User login
Oncology care model reduces cost of supportive care meds
The Oncology Care Model (OCM), launched by the Centers for Medicare & Medicaid Services (CMS) with the goal of reducing spending for Medicare beneficiaries, was “associated with meaningful changes in the use of supportive care medications during chemotherapy treatment episodes,” according to new findings.
The OCM led to a statistically significant reduction in the use of denosumab – a pricier bone-modifying drug – by patients with bone metastases without changing the overall use of bone-modifying medications. The OCM also prompted more rapid adoption of a less expensive white blood cell growth factor agent – the biosimilar filgrastim – and more selective use of costly antiemetics as primary prophylaxis for chemotherapy-induced nausea.
study author Gabriel A. Brooks, MD, MPH, of the Dartmouth Institute for Health Policy and Clinical Practice, Geisel School of Medicine, Lebanon, N.H., and colleagues write.
The study was published online Feb. 25 in the Journal of Clinical Oncology.
Since the OCM was launched in 2016, several studies have evaluated whether the alternative payment model reached its goal of reducing spending while improving or maintaining the quality of cancer care.
The results have been decidedly mixed.
As previously reported by this news organization, one study found that after 4 years, the OCM led to a $155 million net loss to Medicare. During that time, physician participation in the program also declined, with the number of practices dropping almost 30% between 2016 and 2020.
Other studies, however, have highlighted more positive results.
One large community practice reported saving Medicare $3 million over the course of 1 year. Another analysis found that among community practices that adopted the OCM, in the first year of the program, there was less physician-administered drug use by patients with prostate cancer, lower drug costs by patients with lung and prostate cancer, fewer visits by patients with breast or colon cancer, and lower office-based costs in all cancers analyzed. However, these savings were largely offset by the costs of these programs.
In the current study, DR. Brooks and colleagues compared the use of supportive care medications – bone-modifying drugs as well as prophylactic white blood cell (WBC) growth factors and antiemetics – in practices that adopted the OCM and those that didn’t.
More specifically, the authors zeroed in on the bone-modifying agent denosumab for patients with breast, lung, or prostate cancer and the WBC growth factor biosimilar filgrastim for those receiving chemotherapy for breast, lung, or colorectal cancer. Prophylactic use of higher-cost neurokinin-1 (NK1) antagonists and long-acting serotonin antagonists for patients receiving chemotherapy for any type of cancer was also evaluated.
The authors evaluated chemotherapy episodes assigned to OCM (n = 201) and comparison practices (n = 534) using Medicare claims from 2013-2019.
There was a total of 255,638 treatment episodes for bone metastases. The authors found that the OCM led to relative reductions in the use of denosumab but not in the overall use of bone-modifying medications, which included the less costly options zoledronic acid and pamidronate. The use of denosumab was similar for OCM and comparison practices during the baseline period, but during the intervention period, there were statistically significant relative reductions in the use of denosumab at OCM practices for breast (-5.0%), prostate (-4.0%), and lung cancer (-4.1%).
For WBC growth factors, 164,310 episodes were included in analyses. The OCM did not affect the use of prophylactic WBC growth factors during breast cancer chemotherapy for those at high risk of febrile neutropenia but did lead to a relative decrease during intermediate-risk chemotherapy (-7.6%). The authors observed no OCM impact on the use of prophylactic WBC growth factors among intermediate-risk lung or colorectal cancer patients. But, during the intervention period, OCM practices did demonstrate an increased use of originator or biosimilar filgrastim (57.3%) compared to other practices (47.6%), and the quarterly rate of increase in the use of the biosimilar grew 2.6 percentage points faster in OCM practices.
The authors report that there were 414,792 treatment episodes involving the use of prophylactic antiemetics. Overall, among patients receiving chemotherapy with high or moderate emetic risk, the OCM led to reductions in the prophylactic use of NK1 antagonists and long-acting serotonin antagonists. The authors report a 6.0 percentage point reduction in the use of NK1 antagonists during high-emetic-risk chemotherapy.
“We found that OCM was associated with meaningful changes in the use of supportive care medications during chemotherapy treatment episodes consistent with value-based care redesign,” the authors conclude. “These impacts on supportive care medication use align with previously reported spending reductions attributable to OCM and suggest that alternative payment models have potential to drive value-based changes in supportive care during cancer treatment.”
The study was supported by CMS. Several of the coauthors have reported relationships with industry, as noted in the article.
A version of this article first appeared on Medscape.com.
The Oncology Care Model (OCM), launched by the Centers for Medicare & Medicaid Services (CMS) with the goal of reducing spending for Medicare beneficiaries, was “associated with meaningful changes in the use of supportive care medications during chemotherapy treatment episodes,” according to new findings.
The OCM led to a statistically significant reduction in the use of denosumab – a pricier bone-modifying drug – by patients with bone metastases without changing the overall use of bone-modifying medications. The OCM also prompted more rapid adoption of a less expensive white blood cell growth factor agent – the biosimilar filgrastim – and more selective use of costly antiemetics as primary prophylaxis for chemotherapy-induced nausea.
study author Gabriel A. Brooks, MD, MPH, of the Dartmouth Institute for Health Policy and Clinical Practice, Geisel School of Medicine, Lebanon, N.H., and colleagues write.
The study was published online Feb. 25 in the Journal of Clinical Oncology.
Since the OCM was launched in 2016, several studies have evaluated whether the alternative payment model reached its goal of reducing spending while improving or maintaining the quality of cancer care.
The results have been decidedly mixed.
As previously reported by this news organization, one study found that after 4 years, the OCM led to a $155 million net loss to Medicare. During that time, physician participation in the program also declined, with the number of practices dropping almost 30% between 2016 and 2020.
Other studies, however, have highlighted more positive results.
One large community practice reported saving Medicare $3 million over the course of 1 year. Another analysis found that among community practices that adopted the OCM, in the first year of the program, there was less physician-administered drug use by patients with prostate cancer, lower drug costs by patients with lung and prostate cancer, fewer visits by patients with breast or colon cancer, and lower office-based costs in all cancers analyzed. However, these savings were largely offset by the costs of these programs.
In the current study, DR. Brooks and colleagues compared the use of supportive care medications – bone-modifying drugs as well as prophylactic white blood cell (WBC) growth factors and antiemetics – in practices that adopted the OCM and those that didn’t.
More specifically, the authors zeroed in on the bone-modifying agent denosumab for patients with breast, lung, or prostate cancer and the WBC growth factor biosimilar filgrastim for those receiving chemotherapy for breast, lung, or colorectal cancer. Prophylactic use of higher-cost neurokinin-1 (NK1) antagonists and long-acting serotonin antagonists for patients receiving chemotherapy for any type of cancer was also evaluated.
The authors evaluated chemotherapy episodes assigned to OCM (n = 201) and comparison practices (n = 534) using Medicare claims from 2013-2019.
There was a total of 255,638 treatment episodes for bone metastases. The authors found that the OCM led to relative reductions in the use of denosumab but not in the overall use of bone-modifying medications, which included the less costly options zoledronic acid and pamidronate. The use of denosumab was similar for OCM and comparison practices during the baseline period, but during the intervention period, there were statistically significant relative reductions in the use of denosumab at OCM practices for breast (-5.0%), prostate (-4.0%), and lung cancer (-4.1%).
For WBC growth factors, 164,310 episodes were included in analyses. The OCM did not affect the use of prophylactic WBC growth factors during breast cancer chemotherapy for those at high risk of febrile neutropenia but did lead to a relative decrease during intermediate-risk chemotherapy (-7.6%). The authors observed no OCM impact on the use of prophylactic WBC growth factors among intermediate-risk lung or colorectal cancer patients. But, during the intervention period, OCM practices did demonstrate an increased use of originator or biosimilar filgrastim (57.3%) compared to other practices (47.6%), and the quarterly rate of increase in the use of the biosimilar grew 2.6 percentage points faster in OCM practices.
The authors report that there were 414,792 treatment episodes involving the use of prophylactic antiemetics. Overall, among patients receiving chemotherapy with high or moderate emetic risk, the OCM led to reductions in the prophylactic use of NK1 antagonists and long-acting serotonin antagonists. The authors report a 6.0 percentage point reduction in the use of NK1 antagonists during high-emetic-risk chemotherapy.
“We found that OCM was associated with meaningful changes in the use of supportive care medications during chemotherapy treatment episodes consistent with value-based care redesign,” the authors conclude. “These impacts on supportive care medication use align with previously reported spending reductions attributable to OCM and suggest that alternative payment models have potential to drive value-based changes in supportive care during cancer treatment.”
The study was supported by CMS. Several of the coauthors have reported relationships with industry, as noted in the article.
A version of this article first appeared on Medscape.com.
The Oncology Care Model (OCM), launched by the Centers for Medicare & Medicaid Services (CMS) with the goal of reducing spending for Medicare beneficiaries, was “associated with meaningful changes in the use of supportive care medications during chemotherapy treatment episodes,” according to new findings.
The OCM led to a statistically significant reduction in the use of denosumab – a pricier bone-modifying drug – by patients with bone metastases without changing the overall use of bone-modifying medications. The OCM also prompted more rapid adoption of a less expensive white blood cell growth factor agent – the biosimilar filgrastim – and more selective use of costly antiemetics as primary prophylaxis for chemotherapy-induced nausea.
study author Gabriel A. Brooks, MD, MPH, of the Dartmouth Institute for Health Policy and Clinical Practice, Geisel School of Medicine, Lebanon, N.H., and colleagues write.
The study was published online Feb. 25 in the Journal of Clinical Oncology.
Since the OCM was launched in 2016, several studies have evaluated whether the alternative payment model reached its goal of reducing spending while improving or maintaining the quality of cancer care.
The results have been decidedly mixed.
As previously reported by this news organization, one study found that after 4 years, the OCM led to a $155 million net loss to Medicare. During that time, physician participation in the program also declined, with the number of practices dropping almost 30% between 2016 and 2020.
Other studies, however, have highlighted more positive results.
One large community practice reported saving Medicare $3 million over the course of 1 year. Another analysis found that among community practices that adopted the OCM, in the first year of the program, there was less physician-administered drug use by patients with prostate cancer, lower drug costs by patients with lung and prostate cancer, fewer visits by patients with breast or colon cancer, and lower office-based costs in all cancers analyzed. However, these savings were largely offset by the costs of these programs.
In the current study, DR. Brooks and colleagues compared the use of supportive care medications – bone-modifying drugs as well as prophylactic white blood cell (WBC) growth factors and antiemetics – in practices that adopted the OCM and those that didn’t.
More specifically, the authors zeroed in on the bone-modifying agent denosumab for patients with breast, lung, or prostate cancer and the WBC growth factor biosimilar filgrastim for those receiving chemotherapy for breast, lung, or colorectal cancer. Prophylactic use of higher-cost neurokinin-1 (NK1) antagonists and long-acting serotonin antagonists for patients receiving chemotherapy for any type of cancer was also evaluated.
The authors evaluated chemotherapy episodes assigned to OCM (n = 201) and comparison practices (n = 534) using Medicare claims from 2013-2019.
There was a total of 255,638 treatment episodes for bone metastases. The authors found that the OCM led to relative reductions in the use of denosumab but not in the overall use of bone-modifying medications, which included the less costly options zoledronic acid and pamidronate. The use of denosumab was similar for OCM and comparison practices during the baseline period, but during the intervention period, there were statistically significant relative reductions in the use of denosumab at OCM practices for breast (-5.0%), prostate (-4.0%), and lung cancer (-4.1%).
For WBC growth factors, 164,310 episodes were included in analyses. The OCM did not affect the use of prophylactic WBC growth factors during breast cancer chemotherapy for those at high risk of febrile neutropenia but did lead to a relative decrease during intermediate-risk chemotherapy (-7.6%). The authors observed no OCM impact on the use of prophylactic WBC growth factors among intermediate-risk lung or colorectal cancer patients. But, during the intervention period, OCM practices did demonstrate an increased use of originator or biosimilar filgrastim (57.3%) compared to other practices (47.6%), and the quarterly rate of increase in the use of the biosimilar grew 2.6 percentage points faster in OCM practices.
The authors report that there were 414,792 treatment episodes involving the use of prophylactic antiemetics. Overall, among patients receiving chemotherapy with high or moderate emetic risk, the OCM led to reductions in the prophylactic use of NK1 antagonists and long-acting serotonin antagonists. The authors report a 6.0 percentage point reduction in the use of NK1 antagonists during high-emetic-risk chemotherapy.
