User login
FDA grants priority review to sNDA for dasatinib

The US Food and Drug Administration (FDA) has accepted for priority review a supplemental new drug application (sNDA) for dasatinib (Sprycel).
Bristol Myers Squibb is seeking approval for dasatinib as a treatment for children with Philadelphia chromosome-positive (Ph+) chronic phase (CP) chronic myeloid leukemia (CML), as well as approval for a powder formulation of dasatinib for oral suspension.
The FDA grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
The agency’s goal is to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The FDA plans to make a decision on the dasatinib sNDA by November 9, 2017.
The sNDA includes data from CA180-226 (NCT00777036), an ongoing, phase 2 trial of dasatinib in pediatric patients with CP-CML who are resistant to or cannot tolerate imatinib and pediatric patients newly diagnosed with CP-CML.
The trial enrolled patients aged 18 and younger with newly diagnosed CML or Ph+ leukemias resistant to or intolerant of imatinib.
Cohort 1 included 29 CP-CML patients resistant to or intolerant of imatinib. Cohort 2 included patients with accelerated/blast phase CML or Ph+ acute lymphoblastic leukemia. Cohort 3 included 84 patients with newly diagnosed CP-CML.
Data from Cohorts 1 and 3 were recently presented at the 2017 ASCO Annual Meeting.
Three months into treatment with dasatinib, patients with CP-CML who were resistant to or intolerant of imatinib (Cohort 1) had a cumulative major cytogenetic response rate of 55.2%. This response rate increased over time to exceed 90% at 24 months.
Newly diagnosed patients with CP-CML (Cohort 3) received dasatinib orally or as powder for oral suspension once daily. They achieved a cumulative complete cytogenetic response rate of 64% as early as 6 months into treatment. This response rate increased to 94% at 24 months.
The median duration of response was not estimable or not yet reached in each cohort at the time of follow-up.
The estimated progression-free survival at 48 months was greater than 75% for patients in Cohort 1 and greater than 90% for patients in Cohort 3.
The safety profile of dasatinib in this study was deemed comparable to that reported in adults with CP-CML. In this study, there were no reported events of pleural/pericardial effusion, pulmonary edema/hypertension, or pulmonary arterial hypertension related to dasatinib.
Dasatinib first received FDA approval in 2006. The drug is currently approved to treat adults with:
- Newly diagnosed Ph+ CP-CML
- Chronic, accelerated, or blast phase Ph+ CML with resistance or intolerance to prior therapy including imatinib
- Ph+ acute lymphoblastic leukemia with resistance or intolerance to prior therapy.

The US Food and Drug Administration (FDA) has accepted for priority review a supplemental new drug application (sNDA) for dasatinib (Sprycel).
Bristol Myers Squibb is seeking approval for dasatinib as a treatment for children with Philadelphia chromosome-positive (Ph+) chronic phase (CP) chronic myeloid leukemia (CML), as well as approval for a powder formulation of dasatinib for oral suspension.
The FDA grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
The agency’s goal is to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The FDA plans to make a decision on the dasatinib sNDA by November 9, 2017.
The sNDA includes data from CA180-226 (NCT00777036), an ongoing, phase 2 trial of dasatinib in pediatric patients with CP-CML who are resistant to or cannot tolerate imatinib and pediatric patients newly diagnosed with CP-CML.
The trial enrolled patients aged 18 and younger with newly diagnosed CML or Ph+ leukemias resistant to or intolerant of imatinib.
Cohort 1 included 29 CP-CML patients resistant to or intolerant of imatinib. Cohort 2 included patients with accelerated/blast phase CML or Ph+ acute lymphoblastic leukemia. Cohort 3 included 84 patients with newly diagnosed CP-CML.
Data from Cohorts 1 and 3 were recently presented at the 2017 ASCO Annual Meeting.
Three months into treatment with dasatinib, patients with CP-CML who were resistant to or intolerant of imatinib (Cohort 1) had a cumulative major cytogenetic response rate of 55.2%. This response rate increased over time to exceed 90% at 24 months.
Newly diagnosed patients with CP-CML (Cohort 3) received dasatinib orally or as powder for oral suspension once daily. They achieved a cumulative complete cytogenetic response rate of 64% as early as 6 months into treatment. This response rate increased to 94% at 24 months.
The median duration of response was not estimable or not yet reached in each cohort at the time of follow-up.
The estimated progression-free survival at 48 months was greater than 75% for patients in Cohort 1 and greater than 90% for patients in Cohort 3.
The safety profile of dasatinib in this study was deemed comparable to that reported in adults with CP-CML. In this study, there were no reported events of pleural/pericardial effusion, pulmonary edema/hypertension, or pulmonary arterial hypertension related to dasatinib.
Dasatinib first received FDA approval in 2006. The drug is currently approved to treat adults with:
- Newly diagnosed Ph+ CP-CML
- Chronic, accelerated, or blast phase Ph+ CML with resistance or intolerance to prior therapy including imatinib
- Ph+ acute lymphoblastic leukemia with resistance or intolerance to prior therapy.
The US Food and Drug Administration (FDA) has accepted for priority review a supplemental new drug application (sNDA) for dasatinib (Sprycel).
Bristol Myers Squibb is seeking approval for dasatinib as a treatment for children with Philadelphia chromosome-positive (Ph+) chronic phase (CP) chronic myeloid leukemia (CML), as well as approval for a powder formulation of dasatinib for oral suspension.
The FDA grants priority review to applications for products that may provide significant improvements in the treatment, diagnosis, or prevention of serious conditions.
The agency’s goal is to take action on a priority review application within 6 months of receiving it, rather than the standard 10 months.
The FDA plans to make a decision on the dasatinib sNDA by November 9, 2017.
The sNDA includes data from CA180-226 (NCT00777036), an ongoing, phase 2 trial of dasatinib in pediatric patients with CP-CML who are resistant to or cannot tolerate imatinib and pediatric patients newly diagnosed with CP-CML.
The trial enrolled patients aged 18 and younger with newly diagnosed CML or Ph+ leukemias resistant to or intolerant of imatinib.
Cohort 1 included 29 CP-CML patients resistant to or intolerant of imatinib. Cohort 2 included patients with accelerated/blast phase CML or Ph+ acute lymphoblastic leukemia. Cohort 3 included 84 patients with newly diagnosed CP-CML.
Data from Cohorts 1 and 3 were recently presented at the 2017 ASCO Annual Meeting.
Three months into treatment with dasatinib, patients with CP-CML who were resistant to or intolerant of imatinib (Cohort 1) had a cumulative major cytogenetic response rate of 55.2%. This response rate increased over time to exceed 90% at 24 months.
Newly diagnosed patients with CP-CML (Cohort 3) received dasatinib orally or as powder for oral suspension once daily. They achieved a cumulative complete cytogenetic response rate of 64% as early as 6 months into treatment. This response rate increased to 94% at 24 months.
The median duration of response was not estimable or not yet reached in each cohort at the time of follow-up.
The estimated progression-free survival at 48 months was greater than 75% for patients in Cohort 1 and greater than 90% for patients in Cohort 3.
The safety profile of dasatinib in this study was deemed comparable to that reported in adults with CP-CML. In this study, there were no reported events of pleural/pericardial effusion, pulmonary edema/hypertension, or pulmonary arterial hypertension related to dasatinib.
Dasatinib first received FDA approval in 2006. The drug is currently approved to treat adults with:
- Newly diagnosed Ph+ CP-CML
- Chronic, accelerated, or blast phase Ph+ CML with resistance or intolerance to prior therapy including imatinib
- Ph+ acute lymphoblastic leukemia with resistance or intolerance to prior therapy.
Hexavalent hepatitis B vaccination mostly immunogenic 10 years later
results of an Italian study show.
The phase 3 open-label, controlled study included 732 healthy Italian children aged 11-13 years who as infants had received a two-dose primary and booster course with either Hexavac (5 mcg hepatitis B surface antigen [HBsAg]) or Infanrix hexa (10 mcg HBsAg) at 3, 5, and 11 months of age; the last dose was received at least 10 years prior to the challenge dose of a monovalent HB vaccine (HBVaxPro, 5 mcg HBsAg).
Although some of the children had HB surface antigen antibody concentrations below the seroprotection threshold, most of them had an anamnestic response when challenged with the dose of HB vaccine, “indicating the presence of specific immune memory,” the investigators said. There was no evidence of active HB disease in any of the children.
Just what the meaning of the lack of immune memory is, defined as the failure to develop an anamnestic response following an HB vaccine challenge, remains to be determined.
results of an Italian study show.
The phase 3 open-label, controlled study included 732 healthy Italian children aged 11-13 years who as infants had received a two-dose primary and booster course with either Hexavac (5 mcg hepatitis B surface antigen [HBsAg]) or Infanrix hexa (10 mcg HBsAg) at 3, 5, and 11 months of age; the last dose was received at least 10 years prior to the challenge dose of a monovalent HB vaccine (HBVaxPro, 5 mcg HBsAg).
Although some of the children had HB surface antigen antibody concentrations below the seroprotection threshold, most of them had an anamnestic response when challenged with the dose of HB vaccine, “indicating the presence of specific immune memory,” the investigators said. There was no evidence of active HB disease in any of the children.
Just what the meaning of the lack of immune memory is, defined as the failure to develop an anamnestic response following an HB vaccine challenge, remains to be determined.
results of an Italian study show.
The phase 3 open-label, controlled study included 732 healthy Italian children aged 11-13 years who as infants had received a two-dose primary and booster course with either Hexavac (5 mcg hepatitis B surface antigen [HBsAg]) or Infanrix hexa (10 mcg HBsAg) at 3, 5, and 11 months of age; the last dose was received at least 10 years prior to the challenge dose of a monovalent HB vaccine (HBVaxPro, 5 mcg HBsAg).
Although some of the children had HB surface antigen antibody concentrations below the seroprotection threshold, most of them had an anamnestic response when challenged with the dose of HB vaccine, “indicating the presence of specific immune memory,” the investigators said. There was no evidence of active HB disease in any of the children.
Just what the meaning of the lack of immune memory is, defined as the failure to develop an anamnestic response following an HB vaccine challenge, remains to be determined.
FROM VACCINE
Sustained remission on biologics bodes well for children with JIA
MADRID – Many children with juvenile idiopathic arthritis (JIA) who do well on biologics for a prolonged period will stay in remission after the medication is withdrawn, some new real-world data suggest.
A database review found that 70% of those in remission for at least 1.5 years remained in remission after stopping their biologic agent. Patients taking tocilizumab had the best outcomes, with 8 months of sustained, drug-free remission and only a 12% rate of disease flare, Ekaterina Alexeeva, MD, reported at the European Congress of Rheumatology.

“Prolonged therapy with biologic agents may cause adverse events which lead to the necessity of discontinuation of therapy in patients once complete disease quiescence has been achieved,” she said. While long-term drug studies do offer some glimpse into the stability of remission after drug discontinuation, these data don’t often reflect real-world experience.
“Clinical trials are made up of highly selected participants in contorted conditions with limited duration. Real-word data, collected under real-life practical circumstances, provide additional characteristics of patient populations, information on the effectiveness and safety of treatment over time, and the outcomes we can achieve under real-world conditions,” Dr. Alexeeva said.
She plumbed a national JIA database to find 83 patients who had achieved longstanding clinical remission on a biologic therapy, then either rapidly discontinued treatment (61) or went through a tapering protocol (22), according to their doctors’ decision. These children were a mean of 11 years old, with mean disease duration of 2 years before the initiation of a biologic treatment. Systemic JIA was present in 40%; 22% had oligoarthritis, and 38% had polyarthritis.
