User login
Rechallenge ‘reasonable’ for some with small-cell lung cancer
In a phase 3 trial, carboplatin plus etoposide significantly prolonged progression-free survival (PFS), when compared with topotecan, in patients with advanced or relapsed, sensitive SCLC.
All patients had responded to first-line platinum plus etoposide, but they experienced relapse or progression 90 days or more after completing that treatment, according to study author Nathalie Baize, MD, of Angers University Hospital in France, and colleagues.
For this trial, Dr. Baize and colleagues enrolled 164 patients with advanced or relapsed SCLC. The median age of the 162 evaluable patients was 64 years, about two-thirds were men, and about 60% had an Eastern Cooperative Oncology Group performance status of 1.
The patients were randomized 1:1 to intravenous carboplatin (area under the curve 5 mg/mL per min on day 1) plus intravenous etoposide (100 mg/m² from day 1 to day 3) or to oral topotecan (2.3 mg/m² from day 1 to day 5 for six cycles). Primary prophylactic filgrastim was recommended for all patients in both treatment groups.
Results: Survival and adverse events
The median follow-up was 22.7 months. The median PFS was significantly longer in the combination therapy arm, at 4.7 months versus 2.7 months in the topotecan arm (stratified hazard ratio 0.57, P = .0041).
The median overall survival was similar in both arms, at 7.5 months in the carboplatin-etoposide arm and 7.4 months in the topotecan arm.
Patients in the carboplatin-etoposide arm had a significantly higher objective response rate, at 49% versus 25% in the topotecan arm (P = .0024).
The most common grade 3-4 adverse events (in the topotecan and combination arms, respectively) were neutropenia (22% vs. 14%), thrombocytopenia (36% vs. 31%), and anemia (21% vs. 25%).
Serious adverse events with hospitalization were reported in 37% of patients in the carboplatin-etoposide arm 43% in the topotecan arm. Febrile neutropenia with sepsis led to two treatment-related deaths in the topotecan group but none in the carboplatin-etoposide group.
Reasonable option for some
Based on the results of this trial, Dr. Baize and colleagues concluded that carboplatin-etoposide rechallenge “can be considered a reasonable second-line chemotherapy option for patients with sensitive relapsed small-cell lung cancer.”
However, while this trial was enrolling patients, immunotherapy and chemotherapy combinations became the standard of care in SCLC, Oscar Arrieta, MD, of Instituto Nacional de Cancerología in Mexico City, and colleagues noted in a related editorial.
Therefore, “reasonable doubts emerge regarding the application of this strategy in patients receiving immunotherapy,” Dr. Arrieta and colleagues wrote.
The editorialists urged conduct of a randomized trial to evaluate rechallenge with carboplatin plus etoposide versus lurbinectedin, which was approved earlier this year by the Food and Drug Administration for the treatment of sensitive and resistant relapsed SCLC.
Commenting on the choice between a platinum-etoposide combination and lurbinectedin, Sarah Goldberg, MD, of Yale University, New Haven, Conn., noted that she and her colleagues have been using the chemotherapy combination for several years.
“This trial confirms that practice and that it’s still a reasonable option for some patients,” Dr. Goldberg said in an interview.
For patients who had a very good first-line response to platinum-etoposide, longer than 180 days (even longer than the 90-day standard in the current trial), she said, “it seems like a rechallenge with platinum-etoposide would potentially be even more effective, and I’d save lurbinectedin for a later line.
“With refractory disease, less than 90 days, I would consider lurbinectedin,” Dr. Goldberg said.
This study was funded by Amgen and the French Lung Cancer Group (Groupe Français de Pneumo-Cancérologie). The researchers disclosed relationships with Pfizer, Roche, AbbVie, and many other companies. Dr. Arrieta disclosed relationships with AstraZeneca, Boehringer Ingelheim, Roche, Lilly, Merck, Pfizer, and Bristol-Myers Squibb. The other editorialists declared no competing interests. Dr. Goldberg disclosed relationships with AstraZeneca, Boehringer Ingelheim, Eli Lilly, Bristol-Myers Squibb, Genentech, Amgen, Spectrum, Blueprint Medicine, Sanofi Genzyme, Daiichi Sankyo, and Regeneron.
SOURCE: Baize N et al. Lancet Oncol. 2020;21:1224-33.
In a phase 3 trial, carboplatin plus etoposide significantly prolonged progression-free survival (PFS), when compared with topotecan, in patients with advanced or relapsed, sensitive SCLC.
All patients had responded to first-line platinum plus etoposide, but they experienced relapse or progression 90 days or more after completing that treatment, according to study author Nathalie Baize, MD, of Angers University Hospital in France, and colleagues.
For this trial, Dr. Baize and colleagues enrolled 164 patients with advanced or relapsed SCLC. The median age of the 162 evaluable patients was 64 years, about two-thirds were men, and about 60% had an Eastern Cooperative Oncology Group performance status of 1.
The patients were randomized 1:1 to intravenous carboplatin (area under the curve 5 mg/mL per min on day 1) plus intravenous etoposide (100 mg/m² from day 1 to day 3) or to oral topotecan (2.3 mg/m² from day 1 to day 5 for six cycles). Primary prophylactic filgrastim was recommended for all patients in both treatment groups.
Results: Survival and adverse events
The median follow-up was 22.7 months. The median PFS was significantly longer in the combination therapy arm, at 4.7 months versus 2.7 months in the topotecan arm (stratified hazard ratio 0.57, P = .0041).
The median overall survival was similar in both arms, at 7.5 months in the carboplatin-etoposide arm and 7.4 months in the topotecan arm.
Patients in the carboplatin-etoposide arm had a significantly higher objective response rate, at 49% versus 25% in the topotecan arm (P = .0024).
The most common grade 3-4 adverse events (in the topotecan and combination arms, respectively) were neutropenia (22% vs. 14%), thrombocytopenia (36% vs. 31%), and anemia (21% vs. 25%).
Serious adverse events with hospitalization were reported in 37% of patients in the carboplatin-etoposide arm 43% in the topotecan arm. Febrile neutropenia with sepsis led to two treatment-related deaths in the topotecan group but none in the carboplatin-etoposide group.
Reasonable option for some
Based on the results of this trial, Dr. Baize and colleagues concluded that carboplatin-etoposide rechallenge “can be considered a reasonable second-line chemotherapy option for patients with sensitive relapsed small-cell lung cancer.”
However, while this trial was enrolling patients, immunotherapy and chemotherapy combinations became the standard of care in SCLC, Oscar Arrieta, MD, of Instituto Nacional de Cancerología in Mexico City, and colleagues noted in a related editorial.
Therefore, “reasonable doubts emerge regarding the application of this strategy in patients receiving immunotherapy,” Dr. Arrieta and colleagues wrote.
The editorialists urged conduct of a randomized trial to evaluate rechallenge with carboplatin plus etoposide versus lurbinectedin, which was approved earlier this year by the Food and Drug Administration for the treatment of sensitive and resistant relapsed SCLC.
Commenting on the choice between a platinum-etoposide combination and lurbinectedin, Sarah Goldberg, MD, of Yale University, New Haven, Conn., noted that she and her colleagues have been using the chemotherapy combination for several years.
“This trial confirms that practice and that it’s still a reasonable option for some patients,” Dr. Goldberg said in an interview.
For patients who had a very good first-line response to platinum-etoposide, longer than 180 days (even longer than the 90-day standard in the current trial), she said, “it seems like a rechallenge with platinum-etoposide would potentially be even more effective, and I’d save lurbinectedin for a later line.
“With refractory disease, less than 90 days, I would consider lurbinectedin,” Dr. Goldberg said.
This study was funded by Amgen and the French Lung Cancer Group (Groupe Français de Pneumo-Cancérologie). The researchers disclosed relationships with Pfizer, Roche, AbbVie, and many other companies. Dr. Arrieta disclosed relationships with AstraZeneca, Boehringer Ingelheim, Roche, Lilly, Merck, Pfizer, and Bristol-Myers Squibb. The other editorialists declared no competing interests. Dr. Goldberg disclosed relationships with AstraZeneca, Boehringer Ingelheim, Eli Lilly, Bristol-Myers Squibb, Genentech, Amgen, Spectrum, Blueprint Medicine, Sanofi Genzyme, Daiichi Sankyo, and Regeneron.
SOURCE: Baize N et al. Lancet Oncol. 2020;21:1224-33.
In a phase 3 trial, carboplatin plus etoposide significantly prolonged progression-free survival (PFS), when compared with topotecan, in patients with advanced or relapsed, sensitive SCLC.
All patients had responded to first-line platinum plus etoposide, but they experienced relapse or progression 90 days or more after completing that treatment, according to study author Nathalie Baize, MD, of Angers University Hospital in France, and colleagues.
For this trial, Dr. Baize and colleagues enrolled 164 patients with advanced or relapsed SCLC. The median age of the 162 evaluable patients was 64 years, about two-thirds were men, and about 60% had an Eastern Cooperative Oncology Group performance status of 1.
The patients were randomized 1:1 to intravenous carboplatin (area under the curve 5 mg/mL per min on day 1) plus intravenous etoposide (100 mg/m² from day 1 to day 3) or to oral topotecan (2.3 mg/m² from day 1 to day 5 for six cycles). Primary prophylactic filgrastim was recommended for all patients in both treatment groups.
Results: Survival and adverse events
The median follow-up was 22.7 months. The median PFS was significantly longer in the combination therapy arm, at 4.7 months versus 2.7 months in the topotecan arm (stratified hazard ratio 0.57, P = .0041).
The median overall survival was similar in both arms, at 7.5 months in the carboplatin-etoposide arm and 7.4 months in the topotecan arm.
Patients in the carboplatin-etoposide arm had a significantly higher objective response rate, at 49% versus 25% in the topotecan arm (P = .0024).
The most common grade 3-4 adverse events (in the topotecan and combination arms, respectively) were neutropenia (22% vs. 14%), thrombocytopenia (36% vs. 31%), and anemia (21% vs. 25%).
Serious adverse events with hospitalization were reported in 37% of patients in the carboplatin-etoposide arm 43% in the topotecan arm. Febrile neutropenia with sepsis led to two treatment-related deaths in the topotecan group but none in the carboplatin-etoposide group.
Reasonable option for some
Based on the results of this trial, Dr. Baize and colleagues concluded that carboplatin-etoposide rechallenge “can be considered a reasonable second-line chemotherapy option for patients with sensitive relapsed small-cell lung cancer.”
However, while this trial was enrolling patients, immunotherapy and chemotherapy combinations became the standard of care in SCLC, Oscar Arrieta, MD, of Instituto Nacional de Cancerología in Mexico City, and colleagues noted in a related editorial.
Therefore, “reasonable doubts emerge regarding the application of this strategy in patients receiving immunotherapy,” Dr. Arrieta and colleagues wrote.
The editorialists urged conduct of a randomized trial to evaluate rechallenge with carboplatin plus etoposide versus lurbinectedin, which was approved earlier this year by the Food and Drug Administration for the treatment of sensitive and resistant relapsed SCLC.
Commenting on the choice between a platinum-etoposide combination and lurbinectedin, Sarah Goldberg, MD, of Yale University, New Haven, Conn., noted that she and her colleagues have been using the chemotherapy combination for several years.
“This trial confirms that practice and that it’s still a reasonable option for some patients,” Dr. Goldberg said in an interview.
For patients who had a very good first-line response to platinum-etoposide, longer than 180 days (even longer than the 90-day standard in the current trial), she said, “it seems like a rechallenge with platinum-etoposide would potentially be even more effective, and I’d save lurbinectedin for a later line.
“With refractory disease, less than 90 days, I would consider lurbinectedin,” Dr. Goldberg said.
This study was funded by Amgen and the French Lung Cancer Group (Groupe Français de Pneumo-Cancérologie). The researchers disclosed relationships with Pfizer, Roche, AbbVie, and many other companies. Dr. Arrieta disclosed relationships with AstraZeneca, Boehringer Ingelheim, Roche, Lilly, Merck, Pfizer, and Bristol-Myers Squibb. The other editorialists declared no competing interests. Dr. Goldberg disclosed relationships with AstraZeneca, Boehringer Ingelheim, Eli Lilly, Bristol-Myers Squibb, Genentech, Amgen, Spectrum, Blueprint Medicine, Sanofi Genzyme, Daiichi Sankyo, and Regeneron.
SOURCE: Baize N et al. Lancet Oncol. 2020;21:1224-33.
FROM LANCET ONCOLOGY
How should we evaluate the benefit of immunotherapy combinations?
Every medical oncologist who has described a combination chemotherapy regimen to a patient with advanced cancer has likely been asked whether the benefits of tumor shrinkage, disease-free survival (DFS), and overall survival are worth the risks of adverse events (AEs).

Single-agent immunotherapy and, more recently, combinations of immunotherapy drugs have been approved for a variety of metastatic tumors. In general, combination immunotherapy regimens have more AEs and a higher frequency of premature treatment discontinuation for toxicity.
Michael Postow, MD, of Memorial Sloan Kettering Cancer Center in New York, reflected on new ways to evaluate the benefits and risks of immunotherapy combinations during a plenary session on novel combinations at the American Association for Cancer Research’s Virtual Special Conference on Tumor Immunology and Immunotherapy.
Potential targets
As with chemotherapy drugs, immunotherapy combinations make the most sense when drugs targeting independent processes are employed.
As described in a paper published in Nature in 2011, the process for recruiting the immune system to combat cancer is as follows:
- Dendritic cells must sample antigens derived from the tumor.
- The dendritic cells must receive an activation signal so they promote immunity rather than tolerance.
- The tumor antigen–loaded dendritic cells need to generate protective T-cell responses, instead of T-regulatory responses, in lymphoid tissues.
- Cancer antigen–specific T cells must enter tumor tissues.
- Tumor-derived mechanisms for promoting immunosuppression need to be circumvented.
Since each step in the cascade is a potential therapeutic target, there are large numbers of potential drug combinations.
Measuring impact
Conventional measurements of tumor response may not be adequately sensitive to the impact from immunotherapy drugs. A case in point is sipuleucel-T, which is approved to treat advanced prostate cancer.
In the pivotal phase 3 trial, only 1 of 341 patients receiving sipuleucel-T achieved a partial response by RECIST criteria. Only 2.6% of patients had a 50% reduction in prostate-specific antigen levels. Nonetheless, a 4.1-month improvement in median overall survival was achieved. These results were published in the New England Journal of Medicine.
The discrepancy between tumor shrinkage and survival benefit for immunotherapy is not unexpected. As many as 10% of patients treated with ipilimumab (ipi) for stage IV malignant melanoma have progressive disease by tumor size but experience prolongation of survival, according to guidelines published in Clinical Cancer Research.
Accurate assessment of the ultimate efficacy of immunotherapy over time would benefit patients and clinicians since immune checkpoint inhibitors are often administered for several years, are financially costly, and treatment-associated AEs emerge unpredictably at any time.
Curtailing the duration of ineffective treatment could be valuable from many perspectives.
Immunotherapy combinations in metastatic melanoma
In the CheckMate 067 study, there was an improvement in response, progression-free survival (PFS), and overall survival for nivolumab (nivo) plus ipi or nivo alone, in comparison with ipi alone, in patients with advanced melanoma. Initial results from this trial were published in the New England Journal of Medicine in 2017.
At a minimum follow-up of 60 months, the 5-year overall survival was 52% for the nivo/ipi regimen, 44% for nivo alone, and 26% for ipi alone. These results were published in the New England Journal of Medicine in 2019.
The trial was not statistically powered to conclude whether the overall survival for the combination was superior to that of single-agent nivo alone, but both nivo regimens were superior to ipi alone.
Unfortunately, the combination also produced the highest treatment-related AE rates – 59% with nivo/ipi, 23% with nivo, and 28% with ipi in 2019. In the 2017 report, the combination regimen had more than twice as many premature treatment discontinuations as the other two study arms.
Is there a better way to quantify the risk-benefit ratio and explain it to patients?
Alternative strategies for assessing benefit: Treatment-free survival
Researchers have proposed treatment-free survival (TFS) as a potential new metric to characterize not only antitumor activity but also toxicity experienced after the cessation of therapy and before initiation of subsequent systemic therapy or death.
TFS is defined as the area between Kaplan-Meier curves from immunotherapy cessation until the reinitiation of systemic therapy or death. All patients who began immunotherapy are included – not just those achieving response or concluding a predefined number of cycles of treatment.
The curves can be partitioned into states with and without toxicity to establish a unique endpoint: time to cessation of both immunotherapy and toxicity.
Researchers conducted a pooled analysis of 3-year follow-up data from the 1,077 patients who participated in CheckMate 069, testing nivo/ipi versus nivo alone, and CheckMate 067, comparing nivo/ipi, nivo alone, and ipi alone. The results were published in the Journal of Clinical Oncology.
The TFS without grade 3 or higher AEs was 28% for nivo/ipi, 11% for nivo alone, and 23% for ipi alone. The restricted mean time without either treatment or grade 3 or greater AEs was 10.1 months, 4.1 months, and 8.5 months, respectively.
TFS incentivizes the use of regimens that have:
- A short duration of treatment
- Prolonged time to subsequent therapy or death
- Only mild AEs of brief duration.
A higher TFS corresponds with the goals that patients and their providers would have for a treatment regimen.
Adaptive models provide clues about benefit from extended therapy
In contrast to cytotoxic chemotherapy and molecularly targeted agents, benefit from immune-targeted therapy can deepen and persist after treatment discontinuation.
In advanced melanoma, researchers observed that overall survival was similar for patients who discontinued nivo/ipi because of AEs during the induction phase of treatment and those who did not. These results were published in the Journal of Clinical Oncology.
This observation has led to an individualized, adaptive approach to de-escalating combination immunotherapy, described in Clinical Cancer Research. The approach is dubbed “SMART,” which stands for sequential multiple assignment randomized trial designs.
With the SMART approach, each stage of a trial corresponds to an important treatment decision point. The goal is to define the population of patients who can safely discontinue treatment based on response, rather than doing so after the development of AEs.
In the Adapt-IT prospective study, 60 patients with advanced melanoma with poor prognostic features were given two doses of nivo/ipi followed by a CT scan at week 6. They were triaged to stopping ipi and proceeding with maintenance therapy with nivo alone or continuing the combination for an additional two cycles of treatment. Results from this trial were presented at ASCO 2020 (abstract 10003).
The investigators found that 68% of patients had no tumor burden increase at week 6 and could discontinue ipi. For those patients, their response rate of 57% approached the expected results from a full course of ipi.
At median follow-up of 22.3 months, median response duration, PFS, and overall survival had not been reached for the responders who received an abbreviated course of the combination regimen.
