User login
Borrelia mayonii is new cause of Lyme disease variant
A new species of Borrelia has been linked to a variant of Lyme disease with symptoms that differ somewhat from typical Lyme borreliosis.
Of 100,545 routine clinical specimens tested at the Mayo Clinic in Rochester, Minn., for Lyme borreliosis between 2003 and 2014, six clinical specimens – all from 2012 or later – yielded an atypical oppA1 PCR result, according to a study published in Lancet Infectious Diseases.

In patients with specimens yielding atypical results, medical records were reviewed and additional samples were examined by a research team led by Dr. Bobbi Pritt of Mayo Clinic.
The researchers performed DNA sequencing, microscopy, or culturing of the diagnostic specimens (five blood and one synovial), as well as oppA1 PCR testing of Ixodes scapularis ticks (black-legged or “deer” ticks) from regions of suspected patient tick exposure. Among the five blood specimens tested, the median oppA1 copy number was 180 times higher than that found in 13 specimens testing positive for B. burgdorferi during the same time period.
Multigene sequencing identified the spirochete as a novel B. burgdorferi genospecies – the same genospecies detected in ticks collected at a probable patient exposure site.
The newly discovered bacteria, provisionally named Borrelia mayonii, caused Lyme disease with symptoms similar to those caused by B. burgdorferi, but with some distinct clinical features. Similar to classic Lyme disease, fever, headache, rash, and neck pain were experienced in the early stages of infection (days after exposure) and arthritis in the later stages (weeks after exposure). But patients infected with B. mayonii also presented with nausea and vomiting, diffuse rashes (as opposed to the typical “bull’s-eye” rash), and a higher concentration of bacteria in the blood.
“In view of the differing clinical manifestations for patients infected with the novel B. burgdorferi sensu lato genospecies, it is likely that Lyme borreliosis is not being considered – and therefore not diagnosed – in some patients with this infection,” said Dr. Pritt and her colleagues. They added that the clinical range of illness must be better defined in additional patients to ensure the infection is recognized and distinguished from other tick-borne infections, and oppA1 PCR is used for diagnosing infection with B. mayonii.
Read the full study in Lancet Infectious Diseases (doi: 10.1016/S1473-3099[15]00464-8).
On Twitter @richpizzi
A new species of Borrelia has been linked to a variant of Lyme disease with symptoms that differ somewhat from typical Lyme borreliosis.
Of 100,545 routine clinical specimens tested at the Mayo Clinic in Rochester, Minn., for Lyme borreliosis between 2003 and 2014, six clinical specimens – all from 2012 or later – yielded an atypical oppA1 PCR result, according to a study published in Lancet Infectious Diseases.
In patients with specimens yielding atypical results, medical records were reviewed and additional samples were examined by a research team led by Dr. Bobbi Pritt of Mayo Clinic.
The researchers performed DNA sequencing, microscopy, or culturing of the diagnostic specimens (five blood and one synovial), as well as oppA1 PCR testing of Ixodes scapularis ticks (black-legged or “deer” ticks) from regions of suspected patient tick exposure. Among the five blood specimens tested, the median oppA1 copy number was 180 times higher than that found in 13 specimens testing positive for B. burgdorferi during the same time period.
Multigene sequencing identified the spirochete as a novel B. burgdorferi genospecies – the same genospecies detected in ticks collected at a probable patient exposure site.
The newly discovered bacteria, provisionally named Borrelia mayonii, caused Lyme disease with symptoms similar to those caused by B. burgdorferi, but with some distinct clinical features. Similar to classic Lyme disease, fever, headache, rash, and neck pain were experienced in the early stages of infection (days after exposure) and arthritis in the later stages (weeks after exposure). But patients infected with B. mayonii also presented with nausea and vomiting, diffuse rashes (as opposed to the typical “bull’s-eye” rash), and a higher concentration of bacteria in the blood.
“In view of the differing clinical manifestations for patients infected with the novel B. burgdorferi sensu lato genospecies, it is likely that Lyme borreliosis is not being considered – and therefore not diagnosed – in some patients with this infection,” said Dr. Pritt and her colleagues. They added that the clinical range of illness must be better defined in additional patients to ensure the infection is recognized and distinguished from other tick-borne infections, and oppA1 PCR is used for diagnosing infection with B. mayonii.
Read the full study in Lancet Infectious Diseases (doi: 10.1016/S1473-3099[15]00464-8).
On Twitter @richpizzi
A new species of Borrelia has been linked to a variant of Lyme disease with symptoms that differ somewhat from typical Lyme borreliosis.
Of 100,545 routine clinical specimens tested at the Mayo Clinic in Rochester, Minn., for Lyme borreliosis between 2003 and 2014, six clinical specimens – all from 2012 or later – yielded an atypical oppA1 PCR result, according to a study published in Lancet Infectious Diseases.
In patients with specimens yielding atypical results, medical records were reviewed and additional samples were examined by a research team led by Dr. Bobbi Pritt of Mayo Clinic.
The researchers performed DNA sequencing, microscopy, or culturing of the diagnostic specimens (five blood and one synovial), as well as oppA1 PCR testing of Ixodes scapularis ticks (black-legged or “deer” ticks) from regions of suspected patient tick exposure. Among the five blood specimens tested, the median oppA1 copy number was 180 times higher than that found in 13 specimens testing positive for B. burgdorferi during the same time period.
Multigene sequencing identified the spirochete as a novel B. burgdorferi genospecies – the same genospecies detected in ticks collected at a probable patient exposure site.
The newly discovered bacteria, provisionally named Borrelia mayonii, caused Lyme disease with symptoms similar to those caused by B. burgdorferi, but with some distinct clinical features. Similar to classic Lyme disease, fever, headache, rash, and neck pain were experienced in the early stages of infection (days after exposure) and arthritis in the later stages (weeks after exposure). But patients infected with B. mayonii also presented with nausea and vomiting, diffuse rashes (as opposed to the typical “bull’s-eye” rash), and a higher concentration of bacteria in the blood.
“In view of the differing clinical manifestations for patients infected with the novel B. burgdorferi sensu lato genospecies, it is likely that Lyme borreliosis is not being considered – and therefore not diagnosed – in some patients with this infection,” said Dr. Pritt and her colleagues. They added that the clinical range of illness must be better defined in additional patients to ensure the infection is recognized and distinguished from other tick-borne infections, and oppA1 PCR is used for diagnosing infection with B. mayonii.
Read the full study in Lancet Infectious Diseases (doi: 10.1016/S1473-3099[15]00464-8).
On Twitter @richpizzi
FROM LANCET INFECTIOUS DISEASES

New evidence strengthens link between Zika and microcephaly
While scientists can’t say with certainty that congenital Zika virus is causing the massive spike in cases of microcephaly seen in Brazil, evidence of a strong association continues to mount.
Two reports, published Feb. 10 in the Morbidity and Mortality Weekly Report and in the New England Journal of Medicine, confirm through laboratory testing that fetuses and infants with microcephaly also were positive for Zika virus infection.
In the MMWR report, researchers from the United States and Brazil present evidence of a link between Zika virus infection and microcephaly and fetal demise through detection of viral RNA and antigens in brain tissues with infants with microcephaly, as well as placental tissues from early miscarriages.
The findings are based on laboratory testing of tissue samples from two newborns with microcephaly who died within 20 hours of birth and two miscarriages (at 11 and 13 weeks’ gestation). The samples were submitted to the Centers for Disease Control and Prevention from the state of Rio Grande do Norte, Brazil, in December 2015. All four mothers had clinical signs of Zika virus infection during the first trimester but did not have signs of active infection at the time of delivery or miscarriage.
Specimens from all four cases were positive by reverse transcription-polymerase chain reaction (RT-PCR) testing, and sequence analysis provided additional evidence of Zika virus infection (Morb Mortal Wkly Rep. 2016 Feb;65:1-2. doi: 10.15585/mmwr.mm6506e1er).
“To better understand the pathogenesis of Zika virus infection and associated congenital anomalies and fetal death, it is necessary to evaluate autopsy and placental tissues from additional cases, and to determine the effect of gestational age during maternal illness on fetal outcomes,” the researchers wrote.
In the New England Journal of Medicine report, Dr. Jernej Mlakar of the University of Ljubljana, Slovenia, and colleagues, presented the case of a previously healthy 25-year-old pregnant woman who had become ill while living in Brazil. During the 13th week of gestation, she had a high fever, followed by severe musculoskeletal and retro-ocular pain, as well as an itchy generalized maculopapular rash. Zika virus was suspected at the time but virologic diagnostic testing was not performed.
Ultrasound at 14 weeks and 20 weeks showed normal fetal growth and anatomy, but ultrasound at 29 weeks showed signs of fetal abnormalities. At 32 weeks, physicians confirmed intrauterine growth retardation and microcephaly with calcifications in the fetal brain and placenta.
The woman requested termination of the pregnancy and an autopsy was performed on the fetus. Positive results for Zika virus were obtained on RT-PCR assay in the fetal brain sample. All autopsy samples were tested on PCR assay and found to be negative for other flaviviruses, including dengue, yellow fever, West Nile, and tick-borne encephalitis (N Engl J Med. 2016 Feb 10. doi: 10.1056/NEJMoa1600651).
In an editorial accompanying the report, physicians from the Harvard School of Public Health and Massachusetts General Hospital, both in Boston, wrote that there are still many unanswered questions about Zika virus in pregnancy. Assuming the association between Zika virus and microcephaly exists, researchers do not know whether the timing of the infection during pregnancy has an effect on the risk of fetal abnormalities. Additionally, it’s unknown whether asymptomatic or minimally symptomatic disease poses a risk to the fetus (N Engl J Med. 2016 Feb 10. doi: 10.1056/NEJMe1601862).
The researchers for both case reports had no financial disclosures.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
While scientists can’t say with certainty that congenital Zika virus is causing the massive spike in cases of microcephaly seen in Brazil, evidence of a strong association continues to mount.
Two reports, published Feb. 10 in the Morbidity and Mortality Weekly Report and in the New England Journal of Medicine, confirm through laboratory testing that fetuses and infants with microcephaly also were positive for Zika virus infection.
In the MMWR report, researchers from the United States and Brazil present evidence of a link between Zika virus infection and microcephaly and fetal demise through detection of viral RNA and antigens in brain tissues with infants with microcephaly, as well as placental tissues from early miscarriages.
The findings are based on laboratory testing of tissue samples from two newborns with microcephaly who died within 20 hours of birth and two miscarriages (at 11 and 13 weeks’ gestation). The samples were submitted to the Centers for Disease Control and Prevention from the state of Rio Grande do Norte, Brazil, in December 2015. All four mothers had clinical signs of Zika virus infection during the first trimester but did not have signs of active infection at the time of delivery or miscarriage.
Specimens from all four cases were positive by reverse transcription-polymerase chain reaction (RT-PCR) testing, and sequence analysis provided additional evidence of Zika virus infection (Morb Mortal Wkly Rep. 2016 Feb;65:1-2. doi: 10.15585/mmwr.mm6506e1er).
“To better understand the pathogenesis of Zika virus infection and associated congenital anomalies and fetal death, it is necessary to evaluate autopsy and placental tissues from additional cases, and to determine the effect of gestational age during maternal illness on fetal outcomes,” the researchers wrote.
In the New England Journal of Medicine report, Dr. Jernej Mlakar of the University of Ljubljana, Slovenia, and colleagues, presented the case of a previously healthy 25-year-old pregnant woman who had become ill while living in Brazil. During the 13th week of gestation, she had a high fever, followed by severe musculoskeletal and retro-ocular pain, as well as an itchy generalized maculopapular rash. Zika virus was suspected at the time but virologic diagnostic testing was not performed.
Ultrasound at 14 weeks and 20 weeks showed normal fetal growth and anatomy, but ultrasound at 29 weeks showed signs of fetal abnormalities. At 32 weeks, physicians confirmed intrauterine growth retardation and microcephaly with calcifications in the fetal brain and placenta.
The woman requested termination of the pregnancy and an autopsy was performed on the fetus. Positive results for Zika virus were obtained on RT-PCR assay in the fetal brain sample. All autopsy samples were tested on PCR assay and found to be negative for other flaviviruses, including dengue, yellow fever, West Nile, and tick-borne encephalitis (N Engl J Med. 2016 Feb 10. doi: 10.1056/NEJMoa1600651).
In an editorial accompanying the report, physicians from the Harvard School of Public Health and Massachusetts General Hospital, both in Boston, wrote that there are still many unanswered questions about Zika virus in pregnancy. Assuming the association between Zika virus and microcephaly exists, researchers do not know whether the timing of the infection during pregnancy has an effect on the risk of fetal abnormalities. Additionally, it’s unknown whether asymptomatic or minimally symptomatic disease poses a risk to the fetus (N Engl J Med. 2016 Feb 10. doi: 10.1056/NEJMe1601862).
The researchers for both case reports had no financial disclosures.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
While scientists can’t say with certainty that congenital Zika virus is causing the massive spike in cases of microcephaly seen in Brazil, evidence of a strong association continues to mount.
Two reports, published Feb. 10 in the Morbidity and Mortality Weekly Report and in the New England Journal of Medicine, confirm through laboratory testing that fetuses and infants with microcephaly also were positive for Zika virus infection.
In the MMWR report, researchers from the United States and Brazil present evidence of a link between Zika virus infection and microcephaly and fetal demise through detection of viral RNA and antigens in brain tissues with infants with microcephaly, as well as placental tissues from early miscarriages.
