User login
Early childhood vaccines not associated with increased infection risk
There was no significant difference in vaccine antigen exposure through the first 23 months of life between children with non–vaccine-targeted infections and controls between 24 and 47 months of age, according to results published March 6 in JAMA.
This was determined in a nested, matched case-control study of 193 infection cases and 751 controls, in whom estimated mean cumulative vaccine antigen exposure was 240.6 for cases of non–vaccine-targeted infections, and 242.9 for controls, reported Jason M. Glanz, PhD, of Kaiser Permanente Colorado, Denver, and his coauthors. The between-group difference was –2.3 (P = .55), a nonsignificant difference.
Using data from the Centers for Disease Control and Prevention-funded Vaccine Safety Datalink (VSD), the investigators identified children born between Jan. 1, 2003, and Sep. 31, 2013. Exclusion criteria were not having at least two well-child visits before the first birthday, medical contraindications to vaccination, or receiving vaccines not recommended by the Advisory Committee on Immunization Practices. Eligible children were followed through age 47 months or until disenrollment from their health care organization, the authors said.
ICD-9 and ICD-10 codes were used to identify non–vaccine-targeted infections, including upper and lower respiratory infections, gastrointestinal infections, and other viral and bacterial infections from ages 24to 47 months. A medical record review was performed to confirm case status. Cases were included only if it was confirmed that the infection occurred, that it was an incident outcome, that the outcome was the primary reason for the medical visit, that the outcome occurred in the inpatient or emergency department setting, and that there was no evidence that the child was diagnosed as having a vaccine preventable disease (VPD) on the same day as the infection. Controls did not have a VPD or record of a non–vaccine-targeted infection prior to the index date, Dr. Glanz and his colleagues said.
Antigen exposure was measured as the number of immunogenic proteins and polysaccharides in each vaccine, and was estimated from birth through age 23 months in both groups. Cumulative antigen exposure was estimated by adding the number of antigens in each non–vaccine-targeted infection and controls.
Estimated mean cumulative vaccine antigen exposure was 240.6 for cases of non–vaccine-targeted infections, and 242.9 for controls, the authors reported. The matched odds ratio (mOR) for estimated cumulative antigen exposure through age 23 months was not significant in children with infections, compared with controls (mOR = 0.94; 95% confidence interval, 0.84-1.07). The estimated maximum single-day antigen exposure was not significantly associated with non–vaccine-targeted infection (mOR = 1.07; 95% CI, 0.81-1.41).
The findings of this study “did not reveal any beneficial or detrimental associations with estimated cumulative vaccine antigen exposure in young children with non–vaccine-targeted infections in ED and inpatient settings,” wrote Dr. Glanz and coauthors. In addition, the study “did not find evidence that multiple vaccine exposure was associated with the risk for non-targeted infectious diseases.”
The CDC funded the study. The authors reported receiving contracts, grants, and other funding from the CDC.
SOURCE: Glanz JM et al. JAMA. 2018;319(9):906-13.
These results provide “further reassurance about the safety of the U.S. child vaccination schedule,” said Sean T. O’Leary, MD, and Yvonne A. Maldonado, MD.
However, they added, more work must be done to strengthen the public’s trust and confidence in vaccines. Parents long have voiced concerns that vaccines might weaken their children’s immune systems.
“The small but vocal minority of anti-vaccine groups may not be satisfied by the evidence provided through VSD and other vaccine safety surveillance,” they wrote. “Simply providing scientific information and assuming parents will make the decision to vaccinate is not enough.
“Delivering evidence-based information to parents and clinicians in ways that inspire confidence in the robust and safe childhood immunization schedule is critical for maintaining the health of children,” they concluded.
Dr. O’Leary and Dr. Maldonado, both of the University of Colorado, Aurora, commented in an editorial accompanying the article by Glanz et al. (JAMA. 2018 Mar 6;319(9):870-1). Dr. Maldonado reported receiving personal fees for serving on a data and safety monitoring board for Pfizer. Dr. O’Leary reported no relevant financial disclosures.
These results provide “further reassurance about the safety of the U.S. child vaccination schedule,” said Sean T. O’Leary, MD, and Yvonne A. Maldonado, MD.
However, they added, more work must be done to strengthen the public’s trust and confidence in vaccines. Parents long have voiced concerns that vaccines might weaken their children’s immune systems.
“The small but vocal minority of anti-vaccine groups may not be satisfied by the evidence provided through VSD and other vaccine safety surveillance,” they wrote. “Simply providing scientific information and assuming parents will make the decision to vaccinate is not enough.
“Delivering evidence-based information to parents and clinicians in ways that inspire confidence in the robust and safe childhood immunization schedule is critical for maintaining the health of children,” they concluded.
Dr. O’Leary and Dr. Maldonado, both of the University of Colorado, Aurora, commented in an editorial accompanying the article by Glanz et al. (JAMA. 2018 Mar 6;319(9):870-1). Dr. Maldonado reported receiving personal fees for serving on a data and safety monitoring board for Pfizer. Dr. O’Leary reported no relevant financial disclosures.
These results provide “further reassurance about the safety of the U.S. child vaccination schedule,” said Sean T. O’Leary, MD, and Yvonne A. Maldonado, MD.
However, they added, more work must be done to strengthen the public’s trust and confidence in vaccines. Parents long have voiced concerns that vaccines might weaken their children’s immune systems.
“The small but vocal minority of anti-vaccine groups may not be satisfied by the evidence provided through VSD and other vaccine safety surveillance,” they wrote. “Simply providing scientific information and assuming parents will make the decision to vaccinate is not enough.
“Delivering evidence-based information to parents and clinicians in ways that inspire confidence in the robust and safe childhood immunization schedule is critical for maintaining the health of children,” they concluded.
Dr. O’Leary and Dr. Maldonado, both of the University of Colorado, Aurora, commented in an editorial accompanying the article by Glanz et al. (JAMA. 2018 Mar 6;319(9):870-1). Dr. Maldonado reported receiving personal fees for serving on a data and safety monitoring board for Pfizer. Dr. O’Leary reported no relevant financial disclosures.
There was no significant difference in vaccine antigen exposure through the first 23 months of life between children with non–vaccine-targeted infections and controls between 24 and 47 months of age, according to results published March 6 in JAMA.
This was determined in a nested, matched case-control study of 193 infection cases and 751 controls, in whom estimated mean cumulative vaccine antigen exposure was 240.6 for cases of non–vaccine-targeted infections, and 242.9 for controls, reported Jason M. Glanz, PhD, of Kaiser Permanente Colorado, Denver, and his coauthors. The between-group difference was –2.3 (P = .55), a nonsignificant difference.
Using data from the Centers for Disease Control and Prevention-funded Vaccine Safety Datalink (VSD), the investigators identified children born between Jan. 1, 2003, and Sep. 31, 2013. Exclusion criteria were not having at least two well-child visits before the first birthday, medical contraindications to vaccination, or receiving vaccines not recommended by the Advisory Committee on Immunization Practices. Eligible children were followed through age 47 months or until disenrollment from their health care organization, the authors said.
ICD-9 and ICD-10 codes were used to identify non–vaccine-targeted infections, including upper and lower respiratory infections, gastrointestinal infections, and other viral and bacterial infections from ages 24to 47 months. A medical record review was performed to confirm case status. Cases were included only if it was confirmed that the infection occurred, that it was an incident outcome, that the outcome was the primary reason for the medical visit, that the outcome occurred in the inpatient or emergency department setting, and that there was no evidence that the child was diagnosed as having a vaccine preventable disease (VPD) on the same day as the infection. Controls did not have a VPD or record of a non–vaccine-targeted infection prior to the index date, Dr. Glanz and his colleagues said.
Antigen exposure was measured as the number of immunogenic proteins and polysaccharides in each vaccine, and was estimated from birth through age 23 months in both groups. Cumulative antigen exposure was estimated by adding the number of antigens in each non–vaccine-targeted infection and controls.
Estimated mean cumulative vaccine antigen exposure was 240.6 for cases of non–vaccine-targeted infections, and 242.9 for controls, the authors reported. The matched odds ratio (mOR) for estimated cumulative antigen exposure through age 23 months was not significant in children with infections, compared with controls (mOR = 0.94; 95% confidence interval, 0.84-1.07). The estimated maximum single-day antigen exposure was not significantly associated with non–vaccine-targeted infection (mOR = 1.07; 95% CI, 0.81-1.41).
The findings of this study “did not reveal any beneficial or detrimental associations with estimated cumulative vaccine antigen exposure in young children with non–vaccine-targeted infections in ED and inpatient settings,” wrote Dr. Glanz and coauthors. In addition, the study “did not find evidence that multiple vaccine exposure was associated with the risk for non-targeted infectious diseases.”
The CDC funded the study. The authors reported receiving contracts, grants, and other funding from the CDC.
SOURCE: Glanz JM et al. JAMA. 2018;319(9):906-13.
There was no significant difference in vaccine antigen exposure through the first 23 months of life between children with non–vaccine-targeted infections and controls between 24 and 47 months of age, according to results published March 6 in JAMA.
This was determined in a nested, matched case-control study of 193 infection cases and 751 controls, in whom estimated mean cumulative vaccine antigen exposure was 240.6 for cases of non–vaccine-targeted infections, and 242.9 for controls, reported Jason M. Glanz, PhD, of Kaiser Permanente Colorado, Denver, and his coauthors. The between-group difference was –2.3 (P = .55), a nonsignificant difference.
Using data from the Centers for Disease Control and Prevention-funded Vaccine Safety Datalink (VSD), the investigators identified children born between Jan. 1, 2003, and Sep. 31, 2013. Exclusion criteria were not having at least two well-child visits before the first birthday, medical contraindications to vaccination, or receiving vaccines not recommended by the Advisory Committee on Immunization Practices. Eligible children were followed through age 47 months or until disenrollment from their health care organization, the authors said.
ICD-9 and ICD-10 codes were used to identify non–vaccine-targeted infections, including upper and lower respiratory infections, gastrointestinal infections, and other viral and bacterial infections from ages 24to 47 months. A medical record review was performed to confirm case status. Cases were included only if it was confirmed that the infection occurred, that it was an incident outcome, that the outcome was the primary reason for the medical visit, that the outcome occurred in the inpatient or emergency department setting, and that there was no evidence that the child was diagnosed as having a vaccine preventable disease (VPD) on the same day as the infection. Controls did not have a VPD or record of a non–vaccine-targeted infection prior to the index date, Dr. Glanz and his colleagues said.
Antigen exposure was measured as the number of immunogenic proteins and polysaccharides in each vaccine, and was estimated from birth through age 23 months in both groups. Cumulative antigen exposure was estimated by adding the number of antigens in each non–vaccine-targeted infection and controls.
Estimated mean cumulative vaccine antigen exposure was 240.6 for cases of non–vaccine-targeted infections, and 242.9 for controls, the authors reported. The matched odds ratio (mOR) for estimated cumulative antigen exposure through age 23 months was not significant in children with infections, compared with controls (mOR = 0.94; 95% confidence interval, 0.84-1.07). The estimated maximum single-day antigen exposure was not significantly associated with non–vaccine-targeted infection (mOR = 1.07; 95% CI, 0.81-1.41).
The findings of this study “did not reveal any beneficial or detrimental associations with estimated cumulative vaccine antigen exposure in young children with non–vaccine-targeted infections in ED and inpatient settings,” wrote Dr. Glanz and coauthors. In addition, the study “did not find evidence that multiple vaccine exposure was associated with the risk for non-targeted infectious diseases.”
The CDC funded the study. The authors reported receiving contracts, grants, and other funding from the CDC.
SOURCE: Glanz JM et al. JAMA. 2018;319(9):906-13.
FROM JAMA
Key clinical point: No significant difference was found in vaccine antigen exposure between controls and children with infectious diseases not targeted by vaccines.
Major finding: Estimated mean cumulative vaccine antigen exposure was 240.6 for cases and 242.9 for controls.
Study details: A matched case-control study of 944 patients enrolled in six integrated health care organizations as part of the Vaccine Safety Datalink (VSD).
Disclosures: The Centers for Disease Control and Prevention funded the study. The authors reported receiving contracts, grants, and other funding from the CDC.
Source: Glanz JM et al. JAMA. 2018;319(9):906-13.
PICU, hospital admissions up due to opioid ingestion
Hospitalization and pediatric ICU admission rates for pediatric opioid-related ingestion are increasing, along with hospitalization costs, according to a retrospective cohort study.
“In this study, we demonstrate a significant and steady increase in the diagnosis of opioid ingestion and poisoning across all age groups in U.S. children’s hospitals from 2004 to 2015,” wrote Jason Kane, MD, of the University of Chicago, and his associates. “Not only did the absolute number of opioid-related admissions increase but the rate of both hospital and PICU [pediatric ICU] admissions increased as well.”

Using the Pediatric Health Information System database, the research team performed a retrospective cohort study of children aged 1-17 years who had been admitted to a PICU between Jan. 1, 2004, and Sep. 30, 2015. For statistical analysis, the years were grouped into separate epochs: 2004-2007, 2008-2011, and 2012-2015.
Of the 4,175,624 admissions to 31 different children’s hospitals around the United States, 3,647 (0.09%) were due to opioid-related conditions. Across the three epochs of the study, the number of opioid-related hospitalizations more than doubled from 797 to 1,504 and concurrently increased the rate of hospital admissions from 6.7 per 10,000 in 2004 to 10.9 per 10,000 in 2015 (P less than .001).
Similar to the trends in overall hospital admissions and hospital admission rates, admission to the PICU and PICU admission rates also increased. Of the 3,647 children admitted for opioid-related issues, 1,564 (43%) were subsequently admitted to the PICU. PICU admission rates also increased from 25 to 36 per 10,000 admissions (P less than .001).While the majority of opioid-related hospitalizations are associated with children aged 12-17 years, children under the age of 6 years accounted for one-third of these hospitalizations. Many PICU admissions are severe enough to warrant mechanical ventilator support (37%, P less than .001) and vasopressors (20%, P less than .001).
The opioids ingested prior to hospital admission varied between age groups, with 20% (243 of 1,249) patients aged 1-5 years ingesting methadone, compared with 10% (218 of 2,223) of patients aged 12-17 years. Heroin was much more common in this group, accounting for 4.4% (99 of 2,223) of patient hospitalizations.
In addition to the human cost of pediatric hospital admissions, there is a significant economic cost on the health care system. The median cost for PICU admission was $4,931. Although these costs have been dropping for the better part of a decade ($6,523 in 2004-2007 to $4,552 in 2012-2015, P less than .001), it still represents a substantial problem. In addition, admission rates are increasing, which will only place a heavier burden on the health care system, according to Dr. Kane and his associates.
Perhaps one positive point from this study is that although hospitalizations and intensive care rates have gone up, mortality decreased over time from 2.8% in 2004-2007 to 1.3% in 2012-2015.
A possible limitation of the data in this study is that it provides data from subjects whose data is accessible to the researcher, rather than those strategically selected. In addition, referral bias may reduce the ability to generalize the information to non–tertiary care children’s hospitals.
“The current U.S. opioid crisis is negatively impacting pediatric patients as the rate of hospitalization and PICU care for the ingestion of opioids by children continues to increase over time,” wrote Dr. Kane and his associates. “Current efforts to reduce prescription opioid use in adults have not curtailed the incidence of pediatric opioid ingestion, and additional efforts are needed to reduce preventable opioid exposure in children.”
This study had no external funding. Dr. Allison H. Bartlett has served as a consultant member of the CVS Caremark National Pharmacy and Therapeutics Committee. All other authors had no relevant financial disclosures to report.
SOURCE: Kane JM et al. Pediatrics. 2018 Mar 5;141(4):e20173335.
The opioid crisis in the United States is staggering. As of 2016, an estimated 2.4 million Americans were considered to have an opioid use disorder, either from prescription drug misuse or heroin addiction. This number includes 0.6% of adolescents (12- to 17-year-olds) and 1.1% of young adults (18- to 25-year-olds). And 33,000 Americans died from opioid overdose in 2015. Despite the best attempts to control the supply of drugs and increase access to treatment, overdose deaths have doubled in the past 10 years. While the overdose death rate has plateaued among children under the age of 18, and misuse rates have dropped among 12th graders, opioid-related hospitalizations are increasing in preschool-age children and adolescents.
Prior to the work of Kane et al., little was known about critical care resource usage among pediatric patients admitted to pediatric ICUs across the country. They found that hospitalization rates were up, with over one-third of patients requiring mechanical ventilation and about 20% needing vasopressors. Perhaps one of the most important findings is that methadone accounted for nearly 20% of opioids ingested, displaying how adults being treated for their own opioid use disorder can put the children they live with at risk.
As the opioid crisis has worsened and overdoses have increased, the Council of Economic Advisers attempted to measure the societal costs of opioid overdoses using the “value of a statistical life” analytic method. This considers activities other than just lost work productivity and earnings, such as volunteering and raising a family. Using the value of a statistical life method, the Council determined that the true cost to society was nearly $504 billion, which included both fatal and nonfatal overdoses, and is approximately 2.8% of the 2015 U.S. gross domestic product.
Clearly, opioid abuse is both an emotional and financial burden to individual families and society as a whole. Pediatricians must help combat the ongoing opioid crisis in this country by addressing the needs of pediatric patients.
Sheryl A. Ryan, MD, is a pediatrician at Penn State Health Children’s Hospital, Milton S. Hershey Medical Center in Hershey, Pa. She wrote this commentary to the article by Kane et al. (Pediatrics. 2018 Mar. 5;41(4):e20174129). There was no external funding for this commentary, and Dr. Ryan said she had no relevant financial disclosures.
The opioid crisis in the United States is staggering. As of 2016, an estimated 2.4 million Americans were considered to have an opioid use disorder, either from prescription drug misuse or heroin addiction. This number includes 0.6% of adolescents (12- to 17-year-olds) and 1.1% of young adults (18- to 25-year-olds). And 33,000 Americans died from opioid overdose in 2015. Despite the best attempts to control the supply of drugs and increase access to treatment, overdose deaths have doubled in the past 10 years. While the overdose death rate has plateaued among children under the age of 18, and misuse rates have dropped among 12th graders, opioid-related hospitalizations are increasing in preschool-age children and adolescents.
Prior to the work of Kane et al., little was known about critical care resource usage among pediatric patients admitted to pediatric ICUs across the country. They found that hospitalization rates were up, with over one-third of patients requiring mechanical ventilation and about 20% needing vasopressors. Perhaps one of the most important findings is that methadone accounted for nearly 20% of opioids ingested, displaying how adults being treated for their own opioid use disorder can put the children they live with at risk.
