User login
Antibiotic course durations for uncomplicated SSTIs reduced by hospital initiative
Using targeted quality improvement methods, a hospital more than tripled the proportion of short courses of antibiotics prescribed for children discharged from hospitalization for uncomplicated skin and soft tissue infections (SSTIs), according to a recent study.
“Short courses of antibiotics may be beneficial to help prevent development of resistant bacteria, lessen cost, and reduce the chances of unintended effects of antimicrobial therapy,” explained Dr. Christine L. Schuler and her associates at the Cincinnati Children’s Hospital Medical Center (Pediatrics. 2016 Jan 18. doi: 10.1542/peds.2015-1223). They aimed specifically to increase the percentage of patients receiving antibiotic prescriptions for 7 days or fewer from their baseline of 23% to 80% over 6 months.
For nonpurulent cellulitis, 5-day courses of antibiotics are recommended as sufficiently effective by the Infectious Diseases Society of America, which recommends an extension only if the patient hasn’t improved in that time. Awareness of these guidelines and relevant evidence through two 15-minute education sessions comprised one of the four key components for the initiative’s implementation. The three other components involved “changing the culture of physician prescribing to include discussion of duration of therapy at admission, buy in from prescribers, and effective monitoring of prescribing,” Dr. Schuler and her associates wrote.
Following the sessions, a second intervention provided clinicians with reminder lanyard cards containing information about recommended treatment regimes. Next, electronic order defaults for antibiotics for SSTIs were changed from 14-day courses of antibiotics to 7-day courses, which then automatically subtracted the days on antibiotics during hospitalization, a median 1.2 days.
Last, the hospital started reviewing medical records daily to identify all patients admitted with SSTIs. An intern or senior resident then contacted the patient’s medical team and reminded them that the patient may be appropriate for a short course of antibiotics, that the lanyard card provided therapy recommendations, and that the medical team could contact the project team with questions.
Of 641 patients – aged 3 months to 18 years – admitted for SSTIs between January 2012 and November 2013, one-third occurred before the intervention and two-thirds after. Clindamycin was prescribed in 88% of cases, trimethoprim-sulfamethoxazole in 8%, and cephalexin in 4%.
The proportion of short courses of antibiotics prescribed increased from a baseline of 23% to 74% by February 2013, where it remained for the next 6 months. From March to November 2013, the median duration of antibiotic courses prescribed was 7 days. A total of 2% of the patients were readmitted for recurrence, and 2% were admitted for treatment failure, but these numbers were similar before and after the intervention.
“We suspect that our sustained improvement in prescriptions for short courses of antibiotics over multiple months was in large part due to modification of our electronic order set used to generate outpatient prescriptions,” the authors wrote.
Using targeted quality improvement methods, a hospital more than tripled the proportion of short courses of antibiotics prescribed for children discharged from hospitalization for uncomplicated skin and soft tissue infections (SSTIs), according to a recent study.
“Short courses of antibiotics may be beneficial to help prevent development of resistant bacteria, lessen cost, and reduce the chances of unintended effects of antimicrobial therapy,” explained Dr. Christine L. Schuler and her associates at the Cincinnati Children’s Hospital Medical Center (Pediatrics. 2016 Jan 18. doi: 10.1542/peds.2015-1223). They aimed specifically to increase the percentage of patients receiving antibiotic prescriptions for 7 days or fewer from their baseline of 23% to 80% over 6 months.
For nonpurulent cellulitis, 5-day courses of antibiotics are recommended as sufficiently effective by the Infectious Diseases Society of America, which recommends an extension only if the patient hasn’t improved in that time. Awareness of these guidelines and relevant evidence through two 15-minute education sessions comprised one of the four key components for the initiative’s implementation. The three other components involved “changing the culture of physician prescribing to include discussion of duration of therapy at admission, buy in from prescribers, and effective monitoring of prescribing,” Dr. Schuler and her associates wrote.
Following the sessions, a second intervention provided clinicians with reminder lanyard cards containing information about recommended treatment regimes. Next, electronic order defaults for antibiotics for SSTIs were changed from 14-day courses of antibiotics to 7-day courses, which then automatically subtracted the days on antibiotics during hospitalization, a median 1.2 days.
Last, the hospital started reviewing medical records daily to identify all patients admitted with SSTIs. An intern or senior resident then contacted the patient’s medical team and reminded them that the patient may be appropriate for a short course of antibiotics, that the lanyard card provided therapy recommendations, and that the medical team could contact the project team with questions.
Of 641 patients – aged 3 months to 18 years – admitted for SSTIs between January 2012 and November 2013, one-third occurred before the intervention and two-thirds after. Clindamycin was prescribed in 88% of cases, trimethoprim-sulfamethoxazole in 8%, and cephalexin in 4%.
The proportion of short courses of antibiotics prescribed increased from a baseline of 23% to 74% by February 2013, where it remained for the next 6 months. From March to November 2013, the median duration of antibiotic courses prescribed was 7 days. A total of 2% of the patients were readmitted for recurrence, and 2% were admitted for treatment failure, but these numbers were similar before and after the intervention.
“We suspect that our sustained improvement in prescriptions for short courses of antibiotics over multiple months was in large part due to modification of our electronic order set used to generate outpatient prescriptions,” the authors wrote.
Using targeted quality improvement methods, a hospital more than tripled the proportion of short courses of antibiotics prescribed for children discharged from hospitalization for uncomplicated skin and soft tissue infections (SSTIs), according to a recent study.
“Short courses of antibiotics may be beneficial to help prevent development of resistant bacteria, lessen cost, and reduce the chances of unintended effects of antimicrobial therapy,” explained Dr. Christine L. Schuler and her associates at the Cincinnati Children’s Hospital Medical Center (Pediatrics. 2016 Jan 18. doi: 10.1542/peds.2015-1223). They aimed specifically to increase the percentage of patients receiving antibiotic prescriptions for 7 days or fewer from their baseline of 23% to 80% over 6 months.
For nonpurulent cellulitis, 5-day courses of antibiotics are recommended as sufficiently effective by the Infectious Diseases Society of America, which recommends an extension only if the patient hasn’t improved in that time. Awareness of these guidelines and relevant evidence through two 15-minute education sessions comprised one of the four key components for the initiative’s implementation. The three other components involved “changing the culture of physician prescribing to include discussion of duration of therapy at admission, buy in from prescribers, and effective monitoring of prescribing,” Dr. Schuler and her associates wrote.
Following the sessions, a second intervention provided clinicians with reminder lanyard cards containing information about recommended treatment regimes. Next, electronic order defaults for antibiotics for SSTIs were changed from 14-day courses of antibiotics to 7-day courses, which then automatically subtracted the days on antibiotics during hospitalization, a median 1.2 days.
Last, the hospital started reviewing medical records daily to identify all patients admitted with SSTIs. An intern or senior resident then contacted the patient’s medical team and reminded them that the patient may be appropriate for a short course of antibiotics, that the lanyard card provided therapy recommendations, and that the medical team could contact the project team with questions.
Of 641 patients – aged 3 months to 18 years – admitted for SSTIs between January 2012 and November 2013, one-third occurred before the intervention and two-thirds after. Clindamycin was prescribed in 88% of cases, trimethoprim-sulfamethoxazole in 8%, and cephalexin in 4%.
The proportion of short courses of antibiotics prescribed increased from a baseline of 23% to 74% by February 2013, where it remained for the next 6 months. From March to November 2013, the median duration of antibiotic courses prescribed was 7 days. A total of 2% of the patients were readmitted for recurrence, and 2% were admitted for treatment failure, but these numbers were similar before and after the intervention.
“We suspect that our sustained improvement in prescriptions for short courses of antibiotics over multiple months was in large part due to modification of our electronic order set used to generate outpatient prescriptions,” the authors wrote.
FROM PEDIATRICS
Key clinical point: Quality improvement methods effectively decreased duration of antibiotic courses prescribed for uncomplicated skin and soft tissue infections.
Major finding: A hospital increased its 5-day course antibiotic prescriptions at discharge from 23% to 74% over 13 months.
Data source: The findings are based on one hospital’s data on short courses of antibiotics prescribed between January 2012 and November 2013.
Disclosures: The research did not use external funding, and the authors reported no disclosures.
Antipsychotics may double to triple diabetes risk in youth
Youth who received at least 3 months of antipsychotics were about two to three times more likely to develop type 2 diabetes, compared with controls, a meta-analysis of 13 studies shows.
The risk was especially apparent for olanzapine, confirming “that [type 2 diabetes] risk with second-generation antipsychotics is not homogeneous, and that olanzapine treatment is a major modifiable risk factor,” said Dr. Britta Galling of Zucker Hillside Hospital in Glen Oaks, N.Y., and her associates. Youth should receive antipsychotics only if safer treatments have failed, for the shortest possible effective duration, with proactive monitoring of cardiovascular risk factors and counseling about possible adverse effects, healthy nutrition, and physical activity, according to the meta-analysis, published online Jan. 19.

The researchers searched PubMed and PsycINFO through May 2015 for longitudinal studies of antipsychotics and type 2 diabetes in children, adolescents, and young adults who did not have diabetes at baseline. The resulting studies included 185,105 individuals and 310,438 patient-years. Patients averaged 14.1 years of age (range, 2-24 years), were followed for an average of 1.7 years, and 60% were male (JAMA Psychiatry. 2016 Jan 20. doi: 10.1001/jamapsychiatry.2015.2923).
Antipsychotic exposure doubled the odds (95% confidence interval, 1.56-4.24; P less than .0001) and tripled the incidence (95% CI, 1.7-5.3; P less than .0001) of type 2 diabetes, compared with healthy controls. Antipsychotic-exposed youth also had double the odds and 1.8 times the incidence of type 2 diabetes, compared with psychiatric controls.
The multivariate analysis linked greater cumulative type 2 diabetes risk with longer follow-up (P less than .001), olanzapine exposure (P less than .001), and male sex (P = .002). However, the incidence of type 2 diabetes was lower in youth with autism spectrum disorders (P = .048), perhaps because of other medications or the fact that other psychiatric disorders have a higher type 2 diabetes risk, compared with ASDs, the researchers said.
“These risks should be considered in the clinical risk-benefit evaluation when initiating or continuing antipsychotic treatment in this age group,” they wrote.
The research was funded by the Zucker Hillside Hospital, the National Institute of Mental Health–funded Advanced Center for Interventions and Services Research in Schizophrenia, and the Agency for Healthcare Research & Quality. Dr. Galling had no disclosures. Senior author Dr. Christoph U. Correll, medical director of the recognition and prevention program at the Zucker Hillside Hospital, and his 11 coauthors reported financial relationships the numerous pharmaceutical companies and nonprofit institutions.