“We found that OCM was associated with meaningful changes in the use of supportive care medications during chemotherapy treatment episodes consistent with value-based care redesign,” the authors conclude. “These impacts on supportive care medication use align with previously reported spending reductions attributable to OCM and suggest that alternative payment models have potential to drive value-based changes in supportive care during cancer treatment.”
The study was supported by CMS. Several of the coauthors have reported relationships with industry, as noted in the article.
A version of this article first appeared on Medscape.com.
FROM JOURNAL OF CLINICAL ONCOLOGY
AGA helps break down barriers to CRC screening
The new year has already marked major progress for colorectal cancer (CRC) screening with the implementation of the Removing Barriers to Colorectal Cancer Screening Act by the Centers for Medicare & Medicaid Services, which will protect Medicare beneficiaries from an unexpected bill if a polyp is detected and removed during a screening colonoscopy, as well as new guidance from the federal government requiring private insurers to cover colonoscopy as a follow-up to a noninvasive CRC screening test without imposing cost sharing for patients.
The American Gastroenterological Association is strongly committed to reducing the incidence of and mortality from colorectal cancer. There is strong evidence that CRC screening is effective, but only 65% of eligible individuals have been screened. A. Mark Fendrick, MD, and colleagues recently found that cost sharing for CRC screening occurred in 48.2% of patients with commercial insurance and 77.9% of patients with Medicare coverage. The elimination of these barriers to CRC screening should improve adherence and reduce the burden of CRC.

As one of AGA President John M. Inadomi’s initiatives, the AGA created the CRC Screening Continuum Executive Committee in 2021 to develop AGA Position Statements that highlight the continuum of CRC screening and identify barriers, as well as work with stakeholders to eliminate known barriers. Chaired by former AGA President, David Lieberman, MD, AGAF, and with public policy guidance from Kathleen Teixeira, AGA Vice President of Public Policy and Government Affairs at the AGA, the committee identified that, at that time, colonoscopies after positive stool tests had often been considered “diagnostic” and, therefore, were not covered in full the way a preventive screening is required to be covered by the Affordable Care Act (ACA). The committee recognized that copays and deductibles are barriers to CRC screening and contribute to health inequity and socio-economic disparities. Noninvasive screening should be considered a part of programs with multiple steps, all of which – including follow-up colonoscopy if the test is positive – should be covered by payers without cost sharing as part of the screening continuum. Further, screening with high-quality colonoscopy should be covered by payers without cost sharing, consistent with the aims of the ACA. The committee recommended that the full cost of screening, including the bowel prep, facility and professional fees, anesthesia, and pathology, should be covered by payers without cost sharing.

Over the past decade, the AGA and other organizations have spent countless hours advocating for closing the gap. In September 2021, Dr. Inadomi and Dr. Lieberman, along with the American Cancer Society Cancer Action Network and Fight CRC, met with Assistant Secretary of Labor, Ali Khawar, and representatives from the U.S. Department of Health & Human Services and U.S. Department of Treasury to request they direct private health plans to cover colonoscopy after a positive noninvasive CRC screening. In January 2022, guidance from the United States Department of Labor, HHS, and the USDT clarified that private insurance plans must cover follow-up colonoscopies after a positive noninvasive stool test. In the Frequently Asked Questions (FAQs) about the Affordable Care Act Implementation, Part 51, the departments affirmed that a plan or issuer must cover and may not impose cost sharing with respect to a colonoscopy conducted after a positive noninvasive stool-based screening test or direct visualization screening test for colorectal cancer for individuals described in a U.S. Preventive Services Task Force (USPSTF) recommendation from May 18, 2021. As stated in that USPSTF recommendation, the follow-up colonoscopy is an integral part of the preventive screening without which the screening would not be complete . The follow-up colonoscopy after a positive noninvasive stool-based screening test or direct visualization screening test is therefore required to be covered without cost sharing in accordance with the requirements of Public Health Service Act section 2713 and its implementing regulations.
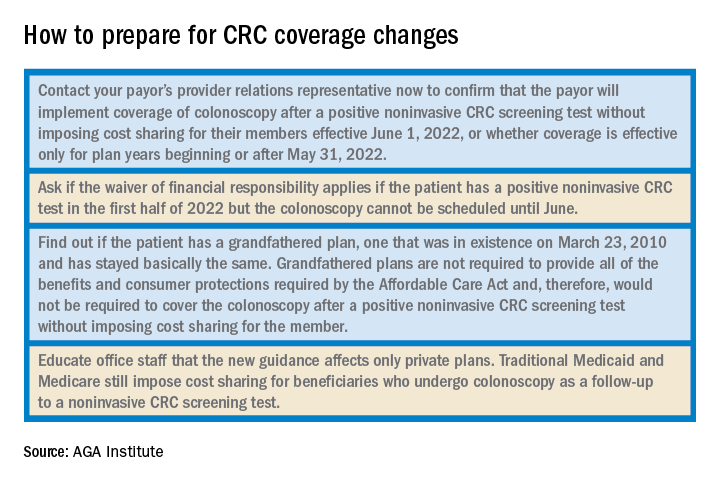
Plans and issuers must provide coverage without cost sharing for plan or policy years beginning on or after May 31, 2022. While this new guidance will expand coverage of follow-up colonoscopies to many more individuals nationwide, including individuals who have coverage through Medicaid expansion, it does not apply to traditional Medicaid and Medicare plans.
The members of the CRC Screening Continuum Executive Committee includes Dr. Brill and Lieberman, as well as Uri Ladabaum, MD; Larry Kim, MD; Folasade May, MD, PhD, MPhil; Caitlin Murphy, MD; and Richard Wender, MD. Disclosures are on file with the AGA National Office.
Dr. Brill is chief medical officer, Predictive Health, Phoenix. Dr. Lieberman is professor of medicine, division of gastroenterology and hepatology, Oregon Health & Science University, Portland, as well as a past president of the AGA. Dr. Brill discloses consulting for Accomplish Health, Alimetry, Allara Health, AnX Robotica, Arch Therapeutics, Biotax, Boomerang Medical, Brightline, Calyx, Capsovision, Check Cap, Clexio, Curology, Docbot, Echosens, Endogastric Solutions, evoEndo, Family First, FDNA, Food Marble, Freespira, Gala Therapeutics, Glaukos, gTech Medical, Gynesonics, Hbox, Hello Heart, HyGIeaCare, Innovative Health Solutions, IronRod Health, Johnson & Johnson, Lantheus, LeMinou, Lumen, Mainstay Medical, MaternaMed, Medtronic, Mightier, Motus GI, OncoSil Medical, Palette Life Sciences, Perry Health, Perspectum, Red Ventures, Reflexion, Respira Labs, Salaso, Smith+Nephew, SonarMD, Stage Zero Life Sciences, Steris, Sword Health, Tabula Rosa Health Care, Ultrasight, Vertos Medical, WL Gore, and holds options/warrants in Accomplish Health, AnX Robotica, Capsovision, Donsini Health, Hbox, Hello Heart, HyGIeaCare, Restech, Perry Health, StageZero Life Sciences, SonarMD. Dr. Lieberman is a consultant to Geneoscopy.
The new year has already marked major progress for colorectal cancer (CRC) screening with the implementation of the Removing Barriers to Colorectal Cancer Screening Act by the Centers for Medicare & Medicaid Services, which will protect Medicare beneficiaries from an unexpected bill if a polyp is detected and removed during a screening colonoscopy, as well as new guidance from the federal government requiring private insurers to cover colonoscopy as a follow-up to a noninvasive CRC screening test without imposing cost sharing for patients.
The American Gastroenterological Association is strongly committed to reducing the incidence of and mortality from colorectal cancer. There is strong evidence that CRC screening is effective, but only 65% of eligible individuals have been screened. A. Mark Fendrick, MD, and colleagues recently found that cost sharing for CRC screening occurred in 48.2% of patients with commercial insurance and 77.9% of patients with Medicare coverage. The elimination of these barriers to CRC screening should improve adherence and reduce the burden of CRC.
As one of AGA President John M. Inadomi’s initiatives, the AGA created the CRC Screening Continuum Executive Committee in 2021 to develop AGA Position Statements that highlight the continuum of CRC screening and identify barriers, as well as work with stakeholders to eliminate known barriers. Chaired by former AGA President, David Lieberman, MD, AGAF, and with public policy guidance from Kathleen Teixeira, AGA Vice President of Public Policy and Government Affairs at the AGA, the committee identified that, at that time, colonoscopies after positive stool tests had often been considered “diagnostic” and, therefore, were not covered in full the way a preventive screening is required to be covered by the Affordable Care Act (ACA). The committee recognized that copays and deductibles are barriers to CRC screening and contribute to health inequity and socio-economic disparities. Noninvasive screening should be considered a part of programs with multiple steps, all of which – including follow-up colonoscopy if the test is positive – should be covered by payers without cost sharing as part of the screening continuum. Further, screening with high-quality colonoscopy should be covered by payers without cost sharing, consistent with the aims of the ACA. The committee recommended that the full cost of screening, including the bowel prep, facility and professional fees, anesthesia, and pathology, should be covered by payers without cost sharing.
Over the past decade, the AGA and other organizations have spent countless hours advocating for closing the gap. In September 2021, Dr. Inadomi and Dr. Lieberman, along with the American Cancer Society Cancer Action Network and Fight CRC, met with Assistant Secretary of Labor, Ali Khawar, and representatives from the U.S. Department of Health & Human Services and U.S. Department of Treasury to request they direct private health plans to cover colonoscopy after a positive noninvasive CRC screening. In January 2022, guidance from the United States Department of Labor, HHS, and the USDT clarified that private insurance plans must cover follow-up colonoscopies after a positive noninvasive stool test. In the Frequently Asked Questions (FAQs) about the Affordable Care Act Implementation, Part 51, the departments affirmed that a plan or issuer must cover and may not impose cost sharing with respect to a colonoscopy conducted after a positive noninvasive stool-based screening test or direct visualization screening test for colorectal cancer for individuals described in a U.S. Preventive Services Task Force (USPSTF) recommendation from May 18, 2021. As stated in that USPSTF recommendation, the follow-up colonoscopy is an integral part of the preventive screening without which the screening would not be complete . The follow-up colonoscopy after a positive noninvasive stool-based screening test or direct visualization screening test is therefore required to be covered without cost sharing in accordance with the requirements of Public Health Service Act section 2713 and its implementing regulations.
Plans and issuers must provide coverage without cost sharing for plan or policy years beginning on or after May 31, 2022. While this new guidance will expand coverage of follow-up colonoscopies to many more individuals nationwide, including individuals who have coverage through Medicaid expansion, it does not apply to traditional Medicaid and Medicare plans.
The members of the CRC Screening Continuum Executive Committee includes Dr. Brill and Lieberman, as well as Uri Ladabaum, MD; Larry Kim, MD; Folasade May, MD, PhD, MPhil; Caitlin Murphy, MD; and Richard Wender, MD. Disclosures are on file with the AGA National Office.
Dr. Brill is chief medical officer, Predictive Health, Phoenix. Dr. Lieberman is professor of medicine, division of gastroenterology and hepatology, Oregon Health & Science University, Portland, as well as a past president of the AGA. Dr. Brill discloses consulting for Accomplish Health, Alimetry, Allara Health, AnX Robotica, Arch Therapeutics, Biotax, Boomerang Medical, Brightline, Calyx, Capsovision, Check Cap, Clexio, Curology, Docbot, Echosens, Endogastric Solutions, evoEndo, Family First, FDNA, Food Marble, Freespira, Gala Therapeutics, Glaukos, gTech Medical, Gynesonics, Hbox, Hello Heart, HyGIeaCare, Innovative Health Solutions, IronRod Health, Johnson & Johnson, Lantheus, LeMinou, Lumen, Mainstay Medical, MaternaMed, Medtronic, Mightier, Motus GI, OncoSil Medical, Palette Life Sciences, Perry Health, Perspectum, Red Ventures, Reflexion, Respira Labs, Salaso, Smith+Nephew, SonarMD, Stage Zero Life Sciences, Steris, Sword Health, Tabula Rosa Health Care, Ultrasight, Vertos Medical, WL Gore, and holds options/warrants in Accomplish Health, AnX Robotica, Capsovision, Donsini Health, Hbox, Hello Heart, HyGIeaCare, Restech, Perry Health, StageZero Life Sciences, SonarMD. Dr. Lieberman is a consultant to Geneoscopy.
The new year has already marked major progress for colorectal cancer (CRC) screening with the implementation of the Removing Barriers to Colorectal Cancer Screening Act by the Centers for Medicare & Medicaid Services, which will protect Medicare beneficiaries from an unexpected bill if a polyp is detected and removed during a screening colonoscopy, as well as new guidance from the federal government requiring private insurers to cover colonoscopy as a follow-up to a noninvasive CRC screening test without imposing cost sharing for patients.
