User login
Don’t let a foodborne illness dampen the holiday season
According to the Centers for Disease Control and Prevention, a foodborne disease occurs in one in six persons (48 million), resulting in 128,000 hospitalizations and 3,000 deaths annually in the United States. The Foodborne Active Surveillance Network (FoodNet) of the CDC’s Emerging Infections Program monitors cases of eight laboratory diagnosed infections from 10 U.S. sites (covering 15% of the U.S. population). Monitored organisms include Campylobacter, Cyclospora, Listeria, Salmonella, Shiga toxin–producing Escherichia coli (STEC), Shigella, Vibrio, and Yersinia. In 2018, FoodNet identified 25,606 cases of infection, 5,893 hospitalizations, and 120 deaths. The incidence of infection (cases/100,000) was highest for Campylobacter (20), Salmonella (18), STEC (6), Shigella (5), Vibrio (1), Yersinia (0.9), Cyclospora (0.7), and Listeria (0.3). How might these pathogens affect your patients? First, a quick review about the four more common infections. Treatment is beyond the scope of our discussion and you are referred to the 2018-2021 Red Book for assistance. The goal of this column is to prevent your patients from becoming a statistic this holiday season.

Campylobacter
It has been the most common infection reported in FoodNet since 2013. Clinically, patients present with fever, abdominal pain, and nonbloody diarrhea. However, bloody diarrhea maybe the only symptom in neonates and young infants. Abdominal pain can mimic acute appendicitis or intussusception. Bacteremia is rare but has been reported in the elderly and in some patients with underlying conditions. During convalescence, immunoreactive complications including Guillain-Barré syndrome, reactive arthritis, and erythema nodosum may occur. In patients with diarrhea, Campylobacter jejuni and C. coli are the most frequently isolated species.
Campylobacter is present in the intestinal tract of both domestic and wild birds and animals. Transmission is via consumption of contaminated food or water. Undercooked poultry, untreated water, and unpasteurized milk are the three main vehicles of transmission. Campylobacter can be isolated in stool and blood, however isolation from stool requires special media. Rehydration is the primary therapy. Use of azithromycin or erythromycin can shorten both the duration of symptoms and bacterial shedding.
Salmonella
Nontyphoidal salmonella (NTS) are responsible for a variety of infections including asymptomatic carriage, gastroenteritis, bacteremia, and serious focal infections. Gastroenteritis is the most common illness and is manifested as diarrhea, abdominal pain, and fever. If bacteremia occurs, up to 10% of patients will develop focal infections. Invasive disease occurs most frequently in infants, persons with hemoglobinopathies, immunosuppressive disorders, and malignancies. The genus Salmonella is divided into two species, S. enterica and S. bongori with S. enterica subspecies accounting for about half of culture-confirmed Salmonella isolates reported by public health laboratories.
Although infections are more common in the summer, infections can occur year-round. In 2018, the CDC investigated at least 15 food-related NTS outbreaks and 6 have been investigated so far in 2019. In industrialized countries, acquisition usually occurs from ingestion of poultry, eggs, and milk products. Infection also has been reported after animal contact and consumption of fresh produce, meats, and contaminated water. Ground beef is the source of the November 2019 outbreak of S. dublin. Diarrhea develops within 12-72 hours. Salmonella can be isolated from stool, blood, and urine. Treatment usually is not indicated for uncomplicated gastroenteritis. While benefit has not been proven, it is recommended for those at increased risk for developing invasive disease.
Shigella
Shigella is the classic cause of colonic or dysenteric diarrhea. Humans are the primary hosts but other primates can be infected. Transmission occurs through direct person-to-person spread, from ingestion of contaminated food and water, and contact with contaminated inanimate objects. Bacteria can survive up to 6 months in food and 30 days in water. As few as 10 organisms can initiate disease. Typically mucoid or bloody diarrhea with abdominal cramps and fever occurs 1-7 days following exposure. Isolation is from stool. Bacteremia is unusual. Therapy is recommended for severe disease.
Shiga toxin–producing Escherichia coli (STEC)
STEC causes hemorrhagic colitis, which can be complicated by hemolytic uremic syndrome. While E. coli O157:H7 is the serotype most often implicated, other serotypes can cause disease. STEC is shed in feces of cattle and other animals. Infection most often is associated with ingestion of undercooked ground beef, but outbreaks also have confirmed that contaminated leafy vegetables, drinking water, peanut butter, and unpasteurized milk have been the source. Symptoms usually develop 3 to 4 days after exposure. Stools initially may be nonbloody. Abdominal pain and bloody diarrhea occur over the next 2-3 days. Fever often is absent or low grade. Stools should be sent for culture and Shiga toxin for diagnosis. Antimicrobial treatment generally is not warranted if STEC is suspected or diagnosed.
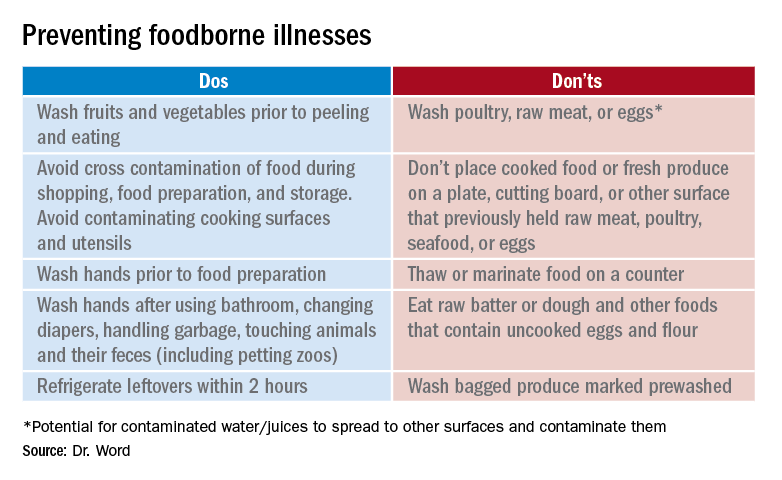
Prevention
It seems so simple. Here are the basic guidelines:
- Clean. Wash hands and surfaces frequently.
- Separate. Separate raw meats and eggs from other foods.
- Cook. Cook all meats to the right temperature.
- Chill. Refrigerate food properly.
Finally, two comments about food poisoning:

Abrupt onset of nausea, vomiting and abdominal cramping due to staphylococcal food poisoning begins 30 minutes to 6 hours after ingestion of food contaminated by enterotoxigenic strains of Staphylococcus aureus which is usually introduced by a food preparer with a purulent lesion. Food left at room temperature allows bacteria to multiply and produce a heat stable toxin. Individuals with purulent lesions of the hands, face, eyes, or nose should not be involved with food preparation.
Clostridium perfringens is the second most common bacterial cause of food poisoning. Symptoms (watery diarrhea and cramping) begin 6-24 hours after ingestion of C. perfringens spores not killed during cooking, which now have multiplied in food left at room temperature that was inadequately reheated. Illness is caused by the production of enterotoxin in the intestine. Outbreaks occur most often in November and December.
This article was updated on 11/12/19.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Information sources
1. foodsafety.gov
2. cdc.gov/foodsafety
3. The United States Department of Agriculture Meat and Poultry Hotline: 888-674-6854
4. Appendix VII: Clinical syndromes associated with foodborne diseases, Red Book online, 31st ed. (Washington DC: Red Book online, 2018, pp. 1086-92).
5. Foodkeeper App available at the App store. Provides appropriate food storage information; food recalls also are available.
According to the Centers for Disease Control and Prevention, a foodborne disease occurs in one in six persons (48 million), resulting in 128,000 hospitalizations and 3,000 deaths annually in the United States. The Foodborne Active Surveillance Network (FoodNet) of the CDC’s Emerging Infections Program monitors cases of eight laboratory diagnosed infections from 10 U.S. sites (covering 15% of the U.S. population). Monitored organisms include Campylobacter, Cyclospora, Listeria, Salmonella, Shiga toxin–producing Escherichia coli (STEC), Shigella, Vibrio, and Yersinia. In 2018, FoodNet identified 25,606 cases of infection, 5,893 hospitalizations, and 120 deaths. The incidence of infection (cases/100,000) was highest for Campylobacter (20), Salmonella (18), STEC (6), Shigella (5), Vibrio (1), Yersinia (0.9), Cyclospora (0.7), and Listeria (0.3). How might these pathogens affect your patients? First, a quick review about the four more common infections. Treatment is beyond the scope of our discussion and you are referred to the 2018-2021 Red Book for assistance. The goal of this column is to prevent your patients from becoming a statistic this holiday season.
Campylobacter
It has been the most common infection reported in FoodNet since 2013. Clinically, patients present with fever, abdominal pain, and nonbloody diarrhea. However, bloody diarrhea maybe the only symptom in neonates and young infants. Abdominal pain can mimic acute appendicitis or intussusception. Bacteremia is rare but has been reported in the elderly and in some patients with underlying conditions. During convalescence, immunoreactive complications including Guillain-Barré syndrome, reactive arthritis, and erythema nodosum may occur. In patients with diarrhea, Campylobacter jejuni and C. coli are the most frequently isolated species.
Campylobacter is present in the intestinal tract of both domestic and wild birds and animals. Transmission is via consumption of contaminated food or water. Undercooked poultry, untreated water, and unpasteurized milk are the three main vehicles of transmission. Campylobacter can be isolated in stool and blood, however isolation from stool requires special media. Rehydration is the primary therapy. Use of azithromycin or erythromycin can shorten both the duration of symptoms and bacterial shedding.
Salmonella
Nontyphoidal salmonella (NTS) are responsible for a variety of infections including asymptomatic carriage, gastroenteritis, bacteremia, and serious focal infections. Gastroenteritis is the most common illness and is manifested as diarrhea, abdominal pain, and fever. If bacteremia occurs, up to 10% of patients will develop focal infections. Invasive disease occurs most frequently in infants, persons with hemoglobinopathies, immunosuppressive disorders, and malignancies. The genus Salmonella is divided into two species, S. enterica and S. bongori with S. enterica subspecies accounting for about half of culture-confirmed Salmonella isolates reported by public health laboratories.
Although infections are more common in the summer, infections can occur year-round. In 2018, the CDC investigated at least 15 food-related NTS outbreaks and 6 have been investigated so far in 2019. In industrialized countries, acquisition usually occurs from ingestion of poultry, eggs, and milk products. Infection also has been reported after animal contact and consumption of fresh produce, meats, and contaminated water. Ground beef is the source of the November 2019 outbreak of S. dublin. Diarrhea develops within 12-72 hours. Salmonella can be isolated from stool, blood, and urine. Treatment usually is not indicated for uncomplicated gastroenteritis. While benefit has not been proven, it is recommended for those at increased risk for developing invasive disease.
Shigella
Shigella is the classic cause of colonic or dysenteric diarrhea. Humans are the primary hosts but other primates can be infected. Transmission occurs through direct person-to-person spread, from ingestion of contaminated food and water, and contact with contaminated inanimate objects. Bacteria can survive up to 6 months in food and 30 days in water. As few as 10 organisms can initiate disease. Typically mucoid or bloody diarrhea with abdominal cramps and fever occurs 1-7 days following exposure. Isolation is from stool. Bacteremia is unusual. Therapy is recommended for severe disease.
Shiga toxin–producing Escherichia coli (STEC)
STEC causes hemorrhagic colitis, which can be complicated by hemolytic uremic syndrome. While E. coli O157:H7 is the serotype most often implicated, other serotypes can cause disease. STEC is shed in feces of cattle and other animals. Infection most often is associated with ingestion of undercooked ground beef, but outbreaks also have confirmed that contaminated leafy vegetables, drinking water, peanut butter, and unpasteurized milk have been the source. Symptoms usually develop 3 to 4 days after exposure. Stools initially may be nonbloody. Abdominal pain and bloody diarrhea occur over the next 2-3 days. Fever often is absent or low grade. Stools should be sent for culture and Shiga toxin for diagnosis. Antimicrobial treatment generally is not warranted if STEC is suspected or diagnosed.
Prevention
It seems so simple. Here are the basic guidelines:
- Clean. Wash hands and surfaces frequently.
- Separate. Separate raw meats and eggs from other foods.
- Cook. Cook all meats to the right temperature.
- Chill. Refrigerate food properly.
Finally, two comments about food poisoning:
Abrupt onset of nausea, vomiting and abdominal cramping due to staphylococcal food poisoning begins 30 minutes to 6 hours after ingestion of food contaminated by enterotoxigenic strains of Staphylococcus aureus which is usually introduced by a food preparer with a purulent lesion. Food left at room temperature allows bacteria to multiply and produce a heat stable toxin. Individuals with purulent lesions of the hands, face, eyes, or nose should not be involved with food preparation.
Clostridium perfringens is the second most common bacterial cause of food poisoning. Symptoms (watery diarrhea and cramping) begin 6-24 hours after ingestion of C. perfringens spores not killed during cooking, which now have multiplied in food left at room temperature that was inadequately reheated. Illness is caused by the production of enterotoxin in the intestine. Outbreaks occur most often in November and December.
This article was updated on 11/12/19.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Information sources
1. foodsafety.gov
2. cdc.gov/foodsafety
3. The United States Department of Agriculture Meat and Poultry Hotline: 888-674-6854
4. Appendix VII: Clinical syndromes associated with foodborne diseases, Red Book online, 31st ed. (Washington DC: Red Book online, 2018, pp. 1086-92).
5. Foodkeeper App available at the App store. Provides appropriate food storage information; food recalls also are available.
According to the Centers for Disease Control and Prevention, a foodborne disease occurs in one in six persons (48 million), resulting in 128,000 hospitalizations and 3,000 deaths annually in the United States. The Foodborne Active Surveillance Network (FoodNet) of the CDC’s Emerging Infections Program monitors cases of eight laboratory diagnosed infections from 10 U.S. sites (covering 15% of the U.S. population). Monitored organisms include Campylobacter, Cyclospora, Listeria, Salmonella, Shiga toxin–producing Escherichia coli (STEC), Shigella, Vibrio, and Yersinia. In 2018, FoodNet identified 25,606 cases of infection, 5,893 hospitalizations, and 120 deaths. The incidence of infection (cases/100,000) was highest for Campylobacter (20), Salmonella (18), STEC (6), Shigella (5), Vibrio (1), Yersinia (0.9), Cyclospora (0.7), and Listeria (0.3). How might these pathogens affect your patients? First, a quick review about the four more common infections. Treatment is beyond the scope of our discussion and you are referred to the 2018-2021 Red Book for assistance. The goal of this column is to prevent your patients from becoming a statistic this holiday season.
Campylobacter
It has been the most common infection reported in FoodNet since 2013. Clinically, patients present with fever, abdominal pain, and nonbloody diarrhea. However, bloody diarrhea maybe the only symptom in neonates and young infants. Abdominal pain can mimic acute appendicitis or intussusception. Bacteremia is rare but has been reported in the elderly and in some patients with underlying conditions. During convalescence, immunoreactive complications including Guillain-Barré syndrome, reactive arthritis, and erythema nodosum may occur. In patients with diarrhea, Campylobacter jejuni and C. coli are the most frequently isolated species.
Campylobacter is present in the intestinal tract of both domestic and wild birds and animals. Transmission is via consumption of contaminated food or water. Undercooked poultry, untreated water, and unpasteurized milk are the three main vehicles of transmission. Campylobacter can be isolated in stool and blood, however isolation from stool requires special media. Rehydration is the primary therapy. Use of azithromycin or erythromycin can shorten both the duration of symptoms and bacterial shedding.
Salmonella
Nontyphoidal salmonella (NTS) are responsible for a variety of infections including asymptomatic carriage, gastroenteritis, bacteremia, and serious focal infections. Gastroenteritis is the most common illness and is manifested as diarrhea, abdominal pain, and fever. If bacteremia occurs, up to 10% of patients will develop focal infections. Invasive disease occurs most frequently in infants, persons with hemoglobinopathies, immunosuppressive disorders, and malignancies. The genus Salmonella is divided into two species, S. enterica and S. bongori with S. enterica subspecies accounting for about half of culture-confirmed Salmonella isolates reported by public health laboratories.
Although infections are more common in the summer, infections can occur year-round. In 2018, the CDC investigated at least 15 food-related NTS outbreaks and 6 have been investigated so far in 2019. In industrialized countries, acquisition usually occurs from ingestion of poultry, eggs, and milk products. Infection also has been reported after animal contact and consumption of fresh produce, meats, and contaminated water. Ground beef is the source of the November 2019 outbreak of S. dublin. Diarrhea develops within 12-72 hours. Salmonella can be isolated from stool, blood, and urine. Treatment usually is not indicated for uncomplicated gastroenteritis. While benefit has not been proven, it is recommended for those at increased risk for developing invasive disease.
Shigella
Shigella is the classic cause of colonic or dysenteric diarrhea. Humans are the primary hosts but other primates can be infected. Transmission occurs through direct person-to-person spread, from ingestion of contaminated food and water, and contact with contaminated inanimate objects. Bacteria can survive up to 6 months in food and 30 days in water. As few as 10 organisms can initiate disease. Typically mucoid or bloody diarrhea with abdominal cramps and fever occurs 1-7 days following exposure. Isolation is from stool. Bacteremia is unusual. Therapy is recommended for severe disease.
Shiga toxin–producing Escherichia coli (STEC)
STEC causes hemorrhagic colitis, which can be complicated by hemolytic uremic syndrome. While E. coli O157:H7 is the serotype most often implicated, other serotypes can cause disease. STEC is shed in feces of cattle and other animals. Infection most often is associated with ingestion of undercooked ground beef, but outbreaks also have confirmed that contaminated leafy vegetables, drinking water, peanut butter, and unpasteurized milk have been the source. Symptoms usually develop 3 to 4 days after exposure. Stools initially may be nonbloody. Abdominal pain and bloody diarrhea occur over the next 2-3 days. Fever often is absent or low grade. Stools should be sent for culture and Shiga toxin for diagnosis. Antimicrobial treatment generally is not warranted if STEC is suspected or diagnosed.
Prevention
It seems so simple. Here are the basic guidelines:
- Clean. Wash hands and surfaces frequently.
- Separate. Separate raw meats and eggs from other foods.
- Cook. Cook all meats to the right temperature.
- Chill. Refrigerate food properly.
Finally, two comments about food poisoning:
Abrupt onset of nausea, vomiting and abdominal cramping due to staphylococcal food poisoning begins 30 minutes to 6 hours after ingestion of food contaminated by enterotoxigenic strains of Staphylococcus aureus which is usually introduced by a food preparer with a purulent lesion. Food left at room temperature allows bacteria to multiply and produce a heat stable toxin. Individuals with purulent lesions of the hands, face, eyes, or nose should not be involved with food preparation.
