User login
Mavoglurant disappoints in fragile X trials
The selective metabotropic glutamate receptor 5 (mGluR5) antagonist mavoglurant failed to improve behavioral symptoms in patients with fragile X syndrome in two phase IIb, multicenter, randomized, placebo-controlled studies.
A post hoc analysis of a prior phase II trial suggested that mavoglurant improved such symptoms in fragile X syndrome patients with completely methylated FMR1 genes, and the current trials were designed to confirm the findings in 175 adults and 139 adolescents, respectively.
But no change in maladaptive behavior, as measured using the Aberrant Behavior Checklist–Community Edition and fragile X syndrome-specific algorithm (ABC-Cfx), was seen 12 weeks after treatment with either 25, 50, or 100 mg of mavoglurant or placebo twice daily for 12 weeks, Dr. Elizabeth Berry-Kravis of Rush University Medical Center, Chicago, and her colleagues reported online Jan. 13 in Science Translational Medicine.
In completely methylated adults, the change in ABC-Cfx score at 12 weeks was similar with placebo and 25 mg mavoglurant (–11.4 and –14.3), and nearly unchanged with 50 and 100 mg of mavoglurant (1.8, -1.8). In adolescents, the corresponding changes were –9.4, –11.8, –3.4, and 8.6 (a statistically significant deterioration vs. placebo). Outcomes were similar in partially methylated adults and adolescents.
Since the primary efficacy endpoint of improvement in behavioral symptoms was not met, the mGluR theory of fragile X syndrome as suggested by animal models – namely that the absence of fragile X mental retardation protein can cause overactivation of mGluR signaling, contributing to the features of the fragile X syndrome phenotype – could not be confirmed, nor could the ability of the methylation state of the FMR1 promoter to predict mavoglurant efficacy, the investigators wrote (Sci Transl Med. 2016 Jan. 13. doi:10.1126/scitranslmed.aab4109).
“One of the most plausible explanations for the negative results is that the mGluR theory on which the studies were based may not be valid or may manifest itself differently in humans, compared to rodents,” they wrote, noting that a combination of targeted treatments may be needed for optimal treatment of fragile X syndrome. Further, preclinical trials suggested that treatment at a younger age and for longer durations might have a greater effect; this approach warrants evaluation in a future trial, they wrote.
This study was supported by Novartis Pharma AG. Dr. Berry-Kravis has served on the Novartis Fragile X Advisory Board and has consulted for Novartis. Other authors also served on the board and have consulted for Novartis and/or Roche, or are employed by Novartis.
The findings of Dr. Berry-Kravis et al. yield important lessons for clinical trial design. Rather than concluding that the negative findings prove that a treatment is ineffective or that presumed underlying pathophysiological mechanisms are invalid, trials like this one provide an opportunity to reflect on clinical trial design and implementation, as well as the underlying mechanistic motivations, and provide lessons for treatment studies of neurodevelopmental disorders in general. This trial highlights key themes to consider in clinical trials, including choice of treatment group, target engagement, selection of outcome measures, and the impact of the placebo effect.
We stand at a therapeutic frontier, with much more to learn. While the result of negative trials are disappointing, they also can be crucial for refining hypotheses and encouraging dialogue to accelerate the process of bringing effective treatments to our patients.
Dr. Shafali S. Jeste and Dr. Daniel H. Geschwind are with the University of California at Los Angeles. These comments are adapted from an accompanying editorial (Sci Transl Med. 2016 Jan 13. doi:10.1126/scitranslmed.aab4109.). The authors did not report financial disclosures.
The findings of Dr. Berry-Kravis et al. yield important lessons for clinical trial design. Rather than concluding that the negative findings prove that a treatment is ineffective or that presumed underlying pathophysiological mechanisms are invalid, trials like this one provide an opportunity to reflect on clinical trial design and implementation, as well as the underlying mechanistic motivations, and provide lessons for treatment studies of neurodevelopmental disorders in general. This trial highlights key themes to consider in clinical trials, including choice of treatment group, target engagement, selection of outcome measures, and the impact of the placebo effect.
We stand at a therapeutic frontier, with much more to learn. While the result of negative trials are disappointing, they also can be crucial for refining hypotheses and encouraging dialogue to accelerate the process of bringing effective treatments to our patients.
Dr. Shafali S. Jeste and Dr. Daniel H. Geschwind are with the University of California at Los Angeles. These comments are adapted from an accompanying editorial (Sci Transl Med. 2016 Jan 13. doi:10.1126/scitranslmed.aab4109.). The authors did not report financial disclosures.
The findings of Dr. Berry-Kravis et al. yield important lessons for clinical trial design. Rather than concluding that the negative findings prove that a treatment is ineffective or that presumed underlying pathophysiological mechanisms are invalid, trials like this one provide an opportunity to reflect on clinical trial design and implementation, as well as the underlying mechanistic motivations, and provide lessons for treatment studies of neurodevelopmental disorders in general. This trial highlights key themes to consider in clinical trials, including choice of treatment group, target engagement, selection of outcome measures, and the impact of the placebo effect.
We stand at a therapeutic frontier, with much more to learn. While the result of negative trials are disappointing, they also can be crucial for refining hypotheses and encouraging dialogue to accelerate the process of bringing effective treatments to our patients.
Dr. Shafali S. Jeste and Dr. Daniel H. Geschwind are with the University of California at Los Angeles. These comments are adapted from an accompanying editorial (Sci Transl Med. 2016 Jan 13. doi:10.1126/scitranslmed.aab4109.). The authors did not report financial disclosures.
The selective metabotropic glutamate receptor 5 (mGluR5) antagonist mavoglurant failed to improve behavioral symptoms in patients with fragile X syndrome in two phase IIb, multicenter, randomized, placebo-controlled studies.
A post hoc analysis of a prior phase II trial suggested that mavoglurant improved such symptoms in fragile X syndrome patients with completely methylated FMR1 genes, and the current trials were designed to confirm the findings in 175 adults and 139 adolescents, respectively.
But no change in maladaptive behavior, as measured using the Aberrant Behavior Checklist–Community Edition and fragile X syndrome-specific algorithm (ABC-Cfx), was seen 12 weeks after treatment with either 25, 50, or 100 mg of mavoglurant or placebo twice daily for 12 weeks, Dr. Elizabeth Berry-Kravis of Rush University Medical Center, Chicago, and her colleagues reported online Jan. 13 in Science Translational Medicine.
In completely methylated adults, the change in ABC-Cfx score at 12 weeks was similar with placebo and 25 mg mavoglurant (–11.4 and –14.3), and nearly unchanged with 50 and 100 mg of mavoglurant (1.8, -1.8). In adolescents, the corresponding changes were –9.4, –11.8, –3.4, and 8.6 (a statistically significant deterioration vs. placebo). Outcomes were similar in partially methylated adults and adolescents.
Since the primary efficacy endpoint of improvement in behavioral symptoms was not met, the mGluR theory of fragile X syndrome as suggested by animal models – namely that the absence of fragile X mental retardation protein can cause overactivation of mGluR signaling, contributing to the features of the fragile X syndrome phenotype – could not be confirmed, nor could the ability of the methylation state of the FMR1 promoter to predict mavoglurant efficacy, the investigators wrote (Sci Transl Med. 2016 Jan. 13. doi:10.1126/scitranslmed.aab4109).
“One of the most plausible explanations for the negative results is that the mGluR theory on which the studies were based may not be valid or may manifest itself differently in humans, compared to rodents,” they wrote, noting that a combination of targeted treatments may be needed for optimal treatment of fragile X syndrome. Further, preclinical trials suggested that treatment at a younger age and for longer durations might have a greater effect; this approach warrants evaluation in a future trial, they wrote.
This study was supported by Novartis Pharma AG. Dr. Berry-Kravis has served on the Novartis Fragile X Advisory Board and has consulted for Novartis. Other authors also served on the board and have consulted for Novartis and/or Roche, or are employed by Novartis.
The selective metabotropic glutamate receptor 5 (mGluR5) antagonist mavoglurant failed to improve behavioral symptoms in patients with fragile X syndrome in two phase IIb, multicenter, randomized, placebo-controlled studies.
A post hoc analysis of a prior phase II trial suggested that mavoglurant improved such symptoms in fragile X syndrome patients with completely methylated FMR1 genes, and the current trials were designed to confirm the findings in 175 adults and 139 adolescents, respectively.
But no change in maladaptive behavior, as measured using the Aberrant Behavior Checklist–Community Edition and fragile X syndrome-specific algorithm (ABC-Cfx), was seen 12 weeks after treatment with either 25, 50, or 100 mg of mavoglurant or placebo twice daily for 12 weeks, Dr. Elizabeth Berry-Kravis of Rush University Medical Center, Chicago, and her colleagues reported online Jan. 13 in Science Translational Medicine.
In completely methylated adults, the change in ABC-Cfx score at 12 weeks was similar with placebo and 25 mg mavoglurant (–11.4 and –14.3), and nearly unchanged with 50 and 100 mg of mavoglurant (1.8, -1.8). In adolescents, the corresponding changes were –9.4, –11.8, –3.4, and 8.6 (a statistically significant deterioration vs. placebo). Outcomes were similar in partially methylated adults and adolescents.
Since the primary efficacy endpoint of improvement in behavioral symptoms was not met, the mGluR theory of fragile X syndrome as suggested by animal models – namely that the absence of fragile X mental retardation protein can cause overactivation of mGluR signaling, contributing to the features of the fragile X syndrome phenotype – could not be confirmed, nor could the ability of the methylation state of the FMR1 promoter to predict mavoglurant efficacy, the investigators wrote (Sci Transl Med. 2016 Jan. 13. doi:10.1126/scitranslmed.aab4109).
“One of the most plausible explanations for the negative results is that the mGluR theory on which the studies were based may not be valid or may manifest itself differently in humans, compared to rodents,” they wrote, noting that a combination of targeted treatments may be needed for optimal treatment of fragile X syndrome. Further, preclinical trials suggested that treatment at a younger age and for longer durations might have a greater effect; this approach warrants evaluation in a future trial, they wrote.
This study was supported by Novartis Pharma AG. Dr. Berry-Kravis has served on the Novartis Fragile X Advisory Board and has consulted for Novartis. Other authors also served on the board and have consulted for Novartis and/or Roche, or are employed by Novartis.
FROM SCIENCE TRANSLATIONAL MEDICINE
Key clinical point: The selective metabotropic glutamate receptor 5 (mGluR5) antagonist mavoglurant failed to improve behavioral symptoms in patients with fragile X syndrome in two phase 2b, multicenter, randomized, placebo-controlled studies.
Major finding: Change in ABC-Cfx score in completely methylated adults was –11.4, –14.3, 1.8 and –1.8 with placebo, 25, 50 and 100 mg of mavoglurant, respectively. In adolescents, the corresponding changes were –9.4, –11.8, –3.4, and 8.6.
Data source: A phase 2b randomized placebo-controlled trial involving 175 adults and 139 adolescents.
Disclosures: This study was supported by Novartis Pharma AG. Dr. Berry-Kravis has served on the Novartis Fragile X Advisory Board and has consulted for Novartis. Other authors also served on the board and have consulted for Novartis and/or Roche, or are employed by Novartis.
Pertussis Vaccine Possibly Ineffective in Preschoolers
Preschool-age children who have been fully vaccinated against pertussis can still develop symptoms of illness consistent with a whooping cough diagnosis, according to a study of toddlers in a Tallahassee, Fla., school that experienced an outbreak of pertussis in late 2013 (Emerg Infect Dis. 2016 Feb;22[2]. doi: 10.3201/eid2202.150325)
The study, published in Emerging Infectious Diseases by the Centers for Disease Control and Prevention, is the result of an outbreak investigation at the preschool that began after a 1-year-old and two 3-year-old children developed illness consistent with pertussis, and were confirmed to have pertussis after undergoing a polymerase chain reaction (PCR) test.

The Florida Department of Health administered a questionnaire to be completed by families of the 117 students (ages 10 months to 6 years) and 26 staff members. Questionnaire completion rate was 98%, with three student households and one staff household failing to complete it.
Overall, 28 cases were determined to be “probable” pertussis and 11 were confirmed as pertussis via PCR or other laboratory testing methods. Of these, 26 were students aged 1-5 years (22% of total student population), 2 were attributed to the staff (7%), and 11 were linked to the preschool, of which 9 originated from the households of the individual students and 2 from “camp counselors who had contact with a sibling of a laboratory-confirmed case-patient who attended the preschool.”
However, 28 of the students who had pertussis had received at least three vaccinations, with 23 of them having received at least four vaccinations, meaning they were classified as being fully vaccinated against the disease. Only 5 out of the school’s 117 children had not received the complete series of vaccinations, out of which 2 ended up being case-patients; both of those children, however, had received at least one vaccination prior to falling sick.
“Poor performance of a vaccine in a defined cohort might suggest a provider-level failure to store, use, and administer the vaccine properly,” noted the researchers, led by Dr. James Matthias of the Florida Department of Health. “Although we did not assess vaccine storage and handling practices, children from this investigation were seen by multiple providers in the community [and] no general increase in reported pertussis incidence was observed in the county at the same time as this outbreak.”
The bottom line, the authors concluded, is for pediatricians and primary care doctors to be wary that vaccination against pertussis doesn’t necessarily mean patients can’t ever get it. If pertussis symptoms arise in a vaccinated child, especially one 5 years old or younger, it may still be whooping cough.
The CDC supported the study. Dr. Matthias and his coauthors are all affiliated with the Florida Department of Health and the CDC, but reported no other relevant financial disclosures.
Preschool-age children who have been fully vaccinated against pertussis can still develop symptoms of illness consistent with a whooping cough diagnosis, according to a study of toddlers in a Tallahassee, Fla., school that experienced an outbreak of pertussis in late 2013 (Emerg Infect Dis. 2016 Feb;22[2]. doi: 10.3201/eid2202.150325)
The study, published in Emerging Infectious Diseases by the Centers for Disease Control and Prevention, is the result of an outbreak investigation at the preschool that began after a 1-year-old and two 3-year-old children developed illness consistent with pertussis, and were confirmed to have pertussis after undergoing a polymerase chain reaction (PCR) test.
