’s bad luck, I say. It’s a genetic mutation causing a cell to replicate.
My answers do not always satisfy their questions. Because it’s not a question seeking an informational answer. The truth is, medically and existentially, I don’t know. None of us do. The question is an existential itch no medical jargon can scratch.
I have a modern Hippocratic oath tacked to a wall in my room. “I will prevent disease whenever I can, because prevention is preferable to cure,” it says. True, but that offers little solace to those who already have the illness. Yes, we need prevention. And we need a path forward when tragedy has already struck.
I am humbled when I meet a new cancer patient because the visit is a metaphor for a nonjudgmental life. There’s something beautiful about meeting someone exactly where they are, where decisions made in the past are as irrelevant to me now as they were to the cancer.
When they inevitably ask “how did I get this?” and I answer, what I’m really saying is this: I don’t care what you did, or didn’t do, or how we got here. But we are here, and so I am here with you, and from now on the only place we care about is here and now, the only direction forward.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz and listen to her each week on the Blood & Cancer podcast.
We are 20 minutes into the visit. My patient is 77 years old, a retired school administrator. She was sent to the oncology clinic for a new diagnosis of lung cancer with metastases to the liver and bones.
I was asking my usual questions – how did this all begin? – and I was hearing the usual answers. The cough that didn’t get better with antibiotics. The unintentional weight loss. The chest x-ray that looked “fuzzy.”
I continue: How many packs of cigarettes a day, and for how many years? Any family history of cancer?
These were my standard questions. They were met by hers: “How did I get this?”
I recently hosted a podcast on common, difficult questions we hear in hematology and oncology. How long do I have to live? What would you do if this were your family member?
This was another. There are variations to be sure. How, why, why me, what did I do, what didn’t I do, did my doctor miss it, if I had this or that test would they have caught it sooner?
When I was an internist, I talked about prevention. Meeting a new patient meant sizing them up for risk factors. In their habits I saw opportunities for healthier choices. In their family histories I gathered warning signs.
Now, I ask the same probing questions, but the purpose is not the same. Smoking, alcohol, family history, I ask these of everyone, I reassure them. It’s no longer about assessing risk. It’s not to place blame. But they read into the fact that I am asking, because they have asked themselves the same.
They ask why.
I try not to overdo the pity. I say that I’m sorry this is happening, but I don’t dwell. What I want to convey is the opposite – it’s normalcy. What I want to convey is: I’ve seen this a million times. This is where we are, and here is where we go. We don’t dwell or regret or wonder what if. My patients don’t want sympathy – at least, not from their doctor. They want a plan.
They ask: How did I get this?
It’s bad luck, I say. It’s a genetic mutation causing a cell to replicate.
My answers do not always satisfy their questions. Because it’s not a question seeking an informational answer. The truth is, medically and existentially, I don’t know. None of us do. The question is an existential itch no medical jargon can scratch.
I have a modern Hippocratic oath tacked to a wall in my room. “I will prevent disease whenever I can, because prevention is preferable to cure,” it says. True, but that offers little solace to those who already have the illness. Yes, we need prevention. And we need a path forward when tragedy has already struck.
I am humbled when I meet a new cancer patient because the visit is a metaphor for a nonjudgmental life. There’s something beautiful about meeting someone exactly where they are, where decisions made in the past are as irrelevant to me now as they were to the cancer.
When they inevitably ask “how did I get this?” and I answer, what I’m really saying is this: I don’t care what you did, or didn’t do, or how we got here. But we are here, and so I am here with you, and from now on the only place we care about is here and now, the only direction forward.
Dr. Yurkiewicz is a fellow in hematology and oncology at Stanford (Calif.) University. Follow her on Twitter @ilanayurkiewicz and listen to her each week on the Blood & Cancer podcast.
Taking the editorial torch
Dear colleagues,
I am excited to introduce the November issue of The New Gastroenterologist – which is also my first issue as the new Editor in Chief! First, I am incredibly grateful for this opportunity to be a part of the only existing publication tailored toward trainees and early-career gastroenterologists. Bryson Katona has done a remarkable job for the last 5 years as the publication’s inaugural EIC, as he has laid a great deal of groundwork and really set the standard going forward. Each issue has been a multifaceted compilation of salient clinical topics paired with brief but high-yield articles to help guide personal and professional growth; I hope to continue to do the same and maintain a high level of interest in our newsletter.

In this issue, the In Focus article, brought to you by Adeeti Chiplunker and Christina Ha (Cedars Sinai), discusses inpatient management of acute severe ulcerative colitis. It is an excellent review of the diagnostic workup and therapeutic options, and an important one, as therapies are quickly evolving in inflammatory bowel disease. We also have Manol Jovani (Johns Hopkins) help us navigate the daunting world of statistics, specifically focusing on the interpretation of the P value.
For those interested in or already pursuing careers in private practice but would not like to relinquish their research interests, Chris Fourment (Texas Digestive Disease Consultants) provides a series of helpful tips on how to be effective in conducting clinical research endeavors. In the realm of basic science, Melinda Engevik (Baylor College of Medicine) gives an informative breakdown on how to choose a lab that is the right fit for you.
Also in this issue, Sadeea Abbasi (Cedars Sinai) provides an array of tangible ways for gastroenterologists to become involved in health policy advocacy. Byron Cryer (UT Southwestern), Jesus Rivera-Nieves (UCSD), and Celena NuQuay (AGA) describe how the AGA has been promoting workforce diversity in academic gastroenterology via the FORWARD (Fostering Opportunities Resulting in Workforce and Research Diversity) program.
Finally, as the submission deadline for DDW® 2020 approaches, abstract reviewers for the fellow-directed quality improvement (QI) projects from this past year share helpful tips on crafting memorable QI abstracts (Mohammad Bilal, UT-Galveston; Chung Sang Tse, Brown University; Manol Jovani, Johns Hopkins; and Mer Mietzelfeld, AGA).
If you are interested in contributing or have ideas for future TNG topics, please contact me (vijayarao@medicine.bsd.uchicago.edu), or Ryan Farrell (rfarrell@gastro.org), managing editor of TNG.
Sincerely,
Vijaya L. Rao, MD
Editor in Chief
Dr. Rao is assistant professor of medicine, University of Chicago, section of gastroenterology, hepatology & nutrition.
Dear colleagues,
I am excited to introduce the November issue of The New Gastroenterologist – which is also my first issue as the new Editor in Chief! First, I am incredibly grateful for this opportunity to be a part of the only existing publication tailored toward trainees and early-career gastroenterologists. Bryson Katona has done a remarkable job for the last 5 years as the publication’s inaugural EIC, as he has laid a great deal of groundwork and really set the standard going forward. Each issue has been a multifaceted compilation of salient clinical topics paired with brief but high-yield articles to help guide personal and professional growth; I hope to continue to do the same and maintain a high level of interest in our newsletter.
In this issue, the In Focus article, brought to you by Adeeti Chiplunker and Christina Ha (Cedars Sinai), discusses inpatient management of acute severe ulcerative colitis. It is an excellent review of the diagnostic workup and therapeutic options, and an important one, as therapies are quickly evolving in inflammatory bowel disease. We also have Manol Jovani (Johns Hopkins) help us navigate the daunting world of statistics, specifically focusing on the interpretation of the P value.
For those interested in or already pursuing careers in private practice but would not like to relinquish their research interests, Chris Fourment (Texas Digestive Disease Consultants) provides a series of helpful tips on how to be effective in conducting clinical research endeavors. In the realm of basic science, Melinda Engevik (Baylor College of Medicine) gives an informative breakdown on how to choose a lab that is the right fit for you.
Also in this issue, Sadeea Abbasi (Cedars Sinai) provides an array of tangible ways for gastroenterologists to become involved in health policy advocacy. Byron Cryer (UT Southwestern), Jesus Rivera-Nieves (UCSD), and Celena NuQuay (AGA) describe how the AGA has been promoting workforce diversity in academic gastroenterology via the FORWARD (Fostering Opportunities Resulting in Workforce and Research Diversity) program.
Finally, as the submission deadline for DDW® 2020 approaches, abstract reviewers for the fellow-directed quality improvement (QI) projects from this past year share helpful tips on crafting memorable QI abstracts (Mohammad Bilal, UT-Galveston; Chung Sang Tse, Brown University; Manol Jovani, Johns Hopkins; and Mer Mietzelfeld, AGA).
If you are interested in contributing or have ideas for future TNG topics, please contact me (vijayarao@medicine.bsd.uchicago.edu), or Ryan Farrell (rfarrell@gastro.org), managing editor of TNG.
Sincerely,
Vijaya L. Rao, MD
Editor in Chief
Dr. Rao is assistant professor of medicine, University of Chicago, section of gastroenterology, hepatology & nutrition.
Dear colleagues,
I am excited to introduce the November issue of The New Gastroenterologist – which is also my first issue as the new Editor in Chief! First, I am incredibly grateful for this opportunity to be a part of the only existing publication tailored toward trainees and early-career gastroenterologists. Bryson Katona has done a remarkable job for the last 5 years as the publication’s inaugural EIC, as he has laid a great deal of groundwork and really set the standard going forward. Each issue has been a multifaceted compilation of salient clinical topics paired with brief but high-yield articles to help guide personal and professional growth; I hope to continue to do the same and maintain a high level of interest in our newsletter.
In this issue, the In Focus article, brought to you by Adeeti Chiplunker and Christina Ha (Cedars Sinai), discusses inpatient management of acute severe ulcerative colitis. It is an excellent review of the diagnostic workup and therapeutic options, and an important one, as therapies are quickly evolving in inflammatory bowel disease. We also have Manol Jovani (Johns Hopkins) help us navigate the daunting world of statistics, specifically focusing on the interpretation of the P value.
For those interested in or already pursuing careers in private practice but would not like to relinquish their research interests, Chris Fourment (Texas Digestive Disease Consultants) provides a series of helpful tips on how to be effective in conducting clinical research endeavors. In the realm of basic science, Melinda Engevik (Baylor College of Medicine) gives an informative breakdown on how to choose a lab that is the right fit for you.
Also in this issue, Sadeea Abbasi (Cedars Sinai) provides an array of tangible ways for gastroenterologists to become involved in health policy advocacy. Byron Cryer (UT Southwestern), Jesus Rivera-Nieves (UCSD), and Celena NuQuay (AGA) describe how the AGA has been promoting workforce diversity in academic gastroenterology via the FORWARD (Fostering Opportunities Resulting in Workforce and Research Diversity) program.
Finally, as the submission deadline for DDW® 2020 approaches, abstract reviewers for the fellow-directed quality improvement (QI) projects from this past year share helpful tips on crafting memorable QI abstracts (Mohammad Bilal, UT-Galveston; Chung Sang Tse, Brown University; Manol Jovani, Johns Hopkins; and Mer Mietzelfeld, AGA).
If you are interested in contributing or have ideas for future TNG topics, please contact me (vijayarao@medicine.bsd.uchicago.edu), or Ryan Farrell (rfarrell@gastro.org), managing editor of TNG.
Sincerely,
Vijaya L. Rao, MD
Editor in Chief
Dr. Rao is assistant professor of medicine, University of Chicago, section of gastroenterology, hepatology & nutrition.
Digital disruption
One of our lead articles stems from the annual Partners in Value meeting, which was developed by the AGA in partnership with the Digestive Health Physicians Association (Chicago, Oct. 4, 2019). This is an annual meeting about innovations and “what’s next” for GI practices. Anton Decker, MD, an expert in the business of GI and Chair of the Practice Management and Economics Committee, discussed “digital disruption.”

When we discuss digital innovations in health care, most think of telehealth, social media, self-care apps, and remote patient monitoring. As a health system executive, my viewpoint about digital technology has been expanded by other critical needs. At the University of Michigan, we are space constrained (land locked without sufficient parking) and are living with shrinking clinical margins. We see digital technology as a solution to both. As we consolidate our call centers from 27 sites to 1, we plan for 30% of our staff to work from home. Setting up a home work station costs $3,000, compared with office space costs (about $5,000/year). A new clinical site might cost $20 million to build, but that is a fraction of the true life-cycle cost of the building. We have a widely distributed patient base (imagine traveling from Michigan’s Upper Penisula to Ann Arbor for a 20-minute clinic visit).
Many people appreciate “seeing” their doctor from the comfort of their living room. We plan to convert at least 15% of patient visits to telehealth over the next few years although reimbursement rules are still limiting. This year, more than 80% of postsurgical visits (90-day bundled payment) were conducted virtually – mostly by NPs or PAs. Our GI psychologist converted 1,500 patient visit hours to virtual visits last year. In 2019, we completed over 4,000 evisits (management of simple conditions initiated by a patient – essential during flu season) and an increasing number of econsults (primary consultations to specialists). Project ECHO (N Engl J Med. 2011;364:2199) remains the star example of how digital health can improve access, especially for underserved communities.
Virtual care, telehealth, remote patient monitoring, telecommuting and other digital innovations are becoming standards for health systems. Now is the time to think of “face-to-face” visits as option B.