Clostridium perfringens is the second most common bacterial cause of food poisoning. Symptoms (watery diarrhea and cramping) begin 6-24 hours after ingestion of C. perfringens spores not killed during cooking, which now have multiplied in food left at room temperature that was inadequately reheated. Illness is caused by the production of enterotoxin in the intestine. Outbreaks occur most often in November and December.
This article was updated on 11/12/19.
Dr. Word is a pediatric infectious disease specialist and director of the Houston Travel Medicine Clinic. She said she had no relevant financial disclosures. Email her at pdnews@mdedge.com.
Information sources
1. foodsafety.gov
2. cdc.gov/foodsafety
3. The United States Department of Agriculture Meat and Poultry Hotline: 888-674-6854
4. Appendix VII: Clinical syndromes associated with foodborne diseases, Red Book online, 31st ed. (Washington DC: Red Book online, 2018, pp. 1086-92).
5. Foodkeeper App available at the App store. Provides appropriate food storage information; food recalls also are available.
‘You had me at hello’: ESMO studies confirm survival benefits in NSCLC and breast cancer
In this edition of “How I will treat my next patient,” I highlight two studies that previously reported significant progression-free survival (PFS) improvements and more recently, at the European Society for Medical Oncology Congress, overall survival (OS) benefit. I reflect on the significance of these new reports in the wake of previously reported data and guidelines from the National Comprehensive Cancer Network (NCCN).

Osimertinib in advanced NSCLC
In the double-blind, phase 3 FLAURA trial, 556 patients with EGFR-mutated (EGFRm), advanced non–small cell lung cancer (NSCLC) received osimertinib or a standard tyrosine kinase inhibitor (TKI) as initial treatment. PFS, the primary endpoint, was clinically and statistically better for osimertinib (18.9 months vs. 10.2 months; hazard ratio 0.46; P less than .001), overall and in all major subgroups. There were fewer grade 3-4 adverse events and fewer permanent treatment discontinuations with osimertinib.
At the time of initial publication, OS data were immature, but because of the substantial survival improvements previously noted, osimertinib was approved by the Food and Drug Administration for first-line treatment of EGFRm stage IV NSCLC patients in April 2018 (N Engl J Med. 2018; 378:113-25).
More recently, at ESMO 2019, Suresh Ramalingam, MD, of the department of hematology and medical oncology at Emory University, Atlanta, and colleagues reported the OS results. Crossover to osimertinib was allowed for patients on the standard TKI arm when they had progressive disease and a T790M mutation. Osimertinib produced a median OS of 38.6 months, compared with 31.8 months for standard TKI (HR, 0.799; P = .0462), a 24-month OS rate of 74% vs. 59% (with no overlap in the 95% confidence intervals), and a 36-month OS rate of 54% vs. 44%. These benefits were interpreted to be statistically significant and clinically meaningful.
The 31.8-month median OS for standard TKI was competitive with the highest reported OS for standard therapy, perhaps because crossover to osimertinib was permitted.
What this means in clinical practice
The report by Dr. Ramalingam and colleagues – and the next abstract I will review – remind me of the famous “You had me at Hello” line from “Jerry Maguire.”
For patient education – and perhaps for some national regulatory agencies – it is good that we now have definition of what the average OS is with osimertinib, compared with standard TKI followed by osimertinib. However, very few oncologists in the United States likely use the latter strategy anymore. It was clear when the impressive PFS and toxicity information appeared in 2018 in the New England Journal of Medicine that osimertinib is the best tolerated, most durably effective front-line treatment for EGFRm mNSCLC, regardless of disease extent, sex, nationality, type of EGFRm (L858R amino acid substitution in exon 21 or exon 19 deletion), or presence/absence of central nervous system metastases.
In NCCN guidelines, osimertinib was listed as the preferred TKI, prior to the OS report at ESMO 2019. The challenges going forward will be to identify high-risk patient subsets who might benefit from drug combinations or novel new agents.
MONARCH 2: Abemaciclib plus fulvestrant
In the MONARCH 2, randomized, placebo-controlled, phase 3 trial, abemaciclib plus fulvestrant (abema-F) significantly improved PFS, in comparison with placebo plus fulvestrant (placebo-F; 16.9 months vs. 9.3 months; HR, 0.563) in 669 premenopausal (with concurrent ovarian function suppression) and postmenopausal women with metastatic breast cancer (mBC) who had disease progression on one to two lines of prior hormonal therapy (J Clin Oncol. 2017;35[25]:2875-84).
At ESMO 2019, George W. Sledge Jr., MD, of Stanford (Calif.) Medical Center, and colleagues reported the OS results, a secondary endpoint for the trial (JAMA Oncol. 2019 Sep 29. doi. 10.1001/jamaoncol.2019.4782). At the prespecified interim analysis point, median OS for abema-F was 46.7 months vs. 37.3 months for placebo-F (HR, 0.757; 95% CI 0.505-0.945; P = .0137). Patients with greatest benefit from abema-F were exactly the patients who needed the most help – those with visceral metastases (HR 0.675) and with primary resistance to prior hormonal therapy (HR, 0.686).
At 3 years, at least three times as many patients remained progression free with abema-F, compared with placebo-F, and the abema-F patients experienced prolongation in time to eventual chemotherapy (50.2 months vs. 22.1 months; HR, 0.625).
What this means in clinical practice
Many times I find myself sitting at the annual meeting of the American Society of Clinical Oncology and thinking, “Only a medical oncologist like me would find this result exciting.” Prior to ESMO 2019, MONARCH 2 (and a similar study presented at ESMO 2019, MONALEESA-3, which employed an alternative CDK 4/6 inhibitor, ribociclib, with similar OS results) added to the body of literature that caused NCCN guidelines to list all of the approved CDK 4/6 inhibitors plus endocrine therapy for first- or second-line use in patients with hormone-receptor positive, HER2/neu-negative mBC. NCCN guidelines have the caveat that, among patients with disease progression on CDK 4/6 inhibitors in the first-line setting, there are no data to support continuing the CDK 4/6 inhibitor or switching to an alternative CDK 4/6 inhibitor thereafter.
For that shrinking group of patients and doctors who choose to avoid CDK 4/6 inhibitors for first-line treatment, as we describe risks and benefits of using a CDK 4/6 inhibitor for second- or third-line therapy, we have high-quality OS information from ESMO 2019 to answer the “Is it worth it?” question.
Are the results of MONARCH 2 and MONALEESA-3 practice changing? No. We were already convinced. Should we be excited that we have this new information for discussions with our patients? Absolutely.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I highlight two studies that previously reported significant progression-free survival (PFS) improvements and more recently, at the European Society for Medical Oncology Congress, overall survival (OS) benefit. I reflect on the significance of these new reports in the wake of previously reported data and guidelines from the National Comprehensive Cancer Network (NCCN).
Osimertinib in advanced NSCLC
In the double-blind, phase 3 FLAURA trial, 556 patients with EGFR-mutated (EGFRm), advanced non–small cell lung cancer (NSCLC) received osimertinib or a standard tyrosine kinase inhibitor (TKI) as initial treatment. PFS, the primary endpoint, was clinically and statistically better for osimertinib (18.9 months vs. 10.2 months; hazard ratio 0.46; P less than .001), overall and in all major subgroups. There were fewer grade 3-4 adverse events and fewer permanent treatment discontinuations with osimertinib.
At the time of initial publication, OS data were immature, but because of the substantial survival improvements previously noted, osimertinib was approved by the Food and Drug Administration for first-line treatment of EGFRm stage IV NSCLC patients in April 2018 (N Engl J Med. 2018; 378:113-25).
More recently, at ESMO 2019, Suresh Ramalingam, MD, of the department of hematology and medical oncology at Emory University, Atlanta, and colleagues reported the OS results. Crossover to osimertinib was allowed for patients on the standard TKI arm when they had progressive disease and a T790M mutation. Osimertinib produced a median OS of 38.6 months, compared with 31.8 months for standard TKI (HR, 0.799; P = .0462), a 24-month OS rate of 74% vs. 59% (with no overlap in the 95% confidence intervals), and a 36-month OS rate of 54% vs. 44%. These benefits were interpreted to be statistically significant and clinically meaningful.
The 31.8-month median OS for standard TKI was competitive with the highest reported OS for standard therapy, perhaps because crossover to osimertinib was permitted.
What this means in clinical practice
The report by Dr. Ramalingam and colleagues – and the next abstract I will review – remind me of the famous “You had me at Hello” line from “Jerry Maguire.”
For patient education – and perhaps for some national regulatory agencies – it is good that we now have definition of what the average OS is with osimertinib, compared with standard TKI followed by osimertinib. However, very few oncologists in the United States likely use the latter strategy anymore. It was clear when the impressive PFS and toxicity information appeared in 2018 in the New England Journal of Medicine that osimertinib is the best tolerated, most durably effective front-line treatment for EGFRm mNSCLC, regardless of disease extent, sex, nationality, type of EGFRm (L858R amino acid substitution in exon 21 or exon 19 deletion), or presence/absence of central nervous system metastases.
In NCCN guidelines, osimertinib was listed as the preferred TKI, prior to the OS report at ESMO 2019. The challenges going forward will be to identify high-risk patient subsets who might benefit from drug combinations or novel new agents.
MONARCH 2: Abemaciclib plus fulvestrant
In the MONARCH 2, randomized, placebo-controlled, phase 3 trial, abemaciclib plus fulvestrant (abema-F) significantly improved PFS, in comparison with placebo plus fulvestrant (placebo-F; 16.9 months vs. 9.3 months; HR, 0.563) in 669 premenopausal (with concurrent ovarian function suppression) and postmenopausal women with metastatic breast cancer (mBC) who had disease progression on one to two lines of prior hormonal therapy (J Clin Oncol. 2017;35[25]:2875-84).
At ESMO 2019, George W. Sledge Jr., MD, of Stanford (Calif.) Medical Center, and colleagues reported the OS results, a secondary endpoint for the trial (JAMA Oncol. 2019 Sep 29. doi. 10.1001/jamaoncol.2019.4782). At the prespecified interim analysis point, median OS for abema-F was 46.7 months vs. 37.3 months for placebo-F (HR, 0.757; 95% CI 0.505-0.945; P = .0137). Patients with greatest benefit from abema-F were exactly the patients who needed the most help – those with visceral metastases (HR 0.675) and with primary resistance to prior hormonal therapy (HR, 0.686).
At 3 years, at least three times as many patients remained progression free with abema-F, compared with placebo-F, and the abema-F patients experienced prolongation in time to eventual chemotherapy (50.2 months vs. 22.1 months; HR, 0.625).
What this means in clinical practice
Many times I find myself sitting at the annual meeting of the American Society of Clinical Oncology and thinking, “Only a medical oncologist like me would find this result exciting.” Prior to ESMO 2019, MONARCH 2 (and a similar study presented at ESMO 2019, MONALEESA-3, which employed an alternative CDK 4/6 inhibitor, ribociclib, with similar OS results) added to the body of literature that caused NCCN guidelines to list all of the approved CDK 4/6 inhibitors plus endocrine therapy for first- or second-line use in patients with hormone-receptor positive, HER2/neu-negative mBC. NCCN guidelines have the caveat that, among patients with disease progression on CDK 4/6 inhibitors in the first-line setting, there are no data to support continuing the CDK 4/6 inhibitor or switching to an alternative CDK 4/6 inhibitor thereafter.
For that shrinking group of patients and doctors who choose to avoid CDK 4/6 inhibitors for first-line treatment, as we describe risks and benefits of using a CDK 4/6 inhibitor for second- or third-line therapy, we have high-quality OS information from ESMO 2019 to answer the “Is it worth it?” question.
Are the results of MONARCH 2 and MONALEESA-3 practice changing? No. We were already convinced. Should we be excited that we have this new information for discussions with our patients? Absolutely.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
In this edition of “How I will treat my next patient,” I highlight two studies that previously reported significant progression-free survival (PFS) improvements and more recently, at the European Society for Medical Oncology Congress, overall survival (OS) benefit. I reflect on the significance of these new reports in the wake of previously reported data and guidelines from the National Comprehensive Cancer Network (NCCN).
Osimertinib in advanced NSCLC
In the double-blind, phase 3 FLAURA trial, 556 patients with EGFR-mutated (EGFRm), advanced non–small cell lung cancer (NSCLC) received osimertinib or a standard tyrosine kinase inhibitor (TKI) as initial treatment. PFS, the primary endpoint, was clinically and statistically better for osimertinib (18.9 months vs. 10.2 months; hazard ratio 0.46; P less than .001), overall and in all major subgroups. There were fewer grade 3-4 adverse events and fewer permanent treatment discontinuations with osimertinib.
At the time of initial publication, OS data were immature, but because of the substantial survival improvements previously noted, osimertinib was approved by the Food and Drug Administration for first-line treatment of EGFRm stage IV NSCLC patients in April 2018 (N Engl J Med. 2018; 378:113-25).
More recently, at ESMO 2019, Suresh Ramalingam, MD, of the department of hematology and medical oncology at Emory University, Atlanta, and colleagues reported the OS results. Crossover to osimertinib was allowed for patients on the standard TKI arm when they had progressive disease and a T790M mutation. Osimertinib produced a median OS of 38.6 months, compared with 31.8 months for standard TKI (HR, 0.799; P = .0462), a 24-month OS rate of 74% vs. 59% (with no overlap in the 95% confidence intervals), and a 36-month OS rate of 54% vs. 44%. These benefits were interpreted to be statistically significant and clinically meaningful.
The 31.8-month median OS for standard TKI was competitive with the highest reported OS for standard therapy, perhaps because crossover to osimertinib was permitted.
What this means in clinical practice
The report by Dr. Ramalingam and colleagues – and the next abstract I will review – remind me of the famous “You had me at Hello” line from “Jerry Maguire.”
For patient education – and perhaps for some national regulatory agencies – it is good that we now have definition of what the average OS is with osimertinib, compared with standard TKI followed by osimertinib. However, very few oncologists in the United States likely use the latter strategy anymore. It was clear when the impressive PFS and toxicity information appeared in 2018 in the New England Journal of Medicine that osimertinib is the best tolerated, most durably effective front-line treatment for EGFRm mNSCLC, regardless of disease extent, sex, nationality, type of EGFRm (L858R amino acid substitution in exon 21 or exon 19 deletion), or presence/absence of central nervous system metastases.
In NCCN guidelines, osimertinib was listed as the preferred TKI, prior to the OS report at ESMO 2019. The challenges going forward will be to identify high-risk patient subsets who might benefit from drug combinations or novel new agents.
MONARCH 2: Abemaciclib plus fulvestrant
In the MONARCH 2, randomized, placebo-controlled, phase 3 trial, abemaciclib plus fulvestrant (abema-F) significantly improved PFS, in comparison with placebo plus fulvestrant (placebo-F; 16.9 months vs. 9.3 months; HR, 0.563) in 669 premenopausal (with concurrent ovarian function suppression) and postmenopausal women with metastatic breast cancer (mBC) who had disease progression on one to two lines of prior hormonal therapy (J Clin Oncol. 2017;35[25]:2875-84).
At ESMO 2019, George W. Sledge Jr., MD, of Stanford (Calif.) Medical Center, and colleagues reported the OS results, a secondary endpoint for the trial (JAMA Oncol. 2019 Sep 29. doi. 10.1001/jamaoncol.2019.4782). At the prespecified interim analysis point, median OS for abema-F was 46.7 months vs. 37.3 months for placebo-F (HR, 0.757; 95% CI 0.505-0.945; P = .0137). Patients with greatest benefit from abema-F were exactly the patients who needed the most help – those with visceral metastases (HR 0.675) and with primary resistance to prior hormonal therapy (HR, 0.686).
At 3 years, at least three times as many patients remained progression free with abema-F, compared with placebo-F, and the abema-F patients experienced prolongation in time to eventual chemotherapy (50.2 months vs. 22.1 months; HR, 0.625).
What this means in clinical practice
Many times I find myself sitting at the annual meeting of the American Society of Clinical Oncology and thinking, “Only a medical oncologist like me would find this result exciting.” Prior to ESMO 2019, MONARCH 2 (and a similar study presented at ESMO 2019, MONALEESA-3, which employed an alternative CDK 4/6 inhibitor, ribociclib, with similar OS results) added to the body of literature that caused NCCN guidelines to list all of the approved CDK 4/6 inhibitors plus endocrine therapy for first- or second-line use in patients with hormone-receptor positive, HER2/neu-negative mBC. NCCN guidelines have the caveat that, among patients with disease progression on CDK 4/6 inhibitors in the first-line setting, there are no data to support continuing the CDK 4/6 inhibitor or switching to an alternative CDK 4/6 inhibitor thereafter.
For that shrinking group of patients and doctors who choose to avoid CDK 4/6 inhibitors for first-line treatment, as we describe risks and benefits of using a CDK 4/6 inhibitor for second- or third-line therapy, we have high-quality OS information from ESMO 2019 to answer the “Is it worth it?” question.
Are the results of MONARCH 2 and MONALEESA-3 practice changing? No. We were already convinced. Should we be excited that we have this new information for discussions with our patients? Absolutely.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers and in expanding access to clinical trials to medically underserved populations.
How I became a better doctor
I became a better doctor on the day I became a cardiac patient. On that day, I experienced the helpless, vulnerable, and needy feelings of a patient’s dependency and blind trust of a physician whom I did not know. I suddenly realized how it feels to be a patient.

My entire life, I had always been an athlete in excellent shape. My 7-day-a-week daily schedule included seeing patients, being an expert psychiatric witness for disability cases, playing 2 hours of tennis, walking/running for 1 hour, and ending the night with 1 hour on a stationary bike.
I get to see my children all the time. I am so fortunate to get to travel with them and play national father-son and father-daughter tennis tournaments. We have been ranked No. 1 in the country many times. I have won 16 gold balls in these tournaments, each symbolic of a U.S. championship.
As a busy board-certified psychiatrist, I had been featured in an article, “Well being: Tennis is doctor’s favorite medicine,” by Art Carey, in the Philadelphia Inquirer, posted May 2, 2011. The author discussed my diet and exercise regime, and how I used exercise to stay healthy and to deal with the stress of being a physician.
‘Take me to the hospital’
At the end of 2018, I had a complete blood count performed, and the results indicated that I had a lipid panel of a healthy 30-year-old; however, my delusional bubble burst in March 2019. I was the No. 1 seed in a National Father-Daughter Tennis Tournament in Chicago. We were in the semifinal match, we had won the first set, and we were up 3-0. I fell, hit my head on the net post, and was feeling nauseated. I checked for bleeding and continued playing, though I was not feeling well. Five minutes later, I experienced symptoms of very extreme gastrointestinal pain and nausea. I ran off the tennis court wanting to vomit and get rid of the symptom so I could go back and finish the match. I wanted to play in the finals the following day and try to win the tournament.
