User login
Prazosin falls short for veterans’ PTSD-related sleep problems
The alpha-1 adrenergic receptor prazosin failed to improve recurring nightmares or sleep quality compared with placebo in veterans with PTSD in a 26-week randomized trial of 304 adult veterans.
In several previous randomized trials lasting fewer than 15 weeks, veterans with PTSD and recurring nightmares who received prazosin showed benefits, including improved sleep quality and PTSD symptoms, compared with placebo patients, wrote Murray A. Raskind, MD, of the Department of Veterans Affairs Puget Sound Health Care System, Seattle, and his colleagues.
In a study published in the New England Journal of Medicine, the researchers randomized 152 veterans with sleep problems and PTSD to prazosin and 152 to a placebo. The participants were recruited from 12 VA medical centers. The average age of the participants was 52 years, more than 96% were male, and about two-thirds were white. Demographics were similar between the two groups.
After 10 weeks and after 26 weeks, there were no significant differences between the two groups in changes from baseline measures of recurring nightmares, using the mean change from baseline in Clinician-Administered PTSD Score item B2 (recurrent distressing dreams). Similarly, no significant differences appeared between the two groups based on Pittsburgh Sleep Quality Index scores.
“A possible explanation for these negative results is selection bias resulting from recruitment of patients who were mainly in clinically stable condition, since symptoms in such patients were less likely to be ameliorated with antiadrenergic treatment,” reported Dr. Raskind and his colleagues.
The average maintenance dose of prazosin was 14.8 mg, compared with 16.4 mg in the placebo group; 187 male study participants reached the maximum dose of 20 mg/day (54% of the prazosin group and 70% of the placebo group).
After 10 weeks, no significant differences were found between the two groups in changes from baseline measures of “recurring distressing dreams,” using the mean change from baseline in Clinician-Administered PTSD Score item B2 (recurrent distressing dreams). The between group difference was 0.2. In addition, no significant differences were found at 10 weeks in the average change from baseline Pittsburgh Sleep Quality Index scores.
Similarly, no significant differences appeared between the two groups at 26 weeks. “ since symptoms in such patients were less likely to be ameliorated with antiadrenergic treatment,” the researchers said.
On average, patients in the prazosin group had significantly greater decreases in blood pressure, compared with the placebo group. In addition, they had fewer reports of new or worsening suicidal ideation, compared with the placebo group (8% vs.15%).
“Given the concern about suicide among veterans, it is noteworthy that the specifically solicited adverse event of new or worsening suicidal ideation was less common in the prazosin group than in the placebo group, but the absolute number of events was small; this issue warrants further study,” the researchers said.
The study was limited by several factors, including the absence of screening for sleep apnea or sleep-disordered breathing, Dr. Raskind and his colleagues noted. However, the results suggest that “further studies with more refined characterization of autonomic nervous system activity and nocturnal behaviors are needed to determine whether there might be subgroups of veterans with PTSD who can benefit from prazosin.”
Dr. Raskind had no financial conflicts to disclose. The study was supported by the Department of Veterans Affairs Cooperative Studies Program.
SOURCE: Raskind MA et al. N Engl J Med. 2018 Feb 8;378:507-17. doi: 10.1056/NEJMoa1507598.
The alpha-1 adrenergic receptor prazosin failed to improve recurring nightmares or sleep quality compared with placebo in veterans with PTSD in a 26-week randomized trial of 304 adult veterans.
In several previous randomized trials lasting fewer than 15 weeks, veterans with PTSD and recurring nightmares who received prazosin showed benefits, including improved sleep quality and PTSD symptoms, compared with placebo patients, wrote Murray A. Raskind, MD, of the Department of Veterans Affairs Puget Sound Health Care System, Seattle, and his colleagues.
In a study published in the New England Journal of Medicine, the researchers randomized 152 veterans with sleep problems and PTSD to prazosin and 152 to a placebo. The participants were recruited from 12 VA medical centers. The average age of the participants was 52 years, more than 96% were male, and about two-thirds were white. Demographics were similar between the two groups.
After 10 weeks and after 26 weeks, there were no significant differences between the two groups in changes from baseline measures of recurring nightmares, using the mean change from baseline in Clinician-Administered PTSD Score item B2 (recurrent distressing dreams). Similarly, no significant differences appeared between the two groups based on Pittsburgh Sleep Quality Index scores.
“A possible explanation for these negative results is selection bias resulting from recruitment of patients who were mainly in clinically stable condition, since symptoms in such patients were less likely to be ameliorated with antiadrenergic treatment,” reported Dr. Raskind and his colleagues.
The average maintenance dose of prazosin was 14.8 mg, compared with 16.4 mg in the placebo group; 187 male study participants reached the maximum dose of 20 mg/day (54% of the prazosin group and 70% of the placebo group).
After 10 weeks, no significant differences were found between the two groups in changes from baseline measures of “recurring distressing dreams,” using the mean change from baseline in Clinician-Administered PTSD Score item B2 (recurrent distressing dreams). The between group difference was 0.2. In addition, no significant differences were found at 10 weeks in the average change from baseline Pittsburgh Sleep Quality Index scores.
Similarly, no significant differences appeared between the two groups at 26 weeks. “ since symptoms in such patients were less likely to be ameliorated with antiadrenergic treatment,” the researchers said.
On average, patients in the prazosin group had significantly greater decreases in blood pressure, compared with the placebo group. In addition, they had fewer reports of new or worsening suicidal ideation, compared with the placebo group (8% vs.15%).
“Given the concern about suicide among veterans, it is noteworthy that the specifically solicited adverse event of new or worsening suicidal ideation was less common in the prazosin group than in the placebo group, but the absolute number of events was small; this issue warrants further study,” the researchers said.
The study was limited by several factors, including the absence of screening for sleep apnea or sleep-disordered breathing, Dr. Raskind and his colleagues noted. However, the results suggest that “further studies with more refined characterization of autonomic nervous system activity and nocturnal behaviors are needed to determine whether there might be subgroups of veterans with PTSD who can benefit from prazosin.”
Dr. Raskind had no financial conflicts to disclose. The study was supported by the Department of Veterans Affairs Cooperative Studies Program.
SOURCE: Raskind MA et al. N Engl J Med. 2018 Feb 8;378:507-17. doi: 10.1056/NEJMoa1507598.
The alpha-1 adrenergic receptor prazosin failed to improve recurring nightmares or sleep quality compared with placebo in veterans with PTSD in a 26-week randomized trial of 304 adult veterans.
In several previous randomized trials lasting fewer than 15 weeks, veterans with PTSD and recurring nightmares who received prazosin showed benefits, including improved sleep quality and PTSD symptoms, compared with placebo patients, wrote Murray A. Raskind, MD, of the Department of Veterans Affairs Puget Sound Health Care System, Seattle, and his colleagues.
In a study published in the New England Journal of Medicine, the researchers randomized 152 veterans with sleep problems and PTSD to prazosin and 152 to a placebo. The participants were recruited from 12 VA medical centers. The average age of the participants was 52 years, more than 96% were male, and about two-thirds were white. Demographics were similar between the two groups.
After 10 weeks and after 26 weeks, there were no significant differences between the two groups in changes from baseline measures of recurring nightmares, using the mean change from baseline in Clinician-Administered PTSD Score item B2 (recurrent distressing dreams). Similarly, no significant differences appeared between the two groups based on Pittsburgh Sleep Quality Index scores.
“A possible explanation for these negative results is selection bias resulting from recruitment of patients who were mainly in clinically stable condition, since symptoms in such patients were less likely to be ameliorated with antiadrenergic treatment,” reported Dr. Raskind and his colleagues.
The average maintenance dose of prazosin was 14.8 mg, compared with 16.4 mg in the placebo group; 187 male study participants reached the maximum dose of 20 mg/day (54% of the prazosin group and 70% of the placebo group).
After 10 weeks, no significant differences were found between the two groups in changes from baseline measures of “recurring distressing dreams,” using the mean change from baseline in Clinician-Administered PTSD Score item B2 (recurrent distressing dreams). The between group difference was 0.2. In addition, no significant differences were found at 10 weeks in the average change from baseline Pittsburgh Sleep Quality Index scores.
Similarly, no significant differences appeared between the two groups at 26 weeks. “ since symptoms in such patients were less likely to be ameliorated with antiadrenergic treatment,” the researchers said.
On average, patients in the prazosin group had significantly greater decreases in blood pressure, compared with the placebo group. In addition, they had fewer reports of new or worsening suicidal ideation, compared with the placebo group (8% vs.15%).
“Given the concern about suicide among veterans, it is noteworthy that the specifically solicited adverse event of new or worsening suicidal ideation was less common in the prazosin group than in the placebo group, but the absolute number of events was small; this issue warrants further study,” the researchers said.
The study was limited by several factors, including the absence of screening for sleep apnea or sleep-disordered breathing, Dr. Raskind and his colleagues noted. However, the results suggest that “further studies with more refined characterization of autonomic nervous system activity and nocturnal behaviors are needed to determine whether there might be subgroups of veterans with PTSD who can benefit from prazosin.”
Dr. Raskind had no financial conflicts to disclose. The study was supported by the Department of Veterans Affairs Cooperative Studies Program.
SOURCE: Raskind MA et al. N Engl J Med. 2018 Feb 8;378:507-17. doi: 10.1056/NEJMoa1507598.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Key clinical point: Prazosin had no apparent effect on recurrent distressing dreams or sleep quality in veterans with PTSD.
Major finding: The between-group difference in scores on a measure of “recurrent distressing dreams” between the prazosin and placebo groups was a nonsignificant 0.2.
Study details: The data come from a randomized trial of 304 military veterans with PTSD who reported frequent nightmares.
Disclosures: Dr. Raskind had no financial conflicts to disclose. The study was supported by the Department of Veterans Affairs Cooperative Studies Program.
Source: Raskind MA et al. N Engl J Med. 2018;378:507-17.
Mental health stressors still loom for Puerto Ricans after Maria
The physical and mental health needs of the people of Puerto Rico cannot be underestimated. Just think of what they have been through over the last few months.
When Hurricane Maria barreled onto the island on Sept. 20, 2017 – just 2 weeks after Hurricane Irma reportedly left more than 1 million residents without power – it ripped off roofs and left behind massive flooding, roads washed out, and utility poles and transmission lines knocked down. Whole forests were defoliated, a massive loss of flora and fauna occurred, and 80% of the crop value was destroyed, along with massive loss of stray dogs and cats, dairy cows, industrial chicken coops, and tropical birds, including endangered species. Beloved pets were displaced.

The official death toll as a result of Maria was 64 in December, but according to reporting by The New York Times, that number could be as high as 1,052. Most of the people who died reportedly were men and women over age 50 in hospitals and nursing homes suffering from illnesses such as diabetes, Alzheimer’s, kidney disease, hypertension, pneumonia, and other respiratory diseases.
One grassroots organization that mobilized to provide supplies and medical assistance was Doctoras Boricuas, a group of all-female doctors in the United States and Puerto Rico that formed after the hurricanes to coordinate the delivery and distribution of supplies directly to Puerto Rico and the Virgin Islands. Two groups affiliated with the University of Missouri at Columbia joined forces to help: Global First Responder or GFR, a nonprofit, secular international medical relief organization founded in 2011 by Adam Beckett, MD, and the International Center for Psychosocial Trauma, or ICPT, a group established in 1995 by Syed Arshad Husain, MD, to help war-traumatized children in Bosnia. I joined Dr. Husain’s group of professionals – Kathryn Dewein, PhD; Andra Ferguson, PhD; and Cathy Grigg, PsyD, – all of whom have traveled broadly in the field of disaster psychiatry – to see how we could help the people of Puerto Rico in Maria’s aftermath.
What we did
ICPT and GFR were a combined team, but we served different functions. As part of ICPT, I focused on the mental health component and helped to train doctors, psychologists, social workers, and other mental health workers in both San Juan and Ponce. All told, we worked with about 50 people using the model of “Training the Trainers.” Many of our students were participants in the outreach teams. Our hope is that they will be able to train their peers to recognize and alleviate symptoms of acute and chronic stress disorders. Some of the techniques taught include patient education, relaxation training, breath work, visualization techniques, mindfulness training, narrative therapy, art therapy, and other expressive techniques.
What the PMSF did
Before Maria, the Ponce Medical School Foundation was in the process of facilitating the transfer of medical records into an electronic format. After the hurricane hit, however, PMSF’s program director, Antonio Fernandez, led a shift to disaster recovery work. PMSF got involved in airlifting dialysis patients off the island to safety, provided health care, and also collaborated with the Primary Care Psychology Program at Ponce Health Services University to assist in locating patients, identifying their health needs – including mental health – and providing for those needs to the extent possible.
At the time of our visit, Puerto Rico’s network of more than 90 largely rural federally funded primary care clinics mostly had reopened, but nearly half remained on back-up generators. Even with the medical centers open, patients were not coming in for one reason or another. People had medical problems, but the daily reality of survival, obtaining food and water, took precedence. Some patients were not showing up because they had left the country, or they were in shelters without transportation. Some people did not have fuel. Some could not keep track of their appointments without cell phones and electricity allowing them to access electronic planners. Some, having been without their medications since the storms, were too sick to travel. Outreach teams were necessary to locate patients, identify their needs, and provide medical and psychological care.
Community outreach
Nydia M. Cappas, PsyD, director of the Primary Care Psychology Program, told us that the outreach teams – consisting of doctors or other medical professionals, social workers, and psychologists, were being sent out to communities once a week. They visited homes for the elderly, orphans’ homes, and children in foster care, as well as individual patients. A similar service was provided by Vargas Medicine (VARMED) in the San Juan area.
Team members found that many people were suffering symptoms of posttraumatic stress disorder, even people who did not have prior psychiatric symptoms. They were having flashbacks and nightmares. Those flashbacks and nightmares were being triggered by clouds, by rain, by supplies beginning to run out.

Another trend we observed is that terrain changes prompted by Maria triggered PTSD symptoms among many veterans. The defoliated trees and brown earth were causing them to have flashbacks to the deserts of Afghanistan and Iraq. Children were showing regressive behaviors, loss of developmental milestones, and symptoms of separation anxiety such as wanting to sleep with their parents. In severe cases, they were having psychotic symptoms and auditory hallucinations. The children were grieving the loss of their homes, toys, pets, and family members, in some cases. , including medications, food, toiletries, and other household goods.
Puerto Rico’s future
Two and a half months after Maria, we learned from our students that things gradually had begun to improve. For example, the public schools had just reopened, and that change was expected to have a stabilizing effect on the children. We also learned that, of the 80 shelters that had been set up housing about 12,500 people, 40 shelters had closed. The five medical shelters that had been set up and funded by FEMA also were in the process of closing, and private donations were beginning to slow down. People were slowly returning to their tarped or otherwise repaired homes, albeit all too often without power.
During the storm, nearly 500,000* homes were destroyed. FEMA offered to airlift about 3,000 people who had no home 2 months past Maria to the U.S. mainland – either Florida or New York.
According to our students, people living in the mountains, mainly coffee growers and retired people and comprising about one-third of the population, remain in acute crisis. Part of the challenge is being able to reach this population: Some roads are still impassable, and supplies – such as drinking water – can be delivered only by helicopter. Despite current conditions, FEMA reportedly has announced that it would end emergency operations on the island.
Our team is currently involved in applying for grant funding that will enable us to return to provide additional training to physicians’ and teachers’ groups. Over the course of the next year, we would like to make six trips to Puerto Rico and focus each trip on a different region and different group of professionals so that the entire island has resources. In addition, we will offer follow-up consultations to professionals we trained previously. The regions to be trained would be San Juan, Ponce, Utuado, Mayagüez, Guayama, and a sixth to be determined upon need. We also would like to address the needs of any ongoing relief workers so that they will be more effective in their ongoing role. Meanwhile, financial assistance from the mainland remains uneven.
Many months after Maria (and Irma), the physical and mental health needs of the Puerto Rican people remain great. However, as mental health professionals, we have the tools to help them move forward.
Judith R. Milner, MD, MEd, SpecEd, is a general, child, and adolescent psychiatrist in private practice in Everett, Wash. She has traveled with various groups over the years in an effort to alleviate some of the suffering caused by war and natural disaster. Her predominant association has been with the International Center for Psychosocial Trauma. She also has worked with Step Up Rwanda Women and Pygmy Survival Alliance, as well as on the Committee for Women at the American Psychiatric Association and the Consumer Issues Committee and Membership Committee for the American Academy of Child and Adolescent Psychiatry.
*Correction, 2/12/2018: An earlier version of this story misstated the number of homes reportedly destroyed by Hurricane Maria.
The physical and mental health needs of the people of Puerto Rico cannot be underestimated. Just think of what they have been through over the last few months.
When Hurricane Maria barreled onto the island on Sept. 20, 2017 – just 2 weeks after Hurricane Irma reportedly left more than 1 million residents without power – it ripped off roofs and left behind massive flooding, roads washed out, and utility poles and transmission lines knocked down. Whole forests were defoliated, a massive loss of flora and fauna occurred, and 80% of the crop value was destroyed, along with massive loss of stray dogs and cats, dairy cows, industrial chicken coops, and tropical birds, including endangered species. Beloved pets were displaced.
The official death toll as a result of Maria was 64 in December, but according to reporting by The New York Times, that number could be as high as 1,052. Most of the people who died reportedly were men and women over age 50 in hospitals and nursing homes suffering from illnesses such as diabetes, Alzheimer’s, kidney disease, hypertension, pneumonia, and other respiratory diseases.
One grassroots organization that mobilized to provide supplies and medical assistance was Doctoras Boricuas, a group of all-female doctors in the United States and Puerto Rico that formed after the hurricanes to coordinate the delivery and distribution of supplies directly to Puerto Rico and the Virgin Islands. Two groups affiliated with the University of Missouri at Columbia joined forces to help: Global First Responder or GFR, a nonprofit, secular international medical relief organization founded in 2011 by Adam Beckett, MD, and the International Center for Psychosocial Trauma, or ICPT, a group established in 1995 by Syed Arshad Husain, MD, to help war-traumatized children in Bosnia. I joined Dr. Husain’s group of professionals – Kathryn Dewein, PhD; Andra Ferguson, PhD; and Cathy Grigg, PsyD, – all of whom have traveled broadly in the field of disaster psychiatry – to see how we could help the people of Puerto Rico in Maria’s aftermath.
