User login
A Practical Overview of Pediatric Atopic Dermatitis, Part 3: Differential Diagnosis, Comorbidities, and Measurement of Disease Burden
In parts 1 and 2 of this series on atopic dermatitis (AD),1,2 the current putative pathogenesis, scoring systems for severity grading, and epidemiology were reviewed. Part 3 reviews the differential diagnosis, with an emphasis on the difficulty of differentiation from some rare but notable illnesses, as well as the recently expanding data on comorbidities that identify AD as a multisystem disorder with widespread health implications for the patient.
Differential Diagnosis for Pediatric AD
The differential diagnosis for pediatric AD includes chronic dermatoses (eg, seborrheic dermatitis, psoriasis), congenital disorders (eg, Netherton syndrome), malignant diseases (eg, cutaneous T-cell lymphoma [CTCL]), immunodeficiencies, infections, and metabolic disorders.3 Netherton syndrome must be ruled out to prevent extensive drug absorption when treating with topical calcineurin inhibitors (TCIs).4 Due to the presence of bamboo hairs in these patients, a hair mount may aid in the diagnosis of Netherton syndrome. Misdiagnosis of CTCL as AD may complicate the analysis of safety data on TCIs.4,5 Multiple skin biopsies are essential in cases of suspected CTCL to provide an accurate diagnosis. Biopsy can be considered in AD cases with changing and/or unusual morphology, erythrodermic skin changes, and disease that is poorly responsive to multiple therapeutic modalities.
Comorbidities in Pediatric AD
Psychosocial Comorbidities
Pediatric AD often takes a psychological toll on patients as well as household members. Almost half of children with AD are reported to have a severely impaired quality of life (QOL).6 Contributing factors include fatigue, sleep disturbance, activity restriction (eg, inability to participate in sports), and depression.7
Chamlin et al8 developed the Childhood Atopic Dermatitis Impact Scale (CADIS), a 45-item instrument (refined from a 62-item prototype), to measure QOL in young children with AD and their family members. Responses were evaluated with consideration of 5 domains: symptoms and activity limitations/behaviors in children, as well as family/social function, sleep, and emotions in parents. The top 12 factors that parents found most bothersome about AD included itching/scratching, child’s pain/discomfort, sleep issues, embarrassment or worry about appearance, child’s fussiness/irritability/crying/unhappiness, helplessness/can’t control it/predict it, worry about skin infection, dryness of skin/nonsmooth skin, skin bleeding, worry about damage/scars, stares/comments of strangers and other children, and rashes/redness of skin/discoloration. Parents were asked to respond to items about their emotional health and social functioning, such as “My child’s skin condition has strained my relationship with my spouse or partner,” “My child’s skin condition makes me feel sad or depressed,” and “I am bothered by the reaction of strangers to this skin condition.”8
Kiebert et al9 found that AD patients had lower scores on the Short Form-36 Health Survey’s vitality, social functioning, and mental health subscales compared to individuals in the general population. The authors noted that anxiety in AD patients is of particular concern, as stress has been found to trigger the itch-scratch cycle, potentially setting off AD flare-ups.9 Family impact of AD is aggravated by disease severity. Sleeplessness, relationship stress, and time management can all cause family problems in patients with AD.8
In a survey of 3775 older teenagers aged 18 to 19 years (80% response rate out of 4774 prospective participants), 9.7% of participants reported having current AD.10 Suicidal ideation was higher in those with current AD than those without AD (15.5% vs 9.1%). The prevalence of suicidal ideation rose to 23.8% in those with both AD and itch. Diagnosis of AD (as determined through participant responses to the question, ‘‘Do you have, or have you had eczema?’’) was associated with mental health problems in 16.0% of those with AD compared to 10.1% of those without AD, with an especially reduced likelihood of romantic relationships for adolescent boys with AD, as measured using the Strength and Difficulties Questionnaire, which measures 4 problem domains and assesses presence of mental health issues in the past 6 months, and the Hopkins Symptom Checklist 10, which uses 10 questions to measure anxiety and depression symptoms in the past week.10
Dalgard et al11 assessed whether the psychological burden of AD persists in adulthood in an international, multicenter, observational, cross-sectional study conducted in 13 European countries. Each dermatology clinic recruited 250 consecutive adult outpatients to complete a questionnaire along with a control group of 125 hospital employees without skin disease from the same institution but from different departments. The study included a total of 4994 participants (3635 patients and 1359 controls). Clinical depression and anxiety were present in 10.1% and 17.6% of patients, respectively, versus 4.3% and 11.1% of controls, respectively. The prevalence of depression and anxiety was highest in patients with leg ulcers, hand eczema, psoriasis, and AD.11 This study demonstrated that the psychological comorbidities of childhood conditions such as AD may persist into adulthood.
Lymphoma
In a systematic review of the literature and a separate meta-analysis, Legendre et al12 identified a slight increase in lymphoma among AD patients, with an uncertain but potential increase associated with topical corticosteroid application. This finding is similar to trends seen in other systemic inflammatory conditions that involve the skin, such as psoriasis, and is felt to relate to long-term inflammation.
Obesity
Obesity has been associated with a greater risk for moderate to severe AD in children.13,14
Infections
Children with AD are at a higher risk for cutaneous infections and generalization of these infections. The leading infections would be with Staphylococcus aureus, but group A streptococci infections do occur. Herpes simplex virus, vaccinia virus or Kaposi varicelliform eruption (KVE), molluscum with or without dermatitis, and fungal infections occur less commonly but with greater morbidity, largely due to the impaired barrier and some innate reduction in cutaneous immunity.15
Atopic dermatitis in children also is associated with a higher prevalence of extracutaneous infections such as influenza, pneumonia, urinary tract infections, varicella-zoster virus, recurrent ear infections, sinus infections, sore throat, and head or chest colds.16 Children with AD and warts (human papillomavirus infection) have an even greater risk for these comorbidities.17 Warts and molluscum infections may become more extensive in children with AD.18 Generalization of herpetic infections occurs more easily in AD patients due to the impaired skin barrier, which includes generalized skin surface extension of herpes simplex virus type 1, varicella-zoster virus, and historically smallpox. A similar clinical appearance of generalized vesiculopustular lesions with fever can be seen when coxsackievirus A6 infections occur in AD patients; these conditions are called eczema herpeticum due to herpes simplex virus, KVE due to varicella-zoster virus and smallpox, and eczema coxsackium due to coxsackievirus A6,19 though some authors refer to all of these as KVE.20 These generalized viral illnesses overlying AD often result in fever, malaise, pain, and life-threatening skin denudation with risk for dehydration and superinfection with S aureus.7,18 It has been shown that the occurrence of eczema herpeticum in AD is associated with and may be caused by an inability to induce human β-defensin 2 and 3 as well as cathelicidin.21
Staphylococcus aureus colonization has been noted in 90% to 100% of AD cases, which can be associated with a higher eczema area and severity index score.22-24 The role of S aureus in AD includes flare triggering through release of superantigens, leading to IL-31–induced pruritis.25 Recurrent infection with either methicillin-sensitive or methicillin-resistant S aureus has been noted in AD.18,26 Skin infections also occur in AD and appear as erosions and pustules, and coinfection with Streptococcus and Staphylococcus does occur; therefore, cultures often are needed to determine the type of bacteria present on the skin in severe cases and when infection is suspected.27 Perianal bacterial dermatitis is a variant of infected AD occurring in the anal/groin area that is associated with S aureus and/or streptococcal superinfection in which topical corticosteroids and topical anti-infectives can be used. In some severe cases, oral antibiotics may be needed.28
Injury/Hyperactivity
Children aged 0 to 5 years with AD carry an increased risk for injuries requiring medical attention, with association in part due to attention deficit disorder, depression, and anxiety. Antihistamines are believed to aggravate this issue by promoting daytime somnolence29; however, pruritus-induced sleep disturbances in AD also may be responsible for daytime somnolence.30
Contact Allergy and Sensitization
Children with AD may become sensitized to environmental allergens through delayed-type hypersensitivity. The presumed mechanism is that these agents include ingredients added into applied medicaments and application occurs over an impaired skin barrier allowing for absorption and greater risk of antigen presentation. Approximately 50% of children with difficult-to-control AD will react to 1 or more epicutaneous allergens, and patch testing can be performed to identify relevant allergens that can improve skin severity.7 Severe dermatitis and id generalized hypersensitivity reactions in patients with AD and nickel allergic contact dermatitis have been described and may aggravate underlying AD.31
Family Burden of AD
Parents or caregivers of children with moderate and severe AD spend nearly 3 hours a day caring for their child’s skin and experience QOL impairments including lack of sleep and/or privacy, often due to cosleeping; treatment-related financial expenditures; and feelings of hopelessness, guilt, and depression.7
Steroid Phobia
Steroid phobia is the fear of topical application of corticosteroids resulting in systemic side effects including unrealistic fears (eg, fear that the child will develop muscles such as an anabolic steroid user) as well as realistic but statistically low-risk fears (eg, fear of systemic absorption). These fears often result in underutilization of prescribed topical corticosteroid therapies and undertreatment of children with AD.32,33
Financial Burden
The cost of AD can be high in the United States, with adult data demonstrating costs ranging from $371 to $489 per person.34 The last published cost data for pediatric AD was from 2003, with an average cost of $219 per year.35 Costs include time lost from work, household purchases (eg, skin care products), and co-pays for visits and medication, with an estimated average expenditure per person (SE) of $601.06 ($137.26) annually in 2012.36 The cost of ambulatory care and emergency department visits for AD in children in the United States in 1993 was estimated at $364 million.37-39 In 2002, Ellis et al40 estimated the overall cost of AD to be between $900 million and $3.8 billion in the United States (1997-1998) based on projections from claims, prescriptions, and comorbidities reported to a private insurer and Medicaid. Ellis et al41 further determined that topical tacrolimus was similar in cost to high-potency corticosteroids.
Pediatric AD often progresses to adult hand eczema and leads to further morbidity, especially in health care workers.42 Kemp43 reviewed the cost of AD in children and concluded that AD was a condition with major handicap with personal, financial, and social effects. A cost review of studies conducted in 163,700 children with AD showed that costs related to AD totaled $316.7 million per year. The author concluded that there were substantial psychosocial and financial stresses associated with pediatric AD but no clear path to potential reduction in related costs.43
Sleep Disturbances
Sleep disturbances are common in pediatric AD patients. Pruritus usually is exacerbated at bedtime due to reduced humidity and lack of distractions to prevent scratching. Sleep deprivation has a substantial impact on both the patient and his/her household. Parental frustration increases with sleep disturbance.18,44 Sleep deprivation is associated with greater severity, both because it is one of the most difficult aspects of illness and because the associated pruritus makes for greater damage done to the skin through injurious scratching.
Sleep disturbances also may interfere with growth and overnight release of growth hormones.18,44 This latter issue can result in reduced linear growth velocity. Furthermore, sleep deprivation can cause increased risk of accidents and poor school performance.18,44,45
Many children do not outgrow AD. In adults, AD-associated sleep deprivation has been shown to have an association with fatigue, regular daytime sleepiness, and regular insomnia, correlating to number of sick days, doctor visits, and poorer overall health status.45
Inadequate Disease Control
Inadequate disease control has been described by Eichenfeld46 as an important issue in AD at this time. Untreated, undertreated, and improperly treated AD are important issues affecting long-term AD care. He further cited steroid phobia as a contributor to undertreatment.46 Fleischer47 has cited the black box warning present on TCIs as a further deterrent to adequate therapeutic control in our current therapeutic paradigm. Undertreatment may result in uncontrolled disease activity, impaired QOL, infections, and sleep disturbances. The role of undertreatment as a driver of the atopic march is unknown.
Conclusion
Atopic dermatitis is a multisystem disorder that has wide-reaching comorbidities and may mimic a variety of skin conditions. The topic of comorbidities is new and emerging and bears further review to define risk factors, prevention strategies, and long-term monitoring requirements.
- Silverberg NB. A practical overview of pediatric atopic dermatitis, part 1: epidemiology and pathogenesis. Cutis. 2016;97:267-271.
- Silverberg NB. A practical overview of pediatric atopic dermatitis, part 2: triggers and grading. Cutis. 2016;97:326-329.
- Siegfried EC, Hebert AA. Diagnosis of atopic dermatitis: mimics, overlaps, and complications. J Clin Med. 2015;4:884-917.
- Allen A, Siegfried E, Silverman R, et al. Significant absorption of topical tacrolimus in 3 patients with Netherton syndrome. Arch Dermatol. 2001;137:747-750.
- Carr WW. Topical calcineurin inhibitors for atopic dermatitis: review and treatment recommendations. Paediatr Drugs. 2013;15:303-310.
- Chamlin SL, Lai JS, Cella D, et al. Childhood Atopic Dermatitis Impact Scale: reliability, discriminative and concurrent validity, and responsiveness. Arch Dermatol. 2007;143:768-772.
- Tollefson MM, Bruckner AL. Atopic dermatitis: skin-directed management. Pediatrics. 2014;134:E1735-E1744.
- Chamlin SL, Cella D, Frieden IJ, et al. Development of the Childhood Atopic Dermatitis Impact Scale: initial validation of a quality-of-life measure for young children with atopic dermatitis and their families. J Invest Dermatol. 2005;125:1106-1111.
- Kiebert G, Sorensen SV, Revicki D, et al. Atopic dermatitis is associated with a decrement in health-related quality of life. Int J Dermatol. 2002;41:151-158.
- Halvorsen JA, Lien L, Dalgard F, et al. Suicidal ideation, mental health problems, and social function in adolescents with eczema: a population-based study. J Invest Dermatol. 2014;134:1847-1854.
- Dalgard FJ, Gieler U, Tomas-Aragones L, et al. The psychological burden of skin diseases: a cross-sectional multicenter study among dermatological out-patients in 13 European countries. J Invest Dermatol. 2015;135:984-991.
- Legendre L, Barnetche T, Mazereeuw-Hautier J, et al. Risk of lymphoma in patients with atopic dermatitis and the role of topical treatment: a systematic review and meta-analysis. J Am Acad Dermatol. 2015;72:992-1002.
- Koutroulis I, Magnelli L, Gaughan J, et al. Atopic dermatitis is more severe in children over the age of two who have an increased body mass index. Acta Paediatr. 2015;104:713-717.
- Silverberg JI, Becker L, Kwasny M, et al. Central obesity and high blood pressure in pediatric patients with atopic dermatitis. JAMA Dermatol. 2015;151:144-152.
- De D, Kanwar AJ, Handa S. Comparative efficacy of Hanifin and Rajka’s criteria and the UK working party’s diagnostic criteria in diagnosis of atopic dermatitis in a hospital setting in North India. J Eur Acad Dermatol Venereol. 2006;20:853-859.
- Silverberg JI, Silverberg NB. Childhood atopic dermatitis and warts are associated with increased risk of infection: a US population-based study [published online October 4, 2013]. J Allergy Clin Immunol. 2014;133:1041-1047.
- Silverberg J, Garg N, Silverberg NB. New developments in comorbidities of atopic dermatitis. Cutis. 2014;93:222-224.
- Kiken DA, Silverberg NB. Atopic dermatitis in children, part 1: epidemiology, clinical features, and complications. Cutis. 2006;78:241-247.
- Mathes EF, Oza V, Frieden IJ, et al. “Eczema coxsackium” and unusual cutaneous findings in an enterovirus outbreak. Pediatrics. 2013;132:E149-E157.
- Vora RV, Pilani AP, Jivani NB, et al. Kaposi varicelliform eruption. Indian Dermatol Online J. 2015;6:364-366.
- Hata TR, Kotol P, Boguniewicz M, et al. History of eczema herpeticum is associated with the inability to induce human β-defensin (HBD)-2, HBD-3 and cathelicidin in the skin of patients with atopic dermatitis. Br J Dermatol. 2010;163:659-661.
- Abeck D, Mempel M. Staphylococcus aureus colonization in atopic dermatitis and its therapeutic implications. Br J Dermatol. 1998;139:13-16.
- Leyden JJ, Marples RR, Kligman AM. Staphylococcus aureus in the lesions of atopic dermatitis. Br J Dermatol. 1974;90:525-530.
- Lipnharski C, d’Azevedo PA, Quinto VP, et al. Colonization by S. aureus increases the EASI and the number of appointments by patients with atopic dermatitis: cohort with 93 patients. An Bras Dermatol. 2013;88:518-521.
- Paller AS. Latest approaches to treating atopic dermatitis. Chem Immunol Allergy. 2012;96:132-140.
- Groner A, Laing-Grayman D, Silverberg NB. Outpatient pediatric community-acquired methicillin-resistant Staphylococcus aureus: a polymorphous clinical disease. Cutis. 2008;81:115-122.
- Sugarman JL, Hersh AL, Okamura T, et al. A retrospective review of streptococcal infections in pediatric atopic dermatitis. Pediatr Dermatol. 2011;28:230-234.
- Heath C, Desai N, Silverberg NB. Recent microbiological shifts in perianal bacterial dermatitis: Staphylococcus aureus predominance. Pediatr Dermatol. 2009;26:696-700.