The kind, competent, compassionate, and warm tournament director said I looked gray – and he promptly called 911. The paramedics came and said they thought I may be having a heart attack. I was in denial since I had no chest pain and I thought I was super healthy; therefore, I could not be experiencing an acute myocardial infarction. I finally agreed to let technicians perform an EKG, and they told me that I had ST elevation. Reality finally set in and I realized I was having a heart attack. “Take me to the hospital,” I said.
At the Chicago hospital where I was taken, I told doctors and staff I was a physician. To my surprise, they did not care. I was not going to get any prioritized treatment. Despite all of my devotion to medicine, I was not even getting their top physician to treat me. I was being evaluated by a resident. I felt even more deflated.
They performed a cardiac catheterization and put in one stent in one vessel in the right cardiac vessel. I had many questions to ask, but everyone seemed very impatient and abrupt with me, acting like this was just a very routine procedure. No one ever adequately answered my questions. I was very disillusioned, and I felt very insignificant, scared, and invisible.
I was discharged a few days later and was told my heart problem was fixed. I was instructed to follow up with a cardiologist in Philadelphia when I got home.
The first night home, I experienced chest pain. I was alarmed and thought my stent may have collapsed, so I went to the emergency room of the Philadelphia area hospital I knew had the best cardiac staff. After another blood test, indicating raised troponin levels, I was informed they needed to perform another cardiac catheterization. I learned I had two more coronary artery blockages, each 95%-99%, in the left ventricle.
I was shocked. How could the doctor in Chicago have made such a significant mistake? What happened? I would never know.
The interventional cardiologist in Philadelphia was able to repair one coronary artery, but the other blockage in the LED vessel (yes, the widow maker) had calcified too much for a stent. I would need cardiac bypass surgery. This was very unbelievable to me, and furthermore, I would have to wait 2 long weeks for the anticoagulant effect of the Brilinta to wear off before I could undergo bypass surgery.
While I anxiously waited for the big day, I was calling either my cardiologist, surgeon, or his nurse practitioner almost daily with questions and concerns; after all, this was a life-threatening and momentous event. Thankfully, I was met with great patience, understanding, and promptness of detailed answers and explanations by all involved with my cardiac care. The reactions of the staff made me mindful of the importance of really hearing my patients’ concerns and addressing their issues in a prompt, nonjudgmental, patient, and genuine manner. I am grateful that my robotic cardiac bypass surgery on March 26, 2019, went very well, and I am now back to work, playing tennis, jogging slowly, and riding my stationery bike.
Changed perspective on practice
I had always thought of myself as a warm, caring, and empathic psychiatrist, but my experience as a cardiac patient made me realize that there is always room for improvement in treating my patients.
Remember, every doctor will become a patient one day, and the reality of illness, injury, and mortality may really hit you hard, as it did me. You may not receive any prioritized treatment and you will know what it feels like to be helpless, vulnerable, and at the mercy of a physician while you regress in the service of the ego and become a patient.
You can be a better doctor now if you are mindful that whatever the physical, emotional, or mental issue facing your patients, the problem may be catastrophic to them. They need your undivided attention. Any problem is a significant event to your presenting patient. Really listen to his or her concerns or questions, and address every one with patience, understanding, and accurate information. If you follow these lessons, which I learned the hard way, you can become a better doctor.
I followed my doctor’s instructions and I started hitting tennis balls gradually. I worked myself back into shape and with my daughter Julia Cohen, and we won the USTA National Father Daughter Clay Court Championship in Florida 6 months after I had the heart attack during a national tennis tournament. This is the comeback of the year in tennis!
Dr. Cohen has had a private practice in psychiatry for more than 35 years. He is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University in Philadelphia. Dr. Cohen has been a nationally ranked tennis player from age 12 to the present, served as captain of the University of Pennsylvania tennis team, and ranked No. 1 in tennis in the middle states section and in the country in various categories and times. He was inducted into the Philadelphia Jewish Sports Hall of Fame in 2012.
I became a better doctor on the day I became a cardiac patient. On that day, I experienced the helpless, vulnerable, and needy feelings of a patient’s dependency and blind trust of a physician whom I did not know. I suddenly realized how it feels to be a patient.
My entire life, I had always been an athlete in excellent shape. My 7-day-a-week daily schedule included seeing patients, being an expert psychiatric witness for disability cases, playing 2 hours of tennis, walking/running for 1 hour, and ending the night with 1 hour on a stationary bike.
I get to see my children all the time. I am so fortunate to get to travel with them and play national father-son and father-daughter tennis tournaments. We have been ranked No. 1 in the country many times. I have won 16 gold balls in these tournaments, each symbolic of a U.S. championship.
As a busy board-certified psychiatrist, I had been featured in an article, “Well being: Tennis is doctor’s favorite medicine,” by Art Carey, in the Philadelphia Inquirer, posted May 2, 2011. The author discussed my diet and exercise regime, and how I used exercise to stay healthy and to deal with the stress of being a physician.
‘Take me to the hospital’
At the end of 2018, I had a complete blood count performed, and the results indicated that I had a lipid panel of a healthy 30-year-old; however, my delusional bubble burst in March 2019. I was the No. 1 seed in a National Father-Daughter Tennis Tournament in Chicago. We were in the semifinal match, we had won the first set, and we were up 3-0. I fell, hit my head on the net post, and was feeling nauseated. I checked for bleeding and continued playing, though I was not feeling well. Five minutes later, I experienced symptoms of very extreme gastrointestinal pain and nausea. I ran off the tennis court wanting to vomit and get rid of the symptom so I could go back and finish the match. I wanted to play in the finals the following day and try to win the tournament.
The kind, competent, compassionate, and warm tournament director said I looked gray – and he promptly called 911. The paramedics came and said they thought I may be having a heart attack. I was in denial since I had no chest pain and I thought I was super healthy; therefore, I could not be experiencing an acute myocardial infarction. I finally agreed to let technicians perform an EKG, and they told me that I had ST elevation. Reality finally set in and I realized I was having a heart attack. “Take me to the hospital,” I said.
At the Chicago hospital where I was taken, I told doctors and staff I was a physician. To my surprise, they did not care. I was not going to get any prioritized treatment. Despite all of my devotion to medicine, I was not even getting their top physician to treat me. I was being evaluated by a resident. I felt even more deflated.
They performed a cardiac catheterization and put in one stent in one vessel in the right cardiac vessel. I had many questions to ask, but everyone seemed very impatient and abrupt with me, acting like this was just a very routine procedure. No one ever adequately answered my questions. I was very disillusioned, and I felt very insignificant, scared, and invisible.
I was discharged a few days later and was told my heart problem was fixed. I was instructed to follow up with a cardiologist in Philadelphia when I got home.
The first night home, I experienced chest pain. I was alarmed and thought my stent may have collapsed, so I went to the emergency room of the Philadelphia area hospital I knew had the best cardiac staff. After another blood test, indicating raised troponin levels, I was informed they needed to perform another cardiac catheterization. I learned I had two more coronary artery blockages, each 95%-99%, in the left ventricle.
I was shocked. How could the doctor in Chicago have made such a significant mistake? What happened? I would never know.
The interventional cardiologist in Philadelphia was able to repair one coronary artery, but the other blockage in the LED vessel (yes, the widow maker) had calcified too much for a stent. I would need cardiac bypass surgery. This was very unbelievable to me, and furthermore, I would have to wait 2 long weeks for the anticoagulant effect of the Brilinta to wear off before I could undergo bypass surgery.
While I anxiously waited for the big day, I was calling either my cardiologist, surgeon, or his nurse practitioner almost daily with questions and concerns; after all, this was a life-threatening and momentous event. Thankfully, I was met with great patience, understanding, and promptness of detailed answers and explanations by all involved with my cardiac care. The reactions of the staff made me mindful of the importance of really hearing my patients’ concerns and addressing their issues in a prompt, nonjudgmental, patient, and genuine manner. I am grateful that my robotic cardiac bypass surgery on March 26, 2019, went very well, and I am now back to work, playing tennis, jogging slowly, and riding my stationery bike.
Changed perspective on practice
I had always thought of myself as a warm, caring, and empathic psychiatrist, but my experience as a cardiac patient made me realize that there is always room for improvement in treating my patients.
Remember, every doctor will become a patient one day, and the reality of illness, injury, and mortality may really hit you hard, as it did me. You may not receive any prioritized treatment and you will know what it feels like to be helpless, vulnerable, and at the mercy of a physician while you regress in the service of the ego and become a patient.
You can be a better doctor now if you are mindful that whatever the physical, emotional, or mental issue facing your patients, the problem may be catastrophic to them. They need your undivided attention. Any problem is a significant event to your presenting patient. Really listen to his or her concerns or questions, and address every one with patience, understanding, and accurate information. If you follow these lessons, which I learned the hard way, you can become a better doctor.
I followed my doctor’s instructions and I started hitting tennis balls gradually. I worked myself back into shape and with my daughter Julia Cohen, and we won the USTA National Father Daughter Clay Court Championship in Florida 6 months after I had the heart attack during a national tennis tournament. This is the comeback of the year in tennis!
Dr. Cohen has had a private practice in psychiatry for more than 35 years. He is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University in Philadelphia. Dr. Cohen has been a nationally ranked tennis player from age 12 to the present, served as captain of the University of Pennsylvania tennis team, and ranked No. 1 in tennis in the middle states section and in the country in various categories and times. He was inducted into the Philadelphia Jewish Sports Hall of Fame in 2012.
I became a better doctor on the day I became a cardiac patient. On that day, I experienced the helpless, vulnerable, and needy feelings of a patient’s dependency and blind trust of a physician whom I did not know. I suddenly realized how it feels to be a patient.
My entire life, I had always been an athlete in excellent shape. My 7-day-a-week daily schedule included seeing patients, being an expert psychiatric witness for disability cases, playing 2 hours of tennis, walking/running for 1 hour, and ending the night with 1 hour on a stationary bike.
I get to see my children all the time. I am so fortunate to get to travel with them and play national father-son and father-daughter tennis tournaments. We have been ranked No. 1 in the country many times. I have won 16 gold balls in these tournaments, each symbolic of a U.S. championship.
As a busy board-certified psychiatrist, I had been featured in an article, “Well being: Tennis is doctor’s favorite medicine,” by Art Carey, in the Philadelphia Inquirer, posted May 2, 2011. The author discussed my diet and exercise regime, and how I used exercise to stay healthy and to deal with the stress of being a physician.
‘Take me to the hospital’
At the end of 2018, I had a complete blood count performed, and the results indicated that I had a lipid panel of a healthy 30-year-old; however, my delusional bubble burst in March 2019. I was the No. 1 seed in a National Father-Daughter Tennis Tournament in Chicago. We were in the semifinal match, we had won the first set, and we were up 3-0. I fell, hit my head on the net post, and was feeling nauseated. I checked for bleeding and continued playing, though I was not feeling well. Five minutes later, I experienced symptoms of very extreme gastrointestinal pain and nausea. I ran off the tennis court wanting to vomit and get rid of the symptom so I could go back and finish the match. I wanted to play in the finals the following day and try to win the tournament.
The kind, competent, compassionate, and warm tournament director said I looked gray – and he promptly called 911. The paramedics came and said they thought I may be having a heart attack. I was in denial since I had no chest pain and I thought I was super healthy; therefore, I could not be experiencing an acute myocardial infarction. I finally agreed to let technicians perform an EKG, and they told me that I had ST elevation. Reality finally set in and I realized I was having a heart attack. “Take me to the hospital,” I said.
At the Chicago hospital where I was taken, I told doctors and staff I was a physician. To my surprise, they did not care. I was not going to get any prioritized treatment. Despite all of my devotion to medicine, I was not even getting their top physician to treat me. I was being evaluated by a resident. I felt even more deflated.
They performed a cardiac catheterization and put in one stent in one vessel in the right cardiac vessel. I had many questions to ask, but everyone seemed very impatient and abrupt with me, acting like this was just a very routine procedure. No one ever adequately answered my questions. I was very disillusioned, and I felt very insignificant, scared, and invisible.
I was discharged a few days later and was told my heart problem was fixed. I was instructed to follow up with a cardiologist in Philadelphia when I got home.
The first night home, I experienced chest pain. I was alarmed and thought my stent may have collapsed, so I went to the emergency room of the Philadelphia area hospital I knew had the best cardiac staff. After another blood test, indicating raised troponin levels, I was informed they needed to perform another cardiac catheterization. I learned I had two more coronary artery blockages, each 95%-99%, in the left ventricle.
I was shocked. How could the doctor in Chicago have made such a significant mistake? What happened? I would never know.
The interventional cardiologist in Philadelphia was able to repair one coronary artery, but the other blockage in the LED vessel (yes, the widow maker) had calcified too much for a stent. I would need cardiac bypass surgery. This was very unbelievable to me, and furthermore, I would have to wait 2 long weeks for the anticoagulant effect of the Brilinta to wear off before I could undergo bypass surgery.
While I anxiously waited for the big day, I was calling either my cardiologist, surgeon, or his nurse practitioner almost daily with questions and concerns; after all, this was a life-threatening and momentous event. Thankfully, I was met with great patience, understanding, and promptness of detailed answers and explanations by all involved with my cardiac care. The reactions of the staff made me mindful of the importance of really hearing my patients’ concerns and addressing their issues in a prompt, nonjudgmental, patient, and genuine manner. I am grateful that my robotic cardiac bypass surgery on March 26, 2019, went very well, and I am now back to work, playing tennis, jogging slowly, and riding my stationery bike.
Changed perspective on practice
I had always thought of myself as a warm, caring, and empathic psychiatrist, but my experience as a cardiac patient made me realize that there is always room for improvement in treating my patients.
Remember, every doctor will become a patient one day, and the reality of illness, injury, and mortality may really hit you hard, as it did me. You may not receive any prioritized treatment and you will know what it feels like to be helpless, vulnerable, and at the mercy of a physician while you regress in the service of the ego and become a patient.
You can be a better doctor now if you are mindful that whatever the physical, emotional, or mental issue facing your patients, the problem may be catastrophic to them. They need your undivided attention. Any problem is a significant event to your presenting patient. Really listen to his or her concerns or questions, and address every one with patience, understanding, and accurate information. If you follow these lessons, which I learned the hard way, you can become a better doctor.
I followed my doctor’s instructions and I started hitting tennis balls gradually. I worked myself back into shape and with my daughter Julia Cohen, and we won the USTA National Father Daughter Clay Court Championship in Florida 6 months after I had the heart attack during a national tennis tournament. This is the comeback of the year in tennis!
Dr. Cohen has had a private practice in psychiatry for more than 35 years. He is a former professor of psychiatry, family medicine, and otolaryngology at Thomas Jefferson University in Philadelphia. Dr. Cohen has been a nationally ranked tennis player from age 12 to the present, served as captain of the University of Pennsylvania tennis team, and ranked No. 1 in tennis in the middle states section and in the country in various categories and times. He was inducted into the Philadelphia Jewish Sports Hall of Fame in 2012.
Letters From Maine: Adult ADHD is on the rise
A study of more than 5 million Kaiser Permanente/Northern California patients suggests that the prevalence of adults diagnosed with ADHD has dramatically increased over the last 10 years (JAMA Netw Open. 2019 Nov 1. doi: 10.1001/jamanetworkopen.2019.14344).

Over the interval between 2007 and 2016, the prevalence of ADHD went from 0.43% to 0.96%, an increase of more than 120%. For adults, being white, male, younger, employed, and better educated increased one’s chances of receiving an ADHD diagnosis. Having a comorbid mental health diagnosis such as an eating disorder, anxiety, depression, or being labeled as bipolar also increased the odds of acquiring the ADHD label.
Are our screening tools too coarse, allowing a significant number of children to slip through the cracks only to land in the laps of our colleagues in internal medicine and family practice? If this were the case, does this mean that adult and youth ADHD are basically the same condition, but in some individuals the signs and symptoms become more obvious with aging? Does it also suggest that there is a genetic basis to ADHD with variable expression? Could it be that individuals with adult ADHD exhibited a few of the hallmarks of the diagnosis when they were young, but aggravating factors in the environment such as job stress or marital discord unmasked the signs and symptoms that had been percolating just under our radar for decades?
As usual, there is no simple answer that explains the findings unearthed by these researchers. One gets a sense from reading their paper that the authors feel that ADHD is being diagnosed more often as more individuals have access to physicians and other professionals who are attuned to the diagnosis. The fact that white, better-educated, and employed men are more likely to acquire the diagnosis might support the argument that as segments of the population who have been underserved by the health care system come on board we will continue to see a rise in the number of adults with the diagnosis. The more patients who see health care providers who are primed to make the diagnosis, the more often the diagnosis will be made.

I am sure there is a segment of the population who enter the world with some genetically mediated chemical or structural vulnerability that results in the signs and symptoms of ADHD. Most, but not all, of these individuals have symptoms that are so obvious that they present in childhood. However, a larger number of children and most adults who are labeled with ADHD are exhibiting the symptoms of inattention, distractibility, and impulsiveness as the result of environmental factors such as sleep deprivation, family or job stress, and other comorbid mental health conditions, or simply because they were young for their school cohort.
Pediatricians need not feel that we have missed another opportunity for prevention because the prevalence of the diagnosis of adult ADHD is increasing dramatically. However, that increase should serve as another reminder to us that there can be multiple factors that can result in signs and symptoms that attract the label of ADHD. We must be careful and look long and hard before we diagnose and reach for our prescription pad.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
A study of more than 5 million Kaiser Permanente/Northern California patients suggests that the prevalence of adults diagnosed with ADHD has dramatically increased over the last 10 years (JAMA Netw Open. 2019 Nov 1. doi: 10.1001/jamanetworkopen.2019.14344).
Over the interval between 2007 and 2016, the prevalence of ADHD went from 0.43% to 0.96%, an increase of more than 120%. For adults, being white, male, younger, employed, and better educated increased one’s chances of receiving an ADHD diagnosis. Having a comorbid mental health diagnosis such as an eating disorder, anxiety, depression, or being labeled as bipolar also increased the odds of acquiring the ADHD label.
Are our screening tools too coarse, allowing a significant number of children to slip through the cracks only to land in the laps of our colleagues in internal medicine and family practice? If this were the case, does this mean that adult and youth ADHD are basically the same condition, but in some individuals the signs and symptoms become more obvious with aging? Does it also suggest that there is a genetic basis to ADHD with variable expression? Could it be that individuals with adult ADHD exhibited a few of the hallmarks of the diagnosis when they were young, but aggravating factors in the environment such as job stress or marital discord unmasked the signs and symptoms that had been percolating just under our radar for decades?