What we did
ICPT and GFR were a combined team, but we served different functions. As part of ICPT, I focused on the mental health component and helped to train doctors, psychologists, social workers, and other mental health workers in both San Juan and Ponce. All told, we worked with about 50 people using the model of “Training the Trainers.” Many of our students were participants in the outreach teams. Our hope is that they will be able to train their peers to recognize and alleviate symptoms of acute and chronic stress disorders. Some of the techniques taught include patient education, relaxation training, breath work, visualization techniques, mindfulness training, narrative therapy, art therapy, and other expressive techniques.
What the PMSF did
Before Maria, the Ponce Medical School Foundation was in the process of facilitating the transfer of medical records into an electronic format. After the hurricane hit, however, PMSF’s program director, Antonio Fernandez, led a shift to disaster recovery work. PMSF got involved in airlifting dialysis patients off the island to safety, provided health care, and also collaborated with the Primary Care Psychology Program at Ponce Health Services University to assist in locating patients, identifying their health needs – including mental health – and providing for those needs to the extent possible.
At the time of our visit, Puerto Rico’s network of more than 90 largely rural federally funded primary care clinics mostly had reopened, but nearly half remained on back-up generators. Even with the medical centers open, patients were not coming in for one reason or another. People had medical problems, but the daily reality of survival, obtaining food and water, took precedence. Some patients were not showing up because they had left the country, or they were in shelters without transportation. Some people did not have fuel. Some could not keep track of their appointments without cell phones and electricity allowing them to access electronic planners. Some, having been without their medications since the storms, were too sick to travel. Outreach teams were necessary to locate patients, identify their needs, and provide medical and psychological care.
Community outreach
Nydia M. Cappas, PsyD, director of the Primary Care Psychology Program, told us that the outreach teams – consisting of doctors or other medical professionals, social workers, and psychologists, were being sent out to communities once a week. They visited homes for the elderly, orphans’ homes, and children in foster care, as well as individual patients. A similar service was provided by Vargas Medicine (VARMED) in the San Juan area.
Team members found that many people were suffering symptoms of posttraumatic stress disorder, even people who did not have prior psychiatric symptoms. They were having flashbacks and nightmares. Those flashbacks and nightmares were being triggered by clouds, by rain, by supplies beginning to run out.
Another trend we observed is that terrain changes prompted by Maria triggered PTSD symptoms among many veterans. The defoliated trees and brown earth were causing them to have flashbacks to the deserts of Afghanistan and Iraq. Children were showing regressive behaviors, loss of developmental milestones, and symptoms of separation anxiety such as wanting to sleep with their parents. In severe cases, they were having psychotic symptoms and auditory hallucinations. The children were grieving the loss of their homes, toys, pets, and family members, in some cases. , including medications, food, toiletries, and other household goods.
Puerto Rico’s future
Two and a half months after Maria, we learned from our students that things gradually had begun to improve. For example, the public schools had just reopened, and that change was expected to have a stabilizing effect on the children. We also learned that, of the 80 shelters that had been set up housing about 12,500 people, 40 shelters had closed. The five medical shelters that had been set up and funded by FEMA also were in the process of closing, and private donations were beginning to slow down. People were slowly returning to their tarped or otherwise repaired homes, albeit all too often without power.
During the storm, nearly 500,000* homes were destroyed. FEMA offered to airlift about 3,000 people who had no home 2 months past Maria to the U.S. mainland – either Florida or New York.
According to our students, people living in the mountains, mainly coffee growers and retired people and comprising about one-third of the population, remain in acute crisis. Part of the challenge is being able to reach this population: Some roads are still impassable, and supplies – such as drinking water – can be delivered only by helicopter. Despite current conditions, FEMA reportedly has announced that it would end emergency operations on the island.
Our team is currently involved in applying for grant funding that will enable us to return to provide additional training to physicians’ and teachers’ groups. Over the course of the next year, we would like to make six trips to Puerto Rico and focus each trip on a different region and different group of professionals so that the entire island has resources. In addition, we will offer follow-up consultations to professionals we trained previously. The regions to be trained would be San Juan, Ponce, Utuado, Mayagüez, Guayama, and a sixth to be determined upon need. We also would like to address the needs of any ongoing relief workers so that they will be more effective in their ongoing role. Meanwhile, financial assistance from the mainland remains uneven.
Many months after Maria (and Irma), the physical and mental health needs of the Puerto Rican people remain great. However, as mental health professionals, we have the tools to help them move forward.
Judith R. Milner, MD, MEd, SpecEd, is a general, child, and adolescent psychiatrist in private practice in Everett, Wash. She has traveled with various groups over the years in an effort to alleviate some of the suffering caused by war and natural disaster. Her predominant association has been with the International Center for Psychosocial Trauma. She also has worked with Step Up Rwanda Women and Pygmy Survival Alliance, as well as on the Committee for Women at the American Psychiatric Association and the Consumer Issues Committee and Membership Committee for the American Academy of Child and Adolescent Psychiatry.
*Correction, 2/12/2018: An earlier version of this story misstated the number of homes reportedly destroyed by Hurricane Maria.
The physical and mental health needs of the people of Puerto Rico cannot be underestimated. Just think of what they have been through over the last few months.
When Hurricane Maria barreled onto the island on Sept. 20, 2017 – just 2 weeks after Hurricane Irma reportedly left more than 1 million residents without power – it ripped off roofs and left behind massive flooding, roads washed out, and utility poles and transmission lines knocked down. Whole forests were defoliated, a massive loss of flora and fauna occurred, and 80% of the crop value was destroyed, along with massive loss of stray dogs and cats, dairy cows, industrial chicken coops, and tropical birds, including endangered species. Beloved pets were displaced.
The official death toll as a result of Maria was 64 in December, but according to reporting by The New York Times, that number could be as high as 1,052. Most of the people who died reportedly were men and women over age 50 in hospitals and nursing homes suffering from illnesses such as diabetes, Alzheimer’s, kidney disease, hypertension, pneumonia, and other respiratory diseases.
One grassroots organization that mobilized to provide supplies and medical assistance was Doctoras Boricuas, a group of all-female doctors in the United States and Puerto Rico that formed after the hurricanes to coordinate the delivery and distribution of supplies directly to Puerto Rico and the Virgin Islands. Two groups affiliated with the University of Missouri at Columbia joined forces to help: Global First Responder or GFR, a nonprofit, secular international medical relief organization founded in 2011 by Adam Beckett, MD, and the International Center for Psychosocial Trauma, or ICPT, a group established in 1995 by Syed Arshad Husain, MD, to help war-traumatized children in Bosnia. I joined Dr. Husain’s group of professionals – Kathryn Dewein, PhD; Andra Ferguson, PhD; and Cathy Grigg, PsyD, – all of whom have traveled broadly in the field of disaster psychiatry – to see how we could help the people of Puerto Rico in Maria’s aftermath.
What we did
ICPT and GFR were a combined team, but we served different functions. As part of ICPT, I focused on the mental health component and helped to train doctors, psychologists, social workers, and other mental health workers in both San Juan and Ponce. All told, we worked with about 50 people using the model of “Training the Trainers.” Many of our students were participants in the outreach teams. Our hope is that they will be able to train their peers to recognize and alleviate symptoms of acute and chronic stress disorders. Some of the techniques taught include patient education, relaxation training, breath work, visualization techniques, mindfulness training, narrative therapy, art therapy, and other expressive techniques.
What the PMSF did
Before Maria, the Ponce Medical School Foundation was in the process of facilitating the transfer of medical records into an electronic format. After the hurricane hit, however, PMSF’s program director, Antonio Fernandez, led a shift to disaster recovery work. PMSF got involved in airlifting dialysis patients off the island to safety, provided health care, and also collaborated with the Primary Care Psychology Program at Ponce Health Services University to assist in locating patients, identifying their health needs – including mental health – and providing for those needs to the extent possible.
At the time of our visit, Puerto Rico’s network of more than 90 largely rural federally funded primary care clinics mostly had reopened, but nearly half remained on back-up generators. Even with the medical centers open, patients were not coming in for one reason or another. People had medical problems, but the daily reality of survival, obtaining food and water, took precedence. Some patients were not showing up because they had left the country, or they were in shelters without transportation. Some people did not have fuel. Some could not keep track of their appointments without cell phones and electricity allowing them to access electronic planners. Some, having been without their medications since the storms, were too sick to travel. Outreach teams were necessary to locate patients, identify their needs, and provide medical and psychological care.
Community outreach
Nydia M. Cappas, PsyD, director of the Primary Care Psychology Program, told us that the outreach teams – consisting of doctors or other medical professionals, social workers, and psychologists, were being sent out to communities once a week. They visited homes for the elderly, orphans’ homes, and children in foster care, as well as individual patients. A similar service was provided by Vargas Medicine (VARMED) in the San Juan area.
Team members found that many people were suffering symptoms of posttraumatic stress disorder, even people who did not have prior psychiatric symptoms. They were having flashbacks and nightmares. Those flashbacks and nightmares were being triggered by clouds, by rain, by supplies beginning to run out.
Another trend we observed is that terrain changes prompted by Maria triggered PTSD symptoms among many veterans. The defoliated trees and brown earth were causing them to have flashbacks to the deserts of Afghanistan and Iraq. Children were showing regressive behaviors, loss of developmental milestones, and symptoms of separation anxiety such as wanting to sleep with their parents. In severe cases, they were having psychotic symptoms and auditory hallucinations. The children were grieving the loss of their homes, toys, pets, and family members, in some cases. , including medications, food, toiletries, and other household goods.
Puerto Rico’s future
Two and a half months after Maria, we learned from our students that things gradually had begun to improve. For example, the public schools had just reopened, and that change was expected to have a stabilizing effect on the children. We also learned that, of the 80 shelters that had been set up housing about 12,500 people, 40 shelters had closed. The five medical shelters that had been set up and funded by FEMA also were in the process of closing, and private donations were beginning to slow down. People were slowly returning to their tarped or otherwise repaired homes, albeit all too often without power.
During the storm, nearly 500,000* homes were destroyed. FEMA offered to airlift about 3,000 people who had no home 2 months past Maria to the U.S. mainland – either Florida or New York.
According to our students, people living in the mountains, mainly coffee growers and retired people and comprising about one-third of the population, remain in acute crisis. Part of the challenge is being able to reach this population: Some roads are still impassable, and supplies – such as drinking water – can be delivered only by helicopter. Despite current conditions, FEMA reportedly has announced that it would end emergency operations on the island.
Our team is currently involved in applying for grant funding that will enable us to return to provide additional training to physicians’ and teachers’ groups. Over the course of the next year, we would like to make six trips to Puerto Rico and focus each trip on a different region and different group of professionals so that the entire island has resources. In addition, we will offer follow-up consultations to professionals we trained previously. The regions to be trained would be San Juan, Ponce, Utuado, Mayagüez, Guayama, and a sixth to be determined upon need. We also would like to address the needs of any ongoing relief workers so that they will be more effective in their ongoing role. Meanwhile, financial assistance from the mainland remains uneven.
Many months after Maria (and Irma), the physical and mental health needs of the Puerto Rican people remain great. However, as mental health professionals, we have the tools to help them move forward.
Judith R. Milner, MD, MEd, SpecEd, is a general, child, and adolescent psychiatrist in private practice in Everett, Wash. She has traveled with various groups over the years in an effort to alleviate some of the suffering caused by war and natural disaster. Her predominant association has been with the International Center for Psychosocial Trauma. She also has worked with Step Up Rwanda Women and Pygmy Survival Alliance, as well as on the Committee for Women at the American Psychiatric Association and the Consumer Issues Committee and Membership Committee for the American Academy of Child and Adolescent Psychiatry.
*Correction, 2/12/2018: An earlier version of this story misstated the number of homes reportedly destroyed by Hurricane Maria.
How to help children process, overcome horrific traumas
Unfathomable. Unspeakable.
These are among the terms used to describe children’s extreme traumatic experiences such as severe abuse and neglect. It is often most shocking when these acts are perpetrated by the children’s parents – the very ones that children should be able to depend on for their protection and safety.
Many believe that, in addition to the cumulative and serious nature of repetitive interpersonal traumas themselves, this betrayal of trust will result in irreparable psychological damage. Fortunately, this does not have to be the case. Children are more resilient than we realize; with safety, support, and effective treatment, they can recover from even the most extreme traumas and live healthy, productive lives.
and allow them to live in safe, stable, supportive settings while minimizing traumatic separation from siblings or further disruptions in their living situation. Acute medical problems need to be stabilized, and a thorough mental health assessment should be conducted.
Evidence-based trauma-focused psychotherapy is the first-line treatment for addressing pediatric posttraumatic stress disorder (J Am Acad Child Adolesc Psychiatry. 2010 Apr;49[4]:414-30). Several treatments are currently available. A few examples are trauma-focused cognitive-behavioral therapy, or TF-CBT, for children aged 3-18 years; child-parent psychotherapy (CPP) for children aged 0-6 years; a group school-based model, cognitive behavioral interventions for trauma in schools (CBITS); and Trauma Affect Regulation: Guide for Education and Therapy for teens (TARGET).
Common elements of evidence-based trauma-focused treatments are: 1) nonperpetrating caregivers are included in therapy to enhance support and understanding of the child’s trauma responses, and to address trauma-related behavioral problems; 2) skills are provided to the youth and caregiver for coping with negative trauma-related thoughts, feelings, and behaviors; and 3) children are supported to directly talk about and make meaning of their trauma experiences.
Through trauma-focused treatment, children become able to cope with their traumatic experiences and memories – make sense out of them. These traumas are no longer “unfathomable or “unspeakable,” but rather, manageable memories of bad experiences that the children have had the courage to face and master.
Children can recover from even extreme trauma experiences when they receive effective trauma-focused treatment in the context of a supportive environment. More information about evidence-based treatments is available from the National Child Traumatic Stress Network at www.nctsn.org/resources/topics/treatments-that-work/promising-practices.

Unfathomable. Unspeakable.
These are among the terms used to describe children’s extreme traumatic experiences such as severe abuse and neglect. It is often most shocking when these acts are perpetrated by the children’s parents – the very ones that children should be able to depend on for their protection and safety.
Many believe that, in addition to the cumulative and serious nature of repetitive interpersonal traumas themselves, this betrayal of trust will result in irreparable psychological damage. Fortunately, this does not have to be the case. Children are more resilient than we realize; with safety, support, and effective treatment, they can recover from even the most extreme traumas and live healthy, productive lives.
and allow them to live in safe, stable, supportive settings while minimizing traumatic separation from siblings or further disruptions in their living situation. Acute medical problems need to be stabilized, and a thorough mental health assessment should be conducted.
Evidence-based trauma-focused psychotherapy is the first-line treatment for addressing pediatric posttraumatic stress disorder (J Am Acad Child Adolesc Psychiatry. 2010 Apr;49[4]:414-30). Several treatments are currently available. A few examples are trauma-focused cognitive-behavioral therapy, or TF-CBT, for children aged 3-18 years; child-parent psychotherapy (CPP) for children aged 0-6 years; a group school-based model, cognitive behavioral interventions for trauma in schools (CBITS); and Trauma Affect Regulation: Guide for Education and Therapy for teens (TARGET).
Common elements of evidence-based trauma-focused treatments are: 1) nonperpetrating caregivers are included in therapy to enhance support and understanding of the child’s trauma responses, and to address trauma-related behavioral problems; 2) skills are provided to the youth and caregiver for coping with negative trauma-related thoughts, feelings, and behaviors; and 3) children are supported to directly talk about and make meaning of their trauma experiences.
Through trauma-focused treatment, children become able to cope with their traumatic experiences and memories – make sense out of them. These traumas are no longer “unfathomable or “unspeakable,” but rather, manageable memories of bad experiences that the children have had the courage to face and master.
Children can recover from even extreme trauma experiences when they receive effective trauma-focused treatment in the context of a supportive environment. More information about evidence-based treatments is available from the National Child Traumatic Stress Network at www.nctsn.org/resources/topics/treatments-that-work/promising-practices.
Unfathomable. Unspeakable.
These are among the terms used to describe children’s extreme traumatic experiences such as severe abuse and neglect. It is often most shocking when these acts are perpetrated by the children’s parents – the very ones that children should be able to depend on for their protection and safety.
Many believe that, in addition to the cumulative and serious nature of repetitive interpersonal traumas themselves, this betrayal of trust will result in irreparable psychological damage. Fortunately, this does not have to be the case. Children are more resilient than we realize; with safety, support, and effective treatment, they can recover from even the most extreme traumas and live healthy, productive lives.
and allow them to live in safe, stable, supportive settings while minimizing traumatic separation from siblings or further disruptions in their living situation. Acute medical problems need to be stabilized, and a thorough mental health assessment should be conducted.
Evidence-based trauma-focused psychotherapy is the first-line treatment for addressing pediatric posttraumatic stress disorder (J Am Acad Child Adolesc Psychiatry. 2010 Apr;49[4]:414-30). Several treatments are currently available. A few examples are trauma-focused cognitive-behavioral therapy, or TF-CBT, for children aged 3-18 years; child-parent psychotherapy (CPP) for children aged 0-6 years; a group school-based model, cognitive behavioral interventions for trauma in schools (CBITS); and Trauma Affect Regulation: Guide for Education and Therapy for teens (TARGET).
Common elements of evidence-based trauma-focused treatments are: 1) nonperpetrating caregivers are included in therapy to enhance support and understanding of the child’s trauma responses, and to address trauma-related behavioral problems; 2) skills are provided to the youth and caregiver for coping with negative trauma-related thoughts, feelings, and behaviors; and 3) children are supported to directly talk about and make meaning of their trauma experiences.
Through trauma-focused treatment, children become able to cope with their traumatic experiences and memories – make sense out of them. These traumas are no longer “unfathomable or “unspeakable,” but rather, manageable memories of bad experiences that the children have had the courage to face and master.
Children can recover from even extreme trauma experiences when they receive effective trauma-focused treatment in the context of a supportive environment. More information about evidence-based treatments is available from the National Child Traumatic Stress Network at www.nctsn.org/resources/topics/treatments-that-work/promising-practices.