The American Gastroenterological Association is strongly committed to reducing the incidence of and mortality from colorectal cancer. There is strong evidence that CRC screening is effective, but only 65% of eligible individuals have been screened. A. Mark Fendrick, MD, and colleagues recently found that cost sharing for CRC screening occurred in 48.2% of patients with commercial insurance and 77.9% of patients with Medicare coverage. The elimination of these barriers to CRC screening should improve adherence and reduce the burden of CRC.
As one of AGA President John M. Inadomi’s initiatives, the AGA created the CRC Screening Continuum Executive Committee in 2021 to develop AGA Position Statements that highlight the continuum of CRC screening and identify barriers, as well as work with stakeholders to eliminate known barriers. Chaired by former AGA President, David Lieberman, MD, AGAF, and with public policy guidance from Kathleen Teixeira, AGA Vice President of Public Policy and Government Affairs at the AGA, the committee identified that, at that time, colonoscopies after positive stool tests had often been considered “diagnostic” and, therefore, were not covered in full the way a preventive screening is required to be covered by the Affordable Care Act (ACA). The committee recognized that copays and deductibles are barriers to CRC screening and contribute to health inequity and socio-economic disparities. Noninvasive screening should be considered a part of programs with multiple steps, all of which – including follow-up colonoscopy if the test is positive – should be covered by payers without cost sharing as part of the screening continuum. Further, screening with high-quality colonoscopy should be covered by payers without cost sharing, consistent with the aims of the ACA. The committee recommended that the full cost of screening, including the bowel prep, facility and professional fees, anesthesia, and pathology, should be covered by payers without cost sharing.
Over the past decade, the AGA and other organizations have spent countless hours advocating for closing the gap. In September 2021, Dr. Inadomi and Dr. Lieberman, along with the American Cancer Society Cancer Action Network and Fight CRC, met with Assistant Secretary of Labor, Ali Khawar, and representatives from the U.S. Department of Health & Human Services and U.S. Department of Treasury to request they direct private health plans to cover colonoscopy after a positive noninvasive CRC screening. In January 2022, guidance from the United States Department of Labor, HHS, and the USDT clarified that private insurance plans must cover follow-up colonoscopies after a positive noninvasive stool test. In the Frequently Asked Questions (FAQs) about the Affordable Care Act Implementation, Part 51, the departments affirmed that a plan or issuer must cover and may not impose cost sharing with respect to a colonoscopy conducted after a positive noninvasive stool-based screening test or direct visualization screening test for colorectal cancer for individuals described in a U.S. Preventive Services Task Force (USPSTF) recommendation from May 18, 2021. As stated in that USPSTF recommendation, the follow-up colonoscopy is an integral part of the preventive screening without which the screening would not be complete . The follow-up colonoscopy after a positive noninvasive stool-based screening test or direct visualization screening test is therefore required to be covered without cost sharing in accordance with the requirements of Public Health Service Act section 2713 and its implementing regulations.
Plans and issuers must provide coverage without cost sharing for plan or policy years beginning on or after May 31, 2022. While this new guidance will expand coverage of follow-up colonoscopies to many more individuals nationwide, including individuals who have coverage through Medicaid expansion, it does not apply to traditional Medicaid and Medicare plans.
The members of the CRC Screening Continuum Executive Committee includes Dr. Brill and Lieberman, as well as Uri Ladabaum, MD; Larry Kim, MD; Folasade May, MD, PhD, MPhil; Caitlin Murphy, MD; and Richard Wender, MD. Disclosures are on file with the AGA National Office.
Dr. Brill is chief medical officer, Predictive Health, Phoenix. Dr. Lieberman is professor of medicine, division of gastroenterology and hepatology, Oregon Health & Science University, Portland, as well as a past president of the AGA. Dr. Brill discloses consulting for Accomplish Health, Alimetry, Allara Health, AnX Robotica, Arch Therapeutics, Biotax, Boomerang Medical, Brightline, Calyx, Capsovision, Check Cap, Clexio, Curology, Docbot, Echosens, Endogastric Solutions, evoEndo, Family First, FDNA, Food Marble, Freespira, Gala Therapeutics, Glaukos, gTech Medical, Gynesonics, Hbox, Hello Heart, HyGIeaCare, Innovative Health Solutions, IronRod Health, Johnson & Johnson, Lantheus, LeMinou, Lumen, Mainstay Medical, MaternaMed, Medtronic, Mightier, Motus GI, OncoSil Medical, Palette Life Sciences, Perry Health, Perspectum, Red Ventures, Reflexion, Respira Labs, Salaso, Smith+Nephew, SonarMD, Stage Zero Life Sciences, Steris, Sword Health, Tabula Rosa Health Care, Ultrasight, Vertos Medical, WL Gore, and holds options/warrants in Accomplish Health, AnX Robotica, Capsovision, Donsini Health, Hbox, Hello Heart, HyGIeaCare, Restech, Perry Health, StageZero Life Sciences, SonarMD. Dr. Lieberman is a consultant to Geneoscopy.
NY radiation oncologist loses license, poses ‘potential danger’
The state Board for Professional Medical Conduct has revoked the medical license of Won Sam Yi, MD, following a lengthy review of the care he provided to seven cancer patients; six of them died.
“He is a danger to potential new patients should he be reinstated as a radiation oncologist,” board members wrote, according to a news report in the Buffalo News.
Dr. Yi’s lawyer said that he is appealing the decision.
Dr. Yi was the former CEO of the now-defunct private cancer practice CCS Oncology, located in western New York.
In 2018, the state health department brought numerous charges of professional misconduct against Dr. Yi, including charges that he had failed to “account for prior doses of radiotherapy” as well as exceeding “appropriate tissue tolerances” during the treatment.
Now, the state’s Board for Professional Medical Conduct has upheld nearly all of the departmental charges that had been levied against him, and also found that Dr. Yi failed to take responsibility or show contrition for his treatment decisions.
However, whistleblower claims from a former CSS Oncology employee were dismissed.
Troubled history
CCS Oncology was once one of the largest private cancer practices in Erie and Niagara counties, both in the Buffalo metropolitan area.
Dr. Yi purchased CCS Oncology in 2008 and was its sole shareholder, and in 2012 he also acquired CCS Medical. As of 2016, the practices provided care to about 30% of cancer patients in the region. CCS also began acquiring other practices as it expanded into noncancer specialties, including primary care.
However, CCS began to struggle financially in late 2016, when health insurance provider Independent Health announced it was removing CCS Oncology from its network, and several vendors and lenders subsequently sued CCS and Dr. Yi for nonpayment.
The announcement from Independent Health was “financially devastating to CCS,” and also was “the direct cause” of the practice defaulting on its Bank of America loan and of the practice’s inability to pay not only its vendors but state and federal tax agencies, the Buffalo News reported. As a result, several vendors and lenders had sued CCS and Dr. Yi for nonpayment.
The FBI raided numerous CCS locations in March 2018, seizing financial and other data as part of an investigation into possible Medicare billing fraud. The following month, CCS filed for Chapter 11 bankruptcy, citing it owed millions of dollars to Bank of America and other creditors. Shortly afterward, the practice closed.
Medical misconduct
The state’s charges of professional misconduct accused Dr. Yi of “gross negligence,” “gross incompetence,” and several other cases of misconduct in treating seven patients between 2009 and 2013 at various CCS locations. The patients ranged in age from 27 to 72. Six of the seven patients died.
In one case, Dr. Yi was accused of providing whole-brain radiation therapy to a 43-year-old woman for about 6 weeks in 2012, but the treatment was “contrary to medical indications” and did not take into account prior doses of such treatment. The patient died in December of that year, and the board concluded that Dr. Yi had improperly treated her with a high dose of radiation that was intended to cure her cancer even though she was at a stage where her disease was incurable.
The state board eventually concluded that for all but one of the patients in question, Dr. Yi was guilty of misconduct in his treatment decisions. They wrote that Dr. Yi had frequently administered radiation doses without taking into account how much radiation therapy the patients had received previously and without considering the risk of serious complications for them.
Dr. Yi plans to appeal the board’s decision in state court, according to his attorney, Anthony Scher.
“Dr Yi has treated over 10,000 patients in his career,” Mr. Scher told the Buffalo News. “These handful of cases don’t represent the thousands of success stories that he’s had.”
A version of this article first appeared on Medscape.com.
The state Board for Professional Medical Conduct has revoked the medical license of Won Sam Yi, MD, following a lengthy review of the care he provided to seven cancer patients; six of them died.
“He is a danger to potential new patients should he be reinstated as a radiation oncologist,” board members wrote, according to a news report in the Buffalo News.
Dr. Yi’s lawyer said that he is appealing the decision.
Dr. Yi was the former CEO of the now-defunct private cancer practice CCS Oncology, located in western New York.
In 2018, the state health department brought numerous charges of professional misconduct against Dr. Yi, including charges that he had failed to “account for prior doses of radiotherapy” as well as exceeding “appropriate tissue tolerances” during the treatment.
Now, the state’s Board for Professional Medical Conduct has upheld nearly all of the departmental charges that had been levied against him, and also found that Dr. Yi failed to take responsibility or show contrition for his treatment decisions.
However, whistleblower claims from a former CSS Oncology employee were dismissed.
Troubled history
CCS Oncology was once one of the largest private cancer practices in Erie and Niagara counties, both in the Buffalo metropolitan area.
Dr. Yi purchased CCS Oncology in 2008 and was its sole shareholder, and in 2012 he also acquired CCS Medical. As of 2016, the practices provided care to about 30% of cancer patients in the region. CCS also began acquiring other practices as it expanded into noncancer specialties, including primary care.
However, CCS began to struggle financially in late 2016, when health insurance provider Independent Health announced it was removing CCS Oncology from its network, and several vendors and lenders subsequently sued CCS and Dr. Yi for nonpayment.
The announcement from Independent Health was “financially devastating to CCS,” and also was “the direct cause” of the practice defaulting on its Bank of America loan and of the practice’s inability to pay not only its vendors but state and federal tax agencies, the Buffalo News reported. As a result, several vendors and lenders had sued CCS and Dr. Yi for nonpayment.
The FBI raided numerous CCS locations in March 2018, seizing financial and other data as part of an investigation into possible Medicare billing fraud. The following month, CCS filed for Chapter 11 bankruptcy, citing it owed millions of dollars to Bank of America and other creditors. Shortly afterward, the practice closed.
Medical misconduct
The state’s charges of professional misconduct accused Dr. Yi of “gross negligence,” “gross incompetence,” and several other cases of misconduct in treating seven patients between 2009 and 2013 at various CCS locations. The patients ranged in age from 27 to 72. Six of the seven patients died.
In one case, Dr. Yi was accused of providing whole-brain radiation therapy to a 43-year-old woman for about 6 weeks in 2012, but the treatment was “contrary to medical indications” and did not take into account prior doses of such treatment. The patient died in December of that year, and the board concluded that Dr. Yi had improperly treated her with a high dose of radiation that was intended to cure her cancer even though she was at a stage where her disease was incurable.
The state board eventually concluded that for all but one of the patients in question, Dr. Yi was guilty of misconduct in his treatment decisions. They wrote that Dr. Yi had frequently administered radiation doses without taking into account how much radiation therapy the patients had received previously and without considering the risk of serious complications for them.
Dr. Yi plans to appeal the board’s decision in state court, according to his attorney, Anthony Scher.
“Dr Yi has treated over 10,000 patients in his career,” Mr. Scher told the Buffalo News. “These handful of cases don’t represent the thousands of success stories that he’s had.”
A version of this article first appeared on Medscape.com.
The state Board for Professional Medical Conduct has revoked the medical license of Won Sam Yi, MD, following a lengthy review of the care he provided to seven cancer patients; six of them died.
“He is a danger to potential new patients should he be reinstated as a radiation oncologist,” board members wrote, according to a news report in the Buffalo News.
Dr. Yi’s lawyer said that he is appealing the decision.
Dr. Yi was the former CEO of the now-defunct private cancer practice CCS Oncology, located in western New York.
In 2018, the state health department brought numerous charges of professional misconduct against Dr. Yi, including charges that he had failed to “account for prior doses of radiotherapy” as well as exceeding “appropriate tissue tolerances” during the treatment.
Now, the state’s Board for Professional Medical Conduct has upheld nearly all of the departmental charges that had been levied against him, and also found that Dr. Yi failed to take responsibility or show contrition for his treatment decisions.
However, whistleblower claims from a former CSS Oncology employee were dismissed.