As the opioid crisis has worsened and overdoses have increased, the Council of Economic Advisers attempted to measure the societal costs of opioid overdoses using the “value of a statistical life” analytic method. This considers activities other than just lost work productivity and earnings, such as volunteering and raising a family. Using the value of a statistical life method, the Council determined that the true cost to society was nearly $504 billion, which included both fatal and nonfatal overdoses, and is approximately 2.8% of the 2015 U.S. gross domestic product.
Clearly, opioid abuse is both an emotional and financial burden to individual families and society as a whole. Pediatricians must help combat the ongoing opioid crisis in this country by addressing the needs of pediatric patients.
Sheryl A. Ryan, MD, is a pediatrician at Penn State Health Children’s Hospital, Milton S. Hershey Medical Center in Hershey, Pa. She wrote this commentary to the article by Kane et al. (Pediatrics. 2018 Mar. 5;41(4):e20174129). There was no external funding for this commentary, and Dr. Ryan said she had no relevant financial disclosures.
The opioid crisis in the United States is staggering. As of 2016, an estimated 2.4 million Americans were considered to have an opioid use disorder, either from prescription drug misuse or heroin addiction. This number includes 0.6% of adolescents (12- to 17-year-olds) and 1.1% of young adults (18- to 25-year-olds). And 33,000 Americans died from opioid overdose in 2015. Despite the best attempts to control the supply of drugs and increase access to treatment, overdose deaths have doubled in the past 10 years. While the overdose death rate has plateaued among children under the age of 18, and misuse rates have dropped among 12th graders, opioid-related hospitalizations are increasing in preschool-age children and adolescents.
Prior to the work of Kane et al., little was known about critical care resource usage among pediatric patients admitted to pediatric ICUs across the country. They found that hospitalization rates were up, with over one-third of patients requiring mechanical ventilation and about 20% needing vasopressors. Perhaps one of the most important findings is that methadone accounted for nearly 20% of opioids ingested, displaying how adults being treated for their own opioid use disorder can put the children they live with at risk.
As the opioid crisis has worsened and overdoses have increased, the Council of Economic Advisers attempted to measure the societal costs of opioid overdoses using the “value of a statistical life” analytic method. This considers activities other than just lost work productivity and earnings, such as volunteering and raising a family. Using the value of a statistical life method, the Council determined that the true cost to society was nearly $504 billion, which included both fatal and nonfatal overdoses, and is approximately 2.8% of the 2015 U.S. gross domestic product.
Clearly, opioid abuse is both an emotional and financial burden to individual families and society as a whole. Pediatricians must help combat the ongoing opioid crisis in this country by addressing the needs of pediatric patients.
Sheryl A. Ryan, MD, is a pediatrician at Penn State Health Children’s Hospital, Milton S. Hershey Medical Center in Hershey, Pa. She wrote this commentary to the article by Kane et al. (Pediatrics. 2018 Mar. 5;41(4):e20174129). There was no external funding for this commentary, and Dr. Ryan said she had no relevant financial disclosures.
Hospitalization and pediatric ICU admission rates for pediatric opioid-related ingestion are increasing, along with hospitalization costs, according to a retrospective cohort study.
“In this study, we demonstrate a significant and steady increase in the diagnosis of opioid ingestion and poisoning across all age groups in U.S. children’s hospitals from 2004 to 2015,” wrote Jason Kane, MD, of the University of Chicago, and his associates. “Not only did the absolute number of opioid-related admissions increase but the rate of both hospital and PICU [pediatric ICU] admissions increased as well.”
Using the Pediatric Health Information System database, the research team performed a retrospective cohort study of children aged 1-17 years who had been admitted to a PICU between Jan. 1, 2004, and Sep. 30, 2015. For statistical analysis, the years were grouped into separate epochs: 2004-2007, 2008-2011, and 2012-2015.
Of the 4,175,624 admissions to 31 different children’s hospitals around the United States, 3,647 (0.09%) were due to opioid-related conditions. Across the three epochs of the study, the number of opioid-related hospitalizations more than doubled from 797 to 1,504 and concurrently increased the rate of hospital admissions from 6.7 per 10,000 in 2004 to 10.9 per 10,000 in 2015 (P less than .001).
Similar to the trends in overall hospital admissions and hospital admission rates, admission to the PICU and PICU admission rates also increased. Of the 3,647 children admitted for opioid-related issues, 1,564 (43%) were subsequently admitted to the PICU. PICU admission rates also increased from 25 to 36 per 10,000 admissions (P less than .001).While the majority of opioid-related hospitalizations are associated with children aged 12-17 years, children under the age of 6 years accounted for one-third of these hospitalizations. Many PICU admissions are severe enough to warrant mechanical ventilator support (37%, P less than .001) and vasopressors (20%, P less than .001).
The opioids ingested prior to hospital admission varied between age groups, with 20% (243 of 1,249) patients aged 1-5 years ingesting methadone, compared with 10% (218 of 2,223) of patients aged 12-17 years. Heroin was much more common in this group, accounting for 4.4% (99 of 2,223) of patient hospitalizations.
In addition to the human cost of pediatric hospital admissions, there is a significant economic cost on the health care system. The median cost for PICU admission was $4,931. Although these costs have been dropping for the better part of a decade ($6,523 in 2004-2007 to $4,552 in 2012-2015, P less than .001), it still represents a substantial problem. In addition, admission rates are increasing, which will only place a heavier burden on the health care system, according to Dr. Kane and his associates.
Perhaps one positive point from this study is that although hospitalizations and intensive care rates have gone up, mortality decreased over time from 2.8% in 2004-2007 to 1.3% in 2012-2015.
A possible limitation of the data in this study is that it provides data from subjects whose data is accessible to the researcher, rather than those strategically selected. In addition, referral bias may reduce the ability to generalize the information to non–tertiary care children’s hospitals.
“The current U.S. opioid crisis is negatively impacting pediatric patients as the rate of hospitalization and PICU care for the ingestion of opioids by children continues to increase over time,” wrote Dr. Kane and his associates. “Current efforts to reduce prescription opioid use in adults have not curtailed the incidence of pediatric opioid ingestion, and additional efforts are needed to reduce preventable opioid exposure in children.”
This study had no external funding. Dr. Allison H. Bartlett has served as a consultant member of the CVS Caremark National Pharmacy and Therapeutics Committee. All other authors had no relevant financial disclosures to report.
SOURCE: Kane JM et al. Pediatrics. 2018 Mar 5;141(4):e20173335.
Hospitalization and pediatric ICU admission rates for pediatric opioid-related ingestion are increasing, along with hospitalization costs, according to a retrospective cohort study.
“In this study, we demonstrate a significant and steady increase in the diagnosis of opioid ingestion and poisoning across all age groups in U.S. children’s hospitals from 2004 to 2015,” wrote Jason Kane, MD, of the University of Chicago, and his associates. “Not only did the absolute number of opioid-related admissions increase but the rate of both hospital and PICU [pediatric ICU] admissions increased as well.”
Using the Pediatric Health Information System database, the research team performed a retrospective cohort study of children aged 1-17 years who had been admitted to a PICU between Jan. 1, 2004, and Sep. 30, 2015. For statistical analysis, the years were grouped into separate epochs: 2004-2007, 2008-2011, and 2012-2015.
Of the 4,175,624 admissions to 31 different children’s hospitals around the United States, 3,647 (0.09%) were due to opioid-related conditions. Across the three epochs of the study, the number of opioid-related hospitalizations more than doubled from 797 to 1,504 and concurrently increased the rate of hospital admissions from 6.7 per 10,000 in 2004 to 10.9 per 10,000 in 2015 (P less than .001).
Similar to the trends in overall hospital admissions and hospital admission rates, admission to the PICU and PICU admission rates also increased. Of the 3,647 children admitted for opioid-related issues, 1,564 (43%) were subsequently admitted to the PICU. PICU admission rates also increased from 25 to 36 per 10,000 admissions (P less than .001).While the majority of opioid-related hospitalizations are associated with children aged 12-17 years, children under the age of 6 years accounted for one-third of these hospitalizations. Many PICU admissions are severe enough to warrant mechanical ventilator support (37%, P less than .001) and vasopressors (20%, P less than .001).
The opioids ingested prior to hospital admission varied between age groups, with 20% (243 of 1,249) patients aged 1-5 years ingesting methadone, compared with 10% (218 of 2,223) of patients aged 12-17 years. Heroin was much more common in this group, accounting for 4.4% (99 of 2,223) of patient hospitalizations.
In addition to the human cost of pediatric hospital admissions, there is a significant economic cost on the health care system. The median cost for PICU admission was $4,931. Although these costs have been dropping for the better part of a decade ($6,523 in 2004-2007 to $4,552 in 2012-2015, P less than .001), it still represents a substantial problem. In addition, admission rates are increasing, which will only place a heavier burden on the health care system, according to Dr. Kane and his associates.
Perhaps one positive point from this study is that although hospitalizations and intensive care rates have gone up, mortality decreased over time from 2.8% in 2004-2007 to 1.3% in 2012-2015.
A possible limitation of the data in this study is that it provides data from subjects whose data is accessible to the researcher, rather than those strategically selected. In addition, referral bias may reduce the ability to generalize the information to non–tertiary care children’s hospitals.
“The current U.S. opioid crisis is negatively impacting pediatric patients as the rate of hospitalization and PICU care for the ingestion of opioids by children continues to increase over time,” wrote Dr. Kane and his associates. “Current efforts to reduce prescription opioid use in adults have not curtailed the incidence of pediatric opioid ingestion, and additional efforts are needed to reduce preventable opioid exposure in children.”
This study had no external funding. Dr. Allison H. Bartlett has served as a consultant member of the CVS Caremark National Pharmacy and Therapeutics Committee. All other authors had no relevant financial disclosures to report.
SOURCE: Kane JM et al. Pediatrics. 2018 Mar 5;141(4):e20173335.
FROM PEDIATRICS
Key clinical point: The rate of hospitalizations and pediatric ICU admissions are up due to opioid ingestion.
Major finding: Over 40% of pediatric patients admitted to hospitals required PICU care.
Study details: A retrospective cohort study of children aged 1-17 years who were admitted to a PICU between Jan. 1, 2004, and Sep. 30, 2015.
Disclosures: This study had no external funding. Dr. Allison H. Bartlett has served as a consultant member of the CVS Caremark National Pharmacy and Therapeutics Committee. All other authors had no relevant financial disclosures to report.
Source: Kane JM et al. Pediatrics. 2018 Mar. 5;141(4):e20173335.
Bullous Eruption in 2 Brothers
The Diagnosis: Bullous Scabies
Scabies infection is caused by the mite Sarcoptes scabiei var hominis. It is commonly transmitted via direct skin-to-skin contact.1 Classic manifestations include pruritus that worsens at night. It commonly presents with burrows and papules in the interdigital web spaces, as well as flexor surfaces of the wrists, elbows, axillae, buttocks, and genitalia. Pruritus occurs from infestation and delayed hypersensitivity reaction to mites. The recommended treatment of classic scabies is permethrin cream 5% for all occupants of the household and a repeat application for just the patients in 1 week. Posttreatment pruritus can last up to 3 weeks.2 At-risk populations include school-aged children and patients in long-term care facilities.
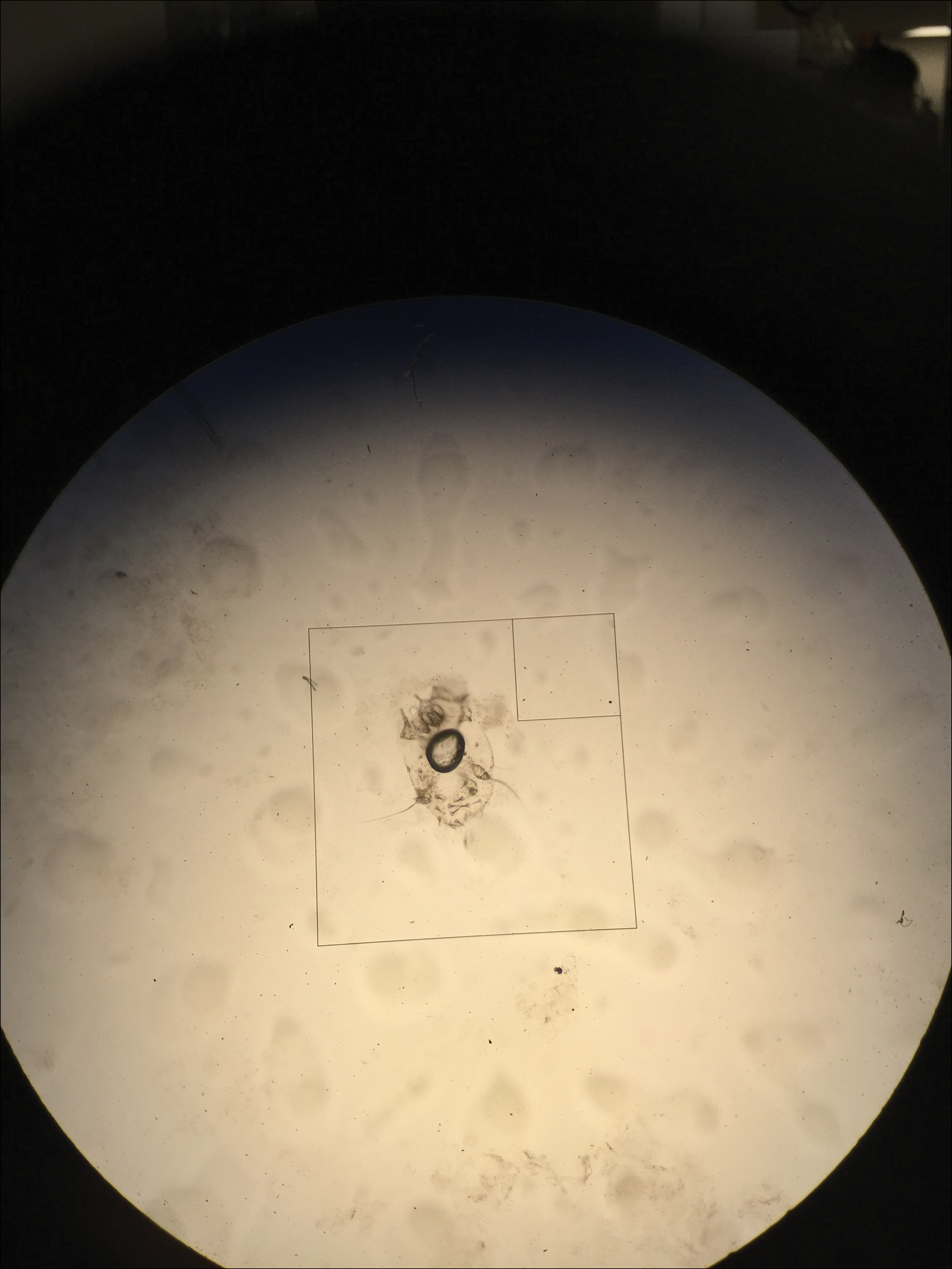
In our case, bullous lesions in a classic distribution with potassium hydroxide preparation of a scabietic mite (Figure) confirmed the diagnosis of bullous scabies. Treatment of bullous scabies is the same as classic scabies. Both patients were treated with 1 application of permethrin cream 5% before we evaluated them. We instructed to repeat application in 7 days for both boys and all family members.
Bullae may be secondary to hypersensitivity response3 or superinfection with Staphylococcus aureus causing bullous impetigo.4 Bullous scabies may present a diagnostic challenge and requires a high index of suspicion. Although childhood bullous pemphigoid can involve the palms and soles, patients usually present in infancy. Diagnoses such as dyshidrotic eczema and bullous tinea can present with pustules on the hands and feet; however, involvement of the genitalia would be uncommon.
- Chosidow O. Clinical practices. scabies. N Engl J Med. 2006;354:1718-1727.
- Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. N Engl J Med. 2010;362:717-725.
- Ansarin H, Jalali MH, Mazloomi S, et al. Scabies presenting with bullous pemphigoid-like lesions. Dermatol Online J. 2006;12:19.
- Herman PS. Letter: scabies and bullae. JAMA. 1975;231:1134.
The Diagnosis: Bullous Scabies
Scabies infection is caused by the mite Sarcoptes scabiei var hominis. It is commonly transmitted via direct skin-to-skin contact.1 Classic manifestations include pruritus that worsens at night. It commonly presents with burrows and papules in the interdigital web spaces, as well as flexor surfaces of the wrists, elbows, axillae, buttocks, and genitalia. Pruritus occurs from infestation and delayed hypersensitivity reaction to mites. The recommended treatment of classic scabies is permethrin cream 5% for all occupants of the household and a repeat application for just the patients in 1 week. Posttreatment pruritus can last up to 3 weeks.2 At-risk populations include school-aged children and patients in long-term care facilities.
In our case, bullous lesions in a classic distribution with potassium hydroxide preparation of a scabietic mite (Figure) confirmed the diagnosis of bullous scabies. Treatment of bullous scabies is the same as classic scabies. Both patients were treated with 1 application of permethrin cream 5% before we evaluated them. We instructed to repeat application in 7 days for both boys and all family members.
Bullae may be secondary to hypersensitivity response3 or superinfection with Staphylococcus aureus causing bullous impetigo.4 Bullous scabies may present a diagnostic challenge and requires a high index of suspicion. Although childhood bullous pemphigoid can involve the palms and soles, patients usually present in infancy. Diagnoses such as dyshidrotic eczema and bullous tinea can present with pustules on the hands and feet; however, involvement of the genitalia would be uncommon.
The Diagnosis: Bullous Scabies
Scabies infection is caused by the mite Sarcoptes scabiei var hominis. It is commonly transmitted via direct skin-to-skin contact.1 Classic manifestations include pruritus that worsens at night. It commonly presents with burrows and papules in the interdigital web spaces, as well as flexor surfaces of the wrists, elbows, axillae, buttocks, and genitalia. Pruritus occurs from infestation and delayed hypersensitivity reaction to mites. The recommended treatment of classic scabies is permethrin cream 5% for all occupants of the household and a repeat application for just the patients in 1 week. Posttreatment pruritus can last up to 3 weeks.2 At-risk populations include school-aged children and patients in long-term care facilities.
In our case, bullous lesions in a classic distribution with potassium hydroxide preparation of a scabietic mite (Figure) confirmed the diagnosis of bullous scabies. Treatment of bullous scabies is the same as classic scabies. Both patients were treated with 1 application of permethrin cream 5% before we evaluated them. We instructed to repeat application in 7 days for both boys and all family members.
Bullae may be secondary to hypersensitivity response3 or superinfection with Staphylococcus aureus causing bullous impetigo.4 Bullous scabies may present a diagnostic challenge and requires a high index of suspicion. Although childhood bullous pemphigoid can involve the palms and soles, patients usually present in infancy. Diagnoses such as dyshidrotic eczema and bullous tinea can present with pustules on the hands and feet; however, involvement of the genitalia would be uncommon.