John I. Allen, MD, MBD, AGAF
Editor in Chief
One of our lead articles stems from the annual Partners in Value meeting, which was developed by the AGA in partnership with the Digestive Health Physicians Association (Chicago, Oct. 4, 2019). This is an annual meeting about innovations and “what’s next” for GI practices. Anton Decker, MD, an expert in the business of GI and Chair of the Practice Management and Economics Committee, discussed “digital disruption.”
When we discuss digital innovations in health care, most think of telehealth, social media, self-care apps, and remote patient monitoring. As a health system executive, my viewpoint about digital technology has been expanded by other critical needs. At the University of Michigan, we are space constrained (land locked without sufficient parking) and are living with shrinking clinical margins. We see digital technology as a solution to both. As we consolidate our call centers from 27 sites to 1, we plan for 30% of our staff to work from home. Setting up a home work station costs $3,000, compared with office space costs (about $5,000/year). A new clinical site might cost $20 million to build, but that is a fraction of the true life-cycle cost of the building. We have a widely distributed patient base (imagine traveling from Michigan’s Upper Penisula to Ann Arbor for a 20-minute clinic visit).
Many people appreciate “seeing” their doctor from the comfort of their living room. We plan to convert at least 15% of patient visits to telehealth over the next few years although reimbursement rules are still limiting. This year, more than 80% of postsurgical visits (90-day bundled payment) were conducted virtually – mostly by NPs or PAs. Our GI psychologist converted 1,500 patient visit hours to virtual visits last year. In 2019, we completed over 4,000 evisits (management of simple conditions initiated by a patient – essential during flu season) and an increasing number of econsults (primary consultations to specialists). Project ECHO (N Engl J Med. 2011;364:2199) remains the star example of how digital health can improve access, especially for underserved communities.
Virtual care, telehealth, remote patient monitoring, telecommuting and other digital innovations are becoming standards for health systems. Now is the time to think of “face-to-face” visits as option B.
John I. Allen, MD, MBD, AGAF
Editor in Chief
One of our lead articles stems from the annual Partners in Value meeting, which was developed by the AGA in partnership with the Digestive Health Physicians Association (Chicago, Oct. 4, 2019). This is an annual meeting about innovations and “what’s next” for GI practices. Anton Decker, MD, an expert in the business of GI and Chair of the Practice Management and Economics Committee, discussed “digital disruption.”
When we discuss digital innovations in health care, most think of telehealth, social media, self-care apps, and remote patient monitoring. As a health system executive, my viewpoint about digital technology has been expanded by other critical needs. At the University of Michigan, we are space constrained (land locked without sufficient parking) and are living with shrinking clinical margins. We see digital technology as a solution to both. As we consolidate our call centers from 27 sites to 1, we plan for 30% of our staff to work from home. Setting up a home work station costs $3,000, compared with office space costs (about $5,000/year). A new clinical site might cost $20 million to build, but that is a fraction of the true life-cycle cost of the building. We have a widely distributed patient base (imagine traveling from Michigan’s Upper Penisula to Ann Arbor for a 20-minute clinic visit).
Many people appreciate “seeing” their doctor from the comfort of their living room. We plan to convert at least 15% of patient visits to telehealth over the next few years although reimbursement rules are still limiting. This year, more than 80% of postsurgical visits (90-day bundled payment) were conducted virtually – mostly by NPs or PAs. Our GI psychologist converted 1,500 patient visit hours to virtual visits last year. In 2019, we completed over 4,000 evisits (management of simple conditions initiated by a patient – essential during flu season) and an increasing number of econsults (primary consultations to specialists). Project ECHO (N Engl J Med. 2011;364:2199) remains the star example of how digital health can improve access, especially for underserved communities.
Virtual care, telehealth, remote patient monitoring, telecommuting and other digital innovations are becoming standards for health systems. Now is the time to think of “face-to-face” visits as option B.
John I. Allen, MD, MBD, AGAF
Editor in Chief
2019 at a glance: Hem-onc U.S. drug approvals
The rapid development and identification of novel drugs has translated into innovative therapies in hematology and oncology. The aim of this piece is to present newly approved drugs and expanded indications to serve as a reference guide for practicing clinicians.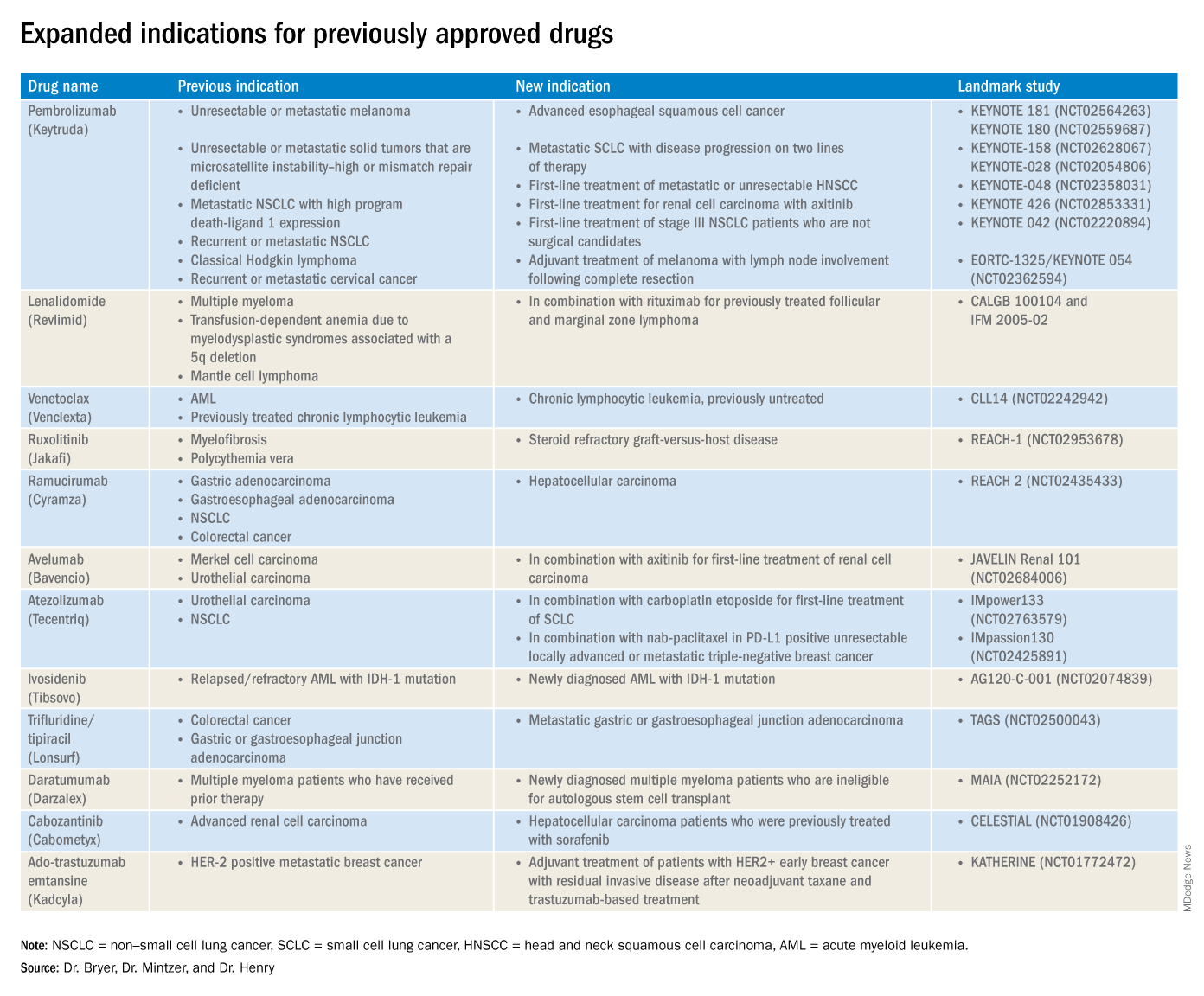
This article reviews therapies that were newly approved so far in 2019, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
New approvals
Fedratinib (Inrebic)
Class: JAK2 and FLT3 selective kinase inhibitor.
Disease: Intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis.
Dose: 400 mg orally once daily, with or without food.
Adverse events (AEs): Black box warning: Fatal encephalopathy, including Wernicke’s (thiamine level monitoring suggested).
Trials: In JAKARTA (NCT01437787), 37% of patients achieved a 35% or greater reduction in spleen volume and 40% received a 50% or greater reduction in myelofibrosis-related symptoms. In Jakarta-2, there was a 55% spleen response in patients resistant or intolerant to ruxolitinib.
Entrectinib (Rozlytrek)
Class: Tropomyosin receptor tyrosine kinase inhibitor.
Disease: Solid tumors that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion and for ROS-1 positive non–small cell lung cancer (NSCLC).
Dose: 600 mg orally once daily.
AEs: Heart failure, QT prolongation, skeletal fractures, hepatotoxicity, central nervous system effects, and hyperuricemia.
Trial: ALKA, STARTRK-1 (NCT02097810) and STARTRK-2 (NCT02568267): Overall response rate of 57% for NTRK positive patients; response rate of 77% in ROS-1 positive NSCLC.
Pexidartinib (Turalio)
Class: Small molecule tyrosine kinase inhibitor targeting CSF1R.
Disease: Symptomatic tenosynovial giant cell tumor.
Dose: 400 mg orally twice daily without food.
AEs: Black box warning on hepatotoxicity.
Trial: ENLIVEN (NCT02371369): Overall response rate of 38% at 25 weeks, with a 15% complete response rate and a 23% partial response rate.
Darolutamide (Nubeqa)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 600 mg orally twice daily with food with concomitant androgen deprivation therapy.
AEs: Fatigue, extremity pain, and rash.
Trial: ARAMIS (NCT02200614): Median metastasis free survival was 40.4 months for patients with darolutamide, compared with 18.4 months for controls.
Selinexor (Xpovio)
Class: Reversible inhibitor of nuclear export of tumor suppressor proteins, growth regulators, and mRNAs of oncogenic proteins.
Disease: Relapsed or refractory multiple myeloma. Indicated for patients who have received at least four prior therapies, including at least two immunomodulatory agents and an anti-CD38 monoclonal antibody.
Dose: 80 mg orally in combination with oral dexamethasone on days 1 and 3 of each week.
AEs: Thrombocytopenia, fatigue, pancytopenia, and hyponatremia.
Trial: STORM (NCT02336815): Overall response rate 25.3% with a median time to first response of 4 weeks and 3.8-month median duration of response.
Polatuzumab vedotin-piiq (Polivy)
Class: CD79b-directed antibody-drug conjugate.
Disease: Relapsed or refractory diffuse large B-cell lymphoma. Indicated for patients who have had at least two prior therapies.
Dose: 1.8 mg/kg intravenous infusion every 21 days for six cycles in combination with bendamustine and a rituximab product.
AEs: Pancytopenia, peripheral neuropathy.
Trial: GO29365 (NCT02257567): Complete response rate was 40% for polatuzumab vedotin-piiq plus bendamustine/rituximab, compared with 18% with bendamustine/rituximab alone.*
Caplacizumab-yhdp (Cablivi)
Class: Monoclonal antibody fragment directed against von Willebrand factor.
Disease: Thrombotic thrombocytopenic purpura.
Dose: 11 mg IV initially, then daily subcutaneously; in combination with plasma exchange and immunosuppressive therapy.
AEs: Epistaxis, headache, and gingival bleeding.
Trial: Hercules trial (NCT02553317): More rapid normalization of platelets, lower incidence of composite TTP-related death, and lower rate of recurrence when added to plasma exchange and steroids.
Alpelisib (Piqray)
Class: Phosphatidylinositol-3-kinase (PI3K) inhibitor.
Disease: Hormone receptor positive HER2-negative PIK3CA-mutated, advanced or metastatic breast cancer.
Dose: 300 mg orally once daily with food with concomitant fulvestrant.
AEs: Hyperglycemia, pancytopenia.
Trial: SOLAR-1 (NCT02437318): 11-month progression-free survival among patients treated with alpelisib and fulvestrant, compared with 5.7 months in fulvestrant alone control arm; overall response rate of 36% versus 16%, respectively.
Erdafitinib (Balversa)
Class: Fibroblast growth factor receptor kinase inhibitor.
Disease: Locally advanced or metastatic urothelial carcinoma with FGFR3 or FGFR2 mutations.
Dose: 8 mg orally once daily, with or without food.
AEs: Ocular disorders including retinopathy or retinal detachment.
Trial: BLC2001 (NCT02365597): Objective response rate of 32.2%, with a complete response in 2.3% of patients and partial response in 29.9% of patients.
Biosimilar approvals
Trastuzumab and hyaluronidase-oysk (Herceptin Hylecta)
Biosimilar to: Trastuzumab.
Indication: HER2-overexpressing breast cancer.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mintzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania.
*Correction, 11/7/2019: An earlier version of this article misstated the drug combination in the GO29365 trial.
The rapid development and identification of novel drugs has translated into innovative therapies in hematology and oncology. The aim of this piece is to present newly approved drugs and expanded indications to serve as a reference guide for practicing clinicians.
