User login
AAAAI: Early peanut consumption brings lasting protection from allergy
LOS ANGELES – A peanut allergy prevention strategy based upon regular consumption of peanut-containing foods from infancy to age 5 continued to provide protection even after peanut intake was halted for a full year from age 5 to 6, according to new results from an extension of the landmark LEAP trial, known as LEAP-On, presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The impetus for LEAP-On was the investigators’ concern that a period of peanut avoidance might cause loss of the protective state. But that didn’t occur.
“I think there is no doubt that we have prevented peanut allergy so far in these high-risk children. Next, the LEAP-Ad Lib study will tell us whether we’ve prevented it by age 10,” said Dr. Gideon Lack of King’s College London, who headed LEAP-On.

A second major randomized trial known as EAT (Enquiring About Tolerance) presented at the meeting provided further support for early dietary introduction of allergenic foods. EAT differed from LEAP (Learning Early About Peanut Allergy) and LEAP-On in that it ambitiously randomized infants to early introduction or avoidance of not one but six allergenic foods: peanut, cooked egg, cow’s milk, fish, sesame, and wheat. Also, while LEAP and LEAP-On involved roughly 600 infants known to be at very high risk for allergy, EAT was conducted in a general population of 1,303 infants who weren’t at increased risk, all of whom were exclusively breast-fed until the intervention beginning at age 3 months.
The presentation of the LEAP-On and EAT results at the AAAAI annual meeting was a major event marked by the National Institute of Allergy and Infectious Diseases by same-day release of new NIAID-sponsored draft recommendations for the diagnosis and management of food allergies.
In a press conference held at the AAAAI annual meeting to announce the start of a 45-day public comment period for the draft update of the 2010 guidelines, Dr. Daniel Rotrosen, director of NIAID’s division of allergy, immunology and transplantation, said the new guidelines were developed largely in response to the compelling LEAP findings. That trial demonstrated that sustained consumption of peanut starting in infancy resulted in an 81% lower rate of peanut allergy at age 5 years compared to a strategy of peanut avoidance (N Engl J Med. 2015;372:803-13).

The draft guidelines, now available on the NIAID website, represent a sharp departure from the former recommendation that physicians encourage exclusive breastfeeding for the first 6 months of life followed by cautious introduction of other foods. Whereas the former orthodoxy was that delayed introduction of allergenic foods protects against development of food allergy, the new evidence-based concept supported by the LEAP and EAT findings is that just the opposite is true: that is, introduction of such foods during the period of immunologic plasticity in infancy induces tolerance.
Thus, the draft guidelines recommend that infants at high risk for peanut allergy because they have severe eczema and/or egg allergy should have introduction of peanut-containing food at 4-6 months of age to reduce their risk of peanut allergy, preceded by evaluation using peanut-specific IgE or skin prick testing to make sure it’s safe. That age window coincides with well-child visits and vaccination schedules, Dr. Rotrosen noted.
These guidelines represent the consensus of 26 organizations that participated in their development. Among them are the American Academy of Pediatrics, the American Academy of Family Physicians, the American Academy of Dermatology, the American College of Gastroenterology, and AAAAI.
“I expect the new guidelines, when finalized, to be endorsed by the leadership of all the participating organizations,” Dr. Rotrosen said.
The new paradigm will require cultural change, said Dr. James R. Baker Jr., CEO and chief medical officer of Food Allergy Research and Education, a nonprofit organization that provided partial funding for LEAP and LEAP-On.

“I think for a long time we’ve vilified these foods. There’s nothing inherently wrong with their intake, and that’s a message we need to get across to parents and physicians so they can start thinking differently,” he said.
“The good news about these studies is that they show there’s no reason not to do this,” Dr. Baker added. “There’s no harm that comes from the early introduction.”
Dr. Lack, who led the EAT trial, noted that the study didn’t meet it’s primary endpoint of a significantly lower prevalence of food allergy to any of the six intervention foods at age 3 years in the intention-to-treat analysis. But adherence to the demanding EAT early-introduction protocol was a problem. Indeed, only 43% of participants adhered to the study protocol. In a per-protocol analysis restricted to the adherent group, however, early introduction was associated with a highly significant 67% reduction in the relative risk of food allergy at 3 years of age compared to controls. And for the two most prevalent food allergies – to peanut and egg – the relative risk reductions in the early-introduction group were 100% and 75%, respectively.
The EAT results suggest that an effective preventive dose of peanut in infants at least 3 months of age is roughly 2 g of peanut protein per week, equivalent to just under 2 tsp of peanut butter, according to Dr. Lack.
Simultaneously with presentation of the LEAP-On and EAT trials in Los Angeles, the studies were published online at NEJM.org (doi: 10.1056/NEJMoa1514210 for LEAP-ON and 10.1056/NEJMoa1514209 for EAT).
LEAP-On was supported primarily by NIAID. EAT was funded mainly by the UK Foods Standards Agency and the Medical Research Council. Dr. Lack reported receiving grants from those agencies as well as Food Allergy Research and Education.
LOS ANGELES – A peanut allergy prevention strategy based upon regular consumption of peanut-containing foods from infancy to age 5 continued to provide protection even after peanut intake was halted for a full year from age 5 to 6, according to new results from an extension of the landmark LEAP trial, known as LEAP-On, presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The impetus for LEAP-On was the investigators’ concern that a period of peanut avoidance might cause loss of the protective state. But that didn’t occur.
“I think there is no doubt that we have prevented peanut allergy so far in these high-risk children. Next, the LEAP-Ad Lib study will tell us whether we’ve prevented it by age 10,” said Dr. Gideon Lack of King’s College London, who headed LEAP-On.
A second major randomized trial known as EAT (Enquiring About Tolerance) presented at the meeting provided further support for early dietary introduction of allergenic foods. EAT differed from LEAP (Learning Early About Peanut Allergy) and LEAP-On in that it ambitiously randomized infants to early introduction or avoidance of not one but six allergenic foods: peanut, cooked egg, cow’s milk, fish, sesame, and wheat. Also, while LEAP and LEAP-On involved roughly 600 infants known to be at very high risk for allergy, EAT was conducted in a general population of 1,303 infants who weren’t at increased risk, all of whom were exclusively breast-fed until the intervention beginning at age 3 months.
The presentation of the LEAP-On and EAT results at the AAAAI annual meeting was a major event marked by the National Institute of Allergy and Infectious Diseases by same-day release of new NIAID-sponsored draft recommendations for the diagnosis and management of food allergies.
In a press conference held at the AAAAI annual meeting to announce the start of a 45-day public comment period for the draft update of the 2010 guidelines, Dr. Daniel Rotrosen, director of NIAID’s division of allergy, immunology and transplantation, said the new guidelines were developed largely in response to the compelling LEAP findings. That trial demonstrated that sustained consumption of peanut starting in infancy resulted in an 81% lower rate of peanut allergy at age 5 years compared to a strategy of peanut avoidance (N Engl J Med. 2015;372:803-13).
The draft guidelines, now available on the NIAID website, represent a sharp departure from the former recommendation that physicians encourage exclusive breastfeeding for the first 6 months of life followed by cautious introduction of other foods. Whereas the former orthodoxy was that delayed introduction of allergenic foods protects against development of food allergy, the new evidence-based concept supported by the LEAP and EAT findings is that just the opposite is true: that is, introduction of such foods during the period of immunologic plasticity in infancy induces tolerance.
Thus, the draft guidelines recommend that infants at high risk for peanut allergy because they have severe eczema and/or egg allergy should have introduction of peanut-containing food at 4-6 months of age to reduce their risk of peanut allergy, preceded by evaluation using peanut-specific IgE or skin prick testing to make sure it’s safe. That age window coincides with well-child visits and vaccination schedules, Dr. Rotrosen noted.
These guidelines represent the consensus of 26 organizations that participated in their development. Among them are the American Academy of Pediatrics, the American Academy of Family Physicians, the American Academy of Dermatology, the American College of Gastroenterology, and AAAAI.
“I expect the new guidelines, when finalized, to be endorsed by the leadership of all the participating organizations,” Dr. Rotrosen said.
The new paradigm will require cultural change, said Dr. James R. Baker Jr., CEO and chief medical officer of Food Allergy Research and Education, a nonprofit organization that provided partial funding for LEAP and LEAP-On.
“I think for a long time we’ve vilified these foods. There’s nothing inherently wrong with their intake, and that’s a message we need to get across to parents and physicians so they can start thinking differently,” he said.
“The good news about these studies is that they show there’s no reason not to do this,” Dr. Baker added. “There’s no harm that comes from the early introduction.”
Dr. Lack, who led the EAT trial, noted that the study didn’t meet it’s primary endpoint of a significantly lower prevalence of food allergy to any of the six intervention foods at age 3 years in the intention-to-treat analysis. But adherence to the demanding EAT early-introduction protocol was a problem. Indeed, only 43% of participants adhered to the study protocol. In a per-protocol analysis restricted to the adherent group, however, early introduction was associated with a highly significant 67% reduction in the relative risk of food allergy at 3 years of age compared to controls. And for the two most prevalent food allergies – to peanut and egg – the relative risk reductions in the early-introduction group were 100% and 75%, respectively.
The EAT results suggest that an effective preventive dose of peanut in infants at least 3 months of age is roughly 2 g of peanut protein per week, equivalent to just under 2 tsp of peanut butter, according to Dr. Lack.
Simultaneously with presentation of the LEAP-On and EAT trials in Los Angeles, the studies were published online at NEJM.org (doi: 10.1056/NEJMoa1514210 for LEAP-ON and 10.1056/NEJMoa1514209 for EAT).
LEAP-On was supported primarily by NIAID. EAT was funded mainly by the UK Foods Standards Agency and the Medical Research Council. Dr. Lack reported receiving grants from those agencies as well as Food Allergy Research and Education.
LOS ANGELES – A peanut allergy prevention strategy based upon regular consumption of peanut-containing foods from infancy to age 5 continued to provide protection even after peanut intake was halted for a full year from age 5 to 6, according to new results from an extension of the landmark LEAP trial, known as LEAP-On, presented at the annual meeting of the American Academy of Allergy, Asthma, and Immunology.
The impetus for LEAP-On was the investigators’ concern that a period of peanut avoidance might cause loss of the protective state. But that didn’t occur.
“I think there is no doubt that we have prevented peanut allergy so far in these high-risk children. Next, the LEAP-Ad Lib study will tell us whether we’ve prevented it by age 10,” said Dr. Gideon Lack of King’s College London, who headed LEAP-On.
A second major randomized trial known as EAT (Enquiring About Tolerance) presented at the meeting provided further support for early dietary introduction of allergenic foods. EAT differed from LEAP (Learning Early About Peanut Allergy) and LEAP-On in that it ambitiously randomized infants to early introduction or avoidance of not one but six allergenic foods: peanut, cooked egg, cow’s milk, fish, sesame, and wheat. Also, while LEAP and LEAP-On involved roughly 600 infants known to be at very high risk for allergy, EAT was conducted in a general population of 1,303 infants who weren’t at increased risk, all of whom were exclusively breast-fed until the intervention beginning at age 3 months.
The presentation of the LEAP-On and EAT results at the AAAAI annual meeting was a major event marked by the National Institute of Allergy and Infectious Diseases by same-day release of new NIAID-sponsored draft recommendations for the diagnosis and management of food allergies.
In a press conference held at the AAAAI annual meeting to announce the start of a 45-day public comment period for the draft update of the 2010 guidelines, Dr. Daniel Rotrosen, director of NIAID’s division of allergy, immunology and transplantation, said the new guidelines were developed largely in response to the compelling LEAP findings. That trial demonstrated that sustained consumption of peanut starting in infancy resulted in an 81% lower rate of peanut allergy at age 5 years compared to a strategy of peanut avoidance (N Engl J Med. 2015;372:803-13).
The draft guidelines, now available on the NIAID website, represent a sharp departure from the former recommendation that physicians encourage exclusive breastfeeding for the first 6 months of life followed by cautious introduction of other foods. Whereas the former orthodoxy was that delayed introduction of allergenic foods protects against development of food allergy, the new evidence-based concept supported by the LEAP and EAT findings is that just the opposite is true: that is, introduction of such foods during the period of immunologic plasticity in infancy induces tolerance.
Thus, the draft guidelines recommend that infants at high risk for peanut allergy because they have severe eczema and/or egg allergy should have introduction of peanut-containing food at 4-6 months of age to reduce their risk of peanut allergy, preceded by evaluation using peanut-specific IgE or skin prick testing to make sure it’s safe. That age window coincides with well-child visits and vaccination schedules, Dr. Rotrosen noted.
These guidelines represent the consensus of 26 organizations that participated in their development. Among them are the American Academy of Pediatrics, the American Academy of Family Physicians, the American Academy of Dermatology, the American College of Gastroenterology, and AAAAI.
“I expect the new guidelines, when finalized, to be endorsed by the leadership of all the participating organizations,” Dr. Rotrosen said.
The new paradigm will require cultural change, said Dr. James R. Baker Jr., CEO and chief medical officer of Food Allergy Research and Education, a nonprofit organization that provided partial funding for LEAP and LEAP-On.
“I think for a long time we’ve vilified these foods. There’s nothing inherently wrong with their intake, and that’s a message we need to get across to parents and physicians so they can start thinking differently,” he said.
“The good news about these studies is that they show there’s no reason not to do this,” Dr. Baker added. “There’s no harm that comes from the early introduction.”
Dr. Lack, who led the EAT trial, noted that the study didn’t meet it’s primary endpoint of a significantly lower prevalence of food allergy to any of the six intervention foods at age 3 years in the intention-to-treat analysis. But adherence to the demanding EAT early-introduction protocol was a problem. Indeed, only 43% of participants adhered to the study protocol. In a per-protocol analysis restricted to the adherent group, however, early introduction was associated with a highly significant 67% reduction in the relative risk of food allergy at 3 years of age compared to controls. And for the two most prevalent food allergies – to peanut and egg – the relative risk reductions in the early-introduction group were 100% and 75%, respectively.
The EAT results suggest that an effective preventive dose of peanut in infants at least 3 months of age is roughly 2 g of peanut protein per week, equivalent to just under 2 tsp of peanut butter, according to Dr. Lack.
Simultaneously with presentation of the LEAP-On and EAT trials in Los Angeles, the studies were published online at NEJM.org (doi: 10.1056/NEJMoa1514210 for LEAP-ON and 10.1056/NEJMoa1514209 for EAT).
LEAP-On was supported primarily by NIAID. EAT was funded mainly by the UK Foods Standards Agency and the Medical Research Council. Dr. Lack reported receiving grants from those agencies as well as Food Allergy Research and Education.
EXPERT ANALYSIS FROM THE 2016 AAAAI ANNUAL MEETING

AAAAI: EpiPen Jr Needles Too Long for Many Children Under 15 kg
LOS ANGELES – For about half of children under 15 kg, pediatric epinephrine autoinjector needles are too long – they’re likely to hit the femur.
If the drug is deposited at the periosteum, it won’t be absorbed properly. If the needle delivers it to the bone marrow, the results could be disastrous.
“I’ve had three patients where the needle came back bent, so this happens,” said Dr. Harold Kim, an allergist in Kitchener, Ont. “Fortunately, there’s a fairly simple workaround. I ask parents to squeeze the [thigh] muscle before they give the shot, so that the muscle doesn’t compress. If the muscle doesn’t compress, you won’t hit bone, and the kid is going to be fine. Parents are really grateful” to learn this, but “they have to be careful not to inject their fingers.”
The findings come from Dr. Kim’s ultrasound study of thigh tissue thickness in 53 children weighing 7.5-15 kg. He and his colleagues found that with 10 pounds of pressure to simulate autoinjector deployment, the mean skin-to-bone distance was 13.3 mm, plus or minus 2.1 mm (J Allergy Clin Immunol. 2016 Feb. doi: 10.1016/j.jaci.2015.12.1167).
The needle length for EpiPen Jr is 12.7 mm, which was long enough to strike bone in 43% of the subjects.
“Epinephrine autoinjectors should be the mainstay of treatment for anaphylaxis, but our data suggest that the optimal needle length” for patients 7.5-15 kg “should be shorter than the needle length in current, commercially available” products. “There may be some modifications that need to be made in the way they are given. I actually ultrasound all the kids in my clinic to see if there will be problems,” Dr. Kim said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The study was done with an ultrasound probe in a housing that mimicked the footprint of Sanofi’s Auvi-Q, which is no longer on the U.S. and Canadian markets. If anything, the problem would be worse with EpiPen Jr because of its smaller footprint, Dr. Kim said.
On average, the subjects were 20 months old and 11 kg. Just over half were boys, and about 80% were white. The mean height was 79 cm and mean body mass index 19 kg/m2. About 60% of the subjects had injectors because of food allergies. Both transverse and longitudinal images of thigh tissue were used in the study, and distances were read by a blinded ultrasound expert.
Dr. Kim and his colleagues became interested after finding that needles may actually be too short to reach muscle in obese patients. While working on that issue, however, they also discovered “that 30% of kids less than 15 kg were at risk of the needle hitting the bone. We were surprised by those findings,” so looked into them further, he said.
EpiPen Jr is off label for children under 15 kg, but still often prescribed for them.
Sanofi funded the work. Dr. Kim is an advisor for the company, as well as for Pfizer, maker of EpiPen.
LOS ANGELES – For about half of children under 15 kg, pediatric epinephrine autoinjector needles are too long – they’re likely to hit the femur.
If the drug is deposited at the periosteum, it won’t be absorbed properly. If the needle delivers it to the bone marrow, the results could be disastrous.
“I’ve had three patients where the needle came back bent, so this happens,” said Dr. Harold Kim, an allergist in Kitchener, Ont. “Fortunately, there’s a fairly simple workaround. I ask parents to squeeze the [thigh] muscle before they give the shot, so that the muscle doesn’t compress. If the muscle doesn’t compress, you won’t hit bone, and the kid is going to be fine. Parents are really grateful” to learn this, but “they have to be careful not to inject their fingers.”
The findings come from Dr. Kim’s ultrasound study of thigh tissue thickness in 53 children weighing 7.5-15 kg. He and his colleagues found that with 10 pounds of pressure to simulate autoinjector deployment, the mean skin-to-bone distance was 13.3 mm, plus or minus 2.1 mm (J Allergy Clin Immunol. 2016 Feb. doi: 10.1016/j.jaci.2015.12.1167).
The needle length for EpiPen Jr is 12.7 mm, which was long enough to strike bone in 43% of the subjects.
“Epinephrine autoinjectors should be the mainstay of treatment for anaphylaxis, but our data suggest that the optimal needle length” for patients 7.5-15 kg “should be shorter than the needle length in current, commercially available” products. “There may be some modifications that need to be made in the way they are given. I actually ultrasound all the kids in my clinic to see if there will be problems,” Dr. Kim said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The study was done with an ultrasound probe in a housing that mimicked the footprint of Sanofi’s Auvi-Q, which is no longer on the U.S. and Canadian markets. If anything, the problem would be worse with EpiPen Jr because of its smaller footprint, Dr. Kim said.
On average, the subjects were 20 months old and 11 kg. Just over half were boys, and about 80% were white. The mean height was 79 cm and mean body mass index 19 kg/m2. About 60% of the subjects had injectors because of food allergies. Both transverse and longitudinal images of thigh tissue were used in the study, and distances were read by a blinded ultrasound expert.
Dr. Kim and his colleagues became interested after finding that needles may actually be too short to reach muscle in obese patients. While working on that issue, however, they also discovered “that 30% of kids less than 15 kg were at risk of the needle hitting the bone. We were surprised by those findings,” so looked into them further, he said.
EpiPen Jr is off label for children under 15 kg, but still often prescribed for them.
Sanofi funded the work. Dr. Kim is an advisor for the company, as well as for Pfizer, maker of EpiPen.
LOS ANGELES – For about half of children under 15 kg, pediatric epinephrine autoinjector needles are too long – they’re likely to hit the femur.
If the drug is deposited at the periosteum, it won’t be absorbed properly. If the needle delivers it to the bone marrow, the results could be disastrous.
“I’ve had three patients where the needle came back bent, so this happens,” said Dr. Harold Kim, an allergist in Kitchener, Ont. “Fortunately, there’s a fairly simple workaround. I ask parents to squeeze the [thigh] muscle before they give the shot, so that the muscle doesn’t compress. If the muscle doesn’t compress, you won’t hit bone, and the kid is going to be fine. Parents are really grateful” to learn this, but “they have to be careful not to inject their fingers.”