Shortened PTSD therapy still effective in active duty military personnel
A compressed 2-week version of prolonged exposure therapy for posttraumatic stress disorder in active duty military personnel delivers results similar to those seen in an 8-week course of treatment, new research suggested.
However, the four-arm clinical trial, published in JAMA, also found that the standard 8-week course of prolonged exposure therapy offered no significant benefits above present-centered therapy, prompting the suggestion that it may be less effective in military personnel.
The trial enrolled 366 military personnel – 12% female – on active duty and with PTSD who had returned from Iraq and/or Afghanistan. They were randomized to prolonged exposure therapy, which is a form of cognitive-behavioral therapy involving repeat exposure to traumatic memories and reminders, delivered in this study as either massed therapy over 2 weeks or spaced therapy over 8 weeks; to non–trauma-focused present-centered therapy over 8 weeks; or to a minimal-contact control consisting of once-weekly telephone calls from therapists for 4 weeks.
At 2 weeks after treatment, individuals who underwent massed exposure therapy showed a mean decrease in PTSD Symptom Scale–Interview (PSS-I) score from baseline of 7.13 points, compared with a mean decrease of 7.29 in the spaced-therapy group, thereby meeting the criteria for noninferiority.
At 12 weeks after treatment, the massed-therapy group showed a 6.32-point mean decrease and the spaced-therapy group had a 6.97-point mean decrease in PSS-I scores.
By comparison, individuals in the minimal-contact control group showed a mean decrease of 3.43 points at 2 weeks after treatment.
When the spaced version of the prolonged exposure therapy was compared with present-centered therapy, researchers saw no significant difference in changes in mean levels of PSS-I between the two groups at posttreatment follow-up.
Edna B. Foa, PhD, from the department of psychiatry at the University of Pennsylvania, Philadelphia, and her coauthors wrote that prolonged exposure therapy for PTSD has been shown to be effective in civilians and veterans, but its use in active duty military personnel has only been explored in case studies.
“One barrier to implementation of prolonged exposure therapy in the military is treatment length (8-15 weeks), which can conflict with military obligations,” they wrote. “A shorter course of therapy could hasten amelioration of PTSD, with the added benefit of facilitating military readiness.”
There had been concerns that the massed-therapy approach would be too emotionally taxing because it involved daily sessions on 10 consecutive weekdays, with patients participating in repeated recounting of the most disturbing traumatic memory followed by processing the thoughts and feelings associated with that memory.
“The noninferiority of massed therapy to spaced therapy is particularly important for the military because 2-week treatment not only is associated with more rapid symptom improvement but also may reduce interference with the demanding military schedule,” the authors wrote.
However, the researchers noted that the effect of both the massed and spaced therapy in this study population was less than that seen in previous studies.
“This suggests that well-established evidence-based treatments for PTSD may be less efficacious for active duty military personnel with PTSD and that modifications to these treatments, or alternative treatments, may be needed to achieve better outcomes.”
The study was conducted with the support of the Department of Defense. Eight authors declared funding from bodies including the Department of Defense, and one author received royalties from books on PTSD treatments.
SOURCE: Foa EB et al. JAMA. 2018 Jan 23. doi: 10.1001/jama.2017.21242.
Guidelines for the management of PTSD currently recommend trauma-focused psychotherapies, such as prolonged exposure therapy and cognitive processing therapy, as the first line of treatment for PTSD ahead of medications. However barriers to care, dropouts, and stigma remain challenges to uptake of these therapies.
The finding that trauma-focused and non–trauma-focused therapy achieve similar outcomes adds to a growing body of evidence that the differences between these approaches are small to negligible. But while current guidelines support present-centered therapy as a second-line approach, recommending it as a primary treatment is a perplexing evolution for a therapy originally developed as a therapy control condition for randomized controlled trials.
It is clear that more substantive evolution in PTSD treatments is needed and that individual variability in mechanisms of recovery and therapeutic preferences – as well as longer-term strategies – must be taken into account when deciding on a therapeutic approach
Charles W. Hoge, MD, is from the Walter Reed Army Institute of Research, Silver Spring, Md., and Kathleen M. Chard, PhD, is from the Trauma Recovery Center at Cincinnati VA Medical Center. These comments are taken from an accompanying editorial (JAMA. 2018 January 23;319:343-5). No conflicts of interest were declared.
Guidelines for the management of PTSD currently recommend trauma-focused psychotherapies, such as prolonged exposure therapy and cognitive processing therapy, as the first line of treatment for PTSD ahead of medications. However barriers to care, dropouts, and stigma remain challenges to uptake of these therapies.
The finding that trauma-focused and non–trauma-focused therapy achieve similar outcomes adds to a growing body of evidence that the differences between these approaches are small to negligible. But while current guidelines support present-centered therapy as a second-line approach, recommending it as a primary treatment is a perplexing evolution for a therapy originally developed as a therapy control condition for randomized controlled trials.
It is clear that more substantive evolution in PTSD treatments is needed and that individual variability in mechanisms of recovery and therapeutic preferences – as well as longer-term strategies – must be taken into account when deciding on a therapeutic approach
Charles W. Hoge, MD, is from the Walter Reed Army Institute of Research, Silver Spring, Md., and Kathleen M. Chard, PhD, is from the Trauma Recovery Center at Cincinnati VA Medical Center. These comments are taken from an accompanying editorial (JAMA. 2018 January 23;319:343-5). No conflicts of interest were declared.
Guidelines for the management of PTSD currently recommend trauma-focused psychotherapies, such as prolonged exposure therapy and cognitive processing therapy, as the first line of treatment for PTSD ahead of medications. However barriers to care, dropouts, and stigma remain challenges to uptake of these therapies.
The finding that trauma-focused and non–trauma-focused therapy achieve similar outcomes adds to a growing body of evidence that the differences between these approaches are small to negligible. But while current guidelines support present-centered therapy as a second-line approach, recommending it as a primary treatment is a perplexing evolution for a therapy originally developed as a therapy control condition for randomized controlled trials.
It is clear that more substantive evolution in PTSD treatments is needed and that individual variability in mechanisms of recovery and therapeutic preferences – as well as longer-term strategies – must be taken into account when deciding on a therapeutic approach
Charles W. Hoge, MD, is from the Walter Reed Army Institute of Research, Silver Spring, Md., and Kathleen M. Chard, PhD, is from the Trauma Recovery Center at Cincinnati VA Medical Center. These comments are taken from an accompanying editorial (JAMA. 2018 January 23;319:343-5). No conflicts of interest were declared.
A compressed 2-week version of prolonged exposure therapy for posttraumatic stress disorder in active duty military personnel delivers results similar to those seen in an 8-week course of treatment, new research suggested.
However, the four-arm clinical trial, published in JAMA, also found that the standard 8-week course of prolonged exposure therapy offered no significant benefits above present-centered therapy, prompting the suggestion that it may be less effective in military personnel.
The trial enrolled 366 military personnel – 12% female – on active duty and with PTSD who had returned from Iraq and/or Afghanistan. They were randomized to prolonged exposure therapy, which is a form of cognitive-behavioral therapy involving repeat exposure to traumatic memories and reminders, delivered in this study as either massed therapy over 2 weeks or spaced therapy over 8 weeks; to non–trauma-focused present-centered therapy over 8 weeks; or to a minimal-contact control consisting of once-weekly telephone calls from therapists for 4 weeks.
At 2 weeks after treatment, individuals who underwent massed exposure therapy showed a mean decrease in PTSD Symptom Scale–Interview (PSS-I) score from baseline of 7.13 points, compared with a mean decrease of 7.29 in the spaced-therapy group, thereby meeting the criteria for noninferiority.
At 12 weeks after treatment, the massed-therapy group showed a 6.32-point mean decrease and the spaced-therapy group had a 6.97-point mean decrease in PSS-I scores.
By comparison, individuals in the minimal-contact control group showed a mean decrease of 3.43 points at 2 weeks after treatment.
When the spaced version of the prolonged exposure therapy was compared with present-centered therapy, researchers saw no significant difference in changes in mean levels of PSS-I between the two groups at posttreatment follow-up.
Edna B. Foa, PhD, from the department of psychiatry at the University of Pennsylvania, Philadelphia, and her coauthors wrote that prolonged exposure therapy for PTSD has been shown to be effective in civilians and veterans, but its use in active duty military personnel has only been explored in case studies.
“One barrier to implementation of prolonged exposure therapy in the military is treatment length (8-15 weeks), which can conflict with military obligations,” they wrote. “A shorter course of therapy could hasten amelioration of PTSD, with the added benefit of facilitating military readiness.”
There had been concerns that the massed-therapy approach would be too emotionally taxing because it involved daily sessions on 10 consecutive weekdays, with patients participating in repeated recounting of the most disturbing traumatic memory followed by processing the thoughts and feelings associated with that memory.
“The noninferiority of massed therapy to spaced therapy is particularly important for the military because 2-week treatment not only is associated with more rapid symptom improvement but also may reduce interference with the demanding military schedule,” the authors wrote.
However, the researchers noted that the effect of both the massed and spaced therapy in this study population was less than that seen in previous studies.
“This suggests that well-established evidence-based treatments for PTSD may be less efficacious for active duty military personnel with PTSD and that modifications to these treatments, or alternative treatments, may be needed to achieve better outcomes.”
The study was conducted with the support of the Department of Defense. Eight authors declared funding from bodies including the Department of Defense, and one author received royalties from books on PTSD treatments.
SOURCE: Foa EB et al. JAMA. 2018 Jan 23. doi: 10.1001/jama.2017.21242.
A compressed 2-week version of prolonged exposure therapy for posttraumatic stress disorder in active duty military personnel delivers results similar to those seen in an 8-week course of treatment, new research suggested.
However, the four-arm clinical trial, published in JAMA, also found that the standard 8-week course of prolonged exposure therapy offered no significant benefits above present-centered therapy, prompting the suggestion that it may be less effective in military personnel.
The trial enrolled 366 military personnel – 12% female – on active duty and with PTSD who had returned from Iraq and/or Afghanistan. They were randomized to prolonged exposure therapy, which is a form of cognitive-behavioral therapy involving repeat exposure to traumatic memories and reminders, delivered in this study as either massed therapy over 2 weeks or spaced therapy over 8 weeks; to non–trauma-focused present-centered therapy over 8 weeks; or to a minimal-contact control consisting of once-weekly telephone calls from therapists for 4 weeks.
At 2 weeks after treatment, individuals who underwent massed exposure therapy showed a mean decrease in PTSD Symptom Scale–Interview (PSS-I) score from baseline of 7.13 points, compared with a mean decrease of 7.29 in the spaced-therapy group, thereby meeting the criteria for noninferiority.
At 12 weeks after treatment, the massed-therapy group showed a 6.32-point mean decrease and the spaced-therapy group had a 6.97-point mean decrease in PSS-I scores.
By comparison, individuals in the minimal-contact control group showed a mean decrease of 3.43 points at 2 weeks after treatment.
When the spaced version of the prolonged exposure therapy was compared with present-centered therapy, researchers saw no significant difference in changes in mean levels of PSS-I between the two groups at posttreatment follow-up.
Edna B. Foa, PhD, from the department of psychiatry at the University of Pennsylvania, Philadelphia, and her coauthors wrote that prolonged exposure therapy for PTSD has been shown to be effective in civilians and veterans, but its use in active duty military personnel has only been explored in case studies.
“One barrier to implementation of prolonged exposure therapy in the military is treatment length (8-15 weeks), which can conflict with military obligations,” they wrote. “A shorter course of therapy could hasten amelioration of PTSD, with the added benefit of facilitating military readiness.”
There had been concerns that the massed-therapy approach would be too emotionally taxing because it involved daily sessions on 10 consecutive weekdays, with patients participating in repeated recounting of the most disturbing traumatic memory followed by processing the thoughts and feelings associated with that memory.
“The noninferiority of massed therapy to spaced therapy is particularly important for the military because 2-week treatment not only is associated with more rapid symptom improvement but also may reduce interference with the demanding military schedule,” the authors wrote.
However, the researchers noted that the effect of both the massed and spaced therapy in this study population was less than that seen in previous studies.
“This suggests that well-established evidence-based treatments for PTSD may be less efficacious for active duty military personnel with PTSD and that modifications to these treatments, or alternative treatments, may be needed to achieve better outcomes.”
The study was conducted with the support of the Department of Defense. Eight authors declared funding from bodies including the Department of Defense, and one author received royalties from books on PTSD treatments.
SOURCE: Foa EB et al. JAMA. 2018 Jan 23. doi: 10.1001/jama.2017.21242.
FROM JAMA
Written exposure therapy rivals cognitive processing therapy for PTSD
Cognitive processing therapy may offer a greater benefit over time for posttraumatic stress disorder, but writing therapy offers a viable treatment in fewer sessions.
“Our results add to mounting research showing that the dose of therapy needed for beneficial outcomes for individuals with PTSD is not as large as what was once previously thought,” wrote Denise M. Sloan, PhD, of the National Center for PTSD, Boston, and her colleagues. “Our findings extend those prior studies by demonstrating that not only can PTSD symptoms be reduced significantly with less therapeutic exposure but that not as many therapy sessions are required.”
In a 1:1 randomized clinical trial, Dr. Sloan and her colleagues compared the effectiveness of written exposure therapy (WET) and cognitive processing therapy (CPT) in treating PTSD in 126 veteran and nonveteran adults, split evenly into the two therapy groups. and focused on details of the event, including thoughts and feelings associated with it. The CPT intervention was a 12-session trauma-focused therapy with a limited take-home writing component. It focused on helping patients recognize and challenge dysfunctional cognitions associated with traumatic events, the investigators wrote in JAMA Psychiatry.
When Dr. Sloan and her colleagues looked at the patients’ mean Clinician Administered PTSD Scale for DSM-5, or CAPS-5 score, a measure of PTSD symptom severity, they found that the WET and CPT groups’ scores were similar at 6 weeks, 12, weeks, and 36 weeks. At the 24-week assessment, the CAPS-5 score for those in the CPT group (20.92) was significantly lower than it was for those in the WET group (25.23) (mean difference, 4.31 points; 95% confidence interval, –1.37 to 9.99).
In addition, the CPT group had a higher dropout rate (31.7%) than did the WET group (6.3%). The investigators concluded, however, that both therapies are effective. “Written exposure therapy should be considered by clinicians to be a viable treatment option that can address some of the barriers to receiving and implementing CPT and prolonged exposure that have been noted in health care settings,” Dr. Sloan and her colleagues wrote.
This study was funded by a grant from the National Institute of Mental Health. None of the authors had financial conflicts to report. Further details on this information can be found here.
SOURCE: Sloan DM. 2018 Jan 17. doi: 10.1001/jamapsychiatry.2017.4249.
Cognitive processing therapy may offer a greater benefit over time for posttraumatic stress disorder, but writing therapy offers a viable treatment in fewer sessions.
“Our results add to mounting research showing that the dose of therapy needed for beneficial outcomes for individuals with PTSD is not as large as what was once previously thought,” wrote Denise M. Sloan, PhD, of the National Center for PTSD, Boston, and her colleagues. “Our findings extend those prior studies by demonstrating that not only can PTSD symptoms be reduced significantly with less therapeutic exposure but that not as many therapy sessions are required.”
In a 1:1 randomized clinical trial, Dr. Sloan and her colleagues compared the effectiveness of written exposure therapy (WET) and cognitive processing therapy (CPT) in treating PTSD in 126 veteran and nonveteran adults, split evenly into the two therapy groups. and focused on details of the event, including thoughts and feelings associated with it. The CPT intervention was a 12-session trauma-focused therapy with a limited take-home writing component. It focused on helping patients recognize and challenge dysfunctional cognitions associated with traumatic events, the investigators wrote in JAMA Psychiatry.
When Dr. Sloan and her colleagues looked at the patients’ mean Clinician Administered PTSD Scale for DSM-5, or CAPS-5 score, a measure of PTSD symptom severity, they found that the WET and CPT groups’ scores were similar at 6 weeks, 12, weeks, and 36 weeks. At the 24-week assessment, the CAPS-5 score for those in the CPT group (20.92) was significantly lower than it was for those in the WET group (25.23) (mean difference, 4.31 points; 95% confidence interval, –1.37 to 9.99).
In addition, the CPT group had a higher dropout rate (31.7%) than did the WET group (6.3%). The investigators concluded, however, that both therapies are effective. “Written exposure therapy should be considered by clinicians to be a viable treatment option that can address some of the barriers to receiving and implementing CPT and prolonged exposure that have been noted in health care settings,” Dr. Sloan and her colleagues wrote.
This study was funded by a grant from the National Institute of Mental Health. None of the authors had financial conflicts to report. Further details on this information can be found here.
SOURCE: Sloan DM. 2018 Jan 17. doi: 10.1001/jamapsychiatry.2017.4249.
Cognitive processing therapy may offer a greater benefit over time for posttraumatic stress disorder, but writing therapy offers a viable treatment in fewer sessions.
“Our results add to mounting research showing that the dose of therapy needed for beneficial outcomes for individuals with PTSD is not as large as what was once previously thought,” wrote Denise M. Sloan, PhD, of the National Center for PTSD, Boston, and her colleagues. “Our findings extend those prior studies by demonstrating that not only can PTSD symptoms be reduced significantly with less therapeutic exposure but that not as many therapy sessions are required.”
In a 1:1 randomized clinical trial, Dr. Sloan and her colleagues compared the effectiveness of written exposure therapy (WET) and cognitive processing therapy (CPT) in treating PTSD in 126 veteran and nonveteran adults, split evenly into the two therapy groups. and focused on details of the event, including thoughts and feelings associated with it. The CPT intervention was a 12-session trauma-focused therapy with a limited take-home writing component. It focused on helping patients recognize and challenge dysfunctional cognitions associated with traumatic events, the investigators wrote in JAMA Psychiatry.
When Dr. Sloan and her colleagues looked at the patients’ mean Clinician Administered PTSD Scale for DSM-5, or CAPS-5 score, a measure of PTSD symptom severity, they found that the WET and CPT groups’ scores were similar at 6 weeks, 12, weeks, and 36 weeks. At the 24-week assessment, the CAPS-5 score for those in the CPT group (20.92) was significantly lower than it was for those in the WET group (25.23) (mean difference, 4.31 points; 95% confidence interval, –1.37 to 9.99).