As usual, there is no simple answer that explains the findings unearthed by these researchers. One gets a sense from reading their paper that the authors feel that ADHD is being diagnosed more often as more individuals have access to physicians and other professionals who are attuned to the diagnosis. The fact that white, better-educated, and employed men are more likely to acquire the diagnosis might support the argument that as segments of the population who have been underserved by the health care system come on board we will continue to see a rise in the number of adults with the diagnosis. The more patients who see health care providers who are primed to make the diagnosis, the more often the diagnosis will be made.
I am sure there is a segment of the population who enter the world with some genetically mediated chemical or structural vulnerability that results in the signs and symptoms of ADHD. Most, but not all, of these individuals have symptoms that are so obvious that they present in childhood. However, a larger number of children and most adults who are labeled with ADHD are exhibiting the symptoms of inattention, distractibility, and impulsiveness as the result of environmental factors such as sleep deprivation, family or job stress, and other comorbid mental health conditions, or simply because they were young for their school cohort.
Pediatricians need not feel that we have missed another opportunity for prevention because the prevalence of the diagnosis of adult ADHD is increasing dramatically. However, that increase should serve as another reminder to us that there can be multiple factors that can result in signs and symptoms that attract the label of ADHD. We must be careful and look long and hard before we diagnose and reach for our prescription pad.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
A study of more than 5 million Kaiser Permanente/Northern California patients suggests that the prevalence of adults diagnosed with ADHD has dramatically increased over the last 10 years (JAMA Netw Open. 2019 Nov 1. doi: 10.1001/jamanetworkopen.2019.14344).
Over the interval between 2007 and 2016, the prevalence of ADHD went from 0.43% to 0.96%, an increase of more than 120%. For adults, being white, male, younger, employed, and better educated increased one’s chances of receiving an ADHD diagnosis. Having a comorbid mental health diagnosis such as an eating disorder, anxiety, depression, or being labeled as bipolar also increased the odds of acquiring the ADHD label.
Are our screening tools too coarse, allowing a significant number of children to slip through the cracks only to land in the laps of our colleagues in internal medicine and family practice? If this were the case, does this mean that adult and youth ADHD are basically the same condition, but in some individuals the signs and symptoms become more obvious with aging? Does it also suggest that there is a genetic basis to ADHD with variable expression? Could it be that individuals with adult ADHD exhibited a few of the hallmarks of the diagnosis when they were young, but aggravating factors in the environment such as job stress or marital discord unmasked the signs and symptoms that had been percolating just under our radar for decades?
As usual, there is no simple answer that explains the findings unearthed by these researchers. One gets a sense from reading their paper that the authors feel that ADHD is being diagnosed more often as more individuals have access to physicians and other professionals who are attuned to the diagnosis. The fact that white, better-educated, and employed men are more likely to acquire the diagnosis might support the argument that as segments of the population who have been underserved by the health care system come on board we will continue to see a rise in the number of adults with the diagnosis. The more patients who see health care providers who are primed to make the diagnosis, the more often the diagnosis will be made.
I am sure there is a segment of the population who enter the world with some genetically mediated chemical or structural vulnerability that results in the signs and symptoms of ADHD. Most, but not all, of these individuals have symptoms that are so obvious that they present in childhood. However, a larger number of children and most adults who are labeled with ADHD are exhibiting the symptoms of inattention, distractibility, and impulsiveness as the result of environmental factors such as sleep deprivation, family or job stress, and other comorbid mental health conditions, or simply because they were young for their school cohort.
Pediatricians need not feel that we have missed another opportunity for prevention because the prevalence of the diagnosis of adult ADHD is increasing dramatically. However, that increase should serve as another reminder to us that there can be multiple factors that can result in signs and symptoms that attract the label of ADHD. We must be careful and look long and hard before we diagnose and reach for our prescription pad.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at pdnews@mdedge.com.
Managing psychosis in youth
Strong feelings – such as intense anxiety, irritability, or depressed mood – may affect every child for brief periods of time during their development. Parents and pediatricians are wise to not treat them as psychiatric disorders unless they persist for weeks, impair functioning, or are dramatically severe. Psychosis – marked by hallucinations, perceptual distortions, or profoundly disorganized thinking and behavior – typically looks dramatically severe. Even when psychotic symptoms are mild or brief, they can cause very serious distress for parents and clinicians. The worry is that they may represent a “first break,” a psychotic episode that requires much work for recovery, or the beginning of a lifelong struggle with schizophrenia or other chronic psychotic illness.

While it is important to recognize schizophrenia early – because early interventions are thought to improve the course of the disease – schizophrenia in childhood is rare. It is not commonly recognized that psychotic or psychoticlike symptoms are much more common than schizophrenia. While it is important to begin a thoughtful evaluation when a child or teenager presents with psychosis, it also is important to know that the majority of young people who experience psychotic symptoms do not have schizophrenia or other psychotic illness.
Psychosis describes symptoms in which there has been some “break with reality,” often in the form of hallucinations (seeing or hearing things which are not objectively present) or of distorted perceptions (such as paranoia or grandiosity). “Subsyndromal psychotic symptoms” occur when a person experiences these perceptual disturbances but has doubt about whether or not they are real. In frank psychosis, patients have a “fixed and firm” belief in the truth or accuracy of their perceptions, no matter the evidence against them. The voices they hear or hallucinations they see are “real” and there is a wholehearted belief that what the voice says or what they are seeing is as true as what you or I see and hear.
Schizophrenia is a diagnosis that requires the presence of both these “positive” psychotic symptoms and “negative” symptoms of flat affect; loss of motivation, social, or motor abilities; and cognitive impairment. These symptoms typically emerge in late adolescence (median age, 18 years) in males and early adulthood (median age, 25 years) in females, with another (smaller) peak in incidence in middle age. Importantly, the negative symptoms often emerge first so there often is a history of subtle cognitive decline and social withdrawal, one of the most common patterns in children, before psychosis emerges. Schizophrenia is quite rare, with a prevalence of slightly under 1% of the global population, an annual incidence of approximately 15 people per 100,000, and 1 in 40,000 in children under 13 years old, according to the National Institute of Mental Health. Psychotic symptoms are much more common than schizophrenia, affecting approximately 5% of the adult population at any point in time. They are even more common in children and adolescents. A meta-analysis of population-based studies of psychotic symptoms in youth demonstrated a median prevalence of 17% in children aged 9-12 years and 7.5% in adolescents aged 13-18 years.1 Of course, as with all statistics, much depends on the definitions used to identify this high prevalence rate.

Children and adolescents who report psychotic symptoms are at increased risk for developing schizophrenia, compared with the general population, but most youth with psychotic symptoms will not go on to develop schizophrenia. They are more likely to indicate other, nonpsychotic psychiatric illnesses, such as anxiety or mood disorders, including depression, obsessive compulsive disorder (OCD), and PTSD. In younger children, these symptoms may prove to be benign, but in adolescents they usually indicate the presence of a psychiatric illness. In one study, 57% of children aged 11-13 years with psychotic symptoms were found to have a nonpsychotic psychiatric illness, but the rate jumped to 80% for those aged 13-15 years with psychotic symptoms.2 So while psychosis in teenagers only rarely indicates schizophrenia, these symptoms usually indicate the presence of a psychiatric illness, and a psychiatric evaluation should be initiated.
If a child in your practice presents with psychotic symptoms, it is appropriate to assess their safety and then start a medical work-up. Find out from your patient or their parents if their behavior has been affected by their perceptual disturbances. Are they frightened and avoiding school? Are they withdrawing from social relationships? Is their sleep disrupted? Have they been more impulsive or unpredictable? If their behavior has been affected, you should refer to a child psychiatrist to perform a full diagnostic evaluation and help with management of these symptoms.
Your medical work-up should include a drug screen, blood count, metabolic panel, and thyroid function test. Medications, particularly stimulants, steroids, and anticholinergics can cause psychotic symptoms in high doses or vulnerable patients (such as those with a developmental disorder or traumatic brain injury). If the physical or neurologic exam are suggestive, further investigation of the many potential medical sources of psychotic symptoms in youth can be pursued to rule out autoimmune illnesses, endocrine disorders, metabolic illnesses, heavy metal poisoning, neurologic diseases, infectious diseases, and nutritional deficits. It is worth noting that childhood sleep disorders also can present with psychosis. Persistent psychotic symptoms in children are very hard to evaluate and may be the harbinger of a serious psychiatric disorder, so even if the medical work-up is negative and the persistent symptoms are mild and not causing a safety concern, a referral to a child psychiatrist for a full mental health evaluation is appropriate.

Psychotic symptoms in an adolescent sometimes are easier to assess, more worrisome for serious mental illness, and are a high-risk category for self-destructive behavior and substance use. Before you begin a medical work-up, you always should assess for safety, including suicide risk, if your adolescent patient presents with psychotic symptoms. Screening for symptoms of mood, anxiety, and substance use disorders also can help reveal the nature of their presenting problem. If your adolescent patient is using drugs, that does not rule out the possibility of an underlying mood, anxiety, or thought disorder. While intoxication with many drugs may precipitate psychotic symptoms (including stimulants, hallucinogens, and marijuana), others may precipitate psychosis in withdrawal states (alcohol, benzodiazepines, and other CNS depressants). It also is important to note that adolescents with emerging schizophrenia have very high rates of comorbid substance abuse (as high as 60%), so their drug use may not be the cause of their psychotic symptoms. There also is emerging evidence that use of certain drugs during sensitive developmental periods can significantly increase the likelihood of developing schizophrenia in vulnerable populations, such as with regular marijuana use in adolescents who have a family history of schizophrenia.
For those rare pediatric patients who present with both negative and positive symptoms of emerging schizophrenia, early diagnosis and treatment has shown promise in improving the course of the disease. Cognitive-behavioral therapy (CBT) for psychosis has shown promise in lowering the rates of conversion to schizophrenia in select patient populations. This therapy teaches strategies for improving reality testing, cognitive flexibility, and social skills. The social skills appear to be especially important for improving adaptive function, even in those patients who progress to schizophrenia. Family therapies, focused on improving family cohesion, communication, and adaptive functioning, appear to improve family well-being and the course of the patient’s illness (such as fewer and less severe psychotic episodes and improved mood and adaptive function). Early use of antipsychotic medications also appears to improve the course of the illness.
While schizophrenia is not curable, early detection (perhaps by a pediatrician), referral, and treatment can be powerfully protective for patients and their families.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
References
1. Psychol Med. 2012 Sep;42(9):1857-63.
2. Br J Psychiatry. 2012 Jul;201(1):26-32.
Strong feelings – such as intense anxiety, irritability, or depressed mood – may affect every child for brief periods of time during their development. Parents and pediatricians are wise to not treat them as psychiatric disorders unless they persist for weeks, impair functioning, or are dramatically severe. Psychosis – marked by hallucinations, perceptual distortions, or profoundly disorganized thinking and behavior – typically looks dramatically severe. Even when psychotic symptoms are mild or brief, they can cause very serious distress for parents and clinicians. The worry is that they may represent a “first break,” a psychotic episode that requires much work for recovery, or the beginning of a lifelong struggle with schizophrenia or other chronic psychotic illness.
While it is important to recognize schizophrenia early – because early interventions are thought to improve the course of the disease – schizophrenia in childhood is rare. It is not commonly recognized that psychotic or psychoticlike symptoms are much more common than schizophrenia. While it is important to begin a thoughtful evaluation when a child or teenager presents with psychosis, it also is important to know that the majority of young people who experience psychotic symptoms do not have schizophrenia or other psychotic illness.
Psychosis describes symptoms in which there has been some “break with reality,” often in the form of hallucinations (seeing or hearing things which are not objectively present) or of distorted perceptions (such as paranoia or grandiosity). “Subsyndromal psychotic symptoms” occur when a person experiences these perceptual disturbances but has doubt about whether or not they are real. In frank psychosis, patients have a “fixed and firm” belief in the truth or accuracy of their perceptions, no matter the evidence against them. The voices they hear or hallucinations they see are “real” and there is a wholehearted belief that what the voice says or what they are seeing is as true as what you or I see and hear.
Schizophrenia is a diagnosis that requires the presence of both these “positive” psychotic symptoms and “negative” symptoms of flat affect; loss of motivation, social, or motor abilities; and cognitive impairment. These symptoms typically emerge in late adolescence (median age, 18 years) in males and early adulthood (median age, 25 years) in females, with another (smaller) peak in incidence in middle age. Importantly, the negative symptoms often emerge first so there often is a history of subtle cognitive decline and social withdrawal, one of the most common patterns in children, before psychosis emerges. Schizophrenia is quite rare, with a prevalence of slightly under 1% of the global population, an annual incidence of approximately 15 people per 100,000, and 1 in 40,000 in children under 13 years old, according to the National Institute of Mental Health. Psychotic symptoms are much more common than schizophrenia, affecting approximately 5% of the adult population at any point in time. They are even more common in children and adolescents. A meta-analysis of population-based studies of psychotic symptoms in youth demonstrated a median prevalence of 17% in children aged 9-12 years and 7.5% in adolescents aged 13-18 years.1 Of course, as with all statistics, much depends on the definitions used to identify this high prevalence rate.
Children and adolescents who report psychotic symptoms are at increased risk for developing schizophrenia, compared with the general population, but most youth with psychotic symptoms will not go on to develop schizophrenia. They are more likely to indicate other, nonpsychotic psychiatric illnesses, such as anxiety or mood disorders, including depression, obsessive compulsive disorder (OCD), and PTSD. In younger children, these symptoms may prove to be benign, but in adolescents they usually indicate the presence of a psychiatric illness. In one study, 57% of children aged 11-13 years with psychotic symptoms were found to have a nonpsychotic psychiatric illness, but the rate jumped to 80% for those aged 13-15 years with psychotic symptoms.2 So while psychosis in teenagers only rarely indicates schizophrenia, these symptoms usually indicate the presence of a psychiatric illness, and a psychiatric evaluation should be initiated.
If a child in your practice presents with psychotic symptoms, it is appropriate to assess their safety and then start a medical work-up. Find out from your patient or their parents if their behavior has been affected by their perceptual disturbances. Are they frightened and avoiding school? Are they withdrawing from social relationships? Is their sleep disrupted? Have they been more impulsive or unpredictable? If their behavior has been affected, you should refer to a child psychiatrist to perform a full diagnostic evaluation and help with management of these symptoms.
Your medical work-up should include a drug screen, blood count, metabolic panel, and thyroid function test. Medications, particularly stimulants, steroids, and anticholinergics can cause psychotic symptoms in high doses or vulnerable patients (such as those with a developmental disorder or traumatic brain injury). If the physical or neurologic exam are suggestive, further investigation of the many potential medical sources of psychotic symptoms in youth can be pursued to rule out autoimmune illnesses, endocrine disorders, metabolic illnesses, heavy metal poisoning, neurologic diseases, infectious diseases, and nutritional deficits. It is worth noting that childhood sleep disorders also can present with psychosis. Persistent psychotic symptoms in children are very hard to evaluate and may be the harbinger of a serious psychiatric disorder, so even if the medical work-up is negative and the persistent symptoms are mild and not causing a safety concern, a referral to a child psychiatrist for a full mental health evaluation is appropriate.
Psychotic symptoms in an adolescent sometimes are easier to assess, more worrisome for serious mental illness, and are a high-risk category for self-destructive behavior and substance use. Before you begin a medical work-up, you always should assess for safety, including suicide risk, if your adolescent patient presents with psychotic symptoms. Screening for symptoms of mood, anxiety, and substance use disorders also can help reveal the nature of their presenting problem. If your adolescent patient is using drugs, that does not rule out the possibility of an underlying mood, anxiety, or thought disorder. While intoxication with many drugs may precipitate psychotic symptoms (including stimulants, hallucinogens, and marijuana), others may precipitate psychosis in withdrawal states (alcohol, benzodiazepines, and other CNS depressants). It also is important to note that adolescents with emerging schizophrenia have very high rates of comorbid substance abuse (as high as 60%), so their drug use may not be the cause of their psychotic symptoms. There also is emerging evidence that use of certain drugs during sensitive developmental periods can significantly increase the likelihood of developing schizophrenia in vulnerable populations, such as with regular marijuana use in adolescents who have a family history of schizophrenia.
For those rare pediatric patients who present with both negative and positive symptoms of emerging schizophrenia, early diagnosis and treatment has shown promise in improving the course of the disease. Cognitive-behavioral therapy (CBT) for psychosis has shown promise in lowering the rates of conversion to schizophrenia in select patient populations. This therapy teaches strategies for improving reality testing, cognitive flexibility, and social skills. The social skills appear to be especially important for improving adaptive function, even in those patients who progress to schizophrenia. Family therapies, focused on improving family cohesion, communication, and adaptive functioning, appear to improve family well-being and the course of the patient’s illness (such as fewer and less severe psychotic episodes and improved mood and adaptive function). Early use of antipsychotic medications also appears to improve the course of the illness.
While schizophrenia is not curable, early detection (perhaps by a pediatrician), referral, and treatment can be powerfully protective for patients and their families.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
References
1. Psychol Med. 2012 Sep;42(9):1857-63.
2. Br J Psychiatry. 2012 Jul;201(1):26-32.
Strong feelings – such as intense anxiety, irritability, or depressed mood – may affect every child for brief periods of time during their development. Parents and pediatricians are wise to not treat them as psychiatric disorders unless they persist for weeks, impair functioning, or are dramatically severe. Psychosis – marked by hallucinations, perceptual distortions, or profoundly disorganized thinking and behavior – typically looks dramatically severe. Even when psychotic symptoms are mild or brief, they can cause very serious distress for parents and clinicians. The worry is that they may represent a “first break,” a psychotic episode that requires much work for recovery, or the beginning of a lifelong struggle with schizophrenia or other chronic psychotic illness.
While it is important to recognize schizophrenia early – because early interventions are thought to improve the course of the disease – schizophrenia in childhood is rare. It is not commonly recognized that psychotic or psychoticlike symptoms are much more common than schizophrenia. While it is important to begin a thoughtful evaluation when a child or teenager presents with psychosis, it also is important to know that the majority of young people who experience psychotic symptoms do not have schizophrenia or other psychotic illness.
Psychosis describes symptoms in which there has been some “break with reality,” often in the form of hallucinations (seeing or hearing things which are not objectively present) or of distorted perceptions (such as paranoia or grandiosity). “Subsyndromal psychotic symptoms” occur when a person experiences these perceptual disturbances but has doubt about whether or not they are real. In frank psychosis, patients have a “fixed and firm” belief in the truth or accuracy of their perceptions, no matter the evidence against them. The voices they hear or hallucinations they see are “real” and there is a wholehearted belief that what the voice says or what they are seeing is as true as what you or I see and hear.
