User login
Better billing privacy protections needed for youth
Better protections of confidential health information of adolescents and young adults in billing and insurance statements are needed, according to a position paper endorsed by the American Academy of Pediatrics, Society for Adolescent Health and Medicine, and the American College of Obstetricians and Gynecologists.
The three societies are calling for policies and procedures to be established “to ensure that health care billing and insurance claims processes such as explanation of benefit (EOB) notifications do not impede the confidential provision of health care services to adolescents” (J Adolesc Health. 2016 Mar. doi: 10.1016/j.jadohealth.2015.12.009).

To reach that objective, the position paper is calling for the Department of Health & Human Services to issue guidance to clarify “endanger” and “endangerment” in the special confidentiality provisions of HIPAA to make it clear that they include “harms that result when access to important sensitive services, such as contraception and STI services, is impeded by fear of loss of confidentiality.”
AAP, ACOG, and SAHM also endorse the idea that sending EOBs and similar notices “should not be required when individuals insured as dependents obtain sensitive services.”
Dr. Lee Savio Beers, medical director for municipal and regional affairs, Child Health Advocacy Institute at Children’s National Medical Center in Washington, said the policy paper is “a nice summary of what has been best practices for a while and what we really should establish more clearly as best practice.”
She recalled experiences in practice where adolescents told her they did not come for treatment because of concerns that “information would show up on the billing statement to their parents, and they would know that they were seeking care for these issues and then surmise that they were sexually active.”
Dr. Beers added that the position paper could go further in establishing requirements for both parents and caregivers on the importance of confidentiality.
“I think that it is sometimes hard for parents to think about there might be something that my child is going to go to the doctor for that I am not going to know about,” she said in an interview.
“When we see patients for visits, when they get close to their teenage years, we start interviewing them, giving them an opportunity to talk without their parent in the room,” she continued. “Some families are surprised by it. Some are glad that you are asking them to step out. Others want to talk about it for a few minutes, but I think there is an important parent and caregiver education component to this as well, particularly when you start talking about things like insurance benefits, which I think parents typically think of as being really fully within their purview.”
Better protections of confidential health information of adolescents and young adults in billing and insurance statements are needed, according to a position paper endorsed by the American Academy of Pediatrics, Society for Adolescent Health and Medicine, and the American College of Obstetricians and Gynecologists.
The three societies are calling for policies and procedures to be established “to ensure that health care billing and insurance claims processes such as explanation of benefit (EOB) notifications do not impede the confidential provision of health care services to adolescents” (J Adolesc Health. 2016 Mar. doi: 10.1016/j.jadohealth.2015.12.009).
To reach that objective, the position paper is calling for the Department of Health & Human Services to issue guidance to clarify “endanger” and “endangerment” in the special confidentiality provisions of HIPAA to make it clear that they include “harms that result when access to important sensitive services, such as contraception and STI services, is impeded by fear of loss of confidentiality.”
AAP, ACOG, and SAHM also endorse the idea that sending EOBs and similar notices “should not be required when individuals insured as dependents obtain sensitive services.”
Dr. Lee Savio Beers, medical director for municipal and regional affairs, Child Health Advocacy Institute at Children’s National Medical Center in Washington, said the policy paper is “a nice summary of what has been best practices for a while and what we really should establish more clearly as best practice.”
She recalled experiences in practice where adolescents told her they did not come for treatment because of concerns that “information would show up on the billing statement to their parents, and they would know that they were seeking care for these issues and then surmise that they were sexually active.”
Dr. Beers added that the position paper could go further in establishing requirements for both parents and caregivers on the importance of confidentiality.
“I think that it is sometimes hard for parents to think about there might be something that my child is going to go to the doctor for that I am not going to know about,” she said in an interview.
“When we see patients for visits, when they get close to their teenage years, we start interviewing them, giving them an opportunity to talk without their parent in the room,” she continued. “Some families are surprised by it. Some are glad that you are asking them to step out. Others want to talk about it for a few minutes, but I think there is an important parent and caregiver education component to this as well, particularly when you start talking about things like insurance benefits, which I think parents typically think of as being really fully within their purview.”
Better protections of confidential health information of adolescents and young adults in billing and insurance statements are needed, according to a position paper endorsed by the American Academy of Pediatrics, Society for Adolescent Health and Medicine, and the American College of Obstetricians and Gynecologists.
The three societies are calling for policies and procedures to be established “to ensure that health care billing and insurance claims processes such as explanation of benefit (EOB) notifications do not impede the confidential provision of health care services to adolescents” (J Adolesc Health. 2016 Mar. doi: 10.1016/j.jadohealth.2015.12.009).
To reach that objective, the position paper is calling for the Department of Health & Human Services to issue guidance to clarify “endanger” and “endangerment” in the special confidentiality provisions of HIPAA to make it clear that they include “harms that result when access to important sensitive services, such as contraception and STI services, is impeded by fear of loss of confidentiality.”
AAP, ACOG, and SAHM also endorse the idea that sending EOBs and similar notices “should not be required when individuals insured as dependents obtain sensitive services.”
Dr. Lee Savio Beers, medical director for municipal and regional affairs, Child Health Advocacy Institute at Children’s National Medical Center in Washington, said the policy paper is “a nice summary of what has been best practices for a while and what we really should establish more clearly as best practice.”
She recalled experiences in practice where adolescents told her they did not come for treatment because of concerns that “information would show up on the billing statement to their parents, and they would know that they were seeking care for these issues and then surmise that they were sexually active.”
Dr. Beers added that the position paper could go further in establishing requirements for both parents and caregivers on the importance of confidentiality.
“I think that it is sometimes hard for parents to think about there might be something that my child is going to go to the doctor for that I am not going to know about,” she said in an interview.
“When we see patients for visits, when they get close to their teenage years, we start interviewing them, giving them an opportunity to talk without their parent in the room,” she continued. “Some families are surprised by it. Some are glad that you are asking them to step out. Others want to talk about it for a few minutes, but I think there is an important parent and caregiver education component to this as well, particularly when you start talking about things like insurance benefits, which I think parents typically think of as being really fully within their purview.”
FROM JOURNAL OF ADOLESCENT HEALTH

No Evidence Supports Hydrolyzed Formula Over Cows’ Milk for Allergy Prevention
Findings on the use of hydrolyzed formula in place of standard cows’ milk formula to prevent allergy in high-risk infants do not support current guidelines, according to Dr. Robert J Boyle of Imperial College London and his associates.
A review and meta-analysis were performed on 28 randomized control trials, 6 quasirandomized trials, and 3 controlled clinical trials describing allergic or autoimmune outcomes, with more than 19,000 participants. Among 13 studies reporting on the risk of food allergy, no significant difference was found in the risk of any food allergy with partially hydrolyzed formula (risk ratio, 1.73; 95% confidence interval, 0.79-3.80) and extensively hydrolyzed formula (RR, 0.86; CI, 0.26-2.82), compared with standard formula at age 0-4 years, and for extensively hydrolyzed formula at age 5-14 years.

The review also examined and found no significant evidence favoring the use of hydrolyzed formula in place of standard cows’ milk formula to avert the risk of eczema, wheeze, allergic rhinitis, or type 1 diabetes mellitus.
The researchers suggest that guidelines be updated and revised to reflect these new findings.
“We found no consistent evidence to support the current recommendations and found evidence of publication bias, methodological biases, and conflict of interest in those studies reporting allergic outcomes,” Dr. Boyle and his associates concluded. “We suggest that any future trials on hydrolyzed formula should be prospectively registered, independently funded, and include adequate oversight to ensure that they do not negatively impact on breastfeeding in study participants”.
Read the full study at the British Medical Journal (doi: 10.1136/bmj.i974)
Findings on the use of hydrolyzed formula in place of standard cows’ milk formula to prevent allergy in high-risk infants do not support current guidelines, according to Dr. Robert J Boyle of Imperial College London and his associates.
A review and meta-analysis were performed on 28 randomized control trials, 6 quasirandomized trials, and 3 controlled clinical trials describing allergic or autoimmune outcomes, with more than 19,000 participants. Among 13 studies reporting on the risk of food allergy, no significant difference was found in the risk of any food allergy with partially hydrolyzed formula (risk ratio, 1.73; 95% confidence interval, 0.79-3.80) and extensively hydrolyzed formula (RR, 0.86; CI, 0.26-2.82), compared with standard formula at age 0-4 years, and for extensively hydrolyzed formula at age 5-14 years.
The review also examined and found no significant evidence favoring the use of hydrolyzed formula in place of standard cows’ milk formula to avert the risk of eczema, wheeze, allergic rhinitis, or type 1 diabetes mellitus.
The researchers suggest that guidelines be updated and revised to reflect these new findings.
“We found no consistent evidence to support the current recommendations and found evidence of publication bias, methodological biases, and conflict of interest in those studies reporting allergic outcomes,” Dr. Boyle and his associates concluded. “We suggest that any future trials on hydrolyzed formula should be prospectively registered, independently funded, and include adequate oversight to ensure that they do not negatively impact on breastfeeding in study participants”.
Read the full study at the British Medical Journal (doi: 10.1136/bmj.i974)
Findings on the use of hydrolyzed formula in place of standard cows’ milk formula to prevent allergy in high-risk infants do not support current guidelines, according to Dr. Robert J Boyle of Imperial College London and his associates.
A review and meta-analysis were performed on 28 randomized control trials, 6 quasirandomized trials, and 3 controlled clinical trials describing allergic or autoimmune outcomes, with more than 19,000 participants. Among 13 studies reporting on the risk of food allergy, no significant difference was found in the risk of any food allergy with partially hydrolyzed formula (risk ratio, 1.73; 95% confidence interval, 0.79-3.80) and extensively hydrolyzed formula (RR, 0.86; CI, 0.26-2.82), compared with standard formula at age 0-4 years, and for extensively hydrolyzed formula at age 5-14 years.
The review also examined and found no significant evidence favoring the use of hydrolyzed formula in place of standard cows’ milk formula to avert the risk of eczema, wheeze, allergic rhinitis, or type 1 diabetes mellitus.
The researchers suggest that guidelines be updated and revised to reflect these new findings.
“We found no consistent evidence to support the current recommendations and found evidence of publication bias, methodological biases, and conflict of interest in those studies reporting allergic outcomes,” Dr. Boyle and his associates concluded. “We suggest that any future trials on hydrolyzed formula should be prospectively registered, independently funded, and include adequate oversight to ensure that they do not negatively impact on breastfeeding in study participants”.
Read the full study at the British Medical Journal (doi: 10.1136/bmj.i974)
FROM BRITISH MEDICAL JOURNAL

No evidence supports hydrolyzed formula over cows’ milk for allergy prevention
Findings on the use of hydrolyzed formula in place of standard cows’ milk formula to prevent allergy in high-risk infants do not support current guidelines, according to Dr. Robert J Boyle of Imperial College London and his associates.
A review and meta-analysis were performed on 28 randomized control trials, 6 quasirandomized trials, and 3 controlled clinical trials describing allergic or autoimmune outcomes, with more than 19,000 participants. Among 13 studies reporting on the risk of food allergy, no significant difference was found in the risk of any food allergy with partially hydrolyzed formula (risk ratio, 1.73; 95% confidence interval, 0.79-3.80) and extensively hydrolyzed formula (RR, 0.86; CI, 0.26-2.82), compared with standard formula at age 0-4 years, and for extensively hydrolyzed formula at age 5-14 years.