All of the patients with systemic JIA were taking tocilizumab, although only 25% took it as monotherapy. Other medications being used were methotrexate (42%), cyclosporine (15%), glucocorticoids (15%), and leflunomide (3%).
For those with oligo- and polyarthritis, etanercept was the most commonly employed biologic (70%), followed by adalimumab (30%). Most (68%) were on monotherapy with their agent; however, 18% of those taking etanercept and 14% of those taking adalimumab were also taking methotrexate.
Before discontinuing their medication, the systemic JIA patients taking tocilizumab had a mean 43 months of inactive disease and a mean 37 months of remission. Among those taking adalimumab, the mean period of inactive disease was 48 months and the mean remission was 40 months. Among those taking etanercept, the mean period of inactive disease was 40 months and the mean remission was 34 months.
After discontinuing the biologic, the mean overall remission length was 6 months for all patients. However, this varied considerably with diagnosis and medication, Dr. Alexeeva noted. For systemic JIA patients taking tocilizumab, remission ranged from a minimum of 1 month to a maximum of 48 months. For those taking adalimumab, remission ranged from 4 to 38 months. Remission ranged from 1 to 20 months among those taking etanercept.
Disease flare occurred in 12% of those taking tocilizumab, at a mean of 8 months after discontinuation; 31% of those taking etanercept at a mean of 5.5 months; and 60% of those taking adalimumab at a mean of 4 months. Time to flare was longest among those taking tocilizumab (6-18 months), followed by etanercept (1.5-12 months) and adalimumab (1-13 months).
Dr. Alexeeva disclosed research funding and support from numerous pharmaceutical companies.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
MADRID – Many children with juvenile idiopathic arthritis (JIA) who do well on biologics for a prolonged period will stay in remission after the medication is withdrawn, some new real-world data suggest.
A database review found that 70% of those in remission for at least 1.5 years remained in remission after stopping their biologic agent. Patients taking tocilizumab had the best outcomes, with 8 months of sustained, drug-free remission and only a 12% rate of disease flare, Ekaterina Alexeeva, MD, reported at the European Congress of Rheumatology.
“Prolonged therapy with biologic agents may cause adverse events which lead to the necessity of discontinuation of therapy in patients once complete disease quiescence has been achieved,” she said. While long-term drug studies do offer some glimpse into the stability of remission after drug discontinuation, these data don’t often reflect real-world experience.
“Clinical trials are made up of highly selected participants in contorted conditions with limited duration. Real-word data, collected under real-life practical circumstances, provide additional characteristics of patient populations, information on the effectiveness and safety of treatment over time, and the outcomes we can achieve under real-world conditions,” Dr. Alexeeva said.
She plumbed a national JIA database to find 83 patients who had achieved longstanding clinical remission on a biologic therapy, then either rapidly discontinued treatment (61) or went through a tapering protocol (22), according to their doctors’ decision. These children were a mean of 11 years old, with mean disease duration of 2 years before the initiation of a biologic treatment. Systemic JIA was present in 40%; 22% had oligoarthritis, and 38% had polyarthritis.
All of the patients with systemic JIA were taking tocilizumab, although only 25% took it as monotherapy. Other medications being used were methotrexate (42%), cyclosporine (15%), glucocorticoids (15%), and leflunomide (3%).
For those with oligo- and polyarthritis, etanercept was the most commonly employed biologic (70%), followed by adalimumab (30%). Most (68%) were on monotherapy with their agent; however, 18% of those taking etanercept and 14% of those taking adalimumab were also taking methotrexate.
Before discontinuing their medication, the systemic JIA patients taking tocilizumab had a mean 43 months of inactive disease and a mean 37 months of remission. Among those taking adalimumab, the mean period of inactive disease was 48 months and the mean remission was 40 months. Among those taking etanercept, the mean period of inactive disease was 40 months and the mean remission was 34 months.
After discontinuing the biologic, the mean overall remission length was 6 months for all patients. However, this varied considerably with diagnosis and medication, Dr. Alexeeva noted. For systemic JIA patients taking tocilizumab, remission ranged from a minimum of 1 month to a maximum of 48 months. For those taking adalimumab, remission ranged from 4 to 38 months. Remission ranged from 1 to 20 months among those taking etanercept.
Disease flare occurred in 12% of those taking tocilizumab, at a mean of 8 months after discontinuation; 31% of those taking etanercept at a mean of 5.5 months; and 60% of those taking adalimumab at a mean of 4 months. Time to flare was longest among those taking tocilizumab (6-18 months), followed by etanercept (1.5-12 months) and adalimumab (1-13 months).
Dr. Alexeeva disclosed research funding and support from numerous pharmaceutical companies.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
MADRID – Many children with juvenile idiopathic arthritis (JIA) who do well on biologics for a prolonged period will stay in remission after the medication is withdrawn, some new real-world data suggest.
A database review found that 70% of those in remission for at least 1.5 years remained in remission after stopping their biologic agent. Patients taking tocilizumab had the best outcomes, with 8 months of sustained, drug-free remission and only a 12% rate of disease flare, Ekaterina Alexeeva, MD, reported at the European Congress of Rheumatology.
“Prolonged therapy with biologic agents may cause adverse events which lead to the necessity of discontinuation of therapy in patients once complete disease quiescence has been achieved,” she said. While long-term drug studies do offer some glimpse into the stability of remission after drug discontinuation, these data don’t often reflect real-world experience.
“Clinical trials are made up of highly selected participants in contorted conditions with limited duration. Real-word data, collected under real-life practical circumstances, provide additional characteristics of patient populations, information on the effectiveness and safety of treatment over time, and the outcomes we can achieve under real-world conditions,” Dr. Alexeeva said.
She plumbed a national JIA database to find 83 patients who had achieved longstanding clinical remission on a biologic therapy, then either rapidly discontinued treatment (61) or went through a tapering protocol (22), according to their doctors’ decision. These children were a mean of 11 years old, with mean disease duration of 2 years before the initiation of a biologic treatment. Systemic JIA was present in 40%; 22% had oligoarthritis, and 38% had polyarthritis.
All of the patients with systemic JIA were taking tocilizumab, although only 25% took it as monotherapy. Other medications being used were methotrexate (42%), cyclosporine (15%), glucocorticoids (15%), and leflunomide (3%).
For those with oligo- and polyarthritis, etanercept was the most commonly employed biologic (70%), followed by adalimumab (30%). Most (68%) were on monotherapy with their agent; however, 18% of those taking etanercept and 14% of those taking adalimumab were also taking methotrexate.
Before discontinuing their medication, the systemic JIA patients taking tocilizumab had a mean 43 months of inactive disease and a mean 37 months of remission. Among those taking adalimumab, the mean period of inactive disease was 48 months and the mean remission was 40 months. Among those taking etanercept, the mean period of inactive disease was 40 months and the mean remission was 34 months.
After discontinuing the biologic, the mean overall remission length was 6 months for all patients. However, this varied considerably with diagnosis and medication, Dr. Alexeeva noted. For systemic JIA patients taking tocilizumab, remission ranged from a minimum of 1 month to a maximum of 48 months. For those taking adalimumab, remission ranged from 4 to 38 months. Remission ranged from 1 to 20 months among those taking etanercept.
Disease flare occurred in 12% of those taking tocilizumab, at a mean of 8 months after discontinuation; 31% of those taking etanercept at a mean of 5.5 months; and 60% of those taking adalimumab at a mean of 4 months. Time to flare was longest among those taking tocilizumab (6-18 months), followed by etanercept (1.5-12 months) and adalimumab (1-13 months).
Dr. Alexeeva disclosed research funding and support from numerous pharmaceutical companies.
msullivan@frontlinemedcom.com
On Twitter @alz_gal
AT THE EULAR 2017 CONGRESS
Key clinical point:
Major finding: Overall, 70% of those who were in remission for at least 1.5 years remained in remission after stopping their biologic.
Data source: A database review comprising 83 children.
Disclosures: Dr. Alexeeva disclosed research and grant support from numerous pharmaceutical companies.
Transcranial magnetic stimulation shows promise in autism spectrum disorder
SAN FRANCISCO – , Eric Hollander, MD, said at the annual conference of the Anxiety and Depression Association of America.
“It’s a promising tool. There’s a lot of hope. There have been a range of scattered studies. But there is still a lot more work that needs to be done in terms of defining the optimal target structures in the brain, the dose and frequency of treatment, and which symptoms respond best,” said Dr. Hollander, director of the autism and obsessive-compulsive spectrum program as well as the anxiety and depression program at Albert Einstein College of Medicine in New York.

The authors characterized transcranial magnetic stimulation (TMS) for autism spectrum disorder (ASD) as “a novel, possibly transformative approach” but added a strong cautionary note.
“The available literature on the TMS use in ASD is preliminary, composed of studies with methodological limitations. Thus, off-label clinical rTMS [repetitive TMS] use for therapeutic interventions in ASD without an investigational device exemption and outside of an IRB [institutional review board]-approved research trial is premature pending further, adequately powered and controlled trials,” according to the white paper by the TMS in ASD Consensus Group (Autism Res. 2016 Feb;9[2]:184-203).
ASD support groups are eager to see TMS developed as a treatment, Dr. Hollander said. This is largely a result of the 2016 publication of a nonfiction book entitled, “Switched On: A Memoir of Brain Change and Emotional Awakening” (New York: Spiegel & Grau, 2016). Author John Elder Robison is a high-functioning individual with ASD who describes his dramatic improvement in response to TMS therapy in an early clinical trial conducted at Boston’s Beth Israel Deaconess Medical Center.
Dr. Hollander has been extensively involved in pioneering studies of TMS for the treatment of depression – currently its only Food and Drug Administration–approved indication – as well as for obsessive-compulsive disorder. His recent work on TMS for the treatment of ASD has focused on the noninvasive therapy’s ability to favorably affect the excitatory/inhibitory imbalance that characterizes ASD. This imbalance is tied chiefly to abnormal glutamatergic and gamma-aminobutyric acid–ergic neurotransmission in the neocortex, cerebellum, hippocampus, and amygdala. The imbalance is thought to be responsible for the cognitive, sensory, learning, memory, and motor deficits, as well as increased propensity for seizures, associated with ASD.
This excitatory/inhibitory imbalance is marked by increased cortical excitability and decreased inhibition within the densely packed cortical minicolumns of neurons, which are organized into pathways and circuits.
“You can use TMS as a treatment, or you can use it as a research probe to look at these mechanisms by turning on or off pathways,” the psychiatrist explained. “These densely packed minicolumns are like wires with poor insulation, which results in impairment in the ability to distinguish a stimulus from background noise. In the pathologic condition, you’re getting a rapid firing which doesn’t really differentiate what’s a true signal from what’s background noise.”
Therapeutically, TMS can be employed to improve that signal-to-noise ratio, either by reducing excitation or increasing inhibition. Potential TMS targets in autism include the anterior cingulate cortex, the supplementary or presupplementary motor area, the dorsal medial prefrontal cortex, the dorsal lateral prefrontal cortex, and the cerebellum. More than a dozen published TMS studies – albeit open-label, uncontrolled, and featuring only handfuls of patients – have demonstrated long-lasting improvements in the two core symptom domains of ASD: reduced repetitive behaviors and improved social relatedness and interpersonal functioning, Dr. Hollander said.
A wide range of associated noncore symptoms, including disruptive behaviors such as self-injury or aggression, impulse control, social anxiety, and depression, also might be targeted.