- Chosidow O. Clinical practices. scabies. N Engl J Med. 2006;354:1718-1727.
- Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. N Engl J Med. 2010;362:717-725.
- Ansarin H, Jalali MH, Mazloomi S, et al. Scabies presenting with bullous pemphigoid-like lesions. Dermatol Online J. 2006;12:19.
- Herman PS. Letter: scabies and bullae. JAMA. 1975;231:1134.
- Chosidow O. Clinical practices. scabies. N Engl J Med. 2006;354:1718-1727.
- Currie BJ, McCarthy JS. Permethrin and ivermectin for scabies. N Engl J Med. 2010;362:717-725.
- Ansarin H, Jalali MH, Mazloomi S, et al. Scabies presenting with bullous pemphigoid-like lesions. Dermatol Online J. 2006;12:19.
- Herman PS. Letter: scabies and bullae. JAMA. 1975;231:1134.

Brothers aged 7 and 8 years with a history of atopic dermatitis presented to the emergency department with similar diffuse pruritic eruptions of 1 week's duration. They previously were treated with permethrin cream 5% without improvement. Two days prior to presentation they developed painful pustules on the hands and feet. No other family members were affected. Physical examination revealed numerous yellow pustules and vesicles in the interdigital web spaces, elbows, and knees. Notably, the penis and scrotum also were involved in both brothers. A potassium hydroxide preparation of small pustules was obtained.

Method may predict relapse at BCP-ALL diagnosis

Researchers say they have developed a technique that can help them determine, at diagnosis, whether children with B-cell precursor acute lymphoblastic leukemia (BCP-ALL) will relapse after treatment.
The method involves examining individual leukemia cells using mass cytometry.
In looking at the cells’ stage of development and signaling behavior, the researchers were able to identify a subset of malignant cells that predispose a patient to relapse.
The team described this method, which they termed “developmentally dependent predictor of relapse (DDPR),” in Nature Medicine.
Prior research suggested relapse may be driven by treatment-resistant cells that are present from the beginning of disease development.
“We wondered, can we identify those cells at the time the patient first presents to the clinic, and can we treat patients with a specific therapy to target them?” said study author Kara Davis, DO, of Stanford University in California.
Dr Davis and her colleagues used mass cytometry to analyze diagnostic bone marrow samples from 60 patients with BCP-ALL.
To pinpoint the problematic cells among the millions of cells in each patient’s sample, the researchers had to figure out how to organize the data.
“Every patient has vastly different features to their cancer,” Dr Davis said, “and we had to ask, ‘Is there any common thread between them?’”
The solution, the researchers found, was to match BCP-ALL cells and healthy B cells according to their developmental states, comparing the leukemic cells to the healthy cells.
The comparison revealed 6 features of leukemic cell populations that were associated with relapse.
Broadly, the features suggested that pro-BII cells with activated mTOR signaling were associated with relapse, as were pre-BI cells with activated and unresponsive pre-B-cell receptor signaling.
“We do not understand the mechanisms by which malignant cells from the pro-BII and pre-BI stages of development resist treatment,” Dr Davis noted.
However, she and her colleagues were able to show the leukemic cell features identified by DDPR could predict relapse in the BCP-ALL patients.
Of the 60 patients analyzed, there were 54 with at least 3 years of follow-up. The researchers divided these patients into a training cohort (n=44) and a validation cohort (n=10).
The team used an integrated cumulative/dynamic area under the curve (iAUC) and a C-statistic to assess DDPR performance in both cohorts.
In the training cohort, DDPR had an iAUC value of 0.92 and a C-statistic of 0.87. In the validation cohort, DDPR had an iAUC value of 0.85 and a C-statistic of 0.87.
The researchers also said DDPR “performed well” in predicting relapse-free survival in a retrospective analysis of both cohorts (P = 2.8 × 10−7).
Now, the researchers plan to validate DDPR in a larger number of patients and evaluate whether the same general approach could predict relapse in other cancers.
Researchers say they have developed a technique that can help them determine, at diagnosis, whether children with B-cell precursor acute lymphoblastic leukemia (BCP-ALL) will relapse after treatment.
The method involves examining individual leukemia cells using mass cytometry.
In looking at the cells’ stage of development and signaling behavior, the researchers were able to identify a subset of malignant cells that predispose a patient to relapse.
The team described this method, which they termed “developmentally dependent predictor of relapse (DDPR),” in Nature Medicine.
Prior research suggested relapse may be driven by treatment-resistant cells that are present from the beginning of disease development.
“We wondered, can we identify those cells at the time the patient first presents to the clinic, and can we treat patients with a specific therapy to target them?” said study author Kara Davis, DO, of Stanford University in California.
Dr Davis and her colleagues used mass cytometry to analyze diagnostic bone marrow samples from 60 patients with BCP-ALL.
To pinpoint the problematic cells among the millions of cells in each patient’s sample, the researchers had to figure out how to organize the data.
“Every patient has vastly different features to their cancer,” Dr Davis said, “and we had to ask, ‘Is there any common thread between them?’”
The solution, the researchers found, was to match BCP-ALL cells and healthy B cells according to their developmental states, comparing the leukemic cells to the healthy cells.
The comparison revealed 6 features of leukemic cell populations that were associated with relapse.
Broadly, the features suggested that pro-BII cells with activated mTOR signaling were associated with relapse, as were pre-BI cells with activated and unresponsive pre-B-cell receptor signaling.
“We do not understand the mechanisms by which malignant cells from the pro-BII and pre-BI stages of development resist treatment,” Dr Davis noted.
However, she and her colleagues were able to show the leukemic cell features identified by DDPR could predict relapse in the BCP-ALL patients.
Of the 60 patients analyzed, there were 54 with at least 3 years of follow-up. The researchers divided these patients into a training cohort (n=44) and a validation cohort (n=10).
The team used an integrated cumulative/dynamic area under the curve (iAUC) and a C-statistic to assess DDPR performance in both cohorts.
In the training cohort, DDPR had an iAUC value of 0.92 and a C-statistic of 0.87. In the validation cohort, DDPR had an iAUC value of 0.85 and a C-statistic of 0.87.
The researchers also said DDPR “performed well” in predicting relapse-free survival in a retrospective analysis of both cohorts (P = 2.8 × 10−7).
Now, the researchers plan to validate DDPR in a larger number of patients and evaluate whether the same general approach could predict relapse in other cancers.
Researchers say they have developed a technique that can help them determine, at diagnosis, whether children with B-cell precursor acute lymphoblastic leukemia (BCP-ALL) will relapse after treatment.
The method involves examining individual leukemia cells using mass cytometry.
In looking at the cells’ stage of development and signaling behavior, the researchers were able to identify a subset of malignant cells that predispose a patient to relapse.
The team described this method, which they termed “developmentally dependent predictor of relapse (DDPR),” in Nature Medicine.
Prior research suggested relapse may be driven by treatment-resistant cells that are present from the beginning of disease development.
“We wondered, can we identify those cells at the time the patient first presents to the clinic, and can we treat patients with a specific therapy to target them?” said study author Kara Davis, DO, of Stanford University in California.
Dr Davis and her colleagues used mass cytometry to analyze diagnostic bone marrow samples from 60 patients with BCP-ALL.
To pinpoint the problematic cells among the millions of cells in each patient’s sample, the researchers had to figure out how to organize the data.
“Every patient has vastly different features to their cancer,” Dr Davis said, “and we had to ask, ‘Is there any common thread between them?’”
The solution, the researchers found, was to match BCP-ALL cells and healthy B cells according to their developmental states, comparing the leukemic cells to the healthy cells.
The comparison revealed 6 features of leukemic cell populations that were associated with relapse.
Broadly, the features suggested that pro-BII cells with activated mTOR signaling were associated with relapse, as were pre-BI cells with activated and unresponsive pre-B-cell receptor signaling.
“We do not understand the mechanisms by which malignant cells from the pro-BII and pre-BI stages of development resist treatment,” Dr Davis noted.
However, she and her colleagues were able to show the leukemic cell features identified by DDPR could predict relapse in the BCP-ALL patients.
Of the 60 patients analyzed, there were 54 with at least 3 years of follow-up. The researchers divided these patients into a training cohort (n=44) and a validation cohort (n=10).
The team used an integrated cumulative/dynamic area under the curve (iAUC) and a C-statistic to assess DDPR performance in both cohorts.
In the training cohort, DDPR had an iAUC value of 0.92 and a C-statistic of 0.87. In the validation cohort, DDPR had an iAUC value of 0.85 and a C-statistic of 0.87.
The researchers also said DDPR “performed well” in predicting relapse-free survival in a retrospective analysis of both cohorts (P = 2.8 × 10−7).
Now, the researchers plan to validate DDPR in a larger number of patients and evaluate whether the same general approach could predict relapse in other cancers.
Interventions ‘key’ when ADHD, conduct disorder, and delinquency overlap
LAS VEGAS – The overlap of ADHD, conduct disorder, substance use disorder, and criminality likely reflect related underlying mechanisms, which may elucidate different developmental pathways of offending.
“Early interventions are key,” Praveen R. Kambam, MD, said at an annual psychopharmacology update held by the Nevada Psychiatric Association.

According to Dr. Kambam, a clinical and forensic psychiatrist at the University of California, Los Angeles, ADHD is overrepresented in correctional settings worldwide, especially the hyperactive-impulsive subtype. “In juvenile settings, ADHD rates are 3-4 times higher than rates in the general population,” he said. “If you combine juvenile and adult prison populations worldwide, the rates are about 2-5 times higher than the general population.”
The risks are increased for comorbid oppositional defiant disorder (ODD) and conduct disorder. In fact, ADHD and conduct disorder co-occur in about 50% of cases. In girls, the prevalence rate of conduct disorder is steady at 0.8% around age 5 years and increases to 2.8% around age 15 years, while in boys, conduct disorder is steady at 2.1% around age 5 years and rises to 5.5% at age 15 years.
According to a literature review of 18 prospective studies, 13 retrospective studies, and four reviews, individuals with ADHD plus or minus conduct disorder had an increased the risk of antisocial personality disorder, and those with ADHD plus conduct disorder had an increased risk of criminality (J Atten Disord. 2016;20[10]:815-24). “So it’s a subtle difference, where antisocial personality disorder and criminality are slightly different,” Dr. Kambam said. “It could be that the diagnostic criteria are catching the same thing. However, the added [conduct disorder] suggests that there may be subpopulations that are vulnerable.”
He went on to note that individuals with ADHD and delinquency tend to have more learning problems, poor academic achievement, peer relationship problems, and risk of social rejection, while individuals with oppositional defiant disorder and delinquency tend to have peer relationship problems, a negative parent-child relationship, and increased risk of developing conduct disorder.
ADHD is associated with alcohol and drug use in adulthood and nicotine use in adolescence. “Comorbidity between ADHD and ODD/[conduct disorder] is robustly related to substance outcomes,” Dr. Kambam said. “However, both initiation and continuation of substance use disorder are more likely when ADHD symptoms are present, even when controlling for ODD/[conduct disorder]. As for substance use disorder [SUD] and delinquency, the onset of delinquency is more likely in children with onset of SUD by age 11, and SUDs are closely linked with criminality in both juveniles and adults.”
Comorbidity of SUD with conduct disorder and ADHD likely reflects multifactorial mechanisms, he said, such as inherent novelty seeking or school failure leading to association with antisocial peers. Risk factors for chronic offending include early onset of criminal behaviors, ADHD plus conduct disorder, and ODD. ADHD has an independent yet weaker relationship with antisocial behaviors as well, while ADHD, conduct disorder, and SUD are independently associated with increased recidivism.
Environmental factors for chronic offending include the home environment, peer response, parenting skills, and in utero exposures and perinatal complications. “Whether ADHD develops into more severe conduct problems depends considerably on exposure to potentiating environmental factors,” Dr. Kambam said. “The converse is also true: Low-risk environments promote desistance from this pathway in impulsive boys.” He added that the chronic offenders/criminality pathway likely stems from underlying mechanisms, such as impulsivity, low self-control, and executive dysfunction.
If left untreated, ADHD is associated with poor academic and employment outcomes, SUDs, depression, bipolar disorder, suicide attempts, vehicular accidents, and use of mental health services. “The economic costs are estimated to be $42.5 billion annually, so it has a large impact,” he said.
Limited evidence exists to support pharmacological treatments for conduct disorder, although stimulants/alpha-agonists, antipsychotics, lithium, and mood stabilizers may offer some benefit for target symptoms. “Most of the treatment data center around multisystemic therapy, including behavioral modification/parent management training, and functional family training,” Dr. Kambam said. “Treating disruptive behavior disorders and SUDs are
likely to reduce criminality and recidivism, particularly if started early. There are many beneficial economic impacts. Think about the cost of having youth detained in the criminal justice systems. In Los Angeles County, that cost is about $230,000 per year per kid. That money can probably be better spent somewhere else.”
Numerous studies show that the nonmedical use of stimulants ranges from 25%-40%. “They’re mostly used to enhance academic and/or work performance, but some are used for euphoric effect,” he said. “Individuals in college and just out of college seem to be at the highest risk. There is a strong relationship between [conduct disorder]/[antisocial personality disorder] or SUDs and nonmedical use.”
Treatment with stimulants in correctional settings is controversial. “Some say try after failure of nonstimulants, while others say never use them due to substance abuse, misuse, intimidation of patients to surrender medication, and security/costs,” Dr. Kambam said. “The protocol for ADHD treatment in Massachusetts prisons calls for use of nonstimulants first, followed by ‘crushable’ stimulants if indicated.” The methylphenidate patch and lisdexamfetamine also can be effective in the incarcerated population.
Dr. Kambam reported having no financial disclosures.
SOURCE: Kambam PR. NPA 2018.
LAS VEGAS – The overlap of ADHD, conduct disorder, substance use disorder, and criminality likely reflect related underlying mechanisms, which may elucidate different developmental pathways of offending.
“Early interventions are key,” Praveen R. Kambam, MD, said at an annual psychopharmacology update held by the Nevada Psychiatric Association.
According to Dr. Kambam, a clinical and forensic psychiatrist at the University of California, Los Angeles, ADHD is overrepresented in correctional settings worldwide, especially the hyperactive-impulsive subtype. “In juvenile settings, ADHD rates are 3-4 times higher than rates in the general population,” he said. “If you combine juvenile and adult prison populations worldwide, the rates are about 2-5 times higher than the general population.”
The risks are increased for comorbid oppositional defiant disorder (ODD) and conduct disorder. In fact, ADHD and conduct disorder co-occur in about 50% of cases. In girls, the prevalence rate of conduct disorder is steady at 0.8% around age 5 years and increases to 2.8% around age 15 years, while in boys, conduct disorder is steady at 2.1% around age 5 years and rises to 5.5% at age 15 years.
According to a literature review of 18 prospective studies, 13 retrospective studies, and four reviews, individuals with ADHD plus or minus conduct disorder had an increased the risk of antisocial personality disorder, and those with ADHD plus conduct disorder had an increased risk of criminality (J Atten Disord. 2016;20[10]:815-24). “So it’s a subtle difference, where antisocial personality disorder and criminality are slightly different,” Dr. Kambam said. “It could be that the diagnostic criteria are catching the same thing. However, the added [conduct disorder] suggests that there may be subpopulations that are vulnerable.”
He went on to note that individuals with ADHD and delinquency tend to have more learning problems, poor academic achievement, peer relationship problems, and risk of social rejection, while individuals with oppositional defiant disorder and delinquency tend to have peer relationship problems, a negative parent-child relationship, and increased risk of developing conduct disorder.
ADHD is associated with alcohol and drug use in adulthood and nicotine use in adolescence. “Comorbidity between ADHD and ODD/[conduct disorder] is robustly related to substance outcomes,” Dr. Kambam said. “However, both initiation and continuation of substance use disorder are more likely when ADHD symptoms are present, even when controlling for ODD/[conduct disorder]. As for substance use disorder [SUD] and delinquency, the onset of delinquency is more likely in children with onset of SUD by age 11, and SUDs are closely linked with criminality in both juveniles and adults.”
Comorbidity of SUD with conduct disorder and ADHD likely reflects multifactorial mechanisms, he said, such as inherent novelty seeking or school failure leading to association with antisocial peers. Risk factors for chronic offending include early onset of criminal behaviors, ADHD plus conduct disorder, and ODD. ADHD has an independent yet weaker relationship with antisocial behaviors as well, while ADHD, conduct disorder, and SUD are independently associated with increased recidivism.
Environmental factors for chronic offending include the home environment, peer response, parenting skills, and in utero exposures and perinatal complications. “Whether ADHD develops into more severe conduct problems depends considerably on exposure to potentiating environmental factors,” Dr. Kambam said. “The converse is also true: Low-risk environments promote desistance from this pathway in impulsive boys.” He added that the chronic offenders/criminality pathway likely stems from underlying mechanisms, such as impulsivity, low self-control, and executive dysfunction.
If left untreated, ADHD is associated with poor academic and employment outcomes, SUDs, depression, bipolar disorder, suicide attempts, vehicular accidents, and use of mental health services. “The economic costs are estimated to be $42.5 billion annually, so it has a large impact,” he said.
Limited evidence exists to support pharmacological treatments for conduct disorder, although stimulants/alpha-agonists, antipsychotics, lithium, and mood stabilizers may offer some benefit for target symptoms. “Most of the treatment data center around multisystemic therapy, including behavioral modification/parent management training, and functional family training,” Dr. Kambam said. “Treating disruptive behavior disorders and SUDs are
likely to reduce criminality and recidivism, particularly if started early. There are many beneficial economic impacts. Think about the cost of having youth detained in the criminal justice systems. In Los Angeles County, that cost is about $230,000 per year per kid. That money can probably be better spent somewhere else.”
Numerous studies show that the nonmedical use of stimulants ranges from 25%-40%. “They’re mostly used to enhance academic and/or work performance, but some are used for euphoric effect,” he said. “Individuals in college and just out of college seem to be at the highest risk. There is a strong relationship between [conduct disorder]/[antisocial personality disorder] or SUDs and nonmedical use.”
Treatment with stimulants in correctional settings is controversial. “Some say try after failure of nonstimulants, while others say never use them due to substance abuse, misuse, intimidation of patients to surrender medication, and security/costs,” Dr. Kambam said. “The protocol for ADHD treatment in Massachusetts prisons calls for use of nonstimulants first, followed by ‘crushable’ stimulants if indicated.” The methylphenidate patch and lisdexamfetamine also can be effective in the incarcerated population.
Dr. Kambam reported having no financial disclosures.
SOURCE: Kambam PR. NPA 2018.
LAS VEGAS – The overlap of ADHD, conduct disorder, substance use disorder, and criminality likely reflect related underlying mechanisms, which may elucidate different developmental pathways of offending.