This article reviews therapies that were newly approved so far in 2019, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
New approvals
Fedratinib (Inrebic)
Class: JAK2 and FLT3 selective kinase inhibitor.
Disease: Intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis.
Dose: 400 mg orally once daily, with or without food.
Adverse events (AEs): Black box warning: Fatal encephalopathy, including Wernicke’s (thiamine level monitoring suggested).
Trials: In JAKARTA (NCT01437787), 37% of patients achieved a 35% or greater reduction in spleen volume and 40% received a 50% or greater reduction in myelofibrosis-related symptoms. In Jakarta-2, there was a 55% spleen response in patients resistant or intolerant to ruxolitinib.
Entrectinib (Rozlytrek)
Class: Tropomyosin receptor tyrosine kinase inhibitor.
Disease: Solid tumors that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion and for ROS-1 positive non–small cell lung cancer (NSCLC).
Dose: 600 mg orally once daily.
AEs: Heart failure, QT prolongation, skeletal fractures, hepatotoxicity, central nervous system effects, and hyperuricemia.
Trial: ALKA, STARTRK-1 (NCT02097810) and STARTRK-2 (NCT02568267): Overall response rate of 57% for NTRK positive patients; response rate of 77% in ROS-1 positive NSCLC.
Pexidartinib (Turalio)
Class: Small molecule tyrosine kinase inhibitor targeting CSF1R.
Disease: Symptomatic tenosynovial giant cell tumor.
Dose: 400 mg orally twice daily without food.
AEs: Black box warning on hepatotoxicity.
Trial: ENLIVEN (NCT02371369): Overall response rate of 38% at 25 weeks, with a 15% complete response rate and a 23% partial response rate.
Darolutamide (Nubeqa)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 600 mg orally twice daily with food with concomitant androgen deprivation therapy.
AEs: Fatigue, extremity pain, and rash.
Trial: ARAMIS (NCT02200614): Median metastasis free survival was 40.4 months for patients with darolutamide, compared with 18.4 months for controls.
Selinexor (Xpovio)
Class: Reversible inhibitor of nuclear export of tumor suppressor proteins, growth regulators, and mRNAs of oncogenic proteins.
Disease: Relapsed or refractory multiple myeloma. Indicated for patients who have received at least four prior therapies, including at least two immunomodulatory agents and an anti-CD38 monoclonal antibody.
Dose: 80 mg orally in combination with oral dexamethasone on days 1 and 3 of each week.
AEs: Thrombocytopenia, fatigue, pancytopenia, and hyponatremia.
Trial: STORM (NCT02336815): Overall response rate 25.3% with a median time to first response of 4 weeks and 3.8-month median duration of response.
Polatuzumab vedotin-piiq (Polivy)
Class: CD79b-directed antibody-drug conjugate.
Disease: Relapsed or refractory diffuse large B-cell lymphoma. Indicated for patients who have had at least two prior therapies.
Dose: 1.8 mg/kg intravenous infusion every 21 days for six cycles in combination with bendamustine and a rituximab product.
AEs: Pancytopenia, peripheral neuropathy.
Trial: GO29365 (NCT02257567): Complete response rate was 40% for polatuzumab vedotin-piiq plus bendamustine/rituximab, compared with 18% with bendamustine/rituximab alone.*
Caplacizumab-yhdp (Cablivi)
Class: Monoclonal antibody fragment directed against von Willebrand factor.
Disease: Thrombotic thrombocytopenic purpura.
Dose: 11 mg IV initially, then daily subcutaneously; in combination with plasma exchange and immunosuppressive therapy.
AEs: Epistaxis, headache, and gingival bleeding.
Trial: Hercules trial (NCT02553317): More rapid normalization of platelets, lower incidence of composite TTP-related death, and lower rate of recurrence when added to plasma exchange and steroids.
Alpelisib (Piqray)
Class: Phosphatidylinositol-3-kinase (PI3K) inhibitor.
Disease: Hormone receptor positive HER2-negative PIK3CA-mutated, advanced or metastatic breast cancer.
Dose: 300 mg orally once daily with food with concomitant fulvestrant.
AEs: Hyperglycemia, pancytopenia.
Trial: SOLAR-1 (NCT02437318): 11-month progression-free survival among patients treated with alpelisib and fulvestrant, compared with 5.7 months in fulvestrant alone control arm; overall response rate of 36% versus 16%, respectively.
Erdafitinib (Balversa)
Class: Fibroblast growth factor receptor kinase inhibitor.
Disease: Locally advanced or metastatic urothelial carcinoma with FGFR3 or FGFR2 mutations.
Dose: 8 mg orally once daily, with or without food.
AEs: Ocular disorders including retinopathy or retinal detachment.
Trial: BLC2001 (NCT02365597): Objective response rate of 32.2%, with a complete response in 2.3% of patients and partial response in 29.9% of patients.
Biosimilar approvals
Trastuzumab and hyaluronidase-oysk (Herceptin Hylecta)
Biosimilar to: Trastuzumab.
Indication: HER2-overexpressing breast cancer.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mintzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania.
*Correction, 11/7/2019: An earlier version of this article misstated the drug combination in the GO29365 trial.
The rapid development and identification of novel drugs has translated into innovative therapies in hematology and oncology. The aim of this piece is to present newly approved drugs and expanded indications to serve as a reference guide for practicing clinicians.
This article reviews therapies that were newly approved so far in 2019, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
New approvals
Fedratinib (Inrebic)
Class: JAK2 and FLT3 selective kinase inhibitor.
Disease: Intermediate or high-risk primary or secondary (postpolycythemia vera or postessential thrombocythemia) myelofibrosis.
Dose: 400 mg orally once daily, with or without food.
Adverse events (AEs): Black box warning: Fatal encephalopathy, including Wernicke’s (thiamine level monitoring suggested).
Trials: In JAKARTA (NCT01437787), 37% of patients achieved a 35% or greater reduction in spleen volume and 40% received a 50% or greater reduction in myelofibrosis-related symptoms. In Jakarta-2, there was a 55% spleen response in patients resistant or intolerant to ruxolitinib.
Entrectinib (Rozlytrek)
Class: Tropomyosin receptor tyrosine kinase inhibitor.
Disease: Solid tumors that have a neurotrophic tyrosine receptor kinase (NTRK) gene fusion and for ROS-1 positive non–small cell lung cancer (NSCLC).
Dose: 600 mg orally once daily.
AEs: Heart failure, QT prolongation, skeletal fractures, hepatotoxicity, central nervous system effects, and hyperuricemia.
Trial: ALKA, STARTRK-1 (NCT02097810) and STARTRK-2 (NCT02568267): Overall response rate of 57% for NTRK positive patients; response rate of 77% in ROS-1 positive NSCLC.
Pexidartinib (Turalio)
Class: Small molecule tyrosine kinase inhibitor targeting CSF1R.
Disease: Symptomatic tenosynovial giant cell tumor.
Dose: 400 mg orally twice daily without food.
AEs: Black box warning on hepatotoxicity.
Trial: ENLIVEN (NCT02371369): Overall response rate of 38% at 25 weeks, with a 15% complete response rate and a 23% partial response rate.
Darolutamide (Nubeqa)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 600 mg orally twice daily with food with concomitant androgen deprivation therapy.
AEs: Fatigue, extremity pain, and rash.
Trial: ARAMIS (NCT02200614): Median metastasis free survival was 40.4 months for patients with darolutamide, compared with 18.4 months for controls.
Selinexor (Xpovio)
Class: Reversible inhibitor of nuclear export of tumor suppressor proteins, growth regulators, and mRNAs of oncogenic proteins.
Disease: Relapsed or refractory multiple myeloma. Indicated for patients who have received at least four prior therapies, including at least two immunomodulatory agents and an anti-CD38 monoclonal antibody.
Dose: 80 mg orally in combination with oral dexamethasone on days 1 and 3 of each week.
AEs: Thrombocytopenia, fatigue, pancytopenia, and hyponatremia.
Trial: STORM (NCT02336815): Overall response rate 25.3% with a median time to first response of 4 weeks and 3.8-month median duration of response.
Polatuzumab vedotin-piiq (Polivy)
Class: CD79b-directed antibody-drug conjugate.
Disease: Relapsed or refractory diffuse large B-cell lymphoma. Indicated for patients who have had at least two prior therapies.
Dose: 1.8 mg/kg intravenous infusion every 21 days for six cycles in combination with bendamustine and a rituximab product.
AEs: Pancytopenia, peripheral neuropathy.
Trial: GO29365 (NCT02257567): Complete response rate was 40% for polatuzumab vedotin-piiq plus bendamustine/rituximab, compared with 18% with bendamustine/rituximab alone.*
Caplacizumab-yhdp (Cablivi)
Class: Monoclonal antibody fragment directed against von Willebrand factor.
Disease: Thrombotic thrombocytopenic purpura.
Dose: 11 mg IV initially, then daily subcutaneously; in combination with plasma exchange and immunosuppressive therapy.
AEs: Epistaxis, headache, and gingival bleeding.
Trial: Hercules trial (NCT02553317): More rapid normalization of platelets, lower incidence of composite TTP-related death, and lower rate of recurrence when added to plasma exchange and steroids.
Alpelisib (Piqray)
Class: Phosphatidylinositol-3-kinase (PI3K) inhibitor.
Disease: Hormone receptor positive HER2-negative PIK3CA-mutated, advanced or metastatic breast cancer.
Dose: 300 mg orally once daily with food with concomitant fulvestrant.
AEs: Hyperglycemia, pancytopenia.
Trial: SOLAR-1 (NCT02437318): 11-month progression-free survival among patients treated with alpelisib and fulvestrant, compared with 5.7 months in fulvestrant alone control arm; overall response rate of 36% versus 16%, respectively.
Erdafitinib (Balversa)
Class: Fibroblast growth factor receptor kinase inhibitor.
Disease: Locally advanced or metastatic urothelial carcinoma with FGFR3 or FGFR2 mutations.
Dose: 8 mg orally once daily, with or without food.
AEs: Ocular disorders including retinopathy or retinal detachment.
Trial: BLC2001 (NCT02365597): Objective response rate of 32.2%, with a complete response in 2.3% of patients and partial response in 29.9% of patients.
Biosimilar approvals
Trastuzumab and hyaluronidase-oysk (Herceptin Hylecta)
Biosimilar to: Trastuzumab.
Indication: HER2-overexpressing breast cancer.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mintzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania.
*Correction, 11/7/2019: An earlier version of this article misstated the drug combination in the GO29365 trial.
Treat or treat
In Charles M. Schulz’s “It’s the Great Pumpkin, Charlie Brown,” the Peanuts gang goes trick or treating door to door. While everyone else gets candy, chewing gum, and chocolate bars, Charlie Brown just gets a bag of rocks. Everyone got treats except Charlie Brown, who only got tricks. Sometimes it seems that my patients are trick or treating, too. Sadly, the tricks come way too often.

Linus tried to avoid tricks by staking out a sincere pumpkin patch in the hope that the Great Pumpkin would rise and deliver him candy and toys. Alas, our patients sometimes sincerely believe things like alkalinization, naturopathy, and antineoplastons will deliver the treats they need to cure their cancer. They will be similarly disappointed.
Most patients depend on us to skew the treat to trick ratio favorably. They trust us to know what to recommend to lengthen life and reduce suffering. Their faith is both a profound privilege and a daunting responsibility.
My patient was hospitalized with hypercalcemia, the latest complication deriving from a decade of progressive multiple myeloma. He was on his 11th line of therapy complicated by at least a grade 3 neuropathy resulting in an unstable gait, chronic pain requiring opioid analgesia, two hospitalizations in the last year for severe infections, and venous thromboembolism on anticoagulation, all resulting in an ECOG performance status no better than a 2. He stabilized and then we needed to talk about next steps.
A clinical trial would be ideal, but he would be excluded from any that we have open and travel isn’t really an option for him. I could choose to treat him with selinexor. It is approved by the Food and Drug Administration and has about a one-in-four chance of producing a short remission in a population of patients that would not include my patient. It also has a three-in-four chance of significant side effects. I could also create a combination regimen with drugs that he has already been exposed to, knowing that response is unlikely and side effects are certain.

This situation is not unique; in fact it is an all too frequent occurrence. The easiest path forward for me would be to recommend treatment. The patient expects treatment and would readily consent to whatever regimen I proposed. He would bear whatever side effects resulted as an expected consequence of therapy. On the surface, this easy path appears to be the proverbial “treat.” But really, further treatment is the “trick” because it is not known to prolong life and would certainly add side effects. The problem, of course, is knowing both when treats become tricks and how to let patients know this, too.
No one knows exactly when treats become tricks, least of all me. Every month I get a report updating me on the status of a former patient being treated elsewhere. This is someone who I thought had no more treatment options. I am humbled every time a colleague, or fellow, recommends a treatment I had never considered. I am not perfect; I do the best I can. My recommendation might be wrong.