“In our clinical practice, we tend to treat adults with ASD who have a lot of OCD [obsessive-compulsive disorder] and repetitive behavior symptoms but also mood or anxiety symptoms or PTSD [posttraumatic stress disorder] symptoms as a result of earlier bullying. You can adapt your treatment to the target symptoms, so if there’s a lot of OCD-type symptoms, you might use low-frequency TMS at 1 Hz to target the supplementary motor area. If people are coming in with depressive symptoms, you can use the dorsolateral prefrontal cortex depression target. If they have a lot of anxiety, you can target the right frontal anxiety loop with low-frequency TMS. Or with a lot of PTSD symptoms, you can use high-frequency stimulation of the dorsolateral prefrontal cortex at 20 Hz,” Dr. Hollander said.
An important caveat, however, is that ASD is associated with an increased risk of seizures and other EEG abnormalities, so low-frequency TMS generally is preferable because of its greater safety.
Another challenge is administering TMS in children.
“Kids move around a lot, so you’re probably going to be using briefer stimulation parameters like theta burst stimulation rather than longer treatment parameters,” Dr. Hollander said.
That being said, there are more than two dozen published studies of TMS for treatment of children and adolescents, and surveys indicate that these patients generally find it quite tolerable. Dr. Hollander noted that in one study, children and adolescents ranked it somewhere between watching television and a long car ride. This placed TMS on the midrange of a tolerability scale: not as good as having a birthday party or playing a game, but better than going to the dentist, throwing up, or, in last place, getting a shot. Of the 39 youngsters, 34 indicated that they would recommend TMS to a friend.
Dr. Hollander reported receiving research funding from the National Institute of Mental Health, the National Institute on Drug Abuse, and the National Institute of Neurological Disorders and Stroke. He serves as a consultant to roughly half a dozen pharmaceutical companies.
SAN FRANCISCO – , Eric Hollander, MD, said at the annual conference of the Anxiety and Depression Association of America.
“It’s a promising tool. There’s a lot of hope. There have been a range of scattered studies. But there is still a lot more work that needs to be done in terms of defining the optimal target structures in the brain, the dose and frequency of treatment, and which symptoms respond best,” said Dr. Hollander, director of the autism and obsessive-compulsive spectrum program as well as the anxiety and depression program at Albert Einstein College of Medicine in New York.
The authors characterized transcranial magnetic stimulation (TMS) for autism spectrum disorder (ASD) as “a novel, possibly transformative approach” but added a strong cautionary note.
“The available literature on the TMS use in ASD is preliminary, composed of studies with methodological limitations. Thus, off-label clinical rTMS [repetitive TMS] use for therapeutic interventions in ASD without an investigational device exemption and outside of an IRB [institutional review board]-approved research trial is premature pending further, adequately powered and controlled trials,” according to the white paper by the TMS in ASD Consensus Group (Autism Res. 2016 Feb;9[2]:184-203).
ASD support groups are eager to see TMS developed as a treatment, Dr. Hollander said. This is largely a result of the 2016 publication of a nonfiction book entitled, “Switched On: A Memoir of Brain Change and Emotional Awakening” (New York: Spiegel & Grau, 2016). Author John Elder Robison is a high-functioning individual with ASD who describes his dramatic improvement in response to TMS therapy in an early clinical trial conducted at Boston’s Beth Israel Deaconess Medical Center.
Dr. Hollander has been extensively involved in pioneering studies of TMS for the treatment of depression – currently its only Food and Drug Administration–approved indication – as well as for obsessive-compulsive disorder. His recent work on TMS for the treatment of ASD has focused on the noninvasive therapy’s ability to favorably affect the excitatory/inhibitory imbalance that characterizes ASD. This imbalance is tied chiefly to abnormal glutamatergic and gamma-aminobutyric acid–ergic neurotransmission in the neocortex, cerebellum, hippocampus, and amygdala. The imbalance is thought to be responsible for the cognitive, sensory, learning, memory, and motor deficits, as well as increased propensity for seizures, associated with ASD.
This excitatory/inhibitory imbalance is marked by increased cortical excitability and decreased inhibition within the densely packed cortical minicolumns of neurons, which are organized into pathways and circuits.
“You can use TMS as a treatment, or you can use it as a research probe to look at these mechanisms by turning on or off pathways,” the psychiatrist explained. “These densely packed minicolumns are like wires with poor insulation, which results in impairment in the ability to distinguish a stimulus from background noise. In the pathologic condition, you’re getting a rapid firing which doesn’t really differentiate what’s a true signal from what’s background noise.”
Therapeutically, TMS can be employed to improve that signal-to-noise ratio, either by reducing excitation or increasing inhibition. Potential TMS targets in autism include the anterior cingulate cortex, the supplementary or presupplementary motor area, the dorsal medial prefrontal cortex, the dorsal lateral prefrontal cortex, and the cerebellum. More than a dozen published TMS studies – albeit open-label, uncontrolled, and featuring only handfuls of patients – have demonstrated long-lasting improvements in the two core symptom domains of ASD: reduced repetitive behaviors and improved social relatedness and interpersonal functioning, Dr. Hollander said.
A wide range of associated noncore symptoms, including disruptive behaviors such as self-injury or aggression, impulse control, social anxiety, and depression, also might be targeted.
“In our clinical practice, we tend to treat adults with ASD who have a lot of OCD [obsessive-compulsive disorder] and repetitive behavior symptoms but also mood or anxiety symptoms or PTSD [posttraumatic stress disorder] symptoms as a result of earlier bullying. You can adapt your treatment to the target symptoms, so if there’s a lot of OCD-type symptoms, you might use low-frequency TMS at 1 Hz to target the supplementary motor area. If people are coming in with depressive symptoms, you can use the dorsolateral prefrontal cortex depression target. If they have a lot of anxiety, you can target the right frontal anxiety loop with low-frequency TMS. Or with a lot of PTSD symptoms, you can use high-frequency stimulation of the dorsolateral prefrontal cortex at 20 Hz,” Dr. Hollander said.
An important caveat, however, is that ASD is associated with an increased risk of seizures and other EEG abnormalities, so low-frequency TMS generally is preferable because of its greater safety.
Another challenge is administering TMS in children.
“Kids move around a lot, so you’re probably going to be using briefer stimulation parameters like theta burst stimulation rather than longer treatment parameters,” Dr. Hollander said.
That being said, there are more than two dozen published studies of TMS for treatment of children and adolescents, and surveys indicate that these patients generally find it quite tolerable. Dr. Hollander noted that in one study, children and adolescents ranked it somewhere between watching television and a long car ride. This placed TMS on the midrange of a tolerability scale: not as good as having a birthday party or playing a game, but better than going to the dentist, throwing up, or, in last place, getting a shot. Of the 39 youngsters, 34 indicated that they would recommend TMS to a friend.
Dr. Hollander reported receiving research funding from the National Institute of Mental Health, the National Institute on Drug Abuse, and the National Institute of Neurological Disorders and Stroke. He serves as a consultant to roughly half a dozen pharmaceutical companies.
SAN FRANCISCO – , Eric Hollander, MD, said at the annual conference of the Anxiety and Depression Association of America.
“It’s a promising tool. There’s a lot of hope. There have been a range of scattered studies. But there is still a lot more work that needs to be done in terms of defining the optimal target structures in the brain, the dose and frequency of treatment, and which symptoms respond best,” said Dr. Hollander, director of the autism and obsessive-compulsive spectrum program as well as the anxiety and depression program at Albert Einstein College of Medicine in New York.
The authors characterized transcranial magnetic stimulation (TMS) for autism spectrum disorder (ASD) as “a novel, possibly transformative approach” but added a strong cautionary note.
“The available literature on the TMS use in ASD is preliminary, composed of studies with methodological limitations. Thus, off-label clinical rTMS [repetitive TMS] use for therapeutic interventions in ASD without an investigational device exemption and outside of an IRB [institutional review board]-approved research trial is premature pending further, adequately powered and controlled trials,” according to the white paper by the TMS in ASD Consensus Group (Autism Res. 2016 Feb;9[2]:184-203).
ASD support groups are eager to see TMS developed as a treatment, Dr. Hollander said. This is largely a result of the 2016 publication of a nonfiction book entitled, “Switched On: A Memoir of Brain Change and Emotional Awakening” (New York: Spiegel & Grau, 2016). Author John Elder Robison is a high-functioning individual with ASD who describes his dramatic improvement in response to TMS therapy in an early clinical trial conducted at Boston’s Beth Israel Deaconess Medical Center.
Dr. Hollander has been extensively involved in pioneering studies of TMS for the treatment of depression – currently its only Food and Drug Administration–approved indication – as well as for obsessive-compulsive disorder. His recent work on TMS for the treatment of ASD has focused on the noninvasive therapy’s ability to favorably affect the excitatory/inhibitory imbalance that characterizes ASD. This imbalance is tied chiefly to abnormal glutamatergic and gamma-aminobutyric acid–ergic neurotransmission in the neocortex, cerebellum, hippocampus, and amygdala. The imbalance is thought to be responsible for the cognitive, sensory, learning, memory, and motor deficits, as well as increased propensity for seizures, associated with ASD.
This excitatory/inhibitory imbalance is marked by increased cortical excitability and decreased inhibition within the densely packed cortical minicolumns of neurons, which are organized into pathways and circuits.
“You can use TMS as a treatment, or you can use it as a research probe to look at these mechanisms by turning on or off pathways,” the psychiatrist explained. “These densely packed minicolumns are like wires with poor insulation, which results in impairment in the ability to distinguish a stimulus from background noise. In the pathologic condition, you’re getting a rapid firing which doesn’t really differentiate what’s a true signal from what’s background noise.”
Therapeutically, TMS can be employed to improve that signal-to-noise ratio, either by reducing excitation or increasing inhibition. Potential TMS targets in autism include the anterior cingulate cortex, the supplementary or presupplementary motor area, the dorsal medial prefrontal cortex, the dorsal lateral prefrontal cortex, and the cerebellum. More than a dozen published TMS studies – albeit open-label, uncontrolled, and featuring only handfuls of patients – have demonstrated long-lasting improvements in the two core symptom domains of ASD: reduced repetitive behaviors and improved social relatedness and interpersonal functioning, Dr. Hollander said.
A wide range of associated noncore symptoms, including disruptive behaviors such as self-injury or aggression, impulse control, social anxiety, and depression, also might be targeted.
“In our clinical practice, we tend to treat adults with ASD who have a lot of OCD [obsessive-compulsive disorder] and repetitive behavior symptoms but also mood or anxiety symptoms or PTSD [posttraumatic stress disorder] symptoms as a result of earlier bullying. You can adapt your treatment to the target symptoms, so if there’s a lot of OCD-type symptoms, you might use low-frequency TMS at 1 Hz to target the supplementary motor area. If people are coming in with depressive symptoms, you can use the dorsolateral prefrontal cortex depression target. If they have a lot of anxiety, you can target the right frontal anxiety loop with low-frequency TMS. Or with a lot of PTSD symptoms, you can use high-frequency stimulation of the dorsolateral prefrontal cortex at 20 Hz,” Dr. Hollander said.
An important caveat, however, is that ASD is associated with an increased risk of seizures and other EEG abnormalities, so low-frequency TMS generally is preferable because of its greater safety.
Another challenge is administering TMS in children.
“Kids move around a lot, so you’re probably going to be using briefer stimulation parameters like theta burst stimulation rather than longer treatment parameters,” Dr. Hollander said.
That being said, there are more than two dozen published studies of TMS for treatment of children and adolescents, and surveys indicate that these patients generally find it quite tolerable. Dr. Hollander noted that in one study, children and adolescents ranked it somewhere between watching television and a long car ride. This placed TMS on the midrange of a tolerability scale: not as good as having a birthday party or playing a game, but better than going to the dentist, throwing up, or, in last place, getting a shot. Of the 39 youngsters, 34 indicated that they would recommend TMS to a friend.
Dr. Hollander reported receiving research funding from the National Institute of Mental Health, the National Institute on Drug Abuse, and the National Institute of Neurological Disorders and Stroke. He serves as a consultant to roughly half a dozen pharmaceutical companies.