The findings come from Dr. Kim’s ultrasound study of thigh tissue thickness in 53 children weighing 7.5-15 kg. He and his colleagues found that with 10 pounds of pressure to simulate autoinjector deployment, the mean skin-to-bone distance was 13.3 mm, plus or minus 2.1 mm (J Allergy Clin Immunol. 2016 Feb. doi: 10.1016/j.jaci.2015.12.1167).
The needle length for EpiPen Jr is 12.7 mm, which was long enough to strike bone in 43% of the subjects.
“Epinephrine autoinjectors should be the mainstay of treatment for anaphylaxis, but our data suggest that the optimal needle length” for patients 7.5-15 kg “should be shorter than the needle length in current, commercially available” products. “There may be some modifications that need to be made in the way they are given. I actually ultrasound all the kids in my clinic to see if there will be problems,” Dr. Kim said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The study was done with an ultrasound probe in a housing that mimicked the footprint of Sanofi’s Auvi-Q, which is no longer on the U.S. and Canadian markets. If anything, the problem would be worse with EpiPen Jr because of its smaller footprint, Dr. Kim said.
On average, the subjects were 20 months old and 11 kg. Just over half were boys, and about 80% were white. The mean height was 79 cm and mean body mass index 19 kg/m2. About 60% of the subjects had injectors because of food allergies. Both transverse and longitudinal images of thigh tissue were used in the study, and distances were read by a blinded ultrasound expert.
Dr. Kim and his colleagues became interested after finding that needles may actually be too short to reach muscle in obese patients. While working on that issue, however, they also discovered “that 30% of kids less than 15 kg were at risk of the needle hitting the bone. We were surprised by those findings,” so looked into them further, he said.
EpiPen Jr is off label for children under 15 kg, but still often prescribed for them.
Sanofi funded the work. Dr. Kim is an advisor for the company, as well as for Pfizer, maker of EpiPen.
AT 2016 AAAAI ANNUAL MEETING
AAAAI: EpiPen Jr needles too long for many children under 15 kg
LOS ANGELES – For about half of children under 15 kg, pediatric epinephrine autoinjector needles are too long – they’re likely to hit the femur.
If the drug is deposited at the periosteum, it won’t be absorbed properly. If the needle delivers it to the bone marrow, the results could be disastrous.
“I’ve had three patients where the needle came back bent, so this happens,” said Dr. Harold Kim, an allergist in Kitchener, Ont. “Fortunately, there’s a fairly simple workaround. I ask parents to squeeze the [thigh] muscle before they give the shot, so that the muscle doesn’t compress. If the muscle doesn’t compress, you won’t hit bone, and the kid is going to be fine. Parents are really grateful” to learn this, but “they have to be careful not to inject their fingers.”
The findings come from Dr. Kim’s ultrasound study of thigh tissue thickness in 53 children weighing 7.5-15 kg. He and his colleagues found that with 10 pounds of pressure to simulate autoinjector deployment, the mean skin-to-bone distance was 13.3 mm, plus or minus 2.1 mm (J Allergy Clin Immunol. 2016 Feb. doi: 10.1016/j.jaci.2015.12.1167).
The needle length for EpiPen Jr is 12.7 mm, which was long enough to strike bone in 43% of the subjects.
“Epinephrine autoinjectors should be the mainstay of treatment for anaphylaxis, but our data suggest that the optimal needle length” for patients 7.5-15 kg “should be shorter than the needle length in current, commercially available” products. “There may be some modifications that need to be made in the way they are given. I actually ultrasound all the kids in my clinic to see if there will be problems,” Dr. Kim said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The study was done with an ultrasound probe in a housing that mimicked the footprint of Sanofi’s Auvi-Q, which is no longer on the U.S. and Canadian markets. If anything, the problem would be worse with EpiPen Jr because of its smaller footprint, Dr. Kim said.
On average, the subjects were 20 months old and 11 kg. Just over half were boys, and about 80% were white. The mean height was 79 cm and mean body mass index 19 kg/m2. About 60% of the subjects had injectors because of food allergies. Both transverse and longitudinal images of thigh tissue were used in the study, and distances were read by a blinded ultrasound expert.
Dr. Kim and his colleagues became interested after finding that needles may actually be too short to reach muscle in obese patients. While working on that issue, however, they also discovered “that 30% of kids less than 15 kg were at risk of the needle hitting the bone. We were surprised by those findings,” so looked into them further, he said.
EpiPen Jr is off label for children under 15 kg, but still often prescribed for them.
Sanofi funded the work. Dr. Kim is an advisor for the company, as well as for Pfizer, maker of EpiPen.
LOS ANGELES – For about half of children under 15 kg, pediatric epinephrine autoinjector needles are too long – they’re likely to hit the femur.
If the drug is deposited at the periosteum, it won’t be absorbed properly. If the needle delivers it to the bone marrow, the results could be disastrous.
“I’ve had three patients where the needle came back bent, so this happens,” said Dr. Harold Kim, an allergist in Kitchener, Ont. “Fortunately, there’s a fairly simple workaround. I ask parents to squeeze the [thigh] muscle before they give the shot, so that the muscle doesn’t compress. If the muscle doesn’t compress, you won’t hit bone, and the kid is going to be fine. Parents are really grateful” to learn this, but “they have to be careful not to inject their fingers.”
The findings come from Dr. Kim’s ultrasound study of thigh tissue thickness in 53 children weighing 7.5-15 kg. He and his colleagues found that with 10 pounds of pressure to simulate autoinjector deployment, the mean skin-to-bone distance was 13.3 mm, plus or minus 2.1 mm (J Allergy Clin Immunol. 2016 Feb. doi: 10.1016/j.jaci.2015.12.1167).
The needle length for EpiPen Jr is 12.7 mm, which was long enough to strike bone in 43% of the subjects.
“Epinephrine autoinjectors should be the mainstay of treatment for anaphylaxis, but our data suggest that the optimal needle length” for patients 7.5-15 kg “should be shorter than the needle length in current, commercially available” products. “There may be some modifications that need to be made in the way they are given. I actually ultrasound all the kids in my clinic to see if there will be problems,” Dr. Kim said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The study was done with an ultrasound probe in a housing that mimicked the footprint of Sanofi’s Auvi-Q, which is no longer on the U.S. and Canadian markets. If anything, the problem would be worse with EpiPen Jr because of its smaller footprint, Dr. Kim said.
On average, the subjects were 20 months old and 11 kg. Just over half were boys, and about 80% were white. The mean height was 79 cm and mean body mass index 19 kg/m2. About 60% of the subjects had injectors because of food allergies. Both transverse and longitudinal images of thigh tissue were used in the study, and distances were read by a blinded ultrasound expert.
Dr. Kim and his colleagues became interested after finding that needles may actually be too short to reach muscle in obese patients. While working on that issue, however, they also discovered “that 30% of kids less than 15 kg were at risk of the needle hitting the bone. We were surprised by those findings,” so looked into them further, he said.
EpiPen Jr is off label for children under 15 kg, but still often prescribed for them.
Sanofi funded the work. Dr. Kim is an advisor for the company, as well as for Pfizer, maker of EpiPen.
LOS ANGELES – For about half of children under 15 kg, pediatric epinephrine autoinjector needles are too long – they’re likely to hit the femur.
If the drug is deposited at the periosteum, it won’t be absorbed properly. If the needle delivers it to the bone marrow, the results could be disastrous.
“I’ve had three patients where the needle came back bent, so this happens,” said Dr. Harold Kim, an allergist in Kitchener, Ont. “Fortunately, there’s a fairly simple workaround. I ask parents to squeeze the [thigh] muscle before they give the shot, so that the muscle doesn’t compress. If the muscle doesn’t compress, you won’t hit bone, and the kid is going to be fine. Parents are really grateful” to learn this, but “they have to be careful not to inject their fingers.”
The findings come from Dr. Kim’s ultrasound study of thigh tissue thickness in 53 children weighing 7.5-15 kg. He and his colleagues found that with 10 pounds of pressure to simulate autoinjector deployment, the mean skin-to-bone distance was 13.3 mm, plus or minus 2.1 mm (J Allergy Clin Immunol. 2016 Feb. doi: 10.1016/j.jaci.2015.12.1167).
The needle length for EpiPen Jr is 12.7 mm, which was long enough to strike bone in 43% of the subjects.
“Epinephrine autoinjectors should be the mainstay of treatment for anaphylaxis, but our data suggest that the optimal needle length” for patients 7.5-15 kg “should be shorter than the needle length in current, commercially available” products. “There may be some modifications that need to be made in the way they are given. I actually ultrasound all the kids in my clinic to see if there will be problems,” Dr. Kim said at the American Academy of Allergy, Asthma, and Immunology annual meeting.
The study was done with an ultrasound probe in a housing that mimicked the footprint of Sanofi’s Auvi-Q, which is no longer on the U.S. and Canadian markets. If anything, the problem would be worse with EpiPen Jr because of its smaller footprint, Dr. Kim said.
On average, the subjects were 20 months old and 11 kg. Just over half were boys, and about 80% were white. The mean height was 79 cm and mean body mass index 19 kg/m2. About 60% of the subjects had injectors because of food allergies. Both transverse and longitudinal images of thigh tissue were used in the study, and distances were read by a blinded ultrasound expert.
Dr. Kim and his colleagues became interested after finding that needles may actually be too short to reach muscle in obese patients. While working on that issue, however, they also discovered “that 30% of kids less than 15 kg were at risk of the needle hitting the bone. We were surprised by those findings,” so looked into them further, he said.
EpiPen Jr is off label for children under 15 kg, but still often prescribed for them.
Sanofi funded the work. Dr. Kim is an advisor for the company, as well as for Pfizer, maker of EpiPen.
AT 2016 AAAAI ANNUAL MEETING
Key clinical point: EpiPen Jr needles are too long for many children under 15 kg.
Major finding: With 10 pounds of pressure to simulate autoinjector deployment, the mean skin-to-bone distance was 13.3 mm, plus or minus 2.1 mm. The needle length for EpiPen Jr is 12.7 mm, which was long enough to strike bone in 43% of the subjects.
Data source: Prospective investigation of 53 children weighing 7.5-15 kg.
Disclosures: Sanofi funded the work. The presenter is an adviser for the company, as well as for Pfizer.
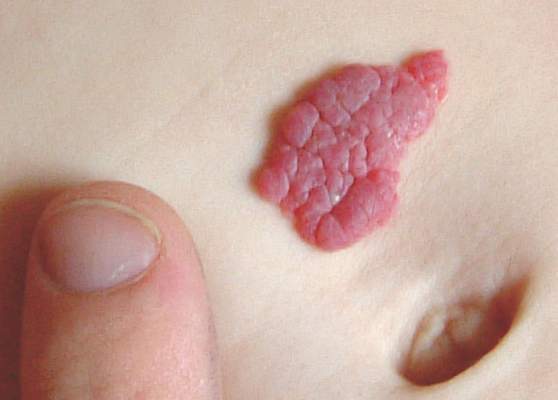
Hemangiomas Recur in 25% of Infants After Propranolol Stopped
Infantile hemangiomas treated with propranolol recurred in 25% of children after discontinuation of propranolol in a retrospective study of nearly 1,000 patients, according to findings published online March 7 in Pediatrics.
“Identifying risk factors for rebound growth could affect treatment strategies, particularly duration of therapy,” wrote Dr. Sonal D. Shah of the University of California, San Francisco, and colleagues.
The study population was the largest to date, the researchers noted, and included 980 children seen at 10 academic centers between 2008 and 2013. Most were term (82%) and female (77%). The average age at the start of treatment was 6 months, and a visual analog scale was used to determine the children’s response to treatment (Pediatrics. 2016. doi: 10.1542/peds.2015-1754). Overall, hemangiomas rebounded in 231 patients (25%). Of these, 191 (83%) required treatment modification. The mean age before initial hemangioma rebound was 17 months, after a mean treatment duration of 11 months.
“The most potent risk factor for rebound was the presence of a deep infantile hemangioma component (i.e., deep or mixed morphology), which was also noted in other studies,” the researchers wrote.
In a multivariate analysis, deep hemangiomas and mixed hemangiomas were significantly more likely (odds ratio, 3.3 and 2.4, respectively) to rebound than superficial hemangiomas, and rebounds were significantly more likely among girls than boys (OR, 1.7).
“The exact reasons for this are uncertain, but it appears that girls are intrinsically more predisposed not only to hemangioma development but also to growth,” Dr. Shah and associates said.
Children least likely to rebound were those who discontinued or tapered propranolol between ages 12 and 18 months, and this group was used as a reference group. By comparison, the odds of rebound were notably high among children who discontinued when they were younger than 9 months (OR, 2.4). The odds ratios for rebound when propranolol was discontinued at ages 18-21 months, 21-24 months, and older than 24 months were 2.0, 1.7, and 2.5, respectively.
The results were limited by the fact that most patients represented more severe cases that were referred for additional treatment, Dr. Shah and associates said. However, the findings suggest that recognizing the risk factors for rebound could aid clinicians when planning therapy.
Lead author Dr. Shah had no relevant financial conflicts to disclose. Several coauthors reported serving as investigators or consultants for Pfizer and for Pierre Fabre Dermatology, which manufactures the propranolol product used in the study. The study was supported by the University of California, San Francisco, Pediatric Dermatology research fund.
“Understanding the phenomenon of postpropranolol rebound, and being able to predict or (better yet) prevent it, will increase clinical success and parental satisfaction with oral propranolol therapy and, in some instances, help prevent morbidity (such as airway blockage resulting from subglottic infantile hemangioma rebound),” Dr. Anthony J. Mancini of Northwestern University in Chicago commented.
The rebound risk factor data in this study expand on and support findings from previous studies, Dr. Mancini noted. Many research questions remain regarding the propranolol dose and duration to manage infantile hemangiomas most effectively. However, “the results of this large cohort review by Shah et al. will help guide clinicians in optimizing oral propranolol therapy and minimizing rebound growth in select higher-risk lesions,” he said.
Dr. Mancini, who commented in an accompanying editorial (Pediatrics. 2016. doi: 10.1542/peds.2015-3739), is a consultant, grant recipient, and speaker for Pierre Fabre Dermatology, and is a member of the Hemangioma Investigator Group, a research consortium that includes several of the study’s coauthors.
“Understanding the phenomenon of postpropranolol rebound, and being able to predict or (better yet) prevent it, will increase clinical success and parental satisfaction with oral propranolol therapy and, in some instances, help prevent morbidity (such as airway blockage resulting from subglottic infantile hemangioma rebound),” Dr. Anthony J. Mancini of Northwestern University in Chicago commented.
The rebound risk factor data in this study expand on and support findings from previous studies, Dr. Mancini noted. Many research questions remain regarding the propranolol dose and duration to manage infantile hemangiomas most effectively. However, “the results of this large cohort review by Shah et al. will help guide clinicians in optimizing oral propranolol therapy and minimizing rebound growth in select higher-risk lesions,” he said.
Dr. Mancini, who commented in an accompanying editorial (Pediatrics. 2016. doi: 10.1542/peds.2015-3739), is a consultant, grant recipient, and speaker for Pierre Fabre Dermatology, and is a member of the Hemangioma Investigator Group, a research consortium that includes several of the study’s coauthors.
“Understanding the phenomenon of postpropranolol rebound, and being able to predict or (better yet) prevent it, will increase clinical success and parental satisfaction with oral propranolol therapy and, in some instances, help prevent morbidity (such as airway blockage resulting from subglottic infantile hemangioma rebound),” Dr. Anthony J. Mancini of Northwestern University in Chicago commented.
The rebound risk factor data in this study expand on and support findings from previous studies, Dr. Mancini noted. Many research questions remain regarding the propranolol dose and duration to manage infantile hemangiomas most effectively. However, “the results of this large cohort review by Shah et al. will help guide clinicians in optimizing oral propranolol therapy and minimizing rebound growth in select higher-risk lesions,” he said.
Dr. Mancini, who commented in an accompanying editorial (Pediatrics. 2016. doi: 10.1542/peds.2015-3739), is a consultant, grant recipient, and speaker for Pierre Fabre Dermatology, and is a member of the Hemangioma Investigator Group, a research consortium that includes several of the study’s coauthors.
Infantile hemangiomas treated with propranolol recurred in 25% of children after discontinuation of propranolol in a retrospective study of nearly 1,000 patients, according to findings published online March 7 in Pediatrics.
“Identifying risk factors for rebound growth could affect treatment strategies, particularly duration of therapy,” wrote Dr. Sonal D. Shah of the University of California, San Francisco, and colleagues.
The study population was the largest to date, the researchers noted, and included 980 children seen at 10 academic centers between 2008 and 2013. Most were term (82%) and female (77%). The average age at the start of treatment was 6 months, and a visual analog scale was used to determine the children’s response to treatment (Pediatrics. 2016. doi: 10.1542/peds.2015-1754). Overall, hemangiomas rebounded in 231 patients (25%). Of these, 191 (83%) required treatment modification. The mean age before initial hemangioma rebound was 17 months, after a mean treatment duration of 11 months.
“The most potent risk factor for rebound was the presence of a deep infantile hemangioma component (i.e., deep or mixed morphology), which was also noted in other studies,” the researchers wrote.
In a multivariate analysis, deep hemangiomas and mixed hemangiomas were significantly more likely (odds ratio, 3.3 and 2.4, respectively) to rebound than superficial hemangiomas, and rebounds were significantly more likely among girls than boys (OR, 1.7).
“The exact reasons for this are uncertain, but it appears that girls are intrinsically more predisposed not only to hemangioma development but also to growth,” Dr. Shah and associates said.
Children least likely to rebound were those who discontinued or tapered propranolol between ages 12 and 18 months, and this group was used as a reference group. By comparison, the odds of rebound were notably high among children who discontinued when they were younger than 9 months (OR, 2.4). The odds ratios for rebound when propranolol was discontinued at ages 18-21 months, 21-24 months, and older than 24 months were 2.0, 1.7, and 2.5, respectively.
The results were limited by the fact that most patients represented more severe cases that were referred for additional treatment, Dr. Shah and associates said. However, the findings suggest that recognizing the risk factors for rebound could aid clinicians when planning therapy.
Lead author Dr. Shah had no relevant financial conflicts to disclose. Several coauthors reported serving as investigators or consultants for Pfizer and for Pierre Fabre Dermatology, which manufactures the propranolol product used in the study. The study was supported by the University of California, San Francisco, Pediatric Dermatology research fund.
Infantile hemangiomas treated with propranolol recurred in 25% of children after discontinuation of propranolol in a retrospective study of nearly 1,000 patients, according to findings published online March 7 in Pediatrics.
“Identifying risk factors for rebound growth could affect treatment strategies, particularly duration of therapy,” wrote Dr. Sonal D. Shah of the University of California, San Francisco, and colleagues.
The study population was the largest to date, the researchers noted, and included 980 children seen at 10 academic centers between 2008 and 2013. Most were term (82%) and female (77%). The average age at the start of treatment was 6 months, and a visual analog scale was used to determine the children’s response to treatment (Pediatrics. 2016. doi: 10.1542/peds.2015-1754). Overall, hemangiomas rebounded in 231 patients (25%). Of these, 191 (83%) required treatment modification. The mean age before initial hemangioma rebound was 17 months, after a mean treatment duration of 11 months.
“The most potent risk factor for rebound was the presence of a deep infantile hemangioma component (i.e., deep or mixed morphology), which was also noted in other studies,” the researchers wrote.
In a multivariate analysis, deep hemangiomas and mixed hemangiomas were significantly more likely (odds ratio, 3.3 and 2.4, respectively) to rebound than superficial hemangiomas, and rebounds were significantly more likely among girls than boys (OR, 1.7).
“The exact reasons for this are uncertain, but it appears that girls are intrinsically more predisposed not only to hemangioma development but also to growth,” Dr. Shah and associates said.
Children least likely to rebound were those who discontinued or tapered propranolol between ages 12 and 18 months, and this group was used as a reference group. By comparison, the odds of rebound were notably high among children who discontinued when they were younger than 9 months (OR, 2.4). The odds ratios for rebound when propranolol was discontinued at ages 18-21 months, 21-24 months, and older than 24 months were 2.0, 1.7, and 2.5, respectively.
The results were limited by the fact that most patients represented more severe cases that were referred for additional treatment, Dr. Shah and associates said. However, the findings suggest that recognizing the risk factors for rebound could aid clinicians when planning therapy.