Schizophrenia is a diagnosis that requires the presence of both these “positive” psychotic symptoms and “negative” symptoms of flat affect; loss of motivation, social, or motor abilities; and cognitive impairment. These symptoms typically emerge in late adolescence (median age, 18 years) in males and early adulthood (median age, 25 years) in females, with another (smaller) peak in incidence in middle age. Importantly, the negative symptoms often emerge first so there often is a history of subtle cognitive decline and social withdrawal, one of the most common patterns in children, before psychosis emerges. Schizophrenia is quite rare, with a prevalence of slightly under 1% of the global population, an annual incidence of approximately 15 people per 100,000, and 1 in 40,000 in children under 13 years old, according to the National Institute of Mental Health. Psychotic symptoms are much more common than schizophrenia, affecting approximately 5% of the adult population at any point in time. They are even more common in children and adolescents. A meta-analysis of population-based studies of psychotic symptoms in youth demonstrated a median prevalence of 17% in children aged 9-12 years and 7.5% in adolescents aged 13-18 years.1 Of course, as with all statistics, much depends on the definitions used to identify this high prevalence rate.
Children and adolescents who report psychotic symptoms are at increased risk for developing schizophrenia, compared with the general population, but most youth with psychotic symptoms will not go on to develop schizophrenia. They are more likely to indicate other, nonpsychotic psychiatric illnesses, such as anxiety or mood disorders, including depression, obsessive compulsive disorder (OCD), and PTSD. In younger children, these symptoms may prove to be benign, but in adolescents they usually indicate the presence of a psychiatric illness. In one study, 57% of children aged 11-13 years with psychotic symptoms were found to have a nonpsychotic psychiatric illness, but the rate jumped to 80% for those aged 13-15 years with psychotic symptoms.2 So while psychosis in teenagers only rarely indicates schizophrenia, these symptoms usually indicate the presence of a psychiatric illness, and a psychiatric evaluation should be initiated.
If a child in your practice presents with psychotic symptoms, it is appropriate to assess their safety and then start a medical work-up. Find out from your patient or their parents if their behavior has been affected by their perceptual disturbances. Are they frightened and avoiding school? Are they withdrawing from social relationships? Is their sleep disrupted? Have they been more impulsive or unpredictable? If their behavior has been affected, you should refer to a child psychiatrist to perform a full diagnostic evaluation and help with management of these symptoms.
Your medical work-up should include a drug screen, blood count, metabolic panel, and thyroid function test. Medications, particularly stimulants, steroids, and anticholinergics can cause psychotic symptoms in high doses or vulnerable patients (such as those with a developmental disorder or traumatic brain injury). If the physical or neurologic exam are suggestive, further investigation of the many potential medical sources of psychotic symptoms in youth can be pursued to rule out autoimmune illnesses, endocrine disorders, metabolic illnesses, heavy metal poisoning, neurologic diseases, infectious diseases, and nutritional deficits. It is worth noting that childhood sleep disorders also can present with psychosis. Persistent psychotic symptoms in children are very hard to evaluate and may be the harbinger of a serious psychiatric disorder, so even if the medical work-up is negative and the persistent symptoms are mild and not causing a safety concern, a referral to a child psychiatrist for a full mental health evaluation is appropriate.
Psychotic symptoms in an adolescent sometimes are easier to assess, more worrisome for serious mental illness, and are a high-risk category for self-destructive behavior and substance use. Before you begin a medical work-up, you always should assess for safety, including suicide risk, if your adolescent patient presents with psychotic symptoms. Screening for symptoms of mood, anxiety, and substance use disorders also can help reveal the nature of their presenting problem. If your adolescent patient is using drugs, that does not rule out the possibility of an underlying mood, anxiety, or thought disorder. While intoxication with many drugs may precipitate psychotic symptoms (including stimulants, hallucinogens, and marijuana), others may precipitate psychosis in withdrawal states (alcohol, benzodiazepines, and other CNS depressants). It also is important to note that adolescents with emerging schizophrenia have very high rates of comorbid substance abuse (as high as 60%), so their drug use may not be the cause of their psychotic symptoms. There also is emerging evidence that use of certain drugs during sensitive developmental periods can significantly increase the likelihood of developing schizophrenia in vulnerable populations, such as with regular marijuana use in adolescents who have a family history of schizophrenia.
For those rare pediatric patients who present with both negative and positive symptoms of emerging schizophrenia, early diagnosis and treatment has shown promise in improving the course of the disease. Cognitive-behavioral therapy (CBT) for psychosis has shown promise in lowering the rates of conversion to schizophrenia in select patient populations. This therapy teaches strategies for improving reality testing, cognitive flexibility, and social skills. The social skills appear to be especially important for improving adaptive function, even in those patients who progress to schizophrenia. Family therapies, focused on improving family cohesion, communication, and adaptive functioning, appear to improve family well-being and the course of the patient’s illness (such as fewer and less severe psychotic episodes and improved mood and adaptive function). Early use of antipsychotic medications also appears to improve the course of the illness.
While schizophrenia is not curable, early detection (perhaps by a pediatrician), referral, and treatment can be powerfully protective for patients and their families.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Email them at pdnews@mdedge.com.
References
1. Psychol Med. 2012 Sep;42(9):1857-63.
2. Br J Psychiatry. 2012 Jul;201(1):26-32.
Was the success of hospital medicine inevitable?
Early on, SHM defined the specialty
When I started at the Society of Hospital Medicine – known then as the National Association of Inpatient Physicians (NAIP) – in January 2000, Bill Clinton was still president. There were probably 500 hospitalists in the United States, and SHM had about 200-250 members.

It was so long ago that the iPhone hadn’t been invented, Twitter wasn’t even an idea, and Amazon was an online book store. SHM’s national offices were a cubicle at the American College of Physicians headquarters in Philadelphia, and our entire staff was me and a part-time assistant.
We have certainly come a long way in my 20 years as CEO of SHM.
When I first became involved with NAIP, it was to help the board with their strategic planning in 1998. At that time, the national thought leaders for the hospitalist movement (the term hospital medicine had not been invented yet) predicted that hospitalists would eventually do the inpatient work for about 25% of family doctors and for 15% of internists. Hospitalists were considered to be a form of “general medicine” without an office-based practice.
One of the first things we set about doing was to define the new specialty of hospital medicine before anyone else (e.g., American Medical Association, ACP, American Academy of Family Physicians, American Academy of Pediatrics, the government) defined us.
Most specialties were defined by a body organ (e.g., cardiology, renal), a population (e.g., pediatrics, geriatrics), or a disease (e.g., oncology), and there were a few other site-specific specialties (e.g., ED medicine, critical care). We felt that, to be a specialty, we needed certain key elements:
- Separate group consciousness
- Professional society
- Distinct residency and fellowship programs
- Separate CME
- Distinct educational materials (e.g., textbooks)
- Definable and distinct competencies
- Separate credentials – certification and/or hospital insurance driven
Early on, SHM defined the Core Competencies for Hospital Medicine for adults in patient care and, eventually, for pediatric patients. We rebranded our specialty as hospital medicine to be more than just inpatient physicians, and to broadly encompass the growing “big tent” of SHM that included those trained in internal medicine, family medicine, pediatrics, med-peds, as well as nurse practitioners, physician assistants, pharmacists, and others.
We were the first and only specialty society to set the standard for hospitalist compensation (how much you are paid) and productivity (what you are expected to do) with our unique State of Hospital Medicine (SOHM) Report. Other specialties left this work to the Medical Group Management Association, the AMA, or commercial companies.
Our specialty was soon being asked to do things that no other group of clinicians was ever asked to do.
Hospitalists were expected to Save Money by reducing length of stay and the use of resources on the sickest patients. Hospitalists were asked to Improve Measurable Quality at a time when most other physicians or even hospitals weren’t even being measured.
We were expected to form and Lead Teams of other clinicians when health care was still seen as a solo enterprise. Hospitalists were expected to Improve Efficiency and to create a Seamless Continuity, both during the hospital stay and in the transitions out of the hospital.
Hospitalists were asked to do things no one else wanted to do, such as taking on the uncompensated patients and extra hospital committee work and just about any new project their hospital wanted to be involved in. Along the way, we were expected to Make Other Physicians’ Lives Better by taking on their inpatients, inpatient calls, comanagement with specialists, and unloading the ED.
And both at medical schools and in the community, hospitalists became the Major Educators of medical students, residents, nurses, and other hospital staff.
At the same time, SHM was focusing on becoming a very unique medical professional society.
SHM built on the energy of our young and innovative hospitalists to forge a different path. We had no reputation to protect. We were not bound like most other specialty societies to over 100 years of “the way it’s always been done.”
While other professional societies thought their role in quality improvement was to pontificate and publish clinical guidelines that often were little used, SHM embarked on an aggressive, hands-on, frontline approach by starting SHM’s Center for Quality Improvement. Over the last 15 years, the center has raised millions of dollars to deliver real change and improvement at hundreds of hospitals nationwide, many times bringing work plans and mentors to support and train local clinicians in quality improvement skills and data collection. This approach was recognized by the National Quality Forum and the Joint Commission with their prestigious John Eisenberg Award for Quality Improvement.
When we went to Washington to help shape the future of health care, we did not ask for more money for hospitalists. We did not ask for more power or to use regulations to protect our new specialty. Instead, we went with ideas of how to make acute medical care more effective and efficient. We could show the politicians and the regulators how we could reduce incidence of deep vein thrombosis and pulmonary emboli, how we could make the hospital discharge process work better, how we could help chart a smoother medication reconciliation process, and so many other ways the system could be improved.
And even the way SHM generated our new ideas was uniquely different than other specialties. Way back in 2000 – long before Twitter and other social media were able to crowdsource and use the Internet to percolate new ideas – SHM relied on our members’ conversations on the SHM electronic mail discussion list to see what hospitalists were worried about, and what everyone was being asked to do, and SHM provided the resources and initiatives to support our nation’s hospitalists.
From these early conversations, SHM heard that hospitalists were being asked to Lead Change without much of an idea of the skills they would need. And so, the SHM leadership academies were born, which have now educated more than 2,700 hospitalist leaders.
Early on, we learned that hospitalists and even their bosses had no idea of how to start or run a successful hospital medicine group. SHM started our practice management courses and webinars and we developed the groundbreaking document, Key Characteristics of Effective Hospital Medicine Groups. In a typical SHM manner, we challenged most of our members to improve and get better rather trying to defend the status quo. At SHM, we have constantly felt that hospital medicine was a “work in progress.” We may not be perfect today, but we will be better in 90 days and even better in a year.
I have more to say about how we got this far and even more to say about where we might go. So, stay tuned and keep contributing to the future and success of SHM and hospital medicine.
Dr. Wellikson is the CEO of SHM. He has announced his plan to retire from SHM in late 2020. This article is the first in a series celebrating Dr. Wellikson’s tenure as CEO.
Early on, SHM defined the specialty
Early on, SHM defined the specialty
When I started at the Society of Hospital Medicine – known then as the National Association of Inpatient Physicians (NAIP) – in January 2000, Bill Clinton was still president. There were probably 500 hospitalists in the United States, and SHM had about 200-250 members.
It was so long ago that the iPhone hadn’t been invented, Twitter wasn’t even an idea, and Amazon was an online book store. SHM’s national offices were a cubicle at the American College of Physicians headquarters in Philadelphia, and our entire staff was me and a part-time assistant.
We have certainly come a long way in my 20 years as CEO of SHM.
When I first became involved with NAIP, it was to help the board with their strategic planning in 1998. At that time, the national thought leaders for the hospitalist movement (the term hospital medicine had not been invented yet) predicted that hospitalists would eventually do the inpatient work for about 25% of family doctors and for 15% of internists. Hospitalists were considered to be a form of “general medicine” without an office-based practice.
One of the first things we set about doing was to define the new specialty of hospital medicine before anyone else (e.g., American Medical Association, ACP, American Academy of Family Physicians, American Academy of Pediatrics, the government) defined us.
Most specialties were defined by a body organ (e.g., cardiology, renal), a population (e.g., pediatrics, geriatrics), or a disease (e.g., oncology), and there were a few other site-specific specialties (e.g., ED medicine, critical care). We felt that, to be a specialty, we needed certain key elements:
- Separate group consciousness
- Professional society
- Distinct residency and fellowship programs
- Separate CME
- Distinct educational materials (e.g., textbooks)
- Definable and distinct competencies
- Separate credentials – certification and/or hospital insurance driven
Early on, SHM defined the Core Competencies for Hospital Medicine for adults in patient care and, eventually, for pediatric patients. We rebranded our specialty as hospital medicine to be more than just inpatient physicians, and to broadly encompass the growing “big tent” of SHM that included those trained in internal medicine, family medicine, pediatrics, med-peds, as well as nurse practitioners, physician assistants, pharmacists, and others.
We were the first and only specialty society to set the standard for hospitalist compensation (how much you are paid) and productivity (what you are expected to do) with our unique State of Hospital Medicine (SOHM) Report. Other specialties left this work to the Medical Group Management Association, the AMA, or commercial companies.
Our specialty was soon being asked to do things that no other group of clinicians was ever asked to do.
Hospitalists were expected to Save Money by reducing length of stay and the use of resources on the sickest patients. Hospitalists were asked to Improve Measurable Quality at a time when most other physicians or even hospitals weren’t even being measured.
We were expected to form and Lead Teams of other clinicians when health care was still seen as a solo enterprise. Hospitalists were expected to Improve Efficiency and to create a Seamless Continuity, both during the hospital stay and in the transitions out of the hospital.
Hospitalists were asked to do things no one else wanted to do, such as taking on the uncompensated patients and extra hospital committee work and just about any new project their hospital wanted to be involved in. Along the way, we were expected to Make Other Physicians’ Lives Better by taking on their inpatients, inpatient calls, comanagement with specialists, and unloading the ED.
And both at medical schools and in the community, hospitalists became the Major Educators of medical students, residents, nurses, and other hospital staff.
At the same time, SHM was focusing on becoming a very unique medical professional society.
SHM built on the energy of our young and innovative hospitalists to forge a different path. We had no reputation to protect. We were not bound like most other specialty societies to over 100 years of “the way it’s always been done.”
While other professional societies thought their role in quality improvement was to pontificate and publish clinical guidelines that often were little used, SHM embarked on an aggressive, hands-on, frontline approach by starting SHM’s Center for Quality Improvement. Over the last 15 years, the center has raised millions of dollars to deliver real change and improvement at hundreds of hospitals nationwide, many times bringing work plans and mentors to support and train local clinicians in quality improvement skills and data collection. This approach was recognized by the National Quality Forum and the Joint Commission with their prestigious John Eisenberg Award for Quality Improvement.
When we went to Washington to help shape the future of health care, we did not ask for more money for hospitalists. We did not ask for more power or to use regulations to protect our new specialty. Instead, we went with ideas of how to make acute medical care more effective and efficient. We could show the politicians and the regulators how we could reduce incidence of deep vein thrombosis and pulmonary emboli, how we could make the hospital discharge process work better, how we could help chart a smoother medication reconciliation process, and so many other ways the system could be improved.
And even the way SHM generated our new ideas was uniquely different than other specialties. Way back in 2000 – long before Twitter and other social media were able to crowdsource and use the Internet to percolate new ideas – SHM relied on our members’ conversations on the SHM electronic mail discussion list to see what hospitalists were worried about, and what everyone was being asked to do, and SHM provided the resources and initiatives to support our nation’s hospitalists.
From these early conversations, SHM heard that hospitalists were being asked to Lead Change without much of an idea of the skills they would need. And so, the SHM leadership academies were born, which have now educated more than 2,700 hospitalist leaders.
Early on, we learned that hospitalists and even their bosses had no idea of how to start or run a successful hospital medicine group. SHM started our practice management courses and webinars and we developed the groundbreaking document, Key Characteristics of Effective Hospital Medicine Groups. In a typical SHM manner, we challenged most of our members to improve and get better rather trying to defend the status quo. At SHM, we have constantly felt that hospital medicine was a “work in progress.” We may not be perfect today, but we will be better in 90 days and even better in a year.
I have more to say about how we got this far and even more to say about where we might go. So, stay tuned and keep contributing to the future and success of SHM and hospital medicine.
Dr. Wellikson is the CEO of SHM. He has announced his plan to retire from SHM in late 2020. This article is the first in a series celebrating Dr. Wellikson’s tenure as CEO.
When I started at the Society of Hospital Medicine – known then as the National Association of Inpatient Physicians (NAIP) – in January 2000, Bill Clinton was still president. There were probably 500 hospitalists in the United States, and SHM had about 200-250 members.
It was so long ago that the iPhone hadn’t been invented, Twitter wasn’t even an idea, and Amazon was an online book store. SHM’s national offices were a cubicle at the American College of Physicians headquarters in Philadelphia, and our entire staff was me and a part-time assistant.
We have certainly come a long way in my 20 years as CEO of SHM.
When I first became involved with NAIP, it was to help the board with their strategic planning in 1998. At that time, the national thought leaders for the hospitalist movement (the term hospital medicine had not been invented yet) predicted that hospitalists would eventually do the inpatient work for about 25% of family doctors and for 15% of internists. Hospitalists were considered to be a form of “general medicine” without an office-based practice.
One of the first things we set about doing was to define the new specialty of hospital medicine before anyone else (e.g., American Medical Association, ACP, American Academy of Family Physicians, American Academy of Pediatrics, the government) defined us.
Most specialties were defined by a body organ (e.g., cardiology, renal), a population (e.g., pediatrics, geriatrics), or a disease (e.g., oncology), and there were a few other site-specific specialties (e.g., ED medicine, critical care). We felt that, to be a specialty, we needed certain key elements:
- Separate group consciousness
- Professional society
- Distinct residency and fellowship programs
- Separate CME
- Distinct educational materials (e.g., textbooks)
- Definable and distinct competencies
- Separate credentials – certification and/or hospital insurance driven
Early on, SHM defined the Core Competencies for Hospital Medicine for adults in patient care and, eventually, for pediatric patients. We rebranded our specialty as hospital medicine to be more than just inpatient physicians, and to broadly encompass the growing “big tent” of SHM that included those trained in internal medicine, family medicine, pediatrics, med-peds, as well as nurse practitioners, physician assistants, pharmacists, and others.
We were the first and only specialty society to set the standard for hospitalist compensation (how much you are paid) and productivity (what you are expected to do) with our unique State of Hospital Medicine (SOHM) Report. Other specialties left this work to the Medical Group Management Association, the AMA, or commercial companies.