EXPERT ANALYSIS FROM THE ANXIETY AND DEPRESSION CONFERENCE 2017
OMV meningococcal vaccine also protected against gonorrhea
A group B meningococcal outer-membrane-vesicle (OMV) vaccine used during a meningitis outbreak in New Zealand also protected against gonorrhea, according to a report published online July 10 in the Lancet.
Even though Neisseria meningitidis and Neisseria gonorrhoeae cause distinctly different diseases, the bacteria are closely related and are genetically and antigenically very similar. Most of the virulence factors present in one pathogen have an equivalent in the other, “providing at least one biologically plausible mechanism for cross-protection,” said Helen Petousis-Harris, PhD, of the department of general practice and primary health care, University of Auckland (New Zealand), and her associates. 
Approximately 1 million people – 81% of the New Zealand population younger than 20 years – received almost 3 million doses of the OMV meningococcal B vaccine (MeNZB) in a 2-year mass immunization program during the outbreak, allowing the investigators to compare the rate of gonorrhea between vaccinated and unvaccinated people. They performed a retrospective case-control study involving 14,730 participants, using information from a national health care database, a national immunization registry, and 11 sexual health clinics covering diverse geographic regions. This included 1,241 cases of gonorrhea (cases), 12,487 cases of chlamydia (controls), and 1,002 cases of gonorrhea plus chlamydia coinfection (categorized as controls or cases in separate analyses).
“The adjusted estimate for vaccine effectiveness of the MeNZB against confirmed cases of gonorrhea” was 31% (95% confidence interval, 21-39; P less than .0001), a finding that remained robust across several sensitivity analyses, Dr. Petousis-Harris and her associates said (Lancet. 2017 July 10. doi: 10.1016/S0140-6736(17)31449-6).
“To our knowledge, ours is the first study to show an association between a vaccine and a reduction in the risk of gonorrhea,” they noted. “The potential ability of an OMV group B meningococcal vaccine to provide even modest protection against gonorrhea would have substantial public health benefits in view of the prevalence of gonorrhea. Modeling suggests that a vaccine with 30% efficacy could decrease the prevalence of gonorrhea by more than 30% within 15 years, if immunity is maintained.”
These findings also are important in view of the organism’s increasing resistance to existing antibiotics. Moreover, if further study confirms that the MeNZB vaccine offers some degree of cross-protection against gonorrhea, these data can inform the development of a gonorrhea vaccine, the investigators added.
This study was funded by GlaxoSmithKline Vaccines and Auckland UniServices. Dr. Petousis-Harris reported serving as a consultant for GSK, Merck, and Pfizer, and one of her associates reported ties to Novartis Vaccines, GSK, Protein Sciences, and Merck.
Over decades of research, all of the attempts to create a vaccine against gonorrhea have failed, largely because of the variable nature of Neisseria gonorrhoeae antigens and the failure of the bacteria to induce a protective immune response, so the findings of Dr. Petousis-Harris and her associates are “a step in the right direction” and should reinvigorate interest and investment in this endeavor.
Although MeNZB is no longer available, another meningococcal vaccine (4CMenB, Bexsero) contains the same outer-membrane-vesicle antigen and three of the same recombinant proteins. As the authors pointed out, immunizing adolescents with this vaccine could reduce the rate of gonorrhea substantially, even if it has only moderate efficacy and duration of effect. In particular, reducing the pool of asymptomatic carriers would decrease both transmission and the severe sequelae that develop when the infection goes undetected.
Kate L. Seib, PhD, is a microbiologist at the Institute for Glycomics at Griffith University in Southport, Australia. She reported support by a career development fellowship from the Australian National Health and Medical Research Council. Dr. Seib made these remarks in an accompanying editorial comment (Lancet. 2017 July 10. doi: 10.1016/S0140-6736(17)31605-7).
Over decades of research, all of the attempts to create a vaccine against gonorrhea have failed, largely because of the variable nature of Neisseria gonorrhoeae antigens and the failure of the bacteria to induce a protective immune response, so the findings of Dr. Petousis-Harris and her associates are “a step in the right direction” and should reinvigorate interest and investment in this endeavor.
Although MeNZB is no longer available, another meningococcal vaccine (4CMenB, Bexsero) contains the same outer-membrane-vesicle antigen and three of the same recombinant proteins. As the authors pointed out, immunizing adolescents with this vaccine could reduce the rate of gonorrhea substantially, even if it has only moderate efficacy and duration of effect. In particular, reducing the pool of asymptomatic carriers would decrease both transmission and the severe sequelae that develop when the infection goes undetected.
Kate L. Seib, PhD, is a microbiologist at the Institute for Glycomics at Griffith University in Southport, Australia. She reported support by a career development fellowship from the Australian National Health and Medical Research Council. Dr. Seib made these remarks in an accompanying editorial comment (Lancet. 2017 July 10. doi: 10.1016/S0140-6736(17)31605-7).
Over decades of research, all of the attempts to create a vaccine against gonorrhea have failed, largely because of the variable nature of Neisseria gonorrhoeae antigens and the failure of the bacteria to induce a protective immune response, so the findings of Dr. Petousis-Harris and her associates are “a step in the right direction” and should reinvigorate interest and investment in this endeavor.
Although MeNZB is no longer available, another meningococcal vaccine (4CMenB, Bexsero) contains the same outer-membrane-vesicle antigen and three of the same recombinant proteins. As the authors pointed out, immunizing adolescents with this vaccine could reduce the rate of gonorrhea substantially, even if it has only moderate efficacy and duration of effect. In particular, reducing the pool of asymptomatic carriers would decrease both transmission and the severe sequelae that develop when the infection goes undetected.
Kate L. Seib, PhD, is a microbiologist at the Institute for Glycomics at Griffith University in Southport, Australia. She reported support by a career development fellowship from the Australian National Health and Medical Research Council. Dr. Seib made these remarks in an accompanying editorial comment (Lancet. 2017 July 10. doi: 10.1016/S0140-6736(17)31605-7).
A group B meningococcal outer-membrane-vesicle (OMV) vaccine used during a meningitis outbreak in New Zealand also protected against gonorrhea, according to a report published online July 10 in the Lancet.
Even though Neisseria meningitidis and Neisseria gonorrhoeae cause distinctly different diseases, the bacteria are closely related and are genetically and antigenically very similar. Most of the virulence factors present in one pathogen have an equivalent in the other, “providing at least one biologically plausible mechanism for cross-protection,” said Helen Petousis-Harris, PhD, of the department of general practice and primary health care, University of Auckland (New Zealand), and her associates.
Approximately 1 million people – 81% of the New Zealand population younger than 20 years – received almost 3 million doses of the OMV meningococcal B vaccine (MeNZB) in a 2-year mass immunization program during the outbreak, allowing the investigators to compare the rate of gonorrhea between vaccinated and unvaccinated people. They performed a retrospective case-control study involving 14,730 participants, using information from a national health care database, a national immunization registry, and 11 sexual health clinics covering diverse geographic regions. This included 1,241 cases of gonorrhea (cases), 12,487 cases of chlamydia (controls), and 1,002 cases of gonorrhea plus chlamydia coinfection (categorized as controls or cases in separate analyses).
“The adjusted estimate for vaccine effectiveness of the MeNZB against confirmed cases of gonorrhea” was 31% (95% confidence interval, 21-39; P less than .0001), a finding that remained robust across several sensitivity analyses, Dr. Petousis-Harris and her associates said (Lancet. 2017 July 10. doi: 10.1016/S0140-6736(17)31449-6).
“To our knowledge, ours is the first study to show an association between a vaccine and a reduction in the risk of gonorrhea,” they noted. “The potential ability of an OMV group B meningococcal vaccine to provide even modest protection against gonorrhea would have substantial public health benefits in view of the prevalence of gonorrhea. Modeling suggests that a vaccine with 30% efficacy could decrease the prevalence of gonorrhea by more than 30% within 15 years, if immunity is maintained.”
These findings also are important in view of the organism’s increasing resistance to existing antibiotics. Moreover, if further study confirms that the MeNZB vaccine offers some degree of cross-protection against gonorrhea, these data can inform the development of a gonorrhea vaccine, the investigators added.
This study was funded by GlaxoSmithKline Vaccines and Auckland UniServices. Dr. Petousis-Harris reported serving as a consultant for GSK, Merck, and Pfizer, and one of her associates reported ties to Novartis Vaccines, GSK, Protein Sciences, and Merck.
A group B meningococcal outer-membrane-vesicle (OMV) vaccine used during a meningitis outbreak in New Zealand also protected against gonorrhea, according to a report published online July 10 in the Lancet.
Even though Neisseria meningitidis and Neisseria gonorrhoeae cause distinctly different diseases, the bacteria are closely related and are genetically and antigenically very similar. Most of the virulence factors present in one pathogen have an equivalent in the other, “providing at least one biologically plausible mechanism for cross-protection,” said Helen Petousis-Harris, PhD, of the department of general practice and primary health care, University of Auckland (New Zealand), and her associates.
Approximately 1 million people – 81% of the New Zealand population younger than 20 years – received almost 3 million doses of the OMV meningococcal B vaccine (MeNZB) in a 2-year mass immunization program during the outbreak, allowing the investigators to compare the rate of gonorrhea between vaccinated and unvaccinated people. They performed a retrospective case-control study involving 14,730 participants, using information from a national health care database, a national immunization registry, and 11 sexual health clinics covering diverse geographic regions. This included 1,241 cases of gonorrhea (cases), 12,487 cases of chlamydia (controls), and 1,002 cases of gonorrhea plus chlamydia coinfection (categorized as controls or cases in separate analyses).
“The adjusted estimate for vaccine effectiveness of the MeNZB against confirmed cases of gonorrhea” was 31% (95% confidence interval, 21-39; P less than .0001), a finding that remained robust across several sensitivity analyses, Dr. Petousis-Harris and her associates said (Lancet. 2017 July 10. doi: 10.1016/S0140-6736(17)31449-6).
“To our knowledge, ours is the first study to show an association between a vaccine and a reduction in the risk of gonorrhea,” they noted. “The potential ability of an OMV group B meningococcal vaccine to provide even modest protection against gonorrhea would have substantial public health benefits in view of the prevalence of gonorrhea. Modeling suggests that a vaccine with 30% efficacy could decrease the prevalence of gonorrhea by more than 30% within 15 years, if immunity is maintained.”
These findings also are important in view of the organism’s increasing resistance to existing antibiotics. Moreover, if further study confirms that the MeNZB vaccine offers some degree of cross-protection against gonorrhea, these data can inform the development of a gonorrhea vaccine, the investigators added.
This study was funded by GlaxoSmithKline Vaccines and Auckland UniServices. Dr. Petousis-Harris reported serving as a consultant for GSK, Merck, and Pfizer, and one of her associates reported ties to Novartis Vaccines, GSK, Protein Sciences, and Merck.
FROM THE LANCET
Key clinical point:
Major finding: The adjusted estimate for the effectiveness of the MeNZB vaccine against cases of gonorrhea was 31%.
Data source: A retrospective case-control study involving 14,730 patients at 11 sexual health clinics across New Zealand.
Disclosures: This study was funded by GlaxoSmithKline Vaccines and Auckland UniServices. Dr. Petousis-Harris reported serving as a consultant for GSK, Merck, and Pfizer, and one of her associates reported ties to Novartis Vaccines, GSK, Protein Sciences, and Merck.
Higher ADHD risk seen in children with migraine
BOSTON – Children aged 5-12 years with signs of migraine headache were as much as seven times as likely as other children to also appear to have attention-deficit/hyperactivity disorder (ADHD), but those with tension-type headaches didn’t face a higher risk of ADHD, a Brazilian study showed.