Lead author Dr. Shah had no relevant financial conflicts to disclose. Several coauthors reported serving as investigators or consultants for Pfizer and for Pierre Fabre Dermatology, which manufactures the propranolol product used in the study. The study was supported by the University of California, San Francisco, Pediatric Dermatology research fund.
FROM PEDIATRICS

Hemangiomas recur in 25% of infants after propranolol stopped
Infantile hemangiomas treated with propranolol recurred in 25% of children after discontinuation of propranolol in a retrospective study of nearly 1,000 patients, according to findings published online March 7 in Pediatrics.
“Identifying risk factors for rebound growth could affect treatment strategies, particularly duration of therapy,” wrote Dr. Sonal D. Shah of the University of California, San Francisco, and colleagues.

The study population was the largest to date, the researchers noted, and included 980 children seen at 10 academic centers between 2008 and 2013. Most were term (82%) and female (77%). The average age at the start of treatment was 6 months, and a visual analog scale was used to determine the children’s response to treatment (Pediatrics. 2016. doi: 10.1542/peds.2015-1754). Overall, hemangiomas rebounded in 231 patients (25%). Of these, 191 (83%) required treatment modification. The mean age before initial hemangioma rebound was 17 months, after a mean treatment duration of 11 months.
“The most potent risk factor for rebound was the presence of a deep infantile hemangioma component (i.e., deep or mixed morphology), which was also noted in other studies,” the researchers wrote.
In a multivariate analysis, deep hemangiomas and mixed hemangiomas were significantly more likely (odds ratio, 3.3 and 2.4, respectively) to rebound than superficial hemangiomas, and rebounds were significantly more likely among girls than boys (OR, 1.7).
“The exact reasons for this are uncertain, but it appears that girls are intrinsically more predisposed not only to hemangioma development but also to growth,” Dr. Shah and associates said.
Children least likely to rebound were those who discontinued or tapered propranolol between ages 12 and 18 months, and this group was used as a reference group. By comparison, the odds of rebound were notably high among children who discontinued when they were younger than 9 months (OR, 2.4). The odds ratios for rebound when propranolol was discontinued at ages 18-21 months, 21-24 months, and older than 24 months were 2.0, 1.7, and 2.5, respectively.
The results were limited by the fact that most patients represented more severe cases that were referred for additional treatment, Dr. Shah and associates said. However, the findings suggest that recognizing the risk factors for rebound could aid clinicians when planning therapy.
Lead author Dr. Shah had no relevant financial conflicts to disclose. Several coauthors reported serving as investigators or consultants for Pfizer and for Pierre Fabre Dermatology, which manufactures the propranolol product used in the study. The study was supported by the University of California, San Francisco, Pediatric Dermatology research fund.
“Understanding the phenomenon of postpropranolol rebound, and being able to predict or (better yet) prevent it, will increase clinical success and parental satisfaction with oral propranolol therapy and, in some instances, help prevent morbidity (such as airway blockage resulting from subglottic infantile hemangioma rebound),” Dr. Anthony J. Mancini of Northwestern University in Chicago commented.
The rebound risk factor data in this study expand on and support findings from previous studies, Dr. Mancini noted. Many research questions remain regarding the propranolol dose and duration to manage infantile hemangiomas most effectively. However, “the results of this large cohort review by Shah et al. will help guide clinicians in optimizing oral propranolol therapy and minimizing rebound growth in select higher-risk lesions,” he said.
Dr. Mancini, who commented in an accompanying editorial (Pediatrics. 2016. doi: 10.1542/peds.2015-3739), is a consultant, grant recipient, and speaker for Pierre Fabre Dermatology, and is a member of the Hemangioma Investigator Group, a research consortium that includes several of the study’s coauthors.
“Understanding the phenomenon of postpropranolol rebound, and being able to predict or (better yet) prevent it, will increase clinical success and parental satisfaction with oral propranolol therapy and, in some instances, help prevent morbidity (such as airway blockage resulting from subglottic infantile hemangioma rebound),” Dr. Anthony J. Mancini of Northwestern University in Chicago commented.
The rebound risk factor data in this study expand on and support findings from previous studies, Dr. Mancini noted. Many research questions remain regarding the propranolol dose and duration to manage infantile hemangiomas most effectively. However, “the results of this large cohort review by Shah et al. will help guide clinicians in optimizing oral propranolol therapy and minimizing rebound growth in select higher-risk lesions,” he said.
Dr. Mancini, who commented in an accompanying editorial (Pediatrics. 2016. doi: 10.1542/peds.2015-3739), is a consultant, grant recipient, and speaker for Pierre Fabre Dermatology, and is a member of the Hemangioma Investigator Group, a research consortium that includes several of the study’s coauthors.
“Understanding the phenomenon of postpropranolol rebound, and being able to predict or (better yet) prevent it, will increase clinical success and parental satisfaction with oral propranolol therapy and, in some instances, help prevent morbidity (such as airway blockage resulting from subglottic infantile hemangioma rebound),” Dr. Anthony J. Mancini of Northwestern University in Chicago commented.
The rebound risk factor data in this study expand on and support findings from previous studies, Dr. Mancini noted. Many research questions remain regarding the propranolol dose and duration to manage infantile hemangiomas most effectively. However, “the results of this large cohort review by Shah et al. will help guide clinicians in optimizing oral propranolol therapy and minimizing rebound growth in select higher-risk lesions,” he said.
Dr. Mancini, who commented in an accompanying editorial (Pediatrics. 2016. doi: 10.1542/peds.2015-3739), is a consultant, grant recipient, and speaker for Pierre Fabre Dermatology, and is a member of the Hemangioma Investigator Group, a research consortium that includes several of the study’s coauthors.
Infantile hemangiomas treated with propranolol recurred in 25% of children after discontinuation of propranolol in a retrospective study of nearly 1,000 patients, according to findings published online March 7 in Pediatrics.
“Identifying risk factors for rebound growth could affect treatment strategies, particularly duration of therapy,” wrote Dr. Sonal D. Shah of the University of California, San Francisco, and colleagues.
The study population was the largest to date, the researchers noted, and included 980 children seen at 10 academic centers between 2008 and 2013. Most were term (82%) and female (77%). The average age at the start of treatment was 6 months, and a visual analog scale was used to determine the children’s response to treatment (Pediatrics. 2016. doi: 10.1542/peds.2015-1754). Overall, hemangiomas rebounded in 231 patients (25%). Of these, 191 (83%) required treatment modification. The mean age before initial hemangioma rebound was 17 months, after a mean treatment duration of 11 months.
“The most potent risk factor for rebound was the presence of a deep infantile hemangioma component (i.e., deep or mixed morphology), which was also noted in other studies,” the researchers wrote.
In a multivariate analysis, deep hemangiomas and mixed hemangiomas were significantly more likely (odds ratio, 3.3 and 2.4, respectively) to rebound than superficial hemangiomas, and rebounds were significantly more likely among girls than boys (OR, 1.7).
“The exact reasons for this are uncertain, but it appears that girls are intrinsically more predisposed not only to hemangioma development but also to growth,” Dr. Shah and associates said.
Children least likely to rebound were those who discontinued or tapered propranolol between ages 12 and 18 months, and this group was used as a reference group. By comparison, the odds of rebound were notably high among children who discontinued when they were younger than 9 months (OR, 2.4). The odds ratios for rebound when propranolol was discontinued at ages 18-21 months, 21-24 months, and older than 24 months were 2.0, 1.7, and 2.5, respectively.
The results were limited by the fact that most patients represented more severe cases that were referred for additional treatment, Dr. Shah and associates said. However, the findings suggest that recognizing the risk factors for rebound could aid clinicians when planning therapy.
Lead author Dr. Shah had no relevant financial conflicts to disclose. Several coauthors reported serving as investigators or consultants for Pfizer and for Pierre Fabre Dermatology, which manufactures the propranolol product used in the study. The study was supported by the University of California, San Francisco, Pediatric Dermatology research fund.
Infantile hemangiomas treated with propranolol recurred in 25% of children after discontinuation of propranolol in a retrospective study of nearly 1,000 patients, according to findings published online March 7 in Pediatrics.
“Identifying risk factors for rebound growth could affect treatment strategies, particularly duration of therapy,” wrote Dr. Sonal D. Shah of the University of California, San Francisco, and colleagues.
The study population was the largest to date, the researchers noted, and included 980 children seen at 10 academic centers between 2008 and 2013. Most were term (82%) and female (77%). The average age at the start of treatment was 6 months, and a visual analog scale was used to determine the children’s response to treatment (Pediatrics. 2016. doi: 10.1542/peds.2015-1754). Overall, hemangiomas rebounded in 231 patients (25%). Of these, 191 (83%) required treatment modification. The mean age before initial hemangioma rebound was 17 months, after a mean treatment duration of 11 months.
“The most potent risk factor for rebound was the presence of a deep infantile hemangioma component (i.e., deep or mixed morphology), which was also noted in other studies,” the researchers wrote.
In a multivariate analysis, deep hemangiomas and mixed hemangiomas were significantly more likely (odds ratio, 3.3 and 2.4, respectively) to rebound than superficial hemangiomas, and rebounds were significantly more likely among girls than boys (OR, 1.7).
“The exact reasons for this are uncertain, but it appears that girls are intrinsically more predisposed not only to hemangioma development but also to growth,” Dr. Shah and associates said.
Children least likely to rebound were those who discontinued or tapered propranolol between ages 12 and 18 months, and this group was used as a reference group. By comparison, the odds of rebound were notably high among children who discontinued when they were younger than 9 months (OR, 2.4). The odds ratios for rebound when propranolol was discontinued at ages 18-21 months, 21-24 months, and older than 24 months were 2.0, 1.7, and 2.5, respectively.
The results were limited by the fact that most patients represented more severe cases that were referred for additional treatment, Dr. Shah and associates said. However, the findings suggest that recognizing the risk factors for rebound could aid clinicians when planning therapy.
Lead author Dr. Shah had no relevant financial conflicts to disclose. Several coauthors reported serving as investigators or consultants for Pfizer and for Pierre Fabre Dermatology, which manufactures the propranolol product used in the study. The study was supported by the University of California, San Francisco, Pediatric Dermatology research fund.
FROM PEDIATRICS
Key clinical point: This large study of nearly 1,000 patients identifies risk factors for hemangioma rebound that may help guide oral propranolol treatment decisions.
Major finding: Infantile hemangiomas recurred in 25% of children after discontinuation of oral propranolol therapy.
Data source: A retrospective study including 980 children seen at 10 academic centers in the United States.
Disclosures: Lead author Dr. Shah had no relevant financial conflicts to disclose. Several coauthors reported serving as investigators or consultants for Pfizer and for Pierre Fabre Dermatology, which manufactures the propranolol product used in the study. The study was supported by the University of California, San Francisco, Pediatric Dermatology research fund.

Recognition and Management of Children with Nonalcoholic Fatty Liver Disease
From the Albert Einstein College of Medicine, Division of Pediatric Gastroenterology and Nutrition, Children’s Hospital at Montefiore, Bronx, NY.
Abstract
- Objective: To review diagnostic challenges and management strategies in children with nonalcoholic fatty liver disease (NAFLD).
- Methods: Review of the literaure.
- Results: NAFLD is common in the United States and should be suspected in overweight or obese children with an elevated serum alanine aminotransferase level. The differential diagnosis for these patients is broad, however, and liver biopsy—the gold standard test—should be undertaken selectively after an appropriate workup. Patients should be counseled on lifestyle modifications, whereas vitamin E therapy can be initiated for those with biopsy-proven disease.
- Conclusion: Providers should have a high degree of suspicion for NAFLD, approaching the workup and diagnosis in an incremental, step-wise fashion. Further research is needed to standardize the diagnostic approach, identify reliable, noninvasive diagnostic measures, and develop novel treatment modalities.
Nonalcoholic fatty liver disease (NAFLD) is the most common liver disease in the Western world, affecting approximately 10% of children and a third of all adults in the United States [1–3]. It is a significant public health challenge and is estimated to soon be the number one indication for liver transplantation in adults.
NAFLD is a generic term encompassing 2 distinct conditions defined by their histopathology: simple steatosis and nonalcoholic steatohepatitis (NASH). Simple steatosis is characterized by predominantly macrovesicular—meaning large droplet—cytoplasmic lipid inclusions found in ≥ 5% of hepatocytes. NASH is defined as hepatic steatosis plus the additional features of inflammation, hepatocyte ballooning, and/or fibrosis. There are some adult data [4-6] and 1 retrospective pediatric study [7] demonstrating that over time, NAFLD may progress. That is, steatosis may progress to NASH and some patients with fibrosis will ultimately develop cirrhosis. If intervention is provided early in the histologic spectrum, NAFLD can be reversed [4,8] and late complications—such as cirrhosis, hepatocellular carcinoma, or liver transplantation—may be prevented.
It is important to highlight that the above definitions are based on histology and that a liver biopsy cannot be reasonably obtained in such a large percentage of the U.S. population. This case-based review will therefore focus primarily on the current diagnostic challenges facing health care providers as well as management strategies in children with presumed NAFLD.
Case Study
Initial Presentation
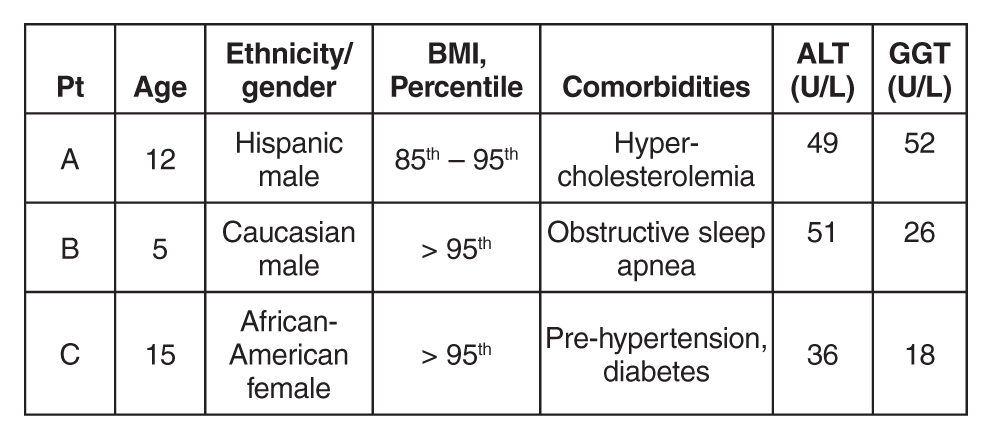
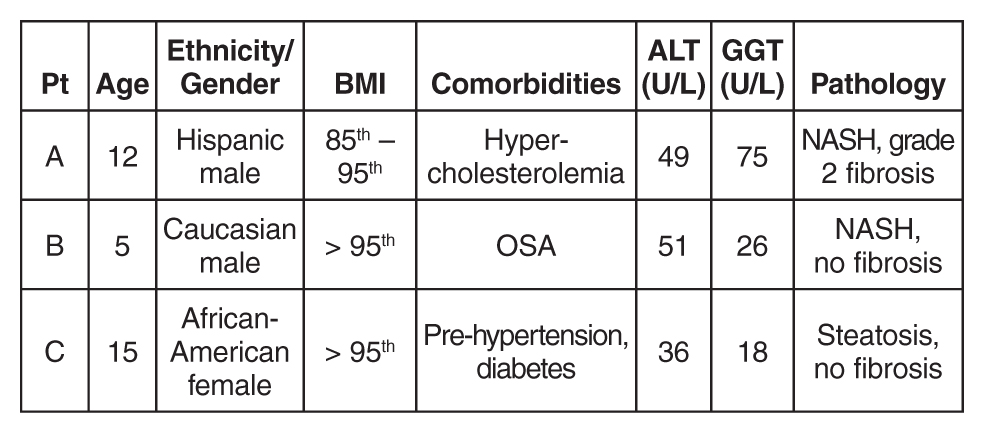
As you finish your charts at the end of a busy clinic day, you identify 3 patients who may have NAFLD:

History
All 3 patients presented to your office for a routine annual physical before the start of the school year and are asymptomatic. None of the patients has a family history of liver disease and their previously diagnosed comorbidities are listed in the table above. No patient is taking medications other than patient C, who is on metformin.
All 3 children have a smooth, velvety rash on their necks consistent with acanthosis nigricans with an otherwise normal physical exam. The liver and spleen are difficult to palpate but are seemingly normal.
What is the typical presentation for a child with NAFLD?
Most children with NAFLD are asymptomatic, though some may present with vague right upper quadrant abdominal pain. It is unclear, however, if the pain is caused by NAFLD or is rather an unrelated symptom that brings the child to the attention of a physician. In addition, hepatomegaly can be found in over 30% to 40% of patients [9]. For children without abdominal pain or hepatomegaly, most are recognized by an elevated serum alanine aminotransferase (ALT) or findings of increased liver echogenicity on ultrasonography.
Serum Alanine Aminotransferase
Serum aminotransferases are one of the more common screening tests for NAFLD. However, ALT is highly insensitive at commonly used thresholds and is also nonspecific. As documented in the SAFETY study, the upper limit of normal for ALT in healthy children should be set around 25 U/L in boys and 22 U/L in girls [10]. Yet even at these thresholds, the sensitivity of ALT to diagnose NAFLD is 80% in boys and 92% in girls, whereas specificity is 79% and 85%, respectively [10]. These findings are largely consistent with adult studies [11–14]. Furthermore, ALT does not correlate well with disease severity and children may still have NASH or significant fibrosis with normal values. In a well-characterized cohort of 91 children with biopsy-proven NAFLD, for example, early fibrosis was identified in 12% of children with a normal ALT (≤ 22 U/L for girls and ≤ 25 U/L in boys) [15]. Advanced fibrosis or cirrhosis was seen in 9% of children with an ALT up to 2 times this upper limit [15]. Thus, reliance on the serum ALT may significantly underestimate the prevalence and severity of liver injury.
Ultrasonography
Children with NAFLD typically have findings of increased hepatic echogenicity on abdominal ultrasonography. However, there are multiple limitations to sonography. First, ultrasound is insensitive for identifying mild steatosis if less than 30% of hepatocytes are affected [16,17]. Second, increased hepatic echogenicity is nonspecific and may be caused by inflammation, fibrosis, or intrahepatic accumulation of iron, copper, or glycogen. Third, there can be considerable inter- and intra-operator variability. And lastly, there is some evidence that ultrasounds do not add benefit to diagnosing children with NAFLD [18].
Which patients are at risk for developing hepatic steatosis and NASH?
Weight, Age, and Gender
There is a strong, direct correlation between body mass index (BMI) and NAFLD. The Study of Child and Adolescent Liver Epidemiology (SCALE)—a sentinel pediatric autopsy study of 742 children—found that 5% of normal weight children, 16% of overweight children, and 38% of obese children had NAFLD. The SCALE study also demonstrated an increasing prevalence with age, such that NAFLD was present in 17.3% of 15- to 19-year-olds but only in 0.2% of 2- to 4-year-olds [1]. With regards to gender, NAFLD is roughly twice as prevalent in males [18–20]. While the exact etiology of this difference is unclear, hormonal differences are a leading hypothesis.
Ethnicity
NAFLD is most common in Hispanics, followed by Asians, Caucasians, and African Americans. Research suggests that genetics may be largely responsible for these ethnic disparities. For example, the I148M allele of PNPLA3 (a single nucleotide polymorphism) is strongly associated with steatosis, NASH, and fibrosis [21] and is most common in Hispanics, with a 50% carrier frequency in some cohorts [22]. Conversely, African Americans are more likely to carry the S453I allele of PNPLA3, which is associated with decreased hepatic steatosis [22]. There is also considerable variability within ethnic groups. For example, Mexican-American children appear to be at the highest risk for steatosis or NASH among Hispanics, whereas Filipino-American children are believed to have higher disease prevalence than Cambodian or Vietnamese Americans [1].
Comorbidities
NAFLD is associated with obesity, insulin resistance and diabetes, cardiovascular disease, the metabolic syndrome [23], decreased quality of life [24,25], and obstructive sleep apnea (OSA). These associations generally hold even after controlling for the other confounders listed. It is important to note that these data come largely from cross-sectional studies and direct causation has yet to be determined.