There were two observations that suggested the first two cycles of treatment drove not only toxicity but also tumor control:
- The rate of grade 3-4 toxicity from only two cycles was high (57%).
- Of the 19 patients (32% of the original 60 patients) who had progressive disease after two cycles of nivo/ipi, there were no responders with continued therapy.
Dr. Postow commented that, in correlative studies conducted as part of Adapt-IT, the Ki-67 of CD8-positive T cells increased after the initial dose of nivo/ipi. However, proliferation did not continue with subsequent cycles (that is, Ki-67 did not continue to rise).
When they examined markers of T-cell stimulation such as inducible costimulator of CD8-positive T cells, the researchers observed the same effect. The “immune boost” occurred with cycle one but not after subsequent doses of the nivo/ipi combination.
Although unproven in clinical trials at this time, these data suggest that response and risks of toxicity may not support giving patients more than one cycle of combination treatment.
More nuanced ways of assessing tumor growth
Dr. Postow noted that judgment about treatment effects over time are often made by displaying spider plots of changes from baseline tumor size from “time zero” – the time at which combination therapy is commenced.
He speculated that it might be worthwhile to give a dose or two of immune-targeted monotherapy (such as a PD-1 or PD-L1 inhibitor alone) before time zero, measure tumor growth prior to and after the single agent, and reserve using combination immunotherapy only for those patients who do not experience a dampening of the growth curve.
Patients whose tumor growth kinetics are improved with single-agent treatment could be spared the additional toxicity (and uncertain additive benefit) from the second agent.
Treatment optimization: More than ‘messaging’
Oncology practice has passed through a long era of “more is better,” an era that gave rise to intensive cytotoxic chemotherapy for hematologic and solid tumors in the metastatic and adjuvant settings. In some cases, that approach proved to be curative, but not in all.
More recently, because of better staging, improved outcomes with newer technology and treatments, and concern about immediate- and late-onset health risks, there has been an effort to deintensify therapy when it can be done safely.
Once a treatment regimen and treatment duration become established, however, patients and their physicians are reluctant to deintensity therapy.
Dr. Postow’s presentation demonstrated that, with regard to immunotherapy combinations – as in other realms of medical practice – science can lead the way to treatment optimization for individual patients.
We have the potential to reassure patients that treatment de-escalation is a rational and personalized component of treatment optimization through the combination of:
- Identifying new endpoints to quantify treatment benefits and risks.
- SMART trial designs.
- Innovative ways to assess tumor response during each phase of a treatment course.
Precision assessment of immunotherapy effect in individual patients can be a key part of precision medicine.
Dr. Postow disclosed relationships with Aduro, Array BioPharma, Bristol Myers Squibb, Eisai, Incyte, Infinity, Merck, NewLink Genetics, Novartis, and RGenix.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Every medical oncologist who has described a combination chemotherapy regimen to a patient with advanced cancer has likely been asked whether the benefits of tumor shrinkage, disease-free survival (DFS), and overall survival are worth the risks of adverse events (AEs).
Single-agent immunotherapy and, more recently, combinations of immunotherapy drugs have been approved for a variety of metastatic tumors. In general, combination immunotherapy regimens have more AEs and a higher frequency of premature treatment discontinuation for toxicity.
Michael Postow, MD, of Memorial Sloan Kettering Cancer Center in New York, reflected on new ways to evaluate the benefits and risks of immunotherapy combinations during a plenary session on novel combinations at the American Association for Cancer Research’s Virtual Special Conference on Tumor Immunology and Immunotherapy.
Potential targets
As with chemotherapy drugs, immunotherapy combinations make the most sense when drugs targeting independent processes are employed.
As described in a paper published in Nature in 2011, the process for recruiting the immune system to combat cancer is as follows:
- Dendritic cells must sample antigens derived from the tumor.
- The dendritic cells must receive an activation signal so they promote immunity rather than tolerance.
- The tumor antigen–loaded dendritic cells need to generate protective T-cell responses, instead of T-regulatory responses, in lymphoid tissues.
- Cancer antigen–specific T cells must enter tumor tissues.
- Tumor-derived mechanisms for promoting immunosuppression need to be circumvented.
Since each step in the cascade is a potential therapeutic target, there are large numbers of potential drug combinations.
Measuring impact
Conventional measurements of tumor response may not be adequately sensitive to the impact from immunotherapy drugs. A case in point is sipuleucel-T, which is approved to treat advanced prostate cancer.
In the pivotal phase 3 trial, only 1 of 341 patients receiving sipuleucel-T achieved a partial response by RECIST criteria. Only 2.6% of patients had a 50% reduction in prostate-specific antigen levels. Nonetheless, a 4.1-month improvement in median overall survival was achieved. These results were published in the New England Journal of Medicine.
The discrepancy between tumor shrinkage and survival benefit for immunotherapy is not unexpected. As many as 10% of patients treated with ipilimumab (ipi) for stage IV malignant melanoma have progressive disease by tumor size but experience prolongation of survival, according to guidelines published in Clinical Cancer Research.
Accurate assessment of the ultimate efficacy of immunotherapy over time would benefit patients and clinicians since immune checkpoint inhibitors are often administered for several years, are financially costly, and treatment-associated AEs emerge unpredictably at any time.
Curtailing the duration of ineffective treatment could be valuable from many perspectives.
Immunotherapy combinations in metastatic melanoma
In the CheckMate 067 study, there was an improvement in response, progression-free survival (PFS), and overall survival for nivolumab (nivo) plus ipi or nivo alone, in comparison with ipi alone, in patients with advanced melanoma. Initial results from this trial were published in the New England Journal of Medicine in 2017.
At a minimum follow-up of 60 months, the 5-year overall survival was 52% for the nivo/ipi regimen, 44% for nivo alone, and 26% for ipi alone. These results were published in the New England Journal of Medicine in 2019.
The trial was not statistically powered to conclude whether the overall survival for the combination was superior to that of single-agent nivo alone, but both nivo regimens were superior to ipi alone.
Unfortunately, the combination also produced the highest treatment-related AE rates – 59% with nivo/ipi, 23% with nivo, and 28% with ipi in 2019. In the 2017 report, the combination regimen had more than twice as many premature treatment discontinuations as the other two study arms.
Is there a better way to quantify the risk-benefit ratio and explain it to patients?
Alternative strategies for assessing benefit: Treatment-free survival
Researchers have proposed treatment-free survival (TFS) as a potential new metric to characterize not only antitumor activity but also toxicity experienced after the cessation of therapy and before initiation of subsequent systemic therapy or death.
TFS is defined as the area between Kaplan-Meier curves from immunotherapy cessation until the reinitiation of systemic therapy or death. All patients who began immunotherapy are included – not just those achieving response or concluding a predefined number of cycles of treatment.
The curves can be partitioned into states with and without toxicity to establish a unique endpoint: time to cessation of both immunotherapy and toxicity.
Researchers conducted a pooled analysis of 3-year follow-up data from the 1,077 patients who participated in CheckMate 069, testing nivo/ipi versus nivo alone, and CheckMate 067, comparing nivo/ipi, nivo alone, and ipi alone. The results were published in the Journal of Clinical Oncology.
The TFS without grade 3 or higher AEs was 28% for nivo/ipi, 11% for nivo alone, and 23% for ipi alone. The restricted mean time without either treatment or grade 3 or greater AEs was 10.1 months, 4.1 months, and 8.5 months, respectively.
TFS incentivizes the use of regimens that have:
- A short duration of treatment
- Prolonged time to subsequent therapy or death
- Only mild AEs of brief duration.
A higher TFS corresponds with the goals that patients and their providers would have for a treatment regimen.
Adaptive models provide clues about benefit from extended therapy
In contrast to cytotoxic chemotherapy and molecularly targeted agents, benefit from immune-targeted therapy can deepen and persist after treatment discontinuation.
In advanced melanoma, researchers observed that overall survival was similar for patients who discontinued nivo/ipi because of AEs during the induction phase of treatment and those who did not. These results were published in the Journal of Clinical Oncology.
This observation has led to an individualized, adaptive approach to de-escalating combination immunotherapy, described in Clinical Cancer Research. The approach is dubbed “SMART,” which stands for sequential multiple assignment randomized trial designs.
With the SMART approach, each stage of a trial corresponds to an important treatment decision point. The goal is to define the population of patients who can safely discontinue treatment based on response, rather than doing so after the development of AEs.
In the Adapt-IT prospective study, 60 patients with advanced melanoma with poor prognostic features were given two doses of nivo/ipi followed by a CT scan at week 6. They were triaged to stopping ipi and proceeding with maintenance therapy with nivo alone or continuing the combination for an additional two cycles of treatment. Results from this trial were presented at ASCO 2020 (abstract 10003).
The investigators found that 68% of patients had no tumor burden increase at week 6 and could discontinue ipi. For those patients, their response rate of 57% approached the expected results from a full course of ipi.
At median follow-up of 22.3 months, median response duration, PFS, and overall survival had not been reached for the responders who received an abbreviated course of the combination regimen.
There were two observations that suggested the first two cycles of treatment drove not only toxicity but also tumor control:
- The rate of grade 3-4 toxicity from only two cycles was high (57%).
- Of the 19 patients (32% of the original 60 patients) who had progressive disease after two cycles of nivo/ipi, there were no responders with continued therapy.
Dr. Postow commented that, in correlative studies conducted as part of Adapt-IT, the Ki-67 of CD8-positive T cells increased after the initial dose of nivo/ipi. However, proliferation did not continue with subsequent cycles (that is, Ki-67 did not continue to rise).
When they examined markers of T-cell stimulation such as inducible costimulator of CD8-positive T cells, the researchers observed the same effect. The “immune boost” occurred with cycle one but not after subsequent doses of the nivo/ipi combination.
Although unproven in clinical trials at this time, these data suggest that response and risks of toxicity may not support giving patients more than one cycle of combination treatment.
More nuanced ways of assessing tumor growth
Dr. Postow noted that judgment about treatment effects over time are often made by displaying spider plots of changes from baseline tumor size from “time zero” – the time at which combination therapy is commenced.
He speculated that it might be worthwhile to give a dose or two of immune-targeted monotherapy (such as a PD-1 or PD-L1 inhibitor alone) before time zero, measure tumor growth prior to and after the single agent, and reserve using combination immunotherapy only for those patients who do not experience a dampening of the growth curve.
Patients whose tumor growth kinetics are improved with single-agent treatment could be spared the additional toxicity (and uncertain additive benefit) from the second agent.
Treatment optimization: More than ‘messaging’
Oncology practice has passed through a long era of “more is better,” an era that gave rise to intensive cytotoxic chemotherapy for hematologic and solid tumors in the metastatic and adjuvant settings. In some cases, that approach proved to be curative, but not in all.
More recently, because of better staging, improved outcomes with newer technology and treatments, and concern about immediate- and late-onset health risks, there has been an effort to deintensify therapy when it can be done safely.
Once a treatment regimen and treatment duration become established, however, patients and their physicians are reluctant to deintensity therapy.
Dr. Postow’s presentation demonstrated that, with regard to immunotherapy combinations – as in other realms of medical practice – science can lead the way to treatment optimization for individual patients.
We have the potential to reassure patients that treatment de-escalation is a rational and personalized component of treatment optimization through the combination of:
- Identifying new endpoints to quantify treatment benefits and risks.
- SMART trial designs.
- Innovative ways to assess tumor response during each phase of a treatment course.
Precision assessment of immunotherapy effect in individual patients can be a key part of precision medicine.
Dr. Postow disclosed relationships with Aduro, Array BioPharma, Bristol Myers Squibb, Eisai, Incyte, Infinity, Merck, NewLink Genetics, Novartis, and RGenix.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
Every medical oncologist who has described a combination chemotherapy regimen to a patient with advanced cancer has likely been asked whether the benefits of tumor shrinkage, disease-free survival (DFS), and overall survival are worth the risks of adverse events (AEs).
Single-agent immunotherapy and, more recently, combinations of immunotherapy drugs have been approved for a variety of metastatic tumors. In general, combination immunotherapy regimens have more AEs and a higher frequency of premature treatment discontinuation for toxicity.
Michael Postow, MD, of Memorial Sloan Kettering Cancer Center in New York, reflected on new ways to evaluate the benefits and risks of immunotherapy combinations during a plenary session on novel combinations at the American Association for Cancer Research’s Virtual Special Conference on Tumor Immunology and Immunotherapy.
Potential targets
As with chemotherapy drugs, immunotherapy combinations make the most sense when drugs targeting independent processes are employed.
As described in a paper published in Nature in 2011, the process for recruiting the immune system to combat cancer is as follows:
- Dendritic cells must sample antigens derived from the tumor.
- The dendritic cells must receive an activation signal so they promote immunity rather than tolerance.
- The tumor antigen–loaded dendritic cells need to generate protective T-cell responses, instead of T-regulatory responses, in lymphoid tissues.
- Cancer antigen–specific T cells must enter tumor tissues.
- Tumor-derived mechanisms for promoting immunosuppression need to be circumvented.
Since each step in the cascade is a potential therapeutic target, there are large numbers of potential drug combinations.
Measuring impact
Conventional measurements of tumor response may not be adequately sensitive to the impact from immunotherapy drugs. A case in point is sipuleucel-T, which is approved to treat advanced prostate cancer.
In the pivotal phase 3 trial, only 1 of 341 patients receiving sipuleucel-T achieved a partial response by RECIST criteria. Only 2.6% of patients had a 50% reduction in prostate-specific antigen levels. Nonetheless, a 4.1-month improvement in median overall survival was achieved. These results were published in the New England Journal of Medicine.
The discrepancy between tumor shrinkage and survival benefit for immunotherapy is not unexpected. As many as 10% of patients treated with ipilimumab (ipi) for stage IV malignant melanoma have progressive disease by tumor size but experience prolongation of survival, according to guidelines published in Clinical Cancer Research.
Accurate assessment of the ultimate efficacy of immunotherapy over time would benefit patients and clinicians since immune checkpoint inhibitors are often administered for several years, are financially costly, and treatment-associated AEs emerge unpredictably at any time.
Curtailing the duration of ineffective treatment could be valuable from many perspectives.
Immunotherapy combinations in metastatic melanoma
In the CheckMate 067 study, there was an improvement in response, progression-free survival (PFS), and overall survival for nivolumab (nivo) plus ipi or nivo alone, in comparison with ipi alone, in patients with advanced melanoma. Initial results from this trial were published in the New England Journal of Medicine in 2017.
At a minimum follow-up of 60 months, the 5-year overall survival was 52% for the nivo/ipi regimen, 44% for nivo alone, and 26% for ipi alone. These results were published in the New England Journal of Medicine in 2019.
The trial was not statistically powered to conclude whether the overall survival for the combination was superior to that of single-agent nivo alone, but both nivo regimens were superior to ipi alone.
Unfortunately, the combination also produced the highest treatment-related AE rates – 59% with nivo/ipi, 23% with nivo, and 28% with ipi in 2019. In the 2017 report, the combination regimen had more than twice as many premature treatment discontinuations as the other two study arms.
Is there a better way to quantify the risk-benefit ratio and explain it to patients?
Alternative strategies for assessing benefit: Treatment-free survival
Researchers have proposed treatment-free survival (TFS) as a potential new metric to characterize not only antitumor activity but also toxicity experienced after the cessation of therapy and before initiation of subsequent systemic therapy or death.
TFS is defined as the area between Kaplan-Meier curves from immunotherapy cessation until the reinitiation of systemic therapy or death. All patients who began immunotherapy are included – not just those achieving response or concluding a predefined number of cycles of treatment.
The curves can be partitioned into states with and without toxicity to establish a unique endpoint: time to cessation of both immunotherapy and toxicity.
Researchers conducted a pooled analysis of 3-year follow-up data from the 1,077 patients who participated in CheckMate 069, testing nivo/ipi versus nivo alone, and CheckMate 067, comparing nivo/ipi, nivo alone, and ipi alone. The results were published in the Journal of Clinical Oncology.
The TFS without grade 3 or higher AEs was 28% for nivo/ipi, 11% for nivo alone, and 23% for ipi alone. The restricted mean time without either treatment or grade 3 or greater AEs was 10.1 months, 4.1 months, and 8.5 months, respectively.
TFS incentivizes the use of regimens that have:
- A short duration of treatment
- Prolonged time to subsequent therapy or death
- Only mild AEs of brief duration.
A higher TFS corresponds with the goals that patients and their providers would have for a treatment regimen.
Adaptive models provide clues about benefit from extended therapy
In contrast to cytotoxic chemotherapy and molecularly targeted agents, benefit from immune-targeted therapy can deepen and persist after treatment discontinuation.
In advanced melanoma, researchers observed that overall survival was similar for patients who discontinued nivo/ipi because of AEs during the induction phase of treatment and those who did not. These results were published in the Journal of Clinical Oncology.
This observation has led to an individualized, adaptive approach to de-escalating combination immunotherapy, described in Clinical Cancer Research. The approach is dubbed “SMART,” which stands for sequential multiple assignment randomized trial designs.
With the SMART approach, each stage of a trial corresponds to an important treatment decision point. The goal is to define the population of patients who can safely discontinue treatment based on response, rather than doing so after the development of AEs.
In the Adapt-IT prospective study, 60 patients with advanced melanoma with poor prognostic features were given two doses of nivo/ipi followed by a CT scan at week 6. They were triaged to stopping ipi and proceeding with maintenance therapy with nivo alone or continuing the combination for an additional two cycles of treatment. Results from this trial were presented at ASCO 2020 (abstract 10003).
The investigators found that 68% of patients had no tumor burden increase at week 6 and could discontinue ipi. For those patients, their response rate of 57% approached the expected results from a full course of ipi.
At median follow-up of 22.3 months, median response duration, PFS, and overall survival had not been reached for the responders who received an abbreviated course of the combination regimen.
There were two observations that suggested the first two cycles of treatment drove not only toxicity but also tumor control:
- The rate of grade 3-4 toxicity from only two cycles was high (57%).
- Of the 19 patients (32% of the original 60 patients) who had progressive disease after two cycles of nivo/ipi, there were no responders with continued therapy.
Dr. Postow commented that, in correlative studies conducted as part of Adapt-IT, the Ki-67 of CD8-positive T cells increased after the initial dose of nivo/ipi. However, proliferation did not continue with subsequent cycles (that is, Ki-67 did not continue to rise).
When they examined markers of T-cell stimulation such as inducible costimulator of CD8-positive T cells, the researchers observed the same effect. The “immune boost” occurred with cycle one but not after subsequent doses of the nivo/ipi combination.
Although unproven in clinical trials at this time, these data suggest that response and risks of toxicity may not support giving patients more than one cycle of combination treatment.
More nuanced ways of assessing tumor growth
Dr. Postow noted that judgment about treatment effects over time are often made by displaying spider plots of changes from baseline tumor size from “time zero” – the time at which combination therapy is commenced.