The Florida Department of Health administered a questionnaire to be completed by families of the 117 students (ages 10 months to 6 years) and 26 staff members. Questionnaire completion rate was 98%, with three student households and one staff household failing to complete it.
Overall, 28 cases were determined to be “probable” pertussis and 11 were confirmed as pertussis via PCR or other laboratory testing methods. Of these, 26 were students aged 1-5 years (22% of total student population), 2 were attributed to the staff (7%), and 11 were linked to the preschool, of which 9 originated from the households of the individual students and 2 from “camp counselors who had contact with a sibling of a laboratory-confirmed case-patient who attended the preschool.”
However, 28 of the students who had pertussis had received at least three vaccinations, with 23 of them having received at least four vaccinations, meaning they were classified as being fully vaccinated against the disease. Only 5 out of the school’s 117 children had not received the complete series of vaccinations, out of which 2 ended up being case-patients; both of those children, however, had received at least one vaccination prior to falling sick.
“Poor performance of a vaccine in a defined cohort might suggest a provider-level failure to store, use, and administer the vaccine properly,” noted the researchers, led by Dr. James Matthias of the Florida Department of Health. “Although we did not assess vaccine storage and handling practices, children from this investigation were seen by multiple providers in the community [and] no general increase in reported pertussis incidence was observed in the county at the same time as this outbreak.”
The bottom line, the authors concluded, is for pediatricians and primary care doctors to be wary that vaccination against pertussis doesn’t necessarily mean patients can’t ever get it. If pertussis symptoms arise in a vaccinated child, especially one 5 years old or younger, it may still be whooping cough.
The CDC supported the study. Dr. Matthias and his coauthors are all affiliated with the Florida Department of Health and the CDC, but reported no other relevant financial disclosures.
Preschool-age children who have been fully vaccinated against pertussis can still develop symptoms of illness consistent with a whooping cough diagnosis, according to a study of toddlers in a Tallahassee, Fla., school that experienced an outbreak of pertussis in late 2013 (Emerg Infect Dis. 2016 Feb;22[2]. doi: 10.3201/eid2202.150325)
The study, published in Emerging Infectious Diseases by the Centers for Disease Control and Prevention, is the result of an outbreak investigation at the preschool that began after a 1-year-old and two 3-year-old children developed illness consistent with pertussis, and were confirmed to have pertussis after undergoing a polymerase chain reaction (PCR) test.
The Florida Department of Health administered a questionnaire to be completed by families of the 117 students (ages 10 months to 6 years) and 26 staff members. Questionnaire completion rate was 98%, with three student households and one staff household failing to complete it.
Overall, 28 cases were determined to be “probable” pertussis and 11 were confirmed as pertussis via PCR or other laboratory testing methods. Of these, 26 were students aged 1-5 years (22% of total student population), 2 were attributed to the staff (7%), and 11 were linked to the preschool, of which 9 originated from the households of the individual students and 2 from “camp counselors who had contact with a sibling of a laboratory-confirmed case-patient who attended the preschool.”
However, 28 of the students who had pertussis had received at least three vaccinations, with 23 of them having received at least four vaccinations, meaning they were classified as being fully vaccinated against the disease. Only 5 out of the school’s 117 children had not received the complete series of vaccinations, out of which 2 ended up being case-patients; both of those children, however, had received at least one vaccination prior to falling sick.
“Poor performance of a vaccine in a defined cohort might suggest a provider-level failure to store, use, and administer the vaccine properly,” noted the researchers, led by Dr. James Matthias of the Florida Department of Health. “Although we did not assess vaccine storage and handling practices, children from this investigation were seen by multiple providers in the community [and] no general increase in reported pertussis incidence was observed in the county at the same time as this outbreak.”
The bottom line, the authors concluded, is for pediatricians and primary care doctors to be wary that vaccination against pertussis doesn’t necessarily mean patients can’t ever get it. If pertussis symptoms arise in a vaccinated child, especially one 5 years old or younger, it may still be whooping cough.
The CDC supported the study. Dr. Matthias and his coauthors are all affiliated with the Florida Department of Health and the CDC, but reported no other relevant financial disclosures.
FROM EMERGING INFECTIOUS DISEASES

Pertussis vaccine possibly ineffective in preschoolers
Preschool-age children who have been fully vaccinated against pertussis can still develop symptoms of illness consistent with a whooping cough diagnosis, according to a study of toddlers in a Tallahassee, Fla., school that experienced an outbreak of pertussis in late 2013 (Emerg Infect Dis. 2016 Feb;22[2]. doi: 10.3201/eid2202.150325)
The study, published in Emerging Infectious Diseases by the Centers for Disease Control and Prevention, is the result of an outbreak investigation at the preschool that began after a 1-year-old and two 3-year-old children developed illness consistent with pertussis, and were confirmed to have pertussis after undergoing a polymerase chain reaction (PCR) test.

The Florida Department of Health administered a questionnaire to be completed by families of the 117 students (ages 10 months to 6 years) and 26 staff members. Questionnaire completion rate was 98%, with three student households and one staff household failing to complete it.
Overall, 28 cases were determined to be “probable” pertussis and 11 were confirmed as pertussis via PCR or other laboratory testing methods. Of these, 26 were students aged 1-5 years (22% of total student population), 2 were attributed to the staff (7%), and 11 were linked to the preschool, of which 9 originated from the households of the individual students and 2 from “camp counselors who had contact with a sibling of a laboratory-confirmed case-patient who attended the preschool.”
However, 28 of the students who had pertussis had received at least three vaccinations, with 23 of them having received at least four vaccinations, meaning they were classified as being fully vaccinated against the disease. Only 5 out of the school’s 117 children had not received the complete series of vaccinations, out of which 2 ended up being case-patients; both of those children, however, had received at least one vaccination prior to falling sick.
“Poor performance of a vaccine in a defined cohort might suggest a provider-level failure to store, use, and administer the vaccine properly,” noted the researchers, led by Dr. James Matthias of the Florida Department of Health. “Although we did not assess vaccine storage and handling practices, children from this investigation were seen by multiple providers in the community [and] no general increase in reported pertussis incidence was observed in the county at the same time as this outbreak.”
The bottom line, the authors concluded, is for pediatricians and primary care doctors to be wary that vaccination against pertussis doesn’t necessarily mean patients can’t ever get it. If pertussis symptoms arise in a vaccinated child, especially one 5 years old or younger, it may still be whooping cough.
The CDC supported the study. Dr. Matthias and his coauthors are all affiliated with the Florida Department of Health and the CDC, but reported no other relevant financial disclosures.
Preschool-age children who have been fully vaccinated against pertussis can still develop symptoms of illness consistent with a whooping cough diagnosis, according to a study of toddlers in a Tallahassee, Fla., school that experienced an outbreak of pertussis in late 2013 (Emerg Infect Dis. 2016 Feb;22[2]. doi: 10.3201/eid2202.150325)
The study, published in Emerging Infectious Diseases by the Centers for Disease Control and Prevention, is the result of an outbreak investigation at the preschool that began after a 1-year-old and two 3-year-old children developed illness consistent with pertussis, and were confirmed to have pertussis after undergoing a polymerase chain reaction (PCR) test.
The Florida Department of Health administered a questionnaire to be completed by families of the 117 students (ages 10 months to 6 years) and 26 staff members. Questionnaire completion rate was 98%, with three student households and one staff household failing to complete it.
Overall, 28 cases were determined to be “probable” pertussis and 11 were confirmed as pertussis via PCR or other laboratory testing methods. Of these, 26 were students aged 1-5 years (22% of total student population), 2 were attributed to the staff (7%), and 11 were linked to the preschool, of which 9 originated from the households of the individual students and 2 from “camp counselors who had contact with a sibling of a laboratory-confirmed case-patient who attended the preschool.”
However, 28 of the students who had pertussis had received at least three vaccinations, with 23 of them having received at least four vaccinations, meaning they were classified as being fully vaccinated against the disease. Only 5 out of the school’s 117 children had not received the complete series of vaccinations, out of which 2 ended up being case-patients; both of those children, however, had received at least one vaccination prior to falling sick.
“Poor performance of a vaccine in a defined cohort might suggest a provider-level failure to store, use, and administer the vaccine properly,” noted the researchers, led by Dr. James Matthias of the Florida Department of Health. “Although we did not assess vaccine storage and handling practices, children from this investigation were seen by multiple providers in the community [and] no general increase in reported pertussis incidence was observed in the county at the same time as this outbreak.”
The bottom line, the authors concluded, is for pediatricians and primary care doctors to be wary that vaccination against pertussis doesn’t necessarily mean patients can’t ever get it. If pertussis symptoms arise in a vaccinated child, especially one 5 years old or younger, it may still be whooping cough.
The CDC supported the study. Dr. Matthias and his coauthors are all affiliated with the Florida Department of Health and the CDC, but reported no other relevant financial disclosures.
Preschool-age children who have been fully vaccinated against pertussis can still develop symptoms of illness consistent with a whooping cough diagnosis, according to a study of toddlers in a Tallahassee, Fla., school that experienced an outbreak of pertussis in late 2013 (Emerg Infect Dis. 2016 Feb;22[2]. doi: 10.3201/eid2202.150325)
The study, published in Emerging Infectious Diseases by the Centers for Disease Control and Prevention, is the result of an outbreak investigation at the preschool that began after a 1-year-old and two 3-year-old children developed illness consistent with pertussis, and were confirmed to have pertussis after undergoing a polymerase chain reaction (PCR) test.
The Florida Department of Health administered a questionnaire to be completed by families of the 117 students (ages 10 months to 6 years) and 26 staff members. Questionnaire completion rate was 98%, with three student households and one staff household failing to complete it.
Overall, 28 cases were determined to be “probable” pertussis and 11 were confirmed as pertussis via PCR or other laboratory testing methods. Of these, 26 were students aged 1-5 years (22% of total student population), 2 were attributed to the staff (7%), and 11 were linked to the preschool, of which 9 originated from the households of the individual students and 2 from “camp counselors who had contact with a sibling of a laboratory-confirmed case-patient who attended the preschool.”
However, 28 of the students who had pertussis had received at least three vaccinations, with 23 of them having received at least four vaccinations, meaning they were classified as being fully vaccinated against the disease. Only 5 out of the school’s 117 children had not received the complete series of vaccinations, out of which 2 ended up being case-patients; both of those children, however, had received at least one vaccination prior to falling sick.
“Poor performance of a vaccine in a defined cohort might suggest a provider-level failure to store, use, and administer the vaccine properly,” noted the researchers, led by Dr. James Matthias of the Florida Department of Health. “Although we did not assess vaccine storage and handling practices, children from this investigation were seen by multiple providers in the community [and] no general increase in reported pertussis incidence was observed in the county at the same time as this outbreak.”
The bottom line, the authors concluded, is for pediatricians and primary care doctors to be wary that vaccination against pertussis doesn’t necessarily mean patients can’t ever get it. If pertussis symptoms arise in a vaccinated child, especially one 5 years old or younger, it may still be whooping cough.
The CDC supported the study. Dr. Matthias and his coauthors are all affiliated with the Florida Department of Health and the CDC, but reported no other relevant financial disclosures.
FROM EMERGING INFECTIOUS DISEASES
Key clinical point: Preschoolers vaccinated against pertussis may still develop whooping cough or similar symptoms.
Major finding: Children who had received full series of pertussis vaccinations still developed whooping cough during an outbreak at a school of 117 children.
Data source: Survey of 117 students and 26 staff members at a Tallahassee, Fla., school in 2014.
Disclosures: The CDC supported the study. Dr. Matthias and his coauthors are all affiliated with the Florida Department of Health and the CDC, but reported no other relevant financial disclosures.

Capital misadventures
A few years ago I wrote a column about what promised to be an exciting development in blood testing technology. Using the money her parents had set aside for her education, a young woman dropped out of Stanford University at age 19 and started a company that she claimed would be able to offer hundreds of lab tests on just a few drops of blood. Results would be available in just minutes instead of hours or days. At the time I wrote the column, the company had just landed a contract with a large drug store chain with an arrangement that would eventually allow nearly every resident of the United States to be within a few miles of a site that would offer rapid response blood tests with nothing more than a finger prick.
It seemed a little hard to believe, but the prospect of pediatricians being able to make a diagnosis without running the risk of exsanguinating our smallest patients sounded appealing. On the other hand, I worried that a quick and easy technology might encourage some physicians to use a shotgun approach to diagnosing illness rather than a more rational and cost-effective process based on the traditional skills of history taking and physical examination. Some patients who foolishly wanted to know “everything” about themselves might be tempted to ask their physicians to order the whole smorgasbord of tests. “Hey, it’s only a few drops of blood.”
Turns out there were enough people with more money than reservations and the company quickly attracted hundreds of millions of dollars in venture capital. The company, now calling itself Theranos, has been valued at nine billion dollars. But, recently this startup star has encountered some serious bumps in the road to a full-scale launch (“Hot Startup Theranos Has Struggled With Its Blood-Test Technology” by John Carreyrou, The Wall Street Journal, updated Oct. 16, 2015). The Wall Street Journal reported that despite promises, only a few of the 240 tests offered by the company are currently performed using their proprietary microtechnique. In the days following the Journal article, the Food and Drug Administration warned Theranos that their “nanotainer” is considered a new medical device that must first clear the agency’s time consuming and costly vetting process (“Hot Startup Theranos Dials Back Lab Tests at FDA’s Behest” by John Carreyrou, The Wall Street Journal, updated Oct. 16, 2015).