Insulin resistance in particular is strongly associated with NAFLD—so much so, in fact, that some consider it to be the hepatic manifestation of the metabolic syndrome. Additionally, children with features of the metabolic syndrome are more likely to have advanced histologic features of NAFLD [23]. There are also intriguing data from small pediatric studies to suggest that OSA may contribute to the development of hepatic fibrosis. In one study of 25 children with biopsy-proven NAFLD, for example, the presence of OSA and hypoxemia correlated with the degree of hepatic fibrosis [26]. In a slightly larger study of 65 children, OSA was also strongly associated with significant hepatic fibrosis (odds ratio, 5.91; 95% confidence interval, 3.23–7.42; P < 0.001). The duration of hypoxemia also correlated with histologic findings of inflammation and circulating biomarkers of apoptosis and fibrogenesis [27].
Other Laboratory Tests
Several studies have documented an association between elevated gamma-glutamyl transferase (GGT) and hepatic fibrosis [28,29], though others have been conflicting [30,31]. Pediatric studies have also demonstrated an inverse correlation between NASH and total bilirubin [32], serum potassium [33], and serum ceruloplasmin [34]. In addition, there are a number of serum biomarkers or biomarker panels commercially available for use in adults. Because similar efficacy data are unavailable in children, however, serum biomarkers should be primarily used for research purposes only.
Who should be screened for NAFLD? And how?
Published professional society recommendations differ significantly with regards to screening. In 2007, the American Academy of Pediatrics suggested screening obese children over 10 years of age or overweight children with additional risk factors with biannual liver tests [35]. There were no management recommendations made for elevated aminotransferase levels other than for subspecialty referral. In 2012, the European Society of Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) recommended obtaining an ultrasound and liver tests in every obese child [36]. One month later, however, the American Gastroenterological Association, American Association for the Study of Liver Disease, and the American College of Gastroenterology published joint guidelines without screening recommendations “due to a paucity of evidence” [37].
Because these statements conflict and are based heavily on expert opinion, one should consider the risks, benefits, and costs to screening large numbers of patients. Until additional research clarifies this controversy, we suggest that providers individualize their screening practices to their population and the risks of each individual patient. For example, we would consider screening children who are obese; Hispanic or Asian; have multiple features of the metabolic syndrome; and/or those who have a family history of NAFLD. Further, we recommend screening children for NAFLD with serum liver enzymes only and not with ultrasonography.
Case Continued: Laboratory Results
ALT and GGT tests are ordered and the results are as follows:
What is the differential for children with suspected NAFLD?
Autoimmune Hepatitis (AIH)
AIH is a progressive necro-inflammatory disorder of the liver characterized by elevated aminotransferases, positive autoantibodies, and distinctive histologic features. AIH is believed to occur in genetically predisposed patients in response to an environmental trigger. There is a female predominance and it can present in any age or ethnic group.
AIH is divided in 2 subtypes. Type 1 disease is characterized by a positive antinuclear (ANA) antibody and anti-smooth muscle antibody. More commonly, it presents in adolescence with an indolent course—many patients are asymptomatic until they develop features of cirrhosis and portal hypertension. Conversely, type 2 AIH is characterized by a positive liver kidney microsomal (LKM) antibody and tends to present acutely in young children. It is important to note that antibody titers can be falsely positive in a significant percentage of patients and, in such cases, are often mildly elevated [38]. We strongly suggest children with positive autoantibody titers be evaluated by a specialist.
Treatment should be started promptly to avoid progression to cirrhosis and should also done so in consultation with a pediatric gastroenterologist or hepatologist. The prognosis of AIH with immunosuppression is favorable, with long-term remission rates of approximately 80%. Transplantation is typically required in the remaining 10% to 20% [39].
Celiac Disease
Celiac disease is an autoimmune, inflammatory enteropathy caused by exposure to gluten in genetically susceptible individuals. Up to a third of all children presenting with celiac will have an elevated serum ALT [40]. Additional symptoms/features are both variable and nonspecific: abdominal pain, poor growth, diarrhea, or constipation, among others. Celiac is diagnosed by duodenal biopsy or a sufficiently elevated tissue transglutaminase antibody level [41]. Treatment with a strict gluten-free diet will resolve the enteropathy and normalize the serum aminotransferases.
Wilson’s Disease
Wilson’s disease is a metabolic disorder leading to copper deposition in the liver, brain, cornea, and kidneys. It is caused by an ATP7B gene mutation and inherited in an autosomal recessive fashion. Patients may present with asymptomatic liver disease, chronic hepatitis, acute liver failure, or with symptoms of portal hypertension. Neuropsychiatric symptoms may also be prominent. Screening tests include a serum ceruloplasmin and 24-hour urinary copper quantification. Because diagnosing Wilson’s disease can be challenging, however, further testing should occur in consultation with a pediatric gastroenterologist or hepatologist.
Viral Hepatitis
Chronic viral infections such as hepatitis B and C are still common etiologies of liver disease in the United States. However, universal vaccination and blood donor screening have reduced the risk of transmission; new antiviral agents will likely further decrease the prevalence and transmission risk over time. Acute viral hepatitis—cytomegalovirus, Epstein-Barr virus, hepatitis A, or hepatitis E—should also be considered in children who present with appropriate symptoms and an elevated ALT.
Drug-Induced
Drug-induced liver injury (DILI) can present with elevated serum aminotransferases (hepatocellular pattern), an elevated bilirubin (cholestatic pattern), or a mixed picture. Idiosyncratic DILI in children is commonly caused by antimicrobial or central nervous system agents and usually presents with a hepatocellular injury pattern. Substance abuse, including alcohol, is common and should also be investigated as the source of underlying liver disease.
Muscle Disease
Aspartate aminotransferase (AST) and ALT are present in hepatocytes, myocytes, and red blood cells, among other tissues. Thus, children with congenital myopathies or myositis can have elevated aminotransferases, typically with the AST higher than the ALT. In these patients, checking a creatine phosphokinase (CPK) level may lead to the correct diagnosis and limit unnecessary testing.
Other Metabolic Disorders
Myriad metabolic disorders present with liver disease and/or elevated serum aminotransferase levels. Individually, these conditions are rare but, collectively, are relatively common. Two of the more occult conditions—lysosomal acid lipase deficiency (LAL-D) and alpha-1 antitrypsin (A1A) deficiency—are discussed in further detail below.
LAL-D is an autosomal recessive disease resulting in the accumulation of cholesterol esters and triglycerides in lysosomes. Patients typically present with hepatomegaly and mildly elevated aminotransferases, an elevated LDL, low HDL cholesterol, and increased hepatic echogenicity on ultrasound. If a biopsy is obtained, microvesicular steatosis is predominant as opposed to macrovesicular steatosis found in NAFLD. The diagnosis of LAL-D can be made on a commercially available dry blood spot enzymatic assay or genetic testing and treatment has recently been FDA approved.
A1A deficiency is an autosomal recessive disease diagnosable by an alpha-1-antitrypsin phenotype. The clinical presentation is characterized by neonatal cholestasis in the infantile form and by hepatitis, cirrhosis and portal hypertension in older children. Classic symptoms of emphysema and chronic lung disease present in adulthood.
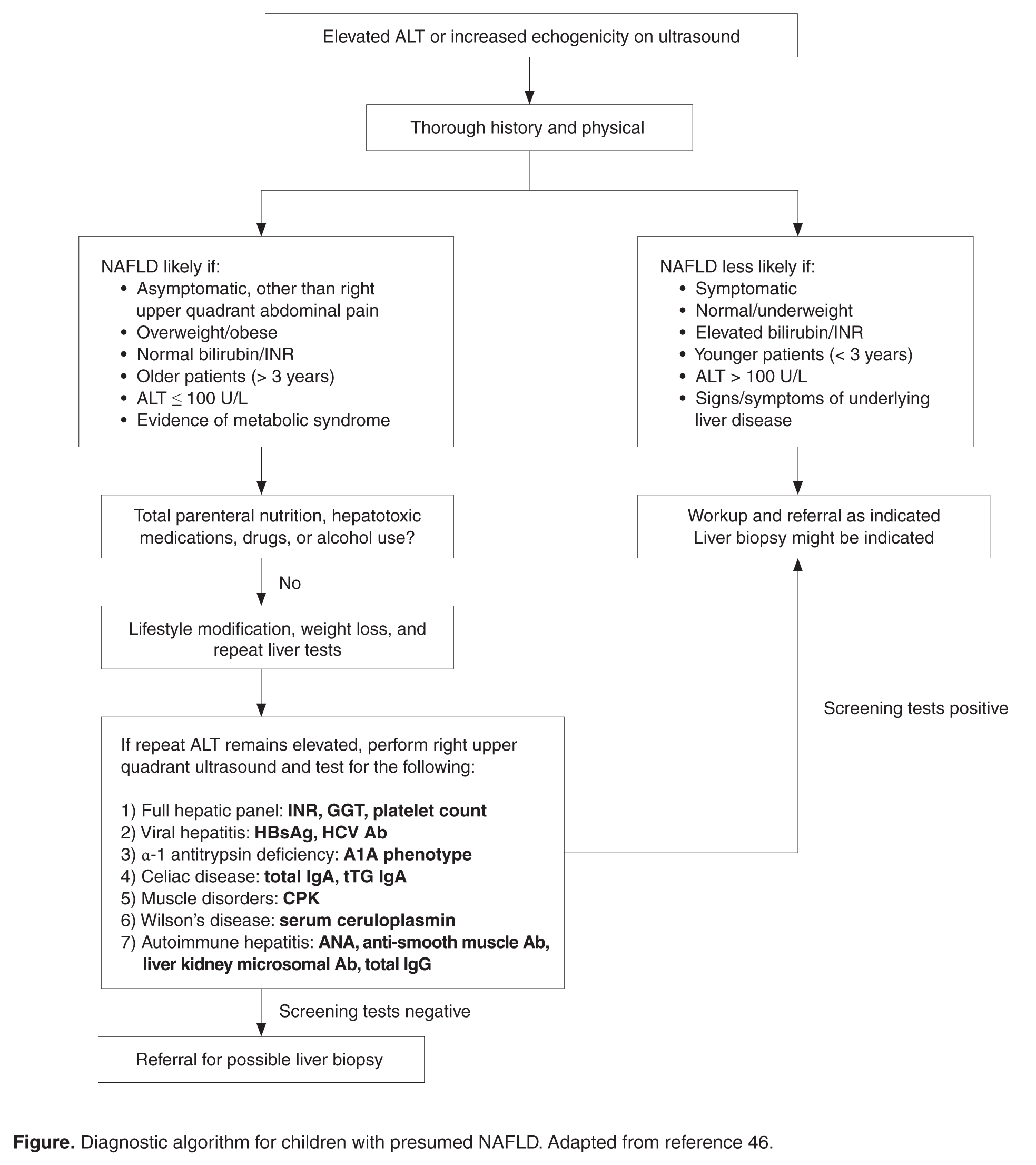
What further testing should be performed in children with suspected NAFLD?
For obese children with an elevated ALT or evidence of increased hepatic echogenicity, ESPGHAN recommends targeting the workup according to the child’s age [36]. According to their consensus statement, they recommend an upfront, thorough laboratory evaluation in children less than 10 years of age and consideration of a liver biopsy upon completion. For children over 10 years of age at low risk for NASH or fibrosis, additional laboratory evaluation is suggested 3 to 6 months after failed lifestyle interventions. In general, the recommended workup includes testing for conditions discussed in the section above such as viral hepatitis, AIH, Wilson’s disease, and others. If negative, ESPGHAN states that a liver biopsy should be “considered.”
The question of whether or not to obtain a liver biopsy is controversial, though there are several clear advantages to doing so. First, biopsy is the gold standard test for diagnosing NAFLD and there are no highly accurate, noninvasive tests currently approved for use in children. Second, biopsy is a more definitive means of ruling out competing diagnoses such as AIH. Third, biopsy may provide prognostic data. In a retrospective adult study of 136 patients, for example, those who presented with simple steatosis had a roughly 3% chance of progressing to cirrhosis within 10 years. If a patient within this cohort presented with NASH, however, the progression risk was approximately 30% within 5 years [42,43]. Fourth, due to potential side effects of medications, position papers recommend obtaining a liver biopsy prior to the initiation of pharmacotherapy [37]. Lastly, the risk for serious morbidity from a liver biopsy is low [44,45]. Alternatively, one must acknowledge the risks of liver biopsy: morbidity, sampling bias, invasiveness, cost, and sedation risks in children.
Case Continued: Biopsy Results
You refer your patients to a gastroenterologist. Tests for viral hepatitis, A1A deficiency, celiac disease, muscle disorders, Wilson’s disease, and AIH are negative. Ultimately, a liver biopsy is performed on all 3 children without complications. The results are presented below.
What is the treatment of NAFLD?
Lifestyle Modification
Lifestyle modifications are the mainstay of treatment for NAFLD. In adult studies, weight loss of more than 5% reduces hepatic steatosis whereas weight loss of more than 9% improves or eliminates NASH [47]. We recommend that children engage in age-appropriate, enjoyable, moderate- or vigorous-intensity aerobic activity for 60 minutes a day [48]. In addition, there should be a focus on reducing sedentary behavior by limiting screen time and a concerted effort to engage the family in lifestyle modifications.
Dietary interventions to treat NAFLD are less concrete but there is a growing body of literature to suggest that dietary fructose is particularly harmful. In adults, for example, fructose consumption is associated with the development of NAFLD [49] and hepatic fibrosis [50]. Recent data in adolescents has similarly documented an association between NAFLD incidence and energy-adjusted fructose intake [51]. It is worth highlighting that these clinical findings are also biologically plausible, as fructose is primarily metabolized within hepatocytes and has recently been shown to increase de novo lipogenesis [52,53]. In general, we suggest a well-balanced diet of unprocessed foods—that is, with limited added sugars—sufficient to induce gradual weight loss in older children or body weight maintenance in younger children.
Medications
Vitamin E is the only medication with proven efficacy in children, as demonstrated in the TONIC trial [20]. TONIC was a double-blind, multicenter, placebo-controlled study with 3 treatment arms: 800 IU of vitamin E daily, 1000 mg of metformin daily, or placebo. Metformin did not reduce the serum ALT or significantly improve liver histology and should therefore not be used for these indications. However, patients treated with vitamin E had a statistically significant improvement in the NAFLD activity score (a histologic grading system comprising steatosis, inflammation, and hepatocyte ballooning) and resolution of NASH when compared to placebo. For these reasons—as well as a paucity of other viable treatment options—vitamin E is routinely prescribed for children with biopsy-proven NASH. However, the long- term risks of high-dose vitamin E therapy in children are largely unknown.
Polyunsaturated fats such as docosahexaenoic acid (DHA) [54] and probiotics such as VSL #3 [55] have showed efficacy reducing hepatic steatosis in small, randomized clinical trials. Both medications need to be further validated before they can be recommended for use in children. Conversely, ursodeoxycholic acid has not been found to be efficacious in children with NAFLD [56], whereas phase IIb data on cysteamine is expected soon. There are currently insufficient data to recommend bariatric surgery as treatment for NAFLD in adolescence.
Case Continued: Follow-up
After their biopsies, both patients with NASH (patients A and B) are started on vitamin E therapy. All 3 patients continue to report for follow-up visits without short-term complications, though they have still been unable to significantly reduce their body mass index and have a persistently elevated serum ALT.
Summary
NAFLD is a common condition in the United States with serious personal and public health ramifications. This case-based review highlights the diagnostic and management challenges in children with NAFLD and the unique role primary care providers play in caring for these patients.
Corresponding author: Bryan Rudolph, MD, Albert Einstein College of Medicine, Division of Pediatric Gastroenterology and Nutrition, Children’s Hospital at Montefiore, 3415 Bainbridge Ave., Bronx, NY 10467, brudolph@montefiore.org.
Financial disclosures: None.
1. Schwimmer JB, Deutsch R, Kahen T, et al. Prevalence of fatty liver in children and adolescents. Pediatrics 2006;118:1388–93.
2. Welsh JA, Karpen S, Vos MB.Increasing prevalence of nonalcoholic fatty liver disease among United States adolescents, 1988-1994 to 2007-2010. J Pediatr 2013;162:496–500.
3. Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther 2011;34:274–85.
4. McPherson S, Hardy T, Henderson E, et al. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for prognosis and clinical management. J Hepatol 2015;62:1148–55.
5. Singh S, Allen AM, Wang Z, et al. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 2015;13:643–54.
6. Pais R, Charlotte F, Fedchuk L, et al. A systematic review of follow-up biopsies reveals disease progression in patients with non-alcoholic fatty liver. J Hepatol 2013;59:550–6.
7. Feldstein AE, Charatcharoenwitthaya P, Treeprasertsuk S, et al. The natural history of non-alcoholic fatty liver disease in children: a follow-up study for up to 20 years. Gut 2009;58:1538–44.
8. Mummadi RR, Kasturi KS, Chennareddygari S, et al. Effect of bariatric surgery on nonalcoholic fatty liver disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol 2008;6:1396–402.
9. Rashid M, Roberts EA. Nonalcoholic steatohepatitis in children. J Pediatr Gastroenterol Nutr 2000;30:48–53.
10. Schwimmer JB, Dunn W, Norman GJ, et al. SAFETY study: alanine aminotransferase cutoff values are set too high for reliable detection of pediatric chronic liver disease. Gastroenterology 2010;138:1357–64.
11. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002;137:1–10.
12. Lee JK, Shim JH, Lee HC, et al. Estimation of the healthy upper limits for serum alanine aminotransferase in Asian populations with normal liver histology. Hepatology 2010;51:1577–83.
13. Kang HS, Um SH, Seo YS, et al. Healthy range for serum ALT and the clinical significance of "unhealthy" normal ALT levels in the Korean population. J Gastroenterol Hepatol 2011;26:292–9.
14. Zheng MH, Shi KQ, Fan YC, et al. Upper limits of normal for serum alanine aminotransferase levels in Chinese Han population. PLoS One 2012;7:e43736.
15. Molleston JP, Schwimmer JB, Yates KP, et al. Histological abnormalities in children with nonalcoholic fatty liver disease and normal or mildly elevated alanine aminotransferase levels. J Pediatr 2014;164:707–13.
16. Dasarathy S, Dasarathy J, Khiyami A, et al. Validity of real time ultrasound in the diagnosis of hepatic steatosis: a prospective study. J Hepatol 2009;51:1061–7.
17. Nobili V, M. Pinzani M. Paediatric non-alcoholic fatty liver disease. Gut 2010;59:561–4.
18. Rudolph B, Rivas Y, Kulak S, et al. Yield of diagnostic tests in obese children with an elevated alanine aminotransferase. Acta Paediatr 2015;104:e557–63.
19. Nobili V, Manco M, Ciampalini P, et al. Metformin use in children with nonalcoholic fatty liver disease: an open-label, 24-month, observational pilot study. Clin Ther 2008;30:1168–76.
20. Lavine JE, Schwimmer JB, Van Natta ML, et al. Effect of vitamin E or metformin for treatment of nonalcoholic fatty liver disease in children and adolescents: the TONIC randomized controlled trial. JAMA 2011;305:1659–68.
21. Krawczyk MP, Portincasa P, Lammert F. PNPLA3-associated steatohepatitis: toward a gene-based classification of fatty liver disease. Semin Liver Dis 2013;33:369–79.
22. Romeo S, Kozlitina J, Xing C, et al. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet 2008;40:1461–5.
23. Patton HM, Yates K, Unalp-Arida A, et al. Association between metabolic syndrome and liver histology among children with nonalcoholic fatty liver disease. Am J Gastroenterol 2010;105:2093–102.
24. Kistler KD, Molleston J, Unalp A, et al., Symptoms and quality of life in obese children and adolescents with non-alcoholic fatty liver disease. Aliment Pharmacol Ther 2010;31:396–406.
25. Kerkar N, D'Urso C, Van Nostrand K, et al. Psychosocial outcomes for children with nonalcoholic fatty liver disease over time and compared with obese controls. J Pediatr Gastroenterol Nutr 2013;56:77–82.
26. Sundaram SS, Sokol RJ, Capocelli KE, et al. Obstructive sleep apnea and hypoxemia are associated with advanced liver histology in pediatric nonalcoholic fatty liver disease. J Pediatr 2014;164:699–706.
27. Nobili V, Cutrera R, Liccardo D, et al. Obstructive sleep apnea syndrome affects liver histology and inflammatory cell activation in pediatric nonalcoholic fatty liver disease, regardless of obesity/insulin resistance. Am J Respir Crit Care Med 2014;189:66–76.