He speculated that it might be worthwhile to give a dose or two of immune-targeted monotherapy (such as a PD-1 or PD-L1 inhibitor alone) before time zero, measure tumor growth prior to and after the single agent, and reserve using combination immunotherapy only for those patients who do not experience a dampening of the growth curve.
Patients whose tumor growth kinetics are improved with single-agent treatment could be spared the additional toxicity (and uncertain additive benefit) from the second agent.
Treatment optimization: More than ‘messaging’
Oncology practice has passed through a long era of “more is better,” an era that gave rise to intensive cytotoxic chemotherapy for hematologic and solid tumors in the metastatic and adjuvant settings. In some cases, that approach proved to be curative, but not in all.
More recently, because of better staging, improved outcomes with newer technology and treatments, and concern about immediate- and late-onset health risks, there has been an effort to deintensify therapy when it can be done safely.
Once a treatment regimen and treatment duration become established, however, patients and their physicians are reluctant to deintensity therapy.
Dr. Postow’s presentation demonstrated that, with regard to immunotherapy combinations – as in other realms of medical practice – science can lead the way to treatment optimization for individual patients.
We have the potential to reassure patients that treatment de-escalation is a rational and personalized component of treatment optimization through the combination of:
- Identifying new endpoints to quantify treatment benefits and risks.
- SMART trial designs.
- Innovative ways to assess tumor response during each phase of a treatment course.
Precision assessment of immunotherapy effect in individual patients can be a key part of precision medicine.
Dr. Postow disclosed relationships with Aduro, Array BioPharma, Bristol Myers Squibb, Eisai, Incyte, Infinity, Merck, NewLink Genetics, Novartis, and RGenix.
Dr. Lyss was a community-based medical oncologist and clinical researcher for more than 35 years before his recent retirement. His clinical and research interests were focused on breast and lung cancers, as well as expanding clinical trial access to medically underserved populations. He is based in St. Louis. He has no conflicts of interest.
FROM AACR: TUMOR IMMUNOLOGY AND IMMUNOTHERAPY
NHS England starts pilot trial of blood test for many cancers
“Early detection, particularly for hard-to-treat conditions like ovarian and pancreatic cancer, has the potential to save many lives,” said NHS Chief Executive Sir Simon Stevens in a statement.
The pilot trial will use the Galleri blood test, developed by Grail. Sir Stevens described the blood test as “promising” and said it could “be a game changer in cancer care, helping thousands more people to get successful treatment.”
However, some clinicians have expressed concerns over the potential for false-positive results with the test.
Results of a study of the Galleri blood test, published earlier this year, showed that the test detected 50 types of cancer with a specificity of 99.3% and a false positive rate of 0.7%.
It also correctly identified the originating tissue in 90% of cases. However, the sensitivity was lower, at 67%, for the 12 most common cancers, as reported at the time.
The senior author of that study, Michael Seiden, MD, PhD, president of the U.S. Oncology Network, The Woodlands, Tex., noted that it was not a screening study: the test had been used in patients with cancer and in healthy volunteers. He said the test “is intended to be complementary to, and not replace, existing guideline-recommended screening tests and might provide new avenues of investigation for cancers that don’t currently have screening tests.”
The Galleri test uses next-generation sequencing to analyze the arrangement of methyl groups on circulating cell-free DNA in a blood sample.
Several other blood tests for cancer are under development, including the CancerSEEK test, which has been reported to be able to identify eight common cancers. It measures circulating tumor DNA from 16 genes and eight protein biomarkers and then uses machine learning to analyze the data.
Improving early detection rates
The pilot trial of the blood test is due to start in mid-2021 and will involve 165,000 people.
The trial will include 140,000 individuals aged 50-79 years who were identified through their health records and who have no cancer symptoms. They will undergo blood tests annually for 3 years and will be referred for investigation if a test result is positive.
A second group will include 25,000 people with potential cancer symptoms. These patients will be offered the blood test to speed up their diagnosis after referral to a hospital via the normal channels.
The results of the pilot are expected in 2023. If successful, the test will be rolled out to 1 million individuals from 2024 to 2025.
The pilot trial is part of the NHS Long Term Plan, which aims to increase early detection of cancer. At present, around half of cancers in England are diagnosed in stage I or II; the NHS aims to increase this to 75% by 2028.
“The NHS has set itself an ambitious target,” commented Peter Johnson, MD, PhD, national clinical director for cancer at NHS England and Improvement.
“Tests like this may help us get there far faster, and I am excited to see how this cutting-edge technology will work out as we test it in clinics across the NHS,” he added.
Lord David Prior, chair of NHS England, noted that almost 200,000 people die from cancer in the United Kingdom every year and that “many of these people are diagnosed too late for treatment to be effective.
“This collaboration between the NHS and Grail offers the chance for a wide range of cancers to be diagnosed much earlier and could fundamentally change the outlook for people with cancer,” he said.
However, some clinicians raised potential concerns.
Stephen Duffy, PhD, Center for Cancer Prevention, Queen Mary University of London, described the pilot as “very exciting,” but cautioned: “We will need to find out just how early the test detects cancers and whether it can it be used in a way which minimizes anxiety from false positives.”
Yong-Jie Lu, MD, PhD, also at Queen Mary University of London, said: “It is not clear how early it aims to catch cancer. For a cancer screen test, it needs very high specificity (>99%), otherwise it may end up in a similar situation as the PSA [prostate-specific antigen] test for prostate cancer, or even worse.”
Mangesh Thorat, MD, Cancer Prevention Trials Unit, King’s College London, warned: “It is likely that for every testing round ... there will be about 1,000 false-positive results, and the test may not be able to pinpoint the location of cancer in 3%-4% of those with a true positive result, necessitating a range of imaging and other investigations in these participants.”
No funding for the study has been declared. The investigators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
“Early detection, particularly for hard-to-treat conditions like ovarian and pancreatic cancer, has the potential to save many lives,” said NHS Chief Executive Sir Simon Stevens in a statement.
The pilot trial will use the Galleri blood test, developed by Grail. Sir Stevens described the blood test as “promising” and said it could “be a game changer in cancer care, helping thousands more people to get successful treatment.”
However, some clinicians have expressed concerns over the potential for false-positive results with the test.
Results of a study of the Galleri blood test, published earlier this year, showed that the test detected 50 types of cancer with a specificity of 99.3% and a false positive rate of 0.7%.
It also correctly identified the originating tissue in 90% of cases. However, the sensitivity was lower, at 67%, for the 12 most common cancers, as reported at the time.
The senior author of that study, Michael Seiden, MD, PhD, president of the U.S. Oncology Network, The Woodlands, Tex., noted that it was not a screening study: the test had been used in patients with cancer and in healthy volunteers. He said the test “is intended to be complementary to, and not replace, existing guideline-recommended screening tests and might provide new avenues of investigation for cancers that don’t currently have screening tests.”
The Galleri test uses next-generation sequencing to analyze the arrangement of methyl groups on circulating cell-free DNA in a blood sample.
Several other blood tests for cancer are under development, including the CancerSEEK test, which has been reported to be able to identify eight common cancers. It measures circulating tumor DNA from 16 genes and eight protein biomarkers and then uses machine learning to analyze the data.
Improving early detection rates
The pilot trial of the blood test is due to start in mid-2021 and will involve 165,000 people.
The trial will include 140,000 individuals aged 50-79 years who were identified through their health records and who have no cancer symptoms. They will undergo blood tests annually for 3 years and will be referred for investigation if a test result is positive.
A second group will include 25,000 people with potential cancer symptoms. These patients will be offered the blood test to speed up their diagnosis after referral to a hospital via the normal channels.
The results of the pilot are expected in 2023. If successful, the test will be rolled out to 1 million individuals from 2024 to 2025.
The pilot trial is part of the NHS Long Term Plan, which aims to increase early detection of cancer. At present, around half of cancers in England are diagnosed in stage I or II; the NHS aims to increase this to 75% by 2028.
“The NHS has set itself an ambitious target,” commented Peter Johnson, MD, PhD, national clinical director for cancer at NHS England and Improvement.
“Tests like this may help us get there far faster, and I am excited to see how this cutting-edge technology will work out as we test it in clinics across the NHS,” he added.
Lord David Prior, chair of NHS England, noted that almost 200,000 people die from cancer in the United Kingdom every year and that “many of these people are diagnosed too late for treatment to be effective.
“This collaboration between the NHS and Grail offers the chance for a wide range of cancers to be diagnosed much earlier and could fundamentally change the outlook for people with cancer,” he said.
However, some clinicians raised potential concerns.
Stephen Duffy, PhD, Center for Cancer Prevention, Queen Mary University of London, described the pilot as “very exciting,” but cautioned: “We will need to find out just how early the test detects cancers and whether it can it be used in a way which minimizes anxiety from false positives.”
Yong-Jie Lu, MD, PhD, also at Queen Mary University of London, said: “It is not clear how early it aims to catch cancer. For a cancer screen test, it needs very high specificity (>99%), otherwise it may end up in a similar situation as the PSA [prostate-specific antigen] test for prostate cancer, or even worse.”
Mangesh Thorat, MD, Cancer Prevention Trials Unit, King’s College London, warned: “It is likely that for every testing round ... there will be about 1,000 false-positive results, and the test may not be able to pinpoint the location of cancer in 3%-4% of those with a true positive result, necessitating a range of imaging and other investigations in these participants.”
No funding for the study has been declared. The investigators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
“Early detection, particularly for hard-to-treat conditions like ovarian and pancreatic cancer, has the potential to save many lives,” said NHS Chief Executive Sir Simon Stevens in a statement.
The pilot trial will use the Galleri blood test, developed by Grail. Sir Stevens described the blood test as “promising” and said it could “be a game changer in cancer care, helping thousands more people to get successful treatment.”
However, some clinicians have expressed concerns over the potential for false-positive results with the test.
Results of a study of the Galleri blood test, published earlier this year, showed that the test detected 50 types of cancer with a specificity of 99.3% and a false positive rate of 0.7%.
It also correctly identified the originating tissue in 90% of cases. However, the sensitivity was lower, at 67%, for the 12 most common cancers, as reported at the time.
The senior author of that study, Michael Seiden, MD, PhD, president of the U.S. Oncology Network, The Woodlands, Tex., noted that it was not a screening study: the test had been used in patients with cancer and in healthy volunteers. He said the test “is intended to be complementary to, and not replace, existing guideline-recommended screening tests and might provide new avenues of investigation for cancers that don’t currently have screening tests.”
The Galleri test uses next-generation sequencing to analyze the arrangement of methyl groups on circulating cell-free DNA in a blood sample.
Several other blood tests for cancer are under development, including the CancerSEEK test, which has been reported to be able to identify eight common cancers. It measures circulating tumor DNA from 16 genes and eight protein biomarkers and then uses machine learning to analyze the data.
Improving early detection rates
The pilot trial of the blood test is due to start in mid-2021 and will involve 165,000 people.
The trial will include 140,000 individuals aged 50-79 years who were identified through their health records and who have no cancer symptoms. They will undergo blood tests annually for 3 years and will be referred for investigation if a test result is positive.
A second group will include 25,000 people with potential cancer symptoms. These patients will be offered the blood test to speed up their diagnosis after referral to a hospital via the normal channels.
The results of the pilot are expected in 2023. If successful, the test will be rolled out to 1 million individuals from 2024 to 2025.
The pilot trial is part of the NHS Long Term Plan, which aims to increase early detection of cancer. At present, around half of cancers in England are diagnosed in stage I or II; the NHS aims to increase this to 75% by 2028.
“The NHS has set itself an ambitious target,” commented Peter Johnson, MD, PhD, national clinical director for cancer at NHS England and Improvement.
“Tests like this may help us get there far faster, and I am excited to see how this cutting-edge technology will work out as we test it in clinics across the NHS,” he added.
Lord David Prior, chair of NHS England, noted that almost 200,000 people die from cancer in the United Kingdom every year and that “many of these people are diagnosed too late for treatment to be effective.
“This collaboration between the NHS and Grail offers the chance for a wide range of cancers to be diagnosed much earlier and could fundamentally change the outlook for people with cancer,” he said.
However, some clinicians raised potential concerns.
Stephen Duffy, PhD, Center for Cancer Prevention, Queen Mary University of London, described the pilot as “very exciting,” but cautioned: “We will need to find out just how early the test detects cancers and whether it can it be used in a way which minimizes anxiety from false positives.”
Yong-Jie Lu, MD, PhD, also at Queen Mary University of London, said: “It is not clear how early it aims to catch cancer. For a cancer screen test, it needs very high specificity (>99%), otherwise it may end up in a similar situation as the PSA [prostate-specific antigen] test for prostate cancer, or even worse.”
Mangesh Thorat, MD, Cancer Prevention Trials Unit, King’s College London, warned: “It is likely that for every testing round ... there will be about 1,000 false-positive results, and the test may not be able to pinpoint the location of cancer in 3%-4% of those with a true positive result, necessitating a range of imaging and other investigations in these participants.”
No funding for the study has been declared. The investigators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Cancer rates on the rise in adolescents and young adults
Rates of cancer increased by 30% from 1973 to 2015 in adolescents and young adults (AYAs) aged 15–39 years in the United States, according to a review of almost a half million cases in the National Institutes of Health’s Surveillance, Epidemiology, and End Results database.
There was an annual increase of 0.537 new cases per 100,000 people, from 57.2 cases per 100,000 in 1973 to 74.2 in 2015.
Kidney carcinoma led with the highest rate increase. There were also marked increases in thyroid and colorectal carcinoma, germ cell and trophoblastic neoplasms, and melanoma, among others.
The report was published online December 1 in JAMA Network Open.
“Clinicians should be on the lookout for these cancers in their adolescent and young adult patients,” said senior investigator Nicholas Zaorsky, MD, an assistant professor of radiation oncology and public health sciences at the Penn State Cancer Institute, Hershey, Pennsylvania.
“Now that there is a better understanding of the types of cancer that are prevalent and rising in this age group, prevention, screening, diagnosis and treatment protocols specifically targeted to this population should be developed,” he said in a press release.
The reasons for the increases are unclear, but environmental and dietary factors, increasing obesity, and changing screening practices are likely in play, the authors comment. In addition, “cancer screening and overdiagnosis are thought to account for much of the increasing rates of thyroid and kidney carcinoma, among others,” they add.
The American Cancer Society (ACS) recently found similar increases in thyroid, kidney, and colorectal cancer among AYAs, as well as an increase in uterine cancer.
It’s important to note, however, that “this phenomenon is largely driven by trends for thyroid cancer, which is thought to be a result of overdiagnosis,” said ACS surveillance researcher Kimberly Miller, MPH, when asked to comment on the new study.
“As such, it is extremely important to also consider trends in cancer mortality rates among this age group, which are declining overall but are increasing for colorectal and uterine cancers. The fact that both incidence and mortality rates are increasing for these two cancers suggests a true increase in disease burden and certainly requires further attention and research,” she said.
Historically, management of cancer in AYAs has fallen somewhere between pediatric and adult oncology, neither of which capture the distinct biological, social, and economic needs of AYAs. Research has also focused on childhood and adult cancers, leaving cancer in AYAs inadequately studied.
The new findings are “valuable to guide more targeted research and interventions specifically to AYAs,” Zaorsky and colleagues say in their report.
Among female patients ― 59.1% of the study population ― incidence increased for 15 cancers, including kidney carcinoma (annual percent change [APC], 3.632), thyroid carcinoma (APC, 3.456), and myeloma, mast cell, and miscellaneous lymphoreticular neoplasms not otherwise specified (APC, 2.805). Rates of five cancers declined, led by astrocytoma not otherwise specified (APC, –3.369) and carcinoma of the gonads (APC, –1.743).
Among male patients, incidence increased for 14 cancers, including kidney carcinoma (APC, 3.572), unspecified soft tissue sarcoma (APC 2.543), and thyroid carcinoma (APC, 2.273). Incidence fell for seven, led by astrocytoma not otherwise specified (APC, –3.759) and carcinoma of the trachea, bronchus, and lung (APC, –2.635).
Increased testicular cancer rates (APC, 1.246) could be related to greater prenatal exposure to estrogen and progesterone or through dairy consumption; increasing survival of premature infants; and greater exposure to cannabis, among other possibilities, the investigators say.
Increases in colorectal cancer might be related to fewer vegetables and more fat and processed meat in the diet; lack of exercise; and increasing obesity. Human papillomavirus infection has also been implicated.
Higher rates of melanoma could be related to tanning bed use.
Declines in some cancers could be related to greater use of oral contraceptives; laws reducing exposure to benzene and other chemicals; and fewer people smoking.
Although kidney carcinoma has increased at the greatest rate, it’s uncommon. Colorectal and thyroid carcinoma, melanoma, non-Hodgkin lymphoma, and germ cell and trophoblastic neoplasms of the gonads contribute more to the overall increase in cancers among AYAs, the investigators note.
Almost 80% of the patients were White; 10.3% were Black.
The study was funded by the National Center for Advancing Translational Sciences. The investigators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Rates of cancer increased by 30% from 1973 to 2015 in adolescents and young adults (AYAs) aged 15–39 years in the United States, according to a review of almost a half million cases in the National Institutes of Health’s Surveillance, Epidemiology, and End Results database.
There was an annual increase of 0.537 new cases per 100,000 people, from 57.2 cases per 100,000 in 1973 to 74.2 in 2015.
Kidney carcinoma led with the highest rate increase. There were also marked increases in thyroid and colorectal carcinoma, germ cell and trophoblastic neoplasms, and melanoma, among others.
The report was published online December 1 in JAMA Network Open.
“Clinicians should be on the lookout for these cancers in their adolescent and young adult patients,” said senior investigator Nicholas Zaorsky, MD, an assistant professor of radiation oncology and public health sciences at the Penn State Cancer Institute, Hershey, Pennsylvania.
“Now that there is a better understanding of the types of cancer that are prevalent and rising in this age group, prevention, screening, diagnosis and treatment protocols specifically targeted to this population should be developed,” he said in a press release.
The reasons for the increases are unclear, but environmental and dietary factors, increasing obesity, and changing screening practices are likely in play, the authors comment. In addition, “cancer screening and overdiagnosis are thought to account for much of the increasing rates of thyroid and kidney carcinoma, among others,” they add.
The American Cancer Society (ACS) recently found similar increases in thyroid, kidney, and colorectal cancer among AYAs, as well as an increase in uterine cancer.
It’s important to note, however, that “this phenomenon is largely driven by trends for thyroid cancer, which is thought to be a result of overdiagnosis,” said ACS surveillance researcher Kimberly Miller, MPH, when asked to comment on the new study.