The review also examined and found no significant evidence favoring the use of hydrolyzed formula in place of standard cows’ milk formula to avert the risk of eczema, wheeze, allergic rhinitis, or type 1 diabetes mellitus.
The researchers suggest that guidelines be updated and revised to reflect these new findings.
“We found no consistent evidence to support the current recommendations and found evidence of publication bias, methodological biases, and conflict of interest in those studies reporting allergic outcomes,” Dr. Boyle and his associates concluded. “We suggest that any future trials on hydrolyzed formula should be prospectively registered, independently funded, and include adequate oversight to ensure that they do not negatively impact on breastfeeding in study participants”.
Read the full study at the British Medical Journal (doi: 10.1136/bmj.i974)
Findings on the use of hydrolyzed formula in place of standard cows’ milk formula to prevent allergy in high-risk infants do not support current guidelines, according to Dr. Robert J Boyle of Imperial College London and his associates.
A review and meta-analysis were performed on 28 randomized control trials, 6 quasirandomized trials, and 3 controlled clinical trials describing allergic or autoimmune outcomes, with more than 19,000 participants. Among 13 studies reporting on the risk of food allergy, no significant difference was found in the risk of any food allergy with partially hydrolyzed formula (risk ratio, 1.73; 95% confidence interval, 0.79-3.80) and extensively hydrolyzed formula (RR, 0.86; CI, 0.26-2.82), compared with standard formula at age 0-4 years, and for extensively hydrolyzed formula at age 5-14 years.
The review also examined and found no significant evidence favoring the use of hydrolyzed formula in place of standard cows’ milk formula to avert the risk of eczema, wheeze, allergic rhinitis, or type 1 diabetes mellitus.
The researchers suggest that guidelines be updated and revised to reflect these new findings.
“We found no consistent evidence to support the current recommendations and found evidence of publication bias, methodological biases, and conflict of interest in those studies reporting allergic outcomes,” Dr. Boyle and his associates concluded. “We suggest that any future trials on hydrolyzed formula should be prospectively registered, independently funded, and include adequate oversight to ensure that they do not negatively impact on breastfeeding in study participants”.
Read the full study at the British Medical Journal (doi: 10.1136/bmj.i974)
Findings on the use of hydrolyzed formula in place of standard cows’ milk formula to prevent allergy in high-risk infants do not support current guidelines, according to Dr. Robert J Boyle of Imperial College London and his associates.
A review and meta-analysis were performed on 28 randomized control trials, 6 quasirandomized trials, and 3 controlled clinical trials describing allergic or autoimmune outcomes, with more than 19,000 participants. Among 13 studies reporting on the risk of food allergy, no significant difference was found in the risk of any food allergy with partially hydrolyzed formula (risk ratio, 1.73; 95% confidence interval, 0.79-3.80) and extensively hydrolyzed formula (RR, 0.86; CI, 0.26-2.82), compared with standard formula at age 0-4 years, and for extensively hydrolyzed formula at age 5-14 years.
The review also examined and found no significant evidence favoring the use of hydrolyzed formula in place of standard cows’ milk formula to avert the risk of eczema, wheeze, allergic rhinitis, or type 1 diabetes mellitus.
The researchers suggest that guidelines be updated and revised to reflect these new findings.
“We found no consistent evidence to support the current recommendations and found evidence of publication bias, methodological biases, and conflict of interest in those studies reporting allergic outcomes,” Dr. Boyle and his associates concluded. “We suggest that any future trials on hydrolyzed formula should be prospectively registered, independently funded, and include adequate oversight to ensure that they do not negatively impact on breastfeeding in study participants”.
Read the full study at the British Medical Journal (doi: 10.1136/bmj.i974)
FROM BRITISH MEDICAL JOURNAL

No extra benefit from infancy booster of MenACWY-TT
Receiving two doses of a combination tetanus and meningococcal vaccine in infancy did not result in additional protection among children 5 years later, a study found.
Researchers followed up on children receiving one or two doses of the quadrivalent meningococcal serogroups A, C, W, and Y tetanus toxoid conjugate vaccine (MenACWY-TT).
“Overall, 5 years after primary vaccination with MenACWY-TT, there was no clear evidence of benefit of receiving two versus one dose of vaccine in infancy,” reported Dr. Nicola P. Klein of the Kaiser Permanente Vaccine Study Center in Oakland, Calif., and her associates online (Pediatr Infect Dis J. 2016 Feb 26. doi: 10.1097/INF.0000000000001123).
In the initial phase II, open multicenter study, the researchers randomized 349 infants to receive either a single dose of MenACWY-TT at 12 months of age or a first dose of MenACWY-TT at 9 months of age followed by a booster dose at 12 months.
Using a per-protocol analysis, the researchers compared the titers of 186 children at 3 years’ follow-up and 135 children at 5 years’ follow-up. In the group that received one dose, 64%-75% of the children had titers of 8 or higher for MenC, MenW, and MenY 5 years later, compared with 75%-86% of the children who received two doses.
Also at 5 years, MenA titers were 8 or higher in 32% of children receiving one dose and 38% of children receiving two doses. Titers for all serotypes had waned by 5 years after vaccination, but only MenA was low enough that most children were seronegative by 1 year after vaccination. Overall average titers were higher in the group that had received two doses than in the group that had received one.
Dr. Klein’s team also evaluated the immune response and safety of a booster dose of MenACWY-TT to 38 children who had received one dose in infancy and 46 children who had received two doses in infancy, and a primary dose in 100 children of the same age who had never received a meningococcal vaccine. All children receiving the booster dose had antibody titers of 8 or higher against all serotypes 1 month after the dose. Among those receiving the vaccine for the first time, titers were 8 or higher at 1 month in 79% of children for MenA, 86% for MenC, 90% for MenW, and 94% for MenY.
No significant differences existed in terms of average titer levels, vaccine response, or titer levels of greater than or equal to 4 or greater than or equal to 8 between the children who received one dose and the children who received two doses in infancy. Children who received one or two vaccine doses in infancy had higher average titers and more vaccine responses to all serogroups than the children receiving a dose at age 5 years for the first time.
The most common adverse event was pain at the injection site and fatigue within 4 days of vaccination, and no fevers or serious adverse events occurred in any children in this time. Within the month after vaccination, 24% of children who received one dose in infancy, 13% of those who received two, and 29% of children receiving the first dose at age 5 years had at least one adverse event. One child had an upper respiratory tract infection and rash, one had diarrhea and vomiting, and one had Raynaud’s phenomenon within the month after vaccination.
The research was funded by GlaxoSmithKline Biologicals SA. Dr. Miller, Dr. Baine, Dr. Van der Wielen, Dr. Baccarini, and Dr. Kolhe are employees of GSK, and all but Dr. Kolhe and Dr. Klein have restricted shares in GSK. Dr. Miller and Dr. Baine coinvented a patent, which, if granted, will be owned by GSK. Dr. Klein has received research grants from GSK, Sanofi Pasteur, Pfizer, Novartis, Merck, Nuron, and Protein Science, outside the submitted work.
Receiving two doses of a combination tetanus and meningococcal vaccine in infancy did not result in additional protection among children 5 years later, a study found.
Researchers followed up on children receiving one or two doses of the quadrivalent meningococcal serogroups A, C, W, and Y tetanus toxoid conjugate vaccine (MenACWY-TT).
“Overall, 5 years after primary vaccination with MenACWY-TT, there was no clear evidence of benefit of receiving two versus one dose of vaccine in infancy,” reported Dr. Nicola P. Klein of the Kaiser Permanente Vaccine Study Center in Oakland, Calif., and her associates online (Pediatr Infect Dis J. 2016 Feb 26. doi: 10.1097/INF.0000000000001123).
In the initial phase II, open multicenter study, the researchers randomized 349 infants to receive either a single dose of MenACWY-TT at 12 months of age or a first dose of MenACWY-TT at 9 months of age followed by a booster dose at 12 months.
Using a per-protocol analysis, the researchers compared the titers of 186 children at 3 years’ follow-up and 135 children at 5 years’ follow-up. In the group that received one dose, 64%-75% of the children had titers of 8 or higher for MenC, MenW, and MenY 5 years later, compared with 75%-86% of the children who received two doses.
Also at 5 years, MenA titers were 8 or higher in 32% of children receiving one dose and 38% of children receiving two doses. Titers for all serotypes had waned by 5 years after vaccination, but only MenA was low enough that most children were seronegative by 1 year after vaccination. Overall average titers were higher in the group that had received two doses than in the group that had received one.
Dr. Klein’s team also evaluated the immune response and safety of a booster dose of MenACWY-TT to 38 children who had received one dose in infancy and 46 children who had received two doses in infancy, and a primary dose in 100 children of the same age who had never received a meningococcal vaccine. All children receiving the booster dose had antibody titers of 8 or higher against all serotypes 1 month after the dose. Among those receiving the vaccine for the first time, titers were 8 or higher at 1 month in 79% of children for MenA, 86% for MenC, 90% for MenW, and 94% for MenY.
No significant differences existed in terms of average titer levels, vaccine response, or titer levels of greater than or equal to 4 or greater than or equal to 8 between the children who received one dose and the children who received two doses in infancy. Children who received one or two vaccine doses in infancy had higher average titers and more vaccine responses to all serogroups than the children receiving a dose at age 5 years for the first time.
The most common adverse event was pain at the injection site and fatigue within 4 days of vaccination, and no fevers or serious adverse events occurred in any children in this time. Within the month after vaccination, 24% of children who received one dose in infancy, 13% of those who received two, and 29% of children receiving the first dose at age 5 years had at least one adverse event. One child had an upper respiratory tract infection and rash, one had diarrhea and vomiting, and one had Raynaud’s phenomenon within the month after vaccination.
The research was funded by GlaxoSmithKline Biologicals SA. Dr. Miller, Dr. Baine, Dr. Van der Wielen, Dr. Baccarini, and Dr. Kolhe are employees of GSK, and all but Dr. Kolhe and Dr. Klein have restricted shares in GSK. Dr. Miller and Dr. Baine coinvented a patent, which, if granted, will be owned by GSK. Dr. Klein has received research grants from GSK, Sanofi Pasteur, Pfizer, Novartis, Merck, Nuron, and Protein Science, outside the submitted work.
Receiving two doses of a combination tetanus and meningococcal vaccine in infancy did not result in additional protection among children 5 years later, a study found.
Researchers followed up on children receiving one or two doses of the quadrivalent meningococcal serogroups A, C, W, and Y tetanus toxoid conjugate vaccine (MenACWY-TT).
“Overall, 5 years after primary vaccination with MenACWY-TT, there was no clear evidence of benefit of receiving two versus one dose of vaccine in infancy,” reported Dr. Nicola P. Klein of the Kaiser Permanente Vaccine Study Center in Oakland, Calif., and her associates online (Pediatr Infect Dis J. 2016 Feb 26. doi: 10.1097/INF.0000000000001123).
In the initial phase II, open multicenter study, the researchers randomized 349 infants to receive either a single dose of MenACWY-TT at 12 months of age or a first dose of MenACWY-TT at 9 months of age followed by a booster dose at 12 months.
Using a per-protocol analysis, the researchers compared the titers of 186 children at 3 years’ follow-up and 135 children at 5 years’ follow-up. In the group that received one dose, 64%-75% of the children had titers of 8 or higher for MenC, MenW, and MenY 5 years later, compared with 75%-86% of the children who received two doses.
Also at 5 years, MenA titers were 8 or higher in 32% of children receiving one dose and 38% of children receiving two doses. Titers for all serotypes had waned by 5 years after vaccination, but only MenA was low enough that most children were seronegative by 1 year after vaccination. Overall average titers were higher in the group that had received two doses than in the group that had received one.
Dr. Klein’s team also evaluated the immune response and safety of a booster dose of MenACWY-TT to 38 children who had received one dose in infancy and 46 children who had received two doses in infancy, and a primary dose in 100 children of the same age who had never received a meningococcal vaccine. All children receiving the booster dose had antibody titers of 8 or higher against all serotypes 1 month after the dose. Among those receiving the vaccine for the first time, titers were 8 or higher at 1 month in 79% of children for MenA, 86% for MenC, 90% for MenW, and 94% for MenY.
No significant differences existed in terms of average titer levels, vaccine response, or titer levels of greater than or equal to 4 or greater than or equal to 8 between the children who received one dose and the children who received two doses in infancy. Children who received one or two vaccine doses in infancy had higher average titers and more vaccine responses to all serogroups than the children receiving a dose at age 5 years for the first time.
The most common adverse event was pain at the injection site and fatigue within 4 days of vaccination, and no fevers or serious adverse events occurred in any children in this time. Within the month after vaccination, 24% of children who received one dose in infancy, 13% of those who received two, and 29% of children receiving the first dose at age 5 years had at least one adverse event. One child had an upper respiratory tract infection and rash, one had diarrhea and vomiting, and one had Raynaud’s phenomenon within the month after vaccination.
The research was funded by GlaxoSmithKline Biologicals SA. Dr. Miller, Dr. Baine, Dr. Van der Wielen, Dr. Baccarini, and Dr. Kolhe are employees of GSK, and all but Dr. Kolhe and Dr. Klein have restricted shares in GSK. Dr. Miller and Dr. Baine coinvented a patent, which, if granted, will be owned by GSK. Dr. Klein has received research grants from GSK, Sanofi Pasteur, Pfizer, Novartis, Merck, Nuron, and Protein Science, outside the submitted work.
FROM PEDIATRIC INFECTIOUS DISEASE JOURNAL
Key clinical point: A booster dose of MenACWY-TT in infancy doesn’t offer additional protection 5 years later.
Major finding: At least 64% of children receiving one dose and at least 75% of children receiving two doses had titers of 8 or higher for MenC, MenW, and MenY at 5 years.
Data source: The findings were based on a 3-year follow-up with 186 children and a 5-year follow-up with 135 children from a prior phase II, open, multicenter study involving 349 infants who received one or two doses of MenACWY-TT.
Disclosures: The research was funded by GlaxoSmithKline Biologicals SA. Dr. Miller, Dr. Baine, Dr. Van der Wielen, Dr. Baccarini, and Dr. Kolhe are employees of GSK, and all but Dr. Kolhe and Dr. Klein have restricted shares in GSK. Dr. Miller and Dr. Baine coinvented a patent, which if granted, will be owned by GSK. Dr. Klein has received research grants from GSK, Sanofi Pasteur, Pfizer, Novartis, Merck, Nuron, and Protein Science, outside the submitted work.
Tool May Help Predict Persistent Postconcussion Symptoms
A new tool – a clinical risk score – may help identify which children and adolescents who recently sustained a head injury are at risk for persistent postconcussion symptoms, according to a report published online March 7 in JAMA.
Approximately one-third of pediatric patients with concussion will have ongoing somatic, cognitive, psychological, and/or behavioral symptoms at 28 days, and at present, there are no tools to help predict which patients will be affected. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Dr. Roger Zemek of Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and his associates (JAMA 2016 Mar 8;315[10]:1014-25).