It’s not clear why the apparent link between migraines and ADHD exists. However, lead study author Marco Antônio Arruda, MD, PhD, a pediatric neurologist in São Paulo (Brazil) University, said in an interview that other research has linked migraine to mental health problems.

The study, presented at the annual meeting of the American Academy of Neurology and published online in the Journal of Attention Disorders (2017. doi: 10.1177/1087054717710767), was launched to better understand the connection between migraine and ADHD, which are thought to each affect as many as 1 in 10 children.
The study analyzes data from mothers and teachers of 5,671 children aged 5-12 years who answered questions as part of a Brazil-wide epidemiologic study called the Attention Brazil Project. Just over half of the participants were boys, and about half were from the Brazilian middle class.
Based on answers from mothers and teachers, the researchers estimated that 9% of the children had episodic migraine and 0.6% had chronic migraine. The level of episodic tension-type headache was estimated at 12.8%, with a lower rate in the two poorest vs. the two richest quintiles (8.6% vs. 14.4%, respectively; relative risk, 0.6; 95% confidence interval, 0.5-0.8).
The researchers estimated that 5.3% of the children overall showed signs of ADHD (7.5% in boys vs. 3.1% in girls; RR, 2.4; 95% CI, 1.9-3.1).
There was no sign that children with tension-type headaches had a significantly higher risk of ADHD than other children. However, compared with controls, those with various types of migraine headaches did have a higher risk of ADHD. Nearly 11% of those with migraine overall showed signs of ADHD, compared with 2.6% of the control group (RR, 4.1; 95% CI, 2.7-6.2). The numbers for episodic migraine were nearly identical to those for migraine overall: 10.2% vs. 2.6% (RR, 3.8; 95% CI, 2.5-5.9).
Just over 19% of kids in a third migraine group – those with chronic migraine, defined as headaches appearing more than 14 days per month for the last 3 months – showed signs of ADHD, compared with just 2.6% of the control group (RR = 7.3; 95% CI, 3.5-15.5).
“A number of risk factors to the association were identified, including male gender, prenatal exposure to tobacco, high headache frequency, and below average school performance,” Dr. Arruda said. “However, we did not find a significant influence of age, race, city density, national region where a child lives, income class, and prenatal exposure to alcohol in the comorbidity of ADHD and migraine in this sample. These results help us to identify risk groups allowing early interventions.”
Regarding an explanation for the links between migraines and ADHD, Dr. Arruda pointed to genetic and epigenetic factors that affect brain neurotransmitters and said he believes that stress and other stimuli could be influencing dopamine and noradrenergic processes.
Dr. Arruda said his next step is to examine whether stimulant drugs – the class used to treat ADHD – may help reduce headaches too.
“My clinical experience strongly indicates that psychostimulants have a highly positive effect on migraine prophylaxis, although headache occurs in the very beginning of the treatment,” Dr. Arruda said. “So, we are looking for financial support to conduct a randomized, double-blind, placebo control study to check this hypothesis.”
The study received no specific funding, and Dr. Arruda reported no relevant financial disclosures.
BOSTON – Children aged 5-12 years with signs of migraine headache were as much as seven times as likely as other children to also appear to have attention-deficit/hyperactivity disorder (ADHD), but those with tension-type headaches didn’t face a higher risk of ADHD, a Brazilian study showed.
It’s not clear why the apparent link between migraines and ADHD exists. However, lead study author Marco Antônio Arruda, MD, PhD, a pediatric neurologist in São Paulo (Brazil) University, said in an interview that other research has linked migraine to mental health problems.
The study, presented at the annual meeting of the American Academy of Neurology and published online in the Journal of Attention Disorders (2017. doi: 10.1177/1087054717710767), was launched to better understand the connection between migraine and ADHD, which are thought to each affect as many as 1 in 10 children.
The study analyzes data from mothers and teachers of 5,671 children aged 5-12 years who answered questions as part of a Brazil-wide epidemiologic study called the Attention Brazil Project. Just over half of the participants were boys, and about half were from the Brazilian middle class.
Based on answers from mothers and teachers, the researchers estimated that 9% of the children had episodic migraine and 0.6% had chronic migraine. The level of episodic tension-type headache was estimated at 12.8%, with a lower rate in the two poorest vs. the two richest quintiles (8.6% vs. 14.4%, respectively; relative risk, 0.6; 95% confidence interval, 0.5-0.8).
The researchers estimated that 5.3% of the children overall showed signs of ADHD (7.5% in boys vs. 3.1% in girls; RR, 2.4; 95% CI, 1.9-3.1).
There was no sign that children with tension-type headaches had a significantly higher risk of ADHD than other children. However, compared with controls, those with various types of migraine headaches did have a higher risk of ADHD. Nearly 11% of those with migraine overall showed signs of ADHD, compared with 2.6% of the control group (RR, 4.1; 95% CI, 2.7-6.2). The numbers for episodic migraine were nearly identical to those for migraine overall: 10.2% vs. 2.6% (RR, 3.8; 95% CI, 2.5-5.9).
Just over 19% of kids in a third migraine group – those with chronic migraine, defined as headaches appearing more than 14 days per month for the last 3 months – showed signs of ADHD, compared with just 2.6% of the control group (RR = 7.3; 95% CI, 3.5-15.5).
“A number of risk factors to the association were identified, including male gender, prenatal exposure to tobacco, high headache frequency, and below average school performance,” Dr. Arruda said. “However, we did not find a significant influence of age, race, city density, national region where a child lives, income class, and prenatal exposure to alcohol in the comorbidity of ADHD and migraine in this sample. These results help us to identify risk groups allowing early interventions.”
Regarding an explanation for the links between migraines and ADHD, Dr. Arruda pointed to genetic and epigenetic factors that affect brain neurotransmitters and said he believes that stress and other stimuli could be influencing dopamine and noradrenergic processes.
Dr. Arruda said his next step is to examine whether stimulant drugs – the class used to treat ADHD – may help reduce headaches too.
“My clinical experience strongly indicates that psychostimulants have a highly positive effect on migraine prophylaxis, although headache occurs in the very beginning of the treatment,” Dr. Arruda said. “So, we are looking for financial support to conduct a randomized, double-blind, placebo control study to check this hypothesis.”
The study received no specific funding, and Dr. Arruda reported no relevant financial disclosures.
BOSTON – Children aged 5-12 years with signs of migraine headache were as much as seven times as likely as other children to also appear to have attention-deficit/hyperactivity disorder (ADHD), but those with tension-type headaches didn’t face a higher risk of ADHD, a Brazilian study showed.
It’s not clear why the apparent link between migraines and ADHD exists. However, lead study author Marco Antônio Arruda, MD, PhD, a pediatric neurologist in São Paulo (Brazil) University, said in an interview that other research has linked migraine to mental health problems.
The study, presented at the annual meeting of the American Academy of Neurology and published online in the Journal of Attention Disorders (2017. doi: 10.1177/1087054717710767), was launched to better understand the connection between migraine and ADHD, which are thought to each affect as many as 1 in 10 children.
The study analyzes data from mothers and teachers of 5,671 children aged 5-12 years who answered questions as part of a Brazil-wide epidemiologic study called the Attention Brazil Project. Just over half of the participants were boys, and about half were from the Brazilian middle class.
Based on answers from mothers and teachers, the researchers estimated that 9% of the children had episodic migraine and 0.6% had chronic migraine. The level of episodic tension-type headache was estimated at 12.8%, with a lower rate in the two poorest vs. the two richest quintiles (8.6% vs. 14.4%, respectively; relative risk, 0.6; 95% confidence interval, 0.5-0.8).
The researchers estimated that 5.3% of the children overall showed signs of ADHD (7.5% in boys vs. 3.1% in girls; RR, 2.4; 95% CI, 1.9-3.1).
There was no sign that children with tension-type headaches had a significantly higher risk of ADHD than other children. However, compared with controls, those with various types of migraine headaches did have a higher risk of ADHD. Nearly 11% of those with migraine overall showed signs of ADHD, compared with 2.6% of the control group (RR, 4.1; 95% CI, 2.7-6.2). The numbers for episodic migraine were nearly identical to those for migraine overall: 10.2% vs. 2.6% (RR, 3.8; 95% CI, 2.5-5.9).
Just over 19% of kids in a third migraine group – those with chronic migraine, defined as headaches appearing more than 14 days per month for the last 3 months – showed signs of ADHD, compared with just 2.6% of the control group (RR = 7.3; 95% CI, 3.5-15.5).
“A number of risk factors to the association were identified, including male gender, prenatal exposure to tobacco, high headache frequency, and below average school performance,” Dr. Arruda said. “However, we did not find a significant influence of age, race, city density, national region where a child lives, income class, and prenatal exposure to alcohol in the comorbidity of ADHD and migraine in this sample. These results help us to identify risk groups allowing early interventions.”
Regarding an explanation for the links between migraines and ADHD, Dr. Arruda pointed to genetic and epigenetic factors that affect brain neurotransmitters and said he believes that stress and other stimuli could be influencing dopamine and noradrenergic processes.
Dr. Arruda said his next step is to examine whether stimulant drugs – the class used to treat ADHD – may help reduce headaches too.
“My clinical experience strongly indicates that psychostimulants have a highly positive effect on migraine prophylaxis, although headache occurs in the very beginning of the treatment,” Dr. Arruda said. “So, we are looking for financial support to conduct a randomized, double-blind, placebo control study to check this hypothesis.”
The study received no specific funding, and Dr. Arruda reported no relevant financial disclosures.
AT AAN 2017
Key clinical point: , but there’s no excess risk in children with tension-type headaches.
Major finding: Of children with chronic migraine, 19.4% (0.6% of the total) showed signs of ADHD, vs. 2.6% of the control group (RR, 7.3; 95% CI, 3.5-15.5).
Data source: Surveys of mothers and teachers of 5,671 Brazilian children aged 5-12 years.
Disclosures: The study received no specific funding, and Dr. Arruda reported no relevant financial disclosures.
How to get through the tough talks about alopecia areata
CHICAGO – If you can’t set the temptation to hurry aside and take the time to listen, things may not go well, said Neil Prose, MD.
With the caveat that Janus kinase inhibitors show promise, Dr. Prose said that “most children who are destined to lose their hair will probably do so despite all of our best efforts.” Figuring out how to engage children and parents and frame a positive conversation about alopecia can present a real challenge, especially in the context of a busy practice, said Dr. Prose, professor of dermatology and medical director of Patterson Place Pediatric Dermatology at Duke University, Durham, N.C.
“These are very culturally-specific suggestions, but see which ones work for you,” said Dr. Prose, speaking to an international audience at the World Congress of Pediatric Dermatology.
Dr. Prose depicted two opposing images. In one, he said, the patient and you are sitting on opposite sides of the table, with the prospect of hair loss looming between them. By contrast, “imagine what it would take to be on the same side of the table, looking at the problem together,” he said.
There are many barriers that stand in the way of getting you and the patient on the same side of the issue of dealing with severe alopecia areata. The high emotional content of the discussion can be big factor, not just for the patient and family members, but also for you.
“We are often dealing with patient disappointment and, frankly, with our own sense of personal failure” when there isn’t always a good set of options, said Dr. Prose. Other specific aspects of severe pediatric alopecia areata that make the conversation difficult include the high degree of uncertainty that any particular treatment will succeed and a knowledge of how to give patients and family members hope without raising expectations unrealistically.
Coming back to the important first steps of not rushing the visit and being sure to listen, Dr. Prose said that, for him, the process begins before he enters the room, when he takes a moment to clear his mind. “It starts for me just before I open the door to the examining room. As human beings, we are infinitely distractible. It’s very hard for us to simply pay attention.”