Youth who received at least 3 months of antipsychotics were about two to three times more likely to develop type 2 diabetes, compared with controls, a meta-analysis of 13 studies shows.
The risk was especially apparent for olanzapine, confirming “that [type 2 diabetes] risk with second-generation antipsychotics is not homogeneous, and that olanzapine treatment is a major modifiable risk factor,” said Dr. Britta Galling of Zucker Hillside Hospital in Glen Oaks, N.Y., and her associates. Youth should receive antipsychotics only if safer treatments have failed, for the shortest possible effective duration, with proactive monitoring of cardiovascular risk factors and counseling about possible adverse effects, healthy nutrition, and physical activity, according to the meta-analysis, published online Jan. 19.
The researchers searched PubMed and PsycINFO through May 2015 for longitudinal studies of antipsychotics and type 2 diabetes in children, adolescents, and young adults who did not have diabetes at baseline. The resulting studies included 185,105 individuals and 310,438 patient-years. Patients averaged 14.1 years of age (range, 2-24 years), were followed for an average of 1.7 years, and 60% were male (JAMA Psychiatry. 2016 Jan 20. doi: 10.1001/jamapsychiatry.2015.2923).
Antipsychotic exposure doubled the odds (95% confidence interval, 1.56-4.24; P less than .0001) and tripled the incidence (95% CI, 1.7-5.3; P less than .0001) of type 2 diabetes, compared with healthy controls. Antipsychotic-exposed youth also had double the odds and 1.8 times the incidence of type 2 diabetes, compared with psychiatric controls.
The multivariate analysis linked greater cumulative type 2 diabetes risk with longer follow-up (P less than .001), olanzapine exposure (P less than .001), and male sex (P = .002). However, the incidence of type 2 diabetes was lower in youth with autism spectrum disorders (P = .048), perhaps because of other medications or the fact that other psychiatric disorders have a higher type 2 diabetes risk, compared with ASDs, the researchers said.
“These risks should be considered in the clinical risk-benefit evaluation when initiating or continuing antipsychotic treatment in this age group,” they wrote.
The research was funded by the Zucker Hillside Hospital, the National Institute of Mental Health–funded Advanced Center for Interventions and Services Research in Schizophrenia, and the Agency for Healthcare Research & Quality. Dr. Galling had no disclosures. Senior author Dr. Christoph U. Correll, medical director of the recognition and prevention program at the Zucker Hillside Hospital, and his 11 coauthors reported financial relationships the numerous pharmaceutical companies and nonprofit institutions.
Youth who received at least 3 months of antipsychotics were about two to three times more likely to develop type 2 diabetes, compared with controls, a meta-analysis of 13 studies shows.
The risk was especially apparent for olanzapine, confirming “that [type 2 diabetes] risk with second-generation antipsychotics is not homogeneous, and that olanzapine treatment is a major modifiable risk factor,” said Dr. Britta Galling of Zucker Hillside Hospital in Glen Oaks, N.Y., and her associates. Youth should receive antipsychotics only if safer treatments have failed, for the shortest possible effective duration, with proactive monitoring of cardiovascular risk factors and counseling about possible adverse effects, healthy nutrition, and physical activity, according to the meta-analysis, published online Jan. 19.
The researchers searched PubMed and PsycINFO through May 2015 for longitudinal studies of antipsychotics and type 2 diabetes in children, adolescents, and young adults who did not have diabetes at baseline. The resulting studies included 185,105 individuals and 310,438 patient-years. Patients averaged 14.1 years of age (range, 2-24 years), were followed for an average of 1.7 years, and 60% were male (JAMA Psychiatry. 2016 Jan 20. doi: 10.1001/jamapsychiatry.2015.2923).
Antipsychotic exposure doubled the odds (95% confidence interval, 1.56-4.24; P less than .0001) and tripled the incidence (95% CI, 1.7-5.3; P less than .0001) of type 2 diabetes, compared with healthy controls. Antipsychotic-exposed youth also had double the odds and 1.8 times the incidence of type 2 diabetes, compared with psychiatric controls.
The multivariate analysis linked greater cumulative type 2 diabetes risk with longer follow-up (P less than .001), olanzapine exposure (P less than .001), and male sex (P = .002). However, the incidence of type 2 diabetes was lower in youth with autism spectrum disorders (P = .048), perhaps because of other medications or the fact that other psychiatric disorders have a higher type 2 diabetes risk, compared with ASDs, the researchers said.
“These risks should be considered in the clinical risk-benefit evaluation when initiating or continuing antipsychotic treatment in this age group,” they wrote.
The research was funded by the Zucker Hillside Hospital, the National Institute of Mental Health–funded Advanced Center for Interventions and Services Research in Schizophrenia, and the Agency for Healthcare Research & Quality. Dr. Galling had no disclosures. Senior author Dr. Christoph U. Correll, medical director of the recognition and prevention program at the Zucker Hillside Hospital, and his 11 coauthors reported financial relationships the numerous pharmaceutical companies and nonprofit institutions.
FROM JAMA PSYCHIATRY
Key clinical point: Antipsychotics, particularly olanzapine, greatly increased the risk of type 2 diabetes mellitus in young people.
Major finding: The increase was about twofold, compared with psychiatric controls, and threefold, compared with healthy controls.
Data source: A meta-analysis of 13 studies of more than 185,000 youth aged 2-24 years who did not have type 2 diabetes at baseline.
Disclosures: The research was funded by the Zucker Hillside Hospital, the National Institute of Mental Health–funded Advanced Center for Interventions and Services Research in Schizophrenia, and the Agency for Healthcare Research & Quality. Dr. Galling had no disclosures. Senior author Dr. Christoph U. Correll, medical director of the recognition and prevention program at the Zucker Hillside Hospital, and 11 coauthors reported financial relationships to the numerous pharmaceutical companies and nonprofit institutions.

Study: Enterovirus 71 had severe neurologic consequences
Neurological disease related to pediatric enterovirus 71 infection was fatal in 7% of cases, and 10% of survivors had persistent brainstem or motor dysfunction 12 months later, investigators reported online Jan. 19 in JAMA Neurology.
The findings underscore the potentially grave consequences of EV71, which “may be considered the new polio” because it causes long-term focal paresis by damaging brainstem and spinal cord grey matter, said Dr. Hooi-Ling Teoh at Sydney Children’s Hospital and her associates. Clinicians can use the World Health Organization guidelines to quickly identify cases and determine which patients need prompt supportive care and immunotherapy during outbreaks, they added.

Enterovirus 71 usually causes uncomplicated hand-foot-and-mouth disease, but patients can develop aseptic meningitis, acute flaccid paralysis, and fatal brainstem encephalitis. This prospective study included 61 children with EV71-related neurologic disease treated at two urban Australian hospitals during an EV71 outbreak in 2013. The 57 survivors were 3 months to 5 years old (median age, 1.5 years) and almost two-thirds were male. Common initial symptoms included fever (100% of cases), myoclonic jerks (86%), ataxia (54%), and vomiting (54%), the researchers said (JAMA Neurol. 2016 Jan 19. doi: 10.1001/jamaneurol.2015.4388).
The most common neurologic diagnoses included encephalomyelitis (40% of patients), brainstem encephalitis (35%), encephalitis (11%), acute flaccid paralysis (7%), and neurogenic pulmonary edema (7%), a particularly severe form of EV71 disease. Characteristic MRI signs included increased T2-weighted signal in the dorsal pons and spinal cord, but pulmonary edema also was associated with dorsal brainstem restricted diffusion (odds ratio, 2.0; 95% confidence interval, 1-4; P = .001). Brainstem or motor dysfunction resolved in 77% of cases by 2 months and in 90% of cases at 12 months. The most common long-term clinical and functional problem was focal paresis, which persisted in five of six patients at 12 months.
Notably, the odds of persistent motor dysfunction were about 15 times higher when patients presented with acute flaccid paralysis or pulmonary edema than when they had other syndromes (OR, 15; 95% CI, 3-79; P < .001). Also, EV RNA was identified far more often from fecal samples and rectal and throat swabs than from cerebrospinal fluid, Dr. Teoh and associates reported.
The research was supported by the Thyne Reid Foundation, National Health and Medical Research Council of Australia, Royal Australasian College of Physicians Paediatrics & Child Health Division, and by a Norah Theresa Hayes-Ratcliffe Paediatric Infectious Diseases fellowship award. The investigators had no disclosures.
Neurological disease related to pediatric enterovirus 71 infection was fatal in 7% of cases, and 10% of survivors had persistent brainstem or motor dysfunction 12 months later, investigators reported online Jan. 19 in JAMA Neurology.
The findings underscore the potentially grave consequences of EV71, which “may be considered the new polio” because it causes long-term focal paresis by damaging brainstem and spinal cord grey matter, said Dr. Hooi-Ling Teoh at Sydney Children’s Hospital and her associates. Clinicians can use the World Health Organization guidelines to quickly identify cases and determine which patients need prompt supportive care and immunotherapy during outbreaks, they added.
Enterovirus 71 usually causes uncomplicated hand-foot-and-mouth disease, but patients can develop aseptic meningitis, acute flaccid paralysis, and fatal brainstem encephalitis. This prospective study included 61 children with EV71-related neurologic disease treated at two urban Australian hospitals during an EV71 outbreak in 2013. The 57 survivors were 3 months to 5 years old (median age, 1.5 years) and almost two-thirds were male. Common initial symptoms included fever (100% of cases), myoclonic jerks (86%), ataxia (54%), and vomiting (54%), the researchers said (JAMA Neurol. 2016 Jan 19. doi: 10.1001/jamaneurol.2015.4388).
The most common neurologic diagnoses included encephalomyelitis (40% of patients), brainstem encephalitis (35%), encephalitis (11%), acute flaccid paralysis (7%), and neurogenic pulmonary edema (7%), a particularly severe form of EV71 disease. Characteristic MRI signs included increased T2-weighted signal in the dorsal pons and spinal cord, but pulmonary edema also was associated with dorsal brainstem restricted diffusion (odds ratio, 2.0; 95% confidence interval, 1-4; P = .001). Brainstem or motor dysfunction resolved in 77% of cases by 2 months and in 90% of cases at 12 months. The most common long-term clinical and functional problem was focal paresis, which persisted in five of six patients at 12 months.