In addition, the CPT group had a higher dropout rate (31.7%) than did the WET group (6.3%). The investigators concluded, however, that both therapies are effective. “Written exposure therapy should be considered by clinicians to be a viable treatment option that can address some of the barriers to receiving and implementing CPT and prolonged exposure that have been noted in health care settings,” Dr. Sloan and her colleagues wrote.
This study was funded by a grant from the National Institute of Mental Health. None of the authors had financial conflicts to report. Further details on this information can be found here.
SOURCE: Sloan DM. 2018 Jan 17. doi: 10.1001/jamapsychiatry.2017.4249.
FROM JAMA Psychiatry
Driving-Related Coping Thoughts in Post-9/11 Combat Veterans With and Without Comorbid PTSD and TBI
Combat veterans who have served in Iraq and Afghanistan in the post-9/11 era face unique reintegration challenges, one being the transition from driving in combat zones to driving at home.1 Relative to previous conflicts, post-9/11 combat involves increased participation in road patrols and convoys along with more prevalent threats of improvised explosive devices (IEDs).1,2 Roadside ambushes designed to destroy or stop vehicles became a common warfare strategy, meaning that driving became an inherently dangerous combat maneuver.3
The modern combat driving framework includes cognitive tools (eg, targeted aggression and tactical awareness) combined with specific behaviors (eg, driving unpredictably fast, using rapid lane changes, and keeping other vehicles at a distance to avoid IEDs).4 This framework is adaptive and lifesaving in combat zones, but it can be maladaptive and dangerous in civilian environments. Service members face difficulty in updating this cognitive framework after leaving combat zones and may continue to experience specific cognitions (eg, “the world is dangerous”; “that car holds an IED”) while driving on civilian roads.3,5-8
The high prevalence of posttraumatic stress disorder (PTSD) and traumatic brain injury (TBI) in post-9/11 veterans may complicate reintegration. Both PTSD and TBI are considered signature wounds of these conflicts.8-11 Traumatic brain injury may be sustained as a result of blast injury or other mechanism, including a closed head injury or penetrating brain injury.10 Previous literature indicated that both PTSD and TBI across all severities are related to deficits in executive functioning, attention, and memory.12-16
In addition to cognitive deficits, veterans with PTSD also may experience cognitive misappraisal, in which they are more likely to perceive ambiguous stimuli as threatening because of an inability to suppress trauma-related schema and associations.5,17,18 Examples of roadside-specific trauma triggers include busy highways, traffic, loud or distracting noises, and vehicles of similar make and model as those commonly rigged with IEDs in Iraq or Afghanistan.2,7
Blast injury
Prior research suggests that veterans with PTSD and/or TBI experience significantly higher levels of anxiety in response to common roadside stimuli (ie, an overpass or stop sign) while driving than do veterans without either PTSD or TBI.3 Cognitive behavioral therapy (CBT) interventions have been developed and systematically evaluated for treating anxiety.21 The goal of CBT is to identify and change dysfunctional cognitions that result in biased information processing. Cognitive restructuring, the process by which problematic cognitions (negative automatic thoughts) are identified and examined for distortions, is one method of accomplishing this goal. Distortions then are disputed and rebutted with assistance from the clinician.22 A strategy for restructuring negative automatic thoughts is coping self-instruction, which centers on identifying when negative automatic thoughts are focused on others’ behavior, accepting that their behavior cannot be changed, and using positive coping behaviors to minimize negative automatic thoughts.23
The link between history of comorbid PTSD and TBI and combat driving, current driving anxiety, and coping strategies has not yet been extensively studied in veterans. Thus, the aim of the current study is to determine whether veterans with comorbid PTSD and TBI utilize coping self-instruction behind the wheel. Driving-specific coping self-instruction involves generating thoughts that are adaptive and accepting of others’ driving behaviors (eg, “Just turn up the radio and tune them out”). It was hypothesized that veterans with comorbid PTSD and TBI would endorse fewer coping self-instruction thoughts than would veterans without either PTSD or TBI.
Methods
The current project is part of a larger study that examines driving behaviors of post-9/11 combat veterans at the Michael J. Crescenz Veterans Affairs Medical Center in Philadelphia, Pennsylvania. Thirty-two male veterans aged between 22 and 48 years (M = 31.6, SD = 6.9) were included in the sample. Twenty-three were diagnosed with comorbid PTSD and TBI and 9 veterans with no major psychiatric or physical 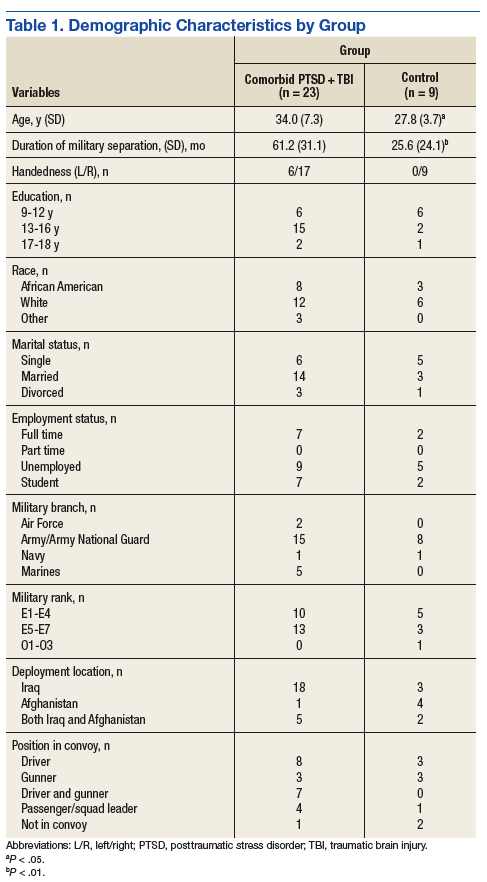
Assessment
All participants completed a battery of questionnaires, including the Driver’s Angry Thoughts Questionnaire (DATQ).23 The DATQ was used to investigate the specific thoughts that veterans experienced while driving.23 Participants indicated on a Likert scale from 1 (not at all) to 5 (all the time) how often they experienced any of 65 thoughts while driving. Each item was categorized into 1 of 5 distinct subscales (Table 2). A frequency score was generated for each of the 5 subscales. Each subscale had good internal consistency and convergent, divergent, and predictive validity. The Coping Self-Instruction subscale, which is defined as engaging in relaxing thoughts to accept others’ driving behaviors, was of primary interest. It is a 9-item scale (frequency score can range from 9 to 45) with good reliability (α = .83).23 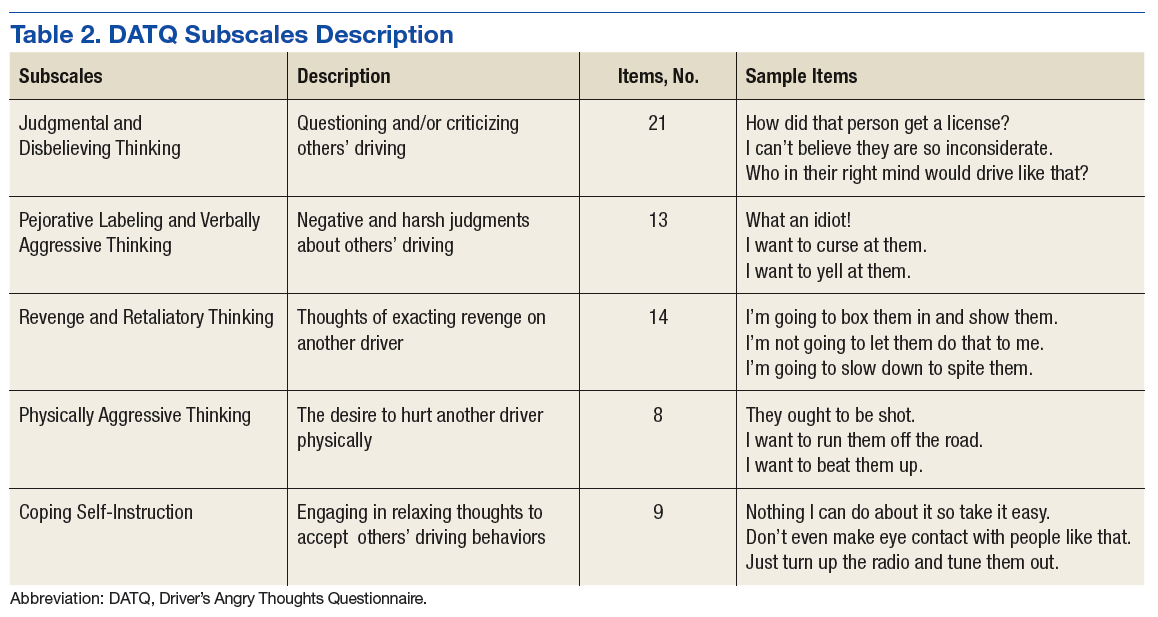
Given the small and unequal sample sizes, nonparametric independent samples Mann-Whitney U-tests were selected to compare frequency of driving-related thoughts across veterans with comorbid PTSD and TBI and those of veterans without either PTSD or TBI.
Results
Descriptive statistics and results for each DATQ subscale are reported in Table 3. Group comparisons revealed that veterans with comorbid PTSD and TBI endorsed statistically significantly fewer coping self-instruction thoughts while driving (M = 11.5, SD = 7.2) than did combat veterans without either PTSD or TBI (M = 18.1, SD = 6.9; U = 56.0, P = .05). Conversely, frequency of angry thoughts were statistically significant in their difference as a function of PTSD or TBI diagnostic status. 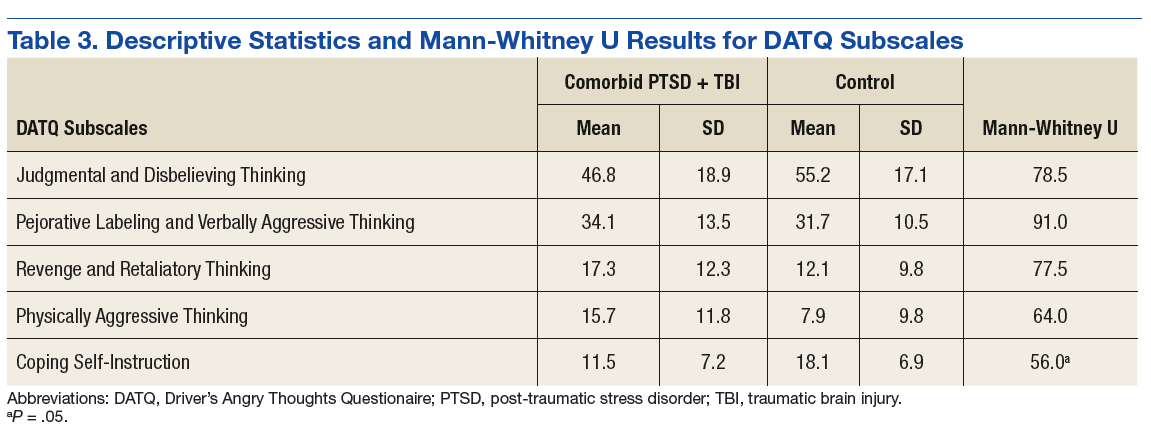
Discussion
While driving, veterans with PTSD or TBI endorsed statistically significantly fewer coping self-instruction thoughts than did veterans without either PTSD or TBI. Prior research suggests that veterans with PTSD or TBI experience greater anxiety than do veterans without either condition while driving.2,3 Taken together, this suggests that veterans with PTSD or TBI may lack efficient cognitive coping strategies related to the anxiety they experience while driving. Furthermore, the groups did not significantly differ in frequency of angry thoughts behind the wheel. This result was expected based on prior analyses that suggested that veterans with and without PTSD or TBI endorsed feelings of aggression, impatience, and frustration while driving at similar frequencies.3
Because all veterans in the current sample were exposed to combat, these results help to parse out the unique contribution of PTSD and TBI diagnoses on driving in civilian environments. Exposure to combat plus diagnoses of PTSD or TBI may be related to veterans’ ability to cope with typical driving situations at home. In the context of prior literature, results suggest that veterans with PTSD or TBI automatically may perceive neutral roadside stimuli as threatening, feel anxious in response to this perceived threat, and be ill-equipped to cope with this anxiety.3,5,17,18 According to CBT models, negative automatic thoughts play a critical role in maintaining anxiety.24 Particular cognitive distortions associated with PTSD symptomatology and combat driving experiences, such as misperceiving ambiguous stimuli as threatening because of an inability to suppress trauma-related schema and associations, may therefore maintain driving anxiety following military separation.
Research on CBT interventions suggests that cognitive restructuring, including coping self-instruction, are effective treatments to reduce anxiety.22,24 The current findings suggest that combat veterans with PTSD and TBI who experience driving anxiety endorse significantly fewer coping self-instruction thoughts than do controls in response to anxiety-provoking driving situations. In fact, prior research suggests that a majority of veterans experiencing driving-related anxiety do not seek help for their symptoms, and many of those who do prefer to reach out to friends rather than mental health professionals.2 However, due to their high levels of anxiety, these veterans likely would benefit from CBT interventions specifically targeted to coping strategies for civilian driving. These coping strategies should focus on recognizing that common roadside stimuli are not necessarily threatening in civilian environments. This type of cognitive restructuring may help veterans better manage anxiety while driving.
Limitations
The current study is limited by its small and unequal sample sizes and lack of a noncombat exposure comparison group. Additionally, while this study highlights a potential relationship between reduced cognitive coping strategies and behind-the-wheel anxiety in veterans with PTSD or TBI, causal inferences cannot be made. It is possible that individuals without coping strategies who are deployed to combat are more likely to develop PTSD or TBI. Being equipped with few coping strategies may then lead these veterans to experience greater anxiety while driving. Conversely, PTSD and TBI symptoms may prevent veterans from developing coping strategies over time.
Furthermore, the comorbid PTSD and TBI group was separated from the military for significantly longer than was the control group. Future studies using a longitudinal design could better examine the potential causal relationship between comorbid PTSD and TBI and coping and determine whether endorsement of coping self-instruction changes as a function of time since military separation.
Veterans in the current study report a variety of deployment experiences and locations. Methods of combat, type of vehicle, driving terrain, and prevalence of IEDs changed over the multiple post-9/11 military campaigns. Veterans who were deployed to Iraq in the mid-2000s were instructed to drive quickly and erratically to avoid IEDs and mortars, whereas veterans deployed in later years were taught to drive slowly and carefully to hunt for IEDs in heavily armored vehicles.3 Seventy-five percent of the veterans with PTSD or TBI in the current sample were deployed to Iraq in the early to mid-2000s, compared with 33% of the veterans without PTSD or TBI. Thus, the 2 groups in the current sample may have experienced different combat environments, which could impact how they perceived roadside stimuli. Future studies should recruit a larger and more balanced sample to better determine whether specific combat experiences impact coping strategies while driving.
Conclusion
To the best of the authors’ knowledge, the current study is the first to examine specific types of thoughts that veterans with and without PTSD or TBI experience while driving on civilian roads. Veterans with PTSD or TBI are not engaging in as many coping self-instruction thoughts behind the wheel, despite experiencing greater anxiety than that of veterans without either PTSD or TBI. Cognitive behavioral therapy interventions for anxiety include engaging in coping self-instruction during anxiety-provoking situations.22 Therefore, veterans with PTSD or TBI may benefit from learning targeted coping self-instruction thoughts that they can utilize when anxiety-provoking situations arise behind the wheel. Results suggest that clinicians should work with veterans with comorbid PTSD and TBI to develop specific coping self-instruction statements that they can utilize internally when faced with anxiety-provoking driving situations.
Acknowledgments
This study is the result of work supported by the Council on Brain Injury (grant #260472). The authors thank Dr. Rosette Biester for her guidance.
1. Belmont PJ, Schoenfeld AJ, Goodman G. Epidemiology of combat wounds in Operation Iraqi Freedom and Operation Enduring Freedom: orthopaedic burden of disease. J Surg Orthop Adv. 2010;19(1):2-7.
2. Zinzow HM, Brooks J, Stern EB. Driving-related anxiety in recently deployed service members: cues, mental health correlates, and help-seeking behavior. Mil Med. 2013;178(3):e357-e361.
3. Whipple EK, Schultheis MT, Robinson KM. Preliminary findings of a novel measure of driving behaviors in veterans with comorbid TBI and PTSD. J Rehabil Res Dev. 2016;53(6):827-838.
4. Adler AB, Bliese PD, McGurk D, Hoge CW, Castro CA. Battlemind debriefing and battlemind training as early interventions with soldiers returning from Iraq: randomization by platoon. J Consult Clin Psychol. 2009;77(5):928-940.
5. Amick MM, Kraft M, McGlinchey R. Driving simulator performance of veterans from the Iraq and Afghanistan wars. J Rehabil Res Dev. 2013;50(4):463-470.
6. Classen S, Cormack NL, Winter SM, et al. Efficacy of an occupational therapy driving intervention for returning combat veterans. OTJR (Thorofare NJ). 2014;34(4):177-182.
7. Hannold EM, Classen S, Winter S, Lanford DN, Levy CE. Exploratory pilot study of driving perceptions among OIF/OEF veterans with mTBI and PTSD. J Rehabil Res Dev. 2013;50(10):1315-1330.
8. Lew HL, Kraft M, Pogoda TK, Amick MM, Woods P, Cifu DX. Prevalence and characteristics of driving difficulties in Operation Iraqi Freedom/Operation Enduring Freedom combat returnees. J Rehabil Res Dev. 2011;48(8):913-925.
9. Arthur DC, MacDermid S, Kiley KC; Defense Health Board Task Force on Mental Health. An Achievable Vision: Report of the Department of Defense Task Force on Mental Health. Falls Church, VA: Defense Health Board; 2007.
10. Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008.
11. Independent Review Group. Rebuilding the Trust: Independent Review Group Report on Rehabilitation Care and Administrative Processes at Walter Reed Army Medical Center and National Naval Medical Center. Arlington, VA: Independent Review Group; 2007
12. Bailie JM, Cole WR, Ivins B, et al. The experience, expression, and control of anger following traumatic brain injury in a military sample. J Head Trauma Rehabil. 2015;30(1):12-20.
