User login
Gone Fishing: A Unique Histologic Pattern in Cutaneous Angiosarcoma
Cutaneous angiosarcoma is a rare malignant tumor of vascular endothelial cells that has the propensity to arise in various clinical settings. This tumor predominantly occurs in the head and neck region in elderly patients, but it also has been reported to develop postradiotherapy or in the setting of chronic lymphedema in the extremities.1-3 In all settings, the diagnosis carries a very poor prognosis with a high likelihood of local recurrence and rapid dissemination. The mortality rate typically is 80% or higher.2,4-6
Making the correct clinical diagnosis of cutaneous angiosarcoma may be difficult given the variety of patient symptoms and clinical appearances that can be demonstrated on presentation. Lesions can appear as bluish or violaceous plaques, macules, or nodules, and ulceration may be present in some advanced cases.5,7 Clinical misdiagnosis is common, as cutaneous angiosarcomas may be mistaken for infectious processes, benign vascular malformations, and other cutaneous malignancies.1 Biopsy often is delayed given the initial benign appearance of the lesions, and this frequently results in aggressive and extensive disease at the time of diagnosis, which is unfortunate given that small tumor size has been shown to be one of the only favorable prognostic indicators in cutaneous angiosarcoma.1,2,6,8
Microscopically, diagnosis of cutaneous angiosarcoma can present a challenge, as the histology varies between a well-differentiated vascular neoplasm and a considerably anaplastic and poorly differentiated malignancy. On low power, some areas may appear as benign hemangiomas with other areas showing frank sarcomatous features.9 As a result, these tumors can be mistaken for a variety of other diseases including melanomas, carcinomas, or other vascular tumors.6,8,9 Previously, electron microscopy has been utilized on undifferentiated tumors to help distinguish cutaneous angiosarcomas from other potential diagnoses. The atypical tumor cells of cutaneous angiosarcoma display common features of endothelial cells (eg, pinocytotic vesicles, tubulated bodies).7 Historically, it has been noted that the histologic findings and tumor grade provide little evidence regarding the aggressiveness of the tumor, and all cutaneous angiosarcoma diagnoses receive a poor prognosis.6,8
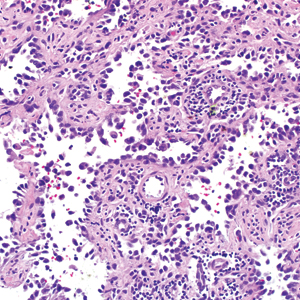
Classically, the histologic findings of cutaneous angiosarcoma include a highly infiltrative neoplasm forming irregular vascular channels that penetrate through the cutaneous soft tissues and frequently extend into the subcutaneous fat. The vascular spaces are lined by hyperchromatic endothelial cells with varying degrees of atypia.1,2,4,6,7,10 Occasionally, prominent endothelial cells lining a papillary structure within the lumen of the neoformed vessel may also be observed. Currently, immunohistochemical staining for MYC, Ki-67, D2-40, and various other markers complement the histologic findings to aid in the diagnosis of cutaneous angiosarcoma.11,12 An additional diagnostic clue that has been described in cases of postirradiation cutaneous angiosarcoma shows free-floating or tufted pleomorphic spindle cells within the vascular lumen (Figure). This finding has been described as “fish in the creek.”11 In this study, we aimed to determine the frequency and subsequent diagnostic utility of the fish-in-the-creek finding in cases of cutaneous angiosarcoma.

Methods
A natural language search of our institutional archives over a 20-year period (1997–2017) using the term angiosarcoma was performed. Fifteen cases of cutaneous angiosarcoma were identified. Fifteen additional benign and malignant vascular tumors with cutaneous angiosarco
Results
The histologic pattern of fish in the creek was identified in all 15 cases of cutaneous angiosarcoma and was absent in the other 15 malignancies examined in this study. This finding shows the potential for the fish-in-the-creek pattern to be used as an additional diagnostic tool for dermatopathologists.
Comment
Cutaneous angiosarcoma is a rare but aggressive malignancy that proves difficult to diagnose both clinically and histologically as well as to treat effectively.1,5-8 Our results indicate that fish in the creek may be a useful and salient histologic feature in cutaneous angiosarcoma. It is important to recognize, however, that this finding should not be the sole feature upon which a diagnosis of cutaneous angiosarcoma is made, as it requires corroboration with positivity of MYC and D2-40 as well as a high Ki-67 proliferation index (>20%).11,12 Finding a fish-in-the-creek pattern should prompt dermatopathologists to consider a diagnosis of cutaneous angiosarcoma in the appropriate clinical and histologic settings.
The chief limitation of this study was the small sample size, with only 15 cases of cutaneous angiosarcoma available in the last 20 years at our institution. The limited sample size did not allow us to make claims on sensitivity and specificity regarding this histologic feature; however, with a larger sample size, the true diagnostic potential could be elucidated. Although the pathologists were blinded to the original diagnoses as they examined it for fish in the creek, it is possible they were able to make the correct diagnosis based on other histopathologic clues and therefore were biased.
Although the fish-in-the-creek pattern is present in cutaneous angiosarcoma, there may be other mimickers to consider. Intraluminal papillary projections lined by endothelial cells may be sectioned in a manner imitating this finding.3 In such a case, these endothelial cells must be differentiated from the free-floating or tufted spindle cells in order to have a positive finding for fish in the creek. There can be confusion if the biopsy cuts through a section of spindled cells, resulting in difficulty differentiating cutaneous angiosarcoma from other spindle tumors such as spindle cell melanoma or spindle cell squamous cell carcinoma.6 In such cases, immunohistochemistry may be helpful, as spindle cell melanoma would stain positive for S100 and SOX10 and spindle cell squamous cell carcinoma would stain positive for p63 and cytokeratin.
Various treatment strategies for cutaneous angiosarcoma have been employed, with the majority still resulting in poor outcomes.2,4-6 The recommended treatment is radical surgical excision of the primary tumor with lymph node clearance if possible. Following excision, the patient should undergo high-dose, wide-field radiotherapy to the region.5,8 Cutaneous angiosarcomas also have the ability to spread extensively through the dermis and can result in subclinical or clinically obvious widespread disease with multifocal or satellite lesions present. Distant metastases occur most frequently in the cervical lymph nodes and lungs.7 In cases where the disease is too extensive for surgery, palliative radiation monotherapy can be used.5,6
As atypical vascular lesions are considered to be a precursor to cutaneous angiosarcoma, it is important to note that the fish-in-the-creek feature was absent in all 6 of the atypical vascular lesions observed in the study. The differentiation generally is made based on MYC, which is present in cutaneous angiosarcomas and absent in atypical vascular lesions.10 The feature of fish in the creek may now be an additional clue for dermatopathologists to differentiate between angiosarcomas and other similar-appearing tumors.
Conclusion
Our study aimed to highlight an important histologic feature of cutaneous angiosarcomas that can aid in the diagnosis of this deceptive malignancy. Our findings warrant further study of the fish-in-the-creek histologic pattern in a larger sample size to determine its success as a diagnostic tool for cutaneous angiosarcomas. As noted previously, tumor grade does not impact survival outcome, but small tumor size has been one of the only features found to result in a more favorable prognosis.1,6,8 Future studies to identify a correlation between the histologic finding of fish in the creek and disease outcome in cutaneous angiosarcoma may be helpful to determine if these histologic findings provide prognostic significance in cases of cutaneous angiosarcoma.
- Aust MR, Olsen KD, Lewis JE, et al. Angiosarcomas of the head and neck: clinical and pathologic characteristics. Ann Otol Rhinol Laryngol. 1997;106:943-951.
- Holden CA, Spittle MF, Jones EW. Angiosarcoma of the face and scalp, prognosis and treatment. Cancer. 1987;59:1046-1057.
- Woodward AH, Ivins JC, Soule EH. Lymphangiosarcoma arising in chronic lymphedematous extremities. Cancer. 1972;30:562-572.
- Calonje E, Brenn T, McKee PH, et al. McKee’s Pathology of the Skin. 4th ed. Edinburgh, Scotland: Elsevier Saunders; 2012.
- Morrison WH, Byers RM, Garden AS, et al. Cutaneous angiosarcoma of the head and neck. a therapeutic dilemma. Cancer. 1995;76:319-327.
- Hodgkinson DJ, Soule EH, Woods JE. Cutaneous angiosarcoma of the head and neck. Cancer. 1979;44:1106-1113.
- Rosai J, Sumner HW, Kostianovsky M, et al. Angiosarcoma of the skin: a clinicopathologic and fine structural study. Hum Pathol. 1976;7:83-109.
- Pawlik TM, Paulino AF, Mcginn CJ, et al. Cutaneous angiosarcoma of the scalp: a multidisciplinary approach. Cancer. 2003;98:1716-1726.
- Haustein UF. Angiosarcoma of the face and scalp. Int J Dermatol. 1991;30:851-856.
- Elston DM, Ferringer T, Ko C, et al. Dermatopathology. 2nd ed. Edinburgh, Scotland: Saunders Elsevier; 2014.
- Requena L, Kutzner H. Cutaneous Soft Tissue Tumors. Philadelphia, PA: Wolters Kluwer; 2015.
- Cuda J, Mirzamani N, Kantipudi R, et al. Diagnostic utility of Fli-1 and D2-40 in distinguishing atypical fibroxanthoma from angiosarcoma. Am J Dermatopathol. 2013;35:316-318.
Cutaneous angiosarcoma is a rare malignant tumor of vascular endothelial cells that has the propensity to arise in various clinical settings. This tumor predominantly occurs in the head and neck region in elderly patients, but it also has been reported to develop postradiotherapy or in the setting of chronic lymphedema in the extremities.1-3 In all settings, the diagnosis carries a very poor prognosis with a high likelihood of local recurrence and rapid dissemination. The mortality rate typically is 80% or higher.2,4-6
Making the correct clinical diagnosis of cutaneous angiosarcoma may be difficult given the variety of patient symptoms and clinical appearances that can be demonstrated on presentation. Lesions can appear as bluish or violaceous plaques, macules, or nodules, and ulceration may be present in some advanced cases.5,7 Clinical misdiagnosis is common, as cutaneous angiosarcomas may be mistaken for infectious processes, benign vascular malformations, and other cutaneous malignancies.1 Biopsy often is delayed given the initial benign appearance of the lesions, and this frequently results in aggressive and extensive disease at the time of diagnosis, which is unfortunate given that small tumor size has been shown to be one of the only favorable prognostic indicators in cutaneous angiosarcoma.1,2,6,8
Microscopically, diagnosis of cutaneous angiosarcoma can present a challenge, as the histology varies between a well-differentiated vascular neoplasm and a considerably anaplastic and poorly differentiated malignancy. On low power, some areas may appear as benign hemangiomas with other areas showing frank sarcomatous features.9 As a result, these tumors can be mistaken for a variety of other diseases including melanomas, carcinomas, or other vascular tumors.6,8,9 Previously, electron microscopy has been utilized on undifferentiated tumors to help distinguish cutaneous angiosarcomas from other potential diagnoses. The atypical tumor cells of cutaneous angiosarcoma display common features of endothelial cells (eg, pinocytotic vesicles, tubulated bodies).7 Historically, it has been noted that the histologic findings and tumor grade provide little evidence regarding the aggressiveness of the tumor, and all cutaneous angiosarcoma diagnoses receive a poor prognosis.6,8
Classically, the histologic findings of cutaneous angiosarcoma include a highly infiltrative neoplasm forming irregular vascular channels that penetrate through the cutaneous soft tissues and frequently extend into the subcutaneous fat. The vascular spaces are lined by hyperchromatic endothelial cells with varying degrees of atypia.1,2,4,6,7,10 Occasionally, prominent endothelial cells lining a papillary structure within the lumen of the neoformed vessel may also be observed. Currently, immunohistochemical staining for MYC, Ki-67, D2-40, and various other markers complement the histologic findings to aid in the diagnosis of cutaneous angiosarcoma.11,12 An additional diagnostic clue that has been described in cases of postirradiation cutaneous angiosarcoma shows free-floating or tufted pleomorphic spindle cells within the vascular lumen (Figure). This finding has been described as “fish in the creek.”11 In this study, we aimed to determine the frequency and subsequent diagnostic utility of the fish-in-the-creek finding in cases of cutaneous angiosarcoma.
Methods
A natural language search of our institutional archives over a 20-year period (1997–2017) using the term angiosarcoma was performed. Fifteen cases of cutaneous angiosarcoma were identified. Fifteen additional benign and malignant vascular tumors with cutaneous angiosarco
Results
The histologic pattern of fish in the creek was identified in all 15 cases of cutaneous angiosarcoma and was absent in the other 15 malignancies examined in this study. This finding shows the potential for the fish-in-the-creek pattern to be used as an additional diagnostic tool for dermatopathologists.
Comment
Cutaneous angiosarcoma is a rare but aggressive malignancy that proves difficult to diagnose both clinically and histologically as well as to treat effectively.1,5-8 Our results indicate that fish in the creek may be a useful and salient histologic feature in cutaneous angiosarcoma. It is important to recognize, however, that this finding should not be the sole feature upon which a diagnosis of cutaneous angiosarcoma is made, as it requires corroboration with positivity of MYC and D2-40 as well as a high Ki-67 proliferation index (>20%).11,12 Finding a fish-in-the-creek pattern should prompt dermatopathologists to consider a diagnosis of cutaneous angiosarcoma in the appropriate clinical and histologic settings.
The chief limitation of this study was the small sample size, with only 15 cases of cutaneous angiosarcoma available in the last 20 years at our institution. The limited sample size did not allow us to make claims on sensitivity and specificity regarding this histologic feature; however, with a larger sample size, the true diagnostic potential could be elucidated. Although the pathologists were blinded to the original diagnoses as they examined it for fish in the creek, it is possible they were able to make the correct diagnosis based on other histopathologic clues and therefore were biased.
Although the fish-in-the-creek pattern is present in cutaneous angiosarcoma, there may be other mimickers to consider. Intraluminal papillary projections lined by endothelial cells may be sectioned in a manner imitating this finding.3 In such a case, these endothelial cells must be differentiated from the free-floating or tufted spindle cells in order to have a positive finding for fish in the creek. There can be confusion if the biopsy cuts through a section of spindled cells, resulting in difficulty differentiating cutaneous angiosarcoma from other spindle tumors such as spindle cell melanoma or spindle cell squamous cell carcinoma.6 In such cases, immunohistochemistry may be helpful, as spindle cell melanoma would stain positive for S100 and SOX10 and spindle cell squamous cell carcinoma would stain positive for p63 and cytokeratin.
Various treatment strategies for cutaneous angiosarcoma have been employed, with the majority still resulting in poor outcomes.2,4-6 The recommended treatment is radical surgical excision of the primary tumor with lymph node clearance if possible. Following excision, the patient should undergo high-dose, wide-field radiotherapy to the region.5,8 Cutaneous angiosarcomas also have the ability to spread extensively through the dermis and can result in subclinical or clinically obvious widespread disease with multifocal or satellite lesions present. Distant metastases occur most frequently in the cervical lymph nodes and lungs.7 In cases where the disease is too extensive for surgery, palliative radiation monotherapy can be used.5,6
As atypical vascular lesions are considered to be a precursor to cutaneous angiosarcoma, it is important to note that the fish-in-the-creek feature was absent in all 6 of the atypical vascular lesions observed in the study. The differentiation generally is made based on MYC, which is present in cutaneous angiosarcomas and absent in atypical vascular lesions.10 The feature of fish in the creek may now be an additional clue for dermatopathologists to differentiate between angiosarcomas and other similar-appearing tumors.
Conclusion
Our study aimed to highlight an important histologic feature of cutaneous angiosarcomas that can aid in the diagnosis of this deceptive malignancy. Our findings warrant further study of the fish-in-the-creek histologic pattern in a larger sample size to determine its success as a diagnostic tool for cutaneous angiosarcomas. As noted previously, tumor grade does not impact survival outcome, but small tumor size has been one of the only features found to result in a more favorable prognosis.1,6,8 Future studies to identify a correlation between the histologic finding of fish in the creek and disease outcome in cutaneous angiosarcoma may be helpful to determine if these histologic findings provide prognostic significance in cases of cutaneous angiosarcoma.
Cutaneous angiosarcoma is a rare malignant tumor of vascular endothelial cells that has the propensity to arise in various clinical settings. This tumor predominantly occurs in the head and neck region in elderly patients, but it also has been reported to develop postradiotherapy or in the setting of chronic lymphedema in the extremities.1-3 In all settings, the diagnosis carries a very poor prognosis with a high likelihood of local recurrence and rapid dissemination. The mortality rate typically is 80% or higher.2,4-6
Making the correct clinical diagnosis of cutaneous angiosarcoma may be difficult given the variety of patient symptoms and clinical appearances that can be demonstrated on presentation. Lesions can appear as bluish or violaceous plaques, macules, or nodules, and ulceration may be present in some advanced cases.5,7 Clinical misdiagnosis is common, as cutaneous angiosarcomas may be mistaken for infectious processes, benign vascular malformations, and other cutaneous malignancies.1 Biopsy often is delayed given the initial benign appearance of the lesions, and this frequently results in aggressive and extensive disease at the time of diagnosis, which is unfortunate given that small tumor size has been shown to be one of the only favorable prognostic indicators in cutaneous angiosarcoma.1,2,6,8
Microscopically, diagnosis of cutaneous angiosarcoma can present a challenge, as the histology varies between a well-differentiated vascular neoplasm and a considerably anaplastic and poorly differentiated malignancy. On low power, some areas may appear as benign hemangiomas with other areas showing frank sarcomatous features.9 As a result, these tumors can be mistaken for a variety of other diseases including melanomas, carcinomas, or other vascular tumors.6,8,9 Previously, electron microscopy has been utilized on undifferentiated tumors to help distinguish cutaneous angiosarcomas from other potential diagnoses. The atypical tumor cells of cutaneous angiosarcoma display common features of endothelial cells (eg, pinocytotic vesicles, tubulated bodies).7 Historically, it has been noted that the histologic findings and tumor grade provide little evidence regarding the aggressiveness of the tumor, and all cutaneous angiosarcoma diagnoses receive a poor prognosis.6,8
Classically, the histologic findings of cutaneous angiosarcoma include a highly infiltrative neoplasm forming irregular vascular channels that penetrate through the cutaneous soft tissues and frequently extend into the subcutaneous fat. The vascular spaces are lined by hyperchromatic endothelial cells with varying degrees of atypia.1,2,4,6,7,10 Occasionally, prominent endothelial cells lining a papillary structure within the lumen of the neoformed vessel may also be observed. Currently, immunohistochemical staining for MYC, Ki-67, D2-40, and various other markers complement the histologic findings to aid in the diagnosis of cutaneous angiosarcoma.11,12 An additional diagnostic clue that has been described in cases of postirradiation cutaneous angiosarcoma shows free-floating or tufted pleomorphic spindle cells within the vascular lumen (Figure). This finding has been described as “fish in the creek.”11 In this study, we aimed to determine the frequency and subsequent diagnostic utility of the fish-in-the-creek finding in cases of cutaneous angiosarcoma.
Methods
A natural language search of our institutional archives over a 20-year period (1997–2017) using the term angiosarcoma was performed. Fifteen cases of cutaneous angiosarcoma were identified. Fifteen additional benign and malignant vascular tumors with cutaneous angiosarco
Results
The histologic pattern of fish in the creek was identified in all 15 cases of cutaneous angiosarcoma and was absent in the other 15 malignancies examined in this study. This finding shows the potential for the fish-in-the-creek pattern to be used as an additional diagnostic tool for dermatopathologists.
