User login
Age influences ED visits for mental health among American Indian children
Age plays an influential role in the number of emergency department (ED) visits for mental health concerns among American Indian children, according to Wyatt J. Pickner and his associates.
The researchers analyzed 26,004 pediatric ED visits by 20,413 patients over a 12-month study period in the Upper Midwest. Among these, there were 1,545 visits (5.94%) by 1,287 patients for mental health reasons.

American Indian children had higher odds of having ED visits for mental health concerns, compared with white children (10.8% vs. 5.1%; P less than .0001), the researchers noted.
Visits by older American Indian children were more likely to be for mental health reasons, compared with younger children (P less than .0001). Within the 5- to 10-year-old group, these children had lower odds of a mental health visit (odds ratio, 0.40), while the 11- to 17-year-old American Indian children had higher odds of a mental health visit (OR, 1.62).
“Visits to the ED for mental health reasons by American Indian children are a complex problem and not fully understood,” the researchers concluded. “We believe our data can help to inform clinicians and policymakers on the appropriate resources and interventions that can be used to improve care for American Indian children.”
Read the study in The Journal of Pediatrics (doi: 10.1016/j.jpeds.2016.03.064).
Age plays an influential role in the number of emergency department (ED) visits for mental health concerns among American Indian children, according to Wyatt J. Pickner and his associates.
The researchers analyzed 26,004 pediatric ED visits by 20,413 patients over a 12-month study period in the Upper Midwest. Among these, there were 1,545 visits (5.94%) by 1,287 patients for mental health reasons.
American Indian children had higher odds of having ED visits for mental health concerns, compared with white children (10.8% vs. 5.1%; P less than .0001), the researchers noted.
Visits by older American Indian children were more likely to be for mental health reasons, compared with younger children (P less than .0001). Within the 5- to 10-year-old group, these children had lower odds of a mental health visit (odds ratio, 0.40), while the 11- to 17-year-old American Indian children had higher odds of a mental health visit (OR, 1.62).
“Visits to the ED for mental health reasons by American Indian children are a complex problem and not fully understood,” the researchers concluded. “We believe our data can help to inform clinicians and policymakers on the appropriate resources and interventions that can be used to improve care for American Indian children.”
Read the study in The Journal of Pediatrics (doi: 10.1016/j.jpeds.2016.03.064).
Age plays an influential role in the number of emergency department (ED) visits for mental health concerns among American Indian children, according to Wyatt J. Pickner and his associates.
The researchers analyzed 26,004 pediatric ED visits by 20,413 patients over a 12-month study period in the Upper Midwest. Among these, there were 1,545 visits (5.94%) by 1,287 patients for mental health reasons.
American Indian children had higher odds of having ED visits for mental health concerns, compared with white children (10.8% vs. 5.1%; P less than .0001), the researchers noted.
Visits by older American Indian children were more likely to be for mental health reasons, compared with younger children (P less than .0001). Within the 5- to 10-year-old group, these children had lower odds of a mental health visit (odds ratio, 0.40), while the 11- to 17-year-old American Indian children had higher odds of a mental health visit (OR, 1.62).
“Visits to the ED for mental health reasons by American Indian children are a complex problem and not fully understood,” the researchers concluded. “We believe our data can help to inform clinicians and policymakers on the appropriate resources and interventions that can be used to improve care for American Indian children.”
Read the study in The Journal of Pediatrics (doi: 10.1016/j.jpeds.2016.03.064).
FROM THE JOURNAL OF PEDIATRICS

Take time to talk to vaccine refusers
I am writing in response to the article titled “Faced with vaccine refusers? Save your breath” by Dr. William G. Wilkoff.
I am a family medicine physician in Spokane, Wash., and have been in practice for the last 12 years. I take care of patients from infancy to old age and through all stages of life between. As a primary care provider, I sympathize with the concerns of Dr. Wilkoff and many others on the front lines of the vaccine debate. It takes much time and energy to talk to patients and parents about the benefits and safety of vaccination and about the sound science behind vaccines. It is exceedingly frustrating to expend so much energy and passion, only to be met with refusal – refusal of interventions that we know to be lifesaving. I take issue, however, with the assertion that it is not worth our time and breath to discuss the importance of vaccination with our questioning patients. I feel this assertion verges on being irresponsible. I worry about the impact that such a statement will have on our primary care providers who are fresh out of training and have yet to experience the positive influence that they can have on patients’ opinions regarding vaccines.
There are a multitude of reasons that people refuse vaccines. The origins of vaccine refusal go back to the beginning of vaccinations themselves, when Edward Jenner introduced the smallpox vaccine in the 1800s. Back then, the refusals most often had to do with the fact that vaccinations were made mandatory, and people felt this government requirement infringed on their personal liberties. Today, however, the most common reason for vaccine refusal, at least in my own practice, seems to stem from fear, pure and simple. Most recently, Dr. Andrew Wakefield, who published an article in the journal The Lancet in the late 1990s suggesting a causal relationship between administration of the MMR vaccine and autism, has stirred up the anti-vaccine movement. Despite the fact that his research has been debunked and he has been stripped of his medical license for falsifying and misrepresenting data, his impact persists. Our efforts are not aided by celebrity figures (actors and politicians) who have a wide-reaching public voice and use their platforms to disseminate misinformation regarding vaccines. There are also the anecdotal reasons that people refuse vaccines – they know someone who had a serious adverse reaction following vaccination or they themselves got sick following vaccination.
We, as primary care clinicians, are charged with determining the reasons behind each individual vaccine refusal so that we can clear up misunderstandings about vaccines. We are asked to do this in a limited time frame, when we have so many other issues to address in an office visit, and we often are speaking to only one or two people at a time. Does fighting this fight often feel like an uphill battle and an impossible task? Yes. Are there other things I could be doing with my time during that office visit? Absolutely! But this is our job. At our core, we are teachers. We are there to educate our patients about health and illness and prevention. Gone are the days of paternalistic medicine. Patients are more involved in their health care than ever before, and they expect to be part of the conversation and decision making process when it comes to interventions such as vaccines.
I completely disagree with the assertion that we should not waste our time discussing vaccinations with patients who initially decline them. Every single day I am able to talk patients into getting vaccines who initially refused them. Perhaps I have success because I come at the task in a nonjudgmental way. We have to remember that patients are not trying to be difficult. They are just trying to make the best decisions for themselves and for their family members. People are more open to hearing what I have to say when I acknowledge their concerns. Perhaps it is just that they respect what their doctor thinks and the fact that I am recommending it, alone, is enough to encourage them. After all, if I, as a doctor who has been through years of training, believe in vaccines, and take them myself, and give them to my own children, then why shouldn’t they feel safe about getting vaccinated? Perhaps it is because I am, as I like to tell my pleasant but challenging patients, annoyingly persistent. I will present the same message over and over again every time we see each other, and eventually they understand how important the issue is – or maybe they just get so tired of hearing me say the same thing repeatedly that they give in, just so I will stop talking. Either way, I win! Or, more seriously, perhaps it is that my patients have had some experience (someone they know had a serious outcome from a vaccine-preventable illness) that changed their minds. If we don’t offer up the topic for conversation, we will never know.
I also take issue with providers who simply refuse to see families who don’t vaccinate. In my mind, this hearkens back to that paternalistic practice of medicine, and it punishes those who are most vulnerable. Children need care, no matter what their parents’ decisions regarding vaccination. It also presumes that the clinician will never be able to impact a family’s opinions regarding vaccination. This is categorically untrue! You’d be amazed at how much you can accomplish if you just take the time to listen, acknowledge, and clarify.
So, if you are one of those new doctors out there, please don’t give up hope that you can make a difference. This is a very worthy fight, and you are up to the task! Keep talking to your patients and their families about the importance of vaccinations. Your voice matters, and patients value what you have to say!
Gretchen LaSalle, M.D.
Spokane, Wash.
Dr. Wilkoff responds: While I have had some successes using the same annoying persistence that Dr. LaSalle suggests, they have been few and far between. I agree that many vaccine-hesitant parents are driven by fear. However, the studies I referred to in my column should give all of us pause as we consider how to invest our limited face-to-face time with patients. Education may be one of the solutions to the vaccine-refusal problem. However, the question remains as to what point in a parent’s development that education should begin. It may be that in many cases we arrive on the scene too late. As pessimistic as this observation may sound, I agree with Dr. LaSalle that discharging vaccine-refusing families doesn’t help the situation and ignores our primary mission.
I am writing in response to the article titled “Faced with vaccine refusers? Save your breath” by Dr. William G. Wilkoff.
I am a family medicine physician in Spokane, Wash., and have been in practice for the last 12 years. I take care of patients from infancy to old age and through all stages of life between. As a primary care provider, I sympathize with the concerns of Dr. Wilkoff and many others on the front lines of the vaccine debate. It takes much time and energy to talk to patients and parents about the benefits and safety of vaccination and about the sound science behind vaccines. It is exceedingly frustrating to expend so much energy and passion, only to be met with refusal – refusal of interventions that we know to be lifesaving. I take issue, however, with the assertion that it is not worth our time and breath to discuss the importance of vaccination with our questioning patients. I feel this assertion verges on being irresponsible. I worry about the impact that such a statement will have on our primary care providers who are fresh out of training and have yet to experience the positive influence that they can have on patients’ opinions regarding vaccines.
There are a multitude of reasons that people refuse vaccines. The origins of vaccine refusal go back to the beginning of vaccinations themselves, when Edward Jenner introduced the smallpox vaccine in the 1800s. Back then, the refusals most often had to do with the fact that vaccinations were made mandatory, and people felt this government requirement infringed on their personal liberties. Today, however, the most common reason for vaccine refusal, at least in my own practice, seems to stem from fear, pure and simple. Most recently, Dr. Andrew Wakefield, who published an article in the journal The Lancet in the late 1990s suggesting a causal relationship between administration of the MMR vaccine and autism, has stirred up the anti-vaccine movement. Despite the fact that his research has been debunked and he has been stripped of his medical license for falsifying and misrepresenting data, his impact persists. Our efforts are not aided by celebrity figures (actors and politicians) who have a wide-reaching public voice and use their platforms to disseminate misinformation regarding vaccines. There are also the anecdotal reasons that people refuse vaccines – they know someone who had a serious adverse reaction following vaccination or they themselves got sick following vaccination.
We, as primary care clinicians, are charged with determining the reasons behind each individual vaccine refusal so that we can clear up misunderstandings about vaccines. We are asked to do this in a limited time frame, when we have so many other issues to address in an office visit, and we often are speaking to only one or two people at a time. Does fighting this fight often feel like an uphill battle and an impossible task? Yes. Are there other things I could be doing with my time during that office visit? Absolutely! But this is our job. At our core, we are teachers. We are there to educate our patients about health and illness and prevention. Gone are the days of paternalistic medicine. Patients are more involved in their health care than ever before, and they expect to be part of the conversation and decision making process when it comes to interventions such as vaccines.
I completely disagree with the assertion that we should not waste our time discussing vaccinations with patients who initially decline them. Every single day I am able to talk patients into getting vaccines who initially refused them. Perhaps I have success because I come at the task in a nonjudgmental way. We have to remember that patients are not trying to be difficult. They are just trying to make the best decisions for themselves and for their family members. People are more open to hearing what I have to say when I acknowledge their concerns. Perhaps it is just that they respect what their doctor thinks and the fact that I am recommending it, alone, is enough to encourage them. After all, if I, as a doctor who has been through years of training, believe in vaccines, and take them myself, and give them to my own children, then why shouldn’t they feel safe about getting vaccinated? Perhaps it is because I am, as I like to tell my pleasant but challenging patients, annoyingly persistent. I will present the same message over and over again every time we see each other, and eventually they understand how important the issue is – or maybe they just get so tired of hearing me say the same thing repeatedly that they give in, just so I will stop talking. Either way, I win! Or, more seriously, perhaps it is that my patients have had some experience (someone they know had a serious outcome from a vaccine-preventable illness) that changed their minds. If we don’t offer up the topic for conversation, we will never know.
I also take issue with providers who simply refuse to see families who don’t vaccinate. In my mind, this hearkens back to that paternalistic practice of medicine, and it punishes those who are most vulnerable. Children need care, no matter what their parents’ decisions regarding vaccination. It also presumes that the clinician will never be able to impact a family’s opinions regarding vaccination. This is categorically untrue! You’d be amazed at how much you can accomplish if you just take the time to listen, acknowledge, and clarify.
So, if you are one of those new doctors out there, please don’t give up hope that you can make a difference. This is a very worthy fight, and you are up to the task! Keep talking to your patients and their families about the importance of vaccinations. Your voice matters, and patients value what you have to say!
Gretchen LaSalle, M.D.
Spokane, Wash.