28. Patton HM, Lavine JE, Van Natta ML, et al., Clinical correlates of histopathology in pediatric nonalcoholic steatohepatitis. Gastroenterology 2008;135:1961–71.
29. Schwimmer JB, Behling C, Newbury R, et al. Histopathology of pediatric nonalcoholic fatty liver disease. Hepatology 2005;42:641–9.
30. Nobili V, Parkes J, Bottazzo G, et al. Performance of ELF serum markers in predicting fibrosis stage in pediatric non-alcoholic fatty liver disease. Gastroenterology 2009;136:160–7.
31. Yang HR, Kim HR, Kim MJ, et al. Noninvasive parameters and hepatic fibrosis scores in children with nonalcoholic fatty liver disease. World J Gastroenterol 2012;18:1525–30.
32. Puri K, Nobili V, Melville K, et al. Serum bilirubin level is inversely associated with nonalcoholic steatohepatitis in children. J Pediatr Gastroenterol Nutr 2013;57:114–8.
33. Tabbaa A, Shaker M, Lopez R, et al. Low serum potassium levels associated with disease severity in children with nonalcoholic fatty liver disease. Pediatr Gastroenterol Hepatol Nutr 2015;18:168–74.
34. Nobili V, Siotto M, Bedogni G, et al. Levels of serum ceruloplasmin associate with pediatric nonalcoholic fatty liver disease. J Pediatr Gastroenterol Nutr 2013;56:370–5.
35. Barlow SE; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 2007;120 Suppl 4:S164–92.
36. Vajro P, Lenta S, Socha P, et al. Diagnosis of nonalcoholic fatty liver disease in children and adolescents: position paper of the ESPGHAN Hepatology Committee. J Pediatr Gastroenterol Nutr 2012;54:700–13.
37. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012;142:1592–609.
38. Vuppalanchi R, Gould RJ, Wilson LA, et al. Clinical significance of serum autoantibodies in patients with NAFLD: results from the nonalcoholic steatohepatitis clinical research network. Hepatol Int 2012;6:379–85.
39. Floreani A, Liberal R, Vergani D, et al. Autoimmune hepatitis: contrasts and comparisons in children and adults - a comprehensive review. J Autoimmun 2013;46:7–16.
40. Vajro P, Paolella G, Maggiore G, et al. Pediatric celiac disease, cryptogenic hypertransaminasemia, and autoimmune hepatitis. J Pediatr Gastroenterol Nutr 2013;56:663–70.
41. Husby S, Koletzko S, Korponay-Szabó IR, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr 2012;54:136–60.
42. Matteoni CA, Younossi ZM, Gramlich T, et al. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 1999;116:1413–9.
43. McCullough AJ. The clinical features, diagnosis and natural history of nonalcoholic fatty liver disease. Clin Liver Dis 2004;8:521–33.
44. Ovchinsky N, Moreira RK, Lefkowitch JH, Lavine JE. Liver biopsy in modern clinical practice: a pediatric point-of-view. Adv Anat Pathol 2012;19:250–62.
45. Dezsőfi A, Baumann U, Dhawan A, et al. Liver biopsy in children: position paper of the ESPGHAN Hepatology Committee. J Pediatr Gastroenterol Nutr 2015;60:408–20.
46. Fusillo S, Rudolph B. Nonalcoholic fatty liver disease. Pediatr Rev 2015;36:198–205.
47. Harrison SA, Fecht W, Brunt EM, Neuschwander-Tetri BA. Orlistat for overweight subjects with nonalcoholic steatohepatitis: A randomized, prospective trial. Hepatology 2009;49:80–6.
48. School health guidelines to promote healthy eating and physical activity. MMWR Recomm Rep 2011;60(Rr-5):1–76.
49. Ouyang X, Cirillo P, Sautin Y, et al. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. J Hepatol 2008;48:993–9.
50. Abdelmalek MF, Suzuki A, Guy C, et al. Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology 2010;51:1961–71.
51. O’Sullivan TA, Oddy WH, Bremner AP, et al. Lower fructose intake may help protect against development of nonalcoholic fatty liver in adolescents with obesity. J Pediatr Gastroenterol Nutr 2014;58:624–31.
52. Parks EJ, Skokan LE, Timlin MT, Dingfelder CS. Dietary sugars stimulate fatty acid synthesis in adults. J Nutr 2008;138:1039–46.
53. Stanhope KL, Schwarz JM, Keim NL, et al. Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans. J Clin Invest 2009;119:1322–34.
54. Nobili V, Alisi A, Della Corte C, et al., Docosahexaenoic acid for the treatment of fatty liver: randomised controlled trial in children. Nutr Metab Cardiovasc Dis 2013;23:1066–70.
55. Alisi A, Bedogni G, Baviera G, et al. Randomised clinical trial: The beneficial effects of VSL#3 in obese children with non-alcoholic steatohepatitis. Aliment Pharmacol Ther 2014;39:1276–85.
56. Vajro P, Franzese A, Valerio G, et al. Lack of efficacy of ursodeoxycholic acid for the treatment of liver abnormalities in obese children. J Pediatr 2000;136:739–43.
From the Albert Einstein College of Medicine, Division of Pediatric Gastroenterology and Nutrition, Children’s Hospital at Montefiore, Bronx, NY.
Abstract
- Objective: To review diagnostic challenges and management strategies in children with nonalcoholic fatty liver disease (NAFLD).
- Methods: Review of the literaure.
- Results: NAFLD is common in the United States and should be suspected in overweight or obese children with an elevated serum alanine aminotransferase level. The differential diagnosis for these patients is broad, however, and liver biopsy—the gold standard test—should be undertaken selectively after an appropriate workup. Patients should be counseled on lifestyle modifications, whereas vitamin E therapy can be initiated for those with biopsy-proven disease.
- Conclusion: Providers should have a high degree of suspicion for NAFLD, approaching the workup and diagnosis in an incremental, step-wise fashion. Further research is needed to standardize the diagnostic approach, identify reliable, noninvasive diagnostic measures, and develop novel treatment modalities.
Nonalcoholic fatty liver disease (NAFLD) is the most common liver disease in the Western world, affecting approximately 10% of children and a third of all adults in the United States [1–3]. It is a significant public health challenge and is estimated to soon be the number one indication for liver transplantation in adults.
NAFLD is a generic term encompassing 2 distinct conditions defined by their histopathology: simple steatosis and nonalcoholic steatohepatitis (NASH). Simple steatosis is characterized by predominantly macrovesicular—meaning large droplet—cytoplasmic lipid inclusions found in ≥ 5% of hepatocytes. NASH is defined as hepatic steatosis plus the additional features of inflammation, hepatocyte ballooning, and/or fibrosis. There are some adult data [4-6] and 1 retrospective pediatric study [7] demonstrating that over time, NAFLD may progress. That is, steatosis may progress to NASH and some patients with fibrosis will ultimately develop cirrhosis. If intervention is provided early in the histologic spectrum, NAFLD can be reversed [4,8] and late complications—such as cirrhosis, hepatocellular carcinoma, or liver transplantation—may be prevented.
It is important to highlight that the above definitions are based on histology and that a liver biopsy cannot be reasonably obtained in such a large percentage of the U.S. population. This case-based review will therefore focus primarily on the current diagnostic challenges facing health care providers as well as management strategies in children with presumed NAFLD.
Case Study
Initial Presentation
As you finish your charts at the end of a busy clinic day, you identify 3 patients who may have NAFLD:
History
All 3 patients presented to your office for a routine annual physical before the start of the school year and are asymptomatic. None of the patients has a family history of liver disease and their previously diagnosed comorbidities are listed in the table above. No patient is taking medications other than patient C, who is on metformin.
All 3 children have a smooth, velvety rash on their necks consistent with acanthosis nigricans with an otherwise normal physical exam. The liver and spleen are difficult to palpate but are seemingly normal.
What is the typical presentation for a child with NAFLD?
Most children with NAFLD are asymptomatic, though some may present with vague right upper quadrant abdominal pain. It is unclear, however, if the pain is caused by NAFLD or is rather an unrelated symptom that brings the child to the attention of a physician. In addition, hepatomegaly can be found in over 30% to 40% of patients [9]. For children without abdominal pain or hepatomegaly, most are recognized by an elevated serum alanine aminotransferase (ALT) or findings of increased liver echogenicity on ultrasonography.
Serum Alanine Aminotransferase
Serum aminotransferases are one of the more common screening tests for NAFLD. However, ALT is highly insensitive at commonly used thresholds and is also nonspecific. As documented in the SAFETY study, the upper limit of normal for ALT in healthy children should be set around 25 U/L in boys and 22 U/L in girls [10]. Yet even at these thresholds, the sensitivity of ALT to diagnose NAFLD is 80% in boys and 92% in girls, whereas specificity is 79% and 85%, respectively [10]. These findings are largely consistent with adult studies [11–14]. Furthermore, ALT does not correlate well with disease severity and children may still have NASH or significant fibrosis with normal values. In a well-characterized cohort of 91 children with biopsy-proven NAFLD, for example, early fibrosis was identified in 12% of children with a normal ALT (≤ 22 U/L for girls and ≤ 25 U/L in boys) [15]. Advanced fibrosis or cirrhosis was seen in 9% of children with an ALT up to 2 times this upper limit [15]. Thus, reliance on the serum ALT may significantly underestimate the prevalence and severity of liver injury.
Ultrasonography
Children with NAFLD typically have findings of increased hepatic echogenicity on abdominal ultrasonography. However, there are multiple limitations to sonography. First, ultrasound is insensitive for identifying mild steatosis if less than 30% of hepatocytes are affected [16,17]. Second, increased hepatic echogenicity is nonspecific and may be caused by inflammation, fibrosis, or intrahepatic accumulation of iron, copper, or glycogen. Third, there can be considerable inter- and intra-operator variability. And lastly, there is some evidence that ultrasounds do not add benefit to diagnosing children with NAFLD [18].
Which patients are at risk for developing hepatic steatosis and NASH?
Weight, Age, and Gender
There is a strong, direct correlation between body mass index (BMI) and NAFLD. The Study of Child and Adolescent Liver Epidemiology (SCALE)—a sentinel pediatric autopsy study of 742 children—found that 5% of normal weight children, 16% of overweight children, and 38% of obese children had NAFLD. The SCALE study also demonstrated an increasing prevalence with age, such that NAFLD was present in 17.3% of 15- to 19-year-olds but only in 0.2% of 2- to 4-year-olds [1]. With regards to gender, NAFLD is roughly twice as prevalent in males [18–20]. While the exact etiology of this difference is unclear, hormonal differences are a leading hypothesis.
Ethnicity
NAFLD is most common in Hispanics, followed by Asians, Caucasians, and African Americans. Research suggests that genetics may be largely responsible for these ethnic disparities. For example, the I148M allele of PNPLA3 (a single nucleotide polymorphism) is strongly associated with steatosis, NASH, and fibrosis [21] and is most common in Hispanics, with a 50% carrier frequency in some cohorts [22]. Conversely, African Americans are more likely to carry the S453I allele of PNPLA3, which is associated with decreased hepatic steatosis [22]. There is also considerable variability within ethnic groups. For example, Mexican-American children appear to be at the highest risk for steatosis or NASH among Hispanics, whereas Filipino-American children are believed to have higher disease prevalence than Cambodian or Vietnamese Americans [1].
Comorbidities
NAFLD is associated with obesity, insulin resistance and diabetes, cardiovascular disease, the metabolic syndrome [23], decreased quality of life [24,25], and obstructive sleep apnea (OSA). These associations generally hold even after controlling for the other confounders listed. It is important to note that these data come largely from cross-sectional studies and direct causation has yet to be determined.
Insulin resistance in particular is strongly associated with NAFLD—so much so, in fact, that some consider it to be the hepatic manifestation of the metabolic syndrome. Additionally, children with features of the metabolic syndrome are more likely to have advanced histologic features of NAFLD [23]. There are also intriguing data from small pediatric studies to suggest that OSA may contribute to the development of hepatic fibrosis. In one study of 25 children with biopsy-proven NAFLD, for example, the presence of OSA and hypoxemia correlated with the degree of hepatic fibrosis [26]. In a slightly larger study of 65 children, OSA was also strongly associated with significant hepatic fibrosis (odds ratio, 5.91; 95% confidence interval, 3.23–7.42; P < 0.001). The duration of hypoxemia also correlated with histologic findings of inflammation and circulating biomarkers of apoptosis and fibrogenesis [27].
Other Laboratory Tests
Several studies have documented an association between elevated gamma-glutamyl transferase (GGT) and hepatic fibrosis [28,29], though others have been conflicting [30,31]. Pediatric studies have also demonstrated an inverse correlation between NASH and total bilirubin [32], serum potassium [33], and serum ceruloplasmin [34]. In addition, there are a number of serum biomarkers or biomarker panels commercially available for use in adults. Because similar efficacy data are unavailable in children, however, serum biomarkers should be primarily used for research purposes only.
Who should be screened for NAFLD? And how?
Published professional society recommendations differ significantly with regards to screening. In 2007, the American Academy of Pediatrics suggested screening obese children over 10 years of age or overweight children with additional risk factors with biannual liver tests [35]. There were no management recommendations made for elevated aminotransferase levels other than for subspecialty referral. In 2012, the European Society of Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) recommended obtaining an ultrasound and liver tests in every obese child [36]. One month later, however, the American Gastroenterological Association, American Association for the Study of Liver Disease, and the American College of Gastroenterology published joint guidelines without screening recommendations “due to a paucity of evidence” [37].
Because these statements conflict and are based heavily on expert opinion, one should consider the risks, benefits, and costs to screening large numbers of patients. Until additional research clarifies this controversy, we suggest that providers individualize their screening practices to their population and the risks of each individual patient. For example, we would consider screening children who are obese; Hispanic or Asian; have multiple features of the metabolic syndrome; and/or those who have a family history of NAFLD. Further, we recommend screening children for NAFLD with serum liver enzymes only and not with ultrasonography.
Case Continued: Laboratory Results
ALT and GGT tests are ordered and the results are as follows:
What is the differential for children with suspected NAFLD?
Autoimmune Hepatitis (AIH)
AIH is a progressive necro-inflammatory disorder of the liver characterized by elevated aminotransferases, positive autoantibodies, and distinctive histologic features. AIH is believed to occur in genetically predisposed patients in response to an environmental trigger. There is a female predominance and it can present in any age or ethnic group.
AIH is divided in 2 subtypes. Type 1 disease is characterized by a positive antinuclear (ANA) antibody and anti-smooth muscle antibody. More commonly, it presents in adolescence with an indolent course—many patients are asymptomatic until they develop features of cirrhosis and portal hypertension. Conversely, type 2 AIH is characterized by a positive liver kidney microsomal (LKM) antibody and tends to present acutely in young children. It is important to note that antibody titers can be falsely positive in a significant percentage of patients and, in such cases, are often mildly elevated [38]. We strongly suggest children with positive autoantibody titers be evaluated by a specialist.
Treatment should be started promptly to avoid progression to cirrhosis and should also done so in consultation with a pediatric gastroenterologist or hepatologist. The prognosis of AIH with immunosuppression is favorable, with long-term remission rates of approximately 80%. Transplantation is typically required in the remaining 10% to 20% [39].
Celiac Disease
Celiac disease is an autoimmune, inflammatory enteropathy caused by exposure to gluten in genetically susceptible individuals. Up to a third of all children presenting with celiac will have an elevated serum ALT [40]. Additional symptoms/features are both variable and nonspecific: abdominal pain, poor growth, diarrhea, or constipation, among others. Celiac is diagnosed by duodenal biopsy or a sufficiently elevated tissue transglutaminase antibody level [41]. Treatment with a strict gluten-free diet will resolve the enteropathy and normalize the serum aminotransferases.
Wilson’s Disease
Wilson’s disease is a metabolic disorder leading to copper deposition in the liver, brain, cornea, and kidneys. It is caused by an ATP7B gene mutation and inherited in an autosomal recessive fashion. Patients may present with asymptomatic liver disease, chronic hepatitis, acute liver failure, or with symptoms of portal hypertension. Neuropsychiatric symptoms may also be prominent. Screening tests include a serum ceruloplasmin and 24-hour urinary copper quantification. Because diagnosing Wilson’s disease can be challenging, however, further testing should occur in consultation with a pediatric gastroenterologist or hepatologist.
Viral Hepatitis
Chronic viral infections such as hepatitis B and C are still common etiologies of liver disease in the United States. However, universal vaccination and blood donor screening have reduced the risk of transmission; new antiviral agents will likely further decrease the prevalence and transmission risk over time. Acute viral hepatitis—cytomegalovirus, Epstein-Barr virus, hepatitis A, or hepatitis E—should also be considered in children who present with appropriate symptoms and an elevated ALT.
Drug-Induced
Drug-induced liver injury (DILI) can present with elevated serum aminotransferases (hepatocellular pattern), an elevated bilirubin (cholestatic pattern), or a mixed picture. Idiosyncratic DILI in children is commonly caused by antimicrobial or central nervous system agents and usually presents with a hepatocellular injury pattern. Substance abuse, including alcohol, is common and should also be investigated as the source of underlying liver disease.
Muscle Disease
Aspartate aminotransferase (AST) and ALT are present in hepatocytes, myocytes, and red blood cells, among other tissues. Thus, children with congenital myopathies or myositis can have elevated aminotransferases, typically with the AST higher than the ALT. In these patients, checking a creatine phosphokinase (CPK) level may lead to the correct diagnosis and limit unnecessary testing.
Other Metabolic Disorders
Myriad metabolic disorders present with liver disease and/or elevated serum aminotransferase levels. Individually, these conditions are rare but, collectively, are relatively common. Two of the more occult conditions—lysosomal acid lipase deficiency (LAL-D) and alpha-1 antitrypsin (A1A) deficiency—are discussed in further detail below.
LAL-D is an autosomal recessive disease resulting in the accumulation of cholesterol esters and triglycerides in lysosomes. Patients typically present with hepatomegaly and mildly elevated aminotransferases, an elevated LDL, low HDL cholesterol, and increased hepatic echogenicity on ultrasound. If a biopsy is obtained, microvesicular steatosis is predominant as opposed to macrovesicular steatosis found in NAFLD. The diagnosis of LAL-D can be made on a commercially available dry blood spot enzymatic assay or genetic testing and treatment has recently been FDA approved.
A1A deficiency is an autosomal recessive disease diagnosable by an alpha-1-antitrypsin phenotype. The clinical presentation is characterized by neonatal cholestasis in the infantile form and by hepatitis, cirrhosis and portal hypertension in older children. Classic symptoms of emphysema and chronic lung disease present in adulthood.
What further testing should be performed in children with suspected NAFLD?
For obese children with an elevated ALT or evidence of increased hepatic echogenicity, ESPGHAN recommends targeting the workup according to the child’s age [36]. According to their consensus statement, they recommend an upfront, thorough laboratory evaluation in children less than 10 years of age and consideration of a liver biopsy upon completion. For children over 10 years of age at low risk for NASH or fibrosis, additional laboratory evaluation is suggested 3 to 6 months after failed lifestyle interventions. In general, the recommended workup includes testing for conditions discussed in the section above such as viral hepatitis, AIH, Wilson’s disease, and others. If negative, ESPGHAN states that a liver biopsy should be “considered.”
The question of whether or not to obtain a liver biopsy is controversial, though there are several clear advantages to doing so. First, biopsy is the gold standard test for diagnosing NAFLD and there are no highly accurate, noninvasive tests currently approved for use in children. Second, biopsy is a more definitive means of ruling out competing diagnoses such as AIH. Third, biopsy may provide prognostic data. In a retrospective adult study of 136 patients, for example, those who presented with simple steatosis had a roughly 3% chance of progressing to cirrhosis within 10 years. If a patient within this cohort presented with NASH, however, the progression risk was approximately 30% within 5 years [42,43]. Fourth, due to potential side effects of medications, position papers recommend obtaining a liver biopsy prior to the initiation of pharmacotherapy [37]. Lastly, the risk for serious morbidity from a liver biopsy is low [44,45]. Alternatively, one must acknowledge the risks of liver biopsy: morbidity, sampling bias, invasiveness, cost, and sedation risks in children.
Case Continued: Biopsy Results
You refer your patients to a gastroenterologist. Tests for viral hepatitis, A1A deficiency, celiac disease, muscle disorders, Wilson’s disease, and AIH are negative. Ultimately, a liver biopsy is performed on all 3 children without complications. The results are presented below.
