User login
PCVs may reduce AOM severity, although they do not decrease incidence
Use of the 7-valent pneumococcal conjugate vaccine (PCV7) may have had a part in reducing the incidence of severe middle ear inflammation of acute otitis media (AOM) in Japanese children, decreasing the rate of myringotomies for AOM, said Atsushi Sasaki, of the Hiroshima (Japan) University, and associates.
To assess whether use of PCV7 and then PCV13 affected AOM incidence, the investigators looked at the incidence of visits to medical institutions (VtMI) due to all-cause AOM in children younger than 15 years in the Japan Medical Data Center Claims Database between January 2005 and December 2015. Data for children aged 10 years to younger than 15 years served as the control. The rate of myringotomies for AOM (MyfA) from January 2007 to December 2015 also was assessed.
Numerous other studies have “concluded that the preventive effect of PCV7 against AOM was very modest,” the researchers said. “In contrast, our study proposes the hypothesis that PCV7 use in 1-year-olds may contribute to the decreased incidence of severe middle ear inflammation of AOM. When evaluating the effectiveness of PCV, measures to evaluate severity may be as important as evaluating disease prevention.”
Read more in Auris Nasus Larynx (2017 Nov 1. doi: 10.1016/j.anl.2017.10.006).
Use of the 7-valent pneumococcal conjugate vaccine (PCV7) may have had a part in reducing the incidence of severe middle ear inflammation of acute otitis media (AOM) in Japanese children, decreasing the rate of myringotomies for AOM, said Atsushi Sasaki, of the Hiroshima (Japan) University, and associates.
To assess whether use of PCV7 and then PCV13 affected AOM incidence, the investigators looked at the incidence of visits to medical institutions (VtMI) due to all-cause AOM in children younger than 15 years in the Japan Medical Data Center Claims Database between January 2005 and December 2015. Data for children aged 10 years to younger than 15 years served as the control. The rate of myringotomies for AOM (MyfA) from January 2007 to December 2015 also was assessed.
Numerous other studies have “concluded that the preventive effect of PCV7 against AOM was very modest,” the researchers said. “In contrast, our study proposes the hypothesis that PCV7 use in 1-year-olds may contribute to the decreased incidence of severe middle ear inflammation of AOM. When evaluating the effectiveness of PCV, measures to evaluate severity may be as important as evaluating disease prevention.”
Read more in Auris Nasus Larynx (2017 Nov 1. doi: 10.1016/j.anl.2017.10.006).
Use of the 7-valent pneumococcal conjugate vaccine (PCV7) may have had a part in reducing the incidence of severe middle ear inflammation of acute otitis media (AOM) in Japanese children, decreasing the rate of myringotomies for AOM, said Atsushi Sasaki, of the Hiroshima (Japan) University, and associates.
To assess whether use of PCV7 and then PCV13 affected AOM incidence, the investigators looked at the incidence of visits to medical institutions (VtMI) due to all-cause AOM in children younger than 15 years in the Japan Medical Data Center Claims Database between January 2005 and December 2015. Data for children aged 10 years to younger than 15 years served as the control. The rate of myringotomies for AOM (MyfA) from January 2007 to December 2015 also was assessed.
Numerous other studies have “concluded that the preventive effect of PCV7 against AOM was very modest,” the researchers said. “In contrast, our study proposes the hypothesis that PCV7 use in 1-year-olds may contribute to the decreased incidence of severe middle ear inflammation of AOM. When evaluating the effectiveness of PCV, measures to evaluate severity may be as important as evaluating disease prevention.”
Read more in Auris Nasus Larynx (2017 Nov 1. doi: 10.1016/j.anl.2017.10.006).
FROM AURIS NASUS LARYNX
Novel biomarker test appears accurate for UTI diagnosis in febrile children under 2 years
Novel test for the urinary neutrophil gelatinase–associated lipocalin (uNGAL) biomarker have good sensitivity and specificity to distinguish whether infants and children younger than 2 years old have a urinary tract infection (UTI), said Tamar R. Lubell, MD, and her associates at Columbia University, New York.
“NGAL is a protein expressed in neutrophils and several other human tissues, including alpha-intercalated cells in the collecting duct of the kidney,” the researchers explained. “The urine and serum contain very low levels of NGAL protein at steady state, with expression of NGAL rising rapidly in response to cell damage caused by ischemia-reperfusion injury, presence of cytotoxins, and sepsis.”
Of the 260 children whose catheterized urine was analyzed, 14% had UTIs. The median uNGAL concentration was 215.1 ng/mL in the UTI group, compared with 4.4 ng/mL in the culture-negative group. Urinalysis and Gram stain also were performed.
“uNGAL had higher sensitivity than [urinalysis], with similar specificity,” the investigators said. “Gram stain had a somewhat lower sensitivity than uNGAL, but with high specificity.”
The researchers identified a cutoff point for uNGAL levels to be 39.1 ng/mL. A previous case-control study of 108 infants with UTI had a cutoff for uNGAL levels of 38 ng/mL, with sensitivity of 93% and specificity of 95%. Most urine samples in that study were obtained by clean catch rather than by catheterization, as in the current study.
“Further studies will need to both confirm our findings and determine the benefit and cost effectiveness of uNGAL testing, compared with [urinalysis],” Dr. Lubell and her associates said.
Read more in Pediatrics (2017 Nov 16. doi: 10.1542/peds.2017-1090).
Novel test for the urinary neutrophil gelatinase–associated lipocalin (uNGAL) biomarker have good sensitivity and specificity to distinguish whether infants and children younger than 2 years old have a urinary tract infection (UTI), said Tamar R. Lubell, MD, and her associates at Columbia University, New York.
“NGAL is a protein expressed in neutrophils and several other human tissues, including alpha-intercalated cells in the collecting duct of the kidney,” the researchers explained. “The urine and serum contain very low levels of NGAL protein at steady state, with expression of NGAL rising rapidly in response to cell damage caused by ischemia-reperfusion injury, presence of cytotoxins, and sepsis.”
Of the 260 children whose catheterized urine was analyzed, 14% had UTIs. The median uNGAL concentration was 215.1 ng/mL in the UTI group, compared with 4.4 ng/mL in the culture-negative group. Urinalysis and Gram stain also were performed.
“uNGAL had higher sensitivity than [urinalysis], with similar specificity,” the investigators said. “Gram stain had a somewhat lower sensitivity than uNGAL, but with high specificity.”
The researchers identified a cutoff point for uNGAL levels to be 39.1 ng/mL. A previous case-control study of 108 infants with UTI had a cutoff for uNGAL levels of 38 ng/mL, with sensitivity of 93% and specificity of 95%. Most urine samples in that study were obtained by clean catch rather than by catheterization, as in the current study.
“Further studies will need to both confirm our findings and determine the benefit and cost effectiveness of uNGAL testing, compared with [urinalysis],” Dr. Lubell and her associates said.
Read more in Pediatrics (2017 Nov 16. doi: 10.1542/peds.2017-1090).
Novel test for the urinary neutrophil gelatinase–associated lipocalin (uNGAL) biomarker have good sensitivity and specificity to distinguish whether infants and children younger than 2 years old have a urinary tract infection (UTI), said Tamar R. Lubell, MD, and her associates at Columbia University, New York.
“NGAL is a protein expressed in neutrophils and several other human tissues, including alpha-intercalated cells in the collecting duct of the kidney,” the researchers explained. “The urine and serum contain very low levels of NGAL protein at steady state, with expression of NGAL rising rapidly in response to cell damage caused by ischemia-reperfusion injury, presence of cytotoxins, and sepsis.”
Of the 260 children whose catheterized urine was analyzed, 14% had UTIs. The median uNGAL concentration was 215.1 ng/mL in the UTI group, compared with 4.4 ng/mL in the culture-negative group. Urinalysis and Gram stain also were performed.
“uNGAL had higher sensitivity than [urinalysis], with similar specificity,” the investigators said. “Gram stain had a somewhat lower sensitivity than uNGAL, but with high specificity.”
The researchers identified a cutoff point for uNGAL levels to be 39.1 ng/mL. A previous case-control study of 108 infants with UTI had a cutoff for uNGAL levels of 38 ng/mL, with sensitivity of 93% and specificity of 95%. Most urine samples in that study were obtained by clean catch rather than by catheterization, as in the current study.
“Further studies will need to both confirm our findings and determine the benefit and cost effectiveness of uNGAL testing, compared with [urinalysis],” Dr. Lubell and her associates said.
Read more in Pediatrics (2017 Nov 16. doi: 10.1542/peds.2017-1090).
FROM PEDIATRICS

After warning, codeine use after tonsillectomy drops, doesn’t stop
– and there has been inappropriate substitution of other opioids rather than nonopioid pain relievers such as ibuprofen, said Kao-Ping Chua, MD, PhD, of the University of Chicago, and his associates.
Codeine has been one of the most commonly prescribed analgesics for children after tonsillectomies and adenoidectomies because it was considered safe.
The FDA issued a boxed warning Feb. 20, 2013, recommending against codeine use in all children undergoing tonsillectomy and/or adenoidectomy. Also, children with obstructive sleep apnea are at risk of opioid-related respiratory depression.
A retrospective study of 362,992 children aged 0-18 years who underwent tonsillectomy and/or adenoidectomy was undertaken in 2010-2015, prior to and after the FDA issued the boxed warning against codeine use. In January 2010, codeine products were prescribed in 47% of cases, compared with 48% for hydrocodone, 4% for oxycodone, and less than 1% for other opioid products. In December 2015, codeine was prescribed in 9% of cases, compared with 73% for hydrocodone, 17% for oxycodone, and less than 1% for other opioid products.
“The unadjusted proportion of children receiving alternative opioids rose substantially during the study period, presumably because of factors other than the investigation itself,” said Dr. Chua and his associates. “This increase deserves further examination, given the abuse liability associated with higher-potency opioids, as well as the growing evidence of genetic variability in the metabolism of many alternative opioids, including oxycodone and tramadol.