Dr. Wilkoff responds: While I have had some successes using the same annoying persistence that Dr. LaSalle suggests, they have been few and far between. I agree that many vaccine-hesitant parents are driven by fear. However, the studies I referred to in my column should give all of us pause as we consider how to invest our limited face-to-face time with patients. Education may be one of the solutions to the vaccine-refusal problem. However, the question remains as to what point in a parent’s development that education should begin. It may be that in many cases we arrive on the scene too late. As pessimistic as this observation may sound, I agree with Dr. LaSalle that discharging vaccine-refusing families doesn’t help the situation and ignores our primary mission.
I am writing in response to the article titled “Faced with vaccine refusers? Save your breath” by Dr. William G. Wilkoff.
I am a family medicine physician in Spokane, Wash., and have been in practice for the last 12 years. I take care of patients from infancy to old age and through all stages of life between. As a primary care provider, I sympathize with the concerns of Dr. Wilkoff and many others on the front lines of the vaccine debate. It takes much time and energy to talk to patients and parents about the benefits and safety of vaccination and about the sound science behind vaccines. It is exceedingly frustrating to expend so much energy and passion, only to be met with refusal – refusal of interventions that we know to be lifesaving. I take issue, however, with the assertion that it is not worth our time and breath to discuss the importance of vaccination with our questioning patients. I feel this assertion verges on being irresponsible. I worry about the impact that such a statement will have on our primary care providers who are fresh out of training and have yet to experience the positive influence that they can have on patients’ opinions regarding vaccines.
There are a multitude of reasons that people refuse vaccines. The origins of vaccine refusal go back to the beginning of vaccinations themselves, when Edward Jenner introduced the smallpox vaccine in the 1800s. Back then, the refusals most often had to do with the fact that vaccinations were made mandatory, and people felt this government requirement infringed on their personal liberties. Today, however, the most common reason for vaccine refusal, at least in my own practice, seems to stem from fear, pure and simple. Most recently, Dr. Andrew Wakefield, who published an article in the journal The Lancet in the late 1990s suggesting a causal relationship between administration of the MMR vaccine and autism, has stirred up the anti-vaccine movement. Despite the fact that his research has been debunked and he has been stripped of his medical license for falsifying and misrepresenting data, his impact persists. Our efforts are not aided by celebrity figures (actors and politicians) who have a wide-reaching public voice and use their platforms to disseminate misinformation regarding vaccines. There are also the anecdotal reasons that people refuse vaccines – they know someone who had a serious adverse reaction following vaccination or they themselves got sick following vaccination.
We, as primary care clinicians, are charged with determining the reasons behind each individual vaccine refusal so that we can clear up misunderstandings about vaccines. We are asked to do this in a limited time frame, when we have so many other issues to address in an office visit, and we often are speaking to only one or two people at a time. Does fighting this fight often feel like an uphill battle and an impossible task? Yes. Are there other things I could be doing with my time during that office visit? Absolutely! But this is our job. At our core, we are teachers. We are there to educate our patients about health and illness and prevention. Gone are the days of paternalistic medicine. Patients are more involved in their health care than ever before, and they expect to be part of the conversation and decision making process when it comes to interventions such as vaccines.
I completely disagree with the assertion that we should not waste our time discussing vaccinations with patients who initially decline them. Every single day I am able to talk patients into getting vaccines who initially refused them. Perhaps I have success because I come at the task in a nonjudgmental way. We have to remember that patients are not trying to be difficult. They are just trying to make the best decisions for themselves and for their family members. People are more open to hearing what I have to say when I acknowledge their concerns. Perhaps it is just that they respect what their doctor thinks and the fact that I am recommending it, alone, is enough to encourage them. After all, if I, as a doctor who has been through years of training, believe in vaccines, and take them myself, and give them to my own children, then why shouldn’t they feel safe about getting vaccinated? Perhaps it is because I am, as I like to tell my pleasant but challenging patients, annoyingly persistent. I will present the same message over and over again every time we see each other, and eventually they understand how important the issue is – or maybe they just get so tired of hearing me say the same thing repeatedly that they give in, just so I will stop talking. Either way, I win! Or, more seriously, perhaps it is that my patients have had some experience (someone they know had a serious outcome from a vaccine-preventable illness) that changed their minds. If we don’t offer up the topic for conversation, we will never know.
I also take issue with providers who simply refuse to see families who don’t vaccinate. In my mind, this hearkens back to that paternalistic practice of medicine, and it punishes those who are most vulnerable. Children need care, no matter what their parents’ decisions regarding vaccination. It also presumes that the clinician will never be able to impact a family’s opinions regarding vaccination. This is categorically untrue! You’d be amazed at how much you can accomplish if you just take the time to listen, acknowledge, and clarify.
So, if you are one of those new doctors out there, please don’t give up hope that you can make a difference. This is a very worthy fight, and you are up to the task! Keep talking to your patients and their families about the importance of vaccinations. Your voice matters, and patients value what you have to say!
Gretchen LaSalle, M.D.
Spokane, Wash.
Dr. Wilkoff responds: While I have had some successes using the same annoying persistence that Dr. LaSalle suggests, they have been few and far between. I agree that many vaccine-hesitant parents are driven by fear. However, the studies I referred to in my column should give all of us pause as we consider how to invest our limited face-to-face time with patients. Education may be one of the solutions to the vaccine-refusal problem. However, the question remains as to what point in a parent’s development that education should begin. It may be that in many cases we arrive on the scene too late. As pessimistic as this observation may sound, I agree with Dr. LaSalle that discharging vaccine-refusing families doesn’t help the situation and ignores our primary mission.
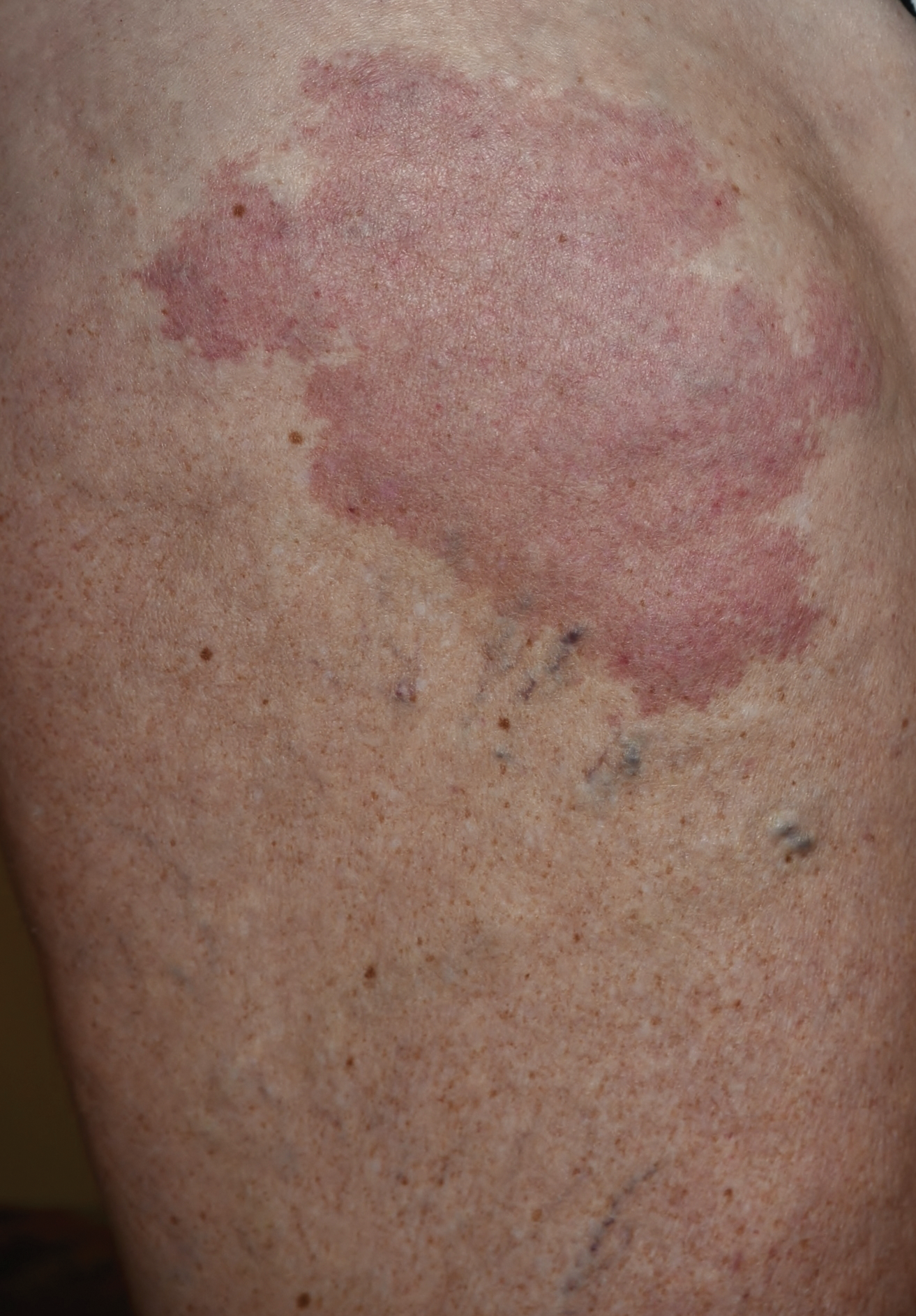
Growing Subcutaneous Mass on the Thigh
The Diagnosis: Eccrine Angiomatous Hamartoma
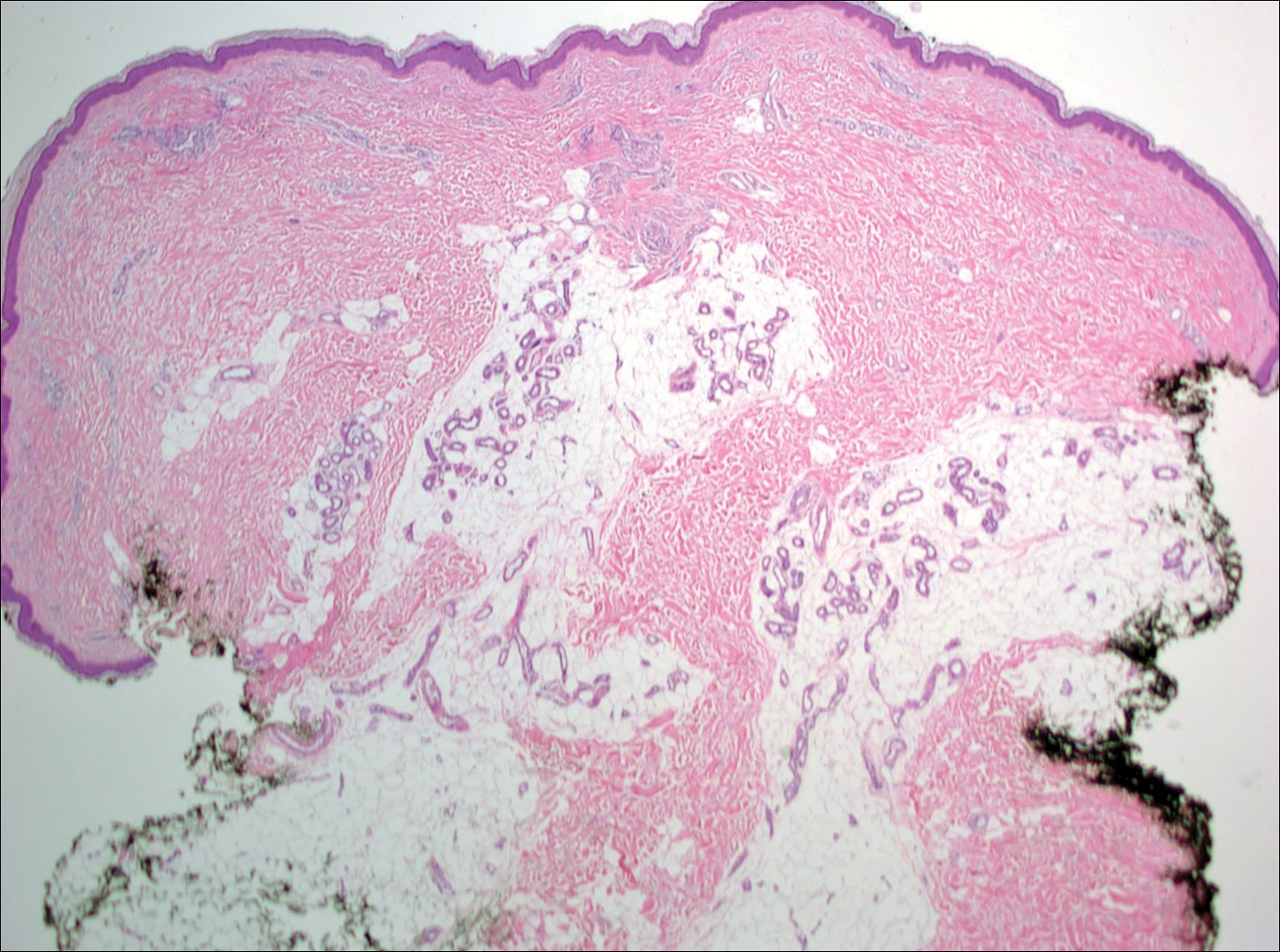
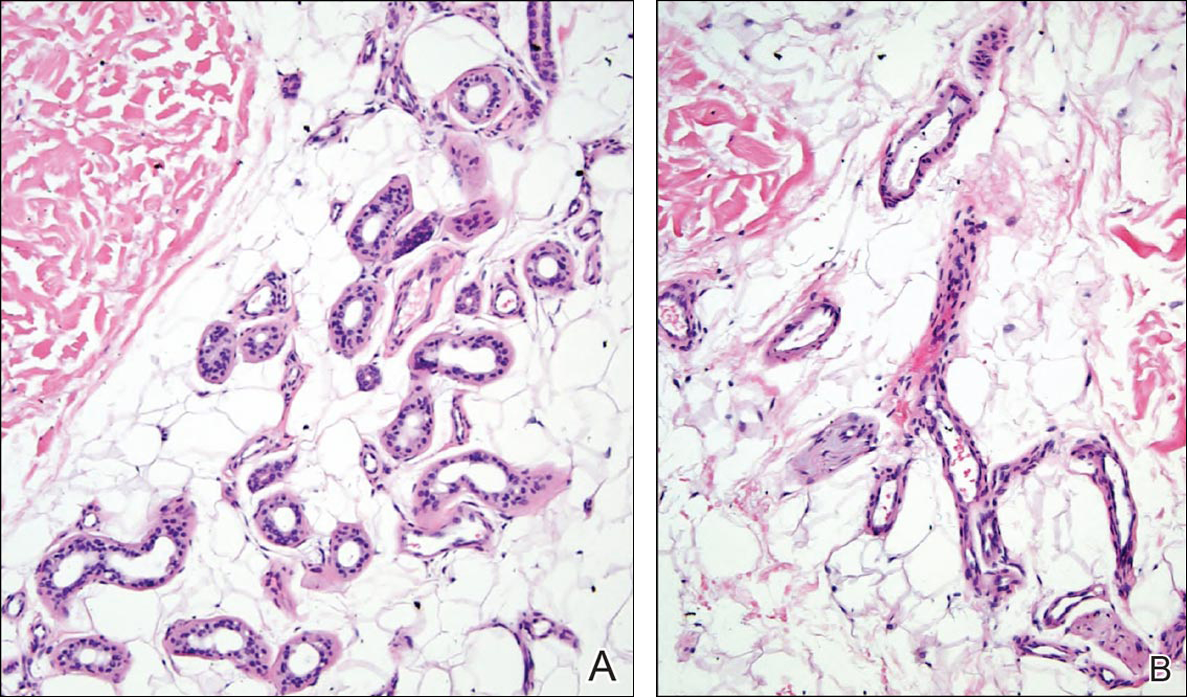
Given the progression of symptoms 3 months prior to presentation, an excisional biopsy was performed (Figure 1). Hematoxylin and eosin staining showed prominent eccrine sweat glands and vessels surrounded by superficially located adipose tissue in the mid and deep dermis (Figure 2).