Comment
Cutaneous angiosarcoma is a rare but aggressive malignancy that proves difficult to diagnose both clinically and histologically as well as to treat effectively.1,5-8 Our results indicate that fish in the creek may be a useful and salient histologic feature in cutaneous angiosarcoma. It is important to recognize, however, that this finding should not be the sole feature upon which a diagnosis of cutaneous angiosarcoma is made, as it requires corroboration with positivity of MYC and D2-40 as well as a high Ki-67 proliferation index (>20%).11,12 Finding a fish-in-the-creek pattern should prompt dermatopathologists to consider a diagnosis of cutaneous angiosarcoma in the appropriate clinical and histologic settings.
The chief limitation of this study was the small sample size, with only 15 cases of cutaneous angiosarcoma available in the last 20 years at our institution. The limited sample size did not allow us to make claims on sensitivity and specificity regarding this histologic feature; however, with a larger sample size, the true diagnostic potential could be elucidated. Although the pathologists were blinded to the original diagnoses as they examined it for fish in the creek, it is possible they were able to make the correct diagnosis based on other histopathologic clues and therefore were biased.
Although the fish-in-the-creek pattern is present in cutaneous angiosarcoma, there may be other mimickers to consider. Intraluminal papillary projections lined by endothelial cells may be sectioned in a manner imitating this finding.3 In such a case, these endothelial cells must be differentiated from the free-floating or tufted spindle cells in order to have a positive finding for fish in the creek. There can be confusion if the biopsy cuts through a section of spindled cells, resulting in difficulty differentiating cutaneous angiosarcoma from other spindle tumors such as spindle cell melanoma or spindle cell squamous cell carcinoma.6 In such cases, immunohistochemistry may be helpful, as spindle cell melanoma would stain positive for S100 and SOX10 and spindle cell squamous cell carcinoma would stain positive for p63 and cytokeratin.
Various treatment strategies for cutaneous angiosarcoma have been employed, with the majority still resulting in poor outcomes.2,4-6 The recommended treatment is radical surgical excision of the primary tumor with lymph node clearance if possible. Following excision, the patient should undergo high-dose, wide-field radiotherapy to the region.5,8 Cutaneous angiosarcomas also have the ability to spread extensively through the dermis and can result in subclinical or clinically obvious widespread disease with multifocal or satellite lesions present. Distant metastases occur most frequently in the cervical lymph nodes and lungs.7 In cases where the disease is too extensive for surgery, palliative radiation monotherapy can be used.5,6
As atypical vascular lesions are considered to be a precursor to cutaneous angiosarcoma, it is important to note that the fish-in-the-creek feature was absent in all 6 of the atypical vascular lesions observed in the study. The differentiation generally is made based on MYC, which is present in cutaneous angiosarcomas and absent in atypical vascular lesions.10 The feature of fish in the creek may now be an additional clue for dermatopathologists to differentiate between angiosarcomas and other similar-appearing tumors.
Conclusion
Our study aimed to highlight an important histologic feature of cutaneous angiosarcomas that can aid in the diagnosis of this deceptive malignancy. Our findings warrant further study of the fish-in-the-creek histologic pattern in a larger sample size to determine its success as a diagnostic tool for cutaneous angiosarcomas. As noted previously, tumor grade does not impact survival outcome, but small tumor size has been one of the only features found to result in a more favorable prognosis.1,6,8 Future studies to identify a correlation between the histologic finding of fish in the creek and disease outcome in cutaneous angiosarcoma may be helpful to determine if these histologic findings provide prognostic significance in cases of cutaneous angiosarcoma.
- Aust MR, Olsen KD, Lewis JE, et al. Angiosarcomas of the head and neck: clinical and pathologic characteristics. Ann Otol Rhinol Laryngol. 1997;106:943-951.
- Holden CA, Spittle MF, Jones EW. Angiosarcoma of the face and scalp, prognosis and treatment. Cancer. 1987;59:1046-1057.
- Woodward AH, Ivins JC, Soule EH. Lymphangiosarcoma arising in chronic lymphedematous extremities. Cancer. 1972;30:562-572.
- Calonje E, Brenn T, McKee PH, et al. McKee’s Pathology of the Skin. 4th ed. Edinburgh, Scotland: Elsevier Saunders; 2012.
- Morrison WH, Byers RM, Garden AS, et al. Cutaneous angiosarcoma of the head and neck. a therapeutic dilemma. Cancer. 1995;76:319-327.
- Hodgkinson DJ, Soule EH, Woods JE. Cutaneous angiosarcoma of the head and neck. Cancer. 1979;44:1106-1113.
- Rosai J, Sumner HW, Kostianovsky M, et al. Angiosarcoma of the skin: a clinicopathologic and fine structural study. Hum Pathol. 1976;7:83-109.
- Pawlik TM, Paulino AF, Mcginn CJ, et al. Cutaneous angiosarcoma of the scalp: a multidisciplinary approach. Cancer. 2003;98:1716-1726.
- Haustein UF. Angiosarcoma of the face and scalp. Int J Dermatol. 1991;30:851-856.
- Elston DM, Ferringer T, Ko C, et al. Dermatopathology. 2nd ed. Edinburgh, Scotland: Saunders Elsevier; 2014.
- Requena L, Kutzner H. Cutaneous Soft Tissue Tumors. Philadelphia, PA: Wolters Kluwer; 2015.
- Cuda J, Mirzamani N, Kantipudi R, et al. Diagnostic utility of Fli-1 and D2-40 in distinguishing atypical fibroxanthoma from angiosarcoma. Am J Dermatopathol. 2013;35:316-318.
- Aust MR, Olsen KD, Lewis JE, et al. Angiosarcomas of the head and neck: clinical and pathologic characteristics. Ann Otol Rhinol Laryngol. 1997;106:943-951.
- Holden CA, Spittle MF, Jones EW. Angiosarcoma of the face and scalp, prognosis and treatment. Cancer. 1987;59:1046-1057.
- Woodward AH, Ivins JC, Soule EH. Lymphangiosarcoma arising in chronic lymphedematous extremities. Cancer. 1972;30:562-572.
- Calonje E, Brenn T, McKee PH, et al. McKee’s Pathology of the Skin. 4th ed. Edinburgh, Scotland: Elsevier Saunders; 2012.
- Morrison WH, Byers RM, Garden AS, et al. Cutaneous angiosarcoma of the head and neck. a therapeutic dilemma. Cancer. 1995;76:319-327.
- Hodgkinson DJ, Soule EH, Woods JE. Cutaneous angiosarcoma of the head and neck. Cancer. 1979;44:1106-1113.
- Rosai J, Sumner HW, Kostianovsky M, et al. Angiosarcoma of the skin: a clinicopathologic and fine structural study. Hum Pathol. 1976;7:83-109.
- Pawlik TM, Paulino AF, Mcginn CJ, et al. Cutaneous angiosarcoma of the scalp: a multidisciplinary approach. Cancer. 2003;98:1716-1726.
- Haustein UF. Angiosarcoma of the face and scalp. Int J Dermatol. 1991;30:851-856.
- Elston DM, Ferringer T, Ko C, et al. Dermatopathology. 2nd ed. Edinburgh, Scotland: Saunders Elsevier; 2014.
- Requena L, Kutzner H. Cutaneous Soft Tissue Tumors. Philadelphia, PA: Wolters Kluwer; 2015.
- Cuda J, Mirzamani N, Kantipudi R, et al. Diagnostic utility of Fli-1 and D2-40 in distinguishing atypical fibroxanthoma from angiosarcoma. Am J Dermatopathol. 2013;35:316-318.
Practice Points
- The histologic finding of “fish in the creek” is characterized by free-floating or tufted pleomorphic spindle cells within the vascular lumen.
- Fish in the creek has only been demonstrated in cutaneous angiosarcoma when compared to histologic findings of other similar vascular malignancies.
- The fish-in-the-creek finding may be an additional diagnostic tool in cases of cutaneous angiosarcoma.
Posttransplant skin conditions vary widely by ethnicity
SAN DIEGO – A new study finds that the risk of skin cancers in organ transplant recipients may vary widely by ethnicity.
“The most important findings from our study are the high rates of keratinocyte neoplasms observed in our white Northern European patients, but also in those of Far East Asian descent. Dermatologists should also appreciate the high risk of Kaposi’s sarcoma (KS) in patients originating from Sub-Saharan Africa,” Jonathan Kentley, MBBS, of Royal London Hospital, said in an interview. He presented the study findings at the annual meeting of the American Academy of Dermatology.

For the study, Dr. Kentley and colleagues sought to better understand .
They analyzed an organ transplant center database for the years 1989-2016, and tracked 1,304 consecutive patients – which included 1,125 with skin problems. The overall population was 64% male with a median age in the early 40s, and almost all (1,276) had undergone renal transplants. A relative handful underwent liver, lung, heart, and pancreas transplants.
The majority of patients (885) were white Northern Europeans, but there were also significant numbers of people with South Asian (202), black African/Caribbean (131) and white/Mediterranean (52) heritage. A small number were Far East Asian (26) and Middle Eastern (8). The median follow-up time for the ethnic groups varied from about 5 years to about 12 years.
The researchers found that basal cell carcinoma was most common in white Northern European patients, at nearly 25%, with other groups under 10%. SCC was common in white Northern European patients and Far East Asians, both at nearly 25%.
By far, KS was the most common in black African/Caribbean patients, at nearly 11%. According to Dr. Kentley, researchers found the number of KS cases to be surprisingly high in this group, “compounded by the fact that we have had a number of additional cases in the past year after we had collected the data for this study.” He attributes the higher number of KS cases in these patients to an increased seroprevalence of its causative agent, human herpesvirus-8, in Sub-Saharan Africa. The rate of KS in the second most commonly affected group – white Mediterranean patients – was almost 2%.
Viral warts were common in most groups, with the rate in both white groups (white Northern European and white Mediterranean) at nearly 60%, and Far East Asians at about 65%. Porokeratosis was by far the most common in white Norther Europeans, at nearly 8%, and sebaceous hyperplasia was common in all groups (more than 20% to about 27%) except in the black African/Caribbean and South Asian groups.
All these results were statistically significant with P values less than .05.
“Our study has confirmed the increased risk of keratinocyte cancers in patients of white Northern European descent, as well as providing more information on the increased risk in patients of Far East Asian descent,” Dr. Kentley said. “We have also confirmed the propensity of black African/Caribbean patients to develop Kaposi’s sarcoma in the first 5 years post transplant and highlighted that white Mediterranean patients are also at high risk. Beyond this, we have been able to review the prevalence of rare malignancies, such as Merkel cell carcinoma and appendageal tumors, and highlight that white Northern European patients remain at high risk of developing these conditions.”
As for the impact on clinical practice, “the patterns of skin disease susceptibility we have identified have important implications for rational design of transplant skin surveillance programs, targeted patient (and provider) education, and optimized clinical management,” Dr. Kentley said. “Ultimately, this is likely to have a significant impact on strategic deployment of limited dermatology health care resources.”
Specifically, the study suggests that all organ transplant patients receive a baseline skin assessment visit and nurse-led targeted education. Black African/Caribbean patients should be followed up for at least 5 years after transplant.
In the United States, at least 724,000 people have undergone organ transplants since 1988, with most getting kidney transplants, according to the United Network for Organ Sharing (UNOS).
No study funding was reported. The authors had no disclosures.
SOURCE: Kentley J et al. AAD 2018, Session F055.
SAN DIEGO – A new study finds that the risk of skin cancers in organ transplant recipients may vary widely by ethnicity.
“The most important findings from our study are the high rates of keratinocyte neoplasms observed in our white Northern European patients, but also in those of Far East Asian descent. Dermatologists should also appreciate the high risk of Kaposi’s sarcoma (KS) in patients originating from Sub-Saharan Africa,” Jonathan Kentley, MBBS, of Royal London Hospital, said in an interview. He presented the study findings at the annual meeting of the American Academy of Dermatology.
For the study, Dr. Kentley and colleagues sought to better understand .
They analyzed an organ transplant center database for the years 1989-2016, and tracked 1,304 consecutive patients – which included 1,125 with skin problems. The overall population was 64% male with a median age in the early 40s, and almost all (1,276) had undergone renal transplants. A relative handful underwent liver, lung, heart, and pancreas transplants.
The majority of patients (885) were white Northern Europeans, but there were also significant numbers of people with South Asian (202), black African/Caribbean (131) and white/Mediterranean (52) heritage. A small number were Far East Asian (26) and Middle Eastern (8). The median follow-up time for the ethnic groups varied from about 5 years to about 12 years.
The researchers found that basal cell carcinoma was most common in white Northern European patients, at nearly 25%, with other groups under 10%. SCC was common in white Northern European patients and Far East Asians, both at nearly 25%.
By far, KS was the most common in black African/Caribbean patients, at nearly 11%. According to Dr. Kentley, researchers found the number of KS cases to be surprisingly high in this group, “compounded by the fact that we have had a number of additional cases in the past year after we had collected the data for this study.” He attributes the higher number of KS cases in these patients to an increased seroprevalence of its causative agent, human herpesvirus-8, in Sub-Saharan Africa. The rate of KS in the second most commonly affected group – white Mediterranean patients – was almost 2%.
Viral warts were common in most groups, with the rate in both white groups (white Northern European and white Mediterranean) at nearly 60%, and Far East Asians at about 65%. Porokeratosis was by far the most common in white Norther Europeans, at nearly 8%, and sebaceous hyperplasia was common in all groups (more than 20% to about 27%) except in the black African/Caribbean and South Asian groups.
All these results were statistically significant with P values less than .05.
“Our study has confirmed the increased risk of keratinocyte cancers in patients of white Northern European descent, as well as providing more information on the increased risk in patients of Far East Asian descent,” Dr. Kentley said. “We have also confirmed the propensity of black African/Caribbean patients to develop Kaposi’s sarcoma in the first 5 years post transplant and highlighted that white Mediterranean patients are also at high risk. Beyond this, we have been able to review the prevalence of rare malignancies, such as Merkel cell carcinoma and appendageal tumors, and highlight that white Northern European patients remain at high risk of developing these conditions.”
As for the impact on clinical practice, “the patterns of skin disease susceptibility we have identified have important implications for rational design of transplant skin surveillance programs, targeted patient (and provider) education, and optimized clinical management,” Dr. Kentley said. “Ultimately, this is likely to have a significant impact on strategic deployment of limited dermatology health care resources.”
Specifically, the study suggests that all organ transplant patients receive a baseline skin assessment visit and nurse-led targeted education. Black African/Caribbean patients should be followed up for at least 5 years after transplant.
In the United States, at least 724,000 people have undergone organ transplants since 1988, with most getting kidney transplants, according to the United Network for Organ Sharing (UNOS).
No study funding was reported. The authors had no disclosures.
SOURCE: Kentley J et al. AAD 2018, Session F055.
SAN DIEGO – A new study finds that the risk of skin cancers in organ transplant recipients may vary widely by ethnicity.
“The most important findings from our study are the high rates of keratinocyte neoplasms observed in our white Northern European patients, but also in those of Far East Asian descent. Dermatologists should also appreciate the high risk of Kaposi’s sarcoma (KS) in patients originating from Sub-Saharan Africa,” Jonathan Kentley, MBBS, of Royal London Hospital, said in an interview. He presented the study findings at the annual meeting of the American Academy of Dermatology.
For the study, Dr. Kentley and colleagues sought to better understand .
They analyzed an organ transplant center database for the years 1989-2016, and tracked 1,304 consecutive patients – which included 1,125 with skin problems. The overall population was 64% male with a median age in the early 40s, and almost all (1,276) had undergone renal transplants. A relative handful underwent liver, lung, heart, and pancreas transplants.
The majority of patients (885) were white Northern Europeans, but there were also significant numbers of people with South Asian (202), black African/Caribbean (131) and white/Mediterranean (52) heritage. A small number were Far East Asian (26) and Middle Eastern (8). The median follow-up time for the ethnic groups varied from about 5 years to about 12 years.
The researchers found that basal cell carcinoma was most common in white Northern European patients, at nearly 25%, with other groups under 10%. SCC was common in white Northern European patients and Far East Asians, both at nearly 25%.
By far, KS was the most common in black African/Caribbean patients, at nearly 11%. According to Dr. Kentley, researchers found the number of KS cases to be surprisingly high in this group, “compounded by the fact that we have had a number of additional cases in the past year after we had collected the data for this study.” He attributes the higher number of KS cases in these patients to an increased seroprevalence of its causative agent, human herpesvirus-8, in Sub-Saharan Africa. The rate of KS in the second most commonly affected group – white Mediterranean patients – was almost 2%.
Viral warts were common in most groups, with the rate in both white groups (white Northern European and white Mediterranean) at nearly 60%, and Far East Asians at about 65%. Porokeratosis was by far the most common in white Norther Europeans, at nearly 8%, and sebaceous hyperplasia was common in all groups (more than 20% to about 27%) except in the black African/Caribbean and South Asian groups.
All these results were statistically significant with P values less than .05.
“Our study has confirmed the increased risk of keratinocyte cancers in patients of white Northern European descent, as well as providing more information on the increased risk in patients of Far East Asian descent,” Dr. Kentley said. “We have also confirmed the propensity of black African/Caribbean patients to develop Kaposi’s sarcoma in the first 5 years post transplant and highlighted that white Mediterranean patients are also at high risk. Beyond this, we have been able to review the prevalence of rare malignancies, such as Merkel cell carcinoma and appendageal tumors, and highlight that white Northern European patients remain at high risk of developing these conditions.”
As for the impact on clinical practice, “the patterns of skin disease susceptibility we have identified have important implications for rational design of transplant skin surveillance programs, targeted patient (and provider) education, and optimized clinical management,” Dr. Kentley said. “Ultimately, this is likely to have a significant impact on strategic deployment of limited dermatology health care resources.”
Specifically, the study suggests that all organ transplant patients receive a baseline skin assessment visit and nurse-led targeted education. Black African/Caribbean patients should be followed up for at least 5 years after transplant.
In the United States, at least 724,000 people have undergone organ transplants since 1988, with most getting kidney transplants, according to the United Network for Organ Sharing (UNOS).
No study funding was reported. The authors had no disclosures.
SOURCE: Kentley J et al. AAD 2018, Session F055.
REPORTING FROM AAD 18
Key clinical point: Skin disorders after organ transplant differ widely by ethnicity.
Major finding: Posttransplant basal cell and squamous cell carcinomas are most common in white Northern Europeans (at nearly 25%), while Kaposi’s sarcoma was higher than expected (nearly 10%) in black African/Caribbean patients.
Study details: Analysis of 1,125 patients from a single transplant center who received organ transplants and developed skin problems over a median follow-up time of 5 to more than 12 years, depending on ethnicity.
Disclosures: No study funding was reported. The authors had no disclosures.
Source: Kentley J et al. AAD 2018, Session F055.
Lenalidomide yields responses in a rare cutaneous lymphoma
The oral immunomodulatory drug lenalidomide is active and may provide prolonged responses in certain patients with a rare and aggressive subtype of primary cutaneous lymphoma, according to results of a phase 2 study.
In the study, which comprised 19 patients with primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL, LT), 5 patients (26.3%) had a response at 6 months, and there were still 3 patients in response at 12 months. The findings were reported in the Journal of Investigative Dermatology.
In an exploratory analysis, reducing the dose of lenalidomide was associated with prolonged response and improved survival, noted lead author Marie Beylot-Barry, MD, of the dermatology department, Hôpital Saint-André, CHU Bordeaux, France, and her colleagues.
“Lenalidomide at reduced doses may allow prolonged responses in few patients, and represents a therapeutic option in relapsing/refractory PCDLBCL, LT,” the researchers wrote.
Found mostly on the lower limbs of elderly patients, PCDLBCL, LT exhibits aggressive behavior and is associated with a high rate of skin recurrences. First-line therapy for the cutaneous lymphoma is typically rituximab and chemotherapy, regardless of clinical stage or patient age, the researchers wrote, though primary resistance or recurrence after treatment occurs in about half of patients. “In such relapsing or refractory cases, no treatment has demonstrated a sustained benefit thus far,” they noted.