“Future quality-improvement efforts should focus on eliminating this residual inappropriate codeine prescribing, and on encouraging the use of effective nonopioid medications such as ibuprofen,” the investigators said.
Read more in Pediatrics (2017 Nov 16. doi: 10.1542/ peds.2017-1765).
– and there has been inappropriate substitution of other opioids rather than nonopioid pain relievers such as ibuprofen, said Kao-Ping Chua, MD, PhD, of the University of Chicago, and his associates.
Codeine has been one of the most commonly prescribed analgesics for children after tonsillectomies and adenoidectomies because it was considered safe.
The FDA issued a boxed warning Feb. 20, 2013, recommending against codeine use in all children undergoing tonsillectomy and/or adenoidectomy. Also, children with obstructive sleep apnea are at risk of opioid-related respiratory depression.
A retrospective study of 362,992 children aged 0-18 years who underwent tonsillectomy and/or adenoidectomy was undertaken in 2010-2015, prior to and after the FDA issued the boxed warning against codeine use. In January 2010, codeine products were prescribed in 47% of cases, compared with 48% for hydrocodone, 4% for oxycodone, and less than 1% for other opioid products. In December 2015, codeine was prescribed in 9% of cases, compared with 73% for hydrocodone, 17% for oxycodone, and less than 1% for other opioid products.
“The unadjusted proportion of children receiving alternative opioids rose substantially during the study period, presumably because of factors other than the investigation itself,” said Dr. Chua and his associates. “This increase deserves further examination, given the abuse liability associated with higher-potency opioids, as well as the growing evidence of genetic variability in the metabolism of many alternative opioids, including oxycodone and tramadol.
“Future quality-improvement efforts should focus on eliminating this residual inappropriate codeine prescribing, and on encouraging the use of effective nonopioid medications such as ibuprofen,” the investigators said.
Read more in Pediatrics (2017 Nov 16. doi: 10.1542/ peds.2017-1765).
– and there has been inappropriate substitution of other opioids rather than nonopioid pain relievers such as ibuprofen, said Kao-Ping Chua, MD, PhD, of the University of Chicago, and his associates.
Codeine has been one of the most commonly prescribed analgesics for children after tonsillectomies and adenoidectomies because it was considered safe.
The FDA issued a boxed warning Feb. 20, 2013, recommending against codeine use in all children undergoing tonsillectomy and/or adenoidectomy. Also, children with obstructive sleep apnea are at risk of opioid-related respiratory depression.
A retrospective study of 362,992 children aged 0-18 years who underwent tonsillectomy and/or adenoidectomy was undertaken in 2010-2015, prior to and after the FDA issued the boxed warning against codeine use. In January 2010, codeine products were prescribed in 47% of cases, compared with 48% for hydrocodone, 4% for oxycodone, and less than 1% for other opioid products. In December 2015, codeine was prescribed in 9% of cases, compared with 73% for hydrocodone, 17% for oxycodone, and less than 1% for other opioid products.
“The unadjusted proportion of children receiving alternative opioids rose substantially during the study period, presumably because of factors other than the investigation itself,” said Dr. Chua and his associates. “This increase deserves further examination, given the abuse liability associated with higher-potency opioids, as well as the growing evidence of genetic variability in the metabolism of many alternative opioids, including oxycodone and tramadol.
“Future quality-improvement efforts should focus on eliminating this residual inappropriate codeine prescribing, and on encouraging the use of effective nonopioid medications such as ibuprofen,” the investigators said.
Read more in Pediatrics (2017 Nov 16. doi: 10.1542/ peds.2017-1765).
FROM PEDIATRICS
DTaP vaccination rate highest in Maryland
, according to the Centers for Disease Control and Prevention.
Maryland’s coverage of required DTaP vaccine doses came in at a national high of 99.6% for children entering kindergarten in 2016-2017, while the District of Columbia had the nation’s lowest rate at 82.2%, Ranee Seither, MPH, of the National Center for Immunization and Respiratory Disease, and associates at the CDC, Atlanta, reported (MMWR. 2017 Oct 13;66[40]:1073-80).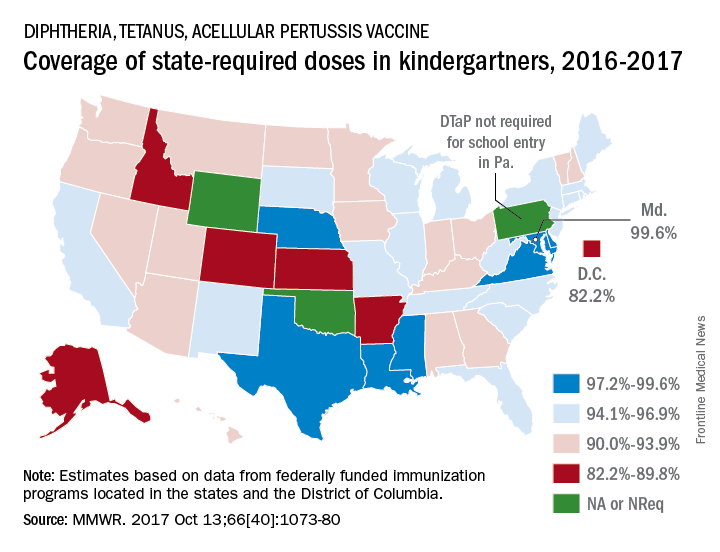
There is also variation among the states in the number of doses required for kindergarten entry: Most require five, but Illinois, Maryland, Virginia, and Wisconsin require four; Nebraska requires three; and Pennsylvania does not require pertussis vaccine. Oklahoma and Wyoming did not report vaccination coverage “because of widespread problems with the quality of data reported by schools,” they noted.
Nationally, median coverage for state-required doses of the DTaP vaccine was 94.5%, according to data from federally funded immunization programs in the 50 states and D.C., which included 3,973,172 kindergartners for the 2016-2017 school year.
, according to the Centers for Disease Control and Prevention.
Maryland’s coverage of required DTaP vaccine doses came in at a national high of 99.6% for children entering kindergarten in 2016-2017, while the District of Columbia had the nation’s lowest rate at 82.2%, Ranee Seither, MPH, of the National Center for Immunization and Respiratory Disease, and associates at the CDC, Atlanta, reported (MMWR. 2017 Oct 13;66[40]:1073-80).
There is also variation among the states in the number of doses required for kindergarten entry: Most require five, but Illinois, Maryland, Virginia, and Wisconsin require four; Nebraska requires three; and Pennsylvania does not require pertussis vaccine. Oklahoma and Wyoming did not report vaccination coverage “because of widespread problems with the quality of data reported by schools,” they noted.
Nationally, median coverage for state-required doses of the DTaP vaccine was 94.5%, according to data from federally funded immunization programs in the 50 states and D.C., which included 3,973,172 kindergartners for the 2016-2017 school year.
, according to the Centers for Disease Control and Prevention.
Maryland’s coverage of required DTaP vaccine doses came in at a national high of 99.6% for children entering kindergarten in 2016-2017, while the District of Columbia had the nation’s lowest rate at 82.2%, Ranee Seither, MPH, of the National Center for Immunization and Respiratory Disease, and associates at the CDC, Atlanta, reported (MMWR. 2017 Oct 13;66[40]:1073-80).
There is also variation among the states in the number of doses required for kindergarten entry: Most require five, but Illinois, Maryland, Virginia, and Wisconsin require four; Nebraska requires three; and Pennsylvania does not require pertussis vaccine. Oklahoma and Wyoming did not report vaccination coverage “because of widespread problems with the quality of data reported by schools,” they noted.
Nationally, median coverage for state-required doses of the DTaP vaccine was 94.5%, according to data from federally funded immunization programs in the 50 states and D.C., which included 3,973,172 kindergartners for the 2016-2017 school year.
FROM MMWR
Higher hospital mortality in pediatric emergency transfer patients
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
I’ve learned so much this summer from working with Dr. Patrick Brady to better understand characteristics of pediatric patients who undergo clinical deterioration and unplanned transfers to the ICU. I’m very grateful to have spent my summer with a mentor who really cared about my growth as a student, and a fantastic group of physicians in the Division of Hospital Medicine at Cincinnati Children’s Hospital Medical Center.

After data analysis, we discovered that children who have had an emergency transfer event spend a longer time in the ICU and in the hospital. After comparing hospital mortality, we can conclude that emergency transfer patients have a higher likelihood of hospital mortality.
From this preliminary research, the emergency transfer metric in children’s hospitals has the potential to enable more rapid learning and systems improvement. We have a few next steps to investigate these next couple months as well. We want to compare medical diagnoses and complex chronic conditions between the emergency transfer cases and controls. We also hope to describe the incidence using a patient-days denominator. Finally, our long term goals are to identify predictors for an emergency transfer event in children.
Farah Hussain is a 2nd-year medical student at University of Cincinnati College of Medicine and student researcher at Cincinnati Children’s Hospital Medical Center. Her research interests involve bettering patient care to vulnerable populations.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
I’ve learned so much this summer from working with Dr. Patrick Brady to better understand characteristics of pediatric patients who undergo clinical deterioration and unplanned transfers to the ICU. I’m very grateful to have spent my summer with a mentor who really cared about my growth as a student, and a fantastic group of physicians in the Division of Hospital Medicine at Cincinnati Children’s Hospital Medical Center.
After data analysis, we discovered that children who have had an emergency transfer event spend a longer time in the ICU and in the hospital. After comparing hospital mortality, we can conclude that emergency transfer patients have a higher likelihood of hospital mortality.
From this preliminary research, the emergency transfer metric in children’s hospitals has the potential to enable more rapid learning and systems improvement. We have a few next steps to investigate these next couple months as well. We want to compare medical diagnoses and complex chronic conditions between the emergency transfer cases and controls. We also hope to describe the incidence using a patient-days denominator. Finally, our long term goals are to identify predictors for an emergency transfer event in children.