The venture capitalists who had climbed on the Theranos bandwagon tempted by the just-a-few-drops promise may end up seeing their bank accounts hemorrhage. But I don’t think we should be too critical of their investment decision. It was and may still be good idea that has simply run afoul of the details. However, I recently learned about another new business that I don’t consider to have even started with a good idea, but still has managed to attract enough capital to get itself off the ground (“Should Breast Milk Be Nutritionally Analyzed?” by Laura Johannes, The Wall Street Journal, Dec. 28, 2015).
I’m sure you have seen some new mothers who were concerned that their breast milk was not enough for their babies. But how many of them would pay $150 for a start-up kit and then more than $300 to find out the nutritional content of their breast milk? What if it meant pumping and freezing three samples 2 or 3 days apart and then shipping them in a cooler to a lab? What if you told them that neither you nor anyone else could reliably interpret the results because there aren’t any published guidelines for the optimal composition of human breast milk? Even if your practice is packed to the rafters with anxiety-driven, irrational parents, I don’t think you would find many takers. But that doesn’t seem to have bothered the folks who have invested in Happy Vitals, a company in Washington that is offering a service similar to the one I have just described.
You and I might not have invested in a company whose business plan was to offer such a service. But I fear there may be enough health care “providers” practicing without the benefit of an evidence-based education that what I consider a capital misadventure may actually be able to pay back its investors.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
A few years ago I wrote a column about what promised to be an exciting development in blood testing technology. Using the money her parents had set aside for her education, a young woman dropped out of Stanford University at age 19 and started a company that she claimed would be able to offer hundreds of lab tests on just a few drops of blood. Results would be available in just minutes instead of hours or days. At the time I wrote the column, the company had just landed a contract with a large drug store chain with an arrangement that would eventually allow nearly every resident of the United States to be within a few miles of a site that would offer rapid response blood tests with nothing more than a finger prick.
It seemed a little hard to believe, but the prospect of pediatricians being able to make a diagnosis without running the risk of exsanguinating our smallest patients sounded appealing. On the other hand, I worried that a quick and easy technology might encourage some physicians to use a shotgun approach to diagnosing illness rather than a more rational and cost-effective process based on the traditional skills of history taking and physical examination. Some patients who foolishly wanted to know “everything” about themselves might be tempted to ask their physicians to order the whole smorgasbord of tests. “Hey, it’s only a few drops of blood.”
Turns out there were enough people with more money than reservations and the company quickly attracted hundreds of millions of dollars in venture capital. The company, now calling itself Theranos, has been valued at nine billion dollars. But, recently this startup star has encountered some serious bumps in the road to a full-scale launch (“Hot Startup Theranos Has Struggled With Its Blood-Test Technology” by John Carreyrou, The Wall Street Journal, updated Oct. 16, 2015). The Wall Street Journal reported that despite promises, only a few of the 240 tests offered by the company are currently performed using their proprietary microtechnique. In the days following the Journal article, the Food and Drug Administration warned Theranos that their “nanotainer” is considered a new medical device that must first clear the agency’s time consuming and costly vetting process (“Hot Startup Theranos Dials Back Lab Tests at FDA’s Behest” by John Carreyrou, The Wall Street Journal, updated Oct. 16, 2015).
The venture capitalists who had climbed on the Theranos bandwagon tempted by the just-a-few-drops promise may end up seeing their bank accounts hemorrhage. But I don’t think we should be too critical of their investment decision. It was and may still be good idea that has simply run afoul of the details. However, I recently learned about another new business that I don’t consider to have even started with a good idea, but still has managed to attract enough capital to get itself off the ground (“Should Breast Milk Be Nutritionally Analyzed?” by Laura Johannes, The Wall Street Journal, Dec. 28, 2015).
I’m sure you have seen some new mothers who were concerned that their breast milk was not enough for their babies. But how many of them would pay $150 for a start-up kit and then more than $300 to find out the nutritional content of their breast milk? What if it meant pumping and freezing three samples 2 or 3 days apart and then shipping them in a cooler to a lab? What if you told them that neither you nor anyone else could reliably interpret the results because there aren’t any published guidelines for the optimal composition of human breast milk? Even if your practice is packed to the rafters with anxiety-driven, irrational parents, I don’t think you would find many takers. But that doesn’t seem to have bothered the folks who have invested in Happy Vitals, a company in Washington that is offering a service similar to the one I have just described.
You and I might not have invested in a company whose business plan was to offer such a service. But I fear there may be enough health care “providers” practicing without the benefit of an evidence-based education that what I consider a capital misadventure may actually be able to pay back its investors.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
A few years ago I wrote a column about what promised to be an exciting development in blood testing technology. Using the money her parents had set aside for her education, a young woman dropped out of Stanford University at age 19 and started a company that she claimed would be able to offer hundreds of lab tests on just a few drops of blood. Results would be available in just minutes instead of hours or days. At the time I wrote the column, the company had just landed a contract with a large drug store chain with an arrangement that would eventually allow nearly every resident of the United States to be within a few miles of a site that would offer rapid response blood tests with nothing more than a finger prick.
It seemed a little hard to believe, but the prospect of pediatricians being able to make a diagnosis without running the risk of exsanguinating our smallest patients sounded appealing. On the other hand, I worried that a quick and easy technology might encourage some physicians to use a shotgun approach to diagnosing illness rather than a more rational and cost-effective process based on the traditional skills of history taking and physical examination. Some patients who foolishly wanted to know “everything” about themselves might be tempted to ask their physicians to order the whole smorgasbord of tests. “Hey, it’s only a few drops of blood.”
Turns out there were enough people with more money than reservations and the company quickly attracted hundreds of millions of dollars in venture capital. The company, now calling itself Theranos, has been valued at nine billion dollars. But, recently this startup star has encountered some serious bumps in the road to a full-scale launch (“Hot Startup Theranos Has Struggled With Its Blood-Test Technology” by John Carreyrou, The Wall Street Journal, updated Oct. 16, 2015). The Wall Street Journal reported that despite promises, only a few of the 240 tests offered by the company are currently performed using their proprietary microtechnique. In the days following the Journal article, the Food and Drug Administration warned Theranos that their “nanotainer” is considered a new medical device that must first clear the agency’s time consuming and costly vetting process (“Hot Startup Theranos Dials Back Lab Tests at FDA’s Behest” by John Carreyrou, The Wall Street Journal, updated Oct. 16, 2015).
The venture capitalists who had climbed on the Theranos bandwagon tempted by the just-a-few-drops promise may end up seeing their bank accounts hemorrhage. But I don’t think we should be too critical of their investment decision. It was and may still be good idea that has simply run afoul of the details. However, I recently learned about another new business that I don’t consider to have even started with a good idea, but still has managed to attract enough capital to get itself off the ground (“Should Breast Milk Be Nutritionally Analyzed?” by Laura Johannes, The Wall Street Journal, Dec. 28, 2015).
I’m sure you have seen some new mothers who were concerned that their breast milk was not enough for their babies. But how many of them would pay $150 for a start-up kit and then more than $300 to find out the nutritional content of their breast milk? What if it meant pumping and freezing three samples 2 or 3 days apart and then shipping them in a cooler to a lab? What if you told them that neither you nor anyone else could reliably interpret the results because there aren’t any published guidelines for the optimal composition of human breast milk? Even if your practice is packed to the rafters with anxiety-driven, irrational parents, I don’t think you would find many takers. But that doesn’t seem to have bothered the folks who have invested in Happy Vitals, a company in Washington that is offering a service similar to the one I have just described.
You and I might not have invested in a company whose business plan was to offer such a service. But I fear there may be enough health care “providers” practicing without the benefit of an evidence-based education that what I consider a capital misadventure may actually be able to pay back its investors.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”

Subcorneal Hematomas in Excessive Video Game Play
Case Report
A 19-year-old man was admitted to our hospital to begin treatment for acute myeloid leukemia that had been diagnosed 2 days prior. Three days after completing a 10-day regimen of induction chemotherapy, he developed bilateral, well-demarcated erythematous patches on the palmar surfaces of the proximal phalanges of the third, fourth, and fifth fingers (Figure 1) and 2 patches on the right palm. The patient was referred to dermatology for evaluation. He recalled no trauma to these sites although he reported pushing his intravenous pole with the right hand when walking. Of note, he had become neutropenic and thrombocytopenic following chemotherapy

On physical examination, the patches measured 1- to 1.5-cm in diameter and were mildly tender to palpation. The 2 patches on the right palm were much smaller than those on the fingers but were otherwise similar in appearance.
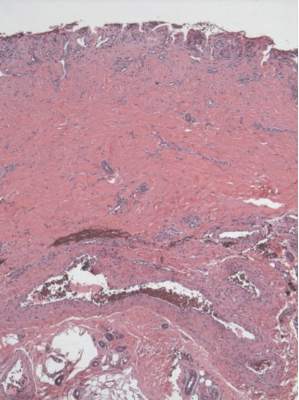
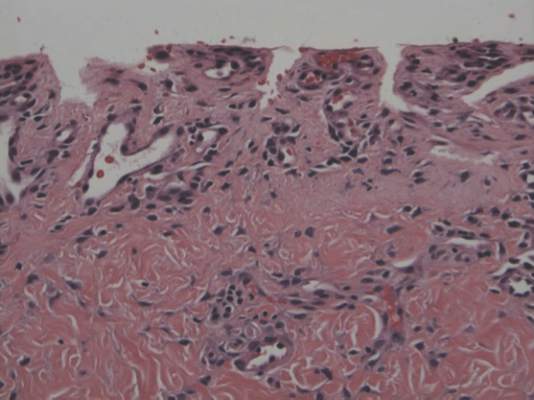
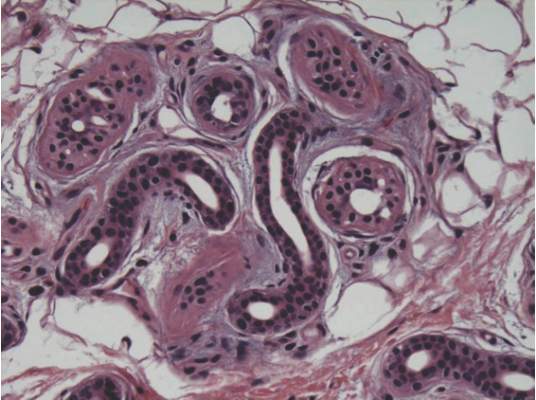
A punch biopsy of the erythematous lesion on the left third digit was performed. Histologic examination revealed extensive epidermal denudation associated with vascular proliferation and congestion as well as hemorrhage and a sparse lymphocytic infiltrate (Figures 2–4). There was no evidence of a leukemic infiltrate, and stains for fungal elements and bacteria were negative. Eccrine ducts appeared normal with no evidence of necrosis or metaplasia. These findings were suggestive of a frictional etiology.
Due to the distribution of the skin lesions on the hands, it was suspected that the source of friction was a video game controller. Although the patient denied playing video games since his admission to the hospital, he reported heavy video game use during the weeks prior to admission. We postulated that the thrombocytopenia the patient developed following chemotherapy along with prior friction injury sustained from heavy video game play led to traumatic subcorneal hemorrhage on the hands at the points of contact with the video game controller (Figure 5). The subcorneal hematomas resolved completely over the next 2 months during which the patient abstained from video game play.

This case demonstrates the importance of obtaining a detailed patient history, as our patient’s history of video game play prior to hospitalization proved to be of major diagnostic importance. Although the location, distribution, and well-demarcated nature of the patient’s lesions suggested an external source of trauma and biopsy definitively ruled out leukemia cutis, Sweet syndrome, and eccrine hidradenitis,1 the final diagnosis of traumatic subcorneal hematomas was only possible with specific knowledge of the patient’s video game controller use.
Comment
History of video game play has been key to the diagnosis of a variety of cutaneous lesions documented in the medical literature. Robertson et al2 attributed a similar case of traumatic subcorneal hematomas of the hands in an otherwise healthy 16-year-old boy to excessive use of a video game controller. Similarly, Kasraee et al3 attributed a case of idiopathic eccrine hidradenitis in an otherwise healthy 12-year-old girl to excessive video game use. In both of these reported cases, bilateral skin lesions on the palms of the hands appeared acutely in a pattern consistent with the points of contact of a video game controller. Excessive video game play has also been associated with unilateral dermatologic lesions on the hands, such as knuckle pads,4 onycholysis,5 friction blisters,6 pressure ulcers,7 and hemorrhagic lesions.5,6,8
Video game–related pathologies are not limited to the skin and have been implicated in a variety of clinical presentations. In 1987, Osterman et al9 published an early account of repetitive strain injury (RSI) related to video game use in which the investigators reported 2 cases of video game–related volar flexor tenosynovitis (or trigger finger), which they termed “joystick digit.” Since that time, video game play has greatly evolved along with the types and nature of RSI cases reported in the medical literature. In 1990, Brasington10 described acute tendinopathy of the extensor pollicis longus tendon caused by excessive video game play, which was termed “Nintendinitis.” This term has since been used in reference to any video game–related RSI and reports have increased over time, likely due to the proliferation of an increasing array of video game systems.5,11-16 In recent years, a number of traumatic injuries including fractures, joint dislocations, head injuries, hemothorax, and lacerations have been attributed to interactive gaming systems.6,11,17-20 In rare cases, video game play also has been associated with enuresis,21 encopresis,22 and epilepsy.23
According to a 2011 report from the Entertainment Software Association, women over the age of 18 years now represent a greater proportion of the video game–playing population than boys aged 17 years and younger.24 This same report also noted that the average video game player is 35 years old; 44% of all players are female; and 27% of Americans over the age of 50 years play video games. This shifting demographic data, including the fact that 80% of American households reportedly play video games, reveals the expanding depth and breadth of the market.24 However, the pediatric population is still a high-volume player demographic. Average time per session peaks between 10 to 12 years of age and then falls through the teenage and adults years.24 Hence, the pediatric population is at high risk for clinical pathology because of the increased repetitive movements associated with video game play. Overall, cognizance of the popularity of video games and related pathologies can be an asset for dermatologists who evaluate pediatric patients.