Notably, the odds of persistent motor dysfunction were about 15 times higher when patients presented with acute flaccid paralysis or pulmonary edema than when they had other syndromes (OR, 15; 95% CI, 3-79; P < .001). Also, EV RNA was identified far more often from fecal samples and rectal and throat swabs than from cerebrospinal fluid, Dr. Teoh and associates reported.
The research was supported by the Thyne Reid Foundation, National Health and Medical Research Council of Australia, Royal Australasian College of Physicians Paediatrics & Child Health Division, and by a Norah Theresa Hayes-Ratcliffe Paediatric Infectious Diseases fellowship award. The investigators had no disclosures.
Neurological disease related to pediatric enterovirus 71 infection was fatal in 7% of cases, and 10% of survivors had persistent brainstem or motor dysfunction 12 months later, investigators reported online Jan. 19 in JAMA Neurology.
The findings underscore the potentially grave consequences of EV71, which “may be considered the new polio” because it causes long-term focal paresis by damaging brainstem and spinal cord grey matter, said Dr. Hooi-Ling Teoh at Sydney Children’s Hospital and her associates. Clinicians can use the World Health Organization guidelines to quickly identify cases and determine which patients need prompt supportive care and immunotherapy during outbreaks, they added.
Enterovirus 71 usually causes uncomplicated hand-foot-and-mouth disease, but patients can develop aseptic meningitis, acute flaccid paralysis, and fatal brainstem encephalitis. This prospective study included 61 children with EV71-related neurologic disease treated at two urban Australian hospitals during an EV71 outbreak in 2013. The 57 survivors were 3 months to 5 years old (median age, 1.5 years) and almost two-thirds were male. Common initial symptoms included fever (100% of cases), myoclonic jerks (86%), ataxia (54%), and vomiting (54%), the researchers said (JAMA Neurol. 2016 Jan 19. doi: 10.1001/jamaneurol.2015.4388).
The most common neurologic diagnoses included encephalomyelitis (40% of patients), brainstem encephalitis (35%), encephalitis (11%), acute flaccid paralysis (7%), and neurogenic pulmonary edema (7%), a particularly severe form of EV71 disease. Characteristic MRI signs included increased T2-weighted signal in the dorsal pons and spinal cord, but pulmonary edema also was associated with dorsal brainstem restricted diffusion (odds ratio, 2.0; 95% confidence interval, 1-4; P = .001). Brainstem or motor dysfunction resolved in 77% of cases by 2 months and in 90% of cases at 12 months. The most common long-term clinical and functional problem was focal paresis, which persisted in five of six patients at 12 months.
Notably, the odds of persistent motor dysfunction were about 15 times higher when patients presented with acute flaccid paralysis or pulmonary edema than when they had other syndromes (OR, 15; 95% CI, 3-79; P < .001). Also, EV RNA was identified far more often from fecal samples and rectal and throat swabs than from cerebrospinal fluid, Dr. Teoh and associates reported.
The research was supported by the Thyne Reid Foundation, National Health and Medical Research Council of Australia, Royal Australasian College of Physicians Paediatrics & Child Health Division, and by a Norah Theresa Hayes-Ratcliffe Paediatric Infectious Diseases fellowship award. The investigators had no disclosures.
FROM JAMA NEUROLOGY
Key clinical point: Enterovirus 71 can have “devastating” neurologic consequences in young patients.
Major finding: Among 61 hospitalized children, the case-fatality rate was 7%, and 10% of survivors had brainstem or motor dysfunctions at 12 months.
Data source: A prospective study of pediatric inpatients at two hospitals in Sydney during an outbreak in 2013.
Disclosures: The research was supported by the Thyne Reid Foundation, the National Health and Medical Research Council of Australia, the Royal Australasian College of Physicians Paediatrics & Child Health Division, and by a Norah Theresa Hayes-Ratcliffe Paediatric Infectious Diseases fellowship award. The investigators had no disclosures.

Meningococcal conjugate vaccine safe, effective with other vaccines
The quadrivalent meningococcal conjugate vaccine MenACWY-CRM can be safely coadministered with other routine vaccines in all age groups, according to Dr. Roberto Gasparini of the University of Genoa, Italy, and his associates.
Infant immune response to diphtheria, tetanus, poliovirus, hepatitis B, Haemophilus influenzae type b, pneumococcal conjugate, measles-mumps-rubella, varicella or pertussis antigens was unaffected by coadministered MenACWY-CRM. In some infants under 7 months old, noninferiority criteria were not met for some pneumococcal serotypes, but no consistent pattern was seen.

In adolescents, a concurrent MenACWY-CRM vaccination did not adversely affect immune responses to tetanus, diphtheria, and human papillomavirus antigens. In adults, the MenACWY-CRM vaccine did not affect immune response to hepatitis A/B, typhoid fever, yellow fever, Japanese encephalitis, and rabies antigens. No group saw an increase in postvaccination adverse events.
“These findings support the concomitant administration of MenACWY-CRM with routine vaccines in all age groups, allowing MenACWY-CRM to be readily incorporated as recommended into existing infant and adolescent vaccination schedules and to be administered with other vaccines as needed in advance of international travel,” the investigators concluded.
Find the full study in the Pediatric Infectious Disease Journal (2016;35[1]:81-93. doi: 10.1097/INF.0000000000000930).
The quadrivalent meningococcal conjugate vaccine MenACWY-CRM can be safely coadministered with other routine vaccines in all age groups, according to Dr. Roberto Gasparini of the University of Genoa, Italy, and his associates.
Infant immune response to diphtheria, tetanus, poliovirus, hepatitis B, Haemophilus influenzae type b, pneumococcal conjugate, measles-mumps-rubella, varicella or pertussis antigens was unaffected by coadministered MenACWY-CRM. In some infants under 7 months old, noninferiority criteria were not met for some pneumococcal serotypes, but no consistent pattern was seen.
In adolescents, a concurrent MenACWY-CRM vaccination did not adversely affect immune responses to tetanus, diphtheria, and human papillomavirus antigens. In adults, the MenACWY-CRM vaccine did not affect immune response to hepatitis A/B, typhoid fever, yellow fever, Japanese encephalitis, and rabies antigens. No group saw an increase in postvaccination adverse events.
“These findings support the concomitant administration of MenACWY-CRM with routine vaccines in all age groups, allowing MenACWY-CRM to be readily incorporated as recommended into existing infant and adolescent vaccination schedules and to be administered with other vaccines as needed in advance of international travel,” the investigators concluded.
Find the full study in the Pediatric Infectious Disease Journal (2016;35[1]:81-93. doi: 10.1097/INF.0000000000000930).
The quadrivalent meningococcal conjugate vaccine MenACWY-CRM can be safely coadministered with other routine vaccines in all age groups, according to Dr. Roberto Gasparini of the University of Genoa, Italy, and his associates.
Infant immune response to diphtheria, tetanus, poliovirus, hepatitis B, Haemophilus influenzae type b, pneumococcal conjugate, measles-mumps-rubella, varicella or pertussis antigens was unaffected by coadministered MenACWY-CRM. In some infants under 7 months old, noninferiority criteria were not met for some pneumococcal serotypes, but no consistent pattern was seen.
In adolescents, a concurrent MenACWY-CRM vaccination did not adversely affect immune responses to tetanus, diphtheria, and human papillomavirus antigens. In adults, the MenACWY-CRM vaccine did not affect immune response to hepatitis A/B, typhoid fever, yellow fever, Japanese encephalitis, and rabies antigens. No group saw an increase in postvaccination adverse events.
“These findings support the concomitant administration of MenACWY-CRM with routine vaccines in all age groups, allowing MenACWY-CRM to be readily incorporated as recommended into existing infant and adolescent vaccination schedules and to be administered with other vaccines as needed in advance of international travel,” the investigators concluded.
Find the full study in the Pediatric Infectious Disease Journal (2016;35[1]:81-93. doi: 10.1097/INF.0000000000000930).
FROM THE PEDIATRIC INFECTIOUS DISEASE JOURNAL

Many Providers Don’t Teach Epinephrine Use for Food Allergies
Many pediatricians and allergists failed to provide instructions for when and how to use epinephrine and a written emergency action plan to the parents of children with food allergies, a study found.
Researchers asked the parents of 859 children with allergies to share their level of satisfaction with the care and delivery of care from the pediatricians and allergists treating their children over the course of the previous 6 months. While more than 75% of the doctors treated the parents courteously and respectfully and provided clear explanations of children’s allergies, a high percentage of the doctors neglected to provide other information essential for caring for children with food allergies, the parents reported.

The parents most often said they were missing explanations on when and how their children should be receiving epinephrine to treat allergic reactions and instructions on exactly what to do if their children had a medical emergency related to their specific allergies and circumstances. More pediatricians than allergists failed to share such information.
Among allergists, 68% explained when to use epinephrine, while 37% of pediatricians provided such information, the parents reported. Instructions on how to use epinephrine were provided to parents by 47% of allergists and 20% of pediatricians. Written emergency health care plans customized to each child were provided by 56% of the allergists and 24% of the pediatricians
“Although pediatricians might be relying on allergists to deliver [an emergency action plan and training in epinephrine autoinjectors use], with the rise in food allergies, guidelines recommend that pediatricians conduct these steps and not rely solely on the allergist,” said Jesse A. Blumenstock of Northwestern University, Chicago, and colleagues. “With our understanding of food allergy and anaphylaxis constantly evolving, guidelines and recommendations for how and when to give epinephrine and the need for an action plan need to be reinforced by physicians.”
Read the study in the Journal of Allergy and Clinical Immunology: In Practice (doi: 10.1016/j.jaip.2015.10.011).
Many pediatricians and allergists failed to provide instructions for when and how to use epinephrine and a written emergency action plan to the parents of children with food allergies, a study found.
Researchers asked the parents of 859 children with allergies to share their level of satisfaction with the care and delivery of care from the pediatricians and allergists treating their children over the course of the previous 6 months. While more than 75% of the doctors treated the parents courteously and respectfully and provided clear explanations of children’s allergies, a high percentage of the doctors neglected to provide other information essential for caring for children with food allergies, the parents reported.
The parents most often said they were missing explanations on when and how their children should be receiving epinephrine to treat allergic reactions and instructions on exactly what to do if their children had a medical emergency related to their specific allergies and circumstances. More pediatricians than allergists failed to share such information.