Troubled history
CCS Oncology was once one of the largest private cancer practices in Erie and Niagara counties, both in the Buffalo metropolitan area.
Dr. Yi purchased CCS Oncology in 2008 and was its sole shareholder, and in 2012 he also acquired CCS Medical. As of 2016, the practices provided care to about 30% of cancer patients in the region. CCS also began acquiring other practices as it expanded into noncancer specialties, including primary care.
However, CCS began to struggle financially in late 2016, when health insurance provider Independent Health announced it was removing CCS Oncology from its network, and several vendors and lenders subsequently sued CCS and Dr. Yi for nonpayment.
The announcement from Independent Health was “financially devastating to CCS,” and also was “the direct cause” of the practice defaulting on its Bank of America loan and of the practice’s inability to pay not only its vendors but state and federal tax agencies, the Buffalo News reported. As a result, several vendors and lenders had sued CCS and Dr. Yi for nonpayment.
The FBI raided numerous CCS locations in March 2018, seizing financial and other data as part of an investigation into possible Medicare billing fraud. The following month, CCS filed for Chapter 11 bankruptcy, citing it owed millions of dollars to Bank of America and other creditors. Shortly afterward, the practice closed.
Medical misconduct
The state’s charges of professional misconduct accused Dr. Yi of “gross negligence,” “gross incompetence,” and several other cases of misconduct in treating seven patients between 2009 and 2013 at various CCS locations. The patients ranged in age from 27 to 72. Six of the seven patients died.
In one case, Dr. Yi was accused of providing whole-brain radiation therapy to a 43-year-old woman for about 6 weeks in 2012, but the treatment was “contrary to medical indications” and did not take into account prior doses of such treatment. The patient died in December of that year, and the board concluded that Dr. Yi had improperly treated her with a high dose of radiation that was intended to cure her cancer even though she was at a stage where her disease was incurable.
The state board eventually concluded that for all but one of the patients in question, Dr. Yi was guilty of misconduct in his treatment decisions. They wrote that Dr. Yi had frequently administered radiation doses without taking into account how much radiation therapy the patients had received previously and without considering the risk of serious complications for them.
Dr. Yi plans to appeal the board’s decision in state court, according to his attorney, Anthony Scher.
“Dr Yi has treated over 10,000 patients in his career,” Mr. Scher told the Buffalo News. “These handful of cases don’t represent the thousands of success stories that he’s had.”
A version of this article first appeared on Medscape.com.
When physicians are the plaintiffs
Have you experienced malpractice?
No, I’m not asking whether you have experienced litigation. I’m asking whether you, as a physician, have actually experienced substandard care from a colleague. I have heard many such experiences over the years, and mistreatment doesn’t seem to be getting any less frequent.
The first is that, unlike the Pope, who has a dedicated confessor trained to minister to his spiritual needs, no one formally trains physicians to treat physicians. As a result, most of us feel slightly uneasy at treating other physicians. We naturally wish to keep our colleagues well, but at the same time realize that our clinical skills are being very closely scrutinized. What if they are found to be wanting? This discomfiture can make a physician treating a physician overly compulsive, or worse, overtly dismissive.
Second, we physicians are famously poor patients. We pretend we don’t need the advice we give others, to monitor our health and promptly seek care when something feels amiss. And, for the period during which we delay a medical encounter, we often attempt to diagnose and treat ourselves.
Sometimes we are successful, which reinforces this approach. Other times, we fail at being our own caregiver and present to someone else either too late, or with avoidable complications. In the former instance, we congratulate ourselves and learn nothing from the experience. In the latter, we may heap shame upon ourselves for our folly, and we may learn; but it could be a lethal lesson. In the worst scenario, our colleague gives in to frustration (or angst), and heaps even more shame onto their late-presenting physician patient.
Third, when we do submit to being a patient, we often demand VIP treatment. This is probably in response to our anxiety that some of the worst things we have seen happen to patients might happen to us if we are not vigilant to ensure we receive a higher level of care. But of course, such hypervigilance can lead to excessive care and testing, with all the attendant hazards, or alternatively to dilution of care if our caregivers decide we are just too much trouble.
Fourth, as a fifth-generation physician myself, I am convinced that physicians and physician family members are either prone to unusual manifestations of common diseases or unusual diseases, or that rare disease entities and complications are actually more common than literature suggests, and they simply aren’t pursued or diagnosed in nonphysician families.
No matter how we may have arrived in a position to need medical care, how often is such care substandard? And how do we respond when we suspect, or know, this to be the case? Are physicians more, or less, likely to take legal action in the face of it?
I certainly don’t know any statistics. Physicians are in an excellent position to take such action, because judges and juries will likely believe that a doctor can recognize negligence when we fall victim to it. But we may also be reluctant to publicly admit the way (or ways) in which we may have contributed to substandard care or outcome.
Based on decades of working with physician clients who have been sued, and having been sued myself (thus witnessing and also experiencing the effects of litigation), I am probably more reluctant than normal patients or physicians to consider taking legal action. This, despite the fact that I am also a lawyer and (through organized medicine) know many colleagues in all specialties who might serve as expert witnesses.
I have experienced serial substandard care, which has left me highly conflicted about the efficacy of my chosen profession. As a resident, I had my first odd pain condition and consulted an “elder statesperson” from my institution, whom I assumed to be a “doctor’s doctor” because he was a superb teacher (wrong!)
He completely missed the diagnosis and further belittled (indeed, libeled) me in the medical record. (Some years later, I learned that, during that period, he was increasingly demented and tended to view all female patients as having “wandering uterus” equivalents.) Fortunately, I found a better diagnostician, or at least one more willing to lend credence to my complaints, who successfully removed the first of several “zebra” lesions I have experienced.
As a young faculty member, I had an odd presentation of a recurring gynecologic condition, which was treated surgically, successfully, except that my fertility was cut in half – a possibility about which I had not been informed when giving operative consent. Would I have sued this fellow faculty member for that? Never, because she invariably treated me with respect as a colleague.
Later in my career after leaving academia, the same condition recurred in a new location. My old-school gynecologist desired to do an extensive procedure, to which I demurred unless specific pathology was found intraoperatively. Affronted, he subjected me to laparoscopy, did nothing but look, and then left the hospital leaving me and the PACU nurse to try to decipher his instructions (which said, basically, “I didn’t find anything; don’t bother me again.”). Several years of pain later, a younger gynecologist performed the correct procedure to address my problem, which has never recurred. Would I have sued him? No, because I believe he had a disability.
At age 59, I developed a new mole. My beloved general practitioner, in the waning years of his practice, forgot to consult a colleague to remove it for several months. When I forced the issue, the mole was removed and turned out to be a rare pediatric condition considered a precursor to melanoma. The same general practitioner had told me I needn’t worry about my “mild hypercalcemia.”
Ten years later I diagnosed my own parathyroid adenoma, in the interim losing 10% of my bone density. Would I have sued him? No, for he always showed he cared. (Though maybe, if I had fractured my spine or hip.)
If you have been the victim of physician malpractice, how did you respond?
Do we serve our profession well by how we handle substandard care – upon ourselves (or our loved ones)?
Dr. Andrew is a former assistant professor in the department of emergency medicine, Johns Hopkins University, Baltimore, and founder and principal of MDMentor, Victoria, B.C.
A version of this article first appeared on Medscape.com.
Have you experienced malpractice?
No, I’m not asking whether you have experienced litigation. I’m asking whether you, as a physician, have actually experienced substandard care from a colleague. I have heard many such experiences over the years, and mistreatment doesn’t seem to be getting any less frequent.
The first is that, unlike the Pope, who has a dedicated confessor trained to minister to his spiritual needs, no one formally trains physicians to treat physicians. As a result, most of us feel slightly uneasy at treating other physicians. We naturally wish to keep our colleagues well, but at the same time realize that our clinical skills are being very closely scrutinized. What if they are found to be wanting? This discomfiture can make a physician treating a physician overly compulsive, or worse, overtly dismissive.
Second, we physicians are famously poor patients. We pretend we don’t need the advice we give others, to monitor our health and promptly seek care when something feels amiss. And, for the period during which we delay a medical encounter, we often attempt to diagnose and treat ourselves.
Sometimes we are successful, which reinforces this approach. Other times, we fail at being our own caregiver and present to someone else either too late, or with avoidable complications. In the former instance, we congratulate ourselves and learn nothing from the experience. In the latter, we may heap shame upon ourselves for our folly, and we may learn; but it could be a lethal lesson. In the worst scenario, our colleague gives in to frustration (or angst), and heaps even more shame onto their late-presenting physician patient.
Third, when we do submit to being a patient, we often demand VIP treatment. This is probably in response to our anxiety that some of the worst things we have seen happen to patients might happen to us if we are not vigilant to ensure we receive a higher level of care. But of course, such hypervigilance can lead to excessive care and testing, with all the attendant hazards, or alternatively to dilution of care if our caregivers decide we are just too much trouble.
Fourth, as a fifth-generation physician myself, I am convinced that physicians and physician family members are either prone to unusual manifestations of common diseases or unusual diseases, or that rare disease entities and complications are actually more common than literature suggests, and they simply aren’t pursued or diagnosed in nonphysician families.
No matter how we may have arrived in a position to need medical care, how often is such care substandard? And how do we respond when we suspect, or know, this to be the case? Are physicians more, or less, likely to take legal action in the face of it?
I certainly don’t know any statistics. Physicians are in an excellent position to take such action, because judges and juries will likely believe that a doctor can recognize negligence when we fall victim to it. But we may also be reluctant to publicly admit the way (or ways) in which we may have contributed to substandard care or outcome.
Based on decades of working with physician clients who have been sued, and having been sued myself (thus witnessing and also experiencing the effects of litigation), I am probably more reluctant than normal patients or physicians to consider taking legal action. This, despite the fact that I am also a lawyer and (through organized medicine) know many colleagues in all specialties who might serve as expert witnesses.
I have experienced serial substandard care, which has left me highly conflicted about the efficacy of my chosen profession. As a resident, I had my first odd pain condition and consulted an “elder statesperson” from my institution, whom I assumed to be a “doctor’s doctor” because he was a superb teacher (wrong!)
He completely missed the diagnosis and further belittled (indeed, libeled) me in the medical record. (Some years later, I learned that, during that period, he was increasingly demented and tended to view all female patients as having “wandering uterus” equivalents.) Fortunately, I found a better diagnostician, or at least one more willing to lend credence to my complaints, who successfully removed the first of several “zebra” lesions I have experienced.
As a young faculty member, I had an odd presentation of a recurring gynecologic condition, which was treated surgically, successfully, except that my fertility was cut in half – a possibility about which I had not been informed when giving operative consent. Would I have sued this fellow faculty member for that? Never, because she invariably treated me with respect as a colleague.
Later in my career after leaving academia, the same condition recurred in a new location. My old-school gynecologist desired to do an extensive procedure, to which I demurred unless specific pathology was found intraoperatively. Affronted, he subjected me to laparoscopy, did nothing but look, and then left the hospital leaving me and the PACU nurse to try to decipher his instructions (which said, basically, “I didn’t find anything; don’t bother me again.”). Several years of pain later, a younger gynecologist performed the correct procedure to address my problem, which has never recurred. Would I have sued him? No, because I believe he had a disability.
At age 59, I developed a new mole. My beloved general practitioner, in the waning years of his practice, forgot to consult a colleague to remove it for several months. When I forced the issue, the mole was removed and turned out to be a rare pediatric condition considered a precursor to melanoma. The same general practitioner had told me I needn’t worry about my “mild hypercalcemia.”
Ten years later I diagnosed my own parathyroid adenoma, in the interim losing 10% of my bone density. Would I have sued him? No, for he always showed he cared. (Though maybe, if I had fractured my spine or hip.)
If you have been the victim of physician malpractice, how did you respond?
Do we serve our profession well by how we handle substandard care – upon ourselves (or our loved ones)?
Dr. Andrew is a former assistant professor in the department of emergency medicine, Johns Hopkins University, Baltimore, and founder and principal of MDMentor, Victoria, B.C.
A version of this article first appeared on Medscape.com.
Have you experienced malpractice?
No, I’m not asking whether you have experienced litigation. I’m asking whether you, as a physician, have actually experienced substandard care from a colleague. I have heard many such experiences over the years, and mistreatment doesn’t seem to be getting any less frequent.
The first is that, unlike the Pope, who has a dedicated confessor trained to minister to his spiritual needs, no one formally trains physicians to treat physicians. As a result, most of us feel slightly uneasy at treating other physicians. We naturally wish to keep our colleagues well, but at the same time realize that our clinical skills are being very closely scrutinized. What if they are found to be wanting? This discomfiture can make a physician treating a physician overly compulsive, or worse, overtly dismissive.
