User login
Increasing eligibility for engineered T-cell therapy

Image courtesy of NIAID
A new study suggests that having a certain type of cancer or receiving certain chemotherapeutic agents
can affect T-cell function and make patients ineligible for engineered T-cell therapy.
However, researchers found that proper timing of T-cell collection can increase the number of patients eiligible for the therapy.
And the team developed a culture technique that can boost T cells’ fitness for expansion, which can increase eligibility as well.
Nathan Singh, MD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Science Translational Medicine.
The researchers set out to determine why some patients’ T cells fail to multiply in culture. The team studied T cells from children with acute lymphoblastic leukemia (ALL) or non-Hodgkin lymphoma (NHL) who were undergoing chemotherapy. (NHL subtypes included Burkitt lymphoma, diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, primary lymphoma of bone, and follicular lymphoma.)
The researchers found that T cells from patients with ALL expanded better in culture than those from patients with NHL.
The team said a threshold of greater than 5-fold expansion during test expansion was associated with a high likelihood of successful clinical expansion.
Nearly 80% of patients with ALL met this threshold at diagnosis, but the rate declined over the course of therapy, falling to about 40% during maintenance therapy.
About 25% of NHL patients met the threshold at diagnosis, but few samples demonstrated any expansion after therapy began (12.5% of samples at all remaining time points tested).
The researchers said the difference in the proportion of ALL and NHL samples that met the expansion threshold was significant at all time points tested.
Analysis revealed that ALL patients had higher numbers of naïve T cells and stem central memory T cells, T cell subtypes known to be highly potent and proliferative with an enhanced capacity for self-renewal.
The researchers also found that certain chemotherapy drugs—namely, cyclophosphamide and cytarabine—selectively depleted early lineage T cells.
Fortunately, the team discovered that poor expansion can be rescued by exposing T cells to signaling molecules that stimulate T-cell activity. Culture with IL-7 and IL-15 boosted the expansion capacity of T cells from patients with NHL and those with ALL.
The researchers therefore concluded that using this culture technique or collecting T cells prior to chemotherapy can increase the number of patients eligible for engineered T-cell therapy. ![]()
Image courtesy of NIAID
A new study suggests that having a certain type of cancer or receiving certain chemotherapeutic agents
can affect T-cell function and make patients ineligible for engineered T-cell therapy.
However, researchers found that proper timing of T-cell collection can increase the number of patients eiligible for the therapy.
And the team developed a culture technique that can boost T cells’ fitness for expansion, which can increase eligibility as well.
Nathan Singh, MD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Science Translational Medicine.
The researchers set out to determine why some patients’ T cells fail to multiply in culture. The team studied T cells from children with acute lymphoblastic leukemia (ALL) or non-Hodgkin lymphoma (NHL) who were undergoing chemotherapy. (NHL subtypes included Burkitt lymphoma, diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, primary lymphoma of bone, and follicular lymphoma.)
The researchers found that T cells from patients with ALL expanded better in culture than those from patients with NHL.
The team said a threshold of greater than 5-fold expansion during test expansion was associated with a high likelihood of successful clinical expansion.
Nearly 80% of patients with ALL met this threshold at diagnosis, but the rate declined over the course of therapy, falling to about 40% during maintenance therapy.
About 25% of NHL patients met the threshold at diagnosis, but few samples demonstrated any expansion after therapy began (12.5% of samples at all remaining time points tested).
The researchers said the difference in the proportion of ALL and NHL samples that met the expansion threshold was significant at all time points tested.
Analysis revealed that ALL patients had higher numbers of naïve T cells and stem central memory T cells, T cell subtypes known to be highly potent and proliferative with an enhanced capacity for self-renewal.
The researchers also found that certain chemotherapy drugs—namely, cyclophosphamide and cytarabine—selectively depleted early lineage T cells.
Fortunately, the team discovered that poor expansion can be rescued by exposing T cells to signaling molecules that stimulate T-cell activity. Culture with IL-7 and IL-15 boosted the expansion capacity of T cells from patients with NHL and those with ALL.
The researchers therefore concluded that using this culture technique or collecting T cells prior to chemotherapy can increase the number of patients eligible for engineered T-cell therapy. ![]()
Image courtesy of NIAID
A new study suggests that having a certain type of cancer or receiving certain chemotherapeutic agents
can affect T-cell function and make patients ineligible for engineered T-cell therapy.
However, researchers found that proper timing of T-cell collection can increase the number of patients eiligible for the therapy.
And the team developed a culture technique that can boost T cells’ fitness for expansion, which can increase eligibility as well.
Nathan Singh, MD, of the University of Pennsylvania in Philadelphia, and his colleagues described this work in Science Translational Medicine.
The researchers set out to determine why some patients’ T cells fail to multiply in culture. The team studied T cells from children with acute lymphoblastic leukemia (ALL) or non-Hodgkin lymphoma (NHL) who were undergoing chemotherapy. (NHL subtypes included Burkitt lymphoma, diffuse large B-cell lymphoma, primary mediastinal large B-cell lymphoma, primary lymphoma of bone, and follicular lymphoma.)
The researchers found that T cells from patients with ALL expanded better in culture than those from patients with NHL.
The team said a threshold of greater than 5-fold expansion during test expansion was associated with a high likelihood of successful clinical expansion.
Nearly 80% of patients with ALL met this threshold at diagnosis, but the rate declined over the course of therapy, falling to about 40% during maintenance therapy.
About 25% of NHL patients met the threshold at diagnosis, but few samples demonstrated any expansion after therapy began (12.5% of samples at all remaining time points tested).
The researchers said the difference in the proportion of ALL and NHL samples that met the expansion threshold was significant at all time points tested.
Analysis revealed that ALL patients had higher numbers of naïve T cells and stem central memory T cells, T cell subtypes known to be highly potent and proliferative with an enhanced capacity for self-renewal.
The researchers also found that certain chemotherapy drugs—namely, cyclophosphamide and cytarabine—selectively depleted early lineage T cells.
Fortunately, the team discovered that poor expansion can be rescued by exposing T cells to signaling molecules that stimulate T-cell activity. Culture with IL-7 and IL-15 boosted the expansion capacity of T cells from patients with NHL and those with ALL.
The researchers therefore concluded that using this culture technique or collecting T cells prior to chemotherapy can increase the number of patients eligible for engineered T-cell therapy. ![]()
US cancer stats: The good and the bad

patient and her father
Photo by Rhoda Baer
The American Cancer Society’s 2016 report on cancer in the US suggests that, in recent years, overall trends in cancer incidence have remained stable for women and declined for men.
However, the rates of certain malignancies are on the rise. This includes some leukemia subtypes for men and women, as well as myeloma for men.
Leukemia is the leading cause of cancer death for men ages 20 to 39, but leukemia is no longer the leading cause of cancer death among children and adolescents (of both genders).
These and other data are included in the report, which is published in CA: A Cancer Journal for Clinicians.
The report estimates there will be 1,685,210 new cancer cases and 595,690 cancer deaths in the US in 2016. This includes 81,080 new lymphoma cases and 21,270 lymphoma deaths, 60,140 new leukemia cases and 24,400 leukemia deaths, and 30,330 new myeloma cases and 12,650 myeloma deaths.
Cancer incidence over time
The report suggests the overall cancer incidence for women has been stable from 1998 to 2012. But the incidence for men has declined by 3.1% per year from 2009 to 2012, with one-half of the drop in men due to recent rapid declines in prostate cancer diagnoses as prostate-specific antigen testing decreases.
Incidence rates increased from 2003 to 2012 among both men and women for some leukemia subtypes and for cancers of the tongue, tonsil, small intestine, liver, pancreas, kidney, renal pelvis, and thyroid.
Incidence rates increased in men for melanoma, myeloma, and cancers of the breast, testis, and oropharynx. Among women, incidence rates increased for cancers of the anus, vulva, and uterine corpus.
Cancer deaths
The rate of cancer deaths in the US has dropped 23% from its peak in 1991 to 2012. The incidence of cancer death was 215.1 per 100,000 in 1991 and 166.4 per 100,000 in 2012.
The decline is larger in men (28% since 1990) than in women (19% since 1991). Over the past decade of data, the rate dropped by 1.8% per year in men and 1.4% per year in women.
The decline in cancer death rates over the past 2 decades is driven by continued decreases in death rates for the 4 major cancer sites: lung, breast, prostate, and colon/rectum.
Breast cancer is the leading cause of cancer death in women ages 20 to 59, while lung cancer is the leading cause of cancer death in women 60 and older.
Among men, leukemia is the leading cause of cancer death for those ages 20 to 39, whereas lung cancer ranks first among men 40 and older.
Among children and adolescents (0-19), brain cancer has surpassed leukemia as the leading cause of cancer death, a result of more rapid therapeutic advances against leukemia.
The report also features an analysis of leading causes of death by state. It shows that, even as cancer remains the second leading cause of death nationwide, steep drops in deaths from heart disease have made cancer the leading cause of death in 21 states: Alaska, Arizona, Colorado, Delaware, Florida, Georgia, Idaho, Kansas, Maine, Massachusetts, Minnesota, Montana, Nebraska, New Hampshire, New Mexico, North Carolina, Oregon, South Carolina, Vermont, Virginia, and Washington.
In addition, cancer is the leading cause of death among adults ages 40 to 79 and among both Hispanics and Asian/Pacific Islanders, who together make up one-quarter of the US population.
Heart disease remains the top cause of death overall in the US. In 2012, there were 599,711 (24%) deaths from heart disease, compared to 582,623 (23%) deaths from cancer.
“We’re gratified to see cancer death rates continuing to drop,” said Otis W. Brawley, MD, chief medical officer of the American Cancer Society.
“But the fact that cancer is nonetheless becoming the top cause of death in many populations is a strong reminder that the fight is not over.” ![]()
patient and her father
Photo by Rhoda Baer
The American Cancer Society’s 2016 report on cancer in the US suggests that, in recent years, overall trends in cancer incidence have remained stable for women and declined for men.
However, the rates of certain malignancies are on the rise. This includes some leukemia subtypes for men and women, as well as myeloma for men.
Leukemia is the leading cause of cancer death for men ages 20 to 39, but leukemia is no longer the leading cause of cancer death among children and adolescents (of both genders).
These and other data are included in the report, which is published in CA: A Cancer Journal for Clinicians.
The report estimates there will be 1,685,210 new cancer cases and 595,690 cancer deaths in the US in 2016. This includes 81,080 new lymphoma cases and 21,270 lymphoma deaths, 60,140 new leukemia cases and 24,400 leukemia deaths, and 30,330 new myeloma cases and 12,650 myeloma deaths.
Cancer incidence over time
The report suggests the overall cancer incidence for women has been stable from 1998 to 2012. But the incidence for men has declined by 3.1% per year from 2009 to 2012, with one-half of the drop in men due to recent rapid declines in prostate cancer diagnoses as prostate-specific antigen testing decreases.
Incidence rates increased from 2003 to 2012 among both men and women for some leukemia subtypes and for cancers of the tongue, tonsil, small intestine, liver, pancreas, kidney, renal pelvis, and thyroid.
Incidence rates increased in men for melanoma, myeloma, and cancers of the breast, testis, and oropharynx. Among women, incidence rates increased for cancers of the anus, vulva, and uterine corpus.
Cancer deaths
The rate of cancer deaths in the US has dropped 23% from its peak in 1991 to 2012. The incidence of cancer death was 215.1 per 100,000 in 1991 and 166.4 per 100,000 in 2012.
The decline is larger in men (28% since 1990) than in women (19% since 1991). Over the past decade of data, the rate dropped by 1.8% per year in men and 1.4% per year in women.
The decline in cancer death rates over the past 2 decades is driven by continued decreases in death rates for the 4 major cancer sites: lung, breast, prostate, and colon/rectum.
Breast cancer is the leading cause of cancer death in women ages 20 to 59, while lung cancer is the leading cause of cancer death in women 60 and older.
Among men, leukemia is the leading cause of cancer death for those ages 20 to 39, whereas lung cancer ranks first among men 40 and older.
Among children and adolescents (0-19), brain cancer has surpassed leukemia as the leading cause of cancer death, a result of more rapid therapeutic advances against leukemia.
The report also features an analysis of leading causes of death by state. It shows that, even as cancer remains the second leading cause of death nationwide, steep drops in deaths from heart disease have made cancer the leading cause of death in 21 states: Alaska, Arizona, Colorado, Delaware, Florida, Georgia, Idaho, Kansas, Maine, Massachusetts, Minnesota, Montana, Nebraska, New Hampshire, New Mexico, North Carolina, Oregon, South Carolina, Vermont, Virginia, and Washington.
In addition, cancer is the leading cause of death among adults ages 40 to 79 and among both Hispanics and Asian/Pacific Islanders, who together make up one-quarter of the US population.
Heart disease remains the top cause of death overall in the US. In 2012, there were 599,711 (24%) deaths from heart disease, compared to 582,623 (23%) deaths from cancer.
“We’re gratified to see cancer death rates continuing to drop,” said Otis W. Brawley, MD, chief medical officer of the American Cancer Society.
“But the fact that cancer is nonetheless becoming the top cause of death in many populations is a strong reminder that the fight is not over.” ![]()
patient and her father
Photo by Rhoda Baer
The American Cancer Society’s 2016 report on cancer in the US suggests that, in recent years, overall trends in cancer incidence have remained stable for women and declined for men.
However, the rates of certain malignancies are on the rise. This includes some leukemia subtypes for men and women, as well as myeloma for men.
Leukemia is the leading cause of cancer death for men ages 20 to 39, but leukemia is no longer the leading cause of cancer death among children and adolescents (of both genders).
These and other data are included in the report, which is published in CA: A Cancer Journal for Clinicians.
The report estimates there will be 1,685,210 new cancer cases and 595,690 cancer deaths in the US in 2016. This includes 81,080 new lymphoma cases and 21,270 lymphoma deaths, 60,140 new leukemia cases and 24,400 leukemia deaths, and 30,330 new myeloma cases and 12,650 myeloma deaths.
Cancer incidence over time
The report suggests the overall cancer incidence for women has been stable from 1998 to 2012. But the incidence for men has declined by 3.1% per year from 2009 to 2012, with one-half of the drop in men due to recent rapid declines in prostate cancer diagnoses as prostate-specific antigen testing decreases.
Incidence rates increased from 2003 to 2012 among both men and women for some leukemia subtypes and for cancers of the tongue, tonsil, small intestine, liver, pancreas, kidney, renal pelvis, and thyroid.
Incidence rates increased in men for melanoma, myeloma, and cancers of the breast, testis, and oropharynx. Among women, incidence rates increased for cancers of the anus, vulva, and uterine corpus.
Cancer deaths
The rate of cancer deaths in the US has dropped 23% from its peak in 1991 to 2012. The incidence of cancer death was 215.1 per 100,000 in 1991 and 166.4 per 100,000 in 2012.
The decline is larger in men (28% since 1990) than in women (19% since 1991). Over the past decade of data, the rate dropped by 1.8% per year in men and 1.4% per year in women.
The decline in cancer death rates over the past 2 decades is driven by continued decreases in death rates for the 4 major cancer sites: lung, breast, prostate, and colon/rectum.
Breast cancer is the leading cause of cancer death in women ages 20 to 59, while lung cancer is the leading cause of cancer death in women 60 and older.
Among men, leukemia is the leading cause of cancer death for those ages 20 to 39, whereas lung cancer ranks first among men 40 and older.
Among children and adolescents (0-19), brain cancer has surpassed leukemia as the leading cause of cancer death, a result of more rapid therapeutic advances against leukemia.
The report also features an analysis of leading causes of death by state. It shows that, even as cancer remains the second leading cause of death nationwide, steep drops in deaths from heart disease have made cancer the leading cause of death in 21 states: Alaska, Arizona, Colorado, Delaware, Florida, Georgia, Idaho, Kansas, Maine, Massachusetts, Minnesota, Montana, Nebraska, New Hampshire, New Mexico, North Carolina, Oregon, South Carolina, Vermont, Virginia, and Washington.
In addition, cancer is the leading cause of death among adults ages 40 to 79 and among both Hispanics and Asian/Pacific Islanders, who together make up one-quarter of the US population.
Heart disease remains the top cause of death overall in the US. In 2012, there were 599,711 (24%) deaths from heart disease, compared to 582,623 (23%) deaths from cancer.
“We’re gratified to see cancer death rates continuing to drop,” said Otis W. Brawley, MD, chief medical officer of the American Cancer Society.
“But the fact that cancer is nonetheless becoming the top cause of death in many populations is a strong reminder that the fight is not over.” ![]()
Redefining care model could improve pediatric obesity prevention, treatment
WASHINGTON – Physicians have a role in combating early childhood obesity, but experts say the clinical setting is not ideal for effective treatment and prevention of this emerging epidemic.
“Pediatricians have high access to kids, parents, and guardians, and we are trusted sources of information for them,” Dr. Ian Paul, professor and chief of academic pediatrics at Penn State University Hershey Medical Center, said at an Institute of Medicine forum on early childhood obesity.