Yet I have watched my patient steadily deteriorate and cognitively decline no matter what treatment I employed, whether or not the monoclonal spike decreased. There is no evidence that treatment under such circumstances benefits the patient at all. Moreover, I have sat through many morbidity and mortality conferences where the conclusion was that we should have consulted hospice sooner. Like so many hematologists and oncologists every day, I needed to have a goals-of-care conversation with my patient knowing that treatment could possibly help, but probably would not.
Crucial conversations like these are difficult for everybody. There are techniques to employ that my palliative care colleagues recommend. I tried to remember them as I started talking to my patient and his wife. He listened and clearly understood the gravity of the situation and the resulting poor prognosis regardless of treatment. I recommended hospice. He declined.
Getting to this point was uncomfortable enough, but then I came to a decision that I am still struggling with – acquiesce to his wishes and treat while feeling that I should not, or decline to treat further and transfer his care to someone more willing? This is not the kind of trick or treat I enjoy.
I look forward to the day when discussions of end of life are less awkward. Small movements have started to bring these conversations into the open. One such movement choreographs a dinner to encourage frank and open discussion of death (https://deathoverdinner.org/). Another reimagines the doula – a childbirth coach – as a coach at the end of life (https://www.agentlerparting.com/). Another provides a step-by-step approach to generating an end-of-life conversation (https://theconversationproject.org/). These, and many other efforts, did not occur in a vacuum. They emerged because of the growing recognition that the modern delivery of health care, and the culture it created, is inadequate for the end of life.
Until our culture changes, though, we are left with tough conversations and tougher decisions with our patients who are at the end of their cancer journey. I wish I could tell my junior colleagues that it gets easier with experience. In many ways it gets worse because of the long relationships we develop. As long as the rewards of treats are greater than the disappointments of tricks, though, I will continue trick or treating in my white coat costume.
Dr. Kalaycio is editor in chief of Hematology News. He is a hematologist-oncologist at the Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
In Charles M. Schulz’s “It’s the Great Pumpkin, Charlie Brown,” the Peanuts gang goes trick or treating door to door. While everyone else gets candy, chewing gum, and chocolate bars, Charlie Brown just gets a bag of rocks. Everyone got treats except Charlie Brown, who only got tricks. Sometimes it seems that my patients are trick or treating, too. Sadly, the tricks come way too often.
Linus tried to avoid tricks by staking out a sincere pumpkin patch in the hope that the Great Pumpkin would rise and deliver him candy and toys. Alas, our patients sometimes sincerely believe things like alkalinization, naturopathy, and antineoplastons will deliver the treats they need to cure their cancer. They will be similarly disappointed.
Most patients depend on us to skew the treat to trick ratio favorably. They trust us to know what to recommend to lengthen life and reduce suffering. Their faith is both a profound privilege and a daunting responsibility.
My patient was hospitalized with hypercalcemia, the latest complication deriving from a decade of progressive multiple myeloma. He was on his 11th line of therapy complicated by at least a grade 3 neuropathy resulting in an unstable gait, chronic pain requiring opioid analgesia, two hospitalizations in the last year for severe infections, and venous thromboembolism on anticoagulation, all resulting in an ECOG performance status no better than a 2. He stabilized and then we needed to talk about next steps.
A clinical trial would be ideal, but he would be excluded from any that we have open and travel isn’t really an option for him. I could choose to treat him with selinexor. It is approved by the Food and Drug Administration and has about a one-in-four chance of producing a short remission in a population of patients that would not include my patient. It also has a three-in-four chance of significant side effects. I could also create a combination regimen with drugs that he has already been exposed to, knowing that response is unlikely and side effects are certain.
This situation is not unique; in fact it is an all too frequent occurrence. The easiest path forward for me would be to recommend treatment. The patient expects treatment and would readily consent to whatever regimen I proposed. He would bear whatever side effects resulted as an expected consequence of therapy. On the surface, this easy path appears to be the proverbial “treat.” But really, further treatment is the “trick” because it is not known to prolong life and would certainly add side effects. The problem, of course, is knowing both when treats become tricks and how to let patients know this, too.
No one knows exactly when treats become tricks, least of all me. Every month I get a report updating me on the status of a former patient being treated elsewhere. This is someone who I thought had no more treatment options. I am humbled every time a colleague, or fellow, recommends a treatment I had never considered. I am not perfect; I do the best I can. My recommendation might be wrong.
Yet I have watched my patient steadily deteriorate and cognitively decline no matter what treatment I employed, whether or not the monoclonal spike decreased. There is no evidence that treatment under such circumstances benefits the patient at all. Moreover, I have sat through many morbidity and mortality conferences where the conclusion was that we should have consulted hospice sooner. Like so many hematologists and oncologists every day, I needed to have a goals-of-care conversation with my patient knowing that treatment could possibly help, but probably would not.
Crucial conversations like these are difficult for everybody. There are techniques to employ that my palliative care colleagues recommend. I tried to remember them as I started talking to my patient and his wife. He listened and clearly understood the gravity of the situation and the resulting poor prognosis regardless of treatment. I recommended hospice. He declined.
Getting to this point was uncomfortable enough, but then I came to a decision that I am still struggling with – acquiesce to his wishes and treat while feeling that I should not, or decline to treat further and transfer his care to someone more willing? This is not the kind of trick or treat I enjoy.
I look forward to the day when discussions of end of life are less awkward. Small movements have started to bring these conversations into the open. One such movement choreographs a dinner to encourage frank and open discussion of death (https://deathoverdinner.org/). Another reimagines the doula – a childbirth coach – as a coach at the end of life (https://www.agentlerparting.com/). Another provides a step-by-step approach to generating an end-of-life conversation (https://theconversationproject.org/). These, and many other efforts, did not occur in a vacuum. They emerged because of the growing recognition that the modern delivery of health care, and the culture it created, is inadequate for the end of life.
Until our culture changes, though, we are left with tough conversations and tougher decisions with our patients who are at the end of their cancer journey. I wish I could tell my junior colleagues that it gets easier with experience. In many ways it gets worse because of the long relationships we develop. As long as the rewards of treats are greater than the disappointments of tricks, though, I will continue trick or treating in my white coat costume.
Dr. Kalaycio is editor in chief of Hematology News. He is a hematologist-oncologist at the Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
In Charles M. Schulz’s “It’s the Great Pumpkin, Charlie Brown,” the Peanuts gang goes trick or treating door to door. While everyone else gets candy, chewing gum, and chocolate bars, Charlie Brown just gets a bag of rocks. Everyone got treats except Charlie Brown, who only got tricks. Sometimes it seems that my patients are trick or treating, too. Sadly, the tricks come way too often.
Linus tried to avoid tricks by staking out a sincere pumpkin patch in the hope that the Great Pumpkin would rise and deliver him candy and toys. Alas, our patients sometimes sincerely believe things like alkalinization, naturopathy, and antineoplastons will deliver the treats they need to cure their cancer. They will be similarly disappointed.
Most patients depend on us to skew the treat to trick ratio favorably. They trust us to know what to recommend to lengthen life and reduce suffering. Their faith is both a profound privilege and a daunting responsibility.
My patient was hospitalized with hypercalcemia, the latest complication deriving from a decade of progressive multiple myeloma. He was on his 11th line of therapy complicated by at least a grade 3 neuropathy resulting in an unstable gait, chronic pain requiring opioid analgesia, two hospitalizations in the last year for severe infections, and venous thromboembolism on anticoagulation, all resulting in an ECOG performance status no better than a 2. He stabilized and then we needed to talk about next steps.
A clinical trial would be ideal, but he would be excluded from any that we have open and travel isn’t really an option for him. I could choose to treat him with selinexor. It is approved by the Food and Drug Administration and has about a one-in-four chance of producing a short remission in a population of patients that would not include my patient. It also has a three-in-four chance of significant side effects. I could also create a combination regimen with drugs that he has already been exposed to, knowing that response is unlikely and side effects are certain.
This situation is not unique; in fact it is an all too frequent occurrence. The easiest path forward for me would be to recommend treatment. The patient expects treatment and would readily consent to whatever regimen I proposed. He would bear whatever side effects resulted as an expected consequence of therapy. On the surface, this easy path appears to be the proverbial “treat.” But really, further treatment is the “trick” because it is not known to prolong life and would certainly add side effects. The problem, of course, is knowing both when treats become tricks and how to let patients know this, too.
No one knows exactly when treats become tricks, least of all me. Every month I get a report updating me on the status of a former patient being treated elsewhere. This is someone who I thought had no more treatment options. I am humbled every time a colleague, or fellow, recommends a treatment I had never considered. I am not perfect; I do the best I can. My recommendation might be wrong.
Yet I have watched my patient steadily deteriorate and cognitively decline no matter what treatment I employed, whether or not the monoclonal spike decreased. There is no evidence that treatment under such circumstances benefits the patient at all. Moreover, I have sat through many morbidity and mortality conferences where the conclusion was that we should have consulted hospice sooner. Like so many hematologists and oncologists every day, I needed to have a goals-of-care conversation with my patient knowing that treatment could possibly help, but probably would not.
Crucial conversations like these are difficult for everybody. There are techniques to employ that my palliative care colleagues recommend. I tried to remember them as I started talking to my patient and his wife. He listened and clearly understood the gravity of the situation and the resulting poor prognosis regardless of treatment. I recommended hospice. He declined.
Getting to this point was uncomfortable enough, but then I came to a decision that I am still struggling with – acquiesce to his wishes and treat while feeling that I should not, or decline to treat further and transfer his care to someone more willing? This is not the kind of trick or treat I enjoy.
I look forward to the day when discussions of end of life are less awkward. Small movements have started to bring these conversations into the open. One such movement choreographs a dinner to encourage frank and open discussion of death (https://deathoverdinner.org/). Another reimagines the doula – a childbirth coach – as a coach at the end of life (https://www.agentlerparting.com/). Another provides a step-by-step approach to generating an end-of-life conversation (https://theconversationproject.org/). These, and many other efforts, did not occur in a vacuum. They emerged because of the growing recognition that the modern delivery of health care, and the culture it created, is inadequate for the end of life.
Until our culture changes, though, we are left with tough conversations and tougher decisions with our patients who are at the end of their cancer journey. I wish I could tell my junior colleagues that it gets easier with experience. In many ways it gets worse because of the long relationships we develop. As long as the rewards of treats are greater than the disappointments of tricks, though, I will continue trick or treating in my white coat costume.
Dr. Kalaycio is editor in chief of Hematology News. He is a hematologist-oncologist at the Cleveland Clinic Taussig Cancer Institute. Contact him at kalaycm@ccf.org.
‘Time lost is brain lost’
Question: Which of the following statements regarding “common knowledge” is correct?

A. In any negligence action absent common knowledge, expert testimony is then required to prove requisite standard of care and causation.
B.
C. An expert is needed in the first place to establish whether something constitutes common knowledge.
D. The jury is the one who determines whether a plaintiff can invoke the common knowledge exception.
E. An example of common knowledge in malpractice law is where a delay in stroke diagnosis results in loss of brain function.
Answer: B. The judge, not the jury or anyone else, makes the decision regarding res ipsa loquitur (the thing speaks for itself) or common knowledge, which exempts a plaintiff from producing an expert witness to testify as to the standard of care and causation. However, this is only true in actions arising out of professional negligence such as medical malpractice, whereas most common negligence actions – for example, slips and falls – do not require expert testimony.
Only a professional, duly qualified by the court as an expert witness, is allowed to offer medical testimony, while the plaintiff will typically be disqualified from playing this role because of the complexity of issues involved unless there is common knowledge. In general, courts are reluctant to grant this exception, which favors the plaintiff.
The best example of res ipsa loquitur is where a surgeon inadvertently leaves behind a sponge or instrument inside a body cavity. Other successfully litigated examples include cardiac arrest in the operating room, hypoxia in the recovery room, burns to the buttock, gangrene after the accidental injection of penicillin into an artery, air trapped subcutaneously from a displaced needle, and a pierced eyeball during a procedure. The factual circumstances of each case are critical to its outcome. For example, in a 2013 New York case, the plaintiff was barred from using the res doctrine.1 The defendant doctor had left a guide wire in the plaintiff’s chest following a biopsy and retrieved it 2 months later. The plaintiff did not call any expert witness, relying instead on the “foreign object” basis for invoking the res doctrine. However, the Court of Appeals reasoned that the object was left behind deliberately, not unintentionally, and that under the circumstances of the case, an expert witness was needed to set out the applicable standard of care, without which a jury could not determine whether the doctor’s professional judgment breached the requisite standard.
The Supreme Court of Kentucky recently rejected the use of common knowledge in a stroke case.2 In 2010, David Shackelford’s rheumatologist referred him to Paul Lewis, MD, an interventional radiologist, for a four-vessel cerebral angiogram to assist with diagnosing the cause of Mr. Shackelford’s chronic headaches. The procedure itself was uneventful, but while in the recovery room, Mr. Shackelford reported a frontal headache and scotoma, which resolved on its own. The headache improved with medication, and the patient experienced no other symptoms. There were no other visual changes, weakness, slurred speech, or facial palsies. Mr. Shackelford was discharged but had to return to the hospital the next morning via ambulance after becoming disoriented at his home. An MRI indicated multiple scattered small infarcts, and he was left with residual short-term memory loss and visual problems.