“Early interventions are key,” Praveen R. Kambam, MD, said at an annual psychopharmacology update held by the Nevada Psychiatric Association.
According to Dr. Kambam, a clinical and forensic psychiatrist at the University of California, Los Angeles, ADHD is overrepresented in correctional settings worldwide, especially the hyperactive-impulsive subtype. “In juvenile settings, ADHD rates are 3-4 times higher than rates in the general population,” he said. “If you combine juvenile and adult prison populations worldwide, the rates are about 2-5 times higher than the general population.”
The risks are increased for comorbid oppositional defiant disorder (ODD) and conduct disorder. In fact, ADHD and conduct disorder co-occur in about 50% of cases. In girls, the prevalence rate of conduct disorder is steady at 0.8% around age 5 years and increases to 2.8% around age 15 years, while in boys, conduct disorder is steady at 2.1% around age 5 years and rises to 5.5% at age 15 years.
According to a literature review of 18 prospective studies, 13 retrospective studies, and four reviews, individuals with ADHD plus or minus conduct disorder had an increased the risk of antisocial personality disorder, and those with ADHD plus conduct disorder had an increased risk of criminality (J Atten Disord. 2016;20[10]:815-24). “So it’s a subtle difference, where antisocial personality disorder and criminality are slightly different,” Dr. Kambam said. “It could be that the diagnostic criteria are catching the same thing. However, the added [conduct disorder] suggests that there may be subpopulations that are vulnerable.”
He went on to note that individuals with ADHD and delinquency tend to have more learning problems, poor academic achievement, peer relationship problems, and risk of social rejection, while individuals with oppositional defiant disorder and delinquency tend to have peer relationship problems, a negative parent-child relationship, and increased risk of developing conduct disorder.
ADHD is associated with alcohol and drug use in adulthood and nicotine use in adolescence. “Comorbidity between ADHD and ODD/[conduct disorder] is robustly related to substance outcomes,” Dr. Kambam said. “However, both initiation and continuation of substance use disorder are more likely when ADHD symptoms are present, even when controlling for ODD/[conduct disorder]. As for substance use disorder [SUD] and delinquency, the onset of delinquency is more likely in children with onset of SUD by age 11, and SUDs are closely linked with criminality in both juveniles and adults.”
Comorbidity of SUD with conduct disorder and ADHD likely reflects multifactorial mechanisms, he said, such as inherent novelty seeking or school failure leading to association with antisocial peers. Risk factors for chronic offending include early onset of criminal behaviors, ADHD plus conduct disorder, and ODD. ADHD has an independent yet weaker relationship with antisocial behaviors as well, while ADHD, conduct disorder, and SUD are independently associated with increased recidivism.
Environmental factors for chronic offending include the home environment, peer response, parenting skills, and in utero exposures and perinatal complications. “Whether ADHD develops into more severe conduct problems depends considerably on exposure to potentiating environmental factors,” Dr. Kambam said. “The converse is also true: Low-risk environments promote desistance from this pathway in impulsive boys.” He added that the chronic offenders/criminality pathway likely stems from underlying mechanisms, such as impulsivity, low self-control, and executive dysfunction.
If left untreated, ADHD is associated with poor academic and employment outcomes, SUDs, depression, bipolar disorder, suicide attempts, vehicular accidents, and use of mental health services. “The economic costs are estimated to be $42.5 billion annually, so it has a large impact,” he said.
Limited evidence exists to support pharmacological treatments for conduct disorder, although stimulants/alpha-agonists, antipsychotics, lithium, and mood stabilizers may offer some benefit for target symptoms. “Most of the treatment data center around multisystemic therapy, including behavioral modification/parent management training, and functional family training,” Dr. Kambam said. “Treating disruptive behavior disorders and SUDs are
likely to reduce criminality and recidivism, particularly if started early. There are many beneficial economic impacts. Think about the cost of having youth detained in the criminal justice systems. In Los Angeles County, that cost is about $230,000 per year per kid. That money can probably be better spent somewhere else.”
Numerous studies show that the nonmedical use of stimulants ranges from 25%-40%. “They’re mostly used to enhance academic and/or work performance, but some are used for euphoric effect,” he said. “Individuals in college and just out of college seem to be at the highest risk. There is a strong relationship between [conduct disorder]/[antisocial personality disorder] or SUDs and nonmedical use.”
Treatment with stimulants in correctional settings is controversial. “Some say try after failure of nonstimulants, while others say never use them due to substance abuse, misuse, intimidation of patients to surrender medication, and security/costs,” Dr. Kambam said. “The protocol for ADHD treatment in Massachusetts prisons calls for use of nonstimulants first, followed by ‘crushable’ stimulants if indicated.” The methylphenidate patch and lisdexamfetamine also can be effective in the incarcerated population.
Dr. Kambam reported having no financial disclosures.
SOURCE: Kambam PR. NPA 2018.
REPORTING FROM NPA 2018

Experts cite five orthopedic tests that physicians and patients should question
The American Academy of Pediatrics–Section on Orthopaedics and the Pediatric Orthopaedic Society of North America (POSNA) provide the following list:
- Do not order a screening hip ultrasound to rule out developmental hip dysplasia or developmental hip dislocation if the baby has no risk factors and has a clinically stable hip examination.
- Do not order radiographs or advise bracing or surgery for a child less than 8 years of age with simple in-toeing gait.
- Do not order custom orthotics or shoe inserts for a child with minimally symptomatic or asymptomatic flat feet.
- Do not order advanced imaging studies (MRI or CT) for most musculoskeletal conditions in a child until all appropriate clinical, laboratory, and plain radiographic examinations have been completed.
- Do not order follow-up x-rays for buckle (or torus) fractures if they are no longer tender or painful.
This list was developed based on data collected from 2014-2015 from the POSNA Evidence Based Committee and Advocacy Committee. Approximately 20 members of the two committees participated in the process. They submitted five items each from their practices and experience of tests or procedures that they found were commonly overutilized. The items were placed in order of number of times listed by each surgeon; a total of 30 items were submitted. The two committees then agreed on a final list of five procedures, based on frequency of responses and importance of the condition. After the list was reviewed and feedback provided, the POSNA board of directors voted on a final list. The AAP Executive Committee then provided final approval.
The committee noted that the list is provided for informational purposes and is not intended as a substitute for consultation with a physician.
Read the full list with more details here.
The American Academy of Pediatrics–Section on Orthopaedics and the Pediatric Orthopaedic Society of North America (POSNA) provide the following list:
- Do not order a screening hip ultrasound to rule out developmental hip dysplasia or developmental hip dislocation if the baby has no risk factors and has a clinically stable hip examination.
- Do not order radiographs or advise bracing or surgery for a child less than 8 years of age with simple in-toeing gait.
- Do not order custom orthotics or shoe inserts for a child with minimally symptomatic or asymptomatic flat feet.
- Do not order advanced imaging studies (MRI or CT) for most musculoskeletal conditions in a child until all appropriate clinical, laboratory, and plain radiographic examinations have been completed.
- Do not order follow-up x-rays for buckle (or torus) fractures if they are no longer tender or painful.
This list was developed based on data collected from 2014-2015 from the POSNA Evidence Based Committee and Advocacy Committee. Approximately 20 members of the two committees participated in the process. They submitted five items each from their practices and experience of tests or procedures that they found were commonly overutilized. The items were placed in order of number of times listed by each surgeon; a total of 30 items were submitted. The two committees then agreed on a final list of five procedures, based on frequency of responses and importance of the condition. After the list was reviewed and feedback provided, the POSNA board of directors voted on a final list. The AAP Executive Committee then provided final approval.
The committee noted that the list is provided for informational purposes and is not intended as a substitute for consultation with a physician.
Read the full list with more details here.
The American Academy of Pediatrics–Section on Orthopaedics and the Pediatric Orthopaedic Society of North America (POSNA) provide the following list:
- Do not order a screening hip ultrasound to rule out developmental hip dysplasia or developmental hip dislocation if the baby has no risk factors and has a clinically stable hip examination.
- Do not order radiographs or advise bracing or surgery for a child less than 8 years of age with simple in-toeing gait.
- Do not order custom orthotics or shoe inserts for a child with minimally symptomatic or asymptomatic flat feet.
- Do not order advanced imaging studies (MRI or CT) for most musculoskeletal conditions in a child until all appropriate clinical, laboratory, and plain radiographic examinations have been completed.
- Do not order follow-up x-rays for buckle (or torus) fractures if they are no longer tender or painful.
This list was developed based on data collected from 2014-2015 from the POSNA Evidence Based Committee and Advocacy Committee. Approximately 20 members of the two committees participated in the process. They submitted five items each from their practices and experience of tests or procedures that they found were commonly overutilized. The items were placed in order of number of times listed by each surgeon; a total of 30 items were submitted. The two committees then agreed on a final list of five procedures, based on frequency of responses and importance of the condition. After the list was reviewed and feedback provided, the POSNA board of directors voted on a final list. The AAP Executive Committee then provided final approval.
The committee noted that the list is provided for informational purposes and is not intended as a substitute for consultation with a physician.
Read the full list with more details here.
Collaboration, consultation part of AAP teen depression guidelines update
The updated information includes recommendations on collaborative care, practice preparation, establishing networks of referrals, and much more.

“These guidelines were developed for PC clinicians who are in a position to identify and assist youth with depression in their practice settings,” they said. The guidelines apply to individuals aged 10-21 years, and support universal depression screening for those aged 12 and older.
Known as the Guidelines for Adolescent Depression in Primary Care (GLAD-PC), they consist of two parts: Practice Preparation, Identification, Assessment, and Initial Management, with Dr. Zuckerbrot as the lead author, and Treatment and Ongoing Management, led by Amy H. Cheung, MD, of the University of Toronto. They were published online in Pediatrics.
“It has been over 10 years since the [last] guidelines were published and they are supposed to be updated every 5,” Dr. Zuckerbrot said in an interview. “Given the new evidence on screening, psychopharmacology, and collaborative care, the guidelines needed to be revised. The USPSTF [United States Preventive Services Task Force ] and the AAP had already supported universal adolescent depression screening, and these guidelines are finally aligned with those positions.
“Different parts of the guidelines will be the go-to for different pediatricians, depending on where they are in their delivery of mental health care,” she explained. “Some may need help with practice preparation while others may need advice on screening; others may already be prescribing and may need advice on ongoing treatment and follow-up. I think there is something for everyone.”
Implementation of the guidelines is difficult in a short visit, Dr. Zuckerbrot acknowledged. “In addition, pediatricians may not have been well trained in the management of adolescent depression during their residencies.” However, the guidelines discuss both “real teams to support the pediatricians in their efforts, as well as virtual teams when staffing is limited.
“The guidelines advise that pediatricians learn about child psychiatry primary care consultation programs in their state and make use of those free telephone consultation programs.” The guidelines also discuss strategies for collaborative or integrative care, she said.
Part I
Part I of the guidelines, “Practice Preparation, Identification, Assessment, and Initial Management,” includes several recommendations for each topic.
For practice preparation, the guidelines recommend that clinicians seek training in the assessment, diagnosis, and treatment of depression, and that they establish a network of referrals and mental health resources in their communities. This network may include not only health professionals, but also current patients and families who are managing teen depression. If available, state-wide or regional child and adolescent psychiatry consultation programs can be included.
The identification and surveillance section of the guidelines calls for screening all patients aged 12 years and older for depression each year, using a formal screening tool on paper or online. The screening could occur at an annual wellness visit or any other medical visit, such as a sports physical. A second recommendation calls for identifying patients at increased risk for depression because of factors such as personal history, family history, substance use, other psychiatric disorders, frequent somatic complaints, or trauma, and monitoring these individuals regularly for signs of depression using a formal screening tool.
The assessment and diagnosis section states that assessment should include interviews with the patients alone as well as with their families or caregivers, and should include screening teens for functional impairment.
Primary care physicians should evaluate for depression not only if an adolescent tests positive on a screening tool, but also in children who present with any emotional problem as the chief complaint, and in those in whom depression is highly suspected even if they test negative on a formal screening tool, the guidelines state.
The three recommendations for initial management of depression in the primary care setting are educating patients and families about depression; developing a treatment plan (if the primary care clinician has had appropriate training) and setting specific treatment goals in areas of functioning such as at home, with peers, and at school; and developing a safety plan that includes restricting access to weapons or other means of self-harm, according to the guidelines.
Part II
Part II of the recommendations, “Treatment and Ongoing Management,” discusses options for managing depression in the primary care setting and utilizing outside resources.
The treatment recommendations emphasize the use of integrated models, if possible. “There is a growing recognition that complex chronic conditions, such as depression, are most successfully managed with proactive, multidisciplinary, patient-centered care teams,” Dr. Cheung and her associates said.
The recommendation for cases of mild depression calls for a period of “active support and monitoring” for 6-8 weeks before reassessing if the teen shows no improvement. By contrast, for cases of moderate to severe depression or cases with evidence of substance abuse or other psychoses, the recommendation calls for potential consultation with a mental health specialist and a discussion of the roles primary and specialty care will play in treatment. The guidelines include a flow chart for PC physicians to follow.
The guidelines suggest that PC clinicians recommend “scientifically tested and proven treatments,” such as psychotherapies, cognitive behavioral therapy (CBT) or interpersonal psychotherapy for adolescents, and/or antidepressant treatment, such as SSRIs, whenever possible and appropriate. It is important to monitor teens on antidepressants regularly to identify adverse events.
Recommendations for the ongoing management of teens with depression in the primary care setting include regular tracking of progress, reassessment if the teen shows no improvement in 6-8 weeks, and consultation with a mental health professional for those who show only partial improvement after exhausting primary care diagnostic and treatment options. Assessment of depressive symptoms is not the only thing to track. Functioning at home, school, and among peers also is important.
The final treatment recommendation is for active support of a depressed teen’s referral to mental health if necessary for best management and sharing care if possible, with an understanding of the roles of the primary and specialty clinicians, the guidelines state.
The guidelines project was funded by the Resource for Advancing Children’s Health Institute and the Bell Canada Chair in Adolescent Mood and Anxiety Disorders.
Dr. Cheung and Dr. Zuckerbrot receive book royalties. Dr Zuckerbrot works for child and adolescent psychiatry for primary care (CAP-PC), now a regional provider for Project TEACH in New York State, and she is on the steering committee as well as faculty for the REACH Institute; both of these institutions are described in the guidelines. Peter S. Jensen, MD, has received royalties from Random House, Oxford University Press, and APPI Inc. He is a part owner of a consulting company, CATCH Services LLC. He is the chief executive officer and president of a nonprofit organization, the Resource for Advancing Children’s Health Institute, but receives no compensation. The other authors indicated they have no financial relationships relevant to the guidelines.
“Mental health disorders have become one of the new morbidities in pediatric care,” Karalyn Kinsella, MD, said in an interview. “With one in five patients having depression, it is an illness that must be within our domain to identify and treat. I think the guidelines will make providers feel more confident in making a diagnosis and providing initial treatment. For those that do not feel comfortable, hopefully the guidelines will encourage them to seek training.

The take-home message for general pediatricians is that a standardized screening tool makes identifying depression relatively easy. “We have been using the PHQ-9 [Patient Health Questionnaire-9] in my office for several years, and it is very easy to administer and score, and is billable,” said Dr. Kinsella. “It can take some practice to tease out some typical teen behaviors, especially on the sleep and fatigue questions, but it provides an opportunity to open up discussion with the teen.
“Treatment [of depression] can be more complicated and time consuming, but rewarding and invaluable to the patient,” she emphasized. “Many states now have psychiatrists available by phone consultation to aid in management of medication. The key is establishing a list of quality counselors for referrals. With those supports and frequent follow-up, pediatricians can play a key role in the treatment of this prevalent and important illness that affects our patients.”
Dr. Kinsella is a pediatrician in Cheshire, Conn., and a member of the Pediatric News editorial advisory board. She was asked to comment on the new AAP teen depression guidelines.
“Mental health disorders have become one of the new morbidities in pediatric care,” Karalyn Kinsella, MD, said in an interview. “With one in five patients having depression, it is an illness that must be within our domain to identify and treat. I think the guidelines will make providers feel more confident in making a diagnosis and providing initial treatment. For those that do not feel comfortable, hopefully the guidelines will encourage them to seek training.
The take-home message for general pediatricians is that a standardized screening tool makes identifying depression relatively easy. “We have been using the PHQ-9 [Patient Health Questionnaire-9] in my office for several years, and it is very easy to administer and score, and is billable,” said Dr. Kinsella. “It can take some practice to tease out some typical teen behaviors, especially on the sleep and fatigue questions, but it provides an opportunity to open up discussion with the teen.
“Treatment [of depression] can be more complicated and time consuming, but rewarding and invaluable to the patient,” she emphasized. “Many states now have psychiatrists available by phone consultation to aid in management of medication. The key is establishing a list of quality counselors for referrals. With those supports and frequent follow-up, pediatricians can play a key role in the treatment of this prevalent and important illness that affects our patients.”
Dr. Kinsella is a pediatrician in Cheshire, Conn., and a member of the Pediatric News editorial advisory board. She was asked to comment on the new AAP teen depression guidelines.
“Mental health disorders have become one of the new morbidities in pediatric care,” Karalyn Kinsella, MD, said in an interview. “With one in five patients having depression, it is an illness that must be within our domain to identify and treat. I think the guidelines will make providers feel more confident in making a diagnosis and providing initial treatment. For those that do not feel comfortable, hopefully the guidelines will encourage them to seek training.
The take-home message for general pediatricians is that a standardized screening tool makes identifying depression relatively easy. “We have been using the PHQ-9 [Patient Health Questionnaire-9] in my office for several years, and it is very easy to administer and score, and is billable,” said Dr. Kinsella. “It can take some practice to tease out some typical teen behaviors, especially on the sleep and fatigue questions, but it provides an opportunity to open up discussion with the teen.
“Treatment [of depression] can be more complicated and time consuming, but rewarding and invaluable to the patient,” she emphasized. “Many states now have psychiatrists available by phone consultation to aid in management of medication. The key is establishing a list of quality counselors for referrals. With those supports and frequent follow-up, pediatricians can play a key role in the treatment of this prevalent and important illness that affects our patients.”
Dr. Kinsella is a pediatrician in Cheshire, Conn., and a member of the Pediatric News editorial advisory board. She was asked to comment on the new AAP teen depression guidelines.
The updated information includes recommendations on collaborative care, practice preparation, establishing networks of referrals, and much more.
“These guidelines were developed for PC clinicians who are in a position to identify and assist youth with depression in their practice settings,” they said. The guidelines apply to individuals aged 10-21 years, and support universal depression screening for those aged 12 and older.