The findings are based on laboratory testing of tissue samples from two newborns with microcephaly who died within 20 hours of birth and two miscarriages (at 11 and 13 weeks’ gestation). The samples were submitted to the Centers for Disease Control and Prevention from the state of Rio Grande do Norte, Brazil, in December 2015. All four mothers had clinical signs of Zika virus infection during the first trimester but did not have signs of active infection at the time of delivery or miscarriage.
Specimens from all four cases were positive by reverse transcription-polymerase chain reaction (RT-PCR) testing, and sequence analysis provided additional evidence of Zika virus infection (Morb Mortal Wkly Rep. 2016 Feb;65:1-2. doi: 10.15585/mmwr.mm6506e1er).
“To better understand the pathogenesis of Zika virus infection and associated congenital anomalies and fetal death, it is necessary to evaluate autopsy and placental tissues from additional cases, and to determine the effect of gestational age during maternal illness on fetal outcomes,” the researchers wrote.
In the New England Journal of Medicine report, Dr. Jernej Mlakar of the University of Ljubljana, Slovenia, and colleagues, presented the case of a previously healthy 25-year-old pregnant woman who had become ill while living in Brazil. During the 13th week of gestation, she had a high fever, followed by severe musculoskeletal and retro-ocular pain, as well as an itchy generalized maculopapular rash. Zika virus was suspected at the time but virologic diagnostic testing was not performed.
Ultrasound at 14 weeks and 20 weeks showed normal fetal growth and anatomy, but ultrasound at 29 weeks showed signs of fetal abnormalities. At 32 weeks, physicians confirmed intrauterine growth retardation and microcephaly with calcifications in the fetal brain and placenta.
The woman requested termination of the pregnancy and an autopsy was performed on the fetus. Positive results for Zika virus were obtained on RT-PCR assay in the fetal brain sample. All autopsy samples were tested on PCR assay and found to be negative for other flaviviruses, including dengue, yellow fever, West Nile, and tick-borne encephalitis (N Engl J Med. 2016 Feb 10. doi: 10.1056/NEJMoa1600651).
In an editorial accompanying the report, physicians from the Harvard School of Public Health and Massachusetts General Hospital, both in Boston, wrote that there are still many unanswered questions about Zika virus in pregnancy. Assuming the association between Zika virus and microcephaly exists, researchers do not know whether the timing of the infection during pregnancy has an effect on the risk of fetal abnormalities. Additionally, it’s unknown whether asymptomatic or minimally symptomatic disease poses a risk to the fetus (N Engl J Med. 2016 Feb 10. doi: 10.1056/NEJMe1601862).
The researchers for both case reports had no financial disclosures.
mschneider@frontlinemedcom.com
On Twitter @maryellenny
Ocular symptoms accompany microcephaly in Brazilian newborns
In a sample of infants born with microcephaly and a presumed diagnosis of congenital Zika virus, about one-third were found to have vision-threatening eye abnormalities, according to researchers working in a Zika hot spot in Brazil.
The group, led by Dr. Bruno de Paula Freitas of the Hospital Geral Roberto Santos, in Salvador, Brazil, evaluated 29 infants with microcephaly born at a single hospital in December following suspected maternal infection with the mosquito-borne Zika virus. In a paper published online Feb 9., Dr. de Paula Freitas and his colleagues reported eye abnormalities in 10 of these children (34.5%) (JAMA Ophthalmol. doi:10.1001/jamaophthalmol.2016.0267.).
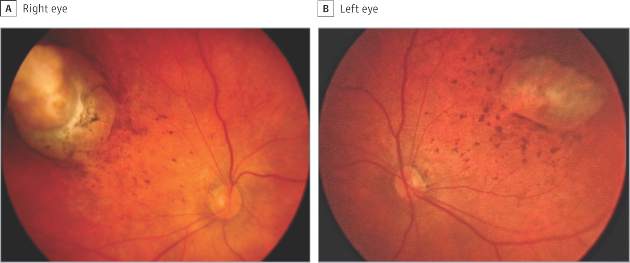
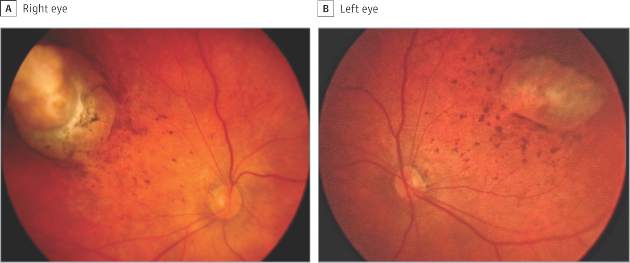
Brazil first reported an outbreak of Zika virus infections in April 2015, followed months later by a spike in the number of infants born with microcephaly, a birth defect defined by a cephalic circumference of 32 cm or less in newborns. The most common ocular abnormalities seen in the cohort of affected infants were pigment mottling of the retina and chorioretinal atrophy (11 of 17 abnormal eyes); optic nerve abnormalities (8 eyes); and iris coloboma (affecting 2 eyes in one infant).
While a previous study of a Zika virus outbreak in Micronesia found conjunctivitis among infected individuals, none of the mothers of the current cohort of infants disclosed having had conjunctivitis. Altogether 23 of the mothers (79%) reported having had any symptoms of Zika virus infection during pregnancy.
Dr. de Paula Freitas and his colleagues acknowledged that their results were limited by a small sample size and single-site study design. However, the investigators noted, the findings suggest the possibility “that even oligosymptomatic or asymptomatic pregnant patients presumably infected [with Zika virus] may have microcephalic newborns with ophthalmoscopic lesions” and those newborns should be routinely evaluated for ocular symptoms.
An important question that requires further investigation, they noted, is whether newborns without microcephaly, but whose mothers may have been infected with the Zika virus, should be screened to identify possible ocular lesions.
Funding for the study came from Hospital Geral Roberto Santos, Federal University of São Paulo, Vision Institute, and Conselho Nacional de Desenvolvimento Científico e Tecnológico in Brasília, Brazil. The authors reported having no financial disclosures.
Ophthalmologic manifestations of congenital Zika virus infection are not yet well described. The report by de Paula Freitas et al. implicates this infection as the cause of chorioretinal scarring and possibly other ocular abnormalities in infants with microcephaly recently born in Brazil.
Microcephaly can be genetic, metabolic, drug related, or caused by perinatal insults such as hypoxia, malnutrition, or infection. The present 20-fold reported increase of microcephaly in parts of Brazil is temporally associated with the outbreak of Zika virus. However, this association is still presumptive because definitive serologic testing for Zika virus was not available in Brazil at the time of the outbreak, and confusion may occur with other causes of microcephaly. Similarly, the currently described eye lesions are presumptively associated with the virus.
Based on current information, in our opinion, clinicians in areas where Zika virus is present should perform ophthalmologic examinations on all microcephalic babies. Because it is still unclear whether the eye lesions occur in the absence of microcephaly, it is premature to suggest ophthalmic screening of all babies born in epidemic areas.
Dr. Lee M. Jampol and Dr. Debra A Goldstein are from the department of ophthalmology, Northwestern University, Chicago. These comments are excerpted from an accompanying editorial (JAMA Ophthalmol. doi:10.1001/jamaopthalmol.2016.0284.). The authors reported having no financial disclosures.
Ophthalmologic manifestations of congenital Zika virus infection are not yet well described. The report by de Paula Freitas et al. implicates this infection as the cause of chorioretinal scarring and possibly other ocular abnormalities in infants with microcephaly recently born in Brazil.
Microcephaly can be genetic, metabolic, drug related, or caused by perinatal insults such as hypoxia, malnutrition, or infection. The present 20-fold reported increase of microcephaly in parts of Brazil is temporally associated with the outbreak of Zika virus. However, this association is still presumptive because definitive serologic testing for Zika virus was not available in Brazil at the time of the outbreak, and confusion may occur with other causes of microcephaly. Similarly, the currently described eye lesions are presumptively associated with the virus.
Based on current information, in our opinion, clinicians in areas where Zika virus is present should perform ophthalmologic examinations on all microcephalic babies. Because it is still unclear whether the eye lesions occur in the absence of microcephaly, it is premature to suggest ophthalmic screening of all babies born in epidemic areas.
Dr. Lee M. Jampol and Dr. Debra A Goldstein are from the department of ophthalmology, Northwestern University, Chicago. These comments are excerpted from an accompanying editorial (JAMA Ophthalmol. doi:10.1001/jamaopthalmol.2016.0284.). The authors reported having no financial disclosures.
Ophthalmologic manifestations of congenital Zika virus infection are not yet well described. The report by de Paula Freitas et al. implicates this infection as the cause of chorioretinal scarring and possibly other ocular abnormalities in infants with microcephaly recently born in Brazil.
Microcephaly can be genetic, metabolic, drug related, or caused by perinatal insults such as hypoxia, malnutrition, or infection. The present 20-fold reported increase of microcephaly in parts of Brazil is temporally associated with the outbreak of Zika virus. However, this association is still presumptive because definitive serologic testing for Zika virus was not available in Brazil at the time of the outbreak, and confusion may occur with other causes of microcephaly. Similarly, the currently described eye lesions are presumptively associated with the virus.
Based on current information, in our opinion, clinicians in areas where Zika virus is present should perform ophthalmologic examinations on all microcephalic babies. Because it is still unclear whether the eye lesions occur in the absence of microcephaly, it is premature to suggest ophthalmic screening of all babies born in epidemic areas.
Dr. Lee M. Jampol and Dr. Debra A Goldstein are from the department of ophthalmology, Northwestern University, Chicago. These comments are excerpted from an accompanying editorial (JAMA Ophthalmol. doi:10.1001/jamaopthalmol.2016.0284.). The authors reported having no financial disclosures.
In a sample of infants born with microcephaly and a presumed diagnosis of congenital Zika virus, about one-third were found to have vision-threatening eye abnormalities, according to researchers working in a Zika hot spot in Brazil.
The group, led by Dr. Bruno de Paula Freitas of the Hospital Geral Roberto Santos, in Salvador, Brazil, evaluated 29 infants with microcephaly born at a single hospital in December following suspected maternal infection with the mosquito-borne Zika virus. In a paper published online Feb 9., Dr. de Paula Freitas and his colleagues reported eye abnormalities in 10 of these children (34.5%) (JAMA Ophthalmol. doi:10.1001/jamaophthalmol.2016.0267.).
Brazil first reported an outbreak of Zika virus infections in April 2015, followed months later by a spike in the number of infants born with microcephaly, a birth defect defined by a cephalic circumference of 32 cm or less in newborns. The most common ocular abnormalities seen in the cohort of affected infants were pigment mottling of the retina and chorioretinal atrophy (11 of 17 abnormal eyes); optic nerve abnormalities (8 eyes); and iris coloboma (affecting 2 eyes in one infant).
While a previous study of a Zika virus outbreak in Micronesia found conjunctivitis among infected individuals, none of the mothers of the current cohort of infants disclosed having had conjunctivitis. Altogether 23 of the mothers (79%) reported having had any symptoms of Zika virus infection during pregnancy.
Dr. de Paula Freitas and his colleagues acknowledged that their results were limited by a small sample size and single-site study design. However, the investigators noted, the findings suggest the possibility “that even oligosymptomatic or asymptomatic pregnant patients presumably infected [with Zika virus] may have microcephalic newborns with ophthalmoscopic lesions” and those newborns should be routinely evaluated for ocular symptoms.
An important question that requires further investigation, they noted, is whether newborns without microcephaly, but whose mothers may have been infected with the Zika virus, should be screened to identify possible ocular lesions.
Funding for the study came from Hospital Geral Roberto Santos, Federal University of São Paulo, Vision Institute, and Conselho Nacional de Desenvolvimento Científico e Tecnológico in Brasília, Brazil. The authors reported having no financial disclosures.
In a sample of infants born with microcephaly and a presumed diagnosis of congenital Zika virus, about one-third were found to have vision-threatening eye abnormalities, according to researchers working in a Zika hot spot in Brazil.
The group, led by Dr. Bruno de Paula Freitas of the Hospital Geral Roberto Santos, in Salvador, Brazil, evaluated 29 infants with microcephaly born at a single hospital in December following suspected maternal infection with the mosquito-borne Zika virus. In a paper published online Feb 9., Dr. de Paula Freitas and his colleagues reported eye abnormalities in 10 of these children (34.5%) (JAMA Ophthalmol. doi:10.1001/jamaophthalmol.2016.0267.).
Brazil first reported an outbreak of Zika virus infections in April 2015, followed months later by a spike in the number of infants born with microcephaly, a birth defect defined by a cephalic circumference of 32 cm or less in newborns. The most common ocular abnormalities seen in the cohort of affected infants were pigment mottling of the retina and chorioretinal atrophy (11 of 17 abnormal eyes); optic nerve abnormalities (8 eyes); and iris coloboma (affecting 2 eyes in one infant).
While a previous study of a Zika virus outbreak in Micronesia found conjunctivitis among infected individuals, none of the mothers of the current cohort of infants disclosed having had conjunctivitis. Altogether 23 of the mothers (79%) reported having had any symptoms of Zika virus infection during pregnancy.
Dr. de Paula Freitas and his colleagues acknowledged that their results were limited by a small sample size and single-site study design. However, the investigators noted, the findings suggest the possibility “that even oligosymptomatic or asymptomatic pregnant patients presumably infected [with Zika virus] may have microcephalic newborns with ophthalmoscopic lesions” and those newborns should be routinely evaluated for ocular symptoms.