1. Bolognia J, Jorizzo J, Rapini R, eds. Dermatology. 2nd ed. Edinburgh, Scotland: Elsevier Health Sciences UK; 2007.
2. Robertson SJ, Leonard J, Chamberlain AJ. PlayStation purpura. Australas J Dermatol. 2010;51:220-222.
3. Kasraee B, Masouyé I, Piguet V. PlayStation palmar hidradenitis. Br J Dermatol. 2009;160:892-894.
4. Rushing ME, Sheehan DJ, Davis LS. Video game induced knuckle pad. Pediatr Dermatol. 2006;23:455-457.
5. Bakos RM, Bakos L. Use of dermoscopy to visualize punctate hemorrhages and onycholysis in “playstation thumb.” Arch Dermatol. 2006;142:1664-1665.
6. Wood DJ. The “How!” sign—a central palmar blister induced by overplaying on a Nintendo console. Arch Dis Child. 2001;84:288.
7. Koh TH. Ulcerative “nintendinitis”: a new kind of repetitive strain injury. Med J Aust. 2000;173:671.
8. Bernabeu-Wittel J, Domínguez-Cruz J, Zulueta T, et al. Hemorrhagic parallel-ridge pattern on dermoscopy in “Playstation fingertip.” J Am Acad Dermatol. 2011;65:238-239.
9. Osterman AL, Weinberg P, Miller G. Joystick digit. JAMA. 1987;257:782.
10. Brasington R. Nintendinitis. N Engl J Med. 1990;322:1473-1474.
11. Sparks DA, Coughlin LM, Chase DM. Did too much Wii cause your patient’s injury? J Fam Pract. 2011;60:404-409.
12. Bright DA, Bringhurst DC. Nintendo elbow. West J Med. 1992;156:667-668.
13. Vaidya HJ. Playstation thumb. Lancet. 2004;363:1080.
14. Bonis J. Acute Wiiitis. N Engl J Med. 2007;356:2431-2432.
15. Boehm KM, Pugh A. A new variant of Wiiitis [published online ahead of print June 13, 2008]. J Emerg Med. 2009;36:80.
16. Beddy P, Dunne R, de Blacam C. Achilles wiiitis. AJR Am J Roentgenol. 2009;192:W79.
17. Eley KA. A Wii fracture. N Engl J Med. 2010;362:473-474.
18. Wells JJ. An 8-year-old girl presented to the ER after accidentally being hit by a Wii remote control swung by her brother. J Trauma. 2008;65:1203.
19. Fysh T, Thompson JF. A Wii problem. J R Soc Med. 2009;102:502.
20. George AJ. Musculo-ske Wii tal medicine. Injury. 2012;43:390-391.
21. Schink JC. Nintendo enuresis. Am J Dis Child. 1991;145:1094.
22. Corkery JC. Nintendo power. Am J Dis Child. 1990;144:959.
23. Hart EJ. Nintendo epilepsy. N Engl J Med. 1990;322:1473.
24. Entertainment Software Association. 2015 sales, demographic, and usage data. essential facts about the computer and video game industry. Entertainment Software Association Web site. http://www.theesa.com/wp-content/uploads/2015/04/ESA-Essential-Facts-2015.pdf. Accessed October 16, 2015.
Case Report
A 19-year-old man was admitted to our hospital to begin treatment for acute myeloid leukemia that had been diagnosed 2 days prior. Three days after completing a 10-day regimen of induction chemotherapy, he developed bilateral, well-demarcated erythematous patches on the palmar surfaces of the proximal phalanges of the third, fourth, and fifth fingers (Figure 1) and 2 patches on the right palm. The patient was referred to dermatology for evaluation. He recalled no trauma to these sites although he reported pushing his intravenous pole with the right hand when walking. Of note, he had become neutropenic and thrombocytopenic following chemotherapy
On physical examination, the patches measured 1- to 1.5-cm in diameter and were mildly tender to palpation. The 2 patches on the right palm were much smaller than those on the fingers but were otherwise similar in appearance.
A punch biopsy of the erythematous lesion on the left third digit was performed. Histologic examination revealed extensive epidermal denudation associated with vascular proliferation and congestion as well as hemorrhage and a sparse lymphocytic infiltrate (Figures 2–4). There was no evidence of a leukemic infiltrate, and stains for fungal elements and bacteria were negative. Eccrine ducts appeared normal with no evidence of necrosis or metaplasia. These findings were suggestive of a frictional etiology.
Due to the distribution of the skin lesions on the hands, it was suspected that the source of friction was a video game controller. Although the patient denied playing video games since his admission to the hospital, he reported heavy video game use during the weeks prior to admission. We postulated that the thrombocytopenia the patient developed following chemotherapy along with prior friction injury sustained from heavy video game play led to traumatic subcorneal hemorrhage on the hands at the points of contact with the video game controller (Figure 5). The subcorneal hematomas resolved completely over the next 2 months during which the patient abstained from video game play.
This case demonstrates the importance of obtaining a detailed patient history, as our patient’s history of video game play prior to hospitalization proved to be of major diagnostic importance. Although the location, distribution, and well-demarcated nature of the patient’s lesions suggested an external source of trauma and biopsy definitively ruled out leukemia cutis, Sweet syndrome, and eccrine hidradenitis,1 the final diagnosis of traumatic subcorneal hematomas was only possible with specific knowledge of the patient’s video game controller use.
Comment
History of video game play has been key to the diagnosis of a variety of cutaneous lesions documented in the medical literature. Robertson et al2 attributed a similar case of traumatic subcorneal hematomas of the hands in an otherwise healthy 16-year-old boy to excessive use of a video game controller. Similarly, Kasraee et al3 attributed a case of idiopathic eccrine hidradenitis in an otherwise healthy 12-year-old girl to excessive video game use. In both of these reported cases, bilateral skin lesions on the palms of the hands appeared acutely in a pattern consistent with the points of contact of a video game controller. Excessive video game play has also been associated with unilateral dermatologic lesions on the hands, such as knuckle pads,4 onycholysis,5 friction blisters,6 pressure ulcers,7 and hemorrhagic lesions.5,6,8
Video game–related pathologies are not limited to the skin and have been implicated in a variety of clinical presentations. In 1987, Osterman et al9 published an early account of repetitive strain injury (RSI) related to video game use in which the investigators reported 2 cases of video game–related volar flexor tenosynovitis (or trigger finger), which they termed “joystick digit.” Since that time, video game play has greatly evolved along with the types and nature of RSI cases reported in the medical literature. In 1990, Brasington10 described acute tendinopathy of the extensor pollicis longus tendon caused by excessive video game play, which was termed “Nintendinitis.” This term has since been used in reference to any video game–related RSI and reports have increased over time, likely due to the proliferation of an increasing array of video game systems.5,11-16 In recent years, a number of traumatic injuries including fractures, joint dislocations, head injuries, hemothorax, and lacerations have been attributed to interactive gaming systems.6,11,17-20 In rare cases, video game play also has been associated with enuresis,21 encopresis,22 and epilepsy.23
According to a 2011 report from the Entertainment Software Association, women over the age of 18 years now represent a greater proportion of the video game–playing population than boys aged 17 years and younger.24 This same report also noted that the average video game player is 35 years old; 44% of all players are female; and 27% of Americans over the age of 50 years play video games. This shifting demographic data, including the fact that 80% of American households reportedly play video games, reveals the expanding depth and breadth of the market.24 However, the pediatric population is still a high-volume player demographic. Average time per session peaks between 10 to 12 years of age and then falls through the teenage and adults years.24 Hence, the pediatric population is at high risk for clinical pathology because of the increased repetitive movements associated with video game play. Overall, cognizance of the popularity of video games and related pathologies can be an asset for dermatologists who evaluate pediatric patients.
Case Report
A 19-year-old man was admitted to our hospital to begin treatment for acute myeloid leukemia that had been diagnosed 2 days prior. Three days after completing a 10-day regimen of induction chemotherapy, he developed bilateral, well-demarcated erythematous patches on the palmar surfaces of the proximal phalanges of the third, fourth, and fifth fingers (Figure 1) and 2 patches on the right palm. The patient was referred to dermatology for evaluation. He recalled no trauma to these sites although he reported pushing his intravenous pole with the right hand when walking. Of note, he had become neutropenic and thrombocytopenic following chemotherapy
On physical examination, the patches measured 1- to 1.5-cm in diameter and were mildly tender to palpation. The 2 patches on the right palm were much smaller than those on the fingers but were otherwise similar in appearance.
A punch biopsy of the erythematous lesion on the left third digit was performed. Histologic examination revealed extensive epidermal denudation associated with vascular proliferation and congestion as well as hemorrhage and a sparse lymphocytic infiltrate (Figures 2–4). There was no evidence of a leukemic infiltrate, and stains for fungal elements and bacteria were negative. Eccrine ducts appeared normal with no evidence of necrosis or metaplasia. These findings were suggestive of a frictional etiology.
Due to the distribution of the skin lesions on the hands, it was suspected that the source of friction was a video game controller. Although the patient denied playing video games since his admission to the hospital, he reported heavy video game use during the weeks prior to admission. We postulated that the thrombocytopenia the patient developed following chemotherapy along with prior friction injury sustained from heavy video game play led to traumatic subcorneal hemorrhage on the hands at the points of contact with the video game controller (Figure 5). The subcorneal hematomas resolved completely over the next 2 months during which the patient abstained from video game play.
This case demonstrates the importance of obtaining a detailed patient history, as our patient’s history of video game play prior to hospitalization proved to be of major diagnostic importance. Although the location, distribution, and well-demarcated nature of the patient’s lesions suggested an external source of trauma and biopsy definitively ruled out leukemia cutis, Sweet syndrome, and eccrine hidradenitis,1 the final diagnosis of traumatic subcorneal hematomas was only possible with specific knowledge of the patient’s video game controller use.
Comment
History of video game play has been key to the diagnosis of a variety of cutaneous lesions documented in the medical literature. Robertson et al2 attributed a similar case of traumatic subcorneal hematomas of the hands in an otherwise healthy 16-year-old boy to excessive use of a video game controller. Similarly, Kasraee et al3 attributed a case of idiopathic eccrine hidradenitis in an otherwise healthy 12-year-old girl to excessive video game use. In both of these reported cases, bilateral skin lesions on the palms of the hands appeared acutely in a pattern consistent with the points of contact of a video game controller. Excessive video game play has also been associated with unilateral dermatologic lesions on the hands, such as knuckle pads,4 onycholysis,5 friction blisters,6 pressure ulcers,7 and hemorrhagic lesions.5,6,8
Video game–related pathologies are not limited to the skin and have been implicated in a variety of clinical presentations. In 1987, Osterman et al9 published an early account of repetitive strain injury (RSI) related to video game use in which the investigators reported 2 cases of video game–related volar flexor tenosynovitis (or trigger finger), which they termed “joystick digit.” Since that time, video game play has greatly evolved along with the types and nature of RSI cases reported in the medical literature. In 1990, Brasington10 described acute tendinopathy of the extensor pollicis longus tendon caused by excessive video game play, which was termed “Nintendinitis.” This term has since been used in reference to any video game–related RSI and reports have increased over time, likely due to the proliferation of an increasing array of video game systems.5,11-16 In recent years, a number of traumatic injuries including fractures, joint dislocations, head injuries, hemothorax, and lacerations have been attributed to interactive gaming systems.6,11,17-20 In rare cases, video game play also has been associated with enuresis,21 encopresis,22 and epilepsy.23
According to a 2011 report from the Entertainment Software Association, women over the age of 18 years now represent a greater proportion of the video game–playing population than boys aged 17 years and younger.24 This same report also noted that the average video game player is 35 years old; 44% of all players are female; and 27% of Americans over the age of 50 years play video games. This shifting demographic data, including the fact that 80% of American households reportedly play video games, reveals the expanding depth and breadth of the market.24 However, the pediatric population is still a high-volume player demographic. Average time per session peaks between 10 to 12 years of age and then falls through the teenage and adults years.24 Hence, the pediatric population is at high risk for clinical pathology because of the increased repetitive movements associated with video game play. Overall, cognizance of the popularity of video games and related pathologies can be an asset for dermatologists who evaluate pediatric patients.
1. Bolognia J, Jorizzo J, Rapini R, eds. Dermatology. 2nd ed. Edinburgh, Scotland: Elsevier Health Sciences UK; 2007.
2. Robertson SJ, Leonard J, Chamberlain AJ. PlayStation purpura. Australas J Dermatol. 2010;51:220-222.
3. Kasraee B, Masouyé I, Piguet V. PlayStation palmar hidradenitis. Br J Dermatol. 2009;160:892-894.
4. Rushing ME, Sheehan DJ, Davis LS. Video game induced knuckle pad. Pediatr Dermatol. 2006;23:455-457.
5. Bakos RM, Bakos L. Use of dermoscopy to visualize punctate hemorrhages and onycholysis in “playstation thumb.” Arch Dermatol. 2006;142:1664-1665.
6. Wood DJ. The “How!” sign—a central palmar blister induced by overplaying on a Nintendo console. Arch Dis Child. 2001;84:288.
7. Koh TH. Ulcerative “nintendinitis”: a new kind of repetitive strain injury. Med J Aust. 2000;173:671.
8. Bernabeu-Wittel J, Domínguez-Cruz J, Zulueta T, et al. Hemorrhagic parallel-ridge pattern on dermoscopy in “Playstation fingertip.” J Am Acad Dermatol. 2011;65:238-239.