This prospective cohort study involved patients aged 5-17 years (median age, 12 years) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms (PPCS). A total of 47 possible predictive variables were assessed for their usefulness in predicting PPCS in this cohort. They were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient/parent responses to weekly follow-up surveys during the month following the injury.
The investigators devised a clinical risk score using the nine predictors they found to be most accurate: patient age, patient gender, the presence or absence of prior concussion, migraine history, the presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to delineate PPCS risk: 0-3 points indicated low risk, 4-8 points indicated intermediate risk, and 9 or more points indicated high risk.
Treating physicians also were asked to predict the likelihood of PPCS.
In the validation cohort, 291 of 883 participants (33%) met the criteria for PPCS.
For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting PPCS. However, in its present form, it is only modestly accurate at distinguishing who will and who will not have the disorder. This tool could be further refined, perhaps by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, Dr. Zemek and his associates wrote.
“Before this score is adopted in clinical practice, further research is needed for external validation, assessment of accuracy in an office setting, and determination of clinical utility,” they concluded.
This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.
The clinical risk score devised by Zemek et al. may facilitate selection of patients who are at highest risk of long-term impairment, both for more intensive monitoring and treatment in the clinical setting and for inclusion in much-needed interventional trials in the research setting. It also may support clinicians in reassuring low-risk patients and their families of the likelihood of full recovery.
However, this tool first must be validated in other settings where children and adolescents are assessed for head injury, including general emergency departments; urgent care centers; and primary care, orthopedic, and sports medicine practices. Its performance should also be evaluated when used in conjunction with bedside vestibular ocular measures, serum biomarkers, genetic factors, and advanced neuroimaging measures. And determining its usefulness in other patient groups excluded from this trial also is warranted, including children younger than age 5, those with multiple trauma, and those found to have structural abnormalities on neuroimaging tests.
Dr. Lynn Babcock is in the division of pediatric emergency medicine at the University of Cincinnati and at the Cincinnati Children’s Hospital Medical Center. Dr. Brad G. Kurowski is in the division of physical medicine and rehabilitation in the department of pediatrics at Cincinnati Children’s Hospital Medical Center. Dr. Kurowski reported receiving grants from the National Institutes of Health and the Centers for Disease Control and Prevention. Dr. Babcock and Dr. Kurowski made these remarks in an editorial accompanying Dr. Zemek’s report (JAMA 2016 Mar 8;315[10]:987-8).
The clinical risk score devised by Zemek et al. may facilitate selection of patients who are at highest risk of long-term impairment, both for more intensive monitoring and treatment in the clinical setting and for inclusion in much-needed interventional trials in the research setting. It also may support clinicians in reassuring low-risk patients and their families of the likelihood of full recovery.
However, this tool first must be validated in other settings where children and adolescents are assessed for head injury, including general emergency departments; urgent care centers; and primary care, orthopedic, and sports medicine practices. Its performance should also be evaluated when used in conjunction with bedside vestibular ocular measures, serum biomarkers, genetic factors, and advanced neuroimaging measures. And determining its usefulness in other patient groups excluded from this trial also is warranted, including children younger than age 5, those with multiple trauma, and those found to have structural abnormalities on neuroimaging tests.
Dr. Lynn Babcock is in the division of pediatric emergency medicine at the University of Cincinnati and at the Cincinnati Children’s Hospital Medical Center. Dr. Brad G. Kurowski is in the division of physical medicine and rehabilitation in the department of pediatrics at Cincinnati Children’s Hospital Medical Center. Dr. Kurowski reported receiving grants from the National Institutes of Health and the Centers for Disease Control and Prevention. Dr. Babcock and Dr. Kurowski made these remarks in an editorial accompanying Dr. Zemek’s report (JAMA 2016 Mar 8;315[10]:987-8).
The clinical risk score devised by Zemek et al. may facilitate selection of patients who are at highest risk of long-term impairment, both for more intensive monitoring and treatment in the clinical setting and for inclusion in much-needed interventional trials in the research setting. It also may support clinicians in reassuring low-risk patients and their families of the likelihood of full recovery.
However, this tool first must be validated in other settings where children and adolescents are assessed for head injury, including general emergency departments; urgent care centers; and primary care, orthopedic, and sports medicine practices. Its performance should also be evaluated when used in conjunction with bedside vestibular ocular measures, serum biomarkers, genetic factors, and advanced neuroimaging measures. And determining its usefulness in other patient groups excluded from this trial also is warranted, including children younger than age 5, those with multiple trauma, and those found to have structural abnormalities on neuroimaging tests.
Dr. Lynn Babcock is in the division of pediatric emergency medicine at the University of Cincinnati and at the Cincinnati Children’s Hospital Medical Center. Dr. Brad G. Kurowski is in the division of physical medicine and rehabilitation in the department of pediatrics at Cincinnati Children’s Hospital Medical Center. Dr. Kurowski reported receiving grants from the National Institutes of Health and the Centers for Disease Control and Prevention. Dr. Babcock and Dr. Kurowski made these remarks in an editorial accompanying Dr. Zemek’s report (JAMA 2016 Mar 8;315[10]:987-8).
A new tool – a clinical risk score – may help identify which children and adolescents who recently sustained a head injury are at risk for persistent postconcussion symptoms, according to a report published online March 7 in JAMA.
Approximately one-third of pediatric patients with concussion will have ongoing somatic, cognitive, psychological, and/or behavioral symptoms at 28 days, and at present, there are no tools to help predict which patients will be affected. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Dr. Roger Zemek of Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and his associates (JAMA 2016 Mar 8;315[10]:1014-25).
This prospective cohort study involved patients aged 5-17 years (median age, 12 years) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms (PPCS). A total of 47 possible predictive variables were assessed for their usefulness in predicting PPCS in this cohort. They were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient/parent responses to weekly follow-up surveys during the month following the injury.
The investigators devised a clinical risk score using the nine predictors they found to be most accurate: patient age, patient gender, the presence or absence of prior concussion, migraine history, the presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to delineate PPCS risk: 0-3 points indicated low risk, 4-8 points indicated intermediate risk, and 9 or more points indicated high risk.
Treating physicians also were asked to predict the likelihood of PPCS.
In the validation cohort, 291 of 883 participants (33%) met the criteria for PPCS.
For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting PPCS. However, in its present form, it is only modestly accurate at distinguishing who will and who will not have the disorder. This tool could be further refined, perhaps by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, Dr. Zemek and his associates wrote.
“Before this score is adopted in clinical practice, further research is needed for external validation, assessment of accuracy in an office setting, and determination of clinical utility,” they concluded.
This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.
A new tool – a clinical risk score – may help identify which children and adolescents who recently sustained a head injury are at risk for persistent postconcussion symptoms, according to a report published online March 7 in JAMA.
Approximately one-third of pediatric patients with concussion will have ongoing somatic, cognitive, psychological, and/or behavioral symptoms at 28 days, and at present, there are no tools to help predict which patients will be affected. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Dr. Roger Zemek of Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and his associates (JAMA 2016 Mar 8;315[10]:1014-25).
This prospective cohort study involved patients aged 5-17 years (median age, 12 years) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms (PPCS). A total of 47 possible predictive variables were assessed for their usefulness in predicting PPCS in this cohort. They were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient/parent responses to weekly follow-up surveys during the month following the injury.
The investigators devised a clinical risk score using the nine predictors they found to be most accurate: patient age, patient gender, the presence or absence of prior concussion, migraine history, the presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to delineate PPCS risk: 0-3 points indicated low risk, 4-8 points indicated intermediate risk, and 9 or more points indicated high risk.
Treating physicians also were asked to predict the likelihood of PPCS.
In the validation cohort, 291 of 883 participants (33%) met the criteria for PPCS.
For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting PPCS. However, in its present form, it is only modestly accurate at distinguishing who will and who will not have the disorder. This tool could be further refined, perhaps by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, Dr. Zemek and his associates wrote.
“Before this score is adopted in clinical practice, further research is needed for external validation, assessment of accuracy in an office setting, and determination of clinical utility,” they concluded.
This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.
FROM JAMA

Tool may help predict persistent postconcussion symptoms
A new tool – a clinical risk score – may help identify which children and adolescents who recently sustained a head injury are at risk for persistent postconcussion symptoms, according to a report published online March 7 in JAMA.
Approximately one-third of pediatric patients with concussion will have ongoing somatic, cognitive, psychological, and/or behavioral symptoms at 28 days, and at present, there are no tools to help predict which patients will be affected. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Dr. Roger Zemek of Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and his associates (JAMA 2016 Mar 8;315[10]:1014-25).