An important question that requires further investigation, they noted, is whether newborns without microcephaly, but whose mothers may have been infected with the Zika virus, should be screened to identify possible ocular lesions.
Funding for the study came from Hospital Geral Roberto Santos, Federal University of São Paulo, Vision Institute, and Conselho Nacional de Desenvolvimento Científico e Tecnológico in Brasília, Brazil. The authors reported having no financial disclosures.
FROM JAMA OPTHALMOLOGY
Key clinical point: Serious ocular abnormalities may accompany microcephaly in babies born to mothers infected with the Zika virus.
Major finding: More than one-third (34.5%) of a cohort of 29 infants born with microcephaly and with a presumed diagnosis of congenital Zika virus had ocular abnormalities in one or both eyes.
Data source: A single-site cohort study evaluating 29 infants born with microcephaly in a single hospital in Salvador, Brazil.
Disclosures: Funding for the study came from Hospital Geral Roberto Santos, Federal University of São Paulo, Vision Institute, and Conselho Nacional de Desenvolvimento Científico e Tecnológico in Brasília, Brazil. The authors reported having no financial disclosures.
A Case of Bloom Syndrome With Uncommon Clinical Manifestations Confirmed on Genetic Testing
Bloom syndrome, also called congenital telangiectatic erythema and stunted growth, was first described by David Bloom in 1954.1 It is a rare autosomal-recessive disorder (Online Mendelian Inheritance in Man 210900) characterized by specific clinical manifestations including photosensitivity, telangiectatic facial erythema, proportionate growth deficiency, hypogonadism, immunodeficiency, and a tendency to develop various malignancies.2 Linkage analysis revealed that the Bloom syndrome gene locus resides on chromosome arm 15q26.1,3 and the BLM gene in this region has been identified as being responsible for the development of Bloom syndrome.4,5 We report the case of a 12-year-old Chinese girl with Bloom syndrome and detected BLM gene. The evaluation was approved by the Institutional Ethical Review Boards of Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College (Beijing, China).
Case Report
We evaluated a Bloom syndrome family, which consisted of the patient and her parents. The patient was a 12-year-old Chinese girl who was apparently healthy until 3 months of age when her parents noticed an erythematous eruption with blisters on the face. Exacerbation after exposure to sunlight is usual, which results in the eruption becoming prominent in summer and fainter in winter.2 Gradually, the patient’s skin lesions became more progressive, extending to the forehead, nose, and ears, with oozing, crusting, atrophy, and telangiectases developing on the face despite treatment. In the last 3 years, no blisters were present on the patient’s face because of her efforts to avoid sun exposure. She had no history of recurrent infections.
On physical examination, the patient was generally healthy with normal intelligence and short stature. She weighed 26 kg and was approximately 122-cm tall. Telangiectatic erythema and slight scaling were noted on the face, which simulated lupus erythematosus (Figures 1A and 1B). She had additional abnormalities including alopecia areata (Figure 1C), eyebrow hair loss, flat nose, reticular pigmentation on the forehead and trunk, and finger swelling. The distal phalanges on all 10 fingers became short and sharpened and the fingernails became wider than they were long (Figure 1D). Laboratory investigations, including a complete blood cell count, liver and kidney function tests, stool examination, serum complement, and albumin and globulin levels, were within reference range.

After informed consent was obtained, a mutation analysis of the BLM gene was performed in the patient and her parents. We used a genomic DNA purification kit to extract genomic DNA from peripheral blood according to the manufacturer’s protocol. Genomic DNA was used to amplify the exons of the BLM gene with intron flanking sequences by polymerase chain reaction with the primer described elsewhere.6 After the amplification, the polymerase chain reaction products were purified and the BLM gene was sequenced. Sequence comparisons and analysis were performed using Phred/Phrap/Consed version 12.0.
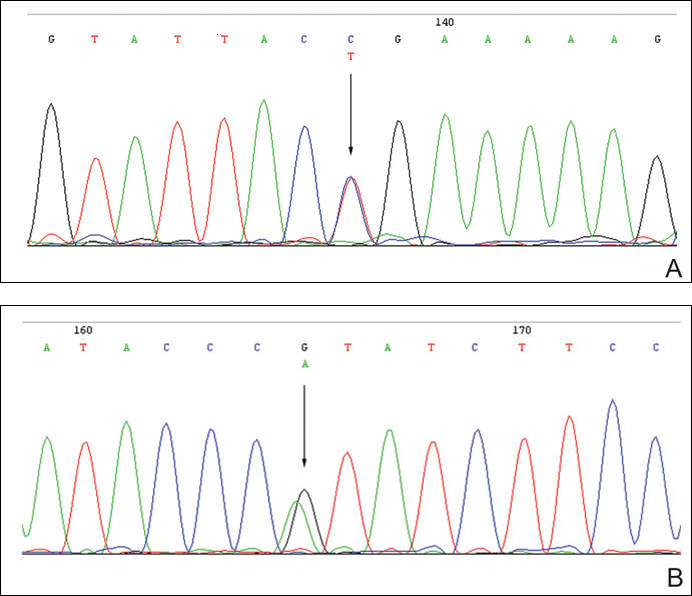
The patient was found to carry changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene. The patient’s father was found to carry c.2603C>T and her mother carried c.3961G>A (Figure 2).
Comment
Patients with Bloom syndrome have a characteristic clinical appearance that typically includes photosensitivity, telangiectatic facial erythema, and growth deficiency. Telangiectatic erythema of the face develops during infancy or early childhood as red macules or plaques and may simulate lupus erythematosus. The lesions are described as a butterfly rash affecting the bridge of the nose and cheeks but also may involve the margins of the eyelids, forehead, ears, and sometimes the dorsa of the hands and forearms. Moderate and proportionate growth deficiencies develop both in utero and postnatally. Patients with Bloom syndrome characteristically have narrow, slender, distinct facial features with micrognathism and a relatively prominent nose. They usually may have mild microcephaly, meaning the head is longer and narrower than normal.2,7-10
German and Takebe11 reported 14 Japanese patients with Bloom syndrome. The phenotype differs somewhat from most cases recognized elsewhere in that dolichocephaly was a less constant feature, the facial skin was less prominent, and life-threatening infections were less common. Our patient had typical telangiectatic facial erythema without microcephaly, dolichocephaly, or any infections. She also had some uncommon manifestations such as alopecia areata, eyebrow hair loss, flat nose, reticular pigmentation, and short sharpened distal phalanges with fingernails that were wider than they were long. Although she had no recurrent infections and laboratory tests were within reference range, the alopecia areata and eyebrow hair loss may be associated with an abnormal immune response. The reasons for the short sharpened distal phalanges and the fingernail findings are unclear. The presence of reticular pigmentation also is unclear but may be associated with photosensitivity. Since the BLM gene was discovered to be the disease-causing gene of Bloom syndrome in 1995,4,5 approximately 70 mutations were reported. The BLM gene encodes for the Bloom syndrome protein, a DNA helicase of the highly conserved RecQ subfamily of helicases, a group of nuclear proteins important in the maintenance of genomic stability.12
Mutation analysis of the BLM gene in our patient showed changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene, which altered proline residue with leucine residue at 868 and valine residue with isoleucine residue at 1321, respectively. According to GenBank,13,14 c.2603C>T and c.3961G>A are single nucleotide polymorphisms of the BLM gene. The genotypic distribution of International HapMap Project15 showed that C=602/602 and T=0/602 on c.2603 in 301 unrelated Chinese patients and G=585/602 and A=17/602 on c.3961 in 301 unrelated Chinese patients. Because of the low prevalence of genotypes c.2603T and c.3961A in China, the relationship between clinical features and c.2603C>T and c.3961G>A of the BLM gene in our patient requires further study.
In conclusion, we report a patient with Bloom syndrome with uncommon clinical manifestations. Our findings indicate that c.2603C>T and c.3961G>A of the BLM gene may be the pathogenic nature for Bloom syndrome in China.
Acknowledgments
The authors would like to thank the patient and her family for their participation in the study. The authors also thank Li Qi, BA, Beijing, China, for his contribution to the review of the data in the literature.
- Bloom D. Congenital telangiectatic erythema resembling lupus erythematosus in dwarfs; probably a syndrome entity. AMA Am J Dis Child. 1954;88:754-758.
- German J. Bloom’s syndrome, I: genetical and clinical observations in the first twenty-seven patients. Am J Hum Genet. 1969;21:196-227.
- German J, Roe AM, Leppert MF, et al. Bloom syndrome: an analysis of consanguineous families assigns the locus mutated to chromosome band 15q26.1. Proc Natl Acad Sci U S A. 1994;91:6669-6673.
- Passarge E. A DNA helicase in full Bloom. Nat Genet. 1995;11:356-357.
- Ellis NA, Groden J, Ye TZ, et al. The Bloom’s syndrome gene product is homologous to RecQ helicases. Cell. 1995;83:655-666.
- German J, Sanz MM, Ciocci S, et al. Syndrome-causing mutations of the BLM gene in persons in the Bloom’s Syndrome Registry. Hum Mutat. 2007;28:743-753.
- Landau JW, Sasaki MS, Newcomer VD, et al. Bloom’s syndrome: the syndrome of telangiectatic erythema and growth retardation. Arch Dermatol. 1966;94:687-694.
- Gretzula JC, Hevia O, Weber PJ. Bloom’s syndrome. J Am Acad Dermatol. 1987;17:479-488.
- Passarge E. Bloom’s syndrome: the German experience. Ann Genet. 1991;34:179-197.
- German J. Bloom’s syndrome. Dermatol Clin. 1995;13:7-18.
- German J, Takebe H. Bloom’s syndrome, XIV: the disorder in Japan. Clin Genet. 1989;35:93-110.
- Bennett RJ, Keck JL. Structure and function of RecQ DNA helicases. Crit Rev Biochem Mol Biol. 2004;39:79-97.
- Reference SNP (refSNP) Cluster Report: rs2227935. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=2227935. Accessed February 3, 2016.
- Reference SNP (refSNP) Cluster Report: rs7167216. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=7167216. Accessed February 3, 2016.
- Homo sapiens:GRCh37.p13 (GCF_000001405.25)Chr 1 (NC_000001.10):1 - 249.3M. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/variationtools/1000genomes/?=%EF%BC%86=. Accessed February 3, 2016.
Bloom syndrome, also called congenital telangiectatic erythema and stunted growth, was first described by David Bloom in 1954.1 It is a rare autosomal-recessive disorder (Online Mendelian Inheritance in Man 210900) characterized by specific clinical manifestations including photosensitivity, telangiectatic facial erythema, proportionate growth deficiency, hypogonadism, immunodeficiency, and a tendency to develop various malignancies.2 Linkage analysis revealed that the Bloom syndrome gene locus resides on chromosome arm 15q26.1,3 and the BLM gene in this region has been identified as being responsible for the development of Bloom syndrome.4,5 We report the case of a 12-year-old Chinese girl with Bloom syndrome and detected BLM gene. The evaluation was approved by the Institutional Ethical Review Boards of Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College (Beijing, China).
Case Report
We evaluated a Bloom syndrome family, which consisted of the patient and her parents. The patient was a 12-year-old Chinese girl who was apparently healthy until 3 months of age when her parents noticed an erythematous eruption with blisters on the face. Exacerbation after exposure to sunlight is usual, which results in the eruption becoming prominent in summer and fainter in winter.2 Gradually, the patient’s skin lesions became more progressive, extending to the forehead, nose, and ears, with oozing, crusting, atrophy, and telangiectases developing on the face despite treatment. In the last 3 years, no blisters were present on the patient’s face because of her efforts to avoid sun exposure. She had no history of recurrent infections.
On physical examination, the patient was generally healthy with normal intelligence and short stature. She weighed 26 kg and was approximately 122-cm tall. Telangiectatic erythema and slight scaling were noted on the face, which simulated lupus erythematosus (Figures 1A and 1B). She had additional abnormalities including alopecia areata (Figure 1C), eyebrow hair loss, flat nose, reticular pigmentation on the forehead and trunk, and finger swelling. The distal phalanges on all 10 fingers became short and sharpened and the fingernails became wider than they were long (Figure 1D). Laboratory investigations, including a complete blood cell count, liver and kidney function tests, stool examination, serum complement, and albumin and globulin levels, were within reference range.
After informed consent was obtained, a mutation analysis of the BLM gene was performed in the patient and her parents. We used a genomic DNA purification kit to extract genomic DNA from peripheral blood according to the manufacturer’s protocol. Genomic DNA was used to amplify the exons of the BLM gene with intron flanking sequences by polymerase chain reaction with the primer described elsewhere.6 After the amplification, the polymerase chain reaction products were purified and the BLM gene was sequenced. Sequence comparisons and analysis were performed using Phred/Phrap/Consed version 12.0.
The patient was found to carry changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene. The patient’s father was found to carry c.2603C>T and her mother carried c.3961G>A (Figure 2).