Among allergists, 68% explained when to use epinephrine, while 37% of pediatricians provided such information, the parents reported. Instructions on how to use epinephrine were provided to parents by 47% of allergists and 20% of pediatricians. Written emergency health care plans customized to each child were provided by 56% of the allergists and 24% of the pediatricians
“Although pediatricians might be relying on allergists to deliver [an emergency action plan and training in epinephrine autoinjectors use], with the rise in food allergies, guidelines recommend that pediatricians conduct these steps and not rely solely on the allergist,” said Jesse A. Blumenstock of Northwestern University, Chicago, and colleagues. “With our understanding of food allergy and anaphylaxis constantly evolving, guidelines and recommendations for how and when to give epinephrine and the need for an action plan need to be reinforced by physicians.”
Read the study in the Journal of Allergy and Clinical Immunology: In Practice (doi: 10.1016/j.jaip.2015.10.011).
Many pediatricians and allergists failed to provide instructions for when and how to use epinephrine and a written emergency action plan to the parents of children with food allergies, a study found.
Researchers asked the parents of 859 children with allergies to share their level of satisfaction with the care and delivery of care from the pediatricians and allergists treating their children over the course of the previous 6 months. While more than 75% of the doctors treated the parents courteously and respectfully and provided clear explanations of children’s allergies, a high percentage of the doctors neglected to provide other information essential for caring for children with food allergies, the parents reported.
The parents most often said they were missing explanations on when and how their children should be receiving epinephrine to treat allergic reactions and instructions on exactly what to do if their children had a medical emergency related to their specific allergies and circumstances. More pediatricians than allergists failed to share such information.
Among allergists, 68% explained when to use epinephrine, while 37% of pediatricians provided such information, the parents reported. Instructions on how to use epinephrine were provided to parents by 47% of allergists and 20% of pediatricians. Written emergency health care plans customized to each child were provided by 56% of the allergists and 24% of the pediatricians
“Although pediatricians might be relying on allergists to deliver [an emergency action plan and training in epinephrine autoinjectors use], with the rise in food allergies, guidelines recommend that pediatricians conduct these steps and not rely solely on the allergist,” said Jesse A. Blumenstock of Northwestern University, Chicago, and colleagues. “With our understanding of food allergy and anaphylaxis constantly evolving, guidelines and recommendations for how and when to give epinephrine and the need for an action plan need to be reinforced by physicians.”
Read the study in the Journal of Allergy and Clinical Immunology: In Practice (doi: 10.1016/j.jaip.2015.10.011).

Many physicians don’t teach epinephrine use for food allergies
Many pediatricians and allergists failed to provide instructions for when and how to use epinephrine and a written emergency action plan to the parents of children with food allergies, a study found.
Researchers asked the parents of 859 children with allergies to share their level of satisfaction with the care and delivery of care from the pediatricians and allergists treating their children over the course of the previous 6 months. While more than 75% of the doctors treated the parents courteously and respectfully and provided clear explanations of children’s allergies, a high percentage of the doctors neglected to provide other information essential for caring for children with food allergies, the parents reported.

The parents most often said they were missing explanations on when and how their children should be receiving epinephrine to treat allergic reactions and instructions on exactly what to do if their children had a medical emergency related to their specific allergies and circumstances. More pediatricians than allergists failed to share such information.
Among allergists, 68% explained when to use epinephrine, while 37% of pediatricians provided such information, the parents reported. Instructions on how to use epinephrine were provided to parents by 47% of allergists and 20% of pediatricians. Written emergency health care plans customized to each child were provided by 56% of the allergists and 24% of the pediatricians
“Although pediatricians might be relying on allergists to deliver [an emergency action plan and training in epinephrine autoinjectors use], with the rise in food allergies, guidelines recommend that pediatricians conduct these steps and not rely solely on the allergist,” said Jesse A. Blumenstock of Northwestern University, Chicago, and colleagues. “With our understanding of food allergy and anaphylaxis constantly evolving, guidelines and recommendations for how and when to give epinephrine and the need for an action plan need to be reinforced by physicians.”
Read the study in the Journal of Allergy and Clinical Immunology: In Practice (doi: 10.1016/j.jaip.2015.10.011).
Many pediatricians and allergists failed to provide instructions for when and how to use epinephrine and a written emergency action plan to the parents of children with food allergies, a study found.
Researchers asked the parents of 859 children with allergies to share their level of satisfaction with the care and delivery of care from the pediatricians and allergists treating their children over the course of the previous 6 months. While more than 75% of the doctors treated the parents courteously and respectfully and provided clear explanations of children’s allergies, a high percentage of the doctors neglected to provide other information essential for caring for children with food allergies, the parents reported.
The parents most often said they were missing explanations on when and how their children should be receiving epinephrine to treat allergic reactions and instructions on exactly what to do if their children had a medical emergency related to their specific allergies and circumstances. More pediatricians than allergists failed to share such information.
Among allergists, 68% explained when to use epinephrine, while 37% of pediatricians provided such information, the parents reported. Instructions on how to use epinephrine were provided to parents by 47% of allergists and 20% of pediatricians. Written emergency health care plans customized to each child were provided by 56% of the allergists and 24% of the pediatricians
“Although pediatricians might be relying on allergists to deliver [an emergency action plan and training in epinephrine autoinjectors use], with the rise in food allergies, guidelines recommend that pediatricians conduct these steps and not rely solely on the allergist,” said Jesse A. Blumenstock of Northwestern University, Chicago, and colleagues. “With our understanding of food allergy and anaphylaxis constantly evolving, guidelines and recommendations for how and when to give epinephrine and the need for an action plan need to be reinforced by physicians.”
Read the study in the Journal of Allergy and Clinical Immunology: In Practice (doi: 10.1016/j.jaip.2015.10.011).
Many pediatricians and allergists failed to provide instructions for when and how to use epinephrine and a written emergency action plan to the parents of children with food allergies, a study found.
Researchers asked the parents of 859 children with allergies to share their level of satisfaction with the care and delivery of care from the pediatricians and allergists treating their children over the course of the previous 6 months. While more than 75% of the doctors treated the parents courteously and respectfully and provided clear explanations of children’s allergies, a high percentage of the doctors neglected to provide other information essential for caring for children with food allergies, the parents reported.
The parents most often said they were missing explanations on when and how their children should be receiving epinephrine to treat allergic reactions and instructions on exactly what to do if their children had a medical emergency related to their specific allergies and circumstances. More pediatricians than allergists failed to share such information.
Among allergists, 68% explained when to use epinephrine, while 37% of pediatricians provided such information, the parents reported. Instructions on how to use epinephrine were provided to parents by 47% of allergists and 20% of pediatricians. Written emergency health care plans customized to each child were provided by 56% of the allergists and 24% of the pediatricians
“Although pediatricians might be relying on allergists to deliver [an emergency action plan and training in epinephrine autoinjectors use], with the rise in food allergies, guidelines recommend that pediatricians conduct these steps and not rely solely on the allergist,” said Jesse A. Blumenstock of Northwestern University, Chicago, and colleagues. “With our understanding of food allergy and anaphylaxis constantly evolving, guidelines and recommendations for how and when to give epinephrine and the need for an action plan need to be reinforced by physicians.”
Read the study in the Journal of Allergy and Clinical Immunology: In Practice (doi: 10.1016/j.jaip.2015.10.011).

Cancer survival tied to reduction in treatment

Photo by Bill Branson
Results of a large study suggest that long-term survivors of childhood cancer are living longer, partly due to a reduction in the use of certain treatments.
The 15-year death rate among the more than 34,000 childhood cancer survivors studied decreased steadily from 1970 onward.
And this decline coincided with changes in pediatric cancer therapy, including reductions in the use and dose of radiation therapy and anthracyclines.
These therapies are known to put cancer survivors at increased risk for developing second malignancies, heart failure, and other serious health problems.
“This study is the first to show that younger survivors from more recent treatment eras are less likely to die from the late effects of cancer treatment and more likely to enjoy longer lives,” said study author Greg Armstrong, MD, of St. Jude Children's Research Hospital in Memphis, Tennessee.
He and his colleagues reported these results in NEJM.
The study included 34,033 subjects who had been diagnosed with cancer and received treatment between 1970 and 1999 when they were age 20 or younger. All patients lived at least 5 years after their cancers were discovered and were considered long-term survivors.
Changes in mortality
At a median follow-up of 21 years (range, 5 to 38), there were 3958 deaths. Forty-one percent of deaths (n=1618) were considered health-related. This included 746 deaths from subsequent neoplasms, 241 from cardiac causes, 137 from pulmonary causes, and 494 from other causes.
The 15-year death rate (death from any cause) fell from 12.4% in the early 1970s to 6% in the 1990s (P<0.001). During the same period, the rate of death from health-related causes fell from 3.5% to 2.1% (P<0.001).
The researchers said there were significant reductions across treatment eras in the rates of death from any health-related cause among patients with acute lymphoblastic leukemia (ALL), Hodgkin lymphoma (HL), Wilms’ tumor, and astrocytoma, but not among patients with other cancers.
The rate of health-related death among ALL patients fell from 3.2% in the early 1970s to 2.1% in the 1990s (P<0.001). The rate fell from 5.3% to 2.6% (P=0.006) for HL patients, from 2.6% to 0.4% (P=0.005) for Wilms’ tumor patients, and from 4.7% to 1.8% (P=0.02) for astrocytoma patients.
The researchers said these reductions in mortality were attributable to decreases in the rates of death from subsequent neoplasm (P<0.001), cardiac causes (P<0.001), and pulmonary causes (P=0.04).
Treatment changes
The overall use of anthracyclines fell from 73% in the 1970s to 42% in the 1990s. And the use of any radiation decreased from 77% to 41%.
The use of cranial radiotherapy for ALL fell from 85% to 19%. The use of abdominal radiotherapy for Wilms’ tumor decreased from 78% to 43%. And the use of chest radiotherapy for HL fell from 87% to 61%.
The researchers noted that temporal reductions in 15-year rates of death from health-related causes followed temporal reductions in therapeutic exposure for patients with ALL, HL, Wilms’ tumor, and astrocytoma.
However, when the team adjusted their analysis for therapy (eg, anthracycline dose), the effect of the treatment era on the relative rate of death from health-related causes was attenuated in ALL (unadjusted relative rate=0.88, adjusted relative rate=1.02) and Wilms’ tumor (0.68 and 0.80, respectively) but not in HL (0.79 in both models) and astrocytoma (0.81 and 0.82, respectively).