What is the treatment of NAFLD?
Lifestyle Modification
Lifestyle modifications are the mainstay of treatment for NAFLD. In adult studies, weight loss of more than 5% reduces hepatic steatosis whereas weight loss of more than 9% improves or eliminates NASH [47]. We recommend that children engage in age-appropriate, enjoyable, moderate- or vigorous-intensity aerobic activity for 60 minutes a day [48]. In addition, there should be a focus on reducing sedentary behavior by limiting screen time and a concerted effort to engage the family in lifestyle modifications.
Dietary interventions to treat NAFLD are less concrete but there is a growing body of literature to suggest that dietary fructose is particularly harmful. In adults, for example, fructose consumption is associated with the development of NAFLD [49] and hepatic fibrosis [50]. Recent data in adolescents has similarly documented an association between NAFLD incidence and energy-adjusted fructose intake [51]. It is worth highlighting that these clinical findings are also biologically plausible, as fructose is primarily metabolized within hepatocytes and has recently been shown to increase de novo lipogenesis [52,53]. In general, we suggest a well-balanced diet of unprocessed foods—that is, with limited added sugars—sufficient to induce gradual weight loss in older children or body weight maintenance in younger children.
Medications
Vitamin E is the only medication with proven efficacy in children, as demonstrated in the TONIC trial [20]. TONIC was a double-blind, multicenter, placebo-controlled study with 3 treatment arms: 800 IU of vitamin E daily, 1000 mg of metformin daily, or placebo. Metformin did not reduce the serum ALT or significantly improve liver histology and should therefore not be used for these indications. However, patients treated with vitamin E had a statistically significant improvement in the NAFLD activity score (a histologic grading system comprising steatosis, inflammation, and hepatocyte ballooning) and resolution of NASH when compared to placebo. For these reasons—as well as a paucity of other viable treatment options—vitamin E is routinely prescribed for children with biopsy-proven NASH. However, the long- term risks of high-dose vitamin E therapy in children are largely unknown.
Polyunsaturated fats such as docosahexaenoic acid (DHA) [54] and probiotics such as VSL #3 [55] have showed efficacy reducing hepatic steatosis in small, randomized clinical trials. Both medications need to be further validated before they can be recommended for use in children. Conversely, ursodeoxycholic acid has not been found to be efficacious in children with NAFLD [56], whereas phase IIb data on cysteamine is expected soon. There are currently insufficient data to recommend bariatric surgery as treatment for NAFLD in adolescence.
Case Continued: Follow-up
After their biopsies, both patients with NASH (patients A and B) are started on vitamin E therapy. All 3 patients continue to report for follow-up visits without short-term complications, though they have still been unable to significantly reduce their body mass index and have a persistently elevated serum ALT.
Summary
NAFLD is a common condition in the United States with serious personal and public health ramifications. This case-based review highlights the diagnostic and management challenges in children with NAFLD and the unique role primary care providers play in caring for these patients.
Corresponding author: Bryan Rudolph, MD, Albert Einstein College of Medicine, Division of Pediatric Gastroenterology and Nutrition, Children’s Hospital at Montefiore, 3415 Bainbridge Ave., Bronx, NY 10467, brudolph@montefiore.org.
Financial disclosures: None.
From the Albert Einstein College of Medicine, Division of Pediatric Gastroenterology and Nutrition, Children’s Hospital at Montefiore, Bronx, NY.
Abstract
- Objective: To review diagnostic challenges and management strategies in children with nonalcoholic fatty liver disease (NAFLD).
- Methods: Review of the literaure.
- Results: NAFLD is common in the United States and should be suspected in overweight or obese children with an elevated serum alanine aminotransferase level. The differential diagnosis for these patients is broad, however, and liver biopsy—the gold standard test—should be undertaken selectively after an appropriate workup. Patients should be counseled on lifestyle modifications, whereas vitamin E therapy can be initiated for those with biopsy-proven disease.
- Conclusion: Providers should have a high degree of suspicion for NAFLD, approaching the workup and diagnosis in an incremental, step-wise fashion. Further research is needed to standardize the diagnostic approach, identify reliable, noninvasive diagnostic measures, and develop novel treatment modalities.
Nonalcoholic fatty liver disease (NAFLD) is the most common liver disease in the Western world, affecting approximately 10% of children and a third of all adults in the United States [1–3]. It is a significant public health challenge and is estimated to soon be the number one indication for liver transplantation in adults.
NAFLD is a generic term encompassing 2 distinct conditions defined by their histopathology: simple steatosis and nonalcoholic steatohepatitis (NASH). Simple steatosis is characterized by predominantly macrovesicular—meaning large droplet—cytoplasmic lipid inclusions found in ≥ 5% of hepatocytes. NASH is defined as hepatic steatosis plus the additional features of inflammation, hepatocyte ballooning, and/or fibrosis. There are some adult data [4-6] and 1 retrospective pediatric study [7] demonstrating that over time, NAFLD may progress. That is, steatosis may progress to NASH and some patients with fibrosis will ultimately develop cirrhosis. If intervention is provided early in the histologic spectrum, NAFLD can be reversed [4,8] and late complications—such as cirrhosis, hepatocellular carcinoma, or liver transplantation—may be prevented.
It is important to highlight that the above definitions are based on histology and that a liver biopsy cannot be reasonably obtained in such a large percentage of the U.S. population. This case-based review will therefore focus primarily on the current diagnostic challenges facing health care providers as well as management strategies in children with presumed NAFLD.
Case Study
Initial Presentation
As you finish your charts at the end of a busy clinic day, you identify 3 patients who may have NAFLD:
History
All 3 patients presented to your office for a routine annual physical before the start of the school year and are asymptomatic. None of the patients has a family history of liver disease and their previously diagnosed comorbidities are listed in the table above. No patient is taking medications other than patient C, who is on metformin.
All 3 children have a smooth, velvety rash on their necks consistent with acanthosis nigricans with an otherwise normal physical exam. The liver and spleen are difficult to palpate but are seemingly normal.
What is the typical presentation for a child with NAFLD?
Most children with NAFLD are asymptomatic, though some may present with vague right upper quadrant abdominal pain. It is unclear, however, if the pain is caused by NAFLD or is rather an unrelated symptom that brings the child to the attention of a physician. In addition, hepatomegaly can be found in over 30% to 40% of patients [9]. For children without abdominal pain or hepatomegaly, most are recognized by an elevated serum alanine aminotransferase (ALT) or findings of increased liver echogenicity on ultrasonography.
Serum Alanine Aminotransferase
Serum aminotransferases are one of the more common screening tests for NAFLD. However, ALT is highly insensitive at commonly used thresholds and is also nonspecific. As documented in the SAFETY study, the upper limit of normal for ALT in healthy children should be set around 25 U/L in boys and 22 U/L in girls [10]. Yet even at these thresholds, the sensitivity of ALT to diagnose NAFLD is 80% in boys and 92% in girls, whereas specificity is 79% and 85%, respectively [10]. These findings are largely consistent with adult studies [11–14]. Furthermore, ALT does not correlate well with disease severity and children may still have NASH or significant fibrosis with normal values. In a well-characterized cohort of 91 children with biopsy-proven NAFLD, for example, early fibrosis was identified in 12% of children with a normal ALT (≤ 22 U/L for girls and ≤ 25 U/L in boys) [15]. Advanced fibrosis or cirrhosis was seen in 9% of children with an ALT up to 2 times this upper limit [15]. Thus, reliance on the serum ALT may significantly underestimate the prevalence and severity of liver injury.
Ultrasonography
Children with NAFLD typically have findings of increased hepatic echogenicity on abdominal ultrasonography. However, there are multiple limitations to sonography. First, ultrasound is insensitive for identifying mild steatosis if less than 30% of hepatocytes are affected [16,17]. Second, increased hepatic echogenicity is nonspecific and may be caused by inflammation, fibrosis, or intrahepatic accumulation of iron, copper, or glycogen. Third, there can be considerable inter- and intra-operator variability. And lastly, there is some evidence that ultrasounds do not add benefit to diagnosing children with NAFLD [18].
Which patients are at risk for developing hepatic steatosis and NASH?
Weight, Age, and Gender
There is a strong, direct correlation between body mass index (BMI) and NAFLD. The Study of Child and Adolescent Liver Epidemiology (SCALE)—a sentinel pediatric autopsy study of 742 children—found that 5% of normal weight children, 16% of overweight children, and 38% of obese children had NAFLD. The SCALE study also demonstrated an increasing prevalence with age, such that NAFLD was present in 17.3% of 15- to 19-year-olds but only in 0.2% of 2- to 4-year-olds [1]. With regards to gender, NAFLD is roughly twice as prevalent in males [18–20]. While the exact etiology of this difference is unclear, hormonal differences are a leading hypothesis.
Ethnicity
NAFLD is most common in Hispanics, followed by Asians, Caucasians, and African Americans. Research suggests that genetics may be largely responsible for these ethnic disparities. For example, the I148M allele of PNPLA3 (a single nucleotide polymorphism) is strongly associated with steatosis, NASH, and fibrosis [21] and is most common in Hispanics, with a 50% carrier frequency in some cohorts [22]. Conversely, African Americans are more likely to carry the S453I allele of PNPLA3, which is associated with decreased hepatic steatosis [22]. There is also considerable variability within ethnic groups. For example, Mexican-American children appear to be at the highest risk for steatosis or NASH among Hispanics, whereas Filipino-American children are believed to have higher disease prevalence than Cambodian or Vietnamese Americans [1].
Comorbidities
NAFLD is associated with obesity, insulin resistance and diabetes, cardiovascular disease, the metabolic syndrome [23], decreased quality of life [24,25], and obstructive sleep apnea (OSA). These associations generally hold even after controlling for the other confounders listed. It is important to note that these data come largely from cross-sectional studies and direct causation has yet to be determined.
Insulin resistance in particular is strongly associated with NAFLD—so much so, in fact, that some consider it to be the hepatic manifestation of the metabolic syndrome. Additionally, children with features of the metabolic syndrome are more likely to have advanced histologic features of NAFLD [23]. There are also intriguing data from small pediatric studies to suggest that OSA may contribute to the development of hepatic fibrosis. In one study of 25 children with biopsy-proven NAFLD, for example, the presence of OSA and hypoxemia correlated with the degree of hepatic fibrosis [26]. In a slightly larger study of 65 children, OSA was also strongly associated with significant hepatic fibrosis (odds ratio, 5.91; 95% confidence interval, 3.23–7.42; P < 0.001). The duration of hypoxemia also correlated with histologic findings of inflammation and circulating biomarkers of apoptosis and fibrogenesis [27].
Other Laboratory Tests
Several studies have documented an association between elevated gamma-glutamyl transferase (GGT) and hepatic fibrosis [28,29], though others have been conflicting [30,31]. Pediatric studies have also demonstrated an inverse correlation between NASH and total bilirubin [32], serum potassium [33], and serum ceruloplasmin [34]. In addition, there are a number of serum biomarkers or biomarker panels commercially available for use in adults. Because similar efficacy data are unavailable in children, however, serum biomarkers should be primarily used for research purposes only.
Who should be screened for NAFLD? And how?
Published professional society recommendations differ significantly with regards to screening. In 2007, the American Academy of Pediatrics suggested screening obese children over 10 years of age or overweight children with additional risk factors with biannual liver tests [35]. There were no management recommendations made for elevated aminotransferase levels other than for subspecialty referral. In 2012, the European Society of Pediatric Gastroenterology, Hepatology, and Nutrition (ESPGHAN) recommended obtaining an ultrasound and liver tests in every obese child [36]. One month later, however, the American Gastroenterological Association, American Association for the Study of Liver Disease, and the American College of Gastroenterology published joint guidelines without screening recommendations “due to a paucity of evidence” [37].
Because these statements conflict and are based heavily on expert opinion, one should consider the risks, benefits, and costs to screening large numbers of patients. Until additional research clarifies this controversy, we suggest that providers individualize their screening practices to their population and the risks of each individual patient. For example, we would consider screening children who are obese; Hispanic or Asian; have multiple features of the metabolic syndrome; and/or those who have a family history of NAFLD. Further, we recommend screening children for NAFLD with serum liver enzymes only and not with ultrasonography.
Case Continued: Laboratory Results
ALT and GGT tests are ordered and the results are as follows:
What is the differential for children with suspected NAFLD?
Autoimmune Hepatitis (AIH)
AIH is a progressive necro-inflammatory disorder of the liver characterized by elevated aminotransferases, positive autoantibodies, and distinctive histologic features. AIH is believed to occur in genetically predisposed patients in response to an environmental trigger. There is a female predominance and it can present in any age or ethnic group.
AIH is divided in 2 subtypes. Type 1 disease is characterized by a positive antinuclear (ANA) antibody and anti-smooth muscle antibody. More commonly, it presents in adolescence with an indolent course—many patients are asymptomatic until they develop features of cirrhosis and portal hypertension. Conversely, type 2 AIH is characterized by a positive liver kidney microsomal (LKM) antibody and tends to present acutely in young children. It is important to note that antibody titers can be falsely positive in a significant percentage of patients and, in such cases, are often mildly elevated [38]. We strongly suggest children with positive autoantibody titers be evaluated by a specialist.
Treatment should be started promptly to avoid progression to cirrhosis and should also done so in consultation with a pediatric gastroenterologist or hepatologist. The prognosis of AIH with immunosuppression is favorable, with long-term remission rates of approximately 80%. Transplantation is typically required in the remaining 10% to 20% [39].
Celiac Disease
Celiac disease is an autoimmune, inflammatory enteropathy caused by exposure to gluten in genetically susceptible individuals. Up to a third of all children presenting with celiac will have an elevated serum ALT [40]. Additional symptoms/features are both variable and nonspecific: abdominal pain, poor growth, diarrhea, or constipation, among others. Celiac is diagnosed by duodenal biopsy or a sufficiently elevated tissue transglutaminase antibody level [41]. Treatment with a strict gluten-free diet will resolve the enteropathy and normalize the serum aminotransferases.
Wilson’s Disease
Wilson’s disease is a metabolic disorder leading to copper deposition in the liver, brain, cornea, and kidneys. It is caused by an ATP7B gene mutation and inherited in an autosomal recessive fashion. Patients may present with asymptomatic liver disease, chronic hepatitis, acute liver failure, or with symptoms of portal hypertension. Neuropsychiatric symptoms may also be prominent. Screening tests include a serum ceruloplasmin and 24-hour urinary copper quantification. Because diagnosing Wilson’s disease can be challenging, however, further testing should occur in consultation with a pediatric gastroenterologist or hepatologist.
Viral Hepatitis
Chronic viral infections such as hepatitis B and C are still common etiologies of liver disease in the United States. However, universal vaccination and blood donor screening have reduced the risk of transmission; new antiviral agents will likely further decrease the prevalence and transmission risk over time. Acute viral hepatitis—cytomegalovirus, Epstein-Barr virus, hepatitis A, or hepatitis E—should also be considered in children who present with appropriate symptoms and an elevated ALT.
Drug-Induced
Drug-induced liver injury (DILI) can present with elevated serum aminotransferases (hepatocellular pattern), an elevated bilirubin (cholestatic pattern), or a mixed picture. Idiosyncratic DILI in children is commonly caused by antimicrobial or central nervous system agents and usually presents with a hepatocellular injury pattern. Substance abuse, including alcohol, is common and should also be investigated as the source of underlying liver disease.
Muscle Disease
Aspartate aminotransferase (AST) and ALT are present in hepatocytes, myocytes, and red blood cells, among other tissues. Thus, children with congenital myopathies or myositis can have elevated aminotransferases, typically with the AST higher than the ALT. In these patients, checking a creatine phosphokinase (CPK) level may lead to the correct diagnosis and limit unnecessary testing.
Other Metabolic Disorders
Myriad metabolic disorders present with liver disease and/or elevated serum aminotransferase levels. Individually, these conditions are rare but, collectively, are relatively common. Two of the more occult conditions—lysosomal acid lipase deficiency (LAL-D) and alpha-1 antitrypsin (A1A) deficiency—are discussed in further detail below.
LAL-D is an autosomal recessive disease resulting in the accumulation of cholesterol esters and triglycerides in lysosomes. Patients typically present with hepatomegaly and mildly elevated aminotransferases, an elevated LDL, low HDL cholesterol, and increased hepatic echogenicity on ultrasound. If a biopsy is obtained, microvesicular steatosis is predominant as opposed to macrovesicular steatosis found in NAFLD. The diagnosis of LAL-D can be made on a commercially available dry blood spot enzymatic assay or genetic testing and treatment has recently been FDA approved.
A1A deficiency is an autosomal recessive disease diagnosable by an alpha-1-antitrypsin phenotype. The clinical presentation is characterized by neonatal cholestasis in the infantile form and by hepatitis, cirrhosis and portal hypertension in older children. Classic symptoms of emphysema and chronic lung disease present in adulthood.
What further testing should be performed in children with suspected NAFLD?
For obese children with an elevated ALT or evidence of increased hepatic echogenicity, ESPGHAN recommends targeting the workup according to the child’s age [36]. According to their consensus statement, they recommend an upfront, thorough laboratory evaluation in children less than 10 years of age and consideration of a liver biopsy upon completion. For children over 10 years of age at low risk for NASH or fibrosis, additional laboratory evaluation is suggested 3 to 6 months after failed lifestyle interventions. In general, the recommended workup includes testing for conditions discussed in the section above such as viral hepatitis, AIH, Wilson’s disease, and others. If negative, ESPGHAN states that a liver biopsy should be “considered.”
The question of whether or not to obtain a liver biopsy is controversial, though there are several clear advantages to doing so. First, biopsy is the gold standard test for diagnosing NAFLD and there are no highly accurate, noninvasive tests currently approved for use in children. Second, biopsy is a more definitive means of ruling out competing diagnoses such as AIH. Third, biopsy may provide prognostic data. In a retrospective adult study of 136 patients, for example, those who presented with simple steatosis had a roughly 3% chance of progressing to cirrhosis within 10 years. If a patient within this cohort presented with NASH, however, the progression risk was approximately 30% within 5 years [42,43]. Fourth, due to potential side effects of medications, position papers recommend obtaining a liver biopsy prior to the initiation of pharmacotherapy [37]. Lastly, the risk for serious morbidity from a liver biopsy is low [44,45]. Alternatively, one must acknowledge the risks of liver biopsy: morbidity, sampling bias, invasiveness, cost, and sedation risks in children.
Case Continued: Biopsy Results
You refer your patients to a gastroenterologist. Tests for viral hepatitis, A1A deficiency, celiac disease, muscle disorders, Wilson’s disease, and AIH are negative. Ultimately, a liver biopsy is performed on all 3 children without complications. The results are presented below.
What is the treatment of NAFLD?
Lifestyle Modification
Lifestyle modifications are the mainstay of treatment for NAFLD. In adult studies, weight loss of more than 5% reduces hepatic steatosis whereas weight loss of more than 9% improves or eliminates NASH [47]. We recommend that children engage in age-appropriate, enjoyable, moderate- or vigorous-intensity aerobic activity for 60 minutes a day [48]. In addition, there should be a focus on reducing sedentary behavior by limiting screen time and a concerted effort to engage the family in lifestyle modifications.
Dietary interventions to treat NAFLD are less concrete but there is a growing body of literature to suggest that dietary fructose is particularly harmful. In adults, for example, fructose consumption is associated with the development of NAFLD [49] and hepatic fibrosis [50]. Recent data in adolescents has similarly documented an association between NAFLD incidence and energy-adjusted fructose intake [51]. It is worth highlighting that these clinical findings are also biologically plausible, as fructose is primarily metabolized within hepatocytes and has recently been shown to increase de novo lipogenesis [52,53]. In general, we suggest a well-balanced diet of unprocessed foods—that is, with limited added sugars—sufficient to induce gradual weight loss in older children or body weight maintenance in younger children.
Medications
Vitamin E is the only medication with proven efficacy in children, as demonstrated in the TONIC trial [20]. TONIC was a double-blind, multicenter, placebo-controlled study with 3 treatment arms: 800 IU of vitamin E daily, 1000 mg of metformin daily, or placebo. Metformin did not reduce the serum ALT or significantly improve liver histology and should therefore not be used for these indications. However, patients treated with vitamin E had a statistically significant improvement in the NAFLD activity score (a histologic grading system comprising steatosis, inflammation, and hepatocyte ballooning) and resolution of NASH when compared to placebo. For these reasons—as well as a paucity of other viable treatment options—vitamin E is routinely prescribed for children with biopsy-proven NASH. However, the long- term risks of high-dose vitamin E therapy in children are largely unknown.