Comment
Patients with Bloom syndrome have a characteristic clinical appearance that typically includes photosensitivity, telangiectatic facial erythema, and growth deficiency. Telangiectatic erythema of the face develops during infancy or early childhood as red macules or plaques and may simulate lupus erythematosus. The lesions are described as a butterfly rash affecting the bridge of the nose and cheeks but also may involve the margins of the eyelids, forehead, ears, and sometimes the dorsa of the hands and forearms. Moderate and proportionate growth deficiencies develop both in utero and postnatally. Patients with Bloom syndrome characteristically have narrow, slender, distinct facial features with micrognathism and a relatively prominent nose. They usually may have mild microcephaly, meaning the head is longer and narrower than normal.2,7-10
German and Takebe11 reported 14 Japanese patients with Bloom syndrome. The phenotype differs somewhat from most cases recognized elsewhere in that dolichocephaly was a less constant feature, the facial skin was less prominent, and life-threatening infections were less common. Our patient had typical telangiectatic facial erythema without microcephaly, dolichocephaly, or any infections. She also had some uncommon manifestations such as alopecia areata, eyebrow hair loss, flat nose, reticular pigmentation, and short sharpened distal phalanges with fingernails that were wider than they were long. Although she had no recurrent infections and laboratory tests were within reference range, the alopecia areata and eyebrow hair loss may be associated with an abnormal immune response. The reasons for the short sharpened distal phalanges and the fingernail findings are unclear. The presence of reticular pigmentation also is unclear but may be associated with photosensitivity. Since the BLM gene was discovered to be the disease-causing gene of Bloom syndrome in 1995,4,5 approximately 70 mutations were reported. The BLM gene encodes for the Bloom syndrome protein, a DNA helicase of the highly conserved RecQ subfamily of helicases, a group of nuclear proteins important in the maintenance of genomic stability.12
Mutation analysis of the BLM gene in our patient showed changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene, which altered proline residue with leucine residue at 868 and valine residue with isoleucine residue at 1321, respectively. According to GenBank,13,14 c.2603C>T and c.3961G>A are single nucleotide polymorphisms of the BLM gene. The genotypic distribution of International HapMap Project15 showed that C=602/602 and T=0/602 on c.2603 in 301 unrelated Chinese patients and G=585/602 and A=17/602 on c.3961 in 301 unrelated Chinese patients. Because of the low prevalence of genotypes c.2603T and c.3961A in China, the relationship between clinical features and c.2603C>T and c.3961G>A of the BLM gene in our patient requires further study.
In conclusion, we report a patient with Bloom syndrome with uncommon clinical manifestations. Our findings indicate that c.2603C>T and c.3961G>A of the BLM gene may be the pathogenic nature for Bloom syndrome in China.
Acknowledgments
The authors would like to thank the patient and her family for their participation in the study. The authors also thank Li Qi, BA, Beijing, China, for his contribution to the review of the data in the literature.
Bloom syndrome, also called congenital telangiectatic erythema and stunted growth, was first described by David Bloom in 1954.1 It is a rare autosomal-recessive disorder (Online Mendelian Inheritance in Man 210900) characterized by specific clinical manifestations including photosensitivity, telangiectatic facial erythema, proportionate growth deficiency, hypogonadism, immunodeficiency, and a tendency to develop various malignancies.2 Linkage analysis revealed that the Bloom syndrome gene locus resides on chromosome arm 15q26.1,3 and the BLM gene in this region has been identified as being responsible for the development of Bloom syndrome.4,5 We report the case of a 12-year-old Chinese girl with Bloom syndrome and detected BLM gene. The evaluation was approved by the Institutional Ethical Review Boards of Institute of Dermatology, Chinese Academy of Medical Sciences and Peking Union Medical College (Beijing, China).
Case Report
We evaluated a Bloom syndrome family, which consisted of the patient and her parents. The patient was a 12-year-old Chinese girl who was apparently healthy until 3 months of age when her parents noticed an erythematous eruption with blisters on the face. Exacerbation after exposure to sunlight is usual, which results in the eruption becoming prominent in summer and fainter in winter.2 Gradually, the patient’s skin lesions became more progressive, extending to the forehead, nose, and ears, with oozing, crusting, atrophy, and telangiectases developing on the face despite treatment. In the last 3 years, no blisters were present on the patient’s face because of her efforts to avoid sun exposure. She had no history of recurrent infections.
On physical examination, the patient was generally healthy with normal intelligence and short stature. She weighed 26 kg and was approximately 122-cm tall. Telangiectatic erythema and slight scaling were noted on the face, which simulated lupus erythematosus (Figures 1A and 1B). She had additional abnormalities including alopecia areata (Figure 1C), eyebrow hair loss, flat nose, reticular pigmentation on the forehead and trunk, and finger swelling. The distal phalanges on all 10 fingers became short and sharpened and the fingernails became wider than they were long (Figure 1D). Laboratory investigations, including a complete blood cell count, liver and kidney function tests, stool examination, serum complement, and albumin and globulin levels, were within reference range.
After informed consent was obtained, a mutation analysis of the BLM gene was performed in the patient and her parents. We used a genomic DNA purification kit to extract genomic DNA from peripheral blood according to the manufacturer’s protocol. Genomic DNA was used to amplify the exons of the BLM gene with intron flanking sequences by polymerase chain reaction with the primer described elsewhere.6 After the amplification, the polymerase chain reaction products were purified and the BLM gene was sequenced. Sequence comparisons and analysis were performed using Phred/Phrap/Consed version 12.0.
The patient was found to carry changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene. The patient’s father was found to carry c.2603C>T and her mother carried c.3961G>A (Figure 2).
Comment
Patients with Bloom syndrome have a characteristic clinical appearance that typically includes photosensitivity, telangiectatic facial erythema, and growth deficiency. Telangiectatic erythema of the face develops during infancy or early childhood as red macules or plaques and may simulate lupus erythematosus. The lesions are described as a butterfly rash affecting the bridge of the nose and cheeks but also may involve the margins of the eyelids, forehead, ears, and sometimes the dorsa of the hands and forearms. Moderate and proportionate growth deficiencies develop both in utero and postnatally. Patients with Bloom syndrome characteristically have narrow, slender, distinct facial features with micrognathism and a relatively prominent nose. They usually may have mild microcephaly, meaning the head is longer and narrower than normal.2,7-10
German and Takebe11 reported 14 Japanese patients with Bloom syndrome. The phenotype differs somewhat from most cases recognized elsewhere in that dolichocephaly was a less constant feature, the facial skin was less prominent, and life-threatening infections were less common. Our patient had typical telangiectatic facial erythema without microcephaly, dolichocephaly, or any infections. She also had some uncommon manifestations such as alopecia areata, eyebrow hair loss, flat nose, reticular pigmentation, and short sharpened distal phalanges with fingernails that were wider than they were long. Although she had no recurrent infections and laboratory tests were within reference range, the alopecia areata and eyebrow hair loss may be associated with an abnormal immune response. The reasons for the short sharpened distal phalanges and the fingernail findings are unclear. The presence of reticular pigmentation also is unclear but may be associated with photosensitivity. Since the BLM gene was discovered to be the disease-causing gene of Bloom syndrome in 1995,4,5 approximately 70 mutations were reported. The BLM gene encodes for the Bloom syndrome protein, a DNA helicase of the highly conserved RecQ subfamily of helicases, a group of nuclear proteins important in the maintenance of genomic stability.12
Mutation analysis of the BLM gene in our patient showed changes in 2 heterozygous nucleotide sites, including c.2603C>T in exon 13 and c.3961G>A in exon 21 of the BLM gene, which altered proline residue with leucine residue at 868 and valine residue with isoleucine residue at 1321, respectively. According to GenBank,13,14 c.2603C>T and c.3961G>A are single nucleotide polymorphisms of the BLM gene. The genotypic distribution of International HapMap Project15 showed that C=602/602 and T=0/602 on c.2603 in 301 unrelated Chinese patients and G=585/602 and A=17/602 on c.3961 in 301 unrelated Chinese patients. Because of the low prevalence of genotypes c.2603T and c.3961A in China, the relationship between clinical features and c.2603C>T and c.3961G>A of the BLM gene in our patient requires further study.
In conclusion, we report a patient with Bloom syndrome with uncommon clinical manifestations. Our findings indicate that c.2603C>T and c.3961G>A of the BLM gene may be the pathogenic nature for Bloom syndrome in China.
Acknowledgments
The authors would like to thank the patient and her family for their participation in the study. The authors also thank Li Qi, BA, Beijing, China, for his contribution to the review of the data in the literature.
- Bloom D. Congenital telangiectatic erythema resembling lupus erythematosus in dwarfs; probably a syndrome entity. AMA Am J Dis Child. 1954;88:754-758.
- German J. Bloom’s syndrome, I: genetical and clinical observations in the first twenty-seven patients. Am J Hum Genet. 1969;21:196-227.
- German J, Roe AM, Leppert MF, et al. Bloom syndrome: an analysis of consanguineous families assigns the locus mutated to chromosome band 15q26.1. Proc Natl Acad Sci U S A. 1994;91:6669-6673.
- Passarge E. A DNA helicase in full Bloom. Nat Genet. 1995;11:356-357.
- Ellis NA, Groden J, Ye TZ, et al. The Bloom’s syndrome gene product is homologous to RecQ helicases. Cell. 1995;83:655-666.
- German J, Sanz MM, Ciocci S, et al. Syndrome-causing mutations of the BLM gene in persons in the Bloom’s Syndrome Registry. Hum Mutat. 2007;28:743-753.
- Landau JW, Sasaki MS, Newcomer VD, et al. Bloom’s syndrome: the syndrome of telangiectatic erythema and growth retardation. Arch Dermatol. 1966;94:687-694.
- Gretzula JC, Hevia O, Weber PJ. Bloom’s syndrome. J Am Acad Dermatol. 1987;17:479-488.
- Passarge E. Bloom’s syndrome: the German experience. Ann Genet. 1991;34:179-197.
- German J. Bloom’s syndrome. Dermatol Clin. 1995;13:7-18.
- German J, Takebe H. Bloom’s syndrome, XIV: the disorder in Japan. Clin Genet. 1989;35:93-110.
- Bennett RJ, Keck JL. Structure and function of RecQ DNA helicases. Crit Rev Biochem Mol Biol. 2004;39:79-97.
- Reference SNP (refSNP) Cluster Report: rs2227935. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=2227935. Accessed February 3, 2016.
- Reference SNP (refSNP) Cluster Report: rs7167216. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=7167216. Accessed February 3, 2016.
- Homo sapiens:GRCh37.p13 (GCF_000001405.25)Chr 1 (NC_000001.10):1 - 249.3M. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/variationtools/1000genomes/?=%EF%BC%86=. Accessed February 3, 2016.
- Bloom D. Congenital telangiectatic erythema resembling lupus erythematosus in dwarfs; probably a syndrome entity. AMA Am J Dis Child. 1954;88:754-758.
- German J. Bloom’s syndrome, I: genetical and clinical observations in the first twenty-seven patients. Am J Hum Genet. 1969;21:196-227.
- German J, Roe AM, Leppert MF, et al. Bloom syndrome: an analysis of consanguineous families assigns the locus mutated to chromosome band 15q26.1. Proc Natl Acad Sci U S A. 1994;91:6669-6673.
- Passarge E. A DNA helicase in full Bloom. Nat Genet. 1995;11:356-357.
- Ellis NA, Groden J, Ye TZ, et al. The Bloom’s syndrome gene product is homologous to RecQ helicases. Cell. 1995;83:655-666.
- German J, Sanz MM, Ciocci S, et al. Syndrome-causing mutations of the BLM gene in persons in the Bloom’s Syndrome Registry. Hum Mutat. 2007;28:743-753.
- Landau JW, Sasaki MS, Newcomer VD, et al. Bloom’s syndrome: the syndrome of telangiectatic erythema and growth retardation. Arch Dermatol. 1966;94:687-694.
- Gretzula JC, Hevia O, Weber PJ. Bloom’s syndrome. J Am Acad Dermatol. 1987;17:479-488.
- Passarge E. Bloom’s syndrome: the German experience. Ann Genet. 1991;34:179-197.
- German J. Bloom’s syndrome. Dermatol Clin. 1995;13:7-18.
- German J, Takebe H. Bloom’s syndrome, XIV: the disorder in Japan. Clin Genet. 1989;35:93-110.
- Bennett RJ, Keck JL. Structure and function of RecQ DNA helicases. Crit Rev Biochem Mol Biol. 2004;39:79-97.
- Reference SNP (refSNP) Cluster Report: rs2227935. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=2227935. Accessed February 3, 2016.
- Reference SNP (refSNP) Cluster Report: rs7167216. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/SNP/snp_ref.cgi?rs=7167216. Accessed February 3, 2016.
- Homo sapiens:GRCh37.p13 (GCF_000001405.25)Chr 1 (NC_000001.10):1 - 249.3M. National Center for Biotechnology Information website. http://www.ncbi.nlm.nih.gov/variationtools/1000genomes/?=%EF%BC%86=. Accessed February 3, 2016.

Childhood Metabolic Syndrome Severity Declined Relative to HDL, Triglyceride Changes
The severity of childhood metabolic syndrome declined in a study of U.S. adolescents relative to increases in high-density lipoproteins (HDL) and decreases in fasting triglyceride measurements among the individuals examined, reported Arthur M. Lee of the University of Virginia, Charlottesville, and his colleagues.
The metabolic syndrome (MetS) is characterized by central obesity, high fasting glucose, high fasting triglycerides, high blood pressure (BP), and low HDL.
The researchers used regression analysis of individual waves of data from 1999 to 2012 to analyze 5,117 individuals aged 12-19 years. The data came from the Centers for Disease Control and Prevention National Health and Nutrition Examination Survey (NHANES, 1999-2012), a cross-sectional, national, stratified, multistage probability survey conducted in 2-year waves. The severity of MetS was calculated using the Pediatric MetS z score. Patients who were pregnant, had an active hepatitis B infection, had physician-diagnosed diabetes, or were currently using antidiabetic or antihyperlipidemic medication were excluded from the study.