Still, the researchers said the results of this study suggest the strategy of lowering therapeutic exposure has contributed to the decline in late mortality among 5-year survivors of childhood cancer. ![]()
Photo by Bill Branson
Results of a large study suggest that long-term survivors of childhood cancer are living longer, partly due to a reduction in the use of certain treatments.
The 15-year death rate among the more than 34,000 childhood cancer survivors studied decreased steadily from 1970 onward.
And this decline coincided with changes in pediatric cancer therapy, including reductions in the use and dose of radiation therapy and anthracyclines.
These therapies are known to put cancer survivors at increased risk for developing second malignancies, heart failure, and other serious health problems.
“This study is the first to show that younger survivors from more recent treatment eras are less likely to die from the late effects of cancer treatment and more likely to enjoy longer lives,” said study author Greg Armstrong, MD, of St. Jude Children's Research Hospital in Memphis, Tennessee.
He and his colleagues reported these results in NEJM.
The study included 34,033 subjects who had been diagnosed with cancer and received treatment between 1970 and 1999 when they were age 20 or younger. All patients lived at least 5 years after their cancers were discovered and were considered long-term survivors.
Changes in mortality
At a median follow-up of 21 years (range, 5 to 38), there were 3958 deaths. Forty-one percent of deaths (n=1618) were considered health-related. This included 746 deaths from subsequent neoplasms, 241 from cardiac causes, 137 from pulmonary causes, and 494 from other causes.
The 15-year death rate (death from any cause) fell from 12.4% in the early 1970s to 6% in the 1990s (P<0.001). During the same period, the rate of death from health-related causes fell from 3.5% to 2.1% (P<0.001).
The researchers said there were significant reductions across treatment eras in the rates of death from any health-related cause among patients with acute lymphoblastic leukemia (ALL), Hodgkin lymphoma (HL), Wilms’ tumor, and astrocytoma, but not among patients with other cancers.
The rate of health-related death among ALL patients fell from 3.2% in the early 1970s to 2.1% in the 1990s (P<0.001). The rate fell from 5.3% to 2.6% (P=0.006) for HL patients, from 2.6% to 0.4% (P=0.005) for Wilms’ tumor patients, and from 4.7% to 1.8% (P=0.02) for astrocytoma patients.
The researchers said these reductions in mortality were attributable to decreases in the rates of death from subsequent neoplasm (P<0.001), cardiac causes (P<0.001), and pulmonary causes (P=0.04).
Treatment changes
The overall use of anthracyclines fell from 73% in the 1970s to 42% in the 1990s. And the use of any radiation decreased from 77% to 41%.
The use of cranial radiotherapy for ALL fell from 85% to 19%. The use of abdominal radiotherapy for Wilms’ tumor decreased from 78% to 43%. And the use of chest radiotherapy for HL fell from 87% to 61%.
The researchers noted that temporal reductions in 15-year rates of death from health-related causes followed temporal reductions in therapeutic exposure for patients with ALL, HL, Wilms’ tumor, and astrocytoma.
However, when the team adjusted their analysis for therapy (eg, anthracycline dose), the effect of the treatment era on the relative rate of death from health-related causes was attenuated in ALL (unadjusted relative rate=0.88, adjusted relative rate=1.02) and Wilms’ tumor (0.68 and 0.80, respectively) but not in HL (0.79 in both models) and astrocytoma (0.81 and 0.82, respectively).
Still, the researchers said the results of this study suggest the strategy of lowering therapeutic exposure has contributed to the decline in late mortality among 5-year survivors of childhood cancer. ![]()
Photo by Bill Branson
Results of a large study suggest that long-term survivors of childhood cancer are living longer, partly due to a reduction in the use of certain treatments.
The 15-year death rate among the more than 34,000 childhood cancer survivors studied decreased steadily from 1970 onward.
And this decline coincided with changes in pediatric cancer therapy, including reductions in the use and dose of radiation therapy and anthracyclines.
These therapies are known to put cancer survivors at increased risk for developing second malignancies, heart failure, and other serious health problems.
“This study is the first to show that younger survivors from more recent treatment eras are less likely to die from the late effects of cancer treatment and more likely to enjoy longer lives,” said study author Greg Armstrong, MD, of St. Jude Children's Research Hospital in Memphis, Tennessee.
He and his colleagues reported these results in NEJM.
The study included 34,033 subjects who had been diagnosed with cancer and received treatment between 1970 and 1999 when they were age 20 or younger. All patients lived at least 5 years after their cancers were discovered and were considered long-term survivors.
Changes in mortality
At a median follow-up of 21 years (range, 5 to 38), there were 3958 deaths. Forty-one percent of deaths (n=1618) were considered health-related. This included 746 deaths from subsequent neoplasms, 241 from cardiac causes, 137 from pulmonary causes, and 494 from other causes.
The 15-year death rate (death from any cause) fell from 12.4% in the early 1970s to 6% in the 1990s (P<0.001). During the same period, the rate of death from health-related causes fell from 3.5% to 2.1% (P<0.001).
The researchers said there were significant reductions across treatment eras in the rates of death from any health-related cause among patients with acute lymphoblastic leukemia (ALL), Hodgkin lymphoma (HL), Wilms’ tumor, and astrocytoma, but not among patients with other cancers.
The rate of health-related death among ALL patients fell from 3.2% in the early 1970s to 2.1% in the 1990s (P<0.001). The rate fell from 5.3% to 2.6% (P=0.006) for HL patients, from 2.6% to 0.4% (P=0.005) for Wilms’ tumor patients, and from 4.7% to 1.8% (P=0.02) for astrocytoma patients.
The researchers said these reductions in mortality were attributable to decreases in the rates of death from subsequent neoplasm (P<0.001), cardiac causes (P<0.001), and pulmonary causes (P=0.04).
Treatment changes
The overall use of anthracyclines fell from 73% in the 1970s to 42% in the 1990s. And the use of any radiation decreased from 77% to 41%.
The use of cranial radiotherapy for ALL fell from 85% to 19%. The use of abdominal radiotherapy for Wilms’ tumor decreased from 78% to 43%. And the use of chest radiotherapy for HL fell from 87% to 61%.
The researchers noted that temporal reductions in 15-year rates of death from health-related causes followed temporal reductions in therapeutic exposure for patients with ALL, HL, Wilms’ tumor, and astrocytoma.
However, when the team adjusted their analysis for therapy (eg, anthracycline dose), the effect of the treatment era on the relative rate of death from health-related causes was attenuated in ALL (unadjusted relative rate=0.88, adjusted relative rate=1.02) and Wilms’ tumor (0.68 and 0.80, respectively) but not in HL (0.79 in both models) and astrocytoma (0.81 and 0.82, respectively).
Still, the researchers said the results of this study suggest the strategy of lowering therapeutic exposure has contributed to the decline in late mortality among 5-year survivors of childhood cancer. ![]()
Therapy, medication together best to treat pediatric mood disorders
Effective management of depression and other mood disorders in children may involve both pharmacotherapy with behavioral recommendations and psychotherapy, according to Stephen P. Whiteside, Ph.D., and Dr. John Huxsahl of the Mayo Clinic in Rochester Minn.
In a presentation at the American Academy of Pediatrics annual meeting in Washington, they reviewed the differences between various mood disorders because accurate diagnosis is a key component to management.

A major depressive episode is among the more common mood disorders among children, but others include disruptive mood dysregulation disorder, persistent depressive disorder, and bipolar I disorder. Because most pediatricians have just 15 minutes or so with patients, Dr. Whiteside and Dr. Huxsahl recommended using screening questionnaires to identify children at risk for a mood disorder. Trying to determine why a child is experiencing these symptoms or feelings can help clinicians determine whether this is a chronic issue or a situational one. Asking about other concerns, such as anxiety or use of substances, also can help with diagnosis.
Depressive episodes
Occurring among approximately 2% of children and 4%-8% of adolescents, a major depressive episode lasts a median of 8 months, but has a very high rate of recurrence: 20%-60% at 1 or 2 years after remission and 70% at 5 years after remission. In a significant proportion of children – about 20%-40% – a major depressive episode forecasts bipolar disorder.
In fact, having a parent with a mood disorder doubles to quadruples a child’s risk of major depressive episodes, and the disorder frequently occurs with anxiety, estimated in approximately 61%-65% of children with a major depressive episode. An episode generally appears to result from a combination of genetic factors and environmental ones, including abuse, neglect, family conflict, childhood adversity, losses, and comorbid disorders.
More heterogeneous than in adults, major depressive episodes in children look different based on a child’s age, according to Dr. Whiteside and Dr. Huxsahl:
• Birth to age 2 years. Symptoms include whining, decreased growth, lack of responsiveness, disrupted sleep, and excessive fears.
• Ages 3-5 years. Symptoms include anxiety, somatic symptoms, tantrums, sadness, weight gain, tiredness/sleepiness, suicidal ideation, anger or irritability, apathy, illness, and social withdrawal
• Ages 6-12 years. Symptoms include sadness, an inability to experience pleasure, decreased energy, low self-esteem, irritability, and suicidal ideation.
• Ages 12-18 years. Symptoms include a volatile mood, rage, acting out, self-consciousness, withdrawal, suicidal ideation, and overeating and/or oversleeping.
Other mood disorders
Disruptive mood dysregulation disorder (DMDD) involves much more acting out at a younger age than major depressive episodes. In children with DMDD, outbursts greatly exceed what would be expected in response to a situation, whether in terms of how long the tantrums last or how intense they are. These outbursts also are unexpected developmentally, with an onset before age 10 years, although the disorder should not be diagnosed earlier than age 6 years. Diagnostic criteria also require that the outbursts occur at least three times weekly, on average, for at least 12 months in at least two settings with a persistently angry or irritable mood between outbursts.
One way to support a diagnosis of DMDD is to rule out what it’s not. DMDD can exist with comorbidities of major depressive disorder (MDD), attention-deficit/hyperactivity disorder (ADHD), conduct disorder, and substance use disorders, and it’s most likely to grow into depression or anxiety. It cannot coexist with oppositional defiant disorder, intermittent explosive disorder, or bipolar disorder, and it does not develop into bipolar disorder.
Persistent depressive disorder resembles MDD, with either a depressed mood lasting at least 2 years or an irritable mood lasting at least 1 year plus at least two of the following symptoms: poor appetite or overeating; insomnia or hypersomnia; low energy or fatigue; poor concretion or difficulty making decisions; feelings of hopelessness; and low self-esteem.