Emerging data underscore obesity’s complex societal components, which include an imbalance of diet and physical activity complicated by less tangible factors such as cultural attitudes, maternal habits, and socio-economic status. And then there is the question of the best way to reimburse physicians for applying the few proven long-term interventions they have.
“I think it’s one of those things where it takes a village,” Dr. Paul said in an interview. “You need multiple people going in the same direction. The pediatrician can give advice, and support what is happening, but it can’t just be the pediatrician by him- or herself.”
The U.S. Centers for Disease Control and Prevention says that pediatric obesity affects a third of the nation’s youth. But there are only vague policies and guidelines for how to intervene in the preschool years, a time when research now shows risk factors present can set the stage for obesity later in a child’s life. This all leaves pediatricians unsure of how to treat young patients who present with signs of overweight and obesity. To date, there are no proven clinical-based obesity interventions for birth to age 5 years, Dr. Paul said. “Pediatricians don’t always feel equipped to handle questions about obesity prevention and treatment,” compounded, by the fact that, “reimbursement for these services has been poor.”
However, through partnerships with community organizations and other clinicians, more effective models of care are emerging, particularly in minority and lower income communities where obesity rates are among the highest nationally (Contemp Clin Trials. 2013 Nov;36[3]:544-54. doi: 10.1016/j.cct.2013.09.015. Epub 2013 Oct 9), noted Dr. Paul.
“In poorer households, high rates of maternal stress and less access to resources such as time with a nutritionist or higher quality produce and other foods, are risk factors for obesity,” Dr. Mary Jo Messito, director of the Starting Early Child Obesity Prevention Program at Bellevue Hospital in New York, said in an interview.
As part of their program, Dr. Messito, clinical associate professor of pediatrics at New York University, and her colleagues conducted a study of a family-based, early obesity intervention and prevention program with nutrition support groups as the central component.
The study involved 534 expectant mothers in their last trimester who were randomly assigned to receive either standard prenatal care followed by standard well-child care, or prenatal nutritional counseling, in addition to well-child visits coupled with continued nutritional counseling in a group setting, which they attend with their babies. The study group met regularly to learn how to make their own minimally processed baby foods, read and understand food labels, and offer peer support for any issues they might be encountering in raising their babies to eat healthfully.
Although many Hispanic families are affected by obesity, there is a need to teach and reinforce these skills in all families of young children affected by poverty, said Dr. Messito. “Middle and upper income people can also be affected by obesity, but they have the resources to deal with it, including education and nutritional support provided by insurance plans.”
The currently unpublished results of the study, based on 3 years of follow-up, are both statistically and clinically significant, said Dr. Messito. Only 6% of the families in the study group prematurely introduced complementary foods such as juices and solids compared with 17% in controls, according to Dr. Messito.
Exclusively breastfed babies in the control group totaled 34% compared with an impressive 46% in the study group, Dr. Messito said.
The potentially devastating consequences of resorting to quick-fixes such as cereal and juice at too young an age to sooth a fussy baby, is that at age 2 or 3 years, when it is still tricky to determine if they’ve exceeded the 95th percentile for their weight, these overfed babies can be on a trajectory that lasts long after they grow up. “If you are obese then, the odds are great you will be for life,” said Dr. Messito.
Much of the Starting Early study’s “plain language” materials, published in both English and Spanish, distributed to families as reinforcement to what they learn in their groups, was based on what is routinely provided by the federal Women, Infants, and Children (WIC) program, said Dr. Messito. “We see ourselves as collaborators with WIC and with primary care.”
This pleases Dr. Paul. “Pediatricians only have a limited amount of time for each visit, and an office setting is not very conducive to get in as in-depth a conversation as you would like, especially in well-child care. By meeting with several families at once, instead of delivering the same information five times, it can be done once in 100 minutes where everyone can be in on the discussion,” he said in an interview.
Partnering with others in the community not only adds another layer of support, it also takes the burden off the physician to do it all.
The NET-Works study (Now Everybody Together for Amazing and Healthful Kids), currently underway at the University of Minnesota, on the Twin Cities campus, includes the families of 500 preschoolers, followed for 3 years after being randomly assigned to standard care or an integrated model that features nutritional counseling, both at the primary care and community level, as well as a home-based intervention, and support from neighborhood and community resources to promote optimal healthful lifestyle habits, including diet and physical activity, and screen time limits. Results from the study are due in 2017.
“What I like about this study is that the pediatrician has a supporting, rather than leading, role in a community-wide effort to prevent and treat childhood obesity,” said Dr. Paul. “I think that’s the answer.”
Another model of community-based care, promoted by the CDC, leverages the time more than 60% of U.S. children spend in early education and care centers by linking various community resources with these early learning facilities to ensure that children learn to consume healthful foods and exercise.
Dr. Dianne Ward, professor of nutrition at the University of North Carolina, Chapel Hill, and a panelist at the IOM roundtable, noted that one hitch is that often the child care providers themselves are often unhealthy. “A number of studies show these women often have poor diets, stress, inactivity, and smoke, yet these are the same women we ask to be role models for our children and lead the healthy eating educational programs. It’s unclear whether their health status has a negative effect on the children.”
Dr. Paul’s own work with others such as Dr. Leann Birch, the William P. “Bill” Flatt Childhood Obesity Professor at the University of Georgia, Athens, focuses on home-based interventions delivered by nurses. By training parents and caregivers in what they call “responsive feeding,” their SLIM-Time study addresses how and why parents feed their children, rather than what they feed them, with the essential byproduct being greater capacity in both parents and children to self-soothe and exert self-control.
Similar to Dr. Messito’s work, SLIM-Time (Sleeping and Intake Methods Taught to Infants and Mothers Early in Life) “teaches people how to respond appropriately to a baby’s cues earlier in life. If you take a baby and give it a bottle, it will stop crying, whether or not [the baby is] hungry. Food should be used for hunger,” Dr. Paul said. “We teach parents to use food for hunger, not comfort.”
The results of the randomly controlled SLIM-Time study of 110 mother-infant dyads, published online in 2010, were that by teaching parents soothing and sleep strategies other than bottle feeding, and helping them to recognize satiety cues, as well as educating them on the appropriate time to introduce solid foods, study babies were encouraged to finish their bottles only half as often as were controls. At 1 year, study babies were in the 35th percentile for weight-for-length compared with 50% of controls. Babies in the test group also required fewer nighttime feedings than did controls at weeks 3, 4, 8, and 16 (P = .003) (Obesity. 2011 Feb; 19[2]: 353-61).
The results led Dr. Paul and his colleagues to create the similarly structured INSIGHT Study (Preventing Obesity Through Interventions During Infancy), the results of which are still in preparation, but preliminarily seem to reinforce SLIM-Time’s results, with 15% of controls being in the 95th or higher weight-per-length percentiles at 1 year compared with 5% of intervention group babies being in that range.
Dr. Birch stated during the IOM round table that the effects in each study group were similar, regardless of whether a child was fed formula or breast milk. “We still have a lot of data to analyze, but at this point, it looks like the effects aren’t limited to intense breastfeeding.” Breastfeeding has been found protective against obesity (Am J Epidemiol. 2005 Sept 1;162[5]:397-403. Epub 2005 Aug 2; Int J Obes Relat Metab Disord. 2004 Oct;28[10]:1247-56.)
Even though the literature for early childhood obesity intervention and prevention is nascent, it’s already evident that to see obesity primarily as a clinical issue is too limiting, according to Dr. Paul.
“This is the focus of my career, and I have state-of-the-art techniques. Yet, I still have plenty of obese patients of all ages in my care,” he said. How should he be reimbursed for treating these patients, particularly if some of them are already on the road to a lifetime of obesity, having been set upon it long before being diagnosed?
“I think a pediatrician should be responsible for delivering content and good advice, and addressing the health issues. That can be documented, and we can be scored on that” said Dr. Paul, but “it might be unfair to judge a pediatrician on the proportion of the number of children who are overweight or obese in his or her practice because there are so many factors that are going to be involved in that outcome.
“There is only so much we can do in the clinic.”
There were no conflicts of interest to report.
On Twitter @whitneymcknight
WASHINGTON – Physicians have a role in combating early childhood obesity, but experts say the clinical setting is not ideal for effective treatment and prevention of this emerging epidemic.
“Pediatricians have high access to kids, parents, and guardians, and we are trusted sources of information for them,” Dr. Ian Paul, professor and chief of academic pediatrics at Penn State University Hershey Medical Center, said at an Institute of Medicine forum on early childhood obesity.
Emerging data underscore obesity’s complex societal components, which include an imbalance of diet and physical activity complicated by less tangible factors such as cultural attitudes, maternal habits, and socio-economic status. And then there is the question of the best way to reimburse physicians for applying the few proven long-term interventions they have.
“I think it’s one of those things where it takes a village,” Dr. Paul said in an interview. “You need multiple people going in the same direction. The pediatrician can give advice, and support what is happening, but it can’t just be the pediatrician by him- or herself.”
The U.S. Centers for Disease Control and Prevention says that pediatric obesity affects a third of the nation’s youth. But there are only vague policies and guidelines for how to intervene in the preschool years, a time when research now shows risk factors present can set the stage for obesity later in a child’s life. This all leaves pediatricians unsure of how to treat young patients who present with signs of overweight and obesity. To date, there are no proven clinical-based obesity interventions for birth to age 5 years, Dr. Paul said. “Pediatricians don’t always feel equipped to handle questions about obesity prevention and treatment,” compounded, by the fact that, “reimbursement for these services has been poor.”
However, through partnerships with community organizations and other clinicians, more effective models of care are emerging, particularly in minority and lower income communities where obesity rates are among the highest nationally (Contemp Clin Trials. 2013 Nov;36[3]:544-54. doi: 10.1016/j.cct.2013.09.015. Epub 2013 Oct 9), noted Dr. Paul.
“In poorer households, high rates of maternal stress and less access to resources such as time with a nutritionist or higher quality produce and other foods, are risk factors for obesity,” Dr. Mary Jo Messito, director of the Starting Early Child Obesity Prevention Program at Bellevue Hospital in New York, said in an interview.
As part of their program, Dr. Messito, clinical associate professor of pediatrics at New York University, and her colleagues conducted a study of a family-based, early obesity intervention and prevention program with nutrition support groups as the central component.
The study involved 534 expectant mothers in their last trimester who were randomly assigned to receive either standard prenatal care followed by standard well-child care, or prenatal nutritional counseling, in addition to well-child visits coupled with continued nutritional counseling in a group setting, which they attend with their babies. The study group met regularly to learn how to make their own minimally processed baby foods, read and understand food labels, and offer peer support for any issues they might be encountering in raising their babies to eat healthfully.
Although many Hispanic families are affected by obesity, there is a need to teach and reinforce these skills in all families of young children affected by poverty, said Dr. Messito. “Middle and upper income people can also be affected by obesity, but they have the resources to deal with it, including education and nutritional support provided by insurance plans.”
The currently unpublished results of the study, based on 3 years of follow-up, are both statistically and clinically significant, said Dr. Messito. Only 6% of the families in the study group prematurely introduced complementary foods such as juices and solids compared with 17% in controls, according to Dr. Messito.
Exclusively breastfed babies in the control group totaled 34% compared with an impressive 46% in the study group, Dr. Messito said.
The potentially devastating consequences of resorting to quick-fixes such as cereal and juice at too young an age to sooth a fussy baby, is that at age 2 or 3 years, when it is still tricky to determine if they’ve exceeded the 95th percentile for their weight, these overfed babies can be on a trajectory that lasts long after they grow up. “If you are obese then, the odds are great you will be for life,” said Dr. Messito.
Much of the Starting Early study’s “plain language” materials, published in both English and Spanish, distributed to families as reinforcement to what they learn in their groups, was based on what is routinely provided by the federal Women, Infants, and Children (WIC) program, said Dr. Messito. “We see ourselves as collaborators with WIC and with primary care.”
This pleases Dr. Paul. “Pediatricians only have a limited amount of time for each visit, and an office setting is not very conducive to get in as in-depth a conversation as you would like, especially in well-child care. By meeting with several families at once, instead of delivering the same information five times, it can be done once in 100 minutes where everyone can be in on the discussion,” he said in an interview.
Partnering with others in the community not only adds another layer of support, it also takes the burden off the physician to do it all.
The NET-Works study (Now Everybody Together for Amazing and Healthful Kids), currently underway at the University of Minnesota, on the Twin Cities campus, includes the families of 500 preschoolers, followed for 3 years after being randomly assigned to standard care or an integrated model that features nutritional counseling, both at the primary care and community level, as well as a home-based intervention, and support from neighborhood and community resources to promote optimal healthful lifestyle habits, including diet and physical activity, and screen time limits. Results from the study are due in 2017.
“What I like about this study is that the pediatrician has a supporting, rather than leading, role in a community-wide effort to prevent and treat childhood obesity,” said Dr. Paul. “I think that’s the answer.”
Another model of community-based care, promoted by the CDC, leverages the time more than 60% of U.S. children spend in early education and care centers by linking various community resources with these early learning facilities to ensure that children learn to consume healthful foods and exercise.
Dr. Dianne Ward, professor of nutrition at the University of North Carolina, Chapel Hill, and a panelist at the IOM roundtable, noted that one hitch is that often the child care providers themselves are often unhealthy. “A number of studies show these women often have poor diets, stress, inactivity, and smoke, yet these are the same women we ask to be role models for our children and lead the healthy eating educational programs. It’s unclear whether their health status has a negative effect on the children.”
Dr. Paul’s own work with others such as Dr. Leann Birch, the William P. “Bill” Flatt Childhood Obesity Professor at the University of Georgia, Athens, focuses on home-based interventions delivered by nurses. By training parents and caregivers in what they call “responsive feeding,” their SLIM-Time study addresses how and why parents feed their children, rather than what they feed them, with the essential byproduct being greater capacity in both parents and children to self-soothe and exert self-control.
Similar to Dr. Messito’s work, SLIM-Time (Sleeping and Intake Methods Taught to Infants and Mothers Early in Life) “teaches people how to respond appropriately to a baby’s cues earlier in life. If you take a baby and give it a bottle, it will stop crying, whether or not [the baby is] hungry. Food should be used for hunger,” Dr. Paul said. “We teach parents to use food for hunger, not comfort.”
The results of the randomly controlled SLIM-Time study of 110 mother-infant dyads, published online in 2010, were that by teaching parents soothing and sleep strategies other than bottle feeding, and helping them to recognize satiety cues, as well as educating them on the appropriate time to introduce solid foods, study babies were encouraged to finish their bottles only half as often as were controls. At 1 year, study babies were in the 35th percentile for weight-for-length compared with 50% of controls. Babies in the test group also required fewer nighttime feedings than did controls at weeks 3, 4, 8, and 16 (P = .003) (Obesity. 2011 Feb; 19[2]: 353-61).
The results led Dr. Paul and his colleagues to create the similarly structured INSIGHT Study (Preventing Obesity Through Interventions During Infancy), the results of which are still in preparation, but preliminarily seem to reinforce SLIM-Time’s results, with 15% of controls being in the 95th or higher weight-per-length percentiles at 1 year compared with 5% of intervention group babies being in that range.
Dr. Birch stated during the IOM round table that the effects in each study group were similar, regardless of whether a child was fed formula or breast milk. “We still have a lot of data to analyze, but at this point, it looks like the effects aren’t limited to intense breastfeeding.” Breastfeeding has been found protective against obesity (Am J Epidemiol. 2005 Sept 1;162[5]:397-403. Epub 2005 Aug 2; Int J Obes Relat Metab Disord. 2004 Oct;28[10]:1247-56.)
Even though the literature for early childhood obesity intervention and prevention is nascent, it’s already evident that to see obesity primarily as a clinical issue is too limiting, according to Dr. Paul.
“This is the focus of my career, and I have state-of-the-art techniques. Yet, I still have plenty of obese patients of all ages in my care,” he said. How should he be reimbursed for treating these patients, particularly if some of them are already on the road to a lifetime of obesity, having been set upon it long before being diagnosed?
“I think a pediatrician should be responsible for delivering content and good advice, and addressing the health issues. That can be documented, and we can be scored on that” said Dr. Paul, but “it might be unfair to judge a pediatrician on the proportion of the number of children who are overweight or obese in his or her practice because there are so many factors that are going to be involved in that outcome.
“There is only so much we can do in the clinic.”
There were no conflicts of interest to report.
On Twitter @whitneymcknight
WASHINGTON – Physicians have a role in combating early childhood obesity, but experts say the clinical setting is not ideal for effective treatment and prevention of this emerging epidemic.
“Pediatricians have high access to kids, parents, and guardians, and we are trusted sources of information for them,” Dr. Ian Paul, professor and chief of academic pediatrics at Penn State University Hershey Medical Center, said at an Institute of Medicine forum on early childhood obesity.
Emerging data underscore obesity’s complex societal components, which include an imbalance of diet and physical activity complicated by less tangible factors such as cultural attitudes, maternal habits, and socio-economic status. And then there is the question of the best way to reimburse physicians for applying the few proven long-term interventions they have.
“I think it’s one of those things where it takes a village,” Dr. Paul said in an interview. “You need multiple people going in the same direction. The pediatrician can give advice, and support what is happening, but it can’t just be the pediatrician by him- or herself.”
The U.S. Centers for Disease Control and Prevention says that pediatric obesity affects a third of the nation’s youth. But there are only vague policies and guidelines for how to intervene in the preschool years, a time when research now shows risk factors present can set the stage for obesity later in a child’s life. This all leaves pediatricians unsure of how to treat young patients who present with signs of overweight and obesity. To date, there are no proven clinical-based obesity interventions for birth to age 5 years, Dr. Paul said. “Pediatricians don’t always feel equipped to handle questions about obesity prevention and treatment,” compounded, by the fact that, “reimbursement for these services has been poor.”
However, through partnerships with community organizations and other clinicians, more effective models of care are emerging, particularly in minority and lower income communities where obesity rates are among the highest nationally (Contemp Clin Trials. 2013 Nov;36[3]:544-54. doi: 10.1016/j.cct.2013.09.015. Epub 2013 Oct 9), noted Dr. Paul.
“In poorer households, high rates of maternal stress and less access to resources such as time with a nutritionist or higher quality produce and other foods, are risk factors for obesity,” Dr. Mary Jo Messito, director of the Starting Early Child Obesity Prevention Program at Bellevue Hospital in New York, said in an interview.
As part of their program, Dr. Messito, clinical associate professor of pediatrics at New York University, and her colleagues conducted a study of a family-based, early obesity intervention and prevention program with nutrition support groups as the central component.
The study involved 534 expectant mothers in their last trimester who were randomly assigned to receive either standard prenatal care followed by standard well-child care, or prenatal nutritional counseling, in addition to well-child visits coupled with continued nutritional counseling in a group setting, which they attend with their babies. The study group met regularly to learn how to make their own minimally processed baby foods, read and understand food labels, and offer peer support for any issues they might be encountering in raising their babies to eat healthfully.
Although many Hispanic families are affected by obesity, there is a need to teach and reinforce these skills in all families of young children affected by poverty, said Dr. Messito. “Middle and upper income people can also be affected by obesity, but they have the resources to deal with it, including education and nutritional support provided by insurance plans.”
The currently unpublished results of the study, based on 3 years of follow-up, are both statistically and clinically significant, said Dr. Messito. Only 6% of the families in the study group prematurely introduced complementary foods such as juices and solids compared with 17% in controls, according to Dr. Messito.
Exclusively breastfed babies in the control group totaled 34% compared with an impressive 46% in the study group, Dr. Messito said.
The potentially devastating consequences of resorting to quick-fixes such as cereal and juice at too young an age to sooth a fussy baby, is that at age 2 or 3 years, when it is still tricky to determine if they’ve exceeded the 95th percentile for their weight, these overfed babies can be on a trajectory that lasts long after they grow up. “If you are obese then, the odds are great you will be for life,” said Dr. Messito.
Much of the Starting Early study’s “plain language” materials, published in both English and Spanish, distributed to families as reinforcement to what they learn in their groups, was based on what is routinely provided by the federal Women, Infants, and Children (WIC) program, said Dr. Messito. “We see ourselves as collaborators with WIC and with primary care.”
This pleases Dr. Paul. “Pediatricians only have a limited amount of time for each visit, and an office setting is not very conducive to get in as in-depth a conversation as you would like, especially in well-child care. By meeting with several families at once, instead of delivering the same information five times, it can be done once in 100 minutes where everyone can be in on the discussion,” he said in an interview.
Partnering with others in the community not only adds another layer of support, it also takes the burden off the physician to do it all.
The NET-Works study (Now Everybody Together for Amazing and Healthful Kids), currently underway at the University of Minnesota, on the Twin Cities campus, includes the families of 500 preschoolers, followed for 3 years after being randomly assigned to standard care or an integrated model that features nutritional counseling, both at the primary care and community level, as well as a home-based intervention, and support from neighborhood and community resources to promote optimal healthful lifestyle habits, including diet and physical activity, and screen time limits. Results from the study are due in 2017.
“What I like about this study is that the pediatrician has a supporting, rather than leading, role in a community-wide effort to prevent and treat childhood obesity,” said Dr. Paul. “I think that’s the answer.”
Another model of community-based care, promoted by the CDC, leverages the time more than 60% of U.S. children spend in early education and care centers by linking various community resources with these early learning facilities to ensure that children learn to consume healthful foods and exercise.
Dr. Dianne Ward, professor of nutrition at the University of North Carolina, Chapel Hill, and a panelist at the IOM roundtable, noted that one hitch is that often the child care providers themselves are often unhealthy. “A number of studies show these women often have poor diets, stress, inactivity, and smoke, yet these are the same women we ask to be role models for our children and lead the healthy eating educational programs. It’s unclear whether their health status has a negative effect on the children.”
Dr. Paul’s own work with others such as Dr. Leann Birch, the William P. “Bill” Flatt Childhood Obesity Professor at the University of Georgia, Athens, focuses on home-based interventions delivered by nurses. By training parents and caregivers in what they call “responsive feeding,” their SLIM-Time study addresses how and why parents feed their children, rather than what they feed them, with the essential byproduct being greater capacity in both parents and children to self-soothe and exert self-control.
Similar to Dr. Messito’s work, SLIM-Time (Sleeping and Intake Methods Taught to Infants and Mothers Early in Life) “teaches people how to respond appropriately to a baby’s cues earlier in life. If you take a baby and give it a bottle, it will stop crying, whether or not [the baby is] hungry. Food should be used for hunger,” Dr. Paul said. “We teach parents to use food for hunger, not comfort.”
The results of the randomly controlled SLIM-Time study of 110 mother-infant dyads, published online in 2010, were that by teaching parents soothing and sleep strategies other than bottle feeding, and helping them to recognize satiety cues, as well as educating them on the appropriate time to introduce solid foods, study babies were encouraged to finish their bottles only half as often as were controls. At 1 year, study babies were in the 35th percentile for weight-for-length compared with 50% of controls. Babies in the test group also required fewer nighttime feedings than did controls at weeks 3, 4, 8, and 16 (P = .003) (Obesity. 2011 Feb; 19[2]: 353-61).
The results led Dr. Paul and his colleagues to create the similarly structured INSIGHT Study (Preventing Obesity Through Interventions During Infancy), the results of which are still in preparation, but preliminarily seem to reinforce SLIM-Time’s results, with 15% of controls being in the 95th or higher weight-per-length percentiles at 1 year compared with 5% of intervention group babies being in that range.
Dr. Birch stated during the IOM round table that the effects in each study group were similar, regardless of whether a child was fed formula or breast milk. “We still have a lot of data to analyze, but at this point, it looks like the effects aren’t limited to intense breastfeeding.” Breastfeeding has been found protective against obesity (Am J Epidemiol. 2005 Sept 1;162[5]:397-403. Epub 2005 Aug 2; Int J Obes Relat Metab Disord. 2004 Oct;28[10]:1247-56.)
Even though the literature for early childhood obesity intervention and prevention is nascent, it’s already evident that to see obesity primarily as a clinical issue is too limiting, according to Dr. Paul.
“This is the focus of my career, and I have state-of-the-art techniques. Yet, I still have plenty of obese patients of all ages in my care,” he said. How should he be reimbursed for treating these patients, particularly if some of them are already on the road to a lifetime of obesity, having been set upon it long before being diagnosed?
“I think a pediatrician should be responsible for delivering content and good advice, and addressing the health issues. That can be documented, and we can be scored on that” said Dr. Paul, but “it might be unfair to judge a pediatrician on the proportion of the number of children who are overweight or obese in his or her practice because there are so many factors that are going to be involved in that outcome.
“There is only so much we can do in the clinic.”
There were no conflicts of interest to report.
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM AN EARLY CHILDHOOD OBESITY ROUNDTABLE