Eccrine angiomatous hamartoma (EAH) is an uncommon benign tumor typically located on the arms and legs or trunk. It is usually solitary, though cases with multiple lesions have been reported.1,2 Most cases are diagnosed in childhood as either congenital or acquired lesions. However, EAHs can develop in adulthood and have been described in patients up to 70 years of age.3 The median age of diagnosis is 10 years,2 indicating that EAH is primarily a pediatric tumor. There is no gender predilection.
Approximately 35% to 66% of patients report pain, pruritus, or hyperhidrosis associated with EAHs, though this incidence may be overrepresented because patients tend to present when the lesions become symptomatic.2-5 The pain is attributed to nerve fibers infiltrating the tumor. Hypertrichosis also has been described and is thought to be due to hair follicles within the hamartoma.
Histologically, EAHs are characterized by normal-appearing eccrine glands mingled with venules and capillaries. Additional variable pathologic findings include lipomatous, pilar, lymphatic, or mucinous features.2 Other vascular anomalies such as hemangiomas or arteriovenous malformations occasionally have been described in association with EAH. The vessels stain for ulex europaeus 1 and factor VIII. Eccrine glands stain for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and cytokeratin CAM 5.2. In light of a publication proposing that EAH is a lymphatic proliferation,6 a D2-40 stain was performed on the specimen and was negative.
Eccrine angiomatous hamartoma has been reported to grow mainly during childhood, puberty, or pregnancy, presumably due to hormonal influences.7 There are few reports of EAH enlarging in middle-aged adults, and even fewer without pain during the growth phase. It is unclear what triggered the growth in our otherwise healthy postmenopausal patient.
Eccrine angiomatous hamartoma does not have malignant potential and thus treatment is optional and based on relief of symptoms. Simple excision of the EAH usually is curative, but recurrences can occur.4 Botulinum toxin also has been used to treat hyperhidrosis in tumors that are too large for resection. Treatment with lasers such as the pulsed dye laser and Nd:YAG laser has not been successful.8 A case of spontaneous regression has been reported.1
Liposuction was considered in our patient given the substantial adipose tissue on biopsy. The patient ultimately declined treatment. This case highlights that EAH can present in adulthood and should be considered in the differential diagnosis of an enlarging but otherwise asymptomatic vascular tumor.
- Tay YK, Sim CS. Eccrine angiomatous hamartoma associated with spontaneous regression. Pediatr Dermatol. 2006;23:516-517.
- Pelle MT, Pride HB, Tyler WB. Eccrine angiomatous hamartoma. J Am Acad Dermatol. 2002;47:429-435.
- Shin J, Jang YH, Kim SC, et al. Eccrine angiomatous hamartoma: a review of ten cases [published online May 10, 2013]. Ann Dermatol. 2013;25:208-212.
- Lin YT, Chen CM, Yang CH, et al. Eccrine angiomatous hamartoma: a retrospective study of 15 cases. Chang Gung Med J. 2012;35:167-177.
- Nakatsui TC, Schloss E, Krol A, et al. Eccrine angiomatous hamartoma: report of a case and literature review. J Am Acad Dermatol. 1999;41:109-111.
- Wang L, Wang S, Gao T, et al. Eccrine angiomatous hamartoma is a lymphatic proliferation. Eur J Dermatol. 2013;23:614-617.
- Kikusawa A, Oka M, Taguchi K, et al. Eccrine angiomatous hamartoma with sudden enlargement and pain in an adolescent girl after menarche [published online October 1, 2011]. Dermatoendocrinol. 2011;3:266-268.
- Barco D, Baselga E, Alegre M, et al. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 2009;145:241-243.
The Diagnosis: Eccrine Angiomatous Hamartoma
Given the progression of symptoms 3 months prior to presentation, an excisional biopsy was performed (Figure 1). Hematoxylin and eosin staining showed prominent eccrine sweat glands and vessels surrounded by superficially located adipose tissue in the mid and deep dermis (Figure 2).
Eccrine angiomatous hamartoma (EAH) is an uncommon benign tumor typically located on the arms and legs or trunk. It is usually solitary, though cases with multiple lesions have been reported.1,2 Most cases are diagnosed in childhood as either congenital or acquired lesions. However, EAHs can develop in adulthood and have been described in patients up to 70 years of age.3 The median age of diagnosis is 10 years,2 indicating that EAH is primarily a pediatric tumor. There is no gender predilection.
Approximately 35% to 66% of patients report pain, pruritus, or hyperhidrosis associated with EAHs, though this incidence may be overrepresented because patients tend to present when the lesions become symptomatic.2-5 The pain is attributed to nerve fibers infiltrating the tumor. Hypertrichosis also has been described and is thought to be due to hair follicles within the hamartoma.
Histologically, EAHs are characterized by normal-appearing eccrine glands mingled with venules and capillaries. Additional variable pathologic findings include lipomatous, pilar, lymphatic, or mucinous features.2 Other vascular anomalies such as hemangiomas or arteriovenous malformations occasionally have been described in association with EAH. The vessels stain for ulex europaeus 1 and factor VIII. Eccrine glands stain for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and cytokeratin CAM 5.2. In light of a publication proposing that EAH is a lymphatic proliferation,6 a D2-40 stain was performed on the specimen and was negative.
Eccrine angiomatous hamartoma has been reported to grow mainly during childhood, puberty, or pregnancy, presumably due to hormonal influences.7 There are few reports of EAH enlarging in middle-aged adults, and even fewer without pain during the growth phase. It is unclear what triggered the growth in our otherwise healthy postmenopausal patient.
Eccrine angiomatous hamartoma does not have malignant potential and thus treatment is optional and based on relief of symptoms. Simple excision of the EAH usually is curative, but recurrences can occur.4 Botulinum toxin also has been used to treat hyperhidrosis in tumors that are too large for resection. Treatment with lasers such as the pulsed dye laser and Nd:YAG laser has not been successful.8 A case of spontaneous regression has been reported.1
Liposuction was considered in our patient given the substantial adipose tissue on biopsy. The patient ultimately declined treatment. This case highlights that EAH can present in adulthood and should be considered in the differential diagnosis of an enlarging but otherwise asymptomatic vascular tumor.
The Diagnosis: Eccrine Angiomatous Hamartoma
Given the progression of symptoms 3 months prior to presentation, an excisional biopsy was performed (Figure 1). Hematoxylin and eosin staining showed prominent eccrine sweat glands and vessels surrounded by superficially located adipose tissue in the mid and deep dermis (Figure 2).
Eccrine angiomatous hamartoma (EAH) is an uncommon benign tumor typically located on the arms and legs or trunk. It is usually solitary, though cases with multiple lesions have been reported.1,2 Most cases are diagnosed in childhood as either congenital or acquired lesions. However, EAHs can develop in adulthood and have been described in patients up to 70 years of age.3 The median age of diagnosis is 10 years,2 indicating that EAH is primarily a pediatric tumor. There is no gender predilection.
Approximately 35% to 66% of patients report pain, pruritus, or hyperhidrosis associated with EAHs, though this incidence may be overrepresented because patients tend to present when the lesions become symptomatic.2-5 The pain is attributed to nerve fibers infiltrating the tumor. Hypertrichosis also has been described and is thought to be due to hair follicles within the hamartoma.
Histologically, EAHs are characterized by normal-appearing eccrine glands mingled with venules and capillaries. Additional variable pathologic findings include lipomatous, pilar, lymphatic, or mucinous features.2 Other vascular anomalies such as hemangiomas or arteriovenous malformations occasionally have been described in association with EAH. The vessels stain for ulex europaeus 1 and factor VIII. Eccrine glands stain for S-100 protein, carcinoembryonic antigen, epithelial membrane antigen, and cytokeratin CAM 5.2. In light of a publication proposing that EAH is a lymphatic proliferation,6 a D2-40 stain was performed on the specimen and was negative.
Eccrine angiomatous hamartoma has been reported to grow mainly during childhood, puberty, or pregnancy, presumably due to hormonal influences.7 There are few reports of EAH enlarging in middle-aged adults, and even fewer without pain during the growth phase. It is unclear what triggered the growth in our otherwise healthy postmenopausal patient.
Eccrine angiomatous hamartoma does not have malignant potential and thus treatment is optional and based on relief of symptoms. Simple excision of the EAH usually is curative, but recurrences can occur.4 Botulinum toxin also has been used to treat hyperhidrosis in tumors that are too large for resection. Treatment with lasers such as the pulsed dye laser and Nd:YAG laser has not been successful.8 A case of spontaneous regression has been reported.1
Liposuction was considered in our patient given the substantial adipose tissue on biopsy. The patient ultimately declined treatment. This case highlights that EAH can present in adulthood and should be considered in the differential diagnosis of an enlarging but otherwise asymptomatic vascular tumor.
- Tay YK, Sim CS. Eccrine angiomatous hamartoma associated with spontaneous regression. Pediatr Dermatol. 2006;23:516-517.
- Pelle MT, Pride HB, Tyler WB. Eccrine angiomatous hamartoma. J Am Acad Dermatol. 2002;47:429-435.
- Shin J, Jang YH, Kim SC, et al. Eccrine angiomatous hamartoma: a review of ten cases [published online May 10, 2013]. Ann Dermatol. 2013;25:208-212.
- Lin YT, Chen CM, Yang CH, et al. Eccrine angiomatous hamartoma: a retrospective study of 15 cases. Chang Gung Med J. 2012;35:167-177.
- Nakatsui TC, Schloss E, Krol A, et al. Eccrine angiomatous hamartoma: report of a case and literature review. J Am Acad Dermatol. 1999;41:109-111.
- Wang L, Wang S, Gao T, et al. Eccrine angiomatous hamartoma is a lymphatic proliferation. Eur J Dermatol. 2013;23:614-617.
- Kikusawa A, Oka M, Taguchi K, et al. Eccrine angiomatous hamartoma with sudden enlargement and pain in an adolescent girl after menarche [published online October 1, 2011]. Dermatoendocrinol. 2011;3:266-268.