This prospective cohort study involved patients aged 5-17 years (median age, 12 years) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms (PPCS). A total of 47 possible predictive variables were assessed for their usefulness in predicting PPCS in this cohort. They were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient/parent responses to weekly follow-up surveys during the month following the injury.
The investigators devised a clinical risk score using the nine predictors they found to be most accurate: patient age, patient gender, the presence or absence of prior concussion, migraine history, the presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to delineate PPCS risk: 0-3 points indicated low risk, 4-8 points indicated intermediate risk, and 9 or more points indicated high risk.
Treating physicians also were asked to predict the likelihood of PPCS.
In the validation cohort, 291 of 883 participants (33%) met the criteria for PPCS.
For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting PPCS. However, in its present form, it is only modestly accurate at distinguishing who will and who will not have the disorder. This tool could be further refined, perhaps by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, Dr. Zemek and his associates wrote.
“Before this score is adopted in clinical practice, further research is needed for external validation, assessment of accuracy in an office setting, and determination of clinical utility,” they concluded.
This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.
The clinical risk score devised by Zemek et al. may facilitate selection of patients who are at highest risk of long-term impairment, both for more intensive monitoring and treatment in the clinical setting and for inclusion in much-needed interventional trials in the research setting. It also may support clinicians in reassuring low-risk patients and their families of the likelihood of full recovery.
However, this tool first must be validated in other settings where children and adolescents are assessed for head injury, including general emergency departments; urgent care centers; and primary care, orthopedic, and sports medicine practices. Its performance should also be evaluated when used in conjunction with bedside vestibular ocular measures, serum biomarkers, genetic factors, and advanced neuroimaging measures. And determining its usefulness in other patient groups excluded from this trial also is warranted, including children younger than age 5, those with multiple trauma, and those found to have structural abnormalities on neuroimaging tests.
Dr. Lynn Babcock is in the division of pediatric emergency medicine at the University of Cincinnati and at the Cincinnati Children’s Hospital Medical Center. Dr. Brad G. Kurowski is in the division of physical medicine and rehabilitation in the department of pediatrics at Cincinnati Children’s Hospital Medical Center. Dr. Kurowski reported receiving grants from the National Institutes of Health and the Centers for Disease Control and Prevention. Dr. Babcock and Dr. Kurowski made these remarks in an editorial accompanying Dr. Zemek’s report (JAMA 2016 Mar 8;315[10]:987-8).
The clinical risk score devised by Zemek et al. may facilitate selection of patients who are at highest risk of long-term impairment, both for more intensive monitoring and treatment in the clinical setting and for inclusion in much-needed interventional trials in the research setting. It also may support clinicians in reassuring low-risk patients and their families of the likelihood of full recovery.
However, this tool first must be validated in other settings where children and adolescents are assessed for head injury, including general emergency departments; urgent care centers; and primary care, orthopedic, and sports medicine practices. Its performance should also be evaluated when used in conjunction with bedside vestibular ocular measures, serum biomarkers, genetic factors, and advanced neuroimaging measures. And determining its usefulness in other patient groups excluded from this trial also is warranted, including children younger than age 5, those with multiple trauma, and those found to have structural abnormalities on neuroimaging tests.
Dr. Lynn Babcock is in the division of pediatric emergency medicine at the University of Cincinnati and at the Cincinnati Children’s Hospital Medical Center. Dr. Brad G. Kurowski is in the division of physical medicine and rehabilitation in the department of pediatrics at Cincinnati Children’s Hospital Medical Center. Dr. Kurowski reported receiving grants from the National Institutes of Health and the Centers for Disease Control and Prevention. Dr. Babcock and Dr. Kurowski made these remarks in an editorial accompanying Dr. Zemek’s report (JAMA 2016 Mar 8;315[10]:987-8).
The clinical risk score devised by Zemek et al. may facilitate selection of patients who are at highest risk of long-term impairment, both for more intensive monitoring and treatment in the clinical setting and for inclusion in much-needed interventional trials in the research setting. It also may support clinicians in reassuring low-risk patients and their families of the likelihood of full recovery.
However, this tool first must be validated in other settings where children and adolescents are assessed for head injury, including general emergency departments; urgent care centers; and primary care, orthopedic, and sports medicine practices. Its performance should also be evaluated when used in conjunction with bedside vestibular ocular measures, serum biomarkers, genetic factors, and advanced neuroimaging measures. And determining its usefulness in other patient groups excluded from this trial also is warranted, including children younger than age 5, those with multiple trauma, and those found to have structural abnormalities on neuroimaging tests.
Dr. Lynn Babcock is in the division of pediatric emergency medicine at the University of Cincinnati and at the Cincinnati Children’s Hospital Medical Center. Dr. Brad G. Kurowski is in the division of physical medicine and rehabilitation in the department of pediatrics at Cincinnati Children’s Hospital Medical Center. Dr. Kurowski reported receiving grants from the National Institutes of Health and the Centers for Disease Control and Prevention. Dr. Babcock and Dr. Kurowski made these remarks in an editorial accompanying Dr. Zemek’s report (JAMA 2016 Mar 8;315[10]:987-8).
A new tool – a clinical risk score – may help identify which children and adolescents who recently sustained a head injury are at risk for persistent postconcussion symptoms, according to a report published online March 7 in JAMA.
Approximately one-third of pediatric patients with concussion will have ongoing somatic, cognitive, psychological, and/or behavioral symptoms at 28 days, and at present, there are no tools to help predict which patients will be affected. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Dr. Roger Zemek of Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and his associates (JAMA 2016 Mar 8;315[10]:1014-25).
This prospective cohort study involved patients aged 5-17 years (median age, 12 years) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms (PPCS). A total of 47 possible predictive variables were assessed for their usefulness in predicting PPCS in this cohort. They were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient/parent responses to weekly follow-up surveys during the month following the injury.
The investigators devised a clinical risk score using the nine predictors they found to be most accurate: patient age, patient gender, the presence or absence of prior concussion, migraine history, the presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to delineate PPCS risk: 0-3 points indicated low risk, 4-8 points indicated intermediate risk, and 9 or more points indicated high risk.
Treating physicians also were asked to predict the likelihood of PPCS.
In the validation cohort, 291 of 883 participants (33%) met the criteria for PPCS.
For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting PPCS. However, in its present form, it is only modestly accurate at distinguishing who will and who will not have the disorder. This tool could be further refined, perhaps by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, Dr. Zemek and his associates wrote.
“Before this score is adopted in clinical practice, further research is needed for external validation, assessment of accuracy in an office setting, and determination of clinical utility,” they concluded.
This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.
A new tool – a clinical risk score – may help identify which children and adolescents who recently sustained a head injury are at risk for persistent postconcussion symptoms, according to a report published online March 7 in JAMA.
Approximately one-third of pediatric patients with concussion will have ongoing somatic, cognitive, psychological, and/or behavioral symptoms at 28 days, and at present, there are no tools to help predict which patients will be affected. The 5P (Preventing Postconcussive Problems in Pediatrics) study was performed to develop and validate a clinical risk score for this purpose, said Dr. Roger Zemek of Children’s Hospital of Eastern Ontario Research Institute, Ottawa, and his associates (JAMA 2016 Mar 8;315[10]:1014-25).
This prospective cohort study involved patients aged 5-17 years (median age, 12 years) who presented to one of nine Canadian pediatric emergency departments within 48 hours of sustaining a concussion.
In the derivation cohort, 510 of 1,701 participants (30%) met the criteria for persistent postconcussion symptoms (PPCS). A total of 47 possible predictive variables were assessed for their usefulness in predicting PPCS in this cohort. They were collected from demographic data, patient history, injury characteristics, physical examination, results on the Acute Concussion Evaluation Inventory and the Postconcussion Symptom Inventory, and patient/parent responses to weekly follow-up surveys during the month following the injury.
The investigators devised a clinical risk score using the nine predictors they found to be most accurate: patient age, patient gender, the presence or absence of prior concussion, migraine history, the presence or absence of current headache, sensitivity to noise, fatigue, slow responses to questions, and an abnormal tandem stance. They then selected three cutoff points to delineate PPCS risk: 0-3 points indicated low risk, 4-8 points indicated intermediate risk, and 9 or more points indicated high risk.
Treating physicians also were asked to predict the likelihood of PPCS.
In the validation cohort, 291 of 883 participants (33%) met the criteria for PPCS.
For low-risk patients, the sensitivity of the clinical risk score was 94%, the specificity was 18%, the negative predictive value was 85%, and the positive predictive value was 36%. For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 94%, the negative predictive value was 70%, and the positive predictive value was 60%.
In both sets of patients, the clinical risk score was significantly better than physician judgment in predicting PPCS. However, in its present form, it is only modestly accurate at distinguishing who will and who will not have the disorder. This tool could be further refined, perhaps by adding information regarding biomarkers, genetic susceptibility, or advanced neuroimaging, Dr. Zemek and his associates wrote.
“Before this score is adopted in clinical practice, further research is needed for external validation, assessment of accuracy in an office setting, and determination of clinical utility,” they concluded.
This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.
FROM JAMA
Key clinical point: A new tool has been developed to help identify children and adolescents at risk for persistent postconcussion symptoms.
Major finding: For high-risk patients, the sensitivity of the clinical risk score was 20%, the specificity was 93%, the negative predictive value was 70%, and the positive predictive value was 60%.
Data source: A prospective, multicenter cohort study involving 1,701 pediatric patients to develop a clinical risk score, and a validation study involving 883 to test the performance of that tool.
Disclosures: This work was supported by the Canadian Institutes of Health Research, the Ontario Neurotrauma Foundation Mild Traumatic Brain Injury Team, and the Alberta Children’s Hospital Foundation. Dr. Zemek and his associates reported having no relevant financial disclosures.