Polyunsaturated fats such as docosahexaenoic acid (DHA) [54] and probiotics such as VSL #3 [55] have showed efficacy reducing hepatic steatosis in small, randomized clinical trials. Both medications need to be further validated before they can be recommended for use in children. Conversely, ursodeoxycholic acid has not been found to be efficacious in children with NAFLD [56], whereas phase IIb data on cysteamine is expected soon. There are currently insufficient data to recommend bariatric surgery as treatment for NAFLD in adolescence.
Case Continued: Follow-up
After their biopsies, both patients with NASH (patients A and B) are started on vitamin E therapy. All 3 patients continue to report for follow-up visits without short-term complications, though they have still been unable to significantly reduce their body mass index and have a persistently elevated serum ALT.
Summary
NAFLD is a common condition in the United States with serious personal and public health ramifications. This case-based review highlights the diagnostic and management challenges in children with NAFLD and the unique role primary care providers play in caring for these patients.
Corresponding author: Bryan Rudolph, MD, Albert Einstein College of Medicine, Division of Pediatric Gastroenterology and Nutrition, Children’s Hospital at Montefiore, 3415 Bainbridge Ave., Bronx, NY 10467, brudolph@montefiore.org.
Financial disclosures: None.
1. Schwimmer JB, Deutsch R, Kahen T, et al. Prevalence of fatty liver in children and adolescents. Pediatrics 2006;118:1388–93.
2. Welsh JA, Karpen S, Vos MB.Increasing prevalence of nonalcoholic fatty liver disease among United States adolescents, 1988-1994 to 2007-2010. J Pediatr 2013;162:496–500.
3. Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther 2011;34:274–85.
4. McPherson S, Hardy T, Henderson E, et al. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for prognosis and clinical management. J Hepatol 2015;62:1148–55.
5. Singh S, Allen AM, Wang Z, et al. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 2015;13:643–54.
6. Pais R, Charlotte F, Fedchuk L, et al. A systematic review of follow-up biopsies reveals disease progression in patients with non-alcoholic fatty liver. J Hepatol 2013;59:550–6.
7. Feldstein AE, Charatcharoenwitthaya P, Treeprasertsuk S, et al. The natural history of non-alcoholic fatty liver disease in children: a follow-up study for up to 20 years. Gut 2009;58:1538–44.
8. Mummadi RR, Kasturi KS, Chennareddygari S, et al. Effect of bariatric surgery on nonalcoholic fatty liver disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol 2008;6:1396–402.
9. Rashid M, Roberts EA. Nonalcoholic steatohepatitis in children. J Pediatr Gastroenterol Nutr 2000;30:48–53.
10. Schwimmer JB, Dunn W, Norman GJ, et al. SAFETY study: alanine aminotransferase cutoff values are set too high for reliable detection of pediatric chronic liver disease. Gastroenterology 2010;138:1357–64.
11. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002;137:1–10.
12. Lee JK, Shim JH, Lee HC, et al. Estimation of the healthy upper limits for serum alanine aminotransferase in Asian populations with normal liver histology. Hepatology 2010;51:1577–83.
13. Kang HS, Um SH, Seo YS, et al. Healthy range for serum ALT and the clinical significance of "unhealthy" normal ALT levels in the Korean population. J Gastroenterol Hepatol 2011;26:292–9.
14. Zheng MH, Shi KQ, Fan YC, et al. Upper limits of normal for serum alanine aminotransferase levels in Chinese Han population. PLoS One 2012;7:e43736.
15. Molleston JP, Schwimmer JB, Yates KP, et al. Histological abnormalities in children with nonalcoholic fatty liver disease and normal or mildly elevated alanine aminotransferase levels. J Pediatr 2014;164:707–13.
16. Dasarathy S, Dasarathy J, Khiyami A, et al. Validity of real time ultrasound in the diagnosis of hepatic steatosis: a prospective study. J Hepatol 2009;51:1061–7.
17. Nobili V, M. Pinzani M. Paediatric non-alcoholic fatty liver disease. Gut 2010;59:561–4.
18. Rudolph B, Rivas Y, Kulak S, et al. Yield of diagnostic tests in obese children with an elevated alanine aminotransferase. Acta Paediatr 2015;104:e557–63.
19. Nobili V, Manco M, Ciampalini P, et al. Metformin use in children with nonalcoholic fatty liver disease: an open-label, 24-month, observational pilot study. Clin Ther 2008;30:1168–76.
20. Lavine JE, Schwimmer JB, Van Natta ML, et al. Effect of vitamin E or metformin for treatment of nonalcoholic fatty liver disease in children and adolescents: the TONIC randomized controlled trial. JAMA 2011;305:1659–68.
21. Krawczyk MP, Portincasa P, Lammert F. PNPLA3-associated steatohepatitis: toward a gene-based classification of fatty liver disease. Semin Liver Dis 2013;33:369–79.
22. Romeo S, Kozlitina J, Xing C, et al. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet 2008;40:1461–5.
23. Patton HM, Yates K, Unalp-Arida A, et al. Association between metabolic syndrome and liver histology among children with nonalcoholic fatty liver disease. Am J Gastroenterol 2010;105:2093–102.
24. Kistler KD, Molleston J, Unalp A, et al., Symptoms and quality of life in obese children and adolescents with non-alcoholic fatty liver disease. Aliment Pharmacol Ther 2010;31:396–406.
25. Kerkar N, D'Urso C, Van Nostrand K, et al. Psychosocial outcomes for children with nonalcoholic fatty liver disease over time and compared with obese controls. J Pediatr Gastroenterol Nutr 2013;56:77–82.
26. Sundaram SS, Sokol RJ, Capocelli KE, et al. Obstructive sleep apnea and hypoxemia are associated with advanced liver histology in pediatric nonalcoholic fatty liver disease. J Pediatr 2014;164:699–706.
27. Nobili V, Cutrera R, Liccardo D, et al. Obstructive sleep apnea syndrome affects liver histology and inflammatory cell activation in pediatric nonalcoholic fatty liver disease, regardless of obesity/insulin resistance. Am J Respir Crit Care Med 2014;189:66–76.
28. Patton HM, Lavine JE, Van Natta ML, et al., Clinical correlates of histopathology in pediatric nonalcoholic steatohepatitis. Gastroenterology 2008;135:1961–71.
29. Schwimmer JB, Behling C, Newbury R, et al. Histopathology of pediatric nonalcoholic fatty liver disease. Hepatology 2005;42:641–9.
30. Nobili V, Parkes J, Bottazzo G, et al. Performance of ELF serum markers in predicting fibrosis stage in pediatric non-alcoholic fatty liver disease. Gastroenterology 2009;136:160–7.
31. Yang HR, Kim HR, Kim MJ, et al. Noninvasive parameters and hepatic fibrosis scores in children with nonalcoholic fatty liver disease. World J Gastroenterol 2012;18:1525–30.
32. Puri K, Nobili V, Melville K, et al. Serum bilirubin level is inversely associated with nonalcoholic steatohepatitis in children. J Pediatr Gastroenterol Nutr 2013;57:114–8.
33. Tabbaa A, Shaker M, Lopez R, et al. Low serum potassium levels associated with disease severity in children with nonalcoholic fatty liver disease. Pediatr Gastroenterol Hepatol Nutr 2015;18:168–74.
34. Nobili V, Siotto M, Bedogni G, et al. Levels of serum ceruloplasmin associate with pediatric nonalcoholic fatty liver disease. J Pediatr Gastroenterol Nutr 2013;56:370–5.
35. Barlow SE; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 2007;120 Suppl 4:S164–92.
36. Vajro P, Lenta S, Socha P, et al. Diagnosis of nonalcoholic fatty liver disease in children and adolescents: position paper of the ESPGHAN Hepatology Committee. J Pediatr Gastroenterol Nutr 2012;54:700–13.
37. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012;142:1592–609.
38. Vuppalanchi R, Gould RJ, Wilson LA, et al. Clinical significance of serum autoantibodies in patients with NAFLD: results from the nonalcoholic steatohepatitis clinical research network. Hepatol Int 2012;6:379–85.
39. Floreani A, Liberal R, Vergani D, et al. Autoimmune hepatitis: contrasts and comparisons in children and adults - a comprehensive review. J Autoimmun 2013;46:7–16.
40. Vajro P, Paolella G, Maggiore G, et al. Pediatric celiac disease, cryptogenic hypertransaminasemia, and autoimmune hepatitis. J Pediatr Gastroenterol Nutr 2013;56:663–70.
41. Husby S, Koletzko S, Korponay-Szabó IR, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr 2012;54:136–60.
42. Matteoni CA, Younossi ZM, Gramlich T, et al. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 1999;116:1413–9.
43. McCullough AJ. The clinical features, diagnosis and natural history of nonalcoholic fatty liver disease. Clin Liver Dis 2004;8:521–33.
44. Ovchinsky N, Moreira RK, Lefkowitch JH, Lavine JE. Liver biopsy in modern clinical practice: a pediatric point-of-view. Adv Anat Pathol 2012;19:250–62.
45. Dezsőfi A, Baumann U, Dhawan A, et al. Liver biopsy in children: position paper of the ESPGHAN Hepatology Committee. J Pediatr Gastroenterol Nutr 2015;60:408–20.
46. Fusillo S, Rudolph B. Nonalcoholic fatty liver disease. Pediatr Rev 2015;36:198–205.
47. Harrison SA, Fecht W, Brunt EM, Neuschwander-Tetri BA. Orlistat for overweight subjects with nonalcoholic steatohepatitis: A randomized, prospective trial. Hepatology 2009;49:80–6.
48. School health guidelines to promote healthy eating and physical activity. MMWR Recomm Rep 2011;60(Rr-5):1–76.
49. Ouyang X, Cirillo P, Sautin Y, et al. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. J Hepatol 2008;48:993–9.
50. Abdelmalek MF, Suzuki A, Guy C, et al. Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology 2010;51:1961–71.
51. O’Sullivan TA, Oddy WH, Bremner AP, et al. Lower fructose intake may help protect against development of nonalcoholic fatty liver in adolescents with obesity. J Pediatr Gastroenterol Nutr 2014;58:624–31.
52. Parks EJ, Skokan LE, Timlin MT, Dingfelder CS. Dietary sugars stimulate fatty acid synthesis in adults. J Nutr 2008;138:1039–46.
53. Stanhope KL, Schwarz JM, Keim NL, et al. Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans. J Clin Invest 2009;119:1322–34.
54. Nobili V, Alisi A, Della Corte C, et al., Docosahexaenoic acid for the treatment of fatty liver: randomised controlled trial in children. Nutr Metab Cardiovasc Dis 2013;23:1066–70.
55. Alisi A, Bedogni G, Baviera G, et al. Randomised clinical trial: The beneficial effects of VSL#3 in obese children with non-alcoholic steatohepatitis. Aliment Pharmacol Ther 2014;39:1276–85.
56. Vajro P, Franzese A, Valerio G, et al. Lack of efficacy of ursodeoxycholic acid for the treatment of liver abnormalities in obese children. J Pediatr 2000;136:739–43.
1. Schwimmer JB, Deutsch R, Kahen T, et al. Prevalence of fatty liver in children and adolescents. Pediatrics 2006;118:1388–93.
2. Welsh JA, Karpen S, Vos MB.Increasing prevalence of nonalcoholic fatty liver disease among United States adolescents, 1988-1994 to 2007-2010. J Pediatr 2013;162:496–500.
3. Vernon G, Baranova A, Younossi ZM. Systematic review: the epidemiology and natural history of non-alcoholic fatty liver disease and non-alcoholic steatohepatitis in adults. Aliment Pharmacol Ther 2011;34:274–85.
4. McPherson S, Hardy T, Henderson E, et al. Evidence of NAFLD progression from steatosis to fibrosing-steatohepatitis using paired biopsies: implications for prognosis and clinical management. J Hepatol 2015;62:1148–55.
5. Singh S, Allen AM, Wang Z, et al. Fibrosis progression in nonalcoholic fatty liver vs nonalcoholic steatohepatitis: a systematic review and meta-analysis of paired-biopsy studies. Clin Gastroenterol Hepatol 2015;13:643–54.
6. Pais R, Charlotte F, Fedchuk L, et al. A systematic review of follow-up biopsies reveals disease progression in patients with non-alcoholic fatty liver. J Hepatol 2013;59:550–6.
7. Feldstein AE, Charatcharoenwitthaya P, Treeprasertsuk S, et al. The natural history of non-alcoholic fatty liver disease in children: a follow-up study for up to 20 years. Gut 2009;58:1538–44.
8. Mummadi RR, Kasturi KS, Chennareddygari S, et al. Effect of bariatric surgery on nonalcoholic fatty liver disease: systematic review and meta-analysis. Clin Gastroenterol Hepatol 2008;6:1396–402.
9. Rashid M, Roberts EA. Nonalcoholic steatohepatitis in children. J Pediatr Gastroenterol Nutr 2000;30:48–53.
10. Schwimmer JB, Dunn W, Norman GJ, et al. SAFETY study: alanine aminotransferase cutoff values are set too high for reliable detection of pediatric chronic liver disease. Gastroenterology 2010;138:1357–64.
11. Prati D, Taioli E, Zanella A, et al. Updated definitions of healthy ranges for serum alanine aminotransferase levels. Ann Intern Med 2002;137:1–10.
12. Lee JK, Shim JH, Lee HC, et al. Estimation of the healthy upper limits for serum alanine aminotransferase in Asian populations with normal liver histology. Hepatology 2010;51:1577–83.
13. Kang HS, Um SH, Seo YS, et al. Healthy range for serum ALT and the clinical significance of "unhealthy" normal ALT levels in the Korean population. J Gastroenterol Hepatol 2011;26:292–9.
14. Zheng MH, Shi KQ, Fan YC, et al. Upper limits of normal for serum alanine aminotransferase levels in Chinese Han population. PLoS One 2012;7:e43736.
15. Molleston JP, Schwimmer JB, Yates KP, et al. Histological abnormalities in children with nonalcoholic fatty liver disease and normal or mildly elevated alanine aminotransferase levels. J Pediatr 2014;164:707–13.
16. Dasarathy S, Dasarathy J, Khiyami A, et al. Validity of real time ultrasound in the diagnosis of hepatic steatosis: a prospective study. J Hepatol 2009;51:1061–7.
17. Nobili V, M. Pinzani M. Paediatric non-alcoholic fatty liver disease. Gut 2010;59:561–4.
18. Rudolph B, Rivas Y, Kulak S, et al. Yield of diagnostic tests in obese children with an elevated alanine aminotransferase. Acta Paediatr 2015;104:e557–63.
19. Nobili V, Manco M, Ciampalini P, et al. Metformin use in children with nonalcoholic fatty liver disease: an open-label, 24-month, observational pilot study. Clin Ther 2008;30:1168–76.
20. Lavine JE, Schwimmer JB, Van Natta ML, et al. Effect of vitamin E or metformin for treatment of nonalcoholic fatty liver disease in children and adolescents: the TONIC randomized controlled trial. JAMA 2011;305:1659–68.
21. Krawczyk MP, Portincasa P, Lammert F. PNPLA3-associated steatohepatitis: toward a gene-based classification of fatty liver disease. Semin Liver Dis 2013;33:369–79.
22. Romeo S, Kozlitina J, Xing C, et al. Genetic variation in PNPLA3 confers susceptibility to nonalcoholic fatty liver disease. Nat Genet 2008;40:1461–5.
23. Patton HM, Yates K, Unalp-Arida A, et al. Association between metabolic syndrome and liver histology among children with nonalcoholic fatty liver disease. Am J Gastroenterol 2010;105:2093–102.
24. Kistler KD, Molleston J, Unalp A, et al., Symptoms and quality of life in obese children and adolescents with non-alcoholic fatty liver disease. Aliment Pharmacol Ther 2010;31:396–406.
25. Kerkar N, D'Urso C, Van Nostrand K, et al. Psychosocial outcomes for children with nonalcoholic fatty liver disease over time and compared with obese controls. J Pediatr Gastroenterol Nutr 2013;56:77–82.
26. Sundaram SS, Sokol RJ, Capocelli KE, et al. Obstructive sleep apnea and hypoxemia are associated with advanced liver histology in pediatric nonalcoholic fatty liver disease. J Pediatr 2014;164:699–706.
27. Nobili V, Cutrera R, Liccardo D, et al. Obstructive sleep apnea syndrome affects liver histology and inflammatory cell activation in pediatric nonalcoholic fatty liver disease, regardless of obesity/insulin resistance. Am J Respir Crit Care Med 2014;189:66–76.
28. Patton HM, Lavine JE, Van Natta ML, et al., Clinical correlates of histopathology in pediatric nonalcoholic steatohepatitis. Gastroenterology 2008;135:1961–71.
29. Schwimmer JB, Behling C, Newbury R, et al. Histopathology of pediatric nonalcoholic fatty liver disease. Hepatology 2005;42:641–9.
30. Nobili V, Parkes J, Bottazzo G, et al. Performance of ELF serum markers in predicting fibrosis stage in pediatric non-alcoholic fatty liver disease. Gastroenterology 2009;136:160–7.
31. Yang HR, Kim HR, Kim MJ, et al. Noninvasive parameters and hepatic fibrosis scores in children with nonalcoholic fatty liver disease. World J Gastroenterol 2012;18:1525–30.
32. Puri K, Nobili V, Melville K, et al. Serum bilirubin level is inversely associated with nonalcoholic steatohepatitis in children. J Pediatr Gastroenterol Nutr 2013;57:114–8.
33. Tabbaa A, Shaker M, Lopez R, et al. Low serum potassium levels associated with disease severity in children with nonalcoholic fatty liver disease. Pediatr Gastroenterol Hepatol Nutr 2015;18:168–74.
34. Nobili V, Siotto M, Bedogni G, et al. Levels of serum ceruloplasmin associate with pediatric nonalcoholic fatty liver disease. J Pediatr Gastroenterol Nutr 2013;56:370–5.
35. Barlow SE; Expert Committee. Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatrics 2007;120 Suppl 4:S164–92.
36. Vajro P, Lenta S, Socha P, et al. Diagnosis of nonalcoholic fatty liver disease in children and adolescents: position paper of the ESPGHAN Hepatology Committee. J Pediatr Gastroenterol Nutr 2012;54:700–13.
37. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice guideline by the American Gastroenterological Association, American Association for the Study of Liver Diseases, and American College of Gastroenterology. Gastroenterology 2012;142:1592–609.
38. Vuppalanchi R, Gould RJ, Wilson LA, et al. Clinical significance of serum autoantibodies in patients with NAFLD: results from the nonalcoholic steatohepatitis clinical research network. Hepatol Int 2012;6:379–85.
39. Floreani A, Liberal R, Vergani D, et al. Autoimmune hepatitis: contrasts and comparisons in children and adults - a comprehensive review. J Autoimmun 2013;46:7–16.
40. Vajro P, Paolella G, Maggiore G, et al. Pediatric celiac disease, cryptogenic hypertransaminasemia, and autoimmune hepatitis. J Pediatr Gastroenterol Nutr 2013;56:663–70.
41. Husby S, Koletzko S, Korponay-Szabó IR, et al. European Society for Pediatric Gastroenterology, Hepatology, and Nutrition guidelines for the diagnosis of coeliac disease. J Pediatr Gastroenterol Nutr 2012;54:136–60.
42. Matteoni CA, Younossi ZM, Gramlich T, et al. Nonalcoholic fatty liver disease: a spectrum of clinical and pathological severity. Gastroenterology 1999;116:1413–9.
43. McCullough AJ. The clinical features, diagnosis and natural history of nonalcoholic fatty liver disease. Clin Liver Dis 2004;8:521–33.
44. Ovchinsky N, Moreira RK, Lefkowitch JH, Lavine JE. Liver biopsy in modern clinical practice: a pediatric point-of-view. Adv Anat Pathol 2012;19:250–62.
45. Dezsőfi A, Baumann U, Dhawan A, et al. Liver biopsy in children: position paper of the ESPGHAN Hepatology Committee. J Pediatr Gastroenterol Nutr 2015;60:408–20.
