User login
Pediatric Heat-Related Illnesses
Heat-related illnesses in children encompass a wide range of disease processes—from minor conditions such as heat rash to life-threatening thermoregulatory emergencies such as heatstroke. Physiological differences in children compared to adults make them particularly susceptible to illnesses caused by heat exposure.
Pediatric heat-related illnesses can usually be prevented if appropriate precautions are taken (see “Taking Steps to Prevent Heat-Related Illnesses” box). In lieu of prevention, early recognition and treatment of heatstroke in children may drastically reduce life-threatening complications related to multisystem organ dysfunction. Management of heatstroke rests primarily on prompt initiation of rapid cooling measures and evaluation for organ dysfunction.
Case Scenarios
Case 1
An obese 10-year-old boy was brought to the ED by emergency medical services (EMS) during the first week of youth football tryouts. It was a hot day in late August, with 100% humidity and temperatures over 95°F. The patient, who weighed approximately 240 lb, was trying out for football but had no previous athletic-conditioning experience. Despite his obesity, he had been generally healthy and only took a stimulant medication for attention-deficit/hyperactivity disorder (ADHD).
At approximately noon, the boy collapsed on the field and had a seizure. When the EMS technicians arrived, they administered a dose of intramuscular (IM) midazolam. Although his seizure ceased, he remained obtunded and was intubated. A rectal temperature revealed a temperature of 105.8°F and paramedics noted that while the patient felt hot, he was no longer sweating. While en route to the ED, EMS technicians removed the patient’s football uniform; placed a fan in front of him; and sprayed cool water on him in an effort to lower his body temperature. At the time of arrival to the ED, his rectal temperature was 104.9°F.
Case 2
A previously healthy 3-month-old female infant was brought to the ED by EMS after she was accidentally left in a car on a summer day with a temperature of 90°F and 100% humidity. The infant’s father said that while running errands, he had forgotten his daughter was in the car and had left her in the rear facing backseat car carrier for approximately 10 minutes. When he returned to the car, he found his daughter awake but crying inconsolably. She had sweated through her clothes, vomited, and felt very hot, so he called 911. Her initial rectal temperature was 102.2°F, and her clothes were removed as she was being transported in an air-conditioned ambulance to the ED for further evaluation. Once undressed, she was noted to have an erythematous rash with multiple papules and pustules on her trunk.
Epidemiology
From 2006 to 2010, an average of 668 heat-related deaths per year occurred among people of all ages in the United States. Of these deaths, approximately 7% occurred in children younger than age 4 years (2.5% in those younger than age 1 year and 4.5% in those age 1-4 years). These figures have remained relatively stable over the last 10 years.1,2 Adolescents are particularly at risk for overexertion, and heatstroke is the third leading cause of death in young athletes, after traumatic and cardiac causes.3 As may be expected, most heat-related deaths (76%) occur in the southern and western regions of the United States.
Pathophysiology of Heat-Related Illnesses
The hypothalamus is the main control center for temperature homeostasis. As the core temperature rises due to either metabolic or environmental causes of heat, the hypothalamus primarily acts on the autonomic nervous system to engage mechanisms of heat dissipation.4 Evaporation of sweat is believed to be the most important mechanism of heat dissipation in humans; however, this method becomes less effective when humidity levels are above 75%.5 Radiation allows heat to transfer from the skin to the air, but is reliant on a temperature gradient. Conduction can allow heat to transfer to a cooler object through physical contact (as seen with cold-water immersion), while convection utilizes air movement to transfer heat (as illustrated by fanning).6
Thermoregulation is disrupted when the body is unable to balance metabolic heat production and heat dissipation. Heat dissipation mechanisms are easily overwhelmed when a person is exposed to excessive heat from the environment. The resulting stress from hyperthermia can directly injure cells, leading to a cytokine storm and endothelial injury. Heat can cause proteins to denature and cells to undergo apoptosis, which, if severe, can result in multisystem organ dysfunction.7
Physiological Differences in Children
Several physiological differences in children compared to adults compromise their ability to manage heat exposure. Thermoregulation in infants is less developed secondary to an immature hypothalamus; therefore, they are less able to utilize compensatory mechanisms to dissipate heat.8 In addition, infants and young children have a decreased sweating capacity, which makes evaporative cooling less effective.9 Children also produce more endogenous heat per kilogram than adults, which is believed to be secondary to a higher basal metabolic rate. They have less blood volume than adults, which decreases their ability to transfer warm blood into the periphery in order to cool the central core. Lastly, children have a higher surface area-to-body mass ratio, which causes increased heat absorption. All of these factors ultimately result in a slower rate of acclimatization in children compared to adults.10
Environmental Factors
Several environmental risk factors predispose children to heat-related illnesses. Infants are completely dependent on their caregivers for hydration and environmental protection from the heat. Infants who are over-bundled or left in a hot car are particularly at risk for heat-related illnesses.11 Older children are at risk for sports-related overexertion and typically must depend on permission from a coach or supervising adult to hydrate or take a break from exercise. Lastly, medications such as stimulants frequently prescribed for ADHD or medications with anticholinergic properties (secondary to decreased sweating) can predispose children to heat intolerance.12
Minor Heat-Related Illnesses
Heat-related illnesses range from benign conditions (eg, heat rash) to life-threatening processes (eg, heatstroke).
Miliaria Rubra
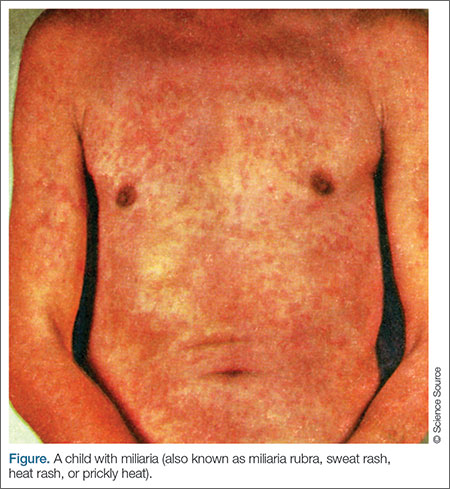
There are several forms of miliaria. Miliaria rubra, also known as heat rash or prickly heat, is a common, benign manifestation of heat exposure in infants and young children. A combination of heat exposure and obstructed sweat glands results in a pruritic, erythematous rash with papules and pustules (Figure). This is often seen in areas of friction from skin rubbing against skin or clothing.13
Heat Edema/Heat Cramps
Heat edema is another benign process related to heat exposure that generally occurs in older adults but can also occur in children. It is the result of peripheral vasodilation as the body attempts to shunt warm blood to the periphery.14 Heat cramps are a common manifestation in young athletes exercising in hot, summer conditions. Although benign, the cramps are very painful spasms that often affect large muscle groups, particularly in the legs, such as the calves, quadriceps, and hamstrings. There is conflicting data regarding the underlying cause of heat cramps. Many believe there is a significant component related to dehydration, while others attribute the cramps to fatigue or a combination
of the two.15
Heat Syncope
Heat syncope secondary to peripheral vasodilation, and venous pooling occurs as the body attempts to dissipate heat by transferring warm blood to the periphery. Relative dehydration plays a role in heat syncope, which is often precipitated by a rapid change in positioning during exercise, such as moving from a sitting to standing position. Heat syncope usually improves after the patient is supine, and children with heat syncope do not have an elevation in core body temperature.14 Some patients who experience heat syncope, however, may also have heat exhaustion.
Heat Exhaustion
Heat exhaustion occurs in patients with a known heat exposure. As opposed to the previously described processes, heat exhaustion is characterized by a body temperature elevated up to 104°F. Heat exhaustion is often accompanied by diffuse, nonspecific symptoms such as tachycardia, sweating, nausea, vomiting, weakness, fatigue, headache, and mild confusion. Dehydration often plays a significant role in heat exhaustion, but in contrast to heatstroke (described in the following section), mentation is normal, or there is a transient, mild confusion.16
Heatstroke
Heatstroke is observed in patients with a known heat exposure who have a temperature greater than 104°F accompanied by central nervous system (CNS) dysfunction.14 The CNS dysfunction involves an alteration in mental status manifested by slurred speech, ataxia, delirium, hallucinations, or seizure activity. In severe cases, obtundation or coma may result in airway compromise.17 Vital signs are unstable, and tachycardia and hypotension are often present. Patients with heatstroke may stop sweating, although the absence of sweating is not required for the diagnosis. Other nonspecific findings such as vomiting and diarrhea are common.6
The hallmark of heatstroke is multisystem organ dysfunction, which is caused by heat-induced tissue damage resulting in a systemic inflammatory response.18 Since the pediatric brain is particularly sensitive to temperature extremes, cerebral edema and herniation are potential complications of heatstroke.17 Damage to myocardial tissue, coupled with dehydration and systemic vasodilation, results in hypotension and poor systemic perfusion.19 Muscle breakdown causes rhabdomyolysis that can lead to kidney failure and hepatic injury. Degradation of clotting factors disrupts the clotting system and can cause disseminated intravascular coagulation (DIC).20 Damage to the mucosal lining of the intestines may result in ischemia and massive hematochezia.21
Heatstroke is classified as either nonexertional or exertional. Nonexertional heatstroke occurs most frequently in younger children who are exposed to a hot environment, such as an infant left in a car on a warm day. Exertional heatstroke occurs primarily in children exercising on a hot day, such as young athletes.6
Due to its significant morbidity and mortality, heatstroke is the most concerning manifestation of excessive heat exposure. The mortality rate for children with heatstroke is significantly lower than for adults; however, approximately 10% of children with heatstroke will not survive,22 and 20% will have long-term neurological disabilities, including permanent impairment in vision, speech, memory, behavior, and coordination.23
Management of Minor Heat-Related Illnesses
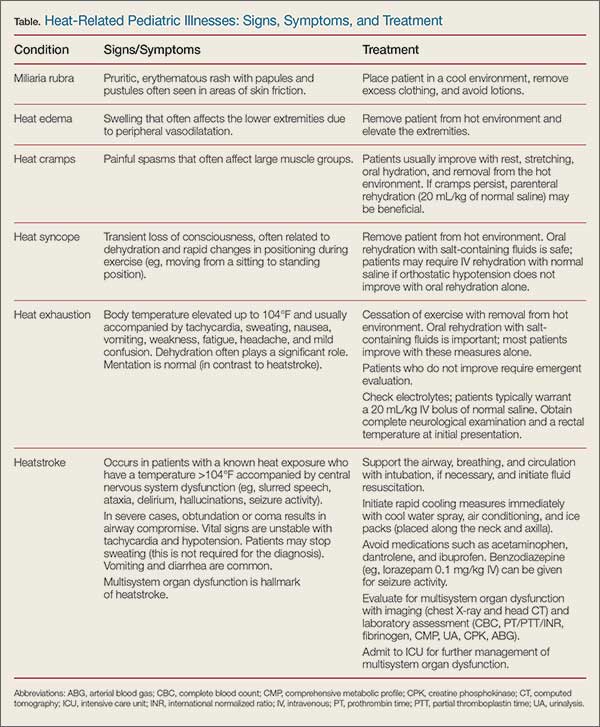
For most minor heat-related illnesses, supportive care is the mainstay of treatment (Table).
Miliaria Rubra
Infants with miliaria rubra typically improve once they are placed in a cool environment and their clothing is removed. In infants, lotions may contribute to sweat gland obstruction and should be used sparingly.13
Heat Edema/Heat Cramps
Similarly, heat edema generally improves once the child is removed from the hot environment and the extremities are elevated.14 Heat cramps are likely the result of fatigue and dehydration; therefore, these painful contractions often improve with rest, stretching, oral hydration, and removal from the hot environment. If cramps persist despite these measures, parenteral rehydration (20 mL/kg of normal saline) may be beneficial.15
Heat Syncope
Patients with orthostatic hypotension from heat syncope usually improve once they are resting in a cool environment and have been rehydrated. Pediatric oral rehydration with salt-containing fluids, such as commercial sports drinks, is safe; nonetheless, these patients may require intravenous (IV) rehydration with normal saline if orthostatic hypotension does not improve with oral rehydration alone.14
Heat Exhaustion
Differentiating heat exhaustion from heatstroke is of upmost importance because the treatment courses vary greatly. The difference in neurological status is the most effective way of differentiating the two diseases. All patients with slurred speech, ataxia, delirium, hallucinations, or seizure activity should be treated for presumptive heatstroke until proven otherwise (see “Management of Heatstroke” section).
Although children with heat exhaustion may have mild confusion, this tends to be transient and resolves with supportive care. Patients with heat exhaustion should stop exercising and be placed in a cool environment without excess clothing. Oral rehydration with salt-containing fluids is important, and most patients improve with these measures alone.
Children with apparent heat exhaustion who do not improve should be evaluated in the hospital setting, and laboratory studies should be obtained to evaluate for electrolyte abnormalities. Such patients typically warrant a 20 mL/kg IV bolus of normal saline. A complete neurological examination and a rectal temperature should be obtained on initial presentation.16
The evaluation of an overbundled infant with hyperthermia may be particularly challenging. Studies have demonstrated that it is possible for an infant to develop core temperature elevation if overbundled and placed in a warm environment.24 Nonetheless, it is important to address these patients with a broad differential diagnosis in mind, and always consider the possibility of sepsis. If the history and examination are consistent with hyperthermia secondary to heat exposure, a period of observation with supportive care may be a reasonable option. Infants should have a rectal temperature assessed every 15 to 30 minutes to monitor for improvement; if they improve with supportive care alone, a septic evaluation can be potentially avoided. Antipyretics will confuse the clinical picture and should be avoided in this situation.24
Management of Heatstroke
Significant morbidity and mortality are associated with heatstroke, and prompt recognition and initiation of therapy are required to prevent or minimize serious complications.22 As in any other life-threatening condition, the initial treatment of heatstroke requires support of the airway, breathing, and circulation. Patients are often neurologically unstable and cannot protect their airway, which should prompt endotracheal intubation. Children who are tachycardic and hypotensive should be resuscitated with normal saline prior to intubation if oxygenation and ventilation are maintained with supplemental oxygen alone. Most patients require at least 20 mL/kg of IV normal saline but many ultimately need up to 60 mL/kg.14 If blood pressure (BP) does not respond adequately to fluid resuscitation alone, vasopressors may be necessary. Seizure activity can be managed with IV benzodiazepines, such as lorazepam (0.1 mg/kg with maximum 4 mg per dose).14
Rapid cooling therapy is the mainstay of treatment for heatstroke and should be initiated as soon as the diagnosis is suspected, since morbidity and mortality correlates directly with the duration of hyperthermia. These measures are ideally started prior to arrival at the hospital. Evaporative cooling can be achieved in the field or ambulance with a cool water spray and air conditioning. Additionally, ice packs can be placed along the neck and axilla to augment rapid cooling measures and can be continued in the ED until the patient’s core temperature decreases to 101.4°F.25
Medications have a limited role in the treatment of heatstroke. Antipyretics such as acetaminophen and ibuprofen have no proven benefit and may exacerbate hepatic, gastrointestinal, clotting, and renal dysfunction.26 Benzodiazepines are helpful for seizure activity and may have a role in seizure prophylaxis. Dantrolene is not recommended for treating heatstroke as studies have not demonstrated a statistical improvement in cooling time, complications, or mortality.14 The use of chilled IV fluids instead of room-temperature fluids is not definitively supported in the literature.27
Further diagnostic evaluation is directed at determining the degree of multisystem organ dysfunction that results from heatstroke. A head computed tomography (CT) scan can evaluate for cerebral edema, whereas a comprehensive metabolic profile (CMP) will screen for electrolyte abnormalities such as hyponatremia (salt loss), hypernatremia (volume depletion), and possible transaminase elevation, which may indicate hepatic injury. Prolonged coagulation studies may reveal DIC and an arterial blood gas (ABG) analysis often may reveal metabolic acidosis. A serum creatine phosphokinase (CPK) and urinalysis (UA) can help to identify rhabdomyolysis or the presence of an acute kidney injury (AKI).16
After their condition is stabilized, children with heatstroke should be monitored in the pediatric intensive care unit (PICU) to effectively address complications of multisystem organ dysfunction.
Case Scenarios Continued
Case 1
[The 10-year-old boy who collapsed during football tryouts.]
The initial evaluation revealed an obese child who was intubated and obtunded. His vital signs included the following: rectal temperature, 104.9°F; heart rate (HR), 149 beats/minute; and BP, 82/36 mm Hg. Heatstroke was diagnosed and rapid cooling measures were initiated.
Evaporative heat loss was maintained with a fan and water spray, and ice packs were placed along the patient’s groin and axillae. Laboratory evaluation included a complete blood count (CBC), CMP, CPK, UA, coagulation panel, and ABG. A normal saline IV bolus at room temperature was given and a postintubation chest X-ray confirmed appropriate position of the endotracheal tube, without any evidence of acute respiratory distress syndrome (ARDS). A head CT scan did not reveal cerebral edema. Since the child’s BP and HR did not improve after the first normal saline bolus, he was given a total of 40 mL/kg of IV normal saline in the ED. The patient’s laboratory results were concerning for an AKI, with elevated CPK, hepatic injury, coagulopathy, and severe metabolic acidosis. He was subsequently admitted to the PICU for further care.
The child’s PICU course was complicated by multisystem organ failure, which ultimately included DIC, ARDS, acute renal failure requiring hemodialysis, and hypotension requiring vasopressors. A repeat head CT scan 3 days after admission revealed marked cerebral edema. The patient subsequently died within a week of presentation.
Case 2
[The 3-month-old girl who was left in a hot vehicle.]
The initial evaluation revealed a fussy infant with dry mucous membranes, elevated HR, and sunken fontanelle. Her rectal temperature on arrival to the ED was 100.7°F after conservative measures were taken (ie, removing her from the hot environment and removing her clothing). A peripheral IV was placed due to her clinical dehydration and she received a 20 mL/kg bolus of normal saline at room temperature. A glucose level was obtained and was normal. The patient’s rectal temperature was monitored every 30 minutes over the next 4 hours, and her temperature and HR gradually normalized.
The patient’s rash appeared consistent with miliaria rubra and improved as her temperature decreased. The infant underwent a brief period of observation in the ED where she continued to look well and tolerated oral fluids without vomiting. Neither a septic work-up nor empiric antibiotics were initiated, since heat exposure was felt to be the likely source of her core temperature elevation. Child Protective Services (CPS) was notified and opened a case for further evaluation of possible child neglect. The patient ultimately returned to her baseline in the ED and was discharged home with a family member, according to the safety plan outlined by CPS, and close follow-up with her pediatrician.
1. Berko J, Ingram DD, Saha S, Parker JD. Deaths attributed to heat, cold, and other weather events in the United States, 2006-2010. National health statistics reports; no 76. Hyattsville, MD: National Center for Health Statistics; 2014. http://www.cdc.gov/nchs/data/nhsr/nhsr076.pdf. Accessed May 22, 2016.
2. Centers for Disease Control and Prevention(CDC). Heat-related deaths--United States, 1999-2003. MMWR Morb Mortal Wkly Rep. 2006;55(29):796-798.
3. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119(8):1085-1092.
4. Romanovsky AA. Thermoregulation: some concepts have changed. Functional architecture of the thermoregulatory system. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R37-R46.
5. Smith CJ, Johnson, JM. Responses to hyperthermia. Optimizing heat dissipation by convection and evaporation: Neural control of skin blood flow and sweating in humans. Auton Neurosci. 2016;196:25-36.
6. Becker JA, Stewart LK. Heat-related illness. Am Fam Physician. 2011;83(11):1325-1330.
7. Aggarwal Y, Karan BM, Das BN, Sinha RK. Prediction of heat-illness symptoms with the prediction of human vascular response in hot environment under resting condition. J Med Syst. 2008;32(2):167-176.
8. Charkoudian N. Human hermoregulation from the autonomic perspective. Auton Neurosci. 2016;196:1-2.
9. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669-682.
10. Falk B, Dotan R. Children’s thermoregulation during exercise in the heat: a revisit. Appl Physiol Nutr Metab. 2008;33(2):420-427.
11. Booth JN 3rd, Davis GG, Waterbor J, McGwin G Jr. Hyperthermia deaths among children in parked vehicles: an analysis of 231 fatalities in the United States, 1999-2007. Forensic Sci Med Pathol. 2010;6(2):99-105.
12. Levine M, LoVecchio F, Ruha AM, Chu G, Roque P. Influence of drug use on morbidity and mortality in heatstroke. J Med Toxicol. 2012;8(3):252-257.
13. O’Connor NR, McLaughlin MR, Ham P. Newborn skin: part I. Common rashes. Am Fam Physician. 2008;77(1):47-52.
14. Howe AS, Boden BP. Heat-related illness in athletes. Am J Sports Med. 2007;35(8):1384-1395.
15. Bergeron MF. Muscle cramps during exercise – Is it fatigue or electrolyte deficit? Curr Sports Med Rep. 2008;7(4):S50-S55.
16. Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician. 2005;71(11):2133-2140.
17. Sharma HS. Methods to produce hyperthermia-induced brain dysfunction. Prog Brain Res. 2007;162:173-199.
18. Leon LR, Helwig BG. Heat stroke: role of the systemic inflammatory response. J Appl Physiol. 2010;109(6):1980-1988.
19. Wilson TE, Crandall CG. Effect of thermal stress on cardiac function. Exerc Sport Sci Rev. 2011;39(1):12-17.
20. Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17-24.
21. Lambert GP. Intestinal barrier dysfunction, endotoxemia, and gastrointestinal symptoms: the ‘canary in the coal mine’ during exercise-heat stress? Med Sport Sci. 2008;53:61-73.
22. Jardine DS. Heat illness and heat stroke. Pediatr Rev. 2007;28(7):249-258
23. Argaud L, Ferry T, Le QH, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007;167(20):2177-2183.
24. Cheng TL, Partridge JC. Effect of bundling and high environmental temperature on neonatal body temperature. Pediatrics. 1993;92(2):238-240.
25. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
26. Walker JS, Hogan DE. Heat emergencies. In: Tintinalli JE, Kelen GD, Stapczynski S. The American College of Emergency Physicians, eds. Emergency Medicine: A Comprehensive Study Guide, Section 15. China: The McGraw-Hill Companies, Inc; 2004:1183-1189.
27. Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39(8):503-507.
28. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-288.
29. National Weather Service, National Oceanic and Atmospheric Administration: NWS Heat Index. http://www.nws.noaa.gov/om/heat/heat_index.shtml. Accessed May 19, 2016.
30. Council on Sports Medicine and Fitness and Council on School Health; Bergeron MF, Devore C, Rice SG; American Academy of Pediatrics. Policy statement—Climatic heat stress and exercising children and adolescents. Pediatrics. 2011;128(3):e741-e777.
Heat-related illnesses in children encompass a wide range of disease processes—from minor conditions such as heat rash to life-threatening thermoregulatory emergencies such as heatstroke. Physiological differences in children compared to adults make them particularly susceptible to illnesses caused by heat exposure.
Pediatric heat-related illnesses can usually be prevented if appropriate precautions are taken (see “Taking Steps to Prevent Heat-Related Illnesses” box). In lieu of prevention, early recognition and treatment of heatstroke in children may drastically reduce life-threatening complications related to multisystem organ dysfunction. Management of heatstroke rests primarily on prompt initiation of rapid cooling measures and evaluation for organ dysfunction.
Case Scenarios
Case 1
An obese 10-year-old boy was brought to the ED by emergency medical services (EMS) during the first week of youth football tryouts. It was a hot day in late August, with 100% humidity and temperatures over 95°F. The patient, who weighed approximately 240 lb, was trying out for football but had no previous athletic-conditioning experience. Despite his obesity, he had been generally healthy and only took a stimulant medication for attention-deficit/hyperactivity disorder (ADHD).
At approximately noon, the boy collapsed on the field and had a seizure. When the EMS technicians arrived, they administered a dose of intramuscular (IM) midazolam. Although his seizure ceased, he remained obtunded and was intubated. A rectal temperature revealed a temperature of 105.8°F and paramedics noted that while the patient felt hot, he was no longer sweating. While en route to the ED, EMS technicians removed the patient’s football uniform; placed a fan in front of him; and sprayed cool water on him in an effort to lower his body temperature. At the time of arrival to the ED, his rectal temperature was 104.9°F.
Case 2
A previously healthy 3-month-old female infant was brought to the ED by EMS after she was accidentally left in a car on a summer day with a temperature of 90°F and 100% humidity. The infant’s father said that while running errands, he had forgotten his daughter was in the car and had left her in the rear facing backseat car carrier for approximately 10 minutes. When he returned to the car, he found his daughter awake but crying inconsolably. She had sweated through her clothes, vomited, and felt very hot, so he called 911. Her initial rectal temperature was 102.2°F, and her clothes were removed as she was being transported in an air-conditioned ambulance to the ED for further evaluation. Once undressed, she was noted to have an erythematous rash with multiple papules and pustules on her trunk.
Epidemiology
From 2006 to 2010, an average of 668 heat-related deaths per year occurred among people of all ages in the United States. Of these deaths, approximately 7% occurred in children younger than age 4 years (2.5% in those younger than age 1 year and 4.5% in those age 1-4 years). These figures have remained relatively stable over the last 10 years.1,2 Adolescents are particularly at risk for overexertion, and heatstroke is the third leading cause of death in young athletes, after traumatic and cardiac causes.3 As may be expected, most heat-related deaths (76%) occur in the southern and western regions of the United States.
Pathophysiology of Heat-Related Illnesses
The hypothalamus is the main control center for temperature homeostasis. As the core temperature rises due to either metabolic or environmental causes of heat, the hypothalamus primarily acts on the autonomic nervous system to engage mechanisms of heat dissipation.4 Evaporation of sweat is believed to be the most important mechanism of heat dissipation in humans; however, this method becomes less effective when humidity levels are above 75%.5 Radiation allows heat to transfer from the skin to the air, but is reliant on a temperature gradient. Conduction can allow heat to transfer to a cooler object through physical contact (as seen with cold-water immersion), while convection utilizes air movement to transfer heat (as illustrated by fanning).6
Thermoregulation is disrupted when the body is unable to balance metabolic heat production and heat dissipation. Heat dissipation mechanisms are easily overwhelmed when a person is exposed to excessive heat from the environment. The resulting stress from hyperthermia can directly injure cells, leading to a cytokine storm and endothelial injury. Heat can cause proteins to denature and cells to undergo apoptosis, which, if severe, can result in multisystem organ dysfunction.7
Physiological Differences in Children
Several physiological differences in children compared to adults compromise their ability to manage heat exposure. Thermoregulation in infants is less developed secondary to an immature hypothalamus; therefore, they are less able to utilize compensatory mechanisms to dissipate heat.8 In addition, infants and young children have a decreased sweating capacity, which makes evaporative cooling less effective.9 Children also produce more endogenous heat per kilogram than adults, which is believed to be secondary to a higher basal metabolic rate. They have less blood volume than adults, which decreases their ability to transfer warm blood into the periphery in order to cool the central core. Lastly, children have a higher surface area-to-body mass ratio, which causes increased heat absorption. All of these factors ultimately result in a slower rate of acclimatization in children compared to adults.10
Environmental Factors
Several environmental risk factors predispose children to heat-related illnesses. Infants are completely dependent on their caregivers for hydration and environmental protection from the heat. Infants who are over-bundled or left in a hot car are particularly at risk for heat-related illnesses.11 Older children are at risk for sports-related overexertion and typically must depend on permission from a coach or supervising adult to hydrate or take a break from exercise. Lastly, medications such as stimulants frequently prescribed for ADHD or medications with anticholinergic properties (secondary to decreased sweating) can predispose children to heat intolerance.12
Minor Heat-Related Illnesses
Heat-related illnesses range from benign conditions (eg, heat rash) to life-threatening processes (eg, heatstroke).
Miliaria Rubra
There are several forms of miliaria. Miliaria rubra, also known as heat rash or prickly heat, is a common, benign manifestation of heat exposure in infants and young children. A combination of heat exposure and obstructed sweat glands results in a pruritic, erythematous rash with papules and pustules (Figure). This is often seen in areas of friction from skin rubbing against skin or clothing.13
Heat Edema/Heat Cramps
Heat edema is another benign process related to heat exposure that generally occurs in older adults but can also occur in children. It is the result of peripheral vasodilation as the body attempts to shunt warm blood to the periphery.14 Heat cramps are a common manifestation in young athletes exercising in hot, summer conditions. Although benign, the cramps are very painful spasms that often affect large muscle groups, particularly in the legs, such as the calves, quadriceps, and hamstrings. There is conflicting data regarding the underlying cause of heat cramps. Many believe there is a significant component related to dehydration, while others attribute the cramps to fatigue or a combination
of the two.15
Heat Syncope
Heat syncope secondary to peripheral vasodilation, and venous pooling occurs as the body attempts to dissipate heat by transferring warm blood to the periphery. Relative dehydration plays a role in heat syncope, which is often precipitated by a rapid change in positioning during exercise, such as moving from a sitting to standing position. Heat syncope usually improves after the patient is supine, and children with heat syncope do not have an elevation in core body temperature.14 Some patients who experience heat syncope, however, may also have heat exhaustion.
Heat Exhaustion
Heat exhaustion occurs in patients with a known heat exposure. As opposed to the previously described processes, heat exhaustion is characterized by a body temperature elevated up to 104°F. Heat exhaustion is often accompanied by diffuse, nonspecific symptoms such as tachycardia, sweating, nausea, vomiting, weakness, fatigue, headache, and mild confusion. Dehydration often plays a significant role in heat exhaustion, but in contrast to heatstroke (described in the following section), mentation is normal, or there is a transient, mild confusion.16
Heatstroke
Heatstroke is observed in patients with a known heat exposure who have a temperature greater than 104°F accompanied by central nervous system (CNS) dysfunction.14 The CNS dysfunction involves an alteration in mental status manifested by slurred speech, ataxia, delirium, hallucinations, or seizure activity. In severe cases, obtundation or coma may result in airway compromise.17 Vital signs are unstable, and tachycardia and hypotension are often present. Patients with heatstroke may stop sweating, although the absence of sweating is not required for the diagnosis. Other nonspecific findings such as vomiting and diarrhea are common.6
The hallmark of heatstroke is multisystem organ dysfunction, which is caused by heat-induced tissue damage resulting in a systemic inflammatory response.18 Since the pediatric brain is particularly sensitive to temperature extremes, cerebral edema and herniation are potential complications of heatstroke.17 Damage to myocardial tissue, coupled with dehydration and systemic vasodilation, results in hypotension and poor systemic perfusion.19 Muscle breakdown causes rhabdomyolysis that can lead to kidney failure and hepatic injury. Degradation of clotting factors disrupts the clotting system and can cause disseminated intravascular coagulation (DIC).20 Damage to the mucosal lining of the intestines may result in ischemia and massive hematochezia.21
Heatstroke is classified as either nonexertional or exertional. Nonexertional heatstroke occurs most frequently in younger children who are exposed to a hot environment, such as an infant left in a car on a warm day. Exertional heatstroke occurs primarily in children exercising on a hot day, such as young athletes.6
Due to its significant morbidity and mortality, heatstroke is the most concerning manifestation of excessive heat exposure. The mortality rate for children with heatstroke is significantly lower than for adults; however, approximately 10% of children with heatstroke will not survive,22 and 20% will have long-term neurological disabilities, including permanent impairment in vision, speech, memory, behavior, and coordination.23
Management of Minor Heat-Related Illnesses
For most minor heat-related illnesses, supportive care is the mainstay of treatment (Table).
Miliaria Rubra
Infants with miliaria rubra typically improve once they are placed in a cool environment and their clothing is removed. In infants, lotions may contribute to sweat gland obstruction and should be used sparingly.13
Heat Edema/Heat Cramps
Similarly, heat edema generally improves once the child is removed from the hot environment and the extremities are elevated.14 Heat cramps are likely the result of fatigue and dehydration; therefore, these painful contractions often improve with rest, stretching, oral hydration, and removal from the hot environment. If cramps persist despite these measures, parenteral rehydration (20 mL/kg of normal saline) may be beneficial.15
Heat Syncope
Patients with orthostatic hypotension from heat syncope usually improve once they are resting in a cool environment and have been rehydrated. Pediatric oral rehydration with salt-containing fluids, such as commercial sports drinks, is safe; nonetheless, these patients may require intravenous (IV) rehydration with normal saline if orthostatic hypotension does not improve with oral rehydration alone.14
Heat Exhaustion