Overall, a linear trend of a decreasing MetS z score (P = .030) was found despite the body mass index z score having increased significantly. While fasting triglyceride measurements declined significantly, HDL levels rose significantly.
The researchers also found temporal trends of decreasing total calorie consumption, decreasing carbohydrate consumption, and increasing unsaturated fat consumption.
“The overall decreasing trend in the MetS z score is likely secondary to the increasing trend in HDL measurements and decreasing trend in fasting triglycerides measurements, ” wrote Mr. Lee and his associates. “The increasing trend in HDL and decreasing fasting triglyceride measurements could be attributable in part to trends of decreasing carbohydrate intake and increasing unsaturated fat intake.”
The researchers recommended future studies on individuals with MetS focus on determining, “the causality of lifestyle factors in improvements of MetS severity.”
Read the study in Pediatrics (doi: 10.1542/peds.2015-3177).
The severity of childhood metabolic syndrome declined in a study of U.S. adolescents relative to increases in high-density lipoproteins (HDL) and decreases in fasting triglyceride measurements among the individuals examined, reported Arthur M. Lee of the University of Virginia, Charlottesville, and his colleagues.
The metabolic syndrome (MetS) is characterized by central obesity, high fasting glucose, high fasting triglycerides, high blood pressure (BP), and low HDL.
The researchers used regression analysis of individual waves of data from 1999 to 2012 to analyze 5,117 individuals aged 12-19 years. The data came from the Centers for Disease Control and Prevention National Health and Nutrition Examination Survey (NHANES, 1999-2012), a cross-sectional, national, stratified, multistage probability survey conducted in 2-year waves. The severity of MetS was calculated using the Pediatric MetS z score. Patients who were pregnant, had an active hepatitis B infection, had physician-diagnosed diabetes, or were currently using antidiabetic or antihyperlipidemic medication were excluded from the study.
Overall, a linear trend of a decreasing MetS z score (P = .030) was found despite the body mass index z score having increased significantly. While fasting triglyceride measurements declined significantly, HDL levels rose significantly.
The researchers also found temporal trends of decreasing total calorie consumption, decreasing carbohydrate consumption, and increasing unsaturated fat consumption.
“The overall decreasing trend in the MetS z score is likely secondary to the increasing trend in HDL measurements and decreasing trend in fasting triglycerides measurements, ” wrote Mr. Lee and his associates. “The increasing trend in HDL and decreasing fasting triglyceride measurements could be attributable in part to trends of decreasing carbohydrate intake and increasing unsaturated fat intake.”
The researchers recommended future studies on individuals with MetS focus on determining, “the causality of lifestyle factors in improvements of MetS severity.”
Read the study in Pediatrics (doi: 10.1542/peds.2015-3177).
The severity of childhood metabolic syndrome declined in a study of U.S. adolescents relative to increases in high-density lipoproteins (HDL) and decreases in fasting triglyceride measurements among the individuals examined, reported Arthur M. Lee of the University of Virginia, Charlottesville, and his colleagues.
The metabolic syndrome (MetS) is characterized by central obesity, high fasting glucose, high fasting triglycerides, high blood pressure (BP), and low HDL.
The researchers used regression analysis of individual waves of data from 1999 to 2012 to analyze 5,117 individuals aged 12-19 years. The data came from the Centers for Disease Control and Prevention National Health and Nutrition Examination Survey (NHANES, 1999-2012), a cross-sectional, national, stratified, multistage probability survey conducted in 2-year waves. The severity of MetS was calculated using the Pediatric MetS z score. Patients who were pregnant, had an active hepatitis B infection, had physician-diagnosed diabetes, or were currently using antidiabetic or antihyperlipidemic medication were excluded from the study.
Overall, a linear trend of a decreasing MetS z score (P = .030) was found despite the body mass index z score having increased significantly. While fasting triglyceride measurements declined significantly, HDL levels rose significantly.
The researchers also found temporal trends of decreasing total calorie consumption, decreasing carbohydrate consumption, and increasing unsaturated fat consumption.
“The overall decreasing trend in the MetS z score is likely secondary to the increasing trend in HDL measurements and decreasing trend in fasting triglycerides measurements, ” wrote Mr. Lee and his associates. “The increasing trend in HDL and decreasing fasting triglyceride measurements could be attributable in part to trends of decreasing carbohydrate intake and increasing unsaturated fat intake.”
The researchers recommended future studies on individuals with MetS focus on determining, “the causality of lifestyle factors in improvements of MetS severity.”
Read the study in Pediatrics (doi: 10.1542/peds.2015-3177).
FROM PEDIATRICS

Childhood metabolic syndrome severity declined relative to HDL, triglyceride changes
The severity of childhood metabolic syndrome declined in a study of U.S. adolescents relative to increases in high-density lipoproteins (HDL) and decreases in fasting triglyceride measurements among the individuals examined, reported Arthur M. Lee of the University of Virginia, Charlottesville, and his colleagues.
The metabolic syndrome (MetS) is characterized by central obesity, high fasting glucose, high fasting triglycerides, high blood pressure (BP), and low HDL.
The researchers used regression analysis of individual waves of data from 1999 to 2012 to analyze 5,117 individuals aged 12-19 years. The data came from the Centers for Disease Control and Prevention National Health and Nutrition Examination Survey (NHANES, 1999-2012), a cross-sectional, national, stratified, multistage probability survey conducted in 2-year waves. The severity of MetS was calculated using the Pediatric MetS z score. Patients who were pregnant, had an active hepatitis B infection, had physician-diagnosed diabetes, or were currently using antidiabetic or antihyperlipidemic medication were excluded from the study.

Overall, a linear trend of a decreasing MetS z score (P = .030) was found despite the body mass index z score having increased significantly. While fasting triglyceride measurements declined significantly, HDL levels rose significantly.
The researchers also found temporal trends of decreasing total calorie consumption, decreasing carbohydrate consumption, and increasing unsaturated fat consumption.
“The overall decreasing trend in the MetS z score is likely secondary to the increasing trend in HDL measurements and decreasing trend in fasting triglycerides measurements, ” wrote Mr. Lee and his associates. “The increasing trend in HDL and decreasing fasting triglyceride measurements could be attributable in part to trends of decreasing carbohydrate intake and increasing unsaturated fat intake.”
The researchers recommended future studies on individuals with MetS focus on determining, “the causality of lifestyle factors in improvements of MetS severity.”
Read the study in Pediatrics (doi: 10.1542/peds.2015-3177).
The severity of childhood metabolic syndrome declined in a study of U.S. adolescents relative to increases in high-density lipoproteins (HDL) and decreases in fasting triglyceride measurements among the individuals examined, reported Arthur M. Lee of the University of Virginia, Charlottesville, and his colleagues.
The metabolic syndrome (MetS) is characterized by central obesity, high fasting glucose, high fasting triglycerides, high blood pressure (BP), and low HDL.
The researchers used regression analysis of individual waves of data from 1999 to 2012 to analyze 5,117 individuals aged 12-19 years. The data came from the Centers for Disease Control and Prevention National Health and Nutrition Examination Survey (NHANES, 1999-2012), a cross-sectional, national, stratified, multistage probability survey conducted in 2-year waves. The severity of MetS was calculated using the Pediatric MetS z score. Patients who were pregnant, had an active hepatitis B infection, had physician-diagnosed diabetes, or were currently using antidiabetic or antihyperlipidemic medication were excluded from the study.
Overall, a linear trend of a decreasing MetS z score (P = .030) was found despite the body mass index z score having increased significantly. While fasting triglyceride measurements declined significantly, HDL levels rose significantly.
The researchers also found temporal trends of decreasing total calorie consumption, decreasing carbohydrate consumption, and increasing unsaturated fat consumption.
“The overall decreasing trend in the MetS z score is likely secondary to the increasing trend in HDL measurements and decreasing trend in fasting triglycerides measurements, ” wrote Mr. Lee and his associates. “The increasing trend in HDL and decreasing fasting triglyceride measurements could be attributable in part to trends of decreasing carbohydrate intake and increasing unsaturated fat intake.”
The researchers recommended future studies on individuals with MetS focus on determining, “the causality of lifestyle factors in improvements of MetS severity.”
Read the study in Pediatrics (doi: 10.1542/peds.2015-3177).
The severity of childhood metabolic syndrome declined in a study of U.S. adolescents relative to increases in high-density lipoproteins (HDL) and decreases in fasting triglyceride measurements among the individuals examined, reported Arthur M. Lee of the University of Virginia, Charlottesville, and his colleagues.
The metabolic syndrome (MetS) is characterized by central obesity, high fasting glucose, high fasting triglycerides, high blood pressure (BP), and low HDL.
The researchers used regression analysis of individual waves of data from 1999 to 2012 to analyze 5,117 individuals aged 12-19 years. The data came from the Centers for Disease Control and Prevention National Health and Nutrition Examination Survey (NHANES, 1999-2012), a cross-sectional, national, stratified, multistage probability survey conducted in 2-year waves. The severity of MetS was calculated using the Pediatric MetS z score. Patients who were pregnant, had an active hepatitis B infection, had physician-diagnosed diabetes, or were currently using antidiabetic or antihyperlipidemic medication were excluded from the study.
Overall, a linear trend of a decreasing MetS z score (P = .030) was found despite the body mass index z score having increased significantly. While fasting triglyceride measurements declined significantly, HDL levels rose significantly.
The researchers also found temporal trends of decreasing total calorie consumption, decreasing carbohydrate consumption, and increasing unsaturated fat consumption.
“The overall decreasing trend in the MetS z score is likely secondary to the increasing trend in HDL measurements and decreasing trend in fasting triglycerides measurements, ” wrote Mr. Lee and his associates. “The increasing trend in HDL and decreasing fasting triglyceride measurements could be attributable in part to trends of decreasing carbohydrate intake and increasing unsaturated fat intake.”
The researchers recommended future studies on individuals with MetS focus on determining, “the causality of lifestyle factors in improvements of MetS severity.”
Read the study in Pediatrics (doi: 10.1542/peds.2015-3177).
FROM PEDIATRICS

Prospective study supports hepatitis A vaccine schedule
Current vaccine recommendations for hepatitis A were endorsed by the findings of a prospective, randomized study of 183 Alaskan Native adolescents followed from infancy to age 15-16 years.
Study participants were randomly assigned to receive two doses of hepatitis A vaccine on three different schedules: at ages 6 and 12 months (group 1); at 12 and 18 months (group 2); or at 15 and 21 months (group 3). Each group was randomized according to maternal anti-HAV status.
Serum samples were collected from study participants at eight sampling time points from 1 month after the second vaccine until age 15-16 years. Those with anti-HAV levels of at least 20 mIU/mL were considered to be seropositive.
Seropositivity was high through age 10 years in all three groups – 100% in groups 2 and 3, and more than 90% in group 1. After age 10 years, however, seropositivity decreased. At age 15-16 years, 50%-75% of those on the 6 and 12 months’ schedule were seropositive as were 67%-87% of the other two groups whose mothers were anti-HAV-positive. Among those who were seropositive at age 15-16 years, 84% are predicted to remain so for at least another 30 years.
The findings that seropositivity was less frequent among those starting vaccination at age 6 months and among those whose mothers were antibody positive and who started vaccination at age 12 months or 15 months support current vaccine recommendations, Dr. Philip Spradling of the Centers for Disease Control and Prevention and his colleagues wrote.
Read the article in Hepatology (2015 Dec 5. doi: 10.1002/hep.28375).
Current vaccine recommendations for hepatitis A were endorsed by the findings of a prospective, randomized study of 183 Alaskan Native adolescents followed from infancy to age 15-16 years.
Study participants were randomly assigned to receive two doses of hepatitis A vaccine on three different schedules: at ages 6 and 12 months (group 1); at 12 and 18 months (group 2); or at 15 and 21 months (group 3). Each group was randomized according to maternal anti-HAV status.
Serum samples were collected from study participants at eight sampling time points from 1 month after the second vaccine until age 15-16 years. Those with anti-HAV levels of at least 20 mIU/mL were considered to be seropositive.
Seropositivity was high through age 10 years in all three groups – 100% in groups 2 and 3, and more than 90% in group 1. After age 10 years, however, seropositivity decreased. At age 15-16 years, 50%-75% of those on the 6 and 12 months’ schedule were seropositive as were 67%-87% of the other two groups whose mothers were anti-HAV-positive. Among those who were seropositive at age 15-16 years, 84% are predicted to remain so for at least another 30 years.
The findings that seropositivity was less frequent among those starting vaccination at age 6 months and among those whose mothers were antibody positive and who started vaccination at age 12 months or 15 months support current vaccine recommendations, Dr. Philip Spradling of the Centers for Disease Control and Prevention and his colleagues wrote.
Read the article in Hepatology (2015 Dec 5. doi: 10.1002/hep.28375).
Current vaccine recommendations for hepatitis A were endorsed by the findings of a prospective, randomized study of 183 Alaskan Native adolescents followed from infancy to age 15-16 years.
Study participants were randomly assigned to receive two doses of hepatitis A vaccine on three different schedules: at ages 6 and 12 months (group 1); at 12 and 18 months (group 2); or at 15 and 21 months (group 3). Each group was randomized according to maternal anti-HAV status.
Serum samples were collected from study participants at eight sampling time points from 1 month after the second vaccine until age 15-16 years. Those with anti-HAV levels of at least 20 mIU/mL were considered to be seropositive.