P. aeruginosa, Serratia have high potential to spread in the NICU
Blood stream infections with Pseudomonas aeruginosa or Serratia subspecies in preterm infants are associated with a markedly elevated risk of same-pathogen bloodstream infections in other infants in the NICU, based on results from a large database in Germany.
Blood stream infections involving P. aeruginosa or Serratia subspecies, while rare, are “exceptional in their potential to spread in the NICU and attack very low birth weight infants. Because they are also those pathogens with the highest reported BSI (blood stream infection)-related mortality rates, vigorous attempts should be made to intensify infection control measures whenever P. aeruginosa or Serratia have been isolated from a patient in the NICU,” researchers led by Dr. Felix Reichert reported online March 8 in Pediatrics.
Dr. Reichert of the department of neonatology at Charité University Medical Center, Berlin, and his associates used data from the German National Neonatal Infection Surveillance System to estimate the probability of a hospitalized very-low-birth-weight infant to develop a bloodstream infection with a particular pathogen when another infant previously diagnosed with a bloodstream infection from the same pathogen was being cared for in the same unit (Pediatrics 2016 Mar 8. doi: 10.1542/peds.2015-2860). They limited their search to 44,818 very-low-birth-weight infants (defined as less than 1,500 g) who were born between Jan. 1, 2000, and Dec. 31, 2011.
The researchers found 2004 culture-positive bloodstream infections; 407 were from methicillin-sensitive Staphylococcus aureus; 246 to Enterobacter spp; 243 to vancomycin-sensitive Enterococcus spp; 210 to cefotaxime-sensitive Escherichia coli; 190 to cefotaxime-sensitive Klebsiella spp; 138 to Candida albicans; 58 to Serratia; and 38 to P. aeruginosa. Pathogens with 30 or fewer bloodstream infections were not analyzed further.
Rates of bloodstream infections acquired while another infant with a same-pathogen infection was being cared for in the unit varied between 2.2 (Enterococcus) and 8.2 (Serratia) per 100 exposed infants. The relative risk for acquiring a bloodstream infection in the presence or absence of an infant with a preceding same-pathogen bloodstream infection varied between 4.3 (Enterococcus) and 77.5 (Serratia).
When a same-pathogen bloodstream infection was observed in the same unit during the preceding 30 days, rates of blood stream infection per 100 exposed infants varied between 1.4 (C. albicans) and 6.5 (Serratia). The relative risk for acquiring a bloodstream infection while a same-pathogen infection had been diagnosed in the preceding 30 days in the same department varied between 2.3 (Enterococcus) and 59.5 (Serratia)
The authors acknowledged certain limitations of the study, including the fact that the reporting system used “made no distinction between various strains of Enterococcus, Enterobacter, or Serratia, and there was no genotyping of the pathogens involved. Thus, two temporally related BSIs [blood stream infections] in the same department might well be a coincidence.”
The German National Neonatal Infection Surveillance System is supported by the Federal Department of Health and funds from the Charité University Medical Center. The authors reported having no financial disclosures.
Blood stream infections with Pseudomonas aeruginosa or Serratia subspecies in preterm infants are associated with a markedly elevated risk of same-pathogen bloodstream infections in other infants in the NICU, based on results from a large database in Germany.
Blood stream infections involving P. aeruginosa or Serratia subspecies, while rare, are “exceptional in their potential to spread in the NICU and attack very low birth weight infants. Because they are also those pathogens with the highest reported BSI (blood stream infection)-related mortality rates, vigorous attempts should be made to intensify infection control measures whenever P. aeruginosa or Serratia have been isolated from a patient in the NICU,” researchers led by Dr. Felix Reichert reported online March 8 in Pediatrics.
Dr. Reichert of the department of neonatology at Charité University Medical Center, Berlin, and his associates used data from the German National Neonatal Infection Surveillance System to estimate the probability of a hospitalized very-low-birth-weight infant to develop a bloodstream infection with a particular pathogen when another infant previously diagnosed with a bloodstream infection from the same pathogen was being cared for in the same unit (Pediatrics 2016 Mar 8. doi: 10.1542/peds.2015-2860). They limited their search to 44,818 very-low-birth-weight infants (defined as less than 1,500 g) who were born between Jan. 1, 2000, and Dec. 31, 2011.
The researchers found 2004 culture-positive bloodstream infections; 407 were from methicillin-sensitive Staphylococcus aureus; 246 to Enterobacter spp; 243 to vancomycin-sensitive Enterococcus spp; 210 to cefotaxime-sensitive Escherichia coli; 190 to cefotaxime-sensitive Klebsiella spp; 138 to Candida albicans; 58 to Serratia; and 38 to P. aeruginosa. Pathogens with 30 or fewer bloodstream infections were not analyzed further.
Rates of bloodstream infections acquired while another infant with a same-pathogen infection was being cared for in the unit varied between 2.2 (Enterococcus) and 8.2 (Serratia) per 100 exposed infants. The relative risk for acquiring a bloodstream infection in the presence or absence of an infant with a preceding same-pathogen bloodstream infection varied between 4.3 (Enterococcus) and 77.5 (Serratia).
When a same-pathogen bloodstream infection was observed in the same unit during the preceding 30 days, rates of blood stream infection per 100 exposed infants varied between 1.4 (C. albicans) and 6.5 (Serratia). The relative risk for acquiring a bloodstream infection while a same-pathogen infection had been diagnosed in the preceding 30 days in the same department varied between 2.3 (Enterococcus) and 59.5 (Serratia)
The authors acknowledged certain limitations of the study, including the fact that the reporting system used “made no distinction between various strains of Enterococcus, Enterobacter, or Serratia, and there was no genotyping of the pathogens involved. Thus, two temporally related BSIs [blood stream infections] in the same department might well be a coincidence.”
The German National Neonatal Infection Surveillance System is supported by the Federal Department of Health and funds from the Charité University Medical Center. The authors reported having no financial disclosures.
Blood stream infections with Pseudomonas aeruginosa or Serratia subspecies in preterm infants are associated with a markedly elevated risk of same-pathogen bloodstream infections in other infants in the NICU, based on results from a large database in Germany.
Blood stream infections involving P. aeruginosa or Serratia subspecies, while rare, are “exceptional in their potential to spread in the NICU and attack very low birth weight infants. Because they are also those pathogens with the highest reported BSI (blood stream infection)-related mortality rates, vigorous attempts should be made to intensify infection control measures whenever P. aeruginosa or Serratia have been isolated from a patient in the NICU,” researchers led by Dr. Felix Reichert reported online March 8 in Pediatrics.
Dr. Reichert of the department of neonatology at Charité University Medical Center, Berlin, and his associates used data from the German National Neonatal Infection Surveillance System to estimate the probability of a hospitalized very-low-birth-weight infant to develop a bloodstream infection with a particular pathogen when another infant previously diagnosed with a bloodstream infection from the same pathogen was being cared for in the same unit (Pediatrics 2016 Mar 8. doi: 10.1542/peds.2015-2860). They limited their search to 44,818 very-low-birth-weight infants (defined as less than 1,500 g) who were born between Jan. 1, 2000, and Dec. 31, 2011.
The researchers found 2004 culture-positive bloodstream infections; 407 were from methicillin-sensitive Staphylococcus aureus; 246 to Enterobacter spp; 243 to vancomycin-sensitive Enterococcus spp; 210 to cefotaxime-sensitive Escherichia coli; 190 to cefotaxime-sensitive Klebsiella spp; 138 to Candida albicans; 58 to Serratia; and 38 to P. aeruginosa. Pathogens with 30 or fewer bloodstream infections were not analyzed further.
Rates of bloodstream infections acquired while another infant with a same-pathogen infection was being cared for in the unit varied between 2.2 (Enterococcus) and 8.2 (Serratia) per 100 exposed infants. The relative risk for acquiring a bloodstream infection in the presence or absence of an infant with a preceding same-pathogen bloodstream infection varied between 4.3 (Enterococcus) and 77.5 (Serratia).
When a same-pathogen bloodstream infection was observed in the same unit during the preceding 30 days, rates of blood stream infection per 100 exposed infants varied between 1.4 (C. albicans) and 6.5 (Serratia). The relative risk for acquiring a bloodstream infection while a same-pathogen infection had been diagnosed in the preceding 30 days in the same department varied between 2.3 (Enterococcus) and 59.5 (Serratia)
The authors acknowledged certain limitations of the study, including the fact that the reporting system used “made no distinction between various strains of Enterococcus, Enterobacter, or Serratia, and there was no genotyping of the pathogens involved. Thus, two temporally related BSIs [blood stream infections] in the same department might well be a coincidence.”
The German National Neonatal Infection Surveillance System is supported by the Federal Department of Health and funds from the Charité University Medical Center. The authors reported having no financial disclosures.
FROM PEDIATRICS
Key clinical point: Blood stream infection with P. aeruginosa or Serratia spp. in a very-low-birth-weight infant confers a markedly high risk of same-pathogen infection to other NICU infants.
Major finding: Rates of bloodstream infections acquired while another infant with a same-pathogen infection was being cared for in the unit varied between 2.2 (Enterococcus) and 8.2 (Serratia) per 100 exposed infants.
Data source: An analysis of data from 44,818 very-low-birth-weight infants who were born in Germany between Jan. 1, 2000, and Dec. 31, 2011.
Disclosures: The German National Neonatal Infection Surveillance System is supported by the Federal Department of Health and funds from the Charité University Medical Center. The authors reported having no financial disclosures.
Diagnosing Porokeratosis of Mibelli Every Time: A Novel Biopsy Technique to Maximize Histopathologic Confirmation
Porokeratosis of Mibelli (PM) is a lesion characterized by a surrounding cornoid lamella with variable nonspecific findings (eg, atrophy, acanthosis, verrucous hyperplasia) in the center of the lesion that typically presents in infancy to early childhood.1 We report a case of PM in which a prior biopsy from the center of the lesion demonstrated papulosquamous dermatitis. We propose a 3-step technique to ensure proper orientation of a punch biopsy in cases of suspected PM.
Case Report
A 3-year-old girl presented with an erythematous, hypopigmented, scaling plaque on the posterior aspect of the left ankle surrounded by a hard rim. The plaque was first noted at 12 months of age and had slowly enlarged as the patient grew. Six months prior, a biopsy from the center of the lesion performed at another facility demonstrated a papulosquamous dermatitis.
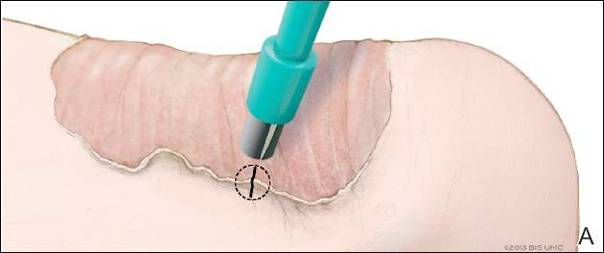
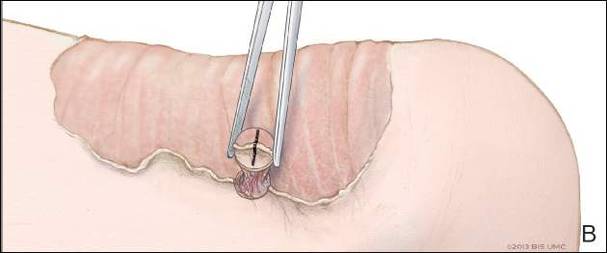
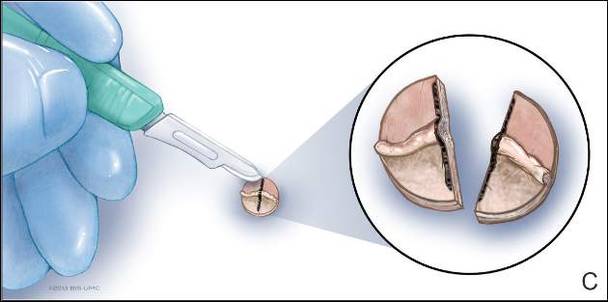
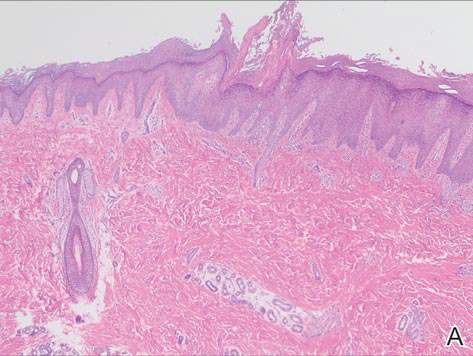
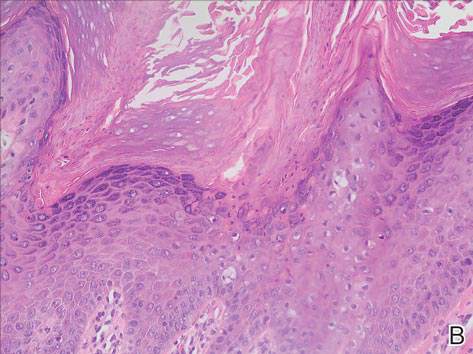
Physical examination revealed a lesion that was 4.2-cm long, 2.2-cm wide at the superior pole, and 3.5-cm wide at the inferior pole (Figure 1). A line was drawn with a skin marker perpendicular to the rim of the lesion (Figure 2A) and a 6-mm punch biopsy was performed, centered at the intersection of the drawn line and the cornoid lamella (Figure 2B). The tissue was then bisected at the bedside along the skin marker line with a #15 blade (Figure 2C) and submitted in formalin for histologic processing. Histologic examination revealed an invagination of the epidermis producing a tier of parakeratotic cells with its apex pointed away from the center of the lesion. Dyskeratotic cells were noted at the base of the parakeratosis (Figure 3). Verrucous hyperplasia was present in the central portion of the specimen adjacent to the cornoid lamella. Based on these histopathologic findings, the correct diagnosis of PM was made.