Differentiating heat exhaustion from heatstroke is of upmost importance because the treatment courses vary greatly. The difference in neurological status is the most effective way of differentiating the two diseases. All patients with slurred speech, ataxia, delirium, hallucinations, or seizure activity should be treated for presumptive heatstroke until proven otherwise (see “Management of Heatstroke” section).
Although children with heat exhaustion may have mild confusion, this tends to be transient and resolves with supportive care. Patients with heat exhaustion should stop exercising and be placed in a cool environment without excess clothing. Oral rehydration with salt-containing fluids is important, and most patients improve with these measures alone.
Children with apparent heat exhaustion who do not improve should be evaluated in the hospital setting, and laboratory studies should be obtained to evaluate for electrolyte abnormalities. Such patients typically warrant a 20 mL/kg IV bolus of normal saline. A complete neurological examination and a rectal temperature should be obtained on initial presentation.16
The evaluation of an overbundled infant with hyperthermia may be particularly challenging. Studies have demonstrated that it is possible for an infant to develop core temperature elevation if overbundled and placed in a warm environment.24 Nonetheless, it is important to address these patients with a broad differential diagnosis in mind, and always consider the possibility of sepsis. If the history and examination are consistent with hyperthermia secondary to heat exposure, a period of observation with supportive care may be a reasonable option. Infants should have a rectal temperature assessed every 15 to 30 minutes to monitor for improvement; if they improve with supportive care alone, a septic evaluation can be potentially avoided. Antipyretics will confuse the clinical picture and should be avoided in this situation.24
Management of Heatstroke
Significant morbidity and mortality are associated with heatstroke, and prompt recognition and initiation of therapy are required to prevent or minimize serious complications.22 As in any other life-threatening condition, the initial treatment of heatstroke requires support of the airway, breathing, and circulation. Patients are often neurologically unstable and cannot protect their airway, which should prompt endotracheal intubation. Children who are tachycardic and hypotensive should be resuscitated with normal saline prior to intubation if oxygenation and ventilation are maintained with supplemental oxygen alone. Most patients require at least 20 mL/kg of IV normal saline but many ultimately need up to 60 mL/kg.14 If blood pressure (BP) does not respond adequately to fluid resuscitation alone, vasopressors may be necessary. Seizure activity can be managed with IV benzodiazepines, such as lorazepam (0.1 mg/kg with maximum 4 mg per dose).14
Rapid cooling therapy is the mainstay of treatment for heatstroke and should be initiated as soon as the diagnosis is suspected, since morbidity and mortality correlates directly with the duration of hyperthermia. These measures are ideally started prior to arrival at the hospital. Evaporative cooling can be achieved in the field or ambulance with a cool water spray and air conditioning. Additionally, ice packs can be placed along the neck and axilla to augment rapid cooling measures and can be continued in the ED until the patient’s core temperature decreases to 101.4°F.25
Medications have a limited role in the treatment of heatstroke. Antipyretics such as acetaminophen and ibuprofen have no proven benefit and may exacerbate hepatic, gastrointestinal, clotting, and renal dysfunction.26 Benzodiazepines are helpful for seizure activity and may have a role in seizure prophylaxis. Dantrolene is not recommended for treating heatstroke as studies have not demonstrated a statistical improvement in cooling time, complications, or mortality.14 The use of chilled IV fluids instead of room-temperature fluids is not definitively supported in the literature.27
Further diagnostic evaluation is directed at determining the degree of multisystem organ dysfunction that results from heatstroke. A head computed tomography (CT) scan can evaluate for cerebral edema, whereas a comprehensive metabolic profile (CMP) will screen for electrolyte abnormalities such as hyponatremia (salt loss), hypernatremia (volume depletion), and possible transaminase elevation, which may indicate hepatic injury. Prolonged coagulation studies may reveal DIC and an arterial blood gas (ABG) analysis often may reveal metabolic acidosis. A serum creatine phosphokinase (CPK) and urinalysis (UA) can help to identify rhabdomyolysis or the presence of an acute kidney injury (AKI).16
After their condition is stabilized, children with heatstroke should be monitored in the pediatric intensive care unit (PICU) to effectively address complications of multisystem organ dysfunction.
Case Scenarios Continued
Case 1
[The 10-year-old boy who collapsed during football tryouts.]
The initial evaluation revealed an obese child who was intubated and obtunded. His vital signs included the following: rectal temperature, 104.9°F; heart rate (HR), 149 beats/minute; and BP, 82/36 mm Hg. Heatstroke was diagnosed and rapid cooling measures were initiated.
Evaporative heat loss was maintained with a fan and water spray, and ice packs were placed along the patient’s groin and axillae. Laboratory evaluation included a complete blood count (CBC), CMP, CPK, UA, coagulation panel, and ABG. A normal saline IV bolus at room temperature was given and a postintubation chest X-ray confirmed appropriate position of the endotracheal tube, without any evidence of acute respiratory distress syndrome (ARDS). A head CT scan did not reveal cerebral edema. Since the child’s BP and HR did not improve after the first normal saline bolus, he was given a total of 40 mL/kg of IV normal saline in the ED. The patient’s laboratory results were concerning for an AKI, with elevated CPK, hepatic injury, coagulopathy, and severe metabolic acidosis. He was subsequently admitted to the PICU for further care.
The child’s PICU course was complicated by multisystem organ failure, which ultimately included DIC, ARDS, acute renal failure requiring hemodialysis, and hypotension requiring vasopressors. A repeat head CT scan 3 days after admission revealed marked cerebral edema. The patient subsequently died within a week of presentation.
Case 2
[The 3-month-old girl who was left in a hot vehicle.]
The initial evaluation revealed a fussy infant with dry mucous membranes, elevated HR, and sunken fontanelle. Her rectal temperature on arrival to the ED was 100.7°F after conservative measures were taken (ie, removing her from the hot environment and removing her clothing). A peripheral IV was placed due to her clinical dehydration and she received a 20 mL/kg bolus of normal saline at room temperature. A glucose level was obtained and was normal. The patient’s rectal temperature was monitored every 30 minutes over the next 4 hours, and her temperature and HR gradually normalized.
The patient’s rash appeared consistent with miliaria rubra and improved as her temperature decreased. The infant underwent a brief period of observation in the ED where she continued to look well and tolerated oral fluids without vomiting. Neither a septic work-up nor empiric antibiotics were initiated, since heat exposure was felt to be the likely source of her core temperature elevation. Child Protective Services (CPS) was notified and opened a case for further evaluation of possible child neglect. The patient ultimately returned to her baseline in the ED and was discharged home with a family member, according to the safety plan outlined by CPS, and close follow-up with her pediatrician.
Heat-related illnesses in children encompass a wide range of disease processes—from minor conditions such as heat rash to life-threatening thermoregulatory emergencies such as heatstroke. Physiological differences in children compared to adults make them particularly susceptible to illnesses caused by heat exposure.
Pediatric heat-related illnesses can usually be prevented if appropriate precautions are taken (see “Taking Steps to Prevent Heat-Related Illnesses” box). In lieu of prevention, early recognition and treatment of heatstroke in children may drastically reduce life-threatening complications related to multisystem organ dysfunction. Management of heatstroke rests primarily on prompt initiation of rapid cooling measures and evaluation for organ dysfunction.
Case Scenarios
Case 1
An obese 10-year-old boy was brought to the ED by emergency medical services (EMS) during the first week of youth football tryouts. It was a hot day in late August, with 100% humidity and temperatures over 95°F. The patient, who weighed approximately 240 lb, was trying out for football but had no previous athletic-conditioning experience. Despite his obesity, he had been generally healthy and only took a stimulant medication for attention-deficit/hyperactivity disorder (ADHD).
At approximately noon, the boy collapsed on the field and had a seizure. When the EMS technicians arrived, they administered a dose of intramuscular (IM) midazolam. Although his seizure ceased, he remained obtunded and was intubated. A rectal temperature revealed a temperature of 105.8°F and paramedics noted that while the patient felt hot, he was no longer sweating. While en route to the ED, EMS technicians removed the patient’s football uniform; placed a fan in front of him; and sprayed cool water on him in an effort to lower his body temperature. At the time of arrival to the ED, his rectal temperature was 104.9°F.
Case 2
A previously healthy 3-month-old female infant was brought to the ED by EMS after she was accidentally left in a car on a summer day with a temperature of 90°F and 100% humidity. The infant’s father said that while running errands, he had forgotten his daughter was in the car and had left her in the rear facing backseat car carrier for approximately 10 minutes. When he returned to the car, he found his daughter awake but crying inconsolably. She had sweated through her clothes, vomited, and felt very hot, so he called 911. Her initial rectal temperature was 102.2°F, and her clothes were removed as she was being transported in an air-conditioned ambulance to the ED for further evaluation. Once undressed, she was noted to have an erythematous rash with multiple papules and pustules on her trunk.
Epidemiology
From 2006 to 2010, an average of 668 heat-related deaths per year occurred among people of all ages in the United States. Of these deaths, approximately 7% occurred in children younger than age 4 years (2.5% in those younger than age 1 year and 4.5% in those age 1-4 years). These figures have remained relatively stable over the last 10 years.1,2 Adolescents are particularly at risk for overexertion, and heatstroke is the third leading cause of death in young athletes, after traumatic and cardiac causes.3 As may be expected, most heat-related deaths (76%) occur in the southern and western regions of the United States.
Pathophysiology of Heat-Related Illnesses
The hypothalamus is the main control center for temperature homeostasis. As the core temperature rises due to either metabolic or environmental causes of heat, the hypothalamus primarily acts on the autonomic nervous system to engage mechanisms of heat dissipation.4 Evaporation of sweat is believed to be the most important mechanism of heat dissipation in humans; however, this method becomes less effective when humidity levels are above 75%.5 Radiation allows heat to transfer from the skin to the air, but is reliant on a temperature gradient. Conduction can allow heat to transfer to a cooler object through physical contact (as seen with cold-water immersion), while convection utilizes air movement to transfer heat (as illustrated by fanning).6
Thermoregulation is disrupted when the body is unable to balance metabolic heat production and heat dissipation. Heat dissipation mechanisms are easily overwhelmed when a person is exposed to excessive heat from the environment. The resulting stress from hyperthermia can directly injure cells, leading to a cytokine storm and endothelial injury. Heat can cause proteins to denature and cells to undergo apoptosis, which, if severe, can result in multisystem organ dysfunction.7
Physiological Differences in Children
Several physiological differences in children compared to adults compromise their ability to manage heat exposure. Thermoregulation in infants is less developed secondary to an immature hypothalamus; therefore, they are less able to utilize compensatory mechanisms to dissipate heat.8 In addition, infants and young children have a decreased sweating capacity, which makes evaporative cooling less effective.9 Children also produce more endogenous heat per kilogram than adults, which is believed to be secondary to a higher basal metabolic rate. They have less blood volume than adults, which decreases their ability to transfer warm blood into the periphery in order to cool the central core. Lastly, children have a higher surface area-to-body mass ratio, which causes increased heat absorption. All of these factors ultimately result in a slower rate of acclimatization in children compared to adults.10
Environmental Factors
Several environmental risk factors predispose children to heat-related illnesses. Infants are completely dependent on their caregivers for hydration and environmental protection from the heat. Infants who are over-bundled or left in a hot car are particularly at risk for heat-related illnesses.11 Older children are at risk for sports-related overexertion and typically must depend on permission from a coach or supervising adult to hydrate or take a break from exercise. Lastly, medications such as stimulants frequently prescribed for ADHD or medications with anticholinergic properties (secondary to decreased sweating) can predispose children to heat intolerance.12
Minor Heat-Related Illnesses
Heat-related illnesses range from benign conditions (eg, heat rash) to life-threatening processes (eg, heatstroke).
Miliaria Rubra
There are several forms of miliaria. Miliaria rubra, also known as heat rash or prickly heat, is a common, benign manifestation of heat exposure in infants and young children. A combination of heat exposure and obstructed sweat glands results in a pruritic, erythematous rash with papules and pustules (Figure). This is often seen in areas of friction from skin rubbing against skin or clothing.13
Heat Edema/Heat Cramps
Heat edema is another benign process related to heat exposure that generally occurs in older adults but can also occur in children. It is the result of peripheral vasodilation as the body attempts to shunt warm blood to the periphery.14 Heat cramps are a common manifestation in young athletes exercising in hot, summer conditions. Although benign, the cramps are very painful spasms that often affect large muscle groups, particularly in the legs, such as the calves, quadriceps, and hamstrings. There is conflicting data regarding the underlying cause of heat cramps. Many believe there is a significant component related to dehydration, while others attribute the cramps to fatigue or a combination
of the two.15
Heat Syncope
Heat syncope secondary to peripheral vasodilation, and venous pooling occurs as the body attempts to dissipate heat by transferring warm blood to the periphery. Relative dehydration plays a role in heat syncope, which is often precipitated by a rapid change in positioning during exercise, such as moving from a sitting to standing position. Heat syncope usually improves after the patient is supine, and children with heat syncope do not have an elevation in core body temperature.14 Some patients who experience heat syncope, however, may also have heat exhaustion.
Heat Exhaustion
Heat exhaustion occurs in patients with a known heat exposure. As opposed to the previously described processes, heat exhaustion is characterized by a body temperature elevated up to 104°F. Heat exhaustion is often accompanied by diffuse, nonspecific symptoms such as tachycardia, sweating, nausea, vomiting, weakness, fatigue, headache, and mild confusion. Dehydration often plays a significant role in heat exhaustion, but in contrast to heatstroke (described in the following section), mentation is normal, or there is a transient, mild confusion.16
Heatstroke
Heatstroke is observed in patients with a known heat exposure who have a temperature greater than 104°F accompanied by central nervous system (CNS) dysfunction.14 The CNS dysfunction involves an alteration in mental status manifested by slurred speech, ataxia, delirium, hallucinations, or seizure activity. In severe cases, obtundation or coma may result in airway compromise.17 Vital signs are unstable, and tachycardia and hypotension are often present. Patients with heatstroke may stop sweating, although the absence of sweating is not required for the diagnosis. Other nonspecific findings such as vomiting and diarrhea are common.6
The hallmark of heatstroke is multisystem organ dysfunction, which is caused by heat-induced tissue damage resulting in a systemic inflammatory response.18 Since the pediatric brain is particularly sensitive to temperature extremes, cerebral edema and herniation are potential complications of heatstroke.17 Damage to myocardial tissue, coupled with dehydration and systemic vasodilation, results in hypotension and poor systemic perfusion.19 Muscle breakdown causes rhabdomyolysis that can lead to kidney failure and hepatic injury. Degradation of clotting factors disrupts the clotting system and can cause disseminated intravascular coagulation (DIC).20 Damage to the mucosal lining of the intestines may result in ischemia and massive hematochezia.21
Heatstroke is classified as either nonexertional or exertional. Nonexertional heatstroke occurs most frequently in younger children who are exposed to a hot environment, such as an infant left in a car on a warm day. Exertional heatstroke occurs primarily in children exercising on a hot day, such as young athletes.6
Due to its significant morbidity and mortality, heatstroke is the most concerning manifestation of excessive heat exposure. The mortality rate for children with heatstroke is significantly lower than for adults; however, approximately 10% of children with heatstroke will not survive,22 and 20% will have long-term neurological disabilities, including permanent impairment in vision, speech, memory, behavior, and coordination.23
Management of Minor Heat-Related Illnesses
For most minor heat-related illnesses, supportive care is the mainstay of treatment (Table).
Miliaria Rubra
Infants with miliaria rubra typically improve once they are placed in a cool environment and their clothing is removed. In infants, lotions may contribute to sweat gland obstruction and should be used sparingly.13
Heat Edema/Heat Cramps
Similarly, heat edema generally improves once the child is removed from the hot environment and the extremities are elevated.14 Heat cramps are likely the result of fatigue and dehydration; therefore, these painful contractions often improve with rest, stretching, oral hydration, and removal from the hot environment. If cramps persist despite these measures, parenteral rehydration (20 mL/kg of normal saline) may be beneficial.15
Heat Syncope
Patients with orthostatic hypotension from heat syncope usually improve once they are resting in a cool environment and have been rehydrated. Pediatric oral rehydration with salt-containing fluids, such as commercial sports drinks, is safe; nonetheless, these patients may require intravenous (IV) rehydration with normal saline if orthostatic hypotension does not improve with oral rehydration alone.14
Heat Exhaustion
Differentiating heat exhaustion from heatstroke is of upmost importance because the treatment courses vary greatly. The difference in neurological status is the most effective way of differentiating the two diseases. All patients with slurred speech, ataxia, delirium, hallucinations, or seizure activity should be treated for presumptive heatstroke until proven otherwise (see “Management of Heatstroke” section).
Although children with heat exhaustion may have mild confusion, this tends to be transient and resolves with supportive care. Patients with heat exhaustion should stop exercising and be placed in a cool environment without excess clothing. Oral rehydration with salt-containing fluids is important, and most patients improve with these measures alone.
Children with apparent heat exhaustion who do not improve should be evaluated in the hospital setting, and laboratory studies should be obtained to evaluate for electrolyte abnormalities. Such patients typically warrant a 20 mL/kg IV bolus of normal saline. A complete neurological examination and a rectal temperature should be obtained on initial presentation.16
The evaluation of an overbundled infant with hyperthermia may be particularly challenging. Studies have demonstrated that it is possible for an infant to develop core temperature elevation if overbundled and placed in a warm environment.24 Nonetheless, it is important to address these patients with a broad differential diagnosis in mind, and always consider the possibility of sepsis. If the history and examination are consistent with hyperthermia secondary to heat exposure, a period of observation with supportive care may be a reasonable option. Infants should have a rectal temperature assessed every 15 to 30 minutes to monitor for improvement; if they improve with supportive care alone, a septic evaluation can be potentially avoided. Antipyretics will confuse the clinical picture and should be avoided in this situation.24
Management of Heatstroke
Significant morbidity and mortality are associated with heatstroke, and prompt recognition and initiation of therapy are required to prevent or minimize serious complications.22 As in any other life-threatening condition, the initial treatment of heatstroke requires support of the airway, breathing, and circulation. Patients are often neurologically unstable and cannot protect their airway, which should prompt endotracheal intubation. Children who are tachycardic and hypotensive should be resuscitated with normal saline prior to intubation if oxygenation and ventilation are maintained with supplemental oxygen alone. Most patients require at least 20 mL/kg of IV normal saline but many ultimately need up to 60 mL/kg.14 If blood pressure (BP) does not respond adequately to fluid resuscitation alone, vasopressors may be necessary. Seizure activity can be managed with IV benzodiazepines, such as lorazepam (0.1 mg/kg with maximum 4 mg per dose).14
Rapid cooling therapy is the mainstay of treatment for heatstroke and should be initiated as soon as the diagnosis is suspected, since morbidity and mortality correlates directly with the duration of hyperthermia. These measures are ideally started prior to arrival at the hospital. Evaporative cooling can be achieved in the field or ambulance with a cool water spray and air conditioning. Additionally, ice packs can be placed along the neck and axilla to augment rapid cooling measures and can be continued in the ED until the patient’s core temperature decreases to 101.4°F.25
Medications have a limited role in the treatment of heatstroke. Antipyretics such as acetaminophen and ibuprofen have no proven benefit and may exacerbate hepatic, gastrointestinal, clotting, and renal dysfunction.26 Benzodiazepines are helpful for seizure activity and may have a role in seizure prophylaxis. Dantrolene is not recommended for treating heatstroke as studies have not demonstrated a statistical improvement in cooling time, complications, or mortality.14 The use of chilled IV fluids instead of room-temperature fluids is not definitively supported in the literature.27
Further diagnostic evaluation is directed at determining the degree of multisystem organ dysfunction that results from heatstroke. A head computed tomography (CT) scan can evaluate for cerebral edema, whereas a comprehensive metabolic profile (CMP) will screen for electrolyte abnormalities such as hyponatremia (salt loss), hypernatremia (volume depletion), and possible transaminase elevation, which may indicate hepatic injury. Prolonged coagulation studies may reveal DIC and an arterial blood gas (ABG) analysis often may reveal metabolic acidosis. A serum creatine phosphokinase (CPK) and urinalysis (UA) can help to identify rhabdomyolysis or the presence of an acute kidney injury (AKI).16
After their condition is stabilized, children with heatstroke should be monitored in the pediatric intensive care unit (PICU) to effectively address complications of multisystem organ dysfunction.
Case Scenarios Continued
Case 1
[The 10-year-old boy who collapsed during football tryouts.]
The initial evaluation revealed an obese child who was intubated and obtunded. His vital signs included the following: rectal temperature, 104.9°F; heart rate (HR), 149 beats/minute; and BP, 82/36 mm Hg. Heatstroke was diagnosed and rapid cooling measures were initiated.
Evaporative heat loss was maintained with a fan and water spray, and ice packs were placed along the patient’s groin and axillae. Laboratory evaluation included a complete blood count (CBC), CMP, CPK, UA, coagulation panel, and ABG. A normal saline IV bolus at room temperature was given and a postintubation chest X-ray confirmed appropriate position of the endotracheal tube, without any evidence of acute respiratory distress syndrome (ARDS). A head CT scan did not reveal cerebral edema. Since the child’s BP and HR did not improve after the first normal saline bolus, he was given a total of 40 mL/kg of IV normal saline in the ED. The patient’s laboratory results were concerning for an AKI, with elevated CPK, hepatic injury, coagulopathy, and severe metabolic acidosis. He was subsequently admitted to the PICU for further care.
The child’s PICU course was complicated by multisystem organ failure, which ultimately included DIC, ARDS, acute renal failure requiring hemodialysis, and hypotension requiring vasopressors. A repeat head CT scan 3 days after admission revealed marked cerebral edema. The patient subsequently died within a week of presentation.
Case 2
[The 3-month-old girl who was left in a hot vehicle.]
The initial evaluation revealed a fussy infant with dry mucous membranes, elevated HR, and sunken fontanelle. Her rectal temperature on arrival to the ED was 100.7°F after conservative measures were taken (ie, removing her from the hot environment and removing her clothing). A peripheral IV was placed due to her clinical dehydration and she received a 20 mL/kg bolus of normal saline at room temperature. A glucose level was obtained and was normal. The patient’s rectal temperature was monitored every 30 minutes over the next 4 hours, and her temperature and HR gradually normalized.
The patient’s rash appeared consistent with miliaria rubra and improved as her temperature decreased. The infant underwent a brief period of observation in the ED where she continued to look well and tolerated oral fluids without vomiting. Neither a septic work-up nor empiric antibiotics were initiated, since heat exposure was felt to be the likely source of her core temperature elevation. Child Protective Services (CPS) was notified and opened a case for further evaluation of possible child neglect. The patient ultimately returned to her baseline in the ED and was discharged home with a family member, according to the safety plan outlined by CPS, and close follow-up with her pediatrician.
1. Berko J, Ingram DD, Saha S, Parker JD. Deaths attributed to heat, cold, and other weather events in the United States, 2006-2010. National health statistics reports; no 76. Hyattsville, MD: National Center for Health Statistics; 2014. http://www.cdc.gov/nchs/data/nhsr/nhsr076.pdf. Accessed May 22, 2016.
2. Centers for Disease Control and Prevention(CDC). Heat-related deaths--United States, 1999-2003. MMWR Morb Mortal Wkly Rep. 2006;55(29):796-798.
3. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119(8):1085-1092.
4. Romanovsky AA. Thermoregulation: some concepts have changed. Functional architecture of the thermoregulatory system. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R37-R46.
5. Smith CJ, Johnson, JM. Responses to hyperthermia. Optimizing heat dissipation by convection and evaporation: Neural control of skin blood flow and sweating in humans. Auton Neurosci. 2016;196:25-36.
6. Becker JA, Stewart LK. Heat-related illness. Am Fam Physician. 2011;83(11):1325-1330.
7. Aggarwal Y, Karan BM, Das BN, Sinha RK. Prediction of heat-illness symptoms with the prediction of human vascular response in hot environment under resting condition. J Med Syst. 2008;32(2):167-176.
8. Charkoudian N. Human hermoregulation from the autonomic perspective. Auton Neurosci. 2016;196:1-2.
9. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669-682.
10. Falk B, Dotan R. Children’s thermoregulation during exercise in the heat: a revisit. Appl Physiol Nutr Metab. 2008;33(2):420-427.
11. Booth JN 3rd, Davis GG, Waterbor J, McGwin G Jr. Hyperthermia deaths among children in parked vehicles: an analysis of 231 fatalities in the United States, 1999-2007. Forensic Sci Med Pathol. 2010;6(2):99-105.
12. Levine M, LoVecchio F, Ruha AM, Chu G, Roque P. Influence of drug use on morbidity and mortality in heatstroke. J Med Toxicol. 2012;8(3):252-257.
13. O’Connor NR, McLaughlin MR, Ham P. Newborn skin: part I. Common rashes. Am Fam Physician. 2008;77(1):47-52.
14. Howe AS, Boden BP. Heat-related illness in athletes. Am J Sports Med. 2007;35(8):1384-1395.
15. Bergeron MF. Muscle cramps during exercise – Is it fatigue or electrolyte deficit? Curr Sports Med Rep. 2008;7(4):S50-S55.
16. Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician. 2005;71(11):2133-2140.
17. Sharma HS. Methods to produce hyperthermia-induced brain dysfunction. Prog Brain Res. 2007;162:173-199.
18. Leon LR, Helwig BG. Heat stroke: role of the systemic inflammatory response. J Appl Physiol. 2010;109(6):1980-1988.
19. Wilson TE, Crandall CG. Effect of thermal stress on cardiac function. Exerc Sport Sci Rev. 2011;39(1):12-17.
20. Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17-24.
21. Lambert GP. Intestinal barrier dysfunction, endotoxemia, and gastrointestinal symptoms: the ‘canary in the coal mine’ during exercise-heat stress? Med Sport Sci. 2008;53:61-73.
22. Jardine DS. Heat illness and heat stroke. Pediatr Rev. 2007;28(7):249-258
23. Argaud L, Ferry T, Le QH, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007;167(20):2177-2183.
24. Cheng TL, Partridge JC. Effect of bundling and high environmental temperature on neonatal body temperature. Pediatrics. 1993;92(2):238-240.
25. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
26. Walker JS, Hogan DE. Heat emergencies. In: Tintinalli JE, Kelen GD, Stapczynski S. The American College of Emergency Physicians, eds. Emergency Medicine: A Comprehensive Study Guide, Section 15. China: The McGraw-Hill Companies, Inc; 2004:1183-1189.
27. Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39(8):503-507.
28. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-288.
29. National Weather Service, National Oceanic and Atmospheric Administration: NWS Heat Index. http://www.nws.noaa.gov/om/heat/heat_index.shtml. Accessed May 19, 2016.
30. Council on Sports Medicine and Fitness and Council on School Health; Bergeron MF, Devore C, Rice SG; American Academy of Pediatrics. Policy statement—Climatic heat stress and exercising children and adolescents. Pediatrics. 2011;128(3):e741-e777.
1. Berko J, Ingram DD, Saha S, Parker JD. Deaths attributed to heat, cold, and other weather events in the United States, 2006-2010. National health statistics reports; no 76. Hyattsville, MD: National Center for Health Statistics; 2014. http://www.cdc.gov/nchs/data/nhsr/nhsr076.pdf. Accessed May 22, 2016.
2. Centers for Disease Control and Prevention(CDC). Heat-related deaths--United States, 1999-2003. MMWR Morb Mortal Wkly Rep. 2006;55(29):796-798.
3. Maron BJ, Doerer JJ, Haas TS, Tierney DM, Mueller FO. Sudden deaths in young competitive athletes: analysis of 1866 deaths in the United States, 1980-2006. Circulation. 2009;119(8):1085-1092.
4. Romanovsky AA. Thermoregulation: some concepts have changed. Functional architecture of the thermoregulatory system. Am J Physiol Regul Integr Comp Physiol. 2007;292(1):R37-R46.
5. Smith CJ, Johnson, JM. Responses to hyperthermia. Optimizing heat dissipation by convection and evaporation: Neural control of skin blood flow and sweating in humans. Auton Neurosci. 2016;196:25-36.
6. Becker JA, Stewart LK. Heat-related illness. Am Fam Physician. 2011;83(11):1325-1330.
7. Aggarwal Y, Karan BM, Das BN, Sinha RK. Prediction of heat-illness symptoms with the prediction of human vascular response in hot environment under resting condition. J Med Syst. 2008;32(2):167-176.
8. Charkoudian N. Human hermoregulation from the autonomic perspective. Auton Neurosci. 2016;196:1-2.
9. Wendt D, van Loon LJ, Lichtenbelt WD. Thermoregulation during exercise in the heat: strategies for maintaining health and performance. Sports Med. 2007;37(8):669-682.
10. Falk B, Dotan R. Children’s thermoregulation during exercise in the heat: a revisit. Appl Physiol Nutr Metab. 2008;33(2):420-427.
11. Booth JN 3rd, Davis GG, Waterbor J, McGwin G Jr. Hyperthermia deaths among children in parked vehicles: an analysis of 231 fatalities in the United States, 1999-2007. Forensic Sci Med Pathol. 2010;6(2):99-105.
12. Levine M, LoVecchio F, Ruha AM, Chu G, Roque P. Influence of drug use on morbidity and mortality in heatstroke. J Med Toxicol. 2012;8(3):252-257.
13. O’Connor NR, McLaughlin MR, Ham P. Newborn skin: part I. Common rashes. Am Fam Physician. 2008;77(1):47-52.
14. Howe AS, Boden BP. Heat-related illness in athletes. Am J Sports Med. 2007;35(8):1384-1395.
15. Bergeron MF. Muscle cramps during exercise – Is it fatigue or electrolyte deficit? Curr Sports Med Rep. 2008;7(4):S50-S55.
16. Glazer JL. Management of heatstroke and heat exhaustion. Am Fam Physician. 2005;71(11):2133-2140.
17. Sharma HS. Methods to produce hyperthermia-induced brain dysfunction. Prog Brain Res. 2007;162:173-199.
18. Leon LR, Helwig BG. Heat stroke: role of the systemic inflammatory response. J Appl Physiol. 2010;109(6):1980-1988.
19. Wilson TE, Crandall CG. Effect of thermal stress on cardiac function. Exerc Sport Sci Rev. 2011;39(1):12-17.
20. Chapin JC, Hajjar KA. Fibrinolysis and the control of blood coagulation. Blood Rev. 2015;29(1):17-24.
21. Lambert GP. Intestinal barrier dysfunction, endotoxemia, and gastrointestinal symptoms: the ‘canary in the coal mine’ during exercise-heat stress? Med Sport Sci. 2008;53:61-73.
22. Jardine DS. Heat illness and heat stroke. Pediatr Rev. 2007;28(7):249-258
23. Argaud L, Ferry T, Le QH, et al. Short- and long-term outcomes of heatstroke following the 2003 heat wave in Lyon, France. Arch Intern Med. 2007;167(20):2177-2183.
24. Cheng TL, Partridge JC. Effect of bundling and high environmental temperature on neonatal body temperature. Pediatrics. 1993;92(2):238-240.
25. Bouchama A, Dehbi M, Chaves-Carballo E. Cooling and hemodynamic management in heatstroke: practical recommendations. Crit Care. 2007;11(3):R54.
26. Walker JS, Hogan DE. Heat emergencies. In: Tintinalli JE, Kelen GD, Stapczynski S. The American College of Emergency Physicians, eds. Emergency Medicine: A Comprehensive Study Guide, Section 15. China: The McGraw-Hill Companies, Inc; 2004:1183-1189.
27. Smith JE. Cooling methods used in the treatment of exertional heat illness. Br J Sports Med. 2005;39(8):503-507.
28. Rowland T. Fluid replacement requirements for child athletes. Sports Med. 2011;41(4):279-288.
29. National Weather Service, National Oceanic and Atmospheric Administration: NWS Heat Index. http://www.nws.noaa.gov/om/heat/heat_index.shtml. Accessed May 19, 2016.
30. Council on Sports Medicine and Fitness and Council on School Health; Bergeron MF, Devore C, Rice SG; American Academy of Pediatrics. Policy statement—Climatic heat stress and exercising children and adolescents. Pediatrics. 2011;128(3):e741-e777.