Farah Hussain is a 2nd-year medical student at University of Cincinnati College of Medicine and student researcher at Cincinnati Children’s Hospital Medical Center. Her research interests involve bettering patient care to vulnerable populations.
Editor’s Note: The Society of Hospital Medicine’s (SHM’s) Physician in Training Committee launched a scholarship program in 2015 for medical students to help transform health care and revolutionize patient care. The program has been expanded for the 2017-2018 year, offering two options for students to receive funding and engage in scholarly work during their first, second, and third years of medical school. As a part of the program, recipients are required to write about their experience on a biweekly basis.
I’ve learned so much this summer from working with Dr. Patrick Brady to better understand characteristics of pediatric patients who undergo clinical deterioration and unplanned transfers to the ICU. I’m very grateful to have spent my summer with a mentor who really cared about my growth as a student, and a fantastic group of physicians in the Division of Hospital Medicine at Cincinnati Children’s Hospital Medical Center.
After data analysis, we discovered that children who have had an emergency transfer event spend a longer time in the ICU and in the hospital. After comparing hospital mortality, we can conclude that emergency transfer patients have a higher likelihood of hospital mortality.
From this preliminary research, the emergency transfer metric in children’s hospitals has the potential to enable more rapid learning and systems improvement. We have a few next steps to investigate these next couple months as well. We want to compare medical diagnoses and complex chronic conditions between the emergency transfer cases and controls. We also hope to describe the incidence using a patient-days denominator. Finally, our long term goals are to identify predictors for an emergency transfer event in children.
Farah Hussain is a 2nd-year medical student at University of Cincinnati College of Medicine and student researcher at Cincinnati Children’s Hospital Medical Center. Her research interests involve bettering patient care to vulnerable populations.
OCD linked to lower education attainment
Obsessive-compulsive disorder could be detrimental to educational attainment, particularly if diagnosed before the age of 18 years, according to a study published online Nov. 15.
A Swedish population-based birth cohort study identified 15,120 individuals who had been diagnosed with obsessive-compulsive disorder (OCD, 11,482 of whom were in families with full siblings discordant for OCD.
Individuals with OCD were also 57% less likely to complete upper secondary school, 28% less likely to start a university degree, 41% less likely to finish that degree, and 48% less likely to complete postgraduate education, compared to individuals without OCD.
“The association was global rather than being limited to a particular course; patients were more likely to fail each of the core and additional courses in compulsory school and less likely to achieve each level of education, from primary school to postgraduate education,” wrote Ana Pérez-Vigil, MD, of the Center for Psychiatry Research at Karolinska Institutet, Stockholm, and her coauthors.
The authors noted that as the education impairment seemed greatest at the end of upper secondary school but reduced during university, individuals with OCD might cope better with their symptoms as they age or receive evidence-based treatment.
“These individuals might be able to find alternative routes to access university, such as the locally funded school system for adults who have failed to complete primary or secondary school (known as komvux in Sweden),” they wrote. “Thus, early educational failure does not necessarily condemn individuals to lifelong educational ostracism.”
People with OCD also were 53% less likely to be eligible to access a vocational program (95% confidence interval, 0.45-0.50) and 49% less likely to be eligible for an academic program in upper secondary school (95% CI, 0.58-0.63), compared with the general population, after adjustment for factors such as sex, year of birth, and parental age at birth of the participant.
Early diagnosis – before the age of 18 years – was associated with even worse educational outcomes, compared with those diagnosed after the age of 18.
Excluding individuals with other comorbidities such as attention-deficit/hyperactivity disorder attenuated the results slightly, but individuals with OCD still showed significantly worse educational attainment than that of the general population.
Dr. Pérez-Vigil and her coauthors said detecting and treating OCD early might help patients “fulfill their educational potential.”
Several authors of the study were supported by grants from the International OCD Foundation; the Alicia Koplowitz Foundation; the Swedish Research Council for Health, Working Life, and Welfare; and the Karolinska Institute. Two authors declared royalties from a publishing company, and one declared speaking fees and a research grant from Shire Pharmaceuticals, all of which were outside the submitted work. No other conflicts of interest were declared.
Obsessive-compulsive disorder could be detrimental to educational attainment, particularly if diagnosed before the age of 18 years, according to a study published online Nov. 15.
A Swedish population-based birth cohort study identified 15,120 individuals who had been diagnosed with obsessive-compulsive disorder (OCD, 11,482 of whom were in families with full siblings discordant for OCD.
Individuals with OCD were also 57% less likely to complete upper secondary school, 28% less likely to start a university degree, 41% less likely to finish that degree, and 48% less likely to complete postgraduate education, compared to individuals without OCD.
“The association was global rather than being limited to a particular course; patients were more likely to fail each of the core and additional courses in compulsory school and less likely to achieve each level of education, from primary school to postgraduate education,” wrote Ana Pérez-Vigil, MD, of the Center for Psychiatry Research at Karolinska Institutet, Stockholm, and her coauthors.
The authors noted that as the education impairment seemed greatest at the end of upper secondary school but reduced during university, individuals with OCD might cope better with their symptoms as they age or receive evidence-based treatment.
“These individuals might be able to find alternative routes to access university, such as the locally funded school system for adults who have failed to complete primary or secondary school (known as komvux in Sweden),” they wrote. “Thus, early educational failure does not necessarily condemn individuals to lifelong educational ostracism.”
People with OCD also were 53% less likely to be eligible to access a vocational program (95% confidence interval, 0.45-0.50) and 49% less likely to be eligible for an academic program in upper secondary school (95% CI, 0.58-0.63), compared with the general population, after adjustment for factors such as sex, year of birth, and parental age at birth of the participant.
Early diagnosis – before the age of 18 years – was associated with even worse educational outcomes, compared with those diagnosed after the age of 18.
Excluding individuals with other comorbidities such as attention-deficit/hyperactivity disorder attenuated the results slightly, but individuals with OCD still showed significantly worse educational attainment than that of the general population.
Dr. Pérez-Vigil and her coauthors said detecting and treating OCD early might help patients “fulfill their educational potential.”
Several authors of the study were supported by grants from the International OCD Foundation; the Alicia Koplowitz Foundation; the Swedish Research Council for Health, Working Life, and Welfare; and the Karolinska Institute. Two authors declared royalties from a publishing company, and one declared speaking fees and a research grant from Shire Pharmaceuticals, all of which were outside the submitted work. No other conflicts of interest were declared.
Obsessive-compulsive disorder could be detrimental to educational attainment, particularly if diagnosed before the age of 18 years, according to a study published online Nov. 15.
A Swedish population-based birth cohort study identified 15,120 individuals who had been diagnosed with obsessive-compulsive disorder (OCD, 11,482 of whom were in families with full siblings discordant for OCD.
Individuals with OCD were also 57% less likely to complete upper secondary school, 28% less likely to start a university degree, 41% less likely to finish that degree, and 48% less likely to complete postgraduate education, compared to individuals without OCD.
“The association was global rather than being limited to a particular course; patients were more likely to fail each of the core and additional courses in compulsory school and less likely to achieve each level of education, from primary school to postgraduate education,” wrote Ana Pérez-Vigil, MD, of the Center for Psychiatry Research at Karolinska Institutet, Stockholm, and her coauthors.
The authors noted that as the education impairment seemed greatest at the end of upper secondary school but reduced during university, individuals with OCD might cope better with their symptoms as they age or receive evidence-based treatment.
“These individuals might be able to find alternative routes to access university, such as the locally funded school system for adults who have failed to complete primary or secondary school (known as komvux in Sweden),” they wrote. “Thus, early educational failure does not necessarily condemn individuals to lifelong educational ostracism.”
People with OCD also were 53% less likely to be eligible to access a vocational program (95% confidence interval, 0.45-0.50) and 49% less likely to be eligible for an academic program in upper secondary school (95% CI, 0.58-0.63), compared with the general population, after adjustment for factors such as sex, year of birth, and parental age at birth of the participant.
Early diagnosis – before the age of 18 years – was associated with even worse educational outcomes, compared with those diagnosed after the age of 18.
Excluding individuals with other comorbidities such as attention-deficit/hyperactivity disorder attenuated the results slightly, but individuals with OCD still showed significantly worse educational attainment than that of the general population.
Dr. Pérez-Vigil and her coauthors said detecting and treating OCD early might help patients “fulfill their educational potential.”
Several authors of the study were supported by grants from the International OCD Foundation; the Alicia Koplowitz Foundation; the Swedish Research Council for Health, Working Life, and Welfare; and the Karolinska Institute. Two authors declared royalties from a publishing company, and one declared speaking fees and a research grant from Shire Pharmaceuticals, all of which were outside the submitted work. No other conflicts of interest were declared.
FROM JAMA PSYCHIATRY
Key clinical point: Obsessive-compulsive disorder is associated with a decrease in education attainment, particularly if diagnosed before the age of 18 years.
Major finding: Individuals with obsessive-compulsive disorder are significantly less likely to complete upper secondary school and significantly less likely to pass courses in the last year of compulsory education.
Data source: A Swedish population-based birth cohort study of 15,120 individuals who had been diagnosed with obsessive-compulsive disorder.
Disclosures: Several authors of the study were supported by grants from the International OCD Foundation; the Alicia Koplowitz Foundation; the Swedish Research Council for Health, Working Life, and Welfare; and the Karolinska Institute. Two authors declared royalties from a publishing company, and one declared speaking fees and a research grant from Shire Pharmaceuticals, all of which were outside the submitted work. No other conflicts of interest were declared.
Stem cells spark successful skin regeneration
Junctional epidermolysis bullosa is a genetic disease characterized by chronic skin wounds, blisters, and erosions. The chronic wounds not only increase a patient’s risk of skin cancer, they also can cause itching, pain, limited mobility, and poor quality of life, wrote Tobias Hirsch, MD, of BG University Hospital Bergmannsheil, Bochum, Germany, and colleagues (Nature. 2017. doi: 10.1038/nature24487). There is no cure for the disease, and more than 40% of patients die prior to adolescence.