Second, we physicians are famously poor patients. We pretend we don’t need the advice we give others, to monitor our health and promptly seek care when something feels amiss. And, for the period during which we delay a medical encounter, we often attempt to diagnose and treat ourselves.
Sometimes we are successful, which reinforces this approach. Other times, we fail at being our own caregiver and present to someone else either too late, or with avoidable complications. In the former instance, we congratulate ourselves and learn nothing from the experience. In the latter, we may heap shame upon ourselves for our folly, and we may learn; but it could be a lethal lesson. In the worst scenario, our colleague gives in to frustration (or angst), and heaps even more shame onto their late-presenting physician patient.
Third, when we do submit to being a patient, we often demand VIP treatment. This is probably in response to our anxiety that some of the worst things we have seen happen to patients might happen to us if we are not vigilant to ensure we receive a higher level of care. But of course, such hypervigilance can lead to excessive care and testing, with all the attendant hazards, or alternatively to dilution of care if our caregivers decide we are just too much trouble.
Fourth, as a fifth-generation physician myself, I am convinced that physicians and physician family members are either prone to unusual manifestations of common diseases or unusual diseases, or that rare disease entities and complications are actually more common than literature suggests, and they simply aren’t pursued or diagnosed in nonphysician families.
No matter how we may have arrived in a position to need medical care, how often is such care substandard? And how do we respond when we suspect, or know, this to be the case? Are physicians more, or less, likely to take legal action in the face of it?
I certainly don’t know any statistics. Physicians are in an excellent position to take such action, because judges and juries will likely believe that a doctor can recognize negligence when we fall victim to it. But we may also be reluctant to publicly admit the way (or ways) in which we may have contributed to substandard care or outcome.
Based on decades of working with physician clients who have been sued, and having been sued myself (thus witnessing and also experiencing the effects of litigation), I am probably more reluctant than normal patients or physicians to consider taking legal action. This, despite the fact that I am also a lawyer and (through organized medicine) know many colleagues in all specialties who might serve as expert witnesses.
I have experienced serial substandard care, which has left me highly conflicted about the efficacy of my chosen profession. As a resident, I had my first odd pain condition and consulted an “elder statesperson” from my institution, whom I assumed to be a “doctor’s doctor” because he was a superb teacher (wrong!)
He completely missed the diagnosis and further belittled (indeed, libeled) me in the medical record. (Some years later, I learned that, during that period, he was increasingly demented and tended to view all female patients as having “wandering uterus” equivalents.) Fortunately, I found a better diagnostician, or at least one more willing to lend credence to my complaints, who successfully removed the first of several “zebra” lesions I have experienced.
As a young faculty member, I had an odd presentation of a recurring gynecologic condition, which was treated surgically, successfully, except that my fertility was cut in half – a possibility about which I had not been informed when giving operative consent. Would I have sued this fellow faculty member for that? Never, because she invariably treated me with respect as a colleague.
Later in my career after leaving academia, the same condition recurred in a new location. My old-school gynecologist desired to do an extensive procedure, to which I demurred unless specific pathology was found intraoperatively. Affronted, he subjected me to laparoscopy, did nothing but look, and then left the hospital leaving me and the PACU nurse to try to decipher his instructions (which said, basically, “I didn’t find anything; don’t bother me again.”). Several years of pain later, a younger gynecologist performed the correct procedure to address my problem, which has never recurred. Would I have sued him? No, because I believe he had a disability.
At age 59, I developed a new mole. My beloved general practitioner, in the waning years of his practice, forgot to consult a colleague to remove it for several months. When I forced the issue, the mole was removed and turned out to be a rare pediatric condition considered a precursor to melanoma. The same general practitioner had told me I needn’t worry about my “mild hypercalcemia.”
Ten years later I diagnosed my own parathyroid adenoma, in the interim losing 10% of my bone density. Would I have sued him? No, for he always showed he cared. (Though maybe, if I had fractured my spine or hip.)
If you have been the victim of physician malpractice, how did you respond?
Do we serve our profession well by how we handle substandard care – upon ourselves (or our loved ones)?
Dr. Andrew is a former assistant professor in the department of emergency medicine, Johns Hopkins University, Baltimore, and founder and principal of MDMentor, Victoria, B.C.
A version of this article first appeared on Medscape.com.
Twenty-three percent of health care workers likely to leave industry soon: Poll
according to a new poll.
About half of the respondents to the poll from USA Today/Ipsos reported feeling “burned out,” 43% said they were “anxious,” and 21% said they were “angry” about politics and abuse from patients and families.
“We’re trying to help people here, and we are getting verbally and physically abused for it,” Sarah Fried, a nurse in California who responded to the survey, told USA Today in a follow-up interview.
“Early in this pandemic, people were clapping for us and calling us heroes,” she said. “And what happened to that? What happened to them appreciating what nurses are doing?”
The poll was done Feb. 9-16 among 1,170 adults in the U.S. health care industry, including doctors, nurses, paramedics, therapists, home health aides, dentists, and other medical professionals.
A large majority of workers still reported being satisfied with their jobs, although that optimism has declined somewhat since early 2021 when the COVID-19 vaccine rollout was underway. About 80% of those in the recent poll said they were somewhat or very satisfied with their current job, which is down from 89% in an April 2021 poll from Kaiser Family Foundation/the Washington Post.
Most health care workers reported feeling “hopeful” (59%), “motivated” (59%), or “optimistic” (56%) about going to work. But “hopeful” is down from 76% and “optimistic” is down from 67%, compared with last year.
If they could pick a career over again, about 16% disagreed with the statement, “I would still decide to go into health care,” and 18% said they didn’t know how they felt about it.
“The pandemic has actually made me realize how important this career is and how I really do make a difference. I still love it,” Christina Rosa, a mental health counselor in Massachusetts, told USA Today.
During the pandemic, about 66% of those polled said they had treated a COVID-19 patient, which increased to 84% among nurses and 86% among hospital workers. Among those, 47% reported having a patient who died from COVID-19, including 53% of nurses and 55% of hospital workers.
What’s more, 81% of those who treated COVID-19 patients have cared for unvaccinated patients. Among those, 67% said their patients continued to express skepticism toward COVID-19 vaccines, and 38% said some patients expressed regret for not getting a vaccine. Beyond that, 26% said unvaccinated patients asked for unproven treatments, and 30% said the patient or family criticized the care they received.
Regarding coronavirus-related policy, most Americans working in health care expressed skepticism or criticism of the nation’s handling of the pandemic. About 39% agreed that the American health care system is “on the verge of collapse.”
Only 21% said the pandemic is mostly or completely under control. About 61% don’t think Americans are taking enough precautions to prevent the spread of the coronavirus.
Health care workers were slightly positive when it comes to the Centers for Disease Control and Prevention (54% approve, 34% disapprove), divided on the Biden administration (41% approve, 40% disapprove), and critical of the news media (20% approve, 61% disapprove) and the American public (18% approve, 68% disapprove).
Broadly, though, health care workers support public health efforts. About 85% back measures that provide N95 masks, and 83% back measures that provide COVID-19 tests.
A version of this article first appeared on WebMD.com.
according to a new poll.
About half of the respondents to the poll from USA Today/Ipsos reported feeling “burned out,” 43% said they were “anxious,” and 21% said they were “angry” about politics and abuse from patients and families.
“We’re trying to help people here, and we are getting verbally and physically abused for it,” Sarah Fried, a nurse in California who responded to the survey, told USA Today in a follow-up interview.
“Early in this pandemic, people were clapping for us and calling us heroes,” she said. “And what happened to that? What happened to them appreciating what nurses are doing?”
The poll was done Feb. 9-16 among 1,170 adults in the U.S. health care industry, including doctors, nurses, paramedics, therapists, home health aides, dentists, and other medical professionals.
A large majority of workers still reported being satisfied with their jobs, although that optimism has declined somewhat since early 2021 when the COVID-19 vaccine rollout was underway. About 80% of those in the recent poll said they were somewhat or very satisfied with their current job, which is down from 89% in an April 2021 poll from Kaiser Family Foundation/the Washington Post.
Most health care workers reported feeling “hopeful” (59%), “motivated” (59%), or “optimistic” (56%) about going to work. But “hopeful” is down from 76% and “optimistic” is down from 67%, compared with last year.
If they could pick a career over again, about 16% disagreed with the statement, “I would still decide to go into health care,” and 18% said they didn’t know how they felt about it.
“The pandemic has actually made me realize how important this career is and how I really do make a difference. I still love it,” Christina Rosa, a mental health counselor in Massachusetts, told USA Today.
During the pandemic, about 66% of those polled said they had treated a COVID-19 patient, which increased to 84% among nurses and 86% among hospital workers. Among those, 47% reported having a patient who died from COVID-19, including 53% of nurses and 55% of hospital workers.
What’s more, 81% of those who treated COVID-19 patients have cared for unvaccinated patients. Among those, 67% said their patients continued to express skepticism toward COVID-19 vaccines, and 38% said some patients expressed regret for not getting a vaccine. Beyond that, 26% said unvaccinated patients asked for unproven treatments, and 30% said the patient or family criticized the care they received.
Regarding coronavirus-related policy, most Americans working in health care expressed skepticism or criticism of the nation’s handling of the pandemic. About 39% agreed that the American health care system is “on the verge of collapse.”
Only 21% said the pandemic is mostly or completely under control. About 61% don’t think Americans are taking enough precautions to prevent the spread of the coronavirus.
Health care workers were slightly positive when it comes to the Centers for Disease Control and Prevention (54% approve, 34% disapprove), divided on the Biden administration (41% approve, 40% disapprove), and critical of the news media (20% approve, 61% disapprove) and the American public (18% approve, 68% disapprove).
Broadly, though, health care workers support public health efforts. About 85% back measures that provide N95 masks, and 83% back measures that provide COVID-19 tests.
A version of this article first appeared on WebMD.com.
according to a new poll.
About half of the respondents to the poll from USA Today/Ipsos reported feeling “burned out,” 43% said they were “anxious,” and 21% said they were “angry” about politics and abuse from patients and families.
“We’re trying to help people here, and we are getting verbally and physically abused for it,” Sarah Fried, a nurse in California who responded to the survey, told USA Today in a follow-up interview.
“Early in this pandemic, people were clapping for us and calling us heroes,” she said. “And what happened to that? What happened to them appreciating what nurses are doing?”
The poll was done Feb. 9-16 among 1,170 adults in the U.S. health care industry, including doctors, nurses, paramedics, therapists, home health aides, dentists, and other medical professionals.
A large majority of workers still reported being satisfied with their jobs, although that optimism has declined somewhat since early 2021 when the COVID-19 vaccine rollout was underway. About 80% of those in the recent poll said they were somewhat or very satisfied with their current job, which is down from 89% in an April 2021 poll from Kaiser Family Foundation/the Washington Post.
Most health care workers reported feeling “hopeful” (59%), “motivated” (59%), or “optimistic” (56%) about going to work. But “hopeful” is down from 76% and “optimistic” is down from 67%, compared with last year.
If they could pick a career over again, about 16% disagreed with the statement, “I would still decide to go into health care,” and 18% said they didn’t know how they felt about it.
“The pandemic has actually made me realize how important this career is and how I really do make a difference. I still love it,” Christina Rosa, a mental health counselor in Massachusetts, told USA Today.
During the pandemic, about 66% of those polled said they had treated a COVID-19 patient, which increased to 84% among nurses and 86% among hospital workers. Among those, 47% reported having a patient who died from COVID-19, including 53% of nurses and 55% of hospital workers.
What’s more, 81% of those who treated COVID-19 patients have cared for unvaccinated patients. Among those, 67% said their patients continued to express skepticism toward COVID-19 vaccines, and 38% said some patients expressed regret for not getting a vaccine. Beyond that, 26% said unvaccinated patients asked for unproven treatments, and 30% said the patient or family criticized the care they received.
Regarding coronavirus-related policy, most Americans working in health care expressed skepticism or criticism of the nation’s handling of the pandemic. About 39% agreed that the American health care system is “on the verge of collapse.”
Only 21% said the pandemic is mostly or completely under control. About 61% don’t think Americans are taking enough precautions to prevent the spread of the coronavirus.
Health care workers were slightly positive when it comes to the Centers for Disease Control and Prevention (54% approve, 34% disapprove), divided on the Biden administration (41% approve, 40% disapprove), and critical of the news media (20% approve, 61% disapprove) and the American public (18% approve, 68% disapprove).