9. Osterman AL, Weinberg P, Miller G. Joystick digit. JAMA. 1987;257:782.
10. Brasington R. Nintendinitis. N Engl J Med. 1990;322:1473-1474.
11. Sparks DA, Coughlin LM, Chase DM. Did too much Wii cause your patient’s injury? J Fam Pract. 2011;60:404-409.
12. Bright DA, Bringhurst DC. Nintendo elbow. West J Med. 1992;156:667-668.
13. Vaidya HJ. Playstation thumb. Lancet. 2004;363:1080.
14. Bonis J. Acute Wiiitis. N Engl J Med. 2007;356:2431-2432.
15. Boehm KM, Pugh A. A new variant of Wiiitis [published online ahead of print June 13, 2008]. J Emerg Med. 2009;36:80.
16. Beddy P, Dunne R, de Blacam C. Achilles wiiitis. AJR Am J Roentgenol. 2009;192:W79.
17. Eley KA. A Wii fracture. N Engl J Med. 2010;362:473-474.
18. Wells JJ. An 8-year-old girl presented to the ER after accidentally being hit by a Wii remote control swung by her brother. J Trauma. 2008;65:1203.
19. Fysh T, Thompson JF. A Wii problem. J R Soc Med. 2009;102:502.
20. George AJ. Musculo-ske Wii tal medicine. Injury. 2012;43:390-391.
21. Schink JC. Nintendo enuresis. Am J Dis Child. 1991;145:1094.
22. Corkery JC. Nintendo power. Am J Dis Child. 1990;144:959.
23. Hart EJ. Nintendo epilepsy. N Engl J Med. 1990;322:1473.
24. Entertainment Software Association. 2015 sales, demographic, and usage data. essential facts about the computer and video game industry. Entertainment Software Association Web site. http://www.theesa.com/wp-content/uploads/2015/04/ESA-Essential-Facts-2015.pdf. Accessed October 16, 2015.
1. Bolognia J, Jorizzo J, Rapini R, eds. Dermatology. 2nd ed. Edinburgh, Scotland: Elsevier Health Sciences UK; 2007.
2. Robertson SJ, Leonard J, Chamberlain AJ. PlayStation purpura. Australas J Dermatol. 2010;51:220-222.
3. Kasraee B, Masouyé I, Piguet V. PlayStation palmar hidradenitis. Br J Dermatol. 2009;160:892-894.
4. Rushing ME, Sheehan DJ, Davis LS. Video game induced knuckle pad. Pediatr Dermatol. 2006;23:455-457.
5. Bakos RM, Bakos L. Use of dermoscopy to visualize punctate hemorrhages and onycholysis in “playstation thumb.” Arch Dermatol. 2006;142:1664-1665.
6. Wood DJ. The “How!” sign—a central palmar blister induced by overplaying on a Nintendo console. Arch Dis Child. 2001;84:288.
7. Koh TH. Ulcerative “nintendinitis”: a new kind of repetitive strain injury. Med J Aust. 2000;173:671.
8. Bernabeu-Wittel J, Domínguez-Cruz J, Zulueta T, et al. Hemorrhagic parallel-ridge pattern on dermoscopy in “Playstation fingertip.” J Am Acad Dermatol. 2011;65:238-239.
9. Osterman AL, Weinberg P, Miller G. Joystick digit. JAMA. 1987;257:782.
10. Brasington R. Nintendinitis. N Engl J Med. 1990;322:1473-1474.
11. Sparks DA, Coughlin LM, Chase DM. Did too much Wii cause your patient’s injury? J Fam Pract. 2011;60:404-409.
12. Bright DA, Bringhurst DC. Nintendo elbow. West J Med. 1992;156:667-668.
13. Vaidya HJ. Playstation thumb. Lancet. 2004;363:1080.
14. Bonis J. Acute Wiiitis. N Engl J Med. 2007;356:2431-2432.
15. Boehm KM, Pugh A. A new variant of Wiiitis [published online ahead of print June 13, 2008]. J Emerg Med. 2009;36:80.
16. Beddy P, Dunne R, de Blacam C. Achilles wiiitis. AJR Am J Roentgenol. 2009;192:W79.
17. Eley KA. A Wii fracture. N Engl J Med. 2010;362:473-474.
18. Wells JJ. An 8-year-old girl presented to the ER after accidentally being hit by a Wii remote control swung by her brother. J Trauma. 2008;65:1203.
19. Fysh T, Thompson JF. A Wii problem. J R Soc Med. 2009;102:502.
20. George AJ. Musculo-ske Wii tal medicine. Injury. 2012;43:390-391.
21. Schink JC. Nintendo enuresis. Am J Dis Child. 1991;145:1094.
22. Corkery JC. Nintendo power. Am J Dis Child. 1990;144:959.
23. Hart EJ. Nintendo epilepsy. N Engl J Med. 1990;322:1473.
24. Entertainment Software Association. 2015 sales, demographic, and usage data. essential facts about the computer and video game industry. Entertainment Software Association Web site. http://www.theesa.com/wp-content/uploads/2015/04/ESA-Essential-Facts-2015.pdf. Accessed October 16, 2015.
Practice Points
- Video game play has been reported as an etiologic factor in multiple musculoskeletal and dermatologic conditions.
- More than two-thirds of US children aged 2 to 18 years live in a home with a video game system.
- Cognizance of the popularity of video games and related pathologies can be an asset for dermatologists who evaluate pediatric patients.

Forces driving leukemia differ in kids and adults

New research suggests childhood leukemias are forged by different evolutionary forces than leukemias in older adults.
Researchers used a computational model to characterize the population dynamics of hematopoietic stem cells (HSCs) that give rise to leukemias.
And they found the evolutionary force known as “drift” contributes to leukemia development in young children but not in older adults.
“Basically, leukemia risk early in life may be more dictated by chance than by the typical ‘survival of the fittest’ that characterizes leukemia formation in older adults,” explained study author James DeGregori, PhD, of the University of Colorado School of Medicine in Aurora.
He and his colleagues recounted this discovery in PNAS.
With previous work, the DeGregori lab showed that the inevitable tissue decline associated with aging benefits HSCs with mutations that allow the cells to better adapt to the new ecosystem.
In contrast, the ecosystem of young tissue favors healthy cells. Optimized by millions of years of co-evolution, most mutations make cells less fit for the ecosystem of young, healthy tissue and lead to purging of mutant cells from the tissue.
With the current study, Dr DeGregori and his colleagues made a surprising discovery. Despite the ability of young tissue to select against cells with cancer-causing mutations, the computational model showed increased proportions of specific, mutation-bearing HSCs in the first few years after birth.
And these mutated cells were not dependent on the effect of the mutation on cell fitness. In other words, the mutation-bearing cells were not more fit than cells without the mutations. Instead of the survival-of-the-fittest form of natural selection that drives the evolution of cancer in older adults, there was another force at work.
In fact, the researchers discovered 2 factors that influence the development of childhood leukemia: the small HSC pool size at birth and the high rate of cell division necessary for body growth early in life.
The high rate of cell division increases the risk of leukemia because mutations largely happen during cell divisions. More cell divisions mean more mutations, and this increases the risk that some of these mutations could contribute to leukemia development.
The small HSC pool size influences leukemia development via the evolutionary force known as drift. Drift is the role of chance—the possibility that, despite being less fit, an animal, organism, or HSC with an oncogenic mutation will survive to shift the genetic makeup of the population.
The influence of drift is greater in small populations and, in this case, small stem cell pools. In the small HSC pools of young children, drift becomes important as a lucky genotype may end up with a larger share of the total HSC pool than warranted by its fitness status.
If this lucky cell clone happens to have a mutation that can start the HSC down the path toward leukemia, this drift-driven expansion should increase the risk of leukemia by increasing the number of HSCs with this mutation.
“Thus, early somatic evolution in HSC pools is significantly impacted by drift, with selection playing a lesser role,” Dr DeGregori and his colleagues wrote.
On the other hand, the impact of drift lessens as the HSC pool grows along with an infant’s body to reach adult size. The larger HSC pool size decreases the role of drift in the success of particular cells in the tissue.
In addition, as the pool size reaches its maximum, the HSC division rate slows to a crawl (as these stem cells enter the maintenance rather than growth phase). With a landscape of healthy, youthful tissues and low rates of mutation due to low cell division rates, the odds of leukemia diminish.
“With a large population of healthy cells optimized to young, healthy tissue, the ability of mutations, including cancerous mutations, to drive uncontrolled cell proliferation is reduced,” Dr DeGregori said.
However, in old age, tissue decline promotes selection for adaptive mutations, leading to the expansion of potentially oncogenic HSC clones that will again increase the risk of leukemia.
Thus, this research shows that, in early life, leukemias are driven by mutation and drift. And in later life, leukemias are driven by mutation and selection.
“We show that leukemias of children and older adults are different diseases, forged by different evolutionary forces and propagated under different circumstances,” Dr DeGregori said.
He and his colleagues believe this understanding raises the possibility of a new approach to cancer treatment. Perhaps researchers could find a way to manipulate the parameters of cell evolution or manipulate the tissue ecosystem to decrease cancer risk. ![]()
New research suggests childhood leukemias are forged by different evolutionary forces than leukemias in older adults.
Researchers used a computational model to characterize the population dynamics of hematopoietic stem cells (HSCs) that give rise to leukemias.
And they found the evolutionary force known as “drift” contributes to leukemia development in young children but not in older adults.
“Basically, leukemia risk early in life may be more dictated by chance than by the typical ‘survival of the fittest’ that characterizes leukemia formation in older adults,” explained study author James DeGregori, PhD, of the University of Colorado School of Medicine in Aurora.
He and his colleagues recounted this discovery in PNAS.
With previous work, the DeGregori lab showed that the inevitable tissue decline associated with aging benefits HSCs with mutations that allow the cells to better adapt to the new ecosystem.
In contrast, the ecosystem of young tissue favors healthy cells. Optimized by millions of years of co-evolution, most mutations make cells less fit for the ecosystem of young, healthy tissue and lead to purging of mutant cells from the tissue.
With the current study, Dr DeGregori and his colleagues made a surprising discovery. Despite the ability of young tissue to select against cells with cancer-causing mutations, the computational model showed increased proportions of specific, mutation-bearing HSCs in the first few years after birth.
And these mutated cells were not dependent on the effect of the mutation on cell fitness. In other words, the mutation-bearing cells were not more fit than cells without the mutations. Instead of the survival-of-the-fittest form of natural selection that drives the evolution of cancer in older adults, there was another force at work.
In fact, the researchers discovered 2 factors that influence the development of childhood leukemia: the small HSC pool size at birth and the high rate of cell division necessary for body growth early in life.
The high rate of cell division increases the risk of leukemia because mutations largely happen during cell divisions. More cell divisions mean more mutations, and this increases the risk that some of these mutations could contribute to leukemia development.
The small HSC pool size influences leukemia development via the evolutionary force known as drift. Drift is the role of chance—the possibility that, despite being less fit, an animal, organism, or HSC with an oncogenic mutation will survive to shift the genetic makeup of the population.
The influence of drift is greater in small populations and, in this case, small stem cell pools. In the small HSC pools of young children, drift becomes important as a lucky genotype may end up with a larger share of the total HSC pool than warranted by its fitness status.
If this lucky cell clone happens to have a mutation that can start the HSC down the path toward leukemia, this drift-driven expansion should increase the risk of leukemia by increasing the number of HSCs with this mutation.
“Thus, early somatic evolution in HSC pools is significantly impacted by drift, with selection playing a lesser role,” Dr DeGregori and his colleagues wrote.
On the other hand, the impact of drift lessens as the HSC pool grows along with an infant’s body to reach adult size. The larger HSC pool size decreases the role of drift in the success of particular cells in the tissue.
In addition, as the pool size reaches its maximum, the HSC division rate slows to a crawl (as these stem cells enter the maintenance rather than growth phase). With a landscape of healthy, youthful tissues and low rates of mutation due to low cell division rates, the odds of leukemia diminish.
“With a large population of healthy cells optimized to young, healthy tissue, the ability of mutations, including cancerous mutations, to drive uncontrolled cell proliferation is reduced,” Dr DeGregori said.
However, in old age, tissue decline promotes selection for adaptive mutations, leading to the expansion of potentially oncogenic HSC clones that will again increase the risk of leukemia.
Thus, this research shows that, in early life, leukemias are driven by mutation and drift. And in later life, leukemias are driven by mutation and selection.
“We show that leukemias of children and older adults are different diseases, forged by different evolutionary forces and propagated under different circumstances,” Dr DeGregori said.
He and his colleagues believe this understanding raises the possibility of a new approach to cancer treatment. Perhaps researchers could find a way to manipulate the parameters of cell evolution or manipulate the tissue ecosystem to decrease cancer risk. ![]()
New research suggests childhood leukemias are forged by different evolutionary forces than leukemias in older adults.
Researchers used a computational model to characterize the population dynamics of hematopoietic stem cells (HSCs) that give rise to leukemias.
And they found the evolutionary force known as “drift” contributes to leukemia development in young children but not in older adults.
“Basically, leukemia risk early in life may be more dictated by chance than by the typical ‘survival of the fittest’ that characterizes leukemia formation in older adults,” explained study author James DeGregori, PhD, of the University of Colorado School of Medicine in Aurora.
He and his colleagues recounted this discovery in PNAS.
With previous work, the DeGregori lab showed that the inevitable tissue decline associated with aging benefits HSCs with mutations that allow the cells to better adapt to the new ecosystem.
In contrast, the ecosystem of young tissue favors healthy cells. Optimized by millions of years of co-evolution, most mutations make cells less fit for the ecosystem of young, healthy tissue and lead to purging of mutant cells from the tissue.
With the current study, Dr DeGregori and his colleagues made a surprising discovery. Despite the ability of young tissue to select against cells with cancer-causing mutations, the computational model showed increased proportions of specific, mutation-bearing HSCs in the first few years after birth.
And these mutated cells were not dependent on the effect of the mutation on cell fitness. In other words, the mutation-bearing cells were not more fit than cells without the mutations. Instead of the survival-of-the-fittest form of natural selection that drives the evolution of cancer in older adults, there was another force at work.