Does poverty predetermine pediatric obesity?
WASHINGTON – Childhood obesity is soaring in the United States, especially among Hispanic and African-American children. At the heart of this “epidemic” are dietary and behavioral factors that are linked to stress and poverty rather than race and ethnicity, and the risks may even begin prenatally, according to experts attending an Institute of Medicine forum on early childhood obesity.
Based on data from the 2009-2010 NHANES (National Health and Nutrition Examination Survey), over 8% of children aged 2-5 years in the United States are obese; based on ethnicity, 18% of Hispanic boys and 15% of Hispanic girls in this age group are obese. Nearly 18% of U.S. children aged 6-11 years are obese; nearly 29% of Hispanic boys and 26% of non-Hispanic black girls in this age group are obese.
“If we’re looking for reasons why black and Hispanic children have these disparities ... then we’re looking at what happens in their early years and during pregnancy,” Dr. Elsie Taveras, chief of general academic pediatrics at Massachusetts General Hospital, Boston, said at the IOM meeting.

Chief among the culprits responsible for the “metabolic programming of risk” is the mother’s pregestational weight, according to Dr. Lisa Bodnar, associate professor of endocrinology at the University of Pittsburgh. “Children may already be programmed to become obese as a result of their intrauterine exposure to an obesogenic environment.”
A 2013 report from the Centers for Disease Control and Prevention found that about 1 in 5 women aged 20 years and older who delivered a live-born infant in 2009 were obese prior to becoming pregnant. The prevalence of obesity was highest among women who were 35 years of age and older (24%); were black, non-Hispanic (32%); had a high school education (28%); and reported Medicaid as their source of insurance coverage before pregnancy (30%). The prevalence of obesity was lowest among women who were 20-34 years of age (22%); were of “other” race/ethnicity (13%); had more than a high school education (20%); and who reported having private insurance coverage before pregnancy (20%), according to the report.
Studies have established that pre-pregnancy body mass index is highly correlated with rates of childhood obesity, but Dr. Bodnar believes the most elegant study, published in Pediatrics in 2004, links the birth records of 8,500 children born to low-income mothers in Ohio with corresponding Women, Infants, and Children data for their children’s respective weights and heights at ages 2, 3, and 4 years. Mothers with pre-pregnancy BMIs in the obese and severely obese ranges had a 3-4 times greater probability that their children had similar BMIs.
More recent U.S. data show that nearly half of all expectant mothers with normal pregravid weights also gain more weight prenatally than the IOM-recommended amounts. The tendency is even more prevalent in those with BMIs in the overweight and obese ranges: 70% of women with pre-gestational BMIs between 25 and 29.9, and 65% of those with BMIs of 30 and over gain too much weight. A 2013 meta-analysis published in JAMA correlated these weight gain patterns with a 90% increased risk of children being obese before the age of 5 years, and a 40% overall lifetime increased risk of obesity.
Stress and sociodemographic factors also can contribute to overeating and unhealthy eating, Dr. Mary Jo Messito, director of the Starting Early Child Obesity Prevention Program at Bellevue Hospital, New York, said in an interview. “High stress can lead to eating higher levels of sugary and processed food.” In lower socioeconomic neighborhoods, processed and fast foods can also be more affordable and more readily available, she added.
At least one study (Sleep Med Rev. 2012 Jun;16[3]:203-11) has established a link between later bedtimes and obesity.
This generation of children sleeps nearly a half hour less per night than did their parents, Dr. Taveras said, and the culprits include later bedtimes, the intake of caffeinated and sugary beverages, and electronic intrusions. A television left on in the room where the child sleeps can make the child dependent upon external means rather than self regulation for putting themselves to sleep, according to Dr. Taveras’ research, published in Pediatrics.
Dr. Taveras also lead a 7-year prospective prebirth cohort study (JAMA Pediatr. 2013 Aug 1;167[8]:731-8) of 1,116 mother and child dyads. In that study, the higher levels of obesity in racial and ethnic minority children were linked to modifiable risk factors. Black and Hispanic 2-year-olds were twice as likely as white ones to have had a cola or other sweetened or caffeinated drink prior to bedtime. By age 4 years, 6.4% of white children, 53% of black children, and 61% of Hispanic children in the study fell to sleep with a television on.
“Dietary patterns in the U.S. are poor, start early, and persist,” Dr. Jose M. Saavedra, chief medical officer for the nutrition division of Nestle USA, said at the meeting. Recently published data in Journal of Obesity (doi: 10.1155/2012/123023) indicate that children who consume sugar-sweetened beverages during infancy are twice as likely to consume them at age 6 years. Similarly, children who do not consume fruits and vegetables daily in infancy were also found to consume them infrequently at the age of 6.
“The patterns start much earlier than what we’ve been paying attention to,” said Dr. Saavedra. He thinks that the window of behavioral plasticity is widest at age 20 months, and urged his peers to find ways to help parents to establish good habits in their children during that time.
Discussing healthy behaviors with parents can help, and may elicit some parental behaviors that can be corrected. During the question and answer session at the meeting, for example, an audience member shared an anecdote about a mother who would only serve her children soda because she’d come from an island nation where the water supply was often unsafe.
Others noted that parents and grandparents who have grown up under conditions of food scarcity can view a “chubby” baby as a healthy baby. Mothers also can feel pressured into overfeeding infants, beginning with supplementing formula.
Also, food is often used as a quick and easy reward, Dr. Messito said. When money is tight, a cookie is an inexpensive treat.
On Twitter @whitneymcknight
WASHINGTON – Childhood obesity is soaring in the United States, especially among Hispanic and African-American children. At the heart of this “epidemic” are dietary and behavioral factors that are linked to stress and poverty rather than race and ethnicity, and the risks may even begin prenatally, according to experts attending an Institute of Medicine forum on early childhood obesity.
Based on data from the 2009-2010 NHANES (National Health and Nutrition Examination Survey), over 8% of children aged 2-5 years in the United States are obese; based on ethnicity, 18% of Hispanic boys and 15% of Hispanic girls in this age group are obese. Nearly 18% of U.S. children aged 6-11 years are obese; nearly 29% of Hispanic boys and 26% of non-Hispanic black girls in this age group are obese.
“If we’re looking for reasons why black and Hispanic children have these disparities ... then we’re looking at what happens in their early years and during pregnancy,” Dr. Elsie Taveras, chief of general academic pediatrics at Massachusetts General Hospital, Boston, said at the IOM meeting.
Chief among the culprits responsible for the “metabolic programming of risk” is the mother’s pregestational weight, according to Dr. Lisa Bodnar, associate professor of endocrinology at the University of Pittsburgh. “Children may already be programmed to become obese as a result of their intrauterine exposure to an obesogenic environment.”
A 2013 report from the Centers for Disease Control and Prevention found that about 1 in 5 women aged 20 years and older who delivered a live-born infant in 2009 were obese prior to becoming pregnant. The prevalence of obesity was highest among women who were 35 years of age and older (24%); were black, non-Hispanic (32%); had a high school education (28%); and reported Medicaid as their source of insurance coverage before pregnancy (30%). The prevalence of obesity was lowest among women who were 20-34 years of age (22%); were of “other” race/ethnicity (13%); had more than a high school education (20%); and who reported having private insurance coverage before pregnancy (20%), according to the report.
Studies have established that pre-pregnancy body mass index is highly correlated with rates of childhood obesity, but Dr. Bodnar believes the most elegant study, published in Pediatrics in 2004, links the birth records of 8,500 children born to low-income mothers in Ohio with corresponding Women, Infants, and Children data for their children’s respective weights and heights at ages 2, 3, and 4 years. Mothers with pre-pregnancy BMIs in the obese and severely obese ranges had a 3-4 times greater probability that their children had similar BMIs.
More recent U.S. data show that nearly half of all expectant mothers with normal pregravid weights also gain more weight prenatally than the IOM-recommended amounts. The tendency is even more prevalent in those with BMIs in the overweight and obese ranges: 70% of women with pre-gestational BMIs between 25 and 29.9, and 65% of those with BMIs of 30 and over gain too much weight. A 2013 meta-analysis published in JAMA correlated these weight gain patterns with a 90% increased risk of children being obese before the age of 5 years, and a 40% overall lifetime increased risk of obesity.
Stress and sociodemographic factors also can contribute to overeating and unhealthy eating, Dr. Mary Jo Messito, director of the Starting Early Child Obesity Prevention Program at Bellevue Hospital, New York, said in an interview. “High stress can lead to eating higher levels of sugary and processed food.” In lower socioeconomic neighborhoods, processed and fast foods can also be more affordable and more readily available, she added.
At least one study (Sleep Med Rev. 2012 Jun;16[3]:203-11) has established a link between later bedtimes and obesity.
This generation of children sleeps nearly a half hour less per night than did their parents, Dr. Taveras said, and the culprits include later bedtimes, the intake of caffeinated and sugary beverages, and electronic intrusions. A television left on in the room where the child sleeps can make the child dependent upon external means rather than self regulation for putting themselves to sleep, according to Dr. Taveras’ research, published in Pediatrics.
Dr. Taveras also lead a 7-year prospective prebirth cohort study (JAMA Pediatr. 2013 Aug 1;167[8]:731-8) of 1,116 mother and child dyads. In that study, the higher levels of obesity in racial and ethnic minority children were linked to modifiable risk factors. Black and Hispanic 2-year-olds were twice as likely as white ones to have had a cola or other sweetened or caffeinated drink prior to bedtime. By age 4 years, 6.4% of white children, 53% of black children, and 61% of Hispanic children in the study fell to sleep with a television on.
“Dietary patterns in the U.S. are poor, start early, and persist,” Dr. Jose M. Saavedra, chief medical officer for the nutrition division of Nestle USA, said at the meeting. Recently published data in Journal of Obesity (doi: 10.1155/2012/123023) indicate that children who consume sugar-sweetened beverages during infancy are twice as likely to consume them at age 6 years. Similarly, children who do not consume fruits and vegetables daily in infancy were also found to consume them infrequently at the age of 6.
“The patterns start much earlier than what we’ve been paying attention to,” said Dr. Saavedra. He thinks that the window of behavioral plasticity is widest at age 20 months, and urged his peers to find ways to help parents to establish good habits in their children during that time.
Discussing healthy behaviors with parents can help, and may elicit some parental behaviors that can be corrected. During the question and answer session at the meeting, for example, an audience member shared an anecdote about a mother who would only serve her children soda because she’d come from an island nation where the water supply was often unsafe.
Others noted that parents and grandparents who have grown up under conditions of food scarcity can view a “chubby” baby as a healthy baby. Mothers also can feel pressured into overfeeding infants, beginning with supplementing formula.
Also, food is often used as a quick and easy reward, Dr. Messito said. When money is tight, a cookie is an inexpensive treat.
On Twitter @whitneymcknight
WASHINGTON – Childhood obesity is soaring in the United States, especially among Hispanic and African-American children. At the heart of this “epidemic” are dietary and behavioral factors that are linked to stress and poverty rather than race and ethnicity, and the risks may even begin prenatally, according to experts attending an Institute of Medicine forum on early childhood obesity.
Based on data from the 2009-2010 NHANES (National Health and Nutrition Examination Survey), over 8% of children aged 2-5 years in the United States are obese; based on ethnicity, 18% of Hispanic boys and 15% of Hispanic girls in this age group are obese. Nearly 18% of U.S. children aged 6-11 years are obese; nearly 29% of Hispanic boys and 26% of non-Hispanic black girls in this age group are obese.
“If we’re looking for reasons why black and Hispanic children have these disparities ... then we’re looking at what happens in their early years and during pregnancy,” Dr. Elsie Taveras, chief of general academic pediatrics at Massachusetts General Hospital, Boston, said at the IOM meeting.
Chief among the culprits responsible for the “metabolic programming of risk” is the mother’s pregestational weight, according to Dr. Lisa Bodnar, associate professor of endocrinology at the University of Pittsburgh. “Children may already be programmed to become obese as a result of their intrauterine exposure to an obesogenic environment.”
A 2013 report from the Centers for Disease Control and Prevention found that about 1 in 5 women aged 20 years and older who delivered a live-born infant in 2009 were obese prior to becoming pregnant. The prevalence of obesity was highest among women who were 35 years of age and older (24%); were black, non-Hispanic (32%); had a high school education (28%); and reported Medicaid as their source of insurance coverage before pregnancy (30%). The prevalence of obesity was lowest among women who were 20-34 years of age (22%); were of “other” race/ethnicity (13%); had more than a high school education (20%); and who reported having private insurance coverage before pregnancy (20%), according to the report.
Studies have established that pre-pregnancy body mass index is highly correlated with rates of childhood obesity, but Dr. Bodnar believes the most elegant study, published in Pediatrics in 2004, links the birth records of 8,500 children born to low-income mothers in Ohio with corresponding Women, Infants, and Children data for their children’s respective weights and heights at ages 2, 3, and 4 years. Mothers with pre-pregnancy BMIs in the obese and severely obese ranges had a 3-4 times greater probability that their children had similar BMIs.
More recent U.S. data show that nearly half of all expectant mothers with normal pregravid weights also gain more weight prenatally than the IOM-recommended amounts. The tendency is even more prevalent in those with BMIs in the overweight and obese ranges: 70% of women with pre-gestational BMIs between 25 and 29.9, and 65% of those with BMIs of 30 and over gain too much weight. A 2013 meta-analysis published in JAMA correlated these weight gain patterns with a 90% increased risk of children being obese before the age of 5 years, and a 40% overall lifetime increased risk of obesity.
Stress and sociodemographic factors also can contribute to overeating and unhealthy eating, Dr. Mary Jo Messito, director of the Starting Early Child Obesity Prevention Program at Bellevue Hospital, New York, said in an interview. “High stress can lead to eating higher levels of sugary and processed food.” In lower socioeconomic neighborhoods, processed and fast foods can also be more affordable and more readily available, she added.
At least one study (Sleep Med Rev. 2012 Jun;16[3]:203-11) has established a link between later bedtimes and obesity.
This generation of children sleeps nearly a half hour less per night than did their parents, Dr. Taveras said, and the culprits include later bedtimes, the intake of caffeinated and sugary beverages, and electronic intrusions. A television left on in the room where the child sleeps can make the child dependent upon external means rather than self regulation for putting themselves to sleep, according to Dr. Taveras’ research, published in Pediatrics.
Dr. Taveras also lead a 7-year prospective prebirth cohort study (JAMA Pediatr. 2013 Aug 1;167[8]:731-8) of 1,116 mother and child dyads. In that study, the higher levels of obesity in racial and ethnic minority children were linked to modifiable risk factors. Black and Hispanic 2-year-olds were twice as likely as white ones to have had a cola or other sweetened or caffeinated drink prior to bedtime. By age 4 years, 6.4% of white children, 53% of black children, and 61% of Hispanic children in the study fell to sleep with a television on.
“Dietary patterns in the U.S. are poor, start early, and persist,” Dr. Jose M. Saavedra, chief medical officer for the nutrition division of Nestle USA, said at the meeting. Recently published data in Journal of Obesity (doi: 10.1155/2012/123023) indicate that children who consume sugar-sweetened beverages during infancy are twice as likely to consume them at age 6 years. Similarly, children who do not consume fruits and vegetables daily in infancy were also found to consume them infrequently at the age of 6.
“The patterns start much earlier than what we’ve been paying attention to,” said Dr. Saavedra. He thinks that the window of behavioral plasticity is widest at age 20 months, and urged his peers to find ways to help parents to establish good habits in their children during that time.
Discussing healthy behaviors with parents can help, and may elicit some parental behaviors that can be corrected. During the question and answer session at the meeting, for example, an audience member shared an anecdote about a mother who would only serve her children soda because she’d come from an island nation where the water supply was often unsafe.
Others noted that parents and grandparents who have grown up under conditions of food scarcity can view a “chubby” baby as a healthy baby. Mothers also can feel pressured into overfeeding infants, beginning with supplementing formula.
Also, food is often used as a quick and easy reward, Dr. Messito said. When money is tight, a cookie is an inexpensive treat.
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM AN EARLY CHILDHOOD OBESITY ROUNDTABLE