Previous studies have shown that epidermal stem cells can be used to repair a damaged epidermis, they noted. However, the technique has been criticized for being insufficient to treat the large lesions common to this disease.
The researchers described the case of a 7-year-old boy who was admitted to a children’s hospital in Germany in June 2015 with junctional epidermolysis bullosa so severe that approximately 80% of his total body surface area was affected. The patient had a genetic mutation that had resulted in blisters on much of his body since birth. Approximately 6 weeks prior to his hospital admission, he developed Staphylococcus aureus and Pseudomonas aeruginosa infections that worsened his condition. After other treatments failed, the patient’s parents consented to a combination of ex vivo cell and gene therapy, in which cultures taken from a biopsy of uninvolved skin were used to develop transgenic epidermal grafts. The grafts were applied sequentially on a dermal wound bed.
“Virtually complete epidermal regeneration was observed after 1 month,” Dr. Hirsch and associates wrote. Over 21 months, the regenerated epidermis healed and remained stable even when subjected to mechanical stress.
For follow-up, the researchers reported on 10 punch biopsies taken at 4, 8, and 21 months after the grafting procedure. “The epidermis had normal morphology and we could not detect blisters, erosions, or epidermal detachment from the underlying dermis,” they noted.
The patient has remained stable since being discharged from the hospital in February 2016, and requires no ointment or medications to maintain a healthy epidermis, they said.
“This approach would be optimal for newly diagnosed patients early in their childhood,” Dr. Hirsch and associates noted. “A bank of transduced epidermal stem cells taken at birth could be used to treat skin lesions while they develop, thus preventing, rather than restoring, the devastating clinical manifestation that arise in these patients.
The study was supported in part by several government grants from organizations including the Italian Ministry of Education and the European Research. Two of the researchers are cofounders and members of the Board of Directors of Holostem Terapie Avanzate, which met all costs of good manufacturing practice production and procedures of transgenic epidermal grafts.
Junctional epidermolysis bullosa is a genetic disease characterized by chronic skin wounds, blisters, and erosions. The chronic wounds not only increase a patient’s risk of skin cancer, they also can cause itching, pain, limited mobility, and poor quality of life, wrote Tobias Hirsch, MD, of BG University Hospital Bergmannsheil, Bochum, Germany, and colleagues (Nature. 2017. doi: 10.1038/nature24487). There is no cure for the disease, and more than 40% of patients die prior to adolescence.
Previous studies have shown that epidermal stem cells can be used to repair a damaged epidermis, they noted. However, the technique has been criticized for being insufficient to treat the large lesions common to this disease.
The researchers described the case of a 7-year-old boy who was admitted to a children’s hospital in Germany in June 2015 with junctional epidermolysis bullosa so severe that approximately 80% of his total body surface area was affected. The patient had a genetic mutation that had resulted in blisters on much of his body since birth. Approximately 6 weeks prior to his hospital admission, he developed Staphylococcus aureus and Pseudomonas aeruginosa infections that worsened his condition. After other treatments failed, the patient’s parents consented to a combination of ex vivo cell and gene therapy, in which cultures taken from a biopsy of uninvolved skin were used to develop transgenic epidermal grafts. The grafts were applied sequentially on a dermal wound bed.
“Virtually complete epidermal regeneration was observed after 1 month,” Dr. Hirsch and associates wrote. Over 21 months, the regenerated epidermis healed and remained stable even when subjected to mechanical stress.
For follow-up, the researchers reported on 10 punch biopsies taken at 4, 8, and 21 months after the grafting procedure. “The epidermis had normal morphology and we could not detect blisters, erosions, or epidermal detachment from the underlying dermis,” they noted.
The patient has remained stable since being discharged from the hospital in February 2016, and requires no ointment or medications to maintain a healthy epidermis, they said.
“This approach would be optimal for newly diagnosed patients early in their childhood,” Dr. Hirsch and associates noted. “A bank of transduced epidermal stem cells taken at birth could be used to treat skin lesions while they develop, thus preventing, rather than restoring, the devastating clinical manifestation that arise in these patients.
The study was supported in part by several government grants from organizations including the Italian Ministry of Education and the European Research. Two of the researchers are cofounders and members of the Board of Directors of Holostem Terapie Avanzate, which met all costs of good manufacturing practice production and procedures of transgenic epidermal grafts.
Junctional epidermolysis bullosa is a genetic disease characterized by chronic skin wounds, blisters, and erosions. The chronic wounds not only increase a patient’s risk of skin cancer, they also can cause itching, pain, limited mobility, and poor quality of life, wrote Tobias Hirsch, MD, of BG University Hospital Bergmannsheil, Bochum, Germany, and colleagues (Nature. 2017. doi: 10.1038/nature24487). There is no cure for the disease, and more than 40% of patients die prior to adolescence.
Previous studies have shown that epidermal stem cells can be used to repair a damaged epidermis, they noted. However, the technique has been criticized for being insufficient to treat the large lesions common to this disease.
The researchers described the case of a 7-year-old boy who was admitted to a children’s hospital in Germany in June 2015 with junctional epidermolysis bullosa so severe that approximately 80% of his total body surface area was affected. The patient had a genetic mutation that had resulted in blisters on much of his body since birth. Approximately 6 weeks prior to his hospital admission, he developed Staphylococcus aureus and Pseudomonas aeruginosa infections that worsened his condition. After other treatments failed, the patient’s parents consented to a combination of ex vivo cell and gene therapy, in which cultures taken from a biopsy of uninvolved skin were used to develop transgenic epidermal grafts. The grafts were applied sequentially on a dermal wound bed.
“Virtually complete epidermal regeneration was observed after 1 month,” Dr. Hirsch and associates wrote. Over 21 months, the regenerated epidermis healed and remained stable even when subjected to mechanical stress.
For follow-up, the researchers reported on 10 punch biopsies taken at 4, 8, and 21 months after the grafting procedure. “The epidermis had normal morphology and we could not detect blisters, erosions, or epidermal detachment from the underlying dermis,” they noted.
The patient has remained stable since being discharged from the hospital in February 2016, and requires no ointment or medications to maintain a healthy epidermis, they said.
“This approach would be optimal for newly diagnosed patients early in their childhood,” Dr. Hirsch and associates noted. “A bank of transduced epidermal stem cells taken at birth could be used to treat skin lesions while they develop, thus preventing, rather than restoring, the devastating clinical manifestation that arise in these patients.
The study was supported in part by several government grants from organizations including the Italian Ministry of Education and the European Research. Two of the researchers are cofounders and members of the Board of Directors of Holostem Terapie Avanzate, which met all costs of good manufacturing practice production and procedures of transgenic epidermal grafts.
FROM NATURE
Herbal supplements offer value with cautions, caveats
CHICAGO – Nearly one in five people who take prescription medications also take herbal or mineral supplements, so emphasized Cora Breuner, MD, MPH, a professor of pediatrics at the University of Washington in Seattle.
“In chronically ill children, almost 80% to 90% of kids are using supplements, so it’s really almost imperative that this be asked when you’re taking your histories, not in the social history, but when you’re asking about medications,” Dr. Breuner told attendees at the annual meeting of the American Academy of Pediatrics. “Remember to ask it, and remember to ask it every time because it makes the patient actually realize it’s something like a medication, and so you can get the drug-herb interactions.”
Providers also should be familiar with the evidence base for complementary and alternative medicine (CAM). According to the 2012 U.S. National Health Interview Survey, which included 10,218 youths, 11.6% of those aged 4-17 years had taken or used some type of complementary health product within the previous year. Fish oil/omega-3 fatty acid supplements, melatonin, probiotics/prebiotics, and echinacea topped the list.
“For children, complementary approaches were most often used for back or neck pain, other musculoskeletal conditions, head or chest colds, anxiety or stress, attention-deficit hyperactivity disorder [ADHD], and insomnia or trouble sleeping,” Dr. Breuner said.
Regulation of herbal and other supplements
Dietary supplements, including vitamins, minerals, and herbal remedies, are regulated under the Dietary Supplement Health and Education Act of 1994 (DSHEA) – not the Food and Drug Administration. Not only can products enter the market without any testing for efficacy, but companies only have to provide “reasonable assurance” of a product’s safety, not proof.
“Supplements do not have to be manufactured according to any standards,” Dr. Breuner said, although reputable manufacturers support standards. “It’s basically up to the company that manufactures it to make sure the product is not contaminated and that the product is basically consistent. There’s no need whatsoever for the company to make sure it works.”
Yet many patients and parents don’t realize that, she said.
“It’s important for people to be aware that this is not a regulated industry per se by the federal government,” she said. “Patients really do think that it is.”
One voluntary quality indicator is the United States Pharmacopeia Dietary Supplement Verification Program, identified by a USP “dietary supplement verified” logo. ConsumerLab.com also provides an “approved quality” logo, tests samples voluntarily sent by manufacturers, and rates the quality of different brands.
“Supplements may not claim to cure or prevent a disease, but they can say how it affects the body’s structure and function,” she said, and companies do not need FDA approval for packaging or marketing claims. In this low regulatory environment, substantial variations exist in the quality and quantity of biological ingredients in marketed supplements.
Risks from herbal supplements
Dr. Breuner cited a 2011 study finding that 75% of 68 products tested had no key safety messages, including all 12 ginkgo products and all but 1 of the 21 garlic and seven Asian ginseng products tested. Most of the 13 echinacea products also lacked safety messages, but two-thirds of the 12 St John’s wort products did have safety information.
Risks can include contamination, inadequate packaging information, and unknown toxicities and interactions. Adverse reactions should be reported to the Food and Drug Administration’s MedWatch at 800-FDA-1088 (fax: 800-FDA-0178) and to Poison Control at 800-222-1222.
Two popular herbal remedies that are unsafe for children include licorice and ephedra. Although it is used for peptic ulcers, licorice lacks much evidence backing it and also shouldn’t be used (or eaten) during pregnancy. Ephedra (ma huang), an appetite suppressant and decongestant, can cause heart palpitations, heart attacks, and death.