“As such, it is extremely important to also consider trends in cancer mortality rates among this age group, which are declining overall but are increasing for colorectal and uterine cancers. The fact that both incidence and mortality rates are increasing for these two cancers suggests a true increase in disease burden and certainly requires further attention and research,” she said.
Historically, management of cancer in AYAs has fallen somewhere between pediatric and adult oncology, neither of which capture the distinct biological, social, and economic needs of AYAs. Research has also focused on childhood and adult cancers, leaving cancer in AYAs inadequately studied.
The new findings are “valuable to guide more targeted research and interventions specifically to AYAs,” Zaorsky and colleagues say in their report.
Among female patients ― 59.1% of the study population ― incidence increased for 15 cancers, including kidney carcinoma (annual percent change [APC], 3.632), thyroid carcinoma (APC, 3.456), and myeloma, mast cell, and miscellaneous lymphoreticular neoplasms not otherwise specified (APC, 2.805). Rates of five cancers declined, led by astrocytoma not otherwise specified (APC, –3.369) and carcinoma of the gonads (APC, –1.743).
Among male patients, incidence increased for 14 cancers, including kidney carcinoma (APC, 3.572), unspecified soft tissue sarcoma (APC 2.543), and thyroid carcinoma (APC, 2.273). Incidence fell for seven, led by astrocytoma not otherwise specified (APC, –3.759) and carcinoma of the trachea, bronchus, and lung (APC, –2.635).
Increased testicular cancer rates (APC, 1.246) could be related to greater prenatal exposure to estrogen and progesterone or through dairy consumption; increasing survival of premature infants; and greater exposure to cannabis, among other possibilities, the investigators say.
Increases in colorectal cancer might be related to fewer vegetables and more fat and processed meat in the diet; lack of exercise; and increasing obesity. Human papillomavirus infection has also been implicated.
Higher rates of melanoma could be related to tanning bed use.
Declines in some cancers could be related to greater use of oral contraceptives; laws reducing exposure to benzene and other chemicals; and fewer people smoking.
Although kidney carcinoma has increased at the greatest rate, it’s uncommon. Colorectal and thyroid carcinoma, melanoma, non-Hodgkin lymphoma, and germ cell and trophoblastic neoplasms of the gonads contribute more to the overall increase in cancers among AYAs, the investigators note.
Almost 80% of the patients were White; 10.3% were Black.
The study was funded by the National Center for Advancing Translational Sciences. The investigators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Rates of cancer increased by 30% from 1973 to 2015 in adolescents and young adults (AYAs) aged 15–39 years in the United States, according to a review of almost a half million cases in the National Institutes of Health’s Surveillance, Epidemiology, and End Results database.
There was an annual increase of 0.537 new cases per 100,000 people, from 57.2 cases per 100,000 in 1973 to 74.2 in 2015.
Kidney carcinoma led with the highest rate increase. There were also marked increases in thyroid and colorectal carcinoma, germ cell and trophoblastic neoplasms, and melanoma, among others.
The report was published online December 1 in JAMA Network Open.
“Clinicians should be on the lookout for these cancers in their adolescent and young adult patients,” said senior investigator Nicholas Zaorsky, MD, an assistant professor of radiation oncology and public health sciences at the Penn State Cancer Institute, Hershey, Pennsylvania.
“Now that there is a better understanding of the types of cancer that are prevalent and rising in this age group, prevention, screening, diagnosis and treatment protocols specifically targeted to this population should be developed,” he said in a press release.
The reasons for the increases are unclear, but environmental and dietary factors, increasing obesity, and changing screening practices are likely in play, the authors comment. In addition, “cancer screening and overdiagnosis are thought to account for much of the increasing rates of thyroid and kidney carcinoma, among others,” they add.
The American Cancer Society (ACS) recently found similar increases in thyroid, kidney, and colorectal cancer among AYAs, as well as an increase in uterine cancer.
It’s important to note, however, that “this phenomenon is largely driven by trends for thyroid cancer, which is thought to be a result of overdiagnosis,” said ACS surveillance researcher Kimberly Miller, MPH, when asked to comment on the new study.
“As such, it is extremely important to also consider trends in cancer mortality rates among this age group, which are declining overall but are increasing for colorectal and uterine cancers. The fact that both incidence and mortality rates are increasing for these two cancers suggests a true increase in disease burden and certainly requires further attention and research,” she said.
Historically, management of cancer in AYAs has fallen somewhere between pediatric and adult oncology, neither of which capture the distinct biological, social, and economic needs of AYAs. Research has also focused on childhood and adult cancers, leaving cancer in AYAs inadequately studied.
The new findings are “valuable to guide more targeted research and interventions specifically to AYAs,” Zaorsky and colleagues say in their report.
Among female patients ― 59.1% of the study population ― incidence increased for 15 cancers, including kidney carcinoma (annual percent change [APC], 3.632), thyroid carcinoma (APC, 3.456), and myeloma, mast cell, and miscellaneous lymphoreticular neoplasms not otherwise specified (APC, 2.805). Rates of five cancers declined, led by astrocytoma not otherwise specified (APC, –3.369) and carcinoma of the gonads (APC, –1.743).
Among male patients, incidence increased for 14 cancers, including kidney carcinoma (APC, 3.572), unspecified soft tissue sarcoma (APC 2.543), and thyroid carcinoma (APC, 2.273). Incidence fell for seven, led by astrocytoma not otherwise specified (APC, –3.759) and carcinoma of the trachea, bronchus, and lung (APC, –2.635).
Increased testicular cancer rates (APC, 1.246) could be related to greater prenatal exposure to estrogen and progesterone or through dairy consumption; increasing survival of premature infants; and greater exposure to cannabis, among other possibilities, the investigators say.
Increases in colorectal cancer might be related to fewer vegetables and more fat and processed meat in the diet; lack of exercise; and increasing obesity. Human papillomavirus infection has also been implicated.
Higher rates of melanoma could be related to tanning bed use.
Declines in some cancers could be related to greater use of oral contraceptives; laws reducing exposure to benzene and other chemicals; and fewer people smoking.
Although kidney carcinoma has increased at the greatest rate, it’s uncommon. Colorectal and thyroid carcinoma, melanoma, non-Hodgkin lymphoma, and germ cell and trophoblastic neoplasms of the gonads contribute more to the overall increase in cancers among AYAs, the investigators note.
Almost 80% of the patients were White; 10.3% were Black.
The study was funded by the National Center for Advancing Translational Sciences. The investigators have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
Lung cancer CT scan is chance for ‘opportunistic’ osteoporosis check
Low-dose chest CT for lung cancer screening provides the opportunity to simultaneously screen patients for osteoporosis, detecting notably higher rates of osteoporosis in men than the traditional tool of DXA, research published in the Journal of Bone and Mineral Research shows.
“Our large-scale, multicenter study of bone density measured from routine low-dose CT scans demonstrated the great potential of using low-dose CT for the opportunistic screening of osteoporosis as an alternative to standard DXA scans,” said senior author Wei Tian, MD, of the Chinese Academy of Engineering and Peking University, in a press statement from the journal.
“Our study revealed the unexpectedly high prevalence of osteoporosis in men, which may impact on the management strategy of men in the future,” Dr. Tian added.
Josephine Therkildsen, MD, of Herning Hospital, Denmark, who has conducted similar research using cardiac CT scans, said the findings add important new insights into the issue of opportunistic screening.
“The results are highly interesting, as they show that low-dose CT-based opportunistic screening could identify a substantial number of patients with low lumbar bone mineral density (BMD) with the future potential to diagnose osteoporosis and initiate relevant treatment before a fracture occurs,” she told this news organization.
Perry J. Pickhardt, MD, chief of gastrointestinal imaging at the University of Wisconsin School of Medicine and Public Health in Madison, agrees. He said in an interview that CT scans of the chest and abdomen, commonly performed for a variety of clinical indications and widespread in most developed countries, can in fact be essential for the detection of a multitude of other concerns – yet are underused for those other purposes.
Use of CT in this way “would likely be very cost effective and clinically efficacious,” he said, adding: “We are seeing greatly increased interest in leveraging this extra information that is contained within every CT scan.” And, “Importantly, artificial intelligence advances now allow for automated approaches, which should allow for expanded use.”
Lung cancer CT scans shed light on osteoporosis prevalence
In the study, led by Xiaoguang Cheng, MD, PhD, of the department of radiology, Beijing Jishuitan Hospital, China, researchers examined lung cancer CT screening data from the prospective China Biobank Project to determine the prevalence of osteoporosis in China.
This included the thoracic low-dose CT scans of 69,095 adults, including 40,733 men and 28,362 women, taken between 2018 and 2019.
To screen for osteoporosis, they used quantitative CT software to evaluate lumbar spine (L1-L2) trabecular volume BMD (vBMD) and diagnostic criteria from the American College of Radiology. Using the vBMD measures from the CT imaging, they found the prevalence of osteoporosis among those over 50 years of age in the Chinese population to be 29% for women (49 million) and 13.5% for men (22.8 million).
Interestingly, the osteoporosis prevalence rate among women was comparable to estimates in the population derived from DXA (29.1%); however, the rate in men was twice that estimated from DXA scans (6.5%).
Decreases in trabecular vBMD with age were observed in both genders. However, declines were steeper among women, who had higher peak trabecular vBMD (185.4 mg/cm3), compared with men (176.6 mg/cm3) at age 30-34 years, but significantly lower measures (62.4 mg/cm3) than men (92.1 mg/cm3) at age 80 years.
The prevalence of osteoporosis in women increased from 2.8% at age 50-54 years to 79.8% at age 85 or older, while in men, the prevalence was 3.2% at age 50-54 years and 44.1% at age 85 or older.
“This is the first study to establish Chinese reference data for vBMD using opportunistic screening from low-dose chest CT in a large population cohort,” the authors write.
“The opportunistic screening of osteoporosis using low-dose CT is clinically feasible and requires no additional exposure to ionizing radiation.”
In addition, no additional equipment or patient time was required, suggesting that “this approach has potential for opportunistic screening for osteoporosis.”
They note, however, that further cohort studies are needed to assess clinical utility of this method.
CT ‘likely a more accurate measure’ of volumetric BMD
Dr. Pickhardt said the differences in osteoporosis prevalence observed between DXA and CT-derived measures in men likely reflect the greater accuracy of CT.
“DXA is a planar technique with a number of drawbacks,” he said in an interview. “CT provides a more direct volumetric measure and is likely a more accurate method for BMD assessment.”
He speculated that the greater differences between DXA versus CT seen in men than women “may relate to sex differences in cortical bone of vertebral bodies, which cannot be separated from the underlying trabecular bone with DXA (whereas CT directly measures the inner trabecular bone).”
The authors note that, although areal BMD (aBMD) derived from DXA is required for osteoporosis diagnosis according to World Health Organization criteria, “trabecular vBMD derived from CT can be also used for diagnosis based on thresholds published by the American College of Radiology of 120 mg/cm3 and 80 mg/cm3 to define osteopenia and osteoporosis, respectively, thresholds that were subsequently confirmed for the Chinese population.”
Furthermore, vBMD has been shown in some studies to be more strongly related to fracture risk, compared with DXA aBMD measures.
Importantly, in another recent study involving 9,223 adults, Dr. Pickhardt and colleagues reported that bone and muscle biomarkers derived from CT were comparable to the Fracture Risk Assessment Tool score for the presymptomatic prediction of future osteoporotic fractures.
Dr. Pickhardt is an advisor to Bracco Imaging and Zebra Medical Vision. Dr. Therkildsen has reported no relevant financial relationships.
This article first appeared on Medscape.com.
Low-dose chest CT for lung cancer screening provides the opportunity to simultaneously screen patients for osteoporosis, detecting notably higher rates of osteoporosis in men than the traditional tool of DXA, research published in the Journal of Bone and Mineral Research shows.
“Our large-scale, multicenter study of bone density measured from routine low-dose CT scans demonstrated the great potential of using low-dose CT for the opportunistic screening of osteoporosis as an alternative to standard DXA scans,” said senior author Wei Tian, MD, of the Chinese Academy of Engineering and Peking University, in a press statement from the journal.
“Our study revealed the unexpectedly high prevalence of osteoporosis in men, which may impact on the management strategy of men in the future,” Dr. Tian added.
Josephine Therkildsen, MD, of Herning Hospital, Denmark, who has conducted similar research using cardiac CT scans, said the findings add important new insights into the issue of opportunistic screening.
“The results are highly interesting, as they show that low-dose CT-based opportunistic screening could identify a substantial number of patients with low lumbar bone mineral density (BMD) with the future potential to diagnose osteoporosis and initiate relevant treatment before a fracture occurs,” she told this news organization.
Perry J. Pickhardt, MD, chief of gastrointestinal imaging at the University of Wisconsin School of Medicine and Public Health in Madison, agrees. He said in an interview that CT scans of the chest and abdomen, commonly performed for a variety of clinical indications and widespread in most developed countries, can in fact be essential for the detection of a multitude of other concerns – yet are underused for those other purposes.
Use of CT in this way “would likely be very cost effective and clinically efficacious,” he said, adding: “We are seeing greatly increased interest in leveraging this extra information that is contained within every CT scan.” And, “Importantly, artificial intelligence advances now allow for automated approaches, which should allow for expanded use.”
Lung cancer CT scans shed light on osteoporosis prevalence
In the study, led by Xiaoguang Cheng, MD, PhD, of the department of radiology, Beijing Jishuitan Hospital, China, researchers examined lung cancer CT screening data from the prospective China Biobank Project to determine the prevalence of osteoporosis in China.
This included the thoracic low-dose CT scans of 69,095 adults, including 40,733 men and 28,362 women, taken between 2018 and 2019.
To screen for osteoporosis, they used quantitative CT software to evaluate lumbar spine (L1-L2) trabecular volume BMD (vBMD) and diagnostic criteria from the American College of Radiology. Using the vBMD measures from the CT imaging, they found the prevalence of osteoporosis among those over 50 years of age in the Chinese population to be 29% for women (49 million) and 13.5% for men (22.8 million).
Interestingly, the osteoporosis prevalence rate among women was comparable to estimates in the population derived from DXA (29.1%); however, the rate in men was twice that estimated from DXA scans (6.5%).
Decreases in trabecular vBMD with age were observed in both genders. However, declines were steeper among women, who had higher peak trabecular vBMD (185.4 mg/cm3), compared with men (176.6 mg/cm3) at age 30-34 years, but significantly lower measures (62.4 mg/cm3) than men (92.1 mg/cm3) at age 80 years.
The prevalence of osteoporosis in women increased from 2.8% at age 50-54 years to 79.8% at age 85 or older, while in men, the prevalence was 3.2% at age 50-54 years and 44.1% at age 85 or older.
“This is the first study to establish Chinese reference data for vBMD using opportunistic screening from low-dose chest CT in a large population cohort,” the authors write.
“The opportunistic screening of osteoporosis using low-dose CT is clinically feasible and requires no additional exposure to ionizing radiation.”
In addition, no additional equipment or patient time was required, suggesting that “this approach has potential for opportunistic screening for osteoporosis.”
They note, however, that further cohort studies are needed to assess clinical utility of this method.
CT ‘likely a more accurate measure’ of volumetric BMD
Dr. Pickhardt said the differences in osteoporosis prevalence observed between DXA and CT-derived measures in men likely reflect the greater accuracy of CT.
“DXA is a planar technique with a number of drawbacks,” he said in an interview. “CT provides a more direct volumetric measure and is likely a more accurate method for BMD assessment.”
He speculated that the greater differences between DXA versus CT seen in men than women “may relate to sex differences in cortical bone of vertebral bodies, which cannot be separated from the underlying trabecular bone with DXA (whereas CT directly measures the inner trabecular bone).”
The authors note that, although areal BMD (aBMD) derived from DXA is required for osteoporosis diagnosis according to World Health Organization criteria, “trabecular vBMD derived from CT can be also used for diagnosis based on thresholds published by the American College of Radiology of 120 mg/cm3 and 80 mg/cm3 to define osteopenia and osteoporosis, respectively, thresholds that were subsequently confirmed for the Chinese population.”
Furthermore, vBMD has been shown in some studies to be more strongly related to fracture risk, compared with DXA aBMD measures.
Importantly, in another recent study involving 9,223 adults, Dr. Pickhardt and colleagues reported that bone and muscle biomarkers derived from CT were comparable to the Fracture Risk Assessment Tool score for the presymptomatic prediction of future osteoporotic fractures.
Dr. Pickhardt is an advisor to Bracco Imaging and Zebra Medical Vision. Dr. Therkildsen has reported no relevant financial relationships.
This article first appeared on Medscape.com.
Low-dose chest CT for lung cancer screening provides the opportunity to simultaneously screen patients for osteoporosis, detecting notably higher rates of osteoporosis in men than the traditional tool of DXA, research published in the Journal of Bone and Mineral Research shows.
“Our large-scale, multicenter study of bone density measured from routine low-dose CT scans demonstrated the great potential of using low-dose CT for the opportunistic screening of osteoporosis as an alternative to standard DXA scans,” said senior author Wei Tian, MD, of the Chinese Academy of Engineering and Peking University, in a press statement from the journal.
“Our study revealed the unexpectedly high prevalence of osteoporosis in men, which may impact on the management strategy of men in the future,” Dr. Tian added.
Josephine Therkildsen, MD, of Herning Hospital, Denmark, who has conducted similar research using cardiac CT scans, said the findings add important new insights into the issue of opportunistic screening.
“The results are highly interesting, as they show that low-dose CT-based opportunistic screening could identify a substantial number of patients with low lumbar bone mineral density (BMD) with the future potential to diagnose osteoporosis and initiate relevant treatment before a fracture occurs,” she told this news organization.
Perry J. Pickhardt, MD, chief of gastrointestinal imaging at the University of Wisconsin School of Medicine and Public Health in Madison, agrees. He said in an interview that CT scans of the chest and abdomen, commonly performed for a variety of clinical indications and widespread in most developed countries, can in fact be essential for the detection of a multitude of other concerns – yet are underused for those other purposes.
Use of CT in this way “would likely be very cost effective and clinically efficacious,” he said, adding: “We are seeing greatly increased interest in leveraging this extra information that is contained within every CT scan.” And, “Importantly, artificial intelligence advances now allow for automated approaches, which should allow for expanded use.”
Lung cancer CT scans shed light on osteoporosis prevalence
In the study, led by Xiaoguang Cheng, MD, PhD, of the department of radiology, Beijing Jishuitan Hospital, China, researchers examined lung cancer CT screening data from the prospective China Biobank Project to determine the prevalence of osteoporosis in China.
This included the thoracic low-dose CT scans of 69,095 adults, including 40,733 men and 28,362 women, taken between 2018 and 2019.