13. Campbell TA, Nelson LA, Lumpkin R, Yoash-Gantz RE, Pickett TC, McCormick CL. Neuropsychological measures of processing speed and executive functioning in combat veterans with PTSD, TBI, and comorbid TBI/PTSD. Psychiatr Ann. 2009;39(8):796-803.
14. Classen S, Levy C, Meyer DL, Bewernitz M, Lanford DN, Mann WC. Simulated driving performance of combat veterans with mild tramatic brain injury and posttraumatic stress disorder: a pilot study. Am J Occup Ther. 2011;65(4):419-427.
15. Lew HL, Amick MM, Kraft M, Stein MB, Cifu DX. Potential driving issues in combat returnees. NeuroRehabilitation. 2010;26(3):271-278.
16. Vasterling JL, Brailey K, Allain AN, Duke LM, Constans JI, Sutker PB. Attention, learning, and memory performances and intellectual resources in Vietnam veterans: PTSD and no disorder comparisons. Neuropsychology. 2002;16(1):5-14.
17. Kimble MO, Kaufman ML, Leonard LL, et al. Sentence completion test in veterans with and without PTSD: preliminary findings. Psychiatry Res. 2002;113(3):303-307.
18. Kuhn E, Drescher K, Ruzek J, Rosen C. Aggressive and unsafe driving in male veterans receiving residential treatment for PTSD. J Trauma Stress. 2010;23(3):399-402.
19. Stein MB, McAllister TW. Exploring the convergence of posttraumatic stress disorder and mild traumatic brain injury. Am J Psychiatry. 2009;166(7):768-776.
20. Hill JJ III, Mobo BH Jr, Cullen MR. Separating deployment-related traumatic brain injury and posttraumatic stress disorder in veterans: preliminary findings from the Veterans Affairs traumatic brain injury screening program. Am J Phys Med Rehabil. 2009;88(8):605-614.
21. Hofmann SG, Smits JA. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J Clin Psychiatry. 2008;69(4):621-632.
22. Hope DA, Burns JA, Hayes SA, Herbert JD, Warner MD. Automatic thoughts and cognitive restructuring in cognitive behavioral group therapy for social anxiety disorder. Cognit Ther Res. 2010;34(1):1-12.
23. Deffenbacher JL, Petrilli RT, Lynch RS, Oetting ER, Swaim RC. The driver’s angry thoughts questionnaire: a measure of angry cognitions when driving. Cognit Ther Res. 2003;27(4):383-402.
24. Beck AT, Emery G, Greenberg RL. Anxiety Disorders and Phobias: A Cognitive Perspective. Rev. paperback ed. New York, NY: Basic Books; 2005.
Combat veterans who have served in Iraq and Afghanistan in the post-9/11 era face unique reintegration challenges, one being the transition from driving in combat zones to driving at home.1 Relative to previous conflicts, post-9/11 combat involves increased participation in road patrols and convoys along with more prevalent threats of improvised explosive devices (IEDs).1,2 Roadside ambushes designed to destroy or stop vehicles became a common warfare strategy, meaning that driving became an inherently dangerous combat maneuver.3
The modern combat driving framework includes cognitive tools (eg, targeted aggression and tactical awareness) combined with specific behaviors (eg, driving unpredictably fast, using rapid lane changes, and keeping other vehicles at a distance to avoid IEDs).4 This framework is adaptive and lifesaving in combat zones, but it can be maladaptive and dangerous in civilian environments. Service members face difficulty in updating this cognitive framework after leaving combat zones and may continue to experience specific cognitions (eg, “the world is dangerous”; “that car holds an IED”) while driving on civilian roads.3,5-8
The high prevalence of posttraumatic stress disorder (PTSD) and traumatic brain injury (TBI) in post-9/11 veterans may complicate reintegration. Both PTSD and TBI are considered signature wounds of these conflicts.8-11 Traumatic brain injury may be sustained as a result of blast injury or other mechanism, including a closed head injury or penetrating brain injury.10 Previous literature indicated that both PTSD and TBI across all severities are related to deficits in executive functioning, attention, and memory.12-16
In addition to cognitive deficits, veterans with PTSD also may experience cognitive misappraisal, in which they are more likely to perceive ambiguous stimuli as threatening because of an inability to suppress trauma-related schema and associations.5,17,18 Examples of roadside-specific trauma triggers include busy highways, traffic, loud or distracting noises, and vehicles of similar make and model as those commonly rigged with IEDs in Iraq or Afghanistan.2,7
Blast injury
Prior research suggests that veterans with PTSD and/or TBI experience significantly higher levels of anxiety in response to common roadside stimuli (ie, an overpass or stop sign) while driving than do veterans without either PTSD or TBI.3 Cognitive behavioral therapy (CBT) interventions have been developed and systematically evaluated for treating anxiety.21 The goal of CBT is to identify and change dysfunctional cognitions that result in biased information processing. Cognitive restructuring, the process by which problematic cognitions (negative automatic thoughts) are identified and examined for distortions, is one method of accomplishing this goal. Distortions then are disputed and rebutted with assistance from the clinician.22 A strategy for restructuring negative automatic thoughts is coping self-instruction, which centers on identifying when negative automatic thoughts are focused on others’ behavior, accepting that their behavior cannot be changed, and using positive coping behaviors to minimize negative automatic thoughts.23
The link between history of comorbid PTSD and TBI and combat driving, current driving anxiety, and coping strategies has not yet been extensively studied in veterans. Thus, the aim of the current study is to determine whether veterans with comorbid PTSD and TBI utilize coping self-instruction behind the wheel. Driving-specific coping self-instruction involves generating thoughts that are adaptive and accepting of others’ driving behaviors (eg, “Just turn up the radio and tune them out”). It was hypothesized that veterans with comorbid PTSD and TBI would endorse fewer coping self-instruction thoughts than would veterans without either PTSD or TBI.
Methods
The current project is part of a larger study that examines driving behaviors of post-9/11 combat veterans at the Michael J. Crescenz Veterans Affairs Medical Center in Philadelphia, Pennsylvania. Thirty-two male veterans aged between 22 and 48 years (M = 31.6, SD = 6.9) were included in the sample. Twenty-three were diagnosed with comorbid PTSD and TBI and 9 veterans with no major psychiatric or physical
Assessment
All participants completed a battery of questionnaires, including the Driver’s Angry Thoughts Questionnaire (DATQ).23 The DATQ was used to investigate the specific thoughts that veterans experienced while driving.23 Participants indicated on a Likert scale from 1 (not at all) to 5 (all the time) how often they experienced any of 65 thoughts while driving. Each item was categorized into 1 of 5 distinct subscales (Table 2). A frequency score was generated for each of the 5 subscales. Each subscale had good internal consistency and convergent, divergent, and predictive validity. The Coping Self-Instruction subscale, which is defined as engaging in relaxing thoughts to accept others’ driving behaviors, was of primary interest. It is a 9-item scale (frequency score can range from 9 to 45) with good reliability (α = .83).23
Given the small and unequal sample sizes, nonparametric independent samples Mann-Whitney U-tests were selected to compare frequency of driving-related thoughts across veterans with comorbid PTSD and TBI and those of veterans without either PTSD or TBI.
Results
Descriptive statistics and results for each DATQ subscale are reported in Table 3. Group comparisons revealed that veterans with comorbid PTSD and TBI endorsed statistically significantly fewer coping self-instruction thoughts while driving (M = 11.5, SD = 7.2) than did combat veterans without either PTSD or TBI (M = 18.1, SD = 6.9; U = 56.0, P = .05). Conversely, frequency of angry thoughts were statistically significant in their difference as a function of PTSD or TBI diagnostic status.
Discussion
While driving, veterans with PTSD or TBI endorsed statistically significantly fewer coping self-instruction thoughts than did veterans without either PTSD or TBI. Prior research suggests that veterans with PTSD or TBI experience greater anxiety than do veterans without either condition while driving.2,3 Taken together, this suggests that veterans with PTSD or TBI may lack efficient cognitive coping strategies related to the anxiety they experience while driving. Furthermore, the groups did not significantly differ in frequency of angry thoughts behind the wheel. This result was expected based on prior analyses that suggested that veterans with and without PTSD or TBI endorsed feelings of aggression, impatience, and frustration while driving at similar frequencies.3
Because all veterans in the current sample were exposed to combat, these results help to parse out the unique contribution of PTSD and TBI diagnoses on driving in civilian environments. Exposure to combat plus diagnoses of PTSD or TBI may be related to veterans’ ability to cope with typical driving situations at home. In the context of prior literature, results suggest that veterans with PTSD or TBI automatically may perceive neutral roadside stimuli as threatening, feel anxious in response to this perceived threat, and be ill-equipped to cope with this anxiety.3,5,17,18 According to CBT models, negative automatic thoughts play a critical role in maintaining anxiety.24 Particular cognitive distortions associated with PTSD symptomatology and combat driving experiences, such as misperceiving ambiguous stimuli as threatening because of an inability to suppress trauma-related schema and associations, may therefore maintain driving anxiety following military separation.
Research on CBT interventions suggests that cognitive restructuring, including coping self-instruction, are effective treatments to reduce anxiety.22,24 The current findings suggest that combat veterans with PTSD and TBI who experience driving anxiety endorse significantly fewer coping self-instruction thoughts than do controls in response to anxiety-provoking driving situations. In fact, prior research suggests that a majority of veterans experiencing driving-related anxiety do not seek help for their symptoms, and many of those who do prefer to reach out to friends rather than mental health professionals.2 However, due to their high levels of anxiety, these veterans likely would benefit from CBT interventions specifically targeted to coping strategies for civilian driving. These coping strategies should focus on recognizing that common roadside stimuli are not necessarily threatening in civilian environments. This type of cognitive restructuring may help veterans better manage anxiety while driving.
Limitations
The current study is limited by its small and unequal sample sizes and lack of a noncombat exposure comparison group. Additionally, while this study highlights a potential relationship between reduced cognitive coping strategies and behind-the-wheel anxiety in veterans with PTSD or TBI, causal inferences cannot be made. It is possible that individuals without coping strategies who are deployed to combat are more likely to develop PTSD or TBI. Being equipped with few coping strategies may then lead these veterans to experience greater anxiety while driving. Conversely, PTSD and TBI symptoms may prevent veterans from developing coping strategies over time.
Furthermore, the comorbid PTSD and TBI group was separated from the military for significantly longer than was the control group. Future studies using a longitudinal design could better examine the potential causal relationship between comorbid PTSD and TBI and coping and determine whether endorsement of coping self-instruction changes as a function of time since military separation.
Veterans in the current study report a variety of deployment experiences and locations. Methods of combat, type of vehicle, driving terrain, and prevalence of IEDs changed over the multiple post-9/11 military campaigns. Veterans who were deployed to Iraq in the mid-2000s were instructed to drive quickly and erratically to avoid IEDs and mortars, whereas veterans deployed in later years were taught to drive slowly and carefully to hunt for IEDs in heavily armored vehicles.3 Seventy-five percent of the veterans with PTSD or TBI in the current sample were deployed to Iraq in the early to mid-2000s, compared with 33% of the veterans without PTSD or TBI. Thus, the 2 groups in the current sample may have experienced different combat environments, which could impact how they perceived roadside stimuli. Future studies should recruit a larger and more balanced sample to better determine whether specific combat experiences impact coping strategies while driving.
Conclusion
To the best of the authors’ knowledge, the current study is the first to examine specific types of thoughts that veterans with and without PTSD or TBI experience while driving on civilian roads. Veterans with PTSD or TBI are not engaging in as many coping self-instruction thoughts behind the wheel, despite experiencing greater anxiety than that of veterans without either PTSD or TBI. Cognitive behavioral therapy interventions for anxiety include engaging in coping self-instruction during anxiety-provoking situations.22 Therefore, veterans with PTSD or TBI may benefit from learning targeted coping self-instruction thoughts that they can utilize when anxiety-provoking situations arise behind the wheel. Results suggest that clinicians should work with veterans with comorbid PTSD and TBI to develop specific coping self-instruction statements that they can utilize internally when faced with anxiety-provoking driving situations.
Acknowledgments
This study is the result of work supported by the Council on Brain Injury (grant #260472). The authors thank Dr. Rosette Biester for her guidance.
Combat veterans who have served in Iraq and Afghanistan in the post-9/11 era face unique reintegration challenges, one being the transition from driving in combat zones to driving at home.1 Relative to previous conflicts, post-9/11 combat involves increased participation in road patrols and convoys along with more prevalent threats of improvised explosive devices (IEDs).1,2 Roadside ambushes designed to destroy or stop vehicles became a common warfare strategy, meaning that driving became an inherently dangerous combat maneuver.3
The modern combat driving framework includes cognitive tools (eg, targeted aggression and tactical awareness) combined with specific behaviors (eg, driving unpredictably fast, using rapid lane changes, and keeping other vehicles at a distance to avoid IEDs).4 This framework is adaptive and lifesaving in combat zones, but it can be maladaptive and dangerous in civilian environments. Service members face difficulty in updating this cognitive framework after leaving combat zones and may continue to experience specific cognitions (eg, “the world is dangerous”; “that car holds an IED”) while driving on civilian roads.3,5-8
The high prevalence of posttraumatic stress disorder (PTSD) and traumatic brain injury (TBI) in post-9/11 veterans may complicate reintegration. Both PTSD and TBI are considered signature wounds of these conflicts.8-11 Traumatic brain injury may be sustained as a result of blast injury or other mechanism, including a closed head injury or penetrating brain injury.10 Previous literature indicated that both PTSD and TBI across all severities are related to deficits in executive functioning, attention, and memory.12-16
In addition to cognitive deficits, veterans with PTSD also may experience cognitive misappraisal, in which they are more likely to perceive ambiguous stimuli as threatening because of an inability to suppress trauma-related schema and associations.5,17,18 Examples of roadside-specific trauma triggers include busy highways, traffic, loud or distracting noises, and vehicles of similar make and model as those commonly rigged with IEDs in Iraq or Afghanistan.2,7
Blast injury
Prior research suggests that veterans with PTSD and/or TBI experience significantly higher levels of anxiety in response to common roadside stimuli (ie, an overpass or stop sign) while driving than do veterans without either PTSD or TBI.3 Cognitive behavioral therapy (CBT) interventions have been developed and systematically evaluated for treating anxiety.21 The goal of CBT is to identify and change dysfunctional cognitions that result in biased information processing. Cognitive restructuring, the process by which problematic cognitions (negative automatic thoughts) are identified and examined for distortions, is one method of accomplishing this goal. Distortions then are disputed and rebutted with assistance from the clinician.22 A strategy for restructuring negative automatic thoughts is coping self-instruction, which centers on identifying when negative automatic thoughts are focused on others’ behavior, accepting that their behavior cannot be changed, and using positive coping behaviors to minimize negative automatic thoughts.23
The link between history of comorbid PTSD and TBI and combat driving, current driving anxiety, and coping strategies has not yet been extensively studied in veterans. Thus, the aim of the current study is to determine whether veterans with comorbid PTSD and TBI utilize coping self-instruction behind the wheel. Driving-specific coping self-instruction involves generating thoughts that are adaptive and accepting of others’ driving behaviors (eg, “Just turn up the radio and tune them out”). It was hypothesized that veterans with comorbid PTSD and TBI would endorse fewer coping self-instruction thoughts than would veterans without either PTSD or TBI.
Methods
The current project is part of a larger study that examines driving behaviors of post-9/11 combat veterans at the Michael J. Crescenz Veterans Affairs Medical Center in Philadelphia, Pennsylvania. Thirty-two male veterans aged between 22 and 48 years (M = 31.6, SD = 6.9) were included in the sample. Twenty-three were diagnosed with comorbid PTSD and TBI and 9 veterans with no major psychiatric or physical
Assessment
All participants completed a battery of questionnaires, including the Driver’s Angry Thoughts Questionnaire (DATQ).23 The DATQ was used to investigate the specific thoughts that veterans experienced while driving.23 Participants indicated on a Likert scale from 1 (not at all) to 5 (all the time) how often they experienced any of 65 thoughts while driving. Each item was categorized into 1 of 5 distinct subscales (Table 2). A frequency score was generated for each of the 5 subscales. Each subscale had good internal consistency and convergent, divergent, and predictive validity. The Coping Self-Instruction subscale, which is defined as engaging in relaxing thoughts to accept others’ driving behaviors, was of primary interest. It is a 9-item scale (frequency score can range from 9 to 45) with good reliability (α = .83).23
Given the small and unequal sample sizes, nonparametric independent samples Mann-Whitney U-tests were selected to compare frequency of driving-related thoughts across veterans with comorbid PTSD and TBI and those of veterans without either PTSD or TBI.
Results
Descriptive statistics and results for each DATQ subscale are reported in Table 3. Group comparisons revealed that veterans with comorbid PTSD and TBI endorsed statistically significantly fewer coping self-instruction thoughts while driving (M = 11.5, SD = 7.2) than did combat veterans without either PTSD or TBI (M = 18.1, SD = 6.9; U = 56.0, P = .05). Conversely, frequency of angry thoughts were statistically significant in their difference as a function of PTSD or TBI diagnostic status.
Discussion
While driving, veterans with PTSD or TBI endorsed statistically significantly fewer coping self-instruction thoughts than did veterans without either PTSD or TBI. Prior research suggests that veterans with PTSD or TBI experience greater anxiety than do veterans without either condition while driving.2,3 Taken together, this suggests that veterans with PTSD or TBI may lack efficient cognitive coping strategies related to the anxiety they experience while driving. Furthermore, the groups did not significantly differ in frequency of angry thoughts behind the wheel. This result was expected based on prior analyses that suggested that veterans with and without PTSD or TBI endorsed feelings of aggression, impatience, and frustration while driving at similar frequencies.3
Because all veterans in the current sample were exposed to combat, these results help to parse out the unique contribution of PTSD and TBI diagnoses on driving in civilian environments. Exposure to combat plus diagnoses of PTSD or TBI may be related to veterans’ ability to cope with typical driving situations at home. In the context of prior literature, results suggest that veterans with PTSD or TBI automatically may perceive neutral roadside stimuli as threatening, feel anxious in response to this perceived threat, and be ill-equipped to cope with this anxiety.3,5,17,18 According to CBT models, negative automatic thoughts play a critical role in maintaining anxiety.24 Particular cognitive distortions associated with PTSD symptomatology and combat driving experiences, such as misperceiving ambiguous stimuli as threatening because of an inability to suppress trauma-related schema and associations, may therefore maintain driving anxiety following military separation.