“You can still get ephedra over the Internet, but it’s very, very dangerous,” Dr. Breuner said.
Dr. Breuner listed other herbal products available online but deemed unsafe for children: aconite (also known as bushi), species from the genus Aristolochia, belladonna, blue cohosh, borage, broom, calamus, chaparral, coltsfoot, comfrey, germander, life root, lobelia, pennyroyal, poke root, sassafras, skullcap, tansy ragwort, and wormwood.
Another set of herbs can be dangerous prior to surgery, she said, noting that an estimated 26% of patients scheduled for surgery use herbal products.
“Many, many of the herbs cause platelet aggregation issues,” Dr. Breuner said, so it’s very important to ask about different herbs before surgeries. Patients should discontinue echinacea, ephedra, garlic, ginkgo, ginseng, kava, St. John’s wort, and valerian before surgery. Risks include cardiovascular instability, prolonged sedation, bleeding, electrolyte disturbances, and immunosuppression. Additionally, four supplements also adversely interact with warfarin: garlic, ginger, and feverfew have additive effects (although small dietary amounts of ginger and garlic are fine), and St. John’s wort can decrease warfarin’s effects.
Dr. Breuner urged attendees to use resources like PubMed Dietary Supplement Subset to find out more about supplements; this subset limits results of a PubMed search of citations and abstracts to just those related to dietary supplements. It was created through a partnership between the Office of Dietary Supplements and the National Library of Medicine, both parts of the National Institutes of Health.
Information on specific herbs
Ginkgo. Although commonly used to boost memory and concentration, only limited studies in adults shows some potential benefit from ginkgo at 40 mg three times a day. “There isn’t any evidence to show any reason to use it in children,” Dr. Breuner said. Adverse effects can include gastrointestinal irritation, headache, bleeding, and contact dermatitis.
Echinacea. Although people use echinacea to treat or prevent the common cold or upper respiratory infections, the evidence does not show significant reductions of incidence, duration, or severity of upper respiratory infections and common colds. Anyone immunocompromised with an allergy or autoimmune disease should not take it.
Zinc. Some evidence from a pediatric Cochrane Review, albeit with heterogeneous studies, supports using 75 mg of zinc a day to reduce duration of common cold and sore throat symptoms in healthy people. Adverse effects include a bad taste, nausea, and anosmia.
Valerian. Children can take 400 mg nightly of valerian to help with sleep, although there are some caveats.
“The problem with Valerian is that it takes 2-6 weeks before it has any effect,” Breuner said. “It tastes terrible, and it’s only in a capsule form. It isn’t dosed for age at all, so you have to be careful about this, and it’s not like Ambien,” she added. It does not work instantaneously, and stopping it abruptly can cause withdrawal symptoms, although she would recommend it over melatonin. Despite its use for sleep, it can have adverse effects, such as anxiety, restlessness, and heart palpitations, and it can interfere with barbiturates.
St. John’s wort. No one is quite sure how it works, but research has shown St. John’s wort extracts can treat mild to moderate depression about as well as standard antidepressants. However, the dose is 300 mg three times a day. “There’s no St. John’s XL,” Dr. Breuner joked. It can also interfere with a wide range of prescribed medications, including oral contraception.
Butterbur. Those taking pyrrolizidine alkaloids should avoid butterbur, but it otherwise can help prevent migraine when dosed at 50-75 mg daily divided up into 2-3 for ages 8-9 years and 100-150 mg daily divided up into 2-3 for ages 10-17 years. “Most of the neurologists at my institution are recommending butterbur,” Dr. Breuner said. “It’s not an abortive, but it’s a preventive, with decreased intensity and severity in childhood migraine 6 weeks after using it. This is absolutely something to consider in your patients with chronic headaches.” Adverse effects include diarrhea, stomach upset, belching, and dermal and allergic symptoms, such as itchy eyes, asthma, and rash.
Magnesium. Also recommended by pediatric neurologists at her institution, 300-500 mg daily of magnesium can reduce migraine incidence, but doses should be titrated up at first. “Don’t start with the higher doses,” she said. “You have to be careful about starting at too high of a dose because of diarrhea,” which is its primary adverse effect. Magnesium also can interfere with bisphosphonates, antibiotics, and diuretics; proton pump inhibitors may reduce magnesium levels.
Melatonin. Unlike most supplements that are herbal or mineral, melatonin is a synthetic hormone, but Dr. Breuner said many patients don’t realize that. “Because it’s a hormone, I’m very, very careful about it,” she said, never recommending more than 0.5 to 5 mg a night for help falling asleep. “I’m really not a fan of melatonin,” she said. “You develop a tolerance to it, and this is not something parents or children should be taking chronically because we do not know long-term outcomes at all. It’s not benign even though you can just toss it into your grocery basket.”
She briefly wrapped up with mentions of omega-3 fatty acid supplements (docosahexaenoic acid and eicosapentaenoic acid); most of the evidence for these supplements comes from adults with psychiatric disorders. However, one study showed reduced tics in children with Tourette’s – if they can stand the fishy taste. It also can cause belching, nosebleeds, nausea, loose stools, and, at higher doses, decreased blood coagulation.
Peppermint can be used to reduce nausea, coughs, anxiety, and irritable bowel syndrome symptoms, but it needs to be taken as 1-2 enteric capsules, not as tea or another form.
“Chamomile is very helpful for generalized colic and also for those with chronic anxiety,” Dr. Breuner said, and arnica can be used topically for bruising. Ginger also can be used to reduce nausea but can cause heartburn. A combination of peppermint, chamomile, arnica, and ginger may be appropriate to address various chemotherapy symptoms in a child, she said.
Several articles are useful for looking up interactions between herbs and drugs, including Pediatrics. 2017. doi: 10.1542/peds.2010-2720C; J Emerg Med. 2005 Apr;28(3):267-71; and Clin Med (Lond). 2013 Feb;13(1):7-12.
No funding was used for this presentation, and Dr. Breuner reported having no disclosures.
CHICAGO – Nearly one in five people who take prescription medications also take herbal or mineral supplements, so emphasized Cora Breuner, MD, MPH, a professor of pediatrics at the University of Washington in Seattle.
“In chronically ill children, almost 80% to 90% of kids are using supplements, so it’s really almost imperative that this be asked when you’re taking your histories, not in the social history, but when you’re asking about medications,” Dr. Breuner told attendees at the annual meeting of the American Academy of Pediatrics. “Remember to ask it, and remember to ask it every time because it makes the patient actually realize it’s something like a medication, and so you can get the drug-herb interactions.”
Providers also should be familiar with the evidence base for complementary and alternative medicine (CAM). According to the 2012 U.S. National Health Interview Survey, which included 10,218 youths, 11.6% of those aged 4-17 years had taken or used some type of complementary health product within the previous year. Fish oil/omega-3 fatty acid supplements, melatonin, probiotics/prebiotics, and echinacea topped the list.
“For children, complementary approaches were most often used for back or neck pain, other musculoskeletal conditions, head or chest colds, anxiety or stress, attention-deficit hyperactivity disorder [ADHD], and insomnia or trouble sleeping,” Dr. Breuner said.
Regulation of herbal and other supplements
Dietary supplements, including vitamins, minerals, and herbal remedies, are regulated under the Dietary Supplement Health and Education Act of 1994 (DSHEA) – not the Food and Drug Administration. Not only can products enter the market without any testing for efficacy, but companies only have to provide “reasonable assurance” of a product’s safety, not proof.
“Supplements do not have to be manufactured according to any standards,” Dr. Breuner said, although reputable manufacturers support standards. “It’s basically up to the company that manufactures it to make sure the product is not contaminated and that the product is basically consistent. There’s no need whatsoever for the company to make sure it works.”
Yet many patients and parents don’t realize that, she said.
“It’s important for people to be aware that this is not a regulated industry per se by the federal government,” she said. “Patients really do think that it is.”
One voluntary quality indicator is the United States Pharmacopeia Dietary Supplement Verification Program, identified by a USP “dietary supplement verified” logo. ConsumerLab.com also provides an “approved quality” logo, tests samples voluntarily sent by manufacturers, and rates the quality of different brands.
“Supplements may not claim to cure or prevent a disease, but they can say how it affects the body’s structure and function,” she said, and companies do not need FDA approval for packaging or marketing claims. In this low regulatory environment, substantial variations exist in the quality and quantity of biological ingredients in marketed supplements.
Risks from herbal supplements
Dr. Breuner cited a 2011 study finding that 75% of 68 products tested had no key safety messages, including all 12 ginkgo products and all but 1 of the 21 garlic and seven Asian ginseng products tested. Most of the 13 echinacea products also lacked safety messages, but two-thirds of the 12 St John’s wort products did have safety information.
Risks can include contamination, inadequate packaging information, and unknown toxicities and interactions. Adverse reactions should be reported to the Food and Drug Administration’s MedWatch at 800-FDA-1088 (fax: 800-FDA-0178) and to Poison Control at 800-222-1222.
Two popular herbal remedies that are unsafe for children include licorice and ephedra. Although it is used for peptic ulcers, licorice lacks much evidence backing it and also shouldn’t be used (or eaten) during pregnancy. Ephedra (ma huang), an appetite suppressant and decongestant, can cause heart palpitations, heart attacks, and death.
“You can still get ephedra over the Internet, but it’s very, very dangerous,” Dr. Breuner said.
Dr. Breuner listed other herbal products available online but deemed unsafe for children: aconite (also known as bushi), species from the genus Aristolochia, belladonna, blue cohosh, borage, broom, calamus, chaparral, coltsfoot, comfrey, germander, life root, lobelia, pennyroyal, poke root, sassafras, skullcap, tansy ragwort, and wormwood.
Another set of herbs can be dangerous prior to surgery, she said, noting that an estimated 26% of patients scheduled for surgery use herbal products.