- Garg N, Silverberg JI. Association between childhood allergic disease, psychological comorbidity, and injury requiring medical attention. Ann Allergy Asthma Immunol. 2014;112:525-532.
- Lavery MJ, Stull C, Kinney MO, et al. Nocturnal pruritus: the battle for a peaceful night’s sleep. Int J Mol Sci. 2016;17:E425.
- Silverberg NB, Licht J, Friedler S, et al. Nickel contact hypersensitivity in children. Pediatr Dermatol. 2002;19:110-113.
- Aubert-Wastiaux H, Moret L, Le Rhun A, et al. Topical corticosteroid phobia in atopic dermatitis: a study of its nature, origins and frequency. Br J Dermatol. 2011;165:808-814.
- Kojima R, Fujiwara T, Matsuda A, et al. Factors associated with steroid phobia in caregivers of children with atopic dermatitis. Pediatr Dermatol. 2013;30:29-35.
- Silverberg JI. Health care utilization, patient costs, and access to care in US adults with eczema: a population-based study. JAMA Dermatol. 2015;151:743-752.
- Weinmann S, Kamtsiuris P, Henke KD, et al. The costs of atopy and asthma in children: assessment of direct costs and their determinants in a birth cohort. Pediatr Allergy Immunol. 2003;14:18-26.
- Fivenson D, Arnold RJ, Kaniecki DJ, et al. The effect of atopic dermatitis on total burden of illness and quality of life on adults and children in a large managed care organization. J Manag Care Pharm. 2002;8:333-342.
- Verboom P, Hakkaart-Van L, Sturkenboom M, et al. The cost of atopic dermatitis in the Netherlands: an international comparison. Br J Dermatol. 2002;147:716-724.
- Lapidus CS, Schwarz DF, Honig PJ. Atopic dermatitis in children: who cares? who pays? J Am Acad Dermatol. 1993;28:699-703.
- Carroll CL, Balkrishnan R, Feldman SR, et al. The burden of atopic dermatitis: impact on the patient, family, and society. Pediatr Dermatol. 2005;22:192-199.
- Ellis CN, Drake LA, Prendergast MM, et al. Cost of atopic dermatitis and eczema in the United States. J Am Acad Dermatol. 2002;46:361-370.
- Ellis CN, Prendergast MM, Tokar M, et al. Quantifying costs associated with atopic dermatitis. J Manag Care Pharm. 2003;9:278.
- Lee SW, Cheong SH, Byun JY, et al. Occupational hand eczema among nursing staffs in Korea: self-reported hand eczema and contact sensitization of hospital nursing staffs. J Dermatol. 2013;40:182-187.
- Kemp AS. Cost of illness of atopic dermatitis in children: a societal perspective. Pharmacoeconomics. 2003;21:105-113.
- Munro DD. Topical corticosteroid therapy and its effect on the hypothalamic-pituitary-adrenal axis. Dermatologica. 1976;152:173-180.
- Silverberg JI, Garg NK, Paller AS, et al. Sleep disturbances in adults with eczema are associated with impaired overall health: a US population-based study. J Invest Dermatol. 2015;135:56-66.
- Eichenfield LF. Improving outcomes in atopic dermatitis. for advances in dermatology. Dermatology Focus. 2015;34:1-6.
- Fleischer AB Jr. Black box warning for topical calcineurin inhibitors and the death of common sense. Dermatol Online J. 2006;12:2.
In parts 1 and 2 of this series on atopic dermatitis (AD),1,2 the current putative pathogenesis, scoring systems for severity grading, and epidemiology were reviewed. Part 3 reviews the differential diagnosis, with an emphasis on the difficulty of differentiation from some rare but notable illnesses, as well as the recently expanding data on comorbidities that identify AD as a multisystem disorder with widespread health implications for the patient.
Differential Diagnosis for Pediatric AD
The differential diagnosis for pediatric AD includes chronic dermatoses (eg, seborrheic dermatitis, psoriasis), congenital disorders (eg, Netherton syndrome), malignant diseases (eg, cutaneous T-cell lymphoma [CTCL]), immunodeficiencies, infections, and metabolic disorders.3 Netherton syndrome must be ruled out to prevent extensive drug absorption when treating with topical calcineurin inhibitors (TCIs).4 Due to the presence of bamboo hairs in these patients, a hair mount may aid in the diagnosis of Netherton syndrome. Misdiagnosis of CTCL as AD may complicate the analysis of safety data on TCIs.4,5 Multiple skin biopsies are essential in cases of suspected CTCL to provide an accurate diagnosis. Biopsy can be considered in AD cases with changing and/or unusual morphology, erythrodermic skin changes, and disease that is poorly responsive to multiple therapeutic modalities.
Comorbidities in Pediatric AD
Psychosocial Comorbidities
Pediatric AD often takes a psychological toll on patients as well as household members. Almost half of children with AD are reported to have a severely impaired quality of life (QOL).6 Contributing factors include fatigue, sleep disturbance, activity restriction (eg, inability to participate in sports), and depression.7
Chamlin et al8 developed the Childhood Atopic Dermatitis Impact Scale (CADIS), a 45-item instrument (refined from a 62-item prototype), to measure QOL in young children with AD and their family members. Responses were evaluated with consideration of 5 domains: symptoms and activity limitations/behaviors in children, as well as family/social function, sleep, and emotions in parents. The top 12 factors that parents found most bothersome about AD included itching/scratching, child’s pain/discomfort, sleep issues, embarrassment or worry about appearance, child’s fussiness/irritability/crying/unhappiness, helplessness/can’t control it/predict it, worry about skin infection, dryness of skin/nonsmooth skin, skin bleeding, worry about damage/scars, stares/comments of strangers and other children, and rashes/redness of skin/discoloration. Parents were asked to respond to items about their emotional health and social functioning, such as “My child’s skin condition has strained my relationship with my spouse or partner,” “My child’s skin condition makes me feel sad or depressed,” and “I am bothered by the reaction of strangers to this skin condition.”8
Kiebert et al9 found that AD patients had lower scores on the Short Form-36 Health Survey’s vitality, social functioning, and mental health subscales compared to individuals in the general population. The authors noted that anxiety in AD patients is of particular concern, as stress has been found to trigger the itch-scratch cycle, potentially setting off AD flare-ups.9 Family impact of AD is aggravated by disease severity. Sleeplessness, relationship stress, and time management can all cause family problems in patients with AD.8
In a survey of 3775 older teenagers aged 18 to 19 years (80% response rate out of 4774 prospective participants), 9.7% of participants reported having current AD.10 Suicidal ideation was higher in those with current AD than those without AD (15.5% vs 9.1%). The prevalence of suicidal ideation rose to 23.8% in those with both AD and itch. Diagnosis of AD (as determined through participant responses to the question, ‘‘Do you have, or have you had eczema?’’) was associated with mental health problems in 16.0% of those with AD compared to 10.1% of those without AD, with an especially reduced likelihood of romantic relationships for adolescent boys with AD, as measured using the Strength and Difficulties Questionnaire, which measures 4 problem domains and assesses presence of mental health issues in the past 6 months, and the Hopkins Symptom Checklist 10, which uses 10 questions to measure anxiety and depression symptoms in the past week.10
Dalgard et al11 assessed whether the psychological burden of AD persists in adulthood in an international, multicenter, observational, cross-sectional study conducted in 13 European countries. Each dermatology clinic recruited 250 consecutive adult outpatients to complete a questionnaire along with a control group of 125 hospital employees without skin disease from the same institution but from different departments. The study included a total of 4994 participants (3635 patients and 1359 controls). Clinical depression and anxiety were present in 10.1% and 17.6% of patients, respectively, versus 4.3% and 11.1% of controls, respectively. The prevalence of depression and anxiety was highest in patients with leg ulcers, hand eczema, psoriasis, and AD.11 This study demonstrated that the psychological comorbidities of childhood conditions such as AD may persist into adulthood.
Lymphoma
In a systematic review of the literature and a separate meta-analysis, Legendre et al12 identified a slight increase in lymphoma among AD patients, with an uncertain but potential increase associated with topical corticosteroid application. This finding is similar to trends seen in other systemic inflammatory conditions that involve the skin, such as psoriasis, and is felt to relate to long-term inflammation.
Obesity
Obesity has been associated with a greater risk for moderate to severe AD in children.13,14
Infections
Children with AD are at a higher risk for cutaneous infections and generalization of these infections. The leading infections would be with Staphylococcus aureus, but group A streptococci infections do occur. Herpes simplex virus, vaccinia virus or Kaposi varicelliform eruption (KVE), molluscum with or without dermatitis, and fungal infections occur less commonly but with greater morbidity, largely due to the impaired barrier and some innate reduction in cutaneous immunity.15
Atopic dermatitis in children also is associated with a higher prevalence of extracutaneous infections such as influenza, pneumonia, urinary tract infections, varicella-zoster virus, recurrent ear infections, sinus infections, sore throat, and head or chest colds.16 Children with AD and warts (human papillomavirus infection) have an even greater risk for these comorbidities.17 Warts and molluscum infections may become more extensive in children with AD.18 Generalization of herpetic infections occurs more easily in AD patients due to the impaired skin barrier, which includes generalized skin surface extension of herpes simplex virus type 1, varicella-zoster virus, and historically smallpox. A similar clinical appearance of generalized vesiculopustular lesions with fever can be seen when coxsackievirus A6 infections occur in AD patients; these conditions are called eczema herpeticum due to herpes simplex virus, KVE due to varicella-zoster virus and smallpox, and eczema coxsackium due to coxsackievirus A6,19 though some authors refer to all of these as KVE.20 These generalized viral illnesses overlying AD often result in fever, malaise, pain, and life-threatening skin denudation with risk for dehydration and superinfection with S aureus.7,18 It has been shown that the occurrence of eczema herpeticum in AD is associated with and may be caused by an inability to induce human β-defensin 2 and 3 as well as cathelicidin.21
Staphylococcus aureus colonization has been noted in 90% to 100% of AD cases, which can be associated with a higher eczema area and severity index score.22-24 The role of S aureus in AD includes flare triggering through release of superantigens, leading to IL-31–induced pruritis.25 Recurrent infection with either methicillin-sensitive or methicillin-resistant S aureus has been noted in AD.18,26 Skin infections also occur in AD and appear as erosions and pustules, and coinfection with Streptococcus and Staphylococcus does occur; therefore, cultures often are needed to determine the type of bacteria present on the skin in severe cases and when infection is suspected.27 Perianal bacterial dermatitis is a variant of infected AD occurring in the anal/groin area that is associated with S aureus and/or streptococcal superinfection in which topical corticosteroids and topical anti-infectives can be used. In some severe cases, oral antibiotics may be needed.28
Injury/Hyperactivity
Children aged 0 to 5 years with AD carry an increased risk for injuries requiring medical attention, with association in part due to attention deficit disorder, depression, and anxiety. Antihistamines are believed to aggravate this issue by promoting daytime somnolence29; however, pruritus-induced sleep disturbances in AD also may be responsible for daytime somnolence.30
Contact Allergy and Sensitization
Children with AD may become sensitized to environmental allergens through delayed-type hypersensitivity. The presumed mechanism is that these agents include ingredients added into applied medicaments and application occurs over an impaired skin barrier allowing for absorption and greater risk of antigen presentation. Approximately 50% of children with difficult-to-control AD will react to 1 or more epicutaneous allergens, and patch testing can be performed to identify relevant allergens that can improve skin severity.7 Severe dermatitis and id generalized hypersensitivity reactions in patients with AD and nickel allergic contact dermatitis have been described and may aggravate underlying AD.31
Family Burden of AD
Parents or caregivers of children with moderate and severe AD spend nearly 3 hours a day caring for their child’s skin and experience QOL impairments including lack of sleep and/or privacy, often due to cosleeping; treatment-related financial expenditures; and feelings of hopelessness, guilt, and depression.7
Steroid Phobia
Steroid phobia is the fear of topical application of corticosteroids resulting in systemic side effects including unrealistic fears (eg, fear that the child will develop muscles such as an anabolic steroid user) as well as realistic but statistically low-risk fears (eg, fear of systemic absorption). These fears often result in underutilization of prescribed topical corticosteroid therapies and undertreatment of children with AD.32,33
Financial Burden
The cost of AD can be high in the United States, with adult data demonstrating costs ranging from $371 to $489 per person.34 The last published cost data for pediatric AD was from 2003, with an average cost of $219 per year.35 Costs include time lost from work, household purchases (eg, skin care products), and co-pays for visits and medication, with an estimated average expenditure per person (SE) of $601.06 ($137.26) annually in 2012.36 The cost of ambulatory care and emergency department visits for AD in children in the United States in 1993 was estimated at $364 million.37-39 In 2002, Ellis et al40 estimated the overall cost of AD to be between $900 million and $3.8 billion in the United States (1997-1998) based on projections from claims, prescriptions, and comorbidities reported to a private insurer and Medicaid. Ellis et al41 further determined that topical tacrolimus was similar in cost to high-potency corticosteroids.
Pediatric AD often progresses to adult hand eczema and leads to further morbidity, especially in health care workers.42 Kemp43 reviewed the cost of AD in children and concluded that AD was a condition with major handicap with personal, financial, and social effects. A cost review of studies conducted in 163,700 children with AD showed that costs related to AD totaled $316.7 million per year. The author concluded that there were substantial psychosocial and financial stresses associated with pediatric AD but no clear path to potential reduction in related costs.43
Sleep Disturbances
Sleep disturbances are common in pediatric AD patients. Pruritus usually is exacerbated at bedtime due to reduced humidity and lack of distractions to prevent scratching. Sleep deprivation has a substantial impact on both the patient and his/her household. Parental frustration increases with sleep disturbance.18,44 Sleep deprivation is associated with greater severity, both because it is one of the most difficult aspects of illness and because the associated pruritus makes for greater damage done to the skin through injurious scratching.
Sleep disturbances also may interfere with growth and overnight release of growth hormones.18,44 This latter issue can result in reduced linear growth velocity. Furthermore, sleep deprivation can cause increased risk of accidents and poor school performance.18,44,45
Many children do not outgrow AD. In adults, AD-associated sleep deprivation has been shown to have an association with fatigue, regular daytime sleepiness, and regular insomnia, correlating to number of sick days, doctor visits, and poorer overall health status.45
Inadequate Disease Control
Inadequate disease control has been described by Eichenfeld46 as an important issue in AD at this time. Untreated, undertreated, and improperly treated AD are important issues affecting long-term AD care. He further cited steroid phobia as a contributor to undertreatment.46 Fleischer47 has cited the black box warning present on TCIs as a further deterrent to adequate therapeutic control in our current therapeutic paradigm. Undertreatment may result in uncontrolled disease activity, impaired QOL, infections, and sleep disturbances. The role of undertreatment as a driver of the atopic march is unknown.
Conclusion
Atopic dermatitis is a multisystem disorder that has wide-reaching comorbidities and may mimic a variety of skin conditions. The topic of comorbidities is new and emerging and bears further review to define risk factors, prevention strategies, and long-term monitoring requirements.
In parts 1 and 2 of this series on atopic dermatitis (AD),1,2 the current putative pathogenesis, scoring systems for severity grading, and epidemiology were reviewed. Part 3 reviews the differential diagnosis, with an emphasis on the difficulty of differentiation from some rare but notable illnesses, as well as the recently expanding data on comorbidities that identify AD as a multisystem disorder with widespread health implications for the patient.
Differential Diagnosis for Pediatric AD
The differential diagnosis for pediatric AD includes chronic dermatoses (eg, seborrheic dermatitis, psoriasis), congenital disorders (eg, Netherton syndrome), malignant diseases (eg, cutaneous T-cell lymphoma [CTCL]), immunodeficiencies, infections, and metabolic disorders.3 Netherton syndrome must be ruled out to prevent extensive drug absorption when treating with topical calcineurin inhibitors (TCIs).4 Due to the presence of bamboo hairs in these patients, a hair mount may aid in the diagnosis of Netherton syndrome. Misdiagnosis of CTCL as AD may complicate the analysis of safety data on TCIs.4,5 Multiple skin biopsies are essential in cases of suspected CTCL to provide an accurate diagnosis. Biopsy can be considered in AD cases with changing and/or unusual morphology, erythrodermic skin changes, and disease that is poorly responsive to multiple therapeutic modalities.