Lenalidomide has already demonstrated efficacy in relapsed/refractory diffuse large B-cell lymphoma (DLBCL) and it induces inhibition of cell signaling, engaging NF-kappaB signaling. PCDLBCL, LT is marked by genetic alterations leading to the NF-kappaB pathway, which represents a therapeutic target.
Dr. Beylot-Barry and her colleagues initiated a multicenter, single-arm, phase 2 trial of 19 patients refractory/relapsing PCDLBCL, LT. Median progression-free survival in the trial was 4.9 months. The 6-month overall response rate – the primary endpoint of the trial – was 26.3%, which was not significantly superior to a prespecified 20% minimal response rate, according to the researchers.
“However, it was a stringent goal, and other secondary evaluations have to be considered in this context, such as a 6-month disease control rate at 42%,” they wrote.
Reduced doses were associated with improved outcomes, they added. Comparing the nine patients who had lenalidomide dose reductions to those who did not, there was a higher likelihood of 6- to 11-month overall response rate (44.4% vs. 10.0%; P = .11) and lower risk of disease progression or death (hazard ratio, 0.54; 95% confidence interval, 0.19-1.59; P = .27).
Grade 3 adverse events were primarily hematologic, and two deaths occurred (pulmonary embolism and sepsis).
Taken together, the encouraging results at reduced doses, the advanced age of the patients, and the high rate of adverse events suggests a role for lenalidomide as a part of combination treatment for PCDLBCL, LT in future trials, the researchers concluded.
The study was supported by grants from the French Ministry of Health and Celgene. The researchers reported having no financial disclosures.
SOURCE: Beylot-Barry M et al. J Invest Dermatol. 2018 Mar 26. doi: 10.1016/j.jid.2018.03.1516.
The oral immunomodulatory drug lenalidomide is active and may provide prolonged responses in certain patients with a rare and aggressive subtype of primary cutaneous lymphoma, according to results of a phase 2 study.
In the study, which comprised 19 patients with primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL, LT), 5 patients (26.3%) had a response at 6 months, and there were still 3 patients in response at 12 months. The findings were reported in the Journal of Investigative Dermatology.
In an exploratory analysis, reducing the dose of lenalidomide was associated with prolonged response and improved survival, noted lead author Marie Beylot-Barry, MD, of the dermatology department, Hôpital Saint-André, CHU Bordeaux, France, and her colleagues.
“Lenalidomide at reduced doses may allow prolonged responses in few patients, and represents a therapeutic option in relapsing/refractory PCDLBCL, LT,” the researchers wrote.
Found mostly on the lower limbs of elderly patients, PCDLBCL, LT exhibits aggressive behavior and is associated with a high rate of skin recurrences. First-line therapy for the cutaneous lymphoma is typically rituximab and chemotherapy, regardless of clinical stage or patient age, the researchers wrote, though primary resistance or recurrence after treatment occurs in about half of patients. “In such relapsing or refractory cases, no treatment has demonstrated a sustained benefit thus far,” they noted.
Lenalidomide has already demonstrated efficacy in relapsed/refractory diffuse large B-cell lymphoma (DLBCL) and it induces inhibition of cell signaling, engaging NF-kappaB signaling. PCDLBCL, LT is marked by genetic alterations leading to the NF-kappaB pathway, which represents a therapeutic target.
Dr. Beylot-Barry and her colleagues initiated a multicenter, single-arm, phase 2 trial of 19 patients refractory/relapsing PCDLBCL, LT. Median progression-free survival in the trial was 4.9 months. The 6-month overall response rate – the primary endpoint of the trial – was 26.3%, which was not significantly superior to a prespecified 20% minimal response rate, according to the researchers.
“However, it was a stringent goal, and other secondary evaluations have to be considered in this context, such as a 6-month disease control rate at 42%,” they wrote.
Reduced doses were associated with improved outcomes, they added. Comparing the nine patients who had lenalidomide dose reductions to those who did not, there was a higher likelihood of 6- to 11-month overall response rate (44.4% vs. 10.0%; P = .11) and lower risk of disease progression or death (hazard ratio, 0.54; 95% confidence interval, 0.19-1.59; P = .27).
Grade 3 adverse events were primarily hematologic, and two deaths occurred (pulmonary embolism and sepsis).
Taken together, the encouraging results at reduced doses, the advanced age of the patients, and the high rate of adverse events suggests a role for lenalidomide as a part of combination treatment for PCDLBCL, LT in future trials, the researchers concluded.
The study was supported by grants from the French Ministry of Health and Celgene. The researchers reported having no financial disclosures.
SOURCE: Beylot-Barry M et al. J Invest Dermatol. 2018 Mar 26. doi: 10.1016/j.jid.2018.03.1516.
The oral immunomodulatory drug lenalidomide is active and may provide prolonged responses in certain patients with a rare and aggressive subtype of primary cutaneous lymphoma, according to results of a phase 2 study.
In the study, which comprised 19 patients with primary cutaneous diffuse large B-cell lymphoma, leg type (PCDLBCL, LT), 5 patients (26.3%) had a response at 6 months, and there were still 3 patients in response at 12 months. The findings were reported in the Journal of Investigative Dermatology.
In an exploratory analysis, reducing the dose of lenalidomide was associated with prolonged response and improved survival, noted lead author Marie Beylot-Barry, MD, of the dermatology department, Hôpital Saint-André, CHU Bordeaux, France, and her colleagues.
“Lenalidomide at reduced doses may allow prolonged responses in few patients, and represents a therapeutic option in relapsing/refractory PCDLBCL, LT,” the researchers wrote.
Found mostly on the lower limbs of elderly patients, PCDLBCL, LT exhibits aggressive behavior and is associated with a high rate of skin recurrences. First-line therapy for the cutaneous lymphoma is typically rituximab and chemotherapy, regardless of clinical stage or patient age, the researchers wrote, though primary resistance or recurrence after treatment occurs in about half of patients. “In such relapsing or refractory cases, no treatment has demonstrated a sustained benefit thus far,” they noted.
Lenalidomide has already demonstrated efficacy in relapsed/refractory diffuse large B-cell lymphoma (DLBCL) and it induces inhibition of cell signaling, engaging NF-kappaB signaling. PCDLBCL, LT is marked by genetic alterations leading to the NF-kappaB pathway, which represents a therapeutic target.
Dr. Beylot-Barry and her colleagues initiated a multicenter, single-arm, phase 2 trial of 19 patients refractory/relapsing PCDLBCL, LT. Median progression-free survival in the trial was 4.9 months. The 6-month overall response rate – the primary endpoint of the trial – was 26.3%, which was not significantly superior to a prespecified 20% minimal response rate, according to the researchers.
“However, it was a stringent goal, and other secondary evaluations have to be considered in this context, such as a 6-month disease control rate at 42%,” they wrote.
Reduced doses were associated with improved outcomes, they added. Comparing the nine patients who had lenalidomide dose reductions to those who did not, there was a higher likelihood of 6- to 11-month overall response rate (44.4% vs. 10.0%; P = .11) and lower risk of disease progression or death (hazard ratio, 0.54; 95% confidence interval, 0.19-1.59; P = .27).
Grade 3 adverse events were primarily hematologic, and two deaths occurred (pulmonary embolism and sepsis).
Taken together, the encouraging results at reduced doses, the advanced age of the patients, and the high rate of adverse events suggests a role for lenalidomide as a part of combination treatment for PCDLBCL, LT in future trials, the researchers concluded.
The study was supported by grants from the French Ministry of Health and Celgene. The researchers reported having no financial disclosures.
SOURCE: Beylot-Barry M et al. J Invest Dermatol. 2018 Mar 26. doi: 10.1016/j.jid.2018.03.1516.
FROM THE JOURNAL OF INVESTIGATIVE DERMATOLOGY
Key clinical point:
Major finding: Five of 19 patients (26.3%) had a response at 6 months, and there were still 3 patients in response at 12 months.
Study details: A multicenter, single-arm, phase 2 trial of 19 patients refractory/relapsing PCDLBCL, LT.
Disclosures: The study was supported by grants from the French Ministry of Health and Celgene. The researchers reported having no financial disclosures.
Source: Beylot-Barry M et al. J Invest Dermatol. 2018 Mar 26. doi: 10.1016/j.jid.2018.03.1516.
Counsel children and young adults on skin cancer prevention
(USPSTF). The recommendations, published online March 20 in JAMA, advise clinicians to counsel young adults, children, and parents of young children who are aged 6 months to 24 years and have fair skin types about skin cancer prevention. Counseling for individuals aged 24 years and older should be based on a clinician’s assessment of patient risk.
The recommendations target asymptomatic individuals with no history of skin cancer who might be likely to sunburn easily, wrote David C. Grossman, MD, of Kaiser Permanente Washington Health Research Institute, Seattle, the corresponding author of the USPSTF recommendation statement, and his associates.
The task force found adequate (grade B) evidence to support behavioral counseling for children and young adults aged 6 months to 24 years with no notable risk of harm from this intervention. The task force gave a grade C recommendation for routine skin cancer counseling for adults older than 24 years, citing a small net benefit. In addition, the USPSTF found insufficient evidence (I statement) to evaluate the risks versus benefits of counseling adults about skin self-examination as a way to reduce skin cancer risk.
In the evidence report, lead author Nora B. Henrikson, PhD, of Kaiser Permanente Washington Health Research Institute, Seattle, and her colleagues addressed five topics: the effects of skin cancer prevention counseling on short- and long-term outcomes, the effects of primary care counseling interventions on skin cancer prevention behavior, the association between skin self-examination and skin cancer outcomes, the potential harms of counseling interventions, and the potential harms of skin self-examinations.
“Small to moderate effects of behavioral interventions on increased sun protection behaviors were observed in studies of all age groups, though overall, adult trial results were mixed and fewer studies demonstrated an intervention effect,” the researchers said.
The evidence review was limited by several factors including a focus on primary care intervention only and an exclusion of skin cancer survivors, the researchers noted. Although evidence does not show that sunburns are less frequent as a result of interventions, behavioral intervention can improve sun protection behavior, they said. However, intervention in adults “may lead to increased skin procedures without detecting additional atypical nevi or skin cancers,” they noted.
The recommendations are consistent with the draft recommendations published in 2017 and expand the recommendations from 2012 that advised counseling for individuals aged 10-24 years.
The research was funded by the Agency for Healthcare Research and Quality. The authors had no financial conflicts to disclose.
SOURCE: Grossman DC et al. JAMA. 2018;319(11):1134-42.
The term “fair skin types” as used in the USPSTF recommendations is not necessarily helpful in identifying individuals who could benefit from skin cancer prevention counseling, June K. Robinson, MD, and Nina G. Jablonski, PhD, wrote in an accompanying editorial (JAMA. 2018;319[11]:1101-2). Hair and eye color do not predict sun sensitivity, and in general, men and individuals with darker skin don’t think they are at risk for skin cancer even when they sunburn, they noted.
“The terminology that is used by investigators and then incorporated into the USPSTF evidence base needs to evolve to include all persons at risk, without disenfranchising portions of the diverse U.S. population,” they said. In addition to skin type, physicians need to evaluate a patient’s melanoma risk based on lifestyle factors, such as time spent outdoors, photosensitizing medications, and sun protection habits, they added, but primary care clinicians often lack the time to offer personalized sun protection counseling.
“It would be better to encourage people to check the UV Index daily – or consider a mobile application that automatically provides it – and plan outdoor activities, especially physical activities, to be sun safe,” they said. In addition, individuals may be more likely to manage skin cancer risk with a mix of supportive messages via social media to augment in-person counseling from a clinician; furthermore, “normative approval by friends and peers can have a strong reinforcing influence on sun safety behaviors, particularly among youth, who are at a vulnerable age for acquiring melanoma risk,” they emphasized.
Dr. Robinson is a research professor of dermatology at Northwestern University, Chicago, and is the editor of JAMA Dermatology. She is supported in part by the National Cancer Institute. Dr. Jablonski is a professor of anthropology at Pennsylvania State University, University Park. Dr. Robinson had no financial conflicts to disclose; Dr. Jablonski has served on the scientific advisory board of the L’Oreal Group.
The term “fair skin types” as used in the USPSTF recommendations is not necessarily helpful in identifying individuals who could benefit from skin cancer prevention counseling, June K. Robinson, MD, and Nina G. Jablonski, PhD, wrote in an accompanying editorial (JAMA. 2018;319[11]:1101-2). Hair and eye color do not predict sun sensitivity, and in general, men and individuals with darker skin don’t think they are at risk for skin cancer even when they sunburn, they noted.
“The terminology that is used by investigators and then incorporated into the USPSTF evidence base needs to evolve to include all persons at risk, without disenfranchising portions of the diverse U.S. population,” they said. In addition to skin type, physicians need to evaluate a patient’s melanoma risk based on lifestyle factors, such as time spent outdoors, photosensitizing medications, and sun protection habits, they added, but primary care clinicians often lack the time to offer personalized sun protection counseling.
“It would be better to encourage people to check the UV Index daily – or consider a mobile application that automatically provides it – and plan outdoor activities, especially physical activities, to be sun safe,” they said. In addition, individuals may be more likely to manage skin cancer risk with a mix of supportive messages via social media to augment in-person counseling from a clinician; furthermore, “normative approval by friends and peers can have a strong reinforcing influence on sun safety behaviors, particularly among youth, who are at a vulnerable age for acquiring melanoma risk,” they emphasized.
Dr. Robinson is a research professor of dermatology at Northwestern University, Chicago, and is the editor of JAMA Dermatology. She is supported in part by the National Cancer Institute. Dr. Jablonski is a professor of anthropology at Pennsylvania State University, University Park. Dr. Robinson had no financial conflicts to disclose; Dr. Jablonski has served on the scientific advisory board of the L’Oreal Group.
The term “fair skin types” as used in the USPSTF recommendations is not necessarily helpful in identifying individuals who could benefit from skin cancer prevention counseling, June K. Robinson, MD, and Nina G. Jablonski, PhD, wrote in an accompanying editorial (JAMA. 2018;319[11]:1101-2). Hair and eye color do not predict sun sensitivity, and in general, men and individuals with darker skin don’t think they are at risk for skin cancer even when they sunburn, they noted.
“The terminology that is used by investigators and then incorporated into the USPSTF evidence base needs to evolve to include all persons at risk, without disenfranchising portions of the diverse U.S. population,” they said. In addition to skin type, physicians need to evaluate a patient’s melanoma risk based on lifestyle factors, such as time spent outdoors, photosensitizing medications, and sun protection habits, they added, but primary care clinicians often lack the time to offer personalized sun protection counseling.
“It would be better to encourage people to check the UV Index daily – or consider a mobile application that automatically provides it – and plan outdoor activities, especially physical activities, to be sun safe,” they said. In addition, individuals may be more likely to manage skin cancer risk with a mix of supportive messages via social media to augment in-person counseling from a clinician; furthermore, “normative approval by friends and peers can have a strong reinforcing influence on sun safety behaviors, particularly among youth, who are at a vulnerable age for acquiring melanoma risk,” they emphasized.
Dr. Robinson is a research professor of dermatology at Northwestern University, Chicago, and is the editor of JAMA Dermatology. She is supported in part by the National Cancer Institute. Dr. Jablonski is a professor of anthropology at Pennsylvania State University, University Park. Dr. Robinson had no financial conflicts to disclose; Dr. Jablonski has served on the scientific advisory board of the L’Oreal Group.
(USPSTF). The recommendations, published online March 20 in JAMA, advise clinicians to counsel young adults, children, and parents of young children who are aged 6 months to 24 years and have fair skin types about skin cancer prevention. Counseling for individuals aged 24 years and older should be based on a clinician’s assessment of patient risk.
The recommendations target asymptomatic individuals with no history of skin cancer who might be likely to sunburn easily, wrote David C. Grossman, MD, of Kaiser Permanente Washington Health Research Institute, Seattle, the corresponding author of the USPSTF recommendation statement, and his associates.
The task force found adequate (grade B) evidence to support behavioral counseling for children and young adults aged 6 months to 24 years with no notable risk of harm from this intervention. The task force gave a grade C recommendation for routine skin cancer counseling for adults older than 24 years, citing a small net benefit. In addition, the USPSTF found insufficient evidence (I statement) to evaluate the risks versus benefits of counseling adults about skin self-examination as a way to reduce skin cancer risk.
In the evidence report, lead author Nora B. Henrikson, PhD, of Kaiser Permanente Washington Health Research Institute, Seattle, and her colleagues addressed five topics: the effects of skin cancer prevention counseling on short- and long-term outcomes, the effects of primary care counseling interventions on skin cancer prevention behavior, the association between skin self-examination and skin cancer outcomes, the potential harms of counseling interventions, and the potential harms of skin self-examinations.
“Small to moderate effects of behavioral interventions on increased sun protection behaviors were observed in studies of all age groups, though overall, adult trial results were mixed and fewer studies demonstrated an intervention effect,” the researchers said.
The evidence review was limited by several factors including a focus on primary care intervention only and an exclusion of skin cancer survivors, the researchers noted. Although evidence does not show that sunburns are less frequent as a result of interventions, behavioral intervention can improve sun protection behavior, they said. However, intervention in adults “may lead to increased skin procedures without detecting additional atypical nevi or skin cancers,” they noted.
The recommendations are consistent with the draft recommendations published in 2017 and expand the recommendations from 2012 that advised counseling for individuals aged 10-24 years.
The research was funded by the Agency for Healthcare Research and Quality. The authors had no financial conflicts to disclose.
SOURCE: Grossman DC et al. JAMA. 2018;319(11):1134-42.
(USPSTF). The recommendations, published online March 20 in JAMA, advise clinicians to counsel young adults, children, and parents of young children who are aged 6 months to 24 years and have fair skin types about skin cancer prevention. Counseling for individuals aged 24 years and older should be based on a clinician’s assessment of patient risk.
The recommendations target asymptomatic individuals with no history of skin cancer who might be likely to sunburn easily, wrote David C. Grossman, MD, of Kaiser Permanente Washington Health Research Institute, Seattle, the corresponding author of the USPSTF recommendation statement, and his associates.
The task force found adequate (grade B) evidence to support behavioral counseling for children and young adults aged 6 months to 24 years with no notable risk of harm from this intervention. The task force gave a grade C recommendation for routine skin cancer counseling for adults older than 24 years, citing a small net benefit. In addition, the USPSTF found insufficient evidence (I statement) to evaluate the risks versus benefits of counseling adults about skin self-examination as a way to reduce skin cancer risk.
In the evidence report, lead author Nora B. Henrikson, PhD, of Kaiser Permanente Washington Health Research Institute, Seattle, and her colleagues addressed five topics: the effects of skin cancer prevention counseling on short- and long-term outcomes, the effects of primary care counseling interventions on skin cancer prevention behavior, the association between skin self-examination and skin cancer outcomes, the potential harms of counseling interventions, and the potential harms of skin self-examinations.
“Small to moderate effects of behavioral interventions on increased sun protection behaviors were observed in studies of all age groups, though overall, adult trial results were mixed and fewer studies demonstrated an intervention effect,” the researchers said.
The evidence review was limited by several factors including a focus on primary care intervention only and an exclusion of skin cancer survivors, the researchers noted. Although evidence does not show that sunburns are less frequent as a result of interventions, behavioral intervention can improve sun protection behavior, they said. However, intervention in adults “may lead to increased skin procedures without detecting additional atypical nevi or skin cancers,” they noted.
The recommendations are consistent with the draft recommendations published in 2017 and expand the recommendations from 2012 that advised counseling for individuals aged 10-24 years.