In fact, the researchers discovered 2 factors that influence the development of childhood leukemia: the small HSC pool size at birth and the high rate of cell division necessary for body growth early in life.
The high rate of cell division increases the risk of leukemia because mutations largely happen during cell divisions. More cell divisions mean more mutations, and this increases the risk that some of these mutations could contribute to leukemia development.
The small HSC pool size influences leukemia development via the evolutionary force known as drift. Drift is the role of chance—the possibility that, despite being less fit, an animal, organism, or HSC with an oncogenic mutation will survive to shift the genetic makeup of the population.
The influence of drift is greater in small populations and, in this case, small stem cell pools. In the small HSC pools of young children, drift becomes important as a lucky genotype may end up with a larger share of the total HSC pool than warranted by its fitness status.
If this lucky cell clone happens to have a mutation that can start the HSC down the path toward leukemia, this drift-driven expansion should increase the risk of leukemia by increasing the number of HSCs with this mutation.
“Thus, early somatic evolution in HSC pools is significantly impacted by drift, with selection playing a lesser role,” Dr DeGregori and his colleagues wrote.
On the other hand, the impact of drift lessens as the HSC pool grows along with an infant’s body to reach adult size. The larger HSC pool size decreases the role of drift in the success of particular cells in the tissue.
In addition, as the pool size reaches its maximum, the HSC division rate slows to a crawl (as these stem cells enter the maintenance rather than growth phase). With a landscape of healthy, youthful tissues and low rates of mutation due to low cell division rates, the odds of leukemia diminish.
“With a large population of healthy cells optimized to young, healthy tissue, the ability of mutations, including cancerous mutations, to drive uncontrolled cell proliferation is reduced,” Dr DeGregori said.
However, in old age, tissue decline promotes selection for adaptive mutations, leading to the expansion of potentially oncogenic HSC clones that will again increase the risk of leukemia.
Thus, this research shows that, in early life, leukemias are driven by mutation and drift. And in later life, leukemias are driven by mutation and selection.
“We show that leukemias of children and older adults are different diseases, forged by different evolutionary forces and propagated under different circumstances,” Dr DeGregori said.
He and his colleagues believe this understanding raises the possibility of a new approach to cancer treatment. Perhaps researchers could find a way to manipulate the parameters of cell evolution or manipulate the tissue ecosystem to decrease cancer risk. ![]()
Investigational maternal group B strep vaccine well tolerated
An investigational trivalent group B streptococcal vaccine given to pregnant women produced elevated antibody levels in their infants, indicating that the infants likely were protected by passive immunity, according to a report published online Jan. 11 in Obstetrics & Gynecology.
A maternally administered vaccine was proposed as possibly the most effective means of preventing group B strep disease “across the entire period of vulnerability in newborns.” In this phase II randomized study performed at two sites in Belgium and three in Canada, levels of GBS-specific antibodies were assessed in infants of 86 healthy women vaccinated at 24-35 weeks’ gestation.
A total of 51 women received active vaccine and 35 received a placebo injection in the 2-year trial, which was supported by Novartis Vaccines and Diagnostics, maker of this investigational vaccine, according to Dr. Gilbert G.G. Donders of Femicare Clinical Research for Women, Tienen, Belgium, and his associates.
Mean maternal antibody levels increased by 16-fold to 23-fold after vaccination. Levels of antibody transfer, as measured in cord blood samples or needlestick samples from the neonate at birth, ranged from 66% to 79% – which is comparable to levels seen after maternal immunization with other vaccines such as those against Haemophilus influenzae type b or meningococcal disease.
At 3 months of age, antibody levels in the infants had decreased to approximately 22%-25% of what they had been at birth, but this was still 5-8 times higher than antibody levels in the placebo group, the investigators reported (Obstet Gynecol. 2016;127:214-22. doi: 10.1097/AOG.0000000000001190).
Neither the mothers nor the infants showed any “concerning safety signals.” One-minute and 5-minute Apgar scores were similar between the two study groups, and the percentage of infants who achieved “normal” scores on developmental measures also was similar: 71%-96% at 5 months and 93%-100% at 7 months in both groups. One newborn developed perinatal asphyxia, “which was considered possibly related to vaccination because no other obvious cause was present,” the researchers noted.
In addition, there was a possibility that the investigational vaccine contained a compound that might interfere with the infant’s response to routine diphtheria immunization. But no such interference was detected when these responses were measured after the infants received their final diphtheria vaccination, according to the researchers.
Novartis Vaccines and Diagnostics, whose non-influenza human vaccine business was recently transferred to GlaxoSmithKline, sponsored the study. Dr. Donders received research fees for undertaking the trial, other coauthors received research funding from Novartis, and four coauthors were employed by Novartis at the time of the study.
An investigational trivalent group B streptococcal vaccine given to pregnant women produced elevated antibody levels in their infants, indicating that the infants likely were protected by passive immunity, according to a report published online Jan. 11 in Obstetrics & Gynecology.
A maternally administered vaccine was proposed as possibly the most effective means of preventing group B strep disease “across the entire period of vulnerability in newborns.” In this phase II randomized study performed at two sites in Belgium and three in Canada, levels of GBS-specific antibodies were assessed in infants of 86 healthy women vaccinated at 24-35 weeks’ gestation.
A total of 51 women received active vaccine and 35 received a placebo injection in the 2-year trial, which was supported by Novartis Vaccines and Diagnostics, maker of this investigational vaccine, according to Dr. Gilbert G.G. Donders of Femicare Clinical Research for Women, Tienen, Belgium, and his associates.
Mean maternal antibody levels increased by 16-fold to 23-fold after vaccination. Levels of antibody transfer, as measured in cord blood samples or needlestick samples from the neonate at birth, ranged from 66% to 79% – which is comparable to levels seen after maternal immunization with other vaccines such as those against Haemophilus influenzae type b or meningococcal disease.
At 3 months of age, antibody levels in the infants had decreased to approximately 22%-25% of what they had been at birth, but this was still 5-8 times higher than antibody levels in the placebo group, the investigators reported (Obstet Gynecol. 2016;127:214-22. doi: 10.1097/AOG.0000000000001190).
Neither the mothers nor the infants showed any “concerning safety signals.” One-minute and 5-minute Apgar scores were similar between the two study groups, and the percentage of infants who achieved “normal” scores on developmental measures also was similar: 71%-96% at 5 months and 93%-100% at 7 months in both groups. One newborn developed perinatal asphyxia, “which was considered possibly related to vaccination because no other obvious cause was present,” the researchers noted.
In addition, there was a possibility that the investigational vaccine contained a compound that might interfere with the infant’s response to routine diphtheria immunization. But no such interference was detected when these responses were measured after the infants received their final diphtheria vaccination, according to the researchers.
Novartis Vaccines and Diagnostics, whose non-influenza human vaccine business was recently transferred to GlaxoSmithKline, sponsored the study. Dr. Donders received research fees for undertaking the trial, other coauthors received research funding from Novartis, and four coauthors were employed by Novartis at the time of the study.
An investigational trivalent group B streptococcal vaccine given to pregnant women produced elevated antibody levels in their infants, indicating that the infants likely were protected by passive immunity, according to a report published online Jan. 11 in Obstetrics & Gynecology.
A maternally administered vaccine was proposed as possibly the most effective means of preventing group B strep disease “across the entire period of vulnerability in newborns.” In this phase II randomized study performed at two sites in Belgium and three in Canada, levels of GBS-specific antibodies were assessed in infants of 86 healthy women vaccinated at 24-35 weeks’ gestation.
A total of 51 women received active vaccine and 35 received a placebo injection in the 2-year trial, which was supported by Novartis Vaccines and Diagnostics, maker of this investigational vaccine, according to Dr. Gilbert G.G. Donders of Femicare Clinical Research for Women, Tienen, Belgium, and his associates.
Mean maternal antibody levels increased by 16-fold to 23-fold after vaccination. Levels of antibody transfer, as measured in cord blood samples or needlestick samples from the neonate at birth, ranged from 66% to 79% – which is comparable to levels seen after maternal immunization with other vaccines such as those against Haemophilus influenzae type b or meningococcal disease.
At 3 months of age, antibody levels in the infants had decreased to approximately 22%-25% of what they had been at birth, but this was still 5-8 times higher than antibody levels in the placebo group, the investigators reported (Obstet Gynecol. 2016;127:214-22. doi: 10.1097/AOG.0000000000001190).
Neither the mothers nor the infants showed any “concerning safety signals.” One-minute and 5-minute Apgar scores were similar between the two study groups, and the percentage of infants who achieved “normal” scores on developmental measures also was similar: 71%-96% at 5 months and 93%-100% at 7 months in both groups. One newborn developed perinatal asphyxia, “which was considered possibly related to vaccination because no other obvious cause was present,” the researchers noted.
In addition, there was a possibility that the investigational vaccine contained a compound that might interfere with the infant’s response to routine diphtheria immunization. But no such interference was detected when these responses were measured after the infants received their final diphtheria vaccination, according to the researchers.
Novartis Vaccines and Diagnostics, whose non-influenza human vaccine business was recently transferred to GlaxoSmithKline, sponsored the study. Dr. Donders received research fees for undertaking the trial, other coauthors received research funding from Novartis, and four coauthors were employed by Novartis at the time of the study.
FROM OBSTETRICS & GYNECOLOGY
Key clinical point: An investigational trivalent group B strep vaccine for pregnant women raised antibody levels in their infants, indicating that the infants likely were protected by passive immunity.
Major finding: Mean maternal antibody levels increased by 16-fold to 23-fold after vaccination, and levels of antibody transfer, as measured in cord blood samples or needlestick samples from the neonate at birth, ranged from 66% to 79%.
Data source: A manufacturer-sponsored phase II randomized placebo-controlled single-blinded study involving 86 healthy pregnant women in Belgium and Canada.
Disclosures: Novartis Vaccines and Diagnostics, whose non-influenza human vaccine business was recently transferred to GlaxoSmithKline, sponsored the study. Dr. Donders received research fees for undertaking the trial, other coauthors received research funding from Novartis, and four coauthors were employed by Novartis at the time of the study.

Save your breath
If you haven’t already stopped investing your limited supply of office time in fruitless attempts to convince vaccine-hesitant parents to immunize their children, a small study at the University of North Carolina Women’s Hospital in Chapel Hill might finally convince you it’s time to save your breath for other more achievable goals. In a survey of 171 parents, 72% reported that they already had settled on their vaccine preferences prior to pregnancy.
This was a limited survey and may not reflect the responses of a national sample of parents, but it is concerning in light of several other studies that paint a similar gloomy picture. One such study found that even when vaccine-denying parents were presented with educational materials that they acknowledged seemed valid, they continued to withhold vaccines by falling back on other arguments to support their views (“Effective Messages in Vaccine Promotion: A Randomized Trial” by Nyhan et al. [Pediatrics. 2014 Apr;133(4):e835-42]).

If a larger and more geographically diverse study continues to find that the die is cast well before pediatricians have gotten our chance to discuss vaccines with parents-to-be, we will need to rethink our strategies for dealing with vaccine refusers. For those pediatricians who already ask vaccine decliners to find another practice, this new study suggests that they could save themselves time and trouble by advertising their policy to the obstetricians in their communities. This proactive advertising would require some courage, but in the long run it probably makes economic sense.
However, for most pediatricians it may be better to wait in hopes that future research can determine exactly when and under what circumstances most vaccine decliners arrive at their unfortunate decisions. How often was it a philosophy that they inherited from their parents? How often did it reflect their religious views? How often did it evolve from something they heard in school? Junior high, high school, college? Was it a science class, or history, or philosophy?
Was it the result of some media story? TV? Print? Internet? If they can recall a particular show or website, what was it that made it sound so convincing? If it was an individual, was it a friend, celebrity, or a teacher?
A study this detailed would be time consuming and labor intensive, as it would be best done in face-to-face structured interviews by someone who could project a nonjudgmental aura. It would necessarily be retrospective. But it might yield some surprising and helpful information that could be used to target our attack on the epidemic of vaccine refusal.
We know that outbreaks of certain infectious diseases, smallpox being the prime example, do not respond to media blitzes and immunization campaigns. Epidemics will continue to roll along unchecked until a labor-intensive, boots-on-the-ground, door-to-door case-finding effort is undertaken. Vaccine refusal may be similar to smallpox. It appears to be unresponsive to mass media and educational initiatives. It may continue to plague us until we chase down its roots.
Whatever strategy we try next, it is clear that although most parents report that they consider pediatricians among their most trusted sources of health information for their children, we are failing to reach a segment of our target audience. We are too late, long after the die is cast.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
*This story was updated 1/28/2016.
If you haven’t already stopped investing your limited supply of office time in fruitless attempts to convince vaccine-hesitant parents to immunize their children, a small study at the University of North Carolina Women’s Hospital in Chapel Hill might finally convince you it’s time to save your breath for other more achievable goals. In a survey of 171 parents, 72% reported that they already had settled on their vaccine preferences prior to pregnancy.
This was a limited survey and may not reflect the responses of a national sample of parents, but it is concerning in light of several other studies that paint a similar gloomy picture. One such study found that even when vaccine-denying parents were presented with educational materials that they acknowledged seemed valid, they continued to withhold vaccines by falling back on other arguments to support their views (“Effective Messages in Vaccine Promotion: A Randomized Trial” by Nyhan et al. [Pediatrics. 2014 Apr;133(4):e835-42]).
If a larger and more geographically diverse study continues to find that the die is cast well before pediatricians have gotten our chance to discuss vaccines with parents-to-be, we will need to rethink our strategies for dealing with vaccine refusers. For those pediatricians who already ask vaccine decliners to find another practice, this new study suggests that they could save themselves time and trouble by advertising their policy to the obstetricians in their communities. This proactive advertising would require some courage, but in the long run it probably makes economic sense.