Comment
Porokeratosis of Mibelli is a rare condition that typically presents in infancy to early childhood.1 It may appear as small keratotic papules or larger plaques that reach several centimeters in diameter.2 There is a 7.5% risk for malignant transformation (eg, basal cell carcinoma, squamous cell carcinoma, Bowen disease).3 Variable nonspecific findings (eg, atrophy, acanthosis, verrucous hyperplasia) typically are present in the center of the lesion. In our case, a biopsy from the center of the plaque demonstrated verrucous hyperplasia. The incorrect diagnosis of PM as psoriasis also has been reported.4
We propose a 3-step technique to ensure proper orientation of a punch biopsy in cases of suspected PM. First, draw a line perpendicular to the rim of the lesion to mark the biopsy site (Figure 2A). Second, perform a punch biopsy centered at the intersection of the drawn line and the cornoid lamella (Figure 2B). Third, section the biopsied tissue with a #15 blade along the perpendicular line at the bedside (Figure 2C). The surgical pathology requisition should mention that the specimen has been transected and the cut edges should be placed down in the cassette, ensuring that the cornoid lamella will be present in cross-section on the slides.
If the punch biopsy specimen is not bisected, it can be difficult to orient it in the pathology laboratory, especially if the cornoid lamellae are not prominent. Furthermore, the technician processing the tissue may not be aware of the importance of sectioning the specimen perpendicular to the cornoid lamella. Following this procedure, diagnosis can be confirmed in virtually every case of PM.
- Richard G, Irvine A, Traupe H, et al. Ichthyosis and disorders of other conification. In: Schachner L, Hansen R, Krafchik B, et al, eds. Pediatric Dermatology. Philadelphia, PA: Elsevier Health Sciences; 2011:640-643.
- Pierson D, Bandel C, Ehrig, et al. Benign epidermal tumors and proliferations. In: Bolognia J, Jorizzo J, Rapini R, et al, eds. Dermatology. 1st ed. Vol 2. Edinburgh, Scotland: Elsevier; 2003:1707-1709.
- Cort DF, Abdel-Aziz AH. Epithelioma arising in porokeratosis of Mibelli. Br J Plast Surg. 1972;25:318-328.
- De Simone C, Paradisi A, Massi G, et al. Giant verrucous porokeratosis of Mibelli mimicking psoriasis in a patient with psoriasis. J Am Acad Dermatol. 2007;57:665-668.
Porokeratosis of Mibelli (PM) is a lesion characterized by a surrounding cornoid lamella with variable nonspecific findings (eg, atrophy, acanthosis, verrucous hyperplasia) in the center of the lesion that typically presents in infancy to early childhood.1 We report a case of PM in which a prior biopsy from the center of the lesion demonstrated papulosquamous dermatitis. We propose a 3-step technique to ensure proper orientation of a punch biopsy in cases of suspected PM.
Case Report
A 3-year-old girl presented with an erythematous, hypopigmented, scaling plaque on the posterior aspect of the left ankle surrounded by a hard rim. The plaque was first noted at 12 months of age and had slowly enlarged as the patient grew. Six months prior, a biopsy from the center of the lesion performed at another facility demonstrated a papulosquamous dermatitis.
Physical examination revealed a lesion that was 4.2-cm long, 2.2-cm wide at the superior pole, and 3.5-cm wide at the inferior pole (Figure 1). A line was drawn with a skin marker perpendicular to the rim of the lesion (Figure 2A) and a 6-mm punch biopsy was performed, centered at the intersection of the drawn line and the cornoid lamella (Figure 2B). The tissue was then bisected at the bedside along the skin marker line with a #15 blade (Figure 2C) and submitted in formalin for histologic processing. Histologic examination revealed an invagination of the epidermis producing a tier of parakeratotic cells with its apex pointed away from the center of the lesion. Dyskeratotic cells were noted at the base of the parakeratosis (Figure 3). Verrucous hyperplasia was present in the central portion of the specimen adjacent to the cornoid lamella. Based on these histopathologic findings, the correct diagnosis of PM was made.
Comment
Porokeratosis of Mibelli is a rare condition that typically presents in infancy to early childhood.1 It may appear as small keratotic papules or larger plaques that reach several centimeters in diameter.2 There is a 7.5% risk for malignant transformation (eg, basal cell carcinoma, squamous cell carcinoma, Bowen disease).3 Variable nonspecific findings (eg, atrophy, acanthosis, verrucous hyperplasia) typically are present in the center of the lesion. In our case, a biopsy from the center of the plaque demonstrated verrucous hyperplasia. The incorrect diagnosis of PM as psoriasis also has been reported.4
We propose a 3-step technique to ensure proper orientation of a punch biopsy in cases of suspected PM. First, draw a line perpendicular to the rim of the lesion to mark the biopsy site (Figure 2A). Second, perform a punch biopsy centered at the intersection of the drawn line and the cornoid lamella (Figure 2B). Third, section the biopsied tissue with a #15 blade along the perpendicular line at the bedside (Figure 2C). The surgical pathology requisition should mention that the specimen has been transected and the cut edges should be placed down in the cassette, ensuring that the cornoid lamella will be present in cross-section on the slides.
If the punch biopsy specimen is not bisected, it can be difficult to orient it in the pathology laboratory, especially if the cornoid lamellae are not prominent. Furthermore, the technician processing the tissue may not be aware of the importance of sectioning the specimen perpendicular to the cornoid lamella. Following this procedure, diagnosis can be confirmed in virtually every case of PM.
Porokeratosis of Mibelli (PM) is a lesion characterized by a surrounding cornoid lamella with variable nonspecific findings (eg, atrophy, acanthosis, verrucous hyperplasia) in the center of the lesion that typically presents in infancy to early childhood.1 We report a case of PM in which a prior biopsy from the center of the lesion demonstrated papulosquamous dermatitis. We propose a 3-step technique to ensure proper orientation of a punch biopsy in cases of suspected PM.
Case Report
A 3-year-old girl presented with an erythematous, hypopigmented, scaling plaque on the posterior aspect of the left ankle surrounded by a hard rim. The plaque was first noted at 12 months of age and had slowly enlarged as the patient grew. Six months prior, a biopsy from the center of the lesion performed at another facility demonstrated a papulosquamous dermatitis.
Physical examination revealed a lesion that was 4.2-cm long, 2.2-cm wide at the superior pole, and 3.5-cm wide at the inferior pole (Figure 1). A line was drawn with a skin marker perpendicular to the rim of the lesion (Figure 2A) and a 6-mm punch biopsy was performed, centered at the intersection of the drawn line and the cornoid lamella (Figure 2B). The tissue was then bisected at the bedside along the skin marker line with a #15 blade (Figure 2C) and submitted in formalin for histologic processing. Histologic examination revealed an invagination of the epidermis producing a tier of parakeratotic cells with its apex pointed away from the center of the lesion. Dyskeratotic cells were noted at the base of the parakeratosis (Figure 3). Verrucous hyperplasia was present in the central portion of the specimen adjacent to the cornoid lamella. Based on these histopathologic findings, the correct diagnosis of PM was made.
Comment
Porokeratosis of Mibelli is a rare condition that typically presents in infancy to early childhood.1 It may appear as small keratotic papules or larger plaques that reach several centimeters in diameter.2 There is a 7.5% risk for malignant transformation (eg, basal cell carcinoma, squamous cell carcinoma, Bowen disease).3 Variable nonspecific findings (eg, atrophy, acanthosis, verrucous hyperplasia) typically are present in the center of the lesion. In our case, a biopsy from the center of the plaque demonstrated verrucous hyperplasia. The incorrect diagnosis of PM as psoriasis also has been reported.4
We propose a 3-step technique to ensure proper orientation of a punch biopsy in cases of suspected PM. First, draw a line perpendicular to the rim of the lesion to mark the biopsy site (Figure 2A). Second, perform a punch biopsy centered at the intersection of the drawn line and the cornoid lamella (Figure 2B). Third, section the biopsied tissue with a #15 blade along the perpendicular line at the bedside (Figure 2C). The surgical pathology requisition should mention that the specimen has been transected and the cut edges should be placed down in the cassette, ensuring that the cornoid lamella will be present in cross-section on the slides.
If the punch biopsy specimen is not bisected, it can be difficult to orient it in the pathology laboratory, especially if the cornoid lamellae are not prominent. Furthermore, the technician processing the tissue may not be aware of the importance of sectioning the specimen perpendicular to the cornoid lamella. Following this procedure, diagnosis can be confirmed in virtually every case of PM.
- Richard G, Irvine A, Traupe H, et al. Ichthyosis and disorders of other conification. In: Schachner L, Hansen R, Krafchik B, et al, eds. Pediatric Dermatology. Philadelphia, PA: Elsevier Health Sciences; 2011:640-643.
- Pierson D, Bandel C, Ehrig, et al. Benign epidermal tumors and proliferations. In: Bolognia J, Jorizzo J, Rapini R, et al, eds. Dermatology. 1st ed. Vol 2. Edinburgh, Scotland: Elsevier; 2003:1707-1709.
- Cort DF, Abdel-Aziz AH. Epithelioma arising in porokeratosis of Mibelli. Br J Plast Surg. 1972;25:318-328.
- De Simone C, Paradisi A, Massi G, et al. Giant verrucous porokeratosis of Mibelli mimicking psoriasis in a patient with psoriasis. J Am Acad Dermatol. 2007;57:665-668.
- Richard G, Irvine A, Traupe H, et al. Ichthyosis and disorders of other conification. In: Schachner L, Hansen R, Krafchik B, et al, eds. Pediatric Dermatology. Philadelphia, PA: Elsevier Health Sciences; 2011:640-643.
- Pierson D, Bandel C, Ehrig, et al. Benign epidermal tumors and proliferations. In: Bolognia J, Jorizzo J, Rapini R, et al, eds. Dermatology. 1st ed. Vol 2. Edinburgh, Scotland: Elsevier; 2003:1707-1709.
- Cort DF, Abdel-Aziz AH. Epithelioma arising in porokeratosis of Mibelli. Br J Plast Surg. 1972;25:318-328.
- De Simone C, Paradisi A, Massi G, et al. Giant verrucous porokeratosis of Mibelli mimicking psoriasis in a patient with psoriasis. J Am Acad Dermatol. 2007;57:665-668.
Practice Points
- A biopsy from the center of a plaque of porokeratosis will produce nonspecific findings.
- Bisecting the punch specimen at the bedside along a line drawn perpendicular to the cornoid lamella guarantees proper orientation of the specimen.