Yet, this is vitally important, he said, because families need to be heard. Citing the oft-quoted statistic that, on average, a physician interrupts a patient in the first 17 seconds of the office visit, Dr. Prose said, “Many of us are ‘explainaholics,’ ’’ spending precious visit time talking about what the physician thinks is important.
Still, it’s important to validate parents’ concerns and to alleviate guilt. “Patients’ families sometimes feel guilty because they are so upset and worried – and it’s not cancer,” said Dr. Prose. Potential impacts on quality of life are still huge, and all parents want the best for their children, he pointed out.
One way he likes to begin a follow-up visit is simply to ask, “So, how’s everyone doing?” This opens the door to allow the child and the family to talk about what’s important to them. These may be symptom-related, but social issues also may be what’s looming largest.
In order to decipher how hair loss is affecting a particular child, Dr. Prose said he likes to say, “I need to understand how this is affecting you, so we can decide together where to go from here.” This gives the family control in setting the agenda and begins the process of bringing you to the same side of the table.
Specific prompts that can help you understand how alopecia is affecting a child can include asking about how things are going at school, what the child’s friends know about his or her alopecia, whether there is mocking or bullying occurring, and how the patient, family, and teachers are addressing the global picture.
Parents can be asked whether they are noticing changes in behavior, and it’s a good idea to check in on how parents are coping as well, said Dr. Prose.
To ensure that families feel they’re being heard, and to make sure you are understanding correctly, it’s useful to mirror what’s been said, beginning with a phrase like, “So, what you’re saying is …” Putting a name to the emotions that emerge during the visit also can be useful, using phrases like, “I can imagine that this has been disappointing,” or “It feels like everyone is very worried.”
But, said Dr. Prose, don’t forget about opportunities to praise patients and their families when they’ve come through a tough time well. This validation is important, he said.
When treatment isn’t working, a first place to start is to acknowledge that you, along with the family, wish that things were turning out differently. Then, said Dr. Prose, it can be really important to reappraise treatment goals. After taking the emotional temperature of the room, it may be appropriate to ask, “Is it time to talk about not doing any more treatments?” This question can be put within the framework that hair may or may not regrow spontaneously anyway and that new treatments are emerging that may help in future.
When giving advice or talking about difficult issues, it can be helpful to ask permission, said Dr. Prose. He likes to begin with, “Would it be okay if I ...?” Then, he said, the door can be opened to give advice about school issues, to ask about difficult treatment decisions, or even to share tips learned from other families’ coping methods.
Don’t forget, said Dr. Prose, to refer patients to high-quality information and online support resources, such as the National Alopecia Areata Foundation. The Internet is full of inaccurate and scary information, and patients and families need help with this navigation, he said.
The very last question Dr. Prose asks during a visit is “What other questions do you have?” The question is always framed exactly like this, he said, because it assumes there will be more questions, and it gives families permission to ask more. Although most of the time there aren’t any further questions, Dr. Prose said, “Do not ask the question with your hand on the doorknob!”
Dr. Prose had no relevant financial disclosures.
koakes@frontlinemedcom.com
On Twitter @karioakes
CHICAGO – If you can’t set the temptation to hurry aside and take the time to listen, things may not go well, said Neil Prose, MD.
With the caveat that Janus kinase inhibitors show promise, Dr. Prose said that “most children who are destined to lose their hair will probably do so despite all of our best efforts.” Figuring out how to engage children and parents and frame a positive conversation about alopecia can present a real challenge, especially in the context of a busy practice, said Dr. Prose, professor of dermatology and medical director of Patterson Place Pediatric Dermatology at Duke University, Durham, N.C.
“These are very culturally-specific suggestions, but see which ones work for you,” said Dr. Prose, speaking to an international audience at the World Congress of Pediatric Dermatology.
Dr. Prose depicted two opposing images. In one, he said, the patient and you are sitting on opposite sides of the table, with the prospect of hair loss looming between them. By contrast, “imagine what it would take to be on the same side of the table, looking at the problem together,” he said.
There are many barriers that stand in the way of getting you and the patient on the same side of the issue of dealing with severe alopecia areata. The high emotional content of the discussion can be big factor, not just for the patient and family members, but also for you.
“We are often dealing with patient disappointment and, frankly, with our own sense of personal failure” when there isn’t always a good set of options, said Dr. Prose. Other specific aspects of severe pediatric alopecia areata that make the conversation difficult include the high degree of uncertainty that any particular treatment will succeed and a knowledge of how to give patients and family members hope without raising expectations unrealistically.
Coming back to the important first steps of not rushing the visit and being sure to listen, Dr. Prose said that, for him, the process begins before he enters the room, when he takes a moment to clear his mind. “It starts for me just before I open the door to the examining room. As human beings, we are infinitely distractible. It’s very hard for us to simply pay attention.”
Yet, this is vitally important, he said, because families need to be heard. Citing the oft-quoted statistic that, on average, a physician interrupts a patient in the first 17 seconds of the office visit, Dr. Prose said, “Many of us are ‘explainaholics,’ ’’ spending precious visit time talking about what the physician thinks is important.
Still, it’s important to validate parents’ concerns and to alleviate guilt. “Patients’ families sometimes feel guilty because they are so upset and worried – and it’s not cancer,” said Dr. Prose. Potential impacts on quality of life are still huge, and all parents want the best for their children, he pointed out.
One way he likes to begin a follow-up visit is simply to ask, “So, how’s everyone doing?” This opens the door to allow the child and the family to talk about what’s important to them. These may be symptom-related, but social issues also may be what’s looming largest.
In order to decipher how hair loss is affecting a particular child, Dr. Prose said he likes to say, “I need to understand how this is affecting you, so we can decide together where to go from here.” This gives the family control in setting the agenda and begins the process of bringing you to the same side of the table.
Specific prompts that can help you understand how alopecia is affecting a child can include asking about how things are going at school, what the child’s friends know about his or her alopecia, whether there is mocking or bullying occurring, and how the patient, family, and teachers are addressing the global picture.
Parents can be asked whether they are noticing changes in behavior, and it’s a good idea to check in on how parents are coping as well, said Dr. Prose.
To ensure that families feel they’re being heard, and to make sure you are understanding correctly, it’s useful to mirror what’s been said, beginning with a phrase like, “So, what you’re saying is …” Putting a name to the emotions that emerge during the visit also can be useful, using phrases like, “I can imagine that this has been disappointing,” or “It feels like everyone is very worried.”
But, said Dr. Prose, don’t forget about opportunities to praise patients and their families when they’ve come through a tough time well. This validation is important, he said.
When treatment isn’t working, a first place to start is to acknowledge that you, along with the family, wish that things were turning out differently. Then, said Dr. Prose, it can be really important to reappraise treatment goals. After taking the emotional temperature of the room, it may be appropriate to ask, “Is it time to talk about not doing any more treatments?” This question can be put within the framework that hair may or may not regrow spontaneously anyway and that new treatments are emerging that may help in future.
When giving advice or talking about difficult issues, it can be helpful to ask permission, said Dr. Prose. He likes to begin with, “Would it be okay if I ...?” Then, he said, the door can be opened to give advice about school issues, to ask about difficult treatment decisions, or even to share tips learned from other families’ coping methods.
Don’t forget, said Dr. Prose, to refer patients to high-quality information and online support resources, such as the National Alopecia Areata Foundation. The Internet is full of inaccurate and scary information, and patients and families need help with this navigation, he said.
The very last question Dr. Prose asks during a visit is “What other questions do you have?” The question is always framed exactly like this, he said, because it assumes there will be more questions, and it gives families permission to ask more. Although most of the time there aren’t any further questions, Dr. Prose said, “Do not ask the question with your hand on the doorknob!”
Dr. Prose had no relevant financial disclosures.
koakes@frontlinemedcom.com
On Twitter @karioakes
CHICAGO – If you can’t set the temptation to hurry aside and take the time to listen, things may not go well, said Neil Prose, MD.
With the caveat that Janus kinase inhibitors show promise, Dr. Prose said that “most children who are destined to lose their hair will probably do so despite all of our best efforts.” Figuring out how to engage children and parents and frame a positive conversation about alopecia can present a real challenge, especially in the context of a busy practice, said Dr. Prose, professor of dermatology and medical director of Patterson Place Pediatric Dermatology at Duke University, Durham, N.C.
“These are very culturally-specific suggestions, but see which ones work for you,” said Dr. Prose, speaking to an international audience at the World Congress of Pediatric Dermatology.
Dr. Prose depicted two opposing images. In one, he said, the patient and you are sitting on opposite sides of the table, with the prospect of hair loss looming between them. By contrast, “imagine what it would take to be on the same side of the table, looking at the problem together,” he said.
There are many barriers that stand in the way of getting you and the patient on the same side of the issue of dealing with severe alopecia areata. The high emotional content of the discussion can be big factor, not just for the patient and family members, but also for you.
“We are often dealing with patient disappointment and, frankly, with our own sense of personal failure” when there isn’t always a good set of options, said Dr. Prose. Other specific aspects of severe pediatric alopecia areata that make the conversation difficult include the high degree of uncertainty that any particular treatment will succeed and a knowledge of how to give patients and family members hope without raising expectations unrealistically.
Coming back to the important first steps of not rushing the visit and being sure to listen, Dr. Prose said that, for him, the process begins before he enters the room, when he takes a moment to clear his mind. “It starts for me just before I open the door to the examining room. As human beings, we are infinitely distractible. It’s very hard for us to simply pay attention.”
Yet, this is vitally important, he said, because families need to be heard. Citing the oft-quoted statistic that, on average, a physician interrupts a patient in the first 17 seconds of the office visit, Dr. Prose said, “Many of us are ‘explainaholics,’ ’’ spending precious visit time talking about what the physician thinks is important.
Still, it’s important to validate parents’ concerns and to alleviate guilt. “Patients’ families sometimes feel guilty because they are so upset and worried – and it’s not cancer,” said Dr. Prose. Potential impacts on quality of life are still huge, and all parents want the best for their children, he pointed out.
One way he likes to begin a follow-up visit is simply to ask, “So, how’s everyone doing?” This opens the door to allow the child and the family to talk about what’s important to them. These may be symptom-related, but social issues also may be what’s looming largest.
In order to decipher how hair loss is affecting a particular child, Dr. Prose said he likes to say, “I need to understand how this is affecting you, so we can decide together where to go from here.” This gives the family control in setting the agenda and begins the process of bringing you to the same side of the table.
Specific prompts that can help you understand how alopecia is affecting a child can include asking about how things are going at school, what the child’s friends know about his or her alopecia, whether there is mocking or bullying occurring, and how the patient, family, and teachers are addressing the global picture.
Parents can be asked whether they are noticing changes in behavior, and it’s a good idea to check in on how parents are coping as well, said Dr. Prose.
To ensure that families feel they’re being heard, and to make sure you are understanding correctly, it’s useful to mirror what’s been said, beginning with a phrase like, “So, what you’re saying is …” Putting a name to the emotions that emerge during the visit also can be useful, using phrases like, “I can imagine that this has been disappointing,” or “It feels like everyone is very worried.”
But, said Dr. Prose, don’t forget about opportunities to praise patients and their families when they’ve come through a tough time well. This validation is important, he said.
When treatment isn’t working, a first place to start is to acknowledge that you, along with the family, wish that things were turning out differently. Then, said Dr. Prose, it can be really important to reappraise treatment goals. After taking the emotional temperature of the room, it may be appropriate to ask, “Is it time to talk about not doing any more treatments?” This question can be put within the framework that hair may or may not regrow spontaneously anyway and that new treatments are emerging that may help in future.
When giving advice or talking about difficult issues, it can be helpful to ask permission, said Dr. Prose. He likes to begin with, “Would it be okay if I ...?” Then, he said, the door can be opened to give advice about school issues, to ask about difficult treatment decisions, or even to share tips learned from other families’ coping methods.