Novel polio vaccine strains promise improved post-eradication safety
Newly developed polio vaccine strains could replace currently used risky inactivated vaccines, thereby allowing for safer vaccine production in a post-polio eradication environment, according to researchers at the National Institute for Biological Standards and Control (NIBSC).
Polio eradication is in sight, and these new strains are safer than the attenuated Sabin strain currently used for developing inactivated vaccine. The Sabin strain is unstable and thus could repopulate the environment, Sarah Knowlson and her colleagues from the NIBSC, Potters Bar, Hertfordshire, England, argue in an article published Dec. 31 in PLOS Pathogens.
“The Global Polio Eradication Initiative is ... very close to eliminating naturally occurring wild poliovirus from the planet. It has involved the extensive use of both the live attenuated vaccines that can revert to a wild type phenotype, and inactivated polio vaccines (IPV) whose production in the main currently requires the growth of very large amounts of virulent wild type poliovirus, ” they explain, noting that the vaccines are therefore a possible source for re-emergence of poliomyelitis following eradication. (PLoS Pathog. 2015 Dec 31;11. doi: 10.1371/journal.ppat.1005316).
To develop the new strains, the researchers started with the well-understood Sabin strain and modified a region of its viral RNA to promote greater genetic stability. The new strains were then compared with the original Sabin vaccine strain and the wild-type strain currently used to produce inactivated vaccine.
The new strains were “extremely attenuated and genetically stable in cell culture by rational design based on understanding of the attenuation of the Sabin vaccine strains of poliovirus. The viruses grow to titers acceptable for IPV production under appropriate conditions of temperature and cell substrate and have the same antigenic properties based on reactions with panels of monoclonal antibodies in ELISA as well as in regulatory assays for antigen and immunogen content as the strains from which their capsids were derived,” the investigators wrote.
The strains were tested in mice and primates and behaved as predicted in that they were “effective, suitable to mass production, and safer than the alternatives,” according to a press statement.
This work was supported by NIBSC. The investigators reported having no disclosures.
Newly developed polio vaccine strains could replace currently used risky inactivated vaccines, thereby allowing for safer vaccine production in a post-polio eradication environment, according to researchers at the National Institute for Biological Standards and Control (NIBSC).
Polio eradication is in sight, and these new strains are safer than the attenuated Sabin strain currently used for developing inactivated vaccine. The Sabin strain is unstable and thus could repopulate the environment, Sarah Knowlson and her colleagues from the NIBSC, Potters Bar, Hertfordshire, England, argue in an article published Dec. 31 in PLOS Pathogens.
“The Global Polio Eradication Initiative is ... very close to eliminating naturally occurring wild poliovirus from the planet. It has involved the extensive use of both the live attenuated vaccines that can revert to a wild type phenotype, and inactivated polio vaccines (IPV) whose production in the main currently requires the growth of very large amounts of virulent wild type poliovirus, ” they explain, noting that the vaccines are therefore a possible source for re-emergence of poliomyelitis following eradication. (PLoS Pathog. 2015 Dec 31;11. doi: 10.1371/journal.ppat.1005316).
To develop the new strains, the researchers started with the well-understood Sabin strain and modified a region of its viral RNA to promote greater genetic stability. The new strains were then compared with the original Sabin vaccine strain and the wild-type strain currently used to produce inactivated vaccine.
The new strains were “extremely attenuated and genetically stable in cell culture by rational design based on understanding of the attenuation of the Sabin vaccine strains of poliovirus. The viruses grow to titers acceptable for IPV production under appropriate conditions of temperature and cell substrate and have the same antigenic properties based on reactions with panels of monoclonal antibodies in ELISA as well as in regulatory assays for antigen and immunogen content as the strains from which their capsids were derived,” the investigators wrote.
The strains were tested in mice and primates and behaved as predicted in that they were “effective, suitable to mass production, and safer than the alternatives,” according to a press statement.
This work was supported by NIBSC. The investigators reported having no disclosures.
Newly developed polio vaccine strains could replace currently used risky inactivated vaccines, thereby allowing for safer vaccine production in a post-polio eradication environment, according to researchers at the National Institute for Biological Standards and Control (NIBSC).
Polio eradication is in sight, and these new strains are safer than the attenuated Sabin strain currently used for developing inactivated vaccine. The Sabin strain is unstable and thus could repopulate the environment, Sarah Knowlson and her colleagues from the NIBSC, Potters Bar, Hertfordshire, England, argue in an article published Dec. 31 in PLOS Pathogens.
“The Global Polio Eradication Initiative is ... very close to eliminating naturally occurring wild poliovirus from the planet. It has involved the extensive use of both the live attenuated vaccines that can revert to a wild type phenotype, and inactivated polio vaccines (IPV) whose production in the main currently requires the growth of very large amounts of virulent wild type poliovirus, ” they explain, noting that the vaccines are therefore a possible source for re-emergence of poliomyelitis following eradication. (PLoS Pathog. 2015 Dec 31;11. doi: 10.1371/journal.ppat.1005316).
To develop the new strains, the researchers started with the well-understood Sabin strain and modified a region of its viral RNA to promote greater genetic stability. The new strains were then compared with the original Sabin vaccine strain and the wild-type strain currently used to produce inactivated vaccine.
The new strains were “extremely attenuated and genetically stable in cell culture by rational design based on understanding of the attenuation of the Sabin vaccine strains of poliovirus. The viruses grow to titers acceptable for IPV production under appropriate conditions of temperature and cell substrate and have the same antigenic properties based on reactions with panels of monoclonal antibodies in ELISA as well as in regulatory assays for antigen and immunogen content as the strains from which their capsids were derived,” the investigators wrote.
The strains were tested in mice and primates and behaved as predicted in that they were “effective, suitable to mass production, and safer than the alternatives,” according to a press statement.
This work was supported by NIBSC. The investigators reported having no disclosures.
FROM PLOS PATHOGENS
LAIV, IIV almost equally effective against influenza
When vaccinating children against influenza, inactivated and live attenuated influenza vaccines show little significant difference in effectiveness against nearly all strains of the virus, according to a new study in Pediatrics.
However, the study – which examined the effectiveness of IIV and LAIV across four consecutive influenza seasons between 2010 and 2014 – cautions that the 2013-2014 season’s A/(H1N1)pdm09 showed an uncharacteristically large gap in effectiveness favoring IIV, a discrepancy likely due to a problem with a vaccine component in LAIV. (Pediatrics. 2016;137(2):e20153279)
“We found that lower LAIV effectiveness in 2013-2014 was specific to the A/(H1N1)pdm09 vaccine component and was consistent with a previously unexamined effect during the 2010-2011 influenza season,” Jessie R. Chung of the influenza division at the Centers for Disease Control and Prevention and associates wrote, adding that the impetus for the study was the lack of available data “from observational studies after the 2009 pandemic on relative effectiveness of LAIV and IIV in children and adolescents.”
Ms. Chung* and coinvestigators enrolled children aged 2-17 years from clinics and hospitals in Michigan, New York, Pennsylvania, Tennessee, Texas, Washington, and Wisconsin during the 2010-2011, 2011-2012, 2012-2013, and 2013-2014 influenza seasons. Children brought in with symptoms of acute respiratory illness – cough, fever, or feverishness – had nasal and throat swabs collected to test for presence and type of influenza.
In total, 7,718 subjects were evaluated across the four influenza seasons, but after excluding subjects for various reasons – unknown vaccine type, indeterminate vaccine status, and inconclusive reverse transcription polymerase chain reaction results, among others – 6,819 subjects were included for vaccine effectiveness analysis, of which 2,703 were ultimately matched age appropriately and placed into IIV and LAIV cohorts for comparison. The IIV cohort consisted of 2,066 individuals (76.4%), while the LAIV cohort had 637 (23.6%).
During the 2010-2011 season, 66 of the 477 IIV subjects contracted influenza, versus 21 of 116 who received LAIV (14% vs. 18%, respectively). In the 2011-2012 season, 51 of the 499 IIV subjects (10%) contracted influenza, compared with 12 of the 152 LAIV subjects (8%). In the 2012-2013 season, 198 of the 622 IIV subjects (32%) contracted influenza, versus 61 of the 205 LAIV subjects (30%). But, in the 2013-2014 season, 36 of the 468 IIV subjects (8%) contracted influenza, versus 34 of the 164 LAIV subjects (21%).
After adjustment for age and season, the odds ratio for the 2013-2014 season was significantly higher than those of the other seasons across the entire age spectrum of 2-17 years: 2.88, compared with 1.49 (2010-2011), 0.67 (2011-2012), and 0.92 (2012-2013).
When comparing influenza type/subtype, adjusted odds ratio was 5.53 for those with A/(H1N1)pdm09 in the 2010-2011 season, compared with 2.65 for those with the same in the 2013-2014 season. Those with A/H3N2 did not show as significant a difference across seasons (2010-2013), nor did those with influenza type B (2010-2011, 2012-2013).
“We found no statistically significant difference in LAIV effectiveness compared with IIV against medically attended, laboratory-confirmed influenza illness due to A/H3N2 or B viruses,” Ms. Chung and colleagues concluded. “We found significantly higher odds of influenza A/(H1N1)pdm09 among participants vaccinated with LAIV, compared with IIV, [but] reasons for lower effectiveness of LAIV against the A/(H1N1)pdm09 virus, compared with IIV are not fully understood.”
The investigators added that “the finding appears to be specific to the A/(H1N1)pdm09 vaccine component; we did not detect any statistically significant differences in effectiveness for the other components.” Three previous randomized controlled trials indicated that trivalent LAIV was just as effective, if not more so, than IIV, making the findings of this study surprising and “unexpected,” the authors noted.
This study was supported by the CDC through cooperative agreements with a variety of universities and foundations, and funded by the National Institutes of Health. Ms. Chung and associates reported no relevant financial disclosures.
*A previous version of this story misstated Jessie Chung’s academic title. Ms. Chung holds a Master’s in public health.
Influenza vaccination has been recommended for everyone for the past few years. Acceptance of this recommendation has been variable, and vaccine failures do not help the cause of convincing our patients to accept vaccination. In the paper by Chung et al. from the CDC and other coinvestigators who are prominent in influenza research, we learn that the live attenuated intranasally administered flu vaccine was significantly inferior to the killed injection administered flu vaccine for one of the type A flu strains. As a consequence, more kids vaccinated with the live attenuated vaccine got the flu. So parents who claim “the flu shot does not work” were partially correct more often since the 2009 flu season, if their child got the intranasal flu vaccine. However, neither the intranasal nor the injectable flu vaccine have an exceptionally high efficacy because the calculations by the authors for the study described and by citation of prior studies we are reminded that vaccine efficacy varies by strain and yearly by the season between 45% and 71%. We need to have better flu vaccines.