The research was funded by the Agency for Healthcare Research and Quality. The authors had no financial conflicts to disclose.
SOURCE: Grossman DC et al. JAMA. 2018;319(11):1134-42.
FROM JAMA
Key clinical point: Moderate evidence supports behavioral counseling to help reduce skin cancer risk in children and young adults.
Major finding: One trial that included 1,356 adults showed no difference in the number of skin cancers and atypical nevi between a control group and patients who received counseling to encourage skin examination.
Study details: The evidence review included 21 trials in 27 publications for a total of 20,561 individuals.
Disclosures: The review was funded by the Agency for Healthcare Research and Quality.
Source: Grossman DC et al. JAMA. 2018;319(11):1134-42.
cSCC staging systems poorly determine metastasis risk
Current staging systems for cutaneous squamous cell carcinoma (cSCC) poorly discerned between patients with and without metastases, according to researchers.
In a population-based case-control study of 6,721 cSCC patients, the American Joint Committee on Cancer, 7th edition (AJCC 7) staging system had the lowest rate of correctly classified cases (61.8%), followed by the AJCC 8 (68.2%), the Brigham and Women’s Hospital (BWH) system (72.3%), and the Breuninger system (76.2%). The Breuninger system performed best, with sensitivity of 77.3%, specificity of 75%, correctly classified tumor rate of 76.2%, and concordance index (C-index) of 0.81, reported Ingrid Roscher, MD, of the department of dermatology at Oslo University Hospital, and her coauthors. The report was published in JAMA Dermatology.
Investigators used data from the Cancer Registry of Norway to identify 6,721 patients with a first cSCC diagnosis between Jan. 1, 2000, and Dec. 31, 2004. Metastasis status was split into one of two categories: no metastases (local disease only) and metastasis (regional lymph node or distant metastasis).
Within 5 years follow-up, 112 patients had developed metastasis, and 112 patients without metastasis were selected at random as controls. Tumor tissue was collected for all 224 patients and checked by a pathologist. Tumors were classified under all four staging systems, and a chi-squared test was performed to compare patients with and without metastasis. Relative risk of metastasis was calculated via logistic regression analyses.
Sensitivity, specificity, and correctly identified cases were used to evaluate performance of the staging systems, and C-index was used to measure discriminatory ability, wrote Dr. Roscher and her colleagues.
AJCC 7 had a sensitivity of 85.6%, specificity of 33.3%, and C-index value of 0.59; compared with AJCC scores of 67.1%, 69.6%, and 0.70 for sensitivity, specificity, and C-index, respectively. BWH had a sensitivity of 68.9%, specificity of 76.5%, and C-index of 0.75.
Within the AJCC 7 system, 85.6% of patients with metastasis and 66.7% without metastasis fell into the T2 category, and no patients were grouped into T3 or T4 (P = .003). Under the BWH system, patients without metastasis fell mostly into the T1 category, while those with metastasis were about equally distributed among T1, T2a, and T2b (P less than .001). With the Breuninger system, more patients with metastasis than without metastasis fell into the high-risk categories for tumor diameter and depth (P less than .001). Lastly, under AJCC 8, 10% of all patients fell into the T2 category, while less than 20% of patients without metastasis and more than 50% of patients with metastasis fell into the T3 category (P less than .001).
Risk of metastasis for T2 patients was greater than for T1 patients under the AJCC 7 system (odds ratio = 2.96; 95% confidence interval, 1.43-6.15). Under BWH, OR for metastasis were 4.6 (95% CI, 2.23-9.49) for T2a patients and 21.31 (95% CI, 6.07-74.88) for T2b patients. Under the Breuninger system, tumor diameter greater than 2 cm (OR = 5.92; 95% CI, 2.18-16.07) and depth of invasion greater than 6 mm (OR = 9.00; 95% CI, 3.51-32.31) increased risk of metastasis. The AJCC 8 system showed increased metastasis risk for T2 (OR = 2.00; 95% CI, 0.62-6.44) and T3 (OR = 6.14; 95% CI, 0.41-1.09) patients, the authors reported.
The results suggest that the current staging systems “distinguished poorly to moderately between patients who developed metastases and those who did not,” Dr. Roscher and her coauthors wrote. Moreover, “the poorest results were found for the AJCC 7 system, which is most widely used,” they added.
“Our findings indicate a need for a more reliable, easy-to-perform, and clinically useful staging system than those presently available,” they concluded.
Oslo University Hospital and the Cancer Registry of Norway funded the study. No other disclosures were reported.
SOURCE: Roscher et al. JAMA Dermatol. 2018 March 7 doi: 10.1001/jamadermatol.2017.6428.
Current staging systems for cutaneous squamous cell carcinoma (cSCC) poorly discerned between patients with and without metastases, according to researchers.
In a population-based case-control study of 6,721 cSCC patients, the American Joint Committee on Cancer, 7th edition (AJCC 7) staging system had the lowest rate of correctly classified cases (61.8%), followed by the AJCC 8 (68.2%), the Brigham and Women’s Hospital (BWH) system (72.3%), and the Breuninger system (76.2%). The Breuninger system performed best, with sensitivity of 77.3%, specificity of 75%, correctly classified tumor rate of 76.2%, and concordance index (C-index) of 0.81, reported Ingrid Roscher, MD, of the department of dermatology at Oslo University Hospital, and her coauthors. The report was published in JAMA Dermatology.
Investigators used data from the Cancer Registry of Norway to identify 6,721 patients with a first cSCC diagnosis between Jan. 1, 2000, and Dec. 31, 2004. Metastasis status was split into one of two categories: no metastases (local disease only) and metastasis (regional lymph node or distant metastasis).
Within 5 years follow-up, 112 patients had developed metastasis, and 112 patients without metastasis were selected at random as controls. Tumor tissue was collected for all 224 patients and checked by a pathologist. Tumors were classified under all four staging systems, and a chi-squared test was performed to compare patients with and without metastasis. Relative risk of metastasis was calculated via logistic regression analyses.
Sensitivity, specificity, and correctly identified cases were used to evaluate performance of the staging systems, and C-index was used to measure discriminatory ability, wrote Dr. Roscher and her colleagues.
AJCC 7 had a sensitivity of 85.6%, specificity of 33.3%, and C-index value of 0.59; compared with AJCC scores of 67.1%, 69.6%, and 0.70 for sensitivity, specificity, and C-index, respectively. BWH had a sensitivity of 68.9%, specificity of 76.5%, and C-index of 0.75.
Within the AJCC 7 system, 85.6% of patients with metastasis and 66.7% without metastasis fell into the T2 category, and no patients were grouped into T3 or T4 (P = .003). Under the BWH system, patients without metastasis fell mostly into the T1 category, while those with metastasis were about equally distributed among T1, T2a, and T2b (P less than .001). With the Breuninger system, more patients with metastasis than without metastasis fell into the high-risk categories for tumor diameter and depth (P less than .001). Lastly, under AJCC 8, 10% of all patients fell into the T2 category, while less than 20% of patients without metastasis and more than 50% of patients with metastasis fell into the T3 category (P less than .001).
Risk of metastasis for T2 patients was greater than for T1 patients under the AJCC 7 system (odds ratio = 2.96; 95% confidence interval, 1.43-6.15). Under BWH, OR for metastasis were 4.6 (95% CI, 2.23-9.49) for T2a patients and 21.31 (95% CI, 6.07-74.88) for T2b patients. Under the Breuninger system, tumor diameter greater than 2 cm (OR = 5.92; 95% CI, 2.18-16.07) and depth of invasion greater than 6 mm (OR = 9.00; 95% CI, 3.51-32.31) increased risk of metastasis. The AJCC 8 system showed increased metastasis risk for T2 (OR = 2.00; 95% CI, 0.62-6.44) and T3 (OR = 6.14; 95% CI, 0.41-1.09) patients, the authors reported.
The results suggest that the current staging systems “distinguished poorly to moderately between patients who developed metastases and those who did not,” Dr. Roscher and her coauthors wrote. Moreover, “the poorest results were found for the AJCC 7 system, which is most widely used,” they added.
“Our findings indicate a need for a more reliable, easy-to-perform, and clinically useful staging system than those presently available,” they concluded.
Oslo University Hospital and the Cancer Registry of Norway funded the study. No other disclosures were reported.
SOURCE: Roscher et al. JAMA Dermatol. 2018 March 7 doi: 10.1001/jamadermatol.2017.6428.
Current staging systems for cutaneous squamous cell carcinoma (cSCC) poorly discerned between patients with and without metastases, according to researchers.
In a population-based case-control study of 6,721 cSCC patients, the American Joint Committee on Cancer, 7th edition (AJCC 7) staging system had the lowest rate of correctly classified cases (61.8%), followed by the AJCC 8 (68.2%), the Brigham and Women’s Hospital (BWH) system (72.3%), and the Breuninger system (76.2%). The Breuninger system performed best, with sensitivity of 77.3%, specificity of 75%, correctly classified tumor rate of 76.2%, and concordance index (C-index) of 0.81, reported Ingrid Roscher, MD, of the department of dermatology at Oslo University Hospital, and her coauthors. The report was published in JAMA Dermatology.
Investigators used data from the Cancer Registry of Norway to identify 6,721 patients with a first cSCC diagnosis between Jan. 1, 2000, and Dec. 31, 2004. Metastasis status was split into one of two categories: no metastases (local disease only) and metastasis (regional lymph node or distant metastasis).
Within 5 years follow-up, 112 patients had developed metastasis, and 112 patients without metastasis were selected at random as controls. Tumor tissue was collected for all 224 patients and checked by a pathologist. Tumors were classified under all four staging systems, and a chi-squared test was performed to compare patients with and without metastasis. Relative risk of metastasis was calculated via logistic regression analyses.
Sensitivity, specificity, and correctly identified cases were used to evaluate performance of the staging systems, and C-index was used to measure discriminatory ability, wrote Dr. Roscher and her colleagues.
AJCC 7 had a sensitivity of 85.6%, specificity of 33.3%, and C-index value of 0.59; compared with AJCC scores of 67.1%, 69.6%, and 0.70 for sensitivity, specificity, and C-index, respectively. BWH had a sensitivity of 68.9%, specificity of 76.5%, and C-index of 0.75.
Within the AJCC 7 system, 85.6% of patients with metastasis and 66.7% without metastasis fell into the T2 category, and no patients were grouped into T3 or T4 (P = .003). Under the BWH system, patients without metastasis fell mostly into the T1 category, while those with metastasis were about equally distributed among T1, T2a, and T2b (P less than .001). With the Breuninger system, more patients with metastasis than without metastasis fell into the high-risk categories for tumor diameter and depth (P less than .001). Lastly, under AJCC 8, 10% of all patients fell into the T2 category, while less than 20% of patients without metastasis and more than 50% of patients with metastasis fell into the T3 category (P less than .001).
Risk of metastasis for T2 patients was greater than for T1 patients under the AJCC 7 system (odds ratio = 2.96; 95% confidence interval, 1.43-6.15). Under BWH, OR for metastasis were 4.6 (95% CI, 2.23-9.49) for T2a patients and 21.31 (95% CI, 6.07-74.88) for T2b patients. Under the Breuninger system, tumor diameter greater than 2 cm (OR = 5.92; 95% CI, 2.18-16.07) and depth of invasion greater than 6 mm (OR = 9.00; 95% CI, 3.51-32.31) increased risk of metastasis. The AJCC 8 system showed increased metastasis risk for T2 (OR = 2.00; 95% CI, 0.62-6.44) and T3 (OR = 6.14; 95% CI, 0.41-1.09) patients, the authors reported.
The results suggest that the current staging systems “distinguished poorly to moderately between patients who developed metastases and those who did not,” Dr. Roscher and her coauthors wrote. Moreover, “the poorest results were found for the AJCC 7 system, which is most widely used,” they added.
“Our findings indicate a need for a more reliable, easy-to-perform, and clinically useful staging system than those presently available,” they concluded.
Oslo University Hospital and the Cancer Registry of Norway funded the study. No other disclosures were reported.
SOURCE: Roscher et al. JAMA Dermatol. 2018 March 7 doi: 10.1001/jamadermatol.2017.6428.
FROM JAMA DERMATOLOGY
Key clinical point: The four cSCC staging systems, especially the AJCC 7, poorly identified metastasis risk.
Major finding: The AJCC 7 staging system had the lowest rate of correctly classified cases (61.8%), followed by the AJCC 8 (68.2%), the Brigham and Women’s Hospital (BWH) system (72.3%), and the Breuninger system (76.2%).
Data source: A population-based case-control study of 6,721 patients with cSCC.
Disclosures: Oslo University Hospital and the Cancer Registry of Norway funded the study.
Source: Roscher et al. JAMA Dermatol. 2018 Mar 7. doi: 10.1001/jamadermatol.2017.6428.
Invasive Penile Squamous Cell Carcinoma
Invasive penile cancer is a rare malignancy with considerable morbidity and mortality. The American Cancer Society estimates that there will be 2320 new cases of invasive penile cancer in the United States in 2018, of which primary penile squamous cell carcinoma (PSCC) represents the majority.1 In one study, the mean age at diagnosis was 60 years, with PSCC occurring only rarely in men younger than 35 years of age (estimated incidence, 0.01 cases per 100,000 individuals).2 Presentation to a physician generally occurs more than 1 year after initial onset of symptoms or clinical lesion(s). This delay in diagnosis and treatment often results in disease progression,3 which can have a devastating outcome.4 Therefore, physicians should maintain a high index of clinical suspicion for PSCC, particularly in young or middle-aged patients in whom presentation of PSCC is uncommon. The most commonly associated risk factors for PSCC include lack of circumcision (specifically during the neonatal period), high-risk human papillomavirus (HPV) infection, and tobacco use.5 Chronic alcoholism also has been linked to PSCC.6 It also is common in patients without health insurance.7 We report the case of a 27-year-old circumcised man who presented with invasive PSCC following a diagnosis of condyloma 8 years prior by an outside physician.
Case Report
A 27-year-old man presented for evaluation of persistent genital warts that had been diagnosed 8 years prior. His medical history was remarkable for intravenous drug use, active hepatitis C infection, tobacco smoking, chronic alcohol use, and mild asthma. Eight years prior to the current presentation, 7 lesions had developed on the penis and were diagnosed by an outside physician as condyloma, which was treated with cryotherapy and topical imiquimod. All of the lesions except for 1 responded to treatment. The residual lesion continued to grow until the size prompted him to contact his primary care physician, who referred him for dermatologic evaluation. The patient cited lack of health insurance as the primary reason he did not seek follow-up treatment after the initial evaluation and treatment 8 years prior.
Physical examination at the current presentation revealed a circumcised man with an asymptomatic, 2.6-cm, pink, friable, verrucous mass on the left lateral penile shaft (Figure 1) and otherwise unremarkable penile architecture. A clinically enlarged, nontender right inguinal lymph node was noted as well as subtle enlargement of a left inguinal lymph node. An excisional biopsy was performed with pathologic evaluation confirming a diagnosis of high-grade invasive squamous cell carcinoma (SCC) arising in the setting of squamous cell carcinoma in situ (Figure 2). Lymphovascular invasion was highlighted on cluster of differentiation 31 and podoplanin immunostaining (Figure 3). The patient was subsequently referred to urology and hematology-oncology specialists for further evaluation. Computed tomography (CT) of the abdomen and pelvis confirmed the contralaterally enlarged right inguinal lymph node discovered during physical examination and mildly enlarged ipsilateral inguinal, obturator, and external iliac nodes. Computed tomography–guided fine-needle aspiration of the right inguinal node confirmed the diagnosis of contralateral locoregional metastasis. Further evaluation with positron emission tomography/CT imaging revealed only a single metabolically active region confined to the right inguinal node. The patient’s history of active hepatitis C complicated proposed neoadjuvant chemotherapy regimens. Ultimately, after discussion with multiple surgical and oncologist specialties within our institution and others, a treatment plan was formulated. The patient underwent robotic laparoscopic bilateral pelvic and inguinal lymph node dissection and re-excision of the primary PSCC, with one of 15 right superficial inguinal nodes testing positive for tumor cells; the left superficial and bilateral deep inguinal lymph nodes were negative for SCC.