However, for most pediatricians it may be better to wait in hopes that future research can determine exactly when and under what circumstances most vaccine decliners arrive at their unfortunate decisions. How often was it a philosophy that they inherited from their parents? How often did it reflect their religious views? How often did it evolve from something they heard in school? Junior high, high school, college? Was it a science class, or history, or philosophy?
Was it the result of some media story? TV? Print? Internet? If they can recall a particular show or website, what was it that made it sound so convincing? If it was an individual, was it a friend, celebrity, or a teacher?
A study this detailed would be time consuming and labor intensive, as it would be best done in face-to-face structured interviews by someone who could project a nonjudgmental aura. It would necessarily be retrospective. But it might yield some surprising and helpful information that could be used to target our attack on the epidemic of vaccine refusal.
We know that outbreaks of certain infectious diseases, smallpox being the prime example, do not respond to media blitzes and immunization campaigns. Epidemics will continue to roll along unchecked until a labor-intensive, boots-on-the-ground, door-to-door case-finding effort is undertaken. Vaccine refusal may be similar to smallpox. It appears to be unresponsive to mass media and educational initiatives. It may continue to plague us until we chase down its roots.
Whatever strategy we try next, it is clear that although most parents report that they consider pediatricians among their most trusted sources of health information for their children, we are failing to reach a segment of our target audience. We are too late, long after the die is cast.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
*This story was updated 1/28/2016.
If you haven’t already stopped investing your limited supply of office time in fruitless attempts to convince vaccine-hesitant parents to immunize their children, a small study at the University of North Carolina Women’s Hospital in Chapel Hill might finally convince you it’s time to save your breath for other more achievable goals. In a survey of 171 parents, 72% reported that they already had settled on their vaccine preferences prior to pregnancy.
This was a limited survey and may not reflect the responses of a national sample of parents, but it is concerning in light of several other studies that paint a similar gloomy picture. One such study found that even when vaccine-denying parents were presented with educational materials that they acknowledged seemed valid, they continued to withhold vaccines by falling back on other arguments to support their views (“Effective Messages in Vaccine Promotion: A Randomized Trial” by Nyhan et al. [Pediatrics. 2014 Apr;133(4):e835-42]).
If a larger and more geographically diverse study continues to find that the die is cast well before pediatricians have gotten our chance to discuss vaccines with parents-to-be, we will need to rethink our strategies for dealing with vaccine refusers. For those pediatricians who already ask vaccine decliners to find another practice, this new study suggests that they could save themselves time and trouble by advertising their policy to the obstetricians in their communities. This proactive advertising would require some courage, but in the long run it probably makes economic sense.
However, for most pediatricians it may be better to wait in hopes that future research can determine exactly when and under what circumstances most vaccine decliners arrive at their unfortunate decisions. How often was it a philosophy that they inherited from their parents? How often did it reflect their religious views? How often did it evolve from something they heard in school? Junior high, high school, college? Was it a science class, or history, or philosophy?
Was it the result of some media story? TV? Print? Internet? If they can recall a particular show or website, what was it that made it sound so convincing? If it was an individual, was it a friend, celebrity, or a teacher?
A study this detailed would be time consuming and labor intensive, as it would be best done in face-to-face structured interviews by someone who could project a nonjudgmental aura. It would necessarily be retrospective. But it might yield some surprising and helpful information that could be used to target our attack on the epidemic of vaccine refusal.
We know that outbreaks of certain infectious diseases, smallpox being the prime example, do not respond to media blitzes and immunization campaigns. Epidemics will continue to roll along unchecked until a labor-intensive, boots-on-the-ground, door-to-door case-finding effort is undertaken. Vaccine refusal may be similar to smallpox. It appears to be unresponsive to mass media and educational initiatives. It may continue to plague us until we chase down its roots.
Whatever strategy we try next, it is clear that although most parents report that they consider pediatricians among their most trusted sources of health information for their children, we are failing to reach a segment of our target audience. We are too late, long after the die is cast.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics including “How to Say No to Your Toddler.”
*This story was updated 1/28/2016.

How new dietary guidelines affect health care providers
The U.S. Department of Health and Human Services and the U.S. Department of Agriculture have released the eighth iteration of the Dietary Guidelines for Americans, a set of recommendations for healthy eating habits Americans should adopt to prevent development of hypertension, heart disease, and type 2 diabetes, among other conditions.
The new guidelines, effective through 2020, highlight the importance of eating a wide variety of fruits, vegetables, grains, and dairy products, while staying away from processed foods heavy in saturated fats, sugar, and cholesterol as much as possible. The difference between this and earlier editions of the guidelines, the health agencies say, is to promote the importance of a wider variety of foods Americans should be consuming, rather than focusing on just a few isolated foods that should be integrated into an otherwise inadequate diet.

“Protecting the health of the American public includes empowering them with the tools they need to make healthy choices in their daily lives,” Secretary of Health and Human Services Sylvia M. Burwell said in a statement. “By focusing on small shifts in what we eat and drink, eating healthy becomes more manageable. The Dietary Guidelines provide science-based recommendations on food and nutrition so people can make decisions that may help keep their weight under control, and prevent chronic conditions, like Type 2 diabetes, hypertension, and heart disease.”
The American Medical Association voiced their support of the new guidelines, saying that they are “extremely pleased that the new recommendations call for significantly reducing the amount of added sugars and sugar sweetened beverages from the American diet.” Similarly, the American College of Cardiology issued a statement saying that the existence of “a source of clear science-based information about diet” is more important than ever for Americans in the face of increasingly omnipresent and often confusing information available; the college also lauded the recommendations to limit the intake of added sugars, saturated and trans fats, and sodium. The American Heart Association released a new Authoritative Review of data on the topic of nutritional balance as it related to chronic diseases.
While the recommendations may seem common sense and geared more towards patients and laymen, they are of equal importance to health care providers. Dr. Carolyn Lopez – a Chicago-area family physician and adjunct professor of medicine at Northwestern University – called the guidelines an important resource for physicians, with several elements that will be of particular benefit to physicians and clinicians looking to improve the quality of care given to their patients.
“People [should] understand that while individual food choices are important, the pattern of eating is paramount,” Dr. Lopez explained in an interview. “It’s not impossible to bring vegetables into breakfast – veggie omelettes are great – but it’s hard to imagine bringing a vegetable into the whole grain cereals with skim milk breakfast.”
As a family practitioner, however, Dr. Lopez stressed the difficulty of any doctor having a significant enough amount of time with each patient to really go in-depth into what needs to be done to enact meaningful nutritional and lifestyle changes. “These guidelines can only be effective if the whole team is talking to patients,” she explained. “On its own, it would be extraordinarily difficult [or] impossible to accomplish.
Dr. Nazrat Mirza, a pediatrician who is medical director of the IDEAL Pediatric Weight Management Clinic at Children’s National Health System, Washington, said in an interview that the guidelines are “significant in that they are leading us even closer to healthier dietary living – and from my pediatric perspective, healthier children who will grow into healthier adults. We must keep in mind that these guidelines are not prescriptive – but generalized to relatively healthy people. In particular, the recommendation to reduce sugar intake with specification of an upper limit of 10% of calories from added sugar factored into the suggested daily nutritional intake is an excellent update. Added sugar consumption is linked to diabetes, so any reduction in recommended intake will steer people away from potentially developing diabetes.”
She continued, “In my clinic and day-to-day counseling of patients, being able to point to helpful resources such as these guidelines is crucial. These guidelines will continue to serve as yet another way to reach parents and affect the daily dietary habits they practice at home. I was happy to see resources such as MyPlate.gov referenced in the guidelines; that is a tool I use regularly. When educating families on what a healthy plate looks like, I’m able to point directly to the MyPlate.gov posters hanging in the clinic. Comprehensive resources such as these guidelines, [which] give parents actual examples of foods, and deliver the information in a clear, concise, implementable way, are the best methods to reach parents and kids.”
“As a medical provider, such guidelines provide us with tools and reinforcement to say ‘this is policy,’ when approaching schools about the food and drink options they offer children on a daily basis – because the schools are going to have to follow these guidelines. If these guidelines can enforce public policy for the kids to eat healthy, ... and we can implement changes according to the guidelines, that would help greatly in the prevention of chronic disorders such as obesity, hypertension and diabetes – which is a step in the right direction,” said Dr. Mirza, also of George Washington University, Washington.
“Most physicians are so rushed nowadays by the health care system that they typically do not have adequate time to discuss these very important issues,” Dr. Rodbard said in an interview. “It takes time and perseverance to educate the patient and provide individualized care, assessing their current diet, assessing their willingness or potential for changing their diet or increasing their physical activity.”
On that last point. Dr. Rodbard criticized the new guidelines for not emphasizing the importance of exercise enough. “More clarity and emphasis on physical activity should have been provided,” she said, adding that “people need continual, gentle reminders with repetition and long-term follow-up.” Dr. Rodbard summed up the guidelines as “marginally adequate” but “a step in the right direction.”
An endocrinologist who practices in Winter Park, Fla., Dr. Victor L. Roberts – a Fellow of the ACP and ACE – agreed that time with the patients is critical in order for these guidelines to have any effect, calling the guidelines “just the GPS, not the destination.”
Preaching an ABC strategy – accountability, behavior, and calories, the latter of which he stressed is the most important part of any dietary strategy – Dr. Roberts explained that clinicians and physicians should leave the more specific dietary advice to nutritional experts and focus on telling their patients to watch calories, watch the amount of food they’re eating of any given type, and to exercise more.
“These guidelines crystallize and summarize what we’ve already known, and what we should have been practicing and advocating, for decades,” Dr. Roberts said in an interview, adding that “the difficulty is putting these recommendations into practice and having patients and doctors accept responsibility.”
Ultimately, the three doctors who treat adult patients concurred that the new guidelines are imperfect, and likely won’t result in any automatic widespread change. Dr. Rodbard admitted that she does not anticipate the guidelines affecting the way she treats her patients very much, if at all, while Dr. Lopez said that she’s “not sure it’s going to have a major effect.” Furthermore, the sheer volume of data and information available often leads to patients simply not knowing what to believe, which Dr. Roberts described as a “glazed over” effect of being told so many different things from so many different sources, patients just tune everything out.
Ultimately, while it’s important for health care providers to give advice and recommendations as necessary, these should be done on an individual basis. And, if a patient requires extensive dietary and nutritional intervention, that should be left in the hands of specialist who can accurately determine what the patient is capable of, what their goals should be, and how to tailor a plan specifically for them.
“I don’t know many clinicians, even in my own specialty, who know much about what specifically to eat,” said Dr. Roberts. “That should come from nutritional medicine people, not us.”
Dr. Lopez, Dr. Rodbard, and Dr. Roberts did not report any relevant financial disclosures.
*This article was updated 1/12/2016.
The U.S. Department of Health and Human Services and the U.S. Department of Agriculture have released the eighth iteration of the Dietary Guidelines for Americans, a set of recommendations for healthy eating habits Americans should adopt to prevent development of hypertension, heart disease, and type 2 diabetes, among other conditions.
The new guidelines, effective through 2020, highlight the importance of eating a wide variety of fruits, vegetables, grains, and dairy products, while staying away from processed foods heavy in saturated fats, sugar, and cholesterol as much as possible. The difference between this and earlier editions of the guidelines, the health agencies say, is to promote the importance of a wider variety of foods Americans should be consuming, rather than focusing on just a few isolated foods that should be integrated into an otherwise inadequate diet.
“Protecting the health of the American public includes empowering them with the tools they need to make healthy choices in their daily lives,” Secretary of Health and Human Services Sylvia M. Burwell said in a statement. “By focusing on small shifts in what we eat and drink, eating healthy becomes more manageable. The Dietary Guidelines provide science-based recommendations on food and nutrition so people can make decisions that may help keep their weight under control, and prevent chronic conditions, like Type 2 diabetes, hypertension, and heart disease.”
The American Medical Association voiced their support of the new guidelines, saying that they are “extremely pleased that the new recommendations call for significantly reducing the amount of added sugars and sugar sweetened beverages from the American diet.” Similarly, the American College of Cardiology issued a statement saying that the existence of “a source of clear science-based information about diet” is more important than ever for Americans in the face of increasingly omnipresent and often confusing information available; the college also lauded the recommendations to limit the intake of added sugars, saturated and trans fats, and sodium. The American Heart Association released a new Authoritative Review of data on the topic of nutritional balance as it related to chronic diseases.
While the recommendations may seem common sense and geared more towards patients and laymen, they are of equal importance to health care providers. Dr. Carolyn Lopez – a Chicago-area family physician and adjunct professor of medicine at Northwestern University – called the guidelines an important resource for physicians, with several elements that will be of particular benefit to physicians and clinicians looking to improve the quality of care given to their patients.
“People [should] understand that while individual food choices are important, the pattern of eating is paramount,” Dr. Lopez explained in an interview. “It’s not impossible to bring vegetables into breakfast – veggie omelettes are great – but it’s hard to imagine bringing a vegetable into the whole grain cereals with skim milk breakfast.”
As a family practitioner, however, Dr. Lopez stressed the difficulty of any doctor having a significant enough amount of time with each patient to really go in-depth into what needs to be done to enact meaningful nutritional and lifestyle changes. “These guidelines can only be effective if the whole team is talking to patients,” she explained. “On its own, it would be extraordinarily difficult [or] impossible to accomplish.
Dr. Nazrat Mirza, a pediatrician who is medical director of the IDEAL Pediatric Weight Management Clinic at Children’s National Health System, Washington, said in an interview that the guidelines are “significant in that they are leading us even closer to healthier dietary living – and from my pediatric perspective, healthier children who will grow into healthier adults. We must keep in mind that these guidelines are not prescriptive – but generalized to relatively healthy people. In particular, the recommendation to reduce sugar intake with specification of an upper limit of 10% of calories from added sugar factored into the suggested daily nutritional intake is an excellent update. Added sugar consumption is linked to diabetes, so any reduction in recommended intake will steer people away from potentially developing diabetes.”