Spontaneous Repigmentation of Silvery Hair in an Infant With Congenital Hydrops Fetalis and Hypoproteinemia
Silvery hair is characteristic of 3 rare autosomal-recessive disorders—Chédiak-Higashi syndrome (CHS), Elejalde syndrome (ES), and Griscelli syndrome (GS)—which are associated with mutations in various genes that encode several proteins involved in the intracellular processing and movement of melanosomes. We report the case of a 2-month-old male infant with transient silvery hair and generalized hypopigmentation of the skin and eyes who did not have any genetic mutations associated with the classic syndromes that usually are characterized by transient silvery hair.
Case Report
A 2-month-old male infant presented to the dermatology department for evaluation of silvery hair with generalized hypopigmentation of the skin and eyes (Figure 1) that had developed at 1 month of age. His parents were healthy, nonconsanguineous, and reported no family history of silvery hair. The patient was delivered by cesarean section at 35 weeks’ gestation. His medical history was remarkable for congenital hydrops fetalis with pleuropericardial effusion, ascites, soft-tissue edema, and hydrocele with no signs of any congenital infection. Both the patient and his mother were O Rh +.

Several studies were performed following delivery. A direct Coombs test was negative. Blood studies revealed hypothyroidism and hypoalbuminemia secondary to protein loss associated with fetal hydrops. Cerebral, abdominal, and renal ultrasound; echocardiogram; thoracic and abdominal computed tomography; and cerebral magnetic resonance imaging revealed no abnormalities.
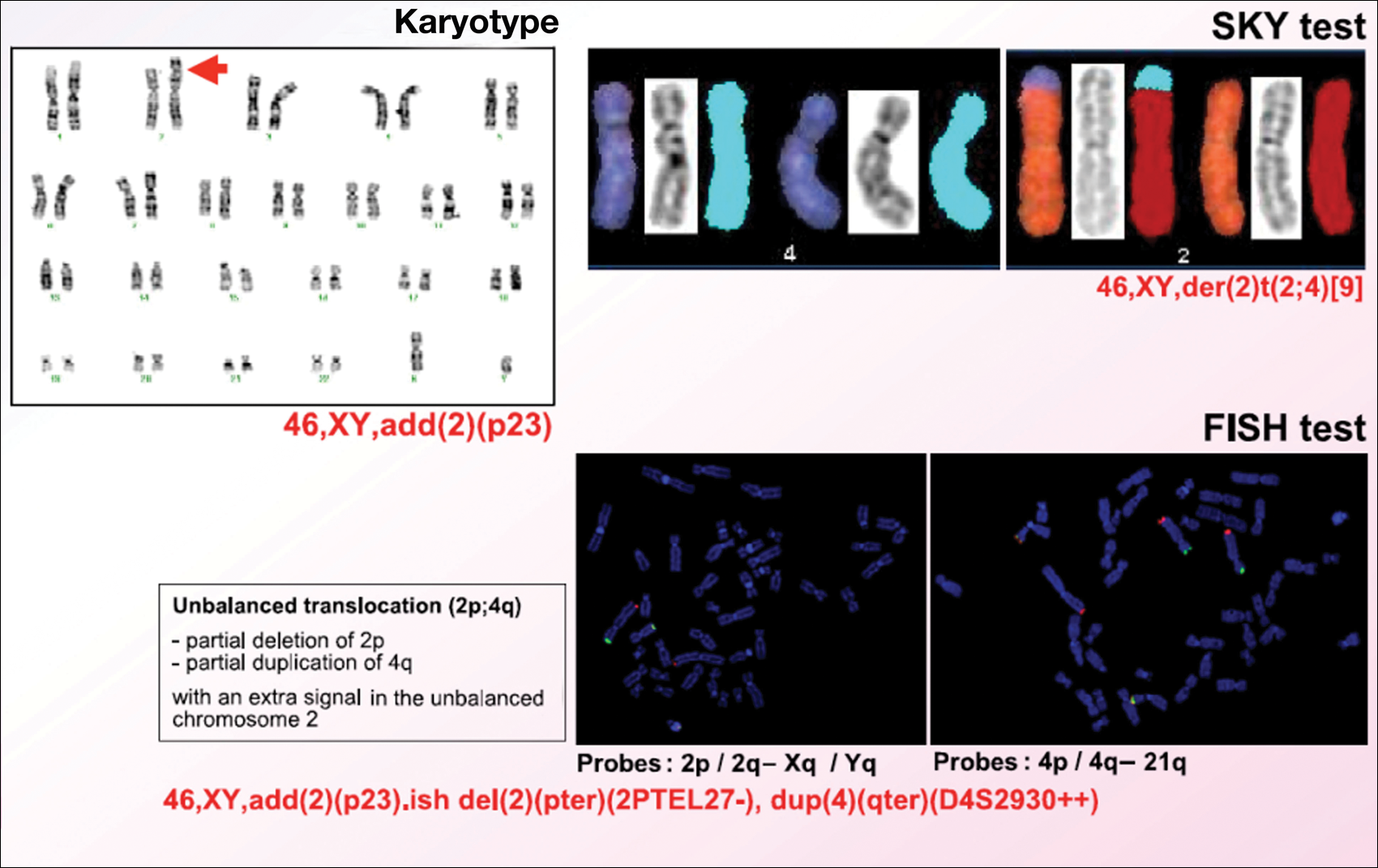
Karyotype results showed 46,XY,add(2)(p23), and subsequent spectral karyotyping and fluorescence in situ hybridization tests identified a chromosomal abnormality (46,XY,add[2][p23].ish del[2][pter][2PTEL27‒], dup[4][qter][D4S2930++])(Figure 2). Parental karyotypes were normal.
After birth, the infant was admitted to the neonatal intensive care unit for 50 days and received pleural and peritoneal drainages, mechanical ventilation, vasoactive drugs, parenteral nutrition with resolution of the hypoalbuminemia, levothyroxine, and intravenous antibiotics for central venous catheter infection. No drugs known to be associated with hypopigmentation of the hair, skin, or eyes were administered.
Two weeks after discharge from the neonatal intensive care unit, the patient was referred to our department. Physical examination revealed silvery hair on the scalp, eyebrows, and eyelashes, along with generalized hypopigmentation of the skin and eyes. Abdominal, cardiovascular, respiratory, and neurologic examination revealed no abnormalities, and no hepatosplenomegaly, lymphadenopathy, nystagmus, or strabismus was noted.
Light microscopy of the hair revealed small and regular aggregates of melanin along the hair shaft, predominantly in the medulla (Figure 3). Light microscopy of a skin biopsy specimen showed normal pigmentation in the melanocytes and no giant melanosomes. The melanocyte count was within reference range. A peripheral blood smear showed no giant granules in the granulocytes. No treatment was administered and the patient was followed closely every month. When the patient returned for follow-up at 9 months of age, physical examination revealed brown hair on the head, eyebrows, and eyelashes, as well as normal pigmentation of the skin and eyes (Figure 4). Thyroid function was normal and no recurrent infections of any type were noted. At follow-up at the age of 4 years, he showed normal neurological and psychological development with brown hair, no recurrent infections, and normal thyroid function. Given that CHS, ES, and GS had been ruled out, the clinical presentation and the genetic mutation detected may indicate that this case represents a new entity characterized by transient silvery hair.