There was no allegation that the stroke itself was caused by negligence; rather, Mr. Shackelford alleged that the failure to examine and diagnose the stroke after the angiogram was negligent and caused injury greater than that which the stroke would have caused with earlier intervention. To support his claims, Mr. Shackelford’s expert, Michael David Khoury, MD, a vascular surgeon, criticized Dr. Lewis’s failure to examine Mr. Shackelford when his symptoms were consistent with a stroke. However, Dr. Khoury did not opine that Dr. Lewis could have limited the effects of the stroke through earlier intervention. When asked specifically whether he could state within a reasonable degree of medical probability that Dr. Lewis’s postprocedure care was a substantial factor in causing harm to Mr. Shackelford, Dr. Khoury responded that it was “impossible to tell.”
Based largely upon Dr. Khoury’s deposition testimony, the defendants successfully moved for summary judgment on the basis that the expert had failed to opine that the alleged negligence caused any injury to Mr. Shackelford. As a result, Mr. Shackelford could not prove an essential element of his medical malpractice claim. Defense expert Peter J. Pema, MD, a neuroradiologist, acknowledged the general proposition that strokes require timely diagnosis and treatment but did not provide an opinion on causation under the specific facts of this case. Another defense expert, Gregory Postal, MD, opined that Mr. Shackelford began to present symptoms of a stroke after leaving the hospital.
Notwithstanding the lower court’s ruling to summarily dismiss the case, the Court of Appeals found that, in this case, the issue of causation did not require expert medical testimony. It explained that given the ubiquity of information regarding stroke symptom identification and the necessity of prompt treatment, it had become common knowledge that “time lost is brain lost” as to timely medical intervention. In other words, a jury of laymen with this general knowledge could resolve the causation issue without the aid of expert testimony.
However, the Supreme Court of Kentucky held otherwise, writing: “We disagree with the Court of Appeals’ analysis. Although public service campaigns have increased public awareness and knowledge about stroke symptoms and timely intervention, that general information cannot provide the medical expertise necessary to evaluate this particular claim of medical malpractice. In other words, the question is not simply whether ‘time lost is brain lost.’ Rather, the specific facts and circumstances of this case play a significant role in determining whether the alleged negligent conduct was a substantial factor in Shackelford’s injuries, and to what extent. For example, as Dr. Lewis’s deposition testimony illustrates, a variety of factors influenced his diagnosis and treatment of Shackelford, including Shackelford’s medical history and history of cluster headaches; the common side effects of the angiogram procedure, including headache and scotoma; and the manner in which Shackelford’s headache and scotoma presented, as well as their timing. The complexities of these factors and how they affected Dr. Lewis’s evaluation of Shackelford may have also influenced the severity of the injury. These matters are clearly relevant to the determination of an alleged breach of the standard of care. Despite public perception about timely intervention, the average layperson cannot properly weigh such complex medical evidence without the aid of expert opinion. … To conclude otherwise is to drastically expand the res ipsa loquitor exception and to virtually eliminate the need for expert opinion evidence in similar medical malpractice actions that involve common or highly publicized conditions (e.g., stroke, heart attack, and even some cancers).”
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical or legal advice. The author published an earlier version of this topic in the April 19, 2016, issue of Internal Medicine News, available at https://www.mdedge.com/internalmedicine/law-medicine. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. James v. Wormuth, 997 N.E.2d 133 (N.Y. 2013).
2. Lewis/Ashland Hospital v. Shackelford, Supreme Court of Kentucky, Opinion of the Court by Justice Keller, rendered August 29, 2019.
Question: Which of the following statements regarding “common knowledge” is correct?
A. In any negligence action absent common knowledge, expert testimony is then required to prove requisite standard of care and causation.
B.
C. An expert is needed in the first place to establish whether something constitutes common knowledge.
D. The jury is the one who determines whether a plaintiff can invoke the common knowledge exception.
E. An example of common knowledge in malpractice law is where a delay in stroke diagnosis results in loss of brain function.
Answer: B. The judge, not the jury or anyone else, makes the decision regarding res ipsa loquitur (the thing speaks for itself) or common knowledge, which exempts a plaintiff from producing an expert witness to testify as to the standard of care and causation. However, this is only true in actions arising out of professional negligence such as medical malpractice, whereas most common negligence actions – for example, slips and falls – do not require expert testimony.
Only a professional, duly qualified by the court as an expert witness, is allowed to offer medical testimony, while the plaintiff will typically be disqualified from playing this role because of the complexity of issues involved unless there is common knowledge. In general, courts are reluctant to grant this exception, which favors the plaintiff.
The best example of res ipsa loquitur is where a surgeon inadvertently leaves behind a sponge or instrument inside a body cavity. Other successfully litigated examples include cardiac arrest in the operating room, hypoxia in the recovery room, burns to the buttock, gangrene after the accidental injection of penicillin into an artery, air trapped subcutaneously from a displaced needle, and a pierced eyeball during a procedure. The factual circumstances of each case are critical to its outcome. For example, in a 2013 New York case, the plaintiff was barred from using the res doctrine.1 The defendant doctor had left a guide wire in the plaintiff’s chest following a biopsy and retrieved it 2 months later. The plaintiff did not call any expert witness, relying instead on the “foreign object” basis for invoking the res doctrine. However, the Court of Appeals reasoned that the object was left behind deliberately, not unintentionally, and that under the circumstances of the case, an expert witness was needed to set out the applicable standard of care, without which a jury could not determine whether the doctor’s professional judgment breached the requisite standard.
The Supreme Court of Kentucky recently rejected the use of common knowledge in a stroke case.2 In 2010, David Shackelford’s rheumatologist referred him to Paul Lewis, MD, an interventional radiologist, for a four-vessel cerebral angiogram to assist with diagnosing the cause of Mr. Shackelford’s chronic headaches. The procedure itself was uneventful, but while in the recovery room, Mr. Shackelford reported a frontal headache and scotoma, which resolved on its own. The headache improved with medication, and the patient experienced no other symptoms. There were no other visual changes, weakness, slurred speech, or facial palsies. Mr. Shackelford was discharged but had to return to the hospital the next morning via ambulance after becoming disoriented at his home. An MRI indicated multiple scattered small infarcts, and he was left with residual short-term memory loss and visual problems.
There was no allegation that the stroke itself was caused by negligence; rather, Mr. Shackelford alleged that the failure to examine and diagnose the stroke after the angiogram was negligent and caused injury greater than that which the stroke would have caused with earlier intervention. To support his claims, Mr. Shackelford’s expert, Michael David Khoury, MD, a vascular surgeon, criticized Dr. Lewis’s failure to examine Mr. Shackelford when his symptoms were consistent with a stroke. However, Dr. Khoury did not opine that Dr. Lewis could have limited the effects of the stroke through earlier intervention. When asked specifically whether he could state within a reasonable degree of medical probability that Dr. Lewis’s postprocedure care was a substantial factor in causing harm to Mr. Shackelford, Dr. Khoury responded that it was “impossible to tell.”
Based largely upon Dr. Khoury’s deposition testimony, the defendants successfully moved for summary judgment on the basis that the expert had failed to opine that the alleged negligence caused any injury to Mr. Shackelford. As a result, Mr. Shackelford could not prove an essential element of his medical malpractice claim. Defense expert Peter J. Pema, MD, a neuroradiologist, acknowledged the general proposition that strokes require timely diagnosis and treatment but did not provide an opinion on causation under the specific facts of this case. Another defense expert, Gregory Postal, MD, opined that Mr. Shackelford began to present symptoms of a stroke after leaving the hospital.
Notwithstanding the lower court’s ruling to summarily dismiss the case, the Court of Appeals found that, in this case, the issue of causation did not require expert medical testimony. It explained that given the ubiquity of information regarding stroke symptom identification and the necessity of prompt treatment, it had become common knowledge that “time lost is brain lost” as to timely medical intervention. In other words, a jury of laymen with this general knowledge could resolve the causation issue without the aid of expert testimony.
However, the Supreme Court of Kentucky held otherwise, writing: “We disagree with the Court of Appeals’ analysis. Although public service campaigns have increased public awareness and knowledge about stroke symptoms and timely intervention, that general information cannot provide the medical expertise necessary to evaluate this particular claim of medical malpractice. In other words, the question is not simply whether ‘time lost is brain lost.’ Rather, the specific facts and circumstances of this case play a significant role in determining whether the alleged negligent conduct was a substantial factor in Shackelford’s injuries, and to what extent. For example, as Dr. Lewis’s deposition testimony illustrates, a variety of factors influenced his diagnosis and treatment of Shackelford, including Shackelford’s medical history and history of cluster headaches; the common side effects of the angiogram procedure, including headache and scotoma; and the manner in which Shackelford’s headache and scotoma presented, as well as their timing. The complexities of these factors and how they affected Dr. Lewis’s evaluation of Shackelford may have also influenced the severity of the injury. These matters are clearly relevant to the determination of an alleged breach of the standard of care. Despite public perception about timely intervention, the average layperson cannot properly weigh such complex medical evidence without the aid of expert opinion. … To conclude otherwise is to drastically expand the res ipsa loquitor exception and to virtually eliminate the need for expert opinion evidence in similar medical malpractice actions that involve common or highly publicized conditions (e.g., stroke, heart attack, and even some cancers).”
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical or legal advice. The author published an earlier version of this topic in the April 19, 2016, issue of Internal Medicine News, available at https://www.mdedge.com/internalmedicine/law-medicine. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. James v. Wormuth, 997 N.E.2d 133 (N.Y. 2013).
2. Lewis/Ashland Hospital v. Shackelford, Supreme Court of Kentucky, Opinion of the Court by Justice Keller, rendered August 29, 2019.
Question: Which of the following statements regarding “common knowledge” is correct?
A. In any negligence action absent common knowledge, expert testimony is then required to prove requisite standard of care and causation.
B.
C. An expert is needed in the first place to establish whether something constitutes common knowledge.
D. The jury is the one who determines whether a plaintiff can invoke the common knowledge exception.
E. An example of common knowledge in malpractice law is where a delay in stroke diagnosis results in loss of brain function.
Answer: B. The judge, not the jury or anyone else, makes the decision regarding res ipsa loquitur (the thing speaks for itself) or common knowledge, which exempts a plaintiff from producing an expert witness to testify as to the standard of care and causation. However, this is only true in actions arising out of professional negligence such as medical malpractice, whereas most common negligence actions – for example, slips and falls – do not require expert testimony.
Only a professional, duly qualified by the court as an expert witness, is allowed to offer medical testimony, while the plaintiff will typically be disqualified from playing this role because of the complexity of issues involved unless there is common knowledge. In general, courts are reluctant to grant this exception, which favors the plaintiff.
The best example of res ipsa loquitur is where a surgeon inadvertently leaves behind a sponge or instrument inside a body cavity. Other successfully litigated examples include cardiac arrest in the operating room, hypoxia in the recovery room, burns to the buttock, gangrene after the accidental injection of penicillin into an artery, air trapped subcutaneously from a displaced needle, and a pierced eyeball during a procedure. The factual circumstances of each case are critical to its outcome. For example, in a 2013 New York case, the plaintiff was barred from using the res doctrine.1 The defendant doctor had left a guide wire in the plaintiff’s chest following a biopsy and retrieved it 2 months later. The plaintiff did not call any expert witness, relying instead on the “foreign object” basis for invoking the res doctrine. However, the Court of Appeals reasoned that the object was left behind deliberately, not unintentionally, and that under the circumstances of the case, an expert witness was needed to set out the applicable standard of care, without which a jury could not determine whether the doctor’s professional judgment breached the requisite standard.
The Supreme Court of Kentucky recently rejected the use of common knowledge in a stroke case.2 In 2010, David Shackelford’s rheumatologist referred him to Paul Lewis, MD, an interventional radiologist, for a four-vessel cerebral angiogram to assist with diagnosing the cause of Mr. Shackelford’s chronic headaches. The procedure itself was uneventful, but while in the recovery room, Mr. Shackelford reported a frontal headache and scotoma, which resolved on its own. The headache improved with medication, and the patient experienced no other symptoms. There were no other visual changes, weakness, slurred speech, or facial palsies. Mr. Shackelford was discharged but had to return to the hospital the next morning via ambulance after becoming disoriented at his home. An MRI indicated multiple scattered small infarcts, and he was left with residual short-term memory loss and visual problems.
There was no allegation that the stroke itself was caused by negligence; rather, Mr. Shackelford alleged that the failure to examine and diagnose the stroke after the angiogram was negligent and caused injury greater than that which the stroke would have caused with earlier intervention. To support his claims, Mr. Shackelford’s expert, Michael David Khoury, MD, a vascular surgeon, criticized Dr. Lewis’s failure to examine Mr. Shackelford when his symptoms were consistent with a stroke. However, Dr. Khoury did not opine that Dr. Lewis could have limited the effects of the stroke through earlier intervention. When asked specifically whether he could state within a reasonable degree of medical probability that Dr. Lewis’s postprocedure care was a substantial factor in causing harm to Mr. Shackelford, Dr. Khoury responded that it was “impossible to tell.”