“Many, many of the herbs cause platelet aggregation issues,” Dr. Breuner said, so it’s very important to ask about different herbs before surgeries. Patients should discontinue echinacea, ephedra, garlic, ginkgo, ginseng, kava, St. John’s wort, and valerian before surgery. Risks include cardiovascular instability, prolonged sedation, bleeding, electrolyte disturbances, and immunosuppression. Additionally, four supplements also adversely interact with warfarin: garlic, ginger, and feverfew have additive effects (although small dietary amounts of ginger and garlic are fine), and St. John’s wort can decrease warfarin’s effects.
Dr. Breuner urged attendees to use resources like PubMed Dietary Supplement Subset to find out more about supplements; this subset limits results of a PubMed search of citations and abstracts to just those related to dietary supplements. It was created through a partnership between the Office of Dietary Supplements and the National Library of Medicine, both parts of the National Institutes of Health.
Information on specific herbs
Ginkgo. Although commonly used to boost memory and concentration, only limited studies in adults shows some potential benefit from ginkgo at 40 mg three times a day. “There isn’t any evidence to show any reason to use it in children,” Dr. Breuner said. Adverse effects can include gastrointestinal irritation, headache, bleeding, and contact dermatitis.
Echinacea. Although people use echinacea to treat or prevent the common cold or upper respiratory infections, the evidence does not show significant reductions of incidence, duration, or severity of upper respiratory infections and common colds. Anyone immunocompromised with an allergy or autoimmune disease should not take it.
Zinc. Some evidence from a pediatric Cochrane Review, albeit with heterogeneous studies, supports using 75 mg of zinc a day to reduce duration of common cold and sore throat symptoms in healthy people. Adverse effects include a bad taste, nausea, and anosmia.
Valerian. Children can take 400 mg nightly of valerian to help with sleep, although there are some caveats.
“The problem with Valerian is that it takes 2-6 weeks before it has any effect,” Breuner said. “It tastes terrible, and it’s only in a capsule form. It isn’t dosed for age at all, so you have to be careful about this, and it’s not like Ambien,” she added. It does not work instantaneously, and stopping it abruptly can cause withdrawal symptoms, although she would recommend it over melatonin. Despite its use for sleep, it can have adverse effects, such as anxiety, restlessness, and heart palpitations, and it can interfere with barbiturates.
St. John’s wort. No one is quite sure how it works, but research has shown St. John’s wort extracts can treat mild to moderate depression about as well as standard antidepressants. However, the dose is 300 mg three times a day. “There’s no St. John’s XL,” Dr. Breuner joked. It can also interfere with a wide range of prescribed medications, including oral contraception.
Butterbur. Those taking pyrrolizidine alkaloids should avoid butterbur, but it otherwise can help prevent migraine when dosed at 50-75 mg daily divided up into 2-3 for ages 8-9 years and 100-150 mg daily divided up into 2-3 for ages 10-17 years. “Most of the neurologists at my institution are recommending butterbur,” Dr. Breuner said. “It’s not an abortive, but it’s a preventive, with decreased intensity and severity in childhood migraine 6 weeks after using it. This is absolutely something to consider in your patients with chronic headaches.” Adverse effects include diarrhea, stomach upset, belching, and dermal and allergic symptoms, such as itchy eyes, asthma, and rash.
Magnesium. Also recommended by pediatric neurologists at her institution, 300-500 mg daily of magnesium can reduce migraine incidence, but doses should be titrated up at first. “Don’t start with the higher doses,” she said. “You have to be careful about starting at too high of a dose because of diarrhea,” which is its primary adverse effect. Magnesium also can interfere with bisphosphonates, antibiotics, and diuretics; proton pump inhibitors may reduce magnesium levels.
Melatonin. Unlike most supplements that are herbal or mineral, melatonin is a synthetic hormone, but Dr. Breuner said many patients don’t realize that. “Because it’s a hormone, I’m very, very careful about it,” she said, never recommending more than 0.5 to 5 mg a night for help falling asleep. “I’m really not a fan of melatonin,” she said. “You develop a tolerance to it, and this is not something parents or children should be taking chronically because we do not know long-term outcomes at all. It’s not benign even though you can just toss it into your grocery basket.”
She briefly wrapped up with mentions of omega-3 fatty acid supplements (docosahexaenoic acid and eicosapentaenoic acid); most of the evidence for these supplements comes from adults with psychiatric disorders. However, one study showed reduced tics in children with Tourette’s – if they can stand the fishy taste. It also can cause belching, nosebleeds, nausea, loose stools, and, at higher doses, decreased blood coagulation.
Peppermint can be used to reduce nausea, coughs, anxiety, and irritable bowel syndrome symptoms, but it needs to be taken as 1-2 enteric capsules, not as tea or another form.
“Chamomile is very helpful for generalized colic and also for those with chronic anxiety,” Dr. Breuner said, and arnica can be used topically for bruising. Ginger also can be used to reduce nausea but can cause heartburn. A combination of peppermint, chamomile, arnica, and ginger may be appropriate to address various chemotherapy symptoms in a child, she said.
Several articles are useful for looking up interactions between herbs and drugs, including Pediatrics. 2017. doi: 10.1542/peds.2010-2720C; J Emerg Med. 2005 Apr;28(3):267-71; and Clin Med (Lond). 2013 Feb;13(1):7-12.
No funding was used for this presentation, and Dr. Breuner reported having no disclosures.
CHICAGO – Nearly one in five people who take prescription medications also take herbal or mineral supplements, so emphasized Cora Breuner, MD, MPH, a professor of pediatrics at the University of Washington in Seattle.
“In chronically ill children, almost 80% to 90% of kids are using supplements, so it’s really almost imperative that this be asked when you’re taking your histories, not in the social history, but when you’re asking about medications,” Dr. Breuner told attendees at the annual meeting of the American Academy of Pediatrics. “Remember to ask it, and remember to ask it every time because it makes the patient actually realize it’s something like a medication, and so you can get the drug-herb interactions.”
Providers also should be familiar with the evidence base for complementary and alternative medicine (CAM). According to the 2012 U.S. National Health Interview Survey, which included 10,218 youths, 11.6% of those aged 4-17 years had taken or used some type of complementary health product within the previous year. Fish oil/omega-3 fatty acid supplements, melatonin, probiotics/prebiotics, and echinacea topped the list.
“For children, complementary approaches were most often used for back or neck pain, other musculoskeletal conditions, head or chest colds, anxiety or stress, attention-deficit hyperactivity disorder [ADHD], and insomnia or trouble sleeping,” Dr. Breuner said.
Regulation of herbal and other supplements
Dietary supplements, including vitamins, minerals, and herbal remedies, are regulated under the Dietary Supplement Health and Education Act of 1994 (DSHEA) – not the Food and Drug Administration. Not only can products enter the market without any testing for efficacy, but companies only have to provide “reasonable assurance” of a product’s safety, not proof.
“Supplements do not have to be manufactured according to any standards,” Dr. Breuner said, although reputable manufacturers support standards. “It’s basically up to the company that manufactures it to make sure the product is not contaminated and that the product is basically consistent. There’s no need whatsoever for the company to make sure it works.”
Yet many patients and parents don’t realize that, she said.
“It’s important for people to be aware that this is not a regulated industry per se by the federal government,” she said. “Patients really do think that it is.”
One voluntary quality indicator is the United States Pharmacopeia Dietary Supplement Verification Program, identified by a USP “dietary supplement verified” logo. ConsumerLab.com also provides an “approved quality” logo, tests samples voluntarily sent by manufacturers, and rates the quality of different brands.
“Supplements may not claim to cure or prevent a disease, but they can say how it affects the body’s structure and function,” she said, and companies do not need FDA approval for packaging or marketing claims. In this low regulatory environment, substantial variations exist in the quality and quantity of biological ingredients in marketed supplements.
Risks from herbal supplements
Dr. Breuner cited a 2011 study finding that 75% of 68 products tested had no key safety messages, including all 12 ginkgo products and all but 1 of the 21 garlic and seven Asian ginseng products tested. Most of the 13 echinacea products also lacked safety messages, but two-thirds of the 12 St John’s wort products did have safety information.
Risks can include contamination, inadequate packaging information, and unknown toxicities and interactions. Adverse reactions should be reported to the Food and Drug Administration’s MedWatch at 800-FDA-1088 (fax: 800-FDA-0178) and to Poison Control at 800-222-1222.
Two popular herbal remedies that are unsafe for children include licorice and ephedra. Although it is used for peptic ulcers, licorice lacks much evidence backing it and also shouldn’t be used (or eaten) during pregnancy. Ephedra (ma huang), an appetite suppressant and decongestant, can cause heart palpitations, heart attacks, and death.
“You can still get ephedra over the Internet, but it’s very, very dangerous,” Dr. Breuner said.
Dr. Breuner listed other herbal products available online but deemed unsafe for children: aconite (also known as bushi), species from the genus Aristolochia, belladonna, blue cohosh, borage, broom, calamus, chaparral, coltsfoot, comfrey, germander, life root, lobelia, pennyroyal, poke root, sassafras, skullcap, tansy ragwort, and wormwood.
Another set of herbs can be dangerous prior to surgery, she said, noting that an estimated 26% of patients scheduled for surgery use herbal products.
“Many, many of the herbs cause platelet aggregation issues,” Dr. Breuner said, so it’s very important to ask about different herbs before surgeries. Patients should discontinue echinacea, ephedra, garlic, ginkgo, ginseng, kava, St. John’s wort, and valerian before surgery. Risks include cardiovascular instability, prolonged sedation, bleeding, electrolyte disturbances, and immunosuppression. Additionally, four supplements also adversely interact with warfarin: garlic, ginger, and feverfew have additive effects (although small dietary amounts of ginger and garlic are fine), and St. John’s wort can decrease warfarin’s effects.
Dr. Breuner urged attendees to use resources like PubMed Dietary Supplement Subset to find out more about supplements; this subset limits results of a PubMed search of citations and abstracts to just those related to dietary supplements. It was created through a partnership between the Office of Dietary Supplements and the National Library of Medicine, both parts of the National Institutes of Health.