Comment
Silvery hair is a known feature of CHS, ES, and GS (Table). The characteristic hypopigmentation associated with these autosomal-recessive disorders is the result of impaired melanosome transport leading to failed transfer of melanin to keratinocytes. These disorders differ from oculocutaneous albinism in that melanin synthesis is unaffected.
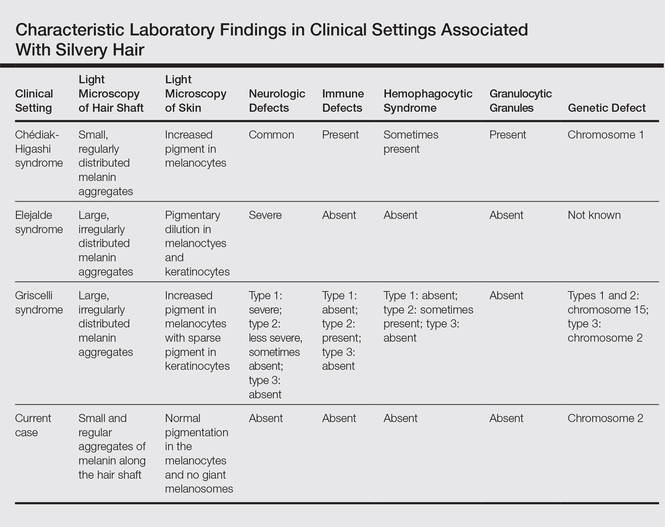
Chédiak-Higashi syndrome is characterized by generalized hypopigmentation of the skin and eyes, silvery hair, neurologic and immune dysfunction, lymphoproliferative disorders, and large granules in granulocytes and other cell types.1-3 A common complication of CHS is hemophagocytic lymphohistiocytosis, which is characterized by fever, jaundice, lymphadenopathy, hepatosplenomegaly, and pancytopenia.4 Pigmentary dilution of the irises also may be present, along with photophobia, strabismus, nystagmus, and impaired visual acuity. Chédiak-Higashi syndrome is the result of a genetic defect in the lysosomal trafficking regulator gene, also known as CHS1 (located on chromosome 1q42.1‒q42.2).5 Melanin in the hair shaft is distributed uniformly in multiple small aggregates. Light microscopy of the skin typically shows giant melanosomes in melanocytes and aberrant keratinocyte maturation.
Elejalde syndrome is characterized by silvery hair (eyelashes and eyebrows), neurologic defects, and normal immunologic function.6,7 The underlying molecular basis remains unknown. It appears related to or allelic to GS type 1 and thus associated with mutations in MYO5A (myosin VA); however, the gene mutation responsible has yet to be defined.8 Light microscopy of the hair shaft usually shows an irregular distribution of large melanin aggregates, primarily in the medulla.9,10 Skin biopsy generally shows irregular distribution and irregular size of melanin granules in the basal layer.11 Leukocytes usually show no abnormal cytoplasmic granules. Ocular involvement is common and may present as nystagmus, diplopia, hypopigmented retinas, and/or papilledema.
In GS, hair microscopy generally reveals large aggregates of melanin pigment distributed irregularly along the hair shaft. Granulocytes typically show no giant granules. Light microscopy of the skin usually shows increased pigment in melanocytes with sparse pigment in keratinocytes. Griscelli syndrome is classified into 3 types.12 In GS type 1, patients have silvery gray hair, light-colored skin, severe neurologic defects,13 and normal immune status. This variant is caused by a mutation in the MYO5A gene located on chromosome 15q21. In GS type 2, patients have silvery gray hair, pyogenic infections, an accelerated phase of hemophagocytic lymphohistiocytosis, and variable neurologic defects in the absence of primary neurologic disease.14,15 This variant is caused by a mutation in the RAB27A (member RAS oncogene family) gene located on chromosome 15q21. In GS type 3, patients exhibit generalized hypopigmentation of the skin and hair with no abnormalities of the nervous or immune systems. There are 2 different mutations associated with GS type 3: the first is located on chromosome 2q37.3, causing a mutation in MLPH (melanophilin), and the second is caused by an F-exon deletion in the MYO5A gene.14
Our patient had silvery hair, generalized hypopigmentation of the skin and eyes, and normal central nervous system function with no other ocular involvement and no evidence of recurrent infections of any kind. Light microscopy showed small and regular melanin pigment aggregates in the hair shaft, which differs from the irregular pigment aggregates in GS and ES.
The regular melanin pigment aggregates observed along the hair shaft were consistent with CHS, but other manifestations of this syndrome were absent: ocular, neurologic, hematologic, and immunologic abnormalities with presence of giant intracytoplasmic granules in leukocytes, and giant melanosomes in melanocytes. In our patient, the absence of these features along with the spontaneous repigmentation of the silvery hair, improvement of thyroid function, reversal of hypoalbuminemia, and the chromosomopathy detected make a diagnosis of CHS highly improbable.
We concluded that the silvery hair noted in our patient resulted from the 46,XY,add(2)(p23) chromosomal abnormality. This mutation could affect some of the genes that control the trafficking of melanosomes or could induce hypothyroidism and hypoproteinemia associated with congenital hydrops fetalis (Figure 5).
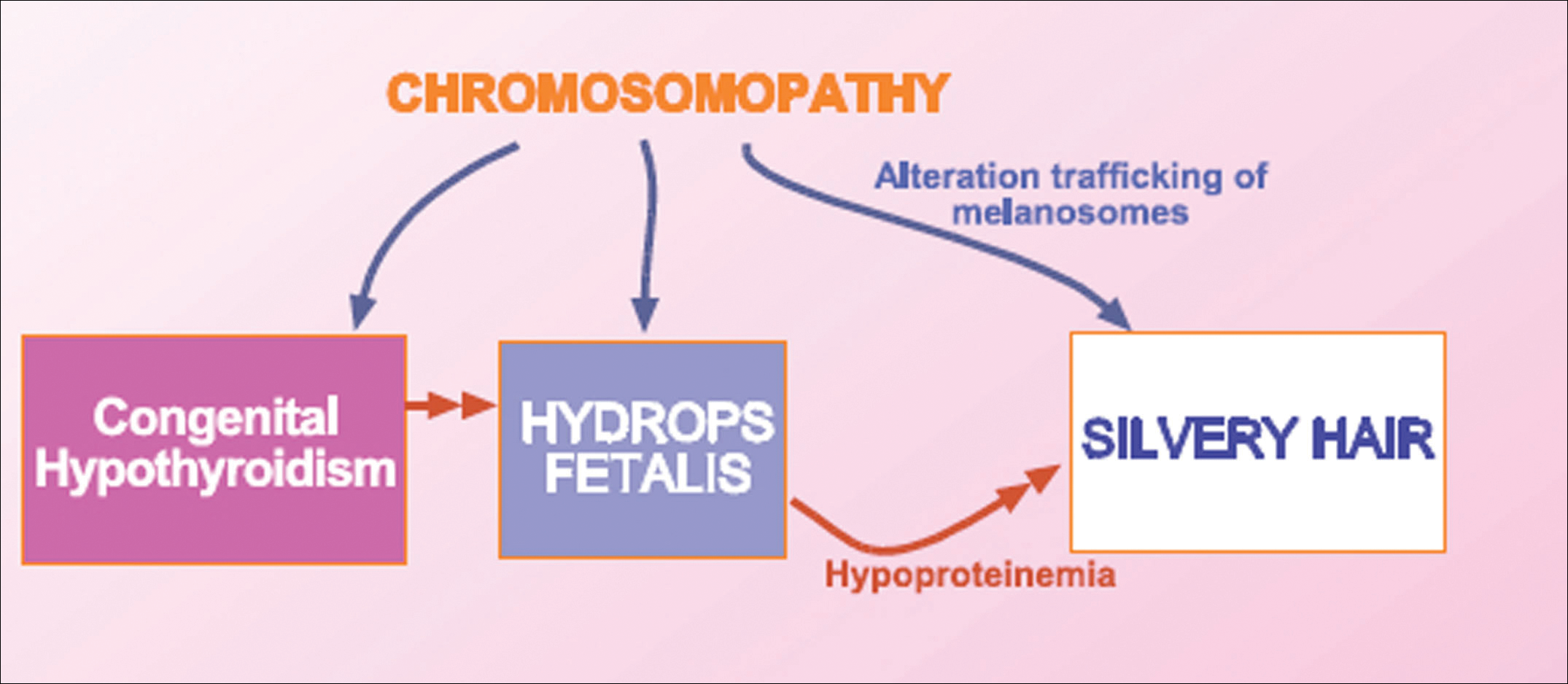
Hydrops fetalis is a potentially fatal condition characterized by severe edema (swelling) in a fetus or neonate. There are 2 types of hydrops fetalis: immune and nonimmune. Immune hydrops fetalis may develop in an Rh+ fetus with an Rh– mother, as the mother’s immune cells begin to break down the red blood cells of the fetus, resulting in anemia in the fetus with subsequent fetal heart failure, leading to an accumulation of large amounts of fluid in the tissues and organs. Nonimmune hydrops fetalis can occur secondary to diseases that interfere with the fetus’s ability to manage fluid (eg, severe anemia; congenital infections; urinary, lymphatic, heart, or thoracic defects; inborn errors of metabolism; chromosomal abnormalities). Case studies have suggested that congenital hypothyroidism could be a cause of nonimmune hydrops fetalis.16,17 Thyroid hormone deficiency reduces stimulation of adrenergic receptors in the lymphatic system and lungs, thereby decreasing lymph flow and protein efflux to the lymphatic system and decreasing clearance of liquid from the lungs. The final result is lymph vessel engorgement and subsequent leakage of lymphatic fluid to pleural spaces, causing hydrops fetalis and chylothorax.
The 46,XY,add(2)(p23) chromosomal abnormality has not been commonly associated with hypothyroidism and hydrops fetalis. The silvery hair in our patient was transient and spontaneously repigmented to brown over the course of follow-up in conjunction with improved physiologic changes. We concluded that the silvery hair in our patient was induced by his hypoproteinemic status secondary to hydrops fetalis and hypothyroidism.
Conclusion
In addition to CHS, ES, and GS, the differential diagnosis for silvery hair with abnormal skin pigmentation in children should include 46,XY,add(2)(p23) mutation, as was detected in our patient. Evaluation should include light microscopy of the hair shaft, skin biopsy, assessment of immune function, peripheral blood smear, and neurologic and eye examinations.
- White JG. The Chédiak-Higashi syndrome: a possible lysosomal disease. Blood. 1966;28:143-156.
- Introne W, Boissy RE, Gahl WA. Clinical, molecular, and cell biological aspects of Chédiak-Higashi syndrome. Mol Genet Metab. 1999;68:283-303.
- Kaplan J, De Domenico I, Ward DM. Chédiak-Higashi syndrome. Curr Opin Hematol. 2008;15:22-29.
- Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis [published online December 7, 2006]. Eur J Pediatr. 2007;166:95-109.
- Morrone K, Wang Y, Huizing M, et al. Two novel mutations identified in an African-American child with Chédiak-Higashi syndrome [published online March 24, 2010]. Case Report Med. 2010;2010:967535.
- Ivanovich J, Mallory S, Storer T, et al. 12-year-old male with Elejalde syndrome (neuroectodermal melanolysosomal disease). Am J Med Genet. 2001;98:313-316.
- Cahali JB, Fernandez SA, Oliveira ZN, et al. Elejalde syndrome: report of a case and review of the literature. Pediatr Dermatol. 2004;21:479-482.
- Bahadoran P, Ortonne JP, Ballotti R, et al. Comment on Elejalde syndrome and relationship with Griscelli syndrome. Am J Med Genet. 2003;116:408-409.
- Duran-McKinster C, Rodriguez-Jurado R, Ridaura C, et al. Elejalde syndrome—a melanolysosomal neurocutaneous syndrome: clinical and morphological findings in 7 patients. Arch Dermatol. 1999;135:182-186.
- Happle R. Neurocutaneous diseases. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Dermatology in General Medicine. 5th ed. New York, NY: McGraw-Hill; 1999:2131-2148.
- Sanal O, Yel L, Kucukali T, et al. An allelic variant of Griscelli disease: presentation with severe hypotonia, mental-motor retardation, and hypopigmentation consistent with Elejalde syndrome (neuroectodermal melanolysosomal disorder). J Neurol. 2000;247:570-572.
- Malhotra AK, Bhaskar G, Nanda M, et al. Griscelli syndrome. J Am Acad Dermatol. 2006;55:337-340.
- Al-Idrissi E, ElGhazali G, Alzahrani M, et al. Premature birth, respiratory distress, intracerebral hemorrhage, and silvery-gray hair: differential diagnosis of the 3 types of Griscelli syndrome. J Pediatr Hematol Oncol. 2010;32:494-496.
- Ménasché G, Ho CH, Sanal O, et al. Griscelli syndrome restricted to hypopigmentation results from a melanophilin defect (GS3) or a MYO5A F-exon deletion (GS1). J Clin Invest. 2003;112:450-456.
- Griscelli C, Durandy A, Guy-Grand D, et al. A syndrome associating partial albinism and immunodeficiency. Am J Med. 1978;65:691-702.
- Narchi H. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;104:1416-1417.
- Kessel I, Makhoul IR, Sujov P. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;103:E9.
Silvery hair is characteristic of 3 rare autosomal-recessive disorders—Chédiak-Higashi syndrome (CHS), Elejalde syndrome (ES), and Griscelli syndrome (GS)—which are associated with mutations in various genes that encode several proteins involved in the intracellular processing and movement of melanosomes. We report the case of a 2-month-old male infant with transient silvery hair and generalized hypopigmentation of the skin and eyes who did not have any genetic mutations associated with the classic syndromes that usually are characterized by transient silvery hair.
Case Report
A 2-month-old male infant presented to the dermatology department for evaluation of silvery hair with generalized hypopigmentation of the skin and eyes (Figure 1) that had developed at 1 month of age. His parents were healthy, nonconsanguineous, and reported no family history of silvery hair. The patient was delivered by cesarean section at 35 weeks’ gestation. His medical history was remarkable for congenital hydrops fetalis with pleuropericardial effusion, ascites, soft-tissue edema, and hydrocele with no signs of any congenital infection. Both the patient and his mother were O Rh +.
Several studies were performed following delivery. A direct Coombs test was negative. Blood studies revealed hypothyroidism and hypoalbuminemia secondary to protein loss associated with fetal hydrops. Cerebral, abdominal, and renal ultrasound; echocardiogram; thoracic and abdominal computed tomography; and cerebral magnetic resonance imaging revealed no abnormalities.
Karyotype results showed 46,XY,add(2)(p23), and subsequent spectral karyotyping and fluorescence in situ hybridization tests identified a chromosomal abnormality (46,XY,add[2][p23].ish del[2][pter][2PTEL27‒], dup[4][qter][D4S2930++])(Figure 2). Parental karyotypes were normal.
After birth, the infant was admitted to the neonatal intensive care unit for 50 days and received pleural and peritoneal drainages, mechanical ventilation, vasoactive drugs, parenteral nutrition with resolution of the hypoalbuminemia, levothyroxine, and intravenous antibiotics for central venous catheter infection. No drugs known to be associated with hypopigmentation of the hair, skin, or eyes were administered.
Two weeks after discharge from the neonatal intensive care unit, the patient was referred to our department. Physical examination revealed silvery hair on the scalp, eyebrows, and eyelashes, along with generalized hypopigmentation of the skin and eyes. Abdominal, cardiovascular, respiratory, and neurologic examination revealed no abnormalities, and no hepatosplenomegaly, lymphadenopathy, nystagmus, or strabismus was noted.
Light microscopy of the hair revealed small and regular aggregates of melanin along the hair shaft, predominantly in the medulla (Figure 3). Light microscopy of a skin biopsy specimen showed normal pigmentation in the melanocytes and no giant melanosomes. The melanocyte count was within reference range. A peripheral blood smear showed no giant granules in the granulocytes. No treatment was administered and the patient was followed closely every month. When the patient returned for follow-up at 9 months of age, physical examination revealed brown hair on the head, eyebrows, and eyelashes, as well as normal pigmentation of the skin and eyes (Figure 4). Thyroid function was normal and no recurrent infections of any type were noted. At follow-up at the age of 4 years, he showed normal neurological and psychological development with brown hair, no recurrent infections, and normal thyroid function. Given that CHS, ES, and GS had been ruled out, the clinical presentation and the genetic mutation detected may indicate that this case represents a new entity characterized by transient silvery hair.
Comment
Silvery hair is a known feature of CHS, ES, and GS (Table). The characteristic hypopigmentation associated with these autosomal-recessive disorders is the result of impaired melanosome transport leading to failed transfer of melanin to keratinocytes. These disorders differ from oculocutaneous albinism in that melanin synthesis is unaffected.
Chédiak-Higashi syndrome is characterized by generalized hypopigmentation of the skin and eyes, silvery hair, neurologic and immune dysfunction, lymphoproliferative disorders, and large granules in granulocytes and other cell types.1-3 A common complication of CHS is hemophagocytic lymphohistiocytosis, which is characterized by fever, jaundice, lymphadenopathy, hepatosplenomegaly, and pancytopenia.4 Pigmentary dilution of the irises also may be present, along with photophobia, strabismus, nystagmus, and impaired visual acuity. Chédiak-Higashi syndrome is the result of a genetic defect in the lysosomal trafficking regulator gene, also known as CHS1 (located on chromosome 1q42.1‒q42.2).5 Melanin in the hair shaft is distributed uniformly in multiple small aggregates. Light microscopy of the skin typically shows giant melanosomes in melanocytes and aberrant keratinocyte maturation.
Elejalde syndrome is characterized by silvery hair (eyelashes and eyebrows), neurologic defects, and normal immunologic function.6,7 The underlying molecular basis remains unknown. It appears related to or allelic to GS type 1 and thus associated with mutations in MYO5A (myosin VA); however, the gene mutation responsible has yet to be defined.8 Light microscopy of the hair shaft usually shows an irregular distribution of large melanin aggregates, primarily in the medulla.9,10 Skin biopsy generally shows irregular distribution and irregular size of melanin granules in the basal layer.11 Leukocytes usually show no abnormal cytoplasmic granules. Ocular involvement is common and may present as nystagmus, diplopia, hypopigmented retinas, and/or papilledema.
In GS, hair microscopy generally reveals large aggregates of melanin pigment distributed irregularly along the hair shaft. Granulocytes typically show no giant granules. Light microscopy of the skin usually shows increased pigment in melanocytes with sparse pigment in keratinocytes. Griscelli syndrome is classified into 3 types.12 In GS type 1, patients have silvery gray hair, light-colored skin, severe neurologic defects,13 and normal immune status. This variant is caused by a mutation in the MYO5A gene located on chromosome 15q21. In GS type 2, patients have silvery gray hair, pyogenic infections, an accelerated phase of hemophagocytic lymphohistiocytosis, and variable neurologic defects in the absence of primary neurologic disease.14,15 This variant is caused by a mutation in the RAB27A (member RAS oncogene family) gene located on chromosome 15q21. In GS type 3, patients exhibit generalized hypopigmentation of the skin and hair with no abnormalities of the nervous or immune systems. There are 2 different mutations associated with GS type 3: the first is located on chromosome 2q37.3, causing a mutation in MLPH (melanophilin), and the second is caused by an F-exon deletion in the MYO5A gene.14
Our patient had silvery hair, generalized hypopigmentation of the skin and eyes, and normal central nervous system function with no other ocular involvement and no evidence of recurrent infections of any kind. Light microscopy showed small and regular melanin pigment aggregates in the hair shaft, which differs from the irregular pigment aggregates in GS and ES.
The regular melanin pigment aggregates observed along the hair shaft were consistent with CHS, but other manifestations of this syndrome were absent: ocular, neurologic, hematologic, and immunologic abnormalities with presence of giant intracytoplasmic granules in leukocytes, and giant melanosomes in melanocytes. In our patient, the absence of these features along with the spontaneous repigmentation of the silvery hair, improvement of thyroid function, reversal of hypoalbuminemia, and the chromosomopathy detected make a diagnosis of CHS highly improbable.
We concluded that the silvery hair noted in our patient resulted from the 46,XY,add(2)(p23) chromosomal abnormality. This mutation could affect some of the genes that control the trafficking of melanosomes or could induce hypothyroidism and hypoproteinemia associated with congenital hydrops fetalis (Figure 5).
Hydrops fetalis is a potentially fatal condition characterized by severe edema (swelling) in a fetus or neonate. There are 2 types of hydrops fetalis: immune and nonimmune. Immune hydrops fetalis may develop in an Rh+ fetus with an Rh– mother, as the mother’s immune cells begin to break down the red blood cells of the fetus, resulting in anemia in the fetus with subsequent fetal heart failure, leading to an accumulation of large amounts of fluid in the tissues and organs. Nonimmune hydrops fetalis can occur secondary to diseases that interfere with the fetus’s ability to manage fluid (eg, severe anemia; congenital infections; urinary, lymphatic, heart, or thoracic defects; inborn errors of metabolism; chromosomal abnormalities). Case studies have suggested that congenital hypothyroidism could be a cause of nonimmune hydrops fetalis.16,17 Thyroid hormone deficiency reduces stimulation of adrenergic receptors in the lymphatic system and lungs, thereby decreasing lymph flow and protein efflux to the lymphatic system and decreasing clearance of liquid from the lungs. The final result is lymph vessel engorgement and subsequent leakage of lymphatic fluid to pleural spaces, causing hydrops fetalis and chylothorax.
The 46,XY,add(2)(p23) chromosomal abnormality has not been commonly associated with hypothyroidism and hydrops fetalis. The silvery hair in our patient was transient and spontaneously repigmented to brown over the course of follow-up in conjunction with improved physiologic changes. We concluded that the silvery hair in our patient was induced by his hypoproteinemic status secondary to hydrops fetalis and hypothyroidism.
Conclusion
In addition to CHS, ES, and GS, the differential diagnosis for silvery hair with abnormal skin pigmentation in children should include 46,XY,add(2)(p23) mutation, as was detected in our patient. Evaluation should include light microscopy of the hair shaft, skin biopsy, assessment of immune function, peripheral blood smear, and neurologic and eye examinations.
Silvery hair is characteristic of 3 rare autosomal-recessive disorders—Chédiak-Higashi syndrome (CHS), Elejalde syndrome (ES), and Griscelli syndrome (GS)—which are associated with mutations in various genes that encode several proteins involved in the intracellular processing and movement of melanosomes. We report the case of a 2-month-old male infant with transient silvery hair and generalized hypopigmentation of the skin and eyes who did not have any genetic mutations associated with the classic syndromes that usually are characterized by transient silvery hair.
Case Report
A 2-month-old male infant presented to the dermatology department for evaluation of silvery hair with generalized hypopigmentation of the skin and eyes (Figure 1) that had developed at 1 month of age. His parents were healthy, nonconsanguineous, and reported no family history of silvery hair. The patient was delivered by cesarean section at 35 weeks’ gestation. His medical history was remarkable for congenital hydrops fetalis with pleuropericardial effusion, ascites, soft-tissue edema, and hydrocele with no signs of any congenital infection. Both the patient and his mother were O Rh +.
Several studies were performed following delivery. A direct Coombs test was negative. Blood studies revealed hypothyroidism and hypoalbuminemia secondary to protein loss associated with fetal hydrops. Cerebral, abdominal, and renal ultrasound; echocardiogram; thoracic and abdominal computed tomography; and cerebral magnetic resonance imaging revealed no abnormalities.
Karyotype results showed 46,XY,add(2)(p23), and subsequent spectral karyotyping and fluorescence in situ hybridization tests identified a chromosomal abnormality (46,XY,add[2][p23].ish del[2][pter][2PTEL27‒], dup[4][qter][D4S2930++])(Figure 2). Parental karyotypes were normal.
After birth, the infant was admitted to the neonatal intensive care unit for 50 days and received pleural and peritoneal drainages, mechanical ventilation, vasoactive drugs, parenteral nutrition with resolution of the hypoalbuminemia, levothyroxine, and intravenous antibiotics for central venous catheter infection. No drugs known to be associated with hypopigmentation of the hair, skin, or eyes were administered.
Two weeks after discharge from the neonatal intensive care unit, the patient was referred to our department. Physical examination revealed silvery hair on the scalp, eyebrows, and eyelashes, along with generalized hypopigmentation of the skin and eyes. Abdominal, cardiovascular, respiratory, and neurologic examination revealed no abnormalities, and no hepatosplenomegaly, lymphadenopathy, nystagmus, or strabismus was noted.
Light microscopy of the hair revealed small and regular aggregates of melanin along the hair shaft, predominantly in the medulla (Figure 3). Light microscopy of a skin biopsy specimen showed normal pigmentation in the melanocytes and no giant melanosomes. The melanocyte count was within reference range. A peripheral blood smear showed no giant granules in the granulocytes. No treatment was administered and the patient was followed closely every month. When the patient returned for follow-up at 9 months of age, physical examination revealed brown hair on the head, eyebrows, and eyelashes, as well as normal pigmentation of the skin and eyes (Figure 4). Thyroid function was normal and no recurrent infections of any type were noted. At follow-up at the age of 4 years, he showed normal neurological and psychological development with brown hair, no recurrent infections, and normal thyroid function. Given that CHS, ES, and GS had been ruled out, the clinical presentation and the genetic mutation detected may indicate that this case represents a new entity characterized by transient silvery hair.
Comment
Silvery hair is a known feature of CHS, ES, and GS (Table). The characteristic hypopigmentation associated with these autosomal-recessive disorders is the result of impaired melanosome transport leading to failed transfer of melanin to keratinocytes. These disorders differ from oculocutaneous albinism in that melanin synthesis is unaffected.
Chédiak-Higashi syndrome is characterized by generalized hypopigmentation of the skin and eyes, silvery hair, neurologic and immune dysfunction, lymphoproliferative disorders, and large granules in granulocytes and other cell types.1-3 A common complication of CHS is hemophagocytic lymphohistiocytosis, which is characterized by fever, jaundice, lymphadenopathy, hepatosplenomegaly, and pancytopenia.4 Pigmentary dilution of the irises also may be present, along with photophobia, strabismus, nystagmus, and impaired visual acuity. Chédiak-Higashi syndrome is the result of a genetic defect in the lysosomal trafficking regulator gene, also known as CHS1 (located on chromosome 1q42.1‒q42.2).5 Melanin in the hair shaft is distributed uniformly in multiple small aggregates. Light microscopy of the skin typically shows giant melanosomes in melanocytes and aberrant keratinocyte maturation.
Elejalde syndrome is characterized by silvery hair (eyelashes and eyebrows), neurologic defects, and normal immunologic function.6,7 The underlying molecular basis remains unknown. It appears related to or allelic to GS type 1 and thus associated with mutations in MYO5A (myosin VA); however, the gene mutation responsible has yet to be defined.8 Light microscopy of the hair shaft usually shows an irregular distribution of large melanin aggregates, primarily in the medulla.9,10 Skin biopsy generally shows irregular distribution and irregular size of melanin granules in the basal layer.11 Leukocytes usually show no abnormal cytoplasmic granules. Ocular involvement is common and may present as nystagmus, diplopia, hypopigmented retinas, and/or papilledema.
In GS, hair microscopy generally reveals large aggregates of melanin pigment distributed irregularly along the hair shaft. Granulocytes typically show no giant granules. Light microscopy of the skin usually shows increased pigment in melanocytes with sparse pigment in keratinocytes. Griscelli syndrome is classified into 3 types.12 In GS type 1, patients have silvery gray hair, light-colored skin, severe neurologic defects,13 and normal immune status. This variant is caused by a mutation in the MYO5A gene located on chromosome 15q21. In GS type 2, patients have silvery gray hair, pyogenic infections, an accelerated phase of hemophagocytic lymphohistiocytosis, and variable neurologic defects in the absence of primary neurologic disease.14,15 This variant is caused by a mutation in the RAB27A (member RAS oncogene family) gene located on chromosome 15q21. In GS type 3, patients exhibit generalized hypopigmentation of the skin and hair with no abnormalities of the nervous or immune systems. There are 2 different mutations associated with GS type 3: the first is located on chromosome 2q37.3, causing a mutation in MLPH (melanophilin), and the second is caused by an F-exon deletion in the MYO5A gene.14
Our patient had silvery hair, generalized hypopigmentation of the skin and eyes, and normal central nervous system function with no other ocular involvement and no evidence of recurrent infections of any kind. Light microscopy showed small and regular melanin pigment aggregates in the hair shaft, which differs from the irregular pigment aggregates in GS and ES.
The regular melanin pigment aggregates observed along the hair shaft were consistent with CHS, but other manifestations of this syndrome were absent: ocular, neurologic, hematologic, and immunologic abnormalities with presence of giant intracytoplasmic granules in leukocytes, and giant melanosomes in melanocytes. In our patient, the absence of these features along with the spontaneous repigmentation of the silvery hair, improvement of thyroid function, reversal of hypoalbuminemia, and the chromosomopathy detected make a diagnosis of CHS highly improbable.
We concluded that the silvery hair noted in our patient resulted from the 46,XY,add(2)(p23) chromosomal abnormality. This mutation could affect some of the genes that control the trafficking of melanosomes or could induce hypothyroidism and hypoproteinemia associated with congenital hydrops fetalis (Figure 5).
Hydrops fetalis is a potentially fatal condition characterized by severe edema (swelling) in a fetus or neonate. There are 2 types of hydrops fetalis: immune and nonimmune. Immune hydrops fetalis may develop in an Rh+ fetus with an Rh– mother, as the mother’s immune cells begin to break down the red blood cells of the fetus, resulting in anemia in the fetus with subsequent fetal heart failure, leading to an accumulation of large amounts of fluid in the tissues and organs. Nonimmune hydrops fetalis can occur secondary to diseases that interfere with the fetus’s ability to manage fluid (eg, severe anemia; congenital infections; urinary, lymphatic, heart, or thoracic defects; inborn errors of metabolism; chromosomal abnormalities). Case studies have suggested that congenital hypothyroidism could be a cause of nonimmune hydrops fetalis.16,17 Thyroid hormone deficiency reduces stimulation of adrenergic receptors in the lymphatic system and lungs, thereby decreasing lymph flow and protein efflux to the lymphatic system and decreasing clearance of liquid from the lungs. The final result is lymph vessel engorgement and subsequent leakage of lymphatic fluid to pleural spaces, causing hydrops fetalis and chylothorax.
The 46,XY,add(2)(p23) chromosomal abnormality has not been commonly associated with hypothyroidism and hydrops fetalis. The silvery hair in our patient was transient and spontaneously repigmented to brown over the course of follow-up in conjunction with improved physiologic changes. We concluded that the silvery hair in our patient was induced by his hypoproteinemic status secondary to hydrops fetalis and hypothyroidism.
Conclusion
In addition to CHS, ES, and GS, the differential diagnosis for silvery hair with abnormal skin pigmentation in children should include 46,XY,add(2)(p23) mutation, as was detected in our patient. Evaluation should include light microscopy of the hair shaft, skin biopsy, assessment of immune function, peripheral blood smear, and neurologic and eye examinations.
- White JG. The Chédiak-Higashi syndrome: a possible lysosomal disease. Blood. 1966;28:143-156.
- Introne W, Boissy RE, Gahl WA. Clinical, molecular, and cell biological aspects of Chédiak-Higashi syndrome. Mol Genet Metab. 1999;68:283-303.
- Kaplan J, De Domenico I, Ward DM. Chédiak-Higashi syndrome. Curr Opin Hematol. 2008;15:22-29.
- Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis [published online December 7, 2006]. Eur J Pediatr. 2007;166:95-109.
- Morrone K, Wang Y, Huizing M, et al. Two novel mutations identified in an African-American child with Chédiak-Higashi syndrome [published online March 24, 2010]. Case Report Med. 2010;2010:967535.
- Ivanovich J, Mallory S, Storer T, et al. 12-year-old male with Elejalde syndrome (neuroectodermal melanolysosomal disease). Am J Med Genet. 2001;98:313-316.
- Cahali JB, Fernandez SA, Oliveira ZN, et al. Elejalde syndrome: report of a case and review of the literature. Pediatr Dermatol. 2004;21:479-482.
- Bahadoran P, Ortonne JP, Ballotti R, et al. Comment on Elejalde syndrome and relationship with Griscelli syndrome. Am J Med Genet. 2003;116:408-409.
- Duran-McKinster C, Rodriguez-Jurado R, Ridaura C, et al. Elejalde syndrome—a melanolysosomal neurocutaneous syndrome: clinical and morphological findings in 7 patients. Arch Dermatol. 1999;135:182-186.
- Happle R. Neurocutaneous diseases. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Dermatology in General Medicine. 5th ed. New York, NY: McGraw-Hill; 1999:2131-2148.
- Sanal O, Yel L, Kucukali T, et al. An allelic variant of Griscelli disease: presentation with severe hypotonia, mental-motor retardation, and hypopigmentation consistent with Elejalde syndrome (neuroectodermal melanolysosomal disorder). J Neurol. 2000;247:570-572.
- Malhotra AK, Bhaskar G, Nanda M, et al. Griscelli syndrome. J Am Acad Dermatol. 2006;55:337-340.
- Al-Idrissi E, ElGhazali G, Alzahrani M, et al. Premature birth, respiratory distress, intracerebral hemorrhage, and silvery-gray hair: differential diagnosis of the 3 types of Griscelli syndrome. J Pediatr Hematol Oncol. 2010;32:494-496.
- Ménasché G, Ho CH, Sanal O, et al. Griscelli syndrome restricted to hypopigmentation results from a melanophilin defect (GS3) or a MYO5A F-exon deletion (GS1). J Clin Invest. 2003;112:450-456.
- Griscelli C, Durandy A, Guy-Grand D, et al. A syndrome associating partial albinism and immunodeficiency. Am J Med. 1978;65:691-702.
- Narchi H. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;104:1416-1417.
- Kessel I, Makhoul IR, Sujov P. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;103:E9.
- White JG. The Chédiak-Higashi syndrome: a possible lysosomal disease. Blood. 1966;28:143-156.
- Introne W, Boissy RE, Gahl WA. Clinical, molecular, and cell biological aspects of Chédiak-Higashi syndrome. Mol Genet Metab. 1999;68:283-303.
- Kaplan J, De Domenico I, Ward DM. Chédiak-Higashi syndrome. Curr Opin Hematol. 2008;15:22-29.
- Janka GE. Familial and acquired hemophagocytic lymphohistiocytosis [published online December 7, 2006]. Eur J Pediatr. 2007;166:95-109.
- Morrone K, Wang Y, Huizing M, et al. Two novel mutations identified in an African-American child with Chédiak-Higashi syndrome [published online March 24, 2010]. Case Report Med. 2010;2010:967535.
- Ivanovich J, Mallory S, Storer T, et al. 12-year-old male with Elejalde syndrome (neuroectodermal melanolysosomal disease). Am J Med Genet. 2001;98:313-316.
- Cahali JB, Fernandez SA, Oliveira ZN, et al. Elejalde syndrome: report of a case and review of the literature. Pediatr Dermatol. 2004;21:479-482.
- Bahadoran P, Ortonne JP, Ballotti R, et al. Comment on Elejalde syndrome and relationship with Griscelli syndrome. Am J Med Genet. 2003;116:408-409.
- Duran-McKinster C, Rodriguez-Jurado R, Ridaura C, et al. Elejalde syndrome—a melanolysosomal neurocutaneous syndrome: clinical and morphological findings in 7 patients. Arch Dermatol. 1999;135:182-186.
- Happle R. Neurocutaneous diseases. In: Freedberg IM, Eisen AZ, Wolff K, et al, eds. Dermatology in General Medicine. 5th ed. New York, NY: McGraw-Hill; 1999:2131-2148.
- Sanal O, Yel L, Kucukali T, et al. An allelic variant of Griscelli disease: presentation with severe hypotonia, mental-motor retardation, and hypopigmentation consistent with Elejalde syndrome (neuroectodermal melanolysosomal disorder). J Neurol. 2000;247:570-572.
- Malhotra AK, Bhaskar G, Nanda M, et al. Griscelli syndrome. J Am Acad Dermatol. 2006;55:337-340.
- Al-Idrissi E, ElGhazali G, Alzahrani M, et al. Premature birth, respiratory distress, intracerebral hemorrhage, and silvery-gray hair: differential diagnosis of the 3 types of Griscelli syndrome. J Pediatr Hematol Oncol. 2010;32:494-496.
- Ménasché G, Ho CH, Sanal O, et al. Griscelli syndrome restricted to hypopigmentation results from a melanophilin defect (GS3) or a MYO5A F-exon deletion (GS1). J Clin Invest. 2003;112:450-456.
- Griscelli C, Durandy A, Guy-Grand D, et al. A syndrome associating partial albinism and immunodeficiency. Am J Med. 1978;65:691-702.
- Narchi H. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;104:1416-1417.
- Kessel I, Makhoul IR, Sujov P. Congenital hypothyroidism and nonimmune hydrops fetalis: associated? Pediatrics. 1999;103:E9.
Practice Points
- Silvery hair is characteristic of 3 rare autosomal-recessive disorders: Chédiak-Higashi syndrome, Elejalde syndrome, and Griscelli syndrome.
- Hypopigmentation is the result of impaired melanosome transport leading to failed transfer of melanin to keratinocytes.
- Evaluation should include light microscopy of the hair shaft, skin biopsy, assessment of immune function, peripheral blood smear, and neurologic and eye examinations.