Seropositivity was high through age 10 years in all three groups – 100% in groups 2 and 3, and more than 90% in group 1. After age 10 years, however, seropositivity decreased. At age 15-16 years, 50%-75% of those on the 6 and 12 months’ schedule were seropositive as were 67%-87% of the other two groups whose mothers were anti-HAV-positive. Among those who were seropositive at age 15-16 years, 84% are predicted to remain so for at least another 30 years.
The findings that seropositivity was less frequent among those starting vaccination at age 6 months and among those whose mothers were antibody positive and who started vaccination at age 12 months or 15 months support current vaccine recommendations, Dr. Philip Spradling of the Centers for Disease Control and Prevention and his colleagues wrote.
Read the article in Hepatology (2015 Dec 5. doi: 10.1002/hep.28375).
FROM HEPATOLOGY
USPSTF Updates Depression-screening Guidelines for Children, Adolescents
Children aged 12-18 years should be screened for major depressive disorder, but current evidence is insufficient to advise screening children aged 11 years or younger for the condition.
Those are among the key guidelines in updated recommendations from the U.S. Preventive Services Task Force on screening for depression in children and adolescents that were published online Feb. 8 in Pediatrics and in the Annals of Internal Medicine.

“Adolescents who are depressed suffer a lot of adverse consequences from their depression,” task force member Dr. Alexander H. Krist of the department of family medicine and population health at Virginia Commonwealth University, Richmond, said in an interview. “It can affect school, their family life, and their quality of life. Being able to identify adolescents who are depressed [and] making sure that they get the care that they need can have a big benefit for adolescents and their families.”
Although little is known about the prevalence of major depressive disorder (MDD) in children, results from national surveys suggest that about 8% of adolescents have had major depression in the past year, according to the task force members, who were chaired by Dr. Albert L. Siu, an internist and geriatrician in the department of geriatrics and palliative medicine at Mount Sinai School of Medicine, New York (Pediatrics. 2016 Feb 8. doi: 10.1542/peds.2015-4467).
The 2009 USPSTF guidelines recommended screening for MDD in adolescents “when systems for diagnosis, treatment, and follow-up are in place” and concluded that there was not enough evidence to make a recommendation regarding children aged 7-11 years. The updated recommendation reaffirms these positions but removes the mention of specific MDD therapies “in recognition of decreased concern over the harms of pharmacotherapy in adolescents when patients are adequately monitored.” In addition, more studies have been published that support the 2009 guidelines, “so that is one important change,” Dr. Krist said.
Recommendations for the new guidelines were based on a literature review conducted for the USPSTF by researchers led by Valerie Forman-Hoffman, Ph.D., of RTI International in Research Triangle Park, N.C. , and published online Feb. 8 (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M15-2259). Supported by a grant from the Agency for Healthcare Research and Quality, the review involved a search for trials and systematic reviews of treatment, test-retest studies of screening, and trials and large cohort studies for harms that appeared in the medical literature between May 2007 and February 2015. No trials were found that directly assessed the benefits or harms of screening children or adolescents for MDD in primary care settings.
Here are the key recommendations:
• Screen for MDD in adolescents aged 12-18 years. Screening “should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up.” This is a “B” recommendation in the USPSTF grading system, which means that “there is high certainty that the net benefit is moderate or there is moderate certainty the net benefit is moderate to substantial.”
As stated in the recommendations, the phrase “adequate systems in place” refers to “having systems and clinical staff to ensure that patients are screened and, if they screen positive, are appropriately diagnosed and treated with evidence-based care or referred to a setting that can provide the necessary care.” This emphasis was made because “we now recognize that our health systems have evolved, and that it’s more the standard of care to have systems in place to care for adolescents who are depressed,” Dr. Krist explained. “The rewording stresses the importance of being able to make sure that care is given to adolescents after they’re diagnosed.”
The Affordable Care Act provides coverage for A and B recommendations of the USPSTF, so screening for MDD in adolescents would be a recommended service. “Often this type of a service would be delivered during a wellness exam,” Dr. Krist said. “That’s a commonly covered benefit right now with the ACA.”
• Current evidence “is insufficient to assess the balance of benefits and harms of screening for MDD in children aged 11 years or younger.” This is an “I” statement, which means that “evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined.”
The new USPSTF guidelines do no not recommend a specific instrument or screening strategy, but the review commissioned for the task force found that the Patient Health Questionnaire for Adolescents and Beck Depression Inventory outperformed other tools in adolescents.
In the opinion of Dr. Krist, a key challenge for primary care clinicians seeking to implement the recommendations is to establish a way to routinely ask adolescents about depression, “being able to systematize that so it’s done routinely and that it’s done well.” A second challenge is to establish a way to ensure proper diagnosis, proper treatment, and follow-up of adolescents who screen positive for MDD. “A lot of primary care practices may choose to do a lot of those activities themselves, or they might work out collaborations with other mental health providers and have a referral mechanism and a follow-up mechanism,” he said.
In an editorial that appeared online in the Annals of Internal Medicine, Dr. John W. Williams Jr. of the Durham (N.C.) Veterans Affairs Medical Center and Dr. Gary Maslow of Duke University, also in Durham, advised generalist physicians to “seize the day and act to implement these guidelines” (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M16-0104). “Implementing high-quality depression care is not easy, but trials and demonstration projects show that it is possible and rewarding.”
Dr. Williams and Dr. Maslow went on to suggest ways that clinicians might incorporate the guidelines into their own practices. “For practices initiating screening for the first time, a pragmatic strategy might be to screen in conjunction with routine health visits and target persons with symptoms associated with depression (for example, insomnia) or risk factors, which in adolescents include female sex, older age, family history of depression, other mental health or behavioral problems, chronic medical illness, and overweight or obesity,” they wrote. “For practices with electronic health records, clinical reminders can be used to prompt staff to distribute screening questionnaires or verbally administer questions along with assessment of vital signs. The Guidelines for Adolescent Depression in Primary Care toolkit includes screening measures, screening procedures, and patient education materials to support the screening and treatment.”
The way Dr. Krist sees it, the overall message of the new recommendations is simple: Screening adolescents for depression has benefits. “We want primary care clinicians to do this, and we want to make sure that primary care practices put systems in place to care for adolescents with identified needs,” he said.
The Agency for Healthcare Research and Quality funded the review that formed the basis of the recommendations. The authors of the recommendation statement reported having no relevant financial disclosures.
Children aged 12-18 years should be screened for major depressive disorder, but current evidence is insufficient to advise screening children aged 11 years or younger for the condition.
Those are among the key guidelines in updated recommendations from the U.S. Preventive Services Task Force on screening for depression in children and adolescents that were published online Feb. 8 in Pediatrics and in the Annals of Internal Medicine.
“Adolescents who are depressed suffer a lot of adverse consequences from their depression,” task force member Dr. Alexander H. Krist of the department of family medicine and population health at Virginia Commonwealth University, Richmond, said in an interview. “It can affect school, their family life, and their quality of life. Being able to identify adolescents who are depressed [and] making sure that they get the care that they need can have a big benefit for adolescents and their families.”
Although little is known about the prevalence of major depressive disorder (MDD) in children, results from national surveys suggest that about 8% of adolescents have had major depression in the past year, according to the task force members, who were chaired by Dr. Albert L. Siu, an internist and geriatrician in the department of geriatrics and palliative medicine at Mount Sinai School of Medicine, New York (Pediatrics. 2016 Feb 8. doi: 10.1542/peds.2015-4467).
The 2009 USPSTF guidelines recommended screening for MDD in adolescents “when systems for diagnosis, treatment, and follow-up are in place” and concluded that there was not enough evidence to make a recommendation regarding children aged 7-11 years. The updated recommendation reaffirms these positions but removes the mention of specific MDD therapies “in recognition of decreased concern over the harms of pharmacotherapy in adolescents when patients are adequately monitored.” In addition, more studies have been published that support the 2009 guidelines, “so that is one important change,” Dr. Krist said.
Recommendations for the new guidelines were based on a literature review conducted for the USPSTF by researchers led by Valerie Forman-Hoffman, Ph.D., of RTI International in Research Triangle Park, N.C. , and published online Feb. 8 (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M15-2259). Supported by a grant from the Agency for Healthcare Research and Quality, the review involved a search for trials and systematic reviews of treatment, test-retest studies of screening, and trials and large cohort studies for harms that appeared in the medical literature between May 2007 and February 2015. No trials were found that directly assessed the benefits or harms of screening children or adolescents for MDD in primary care settings.
Here are the key recommendations:
• Screen for MDD in adolescents aged 12-18 years. Screening “should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up.” This is a “B” recommendation in the USPSTF grading system, which means that “there is high certainty that the net benefit is moderate or there is moderate certainty the net benefit is moderate to substantial.”
As stated in the recommendations, the phrase “adequate systems in place” refers to “having systems and clinical staff to ensure that patients are screened and, if they screen positive, are appropriately diagnosed and treated with evidence-based care or referred to a setting that can provide the necessary care.” This emphasis was made because “we now recognize that our health systems have evolved, and that it’s more the standard of care to have systems in place to care for adolescents who are depressed,” Dr. Krist explained. “The rewording stresses the importance of being able to make sure that care is given to adolescents after they’re diagnosed.”
The Affordable Care Act provides coverage for A and B recommendations of the USPSTF, so screening for MDD in adolescents would be a recommended service. “Often this type of a service would be delivered during a wellness exam,” Dr. Krist said. “That’s a commonly covered benefit right now with the ACA.”
• Current evidence “is insufficient to assess the balance of benefits and harms of screening for MDD in children aged 11 years or younger.” This is an “I” statement, which means that “evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined.”
The new USPSTF guidelines do no not recommend a specific instrument or screening strategy, but the review commissioned for the task force found that the Patient Health Questionnaire for Adolescents and Beck Depression Inventory outperformed other tools in adolescents.
In the opinion of Dr. Krist, a key challenge for primary care clinicians seeking to implement the recommendations is to establish a way to routinely ask adolescents about depression, “being able to systematize that so it’s done routinely and that it’s done well.” A second challenge is to establish a way to ensure proper diagnosis, proper treatment, and follow-up of adolescents who screen positive for MDD. “A lot of primary care practices may choose to do a lot of those activities themselves, or they might work out collaborations with other mental health providers and have a referral mechanism and a follow-up mechanism,” he said.
In an editorial that appeared online in the Annals of Internal Medicine, Dr. John W. Williams Jr. of the Durham (N.C.) Veterans Affairs Medical Center and Dr. Gary Maslow of Duke University, also in Durham, advised generalist physicians to “seize the day and act to implement these guidelines” (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M16-0104). “Implementing high-quality depression care is not easy, but trials and demonstration projects show that it is possible and rewarding.”
Dr. Williams and Dr. Maslow went on to suggest ways that clinicians might incorporate the guidelines into their own practices. “For practices initiating screening for the first time, a pragmatic strategy might be to screen in conjunction with routine health visits and target persons with symptoms associated with depression (for example, insomnia) or risk factors, which in adolescents include female sex, older age, family history of depression, other mental health or behavioral problems, chronic medical illness, and overweight or obesity,” they wrote. “For practices with electronic health records, clinical reminders can be used to prompt staff to distribute screening questionnaires or verbally administer questions along with assessment of vital signs. The Guidelines for Adolescent Depression in Primary Care toolkit includes screening measures, screening procedures, and patient education materials to support the screening and treatment.”
The way Dr. Krist sees it, the overall message of the new recommendations is simple: Screening adolescents for depression has benefits. “We want primary care clinicians to do this, and we want to make sure that primary care practices put systems in place to care for adolescents with identified needs,” he said.
The Agency for Healthcare Research and Quality funded the review that formed the basis of the recommendations. The authors of the recommendation statement reported having no relevant financial disclosures.
Children aged 12-18 years should be screened for major depressive disorder, but current evidence is insufficient to advise screening children aged 11 years or younger for the condition.
Those are among the key guidelines in updated recommendations from the U.S. Preventive Services Task Force on screening for depression in children and adolescents that were published online Feb. 8 in Pediatrics and in the Annals of Internal Medicine.
“Adolescents who are depressed suffer a lot of adverse consequences from their depression,” task force member Dr. Alexander H. Krist of the department of family medicine and population health at Virginia Commonwealth University, Richmond, said in an interview. “It can affect school, their family life, and their quality of life. Being able to identify adolescents who are depressed [and] making sure that they get the care that they need can have a big benefit for adolescents and their families.”
Although little is known about the prevalence of major depressive disorder (MDD) in children, results from national surveys suggest that about 8% of adolescents have had major depression in the past year, according to the task force members, who were chaired by Dr. Albert L. Siu, an internist and geriatrician in the department of geriatrics and palliative medicine at Mount Sinai School of Medicine, New York (Pediatrics. 2016 Feb 8. doi: 10.1542/peds.2015-4467).
The 2009 USPSTF guidelines recommended screening for MDD in adolescents “when systems for diagnosis, treatment, and follow-up are in place” and concluded that there was not enough evidence to make a recommendation regarding children aged 7-11 years. The updated recommendation reaffirms these positions but removes the mention of specific MDD therapies “in recognition of decreased concern over the harms of pharmacotherapy in adolescents when patients are adequately monitored.” In addition, more studies have been published that support the 2009 guidelines, “so that is one important change,” Dr. Krist said.
Recommendations for the new guidelines were based on a literature review conducted for the USPSTF by researchers led by Valerie Forman-Hoffman, Ph.D., of RTI International in Research Triangle Park, N.C. , and published online Feb. 8 (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M15-2259). Supported by a grant from the Agency for Healthcare Research and Quality, the review involved a search for trials and systematic reviews of treatment, test-retest studies of screening, and trials and large cohort studies for harms that appeared in the medical literature between May 2007 and February 2015. No trials were found that directly assessed the benefits or harms of screening children or adolescents for MDD in primary care settings.