Based largely upon Dr. Khoury’s deposition testimony, the defendants successfully moved for summary judgment on the basis that the expert had failed to opine that the alleged negligence caused any injury to Mr. Shackelford. As a result, Mr. Shackelford could not prove an essential element of his medical malpractice claim. Defense expert Peter J. Pema, MD, a neuroradiologist, acknowledged the general proposition that strokes require timely diagnosis and treatment but did not provide an opinion on causation under the specific facts of this case. Another defense expert, Gregory Postal, MD, opined that Mr. Shackelford began to present symptoms of a stroke after leaving the hospital.
Notwithstanding the lower court’s ruling to summarily dismiss the case, the Court of Appeals found that, in this case, the issue of causation did not require expert medical testimony. It explained that given the ubiquity of information regarding stroke symptom identification and the necessity of prompt treatment, it had become common knowledge that “time lost is brain lost” as to timely medical intervention. In other words, a jury of laymen with this general knowledge could resolve the causation issue without the aid of expert testimony.
However, the Supreme Court of Kentucky held otherwise, writing: “We disagree with the Court of Appeals’ analysis. Although public service campaigns have increased public awareness and knowledge about stroke symptoms and timely intervention, that general information cannot provide the medical expertise necessary to evaluate this particular claim of medical malpractice. In other words, the question is not simply whether ‘time lost is brain lost.’ Rather, the specific facts and circumstances of this case play a significant role in determining whether the alleged negligent conduct was a substantial factor in Shackelford’s injuries, and to what extent. For example, as Dr. Lewis’s deposition testimony illustrates, a variety of factors influenced his diagnosis and treatment of Shackelford, including Shackelford’s medical history and history of cluster headaches; the common side effects of the angiogram procedure, including headache and scotoma; and the manner in which Shackelford’s headache and scotoma presented, as well as their timing. The complexities of these factors and how they affected Dr. Lewis’s evaluation of Shackelford may have also influenced the severity of the injury. These matters are clearly relevant to the determination of an alleged breach of the standard of care. Despite public perception about timely intervention, the average layperson cannot properly weigh such complex medical evidence without the aid of expert opinion. … To conclude otherwise is to drastically expand the res ipsa loquitor exception and to virtually eliminate the need for expert opinion evidence in similar medical malpractice actions that involve common or highly publicized conditions (e.g., stroke, heart attack, and even some cancers).”
Dr. Tan is professor emeritus of medicine and former adjunct professor of law at the University of Hawaii, Honolulu. This article is meant to be educational and does not constitute medical, ethical or legal advice. The author published an earlier version of this topic in the April 19, 2016, issue of Internal Medicine News, available at https://www.mdedge.com/internalmedicine/law-medicine. For additional information, readers may contact the author at siang@hawaii.edu.
References
1. James v. Wormuth, 997 N.E.2d 133 (N.Y. 2013).
2. Lewis/Ashland Hospital v. Shackelford, Supreme Court of Kentucky, Opinion of the Court by Justice Keller, rendered August 29, 2019.
USPSTF recommendations on risk assessment, genetic counseling, and genetic testing for BRCA-related cancer
Breast cancer screening recommendations have evolved over the past decade. BRCA1/2 genes are tumor-suppressor genes. Mutations in these genes place women at an increased risk for developing breast, ovarian, fallopian tube, and peritoneal cancer. Detection of BRCA1/2 mutations through genetic screening can provide patients with more information about their cancer risk and can lead to discussion of prophylactic therapies. This includes increased screening frequency, medical therapy, and surgical interventions.
New USPSTF recommendations address who is at an increased risk for BRCA1/2 mutations. They recommend using screening tools focusing on family history that primary care physicians can utilize to determine who should be referred for genetic counseling to discuss the risks and benefits of genetic screening. The following are the task force’s two primary recommendations:
The USPSTF recommends that primary care clinicians assess women with a personal or family history of breast, ovarian, tubal, or peritoneal cancer or who have an ancestry associated with BRCA1/2 gene mutations with an appropriate brief familial risk assessment tool. Women with a positive result on the risk assessment tool should receive genetic counseling and, if indicated after counseling, genetic testing. (B recommendation)
The USPSTF recommends against routine risk assessment, genetic counseling, or genetic testing for women whose personal or family history or ancestry is not associated with potentially harmful BRCA1/2 gene mutations. (D recommendation)
Breast cancer is the second leading cause of cancer and cancer death for women in the United States. Ovarian cancer ranks fifth in cancer deaths for women in the U.S. By age 70, women with BRCA1/2 mutations have a 45%-65% cumulative lifetime risk of developing breast cancer.
Mutations in BRCA1, specifically, are associated with a 39% lifetime risk for ovarian, fallopian tube, and peritoneal cancer. In contrast, mutations in BRCA2 are associated with a 10%-17% lifetime risk.
The USPSTF also underscores the increased prevalence of BRCA1/2 mutations in the Ashkenazi Jewish population. Three out of seven familial risk assessment tools inquire about Jewish ancestry. This is because the Ashkenazi Jewish population have a higher prevalence of three founder mutations in the BRCA1/2 gene. A member of this population has a 1 in 40 chance of carrying one of these three mutations, whereas the general population has a 1 in 300 chance.
The USPSTF recommends a multistep process of screening. The first step is taking a family history of cancer. For women who have a family history of breast, ovarian, tubal, or peritoneal cancer or a personal history of these cancers, a brief familial risk assessment tool should be used to determine the need for referral for in-depth genetic counseling to determine the need for genetic testing.
It is important to recognize that the validated tools recommended by the USPSTF are specific for genetic risk assessment. General breast cancer risk assessment tools, including the National Cancer Institute Breast Cancer Risk Assessment Tool, which is based on the Gail model, are not recommended.
The sensitivity of the tools recommended by the USPSTF range between 77% and 100%. A number of tools are given as an option with no one tool being better than the other. Perhaps the easiest to implement of the validated tools recommended is the Pedigree Assessment Tool. For this tool, points are assigned for every family member with breast or ovarian cancer as indicated in the table below.
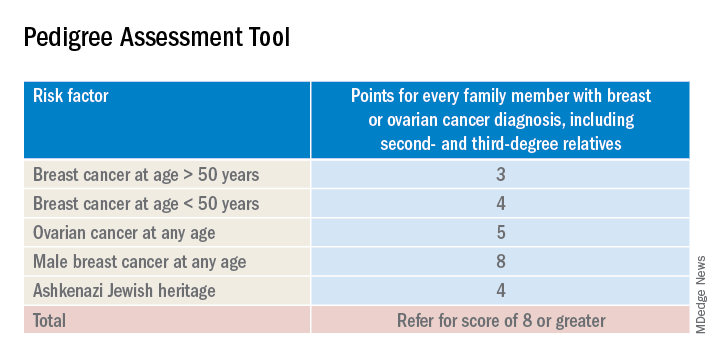
A positive result on a screening tool will lead primary care physicians to appropriately refer patients for genetic counseling. Genetic testing for BRCA1/2 mutations should be limited to those individuals whose personal and/or family history reflects an increased risk for gene mutations after detailed genetic assessment and counseling. The results of the genetic screening should assist a patient in their decision making.
Prophylactic treatment for BRCA1/2 mutation carriers are outside the scope of this recommendation. However the guidelines briefly review risk-reducing therapies including screening, medical, and surgical options. Medical therapy for patients who have BRCA1/2 mutations include the use of tamoxifen, raloxifene, and aromatase inhibitors. Surgical interventions include bilateral mastectomy and salpingo-oopherectomy.
Screening options include earlier and more frequent mammograms and breast MRIs. Screening is largely based on family history and the USPSTF acknowledges their uncertainty when screening women with an unknown family history. Male breast cancer, pancreatic cancer, prostate cancer, and melanoma are also associated with BRCA1/2 mutations. They are not included in this recommendation.
The bottom line
USPSTF recommended that primary care physicians should use familial risk assessment tools to screen women for BRCA1/2 mutations. This includes women with a personal and/or family history of breast, ovarian, tubal, or peritoneal cancer or women with a family history of BRCA1/2 gene mutations. Patients who test positive through one of the suggested screening tools should be referred for genetic counseling. This could lead to genetic testing and subsequent prophylactic therapies and/or increased screenings if the patient so desires. It is of importance to note the USPSTF recommends against routine screening of BRCA1/2 gene mutations for women who do not meet the above requirements.
Reference
USPSTF Recommendation: Assessment, counseling, and testing for BRCA-related cancer. JAMA. 2019;322(7):652-65. doi: 10.1001/jama.2019.10987.
Dr. Style is a second-year resident in the Family Medicine Residency Program at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Jefferson Health.
Breast cancer screening recommendations have evolved over the past decade. BRCA1/2 genes are tumor-suppressor genes. Mutations in these genes place women at an increased risk for developing breast, ovarian, fallopian tube, and peritoneal cancer. Detection of BRCA1/2 mutations through genetic screening can provide patients with more information about their cancer risk and can lead to discussion of prophylactic therapies. This includes increased screening frequency, medical therapy, and surgical interventions.
New USPSTF recommendations address who is at an increased risk for BRCA1/2 mutations. They recommend using screening tools focusing on family history that primary care physicians can utilize to determine who should be referred for genetic counseling to discuss the risks and benefits of genetic screening. The following are the task force’s two primary recommendations:
The USPSTF recommends that primary care clinicians assess women with a personal or family history of breast, ovarian, tubal, or peritoneal cancer or who have an ancestry associated with BRCA1/2 gene mutations with an appropriate brief familial risk assessment tool. Women with a positive result on the risk assessment tool should receive genetic counseling and, if indicated after counseling, genetic testing. (B recommendation)
The USPSTF recommends against routine risk assessment, genetic counseling, or genetic testing for women whose personal or family history or ancestry is not associated with potentially harmful BRCA1/2 gene mutations. (D recommendation)
Breast cancer is the second leading cause of cancer and cancer death for women in the United States. Ovarian cancer ranks fifth in cancer deaths for women in the U.S. By age 70, women with BRCA1/2 mutations have a 45%-65% cumulative lifetime risk of developing breast cancer.
Mutations in BRCA1, specifically, are associated with a 39% lifetime risk for ovarian, fallopian tube, and peritoneal cancer. In contrast, mutations in BRCA2 are associated with a 10%-17% lifetime risk.
The USPSTF also underscores the increased prevalence of BRCA1/2 mutations in the Ashkenazi Jewish population. Three out of seven familial risk assessment tools inquire about Jewish ancestry. This is because the Ashkenazi Jewish population have a higher prevalence of three founder mutations in the BRCA1/2 gene. A member of this population has a 1 in 40 chance of carrying one of these three mutations, whereas the general population has a 1 in 300 chance.
The USPSTF recommends a multistep process of screening. The first step is taking a family history of cancer. For women who have a family history of breast, ovarian, tubal, or peritoneal cancer or a personal history of these cancers, a brief familial risk assessment tool should be used to determine the need for referral for in-depth genetic counseling to determine the need for genetic testing.
It is important to recognize that the validated tools recommended by the USPSTF are specific for genetic risk assessment. General breast cancer risk assessment tools, including the National Cancer Institute Breast Cancer Risk Assessment Tool, which is based on the Gail model, are not recommended.
The sensitivity of the tools recommended by the USPSTF range between 77% and 100%. A number of tools are given as an option with no one tool being better than the other. Perhaps the easiest to implement of the validated tools recommended is the Pedigree Assessment Tool. For this tool, points are assigned for every family member with breast or ovarian cancer as indicated in the table below.
A positive result on a screening tool will lead primary care physicians to appropriately refer patients for genetic counseling. Genetic testing for BRCA1/2 mutations should be limited to those individuals whose personal and/or family history reflects an increased risk for gene mutations after detailed genetic assessment and counseling. The results of the genetic screening should assist a patient in their decision making.
Prophylactic treatment for BRCA1/2 mutation carriers are outside the scope of this recommendation. However the guidelines briefly review risk-reducing therapies including screening, medical, and surgical options. Medical therapy for patients who have BRCA1/2 mutations include the use of tamoxifen, raloxifene, and aromatase inhibitors. Surgical interventions include bilateral mastectomy and salpingo-oopherectomy.
Screening options include earlier and more frequent mammograms and breast MRIs. Screening is largely based on family history and the USPSTF acknowledges their uncertainty when screening women with an unknown family history. Male breast cancer, pancreatic cancer, prostate cancer, and melanoma are also associated with BRCA1/2 mutations. They are not included in this recommendation.
The bottom line
USPSTF recommended that primary care physicians should use familial risk assessment tools to screen women for BRCA1/2 mutations. This includes women with a personal and/or family history of breast, ovarian, tubal, or peritoneal cancer or women with a family history of BRCA1/2 gene mutations. Patients who test positive through one of the suggested screening tools should be referred for genetic counseling. This could lead to genetic testing and subsequent prophylactic therapies and/or increased screenings if the patient so desires. It is of importance to note the USPSTF recommends against routine screening of BRCA1/2 gene mutations for women who do not meet the above requirements.