|
Dr. Michael E. Pichichero |
At Legacy Pediatrics, where I am in part-time private practice, we have seen increasing requests for the intranasal flu vaccine each year because parents and kids who can voice their wishes don’t want the shot. Our nurses like it, too, because the crying, wailing, and fighting to hold the kid down is avoided. There had been some reports before 2009 that the intranasal flu vaccine was more effective than the shot. But those of us who have been around long enough practicing medicine have learned about the pendulum of data and opinion sometimes swings back and forth. The article by Chung et al. reminds us once again of this reality.
Dr. Michael E. Pichichero is at the University of Rochester (N.Y.) Medical Center. He has received investigator-initiated grants from Sanofi Pasteur to study novel pneumococcal protein vaccines over the past 3 years and currently but has received no funding from Sanofi regarding injectable influenza vaccine. He also has conducted research with study coauthor Dr. John J. Treanor that was supported by MedImmune, who makes the intranasal flu vaccine.
Influenza vaccination has been recommended for everyone for the past few years. Acceptance of this recommendation has been variable, and vaccine failures do not help the cause of convincing our patients to accept vaccination. In the paper by Chung et al. from the CDC and other coinvestigators who are prominent in influenza research, we learn that the live attenuated intranasally administered flu vaccine was significantly inferior to the killed injection administered flu vaccine for one of the type A flu strains. As a consequence, more kids vaccinated with the live attenuated vaccine got the flu. So parents who claim “the flu shot does not work” were partially correct more often since the 2009 flu season, if their child got the intranasal flu vaccine. However, neither the intranasal nor the injectable flu vaccine have an exceptionally high efficacy because the calculations by the authors for the study described and by citation of prior studies we are reminded that vaccine efficacy varies by strain and yearly by the season between 45% and 71%. We need to have better flu vaccines.
|
|
Dr. Michael E. Pichichero |
At Legacy Pediatrics, where I am in part-time private practice, we have seen increasing requests for the intranasal flu vaccine each year because parents and kids who can voice their wishes don’t want the shot. Our nurses like it, too, because the crying, wailing, and fighting to hold the kid down is avoided. There had been some reports before 2009 that the intranasal flu vaccine was more effective than the shot. But those of us who have been around long enough practicing medicine have learned about the pendulum of data and opinion sometimes swings back and forth. The article by Chung et al. reminds us once again of this reality.
Dr. Michael E. Pichichero is at the University of Rochester (N.Y.) Medical Center. He has received investigator-initiated grants from Sanofi Pasteur to study novel pneumococcal protein vaccines over the past 3 years and currently but has received no funding from Sanofi regarding injectable influenza vaccine. He also has conducted research with study coauthor Dr. John J. Treanor that was supported by MedImmune, who makes the intranasal flu vaccine.
Influenza vaccination has been recommended for everyone for the past few years. Acceptance of this recommendation has been variable, and vaccine failures do not help the cause of convincing our patients to accept vaccination. In the paper by Chung et al. from the CDC and other coinvestigators who are prominent in influenza research, we learn that the live attenuated intranasally administered flu vaccine was significantly inferior to the killed injection administered flu vaccine for one of the type A flu strains. As a consequence, more kids vaccinated with the live attenuated vaccine got the flu. So parents who claim “the flu shot does not work” were partially correct more often since the 2009 flu season, if their child got the intranasal flu vaccine. However, neither the intranasal nor the injectable flu vaccine have an exceptionally high efficacy because the calculations by the authors for the study described and by citation of prior studies we are reminded that vaccine efficacy varies by strain and yearly by the season between 45% and 71%. We need to have better flu vaccines.
|
|
Dr. Michael E. Pichichero |
At Legacy Pediatrics, where I am in part-time private practice, we have seen increasing requests for the intranasal flu vaccine each year because parents and kids who can voice their wishes don’t want the shot. Our nurses like it, too, because the crying, wailing, and fighting to hold the kid down is avoided. There had been some reports before 2009 that the intranasal flu vaccine was more effective than the shot. But those of us who have been around long enough practicing medicine have learned about the pendulum of data and opinion sometimes swings back and forth. The article by Chung et al. reminds us once again of this reality.
Dr. Michael E. Pichichero is at the University of Rochester (N.Y.) Medical Center. He has received investigator-initiated grants from Sanofi Pasteur to study novel pneumococcal protein vaccines over the past 3 years and currently but has received no funding from Sanofi regarding injectable influenza vaccine. He also has conducted research with study coauthor Dr. John J. Treanor that was supported by MedImmune, who makes the intranasal flu vaccine.
When vaccinating children against influenza, inactivated and live attenuated influenza vaccines show little significant difference in effectiveness against nearly all strains of the virus, according to a new study in Pediatrics.
However, the study – which examined the effectiveness of IIV and LAIV across four consecutive influenza seasons between 2010 and 2014 – cautions that the 2013-2014 season’s A/(H1N1)pdm09 showed an uncharacteristically large gap in effectiveness favoring IIV, a discrepancy likely due to a problem with a vaccine component in LAIV. (Pediatrics. 2016;137(2):e20153279)
“We found that lower LAIV effectiveness in 2013-2014 was specific to the A/(H1N1)pdm09 vaccine component and was consistent with a previously unexamined effect during the 2010-2011 influenza season,” Jessie R. Chung of the influenza division at the Centers for Disease Control and Prevention and associates wrote, adding that the impetus for the study was the lack of available data “from observational studies after the 2009 pandemic on relative effectiveness of LAIV and IIV in children and adolescents.”
Ms. Chung* and coinvestigators enrolled children aged 2-17 years from clinics and hospitals in Michigan, New York, Pennsylvania, Tennessee, Texas, Washington, and Wisconsin during the 2010-2011, 2011-2012, 2012-2013, and 2013-2014 influenza seasons. Children brought in with symptoms of acute respiratory illness – cough, fever, or feverishness – had nasal and throat swabs collected to test for presence and type of influenza.
In total, 7,718 subjects were evaluated across the four influenza seasons, but after excluding subjects for various reasons – unknown vaccine type, indeterminate vaccine status, and inconclusive reverse transcription polymerase chain reaction results, among others – 6,819 subjects were included for vaccine effectiveness analysis, of which 2,703 were ultimately matched age appropriately and placed into IIV and LAIV cohorts for comparison. The IIV cohort consisted of 2,066 individuals (76.4%), while the LAIV cohort had 637 (23.6%).
During the 2010-2011 season, 66 of the 477 IIV subjects contracted influenza, versus 21 of 116 who received LAIV (14% vs. 18%, respectively). In the 2011-2012 season, 51 of the 499 IIV subjects (10%) contracted influenza, compared with 12 of the 152 LAIV subjects (8%). In the 2012-2013 season, 198 of the 622 IIV subjects (32%) contracted influenza, versus 61 of the 205 LAIV subjects (30%). But, in the 2013-2014 season, 36 of the 468 IIV subjects (8%) contracted influenza, versus 34 of the 164 LAIV subjects (21%).
After adjustment for age and season, the odds ratio for the 2013-2014 season was significantly higher than those of the other seasons across the entire age spectrum of 2-17 years: 2.88, compared with 1.49 (2010-2011), 0.67 (2011-2012), and 0.92 (2012-2013).
When comparing influenza type/subtype, adjusted odds ratio was 5.53 for those with A/(H1N1)pdm09 in the 2010-2011 season, compared with 2.65 for those with the same in the 2013-2014 season. Those with A/H3N2 did not show as significant a difference across seasons (2010-2013), nor did those with influenza type B (2010-2011, 2012-2013).
“We found no statistically significant difference in LAIV effectiveness compared with IIV against medically attended, laboratory-confirmed influenza illness due to A/H3N2 or B viruses,” Ms. Chung and colleagues concluded. “We found significantly higher odds of influenza A/(H1N1)pdm09 among participants vaccinated with LAIV, compared with IIV, [but] reasons for lower effectiveness of LAIV against the A/(H1N1)pdm09 virus, compared with IIV are not fully understood.”
The investigators added that “the finding appears to be specific to the A/(H1N1)pdm09 vaccine component; we did not detect any statistically significant differences in effectiveness for the other components.” Three previous randomized controlled trials indicated that trivalent LAIV was just as effective, if not more so, than IIV, making the findings of this study surprising and “unexpected,” the authors noted.
This study was supported by the CDC through cooperative agreements with a variety of universities and foundations, and funded by the National Institutes of Health. Ms. Chung and associates reported no relevant financial disclosures.
*A previous version of this story misstated Jessie Chung’s academic title. Ms. Chung holds a Master’s in public health.
When vaccinating children against influenza, inactivated and live attenuated influenza vaccines show little significant difference in effectiveness against nearly all strains of the virus, according to a new study in Pediatrics.
However, the study – which examined the effectiveness of IIV and LAIV across four consecutive influenza seasons between 2010 and 2014 – cautions that the 2013-2014 season’s A/(H1N1)pdm09 showed an uncharacteristically large gap in effectiveness favoring IIV, a discrepancy likely due to a problem with a vaccine component in LAIV. (Pediatrics. 2016;137(2):e20153279)
“We found that lower LAIV effectiveness in 2013-2014 was specific to the A/(H1N1)pdm09 vaccine component and was consistent with a previously unexamined effect during the 2010-2011 influenza season,” Jessie R. Chung of the influenza division at the Centers for Disease Control and Prevention and associates wrote, adding that the impetus for the study was the lack of available data “from observational studies after the 2009 pandemic on relative effectiveness of LAIV and IIV in children and adolescents.”
Ms. Chung* and coinvestigators enrolled children aged 2-17 years from clinics and hospitals in Michigan, New York, Pennsylvania, Tennessee, Texas, Washington, and Wisconsin during the 2010-2011, 2011-2012, 2012-2013, and 2013-2014 influenza seasons. Children brought in with symptoms of acute respiratory illness – cough, fever, or feverishness – had nasal and throat swabs collected to test for presence and type of influenza.
In total, 7,718 subjects were evaluated across the four influenza seasons, but after excluding subjects for various reasons – unknown vaccine type, indeterminate vaccine status, and inconclusive reverse transcription polymerase chain reaction results, among others – 6,819 subjects were included for vaccine effectiveness analysis, of which 2,703 were ultimately matched age appropriately and placed into IIV and LAIV cohorts for comparison. The IIV cohort consisted of 2,066 individuals (76.4%), while the LAIV cohort had 637 (23.6%).
During the 2010-2011 season, 66 of the 477 IIV subjects contracted influenza, versus 21 of 116 who received LAIV (14% vs. 18%, respectively). In the 2011-2012 season, 51 of the 499 IIV subjects (10%) contracted influenza, compared with 12 of the 152 LAIV subjects (8%). In the 2012-2013 season, 198 of the 622 IIV subjects (32%) contracted influenza, versus 61 of the 205 LAIV subjects (30%). But, in the 2013-2014 season, 36 of the 468 IIV subjects (8%) contracted influenza, versus 34 of the 164 LAIV subjects (21%).
After adjustment for age and season, the odds ratio for the 2013-2014 season was significantly higher than those of the other seasons across the entire age spectrum of 2-17 years: 2.88, compared with 1.49 (2010-2011), 0.67 (2011-2012), and 0.92 (2012-2013).
When comparing influenza type/subtype, adjusted odds ratio was 5.53 for those with A/(H1N1)pdm09 in the 2010-2011 season, compared with 2.65 for those with the same in the 2013-2014 season. Those with A/H3N2 did not show as significant a difference across seasons (2010-2013), nor did those with influenza type B (2010-2011, 2012-2013).
“We found no statistically significant difference in LAIV effectiveness compared with IIV against medically attended, laboratory-confirmed influenza illness due to A/H3N2 or B viruses,” Ms. Chung and colleagues concluded. “We found significantly higher odds of influenza A/(H1N1)pdm09 among participants vaccinated with LAIV, compared with IIV, [but] reasons for lower effectiveness of LAIV against the A/(H1N1)pdm09 virus, compared with IIV are not fully understood.”
The investigators added that “the finding appears to be specific to the A/(H1N1)pdm09 vaccine component; we did not detect any statistically significant differences in effectiveness for the other components.” Three previous randomized controlled trials indicated that trivalent LAIV was just as effective, if not more so, than IIV, making the findings of this study surprising and “unexpected,” the authors noted.
This study was supported by the CDC through cooperative agreements with a variety of universities and foundations, and funded by the National Institutes of Health. Ms. Chung and associates reported no relevant financial disclosures.
*A previous version of this story misstated Jessie Chung’s academic title. Ms. Chung holds a Master’s in public health.
FROM PEDIATRICS
Key clinical point: Inactivated influenza vaccine was significantly more effective against at least one strain of influenza than live attenuated influenza vaccine in 2013-2014.
Major finding: While no significant differences were seen in influenza rates between the IIV and LAIV cohorts for three consecutive seasons (2010-2013), the A/(H1N1)pdm09 strain of 2013-2014 affected subjects with LAIV at a significantly higher rate than did those with IIV.
Data source: Prospective cohort study of 2,703 children aged 2-17 years vaccinated between 2010 and 2014 with either IIV or LAIV.
Disclosures: This study was supported by the CDC through cooperative agreements with a variety of universities and foundations, and funded by the National Institutes of Health. Dr. Chung and his associates reported no relevant financial disclosures.

Combined Tibial Tubercle Avulsion Fracture and Patellar Avulsion Fracture: An Unusual Variant in an Adolescent Patient
Tibial tubercle fractures are rare injuries accounting for less than 1% of all pediatric physeal injuries.1 The original classification scheme for such fractures was proposed by Watson-Jones.2 Initially modified by Ogden and colleagues,3 the classification system has had numerous additions and modifications as new patterns of injury have been identified.4-6 Patellar fractures are also rare in children, making up 1% of all pediatric fractures, with less than 2% of these occurring in skeletally immature children.7
We present a case of an unreported combined tibial tubercle avulsion fracture and patellar avulsion fracture in an adolescent boy. The patient and his guardian provided written informed consent for print and electronic publication of this case report.
Case Report
A 12-year-old boy presented to the emergency department with acute onset of right-knee pain and inability to ambulate after falling off a skateboard on the day of the injury. The patient was otherwise healthy and had no noteworthy medical or surgical history, including no prior fractures. On physical examination, he was noted to have a large right-knee effusion presumed to be hemarthrosis, and inability to perform a straight-leg raise against gravity. There were no neurologic deficits and his leg compartments were soft. Plain radiographs showed patella alta and numerous bony fragments believed to represent a complex tibial tubercle fracture. One bony fragment was identified closer to the patella, suggesting a possible concurrent patellar fracture (Figures 1A, 1B). A computed tomography (CT) scan further characterized both the tibial tubercle avulsion fracture and the lateral inferior pole patellar avulsion fracture (Figures 2A, 2B). The patient’s knee was immobilized, and he was admitted for soft-tissue rest and overnight observation to ensure that compartment syndrome did not develop.
Five days after injury, open reduction and internal fixation were performed. After limb exsanguination and tourniquet insufflation, the fracture was visualized through a direct midline approach. The patient was found to have a Z-type injury pattern to the extensor mechanism: an inferior lateral patellar avulsion fracture, longitudinal splits of the patellar tendon, and 2 large, mainly cartilaginous tibial tubercle fracture fragments, 1 of which extended into the proximal tibial epiphysis (Ogden type III) (Figures 3A-3C). Under direct visualization, the tibial tubercle fragments were reduced and stabilized with 3 cannulated 3.5-mm titanium, partially threaded screws with washers. Smaller screws were used to prevent fragmentation of these mostly cartilaginous fragments. Anatomic reduction was ensured along the articular surface, visualized through an arthrotomy, as well as on the distal cortex (Figures 4A, 4B). The patellar avulsion fracture included a very small section of articular surface and the decision was made to preserve the fragment. Because the patellar fragment was too small for screw fixation, the fracture was secured with suture fixation through bone tunnels over a patellar bony bridge using size 2 Phantom Fiber suture (Tornier) (Figure 5). Vicryl was used to repair the longitudinal patellar tendon split as well as the capsular and paratenon traumatic tears. Layered closure was completed and intraoperative radiographs were obtained (Figures 6A, 6B) prior to placement of a cylinder cast in full extension. Postoperatively, the patient remained overnight for observation and physical therapy evaluation. He was encouraged to bear weight in his cylinder cast as tolerated with crutches to assist with ambulation.
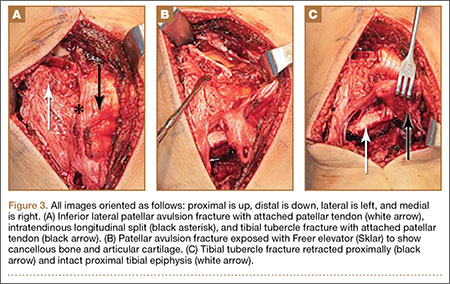
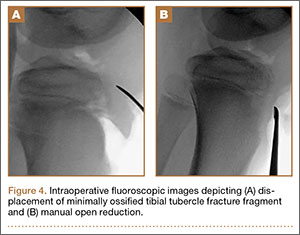