Don’t forget, said Dr. Prose, to refer patients to high-quality information and online support resources, such as the National Alopecia Areata Foundation. The Internet is full of inaccurate and scary information, and patients and families need help with this navigation, he said.
The very last question Dr. Prose asks during a visit is “What other questions do you have?” The question is always framed exactly like this, he said, because it assumes there will be more questions, and it gives families permission to ask more. Although most of the time there aren’t any further questions, Dr. Prose said, “Do not ask the question with your hand on the doorknob!”
Dr. Prose had no relevant financial disclosures.
koakes@frontlinemedcom.com
On Twitter @karioakes
EXPERT ANALYSIS FROM WCPD 2017
Study spotlights pediatric dermatology workplace trends
CHICAGO – Geographic maldistribution of trained pediatric dermatologists and long wait times for new-patient appointments are two key hurdles impacting patient access to pediatric dermatology care, according to a survey of workforce trends.
“There are large areas of the country that don’t have any pediatric dermatologists, which influences how we can train dermatologists, pediatricians, and medical students who want to do pediatric dermatology,” study author Brea Prindaville, MD, said in an interview at the World Congress for Pediatric Dermatology. “We’re trying to keep an eye on how that’s going, and how we can improve not only the geographic distribution, but also the numbers that we have in the workforce.”
In a project spearheaded by the Society for Pediatric Dermatology (SPD) workforce committee, Dr. Prindaville of Children’s Mercy-Kansas City (Mo.) and her associates emailed a nine-question survey to the 484 SPD members in the United States to determine practice location, number and types of patients seen, wait times, and association with advance practice providers between November and December of 2016. In all, 146 surveys were completed, for a response rate of 30%. Of these, 75% were from board-certified pediatric dermatologists. The majority of survey respondents were practicing in and around large cities, while 60% of all respondents and 68% of board-certified respondents were practicing full-time, seeing pediatric patients exclusively. An additional 30% were practicing part-time or also seeing adults. Board-certified pediatric dermatologists saw an average of 80 pediatric patients per week.
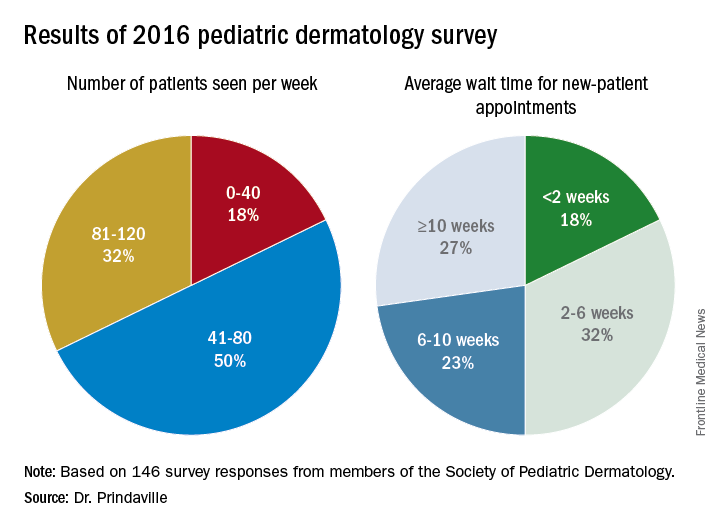
Only 10% of survey respondents did not accept Medicaid, and about 50% of patients seen by board-certified pediatric dermatologists were insured by Medicaid. In addition, about half of respondents worked with one to three advanced practice providers.
Dr. Prindaville, who helped conduct the study during her pediatric dermatology fellowship at the University of Massachusetts, Worcester, acknowledged certain limitations of the analysis, including its low response rate, the limited number of survey questions, and the question design. Going forward, she and her associates hope to keep a pulse on workplace trends by surveying SPD members annually, perhaps with membership renewal.
The survey was supported by the SPD. Dr. Prindaville reported having no relevant financial disclosures.
CHICAGO – Geographic maldistribution of trained pediatric dermatologists and long wait times for new-patient appointments are two key hurdles impacting patient access to pediatric dermatology care, according to a survey of workforce trends.
“There are large areas of the country that don’t have any pediatric dermatologists, which influences how we can train dermatologists, pediatricians, and medical students who want to do pediatric dermatology,” study author Brea Prindaville, MD, said in an interview at the World Congress for Pediatric Dermatology. “We’re trying to keep an eye on how that’s going, and how we can improve not only the geographic distribution, but also the numbers that we have in the workforce.”
In a project spearheaded by the Society for Pediatric Dermatology (SPD) workforce committee, Dr. Prindaville of Children’s Mercy-Kansas City (Mo.) and her associates emailed a nine-question survey to the 484 SPD members in the United States to determine practice location, number and types of patients seen, wait times, and association with advance practice providers between November and December of 2016. In all, 146 surveys were completed, for a response rate of 30%. Of these, 75% were from board-certified pediatric dermatologists. The majority of survey respondents were practicing in and around large cities, while 60% of all respondents and 68% of board-certified respondents were practicing full-time, seeing pediatric patients exclusively. An additional 30% were practicing part-time or also seeing adults. Board-certified pediatric dermatologists saw an average of 80 pediatric patients per week.
Only 10% of survey respondents did not accept Medicaid, and about 50% of patients seen by board-certified pediatric dermatologists were insured by Medicaid. In addition, about half of respondents worked with one to three advanced practice providers.
Dr. Prindaville, who helped conduct the study during her pediatric dermatology fellowship at the University of Massachusetts, Worcester, acknowledged certain limitations of the analysis, including its low response rate, the limited number of survey questions, and the question design. Going forward, she and her associates hope to keep a pulse on workplace trends by surveying SPD members annually, perhaps with membership renewal.
The survey was supported by the SPD. Dr. Prindaville reported having no relevant financial disclosures.
CHICAGO – Geographic maldistribution of trained pediatric dermatologists and long wait times for new-patient appointments are two key hurdles impacting patient access to pediatric dermatology care, according to a survey of workforce trends.
“There are large areas of the country that don’t have any pediatric dermatologists, which influences how we can train dermatologists, pediatricians, and medical students who want to do pediatric dermatology,” study author Brea Prindaville, MD, said in an interview at the World Congress for Pediatric Dermatology. “We’re trying to keep an eye on how that’s going, and how we can improve not only the geographic distribution, but also the numbers that we have in the workforce.”
In a project spearheaded by the Society for Pediatric Dermatology (SPD) workforce committee, Dr. Prindaville of Children’s Mercy-Kansas City (Mo.) and her associates emailed a nine-question survey to the 484 SPD members in the United States to determine practice location, number and types of patients seen, wait times, and association with advance practice providers between November and December of 2016. In all, 146 surveys were completed, for a response rate of 30%. Of these, 75% were from board-certified pediatric dermatologists. The majority of survey respondents were practicing in and around large cities, while 60% of all respondents and 68% of board-certified respondents were practicing full-time, seeing pediatric patients exclusively. An additional 30% were practicing part-time or also seeing adults. Board-certified pediatric dermatologists saw an average of 80 pediatric patients per week.
Only 10% of survey respondents did not accept Medicaid, and about 50% of patients seen by board-certified pediatric dermatologists were insured by Medicaid. In addition, about half of respondents worked with one to three advanced practice providers.
Dr. Prindaville, who helped conduct the study during her pediatric dermatology fellowship at the University of Massachusetts, Worcester, acknowledged certain limitations of the analysis, including its low response rate, the limited number of survey questions, and the question design. Going forward, she and her associates hope to keep a pulse on workplace trends by surveying SPD members annually, perhaps with membership renewal.
The survey was supported by the SPD. Dr. Prindaville reported having no relevant financial disclosures.
AT WCPD 2017
Key clinical point:
Major finding: The majority of survey respondents were practicing in and around large cities, and the average wait time for a new-patient appointment for all respondents was about 6 weeks.
Data source: Online survey completed by 146 Society for Pediatric Dermatology (SPD) members in the United States.
Disclosures: The survey was supported by the SPD. Dr. Prindaville reported having no relevant financial disclosures.
Vaccination does not eliminate risk for meningococcal disease in eculizumab recipients
Patients taking eculizumab are at a significant risk for meningococcal disease even if they have received the quadrivalent meningococcal conjugate (MenACWY) and serogroup B (MenB) meningococcal vaccines, according to the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report, released July 7.
Between 2008 and 2016, 16 cases of meningococcal disease were reported in eculizumab users in 10 jurisdictions within the United States. Of those infected, 14 had received MenACWY and MenB vaccines as recommended by the Advisory Committee on Immunization Practices, according to the CDC report.
Required vaccination plus antimicrobial prophylaxis for the duration of eculizumab treatment might reduce the risk for meningococcal disease in these patients, but the addition of antibiotic prophylaxis is no guarantee that all cases of meningococcal disease would be prevented, wrote Lucy A. McNamara, PhD, of the division of bacterial diseases, National Center for Immunization and Respiratory Diseases, CDC, and her colleagues.
They advised physician and patient vigilance regarding meningococcal disease symptoms and urged that patients be advised to seek immediate care and be rapidly treated, regardless of meningococcal vaccination or antimicrobial prophylaxis status.
Health organizations in Europe, including France and the United Kingdom, are recommending eculizumab users receive penicillin during eculizumab treatment. A recent study of invasive meningococcal isolates in the United States found most were susceptible to penicillin, according to the report.
In the 16 U.S. cases reported, nongroupable Neisseria meningitidis caused meningococcal disease in 11 of the patients, serogroup Y was the cause in 4 patients, and the cause was not identified in 1 patient.
Ten patients had meningococcemia without meningitis, the researchers noted. “Initial symptoms of meningococcemia are often relatively mild and nonspecific and might include fever, chills, fatigue, vomiting, diarrhea, and aches or pains in the muscles, joints, chest, or abdomen; however, these symptoms can progress to severe illness and death within hours.”
Eculizumab (Soliris, Alexion Pharmaceuticals) is licensed in the United States for treatment of paroxysmal nocturnal hemoglobinuria and atypical hemolytic uremic syndrome, two diseases that are rare and can be fatal.
Eculizumab is associated with a 1,000-fold to 2,000-fold increased incidence of meningococcal disease among persons receiving the drug. The Food and Drug Administration–approved prescribing information includes a boxed warning regarding increased risk for meningococcal disease.
The CDC is collecting reports from state health departments for further analysis of the risk among eculizumab recipients.
The researchers reported having no conflicts of interest.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
Patients taking eculizumab are at a significant risk for meningococcal disease even if they have received the quadrivalent meningococcal conjugate (MenACWY) and serogroup B (MenB) meningococcal vaccines, according to the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report, released July 7.
Between 2008 and 2016, 16 cases of meningococcal disease were reported in eculizumab users in 10 jurisdictions within the United States. Of those infected, 14 had received MenACWY and MenB vaccines as recommended by the Advisory Committee on Immunization Practices, according to the CDC report.
Required vaccination plus antimicrobial prophylaxis for the duration of eculizumab treatment might reduce the risk for meningococcal disease in these patients, but the addition of antibiotic prophylaxis is no guarantee that all cases of meningococcal disease would be prevented, wrote Lucy A. McNamara, PhD, of the division of bacterial diseases, National Center for Immunization and Respiratory Diseases, CDC, and her colleagues.
They advised physician and patient vigilance regarding meningococcal disease symptoms and urged that patients be advised to seek immediate care and be rapidly treated, regardless of meningococcal vaccination or antimicrobial prophylaxis status.
Health organizations in Europe, including France and the United Kingdom, are recommending eculizumab users receive penicillin during eculizumab treatment. A recent study of invasive meningococcal isolates in the United States found most were susceptible to penicillin, according to the report.