Broadly, though, health care workers support public health efforts. About 85% back measures that provide N95 masks, and 83% back measures that provide COVID-19 tests.
A version of this article first appeared on WebMD.com.
CMS updates lung screening criteria, more aligned with USPSTF
for Medicare recipients.
According to the final decision, announced February 10, CMS will lower the age for screening from 55 to 50 years up to 77 years and reduce criteria for tobacco smoking history from at least 30 pack-years to 20 pack-years. The expanded Medicare recommendation will address racial disparities associated with lung cancer, given evidence that one third of Black patients are diagnosed with lung cancer before age 55.
The updated CMS guidelines align closely with recommendations made by the U.S. Preventive Services Task Force (USPSTF) in March 2021. The USPSTF expanded its guidelines for screening to include individuals ages 50 to 80 years, as well as those who have a 20–pack-year smoking history and who currently smoke or have quit within the past 15 years.
Overall, the expanded guidelines will nearly double the number of individuals who are eligible for screening and have the potential to save significantly more lives by identifying cancers at an earlier, more treatable stage.
“Expanding coverage broadens access for lung cancer screening to at-risk populations,” said Lee Felisher, MD, CMS chief medical officer and director of the Center for Clinical Standards and Quality, in a statement. “Today’s decision not only expands access to quality care but is also critical to improving health outcomes for people by helping to detect lung cancer earlier.”
CMS’s decision also simplifies requirements for counseling and shared decision-making visits and removes an initial requirement for the reading radiologist to document participation in continuing medical education, which will reduce administrative burden. CMS also added a requirement back to the National Coverage Determination criteria that requires radiology imaging facilities to use a standardized lung nodule identification, classification, and reporting system.
The American Lung Association applauds the decision to update eligibility.
“[The] announcement from CMS will give more people enrolled in Medicare access to lifesaving lung cancer screening. Screening for individuals at high risk is the only tool to catch this disease early when it is more curable,” Harold Wimmer, president and CEO of the American Lung Association, said in a statement. “Unfortunately, only 5.7% of people who are eligible have been screened, so it’s important that we talk with our friends and family who are at high risk about getting screened.”
While access to screening will significantly increase, the American Lung Association recommends CMS go a step further and expand eligibility to individuals up to 80 years of age, as the USPSTF recommendations do, as well as remove the recommendation that individuals cease screening once they have stopped smoking for 15 years.
Given the new guidelines, most private insurance plans will need to update screening coverage policies to reflect the updated guidelines for plan years beginning after March 31.
To read the final decision, visit the CMS website.
A version of this article first appeared on Medscape.com.
for Medicare recipients.
According to the final decision, announced February 10, CMS will lower the age for screening from 55 to 50 years up to 77 years and reduce criteria for tobacco smoking history from at least 30 pack-years to 20 pack-years. The expanded Medicare recommendation will address racial disparities associated with lung cancer, given evidence that one third of Black patients are diagnosed with lung cancer before age 55.
The updated CMS guidelines align closely with recommendations made by the U.S. Preventive Services Task Force (USPSTF) in March 2021. The USPSTF expanded its guidelines for screening to include individuals ages 50 to 80 years, as well as those who have a 20–pack-year smoking history and who currently smoke or have quit within the past 15 years.
Overall, the expanded guidelines will nearly double the number of individuals who are eligible for screening and have the potential to save significantly more lives by identifying cancers at an earlier, more treatable stage.
“Expanding coverage broadens access for lung cancer screening to at-risk populations,” said Lee Felisher, MD, CMS chief medical officer and director of the Center for Clinical Standards and Quality, in a statement. “Today’s decision not only expands access to quality care but is also critical to improving health outcomes for people by helping to detect lung cancer earlier.”
CMS’s decision also simplifies requirements for counseling and shared decision-making visits and removes an initial requirement for the reading radiologist to document participation in continuing medical education, which will reduce administrative burden. CMS also added a requirement back to the National Coverage Determination criteria that requires radiology imaging facilities to use a standardized lung nodule identification, classification, and reporting system.
The American Lung Association applauds the decision to update eligibility.
“[The] announcement from CMS will give more people enrolled in Medicare access to lifesaving lung cancer screening. Screening for individuals at high risk is the only tool to catch this disease early when it is more curable,” Harold Wimmer, president and CEO of the American Lung Association, said in a statement. “Unfortunately, only 5.7% of people who are eligible have been screened, so it’s important that we talk with our friends and family who are at high risk about getting screened.”
While access to screening will significantly increase, the American Lung Association recommends CMS go a step further and expand eligibility to individuals up to 80 years of age, as the USPSTF recommendations do, as well as remove the recommendation that individuals cease screening once they have stopped smoking for 15 years.
Given the new guidelines, most private insurance plans will need to update screening coverage policies to reflect the updated guidelines for plan years beginning after March 31.
To read the final decision, visit the CMS website.
A version of this article first appeared on Medscape.com.
for Medicare recipients.
According to the final decision, announced February 10, CMS will lower the age for screening from 55 to 50 years up to 77 years and reduce criteria for tobacco smoking history from at least 30 pack-years to 20 pack-years. The expanded Medicare recommendation will address racial disparities associated with lung cancer, given evidence that one third of Black patients are diagnosed with lung cancer before age 55.
The updated CMS guidelines align closely with recommendations made by the U.S. Preventive Services Task Force (USPSTF) in March 2021. The USPSTF expanded its guidelines for screening to include individuals ages 50 to 80 years, as well as those who have a 20–pack-year smoking history and who currently smoke or have quit within the past 15 years.
Overall, the expanded guidelines will nearly double the number of individuals who are eligible for screening and have the potential to save significantly more lives by identifying cancers at an earlier, more treatable stage.
“Expanding coverage broadens access for lung cancer screening to at-risk populations,” said Lee Felisher, MD, CMS chief medical officer and director of the Center for Clinical Standards and Quality, in a statement. “Today’s decision not only expands access to quality care but is also critical to improving health outcomes for people by helping to detect lung cancer earlier.”
CMS’s decision also simplifies requirements for counseling and shared decision-making visits and removes an initial requirement for the reading radiologist to document participation in continuing medical education, which will reduce administrative burden. CMS also added a requirement back to the National Coverage Determination criteria that requires radiology imaging facilities to use a standardized lung nodule identification, classification, and reporting system.
The American Lung Association applauds the decision to update eligibility.
“[The] announcement from CMS will give more people enrolled in Medicare access to lifesaving lung cancer screening. Screening for individuals at high risk is the only tool to catch this disease early when it is more curable,” Harold Wimmer, president and CEO of the American Lung Association, said in a statement. “Unfortunately, only 5.7% of people who are eligible have been screened, so it’s important that we talk with our friends and family who are at high risk about getting screened.”
While access to screening will significantly increase, the American Lung Association recommends CMS go a step further and expand eligibility to individuals up to 80 years of age, as the USPSTF recommendations do, as well as remove the recommendation that individuals cease screening once they have stopped smoking for 15 years.
Given the new guidelines, most private insurance plans will need to update screening coverage policies to reflect the updated guidelines for plan years beginning after March 31.
To read the final decision, visit the CMS website.
A version of this article first appeared on Medscape.com.
FDA hints at deadlines to meet accelerated approval requirements
The FDA launched its accelerated approval program in 1992 in response to the AIDS crisis, but the bulk of approvals since then have been for cancer drugs, wrote the authors who included Gautam U. Mehta, MD, a clinical reviewer with the FDA’s Center for Drug Evaluation and Research; R. Angelo de Claro, MD, associate director of the FDA’s Global Clinical Sciences division within the Oncology Center of Excellence; and Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence.
Accelerated approvals are typically granted in oncology based on overall response rate with a requirement that companies confirm that there’s actually a clinical benefit in postmarketing studies.
The system has inspired European nations and Australia to launch their own programs, but with a key difference: Conditional approvals expire within 1 year or 2.
To be reinstated and remain on the market, companies have to submit a timeline for when they’ll meet their outstanding obligations and demonstrate that the benefit of leaving their product on the market outweighs the risk.
The approach puts “the onus of timely completion of confirmatory trials and verification of benefit” on the drug maker. In the meantime, the system limits “public exposure to stale claims of effectiveness that cannot be expeditiously substantiated,” Dr. Mehta and colleagues wrote.
There aren’t any deadlines in the United States, however, so the FDA has “to initiate a resource-intensive withdrawal process” when proof of clinical benefit is not forthcoming, they said.
In the United States, only 14 of 167 oncology indications granted accelerated approval since 1992 were withdrawn voluntarily and one was withdrawn by FDA request, and one was forced by the agency. The median time from accelerated approval to withdrawal was 8.8 years.
The actual withdrawal process itself took 11 months when bevacizumab’s breast cancer indication was canceled in 2011.
The authors didn’t call for change outright, but they did say that “future discussions of the accelerated approval program in the U.S.” will seek “to coordinate regulatory processes” with other countries, with an eye towards building “harmony between” agencies.
Among other targets for possible harmonization, they noted that only new molecular entities are eligible for accelerated approval in Europe, whereas supplemental indications are also eligible in the United States
Europe also requires a risk-benefit assessment for conditional approvals, which “has led to relatively few approvals based on single-arm clinical trial data,” the authors said.
Dr. Mehta, Dr. de Claro, and Dr. Pazdur had no conflicts of interest.
The FDA launched its accelerated approval program in 1992 in response to the AIDS crisis, but the bulk of approvals since then have been for cancer drugs, wrote the authors who included Gautam U. Mehta, MD, a clinical reviewer with the FDA’s Center for Drug Evaluation and Research; R. Angelo de Claro, MD, associate director of the FDA’s Global Clinical Sciences division within the Oncology Center of Excellence; and Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence.
Accelerated approvals are typically granted in oncology based on overall response rate with a requirement that companies confirm that there’s actually a clinical benefit in postmarketing studies.
The system has inspired European nations and Australia to launch their own programs, but with a key difference: Conditional approvals expire within 1 year or 2.
To be reinstated and remain on the market, companies have to submit a timeline for when they’ll meet their outstanding obligations and demonstrate that the benefit of leaving their product on the market outweighs the risk.
The approach puts “the onus of timely completion of confirmatory trials and verification of benefit” on the drug maker. In the meantime, the system limits “public exposure to stale claims of effectiveness that cannot be expeditiously substantiated,” Dr. Mehta and colleagues wrote.
There aren’t any deadlines in the United States, however, so the FDA has “to initiate a resource-intensive withdrawal process” when proof of clinical benefit is not forthcoming, they said.
In the United States, only 14 of 167 oncology indications granted accelerated approval since 1992 were withdrawn voluntarily and one was withdrawn by FDA request, and one was forced by the agency. The median time from accelerated approval to withdrawal was 8.8 years.
The actual withdrawal process itself took 11 months when bevacizumab’s breast cancer indication was canceled in 2011.
The authors didn’t call for change outright, but they did say that “future discussions of the accelerated approval program in the U.S.” will seek “to coordinate regulatory processes” with other countries, with an eye towards building “harmony between” agencies.
Among other targets for possible harmonization, they noted that only new molecular entities are eligible for accelerated approval in Europe, whereas supplemental indications are also eligible in the United States
Europe also requires a risk-benefit assessment for conditional approvals, which “has led to relatively few approvals based on single-arm clinical trial data,” the authors said.
Dr. Mehta, Dr. de Claro, and Dr. Pazdur had no conflicts of interest.
The FDA launched its accelerated approval program in 1992 in response to the AIDS crisis, but the bulk of approvals since then have been for cancer drugs, wrote the authors who included Gautam U. Mehta, MD, a clinical reviewer with the FDA’s Center for Drug Evaluation and Research; R. Angelo de Claro, MD, associate director of the FDA’s Global Clinical Sciences division within the Oncology Center of Excellence; and Richard Pazdur, MD, director of the FDA’s Oncology Center of Excellence.
Accelerated approvals are typically granted in oncology based on overall response rate with a requirement that companies confirm that there’s actually a clinical benefit in postmarketing studies.
The system has inspired European nations and Australia to launch their own programs, but with a key difference: Conditional approvals expire within 1 year or 2.
To be reinstated and remain on the market, companies have to submit a timeline for when they’ll meet their outstanding obligations and demonstrate that the benefit of leaving their product on the market outweighs the risk.
The approach puts “the onus of timely completion of confirmatory trials and verification of benefit” on the drug maker. In the meantime, the system limits “public exposure to stale claims of effectiveness that cannot be expeditiously substantiated,” Dr. Mehta and colleagues wrote.
There aren’t any deadlines in the United States, however, so the FDA has “to initiate a resource-intensive withdrawal process” when proof of clinical benefit is not forthcoming, they said.