Our specialty was soon being asked to do things that no other group of clinicians was ever asked to do.
Hospitalists were expected to Save Money by reducing length of stay and the use of resources on the sickest patients. Hospitalists were asked to Improve Measurable Quality at a time when most other physicians or even hospitals weren’t even being measured.
We were expected to form and Lead Teams of other clinicians when health care was still seen as a solo enterprise. Hospitalists were expected to Improve Efficiency and to create a Seamless Continuity, both during the hospital stay and in the transitions out of the hospital.
Hospitalists were asked to do things no one else wanted to do, such as taking on the uncompensated patients and extra hospital committee work and just about any new project their hospital wanted to be involved in. Along the way, we were expected to Make Other Physicians’ Lives Better by taking on their inpatients, inpatient calls, comanagement with specialists, and unloading the ED.
And both at medical schools and in the community, hospitalists became the Major Educators of medical students, residents, nurses, and other hospital staff.
At the same time, SHM was focusing on becoming a very unique medical professional society.
SHM built on the energy of our young and innovative hospitalists to forge a different path. We had no reputation to protect. We were not bound like most other specialty societies to over 100 years of “the way it’s always been done.”
While other professional societies thought their role in quality improvement was to pontificate and publish clinical guidelines that often were little used, SHM embarked on an aggressive, hands-on, frontline approach by starting SHM’s Center for Quality Improvement. Over the last 15 years, the center has raised millions of dollars to deliver real change and improvement at hundreds of hospitals nationwide, many times bringing work plans and mentors to support and train local clinicians in quality improvement skills and data collection. This approach was recognized by the National Quality Forum and the Joint Commission with their prestigious John Eisenberg Award for Quality Improvement.
When we went to Washington to help shape the future of health care, we did not ask for more money for hospitalists. We did not ask for more power or to use regulations to protect our new specialty. Instead, we went with ideas of how to make acute medical care more effective and efficient. We could show the politicians and the regulators how we could reduce incidence of deep vein thrombosis and pulmonary emboli, how we could make the hospital discharge process work better, how we could help chart a smoother medication reconciliation process, and so many other ways the system could be improved.
And even the way SHM generated our new ideas was uniquely different than other specialties. Way back in 2000 – long before Twitter and other social media were able to crowdsource and use the Internet to percolate new ideas – SHM relied on our members’ conversations on the SHM electronic mail discussion list to see what hospitalists were worried about, and what everyone was being asked to do, and SHM provided the resources and initiatives to support our nation’s hospitalists.
From these early conversations, SHM heard that hospitalists were being asked to Lead Change without much of an idea of the skills they would need. And so, the SHM leadership academies were born, which have now educated more than 2,700 hospitalist leaders.
Early on, we learned that hospitalists and even their bosses had no idea of how to start or run a successful hospital medicine group. SHM started our practice management courses and webinars and we developed the groundbreaking document, Key Characteristics of Effective Hospital Medicine Groups. In a typical SHM manner, we challenged most of our members to improve and get better rather trying to defend the status quo. At SHM, we have constantly felt that hospital medicine was a “work in progress.” We may not be perfect today, but we will be better in 90 days and even better in a year.
I have more to say about how we got this far and even more to say about where we might go. So, stay tuned and keep contributing to the future and success of SHM and hospital medicine.
Dr. Wellikson is the CEO of SHM. He has announced his plan to retire from SHM in late 2020. This article is the first in a series celebrating Dr. Wellikson’s tenure as CEO.

The fundamental things apply
Dear Colleagues,
or questions about cosmetic procedures or skin care advice.

Needle nippers were around, but no elaborate, molded-plastic contraptions like the sharps containers now in wide use. You sent pathology specimens in plastic cylinders by U.S. mail; then you called the lab 2 weeks later to ask, “Where’s the report on Jane Smith, with the rule out melanoma,” and the lab said, “Jane who?”
Of course, some things about practice have not changed. Patients with atopic dermatitis still ask why eczema comes back and why we can’t give them something to make it go away once and for all. Some referring physicians still treat scaly rashes with ketoconazole cream (and when that fails, oral fluconazole, which doesn’t work either).
Of course the biggest change between then and now, coincident with the rise of computers and technology, is the advent and ubiquity of that great swindle foisted upon the profession and the public – electronic health records – with their unfulfilled promises of cost-savings and efficiency and unconceded consequences: turning healers into harried data-entry drudges too busy clicking mice to make eye contact with humans. Yes, the Emperor has clothes. The Emperor is wearing Depends.
I wrote my first column for this periodical 22 years ago; this will be my last. My wonderful editor, Elizabeth Mechcatie, has agreed to take under advisement a proposal that I go on sending occasional dispatches under the heading “Pruritus Emeritus.” My family used to refer to those in the anomalous state of being emeritus – it means, roughly, “Forgotten, but not gone” – by rhyming emeritus with sinusitis.
There is no way to remember 40 years of patients. Many came just once, others several times. Some moved away, some passed away, changed primary doctors, changed insurances. Some grew too old to visit, sent regretful notes apologizing for finding the drive too long, the parking too hard. Some returned after an absence of a decade or 3, having forgotten that they had once come for the same problem, or come at all.
But there have been other patients who formed a real bond, whose names and faces still come readily to mind, who visited over long periods, sent their spouses, family members, even children and grandchildren. The stories of their lives became part of mine, and sometimes mine part of theirs.
Though hardly an old-movie buff, I know the famous scene in Casablanca in which a radiant Ingrid Bergman (that skin!) asks Dooley Wilson – the piano player, Sam – to play the song Humphrey Bogart does not want to hear:
“You must remember this
A kiss is just a kiss
A sigh is just a sigh
The fundamental things apply
As time goes by.”
Over the last 40 years there have been substantial advances in the way we treat patients, though perhaps not enough to justify the endless noisy hype about imminent breakthroughs and looming disruptions, therapies, and apps that are sure to change practice and civilization as we know them. Altogether too much noise, at least for my taste. But not inside the examining room.
Outside the room rages the din of demographic updates, of online checks of insurance eligibility, referral status, prior authorizations, the blare of marketing and promotion, the cacophony of metrics and algorithms.
Inside the room, however, quiet reigns. A patient presents with a symptom or a sign, or the fear of a symptom or anxiety over the meaning of a sign, filtered through a jumble of ideas – misremembered, half understood, at times mutually contradictory – that amplify fears common to anyone who visits a practitioner, however minor the presenting complaint: pain, debility, decline, isolation, solitude, death.
And the practitioner attends, considers, contextualizes, counsels, consoles, and conveys a response to the patient’s questions, whether in so many words or by body language or tone of voice, offers answers not just to what the patient has asked but the ones the patient meant to ask but did not know how.
“Yes, sir, death waits for all of us in the end, but for you, perhaps, not today.”
“Yes, madam, illness can be a frightening affair, but your case is not as bad as you think it is and won’t move as fast as you imagine. And as to your being limited and alone – well, not yet. There are those you can rely on, people with a bit of knowledge and a little experience, who are committed to doing what can be done to bend the arc of illness in your favor.”
That fundamental role will, it seems to me, always apply as long people practice medicine.
With all good wishes for personal happiness and professional success,
Alan Rockoff
Dear Colleagues,
or questions about cosmetic procedures or skin care advice.
Needle nippers were around, but no elaborate, molded-plastic contraptions like the sharps containers now in wide use. You sent pathology specimens in plastic cylinders by U.S. mail; then you called the lab 2 weeks later to ask, “Where’s the report on Jane Smith, with the rule out melanoma,” and the lab said, “Jane who?”
Of course, some things about practice have not changed. Patients with atopic dermatitis still ask why eczema comes back and why we can’t give them something to make it go away once and for all. Some referring physicians still treat scaly rashes with ketoconazole cream (and when that fails, oral fluconazole, which doesn’t work either).
Of course the biggest change between then and now, coincident with the rise of computers and technology, is the advent and ubiquity of that great swindle foisted upon the profession and the public – electronic health records – with their unfulfilled promises of cost-savings and efficiency and unconceded consequences: turning healers into harried data-entry drudges too busy clicking mice to make eye contact with humans. Yes, the Emperor has clothes. The Emperor is wearing Depends.
I wrote my first column for this periodical 22 years ago; this will be my last. My wonderful editor, Elizabeth Mechcatie, has agreed to take under advisement a proposal that I go on sending occasional dispatches under the heading “Pruritus Emeritus.” My family used to refer to those in the anomalous state of being emeritus – it means, roughly, “Forgotten, but not gone” – by rhyming emeritus with sinusitis.
There is no way to remember 40 years of patients. Many came just once, others several times. Some moved away, some passed away, changed primary doctors, changed insurances. Some grew too old to visit, sent regretful notes apologizing for finding the drive too long, the parking too hard. Some returned after an absence of a decade or 3, having forgotten that they had once come for the same problem, or come at all.
But there have been other patients who formed a real bond, whose names and faces still come readily to mind, who visited over long periods, sent their spouses, family members, even children and grandchildren. The stories of their lives became part of mine, and sometimes mine part of theirs.
Though hardly an old-movie buff, I know the famous scene in Casablanca in which a radiant Ingrid Bergman (that skin!) asks Dooley Wilson – the piano player, Sam – to play the song Humphrey Bogart does not want to hear:
“You must remember this
A kiss is just a kiss
A sigh is just a sigh
The fundamental things apply
As time goes by.”
Over the last 40 years there have been substantial advances in the way we treat patients, though perhaps not enough to justify the endless noisy hype about imminent breakthroughs and looming disruptions, therapies, and apps that are sure to change practice and civilization as we know them. Altogether too much noise, at least for my taste. But not inside the examining room.
Outside the room rages the din of demographic updates, of online checks of insurance eligibility, referral status, prior authorizations, the blare of marketing and promotion, the cacophony of metrics and algorithms.
Inside the room, however, quiet reigns. A patient presents with a symptom or a sign, or the fear of a symptom or anxiety over the meaning of a sign, filtered through a jumble of ideas – misremembered, half understood, at times mutually contradictory – that amplify fears common to anyone who visits a practitioner, however minor the presenting complaint: pain, debility, decline, isolation, solitude, death.
And the practitioner attends, considers, contextualizes, counsels, consoles, and conveys a response to the patient’s questions, whether in so many words or by body language or tone of voice, offers answers not just to what the patient has asked but the ones the patient meant to ask but did not know how.
“Yes, sir, death waits for all of us in the end, but for you, perhaps, not today.”
“Yes, madam, illness can be a frightening affair, but your case is not as bad as you think it is and won’t move as fast as you imagine. And as to your being limited and alone – well, not yet. There are those you can rely on, people with a bit of knowledge and a little experience, who are committed to doing what can be done to bend the arc of illness in your favor.”
That fundamental role will, it seems to me, always apply as long people practice medicine.
With all good wishes for personal happiness and professional success,
Alan Rockoff
Dear Colleagues,
or questions about cosmetic procedures or skin care advice.
Needle nippers were around, but no elaborate, molded-plastic contraptions like the sharps containers now in wide use. You sent pathology specimens in plastic cylinders by U.S. mail; then you called the lab 2 weeks later to ask, “Where’s the report on Jane Smith, with the rule out melanoma,” and the lab said, “Jane who?”
Of course, some things about practice have not changed. Patients with atopic dermatitis still ask why eczema comes back and why we can’t give them something to make it go away once and for all. Some referring physicians still treat scaly rashes with ketoconazole cream (and when that fails, oral fluconazole, which doesn’t work either).
Of course the biggest change between then and now, coincident with the rise of computers and technology, is the advent and ubiquity of that great swindle foisted upon the profession and the public – electronic health records – with their unfulfilled promises of cost-savings and efficiency and unconceded consequences: turning healers into harried data-entry drudges too busy clicking mice to make eye contact with humans. Yes, the Emperor has clothes. The Emperor is wearing Depends.
I wrote my first column for this periodical 22 years ago; this will be my last. My wonderful editor, Elizabeth Mechcatie, has agreed to take under advisement a proposal that I go on sending occasional dispatches under the heading “Pruritus Emeritus.” My family used to refer to those in the anomalous state of being emeritus – it means, roughly, “Forgotten, but not gone” – by rhyming emeritus with sinusitis.
There is no way to remember 40 years of patients. Many came just once, others several times. Some moved away, some passed away, changed primary doctors, changed insurances. Some grew too old to visit, sent regretful notes apologizing for finding the drive too long, the parking too hard. Some returned after an absence of a decade or 3, having forgotten that they had once come for the same problem, or come at all.
But there have been other patients who formed a real bond, whose names and faces still come readily to mind, who visited over long periods, sent their spouses, family members, even children and grandchildren. The stories of their lives became part of mine, and sometimes mine part of theirs.
Though hardly an old-movie buff, I know the famous scene in Casablanca in which a radiant Ingrid Bergman (that skin!) asks Dooley Wilson – the piano player, Sam – to play the song Humphrey Bogart does not want to hear:
“You must remember this
A kiss is just a kiss
A sigh is just a sigh
The fundamental things apply
As time goes by.”
Over the last 40 years there have been substantial advances in the way we treat patients, though perhaps not enough to justify the endless noisy hype about imminent breakthroughs and looming disruptions, therapies, and apps that are sure to change practice and civilization as we know them. Altogether too much noise, at least for my taste. But not inside the examining room.
Outside the room rages the din of demographic updates, of online checks of insurance eligibility, referral status, prior authorizations, the blare of marketing and promotion, the cacophony of metrics and algorithms.
Inside the room, however, quiet reigns. A patient presents with a symptom or a sign, or the fear of a symptom or anxiety over the meaning of a sign, filtered through a jumble of ideas – misremembered, half understood, at times mutually contradictory – that amplify fears common to anyone who visits a practitioner, however minor the presenting complaint: pain, debility, decline, isolation, solitude, death.
And the practitioner attends, considers, contextualizes, counsels, consoles, and conveys a response to the patient’s questions, whether in so many words or by body language or tone of voice, offers answers not just to what the patient has asked but the ones the patient meant to ask but did not know how.
“Yes, sir, death waits for all of us in the end, but for you, perhaps, not today.”
“Yes, madam, illness can be a frightening affair, but your case is not as bad as you think it is and won’t move as fast as you imagine. And as to your being limited and alone – well, not yet. There are those you can rely on, people with a bit of knowledge and a little experience, who are committed to doing what can be done to bend the arc of illness in your favor.”
That fundamental role will, it seems to me, always apply as long people practice medicine.
With all good wishes for personal happiness and professional success,
Alan Rockoff
Ask about vaping and e-cigarette use
When we studied the knowledge and practice of e-cigarette use among pregnant women in one of our outpatient practices, we found that 43% of more than 300 survey participants believed e-cigarettes are less harmful to a fetus than traditional cigarettes. Just over half – 57% – believed that e-cigarettes contain nicotine.
This study from 5 years ago demonstrated the need for more patient education.1 Today, we have even more clarity that, while there may be health benefits of switching to noncombustible forms of nicotine consumption outside of pregnancy, these potential benefits do not extend to pregnancy. Both human and animal studies have demonstrated that nicotine itself is harmful to the developing fetus; the Centers for Disease Control and Prevention warns against the use of e-cigarettes in pregnancy for this reason.
A 2018 literature review on the use of e-cigarettes in pregnancy and the effects on perinatal/neonatal outcomes reported that the amount of nicotine consumed by e-cigarette users is similar to that of cigarette smokers and that most animal studies suggest a potential danger to the fetus, primarily because of the nicotine.2 Effects on the immune system, neural development, lung function, and cardiac function were all noted in the review. Other research has shown that e-cigarette fluid can contain formaldehyde and other harmful substances.
A new analysis of data from the 2014-2017 National Health Interview Survey shows a significantly lower prevalence of conventional cigarette use among pregnant women than in nonpregnant women, and an almost identical prevalence of e-cigarette use among pregnant and nonpregnant women of reproductive age.3 This discrepancy again suggests that women may not be aware of the potential harms of e-cigarettes in pregnancy, which is not surprising considering that prenatal care clinicians often are not appropriately screening or counseling regarding e-cigarette use.4
and counsel women that the use of e-cigarettes is not a safer alternative to cigarette smoking. I urge patients who have switched to e-cigarettes as a means of smoking cessation or as a choice they perceive to be safer to work together with me to find another way to reduce potential harm to their baby.
References
1. J Addict Med. 2015 Jul-Aug;9(4):266-72.
2. Obstet Gynecol Surv. 2018 Sep;73(9):544-9.
3. JAMA Pediatr. 2019 Jun 1;173(6):600-2.
4. Am J Obstet Gynecol. 2014 Dec;211(6):695.e1-7.
When we studied the knowledge and practice of e-cigarette use among pregnant women in one of our outpatient practices, we found that 43% of more than 300 survey participants believed e-cigarettes are less harmful to a fetus than traditional cigarettes. Just over half – 57% – believed that e-cigarettes contain nicotine.
This study from 5 years ago demonstrated the need for more patient education.1 Today, we have even more clarity that, while there may be health benefits of switching to noncombustible forms of nicotine consumption outside of pregnancy, these potential benefits do not extend to pregnancy. Both human and animal studies have demonstrated that nicotine itself is harmful to the developing fetus; the Centers for Disease Control and Prevention warns against the use of e-cigarettes in pregnancy for this reason.
A 2018 literature review on the use of e-cigarettes in pregnancy and the effects on perinatal/neonatal outcomes reported that the amount of nicotine consumed by e-cigarette users is similar to that of cigarette smokers and that most animal studies suggest a potential danger to the fetus, primarily because of the nicotine.2 Effects on the immune system, neural development, lung function, and cardiac function were all noted in the review. Other research has shown that e-cigarette fluid can contain formaldehyde and other harmful substances.
A new analysis of data from the 2014-2017 National Health Interview Survey shows a significantly lower prevalence of conventional cigarette use among pregnant women than in nonpregnant women, and an almost identical prevalence of e-cigarette use among pregnant and nonpregnant women of reproductive age.3 This discrepancy again suggests that women may not be aware of the potential harms of e-cigarettes in pregnancy, which is not surprising considering that prenatal care clinicians often are not appropriately screening or counseling regarding e-cigarette use.4
and counsel women that the use of e-cigarettes is not a safer alternative to cigarette smoking. I urge patients who have switched to e-cigarettes as a means of smoking cessation or as a choice they perceive to be safer to work together with me to find another way to reduce potential harm to their baby.
References
1. J Addict Med. 2015 Jul-Aug;9(4):266-72.
2. Obstet Gynecol Surv. 2018 Sep;73(9):544-9.
3. JAMA Pediatr. 2019 Jun 1;173(6):600-2.
4. Am J Obstet Gynecol. 2014 Dec;211(6):695.e1-7.
When we studied the knowledge and practice of e-cigarette use among pregnant women in one of our outpatient practices, we found that 43% of more than 300 survey participants believed e-cigarettes are less harmful to a fetus than traditional cigarettes. Just over half – 57% – believed that e-cigarettes contain nicotine.