Known as the Guidelines for Adolescent Depression in Primary Care (GLAD-PC), they consist of two parts: Practice Preparation, Identification, Assessment, and Initial Management, with Dr. Zuckerbrot as the lead author, and Treatment and Ongoing Management, led by Amy H. Cheung, MD, of the University of Toronto. They were published online in Pediatrics.
“It has been over 10 years since the [last] guidelines were published and they are supposed to be updated every 5,” Dr. Zuckerbrot said in an interview. “Given the new evidence on screening, psychopharmacology, and collaborative care, the guidelines needed to be revised. The USPSTF [United States Preventive Services Task Force ] and the AAP had already supported universal adolescent depression screening, and these guidelines are finally aligned with those positions.
“Different parts of the guidelines will be the go-to for different pediatricians, depending on where they are in their delivery of mental health care,” she explained. “Some may need help with practice preparation while others may need advice on screening; others may already be prescribing and may need advice on ongoing treatment and follow-up. I think there is something for everyone.”
Implementation of the guidelines is difficult in a short visit, Dr. Zuckerbrot acknowledged. “In addition, pediatricians may not have been well trained in the management of adolescent depression during their residencies.” However, the guidelines discuss both “real teams to support the pediatricians in their efforts, as well as virtual teams when staffing is limited.
“The guidelines advise that pediatricians learn about child psychiatry primary care consultation programs in their state and make use of those free telephone consultation programs.” The guidelines also discuss strategies for collaborative or integrative care, she said.
Part I
Part I of the guidelines, “Practice Preparation, Identification, Assessment, and Initial Management,” includes several recommendations for each topic.
For practice preparation, the guidelines recommend that clinicians seek training in the assessment, diagnosis, and treatment of depression, and that they establish a network of referrals and mental health resources in their communities. This network may include not only health professionals, but also current patients and families who are managing teen depression. If available, state-wide or regional child and adolescent psychiatry consultation programs can be included.
The identification and surveillance section of the guidelines calls for screening all patients aged 12 years and older for depression each year, using a formal screening tool on paper or online. The screening could occur at an annual wellness visit or any other medical visit, such as a sports physical. A second recommendation calls for identifying patients at increased risk for depression because of factors such as personal history, family history, substance use, other psychiatric disorders, frequent somatic complaints, or trauma, and monitoring these individuals regularly for signs of depression using a formal screening tool.
The assessment and diagnosis section states that assessment should include interviews with the patients alone as well as with their families or caregivers, and should include screening teens for functional impairment.
Primary care physicians should evaluate for depression not only if an adolescent tests positive on a screening tool, but also in children who present with any emotional problem as the chief complaint, and in those in whom depression is highly suspected even if they test negative on a formal screening tool, the guidelines state.
The three recommendations for initial management of depression in the primary care setting are educating patients and families about depression; developing a treatment plan (if the primary care clinician has had appropriate training) and setting specific treatment goals in areas of functioning such as at home, with peers, and at school; and developing a safety plan that includes restricting access to weapons or other means of self-harm, according to the guidelines.
Part II
Part II of the recommendations, “Treatment and Ongoing Management,” discusses options for managing depression in the primary care setting and utilizing outside resources.
The treatment recommendations emphasize the use of integrated models, if possible. “There is a growing recognition that complex chronic conditions, such as depression, are most successfully managed with proactive, multidisciplinary, patient-centered care teams,” Dr. Cheung and her associates said.
The recommendation for cases of mild depression calls for a period of “active support and monitoring” for 6-8 weeks before reassessing if the teen shows no improvement. By contrast, for cases of moderate to severe depression or cases with evidence of substance abuse or other psychoses, the recommendation calls for potential consultation with a mental health specialist and a discussion of the roles primary and specialty care will play in treatment. The guidelines include a flow chart for PC physicians to follow.
The guidelines suggest that PC clinicians recommend “scientifically tested and proven treatments,” such as psychotherapies, cognitive behavioral therapy (CBT) or interpersonal psychotherapy for adolescents, and/or antidepressant treatment, such as SSRIs, whenever possible and appropriate. It is important to monitor teens on antidepressants regularly to identify adverse events.
Recommendations for the ongoing management of teens with depression in the primary care setting include regular tracking of progress, reassessment if the teen shows no improvement in 6-8 weeks, and consultation with a mental health professional for those who show only partial improvement after exhausting primary care diagnostic and treatment options. Assessment of depressive symptoms is not the only thing to track. Functioning at home, school, and among peers also is important.
The final treatment recommendation is for active support of a depressed teen’s referral to mental health if necessary for best management and sharing care if possible, with an understanding of the roles of the primary and specialty clinicians, the guidelines state.
The guidelines project was funded by the Resource for Advancing Children’s Health Institute and the Bell Canada Chair in Adolescent Mood and Anxiety Disorders.
Dr. Cheung and Dr. Zuckerbrot receive book royalties. Dr Zuckerbrot works for child and adolescent psychiatry for primary care (CAP-PC), now a regional provider for Project TEACH in New York State, and she is on the steering committee as well as faculty for the REACH Institute; both of these institutions are described in the guidelines. Peter S. Jensen, MD, has received royalties from Random House, Oxford University Press, and APPI Inc. He is a part owner of a consulting company, CATCH Services LLC. He is the chief executive officer and president of a nonprofit organization, the Resource for Advancing Children’s Health Institute, but receives no compensation. The other authors indicated they have no financial relationships relevant to the guidelines.
The updated information includes recommendations on collaborative care, practice preparation, establishing networks of referrals, and much more.
“These guidelines were developed for PC clinicians who are in a position to identify and assist youth with depression in their practice settings,” they said. The guidelines apply to individuals aged 10-21 years, and support universal depression screening for those aged 12 and older.
Known as the Guidelines for Adolescent Depression in Primary Care (GLAD-PC), they consist of two parts: Practice Preparation, Identification, Assessment, and Initial Management, with Dr. Zuckerbrot as the lead author, and Treatment and Ongoing Management, led by Amy H. Cheung, MD, of the University of Toronto. They were published online in Pediatrics.
“It has been over 10 years since the [last] guidelines were published and they are supposed to be updated every 5,” Dr. Zuckerbrot said in an interview. “Given the new evidence on screening, psychopharmacology, and collaborative care, the guidelines needed to be revised. The USPSTF [United States Preventive Services Task Force ] and the AAP had already supported universal adolescent depression screening, and these guidelines are finally aligned with those positions.
“Different parts of the guidelines will be the go-to for different pediatricians, depending on where they are in their delivery of mental health care,” she explained. “Some may need help with practice preparation while others may need advice on screening; others may already be prescribing and may need advice on ongoing treatment and follow-up. I think there is something for everyone.”
Implementation of the guidelines is difficult in a short visit, Dr. Zuckerbrot acknowledged. “In addition, pediatricians may not have been well trained in the management of adolescent depression during their residencies.” However, the guidelines discuss both “real teams to support the pediatricians in their efforts, as well as virtual teams when staffing is limited.
“The guidelines advise that pediatricians learn about child psychiatry primary care consultation programs in their state and make use of those free telephone consultation programs.” The guidelines also discuss strategies for collaborative or integrative care, she said.
Part I
Part I of the guidelines, “Practice Preparation, Identification, Assessment, and Initial Management,” includes several recommendations for each topic.
For practice preparation, the guidelines recommend that clinicians seek training in the assessment, diagnosis, and treatment of depression, and that they establish a network of referrals and mental health resources in their communities. This network may include not only health professionals, but also current patients and families who are managing teen depression. If available, state-wide or regional child and adolescent psychiatry consultation programs can be included.
The identification and surveillance section of the guidelines calls for screening all patients aged 12 years and older for depression each year, using a formal screening tool on paper or online. The screening could occur at an annual wellness visit or any other medical visit, such as a sports physical. A second recommendation calls for identifying patients at increased risk for depression because of factors such as personal history, family history, substance use, other psychiatric disorders, frequent somatic complaints, or trauma, and monitoring these individuals regularly for signs of depression using a formal screening tool.
The assessment and diagnosis section states that assessment should include interviews with the patients alone as well as with their families or caregivers, and should include screening teens for functional impairment.
Primary care physicians should evaluate for depression not only if an adolescent tests positive on a screening tool, but also in children who present with any emotional problem as the chief complaint, and in those in whom depression is highly suspected even if they test negative on a formal screening tool, the guidelines state.
The three recommendations for initial management of depression in the primary care setting are educating patients and families about depression; developing a treatment plan (if the primary care clinician has had appropriate training) and setting specific treatment goals in areas of functioning such as at home, with peers, and at school; and developing a safety plan that includes restricting access to weapons or other means of self-harm, according to the guidelines.
Part II
Part II of the recommendations, “Treatment and Ongoing Management,” discusses options for managing depression in the primary care setting and utilizing outside resources.
The treatment recommendations emphasize the use of integrated models, if possible. “There is a growing recognition that complex chronic conditions, such as depression, are most successfully managed with proactive, multidisciplinary, patient-centered care teams,” Dr. Cheung and her associates said.
The recommendation for cases of mild depression calls for a period of “active support and monitoring” for 6-8 weeks before reassessing if the teen shows no improvement. By contrast, for cases of moderate to severe depression or cases with evidence of substance abuse or other psychoses, the recommendation calls for potential consultation with a mental health specialist and a discussion of the roles primary and specialty care will play in treatment. The guidelines include a flow chart for PC physicians to follow.
The guidelines suggest that PC clinicians recommend “scientifically tested and proven treatments,” such as psychotherapies, cognitive behavioral therapy (CBT) or interpersonal psychotherapy for adolescents, and/or antidepressant treatment, such as SSRIs, whenever possible and appropriate. It is important to monitor teens on antidepressants regularly to identify adverse events.
Recommendations for the ongoing management of teens with depression in the primary care setting include regular tracking of progress, reassessment if the teen shows no improvement in 6-8 weeks, and consultation with a mental health professional for those who show only partial improvement after exhausting primary care diagnostic and treatment options. Assessment of depressive symptoms is not the only thing to track. Functioning at home, school, and among peers also is important.
The final treatment recommendation is for active support of a depressed teen’s referral to mental health if necessary for best management and sharing care if possible, with an understanding of the roles of the primary and specialty clinicians, the guidelines state.
The guidelines project was funded by the Resource for Advancing Children’s Health Institute and the Bell Canada Chair in Adolescent Mood and Anxiety Disorders.
Dr. Cheung and Dr. Zuckerbrot receive book royalties. Dr Zuckerbrot works for child and adolescent psychiatry for primary care (CAP-PC), now a regional provider for Project TEACH in New York State, and she is on the steering committee as well as faculty for the REACH Institute; both of these institutions are described in the guidelines. Peter S. Jensen, MD, has received royalties from Random House, Oxford University Press, and APPI Inc. He is a part owner of a consulting company, CATCH Services LLC. He is the chief executive officer and president of a nonprofit organization, the Resource for Advancing Children’s Health Institute, but receives no compensation. The other authors indicated they have no financial relationships relevant to the guidelines.
FROM PEDIATRICS

When to worry about congenital melanocytic nevi
KAUAI, HAWAII – according to Jennifer Huang, MD, a pediatric dermatologist at Boston Children’s Hospital.
Two or more nevi increase the risk of CNS involvement, which in turn increases the risk of malignant conversion by more than 16-fold.

Among the studies she cited was a 2017 literature review of 448 children with congenital nevi, 10 of whom developed melanoma: It arose in the skin in 2, the brain in 6, and an unknown location in 2. All 10 children were born with two or more nevi, and not all of them had large or giant nevi, which is a known risk factor for malignant conversion (Br J Dermatol. 2017 May;176[5]:1131-43).
“If the scanning brain MRI is normal, [children] might not have congenital melanocytic nevus syndrome, and would be at low risk for melanoma,” Dr. Huang said. “If it’s abnormal, they might be at high risk for melanoma.” In the 2017 study, the odds ratio for melanoma with an abnormal MRI was 16.7 (P = .001).
Both melanocytes and neuronal cells arise from the embryonic neural crest, which explains the link between congenital nevi and brain lesions. Almost all congenital nevi are associated with early postzygotic mutations in the NRAS gene, and it’s possible the mutations affect other neural crest cell lines, including in the CNS, she said.
It’s also important to remember that childhood melanoma often doesn’t follow the ABCDE (asymmetry, border irregularity, color not uniform, diameter greater than 6 mm, and evolving) signs of melanoma common in adults.
In a retrospective study of 70 children with melanoma or ambiguous melanocytic tumors, 40% of pubertal subjects and 60% of prepubertal participants did not meet conventional adult ABCDE criteria. The majority of cases were raised, even in color, less than 6 mm across, symmetric, and de novo (J Am Acad Dermatol. 2013 Jun;68[6]:913-25).
It turns out that rapid evolution in size, shape, and color is the number one, unifying factor in childhood melanomas. Other key clues include raised lesions with uniform color or no pigmentation at all. A modified ABCDE for pediatric melanoma has been proposed: amelanotic, bump/bleeding, color uniform, diameter variable, de novo, and evolution.
“The lesson to learn is not to ignore the traditional ABCDEs of melanoma, but to recognize that pediatric melanoma may present with different clinical characteristics, and to incorporate this awareness into our practice,” Dr. Huang said.
She did not have any disclosures. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – according to Jennifer Huang, MD, a pediatric dermatologist at Boston Children’s Hospital.
Two or more nevi increase the risk of CNS involvement, which in turn increases the risk of malignant conversion by more than 16-fold.
Among the studies she cited was a 2017 literature review of 448 children with congenital nevi, 10 of whom developed melanoma: It arose in the skin in 2, the brain in 6, and an unknown location in 2. All 10 children were born with two or more nevi, and not all of them had large or giant nevi, which is a known risk factor for malignant conversion (Br J Dermatol. 2017 May;176[5]:1131-43).
“If the scanning brain MRI is normal, [children] might not have congenital melanocytic nevus syndrome, and would be at low risk for melanoma,” Dr. Huang said. “If it’s abnormal, they might be at high risk for melanoma.” In the 2017 study, the odds ratio for melanoma with an abnormal MRI was 16.7 (P = .001).
Both melanocytes and neuronal cells arise from the embryonic neural crest, which explains the link between congenital nevi and brain lesions. Almost all congenital nevi are associated with early postzygotic mutations in the NRAS gene, and it’s possible the mutations affect other neural crest cell lines, including in the CNS, she said.
It’s also important to remember that childhood melanoma often doesn’t follow the ABCDE (asymmetry, border irregularity, color not uniform, diameter greater than 6 mm, and evolving) signs of melanoma common in adults.
In a retrospective study of 70 children with melanoma or ambiguous melanocytic tumors, 40% of pubertal subjects and 60% of prepubertal participants did not meet conventional adult ABCDE criteria. The majority of cases were raised, even in color, less than 6 mm across, symmetric, and de novo (J Am Acad Dermatol. 2013 Jun;68[6]:913-25).
It turns out that rapid evolution in size, shape, and color is the number one, unifying factor in childhood melanomas. Other key clues include raised lesions with uniform color or no pigmentation at all. A modified ABCDE for pediatric melanoma has been proposed: amelanotic, bump/bleeding, color uniform, diameter variable, de novo, and evolution.
“The lesson to learn is not to ignore the traditional ABCDEs of melanoma, but to recognize that pediatric melanoma may present with different clinical characteristics, and to incorporate this awareness into our practice,” Dr. Huang said.
She did not have any disclosures. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – according to Jennifer Huang, MD, a pediatric dermatologist at Boston Children’s Hospital.
Two or more nevi increase the risk of CNS involvement, which in turn increases the risk of malignant conversion by more than 16-fold.
Among the studies she cited was a 2017 literature review of 448 children with congenital nevi, 10 of whom developed melanoma: It arose in the skin in 2, the brain in 6, and an unknown location in 2. All 10 children were born with two or more nevi, and not all of them had large or giant nevi, which is a known risk factor for malignant conversion (Br J Dermatol. 2017 May;176[5]:1131-43).
“If the scanning brain MRI is normal, [children] might not have congenital melanocytic nevus syndrome, and would be at low risk for melanoma,” Dr. Huang said. “If it’s abnormal, they might be at high risk for melanoma.” In the 2017 study, the odds ratio for melanoma with an abnormal MRI was 16.7 (P = .001).
Both melanocytes and neuronal cells arise from the embryonic neural crest, which explains the link between congenital nevi and brain lesions. Almost all congenital nevi are associated with early postzygotic mutations in the NRAS gene, and it’s possible the mutations affect other neural crest cell lines, including in the CNS, she said.
It’s also important to remember that childhood melanoma often doesn’t follow the ABCDE (asymmetry, border irregularity, color not uniform, diameter greater than 6 mm, and evolving) signs of melanoma common in adults.
In a retrospective study of 70 children with melanoma or ambiguous melanocytic tumors, 40% of pubertal subjects and 60% of prepubertal participants did not meet conventional adult ABCDE criteria. The majority of cases were raised, even in color, less than 6 mm across, symmetric, and de novo (J Am Acad Dermatol. 2013 Jun;68[6]:913-25).
It turns out that rapid evolution in size, shape, and color is the number one, unifying factor in childhood melanomas. Other key clues include raised lesions with uniform color or no pigmentation at all. A modified ABCDE for pediatric melanoma has been proposed: amelanotic, bump/bleeding, color uniform, diameter variable, de novo, and evolution.
“The lesson to learn is not to ignore the traditional ABCDEs of melanoma, but to recognize that pediatric melanoma may present with different clinical characteristics, and to incorporate this awareness into our practice,” Dr. Huang said.
She did not have any disclosures. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
An easy approach to obtaining clean-catch urine from infants
ILLUSTRATIVE CASE
A fussy 6-month-old infant is brought into the emergency department (ED) with a rectal temperature of 101.5° F. She is consolable, breathing normally, and appears well hydrated. You find no clear etiology for her fever and suspect that a urinary tract infection (UTI) may be the source of her illness. How do you proceed with obtaining a urine sample?
A febrile infant in the family physician’s office or ED is a familiar clinical situation that may require an invasive diagnostic work-up. Up to 7% of infants ages 2 to 24 months with fever of unknown origin may have a UTI.2 Collecting a urine sample from pre-toilet-trained children can be time consuming. In fact, obtaining a clean-catch urine sample in this age group took an average of more than one hour in one randomized controlled trial (RCT).3 More convenient methods of urine collection, such as placing a cotton ball in the diaper or using a perineal collection bag, have contamination rates of up to 63%.4
The American Academy of Pediatrics (AAP) guidelines for evaluating possible UTI in a febrile child <2 years of age recommend obtaining a sample for urinalysis “through the most convenient means.”5 If urinalysis is positive, only urine obtained by catheterization or suprapubic aspiration should be cultured. Guidelines from the National Institute for Health and Care Excellence in the United Kingdom are similar, but allow for culture of clean-catch urine samples.6
A recent prospective cohort study examined a noninvasive alternating lumbar-bladder tapping method to stimulate voiding in infants ages 0 to 6 months.7 Within 5 minutes, 49% of the infants provided a clean-catch sample, with contamination rates similar to those of samples obtained using invasive methods.7 Younger infants were more likely to void within the time allotted. Another trial of bladder tapping conducted in hospitalized infants <30 days old showed similar results.8
There are, however, no previously reported randomized trials demonstrating the efficacy of a noninvasive urine collection technique in the outpatient setting.