Children who have stem cell transplants need skin exams, sun protection
WASHINGTON – Children who have had a hematopoietic stem cell transplant (HSCT) have an increased risk of benign and atypical nevi, Dr. Johanna Sheu reported at the annual meeting of the American Academy of Dermatology.
These patients need to have routine skin exams and be educated about sun protection needs, she said. Based on her study, these needs are not routinely met.
At least 1 year after undergoing HSCT at Boston Children’s Hospital, 85 posttransplant patients had significantly more nevi and more atypical nevi than did 85 healthy controls who were matched by age, gender, and Fitzpatrick skin type. In addition, 41% of the transplant recipients had at least one actinic keratosis, a basal or squamous cell carcinoma, or a solar lentigo; 11% had at least one nevus spilus.
Moreover, “sun protection … and dermatology follow-up was poor” among the transplant recipients, said Dr. Sheu, of MassGeneral Hospital for Children, Boston. About 40% of the transplant recipients reported having a sunburn since their transplant, only 15% reported daily use of sunscreen, and 53% said they did not recall being told that sunburn could trigger graft-versus-host disease (GVHD).
About one-third of the patients had never seen a dermatologist; of those who had, two-thirds had only seen the dermatologist once, Dr. Sheu reported.
Late skin effects of HSCT are not as well described in children as they are in adults, she said. In adults, late skin effects include vitiligo, psoriasis, nonmelanoma skin cancers, and an increased nevi count.
The children in the study had undergone an HSCT between 1998 and 2013, at a median age of about 7 years (range was 1 month to 19 years). At the time of their skin exams, their mean age was 14 years, and they had been followed for a median of almost 4 years. Nevi were counted on the forearms, backs, legs, palms, and soles.
The median nevi count was 44 nevi, significantly more than the level seen in control subjects. Transplant recipients also had significantly more nevi in sun-exposed areas of the body, as well as on the palms and soles. Transplant recipients were more likely to have atypical nevi and to have nevi greater than 5 mm in diameter.
In addition to fair skin, factors associated with an increase in the overall nevi count included being older than age 10 at the time of the transplant and having total body irradiation, pretransplant chemotherapy, and myeloablative conditioning. Having had a sunburn since the transplant, reported by 40%, was also a risk factor.
Chronic GVHD and chronic GVHD of the skin were associated with the presence of atypical nevi; acute GVHD, the duration of immune suppression, and the use of topical steroids or calcineurin inhibitors were not associated with increased risk of atypical nevi.
She and her coinvestigators are currently analyzing the pathogenesis of these late effects in this population, and autoimmune skin conditions – vitiligo and alopecia – in 25% of the transplant recipients in the study.
In 2013, 1,100 children under aged 16 years in the United States underwent a bone marrow transplant, she noted.
Dr. Sheu had no disclosures.
WASHINGTON – Children who have had a hematopoietic stem cell transplant (HSCT) have an increased risk of benign and atypical nevi, Dr. Johanna Sheu reported at the annual meeting of the American Academy of Dermatology.
These patients need to have routine skin exams and be educated about sun protection needs, she said. Based on her study, these needs are not routinely met.
At least 1 year after undergoing HSCT at Boston Children’s Hospital, 85 posttransplant patients had significantly more nevi and more atypical nevi than did 85 healthy controls who were matched by age, gender, and Fitzpatrick skin type. In addition, 41% of the transplant recipients had at least one actinic keratosis, a basal or squamous cell carcinoma, or a solar lentigo; 11% had at least one nevus spilus.
Moreover, “sun protection … and dermatology follow-up was poor” among the transplant recipients, said Dr. Sheu, of MassGeneral Hospital for Children, Boston. About 40% of the transplant recipients reported having a sunburn since their transplant, only 15% reported daily use of sunscreen, and 53% said they did not recall being told that sunburn could trigger graft-versus-host disease (GVHD).
About one-third of the patients had never seen a dermatologist; of those who had, two-thirds had only seen the dermatologist once, Dr. Sheu reported.
Late skin effects of HSCT are not as well described in children as they are in adults, she said. In adults, late skin effects include vitiligo, psoriasis, nonmelanoma skin cancers, and an increased nevi count.
The children in the study had undergone an HSCT between 1998 and 2013, at a median age of about 7 years (range was 1 month to 19 years). At the time of their skin exams, their mean age was 14 years, and they had been followed for a median of almost 4 years. Nevi were counted on the forearms, backs, legs, palms, and soles.
The median nevi count was 44 nevi, significantly more than the level seen in control subjects. Transplant recipients also had significantly more nevi in sun-exposed areas of the body, as well as on the palms and soles. Transplant recipients were more likely to have atypical nevi and to have nevi greater than 5 mm in diameter.
In addition to fair skin, factors associated with an increase in the overall nevi count included being older than age 10 at the time of the transplant and having total body irradiation, pretransplant chemotherapy, and myeloablative conditioning. Having had a sunburn since the transplant, reported by 40%, was also a risk factor.
Chronic GVHD and chronic GVHD of the skin were associated with the presence of atypical nevi; acute GVHD, the duration of immune suppression, and the use of topical steroids or calcineurin inhibitors were not associated with increased risk of atypical nevi.
She and her coinvestigators are currently analyzing the pathogenesis of these late effects in this population, and autoimmune skin conditions – vitiligo and alopecia – in 25% of the transplant recipients in the study.
In 2013, 1,100 children under aged 16 years in the United States underwent a bone marrow transplant, she noted.
Dr. Sheu had no disclosures.
WASHINGTON – Children who have had a hematopoietic stem cell transplant (HSCT) have an increased risk of benign and atypical nevi, Dr. Johanna Sheu reported at the annual meeting of the American Academy of Dermatology.
These patients need to have routine skin exams and be educated about sun protection needs, she said. Based on her study, these needs are not routinely met.
At least 1 year after undergoing HSCT at Boston Children’s Hospital, 85 posttransplant patients had significantly more nevi and more atypical nevi than did 85 healthy controls who were matched by age, gender, and Fitzpatrick skin type. In addition, 41% of the transplant recipients had at least one actinic keratosis, a basal or squamous cell carcinoma, or a solar lentigo; 11% had at least one nevus spilus.
Moreover, “sun protection … and dermatology follow-up was poor” among the transplant recipients, said Dr. Sheu, of MassGeneral Hospital for Children, Boston. About 40% of the transplant recipients reported having a sunburn since their transplant, only 15% reported daily use of sunscreen, and 53% said they did not recall being told that sunburn could trigger graft-versus-host disease (GVHD).
About one-third of the patients had never seen a dermatologist; of those who had, two-thirds had only seen the dermatologist once, Dr. Sheu reported.
Late skin effects of HSCT are not as well described in children as they are in adults, she said. In adults, late skin effects include vitiligo, psoriasis, nonmelanoma skin cancers, and an increased nevi count.
The children in the study had undergone an HSCT between 1998 and 2013, at a median age of about 7 years (range was 1 month to 19 years). At the time of their skin exams, their mean age was 14 years, and they had been followed for a median of almost 4 years. Nevi were counted on the forearms, backs, legs, palms, and soles.
The median nevi count was 44 nevi, significantly more than the level seen in control subjects. Transplant recipients also had significantly more nevi in sun-exposed areas of the body, as well as on the palms and soles. Transplant recipients were more likely to have atypical nevi and to have nevi greater than 5 mm in diameter.
In addition to fair skin, factors associated with an increase in the overall nevi count included being older than age 10 at the time of the transplant and having total body irradiation, pretransplant chemotherapy, and myeloablative conditioning. Having had a sunburn since the transplant, reported by 40%, was also a risk factor.
Chronic GVHD and chronic GVHD of the skin were associated with the presence of atypical nevi; acute GVHD, the duration of immune suppression, and the use of topical steroids or calcineurin inhibitors were not associated with increased risk of atypical nevi.
She and her coinvestigators are currently analyzing the pathogenesis of these late effects in this population, and autoimmune skin conditions – vitiligo and alopecia – in 25% of the transplant recipients in the study.
In 2013, 1,100 children under aged 16 years in the United States underwent a bone marrow transplant, she noted.
Dr. Sheu had no disclosures.
AT AAD 16
Key clinical point: Children who have had a hematopoietic stem cell transplant need to have routine skin exams and be educated about sun protection needs.
Major finding: 41% of the transplant recipients had at least one actinic keratosis, a basal or squamous cell carcinoma, or a solar lentigo; 11% had at least one nevus spilus.
Data source: A single-center study of 85 posttransplant patients and 85 healthy controls who were matched by age, gender, and Fitzpatrick skin type.
Disclosures: The study was not sponsored and Dr. Sheu had no disclosures.
AAAAI: Early Peanut Consumption Brings Lasting Protection From Allergy
LOS ANGELES – A peanut allergy prevention strategy based upon regular consumption of peanut-containing foods from infancy to age 5 continued to provide protection even after peanut intake was halted for a full year from age 5 to 6, according to new results from an extension of the landmark LEAP trial, known as LEAP-On, presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The impetus for LEAP-On was the investigators’ concern that a period of peanut avoidance might cause loss of the protective state. But that didn’t occur.
“I think there is no doubt that we have prevented peanut allergy so far in these high-risk children. Next, the LEAP-Ad Lib study will tell us whether we’ve prevented it by age 10,” said Dr. Gideon Lack of King’s College London, who headed LEAP-On.

A second major randomized trial known as EAT (Enquiring About Tolerance) presented at the meeting provided further support for early dietary introduction of allergenic foods. EAT differed from LEAP (Learning Early About Peanut Allergy) and LEAP-On in that it ambitiously randomized infants to early introduction or avoidance of not one but six allergenic foods: peanut, cooked egg, cow’s milk, fish, sesame, and wheat. Also, while LEAP and LEAP-On involved roughly 600 infants known to be at very high risk for allergy, EAT was conducted in a general population of 1,303 infants who weren’t at increased risk, all of whom were exclusively breast-fed until the intervention beginning at age 3 months.
The presentation of the LEAP-On and EAT results at the AAAAI annual meeting was a major event marked by the National Institute of Allergy and Infectious Diseases by same-day release of new NIAID-sponsored draft recommendations for the diagnosis and management of food allergies.
In a press conference held at the AAAAI annual meeting to announce the start of a 45-day public comment period for the draft update of the 2010 guidelines, Dr. Daniel Rotrosen, director of NIAID’s division of allergy, immunology and transplantation, said the new guidelines were developed largely in response to the compelling LEAP findings. That trial demonstrated that sustained consumption of peanut starting in infancy resulted in an 81% lower rate of peanut allergy at age 5 years compared to a strategy of peanut avoidance (N Engl J Med. 2015;372:803-13).

The draft guidelines, now available on the NIAID website, represent a sharp departure from the former recommendation that physicians encourage exclusive breastfeeding for the first 6 months of life followed by cautious introduction of other foods. Whereas the former orthodoxy was that delayed introduction of allergenic foods protects against development of food allergy, the new evidence-based concept supported by the LEAP and EAT findings is that just the opposite is true: that is, introduction of such foods during the period of immunologic plasticity in infancy induces tolerance.
Thus, the draft guidelines recommend that infants at high risk for peanut allergy because they have severe eczema and/or egg allergy should have introduction of peanut-containing food at 4-6 months of age to reduce their risk of peanut allergy, preceded by evaluation using peanut-specific IgE or skin prick testing to make sure it’s safe. That age window coincides with well-child visits and vaccination schedules, Dr. Rotrosen noted.
These guidelines represent the consensus of 26 organizations that participated in their development. Among them are the American Academy of Pediatrics, the American Academy of Family Physicians, the American Academy of Dermatology, the American College of Gastroenterology, and AAAAI.
“I expect the new guidelines, when finalized, to be endorsed by the leadership of all the participating organizations,” Dr. Rotrosen said.
The new paradigm will require cultural change, said Dr. James R. Baker Jr., CEO and chief medical officer of Food Allergy Research and Education, a nonprofit organization that provided partial funding for LEAP and LEAP-On.