To screen for osteoporosis, they used quantitative CT software to evaluate lumbar spine (L1-L2) trabecular volume BMD (vBMD) and diagnostic criteria from the American College of Radiology. Using the vBMD measures from the CT imaging, they found the prevalence of osteoporosis among those over 50 years of age in the Chinese population to be 29% for women (49 million) and 13.5% for men (22.8 million).
Interestingly, the osteoporosis prevalence rate among women was comparable to estimates in the population derived from DXA (29.1%); however, the rate in men was twice that estimated from DXA scans (6.5%).
Decreases in trabecular vBMD with age were observed in both genders. However, declines were steeper among women, who had higher peak trabecular vBMD (185.4 mg/cm3), compared with men (176.6 mg/cm3) at age 30-34 years, but significantly lower measures (62.4 mg/cm3) than men (92.1 mg/cm3) at age 80 years.
The prevalence of osteoporosis in women increased from 2.8% at age 50-54 years to 79.8% at age 85 or older, while in men, the prevalence was 3.2% at age 50-54 years and 44.1% at age 85 or older.
“This is the first study to establish Chinese reference data for vBMD using opportunistic screening from low-dose chest CT in a large population cohort,” the authors write.
“The opportunistic screening of osteoporosis using low-dose CT is clinically feasible and requires no additional exposure to ionizing radiation.”
In addition, no additional equipment or patient time was required, suggesting that “this approach has potential for opportunistic screening for osteoporosis.”
They note, however, that further cohort studies are needed to assess clinical utility of this method.
CT ‘likely a more accurate measure’ of volumetric BMD
Dr. Pickhardt said the differences in osteoporosis prevalence observed between DXA and CT-derived measures in men likely reflect the greater accuracy of CT.
“DXA is a planar technique with a number of drawbacks,” he said in an interview. “CT provides a more direct volumetric measure and is likely a more accurate method for BMD assessment.”
He speculated that the greater differences between DXA versus CT seen in men than women “may relate to sex differences in cortical bone of vertebral bodies, which cannot be separated from the underlying trabecular bone with DXA (whereas CT directly measures the inner trabecular bone).”
The authors note that, although areal BMD (aBMD) derived from DXA is required for osteoporosis diagnosis according to World Health Organization criteria, “trabecular vBMD derived from CT can be also used for diagnosis based on thresholds published by the American College of Radiology of 120 mg/cm3 and 80 mg/cm3 to define osteopenia and osteoporosis, respectively, thresholds that were subsequently confirmed for the Chinese population.”
Furthermore, vBMD has been shown in some studies to be more strongly related to fracture risk, compared with DXA aBMD measures.
Importantly, in another recent study involving 9,223 adults, Dr. Pickhardt and colleagues reported that bone and muscle biomarkers derived from CT were comparable to the Fracture Risk Assessment Tool score for the presymptomatic prediction of future osteoporotic fractures.
Dr. Pickhardt is an advisor to Bracco Imaging and Zebra Medical Vision. Dr. Therkildsen has reported no relevant financial relationships.
This article first appeared on Medscape.com.
Black patients with ES-SCLC get less chemo but have better survival
Black patients with extensive-stage small cell lung cancer (ES-SCLC) are less likely to receive chemotherapy but have better survival, compared with White patients, according to a study published in JTO Clinical Research and Reports.
This study provides a large-scale analysis of real-world data identifying racial and socioeconomic factors impacting systemic therapy delivery and survival in ES-SCLC.
“The most important finding was the significant disparity in receipt of chemotherapy,” said study author Umit Tapan, MD, of Boston Medical Center.
“Black individuals with ES-SCLC were less likely to receive chemotherapy compared to Whites and other racial groups. Similarly, elderly, uninsured patients, patients with nonprivate health insurance, and those with lower education levels were less likely to be treated with chemotherapy,” Dr. Tapan said.
Using the National Cancer Data Base (NCDB), Dr. Tapan and colleagues identified 148,961 patients who were diagnosed with stage IV ES-SCLC during 2004-2016. In all, 82,592 patients were included in the study.
Results: Treatment and survival
Compared with White patients, Black patients (adjusted odds ratio, 0.85; P = .0004) and patients from other racial groups (aOR, 0.87; P = .126) had lower odds of receiving chemotherapy on multivariate analysis.
However, survival was superior in Black patients (adjusted hazard ratio, 0.92; P < .0001) and other non-White patients (aHR 0.86; P < .0001).
“We speculate that additional factors, such as performance status, which is not captured by NCDB, might have accounted for better survival for Black patients,” Dr. Tapan said, noting that the analysis was adjusted for known possible confounding factors, such as age, gender, and comorbidity status.
Black patients had higher odds of receiving chemotherapy between 2010 and 2016 compared with 2004 and 2009. “This suggests a positive impact of the Patient Protection and Affordable Care Act (ACA) in 2010,” Dr. Tapan said.
Another surprising finding pertained to patients with nonprivate insurance. These patients had even lower odds of getting chemotherapy after the implementation of ACA, Dr. Tapan said. Patients who had private insurance had higher survival compared with those who were uninsured.
Higher level of education, measured by percentage of residents with a high school degree, increased the odds of receiving chemotherapy.
Age also had a significant impact on receipt of chemotherapy. About 83% of patients over age 80 years received chemotherapy, compared with 94% of patients aged 40-64 years.
Real-world data
Minorities are underrepresented in cancer clinical trials in the United States, with only 2% of National Cancer Institute trials having sufficient minority participants, Dr. Tapan said. A study published in Academic Medicine in 2018 showed that only 13% of 782 National Institute of Health–sponsored clinical trials reported outcomes by race and ethnicity.
As a result, we are missing data on patient care in minority populations, Dr. Tapan said. “Collecting and analyzing real-world data becomes critical to study treatment patterns and outcomes,” he added.
The current real-world study had a somewhat diverse patient population, but 90.6% of patients were White, 7.8% were Black, and 1.7% were other races.
“We would have expected a higher percentage of Black patients considering the most recent U.S. Census Bureau estimates that 76.3% of the U.S. population is White and 13.4% is Black,” Dr. Tapan said. “There are conflicting results in the literature regarding racial disparities in SCLC and survival. Many of these studies were performed via state-based cancer registries instead of on a national level, making prior reports less generalizable.”
‘More work to do’
While the new study showed patients with nonprivate insurance or those with no insurance were less likely to receive chemotherapy, studies have shown that chemotherapy administration was not impacted by insurance status in limited-stage SCLC.
This is in contrast to radiotherapy delivery. Studies have revealed a lower likelihood of radiotherapy delivery in limited-stage SCLC for patients with government health insurance such as Medicare/Medicaid, Dr. Tapan said.
“Access to cancer care has been shown to be one of the most important barriers in racial disparity. Studies analyzing outcomes in the equal access health systems, such as the Veteran Administration, have revealed less racial disparities,” Dr. Tapan said.
Even when Black patients have equal access to care, they might receive suboptimal treatment, Dr. Tapan noted.
“Studies have shown that Black patients are not only more likely to refuse surgery, but also are more likely to be given a negative recommendation by a surgeon as compared to Whites, suggesting potential involvement of miscommunication or bias during patient-physician encounters,” Dr. Tapan said. “In the same vein, physicians would need to acknowledge their patients’ beliefs. Not doing so may lead to unsatisfactory physician-patient interactions and suboptimal decision-making.”
“Measures to reduce physician bias are an important step to reduce disparities,” Dr. Tapan continued. “Studies have shown that Black patients are perceived to be less intelligent and educated, less likely to have social support, and more likely to be at risk of noncompliance. For some patients and oncologists, extra effort is needed so that every patient can access the best possible treatments and outcomes. It is the oncologist’s responsibility to advocate for patients, but, ultimately, further legislative actions are needed to mitigate the disparities around cancer care.”
Dr. Tapan noted that, in 1966, Martin Luther King Jr., PhD, stated that “of all the forms of inequality, injustice in health care is the most shocking and inhumane.”
Dr. Tapan said: “We have overcome some barriers since 1966, but we have more work to do.” He and colleagues had no disclosures related to this study.
SOURCE: Tapan U et al. JTO Clin Res Rep. 2020. doi: 10.1016/j.jtocrr.2020.100109.
Black patients with extensive-stage small cell lung cancer (ES-SCLC) are less likely to receive chemotherapy but have better survival, compared with White patients, according to a study published in JTO Clinical Research and Reports.
This study provides a large-scale analysis of real-world data identifying racial and socioeconomic factors impacting systemic therapy delivery and survival in ES-SCLC.
“The most important finding was the significant disparity in receipt of chemotherapy,” said study author Umit Tapan, MD, of Boston Medical Center.
“Black individuals with ES-SCLC were less likely to receive chemotherapy compared to Whites and other racial groups. Similarly, elderly, uninsured patients, patients with nonprivate health insurance, and those with lower education levels were less likely to be treated with chemotherapy,” Dr. Tapan said.
Using the National Cancer Data Base (NCDB), Dr. Tapan and colleagues identified 148,961 patients who were diagnosed with stage IV ES-SCLC during 2004-2016. In all, 82,592 patients were included in the study.
Results: Treatment and survival
Compared with White patients, Black patients (adjusted odds ratio, 0.85; P = .0004) and patients from other racial groups (aOR, 0.87; P = .126) had lower odds of receiving chemotherapy on multivariate analysis.
However, survival was superior in Black patients (adjusted hazard ratio, 0.92; P < .0001) and other non-White patients (aHR 0.86; P < .0001).
“We speculate that additional factors, such as performance status, which is not captured by NCDB, might have accounted for better survival for Black patients,” Dr. Tapan said, noting that the analysis was adjusted for known possible confounding factors, such as age, gender, and comorbidity status.
Black patients had higher odds of receiving chemotherapy between 2010 and 2016 compared with 2004 and 2009. “This suggests a positive impact of the Patient Protection and Affordable Care Act (ACA) in 2010,” Dr. Tapan said.
Another surprising finding pertained to patients with nonprivate insurance. These patients had even lower odds of getting chemotherapy after the implementation of ACA, Dr. Tapan said. Patients who had private insurance had higher survival compared with those who were uninsured.
Higher level of education, measured by percentage of residents with a high school degree, increased the odds of receiving chemotherapy.
Age also had a significant impact on receipt of chemotherapy. About 83% of patients over age 80 years received chemotherapy, compared with 94% of patients aged 40-64 years.
Real-world data
Minorities are underrepresented in cancer clinical trials in the United States, with only 2% of National Cancer Institute trials having sufficient minority participants, Dr. Tapan said. A study published in Academic Medicine in 2018 showed that only 13% of 782 National Institute of Health–sponsored clinical trials reported outcomes by race and ethnicity.
As a result, we are missing data on patient care in minority populations, Dr. Tapan said. “Collecting and analyzing real-world data becomes critical to study treatment patterns and outcomes,” he added.
The current real-world study had a somewhat diverse patient population, but 90.6% of patients were White, 7.8% were Black, and 1.7% were other races.
“We would have expected a higher percentage of Black patients considering the most recent U.S. Census Bureau estimates that 76.3% of the U.S. population is White and 13.4% is Black,” Dr. Tapan said. “There are conflicting results in the literature regarding racial disparities in SCLC and survival. Many of these studies were performed via state-based cancer registries instead of on a national level, making prior reports less generalizable.”
‘More work to do’
While the new study showed patients with nonprivate insurance or those with no insurance were less likely to receive chemotherapy, studies have shown that chemotherapy administration was not impacted by insurance status in limited-stage SCLC.
This is in contrast to radiotherapy delivery. Studies have revealed a lower likelihood of radiotherapy delivery in limited-stage SCLC for patients with government health insurance such as Medicare/Medicaid, Dr. Tapan said.
“Access to cancer care has been shown to be one of the most important barriers in racial disparity. Studies analyzing outcomes in the equal access health systems, such as the Veteran Administration, have revealed less racial disparities,” Dr. Tapan said.
Even when Black patients have equal access to care, they might receive suboptimal treatment, Dr. Tapan noted.
“Studies have shown that Black patients are not only more likely to refuse surgery, but also are more likely to be given a negative recommendation by a surgeon as compared to Whites, suggesting potential involvement of miscommunication or bias during patient-physician encounters,” Dr. Tapan said. “In the same vein, physicians would need to acknowledge their patients’ beliefs. Not doing so may lead to unsatisfactory physician-patient interactions and suboptimal decision-making.”
“Measures to reduce physician bias are an important step to reduce disparities,” Dr. Tapan continued. “Studies have shown that Black patients are perceived to be less intelligent and educated, less likely to have social support, and more likely to be at risk of noncompliance. For some patients and oncologists, extra effort is needed so that every patient can access the best possible treatments and outcomes. It is the oncologist’s responsibility to advocate for patients, but, ultimately, further legislative actions are needed to mitigate the disparities around cancer care.”
Dr. Tapan noted that, in 1966, Martin Luther King Jr., PhD, stated that “of all the forms of inequality, injustice in health care is the most shocking and inhumane.”
Dr. Tapan said: “We have overcome some barriers since 1966, but we have more work to do.” He and colleagues had no disclosures related to this study.
SOURCE: Tapan U et al. JTO Clin Res Rep. 2020. doi: 10.1016/j.jtocrr.2020.100109.
Black patients with extensive-stage small cell lung cancer (ES-SCLC) are less likely to receive chemotherapy but have better survival, compared with White patients, according to a study published in JTO Clinical Research and Reports.
This study provides a large-scale analysis of real-world data identifying racial and socioeconomic factors impacting systemic therapy delivery and survival in ES-SCLC.
“The most important finding was the significant disparity in receipt of chemotherapy,” said study author Umit Tapan, MD, of Boston Medical Center.
“Black individuals with ES-SCLC were less likely to receive chemotherapy compared to Whites and other racial groups. Similarly, elderly, uninsured patients, patients with nonprivate health insurance, and those with lower education levels were less likely to be treated with chemotherapy,” Dr. Tapan said.
Using the National Cancer Data Base (NCDB), Dr. Tapan and colleagues identified 148,961 patients who were diagnosed with stage IV ES-SCLC during 2004-2016. In all, 82,592 patients were included in the study.
Results: Treatment and survival
Compared with White patients, Black patients (adjusted odds ratio, 0.85; P = .0004) and patients from other racial groups (aOR, 0.87; P = .126) had lower odds of receiving chemotherapy on multivariate analysis.
However, survival was superior in Black patients (adjusted hazard ratio, 0.92; P < .0001) and other non-White patients (aHR 0.86; P < .0001).
“We speculate that additional factors, such as performance status, which is not captured by NCDB, might have accounted for better survival for Black patients,” Dr. Tapan said, noting that the analysis was adjusted for known possible confounding factors, such as age, gender, and comorbidity status.
Black patients had higher odds of receiving chemotherapy between 2010 and 2016 compared with 2004 and 2009. “This suggests a positive impact of the Patient Protection and Affordable Care Act (ACA) in 2010,” Dr. Tapan said.
Another surprising finding pertained to patients with nonprivate insurance. These patients had even lower odds of getting chemotherapy after the implementation of ACA, Dr. Tapan said. Patients who had private insurance had higher survival compared with those who were uninsured.
Higher level of education, measured by percentage of residents with a high school degree, increased the odds of receiving chemotherapy.
Age also had a significant impact on receipt of chemotherapy. About 83% of patients over age 80 years received chemotherapy, compared with 94% of patients aged 40-64 years.
Real-world data
Minorities are underrepresented in cancer clinical trials in the United States, with only 2% of National Cancer Institute trials having sufficient minority participants, Dr. Tapan said. A study published in Academic Medicine in 2018 showed that only 13% of 782 National Institute of Health–sponsored clinical trials reported outcomes by race and ethnicity.
As a result, we are missing data on patient care in minority populations, Dr. Tapan said. “Collecting and analyzing real-world data becomes critical to study treatment patterns and outcomes,” he added.
The current real-world study had a somewhat diverse patient population, but 90.6% of patients were White, 7.8% were Black, and 1.7% were other races.
“We would have expected a higher percentage of Black patients considering the most recent U.S. Census Bureau estimates that 76.3% of the U.S. population is White and 13.4% is Black,” Dr. Tapan said. “There are conflicting results in the literature regarding racial disparities in SCLC and survival. Many of these studies were performed via state-based cancer registries instead of on a national level, making prior reports less generalizable.”
‘More work to do’
While the new study showed patients with nonprivate insurance or those with no insurance were less likely to receive chemotherapy, studies have shown that chemotherapy administration was not impacted by insurance status in limited-stage SCLC.
This is in contrast to radiotherapy delivery. Studies have revealed a lower likelihood of radiotherapy delivery in limited-stage SCLC for patients with government health insurance such as Medicare/Medicaid, Dr. Tapan said.
“Access to cancer care has been shown to be one of the most important barriers in racial disparity. Studies analyzing outcomes in the equal access health systems, such as the Veteran Administration, have revealed less racial disparities,” Dr. Tapan said.
Even when Black patients have equal access to care, they might receive suboptimal treatment, Dr. Tapan noted.
“Studies have shown that Black patients are not only more likely to refuse surgery, but also are more likely to be given a negative recommendation by a surgeon as compared to Whites, suggesting potential involvement of miscommunication or bias during patient-physician encounters,” Dr. Tapan said. “In the same vein, physicians would need to acknowledge their patients’ beliefs. Not doing so may lead to unsatisfactory physician-patient interactions and suboptimal decision-making.”
“Measures to reduce physician bias are an important step to reduce disparities,” Dr. Tapan continued. “Studies have shown that Black patients are perceived to be less intelligent and educated, less likely to have social support, and more likely to be at risk of noncompliance. For some patients and oncologists, extra effort is needed so that every patient can access the best possible treatments and outcomes. It is the oncologist’s responsibility to advocate for patients, but, ultimately, further legislative actions are needed to mitigate the disparities around cancer care.”
Dr. Tapan noted that, in 1966, Martin Luther King Jr., PhD, stated that “of all the forms of inequality, injustice in health care is the most shocking and inhumane.”
Dr. Tapan said: “We have overcome some barriers since 1966, but we have more work to do.” He and colleagues had no disclosures related to this study.
SOURCE: Tapan U et al. JTO Clin Res Rep. 2020. doi: 10.1016/j.jtocrr.2020.100109.
FROM JTO CLINICAL AND RESEARCH REPORTS
Immune checkpoint inhibitors don’t increase COVID-19 incidence or mortality, studies suggest
Cytokine storm plays a major role in the pathogenesis of COVID-19, according to research published in The Lancet Respiratory Medicine. This has generated concern about using ICIs during the pandemic, given their immunostimulatory activity and the risk of immune-related adverse effects.
However, two retrospective studies suggest ICIs do not increase the risk of developing COVID-19 or dying from the disease.