46. Fusillo S, Rudolph B. Nonalcoholic fatty liver disease. Pediatr Rev 2015;36:198–205.
47. Harrison SA, Fecht W, Brunt EM, Neuschwander-Tetri BA. Orlistat for overweight subjects with nonalcoholic steatohepatitis: A randomized, prospective trial. Hepatology 2009;49:80–6.
48. School health guidelines to promote healthy eating and physical activity. MMWR Recomm Rep 2011;60(Rr-5):1–76.
49. Ouyang X, Cirillo P, Sautin Y, et al. Fructose consumption as a risk factor for non-alcoholic fatty liver disease. J Hepatol 2008;48:993–9.
50. Abdelmalek MF, Suzuki A, Guy C, et al. Increased fructose consumption is associated with fibrosis severity in patients with nonalcoholic fatty liver disease. Hepatology 2010;51:1961–71.
51. O’Sullivan TA, Oddy WH, Bremner AP, et al. Lower fructose intake may help protect against development of nonalcoholic fatty liver in adolescents with obesity. J Pediatr Gastroenterol Nutr 2014;58:624–31.
52. Parks EJ, Skokan LE, Timlin MT, Dingfelder CS. Dietary sugars stimulate fatty acid synthesis in adults. J Nutr 2008;138:1039–46.
53. Stanhope KL, Schwarz JM, Keim NL, et al. Consuming fructose-sweetened, not glucose-sweetened, beverages increases visceral adiposity and lipids and decreases insulin sensitivity in overweight/obese humans. J Clin Invest 2009;119:1322–34.
54. Nobili V, Alisi A, Della Corte C, et al., Docosahexaenoic acid for the treatment of fatty liver: randomised controlled trial in children. Nutr Metab Cardiovasc Dis 2013;23:1066–70.
55. Alisi A, Bedogni G, Baviera G, et al. Randomised clinical trial: The beneficial effects of VSL#3 in obese children with non-alcoholic steatohepatitis. Aliment Pharmacol Ther 2014;39:1276–85.
56. Vajro P, Franzese A, Valerio G, et al. Lack of efficacy of ursodeoxycholic acid for the treatment of liver abnormalities in obese children. J Pediatr 2000;136:739–43.
Study sheds new light on blood clot structure

Photo by Vera Kratochvil
Researchers say they have discovered significant differences between blood clot structure in adults and newborns, a finding that could help us better understand the challenges in addressing post-operative bleeding in neonatal patients.
The researchers also found evidence to suggest the current standard of care for treating post-operative bleeding may pose an increased risk of thrombosis in newborns as compared to adults.
The team reported these findings in Anesthesiology.
“We knew that neonates—infants less than 1 month old—are more likely than adults to suffer from severe bleeding after heart surgery, which poses a variety of health risks,” said study author Ashley Brown, PhD, of the University of North Carolina at Chapel Hill.
“The current standard of care is to give neonatal patients blood products . . . derived from adult blood, but neonatal blood and adult blood aren’t the same. Many of the components involved in clotting in newborns have differing levels of activity, or effectiveness, compared to the same components in adults. Our goal was to better understand how clotting in neonates differs from that in adults so that we can move closer to developing more effective treatment strategies for these infants.”
The researchers’ hypothesis was that fibrinogen from neonates would form clots that are different from those formed by adult fibrinogen, and this proved correct. However, the team was surprised to find that fibrinogen from adults did not integrate well with fibrinogen from neonates.
To test their hypothesis, the researchers took samples of neonate fibrinogen and adult fibrinogen and compared clot formation. The team looked at clots formed solely of adult fibrinogen, clots formed solely of neonate fibrinogen, and clots made from a mixture of the two.
Neonate fibrinogen formed less dense, more fragile clots than adult fibrinogen. Likewise, a mixture of adult and neonate fibrinogen formed clots that were fragile and less dense, even if there was relatively little neonate fibrinogen in the mixture.
The researchers also evaluated how long it took these clots to dissolve. Clots of neonate fibrinogen dissolved about twice as quickly as clots formed from adult fibrinogen.
Clots formed from an adult and neonate fibrinogen mixture dissolved at approximately the same rate as adult-only clots, regardless of the percentage of neonate fibrinogen in the mixture.
“This suggests that using adult fibrinogen in neonatal patients may pose an increased risk of embolism or other adverse thrombotic events,” said study author Nina Guzzetta, MD, of the Emory University School of Medicine in Atlanta, Georgia.
“This work drives home that newborns are not just small adults, and we still have much to learn about clotting in neonates. It also tells us that there is a great deal of room for improvement in the current standard of care for post-operative bleeding in neonates.”
“We are investigating several approaches that may help address this problem, evaluating various modes of action,” Dr Brown added. “It is possible that we can use various external factors that promote clotting to stimulate the fibrinogen in neonates to form a denser clot.”
“We are investigating possible alternatives to help neonates form a better clot after major surgery without having to use adult fibrinogen. For example, we are investigating the use of synthetic platelet-like particles developed by our team to augment hemostasis . . . in blood samples collected from these patients.” ![]()
Photo by Vera Kratochvil
Researchers say they have discovered significant differences between blood clot structure in adults and newborns, a finding that could help us better understand the challenges in addressing post-operative bleeding in neonatal patients.
The researchers also found evidence to suggest the current standard of care for treating post-operative bleeding may pose an increased risk of thrombosis in newborns as compared to adults.
The team reported these findings in Anesthesiology.
“We knew that neonates—infants less than 1 month old—are more likely than adults to suffer from severe bleeding after heart surgery, which poses a variety of health risks,” said study author Ashley Brown, PhD, of the University of North Carolina at Chapel Hill.
“The current standard of care is to give neonatal patients blood products . . . derived from adult blood, but neonatal blood and adult blood aren’t the same. Many of the components involved in clotting in newborns have differing levels of activity, or effectiveness, compared to the same components in adults. Our goal was to better understand how clotting in neonates differs from that in adults so that we can move closer to developing more effective treatment strategies for these infants.”
The researchers’ hypothesis was that fibrinogen from neonates would form clots that are different from those formed by adult fibrinogen, and this proved correct. However, the team was surprised to find that fibrinogen from adults did not integrate well with fibrinogen from neonates.
To test their hypothesis, the researchers took samples of neonate fibrinogen and adult fibrinogen and compared clot formation. The team looked at clots formed solely of adult fibrinogen, clots formed solely of neonate fibrinogen, and clots made from a mixture of the two.
Neonate fibrinogen formed less dense, more fragile clots than adult fibrinogen. Likewise, a mixture of adult and neonate fibrinogen formed clots that were fragile and less dense, even if there was relatively little neonate fibrinogen in the mixture.
The researchers also evaluated how long it took these clots to dissolve. Clots of neonate fibrinogen dissolved about twice as quickly as clots formed from adult fibrinogen.
Clots formed from an adult and neonate fibrinogen mixture dissolved at approximately the same rate as adult-only clots, regardless of the percentage of neonate fibrinogen in the mixture.
“This suggests that using adult fibrinogen in neonatal patients may pose an increased risk of embolism or other adverse thrombotic events,” said study author Nina Guzzetta, MD, of the Emory University School of Medicine in Atlanta, Georgia.
“This work drives home that newborns are not just small adults, and we still have much to learn about clotting in neonates. It also tells us that there is a great deal of room for improvement in the current standard of care for post-operative bleeding in neonates.”
“We are investigating several approaches that may help address this problem, evaluating various modes of action,” Dr Brown added. “It is possible that we can use various external factors that promote clotting to stimulate the fibrinogen in neonates to form a denser clot.”
“We are investigating possible alternatives to help neonates form a better clot after major surgery without having to use adult fibrinogen. For example, we are investigating the use of synthetic platelet-like particles developed by our team to augment hemostasis . . . in blood samples collected from these patients.” ![]()
Photo by Vera Kratochvil
Researchers say they have discovered significant differences between blood clot structure in adults and newborns, a finding that could help us better understand the challenges in addressing post-operative bleeding in neonatal patients.
The researchers also found evidence to suggest the current standard of care for treating post-operative bleeding may pose an increased risk of thrombosis in newborns as compared to adults.
The team reported these findings in Anesthesiology.
“We knew that neonates—infants less than 1 month old—are more likely than adults to suffer from severe bleeding after heart surgery, which poses a variety of health risks,” said study author Ashley Brown, PhD, of the University of North Carolina at Chapel Hill.
“The current standard of care is to give neonatal patients blood products . . . derived from adult blood, but neonatal blood and adult blood aren’t the same. Many of the components involved in clotting in newborns have differing levels of activity, or effectiveness, compared to the same components in adults. Our goal was to better understand how clotting in neonates differs from that in adults so that we can move closer to developing more effective treatment strategies for these infants.”
The researchers’ hypothesis was that fibrinogen from neonates would form clots that are different from those formed by adult fibrinogen, and this proved correct. However, the team was surprised to find that fibrinogen from adults did not integrate well with fibrinogen from neonates.
To test their hypothesis, the researchers took samples of neonate fibrinogen and adult fibrinogen and compared clot formation. The team looked at clots formed solely of adult fibrinogen, clots formed solely of neonate fibrinogen, and clots made from a mixture of the two.
Neonate fibrinogen formed less dense, more fragile clots than adult fibrinogen. Likewise, a mixture of adult and neonate fibrinogen formed clots that were fragile and less dense, even if there was relatively little neonate fibrinogen in the mixture.
The researchers also evaluated how long it took these clots to dissolve. Clots of neonate fibrinogen dissolved about twice as quickly as clots formed from adult fibrinogen.
Clots formed from an adult and neonate fibrinogen mixture dissolved at approximately the same rate as adult-only clots, regardless of the percentage of neonate fibrinogen in the mixture.
“This suggests that using adult fibrinogen in neonatal patients may pose an increased risk of embolism or other adverse thrombotic events,” said study author Nina Guzzetta, MD, of the Emory University School of Medicine in Atlanta, Georgia.
“This work drives home that newborns are not just small adults, and we still have much to learn about clotting in neonates. It also tells us that there is a great deal of room for improvement in the current standard of care for post-operative bleeding in neonates.”
“We are investigating several approaches that may help address this problem, evaluating various modes of action,” Dr Brown added. “It is possible that we can use various external factors that promote clotting to stimulate the fibrinogen in neonates to form a denser clot.”
“We are investigating possible alternatives to help neonates form a better clot after major surgery without having to use adult fibrinogen. For example, we are investigating the use of synthetic platelet-like particles developed by our team to augment hemostasis . . . in blood samples collected from these patients.” ![]()
VIDEO – Survey: Isolation, rejection is real for acne patients
WASHINGTON – Acne patients are telling the truth when they describe feeling isolated, rejected, and stigmatized – and now there are data to prove it.
Dr. Alexa B. Kimball, professor of dermatology at Harvard Medical School, Boston, found that almost 70% of people surveyed believe that those with acne are unattractive and hesitate to be seen with them. Her survey of 56 people also found that they harbor fears that acne is infectious and can be transmitted, that it’s caused by poor hygiene and diet.
“The widespread misconceptions about acne contribute to negative perceptions, which can affect patients’ quality of life and social interaction,” Dr. Kimball said. “When our patients describe these feelings, they are describing their real, day-to-day life experiences.”
See more of her comments on treating patients with acne in this video.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Acne patients are telling the truth when they describe feeling isolated, rejected, and stigmatized – and now there are data to prove it.
Dr. Alexa B. Kimball, professor of dermatology at Harvard Medical School, Boston, found that almost 70% of people surveyed believe that those with acne are unattractive and hesitate to be seen with them. Her survey of 56 people also found that they harbor fears that acne is infectious and can be transmitted, that it’s caused by poor hygiene and diet.
“The widespread misconceptions about acne contribute to negative perceptions, which can affect patients’ quality of life and social interaction,” Dr. Kimball said. “When our patients describe these feelings, they are describing their real, day-to-day life experiences.”
See more of her comments on treating patients with acne in this video.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – Acne patients are telling the truth when they describe feeling isolated, rejected, and stigmatized – and now there are data to prove it.
Dr. Alexa B. Kimball, professor of dermatology at Harvard Medical School, Boston, found that almost 70% of people surveyed believe that those with acne are unattractive and hesitate to be seen with them. Her survey of 56 people also found that they harbor fears that acne is infectious and can be transmitted, that it’s caused by poor hygiene and diet.
“The widespread misconceptions about acne contribute to negative perceptions, which can affect patients’ quality of life and social interaction,” Dr. Kimball said. “When our patients describe these feelings, they are describing their real, day-to-day life experiences.”
See more of her comments on treating patients with acne in this video.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT AAD 16

Medicaid expansion approved to address Flint water crisis
In direct response to the Flint, Mich., water crisis, an expansion of Medicaid eligibility has been approved by the Department of Health & Human Services.
Under the new expansion, announced March 3, Medicaid will now cover children up to age 21 and pregnant women who were served by the Flint water system from April 2014 up to a date to be specified by the Michigan governor. Those eligible can have incomes up to 400% of the federal poverty level. Under this new waiver agreement, about 15,000 additional children and pregnant women will be eligible for Medicaid coverage and 30,000 current Medicaid beneficiaries in the area will be eligible for expanded services, HHS estimates.

“The expanded benefits available through this Medicaid waiver gives parents in Flint access to this type of care and support that may be needed to help their children overcome possible effects of high lead exposure,” Dr. Nicole Lurie, HHS assistant secretary for preparedness and response, said in a statement.
In addition to full state Medicaid benefits that will not be subjected to cost sharing or premiums, the state will provide to those exposed to lead through the water system targeted case management services that include medical, social, educational, and other services.
The expansion was approved under the Section 1115 process and is approved for 5 years. Michigan Governor Rick Snyder made the request on Feb. 13.
In direct response to the Flint, Mich., water crisis, an expansion of Medicaid eligibility has been approved by the Department of Health & Human Services.
Under the new expansion, announced March 3, Medicaid will now cover children up to age 21 and pregnant women who were served by the Flint water system from April 2014 up to a date to be specified by the Michigan governor. Those eligible can have incomes up to 400% of the federal poverty level. Under this new waiver agreement, about 15,000 additional children and pregnant women will be eligible for Medicaid coverage and 30,000 current Medicaid beneficiaries in the area will be eligible for expanded services, HHS estimates.
“The expanded benefits available through this Medicaid waiver gives parents in Flint access to this type of care and support that may be needed to help their children overcome possible effects of high lead exposure,” Dr. Nicole Lurie, HHS assistant secretary for preparedness and response, said in a statement.
In addition to full state Medicaid benefits that will not be subjected to cost sharing or premiums, the state will provide to those exposed to lead through the water system targeted case management services that include medical, social, educational, and other services.
The expansion was approved under the Section 1115 process and is approved for 5 years. Michigan Governor Rick Snyder made the request on Feb. 13.
In direct response to the Flint, Mich., water crisis, an expansion of Medicaid eligibility has been approved by the Department of Health & Human Services.
Under the new expansion, announced March 3, Medicaid will now cover children up to age 21 and pregnant women who were served by the Flint water system from April 2014 up to a date to be specified by the Michigan governor. Those eligible can have incomes up to 400% of the federal poverty level. Under this new waiver agreement, about 15,000 additional children and pregnant women will be eligible for Medicaid coverage and 30,000 current Medicaid beneficiaries in the area will be eligible for expanded services, HHS estimates.
“The expanded benefits available through this Medicaid waiver gives parents in Flint access to this type of care and support that may be needed to help their children overcome possible effects of high lead exposure,” Dr. Nicole Lurie, HHS assistant secretary for preparedness and response, said in a statement.
In addition to full state Medicaid benefits that will not be subjected to cost sharing or premiums, the state will provide to those exposed to lead through the water system targeted case management services that include medical, social, educational, and other services.
The expansion was approved under the Section 1115 process and is approved for 5 years. Michigan Governor Rick Snyder made the request on Feb. 13.

Publicizing benefits of HPV vaccine may drive uptick in its use
Increased publicizing of the human papillomavirus (HPV) vaccine’s benefits could drive growth in patients’ usage of the vaccine, researchers said in a letter to the editors of the Pediatric Infectious Disease Journal.
Dr. Harry Pellman, clinical professor of pediatrics at the University of California, Irvine, and Brandon Brown, Ph.D., of the division of clinical sciences at the Center for Health Communities at the University of California, Riverside, cited having observed higher rates of HPV vaccinations in their practice, where doctors recommend the vaccine, than were found by a Centers for Disease Control and Prevention study (42% males, 60% females) as an explanation for their hypothesis. In Dr. Pellman’s and Dr. Brown’s study, which included 101 patients, 90% of male and 67% of female patients (P less than .01) received an HPV vaccination.

In an anonymous survey of these patients’ parents, the researchers learned that “strength of the provider recommendation” (85%) and “publicity around the importance of vaccinating against HPV disease” (69%) were the most common reasons parents chose to accept the HPV vaccination for their child. The pediatricians also noted that 89% of the parents surveyed who had a family member or friend diagnosed with cervical or female organ cancer agreed to have their child vaccinated.
Dr. Pellman and Dr. Brown also found that “wanting to learn more about the vaccine” (60%) was the reason given by most parents who opted not to have their child vaccinated to prevent HPV. “This also suggests that publicizing the role of HPV vaccination in preventing HPV disease and its consequences might be an important public health strategy,” they said.
To read the letter, go to (Pediatr Infect Dis J. 2016 Jan;35[1]:119-20 doi: 10.1097/INF.0000000000000941).
Increased publicizing of the human papillomavirus (HPV) vaccine’s benefits could drive growth in patients’ usage of the vaccine, researchers said in a letter to the editors of the Pediatric Infectious Disease Journal.
Dr. Harry Pellman, clinical professor of pediatrics at the University of California, Irvine, and Brandon Brown, Ph.D., of the division of clinical sciences at the Center for Health Communities at the University of California, Riverside, cited having observed higher rates of HPV vaccinations in their practice, where doctors recommend the vaccine, than were found by a Centers for Disease Control and Prevention study (42% males, 60% females) as an explanation for their hypothesis. In Dr. Pellman’s and Dr. Brown’s study, which included 101 patients, 90% of male and 67% of female patients (P less than .01) received an HPV vaccination.
In an anonymous survey of these patients’ parents, the researchers learned that “strength of the provider recommendation” (85%) and “publicity around the importance of vaccinating against HPV disease” (69%) were the most common reasons parents chose to accept the HPV vaccination for their child. The pediatricians also noted that 89% of the parents surveyed who had a family member or friend diagnosed with cervical or female organ cancer agreed to have their child vaccinated.
Dr. Pellman and Dr. Brown also found that “wanting to learn more about the vaccine” (60%) was the reason given by most parents who opted not to have their child vaccinated to prevent HPV. “This also suggests that publicizing the role of HPV vaccination in preventing HPV disease and its consequences might be an important public health strategy,” they said.
To read the letter, go to (Pediatr Infect Dis J. 2016 Jan;35[1]:119-20 doi: 10.1097/INF.0000000000000941).
Increased publicizing of the human papillomavirus (HPV) vaccine’s benefits could drive growth in patients’ usage of the vaccine, researchers said in a letter to the editors of the Pediatric Infectious Disease Journal.
Dr. Harry Pellman, clinical professor of pediatrics at the University of California, Irvine, and Brandon Brown, Ph.D., of the division of clinical sciences at the Center for Health Communities at the University of California, Riverside, cited having observed higher rates of HPV vaccinations in their practice, where doctors recommend the vaccine, than were found by a Centers for Disease Control and Prevention study (42% males, 60% females) as an explanation for their hypothesis. In Dr. Pellman’s and Dr. Brown’s study, which included 101 patients, 90% of male and 67% of female patients (P less than .01) received an HPV vaccination.
In an anonymous survey of these patients’ parents, the researchers learned that “strength of the provider recommendation” (85%) and “publicity around the importance of vaccinating against HPV disease” (69%) were the most common reasons parents chose to accept the HPV vaccination for their child. The pediatricians also noted that 89% of the parents surveyed who had a family member or friend diagnosed with cervical or female organ cancer agreed to have their child vaccinated.
Dr. Pellman and Dr. Brown also found that “wanting to learn more about the vaccine” (60%) was the reason given by most parents who opted not to have their child vaccinated to prevent HPV. “This also suggests that publicizing the role of HPV vaccination in preventing HPV disease and its consequences might be an important public health strategy,” they said.
To read the letter, go to (Pediatr Infect Dis J. 2016 Jan;35[1]:119-20 doi: 10.1097/INF.0000000000000941).
FROM THE PEDIATRIC INFECTIOUS DISEASE JOURNAL