Here are the key recommendations:
• Screen for MDD in adolescents aged 12-18 years. Screening “should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up.” This is a “B” recommendation in the USPSTF grading system, which means that “there is high certainty that the net benefit is moderate or there is moderate certainty the net benefit is moderate to substantial.”
As stated in the recommendations, the phrase “adequate systems in place” refers to “having systems and clinical staff to ensure that patients are screened and, if they screen positive, are appropriately diagnosed and treated with evidence-based care or referred to a setting that can provide the necessary care.” This emphasis was made because “we now recognize that our health systems have evolved, and that it’s more the standard of care to have systems in place to care for adolescents who are depressed,” Dr. Krist explained. “The rewording stresses the importance of being able to make sure that care is given to adolescents after they’re diagnosed.”
The Affordable Care Act provides coverage for A and B recommendations of the USPSTF, so screening for MDD in adolescents would be a recommended service. “Often this type of a service would be delivered during a wellness exam,” Dr. Krist said. “That’s a commonly covered benefit right now with the ACA.”
• Current evidence “is insufficient to assess the balance of benefits and harms of screening for MDD in children aged 11 years or younger.” This is an “I” statement, which means that “evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined.”
The new USPSTF guidelines do no not recommend a specific instrument or screening strategy, but the review commissioned for the task force found that the Patient Health Questionnaire for Adolescents and Beck Depression Inventory outperformed other tools in adolescents.
In the opinion of Dr. Krist, a key challenge for primary care clinicians seeking to implement the recommendations is to establish a way to routinely ask adolescents about depression, “being able to systematize that so it’s done routinely and that it’s done well.” A second challenge is to establish a way to ensure proper diagnosis, proper treatment, and follow-up of adolescents who screen positive for MDD. “A lot of primary care practices may choose to do a lot of those activities themselves, or they might work out collaborations with other mental health providers and have a referral mechanism and a follow-up mechanism,” he said.
In an editorial that appeared online in the Annals of Internal Medicine, Dr. John W. Williams Jr. of the Durham (N.C.) Veterans Affairs Medical Center and Dr. Gary Maslow of Duke University, also in Durham, advised generalist physicians to “seize the day and act to implement these guidelines” (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M16-0104). “Implementing high-quality depression care is not easy, but trials and demonstration projects show that it is possible and rewarding.”
Dr. Williams and Dr. Maslow went on to suggest ways that clinicians might incorporate the guidelines into their own practices. “For practices initiating screening for the first time, a pragmatic strategy might be to screen in conjunction with routine health visits and target persons with symptoms associated with depression (for example, insomnia) or risk factors, which in adolescents include female sex, older age, family history of depression, other mental health or behavioral problems, chronic medical illness, and overweight or obesity,” they wrote. “For practices with electronic health records, clinical reminders can be used to prompt staff to distribute screening questionnaires or verbally administer questions along with assessment of vital signs. The Guidelines for Adolescent Depression in Primary Care toolkit includes screening measures, screening procedures, and patient education materials to support the screening and treatment.”
The way Dr. Krist sees it, the overall message of the new recommendations is simple: Screening adolescents for depression has benefits. “We want primary care clinicians to do this, and we want to make sure that primary care practices put systems in place to care for adolescents with identified needs,” he said.
The Agency for Healthcare Research and Quality funded the review that formed the basis of the recommendations. The authors of the recommendation statement reported having no relevant financial disclosures.
FROM PEDIATRICS AND ANNALS OF INTERNAL MEDICINE

USPSTF updates depression-screening guidelines for children, adolescents
Children aged 12-18 years should be screened for major depressive disorder, but current evidence is insufficient to advise screening children aged 11 years or younger for the condition.
Those are among the key guidelines in updated recommendations from the U.S. Preventive Services Task Force on screening for depression in children and adolescents that were published online Feb. 8 in Pediatrics and in the Annals of Internal Medicine.

“Adolescents who are depressed suffer a lot of adverse consequences from their depression,” task force member Dr. Alexander H. Krist of the department of family medicine and population health at Virginia Commonwealth University, Richmond, said in an interview. “It can affect school, their family life, and their quality of life. Being able to identify adolescents who are depressed [and] making sure that they get the care that they need can have a big benefit for adolescents and their families.”
Although little is known about the prevalence of major depressive disorder (MDD) in children, results from national surveys suggest that about 8% of adolescents have had major depression in the past year, according to the task force members, who were chaired by Dr. Albert L. Siu, an internist and geriatrician in the department of geriatrics and palliative medicine at Mount Sinai School of Medicine, New York (Pediatrics. 2016 Feb 8. doi: 10.1542/peds.2015-4467).
The 2009 USPSTF guidelines recommended screening for MDD in adolescents “when systems for diagnosis, treatment, and follow-up are in place” and concluded that there was not enough evidence to make a recommendation regarding children aged 7-11 years. The updated recommendation reaffirms these positions but removes the mention of specific MDD therapies “in recognition of decreased concern over the harms of pharmacotherapy in adolescents when patients are adequately monitored.” In addition, more studies have been published that support the 2009 guidelines, “so that is one important change,” Dr. Krist said.
Recommendations for the new guidelines were based on a literature review conducted for the USPSTF by researchers led by Valerie Forman-Hoffman, Ph.D., of RTI International in Research Triangle Park, N.C. , and published online Feb. 8 (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M15-2259). Supported by a grant from the Agency for Healthcare Research and Quality, the review involved a search for trials and systematic reviews of treatment, test-retest studies of screening, and trials and large cohort studies for harms that appeared in the medical literature between May 2007 and February 2015. No trials were found that directly assessed the benefits or harms of screening children or adolescents for MDD in primary care settings.
Here are the key recommendations:
• Screen for MDD in adolescents aged 12-18 years. Screening “should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up.” This is a “B” recommendation in the USPSTF grading system, which means that “there is high certainty that the net benefit is moderate or there is moderate certainty the net benefit is moderate to substantial.”
As stated in the recommendations, the phrase “adequate systems in place” refers to “having systems and clinical staff to ensure that patients are screened and, if they screen positive, are appropriately diagnosed and treated with evidence-based care or referred to a setting that can provide the necessary care.” This emphasis was made because “we now recognize that our health systems have evolved, and that it’s more the standard of care to have systems in place to care for adolescents who are depressed,” Dr. Krist explained. “The rewording stresses the importance of being able to make sure that care is given to adolescents after they’re diagnosed.”
The Affordable Care Act provides coverage for A and B recommendations of the USPSTF, so screening for MDD in adolescents would be a recommended service. “Often this type of a service would be delivered during a wellness exam,” Dr. Krist said. “That’s a commonly covered benefit right now with the ACA.”
• Current evidence “is insufficient to assess the balance of benefits and harms of screening for MDD in children aged 11 years or younger.” This is an “I” statement, which means that “evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined.”
The new USPSTF guidelines do no not recommend a specific instrument or screening strategy, but the review commissioned for the task force found that the Patient Health Questionnaire for Adolescents and Beck Depression Inventory outperformed other tools in adolescents.
In the opinion of Dr. Krist, a key challenge for primary care clinicians seeking to implement the recommendations is to establish a way to routinely ask adolescents about depression, “being able to systematize that so it’s done routinely and that it’s done well.” A second challenge is to establish a way to ensure proper diagnosis, proper treatment, and follow-up of adolescents who screen positive for MDD. “A lot of primary care practices may choose to do a lot of those activities themselves, or they might work out collaborations with other mental health providers and have a referral mechanism and a follow-up mechanism,” he said.
In an editorial that appeared online in the Annals of Internal Medicine, Dr. John W. Williams Jr. of the Durham (N.C.) Veterans Affairs Medical Center and Dr. Gary Maslow of Duke University, also in Durham, advised generalist physicians to “seize the day and act to implement these guidelines” (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M16-0104). “Implementing high-quality depression care is not easy, but trials and demonstration projects show that it is possible and rewarding.”
Dr. Williams and Dr. Maslow went on to suggest ways that clinicians might incorporate the guidelines into their own practices. “For practices initiating screening for the first time, a pragmatic strategy might be to screen in conjunction with routine health visits and target persons with symptoms associated with depression (for example, insomnia) or risk factors, which in adolescents include female sex, older age, family history of depression, other mental health or behavioral problems, chronic medical illness, and overweight or obesity,” they wrote. “For practices with electronic health records, clinical reminders can be used to prompt staff to distribute screening questionnaires or verbally administer questions along with assessment of vital signs. The Guidelines for Adolescent Depression in Primary Care toolkit includes screening measures, screening procedures, and patient education materials to support the screening and treatment.”
The way Dr. Krist sees it, the overall message of the new recommendations is simple: Screening adolescents for depression has benefits. “We want primary care clinicians to do this, and we want to make sure that primary care practices put systems in place to care for adolescents with identified needs,” he said.
The Agency for Healthcare Research and Quality funded the review that formed the basis of the recommendations. The authors of the recommendation statement reported having no relevant financial disclosures.
On Twitter @dougbrunk
Children aged 12-18 years should be screened for major depressive disorder, but current evidence is insufficient to advise screening children aged 11 years or younger for the condition.
Those are among the key guidelines in updated recommendations from the U.S. Preventive Services Task Force on screening for depression in children and adolescents that were published online Feb. 8 in Pediatrics and in the Annals of Internal Medicine.
“Adolescents who are depressed suffer a lot of adverse consequences from their depression,” task force member Dr. Alexander H. Krist of the department of family medicine and population health at Virginia Commonwealth University, Richmond, said in an interview. “It can affect school, their family life, and their quality of life. Being able to identify adolescents who are depressed [and] making sure that they get the care that they need can have a big benefit for adolescents and their families.”
Although little is known about the prevalence of major depressive disorder (MDD) in children, results from national surveys suggest that about 8% of adolescents have had major depression in the past year, according to the task force members, who were chaired by Dr. Albert L. Siu, an internist and geriatrician in the department of geriatrics and palliative medicine at Mount Sinai School of Medicine, New York (Pediatrics. 2016 Feb 8. doi: 10.1542/peds.2015-4467).
The 2009 USPSTF guidelines recommended screening for MDD in adolescents “when systems for diagnosis, treatment, and follow-up are in place” and concluded that there was not enough evidence to make a recommendation regarding children aged 7-11 years. The updated recommendation reaffirms these positions but removes the mention of specific MDD therapies “in recognition of decreased concern over the harms of pharmacotherapy in adolescents when patients are adequately monitored.” In addition, more studies have been published that support the 2009 guidelines, “so that is one important change,” Dr. Krist said.
Recommendations for the new guidelines were based on a literature review conducted for the USPSTF by researchers led by Valerie Forman-Hoffman, Ph.D., of RTI International in Research Triangle Park, N.C. , and published online Feb. 8 (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M15-2259). Supported by a grant from the Agency for Healthcare Research and Quality, the review involved a search for trials and systematic reviews of treatment, test-retest studies of screening, and trials and large cohort studies for harms that appeared in the medical literature between May 2007 and February 2015. No trials were found that directly assessed the benefits or harms of screening children or adolescents for MDD in primary care settings.
Here are the key recommendations:
• Screen for MDD in adolescents aged 12-18 years. Screening “should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up.” This is a “B” recommendation in the USPSTF grading system, which means that “there is high certainty that the net benefit is moderate or there is moderate certainty the net benefit is moderate to substantial.”
As stated in the recommendations, the phrase “adequate systems in place” refers to “having systems and clinical staff to ensure that patients are screened and, if they screen positive, are appropriately diagnosed and treated with evidence-based care or referred to a setting that can provide the necessary care.” This emphasis was made because “we now recognize that our health systems have evolved, and that it’s more the standard of care to have systems in place to care for adolescents who are depressed,” Dr. Krist explained. “The rewording stresses the importance of being able to make sure that care is given to adolescents after they’re diagnosed.”
The Affordable Care Act provides coverage for A and B recommendations of the USPSTF, so screening for MDD in adolescents would be a recommended service. “Often this type of a service would be delivered during a wellness exam,” Dr. Krist said. “That’s a commonly covered benefit right now with the ACA.”
• Current evidence “is insufficient to assess the balance of benefits and harms of screening for MDD in children aged 11 years or younger.” This is an “I” statement, which means that “evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined.”
The new USPSTF guidelines do no not recommend a specific instrument or screening strategy, but the review commissioned for the task force found that the Patient Health Questionnaire for Adolescents and Beck Depression Inventory outperformed other tools in adolescents.
In the opinion of Dr. Krist, a key challenge for primary care clinicians seeking to implement the recommendations is to establish a way to routinely ask adolescents about depression, “being able to systematize that so it’s done routinely and that it’s done well.” A second challenge is to establish a way to ensure proper diagnosis, proper treatment, and follow-up of adolescents who screen positive for MDD. “A lot of primary care practices may choose to do a lot of those activities themselves, or they might work out collaborations with other mental health providers and have a referral mechanism and a follow-up mechanism,” he said.
In an editorial that appeared online in the Annals of Internal Medicine, Dr. John W. Williams Jr. of the Durham (N.C.) Veterans Affairs Medical Center and Dr. Gary Maslow of Duke University, also in Durham, advised generalist physicians to “seize the day and act to implement these guidelines” (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M16-0104). “Implementing high-quality depression care is not easy, but trials and demonstration projects show that it is possible and rewarding.”