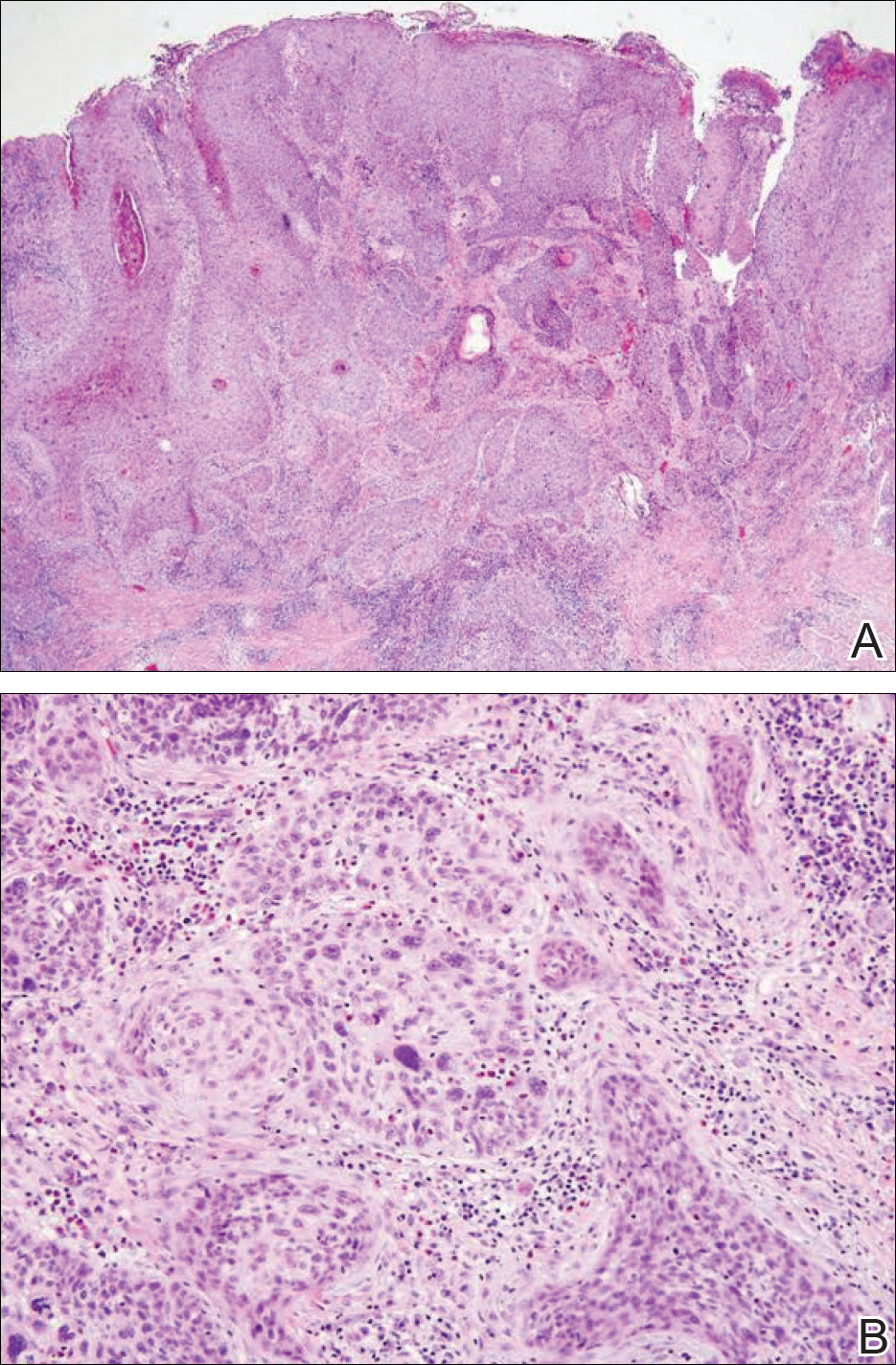
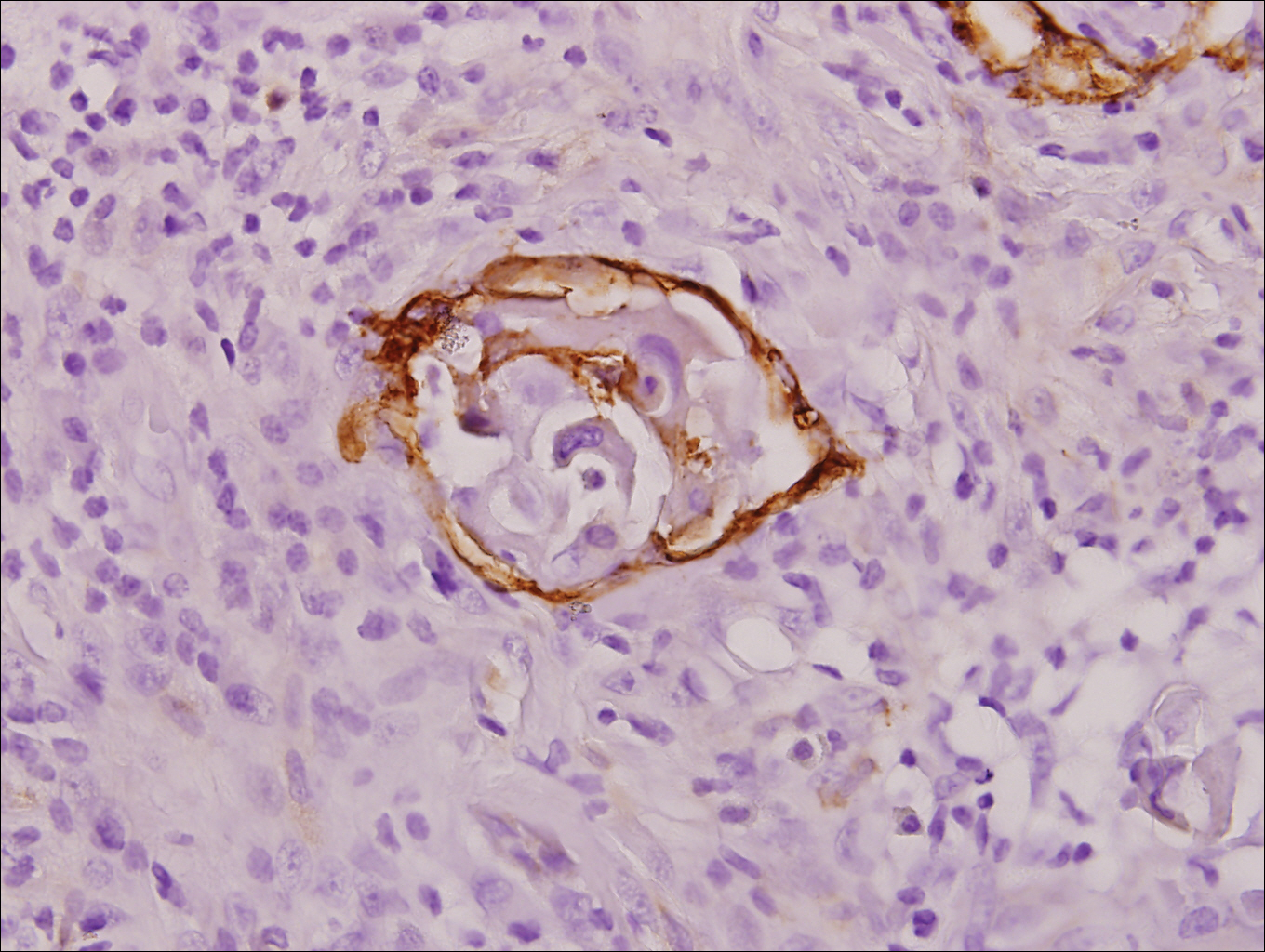
Repeat positron emission tomography/CT imaging at 6 months’ follow-up showed no evidence of active disease. On 1-year follow-up, a CT scan did not show any new or residual disease, but the patient continued to have edema of the bilateral legs, which began after lymph node dissection and was managed with physical therapy and compression stockings.
Comment
Prevalence
Penile cancer is rare in industrialized countries. Early detection is a critical factor for both overall survival and organ function. If successful interventions are to be made, physicians should be familiar with known risk factors as well as unusual presentations, such as lesions presenting in young circumcised men, as reported above. Similarly, tumors located on the shaft of the penis represent an uncommon location for tumor presentation, occurring in less than 5% of PSCC cases.8 Penile SCC most commonly develops as a solitary painless lesion on the glans, balanopreputial sulcus and/or prepuce.9 In our case, histopathology confirmed high-grade invasive SCC arising from squamous cell carcinoma in situ, an entity generally associated with older men with a 10% to 20% rate of progression into invasive SCC.9 Our patient denied any clinical change in the appearance of the tumor in the years prior to the current presentation, making it possible that the condyloma treated 8 years prior was squamous cell carcinoma in situ or PSCC. As many as 25% of premalignant lesions are mistaken for benign lesions, which can thus delay treatment and allow progression to malignancy.10
Diagnosis
Penile SCC often is etiologically subcategorized into 2 pathways based on HPV dependence or independence. Recent research suggests that this distinction often is difficult to make, and accurate laboratory and pathologic confirmation of HPV DNA, intact virions, and viral-related cutaneous changes is not always possible, leading to much speculation regarding the exact role of HPV in tumorigenesis.11 Cancers developing in the absence of HPV DNA often occur secondary to chronic inflammatory conditions such as lichen planus or lichen sclerosus. Human papillomavirus DNA has shown to be present in 70% to 100% of all SCC in situ of the penis11; therefore, the transformation of in situ disease to an invasive tumor in our patient most likely occurred via an HPV-dependent pathway. Viral carcinogenesis in the HPV-dependent pathway involves inactivation of host cell cycle regulatory proteins, specifically the retinoblastoma and p53 regulatory proteins by the viral oncoproteins E7 and E6, respectively.12,13 Human papillomavirus–dependent pathways are related to a patient’s age at first sexual intercourse, number of sexual partners, and history of condyloma and other sexually transmitted diseases.14,15 High-risk HPV types 16 and 18 are the most common viral types found in HPV related premalignant lesions, making it possible to decrease the incidence of PSCC with recently developed vaccines.16 Human papillomavirus vaccines have been shown to reduce the incidence of anal intraepithelial neoplasias and genital warts in men.17 While the effects of the HPV vaccine on reducing PSCC could not be assessed in the study due to low incidence of disease (both in the study population and in general), it is thought that HPV vaccination could potentially decrease the incidence of all PSCCs by one third, making it an important resource in the primary prevention of the disease.18
Management
Contemporary surgical management of PSCC has evolved from organ resection in toto for all PSCCs to a more conservative approach based upon tumor stage and grade. The standard margin for surgical resection of PSCC is 2 cm, a procedure often referred to as a partial penectomy. This remains the most common procedure for surgical resection of PSCC and has achieved good local control, with reported recurrence rates of 4% to 8%.19,20 Complication rates of the procedure are moderate one-third of patients experiencing compromise of sexual activity after surgery.21 With evidence that smaller resection margins may result in good local control and a lower incidence of postoperative functional impairment, resection margins of 5, 10, and 15 mm have been advocated for PSCCs of varying histologic grades and tumor stages.22-24 Treatment options for T1 and in situ tumors have expanded to include glansectomy, margin-controlled Mohs micrographic surgery, and ablative laser therapy for local disease control.5,20 More advanced tumors are still treated with partial or complete penectomy given the high risks for locoregional recurrence and distant spread.
Prognosis
The most important factor predicting survival in patients with PSCC is metastasis to inguinal lymph nodes. The 5-year survival rate for patients without nodal involvement is 85% to 100%, while those with pathologically positive lymph nodes have a 5-year survival rate of 15% to 45%.25 Once distant metastasis occurs, the mean time of survival is 7 to 10 months.26 Our patient presented with high-grade PSCC with histologic lymphovascular spread and palpable inguinal lymph nodes. When stratified with other similar cases at presentation, our patient was at a considerable risk for locoregional as well as distant metastasis. Management with regional nodal dissection with a plan for close observation (and deferment of chemotherapeutics) was based upon evaluations from multiple different medical specialties.
Conclusion
Invasive PSCC is rare in young circumcised adults, and a delay in diagnosis can lead to considerable morbidity and mortality. We present a case of invasive PSCC arising in the setting of squamous cell carcinoma in situ in an area previously treated with cryotherapy and imiquimod. Our patient’s young age, concurrent hepatitis C infection, and contralateral locoregional nodal metastasis made this a complex case, involving evaluation and treatment by multiple medical disciplines. This case highlights the importance of biopsy in any lesion recalcitrant to conventional modalities regardless of the patient’s age. Early detection and treatment of PSCC can prevent organ dysfunction, loss of organ, and even death.
- About penile cancer. American Cancer Society website. https://www.cancer.org/content/dam/CRC/PDF/Public/8783.00.pdf. Revised February 9, 2016. Accessed February 27, 2018.
- Barnholtz-Sloan JS, Maldonado JL, Pow-sang J, et al. Incidence trends in primary malignant penile cancer. Urol Oncol. 2007;25:361-367.
- Koifman L, Vides AJ, Koifman N, et al. Epidemiological aspects of penile cancer in Rio de Janeiro: evaluation of 230 cases. Int Braz J Urol. 2011;37:231-240.
- Kamat AM, Carpenter SM, Czerniak BA, et al. Metastatic penile cancer in a young Caucasian male: impact of delayed diagnosis. Urol Oncol. 2005;23:130-131.
- Deem S, Keane T, Bhavsar R, et al. Contemporary diagnosis and management of squamous cell carcinoma (SCC) of the penis. BJU Int. 2011;108:1378-1392.
- McIntyre M, Weiss A, Wahlquist A, et al. Penile cancer: an analysis of socioeconomic factors at a southeastern tertiary referral center. Can J Urol. 2011;18:5524-5528.
- Maden C, Sherman KJ, Beckmann AM, et al. History of circumcision, medical conditions, and sexual activity and risk of penile cancer. J Natl Cancer Inst. 1993;85:19-24.
- Hernandez BY, Barnholtz-Sloan J, German RR, et al. Burden of invasive squamous cell carcinoma of the penis in the United States, 1998-2003. Cancer. 2008;113(suppl 10):2883-2891.
- Ferrandiz-Pulido C, de Torres I, Garcia-Patos V. Penile squamous cell carcinoma. Actas Dermosifiliogr. 2012;103:478-487.
- Tietjen DN, Malek RS. Laser therapy of squamous cell dysplasia and carcinoma of the penis. Urology. 1998;52:559-565.
- Mannweiler S, Sygulla S, Winter E, et al. Two major pathways of penile carcinogenesis: HPV-induced penile cancers overexpress p16, HPV-negative cancers associated with dermatoses express p53, but lack p16 overexpression. J Am Acad Dermatol. 2013;69:73-81.
- Scheffner M, Werness BA, Huibregtse JM, et al. The E6 oncoprotein encoded by human papillomavirus types 16 and 18 promotes the degradation of p53. Cell. 1990;63:1129-1136.
- Werness BA, Levine AJ, Howley PM. Association of human papillomavirus types 16 and 18 E6 proteins with p53. Science. 1990;248:76-79.
- Daling JR, Madeleine MM, Johnson LG, et al. Penile cancer: importance of circumcision, human papillomavirus and smoking in in situ and invasive disease. Int J Cancer. 2005;116:606-616.
- Bleeker MC, Heideman DA, Snijders PJ, et al. Penile cancer: epidemiology, pathogenesis and prevention. World J Urol. 2009;27:141-150.
- Shabbir M, Barod R, Hegarty PK, et al. Primary prevention and vaccination for penile cancer. Ther Adv Urol. 2013;5:161-169.
- Palefsky J, Giuliano A, Goldstone S, et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N Engl J Med. 2011;365:1576-1585.
- Backes DM, Kurman RJ, Pimenta JM, et al. Systematic review of human papillomavirus prevalence in invasive penile cancer. Cancer Causes Control. 2009;20:449-457.
- Korets R, Koppie TM, Snyder ME, et al. Partial penectomy for patients with squamous cell carcinoma of the penis: the Memorial Sloan-Kettering experience. Ann Surg Oncol. 2007;14:3614-3619.
- Zukiwskyj M, Daly P, Chung E. Penile cancer and phallus preservation strategies: a review of current literature. BJU Int. 2013;112(suppl 2):21-26.
- Romero FR, Romero KR, Mattos MA, et al. Sexual function after partial penectomy for penile cancer. Urology. 2005;66:1292-1295.
- Minhas S, Kayes O, Hegarty P, et al. What surgical resection margins are required to achieve oncological control in men with primary penile cancer? BJU Int. 2005;96:1040-1043.
- Feldman AS, McDougal WS. Long-term outcome of excisional organ sparing surgery for carcinoma of the penis. J Urol. 2011;186:1303-1307.
- Philippou P, Shabbir M, Malone P, et al. Conservative surgery for squamous cell carcinoma of the penis: resection margins and long-term oncological control. J Urol. 2012;188:803-808.
- Brady KL, Mercurio MG, Brown MD. Malignant tumors of the penis. Dermatol Surg. 2013;39:527-547.
- Ornellas AA, Nobrega BL, Wei Kin Chin E, et al. Prognostic factors in invasive squamous cell carcinoma of the penis: analysis of 196 patients treated at the Brazilian National Cancer Institute. J Urol. 2008;180:1354-1359.
Invasive penile cancer is a rare malignancy with considerable morbidity and mortality. The American Cancer Society estimates that there will be 2320 new cases of invasive penile cancer in the United States in 2018, of which primary penile squamous cell carcinoma (PSCC) represents the majority.1 In one study, the mean age at diagnosis was 60 years, with PSCC occurring only rarely in men younger than 35 years of age (estimated incidence, 0.01 cases per 100,000 individuals).2 Presentation to a physician generally occurs more than 1 year after initial onset of symptoms or clinical lesion(s). This delay in diagnosis and treatment often results in disease progression,3 which can have a devastating outcome.4 Therefore, physicians should maintain a high index of clinical suspicion for PSCC, particularly in young or middle-aged patients in whom presentation of PSCC is uncommon. The most commonly associated risk factors for PSCC include lack of circumcision (specifically during the neonatal period), high-risk human papillomavirus (HPV) infection, and tobacco use.5 Chronic alcoholism also has been linked to PSCC.6 It also is common in patients without health insurance.7 We report the case of a 27-year-old circumcised man who presented with invasive PSCC following a diagnosis of condyloma 8 years prior by an outside physician.
Case Report
A 27-year-old man presented for evaluation of persistent genital warts that had been diagnosed 8 years prior. His medical history was remarkable for intravenous drug use, active hepatitis C infection, tobacco smoking, chronic alcohol use, and mild asthma. Eight years prior to the current presentation, 7 lesions had developed on the penis and were diagnosed by an outside physician as condyloma, which was treated with cryotherapy and topical imiquimod. All of the lesions except for 1 responded to treatment. The residual lesion continued to grow until the size prompted him to contact his primary care physician, who referred him for dermatologic evaluation. The patient cited lack of health insurance as the primary reason he did not seek follow-up treatment after the initial evaluation and treatment 8 years prior.
Physical examination at the current presentation revealed a circumcised man with an asymptomatic, 2.6-cm, pink, friable, verrucous mass on the left lateral penile shaft (Figure 1) and otherwise unremarkable penile architecture. A clinically enlarged, nontender right inguinal lymph node was noted as well as subtle enlargement of a left inguinal lymph node. An excisional biopsy was performed with pathologic evaluation confirming a diagnosis of high-grade invasive squamous cell carcinoma (SCC) arising in the setting of squamous cell carcinoma in situ (Figure 2). Lymphovascular invasion was highlighted on cluster of differentiation 31 and podoplanin immunostaining (Figure 3). The patient was subsequently referred to urology and hematology-oncology specialists for further evaluation. Computed tomography (CT) of the abdomen and pelvis confirmed the contralaterally enlarged right inguinal lymph node discovered during physical examination and mildly enlarged ipsilateral inguinal, obturator, and external iliac nodes. Computed tomography–guided fine-needle aspiration of the right inguinal node confirmed the diagnosis of contralateral locoregional metastasis. Further evaluation with positron emission tomography/CT imaging revealed only a single metabolically active region confined to the right inguinal node. The patient’s history of active hepatitis C complicated proposed neoadjuvant chemotherapy regimens. Ultimately, after discussion with multiple surgical and oncologist specialties within our institution and others, a treatment plan was formulated. The patient underwent robotic laparoscopic bilateral pelvic and inguinal lymph node dissection and re-excision of the primary PSCC, with one of 15 right superficial inguinal nodes testing positive for tumor cells; the left superficial and bilateral deep inguinal lymph nodes were negative for SCC.
Repeat positron emission tomography/CT imaging at 6 months’ follow-up showed no evidence of active disease. On 1-year follow-up, a CT scan did not show any new or residual disease, but the patient continued to have edema of the bilateral legs, which began after lymph node dissection and was managed with physical therapy and compression stockings.
Comment
Prevalence
Penile cancer is rare in industrialized countries. Early detection is a critical factor for both overall survival and organ function. If successful interventions are to be made, physicians should be familiar with known risk factors as well as unusual presentations, such as lesions presenting in young circumcised men, as reported above. Similarly, tumors located on the shaft of the penis represent an uncommon location for tumor presentation, occurring in less than 5% of PSCC cases.8 Penile SCC most commonly develops as a solitary painless lesion on the glans, balanopreputial sulcus and/or prepuce.9 In our case, histopathology confirmed high-grade invasive SCC arising from squamous cell carcinoma in situ, an entity generally associated with older men with a 10% to 20% rate of progression into invasive SCC.9 Our patient denied any clinical change in the appearance of the tumor in the years prior to the current presentation, making it possible that the condyloma treated 8 years prior was squamous cell carcinoma in situ or PSCC. As many as 25% of premalignant lesions are mistaken for benign lesions, which can thus delay treatment and allow progression to malignancy.10
Diagnosis
Penile SCC often is etiologically subcategorized into 2 pathways based on HPV dependence or independence. Recent research suggests that this distinction often is difficult to make, and accurate laboratory and pathologic confirmation of HPV DNA, intact virions, and viral-related cutaneous changes is not always possible, leading to much speculation regarding the exact role of HPV in tumorigenesis.11 Cancers developing in the absence of HPV DNA often occur secondary to chronic inflammatory conditions such as lichen planus or lichen sclerosus. Human papillomavirus DNA has shown to be present in 70% to 100% of all SCC in situ of the penis11; therefore, the transformation of in situ disease to an invasive tumor in our patient most likely occurred via an HPV-dependent pathway. Viral carcinogenesis in the HPV-dependent pathway involves inactivation of host cell cycle regulatory proteins, specifically the retinoblastoma and p53 regulatory proteins by the viral oncoproteins E7 and E6, respectively.12,13 Human papillomavirus–dependent pathways are related to a patient’s age at first sexual intercourse, number of sexual partners, and history of condyloma and other sexually transmitted diseases.14,15 High-risk HPV types 16 and 18 are the most common viral types found in HPV related premalignant lesions, making it possible to decrease the incidence of PSCC with recently developed vaccines.16 Human papillomavirus vaccines have been shown to reduce the incidence of anal intraepithelial neoplasias and genital warts in men.17 While the effects of the HPV vaccine on reducing PSCC could not be assessed in the study due to low incidence of disease (both in the study population and in general), it is thought that HPV vaccination could potentially decrease the incidence of all PSCCs by one third, making it an important resource in the primary prevention of the disease.18
Management
Contemporary surgical management of PSCC has evolved from organ resection in toto for all PSCCs to a more conservative approach based upon tumor stage and grade. The standard margin for surgical resection of PSCC is 2 cm, a procedure often referred to as a partial penectomy. This remains the most common procedure for surgical resection of PSCC and has achieved good local control, with reported recurrence rates of 4% to 8%.19,20 Complication rates of the procedure are moderate one-third of patients experiencing compromise of sexual activity after surgery.21 With evidence that smaller resection margins may result in good local control and a lower incidence of postoperative functional impairment, resection margins of 5, 10, and 15 mm have been advocated for PSCCs of varying histologic grades and tumor stages.22-24 Treatment options for T1 and in situ tumors have expanded to include glansectomy, margin-controlled Mohs micrographic surgery, and ablative laser therapy for local disease control.5,20 More advanced tumors are still treated with partial or complete penectomy given the high risks for locoregional recurrence and distant spread.