Primary Herpes Simplex Virus Infection of the Nipple in a Breastfeeding Woman
To the Editor:
A 33-year-old woman presented with tenderness of the left breast and nipple of 2 weeks’ duration and fever of 2 days’ duration. The pain was so severe it precluded nursing. She rented a hospital-grade electric breast pump to continue lactation but only could produce 1 ounce of milk daily. The mother had been breastfeeding her 13-month-old twins since birth and did not report any prior difficulties with breastfeeding. Both twins had a history of mucosal sores 2 months prior and a recent outbreak of perioral vesicles following an upper respiratory tract illness that was consistent with gingivostomatitis, followed by a cutaneous outbreak secondary to herpes simplex virus (HSV) type 1 infection. The patient had no known history of HSV infection. Prior to presentation the patient was treated with oral dicloxacillin and then cephalexin for suspected bacterial mastitis. She also had used combination clotrimazole-betamethasone cream for possible superficial candidiasis. The patient had no relief with these treatments.
Physical examination revealed approximately 20 microvesicles (<1 mm) on an erythematous base clustered around the left areola (Figure). Erythematous streaks were noted from the medial aspect of the areolar margin extending to the central sternum. The left breast was firm and engorged but without apparent plugged lactiferous ducts. There was no lymphadenopathy. No lesions were present on the palms, soles, and oral mucosa.