Comorbidities in Pediatric AD
Psychosocial Comorbidities
Pediatric AD often takes a psychological toll on patients as well as household members. Almost half of children with AD are reported to have a severely impaired quality of life (QOL).6 Contributing factors include fatigue, sleep disturbance, activity restriction (eg, inability to participate in sports), and depression.7
Chamlin et al8 developed the Childhood Atopic Dermatitis Impact Scale (CADIS), a 45-item instrument (refined from a 62-item prototype), to measure QOL in young children with AD and their family members. Responses were evaluated with consideration of 5 domains: symptoms and activity limitations/behaviors in children, as well as family/social function, sleep, and emotions in parents. The top 12 factors that parents found most bothersome about AD included itching/scratching, child’s pain/discomfort, sleep issues, embarrassment or worry about appearance, child’s fussiness/irritability/crying/unhappiness, helplessness/can’t control it/predict it, worry about skin infection, dryness of skin/nonsmooth skin, skin bleeding, worry about damage/scars, stares/comments of strangers and other children, and rashes/redness of skin/discoloration. Parents were asked to respond to items about their emotional health and social functioning, such as “My child’s skin condition has strained my relationship with my spouse or partner,” “My child’s skin condition makes me feel sad or depressed,” and “I am bothered by the reaction of strangers to this skin condition.”8
Kiebert et al9 found that AD patients had lower scores on the Short Form-36 Health Survey’s vitality, social functioning, and mental health subscales compared to individuals in the general population. The authors noted that anxiety in AD patients is of particular concern, as stress has been found to trigger the itch-scratch cycle, potentially setting off AD flare-ups.9 Family impact of AD is aggravated by disease severity. Sleeplessness, relationship stress, and time management can all cause family problems in patients with AD.8
In a survey of 3775 older teenagers aged 18 to 19 years (80% response rate out of 4774 prospective participants), 9.7% of participants reported having current AD.10 Suicidal ideation was higher in those with current AD than those without AD (15.5% vs 9.1%). The prevalence of suicidal ideation rose to 23.8% in those with both AD and itch. Diagnosis of AD (as determined through participant responses to the question, ‘‘Do you have, or have you had eczema?’’) was associated with mental health problems in 16.0% of those with AD compared to 10.1% of those without AD, with an especially reduced likelihood of romantic relationships for adolescent boys with AD, as measured using the Strength and Difficulties Questionnaire, which measures 4 problem domains and assesses presence of mental health issues in the past 6 months, and the Hopkins Symptom Checklist 10, which uses 10 questions to measure anxiety and depression symptoms in the past week.10
Dalgard et al11 assessed whether the psychological burden of AD persists in adulthood in an international, multicenter, observational, cross-sectional study conducted in 13 European countries. Each dermatology clinic recruited 250 consecutive adult outpatients to complete a questionnaire along with a control group of 125 hospital employees without skin disease from the same institution but from different departments. The study included a total of 4994 participants (3635 patients and 1359 controls). Clinical depression and anxiety were present in 10.1% and 17.6% of patients, respectively, versus 4.3% and 11.1% of controls, respectively. The prevalence of depression and anxiety was highest in patients with leg ulcers, hand eczema, psoriasis, and AD.11 This study demonstrated that the psychological comorbidities of childhood conditions such as AD may persist into adulthood.
Lymphoma
In a systematic review of the literature and a separate meta-analysis, Legendre et al12 identified a slight increase in lymphoma among AD patients, with an uncertain but potential increase associated with topical corticosteroid application. This finding is similar to trends seen in other systemic inflammatory conditions that involve the skin, such as psoriasis, and is felt to relate to long-term inflammation.
Obesity
Obesity has been associated with a greater risk for moderate to severe AD in children.13,14
Infections
Children with AD are at a higher risk for cutaneous infections and generalization of these infections. The leading infections would be with Staphylococcus aureus, but group A streptococci infections do occur. Herpes simplex virus, vaccinia virus or Kaposi varicelliform eruption (KVE), molluscum with or without dermatitis, and fungal infections occur less commonly but with greater morbidity, largely due to the impaired barrier and some innate reduction in cutaneous immunity.15
Atopic dermatitis in children also is associated with a higher prevalence of extracutaneous infections such as influenza, pneumonia, urinary tract infections, varicella-zoster virus, recurrent ear infections, sinus infections, sore throat, and head or chest colds.16 Children with AD and warts (human papillomavirus infection) have an even greater risk for these comorbidities.17 Warts and molluscum infections may become more extensive in children with AD.18 Generalization of herpetic infections occurs more easily in AD patients due to the impaired skin barrier, which includes generalized skin surface extension of herpes simplex virus type 1, varicella-zoster virus, and historically smallpox. A similar clinical appearance of generalized vesiculopustular lesions with fever can be seen when coxsackievirus A6 infections occur in AD patients; these conditions are called eczema herpeticum due to herpes simplex virus, KVE due to varicella-zoster virus and smallpox, and eczema coxsackium due to coxsackievirus A6,19 though some authors refer to all of these as KVE.20 These generalized viral illnesses overlying AD often result in fever, malaise, pain, and life-threatening skin denudation with risk for dehydration and superinfection with S aureus.7,18 It has been shown that the occurrence of eczema herpeticum in AD is associated with and may be caused by an inability to induce human β-defensin 2 and 3 as well as cathelicidin.21
Staphylococcus aureus colonization has been noted in 90% to 100% of AD cases, which can be associated with a higher eczema area and severity index score.22-24 The role of S aureus in AD includes flare triggering through release of superantigens, leading to IL-31–induced pruritis.25 Recurrent infection with either methicillin-sensitive or methicillin-resistant S aureus has been noted in AD.18,26 Skin infections also occur in AD and appear as erosions and pustules, and coinfection with Streptococcus and Staphylococcus does occur; therefore, cultures often are needed to determine the type of bacteria present on the skin in severe cases and when infection is suspected.27 Perianal bacterial dermatitis is a variant of infected AD occurring in the anal/groin area that is associated with S aureus and/or streptococcal superinfection in which topical corticosteroids and topical anti-infectives can be used. In some severe cases, oral antibiotics may be needed.28
Injury/Hyperactivity
Children aged 0 to 5 years with AD carry an increased risk for injuries requiring medical attention, with association in part due to attention deficit disorder, depression, and anxiety. Antihistamines are believed to aggravate this issue by promoting daytime somnolence29; however, pruritus-induced sleep disturbances in AD also may be responsible for daytime somnolence.30
Contact Allergy and Sensitization
Children with AD may become sensitized to environmental allergens through delayed-type hypersensitivity. The presumed mechanism is that these agents include ingredients added into applied medicaments and application occurs over an impaired skin barrier allowing for absorption and greater risk of antigen presentation. Approximately 50% of children with difficult-to-control AD will react to 1 or more epicutaneous allergens, and patch testing can be performed to identify relevant allergens that can improve skin severity.7 Severe dermatitis and id generalized hypersensitivity reactions in patients with AD and nickel allergic contact dermatitis have been described and may aggravate underlying AD.31
Family Burden of AD
Parents or caregivers of children with moderate and severe AD spend nearly 3 hours a day caring for their child’s skin and experience QOL impairments including lack of sleep and/or privacy, often due to cosleeping; treatment-related financial expenditures; and feelings of hopelessness, guilt, and depression.7
Steroid Phobia
Steroid phobia is the fear of topical application of corticosteroids resulting in systemic side effects including unrealistic fears (eg, fear that the child will develop muscles such as an anabolic steroid user) as well as realistic but statistically low-risk fears (eg, fear of systemic absorption). These fears often result in underutilization of prescribed topical corticosteroid therapies and undertreatment of children with AD.32,33
Financial Burden
The cost of AD can be high in the United States, with adult data demonstrating costs ranging from $371 to $489 per person.34 The last published cost data for pediatric AD was from 2003, with an average cost of $219 per year.35 Costs include time lost from work, household purchases (eg, skin care products), and co-pays for visits and medication, with an estimated average expenditure per person (SE) of $601.06 ($137.26) annually in 2012.36 The cost of ambulatory care and emergency department visits for AD in children in the United States in 1993 was estimated at $364 million.37-39 In 2002, Ellis et al40 estimated the overall cost of AD to be between $900 million and $3.8 billion in the United States (1997-1998) based on projections from claims, prescriptions, and comorbidities reported to a private insurer and Medicaid. Ellis et al41 further determined that topical tacrolimus was similar in cost to high-potency corticosteroids.
Pediatric AD often progresses to adult hand eczema and leads to further morbidity, especially in health care workers.42 Kemp43 reviewed the cost of AD in children and concluded that AD was a condition with major handicap with personal, financial, and social effects. A cost review of studies conducted in 163,700 children with AD showed that costs related to AD totaled $316.7 million per year. The author concluded that there were substantial psychosocial and financial stresses associated with pediatric AD but no clear path to potential reduction in related costs.43
Sleep Disturbances
Sleep disturbances are common in pediatric AD patients. Pruritus usually is exacerbated at bedtime due to reduced humidity and lack of distractions to prevent scratching. Sleep deprivation has a substantial impact on both the patient and his/her household. Parental frustration increases with sleep disturbance.18,44 Sleep deprivation is associated with greater severity, both because it is one of the most difficult aspects of illness and because the associated pruritus makes for greater damage done to the skin through injurious scratching.
Sleep disturbances also may interfere with growth and overnight release of growth hormones.18,44 This latter issue can result in reduced linear growth velocity. Furthermore, sleep deprivation can cause increased risk of accidents and poor school performance.18,44,45
Many children do not outgrow AD. In adults, AD-associated sleep deprivation has been shown to have an association with fatigue, regular daytime sleepiness, and regular insomnia, correlating to number of sick days, doctor visits, and poorer overall health status.45
Inadequate Disease Control
Inadequate disease control has been described by Eichenfeld46 as an important issue in AD at this time. Untreated, undertreated, and improperly treated AD are important issues affecting long-term AD care. He further cited steroid phobia as a contributor to undertreatment.46 Fleischer47 has cited the black box warning present on TCIs as a further deterrent to adequate therapeutic control in our current therapeutic paradigm. Undertreatment may result in uncontrolled disease activity, impaired QOL, infections, and sleep disturbances. The role of undertreatment as a driver of the atopic march is unknown.
Conclusion
Atopic dermatitis is a multisystem disorder that has wide-reaching comorbidities and may mimic a variety of skin conditions. The topic of comorbidities is new and emerging and bears further review to define risk factors, prevention strategies, and long-term monitoring requirements.
- Silverberg NB. A practical overview of pediatric atopic dermatitis, part 1: epidemiology and pathogenesis. Cutis. 2016;97:267-271.
- Silverberg NB. A practical overview of pediatric atopic dermatitis, part 2: triggers and grading. Cutis. 2016;97:326-329.
- Siegfried EC, Hebert AA. Diagnosis of atopic dermatitis: mimics, overlaps, and complications. J Clin Med. 2015;4:884-917.
- Allen A, Siegfried E, Silverman R, et al. Significant absorption of topical tacrolimus in 3 patients with Netherton syndrome. Arch Dermatol. 2001;137:747-750.
- Carr WW. Topical calcineurin inhibitors for atopic dermatitis: review and treatment recommendations. Paediatr Drugs. 2013;15:303-310.
- Chamlin SL, Lai JS, Cella D, et al. Childhood Atopic Dermatitis Impact Scale: reliability, discriminative and concurrent validity, and responsiveness. Arch Dermatol. 2007;143:768-772.
- Tollefson MM, Bruckner AL. Atopic dermatitis: skin-directed management. Pediatrics. 2014;134:E1735-E1744.
- Chamlin SL, Cella D, Frieden IJ, et al. Development of the Childhood Atopic Dermatitis Impact Scale: initial validation of a quality-of-life measure for young children with atopic dermatitis and their families. J Invest Dermatol. 2005;125:1106-1111.
- Kiebert G, Sorensen SV, Revicki D, et al. Atopic dermatitis is associated with a decrement in health-related quality of life. Int J Dermatol. 2002;41:151-158.
- Halvorsen JA, Lien L, Dalgard F, et al. Suicidal ideation, mental health problems, and social function in adolescents with eczema: a population-based study. J Invest Dermatol. 2014;134:1847-1854.
- Dalgard FJ, Gieler U, Tomas-Aragones L, et al. The psychological burden of skin diseases: a cross-sectional multicenter study among dermatological out-patients in 13 European countries. J Invest Dermatol. 2015;135:984-991.
- Legendre L, Barnetche T, Mazereeuw-Hautier J, et al. Risk of lymphoma in patients with atopic dermatitis and the role of topical treatment: a systematic review and meta-analysis. J Am Acad Dermatol. 2015;72:992-1002.
- Koutroulis I, Magnelli L, Gaughan J, et al. Atopic dermatitis is more severe in children over the age of two who have an increased body mass index. Acta Paediatr. 2015;104:713-717.
- Silverberg JI, Becker L, Kwasny M, et al. Central obesity and high blood pressure in pediatric patients with atopic dermatitis. JAMA Dermatol. 2015;151:144-152.
- De D, Kanwar AJ, Handa S. Comparative efficacy of Hanifin and Rajka’s criteria and the UK working party’s diagnostic criteria in diagnosis of atopic dermatitis in a hospital setting in North India. J Eur Acad Dermatol Venereol. 2006;20:853-859.
- Silverberg JI, Silverberg NB. Childhood atopic dermatitis and warts are associated with increased risk of infection: a US population-based study [published online October 4, 2013]. J Allergy Clin Immunol. 2014;133:1041-1047.
- Silverberg J, Garg N, Silverberg NB. New developments in comorbidities of atopic dermatitis. Cutis. 2014;93:222-224.
- Kiken DA, Silverberg NB. Atopic dermatitis in children, part 1: epidemiology, clinical features, and complications. Cutis. 2006;78:241-247.
- Mathes EF, Oza V, Frieden IJ, et al. “Eczema coxsackium” and unusual cutaneous findings in an enterovirus outbreak. Pediatrics. 2013;132:E149-E157.
- Vora RV, Pilani AP, Jivani NB, et al. Kaposi varicelliform eruption. Indian Dermatol Online J. 2015;6:364-366.
- Hata TR, Kotol P, Boguniewicz M, et al. History of eczema herpeticum is associated with the inability to induce human β-defensin (HBD)-2, HBD-3 and cathelicidin in the skin of patients with atopic dermatitis. Br J Dermatol. 2010;163:659-661.
- Abeck D, Mempel M. Staphylococcus aureus colonization in atopic dermatitis and its therapeutic implications. Br J Dermatol. 1998;139:13-16.
- Leyden JJ, Marples RR, Kligman AM. Staphylococcus aureus in the lesions of atopic dermatitis. Br J Dermatol. 1974;90:525-530.
- Lipnharski C, d’Azevedo PA, Quinto VP, et al. Colonization by S. aureus increases the EASI and the number of appointments by patients with atopic dermatitis: cohort with 93 patients. An Bras Dermatol. 2013;88:518-521.
- Paller AS. Latest approaches to treating atopic dermatitis. Chem Immunol Allergy. 2012;96:132-140.
- Groner A, Laing-Grayman D, Silverberg NB. Outpatient pediatric community-acquired methicillin-resistant Staphylococcus aureus: a polymorphous clinical disease. Cutis. 2008;81:115-122.
- Sugarman JL, Hersh AL, Okamura T, et al. A retrospective review of streptococcal infections in pediatric atopic dermatitis. Pediatr Dermatol. 2011;28:230-234.
- Heath C, Desai N, Silverberg NB. Recent microbiological shifts in perianal bacterial dermatitis: Staphylococcus aureus predominance. Pediatr Dermatol. 2009;26:696-700.
- Garg N, Silverberg JI. Association between childhood allergic disease, psychological comorbidity, and injury requiring medical attention. Ann Allergy Asthma Immunol. 2014;112:525-532.
- Lavery MJ, Stull C, Kinney MO, et al. Nocturnal pruritus: the battle for a peaceful night’s sleep. Int J Mol Sci. 2016;17:E425.
- Silverberg NB, Licht J, Friedler S, et al. Nickel contact hypersensitivity in children. Pediatr Dermatol. 2002;19:110-113.
- Aubert-Wastiaux H, Moret L, Le Rhun A, et al. Topical corticosteroid phobia in atopic dermatitis: a study of its nature, origins and frequency. Br J Dermatol. 2011;165:808-814.
- Kojima R, Fujiwara T, Matsuda A, et al. Factors associated with steroid phobia in caregivers of children with atopic dermatitis. Pediatr Dermatol. 2013;30:29-35.
- Silverberg JI. Health care utilization, patient costs, and access to care in US adults with eczema: a population-based study. JAMA Dermatol. 2015;151:743-752.
- Weinmann S, Kamtsiuris P, Henke KD, et al. The costs of atopy and asthma in children: assessment of direct costs and their determinants in a birth cohort. Pediatr Allergy Immunol. 2003;14:18-26.
- Fivenson D, Arnold RJ, Kaniecki DJ, et al. The effect of atopic dermatitis on total burden of illness and quality of life on adults and children in a large managed care organization. J Manag Care Pharm. 2002;8:333-342.
- Verboom P, Hakkaart-Van L, Sturkenboom M, et al. The cost of atopic dermatitis in the Netherlands: an international comparison. Br J Dermatol. 2002;147:716-724.
- Lapidus CS, Schwarz DF, Honig PJ. Atopic dermatitis in children: who cares? who pays? J Am Acad Dermatol. 1993;28:699-703.
- Carroll CL, Balkrishnan R, Feldman SR, et al. The burden of atopic dermatitis: impact on the patient, family, and society. Pediatr Dermatol. 2005;22:192-199.
- Ellis CN, Drake LA, Prendergast MM, et al. Cost of atopic dermatitis and eczema in the United States. J Am Acad Dermatol. 2002;46:361-370.