In a study of 1,545 cancer patients prescribed ICIs and 20,418 matched controls, the incidence of COVID-19 was 1.4% with ICI therapy and 1.0% without it (odds ratio, 1.38; P = .15).
In a case-control study of 50 patients with cancer and COVID-19, 28% of patients who had received ICIs died from COVID-19, compared with 36% of patients who had not received ICIs (OR, 0.36; P = .23).
Vartan Pahalyants and Kevin Tyan, both students in Harvard University’s joint MD/MBA program in Boston, presented these studies at the meeting.
COVID-19 incidence with ICIs
Mr. Pahalyants and colleagues analyzed data from cancer patients treated in the Mass General Brigham health care system. The researchers compared 1,545 patients with at least one ICI prescription between July 1, 2019, and Feb. 29, 2020, with 20,418 matched cancer patients not prescribed ICIs. The team assessed COVID-19 incidence based on positive test results through June 19, 2020, from public health data.

The incidence of COVID-19 was low in both groups – 1.4% in the ICI group and 1.0% in the matched control group (P = .16). Among COVID-19–positive patients, the all-cause death rate was 40.9% in the ICI group and 28.6% in the control group (P = .23).
In multivariate analysis, patients prescribed ICIs did not have a significantly elevated risk for COVID-19 relative to peers not prescribed ICIs (OR, 1.38; P = .15). However, risk was significantly increased for female patients (OR, 1.74; P < .001), those living in a town or county with higher COVID-19 positivity rate (OR, 1.59; P < .001), and those with severe comorbidity (vs. mild or moderate; OR, 9.77; P = .02).
Among COVID-19–positive patients, those prescribed ICIs did not have a significantly elevated risk for all-cause mortality (OR, 1.60; P = .71), but male sex and lower income were associated with an increased risk of death.
“We did not identify an increased risk of [COVID-19] diagnosis among patients prescribed ICIs compared to the controls,” Mr. Pahalyants said. “This information may assist patients and their providers in decision-making around continuation of therapy during this protracted pandemic. However, more research needs to be conducted to determine potential behavioral and testing factors that may have affected COVID-19 diagnosis susceptibility among patients included in the study.”
COVID-19 mortality with ICIs
For their study, Mr. Tyan and colleagues identified 25 cancer patients who had received ICIs in the year before a COVID-19 diagnosis between March 20, 2020, and June 3, 2020, at the Dana-Farber Cancer Institute and Mass General Brigham network. The researchers then matched each patient with a cancer patient having a COVID-19 diagnosis who had not received ICIs during the preceding year.
Overall, 28% of patients who had received ICIs before their COVID-19 diagnosis died from COVID-19, compared with 36% of those who had not received ICIs.
In multivariate analysis, ICI therapy did not predict COVID-19 mortality (OR, 0.36; P = .23). However, the risk of death from COVID-19 increased with age (OR, 1.14; P = .01) and for patients with chronic obstructive pulmonary disease (OR, 12.26; P = .01), and risk was lower for statin users (OR, 0.08; P = .02). Findings were similar in an analysis restricted to hospitalized patients in the ICI group and their matched controls.
Two ICI-treated patients with COVID-19 had persistent immune-related adverse events (hypophysitis in both cases), and one ICI-treated patient developed a new immune-related adverse event (hypothyroidism).
At COVID-19 presentation, relative to counterparts who had not received ICIs, patients who had received ICIs had higher platelet counts (P = .017) and higher D-dimer levels (P = .037). In the context of similar levels of other biomarkers, this finding is “of unclear significance, as all deaths in the cohort were due to respiratory failure as opposed to hypercoagulability,” Mr. Tyan said.
The patients treated with ICIs were more likely to die from COVID-19 if they had elevated troponin levels (P = .01), whereas no such association was seen for those not treated with ICIs.
“We found that ICI therapy is not associated with greater risk for COVID-19 mortality. Our period of follow-up was relatively short, but we did not observe a high incidence of new or persistent immune-related adverse events among our patients taking ICIs,” Mr. Tyan said.
“While larger prospective trials are needed to evaluate long-term safety in the context of COVID-19 infection, our findings support the continuation of ICI therapy during the pandemic as it does not appear to worsen outcomes for cancer patients,” he concluded.
ICI therapy can continue, with precautions
“The question of susceptibility to COVID-19 has been unclear as ICIs do not necessarily cause immunosuppression but certainly result in modulation of a patient’s immune system,” said Deborah Doroshow, MD, PhD, assistant professor at the Tisch Cancer Institute Icahn School of Medicine at Mount Sinai, New York. She was not involved in these studies.
“The findings of the study by Pahalyants and colleagues, which used a very large sample size, appear to convincingly demonstrate that ICI receipt is not associated with an increased susceptibility to COVID-19,” Dr. Doroshow said in an interview.

However, the findings of the study by Tyan and colleagues are more “thought-provoking,” Dr. Doroshow said. She noted that a large study published in Nature Medicine showed previous ICI therapy in cancer patients with COVID-19 increased the risk for hospitalization or severe COVID-19 requiring high-flow oxygen or mechanical ventilation. The new study was much smaller and did not perform statistical comparisons for outcomes such as oxygen requirements.
“I would feel comfortable telling patients that the data suggests that ICI treatment does not increase their risk of COVID-19. However, if they were to be diagnosed with COVID-19, it is unclear whether their previous ICI treatment increases their risk for poor outcomes,” Dr. Doroshow said.
“I would feel comfortable continuing to treat patients with ICIs at this time, but because we know that patients with cancer are generally more likely to develop COVID-19 and have poor outcomes, it is critical that our patients be educated about social distancing and mask wearing to the extent that their living and working situations permit,” she added.
Mr. Pahalyants disclosed no relevant conflicts of interest, and his study did not receive any specific funding. Mr. Tyan disclosed that he is cofounder and chief science officer of Kinnos, and his study did not receive any specific funding. Dr. Doroshow disclosed no relevant conflicts of interest.
SOURCE: Pahalyants V et al. SITC 2020, Abstract 826. Tyan K et al. SITC 2020, Abstract 481.
Cytokine storm plays a major role in the pathogenesis of COVID-19, according to research published in The Lancet Respiratory Medicine. This has generated concern about using ICIs during the pandemic, given their immunostimulatory activity and the risk of immune-related adverse effects.
However, two retrospective studies suggest ICIs do not increase the risk of developing COVID-19 or dying from the disease.
In a study of 1,545 cancer patients prescribed ICIs and 20,418 matched controls, the incidence of COVID-19 was 1.4% with ICI therapy and 1.0% without it (odds ratio, 1.38; P = .15).
In a case-control study of 50 patients with cancer and COVID-19, 28% of patients who had received ICIs died from COVID-19, compared with 36% of patients who had not received ICIs (OR, 0.36; P = .23).
Vartan Pahalyants and Kevin Tyan, both students in Harvard University’s joint MD/MBA program in Boston, presented these studies at the meeting.
COVID-19 incidence with ICIs
Mr. Pahalyants and colleagues analyzed data from cancer patients treated in the Mass General Brigham health care system. The researchers compared 1,545 patients with at least one ICI prescription between July 1, 2019, and Feb. 29, 2020, with 20,418 matched cancer patients not prescribed ICIs. The team assessed COVID-19 incidence based on positive test results through June 19, 2020, from public health data.
The incidence of COVID-19 was low in both groups – 1.4% in the ICI group and 1.0% in the matched control group (P = .16). Among COVID-19–positive patients, the all-cause death rate was 40.9% in the ICI group and 28.6% in the control group (P = .23).
In multivariate analysis, patients prescribed ICIs did not have a significantly elevated risk for COVID-19 relative to peers not prescribed ICIs (OR, 1.38; P = .15). However, risk was significantly increased for female patients (OR, 1.74; P < .001), those living in a town or county with higher COVID-19 positivity rate (OR, 1.59; P < .001), and those with severe comorbidity (vs. mild or moderate; OR, 9.77; P = .02).
Among COVID-19–positive patients, those prescribed ICIs did not have a significantly elevated risk for all-cause mortality (OR, 1.60; P = .71), but male sex and lower income were associated with an increased risk of death.
“We did not identify an increased risk of [COVID-19] diagnosis among patients prescribed ICIs compared to the controls,” Mr. Pahalyants said. “This information may assist patients and their providers in decision-making around continuation of therapy during this protracted pandemic. However, more research needs to be conducted to determine potential behavioral and testing factors that may have affected COVID-19 diagnosis susceptibility among patients included in the study.”
COVID-19 mortality with ICIs
For their study, Mr. Tyan and colleagues identified 25 cancer patients who had received ICIs in the year before a COVID-19 diagnosis between March 20, 2020, and June 3, 2020, at the Dana-Farber Cancer Institute and Mass General Brigham network. The researchers then matched each patient with a cancer patient having a COVID-19 diagnosis who had not received ICIs during the preceding year.
Overall, 28% of patients who had received ICIs before their COVID-19 diagnosis died from COVID-19, compared with 36% of those who had not received ICIs.
In multivariate analysis, ICI therapy did not predict COVID-19 mortality (OR, 0.36; P = .23). However, the risk of death from COVID-19 increased with age (OR, 1.14; P = .01) and for patients with chronic obstructive pulmonary disease (OR, 12.26; P = .01), and risk was lower for statin users (OR, 0.08; P = .02). Findings were similar in an analysis restricted to hospitalized patients in the ICI group and their matched controls.
Two ICI-treated patients with COVID-19 had persistent immune-related adverse events (hypophysitis in both cases), and one ICI-treated patient developed a new immune-related adverse event (hypothyroidism).
At COVID-19 presentation, relative to counterparts who had not received ICIs, patients who had received ICIs had higher platelet counts (P = .017) and higher D-dimer levels (P = .037). In the context of similar levels of other biomarkers, this finding is “of unclear significance, as all deaths in the cohort were due to respiratory failure as opposed to hypercoagulability,” Mr. Tyan said.
The patients treated with ICIs were more likely to die from COVID-19 if they had elevated troponin levels (P = .01), whereas no such association was seen for those not treated with ICIs.
“We found that ICI therapy is not associated with greater risk for COVID-19 mortality. Our period of follow-up was relatively short, but we did not observe a high incidence of new or persistent immune-related adverse events among our patients taking ICIs,” Mr. Tyan said.
“While larger prospective trials are needed to evaluate long-term safety in the context of COVID-19 infection, our findings support the continuation of ICI therapy during the pandemic as it does not appear to worsen outcomes for cancer patients,” he concluded.
ICI therapy can continue, with precautions
“The question of susceptibility to COVID-19 has been unclear as ICIs do not necessarily cause immunosuppression but certainly result in modulation of a patient’s immune system,” said Deborah Doroshow, MD, PhD, assistant professor at the Tisch Cancer Institute Icahn School of Medicine at Mount Sinai, New York. She was not involved in these studies.
“The findings of the study by Pahalyants and colleagues, which used a very large sample size, appear to convincingly demonstrate that ICI receipt is not associated with an increased susceptibility to COVID-19,” Dr. Doroshow said in an interview.
However, the findings of the study by Tyan and colleagues are more “thought-provoking,” Dr. Doroshow said. She noted that a large study published in Nature Medicine showed previous ICI therapy in cancer patients with COVID-19 increased the risk for hospitalization or severe COVID-19 requiring high-flow oxygen or mechanical ventilation. The new study was much smaller and did not perform statistical comparisons for outcomes such as oxygen requirements.
“I would feel comfortable telling patients that the data suggests that ICI treatment does not increase their risk of COVID-19. However, if they were to be diagnosed with COVID-19, it is unclear whether their previous ICI treatment increases their risk for poor outcomes,” Dr. Doroshow said.
“I would feel comfortable continuing to treat patients with ICIs at this time, but because we know that patients with cancer are generally more likely to develop COVID-19 and have poor outcomes, it is critical that our patients be educated about social distancing and mask wearing to the extent that their living and working situations permit,” she added.
Mr. Pahalyants disclosed no relevant conflicts of interest, and his study did not receive any specific funding. Mr. Tyan disclosed that he is cofounder and chief science officer of Kinnos, and his study did not receive any specific funding. Dr. Doroshow disclosed no relevant conflicts of interest.
SOURCE: Pahalyants V et al. SITC 2020, Abstract 826. Tyan K et al. SITC 2020, Abstract 481.
Cytokine storm plays a major role in the pathogenesis of COVID-19, according to research published in The Lancet Respiratory Medicine. This has generated concern about using ICIs during the pandemic, given their immunostimulatory activity and the risk of immune-related adverse effects.
However, two retrospective studies suggest ICIs do not increase the risk of developing COVID-19 or dying from the disease.
In a study of 1,545 cancer patients prescribed ICIs and 20,418 matched controls, the incidence of COVID-19 was 1.4% with ICI therapy and 1.0% without it (odds ratio, 1.38; P = .15).
In a case-control study of 50 patients with cancer and COVID-19, 28% of patients who had received ICIs died from COVID-19, compared with 36% of patients who had not received ICIs (OR, 0.36; P = .23).
Vartan Pahalyants and Kevin Tyan, both students in Harvard University’s joint MD/MBA program in Boston, presented these studies at the meeting.
COVID-19 incidence with ICIs
Mr. Pahalyants and colleagues analyzed data from cancer patients treated in the Mass General Brigham health care system. The researchers compared 1,545 patients with at least one ICI prescription between July 1, 2019, and Feb. 29, 2020, with 20,418 matched cancer patients not prescribed ICIs. The team assessed COVID-19 incidence based on positive test results through June 19, 2020, from public health data.
The incidence of COVID-19 was low in both groups – 1.4% in the ICI group and 1.0% in the matched control group (P = .16). Among COVID-19–positive patients, the all-cause death rate was 40.9% in the ICI group and 28.6% in the control group (P = .23).
In multivariate analysis, patients prescribed ICIs did not have a significantly elevated risk for COVID-19 relative to peers not prescribed ICIs (OR, 1.38; P = .15). However, risk was significantly increased for female patients (OR, 1.74; P < .001), those living in a town or county with higher COVID-19 positivity rate (OR, 1.59; P < .001), and those with severe comorbidity (vs. mild or moderate; OR, 9.77; P = .02).
Among COVID-19–positive patients, those prescribed ICIs did not have a significantly elevated risk for all-cause mortality (OR, 1.60; P = .71), but male sex and lower income were associated with an increased risk of death.
“We did not identify an increased risk of [COVID-19] diagnosis among patients prescribed ICIs compared to the controls,” Mr. Pahalyants said. “This information may assist patients and their providers in decision-making around continuation of therapy during this protracted pandemic. However, more research needs to be conducted to determine potential behavioral and testing factors that may have affected COVID-19 diagnosis susceptibility among patients included in the study.”
COVID-19 mortality with ICIs
For their study, Mr. Tyan and colleagues identified 25 cancer patients who had received ICIs in the year before a COVID-19 diagnosis between March 20, 2020, and June 3, 2020, at the Dana-Farber Cancer Institute and Mass General Brigham network. The researchers then matched each patient with a cancer patient having a COVID-19 diagnosis who had not received ICIs during the preceding year.
Overall, 28% of patients who had received ICIs before their COVID-19 diagnosis died from COVID-19, compared with 36% of those who had not received ICIs.
In multivariate analysis, ICI therapy did not predict COVID-19 mortality (OR, 0.36; P = .23). However, the risk of death from COVID-19 increased with age (OR, 1.14; P = .01) and for patients with chronic obstructive pulmonary disease (OR, 12.26; P = .01), and risk was lower for statin users (OR, 0.08; P = .02). Findings were similar in an analysis restricted to hospitalized patients in the ICI group and their matched controls.
Two ICI-treated patients with COVID-19 had persistent immune-related adverse events (hypophysitis in both cases), and one ICI-treated patient developed a new immune-related adverse event (hypothyroidism).
At COVID-19 presentation, relative to counterparts who had not received ICIs, patients who had received ICIs had higher platelet counts (P = .017) and higher D-dimer levels (P = .037). In the context of similar levels of other biomarkers, this finding is “of unclear significance, as all deaths in the cohort were due to respiratory failure as opposed to hypercoagulability,” Mr. Tyan said.
The patients treated with ICIs were more likely to die from COVID-19 if they had elevated troponin levels (P = .01), whereas no such association was seen for those not treated with ICIs.
“We found that ICI therapy is not associated with greater risk for COVID-19 mortality. Our period of follow-up was relatively short, but we did not observe a high incidence of new or persistent immune-related adverse events among our patients taking ICIs,” Mr. Tyan said.
“While larger prospective trials are needed to evaluate long-term safety in the context of COVID-19 infection, our findings support the continuation of ICI therapy during the pandemic as it does not appear to worsen outcomes for cancer patients,” he concluded.
ICI therapy can continue, with precautions
“The question of susceptibility to COVID-19 has been unclear as ICIs do not necessarily cause immunosuppression but certainly result in modulation of a patient’s immune system,” said Deborah Doroshow, MD, PhD, assistant professor at the Tisch Cancer Institute Icahn School of Medicine at Mount Sinai, New York. She was not involved in these studies.
“The findings of the study by Pahalyants and colleagues, which used a very large sample size, appear to convincingly demonstrate that ICI receipt is not associated with an increased susceptibility to COVID-19,” Dr. Doroshow said in an interview.
However, the findings of the study by Tyan and colleagues are more “thought-provoking,” Dr. Doroshow said. She noted that a large study published in Nature Medicine showed previous ICI therapy in cancer patients with COVID-19 increased the risk for hospitalization or severe COVID-19 requiring high-flow oxygen or mechanical ventilation. The new study was much smaller and did not perform statistical comparisons for outcomes such as oxygen requirements.
“I would feel comfortable telling patients that the data suggests that ICI treatment does not increase their risk of COVID-19. However, if they were to be diagnosed with COVID-19, it is unclear whether their previous ICI treatment increases their risk for poor outcomes,” Dr. Doroshow said.
“I would feel comfortable continuing to treat patients with ICIs at this time, but because we know that patients with cancer are generally more likely to develop COVID-19 and have poor outcomes, it is critical that our patients be educated about social distancing and mask wearing to the extent that their living and working situations permit,” she added.
Mr. Pahalyants disclosed no relevant conflicts of interest, and his study did not receive any specific funding. Mr. Tyan disclosed that he is cofounder and chief science officer of Kinnos, and his study did not receive any specific funding. Dr. Doroshow disclosed no relevant conflicts of interest.
SOURCE: Pahalyants V et al. SITC 2020, Abstract 826. Tyan K et al. SITC 2020, Abstract 481.
FROM SITC 2020
Reduced cancer mortality with Medicaid expansion
Researchers reviewed data on 523,802 patients in the National Cancer Database who were diagnosed with cancer from 2012 through 2015. Slightly more than half of patients (55.2%) lived in Medicaid expansion states.