Dr. Williams and Dr. Maslow went on to suggest ways that clinicians might incorporate the guidelines into their own practices. “For practices initiating screening for the first time, a pragmatic strategy might be to screen in conjunction with routine health visits and target persons with symptoms associated with depression (for example, insomnia) or risk factors, which in adolescents include female sex, older age, family history of depression, other mental health or behavioral problems, chronic medical illness, and overweight or obesity,” they wrote. “For practices with electronic health records, clinical reminders can be used to prompt staff to distribute screening questionnaires or verbally administer questions along with assessment of vital signs. The Guidelines for Adolescent Depression in Primary Care toolkit includes screening measures, screening procedures, and patient education materials to support the screening and treatment.”
The way Dr. Krist sees it, the overall message of the new recommendations is simple: Screening adolescents for depression has benefits. “We want primary care clinicians to do this, and we want to make sure that primary care practices put systems in place to care for adolescents with identified needs,” he said.
The Agency for Healthcare Research and Quality funded the review that formed the basis of the recommendations. The authors of the recommendation statement reported having no relevant financial disclosures.
On Twitter @dougbrunk
Children aged 12-18 years should be screened for major depressive disorder, but current evidence is insufficient to advise screening children aged 11 years or younger for the condition.
Those are among the key guidelines in updated recommendations from the U.S. Preventive Services Task Force on screening for depression in children and adolescents that were published online Feb. 8 in Pediatrics and in the Annals of Internal Medicine.
“Adolescents who are depressed suffer a lot of adverse consequences from their depression,” task force member Dr. Alexander H. Krist of the department of family medicine and population health at Virginia Commonwealth University, Richmond, said in an interview. “It can affect school, their family life, and their quality of life. Being able to identify adolescents who are depressed [and] making sure that they get the care that they need can have a big benefit for adolescents and their families.”
Although little is known about the prevalence of major depressive disorder (MDD) in children, results from national surveys suggest that about 8% of adolescents have had major depression in the past year, according to the task force members, who were chaired by Dr. Albert L. Siu, an internist and geriatrician in the department of geriatrics and palliative medicine at Mount Sinai School of Medicine, New York (Pediatrics. 2016 Feb 8. doi: 10.1542/peds.2015-4467).
The 2009 USPSTF guidelines recommended screening for MDD in adolescents “when systems for diagnosis, treatment, and follow-up are in place” and concluded that there was not enough evidence to make a recommendation regarding children aged 7-11 years. The updated recommendation reaffirms these positions but removes the mention of specific MDD therapies “in recognition of decreased concern over the harms of pharmacotherapy in adolescents when patients are adequately monitored.” In addition, more studies have been published that support the 2009 guidelines, “so that is one important change,” Dr. Krist said.
Recommendations for the new guidelines were based on a literature review conducted for the USPSTF by researchers led by Valerie Forman-Hoffman, Ph.D., of RTI International in Research Triangle Park, N.C. , and published online Feb. 8 (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M15-2259). Supported by a grant from the Agency for Healthcare Research and Quality, the review involved a search for trials and systematic reviews of treatment, test-retest studies of screening, and trials and large cohort studies for harms that appeared in the medical literature between May 2007 and February 2015. No trials were found that directly assessed the benefits or harms of screening children or adolescents for MDD in primary care settings.
Here are the key recommendations:
• Screen for MDD in adolescents aged 12-18 years. Screening “should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up.” This is a “B” recommendation in the USPSTF grading system, which means that “there is high certainty that the net benefit is moderate or there is moderate certainty the net benefit is moderate to substantial.”
As stated in the recommendations, the phrase “adequate systems in place” refers to “having systems and clinical staff to ensure that patients are screened and, if they screen positive, are appropriately diagnosed and treated with evidence-based care or referred to a setting that can provide the necessary care.” This emphasis was made because “we now recognize that our health systems have evolved, and that it’s more the standard of care to have systems in place to care for adolescents who are depressed,” Dr. Krist explained. “The rewording stresses the importance of being able to make sure that care is given to adolescents after they’re diagnosed.”
The Affordable Care Act provides coverage for A and B recommendations of the USPSTF, so screening for MDD in adolescents would be a recommended service. “Often this type of a service would be delivered during a wellness exam,” Dr. Krist said. “That’s a commonly covered benefit right now with the ACA.”
• Current evidence “is insufficient to assess the balance of benefits and harms of screening for MDD in children aged 11 years or younger.” This is an “I” statement, which means that “evidence is lacking, of poor quality, or conflicting, and the balance of benefits and harms cannot be determined.”
The new USPSTF guidelines do no not recommend a specific instrument or screening strategy, but the review commissioned for the task force found that the Patient Health Questionnaire for Adolescents and Beck Depression Inventory outperformed other tools in adolescents.
In the opinion of Dr. Krist, a key challenge for primary care clinicians seeking to implement the recommendations is to establish a way to routinely ask adolescents about depression, “being able to systematize that so it’s done routinely and that it’s done well.” A second challenge is to establish a way to ensure proper diagnosis, proper treatment, and follow-up of adolescents who screen positive for MDD. “A lot of primary care practices may choose to do a lot of those activities themselves, or they might work out collaborations with other mental health providers and have a referral mechanism and a follow-up mechanism,” he said.
In an editorial that appeared online in the Annals of Internal Medicine, Dr. John W. Williams Jr. of the Durham (N.C.) Veterans Affairs Medical Center and Dr. Gary Maslow of Duke University, also in Durham, advised generalist physicians to “seize the day and act to implement these guidelines” (Ann Intern Med. 2016 Feb 8. doi: 10.7326/M16-0104). “Implementing high-quality depression care is not easy, but trials and demonstration projects show that it is possible and rewarding.”
Dr. Williams and Dr. Maslow went on to suggest ways that clinicians might incorporate the guidelines into their own practices. “For practices initiating screening for the first time, a pragmatic strategy might be to screen in conjunction with routine health visits and target persons with symptoms associated with depression (for example, insomnia) or risk factors, which in adolescents include female sex, older age, family history of depression, other mental health or behavioral problems, chronic medical illness, and overweight or obesity,” they wrote. “For practices with electronic health records, clinical reminders can be used to prompt staff to distribute screening questionnaires or verbally administer questions along with assessment of vital signs. The Guidelines for Adolescent Depression in Primary Care toolkit includes screening measures, screening procedures, and patient education materials to support the screening and treatment.”
The way Dr. Krist sees it, the overall message of the new recommendations is simple: Screening adolescents for depression has benefits. “We want primary care clinicians to do this, and we want to make sure that primary care practices put systems in place to care for adolescents with identified needs,” he said.
The Agency for Healthcare Research and Quality funded the review that formed the basis of the recommendations. The authors of the recommendation statement reported having no relevant financial disclosures.
On Twitter @dougbrunk
FROM PEDIATRICS AND ANNALS OF INTERNAL MEDICINE
Key clinical point: Adolescents should be routinely screened for major depressive disorder.
Major finding: Screening for major depressive disorder in adolescents should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up, but such evidence is lacking to recommend screening in children.
Data source: An update of 2009 recommendations from the U.S. Preventive Services Task Force on screening for depression in children and adolescents, based on a review of current evidence.
Disclosures: The Agency for Healthcare Research and Quality funded the review that formed the basis of the recommendations. The authors of the recommendation statement reported having no relevant financial disclosures.

More children getting vaccinated since Vaccines for Children inception
Vaccination rates have been improving since the introduction of the federal Vaccines for Children program, new research in Health Affairs showed.
Since the start of the VFC program in 1995, racial and ethnic disparities also have narrowed, as have income-related disparities – although at different rates, based on analysis of data from the National Immunization Survey.

“These gains may well be attributed to the impact of the program in reducing financial barriers to access,” Brendan Walsh, Ph.D., research fellow at City University London, and his colleagues wrote, although they are calling for a deeper investigation because the pattern of uptake “varied within groups differentiated by race and ethnicity over time.” The data analysis appears in the February 2016 issue of Health Affairs (2016;35[2]:356-64. doi: 10.1377/hlthaff.2015.1019).
For example, vaccination rates for polio among white children aged 19-35 months grew from 91% in the 1995-1997 survey period to 93% in 2011-2013. For black children, the rate grew from 87% to 92%, and for Hispanics, the rate improved from 87% to 92%.
“The largest increase in overall vaccination rates over time was observed among low-income Hispanic children,” the researchers noted. “While these children consistently had the lowest vaccination rates of all groups at the beginning of the VFC program, this was not the case in the later periods.”
The data, however, also revealed a need for more nuanced research into racial, ethnic, and income disparities.
“As the VFC program developed, disparities between blacks and Hispanics relative to whites decreased,” Dr. Walsh and his associates said. “However, among blacks, income-related disparities increased, while those among Hispanics decreased.”
The report’s authors also observed that reductions in disparities did not occur evenly over time, which demonstrates a need to understand how factors other than financial barriers, such as disease outbreaks and increased public awareness, are influencing vaccination rates, which in turn will provide “a fuller understanding of the contribution of the VFC program to the increase in uptake and reductions in disparities.”
“One potential future avenue of research may be to study the perceived benefit of some vaccines, the perceived severity of illness that vaccines prevent, and to what extent these perceptions influence the decisions of parents and vaccination providers (that is, physicians) to request or suggest vaccination,” the researchers said.
Coauthor Ciaran O’Neill was supported by a Health Research Board (Ireland) Research Leaders Award 2013.
Vaccination rates have been improving since the introduction of the federal Vaccines for Children program, new research in Health Affairs showed.
Since the start of the VFC program in 1995, racial and ethnic disparities also have narrowed, as have income-related disparities – although at different rates, based on analysis of data from the National Immunization Survey.
“These gains may well be attributed to the impact of the program in reducing financial barriers to access,” Brendan Walsh, Ph.D., research fellow at City University London, and his colleagues wrote, although they are calling for a deeper investigation because the pattern of uptake “varied within groups differentiated by race and ethnicity over time.” The data analysis appears in the February 2016 issue of Health Affairs (2016;35[2]:356-64. doi: 10.1377/hlthaff.2015.1019).
For example, vaccination rates for polio among white children aged 19-35 months grew from 91% in the 1995-1997 survey period to 93% in 2011-2013. For black children, the rate grew from 87% to 92%, and for Hispanics, the rate improved from 87% to 92%.
“The largest increase in overall vaccination rates over time was observed among low-income Hispanic children,” the researchers noted. “While these children consistently had the lowest vaccination rates of all groups at the beginning of the VFC program, this was not the case in the later periods.”
The data, however, also revealed a need for more nuanced research into racial, ethnic, and income disparities.
“As the VFC program developed, disparities between blacks and Hispanics relative to whites decreased,” Dr. Walsh and his associates said. “However, among blacks, income-related disparities increased, while those among Hispanics decreased.”
The report’s authors also observed that reductions in disparities did not occur evenly over time, which demonstrates a need to understand how factors other than financial barriers, such as disease outbreaks and increased public awareness, are influencing vaccination rates, which in turn will provide “a fuller understanding of the contribution of the VFC program to the increase in uptake and reductions in disparities.”
“One potential future avenue of research may be to study the perceived benefit of some vaccines, the perceived severity of illness that vaccines prevent, and to what extent these perceptions influence the decisions of parents and vaccination providers (that is, physicians) to request or suggest vaccination,” the researchers said.
Coauthor Ciaran O’Neill was supported by a Health Research Board (Ireland) Research Leaders Award 2013.
Vaccination rates have been improving since the introduction of the federal Vaccines for Children program, new research in Health Affairs showed.
Since the start of the VFC program in 1995, racial and ethnic disparities also have narrowed, as have income-related disparities – although at different rates, based on analysis of data from the National Immunization Survey.
“These gains may well be attributed to the impact of the program in reducing financial barriers to access,” Brendan Walsh, Ph.D., research fellow at City University London, and his colleagues wrote, although they are calling for a deeper investigation because the pattern of uptake “varied within groups differentiated by race and ethnicity over time.” The data analysis appears in the February 2016 issue of Health Affairs (2016;35[2]:356-64. doi: 10.1377/hlthaff.2015.1019).
For example, vaccination rates for polio among white children aged 19-35 months grew from 91% in the 1995-1997 survey period to 93% in 2011-2013. For black children, the rate grew from 87% to 92%, and for Hispanics, the rate improved from 87% to 92%.
“The largest increase in overall vaccination rates over time was observed among low-income Hispanic children,” the researchers noted. “While these children consistently had the lowest vaccination rates of all groups at the beginning of the VFC program, this was not the case in the later periods.”
The data, however, also revealed a need for more nuanced research into racial, ethnic, and income disparities.
“As the VFC program developed, disparities between blacks and Hispanics relative to whites decreased,” Dr. Walsh and his associates said. “However, among blacks, income-related disparities increased, while those among Hispanics decreased.”
The report’s authors also observed that reductions in disparities did not occur evenly over time, which demonstrates a need to understand how factors other than financial barriers, such as disease outbreaks and increased public awareness, are influencing vaccination rates, which in turn will provide “a fuller understanding of the contribution of the VFC program to the increase in uptake and reductions in disparities.”
“One potential future avenue of research may be to study the perceived benefit of some vaccines, the perceived severity of illness that vaccines prevent, and to what extent these perceptions influence the decisions of parents and vaccination providers (that is, physicians) to request or suggest vaccination,” the researchers said.
Coauthor Ciaran O’Neill was supported by a Health Research Board (Ireland) Research Leaders Award 2013.
FROM HEALTH AFFAIRS