- Ellis CN, Prendergast MM, Tokar M, et al. Quantifying costs associated with atopic dermatitis. J Manag Care Pharm. 2003;9:278.
- Lee SW, Cheong SH, Byun JY, et al. Occupational hand eczema among nursing staffs in Korea: self-reported hand eczema and contact sensitization of hospital nursing staffs. J Dermatol. 2013;40:182-187.
- Kemp AS. Cost of illness of atopic dermatitis in children: a societal perspective. Pharmacoeconomics. 2003;21:105-113.
- Munro DD. Topical corticosteroid therapy and its effect on the hypothalamic-pituitary-adrenal axis. Dermatologica. 1976;152:173-180.
- Silverberg JI, Garg NK, Paller AS, et al. Sleep disturbances in adults with eczema are associated with impaired overall health: a US population-based study. J Invest Dermatol. 2015;135:56-66.
- Eichenfield LF. Improving outcomes in atopic dermatitis. for advances in dermatology. Dermatology Focus. 2015;34:1-6.
- Fleischer AB Jr. Black box warning for topical calcineurin inhibitors and the death of common sense. Dermatol Online J. 2006;12:2.
- Silverberg NB. A practical overview of pediatric atopic dermatitis, part 1: epidemiology and pathogenesis. Cutis. 2016;97:267-271.
- Silverberg NB. A practical overview of pediatric atopic dermatitis, part 2: triggers and grading. Cutis. 2016;97:326-329.
- Siegfried EC, Hebert AA. Diagnosis of atopic dermatitis: mimics, overlaps, and complications. J Clin Med. 2015;4:884-917.
- Allen A, Siegfried E, Silverman R, et al. Significant absorption of topical tacrolimus in 3 patients with Netherton syndrome. Arch Dermatol. 2001;137:747-750.
- Carr WW. Topical calcineurin inhibitors for atopic dermatitis: review and treatment recommendations. Paediatr Drugs. 2013;15:303-310.
- Chamlin SL, Lai JS, Cella D, et al. Childhood Atopic Dermatitis Impact Scale: reliability, discriminative and concurrent validity, and responsiveness. Arch Dermatol. 2007;143:768-772.
- Tollefson MM, Bruckner AL. Atopic dermatitis: skin-directed management. Pediatrics. 2014;134:E1735-E1744.
- Chamlin SL, Cella D, Frieden IJ, et al. Development of the Childhood Atopic Dermatitis Impact Scale: initial validation of a quality-of-life measure for young children with atopic dermatitis and their families. J Invest Dermatol. 2005;125:1106-1111.
- Kiebert G, Sorensen SV, Revicki D, et al. Atopic dermatitis is associated with a decrement in health-related quality of life. Int J Dermatol. 2002;41:151-158.
- Halvorsen JA, Lien L, Dalgard F, et al. Suicidal ideation, mental health problems, and social function in adolescents with eczema: a population-based study. J Invest Dermatol. 2014;134:1847-1854.
- Dalgard FJ, Gieler U, Tomas-Aragones L, et al. The psychological burden of skin diseases: a cross-sectional multicenter study among dermatological out-patients in 13 European countries. J Invest Dermatol. 2015;135:984-991.
- Legendre L, Barnetche T, Mazereeuw-Hautier J, et al. Risk of lymphoma in patients with atopic dermatitis and the role of topical treatment: a systematic review and meta-analysis. J Am Acad Dermatol. 2015;72:992-1002.
- Koutroulis I, Magnelli L, Gaughan J, et al. Atopic dermatitis is more severe in children over the age of two who have an increased body mass index. Acta Paediatr. 2015;104:713-717.
- Silverberg JI, Becker L, Kwasny M, et al. Central obesity and high blood pressure in pediatric patients with atopic dermatitis. JAMA Dermatol. 2015;151:144-152.
- De D, Kanwar AJ, Handa S. Comparative efficacy of Hanifin and Rajka’s criteria and the UK working party’s diagnostic criteria in diagnosis of atopic dermatitis in a hospital setting in North India. J Eur Acad Dermatol Venereol. 2006;20:853-859.
- Silverberg JI, Silverberg NB. Childhood atopic dermatitis and warts are associated with increased risk of infection: a US population-based study [published online October 4, 2013]. J Allergy Clin Immunol. 2014;133:1041-1047.
- Silverberg J, Garg N, Silverberg NB. New developments in comorbidities of atopic dermatitis. Cutis. 2014;93:222-224.
- Kiken DA, Silverberg NB. Atopic dermatitis in children, part 1: epidemiology, clinical features, and complications. Cutis. 2006;78:241-247.
- Mathes EF, Oza V, Frieden IJ, et al. “Eczema coxsackium” and unusual cutaneous findings in an enterovirus outbreak. Pediatrics. 2013;132:E149-E157.
- Vora RV, Pilani AP, Jivani NB, et al. Kaposi varicelliform eruption. Indian Dermatol Online J. 2015;6:364-366.
- Hata TR, Kotol P, Boguniewicz M, et al. History of eczema herpeticum is associated with the inability to induce human β-defensin (HBD)-2, HBD-3 and cathelicidin in the skin of patients with atopic dermatitis. Br J Dermatol. 2010;163:659-661.
- Abeck D, Mempel M. Staphylococcus aureus colonization in atopic dermatitis and its therapeutic implications. Br J Dermatol. 1998;139:13-16.
- Leyden JJ, Marples RR, Kligman AM. Staphylococcus aureus in the lesions of atopic dermatitis. Br J Dermatol. 1974;90:525-530.
- Lipnharski C, d’Azevedo PA, Quinto VP, et al. Colonization by S. aureus increases the EASI and the number of appointments by patients with atopic dermatitis: cohort with 93 patients. An Bras Dermatol. 2013;88:518-521.
- Paller AS. Latest approaches to treating atopic dermatitis. Chem Immunol Allergy. 2012;96:132-140.
- Groner A, Laing-Grayman D, Silverberg NB. Outpatient pediatric community-acquired methicillin-resistant Staphylococcus aureus: a polymorphous clinical disease. Cutis. 2008;81:115-122.
- Sugarman JL, Hersh AL, Okamura T, et al. A retrospective review of streptococcal infections in pediatric atopic dermatitis. Pediatr Dermatol. 2011;28:230-234.
- Heath C, Desai N, Silverberg NB. Recent microbiological shifts in perianal bacterial dermatitis: Staphylococcus aureus predominance. Pediatr Dermatol. 2009;26:696-700.
- Garg N, Silverberg JI. Association between childhood allergic disease, psychological comorbidity, and injury requiring medical attention. Ann Allergy Asthma Immunol. 2014;112:525-532.
- Lavery MJ, Stull C, Kinney MO, et al. Nocturnal pruritus: the battle for a peaceful night’s sleep. Int J Mol Sci. 2016;17:E425.
- Silverberg NB, Licht J, Friedler S, et al. Nickel contact hypersensitivity in children. Pediatr Dermatol. 2002;19:110-113.
- Aubert-Wastiaux H, Moret L, Le Rhun A, et al. Topical corticosteroid phobia in atopic dermatitis: a study of its nature, origins and frequency. Br J Dermatol. 2011;165:808-814.
- Kojima R, Fujiwara T, Matsuda A, et al. Factors associated with steroid phobia in caregivers of children with atopic dermatitis. Pediatr Dermatol. 2013;30:29-35.
- Silverberg JI. Health care utilization, patient costs, and access to care in US adults with eczema: a population-based study. JAMA Dermatol. 2015;151:743-752.
- Weinmann S, Kamtsiuris P, Henke KD, et al. The costs of atopy and asthma in children: assessment of direct costs and their determinants in a birth cohort. Pediatr Allergy Immunol. 2003;14:18-26.
- Fivenson D, Arnold RJ, Kaniecki DJ, et al. The effect of atopic dermatitis on total burden of illness and quality of life on adults and children in a large managed care organization. J Manag Care Pharm. 2002;8:333-342.
- Verboom P, Hakkaart-Van L, Sturkenboom M, et al. The cost of atopic dermatitis in the Netherlands: an international comparison. Br J Dermatol. 2002;147:716-724.
- Lapidus CS, Schwarz DF, Honig PJ. Atopic dermatitis in children: who cares? who pays? J Am Acad Dermatol. 1993;28:699-703.
- Carroll CL, Balkrishnan R, Feldman SR, et al. The burden of atopic dermatitis: impact on the patient, family, and society. Pediatr Dermatol. 2005;22:192-199.
- Ellis CN, Drake LA, Prendergast MM, et al. Cost of atopic dermatitis and eczema in the United States. J Am Acad Dermatol. 2002;46:361-370.
- Ellis CN, Prendergast MM, Tokar M, et al. Quantifying costs associated with atopic dermatitis. J Manag Care Pharm. 2003;9:278.
- Lee SW, Cheong SH, Byun JY, et al. Occupational hand eczema among nursing staffs in Korea: self-reported hand eczema and contact sensitization of hospital nursing staffs. J Dermatol. 2013;40:182-187.
- Kemp AS. Cost of illness of atopic dermatitis in children: a societal perspective. Pharmacoeconomics. 2003;21:105-113.
- Munro DD. Topical corticosteroid therapy and its effect on the hypothalamic-pituitary-adrenal axis. Dermatologica. 1976;152:173-180.
- Silverberg JI, Garg NK, Paller AS, et al. Sleep disturbances in adults with eczema are associated with impaired overall health: a US population-based study. J Invest Dermatol. 2015;135:56-66.
- Eichenfield LF. Improving outcomes in atopic dermatitis. for advances in dermatology. Dermatology Focus. 2015;34:1-6.
- Fleischer AB Jr. Black box warning for topical calcineurin inhibitors and the death of common sense. Dermatol Online J. 2006;12:2.
Practice Points
- Atopic dermatitis (AD) has a variety of comorbidities including psychosocial disorders, obesity, and infection.
- A variety of skin conditions can mimic AD.
- Atopic dermatitis can be complicated by coinfections.

Large plaques on a baby boy
A 25-year-old G2P1 mother gave birth to a boy at 40 and 6/7 weeks by vaginal delivery. Labor was induced because of oligohydramnios complicated by chorioamnionitis. The mother was treated with vancomycin and gentamicin. Prenatal lab work and delivery were otherwise unremarkable.
The delivering physician (CG) noted that the neonate had numerous brown, red, and black plaques distributed over his abdomen, lower back, groin, and thighs (FIGURE). Some plaques were hypertrichotic and other areas, apart from the plaques, were thinly desquamated. Apgar scores were 8 and 9 and the remainder of the exam, including the neurologic exam, was normal. The Dermatology Service (JK) was consulted.

WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Giant congenital nevus
Congenital melanocytic nevi (CMN) are pigmented lesions that are present at birth and created by the abnormal migration of neural crest cells during embryogenesis.1 Nevi are categorized by size as small (<1.5 cm), medium (1.5-20 cm), large (>20 cm), and giant (>40 cm).2 Congenital nevi tend to start out flat, with uniform pigmentation, but can become more variegated in texture and color as normal growth and development continue. Giant congenital nevi are likely to thicken, darken, and enlarge as the patient grows. Some nevi may develop very coarse or dark hair.
CMN can cover any part of the body and occur independent of skin color and other ethnic factors.3 Giant congenital nevi are rare, with an incidence of approximately one in 50,000 live births and with males and females equally affected.3,4 The condition is diagnosed at birth, based on the appearance of the lesions.
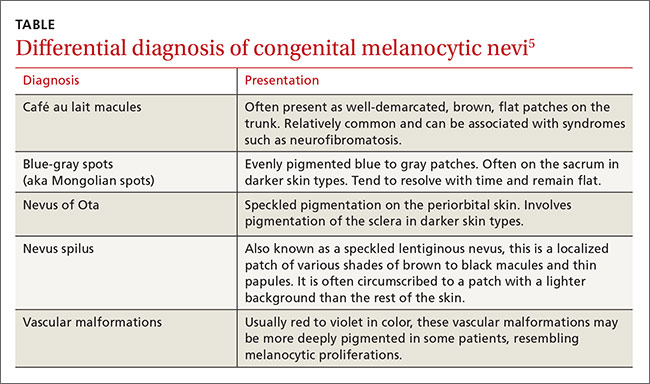
The differential diagnosis for CMN includes café au lait macules, blue-gray spots (aka Mongolian spots), nevus of Ota, nevus spilus, and vascular malformations (TABLE).5 CMN may present in almost any location and may be brown, black, pink, or purple in color. Café au lait macules, blue-gray spots, nevus of Ota, nevus spilus, and vascular malformations have individual location and color characteristics that set them apart clinically.
Monitor patients for melanoma, CNS complications
Patients with CMN are at increased risk of neurocutaneous melanosis (NCM) and cutaneous melanoma.
Neurocutaneous melanosis, a complication of giant congenital nevi, is a melanocyte proliferation in the central nervous system (CNS). Between 6% and 11% of patients with giant congenital nevi develop symptomatic NCM in childhood. Thus, any CNS symptoms should be fully evaluated.4,6 NCM can result in seizures, cranial nerve palsy, hydrocephalus, and leptomeningeal melanoma.
Besides giant congenital nevi, risk factors for NCM include male sex, large numbers of satellite nevi, and the presence of nevi over the posterior midline or head and neck.7 The prognosis is poor for patients who develop neurologic symptoms. NCM is associated with other malignancies, including rhadomyosarcoma, liposarcoma, and malignant peripheral nerve sheath tumors.4
Magnetic resonance imaging (MRI) is helpful to exclude NCM. Ideally, an MRI should be ordered before 4 months of age, at which time myelination begins to make the identification of melanin deposits in the CNS more challenging.7 Not all patients with imaging findings that are consistent with NCM will develop symptoms.8
Melanoma. By age 10, up to 8% of patients with giant congenital nevi will develop melanoma within the nevi; most of these cases occur during the first 2 years of life.7,9 Patients with NCM are at even greater risk: their rate of malignant melanoma is between 40% and 60%.6 As a result, patients should be monitored closely for any signs of the disease. Total body photography, serial clinical photos, and patient self-exam are helpful to detect changes and de novo lesions. New lesions or ulcerations superimposed on existing nevi may indicate malignancy.7 Sun protection is critical to reduce the risk of melanogenesis.
Should patients pursue surgery? It’s debatable
Options for patients with large and giant CMN include early curettage (prior to 2 weeks of life), local excision (often with tissue expansion), dermabrasion, and laser therapy.2 There is considerable debate about surgery. Advocates of surgery cite psychosocial relief as a major treatment benefit and speculate about prevention of melanoma. Opponents worry that excessive surgical intervention may cause melanogenesis in a scar or deep in an area of treatment. And, while smaller congenital nevi are easier to surgically remove, they have a low associated risk of developing melanoma and are typically monitored clinically.
Children with congenital nevi will need support
Several nonprofit organizations offer resources for children with congenital nevi and their families. Nevus Outreach (www.nevus.org) is an organization devoted to improving awareness and providing support for people with CMN and NCM. The group maintains a registry of patients with large nevi in an effort to help researchers improve treatment and identify a cure.
For children with congenital nevi and other skin conditions, the American Academy of Dermatology offers its “Camp Discovery” at locations across the country (https://www.aad.org/public/kids/camp-discovery). Camp Discovery provides full scholarships and includes transportation to each of the individual camps for attendees.
Our patient underwent an MRI on his fifth day of life. The results were normal and he hadn’t developed any neurologic symptoms at 4 months of age. The child sees his family physician for routine well-child visits and a dermatologist annually. The dermatologist is carefully monitoring the nevi, which continue to grow.
CORRESPONDENCE
Jonathan Karnes, MD, 6 East Chestnut Street, Suite 340, Augusta, ME 04330; jonathan.karnes@mainegeneral.org.
1. Sarnat HB, Flores-Sarnat L. Embryology of the neural crest: its inductive role in the neurocutaneous syndromes. J Child Neurol. 2005:20:637-643.
2. Gosain AK, Santoro TD, Larson DL, et al. Giant congenital nevi: a 20-year experience and an algorithm for their management. Plast Reconstr Surg. 2001;108:622-636.
3. National Organization for Rare Disorders. Giant congenital melanocytic nevus. National Organization for Rare Disorders Web site. Available at: http://rarediseases.org/rare-diseases/giant-congenital-melanocytic-nevus. Accessed April 29, 2016.
4. Vourc’h-Jourdain M, Martin L, Barbarot S; aRED. Large congenital melanocytic nevi: therapeutic management and melanoma risk: a systematic review. J Am Acad Dermatol. 2013;68:493-498.e1-e14.
5. Jackson SM, Nesbitt LT. Differential Diagnosis for the Dermatologist. 2nd ed. Berlin: Springer; 2012.
6. Jain P, Kannan L, Kumar A, et al. Symptomatic neurocutaneous melanosis in a child. JAMA Neurol. 2013;70:516.
7. Kinsler VA, Chong WK, Aylett SE, et al. Complications of congenital melanocytic naevi in children: analysis of 16 years’ experience and clinical practice. Br J Dermatol. 2008;159:907-914.