Bipolar disorder
“The most important part of managing bipolar I is episodes, episodes, episodes,” Dr. Whiteside said. Alternating with either hypomanic or major depressive episodes are manic episodes, in which a child experiences an abnormal “high,” a period of at least a week of extremely high energy nearly all day, every day, with a “persistently elevated, expansive, or irritable mood.”
For an episode to be considered manic, however, at least three of the following seven other symptoms must be present, and deviate from the patient’s otherwise normal behavior: grandiosity or an especially inflated sense of self-esteem; a decreased need for sleep (not just that the patient doesn’t sleep but doesn’t actually seem to need to); extreme talkativeness or use of pressured speech; a feeling of having racing thoughts or ideas flying about; a tendency to be easily distracted or unfocused; an increase in activities aimed at accomplishing certain goals (in any sphere, for example, school, work, social, or sexual); and risky behaviors with potentially severe, long-term consequences, such as more frequent sexual behavior or shopping sprees.
Dr. Whiteside compared bipolar disorder to ADHD to help clinicians appreciate how to best understand it. Key differences with ADHD are an earlier age of onset, a more consistent presence of symptoms without episodes, a need for sleep despite possible insomnia, and only situational depression. In a 1998 study, a comparison of bipolar I and ADHD revealed that 89% of bipolar children had an elevated mood, compared with just 14% of those with ADHD. A similar gulf existed with grandiose thoughts, occurring in 86% of children with bipolar disorder and 5% of those with ADHD. Likewise, a much greater proportion of children with bipolar disorder experienced “flights of ideas,” decreased sleep, or hypersexuality, compared with these symptoms in children with ADHD.
Treating depression: Behavioral interventions
Psychopharmacology can be beneficial, but it works best when combined with behavioral interventions and simply explaining the disorder, said Dr. Whiteside. “There’s a lot of evidence that exercise can be a powerful treatment with depression,” he said. “Education is especially important since one of the four features of depression is a sense of hopelessness and belief that nothing is going to [get] better, so for them to know there are steps they can take is a very powerful intervention itself.”
The most effective intervention, however, is cognitive-behavioral therapy, with an 81% success rate 1 year out and a 98% success rate 2 years out. After the initial intervention, however, the numbers are more modest, with 67% of children no longer meeting major depressive disorder criteria when undergoing cognitive-behavioral therapy, compared with 48% in the waiting-list control group.
An important aspect to education starts with developing an alliance with a family so that the clinician can explain the condition and its treatment, build trust, and instill hope. In doing so, both parents’ and children’s expectations can be adjusted so that children feel less guilty and parents respond less negatively to their children.
Treatment with medication
Although only fluoxetine and escitalopram have Food and Drug Administration approval for MDD, Dr. Huxsahl recommended starting kids with mixed anxiety and depression on fluoxetine, fluvoxamine, or sertraline, and suggested clinicians not shy away from the target doses recommended for each drug. After 2-4 months of acute treatment, clinicians also should help families understand that continuing the treatment for at least 4-9 months and then potentially taking a maintenance dose for up to 3 years may be recommended.
“I would encourage you to educate the parents, and especially the teenagers, that they need to take the medication beyond the time that they are depressed,” he explained. Initially, however, start with a low dose and then increase it within 4 weeks if no response occurs. After 8 weeks, switch agents if no response has occurred, a process that requires monthly visits for the first 3-6 months of treatment.
Another question families and clinicians face is when to taper off medication when moving to a maintenance dose or working toward no longer taking the medication.
“In at least one study where they randomized kids to tapering during the school year or in the summer, the findings showed that the kids actually did better in the summer,” said Dr. Huxsahl. But follow-up is important during cessation because during the first 2-3 months is when there is the greatest risk for relapse or recurrence.
Dr. Whiteside and Dr. Huxsahl said they had no relevant financial disclosures.
Effective management of depression and other mood disorders in children may involve both pharmacotherapy with behavioral recommendations and psychotherapy, according to Stephen P. Whiteside, Ph.D., and Dr. John Huxsahl of the Mayo Clinic in Rochester Minn.
In a presentation at the American Academy of Pediatrics annual meeting in Washington, they reviewed the differences between various mood disorders because accurate diagnosis is a key component to management.
A major depressive episode is among the more common mood disorders among children, but others include disruptive mood dysregulation disorder, persistent depressive disorder, and bipolar I disorder. Because most pediatricians have just 15 minutes or so with patients, Dr. Whiteside and Dr. Huxsahl recommended using screening questionnaires to identify children at risk for a mood disorder. Trying to determine why a child is experiencing these symptoms or feelings can help clinicians determine whether this is a chronic issue or a situational one. Asking about other concerns, such as anxiety or use of substances, also can help with diagnosis.
Depressive episodes
Occurring among approximately 2% of children and 4%-8% of adolescents, a major depressive episode lasts a median of 8 months, but has a very high rate of recurrence: 20%-60% at 1 or 2 years after remission and 70% at 5 years after remission. In a significant proportion of children – about 20%-40% – a major depressive episode forecasts bipolar disorder.
In fact, having a parent with a mood disorder doubles to quadruples a child’s risk of major depressive episodes, and the disorder frequently occurs with anxiety, estimated in approximately 61%-65% of children with a major depressive episode. An episode generally appears to result from a combination of genetic factors and environmental ones, including abuse, neglect, family conflict, childhood adversity, losses, and comorbid disorders.
More heterogeneous than in adults, major depressive episodes in children look different based on a child’s age, according to Dr. Whiteside and Dr. Huxsahl:
• Birth to age 2 years. Symptoms include whining, decreased growth, lack of responsiveness, disrupted sleep, and excessive fears.
• Ages 3-5 years. Symptoms include anxiety, somatic symptoms, tantrums, sadness, weight gain, tiredness/sleepiness, suicidal ideation, anger or irritability, apathy, illness, and social withdrawal
• Ages 6-12 years. Symptoms include sadness, an inability to experience pleasure, decreased energy, low self-esteem, irritability, and suicidal ideation.
• Ages 12-18 years. Symptoms include a volatile mood, rage, acting out, self-consciousness, withdrawal, suicidal ideation, and overeating and/or oversleeping.
Other mood disorders
Disruptive mood dysregulation disorder (DMDD) involves much more acting out at a younger age than major depressive episodes. In children with DMDD, outbursts greatly exceed what would be expected in response to a situation, whether in terms of how long the tantrums last or how intense they are. These outbursts also are unexpected developmentally, with an onset before age 10 years, although the disorder should not be diagnosed earlier than age 6 years. Diagnostic criteria also require that the outbursts occur at least three times weekly, on average, for at least 12 months in at least two settings with a persistently angry or irritable mood between outbursts.
One way to support a diagnosis of DMDD is to rule out what it’s not. DMDD can exist with comorbidities of major depressive disorder (MDD), attention-deficit/hyperactivity disorder (ADHD), conduct disorder, and substance use disorders, and it’s most likely to grow into depression or anxiety. It cannot coexist with oppositional defiant disorder, intermittent explosive disorder, or bipolar disorder, and it does not develop into bipolar disorder.
Persistent depressive disorder resembles MDD, with either a depressed mood lasting at least 2 years or an irritable mood lasting at least 1 year plus at least two of the following symptoms: poor appetite or overeating; insomnia or hypersomnia; low energy or fatigue; poor concretion or difficulty making decisions; feelings of hopelessness; and low self-esteem.
Bipolar disorder
“The most important part of managing bipolar I is episodes, episodes, episodes,” Dr. Whiteside said. Alternating with either hypomanic or major depressive episodes are manic episodes, in which a child experiences an abnormal “high,” a period of at least a week of extremely high energy nearly all day, every day, with a “persistently elevated, expansive, or irritable mood.”
For an episode to be considered manic, however, at least three of the following seven other symptoms must be present, and deviate from the patient’s otherwise normal behavior: grandiosity or an especially inflated sense of self-esteem; a decreased need for sleep (not just that the patient doesn’t sleep but doesn’t actually seem to need to); extreme talkativeness or use of pressured speech; a feeling of having racing thoughts or ideas flying about; a tendency to be easily distracted or unfocused; an increase in activities aimed at accomplishing certain goals (in any sphere, for example, school, work, social, or sexual); and risky behaviors with potentially severe, long-term consequences, such as more frequent sexual behavior or shopping sprees.
Dr. Whiteside compared bipolar disorder to ADHD to help clinicians appreciate how to best understand it. Key differences with ADHD are an earlier age of onset, a more consistent presence of symptoms without episodes, a need for sleep despite possible insomnia, and only situational depression. In a 1998 study, a comparison of bipolar I and ADHD revealed that 89% of bipolar children had an elevated mood, compared with just 14% of those with ADHD. A similar gulf existed with grandiose thoughts, occurring in 86% of children with bipolar disorder and 5% of those with ADHD. Likewise, a much greater proportion of children with bipolar disorder experienced “flights of ideas,” decreased sleep, or hypersexuality, compared with these symptoms in children with ADHD.
Treating depression: Behavioral interventions
Psychopharmacology can be beneficial, but it works best when combined with behavioral interventions and simply explaining the disorder, said Dr. Whiteside. “There’s a lot of evidence that exercise can be a powerful treatment with depression,” he said. “Education is especially important since one of the four features of depression is a sense of hopelessness and belief that nothing is going to [get] better, so for them to know there are steps they can take is a very powerful intervention itself.”
The most effective intervention, however, is cognitive-behavioral therapy, with an 81% success rate 1 year out and a 98% success rate 2 years out. After the initial intervention, however, the numbers are more modest, with 67% of children no longer meeting major depressive disorder criteria when undergoing cognitive-behavioral therapy, compared with 48% in the waiting-list control group.
An important aspect to education starts with developing an alliance with a family so that the clinician can explain the condition and its treatment, build trust, and instill hope. In doing so, both parents’ and children’s expectations can be adjusted so that children feel less guilty and parents respond less negatively to their children.
Treatment with medication
Although only fluoxetine and escitalopram have Food and Drug Administration approval for MDD, Dr. Huxsahl recommended starting kids with mixed anxiety and depression on fluoxetine, fluvoxamine, or sertraline, and suggested clinicians not shy away from the target doses recommended for each drug. After 2-4 months of acute treatment, clinicians also should help families understand that continuing the treatment for at least 4-9 months and then potentially taking a maintenance dose for up to 3 years may be recommended.
“I would encourage you to educate the parents, and especially the teenagers, that they need to take the medication beyond the time that they are depressed,” he explained. Initially, however, start with a low dose and then increase it within 4 weeks if no response occurs. After 8 weeks, switch agents if no response has occurred, a process that requires monthly visits for the first 3-6 months of treatment.