This study from 5 years ago demonstrated the need for more patient education.1 Today, we have even more clarity that, while there may be health benefits of switching to noncombustible forms of nicotine consumption outside of pregnancy, these potential benefits do not extend to pregnancy. Both human and animal studies have demonstrated that nicotine itself is harmful to the developing fetus; the Centers for Disease Control and Prevention warns against the use of e-cigarettes in pregnancy for this reason.
A 2018 literature review on the use of e-cigarettes in pregnancy and the effects on perinatal/neonatal outcomes reported that the amount of nicotine consumed by e-cigarette users is similar to that of cigarette smokers and that most animal studies suggest a potential danger to the fetus, primarily because of the nicotine.2 Effects on the immune system, neural development, lung function, and cardiac function were all noted in the review. Other research has shown that e-cigarette fluid can contain formaldehyde and other harmful substances.
A new analysis of data from the 2014-2017 National Health Interview Survey shows a significantly lower prevalence of conventional cigarette use among pregnant women than in nonpregnant women, and an almost identical prevalence of e-cigarette use among pregnant and nonpregnant women of reproductive age.3 This discrepancy again suggests that women may not be aware of the potential harms of e-cigarettes in pregnancy, which is not surprising considering that prenatal care clinicians often are not appropriately screening or counseling regarding e-cigarette use.4
and counsel women that the use of e-cigarettes is not a safer alternative to cigarette smoking. I urge patients who have switched to e-cigarettes as a means of smoking cessation or as a choice they perceive to be safer to work together with me to find another way to reduce potential harm to their baby.
References
1. J Addict Med. 2015 Jul-Aug;9(4):266-72.
2. Obstet Gynecol Surv. 2018 Sep;73(9):544-9.
3. JAMA Pediatr. 2019 Jun 1;173(6):600-2.
4. Am J Obstet Gynecol. 2014 Dec;211(6):695.e1-7.
Cannabis and prenatal care
We know that the environment significantly impacts our health. People who live in areas prone to industrial waste, poor air or water quality, and crime have higher risks for cardiovascular disease, severe asthma, and stress-induced illnesses. Children who grow up under these conditions can experience a failure to thrive.

As ob.gyns., we also recognize that the intrauterine environment plays a key role in influencing embryonic and fetal development. For this reason, we counsel our pregnant patients to eat well-balanced diets, drink healthy amounts of water, get plenty of rest, and incorporate physical activity into their daily routines. Indeed, the seminal work by Sir David Barker demonstrated that the roots of chronic diseases – including hypertension, stroke, and type 2 diabetes – begin in utero. We truly are where we live – from before birth up through adulthood.
Because the womb environment, where we spend the first critical 9 months of life, dramatically affects our lifelong health, we advise against the use of certain medications and other substances during pregnancy. Some of these recommendations seem clear-cut: Don’t smoke and significantly reduce or abstain from alcohol consumption; illicit drugs – such as cocaine or heroin – should never be used. However, gray areas exist. For example, although anticonvulsants carry higher risks for congenital malformations, patients who experience seizures may need to continue taking antiepileptic drugs during pregnancy, especially those with long safety records.
One of the newer challenges the medical community in general must face is the broadened use and wider societal acceptance of cannabis. Currently legal in 33 U.S. states and Washington, D.C., medical marijuana now is viewed as another legitimate tool in the health care arsenal, rather than the off-limits, off-label substance it was less than a generation ago.
Although proponents may tout the health benefits of cannabis and related products like cannabidiol, it remains unclear what the long-term effects of routine use may have on development, especially fetal development. However, how we as ob.gyns. navigate conversations with our patients around substance use remains crucial to our delivery of the best possible prenatal care.
We have invited Katrina S. Mark, MD, associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, to examine use of cannabis in pregnancy and the need for maintaining trust in the patient-practitioner relationship when discussing substance use during prenatal counseling.
Dr. Reece, who specializes in maternal-fetal medicine, is executive vice president for medical affairs at the University of Maryland School of Medicine as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. He is the medical editor of this column. He said he had no relevant financial disclosures. Contact him at obnews@mdedge.com.
We know that the environment significantly impacts our health. People who live in areas prone to industrial waste, poor air or water quality, and crime have higher risks for cardiovascular disease, severe asthma, and stress-induced illnesses. Children who grow up under these conditions can experience a failure to thrive.
As ob.gyns., we also recognize that the intrauterine environment plays a key role in influencing embryonic and fetal development. For this reason, we counsel our pregnant patients to eat well-balanced diets, drink healthy amounts of water, get plenty of rest, and incorporate physical activity into their daily routines. Indeed, the seminal work by Sir David Barker demonstrated that the roots of chronic diseases – including hypertension, stroke, and type 2 diabetes – begin in utero. We truly are where we live – from before birth up through adulthood.
Because the womb environment, where we spend the first critical 9 months of life, dramatically affects our lifelong health, we advise against the use of certain medications and other substances during pregnancy. Some of these recommendations seem clear-cut: Don’t smoke and significantly reduce or abstain from alcohol consumption; illicit drugs – such as cocaine or heroin – should never be used. However, gray areas exist. For example, although anticonvulsants carry higher risks for congenital malformations, patients who experience seizures may need to continue taking antiepileptic drugs during pregnancy, especially those with long safety records.
One of the newer challenges the medical community in general must face is the broadened use and wider societal acceptance of cannabis. Currently legal in 33 U.S. states and Washington, D.C., medical marijuana now is viewed as another legitimate tool in the health care arsenal, rather than the off-limits, off-label substance it was less than a generation ago.
Although proponents may tout the health benefits of cannabis and related products like cannabidiol, it remains unclear what the long-term effects of routine use may have on development, especially fetal development. However, how we as ob.gyns. navigate conversations with our patients around substance use remains crucial to our delivery of the best possible prenatal care.
We have invited Katrina S. Mark, MD, associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, to examine use of cannabis in pregnancy and the need for maintaining trust in the patient-practitioner relationship when discussing substance use during prenatal counseling.
Dr. Reece, who specializes in maternal-fetal medicine, is executive vice president for medical affairs at the University of Maryland School of Medicine as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. He is the medical editor of this column. He said he had no relevant financial disclosures. Contact him at obnews@mdedge.com.
We know that the environment significantly impacts our health. People who live in areas prone to industrial waste, poor air or water quality, and crime have higher risks for cardiovascular disease, severe asthma, and stress-induced illnesses. Children who grow up under these conditions can experience a failure to thrive.
As ob.gyns., we also recognize that the intrauterine environment plays a key role in influencing embryonic and fetal development. For this reason, we counsel our pregnant patients to eat well-balanced diets, drink healthy amounts of water, get plenty of rest, and incorporate physical activity into their daily routines. Indeed, the seminal work by Sir David Barker demonstrated that the roots of chronic diseases – including hypertension, stroke, and type 2 diabetes – begin in utero. We truly are where we live – from before birth up through adulthood.
Because the womb environment, where we spend the first critical 9 months of life, dramatically affects our lifelong health, we advise against the use of certain medications and other substances during pregnancy. Some of these recommendations seem clear-cut: Don’t smoke and significantly reduce or abstain from alcohol consumption; illicit drugs – such as cocaine or heroin – should never be used. However, gray areas exist. For example, although anticonvulsants carry higher risks for congenital malformations, patients who experience seizures may need to continue taking antiepileptic drugs during pregnancy, especially those with long safety records.
One of the newer challenges the medical community in general must face is the broadened use and wider societal acceptance of cannabis. Currently legal in 33 U.S. states and Washington, D.C., medical marijuana now is viewed as another legitimate tool in the health care arsenal, rather than the off-limits, off-label substance it was less than a generation ago.
Although proponents may tout the health benefits of cannabis and related products like cannabidiol, it remains unclear what the long-term effects of routine use may have on development, especially fetal development. However, how we as ob.gyns. navigate conversations with our patients around substance use remains crucial to our delivery of the best possible prenatal care.
We have invited Katrina S. Mark, MD, associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine, to examine use of cannabis in pregnancy and the need for maintaining trust in the patient-practitioner relationship when discussing substance use during prenatal counseling.
Dr. Reece, who specializes in maternal-fetal medicine, is executive vice president for medical affairs at the University of Maryland School of Medicine as well as the John Z. and Akiko K. Bowers Distinguished Professor and dean of the school of medicine. He is the medical editor of this column. He said he had no relevant financial disclosures. Contact him at obnews@mdedge.com.
Counseling on cannabis use in pregnancy
A flurry of research papers published this year has simultaneously documented a rise in the use of cannabis during pregnancy and offered more data about its potential harms. This confluence of findings is concerning and highlights the importance of screening our patients for cannabis use and engaging with them in a way in which we can maintain their trust and their commitment to prenatal care.

A retrospective cohort study involving 661,617 women in Ontario found a significant association between self-reported cannabis use in pregnancy and an increased risk of preterm birth (relative risk, 1.41), as well as a greater likelihood of small-for-gestational-age babies (RR, 1.53), placental abruption (RR, 1.72), and transfer to neonatal intensive care (RR, 1.40).1 The study, reported in JAMA in July 2019, carefully matched users with nonusers who had the same characteristics – for example, tobacco use or not.
This new information builds upon other meta-analyses that have demonstrated a decrease in birth weight and greater admittance to the neonatal ICU associated with cannabis use in pregnancy – and it supplements what some research suggests about long-term neurologic development and a potentially increased risk of attention and behavioral problems. Other outcomes that have been noted in long-term neurologic studies of children who were exposed to cannabis in utero include impaired visual acuity, verbal reasoning and comprehension, and short-term memory.2
Increases in use were recently documented in two studies. One, an analysis of data from the National Survey on Drug Use and Health (NSDUH) published in JAMA in June 2019, showed that, between 2002-2003 and 2016-2017, the use of cannabis “in the past month” increased from 3.4% to 7.0% among pregnant women overall, and from 6% to 12% during the first trimester.3
The use of cannabis on a daily or near-daily basis, moreover, increased from 0.9% to 3% among pregnant women overall and from 2% to 5% during the first trimester. The data were collected during face-to-face interviews and were adjusted for age, race/ethnicity, and family income.
In the second study – a cross-sectional study of 367,403 pregnancies among women who filled out a questionnaire on cannabis use during standard prenatal care at Kaiser Permanente Northern California – the adjusted prevalence of use in the year before pregnancy increased from 7% in 2009 to 13% in 2017, and the adjusted prevalence during pregnancy increased from 2% to 3%.4
As in the NSDUH analysis, daily use increased most rapidly (compared with weekly or monthly) such that, by 2017, 25% of those who reported using cannabis in the year before pregnancy – and 21% of those who used cannabis during pregnancy – were daily users. It is notable that Kaiser’s population is diverse in all respects, and that the annual relative rates of increase in cannabis use before and during pregnancy (at each level of frequency) were consistent across racial/ethnic and household income groups.
It’s also worth noting that, in earlier research covering a similar time period (2009-2016), the investigators found significant increases in use via urine toxicology testing that occurs at the first prenatal visit at Kaiser. The increase found through questionnaires, therefore, reflects more than a greater willingness to self-report.
Choosing a screening tool
Universal prenatal substance use screening is recommended by the American College of Obstetricians and Gynecologists and the Centers for Disease Control and Prevention, but we don’t have any specific recommendations on what this means. Who should be screening, and what should that screening look like? Should we use a biologic screen, a standardized screening tool, or simply ask patients whether they use illicit substances?
Screening tools seem advantageous in that they are low cost, noninvasive, potentially comprehensive, and not subject to false-positive results as biologic screens can be – but which tool or tools are best? There are several validated screening tools that can be used outside of pregnancy to determine an individual’s use of illicit substances and whether or not that use is problematic, but previous studies have not used biologic markers to validate substance use screeners in pregnancy. Nor have studies compared screeners in pregnancy.
In our prenatal population in Baltimore, we have not been getting the answers we want using various nonvalidated screening tools. Approximately 30% of patients are positive for cannabis by urine screen, but only half tell us about their use.
Through research in our two prenatal care practices (one serving mostly privately insured and the other serving primarily Medicaid-eligible patients), we assessed both the accuracy and the acceptability of three substance use screening tools that are brief and that have been validated (for the general population) by the World Health Organization for screening of multiple substances: the 4P’s Plus (Parents, Partner, Past, and Pregnancy), the National Institute on Drug Abuse Quick Screen–ASSIST (Modified Alcohol, Smoking and Substance Involvement Screening Test), and the SURP-P (Substance Use Risk Profile–Pregnancy) scale.
In one study, published in May 2019 in Obstetrics & Gynecology, we recruited 500 pregnant women and administered these three tests to each of them.5 We then compared results with those of urine and hair drug testing, and checked the test-retest reliability of each test by readministering them (albeit by telephone) a week later. Although hair testing is not an indicator of current substance use, we used it to validate the screening tools on less-recent use.
The tests with the highest sensitivity and negative predictive values – the qualities we most want for screening – were the SURP-P and the 4P’s Plus (sensitivity of 92.4% and 90.2%, respectively). Overall they were highly sensitive screening tools across all trimesters, races, and age groups, making them more ideal screening tests than the NIDA Quick Screen–ASSIST.
Of the two tests, the 4P’s Plus screening tool was the one preferred by staff from both practices. In a companion qualitative study, we conducted focus-group discussions with 40 practice staff who were responsible for administering or overseeing patient screening.6 The staff, who were unaware of the sensitivity findings, were asked what they thought about the acceptability to patients of each of the three tools and their usability in practice.
Most of the participating staff preferred the 4P’s Plus screening tool for several reasons: It is easy to understand, is brief and to the point, and it has nonjudgmental language and tone. The screener first asks the patient about her parents’ and her partner’s use of alcohol and drugs, and then asks the patient about her own use of alcohol and tobacco. Affirmative responses to these questions lead to additional questions.
The premise is that one’s genetics, history, and current exposures – as well as one’s own use of tobacco and alcohol – are significantly associated with the use of illicit substances. If the patient reports no parental history or partner usage, and has never drank or smoked before, it’s extremely unlikely that she is using other drugs. The progression of questions does indeed seem less judgmental than immediately asking: “Do you use drugs?”
For us, the insight from this staff perception study combined with the findings on accuracy mean that the 4P’s Plus may be the most useful and acceptable screening tool for routine use in prenatal care.
Talking with our patients
The increase in the use of cannabis before and after pregnancy parallels the movement toward state legalization and decriminalization. Historically, clinicians often have relied on illegality as their main focus of counseling when giving recommendations for cessation and abstinence in pregnancy.2 This approach not only leads to punitive counseling, which can fracture the doctor-patient relationship, but increasingly it is no longer valid. In our changing legal climate, we need to provide medically based counseling and be very clear with our patients that legalization does not equate to safety.
It is important that we neither minimize nor overstate the risks. The evidence base for adverse birth outcomes of cannabis use in pregnancy is quite robust, but the associations can be subtle and are moderated by other behaviors and environmental factors that continue to challenge researchers.
As with alcohol, there likely are dose-or trimester-dependent differences in perinatal outcomes, and it’s quite possible that different cannabis products and routes of consumption have different effects. At this point, however, we don’t know the full story, nor do we know the extent to which the literature is biased toward positive correlations – the reporting of adverse effects – compared with negative findings. It is our job as medical care providers to be comfortable in that gray area and to still counsel patients on what we do know, providing the best-possible medical advice based on the information available to us.
In talking with patients, I explain that cannabis may cause a spectrum of problems and that there certainly are risks. I also tell them that we’re uncertain about the conditions and magnitude of that risk and that some babies who are exposed to cannabis in utero may have no perceivable consequences. Such honesty is important for maintaining trust, especially as some patients may see friends and relatives who also are cannabis users have normal pregnancy outcomes.
Much of my concern about cannabis in pregnancy centers on its effect on the developing brain and on long-term neurologic development. I share this with patients – I tell them that cannabis crosses the placenta and may well affect their baby’s brain as it is developing. I explain that I do not know whether this effect would be big or small, but that it’s not a chance I’m willing to take for their baby.
It is also important to educate patients that cannabis products are untested and unregulated and that they may be contaminated with heavy metals, pesticides, and other toxins that may be harmful to themselves and their babies. Patients also should know that the potency of cannabis has been dramatically increasing; research shows that the tetrahydrocannabinol – the psychoactive component – concentration has tripled over the past 2 decades.7
Research tells us that women who use illicit drugs and alcohol categorically engage in some form of harm reduction once they learn they are pregnant, and the same is true for cannabis. This is seen in dramatically different rates of first- and third-trimester use in the new analysis of NSDUH data; third-trimester use is approximately halved.
Some women will not be able to discontinue use, however, or they may try to quit and fail in their attempts. As we should with substance use more broadly, we must meet patients where they are, view cannabis use as a chronic medical problem, offer our assistance in helping them reduce harms of their use, and understand that quitting is a process.
Screening for mental health disorders and trauma is, of course, especially important in patients who use cannabis and other substances recreationally. In cases of medical marijuana usage, I recommend, as ACOG and other have done, that we discuss the risks and benefits of continuing cannabis versus shifting to alternative medications if options exist.
All patients should be welcomed, congratulated on their pregnancy and on coming for prenatal care, and engaged in the overall process of optimizing their health and the health of their baby. Like any other health issue during pregnancy, cannabis use needs to be screened for and treated in an evidence-based manner, but it does not define the trajectory or success of a woman’s pregnancy or her ability to be a successful parent.
Dr. Mark is associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine.
References
1. JAMA. 2019 Jul 9;322(2):145-52.
2. Preventive Medicine 2017 May 18;104:46-9.
3. JAMA. 2019 Jul 9;322(2):167-9.
4. JAMA Netw Open. 2019 Jul 3;2(7):e196471.
5. Obstet Gynecol. 2019 May;133(5):952-61.
6. J. Addict Med. 2019 May 10. doi: 10.1097/ADM.0000000000000543.
7. Biol Psychiatry. 2016 Apr 1;79(7):613-9.
A flurry of research papers published this year has simultaneously documented a rise in the use of cannabis during pregnancy and offered more data about its potential harms. This confluence of findings is concerning and highlights the importance of screening our patients for cannabis use and engaging with them in a way in which we can maintain their trust and their commitment to prenatal care.
A retrospective cohort study involving 661,617 women in Ontario found a significant association between self-reported cannabis use in pregnancy and an increased risk of preterm birth (relative risk, 1.41), as well as a greater likelihood of small-for-gestational-age babies (RR, 1.53), placental abruption (RR, 1.72), and transfer to neonatal intensive care (RR, 1.40).1 The study, reported in JAMA in July 2019, carefully matched users with nonusers who had the same characteristics – for example, tobacco use or not.