8. Agero AL, B envenuto-Andrade C, Dusza SW, et al. Asymptomatic neurocutaneous melanocytosis in patients with large congenital melanocytic nevi: a study of cases from an Internet-based registry. J Am Acad Dermatol. 2005;53:959-965.
9. Zayour M, Lazova R. Congenital melanocytic nevi. Clin Lab Med. 2011;31:267-280.
A 25-year-old G2P1 mother gave birth to a boy at 40 and 6/7 weeks by vaginal delivery. Labor was induced because of oligohydramnios complicated by chorioamnionitis. The mother was treated with vancomycin and gentamicin. Prenatal lab work and delivery were otherwise unremarkable.
The delivering physician (CG) noted that the neonate had numerous brown, red, and black plaques distributed over his abdomen, lower back, groin, and thighs (FIGURE). Some plaques were hypertrichotic and other areas, apart from the plaques, were thinly desquamated. Apgar scores were 8 and 9 and the remainder of the exam, including the neurologic exam, was normal. The Dermatology Service (JK) was consulted.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Giant congenital nevus
Congenital melanocytic nevi (CMN) are pigmented lesions that are present at birth and created by the abnormal migration of neural crest cells during embryogenesis.1 Nevi are categorized by size as small (<1.5 cm), medium (1.5-20 cm), large (>20 cm), and giant (>40 cm).2 Congenital nevi tend to start out flat, with uniform pigmentation, but can become more variegated in texture and color as normal growth and development continue. Giant congenital nevi are likely to thicken, darken, and enlarge as the patient grows. Some nevi may develop very coarse or dark hair.
CMN can cover any part of the body and occur independent of skin color and other ethnic factors.3 Giant congenital nevi are rare, with an incidence of approximately one in 50,000 live births and with males and females equally affected.3,4 The condition is diagnosed at birth, based on the appearance of the lesions.
The differential diagnosis for CMN includes café au lait macules, blue-gray spots (aka Mongolian spots), nevus of Ota, nevus spilus, and vascular malformations (TABLE).5 CMN may present in almost any location and may be brown, black, pink, or purple in color. Café au lait macules, blue-gray spots, nevus of Ota, nevus spilus, and vascular malformations have individual location and color characteristics that set them apart clinically.
Monitor patients for melanoma, CNS complications
Patients with CMN are at increased risk of neurocutaneous melanosis (NCM) and cutaneous melanoma.
Neurocutaneous melanosis, a complication of giant congenital nevi, is a melanocyte proliferation in the central nervous system (CNS). Between 6% and 11% of patients with giant congenital nevi develop symptomatic NCM in childhood. Thus, any CNS symptoms should be fully evaluated.4,6 NCM can result in seizures, cranial nerve palsy, hydrocephalus, and leptomeningeal melanoma.
Besides giant congenital nevi, risk factors for NCM include male sex, large numbers of satellite nevi, and the presence of nevi over the posterior midline or head and neck.7 The prognosis is poor for patients who develop neurologic symptoms. NCM is associated with other malignancies, including rhadomyosarcoma, liposarcoma, and malignant peripheral nerve sheath tumors.4
Magnetic resonance imaging (MRI) is helpful to exclude NCM. Ideally, an MRI should be ordered before 4 months of age, at which time myelination begins to make the identification of melanin deposits in the CNS more challenging.7 Not all patients with imaging findings that are consistent with NCM will develop symptoms.8
Melanoma. By age 10, up to 8% of patients with giant congenital nevi will develop melanoma within the nevi; most of these cases occur during the first 2 years of life.7,9 Patients with NCM are at even greater risk: their rate of malignant melanoma is between 40% and 60%.6 As a result, patients should be monitored closely for any signs of the disease. Total body photography, serial clinical photos, and patient self-exam are helpful to detect changes and de novo lesions. New lesions or ulcerations superimposed on existing nevi may indicate malignancy.7 Sun protection is critical to reduce the risk of melanogenesis.
Should patients pursue surgery? It’s debatable
Options for patients with large and giant CMN include early curettage (prior to 2 weeks of life), local excision (often with tissue expansion), dermabrasion, and laser therapy.2 There is considerable debate about surgery. Advocates of surgery cite psychosocial relief as a major treatment benefit and speculate about prevention of melanoma. Opponents worry that excessive surgical intervention may cause melanogenesis in a scar or deep in an area of treatment. And, while smaller congenital nevi are easier to surgically remove, they have a low associated risk of developing melanoma and are typically monitored clinically.
Children with congenital nevi will need support
Several nonprofit organizations offer resources for children with congenital nevi and their families. Nevus Outreach (www.nevus.org) is an organization devoted to improving awareness and providing support for people with CMN and NCM. The group maintains a registry of patients with large nevi in an effort to help researchers improve treatment and identify a cure.
For children with congenital nevi and other skin conditions, the American Academy of Dermatology offers its “Camp Discovery” at locations across the country (https://www.aad.org/public/kids/camp-discovery). Camp Discovery provides full scholarships and includes transportation to each of the individual camps for attendees.
Our patient underwent an MRI on his fifth day of life. The results were normal and he hadn’t developed any neurologic symptoms at 4 months of age. The child sees his family physician for routine well-child visits and a dermatologist annually. The dermatologist is carefully monitoring the nevi, which continue to grow.
CORRESPONDENCE
Jonathan Karnes, MD, 6 East Chestnut Street, Suite 340, Augusta, ME 04330; jonathan.karnes@mainegeneral.org.
A 25-year-old G2P1 mother gave birth to a boy at 40 and 6/7 weeks by vaginal delivery. Labor was induced because of oligohydramnios complicated by chorioamnionitis. The mother was treated with vancomycin and gentamicin. Prenatal lab work and delivery were otherwise unremarkable.
The delivering physician (CG) noted that the neonate had numerous brown, red, and black plaques distributed over his abdomen, lower back, groin, and thighs (FIGURE). Some plaques were hypertrichotic and other areas, apart from the plaques, were thinly desquamated. Apgar scores were 8 and 9 and the remainder of the exam, including the neurologic exam, was normal. The Dermatology Service (JK) was consulted.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Giant congenital nevus
Congenital melanocytic nevi (CMN) are pigmented lesions that are present at birth and created by the abnormal migration of neural crest cells during embryogenesis.1 Nevi are categorized by size as small (<1.5 cm), medium (1.5-20 cm), large (>20 cm), and giant (>40 cm).2 Congenital nevi tend to start out flat, with uniform pigmentation, but can become more variegated in texture and color as normal growth and development continue. Giant congenital nevi are likely to thicken, darken, and enlarge as the patient grows. Some nevi may develop very coarse or dark hair.
CMN can cover any part of the body and occur independent of skin color and other ethnic factors.3 Giant congenital nevi are rare, with an incidence of approximately one in 50,000 live births and with males and females equally affected.3,4 The condition is diagnosed at birth, based on the appearance of the lesions.
The differential diagnosis for CMN includes café au lait macules, blue-gray spots (aka Mongolian spots), nevus of Ota, nevus spilus, and vascular malformations (TABLE).5 CMN may present in almost any location and may be brown, black, pink, or purple in color. Café au lait macules, blue-gray spots, nevus of Ota, nevus spilus, and vascular malformations have individual location and color characteristics that set them apart clinically.
Monitor patients for melanoma, CNS complications
Patients with CMN are at increased risk of neurocutaneous melanosis (NCM) and cutaneous melanoma.
Neurocutaneous melanosis, a complication of giant congenital nevi, is a melanocyte proliferation in the central nervous system (CNS). Between 6% and 11% of patients with giant congenital nevi develop symptomatic NCM in childhood. Thus, any CNS symptoms should be fully evaluated.4,6 NCM can result in seizures, cranial nerve palsy, hydrocephalus, and leptomeningeal melanoma.
Besides giant congenital nevi, risk factors for NCM include male sex, large numbers of satellite nevi, and the presence of nevi over the posterior midline or head and neck.7 The prognosis is poor for patients who develop neurologic symptoms. NCM is associated with other malignancies, including rhadomyosarcoma, liposarcoma, and malignant peripheral nerve sheath tumors.4
Magnetic resonance imaging (MRI) is helpful to exclude NCM. Ideally, an MRI should be ordered before 4 months of age, at which time myelination begins to make the identification of melanin deposits in the CNS more challenging.7 Not all patients with imaging findings that are consistent with NCM will develop symptoms.8
Melanoma. By age 10, up to 8% of patients with giant congenital nevi will develop melanoma within the nevi; most of these cases occur during the first 2 years of life.7,9 Patients with NCM are at even greater risk: their rate of malignant melanoma is between 40% and 60%.6 As a result, patients should be monitored closely for any signs of the disease. Total body photography, serial clinical photos, and patient self-exam are helpful to detect changes and de novo lesions. New lesions or ulcerations superimposed on existing nevi may indicate malignancy.7 Sun protection is critical to reduce the risk of melanogenesis.
Should patients pursue surgery? It’s debatable
Options for patients with large and giant CMN include early curettage (prior to 2 weeks of life), local excision (often with tissue expansion), dermabrasion, and laser therapy.2 There is considerable debate about surgery. Advocates of surgery cite psychosocial relief as a major treatment benefit and speculate about prevention of melanoma. Opponents worry that excessive surgical intervention may cause melanogenesis in a scar or deep in an area of treatment. And, while smaller congenital nevi are easier to surgically remove, they have a low associated risk of developing melanoma and are typically monitored clinically.
Children with congenital nevi will need support
Several nonprofit organizations offer resources for children with congenital nevi and their families. Nevus Outreach (www.nevus.org) is an organization devoted to improving awareness and providing support for people with CMN and NCM. The group maintains a registry of patients with large nevi in an effort to help researchers improve treatment and identify a cure.
For children with congenital nevi and other skin conditions, the American Academy of Dermatology offers its “Camp Discovery” at locations across the country (https://www.aad.org/public/kids/camp-discovery). Camp Discovery provides full scholarships and includes transportation to each of the individual camps for attendees.
Our patient underwent an MRI on his fifth day of life. The results were normal and he hadn’t developed any neurologic symptoms at 4 months of age. The child sees his family physician for routine well-child visits and a dermatologist annually. The dermatologist is carefully monitoring the nevi, which continue to grow.
CORRESPONDENCE
Jonathan Karnes, MD, 6 East Chestnut Street, Suite 340, Augusta, ME 04330; jonathan.karnes@mainegeneral.org.
1. Sarnat HB, Flores-Sarnat L. Embryology of the neural crest: its inductive role in the neurocutaneous syndromes. J Child Neurol. 2005:20:637-643.
2. Gosain AK, Santoro TD, Larson DL, et al. Giant congenital nevi: a 20-year experience and an algorithm for their management. Plast Reconstr Surg. 2001;108:622-636.
3. National Organization for Rare Disorders. Giant congenital melanocytic nevus. National Organization for Rare Disorders Web site. Available at: http://rarediseases.org/rare-diseases/giant-congenital-melanocytic-nevus. Accessed April 29, 2016.
4. Vourc’h-Jourdain M, Martin L, Barbarot S; aRED. Large congenital melanocytic nevi: therapeutic management and melanoma risk: a systematic review. J Am Acad Dermatol. 2013;68:493-498.e1-e14.
5. Jackson SM, Nesbitt LT. Differential Diagnosis for the Dermatologist. 2nd ed. Berlin: Springer; 2012.
6. Jain P, Kannan L, Kumar A, et al. Symptomatic neurocutaneous melanosis in a child. JAMA Neurol. 2013;70:516.
7. Kinsler VA, Chong WK, Aylett SE, et al. Complications of congenital melanocytic naevi in children: analysis of 16 years’ experience and clinical practice. Br J Dermatol. 2008;159:907-914.
8. Agero AL, B envenuto-Andrade C, Dusza SW, et al. Asymptomatic neurocutaneous melanocytosis in patients with large congenital melanocytic nevi: a study of cases from an Internet-based registry. J Am Acad Dermatol. 2005;53:959-965.
9. Zayour M, Lazova R. Congenital melanocytic nevi. Clin Lab Med. 2011;31:267-280.
1. Sarnat HB, Flores-Sarnat L. Embryology of the neural crest: its inductive role in the neurocutaneous syndromes. J Child Neurol. 2005:20:637-643.
2. Gosain AK, Santoro TD, Larson DL, et al. Giant congenital nevi: a 20-year experience and an algorithm for their management. Plast Reconstr Surg. 2001;108:622-636.
3. National Organization for Rare Disorders. Giant congenital melanocytic nevus. National Organization for Rare Disorders Web site. Available at: http://rarediseases.org/rare-diseases/giant-congenital-melanocytic-nevus. Accessed April 29, 2016.
4. Vourc’h-Jourdain M, Martin L, Barbarot S; aRED. Large congenital melanocytic nevi: therapeutic management and melanoma risk: a systematic review. J Am Acad Dermatol. 2013;68:493-498.e1-e14.
5. Jackson SM, Nesbitt LT. Differential Diagnosis for the Dermatologist. 2nd ed. Berlin: Springer; 2012.
6. Jain P, Kannan L, Kumar A, et al. Symptomatic neurocutaneous melanosis in a child. JAMA Neurol. 2013;70:516.
7. Kinsler VA, Chong WK, Aylett SE, et al. Complications of congenital melanocytic naevi in children: analysis of 16 years’ experience and clinical practice. Br J Dermatol. 2008;159:907-914.
8. Agero AL, B envenuto-Andrade C, Dusza SW, et al. Asymptomatic neurocutaneous melanocytosis in patients with large congenital melanocytic nevi: a study of cases from an Internet-based registry. J Am Acad Dermatol. 2005;53:959-965.
9. Zayour M, Lazova R. Congenital melanocytic nevi. Clin Lab Med. 2011;31:267-280.

Register for Pediatric Hospital Medicine 2016

PHM16 will provide in-depth review and challenge participants in various areas, including clinical practice, medical education, quality improvement, and professional development. Time will also be dedicated to networking and meeting with leaders in the field.
Register, book your hotel, and see the full course schedule at www.phmmeeting.org.
Brett Radler is SHM’s communications coordinator.
PHM16 will provide in-depth review and challenge participants in various areas, including clinical practice, medical education, quality improvement, and professional development. Time will also be dedicated to networking and meeting with leaders in the field.
Register, book your hotel, and see the full course schedule at www.phmmeeting.org.
Brett Radler is SHM’s communications coordinator.
PHM16 will provide in-depth review and challenge participants in various areas, including clinical practice, medical education, quality improvement, and professional development. Time will also be dedicated to networking and meeting with leaders in the field.
Register, book your hotel, and see the full course schedule at www.phmmeeting.org.
Brett Radler is SHM’s communications coordinator.
Long-term benefits seen in sacral nerve stimulation for constipation in kids
SAN DIEGO – Children with refractory constipation may benefit from sacral nerve stimulation, although complications are common, according to a study that found benefits over more than 2 years, as well as evidence that parents like the treatment.
Sacral nerve stimulation is an accepted treatment for refractory constipation in adults, but long-term research in kids has been lacking.
The current study showed that sacral nerve stimulation (SNS) “can be used successfully for some children with intractable constipation, and the improvement seen with SNS treatment can be durable,” said study lead author Dr. Peter Lu, a pediatric gastroenterology fellow with Nationwide Children’s Hospital in Columbus, Ohio. “However, much more research is needed before more widespread adoption of SNS for treatment of this population.”

An estimated 12% of children suffer from constipation, and about 10% of those will still have symptoms despite laxative use, said Dr. Lu, who presented the findings at the annual Digestive Disease Week.
“We regularly see children in our GI clinic who have severe constipation leading to frequent episodes of overflow fecal incontinence, often throughout the day at school,” Dr. Lu said. “As you might imagine, this is incredibly embarrassing and isolating.”
According to Dr. Lu, treatments include anal sphincter botulinum injection, antegrade continence enema (ACE), colonic resection, and SNS.
Adult research has shown that SNS is effective in the treatment of constipation and fetal incontinence, Dr. Lu said, but research in children is limited and only looked at effects over a period of 4-12 months. “The durability of symptom improvement has not been really shown,” he said.
Dr. Lu and associates tracked 25 children (52% male; mean age, 14.0 years) with refractory constipation: 17 had functional constipation, 6 had an anorectal malformation, 1 had Hirschsprung’s disease, and 1 had a tethered cord. Comorbid conditions included fecal incontinence (18, 72%) and urinary symptoms (16, 64%). Thirteen (52%) used ACEs at baseline.
At the most recent follow-up, the number using laxatives fell from 16/64% to 11/44% (P = .16).
Of 13 subjects using ACEs, 8 (62%) had undergone closure of their appendicostomy or cecostomy and the other 5 (38%) had reduced ACE frequency by follow-up. ACE use fell from 12/48% to 5/20% (P = .03).
Scores on the PedsQL GI Symptom Scale and Fecal Incontinence Severity Index and on most Fecal Incontinence Quality of Life Scale domains had improved at follow-up.