Another question families and clinicians face is when to taper off medication when moving to a maintenance dose or working toward no longer taking the medication.
“In at least one study where they randomized kids to tapering during the school year or in the summer, the findings showed that the kids actually did better in the summer,” said Dr. Huxsahl. But follow-up is important during cessation because during the first 2-3 months is when there is the greatest risk for relapse or recurrence.
Dr. Whiteside and Dr. Huxsahl said they had no relevant financial disclosures.
Effective management of depression and other mood disorders in children may involve both pharmacotherapy with behavioral recommendations and psychotherapy, according to Stephen P. Whiteside, Ph.D., and Dr. John Huxsahl of the Mayo Clinic in Rochester Minn.
In a presentation at the American Academy of Pediatrics annual meeting in Washington, they reviewed the differences between various mood disorders because accurate diagnosis is a key component to management.
A major depressive episode is among the more common mood disorders among children, but others include disruptive mood dysregulation disorder, persistent depressive disorder, and bipolar I disorder. Because most pediatricians have just 15 minutes or so with patients, Dr. Whiteside and Dr. Huxsahl recommended using screening questionnaires to identify children at risk for a mood disorder. Trying to determine why a child is experiencing these symptoms or feelings can help clinicians determine whether this is a chronic issue or a situational one. Asking about other concerns, such as anxiety or use of substances, also can help with diagnosis.
Depressive episodes
Occurring among approximately 2% of children and 4%-8% of adolescents, a major depressive episode lasts a median of 8 months, but has a very high rate of recurrence: 20%-60% at 1 or 2 years after remission and 70% at 5 years after remission. In a significant proportion of children – about 20%-40% – a major depressive episode forecasts bipolar disorder.
In fact, having a parent with a mood disorder doubles to quadruples a child’s risk of major depressive episodes, and the disorder frequently occurs with anxiety, estimated in approximately 61%-65% of children with a major depressive episode. An episode generally appears to result from a combination of genetic factors and environmental ones, including abuse, neglect, family conflict, childhood adversity, losses, and comorbid disorders.
More heterogeneous than in adults, major depressive episodes in children look different based on a child’s age, according to Dr. Whiteside and Dr. Huxsahl:
• Birth to age 2 years. Symptoms include whining, decreased growth, lack of responsiveness, disrupted sleep, and excessive fears.
• Ages 3-5 years. Symptoms include anxiety, somatic symptoms, tantrums, sadness, weight gain, tiredness/sleepiness, suicidal ideation, anger or irritability, apathy, illness, and social withdrawal
• Ages 6-12 years. Symptoms include sadness, an inability to experience pleasure, decreased energy, low self-esteem, irritability, and suicidal ideation.
• Ages 12-18 years. Symptoms include a volatile mood, rage, acting out, self-consciousness, withdrawal, suicidal ideation, and overeating and/or oversleeping.
Other mood disorders
Disruptive mood dysregulation disorder (DMDD) involves much more acting out at a younger age than major depressive episodes. In children with DMDD, outbursts greatly exceed what would be expected in response to a situation, whether in terms of how long the tantrums last or how intense they are. These outbursts also are unexpected developmentally, with an onset before age 10 years, although the disorder should not be diagnosed earlier than age 6 years. Diagnostic criteria also require that the outbursts occur at least three times weekly, on average, for at least 12 months in at least two settings with a persistently angry or irritable mood between outbursts.
One way to support a diagnosis of DMDD is to rule out what it’s not. DMDD can exist with comorbidities of major depressive disorder (MDD), attention-deficit/hyperactivity disorder (ADHD), conduct disorder, and substance use disorders, and it’s most likely to grow into depression or anxiety. It cannot coexist with oppositional defiant disorder, intermittent explosive disorder, or bipolar disorder, and it does not develop into bipolar disorder.
Persistent depressive disorder resembles MDD, with either a depressed mood lasting at least 2 years or an irritable mood lasting at least 1 year plus at least two of the following symptoms: poor appetite or overeating; insomnia or hypersomnia; low energy or fatigue; poor concretion or difficulty making decisions; feelings of hopelessness; and low self-esteem.
Bipolar disorder
“The most important part of managing bipolar I is episodes, episodes, episodes,” Dr. Whiteside said. Alternating with either hypomanic or major depressive episodes are manic episodes, in which a child experiences an abnormal “high,” a period of at least a week of extremely high energy nearly all day, every day, with a “persistently elevated, expansive, or irritable mood.”
For an episode to be considered manic, however, at least three of the following seven other symptoms must be present, and deviate from the patient’s otherwise normal behavior: grandiosity or an especially inflated sense of self-esteem; a decreased need for sleep (not just that the patient doesn’t sleep but doesn’t actually seem to need to); extreme talkativeness or use of pressured speech; a feeling of having racing thoughts or ideas flying about; a tendency to be easily distracted or unfocused; an increase in activities aimed at accomplishing certain goals (in any sphere, for example, school, work, social, or sexual); and risky behaviors with potentially severe, long-term consequences, such as more frequent sexual behavior or shopping sprees.
Dr. Whiteside compared bipolar disorder to ADHD to help clinicians appreciate how to best understand it. Key differences with ADHD are an earlier age of onset, a more consistent presence of symptoms without episodes, a need for sleep despite possible insomnia, and only situational depression. In a 1998 study, a comparison of bipolar I and ADHD revealed that 89% of bipolar children had an elevated mood, compared with just 14% of those with ADHD. A similar gulf existed with grandiose thoughts, occurring in 86% of children with bipolar disorder and 5% of those with ADHD. Likewise, a much greater proportion of children with bipolar disorder experienced “flights of ideas,” decreased sleep, or hypersexuality, compared with these symptoms in children with ADHD.
Treating depression: Behavioral interventions
Psychopharmacology can be beneficial, but it works best when combined with behavioral interventions and simply explaining the disorder, said Dr. Whiteside. “There’s a lot of evidence that exercise can be a powerful treatment with depression,” he said. “Education is especially important since one of the four features of depression is a sense of hopelessness and belief that nothing is going to [get] better, so for them to know there are steps they can take is a very powerful intervention itself.”
The most effective intervention, however, is cognitive-behavioral therapy, with an 81% success rate 1 year out and a 98% success rate 2 years out. After the initial intervention, however, the numbers are more modest, with 67% of children no longer meeting major depressive disorder criteria when undergoing cognitive-behavioral therapy, compared with 48% in the waiting-list control group.
An important aspect to education starts with developing an alliance with a family so that the clinician can explain the condition and its treatment, build trust, and instill hope. In doing so, both parents’ and children’s expectations can be adjusted so that children feel less guilty and parents respond less negatively to their children.
Treatment with medication
Although only fluoxetine and escitalopram have Food and Drug Administration approval for MDD, Dr. Huxsahl recommended starting kids with mixed anxiety and depression on fluoxetine, fluvoxamine, or sertraline, and suggested clinicians not shy away from the target doses recommended for each drug. After 2-4 months of acute treatment, clinicians also should help families understand that continuing the treatment for at least 4-9 months and then potentially taking a maintenance dose for up to 3 years may be recommended.
“I would encourage you to educate the parents, and especially the teenagers, that they need to take the medication beyond the time that they are depressed,” he explained. Initially, however, start with a low dose and then increase it within 4 weeks if no response occurs. After 8 weeks, switch agents if no response has occurred, a process that requires monthly visits for the first 3-6 months of treatment.
Another question families and clinicians face is when to taper off medication when moving to a maintenance dose or working toward no longer taking the medication.
“In at least one study where they randomized kids to tapering during the school year or in the summer, the findings showed that the kids actually did better in the summer,” said Dr. Huxsahl. But follow-up is important during cessation because during the first 2-3 months is when there is the greatest risk for relapse or recurrence.
Dr. Whiteside and Dr. Huxsahl said they had no relevant financial disclosures.

Death from late effects of childhood cancer on decline
The rate of death from treatment-related late effects such as subsequent cancers and cardiopulmonary conditions has decreased among childhood cancer survivors, according to researchers.
At 15 years post diagnosis, the cumulative incidence of death from any cause for survivors diagnosed in the 1970s was 10.7%, 7.9% for those diagnosed in the 1980s, and 5.8% for those diagnosed in the 1990s (P less than .001). The cumulative incidence of death due to health-related causes, which include late effects of cancer therapy, were 3.1%, 2.4%, and 1.9%, respectively (P less than .001).
Results indicate that “the strategy of reducing treatment exposures in order to decrease the frequency of late effects is translating into a significant reduction in observed late mortality and an extension of the life span of children and adolescents who are successfully treated for cancer,” wrote Dr. Gregory Armstrong of St. Jude Children’s Research Hospital, Memphis, Tenn., and colleagues (N Engl J Med. 2016 Jan 13. doi: 10.1056/NEJMoa1510795).
A multivariate model showed that more recent treatment eras were associated with a reduced rate of death. The adjusted relative rate per every 5 years for death due to subsequent neoplasms was 0.83 (95% CI, 0.78-0.88), for cardiac causes, 0.77 (0.68-0.86), and for pulmonary causes, 0.77 (0.66-0.89).
Reductions across treatment eras in the rate of death from health-related causes were observed among survivors of acute lymphoblastic leukemia (3.2% in the early 1970s to 2.1% in the 1990s, P less than .001), Hodgkin lymphoma (5.3% to 2.6%, P = .006), Wilms tumor (2.6% to 0.4%, P = .005), and astrocytoma (4.7% to 1.8%, P = .02).
Temporal reductions in exposure to radiotherapy and anthracyclines occurred in treatment for acute lymphoblastic leukemia, Hodgkin lymphoma, Wilms tumor, and astrocytoma. Health-related mortality reductions were observed concurrently with reduced therapeutic exposures for acute lymphoblastic leukemia and Wilms tumor. For Hodgkin lymphoma and astrocytoma, other factors such as improved screening for late effects of cancer treatment appear to account for reductions in late health-related mortality.
For certain cancers, primarily neuroblastoma, late mortality has increased in recent decades. Increased therapeutic intensity has improved 5-year survival but increased the risk of late effects.
The reduced rate of death from recurrence or progression of primary cancers is the main driver to reductions in all-cause mortality, consistent with results from previous studies.
The retrospective Childhood Cancer Survivor Study evaluated 34,033 patients diagnosed at 31 hospitals in the United States and Canada from 1970 through 1999. In total, 3,958 deaths occurred, 2,002 due to primary cancer and 1,618 due to health-related causes: 746 subsequent neoplasms, 241 cardiac causes, 137 pulmonary causes, and 494 from other causes.