Reference
USPSTF Recommendation: Assessment, counseling, and testing for BRCA-related cancer. JAMA. 2019;322(7):652-65. doi: 10.1001/jama.2019.10987.
Dr. Style is a second-year resident in the Family Medicine Residency Program at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Jefferson Health.
Breast cancer screening recommendations have evolved over the past decade. BRCA1/2 genes are tumor-suppressor genes. Mutations in these genes place women at an increased risk for developing breast, ovarian, fallopian tube, and peritoneal cancer. Detection of BRCA1/2 mutations through genetic screening can provide patients with more information about their cancer risk and can lead to discussion of prophylactic therapies. This includes increased screening frequency, medical therapy, and surgical interventions.
New USPSTF recommendations address who is at an increased risk for BRCA1/2 mutations. They recommend using screening tools focusing on family history that primary care physicians can utilize to determine who should be referred for genetic counseling to discuss the risks and benefits of genetic screening. The following are the task force’s two primary recommendations:
The USPSTF recommends that primary care clinicians assess women with a personal or family history of breast, ovarian, tubal, or peritoneal cancer or who have an ancestry associated with BRCA1/2 gene mutations with an appropriate brief familial risk assessment tool. Women with a positive result on the risk assessment tool should receive genetic counseling and, if indicated after counseling, genetic testing. (B recommendation)
The USPSTF recommends against routine risk assessment, genetic counseling, or genetic testing for women whose personal or family history or ancestry is not associated with potentially harmful BRCA1/2 gene mutations. (D recommendation)
Breast cancer is the second leading cause of cancer and cancer death for women in the United States. Ovarian cancer ranks fifth in cancer deaths for women in the U.S. By age 70, women with BRCA1/2 mutations have a 45%-65% cumulative lifetime risk of developing breast cancer.
Mutations in BRCA1, specifically, are associated with a 39% lifetime risk for ovarian, fallopian tube, and peritoneal cancer. In contrast, mutations in BRCA2 are associated with a 10%-17% lifetime risk.
The USPSTF also underscores the increased prevalence of BRCA1/2 mutations in the Ashkenazi Jewish population. Three out of seven familial risk assessment tools inquire about Jewish ancestry. This is because the Ashkenazi Jewish population have a higher prevalence of three founder mutations in the BRCA1/2 gene. A member of this population has a 1 in 40 chance of carrying one of these three mutations, whereas the general population has a 1 in 300 chance.
The USPSTF recommends a multistep process of screening. The first step is taking a family history of cancer. For women who have a family history of breast, ovarian, tubal, or peritoneal cancer or a personal history of these cancers, a brief familial risk assessment tool should be used to determine the need for referral for in-depth genetic counseling to determine the need for genetic testing.
It is important to recognize that the validated tools recommended by the USPSTF are specific for genetic risk assessment. General breast cancer risk assessment tools, including the National Cancer Institute Breast Cancer Risk Assessment Tool, which is based on the Gail model, are not recommended.
The sensitivity of the tools recommended by the USPSTF range between 77% and 100%. A number of tools are given as an option with no one tool being better than the other. Perhaps the easiest to implement of the validated tools recommended is the Pedigree Assessment Tool. For this tool, points are assigned for every family member with breast or ovarian cancer as indicated in the table below.
A positive result on a screening tool will lead primary care physicians to appropriately refer patients for genetic counseling. Genetic testing for BRCA1/2 mutations should be limited to those individuals whose personal and/or family history reflects an increased risk for gene mutations after detailed genetic assessment and counseling. The results of the genetic screening should assist a patient in their decision making.
Prophylactic treatment for BRCA1/2 mutation carriers are outside the scope of this recommendation. However the guidelines briefly review risk-reducing therapies including screening, medical, and surgical options. Medical therapy for patients who have BRCA1/2 mutations include the use of tamoxifen, raloxifene, and aromatase inhibitors. Surgical interventions include bilateral mastectomy and salpingo-oopherectomy.
Screening options include earlier and more frequent mammograms and breast MRIs. Screening is largely based on family history and the USPSTF acknowledges their uncertainty when screening women with an unknown family history. Male breast cancer, pancreatic cancer, prostate cancer, and melanoma are also associated with BRCA1/2 mutations. They are not included in this recommendation.
The bottom line
USPSTF recommended that primary care physicians should use familial risk assessment tools to screen women for BRCA1/2 mutations. This includes women with a personal and/or family history of breast, ovarian, tubal, or peritoneal cancer or women with a family history of BRCA1/2 gene mutations. Patients who test positive through one of the suggested screening tools should be referred for genetic counseling. This could lead to genetic testing and subsequent prophylactic therapies and/or increased screenings if the patient so desires. It is of importance to note the USPSTF recommends against routine screening of BRCA1/2 gene mutations for women who do not meet the above requirements.
Reference
USPSTF Recommendation: Assessment, counseling, and testing for BRCA-related cancer. JAMA. 2019;322(7):652-65. doi: 10.1001/jama.2019.10987.
Dr. Style is a second-year resident in the Family Medicine Residency Program at Abington (Pa.) Jefferson Health. Dr. Skolnik is professor of family and community medicine at Jefferson Medical College, Philadelphia, and an associate director of the family medicine residency program at Abington Jefferson Health.
CBD: What physicians need to know about it
Cannabidiol is a derivative of marijuana that is sold everywhere from medical marijuana stores to health food markets to gas stations. While this chemical is derived from marijuana plants, it can be sold in many states as a supplement and is largely unregulated. The ubiquity of cannabidiol (CBD) and its potential benefits means that doctors need to be able to counsel patients about what we know, what we don’t, and how to use it safely. For conditions such as chronic pain and addiction, where we have few safe and effective alternatives, CBD may be reasonable to recommend.

To find out what physicians need to know about CBD, Elisabeth Poorman, MD, a general internist at a University of Washington neighborhood clinic in Kent and member of the editorial advisory board of Internal Medicine News, interviewed Peter Grinspoon, MD, who provides free consultation to primary care patients on the benefits and risks of using various forms of cannabis, including CBD. Dr. Grinspoon is an internist at Massachusetts General Hospital Chelsea Healthcare Center and is an instructor at Harvard Medical School, Boston. He has contributed to the Harvard Health Blog on the topic of medical marijuana, delivered grand rounds on cannabis at Massachusetts General Hospital, and lectured at the American College of Physicians. Dr. Grinspoon is also medical director for Galenas, a medical marijuana company.
Dr. Grinspoon is the son of Lester Grinspoon, MD, associate professor emeritus of psychiatry at Harvard Medical School, who researched the medicinal legitimacy of marijuana prohibition and has authored books on the medical benefits of marijuana.
and his knowledge of CBD’s efficacy for various medical conditions. Below are excerpts from that conversation.
Dr. Poorman: How do you explain the difference between THC and CBD to patients?
Dr. Grinspoon: Cannabis contains at least a hundred different chemicals called cannabinoids, of which tetrahydrocannabinol (THC) and CBD are the most prevalent. THC is the one that gets you high and can be used recreationally and medically. The CBD molecule is not intoxicating, and people use it for a variety of medical purposes, most commonly to treat anxiety, insomnia, and pain.
Dr. Poorman: There are a lot of gaps in what we now about CBD’s potential benefits. Why don’t we know more?
Dr. Grinspoon: CBD has no abuse liability according to the World Health Organization, but because it is a cannabinoid, it is still technically a schedule I substance under the Controlled Substances Act, and that makes it difficult to study.
Dr. Poorman: What kinds of conditions can CBD treat?
Dr. Grinspoon: In anxiety, the enthusiasm has outpaced the science; there’s no question about that. And most of the studies have done in animals. That said, some studies have shown that CBD helps treat components of anxiety, like public speaking. Unlike THC, it is nonintoxicating and non–habit forming. But we don’t have the wealth of randomized controlled trials that we have for official psychiatric medications.
CBD’s benefits have been most extensively studied in pediatric epilepsy. The one Food and Drug Administration–approved drug derived from cannabis is Epidiolex, used to treat rare forms of childhood epilepsy. There is some evidence that as an adjunct, it can be used for glioblastoma multiforme in patients receiving other appropriate therapy. There is also some preliminary evidence that it can be used for addiction, including to opioids, cannabis, tobacco, and stimulants.
Most of the evidence for using CBD in chronic pain comes from animal studies, including a study published in the European Journal of Pain in 2016. Among my patients to whom I have suggested CBD for chronic pain, a few have noticed great benefit, a few have noticed some benefit, and a lot have noticed no benefit. For those who have said they noticed benefit it is unclear whether that benefit was just the placebo effect.
In insomnia, I usually have them take CBD under the tongue half an hour time before bedtime, or if it’s an edible, an hour before bedtime. I start with a lower dose and slowly try higher doses. I also encourage them to do the other sleep hygiene things, like no screens, increasing exercise, and decreasing caffeine. It seems that CBD helps them fall asleep, though it’s hard to know if it’s the CBD or the fact that they have started taking something, and have simultaneously made various lifestyle changes.
Dr. Poorman: Can CBD interfere with your normal sleep architecture, the way benzodiazepines and Benadryl can?
Dr. Grinspoon: We know that THC affects your sleep architecture and affects what percentage of REM sleep you have. But I don’t know if the effects of CBD on sleep architecture have been studied.
Dr. Poorman: What harms do you counsel patients about when discussing CBD?
Dr. Grinspoon: There are four main harms. The first is the price. It’s overpriced, and the doses are very low. In most animal studies, the doses are about 20 milligrams per kilogram of weight. And you go to the market, and it’s like a dollar for a hundredth of that.
Number two is that it’s not regulated; it’s a supplement. A few years ago, the government tested a bunch of samples of CBD, and some didn’t actually contain CBD, some didn’t have the right amount; and worse, some contained THC that had not been disclosed in the packaging. So you can’t just go to a roadside gas station and assume that if you buy CBD, it’s actually that. You want a place that has a certificate of assurance. Make sure third-party testing was done, including testing for pesticides and other heavy metals.
The third thing is drug interactions. It affects the body like grapefruit and inhibits the cytochrome P450 system. The medications doctors should be most concerned about are blood thinners like Coumadin. And if you’re on blood thinners, you definitely want to tell your doctor that you are on CBD and he or she might want to check your blood levels more frequently than they usually do.
The fourth concern is liver inflammation. In the childhood epilepsy studies, a bump in some liver enzymes was seen, although I haven’t heard of any clinically significant cases of chemical hepatitis related to CBD. But if someone has liver disease you want to keep an eye on their liver enzymes.
Dr. Poorman: What methods of ingestion do you recommend or not recommend?
Dr. Grinspoon: It’s basically trial and error, but I usually recommend oral form. If people feel comfortable taking a gummy bear, or a pill, I’m not particular about that. If the product being taken contains less than 0.3% THC, it won’t get you high.
The topical form probably works better for treating chronic pain if it contains some THC, suggests a review article published in the Cleveland Clinic Journal of Medicine. Topical THC is nonintoxicating, unless you managed to sit in a bathtub for 8 hours after applying it.
I don’t recommend smoking CBD, and right now, I don’t recommend vaping anything.
If people have severe pain, like moderately severe arthritis, CBD may not be enough, whereas medical cannabis with THC could help, a report suggests.
Dr. Poorman: Do you ever encourage patients to stop using CBD products?
Dr. Grinspoon: I work in a low-income area, and my patients don’t have a ton of disposable income. If it’s not working, I worry about the expense.
Dr. Poorman: The CBD industry is growing quickly. What changes are you seeing in what products are out there, and what changes would you like to see?
Dr. Grinspoon: CBD is being put in everything, and it’s comical. On the one hand, you can say if people want to waste their money on a CBD emitting pillowcase, that’s fine. On the other hand, you can say that certainly seems like misleading advertising, because a CBD emitting pillowcase isn’t going to help you sleep any better.
I think the purported benefits are far beyond what we can say scientifically. We do know that CBD has anti-inflammatory characteristics. But that doesn’t mean that putting CBD in all skin products is good for your skin. It’s bad for your pocketbook, though. I would like there to be less of a gap between the claims and the science.
Dr. Elisabeth Poorman has no conflicts to disclose.
Cannabidiol is a derivative of marijuana that is sold everywhere from medical marijuana stores to health food markets to gas stations. While this chemical is derived from marijuana plants, it can be sold in many states as a supplement and is largely unregulated. The ubiquity of cannabidiol (CBD) and its potential benefits means that doctors need to be able to counsel patients about what we know, what we don’t, and how to use it safely. For conditions such as chronic pain and addiction, where we have few safe and effective alternatives, CBD may be reasonable to recommend.
To find out what physicians need to know about CBD, Elisabeth Poorman, MD, a general internist at a University of Washington neighborhood clinic in Kent and member of the editorial advisory board of Internal Medicine News, interviewed Peter Grinspoon, MD, who provides free consultation to primary care patients on the benefits and risks of using various forms of cannabis, including CBD. Dr. Grinspoon is an internist at Massachusetts General Hospital Chelsea Healthcare Center and is an instructor at Harvard Medical School, Boston. He has contributed to the Harvard Health Blog on the topic of medical marijuana, delivered grand rounds on cannabis at Massachusetts General Hospital, and lectured at the American College of Physicians. Dr. Grinspoon is also medical director for Galenas, a medical marijuana company.