At a mean of 2.4 years for constipation scores and 1.8 years for symptom scores, 16 parents completed questionnaires. Median Glasgow Children’s Benefit Inventory (GCBI) scores were +42.7 (interquartile range, 23.4-77.1), and 15 (94%) reported GCBI scores greater than 0. Fourteen (88%) said they’d allow their children to undergo SNS again if they could make the choice once more.
“Almost all reported benefit from SNS,” Dr. Lu said, “and all would still recommend SNS to other families with children who have similar symptoms.”
However, six patients (24%) had complications requiring surgery; four of those needed SNS replacement.
There are remaining questions. For one, “the mechanism of SNS treatment remains unclear,” Dr. Lu said. “We suspect that SNS leads to improvement by modulating anorectal function, and there has also been evidence that SNS can affect colonic motility. We are currently studying this further and hope to have a better understanding of how the treatment works soon.”
Dr. Lu and colleagues are also studying why patients have complications, with an eye toward identifying risk factors.
In a question and answer session, Dr. Lu acknowledged that many patients were lost to follow-up; some moved away. “Part of it was that we didn’t have the time to really track them down,” he said. “That’s something we definitely have to look at.” However, he noted that the 16 parents who did respond accounted for 5 of the 6 children who encountered complications.
Dr. Lu said he doesn’t recommend widespread use of SNS in children. “We need to have a better understanding of which patients will benefit from SNS and which patients will not,” Dr. Lu said.
No funding was reported. Dr. Lu had no relevant financial disclosures.
SAN DIEGO – Children with refractory constipation may benefit from sacral nerve stimulation, although complications are common, according to a study that found benefits over more than 2 years, as well as evidence that parents like the treatment.
Sacral nerve stimulation is an accepted treatment for refractory constipation in adults, but long-term research in kids has been lacking.
The current study showed that sacral nerve stimulation (SNS) “can be used successfully for some children with intractable constipation, and the improvement seen with SNS treatment can be durable,” said study lead author Dr. Peter Lu, a pediatric gastroenterology fellow with Nationwide Children’s Hospital in Columbus, Ohio. “However, much more research is needed before more widespread adoption of SNS for treatment of this population.”
An estimated 12% of children suffer from constipation, and about 10% of those will still have symptoms despite laxative use, said Dr. Lu, who presented the findings at the annual Digestive Disease Week.
“We regularly see children in our GI clinic who have severe constipation leading to frequent episodes of overflow fecal incontinence, often throughout the day at school,” Dr. Lu said. “As you might imagine, this is incredibly embarrassing and isolating.”
According to Dr. Lu, treatments include anal sphincter botulinum injection, antegrade continence enema (ACE), colonic resection, and SNS.
Adult research has shown that SNS is effective in the treatment of constipation and fetal incontinence, Dr. Lu said, but research in children is limited and only looked at effects over a period of 4-12 months. “The durability of symptom improvement has not been really shown,” he said.
Dr. Lu and associates tracked 25 children (52% male; mean age, 14.0 years) with refractory constipation: 17 had functional constipation, 6 had an anorectal malformation, 1 had Hirschsprung’s disease, and 1 had a tethered cord. Comorbid conditions included fecal incontinence (18, 72%) and urinary symptoms (16, 64%). Thirteen (52%) used ACEs at baseline.
At the most recent follow-up, the number using laxatives fell from 16/64% to 11/44% (P = .16).
Of 13 subjects using ACEs, 8 (62%) had undergone closure of their appendicostomy or cecostomy and the other 5 (38%) had reduced ACE frequency by follow-up. ACE use fell from 12/48% to 5/20% (P = .03).
Scores on the PedsQL GI Symptom Scale and Fecal Incontinence Severity Index and on most Fecal Incontinence Quality of Life Scale domains had improved at follow-up.
At a mean of 2.4 years for constipation scores and 1.8 years for symptom scores, 16 parents completed questionnaires. Median Glasgow Children’s Benefit Inventory (GCBI) scores were +42.7 (interquartile range, 23.4-77.1), and 15 (94%) reported GCBI scores greater than 0. Fourteen (88%) said they’d allow their children to undergo SNS again if they could make the choice once more.
“Almost all reported benefit from SNS,” Dr. Lu said, “and all would still recommend SNS to other families with children who have similar symptoms.”
However, six patients (24%) had complications requiring surgery; four of those needed SNS replacement.
There are remaining questions. For one, “the mechanism of SNS treatment remains unclear,” Dr. Lu said. “We suspect that SNS leads to improvement by modulating anorectal function, and there has also been evidence that SNS can affect colonic motility. We are currently studying this further and hope to have a better understanding of how the treatment works soon.”
Dr. Lu and colleagues are also studying why patients have complications, with an eye toward identifying risk factors.
In a question and answer session, Dr. Lu acknowledged that many patients were lost to follow-up; some moved away. “Part of it was that we didn’t have the time to really track them down,” he said. “That’s something we definitely have to look at.” However, he noted that the 16 parents who did respond accounted for 5 of the 6 children who encountered complications.
Dr. Lu said he doesn’t recommend widespread use of SNS in children. “We need to have a better understanding of which patients will benefit from SNS and which patients will not,” Dr. Lu said.
No funding was reported. Dr. Lu had no relevant financial disclosures.
SAN DIEGO – Children with refractory constipation may benefit from sacral nerve stimulation, although complications are common, according to a study that found benefits over more than 2 years, as well as evidence that parents like the treatment.
Sacral nerve stimulation is an accepted treatment for refractory constipation in adults, but long-term research in kids has been lacking.
The current study showed that sacral nerve stimulation (SNS) “can be used successfully for some children with intractable constipation, and the improvement seen with SNS treatment can be durable,” said study lead author Dr. Peter Lu, a pediatric gastroenterology fellow with Nationwide Children’s Hospital in Columbus, Ohio. “However, much more research is needed before more widespread adoption of SNS for treatment of this population.”
An estimated 12% of children suffer from constipation, and about 10% of those will still have symptoms despite laxative use, said Dr. Lu, who presented the findings at the annual Digestive Disease Week.
“We regularly see children in our GI clinic who have severe constipation leading to frequent episodes of overflow fecal incontinence, often throughout the day at school,” Dr. Lu said. “As you might imagine, this is incredibly embarrassing and isolating.”
According to Dr. Lu, treatments include anal sphincter botulinum injection, antegrade continence enema (ACE), colonic resection, and SNS.
Adult research has shown that SNS is effective in the treatment of constipation and fetal incontinence, Dr. Lu said, but research in children is limited and only looked at effects over a period of 4-12 months. “The durability of symptom improvement has not been really shown,” he said.
Dr. Lu and associates tracked 25 children (52% male; mean age, 14.0 years) with refractory constipation: 17 had functional constipation, 6 had an anorectal malformation, 1 had Hirschsprung’s disease, and 1 had a tethered cord. Comorbid conditions included fecal incontinence (18, 72%) and urinary symptoms (16, 64%). Thirteen (52%) used ACEs at baseline.
At the most recent follow-up, the number using laxatives fell from 16/64% to 11/44% (P = .16).
Of 13 subjects using ACEs, 8 (62%) had undergone closure of their appendicostomy or cecostomy and the other 5 (38%) had reduced ACE frequency by follow-up. ACE use fell from 12/48% to 5/20% (P = .03).
Scores on the PedsQL GI Symptom Scale and Fecal Incontinence Severity Index and on most Fecal Incontinence Quality of Life Scale domains had improved at follow-up.
At a mean of 2.4 years for constipation scores and 1.8 years for symptom scores, 16 parents completed questionnaires. Median Glasgow Children’s Benefit Inventory (GCBI) scores were +42.7 (interquartile range, 23.4-77.1), and 15 (94%) reported GCBI scores greater than 0. Fourteen (88%) said they’d allow their children to undergo SNS again if they could make the choice once more.
“Almost all reported benefit from SNS,” Dr. Lu said, “and all would still recommend SNS to other families with children who have similar symptoms.”
However, six patients (24%) had complications requiring surgery; four of those needed SNS replacement.
There are remaining questions. For one, “the mechanism of SNS treatment remains unclear,” Dr. Lu said. “We suspect that SNS leads to improvement by modulating anorectal function, and there has also been evidence that SNS can affect colonic motility. We are currently studying this further and hope to have a better understanding of how the treatment works soon.”
Dr. Lu and colleagues are also studying why patients have complications, with an eye toward identifying risk factors.
In a question and answer session, Dr. Lu acknowledged that many patients were lost to follow-up; some moved away. “Part of it was that we didn’t have the time to really track them down,” he said. “That’s something we definitely have to look at.” However, he noted that the 16 parents who did respond accounted for 5 of the 6 children who encountered complications.
Dr. Lu said he doesn’t recommend widespread use of SNS in children. “We need to have a better understanding of which patients will benefit from SNS and which patients will not,” Dr. Lu said.
No funding was reported. Dr. Lu had no relevant financial disclosures.
AT DDW 2016
Key clinical point: Children with refractory constipation may benefit from sacral nerve stimulation although complications are common.
Major finding: The use of laxatives fell from 64% to 44% by follow-up (P =.16), as did ACE use, which went from 48% to 20% (P = .03). All parents who weren’t lost to follow-up said they’d recommend the treatment.
Data source: A prospective cohort of 25 children (52% male; mean age, 14 years; all under 21) with refractory constipation who were treated for more than 2 years.
Disclosures: No funding was reported. Dr. Lu had no relevant financial disclosures.

Don’t touch that! You’ll get hurt! Fear in childhood
Fear is an intrinsic reaction evolved to protect us from harm. Unsurprisingly, anxiety disorders are common, affecting as many as 25% of children. On average, children have 2-14 fears typical for thinking at their age, from separation (1 year), animals (6 years), environment (dark or storms), medical intrusions or injury (9 years) to social disgrace (16 years). But about one-fifth of children with typical fear topics qualify as having a disorder; that is, they have impairment in functioning.
I wonder daily in my care of anxious children: Is this amount of fear really inevitable? Are there things we can do to avoid this burden on children?

For everyone, genetics predispose fear of things that are dangerous, such as snakes. (Tell me that they don’t make you startle!) Genetic influences account for about 50% of the variance in significant fearfulness as evidenced by parent-child patterns, and the fact that monozygotic twins are more highly concordant in fearfulness than dizygotic. Not much we can do about that!
So, if evolution armed humans with fear for protection, how is it that everyone is not impaired?
In combination with genetic vulnerabilities, fears are learned in three ways: experiential conditioning, modeling, and threat information transmission. These frequently co-occur because bad things happen, genetically anxious parents show a fear reaction, and the same parents warn their children frequently and expressively about potential dangers.
As for avoiding fear conditioning, all parents want to protect their children from scary experiences, but it is not always possible. Car crashes and other bad things happen. Even viewing events that threaten injury or death, such as 9/11, can be sufficient to induce post-traumatic stress disorder (18% of children in New York City). The closer and more severe a scary event is, the more it injures or has potential to injure the child or the child’s loved ones; the more expressive the family members are and the more it is repeated (abuse, for example), the greater the likelihood of it lasting and having impairing effects.
Conditioned fears from real experiences are not entirely random. Low-income children are more likely to experience frightening events from rat bites to house fires to domestic violence to gunshots. Asking about environmental factors or using screening tools such as Safe Environment for Every Kid to evaluate the home environment, and referring families for assistance are steps relevant to every child, but especially anxious ones.
You and I need to continue to advocate for safer communities for all children. In the meantime, it is important to know that encouraging a child to describe in detail to a caring adult – verbally and/or by drawing – traumas they experienced is significantly therapeutic. It might not seem intuitive to parents to promote “reliving the experience,” especially because they may have been traumatized themselves. So providing this opportunity ourselves or through a friend, teacher, or counselor who can calmly answer questions and put the event in perspective, is important advice.
But even simply viewing disasters, violence, or artificial frightening events on television or film can produce lasting fears. While inherently anxious children are more vulnerable to fears induced by media, 90% of undergraduates report at least one enduring fear that started this way, and 26% report persistence to the present. At least one-third of youth have fear reactions to media. Simply the number of hours watching television is associated with a child’s increased perception of personal vulnerability. While 8- to 10-year-olds had reduced fear when parents explained news events, more realistic and serious coverage (the Iraq War, for example) and older age predicted more severe fear reactions not similarly reassured. With this high prevalence of anxiety, I encourage parents to avoid media whose content is not known to them for all children, but especially for those already anxious or traumatized. It amazes me how many families of anxious children have the Weather Channel on constantly, showing devastation all over the world, oblivious that the child is internalizing the risk as though it was outside their window! When media trauma exposure can’t be avoided, parents need to show calm and provide explanation to the child to put it in perspective, as we saw the father do on TV after the Paris massacre.
Modeling of fearful reactions is the second powerful influence on the development of fears. How caregivers react when they encounter a situation such as an approaching dog is quickly modeled by the child. This vicarious learning by watching others’ reactions evolved as preferable to having to chance it yourself. Mothers’ voices and actions are especially salient to children, compared with fathers’ voices and actions. Unfortunately, females tend to be both more fearful and more expressive of fear than males. Some approaches you can suggest regarding modeling include coaching parents (sometimes even sitters) to dampen or mask their reactions, provide other adults without a similar fear to model for the child, or at least not tell the child why they are walking a different route to avoid a dog!
How information about threats is transmitted is the third and perhaps most modifiable influence on a child’s development of fears. Parents talk to children constantly, and a lot of it is warnings! This too may be genetic/cultural as evidenced by the 41% of nursery rhymes across cultures that include violence! Children who have been told potentially bad things about an animal, person, or event show a stronger fear response as measured by self-report, physiological reaction, and behavioral avoidance than when not primed. Conversely, children told positive things react with less fear immediately and are less likely to learn a fear response at later exposures. Once fear has been promoted by negative information, the child’s actual ways of thinking (cognitive biases) are shifted. Attention to forewarned stimuli is increased, the use of reasoning is limited to verifying that fear was warranted rather than alternatively looking for evidence against it, and over estimation of the likelihood of bad outcomes occurs. Children with an overly aroused brain behavioral inhibition system (inherent tendency to react to novelty with physiological arousal and fear) are more influenced by negative verbal information to have fear, cognitive distortions, and avoidance.1
Not surprisingly, anxious parents give more negative information, particularly about ambiguous situations, than other parents. Children living in homes with more negative interactions with fathers or more punitive or neglectful mothers also are more susceptible to increased fears from verbal threat information. Unfortunately, parents generally do not perceive their own role in transmitting threat information. In contrast, one-quarter to one-third of children with significant fears relate onset or intensification of their fears to things they heard. While possibly not relevant for innate fears such as of spiders, this is important information for prevention of fears in general. A child’s development of excessive fear can be somewhat dampened by adult verbal explanations, a focus on the positives, and reassurance, especially if this is done routinely.
The “30 Million Word Gap”2 in total word exposure before age 3 years of children in families on welfare vs. professionals found that higher-income parents provided far more words of praise and six encouragements for every discouragement vs. more total negative vocabulary and two discouragements for every encouragement. The same children more likely to be exposed to trauma also may have less positive preparation to reduce their development of significant fears with the associated stress effects. You and I see this during visits – take the opportunity to discuss and model an alternative.
References
1. Clin Child Fam Psychol Rev. 2010 Jun;13(2):129-50.
2. “The Early Catastrophe: The 30 Million Word Gap by Age 3” (Washington: American Educator, Spring 2003).
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
Fear is an intrinsic reaction evolved to protect us from harm. Unsurprisingly, anxiety disorders are common, affecting as many as 25% of children. On average, children have 2-14 fears typical for thinking at their age, from separation (1 year), animals (6 years), environment (dark or storms), medical intrusions or injury (9 years) to social disgrace (16 years). But about one-fifth of children with typical fear topics qualify as having a disorder; that is, they have impairment in functioning.
I wonder daily in my care of anxious children: Is this amount of fear really inevitable? Are there things we can do to avoid this burden on children?
For everyone, genetics predispose fear of things that are dangerous, such as snakes. (Tell me that they don’t make you startle!) Genetic influences account for about 50% of the variance in significant fearfulness as evidenced by parent-child patterns, and the fact that monozygotic twins are more highly concordant in fearfulness than dizygotic. Not much we can do about that!
So, if evolution armed humans with fear for protection, how is it that everyone is not impaired?
In combination with genetic vulnerabilities, fears are learned in three ways: experiential conditioning, modeling, and threat information transmission. These frequently co-occur because bad things happen, genetically anxious parents show a fear reaction, and the same parents warn their children frequently and expressively about potential dangers.
As for avoiding fear conditioning, all parents want to protect their children from scary experiences, but it is not always possible. Car crashes and other bad things happen. Even viewing events that threaten injury or death, such as 9/11, can be sufficient to induce post-traumatic stress disorder (18% of children in New York City). The closer and more severe a scary event is, the more it injures or has potential to injure the child or the child’s loved ones; the more expressive the family members are and the more it is repeated (abuse, for example), the greater the likelihood of it lasting and having impairing effects.