The patient was empirically treated with valacyclovir, trimethoprim-sulfamethoxazole, and nonsteroidal anti-inflammatory drugs while awaiting laboratory results. Bacterial cultures were negative. Viral titers revealed positive combination HSV-1 and HSV-2 IgM (4.64 [<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]) and negative HSV-1 and HSV-2 IgG (<0.91[<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]), which confirmed the diagnosis of primary HSV infection. Two months later viral titers were positive for HSV-1 IgG (1.3) and negative for HSV-2 IgG (<0.91).
At 1-week follow-up the patient reported that the fever had subsided 1 day after initial presentation. After commencement of antiviral therapy, she continued to have some mild residual tenderness, but the vesicles had crusted over and markedly improved. Upon further questioning, the patient’s husband had a history of oral HSV-1 and was likely the primary source for the infection in the infants.
Herpes simplex virus infection primarily is transmitted through direct mucocutaneous contact with either oral or genital lesions of an infected individual. Transmission of HSV from infant to mother rarely is described. A PubMed search of articles indexed for MEDLINE using the terms herpes mastitis, herpes of the breast, infant to maternal transmission, gingivostomatitis, primary herpes, and breastfeeding yielded 4 reported cases of HSV of the nipple in breastfeeding women from children with herpetic gingivostomatitis.1-4
Herpes simplex virus infection is common in neonatal and pediatric populations. In the United States, more than 30% of children (aged <14 years) have evidence of HSV-1 infection on serology. Herpes simplex virus infections in children can range from uncomplicated mucocutaneous diseases to severe life-threatening infections involving the central nervous system. In children, antivirals should be initiated within 72 hours of symptom onset to prevent more serious complications. Diagnostic testing was not performed on the infants in this case because the 72-hour treatment window had passed. In particular, neonates (aged <3 months) will require intravenous antivirals to prevent the development of central nervous system disease, which occurs in 33% of neonatal HSV infections.5 It is critically important to confirm the diagnosis of HSV in a breastfeeding woman, when clinically indicated, with a viral culture, serology, direct immunofluorescence assay, polymerase chain reaction, or Tzanck smear because other conditions such as plugged lactiferous ducts, candidal mastitis, or bacterial mastitis may mimic HSV. Rapid and accurate diagnosis of the breastfeeding woman with HSV of the nipple can help identify children with herpetic gingivostomatitis that is not readily apparent.
- Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust. 1978;2:411-412.
- Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol. 1986;11:664-666.
- Sealander JY, Kerr CP. Herpes simplex of the nipple: infant-to-mother transmission. Am Fam Physician. 1989;39:111-113.
- Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol. 2008;22:878-879.
- James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther. 2010;88:720-724.
To the Editor:
A 33-year-old woman presented with tenderness of the left breast and nipple of 2 weeks’ duration and fever of 2 days’ duration. The pain was so severe it precluded nursing. She rented a hospital-grade electric breast pump to continue lactation but only could produce 1 ounce of milk daily. The mother had been breastfeeding her 13-month-old twins since birth and did not report any prior difficulties with breastfeeding. Both twins had a history of mucosal sores 2 months prior and a recent outbreak of perioral vesicles following an upper respiratory tract illness that was consistent with gingivostomatitis, followed by a cutaneous outbreak secondary to herpes simplex virus (HSV) type 1 infection. The patient had no known history of HSV infection. Prior to presentation the patient was treated with oral dicloxacillin and then cephalexin for suspected bacterial mastitis. She also had used combination clotrimazole-betamethasone cream for possible superficial candidiasis. The patient had no relief with these treatments.
Physical examination revealed approximately 20 microvesicles (<1 mm) on an erythematous base clustered around the left areola (Figure). Erythematous streaks were noted from the medial aspect of the areolar margin extending to the central sternum. The left breast was firm and engorged but without apparent plugged lactiferous ducts. There was no lymphadenopathy. No lesions were present on the palms, soles, and oral mucosa.
The patient was empirically treated with valacyclovir, trimethoprim-sulfamethoxazole, and nonsteroidal anti-inflammatory drugs while awaiting laboratory results. Bacterial cultures were negative. Viral titers revealed positive combination HSV-1 and HSV-2 IgM (4.64 [<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]) and negative HSV-1 and HSV-2 IgG (<0.91[<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]), which confirmed the diagnosis of primary HSV infection. Two months later viral titers were positive for HSV-1 IgG (1.3) and negative for HSV-2 IgG (<0.91).
At 1-week follow-up the patient reported that the fever had subsided 1 day after initial presentation. After commencement of antiviral therapy, she continued to have some mild residual tenderness, but the vesicles had crusted over and markedly improved. Upon further questioning, the patient’s husband had a history of oral HSV-1 and was likely the primary source for the infection in the infants.
Herpes simplex virus infection primarily is transmitted through direct mucocutaneous contact with either oral or genital lesions of an infected individual. Transmission of HSV from infant to mother rarely is described. A PubMed search of articles indexed for MEDLINE using the terms herpes mastitis, herpes of the breast, infant to maternal transmission, gingivostomatitis, primary herpes, and breastfeeding yielded 4 reported cases of HSV of the nipple in breastfeeding women from children with herpetic gingivostomatitis.1-4
Herpes simplex virus infection is common in neonatal and pediatric populations. In the United States, more than 30% of children (aged <14 years) have evidence of HSV-1 infection on serology. Herpes simplex virus infections in children can range from uncomplicated mucocutaneous diseases to severe life-threatening infections involving the central nervous system. In children, antivirals should be initiated within 72 hours of symptom onset to prevent more serious complications. Diagnostic testing was not performed on the infants in this case because the 72-hour treatment window had passed. In particular, neonates (aged <3 months) will require intravenous antivirals to prevent the development of central nervous system disease, which occurs in 33% of neonatal HSV infections.5 It is critically important to confirm the diagnosis of HSV in a breastfeeding woman, when clinically indicated, with a viral culture, serology, direct immunofluorescence assay, polymerase chain reaction, or Tzanck smear because other conditions such as plugged lactiferous ducts, candidal mastitis, or bacterial mastitis may mimic HSV. Rapid and accurate diagnosis of the breastfeeding woman with HSV of the nipple can help identify children with herpetic gingivostomatitis that is not readily apparent.
To the Editor:
A 33-year-old woman presented with tenderness of the left breast and nipple of 2 weeks’ duration and fever of 2 days’ duration. The pain was so severe it precluded nursing. She rented a hospital-grade electric breast pump to continue lactation but only could produce 1 ounce of milk daily. The mother had been breastfeeding her 13-month-old twins since birth and did not report any prior difficulties with breastfeeding. Both twins had a history of mucosal sores 2 months prior and a recent outbreak of perioral vesicles following an upper respiratory tract illness that was consistent with gingivostomatitis, followed by a cutaneous outbreak secondary to herpes simplex virus (HSV) type 1 infection. The patient had no known history of HSV infection. Prior to presentation the patient was treated with oral dicloxacillin and then cephalexin for suspected bacterial mastitis. She also had used combination clotrimazole-betamethasone cream for possible superficial candidiasis. The patient had no relief with these treatments.
Physical examination revealed approximately 20 microvesicles (<1 mm) on an erythematous base clustered around the left areola (Figure). Erythematous streaks were noted from the medial aspect of the areolar margin extending to the central sternum. The left breast was firm and engorged but without apparent plugged lactiferous ducts. There was no lymphadenopathy. No lesions were present on the palms, soles, and oral mucosa.
The patient was empirically treated with valacyclovir, trimethoprim-sulfamethoxazole, and nonsteroidal anti-inflammatory drugs while awaiting laboratory results. Bacterial cultures were negative. Viral titers revealed positive combination HSV-1 and HSV-2 IgM (4.64 [<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]) and negative HSV-1 and HSV-2 IgG (<0.91[<0.91=negative, 0.91–1.09=equivocal, >1.09=positive]), which confirmed the diagnosis of primary HSV infection. Two months later viral titers were positive for HSV-1 IgG (1.3) and negative for HSV-2 IgG (<0.91).
At 1-week follow-up the patient reported that the fever had subsided 1 day after initial presentation. After commencement of antiviral therapy, she continued to have some mild residual tenderness, but the vesicles had crusted over and markedly improved. Upon further questioning, the patient’s husband had a history of oral HSV-1 and was likely the primary source for the infection in the infants.
Herpes simplex virus infection primarily is transmitted through direct mucocutaneous contact with either oral or genital lesions of an infected individual. Transmission of HSV from infant to mother rarely is described. A PubMed search of articles indexed for MEDLINE using the terms herpes mastitis, herpes of the breast, infant to maternal transmission, gingivostomatitis, primary herpes, and breastfeeding yielded 4 reported cases of HSV of the nipple in breastfeeding women from children with herpetic gingivostomatitis.1-4
Herpes simplex virus infection is common in neonatal and pediatric populations. In the United States, more than 30% of children (aged <14 years) have evidence of HSV-1 infection on serology. Herpes simplex virus infections in children can range from uncomplicated mucocutaneous diseases to severe life-threatening infections involving the central nervous system. In children, antivirals should be initiated within 72 hours of symptom onset to prevent more serious complications. Diagnostic testing was not performed on the infants in this case because the 72-hour treatment window had passed. In particular, neonates (aged <3 months) will require intravenous antivirals to prevent the development of central nervous system disease, which occurs in 33% of neonatal HSV infections.5 It is critically important to confirm the diagnosis of HSV in a breastfeeding woman, when clinically indicated, with a viral culture, serology, direct immunofluorescence assay, polymerase chain reaction, or Tzanck smear because other conditions such as plugged lactiferous ducts, candidal mastitis, or bacterial mastitis may mimic HSV. Rapid and accurate diagnosis of the breastfeeding woman with HSV of the nipple can help identify children with herpetic gingivostomatitis that is not readily apparent.
- Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust. 1978;2:411-412.
- Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol. 1986;11:664-666.
- Sealander JY, Kerr CP. Herpes simplex of the nipple: infant-to-mother transmission. Am Fam Physician. 1989;39:111-113.
- Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol. 2008;22:878-879.
- James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther. 2010;88:720-724.
- Quinn PT, Lofberg JV. Maternal herpetic breast infection: another hazard of neonatal herpes simplex. Med J Aust. 1978;2:411-412.
- Dekio S, Kawasaki Y, Jidoi J. Herpes simplex on nipples inoculated from herpetic gingivostomatitis of a baby. Clin Exp Dermatol. 1986;11:664-666.
- Sealander JY, Kerr CP. Herpes simplex of the nipple: infant-to-mother transmission. Am Fam Physician. 1989;39:111-113.
- Gupta S, Malhotra AK, Dash SS. Child to mother transmission of herpes simplex virus-1 infection at an unusual site. J Eur Acad Dermatol Venereol. 2008;22:878-879.
- James SH, Whitley RJ. Treatment of herpes simplex virus infections in pediatric patients: current status and future needs. Clin Pharmacol Ther. 2010;88:720-724.
Practice Points
- Herpes mastitis should be included in the differential diagnosis for breast pain during lactation.
- Children of breastfeeding women diagnosed with herpes mastitis require immediate evaluation for a possible source of the infection, as complications of herpes viral infection in infants can be severe and life threatening.

Behavioral interventions better than sleep education for infants
Graduated extinction and bedtime fading significantly reduced nocturnal wakefulness in infants and maternal stress, according to Michael Gradisar, Ph.D., of Flinders University, Adelaide, South Australia, and his associates.

For the study, a group of 43 infants aged 6-16 months received either graduated extinction, bedtime fading, or sleep education. Compared with the control group of sleep education, sleep latency was significantly decreased in both the graduated extinction and bedtime fading groups. A significant reduction in number of awakenings and wake after sleep onset was seen in the graduated extinction group.
Maternal stress decreased over time in all groups, however, compared with the control group; stress was moderately reduced in the graduated extinction group and was significantly reduced in the bedtime fading group. After 12 months, no significant difference in parent-child attachment was seen between the control and noncontrol groups.
“Our data suggest introducing bedtime fading will provide quick results for improving sleep-onset latency. Graduated extinction may then be introduced to reduce nocturnal wakefulness during the night (if needed). Our data suggest sleep education alone may not be enough to help most families with an infant who has a sleep problem,” the investigators noted.
Find the full study in Pediatrics (doi: 10.1542/peds.2015-1486).
Graduated extinction and bedtime fading significantly reduced nocturnal wakefulness in infants and maternal stress, according to Michael Gradisar, Ph.D., of Flinders University, Adelaide, South Australia, and his associates.
For the study, a group of 43 infants aged 6-16 months received either graduated extinction, bedtime fading, or sleep education. Compared with the control group of sleep education, sleep latency was significantly decreased in both the graduated extinction and bedtime fading groups. A significant reduction in number of awakenings and wake after sleep onset was seen in the graduated extinction group.
Maternal stress decreased over time in all groups, however, compared with the control group; stress was moderately reduced in the graduated extinction group and was significantly reduced in the bedtime fading group. After 12 months, no significant difference in parent-child attachment was seen between the control and noncontrol groups.
“Our data suggest introducing bedtime fading will provide quick results for improving sleep-onset latency. Graduated extinction may then be introduced to reduce nocturnal wakefulness during the night (if needed). Our data suggest sleep education alone may not be enough to help most families with an infant who has a sleep problem,” the investigators noted.
Find the full study in Pediatrics (doi: 10.1542/peds.2015-1486).
Graduated extinction and bedtime fading significantly reduced nocturnal wakefulness in infants and maternal stress, according to Michael Gradisar, Ph.D., of Flinders University, Adelaide, South Australia, and his associates.
For the study, a group of 43 infants aged 6-16 months received either graduated extinction, bedtime fading, or sleep education. Compared with the control group of sleep education, sleep latency was significantly decreased in both the graduated extinction and bedtime fading groups. A significant reduction in number of awakenings and wake after sleep onset was seen in the graduated extinction group.
Maternal stress decreased over time in all groups, however, compared with the control group; stress was moderately reduced in the graduated extinction group and was significantly reduced in the bedtime fading group. After 12 months, no significant difference in parent-child attachment was seen between the control and noncontrol groups.
“Our data suggest introducing bedtime fading will provide quick results for improving sleep-onset latency. Graduated extinction may then be introduced to reduce nocturnal wakefulness during the night (if needed). Our data suggest sleep education alone may not be enough to help most families with an infant who has a sleep problem,” the investigators noted.
Find the full study in Pediatrics (doi: 10.1542/peds.2015-1486).
FROM PEDIATRICS

Rooming in cuts costs and improves care for neonatal abstinence syndrome
A neonatal abstinence syndrome program that focused on rooming in significantly decreased hospital costs, drug use, and length of hospital stay, based on data from a program in a single hospital in a rural academic tertiary care center.
“The aim of this project was to improve the care of opioid-exposed newborns by involving families, standardizing assessment and treatment, and transitioning to rooming-in for the full hospital stay,” reported Dr. Alison Volpe Holmes of the Geisel School of Medicine at Dartmouth, Hanover, N.H., and colleagues.

The researchers reviewed data from 163 newborns with neonatal abstinence syndrome (NAS) treated at Children’s Hospital at Dartmouth-Hitchcock between March 2012 and February 2015. Between the preintervention period and the study’s end, cumulative morphine exposure per infant dropped from 13.7 mg to 6.6 mg, length of hospital stay for newborns needing pharmacologic care dropped from 16.9 days to 12.3 days, and the average cost for newborns needing pharmacologic care dropped from $19,737 to $8,755. No adverse events were reported during the study period.
“We reduced system costs by more than half by caring for infants with prenatal opioid exposure and NAS in a rooming-in model, safely eliminating the use of critical care beds for this condition,” they noted.
Read the full study in Pediatrics (2016;137[6]:e20152929).
A neonatal abstinence syndrome program that focused on rooming in significantly decreased hospital costs, drug use, and length of hospital stay, based on data from a program in a single hospital in a rural academic tertiary care center.
“The aim of this project was to improve the care of opioid-exposed newborns by involving families, standardizing assessment and treatment, and transitioning to rooming-in for the full hospital stay,” reported Dr. Alison Volpe Holmes of the Geisel School of Medicine at Dartmouth, Hanover, N.H., and colleagues.
The researchers reviewed data from 163 newborns with neonatal abstinence syndrome (NAS) treated at Children’s Hospital at Dartmouth-Hitchcock between March 2012 and February 2015. Between the preintervention period and the study’s end, cumulative morphine exposure per infant dropped from 13.7 mg to 6.6 mg, length of hospital stay for newborns needing pharmacologic care dropped from 16.9 days to 12.3 days, and the average cost for newborns needing pharmacologic care dropped from $19,737 to $8,755. No adverse events were reported during the study period.
“We reduced system costs by more than half by caring for infants with prenatal opioid exposure and NAS in a rooming-in model, safely eliminating the use of critical care beds for this condition,” they noted.
Read the full study in Pediatrics (2016;137[6]:e20152929).
A neonatal abstinence syndrome program that focused on rooming in significantly decreased hospital costs, drug use, and length of hospital stay, based on data from a program in a single hospital in a rural academic tertiary care center.
“The aim of this project was to improve the care of opioid-exposed newborns by involving families, standardizing assessment and treatment, and transitioning to rooming-in for the full hospital stay,” reported Dr. Alison Volpe Holmes of the Geisel School of Medicine at Dartmouth, Hanover, N.H., and colleagues.
The researchers reviewed data from 163 newborns with neonatal abstinence syndrome (NAS) treated at Children’s Hospital at Dartmouth-Hitchcock between March 2012 and February 2015. Between the preintervention period and the study’s end, cumulative morphine exposure per infant dropped from 13.7 mg to 6.6 mg, length of hospital stay for newborns needing pharmacologic care dropped from 16.9 days to 12.3 days, and the average cost for newborns needing pharmacologic care dropped from $19,737 to $8,755. No adverse events were reported during the study period.
“We reduced system costs by more than half by caring for infants with prenatal opioid exposure and NAS in a rooming-in model, safely eliminating the use of critical care beds for this condition,” they noted.
Read the full study in Pediatrics (2016;137[6]:e20152929).
FROM PEDIATRICS

Two-step UTI screening cuts catheterization rate in half
After implementation of a quality improvement initiative to more effectively screen febrile children for urinary tract infections (UTIs) in the emergency department, catheterization rates dropped from 63% to 30% over a 6-month period, a study found.
The sustained drop prevented more than 350 young children from catheterization without increasing revisit rates or missing UTIs in the 39% of children who were followed in the care network. This was in a study that compared catheterization rates in 1,520 children aged 6-24 months in the year before the intervention and 828 children in the 6 months during the intervention.
“Although urine catheterization remains the gold standard in diagnosing UTIs, it is an invasive procedure that may be avoided in most patients who are being screened,” wrote Dr. Jane M. Lavelle of Children’s Hospital of Philadelphia (CHOP) and her associates. UTI screening by this method can be “painful, time consuming, and costly,” they added (Pediatrics. 2016 June 2. doi: 10.1542/peds.2015-3023).