Prognosis
The most important factor predicting survival in patients with PSCC is metastasis to inguinal lymph nodes. The 5-year survival rate for patients without nodal involvement is 85% to 100%, while those with pathologically positive lymph nodes have a 5-year survival rate of 15% to 45%.25 Once distant metastasis occurs, the mean time of survival is 7 to 10 months.26 Our patient presented with high-grade PSCC with histologic lymphovascular spread and palpable inguinal lymph nodes. When stratified with other similar cases at presentation, our patient was at a considerable risk for locoregional as well as distant metastasis. Management with regional nodal dissection with a plan for close observation (and deferment of chemotherapeutics) was based upon evaluations from multiple different medical specialties.
Conclusion
Invasive PSCC is rare in young circumcised adults, and a delay in diagnosis can lead to considerable morbidity and mortality. We present a case of invasive PSCC arising in the setting of squamous cell carcinoma in situ in an area previously treated with cryotherapy and imiquimod. Our patient’s young age, concurrent hepatitis C infection, and contralateral locoregional nodal metastasis made this a complex case, involving evaluation and treatment by multiple medical disciplines. This case highlights the importance of biopsy in any lesion recalcitrant to conventional modalities regardless of the patient’s age. Early detection and treatment of PSCC can prevent organ dysfunction, loss of organ, and even death.
Invasive penile cancer is a rare malignancy with considerable morbidity and mortality. The American Cancer Society estimates that there will be 2320 new cases of invasive penile cancer in the United States in 2018, of which primary penile squamous cell carcinoma (PSCC) represents the majority.1 In one study, the mean age at diagnosis was 60 years, with PSCC occurring only rarely in men younger than 35 years of age (estimated incidence, 0.01 cases per 100,000 individuals).2 Presentation to a physician generally occurs more than 1 year after initial onset of symptoms or clinical lesion(s). This delay in diagnosis and treatment often results in disease progression,3 which can have a devastating outcome.4 Therefore, physicians should maintain a high index of clinical suspicion for PSCC, particularly in young or middle-aged patients in whom presentation of PSCC is uncommon. The most commonly associated risk factors for PSCC include lack of circumcision (specifically during the neonatal period), high-risk human papillomavirus (HPV) infection, and tobacco use.5 Chronic alcoholism also has been linked to PSCC.6 It also is common in patients without health insurance.7 We report the case of a 27-year-old circumcised man who presented with invasive PSCC following a diagnosis of condyloma 8 years prior by an outside physician.
Case Report
A 27-year-old man presented for evaluation of persistent genital warts that had been diagnosed 8 years prior. His medical history was remarkable for intravenous drug use, active hepatitis C infection, tobacco smoking, chronic alcohol use, and mild asthma. Eight years prior to the current presentation, 7 lesions had developed on the penis and were diagnosed by an outside physician as condyloma, which was treated with cryotherapy and topical imiquimod. All of the lesions except for 1 responded to treatment. The residual lesion continued to grow until the size prompted him to contact his primary care physician, who referred him for dermatologic evaluation. The patient cited lack of health insurance as the primary reason he did not seek follow-up treatment after the initial evaluation and treatment 8 years prior.
Physical examination at the current presentation revealed a circumcised man with an asymptomatic, 2.6-cm, pink, friable, verrucous mass on the left lateral penile shaft (Figure 1) and otherwise unremarkable penile architecture. A clinically enlarged, nontender right inguinal lymph node was noted as well as subtle enlargement of a left inguinal lymph node. An excisional biopsy was performed with pathologic evaluation confirming a diagnosis of high-grade invasive squamous cell carcinoma (SCC) arising in the setting of squamous cell carcinoma in situ (Figure 2). Lymphovascular invasion was highlighted on cluster of differentiation 31 and podoplanin immunostaining (Figure 3). The patient was subsequently referred to urology and hematology-oncology specialists for further evaluation. Computed tomography (CT) of the abdomen and pelvis confirmed the contralaterally enlarged right inguinal lymph node discovered during physical examination and mildly enlarged ipsilateral inguinal, obturator, and external iliac nodes. Computed tomography–guided fine-needle aspiration of the right inguinal node confirmed the diagnosis of contralateral locoregional metastasis. Further evaluation with positron emission tomography/CT imaging revealed only a single metabolically active region confined to the right inguinal node. The patient’s history of active hepatitis C complicated proposed neoadjuvant chemotherapy regimens. Ultimately, after discussion with multiple surgical and oncologist specialties within our institution and others, a treatment plan was formulated. The patient underwent robotic laparoscopic bilateral pelvic and inguinal lymph node dissection and re-excision of the primary PSCC, with one of 15 right superficial inguinal nodes testing positive for tumor cells; the left superficial and bilateral deep inguinal lymph nodes were negative for SCC.
Repeat positron emission tomography/CT imaging at 6 months’ follow-up showed no evidence of active disease. On 1-year follow-up, a CT scan did not show any new or residual disease, but the patient continued to have edema of the bilateral legs, which began after lymph node dissection and was managed with physical therapy and compression stockings.
Comment
Prevalence
Penile cancer is rare in industrialized countries. Early detection is a critical factor for both overall survival and organ function. If successful interventions are to be made, physicians should be familiar with known risk factors as well as unusual presentations, such as lesions presenting in young circumcised men, as reported above. Similarly, tumors located on the shaft of the penis represent an uncommon location for tumor presentation, occurring in less than 5% of PSCC cases.8 Penile SCC most commonly develops as a solitary painless lesion on the glans, balanopreputial sulcus and/or prepuce.9 In our case, histopathology confirmed high-grade invasive SCC arising from squamous cell carcinoma in situ, an entity generally associated with older men with a 10% to 20% rate of progression into invasive SCC.9 Our patient denied any clinical change in the appearance of the tumor in the years prior to the current presentation, making it possible that the condyloma treated 8 years prior was squamous cell carcinoma in situ or PSCC. As many as 25% of premalignant lesions are mistaken for benign lesions, which can thus delay treatment and allow progression to malignancy.10
Diagnosis
Penile SCC often is etiologically subcategorized into 2 pathways based on HPV dependence or independence. Recent research suggests that this distinction often is difficult to make, and accurate laboratory and pathologic confirmation of HPV DNA, intact virions, and viral-related cutaneous changes is not always possible, leading to much speculation regarding the exact role of HPV in tumorigenesis.11 Cancers developing in the absence of HPV DNA often occur secondary to chronic inflammatory conditions such as lichen planus or lichen sclerosus. Human papillomavirus DNA has shown to be present in 70% to 100% of all SCC in situ of the penis11; therefore, the transformation of in situ disease to an invasive tumor in our patient most likely occurred via an HPV-dependent pathway. Viral carcinogenesis in the HPV-dependent pathway involves inactivation of host cell cycle regulatory proteins, specifically the retinoblastoma and p53 regulatory proteins by the viral oncoproteins E7 and E6, respectively.12,13 Human papillomavirus–dependent pathways are related to a patient’s age at first sexual intercourse, number of sexual partners, and history of condyloma and other sexually transmitted diseases.14,15 High-risk HPV types 16 and 18 are the most common viral types found in HPV related premalignant lesions, making it possible to decrease the incidence of PSCC with recently developed vaccines.16 Human papillomavirus vaccines have been shown to reduce the incidence of anal intraepithelial neoplasias and genital warts in men.17 While the effects of the HPV vaccine on reducing PSCC could not be assessed in the study due to low incidence of disease (both in the study population and in general), it is thought that HPV vaccination could potentially decrease the incidence of all PSCCs by one third, making it an important resource in the primary prevention of the disease.18
Management
Contemporary surgical management of PSCC has evolved from organ resection in toto for all PSCCs to a more conservative approach based upon tumor stage and grade. The standard margin for surgical resection of PSCC is 2 cm, a procedure often referred to as a partial penectomy. This remains the most common procedure for surgical resection of PSCC and has achieved good local control, with reported recurrence rates of 4% to 8%.19,20 Complication rates of the procedure are moderate one-third of patients experiencing compromise of sexual activity after surgery.21 With evidence that smaller resection margins may result in good local control and a lower incidence of postoperative functional impairment, resection margins of 5, 10, and 15 mm have been advocated for PSCCs of varying histologic grades and tumor stages.22-24 Treatment options for T1 and in situ tumors have expanded to include glansectomy, margin-controlled Mohs micrographic surgery, and ablative laser therapy for local disease control.5,20 More advanced tumors are still treated with partial or complete penectomy given the high risks for locoregional recurrence and distant spread.
Prognosis
The most important factor predicting survival in patients with PSCC is metastasis to inguinal lymph nodes. The 5-year survival rate for patients without nodal involvement is 85% to 100%, while those with pathologically positive lymph nodes have a 5-year survival rate of 15% to 45%.25 Once distant metastasis occurs, the mean time of survival is 7 to 10 months.26 Our patient presented with high-grade PSCC with histologic lymphovascular spread and palpable inguinal lymph nodes. When stratified with other similar cases at presentation, our patient was at a considerable risk for locoregional as well as distant metastasis. Management with regional nodal dissection with a plan for close observation (and deferment of chemotherapeutics) was based upon evaluations from multiple different medical specialties.
Conclusion
Invasive PSCC is rare in young circumcised adults, and a delay in diagnosis can lead to considerable morbidity and mortality. We present a case of invasive PSCC arising in the setting of squamous cell carcinoma in situ in an area previously treated with cryotherapy and imiquimod. Our patient’s young age, concurrent hepatitis C infection, and contralateral locoregional nodal metastasis made this a complex case, involving evaluation and treatment by multiple medical disciplines. This case highlights the importance of biopsy in any lesion recalcitrant to conventional modalities regardless of the patient’s age. Early detection and treatment of PSCC can prevent organ dysfunction, loss of organ, and even death.
- About penile cancer. American Cancer Society website. https://www.cancer.org/content/dam/CRC/PDF/Public/8783.00.pdf. Revised February 9, 2016. Accessed February 27, 2018.
- Barnholtz-Sloan JS, Maldonado JL, Pow-sang J, et al. Incidence trends in primary malignant penile cancer. Urol Oncol. 2007;25:361-367.
- Koifman L, Vides AJ, Koifman N, et al. Epidemiological aspects of penile cancer in Rio de Janeiro: evaluation of 230 cases. Int Braz J Urol. 2011;37:231-240.
- Kamat AM, Carpenter SM, Czerniak BA, et al. Metastatic penile cancer in a young Caucasian male: impact of delayed diagnosis. Urol Oncol. 2005;23:130-131.
- Deem S, Keane T, Bhavsar R, et al. Contemporary diagnosis and management of squamous cell carcinoma (SCC) of the penis. BJU Int. 2011;108:1378-1392.
- McIntyre M, Weiss A, Wahlquist A, et al. Penile cancer: an analysis of socioeconomic factors at a southeastern tertiary referral center. Can J Urol. 2011;18:5524-5528.
- Maden C, Sherman KJ, Beckmann AM, et al. History of circumcision, medical conditions, and sexual activity and risk of penile cancer. J Natl Cancer Inst. 1993;85:19-24.
- Hernandez BY, Barnholtz-Sloan J, German RR, et al. Burden of invasive squamous cell carcinoma of the penis in the United States, 1998-2003. Cancer. 2008;113(suppl 10):2883-2891.
- Ferrandiz-Pulido C, de Torres I, Garcia-Patos V. Penile squamous cell carcinoma. Actas Dermosifiliogr. 2012;103:478-487.
- Tietjen DN, Malek RS. Laser therapy of squamous cell dysplasia and carcinoma of the penis. Urology. 1998;52:559-565.
- Mannweiler S, Sygulla S, Winter E, et al. Two major pathways of penile carcinogenesis: HPV-induced penile cancers overexpress p16, HPV-negative cancers associated with dermatoses express p53, but lack p16 overexpression. J Am Acad Dermatol. 2013;69:73-81.
- Scheffner M, Werness BA, Huibregtse JM, et al. The E6 oncoprotein encoded by human papillomavirus types 16 and 18 promotes the degradation of p53. Cell. 1990;63:1129-1136.
- Werness BA, Levine AJ, Howley PM. Association of human papillomavirus types 16 and 18 E6 proteins with p53. Science. 1990;248:76-79.
- Daling JR, Madeleine MM, Johnson LG, et al. Penile cancer: importance of circumcision, human papillomavirus and smoking in in situ and invasive disease. Int J Cancer. 2005;116:606-616.
- Bleeker MC, Heideman DA, Snijders PJ, et al. Penile cancer: epidemiology, pathogenesis and prevention. World J Urol. 2009;27:141-150.
- Shabbir M, Barod R, Hegarty PK, et al. Primary prevention and vaccination for penile cancer. Ther Adv Urol. 2013;5:161-169.
- Palefsky J, Giuliano A, Goldstone S, et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N Engl J Med. 2011;365:1576-1585.
- Backes DM, Kurman RJ, Pimenta JM, et al. Systematic review of human papillomavirus prevalence in invasive penile cancer. Cancer Causes Control. 2009;20:449-457.
- Korets R, Koppie TM, Snyder ME, et al. Partial penectomy for patients with squamous cell carcinoma of the penis: the Memorial Sloan-Kettering experience. Ann Surg Oncol. 2007;14:3614-3619.
- Zukiwskyj M, Daly P, Chung E. Penile cancer and phallus preservation strategies: a review of current literature. BJU Int. 2013;112(suppl 2):21-26.
- Romero FR, Romero KR, Mattos MA, et al. Sexual function after partial penectomy for penile cancer. Urology. 2005;66:1292-1295.
- Minhas S, Kayes O, Hegarty P, et al. What surgical resection margins are required to achieve oncological control in men with primary penile cancer? BJU Int. 2005;96:1040-1043.
- Feldman AS, McDougal WS. Long-term outcome of excisional organ sparing surgery for carcinoma of the penis. J Urol. 2011;186:1303-1307.
- Philippou P, Shabbir M, Malone P, et al. Conservative surgery for squamous cell carcinoma of the penis: resection margins and long-term oncological control. J Urol. 2012;188:803-808.
- Brady KL, Mercurio MG, Brown MD. Malignant tumors of the penis. Dermatol Surg. 2013;39:527-547.
- Ornellas AA, Nobrega BL, Wei Kin Chin E, et al. Prognostic factors in invasive squamous cell carcinoma of the penis: analysis of 196 patients treated at the Brazilian National Cancer Institute. J Urol. 2008;180:1354-1359.
- About penile cancer. American Cancer Society website. https://www.cancer.org/content/dam/CRC/PDF/Public/8783.00.pdf. Revised February 9, 2016. Accessed February 27, 2018.
- Barnholtz-Sloan JS, Maldonado JL, Pow-sang J, et al. Incidence trends in primary malignant penile cancer. Urol Oncol. 2007;25:361-367.
- Koifman L, Vides AJ, Koifman N, et al. Epidemiological aspects of penile cancer in Rio de Janeiro: evaluation of 230 cases. Int Braz J Urol. 2011;37:231-240.
- Kamat AM, Carpenter SM, Czerniak BA, et al. Metastatic penile cancer in a young Caucasian male: impact of delayed diagnosis. Urol Oncol. 2005;23:130-131.
- Deem S, Keane T, Bhavsar R, et al. Contemporary diagnosis and management of squamous cell carcinoma (SCC) of the penis. BJU Int. 2011;108:1378-1392.
- McIntyre M, Weiss A, Wahlquist A, et al. Penile cancer: an analysis of socioeconomic factors at a southeastern tertiary referral center. Can J Urol. 2011;18:5524-5528.
- Maden C, Sherman KJ, Beckmann AM, et al. History of circumcision, medical conditions, and sexual activity and risk of penile cancer. J Natl Cancer Inst. 1993;85:19-24.
- Hernandez BY, Barnholtz-Sloan J, German RR, et al. Burden of invasive squamous cell carcinoma of the penis in the United States, 1998-2003. Cancer. 2008;113(suppl 10):2883-2891.
- Ferrandiz-Pulido C, de Torres I, Garcia-Patos V. Penile squamous cell carcinoma. Actas Dermosifiliogr. 2012;103:478-487.
- Tietjen DN, Malek RS. Laser therapy of squamous cell dysplasia and carcinoma of the penis. Urology. 1998;52:559-565.
- Mannweiler S, Sygulla S, Winter E, et al. Two major pathways of penile carcinogenesis: HPV-induced penile cancers overexpress p16, HPV-negative cancers associated with dermatoses express p53, but lack p16 overexpression. J Am Acad Dermatol. 2013;69:73-81.
- Scheffner M, Werness BA, Huibregtse JM, et al. The E6 oncoprotein encoded by human papillomavirus types 16 and 18 promotes the degradation of p53. Cell. 1990;63:1129-1136.
- Werness BA, Levine AJ, Howley PM. Association of human papillomavirus types 16 and 18 E6 proteins with p53. Science. 1990;248:76-79.
- Daling JR, Madeleine MM, Johnson LG, et al. Penile cancer: importance of circumcision, human papillomavirus and smoking in in situ and invasive disease. Int J Cancer. 2005;116:606-616.
- Bleeker MC, Heideman DA, Snijders PJ, et al. Penile cancer: epidemiology, pathogenesis and prevention. World J Urol. 2009;27:141-150.
- Shabbir M, Barod R, Hegarty PK, et al. Primary prevention and vaccination for penile cancer. Ther Adv Urol. 2013;5:161-169.
- Palefsky J, Giuliano A, Goldstone S, et al. HPV vaccine against anal HPV infection and anal intraepithelial neoplasia. N Engl J Med. 2011;365:1576-1585.
- Backes DM, Kurman RJ, Pimenta JM, et al. Systematic review of human papillomavirus prevalence in invasive penile cancer. Cancer Causes Control. 2009;20:449-457.
- Korets R, Koppie TM, Snyder ME, et al. Partial penectomy for patients with squamous cell carcinoma of the penis: the Memorial Sloan-Kettering experience. Ann Surg Oncol. 2007;14:3614-3619.
- Zukiwskyj M, Daly P, Chung E. Penile cancer and phallus preservation strategies: a review of current literature. BJU Int. 2013;112(suppl 2):21-26.
- Romero FR, Romero KR, Mattos MA, et al. Sexual function after partial penectomy for penile cancer. Urology. 2005;66:1292-1295.
- Minhas S, Kayes O, Hegarty P, et al. What surgical resection margins are required to achieve oncological control in men with primary penile cancer? BJU Int. 2005;96:1040-1043.
- Feldman AS, McDougal WS. Long-term outcome of excisional organ sparing surgery for carcinoma of the penis. J Urol. 2011;186:1303-1307.
- Philippou P, Shabbir M, Malone P, et al. Conservative surgery for squamous cell carcinoma of the penis: resection margins and long-term oncological control. J Urol. 2012;188:803-808.