“I think for a long time we’ve vilified these foods. There’s nothing inherently wrong with their intake, and that’s a message we need to get across to parents and physicians so they can start thinking differently,” he said.
“The good news about these studies is that they show there’s no reason not to do this,” Dr. Baker added. “There’s no harm that comes from the early introduction.”
Dr. Lack, who led the EAT trial, noted that the study didn’t meet it’s primary endpoint of a significantly lower prevalence of food allergy to any of the six intervention foods at age 3 years in the intention-to-treat analysis. But adherence to the demanding EAT early-introduction protocol was a problem. Indeed, only 43% of participants adhered to the study protocol. In a per-protocol analysis restricted to the adherent group, however, early introduction was associated with a highly significant 67% reduction in the relative risk of food allergy at 3 years of age compared to controls. And for the two most prevalent food allergies – to peanut and egg – the relative risk reductions in the early-introduction group were 100% and 75%, respectively.
The EAT results suggest that an effective preventive dose of peanut in infants at least 3 months of age is roughly 2 g of peanut protein per week, equivalent to just under 2 tsp of peanut butter, according to Dr. Lack.
Simultaneously with presentation of the LEAP-On and EAT trials in Los Angeles, the studies were published online at NEJM.org (doi: 10.1056/NEJMoa1514210 for LEAP-ON and 10.1056/NEJMoa1514209 for EAT).
LEAP-On was supported primarily by NIAID. EAT was funded mainly by the UK Foods Standards Agency and the Medical Research Council. Dr. Lack reported receiving grants from those agencies as well as Food Allergy Research and Education.
LOS ANGELES – A peanut allergy prevention strategy based upon regular consumption of peanut-containing foods from infancy to age 5 continued to provide protection even after peanut intake was halted for a full year from age 5 to 6, according to new results from an extension of the landmark LEAP trial, known as LEAP-On, presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The impetus for LEAP-On was the investigators’ concern that a period of peanut avoidance might cause loss of the protective state. But that didn’t occur.
“I think there is no doubt that we have prevented peanut allergy so far in these high-risk children. Next, the LEAP-Ad Lib study will tell us whether we’ve prevented it by age 10,” said Dr. Gideon Lack of King’s College London, who headed LEAP-On.
A second major randomized trial known as EAT (Enquiring About Tolerance) presented at the meeting provided further support for early dietary introduction of allergenic foods. EAT differed from LEAP (Learning Early About Peanut Allergy) and LEAP-On in that it ambitiously randomized infants to early introduction or avoidance of not one but six allergenic foods: peanut, cooked egg, cow’s milk, fish, sesame, and wheat. Also, while LEAP and LEAP-On involved roughly 600 infants known to be at very high risk for allergy, EAT was conducted in a general population of 1,303 infants who weren’t at increased risk, all of whom were exclusively breast-fed until the intervention beginning at age 3 months.
The presentation of the LEAP-On and EAT results at the AAAAI annual meeting was a major event marked by the National Institute of Allergy and Infectious Diseases by same-day release of new NIAID-sponsored draft recommendations for the diagnosis and management of food allergies.
In a press conference held at the AAAAI annual meeting to announce the start of a 45-day public comment period for the draft update of the 2010 guidelines, Dr. Daniel Rotrosen, director of NIAID’s division of allergy, immunology and transplantation, said the new guidelines were developed largely in response to the compelling LEAP findings. That trial demonstrated that sustained consumption of peanut starting in infancy resulted in an 81% lower rate of peanut allergy at age 5 years compared to a strategy of peanut avoidance (N Engl J Med. 2015;372:803-13).
The draft guidelines, now available on the NIAID website, represent a sharp departure from the former recommendation that physicians encourage exclusive breastfeeding for the first 6 months of life followed by cautious introduction of other foods. Whereas the former orthodoxy was that delayed introduction of allergenic foods protects against development of food allergy, the new evidence-based concept supported by the LEAP and EAT findings is that just the opposite is true: that is, introduction of such foods during the period of immunologic plasticity in infancy induces tolerance.
Thus, the draft guidelines recommend that infants at high risk for peanut allergy because they have severe eczema and/or egg allergy should have introduction of peanut-containing food at 4-6 months of age to reduce their risk of peanut allergy, preceded by evaluation using peanut-specific IgE or skin prick testing to make sure it’s safe. That age window coincides with well-child visits and vaccination schedules, Dr. Rotrosen noted.
These guidelines represent the consensus of 26 organizations that participated in their development. Among them are the American Academy of Pediatrics, the American Academy of Family Physicians, the American Academy of Dermatology, the American College of Gastroenterology, and AAAAI.
“I expect the new guidelines, when finalized, to be endorsed by the leadership of all the participating organizations,” Dr. Rotrosen said.
The new paradigm will require cultural change, said Dr. James R. Baker Jr., CEO and chief medical officer of Food Allergy Research and Education, a nonprofit organization that provided partial funding for LEAP and LEAP-On.
“I think for a long time we’ve vilified these foods. There’s nothing inherently wrong with their intake, and that’s a message we need to get across to parents and physicians so they can start thinking differently,” he said.
“The good news about these studies is that they show there’s no reason not to do this,” Dr. Baker added. “There’s no harm that comes from the early introduction.”
Dr. Lack, who led the EAT trial, noted that the study didn’t meet it’s primary endpoint of a significantly lower prevalence of food allergy to any of the six intervention foods at age 3 years in the intention-to-treat analysis. But adherence to the demanding EAT early-introduction protocol was a problem. Indeed, only 43% of participants adhered to the study protocol. In a per-protocol analysis restricted to the adherent group, however, early introduction was associated with a highly significant 67% reduction in the relative risk of food allergy at 3 years of age compared to controls. And for the two most prevalent food allergies – to peanut and egg – the relative risk reductions in the early-introduction group were 100% and 75%, respectively.
The EAT results suggest that an effective preventive dose of peanut in infants at least 3 months of age is roughly 2 g of peanut protein per week, equivalent to just under 2 tsp of peanut butter, according to Dr. Lack.
Simultaneously with presentation of the LEAP-On and EAT trials in Los Angeles, the studies were published online at NEJM.org (doi: 10.1056/NEJMoa1514210 for LEAP-ON and 10.1056/NEJMoa1514209 for EAT).
LEAP-On was supported primarily by NIAID. EAT was funded mainly by the UK Foods Standards Agency and the Medical Research Council. Dr. Lack reported receiving grants from those agencies as well as Food Allergy Research and Education.
LOS ANGELES – A peanut allergy prevention strategy based upon regular consumption of peanut-containing foods from infancy to age 5 continued to provide protection even after peanut intake was halted for a full year from age 5 to 6, according to new results from an extension of the landmark LEAP trial, known as LEAP-On, presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The impetus for LEAP-On was the investigators’ concern that a period of peanut avoidance might cause loss of the protective state. But that didn’t occur.
“I think there is no doubt that we have prevented peanut allergy so far in these high-risk children. Next, the LEAP-Ad Lib study will tell us whether we’ve prevented it by age 10,” said Dr. Gideon Lack of King’s College London, who headed LEAP-On.
A second major randomized trial known as EAT (Enquiring About Tolerance) presented at the meeting provided further support for early dietary introduction of allergenic foods. EAT differed from LEAP (Learning Early About Peanut Allergy) and LEAP-On in that it ambitiously randomized infants to early introduction or avoidance of not one but six allergenic foods: peanut, cooked egg, cow’s milk, fish, sesame, and wheat. Also, while LEAP and LEAP-On involved roughly 600 infants known to be at very high risk for allergy, EAT was conducted in a general population of 1,303 infants who weren’t at increased risk, all of whom were exclusively breast-fed until the intervention beginning at age 3 months.
The presentation of the LEAP-On and EAT results at the AAAAI annual meeting was a major event marked by the National Institute of Allergy and Infectious Diseases by same-day release of new NIAID-sponsored draft recommendations for the diagnosis and management of food allergies.
In a press conference held at the AAAAI annual meeting to announce the start of a 45-day public comment period for the draft update of the 2010 guidelines, Dr. Daniel Rotrosen, director of NIAID’s division of allergy, immunology and transplantation, said the new guidelines were developed largely in response to the compelling LEAP findings. That trial demonstrated that sustained consumption of peanut starting in infancy resulted in an 81% lower rate of peanut allergy at age 5 years compared to a strategy of peanut avoidance (N Engl J Med. 2015;372:803-13).
The draft guidelines, now available on the NIAID website, represent a sharp departure from the former recommendation that physicians encourage exclusive breastfeeding for the first 6 months of life followed by cautious introduction of other foods. Whereas the former orthodoxy was that delayed introduction of allergenic foods protects against development of food allergy, the new evidence-based concept supported by the LEAP and EAT findings is that just the opposite is true: that is, introduction of such foods during the period of immunologic plasticity in infancy induces tolerance.
Thus, the draft guidelines recommend that infants at high risk for peanut allergy because they have severe eczema and/or egg allergy should have introduction of peanut-containing food at 4-6 months of age to reduce their risk of peanut allergy, preceded by evaluation using peanut-specific IgE or skin prick testing to make sure it’s safe. That age window coincides with well-child visits and vaccination schedules, Dr. Rotrosen noted.
These guidelines represent the consensus of 26 organizations that participated in their development. Among them are the American Academy of Pediatrics, the American Academy of Family Physicians, the American Academy of Dermatology, the American College of Gastroenterology, and AAAAI.
“I expect the new guidelines, when finalized, to be endorsed by the leadership of all the participating organizations,” Dr. Rotrosen said.
The new paradigm will require cultural change, said Dr. James R. Baker Jr., CEO and chief medical officer of Food Allergy Research and Education, a nonprofit organization that provided partial funding for LEAP and LEAP-On.
“I think for a long time we’ve vilified these foods. There’s nothing inherently wrong with their intake, and that’s a message we need to get across to parents and physicians so they can start thinking differently,” he said.
“The good news about these studies is that they show there’s no reason not to do this,” Dr. Baker added. “There’s no harm that comes from the early introduction.”
Dr. Lack, who led the EAT trial, noted that the study didn’t meet it’s primary endpoint of a significantly lower prevalence of food allergy to any of the six intervention foods at age 3 years in the intention-to-treat analysis. But adherence to the demanding EAT early-introduction protocol was a problem. Indeed, only 43% of participants adhered to the study protocol. In a per-protocol analysis restricted to the adherent group, however, early introduction was associated with a highly significant 67% reduction in the relative risk of food allergy at 3 years of age compared to controls. And for the two most prevalent food allergies – to peanut and egg – the relative risk reductions in the early-introduction group were 100% and 75%, respectively.
The EAT results suggest that an effective preventive dose of peanut in infants at least 3 months of age is roughly 2 g of peanut protein per week, equivalent to just under 2 tsp of peanut butter, according to Dr. Lack.
Simultaneously with presentation of the LEAP-On and EAT trials in Los Angeles, the studies were published online at NEJM.org (doi: 10.1056/NEJMoa1514210 for LEAP-ON and 10.1056/NEJMoa1514209 for EAT).
LEAP-On was supported primarily by NIAID. EAT was funded mainly by the UK Foods Standards Agency and the Medical Research Council. Dr. Lack reported receiving grants from those agencies as well as Food Allergy Research and Education.
EXPERT ANALYSIS FROM THE 2016 AAAAI ANNUAL MEETING