Use of invasive collection methods requires skilled personnel and may cause significant discomfort for patients (and parents). Noninvasive methods, such as bag urine collection, have unacceptable contamination rates. In addition, waiting to catch a potentially cleaner urine sample is time-consuming, so better strategies to collect urine from infants are needed. This RCT is the first to examine the efficacy of a unique stimulation technique to obtain a clean-catch urine sample from infants ages 1 to 12 months.
STUDY SUMMARY
Noninvasive stimulation method triggers faster clean urine samples
A nonblinded, single-center RCT conducted in Australia compared 2 methods for obtaining a clean-catch urine sample within 5 minutes: the Quick-Wee method (suprapubic stimulation with gauze soaked in cold fluid) or usual care (waiting for spontaneous voiding with no stimulation).1 Three hundred fifty-four infants (ages 1-12 months) who required urine sample collection were randomized in a 1:1 ratio; allocation was concealed. Infants with anatomic or neurologic abnormalities and those needing immediate antibiotic therapy were excluded.
The most common reasons for obtaining the urine sample were fever of unknown origin and “unsettled baby,” followed by poor feeding and suspected UTI. The primary outcome was voiding within 5 minutes; secondary outcomes included time to void, whether urine was successfully caught, contamination rate, and parent/clinician satisfaction.
Study personnel removed the diaper, then cleaned the genitals of all patients with room temperature sterile water. A caregiver or clinician was ready and waiting to catch urine when the patient voided. In the Quick-Wee group, a clinician rubbed the patient’s suprapubic area in a circular fashion with gauze soaked in refrigerated saline (2.8° C). At 5 minutes, clinicians recorded the voiding status and decided how to proceed.
Using intention-to-treat analysis, 31% of the patients in the Quick-Wee group voided within 5 minutes, compared with 12% of the usual-care patients. Similarly, 30% of patients in the Quick-Wee group provided a successful clean-catch sample within 5 minutes compared with 9% in the usual-care group (P<.001; number needed to treat=4.7; 95% CI, 3.4-7.7). Contamination rates were no different between the Quick-Wee and usual-care samples. Both parents and clinicians were more satisfied with the Quick-Wee method than with usual care (median score of 2 vs 3 on a 5-point Likert scale, in which 1 is most satisfied; P<.001). There was no difference when results were adjusted for age or sex. No adverse events occurred.
WHAT’S NEW
New method could reduce the need for invasive sampling
A simple suprapubic stimulation technique increased the number of infants who provided a clean-catch voided urine sample within 5 minutes—a clinically relevant and satisfying outcome. In appropriate patients, use of the Quick-Wee method to obtain a clean-catch voided sample for initial urinalysis, rather than attempting methods with known high contamination rates, may potentially reduce the need for invasive sampling using catheterization or suprapubic aspiration.
CAVEATS
Complete age range and ideal storage temperature are unknown
Neonates and pre-continent children older than 12 months were not included in this trial, so these conclusions do not apply to those groups of patients. The intervention period lasted only 5 minutes, but other published studies suggest that this amount of time is adequate for voiding to occur.6,7 Although this study used soaking fluid stored at 2.8° C, the ideal storage temperature is unknown.
CHALLENGES TO IMPLEMENTATION
AAP doesn’t endorse clean-catch urine samples for culture
The Quick-Wee method is simple and easy to implement, and requires no specialized training or equipment. AAP guidelines do not endorse the use of clean-catch voided urine for culture, which may be a barrier to changing urine collection practices in some settings.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Kaufman J, Fitzpatrick P, Tosif S, et al. Faster clean catch urine collection (Quick-Wee method) from infants: randomised controlled trial. BMJ. 2017;357:j1341.
2. Shaikh N, Morone NE, Bost JE, et al. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008;27:302-308.
3. Davies P, Greenwood R, Benger J. Randomised trial of a vibrating bladder stimulator—the time to pee study. Arch Dis Child. 2008;93:423-424.
4. Al-Orifi F, McGillivray D, Tange S, et al. Urine culture from bag specimens in young children: are the risks too high? J Pediatr. 2000;137:221-226.
5. Reaffirmation of AAP clinical practice guideline: the diagnosis and management of the initial urinary tract infection in febrile infants and young children 2-24 months of age. Pediatrics. 2016;138:e20163026.
6. National Institute for Health and Care Excellence. Urinary tract infection in under 16s: diagnosis and management. Clinical guideline CG54. Published August 2007. Available at: https://www.nice.org.uk/guidance/cg54/chapter/1-guidance. Accessed May 30, 2017.
7. Labrosse M, Levy A, Autmizguine J, et al. Evaluation of a new strategy for clean-catch urine in infants. Pediatrics. 2016;138:e20160573.
8. Herreros Fernández ML, González Merino N, Tagarro García A, et al. A new technique for fast and safe collection of urine in newborns. Arch Dis Child. 2013;98:27-29.
ILLUSTRATIVE CASE
A fussy 6-month-old infant is brought into the emergency department (ED) with a rectal temperature of 101.5° F. She is consolable, breathing normally, and appears well hydrated. You find no clear etiology for her fever and suspect that a urinary tract infection (UTI) may be the source of her illness. How do you proceed with obtaining a urine sample?
A febrile infant in the family physician’s office or ED is a familiar clinical situation that may require an invasive diagnostic work-up. Up to 7% of infants ages 2 to 24 months with fever of unknown origin may have a UTI.2 Collecting a urine sample from pre-toilet-trained children can be time consuming. In fact, obtaining a clean-catch urine sample in this age group took an average of more than one hour in one randomized controlled trial (RCT).3 More convenient methods of urine collection, such as placing a cotton ball in the diaper or using a perineal collection bag, have contamination rates of up to 63%.4
The American Academy of Pediatrics (AAP) guidelines for evaluating possible UTI in a febrile child <2 years of age recommend obtaining a sample for urinalysis “through the most convenient means.”5 If urinalysis is positive, only urine obtained by catheterization or suprapubic aspiration should be cultured. Guidelines from the National Institute for Health and Care Excellence in the United Kingdom are similar, but allow for culture of clean-catch urine samples.6
A recent prospective cohort study examined a noninvasive alternating lumbar-bladder tapping method to stimulate voiding in infants ages 0 to 6 months.7 Within 5 minutes, 49% of the infants provided a clean-catch sample, with contamination rates similar to those of samples obtained using invasive methods.7 Younger infants were more likely to void within the time allotted. Another trial of bladder tapping conducted in hospitalized infants <30 days old showed similar results.8
There are, however, no previously reported randomized trials demonstrating the efficacy of a noninvasive urine collection technique in the outpatient setting.
Use of invasive collection methods requires skilled personnel and may cause significant discomfort for patients (and parents). Noninvasive methods, such as bag urine collection, have unacceptable contamination rates. In addition, waiting to catch a potentially cleaner urine sample is time-consuming, so better strategies to collect urine from infants are needed. This RCT is the first to examine the efficacy of a unique stimulation technique to obtain a clean-catch urine sample from infants ages 1 to 12 months.
STUDY SUMMARY
Noninvasive stimulation method triggers faster clean urine samples
A nonblinded, single-center RCT conducted in Australia compared 2 methods for obtaining a clean-catch urine sample within 5 minutes: the Quick-Wee method (suprapubic stimulation with gauze soaked in cold fluid) or usual care (waiting for spontaneous voiding with no stimulation).1 Three hundred fifty-four infants (ages 1-12 months) who required urine sample collection were randomized in a 1:1 ratio; allocation was concealed. Infants with anatomic or neurologic abnormalities and those needing immediate antibiotic therapy were excluded.
The most common reasons for obtaining the urine sample were fever of unknown origin and “unsettled baby,” followed by poor feeding and suspected UTI. The primary outcome was voiding within 5 minutes; secondary outcomes included time to void, whether urine was successfully caught, contamination rate, and parent/clinician satisfaction.
Study personnel removed the diaper, then cleaned the genitals of all patients with room temperature sterile water. A caregiver or clinician was ready and waiting to catch urine when the patient voided. In the Quick-Wee group, a clinician rubbed the patient’s suprapubic area in a circular fashion with gauze soaked in refrigerated saline (2.8° C). At 5 minutes, clinicians recorded the voiding status and decided how to proceed.
Using intention-to-treat analysis, 31% of the patients in the Quick-Wee group voided within 5 minutes, compared with 12% of the usual-care patients. Similarly, 30% of patients in the Quick-Wee group provided a successful clean-catch sample within 5 minutes compared with 9% in the usual-care group (P<.001; number needed to treat=4.7; 95% CI, 3.4-7.7). Contamination rates were no different between the Quick-Wee and usual-care samples. Both parents and clinicians were more satisfied with the Quick-Wee method than with usual care (median score of 2 vs 3 on a 5-point Likert scale, in which 1 is most satisfied; P<.001). There was no difference when results were adjusted for age or sex. No adverse events occurred.
WHAT’S NEW
New method could reduce the need for invasive sampling
A simple suprapubic stimulation technique increased the number of infants who provided a clean-catch voided urine sample within 5 minutes—a clinically relevant and satisfying outcome. In appropriate patients, use of the Quick-Wee method to obtain a clean-catch voided sample for initial urinalysis, rather than attempting methods with known high contamination rates, may potentially reduce the need for invasive sampling using catheterization or suprapubic aspiration.
CAVEATS
Complete age range and ideal storage temperature are unknown
Neonates and pre-continent children older than 12 months were not included in this trial, so these conclusions do not apply to those groups of patients. The intervention period lasted only 5 minutes, but other published studies suggest that this amount of time is adequate for voiding to occur.6,7 Although this study used soaking fluid stored at 2.8° C, the ideal storage temperature is unknown.
CHALLENGES TO IMPLEMENTATION
AAP doesn’t endorse clean-catch urine samples for culture
The Quick-Wee method is simple and easy to implement, and requires no specialized training or equipment. AAP guidelines do not endorse the use of clean-catch voided urine for culture, which may be a barrier to changing urine collection practices in some settings.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
ILLUSTRATIVE CASE
A fussy 6-month-old infant is brought into the emergency department (ED) with a rectal temperature of 101.5° F. She is consolable, breathing normally, and appears well hydrated. You find no clear etiology for her fever and suspect that a urinary tract infection (UTI) may be the source of her illness. How do you proceed with obtaining a urine sample?
A febrile infant in the family physician’s office or ED is a familiar clinical situation that may require an invasive diagnostic work-up. Up to 7% of infants ages 2 to 24 months with fever of unknown origin may have a UTI.2 Collecting a urine sample from pre-toilet-trained children can be time consuming. In fact, obtaining a clean-catch urine sample in this age group took an average of more than one hour in one randomized controlled trial (RCT).3 More convenient methods of urine collection, such as placing a cotton ball in the diaper or using a perineal collection bag, have contamination rates of up to 63%.4
The American Academy of Pediatrics (AAP) guidelines for evaluating possible UTI in a febrile child <2 years of age recommend obtaining a sample for urinalysis “through the most convenient means.”5 If urinalysis is positive, only urine obtained by catheterization or suprapubic aspiration should be cultured. Guidelines from the National Institute for Health and Care Excellence in the United Kingdom are similar, but allow for culture of clean-catch urine samples.6
A recent prospective cohort study examined a noninvasive alternating lumbar-bladder tapping method to stimulate voiding in infants ages 0 to 6 months.7 Within 5 minutes, 49% of the infants provided a clean-catch sample, with contamination rates similar to those of samples obtained using invasive methods.7 Younger infants were more likely to void within the time allotted. Another trial of bladder tapping conducted in hospitalized infants <30 days old showed similar results.8
There are, however, no previously reported randomized trials demonstrating the efficacy of a noninvasive urine collection technique in the outpatient setting.
Use of invasive collection methods requires skilled personnel and may cause significant discomfort for patients (and parents). Noninvasive methods, such as bag urine collection, have unacceptable contamination rates. In addition, waiting to catch a potentially cleaner urine sample is time-consuming, so better strategies to collect urine from infants are needed. This RCT is the first to examine the efficacy of a unique stimulation technique to obtain a clean-catch urine sample from infants ages 1 to 12 months.
STUDY SUMMARY
Noninvasive stimulation method triggers faster clean urine samples
A nonblinded, single-center RCT conducted in Australia compared 2 methods for obtaining a clean-catch urine sample within 5 minutes: the Quick-Wee method (suprapubic stimulation with gauze soaked in cold fluid) or usual care (waiting for spontaneous voiding with no stimulation).1 Three hundred fifty-four infants (ages 1-12 months) who required urine sample collection were randomized in a 1:1 ratio; allocation was concealed. Infants with anatomic or neurologic abnormalities and those needing immediate antibiotic therapy were excluded.
The most common reasons for obtaining the urine sample were fever of unknown origin and “unsettled baby,” followed by poor feeding and suspected UTI. The primary outcome was voiding within 5 minutes; secondary outcomes included time to void, whether urine was successfully caught, contamination rate, and parent/clinician satisfaction.
Study personnel removed the diaper, then cleaned the genitals of all patients with room temperature sterile water. A caregiver or clinician was ready and waiting to catch urine when the patient voided. In the Quick-Wee group, a clinician rubbed the patient’s suprapubic area in a circular fashion with gauze soaked in refrigerated saline (2.8° C). At 5 minutes, clinicians recorded the voiding status and decided how to proceed.
Using intention-to-treat analysis, 31% of the patients in the Quick-Wee group voided within 5 minutes, compared with 12% of the usual-care patients. Similarly, 30% of patients in the Quick-Wee group provided a successful clean-catch sample within 5 minutes compared with 9% in the usual-care group (P<.001; number needed to treat=4.7; 95% CI, 3.4-7.7). Contamination rates were no different between the Quick-Wee and usual-care samples. Both parents and clinicians were more satisfied with the Quick-Wee method than with usual care (median score of 2 vs 3 on a 5-point Likert scale, in which 1 is most satisfied; P<.001). There was no difference when results were adjusted for age or sex. No adverse events occurred.
WHAT’S NEW
New method could reduce the need for invasive sampling
A simple suprapubic stimulation technique increased the number of infants who provided a clean-catch voided urine sample within 5 minutes—a clinically relevant and satisfying outcome. In appropriate patients, use of the Quick-Wee method to obtain a clean-catch voided sample for initial urinalysis, rather than attempting methods with known high contamination rates, may potentially reduce the need for invasive sampling using catheterization or suprapubic aspiration.
CAVEATS
Complete age range and ideal storage temperature are unknown
Neonates and pre-continent children older than 12 months were not included in this trial, so these conclusions do not apply to those groups of patients. The intervention period lasted only 5 minutes, but other published studies suggest that this amount of time is adequate for voiding to occur.6,7 Although this study used soaking fluid stored at 2.8° C, the ideal storage temperature is unknown.
CHALLENGES TO IMPLEMENTATION
AAP doesn’t endorse clean-catch urine samples for culture
The Quick-Wee method is simple and easy to implement, and requires no specialized training or equipment. AAP guidelines do not endorse the use of clean-catch voided urine for culture, which may be a barrier to changing urine collection practices in some settings.
ACKNOWLEDGEMENT
The PURLs Surveillance System was supported in part by Grant Number UL1RR024999 from the National Center For Research Resources, a Clinical Translational Science Award to the University of Chicago. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Center For Research Resources or the National Institutes of Health.
1. Kaufman J, Fitzpatrick P, Tosif S, et al. Faster clean catch urine collection (Quick-Wee method) from infants: randomised controlled trial. BMJ. 2017;357:j1341.
2. Shaikh N, Morone NE, Bost JE, et al. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008;27:302-308.
3. Davies P, Greenwood R, Benger J. Randomised trial of a vibrating bladder stimulator—the time to pee study. Arch Dis Child. 2008;93:423-424.
4. Al-Orifi F, McGillivray D, Tange S, et al. Urine culture from bag specimens in young children: are the risks too high? J Pediatr. 2000;137:221-226.
5. Reaffirmation of AAP clinical practice guideline: the diagnosis and management of the initial urinary tract infection in febrile infants and young children 2-24 months of age. Pediatrics. 2016;138:e20163026.
6. National Institute for Health and Care Excellence. Urinary tract infection in under 16s: diagnosis and management. Clinical guideline CG54. Published August 2007. Available at: https://www.nice.org.uk/guidance/cg54/chapter/1-guidance. Accessed May 30, 2017.
7. Labrosse M, Levy A, Autmizguine J, et al. Evaluation of a new strategy for clean-catch urine in infants. Pediatrics. 2016;138:e20160573.
8. Herreros Fernández ML, González Merino N, Tagarro García A, et al. A new technique for fast and safe collection of urine in newborns. Arch Dis Child. 2013;98:27-29.
1. Kaufman J, Fitzpatrick P, Tosif S, et al. Faster clean catch urine collection (Quick-Wee method) from infants: randomised controlled trial. BMJ. 2017;357:j1341.
2. Shaikh N, Morone NE, Bost JE, et al. Prevalence of urinary tract infection in childhood: a meta-analysis. Pediatr Infect Dis J. 2008;27:302-308.
3. Davies P, Greenwood R, Benger J. Randomised trial of a vibrating bladder stimulator—the time to pee study. Arch Dis Child. 2008;93:423-424.
4. Al-Orifi F, McGillivray D, Tange S, et al. Urine culture from bag specimens in young children: are the risks too high? J Pediatr. 2000;137:221-226.
5. Reaffirmation of AAP clinical practice guideline: the diagnosis and management of the initial urinary tract infection in febrile infants and young children 2-24 months of age. Pediatrics. 2016;138:e20163026.
6. National Institute for Health and Care Excellence. Urinary tract infection in under 16s: diagnosis and management. Clinical guideline CG54. Published August 2007. Available at: https://www.nice.org.uk/guidance/cg54/chapter/1-guidance. Accessed May 30, 2017.
7. Labrosse M, Levy A, Autmizguine J, et al. Evaluation of a new strategy for clean-catch urine in infants. Pediatrics. 2016;138:e20160573.
8. Herreros Fernández ML, González Merino N, Tagarro García A, et al. A new technique for fast and safe collection of urine in newborns. Arch Dis Child. 2013;98:27-29.
Copyright © 2018. The Family Physicians Inquiries Network. All rights reserved.