Research on CBT interventions suggests that cognitive restructuring, including coping self-instruction, are effective treatments to reduce anxiety.22,24 The current findings suggest that combat veterans with PTSD and TBI who experience driving anxiety endorse significantly fewer coping self-instruction thoughts than do controls in response to anxiety-provoking driving situations. In fact, prior research suggests that a majority of veterans experiencing driving-related anxiety do not seek help for their symptoms, and many of those who do prefer to reach out to friends rather than mental health professionals.2 However, due to their high levels of anxiety, these veterans likely would benefit from CBT interventions specifically targeted to coping strategies for civilian driving. These coping strategies should focus on recognizing that common roadside stimuli are not necessarily threatening in civilian environments. This type of cognitive restructuring may help veterans better manage anxiety while driving.
Limitations
The current study is limited by its small and unequal sample sizes and lack of a noncombat exposure comparison group. Additionally, while this study highlights a potential relationship between reduced cognitive coping strategies and behind-the-wheel anxiety in veterans with PTSD or TBI, causal inferences cannot be made. It is possible that individuals without coping strategies who are deployed to combat are more likely to develop PTSD or TBI. Being equipped with few coping strategies may then lead these veterans to experience greater anxiety while driving. Conversely, PTSD and TBI symptoms may prevent veterans from developing coping strategies over time.
Furthermore, the comorbid PTSD and TBI group was separated from the military for significantly longer than was the control group. Future studies using a longitudinal design could better examine the potential causal relationship between comorbid PTSD and TBI and coping and determine whether endorsement of coping self-instruction changes as a function of time since military separation.
Veterans in the current study report a variety of deployment experiences and locations. Methods of combat, type of vehicle, driving terrain, and prevalence of IEDs changed over the multiple post-9/11 military campaigns. Veterans who were deployed to Iraq in the mid-2000s were instructed to drive quickly and erratically to avoid IEDs and mortars, whereas veterans deployed in later years were taught to drive slowly and carefully to hunt for IEDs in heavily armored vehicles.3 Seventy-five percent of the veterans with PTSD or TBI in the current sample were deployed to Iraq in the early to mid-2000s, compared with 33% of the veterans without PTSD or TBI. Thus, the 2 groups in the current sample may have experienced different combat environments, which could impact how they perceived roadside stimuli. Future studies should recruit a larger and more balanced sample to better determine whether specific combat experiences impact coping strategies while driving.
Conclusion
To the best of the authors’ knowledge, the current study is the first to examine specific types of thoughts that veterans with and without PTSD or TBI experience while driving on civilian roads. Veterans with PTSD or TBI are not engaging in as many coping self-instruction thoughts behind the wheel, despite experiencing greater anxiety than that of veterans without either PTSD or TBI. Cognitive behavioral therapy interventions for anxiety include engaging in coping self-instruction during anxiety-provoking situations.22 Therefore, veterans with PTSD or TBI may benefit from learning targeted coping self-instruction thoughts that they can utilize when anxiety-provoking situations arise behind the wheel. Results suggest that clinicians should work with veterans with comorbid PTSD and TBI to develop specific coping self-instruction statements that they can utilize internally when faced with anxiety-provoking driving situations.
Acknowledgments
This study is the result of work supported by the Council on Brain Injury (grant #260472). The authors thank Dr. Rosette Biester for her guidance.
1. Belmont PJ, Schoenfeld AJ, Goodman G. Epidemiology of combat wounds in Operation Iraqi Freedom and Operation Enduring Freedom: orthopaedic burden of disease. J Surg Orthop Adv. 2010;19(1):2-7.
2. Zinzow HM, Brooks J, Stern EB. Driving-related anxiety in recently deployed service members: cues, mental health correlates, and help-seeking behavior. Mil Med. 2013;178(3):e357-e361.
3. Whipple EK, Schultheis MT, Robinson KM. Preliminary findings of a novel measure of driving behaviors in veterans with comorbid TBI and PTSD. J Rehabil Res Dev. 2016;53(6):827-838.
4. Adler AB, Bliese PD, McGurk D, Hoge CW, Castro CA. Battlemind debriefing and battlemind training as early interventions with soldiers returning from Iraq: randomization by platoon. J Consult Clin Psychol. 2009;77(5):928-940.
5. Amick MM, Kraft M, McGlinchey R. Driving simulator performance of veterans from the Iraq and Afghanistan wars. J Rehabil Res Dev. 2013;50(4):463-470.
6. Classen S, Cormack NL, Winter SM, et al. Efficacy of an occupational therapy driving intervention for returning combat veterans. OTJR (Thorofare NJ). 2014;34(4):177-182.
7. Hannold EM, Classen S, Winter S, Lanford DN, Levy CE. Exploratory pilot study of driving perceptions among OIF/OEF veterans with mTBI and PTSD. J Rehabil Res Dev. 2013;50(10):1315-1330.
8. Lew HL, Kraft M, Pogoda TK, Amick MM, Woods P, Cifu DX. Prevalence and characteristics of driving difficulties in Operation Iraqi Freedom/Operation Enduring Freedom combat returnees. J Rehabil Res Dev. 2011;48(8):913-925.
9. Arthur DC, MacDermid S, Kiley KC; Defense Health Board Task Force on Mental Health. An Achievable Vision: Report of the Department of Defense Task Force on Mental Health. Falls Church, VA: Defense Health Board; 2007.
10. Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008.
11. Independent Review Group. Rebuilding the Trust: Independent Review Group Report on Rehabilitation Care and Administrative Processes at Walter Reed Army Medical Center and National Naval Medical Center. Arlington, VA: Independent Review Group; 2007
12. Bailie JM, Cole WR, Ivins B, et al. The experience, expression, and control of anger following traumatic brain injury in a military sample. J Head Trauma Rehabil. 2015;30(1):12-20.
13. Campbell TA, Nelson LA, Lumpkin R, Yoash-Gantz RE, Pickett TC, McCormick CL. Neuropsychological measures of processing speed and executive functioning in combat veterans with PTSD, TBI, and comorbid TBI/PTSD. Psychiatr Ann. 2009;39(8):796-803.
14. Classen S, Levy C, Meyer DL, Bewernitz M, Lanford DN, Mann WC. Simulated driving performance of combat veterans with mild tramatic brain injury and posttraumatic stress disorder: a pilot study. Am J Occup Ther. 2011;65(4):419-427.
15. Lew HL, Amick MM, Kraft M, Stein MB, Cifu DX. Potential driving issues in combat returnees. NeuroRehabilitation. 2010;26(3):271-278.
16. Vasterling JL, Brailey K, Allain AN, Duke LM, Constans JI, Sutker PB. Attention, learning, and memory performances and intellectual resources in Vietnam veterans: PTSD and no disorder comparisons. Neuropsychology. 2002;16(1):5-14.
17. Kimble MO, Kaufman ML, Leonard LL, et al. Sentence completion test in veterans with and without PTSD: preliminary findings. Psychiatry Res. 2002;113(3):303-307.
18. Kuhn E, Drescher K, Ruzek J, Rosen C. Aggressive and unsafe driving in male veterans receiving residential treatment for PTSD. J Trauma Stress. 2010;23(3):399-402.
19. Stein MB, McAllister TW. Exploring the convergence of posttraumatic stress disorder and mild traumatic brain injury. Am J Psychiatry. 2009;166(7):768-776.
20. Hill JJ III, Mobo BH Jr, Cullen MR. Separating deployment-related traumatic brain injury and posttraumatic stress disorder in veterans: preliminary findings from the Veterans Affairs traumatic brain injury screening program. Am J Phys Med Rehabil. 2009;88(8):605-614.
21. Hofmann SG, Smits JA. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J Clin Psychiatry. 2008;69(4):621-632.
22. Hope DA, Burns JA, Hayes SA, Herbert JD, Warner MD. Automatic thoughts and cognitive restructuring in cognitive behavioral group therapy for social anxiety disorder. Cognit Ther Res. 2010;34(1):1-12.
23. Deffenbacher JL, Petrilli RT, Lynch RS, Oetting ER, Swaim RC. The driver’s angry thoughts questionnaire: a measure of angry cognitions when driving. Cognit Ther Res. 2003;27(4):383-402.
24. Beck AT, Emery G, Greenberg RL. Anxiety Disorders and Phobias: A Cognitive Perspective. Rev. paperback ed. New York, NY: Basic Books; 2005.
1. Belmont PJ, Schoenfeld AJ, Goodman G. Epidemiology of combat wounds in Operation Iraqi Freedom and Operation Enduring Freedom: orthopaedic burden of disease. J Surg Orthop Adv. 2010;19(1):2-7.
2. Zinzow HM, Brooks J, Stern EB. Driving-related anxiety in recently deployed service members: cues, mental health correlates, and help-seeking behavior. Mil Med. 2013;178(3):e357-e361.
3. Whipple EK, Schultheis MT, Robinson KM. Preliminary findings of a novel measure of driving behaviors in veterans with comorbid TBI and PTSD. J Rehabil Res Dev. 2016;53(6):827-838.
4. Adler AB, Bliese PD, McGurk D, Hoge CW, Castro CA. Battlemind debriefing and battlemind training as early interventions with soldiers returning from Iraq: randomization by platoon. J Consult Clin Psychol. 2009;77(5):928-940.
5. Amick MM, Kraft M, McGlinchey R. Driving simulator performance of veterans from the Iraq and Afghanistan wars. J Rehabil Res Dev. 2013;50(4):463-470.
6. Classen S, Cormack NL, Winter SM, et al. Efficacy of an occupational therapy driving intervention for returning combat veterans. OTJR (Thorofare NJ). 2014;34(4):177-182.
7. Hannold EM, Classen S, Winter S, Lanford DN, Levy CE. Exploratory pilot study of driving perceptions among OIF/OEF veterans with mTBI and PTSD. J Rehabil Res Dev. 2013;50(10):1315-1330.
8. Lew HL, Kraft M, Pogoda TK, Amick MM, Woods P, Cifu DX. Prevalence and characteristics of driving difficulties in Operation Iraqi Freedom/Operation Enduring Freedom combat returnees. J Rehabil Res Dev. 2011;48(8):913-925.
9. Arthur DC, MacDermid S, Kiley KC; Defense Health Board Task Force on Mental Health. An Achievable Vision: Report of the Department of Defense Task Force on Mental Health. Falls Church, VA: Defense Health Board; 2007.
10. Tanielian T, Jaycox LH, eds. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: RAND Corporation; 2008.
11. Independent Review Group. Rebuilding the Trust: Independent Review Group Report on Rehabilitation Care and Administrative Processes at Walter Reed Army Medical Center and National Naval Medical Center. Arlington, VA: Independent Review Group; 2007
12. Bailie JM, Cole WR, Ivins B, et al. The experience, expression, and control of anger following traumatic brain injury in a military sample. J Head Trauma Rehabil. 2015;30(1):12-20.
13. Campbell TA, Nelson LA, Lumpkin R, Yoash-Gantz RE, Pickett TC, McCormick CL. Neuropsychological measures of processing speed and executive functioning in combat veterans with PTSD, TBI, and comorbid TBI/PTSD. Psychiatr Ann. 2009;39(8):796-803.
14. Classen S, Levy C, Meyer DL, Bewernitz M, Lanford DN, Mann WC. Simulated driving performance of combat veterans with mild tramatic brain injury and posttraumatic stress disorder: a pilot study. Am J Occup Ther. 2011;65(4):419-427.
15. Lew HL, Amick MM, Kraft M, Stein MB, Cifu DX. Potential driving issues in combat returnees. NeuroRehabilitation. 2010;26(3):271-278.
16. Vasterling JL, Brailey K, Allain AN, Duke LM, Constans JI, Sutker PB. Attention, learning, and memory performances and intellectual resources in Vietnam veterans: PTSD and no disorder comparisons. Neuropsychology. 2002;16(1):5-14.
17. Kimble MO, Kaufman ML, Leonard LL, et al. Sentence completion test in veterans with and without PTSD: preliminary findings. Psychiatry Res. 2002;113(3):303-307.
18. Kuhn E, Drescher K, Ruzek J, Rosen C. Aggressive and unsafe driving in male veterans receiving residential treatment for PTSD. J Trauma Stress. 2010;23(3):399-402.
19. Stein MB, McAllister TW. Exploring the convergence of posttraumatic stress disorder and mild traumatic brain injury. Am J Psychiatry. 2009;166(7):768-776.
20. Hill JJ III, Mobo BH Jr, Cullen MR. Separating deployment-related traumatic brain injury and posttraumatic stress disorder in veterans: preliminary findings from the Veterans Affairs traumatic brain injury screening program. Am J Phys Med Rehabil. 2009;88(8):605-614.
21. Hofmann SG, Smits JA. Cognitive-behavioral therapy for adult anxiety disorders: a meta-analysis of randomized placebo-controlled trials. J Clin Psychiatry. 2008;69(4):621-632.
22. Hope DA, Burns JA, Hayes SA, Herbert JD, Warner MD. Automatic thoughts and cognitive restructuring in cognitive behavioral group therapy for social anxiety disorder. Cognit Ther Res. 2010;34(1):1-12.
23. Deffenbacher JL, Petrilli RT, Lynch RS, Oetting ER, Swaim RC. The driver’s angry thoughts questionnaire: a measure of angry cognitions when driving. Cognit Ther Res. 2003;27(4):383-402.
24. Beck AT, Emery G, Greenberg RL. Anxiety Disorders and Phobias: A Cognitive Perspective. Rev. paperback ed. New York, NY: Basic Books; 2005.

Pediatric seclusion and restraint increases with ADHD, decreases with PTSD
NEW ORLEANS – Attention-deficit/hyperactivity disorder and non-suicidal self-harm – cutting and head banging, for instance – strongly predicted longer seclusion and restraint episodes, sometimes past 2 hours, in a review at the University of Missouri, Columbia, pediatric inpatient psychiatric unit.
Meanwhile, children with histories of physical abuse, post-traumatic stress disorder (PTSD), or out-of-home placement were less likely to have multiple seclusion and restraint (SR) episodes during an admission, and had lower numbers of SR events overall. Perhaps hyper-vigilance due to past traumas helped them avoid situations that led to problems. Staff might also have used a lighter touch given the children’s histories.
The investigators reviewed 305 SR episodes from 2011-2014 among 92 children aged 5-18 years old. They plan to expand their study to 2009-2017 and add a prospective arm.

It’s well known that SR, a last-ditch effort to prevent physical harm, traumatizes patients, but research on how to avoid it has mostly focused on adults. The Missouri team wants to change that by identifying the children most at risk, so that something can be done beforehand to prevent it. Maybe extra one-on-one care would help, Dr. Badawy said.
The children in the review were an average of 10.5 years old, and most were admitted for 3-7 days. Fifty-five (60%) had multiple SR episodes, 34 in a single admission and 21 across multiple admissions; 71% of the episodes were in boys, 58% in white children, 27.7% in black children, and the rest in multiracial children. Twenty-one percent of the episodes were in children with intellectual problems. ADHD and oppositional defiant disorder were the most common diagnoses, each diagnosed in more than half of the subjects.
When asked how a 5-year-old child can end up in restraints, Dr. Badawy agreed that bad parenting is a factor. Parents who don’t know any better might escalate normal behavior, and others might simply not care that much about their kids, or have much empathy. “In the 5-10 year-olds, I do think a lot of it is parenting. Neglect is the number one form of abuse,” she said, “and it causes instability in children.”
But parents aren’t always the problem. Dr. Badawy mentioned an “extremely depressed” boy who tried to hang himself again and again, at 8 years old. “His parents were supportive and focused on getting him better,” she said. It’s unknown if anything happened to him when they weren’t around.
If SR is related to children’s own behavior, and if they are able to listen to staff afterward and control it, kids seem able to avoid another episode. Those who have PTSD, or who have been through physical abuse or out-of-home placement, seemed particularly adept in the review.
Avoidance seems less likely, however, when children are set off by other kids.
Sometimes there are clues of impending trouble, like the boy who walked around whistling before he lashed out. Staff at the university quickly learned to swoop in and calm him when they heard the whistling.
The investigators had no industry disclosures.
NEW ORLEANS – Attention-deficit/hyperactivity disorder and non-suicidal self-harm – cutting and head banging, for instance – strongly predicted longer seclusion and restraint episodes, sometimes past 2 hours, in a review at the University of Missouri, Columbia, pediatric inpatient psychiatric unit.
Meanwhile, children with histories of physical abuse, post-traumatic stress disorder (PTSD), or out-of-home placement were less likely to have multiple seclusion and restraint (SR) episodes during an admission, and had lower numbers of SR events overall. Perhaps hyper-vigilance due to past traumas helped them avoid situations that led to problems. Staff might also have used a lighter touch given the children’s histories.
The investigators reviewed 305 SR episodes from 2011-2014 among 92 children aged 5-18 years old. They plan to expand their study to 2009-2017 and add a prospective arm.
It’s well known that SR, a last-ditch effort to prevent physical harm, traumatizes patients, but research on how to avoid it has mostly focused on adults. The Missouri team wants to change that by identifying the children most at risk, so that something can be done beforehand to prevent it. Maybe extra one-on-one care would help, Dr. Badawy said.
The children in the review were an average of 10.5 years old, and most were admitted for 3-7 days. Fifty-five (60%) had multiple SR episodes, 34 in a single admission and 21 across multiple admissions; 71% of the episodes were in boys, 58% in white children, 27.7% in black children, and the rest in multiracial children. Twenty-one percent of the episodes were in children with intellectual problems. ADHD and oppositional defiant disorder were the most common diagnoses, each diagnosed in more than half of the subjects.
When asked how a 5-year-old child can end up in restraints, Dr. Badawy agreed that bad parenting is a factor. Parents who don’t know any better might escalate normal behavior, and others might simply not care that much about their kids, or have much empathy. “In the 5-10 year-olds, I do think a lot of it is parenting. Neglect is the number one form of abuse,” she said, “and it causes instability in children.”