In the 16 U.S. cases reported, nongroupable Neisseria meningitidis caused meningococcal disease in 11 of the patients, serogroup Y was the cause in 4 patients, and the cause was not identified in 1 patient.
Ten patients had meningococcemia without meningitis, the researchers noted. “Initial symptoms of meningococcemia are often relatively mild and nonspecific and might include fever, chills, fatigue, vomiting, diarrhea, and aches or pains in the muscles, joints, chest, or abdomen; however, these symptoms can progress to severe illness and death within hours.”
Eculizumab (Soliris, Alexion Pharmaceuticals) is licensed in the United States for treatment of paroxysmal nocturnal hemoglobinuria and atypical hemolytic uremic syndrome, two diseases that are rare and can be fatal.
Eculizumab is associated with a 1,000-fold to 2,000-fold increased incidence of meningococcal disease among persons receiving the drug. The Food and Drug Administration–approved prescribing information includes a boxed warning regarding increased risk for meningococcal disease.
The CDC is collecting reports from state health departments for further analysis of the risk among eculizumab recipients.
The researchers reported having no conflicts of interest.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
Patients taking eculizumab are at a significant risk for meningococcal disease even if they have received the quadrivalent meningococcal conjugate (MenACWY) and serogroup B (MenB) meningococcal vaccines, according to the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report, released July 7.
Between 2008 and 2016, 16 cases of meningococcal disease were reported in eculizumab users in 10 jurisdictions within the United States. Of those infected, 14 had received MenACWY and MenB vaccines as recommended by the Advisory Committee on Immunization Practices, according to the CDC report.
Required vaccination plus antimicrobial prophylaxis for the duration of eculizumab treatment might reduce the risk for meningococcal disease in these patients, but the addition of antibiotic prophylaxis is no guarantee that all cases of meningococcal disease would be prevented, wrote Lucy A. McNamara, PhD, of the division of bacterial diseases, National Center for Immunization and Respiratory Diseases, CDC, and her colleagues.
They advised physician and patient vigilance regarding meningococcal disease symptoms and urged that patients be advised to seek immediate care and be rapidly treated, regardless of meningococcal vaccination or antimicrobial prophylaxis status.
Health organizations in Europe, including France and the United Kingdom, are recommending eculizumab users receive penicillin during eculizumab treatment. A recent study of invasive meningococcal isolates in the United States found most were susceptible to penicillin, according to the report.
In the 16 U.S. cases reported, nongroupable Neisseria meningitidis caused meningococcal disease in 11 of the patients, serogroup Y was the cause in 4 patients, and the cause was not identified in 1 patient.
Ten patients had meningococcemia without meningitis, the researchers noted. “Initial symptoms of meningococcemia are often relatively mild and nonspecific and might include fever, chills, fatigue, vomiting, diarrhea, and aches or pains in the muscles, joints, chest, or abdomen; however, these symptoms can progress to severe illness and death within hours.”
Eculizumab (Soliris, Alexion Pharmaceuticals) is licensed in the United States for treatment of paroxysmal nocturnal hemoglobinuria and atypical hemolytic uremic syndrome, two diseases that are rare and can be fatal.
Eculizumab is associated with a 1,000-fold to 2,000-fold increased incidence of meningococcal disease among persons receiving the drug. The Food and Drug Administration–approved prescribing information includes a boxed warning regarding increased risk for meningococcal disease.
The CDC is collecting reports from state health departments for further analysis of the risk among eculizumab recipients.
The researchers reported having no conflicts of interest.
ezimmerman@frontlinemedcom.com
On Twitter @eaztweets
FROM MMWR
Subset of pediatric herpes simplex virus entails frequent episodes
There’s a newly identified, atypical, but substantial subset of patients: Young children who have frequent episodes of herpes simplex virus (HSV) that may not affect mucosal tissue, often are multifocal, and may require suppressive therapy, according to a report published in Pediatric Dermatology.
“Most of our knowledge of the clinical manifestations of HSV infections in children derives from cases of common mucosal HSV that present to and are treated by primary care providers,” said Julia K. Gittler, MD, and her associates at New York University. 
These cases comprise primary herpetic gingivostomatitis or the well-known orolabial HSV. To characterize the more atypical presentations in the pediatric population, the investigators reviewed the charts of all 48 patients referred to their pediatric dermatology clinic in a 10-year period after receiving a diagnosis of HSV. Only 19% of these patients were older than 11 years of age, and more than 40% were younger than 2 years of age at presentation.
Dr. Gittler and her associates found a “substantial” subset of 19 patients (approximately 40% of the study sample) who had six or more outbreaks per year. Only four patients (8.3%) had one or fewer outbreaks per year. The mean frequency of outbreaks in their study population was seven per year. “Reported triggers for outbreaks included fever, viral infections, sun, cold, stress, vaccinations, and courses of oral corticosteroids for asthma flares,” the investigators said.
Given this high frequency of outbreaks, antiviral therapy was initiated in 16 patients (33%). The average age of this treatment initiation was only 6 years. “In the general population, only approximately 15%-40% of patients with serologic evidence of HSV-1 have recurrent HSV; most of these will have an average of 2 outbreaks per year, and only 5%-10% have more than 6 outbreaks per year,” the investigators wrote (Pediatr Dermatol. 2017. doi: 10.1111/pde.13190).
The majority of the study participants (29 patients) had no labial or mucosal involvement. Approximately 23% had cutaneous involvement of the cheek, “which may have been because the primary infection was acquired through the kiss of a caregiver,” they said. Other sites of cutaneous lesions that were frequent in this population but are considered atypical in general were the ear, forehead, chest, and knees.
Most commonly, the physical examination findings were vesicles or papulovesicles (52%), but crusting (33%), pustules (6%), and erosions (23%) also occurred.
Fully half of the study population had multifocal rather than unifocal presentations.
Atypical presentation of HSV is frequently misdiagnosed as impetigo or herpes zoster, according to reports in the literature. Fifteen (31%) patients in this study had a previous misdiagnosis of impetigo. “These less typical cutaneous presentations of HSV may evade accurate diagnosis and delay initiation of appropriate treatment,” Dr. Gittler and her associates noted.
No financial disclosures were provided for Dr. Gittler and her associates.
There’s a newly identified, atypical, but substantial subset of patients: Young children who have frequent episodes of herpes simplex virus (HSV) that may not affect mucosal tissue, often are multifocal, and may require suppressive therapy, according to a report published in Pediatric Dermatology.
“Most of our knowledge of the clinical manifestations of HSV infections in children derives from cases of common mucosal HSV that present to and are treated by primary care providers,” said Julia K. Gittler, MD, and her associates at New York University.
These cases comprise primary herpetic gingivostomatitis or the well-known orolabial HSV. To characterize the more atypical presentations in the pediatric population, the investigators reviewed the charts of all 48 patients referred to their pediatric dermatology clinic in a 10-year period after receiving a diagnosis of HSV. Only 19% of these patients were older than 11 years of age, and more than 40% were younger than 2 years of age at presentation.
Dr. Gittler and her associates found a “substantial” subset of 19 patients (approximately 40% of the study sample) who had six or more outbreaks per year. Only four patients (8.3%) had one or fewer outbreaks per year. The mean frequency of outbreaks in their study population was seven per year. “Reported triggers for outbreaks included fever, viral infections, sun, cold, stress, vaccinations, and courses of oral corticosteroids for asthma flares,” the investigators said.
Given this high frequency of outbreaks, antiviral therapy was initiated in 16 patients (33%). The average age of this treatment initiation was only 6 years. “In the general population, only approximately 15%-40% of patients with serologic evidence of HSV-1 have recurrent HSV; most of these will have an average of 2 outbreaks per year, and only 5%-10% have more than 6 outbreaks per year,” the investigators wrote (Pediatr Dermatol. 2017. doi: 10.1111/pde.13190).
The majority of the study participants (29 patients) had no labial or mucosal involvement. Approximately 23% had cutaneous involvement of the cheek, “which may have been because the primary infection was acquired through the kiss of a caregiver,” they said. Other sites of cutaneous lesions that were frequent in this population but are considered atypical in general were the ear, forehead, chest, and knees.
Most commonly, the physical examination findings were vesicles or papulovesicles (52%), but crusting (33%), pustules (6%), and erosions (23%) also occurred.
Fully half of the study population had multifocal rather than unifocal presentations.
Atypical presentation of HSV is frequently misdiagnosed as impetigo or herpes zoster, according to reports in the literature. Fifteen (31%) patients in this study had a previous misdiagnosis of impetigo. “These less typical cutaneous presentations of HSV may evade accurate diagnosis and delay initiation of appropriate treatment,” Dr. Gittler and her associates noted.
No financial disclosures were provided for Dr. Gittler and her associates.
There’s a newly identified, atypical, but substantial subset of patients: Young children who have frequent episodes of herpes simplex virus (HSV) that may not affect mucosal tissue, often are multifocal, and may require suppressive therapy, according to a report published in Pediatric Dermatology.
“Most of our knowledge of the clinical manifestations of HSV infections in children derives from cases of common mucosal HSV that present to and are treated by primary care providers,” said Julia K. Gittler, MD, and her associates at New York University.
These cases comprise primary herpetic gingivostomatitis or the well-known orolabial HSV. To characterize the more atypical presentations in the pediatric population, the investigators reviewed the charts of all 48 patients referred to their pediatric dermatology clinic in a 10-year period after receiving a diagnosis of HSV. Only 19% of these patients were older than 11 years of age, and more than 40% were younger than 2 years of age at presentation.
Dr. Gittler and her associates found a “substantial” subset of 19 patients (approximately 40% of the study sample) who had six or more outbreaks per year. Only four patients (8.3%) had one or fewer outbreaks per year. The mean frequency of outbreaks in their study population was seven per year. “Reported triggers for outbreaks included fever, viral infections, sun, cold, stress, vaccinations, and courses of oral corticosteroids for asthma flares,” the investigators said.
Given this high frequency of outbreaks, antiviral therapy was initiated in 16 patients (33%). The average age of this treatment initiation was only 6 years. “In the general population, only approximately 15%-40% of patients with serologic evidence of HSV-1 have recurrent HSV; most of these will have an average of 2 outbreaks per year, and only 5%-10% have more than 6 outbreaks per year,” the investigators wrote (Pediatr Dermatol. 2017. doi: 10.1111/pde.13190).
The majority of the study participants (29 patients) had no labial or mucosal involvement. Approximately 23% had cutaneous involvement of the cheek, “which may have been because the primary infection was acquired through the kiss of a caregiver,” they said. Other sites of cutaneous lesions that were frequent in this population but are considered atypical in general were the ear, forehead, chest, and knees.
Most commonly, the physical examination findings were vesicles or papulovesicles (52%), but crusting (33%), pustules (6%), and erosions (23%) also occurred.
Fully half of the study population had multifocal rather than unifocal presentations.
Atypical presentation of HSV is frequently misdiagnosed as impetigo or herpes zoster, according to reports in the literature. Fifteen (31%) patients in this study had a previous misdiagnosis of impetigo. “These less typical cutaneous presentations of HSV may evade accurate diagnosis and delay initiation of appropriate treatment,” Dr. Gittler and her associates noted.
No financial disclosures were provided for Dr. Gittler and her associates.
FROM PEDIATRIC DERMATOLOGY
Key clinical point:
Major finding: 19 of 48 (40%) patients had six or more HSV outbreaks per year, and the mean frequency of outbreaks in this study population was seven per year.
Data source: Chart review of 48 cases referred to a single pediatric dermatology clinic in a 10-year period.
Disclosures: No financial disclosures were provided for Dr. Gittler and her associates.