- Brady KL, Mercurio MG, Brown MD. Malignant tumors of the penis. Dermatol Surg. 2013;39:527-547.
- Ornellas AA, Nobrega BL, Wei Kin Chin E, et al. Prognostic factors in invasive squamous cell carcinoma of the penis: analysis of 196 patients treated at the Brazilian National Cancer Institute. J Urol. 2008;180:1354-1359.
Practice Points
- Invasive penile squamous cell carcinoma (PSCC) is a rare malignancy with considerable morbidity and mortality that typically does not present in young men.
- Delayed or incorrect diagnosis of PSCC can have a devastating outcome; therefore, physicians should maintain a high index of clinical suspicion for PSCC in patients presenting with penile lesions, particularly in young or middle-aged patients.

Consider drug holidays for BCC patients on hedgehog inhibitors
KAUAI, HAWAII – according to Kishwer Nehal, MD, director of Mohs micrographic and dermatologic surgery at Memorial Sloan Kettering Cancer Center, New York.
That’s important because, although some patients have a good response to vismodegib, more – about 80% – have side effects that make it necessary to stop treatment, including muscle spasms and weight loss, among other problems. Side effects often come on quickly and can become intolerable after a few months of treatment, so physicians have looked for alternative dosing regimens to hold them off, with some success.

Compared with those on continuous dosing, fewer patients on intermittent dosing discontinued treatment for adverse events (23% versus 31%). Patients on intermittent dosing also experienced fewer grade 3 adverse events (31% versus 44%) and were on treatment for a longer period of time (a median of 71.4 weeks versus 37.6 weeks).
Meanwhile, among those on intermittent dosing, the number of BCCs was reduced in more than half of the patients in both interrupted treatment groups, but more so in the 12-weeks-on/8-weeks-off group (Lancet Oncol. 2017 Mar; 18[3]:404-12).
Other treatment options are being explored for vismodegib, as well as for sonidegib (Odomzo), another hedgehog signaling pathway inhibitor approved for advanced BCC. Ongoing trials are looking at the use of hedgehog inhibitors with radiation, and for shrinking tumors before surgery, Dr. Nehal said
For now, however, surgery remains the mainstay of treatment for BCC; both biologics are indicated for when other treatments fail or are not feasible. For high-risk BCC (meaning high risk for recurrence, based on infiltrative or poorly defined histology, perineural or bony involvement, or location on the face, for instance), “surgery with clear margins remains the goal and is the most effective treatment. For a high-risk [BCC], you pretty much need surgery,” she said.
Recurrence is less likely with Mohs surgery than with standard excision. When Mohs isn’t available, “you should wait for the pathology report before reconstruction,” she said.
“Radiation for high-risk [BCC] is really reserved for nonsurgical candidates,” Dr. Nehal commented. There are only two scenarios to consider radiation in high-risk BCC, “and they really have no proven benefit in any sort of prospective trial. One is if you cannot, after exhaustive surgery, clear your very high risk [BCC].” The other is if there is “really large nerve involvement, greater than 0.1 mm, or such extensive perineural involvement that surgery is unlikely to be successful,” she said.
Dr. Nehal had no relevant disclosures. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – according to Kishwer Nehal, MD, director of Mohs micrographic and dermatologic surgery at Memorial Sloan Kettering Cancer Center, New York.
That’s important because, although some patients have a good response to vismodegib, more – about 80% – have side effects that make it necessary to stop treatment, including muscle spasms and weight loss, among other problems. Side effects often come on quickly and can become intolerable after a few months of treatment, so physicians have looked for alternative dosing regimens to hold them off, with some success.
Compared with those on continuous dosing, fewer patients on intermittent dosing discontinued treatment for adverse events (23% versus 31%). Patients on intermittent dosing also experienced fewer grade 3 adverse events (31% versus 44%) and were on treatment for a longer period of time (a median of 71.4 weeks versus 37.6 weeks).
Meanwhile, among those on intermittent dosing, the number of BCCs was reduced in more than half of the patients in both interrupted treatment groups, but more so in the 12-weeks-on/8-weeks-off group (Lancet Oncol. 2017 Mar; 18[3]:404-12).
Other treatment options are being explored for vismodegib, as well as for sonidegib (Odomzo), another hedgehog signaling pathway inhibitor approved for advanced BCC. Ongoing trials are looking at the use of hedgehog inhibitors with radiation, and for shrinking tumors before surgery, Dr. Nehal said
For now, however, surgery remains the mainstay of treatment for BCC; both biologics are indicated for when other treatments fail or are not feasible. For high-risk BCC (meaning high risk for recurrence, based on infiltrative or poorly defined histology, perineural or bony involvement, or location on the face, for instance), “surgery with clear margins remains the goal and is the most effective treatment. For a high-risk [BCC], you pretty much need surgery,” she said.
Recurrence is less likely with Mohs surgery than with standard excision. When Mohs isn’t available, “you should wait for the pathology report before reconstruction,” she said.
“Radiation for high-risk [BCC] is really reserved for nonsurgical candidates,” Dr. Nehal commented. There are only two scenarios to consider radiation in high-risk BCC, “and they really have no proven benefit in any sort of prospective trial. One is if you cannot, after exhaustive surgery, clear your very high risk [BCC].” The other is if there is “really large nerve involvement, greater than 0.1 mm, or such extensive perineural involvement that surgery is unlikely to be successful,” she said.
Dr. Nehal had no relevant disclosures. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
KAUAI, HAWAII – according to Kishwer Nehal, MD, director of Mohs micrographic and dermatologic surgery at Memorial Sloan Kettering Cancer Center, New York.
That’s important because, although some patients have a good response to vismodegib, more – about 80% – have side effects that make it necessary to stop treatment, including muscle spasms and weight loss, among other problems. Side effects often come on quickly and can become intolerable after a few months of treatment, so physicians have looked for alternative dosing regimens to hold them off, with some success.
Compared with those on continuous dosing, fewer patients on intermittent dosing discontinued treatment for adverse events (23% versus 31%). Patients on intermittent dosing also experienced fewer grade 3 adverse events (31% versus 44%) and were on treatment for a longer period of time (a median of 71.4 weeks versus 37.6 weeks).
Meanwhile, among those on intermittent dosing, the number of BCCs was reduced in more than half of the patients in both interrupted treatment groups, but more so in the 12-weeks-on/8-weeks-off group (Lancet Oncol. 2017 Mar; 18[3]:404-12).
Other treatment options are being explored for vismodegib, as well as for sonidegib (Odomzo), another hedgehog signaling pathway inhibitor approved for advanced BCC. Ongoing trials are looking at the use of hedgehog inhibitors with radiation, and for shrinking tumors before surgery, Dr. Nehal said
For now, however, surgery remains the mainstay of treatment for BCC; both biologics are indicated for when other treatments fail or are not feasible. For high-risk BCC (meaning high risk for recurrence, based on infiltrative or poorly defined histology, perineural or bony involvement, or location on the face, for instance), “surgery with clear margins remains the goal and is the most effective treatment. For a high-risk [BCC], you pretty much need surgery,” she said.
Recurrence is less likely with Mohs surgery than with standard excision. When Mohs isn’t available, “you should wait for the pathology report before reconstruction,” she said.
“Radiation for high-risk [BCC] is really reserved for nonsurgical candidates,” Dr. Nehal commented. There are only two scenarios to consider radiation in high-risk BCC, “and they really have no proven benefit in any sort of prospective trial. One is if you cannot, after exhaustive surgery, clear your very high risk [BCC].” The other is if there is “really large nerve involvement, greater than 0.1 mm, or such extensive perineural involvement that surgery is unlikely to be successful,” she said.
Dr. Nehal had no relevant disclosures. SDEF/Global Academy for Medical Education and this news organization are owned by the same parent company.
EXPERT ANALYSIS FROM SDEF HAWAII DERMATOLOGY SEMINAR
VIDEO: Bioimpedance provides accurate assessment of Mohs surgical margins
SAN DIEGO – In assessing tumor-free margins during Mohs micrographic surgery for skin cancer, of histologic sections, in a single-center, pilot study of bioimpedance in 151 specimens from 50 consecutive patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
If the finding of high diagnostic accuracy using bioimpedance spectroscopy is confirmed in larger numbers of patients and specimens run at multiple sites, this approach could “potentially revolutionize what happens with the way Mohs sections are processed in the future” by potentially shaving many minutes off the duration of a standard procedure, Darrell S. Rigel, MD, said in a video interview during the annual meeting of the American Academy of Dermatology.
Usually, it takes 10-20 minutes to process and examine Mohs specimens at each stage of the surgical procedure to determine whether additional excision must remove residual cancer cells, said Dr. Rigel, a dermatologist at New York University. In contrast, assessment for residual cancer cells in the surgical field takes less than a minute using bioimpedance spectroscopy, which relies on differences in electrical conductivity between benign and cancerous cells to identify cancer cells remaining at the surgical margins.
The results of the study were presented in a poster at the meeting, by a research associate of Dr. Rigel’s, Ryan Svoboda, MD, of the National Society for Cutaneous Medicine, New York.
The researchers used a bioimpedance spectroscopy device made by NovaScan to assess 151 histology slides prepared during Mohs micrographic surgery on patients with nonmelanoma skin cancer, and compared the findings against the gold standard of histological slide examination. By this criterion, bioimpedance spectroscopy identified 105 true negatives and 2 false negatives, and 43 true positives and 1 false positive. Calculations showed that this equated to 95.6% sensitivity, 99.1% specificity, a 97.7% positive predictive value, and a 98.1% negative predictive value.
These may be underestimates of the accuracy of bioimpedance spectroscopy because the calculations presume that conventional histology is always correct, but Dr. Rigel noted that sometimes the histological diagnosis is wrong.
SOURCE: Svoboda R et al. Poster 7304.
SAN DIEGO – In assessing tumor-free margins during Mohs micrographic surgery for skin cancer, of histologic sections, in a single-center, pilot study of bioimpedance in 151 specimens from 50 consecutive patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
If the finding of high diagnostic accuracy using bioimpedance spectroscopy is confirmed in larger numbers of patients and specimens run at multiple sites, this approach could “potentially revolutionize what happens with the way Mohs sections are processed in the future” by potentially shaving many minutes off the duration of a standard procedure, Darrell S. Rigel, MD, said in a video interview during the annual meeting of the American Academy of Dermatology.
Usually, it takes 10-20 minutes to process and examine Mohs specimens at each stage of the surgical procedure to determine whether additional excision must remove residual cancer cells, said Dr. Rigel, a dermatologist at New York University. In contrast, assessment for residual cancer cells in the surgical field takes less than a minute using bioimpedance spectroscopy, which relies on differences in electrical conductivity between benign and cancerous cells to identify cancer cells remaining at the surgical margins.
The results of the study were presented in a poster at the meeting, by a research associate of Dr. Rigel’s, Ryan Svoboda, MD, of the National Society for Cutaneous Medicine, New York.
The researchers used a bioimpedance spectroscopy device made by NovaScan to assess 151 histology slides prepared during Mohs micrographic surgery on patients with nonmelanoma skin cancer, and compared the findings against the gold standard of histological slide examination. By this criterion, bioimpedance spectroscopy identified 105 true negatives and 2 false negatives, and 43 true positives and 1 false positive. Calculations showed that this equated to 95.6% sensitivity, 99.1% specificity, a 97.7% positive predictive value, and a 98.1% negative predictive value.
These may be underestimates of the accuracy of bioimpedance spectroscopy because the calculations presume that conventional histology is always correct, but Dr. Rigel noted that sometimes the histological diagnosis is wrong.
SOURCE: Svoboda R et al. Poster 7304.
SAN DIEGO – In assessing tumor-free margins during Mohs micrographic surgery for skin cancer, of histologic sections, in a single-center, pilot study of bioimpedance in 151 specimens from 50 consecutive patients.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
If the finding of high diagnostic accuracy using bioimpedance spectroscopy is confirmed in larger numbers of patients and specimens run at multiple sites, this approach could “potentially revolutionize what happens with the way Mohs sections are processed in the future” by potentially shaving many minutes off the duration of a standard procedure, Darrell S. Rigel, MD, said in a video interview during the annual meeting of the American Academy of Dermatology.
Usually, it takes 10-20 minutes to process and examine Mohs specimens at each stage of the surgical procedure to determine whether additional excision must remove residual cancer cells, said Dr. Rigel, a dermatologist at New York University. In contrast, assessment for residual cancer cells in the surgical field takes less than a minute using bioimpedance spectroscopy, which relies on differences in electrical conductivity between benign and cancerous cells to identify cancer cells remaining at the surgical margins.
The results of the study were presented in a poster at the meeting, by a research associate of Dr. Rigel’s, Ryan Svoboda, MD, of the National Society for Cutaneous Medicine, New York.
The researchers used a bioimpedance spectroscopy device made by NovaScan to assess 151 histology slides prepared during Mohs micrographic surgery on patients with nonmelanoma skin cancer, and compared the findings against the gold standard of histological slide examination. By this criterion, bioimpedance spectroscopy identified 105 true negatives and 2 false negatives, and 43 true positives and 1 false positive. Calculations showed that this equated to 95.6% sensitivity, 99.1% specificity, a 97.7% positive predictive value, and a 98.1% negative predictive value.
These may be underestimates of the accuracy of bioimpedance spectroscopy because the calculations presume that conventional histology is always correct, but Dr. Rigel noted that sometimes the histological diagnosis is wrong.
SOURCE: Svoboda R et al. Poster 7304.
REPORTING FROM AAD 18
Key clinical point: Bioimpedance spectroscopy showed excellent diagnostic accuracy for cancer cells on Mohs surgical margins.
Major finding: Bioimpedance spectroscopy had a sensitivity of 95.6% and specificity of 99.1% compared with Mohs histology.
Study details: A single-center pilot study with 151 Mohs surgical specimens taken from 50 patients.
Disclosures: The study was funded by NovaScan, the company developing the device tested in the study. Dr. Rigel has been a consultant to NovaScan and to Castle Biosciences, DermTech, Ferndale, Myriad, and Neutrogena, and has received research support from Castle and Neutrogena.
Source: Svoboda R et al. Poster 7304.

Evaluating Dermatology Apps for Patient Education


Study: Test for PD-L1 amplification in solid tumors
SAN FRANCISCO – Amplification of programmed death-ligand 1 (PD-L1), also known as cluster of differentiation 274 (CD274), is rare in most solid tumors, but findings from an analysis in which a majority of patients with the alteration experienced durable responses to PD-1/PD-L1 blockade suggest that testing for it may be warranted.
Of 117,344 deidentified cancer patient samples from a large database, only 0.7% had PD-L1 amplification, which was defined as 6 or more copy number alterations (CNAs). The CNAs were found across more than 100 tumor histologies, Aaron Goodman, MD, reported at the ASCO-SITC Clinical Immuno-Oncology Symposium.
Of a subset of 2,039 clinically annotated patients from the database, who were seen at the University of California, San Diego (UCSD) Center for Personalized Cancer Therapy, 13 (0.6%) had PD-L1 CNAs, and 9 were treated with immune checkpoint blockade, either alone or in combination with another immunotherapeutic or targeted therapy, after a median of four prior systemic therapies.
The PD-1/PD-L1 blockade response rate in those nine patients was 67%, and median progression-free survival was 15.2 months; three objective responses were ongoing for at least 15 months, said Dr. Goodman of UCSD.
The findings are notable, because in unselected patients, the rates of response to immune checkpoint blockade range from 10% to 20%.
Lessons from cHL and solid tumors
“Over the past few years, investigators have identified numerous biomarkers that can select subgroups of patients with increased likelihoods of responding to PD-1 blockade,” he said, adding that biomarkers include PD-L1 expression by immunohistochemistry, microsatellite instability – with microsatellite instability–high tumors responding extremely well to immunotherapy, tumor mutational burden measured by whole exome sequencing and next generation sequencing, and possibly PD-L1 amplification.
Of note, response rates are high in patients with classical Hodgkin lymphoma (cHL). In general, cHL patients respond well to treatment, with the majority being cured by way of multiagent chemotherapy and radiation.
“But for the subpopulation that fails to respond to chemotherapy or relapses, outcomes still remain suboptimal. Remarkably, in the relapsed/refractory population of Hodgkin lymphoma ... response rates to single agent nivolumab and pembrolizumab were 65% to 87% [in recent studies],” he said. “Long-term follow-up demonstrates that the majority of these responses were durable and lasted over a year.”
The question is why relapsed/refractory cHL patients treated with immune checkpoint blockade have such a higher response rate than is typically seen in patients with solid tumors.
One answer might lie in the recent finding that nearly 100% of cHL tumors harbor amplification of 9p24.1; the 9p24.1 amplicon encodes the genes PD-L1, PD-L2, and JAK2, (and thus is also known as the PDJ amplicon), he explained, adding that “through gene dose-dependent increased expression of PD-L1 ligand on the Hodgkin lymphoma Reed-Sternberg cells, there is also JAK-STAT mediation of further expression of PD-L1 on the Reed-Sternberg cells.
An encounter with a patient with metastatic basal cell carcinoma – a “relatively unusual situation, as the majority of patients are cured with local therapy”– led to interest in looking at 9p24.1 alterations in solid tumors.
The patient had extensive metastatic disease, and had progressed through multiple therapies. Given his limited treatment options, next generation sequencing was performed on a biopsy from his tumor, and it revealed the PTCH1 alteration typical in basal cell carcinoma, as well as amplification of 9p24.1 with PD-L1, PD-L2, and JAK2 amplification. Nivolumab monotherapy was initiated.
“Within 2 months, he had an excellent partial response to therapy, and I’m pleased to say that he’s in an ongoing complete response 2 years later,” Dr. Goodman said.
It was that case that sparked the idea for the current study.
9p24.1 alterations and checkpoint blockade
“With my interest in hematologic malignancies, I was unaware that [9p24.1] amplification could occur in solid tumors, so the first aim was to determine the prevalence of chromosome 9p24.1 alterations in solid tumors. The next was to determine if patients with solid tumors and chromosome 9p24.1 alterations respond to PD-1/PD-L1 checkpoint blockade.
“What is astounding is [that PD-L1 amplification] was found in over 100 unique tumor histologies, although rare in most histologies,” Dr. Goodman said, noting that histologies with a statistically increased prevalence of PD-L1 amplification included breast cancer, head and neck squamous cell carcinoma, lung squamous cell carcinoma, and soft tissue sarcoma.
There also were some rare histologies with increased prevalence of PD-L1 amplification, including nasopharyngeal carcinoma, renal sarcomatoid carcinoma, bladder squamous cell carcinoma, and liver mixed hepatocellular cholangiocarcinoma, he said.
Tumors with a paucity of PD-L1 amplification included colorectal cancer, pancreatic cancer, and cutaneous melanoma, although even these still harbored a few patients with amplification, he said.
A closer look at the mutational burden in amplified vs. unamplified tumors showed a median of 7.4 vs. 3.6 mut/mb, but in the PD-L1 amplified group, 85% still had a low-to intermediate mutational burden of 1-20 mut/mb.
“Microsatellite instability and PD-L1 amplification were not mutually exclusive, but a rare event. Five of the 821 cases with PD-L1 amplification were microsatellite high; these included three carcinomas of unknown origin and two cases of gastrointestinal cancer,” he noted.
Treatment outcomes
In the 13 UCSD patients with PD-L1 amplification, nine different malignancies were identified, and all patients had advanced or metastatic disease and were heavily pretreated. Of the nine treated patients, five received anti-PD-1 monotherapy, one received anti-CTLA4/anti-PD-1 combination therapy, and three received a PD-1/PD-L1 inhibitor plus an investigational agent, which was immunotherapeutic, Dr. Goodman said.
The 67% overall response rate was similar to that seen in Hodgkin lymphoma, and many of the responses were durable; median overall survival was not reached.