After expansion, mortality significantly decreased in expansion states (hazard ratio, 0.98; P = .008) but not in nonexpansion states (HR, 1.01; P = .43). The difference was significant in a difference-in-difference analysis (HR, 1.03; P = .01).
Across 69,000 patients with newly diagnosed cancer in Medicaid expansion states, the 2% decrease in the hazard of death would translate to 1,384 lives saved annually.
The benefit was primarily observed in patients with nonmetastatic cancer. For patients with stage I-III cancer, the risk of death was increased in nonexpansion states (HR, 1.05; P < .001) and unchanged in expansion states (HR, 0.99; P = .64). Mortality significantly improved in expansion states vs. nonexpansion states (HR, 1.05; P = .003).
For patients with stage IV cancer, both expansion and nonexpansion states had improvements in mortality, but the differences were not significant.
“Earlier stage at diagnosis appears to explain the mortality improvement,” wrote study author Miranda Lam, MD, of Harvard Medical School, Boston, and colleagues.
Clinical benefits, ‘no economic downside’
Under the Affordable Care Act, passed in 2010, states have the option of expanding Medicaid eligibility to adults with incomes at or below 138% of the federal poverty level. As of March 2020, 36 states and the District of Columbia had expanded Medicaid, with more than 20 million residents obtaining coverage.
Previous studies have associated Medicaid expansion with fewer patients being uninsured, increased cancer screening, and earlier stage of diagnosis, as well as reduced racial disparities in access to high-volume hospitals for cancer surgery and increased rates of cancer surgery among low-income patients.
“This study adds to an increasingly large body of research finding that Medicaid expansion has improved our ability to fight cancer,” said Coleman Drake, PhD, of the University of Pittsburgh, who was not involved in this study.
“Obtaining health insurance through Medicaid allows patients to receive recommended preventive cancer screenings, which explains the increase in early-stage diagnosis rates. Detecting cancer early is critical for successful cancer treatment,” Dr. Drake noted.
“It is hard to overstate the positive effects of Medicaid expansion on health outcomes. At the same time, concerns that Medicaid expansion would be costly to state governments’ budgets have not been realized. In short, Medicaid expansion yields many benefits and has no economic downside for state policymakers. Clinical and economic evidence make an overwhelming case for states to expand Medicaid,” Dr. Drake said.
Significant difference for lung cancer
Most patients in this study were women (73.6%), and the patients’ mean age was 54.8 years (range, 40-64 years). Patients had newly diagnosed breast cancer (52.2%), colorectal cancer (21.3%), and lung cancer (26.5%).
The benefits of Medicaid expansion persisted after adjustment for education, income, insurance, and race.
The lower mortality in expansion states compared with nonexpansion states was similar across all three cancer types. However, in stratified analyses, the difference was significant only for lung cancer (P = .03).
“Lung cancer has a higher mortality rate than breast and colorectal cancer, and with longer follow-up, it is possible that the lower mortality rates seen for breast and colorectal cancer may also become significant,” the authors wrote.
This research was funded by Harvard Catalyst, the Harvard Clinical and Translational Science Center, and the National Center for Advancing Translational Sciences at the National Institutes of Health. The investigators and Dr. Drake had no relevant disclosures.
SOURCE: Lam MB et al. JAMA Netw Open. 2020 Nov 2;3(11):e2024366.
Researchers reviewed data on 523,802 patients in the National Cancer Database who were diagnosed with cancer from 2012 through 2015. Slightly more than half of patients (55.2%) lived in Medicaid expansion states.
After expansion, mortality significantly decreased in expansion states (hazard ratio, 0.98; P = .008) but not in nonexpansion states (HR, 1.01; P = .43). The difference was significant in a difference-in-difference analysis (HR, 1.03; P = .01).
Across 69,000 patients with newly diagnosed cancer in Medicaid expansion states, the 2% decrease in the hazard of death would translate to 1,384 lives saved annually.
The benefit was primarily observed in patients with nonmetastatic cancer. For patients with stage I-III cancer, the risk of death was increased in nonexpansion states (HR, 1.05; P < .001) and unchanged in expansion states (HR, 0.99; P = .64). Mortality significantly improved in expansion states vs. nonexpansion states (HR, 1.05; P = .003).
For patients with stage IV cancer, both expansion and nonexpansion states had improvements in mortality, but the differences were not significant.
“Earlier stage at diagnosis appears to explain the mortality improvement,” wrote study author Miranda Lam, MD, of Harvard Medical School, Boston, and colleagues.
Clinical benefits, ‘no economic downside’
Under the Affordable Care Act, passed in 2010, states have the option of expanding Medicaid eligibility to adults with incomes at or below 138% of the federal poverty level. As of March 2020, 36 states and the District of Columbia had expanded Medicaid, with more than 20 million residents obtaining coverage.
Previous studies have associated Medicaid expansion with fewer patients being uninsured, increased cancer screening, and earlier stage of diagnosis, as well as reduced racial disparities in access to high-volume hospitals for cancer surgery and increased rates of cancer surgery among low-income patients.
“This study adds to an increasingly large body of research finding that Medicaid expansion has improved our ability to fight cancer,” said Coleman Drake, PhD, of the University of Pittsburgh, who was not involved in this study.
“Obtaining health insurance through Medicaid allows patients to receive recommended preventive cancer screenings, which explains the increase in early-stage diagnosis rates. Detecting cancer early is critical for successful cancer treatment,” Dr. Drake noted.
“It is hard to overstate the positive effects of Medicaid expansion on health outcomes. At the same time, concerns that Medicaid expansion would be costly to state governments’ budgets have not been realized. In short, Medicaid expansion yields many benefits and has no economic downside for state policymakers. Clinical and economic evidence make an overwhelming case for states to expand Medicaid,” Dr. Drake said.
Significant difference for lung cancer
Most patients in this study were women (73.6%), and the patients’ mean age was 54.8 years (range, 40-64 years). Patients had newly diagnosed breast cancer (52.2%), colorectal cancer (21.3%), and lung cancer (26.5%).
The benefits of Medicaid expansion persisted after adjustment for education, income, insurance, and race.
The lower mortality in expansion states compared with nonexpansion states was similar across all three cancer types. However, in stratified analyses, the difference was significant only for lung cancer (P = .03).
“Lung cancer has a higher mortality rate than breast and colorectal cancer, and with longer follow-up, it is possible that the lower mortality rates seen for breast and colorectal cancer may also become significant,” the authors wrote.
This research was funded by Harvard Catalyst, the Harvard Clinical and Translational Science Center, and the National Center for Advancing Translational Sciences at the National Institutes of Health. The investigators and Dr. Drake had no relevant disclosures.
SOURCE: Lam MB et al. JAMA Netw Open. 2020 Nov 2;3(11):e2024366.
Researchers reviewed data on 523,802 patients in the National Cancer Database who were diagnosed with cancer from 2012 through 2015. Slightly more than half of patients (55.2%) lived in Medicaid expansion states.
After expansion, mortality significantly decreased in expansion states (hazard ratio, 0.98; P = .008) but not in nonexpansion states (HR, 1.01; P = .43). The difference was significant in a difference-in-difference analysis (HR, 1.03; P = .01).
Across 69,000 patients with newly diagnosed cancer in Medicaid expansion states, the 2% decrease in the hazard of death would translate to 1,384 lives saved annually.
The benefit was primarily observed in patients with nonmetastatic cancer. For patients with stage I-III cancer, the risk of death was increased in nonexpansion states (HR, 1.05; P < .001) and unchanged in expansion states (HR, 0.99; P = .64). Mortality significantly improved in expansion states vs. nonexpansion states (HR, 1.05; P = .003).
For patients with stage IV cancer, both expansion and nonexpansion states had improvements in mortality, but the differences were not significant.
“Earlier stage at diagnosis appears to explain the mortality improvement,” wrote study author Miranda Lam, MD, of Harvard Medical School, Boston, and colleagues.
Clinical benefits, ‘no economic downside’
Under the Affordable Care Act, passed in 2010, states have the option of expanding Medicaid eligibility to adults with incomes at or below 138% of the federal poverty level. As of March 2020, 36 states and the District of Columbia had expanded Medicaid, with more than 20 million residents obtaining coverage.
Previous studies have associated Medicaid expansion with fewer patients being uninsured, increased cancer screening, and earlier stage of diagnosis, as well as reduced racial disparities in access to high-volume hospitals for cancer surgery and increased rates of cancer surgery among low-income patients.
“This study adds to an increasingly large body of research finding that Medicaid expansion has improved our ability to fight cancer,” said Coleman Drake, PhD, of the University of Pittsburgh, who was not involved in this study.
“Obtaining health insurance through Medicaid allows patients to receive recommended preventive cancer screenings, which explains the increase in early-stage diagnosis rates. Detecting cancer early is critical for successful cancer treatment,” Dr. Drake noted.
“It is hard to overstate the positive effects of Medicaid expansion on health outcomes. At the same time, concerns that Medicaid expansion would be costly to state governments’ budgets have not been realized. In short, Medicaid expansion yields many benefits and has no economic downside for state policymakers. Clinical and economic evidence make an overwhelming case for states to expand Medicaid,” Dr. Drake said.
Significant difference for lung cancer
Most patients in this study were women (73.6%), and the patients’ mean age was 54.8 years (range, 40-64 years). Patients had newly diagnosed breast cancer (52.2%), colorectal cancer (21.3%), and lung cancer (26.5%).
The benefits of Medicaid expansion persisted after adjustment for education, income, insurance, and race.
The lower mortality in expansion states compared with nonexpansion states was similar across all three cancer types. However, in stratified analyses, the difference was significant only for lung cancer (P = .03).
“Lung cancer has a higher mortality rate than breast and colorectal cancer, and with longer follow-up, it is possible that the lower mortality rates seen for breast and colorectal cancer may also become significant,” the authors wrote.
This research was funded by Harvard Catalyst, the Harvard Clinical and Translational Science Center, and the National Center for Advancing Translational Sciences at the National Institutes of Health. The investigators and Dr. Drake had no relevant disclosures.
SOURCE: Lam MB et al. JAMA Netw Open. 2020 Nov 2;3(11):e2024366.
FROM JAMA OPEN NETWORK
50.6 million tobacco users are not a homogeneous group
Cigarettes are still the product of choice among U.S. adults who use tobacco, but the youngest adults are more likely to use e-cigarettes than any other product, according to data from the 2019 National Health Interview Survey.
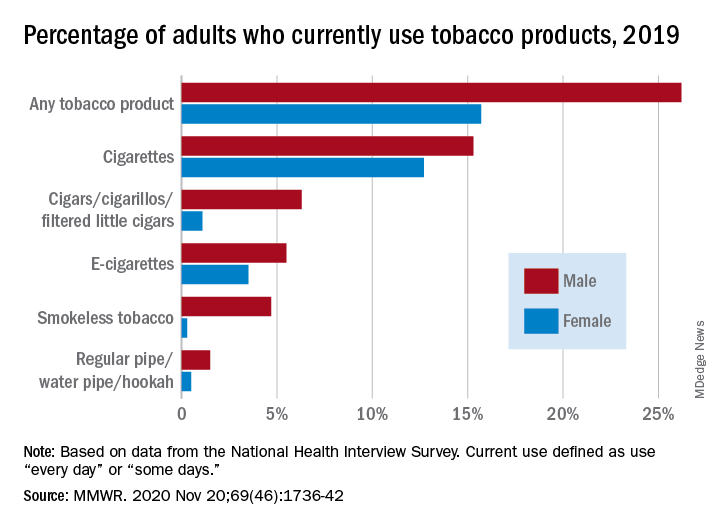
with cigarette use reported by the largest share of respondents (14.0%) and e-cigarettes next at 4.5%, Monica E. Cornelius, PhD, and associates said in the Morbidity and Mortality Weekly Report.
Among adults aged 18-24 years, however, e-cigarettes were used by 9.3% of respondents in 2019, compared with 8.0% who used cigarettes every day or some days. Current e-cigarette use was 6.4% in 25- to 44-year-olds and continued to diminish with increasing age, said Dr. Cornelius and associates at the Centers for Disease Control and Prevention’s National Center for Chronic Disease Prevention and Health Promotion.
Men were more likely than women to use e-cigarettes (5.5% vs. 3.5%), and to use any tobacco product (26.2% vs. 15.7%). Use of other products, including cigarettes (15.3% for men vs. 12.7% for women), followed the same pattern to varying degrees, the national survey data show.
“Differences in prevalence of tobacco use also were also seen across population groups, with higher prevalence among those with a [high school equivalency degree], American Indian/Alaska Natives, uninsured adults and adults with Medicaid, and [lesbian, gay, or bisexual] adults,” the investigators said.
Among those groups, overall tobacco use and cigarette use were highest in those with an equivalency degree (43.8%, 37.1%), while lesbian/gay/bisexual individuals had the highest prevalence of e-cigarette use at 11.5%, they reported.
“As part of a comprehensive approach” to reduce tobacco-related disease and death, Dr. Cornelius and associates suggested, “targeted interventions are also warranted to reach subpopulations with the highest prevalence of use, which might vary by tobacco product type.”
SOURCE: Cornelius ME et al. MMWR. 2020 Nov 20;69(46);1736-42.
Cigarettes are still the product of choice among U.S. adults who use tobacco, but the youngest adults are more likely to use e-cigarettes than any other product, according to data from the 2019 National Health Interview Survey.
with cigarette use reported by the largest share of respondents (14.0%) and e-cigarettes next at 4.5%, Monica E. Cornelius, PhD, and associates said in the Morbidity and Mortality Weekly Report.
Among adults aged 18-24 years, however, e-cigarettes were used by 9.3% of respondents in 2019, compared with 8.0% who used cigarettes every day or some days. Current e-cigarette use was 6.4% in 25- to 44-year-olds and continued to diminish with increasing age, said Dr. Cornelius and associates at the Centers for Disease Control and Prevention’s National Center for Chronic Disease Prevention and Health Promotion.
Men were more likely than women to use e-cigarettes (5.5% vs. 3.5%), and to use any tobacco product (26.2% vs. 15.7%). Use of other products, including cigarettes (15.3% for men vs. 12.7% for women), followed the same pattern to varying degrees, the national survey data show.
“Differences in prevalence of tobacco use also were also seen across population groups, with higher prevalence among those with a [high school equivalency degree], American Indian/Alaska Natives, uninsured adults and adults with Medicaid, and [lesbian, gay, or bisexual] adults,” the investigators said.
Among those groups, overall tobacco use and cigarette use were highest in those with an equivalency degree (43.8%, 37.1%), while lesbian/gay/bisexual individuals had the highest prevalence of e-cigarette use at 11.5%, they reported.
“As part of a comprehensive approach” to reduce tobacco-related disease and death, Dr. Cornelius and associates suggested, “targeted interventions are also warranted to reach subpopulations with the highest prevalence of use, which might vary by tobacco product type.”
SOURCE: Cornelius ME et al. MMWR. 2020 Nov 20;69(46);1736-42.
Cigarettes are still the product of choice among U.S. adults who use tobacco, but the youngest adults are more likely to use e-cigarettes than any other product, according to data from the 2019 National Health Interview Survey.
with cigarette use reported by the largest share of respondents (14.0%) and e-cigarettes next at 4.5%, Monica E. Cornelius, PhD, and associates said in the Morbidity and Mortality Weekly Report.
Among adults aged 18-24 years, however, e-cigarettes were used by 9.3% of respondents in 2019, compared with 8.0% who used cigarettes every day or some days. Current e-cigarette use was 6.4% in 25- to 44-year-olds and continued to diminish with increasing age, said Dr. Cornelius and associates at the Centers for Disease Control and Prevention’s National Center for Chronic Disease Prevention and Health Promotion.
Men were more likely than women to use e-cigarettes (5.5% vs. 3.5%), and to use any tobacco product (26.2% vs. 15.7%). Use of other products, including cigarettes (15.3% for men vs. 12.7% for women), followed the same pattern to varying degrees, the national survey data show.
“Differences in prevalence of tobacco use also were also seen across population groups, with higher prevalence among those with a [high school equivalency degree], American Indian/Alaska Natives, uninsured adults and adults with Medicaid, and [lesbian, gay, or bisexual] adults,” the investigators said.
Among those groups, overall tobacco use and cigarette use were highest in those with an equivalency degree (43.8%, 37.1%), while lesbian/gay/bisexual individuals had the highest prevalence of e-cigarette use at 11.5%, they reported.
“As part of a comprehensive approach” to reduce tobacco-related disease and death, Dr. Cornelius and associates suggested, “targeted interventions are also warranted to reach subpopulations with the highest prevalence of use, which might vary by tobacco product type.”
SOURCE: Cornelius ME et al. MMWR. 2020 Nov 20;69(46);1736-42.
FROM MMWR
New findings on ‘exceptional responders’ to cancer therapies
An ongoing research project is studying why some patients have exceptional responses. The researchers have found particular molecular features in the tumors of about a quarter of these patients. In some cases, there are multiple rare genetic changes in the tumor genome. In other cases, the tumors are infiltrated with certain types of immune cells.
The findings were published online November 19 in Cancer Cell. They come from a genomic analysis of tumor biopsy specimens from 111 patients who were identified by the National Cancer Institute’s (NCI’s) Exceptional Responders Initiative, a national project launched in 2014.
An exceptional responder is defined as an individual who achieves a partial or complete response to a treatment that would be effective in fewer than 10% of similar patients. For exceptional response, the duration of response is at least three times longer than the usual median response time.
In this study of 111 such patients, about one quarter (24%, n = 26 patients) were found to have tumors in which there were molecular features that could potentially explain exceptional responses to treatment.
“We won’t be able to identify, in every patient, which particular drugs will be beneficial,” said Louis Staudt, MD, PhD, director of the NCI’s Center for Cancer Genomics, who co-led the study. “We are nowhere near that. But what it does say is that we have identified particular mutations, some of which we knew about in some types of cancer but can also occur less commonly in other cancer types.”
Staudt noted that these mutations can “illuminate” the path that the cancer will take — and potentially can be used to predict whether the cancer will be aggressive and will require treatment or could be managed with surveillance. This is why this research can be useful in the short term, he said.
“In the longer term, this is the kind of research that inspires future work,” he told Medscape Medical News. “That would encompass clinical trials involving drugs that target some of the pathways we found to be genetically inactivated in some of these responders.”
These results support the use of genetic testing in routine clinical care, he said.
Earlier this year, the NCI team published the results of a pilot study that affirmed the feasibility of this approach. Of the more than 100 cases that were analyzed, six were identified as involving potentially clinically actionable germline mutations.