- Barco D, Baselga E, Alegre M, et al. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 2009;145:241-243.
- Tay YK, Sim CS. Eccrine angiomatous hamartoma associated with spontaneous regression. Pediatr Dermatol. 2006;23:516-517.
- Pelle MT, Pride HB, Tyler WB. Eccrine angiomatous hamartoma. J Am Acad Dermatol. 2002;47:429-435.
- Shin J, Jang YH, Kim SC, et al. Eccrine angiomatous hamartoma: a review of ten cases [published online May 10, 2013]. Ann Dermatol. 2013;25:208-212.
- Lin YT, Chen CM, Yang CH, et al. Eccrine angiomatous hamartoma: a retrospective study of 15 cases. Chang Gung Med J. 2012;35:167-177.
- Nakatsui TC, Schloss E, Krol A, et al. Eccrine angiomatous hamartoma: report of a case and literature review. J Am Acad Dermatol. 1999;41:109-111.
- Wang L, Wang S, Gao T, et al. Eccrine angiomatous hamartoma is a lymphatic proliferation. Eur J Dermatol. 2013;23:614-617.
- Kikusawa A, Oka M, Taguchi K, et al. Eccrine angiomatous hamartoma with sudden enlargement and pain in an adolescent girl after menarche [published online October 1, 2011]. Dermatoendocrinol. 2011;3:266-268.
- Barco D, Baselga E, Alegre M, et al. Successful treatment of eccrine angiomatous hamartoma with botulinum toxin. Arch Dermatol. 2009;145:241-243.
Ontario’s infant rotavirus immunization program found effective
A publicly-funded rotavirus (RV) immunization program designed to prevent hospitalizations and emergency department (ED) visits for RV-specific acute gastroenteritis (AGE) has shown remarkable improvements in direct and indirect effects 1.5 years after implementation, according to the results of a study published in the PLoS ONE.
“On August 8, 2011, Ontario became one of the first Canadian provinces to implement a universal, publicly-funded RV immunization program, using Rotarix vaccine at 2 and 4 months of age,” noted Dr. Sarah E. Wilson of Public Health Ontario in Toronto and the University of Toronto, and her colleagues. The program was subsequently implemented across 10 of 13 Canadian provinces and territories.
Dr. Wilson and colleagues conducted a retrospective longitudinal population-based cohort study examining health care utilization for AGE between the period of Aug. 1, 2005, and March 31, 2013, as identified from individual-level hospitalizations and ED visits present in the Discharge Abstract Database of the Canadian Institutes for Health Information and the National Ambulatory Care Reporting System, respectively. Furthermore, the study was divided into preprogram (Aug. 1, 2005-July 31, 2011) and a public program (Aug. 1, 2011-March 31, 2013) time periods (PLoS ONE 2016 May 11. doi: 10.1371/journal.pone.0154340).
Study results revealed that infants younger than 1 year of age showed the greatest reduction in the rate of RV-AGE hospitalizations after adjustment for secular trends and seasonality during the public program period (79%, rate ratio 0.21). Children 12-23 months of age (RR 0.27), 24-35 months of age (RR 0.48), 3-4 years of age (RR 0.31), and 5-19 years of age (RR 0.25) also showed significant reductions in RV-AGE hospitalizations. Significant decreases indicative of direct and indirect effects of immunization after adjustment for age, secular trends, and seasonality during the public program period also were demonstrated by a 68% reduction in RV-AGE ED visits (RR 0.32) and a 10% reduction in overall AGE ED visits (RR 0.90).
Regarding the greater implications of their study results, Dr. Wilson and colleagues suggested that their findings should help inform vaccine decision makers in regions without publicly funded RV programs as part of their routine immunization schedules.
Public Health Ontario and the Ontario Ministry of Health and Long-Term Care funded the study. The authors reported no conflicts of interest.
A publicly-funded rotavirus (RV) immunization program designed to prevent hospitalizations and emergency department (ED) visits for RV-specific acute gastroenteritis (AGE) has shown remarkable improvements in direct and indirect effects 1.5 years after implementation, according to the results of a study published in the PLoS ONE.
“On August 8, 2011, Ontario became one of the first Canadian provinces to implement a universal, publicly-funded RV immunization program, using Rotarix vaccine at 2 and 4 months of age,” noted Dr. Sarah E. Wilson of Public Health Ontario in Toronto and the University of Toronto, and her colleagues. The program was subsequently implemented across 10 of 13 Canadian provinces and territories.
Dr. Wilson and colleagues conducted a retrospective longitudinal population-based cohort study examining health care utilization for AGE between the period of Aug. 1, 2005, and March 31, 2013, as identified from individual-level hospitalizations and ED visits present in the Discharge Abstract Database of the Canadian Institutes for Health Information and the National Ambulatory Care Reporting System, respectively. Furthermore, the study was divided into preprogram (Aug. 1, 2005-July 31, 2011) and a public program (Aug. 1, 2011-March 31, 2013) time periods (PLoS ONE 2016 May 11. doi: 10.1371/journal.pone.0154340).
Study results revealed that infants younger than 1 year of age showed the greatest reduction in the rate of RV-AGE hospitalizations after adjustment for secular trends and seasonality during the public program period (79%, rate ratio 0.21). Children 12-23 months of age (RR 0.27), 24-35 months of age (RR 0.48), 3-4 years of age (RR 0.31), and 5-19 years of age (RR 0.25) also showed significant reductions in RV-AGE hospitalizations. Significant decreases indicative of direct and indirect effects of immunization after adjustment for age, secular trends, and seasonality during the public program period also were demonstrated by a 68% reduction in RV-AGE ED visits (RR 0.32) and a 10% reduction in overall AGE ED visits (RR 0.90).
Regarding the greater implications of their study results, Dr. Wilson and colleagues suggested that their findings should help inform vaccine decision makers in regions without publicly funded RV programs as part of their routine immunization schedules.
Public Health Ontario and the Ontario Ministry of Health and Long-Term Care funded the study. The authors reported no conflicts of interest.
A publicly-funded rotavirus (RV) immunization program designed to prevent hospitalizations and emergency department (ED) visits for RV-specific acute gastroenteritis (AGE) has shown remarkable improvements in direct and indirect effects 1.5 years after implementation, according to the results of a study published in the PLoS ONE.
“On August 8, 2011, Ontario became one of the first Canadian provinces to implement a universal, publicly-funded RV immunization program, using Rotarix vaccine at 2 and 4 months of age,” noted Dr. Sarah E. Wilson of Public Health Ontario in Toronto and the University of Toronto, and her colleagues. The program was subsequently implemented across 10 of 13 Canadian provinces and territories.
Dr. Wilson and colleagues conducted a retrospective longitudinal population-based cohort study examining health care utilization for AGE between the period of Aug. 1, 2005, and March 31, 2013, as identified from individual-level hospitalizations and ED visits present in the Discharge Abstract Database of the Canadian Institutes for Health Information and the National Ambulatory Care Reporting System, respectively. Furthermore, the study was divided into preprogram (Aug. 1, 2005-July 31, 2011) and a public program (Aug. 1, 2011-March 31, 2013) time periods (PLoS ONE 2016 May 11. doi: 10.1371/journal.pone.0154340).
Study results revealed that infants younger than 1 year of age showed the greatest reduction in the rate of RV-AGE hospitalizations after adjustment for secular trends and seasonality during the public program period (79%, rate ratio 0.21). Children 12-23 months of age (RR 0.27), 24-35 months of age (RR 0.48), 3-4 years of age (RR 0.31), and 5-19 years of age (RR 0.25) also showed significant reductions in RV-AGE hospitalizations. Significant decreases indicative of direct and indirect effects of immunization after adjustment for age, secular trends, and seasonality during the public program period also were demonstrated by a 68% reduction in RV-AGE ED visits (RR 0.32) and a 10% reduction in overall AGE ED visits (RR 0.90).
Regarding the greater implications of their study results, Dr. Wilson and colleagues suggested that their findings should help inform vaccine decision makers in regions without publicly funded RV programs as part of their routine immunization schedules.
Public Health Ontario and the Ontario Ministry of Health and Long-Term Care funded the study. The authors reported no conflicts of interest.
FROM PLOS ONE
Key clinical point: A publicly funded rotavirus immunization program was successful in preventing hospitalizations and ED visits for RV-specific acute gastroenteritis at the population level.
Major finding: Implementation of the program resulted in significantly increased median age at rotavirus-specific acute gastroenteritis hospitalization and significantly reduced rotavirus-specific acute gastroenteritis hospitalizations and ED visits.
Data sources: Discharge Abstract Database of the Canadian Institutes for Health Information and the National Ambulatory Care Reporting System.
Disclosures: Public Health Ontario and the Ontario Ministry of Health and Long-Term Care funded the study. The authors reported no conflicts of interest.
Putting an end to ENDS
Recent legislation to ban the sale of e-cigarettes to persons younger than 18 years of age, and to prevent distribution of free samples and placement in vending machines where teens may be present, was a major win for the fight for the health and well-being of our adolescents.1
The electronic nicotine delivery system, or ENDS, was developed as an alternative to smoking cigarettes, reducing the intake of harmful fumes that lead to lung cancer. It was a great idea for those wishing to decrease or completely stop smoking. Its sleek design and flavor assortment made it very appealing, not only to adults, but to teenagers as well.
The history of e-cigs goes back to the 1960s when first developed, but because smoking was so socially acceptable the idea did not take hold. It wasn’t until 2003 when they started to become popular. Initially, e-cigs were met with resistance from the Food and Drug Administration, which stated that they were dangerous. But as the need for an alternative to smoking increased and preventable deaths continued to rise, there was more pressure to make them available. In 2013, sales started to skyrocket, but no restrictions for sale or product information was required. This made them readily available to teens and heralded the start of a whole new crisis. The Centers for Disease Control and Prevention reported that between 2011 and 2014, e-cig use rose from 0.6% to 5.3% among middle schoolers and from 1.5% to 16% among high school students.2

Because the marketing for e-cigs suggests they carry a reduced risk for cancer and are a healthier alternative to cigarettes, the perception is that they are not harmful. But research shows the contrary. Nicotine exposure of any level to the developing brain has been found to have negative effects, particularly in the prefrontal cortex where altered synapses have been identified.3 Symptoms of nicotine dependence at lower doses of nicotine is evident in adolescents. Long-term effects in adolescents are reported in working memory, attention, and predilection to major depressive disorder, panic disorder, academic problems, and addiction to other substances.3
The American Academy of Pediatrics 2015 statement on e-cigarettes stated increasing use by teens “threatens 5 decades of public health gains in successfully deglamorizing, restricting, and decreasing the use of tobacco products” and called for an FDA ban on the products.4 Although the FDA recently did place new restrictions, it will take several years for them to go fully into effect. A recent incident where a toddler ingested the liquid nicotine from an e-cig and died also brought to light other dangers of nicotine.5 These nicotine solutions come in colors and a variety of flavors, which makes them even more desirable to toddlers.Just one confirmed death has been reported from e-cig solution ingestion, but there has been a significant jump in calls to poison control centers associated with the liquids. Nicotine from these solutions also can be absorbed through the skin.

More than 3 million middle and high school students were current users of e-cigarettes in 2015,1 and e-cigs were the most commonly used tobacco product among middle and high school students that year.2 Early introduction of ENDS causes a combination of early dependence and addiction with long-term impairment of cognitive skills, promoting an even more grim future for the health of our teens. Education and awareness is imperative to slow the current trends and prevent an even worse crisis than the one ENDS was created to improve.
References
1. http://www.fda.gov/TobaccoProducts/Labeling/ProductsIngredientsComponents/ucm456610.htm
2. MMWR Morb Mortal Wkly Rep. 2016 Apr 15;65(14):361-7.
3. Cold Spring Harbor Perspectives in Medicine. 2012;2(12):10.1101/cshperspect.a012120 a012120.
4. Pediatrics. 2015 Nov.10.1542/peds.2015-3222.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
Recent legislation to ban the sale of e-cigarettes to persons younger than 18 years of age, and to prevent distribution of free samples and placement in vending machines where teens may be present, was a major win for the fight for the health and well-being of our adolescents.1
The electronic nicotine delivery system, or ENDS, was developed as an alternative to smoking cigarettes, reducing the intake of harmful fumes that lead to lung cancer. It was a great idea for those wishing to decrease or completely stop smoking. Its sleek design and flavor assortment made it very appealing, not only to adults, but to teenagers as well.