The rate of death from treatment-related late effects such as subsequent cancers and cardiopulmonary conditions has decreased among childhood cancer survivors, according to researchers.
At 15 years post diagnosis, the cumulative incidence of death from any cause for survivors diagnosed in the 1970s was 10.7%, 7.9% for those diagnosed in the 1980s, and 5.8% for those diagnosed in the 1990s (P less than .001). The cumulative incidence of death due to health-related causes, which include late effects of cancer therapy, were 3.1%, 2.4%, and 1.9%, respectively (P less than .001).
Results indicate that “the strategy of reducing treatment exposures in order to decrease the frequency of late effects is translating into a significant reduction in observed late mortality and an extension of the life span of children and adolescents who are successfully treated for cancer,” wrote Dr. Gregory Armstrong of St. Jude Children’s Research Hospital, Memphis, Tenn., and colleagues (N Engl J Med. 2016 Jan 13. doi: 10.1056/NEJMoa1510795).
A multivariate model showed that more recent treatment eras were associated with a reduced rate of death. The adjusted relative rate per every 5 years for death due to subsequent neoplasms was 0.83 (95% CI, 0.78-0.88), for cardiac causes, 0.77 (0.68-0.86), and for pulmonary causes, 0.77 (0.66-0.89).
Reductions across treatment eras in the rate of death from health-related causes were observed among survivors of acute lymphoblastic leukemia (3.2% in the early 1970s to 2.1% in the 1990s, P less than .001), Hodgkin lymphoma (5.3% to 2.6%, P = .006), Wilms tumor (2.6% to 0.4%, P = .005), and astrocytoma (4.7% to 1.8%, P = .02).
Temporal reductions in exposure to radiotherapy and anthracyclines occurred in treatment for acute lymphoblastic leukemia, Hodgkin lymphoma, Wilms tumor, and astrocytoma. Health-related mortality reductions were observed concurrently with reduced therapeutic exposures for acute lymphoblastic leukemia and Wilms tumor. For Hodgkin lymphoma and astrocytoma, other factors such as improved screening for late effects of cancer treatment appear to account for reductions in late health-related mortality.
For certain cancers, primarily neuroblastoma, late mortality has increased in recent decades. Increased therapeutic intensity has improved 5-year survival but increased the risk of late effects.
The reduced rate of death from recurrence or progression of primary cancers is the main driver to reductions in all-cause mortality, consistent with results from previous studies.
The retrospective Childhood Cancer Survivor Study evaluated 34,033 patients diagnosed at 31 hospitals in the United States and Canada from 1970 through 1999. In total, 3,958 deaths occurred, 2,002 due to primary cancer and 1,618 due to health-related causes: 746 subsequent neoplasms, 241 cardiac causes, 137 pulmonary causes, and 494 from other causes.
The rate of death from treatment-related late effects such as subsequent cancers and cardiopulmonary conditions has decreased among childhood cancer survivors, according to researchers.
At 15 years post diagnosis, the cumulative incidence of death from any cause for survivors diagnosed in the 1970s was 10.7%, 7.9% for those diagnosed in the 1980s, and 5.8% for those diagnosed in the 1990s (P less than .001). The cumulative incidence of death due to health-related causes, which include late effects of cancer therapy, were 3.1%, 2.4%, and 1.9%, respectively (P less than .001).
Results indicate that “the strategy of reducing treatment exposures in order to decrease the frequency of late effects is translating into a significant reduction in observed late mortality and an extension of the life span of children and adolescents who are successfully treated for cancer,” wrote Dr. Gregory Armstrong of St. Jude Children’s Research Hospital, Memphis, Tenn., and colleagues (N Engl J Med. 2016 Jan 13. doi: 10.1056/NEJMoa1510795).
A multivariate model showed that more recent treatment eras were associated with a reduced rate of death. The adjusted relative rate per every 5 years for death due to subsequent neoplasms was 0.83 (95% CI, 0.78-0.88), for cardiac causes, 0.77 (0.68-0.86), and for pulmonary causes, 0.77 (0.66-0.89).
Reductions across treatment eras in the rate of death from health-related causes were observed among survivors of acute lymphoblastic leukemia (3.2% in the early 1970s to 2.1% in the 1990s, P less than .001), Hodgkin lymphoma (5.3% to 2.6%, P = .006), Wilms tumor (2.6% to 0.4%, P = .005), and astrocytoma (4.7% to 1.8%, P = .02).
Temporal reductions in exposure to radiotherapy and anthracyclines occurred in treatment for acute lymphoblastic leukemia, Hodgkin lymphoma, Wilms tumor, and astrocytoma. Health-related mortality reductions were observed concurrently with reduced therapeutic exposures for acute lymphoblastic leukemia and Wilms tumor. For Hodgkin lymphoma and astrocytoma, other factors such as improved screening for late effects of cancer treatment appear to account for reductions in late health-related mortality.
For certain cancers, primarily neuroblastoma, late mortality has increased in recent decades. Increased therapeutic intensity has improved 5-year survival but increased the risk of late effects.
The reduced rate of death from recurrence or progression of primary cancers is the main driver to reductions in all-cause mortality, consistent with results from previous studies.
The retrospective Childhood Cancer Survivor Study evaluated 34,033 patients diagnosed at 31 hospitals in the United States and Canada from 1970 through 1999. In total, 3,958 deaths occurred, 2,002 due to primary cancer and 1,618 due to health-related causes: 746 subsequent neoplasms, 241 cardiac causes, 137 pulmonary causes, and 494 from other causes.
Key clinical point: Five-year survivors of childhood cancers have increased lifespans due in part to reduced rates of treatment-related late effects.
Major finding: At 15 years post diagnosis, the cumulative incidence of death from any cause for survivors diagnosed in the 1970s was 10.7%; in the 1980s, 7.9%; and in the 1990s, 5.8% (P less than .001). The cumulative incidence of death due to health-related causes, which include late effects of cancer therapy, were 3.1%, 2.4%, and 1.9%, respectively (P less than .001).
Data source: The retrospective Childhood Cancer Survivor Study, evaluating 34,033 patients diagnosed at 31 hospitals in the United States and Canada from 1970 through 1999; 3,958 deaths occurred.
Disclosures: Dr. Armstrong and coauthors reported having no disclosures.
More children getting well-child checkups
The percentage of all children aged 10-17 years who did not receive a well-child checkup is down since 2008, but there is a considerable gap between those living in metropolitan and nonmetropolitan areas, the Centers for Disease Control and Prevention reported.
In 2014, 21% of all 10- to 17-year-olds had not had a well-child checkup in the past 12 months, compared with 31% in 2008, said Lindsey I. Black and Anjel Vahratian, Ph.D., of the CDC’s National Center for Health Statistics in Hyattsville, Md. (MMWR 2016 Jan 8;64[52]:1410).
Those living in nonmetropolitan areas, however, were at a consistent disadvantage over the 6-year period, compared with their metropolitan counterparts. In 2014, 28% of the children had not had a well-child visit in the past 12 months, compared with just over 20% in metro areas, according to data from the National Health Interview Survey.
The nonmetropolitan areas did show a slightly larger relative decrease from 2008 to 2014 than the metropolitan areas – 33% vs. 31% – so the gap has closed slightly over time.
Metropolitan residences are those located within a county or group of contiguous counties containing at least one urbanized area with a population of 50,000 or more, along with surrounding counties that have strong economic ties to the urbanized area. Nonmetropolitan areas do not include a large urbanized area and are generally more rural, the investigators noted.
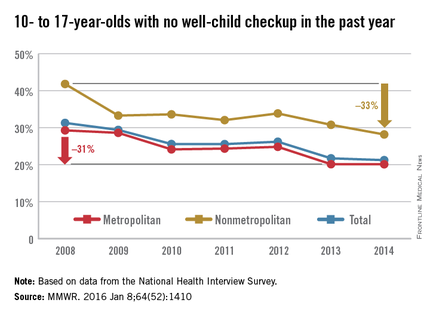
The percentage of all children aged 10-17 years who did not receive a well-child checkup is down since 2008, but there is a considerable gap between those living in metropolitan and nonmetropolitan areas, the Centers for Disease Control and Prevention reported.
In 2014, 21% of all 10- to 17-year-olds had not had a well-child checkup in the past 12 months, compared with 31% in 2008, said Lindsey I. Black and Anjel Vahratian, Ph.D., of the CDC’s National Center for Health Statistics in Hyattsville, Md. (MMWR 2016 Jan 8;64[52]:1410).
Those living in nonmetropolitan areas, however, were at a consistent disadvantage over the 6-year period, compared with their metropolitan counterparts. In 2014, 28% of the children had not had a well-child visit in the past 12 months, compared with just over 20% in metro areas, according to data from the National Health Interview Survey.
The nonmetropolitan areas did show a slightly larger relative decrease from 2008 to 2014 than the metropolitan areas – 33% vs. 31% – so the gap has closed slightly over time.
Metropolitan residences are those located within a county or group of contiguous counties containing at least one urbanized area with a population of 50,000 or more, along with surrounding counties that have strong economic ties to the urbanized area. Nonmetropolitan areas do not include a large urbanized area and are generally more rural, the investigators noted.
The percentage of all children aged 10-17 years who did not receive a well-child checkup is down since 2008, but there is a considerable gap between those living in metropolitan and nonmetropolitan areas, the Centers for Disease Control and Prevention reported.
In 2014, 21% of all 10- to 17-year-olds had not had a well-child checkup in the past 12 months, compared with 31% in 2008, said Lindsey I. Black and Anjel Vahratian, Ph.D., of the CDC’s National Center for Health Statistics in Hyattsville, Md. (MMWR 2016 Jan 8;64[52]:1410).
Those living in nonmetropolitan areas, however, were at a consistent disadvantage over the 6-year period, compared with their metropolitan counterparts. In 2014, 28% of the children had not had a well-child visit in the past 12 months, compared with just over 20% in metro areas, according to data from the National Health Interview Survey.
The nonmetropolitan areas did show a slightly larger relative decrease from 2008 to 2014 than the metropolitan areas – 33% vs. 31% – so the gap has closed slightly over time.
Metropolitan residences are those located within a county or group of contiguous counties containing at least one urbanized area with a population of 50,000 or more, along with surrounding counties that have strong economic ties to the urbanized area. Nonmetropolitan areas do not include a large urbanized area and are generally more rural, the investigators noted.
FROM MMWR