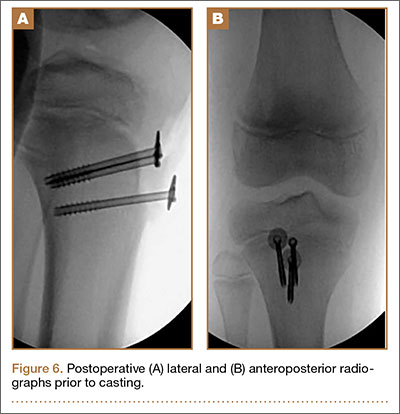
Postoperatively, the patient was maintained in full extension in the cylinder cast for 4 weeks. After cast removal, the patient was placed in a range-of-motion brace locked in extension for ambulation. He started physical therapy and was allowed to perform prone active-knee flexion limited to 90º, with passive extension, for an additional 4 weeks. At 8 weeks, the patient was allowed full-knee motion both active and passive, and the brace was discontinued. At his 18-week follow-up appointment, the patient reported successful return to all his normal activities, including skateboarding, with no apparent limitation in motion or weight-bearing. Examination at that time demonstrated knee range of motion from 5º in hyperextension to 135º in flexion, with his left knee having 5º in hyperextension and 145º in flexion. The patient appeared to have no gait abnormalities, and radiographs showed healed fractures. Because of a concern that continued compression across his tibial physis could lead to greater risk of growth arrest, the decision was made to remove the implants when radiographs showed healing. The patient returned to surgery at 20 weeks for implant removal. At 6 weeks after implant removal, the patient had returned to full activity with no residual pain and full-knee flexion equal to the uninvolved left knee. He was able to perform a stable single-leg squat on his affected leg, and his single-leg hop for distance was the same as his uninvolved leg. He was allowed to return to full sports activity. The patient will be followed with serial radiographs at 4 months, 8 months, and 12 months to look for premature physeal arrest. If an arrest occurs, treatment will be dictated by the extent of the arrest and the potential to cause either limb-length difference or angular deformity.
Discussion
Tibial tubercle fractures typically result from quadriceps contraction during sporting activities, predominantly in adolescent boys with open physes. Numerous modifications and additions have been made to the original classification of such fractures by Watson-Jones,2 most notably by Ogden and colleagues3 in 1980. These additions have included combined tendon avulsions and tubercle fractures as described by Frankl and coauthors,4 complete proximal tibial physeal separation now classified as type 4 by Ryu and Debenham,5 and a “Y” fracture configuration now termed type 5 by McKoy and Stanitski.6 Pandya and colleagues8 reported on 41 tibial tubercle fractures and described a new classification scheme based on the known anatomical closure pattern of the proximal tibial physis and tibial tubercle apophysis. The authors stressed the role of advanced imaging, such as CT or magnetic resonance imaging, in preoperative management of these complex high-energy fractures in adolescents, and the need for intraoperative arthroscopy or arthrotomy to ensure anatomical reduction of the articular involvement.
Tibial tubercle fractures and extensor mechanism injuries that do not fit these classification patterns have also been described. In 1979, Houghton and Ackroyd9 reported 3 cases of acute loss of extensor mechanism secondary to a traumatic patellar sleeve avulsion. In 1995, Berg10 described an ipsilateral inferior pole osteochondral patellar avulsion fracture with patellar tendon avulsion without fracture at the tubercle in a 12-year-old boy. Another variant was described in a 2002 case series of 3 adolescent boys who underwent operative fixation for tibial metaphyseal partial-sleeve avulsion injuries.11
Conclusion
We report a case of combined ipsilateral inferior lateral patellar avulsion fracture and an intra-articular tibial tubercle avulsion fracture with intervening longitudinal patellar tendon split. Preoperative standard radiographs were confusing, given the bony fragment high up by the patella, but use of advanced imaging, in this case CT, allowed us to fully characterize the origin of fracture fragments and realize we were dealing with a unique fracture pattern previously unreported in a pediatric patient. The CT findings allowed us to be better prepared preoperatively by having options for fixation of the patellar fracture, and the extent of articular involvement led us to decide that intra-articular evaluation would be required. Through the use of an open arthrotomy, anatomical articular reduction could be visualized and stabilized with screw fixation of the large, mostly cartilaginous tubercle fracture. Following the principles described by Pandya and colleagues,8 anatomical reduction was achieved, and, 6 months after the original surgery, the patient had return of full motion, clinical and radiographic union, and no clinical pain or limp, with no retained metallic implants across the tibial apophysis. Longer-term follow-up as planned will demonstrate any growth abnormality that would require further surgical intervention.
1. Mosier SM, Stanitski CL. Acute tibial tubercle avulsion fractures. J Pediatr Orthop. 2004;24(2):181-184.
2. Watson-Jones R. Fractures and Joint Injuries. Baltimore, MD: Lippincott Williams & Wilkins; 1955.
3. Ogden JA, Tross RB, Murphy MJ. Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am. 1980;62(2):205-215.
4. Frankl U, Wasilewski SA, Healy WL. Avulsion fracture of the tibial tubercle with avulsion of the patellar ligament. Report of two cases. J Bone Joint Surg Am. 1990;72(9):1411-1413.
5. Ryu RK, Debenham JO. An unusual avulsion fracture of the proximal tibial epiphysis. Case report and proposed addition to the Watson-Jones classification. Clin Orthop Relat Res. 1985;(194):181-184.
6. McKoy BE, Stanitski CL. Acute tibial tubercle avulsion fractures. Orthop Clin North Am. 2003;34(3):397-403.
7. Hunt DM, Somashekar N. A review of sleeve fractures of the patella in children. Knee. 2005;12:3-7.
8. Pandya NK, Edmonds EW, Roocroft JH, Mubarak SJ. Tibial tubercle fractures: complications, classification, and the need for intra-articular assessment. J Pediatr Orthop. 2012;32(8):749-759.
9. Houghton GR, Ackroyd CE. Sleeve fractures of the patella in children: a report of three cases. J Bone Joint Surg Br. 1979;61(2):165-168.
10. Berg EE. Bipolar infrapatellar tendon rupture. J Pediatr Orthop. 1995;15(3):302-303.
11. Davidson D, Letts M. Partial sleeve fractures of the tibia in children: an unusual fracture pattern. J Pediatr Orthop. 2002;22(1):36-40.
Tibial tubercle fractures are rare injuries accounting for less than 1% of all pediatric physeal injuries.1 The original classification scheme for such fractures was proposed by Watson-Jones.2 Initially modified by Ogden and colleagues,3 the classification system has had numerous additions and modifications as new patterns of injury have been identified.4-6 Patellar fractures are also rare in children, making up 1% of all pediatric fractures, with less than 2% of these occurring in skeletally immature children.7
We present a case of an unreported combined tibial tubercle avulsion fracture and patellar avulsion fracture in an adolescent boy. The patient and his guardian provided written informed consent for print and electronic publication of this case report.
Case Report
A 12-year-old boy presented to the emergency department with acute onset of right-knee pain and inability to ambulate after falling off a skateboard on the day of the injury. The patient was otherwise healthy and had no noteworthy medical or surgical history, including no prior fractures. On physical examination, he was noted to have a large right-knee effusion presumed to be hemarthrosis, and inability to perform a straight-leg raise against gravity. There were no neurologic deficits and his leg compartments were soft. Plain radiographs showed patella alta and numerous bony fragments believed to represent a complex tibial tubercle fracture. One bony fragment was identified closer to the patella, suggesting a possible concurrent patellar fracture (Figures 1A, 1B). A computed tomography (CT) scan further characterized both the tibial tubercle avulsion fracture and the lateral inferior pole patellar avulsion fracture (Figures 2A, 2B). The patient’s knee was immobilized, and he was admitted for soft-tissue rest and overnight observation to ensure that compartment syndrome did not develop.
Five days after injury, open reduction and internal fixation were performed. After limb exsanguination and tourniquet insufflation, the fracture was visualized through a direct midline approach. The patient was found to have a Z-type injury pattern to the extensor mechanism: an inferior lateral patellar avulsion fracture, longitudinal splits of the patellar tendon, and 2 large, mainly cartilaginous tibial tubercle fracture fragments, 1 of which extended into the proximal tibial epiphysis (Ogden type III) (Figures 3A-3C). Under direct visualization, the tibial tubercle fragments were reduced and stabilized with 3 cannulated 3.5-mm titanium, partially threaded screws with washers. Smaller screws were used to prevent fragmentation of these mostly cartilaginous fragments. Anatomic reduction was ensured along the articular surface, visualized through an arthrotomy, as well as on the distal cortex (Figures 4A, 4B). The patellar avulsion fracture included a very small section of articular surface and the decision was made to preserve the fragment. Because the patellar fragment was too small for screw fixation, the fracture was secured with suture fixation through bone tunnels over a patellar bony bridge using size 2 Phantom Fiber suture (Tornier) (Figure 5). Vicryl was used to repair the longitudinal patellar tendon split as well as the capsular and paratenon traumatic tears. Layered closure was completed and intraoperative radiographs were obtained (Figures 6A, 6B) prior to placement of a cylinder cast in full extension. Postoperatively, the patient remained overnight for observation and physical therapy evaluation. He was encouraged to bear weight in his cylinder cast as tolerated with crutches to assist with ambulation.
Postoperatively, the patient was maintained in full extension in the cylinder cast for 4 weeks. After cast removal, the patient was placed in a range-of-motion brace locked in extension for ambulation. He started physical therapy and was allowed to perform prone active-knee flexion limited to 90º, with passive extension, for an additional 4 weeks. At 8 weeks, the patient was allowed full-knee motion both active and passive, and the brace was discontinued. At his 18-week follow-up appointment, the patient reported successful return to all his normal activities, including skateboarding, with no apparent limitation in motion or weight-bearing. Examination at that time demonstrated knee range of motion from 5º in hyperextension to 135º in flexion, with his left knee having 5º in hyperextension and 145º in flexion. The patient appeared to have no gait abnormalities, and radiographs showed healed fractures. Because of a concern that continued compression across his tibial physis could lead to greater risk of growth arrest, the decision was made to remove the implants when radiographs showed healing. The patient returned to surgery at 20 weeks for implant removal. At 6 weeks after implant removal, the patient had returned to full activity with no residual pain and full-knee flexion equal to the uninvolved left knee. He was able to perform a stable single-leg squat on his affected leg, and his single-leg hop for distance was the same as his uninvolved leg. He was allowed to return to full sports activity. The patient will be followed with serial radiographs at 4 months, 8 months, and 12 months to look for premature physeal arrest. If an arrest occurs, treatment will be dictated by the extent of the arrest and the potential to cause either limb-length difference or angular deformity.
Discussion
Tibial tubercle fractures typically result from quadriceps contraction during sporting activities, predominantly in adolescent boys with open physes. Numerous modifications and additions have been made to the original classification of such fractures by Watson-Jones,2 most notably by Ogden and colleagues3 in 1980. These additions have included combined tendon avulsions and tubercle fractures as described by Frankl and coauthors,4 complete proximal tibial physeal separation now classified as type 4 by Ryu and Debenham,5 and a “Y” fracture configuration now termed type 5 by McKoy and Stanitski.6 Pandya and colleagues8 reported on 41 tibial tubercle fractures and described a new classification scheme based on the known anatomical closure pattern of the proximal tibial physis and tibial tubercle apophysis. The authors stressed the role of advanced imaging, such as CT or magnetic resonance imaging, in preoperative management of these complex high-energy fractures in adolescents, and the need for intraoperative arthroscopy or arthrotomy to ensure anatomical reduction of the articular involvement.
Tibial tubercle fractures and extensor mechanism injuries that do not fit these classification patterns have also been described. In 1979, Houghton and Ackroyd9 reported 3 cases of acute loss of extensor mechanism secondary to a traumatic patellar sleeve avulsion. In 1995, Berg10 described an ipsilateral inferior pole osteochondral patellar avulsion fracture with patellar tendon avulsion without fracture at the tubercle in a 12-year-old boy. Another variant was described in a 2002 case series of 3 adolescent boys who underwent operative fixation for tibial metaphyseal partial-sleeve avulsion injuries.11
Conclusion
We report a case of combined ipsilateral inferior lateral patellar avulsion fracture and an intra-articular tibial tubercle avulsion fracture with intervening longitudinal patellar tendon split. Preoperative standard radiographs were confusing, given the bony fragment high up by the patella, but use of advanced imaging, in this case CT, allowed us to fully characterize the origin of fracture fragments and realize we were dealing with a unique fracture pattern previously unreported in a pediatric patient. The CT findings allowed us to be better prepared preoperatively by having options for fixation of the patellar fracture, and the extent of articular involvement led us to decide that intra-articular evaluation would be required. Through the use of an open arthrotomy, anatomical articular reduction could be visualized and stabilized with screw fixation of the large, mostly cartilaginous tubercle fracture. Following the principles described by Pandya and colleagues,8 anatomical reduction was achieved, and, 6 months after the original surgery, the patient had return of full motion, clinical and radiographic union, and no clinical pain or limp, with no retained metallic implants across the tibial apophysis. Longer-term follow-up as planned will demonstrate any growth abnormality that would require further surgical intervention.
Tibial tubercle fractures are rare injuries accounting for less than 1% of all pediatric physeal injuries.1 The original classification scheme for such fractures was proposed by Watson-Jones.2 Initially modified by Ogden and colleagues,3 the classification system has had numerous additions and modifications as new patterns of injury have been identified.4-6 Patellar fractures are also rare in children, making up 1% of all pediatric fractures, with less than 2% of these occurring in skeletally immature children.7
We present a case of an unreported combined tibial tubercle avulsion fracture and patellar avulsion fracture in an adolescent boy. The patient and his guardian provided written informed consent for print and electronic publication of this case report.
Case Report
A 12-year-old boy presented to the emergency department with acute onset of right-knee pain and inability to ambulate after falling off a skateboard on the day of the injury. The patient was otherwise healthy and had no noteworthy medical or surgical history, including no prior fractures. On physical examination, he was noted to have a large right-knee effusion presumed to be hemarthrosis, and inability to perform a straight-leg raise against gravity. There were no neurologic deficits and his leg compartments were soft. Plain radiographs showed patella alta and numerous bony fragments believed to represent a complex tibial tubercle fracture. One bony fragment was identified closer to the patella, suggesting a possible concurrent patellar fracture (Figures 1A, 1B). A computed tomography (CT) scan further characterized both the tibial tubercle avulsion fracture and the lateral inferior pole patellar avulsion fracture (Figures 2A, 2B). The patient’s knee was immobilized, and he was admitted for soft-tissue rest and overnight observation to ensure that compartment syndrome did not develop.
Five days after injury, open reduction and internal fixation were performed. After limb exsanguination and tourniquet insufflation, the fracture was visualized through a direct midline approach. The patient was found to have a Z-type injury pattern to the extensor mechanism: an inferior lateral patellar avulsion fracture, longitudinal splits of the patellar tendon, and 2 large, mainly cartilaginous tibial tubercle fracture fragments, 1 of which extended into the proximal tibial epiphysis (Ogden type III) (Figures 3A-3C). Under direct visualization, the tibial tubercle fragments were reduced and stabilized with 3 cannulated 3.5-mm titanium, partially threaded screws with washers. Smaller screws were used to prevent fragmentation of these mostly cartilaginous fragments. Anatomic reduction was ensured along the articular surface, visualized through an arthrotomy, as well as on the distal cortex (Figures 4A, 4B). The patellar avulsion fracture included a very small section of articular surface and the decision was made to preserve the fragment. Because the patellar fragment was too small for screw fixation, the fracture was secured with suture fixation through bone tunnels over a patellar bony bridge using size 2 Phantom Fiber suture (Tornier) (Figure 5). Vicryl was used to repair the longitudinal patellar tendon split as well as the capsular and paratenon traumatic tears. Layered closure was completed and intraoperative radiographs were obtained (Figures 6A, 6B) prior to placement of a cylinder cast in full extension. Postoperatively, the patient remained overnight for observation and physical therapy evaluation. He was encouraged to bear weight in his cylinder cast as tolerated with crutches to assist with ambulation.
Postoperatively, the patient was maintained in full extension in the cylinder cast for 4 weeks. After cast removal, the patient was placed in a range-of-motion brace locked in extension for ambulation. He started physical therapy and was allowed to perform prone active-knee flexion limited to 90º, with passive extension, for an additional 4 weeks. At 8 weeks, the patient was allowed full-knee motion both active and passive, and the brace was discontinued. At his 18-week follow-up appointment, the patient reported successful return to all his normal activities, including skateboarding, with no apparent limitation in motion or weight-bearing. Examination at that time demonstrated knee range of motion from 5º in hyperextension to 135º in flexion, with his left knee having 5º in hyperextension and 145º in flexion. The patient appeared to have no gait abnormalities, and radiographs showed healed fractures. Because of a concern that continued compression across his tibial physis could lead to greater risk of growth arrest, the decision was made to remove the implants when radiographs showed healing. The patient returned to surgery at 20 weeks for implant removal. At 6 weeks after implant removal, the patient had returned to full activity with no residual pain and full-knee flexion equal to the uninvolved left knee. He was able to perform a stable single-leg squat on his affected leg, and his single-leg hop for distance was the same as his uninvolved leg. He was allowed to return to full sports activity. The patient will be followed with serial radiographs at 4 months, 8 months, and 12 months to look for premature physeal arrest. If an arrest occurs, treatment will be dictated by the extent of the arrest and the potential to cause either limb-length difference or angular deformity.
Discussion
Tibial tubercle fractures typically result from quadriceps contraction during sporting activities, predominantly in adolescent boys with open physes. Numerous modifications and additions have been made to the original classification of such fractures by Watson-Jones,2 most notably by Ogden and colleagues3 in 1980. These additions have included combined tendon avulsions and tubercle fractures as described by Frankl and coauthors,4 complete proximal tibial physeal separation now classified as type 4 by Ryu and Debenham,5 and a “Y” fracture configuration now termed type 5 by McKoy and Stanitski.6 Pandya and colleagues8 reported on 41 tibial tubercle fractures and described a new classification scheme based on the known anatomical closure pattern of the proximal tibial physis and tibial tubercle apophysis. The authors stressed the role of advanced imaging, such as CT or magnetic resonance imaging, in preoperative management of these complex high-energy fractures in adolescents, and the need for intraoperative arthroscopy or arthrotomy to ensure anatomical reduction of the articular involvement.
Tibial tubercle fractures and extensor mechanism injuries that do not fit these classification patterns have also been described. In 1979, Houghton and Ackroyd9 reported 3 cases of acute loss of extensor mechanism secondary to a traumatic patellar sleeve avulsion. In 1995, Berg10 described an ipsilateral inferior pole osteochondral patellar avulsion fracture with patellar tendon avulsion without fracture at the tubercle in a 12-year-old boy. Another variant was described in a 2002 case series of 3 adolescent boys who underwent operative fixation for tibial metaphyseal partial-sleeve avulsion injuries.11
Conclusion
We report a case of combined ipsilateral inferior lateral patellar avulsion fracture and an intra-articular tibial tubercle avulsion fracture with intervening longitudinal patellar tendon split. Preoperative standard radiographs were confusing, given the bony fragment high up by the patella, but use of advanced imaging, in this case CT, allowed us to fully characterize the origin of fracture fragments and realize we were dealing with a unique fracture pattern previously unreported in a pediatric patient. The CT findings allowed us to be better prepared preoperatively by having options for fixation of the patellar fracture, and the extent of articular involvement led us to decide that intra-articular evaluation would be required. Through the use of an open arthrotomy, anatomical articular reduction could be visualized and stabilized with screw fixation of the large, mostly cartilaginous tubercle fracture. Following the principles described by Pandya and colleagues,8 anatomical reduction was achieved, and, 6 months after the original surgery, the patient had return of full motion, clinical and radiographic union, and no clinical pain or limp, with no retained metallic implants across the tibial apophysis. Longer-term follow-up as planned will demonstrate any growth abnormality that would require further surgical intervention.
1. Mosier SM, Stanitski CL. Acute tibial tubercle avulsion fractures. J Pediatr Orthop. 2004;24(2):181-184.
2. Watson-Jones R. Fractures and Joint Injuries. Baltimore, MD: Lippincott Williams & Wilkins; 1955.
3. Ogden JA, Tross RB, Murphy MJ. Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am. 1980;62(2):205-215.
4. Frankl U, Wasilewski SA, Healy WL. Avulsion fracture of the tibial tubercle with avulsion of the patellar ligament. Report of two cases. J Bone Joint Surg Am. 1990;72(9):1411-1413.
5. Ryu RK, Debenham JO. An unusual avulsion fracture of the proximal tibial epiphysis. Case report and proposed addition to the Watson-Jones classification. Clin Orthop Relat Res. 1985;(194):181-184.
6. McKoy BE, Stanitski CL. Acute tibial tubercle avulsion fractures. Orthop Clin North Am. 2003;34(3):397-403.
7. Hunt DM, Somashekar N. A review of sleeve fractures of the patella in children. Knee. 2005;12:3-7.
8. Pandya NK, Edmonds EW, Roocroft JH, Mubarak SJ. Tibial tubercle fractures: complications, classification, and the need for intra-articular assessment. J Pediatr Orthop. 2012;32(8):749-759.
9. Houghton GR, Ackroyd CE. Sleeve fractures of the patella in children: a report of three cases. J Bone Joint Surg Br. 1979;61(2):165-168.
10. Berg EE. Bipolar infrapatellar tendon rupture. J Pediatr Orthop. 1995;15(3):302-303.
11. Davidson D, Letts M. Partial sleeve fractures of the tibia in children: an unusual fracture pattern. J Pediatr Orthop. 2002;22(1):36-40.
1. Mosier SM, Stanitski CL. Acute tibial tubercle avulsion fractures. J Pediatr Orthop. 2004;24(2):181-184.
2. Watson-Jones R. Fractures and Joint Injuries. Baltimore, MD: Lippincott Williams & Wilkins; 1955.
3. Ogden JA, Tross RB, Murphy MJ. Fractures of the tibial tuberosity in adolescents. J Bone Joint Surg Am. 1980;62(2):205-215.
4. Frankl U, Wasilewski SA, Healy WL. Avulsion fracture of the tibial tubercle with avulsion of the patellar ligament. Report of two cases. J Bone Joint Surg Am. 1990;72(9):1411-1413.
5. Ryu RK, Debenham JO. An unusual avulsion fracture of the proximal tibial epiphysis. Case report and proposed addition to the Watson-Jones classification. Clin Orthop Relat Res. 1985;(194):181-184.
6. McKoy BE, Stanitski CL. Acute tibial tubercle avulsion fractures. Orthop Clin North Am. 2003;34(3):397-403.
7. Hunt DM, Somashekar N. A review of sleeve fractures of the patella in children. Knee. 2005;12:3-7.
8. Pandya NK, Edmonds EW, Roocroft JH, Mubarak SJ. Tibial tubercle fractures: complications, classification, and the need for intra-articular assessment. J Pediatr Orthop. 2012;32(8):749-759.
9. Houghton GR, Ackroyd CE. Sleeve fractures of the patella in children: a report of three cases. J Bone Joint Surg Br. 1979;61(2):165-168.
10. Berg EE. Bipolar infrapatellar tendon rupture. J Pediatr Orthop. 1995;15(3):302-303.
11. Davidson D, Letts M. Partial sleeve fractures of the tibia in children: an unusual fracture pattern. J Pediatr Orthop. 2002;22(1):36-40.