The history of e-cigs goes back to the 1960s when first developed, but because smoking was so socially acceptable the idea did not take hold. It wasn’t until 2003 when they started to become popular. Initially, e-cigs were met with resistance from the Food and Drug Administration, which stated that they were dangerous. But as the need for an alternative to smoking increased and preventable deaths continued to rise, there was more pressure to make them available. In 2013, sales started to skyrocket, but no restrictions for sale or product information was required. This made them readily available to teens and heralded the start of a whole new crisis. The Centers for Disease Control and Prevention reported that between 2011 and 2014, e-cig use rose from 0.6% to 5.3% among middle schoolers and from 1.5% to 16% among high school students.2
Because the marketing for e-cigs suggests they carry a reduced risk for cancer and are a healthier alternative to cigarettes, the perception is that they are not harmful. But research shows the contrary. Nicotine exposure of any level to the developing brain has been found to have negative effects, particularly in the prefrontal cortex where altered synapses have been identified.3 Symptoms of nicotine dependence at lower doses of nicotine is evident in adolescents. Long-term effects in adolescents are reported in working memory, attention, and predilection to major depressive disorder, panic disorder, academic problems, and addiction to other substances.3
The American Academy of Pediatrics 2015 statement on e-cigarettes stated increasing use by teens “threatens 5 decades of public health gains in successfully deglamorizing, restricting, and decreasing the use of tobacco products” and called for an FDA ban on the products.4 Although the FDA recently did place new restrictions, it will take several years for them to go fully into effect. A recent incident where a toddler ingested the liquid nicotine from an e-cig and died also brought to light other dangers of nicotine.5 These nicotine solutions come in colors and a variety of flavors, which makes them even more desirable to toddlers.Just one confirmed death has been reported from e-cig solution ingestion, but there has been a significant jump in calls to poison control centers associated with the liquids. Nicotine from these solutions also can be absorbed through the skin.
More than 3 million middle and high school students were current users of e-cigarettes in 2015,1 and e-cigs were the most commonly used tobacco product among middle and high school students that year.2 Early introduction of ENDS causes a combination of early dependence and addiction with long-term impairment of cognitive skills, promoting an even more grim future for the health of our teens. Education and awareness is imperative to slow the current trends and prevent an even worse crisis than the one ENDS was created to improve.
References
1. http://www.fda.gov/TobaccoProducts/Labeling/ProductsIngredientsComponents/ucm456610.htm
2. MMWR Morb Mortal Wkly Rep. 2016 Apr 15;65(14):361-7.
3. Cold Spring Harbor Perspectives in Medicine. 2012;2(12):10.1101/cshperspect.a012120 a012120.
4. Pediatrics. 2015 Nov.10.1542/peds.2015-3222.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.
Recent legislation to ban the sale of e-cigarettes to persons younger than 18 years of age, and to prevent distribution of free samples and placement in vending machines where teens may be present, was a major win for the fight for the health and well-being of our adolescents.1
The electronic nicotine delivery system, or ENDS, was developed as an alternative to smoking cigarettes, reducing the intake of harmful fumes that lead to lung cancer. It was a great idea for those wishing to decrease or completely stop smoking. Its sleek design and flavor assortment made it very appealing, not only to adults, but to teenagers as well.
The history of e-cigs goes back to the 1960s when first developed, but because smoking was so socially acceptable the idea did not take hold. It wasn’t until 2003 when they started to become popular. Initially, e-cigs were met with resistance from the Food and Drug Administration, which stated that they were dangerous. But as the need for an alternative to smoking increased and preventable deaths continued to rise, there was more pressure to make them available. In 2013, sales started to skyrocket, but no restrictions for sale or product information was required. This made them readily available to teens and heralded the start of a whole new crisis. The Centers for Disease Control and Prevention reported that between 2011 and 2014, e-cig use rose from 0.6% to 5.3% among middle schoolers and from 1.5% to 16% among high school students.2
Because the marketing for e-cigs suggests they carry a reduced risk for cancer and are a healthier alternative to cigarettes, the perception is that they are not harmful. But research shows the contrary. Nicotine exposure of any level to the developing brain has been found to have negative effects, particularly in the prefrontal cortex where altered synapses have been identified.3 Symptoms of nicotine dependence at lower doses of nicotine is evident in adolescents. Long-term effects in adolescents are reported in working memory, attention, and predilection to major depressive disorder, panic disorder, academic problems, and addiction to other substances.3
The American Academy of Pediatrics 2015 statement on e-cigarettes stated increasing use by teens “threatens 5 decades of public health gains in successfully deglamorizing, restricting, and decreasing the use of tobacco products” and called for an FDA ban on the products.4 Although the FDA recently did place new restrictions, it will take several years for them to go fully into effect. A recent incident where a toddler ingested the liquid nicotine from an e-cig and died also brought to light other dangers of nicotine.5 These nicotine solutions come in colors and a variety of flavors, which makes them even more desirable to toddlers.Just one confirmed death has been reported from e-cig solution ingestion, but there has been a significant jump in calls to poison control centers associated with the liquids. Nicotine from these solutions also can be absorbed through the skin.
More than 3 million middle and high school students were current users of e-cigarettes in 2015,1 and e-cigs were the most commonly used tobacco product among middle and high school students that year.2 Early introduction of ENDS causes a combination of early dependence and addiction with long-term impairment of cognitive skills, promoting an even more grim future for the health of our teens. Education and awareness is imperative to slow the current trends and prevent an even worse crisis than the one ENDS was created to improve.
References
1. http://www.fda.gov/TobaccoProducts/Labeling/ProductsIngredientsComponents/ucm456610.htm
2. MMWR Morb Mortal Wkly Rep. 2016 Apr 15;65(14):361-7.
3. Cold Spring Harbor Perspectives in Medicine. 2012;2(12):10.1101/cshperspect.a012120 a012120.
4. Pediatrics. 2015 Nov.10.1542/peds.2015-3222.
Dr. Pearce is a pediatrician in Frankfort, Ill. Email her at pdnews@frontlinemedcom.com.

Mental health of transgender youth
There has been quite a bit of discussion and controversy lately about transgender individuals. The debate has extended to the diagnosis itself and whether it should be maintained as an official entity. The previous edition of the Diagnostic and Statistical Manual included the diagnosis of gender identity disorder, which was modified to the current diagnosis of gender dysphoria that describes individuals who show a persistent desire to be the “other” gender and/or an insistence that their gender is different from their birth sex.
One question at the heart of this discussion is the degree to which psychiatric symptoms and disorders are inherent in the gender dysphoria itself or whether most, if not all, of the noted links to things like anxiety, depression, and suicidal behavior stem from the hostility and abuse that many of these youth endure.

As has been reported in the Pediatric News column LGBT Youth Consult, research is now focusing on the mental health of transgender youth, although the data are not entirely consistent. One recent study of 298 transgender women between the ages of 16 and 29 years, of whom nearly three-quarters had received crossgender hormones, showed quite high rates of psychiatric disorders including depression (35%), anxiety (8%), and substance abuse (11%).1 Moderate to high levels of suicidality in the past month were found in 20% of the sample. Although one cannot conclude from this study that psychopathology is intrinsic to transgender individuals, it does suggest that difficulties can certainly persist among those who have socially transitioned to their affirmed gender.
In contrast, another study from the TransYouth Project showed much more hopeful results.2 In this younger sample of 73 prepubescent children, 70% of whom were natal males and all of whom had been supported in the social transition to their affirmed gender at a relatively young age, levels of depressed symptoms were no different from those in 73 controls, and scores on an anxiety scale were only slightly elevated, but did not reach clinical or even subclinical levels as a group. The authors of this study concluded that psychiatric symptoms are not “synonymous” with being transgender. They suggest that supporting youth in their transition at earlier ages could possibly prevent the occurrence of mental health problems in the future.
There is wide acknowledgment that gender-nonconforming youth are at much heightened risk from what can be vicious and cruel maltreatment from peers and the wider community. Similarly, there is good consensus that “conversion therapy” approaches that actively try to discourage youth from their affirmed gender are misguided and unethical. What remains in question among well-meaning parents and clinicians alike, however, is at what age should social transition be supported and how encompassing should it be with regard to pronoun use, bathroom and dressing room access, clothing, and so on. Studies have shown that gender atypical behavior can be quite common in young children, with the vast majority eventually developing gender identities that are in line with their natal sex. Parents may worry that promoting a premature gender transition might expose their child to bullying and harassment that could otherwise be avoided. On the other hand, parents may worry that not supporting gender transition will be experienced as rejecting and critical, which could lead to increased feelings of depression and isolation. Although both views represent valid concerns, it is probably fair to say that among clinicians and researchers who work with transgender youth, there seems to be some movement toward more active acceptance and encouragement of a child’s gender expression at the time, with the understanding that for many, there can be continued movement in one’s gender “journey” across development.
Interestingly, these studies are being published in parallel with some neuroimaging research investigating sex differences with regard to the brain. A recent study from the Proceedings of the National Academy of Sciences found that, among many different regions that are known to show some sex differences with regard to size or connectivity to other regions, the typical human brain shows a “mosaic” pattern in which some regions look more typically male while others look more typically female.3
References
1. JAMA Pediatr. 2016 May 1;170(5):481-6.
2. Pediatrics. 2016;137(3):1-8.
3. PNAS. 2015;112(50):15468-73
Dr. Rettew is an associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Follow him on Twitter @pedipsych.
There has been quite a bit of discussion and controversy lately about transgender individuals. The debate has extended to the diagnosis itself and whether it should be maintained as an official entity. The previous edition of the Diagnostic and Statistical Manual included the diagnosis of gender identity disorder, which was modified to the current diagnosis of gender dysphoria that describes individuals who show a persistent desire to be the “other” gender and/or an insistence that their gender is different from their birth sex.
One question at the heart of this discussion is the degree to which psychiatric symptoms and disorders are inherent in the gender dysphoria itself or whether most, if not all, of the noted links to things like anxiety, depression, and suicidal behavior stem from the hostility and abuse that many of these youth endure.
As has been reported in the Pediatric News column LGBT Youth Consult, research is now focusing on the mental health of transgender youth, although the data are not entirely consistent. One recent study of 298 transgender women between the ages of 16 and 29 years, of whom nearly three-quarters had received crossgender hormones, showed quite high rates of psychiatric disorders including depression (35%), anxiety (8%), and substance abuse (11%).1 Moderate to high levels of suicidality in the past month were found in 20% of the sample. Although one cannot conclude from this study that psychopathology is intrinsic to transgender individuals, it does suggest that difficulties can certainly persist among those who have socially transitioned to their affirmed gender.
In contrast, another study from the TransYouth Project showed much more hopeful results.2 In this younger sample of 73 prepubescent children, 70% of whom were natal males and all of whom had been supported in the social transition to their affirmed gender at a relatively young age, levels of depressed symptoms were no different from those in 73 controls, and scores on an anxiety scale were only slightly elevated, but did not reach clinical or even subclinical levels as a group. The authors of this study concluded that psychiatric symptoms are not “synonymous” with being transgender. They suggest that supporting youth in their transition at earlier ages could possibly prevent the occurrence of mental health problems in the future.
There is wide acknowledgment that gender-nonconforming youth are at much heightened risk from what can be vicious and cruel maltreatment from peers and the wider community. Similarly, there is good consensus that “conversion therapy” approaches that actively try to discourage youth from their affirmed gender are misguided and unethical. What remains in question among well-meaning parents and clinicians alike, however, is at what age should social transition be supported and how encompassing should it be with regard to pronoun use, bathroom and dressing room access, clothing, and so on. Studies have shown that gender atypical behavior can be quite common in young children, with the vast majority eventually developing gender identities that are in line with their natal sex. Parents may worry that promoting a premature gender transition might expose their child to bullying and harassment that could otherwise be avoided. On the other hand, parents may worry that not supporting gender transition will be experienced as rejecting and critical, which could lead to increased feelings of depression and isolation. Although both views represent valid concerns, it is probably fair to say that among clinicians and researchers who work with transgender youth, there seems to be some movement toward more active acceptance and encouragement of a child’s gender expression at the time, with the understanding that for many, there can be continued movement in one’s gender “journey” across development.
Interestingly, these studies are being published in parallel with some neuroimaging research investigating sex differences with regard to the brain. A recent study from the Proceedings of the National Academy of Sciences found that, among many different regions that are known to show some sex differences with regard to size or connectivity to other regions, the typical human brain shows a “mosaic” pattern in which some regions look more typically male while others look more typically female.3
References
1. JAMA Pediatr. 2016 May 1;170(5):481-6.
2. Pediatrics. 2016;137(3):1-8.
3. PNAS. 2015;112(50):15468-73
Dr. Rettew is an associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Follow him on Twitter @pedipsych.
There has been quite a bit of discussion and controversy lately about transgender individuals. The debate has extended to the diagnosis itself and whether it should be maintained as an official entity. The previous edition of the Diagnostic and Statistical Manual included the diagnosis of gender identity disorder, which was modified to the current diagnosis of gender dysphoria that describes individuals who show a persistent desire to be the “other” gender and/or an insistence that their gender is different from their birth sex.
One question at the heart of this discussion is the degree to which psychiatric symptoms and disorders are inherent in the gender dysphoria itself or whether most, if not all, of the noted links to things like anxiety, depression, and suicidal behavior stem from the hostility and abuse that many of these youth endure.