Of note, genomic analysis in the 13 UCSD patients found to have PD-L1 amplification showed there were 143 total alterations in 70 different genes. All but one patient had amplification of PD-L1, PD-L2, and JAK2, and that one had amplification of PD-L1 and PD-L2.
Of six tumors with tissue available to test for PD-L1 expression by immunohistochemistry, four (67%) tested positive. None were microsatellite high, and tumor-infiltrating lymphocytes were present in five cases.
The tumors that tested negative for PD-L1 expression were from the patient with the rare basal cell cancer, and another with glioblastoma. Both responded to anti-PD1/PD-L1 therapy.
The glioblastoma patient was a 40-year-old man with progressive disease, who underwent standard surgical debulking followed by concurrent radiation therapy plus temozolomide. He progressed soon after completing the concurrent chemoradiation therapy, and genomic profiling revealed 12 alterations, including 9p24.1 amplification, Dr. Goodman said, adding that nivolumab therapy was initiated.
“By week 12, much of the tumor mass had started to resolve, and by week 26 it continued to decrease further. He continues to be in an ongoing partial response at 5.2 months,” he said.
Recommendations
The findings of this study demonstrate that PD-Ll amplification is rare in solid tumors.
“However, PD-L1 amplification appears to be tissue agnostic, as we have seen in over 100 tumor histologies. We also noted that PD-L1 amplification was enriched in many rare tumors with limited treatment options, including anaplastic thyroid cancer, sarcomatoid carcinoma, and some sarcomas. We believe testing for PD-L1 amplification may be warranted given the frequent responses that were durable and seemed to be independent of mutational burden,” he concluded.
Ravindra Uppaluri, MD, session chair and discussant for Dr. Goodman’s presentation, said that Dr. Goodman’s findings should be considered in the context of “the complex biology [of PD-L1/PD-L2] that has evolved over the last few years.”
He specifically mentioned the two patients without PD-L1 expression despite amplification, but with response to immune checkpoint blockade, and noted that “there are several things going on here ... and we really want to look at all these things.”
The PDJ amplicon, especially given “the ability to look at this with the targeted gene panels that many patients are getting,” is clearly contributing to biomarker stratification, said Dr. Uppaluri of Dana-Farber Cancer Institute and Brigham and Women’s Hospital, Boston.
However, it should be assessed as part of a “global biomarker” that includes tumor-infiltrating lymphocytes and tumor mutational burden, he said.
Dr. Goodman reported having no disclosures. Dr. Uppaluri has received grant/research support from NIH/NIDCR, Merck, and V Foundation, and has received honoraria from Merck.
sworcester@frontlinemedcom.com
SOURCE: Goodman A et al. ASCO-SITC, Abstract 47
SAN FRANCISCO – Amplification of programmed death-ligand 1 (PD-L1), also known as cluster of differentiation 274 (CD274), is rare in most solid tumors, but findings from an analysis in which a majority of patients with the alteration experienced durable responses to PD-1/PD-L1 blockade suggest that testing for it may be warranted.
Of 117,344 deidentified cancer patient samples from a large database, only 0.7% had PD-L1 amplification, which was defined as 6 or more copy number alterations (CNAs). The CNAs were found across more than 100 tumor histologies, Aaron Goodman, MD, reported at the ASCO-SITC Clinical Immuno-Oncology Symposium.
Of a subset of 2,039 clinically annotated patients from the database, who were seen at the University of California, San Diego (UCSD) Center for Personalized Cancer Therapy, 13 (0.6%) had PD-L1 CNAs, and 9 were treated with immune checkpoint blockade, either alone or in combination with another immunotherapeutic or targeted therapy, after a median of four prior systemic therapies.
The PD-1/PD-L1 blockade response rate in those nine patients was 67%, and median progression-free survival was 15.2 months; three objective responses were ongoing for at least 15 months, said Dr. Goodman of UCSD.
The findings are notable, because in unselected patients, the rates of response to immune checkpoint blockade range from 10% to 20%.
Lessons from cHL and solid tumors
“Over the past few years, investigators have identified numerous biomarkers that can select subgroups of patients with increased likelihoods of responding to PD-1 blockade,” he said, adding that biomarkers include PD-L1 expression by immunohistochemistry, microsatellite instability – with microsatellite instability–high tumors responding extremely well to immunotherapy, tumor mutational burden measured by whole exome sequencing and next generation sequencing, and possibly PD-L1 amplification.
Of note, response rates are high in patients with classical Hodgkin lymphoma (cHL). In general, cHL patients respond well to treatment, with the majority being cured by way of multiagent chemotherapy and radiation.
“But for the subpopulation that fails to respond to chemotherapy or relapses, outcomes still remain suboptimal. Remarkably, in the relapsed/refractory population of Hodgkin lymphoma ... response rates to single agent nivolumab and pembrolizumab were 65% to 87% [in recent studies],” he said. “Long-term follow-up demonstrates that the majority of these responses were durable and lasted over a year.”
The question is why relapsed/refractory cHL patients treated with immune checkpoint blockade have such a higher response rate than is typically seen in patients with solid tumors.
One answer might lie in the recent finding that nearly 100% of cHL tumors harbor amplification of 9p24.1; the 9p24.1 amplicon encodes the genes PD-L1, PD-L2, and JAK2, (and thus is also known as the PDJ amplicon), he explained, adding that “through gene dose-dependent increased expression of PD-L1 ligand on the Hodgkin lymphoma Reed-Sternberg cells, there is also JAK-STAT mediation of further expression of PD-L1 on the Reed-Sternberg cells.
An encounter with a patient with metastatic basal cell carcinoma – a “relatively unusual situation, as the majority of patients are cured with local therapy”– led to interest in looking at 9p24.1 alterations in solid tumors.
The patient had extensive metastatic disease, and had progressed through multiple therapies. Given his limited treatment options, next generation sequencing was performed on a biopsy from his tumor, and it revealed the PTCH1 alteration typical in basal cell carcinoma, as well as amplification of 9p24.1 with PD-L1, PD-L2, and JAK2 amplification. Nivolumab monotherapy was initiated.
“Within 2 months, he had an excellent partial response to therapy, and I’m pleased to say that he’s in an ongoing complete response 2 years later,” Dr. Goodman said.
It was that case that sparked the idea for the current study.
9p24.1 alterations and checkpoint blockade
“With my interest in hematologic malignancies, I was unaware that [9p24.1] amplification could occur in solid tumors, so the first aim was to determine the prevalence of chromosome 9p24.1 alterations in solid tumors. The next was to determine if patients with solid tumors and chromosome 9p24.1 alterations respond to PD-1/PD-L1 checkpoint blockade.
“What is astounding is [that PD-L1 amplification] was found in over 100 unique tumor histologies, although rare in most histologies,” Dr. Goodman said, noting that histologies with a statistically increased prevalence of PD-L1 amplification included breast cancer, head and neck squamous cell carcinoma, lung squamous cell carcinoma, and soft tissue sarcoma.
There also were some rare histologies with increased prevalence of PD-L1 amplification, including nasopharyngeal carcinoma, renal sarcomatoid carcinoma, bladder squamous cell carcinoma, and liver mixed hepatocellular cholangiocarcinoma, he said.
Tumors with a paucity of PD-L1 amplification included colorectal cancer, pancreatic cancer, and cutaneous melanoma, although even these still harbored a few patients with amplification, he said.
A closer look at the mutational burden in amplified vs. unamplified tumors showed a median of 7.4 vs. 3.6 mut/mb, but in the PD-L1 amplified group, 85% still had a low-to intermediate mutational burden of 1-20 mut/mb.
“Microsatellite instability and PD-L1 amplification were not mutually exclusive, but a rare event. Five of the 821 cases with PD-L1 amplification were microsatellite high; these included three carcinomas of unknown origin and two cases of gastrointestinal cancer,” he noted.
Treatment outcomes
In the 13 UCSD patients with PD-L1 amplification, nine different malignancies were identified, and all patients had advanced or metastatic disease and were heavily pretreated. Of the nine treated patients, five received anti-PD-1 monotherapy, one received anti-CTLA4/anti-PD-1 combination therapy, and three received a PD-1/PD-L1 inhibitor plus an investigational agent, which was immunotherapeutic, Dr. Goodman said.
The 67% overall response rate was similar to that seen in Hodgkin lymphoma, and many of the responses were durable; median overall survival was not reached.
Of note, genomic analysis in the 13 UCSD patients found to have PD-L1 amplification showed there were 143 total alterations in 70 different genes. All but one patient had amplification of PD-L1, PD-L2, and JAK2, and that one had amplification of PD-L1 and PD-L2.
Of six tumors with tissue available to test for PD-L1 expression by immunohistochemistry, four (67%) tested positive. None were microsatellite high, and tumor-infiltrating lymphocytes were present in five cases.
The tumors that tested negative for PD-L1 expression were from the patient with the rare basal cell cancer, and another with glioblastoma. Both responded to anti-PD1/PD-L1 therapy.
The glioblastoma patient was a 40-year-old man with progressive disease, who underwent standard surgical debulking followed by concurrent radiation therapy plus temozolomide. He progressed soon after completing the concurrent chemoradiation therapy, and genomic profiling revealed 12 alterations, including 9p24.1 amplification, Dr. Goodman said, adding that nivolumab therapy was initiated.
“By week 12, much of the tumor mass had started to resolve, and by week 26 it continued to decrease further. He continues to be in an ongoing partial response at 5.2 months,” he said.
Recommendations
The findings of this study demonstrate that PD-Ll amplification is rare in solid tumors.
“However, PD-L1 amplification appears to be tissue agnostic, as we have seen in over 100 tumor histologies. We also noted that PD-L1 amplification was enriched in many rare tumors with limited treatment options, including anaplastic thyroid cancer, sarcomatoid carcinoma, and some sarcomas. We believe testing for PD-L1 amplification may be warranted given the frequent responses that were durable and seemed to be independent of mutational burden,” he concluded.
Ravindra Uppaluri, MD, session chair and discussant for Dr. Goodman’s presentation, said that Dr. Goodman’s findings should be considered in the context of “the complex biology [of PD-L1/PD-L2] that has evolved over the last few years.”
He specifically mentioned the two patients without PD-L1 expression despite amplification, but with response to immune checkpoint blockade, and noted that “there are several things going on here ... and we really want to look at all these things.”
The PDJ amplicon, especially given “the ability to look at this with the targeted gene panels that many patients are getting,” is clearly contributing to biomarker stratification, said Dr. Uppaluri of Dana-Farber Cancer Institute and Brigham and Women’s Hospital, Boston.
However, it should be assessed as part of a “global biomarker” that includes tumor-infiltrating lymphocytes and tumor mutational burden, he said.
Dr. Goodman reported having no disclosures. Dr. Uppaluri has received grant/research support from NIH/NIDCR, Merck, and V Foundation, and has received honoraria from Merck.
sworcester@frontlinemedcom.com
SOURCE: Goodman A et al. ASCO-SITC, Abstract 47
SAN FRANCISCO – Amplification of programmed death-ligand 1 (PD-L1), also known as cluster of differentiation 274 (CD274), is rare in most solid tumors, but findings from an analysis in which a majority of patients with the alteration experienced durable responses to PD-1/PD-L1 blockade suggest that testing for it may be warranted.
Of 117,344 deidentified cancer patient samples from a large database, only 0.7% had PD-L1 amplification, which was defined as 6 or more copy number alterations (CNAs). The CNAs were found across more than 100 tumor histologies, Aaron Goodman, MD, reported at the ASCO-SITC Clinical Immuno-Oncology Symposium.
Of a subset of 2,039 clinically annotated patients from the database, who were seen at the University of California, San Diego (UCSD) Center for Personalized Cancer Therapy, 13 (0.6%) had PD-L1 CNAs, and 9 were treated with immune checkpoint blockade, either alone or in combination with another immunotherapeutic or targeted therapy, after a median of four prior systemic therapies.
The PD-1/PD-L1 blockade response rate in those nine patients was 67%, and median progression-free survival was 15.2 months; three objective responses were ongoing for at least 15 months, said Dr. Goodman of UCSD.
The findings are notable, because in unselected patients, the rates of response to immune checkpoint blockade range from 10% to 20%.
Lessons from cHL and solid tumors
“Over the past few years, investigators have identified numerous biomarkers that can select subgroups of patients with increased likelihoods of responding to PD-1 blockade,” he said, adding that biomarkers include PD-L1 expression by immunohistochemistry, microsatellite instability – with microsatellite instability–high tumors responding extremely well to immunotherapy, tumor mutational burden measured by whole exome sequencing and next generation sequencing, and possibly PD-L1 amplification.
Of note, response rates are high in patients with classical Hodgkin lymphoma (cHL). In general, cHL patients respond well to treatment, with the majority being cured by way of multiagent chemotherapy and radiation.
“But for the subpopulation that fails to respond to chemotherapy or relapses, outcomes still remain suboptimal. Remarkably, in the relapsed/refractory population of Hodgkin lymphoma ... response rates to single agent nivolumab and pembrolizumab were 65% to 87% [in recent studies],” he said. “Long-term follow-up demonstrates that the majority of these responses were durable and lasted over a year.”
The question is why relapsed/refractory cHL patients treated with immune checkpoint blockade have such a higher response rate than is typically seen in patients with solid tumors.
One answer might lie in the recent finding that nearly 100% of cHL tumors harbor amplification of 9p24.1; the 9p24.1 amplicon encodes the genes PD-L1, PD-L2, and JAK2, (and thus is also known as the PDJ amplicon), he explained, adding that “through gene dose-dependent increased expression of PD-L1 ligand on the Hodgkin lymphoma Reed-Sternberg cells, there is also JAK-STAT mediation of further expression of PD-L1 on the Reed-Sternberg cells.
An encounter with a patient with metastatic basal cell carcinoma – a “relatively unusual situation, as the majority of patients are cured with local therapy”– led to interest in looking at 9p24.1 alterations in solid tumors.
The patient had extensive metastatic disease, and had progressed through multiple therapies. Given his limited treatment options, next generation sequencing was performed on a biopsy from his tumor, and it revealed the PTCH1 alteration typical in basal cell carcinoma, as well as amplification of 9p24.1 with PD-L1, PD-L2, and JAK2 amplification. Nivolumab monotherapy was initiated.
“Within 2 months, he had an excellent partial response to therapy, and I’m pleased to say that he’s in an ongoing complete response 2 years later,” Dr. Goodman said.
It was that case that sparked the idea for the current study.
9p24.1 alterations and checkpoint blockade
“With my interest in hematologic malignancies, I was unaware that [9p24.1] amplification could occur in solid tumors, so the first aim was to determine the prevalence of chromosome 9p24.1 alterations in solid tumors. The next was to determine if patients with solid tumors and chromosome 9p24.1 alterations respond to PD-1/PD-L1 checkpoint blockade.
“What is astounding is [that PD-L1 amplification] was found in over 100 unique tumor histologies, although rare in most histologies,” Dr. Goodman said, noting that histologies with a statistically increased prevalence of PD-L1 amplification included breast cancer, head and neck squamous cell carcinoma, lung squamous cell carcinoma, and soft tissue sarcoma.
There also were some rare histologies with increased prevalence of PD-L1 amplification, including nasopharyngeal carcinoma, renal sarcomatoid carcinoma, bladder squamous cell carcinoma, and liver mixed hepatocellular cholangiocarcinoma, he said.
Tumors with a paucity of PD-L1 amplification included colorectal cancer, pancreatic cancer, and cutaneous melanoma, although even these still harbored a few patients with amplification, he said.
A closer look at the mutational burden in amplified vs. unamplified tumors showed a median of 7.4 vs. 3.6 mut/mb, but in the PD-L1 amplified group, 85% still had a low-to intermediate mutational burden of 1-20 mut/mb.
“Microsatellite instability and PD-L1 amplification were not mutually exclusive, but a rare event. Five of the 821 cases with PD-L1 amplification were microsatellite high; these included three carcinomas of unknown origin and two cases of gastrointestinal cancer,” he noted.
Treatment outcomes
In the 13 UCSD patients with PD-L1 amplification, nine different malignancies were identified, and all patients had advanced or metastatic disease and were heavily pretreated. Of the nine treated patients, five received anti-PD-1 monotherapy, one received anti-CTLA4/anti-PD-1 combination therapy, and three received a PD-1/PD-L1 inhibitor plus an investigational agent, which was immunotherapeutic, Dr. Goodman said.
The 67% overall response rate was similar to that seen in Hodgkin lymphoma, and many of the responses were durable; median overall survival was not reached.
Of note, genomic analysis in the 13 UCSD patients found to have PD-L1 amplification showed there were 143 total alterations in 70 different genes. All but one patient had amplification of PD-L1, PD-L2, and JAK2, and that one had amplification of PD-L1 and PD-L2.
Of six tumors with tissue available to test for PD-L1 expression by immunohistochemistry, four (67%) tested positive. None were microsatellite high, and tumor-infiltrating lymphocytes were present in five cases.
The tumors that tested negative for PD-L1 expression were from the patient with the rare basal cell cancer, and another with glioblastoma. Both responded to anti-PD1/PD-L1 therapy.
The glioblastoma patient was a 40-year-old man with progressive disease, who underwent standard surgical debulking followed by concurrent radiation therapy plus temozolomide. He progressed soon after completing the concurrent chemoradiation therapy, and genomic profiling revealed 12 alterations, including 9p24.1 amplification, Dr. Goodman said, adding that nivolumab therapy was initiated.
“By week 12, much of the tumor mass had started to resolve, and by week 26 it continued to decrease further. He continues to be in an ongoing partial response at 5.2 months,” he said.
Recommendations
The findings of this study demonstrate that PD-Ll amplification is rare in solid tumors.
“However, PD-L1 amplification appears to be tissue agnostic, as we have seen in over 100 tumor histologies. We also noted that PD-L1 amplification was enriched in many rare tumors with limited treatment options, including anaplastic thyroid cancer, sarcomatoid carcinoma, and some sarcomas. We believe testing for PD-L1 amplification may be warranted given the frequent responses that were durable and seemed to be independent of mutational burden,” he concluded.
Ravindra Uppaluri, MD, session chair and discussant for Dr. Goodman’s presentation, said that Dr. Goodman’s findings should be considered in the context of “the complex biology [of PD-L1/PD-L2] that has evolved over the last few years.”
He specifically mentioned the two patients without PD-L1 expression despite amplification, but with response to immune checkpoint blockade, and noted that “there are several things going on here ... and we really want to look at all these things.”
The PDJ amplicon, especially given “the ability to look at this with the targeted gene panels that many patients are getting,” is clearly contributing to biomarker stratification, said Dr. Uppaluri of Dana-Farber Cancer Institute and Brigham and Women’s Hospital, Boston.
However, it should be assessed as part of a “global biomarker” that includes tumor-infiltrating lymphocytes and tumor mutational burden, he said.
Dr. Goodman reported having no disclosures. Dr. Uppaluri has received grant/research support from NIH/NIDCR, Merck, and V Foundation, and has received honoraria from Merck.
sworcester@frontlinemedcom.com
SOURCE: Goodman A et al. ASCO-SITC, Abstract 47
REPORTING FROM THE CLINICAL IMMUNO-ONCOLOGY SYMPOSIUM
Key clinical point: Solid tumor patients with PD-L1 amplification had durable responses to PD-1/PD-L1 blockade.
Major finding: The overall response rate was 67% in nine patients treated with PD-1/PD-L1 blockade.
Study details: An analysis of more than 117,000 patient samples.
Disclosures: Dr. Goodman reported having no disclosures. Dr. Uppaluri has received grant/research support from NIH/NIDCR, Merck, and V Foundation, and has received honoraria from Merck.
Source: Goodman A et al. ASCO-SITC, Abstract 47.