In the United States, only 14 of 167 oncology indications granted accelerated approval since 1992 were withdrawn voluntarily and one was withdrawn by FDA request, and one was forced by the agency. The median time from accelerated approval to withdrawal was 8.8 years.
The actual withdrawal process itself took 11 months when bevacizumab’s breast cancer indication was canceled in 2011.
The authors didn’t call for change outright, but they did say that “future discussions of the accelerated approval program in the U.S.” will seek “to coordinate regulatory processes” with other countries, with an eye towards building “harmony between” agencies.
Among other targets for possible harmonization, they noted that only new molecular entities are eligible for accelerated approval in Europe, whereas supplemental indications are also eligible in the United States
Europe also requires a risk-benefit assessment for conditional approvals, which “has led to relatively few approvals based on single-arm clinical trial data,” the authors said.
Dr. Mehta, Dr. de Claro, and Dr. Pazdur had no conflicts of interest.
FROM JAMA ONCOLOGY
Tips for connecting with your patients
It is a tough time to be a doctor. With the stresses of the pandemic, the continued unfettered rise of insurance company BS, and so many medical groups being bought up that we often don’t even know who makes the decisions, the patient can sometimes be hidden in the equation.

Be curious
When physicians are curious about why patients have symptoms, how those symptoms will affect their lives, and how worried the patient is about them, patients feel cared about.
Ascertaining how concerned patients are about their symptoms will help you make decisions on whether symptoms you are not concerned about actually need to be treated.
Limit use of EHRs when possible
Use of the electronic health record during visits is essential, but focusing on it too much can put a barrier between the physician and the patient.
Marmor and colleagues found there is an inverse relationship between time spent on the EHR by a patient’s physician and the patient’s satisfaction.1
Eye contact with the patient is important, especially when patients are sharing concerns they are scared about and upsetting experiences. There can be awkward pauses when looking things up on the EHR. Fill those pauses by explaining to the patient what you are doing, or chatting with the patient.
Consider teaching medical students
When a medical student works with you, it doubles the time the patient gets with a concerned listener. Students also can do a great job with timely follow-up and checking in with worried patients.
By having the student present in the clinic room, with the patient present, the patient can really feel heard. The student shares all the details the patient shared, and now their physician is hearing an organized, thoughtful report of the patients concerns.
In fact, I was involved in a study that showed that patients preferred in room presentations, and that they were more satisfied when students presented in the room.2
Use healing words
Some words carry loaded emotions. The word chronic, for example, has negative connotations, whereas the term persisting does not.
I will often ask patients how long they have been suffering from a symptom to imply my concern for what they are going through. The term “chief complaint” is outdated, and upsets patients when they see it in their medical record.
As a patient of mine once said to me: “I never complained about that problem, I just brought it to your attention.” No one wants to be seen as a complainer. Substituting the word concern for complaint works well.
Explain as you examine
People love to hear the term normal. When you are examining a patient, let them know when findings are normal.
I also find it helpful to explain to patients why I am doing certain physical exam maneuvers. This helps them assess how thorough we are in our thought process.
When patients feel their physicians are thorough, they have more confidence in them.
In summary
- Be curious.
- Do not overly focus on the EHR.
- Consider teaching a medical student.
- Be careful of word choice.
- “Overexplain” the physical exam.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Marmor RA et al. Appl Clin Inform. 2018 Jan;9(1):11-4.
2. Rogers HD et al. Acad Med. 2003 Sep;78(9):945-9.
It is a tough time to be a doctor. With the stresses of the pandemic, the continued unfettered rise of insurance company BS, and so many medical groups being bought up that we often don’t even know who makes the decisions, the patient can sometimes be hidden in the equation.
Be curious
When physicians are curious about why patients have symptoms, how those symptoms will affect their lives, and how worried the patient is about them, patients feel cared about.
Ascertaining how concerned patients are about their symptoms will help you make decisions on whether symptoms you are not concerned about actually need to be treated.
Limit use of EHRs when possible
Use of the electronic health record during visits is essential, but focusing on it too much can put a barrier between the physician and the patient.
Marmor and colleagues found there is an inverse relationship between time spent on the EHR by a patient’s physician and the patient’s satisfaction.1
Eye contact with the patient is important, especially when patients are sharing concerns they are scared about and upsetting experiences. There can be awkward pauses when looking things up on the EHR. Fill those pauses by explaining to the patient what you are doing, or chatting with the patient.
Consider teaching medical students
When a medical student works with you, it doubles the time the patient gets with a concerned listener. Students also can do a great job with timely follow-up and checking in with worried patients.
By having the student present in the clinic room, with the patient present, the patient can really feel heard. The student shares all the details the patient shared, and now their physician is hearing an organized, thoughtful report of the patients concerns.
In fact, I was involved in a study that showed that patients preferred in room presentations, and that they were more satisfied when students presented in the room.2
Use healing words
Some words carry loaded emotions. The word chronic, for example, has negative connotations, whereas the term persisting does not.
I will often ask patients how long they have been suffering from a symptom to imply my concern for what they are going through. The term “chief complaint” is outdated, and upsets patients when they see it in their medical record.
As a patient of mine once said to me: “I never complained about that problem, I just brought it to your attention.” No one wants to be seen as a complainer. Substituting the word concern for complaint works well.
Explain as you examine
People love to hear the term normal. When you are examining a patient, let them know when findings are normal.
I also find it helpful to explain to patients why I am doing certain physical exam maneuvers. This helps them assess how thorough we are in our thought process.
When patients feel their physicians are thorough, they have more confidence in them.
In summary
- Be curious.
- Do not overly focus on the EHR.
- Consider teaching a medical student.
- Be careful of word choice.
- “Overexplain” the physical exam.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Marmor RA et al. Appl Clin Inform. 2018 Jan;9(1):11-4.
2. Rogers HD et al. Acad Med. 2003 Sep;78(9):945-9.
It is a tough time to be a doctor. With the stresses of the pandemic, the continued unfettered rise of insurance company BS, and so many medical groups being bought up that we often don’t even know who makes the decisions, the patient can sometimes be hidden in the equation.
Be curious
When physicians are curious about why patients have symptoms, how those symptoms will affect their lives, and how worried the patient is about them, patients feel cared about.
Ascertaining how concerned patients are about their symptoms will help you make decisions on whether symptoms you are not concerned about actually need to be treated.
Limit use of EHRs when possible
Use of the electronic health record during visits is essential, but focusing on it too much can put a barrier between the physician and the patient.
Marmor and colleagues found there is an inverse relationship between time spent on the EHR by a patient’s physician and the patient’s satisfaction.1
Eye contact with the patient is important, especially when patients are sharing concerns they are scared about and upsetting experiences. There can be awkward pauses when looking things up on the EHR. Fill those pauses by explaining to the patient what you are doing, or chatting with the patient.
Consider teaching medical students
When a medical student works with you, it doubles the time the patient gets with a concerned listener. Students also can do a great job with timely follow-up and checking in with worried patients.
By having the student present in the clinic room, with the patient present, the patient can really feel heard. The student shares all the details the patient shared, and now their physician is hearing an organized, thoughtful report of the patients concerns.
In fact, I was involved in a study that showed that patients preferred in room presentations, and that they were more satisfied when students presented in the room.2
Use healing words
Some words carry loaded emotions. The word chronic, for example, has negative connotations, whereas the term persisting does not.
I will often ask patients how long they have been suffering from a symptom to imply my concern for what they are going through. The term “chief complaint” is outdated, and upsets patients when they see it in their medical record.
As a patient of mine once said to me: “I never complained about that problem, I just brought it to your attention.” No one wants to be seen as a complainer. Substituting the word concern for complaint works well.
Explain as you examine
People love to hear the term normal. When you are examining a patient, let them know when findings are normal.
I also find it helpful to explain to patients why I am doing certain physical exam maneuvers. This helps them assess how thorough we are in our thought process.
When patients feel their physicians are thorough, they have more confidence in them.
In summary
- Be curious.
- Do not overly focus on the EHR.
- Consider teaching a medical student.
- Be careful of word choice.
- “Overexplain” the physical exam.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as 3rd-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at imnews@mdedge.com.
References
1. Marmor RA et al. Appl Clin Inform. 2018 Jan;9(1):11-4.
2. Rogers HD et al. Acad Med. 2003 Sep;78(9):945-9.
City of Hope completes acquisition of CTCA
The combined group now has 575 physicians and more than 11,000 employees and is expected to care for approximately 115,000 patients each year.
City of Hope, a National Cancer Institute–designated comprehensive cancer center, is located near Los Angeles. It currently comprises its main campus and a network of clinical care locations across Southern California. A new campus is scheduled to open this year in Irvine, California, about 50 miles south of the main center.
The acquisition of CTCA expands its reach into three new states – Arizona, Illinois, and Georgia – with an additional 41 clinical network locations.
Commenting on the completion of the deal, Robert Stone, president and CEO of City of Hope, said in a statement: “With the completion of this acquisition, City of Hope and Cancer Treatment Centers of America are combining complementary strengths. ... Together, we are creating a new model for how cancer care is delivered, leveraging real-world cancer care experience to inform scientific innovation and making tomorrow’s new discoveries available to the people who need them today.”
City of Hope announced in December 2020 that it would acquire CTCA for $390 million, as previously reported by this news organization.
At the time, Pat Basu MD, MBA, president and CEO of CTCA, said that they were excited about the deal. “Through the shared, patient-centric values of both organizations and expanded access as a result of the collaboration, cancer patients across the nation will be the ultimate beneficiaries of this relationship,” he said. Dr. Basu will remain CEO of CTCA and report to Robert Stone.
Controversies and closures
CTCA is a national oncology network of hospitals and outpatient care centers that offers an integrated approach to care, including surgery, radiotherapy, chemotherapy, immunotherapy, and advancements in precision medicine with supportive therapies to manage side effects and enhance quality of life during treatment and into survivorship.
However, it appears to have run into financial problems. During 2021, CTCA closed a center in Tulsa, Oklahoma, and sold off assets from a Philadelphia-based hospital.
In addition, for the past 10 years, CTCA had been involved in a series of controversies. These include a 2013 investigation into alleged questionable practices designed to boost its mortality statistics, as well as an analysis of cancer center advertising practices that showed that CTCA spent $101.7 million on advertising in 2014. More recently, a 2019 report showed that CTCA’s high advertising expenditures did not correlate with better patient outcomes in comparison with other centers.
Now that it has been acquired, CTCA will transition from a private for-profit company to a nonprofit organization, according to City of Hope.
A version of this article first appeared on Medscape.com.
The combined group now has 575 physicians and more than 11,000 employees and is expected to care for approximately 115,000 patients each year.
City of Hope, a National Cancer Institute–designated comprehensive cancer center, is located near Los Angeles. It currently comprises its main campus and a network of clinical care locations across Southern California. A new campus is scheduled to open this year in Irvine, California, about 50 miles south of the main center.
The acquisition of CTCA expands its reach into three new states – Arizona, Illinois, and Georgia – with an additional 41 clinical network locations.
Commenting on the completion of the deal, Robert Stone, president and CEO of City of Hope, said in a statement: “With the completion of this acquisition, City of Hope and Cancer Treatment Centers of America are combining complementary strengths. ... Together, we are creating a new model for how cancer care is delivered, leveraging real-world cancer care experience to inform scientific innovation and making tomorrow’s new discoveries available to the people who need them today.”
City of Hope announced in December 2020 that it would acquire CTCA for $390 million, as previously reported by this news organization.
At the time, Pat Basu MD, MBA, president and CEO of CTCA, said that they were excited about the deal. “Through the shared, patient-centric values of both organizations and expanded access as a result of the collaboration, cancer patients across the nation will be the ultimate beneficiaries of this relationship,” he said. Dr. Basu will remain CEO of CTCA and report to Robert Stone.
Controversies and closures
CTCA is a national oncology network of hospitals and outpatient care centers that offers an integrated approach to care, including surgery, radiotherapy, chemotherapy, immunotherapy, and advancements in precision medicine with supportive therapies to manage side effects and enhance quality of life during treatment and into survivorship.
However, it appears to have run into financial problems. During 2021, CTCA closed a center in Tulsa, Oklahoma, and sold off assets from a Philadelphia-based hospital.
In addition, for the past 10 years, CTCA had been involved in a series of controversies. These include a 2013 investigation into alleged questionable practices designed to boost its mortality statistics, as well as an analysis of cancer center advertising practices that showed that CTCA spent $101.7 million on advertising in 2014. More recently, a 2019 report showed that CTCA’s high advertising expenditures did not correlate with better patient outcomes in comparison with other centers.