Conditioned fears from real experiences are not entirely random. Low-income children are more likely to experience frightening events from rat bites to house fires to domestic violence to gunshots. Asking about environmental factors or using screening tools such as Safe Environment for Every Kid to evaluate the home environment, and referring families for assistance are steps relevant to every child, but especially anxious ones.
You and I need to continue to advocate for safer communities for all children. In the meantime, it is important to know that encouraging a child to describe in detail to a caring adult – verbally and/or by drawing – traumas they experienced is significantly therapeutic. It might not seem intuitive to parents to promote “reliving the experience,” especially because they may have been traumatized themselves. So providing this opportunity ourselves or through a friend, teacher, or counselor who can calmly answer questions and put the event in perspective, is important advice.
But even simply viewing disasters, violence, or artificial frightening events on television or film can produce lasting fears. While inherently anxious children are more vulnerable to fears induced by media, 90% of undergraduates report at least one enduring fear that started this way, and 26% report persistence to the present. At least one-third of youth have fear reactions to media. Simply the number of hours watching television is associated with a child’s increased perception of personal vulnerability. While 8- to 10-year-olds had reduced fear when parents explained news events, more realistic and serious coverage (the Iraq War, for example) and older age predicted more severe fear reactions not similarly reassured. With this high prevalence of anxiety, I encourage parents to avoid media whose content is not known to them for all children, but especially for those already anxious or traumatized. It amazes me how many families of anxious children have the Weather Channel on constantly, showing devastation all over the world, oblivious that the child is internalizing the risk as though it was outside their window! When media trauma exposure can’t be avoided, parents need to show calm and provide explanation to the child to put it in perspective, as we saw the father do on TV after the Paris massacre.
Modeling of fearful reactions is the second powerful influence on the development of fears. How caregivers react when they encounter a situation such as an approaching dog is quickly modeled by the child. This vicarious learning by watching others’ reactions evolved as preferable to having to chance it yourself. Mothers’ voices and actions are especially salient to children, compared with fathers’ voices and actions. Unfortunately, females tend to be both more fearful and more expressive of fear than males. Some approaches you can suggest regarding modeling include coaching parents (sometimes even sitters) to dampen or mask their reactions, provide other adults without a similar fear to model for the child, or at least not tell the child why they are walking a different route to avoid a dog!
How information about threats is transmitted is the third and perhaps most modifiable influence on a child’s development of fears. Parents talk to children constantly, and a lot of it is warnings! This too may be genetic/cultural as evidenced by the 41% of nursery rhymes across cultures that include violence! Children who have been told potentially bad things about an animal, person, or event show a stronger fear response as measured by self-report, physiological reaction, and behavioral avoidance than when not primed. Conversely, children told positive things react with less fear immediately and are less likely to learn a fear response at later exposures. Once fear has been promoted by negative information, the child’s actual ways of thinking (cognitive biases) are shifted. Attention to forewarned stimuli is increased, the use of reasoning is limited to verifying that fear was warranted rather than alternatively looking for evidence against it, and over estimation of the likelihood of bad outcomes occurs. Children with an overly aroused brain behavioral inhibition system (inherent tendency to react to novelty with physiological arousal and fear) are more influenced by negative verbal information to have fear, cognitive distortions, and avoidance.1
Not surprisingly, anxious parents give more negative information, particularly about ambiguous situations, than other parents. Children living in homes with more negative interactions with fathers or more punitive or neglectful mothers also are more susceptible to increased fears from verbal threat information. Unfortunately, parents generally do not perceive their own role in transmitting threat information. In contrast, one-quarter to one-third of children with significant fears relate onset or intensification of their fears to things they heard. While possibly not relevant for innate fears such as of spiders, this is important information for prevention of fears in general. A child’s development of excessive fear can be somewhat dampened by adult verbal explanations, a focus on the positives, and reassurance, especially if this is done routinely.
The “30 Million Word Gap”2 in total word exposure before age 3 years of children in families on welfare vs. professionals found that higher-income parents provided far more words of praise and six encouragements for every discouragement vs. more total negative vocabulary and two discouragements for every encouragement. The same children more likely to be exposed to trauma also may have less positive preparation to reduce their development of significant fears with the associated stress effects. You and I see this during visits – take the opportunity to discuss and model an alternative.
References
1. Clin Child Fam Psychol Rev. 2010 Jun;13(2):129-50.
2. “The Early Catastrophe: The 30 Million Word Gap by Age 3” (Washington: American Educator, Spring 2003).
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.
Fear is an intrinsic reaction evolved to protect us from harm. Unsurprisingly, anxiety disorders are common, affecting as many as 25% of children. On average, children have 2-14 fears typical for thinking at their age, from separation (1 year), animals (6 years), environment (dark or storms), medical intrusions or injury (9 years) to social disgrace (16 years). But about one-fifth of children with typical fear topics qualify as having a disorder; that is, they have impairment in functioning.
I wonder daily in my care of anxious children: Is this amount of fear really inevitable? Are there things we can do to avoid this burden on children?
For everyone, genetics predispose fear of things that are dangerous, such as snakes. (Tell me that they don’t make you startle!) Genetic influences account for about 50% of the variance in significant fearfulness as evidenced by parent-child patterns, and the fact that monozygotic twins are more highly concordant in fearfulness than dizygotic. Not much we can do about that!
So, if evolution armed humans with fear for protection, how is it that everyone is not impaired?
In combination with genetic vulnerabilities, fears are learned in three ways: experiential conditioning, modeling, and threat information transmission. These frequently co-occur because bad things happen, genetically anxious parents show a fear reaction, and the same parents warn their children frequently and expressively about potential dangers.
As for avoiding fear conditioning, all parents want to protect their children from scary experiences, but it is not always possible. Car crashes and other bad things happen. Even viewing events that threaten injury or death, such as 9/11, can be sufficient to induce post-traumatic stress disorder (18% of children in New York City). The closer and more severe a scary event is, the more it injures or has potential to injure the child or the child’s loved ones; the more expressive the family members are and the more it is repeated (abuse, for example), the greater the likelihood of it lasting and having impairing effects.
Conditioned fears from real experiences are not entirely random. Low-income children are more likely to experience frightening events from rat bites to house fires to domestic violence to gunshots. Asking about environmental factors or using screening tools such as Safe Environment for Every Kid to evaluate the home environment, and referring families for assistance are steps relevant to every child, but especially anxious ones.
You and I need to continue to advocate for safer communities for all children. In the meantime, it is important to know that encouraging a child to describe in detail to a caring adult – verbally and/or by drawing – traumas they experienced is significantly therapeutic. It might not seem intuitive to parents to promote “reliving the experience,” especially because they may have been traumatized themselves. So providing this opportunity ourselves or through a friend, teacher, or counselor who can calmly answer questions and put the event in perspective, is important advice.
But even simply viewing disasters, violence, or artificial frightening events on television or film can produce lasting fears. While inherently anxious children are more vulnerable to fears induced by media, 90% of undergraduates report at least one enduring fear that started this way, and 26% report persistence to the present. At least one-third of youth have fear reactions to media. Simply the number of hours watching television is associated with a child’s increased perception of personal vulnerability. While 8- to 10-year-olds had reduced fear when parents explained news events, more realistic and serious coverage (the Iraq War, for example) and older age predicted more severe fear reactions not similarly reassured. With this high prevalence of anxiety, I encourage parents to avoid media whose content is not known to them for all children, but especially for those already anxious or traumatized. It amazes me how many families of anxious children have the Weather Channel on constantly, showing devastation all over the world, oblivious that the child is internalizing the risk as though it was outside their window! When media trauma exposure can’t be avoided, parents need to show calm and provide explanation to the child to put it in perspective, as we saw the father do on TV after the Paris massacre.
Modeling of fearful reactions is the second powerful influence on the development of fears. How caregivers react when they encounter a situation such as an approaching dog is quickly modeled by the child. This vicarious learning by watching others’ reactions evolved as preferable to having to chance it yourself. Mothers’ voices and actions are especially salient to children, compared with fathers’ voices and actions. Unfortunately, females tend to be both more fearful and more expressive of fear than males. Some approaches you can suggest regarding modeling include coaching parents (sometimes even sitters) to dampen or mask their reactions, provide other adults without a similar fear to model for the child, or at least not tell the child why they are walking a different route to avoid a dog!
How information about threats is transmitted is the third and perhaps most modifiable influence on a child’s development of fears. Parents talk to children constantly, and a lot of it is warnings! This too may be genetic/cultural as evidenced by the 41% of nursery rhymes across cultures that include violence! Children who have been told potentially bad things about an animal, person, or event show a stronger fear response as measured by self-report, physiological reaction, and behavioral avoidance than when not primed. Conversely, children told positive things react with less fear immediately and are less likely to learn a fear response at later exposures. Once fear has been promoted by negative information, the child’s actual ways of thinking (cognitive biases) are shifted. Attention to forewarned stimuli is increased, the use of reasoning is limited to verifying that fear was warranted rather than alternatively looking for evidence against it, and over estimation of the likelihood of bad outcomes occurs. Children with an overly aroused brain behavioral inhibition system (inherent tendency to react to novelty with physiological arousal and fear) are more influenced by negative verbal information to have fear, cognitive distortions, and avoidance.1
Not surprisingly, anxious parents give more negative information, particularly about ambiguous situations, than other parents. Children living in homes with more negative interactions with fathers or more punitive or neglectful mothers also are more susceptible to increased fears from verbal threat information. Unfortunately, parents generally do not perceive their own role in transmitting threat information. In contrast, one-quarter to one-third of children with significant fears relate onset or intensification of their fears to things they heard. While possibly not relevant for innate fears such as of spiders, this is important information for prevention of fears in general. A child’s development of excessive fear can be somewhat dampened by adult verbal explanations, a focus on the positives, and reassurance, especially if this is done routinely.
The “30 Million Word Gap”2 in total word exposure before age 3 years of children in families on welfare vs. professionals found that higher-income parents provided far more words of praise and six encouragements for every discouragement vs. more total negative vocabulary and two discouragements for every encouragement. The same children more likely to be exposed to trauma also may have less positive preparation to reduce their development of significant fears with the associated stress effects. You and I see this during visits – take the opportunity to discuss and model an alternative.
References
1. Clin Child Fam Psychol Rev. 2010 Jun;13(2):129-50.
2. “The Early Catastrophe: The 30 Million Word Gap by Age 3” (Washington: American Educator, Spring 2003).
Dr. Howard is assistant professor of pediatrics at Johns Hopkins University School of Medicine, Baltimore, and creator of CHADIS. She has no other relevant disclosures. Dr. Howard’s contribution to this publication was as a paid expert to Frontline Medical News. Email her at pdnews@frontlinemedcom.com.

VIDEO: Integrated care effective in first-episode psychosis
ATLANTA – Increasingly, data support taking an integrated approach to care in the intervention of first-episode psychosis.
But what are the key components of such treatment?
Dr. Charles Schulz, who initiated an integrated care clinic for first-episode psychosis at the University of Minnesota, Minneapolis, outlined the steps in an integrated care approach.
In an interview at the annual meeting of the American Psychiatric Association, Dr. Schulz reviewed the importance of intervening in the prodromal phase whenever possible, as well as offering cognitive-behavioral and remediation therapies along with medication management.
He also addressed the need for family psychoeducation and group therapy. And Dr. Schulz explained what to do when there might be a differential that manifests with psychiatric presentations that are not psychosis.
Dr. Schulz said he has industry relationships with Forum Pharmaceuticals and Myriad.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
ATLANTA – Increasingly, data support taking an integrated approach to care in the intervention of first-episode psychosis.
But what are the key components of such treatment?
Dr. Charles Schulz, who initiated an integrated care clinic for first-episode psychosis at the University of Minnesota, Minneapolis, outlined the steps in an integrated care approach.
In an interview at the annual meeting of the American Psychiatric Association, Dr. Schulz reviewed the importance of intervening in the prodromal phase whenever possible, as well as offering cognitive-behavioral and remediation therapies along with medication management.
He also addressed the need for family psychoeducation and group therapy. And Dr. Schulz explained what to do when there might be a differential that manifests with psychiatric presentations that are not psychosis.
Dr. Schulz said he has industry relationships with Forum Pharmaceuticals and Myriad.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
ATLANTA – Increasingly, data support taking an integrated approach to care in the intervention of first-episode psychosis.
But what are the key components of such treatment?
Dr. Charles Schulz, who initiated an integrated care clinic for first-episode psychosis at the University of Minnesota, Minneapolis, outlined the steps in an integrated care approach.
In an interview at the annual meeting of the American Psychiatric Association, Dr. Schulz reviewed the importance of intervening in the prodromal phase whenever possible, as well as offering cognitive-behavioral and remediation therapies along with medication management.
He also addressed the need for family psychoeducation and group therapy. And Dr. Schulz explained what to do when there might be a differential that manifests with psychiatric presentations that are not psychosis.
Dr. Schulz said he has industry relationships with Forum Pharmaceuticals and Myriad.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
On Twitter @whitneymcknight
EXPERT ANALYSIS FROM THE APA ANNUAL MEETING

Children’s Bone Development Linked to Mothers’ Placenta Size
A larger placenta during pregnancy may lead to larger bones in children, according to a study published in the Journal of Bone and Mineral Research.
Researchers studied 518 children who underwent bone scans at ages 9, 15, and 17. Measurements of thickness, volume, and weight also were taken from their mothers’ placenta. They found that a greater placenta size at birth was associated with larger bones at each age in childhood. This relationship remained robust even after adjusting for factors such as the child’s height, weight, and pubertal status.
Overall, larger bones in early life can lead to larger, stronger bones in older adulthood, thus reducing the risk of osteoporosis and broken bones in later life.
Suggested Reading
Holroyd CR, Osmond C, Barker D, et al. Placental size is associated differentially with postnatal bone size and density. J Bone Miner Res. 2016 Mar 21. [Epub ahead of print]
A larger placenta during pregnancy may lead to larger bones in children, according to a study published in the Journal of Bone and Mineral Research.
Researchers studied 518 children who underwent bone scans at ages 9, 15, and 17. Measurements of thickness, volume, and weight also were taken from their mothers’ placenta. They found that a greater placenta size at birth was associated with larger bones at each age in childhood. This relationship remained robust even after adjusting for factors such as the child’s height, weight, and pubertal status.
Overall, larger bones in early life can lead to larger, stronger bones in older adulthood, thus reducing the risk of osteoporosis and broken bones in later life.
A larger placenta during pregnancy may lead to larger bones in children, according to a study published in the Journal of Bone and Mineral Research.
Researchers studied 518 children who underwent bone scans at ages 9, 15, and 17. Measurements of thickness, volume, and weight also were taken from their mothers’ placenta. They found that a greater placenta size at birth was associated with larger bones at each age in childhood. This relationship remained robust even after adjusting for factors such as the child’s height, weight, and pubertal status.
Overall, larger bones in early life can lead to larger, stronger bones in older adulthood, thus reducing the risk of osteoporosis and broken bones in later life.
Suggested Reading
Holroyd CR, Osmond C, Barker D, et al. Placental size is associated differentially with postnatal bone size and density. J Bone Miner Res. 2016 Mar 21. [Epub ahead of print]
Suggested Reading
Holroyd CR, Osmond C, Barker D, et al. Placental size is associated differentially with postnatal bone size and density. J Bone Miner Res. 2016 Mar 21. [Epub ahead of print]
Why access to public bathrooms matters
Going to the movies is something I have always enjoyed. What I don’t always enjoy is waiting in line to use the bathroom after the movie is over and invariably picking a stall that has run out of toilet paper or that is in need of cleaning. These minor inconveniences in no way compare to the experiences some of my transgender patients have shared with me. Many of my patients tell me that they avoid using bathrooms in public places because of the anxiety they feel at having to pick a bathroom. Do they use the one that matches their sex assigned at birth or the one that matches their gender identity? Will they be safe and free from harassment in either bathroom? Some of my patients tell me they avoid drinking water at school just so they do not have to deal with going to the bathroom there.
Recently there have been bills introduced in several states that seek to deny transgender youth access to sex-segregated spaces including restrooms and locker rooms. These bills stigmatize an already vulnerable population, potentially increasing their risk of negative health outcomes. In a survey of transgender people in Massachusetts, 65% of respondents reported being discriminated against in public accommodations, and this discrimination was associated with poorer mental and physical health outcomes.1

In February of 2016, the American Academy of Pediatrics and several other organizations dedicated to the health and welfare of children came out with a letter to state governors in opposition to these bills.2 It states: “Transgender kids are already at heightened risk for violence, bullying, and harassment, and these bills exacerbate those risks by creating a hostile environment. … In addition, students who would be affected by these bills are among our most vulnerable to experiencing depression and engaging in self-harm, including suicide.”
On May 13, 2016, the U.S. Department of Justice and the U.S. Department of Education jointly issued a letter directing public schools to allow transgender students to use bathrooms that correspond with their gender identity.3 The letter was accompanied by a 25-page document with examples of policies and emerging practices to support transgender students.4
Proponents of these bills state that their purpose is to increase public safety and protect privacy. There are concerns that individuals may take advantage of these policies to sexually harass people in sex-segregated spaces. To date, there are no data to support these claims. In interviews conducted with heads of state police departments in 12 states that have nondiscrimination laws to protect transgender people in public settings, not one of the participants indicated any increase in sexual harassment or abuse in connection with these laws.1 In addition, should any type of harassment occur, it would not be protected under antidiscrimination laws, and perpetrators would be subject to criminal penalties.