Information on specific herbs
Ginkgo. Although commonly used to boost memory and concentration, only limited studies in adults shows some potential benefit from ginkgo at 40 mg three times a day. “There isn’t any evidence to show any reason to use it in children,” Dr. Breuner said. Adverse effects can include gastrointestinal irritation, headache, bleeding, and contact dermatitis.
Echinacea. Although people use echinacea to treat or prevent the common cold or upper respiratory infections, the evidence does not show significant reductions of incidence, duration, or severity of upper respiratory infections and common colds. Anyone immunocompromised with an allergy or autoimmune disease should not take it.
Zinc. Some evidence from a pediatric Cochrane Review, albeit with heterogeneous studies, supports using 75 mg of zinc a day to reduce duration of common cold and sore throat symptoms in healthy people. Adverse effects include a bad taste, nausea, and anosmia.
Valerian. Children can take 400 mg nightly of valerian to help with sleep, although there are some caveats.
“The problem with Valerian is that it takes 2-6 weeks before it has any effect,” Breuner said. “It tastes terrible, and it’s only in a capsule form. It isn’t dosed for age at all, so you have to be careful about this, and it’s not like Ambien,” she added. It does not work instantaneously, and stopping it abruptly can cause withdrawal symptoms, although she would recommend it over melatonin. Despite its use for sleep, it can have adverse effects, such as anxiety, restlessness, and heart palpitations, and it can interfere with barbiturates.
St. John’s wort. No one is quite sure how it works, but research has shown St. John’s wort extracts can treat mild to moderate depression about as well as standard antidepressants. However, the dose is 300 mg three times a day. “There’s no St. John’s XL,” Dr. Breuner joked. It can also interfere with a wide range of prescribed medications, including oral contraception.
Butterbur. Those taking pyrrolizidine alkaloids should avoid butterbur, but it otherwise can help prevent migraine when dosed at 50-75 mg daily divided up into 2-3 for ages 8-9 years and 100-150 mg daily divided up into 2-3 for ages 10-17 years. “Most of the neurologists at my institution are recommending butterbur,” Dr. Breuner said. “It’s not an abortive, but it’s a preventive, with decreased intensity and severity in childhood migraine 6 weeks after using it. This is absolutely something to consider in your patients with chronic headaches.” Adverse effects include diarrhea, stomach upset, belching, and dermal and allergic symptoms, such as itchy eyes, asthma, and rash.
Magnesium. Also recommended by pediatric neurologists at her institution, 300-500 mg daily of magnesium can reduce migraine incidence, but doses should be titrated up at first. “Don’t start with the higher doses,” she said. “You have to be careful about starting at too high of a dose because of diarrhea,” which is its primary adverse effect. Magnesium also can interfere with bisphosphonates, antibiotics, and diuretics; proton pump inhibitors may reduce magnesium levels.
Melatonin. Unlike most supplements that are herbal or mineral, melatonin is a synthetic hormone, but Dr. Breuner said many patients don’t realize that. “Because it’s a hormone, I’m very, very careful about it,” she said, never recommending more than 0.5 to 5 mg a night for help falling asleep. “I’m really not a fan of melatonin,” she said. “You develop a tolerance to it, and this is not something parents or children should be taking chronically because we do not know long-term outcomes at all. It’s not benign even though you can just toss it into your grocery basket.”
She briefly wrapped up with mentions of omega-3 fatty acid supplements (docosahexaenoic acid and eicosapentaenoic acid); most of the evidence for these supplements comes from adults with psychiatric disorders. However, one study showed reduced tics in children with Tourette’s – if they can stand the fishy taste. It also can cause belching, nosebleeds, nausea, loose stools, and, at higher doses, decreased blood coagulation.
Peppermint can be used to reduce nausea, coughs, anxiety, and irritable bowel syndrome symptoms, but it needs to be taken as 1-2 enteric capsules, not as tea or another form.
“Chamomile is very helpful for generalized colic and also for those with chronic anxiety,” Dr. Breuner said, and arnica can be used topically for bruising. Ginger also can be used to reduce nausea but can cause heartburn. A combination of peppermint, chamomile, arnica, and ginger may be appropriate to address various chemotherapy symptoms in a child, she said.
Several articles are useful for looking up interactions between herbs and drugs, including Pediatrics. 2017. doi: 10.1542/peds.2010-2720C; J Emerg Med. 2005 Apr;28(3):267-71; and Clin Med (Lond). 2013 Feb;13(1):7-12.
No funding was used for this presentation, and Dr. Breuner reported having no disclosures.
EXPERT ANALYSIS FROM AAP 2017
Vaccine coverage high among U.S. toddlers in 2016, but gaps remain
, said Holly A. Hill, MD, PhD, and her associates at the National Center for Immunization and Respiratory Diseases, Atlanta.
Coverage still was below 90% for vaccines that needed booster doses during the second year of life (four or more doses of DTaP and pneumococcal conjugate vaccine [PCV] and Haemophilus influenzae type b [Hib] full series) and for other recommended vaccines (hepatitis B [HepB] birth dose, rotavirus, and hepatitis A [HepA]), they reported in Morbidity and Mortality Weekly Report.
Coverage was estimated to be 61% for two or more doses of HepA vaccine, 71% of the HepB birth dose, 74% of a completed series of rotavirus vaccine, and 71% of the combined seven-vaccine series (four or more doses of DTaP; three or more doses of poliovirus vaccine; one or more doses of measles-containing vaccine; three or four doses of Hib [depending upon product type of vaccine]; three or more doses of HepB; one or more doses of varicella vaccine; and four or more doses of PCV).
Fewer than 1% of children received no vaccinations.
Coverage of most vaccines in 2016 was lower in non-Hispanic black children, compared with non-Hispanic white children. It also was lower for children living below the federal poverty level, compared with children living at or above the poverty level. For Medicaid children, vaccination coverage was lower by 3%-13% than among children who had private insurance; for children with no insurance, vaccination coverage was lower by 12%-25% than among children with private insurance, the investigators reported.
Uninsured children “are eligible for the Vaccines for Children (VFC) program, which was designed to increase access to vaccination among children through age 18 years who might not otherwise be vaccinated because of inability to pay,” the researchers said. “Some families might not be aware of the VFC program, be unable to afford fees associated with visits to a vaccine provider, or might need assistance locating a physician who participates in the VFC program. Children living below poverty and up to a certain percentage above the poverty level are eligible for Medicaid … and are entitled to VFC vaccines.”
The investigators cited language barriers, lack of trust in providers, transportation problems, inconvenient office hours, and other provider- and system-level factors as health care–access barriers among publicly insured children.
“These data indicate that the immunization safety net is not reaching all children early in life,” Dr. Hill and her associates said. “Health care providers can increase vaccination coverage using evidence-based strategies such as provider reminders, standing orders to provide vaccination whenever appropriate, and immunization information systems” such as www.thecommunityguide.org/topic/vaccination.
Read more in MMWR (2017 Nov 3;66[43]:1171-7).
, said Holly A. Hill, MD, PhD, and her associates at the National Center for Immunization and Respiratory Diseases, Atlanta.
Coverage still was below 90% for vaccines that needed booster doses during the second year of life (four or more doses of DTaP and pneumococcal conjugate vaccine [PCV] and Haemophilus influenzae type b [Hib] full series) and for other recommended vaccines (hepatitis B [HepB] birth dose, rotavirus, and hepatitis A [HepA]), they reported in Morbidity and Mortality Weekly Report.
Coverage was estimated to be 61% for two or more doses of HepA vaccine, 71% of the HepB birth dose, 74% of a completed series of rotavirus vaccine, and 71% of the combined seven-vaccine series (four or more doses of DTaP; three or more doses of poliovirus vaccine; one or more doses of measles-containing vaccine; three or four doses of Hib [depending upon product type of vaccine]; three or more doses of HepB; one or more doses of varicella vaccine; and four or more doses of PCV).
Fewer than 1% of children received no vaccinations.
Coverage of most vaccines in 2016 was lower in non-Hispanic black children, compared with non-Hispanic white children. It also was lower for children living below the federal poverty level, compared with children living at or above the poverty level. For Medicaid children, vaccination coverage was lower by 3%-13% than among children who had private insurance; for children with no insurance, vaccination coverage was lower by 12%-25% than among children with private insurance, the investigators reported.
Uninsured children “are eligible for the Vaccines for Children (VFC) program, which was designed to increase access to vaccination among children through age 18 years who might not otherwise be vaccinated because of inability to pay,” the researchers said. “Some families might not be aware of the VFC program, be unable to afford fees associated with visits to a vaccine provider, or might need assistance locating a physician who participates in the VFC program. Children living below poverty and up to a certain percentage above the poverty level are eligible for Medicaid … and are entitled to VFC vaccines.”
The investigators cited language barriers, lack of trust in providers, transportation problems, inconvenient office hours, and other provider- and system-level factors as health care–access barriers among publicly insured children.
“These data indicate that the immunization safety net is not reaching all children early in life,” Dr. Hill and her associates said. “Health care providers can increase vaccination coverage using evidence-based strategies such as provider reminders, standing orders to provide vaccination whenever appropriate, and immunization information systems” such as www.thecommunityguide.org/topic/vaccination.
Read more in MMWR (2017 Nov 3;66[43]:1171-7).
, said Holly A. Hill, MD, PhD, and her associates at the National Center for Immunization and Respiratory Diseases, Atlanta.
Coverage still was below 90% for vaccines that needed booster doses during the second year of life (four or more doses of DTaP and pneumococcal conjugate vaccine [PCV] and Haemophilus influenzae type b [Hib] full series) and for other recommended vaccines (hepatitis B [HepB] birth dose, rotavirus, and hepatitis A [HepA]), they reported in Morbidity and Mortality Weekly Report.