As has been reported in the Pediatric News column LGBT Youth Consult, research is now focusing on the mental health of transgender youth, although the data are not entirely consistent. One recent study of 298 transgender women between the ages of 16 and 29 years, of whom nearly three-quarters had received crossgender hormones, showed quite high rates of psychiatric disorders including depression (35%), anxiety (8%), and substance abuse (11%).1 Moderate to high levels of suicidality in the past month were found in 20% of the sample. Although one cannot conclude from this study that psychopathology is intrinsic to transgender individuals, it does suggest that difficulties can certainly persist among those who have socially transitioned to their affirmed gender.
In contrast, another study from the TransYouth Project showed much more hopeful results.2 In this younger sample of 73 prepubescent children, 70% of whom were natal males and all of whom had been supported in the social transition to their affirmed gender at a relatively young age, levels of depressed symptoms were no different from those in 73 controls, and scores on an anxiety scale were only slightly elevated, but did not reach clinical or even subclinical levels as a group. The authors of this study concluded that psychiatric symptoms are not “synonymous” with being transgender. They suggest that supporting youth in their transition at earlier ages could possibly prevent the occurrence of mental health problems in the future.
There is wide acknowledgment that gender-nonconforming youth are at much heightened risk from what can be vicious and cruel maltreatment from peers and the wider community. Similarly, there is good consensus that “conversion therapy” approaches that actively try to discourage youth from their affirmed gender are misguided and unethical. What remains in question among well-meaning parents and clinicians alike, however, is at what age should social transition be supported and how encompassing should it be with regard to pronoun use, bathroom and dressing room access, clothing, and so on. Studies have shown that gender atypical behavior can be quite common in young children, with the vast majority eventually developing gender identities that are in line with their natal sex. Parents may worry that promoting a premature gender transition might expose their child to bullying and harassment that could otherwise be avoided. On the other hand, parents may worry that not supporting gender transition will be experienced as rejecting and critical, which could lead to increased feelings of depression and isolation. Although both views represent valid concerns, it is probably fair to say that among clinicians and researchers who work with transgender youth, there seems to be some movement toward more active acceptance and encouragement of a child’s gender expression at the time, with the understanding that for many, there can be continued movement in one’s gender “journey” across development.
Interestingly, these studies are being published in parallel with some neuroimaging research investigating sex differences with regard to the brain. A recent study from the Proceedings of the National Academy of Sciences found that, among many different regions that are known to show some sex differences with regard to size or connectivity to other regions, the typical human brain shows a “mosaic” pattern in which some regions look more typically male while others look more typically female.3
References
1. JAMA Pediatr. 2016 May 1;170(5):481-6.
2. Pediatrics. 2016;137(3):1-8.
3. PNAS. 2015;112(50):15468-73
Dr. Rettew is an associate professor of psychiatry and pediatrics at the University of Vermont, Burlington. Follow him on Twitter @pedipsych.

Persistent ADHD in early years linked to worse academic, emotional outcomes
BALTIMORE – Persistent attention-deficit/hyperactivity disorder (ADHD) through young childhood is associated with both poorer academic outcomes and an increased risk of other mental health problems, according to a longitudinal study of younger children with ADHD.
An Australian study presented at the annual meeting of the Pediatric Academic Societies found that 67% of children who had ADHD at age 7 years still met the diagnostic criteria 3 years later, when they were 10 years old. Boys were more likely than girls to have retained the diagnosis (74% vs. 50%; odds ratio, 3.4; P = .01).
On average, children with ADHD had lower scores on math and reading tests than their matched peers without ADHD, even after adjustment for socioeconomic variables and comorbidities (mean difference, –7.6 for math and –8.7 for reading, P less than .001 for both).

When Emma Sciberras, Ph.D., and her colleagues examined the longitudinal data, they found that children who had a persistent ADHD diagnosis were more likely to have an externalizing disorder, such as a conduct disorder (57% vs. 33%; OR, 2.8; P = .008). They also were more likely to have a mood disorder (8% vs. 0%; P = .04).
No sex differences were seen, aside from the increased likelihood of a persistent diagnosis.
“Childhood ADHD confers risk for future mental health difficulties,” said Dr. Sciberras, a psychologist at Deakin University, Melbourne. Dr. Sciberras presented preliminary findings from the Children’s Attention Project, a 3-year study of 179 young children with ADHD and 212 children without the diagnosis.
The goal of the Children’s Attention Project, a community-based longitudinal study, was to document the natural history of ADHD. Aspects of the study included assessing the impact of ADHD on the mental health of both children and parents, as well as examining social, academic, and family functioning, and overall quality of life. The study also seeks to tease out both risks and protective factors that can tip outcomes toward the better – or worse – end of the spectrum, said Dr. Sciberras.
The Children’s Attention Project enrolled first graders from 43 primary schools in Melbourne, to compare 3-year outcomes of a sample of children with ADHD with a control group of children who did not have ADHD. In addition to assessing diagnostic stability (the persistence of an ADHD diagnosis), Dr. Sciberras and her collaborators also looked at functional outcomes. Sex differences in outcomes, as well as the effect of ADHD persistence, also were assessed for the community-based sample of children.
Children were enrolled after families and teachers of the first graders completed the Conners 3 ADHD Index. Families of children with positive screens and matched controls were offered enrollment in the study, with intake involving confirmation of the ADHD diagnosis, as well as detailed academic and behavioral assessments and a family survey. Children in the study were assessed at baseline, and then again at 18 and 36 months after enrollment. Longitudinal data were available for 72% of those initially enrolled.
Children in the study averaged 7.3 years old. Of the ADHD group, 124/179 (69%) were male, as were 135/212 (64%) of the control group. For children in the ADHD group, 31 (17%) had previously been diagnosed with ADHD, and 23 children (13%) were on ADHD medication at enrollment; none of the control group had a prior ADHD diagnosis or was taking medication. For 63 (38%) of the children in the ADHD group, their primary caregiver had not completed high school, compared with 39 (19%) in the control group.
“This is really more of a community-based approach to researching ADHD,” Dr. Sciberras said in an interview. Previous longitudinal studies, she said, had a near-exclusive focus on clinical samples, which can “overrepresent boys and children with more severe symptoms,” she said. Age ranges were broad, and follow-up was often infrequent. Most importantly, positive factors that lead to good outcomes for children with ADHD had been understudied, she said, and she and her colleagues are continuing to look for factors, such as resilience, that contribute to better social and emotional functioning.
It’s important to study children with ADHD in a real world manner because “childhood ADHD is associated with poorer academic outcomes, and the risk is evident from the second year of school,” said Dr. Sciberras. “We need to identify which factors lead to improved outcomes over time. The ultimate aim is to map functional impairment and key predictors from age 7 to later adolescence and adulthood.”
The study was funded by Australia’s National Health and Medical Research Council and by the Collier Foundation. Dr. Sciberras and her collaborators had no relevant financial disclosures.
On Twitter @karioakes
BALTIMORE – Persistent attention-deficit/hyperactivity disorder (ADHD) through young childhood is associated with both poorer academic outcomes and an increased risk of other mental health problems, according to a longitudinal study of younger children with ADHD.
An Australian study presented at the annual meeting of the Pediatric Academic Societies found that 67% of children who had ADHD at age 7 years still met the diagnostic criteria 3 years later, when they were 10 years old. Boys were more likely than girls to have retained the diagnosis (74% vs. 50%; odds ratio, 3.4; P = .01).
On average, children with ADHD had lower scores on math and reading tests than their matched peers without ADHD, even after adjustment for socioeconomic variables and comorbidities (mean difference, –7.6 for math and –8.7 for reading, P less than .001 for both).
When Emma Sciberras, Ph.D., and her colleagues examined the longitudinal data, they found that children who had a persistent ADHD diagnosis were more likely to have an externalizing disorder, such as a conduct disorder (57% vs. 33%; OR, 2.8; P = .008). They also were more likely to have a mood disorder (8% vs. 0%; P = .04).
No sex differences were seen, aside from the increased likelihood of a persistent diagnosis.
“Childhood ADHD confers risk for future mental health difficulties,” said Dr. Sciberras, a psychologist at Deakin University, Melbourne. Dr. Sciberras presented preliminary findings from the Children’s Attention Project, a 3-year study of 179 young children with ADHD and 212 children without the diagnosis.
The goal of the Children’s Attention Project, a community-based longitudinal study, was to document the natural history of ADHD. Aspects of the study included assessing the impact of ADHD on the mental health of both children and parents, as well as examining social, academic, and family functioning, and overall quality of life. The study also seeks to tease out both risks and protective factors that can tip outcomes toward the better – or worse – end of the spectrum, said Dr. Sciberras.
The Children’s Attention Project enrolled first graders from 43 primary schools in Melbourne, to compare 3-year outcomes of a sample of children with ADHD with a control group of children who did not have ADHD. In addition to assessing diagnostic stability (the persistence of an ADHD diagnosis), Dr. Sciberras and her collaborators also looked at functional outcomes. Sex differences in outcomes, as well as the effect of ADHD persistence, also were assessed for the community-based sample of children.
Children were enrolled after families and teachers of the first graders completed the Conners 3 ADHD Index. Families of children with positive screens and matched controls were offered enrollment in the study, with intake involving confirmation of the ADHD diagnosis, as well as detailed academic and behavioral assessments and a family survey. Children in the study were assessed at baseline, and then again at 18 and 36 months after enrollment. Longitudinal data were available for 72% of those initially enrolled.
Children in the study averaged 7.3 years old. Of the ADHD group, 124/179 (69%) were male, as were 135/212 (64%) of the control group. For children in the ADHD group, 31 (17%) had previously been diagnosed with ADHD, and 23 children (13%) were on ADHD medication at enrollment; none of the control group had a prior ADHD diagnosis or was taking medication. For 63 (38%) of the children in the ADHD group, their primary caregiver had not completed high school, compared with 39 (19%) in the control group.
“This is really more of a community-based approach to researching ADHD,” Dr. Sciberras said in an interview. Previous longitudinal studies, she said, had a near-exclusive focus on clinical samples, which can “overrepresent boys and children with more severe symptoms,” she said. Age ranges were broad, and follow-up was often infrequent. Most importantly, positive factors that lead to good outcomes for children with ADHD had been understudied, she said, and she and her colleagues are continuing to look for factors, such as resilience, that contribute to better social and emotional functioning.
It’s important to study children with ADHD in a real world manner because “childhood ADHD is associated with poorer academic outcomes, and the risk is evident from the second year of school,” said Dr. Sciberras. “We need to identify which factors lead to improved outcomes over time. The ultimate aim is to map functional impairment and key predictors from age 7 to later adolescence and adulthood.”
The study was funded by Australia’s National Health and Medical Research Council and by the Collier Foundation. Dr. Sciberras and her collaborators had no relevant financial disclosures.
On Twitter @karioakes
BALTIMORE – Persistent attention-deficit/hyperactivity disorder (ADHD) through young childhood is associated with both poorer academic outcomes and an increased risk of other mental health problems, according to a longitudinal study of younger children with ADHD.
An Australian study presented at the annual meeting of the Pediatric Academic Societies found that 67% of children who had ADHD at age 7 years still met the diagnostic criteria 3 years later, when they were 10 years old. Boys were more likely than girls to have retained the diagnosis (74% vs. 50%; odds ratio, 3.4; P = .01).
On average, children with ADHD had lower scores on math and reading tests than their matched peers without ADHD, even after adjustment for socioeconomic variables and comorbidities (mean difference, –7.6 for math and –8.7 for reading, P less than .001 for both).
When Emma Sciberras, Ph.D., and her colleagues examined the longitudinal data, they found that children who had a persistent ADHD diagnosis were more likely to have an externalizing disorder, such as a conduct disorder (57% vs. 33%; OR, 2.8; P = .008). They also were more likely to have a mood disorder (8% vs. 0%; P = .04).
No sex differences were seen, aside from the increased likelihood of a persistent diagnosis.
“Childhood ADHD confers risk for future mental health difficulties,” said Dr. Sciberras, a psychologist at Deakin University, Melbourne. Dr. Sciberras presented preliminary findings from the Children’s Attention Project, a 3-year study of 179 young children with ADHD and 212 children without the diagnosis.
The goal of the Children’s Attention Project, a community-based longitudinal study, was to document the natural history of ADHD. Aspects of the study included assessing the impact of ADHD on the mental health of both children and parents, as well as examining social, academic, and family functioning, and overall quality of life. The study also seeks to tease out both risks and protective factors that can tip outcomes toward the better – or worse – end of the spectrum, said Dr. Sciberras.
The Children’s Attention Project enrolled first graders from 43 primary schools in Melbourne, to compare 3-year outcomes of a sample of children with ADHD with a control group of children who did not have ADHD. In addition to assessing diagnostic stability (the persistence of an ADHD diagnosis), Dr. Sciberras and her collaborators also looked at functional outcomes. Sex differences in outcomes, as well as the effect of ADHD persistence, also were assessed for the community-based sample of children.