PRACTICE CHANGER
Apply gauze soaked in cold sterile saline to the suprapubic area to stimulate infants ages 1 to 12 months to provide a clean-catch urine sample. Doing so produces significantly more clean-catch urine samples within 5 minutes than simply waiting for the patient to void, with no difference in contamination and with increased parental and provider satisfaction.1
STRENGTH OF RECOMMENDATION
B: Based on a single good-quality, randomized controlled trial.
Kaufman J, Fitzpatrick P, Tosif S, et al. Faster clean catch urine collection (Quick-Wee method) from infants: randomised controlled trial. BMJ. 2017;357:j1341.

Depigmented plaques on vulva
A mother brought her 8-year-old daughter to our office for evaluation of vitiligo “down there” (FIGURE). The skin eruption first appeared on her vulva a year earlier and was intermittently pruritic. The lesions were initially smaller and red, but had since lightened in color, coalesced, and had begun to spread to the perianal area. The patient’s mother had received a call from her daughter’s teacher who observed that her daughter was scratching the area and might be masturbating in class.
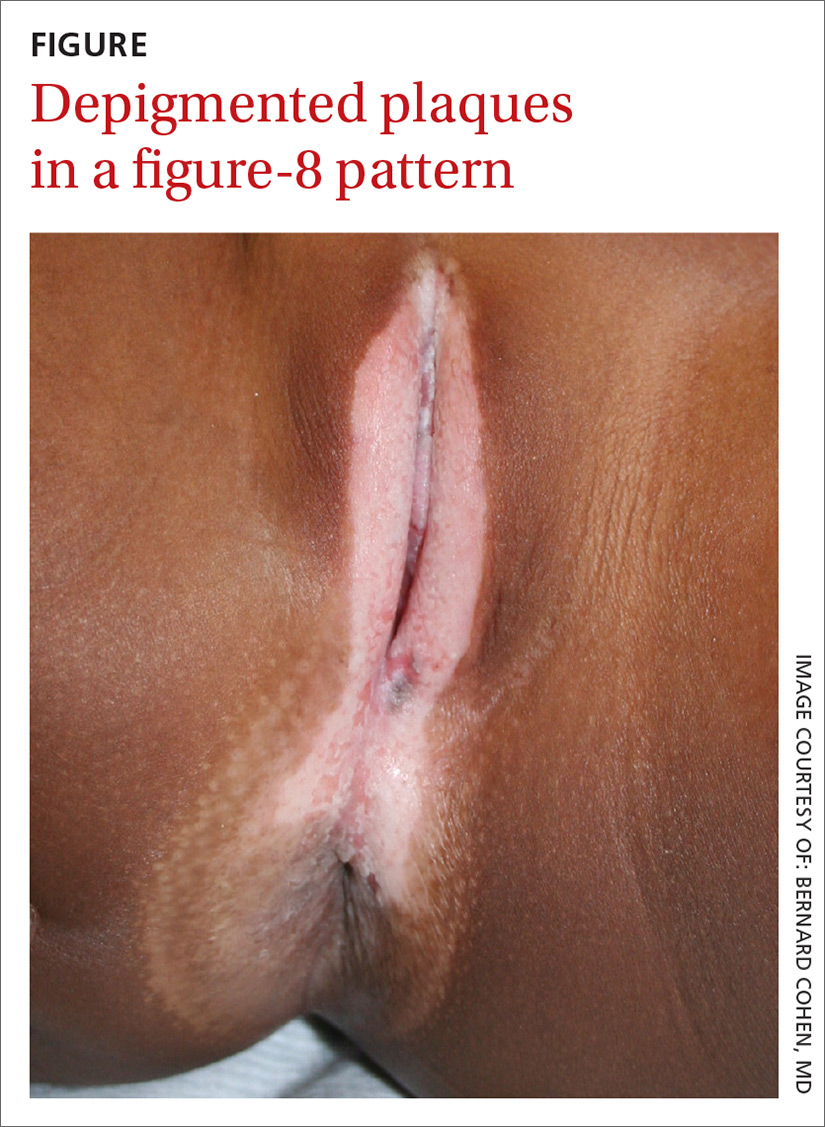
The mother reported that 6 months earlier, her daughter had experienced bloody spots in her underwear accompanied by dysuria. The mother brought her to the emergency department, where she was treated with antibiotics for a urinary tract infection.
Our physical examination revealed well-circumscribed, symmetric, depigmented, confluent, crinkled, parchment-like plaques with small hemorrhagic erosions on the medial labia majora and minora. The lesions had spread to the perianal area with depigmentation superiorly and hypopigmentation inferiorly, creating a figure-8 pattern.
A review of systems was negative for pruritus, pain, dysuria, dyschezia, constipation, and vaginal discharge. The patient denied sexual activity, depression, or anxiety. Her mother denied behavioral changes in her daughter and said that her daughter hadn’t had any one-on-one time alone with any adults besides herself. Her mother was concerned that the white spots might spread to the rest of her daughter’s body, which could affect her socially.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Lichen sclerosus
Based on the history and clinical findings, including the classic figure-8 pattern, we diagnosed childhood lichen sclerosus (LS) in this patient. LS is a chronic inflammatory skin disorder that primarily affects the genital mucosa. The disorder can present at any age, but is most common among postmenopausal women, with a prevalence estimated to be as high as one in 30.1-3 A second incidence peak is observed in prepubescent girls, with a prevalence of one in 900.3,4 LS is less common in men and boys, with a female-to-male ratio that can reach 10:1.5 The classic symptoms of LS are pruritus and pain, which may be intermittent or persistent.
In girls, initial manifestations may be constipation, dysuria, or even behavioral symptoms such as night fears, which can occur because children are less active at night and become more aware of urinary discomfort.1,2,6 Typical signs of LS are thin atrophic plaques that spare the vagina and cervix. The plaques can be ivory-white, erythematous, or violaceous. Some patients have perianal lesions as well, and can display the pathognomonic figure-8 pattern of porcelain plaques around the vulva and anus.5
With more advanced disease, erosions, lichenification, and even distortion of vulvar architecture may occur.2,4,7 In severe cases, labia resorption and clitoral phimosis may develop.5 Complications include secondary infection, dyspareunia, and psychosexual distress. The most worrisome sequela of LS is squamous cell carcinoma of the vulva (SCCV), which occurs in 5% of female patients with LS.4
In men and boys, LS typically involves the foreskin and the glans, while sparing the perianal region.5 Scarring of the foreskin can lead to phimosis, and patients may complain of painful erections and difficulty urinating. LS can also occur away from the genitalia in both males and females.
Autoimmune mechanisms, genetics, and hormones play a role
The exact pathogenesis of LS remains unknown, but multiple factors are likely at work.
Autoimmune mechanisms. Up to 60% of women with LS have an autoimmune disorder, which is most commonly vitiligo, alopecia areata, or thyroid disease.5 In addition, 67% of patients have autoantibodies against extracellular matrix protein 1, and 30% have them against bullous pemphigoid antigen 180.1,8
Genetics. LS is associated with certain human leukocyte antigen class II haplotypes (especially DQ7) and with polymorphisms at the interleukin-1 receptor antagonist gene locus.5,6,9
Hormones. The clear peaks of incidence during times of low estrogen, and a higher incidence in patients with Turner syndrome or kidney disease, suggest that low estrogen may play a role in the development of LS, as well.1,5,6
While it is generally accepted that trauma may trigger LS via the Koebner phenomenon (the appearance of lesions at the site of injury), there is debate as to whether microbes—especially Borrelia burgdorferi and human papillomavirus (HPV)—might play a role.1,5
Diagnosis is often delayed, misdiagnosis is common
The average delay from symptom onset to diagnosis of LS is 1.3 years, and up to 84% of childhood LS is misdiagnosed before referral.2,9 The differential diagnosis includes:
Sexual abuse. In prepubertal girls presenting with genital redness, the can’t-miss diagnosis is sexual abuse, which occurs in more than 25% of children in the United States.10 Initial manifestations may be regression in developmental milestones, such as new-onset bedwetting, or behavioral changes such as social withdrawal or declining academic performance.11
However, physicians must be conscientious about ruling out medical etiologies before prematurely diagnosing abuse. Fourteen percent of girls with LS are incorrectly diagnosed as having been sexually abused.2 A clinical pearl is that while LS may resemble abuse on exam, it rarely affects the hymenal structure.12 It is also important to keep in mind that the 2 entities are not incompatible, as sexual abuse leading to LS via Koebnerization is a well-described phenomenon.12
Lichen planus. LP, which is also an immune-mediated inflammatory disorder affecting the vulva, classically presents with the 6 Ps: pruritic, polygonal, planar, purple papules and plaques.4 LP is distinguished from LS by being rare in childhood, having a predilection for the flexor wrists, and involving the oral and vaginal mucosa.4
Lichen simplex chronicus (LSC) is a chronic, circumscribed, pruritic, eczematous condition that becomes lichenified with thickened skin secondary to repeated scratching.13 Children with atopic dermatitis can develop LSC, but other children can also develop the scratch-itch cycle that results in the thickened plaques of LSC. Like LS, LSC can occur in areas other than the genitalia, including the neck and feet.14
Allergic contact dermatitis can occur in the genital area from diaper creams, soaps, and perfumes. Irritant contact dermatitis can occur from exposure to diarrhea, bedwetting, and other irritants. Contact dermatitis is less likely to have the classic figure-8 pattern seen in LS.
Psoriasis in the genital area can be confused with LS. However, psoriasis favors the groin creases in what is called inverse psoriasis. In addition, psoriasis tends to involve multiple areas, including the extensor surfaces of the elbows and knees, the nails, and the scalp.
Vitiligo can present on the genitals as circumscribed hypopigmented and depigmented patches that are flat. Vitiligo is asymptomatic, and the only pathology is the change in skin color. With LS, there is lichenification, atrophy, and sclerosis.4 Vitiligo often occurs with bilateral symmetric involvement in areas of trauma including the face, neck, scalp, elbows, wrists, hands, knees, ankles, and feet.
Treatment aims to improve symptoms
LS is usually diagnosed clinically (especially in children, as a biopsy is a great challenge to perform). However, when the clinical presentation is unclear, a skin biopsy will demonstrate the diagnostic findings of thinning of the epidermis, loss of rete pegs, hyperkeratosis, and dermal fibrosis with a T-lymphocyte-dominant inflammatory infiltrate.1,2,4,5
LS is a remitting and relapsing condition with no cure. The goals of treatment are to provide symptom relief and minimize scarring and atrophy,2 but it is unknown whether treatment reduces the risk of malignancy.9
First-line treatment for both genders and all ages is ultrapotent topical corticosteroids; clobetasol propionate 0.05% is most commonly used.1,6 Regimens vary, but the vast majority of patients improve within 3 months of once-daily treatment.4
For refractory LS, calcineurin inhibitors such as tacrolimus may be used. Although it has a black box warning regarding a potential cancer risk, long-term studies of children using tacrolimus for atopic dermatitis have not demonstrated an increased risk of malignancy.6,9 Because of a considerable adverse effect profile, oral retinoids are limited to refractory cases in adults.6 Surgery is reserved for scarring and adhesions.4
Follow-up plays an important role in management
Historically, it was believed that pediatric LS had an excellent prognosis, with patients achieving complete resolution after puberty.1,4 Recent findings have shown mixed results, with LS persisting in many patients beyond puberty.2,4 Therefore, regular follow-up is recommended every 6 to 12 months.
For uncomplicated LS, specialist follow-up is not indicated. Female patients should regularly conduct self-examinations and, at a minimum, undergo annual examinations by their primary care physician. Those who require specialist follow-up include patients with difficult-to-control symptoms, hypertrophic lesions, a history of SCCV or differentiated vulvar intraepithelial neoplasia (dVIN), or pathology showing possible dVIN.15
Our patient. We prescribed clobetasol propionate 0.05% ointment to be used once daily for 8 weeks. We stressed the importance of genital self-examinations using a mirror to monitor for any concerning changes such as skin thickening. We showed the patient and her mother photos of normal female genitalia to help normalize the genital exam, and taught the patient how to find her plaques in the mirror. We set expectations by emphasizing the chronic nature of LS and the likelihood of recurrence. We also encouraged HPV vaccination in the upcoming years to prevent both cervical cancer and HPV-related SCCV.
CORRESPONDENCE
Somya Abubucker, MD, University of Hawaii, 1356 Lusitana Street, 7th floor, Honolulu, HI 96813; sabubuck@hawaii.edu.
1. Murphy R. Lichen sclerosus. Dermatol Clin. 2010;28:707-715.
2. Dendrinos ML, Quint EH. Lichen sclerosus in children and adolescents. Curr Opin Obstet Gynecol. 2013;25:370-374.
3. Eva LJ. Screening and follow up of vulval skin disorders. Best Pract Res Clin Obstet Gynaecol. 2012;26:175-188.
4. Focseneanu MA, Gupta M, Squires KC, et al. The course of lichen sclerosus diagnosed prior to puberty. J Pediatr Adolesc Gynecol. 2013;26:153-155.
5. Funaro D. Lichen sclerosus: a review and practical approach. Dermatol Ther. 2004;17:28-37.
6. Heymann WR. Lichen sclerosus. J Am Acad Dermatol. 2007;56:683-684.
7. Tong LX, Sun GS, Teng JM. Pediatric lichen sclerosus: a review of the epidemiology and treatment options. Pediatr Dermatol. 2015;32:593-599.
8. Lagerstedt M, Karvinen K, Joki-Erkkilä M, et al. Childhood lichen sclerosus—a challenge for clinicians. Pediatr Dermatol. 2013;30:444-450.
9. Keith PJ, Wolz MM, Peters MS. Eosinophils in lichen sclerosus et atrophicus. J Cutan Pathol. 2015;42:693-698.
10. National Sexual Violence Resource Center. Child sexual abuse prevention. 2011. Available at: https://www.nsvrc.org/sites/default/files/Publications_NSVRC_Overview_Child-sexual-abuse-prevention_0.pdf. Accessed February 8, 2018.
11. Dubowitz H, Lane WG. Abused and neglected children. In: Kliegman RM, Stanton BF, St. Geme JW, et al, eds. Nelson Textbook of Pediatrics. 20th ed. Philadelphia, PA: Elsevier; 2016:236-249.
12. Powell J, Wojnarowska F. Childhood vulvar lichen sclerosus: an increasingly common problem. J Am Acad Dermatol. 2001;44:803-806.
13. Reamy BV, Bunt CW, Fletcher S. A diagnostic approach to pruritus. Am Fam Physician. 2011;84:195-202.
14. Warshaw E, Hook K. Dermatitis. In: Soutor C, Hordinsky MK, eds. Clinical Dermatology. 1st ed. New York, NY: McGraw-Hill; 2013.
15. Jones RW, Scurry J, Neill S, et al. Guidelines for the follow-up of women with vulvar lichen sclerosus in specialist clinics. Am J Obstet Gynecol. 2008;198:496.e1-e3.
A mother brought her 8-year-old daughter to our office for evaluation of vitiligo “down there” (FIGURE). The skin eruption first appeared on her vulva a year earlier and was intermittently pruritic. The lesions were initially smaller and red, but had since lightened in color, coalesced, and had begun to spread to the perianal area. The patient’s mother had received a call from her daughter’s teacher who observed that her daughter was scratching the area and might be masturbating in class.
The mother reported that 6 months earlier, her daughter had experienced bloody spots in her underwear accompanied by dysuria. The mother brought her to the emergency department, where she was treated with antibiotics for a urinary tract infection.
Our physical examination revealed well-circumscribed, symmetric, depigmented, confluent, crinkled, parchment-like plaques with small hemorrhagic erosions on the medial labia majora and minora. The lesions had spread to the perianal area with depigmentation superiorly and hypopigmentation inferiorly, creating a figure-8 pattern.
A review of systems was negative for pruritus, pain, dysuria, dyschezia, constipation, and vaginal discharge. The patient denied sexual activity, depression, or anxiety. Her mother denied behavioral changes in her daughter and said that her daughter hadn’t had any one-on-one time alone with any adults besides herself. Her mother was concerned that the white spots might spread to the rest of her daughter’s body, which could affect her socially.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Lichen sclerosus
Based on the history and clinical findings, including the classic figure-8 pattern, we diagnosed childhood lichen sclerosus (LS) in this patient. LS is a chronic inflammatory skin disorder that primarily affects the genital mucosa. The disorder can present at any age, but is most common among postmenopausal women, with a prevalence estimated to be as high as one in 30.1-3 A second incidence peak is observed in prepubescent girls, with a prevalence of one in 900.3,4 LS is less common in men and boys, with a female-to-male ratio that can reach 10:1.5 The classic symptoms of LS are pruritus and pain, which may be intermittent or persistent.
In girls, initial manifestations may be constipation, dysuria, or even behavioral symptoms such as night fears, which can occur because children are less active at night and become more aware of urinary discomfort.1,2,6 Typical signs of LS are thin atrophic plaques that spare the vagina and cervix. The plaques can be ivory-white, erythematous, or violaceous. Some patients have perianal lesions as well, and can display the pathognomonic figure-8 pattern of porcelain plaques around the vulva and anus.5
With more advanced disease, erosions, lichenification, and even distortion of vulvar architecture may occur.2,4,7 In severe cases, labia resorption and clitoral phimosis may develop.5 Complications include secondary infection, dyspareunia, and psychosexual distress. The most worrisome sequela of LS is squamous cell carcinoma of the vulva (SCCV), which occurs in 5% of female patients with LS.4
In men and boys, LS typically involves the foreskin and the glans, while sparing the perianal region.5 Scarring of the foreskin can lead to phimosis, and patients may complain of painful erections and difficulty urinating. LS can also occur away from the genitalia in both males and females.
Autoimmune mechanisms, genetics, and hormones play a role
The exact pathogenesis of LS remains unknown, but multiple factors are likely at work.