‘Curiosity drove the research’
“We had these wonderful and gratifying experiences with our patients, so we were immediately curious how that happened, so it was pretty much that curiosity that drove a lot of this work,” said Staudt.
In the current study, Staudt and colleagues used multiple genomic methodologies to detect mutations, copy number changes, aberrant methylation, outlier gene expression, and the cellular makeup of the tumor microenvironment.
The hypothesized mechanisms for exceptional responses were broadly divided into the following four categories: DNA damage response (n = 15), intracellular signaling pathway (n = 9), prognostic genetics (n = 9), and immunologic engagement (n = 16). For many patients, two or more of these mechanisms were involved.
The authors note that the “predominance of plausible DNA damage response mechanisms parallels the frequent use of cytotoxic chemotherapy in routine cancer treatment reflected in this cohort.”
Twenty-six patients were identified as exceptional responders. Among these patients, a variety of cancer types was represented: brain (8); gastrointestinal tract (6); breast (4); cholangiocarcinoma (2); lung (2); pancreas, endometrium, ovarian, and bladder (1 each). Many of these patients (65%, n = 17) were treated with chemotherapy that included DNA-damaging agents. For more than half (54%, n = 14), targeted therapies were used, and some patients received both.
The authors highlight several patients as examples of exceptional responders:
- One patient with glioblastoma multiforme (GBM) was treated sequentially with surgery, localized carmustine, and radiotherapy. When the cancer recurred, temozolomide was administered. This induced a complete response that has lasted for more than a decade.
- A patient with metastatic colon adenocarcinoma has had an ongoing and nearly complete response that has lasted 45 months (last follow-up) after receiving temozolomide in combination with the investigational drug TRC102 (methoxyamine, under development by Tracon) in a phase 1 clinical trial. TRC102 is an inhibitor of the DNA base excision repair pathway, which is a pathway that causes resistance to alkylating and antimetabolite chemotherapeutics.
- A patient with metastatic, estrogen receptor–positive breast cancer received trastuzumab because of a high-level ERBB2 amplification, together with anastrozole. This resulted in an ongoing 2.4-year partial response.
- Although the patient was clinically HER2 positive, her tumor had exceedingly low expression of ERBB2 mRNA. Molecular profiling had classified the tumor as of the basal-like subtype rather than the HER2-enriched subtype. This meant that it was unlikely that trastuzumab contributed to the exceptional response, the authors note. Because the patient was estrogen-receptor positive, she received anastrozole, an inhibitor of aromatase (CYP19A), which converts testosterone into estradiol.
- A patient who had a gastrointestinal stromal tumor with a deletion of KIT exon 11 experienced relapse after an initial response to imatinib, which targets KIT and other tyrosine kinases, but then achieved a complete response with sunitinib. Gene expression profiling revealed high expression not only of KIT but also of genes encoding several tyrosine kinases that are targeted by sunitinib (KDR, FLT1, and FLT3). This may have accounted for the patient’s response.
Favorable genomic characteristics
The authors defined a “prognostic genetics” category of tumors, characterized by genetic lesions that are now known to be associated with a favorable prognosis but that were not addressed through routine care that these patients received when they were first diagnosed. Although the patients experienced relapse after first-line treatment, their exceptional survival after salvage therapy could be linked to favorable genomic characteristics.
For example, several of the patients with high-grade GBMs and astrocytomas had genetic lesions that are generally more common in low-grade glioma and that have been associated with an indolent clinical course following standard therapy.
The authors also assessed immune response. Examining immune cell infiltration in responder tumors in comparison with control cases, the team found that signatures of B cells and activated (CD56dim) natural killer cells were higher in exceptional-responder tumors.
In one patient with metastatic urothelial cancer who experienced disease progression after chemotherapy, radiotherapy, and surgery, treatment with nivolumab produced a complete response that lasted 7 months. Such an outcome occurs in only about 3% of bladder cancer patients. The tumor expressed high mRNA levels of PDCD1, which encodes the nivolumab target PD-1, and CD274, which encodes the PD-1 ligand PD-L1. There was also a high level of amplification of IFNG, which encodes interferon-gamma, a cytokine that has been linked to favorable response to immune checkpoint blockade.
Moving to precision medicine
“It is very valuable to be tested up front and again when the disease progresses, because there may have been some genetic changes, and this may change the treatment,” said co–lead author S. Percy Ivy, MD, of the NCI’s Division of Cancer Treatment and Diagnosis.
“The goal of this study was to understand what was unique about these patients and their genetic makeup that led them to be classified as exceptional responders, and hopefully we will be able to tease that out,” she added.
“As researchers, we have a lot to learn from these patients, and they have a lot to teach us,” she added. “In the future, they will help us as we move closer to the goal of delivering precision oncology to all of our patients. We’re not there yet, but every time we study more deeply and learn more, we are able to provide better care.”
To encourage participation in this effort by investigators around the world, the NCI team and their colleagues have made their molecular profiling results and clinical information publicly available in the NCI Genomic Data Commons.
The study was supported by the NCI’s Intramural Research Program, the National Institutes of Health, the Center for Cancer Research, and the NCI’s Center for Cancer Genomics. Staudt and Ivy have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
An ongoing research project is studying why some patients have exceptional responses. The researchers have found particular molecular features in the tumors of about a quarter of these patients. In some cases, there are multiple rare genetic changes in the tumor genome. In other cases, the tumors are infiltrated with certain types of immune cells.
The findings were published online November 19 in Cancer Cell. They come from a genomic analysis of tumor biopsy specimens from 111 patients who were identified by the National Cancer Institute’s (NCI’s) Exceptional Responders Initiative, a national project launched in 2014.
An exceptional responder is defined as an individual who achieves a partial or complete response to a treatment that would be effective in fewer than 10% of similar patients. For exceptional response, the duration of response is at least three times longer than the usual median response time.
In this study of 111 such patients, about one quarter (24%, n = 26 patients) were found to have tumors in which there were molecular features that could potentially explain exceptional responses to treatment.
“We won’t be able to identify, in every patient, which particular drugs will be beneficial,” said Louis Staudt, MD, PhD, director of the NCI’s Center for Cancer Genomics, who co-led the study. “We are nowhere near that. But what it does say is that we have identified particular mutations, some of which we knew about in some types of cancer but can also occur less commonly in other cancer types.”
Staudt noted that these mutations can “illuminate” the path that the cancer will take — and potentially can be used to predict whether the cancer will be aggressive and will require treatment or could be managed with surveillance. This is why this research can be useful in the short term, he said.
“In the longer term, this is the kind of research that inspires future work,” he told Medscape Medical News. “That would encompass clinical trials involving drugs that target some of the pathways we found to be genetically inactivated in some of these responders.”
These results support the use of genetic testing in routine clinical care, he said.
Earlier this year, the NCI team published the results of a pilot study that affirmed the feasibility of this approach. Of the more than 100 cases that were analyzed, six were identified as involving potentially clinically actionable germline mutations.
‘Curiosity drove the research’
“We had these wonderful and gratifying experiences with our patients, so we were immediately curious how that happened, so it was pretty much that curiosity that drove a lot of this work,” said Staudt.
In the current study, Staudt and colleagues used multiple genomic methodologies to detect mutations, copy number changes, aberrant methylation, outlier gene expression, and the cellular makeup of the tumor microenvironment.
The hypothesized mechanisms for exceptional responses were broadly divided into the following four categories: DNA damage response (n = 15), intracellular signaling pathway (n = 9), prognostic genetics (n = 9), and immunologic engagement (n = 16). For many patients, two or more of these mechanisms were involved.
The authors note that the “predominance of plausible DNA damage response mechanisms parallels the frequent use of cytotoxic chemotherapy in routine cancer treatment reflected in this cohort.”
Twenty-six patients were identified as exceptional responders. Among these patients, a variety of cancer types was represented: brain (8); gastrointestinal tract (6); breast (4); cholangiocarcinoma (2); lung (2); pancreas, endometrium, ovarian, and bladder (1 each). Many of these patients (65%, n = 17) were treated with chemotherapy that included DNA-damaging agents. For more than half (54%, n = 14), targeted therapies were used, and some patients received both.
The authors highlight several patients as examples of exceptional responders:
- One patient with glioblastoma multiforme (GBM) was treated sequentially with surgery, localized carmustine, and radiotherapy. When the cancer recurred, temozolomide was administered. This induced a complete response that has lasted for more than a decade.
- A patient with metastatic colon adenocarcinoma has had an ongoing and nearly complete response that has lasted 45 months (last follow-up) after receiving temozolomide in combination with the investigational drug TRC102 (methoxyamine, under development by Tracon) in a phase 1 clinical trial. TRC102 is an inhibitor of the DNA base excision repair pathway, which is a pathway that causes resistance to alkylating and antimetabolite chemotherapeutics.
- A patient with metastatic, estrogen receptor–positive breast cancer received trastuzumab because of a high-level ERBB2 amplification, together with anastrozole. This resulted in an ongoing 2.4-year partial response.
- Although the patient was clinically HER2 positive, her tumor had exceedingly low expression of ERBB2 mRNA. Molecular profiling had classified the tumor as of the basal-like subtype rather than the HER2-enriched subtype. This meant that it was unlikely that trastuzumab contributed to the exceptional response, the authors note. Because the patient was estrogen-receptor positive, she received anastrozole, an inhibitor of aromatase (CYP19A), which converts testosterone into estradiol.
- A patient who had a gastrointestinal stromal tumor with a deletion of KIT exon 11 experienced relapse after an initial response to imatinib, which targets KIT and other tyrosine kinases, but then achieved a complete response with sunitinib. Gene expression profiling revealed high expression not only of KIT but also of genes encoding several tyrosine kinases that are targeted by sunitinib (KDR, FLT1, and FLT3). This may have accounted for the patient’s response.
Favorable genomic characteristics
The authors defined a “prognostic genetics” category of tumors, characterized by genetic lesions that are now known to be associated with a favorable prognosis but that were not addressed through routine care that these patients received when they were first diagnosed. Although the patients experienced relapse after first-line treatment, their exceptional survival after salvage therapy could be linked to favorable genomic characteristics.
For example, several of the patients with high-grade GBMs and astrocytomas had genetic lesions that are generally more common in low-grade glioma and that have been associated with an indolent clinical course following standard therapy.
The authors also assessed immune response. Examining immune cell infiltration in responder tumors in comparison with control cases, the team found that signatures of B cells and activated (CD56dim) natural killer cells were higher in exceptional-responder tumors.
In one patient with metastatic urothelial cancer who experienced disease progression after chemotherapy, radiotherapy, and surgery, treatment with nivolumab produced a complete response that lasted 7 months. Such an outcome occurs in only about 3% of bladder cancer patients. The tumor expressed high mRNA levels of PDCD1, which encodes the nivolumab target PD-1, and CD274, which encodes the PD-1 ligand PD-L1. There was also a high level of amplification of IFNG, which encodes interferon-gamma, a cytokine that has been linked to favorable response to immune checkpoint blockade.
Moving to precision medicine
“It is very valuable to be tested up front and again when the disease progresses, because there may have been some genetic changes, and this may change the treatment,” said co–lead author S. Percy Ivy, MD, of the NCI’s Division of Cancer Treatment and Diagnosis.
“The goal of this study was to understand what was unique about these patients and their genetic makeup that led them to be classified as exceptional responders, and hopefully we will be able to tease that out,” she added.
“As researchers, we have a lot to learn from these patients, and they have a lot to teach us,” she added. “In the future, they will help us as we move closer to the goal of delivering precision oncology to all of our patients. We’re not there yet, but every time we study more deeply and learn more, we are able to provide better care.”
To encourage participation in this effort by investigators around the world, the NCI team and their colleagues have made their molecular profiling results and clinical information publicly available in the NCI Genomic Data Commons.
The study was supported by the NCI’s Intramural Research Program, the National Institutes of Health, the Center for Cancer Research, and the NCI’s Center for Cancer Genomics. Staudt and Ivy have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.
An ongoing research project is studying why some patients have exceptional responses. The researchers have found particular molecular features in the tumors of about a quarter of these patients. In some cases, there are multiple rare genetic changes in the tumor genome. In other cases, the tumors are infiltrated with certain types of immune cells.
The findings were published online November 19 in Cancer Cell. They come from a genomic analysis of tumor biopsy specimens from 111 patients who were identified by the National Cancer Institute’s (NCI’s) Exceptional Responders Initiative, a national project launched in 2014.
An exceptional responder is defined as an individual who achieves a partial or complete response to a treatment that would be effective in fewer than 10% of similar patients. For exceptional response, the duration of response is at least three times longer than the usual median response time.
In this study of 111 such patients, about one quarter (24%, n = 26 patients) were found to have tumors in which there were molecular features that could potentially explain exceptional responses to treatment.
“We won’t be able to identify, in every patient, which particular drugs will be beneficial,” said Louis Staudt, MD, PhD, director of the NCI’s Center for Cancer Genomics, who co-led the study. “We are nowhere near that. But what it does say is that we have identified particular mutations, some of which we knew about in some types of cancer but can also occur less commonly in other cancer types.”
Staudt noted that these mutations can “illuminate” the path that the cancer will take — and potentially can be used to predict whether the cancer will be aggressive and will require treatment or could be managed with surveillance. This is why this research can be useful in the short term, he said.
“In the longer term, this is the kind of research that inspires future work,” he told Medscape Medical News. “That would encompass clinical trials involving drugs that target some of the pathways we found to be genetically inactivated in some of these responders.”
These results support the use of genetic testing in routine clinical care, he said.
Earlier this year, the NCI team published the results of a pilot study that affirmed the feasibility of this approach. Of the more than 100 cases that were analyzed, six were identified as involving potentially clinically actionable germline mutations.
‘Curiosity drove the research’
“We had these wonderful and gratifying experiences with our patients, so we were immediately curious how that happened, so it was pretty much that curiosity that drove a lot of this work,” said Staudt.
In the current study, Staudt and colleagues used multiple genomic methodologies to detect mutations, copy number changes, aberrant methylation, outlier gene expression, and the cellular makeup of the tumor microenvironment.
The hypothesized mechanisms for exceptional responses were broadly divided into the following four categories: DNA damage response (n = 15), intracellular signaling pathway (n = 9), prognostic genetics (n = 9), and immunologic engagement (n = 16). For many patients, two or more of these mechanisms were involved.
The authors note that the “predominance of plausible DNA damage response mechanisms parallels the frequent use of cytotoxic chemotherapy in routine cancer treatment reflected in this cohort.”
Twenty-six patients were identified as exceptional responders. Among these patients, a variety of cancer types was represented: brain (8); gastrointestinal tract (6); breast (4); cholangiocarcinoma (2); lung (2); pancreas, endometrium, ovarian, and bladder (1 each). Many of these patients (65%, n = 17) were treated with chemotherapy that included DNA-damaging agents. For more than half (54%, n = 14), targeted therapies were used, and some patients received both.
The authors highlight several patients as examples of exceptional responders:
- One patient with glioblastoma multiforme (GBM) was treated sequentially with surgery, localized carmustine, and radiotherapy. When the cancer recurred, temozolomide was administered. This induced a complete response that has lasted for more than a decade.
- A patient with metastatic colon adenocarcinoma has had an ongoing and nearly complete response that has lasted 45 months (last follow-up) after receiving temozolomide in combination with the investigational drug TRC102 (methoxyamine, under development by Tracon) in a phase 1 clinical trial. TRC102 is an inhibitor of the DNA base excision repair pathway, which is a pathway that causes resistance to alkylating and antimetabolite chemotherapeutics.
- A patient with metastatic, estrogen receptor–positive breast cancer received trastuzumab because of a high-level ERBB2 amplification, together with anastrozole. This resulted in an ongoing 2.4-year partial response.
- Although the patient was clinically HER2 positive, her tumor had exceedingly low expression of ERBB2 mRNA. Molecular profiling had classified the tumor as of the basal-like subtype rather than the HER2-enriched subtype. This meant that it was unlikely that trastuzumab contributed to the exceptional response, the authors note. Because the patient was estrogen-receptor positive, she received anastrozole, an inhibitor of aromatase (CYP19A), which converts testosterone into estradiol.
- A patient who had a gastrointestinal stromal tumor with a deletion of KIT exon 11 experienced relapse after an initial response to imatinib, which targets KIT and other tyrosine kinases, but then achieved a complete response with sunitinib. Gene expression profiling revealed high expression not only of KIT but also of genes encoding several tyrosine kinases that are targeted by sunitinib (KDR, FLT1, and FLT3). This may have accounted for the patient’s response.
Favorable genomic characteristics
The authors defined a “prognostic genetics” category of tumors, characterized by genetic lesions that are now known to be associated with a favorable prognosis but that were not addressed through routine care that these patients received when they were first diagnosed. Although the patients experienced relapse after first-line treatment, their exceptional survival after salvage therapy could be linked to favorable genomic characteristics.
For example, several of the patients with high-grade GBMs and astrocytomas had genetic lesions that are generally more common in low-grade glioma and that have been associated with an indolent clinical course following standard therapy.
The authors also assessed immune response. Examining immune cell infiltration in responder tumors in comparison with control cases, the team found that signatures of B cells and activated (CD56dim) natural killer cells were higher in exceptional-responder tumors.
In one patient with metastatic urothelial cancer who experienced disease progression after chemotherapy, radiotherapy, and surgery, treatment with nivolumab produced a complete response that lasted 7 months. Such an outcome occurs in only about 3% of bladder cancer patients. The tumor expressed high mRNA levels of PDCD1, which encodes the nivolumab target PD-1, and CD274, which encodes the PD-1 ligand PD-L1. There was also a high level of amplification of IFNG, which encodes interferon-gamma, a cytokine that has been linked to favorable response to immune checkpoint blockade.
Moving to precision medicine
“It is very valuable to be tested up front and again when the disease progresses, because there may have been some genetic changes, and this may change the treatment,” said co–lead author S. Percy Ivy, MD, of the NCI’s Division of Cancer Treatment and Diagnosis.
“The goal of this study was to understand what was unique about these patients and their genetic makeup that led them to be classified as exceptional responders, and hopefully we will be able to tease that out,” she added.
“As researchers, we have a lot to learn from these patients, and they have a lot to teach us,” she added. “In the future, they will help us as we move closer to the goal of delivering precision oncology to all of our patients. We’re not there yet, but every time we study more deeply and learn more, we are able to provide better care.”
To encourage participation in this effort by investigators around the world, the NCI team and their colleagues have made their molecular profiling results and clinical information publicly available in the NCI Genomic Data Commons.
The study was supported by the NCI’s Intramural Research Program, the National Institutes of Health, the Center for Cancer Research, and the NCI’s Center for Cancer Genomics. Staudt and Ivy have disclosed no relevant financial relationships.
This article first appeared on Medscape.com.