Now that it has been acquired, CTCA will transition from a private for-profit company to a nonprofit organization, according to City of Hope.
A version of this article first appeared on Medscape.com.
The combined group now has 575 physicians and more than 11,000 employees and is expected to care for approximately 115,000 patients each year.
City of Hope, a National Cancer Institute–designated comprehensive cancer center, is located near Los Angeles. It currently comprises its main campus and a network of clinical care locations across Southern California. A new campus is scheduled to open this year in Irvine, California, about 50 miles south of the main center.
The acquisition of CTCA expands its reach into three new states – Arizona, Illinois, and Georgia – with an additional 41 clinical network locations.
Commenting on the completion of the deal, Robert Stone, president and CEO of City of Hope, said in a statement: “With the completion of this acquisition, City of Hope and Cancer Treatment Centers of America are combining complementary strengths. ... Together, we are creating a new model for how cancer care is delivered, leveraging real-world cancer care experience to inform scientific innovation and making tomorrow’s new discoveries available to the people who need them today.”
City of Hope announced in December 2020 that it would acquire CTCA for $390 million, as previously reported by this news organization.
At the time, Pat Basu MD, MBA, president and CEO of CTCA, said that they were excited about the deal. “Through the shared, patient-centric values of both organizations and expanded access as a result of the collaboration, cancer patients across the nation will be the ultimate beneficiaries of this relationship,” he said. Dr. Basu will remain CEO of CTCA and report to Robert Stone.
Controversies and closures
CTCA is a national oncology network of hospitals and outpatient care centers that offers an integrated approach to care, including surgery, radiotherapy, chemotherapy, immunotherapy, and advancements in precision medicine with supportive therapies to manage side effects and enhance quality of life during treatment and into survivorship.
However, it appears to have run into financial problems. During 2021, CTCA closed a center in Tulsa, Oklahoma, and sold off assets from a Philadelphia-based hospital.
In addition, for the past 10 years, CTCA had been involved in a series of controversies. These include a 2013 investigation into alleged questionable practices designed to boost its mortality statistics, as well as an analysis of cancer center advertising practices that showed that CTCA spent $101.7 million on advertising in 2014. More recently, a 2019 report showed that CTCA’s high advertising expenditures did not correlate with better patient outcomes in comparison with other centers.
Now that it has been acquired, CTCA will transition from a private for-profit company to a nonprofit organization, according to City of Hope.
A version of this article first appeared on Medscape.com.
President Biden’s ‘Cancer Moonshot’ to be relaunched
The “Cancer Moonshot” is about to be relaunched.
In a White House briefing, President Joe Biden announced that he is “reigniting” the initiative he spearheaded when he was vice president during the Obama administration.
During the livestreamed event, the president discussed his plans to bring a “fierce sense of urgency” to the fight against cancer and better support patients with cancer and their families.
He emphasized that cancer is one of the truly bipartisan issues. There is strong support from both “sides of the aisle,” he said, and he sees it as an issue that can bring the country together.
“We can do this. I promise you, we can do this. For all those we lost, for all those we miss. We can end cancer as we know it,” he said. “This is a presidential White House priority.”
The aim is to reduce the death rate from cancer by at least 50% over the next 25 years.
There is also a proposal to create the Advanced Research Projects Agency for Health, which would focus on driving cutting-edge innovation in health research.
Part of the plan is to assemble a “cancer cabinet” that includes 18 federal departments, agencies, and offices, including leaders from the departments of Health & Human Services, Veterans Affairs, Defense, Energy, and Agriculture.
At present, there are few details about the new program or how it will be funded.
Presumably more will be revealed at the Cancer Moonshot Summit being planned, as well as on a planned new website where people can track its progress.
President priority
Cancer Moonshot began back in 2016, when during his last State of the Union Address, former President Barack Obama announced the ambitious initiative. A few days later, Obama asked Congress for $1 billion to send cancer to the moon, and he put Biden, then vice president, in charge of “mission control” in the remaining months of the administration.
The new initiative will be headed by Danielle Carnival, PhD, who serves in the White House Office of Science and Technology Policy and has been appointed as White House Cancer Moonshot coordinator.
At the briefing, Mr. Biden and Vice President Kamala Harris spoke about losing family members to cancer. The president spoke about his eldest son, Beau, who died from brain cancer when he was 46 years old, while Ms. Harris spoke about her mother, Shyamala Gopalan, a breast cancer researcher who died of colon cancer in 2009.
Accolades but a bit of caution
The president’s speech was applauded by many cancer groups, both professional organizations and patient advocacy groups.
Karen E. Knudsen, PhD, chief executive officer of the American Cancer Society and its advocacy affiliate, the American Cancer Society Cancer Action Network, commended Mr. Biden for reigniting Cancer Moonshot.
“In 2022 alone, there will be an estimated 1.9 million people diagnosed with cancer and more than 600,000 people in the U.S. will die. Marshaling the resources of the federal government will be critical in our ability to reduce death and suffering from this disease,” she said.
The American Society for Radiation Oncology issued a press release, saying: “On behalf of radiation oncologists who treat people with cancer every day, we support the Biden-Harris administration’s move to drastically reduce the number of cancer deaths in the United States and improve the lives of people diagnosed with this disease.
“We believe the administration’s commitment to expand cancer prevention efforts and to increase equitable access to screenings and treatments will help mitigate some of the negative impact of the COVID-19 pandemic,” the society added.
At the American Association for Cancer Research, Chief Executive Officer Margaret Foti, MD, PhD, said she was thrilled to hear the announcement after the devastating interruptions in cancer research and patient care over the past 2 years.
“The reignited Cancer Moonshot will provide an important framework to help improve cancer prevention strategies, increase cancer screenings and early detection, reduce cancer disparities, and propel new lifesaving cures for patients with cancer,” she said.
However, increased funding from Congress will be needed for these goals to be achieved, she emphasized.
A version of this article first appeared on Medscape.com.
The “Cancer Moonshot” is about to be relaunched.
In a White House briefing, President Joe Biden announced that he is “reigniting” the initiative he spearheaded when he was vice president during the Obama administration.
During the livestreamed event, the president discussed his plans to bring a “fierce sense of urgency” to the fight against cancer and better support patients with cancer and their families.
He emphasized that cancer is one of the truly bipartisan issues. There is strong support from both “sides of the aisle,” he said, and he sees it as an issue that can bring the country together.
“We can do this. I promise you, we can do this. For all those we lost, for all those we miss. We can end cancer as we know it,” he said. “This is a presidential White House priority.”
The aim is to reduce the death rate from cancer by at least 50% over the next 25 years.
There is also a proposal to create the Advanced Research Projects Agency for Health, which would focus on driving cutting-edge innovation in health research.
Part of the plan is to assemble a “cancer cabinet” that includes 18 federal departments, agencies, and offices, including leaders from the departments of Health & Human Services, Veterans Affairs, Defense, Energy, and Agriculture.
At present, there are few details about the new program or how it will be funded.
Presumably more will be revealed at the Cancer Moonshot Summit being planned, as well as on a planned new website where people can track its progress.
President priority
Cancer Moonshot began back in 2016, when during his last State of the Union Address, former President Barack Obama announced the ambitious initiative. A few days later, Obama asked Congress for $1 billion to send cancer to the moon, and he put Biden, then vice president, in charge of “mission control” in the remaining months of the administration.
The new initiative will be headed by Danielle Carnival, PhD, who serves in the White House Office of Science and Technology Policy and has been appointed as White House Cancer Moonshot coordinator.
At the briefing, Mr. Biden and Vice President Kamala Harris spoke about losing family members to cancer. The president spoke about his eldest son, Beau, who died from brain cancer when he was 46 years old, while Ms. Harris spoke about her mother, Shyamala Gopalan, a breast cancer researcher who died of colon cancer in 2009.
Accolades but a bit of caution
The president’s speech was applauded by many cancer groups, both professional organizations and patient advocacy groups.
Karen E. Knudsen, PhD, chief executive officer of the American Cancer Society and its advocacy affiliate, the American Cancer Society Cancer Action Network, commended Mr. Biden for reigniting Cancer Moonshot.
“In 2022 alone, there will be an estimated 1.9 million people diagnosed with cancer and more than 600,000 people in the U.S. will die. Marshaling the resources of the federal government will be critical in our ability to reduce death and suffering from this disease,” she said.
The American Society for Radiation Oncology issued a press release, saying: “On behalf of radiation oncologists who treat people with cancer every day, we support the Biden-Harris administration’s move to drastically reduce the number of cancer deaths in the United States and improve the lives of people diagnosed with this disease.
“We believe the administration’s commitment to expand cancer prevention efforts and to increase equitable access to screenings and treatments will help mitigate some of the negative impact of the COVID-19 pandemic,” the society added.
At the American Association for Cancer Research, Chief Executive Officer Margaret Foti, MD, PhD, said she was thrilled to hear the announcement after the devastating interruptions in cancer research and patient care over the past 2 years.
“The reignited Cancer Moonshot will provide an important framework to help improve cancer prevention strategies, increase cancer screenings and early detection, reduce cancer disparities, and propel new lifesaving cures for patients with cancer,” she said.
However, increased funding from Congress will be needed for these goals to be achieved, she emphasized.
A version of this article first appeared on Medscape.com.
The “Cancer Moonshot” is about to be relaunched.
In a White House briefing, President Joe Biden announced that he is “reigniting” the initiative he spearheaded when he was vice president during the Obama administration.
During the livestreamed event, the president discussed his plans to bring a “fierce sense of urgency” to the fight against cancer and better support patients with cancer and their families.
He emphasized that cancer is one of the truly bipartisan issues. There is strong support from both “sides of the aisle,” he said, and he sees it as an issue that can bring the country together.
“We can do this. I promise you, we can do this. For all those we lost, for all those we miss. We can end cancer as we know it,” he said. “This is a presidential White House priority.”
The aim is to reduce the death rate from cancer by at least 50% over the next 25 years.
There is also a proposal to create the Advanced Research Projects Agency for Health, which would focus on driving cutting-edge innovation in health research.
Part of the plan is to assemble a “cancer cabinet” that includes 18 federal departments, agencies, and offices, including leaders from the departments of Health & Human Services, Veterans Affairs, Defense, Energy, and Agriculture.
At present, there are few details about the new program or how it will be funded.
Presumably more will be revealed at the Cancer Moonshot Summit being planned, as well as on a planned new website where people can track its progress.
President priority
Cancer Moonshot began back in 2016, when during his last State of the Union Address, former President Barack Obama announced the ambitious initiative. A few days later, Obama asked Congress for $1 billion to send cancer to the moon, and he put Biden, then vice president, in charge of “mission control” in the remaining months of the administration.
The new initiative will be headed by Danielle Carnival, PhD, who serves in the White House Office of Science and Technology Policy and has been appointed as White House Cancer Moonshot coordinator.
At the briefing, Mr. Biden and Vice President Kamala Harris spoke about losing family members to cancer. The president spoke about his eldest son, Beau, who died from brain cancer when he was 46 years old, while Ms. Harris spoke about her mother, Shyamala Gopalan, a breast cancer researcher who died of colon cancer in 2009.
Accolades but a bit of caution
The president’s speech was applauded by many cancer groups, both professional organizations and patient advocacy groups.
Karen E. Knudsen, PhD, chief executive officer of the American Cancer Society and its advocacy affiliate, the American Cancer Society Cancer Action Network, commended Mr. Biden for reigniting Cancer Moonshot.
“In 2022 alone, there will be an estimated 1.9 million people diagnosed with cancer and more than 600,000 people in the U.S. will die. Marshaling the resources of the federal government will be critical in our ability to reduce death and suffering from this disease,” she said.
The American Society for Radiation Oncology issued a press release, saying: “On behalf of radiation oncologists who treat people with cancer every day, we support the Biden-Harris administration’s move to drastically reduce the number of cancer deaths in the United States and improve the lives of people diagnosed with this disease.
“We believe the administration’s commitment to expand cancer prevention efforts and to increase equitable access to screenings and treatments will help mitigate some of the negative impact of the COVID-19 pandemic,” the society added.
At the American Association for Cancer Research, Chief Executive Officer Margaret Foti, MD, PhD, said she was thrilled to hear the announcement after the devastating interruptions in cancer research and patient care over the past 2 years.
“The reignited Cancer Moonshot will provide an important framework to help improve cancer prevention strategies, increase cancer screenings and early detection, reduce cancer disparities, and propel new lifesaving cures for patients with cancer,” she said.
However, increased funding from Congress will be needed for these goals to be achieved, she emphasized.
A version of this article first appeared on Medscape.com.