This new information builds upon other meta-analyses that have demonstrated a decrease in birth weight and greater admittance to the neonatal ICU associated with cannabis use in pregnancy – and it supplements what some research suggests about long-term neurologic development and a potentially increased risk of attention and behavioral problems. Other outcomes that have been noted in long-term neurologic studies of children who were exposed to cannabis in utero include impaired visual acuity, verbal reasoning and comprehension, and short-term memory.2
Increases in use were recently documented in two studies. One, an analysis of data from the National Survey on Drug Use and Health (NSDUH) published in JAMA in June 2019, showed that, between 2002-2003 and 2016-2017, the use of cannabis “in the past month” increased from 3.4% to 7.0% among pregnant women overall, and from 6% to 12% during the first trimester.3
The use of cannabis on a daily or near-daily basis, moreover, increased from 0.9% to 3% among pregnant women overall and from 2% to 5% during the first trimester. The data were collected during face-to-face interviews and were adjusted for age, race/ethnicity, and family income.
In the second study – a cross-sectional study of 367,403 pregnancies among women who filled out a questionnaire on cannabis use during standard prenatal care at Kaiser Permanente Northern California – the adjusted prevalence of use in the year before pregnancy increased from 7% in 2009 to 13% in 2017, and the adjusted prevalence during pregnancy increased from 2% to 3%.4
As in the NSDUH analysis, daily use increased most rapidly (compared with weekly or monthly) such that, by 2017, 25% of those who reported using cannabis in the year before pregnancy – and 21% of those who used cannabis during pregnancy – were daily users. It is notable that Kaiser’s population is diverse in all respects, and that the annual relative rates of increase in cannabis use before and during pregnancy (at each level of frequency) were consistent across racial/ethnic and household income groups.
It’s also worth noting that, in earlier research covering a similar time period (2009-2016), the investigators found significant increases in use via urine toxicology testing that occurs at the first prenatal visit at Kaiser. The increase found through questionnaires, therefore, reflects more than a greater willingness to self-report.
Choosing a screening tool
Universal prenatal substance use screening is recommended by the American College of Obstetricians and Gynecologists and the Centers for Disease Control and Prevention, but we don’t have any specific recommendations on what this means. Who should be screening, and what should that screening look like? Should we use a biologic screen, a standardized screening tool, or simply ask patients whether they use illicit substances?
Screening tools seem advantageous in that they are low cost, noninvasive, potentially comprehensive, and not subject to false-positive results as biologic screens can be – but which tool or tools are best? There are several validated screening tools that can be used outside of pregnancy to determine an individual’s use of illicit substances and whether or not that use is problematic, but previous studies have not used biologic markers to validate substance use screeners in pregnancy. Nor have studies compared screeners in pregnancy.
In our prenatal population in Baltimore, we have not been getting the answers we want using various nonvalidated screening tools. Approximately 30% of patients are positive for cannabis by urine screen, but only half tell us about their use.
Through research in our two prenatal care practices (one serving mostly privately insured and the other serving primarily Medicaid-eligible patients), we assessed both the accuracy and the acceptability of three substance use screening tools that are brief and that have been validated (for the general population) by the World Health Organization for screening of multiple substances: the 4P’s Plus (Parents, Partner, Past, and Pregnancy), the National Institute on Drug Abuse Quick Screen–ASSIST (Modified Alcohol, Smoking and Substance Involvement Screening Test), and the SURP-P (Substance Use Risk Profile–Pregnancy) scale.
In one study, published in May 2019 in Obstetrics & Gynecology, we recruited 500 pregnant women and administered these three tests to each of them.5 We then compared results with those of urine and hair drug testing, and checked the test-retest reliability of each test by readministering them (albeit by telephone) a week later. Although hair testing is not an indicator of current substance use, we used it to validate the screening tools on less-recent use.
The tests with the highest sensitivity and negative predictive values – the qualities we most want for screening – were the SURP-P and the 4P’s Plus (sensitivity of 92.4% and 90.2%, respectively). Overall they were highly sensitive screening tools across all trimesters, races, and age groups, making them more ideal screening tests than the NIDA Quick Screen–ASSIST.
Of the two tests, the 4P’s Plus screening tool was the one preferred by staff from both practices. In a companion qualitative study, we conducted focus-group discussions with 40 practice staff who were responsible for administering or overseeing patient screening.6 The staff, who were unaware of the sensitivity findings, were asked what they thought about the acceptability to patients of each of the three tools and their usability in practice.
Most of the participating staff preferred the 4P’s Plus screening tool for several reasons: It is easy to understand, is brief and to the point, and it has nonjudgmental language and tone. The screener first asks the patient about her parents’ and her partner’s use of alcohol and drugs, and then asks the patient about her own use of alcohol and tobacco. Affirmative responses to these questions lead to additional questions.
The premise is that one’s genetics, history, and current exposures – as well as one’s own use of tobacco and alcohol – are significantly associated with the use of illicit substances. If the patient reports no parental history or partner usage, and has never drank or smoked before, it’s extremely unlikely that she is using other drugs. The progression of questions does indeed seem less judgmental than immediately asking: “Do you use drugs?”
For us, the insight from this staff perception study combined with the findings on accuracy mean that the 4P’s Plus may be the most useful and acceptable screening tool for routine use in prenatal care.
Talking with our patients
The increase in the use of cannabis before and after pregnancy parallels the movement toward state legalization and decriminalization. Historically, clinicians often have relied on illegality as their main focus of counseling when giving recommendations for cessation and abstinence in pregnancy.2 This approach not only leads to punitive counseling, which can fracture the doctor-patient relationship, but increasingly it is no longer valid. In our changing legal climate, we need to provide medically based counseling and be very clear with our patients that legalization does not equate to safety.
It is important that we neither minimize nor overstate the risks. The evidence base for adverse birth outcomes of cannabis use in pregnancy is quite robust, but the associations can be subtle and are moderated by other behaviors and environmental factors that continue to challenge researchers.
As with alcohol, there likely are dose-or trimester-dependent differences in perinatal outcomes, and it’s quite possible that different cannabis products and routes of consumption have different effects. At this point, however, we don’t know the full story, nor do we know the extent to which the literature is biased toward positive correlations – the reporting of adverse effects – compared with negative findings. It is our job as medical care providers to be comfortable in that gray area and to still counsel patients on what we do know, providing the best-possible medical advice based on the information available to us.
In talking with patients, I explain that cannabis may cause a spectrum of problems and that there certainly are risks. I also tell them that we’re uncertain about the conditions and magnitude of that risk and that some babies who are exposed to cannabis in utero may have no perceivable consequences. Such honesty is important for maintaining trust, especially as some patients may see friends and relatives who also are cannabis users have normal pregnancy outcomes.
Much of my concern about cannabis in pregnancy centers on its effect on the developing brain and on long-term neurologic development. I share this with patients – I tell them that cannabis crosses the placenta and may well affect their baby’s brain as it is developing. I explain that I do not know whether this effect would be big or small, but that it’s not a chance I’m willing to take for their baby.
It is also important to educate patients that cannabis products are untested and unregulated and that they may be contaminated with heavy metals, pesticides, and other toxins that may be harmful to themselves and their babies. Patients also should know that the potency of cannabis has been dramatically increasing; research shows that the tetrahydrocannabinol – the psychoactive component – concentration has tripled over the past 2 decades.7
Research tells us that women who use illicit drugs and alcohol categorically engage in some form of harm reduction once they learn they are pregnant, and the same is true for cannabis. This is seen in dramatically different rates of first- and third-trimester use in the new analysis of NSDUH data; third-trimester use is approximately halved.
Some women will not be able to discontinue use, however, or they may try to quit and fail in their attempts. As we should with substance use more broadly, we must meet patients where they are, view cannabis use as a chronic medical problem, offer our assistance in helping them reduce harms of their use, and understand that quitting is a process.
Screening for mental health disorders and trauma is, of course, especially important in patients who use cannabis and other substances recreationally. In cases of medical marijuana usage, I recommend, as ACOG and other have done, that we discuss the risks and benefits of continuing cannabis versus shifting to alternative medications if options exist.
All patients should be welcomed, congratulated on their pregnancy and on coming for prenatal care, and engaged in the overall process of optimizing their health and the health of their baby. Like any other health issue during pregnancy, cannabis use needs to be screened for and treated in an evidence-based manner, but it does not define the trajectory or success of a woman’s pregnancy or her ability to be a successful parent.
Dr. Mark is associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine.
References
1. JAMA. 2019 Jul 9;322(2):145-52.
2. Preventive Medicine 2017 May 18;104:46-9.
3. JAMA. 2019 Jul 9;322(2):167-9.
4. JAMA Netw Open. 2019 Jul 3;2(7):e196471.
5. Obstet Gynecol. 2019 May;133(5):952-61.
6. J. Addict Med. 2019 May 10. doi: 10.1097/ADM.0000000000000543.
7. Biol Psychiatry. 2016 Apr 1;79(7):613-9.
A flurry of research papers published this year has simultaneously documented a rise in the use of cannabis during pregnancy and offered more data about its potential harms. This confluence of findings is concerning and highlights the importance of screening our patients for cannabis use and engaging with them in a way in which we can maintain their trust and their commitment to prenatal care.
A retrospective cohort study involving 661,617 women in Ontario found a significant association between self-reported cannabis use in pregnancy and an increased risk of preterm birth (relative risk, 1.41), as well as a greater likelihood of small-for-gestational-age babies (RR, 1.53), placental abruption (RR, 1.72), and transfer to neonatal intensive care (RR, 1.40).1 The study, reported in JAMA in July 2019, carefully matched users with nonusers who had the same characteristics – for example, tobacco use or not.
This new information builds upon other meta-analyses that have demonstrated a decrease in birth weight and greater admittance to the neonatal ICU associated with cannabis use in pregnancy – and it supplements what some research suggests about long-term neurologic development and a potentially increased risk of attention and behavioral problems. Other outcomes that have been noted in long-term neurologic studies of children who were exposed to cannabis in utero include impaired visual acuity, verbal reasoning and comprehension, and short-term memory.2
Increases in use were recently documented in two studies. One, an analysis of data from the National Survey on Drug Use and Health (NSDUH) published in JAMA in June 2019, showed that, between 2002-2003 and 2016-2017, the use of cannabis “in the past month” increased from 3.4% to 7.0% among pregnant women overall, and from 6% to 12% during the first trimester.3
The use of cannabis on a daily or near-daily basis, moreover, increased from 0.9% to 3% among pregnant women overall and from 2% to 5% during the first trimester. The data were collected during face-to-face interviews and were adjusted for age, race/ethnicity, and family income.
In the second study – a cross-sectional study of 367,403 pregnancies among women who filled out a questionnaire on cannabis use during standard prenatal care at Kaiser Permanente Northern California – the adjusted prevalence of use in the year before pregnancy increased from 7% in 2009 to 13% in 2017, and the adjusted prevalence during pregnancy increased from 2% to 3%.4
As in the NSDUH analysis, daily use increased most rapidly (compared with weekly or monthly) such that, by 2017, 25% of those who reported using cannabis in the year before pregnancy – and 21% of those who used cannabis during pregnancy – were daily users. It is notable that Kaiser’s population is diverse in all respects, and that the annual relative rates of increase in cannabis use before and during pregnancy (at each level of frequency) were consistent across racial/ethnic and household income groups.
It’s also worth noting that, in earlier research covering a similar time period (2009-2016), the investigators found significant increases in use via urine toxicology testing that occurs at the first prenatal visit at Kaiser. The increase found through questionnaires, therefore, reflects more than a greater willingness to self-report.
Choosing a screening tool
Universal prenatal substance use screening is recommended by the American College of Obstetricians and Gynecologists and the Centers for Disease Control and Prevention, but we don’t have any specific recommendations on what this means. Who should be screening, and what should that screening look like? Should we use a biologic screen, a standardized screening tool, or simply ask patients whether they use illicit substances?
Screening tools seem advantageous in that they are low cost, noninvasive, potentially comprehensive, and not subject to false-positive results as biologic screens can be – but which tool or tools are best? There are several validated screening tools that can be used outside of pregnancy to determine an individual’s use of illicit substances and whether or not that use is problematic, but previous studies have not used biologic markers to validate substance use screeners in pregnancy. Nor have studies compared screeners in pregnancy.
In our prenatal population in Baltimore, we have not been getting the answers we want using various nonvalidated screening tools. Approximately 30% of patients are positive for cannabis by urine screen, but only half tell us about their use.
Through research in our two prenatal care practices (one serving mostly privately insured and the other serving primarily Medicaid-eligible patients), we assessed both the accuracy and the acceptability of three substance use screening tools that are brief and that have been validated (for the general population) by the World Health Organization for screening of multiple substances: the 4P’s Plus (Parents, Partner, Past, and Pregnancy), the National Institute on Drug Abuse Quick Screen–ASSIST (Modified Alcohol, Smoking and Substance Involvement Screening Test), and the SURP-P (Substance Use Risk Profile–Pregnancy) scale.
In one study, published in May 2019 in Obstetrics & Gynecology, we recruited 500 pregnant women and administered these three tests to each of them.5 We then compared results with those of urine and hair drug testing, and checked the test-retest reliability of each test by readministering them (albeit by telephone) a week later. Although hair testing is not an indicator of current substance use, we used it to validate the screening tools on less-recent use.
The tests with the highest sensitivity and negative predictive values – the qualities we most want for screening – were the SURP-P and the 4P’s Plus (sensitivity of 92.4% and 90.2%, respectively). Overall they were highly sensitive screening tools across all trimesters, races, and age groups, making them more ideal screening tests than the NIDA Quick Screen–ASSIST.
Of the two tests, the 4P’s Plus screening tool was the one preferred by staff from both practices. In a companion qualitative study, we conducted focus-group discussions with 40 practice staff who were responsible for administering or overseeing patient screening.6 The staff, who were unaware of the sensitivity findings, were asked what they thought about the acceptability to patients of each of the three tools and their usability in practice.
Most of the participating staff preferred the 4P’s Plus screening tool for several reasons: It is easy to understand, is brief and to the point, and it has nonjudgmental language and tone. The screener first asks the patient about her parents’ and her partner’s use of alcohol and drugs, and then asks the patient about her own use of alcohol and tobacco. Affirmative responses to these questions lead to additional questions.
The premise is that one’s genetics, history, and current exposures – as well as one’s own use of tobacco and alcohol – are significantly associated with the use of illicit substances. If the patient reports no parental history or partner usage, and has never drank or smoked before, it’s extremely unlikely that she is using other drugs. The progression of questions does indeed seem less judgmental than immediately asking: “Do you use drugs?”
For us, the insight from this staff perception study combined with the findings on accuracy mean that the 4P’s Plus may be the most useful and acceptable screening tool for routine use in prenatal care.
Talking with our patients
The increase in the use of cannabis before and after pregnancy parallels the movement toward state legalization and decriminalization. Historically, clinicians often have relied on illegality as their main focus of counseling when giving recommendations for cessation and abstinence in pregnancy.2 This approach not only leads to punitive counseling, which can fracture the doctor-patient relationship, but increasingly it is no longer valid. In our changing legal climate, we need to provide medically based counseling and be very clear with our patients that legalization does not equate to safety.
It is important that we neither minimize nor overstate the risks. The evidence base for adverse birth outcomes of cannabis use in pregnancy is quite robust, but the associations can be subtle and are moderated by other behaviors and environmental factors that continue to challenge researchers.
As with alcohol, there likely are dose-or trimester-dependent differences in perinatal outcomes, and it’s quite possible that different cannabis products and routes of consumption have different effects. At this point, however, we don’t know the full story, nor do we know the extent to which the literature is biased toward positive correlations – the reporting of adverse effects – compared with negative findings. It is our job as medical care providers to be comfortable in that gray area and to still counsel patients on what we do know, providing the best-possible medical advice based on the information available to us.
In talking with patients, I explain that cannabis may cause a spectrum of problems and that there certainly are risks. I also tell them that we’re uncertain about the conditions and magnitude of that risk and that some babies who are exposed to cannabis in utero may have no perceivable consequences. Such honesty is important for maintaining trust, especially as some patients may see friends and relatives who also are cannabis users have normal pregnancy outcomes.
Much of my concern about cannabis in pregnancy centers on its effect on the developing brain and on long-term neurologic development. I share this with patients – I tell them that cannabis crosses the placenta and may well affect their baby’s brain as it is developing. I explain that I do not know whether this effect would be big or small, but that it’s not a chance I’m willing to take for their baby.
It is also important to educate patients that cannabis products are untested and unregulated and that they may be contaminated with heavy metals, pesticides, and other toxins that may be harmful to themselves and their babies. Patients also should know that the potency of cannabis has been dramatically increasing; research shows that the tetrahydrocannabinol – the psychoactive component – concentration has tripled over the past 2 decades.7
Research tells us that women who use illicit drugs and alcohol categorically engage in some form of harm reduction once they learn they are pregnant, and the same is true for cannabis. This is seen in dramatically different rates of first- and third-trimester use in the new analysis of NSDUH data; third-trimester use is approximately halved.
Some women will not be able to discontinue use, however, or they may try to quit and fail in their attempts. As we should with substance use more broadly, we must meet patients where they are, view cannabis use as a chronic medical problem, offer our assistance in helping them reduce harms of their use, and understand that quitting is a process.
Screening for mental health disorders and trauma is, of course, especially important in patients who use cannabis and other substances recreationally. In cases of medical marijuana usage, I recommend, as ACOG and other have done, that we discuss the risks and benefits of continuing cannabis versus shifting to alternative medications if options exist.
All patients should be welcomed, congratulated on their pregnancy and on coming for prenatal care, and engaged in the overall process of optimizing their health and the health of their baby. Like any other health issue during pregnancy, cannabis use needs to be screened for and treated in an evidence-based manner, but it does not define the trajectory or success of a woman’s pregnancy or her ability to be a successful parent.
Dr. Mark is associate professor of obstetrics, gynecology, and reproductive sciences at the University of Maryland School of Medicine.
References
1. JAMA. 2019 Jul 9;322(2):145-52.
2. Preventive Medicine 2017 May 18;104:46-9.
3. JAMA. 2019 Jul 9;322(2):167-9.
4. JAMA Netw Open. 2019 Jul 3;2(7):e196471.
5. Obstet Gynecol. 2019 May;133(5):952-61.
6. J. Addict Med. 2019 May 10. doi: 10.1097/ADM.0000000000000543.
7. Biol Psychiatry. 2016 Apr 1;79(7):613-9.