Subtly elevated maternal glucose linked to increased risk of tetralogy of Fallot
ORLANDO – Subclinical elevated maternal blood glucose levels during the second trimester are strongly associated with increased risk of tetralogy of Fallot, Dr. James R. Priest reported at the American Heart Association scientific sessions.
It’s well established that maternal type 2 diabetes and gestational diabetes are strong maternal risk factors for structural congenital heart disease in their offspring. But the women in this study didn’t meet criteria for those diagnoses. They were asymptomatic, and their elevations in blood glucose in random nonfasting measurements obtained in the second trimester were below the 200 mg/dL threshold.

Thus, this study provides the first evidence that maternal blood glucose as a continuous variable is associated with increased risk of specific congenital heart defects in offspring, according to Dr. Priest, a pediatric cardiologist at Stanford (Calif.) University.
Of note, in this study of nondiabetic women, an elevated blood glucose was not associated with increased risk of d-transposition of the great arteries (dTGA), which, like tetralogy of Fallot, has been associated with maternal diabetes.
Dr. Priest presented an observational study of 277 pregnant, nondiabetic women, of whom 55 gave birth to a baby with tetralogy of Fallot, 42 had a baby with dTGA, and 180 gave birth to a baby without congenital heart disease or other malformations. Random nonfasting blood glucose and serum insulin levels were obtained from all subjects during weeks 15-18 of pregnancy.
The median maternal blood glucose level was 91.5 mg/dL in controls, similar at 90 mg/dL in the mothers of infants with dTGA, and significantly increased at 97 mg/dL in the mothers of offspring with tetralogy of Fallot. In a multivariate analysis adjusted for maternal age and ethnicity, elevated nonfasting second-trimester maternal glucose was associated with a 7.54-fold increased risk of having an infant with tetralogy of Fallot.
Maternal serum insulin level wasn’t associated with the risk of congenital heart disease.
Dr. Priest emphasized that while this study breaks new ground, the findings must be considered preliminary.
“Maternal blood glucose levels are influenced by diet, exercise, beta-cell function, and insulin resistance. Thus, blood glucose levels may simply be a marker of risk conferred by another physiologic process. The question remains whether elevated blood glucose or a variety of correlated but independent traits is behind the observed association,” he noted.
He plans to answer this key question by studying the relationship between these physiologic traits and blood glucose levels earlier in pregnancy.
This study was funded by the Stanford Cardiovascular Institute and the National Institutes of Health. Dr. Priest reported having no financial conflicts of interest.
ORLANDO – Subclinical elevated maternal blood glucose levels during the second trimester are strongly associated with increased risk of tetralogy of Fallot, Dr. James R. Priest reported at the American Heart Association scientific sessions.
It’s well established that maternal type 2 diabetes and gestational diabetes are strong maternal risk factors for structural congenital heart disease in their offspring. But the women in this study didn’t meet criteria for those diagnoses. They were asymptomatic, and their elevations in blood glucose in random nonfasting measurements obtained in the second trimester were below the 200 mg/dL threshold.
Thus, this study provides the first evidence that maternal blood glucose as a continuous variable is associated with increased risk of specific congenital heart defects in offspring, according to Dr. Priest, a pediatric cardiologist at Stanford (Calif.) University.
Of note, in this study of nondiabetic women, an elevated blood glucose was not associated with increased risk of d-transposition of the great arteries (dTGA), which, like tetralogy of Fallot, has been associated with maternal diabetes.
Dr. Priest presented an observational study of 277 pregnant, nondiabetic women, of whom 55 gave birth to a baby with tetralogy of Fallot, 42 had a baby with dTGA, and 180 gave birth to a baby without congenital heart disease or other malformations. Random nonfasting blood glucose and serum insulin levels were obtained from all subjects during weeks 15-18 of pregnancy.
The median maternal blood glucose level was 91.5 mg/dL in controls, similar at 90 mg/dL in the mothers of infants with dTGA, and significantly increased at 97 mg/dL in the mothers of offspring with tetralogy of Fallot. In a multivariate analysis adjusted for maternal age and ethnicity, elevated nonfasting second-trimester maternal glucose was associated with a 7.54-fold increased risk of having an infant with tetralogy of Fallot.
Maternal serum insulin level wasn’t associated with the risk of congenital heart disease.
Dr. Priest emphasized that while this study breaks new ground, the findings must be considered preliminary.
“Maternal blood glucose levels are influenced by diet, exercise, beta-cell function, and insulin resistance. Thus, blood glucose levels may simply be a marker of risk conferred by another physiologic process. The question remains whether elevated blood glucose or a variety of correlated but independent traits is behind the observed association,” he noted.
He plans to answer this key question by studying the relationship between these physiologic traits and blood glucose levels earlier in pregnancy.
This study was funded by the Stanford Cardiovascular Institute and the National Institutes of Health. Dr. Priest reported having no financial conflicts of interest.
ORLANDO – Subclinical elevated maternal blood glucose levels during the second trimester are strongly associated with increased risk of tetralogy of Fallot, Dr. James R. Priest reported at the American Heart Association scientific sessions.
It’s well established that maternal type 2 diabetes and gestational diabetes are strong maternal risk factors for structural congenital heart disease in their offspring. But the women in this study didn’t meet criteria for those diagnoses. They were asymptomatic, and their elevations in blood glucose in random nonfasting measurements obtained in the second trimester were below the 200 mg/dL threshold.
Thus, this study provides the first evidence that maternal blood glucose as a continuous variable is associated with increased risk of specific congenital heart defects in offspring, according to Dr. Priest, a pediatric cardiologist at Stanford (Calif.) University.
Of note, in this study of nondiabetic women, an elevated blood glucose was not associated with increased risk of d-transposition of the great arteries (dTGA), which, like tetralogy of Fallot, has been associated with maternal diabetes.
Dr. Priest presented an observational study of 277 pregnant, nondiabetic women, of whom 55 gave birth to a baby with tetralogy of Fallot, 42 had a baby with dTGA, and 180 gave birth to a baby without congenital heart disease or other malformations. Random nonfasting blood glucose and serum insulin levels were obtained from all subjects during weeks 15-18 of pregnancy.
The median maternal blood glucose level was 91.5 mg/dL in controls, similar at 90 mg/dL in the mothers of infants with dTGA, and significantly increased at 97 mg/dL in the mothers of offspring with tetralogy of Fallot. In a multivariate analysis adjusted for maternal age and ethnicity, elevated nonfasting second-trimester maternal glucose was associated with a 7.54-fold increased risk of having an infant with tetralogy of Fallot.
Maternal serum insulin level wasn’t associated with the risk of congenital heart disease.
Dr. Priest emphasized that while this study breaks new ground, the findings must be considered preliminary.
“Maternal blood glucose levels are influenced by diet, exercise, beta-cell function, and insulin resistance. Thus, blood glucose levels may simply be a marker of risk conferred by another physiologic process. The question remains whether elevated blood glucose or a variety of correlated but independent traits is behind the observed association,” he noted.
He plans to answer this key question by studying the relationship between these physiologic traits and blood glucose levels earlier in pregnancy.
This study was funded by the Stanford Cardiovascular Institute and the National Institutes of Health. Dr. Priest reported having no financial conflicts of interest.
AT THE AHA SCIENTIFIC SESSIONS
Key clinical point: Second-trimester subclinical elevated maternal blood glucose in nondiabetic women is associated with sharply increased risk of tetralogy of Fallot.
Major finding: Subtly elevated maternal blood glucose in nondiabetic women in their second trimester is associated with a 7.54-fold increased risk of tetralogy of Fallot in the baby.
Data source: This observational study involved prospectively collected data on 277 pregnant women included in California’s birth defects screening program.
Disclosures: This study was funded by the Stanford Cardiovascular Institute and the National Institutes of Health. The presenter reported having no financial conflicts of interest.

AES: Seizure freedom attainable for most epilepsy patients
PHILADELPHIA - Fully optimized antiepilepsy therapy that tries at least a couple of well-chosen and properly dosed antiseizure drugs as well as follow-up with nondrug options for patients who are unresponsive to pharmaceuticals seems able to render about 80%-90% of epilepsy patients seizure free, Dr. Cynthia L. Harden said while summing up a session on epilepsy therapy at the annual meeting of the American Epilepsy Society.
Finding an appropriate and effective treatment for each epilepsy patient can be “labor intensive and expensive”; it depends in part on a patient’s mood, psychosocial profile, and willingness to comply with treatment; and it often needs the multidisciplinary expertise found at epilepsy centers. But the optimistic message from contemporary seizure-management is that by using a drug or two and in selected patients surgery, diet, or an implanted device, the vast majority of epilepsy patients can become seizure free, noted Dr. Harden, system director of clinical epilepsy services at the Mount Sinai Health System in New York and cochair of the session.

“How many of your uncontrolled patients can become seizure free with more vigilance and tender loving care?” she asked the large audience as she concluded the session. A significant fraction of uncontrolled patients become seizure free when their drug dosage is increased, another drug is substituted or added, their compliance improves, their depression diminishes, or a patient’s understanding of their epilepsy and treatment increases through education, Dr. Harden said.
Drugs remain the cornerstone of seizure control for epilepsy patients, with at least 22 agents now available for epilepsy treatment, including 13 with U.S. or European (or both) approval for initial monotherapy of epilepsy. In addition, study results have shown several agents – carbamazepine, lamotrigine, levetiracetam, oxcarbazepine, phenytoin, and zonisamide – to be more or less equally effective for treating newly diagnosed focal epilepsy, which means that clinicians must also consider factors beyond just efficacy, such as adverse effects, impact on a specific patient’s comorbidities, interactions with other drugs a patient takes, and ease of use and cost, said Dr. Emilio Perucca, a neurologist and professor of pharmacology at the University of Pavia (Italy). In general, newer antiepilepsy drugs have not been more effective than older drugs, he noted.

Another feature of drug treatment is that more is usually not better. “Most patients do not need the highest tolerated dosage,” he said, and minimizing dosages to the lowest effective level helps minimize adverse effects. On the other hand, an antiepilepsy drug needs to be administered at an adequate dosage before concluding that it is ineffective for a patient.
Although a majority of patients respond to the first or second antiepilepsy agent they receive, drugs can’t render all patients seizure free. Results from several reported cohorts show that about 45% of patients with newly diagnosed epilepsy respond well to the first drug they receive and about 13% become seizure free on a second drug. After that, the response rates fall off sharply, with roughly 5% of patients responding to a third drug or drug combinations, said Dr. Patrick Kwan, professor and chairman of neurology at the University of Melbourne and head of epilepsy at Royal Melbourne Hospital. “Once a patient has failed two drugs, even if they become seizure free on a subsequent drug, there is a higher rate of relapse,” Dr. Kwan noted.

In general, 60%-65% of newly diagnosed epilepsy patients become seizure free with drug monotherapy, Dr. Kwan summarized. Epilepsy patients who fail to fully respond to the first two antiepilepsy drugs they receive need “prompt” referral to an epilepsy center. A “substantial proportion” of patients like this can become seizure free by further optimization of the dosage they receive or by addressing compliance issues, Dr. Kwan said. In addition, some patients achieve full or partial seizure freedom through multidrug treatment or with other treatments.
Two-drug combinations have generally been more effective than combinations with three or more drugs, said Dr. Josiane LaJoie, a pediatric neurologist at New York University. “Using three or more drugs probably won’t lead to better control, just more adverse events,” she cautioned. Many published study results have documented successful two-drug combinations, such as lamotrigine and valproate, and valproate and clobazam, to name just two combinations. In addition to looking at combinations with successful track records in published studies, she highlighted the importance of combining drugs with distinct mechanisms of action and avoiding combing drugs with similar adverse-event profiles. Combinations also need to be tailored to each patient’s clinical characteristics, taking possible drug-drug interactions into account, Dr. LaJoie said.

When drug treatment fails to produce seizure freedom, other options are resective or ablative surgery, diet, or a neurostimulation implant. “At no time in history have we had as many nonpharmacologic treatment options as we have today,” said Dr. Christopher T. Skidmore, a neurologist in the Comprehensive Epilepsy Center at Thomas Jefferson University in Philadelphia. “With diet or neurostimulation, you get seizure reduction without the adverse effects of addition additional drugs.”
Study results with three different diets indicate that they can each produce a roughly 50% cut in seizure rate in about half the patients who adhere to the diet. The ketogenic diet has the longest track record, but with a 90% fat content, it is notoriously difficult to stick with and requires that patients eat meals that often preclude eating with friends or family members or away from home. Adhering to a modified Atkins diet or a low glycemic load diet seems about as effective as a ketogenic diet while offering more food flexibility and a range of foods more compatible with group meals or meals outside the home, Dr. Skidmore said.