An alternative method to automatic catheterization is a two-step process already included as an option in American Academy of Pediatrics guidelines: Instead of collecting urine through catheterization just once for screening and culture, an emergency department first noninvasively collects urine with a urine bag for screening in those indicated with evidence-based risk factors, and then catheterizes only those who screen positive (Pediatrics. 2011;128[3]:595-610).
“Due to the predictive models’ higher sensitivity than specificity for screening, most urine samples will have a negative screen for pyuria or bacteriuria by urine dipstick or microscopy,” the authors wrote.
At baseline, CHOP’s ED was screening 63% of febrile children under age 24 months using catheterization, but screens were most commonly negative and only 4.3% had positive cultures. The authors therefore initiated a switch to the two-step method as a pilot run in one ED area before educating all ED personnel and expanding to the full department in the second month, using three cycles of Plan-Do-Study-Act protocol.
Children aged 6-24 months comprised approximately 20% of the ED’s more than 90,000 annual patients, and about 22% of these children presented with fever as the primary concern. Children with a history of genitourinary problems or immune deficiency were excluded.
The pilot ran in an “urgent care section of ED where there are typically more children with less complex medical histories and where ‘fever’ is a common complaint,” the investigators said. The staff completed a learning module with assessment and then received in-person and visual reminders of the procedure. Nurse feedback was then used to develop a nursing-specific educational module before expanding the intervention to all ED areas.
While 69% of 828 febrile young children still underwent screening during the 6-month intervention period, only 16% still underwent urethral catheterization as the initial screening step, typically because of strong clinical indications for a UTI. Another 14% underwent catheterization only after a positive urine screen from an initial noninvasive urine collection or because of an inability to get an adequate urine specimen with the bag. The reduction in catheterization dropped to 55% within 2 weeks of the intervention’s start and spread to other hospital departments. The drop to a 30% catheterization rate remained throughout 18 additional months of monitoring.
“Through online education modules, staff meetings, printed and EHR reminders, family involvement, team review of weekly data, individual and group feedback, and nurse scripting, the ED was able to achieve our aim of reducing catheterization rates among febrile young children ages 6-24 months by half over a 6-month period with sustained results,” Dr. Lavelle and her associates reported.
The research did not use external funding, and the researchers reported they had no financial disclosures.
When children are febrile and younger than 24 months old and they go to a pediatric emergency department, a pretty big work-up can be anticipated, taking several hours and including a test for possible UTI.

|
Dr. Michael E. Pichichero |
In this report from investigators at Children’s Hospital of Philadelphia, we learn the results of a study undertaken to reduce the frequency of bladder catheterization by using a urine bag collection as a screening tool. It worked! Before the study, 63% of 1,520 young children got catheterized, and 4.3% had a UTI. With the screening method, only those with a positive screen for a possible UTI (16% of 828) proceeded to be catheterized, reducing catheterization rates significantly. Only 4.4% of the 69% of children screened by either method had a UTI. So by screening with a bag urine specimen first, many of the children who would have been catheterized did not undergo the procedure.
A hidden gem of information in the study was the length of a visit to the emergency department. The kids were there an average of 4.7 hours whether the provider waited for the bag urine and then catheterized or went straight to the procedure! If only they had gone to their primary care provider, I wonder how much time could have been saved?
Dr. Michael E. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he had no relevant financial disclosures.
When children are febrile and younger than 24 months old and they go to a pediatric emergency department, a pretty big work-up can be anticipated, taking several hours and including a test for possible UTI.
|
|
Dr. Michael E. Pichichero |
In this report from investigators at Children’s Hospital of Philadelphia, we learn the results of a study undertaken to reduce the frequency of bladder catheterization by using a urine bag collection as a screening tool. It worked! Before the study, 63% of 1,520 young children got catheterized, and 4.3% had a UTI. With the screening method, only those with a positive screen for a possible UTI (16% of 828) proceeded to be catheterized, reducing catheterization rates significantly. Only 4.4% of the 69% of children screened by either method had a UTI. So by screening with a bag urine specimen first, many of the children who would have been catheterized did not undergo the procedure.
A hidden gem of information in the study was the length of a visit to the emergency department. The kids were there an average of 4.7 hours whether the provider waited for the bag urine and then catheterized or went straight to the procedure! If only they had gone to their primary care provider, I wonder how much time could have been saved?
Dr. Michael E. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he had no relevant financial disclosures.
When children are febrile and younger than 24 months old and they go to a pediatric emergency department, a pretty big work-up can be anticipated, taking several hours and including a test for possible UTI.
|
|
Dr. Michael E. Pichichero |
In this report from investigators at Children’s Hospital of Philadelphia, we learn the results of a study undertaken to reduce the frequency of bladder catheterization by using a urine bag collection as a screening tool. It worked! Before the study, 63% of 1,520 young children got catheterized, and 4.3% had a UTI. With the screening method, only those with a positive screen for a possible UTI (16% of 828) proceeded to be catheterized, reducing catheterization rates significantly. Only 4.4% of the 69% of children screened by either method had a UTI. So by screening with a bag urine specimen first, many of the children who would have been catheterized did not undergo the procedure.
A hidden gem of information in the study was the length of a visit to the emergency department. The kids were there an average of 4.7 hours whether the provider waited for the bag urine and then catheterized or went straight to the procedure! If only they had gone to their primary care provider, I wonder how much time could have been saved?
Dr. Michael E. Pichichero, a specialist in pediatric infectious diseases, is director of the Research Institute, Rochester (N.Y.) General Hospital. He is also a pediatrician at Legacy Pediatrics in Rochester. Dr. Pichichero said he had no relevant financial disclosures.
After implementation of a quality improvement initiative to more effectively screen febrile children for urinary tract infections (UTIs) in the emergency department, catheterization rates dropped from 63% to 30% over a 6-month period, a study found.
The sustained drop prevented more than 350 young children from catheterization without increasing revisit rates or missing UTIs in the 39% of children who were followed in the care network. This was in a study that compared catheterization rates in 1,520 children aged 6-24 months in the year before the intervention and 828 children in the 6 months during the intervention.
“Although urine catheterization remains the gold standard in diagnosing UTIs, it is an invasive procedure that may be avoided in most patients who are being screened,” wrote Dr. Jane M. Lavelle of Children’s Hospital of Philadelphia (CHOP) and her associates. UTI screening by this method can be “painful, time consuming, and costly,” they added (Pediatrics. 2016 June 2. doi: 10.1542/peds.2015-3023).
An alternative method to automatic catheterization is a two-step process already included as an option in American Academy of Pediatrics guidelines: Instead of collecting urine through catheterization just once for screening and culture, an emergency department first noninvasively collects urine with a urine bag for screening in those indicated with evidence-based risk factors, and then catheterizes only those who screen positive (Pediatrics. 2011;128[3]:595-610).
“Due to the predictive models’ higher sensitivity than specificity for screening, most urine samples will have a negative screen for pyuria or bacteriuria by urine dipstick or microscopy,” the authors wrote.
At baseline, CHOP’s ED was screening 63% of febrile children under age 24 months using catheterization, but screens were most commonly negative and only 4.3% had positive cultures. The authors therefore initiated a switch to the two-step method as a pilot run in one ED area before educating all ED personnel and expanding to the full department in the second month, using three cycles of Plan-Do-Study-Act protocol.
Children aged 6-24 months comprised approximately 20% of the ED’s more than 90,000 annual patients, and about 22% of these children presented with fever as the primary concern. Children with a history of genitourinary problems or immune deficiency were excluded.
The pilot ran in an “urgent care section of ED where there are typically more children with less complex medical histories and where ‘fever’ is a common complaint,” the investigators said. The staff completed a learning module with assessment and then received in-person and visual reminders of the procedure. Nurse feedback was then used to develop a nursing-specific educational module before expanding the intervention to all ED areas.
While 69% of 828 febrile young children still underwent screening during the 6-month intervention period, only 16% still underwent urethral catheterization as the initial screening step, typically because of strong clinical indications for a UTI. Another 14% underwent catheterization only after a positive urine screen from an initial noninvasive urine collection or because of an inability to get an adequate urine specimen with the bag. The reduction in catheterization dropped to 55% within 2 weeks of the intervention’s start and spread to other hospital departments. The drop to a 30% catheterization rate remained throughout 18 additional months of monitoring.
“Through online education modules, staff meetings, printed and EHR reminders, family involvement, team review of weekly data, individual and group feedback, and nurse scripting, the ED was able to achieve our aim of reducing catheterization rates among febrile young children ages 6-24 months by half over a 6-month period with sustained results,” Dr. Lavelle and her associates reported.
The research did not use external funding, and the researchers reported they had no financial disclosures.
After implementation of a quality improvement initiative to more effectively screen febrile children for urinary tract infections (UTIs) in the emergency department, catheterization rates dropped from 63% to 30% over a 6-month period, a study found.
The sustained drop prevented more than 350 young children from catheterization without increasing revisit rates or missing UTIs in the 39% of children who were followed in the care network. This was in a study that compared catheterization rates in 1,520 children aged 6-24 months in the year before the intervention and 828 children in the 6 months during the intervention.
“Although urine catheterization remains the gold standard in diagnosing UTIs, it is an invasive procedure that may be avoided in most patients who are being screened,” wrote Dr. Jane M. Lavelle of Children’s Hospital of Philadelphia (CHOP) and her associates. UTI screening by this method can be “painful, time consuming, and costly,” they added (Pediatrics. 2016 June 2. doi: 10.1542/peds.2015-3023).
An alternative method to automatic catheterization is a two-step process already included as an option in American Academy of Pediatrics guidelines: Instead of collecting urine through catheterization just once for screening and culture, an emergency department first noninvasively collects urine with a urine bag for screening in those indicated with evidence-based risk factors, and then catheterizes only those who screen positive (Pediatrics. 2011;128[3]:595-610).
“Due to the predictive models’ higher sensitivity than specificity for screening, most urine samples will have a negative screen for pyuria or bacteriuria by urine dipstick or microscopy,” the authors wrote.
At baseline, CHOP’s ED was screening 63% of febrile children under age 24 months using catheterization, but screens were most commonly negative and only 4.3% had positive cultures. The authors therefore initiated a switch to the two-step method as a pilot run in one ED area before educating all ED personnel and expanding to the full department in the second month, using three cycles of Plan-Do-Study-Act protocol.
Children aged 6-24 months comprised approximately 20% of the ED’s more than 90,000 annual patients, and about 22% of these children presented with fever as the primary concern. Children with a history of genitourinary problems or immune deficiency were excluded.
The pilot ran in an “urgent care section of ED where there are typically more children with less complex medical histories and where ‘fever’ is a common complaint,” the investigators said. The staff completed a learning module with assessment and then received in-person and visual reminders of the procedure. Nurse feedback was then used to develop a nursing-specific educational module before expanding the intervention to all ED areas.
While 69% of 828 febrile young children still underwent screening during the 6-month intervention period, only 16% still underwent urethral catheterization as the initial screening step, typically because of strong clinical indications for a UTI. Another 14% underwent catheterization only after a positive urine screen from an initial noninvasive urine collection or because of an inability to get an adequate urine specimen with the bag. The reduction in catheterization dropped to 55% within 2 weeks of the intervention’s start and spread to other hospital departments. The drop to a 30% catheterization rate remained throughout 18 additional months of monitoring.
“Through online education modules, staff meetings, printed and EHR reminders, family involvement, team review of weekly data, individual and group feedback, and nurse scripting, the ED was able to achieve our aim of reducing catheterization rates among febrile young children ages 6-24 months by half over a 6-month period with sustained results,” Dr. Lavelle and her associates reported.
The research did not use external funding, and the researchers reported they had no financial disclosures.
FROM PEDIATRICS
Key clinical point: Use of a two-step UTI screening process reduced unnecessary catheterizations by half.
Major finding: The ED catheterization rate in febrile children suspected of a UTI dropped from 63% to 30% over a 6-month period.
Data source: An assessment of a quality improvement initiative in the Children’s Hospital of Philadelphia ED that compared catheterization rates in 1,520 children aged 6-24 months in the year before the intervention and 828 children in the 6 months during the intervention.
Disclosures: The research did not use external funding, and the researchers reported they had no financial disclosures.

Maternal vaccination against pertussis can protect premature infants
Maternal immunization in the early third trimester (from 28 weeks’ gestation) may protect premature infants from pertussis, study results found.
This was the finding of an observational substudy of a larger multicenter, randomized, controlled vaccination trial of premature infants (the PUNS trial), which compared pertussis antibody concentrations before and after primary immunization in premature infants born to mothers who were or were not vaccinated with Repevax. Dr. Alison Kent of St George’s, University of London, and colleagues assessed the levels of the five vaccine antigens present in the maternal combination Repevax vaccine (pertussis toxoid, filamentous hemagglutinin, fimbriae types 2 and 3, diphtheria toxoid, tetanus toxoid, and inactivated poliovirus) in premature infants born to mothers who either received or did not receive Repevax from 28 weeks’ gestation. Antigen quantifications were conducted in these premature infants at approximately 2, 5, and 12 months of age.

Thirty-one (19%) of the 160 premature infants in the substudy were born to mothers who had been vaccinated. Two months after their premature birth, infants born to vaccinated mothers had significantly higher concentrations of all five measured antigens, compared with those born to unvaccinated mothers (all P values less than .001). Although fewer infants were sampled at 5 months of age, significantly higher concentrations of filamentous hemagglutinin and diphtheria toxoid were still found in those born to vaccinated mothers (both P = .003). Data collected at the 12-month assessment indicated that only tetanus antibody concentrations remained significantly higher in those born to vaccinated mothers (P = .015). A positive correlation between the number of days from maternal vaccination to delivery was found for all measured antigens, with the exception of fimbriae types 2 and 3.
“The emergency introduction of a maternal immunization program to control a national pertussis outbreak serendipitously provided an opportunity to assess antibody concentrations to maternal vaccine antigens in premature infants,” Dr. Kent and associates noted in Pediatrics (June 2016 doi: 10.1542/peds.2015-3854). This unexpected opportunity resulted in evidence supporting a protective effect against pertussis in the early lives of infants born prematurely to mothers immunized in their early third trimester.
Pfizer and the National Institute for Health Research Clinical Research Network funded the study. Professor Heath and Dr. Ladhani disclosed conducting studies on behalf of St George’s, University of London funded by vaccine manufacturers without receiving personal payments or travel support. The other authors reported no conflicts of interest.
Maternal immunization in the early third trimester (from 28 weeks’ gestation) may protect premature infants from pertussis, study results found.
This was the finding of an observational substudy of a larger multicenter, randomized, controlled vaccination trial of premature infants (the PUNS trial), which compared pertussis antibody concentrations before and after primary immunization in premature infants born to mothers who were or were not vaccinated with Repevax. Dr. Alison Kent of St George’s, University of London, and colleagues assessed the levels of the five vaccine antigens present in the maternal combination Repevax vaccine (pertussis toxoid, filamentous hemagglutinin, fimbriae types 2 and 3, diphtheria toxoid, tetanus toxoid, and inactivated poliovirus) in premature infants born to mothers who either received or did not receive Repevax from 28 weeks’ gestation. Antigen quantifications were conducted in these premature infants at approximately 2, 5, and 12 months of age.
Thirty-one (19%) of the 160 premature infants in the substudy were born to mothers who had been vaccinated. Two months after their premature birth, infants born to vaccinated mothers had significantly higher concentrations of all five measured antigens, compared with those born to unvaccinated mothers (all P values less than .001). Although fewer infants were sampled at 5 months of age, significantly higher concentrations of filamentous hemagglutinin and diphtheria toxoid were still found in those born to vaccinated mothers (both P = .003). Data collected at the 12-month assessment indicated that only tetanus antibody concentrations remained significantly higher in those born to vaccinated mothers (P = .015). A positive correlation between the number of days from maternal vaccination to delivery was found for all measured antigens, with the exception of fimbriae types 2 and 3.
“The emergency introduction of a maternal immunization program to control a national pertussis outbreak serendipitously provided an opportunity to assess antibody concentrations to maternal vaccine antigens in premature infants,” Dr. Kent and associates noted in Pediatrics (June 2016 doi: 10.1542/peds.2015-3854). This unexpected opportunity resulted in evidence supporting a protective effect against pertussis in the early lives of infants born prematurely to mothers immunized in their early third trimester.
Pfizer and the National Institute for Health Research Clinical Research Network funded the study. Professor Heath and Dr. Ladhani disclosed conducting studies on behalf of St George’s, University of London funded by vaccine manufacturers without receiving personal payments or travel support. The other authors reported no conflicts of interest.
Maternal immunization in the early third trimester (from 28 weeks’ gestation) may protect premature infants from pertussis, study results found.
This was the finding of an observational substudy of a larger multicenter, randomized, controlled vaccination trial of premature infants (the PUNS trial), which compared pertussis antibody concentrations before and after primary immunization in premature infants born to mothers who were or were not vaccinated with Repevax. Dr. Alison Kent of St George’s, University of London, and colleagues assessed the levels of the five vaccine antigens present in the maternal combination Repevax vaccine (pertussis toxoid, filamentous hemagglutinin, fimbriae types 2 and 3, diphtheria toxoid, tetanus toxoid, and inactivated poliovirus) in premature infants born to mothers who either received or did not receive Repevax from 28 weeks’ gestation. Antigen quantifications were conducted in these premature infants at approximately 2, 5, and 12 months of age.
Thirty-one (19%) of the 160 premature infants in the substudy were born to mothers who had been vaccinated. Two months after their premature birth, infants born to vaccinated mothers had significantly higher concentrations of all five measured antigens, compared with those born to unvaccinated mothers (all P values less than .001). Although fewer infants were sampled at 5 months of age, significantly higher concentrations of filamentous hemagglutinin and diphtheria toxoid were still found in those born to vaccinated mothers (both P = .003). Data collected at the 12-month assessment indicated that only tetanus antibody concentrations remained significantly higher in those born to vaccinated mothers (P = .015). A positive correlation between the number of days from maternal vaccination to delivery was found for all measured antigens, with the exception of fimbriae types 2 and 3.
“The emergency introduction of a maternal immunization program to control a national pertussis outbreak serendipitously provided an opportunity to assess antibody concentrations to maternal vaccine antigens in premature infants,” Dr. Kent and associates noted in Pediatrics (June 2016 doi: 10.1542/peds.2015-3854). This unexpected opportunity resulted in evidence supporting a protective effect against pertussis in the early lives of infants born prematurely to mothers immunized in their early third trimester.
Pfizer and the National Institute for Health Research Clinical Research Network funded the study. Professor Heath and Dr. Ladhani disclosed conducting studies on behalf of St George’s, University of London funded by vaccine manufacturers without receiving personal payments or travel support. The other authors reported no conflicts of interest.
FROM PEDIATRICS
Key clinical point: Vaccination of pregnant women early in their third trimester may protect premature infants against pertussis.
Major finding: At 2 months after birth, infants born to vaccinated mothers displayed higher antibody concentrations to vaccine antigens than did infants born to unvaccinated mothers.
Data source: Premature infants born to mothers that did or did not receive Repevax from 28 weeks of pregnancy.
Disclosures: Pfizer Ltd. and the National Institute for Health Research Clinical Research Network funded the study. Professor Heath and Dr. Ladhani disclosed conducting studies on behalf of St George’s, University of London funded by vaccine manufacturers without receiving personal payments or travel support. The other authors reported no conflicts of interest.