What can we do as health care providers to support our patients?
• Educate ourselves. Keep up to date with best practice guidelines and evidence on how to promote the health and well-being of all children. The National LGBT Health Education Center has many educational resources to help health care providers provide quality care to LGBT patients and families. It is important to be aware of resources to help patients and families be aware of their rights and advocate for themselves in other settings such as school and work. Two organizations that provide this support and information are Trans Youth Family Allies and Lambda Legal.
• Create safe spaces. Create spaces in our practice settings where children and youth can safely explore their gender identity and gender expression. This can be done by providing access to gender-neutral bathrooms, prominently displaying nondiscrimination policies that are inclusive of gender identity, and modeling recognition of the variety of ways gender can be experienced by asking and using patients’ preferred names and pronouns.
• Advocate. Advocate for gender-inclusive environments within local youth-serving organizations including schools, medical facilities, and child welfare agencies. Share available information about the potential negative health effects of stigmatization and discrimination in transgender youth.
Together we can work to promote the well-being of all children.
Resources
• The National LGBT Health Education Center (www.lgbthealtheducation.org/).
• Trans Youth Family Allies (www.imatyfa.org/).
• Lambda Legal (www.lambdalegal.org/know-your-rights/youth).
References
1. Policy Brief: State Anti-transgender Bathroom Bills Threaten Transgender People’s Health and Participation in Public Life. Fenway Institute and Center for American Progress, 2016.
2. American Academy of Pediatrics letter on sex-segregated spaces (www.aap.org/en-us/advocacy-and-policy/state-advocacy/Documents/AAP_HRCLetter.pdf).
3. Department of Justice and Department of Education Dear Colleague Letter on Transgender Students (www.justice.gov/opa/file/850996/download).
4. Department of Education Examples of Policies and Emerging Practices for Supporting Transgender Students (www2.ed.gov/about/offices/list/oese/oshs/emergingpractices.pdf).
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
Going to the movies is something I have always enjoyed. What I don’t always enjoy is waiting in line to use the bathroom after the movie is over and invariably picking a stall that has run out of toilet paper or that is in need of cleaning. These minor inconveniences in no way compare to the experiences some of my transgender patients have shared with me. Many of my patients tell me that they avoid using bathrooms in public places because of the anxiety they feel at having to pick a bathroom. Do they use the one that matches their sex assigned at birth or the one that matches their gender identity? Will they be safe and free from harassment in either bathroom? Some of my patients tell me they avoid drinking water at school just so they do not have to deal with going to the bathroom there.
Recently there have been bills introduced in several states that seek to deny transgender youth access to sex-segregated spaces including restrooms and locker rooms. These bills stigmatize an already vulnerable population, potentially increasing their risk of negative health outcomes. In a survey of transgender people in Massachusetts, 65% of respondents reported being discriminated against in public accommodations, and this discrimination was associated with poorer mental and physical health outcomes.1
In February of 2016, the American Academy of Pediatrics and several other organizations dedicated to the health and welfare of children came out with a letter to state governors in opposition to these bills.2 It states: “Transgender kids are already at heightened risk for violence, bullying, and harassment, and these bills exacerbate those risks by creating a hostile environment. … In addition, students who would be affected by these bills are among our most vulnerable to experiencing depression and engaging in self-harm, including suicide.”
On May 13, 2016, the U.S. Department of Justice and the U.S. Department of Education jointly issued a letter directing public schools to allow transgender students to use bathrooms that correspond with their gender identity.3 The letter was accompanied by a 25-page document with examples of policies and emerging practices to support transgender students.4
Proponents of these bills state that their purpose is to increase public safety and protect privacy. There are concerns that individuals may take advantage of these policies to sexually harass people in sex-segregated spaces. To date, there are no data to support these claims. In interviews conducted with heads of state police departments in 12 states that have nondiscrimination laws to protect transgender people in public settings, not one of the participants indicated any increase in sexual harassment or abuse in connection with these laws.1 In addition, should any type of harassment occur, it would not be protected under antidiscrimination laws, and perpetrators would be subject to criminal penalties.
What can we do as health care providers to support our patients?
• Educate ourselves. Keep up to date with best practice guidelines and evidence on how to promote the health and well-being of all children. The National LGBT Health Education Center has many educational resources to help health care providers provide quality care to LGBT patients and families. It is important to be aware of resources to help patients and families be aware of their rights and advocate for themselves in other settings such as school and work. Two organizations that provide this support and information are Trans Youth Family Allies and Lambda Legal.
• Create safe spaces. Create spaces in our practice settings where children and youth can safely explore their gender identity and gender expression. This can be done by providing access to gender-neutral bathrooms, prominently displaying nondiscrimination policies that are inclusive of gender identity, and modeling recognition of the variety of ways gender can be experienced by asking and using patients’ preferred names and pronouns.
• Advocate. Advocate for gender-inclusive environments within local youth-serving organizations including schools, medical facilities, and child welfare agencies. Share available information about the potential negative health effects of stigmatization and discrimination in transgender youth.
Together we can work to promote the well-being of all children.
Resources
• The National LGBT Health Education Center (www.lgbthealtheducation.org/).
• Trans Youth Family Allies (www.imatyfa.org/).
• Lambda Legal (www.lambdalegal.org/know-your-rights/youth).
References
1. Policy Brief: State Anti-transgender Bathroom Bills Threaten Transgender People’s Health and Participation in Public Life. Fenway Institute and Center for American Progress, 2016.
2. American Academy of Pediatrics letter on sex-segregated spaces (www.aap.org/en-us/advocacy-and-policy/state-advocacy/Documents/AAP_HRCLetter.pdf).
3. Department of Justice and Department of Education Dear Colleague Letter on Transgender Students (www.justice.gov/opa/file/850996/download).
4. Department of Education Examples of Policies and Emerging Practices for Supporting Transgender Students (www2.ed.gov/about/offices/list/oese/oshs/emergingpractices.pdf).
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.
Going to the movies is something I have always enjoyed. What I don’t always enjoy is waiting in line to use the bathroom after the movie is over and invariably picking a stall that has run out of toilet paper or that is in need of cleaning. These minor inconveniences in no way compare to the experiences some of my transgender patients have shared with me. Many of my patients tell me that they avoid using bathrooms in public places because of the anxiety they feel at having to pick a bathroom. Do they use the one that matches their sex assigned at birth or the one that matches their gender identity? Will they be safe and free from harassment in either bathroom? Some of my patients tell me they avoid drinking water at school just so they do not have to deal with going to the bathroom there.
Recently there have been bills introduced in several states that seek to deny transgender youth access to sex-segregated spaces including restrooms and locker rooms. These bills stigmatize an already vulnerable population, potentially increasing their risk of negative health outcomes. In a survey of transgender people in Massachusetts, 65% of respondents reported being discriminated against in public accommodations, and this discrimination was associated with poorer mental and physical health outcomes.1
In February of 2016, the American Academy of Pediatrics and several other organizations dedicated to the health and welfare of children came out with a letter to state governors in opposition to these bills.2 It states: “Transgender kids are already at heightened risk for violence, bullying, and harassment, and these bills exacerbate those risks by creating a hostile environment. … In addition, students who would be affected by these bills are among our most vulnerable to experiencing depression and engaging in self-harm, including suicide.”
On May 13, 2016, the U.S. Department of Justice and the U.S. Department of Education jointly issued a letter directing public schools to allow transgender students to use bathrooms that correspond with their gender identity.3 The letter was accompanied by a 25-page document with examples of policies and emerging practices to support transgender students.4
Proponents of these bills state that their purpose is to increase public safety and protect privacy. There are concerns that individuals may take advantage of these policies to sexually harass people in sex-segregated spaces. To date, there are no data to support these claims. In interviews conducted with heads of state police departments in 12 states that have nondiscrimination laws to protect transgender people in public settings, not one of the participants indicated any increase in sexual harassment or abuse in connection with these laws.1 In addition, should any type of harassment occur, it would not be protected under antidiscrimination laws, and perpetrators would be subject to criminal penalties.
What can we do as health care providers to support our patients?
• Educate ourselves. Keep up to date with best practice guidelines and evidence on how to promote the health and well-being of all children. The National LGBT Health Education Center has many educational resources to help health care providers provide quality care to LGBT patients and families. It is important to be aware of resources to help patients and families be aware of their rights and advocate for themselves in other settings such as school and work. Two organizations that provide this support and information are Trans Youth Family Allies and Lambda Legal.
• Create safe spaces. Create spaces in our practice settings where children and youth can safely explore their gender identity and gender expression. This can be done by providing access to gender-neutral bathrooms, prominently displaying nondiscrimination policies that are inclusive of gender identity, and modeling recognition of the variety of ways gender can be experienced by asking and using patients’ preferred names and pronouns.
• Advocate. Advocate for gender-inclusive environments within local youth-serving organizations including schools, medical facilities, and child welfare agencies. Share available information about the potential negative health effects of stigmatization and discrimination in transgender youth.
Together we can work to promote the well-being of all children.
Resources
• The National LGBT Health Education Center (www.lgbthealtheducation.org/).
• Trans Youth Family Allies (www.imatyfa.org/).
• Lambda Legal (www.lambdalegal.org/know-your-rights/youth).
References
1. Policy Brief: State Anti-transgender Bathroom Bills Threaten Transgender People’s Health and Participation in Public Life. Fenway Institute and Center for American Progress, 2016.
2. American Academy of Pediatrics letter on sex-segregated spaces (www.aap.org/en-us/advocacy-and-policy/state-advocacy/Documents/AAP_HRCLetter.pdf).
3. Department of Justice and Department of Education Dear Colleague Letter on Transgender Students (www.justice.gov/opa/file/850996/download).
4. Department of Education Examples of Policies and Emerging Practices for Supporting Transgender Students (www2.ed.gov/about/offices/list/oese/oshs/emergingpractices.pdf).
Dr. Chelvakumar is an attending physician in the division of adolescent medicine at Nationwide Children’s Hospital and an assistant professor of clinical pediatrics at the Ohio State University, both in Columbus.

Age Influences ED Visits for Mental Health Among American Indian Children
Age plays an influential role in the number of emergency department (ED) visits for mental health concerns among American Indian children, according to Wyatt J. Pickner and his associates.
The researchers analyzed 26,004 pediatric ED visits by 20,413 patients over a 12-month study period in the Upper Midwest. Among these, there were 1,545 visits (5.94%) by 1,287 patients for mental health reasons.

American Indian children had higher odds of having ED visits for mental health concerns, compared with white children (10.8% vs. 5.1%; P less than .0001), the researchers noted.
Visits by older American Indian children were more likely to be for mental health reasons, compared with younger children (P less than .0001). Within the 5- to 10-year-old group, these children had lower odds of a mental health visit (odds ratio, 0.40), while the 11- to 17-year-old American Indian children had higher odds of a mental health visit (OR, 1.62).
“Visits to the ED for mental health reasons by American Indian children are a complex problem and not fully understood,” the researchers concluded. “We believe our data can help to inform clinicians and policymakers on the appropriate resources and interventions that can be used to improve care for American Indian children.”
Read the study in The Journal of Pediatrics (doi: 10.1016/j.jpeds.2016.03.064).
Age plays an influential role in the number of emergency department (ED) visits for mental health concerns among American Indian children, according to Wyatt J. Pickner and his associates.
The researchers analyzed 26,004 pediatric ED visits by 20,413 patients over a 12-month study period in the Upper Midwest. Among these, there were 1,545 visits (5.94%) by 1,287 patients for mental health reasons.
American Indian children had higher odds of having ED visits for mental health concerns, compared with white children (10.8% vs. 5.1%; P less than .0001), the researchers noted.
Visits by older American Indian children were more likely to be for mental health reasons, compared with younger children (P less than .0001). Within the 5- to 10-year-old group, these children had lower odds of a mental health visit (odds ratio, 0.40), while the 11- to 17-year-old American Indian children had higher odds of a mental health visit (OR, 1.62).
“Visits to the ED for mental health reasons by American Indian children are a complex problem and not fully understood,” the researchers concluded. “We believe our data can help to inform clinicians and policymakers on the appropriate resources and interventions that can be used to improve care for American Indian children.”
Read the study in The Journal of Pediatrics (doi: 10.1016/j.jpeds.2016.03.064).
Age plays an influential role in the number of emergency department (ED) visits for mental health concerns among American Indian children, according to Wyatt J. Pickner and his associates.
The researchers analyzed 26,004 pediatric ED visits by 20,413 patients over a 12-month study period in the Upper Midwest. Among these, there were 1,545 visits (5.94%) by 1,287 patients for mental health reasons.
American Indian children had higher odds of having ED visits for mental health concerns, compared with white children (10.8% vs. 5.1%; P less than .0001), the researchers noted.
Visits by older American Indian children were more likely to be for mental health reasons, compared with younger children (P less than .0001). Within the 5- to 10-year-old group, these children had lower odds of a mental health visit (odds ratio, 0.40), while the 11- to 17-year-old American Indian children had higher odds of a mental health visit (OR, 1.62).
“Visits to the ED for mental health reasons by American Indian children are a complex problem and not fully understood,” the researchers concluded. “We believe our data can help to inform clinicians and policymakers on the appropriate resources and interventions that can be used to improve care for American Indian children.”
Read the study in The Journal of Pediatrics (doi: 10.1016/j.jpeds.2016.03.064).
FROM THE JOURNAL OF PEDIATRICS

Age Influences ED Visits for Mental Health Among American Indian Children
Age plays an influential role in the number of emergency department (ED) visits for mental health concerns among American Indian children, according to Wyatt J. Pickner and his associates.
The researchers analyzed 26,004 pediatric ED visits by 20,413 patients over a 12-month study period in the Upper Midwest. Among these, there were 1,545 visits (5.94%) by 1,287 patients for mental health reasons.
American Indian children had higher odds of having ED visits for mental health concerns, compared with white children (10.8% vs. 5.1%; P less than .0001), the researchers noted.
Visits by older American Indian children were more likely to be for mental health reasons, compared with younger children (P less than .0001). Within the 5- to 10-year-old group, these children had lower odds of a mental health visit (odds ratio, 0.40), while the 11- to 17-year-old American Indian children had higher odds of a mental health visit (OR, 1.62).
“Visits to the ED for mental health reasons by American Indian children are a complex problem and not fully understood,” the researchers concluded. “We believe our data can help to inform clinicians and policymakers on the appropriate resources and interventions that can be used to improve care for American Indian children.”
Read the study in The Journal of Pediatrics (doi: 10.1016/j.jpeds.2016.03.064).
Age plays an influential role in the number of emergency department (ED) visits for mental health concerns among American Indian children, according to Wyatt J. Pickner and his associates.
The researchers analyzed 26,004 pediatric ED visits by 20,413 patients over a 12-month study period in the Upper Midwest. Among these, there were 1,545 visits (5.94%) by 1,287 patients for mental health reasons.
American Indian children had higher odds of having ED visits for mental health concerns, compared with white children (10.8% vs. 5.1%; P less than .0001), the researchers noted.
Visits by older American Indian children were more likely to be for mental health reasons, compared with younger children (P less than .0001). Within the 5- to 10-year-old group, these children had lower odds of a mental health visit (odds ratio, 0.40), while the 11- to 17-year-old American Indian children had higher odds of a mental health visit (OR, 1.62).
“Visits to the ED for mental health reasons by American Indian children are a complex problem and not fully understood,” the researchers concluded. “We believe our data can help to inform clinicians and policymakers on the appropriate resources and interventions that can be used to improve care for American Indian children.”
Read the study in The Journal of Pediatrics (doi: 10.1016/j.jpeds.2016.03.064).
Age plays an influential role in the number of emergency department (ED) visits for mental health concerns among American Indian children, according to Wyatt J. Pickner and his associates.
The researchers analyzed 26,004 pediatric ED visits by 20,413 patients over a 12-month study period in the Upper Midwest. Among these, there were 1,545 visits (5.94%) by 1,287 patients for mental health reasons.
American Indian children had higher odds of having ED visits for mental health concerns, compared with white children (10.8% vs. 5.1%; P less than .0001), the researchers noted.
Visits by older American Indian children were more likely to be for mental health reasons, compared with younger children (P less than .0001). Within the 5- to 10-year-old group, these children had lower odds of a mental health visit (odds ratio, 0.40), while the 11- to 17-year-old American Indian children had higher odds of a mental health visit (OR, 1.62).
“Visits to the ED for mental health reasons by American Indian children are a complex problem and not fully understood,” the researchers concluded. “We believe our data can help to inform clinicians and policymakers on the appropriate resources and interventions that can be used to improve care for American Indian children.”
Read the study in The Journal of Pediatrics (doi: 10.1016/j.jpeds.2016.03.064).
FROM THE JOURNAL OF PEDIATRICS