Even though the modified Atkins and low glycemic load diets offer somewhat more flexibility, both remain a “paradigm shift in food consumption,” compared with what most Americans eat, and when compliance is poor they don’t work. “Diet doesn’t work when people cheat,” Dr. Skidmore noted.
Three forms of nerve stimulation have also shown efficacy for seizure reduction, he said: vagal nerve stimulation, responsive neurostimulation, and deep brain stimulation of the anterior nucleus of the thalamus. “All three devices have proven efficacy,” he noted. “Neurostimulation offers an alternative to medical therapy that does not require daily effort and compliance.”
Discussions with patients about diet, neurostimulation, and surgery options allow each patient to decide whether one or more of these might be a good option. “It takes a certain patient to follow a diet or want an implant,” he said. “There is no one right choice. You need to educate patients and help them make their choice,” Dr. Skidmore advised.
Dr. Harmon had no disclosures. Dr. Perucca has served as a consultant to and received honoraria from Biopharma Solutions, GW Pharma, Takeda, Sun Pharma, and UCB Pharma. Dr. Kwan has been a consultant to Eisai and Novartis and has received research funding from UCB. Dr. LaJoie had no disclosures. Dr. Skidmore has been a consultant to Supernus and a site principal investigator for NeuroPace.
On Twitter @mitchelzoler
PHILADELPHIA - Fully optimized antiepilepsy therapy that tries at least a couple of well-chosen and properly dosed antiseizure drugs as well as follow-up with nondrug options for patients who are unresponsive to pharmaceuticals seems able to render about 80%-90% of epilepsy patients seizure free, Dr. Cynthia L. Harden said while summing up a session on epilepsy therapy at the annual meeting of the American Epilepsy Society.
Finding an appropriate and effective treatment for each epilepsy patient can be “labor intensive and expensive”; it depends in part on a patient’s mood, psychosocial profile, and willingness to comply with treatment; and it often needs the multidisciplinary expertise found at epilepsy centers. But the optimistic message from contemporary seizure-management is that by using a drug or two and in selected patients surgery, diet, or an implanted device, the vast majority of epilepsy patients can become seizure free, noted Dr. Harden, system director of clinical epilepsy services at the Mount Sinai Health System in New York and cochair of the session.
“How many of your uncontrolled patients can become seizure free with more vigilance and tender loving care?” she asked the large audience as she concluded the session. A significant fraction of uncontrolled patients become seizure free when their drug dosage is increased, another drug is substituted or added, their compliance improves, their depression diminishes, or a patient’s understanding of their epilepsy and treatment increases through education, Dr. Harden said.
Drugs remain the cornerstone of seizure control for epilepsy patients, with at least 22 agents now available for epilepsy treatment, including 13 with U.S. or European (or both) approval for initial monotherapy of epilepsy. In addition, study results have shown several agents – carbamazepine, lamotrigine, levetiracetam, oxcarbazepine, phenytoin, and zonisamide – to be more or less equally effective for treating newly diagnosed focal epilepsy, which means that clinicians must also consider factors beyond just efficacy, such as adverse effects, impact on a specific patient’s comorbidities, interactions with other drugs a patient takes, and ease of use and cost, said Dr. Emilio Perucca, a neurologist and professor of pharmacology at the University of Pavia (Italy). In general, newer antiepilepsy drugs have not been more effective than older drugs, he noted.
Another feature of drug treatment is that more is usually not better. “Most patients do not need the highest tolerated dosage,” he said, and minimizing dosages to the lowest effective level helps minimize adverse effects. On the other hand, an antiepilepsy drug needs to be administered at an adequate dosage before concluding that it is ineffective for a patient.
Although a majority of patients respond to the first or second antiepilepsy agent they receive, drugs can’t render all patients seizure free. Results from several reported cohorts show that about 45% of patients with newly diagnosed epilepsy respond well to the first drug they receive and about 13% become seizure free on a second drug. After that, the response rates fall off sharply, with roughly 5% of patients responding to a third drug or drug combinations, said Dr. Patrick Kwan, professor and chairman of neurology at the University of Melbourne and head of epilepsy at Royal Melbourne Hospital. “Once a patient has failed two drugs, even if they become seizure free on a subsequent drug, there is a higher rate of relapse,” Dr. Kwan noted.
In general, 60%-65% of newly diagnosed epilepsy patients become seizure free with drug monotherapy, Dr. Kwan summarized. Epilepsy patients who fail to fully respond to the first two antiepilepsy drugs they receive need “prompt” referral to an epilepsy center. A “substantial proportion” of patients like this can become seizure free by further optimization of the dosage they receive or by addressing compliance issues, Dr. Kwan said. In addition, some patients achieve full or partial seizure freedom through multidrug treatment or with other treatments.
Two-drug combinations have generally been more effective than combinations with three or more drugs, said Dr. Josiane LaJoie, a pediatric neurologist at New York University. “Using three or more drugs probably won’t lead to better control, just more adverse events,” she cautioned. Many published study results have documented successful two-drug combinations, such as lamotrigine and valproate, and valproate and clobazam, to name just two combinations. In addition to looking at combinations with successful track records in published studies, she highlighted the importance of combining drugs with distinct mechanisms of action and avoiding combing drugs with similar adverse-event profiles. Combinations also need to be tailored to each patient’s clinical characteristics, taking possible drug-drug interactions into account, Dr. LaJoie said.
When drug treatment fails to produce seizure freedom, other options are resective or ablative surgery, diet, or a neurostimulation implant. “At no time in history have we had as many nonpharmacologic treatment options as we have today,” said Dr. Christopher T. Skidmore, a neurologist in the Comprehensive Epilepsy Center at Thomas Jefferson University in Philadelphia. “With diet or neurostimulation, you get seizure reduction without the adverse effects of addition additional drugs.”
Study results with three different diets indicate that they can each produce a roughly 50% cut in seizure rate in about half the patients who adhere to the diet. The ketogenic diet has the longest track record, but with a 90% fat content, it is notoriously difficult to stick with and requires that patients eat meals that often preclude eating with friends or family members or away from home. Adhering to a modified Atkins diet or a low glycemic load diet seems about as effective as a ketogenic diet while offering more food flexibility and a range of foods more compatible with group meals or meals outside the home, Dr. Skidmore said.
Even though the modified Atkins and low glycemic load diets offer somewhat more flexibility, both remain a “paradigm shift in food consumption,” compared with what most Americans eat, and when compliance is poor they don’t work. “Diet doesn’t work when people cheat,” Dr. Skidmore noted.
Three forms of nerve stimulation have also shown efficacy for seizure reduction, he said: vagal nerve stimulation, responsive neurostimulation, and deep brain stimulation of the anterior nucleus of the thalamus. “All three devices have proven efficacy,” he noted. “Neurostimulation offers an alternative to medical therapy that does not require daily effort and compliance.”
Discussions with patients about diet, neurostimulation, and surgery options allow each patient to decide whether one or more of these might be a good option. “It takes a certain patient to follow a diet or want an implant,” he said. “There is no one right choice. You need to educate patients and help them make their choice,” Dr. Skidmore advised.
Dr. Harmon had no disclosures. Dr. Perucca has served as a consultant to and received honoraria from Biopharma Solutions, GW Pharma, Takeda, Sun Pharma, and UCB Pharma. Dr. Kwan has been a consultant to Eisai and Novartis and has received research funding from UCB. Dr. LaJoie had no disclosures. Dr. Skidmore has been a consultant to Supernus and a site principal investigator for NeuroPace.
On Twitter @mitchelzoler
PHILADELPHIA - Fully optimized antiepilepsy therapy that tries at least a couple of well-chosen and properly dosed antiseizure drugs as well as follow-up with nondrug options for patients who are unresponsive to pharmaceuticals seems able to render about 80%-90% of epilepsy patients seizure free, Dr. Cynthia L. Harden said while summing up a session on epilepsy therapy at the annual meeting of the American Epilepsy Society.
Finding an appropriate and effective treatment for each epilepsy patient can be “labor intensive and expensive”; it depends in part on a patient’s mood, psychosocial profile, and willingness to comply with treatment; and it often needs the multidisciplinary expertise found at epilepsy centers. But the optimistic message from contemporary seizure-management is that by using a drug or two and in selected patients surgery, diet, or an implanted device, the vast majority of epilepsy patients can become seizure free, noted Dr. Harden, system director of clinical epilepsy services at the Mount Sinai Health System in New York and cochair of the session.
“How many of your uncontrolled patients can become seizure free with more vigilance and tender loving care?” she asked the large audience as she concluded the session. A significant fraction of uncontrolled patients become seizure free when their drug dosage is increased, another drug is substituted or added, their compliance improves, their depression diminishes, or a patient’s understanding of their epilepsy and treatment increases through education, Dr. Harden said.
Drugs remain the cornerstone of seizure control for epilepsy patients, with at least 22 agents now available for epilepsy treatment, including 13 with U.S. or European (or both) approval for initial monotherapy of epilepsy. In addition, study results have shown several agents – carbamazepine, lamotrigine, levetiracetam, oxcarbazepine, phenytoin, and zonisamide – to be more or less equally effective for treating newly diagnosed focal epilepsy, which means that clinicians must also consider factors beyond just efficacy, such as adverse effects, impact on a specific patient’s comorbidities, interactions with other drugs a patient takes, and ease of use and cost, said Dr. Emilio Perucca, a neurologist and professor of pharmacology at the University of Pavia (Italy). In general, newer antiepilepsy drugs have not been more effective than older drugs, he noted.
Another feature of drug treatment is that more is usually not better. “Most patients do not need the highest tolerated dosage,” he said, and minimizing dosages to the lowest effective level helps minimize adverse effects. On the other hand, an antiepilepsy drug needs to be administered at an adequate dosage before concluding that it is ineffective for a patient.
Although a majority of patients respond to the first or second antiepilepsy agent they receive, drugs can’t render all patients seizure free. Results from several reported cohorts show that about 45% of patients with newly diagnosed epilepsy respond well to the first drug they receive and about 13% become seizure free on a second drug. After that, the response rates fall off sharply, with roughly 5% of patients responding to a third drug or drug combinations, said Dr. Patrick Kwan, professor and chairman of neurology at the University of Melbourne and head of epilepsy at Royal Melbourne Hospital. “Once a patient has failed two drugs, even if they become seizure free on a subsequent drug, there is a higher rate of relapse,” Dr. Kwan noted.
In general, 60%-65% of newly diagnosed epilepsy patients become seizure free with drug monotherapy, Dr. Kwan summarized. Epilepsy patients who fail to fully respond to the first two antiepilepsy drugs they receive need “prompt” referral to an epilepsy center. A “substantial proportion” of patients like this can become seizure free by further optimization of the dosage they receive or by addressing compliance issues, Dr. Kwan said. In addition, some patients achieve full or partial seizure freedom through multidrug treatment or with other treatments.
Two-drug combinations have generally been more effective than combinations with three or more drugs, said Dr. Josiane LaJoie, a pediatric neurologist at New York University. “Using three or more drugs probably won’t lead to better control, just more adverse events,” she cautioned. Many published study results have documented successful two-drug combinations, such as lamotrigine and valproate, and valproate and clobazam, to name just two combinations. In addition to looking at combinations with successful track records in published studies, she highlighted the importance of combining drugs with distinct mechanisms of action and avoiding combing drugs with similar adverse-event profiles. Combinations also need to be tailored to each patient’s clinical characteristics, taking possible drug-drug interactions into account, Dr. LaJoie said.
When drug treatment fails to produce seizure freedom, other options are resective or ablative surgery, diet, or a neurostimulation implant. “At no time in history have we had as many nonpharmacologic treatment options as we have today,” said Dr. Christopher T. Skidmore, a neurologist in the Comprehensive Epilepsy Center at Thomas Jefferson University in Philadelphia. “With diet or neurostimulation, you get seizure reduction without the adverse effects of addition additional drugs.”
Study results with three different diets indicate that they can each produce a roughly 50% cut in seizure rate in about half the patients who adhere to the diet. The ketogenic diet has the longest track record, but with a 90% fat content, it is notoriously difficult to stick with and requires that patients eat meals that often preclude eating with friends or family members or away from home. Adhering to a modified Atkins diet or a low glycemic load diet seems about as effective as a ketogenic diet while offering more food flexibility and a range of foods more compatible with group meals or meals outside the home, Dr. Skidmore said.
Even though the modified Atkins and low glycemic load diets offer somewhat more flexibility, both remain a “paradigm shift in food consumption,” compared with what most Americans eat, and when compliance is poor they don’t work. “Diet doesn’t work when people cheat,” Dr. Skidmore noted.
Three forms of nerve stimulation have also shown efficacy for seizure reduction, he said: vagal nerve stimulation, responsive neurostimulation, and deep brain stimulation of the anterior nucleus of the thalamus. “All three devices have proven efficacy,” he noted. “Neurostimulation offers an alternative to medical therapy that does not require daily effort and compliance.”
Discussions with patients about diet, neurostimulation, and surgery options allow each patient to decide whether one or more of these might be a good option. “It takes a certain patient to follow a diet or want an implant,” he said. “There is no one right choice. You need to educate patients and help them make their choice,” Dr. Skidmore advised.
Dr. Harmon had no disclosures. Dr. Perucca has served as a consultant to and received honoraria from Biopharma Solutions, GW Pharma, Takeda, Sun Pharma, and UCB Pharma. Dr. Kwan has been a consultant to Eisai and Novartis and has received research funding from UCB. Dr. LaJoie had no disclosures. Dr. Skidmore has been a consultant to Supernus and a site principal investigator for NeuroPace.
On Twitter @mitchelzoler
EXPERT ANALYSIS FROM AES 2015

Cardiac abnormalities among childhood cancer survivors

Photo by Bill Branson
A new study has provided additional insight into the development of cardiac abnormalities in adult survivors of childhood cancer.
Researchers analyzed more than 1800 cancer survivors who were exposed to cardiotoxic therapies as children.
The team said they found evidence of cardiac abnormalities in a substantial number of these subjects, many of whom were younger and did not exhibit symptoms of abnormalities.
Daniel A. Mulrooney, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee, and his colleagues reported these findings in Annals of Internal Medicine.
The team assessed cardiac outcomes among 1853 subjects who were 18 and older and had received cancer-related cardiotoxic therapy at least 10 years earlier.
The subjects were pretty evenly split along gender lines (52.3% male), their median age at cancer diagnosis was 8 (range, 0 to 24), and their median age at evaluation was 31 (range, 18 to 60).
At evaluation, 7.4% of subjects had cardiomyopathy (newly identified in 4.7%), 3.8% had coronary artery disease (newly identified in 2.2%), 28% had valvular regurgitation or stenosis (newly identified in 24.8%), and 4.4% had conduction or rhythm abnormalities (newly identified in 1.4%). All but 5 subjects were asymptomatic.
Multivariable analysis suggested the odds of developing cardiomyopathy were significantly associated with being male (odds ratio [OR]=1.9), receiving anthracycline doses of 250 mg/m2 or greater (OR=2.7), having cardiac radiation exposure greater than 1500 cGy (OR=1.9), and having hypertension (OR=3.0).
Being younger at diagnosis was associated with higher odds of valvular disease. The ORs were 1.5 for patients who were 0 to 4 years of age at diagnosis and 1.3 for patients who were 5 to 9 at diagnosis.
Receiving higher radiation doses was associated with higher odds of valvular disease as well. But associations between radiation and valvular disease varied according to a patient’s anthracycline exposure (interaction P<0.001). The highest odds were among survivors with the highest doses of radiation exposure and any anthracycline exposure (OR=4.5).
The researchers also noted a reduction in the OR for valvular disease among obese patients (OR=0.4) and those with dyslipidemia (OR=0.7).
The team said there were not enough cases of coronary artery disease and conduction or rhythm abnormalities to support a fully adjusted multivariable model. However, it seemed these outcomes were more common with older age (≥40 years) and among patients with cardiac radiation doses of 1500 cGy or greater.
The researchers said this study revealed “considerable cardiovascular disease” in a large cohort of adult survivors of childhood cancer, which suggests a substantial future healthcare burden.
The team believes their findings could guide stratification of risk factors, screening practices, health counseling, and potential therapeutic measures aimed at changing the disease trajectory in this young adult population. ![]()
Photo by Bill Branson
A new study has provided additional insight into the development of cardiac abnormalities in adult survivors of childhood cancer.
Researchers analyzed more than 1800 cancer survivors who were exposed to cardiotoxic therapies as children.
The team said they found evidence of cardiac abnormalities in a substantial number of these subjects, many of whom were younger and did not exhibit symptoms of abnormalities.
Daniel A. Mulrooney, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee, and his colleagues reported these findings in Annals of Internal Medicine.
The team assessed cardiac outcomes among 1853 subjects who were 18 and older and had received cancer-related cardiotoxic therapy at least 10 years earlier.
The subjects were pretty evenly split along gender lines (52.3% male), their median age at cancer diagnosis was 8 (range, 0 to 24), and their median age at evaluation was 31 (range, 18 to 60).
At evaluation, 7.4% of subjects had cardiomyopathy (newly identified in 4.7%), 3.8% had coronary artery disease (newly identified in 2.2%), 28% had valvular regurgitation or stenosis (newly identified in 24.8%), and 4.4% had conduction or rhythm abnormalities (newly identified in 1.4%). All but 5 subjects were asymptomatic.
Multivariable analysis suggested the odds of developing cardiomyopathy were significantly associated with being male (odds ratio [OR]=1.9), receiving anthracycline doses of 250 mg/m2 or greater (OR=2.7), having cardiac radiation exposure greater than 1500 cGy (OR=1.9), and having hypertension (OR=3.0).
Being younger at diagnosis was associated with higher odds of valvular disease. The ORs were 1.5 for patients who were 0 to 4 years of age at diagnosis and 1.3 for patients who were 5 to 9 at diagnosis.
Receiving higher radiation doses was associated with higher odds of valvular disease as well. But associations between radiation and valvular disease varied according to a patient’s anthracycline exposure (interaction P<0.001). The highest odds were among survivors with the highest doses of radiation exposure and any anthracycline exposure (OR=4.5).
The researchers also noted a reduction in the OR for valvular disease among obese patients (OR=0.4) and those with dyslipidemia (OR=0.7).
The team said there were not enough cases of coronary artery disease and conduction or rhythm abnormalities to support a fully adjusted multivariable model. However, it seemed these outcomes were more common with older age (≥40 years) and among patients with cardiac radiation doses of 1500 cGy or greater.
The researchers said this study revealed “considerable cardiovascular disease” in a large cohort of adult survivors of childhood cancer, which suggests a substantial future healthcare burden.
The team believes their findings could guide stratification of risk factors, screening practices, health counseling, and potential therapeutic measures aimed at changing the disease trajectory in this young adult population. ![]()
Photo by Bill Branson
A new study has provided additional insight into the development of cardiac abnormalities in adult survivors of childhood cancer.
Researchers analyzed more than 1800 cancer survivors who were exposed to cardiotoxic therapies as children.
The team said they found evidence of cardiac abnormalities in a substantial number of these subjects, many of whom were younger and did not exhibit symptoms of abnormalities.
Daniel A. Mulrooney, MD, of St. Jude Children’s Research Hospital in Memphis, Tennessee, and his colleagues reported these findings in Annals of Internal Medicine.
The team assessed cardiac outcomes among 1853 subjects who were 18 and older and had received cancer-related cardiotoxic therapy at least 10 years earlier.
The subjects were pretty evenly split along gender lines (52.3% male), their median age at cancer diagnosis was 8 (range, 0 to 24), and their median age at evaluation was 31 (range, 18 to 60).
At evaluation, 7.4% of subjects had cardiomyopathy (newly identified in 4.7%), 3.8% had coronary artery disease (newly identified in 2.2%), 28% had valvular regurgitation or stenosis (newly identified in 24.8%), and 4.4% had conduction or rhythm abnormalities (newly identified in 1.4%). All but 5 subjects were asymptomatic.
Multivariable analysis suggested the odds of developing cardiomyopathy were significantly associated with being male (odds ratio [OR]=1.9), receiving anthracycline doses of 250 mg/m2 or greater (OR=2.7), having cardiac radiation exposure greater than 1500 cGy (OR=1.9), and having hypertension (OR=3.0).
Being younger at diagnosis was associated with higher odds of valvular disease. The ORs were 1.5 for patients who were 0 to 4 years of age at diagnosis and 1.3 for patients who were 5 to 9 at diagnosis.
Receiving higher radiation doses was associated with higher odds of valvular disease as well. But associations between radiation and valvular disease varied according to a patient’s anthracycline exposure (interaction P<0.001). The highest odds were among survivors with the highest doses of radiation exposure and any anthracycline exposure (OR=4.5).
The researchers also noted a reduction in the OR for valvular disease among obese patients (OR=0.4) and those with dyslipidemia (OR=0.7).
The team said there were not enough cases of coronary artery disease and conduction or rhythm abnormalities to support a fully adjusted multivariable model. However, it seemed these outcomes were more common with older age (≥40 years) and among patients with cardiac radiation doses of 1500 cGy or greater.
The researchers said this study revealed “considerable cardiovascular disease” in a large cohort of adult survivors of childhood cancer, which suggests a substantial future healthcare burden.
The team believes their findings could guide stratification of risk factors, screening practices, health counseling, and potential therapeutic measures aimed at changing the disease trajectory in this young adult population. ![]()