Platelet transfusions do not reduce IVH risk in VLBW infants

A retrospective, multicenter study of 972 very-low-birth-weight (VLBW) infants treated in 6 US neonatal intensive care units (NICUs) has shown that platelet transfusions do not significantly affect the incidence of intraventricular hemorrhage (IVH).
Thrombocytopenia is a risk factor for IVH, but investigators found no correlation between its severity and risk for IVH. Nor did they find platelet transfusions to have a significant effect on the incidence of IVH.
To describe platelet transfusion practices in US NICUs, senior author Martha Sola-Visner, MD, of Boston Children’s Hospital in Massachusetts, and colleagues studied NICU admissions from January 1, 2006, to December 31, 2007. They collected the last data on December 4, 2008.
Of the 972 VLBW infants, 231 (23.8%) received at least 1 platelet transfusion. And more males received transfusions (61%) than females.
Infants who received transfusions were more premature at 26.3 weeks’ gestation age compared with 28.8 weeks for those who did not receive transfusions, P<0.001.
Transfused infants were also smaller, with a mean birth weight of 805 g compared with 1113 g in the group that did not receive a transfusion, P<0.001.
Platelet transfusions
The 231 transfused infants received a total of 1002 platelet transfusions, with a mean of 4.3 per infant (range 1 to 63 transfusions).
Forty-one percent of infants had transfusions during the first 7 days of life only, amounting to 281 transfusions; 32.9% had transfusions after the first 7 days only, and 26.4% had transfusions during both periods. Seven hundred twenty-one transfusions were administered after day 7.
Almost two thirds of the transfusions, 65.4% or 653 of 998 transfusions, were given to infants who had a pre-transfusion platelet count of at least 50,000/μL.
The investigators poined out that this finding “was in contrast to UK NICUs,” where transfusions are administered at a median platelet count of 27,000/μL.
Illness severity
The investigators found significant differences among NICU sites in terms of clinical markers for transfusions.
Overall, 189 VLBW infants had platelet counts less than 100,000/μL in the first 7 days of life for a total of 402 days. And at least 1 platelet transfusion was given on 212 of those days. Of these, 198 transfusions (93.4%) had a marker of severe illness or bleeding.
On the other hand, of the 190 patient days without a transfusion, 113 (59.5%) had at least 1 of these markers (P<0.001).
Thrombocytopenia and IVH risk
The investigators evaluated the risk for IVH based on the lowest platelet count before the diagnosis of IVH was made.
They found that infants with thrombocytopenia were at higher risk for IVH, with a hazard ratio of 2.17 for any platelet count less than 150,000/μL (P<0.001).
Nevertheless, for the 314 infants with at least 1 platelet count less than 150,000/μL during the first 7 days of life, they found no association between severity of thrombocytopenia and the risk for subsequent IVH (P=0.70).
Transfusion and IVH risk
To determine whether platelet transfusions protected VLBW infants from IVH during their first 7 days of life, the investigators performed a Cox regression analysis in 756 infants.
They found that 134 infants (17.7%) had an IVH, including 62 (8.2%) with grade III or IV. So in the unadjusted model, they found a significant association between platelet transfusion and subsequent IVH, P=0.004.
However, when they adjusted the model for clinical covariates, only infants with grade III or IV IVH had a significantly greater risk with platelet transfusion, P=0.01.
Clinical covariates included sex, gestational age less than 28 weeks, 5-minute Apgar score less than 7, antenatal corticosteroid treatment, and pregnancy-induced hypertension as an indication for delivery.
The investigators also adjusted the model for clinical covariates and nadir platelet count of less than 15,000/μL. In this model, platelet transfusion became nonsignificant, even for IVH of grade III or IV.
The investigators noted that the degree to which their results are generalizable to infants with more severe thrombocytopenia is unclear, since infants in this analysis often had transfusions at platelet levels between 50,000/μL and 150,000/μL. They also collected the data approximately 8 years ago, and transfusion practices may have changed since then.
The 6 NICU study sites included Boston Children’s Hospital, Boston, Massachusetts; University of Iowa Children’s Hospital, Iowa City, Iowa; and 4 NICUs affiliated with Intermountain Health Care in Utah.
The investigators published their findings in JAMA Pediatrics. ![]()
A retrospective, multicenter study of 972 very-low-birth-weight (VLBW) infants treated in 6 US neonatal intensive care units (NICUs) has shown that platelet transfusions do not significantly affect the incidence of intraventricular hemorrhage (IVH).
Thrombocytopenia is a risk factor for IVH, but investigators found no correlation between its severity and risk for IVH. Nor did they find platelet transfusions to have a significant effect on the incidence of IVH.
To describe platelet transfusion practices in US NICUs, senior author Martha Sola-Visner, MD, of Boston Children’s Hospital in Massachusetts, and colleagues studied NICU admissions from January 1, 2006, to December 31, 2007. They collected the last data on December 4, 2008.
Of the 972 VLBW infants, 231 (23.8%) received at least 1 platelet transfusion. And more males received transfusions (61%) than females.
Infants who received transfusions were more premature at 26.3 weeks’ gestation age compared with 28.8 weeks for those who did not receive transfusions, P<0.001.
Transfused infants were also smaller, with a mean birth weight of 805 g compared with 1113 g in the group that did not receive a transfusion, P<0.001.
Platelet transfusions
The 231 transfused infants received a total of 1002 platelet transfusions, with a mean of 4.3 per infant (range 1 to 63 transfusions).
Forty-one percent of infants had transfusions during the first 7 days of life only, amounting to 281 transfusions; 32.9% had transfusions after the first 7 days only, and 26.4% had transfusions during both periods. Seven hundred twenty-one transfusions were administered after day 7.
Almost two thirds of the transfusions, 65.4% or 653 of 998 transfusions, were given to infants who had a pre-transfusion platelet count of at least 50,000/μL.
The investigators poined out that this finding “was in contrast to UK NICUs,” where transfusions are administered at a median platelet count of 27,000/μL.
Illness severity
The investigators found significant differences among NICU sites in terms of clinical markers for transfusions.
Overall, 189 VLBW infants had platelet counts less than 100,000/μL in the first 7 days of life for a total of 402 days. And at least 1 platelet transfusion was given on 212 of those days. Of these, 198 transfusions (93.4%) had a marker of severe illness or bleeding.
On the other hand, of the 190 patient days without a transfusion, 113 (59.5%) had at least 1 of these markers (P<0.001).
Thrombocytopenia and IVH risk
The investigators evaluated the risk for IVH based on the lowest platelet count before the diagnosis of IVH was made.
They found that infants with thrombocytopenia were at higher risk for IVH, with a hazard ratio of 2.17 for any platelet count less than 150,000/μL (P<0.001).
Nevertheless, for the 314 infants with at least 1 platelet count less than 150,000/μL during the first 7 days of life, they found no association between severity of thrombocytopenia and the risk for subsequent IVH (P=0.70).
Transfusion and IVH risk
To determine whether platelet transfusions protected VLBW infants from IVH during their first 7 days of life, the investigators performed a Cox regression analysis in 756 infants.
They found that 134 infants (17.7%) had an IVH, including 62 (8.2%) with grade III or IV. So in the unadjusted model, they found a significant association between platelet transfusion and subsequent IVH, P=0.004.
However, when they adjusted the model for clinical covariates, only infants with grade III or IV IVH had a significantly greater risk with platelet transfusion, P=0.01.
Clinical covariates included sex, gestational age less than 28 weeks, 5-minute Apgar score less than 7, antenatal corticosteroid treatment, and pregnancy-induced hypertension as an indication for delivery.
The investigators also adjusted the model for clinical covariates and nadir platelet count of less than 15,000/μL. In this model, platelet transfusion became nonsignificant, even for IVH of grade III or IV.
The investigators noted that the degree to which their results are generalizable to infants with more severe thrombocytopenia is unclear, since infants in this analysis often had transfusions at platelet levels between 50,000/μL and 150,000/μL. They also collected the data approximately 8 years ago, and transfusion practices may have changed since then.
The 6 NICU study sites included Boston Children’s Hospital, Boston, Massachusetts; University of Iowa Children’s Hospital, Iowa City, Iowa; and 4 NICUs affiliated with Intermountain Health Care in Utah.
The investigators published their findings in JAMA Pediatrics. ![]()
A retrospective, multicenter study of 972 very-low-birth-weight (VLBW) infants treated in 6 US neonatal intensive care units (NICUs) has shown that platelet transfusions do not significantly affect the incidence of intraventricular hemorrhage (IVH).
Thrombocytopenia is a risk factor for IVH, but investigators found no correlation between its severity and risk for IVH. Nor did they find platelet transfusions to have a significant effect on the incidence of IVH.
To describe platelet transfusion practices in US NICUs, senior author Martha Sola-Visner, MD, of Boston Children’s Hospital in Massachusetts, and colleagues studied NICU admissions from January 1, 2006, to December 31, 2007. They collected the last data on December 4, 2008.
Of the 972 VLBW infants, 231 (23.8%) received at least 1 platelet transfusion. And more males received transfusions (61%) than females.
Infants who received transfusions were more premature at 26.3 weeks’ gestation age compared with 28.8 weeks for those who did not receive transfusions, P<0.001.
Transfused infants were also smaller, with a mean birth weight of 805 g compared with 1113 g in the group that did not receive a transfusion, P<0.001.
Platelet transfusions
The 231 transfused infants received a total of 1002 platelet transfusions, with a mean of 4.3 per infant (range 1 to 63 transfusions).
Forty-one percent of infants had transfusions during the first 7 days of life only, amounting to 281 transfusions; 32.9% had transfusions after the first 7 days only, and 26.4% had transfusions during both periods. Seven hundred twenty-one transfusions were administered after day 7.
Almost two thirds of the transfusions, 65.4% or 653 of 998 transfusions, were given to infants who had a pre-transfusion platelet count of at least 50,000/μL.
The investigators poined out that this finding “was in contrast to UK NICUs,” where transfusions are administered at a median platelet count of 27,000/μL.
Illness severity
The investigators found significant differences among NICU sites in terms of clinical markers for transfusions.
Overall, 189 VLBW infants had platelet counts less than 100,000/μL in the first 7 days of life for a total of 402 days. And at least 1 platelet transfusion was given on 212 of those days. Of these, 198 transfusions (93.4%) had a marker of severe illness or bleeding.
On the other hand, of the 190 patient days without a transfusion, 113 (59.5%) had at least 1 of these markers (P<0.001).
Thrombocytopenia and IVH risk
The investigators evaluated the risk for IVH based on the lowest platelet count before the diagnosis of IVH was made.
They found that infants with thrombocytopenia were at higher risk for IVH, with a hazard ratio of 2.17 for any platelet count less than 150,000/μL (P<0.001).
Nevertheless, for the 314 infants with at least 1 platelet count less than 150,000/μL during the first 7 days of life, they found no association between severity of thrombocytopenia and the risk for subsequent IVH (P=0.70).
Transfusion and IVH risk
To determine whether platelet transfusions protected VLBW infants from IVH during their first 7 days of life, the investigators performed a Cox regression analysis in 756 infants.
They found that 134 infants (17.7%) had an IVH, including 62 (8.2%) with grade III or IV. So in the unadjusted model, they found a significant association between platelet transfusion and subsequent IVH, P=0.004.
However, when they adjusted the model for clinical covariates, only infants with grade III or IV IVH had a significantly greater risk with platelet transfusion, P=0.01.
Clinical covariates included sex, gestational age less than 28 weeks, 5-minute Apgar score less than 7, antenatal corticosteroid treatment, and pregnancy-induced hypertension as an indication for delivery.
The investigators also adjusted the model for clinical covariates and nadir platelet count of less than 15,000/μL. In this model, platelet transfusion became nonsignificant, even for IVH of grade III or IV.
The investigators noted that the degree to which their results are generalizable to infants with more severe thrombocytopenia is unclear, since infants in this analysis often had transfusions at platelet levels between 50,000/μL and 150,000/μL. They also collected the data approximately 8 years ago, and transfusion practices may have changed since then.
The 6 NICU study sites included Boston Children’s Hospital, Boston, Massachusetts; University of Iowa Children’s Hospital, Iowa City, Iowa; and 4 NICUs affiliated with Intermountain Health Care in Utah.
The investigators published their findings in JAMA Pediatrics. ![]()
Methylphenidate Tied to Greater Risk for Arrhythmia in Children, Adolescents
Children and adolescents with attention-deficit/hyperactivity disorder who are prescribed methylphenidate to manage their conditions stand at a higher risk for arrhythmia and other, more serious, cardiac conditions.
In a study published in the BMJ, Ju-Young Shin, Ph.D., and colleagues examined records of 1,224 patients aged 17 years and younger from a nationwide South Korean health insurance database submitted between January 2007 and December 2011. All of the patients had experienced a cardiovascular event and at least one recorded prescription for methylphenidate to treat attention-deficit/hyperactivity disorder (ADHD) (BMJ 2016;353:i2550 doi:10.1136/bmj.i2550).

Of the 1,224 subjects, 864 (70.5%) had experienced arrhythmias, and the mean duration of exposure to methylphenidate was 0.5 years. During periods of methylphenidate treatment, subjects had an increased risk of arrhythmia, as Dr. Shin and coinvestigators calculated an adjusted incidence rate ratio of 1.61 (95% confidence interval, 1.48-1.74). This incidence rate ratio jumped up to 2.01 (95% CI, 1.74-2.31) during the first 3 days of methylphenidate treatment.
The risk was even higher for subjects with congenital heart disease; this subgroup had an adjusted incidence rate ratio of 3.49 (95% CI, 2.33-5.22), compared with 1.34 (95% CI, 1.23-1.46) in patients without it. Both the median age of first exposure to methylphenidate and occurrence of the first cardiac event were in patients aged 11-13 years, reported Dr. Shin of the Centre for Clinical Epidemiology at Jewish General Hospital and McGill University, both in Montreal, and colleagues in Australia and Korea.
“These results are consistent with the biological plausibility that the mechanism of action relates to the effect of methylphenidate on the heart rate,” the authors concluded. “Delayed effects would be expected with myocardial infarction, while more immediate effects would be expected with arrhythmias, as we observed.”
Dr. Shin and colleagues cited several limitations. For example, coding mistakes and incomplete records could not be ruled out in their study. In addition, they said, the “outcome measures were limited to patients with diagnoses of cardiovascular adverse events, and we could have missed outcomes not diagnosed.”
Nevertheless, they said, in light of the increased use of methylphenidate to treat ADHD across the globe, the benefits of using the drug “should be carefully weighed against potential cardiovascular risks of these drugs in children and adolescents.”
Two of the authors disclosed receiving support via fellowships from Australia’s National Health and Medical Research Council.
Children and adolescents with attention-deficit/hyperactivity disorder who are prescribed methylphenidate to manage their conditions stand at a higher risk for arrhythmia and other, more serious, cardiac conditions.
In a study published in the BMJ, Ju-Young Shin, Ph.D., and colleagues examined records of 1,224 patients aged 17 years and younger from a nationwide South Korean health insurance database submitted between January 2007 and December 2011. All of the patients had experienced a cardiovascular event and at least one recorded prescription for methylphenidate to treat attention-deficit/hyperactivity disorder (ADHD) (BMJ 2016;353:i2550 doi:10.1136/bmj.i2550).
Of the 1,224 subjects, 864 (70.5%) had experienced arrhythmias, and the mean duration of exposure to methylphenidate was 0.5 years. During periods of methylphenidate treatment, subjects had an increased risk of arrhythmia, as Dr. Shin and coinvestigators calculated an adjusted incidence rate ratio of 1.61 (95% confidence interval, 1.48-1.74). This incidence rate ratio jumped up to 2.01 (95% CI, 1.74-2.31) during the first 3 days of methylphenidate treatment.
The risk was even higher for subjects with congenital heart disease; this subgroup had an adjusted incidence rate ratio of 3.49 (95% CI, 2.33-5.22), compared with 1.34 (95% CI, 1.23-1.46) in patients without it. Both the median age of first exposure to methylphenidate and occurrence of the first cardiac event were in patients aged 11-13 years, reported Dr. Shin of the Centre for Clinical Epidemiology at Jewish General Hospital and McGill University, both in Montreal, and colleagues in Australia and Korea.
“These results are consistent with the biological plausibility that the mechanism of action relates to the effect of methylphenidate on the heart rate,” the authors concluded. “Delayed effects would be expected with myocardial infarction, while more immediate effects would be expected with arrhythmias, as we observed.”
Dr. Shin and colleagues cited several limitations. For example, coding mistakes and incomplete records could not be ruled out in their study. In addition, they said, the “outcome measures were limited to patients with diagnoses of cardiovascular adverse events, and we could have missed outcomes not diagnosed.”
Nevertheless, they said, in light of the increased use of methylphenidate to treat ADHD across the globe, the benefits of using the drug “should be carefully weighed against potential cardiovascular risks of these drugs in children and adolescents.”
Two of the authors disclosed receiving support via fellowships from Australia’s National Health and Medical Research Council.
Children and adolescents with attention-deficit/hyperactivity disorder who are prescribed methylphenidate to manage their conditions stand at a higher risk for arrhythmia and other, more serious, cardiac conditions.
In a study published in the BMJ, Ju-Young Shin, Ph.D., and colleagues examined records of 1,224 patients aged 17 years and younger from a nationwide South Korean health insurance database submitted between January 2007 and December 2011. All of the patients had experienced a cardiovascular event and at least one recorded prescription for methylphenidate to treat attention-deficit/hyperactivity disorder (ADHD) (BMJ 2016;353:i2550 doi:10.1136/bmj.i2550).
Of the 1,224 subjects, 864 (70.5%) had experienced arrhythmias, and the mean duration of exposure to methylphenidate was 0.5 years. During periods of methylphenidate treatment, subjects had an increased risk of arrhythmia, as Dr. Shin and coinvestigators calculated an adjusted incidence rate ratio of 1.61 (95% confidence interval, 1.48-1.74). This incidence rate ratio jumped up to 2.01 (95% CI, 1.74-2.31) during the first 3 days of methylphenidate treatment.
The risk was even higher for subjects with congenital heart disease; this subgroup had an adjusted incidence rate ratio of 3.49 (95% CI, 2.33-5.22), compared with 1.34 (95% CI, 1.23-1.46) in patients without it. Both the median age of first exposure to methylphenidate and occurrence of the first cardiac event were in patients aged 11-13 years, reported Dr. Shin of the Centre for Clinical Epidemiology at Jewish General Hospital and McGill University, both in Montreal, and colleagues in Australia and Korea.
“These results are consistent with the biological plausibility that the mechanism of action relates to the effect of methylphenidate on the heart rate,” the authors concluded. “Delayed effects would be expected with myocardial infarction, while more immediate effects would be expected with arrhythmias, as we observed.”
Dr. Shin and colleagues cited several limitations. For example, coding mistakes and incomplete records could not be ruled out in their study. In addition, they said, the “outcome measures were limited to patients with diagnoses of cardiovascular adverse events, and we could have missed outcomes not diagnosed.”
Nevertheless, they said, in light of the increased use of methylphenidate to treat ADHD across the globe, the benefits of using the drug “should be carefully weighed against potential cardiovascular risks of these drugs in children and adolescents.”
Two of the authors disclosed receiving support via fellowships from Australia’s National Health and Medical Research Council.
FROM THE BMJ

Methylphenidate tied to greater risk of arrhythmia in children, adolescents
Children and adolescents with attention-deficit/hyperactivity disorder who are prescribed methylphenidate to manage their conditions stand at a higher risk for arrhythmia and other, more serious, cardiac conditions.
In a study published in the BMJ, Ju-Young Shin, Ph.D., and colleagues examined records of 1,224 patients aged 17 years and younger from a nationwide South Korean health insurance database submitted between January 2007 and December 2011. All of the patients had experienced a cardiovascular event and at least one recorded prescription for methylphenidate to treat attention-deficit/hyperactivity disorder (ADHD) (BMJ 2016;353:i2550 doi:10.1136/bmj.i2550).

Of the 1,224 subjects, 864 (70.5%) had experienced arrhythmias, and the mean duration of exposure to methylphenidate was 0.5 years. During periods of methylphenidate treatment, subjects had an increased risk of arrhythmia, as Dr. Shin and coinvestigators calculated an adjusted incidence rate ratio of 1.61 (95% confidence interval, 1.48-1.74). This incidence rate ratio jumped up to 2.01 (95% CI, 1.74-2.31) during the first 3 days of methylphenidate treatment.
The risk was even higher for subjects with congenital heart disease; this subgroup had an adjusted incidence rate ratio of 3.49 (95% CI, 2.33-5.22), compared with 1.34 (95% CI, 1.23-1.46) in patients without it. Both the median age of first exposure to methylphenidate and occurrence of the first cardiac event were in patients aged 11-13 years, reported Dr. Shin of the Centre for Clinical Epidemiology at Jewish General Hospital and McGill University, both in Montreal, and colleagues in Australia and Korea.
“These results are consistent with the biological plausibility that the mechanism of action relates to the effect of methylphenidate on the heart rate,” the authors concluded. “Delayed effects would be expected with myocardial infarction, while more immediate effects would be expected with arrhythmias, as we observed.”
Dr. Shin and colleagues cited several limitations. For example, coding mistakes and incomplete records could not be ruled out in their study. In addition, they said, the “outcome measures were limited to patients with diagnoses of cardiovascular adverse events, and we could have missed outcomes not diagnosed.”
Nevertheless, they said, in light of the increased use of methylphenidate to treat ADHD across the globe, the benefits of using the drug “should be carefully weighed against potential cardiovascular risks of these drugs in children and adolescents.”
Two of the authors disclosed receiving support via fellowships from Australia’s National Health and Medical Research Council.
Children and adolescents with attention-deficit/hyperactivity disorder who are prescribed methylphenidate to manage their conditions stand at a higher risk for arrhythmia and other, more serious, cardiac conditions.
In a study published in the BMJ, Ju-Young Shin, Ph.D., and colleagues examined records of 1,224 patients aged 17 years and younger from a nationwide South Korean health insurance database submitted between January 2007 and December 2011. All of the patients had experienced a cardiovascular event and at least one recorded prescription for methylphenidate to treat attention-deficit/hyperactivity disorder (ADHD) (BMJ 2016;353:i2550 doi:10.1136/bmj.i2550).
Of the 1,224 subjects, 864 (70.5%) had experienced arrhythmias, and the mean duration of exposure to methylphenidate was 0.5 years. During periods of methylphenidate treatment, subjects had an increased risk of arrhythmia, as Dr. Shin and coinvestigators calculated an adjusted incidence rate ratio of 1.61 (95% confidence interval, 1.48-1.74). This incidence rate ratio jumped up to 2.01 (95% CI, 1.74-2.31) during the first 3 days of methylphenidate treatment.
The risk was even higher for subjects with congenital heart disease; this subgroup had an adjusted incidence rate ratio of 3.49 (95% CI, 2.33-5.22), compared with 1.34 (95% CI, 1.23-1.46) in patients without it. Both the median age of first exposure to methylphenidate and occurrence of the first cardiac event were in patients aged 11-13 years, reported Dr. Shin of the Centre for Clinical Epidemiology at Jewish General Hospital and McGill University, both in Montreal, and colleagues in Australia and Korea.
“These results are consistent with the biological plausibility that the mechanism of action relates to the effect of methylphenidate on the heart rate,” the authors concluded. “Delayed effects would be expected with myocardial infarction, while more immediate effects would be expected with arrhythmias, as we observed.”
Dr. Shin and colleagues cited several limitations. For example, coding mistakes and incomplete records could not be ruled out in their study. In addition, they said, the “outcome measures were limited to patients with diagnoses of cardiovascular adverse events, and we could have missed outcomes not diagnosed.”
Nevertheless, they said, in light of the increased use of methylphenidate to treat ADHD across the globe, the benefits of using the drug “should be carefully weighed against potential cardiovascular risks of these drugs in children and adolescents.”
Two of the authors disclosed receiving support via fellowships from Australia’s National Health and Medical Research Council.
Children and adolescents with attention-deficit/hyperactivity disorder who are prescribed methylphenidate to manage their conditions stand at a higher risk for arrhythmia and other, more serious, cardiac conditions.
In a study published in the BMJ, Ju-Young Shin, Ph.D., and colleagues examined records of 1,224 patients aged 17 years and younger from a nationwide South Korean health insurance database submitted between January 2007 and December 2011. All of the patients had experienced a cardiovascular event and at least one recorded prescription for methylphenidate to treat attention-deficit/hyperactivity disorder (ADHD) (BMJ 2016;353:i2550 doi:10.1136/bmj.i2550).
Of the 1,224 subjects, 864 (70.5%) had experienced arrhythmias, and the mean duration of exposure to methylphenidate was 0.5 years. During periods of methylphenidate treatment, subjects had an increased risk of arrhythmia, as Dr. Shin and coinvestigators calculated an adjusted incidence rate ratio of 1.61 (95% confidence interval, 1.48-1.74). This incidence rate ratio jumped up to 2.01 (95% CI, 1.74-2.31) during the first 3 days of methylphenidate treatment.
The risk was even higher for subjects with congenital heart disease; this subgroup had an adjusted incidence rate ratio of 3.49 (95% CI, 2.33-5.22), compared with 1.34 (95% CI, 1.23-1.46) in patients without it. Both the median age of first exposure to methylphenidate and occurrence of the first cardiac event were in patients aged 11-13 years, reported Dr. Shin of the Centre for Clinical Epidemiology at Jewish General Hospital and McGill University, both in Montreal, and colleagues in Australia and Korea.
“These results are consistent with the biological plausibility that the mechanism of action relates to the effect of methylphenidate on the heart rate,” the authors concluded. “Delayed effects would be expected with myocardial infarction, while more immediate effects would be expected with arrhythmias, as we observed.”
Dr. Shin and colleagues cited several limitations. For example, coding mistakes and incomplete records could not be ruled out in their study. In addition, they said, the “outcome measures were limited to patients with diagnoses of cardiovascular adverse events, and we could have missed outcomes not diagnosed.”
Nevertheless, they said, in light of the increased use of methylphenidate to treat ADHD across the globe, the benefits of using the drug “should be carefully weighed against potential cardiovascular risks of these drugs in children and adolescents.”
Two of the authors disclosed receiving support via fellowships from Australia’s National Health and Medical Research Council.
FROM THE BMJ
Key clinical point: Use of methylphenidate to treat children with attention-deficit/hyperactivity disorder (ADHD) can lead to higher risk for arrhythmia, especially in the first 3 days of use.
Major finding: The risk of arrhythmia increased during periods of treatment with methylphenidate when compared with other treatment periods (incidence rate ratio, 1.61), and reached 2.01 during the first 1-3 days of methylphenidate treatment.
Data source: A retrospective case series analysis of 1,224 patients at or younger than 17 years of age, who had at least one recorded cardiovascular event and one prescription for methylphenidate.
Disclosures: Two coauthors disclosed receiving support via fellowships from Australia’s National Health and Medical Research Council.