Dr. Grinspoon is the son of Lester Grinspoon, MD, associate professor emeritus of psychiatry at Harvard Medical School, who researched the medicinal legitimacy of marijuana prohibition and has authored books on the medical benefits of marijuana.
and his knowledge of CBD’s efficacy for various medical conditions. Below are excerpts from that conversation.
Dr. Poorman: How do you explain the difference between THC and CBD to patients?
Dr. Grinspoon: Cannabis contains at least a hundred different chemicals called cannabinoids, of which tetrahydrocannabinol (THC) and CBD are the most prevalent. THC is the one that gets you high and can be used recreationally and medically. The CBD molecule is not intoxicating, and people use it for a variety of medical purposes, most commonly to treat anxiety, insomnia, and pain.
Dr. Poorman: There are a lot of gaps in what we now about CBD’s potential benefits. Why don’t we know more?
Dr. Grinspoon: CBD has no abuse liability according to the World Health Organization, but because it is a cannabinoid, it is still technically a schedule I substance under the Controlled Substances Act, and that makes it difficult to study.
Dr. Poorman: What kinds of conditions can CBD treat?
Dr. Grinspoon: In anxiety, the enthusiasm has outpaced the science; there’s no question about that. And most of the studies have done in animals. That said, some studies have shown that CBD helps treat components of anxiety, like public speaking. Unlike THC, it is nonintoxicating and non–habit forming. But we don’t have the wealth of randomized controlled trials that we have for official psychiatric medications.
CBD’s benefits have been most extensively studied in pediatric epilepsy. The one Food and Drug Administration–approved drug derived from cannabis is Epidiolex, used to treat rare forms of childhood epilepsy. There is some evidence that as an adjunct, it can be used for glioblastoma multiforme in patients receiving other appropriate therapy. There is also some preliminary evidence that it can be used for addiction, including to opioids, cannabis, tobacco, and stimulants.
Most of the evidence for using CBD in chronic pain comes from animal studies, including a study published in the European Journal of Pain in 2016. Among my patients to whom I have suggested CBD for chronic pain, a few have noticed great benefit, a few have noticed some benefit, and a lot have noticed no benefit. For those who have said they noticed benefit it is unclear whether that benefit was just the placebo effect.
In insomnia, I usually have them take CBD under the tongue half an hour time before bedtime, or if it’s an edible, an hour before bedtime. I start with a lower dose and slowly try higher doses. I also encourage them to do the other sleep hygiene things, like no screens, increasing exercise, and decreasing caffeine. It seems that CBD helps them fall asleep, though it’s hard to know if it’s the CBD or the fact that they have started taking something, and have simultaneously made various lifestyle changes.
Dr. Poorman: Can CBD interfere with your normal sleep architecture, the way benzodiazepines and Benadryl can?
Dr. Grinspoon: We know that THC affects your sleep architecture and affects what percentage of REM sleep you have. But I don’t know if the effects of CBD on sleep architecture have been studied.
Dr. Poorman: What harms do you counsel patients about when discussing CBD?
Dr. Grinspoon: There are four main harms. The first is the price. It’s overpriced, and the doses are very low. In most animal studies, the doses are about 20 milligrams per kilogram of weight. And you go to the market, and it’s like a dollar for a hundredth of that.
Number two is that it’s not regulated; it’s a supplement. A few years ago, the government tested a bunch of samples of CBD, and some didn’t actually contain CBD, some didn’t have the right amount; and worse, some contained THC that had not been disclosed in the packaging. So you can’t just go to a roadside gas station and assume that if you buy CBD, it’s actually that. You want a place that has a certificate of assurance. Make sure third-party testing was done, including testing for pesticides and other heavy metals.
The third thing is drug interactions. It affects the body like grapefruit and inhibits the cytochrome P450 system. The medications doctors should be most concerned about are blood thinners like Coumadin. And if you’re on blood thinners, you definitely want to tell your doctor that you are on CBD and he or she might want to check your blood levels more frequently than they usually do.
The fourth concern is liver inflammation. In the childhood epilepsy studies, a bump in some liver enzymes was seen, although I haven’t heard of any clinically significant cases of chemical hepatitis related to CBD. But if someone has liver disease you want to keep an eye on their liver enzymes.
Dr. Poorman: What methods of ingestion do you recommend or not recommend?
Dr. Grinspoon: It’s basically trial and error, but I usually recommend oral form. If people feel comfortable taking a gummy bear, or a pill, I’m not particular about that. If the product being taken contains less than 0.3% THC, it won’t get you high.
The topical form probably works better for treating chronic pain if it contains some THC, suggests a review article published in the Cleveland Clinic Journal of Medicine. Topical THC is nonintoxicating, unless you managed to sit in a bathtub for 8 hours after applying it.
I don’t recommend smoking CBD, and right now, I don’t recommend vaping anything.
If people have severe pain, like moderately severe arthritis, CBD may not be enough, whereas medical cannabis with THC could help, a report suggests.
Dr. Poorman: Do you ever encourage patients to stop using CBD products?
Dr. Grinspoon: I work in a low-income area, and my patients don’t have a ton of disposable income. If it’s not working, I worry about the expense.
Dr. Poorman: The CBD industry is growing quickly. What changes are you seeing in what products are out there, and what changes would you like to see?
Dr. Grinspoon: CBD is being put in everything, and it’s comical. On the one hand, you can say if people want to waste their money on a CBD emitting pillowcase, that’s fine. On the other hand, you can say that certainly seems like misleading advertising, because a CBD emitting pillowcase isn’t going to help you sleep any better.
I think the purported benefits are far beyond what we can say scientifically. We do know that CBD has anti-inflammatory characteristics. But that doesn’t mean that putting CBD in all skin products is good for your skin. It’s bad for your pocketbook, though. I would like there to be less of a gap between the claims and the science.
Dr. Elisabeth Poorman has no conflicts to disclose.
Cannabidiol is a derivative of marijuana that is sold everywhere from medical marijuana stores to health food markets to gas stations. While this chemical is derived from marijuana plants, it can be sold in many states as a supplement and is largely unregulated. The ubiquity of cannabidiol (CBD) and its potential benefits means that doctors need to be able to counsel patients about what we know, what we don’t, and how to use it safely. For conditions such as chronic pain and addiction, where we have few safe and effective alternatives, CBD may be reasonable to recommend.
To find out what physicians need to know about CBD, Elisabeth Poorman, MD, a general internist at a University of Washington neighborhood clinic in Kent and member of the editorial advisory board of Internal Medicine News, interviewed Peter Grinspoon, MD, who provides free consultation to primary care patients on the benefits and risks of using various forms of cannabis, including CBD. Dr. Grinspoon is an internist at Massachusetts General Hospital Chelsea Healthcare Center and is an instructor at Harvard Medical School, Boston. He has contributed to the Harvard Health Blog on the topic of medical marijuana, delivered grand rounds on cannabis at Massachusetts General Hospital, and lectured at the American College of Physicians. Dr. Grinspoon is also medical director for Galenas, a medical marijuana company.
Dr. Grinspoon is the son of Lester Grinspoon, MD, associate professor emeritus of psychiatry at Harvard Medical School, who researched the medicinal legitimacy of marijuana prohibition and has authored books on the medical benefits of marijuana.
and his knowledge of CBD’s efficacy for various medical conditions. Below are excerpts from that conversation.
Dr. Poorman: How do you explain the difference between THC and CBD to patients?
Dr. Grinspoon: Cannabis contains at least a hundred different chemicals called cannabinoids, of which tetrahydrocannabinol (THC) and CBD are the most prevalent. THC is the one that gets you high and can be used recreationally and medically. The CBD molecule is not intoxicating, and people use it for a variety of medical purposes, most commonly to treat anxiety, insomnia, and pain.
Dr. Poorman: There are a lot of gaps in what we now about CBD’s potential benefits. Why don’t we know more?
Dr. Grinspoon: CBD has no abuse liability according to the World Health Organization, but because it is a cannabinoid, it is still technically a schedule I substance under the Controlled Substances Act, and that makes it difficult to study.
Dr. Poorman: What kinds of conditions can CBD treat?
Dr. Grinspoon: In anxiety, the enthusiasm has outpaced the science; there’s no question about that. And most of the studies have done in animals. That said, some studies have shown that CBD helps treat components of anxiety, like public speaking. Unlike THC, it is nonintoxicating and non–habit forming. But we don’t have the wealth of randomized controlled trials that we have for official psychiatric medications.
CBD’s benefits have been most extensively studied in pediatric epilepsy. The one Food and Drug Administration–approved drug derived from cannabis is Epidiolex, used to treat rare forms of childhood epilepsy. There is some evidence that as an adjunct, it can be used for glioblastoma multiforme in patients receiving other appropriate therapy. There is also some preliminary evidence that it can be used for addiction, including to opioids, cannabis, tobacco, and stimulants.
Most of the evidence for using CBD in chronic pain comes from animal studies, including a study published in the European Journal of Pain in 2016. Among my patients to whom I have suggested CBD for chronic pain, a few have noticed great benefit, a few have noticed some benefit, and a lot have noticed no benefit. For those who have said they noticed benefit it is unclear whether that benefit was just the placebo effect.
In insomnia, I usually have them take CBD under the tongue half an hour time before bedtime, or if it’s an edible, an hour before bedtime. I start with a lower dose and slowly try higher doses. I also encourage them to do the other sleep hygiene things, like no screens, increasing exercise, and decreasing caffeine. It seems that CBD helps them fall asleep, though it’s hard to know if it’s the CBD or the fact that they have started taking something, and have simultaneously made various lifestyle changes.
Dr. Poorman: Can CBD interfere with your normal sleep architecture, the way benzodiazepines and Benadryl can?
Dr. Grinspoon: We know that THC affects your sleep architecture and affects what percentage of REM sleep you have. But I don’t know if the effects of CBD on sleep architecture have been studied.
Dr. Poorman: What harms do you counsel patients about when discussing CBD?
Dr. Grinspoon: There are four main harms. The first is the price. It’s overpriced, and the doses are very low. In most animal studies, the doses are about 20 milligrams per kilogram of weight. And you go to the market, and it’s like a dollar for a hundredth of that.
Number two is that it’s not regulated; it’s a supplement. A few years ago, the government tested a bunch of samples of CBD, and some didn’t actually contain CBD, some didn’t have the right amount; and worse, some contained THC that had not been disclosed in the packaging. So you can’t just go to a roadside gas station and assume that if you buy CBD, it’s actually that. You want a place that has a certificate of assurance. Make sure third-party testing was done, including testing for pesticides and other heavy metals.
The third thing is drug interactions. It affects the body like grapefruit and inhibits the cytochrome P450 system. The medications doctors should be most concerned about are blood thinners like Coumadin. And if you’re on blood thinners, you definitely want to tell your doctor that you are on CBD and he or she might want to check your blood levels more frequently than they usually do.
The fourth concern is liver inflammation. In the childhood epilepsy studies, a bump in some liver enzymes was seen, although I haven’t heard of any clinically significant cases of chemical hepatitis related to CBD. But if someone has liver disease you want to keep an eye on their liver enzymes.
Dr. Poorman: What methods of ingestion do you recommend or not recommend?
Dr. Grinspoon: It’s basically trial and error, but I usually recommend oral form. If people feel comfortable taking a gummy bear, or a pill, I’m not particular about that. If the product being taken contains less than 0.3% THC, it won’t get you high.
The topical form probably works better for treating chronic pain if it contains some THC, suggests a review article published in the Cleveland Clinic Journal of Medicine. Topical THC is nonintoxicating, unless you managed to sit in a bathtub for 8 hours after applying it.
I don’t recommend smoking CBD, and right now, I don’t recommend vaping anything.
If people have severe pain, like moderately severe arthritis, CBD may not be enough, whereas medical cannabis with THC could help, a report suggests.
Dr. Poorman: Do you ever encourage patients to stop using CBD products?
Dr. Grinspoon: I work in a low-income area, and my patients don’t have a ton of disposable income. If it’s not working, I worry about the expense.
Dr. Poorman: The CBD industry is growing quickly. What changes are you seeing in what products are out there, and what changes would you like to see?
Dr. Grinspoon: CBD is being put in everything, and it’s comical. On the one hand, you can say if people want to waste their money on a CBD emitting pillowcase, that’s fine. On the other hand, you can say that certainly seems like misleading advertising, because a CBD emitting pillowcase isn’t going to help you sleep any better.
I think the purported benefits are far beyond what we can say scientifically. We do know that CBD has anti-inflammatory characteristics. But that doesn’t mean that putting CBD in all skin products is good for your skin. It’s bad for your pocketbook, though. I would like there to be less of a gap between the claims and the science.
Dr. Elisabeth Poorman has no conflicts to disclose.