But parents aren’t always the problem. Dr. Badawy mentioned an “extremely depressed” boy who tried to hang himself again and again, at 8 years old. “His parents were supportive and focused on getting him better,” she said. It’s unknown if anything happened to him when they weren’t around.
If SR is related to children’s own behavior, and if they are able to listen to staff afterward and control it, kids seem able to avoid another episode. Those who have PTSD, or who have been through physical abuse or out-of-home placement, seemed particularly adept in the review.
Avoidance seems less likely, however, when children are set off by other kids.
Sometimes there are clues of impending trouble, like the boy who walked around whistling before he lashed out. Staff at the university quickly learned to swoop in and calm him when they heard the whistling.
The investigators had no industry disclosures.
NEW ORLEANS – Attention-deficit/hyperactivity disorder and non-suicidal self-harm – cutting and head banging, for instance – strongly predicted longer seclusion and restraint episodes, sometimes past 2 hours, in a review at the University of Missouri, Columbia, pediatric inpatient psychiatric unit.
Meanwhile, children with histories of physical abuse, post-traumatic stress disorder (PTSD), or out-of-home placement were less likely to have multiple seclusion and restraint (SR) episodes during an admission, and had lower numbers of SR events overall. Perhaps hyper-vigilance due to past traumas helped them avoid situations that led to problems. Staff might also have used a lighter touch given the children’s histories.
The investigators reviewed 305 SR episodes from 2011-2014 among 92 children aged 5-18 years old. They plan to expand their study to 2009-2017 and add a prospective arm.
It’s well known that SR, a last-ditch effort to prevent physical harm, traumatizes patients, but research on how to avoid it has mostly focused on adults. The Missouri team wants to change that by identifying the children most at risk, so that something can be done beforehand to prevent it. Maybe extra one-on-one care would help, Dr. Badawy said.
The children in the review were an average of 10.5 years old, and most were admitted for 3-7 days. Fifty-five (60%) had multiple SR episodes, 34 in a single admission and 21 across multiple admissions; 71% of the episodes were in boys, 58% in white children, 27.7% in black children, and the rest in multiracial children. Twenty-one percent of the episodes were in children with intellectual problems. ADHD and oppositional defiant disorder were the most common diagnoses, each diagnosed in more than half of the subjects.
When asked how a 5-year-old child can end up in restraints, Dr. Badawy agreed that bad parenting is a factor. Parents who don’t know any better might escalate normal behavior, and others might simply not care that much about their kids, or have much empathy. “In the 5-10 year-olds, I do think a lot of it is parenting. Neglect is the number one form of abuse,” she said, “and it causes instability in children.”
But parents aren’t always the problem. Dr. Badawy mentioned an “extremely depressed” boy who tried to hang himself again and again, at 8 years old. “His parents were supportive and focused on getting him better,” she said. It’s unknown if anything happened to him when they weren’t around.
If SR is related to children’s own behavior, and if they are able to listen to staff afterward and control it, kids seem able to avoid another episode. Those who have PTSD, or who have been through physical abuse or out-of-home placement, seemed particularly adept in the review.
Avoidance seems less likely, however, when children are set off by other kids.
Sometimes there are clues of impending trouble, like the boy who walked around whistling before he lashed out. Staff at the university quickly learned to swoop in and calm him when they heard the whistling.
The investigators had no industry disclosures.
AT IPS 2017
Key clinical point:
Major finding: ADHD and non-suicidal self-harm – cutting and head banging – strongly predict longer seclusion and restraint episodes, sometimes past 2 hours.
Data source: A University of Missouri, Columbia, review of 305 seclusion and restraint episodes from 2011-2014 among 92 children aged 5-18 years old.
Disclosures: The investigators had no industry disclosures.
Children and trauma: How Sesame Street can help
Nearly half of American children have faced one adverse childhood experience (ACE), according to new analysis of the 2016 National Survey of Children’s Health, and more than 20% have had two ACEs or more. This may include abuse or neglect, witnessing violence, parental substance abuse, mental illness, or incarceration. And from news headlines, we are all too aware of other traumas children face, such as natural disasters and mass violence.
But we know that children are remarkably resilient, and trauma does not have to define their trajectory. With the right tools and support, the effects of trauma can be mitigated, and children can build coping skills and resiliency for a healthy, promising future.

When we began hearing from community service partners and child development experts that there was a critical need for resources to help children cope with trauma, we felt we could help.
Traumatic experiences can disrupt brain development, but when children have hope, when they feel seen and heard by caring adults who can guide them through those crucial resilience-building techniques, the impact of ACEs can be mitigated, and children can be set on the road to healing and stability.
With support from the Robert Wood Johnson Foundation and other funders, To do this, we enlisted the pediatric community and professionals in the field, grounding our approach in the latest research. Then we used our proven model to produce resources that could engage and comfort children while building coping skills and foster crucial nurturing connections between children and the adults in their lives.
Our free materials – some are targeted for children and others are for providers – include videos, storybooks, and digital activities in English and Spanish. They are all available at sesamestreetincommunities.org/topics/traumatic-experiences.

In one video called “Comfy Cozy Nest,” when Big Bird faces an unspecified difficult situation, he learns to think of his nest as a “safe space” with comforting items like his teddy bear and Granny Bird’s birdseed cookies. This is a place he can go in his imagination to make himself feel safe. In others, Elmo builds a blanket fort to feel secure and the Count teaches Cookie Monster a breathing strategy to help him relax.
In addition to engaging materials for children, providers can find professional development workshops, webinars, and other adult-facing content that includes, as part of our trauma content, a powerful animation to help parents and caregivers understand the impact of domestic violence from a child’s perspective.

No one plays a more vital role in children’s health and well-being than pediatricians, nurse practitioners, and family physicians. Our hope is that Sesame Street in Communities will allow us to work together, to help children everywhere grow smarter, stronger, and kinder.
Dr. Betancourt is the senior vice president for U.S. social impact at Sesame Workshop, the nonprofit media and educational organization behind Sesame Street, in New York.
Nearly half of American children have faced one adverse childhood experience (ACE), according to new analysis of the 2016 National Survey of Children’s Health, and more than 20% have had two ACEs or more. This may include abuse or neglect, witnessing violence, parental substance abuse, mental illness, or incarceration. And from news headlines, we are all too aware of other traumas children face, such as natural disasters and mass violence.
But we know that children are remarkably resilient, and trauma does not have to define their trajectory. With the right tools and support, the effects of trauma can be mitigated, and children can build coping skills and resiliency for a healthy, promising future.
When we began hearing from community service partners and child development experts that there was a critical need for resources to help children cope with trauma, we felt we could help.
Traumatic experiences can disrupt brain development, but when children have hope, when they feel seen and heard by caring adults who can guide them through those crucial resilience-building techniques, the impact of ACEs can be mitigated, and children can be set on the road to healing and stability.
With support from the Robert Wood Johnson Foundation and other funders, To do this, we enlisted the pediatric community and professionals in the field, grounding our approach in the latest research. Then we used our proven model to produce resources that could engage and comfort children while building coping skills and foster crucial nurturing connections between children and the adults in their lives.
Our free materials – some are targeted for children and others are for providers – include videos, storybooks, and digital activities in English and Spanish. They are all available at sesamestreetincommunities.org/topics/traumatic-experiences.
In one video called “Comfy Cozy Nest,” when Big Bird faces an unspecified difficult situation, he learns to think of his nest as a “safe space” with comforting items like his teddy bear and Granny Bird’s birdseed cookies. This is a place he can go in his imagination to make himself feel safe. In others, Elmo builds a blanket fort to feel secure and the Count teaches Cookie Monster a breathing strategy to help him relax.
In addition to engaging materials for children, providers can find professional development workshops, webinars, and other adult-facing content that includes, as part of our trauma content, a powerful animation to help parents and caregivers understand the impact of domestic violence from a child’s perspective.
No one plays a more vital role in children’s health and well-being than pediatricians, nurse practitioners, and family physicians. Our hope is that Sesame Street in Communities will allow us to work together, to help children everywhere grow smarter, stronger, and kinder.
Dr. Betancourt is the senior vice president for U.S. social impact at Sesame Workshop, the nonprofit media and educational organization behind Sesame Street, in New York.
Nearly half of American children have faced one adverse childhood experience (ACE), according to new analysis of the 2016 National Survey of Children’s Health, and more than 20% have had two ACEs or more. This may include abuse or neglect, witnessing violence, parental substance abuse, mental illness, or incarceration. And from news headlines, we are all too aware of other traumas children face, such as natural disasters and mass violence.
But we know that children are remarkably resilient, and trauma does not have to define their trajectory. With the right tools and support, the effects of trauma can be mitigated, and children can build coping skills and resiliency for a healthy, promising future.
When we began hearing from community service partners and child development experts that there was a critical need for resources to help children cope with trauma, we felt we could help.
Traumatic experiences can disrupt brain development, but when children have hope, when they feel seen and heard by caring adults who can guide them through those crucial resilience-building techniques, the impact of ACEs can be mitigated, and children can be set on the road to healing and stability.
With support from the Robert Wood Johnson Foundation and other funders, To do this, we enlisted the pediatric community and professionals in the field, grounding our approach in the latest research. Then we used our proven model to produce resources that could engage and comfort children while building coping skills and foster crucial nurturing connections between children and the adults in their lives.
Our free materials – some are targeted for children and others are for providers – include videos, storybooks, and digital activities in English and Spanish. They are all available at sesamestreetincommunities.org/topics/traumatic-experiences.
In one video called “Comfy Cozy Nest,” when Big Bird faces an unspecified difficult situation, he learns to think of his nest as a “safe space” with comforting items like his teddy bear and Granny Bird’s birdseed cookies. This is a place he can go in his imagination to make himself feel safe. In others, Elmo builds a blanket fort to feel secure and the Count teaches Cookie Monster a breathing strategy to help him relax.
In addition to engaging materials for children, providers can find professional development workshops, webinars, and other adult-facing content that includes, as part of our trauma content, a powerful animation to help parents and caregivers understand the impact of domestic violence from a child’s perspective.
No one plays a more vital role in children’s health and well-being than pediatricians, nurse practitioners, and family physicians. Our hope is that Sesame Street in Communities will allow us to work together, to help children everywhere grow smarter, stronger, and kinder.
Dr. Betancourt is the senior vice president for U.S. social impact at Sesame Workshop, the nonprofit media and educational organization behind Sesame Street, in New York.
When the waters recede: Hurricane Harvey and PTSD through indirect trauma
It’s been 5 days since Texas came under siege from Hurricane Harvey and it left up to 51 inches of rain in its wake. Several Southern cities suffered almost complete loss of homes and businesses. The Houston metropolitan area reported 14 deaths, including one of a police officer who was trying to report for duty. Hundreds of thousands of homes have been damaged or lost, and thousands of people are now in makeshift shelters across the city. We have slowly begun the process of repair and rebuilding, and many Houstonians are returning to work. Many others, including well-known local celebrities like J.J. Watt and MattressMack, are volunteering their time and giving money to help those who were not so fortunate. The rescue and recovery efforts have been lauded for the absence of issues tied to politics, religion, or race.
Despite this, we must not forget that this was a natural disaster unlike anything that’s been seen in recent decades. Much like Katrina and Sandy, Hurricane Harvey brought to the people who have lived through the initial trauma the fear, nightmares, emotional distress, and sleep disturbances associated with posttraumatic stress disorder (PTSD). They will require significant support and monitoring to determine whether there is a need for medical intervention, such as cognitive-behavioral therapy, behavioral modification, or pharmacotherapy. However, we are also witnessing something psychiatrists are just becoming more knowledgeable about – PTSD due to indirect trauma.

Taking early warnings in stride
When the anchors and journalists began reporting about a tropical cyclone heading toward the Gulf of Mexico on Aug. 17, most Houstonians – myself included – flipped the channel. Living off the Southern Coast of the United States meant seeing more than our fair share of storm systems, including hurricanes. Each time, no matter the damage or the loss, Texans would pull themselves up by their bootstraps and band together to rebuild their beloved city.
So, it’s no surprise that even as Harvey was upgraded to a hurricane and prepared to breach land, we went about business as usual. However, less than a week later, countless residents of the Lone Star State prepared for what promised to be one of the worst storms in recent history.
Moving to Houston from Dallas for college back in 1998, I fell in love with the city and made it my home. I was here when Tropical Storm Allison made landfall in 2001, leaving up to 37 inches of rain and massive flooding in its wake. The Texas Medical Center, where I was working at the Baylor Human Genome Lab for the summer, suffered about $2 billion worth of damage.
I watched as the images and videos of the city under water splashed across my television screen. I witnessed the floodwaters firsthand as my friends and I carefully drove to an overpass and found a vast body of water where a convergence of three highways used to be visible. I was fortunate not to have been affected by the flood, but the fear of West Nile virus worried me for days because of the mosquito infestation that followed. Eventually, the city recovered, the water receded, and we persevered.
In 2005, in the wake of Katrina, Southern Texans were warned of an impending Category 3 hurricane named Rita. Having been inundated with local and national news coverage of the devastation, and hearing the personal stories of evacuees from New Orleans, Houstonians definitely took more notice this time. More than 3 million people from Houston and the surrounding areas evacuated inland before it arrived, but the chaos resulted in indirect deaths from panicked people trying to leave.
I, along with my two best friends and my boyfriend, were among the many who made the lengthy drive to Dallas, where my parents were anxiously waiting. What should have been a 4-hour drive turned into 10, and that was the result of all the back roads we took to get around the majority of the traffic. There were mass outages around the city, but within a few days, we were all back home. Rita left behind much less damage than predicted, and after the water receded, we persevered.
My third encounter with a hurricane was the Category 2 Ike 3 years later. There were mixed emotions going into this one, with many citizens split between evacuating and staying behind. I was in residency by then, and with only a voluntary evacuation for Houston (compared with a mandatory one in Galveston and the coastal cities), I opted to remain. I had already prepared for the worst by barricading all the glass and stocking up on supplies. In addition, I was living in a two-story townhome in an area considered part of a 200-year flood plain, so I figured I was safe. When Ike struck the city, I was up for several hours listening to the howl of the wind and the insistent smacks of rain against my windows. I left town once the coast was clear, not because of flooding, but because Ike knocked out power and water for much of Houston in the middle of a horridly hot September. I stayed with my parents for about a week until my complex had fixed everything, and seeing that the water had receded, I persevered.
Harvey’s vast destruction
This past week, when Category 4 Hurricane Harvey struck my beloved city, I could not have imagined the losses that were waiting for us. After finishing up a short workday on Friday, Aug. 25, I made my last run for supplies before the weekend. Like many others, I had been keeping an eye on the news as we heard about the destruction Harvey had wreaked on Rockport, South Padre, and Corpus Christi. We all knew that this one was the real deal, that Harvey was going to challenge us in every way possible. For the next 4 days I hunkered down in my house, waiting out the periods of torrential rain while keeping a close eye on the news. At worst, my neighborhood flooded up to the front sidewalk, but water never entered my home, as it did for so many unfortunate individuals. I never lost power, air conditioning, or Internet access. The most distressing thing to happen to me was the inability to leave my home for fear of being caught in the floodwater.

We are #The CityWithNoLimits.
We are #HoustonStrong.
We are #TexasStrong.
When the waters recede, we will persevere.
Jennifer Yen, MD, is a board-certified child, adolescent, and adult private practice psychiatrist in Houston. She also is a clinical assistant professor of psychiatry at Baylor College of Medicine and serves on the Consumers Issues Committee of the American Academy of Child and Adolescent Psychiatry.
It’s been 5 days since Texas came under siege from Hurricane Harvey and it left up to 51 inches of rain in its wake. Several Southern cities suffered almost complete loss of homes and businesses. The Houston metropolitan area reported 14 deaths, including one of a police officer who was trying to report for duty. Hundreds of thousands of homes have been damaged or lost, and thousands of people are now in makeshift shelters across the city. We have slowly begun the process of repair and rebuilding, and many Houstonians are returning to work. Many others, including well-known local celebrities like J.J. Watt and MattressMack, are volunteering their time and giving money to help those who were not so fortunate. The rescue and recovery efforts have been lauded for the absence of issues tied to politics, religion, or race.
Despite this, we must not forget that this was a natural disaster unlike anything that’s been seen in recent decades. Much like Katrina and Sandy, Hurricane Harvey brought to the people who have lived through the initial trauma the fear, nightmares, emotional distress, and sleep disturbances associated with posttraumatic stress disorder (PTSD). They will require significant support and monitoring to determine whether there is a need for medical intervention, such as cognitive-behavioral therapy, behavioral modification, or pharmacotherapy. However, we are also witnessing something psychiatrists are just becoming more knowledgeable about – PTSD due to indirect trauma.
Taking early warnings in stride
When the anchors and journalists began reporting about a tropical cyclone heading toward the Gulf of Mexico on Aug. 17, most Houstonians – myself included – flipped the channel. Living off the Southern Coast of the United States meant seeing more than our fair share of storm systems, including hurricanes. Each time, no matter the damage or the loss, Texans would pull themselves up by their bootstraps and band together to rebuild their beloved city.
So, it’s no surprise that even as Harvey was upgraded to a hurricane and prepared to breach land, we went about business as usual. However, less than a week later, countless residents of the Lone Star State prepared for what promised to be one of the worst storms in recent history.
Moving to Houston from Dallas for college back in 1998, I fell in love with the city and made it my home. I was here when Tropical Storm Allison made landfall in 2001, leaving up to 37 inches of rain and massive flooding in its wake. The Texas Medical Center, where I was working at the Baylor Human Genome Lab for the summer, suffered about $2 billion worth of damage.
I watched as the images and videos of the city under water splashed across my television screen. I witnessed the floodwaters firsthand as my friends and I carefully drove to an overpass and found a vast body of water where a convergence of three highways used to be visible. I was fortunate not to have been affected by the flood, but the fear of West Nile virus worried me for days because of the mosquito infestation that followed. Eventually, the city recovered, the water receded, and we persevered.