Children were enrolled after families and teachers of the first graders completed the Conners 3 ADHD Index. Families of children with positive screens and matched controls were offered enrollment in the study, with intake involving confirmation of the ADHD diagnosis, as well as detailed academic and behavioral assessments and a family survey. Children in the study were assessed at baseline, and then again at 18 and 36 months after enrollment. Longitudinal data were available for 72% of those initially enrolled.
Children in the study averaged 7.3 years old. Of the ADHD group, 124/179 (69%) were male, as were 135/212 (64%) of the control group. For children in the ADHD group, 31 (17%) had previously been diagnosed with ADHD, and 23 children (13%) were on ADHD medication at enrollment; none of the control group had a prior ADHD diagnosis or was taking medication. For 63 (38%) of the children in the ADHD group, their primary caregiver had not completed high school, compared with 39 (19%) in the control group.
“This is really more of a community-based approach to researching ADHD,” Dr. Sciberras said in an interview. Previous longitudinal studies, she said, had a near-exclusive focus on clinical samples, which can “overrepresent boys and children with more severe symptoms,” she said. Age ranges were broad, and follow-up was often infrequent. Most importantly, positive factors that lead to good outcomes for children with ADHD had been understudied, she said, and she and her colleagues are continuing to look for factors, such as resilience, that contribute to better social and emotional functioning.
It’s important to study children with ADHD in a real world manner because “childhood ADHD is associated with poorer academic outcomes, and the risk is evident from the second year of school,” said Dr. Sciberras. “We need to identify which factors lead to improved outcomes over time. The ultimate aim is to map functional impairment and key predictors from age 7 to later adolescence and adulthood.”
The study was funded by Australia’s National Health and Medical Research Council and by the Collier Foundation. Dr. Sciberras and her collaborators had no relevant financial disclosures.
On Twitter @karioakes
AT THE PAS ANNUAL MEETING
Key clinical point: Persistent ADHD in early childhood was associated with worse academic and emotional outcomes at age 10 years.
Major finding: Young children with persistent ADHD were almost three times more likely to have an externalizing mental health disorder than peers without ADHD (57% vs. 33%; OR, 2.8; P = .008).
Data source: A 3-year longitudinal study of 179 first graders with ADHD and 212 children without ADHD.
Disclosures: The study was funded by Australia’s National Health and Medical Research Council and by the Collier Foundation. Dr. Sciberras and her collaborators had no relevant financial disclosures.

Oxandrolone, propranolol combo increases growth in severely burned children
CHICAGO – Combination therapy with oxandrolone and propranolol can attenuate burn-induced growth arrest and increase growth rate in severely burned children, according to findings from a prospective, randomized clinical trial.
Of 612 children with burns over at least 30% of their total body surface area (average of more than 50%), 103 were randomized to receive treatment with both oxandrolone and propranolol, 67 received oxandrolone alone, 194 received propranolol alone, and 248 served as controls. After a minimum of 1 year of treatment, the average growth rate was 5.9 cm in the control group and 7.6 cm in the group receiving combination therapy, Dr. David N. Herndon of the University of Texas Medical Branch at Galveston reported at the annual meeting of the American Surgical Association.
“The rate of growth with combination therapy was significantly greater than with either of the individual drugs alone,” Dr. Herndon said.
Further, the period of growth arrest was significantly shorter – by 84 days – among those in the combination-treatment group, compared with those in the control group.
Study subjects were children treated at Shriners Hospitals for Children – Galveston from 1997 to 2015. Boys aged 6 months to 14 years and girls aged 6 months to 12 years were included to eliminate the variable onset of postpubescent growth delay. About two-thirds in each group were boys, and the ages in the patient groups were similar. Mortality was low and was similar across the groups, as was hospital length of stay.
Dr. Herndon and his colleagues controlled for heterogeneous burn distribution between the groups in the course of their analyses, as well as age.
In children with severe, extensive burn injury, the hypercatabolic response is mediated by increased production of catecholamines and corticosteroids, coupled with decreased production of testosterone. This contributes to growth arrest and to decreased strength for up to 2 years after burn injury, he explained. Children with burns over 50% of their total body surface routinely survive acute hospitalization but, at 3 months post injury, are thin, have difficulty walking, and require occupational and physical therapy to help them perform even the simplest activities of daily living.
At 1 year, a raised inflammatory mass covers their wounds, they experience itching, and they have, in large part, stunted growth; there is severe loss of lean body mass and strength, and fracture risk is increased, Dr. Herndon said.
In previous work, he and his colleagues showed that administration of propranolol at an average dose of 4 mg/kg per day for 1 year decreased cardiac work and resting energy expenditure while increasing peripheral lean mass. Further, they found that the testosterone analog oxandrolone, given at 0.1 mg/kg twice per day for 1 year, improved lean body mass accretion and bone mineral content.
The current study was conducted to test the effects of administering both agents in combination.
“The combined use of oxandrolone and propranolol in severely burned children confers an additional benefit on growth over either treatment alone,” Dr. Herndon said, adding that the additive effects of combination therapy may be due to the effects of oxandrolone on bone growth and the anti-inflammatory effects of propranolol.
“The additional benefits point out mechanistic changes that may be eventful in the treatment of hypermetabolism generally and in inflammatory states,” he concluded.
Dr. Herndon reported having no disclosures.
CHICAGO – Combination therapy with oxandrolone and propranolol can attenuate burn-induced growth arrest and increase growth rate in severely burned children, according to findings from a prospective, randomized clinical trial.
Of 612 children with burns over at least 30% of their total body surface area (average of more than 50%), 103 were randomized to receive treatment with both oxandrolone and propranolol, 67 received oxandrolone alone, 194 received propranolol alone, and 248 served as controls. After a minimum of 1 year of treatment, the average growth rate was 5.9 cm in the control group and 7.6 cm in the group receiving combination therapy, Dr. David N. Herndon of the University of Texas Medical Branch at Galveston reported at the annual meeting of the American Surgical Association.
“The rate of growth with combination therapy was significantly greater than with either of the individual drugs alone,” Dr. Herndon said.
Further, the period of growth arrest was significantly shorter – by 84 days – among those in the combination-treatment group, compared with those in the control group.
Study subjects were children treated at Shriners Hospitals for Children – Galveston from 1997 to 2015. Boys aged 6 months to 14 years and girls aged 6 months to 12 years were included to eliminate the variable onset of postpubescent growth delay. About two-thirds in each group were boys, and the ages in the patient groups were similar. Mortality was low and was similar across the groups, as was hospital length of stay.
Dr. Herndon and his colleagues controlled for heterogeneous burn distribution between the groups in the course of their analyses, as well as age.
In children with severe, extensive burn injury, the hypercatabolic response is mediated by increased production of catecholamines and corticosteroids, coupled with decreased production of testosterone. This contributes to growth arrest and to decreased strength for up to 2 years after burn injury, he explained. Children with burns over 50% of their total body surface routinely survive acute hospitalization but, at 3 months post injury, are thin, have difficulty walking, and require occupational and physical therapy to help them perform even the simplest activities of daily living.
At 1 year, a raised inflammatory mass covers their wounds, they experience itching, and they have, in large part, stunted growth; there is severe loss of lean body mass and strength, and fracture risk is increased, Dr. Herndon said.
In previous work, he and his colleagues showed that administration of propranolol at an average dose of 4 mg/kg per day for 1 year decreased cardiac work and resting energy expenditure while increasing peripheral lean mass. Further, they found that the testosterone analog oxandrolone, given at 0.1 mg/kg twice per day for 1 year, improved lean body mass accretion and bone mineral content.
The current study was conducted to test the effects of administering both agents in combination.
“The combined use of oxandrolone and propranolol in severely burned children confers an additional benefit on growth over either treatment alone,” Dr. Herndon said, adding that the additive effects of combination therapy may be due to the effects of oxandrolone on bone growth and the anti-inflammatory effects of propranolol.
“The additional benefits point out mechanistic changes that may be eventful in the treatment of hypermetabolism generally and in inflammatory states,” he concluded.
Dr. Herndon reported having no disclosures.
CHICAGO – Combination therapy with oxandrolone and propranolol can attenuate burn-induced growth arrest and increase growth rate in severely burned children, according to findings from a prospective, randomized clinical trial.
Of 612 children with burns over at least 30% of their total body surface area (average of more than 50%), 103 were randomized to receive treatment with both oxandrolone and propranolol, 67 received oxandrolone alone, 194 received propranolol alone, and 248 served as controls. After a minimum of 1 year of treatment, the average growth rate was 5.9 cm in the control group and 7.6 cm in the group receiving combination therapy, Dr. David N. Herndon of the University of Texas Medical Branch at Galveston reported at the annual meeting of the American Surgical Association.
“The rate of growth with combination therapy was significantly greater than with either of the individual drugs alone,” Dr. Herndon said.
Further, the period of growth arrest was significantly shorter – by 84 days – among those in the combination-treatment group, compared with those in the control group.
Study subjects were children treated at Shriners Hospitals for Children – Galveston from 1997 to 2015. Boys aged 6 months to 14 years and girls aged 6 months to 12 years were included to eliminate the variable onset of postpubescent growth delay. About two-thirds in each group were boys, and the ages in the patient groups were similar. Mortality was low and was similar across the groups, as was hospital length of stay.
Dr. Herndon and his colleagues controlled for heterogeneous burn distribution between the groups in the course of their analyses, as well as age.
In children with severe, extensive burn injury, the hypercatabolic response is mediated by increased production of catecholamines and corticosteroids, coupled with decreased production of testosterone. This contributes to growth arrest and to decreased strength for up to 2 years after burn injury, he explained. Children with burns over 50% of their total body surface routinely survive acute hospitalization but, at 3 months post injury, are thin, have difficulty walking, and require occupational and physical therapy to help them perform even the simplest activities of daily living.
At 1 year, a raised inflammatory mass covers their wounds, they experience itching, and they have, in large part, stunted growth; there is severe loss of lean body mass and strength, and fracture risk is increased, Dr. Herndon said.
In previous work, he and his colleagues showed that administration of propranolol at an average dose of 4 mg/kg per day for 1 year decreased cardiac work and resting energy expenditure while increasing peripheral lean mass. Further, they found that the testosterone analog oxandrolone, given at 0.1 mg/kg twice per day for 1 year, improved lean body mass accretion and bone mineral content.
The current study was conducted to test the effects of administering both agents in combination.
“The combined use of oxandrolone and propranolol in severely burned children confers an additional benefit on growth over either treatment alone,” Dr. Herndon said, adding that the additive effects of combination therapy may be due to the effects of oxandrolone on bone growth and the anti-inflammatory effects of propranolol.
“The additional benefits point out mechanistic changes that may be eventful in the treatment of hypermetabolism generally and in inflammatory states,” he concluded.
Dr. Herndon reported having no disclosures.
AT THE ASA ANNUAL MEETING
Key clinical point: Combination therapy with oxandrolone and propranolol can attenuate burn-induced growth arrest and increase growth rate in severely burned children, according to findings from a prospective, randomized clinical trial.
Major finding: After a minimum of 1 year of treatment, the average growth rate was 5.9 cm in the control group and 7.6 cm in the group receiving combination therapy.
Data source: A prospective, randomized clinical trial involving 612 children.
Disclosures: Dr. Herndon reported having no disclosures.
Phototherapy may increase risk of pediatric cancers

phototherapy to treat
neonatal jaundice
Photo by Martin Pot
Two new studies raise questions about a possible link between childhood cancer and phototherapy for newborn jaundice.
One study showed a significant positive association between phototherapy and 2 cancer types—myeloid leukemia and kidney cancer—but the other study did not.
Although these results are inconclusive, researchers say clinicians should exercise caution in prescribing phototherapy for infants whose jaundice is likely to resolve on its own.
However, the findings should not discourage the use of phototherapy in infants who otherwise would be at risk of brain damage or hearing loss.
The studies were published in Pediatrics alongside a related editorial.
“Phototherapy has been perceived by most as causing minimal risk to the infant,” said editorial author A. Lindsay Frazier, MD, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“Although these studies are inconclusive and do not prove a relationship between phototherapy and cancer, they should give us pause. That being said, however, the brain damage and hearing loss from high bilirubin levels are real and well-documented, and the suggested risk of cancer from these new studies is both unclear and very small.”
Kaiser Permanente study
Thomas B. Newman, MD, of University of California, San Francisco, and his colleagues conducted a study of children born in Kaiser Permanente Northern California hospitals from 1995 to 2011. The researchers analyzed data on 499,621 children born at 35 weeks’ gestation or later.
There were 60 cases of cancer among the 39,403 children exposed to phototherapy and 651 cases of cancer among the 460,218 children who were not exposed to phototherapy. That translates to 25 per 100,000 person-years and 18 per 100,000 person-years, respectively, for an incidence rate ratio (IRR) of 1.4 (P=0.01).
In an unadjusted analysis, phototherapy was associated with increased rates of any leukemia (IRR=2.1, P=0.0007), nonlymphocytic leukemia (IRR=4.0, P=0.0004), and liver cancer (IRR=5.2, P=0.04).