Autoimmune mechanisms. Up to 60% of women with LS have an autoimmune disorder, which is most commonly vitiligo, alopecia areata, or thyroid disease.5 In addition, 67% of patients have autoantibodies against extracellular matrix protein 1, and 30% have them against bullous pemphigoid antigen 180.1,8
Genetics. LS is associated with certain human leukocyte antigen class II haplotypes (especially DQ7) and with polymorphisms at the interleukin-1 receptor antagonist gene locus.5,6,9
Hormones. The clear peaks of incidence during times of low estrogen, and a higher incidence in patients with Turner syndrome or kidney disease, suggest that low estrogen may play a role in the development of LS, as well.1,5,6
While it is generally accepted that trauma may trigger LS via the Koebner phenomenon (the appearance of lesions at the site of injury), there is debate as to whether microbes—especially Borrelia burgdorferi and human papillomavirus (HPV)—might play a role.1,5
Diagnosis is often delayed, misdiagnosis is common
The average delay from symptom onset to diagnosis of LS is 1.3 years, and up to 84% of childhood LS is misdiagnosed before referral.2,9 The differential diagnosis includes:
Sexual abuse. In prepubertal girls presenting with genital redness, the can’t-miss diagnosis is sexual abuse, which occurs in more than 25% of children in the United States.10 Initial manifestations may be regression in developmental milestones, such as new-onset bedwetting, or behavioral changes such as social withdrawal or declining academic performance.11
However, physicians must be conscientious about ruling out medical etiologies before prematurely diagnosing abuse. Fourteen percent of girls with LS are incorrectly diagnosed as having been sexually abused.2 A clinical pearl is that while LS may resemble abuse on exam, it rarely affects the hymenal structure.12 It is also important to keep in mind that the 2 entities are not incompatible, as sexual abuse leading to LS via Koebnerization is a well-described phenomenon.12
Lichen planus. LP, which is also an immune-mediated inflammatory disorder affecting the vulva, classically presents with the 6 Ps: pruritic, polygonal, planar, purple papules and plaques.4 LP is distinguished from LS by being rare in childhood, having a predilection for the flexor wrists, and involving the oral and vaginal mucosa.4
Lichen simplex chronicus (LSC) is a chronic, circumscribed, pruritic, eczematous condition that becomes lichenified with thickened skin secondary to repeated scratching.13 Children with atopic dermatitis can develop LSC, but other children can also develop the scratch-itch cycle that results in the thickened plaques of LSC. Like LS, LSC can occur in areas other than the genitalia, including the neck and feet.14
Allergic contact dermatitis can occur in the genital area from diaper creams, soaps, and perfumes. Irritant contact dermatitis can occur from exposure to diarrhea, bedwetting, and other irritants. Contact dermatitis is less likely to have the classic figure-8 pattern seen in LS.
Psoriasis in the genital area can be confused with LS. However, psoriasis favors the groin creases in what is called inverse psoriasis. In addition, psoriasis tends to involve multiple areas, including the extensor surfaces of the elbows and knees, the nails, and the scalp.
Vitiligo can present on the genitals as circumscribed hypopigmented and depigmented patches that are flat. Vitiligo is asymptomatic, and the only pathology is the change in skin color. With LS, there is lichenification, atrophy, and sclerosis.4 Vitiligo often occurs with bilateral symmetric involvement in areas of trauma including the face, neck, scalp, elbows, wrists, hands, knees, ankles, and feet.
Treatment aims to improve symptoms
LS is usually diagnosed clinically (especially in children, as a biopsy is a great challenge to perform). However, when the clinical presentation is unclear, a skin biopsy will demonstrate the diagnostic findings of thinning of the epidermis, loss of rete pegs, hyperkeratosis, and dermal fibrosis with a T-lymphocyte-dominant inflammatory infiltrate.1,2,4,5
LS is a remitting and relapsing condition with no cure. The goals of treatment are to provide symptom relief and minimize scarring and atrophy,2 but it is unknown whether treatment reduces the risk of malignancy.9
First-line treatment for both genders and all ages is ultrapotent topical corticosteroids; clobetasol propionate 0.05% is most commonly used.1,6 Regimens vary, but the vast majority of patients improve within 3 months of once-daily treatment.4
For refractory LS, calcineurin inhibitors such as tacrolimus may be used. Although it has a black box warning regarding a potential cancer risk, long-term studies of children using tacrolimus for atopic dermatitis have not demonstrated an increased risk of malignancy.6,9 Because of a considerable adverse effect profile, oral retinoids are limited to refractory cases in adults.6 Surgery is reserved for scarring and adhesions.4
Follow-up plays an important role in management
Historically, it was believed that pediatric LS had an excellent prognosis, with patients achieving complete resolution after puberty.1,4 Recent findings have shown mixed results, with LS persisting in many patients beyond puberty.2,4 Therefore, regular follow-up is recommended every 6 to 12 months.
For uncomplicated LS, specialist follow-up is not indicated. Female patients should regularly conduct self-examinations and, at a minimum, undergo annual examinations by their primary care physician. Those who require specialist follow-up include patients with difficult-to-control symptoms, hypertrophic lesions, a history of SCCV or differentiated vulvar intraepithelial neoplasia (dVIN), or pathology showing possible dVIN.15
Our patient. We prescribed clobetasol propionate 0.05% ointment to be used once daily for 8 weeks. We stressed the importance of genital self-examinations using a mirror to monitor for any concerning changes such as skin thickening. We showed the patient and her mother photos of normal female genitalia to help normalize the genital exam, and taught the patient how to find her plaques in the mirror. We set expectations by emphasizing the chronic nature of LS and the likelihood of recurrence. We also encouraged HPV vaccination in the upcoming years to prevent both cervical cancer and HPV-related SCCV.
CORRESPONDENCE
Somya Abubucker, MD, University of Hawaii, 1356 Lusitana Street, 7th floor, Honolulu, HI 96813; sabubuck@hawaii.edu.
A mother brought her 8-year-old daughter to our office for evaluation of vitiligo “down there” (FIGURE). The skin eruption first appeared on her vulva a year earlier and was intermittently pruritic. The lesions were initially smaller and red, but had since lightened in color, coalesced, and had begun to spread to the perianal area. The patient’s mother had received a call from her daughter’s teacher who observed that her daughter was scratching the area and might be masturbating in class.
The mother reported that 6 months earlier, her daughter had experienced bloody spots in her underwear accompanied by dysuria. The mother brought her to the emergency department, where she was treated with antibiotics for a urinary tract infection.
Our physical examination revealed well-circumscribed, symmetric, depigmented, confluent, crinkled, parchment-like plaques with small hemorrhagic erosions on the medial labia majora and minora. The lesions had spread to the perianal area with depigmentation superiorly and hypopigmentation inferiorly, creating a figure-8 pattern.
A review of systems was negative for pruritus, pain, dysuria, dyschezia, constipation, and vaginal discharge. The patient denied sexual activity, depression, or anxiety. Her mother denied behavioral changes in her daughter and said that her daughter hadn’t had any one-on-one time alone with any adults besides herself. Her mother was concerned that the white spots might spread to the rest of her daughter’s body, which could affect her socially.
WHAT IS YOUR DIAGNOSIS?
HOW WOULD YOU TREAT THIS PATIENT?
Diagnosis: Lichen sclerosus
Based on the history and clinical findings, including the classic figure-8 pattern, we diagnosed childhood lichen sclerosus (LS) in this patient. LS is a chronic inflammatory skin disorder that primarily affects the genital mucosa. The disorder can present at any age, but is most common among postmenopausal women, with a prevalence estimated to be as high as one in 30.1-3 A second incidence peak is observed in prepubescent girls, with a prevalence of one in 900.3,4 LS is less common in men and boys, with a female-to-male ratio that can reach 10:1.5 The classic symptoms of LS are pruritus and pain, which may be intermittent or persistent.
In girls, initial manifestations may be constipation, dysuria, or even behavioral symptoms such as night fears, which can occur because children are less active at night and become more aware of urinary discomfort.1,2,6 Typical signs of LS are thin atrophic plaques that spare the vagina and cervix. The plaques can be ivory-white, erythematous, or violaceous. Some patients have perianal lesions as well, and can display the pathognomonic figure-8 pattern of porcelain plaques around the vulva and anus.5
With more advanced disease, erosions, lichenification, and even distortion of vulvar architecture may occur.2,4,7 In severe cases, labia resorption and clitoral phimosis may develop.5 Complications include secondary infection, dyspareunia, and psychosexual distress. The most worrisome sequela of LS is squamous cell carcinoma of the vulva (SCCV), which occurs in 5% of female patients with LS.4
In men and boys, LS typically involves the foreskin and the glans, while sparing the perianal region.5 Scarring of the foreskin can lead to phimosis, and patients may complain of painful erections and difficulty urinating. LS can also occur away from the genitalia in both males and females.
Autoimmune mechanisms, genetics, and hormones play a role
The exact pathogenesis of LS remains unknown, but multiple factors are likely at work.
Autoimmune mechanisms. Up to 60% of women with LS have an autoimmune disorder, which is most commonly vitiligo, alopecia areata, or thyroid disease.5 In addition, 67% of patients have autoantibodies against extracellular matrix protein 1, and 30% have them against bullous pemphigoid antigen 180.1,8
Genetics. LS is associated with certain human leukocyte antigen class II haplotypes (especially DQ7) and with polymorphisms at the interleukin-1 receptor antagonist gene locus.5,6,9
Hormones. The clear peaks of incidence during times of low estrogen, and a higher incidence in patients with Turner syndrome or kidney disease, suggest that low estrogen may play a role in the development of LS, as well.1,5,6
While it is generally accepted that trauma may trigger LS via the Koebner phenomenon (the appearance of lesions at the site of injury), there is debate as to whether microbes—especially Borrelia burgdorferi and human papillomavirus (HPV)—might play a role.1,5
Diagnosis is often delayed, misdiagnosis is common
The average delay from symptom onset to diagnosis of LS is 1.3 years, and up to 84% of childhood LS is misdiagnosed before referral.2,9 The differential diagnosis includes:
Sexual abuse. In prepubertal girls presenting with genital redness, the can’t-miss diagnosis is sexual abuse, which occurs in more than 25% of children in the United States.10 Initial manifestations may be regression in developmental milestones, such as new-onset bedwetting, or behavioral changes such as social withdrawal or declining academic performance.11
However, physicians must be conscientious about ruling out medical etiologies before prematurely diagnosing abuse. Fourteen percent of girls with LS are incorrectly diagnosed as having been sexually abused.2 A clinical pearl is that while LS may resemble abuse on exam, it rarely affects the hymenal structure.12 It is also important to keep in mind that the 2 entities are not incompatible, as sexual abuse leading to LS via Koebnerization is a well-described phenomenon.12
Lichen planus. LP, which is also an immune-mediated inflammatory disorder affecting the vulva, classically presents with the 6 Ps: pruritic, polygonal, planar, purple papules and plaques.4 LP is distinguished from LS by being rare in childhood, having a predilection for the flexor wrists, and involving the oral and vaginal mucosa.4
Lichen simplex chronicus (LSC) is a chronic, circumscribed, pruritic, eczematous condition that becomes lichenified with thickened skin secondary to repeated scratching.13 Children with atopic dermatitis can develop LSC, but other children can also develop the scratch-itch cycle that results in the thickened plaques of LSC. Like LS, LSC can occur in areas other than the genitalia, including the neck and feet.14
Allergic contact dermatitis can occur in the genital area from diaper creams, soaps, and perfumes. Irritant contact dermatitis can occur from exposure to diarrhea, bedwetting, and other irritants. Contact dermatitis is less likely to have the classic figure-8 pattern seen in LS.
Psoriasis in the genital area can be confused with LS. However, psoriasis favors the groin creases in what is called inverse psoriasis. In addition, psoriasis tends to involve multiple areas, including the extensor surfaces of the elbows and knees, the nails, and the scalp.
Vitiligo can present on the genitals as circumscribed hypopigmented and depigmented patches that are flat. Vitiligo is asymptomatic, and the only pathology is the change in skin color. With LS, there is lichenification, atrophy, and sclerosis.4 Vitiligo often occurs with bilateral symmetric involvement in areas of trauma including the face, neck, scalp, elbows, wrists, hands, knees, ankles, and feet.
Treatment aims to improve symptoms
LS is usually diagnosed clinically (especially in children, as a biopsy is a great challenge to perform). However, when the clinical presentation is unclear, a skin biopsy will demonstrate the diagnostic findings of thinning of the epidermis, loss of rete pegs, hyperkeratosis, and dermal fibrosis with a T-lymphocyte-dominant inflammatory infiltrate.1,2,4,5
LS is a remitting and relapsing condition with no cure. The goals of treatment are to provide symptom relief and minimize scarring and atrophy,2 but it is unknown whether treatment reduces the risk of malignancy.9
First-line treatment for both genders and all ages is ultrapotent topical corticosteroids; clobetasol propionate 0.05% is most commonly used.1,6 Regimens vary, but the vast majority of patients improve within 3 months of once-daily treatment.4
For refractory LS, calcineurin inhibitors such as tacrolimus may be used. Although it has a black box warning regarding a potential cancer risk, long-term studies of children using tacrolimus for atopic dermatitis have not demonstrated an increased risk of malignancy.6,9 Because of a considerable adverse effect profile, oral retinoids are limited to refractory cases in adults.6 Surgery is reserved for scarring and adhesions.4
Follow-up plays an important role in management
Historically, it was believed that pediatric LS had an excellent prognosis, with patients achieving complete resolution after puberty.1,4 Recent findings have shown mixed results, with LS persisting in many patients beyond puberty.2,4 Therefore, regular follow-up is recommended every 6 to 12 months.
For uncomplicated LS, specialist follow-up is not indicated. Female patients should regularly conduct self-examinations and, at a minimum, undergo annual examinations by their primary care physician. Those who require specialist follow-up include patients with difficult-to-control symptoms, hypertrophic lesions, a history of SCCV or differentiated vulvar intraepithelial neoplasia (dVIN), or pathology showing possible dVIN.15
Our patient. We prescribed clobetasol propionate 0.05% ointment to be used once daily for 8 weeks. We stressed the importance of genital self-examinations using a mirror to monitor for any concerning changes such as skin thickening. We showed the patient and her mother photos of normal female genitalia to help normalize the genital exam, and taught the patient how to find her plaques in the mirror. We set expectations by emphasizing the chronic nature of LS and the likelihood of recurrence. We also encouraged HPV vaccination in the upcoming years to prevent both cervical cancer and HPV-related SCCV.
CORRESPONDENCE
Somya Abubucker, MD, University of Hawaii, 1356 Lusitana Street, 7th floor, Honolulu, HI 96813; sabubuck@hawaii.edu.
1. Murphy R. Lichen sclerosus. Dermatol Clin. 2010;28:707-715.
2. Dendrinos ML, Quint EH. Lichen sclerosus in children and adolescents. Curr Opin Obstet Gynecol. 2013;25:370-374.
3. Eva LJ. Screening and follow up of vulval skin disorders. Best Pract Res Clin Obstet Gynaecol. 2012;26:175-188.
4. Focseneanu MA, Gupta M, Squires KC, et al. The course of lichen sclerosus diagnosed prior to puberty. J Pediatr Adolesc Gynecol. 2013;26:153-155.
5. Funaro D. Lichen sclerosus: a review and practical approach. Dermatol Ther. 2004;17:28-37.
6. Heymann WR. Lichen sclerosus. J Am Acad Dermatol. 2007;56:683-684.
7. Tong LX, Sun GS, Teng JM. Pediatric lichen sclerosus: a review of the epidemiology and treatment options. Pediatr Dermatol. 2015;32:593-599.
8. Lagerstedt M, Karvinen K, Joki-Erkkilä M, et al. Childhood lichen sclerosus—a challenge for clinicians. Pediatr Dermatol. 2013;30:444-450.
9. Keith PJ, Wolz MM, Peters MS. Eosinophils in lichen sclerosus et atrophicus. J Cutan Pathol. 2015;42:693-698.
10. National Sexual Violence Resource Center. Child sexual abuse prevention. 2011. Available at: https://www.nsvrc.org/sites/default/files/Publications_NSVRC_Overview_Child-sexual-abuse-prevention_0.pdf. Accessed February 8, 2018.
11. Dubowitz H, Lane WG. Abused and neglected children. In: Kliegman RM, Stanton BF, St. Geme JW, et al, eds. Nelson Textbook of Pediatrics. 20th ed. Philadelphia, PA: Elsevier; 2016:236-249.
12. Powell J, Wojnarowska F. Childhood vulvar lichen sclerosus: an increasingly common problem. J Am Acad Dermatol. 2001;44:803-806.
13. Reamy BV, Bunt CW, Fletcher S. A diagnostic approach to pruritus. Am Fam Physician. 2011;84:195-202.
14. Warshaw E, Hook K. Dermatitis. In: Soutor C, Hordinsky MK, eds. Clinical Dermatology. 1st ed. New York, NY: McGraw-Hill; 2013.
15. Jones RW, Scurry J, Neill S, et al. Guidelines for the follow-up of women with vulvar lichen sclerosus in specialist clinics. Am J Obstet Gynecol. 2008;198:496.e1-e3.
1. Murphy R. Lichen sclerosus. Dermatol Clin. 2010;28:707-715.
2. Dendrinos ML, Quint EH. Lichen sclerosus in children and adolescents. Curr Opin Obstet Gynecol. 2013;25:370-374.
3. Eva LJ. Screening and follow up of vulval skin disorders. Best Pract Res Clin Obstet Gynaecol. 2012;26:175-188.
4. Focseneanu MA, Gupta M, Squires KC, et al. The course of lichen sclerosus diagnosed prior to puberty. J Pediatr Adolesc Gynecol. 2013;26:153-155.
5. Funaro D. Lichen sclerosus: a review and practical approach. Dermatol Ther. 2004;17:28-37.
6. Heymann WR. Lichen sclerosus. J Am Acad Dermatol. 2007;56:683-684.
7. Tong LX, Sun GS, Teng JM. Pediatric lichen sclerosus: a review of the epidemiology and treatment options. Pediatr Dermatol. 2015;32:593-599.
8. Lagerstedt M, Karvinen K, Joki-Erkkilä M, et al. Childhood lichen sclerosus—a challenge for clinicians. Pediatr Dermatol. 2013;30:444-450.
9. Keith PJ, Wolz MM, Peters MS. Eosinophils in lichen sclerosus et atrophicus. J Cutan Pathol. 2015;42:693-698.
10. National Sexual Violence Resource Center. Child sexual abuse prevention. 2011. Available at: https://www.nsvrc.org/sites/default/files/Publications_NSVRC_Overview_Child-sexual-abuse-prevention_0.pdf. Accessed February 8, 2018.
11. Dubowitz H, Lane WG. Abused and neglected children. In: Kliegman RM, Stanton BF, St. Geme JW, et al, eds. Nelson Textbook of Pediatrics. 20th ed. Philadelphia, PA: Elsevier; 2016:236-249.
12. Powell J, Wojnarowska F. Childhood vulvar lichen sclerosus: an increasingly common problem. J Am Acad Dermatol. 2001;44:803-806.
13. Reamy BV, Bunt CW, Fletcher S. A diagnostic approach to pruritus. Am Fam Physician. 2011;84:195-202.
14. Warshaw E, Hook K. Dermatitis. In: Soutor C, Hordinsky MK, eds. Clinical Dermatology. 1st ed. New York, NY: McGraw-Hill; 2013.
15. Jones RW, Scurry J, Neill S, et al. Guidelines for the follow-up of women with vulvar lichen sclerosus in specialist clinics. Am J Obstet Gynecol. 2008;198:496.e1-e3.