In 2005, in the wake of Katrina, Southern Texans were warned of an impending Category 3 hurricane named Rita. Having been inundated with local and national news coverage of the devastation, and hearing the personal stories of evacuees from New Orleans, Houstonians definitely took more notice this time. More than 3 million people from Houston and the surrounding areas evacuated inland before it arrived, but the chaos resulted in indirect deaths from panicked people trying to leave.
I, along with my two best friends and my boyfriend, were among the many who made the lengthy drive to Dallas, where my parents were anxiously waiting. What should have been a 4-hour drive turned into 10, and that was the result of all the back roads we took to get around the majority of the traffic. There were mass outages around the city, but within a few days, we were all back home. Rita left behind much less damage than predicted, and after the water receded, we persevered.
My third encounter with a hurricane was the Category 2 Ike 3 years later. There were mixed emotions going into this one, with many citizens split between evacuating and staying behind. I was in residency by then, and with only a voluntary evacuation for Houston (compared with a mandatory one in Galveston and the coastal cities), I opted to remain. I had already prepared for the worst by barricading all the glass and stocking up on supplies. In addition, I was living in a two-story townhome in an area considered part of a 200-year flood plain, so I figured I was safe. When Ike struck the city, I was up for several hours listening to the howl of the wind and the insistent smacks of rain against my windows. I left town once the coast was clear, not because of flooding, but because Ike knocked out power and water for much of Houston in the middle of a horridly hot September. I stayed with my parents for about a week until my complex had fixed everything, and seeing that the water had receded, I persevered.
Harvey’s vast destruction
This past week, when Category 4 Hurricane Harvey struck my beloved city, I could not have imagined the losses that were waiting for us. After finishing up a short workday on Friday, Aug. 25, I made my last run for supplies before the weekend. Like many others, I had been keeping an eye on the news as we heard about the destruction Harvey had wreaked on Rockport, South Padre, and Corpus Christi. We all knew that this one was the real deal, that Harvey was going to challenge us in every way possible. For the next 4 days I hunkered down in my house, waiting out the periods of torrential rain while keeping a close eye on the news. At worst, my neighborhood flooded up to the front sidewalk, but water never entered my home, as it did for so many unfortunate individuals. I never lost power, air conditioning, or Internet access. The most distressing thing to happen to me was the inability to leave my home for fear of being caught in the floodwater.
We are #The CityWithNoLimits.
We are #HoustonStrong.
We are #TexasStrong.
When the waters recede, we will persevere.
Jennifer Yen, MD, is a board-certified child, adolescent, and adult private practice psychiatrist in Houston. She also is a clinical assistant professor of psychiatry at Baylor College of Medicine and serves on the Consumers Issues Committee of the American Academy of Child and Adolescent Psychiatry.
It’s been 5 days since Texas came under siege from Hurricane Harvey and it left up to 51 inches of rain in its wake. Several Southern cities suffered almost complete loss of homes and businesses. The Houston metropolitan area reported 14 deaths, including one of a police officer who was trying to report for duty. Hundreds of thousands of homes have been damaged or lost, and thousands of people are now in makeshift shelters across the city. We have slowly begun the process of repair and rebuilding, and many Houstonians are returning to work. Many others, including well-known local celebrities like J.J. Watt and MattressMack, are volunteering their time and giving money to help those who were not so fortunate. The rescue and recovery efforts have been lauded for the absence of issues tied to politics, religion, or race.
Despite this, we must not forget that this was a natural disaster unlike anything that’s been seen in recent decades. Much like Katrina and Sandy, Hurricane Harvey brought to the people who have lived through the initial trauma the fear, nightmares, emotional distress, and sleep disturbances associated with posttraumatic stress disorder (PTSD). They will require significant support and monitoring to determine whether there is a need for medical intervention, such as cognitive-behavioral therapy, behavioral modification, or pharmacotherapy. However, we are also witnessing something psychiatrists are just becoming more knowledgeable about – PTSD due to indirect trauma.
Taking early warnings in stride
When the anchors and journalists began reporting about a tropical cyclone heading toward the Gulf of Mexico on Aug. 17, most Houstonians – myself included – flipped the channel. Living off the Southern Coast of the United States meant seeing more than our fair share of storm systems, including hurricanes. Each time, no matter the damage or the loss, Texans would pull themselves up by their bootstraps and band together to rebuild their beloved city.
So, it’s no surprise that even as Harvey was upgraded to a hurricane and prepared to breach land, we went about business as usual. However, less than a week later, countless residents of the Lone Star State prepared for what promised to be one of the worst storms in recent history.
Moving to Houston from Dallas for college back in 1998, I fell in love with the city and made it my home. I was here when Tropical Storm Allison made landfall in 2001, leaving up to 37 inches of rain and massive flooding in its wake. The Texas Medical Center, where I was working at the Baylor Human Genome Lab for the summer, suffered about $2 billion worth of damage.
I watched as the images and videos of the city under water splashed across my television screen. I witnessed the floodwaters firsthand as my friends and I carefully drove to an overpass and found a vast body of water where a convergence of three highways used to be visible. I was fortunate not to have been affected by the flood, but the fear of West Nile virus worried me for days because of the mosquito infestation that followed. Eventually, the city recovered, the water receded, and we persevered.
In 2005, in the wake of Katrina, Southern Texans were warned of an impending Category 3 hurricane named Rita. Having been inundated with local and national news coverage of the devastation, and hearing the personal stories of evacuees from New Orleans, Houstonians definitely took more notice this time. More than 3 million people from Houston and the surrounding areas evacuated inland before it arrived, but the chaos resulted in indirect deaths from panicked people trying to leave.
I, along with my two best friends and my boyfriend, were among the many who made the lengthy drive to Dallas, where my parents were anxiously waiting. What should have been a 4-hour drive turned into 10, and that was the result of all the back roads we took to get around the majority of the traffic. There were mass outages around the city, but within a few days, we were all back home. Rita left behind much less damage than predicted, and after the water receded, we persevered.
My third encounter with a hurricane was the Category 2 Ike 3 years later. There were mixed emotions going into this one, with many citizens split between evacuating and staying behind. I was in residency by then, and with only a voluntary evacuation for Houston (compared with a mandatory one in Galveston and the coastal cities), I opted to remain. I had already prepared for the worst by barricading all the glass and stocking up on supplies. In addition, I was living in a two-story townhome in an area considered part of a 200-year flood plain, so I figured I was safe. When Ike struck the city, I was up for several hours listening to the howl of the wind and the insistent smacks of rain against my windows. I left town once the coast was clear, not because of flooding, but because Ike knocked out power and water for much of Houston in the middle of a horridly hot September. I stayed with my parents for about a week until my complex had fixed everything, and seeing that the water had receded, I persevered.
Harvey’s vast destruction
This past week, when Category 4 Hurricane Harvey struck my beloved city, I could not have imagined the losses that were waiting for us. After finishing up a short workday on Friday, Aug. 25, I made my last run for supplies before the weekend. Like many others, I had been keeping an eye on the news as we heard about the destruction Harvey had wreaked on Rockport, South Padre, and Corpus Christi. We all knew that this one was the real deal, that Harvey was going to challenge us in every way possible. For the next 4 days I hunkered down in my house, waiting out the periods of torrential rain while keeping a close eye on the news. At worst, my neighborhood flooded up to the front sidewalk, but water never entered my home, as it did for so many unfortunate individuals. I never lost power, air conditioning, or Internet access. The most distressing thing to happen to me was the inability to leave my home for fear of being caught in the floodwater.
We are #The CityWithNoLimits.
We are #HoustonStrong.
We are #TexasStrong.
When the waters recede, we will persevere.
Jennifer Yen, MD, is a board-certified child, adolescent, and adult private practice psychiatrist in Houston. She also is a clinical assistant professor of psychiatry at Baylor College of Medicine and serves on the Consumers Issues Committee of the American Academy of Child and Adolescent Psychiatry.
More data show value of CBT for PTSD, anxiety, depression
So often in clinical practice, guidelines and directives about psychiatric treatments lag behind the results we see every day in our offices. Such is the case with cognitive-behavioral therapy.
Earlier this summer, the departments of Veterans Affairs and Defense deemed trauma-focused psychotherapies, such as CBT, as first-line treatments for posttraumatic stress disorder over medication management. Was I surprised by these findings? Absolutely not. Likewise, last year, the American College of Physicians released a guideline recommending CBT as first-line treatment for chronic insomnia disorder in adults. Surprising? Again, not in the least.
Pierre Janet, PhD, MD, the French psychiatrist, psychologist, and neurologist, more than a hundred years ago in his L’Automatisme Psychologique, advanced the idea that thoughts can be challenged and that perceptions leading to mental problems can be reversed. Dr. Janet completed his pioneering work, including an exploration of the power of hypnosis, even though the psychoanalytic movement was in full force and many parallel ideas about treating mental disorders were barely recognized.
By the middle of the 20th century, Albert Ellis, PhD, developed rational emotive behavior therapy, which focused on thoughtfully restructuring irrational beliefs into rational ones that led to improved skills and behaviors. A decade later, the great Aaron T. Beck, MD, developed a true form of CBT. Over the years, Dr. Beck went on to develop controlled clinical trials showing CBT to be more effective in treating a variety of psychiatric disorders, including depression, panic attacks, anxiety disorders, obsessive-compulsive disorders, various phobic disorders, and PTSD.
Yet, despite the effectiveness of CBT, too few young psychiatrists and mental health professionals learn how to use it, and fewer appear to practice it. Traditional psychiatric training, by and large, continues to rely on more psychodynamic approaches, which do have value but take longer to get results than does CBT.
Clearly, partnering with patients and helping them learn new constructs can lead to positive results. More and more research shows that CBT is efficacious for patients across many age and demographic groups.
In one randomized, controlled study of 96 Latino patients with depression, for example, researchers at the University of California, Berkeley, found that group CBT administered in a primary care setting led to a significant decrease in depressive symptoms as measured by the Spanish-language version of the Patient Health Questionnaire (PHQ-9) (Cog Behav Prac. 2017 Apr 17; doi: 10.1016/j.cbpra.2017.03.02). Of the 96 patients, 92 completed the PHQ-9 at least once, and 76 completed a baseline measure of the questionnaire on day 1 of group therapy, the researchers reported. At baseline, the average PHQ-9 score was 13.88, which points to the high end of moderate depression, moving toward moderately severe depression. For every week the patients were enrolled in the therapy, PHQ-9 scores fell by 0.15 points.
The spin on CBT that I created – which I call the learning, philosophizing, and action (LPA) technique – helps patients think through problematic issues and come away with new narratives. I developed and used the LPA technique as part of a smoking-cessation program I ran for many years at the New York University Langone Medical Center. In turn, that program developed into a short-term psychotherapy program with a focus on CBT and hypnosis/relaxation techniques.

We need better codification and organization on what kinds of therapies are and are not suited for specific diagnosable problems. It is hoped that a clearer understanding of genetics, laboratory testing, and imaging, as emphasized by the National Institute of Mental Health’s Research Domain Criteria, will better equip us to decide what works best. Again, for now, helping patients learn and relearn new ways of thinking and behaving, as developed through CBT, is among the best treatments available for many mental health problems.
Dr. London, a psychiatrist who practices in New York, developed and ran a short-term psychotherapy program for 20 years at NYU Langone Medical Center and has been writing columns for 35 years. His new book about helping people feel better fast is expected to be published in fall 2017. He has no disclosures.
So often in clinical practice, guidelines and directives about psychiatric treatments lag behind the results we see every day in our offices. Such is the case with cognitive-behavioral therapy.
Earlier this summer, the departments of Veterans Affairs and Defense deemed trauma-focused psychotherapies, such as CBT, as first-line treatments for posttraumatic stress disorder over medication management. Was I surprised by these findings? Absolutely not. Likewise, last year, the American College of Physicians released a guideline recommending CBT as first-line treatment for chronic insomnia disorder in adults. Surprising? Again, not in the least.
Pierre Janet, PhD, MD, the French psychiatrist, psychologist, and neurologist, more than a hundred years ago in his L’Automatisme Psychologique, advanced the idea that thoughts can be challenged and that perceptions leading to mental problems can be reversed. Dr. Janet completed his pioneering work, including an exploration of the power of hypnosis, even though the psychoanalytic movement was in full force and many parallel ideas about treating mental disorders were barely recognized.
By the middle of the 20th century, Albert Ellis, PhD, developed rational emotive behavior therapy, which focused on thoughtfully restructuring irrational beliefs into rational ones that led to improved skills and behaviors. A decade later, the great Aaron T. Beck, MD, developed a true form of CBT. Over the years, Dr. Beck went on to develop controlled clinical trials showing CBT to be more effective in treating a variety of psychiatric disorders, including depression, panic attacks, anxiety disorders, obsessive-compulsive disorders, various phobic disorders, and PTSD.
Yet, despite the effectiveness of CBT, too few young psychiatrists and mental health professionals learn how to use it, and fewer appear to practice it. Traditional psychiatric training, by and large, continues to rely on more psychodynamic approaches, which do have value but take longer to get results than does CBT.
Clearly, partnering with patients and helping them learn new constructs can lead to positive results. More and more research shows that CBT is efficacious for patients across many age and demographic groups.
In one randomized, controlled study of 96 Latino patients with depression, for example, researchers at the University of California, Berkeley, found that group CBT administered in a primary care setting led to a significant decrease in depressive symptoms as measured by the Spanish-language version of the Patient Health Questionnaire (PHQ-9) (Cog Behav Prac. 2017 Apr 17; doi: 10.1016/j.cbpra.2017.03.02). Of the 96 patients, 92 completed the PHQ-9 at least once, and 76 completed a baseline measure of the questionnaire on day 1 of group therapy, the researchers reported. At baseline, the average PHQ-9 score was 13.88, which points to the high end of moderate depression, moving toward moderately severe depression. For every week the patients were enrolled in the therapy, PHQ-9 scores fell by 0.15 points.
The spin on CBT that I created – which I call the learning, philosophizing, and action (LPA) technique – helps patients think through problematic issues and come away with new narratives. I developed and used the LPA technique as part of a smoking-cessation program I ran for many years at the New York University Langone Medical Center. In turn, that program developed into a short-term psychotherapy program with a focus on CBT and hypnosis/relaxation techniques.
We need better codification and organization on what kinds of therapies are and are not suited for specific diagnosable problems. It is hoped that a clearer understanding of genetics, laboratory testing, and imaging, as emphasized by the National Institute of Mental Health’s Research Domain Criteria, will better equip us to decide what works best. Again, for now, helping patients learn and relearn new ways of thinking and behaving, as developed through CBT, is among the best treatments available for many mental health problems.
Dr. London, a psychiatrist who practices in New York, developed and ran a short-term psychotherapy program for 20 years at NYU Langone Medical Center and has been writing columns for 35 years. His new book about helping people feel better fast is expected to be published in fall 2017. He has no disclosures.
So often in clinical practice, guidelines and directives about psychiatric treatments lag behind the results we see every day in our offices. Such is the case with cognitive-behavioral therapy.
Earlier this summer, the departments of Veterans Affairs and Defense deemed trauma-focused psychotherapies, such as CBT, as first-line treatments for posttraumatic stress disorder over medication management. Was I surprised by these findings? Absolutely not. Likewise, last year, the American College of Physicians released a guideline recommending CBT as first-line treatment for chronic insomnia disorder in adults. Surprising? Again, not in the least.
Pierre Janet, PhD, MD, the French psychiatrist, psychologist, and neurologist, more than a hundred years ago in his L’Automatisme Psychologique, advanced the idea that thoughts can be challenged and that perceptions leading to mental problems can be reversed. Dr. Janet completed his pioneering work, including an exploration of the power of hypnosis, even though the psychoanalytic movement was in full force and many parallel ideas about treating mental disorders were barely recognized.
By the middle of the 20th century, Albert Ellis, PhD, developed rational emotive behavior therapy, which focused on thoughtfully restructuring irrational beliefs into rational ones that led to improved skills and behaviors. A decade later, the great Aaron T. Beck, MD, developed a true form of CBT. Over the years, Dr. Beck went on to develop controlled clinical trials showing CBT to be more effective in treating a variety of psychiatric disorders, including depression, panic attacks, anxiety disorders, obsessive-compulsive disorders, various phobic disorders, and PTSD.
Yet, despite the effectiveness of CBT, too few young psychiatrists and mental health professionals learn how to use it, and fewer appear to practice it. Traditional psychiatric training, by and large, continues to rely on more psychodynamic approaches, which do have value but take longer to get results than does CBT.
Clearly, partnering with patients and helping them learn new constructs can lead to positive results. More and more research shows that CBT is efficacious for patients across many age and demographic groups.
In one randomized, controlled study of 96 Latino patients with depression, for example, researchers at the University of California, Berkeley, found that group CBT administered in a primary care setting led to a significant decrease in depressive symptoms as measured by the Spanish-language version of the Patient Health Questionnaire (PHQ-9) (Cog Behav Prac. 2017 Apr 17; doi: 10.1016/j.cbpra.2017.03.02). Of the 96 patients, 92 completed the PHQ-9 at least once, and 76 completed a baseline measure of the questionnaire on day 1 of group therapy, the researchers reported. At baseline, the average PHQ-9 score was 13.88, which points to the high end of moderate depression, moving toward moderately severe depression. For every week the patients were enrolled in the therapy, PHQ-9 scores fell by 0.15 points.
The spin on CBT that I created – which I call the learning, philosophizing, and action (LPA) technique – helps patients think through problematic issues and come away with new narratives. I developed and used the LPA technique as part of a smoking-cessation program I ran for many years at the New York University Langone Medical Center. In turn, that program developed into a short-term psychotherapy program with a focus on CBT and hypnosis/relaxation techniques.
We need better codification and organization on what kinds of therapies are and are not suited for specific diagnosable problems. It is hoped that a clearer understanding of genetics, laboratory testing, and imaging, as emphasized by the National Institute of Mental Health’s Research Domain Criteria, will better equip us to decide what works best. Again, for now, helping patients learn and relearn new ways of thinking and behaving, as developed through CBT, is among the best treatments available for many mental health problems.
Dr. London, a psychiatrist who practices in New York, developed and ran a short-term psychotherapy program for 20 years at NYU Langone Medical Center and has been writing columns for 35 years. His new book about helping people feel better fast is expected to be published in fall 2017. He has no disclosures.