However, when the researchers adjusted for bilirubin levels, chromosomal disorders, congenital anomalies, and other covariates, these associations were no longer statistically significant.
Study of California hospitals
Andrea C. Wickremasinghe, MD, of Kaiser Permanente Northern California in Santa Clara, and her colleagues conducted a study of children born in California hospitals from 1998 to 2007.
The team analyzed data from the California Office of Statewide Health Planning and Development, which included 5,144,849 infants born at 35 weeks’ gestation or later.
There were 58 cases of cancer among the 178,017 infants exposed to phototherapy and 1042 cancer cases among the 4,966,832 infants who were not exposed to phototherapy. That translated to 32.6 per 100,000 and 21.0 per 100,000, respectively, for a relative risk of 1.6 (95% confidence interval [CI], 1.2–2.0; P=0.002).
In propensity-adjusted analyses, there were significant positive associations between phototherapy and overall cancer (adjusted odds ratio [aOR]=1.4; 95% CI, 1.1–1.9; P=0.007), myeloid leukemia (aOR=2.6; 95% CI, 1.3–5.0; P=0.005), and kidney cancer (aOR=2.5; 95% CI, 1.2–5.1; P=0.02).
Dr Frazier noted that these studies come at a time when the number of infants receiving phototherapy is increasing, perhaps because of the availability of light therapy units that can be used in the home. In the Kaiser Permanente study, 15.9% of infants received phototherapy in 2011, compared to 2.7% in 1995.
“What is concerning is the fact that, at least in the Kaiser Permanente Northern California healthcare system, the number of children receiving phototherapy has dramatically increased,” Dr Frazier said.
“The risks associated with such a prevalent exposure require close scrutiny. If I were the one prescribing phototherapy today, I would want to be sure it was indicated.” ![]()
phototherapy to treat
neonatal jaundice
Photo by Martin Pot
Two new studies raise questions about a possible link between childhood cancer and phototherapy for newborn jaundice.
One study showed a significant positive association between phototherapy and 2 cancer types—myeloid leukemia and kidney cancer—but the other study did not.
Although these results are inconclusive, researchers say clinicians should exercise caution in prescribing phototherapy for infants whose jaundice is likely to resolve on its own.
However, the findings should not discourage the use of phototherapy in infants who otherwise would be at risk of brain damage or hearing loss.
The studies were published in Pediatrics alongside a related editorial.
“Phototherapy has been perceived by most as causing minimal risk to the infant,” said editorial author A. Lindsay Frazier, MD, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“Although these studies are inconclusive and do not prove a relationship between phototherapy and cancer, they should give us pause. That being said, however, the brain damage and hearing loss from high bilirubin levels are real and well-documented, and the suggested risk of cancer from these new studies is both unclear and very small.”
Kaiser Permanente study
Thomas B. Newman, MD, of University of California, San Francisco, and his colleagues conducted a study of children born in Kaiser Permanente Northern California hospitals from 1995 to 2011. The researchers analyzed data on 499,621 children born at 35 weeks’ gestation or later.
There were 60 cases of cancer among the 39,403 children exposed to phototherapy and 651 cases of cancer among the 460,218 children who were not exposed to phototherapy. That translates to 25 per 100,000 person-years and 18 per 100,000 person-years, respectively, for an incidence rate ratio (IRR) of 1.4 (P=0.01).
In an unadjusted analysis, phototherapy was associated with increased rates of any leukemia (IRR=2.1, P=0.0007), nonlymphocytic leukemia (IRR=4.0, P=0.0004), and liver cancer (IRR=5.2, P=0.04).
However, when the researchers adjusted for bilirubin levels, chromosomal disorders, congenital anomalies, and other covariates, these associations were no longer statistically significant.
Study of California hospitals
Andrea C. Wickremasinghe, MD, of Kaiser Permanente Northern California in Santa Clara, and her colleagues conducted a study of children born in California hospitals from 1998 to 2007.
The team analyzed data from the California Office of Statewide Health Planning and Development, which included 5,144,849 infants born at 35 weeks’ gestation or later.
There were 58 cases of cancer among the 178,017 infants exposed to phototherapy and 1042 cancer cases among the 4,966,832 infants who were not exposed to phototherapy. That translated to 32.6 per 100,000 and 21.0 per 100,000, respectively, for a relative risk of 1.6 (95% confidence interval [CI], 1.2–2.0; P=0.002).
In propensity-adjusted analyses, there were significant positive associations between phototherapy and overall cancer (adjusted odds ratio [aOR]=1.4; 95% CI, 1.1–1.9; P=0.007), myeloid leukemia (aOR=2.6; 95% CI, 1.3–5.0; P=0.005), and kidney cancer (aOR=2.5; 95% CI, 1.2–5.1; P=0.02).
Dr Frazier noted that these studies come at a time when the number of infants receiving phototherapy is increasing, perhaps because of the availability of light therapy units that can be used in the home. In the Kaiser Permanente study, 15.9% of infants received phototherapy in 2011, compared to 2.7% in 1995.
“What is concerning is the fact that, at least in the Kaiser Permanente Northern California healthcare system, the number of children receiving phototherapy has dramatically increased,” Dr Frazier said.
“The risks associated with such a prevalent exposure require close scrutiny. If I were the one prescribing phototherapy today, I would want to be sure it was indicated.” ![]()
phototherapy to treat
neonatal jaundice
Photo by Martin Pot
Two new studies raise questions about a possible link between childhood cancer and phototherapy for newborn jaundice.
One study showed a significant positive association between phototherapy and 2 cancer types—myeloid leukemia and kidney cancer—but the other study did not.
Although these results are inconclusive, researchers say clinicians should exercise caution in prescribing phototherapy for infants whose jaundice is likely to resolve on its own.
However, the findings should not discourage the use of phototherapy in infants who otherwise would be at risk of brain damage or hearing loss.
The studies were published in Pediatrics alongside a related editorial.
“Phototherapy has been perceived by most as causing minimal risk to the infant,” said editorial author A. Lindsay Frazier, MD, of the Dana-Farber Cancer Institute in Boston, Massachusetts.
“Although these studies are inconclusive and do not prove a relationship between phototherapy and cancer, they should give us pause. That being said, however, the brain damage and hearing loss from high bilirubin levels are real and well-documented, and the suggested risk of cancer from these new studies is both unclear and very small.”
Kaiser Permanente study
Thomas B. Newman, MD, of University of California, San Francisco, and his colleagues conducted a study of children born in Kaiser Permanente Northern California hospitals from 1995 to 2011. The researchers analyzed data on 499,621 children born at 35 weeks’ gestation or later.
There were 60 cases of cancer among the 39,403 children exposed to phototherapy and 651 cases of cancer among the 460,218 children who were not exposed to phototherapy. That translates to 25 per 100,000 person-years and 18 per 100,000 person-years, respectively, for an incidence rate ratio (IRR) of 1.4 (P=0.01).
In an unadjusted analysis, phototherapy was associated with increased rates of any leukemia (IRR=2.1, P=0.0007), nonlymphocytic leukemia (IRR=4.0, P=0.0004), and liver cancer (IRR=5.2, P=0.04).
However, when the researchers adjusted for bilirubin levels, chromosomal disorders, congenital anomalies, and other covariates, these associations were no longer statistically significant.
Study of California hospitals
Andrea C. Wickremasinghe, MD, of Kaiser Permanente Northern California in Santa Clara, and her colleagues conducted a study of children born in California hospitals from 1998 to 2007.
The team analyzed data from the California Office of Statewide Health Planning and Development, which included 5,144,849 infants born at 35 weeks’ gestation or later.
There were 58 cases of cancer among the 178,017 infants exposed to phototherapy and 1042 cancer cases among the 4,966,832 infants who were not exposed to phototherapy. That translated to 32.6 per 100,000 and 21.0 per 100,000, respectively, for a relative risk of 1.6 (95% confidence interval [CI], 1.2–2.0; P=0.002).
In propensity-adjusted analyses, there were significant positive associations between phototherapy and overall cancer (adjusted odds ratio [aOR]=1.4; 95% CI, 1.1–1.9; P=0.007), myeloid leukemia (aOR=2.6; 95% CI, 1.3–5.0; P=0.005), and kidney cancer (aOR=2.5; 95% CI, 1.2–5.1; P=0.02).
Dr Frazier noted that these studies come at a time when the number of infants receiving phototherapy is increasing, perhaps because of the availability of light therapy units that can be used in the home. In the Kaiser Permanente study, 15.9% of infants received phototherapy in 2011, compared to 2.7% in 1995.
“What is concerning is the fact that, at least in the Kaiser Permanente Northern California healthcare system, the number of children receiving phototherapy has dramatically increased,” Dr Frazier said.
“The risks associated with such a prevalent exposure require close scrutiny. If I were the one prescribing phototherapy today, I would want to be sure it was indicated.” ![]()
VIDEO: Post legalization, what effect is recreational marijuana use having on children?
BALTIMORE – Experts from Colorado and Washington – two states which have legalized recreational use of the drug – came together at the annual meeting of the Pediatric Academic Societies to discuss the challenges of treating and preventing short-term and long-term illness brought on by marijuana use.
“In Colorado, a lot of [mothers] use [marijuana] for depression, anxiety, as well as for nausea, and they’re not disclosing that” to their primary care doctors, explained Dr. Maya Bunik of the University of Colorado in Aurora. “Then they’re sort of surprised at birth when we tell them that we don’t know what [marijuana] does in terms of affecting [their] baby.”
In a series of interviews, presenters at the roundtable discussed the importance of talking to parents – particularly pregnant mothers – about the dangers of marijuana use around kids, keeping marijuana and related products away from children, what’s being done on the legislative side to keep marijuana away from children and adolescents, and the long-term ramifications of marijuana use by children and their parents.
Joining Dr. Bunik for this discussion are Dr. George Sam Wang, Ayelet Talmi, Ph.D., Dr. Karen M. Wilson, Dr. Kathryn M. Wells, and Dr. Erica M. Wymore of the University of Colorado at Aurora, and Dr. Leslie R. Walker of the University of Washington in Seattle.
Dr. Wang disclosed receiving a grant from the Colorado Department of Public Health and Environments, and royalties from author contributions. The other presenters had no relevant financial disclosures.
BALTIMORE – Experts from Colorado and Washington – two states which have legalized recreational use of the drug – came together at the annual meeting of the Pediatric Academic Societies to discuss the challenges of treating and preventing short-term and long-term illness brought on by marijuana use.
“In Colorado, a lot of [mothers] use [marijuana] for depression, anxiety, as well as for nausea, and they’re not disclosing that” to their primary care doctors, explained Dr. Maya Bunik of the University of Colorado in Aurora. “Then they’re sort of surprised at birth when we tell them that we don’t know what [marijuana] does in terms of affecting [their] baby.”
In a series of interviews, presenters at the roundtable discussed the importance of talking to parents – particularly pregnant mothers – about the dangers of marijuana use around kids, keeping marijuana and related products away from children, what’s being done on the legislative side to keep marijuana away from children and adolescents, and the long-term ramifications of marijuana use by children and their parents.
Joining Dr. Bunik for this discussion are Dr. George Sam Wang, Ayelet Talmi, Ph.D., Dr. Karen M. Wilson, Dr. Kathryn M. Wells, and Dr. Erica M. Wymore of the University of Colorado at Aurora, and Dr. Leslie R. Walker of the University of Washington in Seattle.
Dr. Wang disclosed receiving a grant from the Colorado Department of Public Health and Environments, and royalties from author contributions. The other presenters had no relevant financial disclosures.
BALTIMORE – Experts from Colorado and Washington – two states which have legalized recreational use of the drug – came together at the annual meeting of the Pediatric Academic Societies to discuss the challenges of treating and preventing short-term and long-term illness brought on by marijuana use.
“In Colorado, a lot of [mothers] use [marijuana] for depression, anxiety, as well as for nausea, and they’re not disclosing that” to their primary care doctors, explained Dr. Maya Bunik of the University of Colorado in Aurora. “Then they’re sort of surprised at birth when we tell them that we don’t know what [marijuana] does in terms of affecting [their] baby.”
In a series of interviews, presenters at the roundtable discussed the importance of talking to parents – particularly pregnant mothers – about the dangers of marijuana use around kids, keeping marijuana and related products away from children, what’s being done on the legislative side to keep marijuana away from children and adolescents, and the long-term ramifications of marijuana use by children and their parents.
Joining Dr. Bunik for this discussion are Dr. George Sam Wang, Ayelet Talmi, Ph.D., Dr. Karen M. Wilson, Dr. Kathryn M. Wells, and Dr. Erica M. Wymore of the University of Colorado at Aurora, and Dr. Leslie R. Walker of the University of Washington in Seattle.
Dr. Wang disclosed receiving a grant from the Colorado Department of Public Health and Environments, and royalties from author contributions. The other presenters had no relevant financial disclosures.
AT THE PAS ANNUAL MEETING