Coverage was estimated to be 61% for two or more doses of HepA vaccine, 71% of the HepB birth dose, 74% of a completed series of rotavirus vaccine, and 71% of the combined seven-vaccine series (four or more doses of DTaP; three or more doses of poliovirus vaccine; one or more doses of measles-containing vaccine; three or four doses of Hib [depending upon product type of vaccine]; three or more doses of HepB; one or more doses of varicella vaccine; and four or more doses of PCV).
Fewer than 1% of children received no vaccinations.
Coverage of most vaccines in 2016 was lower in non-Hispanic black children, compared with non-Hispanic white children. It also was lower for children living below the federal poverty level, compared with children living at or above the poverty level. For Medicaid children, vaccination coverage was lower by 3%-13% than among children who had private insurance; for children with no insurance, vaccination coverage was lower by 12%-25% than among children with private insurance, the investigators reported.
Uninsured children “are eligible for the Vaccines for Children (VFC) program, which was designed to increase access to vaccination among children through age 18 years who might not otherwise be vaccinated because of inability to pay,” the researchers said. “Some families might not be aware of the VFC program, be unable to afford fees associated with visits to a vaccine provider, or might need assistance locating a physician who participates in the VFC program. Children living below poverty and up to a certain percentage above the poverty level are eligible for Medicaid … and are entitled to VFC vaccines.”
The investigators cited language barriers, lack of trust in providers, transportation problems, inconvenient office hours, and other provider- and system-level factors as health care–access barriers among publicly insured children.
“These data indicate that the immunization safety net is not reaching all children early in life,” Dr. Hill and her associates said. “Health care providers can increase vaccination coverage using evidence-based strategies such as provider reminders, standing orders to provide vaccination whenever appropriate, and immunization information systems” such as www.thecommunityguide.org/topic/vaccination.
Read more in MMWR (2017 Nov 3;66[43]:1171-7).
FROM MMWR
In children with ALL, physical and emotional effects persist
Among children with average-risk acute lymphoblastic leukemia (ALL), those with impairments in physical and emotional functioning at 2 months after diagnosis are likely to have continuing difficulties over 2 years later, based on the results of a 594-patient study published online in Cancer (2017 Nov 7. doi: 10.1002/cncr.31085).
Evaluations of quality of life and family functioning as early as 2 months after diagnosis identified those at highest risk of continued impairment, and can be used to target patients and their families for interventions and risk factor modification, the researchers said.
“These results provide a compelling rationale to screen patients for physical and emotional functioning early in therapy to target interventions toward patients at the highest risk of later impairment,” wrote lead author Daniel J. Zheng, MD, of the section of pediatric hematology-oncology at Yale University, New Haven, Conn., and coauthors.
Dr. Zheng and his colleagues measured impairments in children with average-risk ALL using the Pediatric Quality of Life Inventory Generic Core Scales Version 4.0 (PedsQL4.0), a 23-item survey that measures a child’s quality of life, and the 12-question General Functioning subscale of the McMaster Family Assessment Device (FAD-GF). Both are quick and low-cost screening measures that can be conducted in the clinic, they added. Evaluations occurred at approximately 2 months, 8 months, 17 months, 26 months, and 38 months (boys only) after diagnosis. The mean age of participants at diagnosis was 6.0 years (standard deviation, 1.6 years).
At 2 months after diagnosis, 36.5% of the children had impairments in physical functioning, and 26.2% had impairments in emotional functioning. The population norms for these measures are 2.3% for both scales, investigators wrote. At a 26-month evaluation, levels of impairment were still 11.9% for physical and 9.8% for emotional functioning.
Boys had an additional 38-month evaluation, at which time there were no significant differences in quality of life outcomes versus those observed at 26 months in the girls.
Unhealthy family functioning was a significant predictor of emotional impairment (odds ratio, 1.5; 95% confidence interval, 1.1-2.1) in multivariate models controlling for age and sex.
Strategies are needed to “intervene early and help the substantial proportion of children” with quality of life impairments, the researchers said. In particular, family functioning is “potentially modifiable with early intervention,” as suggested by a series of promising studies of techniques such as stress management sessions for parents. Most techniques feature a “targeted family-centered approach to psychosocial needs” that includes “embedded psychologists” as part of the multidisciplinary cancer care team.
Study funding came from the National Institutes of Health, National Cancer Institute, and the St. Baldrick’s Foundation. Dr. Zheng reported funding from a Yale Medical Student research fellowship, while coauthors reported conflict of interest disclosures from entities including Amgen, Takeda Pharmaceuticals International, and Shire Pharmaceuticals.
Among children with average-risk acute lymphoblastic leukemia (ALL), those with impairments in physical and emotional functioning at 2 months after diagnosis are likely to have continuing difficulties over 2 years later, based on the results of a 594-patient study published online in Cancer (2017 Nov 7. doi: 10.1002/cncr.31085).
Evaluations of quality of life and family functioning as early as 2 months after diagnosis identified those at highest risk of continued impairment, and can be used to target patients and their families for interventions and risk factor modification, the researchers said.
“These results provide a compelling rationale to screen patients for physical and emotional functioning early in therapy to target interventions toward patients at the highest risk of later impairment,” wrote lead author Daniel J. Zheng, MD, of the section of pediatric hematology-oncology at Yale University, New Haven, Conn., and coauthors.
Dr. Zheng and his colleagues measured impairments in children with average-risk ALL using the Pediatric Quality of Life Inventory Generic Core Scales Version 4.0 (PedsQL4.0), a 23-item survey that measures a child’s quality of life, and the 12-question General Functioning subscale of the McMaster Family Assessment Device (FAD-GF). Both are quick and low-cost screening measures that can be conducted in the clinic, they added. Evaluations occurred at approximately 2 months, 8 months, 17 months, 26 months, and 38 months (boys only) after diagnosis. The mean age of participants at diagnosis was 6.0 years (standard deviation, 1.6 years).
At 2 months after diagnosis, 36.5% of the children had impairments in physical functioning, and 26.2% had impairments in emotional functioning. The population norms for these measures are 2.3% for both scales, investigators wrote. At a 26-month evaluation, levels of impairment were still 11.9% for physical and 9.8% for emotional functioning.
Boys had an additional 38-month evaluation, at which time there were no significant differences in quality of life outcomes versus those observed at 26 months in the girls.
Unhealthy family functioning was a significant predictor of emotional impairment (odds ratio, 1.5; 95% confidence interval, 1.1-2.1) in multivariate models controlling for age and sex.
Strategies are needed to “intervene early and help the substantial proportion of children” with quality of life impairments, the researchers said. In particular, family functioning is “potentially modifiable with early intervention,” as suggested by a series of promising studies of techniques such as stress management sessions for parents. Most techniques feature a “targeted family-centered approach to psychosocial needs” that includes “embedded psychologists” as part of the multidisciplinary cancer care team.
Study funding came from the National Institutes of Health, National Cancer Institute, and the St. Baldrick’s Foundation. Dr. Zheng reported funding from a Yale Medical Student research fellowship, while coauthors reported conflict of interest disclosures from entities including Amgen, Takeda Pharmaceuticals International, and Shire Pharmaceuticals.
Among children with average-risk acute lymphoblastic leukemia (ALL), those with impairments in physical and emotional functioning at 2 months after diagnosis are likely to have continuing difficulties over 2 years later, based on the results of a 594-patient study published online in Cancer (2017 Nov 7. doi: 10.1002/cncr.31085).
Evaluations of quality of life and family functioning as early as 2 months after diagnosis identified those at highest risk of continued impairment, and can be used to target patients and their families for interventions and risk factor modification, the researchers said.
“These results provide a compelling rationale to screen patients for physical and emotional functioning early in therapy to target interventions toward patients at the highest risk of later impairment,” wrote lead author Daniel J. Zheng, MD, of the section of pediatric hematology-oncology at Yale University, New Haven, Conn., and coauthors.
Dr. Zheng and his colleagues measured impairments in children with average-risk ALL using the Pediatric Quality of Life Inventory Generic Core Scales Version 4.0 (PedsQL4.0), a 23-item survey that measures a child’s quality of life, and the 12-question General Functioning subscale of the McMaster Family Assessment Device (FAD-GF). Both are quick and low-cost screening measures that can be conducted in the clinic, they added. Evaluations occurred at approximately 2 months, 8 months, 17 months, 26 months, and 38 months (boys only) after diagnosis. The mean age of participants at diagnosis was 6.0 years (standard deviation, 1.6 years).
At 2 months after diagnosis, 36.5% of the children had impairments in physical functioning, and 26.2% had impairments in emotional functioning. The population norms for these measures are 2.3% for both scales, investigators wrote. At a 26-month evaluation, levels of impairment were still 11.9% for physical and 9.8% for emotional functioning.
Boys had an additional 38-month evaluation, at which time there were no significant differences in quality of life outcomes versus those observed at 26 months in the girls.
Unhealthy family functioning was a significant predictor of emotional impairment (odds ratio, 1.5; 95% confidence interval, 1.1-2.1) in multivariate models controlling for age and sex.
Strategies are needed to “intervene early and help the substantial proportion of children” with quality of life impairments, the researchers said. In particular, family functioning is “potentially modifiable with early intervention,” as suggested by a series of promising studies of techniques such as stress management sessions for parents. Most techniques feature a “targeted family-centered approach to psychosocial needs” that includes “embedded psychologists” as part of the multidisciplinary cancer care team.
Study funding came from the National Institutes of Health, National Cancer Institute, and the St. Baldrick’s Foundation. Dr. Zheng reported funding from a Yale Medical Student research fellowship, while coauthors reported conflict of interest disclosures from entities including Amgen, Takeda Pharmaceuticals International, and Shire Pharmaceuticals.
FROM CANCER
Key clinical point: Simple
Major finding: At 26 months after diagnosis, a considerable proportion of children identified at 2 months after diagnosis still had impairments in physical functioning (11.9%) and emotional functioning (9.8%).
Data source: A prospective cohort study of 594 participants with average-risk ALL in the Children’s Oncology Group AALL0932 trial.
Disclosures: The National Institutes of Health, National Cancer Institute, and St. Baldrick’s Foundation provided funding for the study.