She continued, “In my clinic and day-to-day counseling of patients, being able to point to helpful resources such as these guidelines is crucial. These guidelines will continue to serve as yet another way to reach parents and affect the daily dietary habits they practice at home. I was happy to see resources such as MyPlate.gov referenced in the guidelines; that is a tool I use regularly. When educating families on what a healthy plate looks like, I’m able to point directly to the MyPlate.gov posters hanging in the clinic. Comprehensive resources such as these guidelines, [which] give parents actual examples of foods, and deliver the information in a clear, concise, implementable way, are the best methods to reach parents and kids.”
“As a medical provider, such guidelines provide us with tools and reinforcement to say ‘this is policy,’ when approaching schools about the food and drink options they offer children on a daily basis – because the schools are going to have to follow these guidelines. If these guidelines can enforce public policy for the kids to eat healthy, ... and we can implement changes according to the guidelines, that would help greatly in the prevention of chronic disorders such as obesity, hypertension and diabetes – which is a step in the right direction,” said Dr. Mirza, also of George Washington University, Washington.
“Most physicians are so rushed nowadays by the health care system that they typically do not have adequate time to discuss these very important issues,” Dr. Rodbard said in an interview. “It takes time and perseverance to educate the patient and provide individualized care, assessing their current diet, assessing their willingness or potential for changing their diet or increasing their physical activity.”
On that last point. Dr. Rodbard criticized the new guidelines for not emphasizing the importance of exercise enough. “More clarity and emphasis on physical activity should have been provided,” she said, adding that “people need continual, gentle reminders with repetition and long-term follow-up.” Dr. Rodbard summed up the guidelines as “marginally adequate” but “a step in the right direction.”
An endocrinologist who practices in Winter Park, Fla., Dr. Victor L. Roberts – a Fellow of the ACP and ACE – agreed that time with the patients is critical in order for these guidelines to have any effect, calling the guidelines “just the GPS, not the destination.”
Preaching an ABC strategy – accountability, behavior, and calories, the latter of which he stressed is the most important part of any dietary strategy – Dr. Roberts explained that clinicians and physicians should leave the more specific dietary advice to nutritional experts and focus on telling their patients to watch calories, watch the amount of food they’re eating of any given type, and to exercise more.
“These guidelines crystallize and summarize what we’ve already known, and what we should have been practicing and advocating, for decades,” Dr. Roberts said in an interview, adding that “the difficulty is putting these recommendations into practice and having patients and doctors accept responsibility.”
Ultimately, the three doctors who treat adult patients concurred that the new guidelines are imperfect, and likely won’t result in any automatic widespread change. Dr. Rodbard admitted that she does not anticipate the guidelines affecting the way she treats her patients very much, if at all, while Dr. Lopez said that she’s “not sure it’s going to have a major effect.” Furthermore, the sheer volume of data and information available often leads to patients simply not knowing what to believe, which Dr. Roberts described as a “glazed over” effect of being told so many different things from so many different sources, patients just tune everything out.
Ultimately, while it’s important for health care providers to give advice and recommendations as necessary, these should be done on an individual basis. And, if a patient requires extensive dietary and nutritional intervention, that should be left in the hands of specialist who can accurately determine what the patient is capable of, what their goals should be, and how to tailor a plan specifically for them.
“I don’t know many clinicians, even in my own specialty, who know much about what specifically to eat,” said Dr. Roberts. “That should come from nutritional medicine people, not us.”
Dr. Lopez, Dr. Rodbard, and Dr. Roberts did not report any relevant financial disclosures.
*This article was updated 1/12/2016.
The U.S. Department of Health and Human Services and the U.S. Department of Agriculture have released the eighth iteration of the Dietary Guidelines for Americans, a set of recommendations for healthy eating habits Americans should adopt to prevent development of hypertension, heart disease, and type 2 diabetes, among other conditions.
The new guidelines, effective through 2020, highlight the importance of eating a wide variety of fruits, vegetables, grains, and dairy products, while staying away from processed foods heavy in saturated fats, sugar, and cholesterol as much as possible. The difference between this and earlier editions of the guidelines, the health agencies say, is to promote the importance of a wider variety of foods Americans should be consuming, rather than focusing on just a few isolated foods that should be integrated into an otherwise inadequate diet.
“Protecting the health of the American public includes empowering them with the tools they need to make healthy choices in their daily lives,” Secretary of Health and Human Services Sylvia M. Burwell said in a statement. “By focusing on small shifts in what we eat and drink, eating healthy becomes more manageable. The Dietary Guidelines provide science-based recommendations on food and nutrition so people can make decisions that may help keep their weight under control, and prevent chronic conditions, like Type 2 diabetes, hypertension, and heart disease.”
The American Medical Association voiced their support of the new guidelines, saying that they are “extremely pleased that the new recommendations call for significantly reducing the amount of added sugars and sugar sweetened beverages from the American diet.” Similarly, the American College of Cardiology issued a statement saying that the existence of “a source of clear science-based information about diet” is more important than ever for Americans in the face of increasingly omnipresent and often confusing information available; the college also lauded the recommendations to limit the intake of added sugars, saturated and trans fats, and sodium. The American Heart Association released a new Authoritative Review of data on the topic of nutritional balance as it related to chronic diseases.
While the recommendations may seem common sense and geared more towards patients and laymen, they are of equal importance to health care providers. Dr. Carolyn Lopez – a Chicago-area family physician and adjunct professor of medicine at Northwestern University – called the guidelines an important resource for physicians, with several elements that will be of particular benefit to physicians and clinicians looking to improve the quality of care given to their patients.
“People [should] understand that while individual food choices are important, the pattern of eating is paramount,” Dr. Lopez explained in an interview. “It’s not impossible to bring vegetables into breakfast – veggie omelettes are great – but it’s hard to imagine bringing a vegetable into the whole grain cereals with skim milk breakfast.”
As a family practitioner, however, Dr. Lopez stressed the difficulty of any doctor having a significant enough amount of time with each patient to really go in-depth into what needs to be done to enact meaningful nutritional and lifestyle changes. “These guidelines can only be effective if the whole team is talking to patients,” she explained. “On its own, it would be extraordinarily difficult [or] impossible to accomplish.
Dr. Nazrat Mirza, a pediatrician who is medical director of the IDEAL Pediatric Weight Management Clinic at Children’s National Health System, Washington, said in an interview that the guidelines are “significant in that they are leading us even closer to healthier dietary living – and from my pediatric perspective, healthier children who will grow into healthier adults. We must keep in mind that these guidelines are not prescriptive – but generalized to relatively healthy people. In particular, the recommendation to reduce sugar intake with specification of an upper limit of 10% of calories from added sugar factored into the suggested daily nutritional intake is an excellent update. Added sugar consumption is linked to diabetes, so any reduction in recommended intake will steer people away from potentially developing diabetes.”
She continued, “In my clinic and day-to-day counseling of patients, being able to point to helpful resources such as these guidelines is crucial. These guidelines will continue to serve as yet another way to reach parents and affect the daily dietary habits they practice at home. I was happy to see resources such as MyPlate.gov referenced in the guidelines; that is a tool I use regularly. When educating families on what a healthy plate looks like, I’m able to point directly to the MyPlate.gov posters hanging in the clinic. Comprehensive resources such as these guidelines, [which] give parents actual examples of foods, and deliver the information in a clear, concise, implementable way, are the best methods to reach parents and kids.”
“As a medical provider, such guidelines provide us with tools and reinforcement to say ‘this is policy,’ when approaching schools about the food and drink options they offer children on a daily basis – because the schools are going to have to follow these guidelines. If these guidelines can enforce public policy for the kids to eat healthy, ... and we can implement changes according to the guidelines, that would help greatly in the prevention of chronic disorders such as obesity, hypertension and diabetes – which is a step in the right direction,” said Dr. Mirza, also of George Washington University, Washington.
“Most physicians are so rushed nowadays by the health care system that they typically do not have adequate time to discuss these very important issues,” Dr. Rodbard said in an interview. “It takes time and perseverance to educate the patient and provide individualized care, assessing their current diet, assessing their willingness or potential for changing their diet or increasing their physical activity.”
On that last point. Dr. Rodbard criticized the new guidelines for not emphasizing the importance of exercise enough. “More clarity and emphasis on physical activity should have been provided,” she said, adding that “people need continual, gentle reminders with repetition and long-term follow-up.” Dr. Rodbard summed up the guidelines as “marginally adequate” but “a step in the right direction.”
An endocrinologist who practices in Winter Park, Fla., Dr. Victor L. Roberts – a Fellow of the ACP and ACE – agreed that time with the patients is critical in order for these guidelines to have any effect, calling the guidelines “just the GPS, not the destination.”
Preaching an ABC strategy – accountability, behavior, and calories, the latter of which he stressed is the most important part of any dietary strategy – Dr. Roberts explained that clinicians and physicians should leave the more specific dietary advice to nutritional experts and focus on telling their patients to watch calories, watch the amount of food they’re eating of any given type, and to exercise more.
“These guidelines crystallize and summarize what we’ve already known, and what we should have been practicing and advocating, for decades,” Dr. Roberts said in an interview, adding that “the difficulty is putting these recommendations into practice and having patients and doctors accept responsibility.”
Ultimately, the three doctors who treat adult patients concurred that the new guidelines are imperfect, and likely won’t result in any automatic widespread change. Dr. Rodbard admitted that she does not anticipate the guidelines affecting the way she treats her patients very much, if at all, while Dr. Lopez said that she’s “not sure it’s going to have a major effect.” Furthermore, the sheer volume of data and information available often leads to patients simply not knowing what to believe, which Dr. Roberts described as a “glazed over” effect of being told so many different things from so many different sources, patients just tune everything out.
Ultimately, while it’s important for health care providers to give advice and recommendations as necessary, these should be done on an individual basis. And, if a patient requires extensive dietary and nutritional intervention, that should be left in the hands of specialist who can accurately determine what the patient is capable of, what their goals should be, and how to tailor a plan specifically for them.
“I don’t know many clinicians, even in my own specialty, who know much about what specifically to eat,” said Dr. Roberts. “That should come from nutritional medicine people, not us.”
Dr. Lopez, Dr. Rodbard, and Dr. Roberts did not report any relevant financial disclosures.
*This article was updated 1/12/2016.
FROM THE USDA AND HHS

Consider reimmunizing with MMR after HIV-infected children undergo antiretroviral treatment
Reimmunization with a single dose of MMR in children with HIV who have undergone antiretroviral therapy in most cases leads to seroconversion to the measles component, Dr. Anju Seth, professor of pediatrics at Lady Hardinge Medical College, New Delhi, and her associates found.
HIV-infected children don’t respond well to primary immunization with measles, mumps and rubella (MMR) vaccine, and those who do respond tend to lose a protective titer of measles antibodies by age 2-3 years. Revaccinating these children after they undergo antiretroviral therapy (ART) might result in good seroconversion, so Dr. Seth and her associates enrolled 66 children with HIV aged 5-18 years who had undergone antiretroviral therapy for a mean 3.4 years whose mean CD4 count was 716 mcg/L.
At enrollment, 16 children tested positive for measles antibodies, 8 were equivocal, and 42 tested negative. Testing 8-12 weeks after reimmmunization with a single dose of MMR, 62 tested positive, 1 equivocal, and 3 tested negative. Between the seropositive and seronegative children, there was no difference in age, gender, duration of ART, CD4 count, or clinical stage. There were no serious adverse reactions to reimmunizations, the investigators reported. Read the full study at the Pediatric Infectious Disease Journal (2016 Jan;35[1]:e8-11).
Reimmunization with a single dose of MMR in children with HIV who have undergone antiretroviral therapy in most cases leads to seroconversion to the measles component, Dr. Anju Seth, professor of pediatrics at Lady Hardinge Medical College, New Delhi, and her associates found.
HIV-infected children don’t respond well to primary immunization with measles, mumps and rubella (MMR) vaccine, and those who do respond tend to lose a protective titer of measles antibodies by age 2-3 years. Revaccinating these children after they undergo antiretroviral therapy (ART) might result in good seroconversion, so Dr. Seth and her associates enrolled 66 children with HIV aged 5-18 years who had undergone antiretroviral therapy for a mean 3.4 years whose mean CD4 count was 716 mcg/L.
At enrollment, 16 children tested positive for measles antibodies, 8 were equivocal, and 42 tested negative. Testing 8-12 weeks after reimmmunization with a single dose of MMR, 62 tested positive, 1 equivocal, and 3 tested negative. Between the seropositive and seronegative children, there was no difference in age, gender, duration of ART, CD4 count, or clinical stage. There were no serious adverse reactions to reimmunizations, the investigators reported. Read the full study at the Pediatric Infectious Disease Journal (2016 Jan;35[1]:e8-11).
Reimmunization with a single dose of MMR in children with HIV who have undergone antiretroviral therapy in most cases leads to seroconversion to the measles component, Dr. Anju Seth, professor of pediatrics at Lady Hardinge Medical College, New Delhi, and her associates found.
HIV-infected children don’t respond well to primary immunization with measles, mumps and rubella (MMR) vaccine, and those who do respond tend to lose a protective titer of measles antibodies by age 2-3 years. Revaccinating these children after they undergo antiretroviral therapy (ART) might result in good seroconversion, so Dr. Seth and her associates enrolled 66 children with HIV aged 5-18 years who had undergone antiretroviral therapy for a mean 3.4 years whose mean CD4 count was 716 mcg/L.
At enrollment, 16 children tested positive for measles antibodies, 8 were equivocal, and 42 tested negative. Testing 8-12 weeks after reimmmunization with a single dose of MMR, 62 tested positive, 1 equivocal, and 3 tested negative. Between the seropositive and seronegative children, there was no difference in age, gender, duration of ART, CD4 count, or clinical stage. There were no serious adverse reactions to reimmunizations, the investigators reported. Read the full study at the Pediatric Infectious Disease Journal (2016 Jan;35[1]:e8-11).